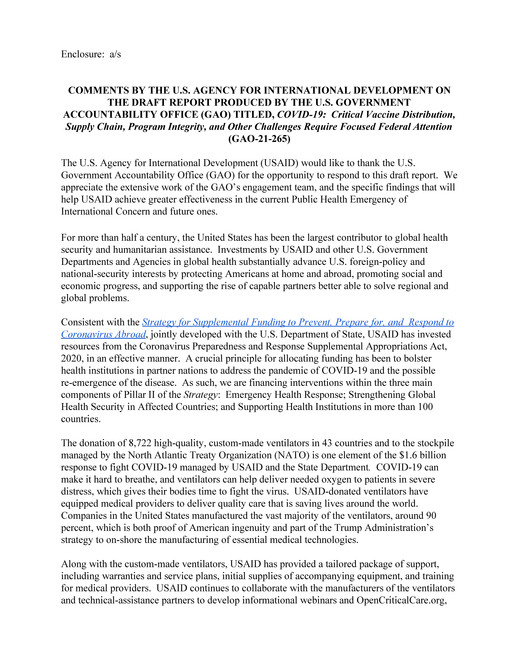
Since November 2020, the number of COVID-19 cases in the U.S. has rapidly increased, further straining health care systems across the country. Between December 31, 2020, and January 13, 2021, new reported COVID-19 cases averaged about 225,000 per day—over 7 and 3 times higher than the surges the nation experienced during the spring and summer of 2020, respectively. (See figure.) The country also continues to experience serious economic repercussions and turmoil as a result of the pandemic. As of December 2020, there were more than 10.7 million unemployed individuals, compared to nearly 5.8 million individuals at the beginning of the calendar year. Until the country better contains the spread of the virus, the pandemic will likely remain a significant obstacle to more robust economic activity.
Reported COVID-19 Cases per Day in the U.S., through January 13, 2021
In this report, GAO is making 13 recommendations to federal agencies to improve the ongoing response and recovery efforts in the areas of public health and the economy. As the new Congress and administration establish their policies and priorities for the federal government’s COVID-19 response, GAO urges swift action on these 13 recommendations, as well as on the additional recommendations that GAO has made since June 2020.
As of January 2021, 27 of GAO’s 31 previous recommendations remained unimplemented. GAO remains deeply troubled that agencies have not acted on recommendations to more fully address critical gaps in the medical supply chain. While GAO recognizes federal agencies continue to take some steps, GAO underscores the importance of developing a well-formulated plan to address critical gaps for the remainder of the pandemic, especially in light of the recent surge in cases. In addition, implementation of GAO’s recommendation concerning the importance of clear and comprehensive vaccine distribution and communication plans remains a work in progress. Moreover, slow implementation of GAO’s recommendations relating to program integrity, in particular those made to the Small Business Administration (SBA) and Department of Labor (DOL), creates risk of considerable improper payments, including those related to fraud, and falls far short of transparency and accountability expectations. See appendix III for the status of GAO’s past recommendations.
GAO is pleased that the Consolidated Appropriations Act, 2021—enacted in December of 2020—requires a number of actions that are consistent with several of GAO’s prior recommendations, including those related to the medical supply chain, vaccines and therapeutics, and COVID-19 testing. GAO will monitor the implementation of the act’s requirements.
GAO’s new recommendations are discussed below.
COVID-19 Testing
Diagnostic testing for COVID-19 is critical to controlling the spread of the virus, according to the Centers for Disease Control and Prevention. GAO found that the Department of Health and Human Services (HHS) has not issued a comprehensive and publicly available national testing strategy. HHS’s national strategy documents are not comprehensive because they only partially address the characteristics that GAO has found to be desirable in an effective national strategy. For example, testing strategy documents do not always provide consistent definitions and benchmarks to measure progress, not all documents clearly define the problem and risks, and there is limited information on the types of resources required for future needs.
Furthermore, some of the documents have not been made public. While the national testing strategy is formally outlined in a publicly available document, HHS has provided only Congress with the COVID-19 Testing Strategy Reports, which detail the implementation of the testing strategy. Stakeholders who are involved in the response efforts told GAO they were unaware of the existence of a national strategy or did not have a clear understanding of the strategy. Without a comprehensive, publicly available national strategy, HHS is at risk of key stakeholders and the public lacking crucial information to support an informed and coordinated testing response. GAO is recommending that HHS develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that HHS has produced for the public and Congress to allow for a more coordinated pandemic testing approach. HHS partially concurred with this recommendation and agreed that it should take steps to more directly incorporate some of the elements of an effective national strategy.
Vaccines and Therapeutics
Multiple federal agencies, through Operation Warp Speed, continue to support the development and manufacturing of vaccines and therapeutics to prevent and treat COVID-19. As of January 8, 2021, two of the six vaccines supported by Operation Warp Speed have been authorized for emergency use, and vaccine distribution and administration have begun. (See figure below). However, distribution and administration fell short of expectations set for the end of the year. As of December 30, 2020, Operation Warp Speed had distributed (shipped) about 12.4 million doses of COVID-19 vaccine and providers reported administering about 2.8 million initial doses, according to Centers for Disease Control and Prevention data. In September 2020, GAO stressed the importance of having a plan that focused on coordination and communication and recommended that HHS, with the support of the Department of Defense, establish a time frame for documenting and sharing a national plan for distributing and administering COVID-19 vaccine, and among other things, outline an approach for how efforts would be coordinated across federal agencies and nonfederal entities. To date, this recommendation has not been fully implemented. GAO reiterates the importance of doing so. Effective coordination and communication among federal agencies, commercial partners, jurisdictions, and providers is critical to successfully deploying COVID-19 vaccines and managing public expectations, especially because the initial supply of vaccine has been limited.
Status of Development of Six Operation Warp Speed COVID-19 Vaccine Candidates, as of January 8, 2021
Medical Supply Chain
The pandemic has highlighted vulnerabilities in the nation’s medical supply chain, which includes personal protective equipment and other supplies necessary to treat individuals with COVID-19. The Strategic National Stockpile (SNS) is an important piece of HHS’s recently developed strategy to improve the medical supply chain to enhance pandemic response capabilities. However, the department has yet to develop a process for engaging about the strategy with key nonfederal stakeholders that have a shared role for providing supplies during a pandemic, such as state and territorial governments and the private sector. GAO’s work has noted the importance of directly and continuously involving key stakeholders, including Congress, in the development of successful agency reforms and helping to harness ideas, expertise, and resources.
To improve the nation’s response and preparedness for pandemics, GAO recommends that HHS establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as the agency refines and implements its supply chain strategy for pandemic preparedness, to include the role of the SNS. HHS generally concurred with this recommendation and noted that the department regularly engages with Congress and nonfederal stakeholders. GAO maintains that capitalizing on existing relationships to engage these critical stakeholders as HHS refines and implements a supply chain strategy, to include the role of the SNS, will improve a whole-of-government response to, and preparedness for, pandemics.
In August 2020, the President issued an Executive Order directing agencies to take steps toward the goal of strengthening domestic drug manufacturing and supply chains. Federal agencies have started implementing the Executive Order, but expressed concerns about their ability to implement some of the provisions. In particular, GAO found that federal agencies do not have complete and accessible information to identify supply chain vulnerabilities and to report the manufacturing supply chains of drugs that were procured by the agency.
To help it identify and mitigate vulnerabilities in the U.S. drug supply chain, GAO recommends that the Food and Drug Administration (FDA) ensure drug manufacturing data obtained are complete and accessible, including by working with manufacturers and other federal agencies, such as the Department of Defense and the Department of Veterans Affairs and, if necessary, seek authority to obtain complete and accessible information. HHS neither agreed nor disagreed with this recommendation.
COVID-19 Data for Health Care Indicators
The federal government does not have a process to help systematically define and ensure the collection of standardized data across the relevant federal agencies and related stakeholders to help respond to COVID-19, communicate the status of the pandemic with citizens, or prepare for future pandemics. As a result, COVID-19 information that is collected and reported by states and other entities to the federal government is often incomplete and inconsistent. The lack of complete and consistent data limits HHS’s and others’ ability to monitor trends in the burden of the pandemic across states and regions, make informed comparisons between such areas, and assess the impact of public health actions to prevent and mitigate the spread of COVID-19. Further, incomplete and inconsistent data have limited HHS’s and others’ ability to prioritize the allocation of health resources in specific geographic areas or among certain populations most affected by the pandemic.
To improve the federal government’s response to COVID-19 and preparedness for future pandemics, GAO recommends that HHS immediately establish an expert committee comprised of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. HHS partially concurred with this recommendation and agreed that it should establish a dedicated working group or other mechanism with a focus on addressing COVID-19 data collection shortcomings.
Drug Manufacturing Inspections
FDA is responsible for overseeing the safety and effectiveness of all drugs marketed in the U.S., including those manufactured overseas, and typically conducts more than 1,600 inspections of foreign and domestic drug manufacturing establishments every year. In light of the COVID-19 pandemic, since March 2020, FDA has limited domestic and foreign inspections for the safety of its employees. (See figure below.)
FDA has used alternative inspection tools to maintain some oversight of drug manufacturing quality while inspections are paused, including inspections conducted by foreign regulators, requesting and reviewing records and other information, and sampling and testing. Although FDA has determined that inspections conducted by certain European regulators are equivalent to an FDA inspection, other tools provide useful information but are not equivalent to an FDA inspection. As a result, FDA could be faced with a backlog of inspections, threatening the agency’s goal to maximize inspections prioritized by its risk-based site selection model each year.
GAO recommends that FDA (1) ensure that inspection plans for future fiscal years identify, analyze, and respond to the issues presented by the backlog of inspections that could jeopardize its goal of risk-driven inspections, and (2) fully assess the agency’s alternative inspection tools and consider whether these tools or others could provide the information needed to supplement regular inspection activities or help meet the agency’s drug oversight objectives when inspections are not possible in the future. FDA concurred with both recommendations.
Number of FDA-Conducted Domestic and Foreign Drug Manufacturing Establishment Inspections, Fiscal Years 2019–2020, by Month
Federal Contracting
Federal agencies are using other transaction agreements to respond to the pandemic, which are contracting mechanisms that can enable agencies to negotiate terms and conditions specific to a project. GAO found that HHS misreports its other transaction agreements related to COVID-19 as procurement contracts, including other transaction agreements with about $1.5 billion obligated for Operation Warp Speed and other medical countermeasures. HHS’s approach is inconsistent with federal acquisition regulations and limits the public’s insight into the agency’s contract spending. To ensure consistent tracking and transparency of federal contracting activity related to the pandemic, GAO recommends that HHS accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts. HHS concurred with this recommendation.
Oversight of Worker Safety and Health
GAO identified concerns about federal oversight of worker safety and health amid the COVID-19 pandemic. Specifically, the Occupational Safety and Health Administration (OSHA) has adapted its enforcement methods for COVID-19 to help protect agency employees from the virus and address resource constraints, such as by permitting remote inspections in place of on-site inspections of workplaces. However, gaps in OSHA’s oversight and tracking of its adapted enforcement methods prevent the agency from assessing the effectiveness of its enforcement methods during the pandemic, ensuring that its adapted enforcement methods do not miss violations, and ensuring that employers are addressing certain identified violations.
To improve its oversight, GAO recommends that OSHA (1) develop a plan, with time frames, to implement the agency’s oversight processes for COVID-19-adapted enforcement methods, and (2) ensure that its data system includes comprehensive information on use of these enforcement methods to inform these processes. The agency neither agreed nor disagreed with these recommendations.
Additionally, OSHA’s data do not include comprehensive information on workplace exposure to COVID-19. For example, OSHA does not receive employer reports of all work-related hospitalizations related to COVID-19, as disease symptoms do not appear within the required reporting time frames. Employers may also face challenges determining whether COVID-19 hospitalizations or fatalities are work-related because of COVID-19’s incubation period and the difficulties in tracking the source of exposure. GAO recommends that OSHA determine what additional data may be needed from employers or other sources to better target the agency’s COVID-19 enforcement efforts. The agency neither agreed nor disagreed with this recommendation.
Assistance for Fishery Participants
The CARES Act appropriated $300 million in March 2020 to the Department of Commerce (Commerce) to assist eligible tribal, subsistence, commercial, and charter fishery participants affected by COVID-19, which may include direct relief payments. After administrative fees were assessed, $298 million of the $300 million appropriated was obligated for fishery participants. Widespread restaurant closures in the spring of 2020 led to a decrease in demand for seafood, adversely affecting the fisheries industry.
As of December 4, 2020, all funds had been obligated and only about 18 percent ($53.9 million) of the CARES Act funding obligated for fishery participants had been disbursed, which is inconsistent with Office of Management and Budget guidance on the importance of agencies distributing CARES Act funds in an expedient manner. Commerce’s National Oceanic and Atmospheric Administration (NOAA) officials said they expect that the vast majority of funds will be disbursed to fisheries participants by early 2021. However, the agency does not have the needed information centralized to help ensure that funds are being disbursed expeditiously and efficiently. GAO recommends that NOAA develop a mechanism to track the progress of states, tribes, and territories in meeting established timelines to disburse funds in an expedited and efficient manner. NOAA concurred with this recommendation.
Program Integrity
GAO continues to identify areas to improve program integrity and reduce the risk of improper payments for programs funded by the COVID-19 relief laws now that federal agencies have obligated a total of $1.9 trillion and expended $1.7 trillion of the $2.7 trillion appropriated for response and recovery efforts as of November 30, 2020. Federal relief programs remain vulnerable to significant risk of fraudulent activities because of the need to quickly provide funds and other assistance to those affected by COVID-19 and its economic effects.
In this report, GAO identifies concerns about overpayments and potential fraud in the unemployment insurance (UI) system, specifically in the federally funded Pandemic Unemployment Assistance (PUA) program, which provides UI benefits to individuals not otherwise eligible for these benefits, such as self-employed and certain gig economy workers. As of January 11, 2021, states that had submitted data to DOL reported more than $1.1 billion in PUA overpayments from March through December 2020. While DOL requires states to report data on PUA overpayments, as of the beginning of 2021, the agency was not tracking the amount of overpayments recovered, limiting insight into the effectiveness of states’ efforts to recoup federal funds. To better track the recovery of federal funds, GAO recommends that DOL collect data from states on the amount of PUA overpayments recovered. DOL concurred with this recommendation, and has taken the first step toward implementing it by issuing new guidance and updated instructions for states to report PUA overpayment recovery data.
GAO also remains concerned about SBA’s management of internal controls and fraud risks in the Economic Injury Disaster Loans (EIDL) program. COVID-19 relief laws made qualifying small businesses and nonprofit organizations adversely affected by COVID-19 eligible for financial assistance from the EIDL program. Some approval requirements were also relaxed, such as requiring each applicant to demonstrate that it could not obtain credit elsewhere, through December 31, 2021. As of December 31, 2020, SBA officials said they had approved about 3.7 million applications for loans related to COVID-19, totaling about $200 billion. SBA rapidly processed loans and advances to millions of small businesses affected by COVID-19. GAO’s analysis of SBA data shows that the agency approved EIDL loans and advances for potentially ineligible businesses. For example, SBA approved at least 3,000 loans totaling about $156 million to potentially ineligible businesses in industries that SBA policies state were ineligible for the EIDL program, such as insurance and real estate development, as of September 30, 2020. GAO recommends that SBA develop and implement portfolio-level data analytics across EIDL loans and advances made in response to COVID-19as a means to detect potentially ineligible and fraudulent applications. SBA neither agreed nor disagreed with this recommendation.
Why GAO Did This Study
As of January 15, 2021, the U.S. had about 23 million cumulative reported cases of COVID-19 and more than 387,000 reported deaths, according to the Centers for Disease Control and Prevention. The country also continues to experience serious economic repercussions.
Four relief laws, including the CARES Act, were enacted as of November 2020 to provide appropriations to address the public health and economic threats posed by COVID-19. As of November 30, 2020, of the $2.7 trillion appropriated by these four laws, the federal government had obligated a total of $1.9 trillion and expended $1.7 trillion of the COVID-19 relief funds, as reported by federal agencies.
In December 2020, the Consolidated Appropriations Act, 2021, provided additional federal assistance for the ongoing response and recovery.
The CARES Act includes a provision for GAO to report on its ongoing monitoring and oversight efforts related to the COVID-19 pandemic. This report examines the federal government’s continued efforts to respond to and recover from the COVID-19 pandemic.
GAO reviewed data, documents, and guidance from federal agencies about their activities and interviewed federal and state officials and stakeholders. GAO completed its audit work on January 15, 2021.
What GAO Recommends
GAO is making 13 new recommendations for agencies that are detailed in this Highlights and in the report.
Recommendations
Recommendations for Executive Action
Recommendations for Executive Action
We are making a total of 13 recommendations to federal agencies:
Number
Agency
Recommendation
1
Department of Health and Human Services : Office of the Assistant Secretary for Preparedness and Response
To improve the nation’s response to and preparedness for pandemics, the Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as the Department of Health and Human Services refines and implements a supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile. (Recommendation 1)
2
Department of Health and Human Services : Food and Drug Administration
The Commissioner of the Food and Drug Administration should, as the agency makes changes to its collection of drug manufacturing data, ensure the information obtained is complete and accessible to help it identify and mitigate supply chain vulnerabilities, including by working with manufacturers and other federal agencies (e.g., the Departments of Defense and Veterans Affairs), and, if necessary, seek authority to obtain complete and accessible information. (Recommendation 2)
3
Department of Health and Human Services
The Secretary of Health and Human Services should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that the Department of Health and Human Services has produced for the public and Congress to allow for a more coordinated pandemic testing approach. (Recommendation 3)
4
Department of Health and Human Services : Food and Drug Administration
The Commissioner of the Food and Drug Administration should, as inspection plans for future fiscal years are developed, ensure that such plans identify, analyze, and respond to the issues presented by the backlog of inspections that could jeopardize the goal of risk-driven inspections. (Recommendation 4)
5
Department of Health and Human Services : Food and Drug Administration
The Commissioner of the Food and Drug Administration should fully assess the agency’s alternative inspection tools and consider whether these tools or others could provide the information needed to supplement regular inspection activities or help meet its drug oversight objectives when inspections are not possible in the future. (Recommendation 5)
6
Department of Health and Human Services
To improve the federal government’s response to COVID-19 and preparedness for future pandemics, the Secretary of Health and Human Services should immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. This committee should include a broad representation of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits. (Recommendation 6)
7
Department of Health and Human Services : Office of the Assistant Secretary for Preparedness and Response
The Assistant Secretary for Preparedness and Response, in coordination with the appropriate offices within the Department of Health and Human Services, should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts. (Recommendation 7)
8
Department of Labor : Occupational Safety and Health Administration
The Assistant Secretary of Labor for Occupational Safety and Health should develop a plan, with time frames, to implement the agency’s oversight processes for COVID-19-adapted enforcement methods, as described in its pandemic enforcement policies. (Recommendation 8)
9
Department of Labor : Occupational Safety and Health Administration
The Assistant Secretary of Labor for Occupational Safety and Health should ensure that the Occupational Safety and Health Administration Information System includes comprehensive information on use of the agency’s COVID-19-adapted enforcement methods sufficient to inform its oversight processes for these methods. (Recommendation 9)
10
Department of Labor : Occupational Safety and Health Administration
The Assistant Secretary of Labor for Occupational Safety and Health should determine what additional data may be needed from employers or other sources to better target the agency’s COVID-19 enforcement efforts. (Recommendation 10)
11
Department of Commerce : National Oceanic and Atmospheric Administration : National Marine Fisheries Service
The Assistant Administrator for the National Oceanic and Atmospheric Administration Fisheries should develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner. (Recommendation 11)
12
Department of Labor : Employment and Training Administration : Office of Unemployment Insurance
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments recovered in the Pandemic Unemployment Assistance program, similar to the regular unemployment insurance program. (Recommendation 12)
13
Small Business Administration
The Administrator of the Small Business Administration should develop and implement portfolio-level data analytics across Economic Injury Disaster Loan program loans and advances made in response to COVID-19 as a means to detect potentially ineligible and fraudulent applications. (Recommendation 13)
The Coronavirus Disease 2019 (COVID-19) pandemic has resulted in catastrophic loss of life and substantial damage to the global economy, stability, and security. Worldwide, as of January 15, 2021, there were about 91,816,000 cumulative reported cases and more than 1,986,000 reported deaths due to COVID-19; within the U.S., there were about 23,194,000 cumulative reported cases and more than 387,000 reported deaths.[1]
The country also continues to experience serious economic repercussions and turmoil as a result of the pandemic. As of December 2020, there were more than 10.7 million unemployed individuals, compared to nearly 5.8 million individuals at the beginning of the calendar year.[2]
In response to this unprecedented global crisis, Congress and the administration have taken a series of actions to protect the health and well-being of Americans. Notably, in March 2020, Congress passed, and the President signed into law, the CARES Act, which provided over $2 trillion in emergency assistance and health care response for individuals, families, and businesses affected by COVID-19.[3]
The CARES Act includes a provision for us to conduct monitoring and oversight of the federal government’s efforts to prepare for, respond to, and recover from the COVID-19 pandemic.[4] We are to report on, among other things, the effect of the pandemic on public health and the economy. To date, we have issued five reports in response to this provision, made 31 recommendations to federal agencies, and raised four matters for congressional consideration to improve the federal government’s response efforts.[5] We also have many other targeted reports in areas such as Federal Reserve lending programs supported by CARES Act funds, the Defense Production Act, and the CARES Act loan program for aviation and other eligible businesses.
This report examines the federal government’s continued efforts to respond to and recover from the COVID-19 pandemic, and makes 13 new recommendations to federal agencies. Areas covered include the Strategic National Stockpile, drug supply chain, COVID-19 testing, drug manufacturing inspections, nursing homes, federal contracts and agreements for COVID-19, worker safety, and unemployment insurance programs.
This report also includes 26 enclosures about a range of federal programs and activities across the government, including the status of health care and economic indicators that could help monitor the nation’s response to and recovery from the COVID-19 pandemic. (See Appendix I) Figure 1 lists these enclosures by topic area and highlights those with new recommendations.
Figure 1: Report Enclosures by Topic Area
Given the government-wide scope of this report, we undertook a variety of methodologies to complete our work, including examining a wide range of data sources and conducting interviews with federal and state officials, and representatives from stakeholder groups and other entities. Among other things, we examined federal laws, agency documents, and guidance. In each enclosure, we include a summary of the methodology specific to the work conducted.
See Appendix II for a list of ongoing GAO work related to COVID-19 and Appendix III for the status of matters for congressional consideration and recommendations for executive action made in our June, September, and November 2020 CARES Act reports and in our November 2020 report on vaccines and therapeutics.
We conducted this performance audit from August 2020 to January 15, 2021 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Since November, the number of COVID-19 cases has rapidly increased, further straining the health care system across the country. Between December 31 and January 13, 2021, new reported COVID-19 cases averaged about 225,000 per day—over 7 and 3 times higher than the surges the nation experienced during the spring and summer of 2020, respectively (see fig. 2).[6] During this same two-week time period, reported new COVID-19 cases per day, on average, increased in 45 states and jurisdictions, held steady in 6 , and decreased in 1.[7]
Figure 2: Reported COVID-19 Cases per Day in the United States, through January 13, 2021
Note: Reported COVID-19 cases include confirmed and probable cases. Beginning April 14, 2020, states could include probable as well as confirmed COVID-19 cases in their reports to CDC. Prior to that time, counts only included confirmed cases. According to CDC, the actual number of cases is unknown for a variety of reasons, including that people who have been infected may not have been tested or may have not sought medical care.
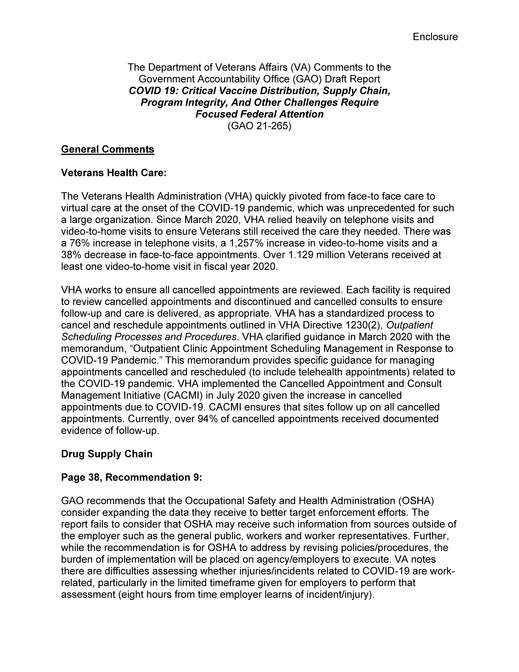
According to data from the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics, about 341,000 more deaths occurred from all causes (COVID-19 and other causes) than would be normally expected from January through mid-December 2020, highlighting the effect of the pandemic on U.S. mortality (see fig. 3).
Figure 3: Higher-Than-Expected Weekly Mortality, January through mid-December 2020
Note: The figure shows the number of deaths from all causes in a given week through December 19, 2020, reported in the U.S. that exceeded the upper bound threshold of expected deaths calculated by CDC’s National Center for Health Statistics on the basis of variation in mortality experienced in prior years. See CDC’s National Center for Health Statistics webpage on excess deaths for further details on how CDC estimates this upper bound threshold: https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm, accessed on January 14, 2021. The number of deaths in recent weeks should be interpreted cautiously as this figure relies on provisional data that are generally less complete.
In December 2020, the Food and Drug Administration (FDA) authorized two vaccines (Pfizer and Moderna) for emergency use in the U.S., which both require two doses administered three to four weeks apart. According to CDC data, more than 30.6 million doses of COVID-19 vaccine had been distributed across the U.S., and about 11.1 million doses of vaccine had been administered as of January 14, 2021 (see fig. 4).[8]
These initial numbers fell short of expectations set by Operation Warp Speed and the Secretary of Health and Human Services for the end of the year. Specifically, an Operation Warp Speed official and the Secretary of the Department of Health and Human Services (HHS) made statements indicating that 40 million doses would be available by the end of 2020, enough to vaccinate about 20 million people.
Figure 4: U.S. COVID-19 Vaccine Distribution and Administration, as of January 14, 2021
Note: According to CDC, doses distributed are cumulative counts of COVID-19 vaccine doses recorded as shipped in CDC’s Vaccine Tracking System since December 13, 2020. Total doses administered are cumulative counts of individual COVID-19 vaccine doses administered as reported to CDC by state, territorial, and local public health agencies and federal entities since December 14, 2020. CDC is requiring health care providers participating in COVID-19 vaccination efforts to report doses to federal, state, territorial, and local agencies up to 72 hours after administration. There may be additional lag for data to be transmitted from the federal, state, territorial, or local agency to CDC. See CDC’s COVID Data Tracker webpage for further details: https://covid.cdc.gov/covid-data-tracker/#vaccinations.
In addition to the public health effects, the pandemic continues to cause economic challenges. For example, based on trends in initial claims for unemployment insurance and surveys of households and businesses conducted by the Bureau of Labor Statistics (BLS), improvements in labor market conditions that were evident during the summer plateaued from October through December 2020. Moreover, both BLS surveys indicate that employment remains substantially below its level before the pandemic.[9] For example, the employment-to-population ratio, based on the BLS survey of households, was flat at 57.4 percent from October through December 2020, and remains 3.7 percentage points below its level in February 2020 (see fig. 5).[10]
Figure 5: Employment Remains below Its Pre-pandemic Level, as of December 2020
In response to the far-reaching public health and economic crisis, Congress has passed, and the President has signed, legislation to fund recovery efforts for COVID-19 (COVID-19 relief laws). Figure 6 shows the COVID-19 relief laws enacted from March 2020 through January 1, 2021.
Figure 6: COVID-19 Relief Laws Enacted, as of January 1, 2021
Note: The selected federal actions included in this figure are examples of the types of COVID-19-related actions taken by the Congress and the administration. The list is not all-inclusive. Additional federal actions, such as the enactment of legislation providing limited and targeted relief to certain individuals and presidential actions authorizing federal support for states and individuals, also occurred during this time frame.aThe Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 provided $7.8 billion to agencies for health emergency prevention, preparedness, and response activities related to COVID-19, with HHS appropriating a majority of the funds. Pub. L. No. 116-123, 134 Stat. 146bThe Families First Coronavirus Response Act provided supplemental appropriations for nutrition assistance programs and public health services and authorized the Internal Revenue Service to provide tax credits for paid emergency sick leave and expanded family medical leave that the act required certain employers to provide. In addition, the act provided states with flexibility to temporarily modify provisions of their unemployment insurance laws and policies related to certain eligibility requirements and provided additional federal financial support to the states. Pub. L. No. 116-127, 134 Stat. 178 (2020).cThe CARES Act provided supplemental appropriations for federal agencies to respond to COVID-19. In addition, it also funded various loans, grants, and other forms of assistance for businesses, industries, states, local governments, and hospitals; provided tax rebates for certain individuals; temporarily expanded unemployment benefits; and suspended payments and interest on federal student loans. Pub. L. No. 116-136, 134 Stat. 281 (2020). dThe Paycheck Protection Program and Health Care Enhancement Act provided additional appropriations for small business loans, grants to health care providers, and COVID-19 testing. Pub. L. No. 116-139, 134 Stat. 620 (2020).eThe Consolidated Appropriations Act, 2021, expanded several CARES Act programs, including appropriating additional funds for targeted advances for the Economic Injury Disaster Loan Program and authorizing additional Paycheck Protection Program loans. Pub. L. No. 116-260, 134 Stat. 1182 (2020). Appropriations warrant information issued by the Department of the Treasury was not available at the time of our analysis. The House Committee on Appropriations estimates that provisions of the Consolidated Appropriations Act, 2021 provide an additional $900 billion in appropriations for emergency coronavirus relief, and the Congressional Budget Office estimates that outlays for coronavirus response and relief provided in divisions M and N of the Act will total about $868 billion. An outlay refers to the issuance of checks, disbursement of cash, or electronic transfer of funds made to liquidate a federal obligation. We will examine and report appropriations enacted in the Consolidated Appropriations Act, 2021 in future reporting.
As of November 30, 2020, about $2.7 trillion had been appropriated to fund response and recovery efforts for—as well as to mitigate the public health, economic, and homeland security effects of—COVID-19.[11] As of November 30, 2020, the most recent date for which government-wide information was available at the time of our analysis, the federal government had obligated a total of $1.9 trillion and expended $1.7 trillion of the COVID-19 relief funds as reported by federal agencies to the Department of the Treasury’s (Treasury) Governmentwide Treasury Account Symbol Adjusted Trial Balance System (GTAS).[12]
The Business Loan Programs, Economic Stabilization and Assistance to Distressed Sectors programs, unemployment insurance, economic impact payments, the Public Health and Social Services Emergency Fund, and the Coronavirus Relief Fund represent $2.3 trillion, or 85 percent, of the total amounts appropriated.[13] For these six largest spending areas, agencies reported obligations totaling $1.5 trillion and expenditures totaling $1.5 trillion as of November 30, 2020. Table 1 provides additional details on appropriations, obligations, and expenditures of government-wide COVID-19 relief funds, including the six largest spending areas.[14]
Table 1: COVID-19 Relief Appropriations, Obligations, and Expenditures, as of November 30, 2020
Major spending area
Total appropriationsa ($ billions)
Total obligationsb ($ billions)
Total expendituresb ($ billions)
Business Loan Programs (Small Business Administration)
687.3
540.1
536.0c
Economic Stabilization and Assistance to Distressed Sectors (Department of the Treasury)
500.0
32.2
19.4c
Unemployment Insurance (Department of Labor)
450.9
393.6
379.6
Economic Impact Payments (Department of the Treasury)
289.3
276.8
276.8
Public Health and Social Services Emergency Fund (Department of Health and Human Services)
231.7
153.5
114.6
Coronavirus Relief Fund (Department of the Treasury)
150.0
150.0
149.5
Other Areas
412.6
311.1
215.5
Totald
2,721.9
1,857.3
1,691.3
Source: GAO analysis of data from the Department of the Treasury and applicable agencies. | GAO-21-265
aCOVID-19 relief appropriations reflect amounts appropriated under the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146; Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); and Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020). These data are based on appropriation warrant information provided by the Department of the Treasury as of November 30, 2020. These amounts have increased over time and could increase in the future for programs with indefinite appropriations, which are appropriations that, at the time of enactment, are for an unspecified amount. In addition, this table does not represent transfers of funds that federal agencies may make between appropriation accounts or transfers of funds they may make to other agencies. bObligation and expenditure data are based on data reported by applicable agencies. cThese expenditures relate mostly to the loan subsidy costs (the loan’s estimated long-term costs to the U.S. government). dThe sum of amounts may not agree due to rounding.
In February 2020, at the outset of the COVID-19 pandemic, we identified key actions that are essential for an effective federal response.[15] Specifically, based on our prior work examining responses to public health emergencies, we emphasized the need for federal agencies to coordinate, establish, and define roles and responsibilities among those responding to the crisis, and provide clear, consistent communication. In our June 2020 bimonthly CARES Act report, we reinforced the importance of these key actions. We also emphasized the need to collect and analyze data to inform decision-making and future preparedness; establish clear goals; establish mechanisms early on for accountability and transparency to help ensure program integrity; and address fraud risks.
In this report, GAO is making 13 recommendations to federal agencies to improve the ongoing federal response and recovery efforts in the areas of public health, the economy, and program integrity. As the new Congress and administration establish their policies and priorities for the federal government’s COVID-19 response, GAO urges swift action on these 13 recommendations, as well as the 27 of the agency’s 31 prior recommendations that have not been implemented from our June, September, and November 2020 CARES Act reports, and our November 2020 report on vaccines and therapeutics. The Consolidated Appropriations Act, 2021—enacted in December of 2020—requires a number of actions that are consistent with several of our prior recommendations, including those related to the medical supply chain, vaccines and therapeutics, COVID-19 testing, and the Paycheck Protection Program.[16]
COVID-19 Vaccines and Therapeutics
Multiple federal agencies continue to support the development, manufacturing, and distribution of vaccines and therapeutics to prevent and treat COVID-19. Through Operation Warp Speed—a partnership between the Department of Defense (DOD) and HHS—the federal government, along with private industry stakeholders, has been working to simultaneously develop and manufacture COVID-19 vaccine and therapeutic candidates at an unusually fast pace, so that they can be distributed as quickly as possible once authorized, licensed, or approved.[17] As of December 31, 2020, DOD and HHS had obligated at least $16.3 billion to develop, manufacture, and distribute vaccines and therapeutics for COVID-19 through Operation Warp Speed.
