The nation is concurrently responding to, and recovering from, the COVID-19 pandemic, as the number of cases, hospitalizations, and deaths have declined in recent months. Among the factors that have contributed to the decline in these metrics, the development and administration of multiple vaccines across the nation have been key. About 53.1 percent of the U.S. population 12 years and older—almost 150.7 million individuals—had been fully vaccinated as of June 23, 2021, according to the Centers for Disease Control and Prevention (CDC).
Continuing to deliver “shots in arms” will be a priority for the federal government, as individuals yet to be vaccinated remain at risk from COVID-19 and as new variants of the virus continue to emerge. A successful vaccination program is seen as essential to further stabilizing the economy and safely returning to prepandemic activities, such as in-person learning for students in the 2021–22 school year.
The economic and public health recovery from the pandemic and its effects remains fragile. Data from the Department of Labor show that labor market conditions improved in March, April, May, and June 2021 but remained worse relative to the prepandemic period. Additionally, new reported COVID-19 cases from June 5 to June 18, 2021, averaged about 13,000 per day—less than a tenth of the peak reported in January 2021 (see figure).
Reported COVID-19 Cases per Day in the U.S., Mar. 1, 2020–June 18, 2021
Since GAO began reporting on the federal response to the pandemic in June 2020, it has made 72 recommendations. The agencies generally agreed with 57 of these recommendations and are in the process of implementing a majority of them; 16 of these recommendations have been fully implemented. GAO also made four matters for congressional consideration, three of which remain open. In this report, GAO is making 15 new recommendations in the areas of federal preparedness and response, delivery of benefits and services, and program integrity. GAO’s recommendations, if effectively implemented, can help improve the government’s ongoing response and recovery efforts as well as help it to prepare for future public health emergencies.
GAO’s new recommendations are discussed below.
COVID-19 Testing
CDC has opportunities to improve collaboration and communication with stakeholders. Prior to the COVID-19 response, CDC had not developed a plan for enhancing laboratory testing capacity that identifies objectives and outlines agency and stakeholder roles and responsibilities for achieving these objectives within defined time frames. Doing so would be consistent with the stated goal of its own memorandum of understanding with public health and private laboratory partners and would also be consistent with other leading principles on sound planning that GAO has identified in its prior work. GAO recommends that CDC work with appropriate stakeholders to develop a plan to enhance surge capacity for laboratory testing. CDC agreed with this recommendation.
CDC initially developed a flawed COVID-19 diagnostic test, which caused challenges for the rollout of testing nationwide. CDC has taken steps to improve its process for developing tests, but additional actions could help strengthen CDC’s preparedness and enhance the nation’s testing capacity during a future infectious disease outbreak. For example, establishing contracts with test kit manufacturers prior to a public health emergency could allow CDC to supplement the supply produced by CDC and aid in the rapid manufacturing and deployment of test kits during a future public health emergency. GAO recommends that CDC assess the agency’s needs for goods and services for the manufacturing and deployment of diagnostic test kits in public health emergencies,including the potential role of establishing contracts in advance of an emergency. CDC agreed with this recommendation.
Strategic National Stockpile
The Strategic National Stockpile (SNS) contains a multibillion dollar inventory of medical countermeasures—drugs, vaccines, supplies, and other materials—to respond to a broad range of public health emergencies. The SNS can be used as a short-term stopgap buffer when the supply of materials may not be immediately available in affected areas during a public health emergency. The Department of Health and Humans Services’ (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR) oversees the SNS.
The Public Health Emergency Medical Countermeasures Enterprise (PHEMCE), an interagency group of experts, advises the Secretary of Health and Human Services in prioritizing, developing, procuring, deploying, and effectively using medical supplies and other countermeasures for the SNS. In the years before the COVID-19 pandemic, ASPR began restructuring the PHEMCE. This led to concerns from interagency partners regarding the effectiveness of interagency collaboration and transparency, such as a lack of clarity on how ASPR makes decisions about medical countermeasure issues, including for the SNS inventory. In addition, while the PHEMCE was being restructured, ASPR did not conduct SNS annual reviews from 2017 through 2019; these reviews result in recommendations to HHS regarding SNS procurement and are provided to Congress.
According to the former Assistant Secretary who initiated the restructure, although PHEMCE was successful in advancing the development of medical countermeasures, its consensus-driven process did not reflect the urgency needed and PHEMCE proceedings created security vulnerabilities. ASPR officials acknowledged that the changes ASPR made to the PHEMCE from 2018 to 2020 did not fully achieve the desired aims and created other challenges. The office is in the process of reassessing and reestablishing new organizational processes for the PHEMCE, but it has not yet finalized planning documents, including an organizational charter and implementation plan, to guide those efforts. GAO recommends that ASPR develop and document its plans for restructuring the PHEMCE. The plans should describe how ASPR will ensure a transparent and deliberative process that engages interagency partners in PHEMCE responsibilities outlined in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, including those related to SNS annual reviews. These plans should also incorporate GAO’s leading practices to foster more effective collaboration, while ensuring that sensitive information is appropriately protected. HHS—which includes ASPR—agreed with this recommendation.
PHEMCE interagency partners raised concerns about the transparency of PHEMCE activities and deliberations, and ASPR lacked documentation of PHEMCE activities and deliberations after 2017. ASPR was unable to provide documentation to GAO regarding PHEMCE decisions or recommendations made from 2018 to 2020; the rationale for the changes to the PHEMCE; or PHEMCE meeting agendas and minutes from 2018 to 2020. Not maintaining such documentation is inconsistent with HHS’s policy for records management and leaves Congress and key stakeholders without assurance that steps taken are advancing national preparedness for natural, accidental, and intentional threats. GAO recommends that ASPR implement records management practices that include developing, maintaining, and securing documentation related to PHEMCE activities and deliberations, including those related to the SNS. HHS, including ASPR, agreed with this recommendation.
The nationwide need for supplies to respond to COVID-19 quickly exceeded the quantity of supplies contained in the SNS. Thus, ASPR used procurement processes in addition to its standard process, including direct shipment of supplies from vendors. Through this direct shipment process, supplies purchased by ASPR were not used to replenish the SNS but instead were primarily distributed from vendors directly to state, local, territorial, and tribal governments.
Although ASPR has documented policies and procedures for its standard procurement process, ASPR did not have documented policies and procedures, including related control and monitoring activities, to address payment integrity risks for its direct shipment procurement process. Without written policies and procedures documenting how ASPR tracks the direct shipment and receipt of supplies before issuing payments, there is an increased risk that ASPR may make improper payments to vendors for incorrect supplies or quantities or for supplies that the intended recipients did not receive. In addition, it is difficult for management to assess the adequacy of controls over the direct shipment procurement process, and ASPR lacks assurance that its staff fully understand the process and properly and consistently perform their duties. GAO recommends that, to strengthen the current procedures for the SNS, HHS update its policies and procedures for the SNS, including related control and monitoring activities, to document the direct shipment procurement process and address payment integrity risks. Although HHS, including ASPR, did not agree with GAO regarding the need to address payment integrity risks, it stated that HHS will update its policies and procedures, including related control and monitoring activities to document the direct shipment procurement process.
Domestic Medical Supply Manufacturing
Before the pandemic, the U.S. generally depended on foreign suppliers for certain types of personal protective equipment (PPE), including nitrile gloves and surgical gowns. Multiple stakeholders representing manufacturers, distributors, and other purchasers noted that meaningful, transparent federal engagement with industry could enhance the resilience of domestic manufacturing and the supply chain. According to some stakeholders, such engagement with the private sector could help ramp up private investment in domestic PPE manufacturing, among other things.
In January 2021, GAO reported that HHS had not developed a process for engaging with key nonfederal stakeholders and Congress for development of a supply chain strategy for pandemic preparedness, including the role of the SNS. GAO recommended that HHS do so, and the department generally agreed with GAO’s recommendation. However, as of May 2021, HHS had not implemented this recommendation. GAO continues to underscore that engaging with key nonfederal stakeholders—in meaningful, proactive ways to obtain their business and industry expertise—and with Congress is critical for developing strategies to build a sustainable domestic medical supply manufacturing base.
HHS COVID-19 Funding
As of May 31, 2021, Congress had appropriated to HHS approximately $484 billion in COVID-19 funds in six relief laws. The majority of HHS’s appropriations from the first five relief laws had been obligated and about half had been expended. Specifically, as of May 31, 2021, the department reported the following (see figure):
Of the $324 billion appropriated in the first five COVID-19 relief laws, about $253 billion had been obligated (about 78 percent) and about $168 billion had been expended (about 52 percent).
Of the $160 billion appropriated in the sixth law, the American Rescue Plan Act of 2021 (ARPA), about $75 billion had been obligated (about 47 percent) and about $3 billion had been expended (about 2 percent).
HHS’s Reported COVID-19 Relief Appropriations, Obligations, and Expenditures from COVID-19 Relief Laws, as of May 31, 2021
The percentage of obligations and expenditures varied across selected COVID-19 response activities for a variety of reasons, including the nature of the activities, their planned uses, and the timing of the funds provided through the six COVID-19 relief laws.
HHS uses spend plans to communicate information about its COVID-19 spending. The first five COVID-19 relief laws generally require the department to develop, update, and provide these spend plans to Congress every 60 days. The sixth relief law, ARPA, does not require a spend plan, but according to HHS officials, the department is preparing a consolidated plan that captures the first five relief laws and a separate spend plan for funding provided through ARPA. The consolidated spend plan is under internal review at HHS and the ARPA spend plan is still being finalized. As of May 2021, GAO had received and reviewed a total of 15 spend plans—the original spend plans and subsequent updates—provided by HHS. GAO found that the most current spend plans generally do not include time frames for obligating the remaining funds, which is useful information for oversight and informing future funding decisions by Congress.
Guidance from the Office of Management and Budget to federal agencies, including HHS, noted the importance of spending transparency and regular reporting to help safeguard taxpayer dollars. GAO recommends that HHS communicate information about, and facilitate oversight of, the department’s use of COVID-19 relief funds by providing projected time frames for its planned spending in the spend plans it submits to Congress. HHS partially concurred with the recommendation and stated that the department would aim to incorporate some time frames on planned spending where that information may be available such as time frames for select grants to states.
Higher Education Grants
The Department of Education (Education) has faced inherent challenges that increase the risk of improper payments for its Higher Education Emergency Relief Fund (HEERF) grants to institutions of higher education to prevent, prepare for, and respond to COVID-19. For example, funding needed to be processed and distributed expeditiously because of health and economic threats to institutions of higher education posed by the COVID-19 pandemic. GAO tested Education’s procedures for approving and processing HEERF grants through a sample of obligations and found that the department had not effectively designed and implemented procedures needed to identify erroneous obligations after awarding the grants. GAO estimated that for 5.5 percent of schools receiving HEERF grants (about 262 of 4,764 schools in GAO’s sample), Education awarded grants that exceeded the amounts allocated—including three instances in GAO’s sample for which Education obligated $20 million more than was allocated.
Officials from Education’s Office of Postsecondary Education stated that because of time and staffing constraints and the high volume of grants administered, they did not regularly perform quality assurance reviews after obligation to identify and correct erroneous obligations. GAO recommends Education design and implement procedures for regularly conducting quality assurance reviews of obligated amounts for higher education grants, including HEERF, to help identify and correct erroneous obligations in a timely manner. Education agreed with this recommendation.
Coronavirus State and Local Relief and Recovery Funds
COVID-19 relief laws appropriated $500 billion to the Department of the Treasury (Treasury) to provide direct funding to states, localities, tribal governments, the District of Columbia, and U.S. territories to help them respond to, and recover from, the COVID-19 pandemic. This amount includes $150 billion that the CARES Act appropriated to Treasury for the Coronavirus Relief Fund (CRF) in March 2020 as well as $350 billion that ARPA appropriated to Treasury for the Coronavirus State and Local Fiscal Recovery Funds (CSLFRF) in March 2021. Recipients can use CRF payments to offset costs related to either the pandemic’s direct effects (e.g., public health needs) or its indirect effects (e.g., harm to individuals or businesses as a result of COVID-19-related closures). The CSLFRF provides payments to these recipients to cover a broader range of costs stemming from the fiscal effects of the COVID-19 pandemic.
The Single Audit Act establishes requirements for states, localities, Indian tribes, the District of Columbia, U.S. territories, and nonprofit organizations that receive federal awards to undergo single audits of those awards annually when their expenditures meet a certain dollar threshold. Single audits are critical to the federal government’s ability to help safeguard the use of the billions of dollars distributed through the CRF and CSLFRF. Auditors who conduct single audits follow guidance in the Single Audit Act’s Compliance Supplement, which provides guidelines and policy for performing single audits. After consultation with federal agencies, OMB annually updates and issues the supplement. Auditors have reported that the timing of the supplement is critical in allowing them to effectively plan their work.
The timely issuance of single audit guidance is critical to ensuring timely completion and reporting of single audits to inform the federal government about actions needed to help safeguard the use of the billions of dollars distributed through the CRF and CSLFRF. GAO recommends that OMB, in consultation with Treasury, issue timely and sufficient single audit guidance for auditing recipients’ uses of payments from the CSLFRF. OMB neither agreed nor disagreed with this recommendation.
Economic Impact Payments
The CARES Act, the Consolidated Appropriations Act, 2021, and ARPA authorized Treasury and the Internal Revenue Service (IRS) to issue three rounds of economic impact payments (EIP) as direct payments to help individuals alleviate financial stress due to the pandemic. (See figure.) To publicize information about how to file a tax return with the IRS to receive an EIP, IRS partners with organizations that work with communities that may not traditionally interact with IRS, such as lower-income families, senior citizens, veterans, tribal communities, and families with mixed-immigration status. According to officials from IRS partner organizations, ensuring eligible nonfilers receive their payments continues to be a challenge. Partners also told GAO their outreach efforts to nonfilers could be more effective if the partners had current data that could help identify specific communities of nonfilers who may need assistance.
Total Number and Amount of Economic Impact Payments (EIP) Disbursed, Rounds 1, 2, and 3, as of May 28, 2021
In January 2021, Treasury began analyzing nearly 9 million notices it had sent to nonfilers who may be eligible for the first round of EIP payments. However, Treasury does not plan to complete this analysis until fall 2021, more than 6 months after the third round of EIP payments began to be issued. This timing would limit the findings’ usefulness for informing EIP outreach efforts. By waiting to complete the analysis, Treasury and IRS are missing an opportunity to identify communities that may have a higher number of nonfilers and to use that information to inform their outreach efforts as well as the efforts of their outreach partners. GAO recommends that Treasury, in coordination with IRS, release interim findings on the effectiveness of the notices it sent in September 2020 to potentially EIP-eligible nonfilers; incorporate that analysis into IRS outreach efforts as appropriate; and then, if necessary, release an update based on new analysis after the 2021 filing season. Treasury neither agreed nor disagreed with this recommendation.
Tax Relief for Businesses
To provide liquidity to businesses during the COVID-19 pandemic, the CARES Act and other COVID-19 relief laws included tax measures to reduce certain tax obligations, including measures related to net operating loss carryback claims. In some cases, these reductions of obligations led to cash refunds. The Internal Revenue Code and the CARES Act generally require IRS to issue certain refunds within 90 days from the date when a complete application for a tentative carryback adjustment is filed or 90 days from the last day of the month in which the return is due, whichever is later. IRS data show that the agency is not meeting the statutory refund requirement for these relief measures and that as of May 1, 2021, the average processing time for refunds was 154 days, excluding additional time for final processing and distribution.
IRS officials said it is taking longer to process returns because IRS facilities that process paper returns continue to operate at reduced capacity to accommodate social distancing. In the meantime, transparent communication about these issues could help taxpayers know when to expect their refunds. Specifically, an explanation on IRS’s website that processing times for tentative refunds may exceed the expected 90 days because of service disruptions would provide taxpayers with more accurate information and expectations for receiving a refund. GAO recommends that IRS clearly communicate on its website that there are delays beyond the statutory 90-day timeline in processing tentative refunds. IRS neither agreed nor disagreed with this recommendation.
2021 Tax Filing Season
IRS is experiencing delays in processing certain returns received in 2021, resulting in extended time frames for processing returns for some taxpayers. IRS reported that it is taking longer than usual to manually review some of these returns. Specifically, as of the end of the 2021 filing season, IRS had about 25.5 million unprocessed individual and business returns, including about 1.2 million returns from its 2020 backlog, and 13.7 million returns that it had suspended because of errors. IRS staff must manually review these returns with errors. IRS typically has unprocessed returns in its inventory at the end of the filing season, but not to this extent. For example, at the end of the 2019 filing season, IRS had 8.3 million unprocessed individual and business returns, including 2.7 million returns suspended for errors. IRS’s annual tax filing activities include processing more than 150 million individual and business tax returns electronically or on paper.
With significantly more returns currently being held for manual review than in prior years, more taxpayers are trying to get information about the status of their returns and refunds. However, taxpayers have had difficulty obtaining status updates on their refunds from IRS, either by phone or online. IRS’s website does not contain all of the relevant information regarding delays in processing 2021 returns and issuing taxpayers’ refunds. Additionally, IRS’s automated message on its toll-free telephone line for individual taxpayers has not been updated to explain refund delays or to include any other alerts associated with the 2021 filing season. GAO recommends that IRS update relevant pages of its website and, if feasible, add alerts to its toll-free telephone lines to more clearly and prominently explain the nature and extent of individual refund delays occurring for returns that taxpayers filed in 2021. IRS neither agreed nor disagreed with this recommendation.
This report contains additional recommendations related to disseminating information related to leave benefits for employees.
Why GAO Did This Study
As of mid-June 2021, the U.S. had about 33.4 million reported cases of COVID-19 and about 593,000 reported deaths, according to CDC. The country also continues to experience serious economic repercussions from the pandemic.
Six relief laws, including the CARES Act, had been enacted as of May 31, 2021, to address the public health and economic threats posed by COVID-19. As of May 31, 2021, of the $4.7 trillion appropriated by these six laws for COVID-19 relief—including about $1.6 trillion appropriated by ARPA, which was enacted in March 2021—the federal government had obligated a total of $3.5 trillion and had expended $3.0 trillion, as reported by federal agencies.
The CARES Act includes a provision for GAO to report on its ongoing monitoring and oversight efforts related to the COVID-19 pandemic. This report examines the federal government’s continued efforts to respond to, and recover from, the COVID-19 pandemic.
GAO reviewed data, documents, and guidance from federal agencies about their activities. GAO also interviewed federal officials; representatives from organizations for states and localities; and other stakeholders, including manufacturers of PPE (e.g., N95 respirators, surgical masks, and nitrile gloves).
What GAO Recommends
GAO is making 15 new recommendations for agencies that are detailed in this Highlights and in the report.
Recommendations
Recommendations for Executive Action
Recommendations for Executive Action
We are making a total of 15 recommendations to federal agencies:
Number
Agency
Recommendation
1
Department of Health and Human Services : Public Health Service : Centers for Disease Control and Prevention
The Director of the Centers for Disease Control and Prevention should work with appropriate stakeholders—including public health and private laboratories—to develop a plan to enhance laboratory surge testing capacity. This plan should include timelines, define agency and stakeholder roles and responsibilities, and address any identified gaps from preparedness exercises. See the COVID-19 Testing enclosure. (Recommendation 1)
2
Department of Health and Human Services : Public Health Service : Centers for Disease Control and Prevention
The Director of the Centers for Disease Control and Prevention should assess the agency’s needs for goods and services for the manufacturing and deployment of diagnostic test kits in public health emergencies. This assessment should evaluate how establishing contracts in advance of an emergency could help the Centers for Disease Control and Prevention quickly and cost-effectively acquire these capabilities when responding to future public health emergencies, including those caused by novel pathogens, and should incorporate lessons learned from the COVID-19 emergency. See the COVID-19 Testing enclosure. (Recommendation 2)
3
Department of Health and Human Services : Office of the Assistant Secretary for Preparedness and Response
To improve the nation’s preparedness for a wide range of threats, including pandemics, the Office of the Assistant Secretary for Preparedness and Response should develop and document plans for restructuring the Public Health Emergency Medical Countermeasures Enterprise. These plans should describe how the Assistant Secretary will ensure a transparent and deliberative process that engages interagency partners in the full range of responsibilities for the Public Health Emergency Medical Countermeasures Enterprise outlined in the Pandemic and All-Hazards Preparedness and Innovation Act of 2019, including the annual Strategic National Stockpile Threat-Based Reviews. These plans should also incorporate GAO’s leading practices to foster more effective collaboration, while ensuring that sensitive information is appropriately protected. See the Strategic National Stockpile enclosure. (Recommendation 3)
4
Department of Health and Human Services : Office of the Assistant Secretary for Preparedness and Response
To improve organizational accountability, the Office of the Assistant Secretary for Preparedness and Response should implement records management practices that include developing and maintaining, and securing documentation related to Public Health Emergency Medical Countermeasures Enterprise activities and deliberations, including those related to the Strategic National Stockpile. Documentation should include information such as the factors considered, the rationale for the action or decision, and the final outcomes of the Public Health Emergency Medical Countermeasures Enterprise processes. See the Strategic National Stockpile enclosure. (Recommendation 4)
5
Department of Health and Human Services : Office of the Assistant Secretary for Preparedness and Response
To strengthen the current procedures, the Assistant Secretary for Preparedness and Response should update policies and procedures, including related control and monitoring activities, for the Strategic National Stockpile to document the direct shipment procurement process and to address payment integrity risks. See the Strategic National Stockpile Payment Integrity enclosure. (Recommendation 5)
6
Department of Health and Human Services
To communicate information about and facilitate oversight of the agency’s use of COVID-19 relief funds, the Secretary of Health and Human Services should provide projected time frames for the planned spending of COVID-19 relief funds in the Department of Health and Human Services’ spend plans submitted to Congress. See the HHS COVID-19 Funding enclosure. (Recommendation 6)
7
Department of Education : Office of the Assistant Secretary for Postsecondary Education
The Assistant Secretary for Postsecondary Education should design and implement procedures for regularly conducting quality assurance reviews of obligated amounts for higher education grants, including the Higher Education Emergency Relief Fund, to help identify and correct erroneous obligations in a timely manner. See the Higher Education Grants enclosure. (Recommendation 7)
8
Executive Office of the President : Office of Management and Budget
The Director of the Office of Management and Budget, in consultation with the Secretary of the Treasury, should issue timely and sufficient single audit guidance for auditing recipients’ uses of payments from the Coronavirus State and Local Fiscal Recovery Funds. See the Coronavirus State and Local Relief and Recovery Funds enclosure. (Recommendation 8)
9
Department of the Treasury
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should release interim findings on the effectiveness of the notices it sent in September 2020 to nonfilers who are potentially eligible for economic impact payments; incorporate that analysis into Internal Revenue Service outreach efforts as appropriate; and then, if necessary, release an update based on new analysis after the 2021 filing season. See the Economic Impact Payments enclosure. (Recommendation 9)
10
Department of Labor : Wage and Hour Division
The Administrator of the Department of Labor’s Wage and Hour Division should better monitor data across all statutes that the Wage and Hour Division enforces to ensure the division’s case management is consistent with established policies for assigning and prioritizing cases. See the Leave Benefits for Employees enclosure. (Recommendation 10)
11
Department of Labor : Wage and Hour Division
The Administrator of the Department of Labor’s Wage and Hour Division should ensure that the new data system under development includes mechanisms to prevent staff from assigning and prioritizing cases in a manner inconsistent with established policies. See the Leave Benefits for Employees enclosure. (Recommendation 11)
12
Department of Labor : Wage and Hour Division
The Administrator of the Department of Labor’s Wage and Hour Division should expand the Essential Workers, Essential Protections initiative on pandemic-related worker protections to include information about filing a complaint related to paid leave provided under the Families First Coronavirus Response Act. See the Leave Benefits for Employees enclosure. (Recommendation 12)
13
Department of Labor : Wage and Hour Division
The Administrator of the Department of Labor’s Wage and Hour Division should engage in a comprehensive and timely effort to consult with employers, workers, and organizations that represent them, to identify and document lessons learned from the Wage and Hour Division’s administration and enforcement of COVID-19-related paid leave. See the Leave Benefits for Employees enclosure. (Recommendation 13)
14
Department of the Treasury : Internal Revenue Service
The Commissioner of Internal Revenue should clearly communicate on the Internal Revenue Service’s website that there are delays, beyond the statutory 90-day timeline, in processing net operating loss and alternative minimum tax tentative refunds. See the Tax Relief for Businesses enclosure. (Recommendation 14)
15
Department of the Treasury : Internal Revenue Service
The Commissioner of Internal Revenue should direct the appropriate officials to update relevant pages of irs.gov and, if feasible, add alerts to the Internal Revenue Service’s toll-free telephone lines to more clearly and prominently explain the nature and extent of individual refund delays occurring for returns taxpayers filed in 2021. See the 2021 Tax Filing Season enclosure. (Recommendation 15)
The nation is concurrently responding to, and recovering from, the Coronavirus Disease 2019 (COVID-19) pandemic, as the number of cases, hospitalizations, and deaths have seen overall declines nationally in recent months. While the decline in these metrics is attributable to a number of factors, the development and administration of multiple vaccines across the nation have been key among them.
About 53.1 percent of the U.S. population age 12 and over—almost 150.7 million individuals—had been fully vaccinated as of June 23, 2021, according to the Centers for Disease Control and Prevention (CDC).[1] Continuing to get “shots in arms” will be a priority for the federal government, as those yet to be vaccinated remain at higher risk from COVID-19 and as new variants of the virus continue to emerge. A successful vaccination program is seen as essential to further stabilizing the economy and safely returning to prepandemic activities, such as in-person learning for students for the 2021–22 school year.
As part of its recovery efforts, Congress passed, and the President signed into law, the American Rescue Plan Act of 2021 (ARPA) in March 2021.[2] The law provided, among other things, about $1.6 trillion to address the continued impact of COVID-19 on the economy, public health, state and local governments, individuals, and businesses. Since March 2020, Congress has provided about $4.7 trillion through ARPA as well as five other laws, including the CARES Act, that were previously enacted to fund efforts to help the nation respond to, and recover from, the COVID-19 pandemic (COVID-19 relief laws).[3]
As the administration implements the provisions in the COVID-19 relief laws, the size and scope of these efforts—from distributing the funding to implementing new programs—demand strong accountability and oversight. Furthermore, the government must remain vigilant and agile to address new COVID-19 variants and potential unexpected events or unintended consequences of recovery and response efforts while concurrently preparing for future public health emergencies.
Recognizing the need for robust monitoring and oversight of new authorities and funding, the CARES Act includes a provision for us to report regularly on the federal response to the pandemic. Specifically, the act requires us to monitor and oversee the federal government’s efforts to prepare for, respond to, and recover from the COVID-19 pandemic.[4] To date, we have issued seven recurring oversight reports in response to this provision; in these reports, we have made 72 recommendations to federal agencies, and raised four matters for congressional consideration to improve the federal government’s response efforts.[5] The agencies generally agreed with 57 of these recommendations, and are in the process of implementing a majority of those recommendations.
This report examines the federal government’s continued efforts to respond to, and recover from, the COVID-19 pandemic. We are making 15 new recommendations to federal agencies in areas including COVID-19 testing, the Strategic National Stockpile, tax relief, higher education grants, leave benefits for employees, and state and local funding.
This report also includes 28 enclosures about a range of federal programs and activities across the government concerning public health and the economy (see app. I). Figure 1 lists these enclosures by topic area and highlights those with new recommendations.
Figure 1: Report Enclosures by Topic Area
Given the government-wide scope of this report, we undertook a variety of methodologies to complete our work, including examining a wide range of data sources and conducting interviews with federal officials, representatives from organizations for state and local entities, and other stakeholder groups such as manufacturers of personal protective equipment (e.g., N95 respirators, surgical masks, and nitrile gloves). We examined federal laws and agency documents and guidance, among other things. In each enclosure, we include a summary of the methodology specific to the work conducted.
We have issued other targeted COVID-19-related reports in areas such as biomedical research, emergency financial aid for college students, and global health security, and we have reviews ongoing in other areas.[6] See appendix II for highlights pages from our recently issued work on COVID-19. See appendix III for a list of our ongoing work related to COVID-19, and see appendix IV for the status of matters for congressional consideration and recommendations for executive action presented in our June 2020, September 2020, November 2020, January 2021, and March 2021 CARES Act reports and in our November 2020 report on vaccines and therapeutics.
We conducted this performance audit from February 2021 to July 2021 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
The effects of the COVID-19 pandemic on public health and the economy over the past 17 months have been devastating, and recovery from the pandemic and its effects remains fragile. As of mid-June 2021, about 33.4 million cases and about 593,000 deaths had been reported in the U.S.[7] Since the pandemic began, the country has also continued to experience higher unemployment. As of May 2021, about 9.3 million individuals were unemployed, compared with nearly 5.8 million at the beginning of 2020.[8]
According to data from CDC’s National Center for Health Statistics, about 584,000 more deaths occurred from all causes (i.e., COVID-19 and other causes) in the U.S. from January 2020, through May 29, 2021, than would normally be expected (see fig. 2).
Figure 2: Higher-Than-Expected Weekly Mortality in the U.S., January 2020–May 29, 2021
Note: The data shown represent the number of deaths from all causes in a given week through May 29, 2021, reported in the U.S. that exceeded the upper-bound threshold of expected deaths calculated by CDC’s NCHS on the basis of variation in mortality in prior years. For further details of CDC’s methodology for estimating this upper-bound threshold, see CDC, National Center for Health Statistics, “Excess Deaths Associated with COVID-19,” accessed June 24, 2021, https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm. The number of deaths in recent weeks should be interpreted cautiously, as this figure relies on provisional data that are generally less complete.
However, recent trends in reported new cases indicate that the country is making progress in its response to the pandemic. The number of new reported COVID-19 cases has decreased since the peak in January 2021. From June 5 to June 18, 2021, new reported COVID-19 cases averaged about 13,000 per day—less than a tenth of the peak reported in January 2021 (see fig. 3).[9] During the same 2-week period, reported new COVID-19 cases per day, on average, increased in four jurisdictions, held steady in 11 jurisdictions, and decreased in 37 jurisdictions.[10] Further, deaths from all causes were within the estimated upper bound of expected variation in March 2021 for the first time since March 2020.
Figure 3: Reported COVID-19 Cases per Day in the U.S., Mar. 1, 2020–June 18, 2021
Note: Reported COVID-19 cases include confirmed and probable cases. Beginning April 14, 2020, states could include probable as well as confirmed COVID-19 cases in their reports to CDC. Previously, counts included only confirmed cases. According to CDC, the actual number of cases is unknown for a variety of reasons, including the fact that people who have been infected may not have been tested or may not have sought medical care. See CDC, “COVID Data Tracker: Trends in Number of COVID-19 Cases and Deaths in the U.S. Reported to CDC, by State/Territory,” accessed June 24, 2021, https://covid.cdc.gov/covid-data-tracker/#trends_dailytrendscases.
Providing the public with safe and effective vaccines to protect people from getting sick with COVID-19 is crucial to mitigating the public health and economic impacts of the virus and ending the pandemic. Two COVID-19 vaccines using a two-dose regimen were authorized for emergency use in December 2020 and a third, one-dose vaccine was authorized in February 2021.[11] Doses of COVID-19 vaccine administered each day have decreased from a peak in early April 2021, with a temporary dip in February due to severe weather across the country (see fig. 4). As of June 23, 2021, about 323 million doses had been administered, according to data reported to CDC. See the Vaccine Implementation enclosure in appendix I for more information.
Figure 4: Daily Count of COVID-19 Vaccine Doses Administered in the U.S. and Reported to CDC, Dec. 14, 2020–June 23, 2021
Notes: The data shown reflect COVID-19 vaccine doses administered in the U.S. as reported to CDC by state, territorial, and local public health agencies and by federal entities since the national vaccine program began on December 14, 2020. The data include doses administered through all vaccine partners, including jurisdictional partner clinics, retail pharmacies, long-term care facilities, Federal Emergency Management Agency and Health Resources and Services Administration partner sites, and federal entity facilities. See CDC, “COVID Data Tracker: COVID-19 Vaccinations in the United States,” accessed on June 28, 2021, https://covid.cdc.gov/covid-data-tracker/#vaccinations.As of June 23, 2021, three COVID-19 vaccines were authorized for emergency use; two of these vaccines are two-dose regimens and the third vaccine requires one dose. The number of doses administered on a given day may be affected by several factors, such as weekend days, holidays, weather, and vaccine availability. The most recent days of reporting may be more impacted by reporting delays, and all reported numbers may change over time as historical data are reported to CDC.
In addition to affecting public health, the pandemic continues to cause economic challenges, particularly for the labor market, though the economy has improved in recent months. Monthly and weekly data from the Department of Labor (DOL) indicate that labor market conditions improved in March, April, May, and June 2021 but remained worse relative to the prepandemic period. Weekly initial unemployment insurance claims fell from March to June 2021, indicating improvements in the labor market in recent months. For example, in May 2021, the employment-to-population ratio, which measures the share of the population employed, was 58.0 percent—a slight increase from the previous month, but 3.1 percentage points lower than in the prepandemic period (see fig. 5).[12] See the Economic Indicators enclosure in appendix I for more information.
Figure 5: Employment-to-Population Ratio, January 2019–May 2021
In response to the far-reaching public health and economic crises resulting from the COVID-19 pandemic, Congress has passed, and the President has signed, six COVID-19 relief laws. Figure 6 shows the COVID-19 relief laws enacted from March 2020, through May 31, 2021.
Figure 6: COVID-19 Relief Laws Enacted as of May 31, 2021
Note: The laws shown are those providing comprehensive COVID-19 relief. Additional COVID-19 relief legislation, such as legislation providing limited and targeted relief to certain individuals, also was enacted during this period. Amounts shown for the six COVID-19 relief laws are based on appropriation warrant information provided by the Department of the Treasury as of May 31, 2021. These amounts have increased over time and could increase in the future for programs with indefinite appropriations, which are appropriations that, at the time of enactment, are for an unspecified amount. aThe Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, provided $7.8 billion to agencies for health emergency prevention, preparedness, and response activities related to the COVID-19 pandemic, with the Department of Health and Human Services receiving a majority of the funds. Pub. L. No. 116-123, 134 Stat. 146.bThe Families First Coronavirus Response Act provided supplemental appropriations for nutrition assistance programs and public health services and authorized the Internal Revenue Service to provide tax credits for paid emergency sick leave and expanded family medical leave that the act required certain employers to provide. In addition, the act provided states with flexibility to temporarily modify provisions of their unemployment insurance laws and policies related to certain eligibility requirements and provided additional federal financial support to the states. Pub. L. No. 116-127, 134 Stat. 178 (2020).cThe CARES Act provided supplemental appropriations for federal agencies to respond to the COVID-19 pandemic. In addition, the act funded various loans, grants, and other forms of federal financial assistance for businesses, industries, states, local governments, and hospitals; provided tax rebates for certain individuals; temporarily expanded unemployment benefits; and suspended payments and interest on federal student loans. Pub. L. No. 116-136, 134 Stat. 281 (2020). dThe Paycheck Protection Program and Health Care Enhancement Act provided additional appropriations for small business loans, grants to health care providers, and COVID-19 testing. Pub. L. No. 116-139, 134 Stat. 620 (2020).eThe Consolidated Appropriations Act, 2021, expanded or extended several CARES Act programs, including unemployment insurance programs, economic impact payments, and Paycheck Protection Program loans and rescinded unobligated funds for certain programs. Pub. L. No. 116-260, 134 Stat. 1182 (2020). fThe American Rescue Plan Act of 2021 provided additional relief to address the continued impact of the COVID-19 pandemic on the economy, public health, state and local governments, individuals, and businesses. Pub. L. No. 117-2, 135 Stat. 4.
As of May 31, 2021, about $4.7 trillion had been appropriated to fund response and recovery efforts for—as well as to mitigate the public health, economic, and homeland security effects of—the COVID-19 pandemic.[13] As of May 31, 2021, the most recent date for which government-wide information was available at the time of our analysis, the federal government had obligated a total of $3.5 trillion and expended $3.0 trillion of the COVID-19 relief funds as reported by federal agencies to the Department of the Treasury’s (Treasury) Governmentwide Treasury Account Symbol Adjusted Trial Balance System (GTAS).[14] Obligations and expenditures relative to the amounts appropriated through COVID-19 relief laws have varied over time, as new relief laws have been enacted, appropriating additional relief funds, and as the federal government has obligated and expended these relief funds (see fig. 7).
Figure 7: Percentage of COVID-19 Relief Appropriations Obligated and Expended, July 31, 2020–May 31, 2021
Note: The percentages shown represent the portions of appropriated funds available as of each date shown that had been obligated and expended. An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes. Appropriation amounts are based on appropriation warrant information provided by the Department of the Treasury as of July 31, 2020; September 30, 2020; November 30, 2020; January 31, 2021; and May 31, 2021, for the six COVID-19 relief laws, four of which were enacted before July 2020. These amounts have increased over time and could increase in the future for programs with indefinite appropriations, which are appropriations that, at the time of enactment, are for an unspecified amount. An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of the other party beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures reflected in the percentages shown include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. Increased spending in Medicaid and Medicare is not accounted for in the appropriations provided by the COVID-19 relief laws. Under Office of Management and Budget (OMB) guidance, federal agencies were not directed to report COVID-19 related obligations and expenditures until July 2020.
The 13 major spending areas shown in table 1 represent $4.1 trillion, or 87 percent, of the total amounts appropriated. For these 13 spending areas, agencies reported obligations totaling $3.2 trillion and expenditures totaling $2.8 trillion as of May 31, 2021. Table 1 provides additional details on appropriations, obligations, and expenditures of government-wide COVID-19 relief funds, including the 13 major spending areas.
Table 1: COVID-19 Relief Appropriations, Obligations, and Expenditures, as of May 31, 2021
Major spending areaa
Total appropriationsb ($ billions)
Total obligationsc ($ billions)
Total expendituresc ($ billions)
Unemployment Insurance (Department of Labor)
858.6
575.6
566.2
Economic Impact Payments (Department of the Treasury)
855.3
829.9
829.9
Business Loan Programs (Small Business Administration)
838.0
834.6
805.4d
Public Health and Social Services Emergency Fund (Department of Health and Human Services)
350.1
228.7
154.5
Coronavirus State and Local Fiscal Recovery Funds (Department of the Treasury) e
350.0
140.2
131.0
Education Stabilization Fund (Department of Education)
278.6
224.0
30.9
Coronavirus Relief Fund (Department of the Treasury)
150.0
149.9
149.5
Disaster Relief Fundf (Department of Homeland Security)
97.0
58.1
2.2
Transit Infrastructure Grants (Department of Transportation)
69.5
27.1
19.6
Supplemental Nutrition Assistance Programs (Department of Agriculture)
69.4
26.9
26.8
Emergency Economic Injury Disaster Loan (EIDL) Grants (Small Business Administration)
55.0
21.4
21.1
Payment to States for the Child Care and Development Block Grant (Department of Health and Human Services)
52.5
51.9
3.9
Disaster Loans Programs (Small Business Administration)
51.0
27.1
25.5d
Other areasg,h
630.6
303.6
233.3
Totali
4,705.6
3,499.0
2,999.8
Source: GAO analysis of data from the Department of the Treasury (Treasury) and applicable agencies. | GAO-21-551
aMajor spending areas shown are based on federal accounts in Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System (GTAS). Each spending area may include multiple programs. bCOVID-19 relief appropriations shown reflect amounts appropriated under the American Rescue Plan Act of 2021 (ARPA), Pub. L. No. 117-2, 135 Stat. 4; Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146. These amounts are based on appropriation warrant information provided by Treasury as of May 31, 2021. These amounts have increased over time and could increase in the future for programs with indefinite appropriations, which are appropriations that, at the time of enactment, are for an unspecified amount. The amounts shown do not include transfers of funds that federal agencies may make between appropriation accounts or transfers of funds they may make to other agencies. cObligation and expenditure data shown are based on data reported by applicable agencies. An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of the other party beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures shown include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. dThe Small Business Administration’s Business Loan Program account includes activity for the Paycheck Protection Program loan guarantees and certain other loan subsidies, and the Disaster Loans Program account includes activity for direct loans. Both of these expenditures relate mostly to the loan subsidy costs (i.e., the loan’s estimated long-term costs to the U.S. government). eThe Coronavirus State and Local Fiscal Recovery Funds were established by section 9901 of ARPA, enacted on March 11, 2021, and are codified at 42 U.S.C. §§ 802, 803. fAppropriations to the Disaster Relief Fund are generally not specific to individual disasters or events, including the COVID-19 response. The Disaster Relief Fund’s COVID-19-related spending includes funding from appropriations in addition to those in the six COVID-19 relief laws. Treasury’s methodology for determining COVID-19-related obligations and expenditures does not include obligations and expenditures from these other appropriations. In its Disaster Relief Fund Monthly Report dated June 10, 2021, the Department of Homeland Security reported COVID-19-related obligations totaling $75.2 billion and expenditures totaling $52.9 billion as of May 31, 2021. gWe previously included Treasury’s Economic Stabilization and Assistance to Distressed Sectors in the major spending areas. Economic Stabilization and Assistance to Distressed Sectors programs received $500 billion in appropriations from the CARES Act, of which approximately $478.8 billion was rescinded in response to the Consolidated Appropriations Act, 2021. Therefore, Economic Stabilization and Assistance to Distressed Sectors is no longer included in our list of major spending areas. hSeveral provisions in the Families First Coronavirus Response Act and ARPA authorized increases in Medicaid payments to states and U.S. territories. The Congressional Budget Office estimated that federal expenditures from these provisions would total approximately $76.9 billion through fiscal year 2030. The largest increase to federal Medicaid spending is based on a temporary formula change rather than a specific appropriated amount. Some of the estimated costs in this total are for the Children’s Health Insurance Program, permanent changes to Medicaid, and changes not specifically related to COVID-19. This increased spending is not accounted for in the appropriations provided by the COVID-19 relief laws and therefore not included in this table. iThe sum of amounts shown may not agree due to rounding.
The COVID-19 relief laws provided more than $1 trillion to federal agencies to provide assistance related to the COVID-19 pandemic to U.S. states, the District of Columbia, localities, U.S. territories, Indian tribes (tribes), and tribal governments through existing and newly created programs and funds.[15]Table 2 lists programs and funds that each received $10 billion or more—exclusively or primarily for states, D.C., localities, U.S. territories, tribes, and tribal governments—in at least one of the six laws.
Table 2: Federal Programs and Funds Receiving $10 Billion or More in COVID-19 Pandemic-Related Aid for States, the District of Columbia, Localities, U.S. Territories, Tribes, and Tribal Governments, as of May 31, 2021
Program/fund and description
Appropriations ($ in billions)
Coronavirus State and Local Fiscal Recovery Funds
Administered by the Department of the Treasury (Treasury), these funds provide payments to states, the District of Columbia (D.C.), U.S. territories, tribal governments, and localities to mitigate the fiscal effects stemming from the COVID-19 pandemic, among other things.
350.0
Elementary and Secondary School Emergency Relief Fund
Administered by the Department of Education, this fund generally provides formula grants to states (including D.C. and Puerto Rico) for education-related needs to address the impact of the COVID-19 pandemic.
190.3
Coronavirus Relief Fund
Administered by Treasury, this fund provides payments to states, D.C., localities, U.S. territories, and tribal governments to help offset costs of their response to the COVID-19 pandemic.
150.0
Disaster Relief Fund
Administered by the Federal Emergency Management Agency, this fund provides federal disaster recovery assistance for state, local, and territorial governments when a major disaster occurs.a
95.0
Medicaid
Administered by states and U.S. territories according to plans approved by the Centers for Medicare & Medicaid Services, which oversees Medicaid at the federal level. This program finances health care for certain low-income and medically needy individuals through federal matching of states’ and U.S. territories’ health care expenditures. The Families First Coronavirus Response Act and American Rescue Plan Act of 2021 temporarily increased federal Medicaid matching rates under specified circumstances, among other changes.
76.9b
Transit grants
Administered by the Federal Transit Administration, these funds are distributed through existing grant programs to provide assistance to states, localities, U.S. territories, and tribes to prevent, prepare for, and respond to the COVID-19 pandemic.
69.5
Child Care and Development Block Grant
Administered by the Department of Health and Human Services (HHS), this block grant provides funds to states, D.C., territories, and tribes to subsidize the cost of child care for low-income families. Funding permits assistance to health care and other essential workers without regard to income eligibility requirements. Additional child care stabilization funding was provided for subgrants to eligible child care providers to support the stability of the child care sector during and after the COVID-19 pandemic.
52.5
Emergency Rental Assistance
Administered by Treasury, this program provides grants to states, D.C., U.S. territories, localities, and tribes to provide rental assistance to eligible households.
46.6
Public Health and Social Services Emergency Fund
Administered by HHS, this fund provides for grants to states, U.S. territories, localities, and tribal governments to support COVID-19 testing, surveillance, and contact tracing, among other uses.
33.4
Airport grants
Administered by the Federal Aviation Administration, these grants provide funds for eligible airports to prevent, prepare for, and respond to the effects of the COVID-19 pandemic.c
20.0
Highway infrastructure programs
Administered by the Federal Highway Administration, these programs provide funds to states, D.C., U.S. territories, and tribes for highway construction and authorize the use of these funds for maintenance, personnel, and other purposes to prevent, prepare for, and respond to the COVID-19 pandemic.
10.0
Coronavirus Capital Projects Fund
Administered by Treasury, this fund provides payments to states, D.C., U.S. territories, and tribal governments for critical capital projects that directly enable work, education, and health monitoring, in response to the COVID-19 pandemic.
10.0
State Small Business Credit Initiative
Administered by Treasury, this program provides funds to states, D.C., U.S. territories, tribal governments, and eligible localities to fund small business credit support and investment programs.
10.0
Source: GAO analysis of federal laws and data from the Congressional Budget Office. | GAO-21-551.
Note: The COVID-19 relief laws providing the amounts shown are the American Rescue Plan Act of 2021 (ARPA), Pub. L. No. 117-2, 135 Stat. 4 (2021), the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M and N, 134 Stat. 1182 (2020), the Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020), the CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020), and the Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020). The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 did not provide any specified amounts for these programs or funds for states, D.C., localities, territories, tribes, or tribal governments. The amounts shown are the cumulative amounts for each program or fund under the other five laws. Some appropriation amounts include an amount available for administration expenses or for the relevant inspectors general. Numbers are rounded to the nearest hundred million. aThe Disaster Relief Fund may be used for various disaster assistance programs, including the Public Assistance program, which provides assistance to states, U.S. territories, and localities. bSeveral provisions in the Families First Coronavirus Response Act and ARPA authorized increases in Medicaid payments to states and U.S. territories. The Congressional Budget Office estimated that federal expenditures from these provisions would be approximately $76.9 billion through fiscal year 2030. The largest increase to federal Medicaid spending is based on a temporary formula change rather than a specific appropriated amount. Some of the estimated costs in this total are for the Children’s Health Insurance Program, permanent changes to Medicaid, and changes not specifically related to COVID-19. cFunds are available to eligible sponsors of airports. Nearly all of these airports are under city, state, county, or public-authority ownership.
As COVID-19 case and death counts decline and the nation looks toward fully reopening, we identify key considerations for the federal government moving forward. In this report, we are making 15 new recommendations across the federal government in the areas of public health and the economy, specifically aimed at enhancing pandemic preparedness and response, program integrity, and the delivery of benefits and services to the public.
In our prior seven CARES Act reports, we made 72 recommendations to agencies. Agencies have fully implemented 16 of these recommendations in areas such as inspections of state veterans homes, data on nursing home vaccination rates, and guidance on reassessing schools’ operating status.[16] As Congress and the administration carry out the federal government’s ongoing COVID-19 response, including the use of funding from ARPA, we urge action on our prior 55 recommendations that have not been fully implemented, as well as our 15 new recommendations. We continue to believe that these recommendations would enhance transparency and accountability over the federal government’s response to, and recovery from, the COVID-19 pandemic. For a summary and the status of all prior recommendations from these reports, see appendix IV.
COVID-19 Testing
CDC developed a COVID-19 test, which received an emergency use authorization (EUA) from the Food and Drug Administration (FDA) on February 4, 2020, and was distributed to public health and Department of Defense laboratories from February 6 to 10, 2020.[17] However, immediately after receiving the CDC test, many public health laboratories reported to CDC that the test was not working properly.[18] Following these reports, CDC worked to correct the issue and, by February 28, 2020, began distributing new test kits to the laboratories. The failure of CDC’s COVID-19 test limited testing capacity in the U.S. during the critical early weeks of the pandemic, when the nation needed to understand the spread of the novel virus.
CDC’s was the only COVID-19 test available in the U.S. until February 29, 2020, when FDA announced that it did not intend to object if certain laboratories began using their own tests while they prepared EUA requests. According to CDC, by February 29, 2020, its laboratory had tested a total of 3,291 specimens, representing approximately 1,195 individuals. In contrast, other countries around the world quickly scaled up testing in late January and early February. For example, the South Korean government reported that South Korea was conducting about 20,000 tests each day by the middle of February 2020.[19]
While CDC has begun making improvements to its process for developing diagnostic tests, additional actions could help strengthen CDC’s preparedness and enhance the nation’s testing capacity during a future infectious disease outbreak. For example, CDC has opportunities to improve communication and collaboration. The agency collaborated with public health and private stakeholders—including public health and private laboratories—beginning in 2018 to identify potential opportunities to enhance laboratory capacity to respond to a needed surge in testing. However, CDC has not yet developed a plan for enhancing laboratory surge testing capacity that identifies objectives and outlines agency and stakeholder roles and responsibilities for achieving these objectives within defined time frames.
We are recommending that CDC work with appropriate stakeholders to develop a plan to enhance surge capacity for laboratory testing. This plan should include timelines, define agency and stakeholder roles and responsibilities, and address any identified gaps from preparedness exercises. CDC agreed with this recommendation.
The COVID-19 pandemic demonstrated potential opportunities for CDC to improve its testing capacity for future public health emergencies by improving test kit manufacturing capacity. For example, if surge testing is required at the beginning of a future emergency, CDC could benefit from establishing contracts for the manufacturing of test kits before a public health emergency occurs. Establishing contracts with test kit manufacturers in advance of a public health emergency could allow CDC to supplement the supply produced by CDC and aid in the rapid manufacturing and deployment of test kits during a future public health emergency. CDC officials told us that responding to COVID-19 required surge capacity for additional laboratory testing. However, the agency did not have manufacturing contracts in place prior to the COVID-19 pandemic that could have supported the testing response.
We are recommending that CDC assess the agency’s needs for goods and services for the manufacturing and deployment of diagnostic test kits in public health emergencies. This assessment should evaluate how establishing contracts in advance of an emergency could help CDC quickly and cost-effectively acquire these capabilities when responding to future public health emergencies and incorporate lessons learned from the COVID-19 emergency. CDC agreed with this recommendation. See the COVID-19 Testing enclosure in appendix I for more information.
Domestic Medical Supply Manufacturing
Personal protective equipment (PPE)—safety products designed to help prevent the spread of infectious disease—has been critical to the COVID-19 response. Before the pandemic, the U.S. generally depended on foreign suppliers for certain PPE types, including nitrile gloves and surgical gowns. U.S. dependence on foreign manufacturers has increased over the past several decades in part because foreign manufacturers can produce their products at a lower cost.[20] Federal agencies have identified this dependence as a national security issue.
Multiple stakeholders representing manufacturers, distributors, and other purchasers we interviewed noted that meaningful, transparent federal engagement with industry could enhance domestic manufacturing and supply chain resilience and help ensure these perspectives are considered in strategies to support and sustain the domestic PPE industry. According to some stakeholders, such engagement with the private sector could help ramp up private investment in domestic PPE manufacturing, among other things.
In January 2021, we reported that the Department of Health and Human Services (HHS) had not developed a process for engaging with key nonfederal stakeholders and Congress for development of a supply chain strategy for pandemic preparedness, including the role of the Strategic National Stockpile (SNS). We recommended that HHS do so, and the department generally agreed with our recommendation. However, as of May 2021, the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR)—which leads the nation’s medical and public health preparedness for, response to, and recovery from disasters and public health emergencies—had not proactively engaged any private or public partners in strategic discussions to implement this recommendation. However, ASPR officials told us that such discussions are important and that they are considering how to better engage their public and private partners.
We continue to underscore that engaging with key nonfederal stakeholders in meaningful, proactive ways to obtain their business and industry expertise, as well as engaging with Congress, is critical for developing strategies to build a sustainable domestic medical supply manufacturing base. See the Domestic Medical Supply Manufacturing enclosure in appendix I for more information.
Strategic National Stockpile
The SNS contains a multibillion dollar inventory of medical countermeasures—drugs, vaccines, supplies, and other materials—to respond to a broad range of public health emergencies. The SNS can be used as a short-term stopgap buffer when the supply of materials may not be immediately available in affected areas during a public health emergency. ASPR oversees the SNS. As of May 31, 2021, HHS reported it had obligated about $10.2 billion of the $13.9 billion it planned to use for the SNS and had expended about $6.3 billion.
ASPR leads an interagency group of experts, the Public Health Emergency Medical Countermeasures Enterprise (PHEMCE). The PHEMCE advises the Secretary of Health and Human Services in prioritizing, developing, procuring, deploying, and effectively using medical countermeasures held in the SNS. Comprising representatives from multiple agencies within HHS and other federal departments such as the Departments of Defense and Homeland Security, the PHEMCE also manages the SNS annual review, a year-long, multistep process that starts with an examination of the SNS inventory and results in recommendations to HHS on SNS medical countermeasure procurements and a report to Congress.
The Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 specified that the PHEMCE is to use a process to make recommendations to the Secretary of Health and Human Services regarding research, procurement, and stockpiling of medical countermeasures.[21] The PHEMCE is also to assist the Secretary in developing strategies for logistics, deployment, distribution, dispensing, and use of countermeasures that may be applicable to SNS activities.
In the years before the COVID-19 pandemic, ASPR began restructuring the PHEMCE. The changes, which began after December 2017, narrowed the scope of PHEMCE deliberations about medical countermeasures from a comprehensive range of issues to a focus on development and procurement. According to the former Assistant Secretary, in future iterations of the PHEMCE restructure, ASPR planned to broaden the PHEMCE’s scope to also focus on issues such as the deployment and utilization of medical countermeasures. The changes also shifted the structure of the deliberation process from bottom up to top down. According to the former Assistant Secretary, this shift was made to make the process more efficient and ensure medical countermeasure development focused on national security vulnerabilities.
However, the restructuring has led to concerns about:
the effectiveness of interagency collaboration and transparency and
lapses in SNS annual reviews, as ASPR did not complete statutorily required annual reviews for 2017, 2018, and 2019.[22]
ASPR is in the process of reassessing and reestablishing new organizational processes for the PHEMCE but, has not yet finalized planning documents, including an organizational charter and implementation plan, to guide those efforts. ASPR officials acknowledged that the changes made to the PHEMCE from 2018 to 2020 did not fully achieve the desired aims and created other challenges.
We are recommending that ASPR develop and document plans for restructuring the PHEMCE. These plans should describe how ASPR will ensure a transparent and deliberative process that engages interagency partners in the full range of responsibilities for the PHEMCE outlined in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, including those related to the SNS annual reviews. These plans should also incorporate GAO’s leading practices to foster more effective collaboration, while ensuring that sensitive information is appropriately protected. HHS—which includes ASPR—agreed with this recommendation. See the Strategic National Stockpile enclosure in appendix I for more information.
ASPR lacked documentation of PHEMCE activities and deliberations after 2017, raising concerns about its records management practices. For example, ASPR was unable to provide us with documentation related to PHEMCE decisions or recommendations made from 2018 to 2020; the rationale for the changes to the PHEMCE; or PHEMCE meeting agendas and minutes from 2018 to 2020. Not maintaining such documentation is inconsistent with HHS’s policy for records management and also leaves Congress and key stakeholders without assurances that steps taken are advancing national preparedness for natural, accidental, and intentional threats.[23]
We are recommending that ASPR implement records management practices that include developing, maintaining, and securing documentation related to PHEMCE activities and deliberations, including those related to the SNS. Documentation should include information such as the factors considered, the rationale for the action or decision, and the final outcomes of PHEMCE processes. HHS, including ASPR, agreed with this recommendation. See the Strategic National Stockpile enclosure in appendix I for more information.
ASPR procures supplies to maintain SNS inventory in preparation for bioterrorist attacks and other public health emergencies, using a standard procurement process. Because the nationwide need for critical supplies to respond to COVID-19 quickly exceeded the quantity of supplies contained in the SNS, ASPR also used additional procurement processes, including direct shipment of supplies from vendors. Under this direct shipment procurement, supplies purchased by ASPR were not used to replenish the SNS but instead were primarily distributed from vendors directly to state, local, territorial, and tribal governments.
Although ASPR has documented policies and procedures for its standard procurement process, ASPR did not have documented policies and procedures, including related control and monitoring activities, to address payment integrity risks for its direct shipment procurement process. Guidance from the Office of Management and Budget (OMB) states that agency management is responsible for managing payment integrity risks to reduce improper payments and protect taxpayer funds.[24]
Without written policies and procedures documenting how ASPR tracks the direct shipment and receipt of supplies prior to issuing payments, there is an increased risk that ASPR may make improper payments to vendors for incorrect supplies or quantities or for supplies the intended recipients did not receive. In addition, it is difficult for management to assess the adequacy of controls over the direct shipment procurement process, and ASPR lacks assurance that its staff fully understand the process and properly and consistently perform their duties.
We are recommending that, to strengthen the current procedures, ASPR update policies and procedures for the SNS, including related control and monitoring activities, to document the direct shipment procurement process and address payment integrity risks. Although HHS, including ASPR, did not agree with us regarding the need to address payment integrity risks, it stated that HHS will update its policies and procedures, including related control and monitoring activities to document the direct shipment procurement process. See the Strategic National Stockpile Payment Integrity enclosure in appendix I for more information.
HHS COVID-19 Funding
As of May 31, 2021, Congress had appropriated HHS approximately $484 billion in COVID-19 funds in six relief laws. The majority of HHS’s appropriations from the first five relief laws have been obligated and about half have been expended. Specifically, as of May 31, 2021, the department reported the following:
Of the $324 billion appropriated in the first five COVID-19 relief laws, about $253 billion had been obligated (about 78 percent) and about $168 billion had been expended (about 52 percent).
Of the $160 billion appropriated in the sixth law, ARPA, about $75 billion had been obligated (about 47 percent) and about $3 billion had been expended (about 2 percent).
The percentage of obligations and expenditures varied across selected COVID-19 response activities for a variety of reasons, including the nature of the activities, their planned uses, and the timing of the funds provided through the six COVID-19 relief laws.
HHS uses “spend plans” to communicate information about its COVID-19 spending. The first five COVID-19 relief laws generally require the department to develop, update, and provide these spend plans to Congress every 60 days.[25] The sixth relief law, ARPA, does not require a spend plan; however, according to HHS officials, the department is preparing a consolidated plan that captures the first five relief laws and a separate spend plan for funding provided through ARPA. The consolidated spend plan is under internal review at HHS, and the ARPA spend plan is still being finalized. As of May 2021, we had received and reviewed a total of 15 spend plans—the original spend plans and subsequent updates—provided by HHS. However, we found that the most current spend plans generally do not include time frames for obligating the remaining relief funds, which is useful information for oversight and for informing Congress’s future funding decisions.
Guidance from OMB encouraged federal agencies, including HHS, to act quickly to disburse relief funds and noted the importance of spending transparency and regular reporting to help safeguard taxpayer dollars.[26] To communicate information about, and facilitate oversight of, the department’s use of COVID-19 relief funds, we are recommending that HHS provide projected time frames for the planned spending of COVID-19 relief funds in the spend plans it submits to Congress. HHS partially concurred with the recommendation and stated that the department would aim to incorporate some time frames on planned spending where that information may be available such as time frames for select grants to states. However, HHS officials stated that the department would not be able to provide specific time frames for all relief funds since the evolving environment requires the department to remain flexible in responding to incoming requests for response activities. See the HHS COVID-19 Funding enclosure in appendix I for more information.
Higher Education Grants
Since March 2020, approximately $76.2 billion in relief funding has been appropriated for the Higher Education Emergency Relief Fund (HEERF), which provides grants to institutions of higher education to prevent, prepare for, and respond to COVID-19.[27] The Department of Education’s (Education) Office of Postsecondary Education (OPE) is responsible for administering HEERF.
In April 2020, Education notified schools of their individual funding allocations provided by the CARES Act and also began awarding HEERF grants to schools.[28] As of May 31, 2021, 14 months after the enactment of the CARES Act, OPE had obligated $66 billion in HEERF funding provided by the COVID-19 relief laws—more than 33 times the average of $2 billion in grants that OPE normally administers annually.
To administer HEERF grants, OPE relied primarily on existing staffing levels and its existing grant policies and procedures, including those documented in its Guide for Managing Formula Grant Programs. This guide establishes the structure and oversight responsibility for grant funding, including the requirement that OPE staff review the accuracy of award information, such as allocation information, before awarding the grants and recording the obligations.
Although OPE had policies and procedures in place, Education faced inherent challenges that increase the risk of improper payments—specifically, an unusually large volume of funding and a needed urgency to process and distribute the funding expeditiously because of health and economic threats posed by the COVID-19 pandemic. We tested Education’s procedures for approving and processing HEERF grants through a sample of obligations and determined that Education did not effectively design and implement procedures needed to identify erroneous obligations. We estimate that for 5.5 percent of schools receiving HEERF grants, (about 262 of the 4,764 schools included in our sample population), Education awarded grants in excess of the amounts allocated to those schools. We identified three such instances, totaling $20 million, in our sample of obligations.
OPE officials stated that because of time constraints and having the same staffing level to administer a significantly higher volume of grants, they did not regularly perform quality assurance reviews after obligating funding to identify and correct erroneous obligations, such as additional quality assurance reviews of HEERF grants. OPE officials told us that in some instances, schools have identified and self-reported discrepancies in their awards. Once noted, OPE then verified those errors and corrected them.
We are recommending that Education design and implement procedures for regularly conducting quality assurance reviews of obligated amounts for higher education grants, including HEERF grants, to help identify and correct erroneous obligations in a timely manner. Education agreed with this recommendation. See the Higher Education Grants enclosure in appendix I for more information.
Coronavirus State and Local Relief and Recovery Funds
COVID-19 relief laws appropriated $500 billion to Treasury to provide direct funding to states, localities, tribal governments, the District of Columbia, and U.S. territories to help them respond to, and recover from, the COVID-19 pandemic. This amount includes $150 billion that the CARES Act appropriated to Treasury for the Coronavirus Relief Fund (CRF) in March 2020, as well as $350 billion that ARPA appropriated to Treasury for the Coronavirus State and Local Fiscal Recovery Funds (CSLFRF) in March 2021.[29]
As of July 31, 2020, Treasury had disbursed $149.5 billion of the $150 billion appropriated for the CRF—$142 billion to states, localities, the District of Columbia, and U.S. territories and approximately $7.5 billion to tribal governments.[30] These recipients can use CRF payments to offset costs related to either the pandemic’s direct effects (e.g., public health needs) or its indirect effects (e.g., harm to individuals or businesses as a result of COVID-19 pandemic-related closures).[31] The CSLFRF provides payments to these recipients to cover a broader range of costs stemming from the fiscal effects of the COVID-19 pandemic.[32]
The Single Audit Act establishes requirements for states, localities, Indian tribes, the District of Columbia, U.S. territories, and nonprofit organizations that receive federal awards to undergo single audits of those awards annually (unless a specific exception applies) when their expenditures meet a certain dollar threshold.[33] Single audits are critical to the federal government’s ability to help safeguard the use of the billions of dollars distributed through the CRF and CSLFRF. Specifically, a single audit may identify deficiencies in an award recipient’s compliance with applicable provisions of laws, regulations, contracts, or grant agreements and in its financial management and internal control systems. Correcting such deficiencies can help to reasonably assure award recipients’ appropriate use of federal funds and reduce the likelihood of federal improper payments.
Auditors who conduct single audits follow guidance in the Single Audit Act’s Compliance Supplement, which provides guidelines and policy for performing single audits. After consultation with federal agencies, OMB annually updates and issues the supplement.[34] Auditors have reported that the timing of the supplement is critical in allowing them to plan their work effectively.
The timely issuance of single audit guidance is critical to ensuring timely completion and reporting of single audits to inform the federal government about actions needed to help safeguard the use of the billions of dollars distributed through the CRF and CSLFRF. We are recommending that OMB, in consultation with Treasury, issue timely and sufficient single audit guidance for auditing recipients’ uses of payments from the CSLFRF. OMB neither agreed nor disagreed with this recommendation. For more information about state and local relief and recovery funds, see the Coronavirus State and Local Relief and Recovery Funds enclosure in appendix I.
Economic Impact Payments
The CARES Act, the Consolidated Appropriations Act, 2021, and ARPA authorized Treasury and the Internal Revenue Service (IRS) to issue economic impact payments (EIP) as direct payments to help individuals address financial stress due to the pandemic. Starting on March 17, 2021, Treasury and IRS quickly issued a third round of direct payments (EIP 3) to most eligible individuals.[35] IRS reported that as of May 28, 2021, it had disbursed over 168.2 million payments totaling more than $394.3 billion.
To publicize information about how to file a tax return with IRS to receive an EIP, IRS partners with other organizations that work with communities that may not traditionally interact with IRS, such as lower-income families, senior citizens, veterans, tribal communities, and families with mixed-immigration status.[36] According to officials from IRS partner organizations, ensuring that eligible nonfilers—particularly among hard-to-reach groups such as those experiencing homelessness—receive their payments continues to be a challenge. Partners also told us their outreach efforts to nonfilers could be more effective if the partners had current data that helped identify specific communities of nonfilers who may need assistance. Treasury and IRS could also ensure any partial data releases were structured to not disclose taxpayer data.
Following our November 2020 recommendation, in January 2021, Treasury began analyzing nearly 9 million notices it had sent to nonfilers who may be eligible for an earlier round of EIPs. However, Treasury does not plan to complete this analysis until fall 2021, more than 6 months after the first EIP 3 payments were issued. This timing will limit the usefulness of the analysis for informing EIP 3 outreach efforts. By waiting to complete the analysis, Treasury and IRS are missing an opportunity to identify communities that may have a higher number of nonfilers and to use that information to inform their outreach efforts as well as the efforts of their outreach partners, and distribute payments to qualified individuals in a more timely manner.
We are recommending that Treasury, in coordination with IRS, release interim findings on the effectiveness of the notices it sent in September 2020 to potentially EIP-eligible nonfilers; incorporate that analysis into IRS outreach efforts as appropriate; and then, if necessary, release an update based on new analysis after the 2021 filing season. Treasury neither agreed nor disagreed with this recommendation and stated that it shares the underlying goal of reaching as many non-filers as possible to encourage them to claim economic impact payments online. However, Treasury does not plan to release any interim findings until it completes its analysis. See the Economic Impact Payments enclosure in appendix I for more information.
Leave Benefits for Employees
The Families First Coronavirus Response Act (FFCRA), as amended by the CARES Act, required employers covered under the act (covered employers) to provide emergency paid sick leave and expanded family and medical leave to eligible employees affected by COVID-19.[37] DOL’s Wage and Hour Division (WHD) administers and enforces FFCRA paid leave requirements for most employees. Covered employers generally face liability if they did not provide or improperly denied emergency paid sick leave or expanded family and medical leave or if they discharged, disciplined, or discriminated against any employee for taking either type of leave.[38] The requirements to provide paid leave benefits under the law were in effect from April 1, 2020, through December 31, 2020. Though the requirement for covered employers to provide paid leave has ended, employees can file a complaint against their employer up to 2 years after the date of an alleged violation or up to 3 years after an alleged willful violation. We identified several areas where WHD can improve its enforcement of FFCRA paid leave requirements:
WHD officials did not design or monitor its data system to support enforcement. WHD officials said they monitor the time taken to process FFCRA cases, but this monitoring did not include whether office audits and limited investigations were properly prioritized.[39] In addition, WHD did not include controls in its data system to prevent staff from incorrectly assigning cases to themselves or from assigning cases to an incorrect priority level. As a result, we identified cases that either were not assigned to a priority level because staff incorrectly assigned cases to themselves, or were assigned to an incorrect priority level. WHD officials said that all of the cases not assigned to a priority level or incorrectly assigned were ultimately investigated and concluded. The officials also said that nearly all of the cases were isolated to three offices in one region. The officials added that as of May 12, 2021, they had not yet determined whether any ongoing cases had also been assigned incorrectly.
In addition, although the number of affected FFCRA paid leave cases may be relatively small, WHD officials acknowledged there may be cases under other statutes enforced by WHD that have not been assigned to a priority level because staff incorrectly assigned cases to themselves. In addition, cases under other statutes enforced by WHD may have been assigned to an incorrect priority level. By not regularly examining data on the assignment of cases or including controls to prevent errors in case assignment and prioritization, WHD may have failed to prioritize ongoing cases under FFCRA and other statutes and may continue making such errors in future cases. Cases that were not assigned to a priority level or were assigned to the wrong priority level may not have been investigated or concluded as rapidly as other cases that were properly assigned.
WHD lacks data that it can easily aggregate to identify the reasons FFCRA complaints were filed with no compliance action and the reasons FFCRA cases were dropped.[40] In December 2020, we reported the same concern with respect to Fair Labor Standards Act of 1938 complaint data and recommended that WHD develop a method for systematically collecting this information to ensure complaints are handled consistently and resources are allocated appropriately. WHD officials agreed with our recommendation and said that WHD’s new case management system will incorporate the ability to categorize, aggregate, and review data on the types of cases that are not investigated. According to the officials, changes to the enforcement database will apply to future cases filed under all statutes WHD enforces but will not apply retroactively.
WHD has done some outreach to stakeholders, including employers and employees, since the FFCRA paid leave requirements expired. However, WHD’s new Essential Workers, Essential Protections (EWEP) initiative about pandemic-related worker protections does not include information on filing a complaint related to FFCRA paid leave, even though employees can continue to file complaints for up to 2 years from the date of an alleged violation, or up to 3 years from the date of an alleged willful violation. According to WHD documents, WHD promotes compliance with the statutes it enforces by conducting education and outreach to ensure that employers are aware of their responsibilities and that employees understand and exercise their rights. By not including information about how to file a complaint about FFCRA paid leave in the scope of its EWEP initiative, WHD may be missing an opportunity to reach employees who did not obtain paid leave to which they were entitled but who could still file a complaint and receive benefits.
WHD officials said they had not actively sought information from stakeholders about their experiences with FFCRA paid leave. As a result, the information WHD is obtaining about stakeholder experiences with FFCRA paid leave will not be comprehensive. By not engaging with stakeholder organizations specifically about their experiences with FFCRA paid leave in a comprehensive and timely manner, WHD may be missing an opportunity to improve its administration and enforcement—including its education and outreach—for future emergencies that might require a rapid response.
We are recommending that DOL’s WHD (1) better monitor data across all statutes that WHD enforces, to ensure the division’s case management is consistent with established policies for assigning and prioritizing cases; (2) ensure that the new data system under development includes mechanisms to prevent staff from assigning and prioritizing cases in a manner inconsistent with established policies; (3) expand the EWEP initiative on pandemic-related worker protections to include information about filing a complaint related to paid leave provided under FFCRA; and (4) engage in a comprehensive and timely effort to consult with employers, workers, and organizations that represent them, to identify and document lessons learned from WHD’s administration and enforcement of COVID-19-related paid leave. DOL’s WHD agreed with these recommendations. See the Leave Benefits for Employees enclosure in appendix I for more information.
Tax Relief for Businesses
To provide liquidity to businesses during the COVID-19 pandemic, the CARES Act and other COVID-19 relief laws included tax measures to help businesses—including sole proprietors, estates, and trusts—by reducing certain tax obligations, which, in some cases, led to cash refunds.[41] These tax measures included expanded net operating loss (NOL) carrybacks and the acceleration of alternative minimum tax (AMT) credit refunds.[42]
The Internal Revenue Code and the CARES Act generally require IRS to issue certain refunds within a period of 90 days from the date on which a complete application for a tentative carryback adjustment is filed or 90 days from the last day of the month in which the return is due, whichever is later.[43]
According to IRS data, the agency is not meeting the statutory refund requirement and, as of May 1, 2021, the average processing time in 2021 was 154 days, excluding additional time for final processing and distribution. IRS officials said it is taking longer to process returns because IRS facilities that process paper returns continue to operate at reduced capacity to accommodate social distancing. IRS had about 11.7 million unprocessed returns as of May 11, 2021, and its processing backlog of tentative refund claims was about 15,000. Delays in processing refunds may continue until the backlog has reduced further.
In the meantime, transparent communication about these issues and delays could help the IRS follow the Taxpayer Bill of Rights and help taxpayers know when to expect their refunds. According to IRS’s Taxpayer Bill of Rights, taxpayers are entitled to clear explanations of the laws and IRS procedures. An explanation on IRS’s website that processing times for tentative refunds may exceed the expected 90 days because of service disruptions would provide taxpayers with more accurate information and expectations for receiving a refund.[44]
We are recommending that IRS clearly communicate on its website that there are delays beyond the statutory 90-day timeline in processing NOL and AMT tentative refunds. IRS neither agreed nor disagreed with this recommendation. However, IRS did say it would review messaging addressing tentative refund processing times and update it as necessary. See the Tax Relief for Businesses enclosure in appendix I for more information.
2021 Tax Filing Season
IRS’s annual tax filing activities include processing more than 150 million individual and business tax returns electronically or on paper; issuing hundreds of billions of dollars in refunds; and providing customer service to tens of millions of taxpayers on return processing issues, such as suspected identity theft and math errors. IRS is experiencing delays in processing certain returns received in 2021, resulting in extended time frames for some taxpayers. Specifically, as of the end of the 2021 filing season, IRS had about 25.5 million unprocessed individual and business returns, including about 1.2 million returns from its 2020 backlog, and 13.7 million returns that it had suspended because of errors. IRS staff must manually review these returns with errors. IRS typically has unprocessed returns in its inventory at the end of the filing season, but not to this extent. For example, at the end of the 2019 filing season, IRS had 8.3 million unprocessed individual and business returns, including 2.7 million returns suspended for errors. IRS reported that it is taking longer than usual to manually review some of the returns received in 2021.
Because IRS is holding significantly more returns for manual review than in prior years, more taxpayers are trying to get information about the status of their returns and refunds. However, taxpayers have had difficulty obtaining status updates on their refunds from IRS, either by telephone or online. For example, IRS’s website (https://www.irs.gov) does not provide all of the relevant information regarding delays in processing 2021 returns and in issuing taxpayers’ refunds. Additionally, IRS’s automated message on its toll-free telephone line for individual taxpayers has not been updated to explain refund delays or to include any other alerts associated with the 2021 filing season.
We are recommending that IRS update relevant pages of its website and, if feasible, add alerts to its toll-free telephone lines to more clearly and prominently explain the nature and extent of individual refund delays occurring for returns taxpayers filed in 2021. IRS neither agreed nor disagreed with our recommendation; however, IRS made some changes to its website and telephone line after it provided comments on our report. We will follow up with IRS on other planned updates to its website and taxpayer telephone line to determine if the agency’s actions are sufficient to fully address our recommendation. See the 2021 Tax Filing Season enclosure in appendix I for more information.
The last 17 months of the COVID-19 pandemic have shown the devastating effects that a pandemic can have on public health and the economy. As the administration continues to respond to, and the nation recovers from, the current pandemic, the administration also needs to simultaneously prepare for the next public health emergency. We are pleased to see that 16 of our recommendations have been implemented. Our 70 remaining recommendations to federal agencies and three matters for congressional consideration, if swiftly and effectively implemented, can help further enhance these efforts.[45] We will continue to monitor the status of these recommendations as part of our ongoing oversight of the federal government’s COVID-19 response and recovery efforts.
We are sending copies of this report to the appropriate congressional committees, the Office of Management and Budget, and other relevant agencies. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at (202) 512-5500 or dodarog@gao.gov. Questions can also be directed to Kate Siggerud, Chief Operating Officer, at (202) 512-5600; A. Nicole Clowers, Managing Director, Health Care, at (202) 512-7114 or clowersa@gao.gov; or Orice Williams Brown, Managing Director, Congressional Relations, at (202) 512-4400 or williamso@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report.
Gene L. Dodaro Comptroller General of the United States
Congressional Addressees
The Honorable Patrick Leahy Chairman The Honorable Richard Shelby Vice Chairman Committee on Appropriations United States Senate
The Honorable Ron Wyden Chairman The Honorable Mike Crapo Ranking Member Committee on Finance United States Senate
The Honorable Patty Murray Chair The Honorable Richard Burr Ranking Member Committee on Health, Education, Labor, and Pensions United States Senate
The Honorable Gary C. Peters Chairman The Honorable Rob Portman Ranking Member Committee on Homeland Security and Governmental Affairs United States Senate
The Honorable Rosa L. DeLauro Chairwoman The Honorable Kay Granger Ranking Member Committee on Appropriations House of Representatives
The Honorable Frank Pallone, Jr. Chair The Honorable Cathy McMorris Rodgers Republican Leader Committee on Energy and Commerce House of Representatives
The Honorable Bennie G. Thompson Chair The Honorable John Katko Ranking Member Committee on Homeland Security House of Representatives
The Honorable Carolyn B. Maloney Chairwoman The Honorable James Comer Ranking Member Committee on Oversight and Reform House of Representatives
The Honorable Richard Neal Chair The Honorable Kevin Brady Republican Leader Committee on Ways and Means House of Representatives
Based on data available in June 2021, the national economy continued to recover, and areas of the economy we are monitoring saw broad-based improvement in recent months. Gross domestic product (GDP) grew at a 6.4 percent annual rate in the 1st quarter of 2021, to a level that was about 1 percent smaller than the size of the economy in 4th quarter 2019. Indicators for areas of the economy supported by the federal pandemic response saw broad-based improvement in recent months, with notable gains in employment, particularly in the leisure and hospitality sector, and in state and local government finances (see table).[46] The strength of the economic recovery will continue to depend on the success of public health measures against the COVID-19 pandemic, particularly vaccinations.
Indicators for Areas of the Economy Supported by the Federal COVID-19 Pandemic Response, Feb.–May 2021, Cumulative Changes since Feb. 2020
aThe employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population 16 years and over. The ratio is subject to a misclassification error with respect to identifying workers as employed and absent from work who are likely unemployed on temporary layoff. bHigher levels in the Consumer Credit Default Composite Index rate indicate more defaults on consumer loans, including auto loans, bank cards, and mortgages. The Consumer Credit Default Composite Index could be subject to seasonal variation but is not seasonally adjusted.cSeriously delinquent loans are 3 months or more past due or in foreclosure, based on mortgages insured by the Federal Housing Administration (FHA). Increases in serious delinquency rates on FHA loans could, to some extent, reflect borrowers taking advantage of mortgage forbearance provisions of the CARES Act, but may also indicate financial challenges facing the minority and low-to-moderate income households that disproportionately take out mortgages insured by FHA. We excluded February 2021 data from the figure because the delinquency rates for February 2021 are likely understated due to late reporting by a large servicer, according to FHA.dLower levels of the small business credit card delinquency index indicate more delayed payments on credit. The small business credit card delinquency index is published under license and with permission from Dun & Bradstreet, and no commercial use can be made of these data.eCorporate bond spreads are option-adjusted spreads on dollar-denominated investment grade corporate bonds from Bloomberg and are measured in basis points or 1/100th of a percentage point. Higher spreads reflect higher perceived risk among corporate borrowers by investors.fSpreads on municipal bonds are calculated relative to interest rates on Treasury securities based on the Bloomberg-Barclays Municipal Bond Index and are measured in basis points or 1/100th of a percentage point. Higher spreads reflect higher perceived risk among municipal borrowers by investors.gState and local government employment data from April 2021 and May 2021 are preliminary.
Key drivers of the economic outlook. The American Rescue Plan Act (ARPA), enacted in March 2021, includes economic provisions that are likely to influence supply and demand throughout the economy. Similar to the CARES Act, ARPA includes assistance for the unemployed and low-to-moderate income families through expanded unemployment benefits (see the Unemployment Insurance Programs enclosure in appendix I) and economic impact payments (see the Economic Impact Payments enclosure in appendix I), while offering further income support through child tax credits starting in July 2021.[47] These provisions of ARPA may reduce household financial stress and could increase demand for goods and services.
The act also includes financial support to state and local governments (see the Coronavirus State and Local Fiscal Recovery Funds enclosure in appendix I) to spend on services and infrastructure, which may boost demand and supply, as well as employment in this sector of the economy.[48] Other provisions of the act may reduce supply-chain disruptions in the agricultural and health care sectors. To the extent that these provisions are effective or that ARPA increases overall economic growth, we could see these effects reflected in the economic indicators we are monitoring.
The increasing availability of COVID-19 vaccinations has become a key aspect of the public health response to the pandemic and is likely to be an important driver of economic activity. The International Monetary Fund increased its 2021 forecast for the U.S. gross domestic product by 1.3 percentage points relative to the previous forecast, reflecting in part the impact of vaccinations on economic activity in the year.[49] For example, widespread vaccinations could increase consumer demand as concerns about COVID-19 decline.[50] In addition, as the number of people vaccinated has increased and COVID-19 cases and hospitalizations have declined, many states have lifted pandemic-related restrictions, including indoor capacity limitations.[51] Altogether, the easing of pandemic-related restrictions, declining health concerns, and the opening of schools and daycare centers following more widespread vaccinations could increase the number of individuals able to return to work and allow businesses to more effectively supply goods and services.[52] See the Vaccine Implementation enclosure in appendix I for more information on COVID-19 vaccinations.
The impact of ARPA and more widespread vaccinations against COVID-19 on supply and demand will have an important influence on the average level of prices in the economy and how fast those prices grow, known as inflation. A number of measures of actual and expected inflation have risen notably in recent months. For example, inflation forecasted for 2021 has risen from 1.7 percent to 3.5 percent over the last year.[53] Public debate is ongoing regarding whether such increases in inflation will be transitory or longer lasting, and how to address any persistent increases in inflation. If demand grows considerably faster than supply for an extended period of time, for example, then inflation could rise to levels that reduce long-term economic growth and exacerbate economic challenges facing low-income households.[54] While the level of inflation that is currently expected is unlikely to cause such problems, additional monitoring is warranted. Federal Reserve officials told us that the Federal Open Market Committee (FOMC) is acutely aware of the issues and has stated it feels well-prepared to act as necessary to achieve its monetary policy objectives. The FOMC is charged with conducting monetary policy to attain stable prices and maximum employment, and, in doing so, expects to achieve a rate of inflation that averages 2 percent over time.
Key trends in economic indicators. Federal debt held by the public rose to $22.0 trillion in May 2021 from $21.6 trillion in December 2020, but fell slightly as a share of GDP, from 100.6 percent in the 4th quarter of 2020 to 99.7 percent of GDP in 1st quarter 2021. Interest rates on 3-month Treasury securities were relatively stable, falling to 0.02 percent in May 2021 from 0.04 percent in February 2021. Interest rates on 10-year Treasury securities, in contrast, increased from 1.26 percent to 1.62 percent over the same period. As we have noted in previous CARES Act reports, the long-term fiscal challenges facing the U.S. have been exacerbated by the pandemic and will require attention once the economy has returned to consistent growth and public health goals have been attained.
Based on monthly and weekly data from the Department of Labor, labor market conditions improved in March, April, May, and June 2021 but remained worse relative to the prepandemic period. Weekly initial unemployment insurance claims fell from March to June 2021, indicating improvements in the labor market in recent months. The employment-to-population ratio in May 2021 was 58.0 percent, which was a slight increase from the previous month, but 3.1 percentage points lower than the prepandemic period (see figure).
Job growth across sectors continues to reflect the differential impact of the pandemic on different parts of the economy. For example, the industry responsible for much of the improvement in the labor market in March through May 2021 was the leisure and hospitality sector. Interest in leisure activities has improved as vaccinations have become more widespread, cases have fallen, and state and local governments have relaxed restrictions. However, despite job growth in the industry in the last few months, employment in the leisure and hospitality sector is still 15.0 percent lower than it was in February 2020.
Serious delinquency rates—loans that are 90 or more days past due or in foreclosure—for single-family mortgage loans insured by the Federal Housing Administration (FHA) decreased slightly from March to April 2021, to 10.58 percent of loans, but remained much higher than rates prior to the pandemic (see figure). FHA loans disproportionately serve minority and low-to-moderate income borrowers.[55] Falling delinquencies may to some extent reflect fewer borrowers taking advantage of mortgage forbearance provisions of the CARES Act.[56] In addition, falling delinquencies may indicate that FHA borrowers have seen some improvement in household finances in recent months.
Serious Delinquency Rates on Single-Family Residential Mortgages, Jan. 2019–Apr. 2021
Note: Seriously delinquent single-family loans are 3 months or more past due or in the foreclosure process. We excluded February 2021 data from the figure because the delinquency rates for February 2021 are likely understated due to late reporting by a large servicer, according to FHA.
Employment by state and local governments increased in March through May 2021 (see figure), and spreads on municipal bonds fell over the same period, suggesting some improvement in state and local government finances.[57]
State and Local Government Employment, Jan. 2019–May 2021
Methodology
To identify indicators for monitoring areas of the economy supported by the federal response to the COVID-19 pandemic, in particular by the six COVID-19 relief laws, we reviewed prior GAO work, data from federal statistical agencies, information from the Board of Governors of the Federal Reserve System (Federal Reserve) and relevant federal agencies responsible for the pandemic response and oversight of the health care system, data available on the Bloomberg Terminal, and input from internal GAO experts. We reviewed the most recent data from these sources as of April, May, or June 2021, depending on availability.
We assessed the reliability of the economic indicators we used through a number of steps, including reviewing relevant documentation, reviewing prior GAO work, and interviewing data providers. Collectively, we determined the indicators were sufficiently reliable to provide a general sense of how the areas of the economy supported by the federal pandemic response were performing.
Agency Comments
We provided the Department of Housing and Urban Development (HUD), the Department of Labor (Labor), the Department of the Treasury (Treasury), the Federal Reserve, and the Office of Management and Budget (OMB) with a draft of this enclosure. Labor and the Federal Reserve provided technical comments, which we incorporated as appropriate. HUD, Treasury, and OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
We plan to monitor and report on changes in economic indicators, including developments in inflation, in future quarterly reports.
Contact information: Lawrance L. Evans, Jr., (202) 512-8678, evansl@gao.gov
To increase access to COVID-19 vaccination, the federal government has expanded the number of vaccine distribution channels and administration sites since COVID-19 vaccination began, and as of June 10, 2021, more than 372 million vaccine doses had been distributed in the United States.
Entities involved: Department of Defense; Department of Health and Human Services, including the Centers for Disease Control and Prevention, Food and Drug Administration, and Health Resources and Services Administration; Federal Emergency Management Agency within the Department of Homeland Security; and the White House COVID-19 Response Team.
Background
Since the pandemic’s start, the federal government has played a key role in the development and manufacturing of COVID-19 vaccines and the implementation of a vaccination program. Federal efforts to support vaccine development, manufacturing, and distribution to states and other jurisdictions have been led at the federal level by a partnership between the Department of Defense (DOD) and the Department of Health and Human Services (HHS). This partnership was formerly known as Operation Warp Speed, but since May 2021 it has been called the HHS-DOD COVID-19 Countermeasures Acceleration Group.[58]
COVID-19 vaccine implementation, which involves the prioritization, allocation, distribution, and administration of vaccine doses, relies on communication and coordination among various stakeholders. Stakeholders include federal agencies, private industry, states and other jurisdictions, local health departments, tribal officials, and health care providers, among others.
Since January 2021, the White House COVID-19 Response Team has been responsible for coordinating across the U.S. government on the COVID-19 response, including COVID-19 vaccine implementation, and for communicating to the public, state and local public health officials, and other stakeholders about these efforts. For example, since January 27, 2021, members of the Response Team have held regular public briefings to provide updates on the status of COVID-19 vaccine implementation, among other information on the federal response.
Status of COVID-19 vaccines. As of June 15, 2021, three COVID-19 vaccines were available in the U.S. under an emergency use authorization (EUA), which allows for the temporary use of vaccines without Food and Drug Administration (FDA) licensure, provided certain statutory criteria are met. [59] Two of the three vaccines—those from Moderna and Janssen—were authorized for individuals 18 years and older; the Pfizer vaccine was authorized for individuals aged 12 years and older.[60]
On May 7, 2021, the first biologics license application (BLA) for a COVID-19 vaccine was submitted to FDA, when Pfizer applied for licensure of its vaccine to prevent COVID-19 in individuals 16 years of age and older.[61] On June 1, 2021, Moderna submitted a BLA to FDA for its vaccine to prevent COVID-19 in individuals 18 years of age and older.[62]
All three companies with authorized vaccines have announced clinical trials for children and adolescents. On May 10, 2021, FDA granted Pfizer’s request to amend its EUA to expand use of its vaccine to adolescents 12 through 15 years of age.[63] Moderna submitted a similar request on June 10, 2021, asking FDA to amend the EUA for its COVID-19 vaccine to expand its use to adolescents 12 through 17 years of age, and as of June 15, 2021, was awaiting a decision from FDA.
The three authorized vaccines have varying storage requirements that may affect the type of setting where each vaccine can be administered. For example, some vaccine administration settings may not have equipment such as freezers that have the capability to store vaccine doses at ultra-cold temperatures, the recommended storage method for the Pfizer vaccine prior to use.[64] Additional research continues on storage and handling requirements to improve the vaccines’ stability and ease storage requirements, such as by increasing the amount of time the vaccine can be stored at a refrigerated temperature.[65] See table.
COVID-19 Vaccines FDA Authorized for Emergency Use, as of June 15, 2021
Vaccine company
Date FDA initially issued emergency use authorization (EUA)a
Individuals for whom vaccine is permitted for emergency use
Dosing and schedule
Storage requirements
(doses per vial and minimum lot size)
Pfizerb
12/11/2020
12 years of age and olderc
2 doses, 3 weeks apart
Stored frozen at ultra-cold temperatures.
Once thawed and diluted, must be used within 6 hours.
(6 doses per vial, minimum lot size 450 doses)
Moderna
12/18/2020
18 years of age and olderd
2 doses, 1 month apart
Stored frozen, but may be refrigerated for up to 30 days once thawed.
Once first dose is withdrawn from vial, other doses must be used within 12 hours.
(2 vial sizes: maximum 11 doses per vial (range 10-11) or 15 doses per vial (range 13-15), minimum lot size 10-multi-dose vials)
Janssene
2/27/2021f
18 years of age and older
1 dose
Refrigerated, but may be stored at room temperature for up to 12 hours.
After first dose is withdrawn may be stored at 36 to 46 degrees Fahrenheit for up to 6 hours or at room temperature for up to 2 hours.
(5 doses per vial, minimum lot size 100 doses)
Source: GAO analysis of vaccine company and Food and Drug Administration (FDA) information. | GAO-21-551
aDuring an emergency, as declared by the Secretary of Health and Human Services under 21 U.S.C. § 360bbb-3(b), FDA may temporarily authorize unlicensed vaccines through an EUA, provided certain statutory criteria are met. FDA has indicated that issuance of an EUA for a COVID-19 vaccine for which there is adequate manufacturing information would require a determination by FDA that the vaccine’s benefits outweigh its risks based on data from at least one well-designed phase 3 clinical trial that demonstrates the vaccine’s safety and efficacy in a clear and compelling manner. Any COVID-19 vaccine that initially receives an EUA from FDA is expected to ultimately be reviewed and receive licensure through a biologics license application (BLA), according to FDA guidance. As of June 15, 2021, Pfizer and Moderna had submitted BLAs for their COVID-19 vaccines. bPfizer and BioNTech developed a COVID-19 vaccine together; for the purposes of this report we refer to it as the Pfizer vaccine. cOn December 11, 2020, FDA authorized the Pfizer vaccine for emergency use in individuals 16 years of age and older, and on May 10, 2021, FDA amended the EUA to include adolescents 12 through 15 years of age. dOn June 10, 2021, Moderna requested that FDA amend the EUA for its vaccine to include adolescents 12 through 17 years of age. eJanssen Pharmaceutical Companies are a part of Johnson & Johnson. fOn April 13, 2021, the Centers for Disease Control and Prevention (CDC) and FDA recommended a pause in use of the Janssen COVID-19 vaccine so the agencies could review data involving six reported U.S. cases of a rare and severe type of blood clot in individuals after receiving this vaccine. CDC and FDA lifted the pause on April 23, 2021, following a safety review, and revised the Janssen COVID-19 vaccine fact sheets for vaccination providers and recipients and caregivers to include information about the risk.
As we have previously reported, the federal government has also contracted to purchase COVID-19 vaccine doses from three other vaccine companies. As of June 15, 2021, none of these companies had submitted an EUA request to FDA.[66]
COVID-19 vaccine administration. COVID-19 vaccinations began on December 14, 2020, in the United States. As of June 10, 2021, data from the Centers for Disease Control and Prevention (CDC) showed the federal government had distributed about 372.8 million COVID-19 vaccine doses, and about 305.7 million doses had been administered, including both first and second doses of the three vaccines authorized for emergency use.[67] About 61 percent of the U.S. population aged 12 and older had received at least one dose of a COVID-19 vaccine and about 50 percent were fully vaccinated, as of June 10, 2021.[68]See figure for the number of vaccine doses administered each month since COVID-19 vaccine implementation began.
Number of COVID-19 Vaccine Doses Administered by Month in the United States, as of June 10, 2021
Note: Data show the number of COVID-19 vaccine doses administered in the U.S. as reported to CDC by state, territorial, and local public health agencies; and federal entities, since the national vaccine program began on December 14, 2020, and include doses administered through all vaccine partners including jurisdictional partner clinics, retail pharmacies, long-term care facilities, dialysis centers participating in the Federal Dialysis Center Program, Federal Emergency Management Agency partner sites, Health Resources and Services Administration-supported health centers, and federal entity facilities. According to CDC the most recent days of reporting may be more impacted by reporting delays, and all reported numbers may change over time as historical data are reported to CDC. As of June 10, 2021, three COVID-19 vaccines were authorized for emergency use; two vaccines were two-dose regimens and the third vaccine required one dose.
More than 70 percent of people in two age groups –those aged 75 and older and those aged 65 through 74–were fully vaccinated as of June 10, 2021. For those under 65, the percentage of people in each age group who were fully vaccinated decreased as age decreased. See figure.
Percentage of Age Group That Was Fully Vaccinated, by Age Group, in the U.S., as of June 10, 2021
Notes: Texas does not report demographic-specific dose number information to CDC, so data for Texas are not represented in this figure. As of June 10, 2021, the only COVID-19 vaccine authorized for emergency use in individuals under age 18 years of age was the Pfizer vaccine. On December 11, 2020, FDA authorized the Pfizer vaccine for emergency use in individuals 16 years of age and older, and on May 10, 2021, FDA expanded the emergency use authorization to include adolescents 12 through 15 years of age. As of June 10, 2021, of the three COVID-19 vaccines authorized for emergency use, two vaccines were two-dose regimens and the third vaccine required one dose. In this figure, fully vaccinated is defined as having received the second dose in a two-dose COVID-19 vaccine regimen or one dose of the single-dose vaccine.
CDC data, though incomplete, showed disparities in vaccine administration by race and ethnicity. Data on race and ethnicity were limited to about 61 percent of the individuals who were fully vaccinated as of June 10, 2021, or about 87 million people. These data indicated that of those who were fully vaccinated:
62.7 percent were non-Hispanic White (compared to 61.2 percent of the U.S. population),
13.4 percent were Hispanic or Latino (compared to 17.2 percent of the U.S. population),
8.7 percent were non-Hispanic Black (compared to 12.4 percent of the U.S. population), and
6 percent were non-Hispanic Asian (compared to 5.8 percent of the U.S. population).[69]
Funding for COVID-19 vaccine implementation. As of April 2021, CDC had awarded about $6.8 billion in funding, provided in three COVID-19 relief laws, to 64 jurisdictions for COVID-19 vaccine preparedness.[70] (See table.)
Department of Health and Human Services Centers for Disease Control and Prevention (CDC) COVID-19 Vaccine Implementation Funding for 64 Jurisdictions, as of April 2021
Legislation
Description of award
Month funds awarded
Amount awarded ($ millions)
CARES Act (Pub. L. No. 116-136)
To plan for and implement COVID-19 vaccine programs.
September 2020 ($200M)
December 2020 ($140M)
340
Consolidated Appropriations Act, 2021 (Pub. L. No. 116-260)
To support a range of COVID-19 vaccination activities. According to CDC, it allocated funds using the population-based formula specified in the act.
January 2021 ($3B)
April 2021 ($1.29B)
4,290
American Rescue Plan Act of 2021 (ARPA) (Pub. L. No. 117-2)
To support COVID-19 vaccine distribution, access, and administration efforts and to increase vaccine uptake. According to CDC, these funds are intended to ensure health equity as guided in the CDC COVID-19 Health Equity Strategy and expanded access to COVID-19 vaccines.b For example, funds could be used to identify and train trusted community members to conduct outreach to raise awareness about COVID-19 vaccines and help individuals sign up for appointments.
April 2021
2,189a
Total
6,819
Source: GAO analysis of CDC information and data. | GAO-21-551.
Notes: Total may not sum to exact amount awarded due to rounding. CDC awarded funds to 64 jurisdictions, including all 50 states, the District of Columbia, five major U.S. cities (Chicago, Houston, New York City, Philadelphia, and San Antonio), and eight territories (American Samoa, Guam, the Marshall Islands, the Federated States of Micronesia, the Northern Mariana Islands, Palau, Puerto Rico, and the U.S. Virgin Islands). aThis total includes about $329.1 million in funding awarded to certain immunization grant recipients by using an alternative allocation formula established under ARPA, which is to be applied in addition to the base formula specified in the Consolidated Appropriations Act, 2021.This funding was awarded to 39 jurisdictions. bSee CDC. “CDC Awards $3 Billion to Expand COVID-19 Vaccine Programs,” April 6, 2021, accessed on April 20, 2021 at https://www.cdc.gov/media/releases/2021/p0407-covid-19-vaccine-programs.html.
In addition to the awards provided by CDC to the 64 jurisdictions, other funding related to COVID-19 vaccination has been made available and includes but is not limited to the following examples:
In April 2021, HHS, through the Health Resources and Services Administration (HRSA), awarded about $6.1 billion in funds appropriated under the American Rescue Plan Act of 2021 to 1,377 health centers nationwide to expand COVID-19 vaccinations, testing, and treatment for vulnerable populations.[71]
As of June 1, 2021, the Federal Emergency Management Agency (FEMA) had provided more than $4.85 billion from the Disaster Relief Fund to states, Washington D.C., tribes, and territories for expenses related to COVID-19 vaccination.[72]
Overview of Key Issues
When COVID-19 vaccination began in December 2020, the federal government allocated and distributed nearly all available vaccine doses primarily to jurisdictions; some of the vaccine doses that went to jurisdictions were used to vaccinate residents and staff of long-term care facilities. The federal government also distributed vaccine doses to select federal entities, including the Department of Defense, Indian Health Service, and Veterans Health Administration. Beginning in February 2021, the federal government started distributing COVID-19 vaccine doses through additional channels, including directly allocating and distributing doses to retail pharmacies and to HRSA-supported health centers.[73] See the table below for a description of these federal distribution channels.