As of January 8, 2021, FDA had authorized two vaccines for emergency use to prevent COVID-19, and several other candidates were in advanced stages of development.[18] An emergency use authorization (EUA) allows for the temporary use of medical products without FDA approval or licensure, provided certain statutory criteria are met.[19]
On December 11, 2020, FDA authorized Pfizer’s COVID-19 vaccine for emergency use in individuals 16 years and older, becoming the first COVID-19 vaccine to receive an EUA.
On December 18, 2020, FDA issued an EUA for Moderna’s COVID-19 vaccine, authorizing it for emergency use in individuals 18 years and older.
As of January 8, 2021, FDA had approved one therapeutic to treat COVID-19 and made certain others available through EUAs.[20]
Federal agencies have identified several necessary steps for COVID-19 vaccine implementation, including the prioritization, allocation, distribution, and administration of any authorized or licensed COVID-19 vaccine. Several of these steps have been taken to implement the Pfizer and Moderna vaccines. For example, in November 2020, Operation Warp Speed provided jurisdictions and federal entities with allocation amounts for estimated initial doses of the Pfizer and Moderna COVID-19 vaccines, which jurisdictions would receive upon FDA’s issuance of EUAs for these vaccines.[21] In early December 2020, CDC’s Advisory Committee on Immunization Practices made a recommendation for the priority groups to be included in the initial phase of vaccination upon FDA’s issuance of EUAs for COVID-19 vaccines.[22]
We have previously noted that coordination and communication are critical to the successful implementation of COVID-19 vaccines. Given that multiple federal agencies support the development, manufacturing, and distribution of COVID-19 vaccines, timely, clear, and consistent communication to state and local health officials, stakeholders, and the public about vaccine availability, efficacy, and safety is important. Vaccine implementation requires federal leadership and coordination among federal agencies and key partners, including commercial entities, jurisdictions, and providers to allocate, distribute, and ultimately administer vaccines to individuals across the country.
In September 2020, we reported that early understanding of planning efforts—such as key assumptions being made about how vaccines will be implemented—is essential to help ensure that coordination takes place across all levels of government and with other stakeholders and that clear and consistent messages are shared with the public on the safety and efficacy of any available vaccines. To facilitate distribution and administration of any licensed or authorized COVID-19 vaccine, we recommended that the Secretary of Health and Human Services, with support from the Secretary of Defense, establish a time frame for documenting and sharing a national plan for distributing and administering COVID-19 vaccines and, among other things, outline an approach for how efforts would be coordinated across federal agencies and nonfederal entities. HHS neither agreed nor disagreed with our recommendation. In November 2020, we reported that HHS and DOD had released initial planning documents for the distribution and administration of COVID-19 vaccines, but stakeholders said they would like to see additional information. For more information on the status of this recommendation see Appendix III.
CDC officials reported that the agency has developed communication resources for the general public, health care providers, health systems, and jurisdictions. For example, CDC has posted training and education materials on its website to help health professionals prepare for COVID-19 vaccination, including information on how to talk to patients about COVID-19 vaccines and make a strong recommendation for COVID-19 vaccination and a COVID-19 vaccination communication toolkit for medical centers, clinics, and clinicians.[23]
Although Operation Warp Speed has distributed COVID-19 vaccines and administration of these vaccines has begun, continued federal planning, leadership, and coordination remain vitally important as initial vaccine rollout has not matched expectations. Initial numbers of distributed and administered COVID-19 vaccines fell short of expectations set by officials, further underscoring the need for careful distribution and administration planning and clear and consistent communication by the federal government in concert with key partners.
We continue to reiterate the importance of our recommendation that HHS, with support from DOD, establish a time frame for documenting and sharing a national plan for distributing and administering COVID-19 vaccines and, among other things, outline an approach for how efforts would be coordinated across federal agencies and nonfederal entities. In finalizing its distribution and administration plans, it will be important for HHS to define the specific roles and responsibilities for the various federal and nonfederal entities involved and include plans for public messaging to help ensure vaccine confidence.
Consistent with our recommendation, the Consolidated Appropriations Act, 2021 requires the CDC Director to provide Congress with an updated and comprehensive COVID-19 vaccine distribution strategy and spend plan within 30 days of enactment (by January 26, 2021).[24] This strategy is to include, among other things, guidance for how jurisdictions and other nonfederal entities should prepare for, store, and administer vaccines; nationwide vaccination targets; and a description of how an informational campaign for the public and health care providers will be executed. We will assess CDC’s strategy and spend plan when they are available and continue to monitor any other federal plans to determine whether such plans address our recommendation.
We are conducting additional work related to COVID-19 vaccines and therapeutics, including federal efforts under Operation Warp Speed, plans for COVID-19 vaccine implementation, and communication to the public about vaccine implementation. See the Vaccines and Therapeutics enclosure in appendix I for more information.
Medical Supply Chain
In September and November 2020, we highlighted medical supply chain issues, including shortages of medical supplies such as personal protective equipment needed to respond to the COVID-19 pandemic.[25] In particular, based on our October 2020 nationwide survey of state health and emergency management offices, we found that states and territories continue to report limitations in the availability of certain medical supplies, such as nitrile gloves and reagents used for COVID-19 testing.
We also reported on steps HHS, in conjunction with federal partners, had taken to replenish and expand the inventory of the Strategic National Stockpile (SNS), an important federal component of the medical supply chain, for the current pandemic. These plans included efforts to build a 90-day supply of certain key items in the SNS to enable HHS to respond to a potential resurgence of COVID-19.
Since November, we have focused on HHS efforts to develop a national supply strategy that, according to Office of the Assistant Secretary for Preparedness and Response officials, outlines the capabilities that HHS must acquire—including, but not limited to, the capacity to quickly resupply the SNS—to address the challenges identified by the pandemic.[26] This strategy is focused on improving the government’s future pandemic response capabilities by enhancing and improving coordination among multiple aspects of the supply chain.
HHS worked with a number of federal agencies to develop the supply chain strategy. However, HHS has yet to establish a process for engaging with key non-federal stakeholders about the strategy, such as state and territorial governments and the private sector which have a shared responsibility for providing supplies during a pandemic. Such a process is important to ensuring that HHS identifies and rectifies issues early on, builds a system that meets the needs of all levels of government, and enhances overall communication. Additionally, consulting with Congress and other stakeholders can help harness ideas, expertise, and resources as HHS develops reforms.
To improve the nation’s response to and preparedness for pandemics, we are recommending that HHS establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as the agency refines and implements its supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile. HHS generally concurred with our recommendation while noting that the term “engage” is vague and unclear, and said that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority. We believe that capitalizing on existing relationships to engage these critical stakeholders as HHS refines and implements a supply chain strategy, to include the role of the SNS, will improve a whole-of-government response to, and preparedness for, pandemics. See the Strategic National Stockpile and the Medical Supply Chain enclosure in appendix I for more information.
The COVID-19 pandemic has called greater attention to the U.S.’s reliance on foreign manufacturing for many marketed drugs. The federal government has taken steps intended to strengthen domestic drug manufacturing and create resilient domestic supply chains. As part of these efforts, in August 2020, the President issued an Executive Order directing federal agencies to take steps toward strengthening domestic drug manufacturing and supply chains.[27]
Federal agencies have started implementing the Executive Order, but expressed concerns about their ability to implement certain provisions. In particular, federal agencies do not have complete and accessible information to identify supply chain vulnerabilities and to report the manufacturing sources of drugs and drug components that they procured, as directed by the Executive Order. As a result, federal efforts to identify and mitigate supply chain vulnerabilities and effectively respond to public health emergencies, such as COVID-19, will remain a challenge.
Although FDA must weigh the benefits of collecting more complete information with the additional burden to manufacturers and the agency, FDA is uniquely positioned to work with its partners to identify ways that it and other federal agencies can obtain manufacturing supply chain information for drugs and their components. Additionally, the Executive Order directs FDA to consider making changes to its collection of manufacturing information and enter into written agreements with other agencies to share information. To help identify and mitigate supply chain vulnerabilities, we are recommending that FDA ensure the information obtained is complete and accessible, including by working with manufacturers and other federal agencies, such as DOD and the Department of Veterans Affairs, and, if necessary, seek authority to obtain complete and accessible information. HHS neither agreed nor disagreed with our recommendation. In HHS’s response, FDA said that as the agency continues efforts to enhance relevant authorities and close data gaps, it will consider GAO’s recommendation. See the Drug Supply Chain enclosure in appendix I for more information.
We previously made three recommendations to address medical supply shortages, all of which remain open (see table 2). We remain deeply troubled that agencies have not acted on our recommendations to more fully address critical gaps in the medical supply chain. While we recognize federal agencies continue to take some steps, we underscore the importance of developing a well-formulated plan to address critical gaps for the remainder of the pandemic, especially in light of the recent surge in cases.
We continue to underscore the critical imperative of implementing these recommendations.
Table 2: Prior GAO Recommendations Related to the Medical Supply Chain
Topic
Recommendation
Status
Medical Supply Chain
In September 2020, we recommended that (1) the Department of Health and Human Services (HHS), in coordination with the Federal Emergency Management Agency (FEMA), document roles and responsibilities for supply chain management functions; (2) HHS further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic; and (3) HHS, in coordination with FEMA, help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the pandemic response. (GAO-20-701)
HHS and the Department of Homeland Security (DHS) disagreed with our recommendations. HHS noted work that the department had done to manage the medical supply chain and increase supply availability, among other things. We maintain that greater action is necessary to address our recommendations, particularly in light of the recent surge in COVID-19 cases.
Related to our recommendation, the Consolidated Appropriations Act, 2021, requires the President to make publicly available a report containing a whole-of-government plan for effective response to subsequent COVID-19 outbreaks and for future global pandemic diseases. The act stipulates that this pandemic plan should address how to improve the role of the federal government with respect to the regulation, acquisition, and disbursement of medical supplies necessary to respond to COVID-19, among other things.
Diagnostic testing for COVID-19 is critical to controlling the spread of the virus, according to CDC. Over the course of the pandemic, the types and volume of available viral diagnostic tests have increased as new testing technologies have emerged.[28] HHS leads the development and implementation of the national COVID-19 testing strategy, whereby states manage their own COVID-19 testing programs with federal support.
HHS has periodically sent to Congress COVID-19 testing strategy implementation plans that outline federal and state testing efforts. However, these plans have not been publicly available, limiting the effectiveness of HHS's communication efforts to stakeholders on testing. In addition, HHS testing strategy documents—individually and collectively—do not fully address the characteristics of effective national strategies that we have found desirable in our prior work.[29] For example, testing strategy documents do not always provide consistent definitions and benchmarks to measure progress, not all documents clearly define the problem and risks, and there is limited information on the types of resources required for future needs. As a result, there is a risk that key stakeholders and the public lack crucial information to support an informed and coordinated testing response.
The Consolidated Appropriations Act, 2021 requires the President to make publicly available a report containing a whole-of-government plan for an effective response to subsequent major outbreaks of COVID-19.[30] This plan, which is required to be completed by late March 2021, is also required to address how to improve diagnostic testing and contact tracing, among other things. In addition, we are recommending that HHS develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that HHS has produced for the public and Congress to allow for a more coordinated pandemic testing approach.
HHS partially concurred with our recommendation and agreed that it should take steps to more directly incorporate some of the elements of an effective national strategy, but expressed concern that producing such a strategy at this time could be overly burdensome on the federal, state, and local entities that are responding to the pandemic, and that a plan would be outdated by the time it was finalized or potentially rendered obsolete by the rate of technological advancement. We maintain that documenting a comprehensive and public national strategy is important so that all participants have the necessary information to accomplish shared goals. Further, a national strategy can be done efficiently and flexibly, without imposing unnecessary burden. See the COVID-19 Testing enclosure in appendix I for more information.
We previously recommended that CDC clearly disclose the scientific rationale for any change to testing guidelines at the time the change is made to improve the transparency of the government’s testing guidance. See table 3 for the status of this recommendation.
Table 3: Prior GAO Recommendation Related to COVID-19 Testing
Topic
Recommendation
Status
Testing Guidance
In November 2020, we recommended that the Centers for Disease Control and Prevention (CDC) clearly disclose the scientific rationale for any change to testing guidelines at the time the change is made. (GAO-21-191)
The Department of Health and Human Services (HHS) concurred with our recommendation, noting that CDC officials typically consult with scientific stakeholders when issuing guidance and that HHS will continue to evaluate its processes in this area. Although CDC stated that they continue outreach to scientific experts when considering scientific recommendations, they have not yet demonstrated that processes are in place for explaining scientific rationale for changes to testing guidelines.
FDA is responsible for overseeing the safety and effectiveness of all drugs marketed in the U.S., including those manufactured overseas, and typically conducts more than 1,600 inspections of foreign and domestic drug manufacturing establishments each year. In light of the COVID-19 pandemic, since March 2020, FDA has limited domestic and foreign inspections for the safety of its employees.
FDA has used alternative inspection tools to maintain some oversight of drug manufacturing quality while inspections are paused, such as reviewing foreign regulator reports. However, these tools are not equivalent to an FDA inspection in all cases. In addition, with one exception, FDA has not yet fully assessed how these tools or others can be used to supplement its regular inspection activities in the future, or as long-term substitutes for an FDA inspection.
Without regular inspections or alternative tools to fully assess whether a drug manufacturing establishment is in compliance with quality standards, FDA could be faced with a backlog of inspections, threatening the agency’s goal of shifting toward exclusively risk-driven surveillance inspections. This creates the risk that FDA may not inspect establishments that it has identified as the highest priority. We are recommending that FDA (1) ensure that inspection plans for future fiscal years identify, analyze, and respond to the issues presented by the backlog of inspections that could jeopardize its goal of risk-driven inspections, and (2) fully assess the agency’s alternative inspection tools and consider whether these tools or others could provide the information needed to supplement the agency’s regular inspection activities or help meet its drug oversight objectives when inspections are not possible in the future. FDA concurred with both of our recommendations and stated that as it pursues continued process improvements, the agency will incorporate both recommendations in its ongoing assessment of these alternative inspection tools. See the Drug Manufacturing Inspections enclosure in appendix I for more information.
COVID-19 Data for Health Care Indicators
The rapid spread and magnitude of the COVID-19 pandemic have underscored the importance of having quality data to help the federal government understand the effects of the disease in the U.S., inform its allocation of resources, and help it make timely and responsive decisions related to public health and safety. Since June 2020, we have identified concerns related to COVID-19 data that inform health care indicators.
Specifically, the federal government does not have a process to help systematically define and ensure the collection of standardized data across the relevant federal agencies and related stakeholders to help respond to COVID-19, communicate the status of the pandemic with citizens, or prepare for future pandemics. As a result, COVID-19 information that is collected and reported by states and other entities to the federal government is often incomplete and inconsistent. For example, we have identified through our prior and current work on COVID-19 examples of specific indicators for which these data are inconsistent or incomplete, including COVID-19 testing and cases and hospital capacity measures.
The lack of complete and consistent data limits HHS’s and others’ ability to monitor trends in the burden of the pandemic across states and regions, such as COVID-19 cases and hospitalizations; make informed comparisons between such areas; and assess the impact of public health actions to prevent and mitigate the spread of COVID-19. Additionally, incomplete and inconsistent data have limited HHS’s and others’ ability to prioritize the allocation of health resources in specific geographic areas or among certain populations most affected by the pandemic.
To improve the federal government’s response to COVID-19 and preparedness for future pandemics, we are recommending that HHS immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. This committee should include a broad representation of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits. HHS partially concurred with our recommendation and agreed that it should establish a dedicated working group or other mechanism with a focus on addressing COVID-19 data collection shortcomings. However, HHS said because of resource constraints and the ongoing response to the pandemic, it could not commit to immediately doing so. Given the current state of the COVID-19 pandemic and the expanded need for complete and consistent data to assist the federal response and to inform the general public (including data on vaccines), we reiterate the importance of immediately establishing an expert committee. See the Health Care Indicators enclosure in appendix I for more information.
We previously made five recommendations to federal agencies to improve the collection of COVID-19 data, all of which remain open (see table 4).
Table 4: Prior GAO Recommendations Related to COVID-19 Data
Topic
Recommendation
Status
Health Disparities
In September 2020, we recommended that the Centers for Disease Control and Prevention (CDC) (1) evaluate whether the authority to require the reporting of race and ethnicity information for COVID-19 data is necessary for ensuring more complete data and, if so, seek authority from Congress to do so, (2) involve key stakeholders to ensure the complete and consistent collection of demographic data, and (3) ensure its ability to assess the long-term health outcomes of persons with COVID-19, including by race and ethnicity. (GAO-20-701)
CDC agreed with our recommendations. CDC stated the agency is working with stakeholders to accelerate the reporting of demographic data and improve data quality. The agency is also developing a plan to monitor the long-term health outcomes of persons with COVID-19 by identifying health care surveillance systems that can electronically report health conditions to state and local health departments. As of December 2020, CDC stated it has various efforts underway such as establishing studies with external partners to assess long-term health outcomes. In addition, CDC stated the agency is analyzing electronic health record data to describe health outcomes after COVID-19 diagnosis as well as analyzing race and ethnicity in any data collected for long-term health effects.
Nursing Homes
In September 2020, we recommended that the Department of Health and Human Services (HHS), in consultation with the Centers for Medicare & Medicaid Services (CMS) and CDC, develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes, and clarify the extent to which nursing homes have reported prior data. (GAO-20-701)
HHS partially agreed with our recommendation. As of October 23, 2020, no specific action had been taken by HHS, although it continues to consider how to implement this recommendation.
State Veterans Homes
In November 2020, we recommended that the Department of Veterans Affairs (VA) collect timely data on COVID-19 cases and deaths in state veterans homes, which provide nursing home care to more than 20,000 veterans in over 150 facilities. (GAO-21-191)
VA concurred in principle with our recommendation.
Consistent with our recommendation, in January 2021, Congress passed and the President signed into law the Johnny Isakson and David P. Roe, M.D. Veterans Health Care and Benefits Improvement Act of 2020, which requires state veterans homes during a covered public health emergency to submit weekly to VA data on the number of (1) suspected and confirmed COVID-19 infections and (2) total deaths and COVID-19 deaths among residents and staff. In addition, the act requires VA to make these data on the total number of residents and staff who are infected with or have died from COVID-19 publically available on its website and to update these data at least weekly.
We will monitor VA’s efforts to implement this requirement.
Agencies are using other transaction agreements to respond to the COVID-19 pandemic, which can enable agencies to negotiate terms and conditions specific to a project.[31] Our analysis found that HHS misreports its other transaction agreements related to COVID-19 as procurement contracts in the federal procurement database system, including other transaction agreements with about $1.5 billion obligated for Operation Warp Speed and other medical countermeasures. HHS’s approach is inconsistent with federal acquisition regulations and limits the public’s insight into the agency’s contract spending.
To ensure consistent tracking and transparency of federal contracting activity related to the pandemic, we are recommending that HHS accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts. HHS concurred with our recommendation and stated that it has taken steps to manually identify its other transaction agreements in its contract writing system to allow the public to distinguish between spending on agreements and procurement contracts. See the Federal Contracts and Agreements for COVID-19 enclosure in appendix I for more information. We previously made recommendations to the Department of Homeland Security and DOD concerning federal contracting, both of which remain open (see table 5).
Table 5: Prior GAO Recommendations Related to Federal Contracting
Topic
Recommendation
Status
Federal Contracting
In September 2020, we recommended that the Department of Homeland Security (DHS) and the Department of Defense (DOD) revise the National Interest Action (NIA) code memorandum of agreement to (1) obtain input from key federal agencies prior to extending or closing an NIA code, (2) establish timelines for evaluating NIA code extensions, and (3) ensure that the criteria for extending or closing the NIA code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic. (GAO-20-701)
DHS and DOD disagreed with our recommendations. However, as of January 2021, DHS and DOD had met to discuss potential revisions to the 2019 NIA code memorandum of agreement. DHS and DOD are in the process of updating the agreement to clarify the steps they take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close an NIA code. When finalized, we will review the updated agreement to determine whether it meets the intent of our recommendation.
In this report, we identify new concerns about federal oversight of worker safety and health amid the COVID-19 pandemic. Specifically, the Occupational Safety and Health Administration (OSHA) has adapted its enforcement methods for COVID-19 to help protect agency employees from the virus and address resource constraints, such as by permitting remote inspections in place of on-site inspections of workplaces. However, OSHA’s oversight and tracking of its adapted enforcement methods contain gaps. For example, the agency lacks plans to implement its oversight and is not tracking certain data related to its adapted enforcement methods. These gaps prevent OSHA from assessing the effectiveness of its enforcement methods during the pandemic, ensuring that these methods do not miss violations, and ensuring that employers are addressing certain identified violations.
To improve its oversight, we are recommending that OSHA (1) develop a plan, with time frames, to implement the agency’s oversight processes for COVID-19-adapted enforcement methods, and (2) ensure that its data system includes comprehensive information on use of these enforcement methods to inform these processes.
Additionally, OSHA’s data do not include comprehensive information on workplace exposure to COVID-19. For example, OSHA does not receive employer reports of all work-related hospitalizations related to COVID-19, as disease symptoms do not appear within the required reporting time frames. Employers may also face challenges determining whether COVID-19 hospitalizations or fatalities are work-related because of COVID-19’s incubation period and the difficulties in tracking the source of exposure.
We are recommending that OSHA determine what additional data may be needed from employers or other sources to better target the agency’s COVID-19 enforcement efforts. The agency neither agreed nor disagreed with our three recommendations. To improve federal efforts to ensure workplace safety and health amid the COVID-19 pandemic, we maintain the importance of developing a plan for oversight, ensuring the data system includes comprehensive information, and determining what additional data may be needed. See the Worker Safety and Health enclosure in appendix I for more information.
Assistance for Fishery Participants
The CARES Act appropriated $300 million in March 2020 to the Department of Commerce (Commerce) to assist eligible tribal, subsistence, commercial, and charter fishery participants affected by COVID-19, which may include direct relief payments.[32] After $2 million in administrative fees were assessed by Commerce’s National Oceanic and Atmospheric Administration (NOAA), $298 million of the $300 million appropriated was obligated for fishery participants. Widespread restaurant closures in the spring of 2020 led to a decrease in demand for seafood, adversely affecting the fisheries industry.
As of December 4, 2020, all funds had been obligated and only about 18 percent ($53.9 million) of the CARES Act funding obligated for fishery participants had been disbursed, which is inconsistent with distributing CARES Act funds in an expedient manner as outlined in Office of Management and Budget guidance.[33] Commerce’s NOAA expects that the vast majority of funds will be disbursed to fisheries participants by early 2021. However, the agency does not have the needed information centralized to help ensure that funds are being disbursed expeditiously and efficiently. We are recommending that NOAA develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner. NOAA concurred with our recommendation. See the Assistance for Fishery Participants enclosure in appendix I for more information.
Program Integrity
We continue to identify areas to improve program integrity and to reduce the risk of improper payments for programs funded by the COVID-19 relief laws which provided $2.7 trillion in appropriations for response and recovery efforts through November 2020. Federal relief programs remain vulnerable to significant risk of fraudulent activities because of the need to quickly provide funds and other assistance to those affected by COVID-19 and its economic effects. The Consolidated Appropriations Act, 2021—enacted in December 2020—includes an expansion of the Small Business Administration’s (SBA) Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program, highlighting the continued need for ensuring program integrity.[34]
Since March 2020, the Department of Justice has publicly announced charges in numerous fraud-related cases across the country, including charges of identity theft, wire and bank fraud, and money laundering. See the Fraud Risks and Federal Response enclosure in appendix I for more information.
Twenty-three individuals have pleaded guilty to federal charges of defrauding COVID-19 relief programs—including SBA’s PPP and EIDL program and the Department of Labor’s (DOL) unemployment insurance (UI) program—from March through November 2020.[35]
Federal charges are pending against 197 individuals for attempting to defraud these programs.[36] Also, one individual pleaded guilty to identity theft in connection with economic impact payments and federal charges are pending against four individuals.
From March 13, 2020, through November 30, 2020, our hotline—known as FraudNet—received over an estimated 1,000 complaints related to the CARES Act, many of which involved SBA’s PPP and EIDL program.
From March through October 2020, 5,344 financial institutions filed 118,625 suspicious activity reports associated with CARES Act programs with the Financial Crimes Enforcement Network under the Bank Secrecy Act.[37] These suspicious activity reports totaled nearly $141 billion in potentially suspicious financial transactions.
An effective federal response to COVID-19 fraud risks should help ensure that federal programs fulfill their intended purpose, funds are spent effectively, and assets are safeguarded. In this report, we identify additional federal programs and efforts where further action is needed to ensure program integrity and reduce the risk of improper payments.
Specifically, we have concerns about overpayments and potential fraud in the UI system, including the federally funded Pandemic Unemployment Assistance (PUA) program, which provides UI benefits to individuals not otherwise eligible for these benefits, such as self-employed and certain gig economy workers.[38] As certain CARES Act UI programs were extended into 2021, the UI system continued to experience high numbers of claims as a result of the COVID-19 pandemic and we remain concerned about overpayments and potential fraud in the UI system. As of January 11, 2021, states that had submitted data to DOL reported more than $1.1 billion in PUA overpayments from March through December 2020. While DOL requires states to report data on PUA overpayments, as of the beginning of 2021, the agency was not tracking the amount of overpayments recovered, limiting insight into states’ efforts to recover federal funds.[39]
To better track the recovery of these funds, we are recommending that DOL collect data from states on the amount of PUA overpayments recovered. DOL agreed with our recommendation and on January 8, 2021, took the first step toward implementing it by issuing new guidance and updated instructions for states to report data on the amount of PUA overpayments recovered. See the Unemployment Insurance Programs enclosure in appendix I for more information.
We also remain concerned about SBA’s management of internal controls and fraud risks in the EIDL program. COVID-19 relief laws made qualifying small businesses and nonprofit organizations adversely affected by COVID-19 eligible for financial assistance from the EIDL program.[40] Some approval requirements were also relaxed, such as requiring each applicant to demonstrate that it could not obtain credit elsewhere. The Consolidated Appropriations Act, 2021 extended the deadline to apply for EIDL loans under the relaxed requirements of the CARES Act from December 31, 2020, to December 31, 2021.[41] However, the act removed the CARES Act provision that prohibited SBA from requiring tax records as part of its eligibility determination. As of December 31, 2020, SBA officials said the agency had approved about 3.7 million loans related to COVID-19, totaling about $200 billion.
SBA rapidly processed loans and advances to millions of small businesses affected by COVID-19. However, our work, as well as that of SBA’s Office of Inspector General and the Department of Justice, indicate potential gaps in SBA’s internal controls may have led to fraud and the provision of EIDL funding to ineligible entities. As we reported in September and October 2020, SBA’s efforts to expedite loan processing may have also contributed to increased fraud risk within the program. For example, between May and October 2020, over 900 U.S. financial institutions filed more than 20,000 suspicious activity reports related to the EIDL program with the Financial Crimes Enforcement Network. In addition, our analysis of SBA data shows that the agency approved EIDL loans and advances for potentially ineligible businesses, including at least 3,000 loans totaling about $156 million to businesses, such as insurance and real estate development businesses, as of September 30, 2020.
Our Fraud Risk Framework cites data analytics as a leading practice in developing specific control activities to prevent and detect fraud—in particular, to mitigate the likelihood and impact of fraud. SBA has not provided evidence that it has conducted portfolio-level data analytics, which could detect potentially ineligible and fraudulent funding to recipients. We are recommending that SBA develop and implement portfolio-level data analytics across EIDL loans and advances made in response to COVID-19. SBA neither agreed nor disagreed with our recommendation, but took issue with our finding that potentially ineligible businesses received EIDL advances and loans, noting actions it is taking to prevent such payments. However, we maintain our recommendation, as SBA has not provided information we have requested on actions it and its contractors take to prevent payments to ineligible businesses. See the Economic Injury Disaster Loan Program enclosure in appendix I for more information.
We previously made seven recommendations to federal agencies and two matters for congressional consideration to identify and respond to risks in key COVID-19 relief programs and reduce improper payments. Recommendations and matters that remain open are listed below (see table 6). Slow implementation of our recommendations related to program integrity to date creates the risk of considerable improper payments, including fraud, and falls far short of transparency and accountability expectations. We again call attention to these critical areas.
Table 6: Prior GAO Matters and Recommendations Related to Program Integrity
Topic
Recommendation or matter for congressional consideration
Status
Economic Impact Payments (EIP)
In June 2020, we urged Congress to amend the Social Security Act to explicitly allow the Social Security Administration (SSA) to share its full death data with the Department of the Treasury (Treasury) for data matching to prevent payments to ineligible individuals.
We also recommended that the Internal Revenue Service (IRS) consider cost-effective options for notifying ineligible recipients on how to return EIPs. (GAO-20-625)
In September 2020, we recommended that Treasury, in coordination with IRS, (1) update and refine estimates of eligible recipients who have yet to file for an EIP and share this information with outreach partners to aid in outreach and communications efforts and (2) make estimates of eligible recipients who have yet to file for an EIP, and other relevant information, available to outreach partners to raise awareness about how and when to file for EIPs. (GAO-20-701)
In November 2020, we recommended that Treasury, in coordination with IRS, begin tracking and publicly reporting the number of individuals who were mailed an EIP notification letter and subsequently filed for and received an EIP, and use that information to inform ongoing outreach and communications efforts. (GAO-21-191)
In December 2020, Congress passed and the President signed into law the Consolidated Appropriations Act, 2021, which requires SSA, to the extent feasible, to share its full death data with Treasury’s Do Not Pay working system for a 3-year period, effective on the date that is 3 years from enactment of this act. Sharing these data will allow agencies to enhance their efforts to identify and prevent improper payments to deceased individuals. Therefore, it will be important for SSA and Treasury to work together, and we will continue to monitor the agencies’ actions to implement this legislation.
IRS agreed with our June 2020 recommendation. Treasury and IRS neither agreed nor disagreed with our September 2020 recommendations, and Treasury agreed with our November 2020 recommendation. Treasury and IRS have taken several actions consistent with our recommendations. Specifically:
IRS provided instructions on its website for individuals to voluntarily return by mail the appropriate EIP amount sent to a decedent.
Treasury and IRS have used tax return information to identify individuals that may be eligible for an EIP and IRS sent a notice to around 9 million individuals who had not received an EIP.
As of December 31, 2020, Treasury and IRS had disbursed 168.2 million payments to individuals, totaling $275.9 billion. According to IRS data, more than 27.7 million non-filers received a payment, including 21.2 million who received an automatic payment and just under 6.5 million non-filers who used the online tool to receive an EIP.
Paycheck Protection Program (PPP)
In June 2020, we recommended that the Small Business Administration (SBA) develop and implement plans to identify and respond to risks in the PPP to ensure program integrity, achieve program effectiveness, and address potential fraud. (GAO-20-625)
In November 2020, we recommended that SBA expeditiously estimate improper payments and report estimates and error rates for the PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread. (GAO-21-191)
SBA neither agreed nor disagreed with our June 2020 recommendation. The agency told us it has completed oversight plans for PPP and provided a draft plan, but it has not yet finalized detailed policies and procedures for some of its plans.
SBA neither agreed nor disagreed with our November 2020 recommendation. SBA stated that it is planning to conduct improper payment testing for the Paycheck Protection Program but it has not finalized the plan for estimating improper payments.
Related to our recommendations, the Consolidated Appropriations Act, 2021, requires SBA to submit to the Senate and House Small Business Committees an audit plan that details the policies and procedures for conducting forgiveness reviews and audits of PPP loans within 45 days of enactment and to provide monthly updates thereafter. We will monitor the extent to which the SBA audit plan implemented in response to this reporting requirement addresses our prior recommendations.
Payroll Support Program (PSP)
In November 2020, we recommended that Treasury finish developing and implement a compliance monitoring plan that identifies and responds to risks in the PSP, which provides payroll support payments and loans to help the aviation industry retain its employees. (GAO-21-191)
Treasury neither agreed nor disagreed with our recommendation.
Improper Payments Government-wide
In November 2020, we suggested that Congress consider, in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments.”
We also recommended that the Office of Management and Budget (OMB) develop and issue guidance directing agencies to include COVID-19 relief funding with associated key risks, such as provisions contained in the CARES Act and other relief legislation that potentially increase the risk of improper payments, as part of their improper payment estimation methodologies. (GAO-21-191)
No new legislation designating executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” has been enacted to date.
In January 2021, OMB staff stated that they believe current OMB guidance sufficiently addresses our recommendation and concerns. Additionally, OMB staff stated that OMB is actively coordinating and engaging with the Pandemic Response Accountability Committee and Inspectors General to share and discuss information relevant to COVID-19 spending risks and improper payment reduction strategies. We do not agree that current OMB guidance sufficiently addressed our recommendation and concerns.
Additionally, while coordination with the Inspectors General is important, federal agencies ultimately maintain the primary responsibility for payment integrity efforts. Therefore, we continue to maintain that without OMB guidance for agencies to include COVID-19 relief funding and associated key risks as part of their improper payment estimation methodologies, agencies are at increased risk that their processes may not result in reliable estimates, calling into question their usefulness for developing effective corrective actions.
Additional Matters for Congress and Agency Recommendations
Beyond the areas discussed above, we previously made recommendations and matters for congressional consideration in other areas throughout the federal government in our prior CARES Act reports on the federal response to COVID-19. Recommendations and matters that remain open are listed below (see table 7).