Description of Federal COVID-19 Vaccine Distribution Channels, as of June 2021
Federal channel for vaccine distribution (responsible agency)
Number of doses delivered, as of June 10, 2021a
Description
States and other jurisdictionsb (HHS and DOD)
First doses delivered: Dec. 2020
Doses delivered: 243.8 million
Allocations of vaccine provided directly from the federal government to 50 states, the District of Columbia, three major cities, and eight territories based on the 62 jurisdictions’ adult population (i.e., those 18 years and older). States and other jurisdictions determine which providers in their jurisdictions are to receive the allocated doses. Vaccine doses may be further redistributed; for example, a state may redistribute its vaccine doses to a local health department or to a health care facility, such as a hospital.
Vaccine doses allocated to states and other jurisdictions may be directed to CDC’s Pharmacy Partnership for Long-Term Care Program or to FEMA-supported community vaccination centers.c
Some states also received additional doses in their state allocations as “sovereign nation” supplements. These additional doses were allocated for American Indian/Alaskan Native populations that elected to receive vaccine doses through the state in which they are located instead of through the Indian Health Service.
Selected federal entities (HHS and DOD)
First doses delivered: Dec. 2020
Doses delivered: 12.2 milliond
Allocations of vaccine provided directly from the federal government to selected federal entities—including the Bureau of Prisons, the Departments of Defense and State, the Indian Health Service, and the Veterans Health Administration—to administer to their respective populations.
Federal Retail Pharmacy Program (CDC)
First doses delivered: Feb. 2021
Doses delivered: 103.4 millione
Allocations of vaccine provided directly from the federal government to 21 national pharmacy and independent pharmacy networks—representing over 40,000 locations nationwide—through a collaboration with the federal government, states, and territories. CDC made recommendations of which pharmacy partners to initially include in the program. States and territories then made the final selections.
Initially, when the program began, allocations were provided on a weekly basis, based on the available vaccine supply and determined on a per capita basis for each jurisdiction, according to CDC. The allocation was then divided among the selected pharmacy partners based on each partner’s number of stores and the store’s reach (the percent of the total U.S. population living within 5 miles of a store location).f
As of June 2021, weekly allocations were based on vaccine availability, with more than half of each pharmacy partner’s vaccine supply proportional to each jurisdiction’s population, according to CDC. As the program has expanded and as vaccine supply has become more readily available, pharmacy partners are able to make additional adjustments to their allocations, according to CDC.
Community Vaccination Center Pilot Site and Mobile Vaccination Program (FEMA and CDC)
First doses delivered: Feb. 2021
Doses delivered: 6.6 million
Allocations of additional vaccine doses are provided to FEMA and FEMA transfers its allocated vaccine doses to the states with pilot community vaccination centers for ordering vaccine doses. According to FEMA, allocations are determined by the size of the particular vaccination center being planned.g
Pilot vaccination centers are a partnership between FEMA, in coordination with CDC and other federal agencies, and states, tribes, territories, and local governments.
Locations for pilot community vaccination centers were chosen based on social vulnerability factors and population, according to FEMA.
As of June 4, 2021, a total of 39 FEMA pilot vaccination centers and 226 satellite sites had been established across the country since the beginning of the initiative, according to FEMA.
Health Center COVID-19 Vaccine Program (HRSA and CDC)
First doses delivered: Feb. 2021
Doses delivered: 6.9 million
Allocations are provided directly from the federal government to HRSA-supported health centers. This program is to increase access to vaccines to the nation’s underserved communities and disproportionately affected populations. Vaccines distributed through HRSA supplement the vaccine supply to the HRSA-supported health centers provided by the state or other jurisdictions, according to CDC.
Allocations are made on a weekly basis and HRSA determines the number of doses that can be ordered by participating health centers based on factors such as the weekly allocation of vaccine the program receives, the number of participating health centers, the number of newly added participating health centers, and health center vaccine distribution capacity data, according to HRSA. Vaccine doses distributed by the program are sent directly to individual health center sites.
Initially 25 health centers were selected based on criteria such as the populations the facility serves, according to HRSA.h The program grew to include 500 health centers as of April 3, 2021, according to HRSA.
On April 7, 2021, HRSA and CDC invited all HRSA-supported health centers, including Health Center Program look-alikes, to participate in the program, increasing its reach to up to 1,470 health centers nationwide.i
Source: GAO analysis of data and information from officials from the Department of Health and Human Services (HHS), the Department of Defense (DOD), the Centers for Disease Control and Prevention (CDC), the Health Resources and Services Administration (HRSA), and the Federal Emergency Management Agency (FEMA). | GAO-21-551
Notes: In addition to the federal channels listed in the table, the federal government also allocates vaccine to two other programs: the HHS/National Institutes of Health Program, which is a small program managing doses allocated to federal departments and agencies for administration to critical federal infrastructure personnel and the Federal Dialysis Center Program, which began on March 29, 2021, and has made allocations directly to participating dialysis center participants to vaccinate patients on dialysis. Additionally, some providers receiving vaccine doses through one of the federal channels may also receive vaccine allocations from their state or other jurisdiction. For example, health centers participating in the Health Center COVID-19 Vaccine Program might receive doses that have been allocated to their jurisdiction, in addition to a direct allocation of vaccine doses from the federal government. aThe Pfizer vaccine is provided in 1,170 dose and 450 dose lots, Moderna’s vaccine is provided in 140 dose lots, and Janssen’s vaccine is provided in 100 dose lots. bFor COVID-19 vaccination, the federal government allocates vaccine doses to 62 jurisdictions, including all 50 states, the District of Columbia, three major cities (Chicago, New York City, and Philadelphia), and eight territories (American Samoa, Guam, the Marshall Islands, the Federated States of Micronesia, the Northern Mariana Islands, Palau, Puerto Rico, and the U.S. Virgin Islands). Although there are 64 jurisdictions implementing COVID-19 vaccination and receiving federal funding for these efforts, allocations of vaccine doses are being made to 62 jurisdictions because two major cities considered jurisdictions—Houston and San Antonio—have their vaccine allocation consolidated with Texas. cFor the Pharmacy Partnership for Long-Term Care Program, states and other jurisdictions allocated some of their doses to pharmacy partners including CVS and Walgreens, which then administered more than 8.3 million vaccine doses to staff and residents of eligible nursing homes and other long-term care facilities between December 2020 and May 2021, according to CDC. Additionally, between February 2021 and as of May 5, 2021, FEMA has supported a total of 1,779 community vaccination centers managed and operated by states and other jurisdictions by providing federal personnel, funding, and material, such as medical equipment and supplies, according to FEMA. See the enclosures on Nursing Homes and FEMA’S Disaster Relief Fund for more information. dData on the number of doses delivered to and administered by these federal entities are available at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/distributing/jurisdiction-portfolios.html, accessed on June 15, 2021. eThis number also includes deliveries provided from states’ and other jurisdictions’ allocations, including as part of the Pharmacy Partnership for Long-Term Care Program. fAccording to CDC, the goal is to have nearly 40,000 pharmacies participating in the program. As the Federal Retail Pharmacy Program expands and supply becomes more readily available, the allocation of vaccine doses to pharmacies may be adjusted to reflect the number of store locations nationwide, the percent of the total U.S. population living within 5 miles of a store location, and the store’s ability to vaccinate. gPilot vaccination centers range in capacity from being able to administer approximately 3,000 vaccinations per day or 6,000 vaccinations per day. According to FEMA officials, one-third of the vaccines allocated to a pilot vaccination center can be redistributed to satellite sites such as mobile vaccination centers. hFor example, HRSA initially included those health centers that served a large volume of disproportionally affected populations, such as individuals experiencing homelessness, public housing residents, migrant or seasonal agricultural workers, or patients with limited English proficiency. iHealth Center Program look-alikes are community-based health care providers that meet the requirements of the HRSA Health Center Program, but do not receive Health Center Program funding.
As of June 10, 2021, CDC data showed that about 65 percent of vaccine doses had been allocated to states and other jurisdictions, and about 35 percent of the doses distributed had been provided through other federal distribution channels.[74] See figure.
Percentage of COVID-19 Vaccine Doses Distributed, by Federal Distribution Channel, as of June 10, 2021
Note: Percentages in figure may not total 100 due to rounding. Vaccine doses distributed include the approximately 373.1 million doses shipped and recorded through the CDC’s vaccine ordering system, Vaccine Tracking System (VTrckS), reported through June 10, 2021. aThis distribution channel includes doses distributed to jurisdictions. Although there are 64 jurisdictions implementing COVID-19 vaccination and receiving federal funding for these efforts, allocations of vaccine doses are being made to 62 jurisdictions because two major cities considered jurisdictions—Houston and San Antonio—have their vaccine allocation consolidated with Texas. For this metric, the three major cities that do receive their own allocations—Chicago, New York City, and Philadelphia—are reported with their respective states. This distribution channel excludes additional doses transferred to jurisdictions by the Federal Emergency Management Agency (FEMA) for use within the Community Vaccination Center Pilot Sites and mobile vaccination program.bThe Federal Retail Pharmacy Program includes vaccine allotments to 21 national pharmacy chains and independent pharmacy networks that represent approximately 48,000 potential vaccination sites across the country. It also includes deliveries provided from the jurisdiction allocations as part of the Pharmacy Partnership for Long-Term Care Program to vaccinate staff and residents of nursing homes and assisted living facilities. Jurisdictions may transfer doses directly to a pharmacy partner, and those doses are included in this category. Doses for states that have allowed vaccine provider pharmacies to order directly from the state are excluded here and included in the jurisdictions total.cThe Health Center COVID-19 Vaccine Program provides allocations directly from the federal government to participating health centers for administration.dFor the FEMA Community Vaccination Center Pilot Site and Mobile Vaccination Program, FEMA receives additional allocations of vaccine doses and transfers these doses to the states with pilot community vaccination centers for ordering and administration. FEMA provides logistical, financial, and other support for vaccination clinics.eThe Other category includes two programs (1): the Department of Health and Human Services/National Institutes of Health Program, which is a small program managing doses allocated to federal departments and agencies for administration to critical federal infrastructure personnel; and (2) the Federal Dialysis Center Program, which began on March 29, 2021, and has made allocations directly to participating dialysis center participants to vaccinate patients on dialysis.fThis distribution channel includes the allocations made to the Bureau of Prisons, Department of Defense, Indian Health Service, and Veterans Health Administration.
Representatives of state, territorial, and local stakeholders we interviewed said they appreciated the extra allocations of vaccine coming into jurisdictions through these different federal distribution channels. However, at the same time, they expressed concern about the level of coordination and communication between the federal government and states and providers regarding these other federal distribution channels for COVID-19 vaccine. For example, in February 2021, the National Governors Association stated that federal decisions to deliver vaccine doses directly to pharmacies and federally qualified health centers should be coordinated with state governments.
Additionally, representatives of state, territorial, and local health officials we interviewed said some pharmacies and health centers receiving direct allocations of vaccine doses from the federal government were also receiving vaccine allocations from their state and local jurisdictions. They said they were unaware when new federal channels were being initiated, resulting in confusion at the state and local levels. Not knowing when or how much vaccine was being distributed to a particular pharmacy or health center prevented state and local health officials from taking that information into consideration when making decisions on how to distribute their own vaccine supply to areas in need.
Vaccine implementation has continued to evolve as the supply of vaccine doses has increased and new distribution channels and groups eligible for vaccination have been added. For example, on May 4, 2021, the President announced plans to ship vaccine doses directly to rural health clinics to increase access to vaccine in rural areas.[75] And on May 10, 2021, FDA granted Pfizer’s request to expand authorized use of its COVID-19 vaccine to adolescents aged 12 through 15 years.[76]
Also, many of the people eligible in the U.S. who wanted to be vaccinated have been, according to some stakeholders we interviewed. These stakeholders said outreach and communication efforts now need to focus on those who remain unvaccinated, such as by targeting messaging to build vaccine confidence among those who may be facing vaccine hesitancy or by making vaccines more accessible.[77] The federal government has expanded its efforts to make COVID-19 vaccinations more accessible. For example, on May 4, 2021, the President announced additional efforts to make it easier for people to get vaccinated. These included plans to direct pharmacies in the Federal Retail Pharmacy Program to offer walk-in appointments and redirecting FEMA resources to support additional smaller vaccination sites and more mobile clinics.
Addressing these continuing changes in COVID-19 vaccine implementation—including vaccinating newly eligible adolescent populations and reaching those who have not yet been vaccinated despite increasing supply—will require continued coordinated efforts across federal, state, territorial, and local governments, and others. Stakeholder representatives we interviewed indicated that overall communication efforts with the federal government, such as calls between the White House COVID-19 Response Team, federal agencies, and state officials have facilitated the exchange of information related to federal vaccine distribution efforts, but often after they were publicly announced. The evolving challenges around COVID-19 vaccination and stakeholder concerns about coordination, reinforce the need for a national plan that clearly outlines how efforts are being coordinated across federal agencies and nonfederal entities, as we recommended in September 2020.
Methodology
To conduct this work, we reviewed CDC’s reported data on the distribution and administration of COVID-19 vaccine doses and reviewed relevant federal laws, agency guidance, and documentation from the DOD and HHS partnership, CDC, FDA, HRSA, and FEMA regarding COVID-19 vaccines and efforts to distribute these vaccines. Documentation we reviewed includes EUA fact sheets for the authorized COVID-19 vaccines, other agency fact sheets and advisories, and information posted on agency websites. We obtained written responses from officials at CDC, HRSA, and FEMA, and reviewed press releases from the vaccine companies. We also conducted interviews in April and May 2021, with organizations that represent state, territorial, and local stakeholders involved in vaccination efforts.[78] To report data on COVID-19 vaccine distribution and administration, we used data from CDC’s COVID Data Tracker. We assessed the reliability of this data by reviewing related documentation and reviewing the data to identify any obvious errors or omissions. We determined that the data were sufficiently reliable for the purpose of analyzing COVID-19 vaccine distribution and administration.
Agency Comments
We provided DOD; CDC, FDA, and HRSA within HHS; FEMA within the Department of Homeland Security; and the Office of Management and Budget (OMB) with a draft of this enclosure. DOD and OMB did not provide comments on this enclosure. CDC, FDA, HRSA, and FEMA provided technical comments, which we incorporated as appropriate.
GAO’s Ongoing Work
We will continue to monitor federal efforts related to COVID-19 vaccines, including the federal government’s COVID-19 vaccine distribution and administration efforts and its communication about these efforts.
GAO’s Prior Recommendations
The table below presents our recommendations on COVID-19 vaccines from prior CARES Act bimonthly/quarterly reports.
Prior GAO Recommendations Related to COVID-19 Vaccines
Recommendation
Status
The Secretary of Health and Human Services, with support from the Secretary of Defense, should establish a time frame for documenting and sharing a national plan for distributing and administering COVID-19 vaccines, and in developing such a plan ensure that it is consistent with best practices for project planning and scheduling and outlines an approach for how efforts will be coordinated across federal agencies and nonfederal entities (September 2020 report).
Open. The Department of Health and Human Services (HHS) neither agreed nor disagreed with our recommendation. In September and October 2020, HHS’ Centers for Disease Control and Prevention (CDC) released initial planning documents, and in January 2021 the White House issued a national COVID-19 response strategy that broadly outlined various channels for vaccine distribution. In addition, CDC provided a high-level description of its activities in a March 2021 COVID-19 vaccine distribution strategy and its June 2021 update. While these documents provide general information on federally supported vaccine distribution activities, they do not outline the approach the federal government is taking to coordinate its efforts or roles of the federal agencies and non-federal entities. We continue to maintain that it is important for HHS to have a national plan that outlines such an approach. We will continue to monitor HHS’ efforts in this area.
The Secretary of Health and Human Services should direct the Commissioner of the Food and Drug Administration (FDA) to identify ways to uniformly disclose to the public the information from FDA’s scientific review of safety and effectiveness data—similar to the public disclosure of the summary safety and effectiveness data supporting the approval of new drugs and biologics—when issuing emergency use authorizations (EUA) for therapeutics and vaccines, and, if necessary, seek the authority to publicly disclose such information (November 2020 report on vaccine and therapeutics).
Closed. In response to our recommendation, FDA said it would explore approaches to achieve the goal of transparency. On November 17, 2020, FDA made an announcement on the agency’s ongoing commitment to transparency for COVID-19 EUAs. FDA also developed a process to disclose its scientific review documents for therapeutic EUAs and released such summaries for one previous therapeutic EUA and the two additional therapeutic EUAs issued from November 2020—when we made our recommendation—through January 2021. These summaries disclosed information similar to what FDA releases to support new drug approvals and biologic licensures. Additionally, for the two vaccine EUAs FDA issued from November 2020—when we made our recommendation—through January 2021, FDA released decision memorandums containing detailed information about FDA’s review of safety and effectiveness data. FDA’s actions meet the intent of our recommendation and will improve transparency.
Nursing homes reported steep declines in COVID-19 cases and deaths starting in mid-December 2020, which generally coincided with the start of federal vaccination efforts through the Partnership for Long-Term Care Program.
Entities involved: Centers for Disease Control and Prevention and Centers for Medicare & Medicaid Services, both within the Department of Health and Human Services.
Background
The health and safety of the 1.4 million elderly or disabled residents in the nation’s more than 15,000 Medicare- and Medicaid-certified nursing homes—who are often in frail health and living in close proximity to one another—has been a particular concern during the COVID-19 pandemic.[79]
The Centers for Medicare and Medicaid Services (CMS), an agency within the Department of Health and Human Services (HHS), is responsible for ensuring that nursing homes meet federal quality standards to participate in the Medicare and Medicaid programs. To monitor compliance with these standards, CMS enters into agreements with state survey agencies within each state to conduct inspections, including recurring comprehensive standard surveys and as-needed investigations.
The CARES Act appropriated $100 million for this oversight, and it directed CMS to prioritize the use of funds for nursing home facilities in localities with community transmission of COVID-19.[80] HHS also designated about $10 billion from the Provider Relief Fund, which was established with funds provided under COVID-19 relief laws, as direct payments to assist nursing homes with responding to COVID-19.[81] Additionally, the American Rescue Plan Act of 2021 appropriated $250 million for the creation of state strike teams that will be deployed to nursing facilities with diagnosed or suspected cases of COVID–19 among residents or staff for the purposes of assisting with clinical care, infection control, or staffing during the COVID-19 emergency period and the following year.[82]
In response to the pandemic, HHS, primarily through CMS and the Centers for Disease Control and Prevention (CDC), has taken a range of actions to address infection prevention and control in nursing homes, which we reported on in five prior reports from June 2020 through March 2021. One of its actions was establishing the Pharmacy Partnership for Long-Term Care Program in October 2020 and agreeing with pharmacy partners to conduct COVID-19 vaccination clinics for residents and staff of long-term care facilities, including nursing homes, beginning in December 2020.[83]
In February 2021, CDC launched the Federal Retail Pharmacy Program for COVID-19 Vaccination, a collaboration between the federal government, pharmacy partners, and states and territories to increase access to COVID-19 vaccination across the U.S., including increased access to vaccines through long-term care pharmacy partners.[84]
COVID-19 cases and deaths in nursing homes. According to CDC case-reporting data, as of May 16, 2021, more than 99 percent of Medicare- and Medicaid-certified U.S. nursing homes had reported at least one confirmed resident or staff case, and more than 80 percent had reported at least one resident or staff COVID-19 death.[85] As we reported in May 2021, nursing homes commonly experienced multiple COVID-19 outbreaks, with 44 percent (5,943 of 13,380 reviewed nursing homes) having experienced four or more outbreaks between May 2020 and January 2021.[86]
New weekly confirmed cases of COVID-19 in nursing homes peaked in December and have since declined by more than 96 percent. The decline in cases for both residents and staff generally coincided with the initiation of the federal government’s nursing home vaccination program, the Pharmacy Partnership for Long-Term Care program, on December 21, 2020.[87] (See figure below.)
Similarly, new weekly resident deaths have steeply declined since peaking in the week ending December 20, 2020, again generally coinciding with the launch of federal vaccination efforts.[88] Combined nursing home resident and staff deaths from COVID-19, as a percentage of total COVID-19 deaths in the U.S., consistently represented about 30 percent of all COVID-19 deaths in the U.S., from May 2020 through February 2021. As of May 16, 2021, the combined percentage of total COVID-19 nursing home resident and staff deaths declined to 22 percent, indicating that the trajectory for nursing home COVID-19 related deaths had declined more than the decline in deaths in the country as a whole. (See figure below.)
New Weekly Confirmed COVID-19 Cases and Deaths among U.S. Nursing Home Residents and Staff, as Reported by Medicare- and Medicaid-Certified Nursing Homes, Weeks Ending May 31, 2020, through May 16, 2021
Notes: Dates refer to the end of a week (e.g., May 31 refers to the entire week from May 25 through May 31). CDC defines a confirmed case as having a positive COVID-19 test resulting from a molecular test, a nucleic acid test, or an antigen test, including antigen point-of-care test results. According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time. Data presented in this enclosure reflect the data downloaded as of May 27, 2021, which includes data through the week ending May 16, 2021. We excluded data for the week ending May 24, 2020, because it is the first week for which data are available from CDC and could include cases and deaths from multiple weeks dating back to January 1, 2020. Weekly and cumulative case and death counts are likely underreported because they do not include data for the nursing homes that did not report COVID-19 data to CDC for that week or from nursing homes that submitted data that failed data quality assurance checks. Additionally, as we previously reported, the Centers for Medicare and Medicaid Services (CMS) does not require nursing homes to report data prior to May 2020, although nursing homes may do so voluntarily. We recommended that the Secretary of Health and Human Services—in consultation with CMS and CDC—develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively to January 1, 2020.Weekly staff deaths reported for the weeks ending May 31, 2020 through May 16, 2021, ranged from 5 (week ending May 16, 2021) to 59 (week ending May 31, 2020).Certain individual nursing homes received their vaccinations outside of the Pharmacy Partnership for Long-Term Care Program. Facilities were not required to participate in the program and could opt to have vaccine supply and management services coordinated by a pharmacy provider of its choice. According to the Department of Health and Human Services (HHS), 2 percent (374 out of 15,727) of nursing homes chose not to enroll in the program, in addition to the state of West Virginia, which opted to use other local pharmacy providers to administer nursing home vaccines starting the week of December 14, 2020.
Two CDC analyses of COVID-19 testing data released in April 2021 showed that vaccination generally protected individuals from COVID-19 infection and symptoms, but both studies identified post-vaccination (breakthrough infections) in a small number of Illinois and Kentucky nursing home residents and staff members.[89] Given that such breakthrough infection can occur, the studies emphasized the need for continued focus on infection prevention and control measures in nursing homes and vaccinating residents and staff.
Nursing home vaccinations through the Pharmacy Partnership for Long-Term Care Program. Vaccination clinics for nursing home residents and staff offered through the pharmacy partnership program, which began in mid-December, were completed in all participating nursing homes as of March 30, 2021. According to CDC, as of March 30, 2021, the program had completed 13,590 first vaccination clinics, 13,521 second vaccination clinics, and 13,145 third vaccination clinics in nursing homes.[90] Further, CDC reported that approximately 3.8 million vaccine doses were administered to residents and staff in nursing homes through the Pharmacy Partnership for Long-Term Care Program—45 percent of all doses administered through the program.[91] See table below.
CDC Data on COVID-19 Vaccinations Conducted through the Pharmacy Partnership for Long-Term Care Program by Recipient Type, as of May 12, 2021
Recipient
Number of vaccine doses administered in nursing homes
Number of vaccine doses administered in all long-term care facility types
Residents
1,926,170
4,564,290
Staff members
1,810,220
3,776,119
Total
3,736,390
8,341,409
Source: Centers for Disease Control and Prevention. | GAO-21-551
Note: According to the Centers for Disease Control and Prevention (CDC), data used in this table are part of a live data set, meaning that data can be corrected by CDC and the pharmacies participating in the pharmacy partnership program at any time. Data presented in this enclosure were reported to us by CDC as of May 12, 2021. Although CDC reports that all nursing home clinics have been completed, as CDC and its participating pharmacies review the data for accuracy, the exact numbers of doses may change. CDC said that the agency anticipates producing final data on the pharmacy partnership program at the end of May.
CDC states that ensuring steady access to vaccine will be necessary after the partnership program ends in order to vaccinate new residents, new staff, and residents or staff who may have initially been hesitant and now wish to be vaccinated.[92] To support these further vaccinations, in mid-March 2021, the federal government started providing a direct allocation of COVID-19 vaccine to long-term care pharmacies participating in the Federal Retail Pharmacy Program through four companies across the country — Managed Health Care Associates, Inc., GeriMed, Innovatix, and Omnicare.[93] These companies receive a proportion of vaccine through the program to distribute to their member long-term care pharmacies that can be accessed by individual facilities.
Methodology
To conduct this work, we reviewed CMS and CDC data, agency guidance, and other relevant information on HHS’s response to the COVID-19 pandemic. We also reviewed written responses from CMS and CDC.
In addition, we analyzed CDC data on COVID-19 reported by nursing homes through the week ending May 16, 2021.[94] We analyzed the CDC data as they were reported by nursing homes to CDC and publicly posted by CMS.
We did not otherwise independently verify the accuracy of the information with these nursing homes. We assessed the reliability of the data sets used in our analyses by checking for missing values and obvious errors and reviewing relevant CMS and CDC documents. We determined the data were sufficiently reliable for the purposes of our reporting objective.
Agency Comments
We provided HHS with a draft of this enclosure. HHS did not provide comments on this enclosure.
GAO’s Ongoing Work
We have released a recent report describing the frequency and duration of COVID-19 outbreaks in nursing homes from May 2020 through January 2021. We also continue to examine the oversight of infection prevention and control as well as emergency preparedness in nursing homes.
GAO’s Prior Recommendations
The table below presents our recommendations on nursing homes from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to COVID-19 Outbreaks in Nursing Homes
Recommendation
Status
The Secretary of Health and Human Services should ensure that the Director of the Centers for Disease Control and Prevention collects data specific to the COVID-19 vaccination rates in nursing homes and makes these data publicly available to better ensure transparency and that the necessary information is available to improve ongoing and future vaccination efforts for nursing home residents and staff. (March 2021 report).
Closed. The Department of Health and Human Services (HHS) neither agreed nor disagreed with our recommendation. In March 2021, HHS said it was working towards better data transparency and noted that nursing homes have an opportunity to voluntarily report data through the National Healthcare Safety Network tracking system.
On May 13, 2021, the Centers for Medicare & Medicaid Services (CMS) issued an interim final rule establishing Long-Term Care Facility Vaccine Immunization Requirements for Residents and Staff, including for nursing homes. The rule requires facilities to report COVID-19 vaccination status of residents and staff to the Centers for Disease Control and Prevention (CDC). According to CDC, the new vaccination reporting requirement will not only assist in monitoring vaccine uptake amongst residents and staff, but will also aid in identifying facilities that may be in need of additional resources and assistance to respond to the COVID-19 pandemic. As of June 10, 2021, CMS has posted resident and staff vaccination rates for over 15,000 Medicare and Medicaid certified nursing homes on a public COVID-19 Nursing Home Data tracking website.
The Secretary of Health and Human Services should ensure that the Administrator of the Centers for Medicare & Medicaid Services, in consultation with the Centers for Disease Control and Prevention, requires nursing homes to offer COVID-19 vaccinations to residents and staff and design and implement associated quality measures (March 2021 report).
Open. HHS neither agreed nor disagreed with our recommendation at the time of publication. However, on April 15, 2021, CMS issued a proposed rule that includes, among other things, a proposal to adopt a new quality measure for skilled nursing facilities. The measure would require facilities to submit data on COVID-19 staff vaccination beginning October 1, 2021 and would be used as part of CMS’s quality reporting program beginning in fiscal year 2023.
On May 13, 2021, CMS also issued an interim final rule that establishes new requirements for nursing homes to develop and implement policies and procedures for educating residents, their representatives, and staff members about the COVID-19 vaccine and for offering these vaccines to each resident and staff member. Facilities will be assessed for compliance with the new requirements, which are effective on May 21, 2021. We will continue to monitor HHS’s progress towards implementing this recommendation.
The Administrator of CMS should quickly develop a plan that further details how the agency intends to respond to and implement, as appropriate, the 27 recommendations in the final report of the Coronavirus Commission on Safety and Quality in Nursing Homes, which CMS released on September 16, 2020.a Such a plan should include milestones that allow the agency to track and report on the status of each recommendation; identify actions taken and planned, including areas where CMS determined not to take action; and identify areas where the agency could coordinate with other federal and nonfederal entities (November 2020 report).
Closed. HHS neither agreed nor disagreed with our recommendation. HHS officials highlighted actions that CMS has taken related to Commission recommendations and said it would refer to and act upon the Commission's recommendations, as appropriate.
As of May 2021, CMS has developed an internal tracking document that notes the status of each of the Nursing Home Commission’s recommendations, the responsible agency for each recommendation, and planned actions for CMS-related recommendations. According to CMS, the agency will be: conducting quarterly reviews of the tracking document, holding interim meetings to discuss the recommendations, and conducting outreach to other Federal agencies to engage them in this work.
The Secretary of Health and Human Services, in consultation with the Centers for Medicare & Medicaid Services (CMS) and the Centers for Disease Control and Prevention (CDC), should develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively back to January 1, 2020, and clarify the extent to which nursing homes had reported data before May 8, 2020. To the extent feasible, this strategy to capture more complete data should incorporate information nursing homes previously reported to CDC or to state or local public health offices (September 2020 report).
Open. HHS partially agreed with our recommendation. As of May 2021, no specific action had been taken by HHS, although according to HHS it continues to consider how to implement our recommendation. We will continue to monitor HHS’s progress towards implementing this recommendation.
aMITRE, Coronavirus Commission on Safety and Quality in Nursing Homes: Commission Final Report, PRS Release Number 20-2382, September 2020.
Related GAO Products
COVID-19 in Nursing Homes: Most Homes Had Multiple Outbreaks and Weeks of Sustained Transmission from May 2020 through January 2021. GAO-21-367. Washington, D.C.: May 19, 2021.
COVID-19 in Nursing Homes: HHS Has Taken Steps in Response to Pandemic, but Several GAO Recommendations Have Not Been Implemented.GAO-21-402T. Washington, D.C.: March 17, 2021.
Infection Control Deficiencies Were Widespread and Persistent in Nursing Homes Prior to COVID-19 Pandemic. GAO-20-576R. Washington, D.C.: May 20, 2020.
The Centers for Disease Control and Prevention initially developed a flawed COVID-19 diagnostic test in January and February 2020, which contributed to the delayed rollout of testing nationwide. The agency has taken steps to improve its process for developing tests, but additional actions could help strengthen its preparedness and enhance the nation’s testing capacity during a future infectious disease outbreak.
Entities involved: The Centers for Disease Control and Prevention and the Food and Drug Administration within the Department of Health and Human Services
Recommendations for Executive Action
The Director of the Centers for Disease Control and Prevention should work with appropriate stakeholders—including public health and private laboratories—to develop a plan to enhance surge capacity for laboratory testing. This plan should include timelines, define agency and stakeholder roles and responsibilities, and address any identified gaps from preparedness exercises.
The Director of the Centers for Disease Control and Prevention should assess the agency’s needs for goods and services for the manufacturing and deployment of diagnostic test kits in public health emergencies. This assessment should evaluate how establishing contracts in advance of an emergency could help CDC quickly and cost-effectively acquire these capabilities when responding to future public health emergencies, including those caused by novel pathogens, and should incorporate lessons learned from the COVID-19 emergency.
The Centers for Disease Control and Prevention agreed with both of these recommendations.
Background
According to the Centers for Disease Control and Prevention (CDC), one of its roles during an emergency response to an emerging infectious disease is to aid and equip public health laboratories around the country to conduct testing during the early stages of a response. CDC typically develops a diagnostic test for an emerging pathogen when no diagnostic test has been cleared by the Food and Drug Administration (FDA) and no adequate alternative is available, as it had during past emergencies, such as with the 2009 H1N1 influenza and Zika.
The FDA issued an emergency use authorization (EUA) for CDC’s COVID-19 test on February 4, 2020.[95] The EUA process allowed CDC to distribute its COVID-19 test kits to public health laboratories more quickly than would typically be necessary for FDA approval or clearance.[96] CDC distributed COVID-19 test kits to 93 public health and Department of Defense (DOD) laboratories between February 6 and 10, 2020.[97]
Immediately after receipt of the CDC test, many public health laboratories reported to CDC that the test was not working properly.[98] Specifically, a number of public health laboratories reported to CDC that they could not validate two of the test’s three primer-probe sets, short fragments of genetic code that can be used to detect a virus’s genetic code, specifically its N1 and N3 primer-probe sets. Following these reports, CDC worked to correct the issue and, by February 28, 2020, began distributing new test kits to the laboratories.
CDC’s was the only COVID-19 test available in the U.S. until February 29, 2020, when FDA announced that it did not intend to object if certain laboratories began using their own tests while they prepared EUA requests, provided the tests were validated and the laboratories notified FDA.[99] FDA played an important role in increasing access to testing during this public health emergency; we have ongoing work examining FDA’s role in authorizing and monitoring COVID-19 tests.
According to CDC, CDC’s laboratory tested 3,291 total specimens, representing approximately 1,195 individuals, on behalf of public health laboratories in January and February, 2020. In contrast, other countries around the world quickly scaled up testing in late January and early February. For example, the South Korean government reported that South Korea was conducting about 20,000 tests each day by the middle of February 2020.[100]
The failure of CDC’s COVID-19 test limited testing capacity in the U.S. during the critical early weeks of the pandemic when the nation needed to understand the spread of the novel virus. In addition, we previously reported that shortages of key testing supplies, such as swabs and testing reagents, also contributed to the delay in broad-scale testing early in the emergency response. These shortages were due to the unprecedented domestic demand and overall global competition.
Overview of Key Issues
The CDC’s test and the test adopted by the World Health Organization were developed concurrently. CDC began work on its first COVID-19 diagnostic test on January 10, 2020—the day that Chinese researchers publicly posted the COVID-19 virus’s genetic code—and had completed the test’s design by January 18.[101] At the same time, a research laboratory in Germany was also designing a diagnostic test. The World Health Organization (WHO) published the protocol of this German test online on January 13, 2020.[102] On January 24, 2020, CDC published its test protocol online. CDC officials told us they did this so that the global laboratory community, including private laboratories in the U.S., could use CDC’s design when developing their own tests. (See figure below.)
Timeline of the Development and Distribution of CDC and WHO COVID-19 Diagnostic Tests in 2020
Although the German laboratory made its test design public on January 13, 2020, CDC officials told us that any effort to use the test designed by the German laboratory would have further delayed testing in the U.S. due to the need to fully validate and manufacture all of the necessary components and obtain the required authorization from FDA. CDC officials told us that CDC developed its own test, in part, to ensure that distribution was not limited by the exercise of intellectual property rights.
On February 3, 2020, WHO announced that it would ship test kits using the German laboratory’s design to qualified laboratories around the world that lacked the materials to produce the test themselves. WHO’s effort helped to quickly scale up testing in some countries, particularly in Africa. However, because CDC possessed the materials to make tests, its laboratories were not among those targeted for assistance by WHO. CDC officials told us that WHO did not raise with CDC the possibility of WHO providing test kits to CDC.
Three primary factors contributed to the failure of CDC’s initial test. According to CDC, the agency’s failure to detect the problems with its test prior to distribution was a “quality process failure of incalculable cost.” The failure of CDC’s first diagnostic test for COVID-19 can largely be attributed to three primary factors, according to information we collected from CDC’s own internal review and interviews with CDC officials: laboratory quality control deficiencies, a lack of clearly defined approval criteria for test release and distribution, and poor communication within CDC about test performance problems.
Laboratory quality control deficiencies. According to CDC’s internal review, the CDC laboratory that developed the test had multiple quality control deficiencies and used incorrect quality control procedures throughout the development process.[103]
For example, according to CDC, because the laboratory used an incorrect testing procedure when it conducted its final quality control check on February 3, 2020, it did not detect problems then. Rather, by February 6, 2020, when problems with the test’s performance were identified, CDC had already manufactured and prepared kits for distribution to public health laboratories. At that time, although laboratory staff had discovered that one of the test’s three primer-probe sets produced some false results, the laboratory accepted the results and approved the test for distribution to public health laboratories that same day.[104]
According to CDC, its laboratory that developed the COVID-19 test had never manufactured a diagnostic test before that one and had not implemented all quality system requirements that pertain to laboratories developing such tests.[105] CDC added that, although the laboratory operated under a quality system that was largely consistent with the requirements under the Clinical Laboratory Improvement Amendments of 1988 (CLIA), the laboratory did not have effective procedures or controls in place to assure that the test kit was fit for its intended purpose, according to the agency.[106] In an internal agency report, CDC acknowledged that the decision to assign manufacturing responsibility to a laboratory that had not implemented quality manufacturing regulatory requirements contributed to the incident.[107]
Centers for Disease Control and Prevention’s (CDC) investigation of the problems with its first COVID-19 test kits
After learning of the problems with its test kits from public health laboratories, CDC investigated the technical reasons for the failure, specifically within the sets of primers and probes—short fragments of genetic code—that could not be validated. CDC determined that the false results from the N1 primer-probe set likely had been caused by contamination during the development process. Problems with the N3 set were likely caused by a design flaw that led to the primers and probes attaching to each other during the reaction—known as a primer-dimer—and not as the result of contamination.
Source: GAO interviews with CDC officials. | GAO-21-551
Lack of clearly defined approval criteria. CDC officials told us the agency proceeded with distributing the test kits on February 6, 2020, even though the laboratory knew of its flaws, because the laboratory had not defined a pass/fail threshold for quality control checks of the test’s components and because there was no independent quality unit in place to oversee the laboratory’s manufacturing process.
Poor communication of test performance problems within CDC. CDC officials told us no one with knowledge of the test’s failure rate communicated the information beyond the laboratory when problems were initially discovered and that CDC’s response leadership was not aware of the failure rate until after CDC began receiving notices from the state public health laboratories that they had been unable to use the test.
In 2016, we reported problems within CDC related to the flow of critical information to leadership about inspections of high containment laboratories that work with hazardous biological agents. Our recommendation that the Secretary of Health and Human Services should develop policies for reporting laboratory incidents to senior department officials or direct the Director of CDC to incorporate these requirements into their policies has not been implemented as of June 25, 2021.[108]
Upon learning of the problems with the test from the public health laboratories, CDC first attempted to re-manufacture test kits using all three primer-probe sets. However, CDC later determined that the third set—N3—was not necessary and that removing it did not affect the test’s overall performance. Thus, the new test kits CDC began distributing to public health laboratories on February 28, 2020, contained only two primer-probe sets.[109]
According to CDC, the test’s design had originally included the N3 set because it was “more broadly reactive and would identify a wider family of coronaviruses, including SARS-CoV and bat-carried strains not known to have infected humans. The inclusion of a broadly reactive primer-probe set was meant to ensure that the test would be partially reactive if sequence variants arose.” During an interview with the Council on Foreign Relations, the Director of CDC at that time, said that CDC added the third set to the test because the agency was being “overly cautious.”
Other CDC actions contributed to slower testing in the early stages of the pandemic. Beyond the failure of the initial version of CDC’s COVID-19 test, three other areas contributed to testing limitations and challenges: CDC’s early testing guidelines, communication with laboratories, and selection of a testing platform.
CDC’s early testing guidelines. COVID-19 testing in the early stages of the pandemic was not widespread, in part, because of CDC’s narrow criteria for who should be tested at that time. Specifically, testing was limited in January 2020 to symptomatic individuals who had recently traveled from Wuhan City, China, or had been in close contact with individuals suspected or confirmed to have COVID-19. By late February, CDC expanded its COVID-19 testing guidelines to include symptomatic individuals who had traveled through multiple international areas and those with severe respiratory illness, regardless of their travel history.[110] According to CDC, these criteria were based on the best available information about the virus at that time and what was known about Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS). CDC officials told us it would not have been appropriate to implement wide-scale testing at that point in the response. CDC’s criteria were generally consistent with the WHO’s criteria in place at that time.
CDC’s communication of test results to public health laboratories. According to the Association of Public Health Laboratories (APHL), which represents state and local-level public health laboratories, communication of test results from CDC back to public health laboratories in the period when they were unable to perform their own tests was inefficient and slow.[111] APHL and CDC attributed the slowness to the CDC laboratory’s lack of a laboratory information management system that could communicate test results back to the public health laboratories electronically and its reliance instead on telephone calls for positive results and emails for negative results.
Further, APHL officials told us that it often took days to receive negative test results from CDC and that it was difficult for laboratories to process the negative results received by email because these laboratories needed to match specimen numbers to separate patient identification numbers—a labor-intensive process for laboratory staff.
CDC’s selection of a testing platform. According to APHL, CDC’s first COVID-19 test kit required the laboratories to use an automated extraction platform that only 12 public health laboratories had in place at the time. CDC officials told us they were unaware of how many public health laboratories had the selected platform in place in early February 2020.
The only alternative to the automated platform CDC had intended for use with its test was manual extraction of viral material, a more time-consuming method for laboratory staff to employ. APHL officials said they believe CDC’s choice of platform indicated that agency officials did not appreciate the need to move quickly to scale up testing at that time.
Officials from APHL told us they worked with the CDC Foundation to purchase the new platform for use by 12 public health laboratories, and on March 15, 2020, the EUA for the CDC test kit was reissued to allow laboratories to use other types of testing platforms.[112] However, according to APHL, had the test worked as intended from the start, CDC’s selection of a platform most public health laboratories did not have would have slowed the testing response because many public health laboratories would have initially been limited in how many specimens they could have processed per day.
CDC has begun taking steps to remediate the problems associated with the development of its first COVID-19 test and communication of test results. CDC has identified and has begun to make improvements to its process for developing diagnostic tests.
To prevent the future distribution of a flawed test, CDC will require all tests it develops to have clearly defined approval criteria and management review. According to information posted on CDC’s website in June 2021 and agency officials, a new process, including specific release criteria and multiple levels of management review and sign-off has been developed.[113] The review process was implemented for the deployment of CDC’s latest COVID-19 test in July 2020, the Influenza SARS-CoV-2 Multiplex Assay, which was designed to test for influenza and COVID-19 simultaneously.
In addition, CDC’s website stated that the agency had begun developing an internal test review board.[114] According to CDC, once developed, the test review board will require all test development and validation data to be reviewed by CDC subject matter experts from infectious disease programs outside of the program developing the test to ensure an objective review and will require multiple levels of management sign-off.[115] If implemented effectively, a review board such as this should help prevent the recurrence of a test being distributed without management having reviewed key information about the test, as occurred with CDC’s first COVID-19 test.
To help ensure CDC laboratories meet high-quality standards, CDC has indicated that it will require laboratories to obtain appropriate accreditation. According to CDC, the agency began efforts in 2020 to require that CDC laboratories become accredited to an appropriate technical standard that assures compliance with regulatory requirements by October 1, 2024.[116] According to CDC officials, this would ensure that its laboratories maintain compliance with applicable regulatory requirements to the extent practicable and that quality practices, integrity and excellence in science are not compromised.[117] CDC is directing funding from the Paycheck Protection Program and Health Care Enhancement Act to support the investments necessary to bring laboratories into compliance with applicable quality system regulations and accreditations.[118]
To improve communication of test results with public health laboratories, CDC plans to upgrade and modernize CDC laboratories’ information management infrastructure. According to CDC officials, CDC plans to spend a combined total of $1.1 billion appropriated through the CARES Act, the American Rescue Plan Act of 2012, and its annual appropriations to support the agency’s data modernization efforts. According to CDC’s road map for these efforts, the agency intends to create interoperable laboratory information systems that will enhance data sharing between federal, state and local governments and the private health care system, and CDC has begun efforts towards this goal. For example, CDC officials told us the agency performed a gap analysis in fiscal year 2021 to identify laboratories’ current and future uses for an information management system and challenges that may hinder adoption of this system. APHL officials told us they believe this new information technology infrastructure will help prevent the inefficient communication of test results from CDC to public health laboratories described above from happening again.
To ensure CDC does not release tests that are incompatible with laboratories’ testing platforms and capabilities, CDC developed a new process that includes an assessment of the platforms available at the laboratories that will use each test. CDC officials told us they employed an improved process for the development of CDC’s Influenza SARS-CoV-2 Multiplex test that included reaching out to public health laboratories to identify the platforms currently in place at those laboratories. APHL officials told us they currently collect this information and provide it to CDC. According to the June 2021 information on CDC’s website, CDC will require that all tests the agency designs for use by public health laboratories are compatible with platforms commonly used by these laboratories.[119]
The COVID-19 pandemic demonstrated potential opportunities for CDC to improve its testing capacity for future public health emergencies. Reducing the spread of infectious diseases may require enhanced collaboration with laboratories across the nation and the rapid deployment of large quantities of test kits. CDC could take additional steps to improve its testing response in future public health emergencies.
Enhancing public-private partnerships for laboratory testing. CDC officials told us that responding to COVID-19 required additional laboratory testing surge capacity. Prior to COVID-19, CDC recognized that the need for diagnostic testing can exceed the capacity of the public health laboratory infrastructure, and that private laboratories can serve to supplement national testing capabilities during an emergency. CDC collaborated with public health and private partners beginning in 2018 to identify potential opportunities to enhance surge capacity for laboratory testing; however, CDC had not taken concrete steps to enable its partners to provide surge capacity by the time of the initial stages of the COVID-19 response. To date, CDC has not yet developed a plan for enhancing laboratory surge testing capacity that identifies objectives and outlines agency and stakeholder roles and responsibilities for achieving these objectives within defined time frames.
Following the Zika outbreak in 2016, CDC initiated three key actions to explore ways to enhance laboratory testing capacity during an emergency response by coordinating with public health and private sector laboratories.
1. CDC entered into a memorandum of understanding (MOU) with CDC, APHL, the American Clinical Laboratory Association (ACLA)—an association of private clinical laboratories, and the Council of State and Territorial Epidemiologists (CSTE), signed in April 2018. [120] CDC established the MOU, in part, in response to our May 2017 report on the 2016 Zika outbreak, which found issues in the transparency of CDC’s processes for the provision of its tests to manufacturers during an emergency.[121]
The stated goal of the MOU was to build a collaborative structure to address testing surge capacity needs during an emergency. However, officials from two of CDC’s three MOU partners told us that while the agreement improved communication ahead of and during the COVID-19 pandemic, it did not have a material effect on how the nation’s testing response unfolded at the beginning of the pandemic. For example, officials from MOU partners commented that:
The MOU represents the “vision” of how enhanced coordination might work. However, officials added that CDC has not used the MOU to change any processes during the COVID-19 emergency response.
The MOU is a good first step, but CDC needs to broaden it to include more organizations. Officials added that CDC’s vision for the role of private laboratories remained unclear to them.
According to CDC officials, the MOU was a low-level agreement with no agency resources provided for its implementation.
Additionally, FDA officials told us FDA is interested in joining CDC’s MOU to enhance communication and coordination related to test development with laboratories. CDC officials told us that adding agencies such as FDA to the MOU would allow for a more thorough and consistent response from the Department of Health and Human Services (HHS). They added that, given FDA’s role in facilitating surge test capacity, both agencies share responsibility in stakeholder engagement and planning for enhanced laboratory testing capacity.
2. CDC held a tabletop training exercise with stakeholders in May 2019 to assess laboratory preparedness during an emergency response that used a scenario where a highly infectious disease emerged that spread both before and after patients began showing symptoms. This exercise included representatives from ACLA, APHL, and CSTE, as well as other agencies in HHS.
During this exercise, participants identified a number of areas for further development, including ensuring early and accurate communication with partners, integrating data more effectively, coordinating the distribution of emergency diagnostic tests and test materials, and building public-private partnerships to support surge-testing capacity during an emergency response.
CDC officials told us that the tabletop exercise helped to open lines of communication with stakeholders that were vital in responding to COVID-19. For example, following this exercise, CDC began hosting quarterly conference calls with commercial laboratories to discuss challenges with electronic reporting and other private sector response-related needs. CDC held two of these calls before the COVID-19 emergency began. CDC added that it is currently hosting calls with laboratories on a monthly basis and will return to a quarterly schedule when the emergency response has ended.
3. CDC began a survey of 1,000 private sector and academic laboratories in January 2021 to identify laboratory testing surge capacity. Officials told us that this survey was originally intended to identify clinical laboratories that would be able to perform CDC-developed tests during an emergency response. They added that based on the large laboratory testing surge capacity needed during the COVID-19 pandemic, CDC has also begun using the survey to identify laboratories with the capability to independently develop diagnostic tests for use during future public health emergencies. CDC officials said they would use the results of this survey to expand partnerships and improve coordination with laboratories that can participate in future response efforts.
The Department of Homeland Security’s Homeland Security Exercise and Evaluation Program outlines principles for preparedness exercise programs, as well as a common approach to program management, design and development, conduct, evaluation, and improvement planning.[122] According to this program, agencies should use improvement planning to turn areas for improvement identified during an exercise into concrete, measurable corrective actions that strengthen capabilities.
Additionally, the National Biodefense Strategy, which explains how the U.S. government will manage its activities when responding to biological threats, states that agencies should develop plans that implement or support surge capabilities across response sectors in coordination with relevant entities, including private sector partners.[123] The strategy states that, among other things, these plans should include:
implementing enhanced surveillance and public health measures for disease control; and
clinical, environmental, food testing, and forensic surge laboratory operations.
Furthermore, in our prior work, we identified key elements of sound planning that can help agencies achieve their goals. Sound plans include elements such as what the plan is trying to achieve and how it will achieve these results, as well as priorities, milestones, and monitoring to assess progress toward achieving goals.
COVID-19 demonstrated that the risk posed by an emerging infectious disease could exceed the testing capacity of CDC and public health laboratories. Until CDC works with appropriate stakeholders—including public health and private laboratories—to develop a plan to enhance laboratory surge testing capacity that includes timelines, defines agency and stakeholder roles and responsibilities to meet objectives, and closes gaps identified in preparedness exercises, CDC and its partners will not be best positioned to fully support diagnostic testing needs during a future infectious disease outbreak.
Improving test kit manufacturing capacity. Enhancing its test kit manufacturing capacity is another way CDC could improve its ability to respond to a future infectious disease outbreak. CDC officials told us they manufactured the first batch of test kits that CDC sent to public health laboratories entirely in-house to allow the agency to make changes to the test during the design and validation process and to ensure that public health laboratories received test kits as quickly as possible. However, CDC officials told us they recognized early in the COVID-19 response that the need for tests exceeded the agency’s manufacturing capacity, and that it needed to engage private manufacturers to increase testing capacity.
According to CDC, the agency awarded a contract in 2018 to support the production and distribution of test kits for a number of pathogens, including, among others, influenza, meningitis, and a 2012 strain of coronavirus. However, this contract did not support the manufacturing of a test kit for COVID-19. Instead, CDC officials told us the agency procured services to supplement its internal test kit manufacturing process using purchase orders, which were issued by January 30, 2020. CDC also reported awarding contracts to two companies on February 20, 2020, for the manufacturing of its test kits. CDC and a contractor jointly manufactured the second batch of corrected test kits that CDC sent to public health laboratories beginning on February 28, 2020.[124] However, CDC did not have manufacturing contracts in place prior to the pandemic that could have supported the COVID-19 testing response.
We have previously reported that contracting during an emergency can pose a unique set of challenges, as officials face a significant amount of pressure to provide life-sustaining goods and services as quickly as possible. We have also previously reported that instead of initiating contracts during an emergency response, some agencies establish contracts and agreements in advance of an emergency or disaster to support their needs for certain goods and services, which could include manufacturing.
Establishing contracts prior to an emergency, also called advance contracting, is a tool that can be leveraged to help federal agencies rapidly and cost-effectively mobilize resources.[125] Further, according to the Federal Emergency Management Administration (FEMA), establishing contracts in advance of an emergency fills a critical gap in the emergency acquisition process and ensures that the agency can provide rapid support during an emergency response.[126] For example, contracts can be structured to include emergency response delivery time frames that require vendors to provide certain goods and services within a specific period of time to meet urgent needs. Additionally, the Office of Management and Budget encourages federal agencies to seek out pre-positioned contractors—which agencies may obtain through advance contracting—to facilitate a timely emergency response.[127]
CDC officials said they recognized that establishing contracts in advance could add some value during an emergency response but that they had not evaluated the potential benefits of establishing contracts in advance or considered how CDC could establish such contracts in the future. Specifically, they noted that having contracts in place before the COVID-19 pandemic could potentially have allowed the agency to distribute the second batch of test kits to public health laboratories one or two days sooner.
While we recognize the challenges of planning for unknown events, we maintain it is critical to think through these issues before, rather than during, the public health emergency to maximize efficiencies and potentially save lives. Further, distributing test kits more quickly, even by only one day, could be valuable because each day is critical for understanding the spread of a novel virus in the early weeks of a pandemic.
Having contracts with outside test kit manufacturers prior to a public health emergency is one tool that could help supplement the supply produced by CDC and aid in the rapid manufacturing and deployment of test kits during a future public health emergency. By assessing the types of goods and services that could be leveraged by advance contracting to support the manufacturing and deployment of diagnostic test kits in public health emergencies, CDC will be prepared to award advance contracts in areas it deems beneficial and be better positioned to respond to future public health emergencies, including those caused by novel pathogens.
Methodology
To conduct this work, we reviewed relevant CDC documents, such as the agency’s internal report summarizing the results of its investigation into the unanticipated failure of its COVID-19 test and its MOU with laboratory stakeholders.[128] We also reviewed transcripts of media briefings by CDC officials, academic publications, and World Health Organization documents describing international COVID-19 testing efforts.
In addition, we interviewed CDC and FDA officials. We also interviewed representatives from associations representing organizations and professionals involved in COVID-19 testing, including the American Clinical Laboratory Association, the Association of Public Health Laboratories, the Council of State and Territorial Epidemiologists, and the Infectious Diseases Society of America. We compared CDC’s efforts to Department of Homeland Security leading practices for exercise planning and improvement planning, the National Biodefense Strategy, Office of Management and Budget and FEMA leading practices for emergency preparedness, and key elements of sound planning from our prior work.
Agency Comments
We provided a draft of this enclosure to HHS for review and comment. Responses from the department, including from CDC and FDA, are reprinted in Appendix VI. CDC and FDA also provided technical comments, which we incorporated as appropriate.
In response to our first recommendation, CDC concurred and noted FDA’s shared role in improving the nation’s laboratory surge testing capacity. We agree and added language to more explicitly state FDA’s role in increasing access to testing by authorizing tests for use during a public health emergency and noted our ongoing work examining FDA’s regulation of COVID-19 tests.
In response to our second recommendation, CDC concurred and stated that CDC will investigate the possibility of setting up a contract mechanism that would allow for rapid capacity to work with commercial manufacturers, or in the event CDC is unable to set up a contract, CDC will draft contract language that can be used as needed for future public health emergencies.
GAO’s Ongoing Work
Our work on COVID-19 testing is ongoing. We are currently examining how FDA regulates COVID-19 tests. We are also planning to examine issues related to the deployment of testing at the beginning of the pandemic, including work to identify lessons learned from COVID-19 testing that can improve the nation’s ability to mount a robust diagnostic testing response in the future.
GAO’s Prior Recommendations
The table below presents our recommendations on testing from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to COVID-19 Testing
Recommendation
Status
The Secretary of Health and Human Services should ensure that the Director of the Centers for Disease Control and Prevention clearly discloses the scientific rationale for any change to testing guidelines at the time the change is made (November report).
Open. The Department of Health and Human Services agreed with our recommendation and has begun to implement it. For example, on February 16, 2021, the Centers for Disease Control and Prevention (CDC) issued Interim Guidance on Testing Healthcare Personnel that stated asymptomatic health care personnel who have recovered from COVID-19 may not need to undergo repeat testing or quarantine in the case of another exposure within 3 months of their initial diagnosis. To support this guidance, CDC's website provided links to studies that explained the scientific rationale. Additionally, CDC told us that it continues to consult with scientific stakeholders when issuing or updating guidance documents, and outlined a series of steps the agency plans to take to strengthen its testing guidance. However, as of May 2021, CDC had not fully completed the recommendation. For example, clear linkage to a scientific rationale for recent changes related to testing after exposure for fully-vaccinated individuals appeared to be missing. We will continue to monitor the implementation of this recommendation to ensure that these efforts continue.
The Secretary of Health and Human Services should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that the Department of Health and Human Services has produced for the public and Congress to allow for a more coordinated pandemic testing approach (January report).
Open. The Department of Health and Human Services (HHS) partially agreed with our recommendation. In January 2021, HHS agreed that the department should take steps to more directly incorporate some of the elements of an effective national strategy, but expressed concern that producing such a strategy at this time could be overly burdensome on the federal, state, and local entities that are responding to the pandemic, and that a plan would be outdated by the time it was finalized or potentially rendered obsolete by the rate of technological advancement. In May 2021, HHS told us that the White House and Department of Health and Human Services plan to execute a National Testing Strategy that will act upon the Administration’s testing goals. According to HHS, a finalized document is forthcoming that includes specific actions as well as timelines to achieve these goals. The National Testing Strategy will speak to the country’s short-term COVID-19 needs as well as the long-term needs associated with the country’s broader bio-preparedness. We will continue to monitor the implementation of this recommendation.
Foreign Assistance: State Department Should Better Assess Results of Efforts to Improve Financial and Some Program Data. GAO-21-373. Washington, D.C.: May 10, 2021.
2017 Disaster Contracting: Action Needed to Better Ensure More Effective Use and Management of Advance Contracts. GAO-19-93. Washington, D.C.: December 6, 2018.
Emerging Infectious Diseases: Actions Needed to Address the Challenges of Responding to Zika Virus Disease Outbreaks. GAO-17-445. Washington, D.C.: May 23, 2017.
High-Containment Laboratories: Comprehensive and Up-to-Date Policies and Stronger Oversight Mechanisms Needed to Improve Safety. GAO-16-305. Washington, D.C.: March 21, 2016.
Disaster Response: Criteria for Developing and Validating Effective Response Plans. GAO-10-969T. Washington, D.C.: September 22, 2010.
As of May 31, 2021, the Department of Health and Human Services had been appropriated approximately $484 billion in COVID-19 relief funds in six relief laws. The department uses spend plans to communicate information to Congress about its COVID-19 relief funds; however, we found that the most recent spend plans generally lack information on projected time frames for obligating the remaining COVID-19 relief funds.
Entity involved: Department of Health and Human Services
Recommendation for Executive Action:
To communicate information about and facilitate oversight of the agency’s use of COVID-19 relief funds, the Secretary of Health and Human Services should provide projected time frames for the planned spending of COVID-19 relief funds in the Department of Health and Human Services’ spend plans submitted to Congress.
HHS partially concurred with the recommendation and stated that the department would aim to incorporate some time frames on planned spending where that information may be available such as time frames for select grants to states. However, HHS officials stated that the department would not be able to provide specific time frames for all relief funds since the evolving environment requires the department to remain flexible in responding to incoming requests for response activities.
Background
To assist the response to the COVID-19 pandemic, the Department of Health and Human Services (HHS) received approximately $484 billion in COVID-19 relief appropriations from six COVID-19 relief laws. Many HHS COVID-19 relief funds are available for a multiyear period or are available until expended. Of the $484 billion, approximately $160 billion (about 33 percent) was appropriated in the sixth COVID-19 relief law, the American Rescue Plan Act of 2021 (ARPA), enacted on March 11, 2021.
Overview of Key Issues
As of May 31, 2021, the department reported that about $253 billion of the $324 billion appropriated in the first five COVID-19 relief laws enacted as of December 27, 2020 had been obligated (about 78 percent) and about $168 billion had been expended (about 52 percent). Of the $160 billion in appropriations from the sixth law enacted on March 11, 2021, about $75 billion had been obligated (47 percent) and about $3 billion had been expended (about 2 percent). In total, approximately $156 billion remained unobligated from all six laws. (See figure.)
HHS’s Reported COVID-19 Relief Appropriations, Obligations, and Expenditures from COVID-19 Relief Laws, as of May 31, 2021
aThese amounts reflect appropriations provided in Divisions M and N of the Consolidated Appropriations Act, 2021 that are specifically designated for COVID-19 relief.
The table below shows HHS appropriations, obligations, and expenditures by COVID-19 relief law that HHS reported as of May 31, 2021. Three quarters of HHS’s appropriations from the first five relief laws have been obligated, and more than half have been expended. HHS also received significant additional appropriations in ARPA, about half of which had not been obligated as of May 31, 2021.
Department of Health and Human Services Reported COVID-19 Relief Appropriations, Obligations, and Expenditures, by Relief Law, as of May 31, 2021
Legislation
Date of enactment
Appropriations ($ millions)
Obligations ($ millions, (% obligated))
Expenditures ($ millions, (% expended))
Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 (Pub. L. No. 116-123)
March 6, 2020
6,497
5,381 (83)
3,202 (49)
Families First Coronavirus Response Act (Pub. L. No. 116-127)
March 18, 2020
1,314
1,288 (98)
1,253 (95)
Coronavirus Aid, Relief, and Economic Security Act. (Pub. L. No. 116-136)
March 27, 2020
142,833
135,532 (95)
112,760 (79)
Paycheck Protection Program and Health Care Enhancement Act (Pub. L. No. 116-139)
April 24, 2020
100,000
56,729 (57)
46,951 (47)
Consolidated Appropriations Act, 2021 (Pub. L. No. 116-260) a
December 27, 2020
73,175
54,140 (74)
3,764 (5)
American Rescue Plan Act of 2021 (Pub. L. No. 117-2)
March 11, 2021
160,494
75,225 (47)
2,642 (2)
Total
484,313
328,294 (68)
170,573 (35)
Source: Department of Health and Human Services (HHS) data. | GAO-21-551
Note: The Department of Health and Human Services (HHS) reported that, of its total appropriations for COVID-19 relief, the agency transferred $289 million to the Department of Homeland Security, and $300 million are not available until HHS has taken certain actions. aThis amount reflects appropriations provided in Divisions M and N of the Consolidated Appropriations Act, 2021 that are specifically designated for COVID-19 relief. An additional $638 million in COVID-19 relief funds were appropriated under Division H to the Administration for Children and Families, an agency within HHS, to prevent, prepare for, and respond to the coronavirus, for necessary expenses for grants to carry out a low-income household drinking water and wastewater emergency assistance program. However, these funds were not included in the HHS-reported data on HHS COVID-19 relief appropriations, obligations, and expenditures, as HHS noted that the funds were not considered COVID-19 relief funding for USAspending.gov reporting purposes.
Appropriations for HHS agencies or key funds. The table below provides COVID-19 relief appropriations to HHS under the six relief laws and the obligations and expenditures of these appropriations by HHS agency or fund as of May 31, 2021. The sixth COVID-19 relief law, ARPA, was enacted on March 11, 2021, and as of May 31, 2021, HHS had obligated $75 billion (47 percent), and expended $3 billion (two percent) of the appropriations provided under this law.
Department of Health and Human Services Reported COVID-19 Relief Appropriations, Obligations, and Expenditures, by Agency or Key Fund, as of May 31, 2021
Agency or key fund
Appropriations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Administration for Children and Families
63,344.0
61,886.3
5,605.3
Administration for Community Living
3,200.0
2,904.7
912.5
Agency for Toxic Substances and Disease Registry
12.5
12.4
7.3
Centers for Disease Control and Prevention (CDC)
26,770.0
12,803.8
2,580.7
Centers for Medicare & Medicaid Servicesa
935.0
124.9
47.4
Enhanced Use of Defense Production Act
10,000.0
0.0
0.0
Food and Drug Administration (FDA)
696.0
64.2
27.6
Health Resources and Services Administration (HRSA)
10,750.0
7,523.3
1,241.3
Indian Health Service (IHS)
7,190.0
3,158.5
3,025.6
National Institutes of Health (NIH)
3,031.4
1,144.7
463.2
Office of Inspector General (OIG)
5.0
0.0
0.0
Public Health and Social Services Emergency Fund (PHSSEF)b
350,144.5
232,162.6
156,506.3
Office of the Assistant Secretary for Healthc
9,532.0
6,913.6
3,373.1
Office of the Assistant Secretary for Preparedness and Responsec
20,497.5
11,776.2
7,595.9
Biomedical Advanced Research and Development Authority c
38,107.3
28,073.3
8,035.4
Provider Relief Fundc, d
178,000.0
134,314.1
127,232.2
CDCc
1,000.0
419.2
204.3
FDAc
22.0
1.9
1.9
HRSAc
979.8
971.1
793.5
IHSc
1,640.0
1,005.9
507.6
NIHc
1,806.0
1,031.8
501.1
OIGc
12.0
3.6
3.1
Other PHSSEFc
98,547.9
47,651.9
8,258.2
Substance Abuse and Mental Health Services Administration
8,235.0
6,508.4
156.2
Grand Total
484,313.4
328,293.8
170,573.4
Source: Department of Health and Human Services (HHS) data. | GAO-21-551
Note: HHS reported that of the total COVID-19 relief appropriations the agency transferred $289 million to the Department of Homeland Security, and that $300 million in appropriations are not available until HHS takes certain actions. HHS’s reported appropriations specifically designated for COVID-19 relief in the Consolidated Appropriations Act, 2021 (Pub. L. No. 116-260) reflect only appropriations provided under Divisions M and N. Of the $324 billion appropriated in the five relief laws enacted as of December 27, 2020, about $253 billion (about 78 percent) had been obligated and about $168 billion (about 52 percent) had been expended, as of May 31, 2021. aThese amounts do not reflect Medicaid and Medicare expenditures that resulted from statutory changes to these programs under the COVID-19 relief laws. bPHSSEF is an account through which funding is provided to certain HHS offices, such as the Office of the Assistant Secretary for Preparedness and Response. Amounts have been appropriated to this fund for the COVID-19 response to support certain HHS agencies and response activities. For example, NIH received about $1.8 billion in transfers from the PHSSEF, and this amount is not included in the approximately $3 billion appropriated directly to NIH. cThe italicized amounts are subtotals of the PHSSEF and are already reflected in the total $350,144.5 million listed for the PHSSEF. Italicized amounts listed under the PHSSEF appropriations column are HHS allocations based on appropriations made in the COVID-19 relief laws and approved allotment decisions made by HHS in coordination with the Office of Management and Budget. Some amounts were appropriated to the PHSSEF for transfer to specified HHS agencies. dThe Provider Relief Fund reimburses eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19. Provider Relief Fund expenditures also may be referred to as disbursements.
Allocations for selected COVID-19 response activities. HHS officials noted that allocations for COVID-19 response activities are determined by appropriations made by Congress in combination with approved spend plan decisions.[129] Some funding—such as funding for testing or vaccine-related activities—could apply to multiple response activity categories, making an exact accounting of the obligations and expenditures in certain areas difficult. For example, certain funds included in the response activity category for support to states, localities, territories, and tribal organizations were designated for testing or vaccine distribution.
As of May 31, 2021, the Provider Relief Fund (PRF), which reimburses eligible health care providers for health care-related expenses or lost revenues attributable to COVID-19, had the largest allocation—comprising about 37 percent ($178 billion) of HHS allocations from the six COVID-19 relief laws. Other activities with high allocations included testing-related activities; the Child Care and Development Block Grant; vaccine-related activities; and support to state, local, territorial, and tribal organizations for preparedness, which together comprised an additional 40 percent ($194.0 billion) of HHS allocations.
The following table provides HHS’s reported allocations, obligations, and expenditures by selected COVID-19 response activity. The sixth COVID-19 relief law, ARPA, was enacted on March 11, 2021, and as of May 31, 2021, HHS had obligated $75 billion (47 percent), and expended $3 billion (two percent) of the appropriations provided under this law.
Department of Health and Human Services (HHS) Reported Allocations, Obligations, and Expenditures by Selected COVID-19 Response Activity, as of May 31, 2021
COVID-19 response activity
Description
Allocations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Provider Relief Fund
Includes reimbursements to eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19.
178,000.0
134,314.1
127,232.2
Testing
Includes procurement and distribution of testing supplies, community-based testing programs, testing in high-risk and underserved populations and Indian Health Services’ programs, implementing a national strategy, Centers for Disease Control and Prevention (CDC) testing-related activities such as technical assistance, and other activities.
61,416.3
21,180.4
5,117.3
Child Care and Development Block Grant
Includes assistance to child care providers to help maintain or resume operations in the case of decreased enrollment or closures related to COVID-19.
52,465.0
52,087.8
4,043.1
Vaccines
Includes Biomedical Advanced Research and Development Authority (BARDA) funding for vaccine development and procurement; National Institutes for Health (NIH) research activities; and CDC vaccine distribution, administration, and technical assistance related activities.
40,221.5
25,063.6
6,387.7
Support to state, local, territorial, and tribal organizations’ preparedness
Includes funding for states and other governments to support testing, contact tracing, and surveillance; vaccines distribution; and other activities.
40,061.5
38,701.3
6,570.4
Strategic National Stockpilea
Includes acquiring, storing, and maintaining ventilators, testing supplies, and personal protective equipment (PPE) and increasing manufacturing capacity for certain PPE.
13,919.9
10,236.7
6,318.9
Drugs and therapeutics
Includes BARDA funding for development and procurement of therapeutics and NIH research activities.
11,379.4
6,874.7
2,049.5
Health centers
Includes support for COVID-19-related activities, such as testing, at health centers, which provide health care services to individuals regardless of their ability to pay.
9,620.0
8,178.1
1,825.4
Rural Provider Payments
Includes assistance for rural providers and suppliers that will be administered using the same mechanism as the Provider Relief Fund, according to HHS officials.
8,500.0
0.0
0.0
Mental health and substance use–related services
Includes substance abuse prevention and treatment, community-based mental health services, and other activities.
8,315.0
6,508.4
156.2
Diagnostics research and development
Includes BARDA diagnostic development programs and NIH projects, such as the Rapid Acceleration of Diagnostics Initiative.
3,321.6
1,761.6
715.1
Head Start
Includes grants to local programs for high-quality learning experiences and to respond to other immediate and ongoing consequences of COVID-19.
2,000.0
1,325.0
460.5
Testing for uninsuredb
Includes reimbursements to eligible providers for COVID-19 testing for individuals who are uninsured.
2,000.0
1,980.9
1,973.0
Global disease detection and emergency response
Includes support to governments and other organizations to rapidly diagnose cases and to ensure readiness to implement vaccines and therapeutics.
1,747.1
432.2
133.5
Telehealth
Includes efforts to support safety-net health care providers transitioning to telehealth, telehealth access—especially for vulnerable maternal and child health populations—and a telehealth website.
307.5
136.5
102.8
Other response activities
Includes additional activities such as activities conducted by the Administration for Community Living, certain CDC-wide activities and program support, and activities conducted by the Food and Drug Administration.
51,038.6
19,512.5
7,487.8
Total
484,313.4
328,293.8
170,573.4
Source: Department of Health and Human Services (HHS) data, written HHS responses, and GAO analysis of HHS spend plans. | GAO-21-551
Note: The selected response activities represent examples of certain targeted activities that fall within particular HHS agencies, such as funding for health centers or Head Start, as well as broader categories of response activities that may span HHS agencies, such as testing-, vaccine-, and therapeutics-related response activities. HHS reported allocations, obligations, and expenditures for these activities based on the primary programmatic recipient organization of the funds, although some activities apply to multiple categories. For example, certain funds in the “support to state, local, territorial, and tribal organizations for preparedness” category were provided for testing but are not reflected in the “testing” category. However, HHS also noted that testing-related funding awarded to states or localities that was appropriated under the American Rescue Plan Act of 2021 (ARPA) was included in the “testing” category. HHS officials explained that the activity names align with how funds were appropriated under different COVID-19 relief laws. According to HHS officials, the allocations reported for the key activities above are based on amounts appropriated for these activities in the COVID-19 relief laws, and on approved spend plan decisions made by HHS in coordination with the Office of Management and Budget. According to HHS, as of June 4, 2021, the agency used about $1.7 billion in appropriations provided under ARPA, including $1.2 billion appropriated for COVID-19 testing, contact tracing, and mitigation activities, for the Administration for Children and Families’ Unaccompanied Children Program, citing the Secretary’s authorities under the Public Health Service Act and the Consolidated Appropriations Act, 2021. See Pub. L. No. 116-260, div. H, tit. II, § 204, 134 Stat. 1182, 1589 (2020); 42 U.S.C. 238j(a).With respect to the Consolidated Appropriations Act, 2021, the amounts reflect appropriations specifically designated for COVID-19 in Divisions M and N of the act. aAccording to HHS, the agency transferred $850 million from the Public Health and Social Services Emergency Fund, Strategic National Stockpile, to the Unaccompanied Children Program within the Administration for Children and Families, citing authority provided in the Consolidated Appropriations Act, 2021. See Pub. L. No. 116-260, div. M, tit. III, § 304, 134 Stat. at 1923 (2020). bAccording to HHS officials, HHS has allocated an additional $4.8 billion to the testing for the uninsured program from section 2401 of ARPA, which HHS included in the “testing” response activity category.
The percentage of obligations and expenditures varied across selected COVID-19 response activities for a variety of reasons including the nature of the activities, their planned uses, and the timing of the funds provided through the six COVID-19 relief laws.
Nature of funded activities. The nature of some funded activities—such as financial assistance grants or awards to state, local, and other jurisdictions—means that the full amount of the grant or award may be obligated at the time of the grant or award, but expended incrementally over time based on the budget period for the activities. For example, support to state, local, territorial, and tribal organizations’ preparedness includes assistance to states and other jurisdictions for testing, contact tracing, laboratory capacity, and vaccine distribution. Centers for Disease Control and Prevention (CDC) officials told us that some expenditures for these awards, such as those for personnel costs, will take place over the time period for which the award is made, some of which are more than 2 years.
Planned use of funds. National Institutes of Health (NIH) officials reported that certain research programs are planned in phases so that additional funds will be obligated after grantees meet certain requirements or integrate new advancements. In addition, officials from the Biomedical Advanced Research and Development Authority told us that funds obligated for vaccine manufacturing and procurement are expended as vaccine doses are shipped to administration or distribution sites. Officials from the Office of the Assistant Secretary for Preparedness and Response said funds obligated for replenishing the Strategic National Stockpile (SNS) are not expended until products are manufactured and delivered into the SNS.
Timing of COVID-relief appropriations: About 34 percent (approximately $21 billion) of funds in the testing category had been obligated as of May 31, 2021. However, a majority of these funds—approximately $49 billion—were allocated from appropriations in the sixth COVID-19 relief law, which was enacted on March 11, 2021. According to HHS data, about 45 percent of allocations in this category from the first five COVID-19 relief laws had been obligated as of February 28, 2021. With respect to expenditures, 19 percent (approximately $1.8 billion) of allocations for health centers had been expended as of May 31, 2021, mostly due to the nearly four-fold increase in funding for this activity that was appropriated in the sixth COVID-19 relief law.
Spend plans. To communicate information about COVID-19 relief funds from the first five COVID-19 relief laws, HHS uses spend plans, which the laws required be developed, updated, and provided to Congress every 60 days.[130] According to HHS officials, the department is also preparing a spend plan for ARPA, which was enacted in March 2021. However, we found that the most current spend plans generally do not include time frames for obligating the remaining relief funds, which is useful information for oversight and for informing future funding decisions by Congress.[131]
Guidance from the Office of Management and Budget (OMB) encouraged federal agencies, including HHS, to act quickly to disburse relief funds and noted the importance of spending transparency and regular reporting to help safeguard taxpayer dollars.[132] In April 2020, OMB issued guidance to agencies noting that “time is of the essence, and the Administration is committed to the rapid delivery of relief funds and response activities” and that “agencies should rapidly issue awards and fund programs to meet crucial needs.” Further, OMB noted that agencies must report information on awards to provide the public with information in a clear, accurate, and timely manner.
In its effort to respond quickly to the pandemic and rapidly issue awards and fund programs consistent with OMB guidance, HHS funded some activities to support relief efforts shortly after funds were appropriated; for example, the Health Resources and Services Administration (HRSA) stated that its goal for the PRF was to distribute funds as quickly as possible. HRSA officials told us the first $30 billion was disbursed to providers by mid-April 2020—about a month after enactment of the first appropriation for provider relief. However, the timing for use of the remaining funds is unknown and highlights the importance of information to help ensure accountability for these funds. According to federal internal control standards, management should communicate quality information to external and internal stakeholders so that they can help the agency achieve its objectives and address related risks. In particular, quality information helps support Congress in making future funding decisions.
As of May 31, 2021, about $156 billion of $484 billion (about 32 percent) of COVID-19 relief funds appropriated to HHS were available to be obligated—this amount includes the funds appropriated in ARPA. By not communicating its plans about when it expects to obligate these remaining funds, HHS is missing an opportunity to provide information for oversight and to guide future congressional funding decisions.[133] The figure below shows obligated and unobligated HHS COVID-19 relief funds as of May 31, 2021.
Department of Health and Human Services (HHS) Obligated and Unobligated COVID-19 Relief Funds, as of May 31, 2021
We found that large amounts of funds for certain activities remained unobligated, and it is not clear when these funds will be obligated or expended. For example:
As of May 31, 2021, about 25 percent of PRF appropriations remained unobligated ($43.7 billion of $178 billion), and HRSA has not provided time frames for obligating this balance. Of the unobligated funds, according to HHS’s October 2020 spend plan, HRSA reserved a portion of the provider relief funds to respond to needs not identified in the spend plan, and in May 2021 HHS officials told us that the reserved funds were approximately $24 billion. HHS has not specified time frames for obligating these reserved funds or for the other $29.1 billion in unobligated provider relief funds. In addition, ARPA appropriated an additional $8.5 billion for rural providers, and as of May 31, 2021, all these funds remained unobligated.[134]
As of May 31, 2021, about 66 percent ($40.2 billion of $61.4 billion) of funds that HHS reported to us for testing activities remained unobligated—most of those allocated funds ($49 billion) were appropriated on March 11, 2021 when ARPA was enacted.[135] We found that the most current spend plans for the first five relief laws do not specify time frames for obligating these funds, and in April 2021 HHS officials told us that they were developing a spend plan for ARPA COVID-19 relief funds, but the plan was not yet completed.[136]
In other cases where funds remained unobligated, agency officials—NIH and CDC—did not provide time frames, but said that unobligated relief funds would be spent according to their spend plans and consistent with legislative requirements. HHS officials told us that the spend plans submitted to Congress contain information about future planned activities, however, officials said that they do not provide information on time frames for obligating relief funds.
Spend plans with information on projected timeframes for obligating the remaining relief funds would give Congress information useful to facilitate oversight of these resources to help ensure that relief funds are spent in an expedient and timely manner, as well as help inform future funding decisions.
Methodology
We requested, and HHS provided, data on appropriations, allocations, obligations, and expenditures of COVID-19 relief funds by HHS agency and by selected response activity, as of May 31, 2021. We also reviewed appropriation warrant information provided by the Department of the Treasury as of May 31, 2021. To assess the reliability of the data reported by HHS, we reviewed HHS documentation; Treasury appropriation warrant information; and information from the federal spending database, www.usaspending.gov; as well as HHS’s spending database, taggs.hhs.gov. We determined that the HHS reported data were sufficiently reliable for the purposes of our reporting objective.[137] We also reviewed the six COVID-19 relief laws to assist the response to COVID-19.
We requested, obtained, and analyzed HHS and agency information, including agency spend plans, and related documentation, to determine HHS and agency plans and information including time frames for spending COVID-19 relief funds on response activities.
Agency Comments
We provided HHS and OMB with a draft of this enclosure. HHS partially concurred with the recommendation and stated that the department would aim to incorporate some time frames on planned spending where such information may be available, such as time frames for select grants to states. However, HHS officials stated that they would not be able to provide specific time frames for all relief funds since the evolving environment requires the department to remain flexible in responding to incoming requests for response activities. For example, HHS cited field management activities that can change quickly depending on the incoming response requests.
We agree that estimating projected time frames can be challenging and subject to changes. However, providing projected time frames would not impinge on the Department’s ability to be flexible as these spend plans are required to be updated every 60 days. Offering projected time frames to spending would give Congress useful information to help ensure relief funds are spent in an expedient and timely manner, as well as help inform future funding decisions. HHS also provided technical comments on this enclosure, which we incorporated as appropriate. OMB did not provide any comments on this enclosure.
GAO’s Ongoing Work
As HHS works to distribute funds for COVID-19 relief activities and to eligible providers, it will continue to be important that HHS officials ensure funds are appropriately distributed and used. We plan to conduct additional work examining HHS’s COVID-19 relief funds.
Related GAO Product
Standards for Internal Control in the Federal Government, GAO-14-704G (Washington, D.C.: September 2014)
Contact information: Carolyn L. Yocom, (202) 512-7114, yocomc@gao.gov
The U.S. faces challenges to building a sustainable domestic manufacturing base for personal protective equipment, including high relative labor costs and limited access to raw materials that make staying competitive with foreign manufacturers difficult. There are a number of factors for the federal government to consider as it moves forward with efforts to build a sustainable manufacturing base, including the broader goal of supply chain resilience, which may call for targeted reliance on foreign manufacturers.
Entities involved: The Department of Defense, the Department of Health and Human Services, and the Federal Emergency Management Agency
Background
Personal protective equipment (PPE)—safety products designed to help prevent the spread of infectious disease—has been critical to the COVID-19 response. Prior to the pandemic, the U.S. generally depended on foreign suppliers for certain types of PPE, such as nitrile gloves and surgical gowns. U.S. dependence on foreign PPE manufacturers has increased over the past several decades in part because foreign manufacturers can produce their products at a lower cost.[138] Federal agencies have identified this dependence as a national security issue.
The COVID-19 pandemic triggered a significant increase in worldwide demand for PPE and disrupted global supply chains, which limited availability of critical equipment for U.S. health care providers. Actions taken by some governments to halt or restrict exports of PPE further affected the availability of medical supplies in the U.S., including N95 respirators, surgical masks, surgical and isolation gowns, and nitrile and other gloves for use in health care settings.[139] Just-in-time supply chain strategies, in which manufacturers and distributors produce and maintain just enough product to meet immediate fulfillment demands, also exacerbated PPE shortages.
Use of the Defense Production Act (DPA) and other actions to address PPE supply chain shortages. Title III of the DPA authorizes the President to provide certain financial incentives to address industrial base capabilities essential for national defense, including maintaining, restoring, and expanding domestic manufacturing, when certain conditions are met.[140] The Department of Defense (DOD) reported awarding contracts and agreements valued at $574.1 million to expand domestic production of PPE during the COVID-19 pandemic, through May 2021.[141] These investments helped manufacturers produce an additional 58 million N95 respirators and 125,000 gowns per month and are expected to result in an additional 38 million nitrile gloves and 44 million surgical masks per month by the fall of 2021.
However, as shown in the figure below, the U.S. remains highly dependent on foreign manufacturers for certain types of PPE such as nitrile gloves and gowns.
Estimated Domestic Production Capacity and Domestic Demand for Select Personal Protective Equipment Types, March 2020 through May 2021
Overview of Key Issues
Federal planning for medical supply domestic industrial base sustainment is in its initial stages. Officials from the Department of Health and Human Services’ (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR), the Department of Homeland Security’s Federal Emergency Management Agency (FEMA), and DOD acknowledged that federal actions are needed to build a sustainable domestic PPE industrial base to respond to future public health emergencies, as well as to enhance the resilience of medical product supply chains more broadly.
Executive Order 14001 called for a national pandemic supply chain resilience strategy, which is due mid-July 2021.[142] ASPR officials told us that the strategy is under development, and they expect to issue it on time. Officials noted that the strategy will include a high-level discussion of the program and policies that may be needed for industrial base sustainment, as well as challenges the government faces. Once the strategy is released, ASPR and its federal partners will develop an implementation plan that includes more specific actions and timelines, as well as roles and responsibilities, according to officials, who did not provide a time frame for development or release of this implementation plan.
The American Rescue Plan Act of 2021 appropriated $10 billion to support the use of the DPA for medical supplies, which agency officials anticipate will result in additional industrial base expansion projects.[143] According to officials, ASPR and the Supply Chain Advisory Group developed and submitted a spend plan for this funding to the White House in April 2021, which is pending approval.[144] This draft spend plan identified $5 billion in medical supply projects for fiscal year 2021, including approximately $2.4 billion for PPE investments, according to an official. ASPR has not yet identified plans for the remaining $5 billion.
Challenges to sustainable domestic PPE manufacturing. The U.S. faces challenges to building a sustainable, competitive domestic PPE manufacturing base primarily due to labor costs and limited access to raw materials.
Higher U.S. labor costs result in higher product costs. Domestically produced PPE typically costs more, in part as a result of higher U.S. labor costs, making it less competitive on the global market, according to the U.S. International Trade Commission (USITC) and many of the stakeholders we interviewed.[145]
Certain PPE types, such as gowns and nitrile gloves, may be particularly challenging to manufacture in the United States because of the amount of labor required to produce them and the cost of labor. For example, according to USITC, surgical gowns, which may require workers to piece gowns together, cost $17 to $20 each for U.S.-made gowns, as compared to $4 to $7 per gown for those made in China.[146] The costs of U.S.-made nitrile gloves may also be higher because of the labor required to manufacture this type of PPE. According to USITC, each glove production line requires 30-40 workers on average, including workers who remove each glove manually from hand-shaped molds. Production also requires chemists, machinists, and quality assurance personnel.
Limited access to raw materials makes scaling production challenging and costly. Each type of PPE requires raw materials that may be difficult to obtain domestically. For example, nitrile rubber, a raw material used to make nitrile gloves, comes predominantly from Malaysia, and domestic production is limited.[147] A representative of one U.S. nitrile glove manufacturer that gets its nitrile rubber from overseas suppliers said the cost of imported nitrile rubber accounts for more than 50 percent of the production costs of the gloves. In addition, this manufacturer cited lengthy delivery delays of nitrile rubber from suppliers in Malaysia as significantly affecting the ability of the federal government to expand domestic manufacturing of gloves in response to ongoing shortages during the pandemic.
In addition, increased domestic manufacturing of PPE may affect access to raw materials also used to manufacture nonmedical products and could result in shortages of raw materials used for both, further increasing product costs. For example, some of the nonwoven fabrics needed to make N95 respirators, masks, and gowns are also used to make diapers and sanitizing wipes and in other industries such as automotive and construction.[148] Significant increases in the demand for N95 respirators and masks at the beginning of COVID-19 also contributed to short supply of these nonwoven fabrics, which contributed to the increased cost of N95 respirators.
Many stakeholders we interviewed, including manufacturers, distributors, and trade associations representing end users, cited additional challenges to building a sustainable domestic PPE manufacturing base. See the below figure for the challenges cited by these stakeholders, as well as USITC, for the four types of PPE included in our review.
Summary of Information from the U.S. International Trade Commission (USITC) and Other Stakeholders on Key Challenges Affecting Domestic Production for Certain Types of Personal Protective Equipment (PPE)
Note: Stakeholders included a nongeneralizable sample of 29 industry stakeholders, including PPE manufacturers; distributors and trade associations representing other purchasers, such as state governments, hospitals, and group purchasing organizations; and researchers.
Stakeholders noted the need for federal actions to help increase long-term demand for domestically made PPE. Without a clear signal of long-term demand for PPE to help ensure a return on investment, some manufacturers—including both those with existing federal domestic industrial base expansion contracts and those who pivoted to making PPE during COVID-19—told us that they were unsure if they would continue to produce PPE after the pandemic because future business longevity seemed too uncertain.
Stakeholders and federal officials provided their perspectives on actions that could help increase federal and nonfederal demand and sustain a long-term domestic base. The options presented below are being explored by ASPR, according to officials, as well as research institutes, such as the National Academies for Science, Education, and Medicine and others. Some of these actions would require regulatory action or legislation. We present the range of stakeholder perspectives on all options, even those that may be deemed less feasible or useful by some, as they may be helpful to HHS and its federal partners in their continued long-term planning.
Federal funding for capital investments and long-term purchases. Funding for capital investments, such as through manufacturing expansion projects like those executed during the pandemic, could help domestic manufacturers achieve economies of scale and be more price competitive, according to some stakeholders we spoke with including manufacturers, distributors, and trade associations. Such investments would allow manufacturers to purchase equipment to expand production capacity or automate manufacturing processes to reduce manual labor costs.[149]
Similarly, long-term federal funding, which could be used for contracts that commit the federal government to purchasing specified volumes of PPE over a number of years, would help create a sustainable base of demand that could justify manufacturers’ capital investments in machinery, technology, and other expansion or facility needs, according to many manufacturers we spoke with, as well as some distributors and trade associations.[150] Without federal purchasing contracts, some manufacturers who received federal contracts or agreements for PPE expansion for the COVID-19 response expressed concern about having idle manufacturing capacity after the pandemic subsides.
Transparent stockpile planning to include domestically manufactured PPE. Some stakeholders, including manufacturers, distributors, trade associations, and researchers, commented that having a clear and transparent understanding of future federal plans for stockpiling would help signal longer-term demand for PPE and help manufacturers with business planning.[151] We have reported on federal actions related to the Strategic National Stockpile during COVID-19 on a regular basis, beginning in June 2020.[152] (See the Strategic National Stockpile enclosure in this report for more information.)
Expanded legal requirements to prioritize federal purchasing of domestically manufactured PPE. Manufacturers, distributors, and trade associations we spoke with had mixed opinions on the effect of expanding federal purchasing requirements for domestically produced goods.
Specifically, one manufacturer suggested that the Berry Amendment, which governs DOD clothing purchases and, according to textile manufacturing stakeholders, is a significant driver of their domestic textile and apparel businesses, could be expanded to include a broader range of PPE.[153] Similarly, one distributor suggested that the amendment could be extended to agencies beyond DOD. However, some other stakeholders noted that even with such expansions, the Berry Amendment may not be feasible for certain PPE types, such as gloves, if raw materials for those products cannot be sourced domestically.
One manufacturer and one trade association representing manufacturers stated that expanding federal purchasing requirements under the Berry Amendment would be unlikely to provide significant or primary support to sustain a domestic manufacturing base because of the small federal share of the domestic medical supply market. One manufacturer and one company that manufactures and distributes PPE noted similar limitations to expanding purchasing requirements under the Buy American Act, which requires federal procurement of domestic products, subject to certain exceptions and waivers.[154]
Use of Medicare to incentivize nonfederal purchasing of domestically manufactured PPE. Some stakeholders, including manufacturers and distributors, also discussed restructuring Medicare in several ways to incentivize health care providers to purchase domestic PPE and help increase the demand signal for such PPE. These suggestions included:
restructuring Medicare conditions of participation to require commitments to domestic medical supply purchasing in order to participate in the program,
restructuring Medicare reimbursement policies to reimburse providers at higher rates for using domestically made PPE, and
requiring hospitals to incorporate plans for purchasing domestically made PPE into their hospital supply inventories.
Officials from the Centers for Medicare & Medicaid Services told us that restructuring Medicare as suggested would be challenging for several reasons. According to officials, the agency lacks the statutory authority to implement such purchasing requirements. Further, officials stated that reimbursement for PPE is bundled into overall service charges.
Officials and other stakeholders, including some manufacturers, distributors, and a trade association representing end users, noted that it would be more feasible to incentivize domestic purchasing by requiring a certain percentage of providers’ PPE to be purchased from domestic manufacturers, or to provide a bonus payment for such purchases on a regular basis. However, they noted that it may be difficult for hospitals and other health care providers, as well as their suppliers, to identify which brands of PPE may be U.S.-made. Officials also agreed with a distributor who told us that any such requirements for purchasing generally higher-priced, domestically made PPE would place a bigger financial burden on smaller providers.
Tax credits for domestic purchases. Some PPE distributors and a manufacturer suggested that tax credits for purchases of domestically produced PPE could help generate demand, but opinions on the utility of such tax credits were mixed. Some stakeholders cited aforementioned difficulties in identifying which PPE products are U.S.-made, which could make such credits hard to obtain. In addition, some distributors noted that tax incentives would not incentivize nonprofit hospitals to purchase domestically manufactured PPE.
Domestic manufacturing is one part of broader supply chain considerations. Building a sustainable domestic PPE manufacturing base is just one part of broader supply chain considerations, according to stakeholders and federal officials we interviewed. Some manufacturers, one distributor, and several trade associations representing manufacturers and end users said that sustaining long-term demand for domestically produced PPE will require a significant shift in the way that U.S. manufacturers and purchasers, including the health care sector, conceive of effective models of just-in-time inventory and other cost control mechanisms. Other stakeholders, including two trade associations, a manufacturer, and a research group noted that investing in or sustaining domestic manufacturing will not necessarily ensure that domestic PPE supply chains alone are sufficient to respond to future public health emergencies.
Stakeholders and federal officials identified several areas for consideration as the federal government moves towards creating a more resilient supply chain for PPE to effectively respond to future public health emergencies.
Supply chain redundancies. Some stakeholders, including trade associations, an advocacy group, and a manufacturer, noted that it will be important to build redundancies into the domestic PPE supply chain, such as having multiple manufacturers of one kind of PPE and multiple manufacturing facilities located in geographically diverse U.S. locations. Several of these stakeholders cited the disruptions to medical supply production caused by the 2017 hurricanes in Puerto Rico and the 2021 winter storms in Texas as examples of the importance of redundant and resilient domestic supply chains that would help the U.S. to respond to future public health emergencies.[155]
Targeted reliance on foreign manufacturers. Some stakeholders, including a manufacturer and two manufacturing trade associations, two distributors, and a research group, as well as federal officials, noted that targeted reliance on, and engagement with, a variety of foreign manufacturers will remain appropriate given existing trade agreements, the U.S.’s participation in complex global supply chains, and challenges in accessing certain raw materials.
Supply chain visibility and mapping. Many stakeholders representing manufacturers, distributors, trade associations, and research groups we spoke with stated that developing a complete picture of the end-to-end supply chain for each type of PPE could help the federal government identify vulnerabilities and risks, determine strategies or actions to mitigate them, and plan for and respond to future disruptions. Supply chain mapping—documenting companies, suppliers, and individuals across the PPE supply chain to create a global map of the supply network—could help the federal government have a more complete picture to respond to disruptions and emergencies, according to stakeholders. However, two stakeholders, including a supply chain research group, acknowledged that such mapping would be complex and laborious.
Industry outreach and engagement. Many stakeholders representing manufacturers and distributors and trade associations representing purchasers and end users noted that meaningful federal engagement with industry will enhance domestic manufacturing and supply chain resilience. In addition, such engagement could help ensure these perspectives are considered in national strategies to support and sustain the domestic PPE industry. According to some of these stakeholders, such engagement with the private sector could help:
ramp up private investment in domestic PPE manufacturing;
connect manufacturers with purchasers;
aid in the collection of data needed for supply chain mapping; and
help the federal government understand the unique challenges of new and small PPE manufacturers, as well as those of veteran and minority-owned businesses, including challenges related to navigating the federal medical device approval or federal contracting processes.
In January 2021, we reported that HHS had not developed a process for engaging with key nonfederal stakeholders and the Congress for development of a supply chain strategy for pandemic preparedness, including the role of the Strategic National Stockpile. We recommended that HHS do so, and the department generally agreed with our recommendation. However, as of May 2021, ASPR had not proactively engaged any private or public partners in strategic discussions to implement this recommendation, although officials told us that such discussions are important and they are considering how to better engage their public and private partners.
We continue to underscore that engaging with key nonfederal stakeholders—in meaningful, proactive ways to obtain their business and industry expertise—as well as engaging with Congress, is critical for developing strategies to build a sustainable domestic medical supply manufacturing base. Such engagement includes for the development of the pandemic supply chain resilience strategy required by Executive Order 14001 and future stockpiling plans.
Methodology
To conduct our work, we reviewed federal strategies and reports, including ASPR’s 2020 draft strategy for modernizing the Strategic National Stockpile and USITC’s December 2020 report on the U.S. market for COVID-related goods.[156] We reviewed written information submitted by PPE industry stakeholders to USITC and the Department of Commerce in the fall of 2020 and early 2021.[157]
We also selected a judgmental sample of industry stakeholders from USITC and Department of Commerce submissions, as well as other sources, to interview for their perspectives on challenges to building a sustainable domestic manufacturing base for PPE and federal efforts that could help support and sustain such a base. Selected stakeholders included PPE manufacturers; distributors and trade associations that represent other purchasers and end users, such as state governments, hospitals, and group purchasing organizations; and researchers and policy advocates.[158]
We interviewed 29 industry stakeholders, including manufacturers that produce textiles for or finished products of each type of PPE (N95 respirators, surgical and procedural masks, reusable and disposable surgical and isolation gowns, and nitrile gloves); distributors; trade associations representing manufacturers, distributors, and other purchasers and end users including state and local government officials; researchers; and standards setting organizations. Our findings from interviews with these stakeholders are not generalizable to the entire PPE industry from manufacturers to end users.
We obtained information on federal domestic PPE industrial base planning efforts, including efforts to address current supply and demand needs from the Supply Chain Advisory Group and relevant federal agencies. We also interviewed officials from ASPR, the Centers for Medicare & Medicaid Services, DOD, FEMA, and USITC about their perspectives on challenges and potential actions, the feasibility of implementing such actions, and any longer-term sustainment planning the relevant agencies have conducted.
Agency Comments
We provided a draft of this enclosure to the Department of Homeland Security, DOD, HHS, Office of Management and Budget, and USITC. We incorporated technical comments from DOD, HHS, and USITC as appropriate. The Department of Homeland Security and Office of Management and Budget did not submit comments.
GAO’s Ongoing Work
We plan to continue to monitor federal funding and actions for domestic medical supply industrial base expansion and sustainment. This work will include evaluating the pandemic supply chain resilience strategy and related implementation plans when they become available and continuing to assess federal efforts to engage key nonfederal stakeholders and Congress to identify ways to overcome many of the challenges we identified in this enclosure.
GAO’s Prior Recommendations
See table below for our past related recommendations on domestic supply manufacturing from prior bimonthly CARES Act reports.
Prior GAO Recommendations Related to Domestic Medical Supply Manufacturing during COVID-19
Recommendation
Status
The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency—who head agencies leading the COVID-19 response through the Unified Coordination Group—should immediately document roles and responsibilities for supply chain management functions transitioning to the Department of Health and Human Services (HHS), including continued support from other federal partners, to ensure sufficient resources exist to sustain and make the necessary progress in stabilizing the supply chain, and address emergent supply issues for the duration of the COVID-19 pandemic (September 2020).
Open. HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability. In May 2021, the Office of the Assistant Secretary for Preparedness and Response (ASPR) noted that since March 2020, supply chain responsibility, coordination, and execution have been incorporated and integrated into ASPR. However, ASPR has not provided us with documentation of roles and responsibilities for these functions. See appendix IV for more information.
The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency—who head agencies leading the COVID-19 response through the Unified Coordination Group—should further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic, including through the use of Defense Production Act authorities. (September 2020 report).
Open. HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability. However, HHS has begun to take steps that help address this recommendation. For example, in May 2021, HHS provided several examples of ASPR’s efforts to restock the Strategic National Stockpile and mitigate potential supply shortages. In addition, ASPR cited its ongoing work to develop the pandemic resilience supply chain strategy called for under Executive Order 14001 and its integration in the interagency supply chain working group run by the White House, both of which are good steps toward developing plans to mitigate supply gaps. See appendix IV for more information.
The Secretary of Health and Human Services—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
Open. Both HHS and the Department of Homeland Security (DHS) disagreed with our recommendation, noting, among other things, the work that the departments had done to manage the medical supply chain and increase supply availability, such as restocking the Strategic National Stockpile (as noted above). In March 2021, DHS reported that the medical supply situation has improved in both the commercial market and at the state level. The agency stated that most states have 30 to 60 days of personal protective equipment to account for spikes in demand or localized critical shortages.
Although both HHS and DHS have reported separate actions taken as part of supply management efforts within their separate purviews, neither has articulated how they have worked with each other and other relevant federal, state, territorial, and tribal stakeholders to devise interim solutions to help states better track, manage, and plan for supply needs for the remainder of the COVID-19 pandemic. See appendix IV for more information.
The Administrator of the Federal Emergency Management Agency—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
The Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders, including state, local, tribal, and territorial governments and private industry, as the Department of Health and Human Services refines and implements a supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile (January 2021 report).
Open. HHS generally agreed with our recommendation, while noting that the term "engage" is vague and unclear, and that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority. However, as of May 2021, HHS has not taken steps to engage with these stakeholders. See appendix IV for more information.
Defense Production Act:Opportunities Exist to Increase Transparency and Identify Future Actions to Mitigate Supply Chain Issues.GAO-21-108. Washington, D.C.: November 19, 2020.
The Department of Defense has provided active-duty servicemembers and National Guard personnel to support the federal government’s COVID-19 response and vaccination efforts and simultaneously vaccinated military servicemembers (active and reserve), dependents, retirees, and civilian and contractor personnel.
Entities involved: Department of Defense, including the Defense Health Agency; the Department of Health and Human Services; and the Federal Emergency Management Agency, within the Department of Homeland Security
Background
The Department of Defense’s (DOD) primary mission is to defend the nation, but the department has also played a prominent role in supporting civil authorities. In that role, DOD has responded rapidly when called on during disasters and during declared natural or manmade emergencies. DOD, which has provided such support through its Defense Support of Civil Authorities mission, is authorized to provide this support when requested by another federal agency, with approval from the Secretary of Defense, or when directed by the President.[159] DOD provides support to civil authorities through military forces (Active-Duty, Reserve, National Guard); DOD civilian and contract personnel; and DOD component assets. To manage both its support for the federal government’s and its own internal COVID-19 response, the department established the DOD COVID-19 Task Force on February 28, 2020.
DOD’s Defense Health Agency (DHA) manages and oversees DOD’s immunization programs, leading efforts to distribute COVID-19 vaccines to eligible DOD personnel.[160] In March 2021, we reported that in mid-December 2020, DHA had begun a phased approach for vaccinating eligible personnel. Using that approach, DOD prioritized vaccination of individuals providing direct medical care, personnel maintaining essential national security and installation functions, deploying forces, and beneficiaries at highest risk for developing severe illness from COVID-19.
Overview of Key Issues
DOD has supported mass vaccination sites and other COVID-19-related civilian missions.
DOD personnel support over time. More than a year after the President declared COVID-19 a national emergency, DOD has consistently provided personnel to assist in the whole-of-government response. The figure below shows the number of DOD active-duty servicemembers and National Guard personnel supporting the response efforts from March 2020 through May 2021.
DOD Personnel Supporting the Federal Government’s COVID-19 Response, Mar. 2020–May 2021
Note: The totals shown are as of the end of each month. The totals refer to active-duty servicemembers—which includes reservists—and National Guard personnel providing support for the federal government’s COVID-19 response at mass vaccination sites and for other COVID-19-related missions. The total number of active-duty servicemembers who provided support in March 2020 is too small to be depicted.
Support at mass vaccination sites. In February 2021, DOD officials stated that the Federal Emergency Management Agency (FEMA) had requested the department to provide personnel to staff mass vaccination sites (i.e., federally supported community vaccination centers).[161] In response, active-duty servicemembers, including medical personnel, from the four military services began supporting community vaccination center operations in mid-February 2021.[162] These servicemembers have assisted with various activities such as registering and screening patients, distributing supplies, and administering COVID-19 vaccines.
From February 14, 2021, through June 22, 2021, more than 5,100 DOD active-duty servicemembers provided vaccine-related support, including administering more than 5 million vaccine doses at centers in 25 states and three territories. During this time, DOD provided active-duty servicemembers to support community vaccination centers on the basis of FEMA’s staffing needs at these centers. The figure below shows information about active-duty servicemembers’ aggregate COVID-19 vaccine support, including administering more than 5 million doses at federally supported community vaccination centers.
Locations Where Active-Duty Servicemembers Provided COVID-19 Vaccine Support at Federally Supported Community Vaccination Centers, Feb. 14, 2021–June 22, 2021
Notes: The shaded states and territories represent the locations where DOD provided active-duty servicemember personnel. From February 14 to June 22, 2021, DOD provided servicemembers on the basis of community vaccination centers’ needs.
National Guard personnel have also been supporting efforts to help vaccinate the civilian population in 47 states and three territories. Approximately 14,000 National Guard personnel have assisted with vaccine activities, including distributing vaccines, planning and coordinating at vaccination centers, providing transportation support, and administering the vaccine across static and mobile vaccination sites. As of June 11, 2021, National Guard personnel had administered about 12 million vaccine doses.
Support for other COVID-19-related missions. At the request of FEMA and the Department of Health and Human Services, DOD provided support for other COVID-19-related missions. From the pandemic’s initial emergency declaration in March 2020 until April 1, 2021, DOD provided more than 4,500 active-duty servicemembers, such as critical care nurses, to support civilian health care providers. These active-duty servicemembers supported 71 hospitals across 51 cities in 14 states and in the Navajo Nation.
Additionally, National Guard personnel continue to broadly support the COVID-19 pandemic response throughout the states and territories. As of June 15, 2021, approximately 28,000 National Guard personnel were providing support in all 50 states, three territories, and the District of Columbia. They continued carrying out a range of broad missions, such as:
testing and screening for COVID-19 cases;
cleaning sites and equipment;
distributing personal protective equipment;
storing and distributing supplies and equipment in warehouses;
collecting COVID-19 specimens;
supporting hospitals, long-term care facilities, food banks, and call centers;
recording data on, and performing contact tracing and mapping of, infected individuals; and
training civilian medical and other personnel.
As of June 9, 2021, DOD had at least partially vaccinated about 53 percent of its 2.1 million military servicemembers and was encouraging vaccinations through outreach and education.
DOD’s progress in vaccinating military servicemembers and others. As of June 9, 2021, DOD had at least partially vaccinated about 53 percent—1,124,624 servicemembers, including about 39 percent or 825,954 fully vaccinated servicemembers—of its 2.1 million active-duty, reserve, and National Guard servicemembers.[163] When considering only active-duty servicemembers, DOD had fully vaccinated about 51 percent (686,915 servicemembers). DOD’s goal was to fully vaccinate 60 percent of its active-duty servicemembers and provide at least one vaccine dose to approximately 70 percent by July 4, 2021.
Additionally, DOD was offering a COVID-19 vaccine to a larger population of 6.7 million individuals, which includes military servicemembers (active-duty, reserve, and National Guard) and their dependents; other uniformed personnel (members of the Coast Guard, U.S. Public Health Service, and National Oceanic and Atmospheric Administration); other beneficiaries (e.g., retired military servicemembers and their dependents); civilian employees; and selected contractor personnel. [164] DOD or a non-DOD vaccine provider had at least partially vaccinated about 45 percent (3,035,474 individuals) of this population as of June 9, 2021. However, the number of vaccinated individuals in this larger population may be higher, because, according to DHA officials, DOD has limited awareness of vaccinations administered to its target vaccine-eligible population at non-DOD sites, such as local retail pharmacies or through local public health vaccination sites.
DOD is tracking data on those who received the COVID-19 vaccine. The DHA Director monitors daily the department’s implementation of its vaccine plan, including vaccine administration, broken out by dose (initial and second) and category of eligibility (e.g., service component, contractors, civilian employees, and other beneficiaries).[165] The figure below shows COVID-19 vaccination rates for military servicemembers and others as of June 9, 2021.
COVID-19 Vaccinations in the Department of Defense (DOD), as of June 9, 2021
Notes: Percentages shown may not sum to 100 because of rounding. The 6.7 million eligible individuals targeted are those DHA assessed as eligible to receive a COVID-19 vaccine through DOD and who live within 40 miles of a DOD vaccination site. The target population includes eligible military servicemembers (those on active duty and members of the reserve component, including the National Guard), other uniformed personnel (those members of the Coast Guard, U.S. Public Health Service, and National Oceanic and Atmospheric Administration), military servicemembers who have retired and their dependent family members, dependent family members of active-duty servicemembers and of certain reserve component members, civilians, and contractors. This data shown refer to individuals vaccinated at DOD and non-DOD vaccination sites. DOD has vaccinated a majority of the individuals.
The percentage of fully vaccinated individuals aged 18 years and older in the U.S. population as of June 10, 2021, was larger than the percentage of fully vaccinated DOD military servicemembers as of June 9, 2021 (about 53 percent and 39 percent, respectively). However, when comparing the percentages of fully vaccinated individuals in the U.S. population and only the fully vaccinated active-duty servicemembers, the rates were more similar (53 percent and 51 percent, respectively).[166] Multiple reasons may account for the vaccination rate differences. For example, because military servicemembers tend to be younger and healthier, the majority of servicemembers did not become eligible for vaccination until April 19, 2021.
DOD officials use the term “vaccine acceptance” to categorize the proportion of individuals who have received a vaccine; however, the remainder of those eligible for the vaccine may not have declined it, as the department does not track or report on the percentage of individuals who declined the COVID-19 vaccine. According to DHA officials, the department does not currently have a reliable method to track and report vaccine declinations or hesitancy. Officials stated that this is due in part to the fact that DOD’s target population is encouraged but not required to receive a COVID-19 vaccine.[167] Individuals who show up for an appointment at a DOD vaccination site and decide not to receive the vaccine after reviewing educational material are asked to record their decision on DHA Form 207–COVID-19 Vaccine Screening and Immunization Document. However, DHA officials noted that this information does not reflect an accurate picture of declinations, because submitting the form is voluntary and the form reflects the individual’s decision at single point in time—that is, the individual may choose to receive the vaccine at a later date.
Outreach initiatives and education. To continue encouraging all of its eligible population to be voluntarily vaccinated, DOD is conducting various efforts designed to communicate the safety and efficacy of the authorized vaccines. Specifically, DOD’s outreach efforts include:
senior DOD leaders’ sharing their own vaccine experiences through social media and video recordings,
press events,
town halls,
internal news articles on TRICARE.mil and Health.mil webpages,[168]
direct email marketing,
scheduling vaccination events for entire military units (e.g., a Navy ship’s crew) and making medical personal available during those events to answer questions or address concerns about the vaccines,
radio and television stories on military broadcast services, and
a "Get the Vax" social media campaign (see figure).
Example of Department of Defense Social Media Graphic
On May 20, 2021, the Deputy Secretary of Defense and Vice Chairman of the Joint Chiefs of Staff published a memo reaffirming support for multiple initiatives to increase vaccination acceptance among all military servicemembers.[169] Further, the memo highlighted multiple techniques that military commanders and leaders at all levels can use to encourage and promote vaccinations. [170] Example of such techniques include:
incorporating vaccination opportunities into training events,
providing educational opportunities with medical professionals,
using routine personnel management tools such as time off for post-vaccination recovery, and
engaging with military servicemembers one-on-one to acknowledge concerns and answer questions.
Methodology
To conduct this work, we reviewed DOD guidance and documentation that DOD’s COVID-19 Task Force and DHA provided. The documentation included the most recent DOD COVID-19-related data available, which the task force and DHA maintained and reported to senior DOD leaders. We also interviewed DOD officials knowledgeable about the department’s COVID-19 response to corroborate our understanding of the data and DOD’s personnel support and vaccination efforts. Although we did not independently verify the accuracy of the data, we assessed their reliability by checking for obvious errors or outliers; discussing the ongoing levels of DOD personnel support and vaccination efforts with agency officials; and reviewing relevant documentation, including publicly available DOD media reports and statements. We determined that the data were sufficiently reliable for the purpose of characterizing DOD’s support to civil authorities and its progress in vaccinating the department’s target population.
Agency Comments
We provided a draft of this enclosure to DOD and the Office of Management and Budget for review and comment. DOD provided technical comments on this enclosure, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
GAO’s Ongoing Work
We plan to continue monitoring DOD’s support of the federal government’s COVID-19 response and progress in vaccinating the department’s eligible military servicemembers, dependents, retirees, and civilian and contractor personnel.
Related GAO Products
COVID-19: DOD Has Focused on Strategy and Oversight to Protect Military Servicemember Health. GAO-21-321. Washington, D.C.: June 3, 2021
Depot Maintenance: DOD Should Improve Pandemic Plans and Publish Working Capital Fund Policy.GAO-21-103. Washington, D.C.: Apr. 06, 2021
The Department of Health and Human Services’ Office of the Assistant Secretary for Preparedness and Response procured and shipped critical Strategic National Stockpile supplies directly from vendors to state, local, territorial, and tribal governments and designated project areas during the COVID-19 pandemic. However, it did not have documented policies and procedures, including related control and monitoring activities, to address the payment integrity risks within the direct shipment procurement process.
Entities involved: The Office of the Assistant Secretary for Preparedness and Response within the Department of Health and Human Services.
Recommendation for Executive Action
To strengthen the current procedures, the Assistant Secretary for Preparedness and Response should update policies and procedures, including related control and monitoring activities, for the Strategic National Stockpile to document the direct shipment procurement process and address payment integrity risks. Although the Department of Health and Human Services did not agree with us regarding the need to address payment integrity risks, it stated that it will update its policies and procedures, including related control and monitoring activities to document the direct shipment procurement process.
Background
Payment integrity is the process of ensuring that a payment is proper, including the legality, propriety, validity, and accuracy of all payments. For procurements, one of the key steps in this process is for agencies to confirm that the goods and services have been received and conform to the requirements of the purchase order. In short, it is the primary means to ensure that the government gets what it pays for. Without this control, the government faces risks including paying for:
goods and services not received;
goods received in the wrong quantity;
goods that are damaged; and
goods that do not meet quality or other specifications.
According to the President’s budget proposal for fiscal year 2021, the Strategic National Stockpile (SNS) is the largest federally owned repository of pharmaceuticals, critical medical supplies, federal medical stations, and medical equipment available for rapid delivery. It is overseen by the Department of Health and Human Services’ (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR).
Through its standard procurement process, ASPR procures supplies to maintain SNS inventory in preparation for bioterrorist attacks and other public health emergencies. The SNS can be used as a short-term stopgap buffer when the supply of materials may not be immediately available in affected areas during a public health emergency.
Because the nationwide need for critical supplies to respond to COVID-19 quickly exceeded the quantity of supplies contained in the SNS, in addition to its standard procurement process, ASPR used two additional procurement processes:
ASPR used a procurement process involving direct shipment from vendors. According to ASPR officials, the office initially established this direct shipment procurement process in response to the 2016 Zika virus outbreak in Puerto Rico. Under this direct shipment process, supplies purchased by ASPR were not used to replenish the SNS, but rather were primarily distributed from vendors directly to state, local, territorial, and tribal governments and designated project areas.
Beginning in April 2020, ASPR worked with interagency partners, such as the Federal Emergency Management Agency and the Department of Defense, through interagency agreements to increase the availability of supplies to respond to COVID-19. Under these reimbursable agreements, contracting staff at interagency partners procured and distributed vital supplies on ASPR’s behalf.
As of May 31, 2021, HHS reported it obligated about $10.2 billion of the $13.9 billion it planned to use for the SNS. The table below summarizes the amount of ASPR’s SNS obligations from appropriations provided by the six COVID-19 relief laws by procurement process from March 16, 2020 through May 31, 2021.
Department of Health and Human Services’ Strategic National Stockpile Obligations from Appropriations Provided by the Six COVID-19 Relief Laws as of May 31, 2021
Procurement process
Obligations ($ millions)
Percent of obligations
Direct shipment
600
6
Interagency agreement
4,700
46
Standard
4,900
48
Totala
10,200
100
Source: GAO summary of Health and Human Services obligations data. | GAO-21-551
aNumbers may not total due to rounding.
Overview of Key Issues
SNS direct shipment procurement process was not documented in policies and procedures. ASPR did not have documented policies and procedures, including related control and monitoring activities, to address payment integrity risks for its direct shipment procurement process. Guidance from the Office of Management and Budget (OMB) states that agency management is responsible for managing payment integrity risks to reduce improper payments and protect taxpayer funds.[171] Accordingly, agencies are to develop control activities to help management achieve payment integrity objectives by establishing policies and procedures related to transaction authorization and approvals of program activities and implementing transaction reviews where detailed criteria are evaluated before funds are expended.
Additionally, federal internal control standards state that management should design control activities to achieve objectives and respond to risks and implement control activities through policies. Accordingly, as part of this internal control principle, agency management is to clearly document internal control, all transactions, and other significant events in a manner that allows the documentation to be readily available for examination. In addition, if there is a significant process change, management is to review the new process in a timely manner after the change to determine that the control activities are designed and implemented appropriately. Management should also establish and operate monitoring activities to monitor the internal control system and evaluate the results.
According to ASPR officials, the office used its direct shipment procurement process to expedite delivery and effectively manage costs during the pandemic. Although ASPR officials verbally explained this procurement process, the office did not have the process and related control and monitoring activities documented in its policies and procedures, in accordance with federal internal control standards.
ASPR officials stated that under the direct shipment procurement process, the office tracks the transportation and delivery of supplies shipped directly from vendors to recipients by requesting that vendors provide ASPR shipment tracking documentation as part of their contracted deliverables. Further, the delivery confirmation will come from an email or phone call from the recipient or a delivery confirmation from the carrier, such as a tracking report from the carrier’s website. ASPR provided examples of email communication with recipients and vendors to confirm delivery of supplies prior to authorizing payment. However, without properly documented procedures for this process, ASPR lacks assurance that this communication would take place consistently.
Although ASPR officials stated that the office’s procedures for invoice receiving apply to all SNS invoices, including those for direct shipment procurements, the policies and procedures did not include specific steps to address payment integrity risks for its direct shipment procurement process, such as to:
confirm vendors provide such shipment tracking documentation, or
verify intended recipients actually received the correct undamaged supplies prior to issuing payment.
Without a properly documented process, we could not determine if the control and monitoring activities were properly designed to provide reasonable assurance that SNS payments are properly authorized and made to eligible vendors at appropriate amounts.
Until ASPR updates its policies and procedures, including related control and monitoring activities, to document its direct shipment procurement process, there is an increased risk that taxpayer funds will not be appropriately protected. For example, without written policies and procedures documenting how ASPR tracks the direct shipment and receipt of supplies prior to issuing payments, there is an increased risk that ASPR may make improper payments to vendors for incorrect supplies or quantities, or supplies the intended recipients did not receive.
In addition, without adequate documentation, it is difficult for management to assess the adequacy of controls over the direct shipment procurement process and ASPR lacks assurance that its staff fully understand the process and properly and consistently perform their duties.
Certain interagency transactions lacked sufficient documentation. In November 2020, HHS’s independent financial statement auditor reported a deficiency, in part due to insufficient documentation to substantiate what was purchased and when it was received for certain SNS COVID-19-related transactions with interagency partners.[172] The auditor stated that HHS is currently reviewing its processes to identify lessons learned so that new processes are developed to address potential future crisis situations similar to the current pandemic.
According to ASPR officials, the office concurred with the interagency finding and is continuing to work with its interagency partners on accountability and documentation for COVID-19 relief funds expended through interagency agreements.[173] Further, according to officials, starting in March 2021, ASPR began meeting weekly with the HHS Corrective Action Planning team to discuss remediation strategies and develop Corrective Action Plans for the auditor’s SNS findings.
SNS designed control activities for its standard procurement process. For supplies purchased through its standard procurement process during the COVID-19 response, ASPR used its existing SNS policies and procedures for purchasing, receiving, distributing, and payment processing activities. ASPR’s policies and procedures for this standard SNS procurement process were designed consistent with federal internal control standards for the key eligibility, processing, and existence control activities we reviewed.
Methodology
We interviewed officials from ASPR, HHS’s Program Support Center, and the HHS Office of Inspector General and reviewed policies and procedures related to the SNS payment process. We also considered HHS’s fiscal year 2020 agency financial report and the accompanying independent auditor’s reports.
Based on HHS provided documentation, we assessed the design of HHS’s policies and procedures related to the SNS payment process against relevant statutory requirements, OMB guidance, and federal internal control standards to determine the extent to which HHS’s key control and monitoring activities are properly designed to achieve the SNS program’s payment integrity objectives and respond to such risks. For any key control and monitoring activities that were not properly designed and documented, we inquired with HHS officials to determine the reasons.
Agency Comments
We provided HHS with a draft of this enclosure. HHS provided written comments, reproduced in Appendix VI and technical comments on this enclosure, which we incorporated as appropriate.
ASPR did not concur with our recommendation. ASPR stated that it did not find that we found or provided evidence to support the statement that there were payment integrity risks for the direct shipment process and noted that ASPR has a three-way matching procedure that is followed for all invoices. However, ASPR acknowledged that it will update its policies and procedures, including related control and monitoring activities, and work to specifically document the direct shipment procurement process.
Although ASPR officials stated that the office’s procedures for invoice receiving apply to all SNS invoices, the policies and procedures did not include specific steps to address payment integrity risks for its direct shipment procurement process, such as procedures to (1) confirm vendors provide shipment tracking documentation, or (2) verify intended recipients actually received the correct undamaged supplies prior to issuing payment. Therefore, we continue to believe the recommendation is needed.
GAO’s Ongoing Work
We will monitor the status of our payment integrity recommendation for the Department of Health and Human Services and continue our oversight of government-wide payment integrity efforts.
Related GAO Product
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
In the years prior to the COVID-19 pandemic, the Office of the Assistant Secretary for Preparedness and Response began restructuring an interagency body that recommends procurement of vaccines, supplies, and other materials for the Strategic National Stockpile to respond to public health threats. Such restructuring has led to concerns about the effectiveness of interagency collaboration, transparency, and a lapse in statutorily required reviews used to inform the contents of the stockpile.
Entities involved: Department of Agriculture; Department of Defense; Department of Health and Human Services, including the Office of the Assistant Secretary for Preparedness and Response, the Centers for Disease Control and Prevention, the Food and Drug Administration, and the National Institutes of Health; Department of Homeland Security; Department of Veterans Affairs; and the Office of the Director of National Intelligence.
Recommendations for Executive Action
To improve the nation’s preparedness for a wide range of threats, including pandemics, the Assistant Secretary for Preparedness and Response should develop and document plans for restructuring the Public Health Emergency Medical Countermeasures Enterprise. These plans should describe how the Assistant Secretary will ensure a transparent and deliberative process that engages interagency partners in the full range of responsibilities for the Public Health Emergency Medical Countermeasures Enterprise outlined in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, including those related to the Strategic National Stockpile annual threat-based reviews. These plans should also incorporate GAO’s leading practices to foster more effective collaboration, while ensuring that sensitive information is appropriately protected.
To improve organizational accountability, the Assistant Secretary for Preparedness and Response should implement records management practices that include developing, maintaining, and securing documentation related to Public Health Emergency Medical Countermeasures Enterprise activities and deliberations, including those related to the Strategic National Stockpile. Documentation should include information such as the factors considered, the rationale for the action or decision, and the final outcomes of the Public Health Emergency Medical Countermeasures Enterprise processes.
The Department of Health and Human Services concurred with the recommendations, noting that its Office of the Assistant Secretary for Preparedness and Response is initiating a review of the Public Health Emergency Medical Countermeasures Enterprise, which will be conducted by the National Academies of Sciences, Engineering, and Medicine. According to the Department of Health and Human Services, the review will examine multiple aspects of the Public Health Emergency Medical Countermeasures Enterprise processes, including interagency coordination, policies and practices, and transparency, with a final report expected in fall 2021.
Background
The COVID-19 pandemic has highlighted the importance of a readily available cache of medical products and supplies to treat patients and protect first responders during public health emergencies. The Strategic National Stockpile (SNS) contains a multibillion dollar inventory of medical countermeasures—drugs, vaccines, supplies, and other materials—to respond to a broad range of public health emergencies resulting from exposure to chemical, biological, radiological, and nuclear agents, as well as emerging infectious diseases, including pandemic influenza.[174]
Overseen by the Office of the Assistant Secretary for Preparedness and Response (ASPR) within the Department of Health and Human Services (HHS), the SNS mission has expanded since its inception in 1999 in response to statutory changes and a growing variety of threats.[175] During public health emergencies like COVID-19, the contents of the stockpile may be deployed to state and local entities when their supplies are depleted or when the necessary medical countermeasures are not commercially available, such as the antitoxin used to treat botulism.
The inventory of the SNS is informed by an interagency group of experts called the Public Health Emergency Medical Countermeasures Enterprise (PHEMCE), which is led by ASPR and comprised of multiple HHS and other federal agencies such as the Departments of Defense and Homeland Security, hereafter referred to as PHEMCE interagency partners. HHS established the PHEMCE in 2006 to advance national preparedness for natural, accidental, and intentional threats by coordinating medical countermeasure efforts within HHS and in cooperation with other federal agencies. Specifically, the key functions of the PHEMCE are to advise the Secretary of Health and Human Services in:
defining and prioritizing requirements for medical countermeasures in public health emergencies;
integrating and coordinating research, product development, and procurement activities; and
setting deployment and use strategies for medical countermeasures held in the SNS.
For example, in 2016, the PHEMCE recommended stockpiling goals for certain personal protective equipment, such as N95 respirators, which were in high demand during the COVID-19 pandemic.
The PHEMCE was later codified in law through the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019.[176] The act specified that the PHEMCE is to use a process to make recommendations to the Secretary of Health and Human Services regarding research, procurement, and stockpiling of medical countermeasures and assist the Secretary in developing strategies for logistics, deployment, distribution, dispensing, and use of countermeasures that may be applicable to the SNS, among other things.
The PHEMCE manages the SNS annual review, a year-long, multistep process that starts with an examination of the inventory. Based on PHEMCE deliberations of the gaps in the stockpile and threat priorities, this process results in recommendations for SNS medical countermeasure procurements. Required to be completed since 2006 and to be submitted to Congress since 2013, these reviews inform medical countermeasure procurements for the SNS inventory 3 years in the future.[177] For example, the 2016 SNS Annual Review examined the SNS’s inventory in 2016, was finalized in 2017, and made recommendations for the procurement of medical countermeasures for fiscal year 2019.
These recommendations are prioritized based on a number of factors, such as how critical the medical countermeasures are to response and life-saving efforts and how usable they are by clinicians or laypersons. They are informed by the anticipated budget of the SNS, and we have reported there have been tensions between the limitations of the budget and procurements in response to identified threats, according to ASPR officials.
As part of our CARES Act reports, we have discussed how the COVID-19 pandemic has highlighted challenges related to SNS funding prior to the pandemic, raising concerns about the SNS’s ability to respond to a wide range of threats in the future. For example, we reported in January and March 2021 that SNS funding has not kept pace with the increasing number of threats for which the SNS may be needed. We also noted that funding requests have not always fully reflected SNS funding needs due to competing priorities and tradeoffs involved in aligning SNS budgetary needs with broader HHS needs and the President’s budget priorities, according to ASPR officials.
We also reported in June 2020 that HHS previously noted the challenge of maintaining a stockpile of medical countermeasures to use against many low-probability, high-consequence threats, while also maintaining the capacity to rapidly respond to novel threats, like emerging infectious diseases.[178] Additionally, we reported in March 2021 that HHS did not replenish personal protective equipment to previous levels following the H1N1 influenza pandemic of 2009 prior to COVID-19 because of a lack of funding.
As of May 31, 2021, six relief laws had been enacted to assist the COVID-19 response.[179] These laws appropriated funding for HHS activities, and, in some cases, specifically authorized their use for the SNS. [180] As of May 31, 2021, HHS reported it obligated about $10.2 billion of the $13.9 billion it planned to use for the SNS to purchase personal protective equipment and ventilators for immediate use as well as to replenish SNS inventory, among other purposes, and had expended about $6.3 billion.
Overview of Key Issues
ASPR significantly changed PHEMCE operations after 2017. According to officials from ASPR and three of six PHEMCE partners, ASPR made changes to the PHEMCE in response to concerns raised by the Assistant Secretary, some of which PHEMCE partners shared, including that the PHEMCE’s decision-making process was too slow.[181] According to the former Assistant Secretary who initiated the PHEMCE changes, while the body was successful in advancing the development of medical countermeasures and a model for interagency coordination and collaboration, its consensus-driven process affected the urgency with which medical countermeasures were developed and, thus, the nation’s preparedness in addressing threats. ASPR officials responsible for the administration of the PHEMCE also noted that some changes made to the PHEMCE were designed to more closely align with the Assistant Secretary’s priorities, as each new Assistant Secretary comes to the position with specific expertise and ideas for how preparedness should be addressed.
The figure below illustrates the PHEMCE operations immediately prior to and after December 2017, including changes that occurred after December 2017, which narrowed the scope of issues on which the PHEMCE primarily focused its deliberations, and shifted the structure of the deliberation process about medical countermeasures from a bottom-up to a top-down approach.[182]
Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) Organization
Note: In addition to the Integrated Program Teams, the PHEMCE also established working groups for specific purposes. For example, the PHEMCE established the Emerging Infectious Disease Working Group in April 2014 to evaluate the public health risks posed by emerging infectious diseases, excluding influenza. This group was sunset in 2016 after it completed its assigned task of developing a framework for prioritizing emerging disease threats, according to an ASPR official.aThe Office of the Director of National Intelligence did not previously participate in the PHEMCE, but was identified as a PHEMCE partner in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. bTen Integrated Program Teams were identified in the July 2015 PHEMCE Integrated Program Team charter; however, the PHEMCE was authorized to establish or disband Integrated Program Teams as needed.cASPR officials told us the PHEMCE discussed other topics as needed. For example, a Botulinum Portfolio Assessment Team was in place for a limited period of time, according to a PHEMCE member who participated on that team.
Scope of PHEMCE deliberations. After 2017, ASPR narrowed the scope of work performed by the PHEMCE in terms of the range of issues for which it provided recommendations, according to officials from ASPR and three of six PHEMCE partners. Historically, the PHEMCE provided input on a comprehensive range of issues related to medical countermeasures, which ASPR officials currently responsible for the administration of the PHEMCE referred to as an end-to-end approach to planning. For example, the PHEMCE provided input on deployment strategies and clinical guidance for the use of medical countermeasures in the SNS for public health emergencies, according to officials from two of six PHEMCE partners.
However, after 2017, ASPR began narrowing the PHEMCE’s scope to focus its efforts on medical countermeasure development and procurement, according to ASPR officials. ASPR and Department of Defense (DOD) officials told us that through these PHEMCE changes, the office sought to better align medical countermeasure development and procurements between HHS and DOD—the primary purchasers of medical countermeasures—including coordinating different priorities for vaccine development. As part of this change, the former Assistant Secretary made DOD a co-chair, along with ASPR, on the Enterprise Governance Board, the most senior leadership level of the PHEMCE structure.
According to the former Assistant Secretary, in future iterations of the PHEMCE restructure, ASPR planned to broaden the PHEMCE’s scope to also focus on issues such as the deployment and utilization of medical countermeasures. In particular, it planned to incorporate the insight of public health organizations that represent states, local governments, tribes, and territories, such as the National Association of County and City Health Officials.
ASPR also aimed to limit access to national-security-sensitive or proprietary information, as part of its scope changes, according to ASPR’s 2020-2023 Strategic Plan and the former Assistant Secretary. According to the former Assistant Secretary, a critical PHEMCE vulnerability that needed to be addressed was the security of PHEMCE proceedings. Prior to 2018, PHEMCE proceedings were conducted in unclassified and unsecured settings which, according to the former Assistant Secretary, could have enabled hostile foreign entities or other individuals to access sensitive or propriety information related to both medical countermeasure vulnerabilities and development innovations.[183] According to officials from ASPR and two of six PHEMCE partners, discussions after 2017 primarily occurred among PHEMCE partners that had appropriate security clearances to enable access to real-time information from the intelligence community. A former senior ASPR official told us that this significantly limited subject matter experts’ ability to participate in discussions. However, according to the former Assistant Secretary, the views of subject matter experts could be communicated through their respective agency representatives who participated in discussions at senior leadership levels of the PHEMCE.
Structure and activities of the PHEMCE. After 2017, PHEMCE deliberations shifted from a bottom-up to a top-down approach. Prior to the reorganization efforts, the PHEMCE process consisted of 10 groups of subject matter experts (known as Integrated Program Teams, as illustrated above), which focused on a specific threat area and its associated medical countermeasures.[184] Among other responsibilities, these teams developed recommendations on the type and number of medical countermeasures HHS should buy for the SNS. These recommendations subsequently underwent further examination by increasingly senior PHEMCE leadership levels, which, according to officials from ASPR and a PHEMCE partner, took a significant amount of time.
To make the process more efficient and ensure medical countermeasure development focused on national security vulnerabilities, the former Assistant Secretary shifted the PHEMCE decision-making structure so that leadership at the highest level, specifically the Assistant Secretary, identified areas of concern related to threats or medical countermeasures and assigned them to subject matter experts for analysis and assessment, according to ASPR officials and the former Assistant Secretary.
Further, as illustrated in the previous figure, ASPR reduced the number of standing subject matter expert groups that convened to deliberate on specific threats and added others that met for a limited period of time. According to ASPR documentation, ASPR established two Portfolio Assessment teams in 2019 to focus on anthrax and smallpox, which have been identified by the PHEMCE as high-priority threats, among other things. The PHEMCE multiyear budget for fiscal years 2018-2022 projected that these threats would account for more than 50 percent of the SNS budget for this period and noted that estimated spending for anthrax and smallpox would increase by 15 and 47 percent, respectively. Senior ASPR officials told us that the PHEMCE also established Portfolio Assessment Teams for other threats, but ASPR did not provide us documentation of the goals of these other teams or evidence that they met regularly.
Additionally, activities and deliberations among the various PHEMCE levels became less frequent and regular after 2017, according to ASPR officials and all PHEMCE partners. The precise number of meetings that occurred at different levels is unclear; ASPR was unable to provide us documentation of these meetings. According to ASPR officials, some of the change in PHEMCE activity between 2017 and 2020 was due to uncertainty about which ASPR division was responsible for the administration of the PHEMCE, the lack of a PHEMCE governance structure, and the COVID-19 pandemic.[185] Consistent with leading collaboration practices we have identified, defining and sustaining leadership is beneficial for collaborative efforts; and as such, leadership transitions and inconsistency can weaken the effectiveness of any interagency collaborative effort.
PHEMCE partners’ concerns about changes. Three of six PHEMCE partners had concerns about changes to the body, including a reduced ability to provide input and reduced transparency of the process. All PHEMCE partners acknowledged that while the previous PHEMCE processes contributed to its inefficiency, these processes were effective in ensuring appropriate input and thorough deliberation on a broad range of medical countermeasure issues that affect all PHEMCE partners. For example, officials from one PHEMCE partner said that under the previous PHEMCE structure, concerns about the purpose and scientific rationale for a plan to purchase a product for the SNS inventory would have been vetted with all PHEMCE partners prior to its acquisition. In addition, two of six PHEMCE partners also told us the PHEMCE restructure resulted in a lack of clarity on how ASPR makes decisions about the medical countermeasure enterprise and the rationale behind decisions made, including for the SNS inventory.
According to the former Assistant Secretary, under the new structure, input of PHEMCE partners was appropriately considered. However, he noted that his responsibility was to make the best use of ASPR resources to advance the nation’s preparedness against threats, not to ensure consensus was reached. ASPR was unable to provide us with documentation to understand the extent PHEMCE partners were involved in deliberations.
Further, officials from two of six PHEMCE partners credited the prior process with enhancing preparedness and producing sound, scientifically based decisions, including recommendations on the SNS inventory. One PHEMCE partner also noted the importance of maintaining connectivity among interagency partners, which existed under the former PHEMCE operational structure. Consistent with leading collaboration practices we have identified, positive working relationships between participants from different organizations build trust and foster communication which facilitates collaboration that is vital in responding to an emergency.
In a hearing before the Senate Committee on Homeland Security and Governmental Affairs on April 14, 2021, the Assistant Secretary for Preparedness and Response from 2009-2017 noted the PHEMCE coordination process led to the development of over 50 medical countermeasures against recognized public health threats. However, she identified the degradation of the PHEMCE process as one of several actions that led to the nation being less ready for the COVID-19 pandemic than we otherwise might have been. In contrast, the former Assistant Secretary said that the revised top-down PHEMCE process was applied successfully during the COVID-19 response for Operation Warp Speed, which focused on portfolios of vaccines, diagnostic tests, and treatments, and were co-led by DOD and HHS.
ASPR did not conduct statutorily required annual reviews of the SNS for 3 years. ASPR did not conduct statutorily required SNS annual reviews for 2017, 2018, and 2019, while the PHEMCE was undergoing operational changes, according to ASPR officials. As noted earlier, the annual reviews examine inventory relative to threat priorities and inform procurements 3 years in the future. Therefore, the first fiscal year affected by the lack of an annual review was 2020.
According to ASPR officials, in the summer of 2020, they made some Congressional staff aware that these annual reviews had not been completed due to the transfer of the SNS from the Centers for Disease Control and Prevention (CDC) to ASPR and the PHEMCE reorganization, among other things. The former Assistant Secretary told us in July 2021 that he recognized the importance of conducting the annual reviews and was not aware that they had not been completed.
In the absence of the annual reviews that would have informed procurements for fiscal years 2020 and 2021, ASPR officials told us that they procured medical countermeasures based on PHEMCE recommendations from SNS annual reviews conducted prior to the PHEMCE restructure and real-time direction from the Assistant Secretary. ASPR plans to use a similar approach for fiscal year 2022. ASPR officials noted that, for many years, much of the annual appropriations for the SNS had been used to replenish medical countermeasures, including anthrax therapeutics and smallpox vaccines, which have always been high priority investments, adding that the SNS’s budget does not enable it to purchase all medical countermeasures identified as priorities in the SNS annual reviews. As a result, there are still many medical countermeasures left over from previous prioritization lists to procure.
Previous SNS annual reviews have identified similar challenges of competing priorities and tradeoffs due to budget limitations. The 2015 SNS Annual Review proposed reducing procurements of both anthrax vaccine and antibiotics to meet budget constraints. Additionally, the 2016 SNS Annual Review reported that the SNS inventory was below the stockpiling goals for several types of medical countermeasures, according to the PHEMCE multiyear budget for fiscal years 2018 to 2022.
ASPR officials stated that the 2020 SNS Annual Threat-Based Review is currently being finalized and will inform SNS procurement priorities for fiscal year 2023.[186] This review was required to be submitted to congressional committees by March 15, 2021, but had not been submitted as of June 21, 2021; ASPR officials told us they communicated this delay to Congress. ASPR officials noted that in comparison with prior SNS annual reviews, the 2020 review was not developed through deliberative discussions of the PHEMCE and will be fairly limited due to the ongoing COVID-19 response; ASPR officials told us they plan to conduct more robust annual threat-based reviews in the future.
New PHEMCE reorganization efforts underway. ASPR is in the process of re-assessing and re-establishing new organizational processes for the PHEMCE, but has not yet finalized planning documents, including an organizational charter and implementation plan, to guide those efforts.
Although ASPR developed some materials outlining the structure it began implementing in 2019, a revised PHEMCE charter was never finalized, according to officials from ASPR and a PHEMCE partner, and therefore, never shared with PHEMCE partners. ASPR officials acknowledged that the changes made to the PHEMCE in the 2018 to 2020 period did not fully achieve the desired aims and created other challenges. As a result, officials said they have paused PHEMCE operations while they assess how best to move forward.
ASPR officials told us they are currently developing the PHEMCE charter and policies that will describe how the PHEMCE will operate going forward, which they hoped to finalize in May 2021. However, as of June 21, 2021, the charter had not been finalized. Additionally, in April 2021, ASPR officials reported that they had engaged with PHEMCE partners to gather feedback and contracted with the National Academies of Sciences, Engineering, and Medicine to develop recommendations on how to improve PHEMCE operations but their review had not yet begun.
According to ASPR’s 2021-2022 PHEMCE Strategy and ASPR officials, the PHEMCE will return to having a broader scope of work, such as helping HHS to develop strategies for the logistics, deployment, distribution, dispensing, and use of medical countermeasures in the SNS.[187] The COVID-19 pandemic illustrated that medical countermeasure planning needs to be comprehensive, according to one ASPR official who noted that discussions among PHEMCE partner officials are underway to determine the best way to evaluate threats and develop strategies to ensure that medical countermeasures to counter those threats are available.
However, responding to the daunting and specific challenges of the COVID-19 response, as well as changes within ASPR (specifically the shifting of the division responsible for PHEMCE administration as recently as July 2020), have contributed to delays in re-establishing the PHEMCE, according to ASPR officials.
Developing and documenting plans for restructuring the PHEMCE would help ASPR to meet the requirements outlined in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. Such plans would help ASPR to ensure that it develops a transparent and deliberative process that also balances the need to protect sensitive, including proprietary information. The act stipulates that the functions of the PHEMCE shall involve several activities, including the following:
Making recommendations to the Secretary of Health and Human Services regarding research, development, procurement, stockpiling, deployment, distribution, and use of medical countermeasures;
Identifying national health security needs, including gaps in public health preparedness and response related to medical countermeasures; and
Assisting the Secretary of Health and Human Services in developing strategies related to logistics, deployment, distribution, dispensing, and use of medical countermeasures that may be applicable to SNS activities.[188]
The act also stipulates that the annual threat-based review should be conducted in consultation with the PHEMCE.[189]
In addition, developing and documenting plans that incorporate GAO’s leading collaboration practices would help ASPR ensure that its current plans for restructuring of the PHEMCE results in an effective interagency collaboration over the long term. Among our leading practices for collaboration ASPR should consider addressing the following in its plans:
identifying a leadership model and detailing how it will be sustained over time,
clearly identifying roles and responsibilities of interagency partners and steps for decision making,
developing ways to update or monitor collaborative agreements, and
establishing ways to operate across participating agencies’ boundaries to build positive relationships and bridge organizational cultures.
Until ASPR develops and documents plans for restructuring the PHEMCE that addresses a number of issues, ASPR risks being unable to fulfill its responsibilities in advancing national preparedness for a wide range of threats, including a pandemic. These include having a transparent and deliberative process that engages interagency partners in the full range of PHEMCE responsibilities outlined in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, including those related to the SNS annual threat-based reviews, and incorporates leading practices to foster more effective collaboration. These plans should also reflect the need to conduct deliberations securely, so as not to risk harming our nation’s homeland security. The completion of the PHEMCE reorganization aided through the development of these plans is crucial to ensuring that the most efficacious medical countermeasures—informed by the PHEMCE partners’ broad range of scientific, regulatory, and logistical expertise—are available for rapid deployment and effective administration and utilization during the next public health emergency.
ASPR lacks documentation of PHEMCE activities and deliberations. ASPR was unable to provide us with documentation of PHEMCE activities and deliberations after 2017, which raises concerns about the office’s records management practices. For example, the office was unable to provide the following items:
Documentation related to PHEMCE decisions or recommendations during the 2018 to 2020 period, which could have provided information on the factors that interagency partners considered when making decisions about the medical countermeasures enterprise, including the SNS.
Documentation that would support ASPR officials’ accounts of the rationale for the changes to the PHEMCE—information that was shared with PHEMCE interagency partners in 2019, according to three of six PHEMCE partner officials we interviewed.
PHEMCE meeting agendas and minutes for 2018 to 2020 to know, for example, who was involved.
For these reasons, we do not know whether PHEMCE partners were aware of the lapse in SNS annual reviews, which historically were managed by the PHEMCE, or if PHEMCE partners discussed the implications of this lapse for the SNS inventory. We also do not know if senior ASPR leadership provided any explicit guidance regarding the approach that should be used to determine medical countermeasure acquisition priorities for the SNS in the absence of SNS annual reviews. ASPR officials told us that several staff transitions during this time period made it challenging for them to locate documentation related to PHEMCE activities and deliberations, and acknowledged the need to improve records management going forward.
Not maintaining such documentation is inconsistent with HHS’s policy for records management, which implements the Federal Records Act of 1950 and other laws and regulations.[190] The policy requires HHS components to:
establish and maintain a records management program that includes managerial activities related to the creation, maintenance and use, and disposition of records, carried out in such a way as to achieve adequate and proper documentation of federal transactions and effective and economical management of agency operations;
implement a records maintenance program so that complete records are filed or otherwise identified and preserved and can easily be found when needed; and
ensure that departing employees’ federal records have been turned over to the appropriate successor or official to permit continued preservation of departmental federal records.[191]
Until ASPR implements records management practices that include developing, maintaining, and securing documentation related to PHEMCE activities and deliberations, including those related to the SNS, Congress and key stakeholders do not have assurance that steps taken are advancing national preparedness for natural, accidental, and intentional threats. Practices should ensure information such as the factors considered, the rationale for the action or decision, and the final outcomes of PHEMCE processes are properly documented. Creation and management of PHEMCE records facilitates transparency and accountability as it provides stakeholders, including interagency partners impacted by decisions and oversight bodies that assess them, with access to information regarding how and why decisions were made. Maintaining these records can also reduce the risks of losing organizational knowledge due to staffing volatility.
Methodology
To conduct this work, we reviewed PHEMCE documentation that described the PHEMCE prior to the restructuring, including charters, a past and current PHEMCE Strategy and Implementation Plan, and information publicly available on the PHEMCE internet site, among other things. We interviewed or obtained written responses from:
current and former ASPR officials that participated in the governance of the PHEMCE and that had responsibility for the administration of the PHEMCE prior to and after December 2017, including the former Assistant Secretary.
seven PHEMCE interagency partners: CDC, Department of Agriculture (USDA), Department of Defense (DOD), Department of Homeland Security (DHS), Department of Veterans Affairs (VA), Food and Drug Administration, and National Institutes of Health, in April and May 2021. One of the seven interagency partners was unable to provide relevant information due to staff turnover. Therefore, we only included responses from the remaining six partners in our findings.
officials within the Division of the Strategic National Stockpile responsible for developing the SNS budget and spend plans for the SNS and ASPR officials that liaised between the PHEMCE and the Division of the Strategic National Stockpile, including the Acting Director of the Division of the Strategic National Stockpile.
Lastly, we assessed ASPR’s actions related to the PHEMCE restructure against our leading practices for effective collaboration and relevant requirements in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, and the Department of Health and Human Services Policy for Records Management, which implements the Federal Records Act of 1950 and other laws and regulations.
Agency Comments
We provided HHS, DOD, DHS, the Office of Management and Budget (OMB), USDA, and VA with a draft of this enclosure. HHS provided comments, which are reproduced in Appendix VI .
In its comments, HHS stated that it concurred with our recommendations and that it is initiating a review of the PHEMCE by the National Academies of Sciences, Engineering, and Medicine to look at a number of issues including interagency coordination, appropriate policies and practices, scope, transparency and ethical conduct. HHS also noted that several meetings will be held to allow for stakeholder input and that the review will culminate in a report, which HHS anticipates receiving in fall 2021.
HHS also provided technical comments, which we incorporated as appropriate. DHS, DOD, OMB, USDA, and VA did not provide comments on this enclosure.
GAO’s Ongoing Work
We are conducting a comprehensive body of work on the SNS in response to the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 and the CARES Act.[192] This work includes examining the contents and management of the SNS to include a review of procurements of medical countermeasures over time, the decisions behind these procurements, and how they help address emergency health security needs. We will also continue to monitor efforts to modernize and restructure the SNS.
GAO’s Prior Recommendation
The table below presents our recommendation on the Strategic National Stockpile from a prior bimonthly CARES Act report.
Prior GAO Recommendation Related to the Strategic National Stockpile
Recommendation
Status
To improve the nation’s response to and preparedness for pandemics, the Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as the Department of Health and Human Services (HHS) refines and implements a supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile (January 2021 report).
Open. HHS generally agreed with our recommendation, while noting that the term “engage” is vague and unclear, and that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority.
As of May 31, 2021, federal agencies reported obligating tens of billions of dollars in support of COVID-19 response efforts through contracts and other transaction agreements, with the predominant types of goods and services procured changing from medical equipment and supplies to drugs and treatments over the course of the pandemic.
Entities involved: U.S. Department of Agriculture; Department of Defense; Department of Health and Human Services; and Department of Homeland Security, among others
Background
Federal agencies have used a variety of contracting mechanisms to provide vital goods and services in support of federal, state, and local COVID-19 response efforts.[193] For example, federal agencies have reported billions of dollars in obligations on contracts subject to the Federal Acquisition Regulation—which provides uniform policies and procedures for acquisitions by all executive agencies.[194] Our prior work on disaster contracting has found that contracts play a key role in federal emergency response efforts, and that contracting during an emergency can present a unique set of challenges as officials can face significant pressure to provide critical goods and services as expeditiously and efficiently as possible. The January 2021 National Strategy for the COVID-19 Response and Pandemic Preparedness emphasizes the important role contracts will continue to play during the response. The strategy states that the federal government will fully leverage contract authorities to strengthen the vaccine supply chain; staff vaccination sites; and fill supply shortages for personal protective equipment, drugs, and therapeutics.
In addition, federal agencies like the Department of Defense (DOD) and Department of Health and Human Services (HHS) have relied on the use of other transaction agreements—which are not subject to the Federal Acquisition Regulation—for activities such as vaccine development and manufacturing in response to COVID-19.[195] Our prior work has noted that the flexibility to tailor other transaction agreements can help agencies attract companies that do not typically do business with the government. However, their use also carries a risk of reduced accountability and transparency. The CARES Act relaxed certain limitations on the use of other transaction agreements in response to COVID-19 for HHS and DOD, such as congressional reporting requirements and requirements for who can approve certain transactions.[196]
As federal contracting activity continues to play a critical role in response to the pandemic, it is important to ensure that contract actions made in response to COVID-19 are accurately reported and visible to congressional decision makers, entities with oversight responsibilities, and taxpayers. National Interest Action (NIA) codes were established in 2005 following Hurricane Katrina to enable the consistent tracking of emergency or contingency-related contracting actions in the Federal Procurement Data System-Next Generation (FPDS-NG). The COVID-19 NIA code—used to track contract actions and associated obligations in response to COVID-19 in FPDS-NG—was originally established on March 13, 2020, and set to expire on July 1, 2020. The Department of Homeland Security (DHS) and DOD subsequently extended the code three times—first to September 30, 2020, then to March 31, 2021, and more recently to September 30, 2021.[197]
Overview of Key Issues
Agencies obligated $61.4 billion on federal contracts, with DOD and HHS accounting for most obligations. In response to the COVID-19 pandemic, contract obligations totaled about $61.4 billion as of May 31, 2021. At the beginning of the response, HHS accounted for the most federal contract obligations. However, as the response has progressed, DOD’s contract obligations surpassed HHS’s, in part due to DOD’s support of interagency acquisition needs, which has included awarding contracts on behalf of HHS for vaccine and therapeutic production and medical supplies.
As of May 31, 2021, DOD accounted for about 40 percent and HHS for about 29 percent of the total obligations made by federal agencies. U.S. Department of Agriculture (USDA) obligations, almost all of which were in support of the Farmers to Families Food Box Program, accounted for $6.1 billion, or 10 percent of total obligations made in response to COVID-19 (see figure).[198]
Contract Obligations in Response to COVID-19 by Federal Agency, as of May 31, 2021
In our March 2021 report, we reported that government-wide contract obligations related to COVID-19 totaled $55.5 billion through February 28, 2021; by May 31, 2021, those obligations had increased by about $5.9 billion—to $61.4 billion. HHS accounted for about $1.9 billion, or about 33 percent of the increase in total contract obligations since February 28, 2021. See figure for government-wide obligations and confirmed COVID-19 cases by month.
Government-wide COVID-19-Related Contract Obligations and Confirmed COVID-19 Cases by Month, February 2020–May 2021
Types of goods and services purchased and extent of competition changed over the course of the pandemic. As the response to the pandemic has progressed, the types of goods and services purchased have shifted from being primarily medical equipment and supplies—such as ventilators and personal protective equipment—to drugs and treatments—such as COVID-19 vaccines and therapeutics.
As we reported in March 2021, drugs and treatments surpassed medical equipment and supplies as the largest area of government-wide obligations, accounting for 23 percent of total obligations. These obligations more than tripled from $3 billion as of November 2020, prior to the Food and Drug Administration’s emergency use authorizations for the Pfizer, Moderna, and Janssen vaccines, to about $14.3 billion as of May 31, 2021.[199] However, these contract obligations hit their peak and have declined by about $333 million since late February.
Medical equipment and supplies—including ventilators and personal protective equipment—increased by about $439.6 million since February 28, 2021, and accounted for about $9.4 billion, or 15 percent of government-wide contract obligations.
Obligations for fruits and vegetables—made primarily in support of the USDA’s Farmers to Families Food Box Program—increased by an additional $732.5 million, to $4.6 billion.
See figure for obligation amounts for the most-procured goods and services over time.
Contract Obligation Amounts for Top Five Goods and Services Procured in Response to COVID-19 by month, Feb. 2020–May 2021
Note: In addition to what is reflected in the figure, agencies canceled, or deobligated, $176.5 million and $335.1 million for drugs and treatments in July 2020 and April 2021, respectively.
As of May 31, 2021, COVID-19-related contracts for goods continued to be competed less frequently than contracts for services. About 69 percent of the obligations for goods were on contracts that were not awarded competitively, compared with about 41 percent of the obligations for services. For example, about $13.8 billion, or 97 percent, of the $14.3 billion in obligations for drugs and treatments and about $8 billion, or 85 percent, of the $9.4 billion in obligations for medical and surgical equipment were on contracts awarded noncompetitively.
The proportion of COVID-19 related contracts identified as having been awarded noncompetitively decreased slightly from about 60 percent of government-wide contract obligations as of February 28, 2021, to about 58 percent as of May 31, 2021—about $35.7 billion.[200] Throughout the course of the pandemic, the percentage of obligations on contracts identified as awarded noncompetitively has fluctuated from a low of 25 percent of obligations in February 2020 to a high of 88 percent of obligations in December 2020. The higher rate of obligations on noncompetitively awarded contracts was driven in part by large noncompetitive awards for vaccine production.
Agencies must provide for full and open competition when awarding contracts, unless one of several limited exceptions applies, such as when there is an unusual and compelling urgency for a needed supply or service. Agencies cited an urgent need for awarding contracts noncompetitively for about 79 percent, or about $28.3 billion, of the contract obligations associated with noncompetitive awards.[201] However, our prior work has noted that promoting competition—even in a limited form—increases the likelihood of acquiring quality goods and services at a lower price in urgent situations.
Federal agencies have obligated about $5 billion on undefinitized contracts. Undefinitized contracts are one technique that agencies have reported using to respond to COVID-19. Undefinitized contracts can enable the government to quickly fulfill requirements that are urgent or need to be met quickly by allowing contractors to begin work before reaching a final agreement with the government on all contract terms and conditions.[202] As of May 31, 2021, undefinitized contract obligations for COVID-19 totaled about $5 billion, and accounted for about 8 percent of government-wide contract obligations on contracts awarded in response to COVID-19. DOD reported the highest amount of undefinitized contract obligations, identifying about $4.1 billion, or about 17 percent of its COVID-19-related contract obligations as being undefinitized for goods and services such as N95 respirator production and constructing alternate care facilities to treat COVID-19 patients. Our prior work has shown that, while undefinitized contract actions can allow the government to fulfill requirements that are urgent or need to be met quickly, these types of contracts can pose risks to the government. For example, contractors may lack incentives to control costs before all contract terms and conditions are defined.
Federal agencies have obligated at least $12.5 billion through other transaction agreements. Three federal agencies—DOD, HHS, and DHS—have continued to report using other transaction agreements in response to COVID-19. From February 28, 2021, through May 31, 2021, obligations associated with other transaction agreements reported by DOD, HHS, and DHS increased from about $12.2 billion to $12.5 billion. Of the $12.5 billion, DOD reported obligating about $10.8 billion through other transaction agreements, including at least $8.5 billion on efforts to manufacture large-scale vaccines and therapeutics in response to COVID-19 through a DOD and HHS partnership formerly known as Operation Warp Speed.
Our analysis of FPDS-NG data and agreement documents found that HHS continues to misreport at least four other transaction agreements with about $1.6 billion in obligations as procurement contracts. These other transaction agreements supported the COVID-19 vaccine manufacturing efforts and other medical countermeasures, which can include therapeutic treatments and testing capabilities. In our January 2021 report, we recommended that HHS should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts. HHS concurred with our recommendation and is exploring ways to address it.
Methodology
To identify agencies’ federal contract and other transaction agreement obligations and competition rate on contracts in response to COVID-19, we reviewed data reported in FPDS-NG through May 31, 2021.[203] We primarily identified contract obligations related to COVID-19 using the NIA code. We supplemented the use of the NIA code by searching for “COVID-19” and “coronavirus” in the contract description field to identify a limited number of additional contract obligations.[204] For contract actions over $1 million, we removed obligations that were identified in the contract description as not related to COVID-19.
We assessed the reliability of federal procurement data by reviewing existing information about FPDS-NG and the data it collects—specifically, the data dictionary and data validation rules—and by performing electronic testing. For the four other transaction agreements that HHS misreported as contracts, we removed the $1.6 billion associated obligations from our reported contract obligations and reported them instead as other transaction agreement obligations. We determined that the data were sufficiently reliable for the purposes of describing agencies’ reported contract obligations in response to COVID-19.
Agency Comments
We provided HHS, DOD, DHS, USDA, and the Office of Management and Budget with a draft of this enclosure. HHS, DHS, USDA, and the Office of Management and Budget did not provide comments. DOD provided technical comments, which we incorporated as appropriate.
GAO’s Ongoing Work
We have work underway related to the federal government’s use of contracts to respond to COVID-19, including assessing contracts awarded by selected agencies in response to COVID-19 and agencies’ efforts to review prospective contractors in advance of awarding a contract.
GAO’s Prior Recommendations
The table below presents our recommendations on federal contracts and agreements for COVID-19 from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to Federal Contracts and Agreements for COVID-19
Recommendation
Status
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to issue guidance—such as an acquisition alert or a reminder to contracting officials—on the use of the COVID-19 National Interest Action code for the Farmers to Families Food Box Program or successor food distribution program to ensure it accurately captures COVID-19-related contract obligations in support of the program (March 2021 report).
Closed-Implemented. The U.S. Department of Agriculture (USDA) neither agreed nor disagreed with our recommendation. In February 2021, following our identification of contract data reporting challenges using the COVID-19 National Interest Action code for the Farmers to Families Food Box Program, Agricultural Marketing Service officials said they conducted training with staff to review National Interest Action code data entry protocols. At that time, a senior Agricultural Marketing Service official also sent an email reminder to procurement division personnel about OMB’s guidance on the use of the COVID-19 National Interest Action code. Following this training and email, officials took action to retroactively report contract actions for the program with the National Interest Action code. In May 2021, the Agricultural Marketing Service updated its instructions for entering contract actions into the Federal Procurement Data System-Next Generation to include a reminder to utilize the proper National Interest Action code, if applicable.
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the Farmers to Families Food Box Program or successor future food distribution program, and take the necessary steps to ensure it has adequate contracting staff in place to award and administer any future contracts for the program (March 2021 report).
Open. USDA neither agreed nor disagreed with our recommendation, and as of May 2021 had not fully assessed the contracting personnel needed to execute and administer contracts in support of the Farmers to Families Food Box Program or successor food distribution program. According to Agricultural Marketing Service officials, they have discontinued the program, and are using other methods of hunger relief, so do not anticipate needing additional permanent staff. Agricultural Marketing Service officials are planning to use an existing contract vehicle to obtain additional staff support for contract documentation needs for the awards that have been made under the Farmers to Families Food Box Program and other food purchasing efforts. However, as of May 2021 Agricultural Marketing Service officials had not yet determined the staffing support levels to be obtained under the contract vehicle.
The Assistant Secretary for Preparedness and Response (ASPR), in coordination with the appropriate offices within the Department of Health and Human Services (HHS), should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts (January 2021 report).
Open. ASPR agreed with our recommendation, and as of April 2021, ASPR officials stated that they have discussed within ASPR the need to consistently identify other transaction agreements in the Federal Procurement Data System-Next Generation (FPDS-NG) and explored how their contract writing system may interface with the FPDS-NG other transaction agreement module in the future. ASPR officials added that in the meantime, they have identified other transaction agreements in the procurement module by manually adding designators such as “other transaction agreement” into the description of requirement data field. We will continue to monitor ASPR’s efforts to implement our recommendation.
The Secretary of Homeland Security, in coordination with the Secretary of Defense, should (1) revise the criteria in the 2019 National Interest Action (NIA) code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Closed-Implemented. The Department of Homeland Security (DHS) did not agree with our recommendation. However, in March 2021, DHS, in coordination with the Department of Defense (DOD), issued a revised memorandum of agreement. The revised agreement establishes a process and timelines for communicating and evaluating NIA code extensions by requiring the General Services Administration to notify other federal agencies no less than seven days before a NIA code is set to expire so that agencies can request an extension as needed. The revised agreement also more clearly defines what constitutes a consistent decrease in contract actions to ensure criteria for extending or closing a NIA code is consistently applied.
The Secretary of Defense, in coordination with the Secretary of Homeland Security, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Closed-Implemented. DOD did not agree with our recommendation. However, in March 2021 DOD, in coordination with DHS, issued a revised memorandum of agreement. The revised agreement establishes a process and timelines for communicating and evaluating NIA code extensions by requiring the General Services Administration to notify other federal agencies no less than seven days before a NIA code is set to expire so that agencies can request an extension as needed. The revised agreement also more clearly defines what constitutes a consistent decrease in contract actions to ensure criteria for extending or closing a NIA code is consistently applied.
COVID-19 Contracting: Observations on Federal Contracting in Response to the Pandemic.GAO-20-632. Washington, D.C.: July 29, 2020.
Defense Acquisitions: DOD’s Use of Other Transactions for Prototype Projects Has Increased. GAO-20-84. Washington, D.C.: November 22, 2019.
DATA Act: Quality of Data Submissions Has Improved but Further Action Is Needed to Disclose Known Data Limitations. GAO-20-75. Washington, D.C.: November 8, 2019.
Disaster Contracting: FEMA Continues to Face Challenges with Its Use of Contracts to Support Response and Recovery. GAO-19-518T. Washington, D.C.: May 9, 2019.
2017 Disaster Contracting: Actions Needed to Improve the Use of Post-Disaster Contracts to Support Response and Recovery. GAO-19-281. Washington, D.C.: April 24, 2019.
2017 Disaster Contracting: Action Needed to Better Ensure More Effective Use and Management of Advance Contracts. GAO-19-93. Washington, D.C.: December 6, 2018.
Federal Contracting: Noncompetitive Contracts Based on Urgency Need Additional Oversight.GAO-14-304. Washington, D.C.: March 26, 2014.
Department of Homeland Security: Further Action Needed to Improve Management of Special Acquisition Authority. GAO-12-557. Washington, D.C.: May 8, 2012.
Defense Contracting: DOD Has Enhanced Insight into Undefinitized Contract Action Use, but Management at Local Commands Needs Improvement. GAO-10-299. Washington, D.C.: January 28, 2010.
Department of Homeland Security: Improvements Could Further Enhance Ability to Acquire Innovative Technologies Using Other Transaction Authority. GAO-08-1088. Washington, D.C.: September 23, 2008.
Contact information: Marie A. Mak, (202) 512-4841, makm@gao.gov
The number of claims for unemployment insurance benefits generally declined during spring 2021, though they remained at a high level into June 2021 as compared to pre-pandemic levels. We continue to focus on the implications of the high number of claims, including timeliness of benefits and program integrity concerns.
Entity involved: Department of Labor
Background
The unemployment insurance (UI) system is a federal-state partnership that provides temporary financial assistance to eligible workers who become unemployed through no fault of their own. States design and administer their own UI programs within federal parameters, and the Department of Labor (DOL) oversees states’ compliance with federal requirements, such as by ensuring states pay benefits when they are due. Regular UI benefits—those provided under the state UI programs in place before the CARES Act was enacted—are funded primarily through state taxes levied on employers and are intended to typically be lower than a claimant’s previous employment earnings, according to DOL.[205]
Three federally funded temporary UI programs that expanded benefit eligibility and enhanced benefits were created by the CARES Act and amended by the Consolidated Appropriations Act, 2021 and the American Rescue Plan Act of 2021.[206]
Pandemic Unemployment Assistance (PUA), generally available through September 6, 2021, generally authorizes up to 79 weeks of UI benefits for individuals not otherwise eligible for UI benefits, such as self-employed and certain gig economy workers, who are unable to work as a result of specified COVID-19 reasons.[207]
Federal Pandemic Unemployment Compensation (FPUC) generally authorized an additional $600 weekly benefit through July 2020 for individuals eligible for weekly benefits under the regular UI and CARES Act UI programs. FPUC also generally authorizes an additional $300 benefit for weeks beginning after December 26, 2020, and ending on or before September 6, 2021, for these individuals.[208]
Pandemic Emergency Unemployment Compensation (PEUC), generally available through September 6, 2021, generally authorizes an additional 53 weeks of UI benefits for those who exhaust their regular UI benefits.[209]
The Consolidated Appropriations Act, 2021 created, and the American Rescue Plan Act of 2021 extended, the Mixed Earner Unemployment Compensation (MEUC) program, which authorizes an additional $100 weekly benefit for certain UI claimants who received at least $5,000 of self-employment income in the most recent tax year prior to their application for UI benefits.[210] The $100 weekly benefit is in addition to other UI benefits received by claimants; however, individuals receiving PUA benefits may not receive MEUC payments. According to DOL, the MEUC program, which is voluntary for states, is intended to cover regular UI claimants whose benefits do not account for significant self-employment income and who thus may receive a lower regular UI benefit than the benefit they would have received had they been eligible for PUA.[211] As of June 8, 2021, 51 of 53 states and territories had elected to participate in the MEUC program, though just 23 had begun paying MEUC benefits, according to DOL.[212]
As of June 8, 2021, 25 states had announced their intention to terminate participation in at least one of the pandemic UI programs before their September 2021 expiration dates.[213] For example, according to DOL, 21 states submitted notice to DOL that they intended to end participation in the FPUC, PEUC, and PUA programs and 3 states submitted notice that they intended to end participation in the FPUC program.[214] In addition, 1 state publicly announced its intention to end participation in the FPUC program, but as of June 8 had not submitted notice to DOL.[215] States’ planned program termination dates range from mid-June through mid-July. In public announcements, states generally cited labor shortages among the reasons for their intended withdrawals from the programs. After the first states’ announcements, the Secretaries of Commerce and Treasury stated that, nationwide, data do not support the argument that unemployment benefits are keeping people from returning to work. They identified caregiving responsibilities and health concerns as key factors in people’s decisions. The Secretary of Commerce also noted that governors had to respond to their regional labor markets, which vary.
In addition to extending and expanding benefits, the Consolidated Appropriations Act, 2021 added new program integrity requirements for the CARES Act UI programs. For example, the act generally requires PUA claimants to provide documentation substantiating their prior employment or self-employment and to recertify with their state each week that they continue to meet the eligibility requirement of not being able to work as a result of COVID-19.[216] In addition, states are required to have procedures for identity verification or validation and for timely payment of PUA benefits, to the extent reasonable and practicable.[217] The American Rescue Plan Act of 2021 also appropriated $2 billion for DOL to detect and prevent fraud, promote equitable access, and ensure the timely payment of UI benefits.[218]
During the pandemic, regular UI claimants in certain states have also had access to the Extended Benefits program. The program, which existed prior to the pandemic and provides up to an additional 13 or 20 weeks of benefits, is activated in states during periods of high unemployment, according to DOL.[219] If unemployment is not high enough to activate the Extended Benefits program in a state, or if regular UI claimants exhaust their PEUC and Extended Benefits, they may be eligible for PUA benefits—provided they also meet PUA eligibility requirements.[220]
Overview of Key Issues
Although weekly numbers of initial and continued claims for UI benefits have declined, their levels suggest that more individuals are still losing jobs on a weekly basis than is typical and that many others are experiencing long-term unemployment. DOL reported that 393,078 initial claims for regular UI benefits and 104,682 initial claims for PUA benefits were submitted nationwide during the week ending June 19, 2021.[221] Weekly initial claims numbers are near their lowest point since the surge at the beginning of the pandemic. However, they remain at a level that indicates that more Americans are still experiencing job losses than was typical in the year before the pandemic. For example, the 393,078 regular UI initial claims submitted during the week ending June 19, 2021, is about 74 percent higher than the number submitted during the corresponding week in 2019.
Weekly Initial Claims Submitted Nationwide for Regular Unemployment Insurance (UI) and Pandemic Unemployment Assistance (PUA) Benefits, Mar. 1, 2020–June 19, 2021
Notes: The weekly counts of initial claims shown are not seasonally adjusted. Counts for weeks through June 5, 2021, are from Department of Labor (DOL) data files that include any adjustments submitted by states as of June 24, 2021. Counts for the weeks ending June 12 and 19, 2021, are from DOL’s weekly report released on June 24, 2021. Counts for the week ending June 19, 2021, reflect advance initial claims, which are preliminary and subject to revision. The number of states and territories reporting PUA claims is out of a potential total of 53. All 53 states and territories reported regular UI claims in each week shown.
The number of initial claims is not intended to measure how many claimants were determined eligible to receive benefits or how many of those who filed for benefits earlier in the pandemic are still unemployed. DOL officials have stated that continued claims (i.e., weeks of unemployment claimed by individuals during a reporting period) may be a better barometer than initial claims for measuring continuing demand for benefits. For example, states reported that about 14.8 million continued claims were submitted in all programs during the week ending June 5, 2021, including:
The number of regular UI continued claims submitted each week has declined overall since the peak in late April and early May 2020 (see figure). Some of this decline is due to claimants’ finding employment, though some of the decline is also likely due to other factors, such as claimants’ exhausting regular UI benefits and beginning to claim PEUC or other benefits.[226] For example, the persistently high numbers of PEUC continued claims since fall 2020 suggest that many individuals may be experiencing long-term unemployment and have likely exhausted their regular UI benefits.[227]
Notably, the combined total of continued claims submitted for regular UI, PEUC, and Extended Benefits remained at a relatively consistent level from the beginning of October 2020 through the beginning of March 2021 (see figure). Since then, the combined total of continued claims submitted in these three programs has generally declined, though the number remains high.
Weekly Continued Claims Submitted Nationwide for Regular Unemployment Insurance, Pandemic Emergency Unemployment Compensation, and Extended Benefits, Mar. 1, 2020–June 5, 2021
Notes: The weekly counts of continued claims shown in the figure are not seasonally adjusted. Counts for weeks through May 29, 2021, are from Department of Labor (DOL) data that include any adjustments submitted by states as of June 24, 2021. The count for the week ending June 5, 2021, is from DOL’s weekly report released on June 24, 2021. The number of states and territories reporting PEUC claims is out of a potential total of 53. All 53 states and territories reported regular UI claims in each week shown. The number of states reporting Extended Benefits claims each week varies, in part based on the number of states with the program activated each week. The Extended Benefits program, which existed before the pandemic, is activated in states during periods of high unemployment, according to DOL.
The persistently high number of claims across all programs suggests continued high demand for benefits. However, as we have previously reported, the number of continued claims has not approximated the number of individuals claiming benefits during the pandemic because of backlogs in processing historic numbers of claims in many states and other data issues. For example, backlogs in claims processing led to individuals claiming multiple weeks of benefits in single reporting periods and thus being counted as multiple claims for that reporting period, particularly in the PUA program. As a result, reliable conclusions about trends in the number of individuals claiming benefits cannot be drawn from data on continued claims.
In November 2020, we recommended that DOL address this issue by (1) revising its weekly news releases to clarify that the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits and (2) pursuing options to report the actual number of distinct individuals claiming benefits from January 2020 onward.
DOL fully agreed with our first recommendation and, starting with the December 10, 2020, weekly UI news release, clarified that the numbers it reports for weeks of unemployment claimed do not represent the number of unique individuals claiming benefits. We consider this recommendation closed.
DOL partially agreed with our second recommendation, taking issue with implementing a retroactive change in state reporting. In a letter dated March 30, 2021, DOL stated that it had begun developing a new state report that would capture data related to distinct individuals claiming regular UI benefits; DOL estimated that this data collection might begin in early 2022. DOL also reiterated its concerns about the feasibility of states’ reporting this information retroactively, including for the pandemic UI programs, without detracting from their primary obligation for timely and accurate claims processing.
We maintain that these data are vital to understanding the size of the population supported by the UI system during the pandemic. Even if the information is unavailable for some time, reporting the number of distinct individuals who claimed benefits for calendar year 2020 and later years will help DOL and policymakers identify lessons learned about the administration and utilization of regular and expanded UI benefit programs during the pandemic. We encourage DOL to pursue options to report this information in the most feasible and least burdensome way and at a time when providing this information retroactively will not detract from states’ primary obligation for timely and accurate claims processing.
Although timeliness of regular UI first payments improved nationally from fall 2020 through early 2021, timeliness has varied since then, including by state, and some claimants still face substantial delays in receiving benefits. The timeliness of first payments of regular UI benefits declined substantially early in the pandemic, as states faced extensive claims-processing backlogs resulting from historically high numbers of claims.[228] When we last reported in March 2021, we observed that, nationwide, first payment timeliness had improved from fall 2020 through January 2021. Since then, regular UI first payment timeliness, nationwide, declined in February 2021, improved again in March and April, and then declined again in May (see figure).[229] In some states, many regular UI claimants continue to face delays before receiving their first payments. For example, in six states, at least half of regular UI claimants who received their first benefits in May 2021 had been waiting longer than 3 weeks. In addition, nationwide, about 10.3 percent of regular UI claimants who received their first benefits in May 2021 had been waiting longer than 10 weeks. By comparison, of the regular UI claimants who received their first benefits in March 2020, nationwide, less than 3 percent had been waiting longer than 3 weeks and less than 1 percent longer than 10 weeks.
Timeliness of First Payments of Regular Unemployment Insurance (UI) Benefits, Jan. 2020–May 2021
Notes: We analyzed first payment timeliness data that states had reported to the Department of Labor (DOL) as of June 21, 2021. At that point, of the 53 states and territories, 46 had reported data for May 2021, 51 had reported data for April 2021, 52 had reported data for January through March 2021, and all 53 had reported data for all months in 2020. One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible, depending on whether the state requires that individuals who are otherwise eligible for benefits serve a waiting period—generally 1 week—before receiving benefits. We focus on payments made within 21 days because in guidance released at the start of the pandemic, DOL recommended that states consider temporarily waiving their waiting week requirements. According to DOL, states must pay at least 87 percent of claims within 14 or 21 days to reach an acceptable level of performance.
As we have previously reported, although DOL has not tracked the timeliness of payments in the temporary PUA program, DOL officials told us that states have struggled with making PUA payments in a timely manner. For example, they said regional officials had observed a number of implementation challenges at the state level that likely contributed to claims processing backlogs and payment delays. In addition, in early 2021, DOL officials said they expected PUA program changes enacted in the Consolidated Appropriations Act, 2021 to slow the payment of PUA benefits as states implemented the new program integrity provisions.
More than half of the 47 states and territories submitting data reported average PUA benefits paid in April 2021 that were close to the minimum amount. Specifically, as of June 21, 2021, 31 states and territories reported average weekly PUA benefits paid in April 2021 that were up to 25 percent above the state’s minimum PUA benefit amount; 13 of these states and territories reported average benefits that were up to 10 percent above the minimum.[230] This suggests that many individuals in these states and territories were receiving the minimum PUA benefit in April 2021—because the average was close to the minimum. As we have previously reported, DOL officials told us that to facilitate implementation of the PUA program, most states decided to initially pay PUA claimants the minimum allowable benefit and then recalculate benefits at a later point based on claimants’ documentation of their prior earnings.[231] DOL officials said that through the regional offices’ monitoring efforts, DOL has found that some states have faced challenges and expressed confusion related to recalculating PUA benefit amounts and that DOL has required some states to implement corrective actions.
Persistently high numbers of UI claims during the pandemic have led some states to take out substantial federal loans to pay UI benefits.[232] As of June 18, 2021, 19 states and territories held federal loans totaling about $53.5 billion—approximately $1.4 billion more than we reported in March 2021. This total loan balance is also greater than the approximately $40.2 billion held by 30 states and territories at the end of 2010, after the 2007-2009 recession and early recovery.[233]
As we reported in March 2021, some states have used their Coronavirus Relief Fund payments, under guidance from the Department of the Treasury, to pay for UI benefits to reduce or prevent loan balances and avoid possible future increases in employer tax rates.[234] Generally, if a state holds a federal loan balance to pay UI benefits for 2 or more years, the rate of the federal tax on employers that is used to fund the UI program will increase.[235] States may continue to use these Coronavirus Relief Fund payments for expenses through the end of 2021.[236] In addition, the American Rescue Plan Act of 2021 provided funds to states, local governments, territories, and tribal governments. States and territories may use these funds, under an interim final rule from the Department of the Treasury, to restore their UI trust funds or to pay back federal loan balances.[237]
DOL and other federal and state agencies continue to take actions to address potential fraud in the UI programs.[238] As we have previously reported, DOL made two allotments of $100 million available to states, in September 2020 and January 2021, respectively, to address potential fraud and identity theft in the PUA and PEUC programs. According to DOL, states have reported using the funds from the September allotment to, among other things, hire additional staff to investigate suspicious claims, connect with the National Association of State Workforce Agencies’ (NASWA) Integrity Data Hub to utilize an identity verification service, and implement integrity tools and software to conduct further identity protections and fraud screening.[239]
The American Rescue Plan Act of 2021, enacted March 11, 2021, subsequently provided DOL with $2 billion to detect and prevent fraud, promote equitable access, and ensure the timely payment of UI benefits. As of May 20, 2021, DOL officials said that DOL was working to develop detailed plans for this $2 billion in coordination with the Office of Management and Budget, and noted that developing spending plans across 53 states and territories involves complex considerations.
In addition to providing funding, DOL continues to assist states with their fraud prevention and detection efforts. For example, on April 13, 2021, DOL issued guidance highlighting the importance of states’ identity verification efforts to stop potentially fraudulent UI claims.[240] The guidance outlines procedures that states must take when processing claims and determining UI eligibility in cases where an individual’s identity is in question. DOL officials also said that DOL is exploring new datasets that states could use to detect potential UI fraud.
In addition, according to DOL officials, DOL has ongoing efforts to connect state workforce agencies with banking institutions and law enforcement to recover potentially fraudulently obtained funds that banks have intercepted. On May 4, 2021, DOL issued guidance encouraging states to work with financial institutions to detect suspicious activity, ensure that accounts are not unduly suspended, and recover overpayments.[241] This guidance also establishes instructions for banks and financial institutions on how to return recovered overpayments, such as in instances when the recovered funds span multiple states.
In March 2021, DOL also launched a website to help the public better understand UI identity theft.[242] The website provides resources for those who may have been victims of identity theft, including a list of contact information for each state and territory to report UI identity theft.
DOL’s Office of Inspector General (OIG), the Department of Justice (DOJ), and the U.S. Secret Service also continue to investigate potential UI fraud and examine program integrity issues. As of June 10, 2021, DOL’s OIG had opened more than 17,000 complaints and investigations involving UI fraud since the pandemic began, according to the agency’s website. According to DOL’s OIG, its efforts have directly resulted in the identification and recovery of more than $160 million in UI fraud. In addition, DOL’s OIG reported that it is currently working on a range of audit work related to UI, covering topics such as DOL’s and states’ efforts to prevent and detect overpayments and states’ capabilities to process UI claims accurately and in a timely manner with outdated information technology systems.
In late May 2021, DOL’s OIG issued a report that found that DOL and states struggled to implement the three CARES Act UI programs (FPUC, PEUC, and PUA) and, among other things, that DOL’s guidance and oversight did not ensure states performed required and recommended improper payment detection and recovery activities.[243] For example, DOL’s OIG found that from March 27, 2020, to July 31, 2020, 20 states did not perform all required cross-matches, which could have prevented improper payments, including fraud.
According to DOJ, from March 2020 through April 2021, DOJ filed federal charges against 207 individuals for defrauding the UI programs, 41 of whom have pleaded guilty.[244] See the enclosure on Federal Fraud-Related Cases in appendix I for more information about DOJ charges.
As we previously reported, the U.S. Secret Service also conducts UI fraud investigations in coordination with various federal, state, and local partners. According to a May 2021 press release, over the last year the Secret Service has initiated more than 690 UI fraud investigations and investigative inquiries and seized more than $640 million in fraudulently obtained funds.[245]
Several state auditors have also issued reports on UI program integrity issues. According to the California State Auditor, California’s Employment Development Department did not take substantive action to bolster its UI fraud detection efforts until months into the pandemic, which resulted in payments of about $10.4 billion that the department has since determined may be potentially fraudulent because it cannot verify claimants’ identities. Also, the Kansas Legislative Division of Post Audit found that the Kansas Department of Labor’s fraud detection process was not designed to detect large-scale fraud. According to this audit, in December 2020, the Kansas Department of Labor reported that it had partnered with a private company to enhance its fraud detection capabilities.
States have continued to identify overpayments in the regular UI and CARES Act UI programs, and some states have begun reporting data to DOL on recovered PUA overpayments. Overpayments are not necessarily a result of fraud, though some may be. As we reported in January 2021, DOL data show that the dollar amount of state-reported overpayments in the regular UI program increased substantially during the pandemic, coinciding with historically high numbers of UI claims. States have also reported large amounts of overpayments in the CARES Act UI programs.
As of June 21, 2021, DOL reported that states and territories had identified approximately $12.9 billion in overpayments made in UI programs during the first four quarters of the pandemic combined (April 2020 through March 2021), including:
$4.3 billion in regular UI and Extended Benefits overpayments,[246]
These amounts are likely to increase as states shift their focus from program implementation and clearing claims processing backlogs to identifying overpayments, according to DOL officials.
States and territories also report the amounts of fraud overpayments—a subset of the total overpayment amounts.[249] During the first four quarters of the pandemic combined (April 2020 through March 2021), states and territories reported about $1.3 billion in overpayments identified as fraud across the UI programs.[250] However, according to DOL, states do not report these overpayments until investigations are complete and fraud has been established, which may take a long time. As a result, it is likely that states and territories have not yet reported substantial amounts of fraud overpayments, which could contribute to increasing amounts reported in the coming months. For example, 7 of the 45 states and territories that have reported PUA overpayments have reported no data on fraud overpayments.
States and territories may waive and not recover overpayments in certain circumstances.[251] States and territories reported waiving about $0.1 billion of regular UI, Extended Benefits, PEUC, and FPUC overpayments during the first four quarters of the pandemic combined (April 2020 through March 2021).[252] In response to a recommendation in our March 2021 report, DOL stated that it was preparing to update its state reporting requirements for the PUA program to include the collection of data on PUA overpayments waived. On June 17, 2021, DOL officials stated that the agency expected to release guidance by mid-July 2021.
States and territories report the amount of overpayments they have recovered in the period the recovery occurs. For example, states and territories have reported recovering about $0.3 billion in the PEUC and FPUC programs combined from April 2020 through March 2021 (i.e., during the first 4 quarters those programs existed).[253] In response to a recommendation in our January 2021 report, DOL updated its state reporting requirements for the PUA program to include the collection of data on PUA overpayments recovered. As of June 21, 2021, 27 states had reported some data on PUA overpayments recovered, reporting a combined total of about $0.2 billion recovered.[254]
Because of the limited number of states and territories reporting data to DOL as of June 21, 2021, our recommendations related to reporting PUA overpayments waived and recovered remain open. Sustained reporting by most states is needed to help inform DOL, policymakers, and the public about the amount of PUA overpayments that states have waived and recovered and about the amount that remains outstanding.
In addition to reporting actual overpayments established, states also conduct independent investigations of samples of regular UI claims to estimate accuracy rates for paid and denied claims. However, estimates of improper payments from this process are not yet available for the pandemic period.[255] We reported in November 2020 that DOL had not included the CARES Act UI programs in its improper payment estimation methods and that it planned to conduct a risk assessment after the first year of each program’s operations. On April 8, 2021, officials told us that DOL would be conducting this risk assessment during the second quarter of 2021. Officials also said that DOL had formed a working group to develop new sampling and investigative methodologies for the PUA program and that DOL planned to extrapolate regular UI data to the FPUC and PEUC programs.
Methodology
To conduct this work, we analyzed regularly reported DOL data for calendar years 2019, 2020, and 2021, having obtained the most recent data on June 24, 2021. We reviewed relevant federal laws, DOL guidance, and DOL OIG reports, and we interviewed DOL officials about program data and agency actions. We also reviewed data file documentation and written responses from DOL officials. In addition, we interviewed DOL officials about the UI database, PUA claims data files, and data on outstanding federal loans to pay UI benefits, specifically related to state-reported data on claims counts, overpayments, payment timeliness, and loan balance amounts by state. We examined the data for outliers, missing values, and errors. We determined the DOL data we used were sufficiently reliable for the purposes of this report.
Agency Comments
We provided DOL and the Office of Management and Budget (OMB) with a draft of this enclosure. DOL provided technical comments on this enclosure, which we incorporated as appropriate. OMB did not have any comments on this enclosure.
GAO’s Ongoing Work
We continue to examine the implementation and administration of CARES Act UI programs and the implications of high claims volumes during the pandemic on the timeliness of benefit payments and on overall program integrity. We plan to conduct additional work to examine selected claimants’ experiences during the pandemic and with accessing CARES Act UI programs. We are also continuing to analyze selected states’ data on PUA benefit receipt by race and ethnicity as part of our ongoing work on the PUA program.
GAO’s Prior Recommendations
The table below presents our recommendations on UI programs from prior bimonthly CARES Act reports.
Prior GAO Recommendations Related to Unemployment Insurance (UI) Programs
Recommendation
Status
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments waived in the Pandemic Unemployment Assistance (PUA) program, similar to the regular UI program (March 2021 report).
Open. The Department of Labor (DOL) agreed with our recommendation and noted that it intended to issue PUA program guidance that would include revised reporting requirements and instructions for states to provide information on the amount of PUA overpayments waived. On June 17, 2021, DOL officials stated that the agency expected to publish guidance by mid-July 2021. As of June 21, 2021, this recommendation remained open, as this guidance had not yet been issued and no states had begun reporting this data. We will continue to monitor state reporting of PUA overpayments waived.
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments recovered in the PUA program, similar to the regular UI program (January 2021 report).
Open. DOL agreed with our recommendation and on January 8, 2021, issued PUA program guidance and updated instructions for states to report PUA overpayments recovered. As of June 21, 2021, this recommendation remained open, as just 27 states had begun reporting some data on the amount of PUA overpayments recovered. Sustained reporting by most states is needed to help inform DOL, policymakers, and the public about the amount of PUA overpayments states have recovered. We will continue to monitor state reporting of PUA overpayment recovery data.
The Secretary of Labor should ensure the Office of Unemployment Insurance pursues options to report the actual number of distinct individuals claiming benefits, such as by collecting these already available data from states, starting from January 2020 onward (November 2020 report).
Open. DOL partially agreed with our recommendation. Specifically, DOL agreed to pursue options to report the actual number of distinct individuals claiming UI benefits. However, DOL did not agree with the retroactive effective date of the reporting. In a letter dated March 30, 2021, DOL stated that it had begun developing a new state report that would capture data related to distinct individuals claiming regular UI benefits; DOL estimated that this data collection might begin in early 2022. DOL also reiterated its concerns about the feasibility of states reporting this information retroactively, including for the pandemic UI programs, without detracting from their primary obligation for timely and accurate claims processing.
As of June 21, 2021, this recommendation remained open. We maintain that DOL should pursue options to report the actual number of distinct individuals claiming UI benefits, retroactive to January 2020. Even if the information is unavailable for some time, these data are vital to understanding how many individuals are receiving UI benefits as well as the size of the population supported by the UI system during the pandemic. Given the substantial investment in UI programs during the pandemic, an accurate accounting of the size of the population supported by this funding may be critical to understanding the efficiency and effectiveness of the nation’s response to unemployment during the pandemic. An accurate accounting may also be critical to helping DOL and policy makers identify lessons learned about the administration and utilization of regular and expanded UI benefit programs.
We encourage DOL to pursue options to report the actual number of individuals claiming benefits in the most feasible and least burdensome way and at a time when providing this information retroactively will not detract from states’ primary obligation for timely and accurate claims processing. Collecting data from states is one way to address the recommendation, but DOL could develop other ways of gathering and reporting this information.
The Secretary of Labor should ensure the Office of Unemployment Insurance revises its weekly news releases to clarify that in the current unemployment environment, the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits (November 2020 report).
Closed. DOL’s weekly news release of December 10, 2020, clarified that the numbers reported for weeks of UI benefits claimed do not represent the number of unique individuals claiming benefits.
The Secretary of Labor should, in consultation with the Small Business Administration (SBA) and the Department of the Treasury, immediately provide information to state unemployment agencies that specifically addresses SBA's Paycheck Protection Program (PPP) loans, and the risk of improper payments associated with these loans (June 2020 report).
Closed. DOL neither agreed nor disagreed with our recommendation. Following our recommendation, DOL issued guidance on August 12, 2020, that clarified that individuals working full-time and being paid through PPP are not eligible for UI, and that individuals working part-time and being paid through PPP would be subject to certain state policies, including state policies on partial unemployment, to determine their eligibility for UI benefits. Further, the guidance clarified that individuals being paid through PPP but not performing any services would similarly be subject to certain provisions of state law, and noted that an individual receiving full compensation would be ineligible for UI.
Management Report: Preliminary Information on Potential Racial and Ethnic Disparities in the Receipt of Unemployment Insurance Benefits during the COVID-19 Pandemic. GAO-21-599R. Washington, D.C.: June 17, 2021.
Contact information: Thomas M. Costa, (202) 512-7215, costat@gao.gov
The Department of the Treasury and the Internal Revenue Service quickly issued the third round of direct payments to most eligible individuals, and have taken steps to begin issuing advance payments of the Child Tax Credit starting in July 2021, but are still not using some available data to improve outreach efforts.
Entities involved: Internal Revenue Service and Bureau of the Fiscal Service, within the Department of the Treasury
Recommendation for Executive Action
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should release interim findings on the effectiveness of the notices it sent in September 2020 to nonfilers who are potentially eligible for economic impact payments; incorporate that analysis into Internal Revenue Service outreach efforts as appropriate; and then, if necessary, release an update based on new analysis after the 2021 filing season.
Treasury neither agreed nor disagreed with this recommendation and stated that it shares the underlying goal of reaching as many nonfilers as possible to encourage them to claim economic impact payments online. However, Treasury does not plan to release any interim findings until it completes its analysis.
Background
The American Rescue Plan Act of 2021 (ARPA) authorized the Internal Revenue Service (IRS) and the Department of the Treasury (Treasury) to issue direct payments, known as economic impact payments (EIP), to eligible individuals to help address financial stress due to the pandemic.[256] Starting on March 17, 2021, Treasury and IRS quickly issued a third round of direct payments (EIP 3) to most eligible individuals.[257] As of May 28, 2021, IRS reported that it had disbursed over 168.2 million payments totaling over $394.3 billion (see figure). From March 2021 through May 2021, the Bureau of the Fiscal Service disbursed the third round of payments in the form of direct deposits, paper checks, and debit cards.
Total Number and Amount of Economic Impact Payments (EIP) Disbursed, Rounds 1, 2, and 3, as of May 28, 2021
Eligible individuals who did not receive EIP 1 or EIP 2—or their maximum amount of the credit for which they were eligible—can claim a recovery rebate credit (RRC) on their tax year 2020 income tax return equal to the amount of the credit for which they are eligible, as reduced by their EIP 1 and EIP 2 amounts. According to IRS data, as of May 26, 2021, 21 million returns, nearly 21 percent of the total number of filed returns, included a claim for the RRC. Of these returns, almost 2.4 million (11 percent) only claimed an RRC; 97 percent of these returns belonged to someone with an adjusted gross income of $15,000 or less. These individuals likely would not have filed a tax return other than to claim an RRC because their income is below the minimum filing threshold or all their income is derived from federal benefits. This very low-income population is one of the groups IRS has been trying to reach through their communications efforts.
ARPA also directed IRS to make supplemental payments to individuals who received an EIP 3 prior to the processing of their 2020 tax return, but who are eligible for an additional payment based on their recently processed 2020 tax returns. For example, in situations where individuals’ adjusted gross income was lower or if they claimed more qualifying dependents on their 2020 tax return than their 2019 tax return, they may be eligible for an additional supplemental payment. As of June 3, 2021, IRS had issued over 8.1 million supplemental payments totaling over $16 billion.
ARPA also made several temporary changes that expand the eligibility of the child tax credit (CTC) to more families and increase the amount. The law makes the following changes:
increases the maximum age of a qualifying child dependent from 16 to 17 years old,
eliminates the earned income requirement, and
increases the maximum amount of the CTC from $2,000 to $3,600 per qualifying child for a young child (0 to 5 years old) and $3,000 per child for an older child (6 to 17 years old).
As part of implementing ARPA, beginning in July 2021, IRS and Treasury are responsible for issuing half of the expected 2021 CTC in periodic advance payments.[258] Eligible individuals can claim the remaining amount of the total 2021 credit for which they are eligible when filing their 2021 income tax return in 2022. The amount of the CTC payments advanced in 2021 is estimated based on the taxpayer’s 2020 income tax data or, if unavailable, the taxpayer’s 2019 income tax data and may be adjusted based on any other information provided by the taxpayer during 2021. IRS is developing an online portal for qualified individuals to update personal information or opt out of the advance payments.
In May 2021, IRS released guidance that provides instructions for individuals who are not otherwise required to file tax returns to receive the advance CTC payments and the third-round EIPs, and also allowed those individuals to claim the 2020 RRC.[259] The guidance outlines two procedures for individuals to follow: The first procedure permits individuals to file simplified returns, while the second procedure enables these individuals to file complete returns electronically even if they have zero adjusted gross income.
Overview of Key Issues
IRS’s EIP communication and outreach efforts. To publicize information about how to file a tax return with IRS to receive an EIP, IRS continued to partner with other organizations that work with communities that may not traditionally interact with IRS, such as lower-income families, senior citizens, veterans, tribal communities, and families with mixed immigration status.[260] However, according to officials from IRS partner organizations with whom we spoke, it continues to be a challenge to ensure that eligible nonfilers, particularly among hard-to-reach groups, such as those experiencing homelessness, receive their payments.
IRS partners reported particular difficulties with reaching underserved communities with limited internet access. Partners said an IRS phone hotline or television and radio advertisements sponsored by IRS could be helpful outreach sources. Most partners we interviewed that have an ongoing relationship with a local IRS office that understands the unique circumstances of the local community—compared with partners that do not traditionally interact with IRS—said they had received IRS materials, that IRS had tailored those materials to meet their constituents’ needs, and that IRS was responsive to their questions and follow-up requests.
Partners also told us their outreach efforts to nonfilers could be more effective if they had current data that help identify specific communities of nonfilers who may need assistance. Following our November 2020 recommendation, in January 2021, Treasury began analyzing nearly 9 million notices it sent to nonfilers who may be eligible for EIP 1 payments. However, Treasury does not plan to complete this analysis until fall 2021, more than 6 months after the first EIP 3 payments were issued. This timing will limit the usefulness of the analysis for informing EIP 3 outreach efforts. According to Treasury officials, they are incorporating information from the 2021 filing season into their analysis. The filing season ended May 17, but there is a 5-month extension to file amended returns, which means complete data would likely not be available until October.
Federal standards for internal control state that management should obtain relevant data from reliable sources in a timely manner based on the identified information requirements. Moreover, Treasury issued a fact sheet in January 2021 outlining efforts Treasury planned to take to help households who had not yet been able to access payments.[261] One action Treasury identified was to analyze and better understand underserved populations to enhance outreach efforts. We acknowledge that having data from the entirety of the filing season will allow for a more robust analysis, which Treasury and IRS could use to inform their outreach efforts for the expanded child tax credit. However, by waiting to complete the analysis, Treasury and IRS are missing an opportunity to identify communities that may have higher numbers of nonfilers, and use that information to inform their outreach efforts and distribute payments to qualified individuals in a more timely manner.
Similar to the previous acts authorizing EIP 1 and 2, ARPA requires Treasury and IRS to carry out a robust and comprehensive outreach program to ensure that all individuals eligible for recovery payments are informed of their eligibility and are provided assistance in applying for these payments.[262] IRS officials said they do not have a new plan to implement this outreach program; rather, they are incorporating the legislative requirements into their current communication strategy. For example, IRS is developing a database to collect feedback from its stakeholders and outreach partners to help update and assess its communication strategy on a quarterly basis.
In our September 2020 report, we recommended that IRS update estimates of eligible recipients who have not received a payment and share that and other relevant information with outreach partners. Fully implementing these recommendations, along with our November 2020 recommendation to analyze notices sent to potentially eligible individuals, would provide Treasury and IRS more information on the nonfiler population and also potentially provide insights into the effectiveness of targeted outreach efforts to reach these populations. Treasury officials said they continue to work on implementing these recommendations but recent changes, such as the extension of the 2020 filing season, have further delayed their efforts.
Payments to federal benefit recipients and incarcerated individuals. Treasury and IRS were able to quickly disburse the majority of EIP 3 payments to most eligible individuals within 3 weeks of the enactment of ARPA. Payments to federal benefit recipients were the last significant batch of payments to be disbursed 3 weeks after the passage of ARPA. These payments arrived later because IRS and the Social Security Administration (SSA) had to work together to put a reimbursable Memorandum of Agreement (agreement) in place to provide funding to SSA to complete non-mission work by providing IRS with up-to-date data on Social Security beneficiaries. SSA officials said they did not receive direct funding to cover any costs associated with preparing the data for IRS. SSA signed the agreement with IRS on March 16, 2021, after starting discussions with IRS in January. According to SSA officials, the agreement could not be signed until ARPA was signed into law on March 11, 2021. The agreement covered SSA’s administrative costs associated with providing SSA benefit recipient data to IRS and conducting a marketing and communication campaign to inform individuals about EIPs. SSA then provided its data to IRS on March 25, 2021.
The fourth batch of payments was issued to recipients of SSA and Railroad Retirement Board benefits. The fifth batch of payments was issued to recipients of Department of Veteran Affairs benefits. According to IRS officials, all three agencies needed to submit updated payments files to IRS, but only SSA had the additional step of a new reimbursable agreement to cover the expenses incurred. SSA does not have the authority to use its funding outside of its mission. SSA officials said that IRS requested information about certain federal benefit recipients in place of using existing tax information within IRS, which required a different file format and transmission process from EIP 1.[263] According to IRS officials, IRS changed the way in which it requested data from the agencies so that it could process their data more quickly.