Table 7: Prior GAO Matters and Recommendations Related to the COVID-19 Response
Topic
Recommendation or matters for congressional consideration
Status
Aviation Preparedness
In June 2020, we urged Congress to take legislative action to require the Department of Transportation (DOT) to work with relevant agencies and stakeholders, such as the Department of Health and Human Services (HHS), the Department of Homeland Security (DHS), members of the aviation and public health sectors, and international organizations, to develop a national aviation-preparedness plan. (GAO-20-625)
In 2020, the House of Representatives and Senate separately introduced or passed legislation related to aviation preparedness. For example, in May 2020, the House of Representatives passed H.R. 6800, referred to as the HEROES Act, which, if enacted, would require DOT, in coordination with HHS, DHS, and other appropriate federal departments and agencies, to develop a national aviation preparedness plan.
Medicaid Funding
In June 2020, we urged Congress to use GAO’s Federal Medical Assistance Percentage formula to determine the timing and increase in Federal Medical Assistance Percentage—which determines the amount of federal Medicaid funding provided to states—for any future changes to the current or any future economic downturn. (GAO-20-625)
No congressional action has been taken to date.
Nursing Homes
In November 2020, we recommended that the Centers for Medicare & Medicaid Services (CMS) quickly develop a plan that further details how it intends to respond to and implement, as appropriate, the recommendations of the Coronavirus Commission on Safety and Quality in Nursing Homes. (GAO-21-191)
HHS neither agreed nor disagreed with our recommendation, and said it would refer to and act upon the Commission’s recommendations, as appropriate.
State Veterans Homes
In November 2020, we recommended that the Department of Veterans Affairs (VA) develop a plan to ensure inspections of state veterans homes occur during the pandemic, which may include using in-person, a mix of virtual and in-person, or fully virtual inspections. (GAO-21-191)
VA agreed with our recommendation, and plans to address it by November 2021. We urge VA to move up its targeted completion date, because it cannot ensure the quality of nursing home care provided to veterans in these facilities until it develops a plan to resume these inspections (virtually, in person, or both). Without these inspections, veterans are at risk of receiving poor quality care.
K-12 School Guidance
In September 2020, we recommended that the Centers for Disease Control and Prevention (CDC) ensure that, as it makes updates to its federal guidance related to reassessing schools' operating status, the guidance is cogent, clear, and internally consistent. (GAO-20-701)
CDC agreed with our recommendation. CDC has made progress, but this recommendation remains open as of January 6, 2021, because the guidance remains inconsistent and unclear in places.
Cybersecurity
In September 2020, we recommended that HHS expedite implementation of our prior recommendations regarding cybersecurity weaknesses at its component agencies, based on imminent cybersecurity threats. (GAO-20-701)
HHS agreed with our recommendation. Since September 2020, the Food and Drug Administration, CMS, and CDC have implemented an additional 54 cybersecurity recommendations. This brings the total number of implemented cybersecurity recommendations to 404 (of 434)—a 12 percent increase of corrective actions taken to bolster cybersecurity at these agencies.
Tax Relief for Businesses
In November 2020, we recommended that the Internal Revenue Service (IRS) update its form instructions to include information on its new electronic filing capability to help taxpayers take advantage of tax provisions included in the CARES Act more effectively. (GAO-21-191)
IRS agreed with our recommendation. As of early December 2020, IRS planned to revise the form instructions by mid-2021—after the deadline for taxpayers to submit a tentative refund application. As a result, taxpayers filing forms before the December 31, 2020, deadline will not find the e-file capability in their form instructions. A timelier update would help taxpayers who file the form before the planned revisions in mid-2021.
Unemployment Insurance
In November 2020, we recommended that the Department of Labor (DOL) pursue options to report the actual number of distinct individuals claiming these benefits starting from January 2020 onward. (GAO-21-191)
DOL partially agreed with our recommendation. DOL did not agree with the retroactive effective date of the reporting.
With the issuance of this report, we have now made 44 recommendations to federal agencies and four matters for congressional consideration to improve the federal response to COVID-19. These recommendations are tailored to specific federal programs and initiatives, and, if implemented, will strengthen the efficiency, effectiveness, and accountability of these federal efforts. In addition to swiftly addressing the open recommendations, we urge the new Congress and administration to consider the principles of an effective federal response that we have previously outlined—clearly defining roles and responsibilities, providing clear and consistent communication, establishing early on accountability and transparency mechanisms, and collecting and analyzing data to drive decisions. Incorporating these principles into ongoing or new COVID-19-related programs and policies will improve the effectiveness of the federal government’s response.
We are sending copies of this report to the appropriate congressional committees, the Office of Management and Budget, and other relevant agencies. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at (202) 512-5500 or dodarog@gao.gov. Questions can also be directed to Kate Siggerud, Chief Operating Officer, at (202) 512-5600; A. Nicole Clowers, Managing Director, Health Care, at (202) 512-7114 or clowersa@gao.gov; or Orice Williams Brown, Managing Director, Congressional Relations, at (202) 512-4400 or williamso@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report.
Gene L. Dodaro Comptroller General of the United States
Congressional Addressees
Chair Vice Chair Committee on Appropriations United States Senate
Chair Ranking Member Committee on Finance United States Senate
Chair Ranking Member Committee on Health, Education, Labor, and Pensions United States Senate
Chair Ranking Member Committee on Homeland Security and Governmental Affairs United States Senate
The Honorable Rosa L. DeLauro Chairwoman The Honorable Kay Granger Ranking Member Committee on Appropriations House of Representatives
The Honorable Frank Pallone, Jr. Chair The Honorable Cathy McMorris Rodgers Republican Leader Committee on Energy and Commerce House of Representatives
The Honorable Bennie G. Thompson Chair The Honorable John Katko Ranking Member Committee on Homeland Security House of Representatives
The Honorable Carolyn B. Maloney Chairwoman The Honorable James Comer Ranking Member Committee on Oversight and Reform House of Representatives
The Honorable Richard Neal Chair The Honorable Kevin Brady Republican Leader Committee on Ways and Means House of Representatives
The federal government does not have a process to help systematically define and ensure the collection of standardized data across the relevant federal agencies and related stakeholders to help respond to COVID-19, communicate the status of the pandemic with citizens, or prepare for future pandemics. As a result, COVID-19 information that is collected and reported by states and other entities to the federal government is often incomplete and inconsistent.
Entity involved: Department of Health and Human Services
Recommendation for Executive Action
To improve the federal government’s response to COVID-19 and preparedness for future pandemics, the Secretary of Health and Human Services should immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. This committee should include a broad representation of knowledgeable health care professionals from the public and private sectors, academia, and non-profits.
Key Considerations and Future GAO Work
More complete and consistent COVID-19 data are needed
to develop and monitor health care indicators to assess trends in the burden of the pandemic on the population and the health care system, nationally and at the state and local level; and
to make informed decisions regarding where to prioritize the allocation of health care resources needed to prevent disease transmission and treat COVID-19 patients.
Since June 2020, we have identified concerns related to COVID-19 data that inform health care indicators and we plan to continue to examine in future CARES Act reporting the Department of Health and Human Services’s (HHS) data collection efforts for COVID-19 and communication of COVID-19 information to the public.[42]
Background
The rapid spread and magnitude of the COVID-19 pandemic have underscored the importance of having quality data to help the federal government understand the effects of the disease in the U.S. and to inform its allocation of resources and help it make timely and responsive decisions related to public health and safety. COVID-19 continues to take a devastating toll on the U.S.
Since 2003, GAO has described challenges related to public health data, including HHS’s lack of progress in establishing an electronic nationwide public health situational awareness network that would incorporate data from different sources and be used to help public health officials make decisions to prepare for and respond to emergencies such as a pandemic. For example, in 2017, we reported that HHS had not defined the minimal data elements needed to establish such a system.
In our September 2020 report, we noted that HHS had developed its HHS Protect platform to help integrate COVID-19 and other types of health information collected by various federal, state, and local public health entities and commercial entities. However, questions have been raised about the completeness and accuracy of some of the COVID-19 data included in HHS Protect that are intended to support the federal government’s response to the pandemic. We have ongoing work examining HHS’s work in establishing the public health situational network and the quality of HHS Protect data.
Overview of Key Issues
The federal government generally lacks consistent and complete COVID-19 data. All of the National Academies of Sciences, Engineering, and Medicine (National Academies) experts we met with since September have emphasized the need for more consistent and complete COVID-19 data than what is currently being collected and reported across states and other entities.[43] Further, through our prior and current work on the COVID-19 pandemic, we have identified examples of specific indicators for which the data currently being collected and reported across states and other entities are inconsistent or incomplete.
COVID-19 testing. As we reported in November 2020, the proportion of COVID-19 viral tests in a given population that are positive for infection (the positivity rate) is one indicator of the sufficiency of testing.[44] We have found that HHS continues to have challenges in collecting complete and consistent COVID-19 testing data. While laboratories must report all COVID-19 test results to HHS, including those for rapid antigen tests, in November 2020, we reported that some states do not require reporting of antigen test results.[45] As a result, the federal government may not have complete and consistent data on testing. (See our COVID-19 Testing enclosure in this report.) In addition, there are also differences in how states report information about antigen tests to the public and whether they include antigen tests in the calculation of positivity rates. We reviewed 56 state and territory websites containing information on COVID-19 data dashboards for November 2020 and found:
40 states and territories reported the numbers or results of antigen tests, while 7 did not publicly report any antigen testing data.
22 states and territories expressly included antigen tests in their percent positivity calculations.
As the use of rapid antigen tests becomes more widespread, HHS may face challenges in understanding the extent of their use and impact on associated positivity rates. A few experts we interviewed also expressed concern that the reporting of COVID-19 testing data is not standardized across states. For example, one expert stated that some states include the results from repeated testing of the same individuals (e.g., college students) over a short period of time to calculate the COVID-19 test positivity rate. This expert explained that including results from successive tests in the calculation of positivity rate in this manner is problematic and could bias the positivity rate toward a lower point if the testing conducted is missing individuals at a higher risk of COVID-19 infection.
COVID-19 cases. We previously reported in July 2020 that data on COVID-19 cases provide insight on the burden of COVID-19 and that data on cases are often incomplete and inconsistent. For example, our work has shown that demographic and other epidemiological information on cases is limited and varies over time and by population and geographic location. As of January 8, 2021, HHS’s Centers for Disease Control and Prevention’s (CDC) COVID-19 Data Tracker stated that race and ethnicity was available for about half of cases (51 percent).[46]
Further, several experts we interviewed expressed concerns about these issues, stating that inconsistent and incomplete case data complicate comparisons of COVID-19 case counts and rates among geographic areas and populations. For example, one expert explained that reported case counts often include several types of cases (probable or not yet lab confirmed, confirmed, recovered), but some states do not specify the type.
In addition, there are also inconsistencies in how states reported dates for cases (e.g., the date of specimen collection, date of illness onset, date reported). Different approaches for counting cases and assigning reporting dates of cases make it harder to compare and interpret trends in cases across states and over time.
Hospital capacity measures. In November 2020, we reported on the importance of monitoring hospitalizations and hospital bed availability, including the proportion of available intensive care unit (ICU) and non-ICU beds, as such information offers insights into our health care system’s capacity to care for patients with COVID-19. Hospitals are required to report data on COVID-19 hospitalizations, bed availability, and other measures to HHS Protect.[47] However, according to several sources, there has been uncertainty about the extent of missing data in the HHS Protect hospital data set and the consistency of interpretations among hospital staff regarding what data they are required to report.
Several experts expressed concerns with the consistency of bed data reported by different hospitals. For example, a few told us that as demand increases, some hospitals may be able to reclassify (for the short term) some of their non-ICU beds as ICU beds and thus may include reclassified and traditional ICU beds in their total counts of ICU beds. In comparison, other hospitals may only include traditional ICU beds in their counts. Further, inconsistent bed data make it challenging to determine and compare the bed capacity (ICU and non-ICU) of hospitals.
Similarly, some hospitals may also be able to utilize surge capacity to provide care for patients (e.g., by using operating beds to provide care). One expert noted that measuring the ability to add capacity could yield consistent information about the resiliency of health systems to move resources and personnel where they are needed. Further, another expert also stated that staffing levels should be tracked as hospitals may not have the necessary staff needed, for example, to treat additional ICU patients even if they are able reclassify some of their non-ICU beds.
Further, a few experts also identified COVID-19 hospitalizations as an indicator of disease burden. One of these experts suggested examining this indicator by race and ethnicity as a way of assessing the disproportionate effects of the pandemic on different subpopulations. CDC collects information on race and ethnicity for COVID-19 hospitalizations through its COVID-19-Associated Hospitalization Surveillance Network (COVID-NET).[48] However, these data are limited to about 250 hospitals in select counties in 14 states and, as we have previously reported, race and ethnicity information are limited.
In addition to ensuring consistent and complete COVID-19 data, a few experts we interviewed stated that the federal government should take additional steps to support its response to the pandemic. For example, one expert stated that the federal government should develop a single national dashboard—based on consistent and complete data—to clearly communicate to the public the current status of the pandemic across different areas (e.g., with a limited number of indicators). Another expert emphasized that the federal government should establish a national surveillance system based on electronic reporting of consistent and complete data across different types of data (e.g., on COVID-19 testing, symptoms).
Other organizations have identified inconsistencies in COVID-19 data. In addition, several organizations, such as Resolve to Save Lives, the COVID Tracking Project, and Duke University’s Margolis Center for Health Policy, have also identified the need for the collection and reporting of more consistent COVID-19 information. For example:
Resolve to Save Lives found that all states maintain COVID-19 data through dashboards, but because state dashboards were developed independently, no two are identical in terms of information presented or usability.[49]
The COVID-19 Tracking Project—a volunteer organization launched to compile COVID-19 data from states—identified inconsistencies in state reporting of COVID-19 information (e.g., cases, completed tests, mortality).
Both of these organizations recommended standardizing these data to improve comparability across states.
Evolving nature of pandemics and future data needs. Given the evolving nature of the pandemic and the potential for future outbreaks, several of the National Academies experts we met with also underscored the importance of having a process in place to ensure that additional data elements (for COVID-19 and future pandemics) are collected and reported consistently. For example, although it is unclear what the long-term health effects of COVID-19 may be, one expert told us it would be important to monitor for these effects. Similarly, a few experts told us it would be important to monitor vaccination rates as vaccines become authorized or licensed, including among different populations (e.g., race, socioeconomic status) to help ensure equitable distribution.
Several experts also described the need for having processes in place to modify the types of information collected because different information may be relevant to different types of outbreaks. For example, one expert said that ICU beds have been important for the COVID-19 pandemic, but might not be as important for future pandemics that involve relatively few infected patients requiring intensive care.
Involving stakeholders with responsibility for data collection in decisions about which data elements to include can help ensure that the collection of additional data elements would be useful and feasible. In particular, decisions about data elements can benefit from including stakeholders such as health systems, providers, hospitals, state public health departments, academia, and non-profits. Our September 2012 work on key considerations for collaboration also stresses the importance of involving key stakeholders in achieving goals.
In September 2020, we reported on the disruption of established data reporting channels that occurred in conjunction with the introduction and expansion of HHS Protect. Specifically, concerns were raised that the lack of communication and involvement by the entities supplying hospital information may have led to problems regarding the accuracy and completeness of the data contained in HHS Protect. Further, a few hospital associations and a public health organization have commented that hospitals raised concerns regarding the clarity of some of the data elements that they report to HHS Protect and as a result, hospitals may have reported information inconsistently.
Lack of standardization in the collection and reporting of COVID-19 data reflects a decentralized public health system. The prevailing lack of standardization across multiple categories of data used to monitor and respond to COVID-19 reflects the longstanding decentralization of public health activities in the U.S. Public health data collection is conducted by state and local health departments in the U.S., with federal agencies such as CDC either aggregating data collected from state and local sources or gathering targeted data on selected topics through individual initiatives. This contrasts with the data that are typically collected for national economic indicators, such as the extensive data on employment that are collected by the U.S. Census Bureau through a monthly nationwide household survey.
In addition, no infectious disease has previously affected population health and stressed health system resources on a national level to the extent of the COVID-19 pandemic since at least the 1918 influenza epidemic. Thus, the existing public health data infrastructure was not prepared to provide the kind of consistent data based on uniform definitions and standardized data collection procedures needed to effectively monitor and respond to a nation-wide pandemic of this magnitude.
According to CDC’s Updated Guidelines for Evaluating Public Health Surveillance Systems, the use of standard definitions for health-related events (such as COVID-19) improves the comparability of such information across different sources of data, including geographic areas (e.g., states).[50] CDC’s guidelines also state that complete data about cases of disease (such as COVID-19) and related information about such cases (e.g., demographic characteristics of persons affected by COVID-19) are needed to ensure that surveillance data are of high quality. Without high-quality data, a surveillance system cannot accurately represent the health-related event under surveillance. Further, our March 2011 work on developing key indicator systems states that standard definitions are needed for the data elements that are used to support indicators, and that without such standards, the usability and comparability of the data are likely limited.
The lack of complete and consistent data limits HHS’s and others’ ability to monitor trends in the burden of the pandemic across states and regions (e.g., cases, hospitalizations), to make informed comparisons between such areas, and to assess the impact of public health actions to prevent and mitigate the spread of COVID-19. Additionally, incomplete and inconsistent data have limited HHS’s and others’ ability to prioritize the allocation of health resources in specific geographic areas or among certain populations most affected by the pandemic.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided general comments, which are reproduced in Appendix IV: Comments from the Department of Health and Human Services. In its comments, HHS partially concurred with our recommendation to immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing COVID-19 data collection and reporting standards for key health indicators. Specifically, HHS agreed that it should establish a dedicated working group or other mechanism with a focus on addressing COVID-19 data collection shortcomings. However, HHS said because of resource constraints and the ongoing response to the pandemic, it could not commit to immediately doing so. Given the current state of the COVID-19 pandemic and the expanded need for complete and consistent data to assist the federal response and to inform the general public (including data on vaccines), we reiterate the importance of immediately establishing an expert committee. Further, we maintain that HHS could use an existing committee, which would help streamline the process and leverage existing resources, to help inform the federal government’s response to the pandemic with more complete and consistent COVID-19 data. OMB did not have comments on this enclosure.
Methodology
To conduct this work, we obtained input from five experts with knowledge in public health, health systems, and health economics.[51] We obtained assistance from the National Academies in identifying these experts to better ensure a breadth of expertise was brought to bear in its preparation; however, all final decisions on the selection of experts for this work are the sole responsibility of GAO.
We asked these experts a core set of questions to obtain their input on data that inform health care indicators. As applicable, we compiled the information we received from these experts with the five National Academies experts we met with for our November report. We also interviewed officials from HHS about the collection of data to inform health care indicators.
We reviewed the websites of 50 states, the District of Columbia, and five territories to examine information related to rapid antigen testing. We also reviewed selected research by organizations with public health and policy researchers who are knowledgeable about the use of COVID-19 data to support decision-making.
COVID-19: Data Quality and Considerations for Modeling and Analysis. GAO-20-635SP. Washington, D.C.: July 30, 2020.
Public Health Information Technology: HHS Has Made Little Progress toward Implementing Enhanced Situational Awareness Network Capabilities, GAO-17-377 Washington, D.C.: September 6, 2017.
Managing for Results: Key Considerations for Implementing Interagency Collaborative Mechanisms. GAO-12-1022. Washington, D.C.: September 27, 2012.
Key Indicator Systems: Experiences of Other National and Subnational Systems Offer Insights for the United States.GAO-11-396. Washington, D.C.: March 31, 2011.
The national economy continued to recover in November and December 2020 while key areas of the economy we are monitoring had mixed performance. Based on the Federal Reserve Bank of New York’s Weekly Economic Index, the national economy continued its gradual recovery in November and December 2020, but the index also indicated notably weaker activity than a year ago (see figure).[52] Indicators for areas of the economy supported by the federal pandemic response saw mixed performance, with some weakness evident in employment, Federal Housing Administration (FHA) mortgage loans, and state and local government finances (see table).[53]
Weekly Economic Index, January 2019 through December 2020
Indicators for Areas of the Economy Supported by the Federal Pandemic Response, September 2020 through December 2020, Cumulative Changes since February 2020
aThe employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population 16 years and over. The ratio is subject to misclassification errors with respect to consistently identifying workers as employed and absent from work or unemployed on temporary layoff.bHigher levels in the Consumer Credit Default Composite Index rate indicate more defaults on consumer loans, including auto loans, bank cards, and mortgages. The Consumer Credit Default Composite Index could be subject to seasonal variation but is not seasonally adjusted.cSeriously delinquent loans are 3 months or more past due or in foreclosure, based on mortgages insured by the Federal Housing Administration (FHA). Increases in serious delinquency rates on FHA loans could to some extent reflect borrowers taking advantage of mortgage forbearance provisions of the CARES Act, but may also indicate financial challenges facing the minority and low-to-moderate income households that disproportionately take out mortgages insured by FHA.dLower levels of the small business credit card delinquency index indicate more delayed payments on credit. The small business credit card delinquency index is published under license and with permission from Dun & Bradstreet, and no commercial use can be made of these data.eCorporate bond spreads are option-adjusted spreads on dollar-denominated investment grade corporate bonds from Bloomberg and are measured in basis points or 1/100th of a percentage point. Higher spreads reflect higher perceived risk among corporate borrowers by investors.fSpreads on municipal bonds are calculated relative to interest rates on Treasury securities based on the Bloomberg-Barclays Municipal Bond Index and are measured in basis points or 1/100th of a percentage point. Higher spreads reflect higher perceived risk among municipal borrowers by investors.gExpenditures are in real (inflation-adjusted) dollars using chained 2012 dollars and are seasonally adjusted at annual rates.
Based on trends in initial claims for unemployment insurance and surveys of households and businesses conducted by the Bureau of Labor Statistics (BLS), improvements in labor market conditions that were evident during the summer have plateaued from October through December 2020. Moreover, both BLS surveys indicate that employment remains substantially below its level before the pandemic.[54] For example, the employment-to-population ratio, based on the BLS survey of households, has been flat at 57.4 percent from October through December 2020, and remains 3.7 percentage points below its level in February 2020 (see figure).
Employment-to-Population Ratio, January 2019 through December 2020
Serious delinquency rates—loans that are 90 or more days past due or in foreclosure—for single family mortgage loans insured by FHA increased slightly from October to November 2020, to 11.3 percent of loans, and remained much higher than rates prior to the pandemic (see figure).[55] Increases in delinquencies to some extent reflect borrowers taking advantage of mortgage forbearance provisions of the CARES Act but may also indicate financial challenges facing households, including minority and low-to-moderate income borrowers disproportionately served by FHA loans.
Serious Delinquency Rates on Single-Family Residential Mortgages, January 2019 through November 2020
Falling spreads on investment grade corporate bonds suggested improved access to credit for investment grade corporations in November and December 2020.[56] Meanwhile, employment by state and local governments increased slightly in November and fell in December, falling three out of the last four months of 2020 (see figure), suggesting some continued weakness in state and local government finances.
State and Local Government Employment, January 2019 through December 2020
Agency Comments
We provided the Department of Housing and Urban Development (HUD), the Department of Labor (Labor), the Department of Treasury (Treasury), the Board of Governors of the Federal Reserve System (Federal Reserve), and the Office of Management and Budget (OMB) with a draft of this enclosure. HUD and the Federal Reserve provided a technical comments, which we incorporated as appropriate. Labor, Treasury and OMB did not provide comments on this enclosure.
Methodology
To identify indicators for monitoring the economy supported by the federal pandemic response, in particular by the COVID-19 relief laws, we reviewed prior GAO work, data from federal statistical agencies, data from Fannie Mae and Freddie Mac, information from the Federal Reserve and relevant federal agencies responsible for the pandemic response and oversight of the health care system, data available on the Bloomberg Terminal, and input from internal GAO experts. We reviewed the most recent data from these sources as of November or December 2020, depending on availability. We assessed the reliability of the economic indicators we used through a number of steps, including reviewing relevant documentation, reviewing prior GAO work, and interviewing data providers. Collectively, we determined the indicators were sufficiently reliable to provide a general sense of how the areas of the economy supported by the federal pandemic response were performing.
Contact information: Lawrance L. Evans, Jr., (202) 512-8678, evansl@gao.gov
As of December 31, 2020, the Department of Health and Human Services had disbursed about $110 billion (about 62 percent) of the $178 billion appropriated by COVID-19 relief laws for the Provider Relief Fund to help support health care providers and finance care for COVID-19 patients and underserved populations. The department also lent about $106.5 billion to health care providers through a program expanded by the CARES Act.
Entities involved: Department of Health and Human Services, including its Centers for Medicare & Medicaid Services and Health Resources and Services Administration
Key Considerations and Future GAO Work
As the Department of Health and Human Services (HHS) works to get funds to eligible providers, it will continue to be important that robust internal controls are in place to help ensure funds are appropriately disbursed and used, notwithstanding the imperative of a quick federal response to the COVID-19 crisis. We plan to conduct additional work to examine HHS’s efforts to provide assistance to providers.
Background
Provider Relief Fund. To respond to the pandemic, the COVID-19 relief laws appropriated $178 billion to reimburse eligible providers for health-care-related expenses or lost revenues attributable to COVID-19, known as the Provider Relief Fund. Specifically, the CARES Act appropriated $100 billion, the Paycheck Protection Program and Health Care Enhancement Act appropriated $75 billion, and the Consolidated Appropriations Act, 2021, appropriated $3 billion for this purpose.[57] The Health Resources and Services Administration (HRSA), within HHS, administers payments from the Provider Relief Fund.
Accelerated and Advance Payments Program. HHS’s Centers for Medicare & Medicaid Services’ (CMS) Accelerated and Advance Payments Program provides loans to providers and suppliers when there is a disruption in claims submission or processing, including during a public health emergency or a presidentially declared disaster.[58] Section 3719 of the CARES Act authorized the expansion of this program due to the COVID-19 pandemic. Under the expanded program, active Medicare providers and suppliers could apply for loans of up to 100 percent or 125 percent of the Medicare payments they received for a prior 3-month or 6-month period, depending on the type of provider or supplier. On April 26, 2020, CMS announced that provider applications for the Advance Payments Program were discontinued in light of grant payments made available for similar purposes through the Provider Relief Fund. The Accelerated Payments Program was discontinued on October 8, 2020.
Overview of Key Issues
Provider Relief Fund. As of December 31, 2020, HHS had allocated about $145 billion from the Provider Relief Fund, with about $33 billion not yet allocated.[59] Of the total allocated (about $145 billion), about $110 billion had been disbursed and about $35 billion was yet to be disbursed. According to HHS officials, the agency allocated about $77 billion for general relief for health care providers and about $67 billion for targeted areas. See table below for a summary of Provider Relief Fund allocations and disbursements.
Summary of the Provider Relief Fund ($178 billion) Allocations and Disbursements, as of December 31, 2020
Description
Allocation ($ billions)
Date of initial disbursement
Disbursement ($ billions)
General distributions
Phase I: Medicare
46.016
April 10, 2020
42.200
Phase II: Medicaid and Children’s Health Insurance Program (CHIP) providers
4.067
July 3, 2020
2.863
Phase II: dental providers
1.290
July 28, 2020
1.001
Phase III: assisted living facilities
0.627
September 25, 2020
0.261
Phase III: general distribution
24.500
November 14, 2020
8.490
Subtotal of general distributions
76.500
54.815
Targeted distributions
Rural health care facilities
11.091
May 6, 2020
10.962
High-impact hospitals
20.751
May 7, 2020
20.668
Skilled nursing facilities
5.000
May 22, 2020
4.764
Indian health care providers
0.520
May 29, 2020
0.479
Safety net hospitals
13.074
June 12, 2020
12.779
Children’s hospitals
1.000
August 20, 2020
1.062
Nursing home infection control, quality, and performance
Source: Summary of Health and Human Services funding data. | GAO-21-265
aHealth Resources and Services Administration (HRSA) officials told us that the amount of unallocated funds/uninsured treatment/vaccine administration is available for treatment of the uninsured and for future allocations. HRSA did not specify the amount available for each purpose. As of December 31, 2020, $1.525 billion had been allocated and disbursed for uninsured treatment.
Summary of fund disbursements. As of December 31, 2020, about $110 billion of the approximately $145 billion allocated from the Provider Relief Fund had been disbursed to providers. The amount disbursed was less than the amount allocated because some of the disbursements were in progress and HRSA told us that providers had declined about $6 billion so far from previous disbursements; those funds are available for subsequent allocations. HRSA told us that the returned funds are not reflected in the above table. According to our analysis of information provided by HRSA, as of December 31, 2020, HHS had disbursed about $55 billion from general distribution allocations and about $56 billion from the targeted allocations.
The amount disbursed over each 2-month reporting period has declined after the initial roll-out of the Provider Relief Fund in March (see figure below). For example, about $65 billion was disbursed from April 10, 2020, the date of the initial disbursement, to May 31, 2020. An additional estimated $27 billion was disbursed from June 1, 2020, through July 31, 2020; about $8 billion was disbursed from August 1, 2020, through September 30, 2020; and about $2 billion from October 1, 2020, through November 30, 2020.[60]
Summary of the Department of Health and Human Services’ (HHS) Reporting Period Disbursements from the Provider Relief Fund through November 30, 2020
Note: Numbers may not be exact due to rounding.
COVID-19 treatment of uninsured. The Provider Relief Fund includes an allocation for the COVID-19 Uninsured Program, although the total amount to be used for this program has not yet been determined by HHS officials. As of December 31, 2020, about $1.5 billion from the Provider Relief Fund had been disbursed. As of December 18, 2020, about 3,660 providers had received reimbursement for COVID-19 treatment of uninsured individuals. HRSA officials reported that future disbursements for this purpose will come out of the approximately $33 billion remaining in unallocated funds in the Provider Relief Fund.
Providers who choose to participate in this program must confirm that the individual treated is uninsured, the provider will accept the program reimbursement as payment in full, the provider will not bill the individual for the balance of the bill, and the provider will agree to program terms and conditions. Reimbursement is generally available at Medicare rates for testing uninsured individuals for COVID-19 and treating uninsured individuals with a COVID-19 diagnosis, as well as the administration of a vaccine authorized, licensed, or approved by the Food and Drug Administration to uninsured individuals. Concerns have been raised that some uninsured individuals may not seek treatment for COVID-19 because they believe they will be liable for the costs of such treatment. HRSA officials noted that health care providers are not obligated to participate in the voluntary HRSA COVID-19 Uninsured Program or to inform uninsured individuals about the program.
Accelerated and Advance Payments Program. Under the expanded Accelerated and Advance Payments Program, amended by the CARES Act, CMS made accelerated and advance payments totaling about $106.5 billion as of October 8, 2020. Initially, recoupment of the accelerated and advance payments, through the offsetting of new Medicare claims, was to begin not more than 120 days after the funds were disbursed. Thus, recoupment was scheduled to begin in late July 2020. However, the Continuing Appropriations Act, 2021 and Other Extensions Act included a provision that delayed repayment until 1 year after the accelerated or advance payment was made, with recoupment of Medicare payments owed to providers beginning at 25 percent for the first 11 months, and at 50 percent for the following 6 months.[61] Accordingly, the provision allows 29 months from the date of the first payment to a provider or a supplier before requiring that the outstanding balance be paid in full.
Additional Relief for Medicare Providers. Among other provisions, the Consolidated Appropriations Act, 2021, also temporarily increased payments to Medicare providers in two ways. First, it suspended the 2-percent Medicare payment cuts required under prior law until March 31, 2021. The CARES Act had previously postponed these cuts through December 31, 2020. Second, the Consolidated Appropriations Act, 2021, increased payments under the Medicare Physician Fee Schedule by 3.75 percent for 2021; it is estimated that this change will increase Medicare payments by $3 billion.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with the draft of this enclosure. HHS provided technical comments on this enclosure, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct our work, we examined publicly released HHS information, and obtained information from CMS and HRSA in the form of written responses to questions, documents, and datasets. Our review of the data sources provides reasonable assurance of the data’s reliability. The Provider Relief Fund dataset came from HRSA, which is the only available source for the disbursement data. The allocation amounts and categories that were provided by HRSA match publicly available information.
Contact information: James Cosgrove, (202) 512-7114, cosgrovej@gao.gov
Nursing homes continue to face COVID-19 challenges many of which have been exacerbated by a surge in cases. Since our November report, nursing homes experienced a third peak in cases and continued to address challenges related to visitation policies, PPE, staffing, and testing, while the federal government outlined vaccination strategies, including for the nursing home population in particular.
Entities involved: Centers for Disease Control and Prevention and Centers for Medicare & Medicaid Services, both within the Department of Health and Human Services.
Key Considerations and Future GAO Work
We have previously made two recommendations related to COVID-19 outbreaks in nursing homes:
In September 2020, we recommended that the Secretary of Health and Human Services, in consultation with the Centers for Medicare & Medicaid Services (CMS) and the Centers for Disease Control and Prevention (CDC), develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively back to January 1, 2020, and clarify the extent to which nursing homes had reported data before May 8, 2020.
While the Department of Health and Human Services (HHS) partially agreed with this recommendation, as of October 23, 2020, it had taken no specific actions. The department indicated that it continues to consider how to implement this recommendation.
In November 2020, we recommended that the Administrator of CMS quickly develop a plan that further detailed how the agency intends to respond to and implement, as appropriate, the 27 recommendations in the final report of the Coronavirus Commission on Safety and Quality in Nursing Homes, which CMS released on September 16, 2020.[62]
HHS neither agreed nor disagreed with our recommendation; instead, it highlighted actions that CMS has taken related to Commission recommendations and indicated that it would refer to and act upon the Commission’s recommendations as appropriate. In December 2020, CMS reiterated this position.
We maintain the importance of our recommendations. Specifically, we maintain that collecting data on COVID-19 cases and deaths from nursing homes retroactively would better inform the government’s continued response and recovery, and we maintain that HHS could ease the burden by incorporating data previously reported to CDC or to state or local public health offices. Additionally, we maintain that developing a plan for how CMS will proceed with the Commission’s recommendations would improve the agency’s ability to systematically consider the Commission’s recommendations going forward.
We have ongoing concerns related to the ability of nursing homes to address challenges related to visitation policies, personal protective equipment (PPE), staffing, and testing as the pandemic surges through the winter months. We will continue to monitor these issues. We also will continue to monitor the management and distribution of vaccinations to nursing home residents. In addition, we have ongoing work on the oversight of infection prevention and control and emergency preparedness in nursing homes.
Background
The health and safety of the 1.4 million elderly or disabled residents in the nation’s more than 15,000 Medicare- and Medicaid-certified nursing homes—who are often in frail health and living in close proximity to one another—has been a particular concern during the COVID-19 pandemic.[63] CMS, an agency within HHS, is responsible for ensuring that nursing homes meet federal quality standards to participate in the Medicare and Medicaid programs. To monitor compliance with these standards, CMS enters into agreements with state survey agencies in each state government to conduct inspections, including recurring comprehensive standard surveys and as-needed investigations.
The CARES Act appropriated $100 million for this oversight, and it directed CMS to prioritize the use of funds for nursing home facilities in localities with community transmission of COVID-19.[64] According to CMS, of this amount, the agency plans to provide state survey agencies approximately $81 million through September 30, 2023, to be used to ensure that all nursing homes receive targeted infection control surveys, among other things.[65] CMS has set aside the remaining $19 million to enhance survey system technology, to fund PPE for federal surveyors, and to implement improvements recommended by the Nursing Home Commission, according to the agency.
In addition, HHS announced in May that it would contribute $4.9 billion from the Provider Relief Fund, established with funds provided under the CARES Act, as direct payments to assist nursing homes with responding to COVID-19. In July, HHS announced that it would provide an additional $5 billion from the fund.
HHS announced in August that $2 billion from the fund would be dedicated to establishing an incentive-based program that rewards nursing homes that create and maintain safe environments for their residents. Payments would be made to nursing homes for their efforts to reduce COVID-19 infection and mortality rates among residents, based on CDC data. In October, HHS announced the first awardees, providing for $331 million in payments to nursing homes, based on data from a 4-week performance period spanning late August 2020 to late September 2020. On December 7, 2020, HHS announced its second round of awardees, providing for $523 million in payments to over 9,000 nursing homes, based on data from a 5-week performance period spanning late September 2020 through November 1, 2020.
In response to the pandemic, HHS, primarily through CMS and CDC, has taken a range of actions to address infection prevention and control in nursing homes, which we reported on in our previous reports from June, September, and November 2020. These actions include taking steps to implement recommendations from the Coronavirus Commission on Safety and Quality in Nursing Homes, requiring testing of nursing home residents and staff, and providing guidance to nursing homes to facilitate safe resident visitation.
Overview of Key Issues
COVID-19 cases and deaths in nursing homes. According to CDC case-reporting data, as of December 6, 2020, about 99 percent of Medicare- and Medicaid-certified U.S. nursing homes had reported at least one confirmed resident or staff case, and about 64 percent had reported at least one resident or staff COVID-19 death.[66] Also as of December 6, 2020, nursing homes had cumulatively reported a total of 409,892 resident and 350,590 staff confirmed cases of COVID-19, along with 81,739 resident and 1,215 staff deaths as a result of the virus—about 30 percent of the total COVID-19 deaths across the U.S. (280,135 as of December 6, 2020, as reported by CDC).[67]
Examining the data over time, for the weeks ending May 31 to December 6, 2020, there have been fluctuations in new weekly confirmed cases. Nursing home data on new weekly COVID-19 cases were not available prior to the week ending May 31, but data since then show that new weekly cases have been in a wave-like pattern. (See figure.) Specifically, after a decline in new cases from May to June, new cases climbed to an initial peak of nearly 12,000 cases for both residents and staff in late July. With some fluctuations, cases again decreased gradually through mid-September. Since the week ending September 13, new cases again have steadily risen to exceed the July peak with almost 26,000 resident cases and almost 23,000 staff cases for the week of December 6, 2020.[68]
Resident deaths have moved in a similar pattern, though data show the subsequent peaks have not reached the same level as in late May. Combined nursing home resident and staff deaths from COVID-19, as a percentage of total COVID-19 deaths in the U.S., remained largely unchanged throughout this time period (increasing slightly from about 28 percent on May 31 to about 30 percent on December 6). The changing weekly COVID-19 death counts in nursing homes generally paralleled changes in the country as a whole.
New Weekly Confirmed COVID-19 Cases and Deaths among U.S. Nursing Home Residents and Staff, as Reported by Medicare- and Medicaid-Certified Nursing Homes, Weeks Ending May 31, 2020, through December 6, 2020
Notes: Dates refer to the end of a week (e.g., May 31 refers to the entire week from May 25 through May 31). According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time. Data presented in this enclosure reflect the data downloaded as of December 17, 2020, which includes data through the week ending December 6, 2020. We excluded data for the week ending May 24, 2020, because it is the first week for which data are available from the Centers for Disease Control and Prevention (CDC) and could include cases and deaths from multiple weeks dating back to January 1, 2020. Weekly and cumulative case and death counts are likely underreported because they do not include data for the nursing homes that did not report COVID-19 data to CDC for that week or from nursing homes that submitted data that failed data quality assurance checks. Additionally, as we previously reported, the Centers for Medicare & Medicaid Services (CMS) does not require nursing homes to report data prior to May 2020, although nursing homes may do so voluntarily. We recommended that the Secretary of Health and Human Services—in consultation with CMS and CDC—develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively to January 1, 2020.Weekly staff deaths reported for the weeks ending May 31 through December 6 ranged from 15 (week ending September 20) to 71 (week ending November 29).
Challenges continue during surge in cases. As the above data reveals, nursing homes experienced a significant surge in COVID-19 cases and many of the previously identified challenges continue, in areas including visitation, PPE, staffing, and testing.
Visitation challenges. The tension between providing residents with important visitation and minimizing the potential for an outbreak continues to be a challenge for nursing homes.
From March through September 2020, CMS guidance focused on reducing the transmission of COVID-19 through restrictions on visitors and non-essential health care personnel in nursing homes. As previously reported, this restriction of visitors has added to the limited oversight of facilities through the exclusion of resident advocates, such as family members and ombudsmen.[69] Additionally, two advocacy organizations and two experts have noted that the isolation resulting from decreased visitation can cause loneliness, anxiety, and depression among residents. According to CDC officials, alterations to daily routines and decreased visitation can worsen outcomes and living conditions particularly for patients with cognitive declines, such as dementia, and can make care more challenging.
The Nursing Home Commission also raised concerns related to visitation, given the potential for unintended harm resulting from residents’ separation from families and loved ones. To help address residents’ physical and emotional needs, CMS relaxed visitation restrictions in September 2020 and released guidance that provided various ways a nursing home can safely facilitate in-person visitation.[70]
However, nursing home associations and an expert we interviewed noted that the colder months and the potential for increased visitation due to the holidays complicate infection control measures and that nursing homes were looking to CMS for additional recommendations and guidance on conducting safe indoor visitation. On November 18, 2020, CMS issued a press release urging nursing home staff, residents, and visitors to follow its September 2020 guidelines for visitation. The agency encouraged nursing homes to educate residents and families of the risks of leaving the facility, the steps they should take to reduce the risk of contracting COVID-19, and how to stay connected through alternative means of communication, such as phone and video communication. In particular, CMS recommended that facilities find innovative ways, such as virtual parties and visits, to recognize the holidays without having gatherings that could increase the risk of COVID-19 transmission. CMS also cautioned that residents who leave nursing homes for outings or family visits may increase their exposure to COVID-19.
PPE challenges. The percentage of nursing homes experiencing PPE shortages has declined from when we reported in November, but shortages remain an issue.[71]
According to data nursing homes self-reported to CDC, as of December 6, 2020, about 10 percent of nursing homes (a decrease of 5 percentage points) did not have a one-week supply of at least one of the following: N95 respirators, surgical masks, gloves, eye protection, or gowns.[72] Of these, N95 respirators were the most needed, with about 8 percent of nursing homes (decrease of 4 percentage points from our November 2020 report) reporting they did not have a one-week supply, followed by surgical gowns (about 5 percent of nursing homes, a decrease of 4 percentage points from our November 2020 report).
Nursing home association officials said nursing homes are reporting increasing shortages in N95 respirators and gloves. These officials noted that while nursing homes typically can meet their current PPE needs, they are unable to stockpile reserves to meet an unexpected surge.
One of the Nursing Home Commission’s PPE recommendations was that CMS assume responsibility for a collaborative process with external stakeholders to ensure that nursing homes can procure and sustain a 3-month supply of high-quality PPE.[73] The Commission also recommended that CMS collaborate with other federal and state agencies to provide additional PPE guidance. According to officials from a nursing home association, it is especially important for CMS to coordinate and clarify guidance on PPE usage to avoid confusion over how to prioritize the use of scarce equipment within nursing homes, such as N95 masks, should PPE become less available during the surge in cases.
According to CMS officials, the agency is coordinating with FEMA to provide adequate PPE to nursing homes, but supply shortages are largely not under their control. CMS guidance on the use of PPE refers to CDC recommended steps that can be used to optimize protection if PPE become scarce.[74]
Staffing challenges. The percentage of nursing homes experiencing staffing shortages did not improve from when we reported in November.[75] According to data nursing homes self-reported to CDC, as of December 6, 2020, approximately
20 percent of nursing homes had a shortage of aides (an increase of 1 percentage point),
18 percent had a shortage of nursing staff (an increase of 2 percentage points),
11 percent had a shortage of other staff (an increase of 1 percentage point), and
3 percent had a shortage of clinical staff (an increase of 1 percentage point).[76]
As COVID-19 cases increase in the communities surrounding nursing homes, researchers predict that staffing shortages could also climb as staff members are increasingly exposed to the virus or take care of family members who may become sick. Officials from one nursing home association said they are concerned about staff burnout and worry that nursing homes have already exhausted many alternative staffing sources to fill critical gaps, such as seeking help from staffing agencies, sharing staff between other local providers, and using emergency waivers to hire nursing aides who had yet to complete their certification.
The Nursing Home Commission made nine recommendations related to the nursing home workforce. The action steps related to these recommendations included short-term solutions, such as that CMS assess how federal relief funds could be used for hazard pay, and long-term solutions, such as increasing wages for nursing home staff to disincentivize staff from working for multiple employers.[77] While CMS has taken some actions related to these recommendations, they have not fully addressed them. For example, the Nursing Home Commission recommended that CMS identify and deploy infection preventionist resources to provide immediate assistance to nursing homes without full-time infection prevention support, prioritizing facilities in COVID-19 hotspots. In response, CMS said that the agency had encouraged collaboration between nursing homes and hospitals to help with infection prevention best practices, adding that deploying additional certified infection preventionists may be outside of its control. While potentially helpful, this action does not directly address the Nursing Home Commission’s concern.
Testing challenges. While nursing homes reported improving testing capacity since we reported in November, challenges in testing equipment remain. (See our related COVID-19 Testing enclosure.)
Nursing homes are required to test all staff and residents for COVID-19 as part of its requirements for the Medicare and Medicaid programs.[78] According to CDC data, the number of nursing homes testing for COVID-19 has continued to increase since the week ending August 16, the first week for which testing data are available. The number of nursing homes testing for COVID-19 has increased by 48 percentage points between August 16, 2020 and November 22, 2020, the last week complete data for overall testing were available.[79]
The number of nursing homes that would be unable to test all staff or residents within the week following their reporting has also declined since August 16. For the week ending December 6, 2020, less than 2 percent (less than 200) nursing homes reported that they would be unable to test all staff or residents within the week following their reporting if that became needed.[80]
However, challenges with utilization of HHS procured tests and testing instruments has continued. We previously reported that CDC data indicate that many nursing homes were not utilizing the tests and testing instruments procured and distributed by HHS beginning in July 2020. Although more nursing homes have begun to use the antigen diagnostic tests and associated point-of-care (POC) testing instruments, as of the week ending December 6, 2020, about 19 percent of nursing homes had reported to CDC that they had never used a POC test for residents or staff.[81]
According to nursing home association officials and an expert we interviewed, conflict between federal and state or local policies creates a disincentive for nursing homes to use the POC tests. For example, some states do not collect POC antigen test data to meet state and federal testing requirements because the states question the accuracy of the test results. In these states, according to the officials and stakeholder we interviewed, nursing homes are unlikely to use the POC tests.[82]
Use of the antigen tests may be more widespread in certain states. For example, officials in one state noted its state was early to mandate weekly testing of all nursing home staff and provided extensive assistance to facilities to ensure testing was conducted, including on the use of POC testing systems. As a result, nursing homes in this state were able to overcome initial challenges related to testing and reporting data. As the surge continues and labs conducting PCR testing may become backlogged, POC tests may become more important to nursing homes that require quick results to screen staff and residents in order to prevent and control COVID-19 outbreaks.
For the week ending December 6, 2020, 87 percent (12,108) of nursing homes reported having a POC testing system available. However, about 28 percent reported that they had not used it to test residents or staff in the prior week, which indicates that many nursing homes are still relying on molecular testing.[83]
Vaccination strategy announced, including prioritization of nursing home residents. On October 16, 2020, HHS announced the Pharmacy Partnership for Long-Term Care Program, an agreement with CVS, Walgreens, and Managed Health Care Associates Inc. to provide and administer COVID-19 vaccines to residents of long-term care facilities, including nursing homes. According to HHS, the program manages the COVID-19 vaccination process, including storage, administration, and reporting, to minimize the burden on facilities and jurisdictional health departments.[84] Nursing home association officials and a knowledgeable stakeholder we interviewed said this agreement is a positive step to centralize the management of vaccine dissemination, including tracking and follow up. These are both essential since a full vaccination course will require multiple doses.
On December 1, 2020, CDC’s Advisory Committee on Immunization Practices recommended prioritizing nursing home residents for vaccinations, in addition to health care personnel and other residents of long-term care facilities, upon authorization or licensing of a COVID-19 vaccine by the Food and Drug Administration.[85] On December 3, 2020, the CDC director accepted the advisory committee’s recommendation for priority groups for the initial phase of the COVID-19 vaccination program. CDC notes that federal, state, and local jurisdictions should use the committee’s recommendations in their COVID-19 vaccination planning and implementation. See our related Vaccines and Therapeutics enclosure for additional information about the availability of vaccine doses and their manufacturing status.
About one month after the pharmacy partnership was announced, officials from one nursing home association said that there was still a lot of uncertainty around certain aspects of vaccination distribution and nursing home requirements. For example, these officials did not know how the vaccine would be prioritized among nursing homes and noted it may be important to ensure vaccinations can reach nursing homes outside of the areas served by CVS and Walgreens.[86] Additionally, these officials said that CMS has not specified whether or how COVID-19 vaccinations will be incorporated into its requirements or quality measures for nursing homes.[87] According to CMS officials, the agency’s primary involvement in the vaccination process for nursing homes is related to Medicare payment for the vaccine and the administration of the vaccine, and CMS will work with vaccine immunizers regarding payment questions and reimbursement for vaccinations. CMS also told us the agency is working with the Food and Drug Administration, CDC, states, and other stakeholders to determine the need for new CMS guidance or changes to existing guidance as the vaccine becomes available to nursing homes, including any impact on infection control requirements.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided technical comments, which we incorporated as appropriate. OMB did not have comments on this enclosure.
Methodology
To conduct this work, we reviewed CMS and CDC data, agency guidance, and other relevant information on HHS’s response to the COVID-19 pandemic. We also reviewed written responses from CMS and CDC and spoke to CMS officials, as well as representatives from two national associations representing nursing homes, an expert with experience in nursing home infection control, and other knowledgeable stakeholders.
In addition, we analyzed CDC data on COVID-19 reported by nursing homes for the week ending December 6, 2020.[88] We analyzed the CDC data as they were reported by nursing homes to CDC and publicly posted by CMS.
We did not otherwise independently verify the accuracy of the information with these nursing homes. We assessed the reliability of the data sets used in our analyses by checking for missing values and obvious errors and reviewing relevant CMS and CDC documents. We determined the data were sufficiently reliable for the purposes of our reporting objective.
Contact information: John E. Dicken, (202) 512-7114, dickenj@gao.gov
Related GAO Products
Infection Control Deficiencies Were Widespread and Persistent in Nursing Homes Prior to COVID-19 Pandemic. GAO-20-576R. Washington, D.C.: May 20, 2020.
The Strategic National Stockpile is an important piece of the Department of Health and Human Services’ recently developed strategy to improve the medical supply chain to enhance pandemic response capabilities; however, the Department has yet to develop a process for engaging key stakeholders—who have a shared role for providing supplies during a pandemic, such as state and territorial governments and the private sector—in the development of the strategy.
Entities involved: The Office of the Assistant Secretary for Preparedness and Response, within the Department of Health and Human Services.
Recommendation for Executive Action
To improve the nation’s response to and preparedness for pandemics, the Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as the agency refines and implements its supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile.
Key Considerations and Future GAO Work
In June 2020, we reported that the Department of Health and Human Services (HHS) planned to restructure the Strategic National Stockpile (SNS), overseen by the Office of the Assistant Secretary for Preparedness and Response (ASPR), based on lessons learned from recent pandemics, including COVID-19.
In September 2020, we recommended that HHS, in coordination with the Federal Emergency Management Agency (FEMA) within the Department of Homeland Security, develop and communicate to stakeholders plans outlining specific federal government actions that will be taken to help mitigate supply gaps for the remainder of COVID-19, which could contribute to ensuring a more effective response. HHS and the Department of Homeland Security disagreed with this recommendation, but more recent federal actions underscore the importance of implementing it.[89] For example:
On December 31, 2020, FEMA issued an extension of its temporary final rule that generally prohibits the export of critical personal protective equipment (PPE), including N95 respirators, surgical masks, nitrile gloves, and surgical gowns, without explicit approval from FEMA. In issuing the rule, the agency noted that “due to a surge in confirmed COVID-19 cases and hospitalizations in October, November, and December 2020, domestic supply of the allocated PPE has not kept pace with demand and is not anticipated to do so.”[90]
The Association of Public Health Laboratories reported in late December that 28 percent of public health laboratories surveyed would run out of reagents or other testing supplies within a week. To support COVID-19 testing demands, the Department of Defense, in coordination with HHS, continue to take action to increase the production of testing supplies. For example, in late December 2020, the Department of Defense awarded new contracts to increase production of pipette tips and reagents used to process tests.
The Consolidated Appropriations Act, 2021—passed in December of 2020—requires the President to make publicly available a report containing a whole-of-government plan for effective response to subsequent COVID-19 outbreaks and for future global pandemic diseases.[91] The act stipulates that this pandemic plan should address how to improve the role of the federal government with respect to the regulation, acquisition, and disbursement of medical supplies necessary to respond to COVID-19 as well as the procurement and distribution of PPE, among other things. Developing and making publicly available a pandemic plan that addresses medical supply needs for the remainder of the current pandemic would be consistent with our September recommendation.
In November 2020, we reported on steps HHS, in conjunction with federal partners, had taken to replenish and expand the SNS inventory to enable HHS to respond to a potential resurgence of COVID-19. With respect to PPE, as of December 18, 2020, the SNS had reached its planned 90-day inventory goal for eye protection or face shields but not for other types of PPE.[92]
We will continue to monitor federal actions to mitigate supply gaps through federal planning and SNS modernization efforts, as well as progress towards SNS 90-day inventory goals, in response to provisions in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 and the CARES Act.[93]
Background
HHS first established a stockpile of vaccines and other pharmaceuticals in 1999 to respond to biological or chemical attacks.[94] This stockpile was initially deployed in response to the terrorist attacks on September 11, 2001, and the anthrax attacks that followed later that year.
Subsequently, the Public Health Security and Bioterrorism Preparedness and Response Act of 2002 named this effort the “Strategic National Stockpile” (SNS) and expanded its mission “to provide for the emergency health security of the United States…in the event of a bioterrorist attack or other public health emergency,” requiring the Secretary of Health and Human Services to stockpile drugs, vaccines and other biologics, medical devices, and other supplies in support of that mission.[95] Since 2006, the Public Health Emergency Medical Countermeasure Enterprise (PHEMCE)—a federal interagency body led by HHS’s ASPR that makes recommendations regarding research, development, procurement, stockpiling, deployment, distribution and utilization with respect to medical countermeasures—has provided guidance and oversight on purchases for the SNS inventory.[96]
To meet its mission the SNS has prepared for a growing variety of threats including chemical, biological, radiological, and nuclear, influenza and other emerging infectious diseases, and natural disasters. For example, the SNS has been deployed to respond to Hurricane Katrina (2005), the H1N1 influenza pandemic (2009), the Ebola outbreak (2014), and Zika virus (2016), among other emergencies. ASPR officials have noted that prior to COVID-19, the SNS had responded primarily to time-limited regional events.
Although funding annually appropriated for the SNS fluctuated between fiscal years 2009 and 2013, it experienced relatively steady annual appropriations with gradual increases from fiscal years 2014 to 2020. (See figure below). In most of the 12 years during this period, appropriations for the SNS were equal to or more than what the administration requested.
However, ASPR officials have noted that annual appropriations have not been sufficient to cover the costs associated with responding to the increase in the threats for which the SNS may be needed. In 2013, a working group comprised of two HHS advisory bodies similarly concluded that the SNS was increasingly confronted with unfunded requirements as its responsibilities expanded and, without action, the working group anticipated a widening gap between the responsibilities of the SNS and the resources available to fulfill them.[97]
Strategic National Stockpile (SNS) Requested and Regular Appropriations
Note: The figure only depicts enacted regular appropriations for the SNS. For the requested amounts, we used the Department of Health and Human Services’ (HHS) congressional budget justification for fiscal years 2019 and 2020 and the President’s budget request for all other fiscal years.
In response to some of the medical supply chain challenges experienced during the COVID-19 response—including that the SNS’s inventory of PPE and other supplies necessary to treat individuals with COVID-19 was not sufficient to effectively respond to the scale of the COVID-19 pandemic—ASPR conducted a review of the SNS with the goal of modernizing it to better respond to future pandemics.[98] ASPR worked with the Logistics, Supply Chain, Next Generation SNS Work Group, comprised of representatives from various federal agencies and the White House, which operated from June through September 2020 to develop and implement objectives and activities that would enable the SNS to “better protect the health and safety of the nation.”[99] One area of focus for this group was refining the strategy and structure of the SNS to enhance future pandemic response.
The five relief laws enacted to assist the COVID-19 response as of January 1, 2021, appropriated funding for HHS activities including, but not limited to, the SNS.[100] As of December 31, 2020, HHS reported it obligated about $8.9 billion of the $10.7 billion it planned to use for the SNS to purchase PPE and ventilators for immediate use as well as to replenish SNS inventory, among other purposes, and had expended about $4.6 billion.[101]
Overview of Key Issues
SNS as part of a national supply chain strategy. In a continuation of its efforts to modernize the SNS and address supply chain vulnerabilities identified by COVID-19, HHS developed a national supply strategy.[102] According to ASPR officials, this strategy outlines the capabilities that HHS must acquire—including, but not limited to, the SNS—to address the challenges identified by the pandemic.
This strategy document, entitled “SNS 2.0 Strategy – Modernize the SNS” is focused on improving the government’s future pandemic response capabilities by enhancing and improving coordination among multiple aspects of the supply chain. The strategy notes that this “whole-of-government” approach is needed to build a capabilities based system—of which the SNS is one component—to proactively address vulnerabilities identified during COVID-19. For example, the strategy states that all levels of government, in addition to partnerships with industry, are needed to better understand the medical countermeasures landscape. The strategy’s goals are:
Develop a supply chain information capability that enables early and informed decisions. This goal includes establishing an information management system that collects, monitors, and forecasts all aspects of the medical supply chain for medical countermeasures—development, deliveries, and inventories—in near real-time.[103]
Increase domestic manufacturing capabilities to ensure national security through manufacturing surge. This goal looks to make the United States a “viable and sustainable” domestic manufacturer of medical supplies and pharmaceuticals by understanding gaps in current supplies and leveraging government contracting options, among other things.
Utilize cost-effective stockpiling and deployment strategies to ensure a timely and effective response. This goal is most closely linked to the SNS and envisions the SNS using the implementation of the above two goals to “streamline” how its inventory is procured, stockpiled and deployed. For example, enhanced supply chain information may allow for the quick identification of those private partners with the capacity to increase production.
ASPR officials told us they are thinking more broadly than the SNS in their pandemic response planning, in an effort to be more strategic and use other solutions that might be more cost effective or efficient in future response efforts. For example, rather than the federal government warehousing supplies, the government might utilize private sector distribution models that allow vendors or end users to hold supplies, rotate stock, and distribute them as needed.
As such, ASPR officials noted that questions about the inventory or future role of the SNS in a pandemic—such as, whether the SNS would serve as a backstop to states in their efforts to acquire supplies or whether the SNS would immediately provide supplies as a first response against pandemic spread—are tied to developing the broader supply chain capability. Currently, ASPR’s website notes that the role of the SNS is to “supplement state and local medical supplies and equipment…and can be used as a short-term, stopgap buffer when the immediate supply of these materials may not be available or sufficient.” ASPR officials noted they are considering whether the SNS should have a broader role by providing supplies as a first response in a pandemic, but that their work on the strategy will guide those decisions.
Additionally, ASPR officials told us that as they work to build the supply chain capability outlined in its broader supply chain strategy, they expect to get to a point where they better understand the lead times needed for private industry to ramp up the production of various medical supplies. They added that this information would allow them to make more strategic decisions about which items should be held in the SNS and which ones private sector partners could manufacture during a pandemic. ASPR officials acknowledged that building the private sector partnerships envisioned in the strategy—such as developing incentives for domestic manufacturers of PPE to ensure a consistent supply chain during a pandemic—are in the early stages and may require the office to develop additional private sector and supply chain expertise.
Although ASPR had not yet determined the role of the SNS within the broader supply strategy, officials stated that they view pandemic response as part of the SNS’s role in meeting its mission. Officials acknowledged that additional actions may be needed to make sure the SNS could be used successfully during future pandemics. Actions identified include ensuring congressional agreement around the role of the SNS, receiving adequate appropriations to support the role of the SNS, clarifying what the states should provide and what the SNS should provide during an emergency response, and determining if any additional statutory authorities are needed.
ASPR officials told us that they have started to consider some of these actions related to the role of the SNS in a pandemic response. For example, they have initiated a legislative analysis to identify any legislative barriers, as well as how proposed legislation may help or create additional challenges. ASPR officials said the office would require new authority to enable supply acquisition through the SNS. For example, officials told us the office does not currently have the authority to enter into joint acquisition agreements with states for the purchase of medical supplies. ASPR officials told us in mid-October that it would be a few months before this legislative analysis is complete. Due to the ongoing COVID-19 response, ASPR has just begun considering how to implement the strategy and the role the SNS might play in future pandemics.
As ASPR continues this work, it will be critical that there is a sustained effort to identify the role of the SNS and how it fits into a broader supply chain strategy. We will continue to monitor any efforts related to modernizing the SNS including implementation of a supply chain strategy, or any other related efforts, as the transition to a new administration takes place
Experts outlined future considerations for the SNS. Several of the 9 experts we interviewed noted that there needs to be a re-examination of the role of the SNS during a pandemic so that there is clarity about what resources and capabilities would be made available to state, local, tribal and territorial governments from the stockpile. Many of these experts also noted that the SNS needs to be part of a broader supply or preparedness strategy or discussion. For example, one expert discussed a model where the SNS—as part of a broader supply strategy—has the ability to rapidly turn on commercial supply chains for needed resources.
Most experts we interviewed also mentioned key considerations for the SNS moving forward including (1) ensuring funding is adequate and flexible enough to match its defined role; (2) developing private sector relationships that help inform and meet supply demand during a pandemic response; and (3) ensuring that expectations between the SNS and states, localities, tribes, and territories are clear about what each can provide during a response.
Several experts stated that during the COVID-19 response thus far, there has been some confusion regarding the role of the SNS and the role of state, local, tribal, and territorial governments. In addition, some experts noted there was a lack of clarity about what the SNS was providing, how supplies were accessed by the states, or how allocations were made by the federal government. Several experts noted that in order for this to be improved in the future, state, local, tribal, and territorial governments should be involved in discussions involving SNS reform and supply strategy moving forward.
Involving stakeholders. Although ASPR worked with a number of federal agencies to develop SNS modernization efforts and the supply chain strategy, it has had limited engagement with non-federal stakeholders, including states, localities, territories, and tribes, in developing the strategy. These stakeholders are a critical part of the response and share in the responsibility for stockpiling and delivering needed supplies to health care entities, including supplies provided by the SNS.
ASPR officials told us they agree that engaging with these non-federal stakeholders about the supply chain strategy will be important. Moreover, the strategy emphasizes the importance of partnerships with state, local, tribal, and territorial governments in executing the goals and objectives outlined in the strategy. The strategy also suggests that greater collaboration with state, local, tribal, and territorial governments—through the Public Health Emergency Medical Countermeasure Enterprise—could help to address concerns that these stakeholders are not well-represented in federal preparedness efforts. Additionally, the strategy emphasizes the importance of private sector partnerships to encourage domestic manufacturing to address shortages in available supplies during a pandemic.
ASPR officials told us they have not yet formally engaged with nonfederal government stakeholders about the strategy because they have been developing it while also responding to the pandemic. They also noted that they were focused on engaging partners at the federal level and determining how to enhance those capabilities.
While no formal process yet exists, APSR officials told us that there had been robust engagement with non-federal partners both before and during the pandemic on logistic and response challenges, which have helped inform the strategy. Additionally, ASPR officials told us that they have provided briefings on SNS modernization efforts to several industry and governmental associations including those that represent state and territorial public health, emergency management, and homeland security officials. In terms of developing a more formal process, the strategy notes that the Public Health Emergency Medical Countermeasure Enterprise will serve as a potential “entity for coordination” with state, local, tribal, and territorial governments.
Coordinating with these key stakeholders on a regular basis as ASPR refines and implements a supply chain strategy for pandemic preparedness would be consistent with Presidential Policy Directive 8, and the National Response Framework, under which the current COVID-19 pandemic is coordinated, and future pandemic response efforts may be coordinated.[104] Presidential Policy Directive 8 stresses that our nation’s preparedness is a shared responsibility and relies on actions by all levels of government, the private and nonprofit sectors, and individual citizens.
Further, as we have previously reported, successful reforms or transitions, including efforts to streamline and improve the effectiveness of government operations, depend upon following change management practices.[105] For example, successful reforms require an integrated approach that involves key stakeholders, and it is important for agencies to directly and continuously involve these key stakeholders—such as state and local governments and private industry—in the development of reform. Additionally, our work has also noted the importance of consulting with Congress and other stakeholders when developing proposed agency reforms to be able to harness ideas, expertise, and resources to address an issue or to achieve a specific goal.
We are at an important crossroads. Reexamining how the U.S. responds to pandemics—including the role of the SNS in such a response—will require difficult policy decisions and tradeoffs about systems, budgets, and authorities. ASPR’s initial efforts are encouraging; however, it is still too early in the strategy’s development and implementation to know whether the office will be able to sufficiently address the challenges of building and modifying such a complex system.
Implementing the supply chain strategy will be multifaceted, requiring both intergovernmental and private sector collaboration. ASPR has begun this process but significant steps lie ahead. Establishing a process for regularly engaging with both Congress and nonfederal stakeholders—to include state, local, tribal, and territorial governments and the private sector—as ASPR refines and implements its supply chain strategy for pandemic preparedness, including the role of the SNS, is key to ensuring the strategy reflects these stakeholders’ input and capabilities, and articulates a shared understanding of the role of the SNS.
Such stakeholder engagement would help to ensure that federal efforts strengthen the nation’s pandemic response capability. It will also help ASPR identify and rectify issues early on in the development cycle and build a system that meets the needs of users at all levels of government and for all participants in the supply chain. Developing such an engagement process could enhance overall communication, improve the likelihood that the strategy will meet stakeholder needs, and strengthen efforts to address any challenges early in the process.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS generally concurred with our recommendation, in comments noted in Appendix IV: Comments from the Department of Health and Human Services, while noting that the term “engage” is vague and unclear, and that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority. As we note in this enclosure, ASPR officials acknowledged they had not yet formally engaged with nonfederal government stakeholders about the strategy. Additionally, the strategy suggests that engagement could occur through the Public Health Emergency Medical Countermeasure Enterprise; however, we recognize there may be other mechanisms that HHS could use to ensure the strategy reflects the input of key stakeholders, such as state and territorial governments and the private sector, which have a shared responsibility for providing supplies during a pandemic. We believe that capitalizing on existing relationships to engage these critical stakeholders as HHS refines and implements a supply chain strategy, to include the role of the SNS, will improve a whole of government response to, and preparedness for, pandemics. HHS did not provide any technical comments. OMB did not provide any comments.
GAO Methodology
To understand federal efforts to define and develop the mission of the SNS, we reviewed the SNS 2.0 strategy document and held interviews with senior officials from ASPR responsible for developing the strategy. We also conducted semi-structured interviews with a non-generalizable sample of 9 individuals with expertise on the operations or activities of the SNS, and an understanding of public health funding, preparedness, and response actions before ASPR’s strategy was publicly released. To obtain a mix of perspectives regarding the actions that might be considered to optimize the SNS for pandemic preparedness and response moving forward, we interviewed former high-ranking ASPR and CDC officials, researchers with expertise in preparedness and response, state emergency management officials, and an association representing domestic manufacturers. We identified these individuals by researching former federal officials with SNS leadership experience, reviewing congressional hearing testimony and relevant literature, and seeking referrals from internal stakeholders and those we interviewed. We also reviewed requested appropriations data available from the President’s budget request for fiscal years 2009 through 2018, and from HHS’s congressional budget justifications for fiscal years 2019 and 2020. To assess the reliability of the data reported in the congressional budget justifications, we confirmed budget amounts with agency officials and conducted comparisons to other sources to check for consistency.