IRS continues to experience challenges in delivering timely payments to incarcerated individuals. According to the attorneys who represented incarcerated individuals in a class action suit against Treasury regarding their eligibility for the payments, there have been several EIP-related challenges that have created confusion among this population. According to IRS data, Treasury and IRS disbursed just over 1.4 million EIP 1 payments to incarcerated individuals in 2020. IRS data also show that nearly 300,000 incarcerated individuals filed tax returns after the deadline for IRS to issue an EIP 1 or EIP 2. Of those individuals, over 70,000 were able to claim an RRC on their 2020 tax return. IRS officials said the remaining 229,000 returns that it reviewed and processed did not claim the RRC or were not eligible for it.
Incarcerated individuals who filed paper returns or who filed after December 31, 2020, may be caught in an IRS backlog of unprocessed returns. IRS is experiencing delays in processing certain returns received in 2021—including millions of returns claiming the RRC—resulting in extended time frames for some taxpayers. For more information about how these errors related to the RRC are affecting the filing season, see the 2021 Filing Season enclosure in appendix I.
Finally, payments to incarcerated individuals are at a higher risk of garnishment. Only statutory authorization for EIP 2 provided protection against garnishment; the statutory authorization for EIP 1 and 3 did not.[264] Federal and state prisons also have different rules regarding how and what portion of payments to incarcerated individuals can be garnished when otherwise permitted by law. According to Treasury and IRS, they have no jurisdiction over the payments once they disburse them, and there is no centralized data on how widespread garnishment is. The Consumer Financial Protection Bureau found fewer than 10 incidents in one state where it investigated garnishments of incarcerated individuals’ payments, upon which the state subsequently returned the EIPs to the recipients. Federal Deposit Insurance Corporation officials said their agency has not received reports that incarcerated individuals’ EIPs were garnished.
Payments in the U.S. territories. Residents of the five U.S. territories are eligible for EIPs from the territory tax authorities if they meet the income thresholds and other eligibility requirements.[265] IRS disbursed three rounds of economic impact funds to the U.S. territory tax administrators totaling $9.7 billion.
Territory residents generally received payments later than mainland residents because territory officials were required to submit payment plans to Treasury for review and approval before receiving funds for each round of payments. The plans specify how the territory tax administrators plan to disburse payments to territory residents. According to IRS officials, improved coordination between Treasury and the territory tax administrators helped expedite the process in subsequent rounds. IRS officials said that once Treasury approved a territory plan, IRS transferred the funds within 24–48 hours.
According to IRS data, over 116,000 duplicate payments—instances where both IRS and the territory tax administrators made the same payment—were issued during the first round of EIP. IRS officials said that as of March 18, 2021, IRS recovered $4.5 million from payments it had issued to 3,632 individuals. IRS does not have data on how much each of the territories has recovered. To the extent provided in the territory plans, each territory tax administrator is responsible for using available methods for recovering duplicate payments and returning the funds to Treasury. IRS is assessing its capability to collect any duplicate payments the territories are unable to recover.
Expired EIP payments. As of May 31, 2021, 583,000 EIP 1 checks, totaling around $822 million, were set to expire if not cashed, representing slightly less than 1 percent of the total number of payments disbursed.[266] The majority of uncashed EIP 1 check payments will expire by July 2021 if they are not cashed. In addition, over 153,000 EIP 1 debit cards remained unactivated as of May 31, 2021. Bureau of the Fiscal Service officials said they did not send notices to remind individuals to cash checks but are considering using social media to remind individuals to activate debit cards. Additionally, around 817,000 EIP 2 checks and over 486,000 EIP 2 debit cards had not been cashed or activated, totaling over $1 billion. Bureau of the Fiscal Service officials said EIP 2 check payments will start expiring in spring 2022.
IRSpreparation for advance child tax credit payments. IRS officials are taking steps to begin issuing advance payments of the CTC starting in July 2021. According to Treasury and IRS, roughly 39 million households—covering 88 percent of children in the U.S.—are slated to automatically begin receiving monthly payments on July 15, 2021. Treasury and IRS also announced that CTC payments will be made on the 15th of each month, unless the 15th falls on a weekend or holiday.
IRS officials are offering three online tools to help individuals with the CTC payments: a Non-filer Sign-Up Tool, a portal (CTC UP) that individuals can use to opt out of the advance payments and update personal information, and an eligibility calculator. On June 14, 2021, IRS opened the Non-filer Sign Up Tool to allow individuals who do not normally file a tax return the opportunity to file a simplified return. This simplified return will allow individuals the opportunity to receive the advance CTC payments and the EIP 3 and to claim the 2020 RRC. IRS officials said the online tool would be similar to the tool established for the first round of EIPs. The new Sign-Up Tool is not available in a mobile friendly version in that it doesn’t scale to fit a phone or tablet screen. Two IRS outreach partners had previously said that the first EIP nonfilers tool could be difficult to access and navigate, particularly on a mobile device, which may be the only device readily available to some individuals.
The CTC Up portal became available on June 21, 2021. Initially, individuals will use the portal to check if they are eligible to receive advance payments and opt out of receiving them. IRS estimates that between 15 and 16 million individuals will opt-out of the advance payments. IRS is planning updates to the portal throughout 2021 to increase its functionality. For example, IRS officials said that starting on June 30, 2021, individuals will be able to update their bank account information. In September 2021, individuals will also be able to update their personal information such as marital status, income, and number of children. Lastly, in November 2021, IRS anticipates launching a Spanish version of the CTC portal, and prior to the start of the 2022 Filing Season, IRS will provide a summary of the advanced payments received to help taxpayers complete their 2021 tax returns.
To raise awareness about CTC advance payments, officials said IRS plans to leverage the outreach channels it established with federal agencies for EIP and work with childcare facilities, educational organizations, and stakeholders who assist individuals experiencing homelessness. On June 14, 2021, IRS published frequently asked questions on the CTC on its website (https://www.irs.gov/credits-deductions/2021-child-tax-credit-and-advance-child-tax-credit-payments-frequently-asked-questions). IRS also sent two notices to alert potentially eligible taxpayers of the advance CTC payments, provide estimated amounts of monthly advance CTC payments, and explain the opt-out option.
The White House declared June 21, 2021 as Child Tax Credit Awareness Day to ensure parents know about the expansion of the CTC and how it will benefit their families. As part of Child Tax Credit Awareness Day, the administration encouraged elected officials, organizations that assist children, and faith-based organizations, to help low-income families use the Non-Filer Sign Up Tool. In addition, Treasury publicly released zip code level data showing the number of children who may be eligible to be claimed for the CTC, but who had not been claimed on a recent tax return. This information could potentially help IRS and its outreach partners tailor outreach efforts for the EIP and CTC to specific communities. IRS also plans to hold in person events in a dozen cities to help eligible families prepare and file tax returns in June and July, 2021.[267]
IRS officials said they are facing multiple challenges as they prepare to issue advance payments, such as the short amount of time between the enactment of ARPA in March and the July start of payments. Staffing is another challenge. The IRS team responsible for the online portal is also responsible for EIP 3, the 2021 filing season, and preparing for the 2022 filing season.
IRS officials said they are also concerned about how to provide sufficient customer support to individuals given the current demands at IRS taxpayer assistance centers and the high number of telephone calls to customer support. IRS reported it intends to set up a dedicated phone line for CTC assistance (1-800-908-4184) and to redirect at least 1,800 customer service representatives and at least 220 bilingual representatives—to provide telephone assistance. As of June 2021, IRS is anticipating 12 million phone calls and expects to be able to answer 17 percent of those calls. IRS officials said that individuals who cannot access the portal can receive assistance at taxpayer assistance centers, however, IRS identified providing sufficient customer service as a risk.
IRS officials said they hope a new authentication process, Secure Access Digital Identity (SADI), will help alleviate some of the pressure on customer support. While IRS has been developing SADI using a third-party service since 2019, the CTC Up portal is the first IRS system that will authenticate users’ identity using SADI. IRS officials estimate that 70 to 80 percent of online users will be able to successfully complete authentication using SADI. IRS officials anticipate that the more people who can successfully authenticate their identity and access the portal will result in fewer people calling the support line for assistance.
In its comments, reproduced in appendix VIII, IRS deferred to Treasury on the recommendation.
Methodology
To review how Treasury and IRS administered EIP 3 payments, we examined Treasury and IRS data as of May 31, 2021, federal laws, and agency guidance. We reviewed the data and interviewed Treasury and IRS officials to determine the data were sufficiently reliable to describe the number and amount of payments disbursed.
We interviewed officials from Treasury and IRS about the administration of EIP 3. We also interviewed officials from the Social Security Administration, Consumer Financial Protection Bureau, and Federal Deposit Insurance Corporation to understand their roles in relation to Treasury and IRS’s administration of the EIP and to understand any support they are providing in preparation for advance payments of the CTC. We interviewed tax administrators from American Samoa, Guam, the Commonwealth of the Northern Mariana Islands, the Commonwealth of Puerto Rico, and the U.S. Virgin Islands to understand how they administered EIP 1, 2, and 3.
We asked representatives from 21 selected IRS outreach partners to provide us with their perspectives on IRS’s outreach coordination with their organizations. We selected 11 partners for their national outreach to underserved populations such as low-income families, veterans, and seniors; we also selected 10 partners for their local outreach to communities in ZIP codes with high numbers of potential nonfilers (based on IRS data). This sample is not representative, but the interviews provided us with illustrative examples of how organizations worked with IRS to reach traditionally underserved communities and what aspects of the IRS communications plan worked well, and they also highlighted potential areas for improvement.
Agency Comments
We provided a draft of this enclosure to Treasury, IRS, the Office of Management and Budget, Social Security Administration, Consumer Financial Protection Bureau, and Federal Deposit Insurance Corporation. Treasury and IRS provided comments, which are summarized below. Treasury also provided technical comments, which we incorporated as appropriate. The Office of Management and Budget, Social Security Administration, Consumer Financial Protection Bureau, and Federal Deposit Insurance Corporation did not provide comments on this enclosure.
In its comments, reproduced in appendix XI, Treasury neither agreed nor disagreed with our recommendation, and stated that it shares the underlying goal of reaching as many nonfilers as possible to encourage them to claim EIPs online. However, Treasury also stated that it is unable to release interim findings and analysis at this time. According to Treasury, the analysis is not yet complete. Moreover, Treasury stated that disclosing partial analysis could limit the extent of its ability to publicize the currently outstanding data (as part of a future, complete data set) because of prohibitions on disclosure of taxpayer data under section 6103 of the Internal Revenue Code.
As stated in the report, we acknowledge that having data from the entirety of the filing season will allow for a more robust analysis. However, by waiting to complete the analysis, Treasury and IRS are missing an opportunity to identify communities that may have higher numbers of nonfilers, and use that information to inform their outreach efforts during the extended 2021 filing season. This type of information could support Treasury and IRS’s ongoing effort to reach eligible families to get them to register for the advance CTC payment before the nonfilers tool closes in October 2021. IRS’s outreach partners told us their outreach efforts to nonfilers could be more effective if they had current data that help identify specific communities of nonfilers who may need assistance. Treasury and IRS could also ensure any partial data releases are structured to not disclose taxpayer data. IRS has existing guidance for preparing statistical tabulations and does not allow releasing data tabulations with fewer than 10 or 20 observations, depending on the circumstances, so that the data cannot be associated with or otherwise identify a particular taxpayer.[268]
GAO’s Ongoing Work
We will continue to monitor IRS and Treasury's efforts to analyze data that could potentially improve communication and outreach to nonfilers. We will also continue to monitor IRS and Treasury’s progress to ensure eligible individuals receive their third EIP, and their efforts to issue the advance payments of the CTC.
GAO’s Prior Recommendations
The table below presents our recommendations on economic impact payments from prior bimonthly CARES Act reports.
GAO’s Prior Recommendations Related to Economic Impact Payments
Recommendation
Status
The Commissioner of Internal Revenue should periodically review control activities for issuing direct payments to individuals to determine that the activities are designed and implemented appropriately as the Internal Revenue Service (IRS) disburses a third round of economic impact payments (EIP) and prepares for advance payments on the child tax credit. These control activities should include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients (March 2021 report).
Open. IRS disagreed with the recommendation. However, IRS acknowledged that it established additional procedures and reviews upon discovering that it had sent millions of payments to the wrong account. IRS also stated that it plans to assess the effectiveness of these new controls during the next round of EIPs and will adjust them as warranted.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed an EIP notification letter and subsequently filed for and received an EIP, and use that information to inform ongoing outreach and communications efforts (November 2020 report).
Open. The Department of the Treasury (Treasury) and IRS agreed with this recommendation. According to Treasury officials, Treasury began analyzing data in January 2021 on those individuals who received a notice and subsequently filed for and received a first-round EIP (EIP 1). However, Treasury does not plan to complete this analysis until fall 2021, more than 6 months after the first payments of the third round of direct payments (EIP 3) were issued, limiting how any findings could inform EIP 3 outreach efforts. According to Treasury officials, they are incorporating information from the 2021 filing season into their analysis. The filing season ended May 17, but there is a 5-month extension to file amended returns.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should make estimates of eligible recipients who have yet to file for an EIP, and other relevant information, available to outreach partners to raise awareness about how and when to file for EIPs (September 2020 report).
Open. Treasury and IRS neither agreed nor disagreed with our recommendation, but did take some actions that are consistent with our recommendation. For example, in September 2020, the agencies used tax return information to identify nearly 9 million individuals who had not received an EIP 1 and then notified these individuals that they may be eligible for a payment. The letters also provided instructions on how to request a payment. In addition, IRS publicly released detailed ZIP code data from the notices to help community outreach partners with their own outreach efforts.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP to help target outreach and communications efforts (September 2020 report).
Open. Treasury and IRS neither agreed nor disagreed with our recommendation, but did take some actions that are consistent with our recommendation. For example, in January 2021, Treasury revised its estimate of eligible recipients who have yet to file for an EIP 1 to 8 million. According to Treasury officials, this estimate is based on the 9 million notices IRS sent in September 2020. Treasury officials stated that it is likely that some of the 9 million recipients have since claimed the EIP, but Treasury did not provide data supporting this claim.
The Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments (June 2020 report).
Closed. Treasury and IRS took steps to implement our recommendation, such as providing instructions on the IRS website requesting that individuals voluntarily mail the appropriate EIP amount sent to the decedent back to IRS, for both electronic and paper check payments. Treasury has also held and canceled payments made to decedents, along with those that have been returned. As of April 30, 2021, around 57 percent (just over $704 million) of the $1.2 billion in EIP 1 sent to deceased individuals had been recovered.
As of March 2021, Treasury and IRS had not taken any further action to recoup payments made to decedents that had not been returned. IRS officials determined that further actions, such as initiating erroneous refund cases against the estates of the decedents to which payments were made and not returned, could be burdensome to taxpayers, the federal court system, and IRS. As such, IRS officials concluded that doing so is not prudent at this time.
The Internal Revenue Service needs to clearly communicate the nature and extent of 2021 tax refund delays to clarify expectations for taxpayers.
Entity involved: Internal Revenue Service, within the Department of the Treasury
Recommendation for Executive Action
The Commissioner of Internal Revenue should direct the appropriate officials to update relevant pages of irs.gov and, if feasible, add alerts to the Internal Revenue Service’s toll-free telephone lines to more clearly and prominently explain the nature and extent of individual refund delays occurring for returns taxpayers filed in 2021. The Internal Revenue Service neither agreed nor disagreed with this recommendation.
Background
The Internal Revenue Service’s (IRS) annual tax filing activities include processing over 150 million individual and business tax returns electronically or on paper, issuing hundreds of billions of dollars in refunds, and providing customer service to tens of millions of taxpayers on return processing issues, such as suspected identity theft and math errors. During the 2021 filing season, IRS was also responsible for issuing a third round of economic impact payments to millions of taxpayers totaling over $388 billion as of May 12, 2021; updating its systems and procedures to incorporate tax law provisions enacted in early 2021; and processing millions of tax returns remaining from the 2020 filing season.[269]
According to IRS officials, these additional responsibilities, coupled with reduced staffing due to ongoing COVID-19 pandemic conditions and an increase in manual work, have impacted IRS’s ability to assist taxpayers and process returns during the 2021 filing season. As a result, taxpayers are experiencing unusually long delays in receiving refunds and difficulty reaching IRS for assistance.
Overview of Key Issues
Returns processing and refund delays. IRS is experiencing delays in processing certain returns received in 2021, resulting in extended time frames for some taxpayers. Specifically, as of the end of the 2021 filing season in mid-May, IRS had about 25.5 million unprocessed individual and business returns, including about 1.2 million returns from its 2020 backlog, and 13.7 million returns IRS suspended due to errors.[270] IRS staff must manually review these returns with errors. IRS typically has unprocessed returns in its inventory at the end of the filing season, but not to this extent. For example, at the end of the 2019 filing season, IRS had 8.3 million unprocessed individual and business returns, including 2.7 million returns suspended for errors.[271]
IRS officials stated that many of the returns are being held due to potential errors in the information taxpayers provided for both the Recovery Rebate Credit, which individuals can claim on their tax year 2020 income tax return if they were eligible for but did not receive their first or second 2020 economic impact payment or did not receive the full amount, and the temporary changes to the Earned Income Tax Credit, which allows taxpayers to use prior year income from 2019 to increase their benefits under this credit. For example, if a taxpayer entered a different amount for the Recovery Rebate Credit than IRS has in its records (such as if the taxpayer had a child since the previous filing season), the return would be suspended for manual review to resolve the discrepancy. IRS reported that it is taking longer than usual to manually review some of these returns, but it has not provided specific time frames. Further, as discussed below, information on the reasons for delayed returns and refunds is not easy for taxpayers to find.
As of May 14, 2021, IRS’s website stated that more than nine out of 10 refunds are issued in less than 21 days. This information provides taxpayers with a general sense of when they will likely receive their refund and at what point they should call IRS for more information. In interviews with representatives of the tax industry, such as software providers and tax preparer organizations, representatives noted that taxpayers were frustrated when they had not received their refunds within IRS’s posted time frames and that they could not get any explanation from IRS’s website, including the Where’s My Refund application, or when calling IRS’s toll-free telephone line.
Taxpayer service limitations. With significantly more returns being held for manual review than in prior years, more taxpayers are trying to get information on the status of their returns and refunds. However, taxpayers have had a difficult time getting a status update on their refund from IRS, either via phone or online:
Phone services. Specifically, during our review between January 1 and May 1, 2021, IRS’s level of telephone service—the percentage of taxpayers seeking and reaching live assistance—was 14.3 percent, compared to an average of about 78 percent level of service for the end of filing seasons 2017 through 2019. IRS’s call volume and demand for live assistors has been unprecedented this year: IRS data show that between January 1 and May 1, 2021, it received about 65.6 million calls from taxpayers, compared to about 15.6 million calls during the same period in 2019.
In addition, IRS’s automated message on its toll-free telephone line for individual taxpayers has not been updated to explain refund delays or to include any other alerts associated with the 2021 filing season. The message as of May 14, 2021, informs taxpayers about refund interest payments they may have received in August 2020. In early May 2021, IRS officials stated that once the filing season starts, it is difficult for IRS to make changes to its telephone system’s automated messages due to scheduled blackout periods and other potential risks to the telephone infrastructure. However, these officials stated that they had no plans to update the recorded messages when the blackout period ends in late May 2021.
Online services. IRS’s website does not contain all of the relevant information regarding 2021 return processing delays and delays in issuing taxpayers’ refunds. Rather, IRS’s webpages devoted to information on refunds state that IRS continues to process and issue refunds and that most of these are issued in 21 days or less.
Further, the information IRS has posted online is not easy for taxpayers to find. While IRS added information on its “IRS Operations and Services” web page about the status of its operations, including a partial explanation for why some refunds have been delayed this filing season, this information is difficult to find because it requires navigating through several pages from the irs.gov home page and is located on a page with information on COVID-19-related tax relief and mission-critical functions. Other web pages that taxpayers might easily access, such as the “Refunds” page or related “Frequently Asked Questions” page, do not include complete information about delays in 2021 returns processing.
After we explained these concerns to IRS officials in early May 2021, IRS updated its “Refunds” and “Frequently Asked Questions” pages to include some information on delays. However, the information IRS posted was inconsistent. For example, one page stated that IRS was experiencing delays in opening mail, and the other page indicated that IRS was current on opening mail. In addition, IRS updated its refund-related pages to include an alert linking to the “IRS Operations and Services” page, which contains status updates on return and refund processing (see figure). However, this alert does not clearly state that a taxpayer will learn about potential refund delays by clicking the link to the “IRS Operations and Services” page.
Internal Revenue Service (IRS) Web Page for Taxpayers on Refund Expectations
When we asked IRS about the limited information online about current refund delays, officials said that they did have some information online and they were not sure what additional information would be helpful. We provided some examples, such as updating specific web pages related to refund information and frequently asked questions. Officials indicated they would consider making changes, but as of May 20, 2021, had not yet done so.
Federal internal control standards state that management should externally communicate necessary quality information to achieve the entity’s objectives. Government entities should report this information to government leaders and regulators, as well as the general public. Without clear, timely information on reasons why some refunds are being delayed during the 2021 filing season, taxpayers lack information on when they should expect to receive their refunds. This may lead taxpayers to continue to call IRS with limited success, due to IRS’s limited ability to answer a high number of incoming calls or lack of information on returns being held for errors. Further, taxpayers that count on their refunds to cover certain expenses do not have essential information to make alternative plans. Providing updated and timely information on irs.gov may help reduce the volume of calls to IRS from taxpayers and help reset taxpayers’ expectations.
Methodology
To conduct this work, we reviewed 2021 filing season return processing and customer service performance data, reviewed federal laws and agency communications, and interviewed IRS officials. To assess the reliability of these data, we interviewed IRS officials and assessed the data for any limitations. Due to disruptions during the 2020 filing season affecting performance, we compared the most recent data available from the 2021 filing season to 2019 filing season data from the same period to determine the extent to which the 2021 filing season differs from a typical year. We determined the data were sufficiently reliable for the purposes of our reporting objective.
Agency Comments
We provided a draft of this enclosure to the Department of the Treasury, IRS, and the Office of Management and Budget. The Department of the Treasury and the Office of Management and Budget had no comments on this enclosure. IRS’s comments are reproduced in appendix VIII and summarized below. IRS also provided technical comments, which we incorporated as appropriate.
In its comments, IRS neither agreed nor disagreed with our recommendation. IRS stated that it will review its messaging on the general state of returns processing and provide clarity as needed. IRS also noted that its “Where’s My Refund” tool provides taxpayers with the most current information on the status of their return and refund. After IRS provided its comments in mid-June 2021, we found that IRS had updated irs.gov to provide clearer information about refund delays. We also found that IRS had removed outdated messaging from its automated toll-free telephone line for taxpayers. We will follow up with IRS on other planned updates to its website and taxpayer telephone line. Based on this information, we will determine if the agency’s actions are sufficient to fully address our recommendation.
GAO’s Ongoing Work
We have ongoing work to evaluate IRS’s 2021 filing season performance, including the ongoing impact of COVID-19.
Related GAO Product
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
Expenditures for key federal nutrition assistance programs remain at record levels because of increased need and the federal response to the pandemic, as the Department of Agriculture works to ensure program integrity.
Entities involved: Food and Nutrition Service, within the Department of Agriculture
Background
Demand and expenditures for key federal nutrition assistance programs have remained high throughout the COVID-19 pandemic. According to the Food and Nutrition Service’s (FNS) most recent data, 42 million individuals participated in the Supplemental Nutrition Assistance Program (SNAP), the largest federal nutrition assistance program, in March 2021. SNAP benefits in that month totaled $9 billion, about 70 percent more than the amount of benefits issued in March 2020.[272] SNAP participation also grew during this period, but to a lesser extent.[273] FNS officials said the agency anticipates it will expend all of the approximately $101.8 billion appropriated for SNAP benefits for fiscal year 2021, which would exceed the previous historic high for the program by more than $25 billion.[274]
FNS, within the Department of Agriculture (USDA), administers SNAP and other federal nutrition assistance programs, including the new Pandemic Electronic Benefits Transfer program (Pandemic EBT); the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC); the Emergency Food Assistance Program (TEFAP); and the Nutrition Assistance Program for the Commonwealth of Puerto Rico, American Samoa, and the Commonwealth of the Northern Mariana Islands. Eligibility criteria vary across FNS’s nutrition assistance programs, and individuals and households may receive assistance from multiple programs.
Throughout the COVID-19 pandemic, legislative and executive actions have resulted in increased funding and expenditures for FNS’s nutrition assistance programs. In March 2021, the American Rescue Plan Act of 2021 (ARPA) extended a temporary 15 percent increase in benefits for all SNAP participants through September 2021.[275] In April 2021, FNS announced that it would begin providing additional SNAP benefits through emergency allotments to households that were already receiving the maximum, or almost the maximum, SNAP benefit for their household size.[276] FNS estimated that this adjustment to eligibility for SNAP emergency allotments would result in approximately 25 million SNAP participants receiving additional benefits and would cost approximately $1 billion per month. FNS’s other nutrition assistance programs have also collectively received and expended billions of dollars in COVID-19 funding. The table below shows total COVID-19 funding and expenditures as of May 2021 for SNAP as well as a selection of other programs.
COVID-19 Funding and Expenditures for Selected Federal Nutrition Assistance Programs as of May 31, 2021
Program
Description
Total COVID-19 funding ($)a
COVID-19 expenditures as of May 31, 2021 ($)
SNAP
Provides low-income individuals and households with benefits to purchase allowed food items and achieve a move nutritious diet.
16.8 billionb
Indefinite appropriationc
15.5 billion
5.7 billion
Pandemic EBT
Provides households with children who would have received free or reduced-price school meals if not for school closures due to COVID-19, as well as eligible children in childcare, with benefits to purchase food.
Indefinite appropriationd
13.3 billione
WIC
Provides eligible low-income women, infants, and children up to age 5 who are at nutrition risk with nutritious foods to supplement diets, information on healthy eating, and referrals to health care.
1.4 billion
475.8 million
TEFAP
Provides low-income individuals with groceries through food banks.
1.25 billion
705.7 million
Nutrition Assistance Program
Provides block grants to Puerto Rico, American Samoa, and the Commonwealth of the Northern Mariana Islands to provide food assistance to low-income households in these territories.
1.9 billion
676.8 million
Legend: Pandemic EBT = Pandemic Electronic Benefits Transfer; SNAP = Supplemental Nutrition Assistance Program; TEFAP = the Emergency Food Assistance Program; WIC = Special Supplemental Nutrition Program for Women, Infants, and Children.
Source: GAO analysis of relevant provisions of the Families First Coronavirus Response Act; the CARES Act; the Consolidated Appropriations Act, 2021; and the American Rescue Plan Act of 2021 as well as information from the Food and Nutrition Service (FNS), within the Department of Agriculture. | GAO-21-551
Note: This table provides information about selected programs and is not intended to provide comprehensive information about all federal nutrition assistance funding provided during the COVID-19 pandemic. aAmounts shown from the Consolidated Appropriations Act, 2021 reflect amounts appropriated in Division N, pertaining to COVID-19 response and relief. bIn some cases, COVID-19 relief laws provided specific amounts of funding to carry out certain SNAP provisions, and in other cases such laws provided an indefinite appropriation for certain SNAP provisions. The $16.8 billion shown reflects total COVID-19 funding for SNAP provisions that included a specific amount in COVID-19 relief laws. cThe Consolidated Appropriations Act, 2021 provided an indefinite appropriation for certain COVID-19 relief provisions, including a provision that temporarily increased SNAP benefits by 15 percent through June 2021. The American Rescue Plan Act of 2021 extended this increase in SNAP benefits through September 2021. dThe Families First Coronavirus Response Act provided an indefinite appropriation for Pandemic EBT. eThe $13.3 billion shown reflects Pandemic EBT expenditures through March 2021, the most recent data available as of June 2021. FNS officials noted that there is a lag in reporting Pandemic EBT expenditures because FNS must manually input state-reported Pandemic EBT data into its accounting system.
Our prior work has highlighted concerns with SNAP improper payments.[277] For example, in April 2020, we recommended that FNS develop and implement a process, documented in policies and procedures, to analyze the root causes of state SNAP estimated improper payments to identify potential similarities among states and develop and implement agency-level corrective actions, if appropriate, to help address them. FNS generally agreed with the recommendation and, in June 2021, officials said the agency had finalized a standard operating procedure to assist FNS in working with states to develop and implement corrective action plans for SNAP improper payments, among other things. We plan to review the standard operating procedure and monitor FNS’s implementation of it. According to the most recent FNS estimate available, the SNAP estimated improper payment rate was 7.36 percent in fiscal year 2019, totaling approximately $4 billion in estimated improper payments that year.
Overview of Key Issues
FNS will assess the susceptibility of Pandemic EBT to significant improper payments. FNS officials said the agency plans to assess Pandemic EBT’s susceptibility to significant improper payments in summer 2021.[278] Pandemic EBT is a new program, authorized in March 2020, to provide benefits to households with children who would have received free or reduced-price school meals if not for school closures due to COVID-19.[279] As of March 2021, Pandemic EBT had expenditures of $13.3 billion. This amount will likely increase significantly during the remainder of fiscal year 2021. For example, FNS estimates that issuing Pandemic EBT benefits in summer 2021 will cost approximately $13 billion. FNS officials previously told us they had not assessed Pandemic EBT for susceptibility to significant improper payments, because it is a temporary program and states have considerable discretion to determine eligibility. However, in April 2021, FNS determined that the agency would perform an improper-payment risk assessment for Pandemic EBT and expects to complete the assessment in summer 2021.
The Payment Integrity Information Act of 2019 (PIIA) directs the head of each executive agency to consider risk factors (examples of which are listed in the law) that are likely to contribute to susceptibility to significant improper payments.[280] See the table for examples of such risk factors that may apply to Pandemic EBT.
Examples of Risk Factors Listed in the Payment Integrity Information Act of 2019 (PIIA) Compared with Characteristics of the Pandemic Electronic Benefits Transfer Program (Pandemic EBT)
PIIA risk factors for improper payments
Characteristics of Pandemic EBT
The program or activity is new to the executive agency.
The program started in March 2020.
The volume of payments made through the program or activity.
The program had expenditures of $13.3 billion as of March 2021.
Payments or payment eligibility decisions are made outside the executive agency, such as by a state or local government.
State agencies make payment eligibility decisions.
There have been recent major changes in program funding, authorities, practices, or procedures.
Several changes have been made to the program since March 2020, including expansion to certain children younger than 6 years and children who are in child care as well as extension through fiscal year 2021.
The program has similarities to other programs or activities that have reported improper payment estimates or been deemed susceptible to significant improper payments.
Program benefits are often loaded onto Supplemental Nutrition Assistance Program (SNAP) electronic benefits transfer cards for households also receiving SNAP. The reported SNAP improper payment rate in fiscal year 2019 was 7.36 percent.
Source: GAO analysis of relevant federal law and information from the Food and Nutrition Service, within the Department of Agriculture. | GAO-21-551
Additionally, the Office of Management and Budget (OMB) issues guidance for federal agencies regarding improper payments.[281] OMB guidance provides that newly established programs should complete an improper payment risk assessment after the first 12 months of the program, a time span that the Pandemic EBT program has exceeded. Also, in general, we and many federal Inspectors General have identified reducing and preventing improper payments as a significant challenge under the COVID-19 relief laws, citing the large amount of money at issue and the need to distribute funds rapidly under emergency conditions.[282]
States have experienced challenges in implementing Pandemic EBT, some of which may indicate the program’s potential susceptibility to significant improper payments. To implement Pandemic EBT, state SNAP officials we interviewed said they needed to work with other state agencies, such as educational agencies, to identify eligible participants. Some state SNAP officials we interviewed identified multiple challenges experienced in securing data to identify and verify eligible participants. For example, officials in one state said state privacy laws impeded data sharing. Officials in another state said the data systems at the SNAP agency and the educational agency were incompatible, making data matching for payment integrity difficult. In that state, the SNAP agency tried to match its data to the list of eligible students from the educational agency’s data to verify addresses and identify any duplication of participants. However, state officials noted that differences between the state SNAP agency’s and the state educational agency’s data systems made this process challenging.
In one instance, a state SNAP official we interviewed noted that the agency had identified some ineligible individuals who had received Pandemic EBT benefits and that the state was unsure what recourse it could take, given the lack of FNS guidance or regulations on the issue. The official said colleagues in other states had identified similar concerns. Officials from the American Public Human Services Association similarly told us that state officials have expressed concern about ineligible individuals’ receiving Pandemic EBT and have also expressed confusion about the steps they should take if they identified ineligible recipients. Unlike for SNAP, FNS has not issued regulations on methods for recovering Pandemic EBT overpayments or states’ ability to disqualify a recipient from Pandemic EBT as a penalty.[283] Instead, for school year 2020–21, FNS’s Pandemic EBT state plan template required states to outline a process to recover or adjust benefits to correct payment accuracy errors.[284]
FNS’s forthcoming assessment of Pandemic EBT’s susceptibility to significant improper payments may inform agency efforts to ensure payment integrity and may guide the agency’s efforts to offer states technical assistance, mitigation strategies, or corrective actions.
FNS cannot calculate SNAP payment error rates for fiscal years 2020 and 2021 but has continued other work to ensure program integrity.
Payment error rate. The payment error rate is integral to SNAP program integrity.[285] In addition to being the basis for establishing the rate of improper payments for SNAP, the error rate is an important factor in FNS oversight of state SNAP agencies. The payment error rate determines state liability for errors that exceed the national target and informs the development of corrective actions to mitigate or reduce payment errors.
In February 2021, FNS announced that it cannot calculate SNAP national and state payment error rates for fiscal years 2020 and 2021.[286] FNS explained that it must develop SNAP payment error rates on the basis of a legislatively mandated Quality Control (QC) review process.[287] However, COVID-19 relief laws and FNS gave states the flexibility to suspend SNAP QC reviews from March 2020 through June 2021 in response to the pandemic.[288] According to FNS officials, all states opted to suspend QC reviews. As a result, FNS determined that it lacked the data necessary to determine error rates. USDA’s Office of General Counsel agreed with FNS’s determination that it could not calculate SNAP payment error rates for fiscal years 2020 and 2021. FNS officials said they also notified OMB of their inability to calculate the SNAP payment error rate.
FNS officials said the agency considered its options for analyzing the SNAP QC data that states submitted in fiscal year 2020 before the pandemic (i.e., from October 2019 through February 2020), but several factors limited the usefulness of these data for publication. For example, FNS officials said that because the available fiscal year 2020 SNAP QC data do not cover any months during the pandemic, FNS and states could not use those data to understand the pandemic’s effect on the SNAP error rate. Officials also explained that calculating a partial-year error rate with incomplete data could expose FNS to the risk of lawsuits from states because states with a high SNAP error rate are subject to sanctions. Last, FNS officials said that using fewer than 12 months of SNAP QC data could result in estimates of the SNAP payment error rate that would be too imprecise to be instructive for FNS and the states.
Oversight of state agencies. Though FNS has determined that it cannot calculate SNAP payment error rates, officials said other SNAP program integrity efforts have continued during the pandemic. Officials said they are currently developing guidance to assist states to resume SNAP QC reviews in July 2021. Several FNS regional officials we interviewed also said that, though all states had opted to suspend SNAP QC reviews, most states continued to perform QC reviews on their own, in some cases using smaller sample sizes as a part of their program integrity efforts. Officials from one regional office said that all states in their region continued to provide QC data to the regional office so that regional officials could review their cases and provide feedback.
Most state SNAP officials we spoke with said they received regular technical assistance regarding payment accuracy from their FNS regional offices during the pandemic. FNS held payment accuracy training for all SNAP QC offices at both the national and regional levels, and FNS regional officials said they were continuing to provide technical assistance on payment accuracy to states both periodically, through conference calls, and on demand. To ensure compliance with program requirements, regional officials also performed scheduled Management Evaluations of states during the pandemic.[289]
Finally, FNS officials told us that the lack of a payment error rate will not impede their work with states currently under sanction for having high SNAP error rates in prior years. Officials further explained that FNS will continue monitoring corrective action plans, including reviewing and updating them.
Demographic information. In addition to calculating the error rate, FNS uses data derived from the SNAP QC reviews to produce the annual report Characteristics of Supplemental Nutrition Assistance Program Households for a given fiscal year. The report describes the demographics of SNAP households and participants nationwide and provides an overview of SNAP benefit levels during that fiscal year. FNS officials said they are assessing the reliability of the available data to determine whether they will be able to produce the report given the SNAP QC suspension during the pandemic. They acknowledged that FNS, policymakers, and other stakeholders use information from this report for many purposes. As long as the agency determines the data are sufficiently reliable, FNS intends to issue Characteristicsof Supplemental Nutrition Assistance Program Households for fiscal year 2020. The agency will follow a similar process to assess the fiscal year 2021 data after the fiscal year ends, according to officials.
Workforce capacity challenges affected states’ implementation of SNAP throughout the COVID-19 pandemic. The COVID-19 pandemic has strained the capacity of most states’ SNAP agency staff and slowed SNAP operations, according to officials we interviewed from each of FNS’s seven regional offices and from five selected state SNAP agencies. Overall, state and regional officials highlighted the following factors that affected the capacity of state SNAP agencies to administer the program during the pandemic:
Higher volume of applications. Many states received and processed substantially higher numbers of SNAP applications, especially at the outset of the pandemic. For example, officials we interviewed in one state said they received double the typical number of applications per week during the early months of the pandemic.
Sudden shift to remote work. Local SNAP offices were unprepared for teleworking and did not have the technology (e.g., laptops) to deliver SNAP services remotely. It was difficult for them to adjust workflow processes typically performed in person.
Shortages of personnel. In some states, COVID-19 caused personnel shortages as staff adjusted work schedules to quarantine and care for children.
Simultaneous operation of other programs. Some states redirected SNAP staff and resources toward planning and implementing Pandemic EBT. In a few states, the pandemic coincided with natural disasters such as hurricanes, causing these states to redirect SNAP staff toward Disaster SNAP operations.[290]
States relied on several strategies to mitigate the challenges of decreased workforce capacity during the pandemic. As we have previously reported, adjustments to SNAP operations allowed by COVID-19 relief laws have helped states streamline program operations and increased their ability to process the large influx of SNAP applications efficiently.[291] For example, officials from six FNS regional offices said states in their regions benefited immensely from adjustments related to certification processes (e.g., to determine participants’ eligibility and benefit levels for SNAP). Some states also pursued innovative technological solutions—such as equipping SNAP websites with chatbots to assist applicants or mass-texting participants and eligible populations about programmatic changes—that increased staff capacity to work on other pressing issues.[292] In addition, FNS officials said that states would spend fiscal year 2021 administrative funds authorized for Pandemic EBT in ways that will reduce SNAP staff’s Pandemic EBT workload. FNS officials anticipate common types of administrative spending will include contracting with call centers to provide customer support and translating program information into multiple languages.
FNS plans to modernize WIC to help promote access to WIC benefits. We have previously reported that FNS is taking steps to provide WIC participants options to purchase food online, similar to SNAP participants. FNS has several ongoing efforts in this area.
WIC Task Force. In response to a Consolidated Appropriations Act, 2021 requirement, FNS established a WIC Task Force in March 2021 to study how to streamline and promote convenience, safety, and equitable access to WIC benefits, including online and phone ordering, curbside pickup, and home delivery. According to FNS officials, although setting up the task force in a short period of time was a challenge, recruiting members who represent various interests (as required by the act) to serve on the task force was not difficult.[293] The task force held a kickoff meeting on March 24, 2021, and is now meeting regularly to complete its study and provide results and recommendations to USDA by September 30, 2021.
Grants to states. In fall 2020, FNS awarded a $2.5 million, 3-year competitive grant to the Gretchen Swanson Center for Nutrition to develop and test a safe and secure model for online ordering in WIC. According to FNS officials, the center plans to begin soliciting grant proposals from states in summer 2021. FNS officials said they are working closely with the center and are on track to award subgrants to states by fall 2021. In addition, FNS officials told us the center worked with experts to develop a document that includes policy, technical, and programmatic information to guide state agencies and other stakeholders as they adopt and implement WIC online ordering.
WIC benefit increase and outreach. ARPA provided $490 million to USDA to offer a temporary increase of up to $35 per month to the WIC cash-value voucher for fruits and vegetables during the pandemic.[294] On March 24, 2021, FNS sent a memo to state WIC agencies to implement this provision, allowing states to provide this increase for up to 4 consecutive months through September 30, 2021. As of June 11, 2021, FNS officials said all states had opted to provide this increase.
In addition, ARPA provided $390 million to USDA for fiscal year 2021 for WIC outreach, innovation, and program modernization efforts, including waivers and flexibilities, to increase participation and benefit redemption.[295] (This funding is available through fiscal year 2024.) FNS officials acknowledged that WIC is underused and said that the agency is giving high priority to conducting outreach to attract eligible people to the program, especially those in underserved populations.[296] Further, FNS officials told us that the agency’s other priorities are to simplify the WIC enrollment process and to support WIC through modernization and technology. They said FNS is currently developing strategic goals for the agency’s efforts to increase access to, and use of, WIC benefits and is also developing plans to engage with stakeholders, such as state and local agencies, on this effort.
FNS plans to offer new food options to help address the continuing challenge of canceled TEFAP orders during the pandemic. FNS plans to offer new food products and ways to buy food as states continue to face challenges with canceled TEFAP orders. We previously reported that TEFAP orders FNS canceled during the pandemic led to shortages of certain products, such as canned meats, soups, and vegetables, in food banks nationwide at a time of increased demand and made it difficult for states to spend TEFAP funds provided through COVID-19 relief laws. We reported that FNS canceled orders for several reasons, including a lack of vendor bids on the orders, unavailability of food due to supply chain issues, and increased costs for transportation and raw materials.
In April 2021, FNS officials told us that these factors continued to contribute to cancelations of TEFAP orders but that there were fewer canceled orders than in the past. According to FNS data from March 2020 to March 2021, the magnitude of canceled TEFAP orders in terms of both the estimated value of the food and total number of truckloads was highest in October 2020, at 33 percent, and decreased by March 2021 to 18 percent. Officials from the American Commodity Distribution Association and Feeding America agreed that canceled TEFAP orders continued to be a challenge and that the causes remained the same.
To address these challenges, according to FNS officials, the agency is working to add new food products and prepackaged, fresh produce to TEFAP to help ensure states can spend COVID-19 funds before they expire on September 30, 2021. On April 9, 2021, USDA announced that it would add prepackaged produce boxes as an option for TEFAP through the rest of fiscal year 2021, as it ends a similar program that provided boxes of food to food banks and other providers.[297] FNS officials told us that, although they believe states and food banks will appreciate the fresh-produce option, the agency is testing this approach to assess demand for prepackaged produce boxes and whether to continue offering them.
Officials from Feeding America said they appreciated how intentional USDA has been in gathering insight from Feeding America’s food bank network regarding adding new food products to TEFAP, including type, size, and method of packaging. Officials from the American Commodity Distribution Association said the box of mixed produce does not replace canceled shelf-stable items, as fresh produce must be distributed within 30 days of receipt and is extremely difficult to move. Further, according to Feeding America officials, although COVID-19 relief funds for TEFAP will help to some extent, they are expecting a 30 to 40 percent drop in USDA foods in Feeding America’s food bank network during 2021, given that a USDA trade mitigation program has ended.[298]
Methodology
To conduct our work, we reviewed FNS data on program participation through March 2021 that were released in June 2021 and FNS data on expenditures as of May 31, 2021—the most recent data available at the time of our analysis. We determined these data were sufficiently reliable for our purposes by reviewing program documentation, discussing the data with knowledgeable FNS officials, and conducting manual testing for outliers or other errors.
In addition, we interviewed officials from FNS’s National Office and all seven FNS regional offices. We also interviewed SNAP officials in five states—California, Illinois, Louisiana, Montana, and Virginia—selected on the basis of a variety of factors, including states’ overall SNAP participation rates, requests for certain SNAP adjustments during the pandemic, methods of issuing Pandemic EBT benefits for school year 2019–20, and geographic diversity. In interviews with FNS and state officials, we discussed their experiences in administering SNAP and Pandemic EBT during the pandemic, FNS’s guidance and assistance to states, and program integrity issues. Further, we reviewed relevant federal laws, FNS guidance, and relevant documents. Finally, we interviewed, or otherwise solicited input from, representatives of the American Commodity Distribution Association, the American Public Human Services Association, Feeding America, and the National WIC Association.
Agency Comments
We provided a draft of this enclosure to FNS and OMB for review and comment. FNS provided technical comments, which we incorporated as appropriate. OMB did not provide comments.
GAO’s Ongoing Work
Our work on FNS’s response to COVID-19 through its nutrition assistance programs is ongoing. We will continue to examine FNS’s use of COVID-19 relief funds, its efforts to ensure program integrity, and its efforts to help vulnerable populations access the programs. In addition, we will continue monitoring FNS’s actions to ensure stakeholders and the public have sufficient context to understand and interpret data on federal nutrition assistance programs during the pandemic. Moreover, we will continue monitoring FNS’s actions to ensure stakeholders and the public are aware of potential sources of error in its data on participation and expenditures for some of its nutrition assistance programs during the pandemic.
GAO’s Prior Recommendations
The table below presents our recommendation from a prior bimonthly CARES Act report.
Prior GAO Recommendation Related to COVID-19 Nutrition Assistance
Recommendation
Status
The Secretary of Agriculture should ensure that the Administrator of the Food and Nutrition Service (1) provides sufficient context to help stakeholders and the public understand and interpret data on federal nutrition assistance programs during the pandemic and (2) discloses potential sources of error that may affect data quality during the pandemic, such as manual processing. For example, the agency could publish key information from its internal communications plan that it developed for the January 2021 data release and include additional table notes in subsequent data releases to help explain these issues (March 2021 report).
Open. As of June 2021, the Food and Nutrition Service (FNS) had taken steps toward implementing this recommendation. For example, the agency added several table notes to data it released in April 2021 to help provide stakeholders and the public with sufficient context to understand and interpret key data. FNS officials said the agency is currently discussing next steps for disclosing potential sources of error, such as manual processing of participation and expenditures data for some programs.
Payment Integrity: Selected Agencies Should Improve Efforts to Evaluate Effectiveness of Corrective Actions to Reduce Improper Payments.GAO-20-336. Washington, D.C.: April 1, 2020.
Contact information: Kathryn A. Larin, (202) 512-7215, larink@gao.gov
The Food and Nutrition Service has taken multiple steps to increase children’s access to meals during the COVID-19 pandemic; however, federal child nutrition programs continue to serve fewer meals than before the pandemic, and schools face ongoing challenges in increasing meal service in the 2021–22 school year.
Entity involved: Food and Nutrition Service, within the U.S. Department of Agriculture
Background
Federal child nutrition programs administered by the U.S. Department of Agriculture’s (USDA) Food and Nutrition Service (FNS) help improve children’s nutrition and combat child hunger by providing cash reimbursements for meals and snacks for eligible children in schools or at other locations when schools are closed. The largest programs, the National School Lunch Program (NSLP) and School Breakfast Program (SBP), subsidize meals for nearly 30 million children in approximately 95,000 elementary and secondary schools nationwide in a typical year.[299] NSLP and SBP typically serve children at school during the school year. In addition, the Summer Food Service Program (SFSP) and Seamless Summer Option (SSO) typically provide meals for school-age children during the summer months. Finally, the Child and Adult Care Food Program (CACFP) provides meals to younger children enrolled for care at participating childcare centers and day care homes, and to school-age children participating in CACFP At-risk Afterschool programs.[300] In general, FNS provides the largest subsidies for free- or reduced-price meals and snacks served to children from low-income households.
According to the Census Household Pulse Survey, from April 2020 through February 2021, the percentage of U.S. households with children reporting that they often or sometimes did not have enough to eat in the last 7 days fluctuated from roughly 12 to 15 percent.[301] As we reported in September 2020 and March 2021, FNS granted various nationwide waivers in response to pandemic-related school closures that began in spring 2020, to facilitate meal provision while limiting potential COVID-19 exposure. For example, these waivers allow meals to be served in noncongregate settings, enable parent and guardian meal pickup, and provide flexibility in foods served and meal times.[302]
In addition to granting the various waiver flexibilities, in spring 2020 FNS began allowing schools and other meal providers to operate under summer meal programs—SFSP and SSO—which are generally more flexible than NSLP. FNS also waived the requirement that summer meal sites providing free meals to all children must be located in areas where at least half of the children are from low-income households. This waiver expanded the population of children eligible for free meals, which eased the administrative burden of tracking and collecting payment for school meals while maintaining social distancing guidelines.
Various COVID-19 relief laws have provided funding or authority to USDA to support child nutrition programs during the pandemic. For example:
The CARES Act provided $8.8 billion in supplemental funds.[303] As of May 31, 2021, FNS had disbursed nearly all of this funding to states and other meal providers, using the majority of the funds, $8.615 billion, to reimburse providers for the cost of meals served during the pandemic. FNS used the remainder of the funds, $185 million, to operate Emergency Meals-to-You, a new partnership that delivered meals to address pandemic-related nutrition needs among children from low-income households in rural areas throughout spring and summer 2020.[304]
The Families First Coronavirus Response Act granted FNS authority to issue nationwide waivers in certain programs for specific purposes.[305] The Continuing Appropriations Act, 2021 and Other Extensions Act, enacted in October 2020, extended this authority and provided an indefinite appropriation to cover the costs incurred as a result of the waiver extensions.[306] As of May 31, 2021, FNS had not obligated any of this funding for child nutrition programs.
The Consolidated Appropriations Act, 2021, enacted in December 2020, provided additional funding to support CACFP childcare providers and school nutrition programs by replacing some of the decline in reimbursement funding in spring 2020.[307] As of May 31, 2021, FNS had not obligated any of this funding for child nutrition programs.
Overview of Key Issues
School districts and other providers served one-third fewer meals in March through November of school year 2020–21 than in the previous year, but changes varied by season. Although waiver flexibilities were in place to facilitate meal provision, according to the most recent available data from FNS, 32 percent—over 2 billion—fewer meals were served under NSLP, SBP, SFSP, and CACFP from March through November 2020 than during the same months in 2019 (see figure). In total, from March through November 2020, meals served under SFSP accounted for 40 percent of all meals served under the four child nutrition programs, compared with 2 percent during the same period in 2019. From March through November 2020, the number of meals served under NSLP, SBP, and CACFP dropped by a combined 58 percent. As we reported in March, school district nutrition officials we interviewed attributed this drop in meals served to several factors, including school closures. The flexibilities allowing operators to use SFSP—which has a higher reimbursement rate and provides free meals—contributed to an increase in meals served under SFSP during the pandemic; however, the increase in meals served under SFSP did not make up for the decreases in the other programs. Although children may be accessing nutrition assistance through food banks, pantries, and other programs, such as the Pandemic EBT program, the extent to which these programs may be filling the gap is not known.
Total Meals Served by Key Federal Child Nutrition Programs, Mar.–Nov. 2019 and Mar.–Nov. 2020
Notes: Totals shown for CACFP include child meals only. Totals shown for SBP and NSLP include meals served through the Seamless Summer Option, a program that allows school districts operating SBP and NSLP to continue using the same meal service rules and claiming procedures as in the regular school year throughout the summer and during unanticipated school closures. According to Food and Nutrition Service, the number of meals reported for any given month is subject to marginal revisions over time for a variety of reasons, including late claims and changes that come as a result of routine monitoring activity.
Although FNS data indicate the number of meals served under each child nutrition program, the expanded eligibility provided by the waivers may make it difficult to determine whether children of certain ages accessed meals through these programs. Specifically, waivers allowed more operators to offer summer meal programs, which can serve all children younger than 18 years rather than only school-age children.[308] As a result, young children who would have typically received meals from day care centers operating CACFP may have accessed meals through summer meal programs during pandemic-related day care closures.[309] At the same time, hunger advocacy officials we interviewed in one state suggested that families whose children were not yet school age may have been unaware of and therefore not accessing these meals, particularly if they did not have school-age siblings.
Differences in the numbers of total meals served through NSLP, SBP, SFSP, and CACFP in school year 2020–21 and in the prior year varied by season. During spring 2020 (March through May) and fall 2020 (September through November), school district nutrition programs and other providers served 42 and 33 percent fewer meals, respectively, than during the same months in 2019. In contrast, meal providers served roughly the same number of meals in the summer 2020 (June through August) as in summer 2019, although the number of meals served in June and July was slightly higher in 2020 than in 2019.
Officials from half of the district nutrition programs and most of the hunger advocacy groups we interviewed told us the flexibilities provided by FNS waivers reduced typical barriers to summer meals and presented an opportunity to expand summer food service.[310] This may explain why, in spite of the pandemic, the number of meals served was roughly the same in summer 2020 as in summer 2019. An official from one hunger advocacy group attributed an increase in meals served in July 2020 specifically to the waiver flexibilities allowing meals to be served in noncongregate settings (i.e., “grab-and-go”). In addition, nutrition program officials from two of the districts told us that schools and other providers in their areas provided more meals during summer 2020 than in prior summers. Officials from two of the hunger advocacy groups agreed, reporting that waiver flexibilities facilitated summer meal service. FNS officials said that after operating summer meal programs during the pandemic, some districts and providers may be more likely to continue to serve meals in future summers. Such an increase in summer meal providers could improve children’s access to summer meals after the pandemic.
FNS leveraged an existing pilot program to distribute meals to high-need children, but participation was regionally concentrated. FNS utilized other programs to serve meals to children whose schools were closed during the pandemic, including Pandemic EBT and Emergency Meals-to-You, which both served high-need children and reduced barriers to accessing food.[311] FNS established the Emergency Meals-to-You program by repurposing an existing summer pilot project (Summer Meals-to-You) to provide boxes of shelf-stable food via mail to children in rural, high-poverty areas in spring and summer 2020.[312] Through its cooperative agreement with FNS, the Baylor Collaborative on Hunger and Poverty operated Emergency Meals-to-You from April through August 2020 and provided approximately 39 million meals to more than 270,000 children in 345 school districts nationwide, according to FNS data.[313]
Access to meals during school closures in rural areas has been a persistent area of concern. For example, in May 2018, we reported challenges with summer meal–site operations that might contribute to underserving of rural communities, including Indian reservations. Officials from hunger advocacy groups whom we interviewed for our current report stated that during the pandemic, rural communities experienced limited access to federal child nutrition programs because of challenges such as lack of transportation. The Emergency Meals-to-You program addressed some of these challenges by shipping boxes of shelf-stable meals directly to eligible children in participating school districts, including several districts serving American Indian and Alaska Native children. According to our analysis, schools funded by the Bureau of Indian Education (BIE), within the Department of the Interior, made up 6 percent of districts participating in Emergency Meals-to-You.[314]
Although the program was available nationwide, almost 90 percent of meals served under Emergency Meals-to-You went to children in the South, and approximately 50 percent were served to children in Louisiana and Texas. Officials from FNS and the Baylor Collaborative on Hunger and Poverty attributed this trend to high rates of rural child poverty in the South and noted that southern state agencies actively encouraged districts to apply for Emergency Meals-to-You.[315] Officials from three of the six school district nutrition programs we interviewed in non-Southern states said they were not aware of Emergency Meals-to-You or of their district’s eligibility to participate while the program was ongoing.
Officials from one FNS regional office told us that state nutrition offices’ level of involvement was an important predictor of districts’ participation in the program. One state nutrition program official suggested states may not have understood that they played a critical role in notifying districts about the program. According to officials from the Baylor Collaborative on Hunger and Poverty, some states were less proactive than others because their resources were already strained during the pandemic.
As school year 2021–22 begins, school learning models and other factors may affect school district nutrition programs’ efforts to return meal service to prepandemic levels.
School learning models. The various learning models—remote, in-person, and hybrid—that schools nationwide adopted during school year 2020–21 may continue in some schools in 2021–22, presenting challenges for school nutrition programs.[316] In its April 2021 handbook on safe reopening of schools, the U.S. Department of Education stated that school leaders should design a variety of meal distribution schedules and feeding models, such as in-person and grab-and-go, to ensure equity among recipients.[317]
Nearly all of the district nutrition and hunger advocacy officials we interviewed described challenges that affected meal service under a hybrid model. For example, one district nutrition official reported that the district could use vans to deliver food when learning was fully remote in spring 2020 but had to stop food delivery when the school changed to hybrid learning, because the vans were needed for more traditional uses. In another district, a nutrition official said that variability in school learning models and student attendance made it difficult to plan meal service and estimate the number of students needing in-person versus grab-and-go meals. In addition, the official reported that the hybrid model required additional resources for serving meals in person while also packing and distributing boxes of meals for remote learners.
Enrollment and staffing. Almost all of the district nutrition and hunger advocacy officials also cited consequences of the pandemic that raised uncertainties for meal service in the coming year. Some district nutrition officials said that the changes in student enrollment, in some cases due to families changing districts or electing homeschooling, would make it difficult to anticipate the number of meals needed. Most district nutrition and hunger advocacy officials described ongoing staffing challenges as a result of the pandemic. For example, nutrition officials in three districts described concerns about staff retention and shortages. In addition, officials in two districts expressed concern that potential furloughs, being considered because of financial constraints, could exacerbate staffing shortages and make it difficult to fill these positions when normal operations resume. In its handbook, the Department of Education noted that schools that are reopening will need sufficient staff to maintain services for in-person, hybrid, and remote students. According to the National CACFP Sponsors Association, staffing may also be a challenge for childcare centers and day care homes that had to let staff go during the pandemic because of low enrollment.[318]
Waivers. Many officials from district offices and hunger advocacy organizations told us that the FNS waivers had been critical in enabling operators to serve meals throughout the pandemic and noted that it would be helpful if the waivers continued through school year 2021–22. In response to state and district requests for continued flexibilities, on April 20, 2021, FNS announced that it would extend through school year 2021–22 several key waivers to aid in social distancing, such as allowing meals to be served in noncongregate settings, enabling parent and guardian meal pickup, and providing flexibility in foods served and meal times. In addition, FNS issued a new waiver allowing schools to operate SSO when school is open during the regular school year.[319] FNS also issued a waiver allowing SSO operators to claim these meals at the higher SFSP reimbursement rate, with the intent of promoting nutritious meals while managing increases in pandemic-related costs. FNS officials noted that they are currently developing guidance related to these new waivers that will include instructions for submitting claims for reimbursements.
FNS did not extend the waiver allowing schools to operate SFSP when school is open during the regular school year. However, because they are allowed to operate SSO, schools may continue to provide free meals to all students in the upcoming school year without the administrative requirement of tracking and collecting payments from students. According to FNS officials, FNS made the decision not to extend the SFSP waivers in part because SFSP has lower nutritional standards than SSO, which emphasizes, among other things, fruits, vegetables, and whole grains.
Methodology
To conduct our work, we analyzed the most recent data available from FNS on meals served through four key child nutrition programs—NSLP, SBP, SFSP, and CACFP—and the Emergency Meals-to-You program. We also used data for school year 2019–20 (the most recent available) from the Department of Education’s CCD, matching and merging these data with the list of school districts participating in Emergency Meals-to-You, to identify school district characteristics, such as BIE status, from the CCD. To assess the reliability of these data, we reviewed existing information about the data and reporting processes, interviewed agency officials, and conducted electronic testing of the data. We determined that these data were sufficiently reliable for our purposes.
We also reviewed relevant federal laws and agency guidance and documents, and we interviewed officials from FNS’s national and regional offices. Additionally, in four states—Georgia, Maine, Texas, and Washington, which we selected in part on the basis of variation in geographic location and school operating policies at the time of selection—we interviewed state nutrition directors and officials from hunger advocacy organizations as well as district nutrition officials from three school districts in each state. Further, we interviewed officials from the School Nutrition Association and National CACFP Sponsors Association. The information presented from these interviews is not intended to be representative but instead to provide examples of meal providers’ experiences during the COVID-19 pandemic.
Agency Comments
We provided a draft of this enclosure to FNS and the Office of Management and Budget for review and comment. They did not provide comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor data on the number of meals served by the child nutrition programs FNS administers, FNS’s use of COVID-19 relief funds, and its efforts to provide flexibilities to states and school districts to support child nutrition. We plan to review FNS’s monitoring and oversight of child nutrition programs in our future work.
Related GAO Product
Summer Meals: Actions Needed to Improve Participation Estimates and Address Program Challenges. GAO-18-369. Washington, D.C.: May 31, 2018.
Contact Information: Kathryn A. Larin, (202) 512-7215 or larink@gao.gov
Employers have claimed about $17.6 billion of employer tax credits, as of May 2021; new information on the Small Business Administration’s Paycheck Protection Program loan forgiveness webpage, posted in response to a proposed recommendation, could help eligible borrowers make decisions to maximize their Employee Retention Credits.
Entities involved: Small Business Administration and Department of the Treasury, including the Internal Revenue Service
Background
The Families First Coronavirus Response Act (FFCRA) and the CARES Act provide tax credits to covered employers to mitigate the cost of paid sick and family leave for employees affected by COVID-19, as well as provide an Employee Retention Credit for all eligible employers, among other tax relief. The Consolidated Appropriations Act, 2021 (CAA, 2021), enacted in December 2020, and the American Rescue Plan Act of 2021 (ARPA), enacted in March 2021, amended and extended some aspects of these credits. The Internal Revenue Service’s (IRS) capacity to implement new initiatives, such as the relief laws’ tax credits, is an ongoing challenge cited in our 2021 High-Risk Report.
Tax credits for employers. The Joint Committee on Taxation (JCT) estimates that the COVID- related tax credit provisions in the four laws will result in about $246 billion in foregone revenue for the federal government for fiscal years 2021-2031.[320]
The paid leave credits and the Employee Retention Credit are both fully refundable payroll tax credits, meaning that they are credited first against certain payroll taxes (also referred to as employment taxes), and any excess over those payroll taxes is refunded to the employer. These payroll tax credits may be claimed on the employer’s employment tax return, typically Form 941, Employer’s Quarterly Federal Tax Return. To receive immediate relief, employers may reduce their semiweekly or monthly payroll tax deposits (or next day deposits, if applicable) by the amount of their anticipated credit.[321] If an anticipated credit amount remains after reducing deposits, employers may receive an advance payment by filing Form 7200, Advance Payment of Employer Credits Due to COVID-19.[322] Form 7200 must be submitted using electronic fax (e-fax). The tax credits include the following:
Leave credits.[323] Businesses and tax-exempt organizations with fewer than 500 employees and certain government entities are eligible for refundable tax credits for sick and family leave.[324] The tax credits under the FFCRA, as amended and extended by the CAA, 2021, for leave taken from April 1, 2020, through March 30, 2021, are equal to qualified leave wages paid to employees, plus the employer share of Medicare taxes paid with respect to qualified wages and allocable health plan expenses. The tax credits under the ARPA for leave taken from April 1, 2021, through September 30, 2021, are equal to qualified leave wages paid to employees, plus the employer share of Medicare tax and the employer share of Social Security tax paid with respect to the qualified leave wages, and allocable health plan expenses and certain collectively bargained contributions as shown below. In the table, we summarize the FFCRA and ARPA paid sick and family leave tax credits. Certain self-employed persons in similar circumstances are allowed equivalent credits.
Comparison of Tax Credits for Paid Leave under the Families First Coronavirus Response Act, as amended and extended by the Consolidated Appropriations Act, 2021 and the American Rescue Plan Act, 2021
Families First Coronavirus Response Act
American Rescue Plan Act of 2021
Periods of leave for which employers may claim credits
Apr. 1, 2020–Mar. 31, 2021
Apr. 1, 2021–Sept. 30, 2021
Eligible entities
Businesses and tax exempt organizations with fewer than 500 employees and self-employed individuals.
Expanded to include state and local governments, as well as 501(c)(1) tax-exempt federal government entities.
Employment tax against which the credit may be applied
Employer share of Social Security tax.
Changed to employer share of Medicare tax for periods of leave taken after March 31, 2021.
Qualifying paid leave definitions
Sick leave: Includes quarantine or isolation order (or caring for someone under these orders), seeking COVID-19 diagnosis, and childcare.
Family leave: Childcare when school or other care is unavailable due to COVID-19.
Sick leave: Expanded to include obtaining a COVID-19 vaccine or illness related to immunization, or waiting for COVID-19 test results.
Family leave: Expanded to include all qualifying reasons for paid sick leave.
Qualifying wages for the credits and credit maximums
Sick leave: Wages paid for up to 80 hours for a full-time employee and allocable health plan expenses and employer share of Medicare taxes. Credit maximum is dependent on the purpose for taking the sick leave.a
Family leave: After 10 days of other leave (unpaid, personal, etc.), employees receive leave that is at least two-thirds of their usual pay (max $200 per day and $10,000 total per employee) and allocable health plan expenses.
Sick leave: Credit also increased for certain collectively bargained contributions and the employer’s share of Social Security tax imposed on the wages.b A new 80-hour period for paid leave eligible for the credits for leave wages after March 31, 2021.
Family leave: Credit also increased for certain collectively bargained contributions and the employer’s share of Social Security tax imposed on the wages. The first 10 days of leave may qualify as paid family leave wages and the per-employee limit is increased to $12,000 and resets for periods of leave after March 31, 2021.
aQualified sick leave wages cannot exceed $511 per day ($5,110 total) for employees if they are taking leave because of a government quarantine or isolation order, self-quarantine, or seeking a COVID-19 diagnosis or related to vaccination when ARPA is in effect. Qualified sick leave wages cannot exceed $200 per day ($2,000 total) for employees if they are caring for someone in quarantine or isolation or caring for a child. bCertain collectively bargained contributions’ includes defined benefit pension plan contributions which are paid or incurred by an employer during the calendar quarter on behalf of its employees to a defined benefit plan which meets certain requirements, are made based on a pension contribution rate, and are required to be made pursuant to the terms of a collective bargaining agreement. The term also includes contributions which are paid or incurred by an employer on behalf of its employees with respect to the calendar quarter to a registered apprenticeship program, are made based on an apprenticeship program contribution rate, and are required to be made pursuant to the terms of a collective bargaining agreement.
Employee Retention Credit. Under the CARES Act as amended by the CAA, 2021 and ARPA, eligible employers of any size—including tax-exempt entities, certain governmental entities, and self-employed individuals with employees—can claim the refundable Employee Retention Credit.[325] The credit amount is based on qualified wages paid to employees, including certain health care expenses. Qualified leave wages for which leave credits are allowed are not included in qualified wages for which an employer may claim the Employee Retention Credit.[326] The table below describes statutory changes made to the Employee Retention Credit.
Selected Changes to the Employee Retention Credit in the American Rescue Plan Act, 2021 and Previous Legislation
CARES Act
Changes in the Consolidated Appropriations Act, 2021
Changes in the American Rescue Plan Act of 2021
Eligibility period for qualified wages paid
Mar. 13–Dec. 31, 2020
Extended Jan. 1–June 30, 2021
Extended through Dec. 31, 2021
Eligible entities
Any employer operating a trade or business or a tax-exempt organization, except governments and their agencies and instrumentalities
Expanded to include:
public colleges or universities,
government entities whose principal purpose is medical or hospital care, and
certain tax-exempt federal entities a
No change
Employment tax offset
Employer portion of Social Security tax
No change
Changed to employer portion of Medicare tax
Eligibility requirements
Employers must experience either:
full or partial suspension of operations due to governmental orders during any quarter or
significant decline in gross receipts, more than 50 percent for the same calendar quarter in 2019b
Amended to require that gross receipts decline to 80 percent of gross receipts for the same quarter in 2019; employers may elect to make the determination using the previous calendar quarterc
Amended to also allow “recovery startup businesses”, who otherwise would not meet eligibility criteria, to be eligible to claim the creditd
Percent of qualified wages eligible for credite
50 percent of qualified wages ($10,000 per employee for the year), including certain health care expenses
100 or fewer employees, all wages count toward qualified wages
Increased maximum to 70 percent ($10,000 per calendar quarter per employee) for wages paid between January 1 and June 30, 2021
500 or fewer employees, all wages count toward qualified wages
Maximums unchanged.
“Severely financially distressed employers” may treat all wages as qualified wages f
No change for small employer qualified wages
Credit maximums
Maximum credit of $5,000 per employee in 2020
Increased the maximum per employee to $7,000 per employee per quarter in 2021
Quarterly maximum unchanged, but extension of dates means $28,000 possible per employee in 2021
“Recovery startup businesses” may receive up to $50,000 per calendar quarter
Interaction with Paycheck Protection Program (PPP)
Generally, an employer receiving a PPP loan is not eligible for the employee retention credit (but see retroactive change for 2020).
PPP borrowers are eligible for the Employee Retention Credit retroactive to 2020. However, employers cannot use the same wages for the credit and to obtain forgiveness of the PPP loan.
aAn organization described in section 501(c)(1) of the Internal Revenue Code can claim the credit. bEmployers are no longer eligible in the first quarter after the one in which gross receipts are more than 80 percent of the same quarter in the previous calendar year. cBusinesses formed in 2020 may use the same quarter in 2020 to establish eligibility. dEmployers which began carrying on any trade or business after February 15, 2020, with average annual gross receipts in the prior three tax years that do not exceed $1 million and that do not experience a full or partial suspension of operations due to a governmental order or a decline in gross receipts. eSmall eligible employers may treat wages paid to employees for providing services and wages paid to employees for not providing services as qualified wages. Large eligible employers may treat only wages that are paid to employees who are not providing services as qualified wages. fSeverely financially distressed employers are those with gross receipts that are less than 10 percent of what they were in the same calendar quarter in 2019.
Consolidated Omnibus Budget Reconciliation Act (COBRA) Premium Assistance Credit. Under federal COBRA requirements and comparable state laws, certain employers must provide employees who experienced specific events with the option for continued health insurance coverage.[327] Under ARPA, eligible individuals are provided with a 100 percent premium subsidy of COBRA coverage for periods of coverage from April 1, 2021, through September 30, 2021.[328] Employers generally are required to cover the costs of the individual’s subsidized COBRA coverage, but can offset costs with a refundable tax credit in certain instances. In other circumstances, a multiemployer plan, or health insurance issuer should cover the subsidized cost and will claim the tax credit. In cases not addressed in the prior two sentences the insurer is eligible for the credit.
Deferred payroll tax payments for employer share of Social Security. The CARES Act granted all employers the option to defer deposits and payments of the employer share of Social Security tax that they would otherwise be required to make during the period beginning March 27 through December 31, 2020.[329] Self-employed individuals could defer half of their Social Security taxes imposed on net earnings from self-employment during the same period.[330] Deferred deposits and payments are to be reported on their employment tax returns, typically on Form 941.[331]
Deferred payroll tax payments for employee share of Social Security. On August 8, 2020, the President signed a presidential memorandum that, in part, directed the Secretary of the Treasury to exercise authority under section 7508A of the Internal Revenue Code.[332] In response, IRS issued Notice 2020-65, which allowed for deferral of the withholding, deposit, and payment of the employee share of certain employment taxes imposed on wages or compensation paid from September 1, 2020, through December 31, 2020, if an employee’s wages or compensation are below a certain amount in a pay period.[333] The presidential memorandum directed the Secretary of the Treasury to make this deferral available to an employer for employees whose earnings during any biweekly pay period generally are less than $4,000 on a pre-tax basis, or the equivalent amount with respect to other pay cycles. Under the CAA, 2021, and Notice 2021-11, payments may be collected until December 31, 2021.[334] Collection of the deferred tax results in a reduction in take-home pay as compared to what would have occurred without the deferral.
Overview of Key Issues
Status of tax credit claim processing. IRS continues to process a paper return backlog, which makes the data on tax credit claims and deferrals incomplete, particularly for small employers who tend to file on paper. Additional claims for the Employee Retention Credit, with regard to 2020 qualified wages, are also being processed as Paycheck Protection Program (PPP) borrowers who became newly eligible for the Employee Retention Credit file retroactively.[335] Most of these newly eligible employers use Form 941-X, Adjusted Employer's Quarterly Federal Tax Return or Claim for Refund, which can be filed only on paper.[336] Several payroll and tax professional industry representatives said refunds from Forms 941-X are delayed. IRS officials said it is taking longer to process returns because IRS facilities that process paper employment tax returns continue to operate at reduced capacity to accommodate social distancing. As of May 2021, IRS officials said they are opening mail in normal time frames but are still processing returns received in 2020. IRS reported about 2.5 million unprocessed Forms 941 as of June 9, 2021.[337]
IRS also continues to process Forms 7200 for tax credit advance refunds. As of May 13, 2021, according to IRS officials, IRS had issued $780.4 million in advance payments.[338] As of May 17, 2021, IRS was taking approximately 7 weeks to process the forms, according to IRS officials. They said they received a higher volume (compared with November and December 2020) of Forms 7200 from January to March 2021, possibly because of CAA, 2021. Six of 10 payroll and tax professional representatives we spoke with said the employers for whom they file employment tax returns were frustrated with the Form 7200 response, and in some cases were using Form 941 instead because the Forms 7200 were not resulting in timely payments. Of the approximately $17.6 billion in claims for the Employee Retention Credit and leave credits claimed, as of May 2021 we found a little over 1 percent were also filed as advance payments through a Form 7200 filing.[339]
IRS designated almost 60 percent (39,722 of 67,310 ) of Form 7200 claims it received as of May 17, 2021, as “rejected,” according to IRS officials. According to IRS officials, the most common reasons for rejecting a Form 7200 claim were that the filer provided an unauthorized signature or filed a Form 7200 after submitting a Form 941 for the quarter or after the due date of the Form 941 for the quarter. Additional rejections resulted from the newly eligible PPP borrowers who submitted Forms 7200 in January 2021 claiming the Employee Retention Credit, when they should have used a Form 941-X instead because those quarters were already closed. IRS said as of May 17, 2021, it had mailed 26,858 letters to employers whose Form 7200 claims were rejected. IRS also continues to process Forms 7200 for claims for advanced payments of employer credits for COVID -19.
IRS issued a “tax tip” in April 2020 outlining common errors on Form 7200 and another tip in May 2021 outlining additional steps that can help employers ensure their Form 7200 is accurate, which can prevent processing delays. IRS officials said they conduct monthly outreach calls with the payroll industry, and the Form 7200 instructions has additional tips. They said they are considering additional outreach.
Data on employer use of tax credits and deferrals. Some data on the use of these tax provisions are available, though data are incomplete due to backlogs and data availability issues on annual filings. At the time of our analysis in May 2021, IRS had processed employer tax return filings claiming about $7.4 billion in leave credits and about $10.2 billion in Employee Retention Credits (see table).[340] Of the approximately 17 million employment tax return filings received, less than 1 percent of employers filed to claim the Employee Retention Credit.[341]
Number and Amount of Leave Credits and Employee Retention Credits Claimed, as of May 2021
Provision
Number of employers claiming
Dollars claimed ($ billions)
Leave credits
766,819
7.4
Employee Retention Credit
146,492
10.2
Source: GAO analysis of Internal Revenue Service data. | GAO-21-551
Notes: The tax credit dollar figures we are reporting are as reported by taxpayers and are subject to taxpayer reporting error. These figures may differ from IRS’s reported figures because we are reporting what was filed without adjustments. The table includes quarterly returns from second through fourth quarter 2020, including electronically filed (e-file) returns and about 6.7 million paper filings. Paper return data are as of May 5, 2021 (main Form 941) and May 19, 2021 (Schedule R), and e-file data are as of May 26, 2021. The second quarter 2020 returns include amounts for the Employee Retention Credit from the end of the first quarter because legislation passed too late in the quarter to be reported then. Dollars claimed as credits include amounts also received as advance payments requested on Form 7200. We did not analyze credits for self-employed individuals, which are reported on their income tax return, and annual employment tax returns. The Internal Revenue Service also continues to process a paper return backlog, which makes the data in the table above incomplete, particularly for small employers.
We found a total of 424,354 employers deferred about $112 billion in Social Security taxes for the employer and employee share together.[342] All 10 of the payroll and tax preparer industry representatives we spoke with said the employer share deferral was the most widely used of the tax-related COVID-19 relief provisions for employee retention. For example, the deferral functioned like an interest free loan, according to one tax professional.
Employee Retention Credit and PPP loan forgiveness. Certain employers who applied for forgiveness of their PPP loans may have included information in the application that subsequently reduced their eligibility for the Employee Retention Credit. Specifically, IRS Notice 2021-20, issued on March 1, 2021, states that employers who include any qualified wages in the amount reported to the Small Business Administration (SBA) as payroll costs when applying for PPP loan forgiveness, unless the loan is not forgiven, are deemed to have elected to not take those qualified wages into account for purposes of the credit.[343] See example.
Example of Tax Implications from Payroll Cost Allocations for Paycheck Protection Program (PPP) Loan Forgiveness
An employer received a PPP loan of $200,000. That employer had $200,000 in payroll costs and $70,000 of other PPP-eligible costs. The $200,000 in payroll costs could also have qualified for the Employee Retention Credit.
Scenario A: The employer submitted a PPP loan forgiveness application and reported the $200,000 of qualified wages as payroll costs, but did not report the other eligible expenses (such as rent or utilities) of $70,000. The employer’s entire loan was forgiven. However because the full $200,000 of qualified wages were reported on the forgiveness application, per IRS Notice 2021-20, no portion of those wages may be treated as qualified wages for the Employee Retention Credit. The employer cannot reduce the deemed election by the amount of the other eligible expenses that it could have reported on its forgiveness application, according to the Notice.
Scenario B: The employer submitted a PPP loan forgiveness application and reported $70,000 of eligible non-payroll expenses and $130,000 of payroll costs. The employer’s entire loan was forgiven. The employer may use the remaining $70,000 in payroll costs not reported on the application as qualified wages for the Employee Retention Credit.
Source: GAO analysis of Internal Revenue Service guidance. | GAO-21-551
To qualify for full PPP loan forgiveness, borrowers must spend at least 60 percent of proceeds on wages and benefits (eligible payroll costs). The remainder may be other eligible non-payroll costs, such as rent and utilities.[344] According to our analysis of SBA data, 911,288 of the approximately 2 million PPP borrowers who applied for PPP loan forgiveness by March 1, 2021, reported more than 60 percent payroll costs on their application for PPP loan forgiveness.[345] Therefore, if they had other potentially eligible expenses that they could have reported, they may have missed opportunities to maximize the qualified wages available to claim the Employee Retention Credit. Borrowers could also make decisions about the covered period for their loan, which may affect availability of qualified wages for the Employee Retention Credit. We are continuing to analyze this situation and any possible options IRS might have for allowing additional credit eligibility, consistent with the law.
As of May 10, 2021, about 37 percent of the forgiveness applications for PPP loans made in 2020 could still be submitted. SBA accepted new loan applications until May 4, 2021, according to SBA officials, and community financial institutions could still enter loan guaranty applications into SBA’s loan portal through May 31, 2021. As of May 2021, neither the loan forgiveness application, its instructions, nor the loan forgiveness frequently asked questions on SBA’s website mentioned how borrowers’ allocations of loan proceeds affect the Employee Retention Credit.
In a draft of this report, we recommended to IRS and SBA that the agencies work together to disseminate information in the SBA loan forgiveness guidance on the tax implications of payroll cost allocations to the PPP loan forgiveness applicants. In response to our draft recommendations and prior to final issuance of this report, SBA worked with Treasury to develop language for its PPP loan forgiveness guidance web page noting the potential tax implications of loan forgiveness applications, and linking to IRS guidance on the Employee Retention Credit. The language was posted on June 11, 2021. This information could help employers—particularly those who do not work with tax professionals—make decisions that allow them to maximize the Employee Retention Credit.
Methodology
To conduct our work, we reviewed federal laws and agency documents; and interviewed officials at IRS and SBA, and representatives from two tax and payroll professional organizations. We selected the organizations because of their members’ prominent role in working with a large number of employers. We interviewed 10 members selected by these organizations. Because these members are from a nongeneralizable sample, we cannot make inferences about the populations of professionals. We also analyzed IRS employment tax data as of May 2021 and SBA data as of May 17, 2021. We determined that the data were sufficiently reliable for our purposes by comparing with other data sources, such as our previous work and other IRS data, and checking for outliers.
Agency Comments
We provided IRS, Treasury, the Office of Management and Budget, and SBA with a draft of this enclosure, which included two recommendations. IRS provided written comments that are summarized below and reproduced in Appendix VIII: Comments from the Internal Revenue Service. IRS, Treasury, and SBA provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not have any comments on this enclosure.
IRS disagreed with our recommendation to work with the SBA to disseminate information in SBA loan forgiveness guidance on the tax implications of payroll cost allocations to PPP loan forgiveness applicants. However, because SBA worked with Treasury and posted IRS guidance on its loan forgiveness website, we removed the recommendations and no further action is required.
GAO’s Ongoing Work
We will continue to monitor information on SBA and IRS guidance. We plan to conduct additional analysis of employment tax returns on the use of these provisions, and on how IRS is adapting to the administration of the credits.
GAO’s Prior Recommendations
The table below presents our recommendations on employer tax relief from prior bimonthly CARES Act reports.
Prior GAO Recommendations Related to Employer Tax Relief
Recommendation
Status
The Commissioner of Internal Revenue should leverage employee counts from Form 941, Employer’s Quarterly Federal Tax Return, and Form 943, Employer’s Annual Federal TaxReturn for Agricultural Employees, to identify potentially ineligible COVID-19 related sick and family leave credit claims, and address discrepancies the Internal Revenue Service deems significant.
Open. IRS agreed with our recommendation. IRS provided an updated compliance plan, as of May 18, 2021. The plan states that IRS is considering Forms 941 and 943 line 1 data in conjunction with W-2 (Wage and Tax Statement) information as well as other data to identify potentially ineligible COVID-19 related credit claims, and address discrepancies IRS deems significant. We will continue to monitor IRS’s plans for evidence that the employee counts will be leveraged.
The Commissioner of Internal Revenue should conduct outreach to employment tax return filers to educate and promote accurate reporting of employee counts on Form 941, Employer’s Quarterly Federal Tax Return, and Form 943, Employer’s Annual Federal Tax Returnfor Agricultural Employees.
Closed-implemented. In May 2021, IRS released a “tax tip” for employment tax return filers reminding them to ensure that line 1 of their return is accurate, and referring employers to the form instructions for details. This information could support compliance efforts, which can result in multiple benefits including—helping taxpayers understand their responsibilities for tax compliance, and a decrease in potentially ineligible credit claims.
The Department of Labor provided information to employers and employees about COVID-19-related paid leave provisions and has continued to enforce them, but gaps in its outreach and case management may limit its efforts to identify and resolve potential violations.
Entity involved: Wage and Hour Division, within the Department of Labor
Recommendations for Executive Action
The Administrator of the Department of Labor’s Wage and Hour Division should:
better monitor data across all statutes that the Wage and Hour Division enforces, to ensure the division’s case management is consistent with established policies for assigning and prioritizing cases;
ensure that the new data system under development includes mechanisms to prevent staff from assigning and prioritizing cases in a manner inconsistent with established policies;
expand the Essential Workers, Essential Protections initiative on pandemic-related worker protections to include information about filing a complaint related to paid leave provided under the Families First Coronavirus Response Act; and
engage in a comprehensive and timely effort to consult with employers, workers, and organizations that represent them, to identify and document lessons learned from the Wage and Hour Division’s administration and enforcement of COVID-19-related paid leave.
The Department of Labor’s Wage and Hour Division agreed with these recommendations.
Background
The Families First Coronavirus Response Act (FFCRA), as amended by the CARES Act, required employers covered under FFCRA—in this report, covered employers—to provide emergency paid sick leave and expanded family and medical leave to eligible employees affected by COVID-19.[346] FFCRA was enacted on March 18, 2020, and the Department of Labor (DOL) developed regulations for the paid leave provisions that went into effect on April 1, 2020, and expired on December 31, 2020.[347] Though the requirement for covered employers to provide paid leave has ended, employees can file a complaint against their employer up to 2 years after the date of an alleged violation or up to 3 years after an alleged willful violation. In addition, employers may continue to provide paid leave voluntarily and, if eligible, can claim paid leave tax credits through September 30, 2021, to offset the cost of employees’ paid leave.[348]
FFCRA paid leave provisions generally required covered employers to provide eligible employees (1) up to 80 hours of emergency paid sick leave, subject to daily and aggregate payment caps, and (2) up to 12 weeks of expanded family and medical leave, including 2 weeks of unpaid and 10 weeks of paid leave at no less than two-thirds of the eligible employee’s regular rate of pay, subject to daily and aggregate payment caps.[349] Covered employers included most public employers and private employers with fewer than 500 employees.[350] Small businesses—those with fewer than 50 employees—may have qualified for an exemption from providing leave to an employee who needed to care for a child because of closure or unavailability of the child’s school, place of care, or child care provider if the requested leave would have jeopardized the business’s viability.[351]
All employees of a covered employer were eligible to take emergency paid sick leave regardless of how long they had been employed, and all employees who had been employed by a covered employer for at least 30 calendar days were eligible to take expanded family and medical leave. However, employers were not required to apply these leave requirements to employees who were health care providers or emergency responders.[352]
The Department of Labor’s (DOL) Wage and Hour Division (WHD) administers and enforces FFCRA paid leave requirements for most employees. Covered employers generally face liability if they did not provide or improperly denied emergency paid sick leave or expanded family and medical leave or if they discharged, disciplined, or discriminated against any employee for taking either type of leave.[353] Employees who believe their covered employer violated FFCRA may call a toll-free number—1-866-4US-WAGE (1-866-487-9243)—for assistance or to file a complaint.
When an employee files an FFCRA paid leave complaint, WHD determines whether the complaint meets its criteria for investigation. If the complaint does not meet the criteria, WHD files the complaint with no compliance action. If the complaint meets the criteria for investigation, WHD registers the complaint as a case, determines the complaint’s priority level, and determines what type of compliance action to take. WHD generally has three priority levels for cases it investigates—tier I, tier II, and tier III. Tier I cases have the highest priority and tier III cases have the lowest priority.[354]
According to internal WHD guidance, all FFCRA cases are to be assigned a priority level of tier I or tier II. Tier I cases are those in which the worker alleges violations that present a danger to safety or health, including both the employees’ safety or health and that of the community at large, or that allege an imminent or recent termination. For example, such violations include situations in which an employee was denied leave even though the employee was subject to a COVID-19 isolation order or was experiencing COVID-19 symptoms. All other FFCRA complaints are to be assigned to tier II. WHD may drop a case after acceptance, even if it meets WHD’s criteria for investigation. For example, WHD may drop a case if an employer went out of business.[355]
WHD can initiate one of four types of compliance actions for FFCRA complaints accepted for investigation—conciliation, office audit, limited investigation, or full investigation. Conciliations use the fewest WHD resources, and full investigations use the most resources. The type of compliance action taken depends on factors such as the number of employees involved, the level of resources involved, or the level of fact finding required to investigate the complaint. In addition to initiating compliance actions in response to complaints, WHD may initiate compliance actions, known as agency-directed investigations, on its own initiative. According to WHD guidance, agency-directed investigations are needed for effective enforcement for vulnerable worker populations, including garment workers, agricultural workers, and workers with disabilities.
Overview of Key Issues
WHD used a variety of mechanisms to increase awareness and understanding of FFCRA paid leave provisions. WHD officials said one of the greatest challenges they faced in administering the paid leave provisions was making employers and employees aware of their responsibilities and rights under FFCRA. WHD officials said their outreach efforts targeted a large cross section of employers and workers, including those in certain vulnerable worker populations. Specifically, WHD reported conducting the following outreach efforts:
Created an FFCRA work group. WHD created an FFCRA work group to oversee FFCRA education and outreach.[356] According to WHD officials, the group’s primary objective was to provide field support to staff responsible for educating employers and employees affected by the COVID-19 pandemic. WHD officials said the work group helped make strategic decisions about outreach.
Conducted outreach efforts. WHD reported that it conducted 3,155 FFCRA outreach events targeting employers and employees from March 17, 2020, to December 31, 2020, when the paid leave requirements ended.[357] WHD officials said these events were facilitated predominantly by Community Outreach and Planning Specialist (CORPS) staff in their district offices.[358] The two most common types of outreach events were compliance consultations (37 percent of events)—meetings requested by an individual or employer to discuss methods of ensuring compliance—and meetings with stakeholder groups or organizations (15 percent). These events, along with webinars and telephone contacts, made up the vast majority of all outreach events (see table). WHD officials noted that these outreach events helped WHD target employees who may have been affected by COVID-19. For example, WHD officials said that WHD exhibits on FFCRA paid leave installed at COVID-19 testing sites reached employees who potentially needed paid leave to quarantine.
Type and Number of Families First Coronavirus Response Act Outreach Events, Mar. 17, 2020–Dec. 31, 2020
Event type
Number of events
Percentage of total events
Compliance consultation
1166
37
Stakeholder meeting
482
15
Webinar
412
13
Telephone contact/call
305
10
Presentation/seminar/speech
268
8
Exhibit booth
172
5
Committee/task force meetings
117
4
Other
233
7
Total
3,155
99a
Source: GAO analysis of Department of Labor data. | GAO-21-551
aPercentages do not sum to 100 because of rounding.
WHD officials said that, in general, CORPS staff determined which outreach events to conduct by targeting specific employer or employee organizations or by responding to requests for information. In addition, the officials said CORPS staff prioritized events expected to reach the largest number of employers and workers.[359] WHD officials said CORPS staff maintained a list of associations and organizations representing employers and workers in their districts, including state and local governments, and regularly sent these groups emails about FFCRA paid leave guidance and outreach events. WHD officials also stated that WHD staff at all levels continually looked for opportunities to collaborate with other federal agencies as well as with state and local governments to disseminate information on FFCRA paid leave, such as by partnering to provide joint presentations.
Conducted a national public awareness campaign. WHD’s national public awareness efforts, which were conducted by a third-party contractor, included disseminating information about FFCRA paid leave through billboards, radio and television public service announcements, and a digital media campaign.[360] WHD officials said the national campaign generally targeted a broad audience. The contractor reported that as a result of this campaign, information about FFCRA paid leave was displayed more than 300 million times. In addition, WHD officials said that after hearing about low use of FFCRA paid leave by agricultural workers, they increased the number of Spanish-language public service announcements in rural areas to target this population.
Disseminated information through other channels. WHD officials also shared information with employers and employees about the paid leave provisions when investigating complaints or responding to questions and by disseminating information on WHD’s website. WHD provides compliance assistance, which includes educating employers about their responsibilities under FFCRA while investigating them for potential violations of the law. WHD’s Operating Plan states that its education efforts play an important role in promoting compliance, because the vast majority of employers want to comply with the law but fail because they do not understand their legal obligations. WHD officials said employers were often willing to comply once WHD made them aware of the paid leave requirements. In addition, WHD provides information to employers and employees who call its toll-free number with questions.[361] WHD also created a COVID-19-related landing page on its website, providing, among other resources, links to its regulations; documents explaining employee rights, including workplace posters and fact sheets; a frequently asked questions page; and a tool to help users determine their eligibility for FFCRA paid leave.[362]
Employers and employees were not always aware of, or did not always understand, the FFCRA paid leave provisions. Representatives of employer and employee organizations we interviewed acknowledged that WHD moved quickly to develop regulations, guidance, and other resources, such as frequently asked questions, fact sheets, posters, and webinars. Several of these organizations’ representatives said that they found WHD’s resources helpful. However, representatives of these organizations also described challenges related to the following areas:
Educating employers about FFCRA paid leave. Like WHD officials, representatives of some employer organizations said it was challenging to ensure that employers were aware of or understood the paid leave provisions. While some representatives said employers may have received information from WHD, a representative of a small business organization with several hundred thousand members across a wide range of industries said that employers were unlikely to have learned about the provisions from the agency. In addition, a representative of a large employer organization representing restaurants across the nation said it seemed the onus was on the organization to educate employers. Representatives from each of the employer organizations we interviewed said they disseminated their own guidance on FFCRA paid leave. Moreover, several representatives noted that employers—particularly small businesses—who did not belong to a membership organization or did not have dedicated staff who knew about the requirements, such as human resources personnel, would likely have found it more difficult to learn about the paid leave requirements.
Educating employees about FFCRA paid leave. Several organizations’ representatives said employees generally learned about FFCRA paid leave from sources other than DOL, including membership organizations—such as unions, trade associations, or community organizations—or by word of mouth. In addition, some representatives of employee organizations said employers may not have effectively informed employees about FFCRA paid leave, in some cases because they may not have wanted to share the information with employees. Moreover, a few organizations’ representatives said they were unaware of public service announcements or other WHD efforts to reach employees directly.
Several organizations’ representatives said that low-wage workers—such as those in food services, restaurants, retail, and construction—are generally harder to reach because they may have less established relationships with their employers or may have limited English proficiency, among other reasons. More specifically, a representative from an organization representing farmworkers said many of these workers did not understand DOL’s guidance and announcements regarding FFCRA paid leave, both because of low levels of education and literacy and because some farmworkers speak indigenous languages rather than English or Spanish.[363]
Complexity of guidance. Several representatives of employer organizations said DOL had provided helpful information and guidance on FFCRA; however, a few of these representatives also said some of DOL’s guidance, such as fact sheets and frequently asked questions, was too long, technical, and challenging to understand. Several organizations’ representatives told us they had created simplified guidance that they said was easier to understand than DOL’s guidance. In addition, a few representatives of employer-related organizations said it would be difficult for a business without legal consultants to follow changes to, and appropriately apply, WHD’s regulations and guidance.
Applying guidance to real-world scenarios. Some employer organizations’ representatives said employers had questions about how to apply FFCRA paid leave provisions to specific scenarios not covered by DOL’s guidance. Examples of such questions included whether employees qualified for FFCRA paid leave when they were required to quarantine because of voluntary out of state travel or when someone in the employee’s household tested positive for COVID-19 but was asymptomatic.
Some organizations’ representatives said employers and employees obtained clarification about FFCRA paid leave requirements from various sources, such as associations to which they belonged or legal counsel, as well as from DOL. A few organizations’ representatives also stated that employers likely used their own judgment to determine what to do in certain situations. As a result, employers may have implemented the requirements unevenly.
Some representatives of both employer and employee organizations said more opportunities to interact with DOL would have been helpful—for example, to submit questions to DOL’s frequently asked questions page or to ask questions during DOL’s webinars. DOL officials said their webinars allowed time for questions, but a representative from one employer organization who attended the webinars expressed concern about the limited amount of time for questions.
Understanding FFCRA exemptions. Several representatives of employer and employee organizations said employers and employees faced obstacles to understanding the health care worker exemption. For example, several representatives of employer and employee organizations said some employers and employees did not understand whether employees such as security guards or administrative personnel employed in a health care setting were covered by the health care exemption and were therefore ineligible to take FFCRA paid leave.
Similarly, some organizations’ representatives said some employers and employees did not understand the small business exemption that applied to businesses with fewer than 50 employees. More specifically, representatives said some employers may have believed—or willfully acted as if—all small businesses with fewer than 50 employees were automatically exempt from providing FFCRA paid leave to any of their workers. In reality, businesses could claim the exemption only under certain circumstances described in DOL regulations.[364] Likewise, a few organizations’ representatives stated that some employees of small businesses either believed all small businesses were exempt from providing FFCRA leave or believed their employers would treat the exemption in this way. Representatives from one employer organization said they did not actively encourage small businesses to use the exemption, because they were worried employers would not understand it or know how to document their use of it.
WHD engaged in a complaint-driven enforcement strategy. WHD relied primarily on employee complaints to identify employers who may have violated requirements to provide FFCRA paid leave. According to WHD officials, when WHD enforces other statutes, such as the Fair Labor Standards Act of 1938 (FLSA), its enforcement is driven in equal parts by complaints and by agency-directed investigations targeting employers in certain industries or employers of vulnerable workers. WHD officials said they initiated a limited number of agency-directed FFCRA paid leave cases based on third-party referrals from federal or state agencies, newspaper articles, or other sources. The officials further said they did not use complaint data or external data sources to identify industries or employers for agency-directed investigations; instead, given short time frames, they focused on responding to, and resolving, the large volume of FFCRA paid leave complaints they received and on conducting outreach to educate employees and generate complaints.
However, many employees were likely unaware of their right to FFCRA paid leave, according to representatives of employee organizations. In addition, interviewees said fear of retaliation may have deterred some low-wage workers, such as those in agriculture or food service, from filing complaints against their employers, even if the employees knew about the enforcement process. As a result, some employees, including those in vulnerable worker populations, may not have received the benefits to which they were entitled.
WHD has concluded more than 80 percent of open FFCRA paid leave cases, primarily through conciliation. The most recent available data show that as of March 31, 2021, WHD had received 8,052 FFCRA paid leave complaints, of which 6,821 (85 percent) resulted in a case that received a compliance action.[365] WHD officials also reported initiating a limited number of agency-directed actions, for a total of 6,929 cases.[366] Of those, 5,500 cases (79 percent) had been concluded as of March 31, 2021 (see table).
Number and Percentage of Concluded Families First Coronavirus Response Act Paid Leave Cases, by Compliance Action, as of Mar. 31, 2021
Compliance action
Total number of registered cases
Number of cases concluded
Percentage of cases concluded
Conciliation
5,525
4,538
82
Office audit
1,350
947
70
Limited investigation
28
14
50
Full investigation
26
1
4
Total
6,929
5,500
79
Source: GAO analysis of Department of Labor data. | GAO-21-551
Note: The data shown are the most recently available.
WHD concluded the vast majority of cases through conciliation.[367] As we reported in our November 2020 CARES Act report, WHD officials said that conciliation is usually the most appropriate action for FFCRA paid leave complaints because most complaints are straightforward and involve one or a few employees. WHD officials further said they have emphasized conciliation because this type of compliance action provides WHD the best way to quickly resolve an employee’s complaint, such as by securing back pay or leave for the employee.[368]
WHD’s data track 11 FFCRA paid leave violations that employers may have committed, on the basis of requirements laid out in the statute. The complaint data show that the most common employer violations among concluded cases were (1) failing to provide up to 2 weeks of paid sick leave—that is, the employer did not pay employees for leave that was granted (50 percent); (2) denying leave (34 percent); and (3) failing to keep accurate records (16 percent).[369]
WHD staff did not correctly prioritize some FFCRA cases. Although WHD guidance calls for FFCRA cases to be assigned to a priority level of tier I or tier II when accepted for investigation, WHD staff did not always follow this guidance. As a result, some concluded cases that should have been assigned to a priority level were not assigned or were incorrectly assigned to tier III (see table).
Number and Percentage of Concluded Families First Coronavirus Response Act Paid Leave Cases, by Priority Level, as of Mar. 31, 2021
Priority level
Number of concluded cases
Percentage of concluded cases
Not assigned
977
18
Tier I
1,313
24
Tier II
3,087
56
Tier III
123
2
Total
5500
100
Source: GAO analysis of Department of Labor data. | GAO-21-551
Notes: The data shown are the most recently available. Tier I denotes highest priority, and tier III denotes lowest priority. According to Department of Labor guidance, all Families First Coronavirus Response Act cases are supposed to be assigned a priority level of tier I or tier II.