Testing has been increasing across the United States, but federal data on the overall volume of testing are incomplete. Furthermore, the Department of Health and Human Services has not issued a publicly available and comprehensive national testing strategy, creating the risk of key stakeholders and the public lacking crucial information to support an informed and coordinated testing response.
Entities involved: Centers for Disease Control and Prevention, the Food and Drug Administration, and the Office of the Assistant Secretary for Health, all within the Department of Health and Human Services
Recommendation: The Secretary of Health and Human Services should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that the Department of Health and Human Services has produced for the public and Congress to allow for a more coordinated pandemic testing approach.
Key Considerations and Future GAO Work
We have included findings related to the federal response to COVID-19 testing in several previous reports.
In June 2020, we reported that while the Department of Health and Human Services (HHS) had taken steps to meet the unprecedented need for COVID-19 testing data, those data were incomplete and inconsistent.
In September 2020, we reported on challenges with testing supply availability, and recommended the development of plans outlining specific actions the federal government could take to help mitigate remaining medical supply gaps—including testing supply shortages.
In November 2020, we reported on issues with the transparency of Centers for Disease Control and Prevention (CDC) testing guidelines and recommended that HHS ensure that the scientific rationale for any changes is included when such changes are made.
Since we reported in November 2020, we have found that data indicate that diagnostic testing has increased. Specifically, HHS testing data suggest that the monthly volume of molecular testing for COVID-19 has roughly doubled from August through December, 2020. However, HHS testing data remain incomplete in part due to gaps in the reporting of newer rapid testing technologies to HHS. In addition, states are inconsistent in whether they report results of rapid antigen tests on their websites, as well as in whether they include these tests when calculating percent positivity—a key public health indicator. For more information and a recommendation on data collection and reporting standards, see the COVID-19 Health Indicators enclosure.
Furthermore, we found that the COVID-19 testing strategy implementation plans periodically sent to Congress to outline federal and state testing efforts have not been publicly available. We also found that the current testing strategy is not comprehensive because it does not fully include all of the characteristics that we have found to be desirable in an effective national strategy, including in our work in February 2004.[106] For example, testing strategy documents provided limited information on the types of resources required for future needs or economic principles guiding the strategy and not all documents clearly defined the problem and risks.
The Consolidated Appropriations Act, 2021 requires the President to make publicly available a report containing a whole-of-government plan for an effective response to subsequent major outbreaks of COVID-19.[107] This plan, which is required to be completed by late March 2021, is also required to address how to improve diagnostic testing and contact tracing, among other things. In addition, we recommend that the Secretary of the Department of Health and Human Services produce a consolidated and comprehensive national strategy document that incorporates all six characteristics of an effective national strategy and is publicly available. We will continue to examine federal testing strategy, data, and reporting issues.
Background
Diagnostic testing for COVID-19 is critical to controlling the spread of the virus, according to the CDC. Over the course of the pandemic, the types and volume of available viral diagnostic tests have increased as new testing technologies have emerged.[108] The Food and Drug Administration (FDA) has issued emergency use authorizations (EUA) for two types of viral diagnostic tests: molecular and antigen.[109] These tests either require processing with specialized laboratory equipment, as is typical with molecular tests, or could be processed rapidly at the point of care (rapid tests), such as in a clinic, nursing home, or school setting.[110] See table below for descriptions of the types of tests and considerations for use.
Types of Viral Diagnostic Tests for COVID-19
Notes: FDA may issue an emergency use authorization if the agency determines that certain medical products, such as a test, “may be effective” at diagnosing, treating, or preventing a disease, among other criteria. See 21 U.S.C. § 360bbb-3. While there are some point-of-care molecular tests, and one fully at-home test, nearly all require laboratory processing with specialized equipment and are not considered to be rapid tests.
As the coordinating agency for the federal response to public health and medical emergencies, HHS leads the development and implementation of the national COVID-19 testing strategy, as discussed below. Under this strategy, states manage their own COVID-19 testing programs with federal support from the Office of the Assistant Secretary for Health (OASH).
According to HHS, the national strategy for testing was formally outlined in the publicly available Testing Blueprint: Opening Up America Again (Blueprint) and the addendum to that Blueprint—issued in April, 2020. [111]
As of December 2020, the implementation of the Blueprint has been detailed in three HHS Testing Strategy Reports to Congress (Testing Strategy Reports) in May, August, and November, 2020—documents that outline the implementation of the national testing strategy.[112] As of January 2021, HHS has not made the Testing Strategy Reports available to the public.
The U.S. Government COVID-19 Response Plan, known as the PanCap Adapted, outlines overall plans for the COVID-19 response, including efforts for communication and public outreach.[113] This document is not publicly available.
According to the November, 2020 Testing Strategy Report, a total of $26.183 billion appropriated by the COVID-19 relief laws was available to HHS to support COVID-19 testing, among other things. HHS reported total testing-related obligations of about $18.9 billion as of December 31, 2020, a majority of which was awarded to states, localities, territories, and tribal organizations, and total expenditures of about $6.4 billion.[114] (See table below.)
HHS’s Reported Obligations and Expenditures for Testing-Related COVID-19 Response Activities, as of December 31, 2020
Key activity
Obligations ($ billions)
Expenditures ($ billions)
Percentage of obligated amounts expended, as of December 31, 2020
Support to state, local, territorial, and tribal organizations’ preparedness
13.355
2.534
19
Testing for uninsured
1.334
1.332
100
Testing
4.186
2.486
59
Total
18.875
6.352
34
Source: GAO analysis of Department of Health and Human Services (HHS) information. | GAO-21-265
Note: the percentages represent the share of obligated amounts for each key activity that were expended as of December 31, 2020. This table includes obligations and expenditures of appropriations provided under the four COVID-19 relief laws enacted in March and April, 2020, and does not include obligations and expenditures of appropriations provided under a fifth relief law, the Consolidated Appropriations Act, 2021, enacted in December 2020.
The Consolidated Appropriations Act, 2021, makes various appropriations to the Public Health and Social Services Emergency Fund, including $22.4 billion that may be used for COVID-19 testing. [115] The funds are to be available to states, localities, territories, and tribal organizations, among others, for necessary expenses for activities to monitor and suppress COVID-19, including testing and contact tracing. Not less than $2.5 billion of this amount is for strategies to improve testing capabilities and other purposes, such as contact tracing in high-risk and underserved populations, including racial and ethnic minority populations and rural communities. This funding will remain available through September 2022.
Overview of Key Issues
We found that molecular testing has increased in recent months. In addition, rapid antigen testing has also likely increased given broader availability and need for faster test results, but the extent of use of antigen tests is unclear because data on rapid antigen testing as reported to HHS are incomplete. In addition, states are inconsistent in whether they report results of rapid antigen tests on their websites, as well as in whether they include these tests when calculating percent positivity—a key public health indicator. Furthermore, we found that the national COVID-19 testing strategy, which could provide coordination on issues like these, has not been publicly available, nor has it been comprehensive.
Data indicate that molecular testing has increased over time, but the overall volume of testing is unknown. HHS testing data suggest that the monthly volume of molecular testing for COVID-19 has roughly doubled from August through December, 2020. Specifically, the number of reported tests increased from roughly 25 million tests in August to over 50 million tests in December. (See table.)
Monthly Volume of Molecular COVID-19 Tests Nationwide, August through December, 2020
Month
Total Number of Molecular Tests Performed (in millions)
August
25.4
September
26.8
October
35.1
November
45.9
December
50.8
Source: GAO analysis of Department of Health and Human Services data. | GAO-21-265
Notes: Data downloaded from https://healthdata.gov/dataset/covid-19-diagnostic-laboratory-testing-pcr-testing-time-series on January 8, 2021. Laboratories and other providers of COVID-19 tests are required to report testing data to the federal government, pursuant to the CARES Act. Laboratory testing data are reported to the Department of Health and Human Services (HHS) through state and jurisdictional health departments. The total number of molecular tests includes tests reported from commercial and reference laboratories, public health laboratories, hospital laboratories, and other testing locations, and does not generally include antigen or antibody tests. Tests include those with positive, negative, and inconclusive results, and is the total number of tests, as opposed to the number of individuals tested. Testing counts are subject to change as data are updated from reporting entities. We compared a selection of five states to the HHS data for those states and identified some discrepancies; we have not determined the reasons for these discrepancies for this report, but we will continue to examine the accuracy and completeness of these data. Regarding completeness of information for tests that are reported to HHS, as of October 30, 2020, HHS reported that 48 of 56 jurisdictions were reporting more detailed data with their test reporting, such as including race and ethnicity information.
Overall testing numbers are unknown in part because those data are incomplete as reported to HHS by the states. Federal testing data reported on the HHS website generally do not include the rapid antigen tests. According to an HHS estimate in its most recent Testing Strategy Report, rapid tests accounted for roughly one-quarter of nationwide testing as of November 30, 2020.
As a result of the incomplete data reporting, HHS does not publicly report the antigen test data the agency receives, nor does it have plans to do so, according to officials we interviewed. This has likely led to an underestimate of the overall amount of testing being done in the U.S. given that more rapid antigen tests have become available on the market and as a result, use of these tests is likely increasing. Some antigen tests do not require specialized laboratory equipment, and in general, they require fewer supplies that have been, at times, constrained. Moreover, antigen tests are considered rapid tests, and some can produce results in less than an hour, making them an attractive alternative to molecular testing despite sensitivity concerns.[116]
The lack of complete data on the number of antigen tests being performed is likely due in part to the challenges associated with the reporting of rapid antigen tests. Rapid antigen tests are being deployed in nursing homes, schools, pharmacies, and correctional facilities—some of which have not had extensive prior experience with testing for COVID-19. According to some public health stakeholder groups we spoke with, some entities offering point-of-care COVID-19 testing, such as rapid antigen tests, may not have the procedures or capabilities necessary for public health reporting. For example, CDC officials told us that some entities submit data through fax machine, which can make federal data reporting even more challenging.
HHS is taking steps to improve the completeness of antigen test data reporting. For example, in October, 2020, CDC introduced an option for long-term care facilities to report point-of-care test results, such as those for rapid antigen tests, through the National Healthcare Safety Network.[117] This new reporting channel facilitates the reporting process to CDC and ultimately HHS for the new antigen tests administered in nursing homes.
Use of rapid antigen tests has likely increased over time, but there is state variation in the planned use and data reporting of antigen tests. While the extent of antigen test use is unknown, use of rapid antigen tests likely has increased over time as HHS has made significant investments in the production and deployment of these rapid antigen tests, and states are planning their respective uses of such tests. For example:
In July 2020, HHS procured and began distributing over 5.3 million Quidel and Becton Dickinson rapid antigen tests to over 15,000 of nursing homes.
In September 2020, HHS began distributing 50 million Abbott rapid antigen tests to long-term care and other settings, as well as 100 million of these tests to states; as of November 30, 2020, over 18 million tests had been sent to nursing homes, over 4.6 million tests had been sent to assisted living facilities, and over 36 million tests had been deployed to states.
In December 2020, HHS announced the launch of a streamlined process for states to purchase point-of-care tests through the federal government at a fixed price, beginning with Abbott rapid antigen tests.
When supplying rapid antigen tests to states, HHS provided information on suggested uses and training from the manufacturer on how to use them.[118] In October 2020, HHS announced that 32 states and the District of Columbia had submitted plans to HHS on how they would use the rapid antigen tests. See figure for highlights from information that states provided to HHS on planned uses.
Planned Uses of Abbott Rapid Antigen Tests Reported by 32 States and the District of Columbia as of October, 2020
Notes: In September, 2020, HHS began providing all states and territories with Abbott rapid antigen tests. In October 2020, HHS announced that 32 states and the District of Columbia had submitted plans on how tests would be used.
In addition to HHS not having complete information on use of rapid antigen tests, there are also inconsistencies in how states report information about antigen tests to the public on their websites. We reviewed 56 state and territory websites containing information on COVID-19 data dashboards for the time period of November 5 through November 29, 2020 and found:
40 states and territories reported the numbers or results of antigen tests, while 7 did not publicly report any antigen testing data.
About 40 percent of states and territories used antigen test results when calculating the percentage of tests with positive results—a key public health indicator known as percent positivity.[119] Specifically, we identified 22 states and territories that expressly included antigen results in their percent positivity calculations.
As the use of antigen and other point-of-care tests continues to increase, including with increased availability of home-based testing, it will be important to capture such use in metrics used for public health decision-making. Furthermore, our work on COVID-19 health care indicators found that more complete and consistent COVID-19 data are needed to monitor health indicators to assess trends in the burden of the pandemic and to make informed decisions regarding resource allocation. For more information and a recommendation on data collection and reporting standards, see the Health Care Indicators enclosure.
HHS has not made all of its national testing strategy documents public. Several stakeholders we spoke with in the summer and fall of 2020 expressed concerns about the national testing strategy for COVID-19. Specifically, stakeholders from several public health and other organizations we spoke with told us they were unaware of the existence of a national strategy, or that they did not have a clear understanding of HHS’s testing strategy. Some stakeholder groups expressed a desire for clear federal communication of a strategy for the best and appropriate use of tests—including, for example, which tests should be used, with which populations, and at what intervals—as well as HHS’s goals for testing. Some stakeholders explained that their efforts to respond to the pandemic could be more effective if they fully understood the administration’s strategy. This would allow them to more effectively coordinate their efforts with the administration’s efforts.
Stakeholders may be unfamiliar with all elements of HHS’s testing strategy, in part, because HHS, as of January 2021, has not made the Testing Strategy Reports public. HHS has stated that its testing strategy can be found in the Blueprint, but this document does not provide the updates that HHS has provided to Congress on implementation of the strategy. To date, these updates have been detailed across three additional documents—the Testing Strategy Reports.[120] As mentioned, while the administration made the Blueprint public, HHS has not made the Testing Strategy Reports public, thus limiting the effectiveness of HHS's strategic communication related to testing.
In September 2020, HHS told us that they did not share Testing Strategy Reports publicly, but conveyed the goals of the reports with states and other stakeholders through regular communication. However, several stakeholders we interviewed said they were unaware of the existence of a testing strategy. Furthermore, CDC officials—key stakeholders given the agency’s role in protecting the country against health threats like COVID-19—told us they were not involved in the development of the August or November Testing Strategy Reports.
HHS testing strategy documents are not comprehensive. HHS strategy documents—individually and collectively—do not include all of the desirable characteristics of an effective national strategy. For example, we found that the current, publicly available, testing strategy is not comprehensive because it does not address all of the characteristics that we have found to be desirable in an effective national strategy. Taken together, all four strategy documents partially address the characteristics that we have found in past work to be desirable in effective national strategies. The six desirable characteristics of an effective national strategy are
clear purpose, scope, and methodology;
problem definition and risk assessment;
goals, subordinate objectives, activities, and performance measures;
resources, investments, and risk management;
organizational roles, responsibilities, and coordination; and
We assessed the extent to which the Blueprint and Testing Strategy Reports addressed the six desirable characteristics of an effective national strategy and found that none of the individual documents fully addressed all six characteristics. For example, both the Blueprint and Testing Strategy Reports provide some information on the purpose, scope and methodology of the strategy. However, information on resources, investments, and risk management is found only in the Testing Strategy Reports, and not in the Blueprint. While the Testing Strategy Reports provided more specific information on the resources associated for the strategy, they provided limited information on the types of resources required for future needs or economic principles guiding the strategy. In addition, only one Testing Strategy Report clearly defined the problem and risks. Therefore, one would need to have access to all of these documents to see a fuller picture of the administration’s testing strategy.
Furthermore, the Blueprint does not contain any performance measures, and the Testing Strategy Reports do not always provide consistent definitions and benchmarks for performance measures. For example, one performance measure HHS uses to assess testing sufficiency is percent positivity, which has not been presented consistently over time.
In its May 2020 Testing Strategy Report, HHS defined percent positivity as the percentage of tests with positive results. The report also noted epidemiological consensus that 10 percent or greater is a possible benchmark of insufficient testing, and reported a nationwide rate from May 8 to May 15, 2020 of 7.5 percent.
In its August 2020 Testing Strategy Report, HHS noted that 5 percent could provide more assurance, and reported a 7-day nationwide rate of 6.38 percent as of August 19, 2020.
In its November 2020 Testing Strategy Report, HHS did not provide a benchmark for percent positivity, nor did it report a nationwide rate, instead reporting state variation in percent positivity.
There is variation in the ways that states measure percent positivity and it is unclear what the federal government is using as its national target. It is important for a national strategy and its associated plans to have clear targets that align with goals and objectives to demonstrate progress.
According to the PanCAP (Adapted), the overall U.S. Government COVID-19 Response Plan, the federal COVID-19 response should facilitate accurate, coordinated, and timely information to affected audiences, including governments, media, the private sector, and the local populace.[122] Additionally, the Consolidated Appropriations Act, 2021 requires the President to make publicly available a report containing a whole-of-government plan for an effective response to subsequent major outbreaks of COVID-19.[123] This plan, which is required to be completed by late March 2021, is also required to address how to improve diagnostic testing and contact tracing, among other things. However, the Act does not prescribe what elements—such as the six characteristics of an effective national strategy—should be included in the plan. Until a comprehensive national testing strategy with all six characteristics of an effective national strategy is publicly available, HHS is at risk of key stakeholders and the public lacking crucial information to support an informed and coordinated testing response.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS partially concurred with our recommendation and provided general comments, which are reproduced in Appendix IV: Comments from the Department of Health and Human Services. OMB did not provide comments on this enclosure.
HHS agreed that the Department should take steps to more directly incorporate some of the elements of an effective national strategy, but expressed concern that producing such a strategy at this time could be overly burdensome on the federal, state, and local entities that are responding to the pandemic, and that a plan would be outdated by the time it was finalized or potentially rendered obsolete by the rate of technological advancement. Additionally, HHS stated that, to be of value to the whole of nation response to COVID-19, testing plans need to establish guidelines and use metrics that are operationally relevant, which necessitates strategic flexibility in testing plans to guide those managing the response in the use of available resources to address local and state conditions rather than a single static nationwide plan.
We believe that documenting a comprehensive and public national strategy is an important and worthwhile investment in resources so that all participants have the necessary information to accomplish shared goals. We also believe this can be done efficiently and flexibly, without imposing unnecessary burden. For example, HHS could make its existing implementation reports publicly available and make certain enhancements to those documents to consistently measure performance on certain metrics.
We also understand the need to be flexible in light of changing technology and information and believe this can be done by producing a strategy that is a living document, which would allow for changes to be made publicly and transparently as more information is gained over the course of the pandemic. Furthermore, we agree that testing plans need to establish guidelines and use metrics that are operationally relevant, and we believe that the current national testing strategy does not do so. We recognize that, by their nature, national strategies are intended to provide broad direction and guidance, however we believe the more detail a strategy provides, the easier it is for the responsible parties to implement it and achieve its goals.
Methodology
To conduct this work, we analyzed HHS data on the number of reported viral molecular COVID-19 tests performed across the country, which we downloaded from https://healthdata.gov/dataset/covid-19-diagnostic-laboratory-testing-pcr-testing-time-series on January 8, 2021. We assessed the reliability of HHS COVID-19 molecular testing data by reviewing related documentation, interviewing knowledgeable agency officials, and comparing a subset of states’ data reported on the HHS website to testing data reported on the states’ websites. We concluded that the data were sufficiently reliable for the purposes of our reporting objective.
We also reviewed agency guidance and other documentation, as well as the websites of 50 states, the District of Columbia, and five territories to examine information and guidance related to rapid antigen testing; interviewed and received written comments from HHS agency officials to obtain information on steps taken to implement, communicate, and update the national testing strategy and other guidance on COVID-19 testing; and interviewed public health and other stakeholder groups to obtain their perspectives on rapid antigen tests, data reporting, and federal COVID-19 testing strategy. To select interviewees, we identified a variety of groups that were impacted by federal testing strategy and guidance and that had broad geographic representation, in addition to practitioners with work in public health. In doing so, we identified 18 stakeholder groups; we spoke with 17 of these groups and obtained written comments from one of them. These groups represent, across the country
over 100,000 state and local public health officials and epidemiologists, as well as public health laboratories and other federal partners;
national, regional, community, and health system clinical laboratories;
state governors’ offices and staff, as well state education officials and school administrators; and
a variety of providers, including nursing home practitioners, physicians, and nurses.
Lastly, we assessed the federal COVID-19 testing strategy (Blueprint) and Testing Strategy Reports from May, August, and November 2020 against each of six characteristics of an effective national strategy and their associated sub-elements.
Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism, GAO-04-408T. Washington, D.C.: February 3, 2004.
The Department of Health and Human Services and Department of Defense, through Operation Warp Speed, continue to support the development and manufacturing of COVID-19 vaccines and therapeutics, and, with FDA’s authorization of two vaccines for emergency use, vaccine distribution and administration has begun, although continued federal planning, leadership, and coordination remains vitally important as initial vaccine rollout has not matched expectations.
Entities involved: Department of Defense, including the Joint Program Executive Office for Chemical, Biological, Radiological, and Nuclear Defense; Department of Health and Human Services, including the Biomedical Advanced Research and Development Authority, Centers for Disease Control and Prevention, Food and Drug Administration, and National Institutes of Health.
Key Considerations and Future GAO Work
In our recent work on COVID-19 vaccines and therapeutics, we identified issues related to the Food and Drug Administration’s (FDA) use of emergency use authorizations (EUA) for therapeutics, as well as the critical importance of planning for COVID-19 vaccine implementation, which includes the prioritization, allocation, distribution, and administration of available vaccines. With FDA’s recent authorization of two vaccines for emergency use as well as additional potential authorizations on the way, it is also important to understand lessons learned from the H1N1 influenza pandemic and their implications for COVID-19 vaccine implementation efforts as discussed later in this enclosure.
In November 2020, we recommended that FDA identify ways to uniformly disclose information from its scientific review of safety and effectiveness data when issuing EUAs for vaccines and therapeutics. This could be similar to the information FDA publicly releases to support approval of new drugs and licensure of new biologics.[124]
In response, FDA said it shared our goal of transparency and would explore approaches to achieving this goal. Further, the FDA Commissioner made an announcement on November 17, 2020, stating that to the extent appropriate and permitted by law, FDA would publicly post its reviews of the scientific data and information supporting the issuance, revision, or revocations of EUAs for all vaccines and therapeutics as part of its COVID-19 response.[125]
Since we made our recommendation, FDA developed a process for working with drug sponsors to disclose its scientific review documents for therapeutic EUAs and has released this information for the EUAs it has already issued. For example, FDA released EUA research review summaries for the previously authorized therapeutic bamlavinimab, as well as for two additional COVID-19 therapeutics.[126] We found the disclosed information was similar to the information the agency has released to support approval of new drugs and licensure of new biologics, as we recommended. For vaccine EUAs, FDA is holding public Vaccines and Related Biological Products Advisory Committee meetings, through which FDA and sponsors are making information from scientific reviews publicly available. FDA also released decision memos for the two vaccine EUAs it issued in December 2020; the decision memos contained detailed information about FDA’s review of clinical safety and effectiveness data.[127]
FDA’s newly developed process and resulting actions meet the intent of our recommendation and will improve the transparency of, and ensure public trust in, FDA’s EUA decisions for COVID-19 vaccines and therapeutics.
We also recommended, in September 2020, that the Secretary of Health and Human Services, with support from the Secretary of Defense, establish a time frame for documenting and sharing a national plan for distributing and administering COVID-19 vaccines, and ensure that such a plan is consistent with best practices for project planning and scheduling and that it outlines an approach for how efforts would be coordinated across federal agencies and nonfederal entities.
In November 2020, we again highlighted the importance of planning for vaccine distribution and clarifying the roles and responsibilities of federal agencies and stakeholders. We reported that the Department of Health and Human Services (HHS) and the Department of Defense (DOD) released initial planning documents in September 2020 for the distribution and administration of COVID-19 vaccines, but that stakeholders indicated the need for additional information as planning continued.
Since our November report, HHS and DOD, through Operation Warp Speed, have continued vaccine distribution planning efforts, including identifying several steps necessary for COVID-19 vaccine implementation. Such implementation requires federal leadership and coordination among federal agencies and key partners, including commercial entities, jurisdictions, and providers to allocate, distribute, and ultimately administer vaccines to individuals across the country.[128]
With FDA’s authorization of two vaccines for emergency use, as of December 30, 2020, Operation Warp Speed had distributed (shipped) about 12.4 million doses of COVID-19 vaccine and providers reported administering about 2.8 million initial doses, according to data from the Centers for Disease Control and Prevention (CDC). However, these initial numbers fell short of expectations set for the end of the year by officials, further underscoring the need for careful distribution and administration planning and clear and consistent communication by the federal government in concert with key partners.[129] By January 14, 2021, about 30.6 million doses had been distributed, and providers had reported administering about 11.1 million doses, according to CDC data.
The Consolidated Appropriations Act, 2021 requires the CDC Director to provide Congress with an updated and comprehensive COVID-19 vaccine distribution strategy and spend plan within 30 days of enactment (by January 26, 2021).[130] This strategy is to include, among other things, guidance for how jurisdictions and other nonfederal entities should prepare for, store, and administer vaccines; nationwide vaccination targets; and a description of how an informational campaign for the public and health care providers will be executed. We will evaluate the CDC’s strategy and spend plan when it is available and continue to monitor any other federal plans to determine whether such plans address our recommendation.
We continue to conduct work related to COVID-19 vaccines and therapeutics, including examining federal efforts under Operation Warp Speed, as well as assessing the federal government’s plans for COVID-19 vaccine implementation for any authorized or licensed vaccine and communication to the public about these implementation efforts.
Background
Vaccination is critical for reducing infection rates and severity of disease and mortality due to COVID-19. As of January 8, 2021, FDA had authorized two vaccines for emergency use to prevent COVID-19, and several other candidates were in advanced stages of development.[131] EUAs allow for the emergency use of medical products without FDA approval or licensure, provided certain statutory criteria are met.[132]
Therapeutics to treat COVID-19 are also critically important, particularly until vaccines become widely available. As of January 8, 2021, FDA had approved one therapeutic and made certain others available through EUAs.[133]
As of January 2021, multiple federal agencies continue to support the development, manufacturing, and implementation, including distribution, of vaccines and therapeutics to prevent and treat COVID-19. Through Operation Warp Speed—a partnership between DOD and HHS that includes several of their components—the federal government, along with private industry stakeholders, has been working to simultaneously develop and manufacture COVID-19 vaccine and therapeutic candidates at an unusually fast pace, so that they can be distributed as quickly as possible once authorized, licensed, or approved.[134] For vaccines in particular, Operation Warp Speed, CDC, commercial partners, and jurisdictions, among others, all have roles in implementing any COVID-19 vaccination program, which encompasses identifying priority groups for vaccination as well as allocating, distributing, and administering available vaccine.
Through Operation Warp Speed, DOD and HHS have obligated at least $16.3 billion as of December 31, 2020, to support the development, manufacture, and distribution of vaccines and therapeutics for COVID-19, as shown in the figure below.[135]
Department of Health and Human Services (HHS) and Department of Defense (DOD) Obligations for COVID-19 Vaccines and Therapeutics under Operation Warp Speed, as of December 31, 2020
Note: We used the HHS Operation Warp Speed website and HHS press releases to determine which contract obligations to include in our analysis. HHS announced two awards related to general manufacturing and distribution for which we could not identify obligations in the Federal Procurement Data System-Next Generation which are not included in the chart above.
Overview of Key Issues
Status of vaccine funding, development, and manufacturing under Operation Warp Speed. Operation Warp Speed aims to accelerate the development and delivery of vaccines for COVID-19. To do so, HHS and DOD awarded contracts and “other transaction agreements” (OTA) for development and manufacturing and began the large-scale manufacturing of vaccines while clinical trials were ongoing.
Vaccine funding status. Through Operation Warp Speed, HHS and DOD have obligated approximately $13 billion as of December 31, 2020, through awards to six pharmaceutical companies for vaccine dose deliverables, with various development and manufacturing activities associated with different awards.
Vaccine development status. The six companies with Operation Warp Speed COVID-19 vaccine candidates were at varying stages of development as of January 8, 2021, as shown in the table below. On December 11, 2020, FDA authorized Pfizer’s COVID-19 vaccine for emergency use in individuals 16 years and older, which was the first COVID-19 vaccine to receive an EUA from FDA. On December 18, 2020, FDA issued an EUA for Moderna’s COVID-19 vaccine, authorizing it for emergency use in individuals 18 years and older.
Status of Development of Six Operation Warp Speed COVID-19 Vaccine Candidates, as of January 8, 2021
Pharmaceutical company
Started phase 3 clinical trialsa
Announced initial findings from phase 3 clinical trials
Submitted emergency use authorization (EUA) request to FDAb
FDA Issued EUA
AstraZeneca
●
●c
Janssen
●
Moderna
●
●
●
●
Novavax
●
Pfizer
●
●
●
●
Sanofi/Glaxo Smith Kline
d
Source: GAO analysis of pharmaceutical company, Operation Warp Speed, and Food and Drug Administration (FDA) information. | GAO-21-265
aPhase 3 clinical trials look at things like whether the product prevents new infections or, if people become infected, if the product helps control the infections so they do not become severe. These trials involve many thousands of volunteers, usually including participants who are at increased risk for infection. Earlier phases generally involve fewer volunteers and test issues such as safety of the product (phase 1) and the maximum tolerated dose or optimal schedule for giving the product (phase 2). bDuring an emergency, as declared by the Secretary of Health and Human Services under 21 U.S.C. § 360bbb-3(b), FDA may temporarily authorize unapproved medical products or unapproved uses of approved medical products through an EUA, provided certain statutory criteria are met. FDA has indicated that issuance of an EUA for a COVID-19 vaccine for which there is adequate manufacturing information would require the submission of certain clinical trial information from phase 3 clinical trials that demonstrate the safety and effectiveness of the vaccine in a clear and compelling manner, among other things. Any COVID-19 vaccine that initially receives an EUA from FDA is expected to ultimately be reviewed and receive licensure through a biologics license application, according to FDA guidance. cAstraZeneca announced findings from an interim analysis of phase 3 clinical trial data from the U.K. and Brazil. As of January 8, 2021, it had not announced findings based on its phase 3 clinical trial in the U.S. dSanofi announced in December 2020 that global phase 3 clinical trials could start during the second quarter of 2021; pending positive data from a phase 2 study expected to start in February 2021.
Vaccine manufacturing status. As of December 31, 2020, the government had at least 800 million vaccine doses under contract expected to be delivered by July 31, 2021, pending any issues with clinical trials, EUA issuance, or other factors.[136] Initial awards made from March through June were generally to fund development efforts, including clinical studies. Later awards made from July to December were generally for vaccine manufacturing, including the purchase of vaccine doses.[137]
While the types of awards, pricing, and delivery dates vary for each company, all six companies were initially expected to deliver 100 million vaccine doses at prices ranging generally from $10 to $19.50 per dose by June 30, 2021, with options for the government to procure additional doses through priced options or follow-on agreements.[138] For example, in December 2020, DOD exercised an option to procure an additional 100 million doses from Moderna by June 30, 2021. In addition, HHS announced an agreement with Pfizer in December for an additional 100 million doses by July 31, 2021. The figure below provides the timeline of initial OWS awards from March to November 2020, based on the acquisition documents we reviewed, and additional information from HHS, DOD, and the pharmaceutical companies.
Timeline of Initial COVID-19 Vaccine Development and Manufacturing Awards from March to November 2020 under Operation Warp Speed
Notes: Initial and final delivery dates are the dates included in the original contracts and supporting acquisition documents we reviewed and may have been adjusted based on subsequent modifications or actions.aAccording to Janssen representatives, approximately 2 million doses will be delivered at the time of emergency use authorization.bDOD exercised an option on December 11, 2020 to acquire an additional 100 million doses from Moderna.cAccording to Sanofi representatives, the potential availability of Sanofi’s vaccine candidate has been delayed until the fourth quarter of 2021.dAccording to AstraZeneca representatives, AstraZeneca is now under contract to provide a total of 300 million doses, which will be provided on a rolling basis. These representatives also noted the dates established in the initial agreement were notional.eAccording to HHS, Pfizer was awarded another agreement in December 2020 to provide an additional 100 million vaccine doses. According to Pfizer representatives, by December 17, Pfizer had shipped 2.9 million doses, 6 days after it received an emergency use authorization for its vaccine. Pfizer representatives stated they expect to deliver 200 million doses by July 31, 2021.
To expedite vaccine manufacturing efforts, HHS partnered with DOD to utilize contracting flexibilities and capacity that HHS lacked, according to HHS officials. Specifically, DOD awarded prototype OTAs to five of the six companies for vaccine manufacturing efforts.[139] Overall, about $8.8 billion of the roughly $13 billion dollars for vaccine development and manufacturing have been obligated through OTA awards as of December 31, 2020.
OTAs are flexible agreements that allow the parties to negotiate terms and conditions specific to the project. This flexibility can help agencies attract and contract with entities that have not done business with federal agencies due to concerns about standard government requirements.[140] However, there may be challenges with their use in terms of a risk of reduced accountability and transparency. OTAs are generally exempt from federal procurement laws and regulations, allowing intellectual property rights under each OTA to be tailored to suit the goals of the project.[141] We have ongoing work to review specific aspects of the contracts and OTAs, including intellectual property rights.
Federal officials report that they are continuing to work with manufacturers to mitigate challenges with scaling up the manufacturing of vaccine candidates. Operation Warp Speed officials stated that the most common challenges experienced by vaccine manufacturers have been gaining timely access to key materials and resources. To help address those challenges, DOD and HHS officials said they have prioritized supply contracts for vaccine manufacturers under the Defense Production Act.[142] Additionally, Operation Warp Speed officials stated that they have worked with U.S. Customs and Border Protection to expedite necessary equipment and goods coming into the U.S. We will continue to examine the federal government’s efforts to manufacture COVID-19 vaccines, including Operation Warp Speed’s activities to further mitigate any manufacturing challenges.