In response to our questions, WHD officials said the 977 concluded cases not assigned to a priority level were “registered to self”—meaning they were self-assigned for investigation to the person who conducted intake. WHD officials said self-assigned cases are not assigned to a priority level because they are investigated immediately. According to WHD guidance, only conciliations—compliance actions that do not involve fact finding and are used to correct minor violations affecting only one or a few employees—can be self-assigned, allowing these cases to be registered and assigned quickly.
According to WHD officials, of the 977 cases not assigned to a priority level, 933 were concluded through conciliation. The remaining 44 cases were concluded through office audits and limited investigations, which, under WHD guidance, should not have been self-assigned and should have been assigned to tier I or tier II. In addition, WHD officials said 123 cases were incorrectly assigned to tier III. Of those, 96 were concluded through conciliation and did not require assignment to a priority level, per WHD’s guidance. The remaining 27 were concluded through office audits and should have been assigned to a priority level of tier I or tier II, according to the guidance.
We found that WHD officials did not monitor data or design its data system to ensure cases were correctly prioritized. WHD officials said they monitor data on the time taken to process FFCRA cases. However, their monitoring did not identify that some office audits or limited investigations either were not assigned to a priority level as they should have been—because staff incorrectly assigned cases to themselves—or were assigned to an incorrect priority level. Standards for internal control in the federal government state that management should perform ongoing monitoring of the design and operating effectiveness of the internal control system as part of the normal course of operations. In addition, WHD did not include controls in its data system to prevent staff from incorrectly assigning cases to themselves or from assigning a case to an invalid tier. Standards for internal control in the federal government state that management should design the entity’s information system and related control activities to achieve objectives and respond to risks.
WHD officials said that all of the cases not assigned to a priority level or incorrectly assigned were ultimately investigated and concluded and that nearly all were isolated to three offices in one region. However, the officials said that as of May 12, 2021, they had not yet determined whether any ongoing cases had also been assigned incorrectly. In addition, although the number of affected FFCRA paid leave cases may be relatively small, WHD officials acknowledged that there may be cases under other statutes enforced by WHD that have not been assigned to a priority level because staff incorrectly assigned cases to themselves. In addition, cases under other statutes enforced by WHD may have been assigned to an incorrect priority level. WHD uses the same general process for prioritizing cases across all statutes it enforces. WHD had not looked into this issue further as of May 10, 2021.
By not regularly examining data on the assignment of cases to priority levels or including features in its data system to prevent errors in case assignment and prioritization, WHD may have failed to prioritize ongoing cases under FFCRA and under other statutes, and it may continue making such errors in future cases. Cases that were not assigned to a priority level or were assigned to the wrong priority level may have not been investigated or concluded as rapidly as other cases that were properly assigned. To address these concerns, WHD officials said they planned to remind staff about WHD’s policies for prioritizing cases and also planned to develop a report to monitor the assignment of cases to priority levels. In addition, WHD officials said its new case management system may include features to prevent future errors.
WHD cannot easily analyze data to show why certain cases are not investigated but plans to address this as it updates its data system. WHD lacks systematic data that it can easily aggregate to identify the reasons FFCRA complaints were filed with no compliance action and the reasons FFCRA cases were dropped.[370] In December 2020, we reported the same concern with respect to FLSA complaint data and recommended that WHD develop a method for systematically collecting this information to ensure complaints are handled consistently and resources are allocated appropriately. WHD agreed with our recommendation and said its new case management system will incorporate the ability to categorize, aggregate, and review data on the types of cases that are not investigated. WHD officials said changes to the enforcement database will apply to future cases filed under all statutes WHD enforces but will not apply retroactively.
WHD has taken limited steps to continue informing employees about their right to file FFCRA paid leave complaints. Although WHD has done some FFCRA outreach since the paid leave provisions expired, WHD’s new Essential Workers, Essential Protections (EWEP) initiative on pandemic-related worker protections does not include information on filing a complaint related to FFCRA paid leave, even though employees can continue to file complaints for up to 2 years from the date of an alleged violation or for up to 3 years from the date of an alleged willful violation.
WHD officials said the EWEP initiative includes presentations to stakeholders—including employers, employees, and organizations who work with or represent them—to share information on WHD’s role, specific worker protections, and general information on how to file a complaint. The specific worker protections included in EWEP are related to FMLA, FLSA, and protections for agricultural workers. WHD officials said they include information on tax credits available to employers who continue to voluntarily provide paid leave through September 30, 2021, but do not include additional information on FFCRA paid leave because the requirements expired in December. WHD officials said that as of April 2021, WHD had conducted 64 outreach events and planned to continue the initiative as long as the pandemic affects industries that employ essential workers.
According to WHD documents, WHD promotes compliance with the statutes it enforces by conducting education and outreach to ensure that employers are aware of their responsibilities and that employees understand and exercise their rights. Standards for internal control in the federal government state that management should externally communicate the necessary quality information to achieve the entity’s objectives. By not including information about how to file a complaint about FFCRA paid leave in the scope of its EWEP initiative, WHD may be missing an opportunity to reach employees who did not obtain paid leave to which they were entitled and who could still file a complaint and receive benefits.
WHD does not have specific plans to engage with stakeholders to generate lessons learned on the administration and enforcement of FFCRA paid leave. WHD officials said they have not actively sought information from stakeholders about their experiences with FFCRA paid leave, though they said some stakeholders have shared this information in the course of WHD’s outreach under the EWEP initiative. As a result, the information WHD is obtaining about stakeholder experiences with FFCRA paid leave will not be comprehensive.
We previously reported that organizations that identify and apply lessons learned can ensure they factor beneficial information into planning for future efforts and limit the recurrence of challenges that can be anticipated in advance. By not engaging with employers, employees, and representative organizations specifically about their experiences with FFCRA paid leave in a comprehensive and timely manner, WHD may be missing an opportunity to improve its administration and enforcement—including its education and outreach—for future emergencies that might require a rapid response.
Methodology
To conduct this work, we reviewed federal laws, regulations, and agency documents; interviewed WHD officials; and reviewed WHD data on FFCRA paid leave outreach and enforcement efforts as of March 31, 2021. On the basis of interviews with WHD officials, we determined the data were sufficiently reliable for the purposes of this report. In addition, we interviewed representatives of 12 organizations that we characterized as either (1) employer organizations (i.e., membership organizations for employers and research entities knowledgeable about employer experiences) or (2) employee organizations (i.e., member organizations for employees, worker advocacy organizations, and research entities knowledgeable about employee experiences). For these interviews, we identified organizations that represented employers and employees in workforce sectors affected by the COVID-19 pandemic, such as agriculture and health care, or that had conducted research on FFCRA paid leave.
We determined that three internal control components identified in Standards for Internal Control in the Federal Government were significant to this audit: (1) the monitoring component and the underlying principle that management should perform ongoing monitoring of the design and operating effectiveness of the internal control system as part of the normal course of operations; (2) the control activities component and the underlying principle that management should design activities for the information system; and (3) the information and communication component and the underlying principle that management should communicate with, and obtain quality information from, external parties. We also reviewed our prior work on key practices of a lessons learned process. We assessed WHD’s efforts against these criteria.
Agency Comments
We provided WHD and the Office of Management and Budget with a draft of this enclosure. WHD provided written comments, reproduced in appendix IX, and technical comments, which we incorporated as appropriate. The Office of Management and Budget did not have comments on this enclosure.
In its comments, WHD agreed with our recommendations. More specifically:
WHD agreed with our recommendation to better monitor data on assigning and prioritizing cases across all statutes WHD enforces. WHD stated that it is in the process of developing a report that will identify the priority level for concluded cases and cases currently under investigation. WHD also plans to include this recommendation in its business requirements for its new case management system.
WHD agreed that its new case management system should include mechanisms to prevent staff from assigning and prioritizing cases in a manner inconsistent with established policies. WHD stated that it plans to include such mechanisms in its business requirements for the new case management system.
WHD agreed that it should expand the EWEP initiative to include information about filing a complaint related to paid leave provided under FFCRA. WHD stated that it is expanding the EWEP initiative into a second phase and will incorporate outreach emphasizing how workers can file a complaint related to their rights to take FFCRA paid leave in 2020.
WHD agreed that it should engage in a comprehensive and timely effort to consult with employers, workers, and organizations that represent them, to identify and document lessons learned from WHD’s administration and enforcement of COVID-19 related paid leave. WHD stated that, as part of the second phase of the EWEP initiative, it plans to conduct stakeholder listening sessions across the country that will include a component on lessons learned from FFCRA.
GAO’s Ongoing Work
We will continue to monitor WHD’s efforts to implement the recommendations we are making in this report.
Related GAO Products
Fair Labor Standards Act: Tracking Additional Complaint Data Could Improve DOL’s Enforcement. GAO-21-13. Washington, D.C.: December 9, 2020.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 2014.
Project Management: DOE and NNSA Should Improve Their Lessons-Learned Process for Capital Asset Projects.GAO-19-25. Washington, D.C.: December 21, 2018.
Contact information: Thomas Costa, (202) 512-7215, costat@gao.gov
The Department of Education did not effectively design and implement procedures for conducting quality assurance reviews of award amounts after they were obligated to help timely identify and correct erroneous obligations, which increased the risk that improper payments could occur.
Entity involved: The Office of Postsecondary Education, within the Department of Education
Recommendation for Executive Action
The Assistant Secretary for Postsecondary Education should design and implement procedures for regularly conducting quality assurance reviews of obligated amounts for higher education grants, including the Higher Education Emergency Relief Fund, to help identify and correct erroneous obligations in a timely manner.
The Department of Education agreed with this recommendation.
Background
Since March 2020, Congress appropriated approximately $76.2 billion in relief funding for the Higher Education Emergency Relief Fund (HEERF), which provides grants to institutions of higher education to prevent, prepare for, and respond to COVID-19.[371] In June 2020, we issued the first of a series of reports on key federal efforts to address the pandemic, which described the timeline of HEERF grants to schools. In April 2021, we issued a report on how schools distributed HEERF emergency financial aid grants to eligible students.
Education’s Office of Postsecondary Education (OPE) is responsible for administering HEERF. The CARES Act directed Education to allocate HEERF funding to eligible schools based on a funding formula.[372] In April 2020, Education notified schools of their individual allocations provided by the CARES Act to help inform their planning,[373] and provided the paperwork required to apply for HEERF grants, which included Certification and Agreement forms that described grantee responsibilities under the program. That same month, Education also began awarding HEERF grants to schools. As of May 31, 2021, 14 months following the enactment of the CARES Act, OPE had obligated $66 billion in HEERF funding provided by the COVID-19 relief laws—33 times the average of $2 billion in grants OPE normally administers annually.[374]
To administer HEERF grants, OPE relied primarily on existing staffing levels and already established grant-management policies and procedures. Although OPE had policies and procedures in place, Education faced inherent challenges—an unusually large volume of funding, and the urgency to process and distribute the funding expeditiously due to the health and economic threats posed by the COVID-19 pandemic—that increase the risk of improper payments.
Overview of Key Issues
Education procedures for approving and processing HEERF grants. Education relied on existing grant policies and procedures, including those documented in its Guide for Managing Formula Grant Programs (the Guide), for awarding HEERF grants, and modified these procedures as necessary given the emergency nature of the funding. The Guide establishes the structure and oversight responsibility over grant funding. OPE developed the process for awarding HEERF grants and provides HEERF-specific guidance, technical assistance, and other communications to grantees, such as responses to frequently asked questions, which OPE posts on its website. As part of administering HEERF, OPE is responsible for designing, implementing, and ensuring the operating effectiveness of procedures so that the funds awarded to grantees are valid and accurate.
The figure below depicts Education’s procedures for approving and processing HEERF grants.
Department of Education (Education) Procedures for Approving and Processing Higher Education Emergency Relief Fund (HEERF) Grants
OPE procedures state that only qualified staff have access to approve grant awards and record obligations in Education’s Grants Management System (G5).[375] Per the Guide, these authorized staff must possess the necessary qualifications, skills, and knowledge, and meet applicable training requirements, to obtain a system license for G5 access. OPE procedures call for staff to verify that the grant applicant adhered to the application requirements and to verify the accuracy of grant amounts prior to awarding the grants and recording obligations. The Guide requires OPE staff to verify that the applicant’s authorized representative signs and dates the applicable Certification and Agreement form(s).[376] This form is a required component of the application package for funding and is the grant recipient’s affirmation of the terms, conditions, and requirements that govern the use of grant award funds.[377]
The Guide requires that OPE staff review the accuracy of award information on the Grant Award Notifications, such as funding period and formula-allocation information, prior to awarding the grant and recording the obligation.[378] The grantee initiates a payment request in G5 to obtain grant funds. The amount the grantee requests cannot exceed the available funds (i.e., obligated amount less any payments already provided) under the grantee’s G5 account. In addition, to help prevent unauthorized access to grant award funds, OPE staff initiate a verification through G5 when reviewing grant applications to validate that: (1) the grant recipient is an active registrant in the System for Award Management and (2) the applicant has an active Data Universal Number System (DUNS) number.[379] If the grantee does not have an active DUNS number, OPE staff manually restrict the grantee’s access to grant funds within G5 until the grantee successfully renews its DUNS number.
We tested Education’s procedures for approving and processing HEERF grants through a sample of obligations and identified exceptions during our testing, described below.
Education changed its process to no longer require that OPE staff verify authorized representative signatures on Certification and Agreement forms for HEERF. Education’s procedures in the Guide require OPE staff to verify that the applicant’s authorized representative signs and dates the required Certification and Agreement form. However, we estimate that 17.8 percent (about 848) of all schools that were awarded HEERF grants as part of the CARES Act have a Certification and Agreement form that cannot be confirmed as signed by an authorized representative from the school.[380] OPE staff told us that in order to expedite the processing of these HEERF grants, Education officials changed the department’s process to allow staff to award them regardless of the type of signature on the Certification and Agreement form submitted. OPE officials told us that applicants submitted HEERF applications, which include the Certification and Agreement form, through Grants.gov.[381] They also stated that schools designate their point of contact or authorized official what their specific roles are in Grants.gov. As such, they accepted all forms submitted through Grants.gov as appropriately authorized by the school because OPE considers applicants registering in Grants.gov as a control measure. In addition, OPE officials stated that only school-designated individuals that are also registered in G5 would have access to obtain grant funds within G5.
The Certification and Agreement forms for HEERF funding provided by the CARES Act included only a signature line and did not require the “authorized representative’s title” or “typed name,” both of which would help OPE verify that the form was signed by an authorized representative. During the course of our testing, OPE updated the Certification and Agreement forms for additional HEERF funding provided by the Consolidated Appropriations Act, 2021 and the American Rescue Plan Act of 2021 to also include a line for the “authorized representative’s title” and “typed name.” OPE officials told us that they added the authorized representative name and title lines to clarify what information they are requesting from the applicant and to verify the identity of the grant applicant.[382]
Standards for internal control in the federal government state that management should identify, analyze, and respond to change. In implementing control activities, management reviews controls for continued relevance and effectiveness in achieving the entity’s objectives and addressing related risks. Education changed its process of verifying an applicant’s authorized representative’s signature given its more immediate objective to process HEERF grants expeditiously. We believe that this change for HEERF was reasonable because of the existing control in G5 that would prevent unauthorized access to grant funds and Education’s subsequent action to revise the Certification and Agreement forms for additional HEERF funding.
Education did not effectively design and implement procedures needed to identify erroneous obligations. We estimate that for 5.5 percent (about 262) of all schools receiving HEERF grants, Education awarded grants in excess of the amount allocated to the school.[383] Within our sample of obligations, we identified three instances, totaling $20 million overobligated. Two of these awards were duplicates and the third award was greater than what was allocated to the school. OPE officials stated that all these instances were due to human error. They also stated that during the initial implementation of HEERF, a team within OPE separately checked all grant awards to mitigate the risk of duplicate obligations and to confirm the accuracy of the obligation. However, this post-obligation quality assurance review was not part of OPE’s policies and procedures and, as the number of grants increased, OPE no longer conducted it on a regular basis. OPE procedures only called for staff approving awards to review the amounts as part of the award-preparation process (pre-obligation).
OPE officials stated that due to time constraints and having the same staffing level to administer a significantly higher volume of grants, OPE did not regularly perform post-obligation reviews to identify and correct erroneous obligations, such as additional quality assurance reviews of HEERF grants. Instead, OPE conducted post-obligation reviews as time permitted and as it deemed appropriate. OPE officials told us that in some instances, schools have identified and self-reported discrepancies in their awards. OPE then verified those errors and processed supplemental Grant Award Notifications to correct them. Subsequent to our inquiry, we verified that OPE processed supplemental Grant Award Notifications to correct the three errors we identified in our testing.
Standards for internal control in the federal government require that management design control activities to achieve objectives and respond to risks. This includes control activities to help ensure that agencies accurately record transactions. In some instances, OPE relied on schools that self-reported to identify errors in award amounts. Absent its own review procedures to identify erroneous obligation amounts such as post-obligation quality assurance reviews, given the significant increase in volume of awards processed, this increased the risk that improper payments could occur.
Methodology
To conduct this work, we interviewed Education officials and reviewed Education’s policies and procedures related to HEERF grant awards (e.g., Education’s Formula Grant Guide, other HEERF-specific guidance, and related Frequently Asked Questions). We evaluated Education’s responses, policies and procedures, and related internal controls, against standards for internal control in the federal government.
We conducted detailed transaction testing of a generalizable random sample of HEERF obligations recorded in G5 representing awards to 4,764 schools (identified by an OPE Identification Number) totaling $13.5 billion from enactment of the CARES Act, March 27, 2020, through September 30, 2020. We selected a stratified random sample of 178 grant recipients representing 514 grant awards. The strata were based on percentiles of the distribution of total obligated dollars in the sampling frame of $13.5 billion, the largest 10 grants by dollar selected with certainty. We used a confidence level of 95 percent and a tolerable error of $89.9 million. For each award in our sample, we reviewed underlying grant documentation to determine whether Education approved and obligated these awards (1) in accordance with established procedures and HEERF-specific guidance and (2) for the correct amounts. We determined the data we used were sufficiently reliable for the purposes of our reporting objective.
We followed a probability procedure based on random selections; as such, our sample is only one of a large number of samples that we might have drawn. Since each sample could have provided different estimates, we expressed our confidence in the precision of our particular sample’s results as a 95 percent confidence interval. While we designed the sample for a 95 percent margin of error for an estimate of total dollars that is within the designed tolerable error of $89.9 million, the estimate for total dollars in error may not follow the same distribution as total dollars. Therefore, we reported our results above with larger margins of error as unweighted actual total dollars in error in the sample, rather than projecting the dollars in error to derive an estimate of erroneous obligations for the sample population.
Agency Comments
We provided Education and the Office of Management and Budget (OMB) with a draft of this enclosure. Education provided written comments, which are reproduced in appendix V. In its comments, Education agreed with our recommendation and with the importance of conducting quality controls throughout the pre- and post-award processing of grant awards to schools. Education stated that it has already established, and will continue to enhance, procedures for quality control of grant obligations. This includes staffing and training program specialists who will have responsibility for quality controls for pre- and post-obligation, as well as for monitoring HEERF grants. Education also stated that it is committed to promptly addressing any error and making corrections to ensure accuracy of obligations. We will continue to monitor Education’s efforts to help reduce the risk of improper payments in this area. Education also provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
As the Department of Education works to provide COVID-19 relief funding to institutions of higher education, it will continue to be important for Education officials to properly award and disburse these funds, and that recipients properly use them.
We plan to monitor the status of our recommendation in future reports and continue our oversight of government-wide payment integrity efforts.
Related GAO Products
COVID-19: Emergency Financial Aid to Students under the CARES Act. GAO-21-312R. Washington, D.C.: April 20, 2021.
COVID-19: Opportunities to Improve Federal Response and Recovery Efforts. GAO-20-625. Washington, D.C.: June 25, 2020
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
Available data indicate the Internal Revenue Service has disbursed approximately $15.8 billion in refunds for net operating loss and alternative minimum tax since the enactment of the CARES Act, but the extent of delays in processing these refunds is not transparent to taxpayers.
Entities involved: Internal Revenue Service, within the Department of the Treasury
Recommendation for Executive Action
The Commissioner of Internal Revenue should clearly communicate on the Internal Revenue Service’s website that there are delays beyond the statutory 90-day timeline in processing net operating loss and alternative minimum tax tentative refunds. IRS neither agreed nor disagreed with this recommendation.
Background
To provide liquidity to businesses during the COVID-19 pandemic, the CARES Act and other COVID-19 relief laws included tax measures to help businesses—including sole proprietors, estates, and trusts—by reducing certain tax obligations, which, in some cases, led to cash refunds.[384] The Internal Revenue Service’s (IRS) capacity to implement new initiatives, such as the many COVID-19 related tax provisions, is an ongoing challenge we cited in our 2021 High Risk Report.
The CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021 modified, among other provisions of the tax law, provisions previously enacted or amended by Public Law 115-97 commonly known as the Tax Cuts and Jobs Act (TCJA).[385] The Joint Committee on Taxation (JCT) estimates the following tax provisions will result in about $211 billion in foregone revenue for the federal government in fiscal years 2020-2030. [386]
Net Operating Loss (NOL) carrybacks. An NOL occurs when a taxpayer's allowable deductions exceed its gross income for a tax year. During an NOL year, a taxpayer generally does not owe any income taxes and may be able to use the NOL to offset income in other tax years.[387] The CARES Act requires, unless waived, carrybacks for 5 years for NOLs arising in tax years beginning in 2018, 2019, and 2020, which may provide a cash refund for certain taxpayers.[388] Tax years prior to 2018 generally had a higher tax rate, so the ability of businesses to carryback post-2018 NOLs to earlier tax years tends to increase the relative value of the carryback amounts. For NOLs arising in tax years beginning after 2017, TCJA limited the deduction of NOL carrybacks and carryforwards to 80 percent of taxable income.[389] The CARES Act temporarily suspended the 80 percent limitation and those NOLs can reduce 100 percent of a taxpayer’s taxable income for tax years beginning before 2021.[390]
NOL carryback refunds are typically claimed on Form 1120-X, an Amended U.S. Corporation Income Tax Return; paper Form 1139, Corporate Application for Tentative Refund; or paper Form 1045, Application for Tentative Refund.[391] From April to December 31, 2020, IRS implemented temporary procedures to allow for e-fax of Forms 1139 and 1045 for a quick tentative refund during the period that IRS campuses were closed and mail was not being processed due to COVID-19.[392]
Acceleration of Alternative Minimum Tax (AMT) Credit refunds. TCJA repealed the corporate AMT, but most corporations could claim their remaining unused minimum tax credits as a refundable credit for tax years 2018 through 2021.[393] Under the CARES Act, corporations with AMT credits may claim a refund for tax years beginning in 2018 and 2019 and may either file Form 1139 or Form 1120-X to receive a refund for some or all of these credits.[394]
Increased limits on business interest. Taxpayers may generally deduct business interest expense in amounts not to exceed the sum of (1) the taxpayer’s business interest income for the tax year, (2) 30 percent of their adjusted taxable income for the tax year, and (3) their floor plan financing interest for the tax year.[395] The CARES Act modified the computation to allow for 50 percent of adjusted taxable income instead of 30 percent for tax years beginning in 2019 and 2020.[396] Taxpayers may still choose to use 30 percent of adjusted taxable income and not 50 percent to calculate and take their 2019 and 2020 business interest expense deduction, as it may affect other credits or deductions. Taxpayers may also elect to use 2019 adjusted taxable income in computing their 2020 business interest expense deduction.
Excess business losses. An excess business loss is the amount by which the total deductions from all of a noncorporate taxpayer’s trades or businesses exceed the sum of the total gross income and gains from those trades or businesses, plus $250,000 ($500,000 for a joint return).[397] Under TCJA, for noncorporate taxpayers, any excess business loss generated in tax years 2018 through 2025 is not allowed as a deduction in that year. Such an amount becomes an NOL, which may lead to NOL deductions in other tax years. The CARES Act temporarily removed this limitation for tax years 2018-2020.[398] Taxpayers that applied the TCJA limits to any excess business loss that arose during the 2018 or 2019 tax year, or during both tax years, can file amended returns to claim refunds. The American Rescue Plan Act of 2021, enacted March 2021, extends the TCJA’s limitation on excess business losses from 2026 to 2027.[399]
Overview of Key Issues
Use of excess business loss provision via amended returns. While complete data on the number of taxpayers taking advantage of the changes to excess business loss tax provisions will not be available until after tax year 2020 returns are processed, initial data are available on claims made so far on processed amended returns. As of April 29, 2021, IRS had received 311 amended returns with excess business loss refund claims. The majority of these claims were for refunds between $100,000 and $999,999. Of the business tax provisions we are monitoring, JCT had estimated that this would be the provision with the largest revenue effect, at $166 billion.
Update on the status of NOL and AMT credit refunds. Initial data are available on refund requests and payments of refunds related to NOL carrybacks and AMT credits (see table).[400] As of April 29, 2021, IRS had received a total of 75,848 NOL carryback and AMT credit refund requests since the start of the CARES Act on March 27, 2020, but we cannot determine if all of these NOL and AMT credit refund requests were specific to CARES Act changes. IRS approved roughly $18.6 billion and dispersed roughly $15.8 billion of NOL and AMT refunds as of April 29, 2021.
Net Operating Loss Carryback and Alternative Minimum Tax Credit Refund Requests Received as of April 29, 2021
Forma
Refund requests receivedb
Number of taxpayers filing
Applications for tentative refund
51,372
40,622
Amended return
24,476
20,457
Totals
75,848
61,079
Source: GAO analysis of Internal Revenue Service data. | GAO-21-551
Notes: “Refund requests” includes applications for tentative refund on Forms 1045 and 1139 as well as amended returns on forms 1040-X and 1120-X. Since these provisions were available prior to the CARES Act, we were unable to distinguish CARES-Act-specific filings for paper applications for tentative refunds and amended returns. aApplications for tentative refund include forms 1045 and 1139 and amended return data includes Forms 1040-X and 1120-X. bA single case may include multiple submissions. Submissions for the same identification number, form, and tax period generally are one case. Submissions for the same number and form, but for different tax periods, are separate cases.
The number of refund requests received via applications for tentative refund has increased by over 10,000 since we last received this data as of December 31, 2020. The general deadlines to file an application for tentative refund for tax year 2018 and 2019 were June 30, 2020, and December 31, 2020, respectively. The deadline for tax year 2020 is December 31, 2021. Since IRS closed the temporary e-fax line for these filings at the end of calendar year 2020, all applications for tentative refund must now be sent by mail.
Transparency around timeliness of issuing tentative refunds. As discussed above, amendments to NOL and AMT tax provisions under the CARES Act can potentially help increase business liquidity during the COVID-19 pandemic. The Internal Revenue Code and the CARES Act generally require IRS to issue certain refunds within a period of 90 days from the date on which a complete application for a tentative carryback adjustment is filed, or from the last day of the month in which the return is due, whichever is later.[401] Form 1139 and 1045 instructions refer to the statutory time frame and IRS’s temporary procedures to e-fax certain Forms 1139 and 1045 due to COVID-19 state that IRS is mindful of taxpayers’ need to get these refunds.[402]
After 45 days, the taxpayer is also owed interest.[403] According to IRS data, 23,236 approved refunds included interest payments totaling nearly $280 million from the enactment of the CARES Act through April 29, 2021. Based on our analysis, nearly 62 percent of approved NOL and AMT refunds included interest payments.
According to IRS data, IRS is not meeting the statutory 90-day refund requirement and the average processing time in 2021 was 154 days as of May 1, 2021. Agency records show that IRS has taken as long as 210 days to process some applications for tentative refunds. IRS officials said that number does not include the additional time it takes for IRS to finalize production and distribution of the refund to the taxpayer, which can take 2 weeks. This could potentially make the total refund processing time as long as 224 days. This would be more than 4 months later than the taxpayer would be expecting, based on the statutory requirement listed on the form instructions and temporary procedures webpage. An industry group has also said that the process to receive a refund is taking longer than expected and several tax professionals we spoke with said most of their clients have waited more than 90 days for their refund.
Based on our analysis of IRS records, the average processing time first consistently surpassed 90 days for Form 1045 in October 2020 and in January 2021 for Form 1139. Prior to that, IRS had been generally meeting the 90-day requirement for the last 3 years.[404] IRS officials said it is taking longer to process returns because IRS facilities that process paper returns continue to operate at reduced capacity to accommodate social distancing. This, combined with the December 31 due date for applications for tentative refund for tax year 2019 and the close of the e-fax line for filing these forms, could be contributing to the slowdown of issuing these tentative refunds.
Delays in processing refunds may continue until the backlog has reduced further. IRS reported being caught up on opening mail in December 2020; however, as of May 2021, IRS officials said they were still processing returns received in 2020.[405] IRS had about 11.7 million unprocessed returns as of May 11, 2021, and its processing backlog of tentative refund claims was roughly 15,000. We are continuing to review data on tentative refund application backlogs to determine the cause, what could have been done to mitigate the delays, and any actions IRS could take to address the issue going forward.
In the meantime, transparent communication on these issues and delays could help the IRS follow the Taxpayer Bill of Rights and help the taxpayer know when to expect their refund. According to IRS’s Taxpayer Bill of Rights, taxpayers are entitled to clear explanations of the laws and IRS procedures. An explanation on IRS’s website that IRS is processing tentative refunds beyond the expected 90 days due to service disruptions would provide taxpayers with more accurate information and expectations for receiving a refund.
In discussions with IRS on the refund delays, we indicated that based on our findings, we are considering a recommendation regarding communication of the issue to taxpayers. In response, on May 21, 2021, IRS added an update to irs.gov indicating that due to the lingering effects of COVID-19, IRS continues to experience inventory backlogs and longer than normal processing times for Forms 1139 and 1045. The update also states that IRS cannot provide a time frame for how long taxpayers will wait for a refund. IRS’s communication effort is an improvement. However, even without an exact time frame, IRS could provide taxpayers a clearer indication of the magnitude of delays.[406] For example, IRS could indicate that processing times may exceed 90 days given current circumstances.[407]
NOL and AMT approved refunds by industry sector. Analysis of IRS data from Form 1120-X and Form 1139 and North American Industry Classification System (NAICS) codes showed that among corporations, the manufacturing; professional, scientific, and technical services; and wholesale trade industries have claimed the highest number of NOL and AMT refunds so far, making up about 37 percent of all approved refunds to corporations (see table).[408] However, the “management of companies and enterprises” industry makes up about 48 percent of all refund dollars approved for corporations, with an average refund size of nearly $6.9 million.[409] Companies under this industry classification can span or overlap with other industry classifications. We will continue to examine refund claim activity across industry types.
Approved Corporate Refunds for Net Operating Loss (NOL) and Alternative Minimum Tax (AMT) Credit by Industry, Mar. 27, 2020–Apr. 29, 2021
Industrya
Average refund size ($ in thousands)b
Number of approved refunds
Percentage of all approved refunds
Amount approved ($ in thousands)
Percentage of total amount approved
Management of Companies and Enterprises
$ 6,872
1,162
5.56%
$ 7,985,785
48.24%
Mining, Quarrying, and Oil and Gas Extraction
$ 1,099
224
1.07%
$ 246,264
1.49%
Manufacturing
$ 837
2,769
13.26%
$ 2,317,482
14.00%
Information
$ 819
489
2.34%
$ 400,662
2.42%
Transportation and Warehousing
$ 669
668
3.20%
$ 446,641
2.70%
Retail Trade
$ 618
1,737
8.32%
$ 1,073,968
6.49%
Wholesale Trade
$ 558
2,159
10.34%
$ 1,204,231
7.27%
Finance and Insurance
$ 532
1,474
7.06%
$ 784,003
4.74%
Administrative and Support and Waste Management and Remediation Services
$ 363
461
2.21%
$ 167,502
1.01%
Accommodation and Food Services
$ 356
375
1.80%
$ 133,444
>1%
Real Estate and Rental and Leasing
$ 302
1,515
7.25%
$ 456,864
2.76%
Arts, Entertainment, and Recreation
$ 300
231
1.11%
$ 69,213
>1%
Utilities
$ 252
57
>1%
$ 14,374
>1%
Professional, Scientific, and Technical Services
$ 210
2,433
11.65%
$ 511,531
3.09%
Health Care and Social Assistance
$ 208
955
4.57%
$ 198,868
1.20%
Educational Services
$ 187
137
>1%
$ 25,574
>1%
Agriculture, Forestry, Fishing and Hunting (not covered in economic census)
$ 121
936
4.48%
$ 113,216
>1%
Construction
$ 114
2,055
9.84%
$ 234,626
1.42%
Other Servicesc
$ 65
586
2.81%
$ 37,894
>1%
Total
N/A
20,423
100%
$16,422,144
100%
Source: GAO analysis of Internal Revenue Service data. | GAO-21-551
Notes: This table includes data from Forms 1120-X and Forms 1139 only, which make up 55 percent of the total number of approved refunds (which is different from the table with applications received found earlier in the document). Forms 1045 and 1040-X are filed by sole proprietors, individuals, estates, and trusts that do not always have an associated NAICS code. We were not able to identify NAICS sectors in IRS data for a small number of Employer Identification Numbers, which made up roughly 2 percent of the corporate records. This does not materially affect our results. a Industry is classified by North American Industry Classification System (NAICS) codes b Companies may receive more than one refund. Average refund size is calculated by dividing the total approved refund dollar amount by the number of approved refunds per industry. c except Public Administration
Insights from public company reporting of provision use. The totality of tax filings reflecting the use of COVID-19 relief provisions will not be filed and processed for a few months. Therefore, to obtain additional preliminary insights on the extent corporations are using these provisions, specifically NOL, we examined a generalizable sample of 185 public company Securities and Exchange Commission (SEC) filings starting with the March 27, 2020, enactment of the CARES Act, through March 26, 2021.[410] Based on our review of annual and quarterly reports for sampled companies, we estimate that about 15 percent of companies said they have or will use the NOL CARES Act provision, and about 5 percent of companies mentioned NOL but were unsure of whether they will use the provision (see table).[411]
Estimated Reported Usage of CARES Act Net Operating Loss Provision Based on a Sample of 185 Public Company Filings, Mar. 27, 2020–Mar. 26, 2021
Estimated percentage of companies that said they did or will usea
Estimated percentage of companies unsure about usage or effectb
Estimated percentage of companies not using or no effectc
Unable to determined
15%
5%
61%
19%
Source: GAO analysis of Securities and Exchange Commission (SEC) data. | GAO-21-551
Note: All estimates in this table have a margin of error, at the 95 percent confidence level, of plus or minus 7 percentage points or fewer. This analysis is not representative of all companies that are eligible for the CARES Act net operating loss (NOL) provision and represents only publicly traded companies, which may have different characteristics than private companies. We reviewed report excerpts with keywords associated with NOL and “CARES Act” within 20-40 words. However, this does not automatically mean that the use of the provision was directly related to the CARES Act. aCompanies that included the specified provision in their SEC filing and said that they either already used it or planned to. bCompanies that mention the specified provision, but are still deciding or unsure if they will ultimately use it or were ambiguous in their mention of NOL. cCompanies that mention the specified provision, but explicitly say they will not use it and companies that did not mention the provision but had populated text related to some of our keywords. dCompanies that mention the specified provision, but that GAO analysts were unable to determine whether or not the company ultimately utilized CARES NOL or the company did not have any text from their filings related to our keywords.
Some companies noted that the provision helped their company, for example, receive a refund or other longer-term tax benefits. Others said that they were still deciding whether to use the NOL provision, due to potential ownership changes that place limitations on the use of net operating losses and other tax attributes.
Based on our analysis of the sampled companies, 37 reported that they did or will use NOL or were unsure if they will use. Of these, we found that businesses in the manufacturing industry mentioned NOL the most, followed by the finance and insurance industry and the information industry.[412] See below for the industry breakdown of companies that mention using or were unsure if they will use NOL.[413]
Sampled Public Company Filings Mentioning CARES Act Net Operating Loss by Industry, From Mar. 27, 2020–Mar. 26, 2021
Sector
Number of sampled companies that said they did or will use
Number of sampled companies unsure if they will use
Manufacturing
16
6
Finance and insurance
2
1
Information
2
1
Retail trade
1
1
Mining, quarrying, and oil and gas extraction
2
0
Utilities
1
0
Transportation & warehousing
1
0
Accommodation and food services
1
0
Professional, scientific, and technical services
1
0
Educational services
0
1
Total:
27
10
Source: GAO analysis of Securities and Exchange Commission data. | GAO-21-551
Note: Industry type was taken from the Standard Industrial Classification codes that appear in Securities and Exchange Commission filings, and translated into the North American Industry Classification System and indicate the company’s type of business.
Methodology
We reviewed IRS data as of April 29, 2021, federal laws, and agency guidance; and interviewed IRS officials and tax professionals. To analyze IRS data, we extracted the data from IRS databases on the use of these provisions from March 27, 2020, through April 29, 2021. We also aligned them with industry codes as reported by taxpayers, using their Employment Identification Number to show which industries took advantage of the tax provisions. Knowledgeable IRS officials confirmed the validity of our methodology. We determined that the data were sufficiently reliable for our purposes.
We selected a generalizable, random sample of 185 publicly traded companies from the Russell 3000 Index, which represents about 98 percent of U.S. incorporated equity securities and lists 3,328 unique companies with an SEC Central Index Key.[414] We computed sample sizes necessary to obtain a precision of at least plus or minus 7 percentage points, at the 95 percent confidence level, for a proportion estimate. We reviewed SEC public company reports filed from March 27, 2020, through March 26, 2021. In our analysis, we reviewed all filed Form 10-Ks and 10-Qs in that time span and ran computer code with a designated list of key terms, and pulled 20 words before and 40 words after the term. We then applied decision rules to manually analyze if the passages indicated whether businesses are using the provisions of the CARES Act. For example, if the SEC company filing provided a monetary value associated with federal NOL carrybacks or carryforwards after any CARES Act mention, we classified the company as using the NOL provision.
As noted above, the sample does not represent all companies that may use the CARES Act NOL provision and only represents publicly traded companies, which may have different characteristics than private companies.[415] Because we followed a probability procedure based on random selections, our sample is only one of a large number of samples that we might have drawn. Since each sample could have provided different estimates, we express our confidence in the precision of our particular sample’s results as a 95 percent confidence interval (e.g., the margin of error is +/- 7 percentage points). This is the interval that would contain the actual population value for 95 percent of the samples we could have drawn. This analysis is similar to the methodology used by authors of a University of Chicago study published in June 2020.[416]
Agency Comments
We provided IRS, Treasury, and the Office of Management and Budget, with a draft of this enclosure. IRS’s written comments are reproduced in appendix VIII , and IRS and Treasury provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not have any comments on this enclosure.
IRS neither agreed nor disagreed with our recommendation to clearly communicate on its website that there are delays beyond the statutory 90-day timeline in processing net operating loss and alternative minimum tax tentative refunds. However, IRS did say it would review messaging addressing tentative refund processing times and update it as necessary. We will monitor IRS actions to address this recommendation.
GAO’s Ongoing Work
We will continue to monitor the use of these COVID-19 related tax provisions and IRS’s efforts to ensure taxpayer compliance with them.
GAO’s Prior Recommendations
The table below presents our recommendation on tax relief for businesses from a prior bimonthly CARES Act report.
Prior GAO Recommendations Related to Tax Relief for Businesses
Recommendation
Status
The Commissioner of Internal Revenue should update the Form 1040-X instructions to include information on the electronic filing capability for tax year 2019 (November 2020 report)
Open. IRS agreed with our recommendation and said that it would start to update the Form 1040-X instructions to include information on the electronic filing (e-file) capability for tax year 2019.
As of early May 2021, IRS still planned to include this information in the next routine annual update of the instructions with an October 31, 2021, release, rather than updating them sooner, out of cycle. According to IRS, the normal revision process takes 10 months to complete properly, and would be difficult to complete in a shorter time frame. IRS’s planned revision will occur after the deadline for submitting an application for a tentative refund via the temporary electronic fax procedures, which for some taxpayers, may require an accompanying Form 1040-X. This means that taxpayers who filed their 1040-X before the December 31 deadline with the temporary procedures did not find the e-file capability in the form instructions. However, some taxpayers will use Form 1040-X for other CARES Act refunds after that deadline, so instructions that are updated in tax year 2021 will still help ensure these taxpayers are aware of this option. A timelier update to the instructions would help taxpayers filing the 1040-X between now and when the annual update to the instructions occurs in October 2021.
In the meantime, IRS previously posted information about the e-file availability on the Form 1040-X product page at IRS.gov, which is referenced in the first paragraph of the Form 1040-X instructions. IRS also added a development article dated February 18, 2021, to www.irs.gov/Form1040X to notify taxpayers that e-filing is available for amending 2019 and 2020 returns that were originally e-filed. We will continue to monitor any updates to the instructions.
By approving nearly $22 billion in loans to aviation and other eligible businesses out of the $46 billion in available funds, the Department of the Treasury provided critical assistance to large passenger air carriers, but smaller businesses did not see the same benefits.
Entity involved: Department of the Treasury
Background
The CARES Act authorized the Department of the Treasury (Treasury) to provide up to $46 billion in loans and loan guarantees to certain aviation businesses and other businesses deemed critical to maintaining national security (national security businesses).[417] This loan program was intended to provide liquidity to targeted sectors. Of the 267 applications submitted, Treasury executed 35 loans to businesses in these targeted sectors, totaling about $22 billion, as shown in the table below.[418]
Loans for the CARES Act Loan Program for Aviation and Other Eligible Businesses
Loan category
Number of applications
Number of loans executed
Assistance provided ($ millions)
Passenger and cargo air carrier
102
17
21,116
Repair station operator
41
5
19
Ticket agent
50
2
21
National security business
74
11
736
Total
267
35
21,891
Source: GAO analysis of Department of the Treasury data. | GAO-21-551
Note: Section 4003 of the CARES Act authorized maximum assistance available through loans in three categories: passenger air carrier, repair station operator, and ticket agent ($25 billion); cargo air carrier ($4 billion); and businesses critical to maintaining national security ($17 billion). CARES Act, Pub. L. No. 116-136, § 4003, 134 Stat. 281, 470 (2020). To match the Department of the Treasury’s reporting on these loans, and because air carriers that received loans could provide both passenger and cargo air services, we combined all air carriers into a single category.
The loan agreements executed by Treasury, as amended, ranged in size from nearly $295,000 to $7.5 billion.[419] Treasury prioritized applications from the largest passenger air carriers and executed loan agreements with seven of them totaling about $20.8 billion.
In December 2020, we reported that Treasury’s policies and procedures to evaluate loan applications were generally consistent with selected standards for internal control, although some practices, such as the quality of external communication with stakeholders, could be improved. Given that Treasury’s authority to make new loans ended on December 31, 2020, we did not make recommendations but identified lessons learned from this program—highlighted below. In March 2021, we further reported that loan applicants did not receive loans for reasons such as not responding to Treasury’s requests for financial data, entering bankruptcy, not meeting Treasury’s credit standards, and—for national security businesses—not meeting Treasury’s criteria for a business critical to maintaining national security. Given our prior work on the implementation of the loan program, we focus below on the initial effects of the loan program on applicants. This enclosure satisfies a provision in the CARES Act that directs us to submit annual reports regarding the loan program.[420]
Overview of Key Issues
Receiving a loan had generally positive effects on employment and operations for the businesses we interviewed. In comparing 16 loan applicants selected to cover the range of business types and sizes that applied, those businesses that received a Treasury loan generally reported positive effects on employment levels and operations, while those that did not receive loans reported negative effects.[421] Of the eight applicants we spoke to that received loans, several said the loan had a positive effect on their employment levels by allowing them to retain employees. Most loan recipients told us they used loan proceeds for payroll and other operational expenses. In contrast, all but one of the eight applicants we spoke to that did not receive loans attributed reductions in employment levels to the inability to receive a loan. Specifically, not receiving the loan funds coupled with reduced revenues meant these applicants had to pause planned hiring or lay off employees.
With regard to businesses’ ability to continue operating, those that received loans generally reported that receiving a loan had a positive effect, and those that did not reported a negative effect. For loan recipients, five said the loan positively affected their operations, in part by enabling them to lease new equipment, keep skilled staff, or take advantage of new contracts. For those that did not receive the loan, seven said the overall effect on operations was negative. The reason was, in part, that they were not able to retain staff or hire new staff and therefore were not able to move forward with planned business activities or not able to take on new contracts.
Treasury officials noted that to make these loans, the CARES Act directed Treasury to determine whether various conditions related to loan risk were met, including that employment levels be maintained and that the loans be prudently incurred and fully secured or made at a rate that reflects the risk of the loan, among other things. As such, officials told us that some businesses that were not in a strong financial position and had a need for financial assistance did not qualify for a loan.
Loan program provided liquidity—the intended goal—to large passenger air carriers that applied. As we reported in December 2020, large passenger carriers viewed the loan program application and review process as responsive and flexible enough to address their financial needs—during a period of unprecedented declines in passenger demand.[422] Representatives from four large passenger air carriers we interviewed—two that received loans and two that did not—told us the existence of the loan program created liquidity in financial markets. The two large passenger air carriers that received the Treasury loan reported it provided critical liquidity to maintain operations. Two large passenger air carriers that applied but did not receive Treasury loans were able to access loans through private financial markets. These air carriers’ representatives credited the Treasury loan program with increasing the confidence of lenders in private financial markets to make loans to air carriers.
According to Treasury officials, the purpose of this loan program was to provide liquidity to the targeted sectors, and they view the continued operations of major airlines as an indicator of the program’s success.
Loan program provided fewer benefits to smaller businesses that we interviewed. Of the 16 loan applicants we interviewed, many of the 12 smaller businesses said the program did not work or did not work as well as it could have.[423] For smaller businesses we interviewed across all application categories (national security and aviation), the application process was long and expensive. For example, several smaller businesses we spoke to said they needed to hire outside legal counsel to assist with their applications. While the six smaller businesses that received loans were positive about the effects on employment and operations, representatives of some of these same businesses raised concerns that the loan amount was too small and the loan terms were, in some cases, too restrictive to allow the businesses to adapt to the post-pandemic environment.
For the six smaller businesses that did not receive loans, representatives generally saw no benefits from applying to the program. Some of these businesses noted they spent significant time and money applying for the Treasury loan, in some cases at the expense of other financing options. Unlike the experience of large passenger air carriers, smaller businesses reported the loan program did not have a positive effect on their ability to receive alternative private financing, with most noting they were not able to find financing to take the place of the Treasury loan.
According to Treasury officials, the concerns highlighted by applicants from smaller businesses reflect the loan program structure and the conditions imposed by statute. For example, they said that in order for Treasury to ensure that loans were sufficiently secured or made at a rate that reflected the risk of the loan as required by the CARES Act, Treasury had to undertake extensive due diligence on each applicant to assess its financial position. Treasury officials said that these requirements and others were unavoidably complex—a situation typical with such transactions. In these situations, it is not unusual for applicants to loan programs, such as this one, to hire a lawyer to assist with the process.
All applicants we spoke to received assistance from other federal programs, including the Paycheck Protection Program, Economic Injury Disaster Loans, and the Payroll Support Program (PSP).[424] These programs offered financial assistance that, for many recipients, does not have to be repaid. However, for those that did not receive Treasury loans, other federal assistance was not generally viewed as a replacement for the Treasury loan program.
As Treasury rolls out new emergency financial assistance programs, it should continue to apply lessons learned from the loan program. Treasury continues to implement emergency financial assistance programs, such as the Coronavirus Economic Relief for Transportation Services (CERTS) and the third extension of PSP (for more information see the Payroll Support Assistance to Aviation Businesses enclosure in app. I).[425] According to Treasury officials, the agency is applying the lessons it has learned from administering the loan program and other financial assistance programs to these newer ones. However, our interviews with loan applicants underscore lessons learned that we reported on in December 2020. Specifically:
Clear communication. In December 2020, we reported concerns from industry associations representing businesses eligible for the loan program about Treasury’s communication with applicants on the status of their application and program timelines. Some loan program applicants we spoke with that did not receive loans were critical of Treasury’s ability to communicate clearly and consistently. Specifically, most of these applicants told us they were not satisfied with the explanations they received from Treasury regarding the status or outcome of their application. For example, two applicants said they thought their application was on track, only to find out within days of closing on the loan that Treasury had changed the loan terms. According to Treasury officials, loan closing dates for all applicants were scheduled at the beginning of the application review process, but approval was subject to the results of this review. In some cases, final decisions on an applicant’s creditworthiness were made close to the previously scheduled closing date.
Multiple paths within a program to better accommodate businesses of varied types and sizes. A wide range of businesses—from large passenger air carriers with tens of thousands of employees to ticket agents, repair station operators, and air carriers with only a handful of employees—were eligible for and applied to this program. According to several applicants we interviewed, the cost of applying, in terms of time, dollars, and missed opportunities, was more onerous for smaller businesses. According to Treasury officials, for smaller businesses a loan program with the terms and conditions as required by the CARES Act may have been less helpful than a program like the Paycheck Protection Program or the Payroll Support Programs, which provided funds that did not need to be repaid. As we reported in December 2020, it is difficult to implement a program quickly for a wide range of businesses, so multiple programs or multiple paths within a program may better accommodate businesses of varied types and sizes.
Leveraging resources from other agencies and external parties. According to some applicants we interviewed and as we previously reported from industry associations, they thought the program was designed for larger businesses, such as large passenger air carriers. For example, several applicants described multiple exchanges with Treasury to clarify the types of collateral available or why certain businesses could not undertake secured loans. Treasury officials said that agency staff, as well as the law firms and financial advisors employed by the agency to help administer this program, had significant experience in financial transactions. As we have reported, Treasury could have made greater use of expertise at the Department of Transportation (DOT) and other entities to design the program and help communicate with eligible businesses, based on the experiences of industry associations we interviewed. According to Treasury officials, the agency is leveraging expertise at DOT and from relevant industry associations as it sets up and rolls out the CERTS program.
Methodology
To conduct this work, we reviewed Treasury reports on the status of loan withdrawals and repayments as of June 1, 2021, and interviewed Treasury officials. We also interviewed 16 loan program applicants, selected based on whether they received a loan or not, the type of business (passenger air carrier, cargo air carrier, ticket agent, repair station operator, or business critical to maintaining national security), amount of loan request, and business size (as measured by number of employees). To enable comparison between those that received and did not receive loans, we selected eight loan recipients that reflected the mix of the factors above and eight applicants that were similar across those factors but did not receive a loan. In conducting these interviews, we used two sets of interview questions—one for those that received loans and one for those that applied but did not receive a loan. The information obtained from our interviews cannot be generalized to all loan program applicants.
Agency Comments
We provided the Department of Transportation (DOT), Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. Treasury provided technical comments, which we incorporated as appropriate. DOT and OMB did not provide comments on the enclosure.
GAO’s Ongoing Work
We continue to review Treasury’s plans to monitor borrowers’ compliance with the terms and conditions of loan agreements. We are also completing a review on the effect of the pandemic on the aviation sector and how those businesses have responded. Further, we will continue to monitor Treasury’s implementation of federal financial assistance programs for the transportation sector authorized by COVID-19 relief laws in December 2020 and March 2021.
Pursuant to Section 4026(f) of the CARES Act, we will provide copies of this enclosure to the following committees: in the House of Representatives, the Committee on Financial Services, the Committee on Transportation and Infrastructure, the Committee on Appropriations, and the Committee on the Budget; and in the Senate, the Committee on Banking, Housing, and Urban Affairs, the Committee on Commerce, Science, and Transportation, the Committee on Appropriations, and the Committee on the Budget.
Related GAO Product
Financial Assistance: Lessons Learned from CARES Act Loan Program for Aviation and Other Eligible Businesses.GAO-21-198. Washington, D.C.: December 10, 2020.
The last of the Federal Reserve’s lending facilities (both CARES Act and non-CARES Act) is scheduled to stop purchasing assets or extending credit on July 30, 2021. As of June 30, 2021, the CARES Act facilities had $30.1 billion in outstanding asset purchases and $36.9 billion in outstanding loans to the Federal Reserve Banks. The Federal Reserve’s oversight of the facilities is ongoing and focuses on previously identified risk areas.
Entities involved: Department of the Treasury, Federal Reserve System
Background
In response to the economic effects of COVID-19, and with the Secretary of the Treasury’s approval, the Board of Governors of the Federal Reserve System (Federal Reserve) established nine facilities supported by CARES Act funding.[426] These programs were established to provide liquidity to the financial system that supports lending to states, tribes, municipalities, eligible businesses, and nonprofit organizations.[427] All nine facilities stopped purchasing assets or extending credit by January 8, 2021. The Federal Reserve also established four facilities with the Treasury Secretary’s approval that did not receive CARES Act-appropriated funds.[428] These facilities were designed to provide liquidity to the financial sector and businesses. The last of these facilities is scheduled to stop extending credit by July 30, 2021.
Overview of Key Issues
As of June 30, 2021, the CARES Act facilities had $30.1 billion in outstanding assets and $36.9 billion in outstanding loans to the Federal Reserve Banks managing the facilities. The Paycheck Protection Program Liquidity Facility was the only non-CARES Act facility that was extended beyond March 31, 2021, to July 30, 2021. This facility conducted an additional $41.6 billion in transactions from April through May 2021.
CARES Act facilities. For the facilities that received CARES Act funds, outstanding assets—that is, assets (for example, corporate and municipal bonds) the facilities purchased and had not disposed of through sale or other means—peaked between November 2020 and January 2021.[429] These outstanding assets have since slightly declined. In June 2021, the Federal Reserve announced that it would begin the process of selling the assets in the Secondary Market Corporate Credit Facility. The Federal Reserve Bank of New York anticipates that it will complete the sale of the facility’s assets by the end of 2021. See the figure below for outstanding assets held by the facilities as of June 2021.
Outstanding Assets of Federal Reserve Lending Facilities Supported by CARES Act Funding, June 2020–June 2021
Note: Beginning on Feb. 24, 2021, the amount of the Main Street Lending Program’s outstanding assets is reported net of an allowance for loan losses, which is updated quarterly.
The Federal Reserve analyzes all of the CARES Act facilities on a quarterly basis to determine if it is necessary to set aside an allowance for potential loan losses in accordance with generally accepted accounting principles. As of March 31, 2021, the most recent financial statement available, only the Main Street Lending Program reflected a loan loss allowance, in the amount of $2.7 billion.[430] Of this amount, a specific allowance of $1.2 billion is for loans for which it has been determined to be probable that the program will be unable to collect all of the contractual interest and principal payments as scheduled in the loan agreement. The remaining $1.5 billion is a general allowance for all other outstanding loans under the program.
As of May 31, 2021, the Main Street facilities had reported about $4 million in actual losses.[431] These, and any future losses, are covered by the Department of the Treasury’s (Treasury) CARES Act funding invested in the Main Street facilities. In its most recent report to Congress in June 2021, the Federal Reserve said it continued to expect that none of the facilities will result in a loss to the Federal Reserve.
Non-CARES Act facilities. As of May 31, 2021, the four non-CARES Act facilities combined had conducted a little more than $377 billion in cumulative transactions—with the Paycheck Protection Program Liquidity Facility and the Primary Dealer Credit Facility accounting for about $182 billion and $132.7 billion, respectively (see figure below).[432] About 60 percent of the transaction volume for non-CARES Act facilities occurred before May 15, 2020. The Paycheck Protection Program Liquidity Facility was the only non-CARES Act facility extended beyond March 31, 2021, through July 30, 2021, and it conducted an additional $41.6 billion in transactions in April and May 2021.[433]
Cumulative Transaction Volume of Federal Reserve Lending Facilities Not Supported by CARES Act Funding, Apr. 2020–May 2021
Note: This figure illustrates the cumulative transaction volume for non-CARES Act facilities. To the extent that loans have been repaid, the outstanding balances will be lower.
As of October 14, 2020, the Commercial Paper Funding Facility had fully repaid all loans used to purchase commercial paper. As of May 9, 2021, the Primary Dealer Credit Facility and the Money Market Mutual Fund Liquidity Facility had also fully repaid all loans to Federal Reserve Banks. None of the three facilities resulted in a loss to the Federal Reserve. According to the Federal Reserve’s quarterly financial reports, as of March 31, 2021, the Paycheck Protection Program Liquidity Facility did not require an allowance for loan losses, and as of May 31, 2021, it had $84.2 billion in outstanding loans.
Oversight of facilities. The Federal Reserve’s Division of Reserve Bank Operations and Payment Systems’ general framework for oversight of all of the facilities consists of three phases. In the initial phase of oversight, the division established oversight approaches and procedures. In the second phase, the division’s reviews assessed the adequacy of the design of the facilities’ controls and processes in ensuring effective operations. The division completed its second-phase reviews for all facilities by December 2020, and found the design of controls and processes to be effective. According to Federal Reserve officials, the division commenced the third and final phase of oversight activities in December 2020, and as of May 2021, the division was still in this phase. For this final phase of review, the division is leveraging findings from second-phase reviews to identify risk areas for continued oversight, including collateral and asset management, conflicts of interest, risk management, and internal controls. According to phase three planning documents, the division will develop and periodically review detailed work plans for each risk area. The division also plans to complete interim reports summarizing the scope of oversight activities at 6-month intervals.
Methodology
To conduct this work, we reviewed Federal Reserve documentation on each facility, including term sheets, reports to Congress, and the most recent Federal Reserve data available on the facilities’ transactions and outstanding loans and assets, as of June 2021. We assessed the reliability of the transaction data and outstanding asset purchases by reviewing published data on the facilities and obtaining information from Federal Reserve officials on the collection, maintenance, and compilation of the data. We found these data to be reliable for our purposes. We also interviewed Federal Reserve and Treasury officials.
Agency Comments
We provided a copy of this enclosure to the Federal Reserve, Treasury, and the Office of Management and Budget (OMB) for review. The Federal Reserve provided technical comments, which we incorporated where appropriate. Treasury and OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
In our ongoing work on the Federal Reserve facilities, we will continue to monitor outstanding assets and loans, and the Federal Reserve’s oversight of the facilities. We also plan to analyze the characteristics of participants of select CARES Act-supported facilities.
In July 2011, we made two recommendations regarding facilities the Federal Reserve established in response to the 2007–2009 financial crisis. Because the Federal Reserve established similar facilities in response to the COVID-19 pandemic, these recommendations are relevant. The two recommendations are for the Federal Reserve to (1) strengthen procedures related to high-risk borrowers and (2) estimate and track losses within and across all facilities. We closed the first recommendation in December 2020 based on the Federal Reserve having established eligibility requirements and terms that applied to all participants, including high-risk borrowers. We closed the second recommendation in May 2021 based on the Federal Reserve conducting scenario-based analyses and documenting a policy for evaluating loan losses, among other things, and using this information to adjust facilities’ terms and inform other facility-related policy decisions.
Related GAO Products
Federal Reserve Lending Programs: Use of CARES Act-Supported Programs Has Been Limited and Flow of Credit Has Generally Improved. GAO-21-180. Washington, D.C.: December 10, 2020.
Federal Reserve System: Opportunities Exist to Strengthen Policies and Processes for Managing Emergency Assistance. GAO-11-696. Washington, D.C.: July 21, 2011.
Contact information: Michael E. Clements, (202) 512-8678, clementsm@gao.gov
The Department of the Treasury continues to provide payroll assistance to the aviation industry and has developed and implemented a risk-based approach to monitoring and overseeing recipients’ compliance with the terms of this assistance.
Entities involved: The Department of Transportation and the Department of the Treasury
Background
In September 2020, November 2020, and March 2021, we reported on the initial rollout of the Payroll Support Program (PSP1), which provided $32 billion that was appropriated by the CARES Act in March 2020, and the Payroll Support Program Extension (PSP2), which provided $16 billion that was appropriated by the Consolidated Appropriations Act, 2021 in December 2020.[434] In March 2021, the American Rescue Plan Act of 2021 extended the program again by appropriating $15 billion to the Department of the Treasury (Treasury) to provide additional financial support to passenger air carriers and contractors that received financial assistance under PSP2.[435] This additional support, known as PSP3, must be used exclusively for employee wages, salaries, and benefits.[436] As was the case with PSP1 and PSP2, Treasury requires passenger air carriers that receive PSP3 payments of more than $100 million and contractors receiving more than $37.5 million to provide warrants or notes as taxpayer protection through Payroll Support Program agreements.[437]
PSP3 recipients—passenger air carriers and contractors—must agree to refrain from conducting involuntary furloughs or terminations and reducing pay rates and benefits until September 30, 2021, or until their funds are exhausted, whichever is later. Other conditions for PSP3 recipients include requirements related to limits on executive compensation and restrictions on dividends or other capital distributions on the recipient’s common stock.
Although passenger demand for air travel seems to be rebounding and leisure travel seems to be leading to an increase in airline bookings, according to industry sources, passenger demand for air travel faces a slow, uneven recovery over the next 3 years or more. The pace of the recovery will depend on many factors, including the COVID-19 vaccination rate globally and the broader economic recovery.
Overview of Key Issues
Treasury has nearly completed making payments for PSP2. Treasury continues to make payments under PSP2, and, as of mid-June 2021, had made payments of about $15.6 billion out of $16 billion available. Treasury has received 520 total applications for PSP2.[438] More specifically:
Of these 520 applications, 317 applications were from passenger air carriers. The 10 largest payments for this category averaged about $1.4 billion. The average for the remaining passenger air carrier payments was about $3.2 million.
The other 203 applications were from aviation contractors. The 10 largest payments for this category averaged about $49.6 million. The average for the remaining contractor payments was about $2.2 million.
Due to the high demand for funds, Treasury prorated the amounts that passenger air carriers and contractors received through PSP2, as authorized by the statute. These prorated amounts represent the percentage of the total approved payment amount that a recipient receives. According to Treasury officials, the prorated amounts for PSP2 payments are 46.0 percent for passenger air carriers and 30.4 percent for aviation contractors.
Treasury has begun making PSP3 payments, and only PSP2 recipients are eligible for PSP3 funds, as directed by statute. PSP2 recipients are eligible for payments under PSP3, as long as they otherwise meet the statutory criteria.[439] Treasury released a guidance document on its website to provide recipients with information about PSP3. Treasury officials said that, at this time, they do not plan to release additional guidance or information about PSP3. Rather, Treasury is communicating directly with PSP2 recipients about PSP3 payments. Treasury sent notifications to all approved PSP2 recipients. According to Treasury officials, these notifications included PSP3 statutory requirements and required that recipients certify that (1) they provided passenger air transportation or performed eligible contractor functions as of March 31, 2021, and (2) they had not involuntarily terminated, furloughed, or reduced pay or benefits between March 31, 2021, and the date the recipient signs a PSP3 agreement.
The terms and conditions of PSP3 are similar to those of PSP2. However, unlike PSP2, PSP3 agreements do not have requirements related to recalling employees who were involuntarily terminated or furloughed. Treasury officials said that the PSP3 notification process was still ongoing because Treasury has not completed making payments of PSP2 funds. However, Treasury officials said they have not provided PSP3 information to PSP2 applicants who have not yet received their PSP2 payment, because these PSP2 applicants cannot qualify for PSP3 unless they receive payroll support under PSP2.
Treasury’s monitoring and oversight of PSP1 funds involve two levels of compliance testing. Treasury uses its monitoring and oversight approach for PSP1 to ensure that recipients are in compliance with the PSP1 agreement’s key terms.[440] Each quarter, recipients submit information to Treasury via a web portal, according to Treasury officials. If a recipient fails to submit a quarterly report, even after Treasury has followed up with the recipient, Treasury will move directly to remediation.
All recipients that have submitted a quarterly report undergo Level 1 testing, which is a set of automated testing rules Treasury has developed. A Level 1 test assesses recipients’ compliance with terms and agreements such as involuntary terminations and furloughs and restrictions on executive compensation. Treasury officials said that, as of May 2021, they were still evaluating the extent to which cash payments to airline executives payable after PSP requirements expire are in compliance with PSP agreement terms. Although Treasury relies primarily on the data from recipients’ quarterly reports for the first level of testing, Treasury may also use supplemental information, such as recall and rehire information that it requests recipients submit via a web portal.
The Level 2 test is a more detailed review conducted by a Treasury analyst, who can communicate with the recipient to obtain additional information. According to Treasury documents and officials, a recipient will be escalated to a Level 2 test if their Level 1 test contains discrepancies.[441] As of May 2021, recipients that have undergone a Level 2 test have been elevated to that level because there were discrepancies in their Level 1 test. According to Treasury officials, most of the issues that are elevated to Level 2 testing are resolved.
However, if a recipient does not clear Level 2 testing and Treasury determines that a recipient is not in compliance with the PSP agreement terms, there is a range of penalties. For example, under the terms and conditions of PSP agreements, Treasury can withhold additional payments or require repayment of previously disbursed payments. Treasury has levied penalties against 23 recipients out of all the recipients it has tested over three quarters, according to Treasury officials.[442] Most instances of noncompliance were due to involuntary terminations or failure to submit quarterly compliance monitoring reports, according to Treasury officials. The penalty amount that a recipient incurs varies based on the infraction. For example, according to Treasury officials, if a large number of employees were terminated or if some funds were used improperly, then Treasury may ask for all PSP funds to be returned, whereas if a recipient terminated one or two employees, then Treasury would request that the recipient return funds equal to the foregone compensation of those employees.
Treasury plans to use the same monitoring and oversight approach for PSP2 and PSP3, with some updates to monitor for specific requirements. Treasury officials said that Treasury will continue to test quarterly reports submitted by recipients through a web portal to monitor PSP2 and PSP3 recipient compliance with agreement terms. As we reported in March 2021, PSP2 required that recipients recall employees who were involuntarily terminated or furloughed between either October 1, 2020, (for recipients that received PSP1 assistance) or March 27, 2020, (for recipients that did not receive PSP1 assistance) and the date of the PSP2 agreement. Each PSP2 payment was allocated in two payments, and prior to making the second payment, Treasury requires recipients to certify that they complied with employee recall-related requirements. After the certification is received and processed, Treasury may make the second PSP2 payment. However, if a recipient is found to be noncompliant with the recall-related requirements or any other requirement, the second PSP2 payment will be delayed until the recipient has been cleared by Treasury. Treasury monitors recipient compliance with these requirements through additional web portals.[443] Treasury also reviews subsequent quarterly reports submitted by the recipient to ensure that all terms are met. Treasury has said that it can also offset PSP2 payment amounts with penalties incurred from a PSP1 monitoring violation.
For PSP3 monitoring and oversight, Treasury officials said that PSP3 recipients will have their payment delayed if they are found to be noncompliant with PSP2 Payroll Support Program agreements. Treasury can also offset PSP3 payment amounts with penalties incurred from a PSP1 or PSP2 monitoring violation.
Methodology
To conduct this work, we reviewed the CARES Act, Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021. We also reviewed agency guidance and documentation, and we interviewed Treasury officials to understand Treasury’s approach to implementing and providing monitoring and oversight of PSP1, PSP2, and PSP3. We also analyzed Treasury data about PSP2 and PSP3 as of June 16, 2021. We reviewed these data for missing information and outliers. We determined that the data were sufficiently reliable for the purposes of summarizing the number and value of PSP2 and PSP3 payments.
Agency Comments
We provided the Department of Transportation (DOT), Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT, Treasury, and OMB did not provide comments on the enclosure.
GAO’s Ongoing Work
As Treasury moves to complete making payments of PSP2 funds and continues making payments of PSP3 funds, we will continue to review Treasury’s implementation and oversight of these programs. We also will continue to monitor Treasury’s implementation of federal financial assistance programs for the transportation sector authorized by COVID-19 relief laws in December 2020 and March 2021.
GAO’s Prior Recommendations
Prior GAO Recommendation Related to Payroll Support Assistance for Aviation Businesses
Recommendation
Status
The Secretary of the Treasury should finish developing and implement a compliance monitoring plan that identifies and responds to risks in the Payroll Support Program (PSP) to ensure program integrity and address potential fraud, including the use of funds for purposes other than for the continuation of employee wages, salaries, and benefits (November 2020 report).
Closed. In April 2021, GAO confirmed that the Department of the Treasury (Treasury) had developed, documented, and implemented a risk-based approach to monitor PSP recipients’ compliance with the terms of the assistance. Treasury’s risk-based approach entails a two level compliance review. In the first level review, automated testing is conducted on all recipients’ quarterly reports using factors/thresholds that can trigger recipients being moved to the next review. In the second level review, Treasury analysts conduct a more detailed review of recipients that failed the first level review or were selected for other reasons. Treasury has also developed penalties and a process for remediating noncompliance with PSP agreement terms through Payroll Support Program agreements. As of April 2021, Treasury has identified noncompliance by recipients and applied penalties, as appropriate.
FEMA’s workforce has been stretched thin as it takes on additional responsibilities to establish mass vaccination sites and provide funeral assistance to families impacted by the COVID-19 pandemic while preparing for the upcoming hurricane season.
Entities involved: Federal Emergency Management Agency, within the Department of Homeland Security
Background
Federal Emergency Management Agency’s (FEMA) Disaster Relief Fund—the primary source of federal disaster assistance for state, local, tribal, and territorial governments—had never before been used during a nationwide public health emergency on the scale of the COVID-19 pandemic.[444] As of May 31, 2021, FEMA had obligated over $75 billion from the Disaster Relief Fund to respond to COVID-19. The Disaster Relief Fund’s balance was over $48 billion and FEMA projected that the balance would be approximately $12.3 billion on September 30, 2021.
FEMA’s Disaster Relief Fund Balance by Month, Feb. 2020–May 2021
FEMA has used the Disaster Relief Fund to respond to the COVID-19 pandemic by providing three primary types of disaster assistance.
Individual Assistance program. FEMA’s Individual Assistance program provides assistance to disaster survivors to cover necessary expenses and serious needs—such as housing assistance, counseling, or funeral assistance—which cannot be met through insurance or low-interest loans. For the COVID-19 response, FEMA has provided lost wages assistance, funeral assistance, and crisis counseling.
Public Assistance program. FEMA’s Public Assistance program provides assistance to state, local, tribal, and territorial governments, and certain types of private nonprofit organizations so that communities can quickly respond to and recover from major disasters or emergencies. For all 59 major disaster declarations for COVID-19, FEMA has authorized Public Assistance for emergency protective measures only. This may include eligible medical care, purchase and distribution of food, non-congregate medical sheltering, operation of Emergency Operations Centers, and the purchase and distribution of personal protective equipment.[445] On February 2, 2021, the President issued a memorandum that directed FEMA to fully reimburse states, territories, and tribes for all work eligible for emergency protective measures assistance.[446]
Mission assignments. FEMA also issues mission assignments—work orders directing other federal agencies to provide direct assistance to state, local, tribal, and territorial governments—to support disaster response and recovery. For the COVID-19 response, for example, FEMA issued a mission assignment to the Department of Defense to fund National Guard deployments to support state and territorial response efforts.
In recent years, we reported on long-standing workforce management, capacity, and training challenges within FEMA. For example, in May 2020, we reported that FEMA had established mechanisms to qualify and deploy staff to disasters. However, FEMA’s qualification and deployment processes did not provide reliable and complete staffing information to field officials to ensure its workforce was effectively deployed and used during the 2017 and 2018 disaster seasons. Further, FEMA’s disaster workforce experienced challenges with receiving staff development through the agency’s existing methods to enhance the skills and competencies needed during disaster deployments—challenges FEMA headquarters officials acknowledged.
Additionally, in 2018, we reported that FEMA’s available workforce was overwhelmed by the response needs of four sequential disasters. While FEMA has taken actions to address several of our workforce management-related recommendations since 2016 that covered topics such as staffing levels and staff development, a number of recommendations remain open. As FEMA continues to address these existing workforce challenges, it is now faced with responding to other missions, including the COVID-19 pandemic and unaccompanied minor children arriving at the Southwest border, which could further stretch its workforce.
Overview of Key Issues
FEMA’s use of the Disaster Relief Fund to support COVID-19 activities. FEMA currently uses the Disaster Relief Fund to provide funding for the three types of disaster assistance mentioned above—(1) Individual Assistance; (2) Public Assistance; and (3) mission assignments––as part of the agency’s COVID-19 response.[447] As of May 31, 2021, FEMA had obligated over $75 billion from the Disaster Relief Fund to respond to COVID-19. Specifically:
Individual Assistance. On August 8, 2020, President Trump issued a presidential memorandum that directed that up to $44 billion be made available from the Disaster Relief Fund to provide lost wages assistance to supplement unemployment insurance compensation.[448] According to FEMA officials, as of April 30, 2021, FEMA had obligated approximately $39 billion for the Lost Wages Assistance program. Further, in December 2020, the Consolidated Appropriations Act, 2021, appropriated $2 billion to the Disaster Relief Fund for eligible funeral expenses for individuals or households with COVID-19-related funeral expenses.[449] On April 12, 2021, FEMA began accepting and processing applications for Funeral Assistance via a dedicated call center number, as discussed further below.
Public Assistance. FEMA officials stated that as of June 4, 2021, FEMA had received 25,168 applications for Public Assistance and awarded $26.9 billion. If all of the remaining approximately 16,000 applicants submits projects, FEMA anticipates it will receive a minimum of approximately 32,000 additional public assistance projects for an estimated additional $27.8 billion as of the end of fiscal year 2021. FEMA officials stated that previous Public Assistance policy indicated that eligibility was limited to response activities and did not extend to operational costs at facilities. However, a January 21, 2021, presidential memorandum expands the definition of eligible goods and services under FEMA’s Public Assistance program to include the costs of opening and operating facilities such as schools, domestic violence shelters, transit systems, and others and may include the funding for the provision of personal protective equipment and disinfecting services and supplies.[450] According to FEMA officials, the memorandum will likely have a significant impact on their resources and operations. Specifically, FEMA officials stated that the eligibility of reopening and operating expenses for schools and other facilities is likely to significantly increase the number of applicants and cost of eligible claims under Public Assistance.
Mission assignments. FEMA has issued mission assignments to multiple federal agencies including the United States Department of Agriculture, Department of Labor, Environmental Protection Agency, and Department of Defense, among others, to assist in the COVID-19 response. For example, FEMA issued a mission assignment to the Department of Defense to fund National Guard deployments to assist in recovery efforts. The presidential memorandum issued on January 21, 2021, provided that FEMA would fully reimburse expenses for National Guard activities to respond to COVID-19, which may include vaccination distribution.[451] According to FEMA, the estimated cost is over $4.2 billion for National Guard assistance as of May 31, 2021.
The figure below shows FEMA’s obligations for COVID-19 by program and activity.
FEMA’s Disaster Relief Fund Obligations and Projections for COVID-19 by Program and Activity through June 2021
Note: This figure includes Disaster Relief Fund obligations through May 31, 2021, and estimated obligations that FEMA projected through June 30, 2021.
FEMA’s workforce and hurricane season preparedness. According to an assessment report issued by FEMA in January 2021, the scale and duration of COVID-19 operations challenged FEMA’s capabilities. The record-breaking response operations included the activation of the National Response Coordination Center for over a year (and counting). Simultaneously, it included FEMA coordinating with the White House Coronavirus Task Force and other federal agencies and supporting its state, local, tribal and territorial partners, while preserving its own workforce from illness. FEMA responded to many disasters in 2020, including a record-breaking hurricane season in the Atlantic Ocean, and the most active fire year on record for the West Coast, with record-breaking wildfires in California, Colorado, Nevada, New Mexico, Oregon, Utah, and Washington.[452] FEMA’s daily operations briefing dated June 14, 2021, shows FEMA’s incident management workforce consisted of 13,789 employees, of which 6,393 were deployed in response to COVID-19 and other natural disasters.
Meteorologists are predicting an above average Atlantic hurricane season this year.[453] With hurricane season approaching and FEMA supporting numerous efforts outside of its normal core responsibilities, such as supporting the COVID-19 response and efforts to address the recent surge in unaccompanied minor children at the Southwest border, we are concerned that FEMA personnel may not be available to deploy or prepared to manage a catastrophic natural disaster or concurrent disasters.
We have made a number of recommendations to FEMA regarding workforce challenges. For example, in May 2020, we recommended that FEMA develop a mechanism to assess how effectively its disaster workforce was deployed to meet mission needs in the field. FEMA officials we spoke with on May 7, 2021, stated that they analyzed past data on deployments and disaster declarations to identify future deployment scenarios and use the results of this analysis to mitigate any workforce shortfalls. Specifically, FEMA’s planned actions to mitigate shortfalls include: (1) replacing reservists and incident management workforce at community vaccination centers with surge capacity forces and the Peace Corps by early June and (2) hiring 600 temporary FEMA employees through its local hire program. Although FEMA has taken action to address our recommendations on staffing levels, staff development and other workforce management-related recommendations since 2016, more than 10 of these recommendations remain open. We will continue to monitor issues related to FEMA’s workforce management.
FEMA is focusing on hurricane season preparation, using the time to coordinate and exercise with state, local, tribal, and territorial governments and other federal agencies. According to FEMA officials, FEMA is working to scale back and provide breaks to staff and teams who are continuously deployed, such as the Incident Management Assistance Teams, before the 2021 hurricane season, while minimizing the impact to current operations. Nevertheless, with the high number of hurricanes predicted, FEMA’s number of deployed staff could be stretched thinner.
Mass vaccination sites. As part of a national effort to speed the pace of COVID-19 vaccination campaigns and ensure equitable access to vaccinations, FEMA was directed by the President to establish Pilot Community Vaccination Centers (CVC). CVCs are a partnership among FEMA, the Centers for Disease Control and Prevention, and other federal agencies, and states, tribal, and territorial governments. After an initial 8-week operational period, CVC pilot sites are closed or transitioned to the state entity to fully operate. As of June 1, 2021, FEMA reported that the Pilot CVCs had given more than 5.5 million doses of vaccines across 39 locations, including sites that have extended their participation in the pilot program.[454]
In addition, FEMA is coordinating with other federal agencies to meet state, local, tribal, and territorial needs to support the distribution of COVID-19 vaccines. Specifically, FEMA officials stated that as of May 31, 2021, it had obligated $4.85 billion to states, tribes, and territories for vaccine distribution.[455] In addition, FEMA is deploying additional personnel to vaccination sites where they will assist people obtaining the vaccine. According to FEMA officials, assistance for vaccine distribution may include but is not limited to:
leasing facilities or equipment to administer and store the vaccine;
providing staffing and training support;
providing personal protective equipment and other administrative supplies; and
using technology to register and track vaccine administration.
FEMA funeral assistance for COVID 19-related deaths. In December 2020, the Consolidated Appropriations Act, 2021, appropriated $2 billion to the Disaster Relief Fund for eligible funeral expenses for individuals or households with COVID-19-related funeral expenses.[456] FEMA began accepting applications on April 12, 2021. According to FEMA data, as of June 28, 2021, the call center had received and is processing 222,862 applications, and as of the same date, FEMA approved 66,798 applications and awarded approximately $447.8 million.
FEMA’s Funeral Assistance by State and Territory as of June 28, 2021
FEMA’s interim policy on COVID-19 funeral assistance states that it will reimburse up to a maximum of $9,000 per funeral in eligible funeral expenses incurred after January 20, 2020, for deaths attributed to the COVID-19 pandemic. The maximum for multiple deaths under the same applicant per state or territory is $35,500. Reimbursements are given for eligible funeral expenses including remains transfer, caskets/urns, burial plots/cremation niches, and markers/headstones.[457]
FEMA does not accept online applications but, according to FEMA officials, hired a contractor to establish a dedicated call center number and staff to accept and support processing applications for COVID-19 related funeral assistance. Currently, the call center is staffed by approximately 3,500 operators across the United States. According to FEMA officials, as of June 30, 2021, the average time to complete an application was about 21 minutes. After completion of the application with a call center representative, applicants are provided an application number that can be used to provide supporting documentation to FEMA online, by fax, or mail. In addition, FEMA sends applicants a letter requesting additional documents to support their application for COVID-19 funeral assistance. Applicants approved for COVID-19 funeral assistance will receive a check by mail or direct deposit, depending on the option chosen when applying for assistance. Applicants who are not approved for COVID-19 funeral assistance are sent a decision letter explaining why they are not approved, their rights to appeal the decision, and information on how to appeal it. Applicants have 60 days from the date of the decision letter to appeal FEMA’s decision. Any U.S. citizen, non-citizen national, or qualified alien who incurred funeral expenses due to a COVID-19 related death after January 20, 2020, can apply for funeral assistance. FEMA has not established a deadline to apply at this time.
The scope of FEMA’s funeral assistance program for COVID-19 related deaths is unprecedented. Prior to COVID-19, FEMA officials stated that approximately 6,000 cases had been processed for funeral assistance for other natural disasters over the past decade. According to FEMA officials, FEMA has internal controls in place to mitigate fraudulent activity. FEMA officials described their internal controls as efficient for preventing and identifying fraud, and to develop them, FEMA relied on numerous sources and lessons learned from previous disasters. Since FEMA only recently began making payments, we have not fully assessed the effectiveness of these controls. However, we will continue to assess the controls FEMA is using to prevent fraud, waste, and abuse in this program. We will continue to report on this program in the next CARES Act report to be issued in October 2021.
Methodology
To conduct this work, we reviewed FEMA’s monthly Disaster Relief Fund reports to obtain FEMA’s obligations data for Individual Assistance, Public Assistance, and mission assignments for March 2020 through May 2021 and projected obligations data through June 2021. We reviewed federal laws and FEMA policies and guidance on how states, local, tribal, and territorial entities may apply for and receive assistance to respond to the COVID-19 pandemic. We also reviewed data from FEMA’s Senior Leadership briefings, FEMA’s Daily Operations Briefings, and FEMA’s advisories on mass vaccination sites, public assistance, FEMA’s workforce, and funeral assistance related to COVID-19. We presented FEMA’s data on funeral assistance, but did not independently review it for accuracy. In addition, we reviewed August 8, 2020, and January 21, 2021, and February 2, 2021 presidential memorandums; FEMA’s fact sheets; and FEMA’s initial assessment of its COVID-19 response report; as well as previous GAO reports on FEMA’s response to the COVID-19 pandemic and other natural disasters. Finally, we interviewed FEMA officials on their initial efforts in implementing the funeral assistance program.
Agency Comments
We provided a draft of this enclosure to the Department of Homeland Security (DHS), FEMA, and the Office of Management and Budget (OMB). In its comments, which are reproduced in appendix VII, DHS outlined various actions it has taken to respond to the COVID 19 pandemic. Specifically, DHS noted that FEMA successfully established federal Community Vaccination Centers to administer vaccines while also accomplishing its commitment to deliver impartial and equitable programs and services to communities. DHS further stated that FEMA adapted its strategy for response and recovery by making resources available for states to fund more on-the ground efforts to promote vaccinations. In addition, FEMA used funds to help individuals with funeral expenses for deaths that were attributed to COVID-19 and noted that funeral assistance at this scale is unprecedented. DHS further stated that FEMA implemented this program with numerous fraud prevention measures to ensure oversight and accountability. DHS also noted steps that FEMA is taking to prepare for hurricane season, including ensuring that the disaster workforce is prepared to address this additional workload. DHS also provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor issues related to FEMA’s Disaster Relief Fund, workforce, and funeral assistance for COVID-19 related deaths. Specifically, we will monitor obligations for Individual Assistance, Public Assistance, and mission assignments, as well as the balance in the fund. In addition, we will monitor FEMA’s workforce challenges and efforts to execute its funeral assistance program and the fraud internal controls established for it.
GAO’s Prior Recommendations
The table below presents our recommendation(s) on FEMA’s response to COVID-19 from prior CARES Act reports.
Prior GAO Recommendations Related to COVID-19
Recommendation
Status
The Federal Emergency Management Agency Administrator should adhere to the agency’s protocols listed in the updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of the tribal consultation process when developing new policies and procedures related to COVID-19 assistance. (March 2021 report).
Open. DHS concurred with our recommendation. DHS stated that FEMA’s National Tribal Affairs Adviser, based in the Office of External Affairs, will coordinate with other FEMA offices and directorates, as appropriate, to review the agency’s adherence to protocols listed in the Tribal Consultation policy.
The Federal Emergency Management Agency Administrator should provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19. (March 2021 report).
Open. DHS concurred with our recommendation. DHS stated that FEMA’s Recovery Directorate will publish a memorandum that will contain direction to FEMA regions regarding the assignment of Public Assistance program delivery managers to promote equitable delivery of Public Assistance to tribal governments. FEMA stated that it plans to send the memorandum to tribal governments in July 2021.
The Administrator of the Federal Emergency Management Agency—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response. (GAO-20-701)
Open. In September 2020, DHS disagreed with this recommendation, noting, among other things, work that FEMA had already done to manage the medical supply chain and increase supply availability. Although DHS disagreed with our recommendation, it began taking some actions in March 2021. As of May 2021, DHS has not demonstrated action to devise interim solutions that would systematically help states, tribes, and territories effectively track, manage, and plan for supplies to carry out the COVID-19 pandemic response in the absence of state-level end-to-end logistics capabilities that would track critical supplies required for a response of this scale. We note that we made this recommendation to both DHS and HHS with the intent that they would work together under the Unified Coordination Group to address challenges reported by state officials with both public health and emergency management responsibilities. Moreover, we recommended they take actions that were consistent with the roles and responsibilities that were to be more clearly defined as HHS took a more central role in leading supply distribution. The recommendation to define those roles and responsibilities remains open. Moreover, although both DHS and HHS have reported separate actions, taken as part of other efforts within each separate purview, neither has articulated how they worked with the other nor how they assessed whether the actions changed the experiences of state officials who reported issues during our prior work. Without systematic and deliberate action to help states ensure they have the support they need to track, manage, and plan for supplies, states, tribes, and territories on the front lines of the whole-of-nation COVID-19 response may continue to face challenges that hamper their effectiveness.
FEMA Disaster Workforce:Actions Needed to Address Deployment and Staff Development Challenges.GAO-20-360. Washington, D.C.: May 4, 2020.
The Nation's Fiscal Health: Action Is Needed to Address the Federal Government's Fiscal Future. GAO-20-403SP. Washington, D.C.: March 12, 2020.
Disaster Response: Federal Assistance and Selected States and Territory Efforts to Identify Deaths from 2017.GAO-19-486. Washington, D.C.: September 13, 2019.
Contact information: Chris Currie, (404) 679-1875, curriec@gao.gov
The Federal Aviation Administration is administering grants to help the nation’s airports respond to and recover from the economic effects of the COVID-19 pandemic.
Entity involved: Federal Aviation Administration, within the Department of Transportation
Background
Historic decreases in passenger demand for air travel due to the COVID-19 pandemic significantly affected U.S. airports’ abilities to generate the revenue needed for operating and infrastructure costs. According to data filed with the Department of Transportation (DOT), U.S. airlines carried about 47 percent fewer passengers in March 2021 than in March 2019. One airport association estimates that U.S. airports will face $40 billion in operating losses and additional costs related to COVID-19 from March 2020 to March 2022. The CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021 provide a combined total of $20 billion in federal funding for U.S. airports to respond to the COVID-19 pandemic, although funding allocation and certain allowable uses differ under each act.
Obligations and expenditures. Of the $20 billion combined total in federal COVID-19 relief funding provided by the CARES Act, Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021 for U.S. airports, about $10.6 billion has been obligated and $6.5 billion expended as of May 14, 2021.
CARES Act. The CARES Act, signed into law on March 27, 2020, provided $10 billion to support U.S. airports of all sizes to prevent, prepare for, and respond to coronavirus.[458] Airport owners—also known as airport sponsors—may use CARES Act funds for any purpose for which airport revenues may be lawfully used, including for airport operating expenses and debt service. As of May 14, 2021, the Federal Aviation Administration (FAA) had obligated about $9.5 billion and expended over $6.5 billion to reimburse airports for eligible costs and to increase the federal share for 2020 Airport Improvement Program (AIP) grants, according to FAA officials (see table). Specifically, for larger airports, FAA has obligated about $6.5 billion, and expended about $5 billion; for smaller airports, FAA has obligated about $3 billion, and expended $1.5 billion in CARES funding.[459] As of May 14, 2021, FAA had processed CARES Act grant applications for 3,230 U.S. airports.
FAA Obligations and Expenditures for CARES Act Airport Grants, as of May 14, 2021
Funding group
Obligations ($ thousands)
Expenditures ($ thousands)
Increase federal share for 2020 Airport Improvement Program (AIP) grantsa
$513,706
$276,390
Commercial service airportsb
$7,134,220
$5,456,731
Primary airportsc
$1,628,724
$665,363
General aviation airportsd
$100,311
$63,846
Reallocated CARES Act fundse
$151,387
$13,795
Total
$9,528,349
$6,476,125
Source: GAO analysis of CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020) and data from the Federal Aviation Administration (FAA). | GAO-21-551
aThe CARES Act directed FAA to allocate funding to these groups through various formulas. Approximately 3,300 airports in the U.S. are part of the national airport system and are eligible to receive federal AIP grants to fund infrastructure projects. The CARES Act appropriated at least $500 million to increase the federal share to 100 percent for grants awarded for airport infrastructure projects under fiscal year 2020 and supplemental discretionary grants. bCommercial service airports are publicly owned airports with at least 2,500 passenger boardings per year and scheduled air service. cPrimary airports are large, medium, and small hub and non-hub airports with more than 10,000 passenger boardings per year. dGeneral aviation airports are public-use airports with fewer than 2,500 passenger boardings per year and no scheduled air service. eUnder the Consolidated Appropriations Act, 2021, unallocated CARES funds as of December 27, 2020 were to be allocated under the Consolidated Appropriations Act, 2021 using the primary commercial service and certain cargo airports allocation formula. According to FAA officials, FAA calculated that $290,774,557 in CARES Act funds are available for reallocation under the Consolidated Appropriations Act, 2021.
Consolidated Appropriations Act, 2021. The Consolidated Appropriations Act, 2021, enacted on December 27, 2020, provided $2 billion in additional federal aid to help eligible airports and certain tenants to prevent, prepare for, and respond to COVID-19.[460] Airports must use Consolidated Appropriations Act, 2021 grant funding for costs related to operations, personnel, cleaning, sanitization, janitorial services, combating the spread of pathogens at the airport, and debt service payments.[461] As of May 14, 2021, FAA had obligated about $1 billion and expended about $53 million to reimburse airports for eligible costs, according to FAA officials (see table). For larger airports, FAA has obligated about $606 million, and expended about $35 million, while for smaller airports, FAA has obligated about $400 million, and expended $14 million in Consolidated Appropriations Act, 2021 funding. As of May 14, 2021, FAA had processed Consolidated Appropriations Act, 2021 grant applications for 2,636 U.S. airports.
FAA Obligations and Expenditures for the Consolidated Appropriations Act, 2021 Airport Grants, as of May 14, 2021
Funding group
Obligations ($ thousands)
Expenditures ($ thousands)
Primary commercial service airports and certain cargo airportsa
$929,416
$48,209
Non-primary commercial service and general aviation airportsb
$8,833
$723
Non-primary airports participating in the Federal Aviation Administration (FAA) Contract Tower programc
$1,264
$11
Tenant relief for primary commercial service airports
$65,921
$0
Small Community Air Service Development Programd
$4,000
$4,000
Total
$1,009,434
$52,943
Source: GAO analysis of the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1939-41 (2020), and data from the Federal Aviation Administration (FAA). | GAO-21-551
aThe Consolidated Appropriations Act, 2021 directed FAA to allocate funding to these groups through various formulas. Primary commercial service airports are publicly owned airports with more than 10,000 passenger boardings per year and scheduled air service. Cargo airports are airports that, in addition to any other air transportation services that may be available, are served by aircraft providing air transportation of only cargo with a total annual landed weight of more than 100 million pounds. bNon-primary commercial service airports have at least 2,500 and no more than 10,000 passenger boardings each year. General aviation airports are public-use airports with fewer than 2,500 passenger boardings per year or no scheduled air service. cNon-primary airports are the same as non-primary commercial service airports, and have at least 2,500 and no more than 10,000 passenger boardings each year. The Federal Contract Tower Program, established in 1982, allows the agency to contract out the operation of certain towers. dThe Small Community Air Service Development Program is a grant program designed to help small communities address air service and airfare issues.
American Rescue Plan Act of 2021. The American Rescue Plan Act of 2021, enacted on March 11, 2021, provided an additional $8 billion for airport assistance (see table).[462] The allowable uses of funds are similar to those for the Consolidated Appropriations Act, 2021, and are available for costs related to operations, personnel, cleaning, sanitization, janitorial services, combating the spread of pathogens at the airport, and debt service payments. Certain amounts are available to increase the federal share for AIP grants, and to provide relief from rent and minimum annual guarantees to airport concessions. As of June 2021, FAA has determined individual airport allocations for airport grants, and has begun obligating and expending funds to increase the federal share for eligible AIP grants. According to officials, FAA has obligated about $12.3 million and expended about $75 thousand in American Rescue Plan Act of 2021 funds to increase the federal share for 2021 and eligible 2020 AIP grants for airports, as of May 14, 2021.
The American Rescue Plan Act, 2021 Airport Grant Allocations
Funding group
Funds appropriated (in dollars)a
Formula applied
Primary commercial service airports and certain cargo airportsb
Up to $6.49 billion
Allocate first based on the statutory Airport Improvement Program (AIP) primary and cargo entitlement formulas. Allocate the remainder based on the number of enplanements the airport had in calendar year 2019, the most recent calendar year of available enplanement data, as a percentage of total 2019 enplanements for all primary airports.
Increase federal share for 2021 and select 2020 AIP grants
Up to $608 million
Increase the federal share to 100 percent for grants awarded for airport infrastructure projects under fiscal year 2021 AIP and supplemental discretionary grants and for airport development projects under fiscal year 2020 which received less than a 100 percent federal share.c
Non-primary commercial service and general aviation airportsd
Up to $100 million
Allocate based on current National Plan of Integrated Airport Systems categories, reflecting the percentage of the aggregate published eligible development costs for each such category, and then dividing the allocated funds evenly among the eligible airports in each category. Any remaining funds are to be allocated to primary commercial service airports and certain cargo airports described in the first funding group.
Tenant relief for primary commercial service airportse
Up to $800 million
Allocate based on the number of airport enplanements in calendar year 2019 as a percentage of total calendar year 2019 enplanements for all primary airports. Of these funds, at least $640 million shall be available to provide relief to eligible small airport concessions, and at least $160 million shall be available to eligible large airport concessions at primary airports.
Source: GAO analysis of the American Rescue Plan Act, 2021, Pub. L. No. 117-2, § 7102, 135 Stat. 4, 96-98. | GAO-21-551
aThe American Rescue Plan Act of 2021 directed FAA to allocate funding to these groups through various formulas. The American Rescue Plan Act of 2021 gives the Federal Aviation Administration (FAA) the authority to retain up to 0.1 percent of the $2 billion (up to $2 million) provided for Relief for Airports to fund the award and oversight by FAA of grants made under the American Rescue Plan Act of 2021. Pub. L. No. 117-2, § 7102(c)(1), 135 Stat. 4, 98. bPrimary commercial service airports are publicly owned airports with more than 10,000 passenger boardings per year and scheduled air service. Cargo airports are airports that, in addition to any other air transportation services that may be available, are served by aircraft providing air transportation of only cargo with a total annual landed weight of more than 100 million pounds. cNational system airports are eligible to receive federal funding from AIP grants for infrastructure development. The distribution of federal AIP grants is based on a combination of formula funds—also referred to as entitlement funds—that are available to national system airports, and discretionary funds that FAA awards for selected eligible projects. Entitlement funds are apportioned by formula to airports and may generally be used for any eligible airport improvement or planning project. Discretionary funds are approved by FAA based on FAA selection criteria and a priority system, which FAA uses to rank projects based on the extent to which they reflect FAA’s nationally identified priorities. The federal share for AIP grants generally ranges from 75 percent to 95 percent. dNon-primary commercial service airports have at least 2,500 and no more than 10,000 passenger boardings each year. General aviation airports are public-use airports with fewer than 2,500 passenger boardings per year or no scheduled air service. ePrimary commercial airport sponsors may only use these funds to provide relief from rent and minimum annual guarantees to in-terminal airport tenants, subject to additional conditions. An eligible large airport concession is one that is in-terminal and has maximum gross receipts, averaged over the previous three fiscal years, of more than $56,420,000. An eligible small airport concession is one that is in-terminal and is a small business with maximum gross receipts, averaged over the previous three fiscal years, of less than $56,420,000, and is a joint venture.
Overview of Key Issues
Airport grant administration, challenges, and oversight. With regard to COVID-19 relief funding appropriated by the CARES Act and Consolidated Appropriations Act, 2021, FAA is processing airport grant applications, obligating funds, and reviewing invoices to reimburse airport sponsors. FAA has also provided guidance on airport grant requirements for these programs, including for workforce retention and tenant relief, which we discuss further below. For funds appropriated by the American Rescue Plan Act of 2021, FAA has established the Airport Rescue Grants Program, and as of June 2021, has determined airport allocations and published guidance.
As we previously reported, FAA has identified challenges to administering CARES Act airport grants, including the need to process grants for over 3,000 airport sponsors under expedited time frames, with expanded eligible uses for these funds. To address the increased workload of processing and monitoring three new airport relief grant programs, FAA has established a dedicated team, including two full-time employees and three annuitants with prior airport grant management experience, to review and process airport payment requests. FAA officials stated they are currently evaluating whether to hire additional employees to assist with the workload.
With regard to monitoring and oversight, FAA officials also reported that the agency hired a contractor in the fall of 2020 to review FAA’s reimbursement processes for CARES Act grants, develop an electronic dashboard to monitor and track funds, and provide recommendations on auditing policies and procedures. As of May 2021, FAA stated that its contractor was reviewing its CARES Act airport grant requirements and reimbursement process, as well as FAA’s process and program controls. FAA said it received a draft of the monitoring dashboard in late April 2021, and is reviewing it to determine if any adjustments are needed. This dashboard will be used to monitor and track funds across all three COVID-19 relief programs, according to FAA officials. Additionally, the contractor is currently auditing a sample of airport payments to determine whether FAA made any improper payments to airport sponsors. FAA is currently working with the contractor to collect data from selected airports to support this effort. In late June 2021, the contractor plans to provide program recommendations and an overall CARES Act airport grant program performance report to FAA. FAA officials said that they plan to apply any recommendations made to improve the CARES Act airport grant program to the Consolidated Appropriations Act, 2021 and American Rescue Plan Act of 2021 airport grant programs.
As non-federal entities, public airport sponsors that receive federal grants are also subject to the Single Audit Act, and they must undergo a single audit of those awards annually when their expenditures meet a certain dollar threshold—currently $750,000 or more in a fiscal year.[463] Single audits of an entity’s financial statements and federal awards can help identify deficiencies in an award recipients’ compliance with applicable laws and regulations, help ensure the appropriate use of federal funds, and reduce the likelihood of federal improper payments. The DOT Office of Inspector General may check compliance and review single audit reports for DOT fund recipients, and is currently reviewing DOT’s processes for verifying that these audits have been completed, among other things.
Workforce retention requirements and monitoring. Certain airport sponsors accepting CARES Act grant funds were required to continue to employ directly by the airport, through December 31, 2020, at least 90 percent of the number of individuals employed as of March 27, 2020.[464] The Consolidated Appropriations Act, 2021 extended these workforce retention requirements through February 15, 2021. Airports that accept American Rescue Plan Act of 2021 grants will be subject to the same workforce retention requirements through September 30, 2021.[465] According to FAA, the 131 largest U.S. airports were subject to this requirement under the Consolidated Appropriations Act, 2021. FAA officials said at the time that airport sponsors execute a COVID-19 relief grant, sponsors certify that they will meet the workforce retention requirements and report their employee numbers.