Status of therapeutic funding, development, and manufacturing under Operation Warp Speed. Through Operation Warp Speed, HHS and DOD have obligated almost $2 billion as of December 31, 2020, for therapeutics. As shown in the figure below, the agencies made initial awards to three pharmaceutical companies from March to November 2020 for therapeutics development and manufacturing activities.[143] Each of the three therapeutics are monoclonal antibody treatments.[144] The figure below provides the timeline of initial OWS awards based on the acquisition documents we reviewed and additional information from HHS and the pharmaceutical companies.
Timeline of Initial COVID-19 Therapeutic Development and Manufacturing Awards from March to November 2020 under Operation Warp Speed
Notes: Initial and final delivery dates are the dates included in the original contracts and supporting acquisition documents we reviewed and may have been adjusted based on subsequent modifications or actions.aAccording to Regeneron representatives, the initial delivery date was July 2020, and later delivery dates included September, October, and November 2020. They noted that the final delivery date for 2020 was in December.bAstraZeneca representatives noted that this date is an estimated delivery date dependent on several factors, including regulatory decisions outside AstraZeneca’s control.cAccording to HHS, Eli Lilly’s agreement was modified to provide the government with a total of 3 million doses. Eli Lilly representatives said initial delivery will take place on January 31, 2021, in the amount of 950,000 doses. They specified that the government has the possibility to acquire up to a maximum of 3 million doses, with any additional quantities above the minimum being dependent upon additional factors, such as available supply as determined by Eli Lilly.
As of January 8, 2021, two of these therapeutics had received an EUA for the treatment of mild-to-moderate COVID-19 in adults and certain pediatric patients: Eli Lily’s bamlanivimab on November 9, 2020 and Regeneron’s antibody treatment of casirivimab and imdevimab, administered together, on November 21, 2020. AstraZeneca’s therapeutic was in phase 3 clinical trials as of January 8, 2021.
Status of federal efforts for COVID-19 vaccine implementation. Federal agencies have identified several necessary steps for COVID-19 vaccine implementation, including the prioritization, allocation, distribution, and administration of any authorized or licensed COVID-19 vaccine. The figure below provides an overview of key components of vaccine implementation for 64 state, local, and territorial jurisdictions from interim planning documents and other information HHS and DOD (under Operation Warp Speed) and CDC have issued since September 2020.[145]
Key Components for COVID-19 Vaccine Implementation for Jurisdictions, as of December 2020
This figure includes the key components for 64 jurisdictions, including all U.S. states, territories, and local health programs in Chicago, the District of Columbia, Houston, New York City, Philadelphia, and San Antonio. It does not apply to the plans for the federal entities receiving direct vaccine allocations, such as the Bureau of Prisons, Department of Defense, Department of State, Indian Health Service, and Department of Veterans Affairs.aThe Centers for Disease Control and Prevention’s (CDC) Advisory Committee on Immunization Practices (ACIP) is comprised of medical and public health experts who make recommendations on the use of vaccines in the civilian population of the United States. Its recommendations serve as public health guidance for safe use of vaccines and other related products. ACIP’s recommendations are not binding and jurisdictions can adopt different approaches.bACIP recommended that in Phase 1b, COVID-19 vaccine should be offered to persons aged ≥75 years and non–health care frontline essential workers, and in Phase 1c, to persons aged 65–74 years, persons aged 16–64 years with high-risk medical conditions, and essential workers not included in Phase 1b. cProviders include organizations such as hospitals, medical practices, pharmacies, Federally Qualified Health Centers, rural health clinics, commercial vaccination service providers, correctional or detention health services, community health centers, home health care providers, long-term care centers, and urgent care as well as federal health agencies and tribal heath centers. Jurisdictions’ immunization information systems (IIS) are confidential, population-based, computerized databases that record all immunization doses administered by participating providers to persons residing within a given geopolitical area. The Vaccine Tracking System is a secure, web-based IT system that integrates the entire publicly funded vaccine supply chain from purchasing and ordering through distribution.dVaccineFinder is a free, online service where users can search for locations that offer vaccinations; providers are expected to update their vaccine inventory daily, according to CDC’s interim playbook.
Several key actions necessary for COVID-19 vaccine implementation are underway for the two COVID-19 vaccines (Pfizer and Moderna) that FDA authorized for emergency use. In November 2020, Operation Warp Speed provided jurisdictions and federal entities with allocation amounts for estimated initial doses of the Pfizer and Moderna COVID-19 vaccines, which jurisdictions were to receive if FDA issued EUAs for these vaccines, as subsequently occurred.[146] Further, CDC’s ACIP met in early December 2020, and made a recommendation for the priority groups to be included in the initial phase of vaccination upon FDA’s issuance of EUAs for COVID-19 vaccines. See the table below for other key actions.
Key Actions of Federal Agencies, Agency Advisory Committees, and Jurisdictions for Two COVID-19 Vaccines Authorized for Emergency Use, as of December 2020, by date
Date
Organization
Action
Oct. 22, 2020
FDA Vaccine and Related Biological Products Advisory Committee (VRBPAC)
Met to discuss, in general, the development, authorization and/or licensure of vaccines to prevent COVID-19; no specific request or application was discussed at this meeting.
Nov. 20, 2020
Operation Warp Speed
Provided 64 jurisdictions and 5 federal entities allocation amounts for estimated initial 6.4 million doses of Pfizer vaccine; allocation based on adult population of jurisdictions.
Nov. 27, 2020
Provided 64 jurisdictions and 5 federal entities allocation amounts for estimated initial 12.5 million doses of Moderna vaccine; allocation based on adult population of jurisdictions.
Dec. 1, 2020
CDC Advisory Committee on Immunization Practices (ACIP)
Met to discuss priority groups for allocation of initial COVID-19 vaccine and recommended that vaccination in the initial phase of the COVID-19 vaccination program (phase 1a) be offered to (1) health care personnel, and (2) residents of long-term care facilities.a
Dec. 2, 2020
CDC
CDC Director adopted ACIP’s recommendation for priority groups for the initial phase of the COVID-19 vaccination program.b
Dec. 4, 2020
64 jurisdictions and 5 federal entities
Microplans for initial Pfizer vaccine allocations due to Operation Warp Speed; deadline for placing orders/locations for initial distribution.
Dec. 10, 2020
VRBPAC
Met to discuss emergency use authorization (EUA) request for Pfizer vaccine. VRBPAC voted to recommend the vaccine for emergency use.
Dec. 11, 2020
64 jurisdictions and 5 federal entities
Microplans for initial Moderna vaccine allocations due to Operation Warp Speed; deadline for placing orders/locations for initial distribution.
Dec. 11, 2020
FDA
Issued EUA for Pfizer vaccine.
Dec. 11-12, 2020
ACIP
Met to discuss Pfizer vaccine and issued an interim recommendation for use of the Pfizer vaccine in persons aged 16 years or older for the prevention of COVID-19.c
Dec. 12, 2020
Operation Warp Speed/Pfizer
Began shipping initial doses of Pfizer vaccine to locations identified by jurisdictions and federal entities in their microplans.
Dec. 13, 2020
CDC
CDC Director adopted ACIP’s interim recommendation for Pfizer vaccine.b
Dec. 14, 2020
jurisdictions and federal entities
First Pfizer vaccinations administered.
Dec. 17, 2020
VRBPAC
Met to discuss EUA request for Moderna vaccine. VRBPAC voted to recommend the vaccine for emergency use.
Dec. 18, 2020
FDA
Issued EUA for Moderna vaccine.
Dec. 19, 2020
ACIP
Met and issued an interim recommendation for the use of the Moderna vaccine in persons aged 18 or older for the prevention of COVID-19.c
Dec. 19, 2020
CDC
CDC Director adopted ACIP’s interim recommendation for Moderna vaccine.b
Dec. 20, 2020
ACIP
Met to update recommendations for priority groups for allocation of COVID-19 vaccine. ACIP recommended that if COVID-19 vaccine supply is limited, after phase 1a, vaccination should be offered in phase 1b to: 1) persons aged 75 and older and 2) frontline essential workers (non-healthcare); and in phase 1c to: 1) persons aged 65-74 years, 2) persons aged 16-64 years with high-risk medical conditions, and 3) other essential workers.d
Dec. 20, 2020
Operation Warp Speed/Distributor
Began shipping initial doses of Moderna vaccine to locations identified by jurisdictions and federal entities in their microplans.
Dec. 21, 2020
CDC
CDC Director adopted ACIP’s updated recommendations for priority groups for allocation of COVID-19 vaccine.b
Dec. 21, 2020
jurisdictions and federal entities
First Moderna vaccinations administered.
Source: GAO Analysis of CDC, FDA, and Operation Warp Speed information and Operation Warp Speed and CDC officials. | GAO-21-265
aHealth care personnel are defined as paid and unpaid persons serving in health care settings who have the potential for direct or indirect exposure to patients or infectious materials. Long-term care facility residents are defined as adults who reside in facilities that provide a verity of services, including medical and personal care, to persons who are unable to live independently. bACIP’s recommendations are reviewed by the CDC Director and, if adopted, are published as official CDC/HHS recommendations in the Morbidity and Mortality Weekly Report. See https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19.html (accessed Jan.11, 2021) for ACIP’s current COVID-19 vaccine recommendations. cThe interim recommendation is based on use of the vaccine under an EUA and might change as more evidence becomes available, according to ACIP. dFor the purposes of ACIP’s recommendation, non-healthcare frontline essential workers include firefighters, police officers, corrections officers, food and agricultural workers, U.S. Postal Service workers, manufacturing workers, grocery story workers, public transit workers, those who are in the education sector (teachers and support staff), as well as daycare workers.
According to HHS and Operation Warp Speed documents, the federal government is leveraging existing IT systems and distribution structures to distribute COVID-19 vaccines to jurisdictions, as shown in the figure below.[147] For example, the Vaccine Tracking System (VTrckS) will match orders from jurisdictions against allocations, and these orders will then be transmitted to the manufacturers and distributors for vaccines and ancillary supplies. According to CDC data, about 30.6 million COVID-19 vaccine doses had been distributed to jurisdictions and federal entities and about 11.1 million doses had been administered, as of January 14, 2021.[148]
Interim Federal Plans for COVID-19 Vaccine Distribution Activities for Jurisdictions, as of December 2020
This is the distribution plan outlined in the Centers for Disease Control and Prevention’s (CDC) interim playbook for 64 jurisdictions, including all U.S. states, territories, and local health programs in Chicago, the District of Columbia, Houston, New York City, Philadelphia, and San Antonio. It does not apply to distribution plans for federal entities receiving direct vaccine allocations, such as the Bureau of Prisons, Department of Defense, Department of State, Indian Health Service, and Veterans Health Administration, and commercial pharmacies. According to Operation Warp Speed, vaccine allocation and centralized distribution utilizes the Vaccine Tracking System (VTrckS), which is a secure, web-based IT system that integrates the entire publicly funded vaccine supply chain. CDC’s interim playbook states these plans are subject to change. aProviders include organizations such as hospitals, medical practices, pharmacies, Federally Qualified Health Centers, rural health clinics, commercial vaccination service providers, correctional or detention health services, community health centers, home health care providers, long-term care centers, and urgent care as well as federal health agencies and tribal heath centers. All providers participating in the COVID-19 Vaccination Program are expected to submit the names, titles, and applicable license numbers to CDC of any licensed health care providers who have prescribing authority. bAdministration sites may include health care provider offices, long-term care facilities, pharmacies, public health clinics, childcare or daycare facilities, community centers, correctional or detention facilities, schools, shelters, temporary or off-site vaccination clinics, mobile clinics, urgent care facilities, or workplaces.
Effective coordination and communication among federal agencies, commercial partners, jurisdictions, providers, and the public is critical to the successful implementation of COVID-19 vaccines. According to DOD officials, there has been ongoing communication between Operation Warp Speed and federal, state, and other jurisdictions, such as discussions with small groups of jurisdictions to help them with planning and to share best practices for vaccine administration. CDC officials reported that the agency has developed communication resources for the general public, health care providers, health systems, and jurisdictions. For example, CDC has posted training and education materials on its website to help health professionals prepare for COVID-19 vaccination, including information on how to talk to patients about COVID-19 vaccines and make a strong recommendation for vaccination and a COVID-19 vaccination communication toolkit for medical centers, clinics, and clinicians.[149]
In addition, the Consolidated Appropriations Act, 2021 appropriated $8.75 billion for CDC-wide activities and program support, including for activities to plan, prepare for, promote, distribute, administer, monitor, and track COVID-19 vaccines.[150] The act provided that “not less than $4.5 billion of this amount shall be for state, local, territorial and tribal public health departments”.[151] The act also requires the Secretary of Health and Human Services, acting through the CDC Director and in coordination with other offices and agencies, to award competitive grants or contracts to one or more public or private entities to develop a national evidence-based campaign to increase awareness and knowledge of the safety and effectiveness of vaccines, among other things.[152]
Lessons learned on vaccine implementation and communication from H1N1 pandemic. The 2009 H1N1 influenza pandemic tested the nation’s ability to distribute and administer a vaccine to millions of Americans and, therefore, can provide important lessons learned for implementing COVID-19 vaccines and communicating to the public about these efforts. Lessons learned from the H1N1 vaccine campaign cover a wide range of areas, including identifying and prioritizing certain groups to receive the vaccine when vaccine availability is limited, distributing and administering available vaccine, and communicating these efforts and the benefits of vaccination to the public. For instance, we found that effective communication about the availability of vaccine was important for managing public expectations during H1N1. Similarly, managing public expectations as COVID-19 vaccine implementation begins is critical especially because initial supplies of vaccine have been limited.
The table below provides examples of lessons learned from the H1N1 influenza pandemic and implications for COVID-19 vaccine implementation and communication to the public, based on our past work examining the H1N1 pandemic as well as our review of reports from the federal government and state and territorial health officials on the H1N1 pandemic, CDC’s interim playbook for COVID-19 vaccination, and other information. In some instances, federal officials have reported taking certain lessons from H1N1 into consideration as they have developed their COVID-19 response efforts, such as using a central distributor for most COVID-19 vaccines.
Selected Lessons Learned from the Federal Response to the 2009 H1N1 Influenza Pandemic, Related to Vaccine Prioritization, Distribution, Administration, and Communication
Lesson learned
Experience during H1N1 pandemic
Implications for implementing COVID-19 vaccine
Prioritization
Differences in how local jurisdictions prioritized groups for vaccination caused confusion
State and local jurisdictions were given flexibility to refine priority groups for H1N1 vaccine to meet local needs. Jurisdictions appreciated this flexibility, but differences in priority groups between neighboring jurisdictions led to confusion or the appearance of inequity.
Because initial supplies of COVID-19 vaccine were expected to be limited, the Centers for Disease Control and Prevention (CDC) and Operation Warp Speed instructed jurisdictions to plan for the need to further refine any CDC recommended priority groups, which could again result in public confusion if neighboring jurisdictions identify differing priority groups.
Distribution
Using a centralized distributor was generally cited as an effective practice
The CDC used a centralized distribution process to distribute H1N1 vaccine to states. Built off CDC’s existing Vaccines for Children program, the distribution process proved to be scalable to also serve adults and used procedures and systems already familiar to many providers.a
For most COVID-19 vaccines, the Department of Health and Human Services (HHS) and Department of Defense (DOD) will use the same central distributor used during the H1N1 pandemic and build off of the CDC Vaccines for Children program. However, one vaccine (Pfizer) requiring ultra-cold storage is being shipped directly from the manufacturer to the vaccination provider site.
Minimum dose requirement for vaccine orders was problematic
CDC’s central distributor required minimum shipments of 100 doses of H1N1 vaccine, which were less suitable for vaccine providers administering vaccine to smaller populations. States had to break down the shipments into smaller increments, which was reported to have required significant staff time, caused storage and handling issues, and delayed when providers received vaccine.
HHS and DOD have determined that the minimum order size for centrally distributed COVID-19 vaccines is 100 doses, and the minimum order size for ultra-cold vaccine distributed from the manufacturer is 975 doses. This could again pose similar or even greater challenges getting vaccine to providers administering vaccine to smaller populations. States have asked for additional guidance on how to redistribute ultra-cold vaccine and officials representing immunization managers said redistributing ultra-cold vaccine will be a challenge for states.
Administration
State and local health departments had success expanding the pool of vaccine administrators
To achieve higher vaccine uptake, state and local jurisdictions used alternative vaccination clinic structures, such as drive-through clinics and retail pharmacies to administer H1N1 vaccine.
HHS and CDC have partnered with large retail pharmacies to administer COVID-19 vaccine in long-term care facilities and to the general public as larger supplies of vaccine becomes available. Participating jurisdictions are expected to have visibility on vaccine supply and uptake data by pharmacies within their respective areas.
Challenges with data collection limited available information on doses administered
Due to variations in states’ immunization tracking systems and capabilities, limited information was available nationally on the number of H1N1 vaccine doses administered. And because requiring data entry into immunization registries can decrease provider participation, states weighed the importance of vaccinating populations against tracking vaccine administration. In the end, according to a state immunization official, just one-quarter of states required patient-level reporting on H1N1 vaccine administration to state registries.
CDC has obtained Data Use Agreements from all 64 jurisdictions, according to the agency. CDC is requiring providers participating in COVID-19 vaccination efforts to report within 72 hours of administration on specific data elements, such as the vaccination site, which vaccine was administered, and information about the person receiving the vaccine. These data will be incorporated into an IT infrastructure that will support CDC analysis, information sharing between jurisdictions, and access to vaccine administration data. State and local health officials have raised concerns about the risks of introducing new data systems and requirements that have yet to be tested to track vaccine distribution and administration.
Vaccine administrators had to work with multiple formulations of the H1N1 vaccine that arrived at different times and had different age and risk-group indications. For example, the first formulation to become available was not appropriate for use in several priority populations. This resulted in confusion and challenges in planning a mass vaccination program.
The multiple COVID-19 vaccines under development and available under emergency use authorizations (EUA) present additional challenges that were not encountered with H1N1 vaccine. COVID-19 vaccines will likely employ different and, in some cases, new technologies that have never been used in a vaccine licensed by the Food and Drug Administration (FDA). In addition to using different technology, the storage and handling requirements for COVID-19 vaccines differ, with some requiring ultra-cold storage that many providers do not have according to two provider groups. Further, unlike the H1N1 vaccine that required a single dose, the two COVID-19 vaccines available under EUAs require two doses, separated by either 21 or 28 days, and FDA may authorize or license different COVID-19 vaccines for different ages and risk groups.
Communication
Effective communication on the availability of vaccine was important for managing public expectations
HHS had conveyed that a robust H1N1 vaccine supply—about 120–160 million doses—was expected to be available in October 2009, but ultimately only about 23 million doses were allocated and fewer than 17 million doses were distributed to states by the end of that month. When vaccine availability was less than anticipated, state and local health departments had to cancel planned and publicized mass vaccination clinics and the credibility of government was diminished.
Delivery of Pfizer and Moderna vaccine doses began in December 2020. The stated goal of HHS and DOD’s Operation Warp Speed partnership is to ultimately deliver 300 million doses of safe and effective COVID-19 vaccines, with initial doses available by January 2021. HHS and DOD have noted that initial vaccine supplies have been limited and anticipate broadening vaccination campaigns as more COVID-19 vaccine becomes available. However, during 2020 federal officials reported differing dates and estimates for when and how much vaccine was estimated to be available.
Effective communication approaches were needed to reach certain communities of color
During the H1N1 pandemic, certain racial and ethnic groups had lower vaccination rates, experienced delays in seeking vaccination, and had disproportionately higher percentages of hospitalizations and deaths compared with other populations. Some state officials observed that more proactive and focused federal vaccine messaging was needed for these groups. State and local health officials also said they wanted CDC to provide more communication materials for non-English speakers, with some state officials noting that it would be more efficient for CDC to provide the translation than having each state spending resources to translate the materials individually.
COVID-19 has affected racial and ethnic minorities disproportionately, and in one survey, a smaller proportion of African-Americans have said they would be willing to get vaccinated compared with other groups.b CDC officials reported that the agency has developed communication resources for the general public, health care providers, health systems, and jurisdictions.
Source: GAO analysis of reports on the 2009 H1N1 pandemic from GAO; the Association of State and Territorial Health Officials; HHS; the Institute of Medicine of the National Academies; other HHS and DOD documentation, including the COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations, Version 2.0; and information from CDC officials. | GAO-21-265
aThe Vaccines for Children program is a federally funded program that provides vaccines at no cost to children who might not otherwise be vaccinated because of their families’ inability to pay. The program, administered by CDC, distributes pediatric vaccines to states and health care providers. bKaiser Family Foundation, “Race, Health, and COVID-19: The Views and Experiences of Black Americans – Key Findings from the KFF/Undefeated Survey on Race and Health” (Washington, D.C.: October 2020), accessed Nov. 25, 2020, http://files.kff.org/attachment/Report-Race-Health-and-COVID-19-The-Views-and-Experiences-of-Black-Americans.pdf
Agency Comments
We provided HHS and DOD with a draft of this enclosure. HHS and DOD provided technical comments, which we incorporated as appropriate.
Methodology
To conduct this work, we reviewed relevant agency documents, including HHS’s and DOD’s Operation Warp Speed fact sheet, Operation Warp Speed’s strategy for distributing a COVID-19 vaccine, and CDC’s COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations, Version 2.0.[153] We also interviewed or received written responses from HHS and DOD officials, including officials working within the Operation Warp Speed partnership and agency officials from the Biomedical Advanced Research and Development Authority, National Institutes of Health, and CDC.
To identify agencies’ federal contract obligations and use of OTAs related to Operation Warp Speed, we reviewed data reported by the Federal Procurement Data System-Next Generation through December 31, 2020, and agreements from DOD, HHS, and Advanced Technology International (ATI).[154] We identified contract obligations related to Operation Warp Speed using the National Interest Action code, the contract description field, and information in agency documents and on an HHS website detailing Operation Warp Speed projects.[155]
We assessed the reliability of federal procurement data by reviewing existing information about the Federal Procurement Data System-Next Generation and the data it collects—specifically, the data dictionary and data validation rules—and by performing electronic testing. We determined that the data were sufficiently reliable for the purposes of describing agencies’ reported contract obligations for Operation Warp Speed. We also interviewed HHS and DOD officials and ATI representatives and reviewed related contract documents.
Further, to identify lessons learned from the federal response to the H1N1 pandemic, we reviewed prior GAO work on the 2009 H1N1 pandemic as well as information and documentation from HHS, DOD, the Association of State and Territorial Health Officials, and the Institute of Medicine of the National Academies.
Contact information: Alyssa M. Hundrup, (202) 512-7114, hundrupa@gao.gov
Related GAO Products
COVID-19: Federal Efforts Accelerate Vaccine and Therapeutic Development, but More Transparency Needed on Emergency Use Authorizations, GAO-21-207. Washington, D.C.: November 17, 2020.
DATA ACT: Quality of Data Submissions Has Improved but Further Action Is Needed to Disclose Known Data Limitations. GAO-20-75. Washington, D.C.: November 8, 2019.
Military Acquisitions: DOD is Taking Steps to Address Challenges Faced by Certain CompaniesGAO-17-644. Washington, D.C.: July 20, 2017.
Influenza Pandemic: Lessons from the H1N1 Pandemic Should Be Incorporated into Future Planning. GAO-11-632. Washington, D.C.: June 27, 2011.
Agencies within the Department of Health and Human Services have taken actions to prevent issuance of duplicate or erroneous payments to providers, but the effectiveness of these actions is limited by lack of needed information. The risk of financial losses may be limited, however, as the few states opting to provide Medicaid coverage of testing services for uninsured individuals have reported modest levels of spending as of December 2020.
Entities involved: Centers for Medicare & Medicaid Services and the Health Resources and Services Administration, within the Department of Health and Human Services.
Key Considerations and Future GAO Work
In our September 2020 report, we found that two entities within the Department of Health and Human Services (HHS)—the Health Resources and Services Administration (HRSA) and the Centers for Medicare & Medicaid Services (CMS)—both make payments to providers for COVID-19 testing of uninsured individuals. According to officials, HRSA has implemented controls to help prevent payment errors, including duplicate payments. The overall effectiveness of these controls, which have identified some payment errors, are limited by the lack of information needed to ensure that individuals are uninsured and thus, qualify for the testing services.
Federal legislation enacted in response to the COVID-19 pandemic provides states the option to enroll the uninsured in Medicaid for the purpose of obtaining COVID-19 testing coverage; however, few states have opted to use this flexibility. Even in these states, providers may bill and receive payment from HRSA for COVID-19 tests of uninsured individuals who have not enrolled in their state’s Medicaid COVID-19 testing coverage. These factors, as well as others, may have contributed to the relatively modest amount—about $7 million—of Medicaid spending on COVID-19 testing for uninsured individuals so far.
Giving states the option to pay for COVID-19 testing using federal Medicaid funds was one of a number of flexibilities Congress and HHS provided to states to respond to the COVID-19 pandemic. We are examining states’ use of Medicaid flexibilities to better understand those that have been most useful to states’ responses to the COVID-19 pandemic.
Background
Medicaid is one of the nation’s largest sources of funding for health care services for low-income and medically needy individuals, covering an estimated 77 million people and spending approximately $673 billion in fiscal year 2020.[156] States and territories administer their Medicaid programs within broad federal rules and according to state plans approved by CMS, which oversees Medicaid at the federal level. The federal government matches states’ spending for Medicaid services according to a statutory formula known as the Federal Medical Assistance Percentage (FMAP).[157]
The Families First Coronavirus Response Act (FFCRA) provides a temporary increase in the FMAP for all qualifying states and territories.[158] FFCRA also created an option for states to provide Medicaid coverage of COVID-19 diagnostic testing and related services to uninsured individuals.[159] CMS has approved 15 states and three territories to make Medicaid payments to providers for COVID-19 testing of uninsured individuals, with the federal government responsible for 100 percent of the cost.[160] Additionally FFCRA and the Paycheck Protection Program and Health Care Enhancement Act each appropriated $1 billion to reimburse providers for conducting COVID-19 testing of uninsured individuals.[161] HRSA is responsible for administering the $2 billion appropriated for paying providers for COVID-19 testing of the uninsured.
As of December 23, 2020, HRSA paid approximately $1.2 billion to providers for COVID-19 testing of uninsured individuals. Of the total, about $432 million, or 36 percent, was paid to providers in the 15 states and two of three territories approved to use 100 percent federal Medicaid funds to pay for testing of uninsured individuals. Medicaid payments for COVID-19 testing for uninsured individuals was an estimated $7 million, as of December 31, 2020.
Overview of Key Issues
Effectiveness of HRSA payment controls is limited by incomplete data.
HRSA has implemented prospective and retrospective controls to prevent erroneous payments; however, the effectiveness of these controls to identify individuals covered by Medicaid’s COVID-19 testing for the uninsured program is limited by incomplete data. As one example HRSA’s controls do not require providers to submit Social Security numbers of patients to HRSA when the providers submit requests for payments. In September 2020, 28 percent of tested individuals in HRSA’s payment database had Social Security numbers listed. Absent a Social Security number, officials from the HRSA contractor that administers payments to providers said that they are unable to comprehensively check for Medicaid coverage. As a result, officials said some individuals deemed to be uninsured may have existing coverage, including Medicaid coverage for COVID-19 testing of the uninsured.
Retrospective payment controls have identified some individuals with insurance coverage who were previously deemed uninsured. As of December 20, 2020, HRSA has recovered about $3.8 million in payments from providers, less than 1 percent of the total payments made. HRSA’s data provides limited reasons for payments identified for recovery. For example, many payments identified for recovery were because the individuals were found to have another source of coverage; however, the data did not specify the type of health insurance or how many of these individuals had Medicaid coverage.
Most Medicaid COVID-19 spending is related to the increased federal matching rate, with modest spending for COVID-19 testing for the uninsured.
As of December 31, 2020, COVID-19-related federal Medicaid expenditures totaled approximately $25 billion, or 7 percent of total federal spending on Medicaid services for this time period.[162] The majority of the COVID-19-related spending is for the 6.2 percent FMAP increase. About $7 million in spending was reported by 10 of the 15 states approved to cover COVID-19 diagnostic testing and related services for uninsured individuals with a 100 percent federal match.
Of those 10 states, California accounted for approximately $6.5 million in spending for testing of uninsured individuals, about 97 percent of the total payments. In the remaining nine states, total Medicaid payments for COVID-19 testing of uninsured individuals ranged from $320 to about $72,000. Several factors may account for the modest Medicaid spending on testing uninsured individuals.
CMS’s reporting of expenditures for COVID-19 testing of uninsured individuals may be delayed because states can report and make adjustments to payments for up to 2 years after a quarter ends.
Officials from one state noted that relatively few people in their state applied for coverage provided through Medicaid’s COVID-19 testing of uninsured individuals, but added that the number of applications has increased over time.
Even in states and territories approved to provide Medicaid coverage of testing of the uninsured, providers may bill HRSA and receive payment for COVID-19 tests of uninsured individuals who have not enrolled in their state’s or territory’s optional Medicaid COVID-19 testing coverage.
The table below summarizes federal Medicaid spending related to the 6.2 percent FMAP increase, COVID-19 expenditures in Medicaid programs approved to cover testing for uninsured individuals, and total Medicaid spending for services as of December 31, 2020.
Federal Medicaid COVID-19 and Total Expenditures, by State and Territory, as of December 31, 2020
State or territory
COVID-19-related federal Medicaid expenditures from the 6.2-percentage-point-increased FMAP ($ in millions)
COVID-19-related federal expenditures for uninsured testing ($ in millions)
Total federal Medicaid services expenditures in 2020 ($ in millions)
Alabamaa
278
N/A
3,546
Alaskaa
49
N/A
1,119
Arizonaa
458
N/A
8,953
Arkansasb
307
N/A
5,059
Californiaa
2,869
6
49,862
Coloradoa
360
< 1 million
4,433
Connecticuta
204
< 1 million
2,836
Delawarea
99
N/A
1,340
District of Columbiaa
125
N/A
1,890
Floridaa
1,254
N/A
13,436
Georgiab
520
N/A
6,275
Hawaiic
82
N/A
1,239
Idahoa
102
N/A
1,549
Illinoisa
835
0
11,220
Indianaa
555
N/A
8,527
Iowaa
212
< 1 million
2,988
Kansasa
182
N/A
1,909
Kentuckyb
379
N/A
7,580
Louisianaa
414
< 1 million
7,330
Mainea
134
< 1 million
1,758
Marylanda
416
N/A
5,700
Massachusettsa
735
N/A
8,474
Michigana
710
N/A
10,792
Minnesotaa
398
< 1 million
3,670
Mississippia
260
N/A
3,487
Missouria
494
N/A
5,976
Montanaa
52
0
1,277
Nebraskab
107
N/A
1,075
Nevadaa
131
0
2,349
New Hampshirea
89
0
1,119
New Jerseya
591
N/A
7,716
New Mexicoa
206
< 1 million
4,055
New Yorka
2,653
N/A
34,823
North Carolinaa
710
< 1 million
8,658
North Dakotaa
48
N/A
625
Ohioa
959
N/A
14,194
Oklahomac
225
N/A
2,827
Oregona
344
N/A
6,268
Pennsylvaniaa
1,348
N/A
16,374
Rhode Islanda
101
N/A
1,367
South Carolinaa
310
0
3,834
South Dakotaa
41
N/A
480
Tennesseea
515
N/A
5,911
Texasa
2,009
N/A
22,459
Utaha
115
< 1 million
1,838
Vermonta
64
N/A
786
Virginiaa,d
313
N/A
4,404
Washingtona
384
N/A
6,631
West Virginiaa
153
0
2,632
Wisconsina
530
N/A
4,826
Wyominga
26
N/A
272
States totale
24,452
7
337,751
American Samoaa
2
N/A
30
Guama
4
N/A
88
Northern Mariana Islandsa
2
0
29
Puerto Ricoa
74
0
1792
Virgin Islandsa
2
0
49
Territories totale
84
0
1,988
Legend: FMAP = federal medical assistance percentage NA = Not applicable. States that did not provide COVID-19 testing for uninsured individuals as of December 31, 2020.
Source: GAO analysis of data from the Centers for Medicare & Medicaid Services. | GAO-21-265
Note: Federal Medicaid payments were available for the second, third and fourth quarters of fiscal year 2020 (January 1, 2020, through September 30, 2020), and for the first quarter of fiscal year 2021 (October 1, 2020, through December 31, 2020). Expenditures do not include expenses for program administration. All the states and territories reported certified expenditures for the second and third quarters of fiscal year 2020. Certified state expenditures have been reviewed by states and are certified as being Medicaid-allowable expenditures. Both certified and uncertified state expenditures are preliminary, as they are subject to further review and are likely to be updated as states continue to report their expenditures and receive federal matching funds. States can report payments and adjustments to payments up to 2 years after a quarter ends. aForty five states and 5 territories did not report any expenditures for the first quarter of fiscal year 2021, as of December 31, 2020. bFour states that reported expenditures for the first quarter of fiscal year 2021, (October 1, 2020, through December 31, 2020), reported uncertified expenditures. cTwo states, Hawaii and Oklahoma, reported certified expenditures for first quarter of fiscal year 2021, as of December 31, 2020. dOne state, Virginia, reported uncertified expenditures for the fourth quarter of fiscal year 2020, as of December 31, 2020. eTotals may not sum exactly due to rounding.
Agency Comments
We provided a draft of this enclosure to HHS and the Office of Management and Budget (OMB) for review and comment. HHS provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed federal laws, CMS data from its Medicaid expenditure reporting system, HRSA’s publicly available data on payments for COVID-19 testing for uninsured individuals, detailed files of HRSA payments, HRSA summary report of payments to be recovered from providers, and Congressional Budget Office spending estimates. We also reviewed CMS Medicaid guidance, including requirements for administering the optional COVID-19 testing for the uninsured; HRSA guidance and requirements for providers to submit claims for COVID-19 testing for uninsured individuals; and our prior work related to Medicaid. We also reviewed CMS guidance to states on reporting COVID-19 expenditures through the Medicaid expenditure reporting system and conducted data reliability checks on state reported-expenditure data and HRSA documentation and written responses from agency officials regarding HRSA’s payment data. We discussed HRSA’s efforts to prevent duplicate or erroneous payments with HRSA officials and the contractor that administers the payment controls. We determined that the CMS and HRSA data were sufficiently reliable for the purpose of this enclosure.