Since we last reported in March 2021, FAA has taken actions to monitor compliance with workforce retention requirements for the 131 affected airports. Officials stated that FAA has compared airport workforce numbers submitted as of February 15, 2021, compared to their baseline number of employees as of March 27, 2020, to ensure airports met the 90 percent employment threshold.[466] FAA officials said that as of May 2021, 117 out of the 131 eligible airports complied with May reporting requirements. Of the 14 remaining, FAA officials said they are in the process of clarifying their submissions, asking for outstanding submissions, or waiting until the grant sponsor has a grant agreement in place. As of May 2021, FAA had not received any waiver requests for the workforce retention requirements. Officials said they will continue to track airport workforce requirements through September 30, 2021, as required by the American Rescue Plan Act of 2021.
Airport grant funding uses. Airport association representatives told us that the federal funding provided has been critical. FAA has begun to collect and consolidate data from airports on general spending categories for CARES Act funding through grant close-out reports, which are completed once all allocated airport funds have been expended. As of May 14, 2021, FAA officials said that 476 CARES Act airport grants, totaling $1.66 billion, have been closed out. For these grants, the majority of airport grant funds have been used for debt service (about 52 percent of these funds, totaling $864 million) and payroll (about 39 percent of these funds, totaling $643 million). While FAA continues to collect these data on airport grant spending, officials said airports are generally using CARES Act funds on payroll, utilities, minor maintenance, and debt service.
As for Consolidated Appropriations Act, 2021 funding, airport associations said that airport sponsors are generally using these grants to pay for operational expenses and costs related to mitigating effects of the COVID-19 pandemic, such as cleaning and sanitation, social distancing measures, and upgrading heating and cooling systems. For the American Rescue Plan Act of 2021, an airport association said airports plan on using these funds to pay for operational costs, debt service, and COVID-19 mitigation related projects, such as changing air conditioning systems with better filters or increasing air flow.
Airport tenant relief. As part of the Consolidated Appropriations Act, 2021 requirements, airport sponsors that accept tenant relief funds will waive rent and minimum annual guarantee obligations for eligible airport tenants beginning December 27, 2020, until the relief equals the total tenant relief allocation amount and to the extent permissible under state and local laws.[467] Eligible airport tenants include on-airport car rental and parking, and in-terminal concession tenants.
To administer the tenant relief portion of the funding, FAA officials have calculated airport allocations and informed airport sponsors of the amount of eligible concessions relief, including funds they can use for administration costs.[468] FAA is requesting that airport sponsors provide tenant relief plans with their payment requests when they are ready to accept their concessions-relief funding. FAA officials said they are reviewing these plans to ensure that airport sponsors are providing relief according to the law and FAA guidance prior to approving payment. According to FAA guidance, FAA requires airport tenants to provide certifications of eligibility directly to airport sponsors, who then keep the documentation on file for possible audits.
Airport association representatives stated that airports are facing challenges with the tenant relief portion of the Consolidated Appropriations Act, 2021, especially related to airports’ roles in determining tenant eligibility and providing relief. Specifically, airport representatives said that determining tenant eligibility can be complex due to varying tenant agreements, and that tenants are not often single entities. To address some of these challenges, FAA has provided guidance on how to administer concession relief through the FAQs posted to FAA’s website, which the agency updated with additional clarifications in April 2021. FAA has also held videoconferences to answer airports’ tenant relief questions, and has established a dedicated email for airports to direct questions to FAA headquarters. FAA officials stated that airports have asked questions about how to determine which tenants are eligible for relief, ways airports can offer relief, and how to equitably apportion the relief. Airport association representatives appreciated FAA’s response to airport inquiries, but noted that airports are continuing to work through questions on how to administer this tenant relief funding.
An airport concessions association told us that while airports have been working to support their tenants, and airports are showing signs of recovery, dedicated tenant relief continues to be important to help respond to the impacts of COVID-19 on airport businesses, many of which have had to permanently or temporarily close, and furlough or lay off employees. An airport tenant employee union stated that while some businesses in airports are beginning to open back up, there are no employee retention requirements associated with the tenant relief funds, and not all companies are calling back or hiring enough workers to meet increasing demand at airport terminals. The airport concessions association and employee union stated that recovery for airport tenants and their employees would likely be uneven, even as passengers begin to return to airports, due to changes in the way people are flying as a result of the pandemic.
The American Rescue Plan Act of 2021 also provides in-terminal concession tenant relief funding for eligible airport sponsors. As of May 2021, FAA was in the process of drafting guidance for airports to administer these funds.
Methodology
To conduct this work, we analyzed FAA data on airport funding as of May 14, 2021. We determined the data were sufficiently reliable for the purposes of our reporting objective by performing interviews with agency officials and reviewing relevant documentation. We also reviewed federal laws and agency guidance related to the CARES Act, the Consolidated Appropriations Act, 2021, and American Rescue Plan Act of 2021 and conducted interviews with agency officials and representatives from airport associations, an airport concessions association, and an airport tenant employee union, selected to represent a wide variety of industry and airport types.
Agency Comments
We provided FAA and the Office of Management and Budget (OMB) with a draft of this enclosure. FAA provided technical comments that we incorporated as appropriate. OMB did not have any comments on this enclosure.
GAO’s Ongoing Work
Our work on aviation industry COVID-19 grants is ongoing. We will continue to monitor FAA’s administration of grants related to the CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021. We will also continue to monitor aviation operations, impacts, and lessons from the COVID-19 pandemic through other ongoing work.
Contact information: Heather Krause, (202) 512-2834 or krauseh@gao.gov
Coronavirus State and Local Relief and Recovery Funds
Lessons from the implementation of the $150 billion Coronavirus Relief Fund can help the federal government ensure that states, localities, tribal governments, the District of Columbia, and U.S. territories appropriately use the $350 billion Coronavirus State and Local Fiscal Recovery Funds to recover from the COVID-19 pandemic.
Entities involved: Department of the Treasury and Office of Management and Budget
Recommendation for Executive Action
The Director of the Office of Management and Budget, in consultation with the Secretary of the Treasury, should issue timely and sufficient single audit guidance for auditing recipients’ uses of payments from the Coronavirus State and Local Fiscal Recovery Funds. The Office of Management and Budget neither agreed nor disagreed with this recommendation.
Background
Congress and the President have appropriated $500 billion to the Department of the Treasury (Treasury) to provide direct funding to states, localities, tribal governments, the District of Columbia, and U.S. territories to help them respond to, and recover from, the COVID-19 pandemic.[469] This amount includes $150 billion that the CARES Act appropriated to Treasury for the Coronavirus Relief Fund (CRF)[470] in March 2020 as well as $350 billion that the American Rescue Plan Act of 2021 (ARPA) appropriated to Treasury for the Coronavirus State and Local Fiscal Recovery Funds (CSLFRF) in March 2021.[471]
As of July 31, 2020, Treasury had disbursed $149.5 billion of the $150 billion CRF—$142 billion to states, localities, the District of Columbia, and U.S. territories and approximately $7.5 billion to tribal governments.[472] These recipients can use CRF payments to offset costs related to either the pandemic’s direct effects (e.g., public health needs) or its indirect effects (e.g., harm to individuals or businesses as a result of COVID-19-related closures).[473]
The CSLFRF provides payments to these recipients to cover a broader range of costs stemming from the fiscal effects of the COVID-19 pandemic.[474] ARPA established four key eligible use categories, providing that recipients may use the CSLFRF payments to cover costs incurred by December 31, 2024, to:
respond to the COVID-19 pandemic or its negative economic impacts, including assistance to households, small businesses, and nonprofits or aid to impacted industries, such as tourism, travel, and hospitality;
respond to workers performing essential work during the COVID-19 pandemic, by providing premium pay to the recipients’ eligible workers or grants to eligible employers that have eligible workers who perform essential work;
provide government services to the extent of any revenue reduction resulting from the COVID-19 pandemic relative to revenues collected in the recipient government’s most recent prepandemic full fiscal year; or
make necessary investments in water, sewer, or broadband infrastructure.
CSLFRF recipients may not use the payments for deposit into any pension fund. Furthermore, states, the District of Columbia, and territories may not use the funds to either directly or indirectly offset a reduction in net tax revenue resulting from a change in law, regulation, or administrative interpretation made between March 3, 2021, and the end of the fiscal year in which the recipient expends the last of the funds it receives.[475] If a recipient fails to comply with these requirements and restrictions, it must repay an amount equal to the amount of funds used in violation of these requirements and restrictions.[476]
Overview of Key Issues
Distribution of CSLFRF. ARPA directs Treasury to allocate and distribute:
$195.3 billion to the states and the District of Columbia;
$130.2 billion to localities, including $65.1 billion to counties, $45.6 billion to metropolitan cities, and $19.5 billion to other cities;[477]
ARPA provides that Treasury shall distribute CSLFRF payments to tribal governments and initial payments to localities within 60 days of ARPA’s enactment, or May 10, 2021, to the extent practicable.[479] To receive the payments, states, the District of Columbia, and U.S. territories must first provide Treasury with a signed certification stating that they require the payments to carry out allowable activities and will comply with relevant requirements when they use the payments.[480] In general, to the extent practicable, ARPA provides that Treasury shall distribute payments to those entities no later than 60 days after it has received their certifications.[481] On May 10, 2021, Treasury announced that all eligible states, territories, metropolitan cities, counties, and tribal governments could request their allocation of the CSLFRF.
According to Treasury, it had distributed $141 billion in CSLFRF payments as of May 28, 2021.
Use of CRF. As of March 31, 2021, state, local, and territorial CRF recipients reported having spent $118 billion (83 percent) of the $142 billion distributed to them.[482] The proportions of the payments that the recipients reported spending varied widely (see figure).
Percentages of Coronavirus Relief Fund (CRF) Payments Recipients Reported Having Spent as of March 31, 2021
Note: The data shown for each state reflect CRF payments to, and spending by, eligible localities in each state. The data shown do not include CRF payments to, and spending by, tribal governments, because complete recipient reporting data for tribal governments were not available at the time of our review. In addition, the data shown do not reflect spending, if any, by Lancaster County, Pa., because that CRF recipient had not reported on its spending at the time of our review.
Guidance from Treasury’s Office of Inspector General (Treasury OIG) requires CRF recipients to report their uses of CRF payments in 17 specific spending categories (e.g., COVID-19 testing and contact tracing) and one unspecified category (i.e., for spending not captured in the other categories).[483] As the figure below shows, spending in the unspecified category made up 46 percent of state, local, and territorial CRF recipients’ reported spending as of March 31, 2021. Consistent with Treasury OIG guidance, the unspecified category includes all spending that CRF recipients report in aggregate—payments of less than $50,000 and payments to individuals, regardless of amount—which made up 78 percent of reported spending in the unspecified category as of March 31, 2021. More than half of the unspecified spending consisted of payments to individuals. According to related Treasury departmental guidance, such payments may include rent, mortgage, or funeral cost assistance to individuals and families directly impacted by a loss of income due to the COVID-19 pandemic.[484] Treasury OIG guidance also directs recipients to report their payroll costs as payments to individuals.[485]
Coronavirus Relief Fund (CRF) Recipient Spending as of March 31, 2021, by Spending Category
Note: CRF spending by tribal governments is not included, because complete recipient reporting data for tribal governments were not available at the time of our review.aCRF recipients reported spending less than 3 percent in each of 10 other specified categories: workers compensation, expenses associated with the issuance of tax anticipation notes, administrative expenses, nursing home expenses, improve telework capabilities of public employees, food programs, budgeted personnel and services diverted to a substantially different use, housing support, unemployment benefits, and medical expenses.
Guidance on eligible uses of the CSLFRF. On May 10, 2021 Treasury released an interim final rule implementing the CSLFRF.[486] This rule includes, among other things, guidance for recipients on the eligible uses of CSLFRF payments.
The rule states that CSLFRF recipients have flexibility, within the four key eligible use categories identified in ARPA, to determine how best to use the payments to meet the needs of their communities and populations. However, the rule provides additional guidance intended to help recipients determine the types of programs and services that are eligible and provides examples of uses they may consider. The rule states that, in general, the CSLFRF’s eligible uses build on the CRF’s eligible uses. However, the rule notes that the eligible uses have been expanded to reflect changed circumstances, such as the need to support vaccination campaigns and address the COVID-19 pandemic’s disproportionate impact on certain populations, geographies, and economic sectors.
For example, the rule states that eligible uses in the category of responding to the COVID-19 pandemic or its negative economic impacts must respond to the disease itself or the harmful consequence of the economic disruptions it caused. The rule directs recipients considering eligible uses in this category to, first, identify a need or negative impact of the pandemic and, second, identify how the program or service addresses the identified need or impact. The rule further identifies a nonexclusive list of programs or services that may be funded under this category. The rule also provides considerations for determining whether additional programs or services meet the eligibility criteria. The nonexclusive list includes the following additional eligible uses:
COVID-19 mitigation and prevention (e.g., vaccinations, testing, contact tracing);
salaries and benefits for public sector staff responding to COVID-19, including health and health care workers;
assistance for small businesses and unemployed workers; and
services for individuals (e.g., affordable housing, child care, education) in communities disproportionately impacted by the pandemic.
The rule provides additional guidance to recipients for using payments in the other three key eligible use categories. For example, the rule:
provides parameters for premium pay programs, such as by defining sectors that constitute essential work and establishing that payments should prioritize lower-income essential workers;
identifies how recipients should measure a reduction in revenue due to the COVID-19 pandemic and describes a broad range of services the payments may be used to support; and
defines necessary infrastructure investments, such as water and sewer projects aligned with existing Environmental Protection Agency–funded programs and broadband projects targeted at underserved populations, to enable households to work or attend school.
Guidance on CSLFRF record keeping and reporting. Treasury’s interim final rule identified preliminary, high-level performance and expenditure reporting requirements for recipients. The rule stated that Treasury would provide additional, specific guidance and instructions for meeting the reporting requirements at a later date.
The rule established that states, territories, metropolitan cities, and counties with populations over 250,000 will be required to submit an annual Recovery Plan Performance Report to Treasury. These recipients must submit initial reports to Treasury by August 31, 2021.[487] The rule stated that the reports are to include a range of Treasury-mandated and recipient-identified performance indicators that, along with other data, are intended to provide Treasury and the public with information about recipients’ projects and about recipients’ planning to achieve outcomes in an effective, efficient, and equitable manner.
The rule also established that recipients must submit quarterly expenditure reports, with an interim report due to Treasury by August 31, 2021.[488] However, the rule did not address the following challenges that affected CRF reporting and that could limit the utility of CSLFRF reporting:
The rule neither listed nor defined the CSLFRF expenditure categories. According to Treasury OIG officials, CRF recipients frequently asked for clarification of the meaning of expenditure categories.
The rule did not include guidance on aggregate CSLFRF reporting or indicate whether CSLFRF expenditure categories would be required for any spending reported in aggregate. In the CRF reporting, a large percentage of spending—most of which was aggregate payments to individuals—did not identify an expenditure category. Aggregate payments to individuals could include, for example, purposes as diverse as recipient payroll costs and rental assistance to those impacted by a loss of income due to the COVID-19 pandemic.
In May 2021, Treasury officials told us that Treasury’s reporting guidance would require CSLFRF prime recipients to report both payments to individuals and payments below a certain dollar threshold in aggregate to ensure that reporting captures all spending. Therefore, in a draft of this report we provided to Treasury in June 2021 for review and comment, we recommended that Treasury, in its guidance, clearly define expenditure categories and require expenditure categories for at least some of the spending to be reported in aggregate, such as payments to individuals. In written comments, Treasury agreed with our recommendation and stated that the guidance would require all CSLFRF spending to be reported by expenditure category.
Treasury subsequently issued reporting guidance on June 17, 2021, that addressed our recommendation. The guidance requires CSLFRF recipients to, among other things, report on CSLFRF-funded projects by expenditure category. Such categories include, for example, “COVID-19 Vaccination,” “Aid to Tourism, Travel, or Hospitality,” and “Education Assistance: Aid to High-Poverty Districts.” In addition, the guidance directs recipients to apply expenditure categories to payments reported in the aggregate—including payments to individuals—at the project level. This information can help ensure that CSLFRF recipients’ reporting will identify the purposes for which they use payments and that their reporting will effectively facilitate oversight and transparency.
Treasury outreach to CSLFRF stakeholders. In September 2020, we reported that Treasury officials, after releasing guidance on eligible uses of the CRF, participated in forums with CRF stakeholders to discuss and answer questions related to the CRF. However, despite this outreach, CRF recipients reported that they found Treasury’s guidance on eligible uses of the funds to be unclear. For example, some states needed additional guidance on eligible uses of the funds, which delayed their transferring funds to subrecipients, such as local governments. In addition, unclear guidance increased the risk of CRF recipients’ noncompliance with spending requirements. Treasury subsequently finalized CRF guidance, which it published in the Federal Register in January 2021.
Treasury has taken steps intended to ensure the clarity of its CSLFRF guidance for recipients. Treasury officials told us that they have consulted with eligible recipients on various aspects of CSLFRF implementation. For example, officials told us that they met with representatives from tribal governments five times in March and early April 2021. According to the officials, tribal participants in these meetings provided feedback on a range of implementation issues, including methodologies for determining allocations and reporting requirements. Treasury officials told us that they plan to continue consultations with recipients as they make payments and recipients begin to use the funds.
Furthermore, Treasury is seeking direct recipient feedback on all aspects of its interim final rule and its work in administering the CSLFRF. To facilitate this feedback, the rule includes specific questions for recipients about ways in which Treasury could improve it. For instance, Treasury asks recipients whether there are additional specific services or costs that it should consider as eligible uses related to responding to the COVID-19 pandemic or its negative economic impacts and how those services or costs could help recipients respond to the pandemic. Treasury has asked for comments on the rule by July 16, 2021.
CRF recipients’ experiences with CRF’s guidance on eligible uses demonstrate how important it will be for Treasury to use the information it collects from recipients to improve the clarity of CSLFRF guidance. Clear guidance can help ensure that recipients use CSLFRF payments appropriately to respond to, and recover from, the COVID-19 pandemic. We will continue to monitor and report on Treasury’s CSLFRF guidance, including the extent to which recipients find it clear and useful, in future reports.
CSLFRF assistance listing number. Treasury initially assigned the same assistance listing number to the CSLFRF that it had previously assigned to the CRF. Assistance listings are detailed public descriptions of federal programs that provide federal financial assistance; the listings include information such as the eligible uses of funding and compliance requirements.[489] Assistance listing numbers are unique numbers assigned to assistance listings.
Local government officials and members of the accountability community told us that Treasury’s use of a single assistance listing number for the CRF and CSLFRF could reduce the transparency of, and accountability for, recipients’ uses of their payments. For example, local government officials reported that many CRF and CSLFRF recipients—such as municipalities with limited financial management capacity—could have difficulty tracking payments from each of the funds separately under a single assistance listing number, according to an official from an association that represents local governments. Such difficulty could increase the risk that a recipient would use inappropriately some of the funding it received—for example, by using its CRF payment for costs incurred after December 31, 2021. We communicated these challenges to Treasury officials.
On May 28, 2021, Treasury issued a new assistance listing number for the CSLFRF that is separate and distinct from the CRF’s number. In June 2021, in technical comments on a draft of this report, Treasury officials told us that they issued initial CSLFRF payments under the CRF assistance listing number to expedite the payments and meet statutory deadlines. They added that feedback that we, Treasury OIG, CSLFRF recipients, and other stakeholders provided had informed their decision to issue a new assistance listing number for the CSLFRF.
Audit guidance. The Single Audit Act establishes requirements for states, localities, tribal governments, the District of Columbia, U.S. territories, and nonprofit organizations that receive federal awards to undergo single audits of those awards annually (unless a specific exception applies) when their expenditures meet a certain dollar threshold.[490] Single audits are critical to the federal government’s ability to help safeguard the use of the billions of dollars distributed through the CRF and CSLFRF. Specifically, a single audit may identify deficiencies in an award recipient’s compliance with applicable provisions of laws, regulations, contracts, or grant agreements and in its financial management and internal control systems. Correcting such deficiencies can help to reasonably assure award recipients’ appropriate use of federal funds and reduce the likelihood of federal improper payments.
Auditors who conduct single audits follow guidance in the Single Audit Act’s Compliance Supplement, which provides guidelines and policy for performing single audits. Auditors rely on the supplement to understand a federal program’s objectives, procedures, and compliance requirements. Without it, auditors would need to research compliance requirements for each program in numerous statutes and regulations. After consultation with federal agencies, OMB annually updates and issues the supplement.[491] Auditors have reported that the timely issuance of the supplement is critical in allowing them to plan their work effectively.
Treasury distributed nearly all CRF funds by July 31, 2020. In August 2020, OMB issued its Compliance Supplement for 2020 audits. However, the supplement did not include guidance for new COVID-19 relief programs, including the CRF. In September 2020, we recommended that OMB, in consultation with Treasury, issue an addendum to the 2020 Compliance Supplement as soon as possible to provide the necessary audit guidance for COVID-19 relief programs. OMB issued the addendum in December 2020. In March 2021, after enactment of two additional COVID-19 relief laws appropriating additional COVID-19 relief funding, we reported that the lag between the distribution of COVID-19 relief funds and OMB’s issuance of relevant single audit guidance had delayed auditors in conducting single audits and reporting results. These delays could affect recipients’ development of corrective action plans and resolution of findings identified during the audits, as well as federal agencies’ formulation of management decisions about single audit findings.
Pursuant to ARPA, Treasury told us that it had distributed $141 billion in CSLFRF funds as of May 28, 2021. In April 2021, OMB officials told us that the 2021 Compliance Supplement will not include guidance for CSLFRF or other ARPA programs. OMB officials stated that they are currently working with agencies to identify single audit requirements for ARPA programs. In addition, OMB officials stated that they will continue to work with Treasury to evaluate the need for CSLFRF audit guidance and will work with agencies to evaluate the need for an addendum to the 2021 Compliance Supplement. OMB did not provide a timeline for issuing the 2021 Compliance Supplement or the related addendum.
Standards for internal control in the federal government require that management identify, analyze, and respond to change—such as by providing timely guidance—to effectively monitor operations. The lack of timely single audit guidance could prevent auditors from completing and issuing timely audit reports, which could in turn limit federal agencies’ ability to ensure their awardees’ appropriate use of the CSLFRF and reduce the likelihood of improper payments.
Given that OMB has not yet issued guidance on the ARPA programs, the audits will need to be delayed. OMB provided a 6-month extension for submitting 2021 single audit reports.[492]
Although deadline extensions may be needed given the delays in issuing audit guidance, it is important to note that such extensions also delay the reporting of audit findings, recipients’ corrective actions, and federal awarding agencies’ management decisions. For example, with a 6-month extension, audit findings that are normally reported within 9 months after an entity’s fiscal year ends will not be due until 15 months after the fiscal year ends (see figure). The reporting delay also affects the development of corrective actions. Specifically, the management decision letter is normally due within 15 months after the fiscal year ends; however, with the 6-month extension, the letter will not be due until 21 months—nearly 2 years—after the fiscal year ends. As we previously reported, auditors normally start in April to conduct interim testing of entities whose fiscal year ends on June 30.
Impact of Extended Deadline for Single Audit Reports on Audit Findings and Development of Corrective Action Plans for Entities Whose Fiscal Year Ends on June 30
To put this in perspective, California expended approximately $7.5 billion of the $9.5 billion CRF payments allocated to the state between July 1, 2020, and December 31, 2020. However, because California’s fiscal year ends June 30, the single audit results of its CRF spending will not be due until September 30, 2022, and the management decision letter regarding such findings will not be due until March 31, 2023—almost 3 years after California started spending the CRF payments.
In light of the late issuance of audit guidance for the COVID-19 programs, OMB’s addendum to the 2020 Compliance Supplement directed awarding agencies to allow a single audit extension to recipients and subrecipients that received COVID-19 funding. However, the addendum also strongly encouraged auditees and auditors to complete and submit their single audit reports as early as possible, given the large size of the COVID-19 programs and the federal government’s dependency on single audit reports to assist with proper oversight over these funds. The timely issuance of single audit guidance is critical to ensuring timely completion and reporting of single audits to inform the federal government of actions needed to help safeguard the use of the billions of dollars distributed through the CRF and CSLFRF.
Methodology
To conduct this work, we reviewed Pandemic Response Accountability Committee data as of March 31, 2021; federal laws; and guidance from Treasury and Treasury OIG. In addition, we interviewed officials from Treasury, Treasury OIG, and the Pandemic Response Accountability Committee. We also collected written responses to questions that we posed to OMB and associations representing different types of CRF and CSLFR recipients. Further, we reviewed our prior work on the implementation of the CRF.
To determine the reliability of the data, we reviewed relevant documentation, tested the data for outliers and obvious errors, and interviewed knowledgeable officials from Treasury OIG and the Pandemic Response Accountability Committee. We found the data were sufficiently reliable for the purposes of our reporting objective.
Agency Comments
We provided a draft of this report to Treasury and OMB for review and comment. Treasury provided written comments, which are summarized below and reproduced in appendix XI. OMB did not provide written comments on this enclosure and neither agreed nor disagreed with our recommendation. Treasury and OMB each provided technical comments, which we incorporated as appropriate.
As described above, in a draft of this report, we recommended that Treasury, when developing recipient reporting guidance for the CSLFRF, clearly define expenditure categories and require expenditure categories for at least some spending reported in aggregate, such as payments to individuals. Treasury agreed with the draft recommendation and stated that forthcoming recipient reporting guidance would require all CSLFRF spending to be reported by expenditure category. We reviewed the guidance that Treasury subsequently issued on June 17, 2021, and determined that it addressed our recommendation. Therefore, we removed that draft recommendation from this report.
In addition, in the draft of this report, we included a second recommendation to Treasury that it issue an assistance listing number for the CSLFRF that was separate and distinct from the assistance listing number for the CRF. As described above, on May 28, 2021, Treasury issued a separate assistance listing number for the CSLFRF. We determined that that action addressed our draft recommendation. Therefore, we removed that draft recommendation from this report.
GAO’s Ongoing Work
We currently have multiple ongoing or planned reviews of the funding that federal COVID-19 relief laws appropriated for agencies across the federal government to provide payments to states, the District of Columbia, localities, territories, and tribal governments in responding to, and recovering from, the COVID-19 pandemic. Our work on the CSLFRF, in particular, is ongoing. We will continue to review the extent to which federal agencies provide effective guidance to help recipients achieve accountability and transparency for their use of payments. We also plan to examine how CSLFRF recipients plan to spend their payments, address challenges they face in managing the funds, and evaluate outcomes of their funded projects.
GAO’s Prior Recommendations
The table below presents our recommendation on single audits from a prior bimonthly CARES Act report.
Prior GAO Recommendation Related to Single Audits
Recommendation
Status
The Director of the Office of Management and Budget (OMB) should work in consultation with federal agencies and the audit community (e.g., agency Offices of Inspector General; National Association of State Auditors, Comptrollers, and Treasurers; and American Institute of Certified Public Accountants), to the extent practicable, to incorporate appropriate measures in OMB’s process for preparing single audit guidance, including the annual Single Audit Compliance Supplement, to better ensure that such guidance is issued in a timely manner and is responsive to users’ input and needs (March 2021 report).
Open. OMB neither agreed nor disagreed with our recommendation. Although OMB stated that it shares the draft Compliance Supplement with the grant and audit communities as part of the Compliance Supplement preparation process, OMB has not taken additional steps to ensure the Compliance Supplement and other single audit guidance is issued in a timely manner and is responsive to users’ input and needs. In April 2021, OMB reached out to us for consultation on the development of single audit guidance for the ARPA. In May, GAO, OMB, and audit community stakeholders met to further discuss single audit guidance needed for ARPA. OMB stated during the meeting that it does not have a planned issuance date for the 2021 Compliance Supplement. We will continue to monitor the actions OMB takes in response to our recommendation.
U.S. imports of COVID-19-related products, such as face masks, ventilators, gloves, and hand sanitizers, have fluctuated.
Background
The COVID-19 pandemic has disrupted businesses around the world as well as international supply chains. According to the United Nations Conference on Trade and Development, world merchandise trade grew by 8 percent in the fourth quarter of 2020 from the end of the third quarter of 2020—a significant improvement from the 21 percent decline in the second quarter of 2020.[493]
Overview of Key Issues
U.S. trade of COVID-19-related products. U.S. imports of COVID-19-related products, such as face masks, ventilators, gloves, and hand sanitizers, have fluctuated. Available data indicate that U.S. imports of products in categories related to the COVID-19 response decreased by 8 percent from December 2020 through February 2021 before rebounding by 18 percent from February through March 2021 (see figure).[494] Imports of these products in March 2021 were 13 percent higher than in March 2020, when transmission of COVID-19 started to become widespread in the U.S., according to the Centers for Disease Control and Prevention (CDC).
Monthly U.S. Imports of COVID-19-Related Products, by Product Type, Jan. 2018–Mar. 2021
Note: U.S. Census Bureau trade statistics—a widely used source analyzing U.S. international trade—do not contain precise data on imports of COVID-19-related products. As a result, we estimated the import value of all product types and categories within those types using Harmonized Tariff Schedule of the United States (HTS) statistical reporting numbers and associated product groupings listed by the U.S. International Trade Commission (USITC). See U.S. International Trade Commission, COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). Revisions to the HTS on July 1, 2020, and January 1, 2021, provided several new HTS-10 statistical reporting numbers for previously identified COVID-19-related product categories. We identified these product categories and included them in our analysis. Some HTS categories represent more than one product, and some categories contain products that are not directly relevant to COVID-19 responses. Product categories that USITC identified as COVID-19 related refer only to the subset of goods considered to be COVID-19 related in each HTS-10 statistical reporting number. Therefore, the values shown may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, the values shown are useful indicators for tracking import trends for such products. For more information about factors influencing import trends in various types of COVID-19-related products, see U.S. International Trade Commission, COVID-19 Related Goods: The U.S. Industry, Market, Trade and Supply Chain Challenges, Investigation No. 332-580 (December 2020).
Many factors affecting product availability—such as supply chain constraints, export restrictions, and product demand—may drive trends in imports of COVID-19-related products. Additionally, total trends in import value are related to changes in import prices. For example, the unit value of nasal swabs increased by 4 percent from March 2020 through March 2021, possibly contributing to a rise in the import values of those products over the same period. Overall, the need for medical supplies in response to the pandemic explains the increase in imports of these products since early 2020. Fluctuations in the number of COVID-19 cases may shift the demand for some COVID-19 products, such as pharmaceuticals and diagnostic equipment, over time.
From December 2020 through March 2021, imports of COVID-19-related products from China—which accounted for 15 percent of such imports in March—increased, and imports of these products from the rest of the world also rose slightly.[495] During this period, imports of COVID-19-related products from China rose by 12 percent (from $2.44 billion to $2.75 billion) and imports of such products from other countries rose by 7 percent (from $15.1 billion to $16.2 billion). Previously, from November through December 2020, imports of COVID-19-related products from China had increased by 2 percent (from $2.39 billion to $2.44 billion) and from other countries by 7 percent (from $14.12 billion to $15.09 billion).[496]
In January and February 2021, total U.S. exports of COVID-19 vaccines to European Union (EU) member countries and the United Kingdom (UK) were almost 10 times greater than the total U.S. imports of the vaccines from those countries.[497] The table below shows the value of U.S. imports and exports of COVID-19 vaccines to and from EU member countries and the UK.
Value of U.S. Trade of COVID-19 Vaccines with European Union Member Countries and United Kingdom in Jan. and Feb. 2021 (U.S. dollars in millions)
Month
U.S. imports of COVID-19 vaccines from EU countries
U.S. exports of COVID-19 vaccines to EU countries
U.S. imports of COVID-19 vaccines from UK
U.S. exports of COVID-19 vaccines to UK
Total imports of COVID-19 vaccines
Total exports of COVID-19 vaccines
January 2021
1.3
61.7
0
0
1.3
61.7
February 2021
5
6.2
.6
0
5.6
6.2
Total
6.4
68.7
.6
0
7
68.7
Legend: EU = European Union, UK = United Kingdom.
Source: GAO analysis of EU Commission and UK trade statistics. | GAO-21-551
Note: We used international trade statistics on goods published by the EU Commission’s Eurostat and Her Majesty’s Revenue and Customs trade in goods statistics to identify imports and exports of vaccines against SARS-related coronaviruses between the U.S. and EU member countries and between the U.S. and the UK. We converted euros and pounds sterling into U.S. dollars using exchange rate data on January 31, 2021, from Federal Economic Reserve Data. The values shown may be underestimated, because the data for some EU member countries were not available. Because of rounding, numbers in columns may not sum to totals shown.
U.S. trade statistics indicate that the EU and UK are the largest exporters of COVID-19 vaccines to the U.S. According to U.S. Census Bureau trade statistics, in January and February 2021, the majority of imports in the product category that contains COVID-19 vaccines were from EU member countries or the UK.[498] The EU Commission reported that member countries had exported 1 million doses of COVID-19 vaccine to the U.S. as of March 11, 2021. However, according to CDC data, more than 275 million doses of COVID-19 vaccines had been administered in the U.S. as of May 19, 2021, which suggests that the majority of these vaccines were produced domestically.
The EU and UK governments have taken steps to regulate exports and liberalize imports of COVID-19 vaccines, which could affect trade flows of these products. On January 29, 2021, the European Commission of the EU issued a regulation imposing an export authorization requirement on certain COVID-19 vaccines and on March 11, 2021, the commission extended this requirement.[499] According to the European Commission, the rationale for the regulation is to ensure timely access to COVID-19 vaccines for all EU citizens and to increase transparency regarding vaccine exports outside the EU. In 2020, the EU and the UK allowed exemptions from value-added taxes on certain imports of COVID-19 vaccines, which will reduce supply chain constraints on acquiring COVID-19 vaccines.
Meanwhile, the U.S. government has taken actions to increase domestic production of the COVID-19 vaccines. For instance, the U.S. government has made efforts to encourage pharmaceutical companies such as Pfizer and Moderna to produce COVID-19 vaccines domestically. In April 2021, we reported that government officials had negotiated with these vaccine companies a requirement for domestic, large-scale manufacturing to ensure, among other things, timely delivery. HHS used the Defense Production Act Title I authorities to ensure sufficient domestic manufacturing capacity to produce the vaccines when the supply chain could have been disrupted.[500]
Methodology
To conduct this work, we reviewed the most recent publicly available U.S. trade statistics from the Census Bureau combined with U.S. International Trade Commission data on product categories that contain COVID-19-related products.[501] To analyze U.S. imports and exports in COVID-19 vaccines, we extracted available EU and UK trade data from the European Commission and Her Majesty’s Revenue and Customs. Specifically, we identified exports and imports of vaccines against SARS-related coronaviruses from and to EU member countries and the UK.[502] We found the trade data sufficiently reliable for our reporting purposes. According to an EU Commission report on the quality of EU trade statistics, data on imports and exports outside the EU from 2016 through 2019 were likely fully accounted for because they rely on customs declarations.[503] Her Majesty’s Revenue and Customs also conducts several validation and credibility checks of its trade data to ensure their accuracy before publication.
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget, which had no comments on this enclosure.
Related GAO Product
COVID-19: Efforts to Increase Vaccine Availability and Perspectives on Initial Implementation. GAO-21-443. Washington, D.C.: April 1, 2021.
Federal agencies’ enforcement actions on fraud-related charges help protect consumers and ensure that taxpayer dollars and government services related to COVID-19 serve their intended purposes.
Entities involved: Government-wide
Background
The public health crisis, economic instability, and increased flow of federal funds associated with the COVID-19 pandemic present increased pressures and opportunities for fraud.[504] By proactively managing fraud risks, federal officials can help safeguard taxpayer dollars to ensure they serve their intended purpose,[505] particularly given that Congress had appropriated about $4.7 trillion as of May 31, 2021, to fund COVID-19 response and recovery efforts.[506] According to GAO’s A Framework for Managing Fraud Risks in Federal Programs, among other things, effective managers of fraud risks refer instances of potential fraud to Offices of Inspector General (OIG) or other appropriate parties, such as law enforcement entities or the Department of Justice, for further investigation.[507]
The extent of fraud associated with the COVID-19 relief funds appropriated to date has not yet been determined. One of the many challenges is that because of fraud’s deceptive nature, programs can incur financial losses related to fraud that are never identified, and such losses are difficult to reliably estimate. However, several individuals have already pleaded guilty to federal charges of defrauding COVID-19 relief programs—including the Small Business Administration’s (SBA) Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program, the Department of Labor’s (DOL) unemployment insurance (UI) program, and economic impact payments (EIP) issued by the Department of the Treasury and Internal Revenue Service. Also, one individual has been convicted at trial of PPP-related fraud.[508] In addition, numerous others faced related federal charges as of April 30, 2021.
Further, federal hotlines have received numerous complaints from the public alleging potential fraud involving COVID-19 relief funds. For example, from March 2020 through April 2021, our hotline—known as FraudNet—received over an estimated 2,000 complaints related to the CARES Act, many of which involve SBA’s PPP and EIDL program, DOL’s UI program, and EIPs (see text box).
Report Fraud, Waste, and Abuse
GAO’s FraudNet supports accountability across the federal government. Allegations of fraud, waste, or abuse can be submitted via the FraudNet portal or by calling the hotline at 1-800-424-5454.
In addition to fraud against federal programs, scammers are also targeting consumers, which can result in financial losses and undermine health and safety. For example, the Federal Trade Commission (FTC) is tracking complaints related to COVID-19 fraud against consumers. According to FTC reporting, the agency had received over 274,000 reports about fraud and over 64,000 reports about identity theft as of May 3, 2021.[509] Also according to FTC reporting, fraud linked to the COVID-19 pandemic has cost Americans over $423 million.
Overview of Key Issues
Since March 2020, the Department of Justice has publicly announced charges in numerous fraud-related cases.[510] The charges—filed across the U.S. and investigated by a range of law enforcement agencies—include making false statements and engaging in identity theft, wire and bank fraud, and money laundering.[511] The number of individuals facing fraud-related charges has continued to grow in the past year and will likely increase, as these cases take time to develop.[512]
Fraud against federal programs. From March 2020 through April 2021, 125 individuals pleaded guilty to federal charges of defrauding COVID-19 relief programs, including SBA’s PPP and EIDL program, DOL’s UI program, and EIPs.[513] For example:
In one case, an individual was sentenced to 41 months in federal prison after fraudulently obtaining nearly $2 million in PPP loans. This individual pleaded guilty to bank fraud and admitted that she had purported to own two businesses, making false representations in PPP loan applications for these two businesses. According to the guilty plea, this individual submitted a PPP application representing that one business had paid more than $1.3 million in wages and compensation, and was approved for and received a PPP loan of more than $1.5 million. Also, this individual submitted a PPP application to a separate bank for the second business and, based on false representations, received a PPP loan for more than $400,000. This individual used the proceeds to make a payment on her personal student loan and to make online retail purchases, among other transactions.
As part of another case, an individual pleaded guilty to major fraud against the U.S. and money laundering conspiracy, associated with a scheme to defraud SBA’s PPP and EIDL program. The individual participated in a scheme to submit more than 20 EIDL loan applications, and submitted a PPP application falsely representing that he had 120 employees on his payroll and over $5 million in payroll expenses when, in fact, he did not operate a business at all. After receiving the funds, this individual withdrew and wired proceeds from the scheme, totaling over $1.2 million, to other individuals.
Two individuals pleaded guilty to wire fraud in connection with defrauding victims using various online scams, including collecting UI in the name of others during the COVID-19 pandemic.[514] One of these individuals was sentenced in March 2021 to 63 months in prison and 3 years of supervised release. For more information on potential fraud in the UI programs, see the enclosure on Unemployment Insurance Programs in appendix I.
One individual pleaded guilty to charges of conspiracy to unlawfully transfer, possess, and use a means of identification in connection with EIPs. This case involved the individual knowingly stealing EIPs issued in the names of other taxpayers and converting them for the individual’s own use.
As of April 30, 2021, one individual had been convicted at trial for COVID-19 relief fraud. A federal jury found this individual guilty of bank fraud, making a false statement to a lending institution, and two counts of money laundering for obtaining a $2.1 million PPP loan and for falsely stating that he intended to use the money to make payroll and pay for rent and utilities for his company.[515] According to the complaint, this individual submitted a loan application that included false and misleading statements that the PPP funds would be used only for business-related purposes, to retain workers, and to maintain payroll or make mortgage payments, lease payments, and utilities payments. The complaint, however, alleges that this individual used a portion of the PPP funds to purchase a catamaran boat, which he registered in his name.
Federal charges were pending against 403 individuals for attempting to defraud COVID-19 relief programs as of April 30, 2021.[516]
Consumer fraud. In addition to fraud against federal programs, fraud can result in financial losses to consumers and undermine health and safety. From March 2020 through April 2021, 11 individuals or entities pleaded guilty to federal charges related to consumer fraud.[517] For example, in one case, an individual was sentenced to 3 years of probation and fined $50,000 for selling a misbranded drug, falsely claiming it would lower a consumer’s risk of contracting COVID-19 by nearly 50 percent. This individual pleaded guilty to the charges.
There were also federal charges pending against 53 individuals or entities related to consumer fraud as of April 30, 2021. For example:
In April 2021, the Department of Justice and FTC announced a civil complaint against one individual and a business in the first enforcement action alleging violations of the COVID-19 Consumer Protection Act.[518] The complaint alleges that these defendants advertised that their products could prevent or treat COVID-19 without competent or reliable scientific evidence to support their claims, and further advertised without scientific support that their products were equally or more effective at preventing COVID-19 than the currently available vaccines.[519]
In another case, one individual was indicted for conspiracy to commit wire fraud by seeking more than $4 million from a purported purchaser of personal protective equipment (PPE) that neither he nor his co-conspirator owned or otherwise had authorization to sell.[520]
In a third case, an individual was indicted for making false and misleading claims in numerous press releases that his company had developed a working, break-through technology that could accurately detect COVID-19 through a quick blood test.[521]
In addition, FTC and the Food and Drug Administration have issued warning letters to companies for allegedly selling fraudulent COVID-19-related products, including those making deceptive or scientifically unsupported claims about their ability to prevent or treat COVID-19. As of April 30, 2021, 64 individuals and entities had pleaded guilty or faced federal charges for different types of consumer fraud, including schemes related to PPE sales, prevention or treatment, and testing (see figure).
Number of Individuals or Entities Who Have Pleaded Guilty to or Faced Federal Charges for Consumer Fraud, as of April 30, 2021
Further, as COVID-19 vaccines become available, potential consumer fraud related to vaccines has emerged. While the extent of vaccine-related fraud is unknown, the Department of Justice has publicly announced charges or other actions in consumer fraud cases involving individuals or entities that claimed to offer vaccines to prevent COVID-19. For example, the Department of Justice issued a permanent injunction to address a fraud scheme in a case where an individual lured customers to “preregister” for a vaccine in exchange for bitcoin. In another case, the Department of Justice seized a domain name for a website that offered COVID-19 vaccines for sale in an effort to seize fraudulent websites that seek to illegally profit from the COVID-19 pandemic.[522]
Other federal cases. The federal government is also pursuing charges including conspiracy, wire fraud, and theft that are related to COVID-19 but separate from consumer fraud—including vaccine-related fraud—and fraud against the federal programs discussed earlier. From March 2020 through April 2021, 12 individuals pleaded guilty to these types of federal charges.[523] For example, one individual pleaded guilty to conspiring to violate the Anti-Kickback Statute and conspiring to commit health care fraud for paying and receiving illegal kickbacks in exchange for referring Medicare beneficiaries for testing, including COVID-19 tests. Another individual was sentenced to 3 years of probation and fined $5,000 after pleading guilty to forging prescriptions and fraudulently obtaining prescription drugs, including hydroxychloroquine sulfate.[524] There were also other federal charges pending against 27 individuals as of April 30, 2021. For example, two individuals were indicted on charges of conspiracy and wire fraud for their roles in a $30 million health care fraud and money laundering scheme in which they exploited Medicare flexibilities that went into effect during the COVID-19 pandemic to submit fraudulent claims for expensive cancer drugs that were never provided, ordered, or authorized by medical professionals.[525]
Federal agency warnings to help prevent future fraud-related cases. As a result of complaints from the public alleging potential fraud involving COVID-19 relief funds received through hotlines and other fraud detection efforts, federal agencies have warned the public about emerging fraud schemes, which can help prevent future fraud-related cases against federal programs and consumers. For example:
According to a December 2020 press release from the Federal Bureau of Investigation (FBI), the FBI, Department of Health and Human Services (HHS) OIG, and Centers for Medicare & Medicaid Services have received complaints of scammers using the public’s interest in COVID-19 vaccines to obtain personally identifiable information and money through various schemes. As a result, these agencies have warned the public about several emerging fraud schemes related to COVID-19 vaccines, including paying to be put on a wait list or to get early access (see figure).[526]
Examples of Consumer Warnings about COVID-19 Vaccine Scams
In March 2021, FTC warned consumers about a bogus COVID-19 vaccine survey that scammers are using to steal money and personal information. According to FTC, consumers are receiving email and text messages asking them to complete a survey about the various COVID-19 vaccines in exchange for a free reward, but are asked to pay shipping fees.
The FBI, HHS OIG, and FTC have all issued warnings to the public about scams involving COVID-19 vaccination cards. Specifically, these agencies have warned the public not to post photos of vaccination cards on social media, as personally identifiable information contained on the cards could be stolen to commit fraud. In addition, the FBI and HHS OIG have warned the public against making or buying fake COVID-19 vaccination cards, noting that individuals misrepresenting themselves as vaccinated put themselves and others around them at risk of contracting COVID-19.
The Federal Emergency Management Agency (FEMA) reported on its website that it has received reports of scammers reaching out to individuals and offering to register them for funeral assistance.[527] In response, FEMA included information on its website to help the public beware of such scams. Specifically, FEMA noted that it will not contact anyone for personal information until they have called FEMA or have applied for assistance, and directed individuals receiving unsolicited calls or emails from anyone claiming to be a federal employee or from FEMA not to disclose personal information and to report the incident to FEMA, the National Center for Disaster Fraud Hotline, or local law enforcement agencies.[528]
Methodology
To conduct this work, we reviewed information from the Department of Justice to identify federal fraud-related charges related to COVID-19 relief funding as of April 30, 2021. We also analyzed related federal court documents. In addition, we reviewed FTC reports on complaints related to fraud and identity theft, and FEMA, FBI, HHS OIG, and FTC alerts about emerging fraud schemes related to COVID-19.
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget, which provided no comments.
GAO’s Ongoing Work
We will continue our oversight of government-wide fraud risk management efforts.
Related GAO Product
A Framework for Managing Fraud Risks in Federal Programs. GAO-15-593SP. Washington, D.C.: July 28, 2015.
The U.S. Postal Service’s mail volume decreased, its on-time performance declined, and its finances improved in the first 3 months of 2021 as compared to the same period in 2020, most of which was just prior to onset of the COVID-19 pandemic.
Entities involved: U.S. Postal Service
Background
The U.S. Postal Service (USPS) plays a critical role in the nation’s communication and commerce, a role highlighted in 2020 as USPS delivered billions of pieces of mail throughout the COVID-19 pandemic including ballots, Census forms, and recovery rebate checks, in addition to an unprecedented surge of packages. As an independent establishment of the executive branch, USPS is expected to provide affordable, quality, and universal postal service. USPS is also expected to be financially self-sufficient by covering its expenses through revenues generated from the sale of its products and services. However, USPS has not been able to cover its expenses since fiscal year 2007 due to long-term declines in its most profitable mail products and rising expenses, such as for compensation and benefits. As a result, USPS’s financial viability has been on our High-Risk List since 2009.
USPS’s mail volume, on-time delivery performance, revenue, and expenses changed significantly since the onset of the COVID-19 pandemic. We reported in April 2021 that when comparing 2020 to 2019, USPS’s:
overall mail volume declined even with increases in the volume of packages;
on-time performance fell with a steep decline nationwide in December 2020; and
net loss grew even though revenue increased by $4.3 billion.
To help USPS respond to the COVID-19 emergency, the CARES Act, as amended in late 2020, provided USPS up to $10 billion in additional funding for COVID-19-related operating expenses.[529]
Overview of Key Issues
Mail volume. In the second quarter of fiscal year 2021, overall mail volume declined by about 3.2 billion pieces (about 9.6 percent) when compared to the same period in fiscal year 2020.[530] This change is attributable to the continuing decline in market dominant products such as First-Class Mail (e.g., letters, cards, billing statements) and Marketing Mail (e.g., advertisements, flyers, newsletters). While the volume of market dominant products has continued to decline since 2007, competitive product (primarily packages) volume has continually increased year over year, with significant increases since the onset of the COVID-19 pandemic. For example, in the second quarter of fiscal year 2021, package volume was about 28.6 percent higher than it was in the same period in fiscal year 2020.
On-time performance. Nationally, while on-time performance for market dominant products was significantly lower during the second quarter of fiscal year 2021 as compared to the same period in fiscal year 2020, performance began rebounding in January from December lows. On-time performance for First-Class Mail averaged 78.1 percent nationally from January through March 2021, as compared to 92.2 percent for the same period in fiscal year 2020. Moreover, the first quarter of fiscal year 2021 ended with a December on-time performance for First Class Mail of 69 percent. However, January 2021 showed an improvement in on-time performance, and was followed by increases in February and March as well. Over the quarter, on-time performance for First Class Mail increased from 74.9 percent in January 2021, to 76.0 percent in February 2021, to 83.8 percent in March 2021, but remained well below 2020 levels.
Revenue and expenses. USPS reported a net loss of $82 million for the second quarter of fiscal year 2021, as compared to a net loss of $4.5 billion for the same period in fiscal year 2020. Excluding non-cash workers' compensation adjustments for each period that vary significantly based on interest rate and other actuarial revaluations, the loss for the 2021 second quarter would have been approximately $1.7 billion, compared to a loss of approximately $1.9 billion for the same quarter last year. USPS earned about $1 billion more in revenue in the second quarter of fiscal year 2021, when compared to the second quarter of fiscal year 2020. Following the trend we reported in April 2021, revenue from USPS’s market-dominant products declined by about $1 billion due to volume decreases while revenue for USPS’s competitive products increased by about $2 billion. USPS’s expenses decreased by approximately $3.4 billion for the second quarter in fiscal year 2021 when compared to the same period in fiscal year 2020. USPS attributed this change to a $4.3 billion decrease in worker’s compensation expenses due to changes in interest rates. USPS reported that this decrease was partially offset by increases in expenses. For example, employee compensation and benefits increased $517 million due to additional work hours needed to process higher package volumes and COVID-19 leave costs, among other things. Transportation expenses also increased $336 million due to more and bigger packages, among other things.
COVID-19 funding. USPS stated that under the CARES Act, as amended, it has received about $7.2 billion in funding for operating expenses incurred due to the COVID-19 emergency from March to December 2020 and about $1.5 billion for expenses incurred from January to February 2021.[531] These expenses included categories such as overtime, hiring and training costs of new employees, absenteeism, and costs of sanitizing work areas (see table).
Amounts Requested by USPS Under the CARES Act, as Amended, for COVID-19-Related Operating Expenses Incurred Mar. 2020–Feb. 2021
Expense category
Mar.– Dec. 2020 ($ in millions)
Jan.–Feb. 2021 ($ in millions)
Supplies & services
254
15
COVID leave
426
31
Transportation
73
0
Hiring/training costs for new employees
121
19
Increase in carriers out after 6 p.m.
47
6
Overall overtime cost increase
1,371
265
Inefficiency factor – general inefficiency of 2 percent of salaries and benefits for time spent managing personal protective equipment, sanitizing work areas, social distancing in postal facilities, among other things.
987
200
Inefficiency Factor – New Hires/Absenteeism
348
24
Additional expenses incurred in providing USPS’s statutorily mandated infrastructure and operations during the COVID-19 emergencya
3,559
902.9
Total (rounded):
7,200
1,500
Source: GAO analysis of U.S. Postal Service (USPS) data. | GAO-21-551
Note: These funds are made available by the CARES Act, Pub. L. No. 116-136, div. A, tit. VI, § 6001, 134 Stat. 281, 504-05 (2020), as amended by the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div, N, tit. VIII, § 801, 134 Stat. 1182, 2119 (2020). USPS requests these funds pursuant to a memorandum of understanding with the Department of the Treasury. aAccording to USPS’s memorandum of understanding with the Department of the Treasury, these additional expenses are due to changes in product volumes attributable to the COVID-19 Emergency versus pre-COVID forecasts in USPS’s financial plans, taking into account (1) the costs captured above for Supplies and Services, (2) the revenue and expenses of all products and services, and (3) the actions USPS was unable to undertake to account for the reduction in volumes because of its statutory mandates, such as the requirement to provide 6-days-a-week delivery. See, e.g., Pub. L. No. 116-260, div. E, tit. V, 134 Stat. 1182, 1423 (2020).
As stated above, USPS has not been able to cover its expenses with its revenues since fiscal year 2007 due to long-term declines in its most profitable mail products and rising expenses, such as for compensation and benefits. USPS has maintained its operations since then through a combination of actions, such as taking on debt and not making required payments for pensions and retiree health care benefits. USPS stated that it took those actions to preserve cash to continue to provide universal postal service.
USPS’s cash balance increased significantly in part due to CARES Act funding and the increase in packages during the pandemic. At the end of December 2020, USPS reported that its cash balance was about $15.7 billion and increased to about $25.5 billion at the end of March 2021. As we reported in April 2021, USPS continued to preserve cash in 2020 by forgoing making required retiree health care and pension payments and by borrowing more from USPS’s existing debt authority with the federal government. However, USPS reported that this increased cash amount is insufficient to support USPS’s annual operating expenses, its capital investments, and to prepare for unexpected contingencies.
USPS’s cash balance could be reduced in the coming years. As stated above, USPS expects to deplete all of its CARES Act funds by the end of 2021. USPS projects that the increased volume of packages may not be sustained, which could reduce USPS’s revenue. USPS also deferred payments of about $1.8 billion for the employer’s share of the Social Security payroll tax on wages from March 27, 2020, through December 31, 2020, as allowed under the CARES Act. Payment of half of this deferred amount is due on December 31, 2021, and payment of the other half is due on December 31, 2022.
Methodology
To conduct this work, we analyzed the most recent USPS volume, on-time performance, and revenue and expense data, as of March 2021, which were the latest data available. We used USPS’s 10-Q financial statement for the second quarter of fiscal year 2021. To determine the reliability of the data we used, we interviewed relevant USPS officials about volume, on-time performance, and financial data that they either provided us directly or that we obtained from publicly available reports. They described where the data came from, how they were collected, and controls in place to provide assurance the data were complete and accurate. Based on these interviews and relevant USPS documents we reviewed, we determined all data used were sufficiently reliable for the purposes of reporting on USPS mail volumes, on-time performance levels, revenues, and expenses.
We also reviewed applicable federal laws and interviewed USPS officials.
Agency Comments
We provided USPS and the Office of Management and Budget (OMB) with a draft of this enclosure for review and comment. USPS provided technical comments that we incorporated as appropriate. USPS also provided general comments, which are reproduced in Appendix XII. In its comments, USPS provided additional context about its financial condition, recent service performance, and anticipated plans to address these issues. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor how USPS uses funds made available by the CARES Act, as amended, as well as its volume, on-time performance, revenue, and expenses. We are currently conducting work on USPS’s strategic plan, its service in rural areas, the resilience of its facilities, and its non-career workforce.
Related GAO Products
U.S. Postal Service: Volume, Performance, and Financial Changes since the Onset of the COVID-19 Pandemic. GAO-21-261. Washington, D.C.: April 2021.
High Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas.GAO-21-119SP. Washington, D.C.: March 2021.
High Risk Series: Restructuring the U.S. Postal Service to Achieve Sustainable Financial Viability. GAO-09-937SP. Washington, D.C.: July 2009.
We issued Grants Management: OMB Should Collect and Share Lessons Learned from Use of COVID-19-Related Grant Flexibilities, GAO-21-318, on March 31, 2021.
We issued Global Health Security: USAID and CDC Funding, Activities, and Assessments of Countries' Capacities to Address Infectious Disease Threats before COVID-19 Onset, GAO-21-359, on April 14, 2021.
We issued COVID-19 in Nursing Homes: Most Homes Had Multiple Outbreaks and Weeks of Sustained Transmission from May 2020 through January 2021, GAO-21-367, on May 19, 2021.
We issued Employee Benefits Security Administration: Enforcement Efforts to Protect Participants' Rights in Employer-Sponsored Retirement and Health Benefit Plans, GAO-21-376, on May 27, 2021.
We issued Management Report: Preliminary Information on Potential Racial and Ethnic Disparities in the Receipt of Unemployment Insurance Benefits during the COVID-19 Pandemic, GAO-21-599R, on June 17, 2021.
We issued Independence Day Celebrations: Estimated Costs and COVID-19 Protective Measures for 2020 Fourth of July Events, GAO-21-458, on June 21, 2021.
We issued Software Development: DOD Faces Risks and Challenges in Implementing Modern Approaches and Addressing Cybersecurity Practices, GAO-21-351, on June 23, 2021.
We issued, Veterans Community Care Program: VA Took Action on Veterans' Access to Care, but COVID-19 Highlighted Continued Scheduling Challenges, GAO-21-476, on June 28, 2021.
We issued COVID-19 Housing Protections: Mortgage Forbearance and Other Federal Efforts have Reduced Default and Foreclosure Risks, GAO-21-554, on July 12, 2021.
We issued COVID-19: The Coast Guard Has Addressed Challenges, but Could Improve Telework Documentation and Personnel Data, GAO-21-539, on July 16, 2021
Appendix III: List of Ongoing GAO Work Related to COVID-19, as of June 23, 2021
In our June 2020 CARES Act report, we made three matters for congressional consideration and three recommendations for executive action; in our September 2020 CARES Act report, we made 16 recommendations; and in our November 2020 CARES Act report, we made one matter for congressional consideration and 11 recommendations. Also, in November 2020, we issued a report on COVID-19 vaccines and therapeutics, in which we made one recommendation. In our January 2021 CARES report, we made 13 recommendations; and in our March 2021 CARES Act report, we made 28 recommendations. Following are the recommendations and their status, by department (see fig. 8).
Figure 8: Status of Prior GAO Recommendations by Department or Agency
Below we list by department or agency our four prior matters for congressional consideration and our 72 prior recommendations, and characterize their implementation status.
Status of Matters for Congressional Consideration and Recommendations Related to the Department of Health and Human Services
Matter. To help ensure that federal funding is targeted and timely, we urge Congress to use our Federal Medical Assistance Percentage formula for any future changes to the Federal Medical Assistance Percentage during the current or any future economic downturn (June 2020 report).
Status: Open
Comments: Our past work has found that during economic downturns—when Medicaid enrollment can increase and state economies weaken—the formula, which is based on each state’s per capita income, does not reflect current state economic conditions. No congressional action has been taken to date.
Recommendation. The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency (FEMA)—who head agencies leading the COVID-19 response through the Unified Coordination Group—should immediately document roles and responsibilities for supply chain management functions transitioning to the Department of Health and Human Services (HHS), including continued support from other federal partners, to ensure sufficient resources exist to sustain and make the necessary progress in stabilizing the supply chain, and address emergent supply issues for the duration of the COVID-19 pandemic (September 2020 report).
Status: Open
Comment: HHS disagreed with our recommendation. In a May 2021 update, the Office of the Assistant Secretary for Preparedness and Response (ASPR) noted that since March 2020, supply chain responsibility, coordination, and execution have been incorporated and integrated into ASPR. HHS stated that ASPR’s supply chain work is divided into three areas: (1) logistics and supply chain management, (2) supply chain and industrial situational awareness, and (3) industrial base expansion. The update noted that this work provides solutions to HHS and other federal partners to address supply chain shortages and vulnerabilities and supports a collaborative approach. Finally, HHS offered several examples of HHS and ASPR’s efforts, including restocking the Strategic National Stockpile; mitigating potential shortages of raw materials; continuing to partner with the Department of Defense (DOD) on supply acquisition; and helping develop the pandemic supply chain resilience strategy. However, HHS has yet to document roles and responsibilities for supply chain management that are transitioning.
We noted in our September 2020 report that complex medical supply management responsibilities that had been shared between many agencies during the nationwide response to COVID-19 were transitioning to HHS. This included procuring testing supplies, monitoring the commercial supply chain, and fulfilling state, local, tribal, and territorial governments’ requests for supplies. We acknowledge the efforts made to date by HHS and ASPR, but as supply chain efforts continue—and ASPR continues to work closely with, and rely on, federal partners—we maintain that our recommendation is warranted to sustain the progress made to date, especially as the pandemic continues and variants circulate.
Recommendation. The Secretary of Health and Human Services in coordination with the Administrator of FEMA—who head agencies leading the COVID-19 response through the Unified Coordination Group—should further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic, including through the use of Defense Production Act authorities (September 2020 report).
Status: Open
Comment: HHS disagreed with our recommendation. However, HHS has taken some action that would implement this recommendation. In a May 2021 update, ASPR noted that since March 2020, supply chain responsibility, coordination, and execution has been incorporated and integrated into ASPR. HHS stated that ASPR’s supply chain work is divided into three areas: (1) logistics and supply chain management, (2) supply chain and industrial situational awareness, and (3) industrial base expansion. The update noted that this work provides solutions to HHS and other federal partners to address supply chain shortages and vulnerabilities and supports a collaborative approach. Finally, HHS offered several examples of HHS and ASPR’s supply chain work, including restocking the Strategic National Stockpile; mitigating potential shortages of raw materials; continuing to partner with DOD on supply acquisition; and helping develop the pandemic supply chain resilience strategy.
We noted in our September 2020 report that HHS and FEMA had not developed plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps needed to respond to the pandemic, including through the use of Defense Production Act authorities. ASPR notes in its May 2021 update that it is the lead agency for HHS for developing the Public Health and Biological Preparedness Industrial Base Report under Executive Order 14001 – A Sustainable Public Health Supply Chain. ASPR also states that it is integrated into the interagency supply chain working groups run by the White House to reconcile and manage public health supply chain constraints and shortages. We believe these are good steps toward developing plans to mitigate supply gaps—both now and for future pandemics—and we will continue to monitor the progress to develop a supply chain strategy.
Recommendation. The Secretary of Health and Human Services—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with its roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
Status: Open
Comment: HHS disagreed with this recommendation, noting, among other things, work that had already been done to manage the medical supply chain and increase supply availability. As of May 2021, HHS has not demonstrated action to devise interim solutions that would systematically help states, tribes, and territories effectively track, manage, and plan for supplies to carry out the COVID-19 pandemic response in the absence of state-level end-to-end logistics capabilities that would track critical supplies required for a response of this scale. We note that we made this recommendation to both HHS and the Department of Homeland Security (DHS) with the intent that they would work together under the Unified Coordination Group to address challenges reported by state officials with both public health and emergency management responsibilities. Moreover, we recommended they take actions that were consistent with the roles and responsibilities that were to be more clearly defined as HHS took a more central role in leading supply distribution.
The recommendation to define those roles and responsibilities remains open. Moreover, although both HHS and DHS have reported separate actions taken as part of other efforts within each separate purview, neither has articulated how it worked with the other nor how it assessed whether the actions changed the experiences of state officials who reported issues during our prior work. Without systematic and deliberate action to help jurisdictions ensure they have the support they need to track, manage, and plan for supplies, those on the front lines of the whole-of-nation COVID-19 response may continue to face challenges that hamper their effectiveness as the pandemic continues and variants circulate.
Recommendation. The Secretary of Health and Human Services, with support from the Secretary of Defense, should establish a time frame for documenting and sharing a national plan for distributing and administering a COVID-19 vaccine and, in developing such a plan, ensure that it is consistent with best practices for project planning and scheduling and outlines an approach for how efforts will be coordinated across federal agencies and nonfederal entities (September 2020 report).
Status: Open
Comment: The Department of Health and Human Services (HHS) neither agreed nor disagreed with our recommendation. In September and October 2020, HHS’ Centers for Disease Control and Prevention (CDC) released initial planning documents, and in January 2021 the White House issued a national COVID-19 response strategy that broadly outlined various channels for vaccine distribution. In addition, CDC provided a high-level description of its activities in a March 2021 COVID-19 vaccine distribution strategy and its June 2021 update. While these documents provide general information on federally supported vaccine distribution activities, they do not outline the approach the federal government is taking to coordinate its efforts or roles of the federal agencies and non-federal entities. We continue to maintain that it is important for HHS to have a national plan that outlines such an approach. We will continue to monitor HHS’ efforts in this area.
Recommendation. Based on the imminent cybersecurity threats, the Secretary of Health and Human Services should expedite the implementation of our prior recommendations regarding cybersecurity weaknesses at its component agencies (September 2020 report).
Status: Open
Comment: HHS agreed with our recommendation and has taken steps to address it. For example, the department’s Office of Information Security has begun planning efforts for the establishment of an audit program intended to identify and centralize audit management capabilities to perform recommendation follow-up activities, among others. Planning efforts for the program are expected to be completed in September 2021. In addition, the Office of Information Security, along with other staff divisions at the department, is planning to join an enterprise effort to increase oversight and reduce the time to resolve recommendations made across HHS through use of audit tracking and storage software. Nevertheless, as of April 2021, the status of the cybersecurity recommendations we issued to the relevant HHS component agencies—the Food and Drug Administration (FDA), the Centers for Medicare & Medicaid Services (CMS), and CDC—remained the same as what we reported in March 2021. Specifically, the component agencies had implemented 421 (about 97 percent) of the total 434 recommendations we made to these agencies.
Recommendation. The Secretary of Health and Human Services should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that HHS has produced for the public and Congress to allow for a more coordinated pandemic testing approach (January 2021 report).
Status: Open
Comment: HHS partially agreed with our recommendation. In January 2021, HHS agreed that the department should take steps to more directly incorporate some of the elements of an effective national strategy, but expressed concern that producing such a strategy at this time could be overly burdensome on the federal, state, and local entities that are responding to the pandemic, and that a plan would be outdated by the time it was finalized or potentially rendered obsolete by the rate of technological advancement. In May 2021, HHS told us that the White House and HHS plan to execute a National Testing Strategy that will act upon the administration’s testing goals. According to HHS, a finalized document is forthcoming that includes specific actions as well as timelines to achieve these goals. HHS said the National Testing Strategy will speak to the country’s short-term COVID-19 needs as well as the long-term needs associated with the country’s broader bio-preparedness. We will continue to monitor the implementation of this recommendation.
Recommendation. To improve the federal government’s response to COVID-19 and preparedness for future pandemics, the Secretary of Health and Human Services should immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. This committee should include a broad representation of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits (January 2021 report).
Status: Open
Comment: HHS partially agreed with our recommendation. In its May 2021 response, HHS stated that it plans to consider ways to establish more permanent work groups to incorporate best practices for ongoing interagency data needs and to scale up as necessary during future public health emergencies. HHS also stated that the Data Strategy and Execution Workgroup, established as part of the HHS COVID-19 response, has helped address the need for a federal interagency coordination process to align ongoing COVID-19 data collection and reporting efforts. We maintain that immediately establishing an expert committee—not limited to federal agency officials—that includes knowledgeable health care professionals from the public and private sectors, academia, and nonprofits is an important and worthwhile effort to help improve the federal government’s response to COVID-19 and its preparedness for future pandemics.
Recommendation. The Secretary of Health and Human Services should make the Department's different sources of publicly available COVID-19 data accessible from a centralized location on the internet. This could improve the federal government's communication with the public about the ongoing pandemic (March 2021 report).
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. In its May 2021 response, HHS stated that it makes COVID-19 content accessible on its website home page, which includes links to specific information that may be contained on other websites. HHS added that CDC’s COVID Data Tracker provides information on community transmission, cases, and vaccination rates. Given the importance of effectively communicating information about the status of the pandemic with the public, we maintain that HHS should make its publicly available COVID-19 data accessible from a centralized online location. Centralizing access to these data in a way that allows individuals to easily locate and obtain the information most relevant to them would improve the ability of the public to fully understand the extent of the pandemic and use the data to best inform their ongoing decision-making.
Recommendation. The Secretary of Health and Human Services should finalize and implement a post-payment review process to validate COVID-19 Uninsured Program claims and to help ensure timely identification of improper payments, including those resulting from potential fraudulent activity, and recovery of overpayments (March 2021 report).
Status: Open
Comment: HHS agreed with our recommendation to finalize and implement a post-payment review process. In response, in May 2021, HHS stated that it had developed a standard operating procedure to initiate a review process to ensure program integrity and compliance with the Uninsured Program’s terms and conditions through a detailed claims review. Additionally, HHS stated that with contractor support, it is currently developing the uninsured audit review strategy, which includes a detailed protocol and procedures for the assessments of the Uninsured Program to be executed by audit contractors. HHS officials added that all claims determined to be paid to an ineligible provider, or a provider that did not maintain supporting documentation to substantiate the claims or in any other way did not comply with the program terms and conditions, will be required to return the funds. We will continue to monitor the implementation of this recommendation to ensure that these efforts continue.
Recommendation. The Secretary of Health and Human Services should ensure that FDA and CDC work with the Assistant Secretary of Labor for Occupational Safety and Health to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with emergency use authorization (March 2021 report).
Status: Open
Comment: HHS agreed with this recommendation. FDA commented that there is an opportunity to build on prior collaboration and lessons learned during the pandemic to ensure that there is a process in place that yields timely and consistent information for stakeholders using and purchasing authorized devices. In May 2021, CDC commented that FDA, CDC’s National Institute for Occupational Safety and Health, and the Occupational Safety and Health Administration had met to discuss how existing informal processes should evolve into formal processes and planned to meet again in coming months to discuss next steps.
HHS CDC
Recommendation. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should determine whether having the authority to require states and jurisdictions to report race and ethnicity information for COVID-19 cases, hospitalizations, and deaths is necessary for ensuring more complete data and, if so, seek such authority from Congress (September 2020 report).
Status: Open
Comment: CDC agreed with our recommendation. In response, in February 2021, CDC stated that it was reviewing race and ethnicity data completeness across its core surveillance systems and engaging stakeholders from across the agency and in state and local health departments to improve the collection of race and ethnicity data. CDC noted that stakeholders include CDC leadership, key task forces from within CDC's COVID-19 emergency response, and data and surveillance experts in CDC and state health agencies. CDC reported that the information derived from this review will be discussed with the CDC Director and used to assess potential opportunities to enhance the collection of race and ethnicity data, including seeking policy changes or legislative authorities. In addition, in May 2021, CDC stated that it was conducting an analysis to determine whether additional authorities given to the agency to mandate the collection of race and ethnicity information could enhance the robustness and completeness of data shared with the agency. We will continue to examine the ongoing work of HHS, CDC, and other component agencies regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should involve key stakeholders to help ensure the complete and consistent collection of demographic data (September 2020 report).
Status: Open
Comment: CDC agreed with our recommendation. In response, in February 2021, CDC stated that it was reviewing the quality of demographic data, including the completeness of race and ethnicity data, across its core surveillance systems and engaging stakeholders from across the agency and in state and local health departments on the issue. CDC noted that stakeholders include CDC leadership, key task forces from within CDC's COVID-19 emergency response, and data and surveillance experts in CDC and state health agencies. CDC reported that the information derived from this review will be discussed with the CDC Director and used to assess potential opportunities to enhance the collection of race and ethnicity data, including seeking policy changes or legislative authorities.
As of May 2021, CDC reported that it had conducted listening sessions with community health workers who serve communities of color and rural populations to seek input on the importance of collecting race and ethnicity data. CDC stated that the information collected will inform the development of appropriate and tailored messages that can be used by community health workers to educate communities about the importance of providing race and ethnicity data when receiving health services, overcome hesitance in sharing this information, and describe how this information is used to promote community health. In addition, CDC stated that it is working with public health partners to automate the generation and transmission to CDC of COVID-19 case reports that contain demographic information, including race and ethnicity. According to CDC, as of May 1, 2021, more than 6,700 facilities were sending COVID-19 electronic case reports to state and jurisdictional health departments. We will continue to examine the ongoing work of HHS, CDC, and other component agencies regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should take steps to help ensure CDC’s ability to comprehensively assess the long-term health outcomes of persons with COVID-19, including by race and ethnicity (September 2020 report).
Status: Open
Comment: CDC agreed with our recommendation. In response to our recommendation, CDC noted in October 2020 that it was convening a team to develop a plan to monitor the long-term health outcomes of persons with COVID-19 by identifying health care surveillance systems that can electronically report health conditions to state and local health departments. CDC said that, as of May 2021, it had various efforts underway with external partners to assess long-term health outcomes. For example, CDC is funding a number of prospective studies in partnership with universities to understand the long-term effects of COVID-19, including a study examining the neurological health outcomes of a large cohort of Black and Hispanic or Latino persons who had COVID-19. In May 2021, CDC reported that its ongoing studies will follow patients for up to 2 years and provide information on the percentage of people who develop post-COVID-19 conditions and assess risk factors for the development of these conditions. According to CDC, these studies will assess different virus strains and antibody responses and the underlying immune response in people who develop post-COVID conditions.
In addition, CDC reported that it is continuing to use multiple de-identified electronic health record databases to examine the persistence of symptoms and incidence of post-COVID conditions. CDC stated that it is also partnering with health systems to perform in-depth medical record reviews, which can provide insight into the patterns of health effects that patients are experiencing and improve its ability to characterize post-COVID conditions. For example, in April 2021 CDC published a Morbidity and Mortality Weekly Report describing patients with post-COVID-19 conditions using electronic health records in an integrated health care system in metropolitan Atlanta. CDC added that it had updated its website on post-COVID conditions in April 2021. We will continue to examine the ongoing work of HHS, CDC, and other component agencies regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. The Director of CDC should ensure that, as it makes updates to its federal guidance related to reassessing schools’ operating status, the guidance is cogent, clear, and internally consistent (September 2020 report).
Status: Closed
Comment: CDC agreed with this recommendation and it is closed as implemented. CDC’s guidance for school operating status during COVID-19 is more cogent, clear, and consistent. On February 12, 2021, CDC released revised guidance for returning to in-person learning, as well as mitigation strategies to help prevent and reduce the spread of COVID-19 in school settings. We found the guidance consolidated much of the earlier guidance into one document that clearly displays all five of CDC’s mitigation strategies and includes steps school officials should consider when deciding to reopen schools. In addition, we identified increased efforts to synchronize content across CDC’s website. We found that CDC had removed some information and updated other information and had begun including summaries of changes made to the guidance at the top of some webpages.
Recommendation. The Secretary of Health and Human Services should ensure that the Director of CDC clearly discloses the scientific rationale for any change to testing guidelines at the time the change is made (November 2020 report).
Status: Open
Comment: HHS agreed with our recommendation and has begun to implement it. For example, on February 16, 2021, CDC issued Interim Guidance on Testing Healthcare Personnel that stated asymptomatic health care personnel who have recovered from COVID-19 may not need to undergo repeat testing or quarantine in the case of another exposure within 3 months of their initial diagnosis. To support this guidance, CDC's website provided links to studies that explained the scientific rationale. Additionally, CDC told us that it continues to consult with scientific stakeholders when issuing or updating guidance documents, and outlined a series of steps the agency plans to take to strengthen its testing guidance. However, as of May 2021, CDC had not fully addressed the recommendation. For example, clear linkage to a scientific rationale for recent changes related to testing after exposure for fully vaccinated individuals appeared to be missing. We will monitor the implementation of this recommendation to ensure that these efforts continue.
Recommendation. The Secretary of Health and Human Services should ensure that the Director of CDC collects data specific to the COVID-19 vaccination rates in nursing homes and makes these data publicly available to better ensure transparency and that the necessary information is available to improve ongoing and future vaccination efforts for nursing home residents and staff (March 2021 report).
Status: Closed
Comment: HHS neither agreed nor disagreed with our recommendation. In March 2021, HHS said it was working towards better data transparency and noted that nursing homes have an opportunity to voluntarily report data through the National Healthcare Safety Network tracking system.
On May 13, 2021, CMS issued an interim final rule establishing Long-Term Care Facility Vaccine Immunization Requirements for Residents and Staff, including for nursing homes. The rule requires facilities to report COVID-19 vaccination status of residents and staff to CDC. According to CDC, the new vaccination reporting requirement will not only assist in monitoring vaccine uptake among residents and staff, but will also aid in identifying facilities that may be in need of additional resources and assistance to respond to the COVID-19 pandemic. As of June 10, 2021, CMS has posted resident and staff vaccination rates for over 15,000 Medicare and Medicaid certified nursing homes on a public COVID-19 Nursing Home Data tracking website.
Recommendation. The Director of CDC should incorporate key elements of a national strategy in the agency's COVID-19 Response Health Equity Strategy. These elements include (1) specific actions to achieve intermediate outcomes, such as increased access to testing; (2) how intermediate outcomes should be prioritized within its four broad priority areas; (3) who will implement actions to achieve intermediate outcomes; and (4) how the strategy relates to other relevant strategies (March 2021 report).
Status: Open
Comment: CDC agreed with this recommendation. CDC stated that it will take steps to include key elements of a national strategy in an internal version of its COVID-19 Response Health Equity Strategy to help with coordination and tracking, among other actions to coordinate health equity activities across various task forces and with federal, state, and local partners. In May 2021, CDC reported that it had implemented the Health Equity Action Tracker as an internal repository of health equity activities related to COVID-19. According to CDC, this tracker includes questions about alignment with the intermediate outcomes in the CDC Health Equity Strategy, as well as questions about additional outcomes and the impact of the activities. CDC added that it launched its Health Equity in Action website in April 2021 to share activities, partnerships, and resources to advance health equity.
In May 2021, CDC also clarified that it does not agree with identifying how intermediate outcomes should be prioritized within the four broad priority areas of CDC’s COVID-19 Response Health Equity Strategy. CDC noted that it does not intend to prioritize its intermediate outcomes because they contribute equally to the achievement of the final outcomes outlined within its COVID-19 Response Health Equity Strategy. Regarding who will implement actions to achieve intermediate outcomes, CDC reported that no one unit is responsible for implementing the strategy as a whole or for implementing each intermediate outcome. CDC added that the strategy provides a guide for the entire CDC response. CDC stated that it will continue to analyze and align key elements of a national strategy into its COVID-19 Response Health Equity Strategy, including identifying areas that are in alignment. We will continue to examine the ongoing work of HHS, CDC, and other component agencies regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. The Director of CDC should take steps to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations, such as working with states and jurisdictions to facilitate consistent collecting and reporting of this information (March 2021 report).
Status: Open
Comment: CDC neither agreed nor disagreed with this recommendation. CDC stated that it is working to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations, such as by requiring providers that participate in CDC’s COVID-19 Vaccination Program to report the race and ethnicity of vaccine recipients. We will continue to examine the ongoing work of HHS, CDC, and other component agencies regarding indicators of COVID-19 and disparities that exist for various populations.
HHS CMS
Recommendation. The Administrator of CMS should quickly develop a plan that further details how the agency intends to respond to and implement, as appropriate, the 27 recommendations in the final report of the Coronavirus Commission on Safety and Quality in Nursing Homes, which CMS released on September 16, 2020. Such a plan should include milestones that allow the agency to track and report on the status of each recommendation; identify actions taken and planned, including areas where CMS determined not to take action; and identify areas where the agency could coordinate with other federal and nonfederal entities (November 2020 report).
Status: Closed
Comment: HHS neither agreed nor disagreed with our recommendation. HHS officials highlighted actions that CMS has taken related to Commission recommendations and said it would refer to and act upon the Commission's recommendations, as appropriate.
As of May 2021, CMS had developed an internal tracking document that notes the status of each of the Nursing Home Commission’s recommendations, the responsible agency for each recommendation, and planned actions for CMS-related recommendations. According to CMS, the agency will be conducting quarterly reviews of the tracking document, holding interim meetings to discuss the recommendations, and conducting outreach to other federal agencies to engage them in this work.
Recommendation. The Secretary of Health and Human Services, in consultation with CMS and CDC, should develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively back to January 1, 2020, and to clarify the extent to which nursing homes have reported data before May 8, 2020. To the extent feasible, this strategy to capture more complete data should incorporate information nursing homes previously reported to CDC or to state or local public health offices (September 2020 report).
Status: Open
Comment: HHS partially agreed with our recommendation. As of May 2021, HHS had taken no specific action, although according to HHS it continues to consider how to implement our recommendation. We will continue to monitor HHS’s progress toward implementing this recommendation.
Recommendation. The Secretary of Health and Human Services should ensure that the Administrator of CMS, in consultation with CDC, requires nursing homes to offer COVID-19 vaccinations to residents and staff and design and implement associated quality measures (March 2021 report).
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. On April 15, 2021, CMS issued a proposed rule that includes, among other things, a proposal to adopt a new quality measure for skilled nursing facilities called COVID-19 Vaccination Coverage among Healthcare Personnel. The measure would require facilities to submit data on COVID-19 staff vaccination beginning on October 1, 2021, and would be used as part of CMS’s quality reporting program beginning in fiscal year 2023.
On May 13, 2021, CMS also issued an interim final rule that establishes new requirements for nursing homes to develop and implement policies and procedures for educating residents, their representatives, and staff members about the COVID-19 vaccine and for offering these vaccines to each resident and staff member. Facilities will be assessed for compliance with the new requirements, which became effective on May 21, 2021. We will continue to monitor HHS’s progress toward implementing this recommendation.
HHS FDA
Recommendation. The Secretary of Health and Human Services should direct the FDA Commissioner to identify ways to uniformly disclose to the public the information from FDA’s scientific review of safety and effectiveness data—similar to the public disclosure of the summary safety and effectiveness data supporting the approval of new drugs and biologics—when issuing emergency use authorizations (EUA) for therapeutics and vaccines, and, if necessary, seek the authority to publicly disclose such information (November 2020 report on vaccine and therapeutics).
Status: Closed
Comment: In response to our recommendation, FDA said it would explore approaches to achieve the goal of transparency. On November 17, 2020, FDA made an announcement on its ongoing commitment to transparency for COVID-19 EUAs. FDA also developed a process to disclose its scientific review documents for therapeutic EUAs and released such summaries for one previous therapeutic EUA and the two additional therapeutic EUAs issued from November 2020—when we made our recommendation—through January 2021. These summaries disclosed information similar to what FDA releases to support new drug approvals and biologic licensures. Additionally, for the two vaccine EUAs FDA issued from November 2020—when we made our recommendation—through January 2021, FDA released decision memorandums containing detailed information about FDA’s review of safety and effectiveness data. FDA’s actions meet the intent of our recommendation and will improve transparency.
Recommendation. The Commissioner of FDA should, as the agency makes changes to its collection of drug manufacturing data, ensure the information obtained is complete and accessible to help it identify and mitigate supply chain vulnerabilities, including by working with manufacturers and other federal agencies (e.g., DOD and the Department of Veterans Affairs (VA)), and, if necessary, seek authority to obtain complete and accessible information (January 2021 report).
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. In HHS's response in January 2021, FDA said that it will consider our recommendation as it continues efforts to enhance relevant authorities and close data gaps. Since then, FDA has taken steps to increase its authority to collect more complete drug manufacturing data. For example, FDA’s budget justification for fiscal year 2022 included a legislative proposal to further clarify the agency’s authority to require more complete and frequent reporting for finished drug products and in-process material. Also, in June 2021, as part of a government-wide review of critical U.S. supply chains that included drugs and active pharmaceutical ingredients, HHS reported that it will develop and make recommendations to Congress to grant FDA authority to obtain additional supply chain data that would include reporting of more comprehensive drug manufacturing information to the agency and require drug labels to include original manufacturers, among other things. We will continue to monitor action on these efforts and, if implemented, determine whether they satisfy the intent of our recommendation.
Recommendation. The Commissioner of FDA should, as inspection plans for future fiscal years are developed, ensure that such plans identify, analyze, and respond to the issues presented by the backlog of inspections that could jeopardize the goal of risk-driven inspections (January 2021 report).
Status: Open
Comment: FDA concurred with our recommendation and stated that it is actively tracking the list of sites that need to be inspected. FDA further noted that the size of the backlog will depend on the extent to which alternative inspection tools are used.
Recommendation. The Commissioner of FDA should fully assess the agency’s alternative inspection tools and consider whether these tools or others could provide the information needed to supplement regular inspection activities or help meet the agency’s drug oversight objectives when inspections are not possible in the future (January 2021 report).
Status: Open
Comment: FDA agreed with our recommendation and, as of January 2021, stated that it would continue to evaluate these alternative tools. FDA stated that the resulting information will help determine how the tools can be used to streamline and supplement regular inspection activities and to prioritize inspections when normal inspection operations are not possible.
Recommendation. As FDA develops a transition plan for devices with emergency use authorizations, the Commissioner should specify a reasonable timeline and process for transitioning authorized devices to clearance, approval, or appropriate disposition that takes into account input from stakeholders (March 2021 report).
Status: Open
Comment: HHS concurred with this recommendation. FDA stated that it believes it is important to provide such a transition period to allow sponsors to meet any additional requirements. In addition, FDA stated it will provide the transition plan in the form of draft guidance for public comment so the agency can work to incorporate suggestions from those impacted by the transition. In May 2021, FDA reiterated its intent to address our recommendation and the agency’s plan to issue draft guidance. FDA stated that given volume of device EUAs, the agency recognizes the need for transparency regarding the timeline and approach for transitioning from EUA to marketing authorization.
HHS ASPR
Recommendation. To improve the nation’s response to and preparedness for pandemics, the Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as HHS refines and implements a supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile (January 2021 report).
Status: Open
Comment: HHS generally agreed with our recommendation, while noting that the term "engage" is vague and unclear, and that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority.
Recommendation. The Assistant Secretary for Preparedness and Response, in coordination with the appropriate offices within HHS, should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts (January 2021 report).
Status: Open
Comment: ASPR agreed with our recommendation. As of April 2021, ASPR officials stated that they had discussed within ASPR the need to consistently identify other transaction agreements in the Federal Procurement Data System-Next Generation and explored how their contract writing system may interface with the other transaction agreement module of the data system in the future. ASPR officials added that in the meantime, they have identified other transaction agreements in the procurement module by manually adding designators such as “OTA” or “other transaction agreement” into the description of requirement data field.
Status of Recommendations Made to the Department of the Treasury
Recommendation. The Secretary of the Treasury should finish developing and implement a compliance monitoring plan that identifies and responds to risks in the Payroll Support Program (PSP) to ensure program integrity and address potential fraud, including the use of funds for purposes other than for the continuation of employee wages, salaries, and benefits (November 2020 report).
Status: Closed
Comment: In April 2021, GAO confirmed that the Department of the Treasury (Treasury) had developed, documented, and implemented a risk-based approach to monitor PSP recipients’ compliance with the terms of the assistance. Treasury’s risk-based approach entails a two-level compliance review. In the first-level review, automated testing is conducted on all recipients’ quarterly reports using factors/thresholds that can trigger recipients being moved to the next review. In the second-level review, Treasury analysts conduct a more detailed review of recipients that failed the first-level review or were selected for other reasons. Treasury has also developed penalties and a process for remediating noncompliance with PSP agreement terms. As of April 2021, Treasury had identified noncompliance by recipients and applied penalties, as appropriate.
Recommendation. The Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments (June 2020 report).
Status: Closed
Comment: Treasury and the Internal Revenue Service (IRS) took steps to implement our recommendation, such as providing instructions on the IRS website requesting that individuals voluntarily mail the appropriate economic impact payment (EIP) amount sent to the decedent back to IRS, for both electronic and paper check payments. Treasury has also held and canceled payments made to decedents, along with those that have been returned. As of April 30, 2021, around 57 percent (just over $704 million) of the $1.2 billion in first-round payments sent to deceased individuals had been recovered.
As of March 2021, Treasury and IRS had not taken any further action to recoup payments made to decedents that had not been returned. IRS officials determined that further actions, such as initiating erroneous refund cases against the estates of the decedents to which payments were made and not returned, could be burdensome to taxpayers, the federal court system, and IRS. As such, IRS officials concluded that doing so is not prudent at this time.
Recommendation. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP to help target outreach and communications efforts (September 2020 report).
Status: Open
Comment: Treasury and IRS neither agreed nor disagreed with our recommendation, but did take some actions that are consistent with our recommendation. For example, in January 2021, Treasury revised its estimate of eligible recipients who have yet to file for a first-round EIP to 8 million. According to Treasury officials, this estimate is based on the 9 million notices IRS sent in September 2020. Treasury officials stated that it is likely that some of the 9 million recipients have since claimed the EIP, but Treasury did not provide data supporting this claim.
Recommendation. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should make estimates of eligible recipients who have yet to file for an EIP, and other relevant information, available to outreach partners to raise awareness about how and when to file for EIPs (September 2020 report).
Status: Open
Comment: Treasury and IRS neither agreed nor disagreed with our recommendation, but did take some actions that are consistent with our recommendation. For example, in September 2020, the agencies used tax return information to identify nearly 9 million individuals who had not received a first-round EIP and then notified these individuals that they may be eligible for a payment. The letters also provided instructions on how to request a payment. In addition, IRS publicly released detailed ZIP code data from the notices to help community outreach partners with their own outreach efforts.
Recommendation. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed an EIP notification letter and subsequently filed for and received an EIP, and use that information to inform ongoing outreach and communications efforts (November 2020 report).
Status: Open
Comment: Treasury and IRS agreed with this recommendation. According to Treasury officials, Treasury began analyzing data in January 2021 on those individuals who received a notice and subsequently filed for and received a first-round EIP. However, Treasury does not plan to complete this analysis until fall 2021, more than 6 months after the first third-round EIP payments were issued, limiting how any findings could inform third-round EIP outreach efforts. According to Treasury officials, they are incorporating information from the 2021 filing season into their analysis. The filing season ended on May 17, but there is a 5-month extension to file amended returns.
Recommendation. The Commissioner of Internal Revenue should update the Form 1040-X instructions to include information on the electronic filing capability for tax year 2019 (November 2020 report).
Status: Open
Comment: IRS agreed with our recommendation and said that it would start to update the Form 1040-X instructions to include information on the electronic filing (e-file) capability for tax year 2019.
As of early May 2021, IRS still planned to include this information in the next routine annual update of the instructions with an October 31, 2021, release, rather than updating them sooner, out of cycle. According to IRS, the normal revision process takes 10 months to complete properly and would be difficult to complete in a shorter time frame. IRS’s planned revision will occur after the deadline for submitting an application for a tentative refund via the temporary electronic fax procedures, which for some taxpayers may require an accompanying Form 1040-X. This means that taxpayers who filed their 1040-X before the December 31 deadline with the temporary procedures did not find the e-file capability in the form instructions. However, some taxpayers will use Form 1040-X for other CARES Act refunds after that deadline, so instructions that are updated in tax year 2021 would still help ensure these taxpayers are aware of this option. A timelier update to the instructions would help taxpayers filing the 1040-X between now and when the annual update to the instructions occurs in October 2021.
In the meantime, IRS previously posted information about the e-file availability on the Form 1040-X product page at IRS.gov, which is referenced in the first paragraph of the Form 1040-X instructions. IRS also added a development article dated February 18, 2021, to www.irs.gov/Form1040X to notify taxpayers that e-filing is available for amending 2019 and 2020 returns that were originally e-filed. We will continue to monitor any updates to the instructions.
Recommendation. The Commissioner of Internal Revenue should periodically review control activities for issuing direct payments to individuals to determine that the activities are designed and implemented appropriately as IRS disburses a third round of economic impact payments and prepares for advance payments on the child tax credit. These control activities should include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients (March 2021 report).
Status: Open
Comment: IRS disagreed with the recommendation. However, IRS acknowledged that it established additional procedures and reviews upon discovering that it had sent millions of payments to the wrong account. IRS also stated that it plans to assess the effectiveness of these new controls during the next round of economic impact payments and will adjust them as warranted.
Recommendation. The Commissioner of Internal Revenue should leverage employee counts from Form 941, Employer’s Quarterly Federal Tax Return, and Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees, to identify potentially ineligible COVID-19-related sick and family leave credit claims, and address discrepancies IRS deems significant (March 2021 report).
Status: Open
Comment: IRS agreed with our recommendation. IRS provided an updated compliance plan, as of May 18, 2021. The plan states that IRS is considering Forms 941 and 943 line 1 data in conjunction with W-2 (Wage and Tax Statement) information, as well as other data, to identify potentially ineligible COVID-19-related credit claims and address discrepancies IRS deems significant. We will continue to monitor IRS’s plans for evidence that the employee counts will be leveraged.
Recommendation. The Commissioner of Internal Revenue should conduct outreach to employment tax return filers to educate and promote accurate reporting of employee counts on Form 941, Employer’s Quarterly Federal Tax Return, and Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees (March 2021 report).
Status: Closed
Comment: In May 2021, IRS released a “tax tip” for employment tax return filers reminding them to ensure that line 1 of their return is accurate and referring employers to the form instructions for details. This information could support compliance efforts, which can result in multiple benefits, including helping taxpayers understand their responsibilities for tax compliance and decreasing potentially ineligible credit claims.
Status of Recommendations Made to the Department of Labor
Recommendation. The Secretary of Labor should, in consultation with the Small Business Administration (SBA) and Department of the Treasury, immediately provide information to state unemployment agencies that specifically addresses SBA's Paycheck Protection Program (PPP) loans, and the risk of improper payments associated with these loans (June 2020 report).
Status: Closed
Comment: The Department of Labor (DOL) neither agreed nor disagreed with our recommendation. Following our recommendation, DOL issued guidance on August 12, 2020, that clarified that individuals working full-time and being paid through PPP are not eligible for unemployment insurance (UI), and that individuals working part-time and being paid through PPP would be subject to certain state policies, including state policies on partial unemployment, to determine their eligibility for UI benefits. Further, the guidance clarified that individuals being paid through PPP but not performing any services would similarly be subject to certain provisions of state law, and noted that an individual receiving full compensation would be ineligible for UI.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance revises its weekly news releases to clarify that in the current unemployment environment, the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits (November 2020 report).
Status: Closed
Comment: DOL’s weekly news release of December 10, 2020, clarified that the numbers reported for weeks of UI benefits claimed do not represent the number of unique individuals claiming benefits.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance pursues options to report the actual number of distinct individuals claiming benefits, such as by collecting these already available data from states, starting from January 2020 onward (November 2020 report).
Status: Open
Comment: DOL partially agreed with our recommendation. Specifically, DOL agreed to pursue options to report the actual number of distinct individuals claiming UI benefits. However, DOL did not agree with the retroactive effective date of the reporting. In a letter dated March 30, 2021, DOL stated that it had begun developing a new state report that would capture data related to distinct individuals claiming regular UI benefits; DOL estimated that this data collection might begin in early 2022. DOL also reiterated its concerns about the feasibility of states reporting this information retroactively, including for the pandemic UI programs, without detracting from their primary obligation for timely and accurate claims processing.
As of June 21, 2021, this recommendation remained open. We maintain that DOL should pursue options to report the actual number of distinct individuals claiming UI benefits, retroactive to January 2020. Even if the information is unavailable for some time, these data are vital to understanding how many individuals are receiving UI benefits, as well as the size of the population supported by the UI system during the pandemic. Given the substantial investment in UI programs during the pandemic, an accurate accounting of the size of the population supported by this funding may be critical to understanding the efficiency and effectiveness of the nation’s response to unemployment during the pandemic. An accurate accounting may also be critical to helping DOL and policymakers identify lessons learned about the administration and utilization of regular and expanded UI benefit programs.
We encourage DOL to pursue options to report the actual number of individuals claiming benefits in the most feasible and least burdensome way and at a time when providing this information retroactively will not detract from states’ primary obligation for timely and accurate claims processing. Collecting data from states is one way to address the recommendation, but DOL could develop other ways of gathering and reporting this information.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should develop a plan, with time frames, to implement the agency’s oversight processes for COVID-19-adapted enforcement methods, as described in its pandemic enforcement policies (January 2021 report).
Status: Open
Comment: DOL neither agreed nor disagreed with our recommendation. In May 2021, the Occupational Safety and Health Administration (OSHA) provided an update on its plans to implement oversight processes for remote inspections, informal inquiries conducted in place of inspections, and citation discretion.
For oversight of remote inspections, OSHA officials said that the agency is no longer planning to conduct the oversight outlined in its May 2020 pandemic-related enforcement policy.[532] Instead, officials said that follow-up for some, but not all, remotely conducted inspections would be performed according to area offices’ discretion as part of OSHA’s COVID-19 national emphasis program that went into effect on March 12, 2021.[533]
For oversight of informal inquiries conducted in place of inspections, in February 2021, OSHA officials said they planned to conduct follow-up inspections for a random sample of cases where COVID-19-related informal inquiries were conducted. However, this plan would target all informal inquiries, and not just those that were conducted in place of inspections because of the pandemic. Therefore, this sampling technique would draw from a larger pool of cases than originally planned in OSHA’s May 2020 enforcement policy, and could make it less likely that the cases meriting further scrutiny would be identified for follow-up. In May 2021, OSHA officials told us they would consider this issue when they make further plans for this oversight.
For oversight of citation discretion, in February 2021, OSHA officials said they would conduct a follow-up inspection for each case coded in the OSHA Information System as having used discretion to not cite violations. OSHA’s COVID-19 national emphasis program includes instructions for conducting these follow-up inspections. However, it is unclear whether all instances where citation discretion was used can be identified in order to conduct follow-up inspections. For example, OSHA officials said that the OSHA Information System code to identify these instances was only intended to be used for discretion related to violations of certain standards, and OSHA has not assessed the extent to which area offices consistently used the code.
Our review of Worker Safety and Health during the COVID-19 pandemic is ongoing. We will continue to examine OSHA’s efforts to implement its oversight processes for COVID-19-adapted enforcement methods, including reviewing the planned oversight that is part of the COVID-19 national emphasis program.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should ensure that the OSHA Information System includes comprehensive information on use of the agency’s COVID-19-adapted enforcement methods sufficient to inform its oversight processes for these methods (January 2021 report).
Status: Open
Comment: DOL neither agreed nor disagreed with our recommendation. In February 2021, OSHA said that the agency believes its current OSHA Information System coding related to COVID-19 and adapted enforcement methods is sufficient to enable agency oversight, and that it will add new coding if and when it is needed. In March 2021, OSHA added a new code related to its new COVID-19 national emphasis program. While adding this code is beneficial, we remain concerned that the system is not collecting comprehensive information. Our work shows that some adapted enforcement methods are not captured in OSHA Information System coding, leaving OSHA unable to reliably track some of these methods, such as citation discretion and informal inquiries used in place of inspections. Our review of Worker Safety and Health during the COVID-19 pandemic is ongoing. We will continue to examine OSHA’s efforts to ensure that the OSHA Information System includes sufficient information to inform its oversight processes.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should determine what additional data may be needed from employers or other sources to better target the agency’s COVID-19 enforcement efforts (January 2021 report).