Contact information: Carolyn L. Yocom, (202) 512-7114, yocomc@gao.gov
The number of veterans accessing the Department of Veterans Affairs health care via telehealth has nearly tripled since February, peaking in April after the department’s Veterans Health Administration issued guidance in March 2020 to avoid all routine or non-urgent face-to-face visits and to shift health care delivery to telehealth. As of December 8, 2020, the Veterans Health Administration rescheduled approximately 17 million of the more than 22 million appointments that were cancelled between March and November 2020; the remaining cancelled appointments have not been rescheduled for a variety of reasons.
Entities involved: Veterans Health Administration, within the Department of Veterans Affairs.
Key Considerations and Future GAO Work
The Department of Veterans Affairs (VA) has used COVID-19 relief funds to increase the availability of telehealth and provide health care to veterans. We will continue to examine VA’s efforts, including ongoing work reviewing how it used COVID-19 funds to expand access to telehealth. We also have ongoing work examining the extent to which COVID-19 affected veterans’ access to care from community providers, including the use of telehealth by these providers in response to the pandemic.
Background
Prior to the pandemic, VA had extensive experience using telehealth. For example, VA invested in technologies used to connect patients with care teams and specialties, including
phone appointments through which veterans receive health care over the phone from providers;
real-time, interactive video conferencing where a veteran, at home, another non-VA site, or at a VA medical facility, receives health care from a VA provider; and
technologies to store clinical information (e.g., data, image, sound, and video) that can be forwarded to a VA provider for clinical evaluation, which VA refers to as “store and forward.”
More than 60 percent of the Department of Veterans Affairs’ Veterans Health Administration’s (VHA) primary care and mental health providers had already used video telehealth prior to the pandemic. VHA delivered more than 2 million episodes of care through telehealth in fiscal year 2019.[163]
In March 2020, VHA issued guidance to veterans and providers to avoid all routine or non-urgent face-to-face visits and to shift health care delivery to telehealth.[164] According to VHA’s COVID-19 Response Plan, telehealth supports continuity of care during the pandemic, by allowing patients to get the care that they need, without exposing themselves or their providers to the risks of COVID-19.
VHA received approximately $17.2 billion in supplemental appropriations from the CARES Act to assist its response to COVID-19, including several provisions to increase the availability and use of telehealth.[165] From this supplemental funding, VHA reported plans to spend $300 million to expand telehealth capacity, such as to purchase tablets to distribute to veterans to facilitate their ability to access telehealth services. According to VHA officials, as of December 1, 2020, VHA’s Office of Connected Care had obligated over $101 million of these funds.[166] In addition, VA’s Office of Information and Technology received $2.15 billion in supplemental appropriations.[167] Between April and September 2020, it had expended approximately $20.3 million to enhance VHA’s telehealth infrastructure, such as for the purchase of equipment to increase bandwidth to allow for additional concurrent telehealth visits.
COVID-19 continues to take a devastating toll on veterans. According to VHA data, as of January 12, 2021, 7,267 veterans have died due to COVID-19. VHA also reported 17,406 active cases as of January 12, 2021—more than double the number of active cases two months prior on November 10, 2020.
Further, as of January 8, 2021 approximately 15 percent of tests performed by VHA were positive.[168] In addition, as of January 12, 2021, VHA reported 4,239 employees with active cases and 105 employee deaths.[169]
Some experts suggest the number of COVID-19 cases and deaths could remain elevated through the remainder of winter. Therefore, it is imperative for VHA to continue to provide and improve upon a range of options through which veterans can access health care, including telehealth.
Veteran outreach. According to VHA officials, at the onset of the COVID-19 response, VHA initiated outreach efforts to increase veterans’ awareness of telehealth services. These efforts included website postings, webinars, published news articles, media interviews, and blog and social media postings. Representatives from a veterans service organization stated that VHA worked with their organization to spread the message regarding telehealth options to their membership.
Telehealth usage. VHA’s total number of monthly telehealth episodes across all modalities tripled during the pandemic—from about 1.5 million episodes during February 2020, to a high of about 4.5 million episodes during April 2020. See figure below.
Total Episodes of VHA Telehealth Care by Month, October 2019 to November 2020
Notes: A veteran may have multiple episodes of care. According to VA, in the context of telehealth, the term “episode(s) of care” is used to express, for example, one real time video conference.
VHA’s telehealth episodes of care increased for telephone and video modalities and decreased slightly for store-and-forward technologies from February 2020 to November 2020. Specifically:
Telephone episodes of care increased from about 1.3 million serving about 860,000 veterans in February 2020 to a high of about 4.1 million serving almost 2 million veterans in April 2020. Monthly telephone episodes of care have declined from a high in April, but remain elevated compared to February.
Video episodes of care generally increased each month from February 2020 to November 2020—from about 130,000 serving about 103,000 veterans in February, to about 718,000 serving about 422,000 veterans in November. VA officials stated that they have encouraged providers to use video telehealth, as evidence has shown added value in this modality.[170]
Store-and-forward episodes of care and the number of veterans served through this modality initially decreased during the first months of the COVID-19 pandemic—from about 38,000 serving about 36,000 veterans in February 2020, to a low of about 14,000 serving about 13,000 veterans in April 2020. However, by September 2020, the number of episodes of care and veterans served approached February 2020 levels, and have generally remained at this level through November 2020. VHA officials attributed the initial decrease to fewer veterans coming to clinics due to the pandemic. Most store-and-forward episodes of care occur between providers and veterans coming to clinics for services.
VHA ongoing efforts to improve telehealth. VHA officials stated that there are several ongoing efforts aimed at removing technology barriers to telehealth use among veterans. For example:
As a pilot program, approximately 50,000 disposable smart phones with unlimited data plans were distributed to veterans in VA homeless programs.
VHA has partnered with major wireless carriers to support veterans’ access to telehealth services by providing more than 50,000 cellular-enabled tablets to veterans across the country.
To ensure that veterans have the digital skills needed to engage in video telehealth, and to increase veterans’ interest and confidence in technology, VHA officials directed facilities to establish programs to help veterans become familiar with the telehealth technology.
VHA continues to reschedule appointments cancelled because of COVID-19. According to VHA data, from March 2020 through November 2020, VHA cancelled about 22.5 million appointments, and as of December 8, 2020, about three-quarters of them (about 17.4 million) had been rescheduled.[171] Of the rescheduled appointments, about 15 million had been completed as of December 8, 2020, either through telehealth or in person.[172]
Although VHA has successfully rescheduled more than 17 million cancelled appointments during the COVID-19 pandemic, about 5 million had not been rescheduled as of December 8, 2020. According to VHA, some of these cancelled in-person appointments did not require rescheduling because veterans received care in the community, a provider determined care was no longer needed, the veteran decided not to get care, or their in-person appointment was converted to a telephone or video visit.[173] Further, according to VHA, due to the large volume of rescheduled appointments and disruption to normal scheduling workflows, there may have been instances in which an in-person appointment was converted to a telehealth visit but not documented in the scheduling system.
VHA officials also told us they are taking steps to reschedule cancelled appointments, including ensuring that all cancelled appointments receive a clinical or administrative review. During these reviews, it may be determined, for example, that care or follow up is not needed, care could be more safely delivered at a later time, or veterans do not respond to attempts to reschedule appointments.
Additionally, a VA Office of Inspector General’s (OIG) review of appointment data found that about 32 percent of the cancelled appointments reviewed by OIG auditors from March 15, 2020, to May 1, 2020, had no indication of follow-up.[174] In response to the OIG’s recommendations, VHA stated it would increase its oversight of appointment cancellations and follow-up, among other actions.
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget (OMB) and VA for review and comment. OMB did not have comments on this enclosure. VA provided technical and general comments on this enclosure, which we incorporated as appropriate. VA’s general comments are reproduced in Appendix X: Comments from the Department of Veterans Affairs.
Methodology
To conduct this work, we reviewed VHA data and guidance, and other relevant information regarding VHA’s response to the COVID-19 pandemic. We also spoke to representatives from a veteran service organization as well as a representative from a national organization representing the larger telehealth industry. In addition, we analyzed VHA data on telehealth usage and appointments cancelled during the COVID-19 pandemic, which included data from October 2019 through December 8, 2020. We assessed the reliability of the data sets used in our analyses by conducting manual checks of it and written responses from agency officials. We determined VHA’s data were sufficiently reliable for the purpose of the audit objectives in this enclosure
As of December 31, 2020, the Department of Health and Human Services reported that it had obligated about $181 billion and expended about $132 billion of the approximately $251 billion appropriated in the first four COVID-19 relief laws—an increase of about 11 percent and 13 percent, respectively, since October 31, 2020.[175]
Entity involved: Department of Health and Human Services
Key Considerations and Future GAO Work
This enclosure examines the Department of Health and Human Services’ (HHS) use of appropriations from four COVID-19 relief laws enacted in March and April 2020.
We will continue to examine HHS’s use of appropriations contained in COVID-19 relief laws enacted to help fund the COVID-19 response, including appropriations in the Consolidated Appropriations Act, 2021, a fifth COVID-19 relief law enacted on December 27, 2020. Specifically, we will examine the status of obligations and expenditures of these COVID-19 relief funds; the activities funded, including how those activities were determined; and efforts to monitor funding use and any related challenges.
Background
HHS received approximately $251 billion in appropriations from the first four relief laws enacted in March and April 2020 to assist the response to COVID-19 (see table below).[176]
Appropriations to HHS for COVID-19 Response from Four COVID-19 Relief Laws
Legislation
Appropriations ($ millions)
Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 (Pub. L. No. 116-123)
6,497.0
Families First Coronavirus Response Act (Pub. L. No. 116-127)
1,314.0
CARES Act (Pub. L. No. 116-136)
142,833.4
Paycheck Protection Program and Health Care Enhancement Act (Pub. L. No. 116-139)
100,000.0
Total
250,644.1
Source: Department of Health and Human Services (HHS) data and GAO analysis of appropriation warrant information provided by the Department of the Treasury. | GAO-21-265
Note: HHS reported that, of the $250.6 billion in COVID-19 relief funds provided by these laws, the agency transferred $289 million to the Department of Homeland Security, and $300 million are not available until HHS has taken certain actions. A fifth law, the Consolidated Appropriations Act, 2021, enacted on December 27, 2020, provided an additional $73 billion in COVID-19 relief funds to HHS. Pub. L. 116-260, 134 Stat. 1182 (2020).
HHS received an additional $73 billion in COVID-19 relief funds from a fifth COVID-19 relief law—Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020)—enacted in December 2020.
Overview of Key Issues
As of December 31, 2020, of the approximately $251 billion in COVID-19 relief funds appropriated in the first four relief laws, HHS reported that it had obligated about $181 billion and expended about $132 billion—an increase of about 11 percent and 13 percent, respectively, since October 31, 2020 (see figure below).
HHS’s COVID-19 Relief Appropriations and HHS’s Reported Obligations and Expenditures from Four COVID-19 Relief Laws, as of December 31, 2020
Note: This figure includes HHS appropriations, obligations, and expenditures from four COVID-19 relief laws enacted in March and April, 2020. It does not include the COVID-19 relief funding from a fifth relief law, the Consolidated Appropriations Act, 2021, enacted on December 27, 2020, which provided $73 billion in appropriations to HHS for COVID-19 response (Pub. L. 116-260, 134 Stat. 1182 (2020)).
HHS reported appropriations, obligations, and expenditures by agency for the first four COVID-19 relief laws. The following table provides HHS’s reported appropriations, obligations, and expenditures by HHS agency.
Department of Health and Human Services Reported Appropriations, Obligations, and Expenditures of Funds for the COVID-19 Response from Four COVID-19 Relief Laws, by Agency or Key Fund, as of December 31, 2020
Agency or key fund
Appropriations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Administration for Children and Families
6,274.0
6,200.0
3,031.2
Administration for Community Living
1,205.0
1,205.0
684.2
Agency for Toxic Substances and Disease Registry
12.5
12.3
2.9
Centers for Disease Control and Prevention
6,500.0
3,945.4
1,314.4
Centers for Medicare & Medicaid Servicesa
200.0
84.1
25.7
Food and Drug Administration
141.0
42.8
15.1
Health Resources and Services Administration
1,320.0
1,319.4
842.3
Indian Health Service
1,096.0
752.5
665.0
National Institutes of Health
1,781.4
928.5
232.9
Public Health and Social Services Emergency Fund (PHSSEF)b
231,689.5
165,884.5
125,572.4
Office of the Assistant Secretary for Preparedness and Responsec
12,393.0
10,416.0
5,713.9
Biomedical Advanced Research and Development Authorityc
17,838.5
16,211.7
2,931.9
Provider Relief Fundc
175,000.0
120,639.7
110,447.0
Testing for uninsuredc
2,000.0
1,333.8
1,332.1
Other PHSSEFc
24,458.0
17,283.3
5,147.5
Substance Abuse and Mental Health Services Administration
425.0
423.3
50.8
Total
250,644.4
180,797.8
132,436.9
Source: Department of Health and Human Services (HHS) data. | GAO-21-265
Notes: This table includes HHS appropriations, obligations, and expenditures from four COVID-19 relief laws enacted in March and April 2020. It does not include COVID-19 relief funding from a fifth relief law, the Consolidated Appropriations Act, 2021, enacted on December 27, 2020, which provided $73 billion in appropriations to HHS for COVID-19 response ( Pub. L. 116-260, 134 Stat. 1182 (2020)). The four COVID-19 relief laws enacted in March and April, 2020, included provisions for HHS to transfer appropriated funds to various HHS agencies. HHS also reported that of the $250.6 billion COVID-19 appropriations, the agency transferred $289 million to the Department of Homeland Security, and $300 million in appropriations are not available until HHS takes certain actions. aThese amounts do not reflect Medicaid and Medicare expenditures. As of December 31, 2020, COVID-19-related federal Medicaid expenditures totaled approximately $25 billion, or 7 percent of total federal spending on Medicaid services for January through December 2020. In addition, the Congressional Budget Office estimated that some provisions of the CARES Act will increase Medicare payments to providers by $8 billion in 2020 and 2021. bThe Public Health and Social Services Emergency Fund (PHSSEF) is an account though which funding is provided to certain HHS offices, such as the Office of the Assistant Secretary for Preparedness and Response. Amounts have been appropriated to this fund for the COVID-19 response to support certain HHS agencies and response activities. PHSSEF appropriations transferred to other HHS agencies or key funds not specifically listed are included under “Other PHSSEF.” For example, the Health Resources and Services Administration received $975 million in transfers from the PHSSEF, and this is represented in the table in “Other PHSSEF.” cThe italicized amounts are subtotals of the PHSSEF and are not added in the total since they are included in the PHSSEF amount. Italicized amounts listed under the PHSSEF appropriations column are HHS allocations based on appropriations made in the four relief laws enacted in March and April 2020, and approved allotment decisions made by HHS in coordination with the Office of Management and Budget. The Provider Relief Fund reimburses eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19. Provider Relief Fund expenditures also may be referred to as disbursements.
HHS reported allocations, obligations, and expenditures for the first four COVID-19 relief laws for a variety of COVID-19 response activities, including activities to support testing, the development of vaccines or therapeutics, and the acquisition of critical supplies. Across these activities, the percentage of allocated funds that had been expended as of December 31, 2020, ranged from about 67 percent for testing for the uninsured to about 5 percent for activities to support telehealth. The following table provides HHS’s reported allocations, obligations, and expenditures by selected key response activity.
Department of Health and Human Services Reported Allocations, Obligations, and Expenditures of Funds for the COVID-19 Response from Four COVID-19 Relief Laws, by Selected Key Response Activity, as of December 31, 2020
Key response activity
Allocations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Health centersa
2,020.0
2,018.3
1,199.4
Head Start
750.0
744.5
275.9
Provider Relief Fundb
175,000.0
120,639.7
110,447.0
Testing for uninsured
2,000.0
1,333.8
1,332.1
Support to state, local, territorial, and tribal organizations for preparedness
13,990.1
13,355.3
2,533.9
Strategic National Stockpile
10,669.9
8,909.7
4,610.6
Telehealth
167.5
40.1
9.6
Testing
6,540.9
4,185.9
2,485.8
Vaccines
13,766.8
13,213.1
1,937.8
Drugs and therapeutics
3,013.0
2,799.7
923.4
Diagnostics research and development
3,000.6
1,317.6
358.2
Global disease detection and emergency response
800.0
265.3
58.9
Other response activitiesc
18,925.6
11,974.8
6,264.3
Total
250,644.4
180,797.8
132,436.9
Source: Department of Health and Human Services (HHS) data. | GAO-21-265
Notes: This table includes HHS allocations, obligations, and expenditures from four COVID-19 relief laws enacted in March and April 2020. It does not include COVID-19 relief funding from a fifth relief law, the Consolidated Appropriations Act, 2021, enacted on December 27, 2020, which provided $73 billion in appropriations to HHS for COVID-19 response (Pub. L. 116-260, 134 Stat. 1182 (2020)). HHS reported allocations, obligations, and expenditures for these activities based on the primary programmatic recipient organization of the funds, although some activities apply to multiple categories. For example, certain funds in the “support to state, local, territorial, and tribal organizations for preparedness” category were provided for testing but are not reflected in the “testing” category. According to HHS officials, the allocations reported for the key activities above are based on amounts appropriated for these activities in the four relief laws enacted in March and April 2020, and approved allotment decisions made by HHS in coordination with the Office of Management and Budget. aHealth centers provide a comprehensive set of primary and preventative health care services to individuals regardless of their ability to pay. Approximately $17 million of this funding is for Health Center Program look-alikes, which are centers that do not receive Health Center Program funding but meet program requirements. bThe Provider Relief Fund reimburses eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19. Provider Relief Fund expenditures may also be referred to as disbursements. cAccording to HHS, other response activities include Centers for Disease Control and Prevention agency-wide activities and program support; health care preparedness and response activities; and certain activities conducted by the National Institutes of Health, among other activities.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
We requested, and HHS provided, data on appropriations, allocations, obligations, and expenditures by HHS agency and by key response activity, as of December 31, 2020.[177] We also obtained and analyzed appropriation warrant information provided by the Department of the Treasury as of May 31, 2020. To assess the reliability of the data reported by HHS, we reviewed information from the federal spending database, USAspending.gov, as well as HHS’s spending database, taggs.hhs.gov, and HHS’s documentation on spending, and we determined that the data were sufficiently reliable for the purposes of our reporting objective.[178] We also reviewed five COVID-19 relief laws enacted as of January 1, 2021, to assist the response to COVID-19.
Contact information: Carolyn L. Yocom, (202) 512-7114, yocomc@gao.gov
Federal agencies do not have complete and accessible drug manufacturing information, inhibiting federal efforts to identify supply chain vulnerabilities and effectively respond to public health emergencies, such as COVID-19.
Entities involved: Department of Defense; Department of Health and Human Services including the Food and Drug Administration and the Office of the Assistant Secretary for Preparedness and Response; Department of Veterans Affairs.
Recommendation for Executive Action
The Commissioner of the Food and Drug Administration should, as the agency makes changes to its collection of drug manufacturing data, ensure the information obtained is complete and accessible to help it identify and mitigate supply chain vulnerabilities, including by working with manufacturers and other federal agencies (e.g., the Departments of Defense and Veterans Affairs) and, if necessary, seek authority to obtain complete and accessible information.
Key Considerations and Future GAO Work
The COVID-19 pandemic has called greater attention to the U.S.’s reliance on foreign manufacturing for many marketed drugs. Concerns with shortages of certain drugs, including for drugs used to treat patients with COVID-19, have further highlighted the importance of ensuring a secure drug supply chain. As such, there has been bipartisan support to identify ways to stabilize the drug supply chain to ensure resilience during times of emergencies, such as the nation is facing now with the COVID-19 pandemic.
In particular, the federal government has taken steps intended to strengthen domestic drug manufacturing and create resilient domestic supply chains. As part of these efforts, in August 2020, the President issued an Executive Order directing agencies to take steps towards the goal of strengthening domestic drug manufacturing and supply chains.[179]
Federal agencies have started implementing the Executive Order, but they expressed concerns about their ability to implement some of the provisions. In particular, federal agencies do not have complete and accessible information to identify supply chain vulnerabilities and to report the manufacturing sources of drugs and drug components that were procured by the agency, as directed by the Executive Order.
Without obtaining the appropriate information on the drug supply chain, and ensuring that these data are complete and accessible, the Food and Drug Administration (FDA) and its federal partners will be challenged to identify and mitigate supply chain vulnerabilities and effectively respond to potential public health emergencies, such as COVID-19. Further, agency officials indicated that the Executive Order’s directive to federal purchasers, to purchase only drugs fully manufactured in the U.S., to the extent possible, could increase the administrative burden and costs of drug purchases for federal agencies if the capacity for domestic manufacturing does not increase.
We will continue to conduct work examining federal efforts to strengthen the resilience of the U.S. drug supply. We also have ongoing work related to federal efforts to enhance the medical device supply chain.
Background
Over the last 30 years, the U.S. drug supply chain has become increasingly dependent on foreign manufacturers, such as those in India and China. Increased reliance on foreign manufacturing has included both the starting materials that are manufactured into the active pharmaceutical ingredients (API), and the eventual combination of the API and other components into a finished drug (see figure below). A number of factors have led to the shift overseas, including the preference for large factory sites; lower labor and energy costs; and fewer environmental regulations governing the buying, handling, and disposing of toxic chemicals involved in drug manufacturing.
Simplified Drug Manufacturing Supply Chain
Note: This figure is a simplified version of the manufacturing supply chain for a drug. The supply chain for an individual drug generally involves multiple different manufacturers of starting materials, active pharmaceutical ingredients, and inactive ingredients.
The federal government generally purchases drugs through the same commercial market as other purchasers, such as hospitals and pharmacies. The largest federal purchasers of drugs by expenditure are the Department of Defense (DOD) and the Department of Veterans Affairs (VA). In addition, the Office of the Assistant Secretary for Preparedness and Response (ASPR) within the Department of Health and Human Services (HHS) oversees and purchases drugs for the Strategic National Stockpile, the largest federally owned repository of drugs and other medical supplies, to provide for the emergency health security of the U.S. in the event of a bioterrorist attack or other public health emergency. While FDA is not a major federal purchaser of drugs, it is responsible for approving drugs for the U.S. market and for conducting surveillance to determine if manufacturers meet quality standards.
The federal government has recently undertaken efforts to increase domestic manufacturing and enhance the U.S. drug supply chain, in some cases in response to the COVID-19 pandemic:
In May 2020, ASPR, through its Biomedical Advanced Research and Development Authority, contracted with Phlow Corporation to manufacture medicines for patients hospitalized with COVID-19.
In July 2020, the U.S. International Development Finance Corporation signed a letter of interest for a loan to Eastman Kodak Company to produce critical pharmaceutical components in the U.S., but in August 2020 it was placed on hold pending a Securities and Exchange Commission investigation of insider trading.
Through ASPR’s efforts to build a more resilient Strategic National Stockpile, the agency has ongoing work to increase supply chain information gathering and enhance domestic manufacturing of drugs and medical supplies (see our Strategic National Stockpile and the Medical Supply Chain enclosure).
As part of these efforts, the August Executive Order 13944, Combating Public Health Emergencies and Strengthening National Security by Ensuring Essential Medicines, Medical Countermeasures, and Critical Inputs Are Made in the United States, instructs federal agencies, including FDA, DOD, and VA to consider actions to
increase domestic procurement of essential medicines, medical countermeasures, and critical inputs, which includes API and API starting materials,[180] and
identify and mitigate vulnerabilities to the domestic supply chains for these products, among other things. (See table below.)
Summary of Selected Provisions of Executive Order No. 13944 to Increase Domestic Production of Essential Medicines, Medical Countermeasures, and Critical Inputs
Agency
Summary
Federal agencies (including the Departments of Defense and of Veterans Affairs)
Procure, as permitted by law, essential medicines, medical countermeasures, and critical inputs produced in the U.S. and divide procurement between two or more domestic manufacturers, unless the limitation is not in public interest, the products are not sufficiently and reasonably available in terms of quantities and quality, or it increases costs by 25 percent or more
Develop and implement procurement strategies to increase U.S. manufacturing of essential medicines, medical countermeasures, and critical inputs, including through the use of long-term contracts to ensure long-term demand (in consultation with the Food and Drug Administration (FDA))
Annually report the manufacturing sources of essential medicines, medical countermeasures, and critical inputs procured by the agency and plans to support domestic production, among other things
FDA
Identify list of essential medicines, medical countermeasures, and critical inputs (in consultation with the Office of Management and Budget (OMB), Office of the Assistant Secretary for Preparedness and Response (within the Department of Health and Human Services), Assistant to the President for Economic Policy, and the Director of the Office of Trade and Manufacturing Policy)
Identify vulnerabilities in the supply chain and mitigate those vulnerabilities, including by
considering proposing regulations or revising guidance on the collection of specified information from manufacturers as part of application approval process
entering into written agreements with other agencies to disclose information regarding the supply chain security and vulnerabilities
recommending necessary changes in law
review and determine whether regulations may be barriers to domestic production and advising on repeal or amendment
(in consultation with OMB)
Department of Defense
Identify and mitigate supply chain vulnerabilities for unique needs of the Armed Forces (in consultation with OMB)
Provide and update a list of medically necessary defense-specific essential medicines, medical countermeasures, and critical inputs
U.S. Trade Representative
Modify U.S. federal procurement products covered under relevant trade agreements to exclude coverage of essential medicines, medical countermeasures, and critical inputs, as permitted by law
Source: GAO summary of Executive Order 13944. | GAO-21-265
Note: Medical countermeasures include drugs, vaccines, and devices to diagnose, treat, prevent, or mitigate potential health effects of exposure to chemical, biological, radiological, and nuclear agents and emerging infectious diseases, pandemics or epidemics, as well as personal protective equipment. Critical inputs are active pharmaceutical ingredients (API), API starting materials, and other drug ingredients and device components that FDA determines to be critical for assessing safety and effectiveness of essential medicines and countermeasures.
The Executive Order is interrelated with existing domestic preference laws governing federal procurement, which include the Buy American Act and Trade Agreements Act. The Buy American Act requires federal procurement of domestic products, including drugs, but permits federal agencies to procure foreign products under certain exceptions, such as in cases in which domestic products are not reasonably available in sufficient quantities of a satisfactory quality. Restrictions also may be waived under international trade agreements so that goods provided by designated countries can compete on an equal footing with domestic products. Under current domestic preference laws, if federal agencies cannot find drugs that meet domestic preference requirements, they may obtain waivers to purchase non-domestic finished drugs or those not substantially transformed in the U.S.
Under the Buy American Act and the Trade Agreements Act, drugs may be treated as if they were domestically sourced even if some or all of the finished drug and drug components are manufactured outside of the U.S. The Executive Order encourages agencies to take advantage of existing procurement authorities to limit competition, when permitted, to maximize the procurement of essential medicines, medical countermeasures, and critical inputs produced in the U.S. Under the Executive Order an essential medicine or medical countermeasure is “produced in the U.S.” if the critical inputs used to produce it were, in turn, produced in the U.S. At this stage, it is unclear how the U.S. Trade Representative and federal agencies will implement these provisions.
Overview of Key Issues
Federal agencies have taken some steps in response to the Executive Order, but gaps in the information available on drug manufacturing location will inhibit federal agencies’ ability to identify vulnerabilities in the supply chain. In addition, federal officials expressed concern that until the capacity for domestic manufacturing increases, the effect of the Executive Order may be limited and may increase federal agencies’ administrative burden and costs.
Federal agencies are taking some steps to identify essential medicines and coordinate efforts to identify vulnerabilities, as directed by the Executive Order. FDA has identified a list of essential medicines and DOD has started to develop its list:
FDA published a list of essential medicines, medical countermeasures, and critical inputs for public comment, in October 2020. In the list, FDA identified those drugs most needed for acute care and that have the largest potential effect on public health. The list includes anticoagulants, antimicrobial, antiviral, and cardiovascular drugs, among others. In publishing this list, FDA also solicited public comment on the list. The agency indicated that the list will be updated periodically.
DOD has begun efforts to develop a defense-specific list of essential medicines, according to the agency. DOD officials said they anticipate releasing this list by February 2021.
Federal agencies indicated they were coordinating with each other to begin implementing provisions in the Executive Order. For example:
FDA reported that it was coordinating with other federal agencies as they develop strategies for acquiring drugs on the essential drug list and increasing domestic manufacturing. FDA noted that it was also evaluating how to accelerate FDA approval for products manufactured domestically and identify and address supply chain vulnerabilities.
DOD contracting officials in the Defense Logistics Agency said they plan to work with FDA to expand interagency coordination to determine the security of the supply chain for essential drugs.
According to ASPR and DOD officials, a White House task force on medical onshoring had begun meeting to coordinate implementation of the Executive Order across the federal government. Officials were unable to provide additional details about the task force’s activities, but ASPR officials noted that the task force was halted in November 2020 in response to the anticipated change in administration.
Limited information on drug manufacturing makes it challenging for federal agencies to identify supply chain vulnerabilities. FDA, DOD, and VA do not have all of the information needed, including the sources of critical inputs and finished drugs, to identify vulnerabilities in the drug supply chain and report on the manufacturing supply chains for purchased drugs. Drug manufacturers provide information on drug manufacturing supply chains to FDA through multiple sources, including drug applications and drug registration and listing data, which each have completeness and accessibility limitations.
Reviewing individual drug applications is labor intensive and has created data accessibility challenges in the past. To review information on starting material and inactive ingredient suppliers, FDA officials explained they would have to search through individual drug application files one-by-one. For example, a widely used drug may have over 50 generic drug applications associated with that one drug, so searching through drug application files individually would be labor intensive, according to FDA officials.
This has created data accessibility challenges for FDA when responding to specific incidents in the past. For example, during FDA’s efforts to recall certain blood pressure medications in 2018 and 2019 due to contamination from a potential carcinogen, FDA staff could not easily identify which finished drug manufacturers potentially used suppliers associated with the contamination and had to manually search electronic and paper drug application documents.
Registration and listing data submitted by manufacturers can be searched more easily electronically, but are incomplete. For example, according to FDA, companies that do not directly ship to the U.S., but may make API used in U.S. marketed products, do not always register with the agency.
Additionally, FDA lacks information to determine which starting materials, API, and inactive ingredient suppliers the finished drug manufacturers are using at any given time. The agency has information only on the potential suppliers that manufacturers listed in their drug applications. For FDA to determine which of these suppliers a finished drug manufacturer is using at any given time, the agency must contact the manufacturer. For example, during the COVID-19 pandemic and in response to concerns of potential supply disruptions and drug shortages, FDA asked more than 180 drug manufacturers to evaluate their supply chains for components manufactured in China and report back to FDA. Agency officials said that it took this step because it was not able to easily access this information from its own data systems.
The CARES Act directs drug manufacturers to annually report to FDA the amount of each drug manufactured at each establishment, which FDA officials said may provide some additional insight into what finished drug manufacturing establishments are being used.[181] However, FDA officials said that this new provision will not likely help provide insight into which suppliers are being used because it does not expressly require manufacturers to identify the sources of API or other ingredients used to manufacture the drugs. FDA officials added that the agency delayed implementation of this provision as it was determining the logistics for electronic reporting, such as whether to incorporate it into existing data systems, and has not indicated when it will begin requiring manufacturers to submit this information.
FDA is not the only agency that lacks information on drug manufacturing supply chains, as DOD and VA also lack information needed to report on the manufacturing supply chains for the drugs they purchase, as directed by the Executive Order.[182]
DOD and VA officials said that their agencies do not have complete information about the manufacturing locations of purchased drugs. Instead of maintaining their own data, agency officials explained that they relied on the companies with which they contract to self-certify that the drugs are manufactured in compliance with the Buy American Act and Trade Agreements Act.[183]
DOD contracting officials said that, in summer 2019, they began to obtain registration and listing data from FDA in an effort to independently identify the manufacturing locations for the drugs they purchase. However, the officials noted that, as a result of the gaps in the data received from FDA, they estimated that for 360 critical drugs purchased by DOD, they were not able to identify manufacturing location information for 75 percent of the API suppliers and 24 percent of the finished drug manufacturers.
These data limitations present federal agencies with challenges in their efforts to identify supply chain vulnerabilities and then to report on the manufacturing locations of purchased drugs, as outlined in the Executive Order. The Executive Order directs federal agencies to collect more complete manufacturing information than in the past, including for the use of identifying vulnerabilities in the U.S. drug supply chain and reporting on the manufacturing supply chains of purchased drugs.
According to FDA, DOD contracting, and VA officials, the agencies have not previously needed manufacturing information for all parts of the supply chain to meet their responsibilities:
FDA has previously obtained manufacturing information for the purposes of drug approvals and ensuring safety, but FDA officials said the agency has not previously had the responsibility to systematically identify vulnerabilities in the U.S. drug supply chain. Further, FDA stated that it may need to clarify its existing authority or request additional authority to require manufacturers to submit the manufacturing supply chain information needed to meet this new responsibility.
DOD and VA do not have their own information on manufacturing locations because it is not needed to determine compliance with the Buy American Act and Trade Agreements Act requirements, according to DOD contracting and VA officials.
Since FDA’s data are not easily accessible in their current state, these data are not a sufficient source of manufacturing information for DOD and VA to use to report on the manufacturing supply chains for the drugs they purchase. Further, officials from DOD and VA noted that additional manufacturing information would be needed to increase domestic purchasing as required in the Executive Order. DOD officials noted that since DOD does not have authority to compel manufacturers to provide such information, it will need to work primarily with FDA to obtain it. VA also noted that FDA should make its manufacturing supply chain information accessible to other federal agencies.