Status: Open
Comment: DOL neither agreed nor disagreed with our recommendation. In February 2021, OSHA said that it had considered our recommendation and determined that it did not need additional information from employers to identify where pandemic-related enforcement should be targeted. OSHA also said that, pursuant to the President’s January 21, 2021, Executive Order on Protecting Worker Health and Safety, OSHA was working to launch a national program to focus its COVID-19-related enforcement efforts on violations that put the largest number of workers at serious risk or that are contrary to anti-retaliation principles. In March 2021, OSHA launched its COVID-19 national emphasis program for this purpose. Our review of Worker Safety and Health during the COVID-19 pandemic is ongoing. We will continue to examine OSHA’s efforts in order to determine whether actions taken, including the implementation of OSHA’s COVID-19 national emphasis program, address our recommendation.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments recovered in the Pandemic Unemployment Assistance (PUA) program, similar to the regular UI program (January 2021 report).
Status: Open
Comment: DOL agreed with our recommendation and on January 8, 2021, issued PUA program guidance and updated instructions for states to report PUA overpayments recovered. As of June 21, 2021, this recommendation remained open, as just 27 states had begun reporting some data on the amount of PUA overpayments recovered. Sustained reporting by most states is needed to help inform DOL, policymakers, and the public about the amount of PUA overpayments states have recovered. We will continue to monitor state reporting of PUA overpayment recovery data.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should work with FDA and CDC to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with emergency use authorization (March 2021 report).
Status: Open
Comment: DOL concurred with the recommendation, and commented that OSHA will work with FDA and CDC to address issues. In April 2021, OSHA, FDA, and CDC’s National Institute for Occupational Safety and Health met to discuss establishing a Memorandum of Understanding for sharing information related to emergency use authorizations, and work on the memorandum is ongoing.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments waived in the PUA program, similar to the regular UI program (March 2021 report).
Status: Open
Comment: DOL agreed with our recommendation and noted that it intended to issue PUA program guidance that would include revised reporting requirements and instructions for states to provide information on the amount of PUA overpayments waived. On June 17, 2021, DOL officials stated that the agency expected to publish guidance by mid-July 2021. As of June 21, 2021, this recommendation remained open, as this guidance had not yet been issued and no states had begun reporting these data. We will continue to monitor state reporting of PUA overpayments waived.
Status of Recommendations Made to the Small Business Administration
Recommendation. The Administrator of SBA should develop and implement plans to identify and respond to risks in PPP to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less (June 2020 report).
Status: Open
Comment: At the time of our report, SBA neither agreed nor disagreed with our recommendation. As we reported in September 2020, SBA has said that it plans to review all PPP loans of $2 million or more and further stated that it may review any PPP loan it deems appropriate, including loans of less than $2 million. In late December 2020, SBA provided a Loan Review Plan outlining steps it planned to take to review PPP loans. The document describes three steps in the process: automated screenings of all loans, manual reviews of selected loans, and quality control reviews to ensure the quality, completeness, and consistency of the review process. In February and April 2021, SBA provided additional documents referenced in the plan that give further details on how SBA and its contractors will conduct the various reviews. However, the documents, and the plan itself, have not been updated to incorporate major changes to the program, such as the additional loans made in 2021. For example, SBA has not determined whether all of the loans made in 2021 will go through the full automatic screening that loans made in 2020 received. In addition, SBA is still implementing its oversight plan and has yet to conduct other critical steps to address potential fraud, including a fraud risk assessment.
Recommendation. The Administrator of SBA should expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread (November 2020 report).
Status: Open
Comment:SBA neither agreed nor disagreed with our recommendation at the time of our report. In response to our recommendation, SBA stated that it was planning to conduct improper payment testing for PPP and that it takes improper payments seriously. SBA officials stated that SBA has submitted the sampling plan to the Office of Management and Budget (OMB) and will use this sampling plan to estimate both improper payments and error rates for PPP in the fourth quarter of fiscal year 2021. We will continue to monitor SBA’s actions to address this recommendation.
Recommendation. The Administrator of SBA should develop and implement portfolio-level data analytics across Economic Injury Disaster Loan program loans and advances made in response to COVID-19 as a means to detect potentially ineligible and fraudulent applications (January 2021 report).
Status: Open
Comment: At the time of our report, SBA neither agreed nor disagreed with this recommendation. As of May 2021, SBA officials stated that the agency was in the process of developing an analysis to apply certain fraud indicators to all application data. These fraud indicators include applicants’ physical address, internet protocol address, email address, phone numbers, bank accounts, and tax identification numbers.
Recommendation. The Administrator of SBA should conduct and document a fraud risk assessment for the Economic Injury Disaster Loan program (March 2021 report).
Status: Open
Comment: SBA agreed with the recommendation, stating that it would work to ensure that a fraud risk assessment for the Economic Injury Disaster Loan program is completed. SBA stated that it has started the work to build a fraud risk framework. We will continue to monitor SBA’s actions to address this recommendation.
Recommendation. The Administrator of SBA should develop a strategy that outlines specific actions to monitor and manage fraud risks in the Economic Injury Disaster Loan program on a continuous basis (March 2021 report).
Status: Open
Comment: SBA agreed with the recommendation, stating that it would work to ensure that fraud risks are monitored on a continuous basis. We will continue to monitor SBA’s actions to address this recommendation.
Recommendation. The Administrator of SBA should implement a comprehensive oversight plan to identify and respond to risks in the Economic Injury Disaster Loan program to help ensure program integrity, achieve program effectiveness, and address potential fraud (March 2021 report).
Status: Open
Comment: SBA agreed with the recommendation, stating that it will implement a comprehensive oversight plan. We will continue to monitor SBA’s actions to address this recommendation.
Recommendation. The Administrator of SBA should conduct and document a fraud risk assessment for the Paycheck Protection Program (March 2021 report).
Status: Open
Comment: SBA agreed with the recommendation, stating that it would work to ensure that a fraud risk assessment for PPP is completed. According to SBA officials, as of May 2021, SBA had begun conducting a formal fraud risk assessment. We will continue to monitor SBA’s actions to address this recommendation.
Recommendation. The Administrator of SBA should develop a strategy that outlines specific actions to monitor and manage fraud risks in the Paycheck Protection Program on a continuous basis (March 2021 report).
Status: Open
Comment: SBA agreed with the recommendation, stating that it would work to ensure that fraud risks are monitored on a continuous basis. We will continue to monitor SBA’s actions to address this recommendation.
Status of Recommendations Made to the Department of Veterans Affairs
Recommendation. The VA Under Secretary for Health should develop a plan to ensure inspections of state veterans homes occur during the COVID-19 pandemic—which may include using in-person, a mix of virtual and in-person, or fully virtual inspections (November 2020 report).
Status: Closed
Comment: On December 7, 2020, VA developed an interim process for reviewing records from state veterans homes, such as evidence that previous corrective action plans were implemented and documentation of infection control assessments, to assess the state veterans homes’ compliance with federal regulations. VA reported it implemented this process until a new inspection contract could be awarded and completed 25 of these record reviews. VA awarded a contract in January 2021 to conduct full virtual, blended virtual, or on-site inspections, and reported that the contractor began conducting inspections on January 19, 2021, which are ongoing.
Recommendation. The VA Under Secretary for Health should collect timely data on COVID-19 cases and deaths in each state veterans home, which may include using data already collected by CMS (November 2020 report).
Status: Open
Comment: As of July 1, 2021, VA is publicly reporting on its website data on COVID-19 cases and deaths among residents and staff at 150 out of 158 state veterans homes. According to VA officials, the eight remaining homes are in the process of enrollment to begin reporting data to CDC’s National Healthcare Safety Network, but have encountered difficulty with the CDC enrollment process. VA officials told us that both VA and CDC staff are working with each home to address enrollment challenges, and that they hope to have all homes successfully reporting by mid-July 2021. We will continue to monitor their progress.
Recommendation. The VA Under Secretary for Health should develop metrics to assess the number of vaccines administered by vaccine rollout phase to better assess progress and make any necessary adjustments as needed (March 2021 report).
Status:Closed
Comment:VA agreed with our recommendation and stated that its goal is to vaccinate all eligible veterans and employees who want to be vaccinated in 2021. In June 2021, VA provided us with evidence that it is tracking the number of vaccines administered by priority group. For example, VA has metrics on the number of vaccinated and unvaccinated veterans aged 75 and older. We are closing this recommendation as implemented.
Recommendation. The VA Under Secretary for Health should develop preliminary vaccination targets for when it will move from one vaccination phase to another; or within one phase, from one group of veterans to another (March 2021 report).
Status: Closed
Comment:VA concurred in principle with our recommendation. VA told us that it did not independently develop vaccination targets for moving from one phase to another. Rather, according to VA, it followed CDC guidance which called for a phased approach and flexibility to ensure efficient use of vaccines while supply was limited. According to VA, it is no longer using a phased approach and vaccine supply in the United States is no longer limited. Therefore, we are closing our recommendation as not implemented because VA is no longer using a phased approach to administer vaccines.
Recommendation. The VA Under Secretary for Health should collect data on the number of staff and veterans who do not show up for a vaccination appointment to better monitor for completion of the second dose of the vaccine (March 2021 report).
Status:Closed
Comment: VA agreed with our recommendation. In June 2021, VA provided us with evidence that is tracking the number of vaccines administered by priority group, including VHA health care staff, VA staff, and veterans. For example, it’s Veteran Outreach Tool includes data on vaccination status, including if a veteran is interested in receiving or refused vaccination, received a vaccine from VA or an outside provider, and if a veteran is overdue for their second dose of Moderna’s or Pfizer’s vaccine. According to VA, providers use these data for individual veteran outreach and scheduling. VA’s actions meet the intent of our recommendation, which was to use data to track vaccine administration and target outreach to improve completion of vaccine regimens. We are closing this recommendation as implemented
Status of Recommendations Made to the Department of Homeland Security
Recommendation. The Administrator of FEMA—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with its roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
Status: Open
Comment: In September 2020, DHS disagreed with this recommendation, noting, among other things, work that FEMA had already done to manage the medical supply chain and increase supply availability. Although DHS disagreed with our recommendation, it began taking some actions in March 2021. As of May 2021, DHS had not demonstrated action to devise interim solutions that would systematically help states, tribes, and territories effectively track, manage, and plan for supplies to carry out the COVID-19 pandemic response in the absence of state-level end-to-end logistics capabilities that would track critical supplies required for a response of this scale.
We note that we made this recommendation to both DHS and HHS with the intent that they would work together under the Unified Coordination Group to address challenges reported by state officials with both public health and emergency management responsibilities. Moreover, we recommended they take actions that were consistent with the roles and responsibilities that were to be more clearly defined as HHS took a more central role in leading supply distribution. The recommendation to define those roles and responsibilities remains open. Moreover, although both DHS and HHS have reported separate actions, taken as part of other efforts within each separate purview, neither has articulated how it worked with the other nor how it assessed whether the actions changed the experiences of state officials who reported issues during our prior work. Without systematic and deliberate action to help states ensure they have the support they need to track, manage, and plan for supplies, states, tribes, and territories on the front lines of the whole-of-nation COVID-19 response may continue to face challenges that hamper their effectiveness.
Recommendation. The Secretary of Homeland Security, in coordination with the Secretary of Defense, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Status: Closed
Comment:DHS did not agree with our recommendation. However, in March 2021, DHS, in coordination with DOD, issued a revised memorandum of agreement. The revised agreement establishes a process and timelines for communicating and evaluating National Interest Action code extensions by requiring the General Services Administration to notify other federal agencies no less than 7 days before a code is set to expire so that agencies can request an extension, as needed. The revised agreement also more clearly defines what constitutes a consistent decrease in contract actions to ensure that criteria for extending or closing a National Interest Action code are consistently applied.
Recommendation. The FEMA Administrator should adhere to the agency’s protocols listed in the updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of the tribal consultation process when developing new policies and procedures related to COVID-19 assistance (March 2021 report).
Status: Open
Comment: DHS concurred with our recommendation. DHS stated that FEMA’s National Tribal Affairs Adviser, based in the Office of External Affairs, would coordinate with other FEMA offices and directorates, as appropriate, to review the agency’s adherence to protocols listed in the Tribal Consultation Policy.
Recommendation. The FEMA Administrator should provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19 (March 2021 report).
Status: Open
Comment: DHS concurred with our recommendation. DHS stated that FEMA’s Recovery Directorate would publish a memorandum that would contain direction to FEMA regions regarding the assignment of Public Assistance program delivery managers to promote equitable delivery of Public Assistance to tribal governments. FEMA stated that it plans to send the draft memo to tribal governments in July 2021.
Status of Recommendations Made to the U.S. Department of Agriculture
Recommendation. The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to issue guidance—such as an acquisition alert or a reminder to contracting officials—on the use of the COVID-19 National Interest Action code for the Farmers to Families Food Box Program or successor food distribution program to ensure it accurately captures COVID-19-related contract obligations in support of the program (March 2021 report).
Status: Closed
Comment: The U.S. Department of Agriculture neither agreed nor disagreed with our recommendation. In February 2021, following our identification of contract data reporting challenges using the COVID-19 National Interest Action code for the Farmers to Families Food Box Program, Agricultural Marketing Service officials said they conducted training with staff to review National Interest Action code data entry protocols. At that time, a senior Agricultural Marketing Service official also sent an email reminder to procurement division personnel about OMB’s guidance on the use of the COVID-19 National Interest Action code. Following this training and email, officials took action to retroactively report contract actions for the program with the National Interest Action code. In May 2021, the Agricultural Marketing Service updated its instructions for entering contract actions into the Federal Procurement Data System-Next Generation to include a reminder to utilize the proper National Interest Action code, if applicable.
Recommendation. The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the Farmers to Families Food Box Program or successor future food distribution program, and take the necessary steps to ensure it has adequate contracting staff in place to award and administer any future contracts for the program (March 2021 report).
Status: Open
Comment: The U.S. Department of Agriculture neither agreed nor disagreed with our recommendation, and as of May 2021 had not fully assessed the contracting personnel needed to execute and administer contracts in support of the Farmers to Families Food Box Program or successor food distribution program. According to Agricultural Marketing Service officials, they have discontinued the program and are using other methods of hunger relief, and so do not anticipate needing additional permanent staff. Agricultural Marketing Service officials are planning to use an existing contract vehicle to obtain additional staff support for contract documentation needs for the awards that have been made under the Farmers to Families Food Box Program and other food purchasing efforts. However, as of May 2021, Agricultural Marketing Service officials had not yet determined the staffing support levels to be obtained under the contract vehicle.
Recommendation. The Secretary of Agriculture should ensure that the Administrator of the Food and Nutrition Service (1) provides sufficient context to help stakeholders and the public understand and interpret data on federal nutrition assistance programs during the pandemic and (2) discloses potential sources of error that may affect data quality during the pandemic, such as manual processing. For example, the agency could publish key information from its internal communications plan that it developed for the January 2021 data release and include additional table notes in subsequent data releases to help explain these issues (March 2021 report).
Status: Open
Comment: As of June 2021, the Food and Nutrition Service had taken steps toward implementing this recommendation. For example, it added several table notes to data it released in April 2021 to help provide stakeholders and the public with sufficient context to understand and interpret key data. Food and Nutrition Service officials said the agency is currently discussing next steps for disclosing potential sources of error, such as manual processing of participation and expenditure data for some programs.
Status of Recommendations Made to the Office of Management and Budget
Recommendation. The Director of OMB, in consultation with Treasury, should issue the addendum to the 2020 Compliance Supplement as soon as possible to provide the necessary audit guidance (September 2020 report).
Status: Closed
Comment: OMB neither agreed nor disagreed with the recommendation. OMB issued the 2020 Compliance Supplement Addendum on December 22, 2020.
Recommendation. The Director of OMB should develop and issue guidance directing agencies to include COVID-19 relief funding with associated key risks, such as provisions contained in the CARES Act and other relief legislation that potentially increase the risk of improper payments or changes to existing program eligibility rules, as part of their improper payment estimation methodologies. This should especially be required for already existing federal programs that received COVID-19 relief funding (November 2020 report).
Status: Open
Comment: OMB neither agreed nor disagreed with our recommendation. In November 2020, we reported that although OMB issued a memorandum providing agencies the option to incorporate new COVID-19 relief funding into their normal sampling processes, it did not specifically direct agencies to do so. In addition, the guidance did not direct agencies to consider associated risks, such as changes to eligibility rules and different payment processes, as part of their improper payment estimation methodologies. Further, OMB staff stated that OMB was actively coordinating and engaging with the Pandemic Response Accountability Committee and Inspectors General to share and discuss information relevant to COVID-19 spending risks and improper payment reduction strategies.
In January 2021, OMB staff stated they believe current OMB guidance sufficiently addresses our recommendation and concerns. In March 2021, OMB issued new guidance on improper payments that implements the requirements from the Payment Integrity Information Act of 2019. This guidance defines a "reliable improper payment and unknown payment estimate" as being produced from accurate sampling populations, testing procedures, and estimation calculations. The OMB guidance discusses a two-phased approach pertaining to assessing programs for susceptibility to significant improper payments and then, if a program is determined to be susceptible, for measuring and reporting improper payments. In phase 1, agencies assess the risk of improper payments, and OMB has added new guidance for how agencies can assess payment integrity risks to identify areas where improper payments may arise. When these risks exceed the established threshold, programs move into phase 2, in which agencies design and submit to OMB a sampling and estimation methodology plan. OMB's guidance states that this plan should have a mechanism for identifying, accounting for, and estimating the annual improper payments and unknown payments separately. However, OMB's guidance does not specifically direct agencies to ensure that all identified payment integrity risks are included as part of their improper payment estimation methodologies.
In April 2021, OMB stated that its position remains the same as communicated to us in January 2021 and reiterated that its current guidance sufficiently addresses the intent of the recommendation. We maintain that without OMB guidance for agencies to include COVID-19 relief funding and associated key risks as part of their improper payment estimation methodologies, agencies are at increased risk that their processes may not result in reliable estimates, calling into question their usefulness for developing effective corrective actions. We will continue to monitor OMB’s actions to address this recommendation.
Recommendation. The Director of OMB should work in consultation with federal agencies and the audit community (e.g., agency Offices of Inspector General; National Association of State Auditors, Comptrollers, and Treasurers; and American Institute of Certified Public Accountants), to the extent practicable, to incorporate appropriate measures in OMB’s process for preparing single audit guidance, including the annual Single Audit Compliance Supplement, to better ensure that such guidance is issued in a timely manner and is responsive to users’ input and needs (March 2021 report).
Status: Open
Comment: OMB neither agreed nor disagreed with our recommendation. Although OMB stated that it shares the draft Compliance Supplement with the grant and audit communities as part of the Compliance Supplement preparation process, OMB has not taken additional steps to ensure the Compliance Supplement and other single audit guidance is issued in a timely manner and is responsive to users’ input and needs. In April 2021, OMB reached out to GAO for consultation on the development of single audit guidance for the American Rescue Plan Act of 2021 (ARPA). In May, GAO, OMB and audit community stakeholders met to further discuss single audit guidance needed for ARPA. OMB stated during the meeting that it does not have a planned issuance date for the 2021 Compliance Supplement. We will continue to monitor the actions OMB takes in response to our recommendation.
Status of Recommendations Made to the Department of Defense
Recommendation. The Secretary of Defense, in coordination with the Secretary of Homeland Security, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Status: Closed
Comment: DOD did not agree with our recommendation. However, in March 2021 DOD, in coordination with DHS, issued a revised memorandum of agreement. The revised agreement establishes a process and timelines for communicating and evaluating National Interest Action code extensions by requiring the General Services Administration to notify other federal agencies no less than 7 days before a National Interest Action code is set to expire so that agencies can request an extension as needed. The revised agreement also more clearly defines what constitutes a consistent decrease in contract actions to ensure criteria for extending or closing a National Interest Action code are consistently applied.
Status of Recommendation Made to the Department of Commerce
Recommendation. The Assistant Administrator for the National Oceanic and Atmospheric Administration Fisheries should develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner (January 2021 report).
Status: Open
Comment: As of February 1, 2021, the agency had developed an electronic tool to track the disbursement of funds and had begun to input data into it based on approved spend plans. The agency plans to update these data on a weekly basis as funds are disbursed. The agency anticipates that all current and relevant data will be entered into the tracking tool by May 2021 and that data will continue to be added to it until all funding has been disbursed.
Status of Recommendation Made to the Department of Education
Recommendation. The Secretary of Education should regularly collect and publicly report information on school districts’ financial commitments (obligations), as well as outlays (expenditures) in order to more completely reflect the status of their use of federal COVID-19 relief funds. For example, the Department of Education (Education) could modify its annual report on state and school district spending data to include obligations data in subsequent reporting cycles (March 2021 report).
Status: Open
Comment:Education agreed with GAO’s recommendation and committed to working collaboratively with states to develop reporting processes that provide greater clarity on state and school district spending. As of June 11, 2021, the Department of Education posted on its website updated information on how most states and school districts spent (i.e., expended) their Elementary and Secondary School Emergency Relief (ESSER) and Governor’s Emergency Education Relief (GEER) funds (https://covid-relief-data.ed.gov/) through September 30, 2020. For example, Education’s website now includes school district expenditures on education technology, activities for underserved students, mental health supports, sanitization, and summer learning and afterschool programs. Education told us that it was following up with states that did not provide valid and reliable data.
On April 21, Education released instructions for states to submit their State Plans for the use of American Rescue Plan Elementary and Secondary School Emergency Relief (ARP ESSER) Funds. As part of these plans, Education also requested that states include in their ARP ESSER State Plans any available information on the amount of funds that have been obligated but not expended by states and school districts from the CARES Act and the Consolidated Appropriations Act, 2021, and information on the extent to which states are able to track school district obligations. States are required to submit their plans to Education by June 7, 2021 and as of June 15, 30 states’ plans were posted on Education’s website. The plans included varying amounts of information on school district obligations and the states’ ability to track them. Education plans to update its website with updated plans from all the states as they become available and Education officials review them.
Education officials told GAO that the agency is taking these efforts to improve transparency and accountability and is committed to effectively administering each of its programs and ensure accountability for all of the resources entrusted to them. We will continue to monitor Education’s efforts to improve tracking of federal COVID-19 relief funds.
Status of Matter for Congressional Consideration Regarding the Social Security Administration
Matter. To provide agencies access to the Social Security Administration’s more complete set of death data, we urge Congress to provide Treasury with access to the Social Security Administration’s full set of death records, and to require that Treasury consistently use it (June 2020 report).
Status: Closed
Comments: In December 2020, Congress passed and the President signed into law the Consolidated Appropriations Act, 2021, section 801(a)(7) of division FF of which requires the Social Security Administration, to the extent feasible, to share its full death data with Treasury’s Do Not Pay working system for a 3-year period through a cooperative arrangement with Treasury. This provision is effective the date that is 3 years from enactment of the act. Sharing these data will allow agencies to enhance their efforts to identify and prevent improper payments to deceased individuals. Therefore, it will be important for the Social Security Administration and Treasury to work together to implement this legislation.
Status of Matter for Congressional Consideration Regarding the Department of Transportation
Matter. We urge Congress to take legislative action to require the Secretary of Transportation to work with relevant agencies and stakeholders, such as HHS and DHS, and members of the aviation and public health sectors, to develop a national aviation preparedness plan to ensure safeguards are in place to limit the spread of communicable disease threats from abroad while at the same time minimizing any unnecessary interference with travel and trade (June 2020 report).
Status: Open
Comment: In May 2020, the House of Representatives passed H.R. 6800, referred to as the HEROES Act, which would require the Department of Transportation, in coordination with HHS, DHS, and other appropriate federal departments and agencies, to develop a national aviation preparedness plan. In September 2020, the Senate passed S. 3681, Ensuring Health Safety in the Skies Act of 2020, which would require HHS, DHS, and the Department of Transportation to form a joint task force on air travel during and after the COVID-19 public health emergency, among other provisions. Also, in October 2020, H.R. 8712, National Aviation Preparedness Plan Act of 2020, was introduced. If enacted, this bill would require the Department of Transportation, in collaboration with DHS, HHS, and other aviation stakeholders, to develop a national plan to prepare the aviation industry for future communicable disease outbreaks. Members of the House and Senate reintroduced similar bills in the new Congress. In February 2021, H.R. 884, the National Aviation Preparedness Plan Act of 2021, was introduced in the House of Representatives, and in May 2021, S. 82, Ensuring Health Safety in the Skies Act of 2021, was reported favorably out of the Senate Committee on Commerce, Science, and Transportation.
We again urge Congress to take swift action to require a national aviation preparedness plan, without which the U.S. will not be as prepared to minimize and quickly respond to ongoing and future communicable disease events.
Status of Matter for Congressional Consideration Regarding Future COVID-19 Relief Funds
Matter. In November 2020, we urged Congress to consider, in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” (November 2020 report).
Status: Open
Comment:No new legislation designating executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” has been enacted to date.
Appendix V: Comments from the Department of Education
[3]The five previously enacted COVID-19 relief laws are the Consolidated Appropriations Act, 2021, Pub. L. No. 116-620, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[4]Pub. L. No. 116-136, § 19010, 134 Stat. at 579–81.
[5]GAO, COVID-19:Sustained Federal Action Is Crucial as Pandemic Enters Its Second Year, GAO-21-387 (Washington, D.C.: Mar. 31, 2021); COVID-19:Critical Vaccine Distribution, Supply Chain, Program Integrity, and Other Challenges Require Focused Federal Attention, GAO-21-265 (Washington, D.C.: Jan. 28, 2021); COVID-19: Urgent Actions Needed to Better Ensure an Effective Federal Response, GAO-21-191 (Washington, D.C.: Nov. 30, 2020); COVID-19: Federal Efforts Accelerate Vaccine and Therapeutics Development, but More Clarity Needed, GAO-21-207 (Washington D.C.: Nov. 17, 2020); COVID-19: Federal Efforts Could Be Strengthened by Timely and Concerted Actions, GAO-20-701 (Washington, D.C.: Sept. 21, 2020); COVID-19: Brief Update on Initial Federal Response to the Pandemic, GAO-20-708 (Washington, D.C.: Aug. 31, 2020); and COVID-19: Opportunities to Improve Federal Response and Recovery Efforts, GAO-20-625 (Washington, D.C.: June 25, 2020).
[7]Data on case counts are through June 18, 2021. Data on COVID-19 cases in the U.S. are based on aggregate case reporting to CDC and include probable and confirmed cases as reported by states and jurisdictions. CDC COVID-19 counts are subject to change due to delays or updates in reported data from states and territories. According to CDC, the actual number of COVID-19 cases is unknown for a variety of reasons, including that people who have been infected may have not been tested or may have not sought medical care. See CDC, “COVID Data Tracker: Trends in Number of COVID-19 Cases and Deaths in the U.S. Reported to CDC, by State/Territory,” accessed June 24, 2021, https://covid.cdc.gov/covid-data-tracker/#trends_dailytrendscases. The number of deaths (about 593,000) include total deaths that occurred through the week ending June 19, 2021. CDC’s National Center for Health Statistics COVID-19 death counts in the U.S. are based on provisional counts from death certificate data, which do not distinguish between laboratory-confirmed and probable COVID-19 deaths. Provisional counts are incomplete due to an average delay of 2 weeks (a range of 1–8 weeks or longer) for death certificate processing. See CDC, National Center for Health Statistics, “Provisional Death Counts for Coronavirus Disease 2019 (COVID-19),” accessed June 24, 2021, https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm. Worldwide, there were more than 179 million cases and about 3.9 million deaths as of June 24, 2021. Worldwide data from the World Health Organization reflect laboratory-confirmed cases and deaths reported by countries and areas. A preliminary assessment from the World Health Organization suggests that the total number of global deaths attributable to the COVID-19 pandemic may be more than officially reported (see World Health Organization, “The True Death Toll of COVID-19: Estimating global excess mortality,” accessed June 24, 2021, https://www.who.int/data/stories/the-true-death-toll-of-covid-19-estimating-global-excess-mortality).
[8]Bureau of Labor Statistics, “Unemployment Level (UNEMPLOY)," retrieved from FRED, Federal Reserve Bank of St. Louis, accessed June 23, 2021, https://fred.stlouisfed.org/series/UNEMPLOY.
[9]CDC’s COVID-19 case counts are subject to change due to delays or updates in reported data from states and territories. We compared the average number of new cases per day between June 5 and June 18, 2021, with the average number of new cases per day during the 14-day window around the peak in January 2021.
[10]The 52 states and jurisdictions include all 50 states, Washington, D.C., and New York City. COVID-19 case counts for New York City are reported separately from New York State. We defined states as holding steady if they had less than a 1 percent increase or decrease in average daily new cases over the time frame. The average percentage change in daily new cases was calculated as the average of the daily rates of change of the 7-day moving average from June 5 to June 18, 2021. (See CDC, “COVID Data Tracker: Trends in Number of COVID-19 Cases and Deaths in the U.S. Reported to CDC, by State/Territory,” accessed June 24, 2021, https://covid.cdc.gov/covid-data-tracker/#trends_dailytrendscases.) These COVID-19 case counts may change as new or updated data are reported by states.
[11]Pfizer’s two-dose COVID-19 vaccine was authorized for emergency use on December 11, 2020, and Moderna’s two-dose COVID-19 vaccine was authorized on December 18, 2020. Janssen’s (Johnson & Johnson) one-dose COVID-19 vaccine was authorized for emergency use on February 27, 2021.
[12]The employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population 16 years and older. The ratio is subject to a misclassification error with respect to consistently identifying workers as employed and absent from work or as unemployed on temporary layoff.
[13]An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes.
[14]An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of the other party beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. Increased spending in Medicaid and Medicare is not accounted for in the appropriations provided by the COVID-19 relief laws. Federal agencies use GTAS to report proprietary financial reporting and budgetary execution information to Treasury.
[15]This total is based on (1) an analysis of the appropriated amounts in the American Rescue Plan Act of 2021, Divisions M and N of the Consolidated Appropriations Act, 2021, the Paycheck Protection Program and Health Care Enhancement Act, the CARES Act, the Families First Coronavirus Response Act, and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 that are available to agencies for assistance to states, D.C., localities, U.S. territories, tribes, and tribal governments, and (2) the Congressional Budget Office’s estimated outlays for Medicaid increases resulting from authorized increases in payments to states and U.S. territories under those laws.
[16]We closed one additional recommendation as unimplemented. This recommendation was for the Department of Veterans Affairs to develop preliminary targets for their phased vaccination rollout. We determined that the recommendation was no longer relevant as the department has discontinued their phased vaccination approach in light of the increased supply of COVID-19 vaccines.
[17]FDA may temporarily allow unapproved products to be used in an emergency through the issuance of EUAs, provided there is evidence that the product may be effective and that the known and potential benefits of the product outweigh known and potential risks, among other statutory criteria. See 21 U.S.C. § 360bbb-3. The EUA authority allows for tests that “may be effective” to be made available in a much shorter time frame than typically would be necessary for approval or clearance because it requires less certainty of effectiveness than is required for FDA product approvals and clearances. Based upon the CDC EUA request, use of the test was limited to qualified laboratories designated by CDC.
[18]According to CDC, before laboratories use a new test on samples from patients, they must verify the test performance to make sure it works as expected. According to CDC, about half of the 93 laboratories had reported the status of their verification of the test to CDC by February 21, 2020, and of these laboratories, 85 percent reported problems with the test. The remaining laboratories did not report their verification status to CDC.
[19]Government of the Republic of Korea, All about Korea’s Response to COVID-19 (Seoul, Republic of Korea: Oct. 13, 2020).
[20]PPE is typically considered to be a low-margin commodity—that is, the selling price is not much higher than the cost to produce. Low-margin commodities like PPE are not highly unique or highly specialized products, making the PPE industry more competitive.
[21]Pub. L No. 116-22, § 402(a), 133 Stat. 905, 942–43 (codified at 42 U.S.C. § 300hh-10a(c)(1)).
[23]See Department of Health and Human Services, HHS Policy for Records Management, HHS-OCIO-PIM-2020-06-004, May 2020.
[24]Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-18-20 (Washington, D.C.: June 26, 2018). In March 2021, OMB issued a revised version of OMB Circular A-123, Appendix C, effective starting in fiscal year 2021. Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-21-19 (Washington, D.C.: Mar. 5, 2021).
[25]The first five COVID-19 relief laws include the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, the Families First Coronavirus Response Act, the CARES Act, the Paycheck Protection Program and Health Care Enhancement Act, and the Consolidated Appropriations Act, 2021.
[26]See Office of Management and Budget, COVID Reporting Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019 (COVID-19), OMB M-20-21 (Apr. 10, 2020).
[27]The total appropriation comprises $13.9 billion from the CARES Act, $22.7 billion from the Consolidated Appropriations Act, 2021, and $39.6 billion from ARPA.
[28]The CARES Act directed the Department of Education (Education) to allocate HEERF funding to eligible schools based on a funding formula. Education used the Office of Postsecondary Education (OPE) Identification Number as the unique identifier for each school that was allocated funding per Education’s formula allocation tables for HEERF, published on OPE’s website. Education subsequently notified schools of additional allocations provided by the other COVID-19 relief laws.
[29]CARES Act, Pub. L. No. 116-136, div. A, tit. V, § 5001, 134 Stat. at 501–04; ARPA, Pub. L. No. 117-2, tit. IX, § 9901, 135 Stat. at 223–36. This section of ARPA appropriated $350 billion for two funds—the Coronavirus State Fiscal Recovery Fund and the Coronavirus Local Fiscal Recovery Fund—as well as $10 billion for the Coronavirus Capital Projects Fund and $2 billion for the Local Assistance and Tribal Consistency Fund, which are codified, respectively, at 42 U.S.C. §§ 802, 803, 804, 805. We focus only on the Coronavirus State Fiscal Recovery Fund and the Coronavirus Local Fiscal Recovery Fund, which we discuss as one for the purposes of this report. Further, this ARPA section appropriated an additional $50 million to the Secretary of the Treasury to administer these four funds as well as the Coronavirus Relief Fund enacted by the CARES Act, as amended. See 42 U.S.C. § 802(a)(2).
[30]Approximately $450 million of the $8 billion Tribal Set-Aside has not been disbursed because of litigation. In 2020, several Indian tribes sued Treasury over its interpretation that Alaska Native regional and village corporations are Indian tribes eligible to receive disbursements from the CRF Tribal Set-Aside. On June 25, 2021, the United States Supreme Court held that Alaska Native regional and village corporations are Indian tribes under the Indian Self-Determination and Education Assistance Act and thus are eligible for disbursements from the CRF Tribal Set-Aside. Yellen v. Confederated Tribes of the Chehalis Reservation, 594 U.S. __ (2021).
[31]The CARES Act established that CRF recipients could use CRF funds to cover costs that they had incurred between March 1, 2020, and December 30, 2020, and had not accounted for in their most recent budget prior to the law’s enactment. Pub. L. No. 116-136, § 5001, 134 Stat. at 503. This time frame was extended to December 31, 2021, by the Consolidated Appropriations Act, 2021. Pub. L. No. 116-260, tit. X, § 1001, 134 Stat. at 2145. Beginning in April 2020, Treasury published guidance on its interpretation of the permissible uses of CRF funds. For example, Treasury stated in guidance to CRF recipients that they may not use the funds to fill shortfalls in government revenue. See 86 Fed. Reg. 4,182, 4,183 (Jan. 15, 2021). For more information on the allocation and disbursement of CRF funds, see GAO, COVID-19: Opportunities to Improve Federal Response and Recovery Efforts, GAO-20-625 (Washington, D.C.: June 25, 2020).
[32]Recipients may use the CSLFRF payments to cover costs incurred by December 31, 2024, to, for example, respond to the COVID-19 pandemic or its negative economic impacts, including assistance to households; small businesses; and nonprofits or aid to impacted industries, such as tourism, travel, and hospitality. ARPA, Pub. L. No. 117-2, § 9901, 135 Stat. at 223.
[33]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing OMB guidance is reprinted in 2 C.F.R. Part 200. Nonfederal entities (states, U.S. territories, tribes, local governments, or nonprofit organizations) that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit—that is, an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[34]To help administer the new COVID-19 relief funding, many federal awarding agencies also issued new guidance to award recipients regarding how those funds should be reported and spent.
[35]In March 2020 and December 2020, respectively, the CARES Act and the Consolidated Appropriations Act, 2021, authorized Treasury and IRS to issue EIP 1 and EIP 2 as direct payments to help individuals address financial stress due to the pandemic. Pub. L. No. 116-136, § 2201, 134 Stat. at 335–340; Pub. L. No. 116-260, § 272, 134 Stat. at 1965–1976. ARPA, enacted in March 2021, authorized a third round of direct payments to individuals. Pub. L. No. 117-2, § 9601, 135 Stat. at 138–44.
[36]IRS partners with nationwide and local organizations by providing outreach material, training, and tax preparation products for taxpayer assistance and education. IRS partner organizations are meant to serve low- to moderate-income populations, older Americans, students, military service members, people with disabilities, and other populations. IRS refers to these organizations as outreach partners.
[37]Pub. L. No. 116-127, §§ 3101-3106, 5101-5111, 134 Stat. at 189–192, 195–201 (2020), as amended by Pub. L. No. 116-136, §§ 3601, 3602, 134 Stat. at 410 (2020). The Family and Medical Leave Act of 1993, as amended, generally requires covered employers to provide up to 12 weeks of unpaid leave per year for eligible employees to, among other things, care for a spouse, child, or parent with a serious health condition or for their own serious health condition. Employees are generally eligible if they meet certain requirements related to length of employment and size of employer. Some state laws also provide paid sick or family leave, with eligibility rules varying by state. Under FFCRA, covered employers included most public employers and private employers with fewer than 500 employees. Small businesses—those with fewer than 50 employees—may have qualified for an exemption from providing leave to an employee who needed to care for a child because of closure or unavailability of the child’s school, place of care, or child care provider if the requested leave would have jeopardized the viability of the business.
[38]Covered employers that failed to provide emergency paid sick leave to eligible employees are considered to have committed minimum wage violations under the Fair Labor Standards Act of 1938, as amended, and are subject to penalties described therein, including being liable to the affected employees. See Pub. L. No. 116-127, § 5105(a), 134 Stat. at 197. Covered employers are subject to additional penalties for discharging, disciplining, or discriminating against any employee for taking emergency paid sick leave. See Pub. L. No. 116-127, § 5105(b), 134 Stat. at 197. The prohibitions and enforcement provisions in the Family and Medical Leave Act apply to leave under the expanded family and medical leave provisions. See 29 U.S.C. §§ 2615, 2617. Employees may also bring a civil action against covered employers that have violated the expanded family and medical leave provisions. See 29 U.S.C. § 2617(a).
[39]WHD generally has three priority levels for cases it investigates—tier I, tier II, and tier III. Tier I cases have the highest priority, and tier III cases have the lowest priority.
[40]WHD filed 14 percent of FFCRA complaints with no compliance action and dropped 16 percent of FFCRA cases that were accepted for investigation.
[41]Pub. L. No. 116-136, §§ 2301–2307, 134 Stat. at 347–359 (2020). The other COVID-19 relief laws include the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021. Pub. L. No. 116-260, 134 Stat. 1182 (2020); Pub. L. No. 117-2, 135 Stat. 4 (2021).
[42]An NOL occurs when a taxpayer's allowable deductions exceed its gross income for a tax year. The CARES Act requires, unless waived, carrybacks for 5 years for NOLs arising in tax years beginning in 2018, 2019, and 2020, which may provide a cash refund for certain taxpayers. Tax years prior to 2018 generally had a higher tax rate, so the ability of businesses to carryback post-2018 NOLs to earlier tax years tends to increase the relative value of the carryback amounts. In general, AMT was an alternative tax regime which applied a lower tax rate to a broader tax base by limiting the use of tax preferences and disallowing credits and deductions. The corporate AMT was repealed in 2017, but most corporations could claim their remaining unused minimum tax credits as a refundable credit for tax years 2018 through 2021. Under the CARES Act, corporations with AMT credits may claim a refund for tax years beginning in 2018 and 2019.
[43]26 U.S.C. § 6411(b), (d)(2); Pub. L. No. 116-136, § 2305(d)(1), 134 Stat. at 357.
[45]As previously mentioned, we closed one recommendation as not implemented.
[46]We identified a number of economic indicators to facilitate ongoing and consistent monitoring of areas of the economy supported by the federal pandemic response, namely labor markets, household finances, small business credit and financial conditions, corporate credit market conditions, and state and local government finances. To the extent that federal pandemic responses are effective, we would expect to see improvements in outcomes related to these indicators. However, while trends in these indicators may be suggestive of the effect of provisions of the COVID-19 relief laws over time, those trends will not on their own provide definitive evidence of effectiveness.
[47]The largest provision of ARPA in terms of dollars provided was the economic impact payments, which totaled $385 billion. In addition, the Congressional Budget Office projects that the budgetary effects of the unemployment insurance provisions will be $195 billion in 2021, while the child tax credit provisions will be $19 billion in 2021 and $65 billion in 2022.
[48]ARPA appropriated $350 billion for the state and local fiscal recovery fund.
[49]Greater progress with vaccinations, for example, can increase expected growth, while new virus variants that evade vaccines can lead to a sharp decrease in expected growth.
[50]As we noted in our November 2020 report, researchers consistently found that a decline in consumer demand related to concerns about COVID-19 had a significant impact on the economy during the initial stages of the pandemic.
[51]As we noted in our November 2020 report, researchers found consistent evidence that the impact of state and local government-mandated restrictions further reduced economic activity.
[52]According to the Bureau of Labor Statistics, past recessions have disrupted employment almost entirely from the demand side, but the COVID-19 pandemic also disrupts labor supply. Health concerns, family demands, and government policies all play roles in who can work and when.
[53]This forecast measures expected consumer price inflation in 2021 based on forecasts collected by Bloomberg.
[54]See, for example, M. Khan and A. Senhadji, “Threshold Effects in the Relationship between Inflation and Growth,” IMF Staff Papers, vol. 48 (2001): 1–21, and William Easterly and Stanley Fischer, “Inflation and the Poor,” Journal of Money, Credit and Banking, vol. 33 (May 2001): 160–178.
[55]According to the January 2021 COVID-19 Survey of Consumers conducted by the Federal Reserve Bank of Philadelphia, Black borrowers reported the highest forbearance rate, at 13.4 percent of borrowers in forbearance at some point during the pandemic. In fiscal year 2020, 34.2 percent of all FHA purchase and refinance borrowers were minorities, 50.4 percent of FHA forward mortgage borrowers were of low-to-moderate income, and 83.1 percent of home purchasers under the FHA forward mortgage insurance program were first-time homebuyers. See Department of Housing and Urban Development, FHA Annual Management Report Fiscal Year 2020.
[56]The CARES Act provided temporary protections for millions of households against foreclosure and eviction, as well as temporary forbearance, suspending mortgage payments for up to 360 days. In addition, FHA allows mortgage servicers to initiate new forbearance through June 30, 2021, and it allows borrowers who requested an initial forbearance on or before June 30, 2020, to request up to two additional 3-month forbearance extensions.
[57]Spreads on municipal bonds relative to benchmark interest rates (e.g., Treasury interest rates) incorporate the favorable tax treatment received by municipal debt and may also reflect any premium state and local borrowers pay to compensate lenders for taking on the risk of loss due to default (risk premium) and for tying up their investment funds for a period of time (liquidity premium). We report spreads calculated based on the Bloomberg Barclays Municipal Bond Index. Spreads are calculated using yield to worst, which results in a conservative—that is, lower—estimate of potential returns on callable bonds.
[58]To accelerate the availability of a vaccine to prevent COVID-19, DOD, on behalf of HHS, awarded contracts and other transaction agreements in 2020 to six vaccine companies for different types of activities, including clinical development and manufacturing activities or the purchase of COVID-19 vaccine doses. There are 64 jurisdictions implementing COVID-19 vaccination, including all 50 states, the District of Columbia, five major U.S. cities (Chicago, Houston, New York City, Philadelphia, and San Antonio), and eight territories (American Samoa, Guam, the Marshall Islands, the Federated States of Micronesia, the Northern Mariana Islands, Palau, Puerto Rico, and the U.S. Virgin Islands).
[59]The Secretary of Health and Human Services may declare that circumstances, prescribed by statute, exist justifying the emergency use of certain medical products, such as vaccines. Once a declaration of an emergency has been made, FDA may temporarily allow use of unlicensed vaccines through an EUA. For FDA to issue an EUA for a vaccine, it must be reasonable to believe that the vaccine may be effective and that the known and potential benefits of the vaccine outweigh the known and potential risks, among other statutory criteria. See 21 U.S.C. § 360bbb-3. Typically, FDA must license a vaccine before it can be marketed in the U.S. See 42 U.S.C. § 262. Any COVID-19 vaccine that initially receives an EUA from FDA is expected to ultimately be reviewed and receive licensure through a biologics license application, according to FDA guidance. See FDA, Emergency Use Authorization for Vaccines to Prevent COVID-19: Guidance for Industry (May 2021).
[60]For the purposes of this report, we refer to the COVID-19 vaccine that Pfizer and BioNTech developed together, as the Pfizer vaccine. In addition, Janssen Pharmaceutical Companies are a part of Johnson & Johnson. On April 23, 2021, the Centers for Disease Control and Prevention (CDC) recommended that pregnant people receive COVID-19 vaccines following publication of preliminary findings of post-COVID-19 vaccine surveillance of about 35,000 pregnant persons. This study found that pregnant people experienced the same side effects as others following vaccination and that no safety concerns were observed for people vaccinated in the third trimester or for their babies. See T.T. Shimabukuro, et al., “Preliminary Findings of mRNA COVID-19 Vaccine Safety in Pregnant Persons” New England Journal of Medicine. (2021) https://www.nejm.org/doi/full/10.1056/NEJMoa2104983.
[61]According to Pfizer, it has requested priority review for its COVID-19 vaccine. A priority review designation directs FDA resources to applications for products that, if approved, would provide significant improvements in the safety or effectiveness of the treatment, diagnosis, or prevention of serious conditions when compared to standard applications. According to FDA, its goal is to take action on a priority BLA within 6 months following a 60-calendar-day filing review period that begins on the date of FDA’s receipt of the BLA (so the goal is a total of 8 months from receipt). For standard BLAs, FDA’s goal is to take action within 10 months following the 60-day filing date (so the goal is a total of 12 months from receipt).
[62]Moderna has also requested priority review for its COVID-19 vaccine BLA.
[63]After FDA’s authorization, CDC’s Advisory Committee on Immunization Practices (ACIP) voted to recommend use of the Pfizer vaccine for adolescents 12 through 15 years of age, and the CDC Director adopted ACIP’s recommendation on May 12, 2021.
[64]Alternatively, Pfizer vaccine vials may be stored frozen prior to use at a slightly higher temperatures of -13 to 5 degrees Fahrenheit for up to 2 weeks.
[65]For example, on May 19, 2021, FDA authorized an increased refrigerated storage time of Pfizer’s vaccine for thawed vials prior to dilution. Thawed, undiluted vials can be stored in the refrigerator at 35 to 46 degrees Fahrenheit for up to 1 month. Previously, such vials could be stored in the refrigerator for up to 5 days.
[66]As of June 15, 2021, AstraZeneca and Novavax had both announced findings from phase 3 clinical trials for their COVID-19 vaccine candidates, while Sanofi announced on May 27, 2021, that it had started enrollment in a global phase 3 clinical trial for its vaccine candidate.
[67]Vaccine doses distributed is the total number that have been delivered to jurisdictions, retail pharmacies, long-term care facilities, dialysis centers participating in the Federal Dialysis Center Program, Federal Emergency Management Agency partner sites, Health Resources and Services Administration-supported health centers, and federal entities. For states; Washington, D.C.; the U.S. Virgin Islands; and Puerto Rico; total counts of COVID-19 vaccine doses distributed include doses delivered since December 14, 2020. However, for Palau, Micronesia, Marshall Islands, Guam, American Samoa, and Northern Marianas Islands, total counts of COVID-19 vaccine doses distributed include doses marked as shipped in CDC’s Vaccine Tracking System since December 13, 2020. The most recent days of reporting for vaccine administrations may be more impacted by reporting delays, and all reported numbers may change over time as historical data are reported to CDC.
[68]As of June 10, 2021, of the three COVID-19 vaccines authorized for emergency use, two vaccines were two-dose regimens and the third vaccine required one dose. For the purpose of this report, fully vaccinated is defined as having received the second dose in a two-dose COVID-19 vaccine regimen or one dose of the single-dose vaccine.
[69]Data from CDC’s COVID Data Tracker also indicated that 0.9 percent of fully vaccinated individuals whose race and ethnicity was known as of June 10, 2021, were non-Hispanic American Indian/Alaska Native (compared to 0.8 percent of the U.S. population), 0.3 percent were non-Hispanic Native Hawaiian or Other Pacific Islander (compared to 0.3 percent of the U.S. population), and 8 percent were non-Hispanic Multiple/Other races (compared to 2.3 percent of the U.S. population).
[70]The 64 jurisdictions, included all 50 states, the District of Columbia, five major U.S. cities (Chicago, Houston, New York City, Philadelphia, and San Antonio), and eight territories (American Samoa, Guam, the Marshall Islands, the Federated States of Micronesia, the Northern Mariana Islands, Palau, Puerto Rico, and the U.S. Virgin Islands). See HHS COVID-19 Funding enclosure for more information on COVID-19 funding.
[71]HRSA’s Bureau of Primary Health Care administers the Health Center Program and makes grants to health centers that primarily serve low-income populations. The majority of health centers serve the general population within a designated area, while other types of health centers provide care to more specific populations, including the homeless, residents of public housing, and migrant and seasonal farmworkers.
[73]The Federal Retail Pharmacy Partnership was initially outlined in CDC’s COVID-19 interim playbook, while the Health Center COVID-19 Vaccine Program was described in the White House’s National Strategy. See Department of Health and Human Services, Centers for Disease Control and Prevention, COVID-19 Vaccination Program Interim Operational Guidance for Jurisdictions Playbook, version 2 (Atlanta, Ga.: Oct. 29, 2020) and White House, National Strategy for the COVID-19 Response and Pandemic Preparedness (Washington, D.C.: Jan. 21, 2021).
[75]Rural health clinics are intended to increase access to primary care services to patients in rural communities and can include public, nonprofit, or for-profit health care facilities.
[77]For the purposes of this report, vaccine hesitancy refers to a delay in acceptance of vaccines despite availability of vaccination services. Those who are vaccine hesitant are a middle group along a continuum that ranges between those who fully accept vaccines on one end and those who are strongly opposed to vaccines on the other. An individual’s level of vaccine hesitancy can vary over time. See also National Academies of Sciences, Engineering, and Medicine, The Critical Public Health Value of Vaccines: Tackling Issues of Access and Hesitancy: Proceedings of a Workshop (Washington, D.C.: 2021).
[78]For perspectives of state, territorial, and local health officials, we interviewed representatives from the Association of State and Territorial Health Officials, Association of Immunization Managers, and the National Association of County and City Health Officials. We also interviewed officials from the National Governors Association. For perspectives of providers, we interviewed representatives from the American Hospital Association, American Medical Association, and the National Association of Community Health Centers.
[79]COVID-19 has affected vulnerable populations in other settings beyond nursing homes, including assisted living facilities. However, as the federal role in oversight of nursing homes is more significant than in other settings such as assisted living facilities, the federal response has been more focused on nursing homes.
[80]Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 557 (2020).According to CMS, of this amount, the agency plans to provide state survey agencies approximately $81 million through September 30, 2023, to be used to ensure that all nursing homes receive targeted infection control surveys, among other things. CMS has set aside the remaining $19 million to enhance survey system technology, to fund purchase of personal protective equipment (PPE) for federal surveyors, and to implement improvements recommended by the Nursing Home Commission, according to the agency.
[81]Specifically, the CARES Act appropriated $100 billion, the Paycheck Protection Program and Health Care Enhancement Act appropriated $75 billion, and the Consolidated Appropriations Act, 2021, appropriated $3 billion for this purpose. Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1920 (2020); Pub. L. No. 116-139, div. B, tit. I, 134 Stat. 620, 622 (2020); Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 563 (2020). Additionally, the American Rescue Plan Act of 2021, signed into law on March 11, 2021, appropriated $8.5 billion for payments to eligible rural health care providers for health care-related expenses and lost revenues that are attributable to COVID–19. Pub. L. No. 117-2, § 9911, 135 Stat. 4, 236-38.
[83]As part of the program, vaccines were provided with no out-of-pocket costs for residents or staff or costs to the facilities. The pharmacy partners—including CVS, Walgreens, and Managed Health Care Associates, Inc.— scheduled and coordinated on-site vaccination clinic dates; ordered vaccines and associated supplies; ensured cold chain management for the vaccine; provided on-site administration; reported required vaccination data to local, state, and federal jurisdictions; while adhering to all applicable CMS COVID-19 testing requirements for facility staff.
[84]According to CDC, a long-term care pharmacy is a specialized pharmacy that is designed specifically to support people living in a long-term care community.
[85]CDC defines a confirmed case as having a positive COVID-19 test resulting from a molecular test, a nucleic acid test, or an antigen test, including antigen point-of-care test results. The percentage of nursing homes reporting at least one confirmed case or death is calculated based on the number of nursing homes that both reported data and passed quality checks for the week ending May 16, 2021.
[86]According to CDC, an outbreak starts the week a nursing home reports a new resident or staff COVID-19 case and ends when there are 2 weeks with no new cases.
[87]According to CDC, some of the decline in resident cases occurred before vaccinations were administered through the partnership program. New weekly resident cases peaked the week ending December 20, 2020, at more than 33,300 resident cases and new weekly staff cases peaked one week prior at more than 28,500 staff cases for the week ending December 13, 2020. New weekly resident cases declined to 700 cases and new weekly staff cases declined to 1,469 cases for the week ending May 16, 2021. New weekly and cumulative case and death counts are likely underreported because they do not include data for the nursing homes that did not report COVID-19 data to CDC for that week or from nursing homes that submitted data that failed data quality assurance checks. Additionally, as we previously reported, CMS does not require nursing homes to report data prior to May 2020, although nursing homes may do so voluntarily. According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time. Data presented in this enclosure reflect the data downloaded as of May 27, 2021, which includes data through the week ending May 16, 2021.
[88]New weekly resident deaths reached a peak of 5,979 for the week ending December, 20, 2020, and have since declined to 197 deaths as of the week ending May 16, 2021—about a 97 percent decline in new weekly deaths since the peak in December 2020.
[89]See A. Cavanaugh et al., “COVID-19 Outbreak Associated with a SARS-CoV-2 R.1 Lineage Variant in a Skilled Nursing Facility After Vaccination Program — Kentucky, March 2021,” Centers for Disease Control and PreventionMorbidity and Mortality Weekly Report, vol. 70 (Apr. 21, 2021) and R. Teran et al., “Postvaccination SARS-CoV-2 Infections Among Skilled Nursing Facility Residents and Staff Members — Chicago, Illinois, December 2020–March 2021,” Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report, vol. 70 (Apr. 21, 2021).
[90]Pharmacies participating in the Pharmacy Partnership for Long-Term Care Program are contracted to provide three vaccination clinics in each long-term care facility enrolled in the program to facilitate safe vaccination of the long-term care population. Certain individual nursing homes are receiving their vaccinations outside of the pharmacy partnership program. Facilities were not required to participate in the program and could opt to have vaccine supply and management services coordinated by a pharmacy provider of its choice. According to HHS, 2 percent (374 out of 15,727) of nursing homes chose not to enroll in the program. CDC does not have complete data on vaccines administered to residents and staff members of nursing homes outside of the Pharmacy Partnership for Long-Term Care Program.
[91]According to CDC, the remaining doses were administered in other long-term care settings, such as assisted living facilities. CDC officials said that when reporting vaccination data, nursing homes generally self-reported their facility type as CMS certified skilled nursing facility, which CDC indicated was the category generally inclusive of nursing homes. CDC’s vaccine distribution and administration tracking website notes that doses administered refers to vaccine administered to long-term care facility residents and staff, as reported to CDC by the pharmacy partners participating in the Pharmacy Partnership for Long-Term Care Program. These data do not include doses administered to long-term care facility residents and staff outside this partnership. A total of 54 out of 55 eligible jurisdictions, including 49 states, four cities, and one territory, participated in the program. Participating jurisdictions did not include West Virginia. The 55 eligible jurisdictions are among a total of 64 jurisdictions which include all U.S. states and territories and some local health programs.
[92]CDC data show that during the week ending May 16, 2021, 243 facilities (about 2 percent) requested assistance related to vaccine access.
[93]The Federal Retail Pharmacy Program for COVID-19 Vaccination, launched on February 11, 2021, is a collaboration between the federal government, states and territories, and 21 national pharmacy partners and independent pharmacy networks to increase access to COVID-19 vaccination across the United States. This program is one component of the federal government’s strategy to expand access to vaccines for the American public.
[94]We analyzed the most recent data available on May 27, 2021. The CDC data on COVID-19 in nursing homes were accessed on May 27, 2021, for the week ending May 16, 2021, from https://data.cms.gov/Covid19-nursing-home-data. For the data on COVID-19 in nursing homes, we analyzed and reported data that had been determined by CDC and CMS to pass quality assurance checks for data entry errors. According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time.
[95]During an emergency, as declared by the Secretary of Health and Human Services, FDA may temporarily authorize unapproved medical products or unapproved uses of approved medical products through an EUA, provided certain statutory criteria are met. See 21 U.S.C. §§ 360bbb-3.CDC submitted its EUA request for the test to FDA on February 3, 2020.
[96]One of the statutory criteria for EUA issuance—evidence that the product “may” be effective—requires less certainty of effectiveness than is required for approval. See 21 U.S.C. § 360bbb-3(c)(2)(A). This allows for products such as tests to be made available through EUAs more quickly than if they were subject to approval.
[97]Based upon the CDC EUA request, use of the test was limited to qualified laboratories designated by CDC.
[98]According to CDC, before laboratories use a new test on samples from patients, they must verify the test performance to make sure it works as expected. According to CDC, about half of the 93 laboratories had reported the status of their verification of the test to CDC by February 21, 2020, and of these laboratories, 85 percent reported problems with the test. The remaining laboratories did not report their verification status to CDC.
[99]Also on February 29, 2020, FDA issued an EUA for the New York State Department of Health’s COVID-19 test.
[100]Government of the Republic of Korea, All about Korea’s Response to COVID-19 (Seoul, Republic of Korea: Oct. 13, 2020).
[101]Chinese researchers posted the virus’s genetic code to the National Institute of Health’s GenBank. CDC’s first COVID-19 test was called the CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. CDC developed a second COVID-19 test in July 2020 called the CDC Influenza SARS-CoV-2 (Flu SC2) Multiplex Assay.
[102]The German laboratory, Charite-Universitatsmedizin Berlin, published a revised version of its test design on January 17, 2020.
[103]The CDC laboratory that developed the test was the Respiratory Viruses Branch laboratory from within CDC’s Division of Viral Diseases, part of the CDC National Center for Immunization and Respiratory Diseases.
[104]CDC’s International Reagent Resource shipped test kits to 93 qualified laboratories including to all 50 state public health laboratories and several DOD laboratories between February 6 and February 10, 2020. Each test kit could test approximately 700 to 800 specimens.
[105]See 21 C.F.R. pt. 820 (2020) (generally referred to as current good manufacturing practice regulations). According to CDC, these regulatory requirements govern the methods, facilities and controls used for the design, manufacture, packaging, labeling, storage, installation, and servicing of all finished in vitro diagnostic devices intended for human use. FDA waived the current good manufacturing practice requirements, including the quality system requirements, under the EUA for the test.
[106]See CLIA of 1988, Pub. L. No. 100-578, 102 Stat. 2903 (codified as amended at 42 U.S.C. § 263a); 42 C.F.R. pt. 493 (2020) (laboratory requirements). Under CLIA, clinical laboratories that perform tests on human specimens to diagnose, prevent, or treat disease must meet certain requirements. The Centers for Medicare & Medicaid Services (CMS) has issued regulations to implement CLIA and is responsible for overseeing and certifying compliance with these regulations.
[107]In addition, according to CDC, the laboratory used an electronic information system that was incompatible with another integral CDC component, which led to a loss of document control that resulted in conflicting versions of laboratory documents and procedures in use at the same time.
[108]In October 2020 CDC established a policy that, among other things, established reporting requirements for laboratory safety events in CDC high containment laboratories and associated areas.
[109]Two days prior, on February 26, 2020, CDC received enforcement discretion from FDA that allowed the CDC test to be used without the N3 primer-probe set.
[110]CDC’s criteria on February 28, 2020, also noted that local health departments, in consultation with clinicians, should determine whether a patient should be investigated or tested for COVID-19.
[111]Additionally, CDC required public health laboratories to send their positive test results to CDC for confirmatory testing until the middle of March, 2020.
[112]According to the foundation’s website, the CDC Foundation is an independent nonprofit that was created by Congress to mobilize philanthropic and private-sector resources to support the CDC’s critical health protection work.
[114]CDC told us it has created a working group to develop a charter and process for this new Test Review Board. CDC expects to complete the Board’s charter by October 2021 and to begin a phased implementation of the Board by early 2022.
[115]CDC officials told us that the Test Review Board will be composed of CDC staff with expertise in statistics, assay development, and assay manufacturing. According to CDC, to ensure independence and safeguard against potential conflicts of interest, the Board’s charter will include a review process that includes input from all board members and a process to recuse members with conflicts of interest from the discussion and voting process. All board members will adhere to CDC ethics requirements and all potential conflicts of interest will be documented within the meeting minutes.
[116]CDC officials told us the agency has initiated the Laboratory Excellence and Accreditation Project, which includes implementation of a quality management system across all of CDC’s laboratories. The goal is for all laboratory programs to achieve accreditation by October 1, 2024.
[117]According to CDC, accreditation is used to verify that laboratories have an appropriate quality management system and can properly develop, deploy, and perform certain test methods that are suitable for their intended purpose, according to their scopes of accreditation.
[118]According to CDC officials, the agency allocated more than $82 million for these efforts.
[120]Memorandum of Understanding between American Clinical Laboratory Association, Association of Public Health Laboratories, Council of State and Territorial Epidemiologists and Centers for Disease Control and Prevention/Center for Surveillance, Epidemiology and Laboratory Services/Division of Laboratory Services. April 30, 2018.
[121]Our May 2017 report on the 2016 Zika outbreak recommended that CDC establish a transparent process to provide CDC diagnostic tests, upon request, to manufacturers in the final stages of diagnostic test authorization. See “Related GAO Products” in this enclosure.
[122]Department of Homeland Security, Homeland Security Exercise and Evaluation Program (Washington, D.C.: January 2020).
[123]Executive Office of the President, National Biodefense Strategy (Washington, D.C.: September 18, 2018).
[124]According to CDC, the agency manufactured all of the chemical components for the second batch, with the manufacturer performing the vialing and labeling. Both contractors were involved in manufacturing the majority of the kits that were distributed to the public health laboratories from that point forward.
[125]For purposes of this report, we refer to advance contracting as an agency’s use of contracts or contracting methods that may offer agencies advance planning, pre-negotiated line items, and special terms and conditions that permit rapid response, such as Federal Supply Schedule contracts, blanket purchase agreements, and indefinite delivery contracts. See e.g., FAR 18.105.
[126]Department of Homeland Security, Federal Emergency Management Agency, Advance Contracting of Goods and Services Report to Congress (December 2007). Under the Federal Acquisition Regulation (FAR), agencies are generally required to use full and open competition when soliciting offers and awarding contracts. During an emergency, contracting officers may use the unusual and compelling urgency exception to full and open competition to support noncompetitive contract awards. See e.g., FAR 6.302-2 and FAR 18.104.
[127]Office of Management and Budget, Office of Federal Procurement Policy, Emergency Acquisitions Guide (Washington, D.C.: January 14, 2011).
[128]Centers for Disease Control and Prevention, Office of Laboratory Science and Safety, Root Cause Analysis: Unanticipated Failure of the ‘CDC 2019-Novel Coronavirus (2019 nCov) Real-Time RT-PCR Diagnostic Panel’ (Atlanta, Ga.: March 24, 2020, updated Oct. 5, 2020)
[129]HHS officials reported that they made spend plan decisions in coordination with the Office of Management and Budget.
[130]The first five COVID-19 relief laws require HHS to provide a detailed spend plan of anticipated uses of funds to the House and Senate Committees on Appropriations and that these plans be updated and submitted to the Committees every 60 days until September 30, 2024, with the exception of the second law, the Families First Coronavirus Response Act, which requires that the plans be updated and submitted until all funds are expended or expire. HHS officials told us that they submit the spend plans to the Office of Management and Budget (OMB) for review. In contrast, spend plans are not required by ARPA, although HHS officials told us in April 2021 that they are developing a spend plan for ARPA COVID-19 relief funds.
[131]As of May 2021, we had received and reviewed a total of 15 spend plans—the original spend plans and subsequent updates—provided by HHS. The spend plans include some limited references to time frames for a small portion of funds; for example, one spend plan notes that an NIH project for additional laboratory space will take 2 years for construction plus 5 to 6 months for move-in time. In April 2021, agency officials told us that HHS is working on a consolidated plan that captures the first five relief laws and a separate spend plan for ARPA. The consolidated spend plan was under internal review at HHS, and the ARPA spend plan was still being finalized as of April 2021.
[132]See OMB M-20-21: COVID Reporting Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019 (COVID-19), Apr.10, 2020.
[133]HHS officials told us that they develop and submit apportionment requests to OMB for the COVID-19 relief funds. These requests may include information on timing of obligations that vary by individual agency, and OMB apportions the funds to HHS either by time period (for example, by quarter) or by purpose, as defined by OMB Circular A-11.
[134]According to HHS, the $8.5 billion for rural providers was appropriated separately from funds for the PRF but will be administered using the same mechanism as the provider relief funds.
[135]The funds HHS reported to us for testing includes various activities (e.g., procurement and distribution of testing supplies, community-based testing programs, testing in high-risk and underserved populations and Indian Health Services’ Programs, implementing a national strategy, and CDC testing-related activities such as technical assistance, and other activities), although this category does not include all funds for testing, such as funds to state and local governments to support testing activities. About 97 percent ($38.7 billion of $40.1 billion) of funds reported for support for state, local, territorial, tribes and tribal organizations’ preparedness was obligated as of May 31, 2021.
[136]HHS’s COVID-19 Strategic Testing Plan, dated November 20, 2020, describes planned uses for $25 billion for testing, research and development, and response, but it does not include time frames for these activities.
[137]We searched HHS’s Tracking Accountability in Government Grants System website and www.usaspending.gov—a publicly available website developed and operated by the Department of the Treasury that includes detailed data on federal spending, including obligations, across the federal government. See https://taggs.hhs.gov/coronavirus, accessed 06/02/2021, and https://www.usaspending.gov, accessed 06/02/2021. We did not independently validate the data provided by HHS.
[138]PPE is typically considered to be a low-margin commodity—that is, the selling price is not much higher than the cost to produce. Low-margin commodities like PPE are not highly unique or highly specialized products, making the industry for them more competitive.
[139]Gloves used in health care settings include latex, vinyl, nitrile, and other rubber synthetic gloves. For the purposes of this information, we are focusing primarily on nitrile gloves. According to the U.S. International Trade Commission (USITC), nitrile gloves are the most common of the four types used in health care settings because of their price, durability, and hypoallergenic properties.
[140]Pub. L. No. 81-774 (1950), codified at 50 U.S.C. §§ 4501 et seq., as amended.
[141]As previously reported, these contracts and agreements were awarded through DPA and other actions.
[142]A Sustainable Public Health Supply Chain, Exec. Order No. 14001, § 4, 86 Fed. Reg. 7,219, 7220-21 (Jan. 21, 2021). The Executive Order directed DOD, HHS, and the Department of Homeland Security, among others, to develop a pandemic supply chain resilience strategy. This strategy, due July 20, 2021, is to include an approach to design, build, and sustain a long-term capability in the U.S. to manufacture medical supplies, including PPE, for future pandemics and biological threats.
[143]Pub. L. No. 117-2, tit. III, § 3101, 135 Stat. 4, 53-54.
[144]The federal interagency Supply Chain Advisory Group, established in March 2020 as the Supply Chain Task Force, was tasked with maximizing the nationwide availability of supplies needed for the COVID-19 response.
[145]U.S. International Trade Commission, COVID-19 Related Goods: The U.S. Industry, Market, Trade, and Supply Challenges (Dec. 2020) (prepared at the request of the U.S. House Committee on Ways and Means and the Senate Committee on finance).
[146]For surgical and isolation gowns, workers are needed to cut gown pieces and sew them together; stitch or weld around seams; and apply any elastic, ties, or other fastening devices.
[147]According to USITC, there are two nitrile rubber manufacturing facilities in the U.S., one owned by a Japanese company and the other owned by a U.S. company.
[148]These nonwoven fabrics are produced in several countries, including the United States.
[149]Tax credits could also help manufacturers offset costs of new equipment or investments in automation technology, according to some manufacturers, distributors, and trade associations. However, other stakeholders noted that such tax credits would provide only nominal cost offsets. Tax credits for qualified research expenses are already available. See 26 U.S.C. § 41.
[150]Contracts to manufacture PPE domestically should be at least 3 years, according to most of the stakeholders that provided suggestions on contract length. Some stakeholders suggested contract lengths as long as 8 to 10 years for both business and resource planning purposes. Preferences for contract lengths also vary based on the type of PPE, as different PPE types require different levels of capital and labor investments.
[151]Two stakeholders also discussed a variety of potential stockpiling strategies, including stockpiling raw materials and using vendor-managed inventory in lieu of federal warehousing. Vendor-managed inventory, which HHS already uses to some extent for the federal stockpile, allows the government to acquire medical supplies, including PPE, only when needed and helps to ensure adequate rotation of stock to avoid costs associated with replacing expired products. While stakeholders primarily discussed stockpiling at the federal level, a few stakeholders from trade associations representing state and local officials suggested building demand through state, or even private, stockpiles.
[152]The Strategic National Stockpile is the federal repository of pharmaceuticals, and medical supplies and devices to be deployed to support responses to public health emergencies.
[153]The Berry Amendment specifically pertains to DOD, generally requiring it to purchase certain products such as clothing and textiles from domestic sources, including components or materials of those products. See 10 U.S.C. § 2533a.
[154]Under the Buy American Act, an end product may be considered domestically made even if it contains foreign components. In addition, the Buy American Act permits federal agencies to procure foreign products under certain exceptions, such as cases in which domestic products are not reasonably available in sufficient quantities of a satisfactory quality. In January 2021, President Biden signed an executive order, Ensuring the Future Is Made in All of America by All of America’s Workers, which directed the Office of Management and Budget and the General Services Administration to make available on a public website information on proposed waivers of Made in America laws including the Buy American Act and whether those waivers have been granted. Exec. Order No. 14005, 86 Fed. Reg. § 6, 7,475, 7,476-7 (Jan. 28, 2021). According to officials from the Office of Management and Budget, this information will help ensure that federal agencies are making all reasonable efforts to source domestically made products. In addition, these officials noted that they hope that this information will encourage additional domestic manufacturers to submit offers in response to solicitations for federal contracts.
[155]Hurricane Maria caused damage to Puerto Rico’s electrical grid, which led to shortages of critical medical supplies from pharmaceutical plants and medical device manufacturing facilities located there during that year’s flu season, as well as delays in transportation and other effects. The Texas winter storms significantly affected the plastics and petrochemicals manufacturers located in the state, which resulted in ongoing shortages of medical supplies made from these items. Medical supplies in shortage during these events included those needed for the COVID-19 response, such as face shields and sharps containers used to dispose of needles like the kind used to administer the COVID-19 vaccine.
[156]See Department of Health and Human Services (HHS), SNS 2.0 Strategy – Modernize the SNS (draft). According to HHS officials, ASPR finalized the strategy in January 2021 under the prior administration but has not released it publicly. For more information on the SNS strategy, see our January 2021 CARES Act report. USITC, COVID-19 Related Goods: The U.S. Industry, Market, Trade, and Supply Challenges.
[157]This information was submitted in response to Executive Order 13944, which directed the Department of Commerce to report on the status of the public health industrial base and provide recommendations for initiatives to strengthen it. Combating Public Health Emergencies and Strengthening National Security by Ensuring Essential Medicines, Medical Countermeasures, and Critical Inputs Are Made in the United States, Exec. Order No. 13944 § 6(b), 85 Fed. Reg. 49,929, 49,933 (Aug. 6, 2020). As part of this work, the department solicited comments from the public. 85 Fed. Reg. 77,428 (Dec. 2, 2020). This report was directed to be completed by February 2021. As of May 2021, the department did not have an anticipated time frame for issuing its report.
[158]We selected stakeholders from the following sources: (1) USITC and the Department of Commerce public written submissions, (2) manufacturers that received DPA Title III or other actions for PPE expansion, (3) related GAO work on medical device authorizations in emergency periods, (4) PPE distributors that share data with the federal Supply Chain Advisory Group, and (5) other relevant stakeholders suggested by selected interviewees. In some instances, we interviewed trade associations representing manufacturers, distributors, and other purchasers of PPE, in lieu of interviewing individual stakeholders.
[159]Requesting agencies may include the Federal Emergency Management Agency (FEMA) within the Department of Homeland Security, the Department of Health and Human Services, and the U.S. Department of Agriculture.
[160]In December 2020, the Food and Drug Administration (FDA) authorized the emergency use of the two-dose Pfizer-BioNTech and Moderna COVID-19 vaccines. On May 10, 2021, the FDA further expanded the emergency use of the two-dose Pfizer-BioNTech COVID-19 vaccines to include adolescents aged 12 to 15 years. In February 2021, the FDA authorized the emergency use of the one-dose Janssen (Johnson & Johnson) COVID-19 vaccine. From April 13 to 23, 2021, the FDA and Centers for Disease Control and Prevention (CDC) recommended a pause in administering the Johnson & Johnson vaccine due to reports of blood clots. However, after conducting a safety review, the FDA and CDC determined that it was safe to resume using the Johnson & Johnson vaccine.
[161]FEMA classifies community vaccination centers by type (i.e., Types 1 through 5) on the basis of facility throughput over a 12-hour period. A Type 1 center can administer about 6,000 doses per day; a Type 2 center, about 3,000 doses per day; a Type 3 center, about 1,000 doses per day; and Types 4 and 5 centers, about 250 doses per day. See Federal Emergency Management Agency, Community Vaccination Centers Playbook (Apr. 23, 2021).
[162]DOD has assigned the servicemembers on the basis of each center’s size and vaccine administration capacity––for example, 222 service members for the larger centers that each administer about 6,000 doses daily.
[163]Partially vaccinated servicemembers received at least one dose of a COVID-19 vaccine. Fully vaccinated servicemembers received both doses of a two-dose COVID-19 vaccine series or one dose of the one-dose COVID-19 vaccine.
[164]According to DHA officials, the target vaccine-eligible population of 6.7 million is the number of individuals whom DHA assessed as eligible to receive a COVID-19 vaccine through DOD and who live within 40 miles of a DOD vaccination site.
[165]Military servicemembers who elect to receive a COVID-19 vaccine through non-DOD sites are to provide proof of vaccination for documentation in their immunization records.
[166]Centers for Disease Control and Prevention, “COVID Data Tracker,” accessed June 11, 2021, https://covid.cdc.gov/covid-data-tracker/#vaccinations. The Centers for Disease Control and Prevention data includes the population vaccinated at or eligible to be vaccinated by DOD.
[167]Federal law states that a vaccine released under an emergency use authorization cannot be made mandatory. 21 U.S.C. § 360bbb-3(e)(1)(A)(ii)(III).
[168]TRICARE is DOD’s regionally structured program that provides purchased health care to beneficiaries through networks of civilian providers.
[169]Deputy Secretary of Defense Memorandum, Methods to Enable and Encourage Vaccination Against Coronavirus Disease 2019 (May 20, 2021).
[170]On May 24, 2021, the Navy updated its COVID-19 Standardized Operational Guidance. For fully vaccinated individuals, the updated guidance relaxes predeployment restrictions of movement, health protection measures when naval ships are underway, and port visits.
[171]Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-18-20 (Washington, D.C.: June 26, 2018). In March 2021, OMB issued a revised version of OMB Circular A-123, Appendix C, effective starting in fiscal year 2021. Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-21-19 (Washington, D.C.: March 5, 2021).
[172]Department of Health and Human Services, Office of Financial Reporting and Policy, Agency Financial Report Fiscal Year 2020, (Washington, D.C.: Nov. 13, 2020), 75-84. A deficiency in internal controls exists when the design or operation of a control does not allow management or employees, in the normal course of performing their assigned functions, to prevent, or detect and correct, misstatements on a timely basis. In addition to the interagency deficiency, the auditor also identified internal control deficiencies, in part due to weaknesses in the timely posting of SNS receiving and issuance activities, and discrepancies between warehouse counts and SNS’s inventory management system. ASPR did not concur with these findings. The auditor did not report any findings specific to the direct shipment procurement process or the standard procurement process.
[173]The Intragovernmental Payment and Collection (IPAC) system is the primary method used by most federal entities to electronically bill or pay for services and supplies within the U.S. government. IPAC is used to communicate between the Treasury and the trading partner entities that the online billing or payment for services and supplies has occurred. While IPAC provides an automated, standardized system for interagency transfers, it does not set documentation requirements for agencies to substantiate purchases, such as receiving reports.
[174]Medical countermeasures refers to drugs, biologics, and devices that can be used to diagnose, treat, prevent, or mitigate harm.
[175]See 42 U.S.C. § 247d-6b. The Secretary of Health and Human Services transferred responsibility for the SNS from the Centers for Disease Control and Prevention to ASPR in 2018.
[176]Pub. L No. 116-22, § 402(a), 133 Stat. 905, 942-43 (codified at 42 U.S.C. § 300hh-10a).
[177]Pandemic and All-Hazards Preparedness Act, Pub. L. No. 109-417, § 102(c)(2), 120 Stat. 2831, 2834 (2006) and Pandemic and All-Hazards Preparedness Reauthorization Act of 2013, Pub. L. No. 113-5, § 403, 127 Stat. 161, 196. The Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 established several new requirements for SNS annual reviews, referred to in the act as “annual threat-based reviews.” For example, the act specified that annual threat-based reviews must provide information regarding quantities of medical countermeasures procured for the SNS, the threat such procurement is intended to address, and planning considerations for appropriate manufacturing capacity, among other information. Pub. L. No. 116-22, § 403(a)(3), 133 Stat. at 944-45 (codified at 42 U.S.C. § 247d-6b(a)(2)).
[178]Department of Health and Human Services, Public Health Emergency Medical Countermeasures Enterprise Multiyear Budget: Fiscal Years 2018-2022 (December 2019).
[179]As of May 31, 2021, the six relief laws enacted to assist the response to COVID-19 were the American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4; Consolidated Appropriations Act, 2021, Pub. L. No. 116-620, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[180]According to HHS, as of April 2, 2021, the agency transferred $850 million from the Public Health and Social Services Emergency Fund, Strategic National Stockpile, to the Unaccompanied Children Program within the Administration for Children and Families, under authority in the Consolidated Appropriations Act, 2021. See Pub. L. No. 116-260, div. M, tit. III, § 304, 134 Stat. at 1923.
[181]While we either interviewed or received written responses from seven PHEMCE partners, one partner was unable to provide relevant information due to staff turnover. Therefore, we only included responses from the remaining six PHEMCE partners.
[182]For the purpose of this report, historical references to PHEMCE operations refer to the structure that existed in 2017; the number and type of work groups could change over time, according to PHEMCE documentation.
[183]ASPR officials noted that while the majority of PHEMCE meetings prior to 2018 were unclassified, classified meetings were held at various levels of the PHEMCE when needed.
[184]Ten Integrated Program Teams were identified in the July 2015 PHEMCE Integrated Program Team charter; however, the PHEMCE was authorized to establish or disband Integrated Program Teams as needed.
[185]ASPR officials told us the office delayed its PHEMCE reorganizational plans while waiting for the enactment of the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, which contained requirements related to the PHEMCE. However, they said the office ultimately began implementing its plans when the legislation was not enacted in the anticipated timeframe. According to ASPR officials, the office expected the legislation to be enacted in June 2018 but it was not enacted until June 2019.
[186]The Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 refers to the SNS annual reviews as “annual threat-based reviews.” Ongoing work will assess the 2020 SNS Annual Threat-Based Review, once complete, against statutory requirements as outlined in the act.
[187]In January 2021, ASPR finalized the 2021-2022 PHEMCE Strategy. The strategy outlines strategic goals to update and strengthen the medical countermeasure enterprise and enhance preparedness. According to the strategy, an associated implementation plan will be created at a later date. The Assistant Secretary is required to develop and submit to appropriate congressional committees a PHEMCE Strategy and Implementation Plan every two years. See 42 U.S.C. § 300hh-10(d).
[190]The Federal Records Act of 1950 requires federal agencies to make and preserve records with adequate and proper documentation of the organization, functions, policies, decisions, procedures, and essential transactions of the agency. Pub. L. No. 81-754, 64 Stat. 578 (codified, as amended, at 44 U.S.C. § 3101 et seq.).
[191]See Department of Health and Human Services, HHS Policy for Records Management, HHS-OCIO-PIM-2020-06-004, May 2020.
[192]Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, Pub. L. No. 116-22, § 403(a)(5), 133 Stat. at 946-47; CARES Act, Pub. L. No. 116-136, § 19010, 134 Stat. at 579-81.
[193]The CARES Act includes a provision for GAO to provide a comprehensive audit and review of federal contracting pursuant to the authorities provided in the Act. In addition to specific contracting reviews, we have reported on federal contracting in response to the pandemic as part of regularly issued government-wide reports on the federal response to COVID-19.
[194]For the purposes of this report, “contract obligations” refers to obligations on procurement contracts that are subject to the Federal Acquisition Regulation and does not include, for example, grants, cooperative agreements, loans, other transactions for research, real property leases, or requisitions from federal stock.
[195]Other transaction authorities allow certain agencies to enter into agreements “other than” standard government contracts or other traditional mechanisms. Agreements under these authorities are generally not subject to federal laws and regulations applicable to federal contracts or financial assistance, allowing agencies to customize their other transaction agreements to help meet project requirements and mission needs.
[197]Based on the memorandum of agreement guiding the management of the NIA code, DHS and DOD are responsible for making determinations about whether to establish or close a code, based on a variety of considerations. The General Services Administration (GSA)—the agency that operates and maintains FPDS-NG—is responsible for adding or updating the NIA code in the system based on DHS’s and DOD’s decisions. The extensions of the code are consistent with our prior recommendations to DHS, DOD, and GSA related to the importance of ensuring federal agencies, the public, and Congress have visibility into contract actions and associated obligations related to emergency response efforts.
[198]In May 2020, USDA implemented the Farmers to Families Food Box Program to assist commodity suppliers impacted by the pandemic and to provide food assistance to the public. To accomplish these goals, USDA contracted with hundreds of distributors to purchase billions of dollars in fresh fruits, vegetables, dairy, and meat products, and package these products into family-sized food boxes for delivery to food banks, community and faith-based organizations, and other non-profit entities across the country.
[199]Emergency use authorizations allow for the temporary use of unapproved medical products. Janssen Pharmaceutical Companies are a part of Johnson & Johnson.
[200]Our methodology for identifying noncompetitive contracts is explained in detail at the end of this enclosure.
[201]For the purposes of this report, obligations on contracts identified as using the unusual and compelling urgency exception include those associated with contracts subject to Federal Acquisition Regulation 6.302-2, as well as orders under multiple award contracts, which are subject to separate requirements under Federal Acquisition Regulation subpart 16.5. Specifically, under Federal Acquisition Regulation 16.505(b)(2), orders on multiple award contracts require contracting officers to give every awardee a fair opportunity to be considered for a delivery order or task order exceeding $3,500, with exceptions, including if the agency need for the supplies or services is so urgent that providing a fair opportunity would result in unacceptable delays. When using the unusual and compelling urgency exception to full and open competition, agencies still must request offers from as many potential sources as is practicable under the circumstances.
[202]Undefinitized contracts include letter contracts, as well as other undefinitized actions.
[203]FPDS-NG data from SAM.gov accessed through May 31, 2021. For purposes of this report, “competition rate” is the percentage of total obligations associated with contracts awarded competitively. We calculated competition rates as the percentages of obligations on competitive contracts and orders over all obligations on contracts and orders. Competitive contracts included contracts and orders coded in the FPDS-NG as “full and open competition,” “full and open after exclusion of sources,” and “competed under simplified acquisition procedures” as well as orders coded as “subject to fair opportunity,” “fair opportunity given,” and “competitive set aside.” Noncompetitive contracts included contracts and orders coded in the FPDS-NG as “not competed,” “not available for competition,” and “not competed under simplified acquisition procedures,” as well as orders coded as an exception to “subject to fair opportunity,” including “urgency,” “only one source,” “minimum guarantee,” “follow-on action following competitive initial action,” “other statutory authority,” and “sole source.” Even for contracts identified as noncompetitive, agencies may have solicited more than one source.
[204]In November 2019 we identified some inconsistencies in the information agencies report in the contract description field in the FPDS-NG. Data on DOD contract obligations based on information in the description field were available only through March 1, 2021, due to differences in the time frames for which DOD data are made publicly available.
[205]To be eligible for regular UI benefits, applicants generally must be able and available to work and actively seeking work. 42 U.S.C. § 503(a)(12). Administration of the regular UI program is financed by a federal tax on employers, according to DOL.
[206]The CARES Act also addressed other aspects of the UI system, such as authorizing certain flexibilities for states to hire additional staff and to participate in Short-Time Compensation programs. In addition to the CARES Act, the Families First Coronavirus Response Act provided up to $1 billion in emergency grant funding to states in fiscal year 2020 for UI administrative purposes. In addition, on August 8, 2020, the President signed a memorandum directing the Department of Homeland Security’s Federal Emergency Management Agency (FEMA) to provide up to $44 billion in lost wages assistance. Pursuant to the presidential memorandum, upon receiving a FEMA grant, states and territories could provide eligible claimants $300 or $400 per week—which included a $300 federal contribution—in addition to their UI benefits. The White House, Memorandum on Authorizing the Other Needs Assistance Program for Major Disaster Declarations Related to Coronavirus Disease 2019 (Aug. 8, 2020). FEMA approved 54 states and territories to provide lost wages assistance to eligible claimants for at most 6 weeks of unemployment experienced from the week ending August 1, 2020, through the week ending September 5, 2020.
[207]Pub. L. No. 117-2, § 9011(a), (b), 135 Stat. 4, 118; Pub. L. No. 116-260, div. N, tit. II, § 201(a), (b), 134 Stat. 1182, 1950-1951 (2020); Pub. L. No. 116-136, § 2102, 134 Stat. 281, 313 (2020). The Consolidated Appropriations Act, 2021 increased the authorized maximum number of weeks of PUA benefits from 39 to 50 and generally extended the expiration of the program from December 31, 2020, to March 14, 2021. The American Rescue Plan Act of 2021 further increased the maximum number of weeks of PUA benefits to 79 and generally extended the expiration of the program to September 6, 2021. The CARES Act also provided funding for up to an additional 7 weeks of PUA benefits in certain states with high rates of unemployment. Department of Labor, CARES Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Operating, Financial and Reporting Instructions, Unemployment Insurance Program Letter (UIPL) 16-20 (Washington, D.C.: Apr. 5, 2020).
[208]Pub. L. No. 117-2, § 9013, 135 Stat. 4, 119; Pub. L. No. 116-260, div. N, tit. II, § 203, 134 Stat. 1182, 1953; Pub. L. No. 116-136, § 2104, 134 Stat. at 318. The Consolidated Appropriations Act, 2021 authorized the $300 benefit initially through March 14, 2021, and the American Rescue Plan Act of 2021 extended that benefit through September 6, 2021.
[209]Pub. L. No. 117-2, § 9016(a), (b), 135 Stat. 4, 119-120; Pub. L. No. 116-260, div. N, tit. II, § 206(a), (b), 134 Stat. 1182, 1954; Pub. L. No. 116-136, § 2107, 134 Stat. at 323. The Consolidated Appropriations Act, 2021 increased the maximum amount of PEUC benefits from 13 to 24 times the individual’s average weekly benefit amount and generally extended the expiration of the PEUC program from December 31, 2020, to March 14, 2021. The American Rescue Plan Act of 2021 further increased the maximum amount to 53 times the individual’s average weekly benefit amount and generally extended the expiration of the program to September 6, 2021. Consistent with the CARES Act and program extension in the Consolidated Appropriations Act, 2021, the increased maximum amount of PEUC benefits translates to 53 weeks of benefits for individuals who are totally unemployed. However, individuals may receive more weeks of benefits if they are receiving a reduced weekly benefit amount for weeks of partial unemployment. See Department of Labor, Continued Assistance for Unemployed Workers Act of 2020—Pandemic Emergency Unemployment Compensation (PEUC) Program: Extension, Transition Rule, Increase in Total Benefits, and Coordination Rules, UIPL 17-20, Change 2 (Washington, D.C.: Dec. 31, 2020).
[210]Pub. L. No. 117-2, § 9013(a), 135 Stat. 4, 119; Pub. L. No. 116-260, div. N, tit. II, § 261(a)(1), 134 Stat. 1182, 1961. The American Rescue Plan Act of 2021 generally extended MEUC through September 6, 2021.
[211]Department of Labor, Continued Assistance for Unemployed Workers (Continued Assistance) Act of 2020 – Federal Pandemic Unemployment Compensation (FPUC) Program Reauthorization and Modification and Mixed Earners Unemployment Compensation (MEUC) Program Operating, Reporting, and Financial Instructions, UIPL 15-20, Change 3 (Washington, D.C.: Jan. 5, 2021).
[212]As of June 8, 2021, Idaho and South Dakota had opted not to participate in the MEUC program, according to DOL.
[213]States participate in these UI programs under agreements with the Secretary of Labor. According to DOL, states are permitted to terminate participation in the FPUC, MEUC, PEUC, and PUA programs before their expiration, upon providing 30 days’ notice to DOL.
[214]The 21 states that submitted notice of their intent to withdraw from FPUC, PEUC, and PUA are Alabama, Arkansas, Georgia, Idaho, Indiana, Iowa, Maryland, Mississippi, Missouri, Montana, Nebraska, New Hampshire, North Dakota, Oklahoma, South Carolina, South Dakota, Tennessee, Texas, Utah, West Virginia, and Wyoming. The 3 states that submitted notice of their intent to withdraw from FPUC are Alaska, Florida, and Ohio. In addition, according to DOL, 22 of these 24 states submitted notice of their intent to withdraw from the MEUC program, and the other two states (Idaho and South Dakota) had not been participating in the MEUC program.
[215]Arizona’s governor announced the state’s intention to withdraw from the FPUC program by early July, but according to DOL, the state had not submitted notice as of June 8, 2021.
[216]Pub. L. No. 116-260, div. N, tit. II, §§ 241(a), 263(a), 134 Stat. 1182, 1959-1960, 1963.
[217]Pub. L. No. 116-260, div. N, tit. II, § 242(a), 134 Stat. 1182, 1960.
[219]DOL reported that as of June 20, 2021, the Extended Benefits program was activated in 11 states and territories because of high levels of unemployment. The Extended Benefits program was activated in all states except South Dakota at some point during the pandemic, according to DOL.
[220]If approved for PUA benefits, the number of weeks of regular UI and Extended Benefits a claimant has already received is subtracted from the duration of PUA benefits. Department of Labor, CARES Act of 2020 – Summary of Key Unemployment Insurance (UI) Provisions and Guidance Regarding Temporary Emergency State Staffing Flexibility, UIPL 14-20 (Washington, D.C.: Apr. 2, 2020).
[221]An initial claim is the first claim filed by an individual to determine eligibility for UI benefits after separating from an employer. Initial claims counts presented are not seasonally adjusted, and counts for the week ending June 19, 2021, reflect advance initial claims, which are preliminary and subject to revision. In some cases, advance initial claims represent estimates submitted by states that are later revised.
[222]Of the 53 states and territories, two did not report PUA continued claims data for the week ending June 5, 2021.
[223]Of the 53 states and territories, two did not report PEUC continued claims data for the week ending June 5, 2021.
[224]According to DOL, during the week ending June 5, 2021, the Extended Benefits program was available in 12 states; however, the total number of continued claims for Extended Benefits was reported by 46 states and territories because some of these claims may have been submitted for previous weeks of unemployment.
[225]Other programs include those for federal employees and newly discharged veterans, state additional benefit programs, and Short-Time Compensation or worksharing.
[226]After exhausting regular UI benefits—generally available for up to 26 weeks in most states, according to DOL—eligible individuals are generally able to apply for (1) PEUC; then (2) the Extended Benefits program, if activated in a state; and finally, in certain circumstances, (3) PUA benefits.
[227]In its Employment Situation news releases, the Bureau of Labor Statistics defines the long-term unemployed population as those who are jobless for 27 weeks or more.
[228]DOL monitors timeliness of benefit payments in the regular UI program. One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible; DOL considers 87 percent to be an acceptable level of performance. DOL uses 14 days as the timeliness goal for states with a waiting week requirement and 21 days for states without a waiting week requirement. According to DOL, some states require individuals who are otherwise eligible for benefits to serve a waiting period—generally 1 week—before receiving benefits. In its guidance released at the start of the pandemic, DOL recommended that states consider temporarily waiving their waiting week requirements. Thus, we focus on payments made within 21 days. We analyzed first payment timeliness data states had reported to DOL as of June 21, 2021. At that point, of the 53 states and territories, 46 had reported data for May 2021, 51 had reported data for April 2021, 52 had reported data for January through March 2021, and all 53 had reported data for all months in 2020.
[229]As we previously reported, the extension of the CARES Act UI programs at the end of 2020 could, according to DOL officials, affect payment timeliness if states had to reassign staff or focus resources on implementing new program requirements. We will continue to monitor regular UI first payment timeliness, including asking DOL about the May 2021 decline in first payment timeliness.
[230]We calculated PUA average benefit amounts by dividing the state-reported monthly amounts for total compensation paid by total weeks compensated, which we compared with each state’s PUA minimum weekly benefit amount set in UIPL 3-20. Benefit amounts are based on data reported by states as of June 21, 2021. At that point, 47 states and territories had reported these PUA data for April 2021 and just 18 had reported for May 2021. Thus, we analyzed PUA benefit payment data for April 2021. The following six states and territories did not report PUA data on weeks or amount compensated for April 2021: Alabama, Florida, Illinois, Oklahoma, Puerto Rico, and Vermont. According to DOL, states must use the amounts set in UIPL 3-20 as the minimum weekly benefit amount for all PUA claims. Department of Labor, Minimum Disaster Unemployment Assistance (DUA) Weekly Benefit Amount: January 1 – March 31, 2020, UIPL 3-20 (Washington, D.C.: Dec. 12, 2019).
[231]According to DOL officials, states have previously used this approach to pay benefits more expediently under the Disaster Unemployment Assistance (DUA) program. Under the CARES Act, the regulations for DUA generally apply to PUA. Pub. L. No. 116-136, § 2102(h), 134 Stat. 281, 317. DOL guidance notes that when individuals submit sufficient documentation of wages, states must immediately recalculate their weekly benefits and pay the full PUA benefit amount with the greatest promptness that is administratively feasible. Department of Labor, Coronavirus Aid, Relief, and Economic Security (CARES) Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Operating, Financial, and Reporting Instructions, UIPL 16-20 (Washington, D.C.: Apr. 5, 2020). According to DOL, guidance also permits states to initially rely on claimant self-attestations to calculate PUA benefit amounts. Department of Labor, Coronavirus Aid, Relief, and Economic Security (CARES) Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Reporting Instructions and Questions and Answers, UIPL 16-20, Change 1 (Washington, D.C.: Apr. 27, 2020); and Coronavirus Aid, Relief, and Economic Security (CARES) Act of 2020 – Pandemic Unemployment Assistance (PUA) Additional Questions and Answers, UIPL 16-20, Change 2 (Washington, D.C.: Jul. 21, 2020).
[232]While the CARES Act UI programs are federally funded, regular UI is primarily funded through state and federal taxes on employers. When a state exhausts the funds available for regular UI benefits, it may borrow from the federal government. According to DOL data, even before the pandemic, many states were not collecting enough UI tax revenue to satisfy the solvency standard specified in DOL regulations providing for interest-free loans to states. See 20 C.F.R. § 606.32 (2019).
[233]According to the National Bureau of Economic Research, the 2007-2009 recession began in December 2007 and ended in June 2009. The total loan balance held by states at the end of 2010 represented the highest year-end balance from the 2007-2009 recession until 2020. Total loan balances fluctuate throughout any given year.
[234]The CARES Act established the $150 billion Coronavirus Relief Fund to provide payments to state, local, territorial, and tribal governments to cover the costs of necessary expenditures incurred due to the COVID-19 pandemic. Pub. L. No. 116-136, § 5001, 134 Stat. 281, 501-504. In its guidance on the Coronavirus Relief Fund, the Department of the Treasury reported that states may use this funding to make payments to their state UI trust funds to prevent expenses related to the COVID-19 public health emergency from causing these UI trust funds to become insolvent. On January 15, 2021, the Department of the Treasury republished in a final form the guidance it had previously made available on its website regarding the Coronavirus Relief Fund. Prior to publication in the Federal Register, the last version of its guidance and frequently asked questions documents were dated September 2, 2020, and October 19, 2020, respectively. 86 Fed. Reg. 4,182 (Jan. 15, 2021).
[235]The regular UI program is primarily funded through state and federal taxes on employers. Under the Federal Unemployment Tax Act (FUTA), employers are generally required to pay a federal unemployment tax at a rate of 6.0 percent on the first $7,000 of wages paid to an employee each year, which funds administrative costs associated with the regular UI program and the federal share of benefits paid under the Extended Benefits program, among other things. FUTA provides a credit of up to 5.4 percent against federal tax liability to employers who pay state taxes timely under an approved state UI program. If a state has outstanding loan balances on January 1 for two consecutive years and does not repay the full amount of its loans by November 10 of the second year, the FUTA credit rate for employers in that state will be reduced. Thus, the federal taxes paid by employers will increase, all else being equal.
[236]The Department of the Treasury reported that as of December 31, 2020, it had obligated all of the $150 billion from the Coronavirus Relief Fund to state, local, territorial, and tribal governments. The Consolidated Appropriations Act, 2021 extended the period for states and other entities to use these funds through December 31, 2021. Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. 1182, 2145.
[237]Coronavirus State and Local Fiscal Recovery Funds, 86 Fed. Reg. 26,786, 26,822 (May 17, 2021).
[238]Fraud involves obtaining something of value through willful misrepresentation. Whether an act is in fact fraud is a determination to be made through the judicial or other adjudicative systems.
[239]DOL is monitoring states’ use of funds and progress in carrying out these efforts through quarterly reports from states. The first round of quarterly reports submitted by states covered the use of the funds made available in September 2020.
[240]Department of Labor, Identity Verification for Unemployment Insurance (UI) Claims, UIPL 16-21 (Washington, D.C.: Apr. 13, 2021).
[241]Department of Labor, Benefits Held by Banks and Financial Institutions as a Result of Suspicious and/or Potentially Fraudulent Activity and the Proportional Distribution Methodology Required to Recovering/Returning Federally Funded Unemployment Compensation (UC) Program Funds, UIPL 19-21 (Washington, D.C.: May 4, 2021).
[243]Department of Labor Office of Inspector General, COVID-19: States Struggled to Implement CARES Act Unemployment Insurance Programs, Report Number 19-21-004-03-315 (Washington, D.C.: May 28, 2021).
[244]Federal charges refer to criminal complaints and indictments. A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[245]These investigations fall within the Secret Service’s jurisdiction to investigate cyber-enabled financial crimes, according to the agency.
[246]States and territories report regular UI, Extended Benefits, PEUC, and FPUC overpayments data to DOL on a quarterly basis. We accessed the data on June 21, 2021. At that point, not all states and territories had reported overpayment amounts for all programs in all quarters. States and territories may revise the amount of overpayments they have identified for 3 years after the reporting quarter, according to DOL. For this report, we excluded overpayments related to emergency unemployment compensation programs prior to the pandemic. Thus, the totals we calculate differ slightly from those available on DOL’s UI overpayment recovery website, which, according to DOL officials, include non-pandemic emergency programs, such as those enacted during the 2007-2009 recession.
[247]States and territories report PUA overpayments data to DOL on a monthly basis, and the total amount shown includes overpayments related to identity theft. This is the first time we have reported total amounts that include data on identity theft overpayments, which DOL began collecting from states and territories in early 2021. We accessed the PUA overpayments data on June 21, 2021; these data are subject to change as more states report data and states revise previously reported data. For consistency with the regular UI overpayment data, which states and territories report on a quarterly basis, the PUA overpayment amount shown is for April 2020 through March 2021. As of June 21, 2021, 40 states and territories had reported an additional approximately $556 million of PUA overpayments identified in April and May 2021. The number of states and territories that have reported PUA overpayments data varies by month; for example, 17 reported overpayment amounts in April 2020 and 40 reported overpayment amounts in March 2021.
[248]FPUC benefits are paid in addition to other UI benefits. About 93 percent of FPUC overpayment amounts were paid on regular UI or PUA claims.
[249]In its data documentation, DOL defines fraud in this context as “an overpayment for which material facts to the determination or payment of a claim are found to be knowingly misrepresented or concealed (i.e., willful misrepresentation) by the claimant in order to obtain benefits to which the individual is not legally entitled.” A nonfraud overpayment is not due to willful misrepresentation and may include overpayments resulting from state agency errors or claimant errors, among other circumstances.
[250]We accessed the fraud overpayments data on June 21, 2021; these data are subject to change as more states and territories report data and states and territories revise previously reported data. Of the $1.3 billion in overpayments identified as fraud, states and territories reported about $208 million from regular UI and Extended Benefits programs, $512 million from PUA, $537 million from FPUC, and $14 million from PEUC.
[251]According to DOL, states generally may waive a nonfraud overpayment, in accordance with state law, if the overpayment was not the fault of the claimant and if requiring repayment would be against equity and good conscience or would otherwise defeat the purpose of the UI law. States were authorized to waive PUA overpayments under the Consolidated Appropriations Act, 2021. According to this act, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount, but the state can waive that requirement if the individual was without fault and repayment would be contrary to equity and good conscience. Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952. According to DOL, states are able to retroactively waive PUA overpayments from the beginning of the program onward.
[252]We accessed the waived overpayments data on June 21, 2021; these data are subject to change as more states and territories report data and states and territories revise previously reported data.
[253]We accessed the recovered overpayments data on June 21, 2021; these data are subject to change as more states and territories report data and states and territories revise previously reported data.
[254]As of June 21, 2021, states and territories had also reported recovering about $1.3 billion in the regular UI and Extended Benefits programs during the first four quarters of the pandemic combined (April 2020 through March 2021). However, the amounts recovered for any quarter may be from overpayments established in many previous periods. Thus, the total amount does not measure the extent to which overpayments made during the pandemic have been recovered.
[255]The performance year for reporting is generally a 12-month period from July through June. For example, improper payment estimates for 2020 would generally cover the period July 1, 2019, through June 30, 2020. However, the sampling and investigation program was suspended for the quarter April 1, 2020, through June 30, 2020, due to operational flexibilities provided to states in response to the pandemic, according to DOL.
[256]On March 10, 2021, Congress passed the American Rescue Plan Act of 2021, which the President signed on March 11, 2021. The statute authorized a third round of direct payments to individuals to help address financial stress due to the pandemic. Pub. L. No. 117-2, § 9601, 135 Stat. 4, 138–144.
[257]The CARES Act (in March 2020) and the Consolidated Appropriations Act, 2021 (in December 2020) authorized Treasury and IRS to issue EIP 1 and EIP 2 as direct payments to help individuals address financial stress due to the pandemic. Pub. L. No. 116-136, § 2201, 134 Stat. 281, 335–340 (2020); Pub. L. No. 116-260, § 272, 134 Stat. 1182, 1965–1976 (2020).
[258]Pub. L. No. 117-2, § 9611(b)(1), 135 Stat. at 145–148, codified at 26 U.S.C. § 7527A. U.S. territory residents are also eligible for the expanded child tax credit. Eligible residents of Puerto Rico will receive the newly expanded child tax credit directly from IRS when they file a 2021 tax return and will not be eligible for advance payments of the credit. The Commonwealth of the Northern Mariana Islands, Guam, and the U.S. Virgin Islands governments are responsible for administering the advance child tax credit payments to their residents and will determine whether or not to disburse advance payments. According to Treasury officials, American Samoa has opted to administer the child tax credit payments for its residents.
[260]IRS partners with nationwide and local organizations by providing outreach material, training, and tax preparation products for taxpayer assistance and education. IRS partner organizations are meant to serve low-to-moderate income populations, older Americans, students, military service members, people with disabilities, and other populations. IRS refers to these organizations as outreach partners.
[262]Pub. L. No. 116-136, § 2201(e), 135 Stat. at 339; Pub. L. No. 116-260, § 272(e), 135 Stat. at 1975; Pub. L. No. 117-2, § 9601(a), 135 Stat. at 142.
[263]For EIP 2, IRS did not request SSA assistance to identify and pay federal benefit recipients and instead used existing tax information and information SSA provided to IRS for EIP 1.
[264]Pub. L. No. 116-260, § 272(d)(2), 134 at 1972. While the statutory authorization for each round of EIPs prohibits Treasury from offsetting EIPs, tax refunds, including refunds based on the RRC, may be subject to offset if the taxpayer has debts owed to government agencies. See, Pub. L. No. 116-136, § 2201(d), 134 Stat. at 338–339; Pub. L. No. 116-260, § 272(d)(1), 134 at 1972; Pub. L. No. 117-2, § 9601(c)(2), 135 Stat. at 143.
[265]The five permanently inhabited U.S. territories are the Commonwealth of Puerto Rico, the U.S. Virgin Islands, American Samoa, Guam, and the Commonwealth of the Northern Mariana Islands.
[266]EIP check payments expire after 14 months after issuance, and debit cards expire after 36 months.
[267]These cities are Atlanta, New York, Detroit, Houston, Las Vegas, Los Angeles, Miami, Milwaukee, Philadelphia, Phoenix, St. Louis, and Washington D.C.
[268]IRS, Tax Information Security Guidelines For Federal, State and Local Agencies, Publication 1075 (Washington, D.C.: September 2016).
[269]As of early June 2021, IRS had largely addressed its 2020 processing backlog—all individual returns had been entered into its processing system and fewer than 1 million business returns remained to be entered. For more information on economic impact payments, see the enclosure on Economic Impact Payments.
[270]Due to the COVID-19 pandemic, the federal government extended this year's federal individual income tax filing deadline from April 15, 2021, to May 17, 2021. Unprocessed returns include those filed on paper or electronically that IRS received but had not fully processed. IRS may suspend a return due to errors such as a miscalculated tax credit or incorrect Social Security number. The 13.7 million returns suspended due to errors may be from the 2021, 2020, or an earlier filing season because, according to officials, IRS cannot differentiate these returns in its systems. The unprocessed returns total does not include those suspended for suspected refund fraud, such as identity theft, or amended returns.
[271]We compare 2021 performance to 2019 because IRS was not impacted by closures during the 2019 filing season due to the COVID-19 pandemic. The 2019 data are based on IRS’s April 17, 2020, Miscellaneous Monitoring Report.
[272]FNS released these preliminary data in June 2021, noting that the data are subject to significant revision.
[273]SNAP participation increased by 14 percent between March 2020 and March 2021. SNAP benefits levels grew more than participation during the pandemic, in part because of legislation that temporarily increased the value of SNAP benefits for all participants.
[274]In nominal terms, SNAP expenditures previously peaked in fiscal year 2013, when benefits totaled $76.1 billion, according to FNS data.
[275]Pub. L. No. 117-2, § 1101(a), 134 Stat. 4, 15.
[276]The Families First Coronavirus Response Act (FFCRA) authorized the issuance of SNAP emergency allotments—additional benefits on top of regular SNAP benefits—during the COVID-19 public health emergency. Pub. L. No. 116-127, § 2302(a), 134 Stat. 178, 188. FNS initially interpreted this provision as providing authority to issue SNAP emergency allotments to increase households’ total monthly benefit to the maximum allowable for their households’ size. In June 2020, we reported that FNS had denied several states’ requests to provide SNAP emergency allotments to households already receiving the maximum benefit. In November 2020, we reported that there was ongoing litigation challenging FNS’s interpretation, and in March 2021, we reported that USDA was reviewing its authority to permit states to issue SNAP emergency allotments to households already receiving the maximum benefit. FNS’s April 2021 announcement explained that the agency had changed its interpretation of FFCRA and would begin providing additional benefits to households that had been receiving less than $95 per month in SNAP emergency allotments, including households that had not received any SNAP emergency allotment before April 2021 because they were already receiving the maximum benefit.
[277]An improper payment is statutorily defined as any payment that should not have been made or that was made in an incorrect amount (including overpayments and underpayments) under statutory, contractual, administrative, or other legally applicable requirements. An improper payment includes any payment to an ineligible recipient, any payment for an ineligible good or service, any duplicate payment, any payment for a good or service not received (except for such payments where authorized by law), and any payment that does not account for credit for applicable discounts. 31 U.S.C. § 3351(4). Further, when an executive agency’s review is unable to discern, because of lacking or insufficient documentation, whether a payment was proper, the agency must treat the payment as improper in conducting risk assessments and producing an improper payment estimate. 31 U.S.C. §§ 3352(a)(3), (c)(2).
[278]Significant improper payments mean that, in a fiscal year, the sum of a program’s or activity’s improper payments and payments whose propriety the agency cannot discern due to lacking or insufficient documentation may have exceeded (1) $10,000,000 of all reported program activity payments made during a given fiscal year and 1.5 percent of program outlays, or (2) $100,000,000. 31 U.S.C. § 3352(a)(3)(A).
[279]Pub. L. No. 116-127, § 1101, 134 Stat. 178, 179-180. FFCRA originally set Pandemic EBT to expire at the end of fiscal year 2020, but the Continuing Appropriations Act, 2021 and Other Extensions Act extended the program through fiscal year 2021 and also expanded it to include younger children affected by day care closures. Pub. L. No. 116-159, § 4601, 134 Stat. 709, 744-745. ARPA amended the duration of the program to continue through the COVID-19 public health emergency, including summer 2021. Pub. L. No. 117-2, § 1108, 135 Stat. 4, 18-19. As such, the Pandemic EBT benefits period stretches more than 12 months, across two fiscal years thus far.
[280]Pub. L. No. 116-117, § 2, 134 Stat. 113, 114-115 (2020), codified at 31 U.S.C. § 3352(a)(3)(B). In November 2020, we suggested that, in future legislation appropriating COVID-19 relief funds, Congress consider designating all executive agency programs and activities making more than $100 million in payments from said funds as “susceptible to significant improper payments.”
[281]Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-21-19 (Washington, D.C.: Mar. 5, 2021).
[282]See, for example, Council of the Inspectors General on Integrity and Efficiency, Pandemic Response Accountability Committee, Top Challenges Facing Federal Agencies: COVID-19 Emergency Relief and Response Efforts (Washington, D.C.: June 2020).
[283]In November 2020, FNS promulgated a Final Rule to help protect Pandemic EBT from retailer trafficking. 85 Fed. Reg. 70,043 (Nov. 4, 2020). Retailer trafficking refers to the practice by which retailers exchange benefits for cash instead of food, often taking a fraudulent profit.
[284]Most states issued Pandemic EBT benefits without receiving an application, thereby automatically providing benefits based on the information they received from other state agencies or collected for other purposes, such as determining SNAP eligibility. Some recipients who automatically received Pandemic EBT benefits may not wish to use them, and states may need to develop a process to recover those benefits.
[285]The error rate measures a state’s ability to determine SNAP eligibility and issue benefits in the correct amount.
[286]In 2014, USDA also identified concerns with the quality of the data used to calculate the SNAP error rate. USDA suspended SNAP error rate reporting for fiscal years 2015 and 2016 to complete a thorough review of quality control systems in all 50 states, the District of Columbia, the U.S. Virgin Islands, and Guam. Through that review, USDA found data integrity issues that required corrective action in 42 states.
[287]FNS uses a two-tier SNAP QC review process. In the first tier, state SNAP agencies randomly select a sample of participating households to confirm eligibility and their receipt of the correct amount of benefits. In the second tier, federal SNAP reviewers select a subsample of each state’s reviews to verify the accuracy of the state’s findings. States must correct errors, and any overpayment of benefits must be paid back to the state. In the case of underpayments, states provide the additional benefits to participants. Federal staff analyze the data from the QC reviews and establish state-level error rates and the national error rate.
[288]Specifically, at the beginning of the pandemic, FNS issued a blanket waiver that allowed states to temporarily waive SNAP QC reviews for March, April, and May 2020. In October 2020, the Continuing Appropriations Act, 2021 and Other Extensions Act allowed states to suspend SNAP QC reviews from June 2020 through September 2021. Pub. L. No. 116-159, § 4603(a)(2), 134 Stat. 709, 746. In December 2020, the Consolidated Appropriations Act, 2021 revised the suspension period to end on June 30, 2021. Pub. L. No. 116-260, div. N, tit. VII, § 702(g), 134 Stat. 1182, 2094.
[289]Management Evaluations are annual reviews to ensure compliance with program requirements. Each year, FNS selects topics for review. FNS regional offices conduct a federal Management Evaluation, while states perform the state evaluation. As part of the Management Evaluation, the regional office selects at least one state in each region for a QC Integrity Review, which evaluates state-level QC processes to ensure state-reported errors are accurate and free from any bias. State agencies receive a QC Integrity Review once every 5 years and more frequently if necessary. States perform a QC Integrity Review of their processes annually.
[290]Disaster SNAP is a separate program from SNAP. FNS officials said that, traditionally, state SNAP agencies conduct Disaster SNAP via an entirely in person application and interview process. Since the onset of the pandemic, states have used fully virtual or hybrid models to ensure social distancing, according to officials.
[291]FFCRA authorized FNS to make certain adjustments to federal requirements for SNAP related to issuing benefits, reviewing applications, and reporting data during the pandemic. Pub. L. No. 116-127, § 2302(a)(2), 134 Stat. 178, 188. The Continuing Appropriations Act, 2021 and Other Extensions Act, among other things, granted states broader authority to adjust some SNAP operations without prior FNS approval. Pub. L. No. 116-159, § 4603(a)(1)(A), 134 Stat. 709, 746. In April 2021, FNS issued guidance on how states could continue to request approval for adjustments authorized by FFCRA through December 2021, or through the month following the month in which the COVID-19 public health emergency ends, whichever comes first. FNS officials said the agency would consider further extensions, depending upon the degree to which the COVID-19 pandemic is under control by the end of 2021. For more information on the successes and challenges states experienced implementing SNAP adjustments during the pandemic, see Johns Hopkins Institute for Health and Social Policy and the American Public Human Services Association, SNAP Waivers and Adaptations During the COVID-19 Pandemic: A Survey of State Agency Perspectives in 2020 (Baltimore, MD: June 2021).
[292]Chatbots are software applications that use artificial intelligence to mimic conversations and provide support that a human customer service agent might otherwise provide.
[293]WIC Task Force members include representatives of manufacturers, retailers, state and local agencies, WIC participants, and other stakeholder organizations.
[294]Pub. L. No. 117-2, § 1105(e), 135 Stat. 4, 17. The WIC cash-value voucher allows participants to purchase fruits and vegetables at grocery stores and farmers’ markets.
[295]Pub. L. No. 117-2, § 1106, 135 Stat. 4, 17. The provision is applicable to WIC and the WIC Farmers’ Market Nutrition Program. The waiver authority provided under the act does not apply to the content of the WIC food packages or to certain regulatory nondiscrimination requirements.
[296]According to a December 2019 FNS report, about 51 percent of eligible individuals participated in WIC in an average month in 2017.
[297]According to the notice, the boxes will include an assortment of fruits and vegetables that meet specific requirements for weight, variety, and shelf life. USDA ended the Farmers to Families Food Box Program on May 31, 2021, and plans to apply lessons learned from this program to inform other activities, such as the TEFAP fresh-produce initiative, according to USDA officials.
[298]According to USDA, most of the food purchased through USDA trade mitigation programs is provided to states for distribution to the network of food banks and food pantries that participate in TEFAP. In fiscal years 2019 and 2020, USDA provided more than $2.2 billion in food through its trade mitigation efforts. The Farmers to Families Food Box Program, which ended on May 31, 2021, is separate from USDA trade mitigation programs.
[299]Congressional Research Service, School Meals and Other Child Nutrition Programs: Background and Funding, R46234 (Washington, D.C.: April 1, 2021).
[300]This review covers meals served under the childcare centers portion of the Child and Adult Care Food Program, which also serves meals to eligible adults enrolled for care at adult day care centers. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) program is not included in this review. The Seamless Summer Option is a program that allows school districts to operate a modified version of the National School Lunch Program and School Breakfast Program in the summer or during unanticipated school closures. The program is reimbursed at the same rate as the National School Lunch Program. In contrast, the Summer Food Service Program has a higher reimbursement rate.
[301]To account for the sample representation and design used in the Household Pulse Survey (HPS), we conducted this analysis using the household weight present in the HPS data These estimates have a margin of error of plus or minus 1.3 percentage points or less at the 95 percent confidence level. The HPS, an experimental data product, is an interagency federal statistical rapid-response survey to measure household experiences during the COVID-19 pandemic. The survey is conducted by the Census Bureau in partnership with seven other agencies from the Federal Statistical System. Response rates have ranged from 1.3 to 10.3 percent. In March 2021, Census published the results of a nonresponse bias analysis that identified evidence of response patterns that could result in biased estimates. The Census Bureau adjusted sampling weights, which can help, but may not completely, mitigate nonresponse bias. See Sandra Peterson, Norilsa Toribio, James Farber, and David Hornick, Nonresponse Bias Report for the 2020 Household Pulse Survey, version 1.0 (U.S. Census Bureau, Mar. 24, 2021), accessed April 23, 2021, https://www2.census.gov/programs-surveys/demo/technical-documentation/hhp/2020_HPS_NR_Bias_Report-final.pdf.
[302]Typically, meals served through federal child nutrition programs must be served in a congregate setting and must be consumed on site. The noncongregate waiver removes these requirements.
[303]Pub. L. No. 116-136, div. B, tit. I, 134 Stat. 281, 507 (2020).
[304]Emergency Meals-to-You was a public–private partnership between USDA, the Baylor University Collaborative on Hunger and Poverty, McLane Global, and PepsiCo. It began as a summer pilot project in 2019 but was expanded in response to the COVID-19 pandemic.
[305]Pub. L. No. 116-127, § 2202(a), 134 Stat. 178, 185 (2020). This act further authorized a new program, Pandemic Electronic Benefits Transfer (Pandemic EBT), which provides benefits for food purchase to households with children who would have received free or reduced-price school meals if not for school closures due to COVID-19. The program also provides these benefits to households with eligible children in childcare. On April 26, 2021, USDA announced that it would offer Pandemic EBT benefits to all low-income children of all ages during the summer of 2021. For more information on the Pandemic EBT program, see the Nutrition Assistance enclosure in appendix I of this report.
[307]Pub. L. No. 116-260, div. N, tit. VII, § 722, 134 Stat. 1182, 2097. This law provided an indefinite appropriation of funds, based on a formula that generally takes into account the difference between reimbursements paid from March through June 2019 and those paid from March through June 2020.
[308]According to FNS officials, FNS does not collect data on program participant age, and changing the type of data collected would require costly and difficult system changes.
[309]According to the National CACFP Sponsors Association, many childcare centers and day care homes have closed permanently because of financial challenges.
[310]In a May 2018 report, we identified challenges affecting summer meal programs, including administrative burdens and lack of community awareness.
[312]In 2019, FNS partnered with Baylor University’s Collaborative on Hunger and Poverty and private partners to create the Summer Meals-to-You pilot project, which provided breakfasts, lunches, and snacks to students in selected school districts during the summer months when schools were closed. Districts were eligible to participate in Emergency Meals-to-You if (1) their schools served rural areas, (2) 50 percent or more of their schools’ students qualified for free or reduced-price lunch, (3) their schools were closed for at least 4 weeks during the pandemic, and (4) their schools participated in the NSLP. During the spring and summer of 2020, the Emergency Meals-to-You program mailed boxes of 10 breakfasts and 10 lunches to eligible students in participating school districts.
[313]This count of school districts participating in the Emergency Meals-to-You Program does not include four private and public schools that participated in the program separately from a school district. However, the count includes schools directly funded by the Bureau of Indian Education (BIE)—known as BIE schools—each of which is considered its own local educational agency (often referred to as a school district) in the U.S. Department of Education’s Common Core of Data (CCD). These data do not include meals served under the Summer Meals-to-You Program.
[314]This analysis is based on CCD data for school year 2019–20 for BIE schools, which represent less than 1 percent of U.S. school districts. According to the CCD, there were 174 BIE schools in school year 2019–20. Officials from the Baylor Collaborative on Hunger and Poverty reported that in addition to serving BIE schools, the Emergency Meals-to-You program served many other schools located on or near reservations that serve American Indian and Alaska Native families.
[315]According to officials from FNS and the Baylor Collaborative on Hunger and Poverty, there was already awareness of the program in Texas because the state was part of the initial Summer Meals-to-You pilot program.
[316]For information on school operating status, see U.S. Department of Education, Institute of Education Sciences, “Monthly Schools Survey Dashboard,” accessed May 6, 2021, https://ies.ed.gov/schoolsurvey/.
[317]U.S. Department of Education, Office of Planning, Evaluation and Policy Development, ED COVID-19 Handbook, Volume 2-2021: Roadmap to Reopening Safely and Meeting All Students’ Needs (Washington, D.C.: 2021), accessed April 20, 2021, https://www2.ed.gov/documents/coronavirus/reopening-2.pdf.
[318]Factors that may have contributed to staff layoffs during the pandemic include limits placed on class size and enrollment as well as families’ removal of children from childcare.
[319]The flexibility to operate the SSO is available to all schools in states that opt to participate under the waiver.
[320]On March 9, 2021, JCT updated estimates for forgone revenue to reflect changes in the American Rescue Plan Act of 2021. JCT’s original estimate for the CARES Act and FFCRA employer provisions was $172 billion for fiscal years 2020-2030.
[322]For 2021, only employers with an average of 500 or fewer full-time employees in 2019 may receive advance payments of the Employee Retention Credit and the amount of any such advance is limited. Pub. L. No. 116-260, § 207(g), 134 Stat. at 3063–3064.
[323]For additional information on FFCRA paid leave provisions, including the Department of Labor’s enforcement of these provisions, see the Leave Benefits for Employees enclosure.
[324]Pub. L. No. 116-127, §§ 7001–7004, 134 Stat. 178, 210–219 (2020); Pub. L. No. 116-136, § 3606, 134 Stat. 281, 411–412 (2020); Pub. L. No. 116-260, § 286, 134 Stat. 1182, 1989 (2020); Pub. L. No. 117-2, § 9641, 135 Stat. 4, 161–172 (2021), codified at 26 U.S.C. §§ 3131–3133. A refundable tax credit reduces tax liability, dollar for dollar; if the credit exceeds tax liability, a refund is due. Full-time and part-time employees are counted. Both credits have maximum payouts. Self-employed individuals may not file for advances on their credit refunds.
[325]Some government entities, including tribal governments, tribal entities, state- or locally-run colleges, universities, and organizations providing medical or hospital care, are also eligible for the Employee Retention Credit. The Employee Retention Credit created by the CARES Act and amended by CAA, 2021, was not made as an amendment to the Internal Revenue Code (IRC) and is classified as a note to section 3111 of the IRC. Pub. L. No. 116-136, § 2301, 134 Stat. at 347–351; Pub. L. No. 116-260, div. EE, § 206, 134 Stat. at 3059–3061.The Employee Retention Credit created by ARPA was added as section 3134 of the IRC. Pub. L. No. 117-2, § 9651, 135 Stat. at 176–182.
[326]There are other wages for which an employer may not claim the Employee Retention Credit. For example, the Employee Retention Credit cannot be claimed for wages for which the Work Opportunity Tax Credit (WOTC) is claimed in the third and fourth quarters of 2021. In the first and second quarters of 2021, the WOTC cannot be claimed on any wages for which the Employee Retention Credit is claimed.
[327]Federal COBRA requirements apply to private sector employers, and state and local government employers that have 20 or more employees and offer their employees employer-sponsored health insurance coverage, and states may impose comparable requirements on other entities. Individuals can receive COBRA premium assistance if they experienced an involuntary termination (except in the case of gross misconduct) or reduction in hours and elect COBRA coverage.
[328]Pub. L. No. 117-2, § 9501, 135 Stat at 127–138. Premium assistance will end earlier if an individual becomes eligible for a different group health plan or Medicare, or the end of the maximum continuation period is reached.
[329]Pub. L. No. 116-136, § 2302, 134 Stat. at 351–352, as amended by the Paycheck Protection Program Flexibility Act, Pub. L. No. 116-142, § 4, 134 Stat. 641, 643 (2020). To be considered timely, deferred payments of 50 percent of tax are to be made by December 31, 2021, with the remainder due December 31, 2022. The employer share of Social Security tax is 6.2 percent of taxable earnings up to the Social Security wage base cap on taxable income.
[330]Self-employed individuals pay the employer and employee tax share, which is 12.4 percent of taxable earnings, up to the Social Security wage base cap on taxable income.
[331]Deferred payments for self-employment taxes are reported on Form 1040, Schedule SE and deferred payments for household employment taxes are reported on Form 1040, Schedule H.
[333]IRS Notice 2020-65, 2020-38 I.R.B. 567 (Sept. 14, 2020), available online at: https://www.irs.gov/irb/2020-38_IRB (accessed May 17, 2021). We were asked to issue a legal decision regarding whether Notice 2020-65 is a rule under the Congressional Review Act. We determined that since IRS submitted Notice 2020-65 to us under the Congressional Review Act, there is no need for a legal decision from our office. See GAO, Request for a Congressional Review Act Opinion on IRS Notice 2020-65, B-332517 (Washington D.C.: September 2020). As noted in our correspondence, on September 4, 2020, Representative John Larson of Connecticut introduced House Joint Resolution 94 which is a resolution of disapproval of the Notice. H. R. J. Res. 94, 116th Cong. (2020).
[334]Pub. L. No. 116-260, div. N, § 274, 134 Stat. at 1978; IRS Notice 2021-11, 2021-6 I.R.B 827 (Feb. 8, 2021). The guidance directs employers to ratably withhold and pay the deferred taxes, meaning, in general, equally apportioned across the period.
[335]The CAA, 2021 amended the CARES Act to allow PPP loan recipients to claim the Employee Retention Credit for qualified wages, although qualified wages for which the credit is claimed cannot be used to support forgiveness of the PPP loan. This change was retroactive to March 27, 2020, the date of the enactment of the CARES Act. Pub. L. No. 116-260, div. N, § 206(c)(2)(B)(i), 134 Stat. at 3061.
[336]Certain employers could have also made claims using the “fourth quarter rule” for certain 2020 second and third quarter credits for which they were previously ineligible. IRS officials said it is not possible to know the number of these claims because they cannot be differentiated from other Employee Retention Credit claims.
[337]In our March 2021 report on the 2020 filing season, we raised concerns about IRS’s paper backlog and also recommended that IRS identify barriers taxpayers face to e-filing business-related returns. IRS agreed with the recommendation and said it will take steps to assess the barriers.
[338]Some of these advances are also included in the table in the next section because employers are to report on employment tax returns the advance payments they have received.
[339]This calculation is based on the amount of advance payments reported by taxpayers on employment tax returns, which differs from the amount of advance payments IRS has issued. For additional details on the data we analyzed, see the next section in this enclosure on credit claims. Additionally, IRS officials said many taxpayers are not reporting advances received. IRS found that of the $631.8 million in advances paid for tax year 2020, for which a return has been filed or processed, taxpayers reported $272.9 million in advances. Therefore, the number we report may be lower than the actual.
[340]The tax credit dollar figures we are reporting are as reported by taxpayers and are subject to taxpayer reporting error. These figures may differ from IRS’s reported figures because we are reporting what was filed without adjustments. These figures represent paper returns as of May 5, 2021 (main Form 941) and May 19, 2021 (Schedule R) and e-file returns, as of May 26, 2021 and include quarterly returns from second quarter through fourth quarter 2020. We did not analyze credits for self-employed individuals, which are reported on their income tax return, and annual employment tax returns.
[341]We calculated this using the number of total unique employer filers (including those listed on Schedule R), and the total number unique employers claiming the Employee Retention Credit.
[342]We could not separate employee and employer share of the deferrals because data from Form 941 that breaks out the two were not available at the time of our analysis.
[343]IRS Notice 2021-20, 2021-11 I.R.B. 922 (Mar. 15, 2021), available online at: https://www.irs.gov/pub/irs-irbs/irb21-11.pdf (accessed May 18, 2021). Eligible employers may elect not to take into account certain qualified wages for purposes of the credit. Pub. L. No. 116-260, div. N, § 206(c)(2)(A), 134 Stat. at 3060–3061.
[344]The first round of PPP loan applications closed on August 8, 2020, and the forgiveness applicants prior to March 1, 2021 were from this round.
[345] Not all PPP borrowers may have paid qualified wages or be an eligible employer that would qualify for the Employee Retention Credit.
[346]Pub. L. No. 116-127, §§ 3101-3106, 5101-5111, 134 Stat. 178, 189-192, 195-201 (2020), as amended by Pub. L. No. 116-136, §§ 3601, 3602, 134 Stat. 281, 410 (2020).The Family and Medical Leave Act of 1993, as amended (FMLA), generally requires covered employers to provide up to 12 weeks of unpaid leave per year for eligible employees to, among other things, care for a spouse, child, or parent with a serious health condition or for their own serious health condition. Employees are generally eligible if they meet certain requirements related to length of employment and size of employer. Some state laws also provide paid sick or family leave, with eligibility rules varying by state.
[347]DOL began enforcement actions related to FFCRA paid leave provisions on April 18, 2020, after a limited stay of enforcement to enable public and private employers who are covered by the act to come into compliance with the new law. During the limited stay of enforcement, DOL reserved its right to exercise its enforcement authority if the employer violated FFCRA willfully, failed to provide a written commitment to future compliance with FFCRA, or failed to remedy a violation after notification by DOL.
[349]The emergency paid sick leave could be used for quarantine and other situations related to COVID-19 that caused employees to be unable to work. Both leave provisions covered care for a child whose school, place of care, or child care provider was closed or unavailable because of COVID-19.
[350]FFCRA paid leave provisions did not apply to private sector employers with 500 or more employees.
[352]DOL revised its definition of “health care provider” in response to a federal court ruling that DOL’s original definition was overly broad. See New York v. U.S. Dep't of Labor, 477 F.Supp. 3d 1 (S.D.N.Y. Aug. 3, 2020). The April 2020 rule defined “health care provider” to include anyone employed at any doctor’s office; hospital; health care center; clinic; postsecondary educational institution offering health care instruction; medical school; local health department or agency; nursing facility; retirement facility; nursing home; home health care provider; any facility that performs laboratory or medical testing; pharmacy; or any similar institution, employer, or entity. DOL revised the definition in September 2020 to include only employees who either (1) met the definition of a health care provider under the FMLA regulations or (2) were employed to provide diagnostic services, preventative services, treatment services, or other services that were integrated with and necessary to the provision of patient care and that if not provided would adversely impact patient care.
[353]Covered employers that failed to provide emergency paid sick leave to eligible employees are considered to have committed minimum wage violations under the Fair Labor Standards Act of 1938, as amended, and are subject to penalties described therein, including being liable to the affected employees. See Pub. L. No. 116-127, § 5105(a), 134 Stat. at 197. Covered employers are subject to additional penalties for discharging, disciplining, or discriminating against any employee for taking emergency paid sick leave. See id. § 5105(b), 134 Stat. at 197. The prohibitions and enforcement provisions in FMLA apply to leave under the expanded family and medical leave provisions. See 29 U.S.C. §§ 2615 and 2617. Employees may also bring civil action against covered employers that have violated the expanded family and medical leave provisions. See 29 U.S.C. § 2617(a).
[354]Tier III is intended for use with cases under other statutes WHD enforces but not for FFCRA cases, according to WHD guidance.
[355]WHD officials said they use their discretion in determining whether to continue an investigation if an employer has filed for bankruptcy or has gone out of business. In the event of bankruptcy, WHD officials said the determining factor in deciding how to proceed is the stage of the investigation when WHD learns of the bankruptcy, as any payment of back wages must be made in accordance with the bankruptcy code. If the court has yet to discharge debts, an employee may have an opportunity to file a claim, according to WHD officials. If an employer has gone out of business and WHD does not perform additional investigative work, WHD officials said they may advise the employee of the employee’s right to bring a private suit in state or federal court.
[356]The work group was also responsible for overseeing FFCRA enforcement. According to WHD documents, the work group includes national and regional representatives with expertise in policy, enforcement, compliance assistance, communications, data analytics, and training.
[357]WHD conducted an additional 66 FFCRA outreach events from January 1 to March 31, 2021.
[358]WHD developed several new fiscal year 2020 performance measures to capture its FFCRA enforcement and outreach efforts. One of these measures is the number of outreach events involving FFCRA. WHD set a goal of 200 events for the first quarter of fiscal year 2021 and exceeded its goal with 683 outreach events in that quarter.
[359]WHD reported that 1,342 of its 3,155 events (43 percent) targeted employee groups and 1,813 events (57 percent) targeted employer groups.
[360]The radio and television public service announcements included more than 2,000 airings on national television networks; more than 24,000 airings on local television stations; and more than 3,000 airings on local radio stations in addition to a smaller number of airings on satellite radio stations, according to a report provided to DOL by the vendor. The digital media campaign included banner displays, social media posts, and other digital advertisements.
[361]WHD established a performance measure in fiscal year 2020 to track the percentage of calls to its toll-free number that were answered live. In the first quarter of fiscal year 2021, WHD live-answered 63 percent of calls to its toll-free number, exceeding its target of 55 percent; however, this measure is not specific to FFCRA and includes all calls received by the call center.
[362]WHD reported more than 12 million visits to its FFCRA paid leave website from March 9, 2020, to February 28, 2021.
[363]FFCRA required that employers post, and keep posted, a notice of the law’s requirements and information concerning procedures for filing complaints of violations of the FFCRA. See Pub. L. No. 116-127, § 5103, 134 Stat. at 196; 29 C.F.R. § 826.80(a)(2020).
[365]Data showing how many employees utilized FFCRA paid leave are not available.
[366]WHD officials said the agency initiated 53 agency-directed cases. In addition, they said that, on further investigation, some cases initially filed under a different statute may have been reclassified as FFCRA cases.
[367]WHD established a performance measure in fiscal year 2020 to track FFCRA enforcement, setting a goal of concluding 70 percent of FFCRA conciliations in 15 days or less. WHD reported that in the first quarter of fiscal year 2021, it concluded 81 percent of FFCRA conciliations within 15 days.
[368]An official from DOL’s Office of Inspector General (OIG) said the OIG is conducting related work on WHD’s enforcement of FFCRA paid leave, which will focus, in part, on WHD’s use of conciliation. The OIG plans to issue a report on its work in the coming months.
[369]WHD’s complaint data show that additional types of FFCRA paid leave violations included failing to display an FFCRA poster (7 percent); failing to provide an additional 10 weeks of paid leave at two-thirds of the regular rate of pay (7 percent); requiring the employee to use other paid leave before using FFCRA paid leave (7 percent); failing to allow the employee to substitute paid leave for the first 2 weeks of expanded family and medical leave (2 percent); terminating the employee (1 percent); discriminating against the employee (1 percent); requiring the employee to search for and find a replacement to cover the employee’s hours (less than 1 percent); and failing to maintain the employee’s health benefits (less than 1 percent). Because an employer may have committed more than one paid leave violation, the sum of the percentages for all 11 violations exceeds 100.
[370]WHD filed 14 percent of FFCRA complaints with no compliance action and dropped 16 percent of FFCRA cases that were accepted for investigation.
[371]The total appropriation comprises $39.6 billion from the American Rescue Plan Act of 2021, Pub. L. No. 117-2, title II, § 2003, 135 Stat. 4, $22.7 billion from the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, title III, §§ 311(b)(3), 314, 134 Stat. 1182 (2020), and $13.9 billion from the CARES Act, Pub. L. No. 116-136, div. B, title VIII, §§ 18001, 18004, 134 Stat. 281, 564, 567-568 (2020).
[372]Education used OPE Identification Number as the unique identifier for each school that was allocated funding per Education’s formula allocation tables for HEERF, published on OPE’s website.
[373]Education notified schools of additional allocations provided by the subsequent COVID-19 relief laws at a later date.
[374]An obligation is a financial commitment to pay the grantee based on the terms and conditions for funding.
[375]G5 is one of the main components of Education’s suite of core financial applications. It performs pre- and post-award processing for grants, including grant payment processing.
[376]Schools may apply for HEERF awards provided by the CARES Act for various purposes or designations (i.e., types of grants). For awards under the CARES Act, these designations included: Institution of Higher Education (IHE)—Student Aid, IHE—Institutional Aid, Historically Black Colleges and Universities, Tribally Controlled Colleges and Universities, Minority Serving Institutions, Strengthening Institutions Program, and Fund of the Improvement of Postsecondary Education. The school must submit a Certification and Agreement form specific to the type of HEERF award for which they are applying.
[377]According to Education’s Instructions for Submitting the Recipient’s Funding Certification and Agreement and Application Form, the institution’s authorized representative, which is typically the institution’s president, chancellor, or chief executive officer, must sign the form. The signature must be handwritten or an electronic signature and it cannot be a typed signature or the typed name of the institution.
[378]When OPE awards a grant, G5 automatically generates a Grant Award Notification and emails it to the grantee as a notice that the grantee has been awarded HEERF funds. Education’s responses to HEERF Frequently Asked Questions state that schools have one calendar year from the date of award to use the funds.
[379]The System for Award Management is a web-based, government-wide application that collects, validates, stores, and disseminates business information about the federal government's trading partners in support of the contract awards, grants, and electronic payment processes. A DUNS number is a unique nine-character number used to identify an organization. The federal government uses it to track how it allocates federal money.
[380]Within our sample of obligations, we could not confirm authorized representative signatures on Certification and Agreement forms for 29 schools (identified by OPE Identification Number) because the signature lines were not legible, not signed, or contained a typed institution name instead of a person’s name. Based on our statistical projection of these testing results, with 95 percent confidence interval of 10.9 percent to 26.6 percent, between 519 to 1267 schools could have this issue.
[381]Grants.gov is a centralized system managed by the Department of Health and Human Services and used by federal agencies to post federal funding opportunities and for grant seekers to find and apply for them.
[382]OPE stated that only new applicants are required to submit the revised forms. Grantees who already received HEERF funding under the CARES Act are not required to re-submit the forms.
[383]Based on our statistical projection of the testing results with 95 percent confidence interval of 0.2 percent to 25.8 percent, about 10 to 1229 schools could have this issue.
[384]Pub. L. No. 116-136, §§ 2301–2307, 134 Stat. 281, 347–359 (2020). Other COVID-19 relief laws include the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021. Pub. L. No. 116-260, 134 Stat. 1182 (2020); Pub. L. No. 117-2, 135 Stat. 4 (2021).
[386]This is an update from our March 2021 CARES Act report estimate and includes the $31 billion estimate for the extension of limitation of excess business loss from the American Rescue Plan Act of 2021.
[387]26 U.S.C. § 172(a). TCJA generally repealed NOL carrybacks and required NOLs to be carried over indefinitely. Pub. L. No. 115-97, § 13302(b), 131 Stat. at 2122. For ease of reporting, we use the term taxpayer to refer to an entity that may use the CARES Act tax relief provisions described in this enclosure.
[388]Pub. L. No. 116-136, § 2303, 134 Stat. at 352–356.
[389]Pub. L. No. 115-97, § 13302(a)(1), 131 Stat. at 2121. Specifically, TCJA’s 80-percent limitation, as amended by section 2303(c) of the CARES Act, limited the deduction of NOL carrybacks and carryforwards (attributable to NOLs generated after 2017) to an amount equal to the lesser of (1) the aggregate of the post-2017 NOL carryovers and carrybacks to that taxable year, or (2) 80 percent of taxable income of the taxpayer computed without regard to any NOL deduction for post-2017 NOLs.
[390]Pub. L. No. 116-136, § 2303(b)(1), 134 Stat. at 353–354.
[391]Corporations file Form 1139, Corporation Application for Tentative Refund. Individuals, estates, and trusts file Form 1045, Application for Tentative Refund. For ease of reporting, we use the term “application for tentative refund” to refer to Form 1139 and Form 1045.
[393]Pub. L. No. 115-97, § 12001(a), 131 Stat. at 2092. More information on AMT is included in our March 2021 CARES Act report. In general, AMT was an alternative tax regime, which applied a lower tax rate to a broader tax base by limiting the use of tax preferences and disallowing credits and deductions.
[394]Pub. L. No. 116-136, § 2305, 134 Stat. at 357. Under the CARES Act, corporations with AMT credits in excess of the credit allowed to offset regular tax liability (excess credit) may claim 50 percent of the excess credit as a refundable credit for the first tax year beginning in 2018 and then claim any remaining excess credit as a refundable credit in 2019. For more information, please see our March 2021 report on the CARES Act.
[395]Pub. L. No. 116-136, § 2306, 134 Stat. at 358. Pub. L. No. 115-97, § 13301, 131 Stat. at 2117. More information, including how partnerships are handled, is included in our March 2021 CARES Act report.
[396]The 50 percent adjusted taxable income limitation did not apply to partnerships for tax years beginning in 2019.
[397]26 U.S.C. § 461(I)(3)(A). These values are 2018 amounts and are indexed for inflation thereafter. The CARES Act clarified that NOL deductions (i.e., losses carried from other years) are not included in the calculation of excess business losses.
[400]Complete data on the number of taxpayers taking advantage of these tax provisions will not be available until after tax year 2020 income tax returns are processed, at the earliest, in late in 2021.
[401]26 U.S.C. § 6411(b), (d)(2); Pub. L. No. 116-136, § 2305(d)(1), 134 Stat. at 357.
[402]According to IRS officials, if an Application for Tentative Refund is deemed unprocessible, IRS does not start counting the 90-day timeline until the application is considered complete. Applications are considered unprocessible for a number of reasons, for example if the name on the form is wrong, or if there is missing supporting documentation, according to IRS officials.
[403]26 U.S.C. § 6611(e), (f). Interest is owed when the refund is not issued within 45 days of the later of the: loss year return due date, delinquent loss year return received date, loss year return processible date, date the application is received by the IRS, or date the application is received by the IRS in processible form.
[404]We reviewed IRS data from October 2016 until present, and this is the first time that the IRS has consistently taken over 90 days to process these forms.
[405]IRS officials said that all 2020 returns have been “opened” by a machine, but not all have been extracted, which is a separate step to extract the paper from the envelope.
[406]The average processing time from 2017-2019 was between 20 and 50 days, making the statement that IRS is experiencing longer than normal processing times misleading given the latest average is over 100 days more than what was considered normal in those years.
[407]For other filings, IRS has shared more information on its website on what time frames taxpayers can expect when filing a form when IRS faces service disruptions, including the size of the current backlog and that it may take longer than a certain specified time frame. For example, see IRS: IRS Operations During COVID-19: Mission-critical functions continue, accessed on June 2, 2021, https://www.irs.gov/newsroom/irs-operations-during-covid-19-mission-critical-functions-continue.
[408]NAICS is the standard used by federal statistical agencies in classifying business establishments for the purpose of collecting, analyzing, and publishing statistical data related to the U.S. business economy. On IRS forms such as the Form 1120, taxpayers are instructed to determine from a provided list which business activity the company derives the largest percentage of its total receipts, to self-report their principal business activity. The list of principal business activity that the IRS uses is based on the NAICS.
[409]This industry comprises of (1) establishments primarily engaged in holding the securities of companies or (2) establishments (except government establishments) that administer, oversee, and manage other establishments of the company or enterprise. This includes a wide range of companies from banks and holding companies, to airlines and freight rail companies.
[410]At this time, we only analyzed the usage of NOL with this methodology, but we will continue to analyze the use of other provisions in future reports. Public companies are required to file annual reports on Form 10-K and quarterly reports on Form 10-Q. The target population of our sample was the largest publicly traded companies with annual or quarterly reports filed. We identified 3,328 companies included in the Russel 3000E index that fit within the scope of our review.
[411]We selected a generalizable, simple random sample of 185 companies from the 3,328 companies that were within the scope of our review. We computed sample sizes necessary to obtain a precision of at least plus or minus 7 percentage points, at the 95 percent confidence level, for a proportion estimate.
[412]This is consistent with our findings in the section above, where we found that the manufacturing industry made up the highest number of approved NOL refunds. The manufacturing sector is comprised of establishments engaged in the mechanical, physical, or chemical transformation of materials, substances, or components into new products, such as food and beverage, textiles, apparel manufacturers, among others. Industry type was taken from the Standard Industrial Classification codes that appear in Securities and Exchange Commission filings, and translated into the North American Industry Classification System and indicate the company’s type of business.
[413]For the purposes of this table, we included only companies that mentioned they did or will use NOL and companies that were unsure if they will use NOL. There were 26 companies who said they did or will use NOL, out of our 185 company sample. There were 10 companies that were unsure if they will use NOL, out of our 185 company sample.
[414]Prior to sample selection, a small number of companies were removed from the population that are not within the scope of this audit.
[415]About 1 percent of the business/corporate population are public companies. In addition to businesses/corporate filers, tax exempt organizations with certain business operations, are eligible for refunds.
[416]Gallemore, John, Stephan Hollander, and Martin Jacobs, “Who CARES? Evidence on the Corporate Tax Provisions of the Coronavirus Aid, Relief, and Economic Security Act from SEC Filings,” Becker Friedman Institute, University of Chicago (June 2020).
[417]CARES Act, Pub. L. No. 116-136, 134 Stat. 281, 470 (2020). The CARES Act did not provide criteria for which businesses were “critical to maintaining national security.” Treasury established the following definition: (1) performing under a “DX”-priority-rated contract or order under the Defense Priorities and Allocations System regulations (15 C.F.R. pt. 700) or (2) operating under a valid top secret facility security clearance under the National Industrial Security Program regulations (32 C.F.R. pt. 2004). Treasury guidance further noted that applicants that did not meet either of these criteria may still be considered for loans if, based on the recommendation and certification by the Secretary of Defense or the Director of National Intelligence, the applicant’s business is critical to maintaining national security.
[418]As directed by the CARES Act, Treasury coordinated with the Department of Transportation (DOT) to determine the eligibility of certain applicants. DOT confirmed that applicants held the appropriate air carrier certificates and the status of their operations, and reported this information to Treasury, according to DOT. Treasury also coordinated with the Department of Defense to determine the eligibility of applicants.
[419]These figures include amendments to loan commitments made to loan agreements after the initial closings. The amendments include increases in loan commitments that reallocated unused funds, according to Treasury.
[420]Specifically, the CARES Act directs GAO to submit a report to specified committees on the Section 4003 loan program within 9 months of the enactment of the Act, and then annually thereafter through the year succeeding the last year for which the loans, loan guarantees, or other investments made from the loan program are outstanding. Pub. L. No. 116-136, § 4026(f), 134 Stat. at 496. Our report in December 2020 (GAO-21-198) satisfied the initial 9 month reporting requirement and this enclosure satisfies our first annual reporting requirement as it pertains to the loans to passenger air carriers (and certain specified related businesses), cargo air carriers, and businesses critical to maintaining national security under Sections 4003(b)(1)-(3).
[421]We selected 16 applicants to interview to ensure variety based on business type (passenger air carrier, cargo air carrier, ticket agent, repair station operator, and business critical to maintaining national security), loan received/not received, amount of loan request, and number of employees. The reasons applicants did not receive loans varied; however, one applicant we interviewed requested that Treasury withdraw its application.
[422]According to Treasury documents, the top 10 large passenger air carriers were identified based on global available seat miles in 2019, which measures how many seats on a plane on a given route are actually available for purchase. These carriers included Alaska Airlines, American Airlines, Delta Air Lines, Frontier Airlines, Hawaiian Airlines, JetBlue Airways, SkyWest Airlines, Spirit Airlines, Southwest Airlines, and United Airlines. In our discussion of large passenger air carriers, we also include another passenger air carrier that applied to the loan program and has several thousand employees.
[423]Those businesses we refer to as “smaller” employed fewer than 200 people and requested loans between $250,000 and $26.1 million.
[424]In addition to the Section 4003 loan program, Treasury also administered PSP. The CARES Act directed Treasury to prioritize PSP, specifically requiring Treasury to publish streamlined and expedited procedures not later than 5 days after the date of enactment of the act (in contrast with 10 days after enactment of the act for the 4003 loan program). Additionally, the CARES Act directed Treasury to make initial payments to air carriers and contractors that submitted requests for financial assistance approved by the Secretary no later than 10 days after enactment of the act, whereas the 4003 loan program did not have such a requirement.
[425]Established by the Consolidated Appropriations Act, 2021, the CERTS program is to provide $2 billion in grants to eligible transportation service providers affected by the COVID-19 pandemic, including motorcoach, school bus, passenger vessel, and pilot vessel companies. Grant funds are primarily to be used to cover payroll costs, but may also be used to cover operating expenses as well. Pub. L. No. 116-260, div. N, tit. IV, 134 Stat. 1182, 2061-68 (2020).
[426]The facilities were authorized under Section 13(3) of the Federal Reserve Act, which permits the Federal Reserve to provide emergency lending, and were approved by the Secretary of the Treasury.
[427]The CARES Act-supported facilities were the Primary Market Corporate Credit Facility, Secondary Market Corporate Credit Facility, Municipal Liquidity Facility, Term Asset-Backed Securities Loan Facility, and five facilities under the Main Street Lending Program—the Main Street New Loan Facility, Main Street Priority Loan Facility, Main Street Expanded Loan Facility, Nonprofit Organization New Loan Facility, and Nonprofit Organization Expanded Loan Facility.
[428]The facilities not supported with CARES Act funds were the Commercial Paper Funding Facility, Money Market Mutual Fund Liquidity Facility, Primary Dealer Credit Facility, and the Paycheck Protection Program Liquidity Facility.
[429]Because all nine CARES Act-supported facilities stopped purchasing assets or extending credit by January 8, 2021, we report on their outstanding assets in this enclosure rather than on their transaction volumes.
[430]The allowance for loan losses is an estimate of potential losses based upon the Main Street Lending Program’s holdings as of March 31, 2021, and does not indicate losses experienced by the program.
[431]According to Federal Reserve officials, these losses involved fewer than five loans, and losses are recognized due to events such as a bankruptcy filing, continued past due payments, or acceleration of a loan by the lender.
[432]Because the non-CARES Act facilities continued conducting transactions in 2021, we report on their transaction volumes in this enclosure.
[433]The Federal Reserve established the Paycheck Protection Program Liquidity Facility under its Section 13(3) authority to encourage lender participation in the Paycheck Protection Program. Although the Paycheck Protection Program was established through the CARES Act, the Paycheck Protection Program Liquidity Facility did not require support through CARES Act funds.
[434]CARES Act, Pub. L. No. 116-136, § 4112, 134 Stat 281, 498 (2020); Pub. L. No. 116-260, div. N, tit. IV, 134 Stat. 1182, 2052-61 (2020).
[435]Pub. L. No. 117-2, § 7301, 135 Stat. 4, 104-107. Treasury guidance defines passenger air carriers as those that derived more than 50 percent of their air transportation revenue from passengers between April 1, 2019, and September 30, 2019. Contractors refer to a person that, under contract with a passenger air carrier conducting operations under 14 C.F.R. pt. 121, performs catering functions or functions on airport property, such as security and airport ticketing, among other things. Under the American Rescue Plan Act of 2021, $14 billion can be made available to eligible passenger air carriers, and $1 billion can be made available to eligible contractors.
[436]Treasury has developed taxpayer protections for certain payments made under PSP1, PSP2, and PSP3. Passenger air carriers receiving over $100 million of payroll support are required to provide notes equal to 30 percent of the payroll support provided over $100 million with a 10-year term. Contractors receiving over $37.5 million of payroll support must provide notes equal to 44 percent of the payroll support provided over $37.5 million with a 10-year term. Warrants provide Treasury with the right to purchase shares of common stock.
[437]As of mid-June 2021, 12 passenger air carriers had received PSP2 payments that required notes, and the total anticipated note principal amount was $3.9 billion. Six contractors received PSP2 payments that required notes, and the total anticipated note principal amount was $45.3 million. Twelve passenger air carriers received PSP2 payments that required warrants, and the total anticipated number of warrants was 14.1 million. No contractors received PSP2 payments that required warrants.
[438]Of the 520 applications Treasury received, 12 have not yet been acted upon. As of mid-May 2021, Treasury officials said they did not know when the review of the 12 outstanding PSP2 applications would be complete due to factors beyond Treasury’s control, such as unresponsive applicants.
[439]For example, recipients must not have conducted involuntary furloughs or reduced pay rates or benefits between March 31, 2021, and the date of the PSP3 agreement. As of mid-June 2021, Treasury had made payments of PSP3 funds to 434 companies—268 passenger air carriers and 166 contractors. The average payment amount for passenger air carriers was $51.3 million, and the average payment amount for contractors was $5 million. Of these 434 companies, 11 received payments greater than $100 million, and four received payments greater than $1 billion. According to Treasury officials, given the authorized amount of funds for PSP3, contractors will receive PSP3 payments equal to their PSP2 payment, and passenger air carriers will receive PSP3 payments equal to 93 percent of their PSP2 payment.
[440]PSP1, PSP2, and PSP3 agreements require that recipients periodically provide Treasury with their financial statements. According to PSP1 and PSP2 guidance, annual financial statements must generally be audited by an independent certified public accountant. However, if a recipient does not prepare audited financial statements as an ordinary part of its business operations, the recipient can submit certified unaudited financial statements. Recipients that sign an agreement with Treasury certify that false, fictitious, or fraudulent statements, including concealing or omitting facts, may result in administrative remedies or civil or criminal penalties. Similarly, for PSP1 compliance reporting, Treasury requires that recipients certify their ongoing compliance with PSP agreement terms, their maintenance of effective internal controls, and the veracity and accuracy of data submitted to Treasury. Treasury officials said that they expect to use the compliance monitoring approach developed for PSP1 for monitoring PSP2 and PSP3.
[441]There are other reasons that a recipient could be escalated to a Level 2 test, such as a whistleblower report.
[442]According to Treasury officials, Treasury tested about 487 recipients in the second quarter of 2020, 603 recipients in the third quarter of 2020, and 610 recipients in the fourth quarter of 2020.
[443]According to Treasury officials, Treasury has made changes to its web portals over time to help ensure that it obtains the information it needs from recipients for its monitoring and compliance process.
[444]The Disaster Relief Fund receives an annual appropriation and has routinely received supplemental appropriations. In March 2020, the CARES Act was enacted, appropriating $45 billion for the Disaster Relief Fund. Pub. L. No. 116-136, div. B, tit. VI, 134 Stat. 281, 543 (2020). The Consolidated Appropriations Act, 2021, appropriated $17 billion to the Disaster Relief Fund for major disasters and an additional $2 billion to provide assistance for COVID19-related funeral expenses. Pub. L. No. 116-260, div. F, tit. III, 134 Stat. 1182, 1462 (2020); Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910. In March 2021, the American Rescue Plan Act of 2021 appropriated $50 billion to the Disaster Relief Fund. Pub. L. No. 117-2, § 4005, 135 Stat. 4, 79.
[445]For natural disasters, Public Assistance tends to be used for emergency cleanup and for permanent reconstruction projects for example, to rebuild damaged public infrastructure.
[446]White House, Memorandum on Maximizing Assistance from the Federal Emergency Management Agency, February 2, 2021.
[447]FEMA continues to play a key role in the ongoing COVID-19 pandemic response effort, including distributing personal protective equipment, supporting Defense Production Act activities, and providing incident management coordination and leadership.
[448]The White House, Memorandum on Authorizing the Other Needs Assistance Program for Major Disaster Declarations Related to Coronavirus Disease 2019 (Aug. 8, 2020). Pursuant to the presidential memorandum, upon receiving a FEMA grant, states and territories may provide eligible claimants $300 or $400 per week—which includes a $300 federal contribution—in addition to their Unemployment Insurance benefits. The presidential memorandum directed that the program would end when $44 billion had been obligated; the balance of the Disaster Relief Fund reached $25 billion; on December 27, 2020; or upon the enactment of legislation providing supplemental federal unemployment compensation, whichever comes first.
[449]Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910.
[450]White House, Memorandum to Extend Federal Support to Governors’ Use of the National Guard to Respond to COVID-19 and to Increase other Federal Assistance Provided to States, January 21, 2021. A subsequent presidential memorandum, issued on February 2, 2021, required FEMA to provide 100 percent cost share reimbursement for work eligible under Public Assistance for emergency protective measures from January 20, 2020, through September 30, 2021, except for the operational expenses made eligible by the January 20, 2021, memorandum, discussed above, which receive 100 percent cost share reimbursement from January 21, 2021 through September 30, 2021. White House, Memorandum on Maximizing Assistance from the Federal Emergency Management Agency, February 2, 2021.
[451]White House, Memorandum to Extend Federal Support to Governors’ Use of the National Guard to Respond to COVID-19 and to Increase other Federal Assistance Provided to States, January 21, 2021.
[452]In addition to supporting the COVID-19 response, FEMA supported California’s largest fire in history and managed the response to 10 named storms in September 2020 alone. As of February 2021, FEMA had personnel deployed to 173 active disasters and was supporting 956 open disasters.
[453]Colorado State University Tropical Weather and Climate Research, Seasonal Hurricane Forecasting: Forecast for 2021 Hurricane Activity (April 8, 2021).
[454]The initial pilot period for each location was eight weeks; however, jurisdictions were able to request an extension of an additional four weeks, during which period of time the site would receive federal staffing and support, but not an additional vaccine allocation.
[455]FEMA officials stated that the almost $5 billion had been obligated through the Public Assistance program.
[456]Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910.
[457]Eligible expenses also include eligible interment expenses that include transportation to identify the deceased for up to two people, interment, funeral services, officiant of the services, and up to five death certificate costs. Costs associated with obituaries and other printed materials, as well as flowers, are not eligible for reimbursement under the funeral assistance program. Applicants must be U.S. citizens, noncitizen nationals, or qualified aliens who paid for funeral expenses that are not covered by other sources, such as burial insurance. The death certificate must directly or indirectly attribute the death to COVID-19 and the death must have occurred in the U.S.
[458]Pub. L. No. 116-136, 134 Stat. 281, 596-97. The CARES Act gives the Federal Aviation Administration (FAA) the authority to retain up to 0.1 percent of the $10 billion (up to $10 million) provided for Grants-in-Aid for Airports to fund the award and oversight by FAA of grants made under the CARES Act.
[459]Consistent with our prior work, we have grouped airports into two broader categories: larger airports, which includes large and medium hubs, and smaller airports, which includes small hubs, non-hubs (also referred to as “non-hub primary”), and non-primary commercial service airports as well as reliever airports and general aviation airports.
[460]Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1939-41 (2020). Division M of the Consolidated Appropriations Act, 2021 is also referred to as the Coronavirus Response and Relief Supplemental Appropriations Act, 2021 (CRRSA). The Consolidated Appropriations Act, 2021, made up to $5 million of the $2 billion in funding available for the Small Community Air Service Development Program.
[461]The 31 airports that received CARES Act funds in excess of four times their annual operating expenses are excluded from receiving Consolidated Appropriations Act, 2021 funding. See Pub. L. No. 116-260, 134 Stat. at 1939. Specific amounts appropriated by the Consolidated Appropriations Act, 2021 are also available to cover lawful expenses to support FAA contract tower operations and to provide relief from rent and minimum annual guarantees to on-airport car rental, on-airport parking, and in-terminal concessions.
[462]American Rescue Plan Act, 2021, Pub. L. No. 117-2, § 7102(a), 135 Stat. 4, 96.
[463]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing Office of Management and Budget guidance is reprinted in 2 C.F.R. part 200. The Single Audit Act establishes requirements for non-federal entities (defined as states, localities, and nonprofit organizations) that receive federal awards to undergo audits of those awards annually (unless a specific exception applies) when their expenditures meet a certain dollar threshold. More specifically, nonfederal entities that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit—that is, an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501. If public airport sponsors do not meet this threshold in a fiscal year, then they are subject to applicable local and state audit requirements. Because private owners of public-use airports are not non-federal entities as defined by the Single Audit Act, private owners of public-use airports are not subject to the Single Audit Act; however, they are still subject to grant assurances that they agree to when they accept federal airport grants. For example, under one grant assurance, a private owner of a public-use airport would agree to keep all project accounts and records which fully disclose the amount and disposition by the recipient of the proceeds of this grant, the total cost of the project in connection with which this grant is given or used, and the amount or nature of that portion of the cost of the project supplied by other sources, and such other financial records pertinent to the project. Additionally, private owners of public-use airports must make any documents pertinent to a grant available to the Comptroller General for the purpose of audit and examination. Finally, DOT may require that an appropriate audit be conducted by a recipient.
[464]Certain airport sponsors that are subject to workforce retention requirements include large, medium, and small-hub airports. As such, airports that were not classified as large, medium, or small-hub airports were exempt from this requirement. More specifically, non-hub and non-primary airports are excluded from the workforce retention requirement. As a result, non-hub primary commercial service airports (airports with more than 10,000 annual passenger boardings, but less than 0.05 percent of total annual passenger boardings); non-primary commercial service airports (airports with at least 2,500 and no more than 10,000 passenger boardings each year); general aviation airports (public-use airports that do not have scheduled service or have scheduled service with fewer than 2,500 passenger boardings each year); and reliever airports (airports designated by FAA to relieve congestion at commercial service airports) are all exempt from the workforce retention requirement. Airports were required to retain 90 percent of full-time equivalent employees working at the airport as of March 27, 2020, as the baseline comparison. According to FAA guidance, airport sponsors did not need to count contractors providing services other than airport management, tenants, or concessionaires. Airport sponsors may make adjustments for retirements or voluntary employee separations when calculating the workforce retention percentage.
[465]As with the CARES Act and the Consolidated Appropriations Act, 2021, DOT could waive the workforce retention requirement under the American Rescue Plan Act of 2021, if DOT determined that the airport was experiencing economic hardship as a direct result of the requirement, or the requirement reduces aviation safety or security.
[466]March 2020 staffing levels have been adjusted for retirements and voluntary separations.
[467]Both the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021 direct airport sponsors to provide such relief to the extent permissible under state laws, local laws, and applicable trust indentures.
[468]Airport tenant relief allocation amounts were calculated based on each airport’s passenger enplanements compared to total passenger enplanements of all airports eligible for concessions relief for calendar year 2019.
[469]Congress and the President have appropriated additional COVID-19 funding to these entities to address specific purposes (see table 2).
[470]CARES Act, Pub. L. No. 116-136, div. A, tit. V, § 5001, 134 Stat. 281, 501 (2020), as amended by the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. 1182, 2145 (2020), codified at 42 U.S.C. § 801.
[471]American Rescue Plan Act of 2021, Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 223. This section of ARPA appropriated $350 billion for two funds—the Coronavirus State Fiscal Recovery Fund and the Coronavirus Local Fiscal Recovery Fund—as well as $10 billion for the Coronavirus Capital Projects Fund and $2 billion for the Local Assistance and Tribal Consistency Fund, which are codified, respectively, at 42 U.S.C. §§ 802, 803, 804, 805. This enclosure focuses only on the Coronavirus State Fiscal Recovery Fund and the Coronavirus Local Fiscal Recovery Fund, which we discuss as one for the purposes of this report. Further, this ARPA section appropriated an additional $50 million to the Secretary of the Treasury to administer these four funds as well as the Coronavirus Relief Fund enacted by the CARES Act, as amended. See 42 U.S.C. § 802(a)(2).
[472]Approximately $450 million of the $8 billion Tribal Set-Aside has not been disbursed because of litigation. In 2020, several tribes sued Treasury over its interpretation that Alaska Native regional and village corporations (ANCs) are Indian tribes eligible to receive disbursements from the CRF Tribal Set-Aside. On June 25, 2021, the Supreme Court held that ANCs are Indian tribes under the Indian Self-Determination and Education Assistance Act and thus are eligible for disbursements from the CRF Tribal Set Aside. Yellen v. Confederated Tribes of the Chehalis Reservation, 594 U.S. __ (2021).
[473]The CARES Act established that CRF recipients could use CRF funds to cover costs that they incurred between March 1, 2020, and December 30, 2020, and had not accounted for in their most recent budget prior to the act’s enactment. This time frame was extended to December 31, 2021, by the Consolidated Appropriations Act, 2021. Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. 1182, 2145 (2020), which is codified at 42 U.S.C. § 801. Beginning in April 2020, Treasury published guidance on its interpretation of the permissible uses of CRF funds. For example, Treasury stated in guidance to CRF recipients that they may not use the funds to fill shortfalls in government revenue. See 86 Fed. Reg. 4,182, 4,183 (Jan. 15, 2021). In June 2020, we described the allocation and disbursement of CRF funds in the first of our series of bimonthly and quarterly reports on the federal response to the COVID-19 pandemic.
[474]Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 223, codified at 42 U.S.C. §§ 802-803.
[475]On May 10, 2021, Treasury issued an Interim Final Rule to implement this and other provisions for the CSLFRF. See 86 Fed. Reg. 26,786 (May 17, 2021), accessed May 24, 2021, https://home.treasury.gov/policy-issues/coronavirus/assistance-for-state-local-and-tribal-governments/state-and-local-fiscal-recovery-funds. Further, multiple state Attorneys General have filed suit against the federal government regarding this provision, alleging that it can be read as prohibiting a state from reducing taxes in any manner and thus impinges on the sovereignty of the states to set their own tax policy. In July 2021, the United States District Court for the Southern District of Ohio found that the provision exceeds Congress’s power under the Constitution and enjoined Treasury from enforcing the provision against Ohio. Ohio v. Yellen, No. 1:21-CV-00181 (S.D. Ohio, July 1, 2021). Cases in other states remain ongoing.
[476]Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 223-33, codified at 42 U.S.C. §§ 802-803.
[477]A metropolitan city is defined as the central city within a metropolitan area (i.e., a standard metropolitan statistical area as established by OMB) or any other city within a metropolitan area that has a population of 50,000 or more. Other cities are nonmetropolitan cities that are units of general local government classified as municipalities by the Census Bureau or any other units of general local government that are towns or townships with certain characteristics. 42 U.S.C. §§ 803(g)(4), (5), 5302(a)(4)-(5). We refer to these recipients as localities.
[478]For states and the District of Columbia, Treasury is to allocate (1) $25.5 billion equally among the entities; (2) an additional amount to the District of Columbia equal to $1.25 billion less the amount allocated to the District of Columbia from the CRF; and (3) remaining funds to each state and the District of Columbia on the basis of the proportion that each entity’s share of the average estimated number of seasonally adjusted unemployed individuals across the entities for a 3-month period ending in December 2020 bears to the average estimate in all of the entities. For localities, ARPA directs Treasury to provide funding directly to most counties and metropolitan cities. For other counties and cities, ARPA directs Treasury to distribute funding to them through the states in which they are located. For tribal governments, ARPA directs Treasury to allocate $1 billion equally among the tribal governments and the remaining $19 billion in a manner it determines. For territories, ARPA directs Treasury to allocate $2.25 billion equally to each territory and to allocate the remaining $2.25 billion among the territories on the basis of the proportion that each territory’s population bears to the share of the total population of all such territories.
[479]ARPA provides that Treasury, to the extent practicable, shall pay a first tranche amount to localities within 60 days of enactment. ARPA then provides that Treasury shall pay a second tranche amount to localities no earlier than 12 months after the date of the first tranche payment. 42 U.S.C. § 803(b)(7).
[480]Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 225-27, codified at 42 U.S.C. § 802(b)(6), (d)(1). The certification requirement applies to funds (1) made available under the Coronavirus State Fiscal Recovery Fund and (2) funds made available under the Coronavirus Local Fiscal Recovery Fund that localities had voluntarily transferred to the state in which the locality is located.
[481]ARPA provides that Treasury shall distribute the additional allocation to the District of Columbia within 15 days of the act’s enactment, or by March 26, 2021. Certification is not required. Treasury made that payment on April 15, 2021. ARPA also provides Treasury the authority to withhold half of each state’s or territory’s payment (with the exception of the additional amount for the District of Columbia) for a period of up to 12 months from the date of the state’s or territory’s certification, based on its unemployment rate as of that date. 42 U.S.C. § 802(b)(6).
[482]The remaining $8 billion of the $150 billion CRF was appropriated for Treasury to distribute to tribal governments. 42 U.S.C. § 801(a)(2)(B). Treasury has distributed $7.5 billion of this amount. Treasury’s Office of Inspector General (OIG), which the CARES Act directed to monitor and oversee the receipt, disbursement, and use of the funds, established a process for recipients to report quarterly on the use of their funds. Since July 2020, the recipients have reported their total funds received, obligated, and expended by spending category. The data have been made publicly available through the website of the Pandemic Response Accountability Committee. The CARES Act established the Pandemic Response Accountability Committee as a committee of the Council of the Inspectors General on Integrity and Efficiency to promote transparency and conduct oversight of COVID-19 relief funds. Pub. L. No. 116-136, div. B, tit. V, § 15010, 134 Stat. 281, 533-42 (2020). At the time of our review, complete recipient reporting data for tribal governments were not available.
[483]Department of the Treasury, Office of Inspector General, Coronavirus Relief Fund Reporting Requirements Update, OIG-CA-20-025, at 2-3 (July 31, 2020). Treasury OIG updated this guidance in Coronavirus Relief Fund Prime Recipient Desk Review Procedures, OIG-CAO-21-004R, at 3 (Mar. 22, 2021).
[485]Department of the Treasury, Office of Inspector General, Coronavirus Relief Fund Frequently Asked Questions Related to Reporting and Recordkeeping (Revised), OIG-CA-20-028R, at 13 (Mar. 2, 2021).
[487]The initial Recovery Plan Performance Report will cover the period from the date of award to July 31, 2021. Thereafter, Recovery Plan Performance reports will cover a 12-month period, and recipients will be required to submit the report to Treasury within 30 days after the end of the 12-month period. The second Recovery Plan Performance report will cover the period from July 1, 2021, to June 30, 2022, and must be submitted to Treasury by July 31, 2022. Each annual Recovery Plan Performance report must be posted on the public-facing website of the recipient. 86 Fed. Reg. 26,786, 26,814-15 (May 17, 2021).
[488]Recipients will be required to submit an interim Project and Expenditure Report to Treasury by August 31, 2021, and thereafter to submit quarterly reports through the end of the award period on Dec. 31, 2026. 86 Fed. Reg. 26,786, 26,814 (May 17, 2021).
[489]Assistance listings were formerly known as the Catalog of Federal Domestic Assistance. The General Services Administration publishes detailed, public descriptions of assistance listings on SAM.gov, its System for Award Management website.
[490]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing OMB guidance is reprinted in 2 C.F.R. part 200. Nonfederal entities (states, U.S. territory and tribal governments, local governments, or nonprofit organizations) that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit—that is, an audit of the entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[491]To help administer the new COVID-19 relief funding, many federal awarding agencies also issued new guidance to award recipients regarding how those funds should be reported and spent.
[492]OMB’s 2020 single audit guidance related to the COVID-19 pandemic directed federal awarding agencies, in their capacity as cognizant or oversight agencies for audit, to provide audit submission extensions of (1) up to 6 months for recipients and subrecipients whose audits were normally due from March 30, 2020, through June 30, 2020; and (2) up to 3 months for those whose audits were normally due from July 31, 2020, through September 30, 2020. See OMB M-20-26, Extension of Administrative Relief for Recipients and Applicants of Federal Financial Assistance Directly Impacted by the Novel Coronavirus (COVID-19) Due to Loss of Operations (June 18, 2020). Similarly, due dates for 2021 single audits for entities whose fiscal year ends on or before June 30, 2021, have been extended by 6 months. See OMB M-21-20, Promoting Public Trust in the Federal Government through Effective Implementation of the American Rescue Plan Act and Stewardship of the Taxpayer Resources (Mar. 19, 2021).
[493]For more information on overall trade trends in 2020, including preliminary data for the fourth quarter, see United Nations Conference on Trade and Development, “East Asian Economies Drive Global Trade Recovery,” accessed May 19, 2021, https://unctad.org/news/east-asian-economies-drive-global-trade-recovery.
[494]U.S. Census Bureau trade statistics—a widely used source analyzing U.S. international trade—do not contain precise data on imports of COVID-19-related products. As a result, we estimated the import value of all product types and categories within those types using Harmonized Tariff Schedule of the United States (HTS) statistical reporting numbers and associated product groupings listed by the U.S. International Trade Commission (USITC) in its report, COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). Revisions to the HTS on July 1, 2020, and January 1, 2021, provided several new HTS-10 statistical reporting numbers for previously identified COVID-19-related product categories. We identified these product categories and included them in our analysis.
[495]Some HTS categories identified in USITC Publication 5073 represent more than one product, and some categories contain products that are not directly relevant to COVID-19 responses. Product categories that USITC identified as COVID-19 related refer only to the subset of goods considered to be COVID-19 related for each HTS-10 statistical reporting number. Therefore, the values we present may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, these values are useful indicators for tracking import trends of such products.
[496]Some imports from China have been subject since 2018 to tariffs imposed by the Office of the U.S. Trade Representative (USTR) at the direction of the President under Section 301 of the Trade Act of 1974. In response to the COVID-19 pandemic, USTR excluded some of these tariffs on certain medical-care-related products. In March 2021, USTR extended 99 tariff exclusions for COVID-19-related products, such as personal protective equipment and other medical care products, through September 30, 2021.
[497]We used statistics on international trade in goods published by the EU Commission’s Eurostat and Her Majesty’s Revenue and Customs to identify imports and exports of vaccines against SARS-related coronaviruses from EU member countries and the United Kingdom.
[498]According to the Census Bureau trade statistics, in January and February 2021, 89 percent of imports of vaccines were classified under the HTS reporting number (3002.20.0080) that includes the FDA approved COVID-19 vaccines. The HTS reporting number also contains several other vaccines not related to COVID-19, such as shingles, whooping cough, and human papillomavirus.
[499]According to the European Commission, only one request for the export of COVID-19 vaccines was denied. Generally, under the regulation, the export authorization shall be granted unless the exports pose a threat to the execution of the EU advance purchase agreements concluded with vaccine manufacturers.
[500]According to the Federal Emergency Management Agency, the Defense Production Act is the primary source of presidential authorities to expedite and expand the supply of materials and services from the U.S. industrial base needed to promote the national defense. Defense Production Act, Pub. L. No. 81-774, 64 Stat. 798 (1950) (codified, as amended, at 50 U.S.C. § 4501, et seq.). The DPA was authorized for use in response to the COVID-19 pandemic as early as March 2020.
[501]We compared COVID-19-related HTS-10 codes both before and after July 1, 2020, and before and after January 1, 2021. If we found no match, we checked USITC guidance to determine whether the original code had been annotated or discontinued. If it had been annotated or discontinued, we included imports of those codes after July 1, 2020, or January 1, 2021, in our analysis. For instance, according to guidance provided by the USITC, products under 4818.50.0000 were to be split into two new HTS-10 product categories, 4818.50.0080 and 4818.50.0020, on July 1, 2020. Therefore, we included imports for products contained in 4818.50.0080 and 4818.50.0020 after July 1, 2020, in our calculations.
[502]Companies may produce FDA-approved COVID-19 vaccines in other countries before shipping to importers in the United States. For example, in September 2020, Pfizer announced that it was producing its COVID-19 vaccine at its production plants in Belgium and that BioNTech’s production would take place in Germany.
[504]Fraud and “fraud risk” are distinct concepts. Fraud—obtaining something of value through willful misrepresentation—is challenging to detect because of its deceptive nature. Fraud risk (which is a function of likelihood and impact) exists when individuals have an opportunity to engage in fraudulent activity, have an incentive or are under pressure to commit fraud, or are able to rationalize committing fraud. Fraud risk management is a process for ensuring program integrity by continuously and strategically mitigating the likelihood and impact of fraud. When fraud risks can be identified and mitigated, fraud may be less likely to occur. Although the occurrence of fraud indicates there is a fraud risk, a fraud risk can exist even if actual fraud has not yet been identified or occurred.
[505]Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-21-19 (Washington, D.C.: Mar. 5, 2021). As outlined in Office of Management and Budget memorandum M-21-19, management is required to manage its payment integrity risk—including fraud risk—to an agency achieving its strategic, operations, reporting, or compliance objectives.
[506]An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes.
[507]On May 17, 2021, the Attorney General established the COVID-19 Fraud Enforcement Task Force to marshal the resources of the Department of Justice in partnership with agencies across the government. According to a related press release, the task force will augment and incorporate the existing coordination mechanisms within the Department of Justice. Also, it will work closely with interagency partners to share information and insights gained from prior enforcement experience to reduce the potential threat to the American people and COVID-19 relief. In addition, it will help agencies increase their fraud prevention efforts by providing information about fraud trends and illicit tactics. Further, it will bolster efforts to investigate and prosecute the most culpable domestic and international criminals, prevent the exploitation of government assistance for personal and financial gain, and recover stolen funds.
[508]We consider convictions to be cases where an individual was convicted of a fraud-related charge at trial. As of April 30, 2021, there had not been any convictions related to UI, EIDL, EIP, or other federal COVID-19 relief programs.
[509]According to FTC, the fraud reports reflect complaints in the Consumer Sentinel Network that mention COVID, stimulus, N95, and related terms. The identity theft reports reflect complaints that mention COVID, stimulus, or related terms, in the following identity theft subtypes: tax, employment and wage, government benefits, and government documents.
[510]In a fact sheet attached to a May 17, 2021, press release, the Department of Justice stated that through its enforcement initiative to detect and disrupt COVID-19-related fraud, it has charged nearly 600 defendants to date with crimes involving over $600 million. A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[511]The federal government may enforce laws through civil or criminal action. Such action may be resolved through a trial, a permanent injunction, a civil settlement, or a guilty plea. For example, in January 2021, the Department of Justice obtained a civil settlement for fraud against PPP. In this case, a company and its president and chief executive officer agreed to pay a combined $100,000 in damages and penalties to resolve allegations.
[512]The statute of limitations for mail fraud and wire fraud prosecutions is 5 years (18 U.S.C. § 3282), except for mail and wire fraud schemes that affect a financial institution, in which case the statute is 10 years (18 U.S.C. § 3293). Also, based on our analysis, these cases can take many years to resolve. For example, the Department of Housing and Urban Development OIG closed cases in 2017–2020 resulting from Hurricane Sandy in 2012.
[513]Fourteen of these individuals had been sentenced as of April 30, 2021. Sentences ranged from time served and 2 years of supervised release to 10 years in prison. Also, some of these individuals pleaded guilty to charges related to more than one federal program. Specifically, 15 individuals pleaded guilty to federal charges related to both PPP and EIDL, two individuals pleaded guilty to federal charges related to both PPP and UI, and one individual pleaded guilty to federal charges related to PPP, EIDL, and UI, as of April 30, 2021.
[514]Officials from the National Association of State Workforce and its UI Integrity Center, funded by and operated in partnership with DOL, said that identity theft remains the biggest challenge for states in addressing potential UI fraud. According to officials, states have recently experienced increases in instances of criminals taking over legitimate claimants’ UI accounts and rerouting benefits to other bank accounts. In January 2021, we reported that states were working to address these account takeovers through communication campaigns that raise public awareness about phishing attempts to steal account information, as well as coordinating with law enforcement and banking institutions. In March 2021, DOL launched a website to help the public better understand UI identity theft. The website also provides resources for those who may have been victims of identity theft, including a list of contact information for each state to report UI identity theft.
[515]This individual faces a maximum penalty of 30 years in federal prison for the bank fraud and false statement charges, and up to 10 years in federal prison for each money laundering charge. A sentencing date had not yet been set as of April 30, 2021.
[516]The majority of these individuals were charged with attempting to defraud SBA’s PPP and EIDL program, DOL’s UI program, or EIPs. Five individuals were charged with attempting to defraud other federal COVID-19 relief programs, including the Accelerated and Advance Payments Program, the Coronavirus Food Assistance Program, the Higher Education Emergency Relief Fund, and the Provider Relief Fund. As of April 30, 2021, there had not been any guilty pleas or convictions related to other federal COVID-19 relief programs. Also, some of these individuals faced charges related to more than one federal program. Specifically, 48 individuals faced federal charges related to both PPP and EIDL, four individuals faced federal charges related to both EIDL and UI, and one individual faced federal charges related to both UI and EIP as of April 30, 2021. One individual also faced federal charges related to PPP, the Accelerated and Advance Payments Program, and the Provider Relief Fund.
[517]Two of the 11 individuals or entities have also pleaded guilty to federal charges of defrauding COVID-19 relief programs. Also, eight of the 11 individuals had been sentenced as of April 30, 2021. Sentences ranged from 1 year of probation and a $1,500 fine to 10 years in prison.
[518]The COVID-19 Consumer Protection Act, which became law in December 2020 as part of the Consolidated Appropriations Act, 2021, gives FTC authority to seek civil penalties on the first offense for scams and deceptive practices related to the COVID-19 pandemic. Pub. L. No. 116-260, div. FF, tit. XIV, § 1401, 134 Stat. 1182, 3275-3276 (2020).
[519]The complaint seeks civil penalties and injunctive relief to stop the defendants from continuing to make deceptive advertising claims.
[520]A co-conspirator in this case was charged in a criminal complaint.
[521]This individual and his company are also parties to a civil complaint.
[522]In a related press release, the Acting U.S. Attorney for this case also clarified that the federal government is providing the vaccine free of charge to people living in the U.S. Individuals visiting a seized website will see a message that the site has been seized by the federal government and be redirected to another site for additional information.
[523]Four individuals had been sentenced as of April 30, 2021. In October 2020, one individual was sentenced to 1 year and 1 day in prison and ordered to pay restitution in the amount of $221,200 for causing damage to a former employer and delaying the shipment of PPE during the COVID-19 pandemic. In January 2021, an individual was sentenced to 3 months in prison and 9 months of home confinement and ordered to pay restitution in the amount of $132,291 for stealing COVID-19-related medical supplies to sell for the individual’s own gain. Two individuals in other cases had been sentenced to 2 to 3 years of probation and ordered to pay fines as of April 30, 2021.
[524]The Food and Drug Administration approved the use of hydroxychloroquine sulfate on an emergency basis for hospitalized COVID-19 patients in March 2020 and revoked this emergency use authorization in June 2020.
[525]One of these individuals was separately charged with concealment money laundering and aggravated identity theft. The other individual was separately charged with concealment money laundering. In May 2021, the Department of Justice announced criminal charges against 14 defendants, including these two, for their alleged participation in various health care fraud schemes resulting in over $143 million in false billings.
[526]In addition to these warnings, in December 2020, FTC, together with the National Association of Attorneys General, issued a blog post warning consumers about these types of scams.
[527]In December 2020, Congress appropriated $2 billion to the Disaster Relief Fund for eligible funeral expenses for individuals or households with COVID-19-related funeral expenses. In April 2021, FEMA began accepting applications for funeral assistance via a dedicated call center. This assistance is limited to a maximum of $9,000 per funeral and a maximum of $35,500 per application.
[528]The National Center for Disaster Fraud, established in 2005, is the result of a partnership between the Department of Justice and various law enforcement and regulatory agencies to form a national coordinating agency to improve and further the detection, prevention, investigation, and prosecution of fraud related to natural and human-made disasters, and to advocate for the victims of such fraud. Among other things, the center operates a hotline to receive reports of disaster-related fraud.
[529]The Consolidated Appropriations Act, 2021 amended CARES Act authority to borrow this amount by providing that USPS shall not be required to repay such amounts borrowed. Pub. L. No. 116-260, div. N, tit. VIII, § 801, 134 Stat. 1182, 2119 (2020) (amending Pub. L. No. 116-136, div. A, tit. VI, § 6001, 134 Stat. 281, 504-05 (2020)). As of March 2021, USPS accessed about $8.7 billion of the $10 billion available. The funds available under the CARES Act, as amended, are in addition to USPS’s borrowing authority under 39 U.S.C. § 2005, which authorizes USPS to borrow up to $3 billion in any one fiscal year and not more than $15 billion in total. On April 2, 2021, USPS repaid $3 billion of its outstanding balance, leaving it with $11 billion borrowed of this $15 billion available.
[530]These data do not include International Mail. This is the most recent data available since we reported in April 2021. Most of the second quarter of fiscal year 2020 was prior to the declaration of a national emergency in March 2020.
[531]USPS can request this funding for COVID-19 related expenses under its memorandum of understanding with the Department of the Treasury. As required by statute, USPS must determine that, due to the COVID-19 emergency, USPS will not be able to fund operating expenses without borrowing money. CARES Act, Pub. L. No. 116-136, div. A, tit. VI, § 6001, 134 Stat. 281, 504-05 (2020). As of March 31, 2021, USPS reported that it has requested and received $8.7 billion of these funds. USPS plans to request the remaining $1.3 billion in CARES Act funding by the end of fiscal year 2021.
[532]OSHA’s May 2020 enforcement policy was replaced in March 2021. See Occupational Safety and Health Administration, Updated Interim Enforcement Response Plan for Coronavirus Disease 2019 (COVID-19) (May 19, 2020) and Updated Interim Enforcement Response Plan for Coronavirus Disease 2019 (COVID-19) (Mar. 12, 2021).
[533]Occupational Safety and Health Administration, OSHA Direction: National Emphasis Program—Coronavirus Disease 2019 (COVID-19), DIR 2021-01 (CPL-03) (Mar. 12, 2021).
Contacts
A. Nicole Clowers
Managing Director, Health Care, clowersa@gao.gov, (202) 512-7114
Congressional Relations
Orice Williams Brown, Managing Director, williamso@gao.gov, (202)-512-4400 U.S. Government Accountability Office 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs
Chuck Young, Managing Director, youngc1@gao.gov, (202)-512-4800 U.S. Government Accountability Office 441 G Street NW, Room 7149, Washington, DC 20548
Strategic Planning and External Liaison
Stephen J. Sanford, Acting Managing Director, spel@gao.gov, (202)-512-4707 U.S. Government Accountability Office 441 G Street NW, Room 7814, Washington, DC 20548
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s cost of production and distribution. Pricing and ordering information is posted on our website.
To Report Fraud, Waste, and Abuse in Federal Programs
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Copyright
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.














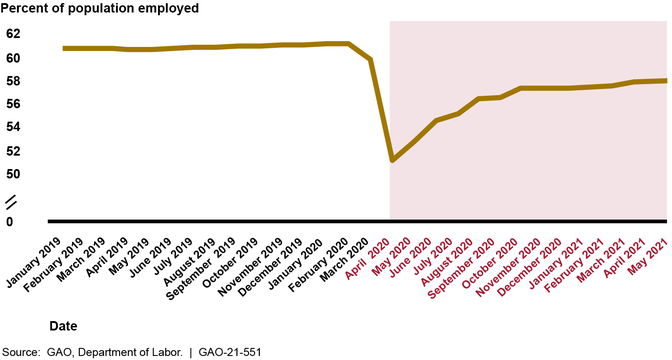



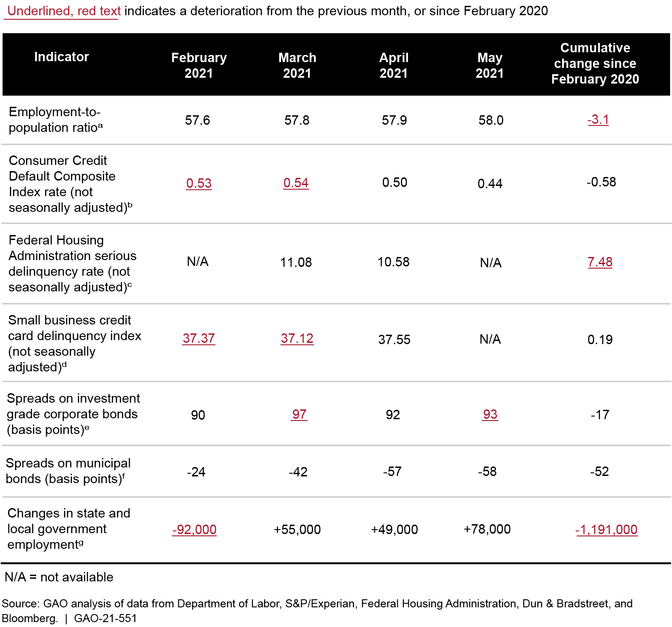









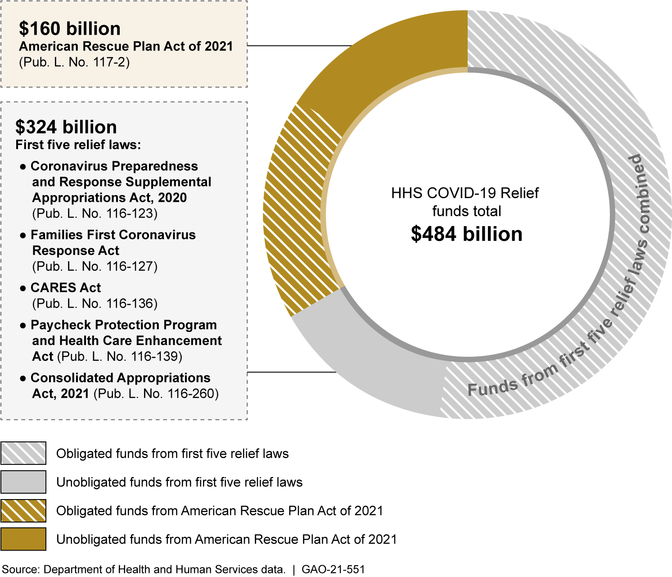







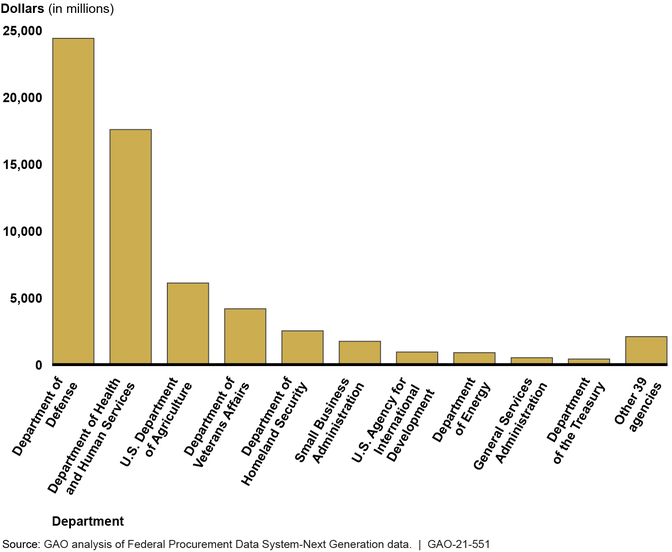


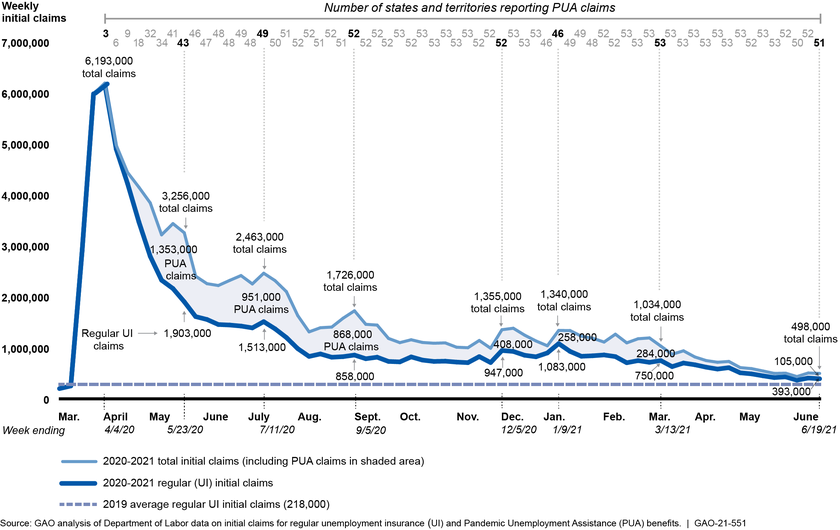











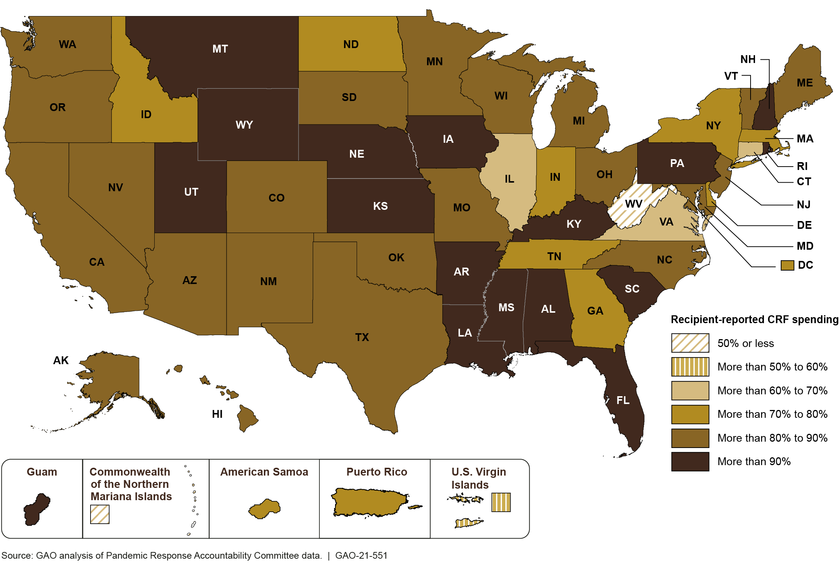



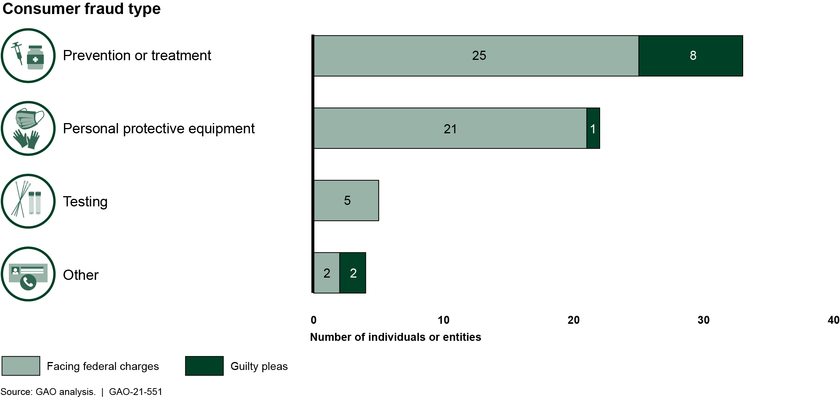






















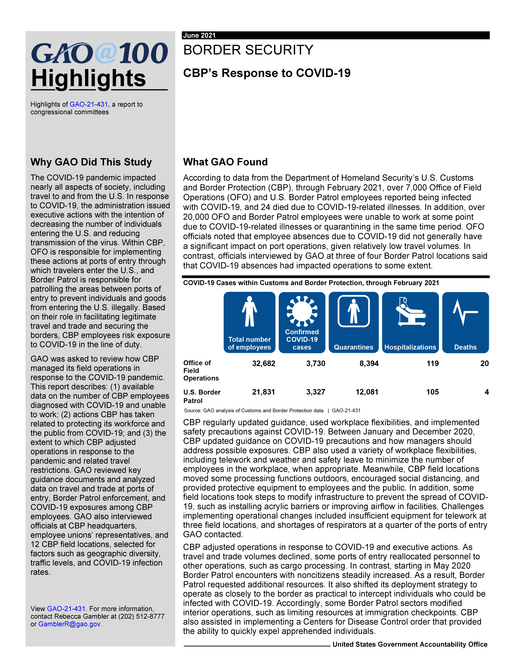




_Page_1-1625273851371.png)
_Page_2-1625273876829.png)
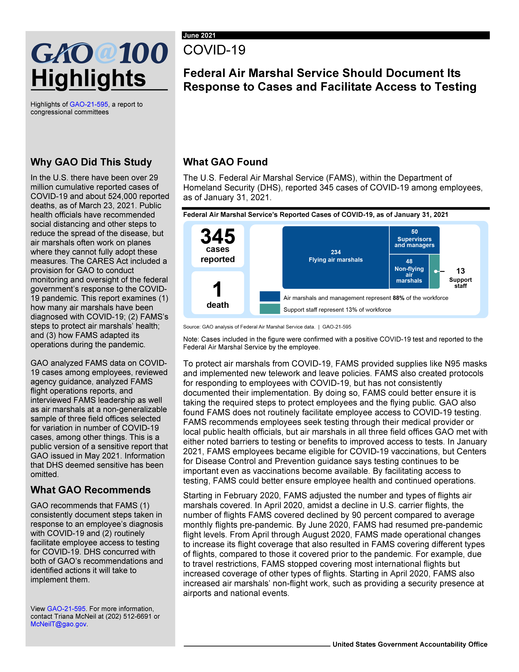








_Page_1_1625796100669.png)
_Page_2_1625796148465.png)
_1_1625796293789.png)
_1_Page_1-1625796346094.png)
_Page_2_1_1625796383102.png)
_Page_3-1625796609302.png)
_Page_1-1625796666108.png)
_Page_2-1625796684204.png)
_Page_3-1625796704515.png)
_Page_1-1625796875027.png)
_Page_2-1625796892330.png)
_Page_3-1625796912161.png)
_Page_1-1625797041072.png)
_Page_2-1625797063155.png)
-1625797117113.png)
_Page_1-1625797153339.png)
_Page_2-1625797170586.png)
_Page_1-1625797207794.png)
_Page_2-1625797226838.png)
-1625797307764.png)