FDA officials stated, however, that collecting more detailed supply chain information for purchasers, such as DOD and VA, will be challenging because it could be burdensome for FDA as well as the manufacturer. According to FDA officials, the information DOD and VA need for reporting information on the supply chains for their purchased drugs may be more detailed than the information FDA will need to identify supply chain vulnerabilities. For example, FDA officials said that DOD and VA would need supply chain information by batch or lot level. However, FDA officials said it would generally not need that level of detail for most drugs because knowing which suppliers were used to make a specific batch or lot is not necessary to identify whether a specific drug has supply chain vulnerabilities. FDA officials added that they were concerned that having FDA routinely collect supply chain information at a level of detail generally only needed for other agencies would be burdensome for them and drug manufacturers.
Although FDA must weigh the benefits of collecting more complete information with the additional burden to manufacturers and the agency, it is uniquely positioned to work with its partners to identify ways that it and other federal agencies can obtain manufacturing supply chain information for drugs and their components. Given FDA’s responsibility for ensuring drug safety and efficacy, the Executive Order directs FDA to consider making changes to its collection of manufacturing information and enter into written agreements with other agencies to share information.
Federal internal control standards for information and communication state that agencies should identify information requirements needed to achieve objectives and address risk and process data into quality information that is complete, accessible, and provided on a timely basis to make informed decisions.[184]
The pandemic has highlighted vulnerabilities in the U.S. drug supply chain and the need to mitigate these risks. Until FDA has manufacturing supply chain information that is complete and accessible, the agency and its federal partners will not be able to effectively identify and mitigate supply chain vulnerabilities and more quickly respond to public health emergencies, such as COVID-19. FDA has acknowledged that this is a new responsibility for the agency, and it may not have access to all of the information that would be needed. Therefore, as FDA considers these changes, it should work with drug manufacturers and other federal agencies, such as DOD and VA, and seek authority to obtain complete and accessible information, if necessary. These actions represent an important first step towards a larger effort to ensure a more resilient drug supply chain.
Effect of the Executive Order may be limited and may increase federal agencies’ administrative burden and costs. Without other efforts, the Executive Order’s provisions to limit drug purchases to solely domestic sources may result in administrative challenges and cost increases, and may have a limited effect on enhancing domestic manufacturing.
Both VA and DOD contracting officials said that efforts to achieve the goal of limiting drug purchases to only those with a domestically manufactured supply chain, as outlined by the Executive Order, could increase the use of waivers to purchase drugs. If the Executive Order is fully implemented, the officials explained that they anticipate that an increased use of waivers will be needed because the drugs that they must purchase will often have some critical inputs—including API and API starting materials—manufactured outside the U.S. Under the provisions of the Buy American Act and Trade Agreements Act, as implemented in federal acquisition regulations, agencies do not necessarily consider where critical inputs such as API are manufactured when determining if a product is domestic.
DOD contracting officials estimated, using FDA’s drug registration and listing data, that 86 percent of the critical drugs purchased are manufactured by, or rely on API suppliers that are non-domestic sources and almost 100 percent reliant on non-domestic sources for at least some critical inputs, such as API starting materials.
DOD contracting officials also said that waivers would be needed when they lack the information to verify all of the locations involved in manufacturing the drugs, from starting materials to the finished drug. According to DOD contracting officials, DOD could not meet standards of clinical care for many indications if they did not have access to non-domestically sourced drugs. DOD contracting officials estimated that the agency would continue to need waivers until drug manufacturers transition to domestic production.
VA and DOD contracting officials also told us that purchasing drugs from only domestic sources would ultimately increase drug procurement costs. DOD contracting officials said that additional staff resources would be necessary to determine the drug manufacturing locations of the drugs they procure and to obtain waivers, especially since the supply chain of drugs is not known and subject to change. Additionally, DOD contracting officials said that additional resources would be needed to implement the Executive Order to cover potential cost increases related to increased workload and drug costs.
In addition, VA officials said that dividing purchasing requirements between two or more domestic manufacturers will likely result in workflow disruptions in VA pharmacies as many of the highly automated medication delivery systems are calibrated for specific drugs. Changing these systems would also result in increased personnel and equipment-related costs, according to VA officials. They also noted that if more than one manufacturer is part of a VA contract then any given manufacturer may be unlikely to offer their best price since they have less incentive to offer the best price to win the contract, which could increase VA’s drug costs.[185]
Federal purchasing alone may not be sufficient to increase domestic manufacturing. According to ASPR and DOD officials, total federal procurement of drugs and medical supplies represents about 5 percent of the commercial market. Some drug manufacturing representatives we spoke to, as well as ASPR officials, said that federal government procurement is such a small portion of the overall commercial drug market that restricting federal agencies to purchase only domestic manufactured drugs will not be enough of an incentive for companies to build new manufacturing establishments in the U.S.
According to one stakeholder’s estimate, building an FDA-approved drug manufacturing facility in the U.S. could cost as much as $2 billion and take 5 to 10 years to build. In addition, Japan and some European countries have similar efforts to bring drug manufacturing to their respective countries, thereby making it more challenging to bring facilities to the U.S. According to stakeholders, drug companies are unable to establish manufacturing facilities in all of these places.
The federal government has initiated other efforts to increase domestic manufacturing in addition to the Executive Order and we will continue to conduct work further examining the extent of federal efforts to strengthen the resilience of the U.S. drug supply chain.
Agency Comments
We provided HHS, DOD, the Office of Management and Budget (OMB), and VA with a draft of this enclosure.
HHS provided general comments, which are reproduced in Appendix IV: Comments from the Department of Health and Human Services. HHS neither agreed nor disagreed with our recommendation. In HHS’s response, FDA said that as the agency continues efforts to enhance relevant authorities and close data gaps, it will consider GAO’s recommendation. FDA also clarified its responsibilities under the Executive Order, and we made edits as appropriate.
HHS and VA provided technical comments, which we incorporated as appropriate. DOD and OMB did not provide comments on this enclosure.
Methodology
To conduct this work we reviewed the Executive Order, federal laws, and agency documents related to information on the drug manufacturing supply chain. We also interviewed or obtained written responses from FDA, ASPR, DOD, and VA officials to identify the actions the agencies have conducted or planned to conduct to implement the Executive Order, including those related to identifying supply chain vulnerabilities and enhancing domestic manufacturing, and any related challenges. We also interviewed the Association for Accessible Medicines, Bulk Pharmaceuticals Task Force, Consumer Healthcare Products Association, Pharmaceutical Research and Manufacturers of America, and Pharma & Biopharma Outsourcing Association to obtain their perspectives on the effect of the Executive Order to enhance domestic drug manufacturing. These groups represent manufacturers of generic drugs, APIs, over-the-counter drugs, and brand drugs; and contract manufacturers, respectively.
Buy American Act: Actions Needed to Improve Exception and Waiver Reporting and Selected Agency Guidance. GAO-19-17. Washington, D.C.: December 18, 2018.
Further assessments are needed to ensure the Food and Drug Administration can carry out its drug manufacturing oversight responsibilities in light of the COVID-19 postponement of most inspections.
Entities involved: Food and Drug Administration, within the Department of Health and Human Services
Recommendations for Executive Action
We are making the following two recommendations to the Food and Drug Administration:
The Commissioner of the Food and Drug Administration should, as inspection plans for future fiscal years are developed, ensure that such plans identify, analyze, and respond to the issues presented by the backlog of inspections that could jeopardize the goal of risk-driven inspections.
The Commissioner of the Food and Drug Administration should fully assess the agency’s alternative inspection tools and consider whether these tools or others could provide the information needed to supplement regular inspection activities or help meet its drug oversight objectives when inspections are not possible in the future.
Key Considerations and Future GAO Work
The Food and Drug Administration (FDA) inspects drug manufacturing establishments for multiple reasons: as part of its drug approval process, to conduct regular surveillance after drugs are marketed in the U.S., and to investigate specific issues.
We have had long-standing concerns about FDA’s ability to oversee drugs manufactured overseas, an issue highlighted in our High Risk series since 2009. Historically, FDA conducted mostly domestic inspections, in spite of a growing number of foreign establishments supplying drugs to the U.S. market. While FDA has increasingly conducted foreign inspections, in June 2020, we reported that both foreign and domestic inspections decreased in recent years.
FDA has postponed most inspections in light of COVID-19. Although FDA has been able to use alternative tools, such as reviewing foreign regulator reports, to maintain some of its oversight activities, these tools are generally not a comprehensive or long-term substitute for inspections. Without regular inspections or alternative tools to fully assess an establishment’s compliance with quality standards, FDA could be faced with a backlog of inspections, threatening the agency’s goal of shifting toward exclusively risk-driven surveillance inspections. While FDA has taken initial steps to evaluate the use of some of its tools to help during the pandemic, it is important that FDA fully assess the value of alternative inspection tools to prepare it for the future.
We have ongoing work examining FDA’s foreign drug inspection program and ongoing work examining both the extent to which federal agencies purchase drugs manufactured overseas and federal efforts to strengthen the resilience of the U.S. drug supply. (See our Drug Supply Chain enclosure in this report.)
Background
FDA is responsible for overseeing the safety and effectiveness of all drugs marketed in the United States, regardless of manufacturing location.[186] As of August 2020, nearly 60 percent of the 4,200 establishments that manufactured drugs for the U.S. market were located overseas. More than one-third of the foreign establishments supplying the U.S. market were in China and India.
Inspections of drug manufacturing establishments are a critical element of FDA’s oversight. FDA typically conducts: 1) preapproval inspections before approving a new brand name or generic drug; 2) surveillance inspections periodically based on a risk analysis after a drug is marketed to ensure continued compliance with applicable laws and regulations; and 3) for-cause inspections to investigate specific issues or follow-up on previous FDA regulatory action.
In recent years, about 70 percent of FDA inspections were surveillance inspections. To prioritize establishments for surveillance inspections each year, FDA applies a risk-based site selection model to its catalog of establishments that supply drugs to the U.S. market to identify those that pose the greatest potential public health risk should they not comply with manufacturing quality standards. This model analyzes several factors—including inherent product risk, establishment type, inspection history, and time since last inspection—to develop a list of establishments that FDA considers to be a priority for inspection. In July of each year, FDA includes this list in its surveillance inspection plan for the following fiscal year.
Overview of Key Issues
Prior to COVID-19, FDA typically conducted more than 1,600 inspections of foreign and domestic drug manufacturing establishments each year, but inspections have been reduced significantly. Alternative tools have helped FDA continue its oversight, but are not a comprehensive or long-term substitute for FDA inspections.
Most foreign inspections postponed and domestic inspections reduced since March 2020. The total number of FDA inspections of foreign and domestic establishments was 56 percent lower in fiscal year 2020 than during each of the previous 2 fiscal years.
Foreign inspections postponed. In early March 2020, FDA announced that, in light of the pandemic and citing the safety of its employees, the agency would temporarily not conduct any foreign inspections other than those deemed mission critical.[187] From the pause in inspections in March to October 1, 2020 (the most recent data available at the time of our analysis), FDA conducted three foreign mission critical inspections (see table below).
In contrast, from March to September of each of the prior 2 years, FDA conducted more than 600 foreign inspections. As of January 2021, FDA had not set a date for resuming regular foreign surveillance inspections in all countries, but said it continues to monitor the global situation and remains in contact with foreign regulators to inform FDA’s assessment of the feasibility of returning to foreign surveillance inspections as conditions improve. For example, according to FDA, in January 2021, staff in the agency’s China office had begun conducting surveillance inspections in China and staff in the agency’s India office would begin conducting surveillance inspections in India shortly.
Foreign Mission Critical Drug Manufacturing Establishment Inspections Conducted by FDA from March 20 to October 1, 2020
Location
Purpose
Drug
Canada
For-cause
Hand sanitizer
Germany
For-cause
Nifurtimox active pharmaceutical ingredient
India
Preapproval
Chloroquine phosphate tablets
Source: GAO analysis of Food and Drug Administration (FDA) data. │ GAO-21-265
Domestic inspections resumed, but at reduced rates. From March to October 1, 2020, FDA conducted 52 domestic inspections, compared to about 400 inspections conducted during this time period in the 2 previous years, as presented in the figure below.
In mid-March 2020, FDA limited domestic inspections to only those deemed mission critical. In July 2020, FDA announced that it planned to resume domestic inspections, contingent on a rating system that incorporates information on COVID-19 infection trends in a geographic area. Depending on an area’s rating, FDA’s inspection activities were to range from mission critical inspections only, to the resumption of all inspections. According to FDA’s area rating data, as of December 3, 2020, conditions were appropriate for conducting routine surveillance inspections in 49 U.S. counties, with regulatory activity limited to mission critical inspections only in the more than 3,000 remaining counties.
FDA also announced that to help assure the safety of inspection staff and establishment employees, for the foreseeable future, domestic inspections will be preannounced, as has typically been done for most foreign inspections. Previously, almost all domestic inspections were unannounced. In June 2020, we testified before Congress about possible risks to preannouncing inspections, including that they can give establishments the opportunity to fix problems before inspection staff arrive.[188]
Domestic and Foreign Drug Manufacturing Establishment Inspections Conducted by FDA, Fiscal Years 2018-2020 by Month
FDA relies on alternative tools, but they are not a comprehensive or long-term substitute for inspections. FDA has used alternative tools for oversight of drug manufacturing quality while inspections are paused, including inspections conducted by foreign regulators, requesting and reviewing records and other information, and sampling and testing. Though FDA has determined that inspections conducted by certain European regulators are equivalent to an FDA inspection, other tools provide useful information, but are not equivalent to an FDA inspection.
Inspections conducted by some foreign regulators, when available, can substitute for FDA inspections. In light of the COVID-19 pause in inspections, FDA established a policy expanding the use of the mutual recognition agreement it has with the European Union to include inspections conducted outside of Europe by European regulators.[189] FDA also began using information from inspections conducted by other regulators—specifically, regulators that are among the 53 members of the Pharmaceutical Inspection Cooperation Scheme (PIC/S), such as Australia, Canada, Japan, and South Africa—though the agency has not determined that inspection reports from such countries are equivalent to FDA inspections. According to FDA officials, in fiscal year 2020, FDA substituted European regulator inspection reports for over 160 FDA inspections in Europe and requested over 30 additional reports from inspections conducted by European regulators or PIC/S members in China, India, Korea, and Japan, among other countries.
FDA had previously determined that European regulators had the capability of conducting inspections in Europe that were equivalent to FDA’s own inspections. In light of the COVID-19 pause in inspections, FDA also evaluated for equivalence inspections conducted outside Europe by European regulators covered under the mutual recognition agreement. According to FDA officials, as of November 2020, FDA deemed that inspections conducted outside of Europe from 19 of 28 European regulators can be substituted for an FDA inspection. However, reports for inspections from the other 9 European regulators conducted outside of Europe and by PIC/S members can only be used to help obtain “surveillance-level oversight” while inspections are paused and are not full substitutes for an FDA inspection. In addition, FDA’s ability to continue to rely on these tools may be limited, as foreign regulators have also postponed inspections due to COVID-19.
Further, many foreign establishments supplying the U.S. market are located where foreign regulator reports may not be available. For example, FDA officials told us that, particularly in China and India (two countries that are not PIC/S members), FDA conducts more foreign inspections than any other regulator. Thus, there may not always be a foreign regulator report to rely on while FDA inspections are paused. In fiscal year 2019, almost half of FDA’s 977 foreign inspections were in China and India, the two countries which also had the largest number of establishments supplying the U.S. market.
FDA can request and review records and other information to substitute for FDA inspections in select circumstances. During the COVID-19 pandemic, FDA substantially increased use of its authority to request that establishments provide records in advance of or in lieu of an inspection, requesting records from establishments in China, India, and the U.S., among others.[190]
FDA can substitute the review of records and other information for conducting a preapproval inspection, but will only do so in certain cases. For example, FDA may choose to do this if the establishment has an acceptable drug inspection history for related manufacturing operations. According to FDA officials, in fiscal year 2020, FDA made over 130 requests for records and other information to support preapproval applications listing establishments in at least 27 countries.
According to FDA’s interim policy, FDA can combine non-European foreign regulator reports with establishment records to support its risk-based surveillance of establishments already manufacturing drugs marketed in the U.S., but establishment records alone cannot be used as a substitute for an FDA surveillance inspection. FDA officials told us that only FDA in-person inspections and European regulator reports can satisfy the agency’s statutory requirements for surveillance inspections. According to FDA officials, in fiscal year 2020, FDA made over 310 requests for records and other information to support surveillance of establishments in at least 36 countries. If needed, FDA can request that the establishment provide translated versions of requested records and provide verification that the translation is complete and accurate.[191]
Sampling and testing are not a substitute for an inspection. FDA noted that in response to the COVID-19 pandemic, the agency has adjusted its approach to selecting drugs for sampling and testing. Specifically, according to FDA officials, the tool it uses to automatically screen drug imports continues to be adjusted during the COVID-19 pandemic to help FDA determine where to focus its sampling at the U.S. border. FDA also has targeted sampling of high-risk and difficult-to-manufacture drugs from foreign establishments that had their inspections postponed.
While FDA’s sampling and testing provides the agency with information about a product’s quality attributes, the agency notes that sampling and testing alone do not specifically confirm adherence to quality standards and thus cannot fully replace an FDA inspection. The agency does not test every drug both because the volume of drugs is not feasible to test and only about 1 percent of the drugs it tests in a given year fail to meet established quality specifications, according to FDA.
Alternative tools allowed FDA to take some regulatory action against foreign drug manufacturing establishments with manufacturing deficiencies during the inspection pause. For instance, to prevent hand sanitizers with methanol contamination from entering the U.S., FDA created a new import alert for drugs that, based on analytic testing, appear to be adulterated. From March 1, 2020, to December 1, 2020, FDA placed 54 foreign establishments on import alert based on sampling.
FDA has also placed establishments on import alert based on information obtained from other alternative tools, such as a finding of non-compliance in a foreign regulator inspection report or for a foreign establishment refusing to provide records in response to a request from FDA. According to FDA officials, from March 1, 2020, to December 1, 2020, FDA placed nine foreign establishments on import alert for refusing FDA records requests or for deficiencies identified during the agency’s review of records provided in response to an FDA records request and one foreign establishment on import alert based on a foreign regulator inspection report.
FDA faces future challenges with its preapproval and surveillance oversight activities. The agency will face challenges with its drug approval and surveillance activities, particularly given that the alternative tools FDA is using while inspections are postponed are not a long-term or comprehensive substitute.
A continued pause in preapproval inspections may lead to future delays in FDA drug approvals. As of November 2020, FDA officials told us that the agency had not experienced a significant impact on approval decisions due to the COVID-19 inspection pause. FDA notes that it is continuing its work to review and approve drug applications and that, as of October, the agency had approved more than 600 brand name and generic drug applications in 2020. Further, as of November 2020, FDA reported that it was operating above its 90 percent on-time action performance goal for approval decisions.
Representatives from three associations representing drug manufacturers stated that, because preapproval inspections may happen months before an application is approved, the postponement of inspections has not had a significant effect on FDA’s ability to make drug approval decisions yet. However, two of these associations noted that the longer inspections are postponed, the more likely the inability to conduct a preapproval inspection could create larger challenges for FDA’s ability to make approval decisions. FDA officials said that they are continuing to expand the use of alternative tools to mitigate the effect of the pandemic on the agency’s ability to make approval decisions when inspections are not possible.
The continued postponement of FDA surveillance inspections may result in a backlog, creating the possibility that FDA may not inspect the establishments prioritized by its risk-based site selection model. As a result of the pause in inspections during the COVID-19 pandemic, FDA was unable to complete more than 1,000 of its fiscal year 2020 surveillance inspections. FDA has a strategic goal of shifting toward exclusively risk-driven surveillance inspections. However, the inspection pause has increased the number of mandatory inspections the agency will have to conduct in 2021, threatening that goal.
In selecting establishments for surveillance inspection each year, FDA prioritizes, as mandatory, those establishments never inspected or not inspected within 5 years. According to FDA officials, such establishments represent significant risks to drug quality, but the extent of the risk is uncertain. With any remaining inspection resources, FDA then inspects those establishments that, based on the model’s application of risk factors, have the greatest potential for public health risk should they not comply with manufacturing quality standards. The percentage of surveillance inspections conducted at establishments that are the highest risk according to the model can thus range from a large to a small percentage of the total depending on the number of mandatory inspections. According to FDA officials, in order to achieve the agency’s strategic goal of risk-driven surveillance inspections, FDA seeks to maximize the number of inspections of establishments prioritized by the model each year. For fiscal years 2019 through 2021, FDA planned for an annual surveillance inspection capacity of about 1,500 inspections and it plans a similar inspection capacity for fiscal year 2022.
Potential Effect of COVID-19 Backlog on Distribution of FDA's Risk-Based Surveillance Inspections over Time if Fiscal Year 2021 Inspections Are Postponed
Note: Fiscal year 2022 percentages are our estimates based on the following assumptions: (1) that FDA will not conduct any inspections of the establishments it has never inspected or for which the inspection is outdated in fiscal year 2021 and so all of those inspections will roll over to fiscal year 2022; (2) that there will be additional establishments that have never been inspected or for which the FDA inspection is outdated (based on the average number of never and outdated inspections FDA identified as mandatory in the last 2 years); and (3) FDA’s inspection capacity of 1,500 surveillance inspections per year will not change. If FDA is able to resume surveillance inspections in fiscal year 2021 or use alternative tools as substitutes for FDA inspections, then it may be able to complete a larger number of inspections of establishments, including those that have never been inspected, that have not been inspected in 5 years, or those that are the highest risk remaining sites than is reflected in our estimates and this figure.
According to FDA officials, in the recent years prior to the pandemic, FDA had been able to inspect both the mandatory establishments and most of the remaining highest risk establishments on its prioritized inspection list. Due to the ongoing COVID-19 pandemic, domestic inspections continue to be limited and the vast majority of foreign surveillance inspections continue to be postponed, as of January 2021. The backlog of mandatory inspections this will create if inspections continue to be postponed could both extend the maximum interval between FDA inspections beyond FDA’s 5-year policy and reduce the resources available in fiscal year 2022 for inspecting the other highest priority establishments identified by its model, as outlined in the figure below.
While FDA is not expected to finalize its surveillance inspection plan for fiscal year 2022 until July 2021, it has noted that for future inspection scheduling, establishments that have never been inspected or that have an outdated inspection should remain the priority. Unless FDA is able to devote more resources to drug inspections, continuing to prioritize establishments that have never been inspected or that have not been inspected in 5 years over those prioritized by FDA’s model would result in such establishments dominating FDA’s surveillance inspection program. This creates a risk that the establishments identified by the model as the highest priority for inspection may not be inspected in a timely manner.
Federal internal control standards call for agencies to identify, analyze, and respond to risks related to achieving defined objectives. FDA officials told us that they have had internal discussions about how the backlog of mandatory inspections could affect the distribution of surveillance inspections in future years and how alternative tools could be used to respond to this risk. However, surveillance inspection plans for fiscal year 2022 have not yet been developed, providing FDA an opportunity to document how it plans to address the backlog of mandatory inspections and assess whether the backlog could jeopardize its strategic goal of shifting toward exclusively risk-driven inspections.
By including such an assessment in its surveillance inspection plan for fiscal year 2022, the agency would have better assurance it could achieve its goal of maximizing the number of inspections of establishments prioritized by its model. This would also help ensure that its inspection resources would be allocated to the establishments that may have the greatest potential for public health risk should they not comply with established manufacturing quality standards. This is particularly important given that we have previously reported that, even prior to COVID-19, FDA faced challenges inspecting the large number of establishments manufacturing drugs for the U.S. market.
FDA has not fully assessed how its alternative tools or others can be used to support its current and future drug oversight activities. With the exception of European regulator inspection reports, FDA has not yet fully assessed how its alternative tools, or others, can be used to supplement its regular inspection activities, or help meet its drug oversight objectives when inspections are not possible in the future. For example, during the COVID-19 pandemic, FDA substantially increased use of its authority to request records and other information from establishments to help obtain surveillance-level oversight, but the agency has not yet finalized a policy for how it can use this information to supplement its inspection activities. In addition, FDA was able to respond quickly to the disruptions caused by the COVID-19 pandemic by establishing an interim policy for expanding its use of foreign regulator reports to include inspections conducted by PIC/S members, when coupled with the review of records and other information, to help FDA obtain surveillance-level oversight while inspections are not feasible. However, FDA has not assessed whether inspections conducted by PIC/S members are equivalent to FDA inspections. Thus, any establishments for which FDA uses PIC/S member reports for surveillance-level oversight during the COVID-19 inspection pause will still require an FDA inspection in the near future to determine their compliance with manufacturing standards.
In contrast, FDA completed a capability assessment of each European regulator over a 5-year period to establish the mutual recognition agreement and enable FDA to use inspection reports from these regulators as a full substitute for an FDA inspection in Europe. As a result, since the start of the COVID-19 pandemic inspection pause, FDA has been able to use European regulator reports from inspections in Europe to continue its oversight of foreign drug establishments.
In addition, there may be additional tools for the agency to utilize when inspections are not possible. For example, four of the five representatives of the pharmaceutical industry we interviewed told us that they are aware of foreign regulators that are conducting remote inspections, allowing those regulators to remotely observe an establishment’s operations. Representatives of one pharmaceutical industry group said that using remote inspections could address the challenges FDA faces when inspections are not possible. According to FDA officials, the agency is in the process of assessing the potential use, including its authority to use, other tools to serve as supplements to FDA inspections, including using remote video and other remote and live interactions with establishment staff and records to evaluate drug manufacturing operations.
Federal internal control standards call for agencies to use quality information to achieve their objectives. In doing so, as changes occur, agencies should identify the information needed to address their modified objectives and risks. FDA has noted that the continued development of tools that can be used in lieu of an FDA inspection is a priority. According to FDA officials, the agency expects that lessons learned from the use of alternative tools during the COVID-19 pandemic will help it evaluate the long-term use of these tools and incorporate best practices into FDA’s normal surveillance activities, as appropriate. However, officials said it is unclear whether FDA can use certain alternative tools as a full substitute for an inspection. For example, FDA officials told us that only FDA in-person inspections and European regulator reports can satisfy its statutory requirements for risk-based surveillance inspections.
While FDA has taken initial steps to evaluate the use of some of its tools to help during the pandemic, it is important that FDA fully assess alternative inspection tools to prepare it for the future. A full assessment will allow the agency to consider whether these tools or others could provide information to supplement FDA’s regular inspection activities, or help address risks to meeting its drug oversight objectives when inspections are not possible, by either substituting for an inspection or providing additional information for surveillance oversight. This assessment would also allow the agency to determine whether statutory changes would allow it to more fully utilize alternative tools to meet its inspection responsibilities.
Such an assessment is an important step to helping FDA manage its inspection activities now and in the future. Specifically, it could help the agency better manage the current challenges it faces resulting from the COVID inspection pause, including helping the agency address the backlog of mandatory surveillance inspections. Importantly, it could also help increase the resilience of its drug manufacturing oversight going forward, including in preparation for any future inspection disruptions.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided comments, which are reproduced in Appendix IV: Comments from the Department of Health and Human Services, and technical comments, which we incorporated as appropriate. OMB did not have comments on this enclosure.
In HHS’s response, FDA concurred with both of our recommendations. Regarding our recommendation to ensure that its future fiscal year drug inspection plans consider the issues presented by the backlog of inspections, FDA stated that it is actively tracking the list of sites that need to be inspected, and noted that the size of the backlog will depend on the extent to which alternative inspection tools are used.
In response to our recommendation to fully assess alternative inspection tools, FDA stated that it would continue to evaluate these alternative tools and that the resulting information will help it determine how such tools can be used to streamline and supplement regular inspection activities and to prioritize inspections when normal inspection operations are not possible. FDA stated that as it pursues continued process improvements, the agency will incorporate both recommendations in its ongoing assessment of these alternative inspection tools.
Methodology
To conduct this work, we reviewed FDA data on inspections through October 1, 2020, from the Field Accomplishments and Compliance Tracking System, agency guidance, public statements, as well as interviews and written responses from FDA officials related to the agency’s drug oversight activities during the COVID-19 pandemic. To assess the reliability of the inspection data, we conducted electronic data testing for missing data and outliers and compared the data to published information from the same database. We found the data sufficiently reliable for our purposes. Further, we interviewed the Association for Accessible Medicines, Bulk Pharmaceuticals Task Force, Consumer Healthcare Products Association, Pharmaceutical Research and Manufacturers of America, and Pharma & Biopharma Outsourcing Association, which represent manufacturers of generic drugs, active ingredients, over-the-counter drugs, brand-name drugs, and contract manufacturers, respectively, on the effects of the temporary postponement of inspections and FDA’s use of alternative tools.
The number of claims for unemployment insurance benefits remained historically high through the beginning of 2021. The extension of CARES Act unemployment insurance programs at the end of 2020 ensured these programs could continue to provide financial support to the many Americans who remain unemployed or who face new job losses as the U.S. economy continues to respond to the COVID-19 pandemic. In addition, state-reported data suggest that many states were paying claimants minimum Pandemic Unemployment Assistance benefits in November 2020. According to the Department of Labor, most states adopted this approach early in the pandemic to facilitate implementation of the new program and to expedite payments.
As of January 2021, Department of Labor officials said they did not know how many states have recalculated and provided back-payments to claimants who provided documentation to support a higher benefit. States have also continued to take out federal loans to pay for unemployment insurance benefits and respond to reports of fraud in the system, and the Department of Labor has continued to monitor and assist states with addressing benefit overpayments and potential fraud, though additional efforts to track the recovery of overpayments are needed.
Entity involved: Department of Labor
Recommendation for Executive Action
We are making the following recommendation to the Department of Labor:
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments recovered in the Pandemic Unemployment Assistance program, similar to the regular unemployment insurance program.
Key Considerations and Future GAO Work
The unemployment insurance (UI) system provides a vital safety net for individuals who become unemployed through no fault of their own, and this support is essential during widespread economic downturns. As certain CARES Act UI programs were extended at the end of 2020, the UI system continued to experience high numbers of claims as a result of the COVID-19 pandemic. The millions of claims submitted each week in CARES Act UI programs suggests that the extension of these programs will provide support for many Americans who remain unemployed or who face new job losses as the U.S. economy continues to respond to the pandemic.
However, as we previously reported, the Department of Labor (DOL) does not collect or report reliable counts of the number of individuals claiming benefits. In November 2020, we recommended that DOL (1) revise its weekly news releases to clarify that in the current unemployment environment, the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits and (2) pursue options to report the actual number of distinct individuals claiming benefits, such as by collecting these already available data from states, starting from January 2020 onward.
DOL agreed with our recommendations, with the exception of collecting data from states retroactively. In its weekly news release published on December 10, 2020, DOL clarified that the numbers it reports for weeks of unemployment claimed do not represent the number of unique individuals claiming benefits.
As of January 14, 2021, DOL had not begun reporting the actual number of unique individuals claiming UI benefits on a weekly basis in its UI news releases. We maintain that these data are vital to understanding the size of the population supported by the UI system during the pandemic. Even if the information is unavailable for some time, reporting numbers for calendar year 2020 and after will help DOL and policymakers identify lessons learned about the administration and utilization of regular and expanded UI benefit programs during the pandemic. We encourage DOL to pursue options to report the actual number of individuals claiming benefits in the most feasible and least burdensome way.
We continue to focus on the implications of persistently high numbers of claims for UI benefits. As a result of backlogs in processing historic numbers of claims, some claimants have faced substantial delays in receiving benefit payments. States also face continued financial pressure in paying a historic volume of claims. As of January 8, 2021, 19 states and territories held $46.3 billion in federal loans taken out to pay UI benefits.
As certain CARES Act UI programs were extended into 2021, we remain concerned about potential fraud throughout the system. As we reported in November, states have identified schemes that reportedly could account for tens of thousands of fraudulent claims involving millions of dollars. DOL continues to support states to help ensure UI program integrity.
We also remain focused on how DOL will account for benefit overpayments and draw lessons learned from the program integrity challenges faced in the CARES Act UI programs throughout 2020 and 2021. For example, although DOL collects data from states on the amount of overpayments made in the federally funded Pandemic Unemployment Assistance program, as of the beginning of 2021, the agency was not tracking the extent to which overpayments in this program had been recovered. DOL officials told us that states are required to recoup these overpayments. However, without additional data collection, the agency, policymakers, and the public cannot know how much federal funding from these benefit overpayments states have been able to recover and how much remains outstanding.
Background
The UI program is a federal-state partnership that provides temporary financial assistance to eligible workers who become unemployed through no fault of their own. States design and administer their own UI programs within federal parameters, and DOL oversees states’ compliance with federal requirements, such as ensuring states pay benefits when they are due. Regular UI benefits—those provided under the state UI programs in place before the CARES Act was enacted—are funded primarily through state taxes levied on employers, and are intended to typically be lower than a claimant’s previous earnings, according to DOL.[192]
The CARES Act created, and the Consolidated Appropriations Act, 2021 amended, three federally funded temporary UI programs that expanded benefit eligibility and enhanced benefits.[193]
Pandemic Unemployment Assistance (PUA), generally available through March 14, 2021, generally authorizes up to 50 weeks of UI benefits to individuals not otherwise eligible for UI benefits, such as self-employed and certain gig economy workers, who are unable to work as a result of specified COVID-19 reasons.[194]
Federal Pandemic Unemployment Compensation (FPUC) generally authorized an additional $600 weekly benefit through July 2020, and authorizes a $300 benefit for weeks beginning after December 26, 2020 and ending on or before March 14, 2021, for individuals eligible for weekly benefits under the regular UI and CARES Act UI programs.[195]
Pandemic Emergency Unemployment Compensation (PEUC), generally available through March 14, 2021, authorizes an additional 24 weeks of UI benefits to those who exhaust their regular UI benefits.[196]
The Consolidated Appropriations Act, 2021 also created the new Mixed Earner Unemployment Compensation (MEUC) program, which authorizes an additional $100 weekly benefit for certain individuals.[197] To be eligible, claimants must have received at least $5,000 of self-employment income in the most recent tax year. The $100 weekly benefit is in addition to other UI benefits received by claimants; however, individuals receiving PUA benefits may not receive MEUC payments.[198]
In addition to the extensions of PUA and PEUC benefits and the reauthorization of FPUC benefits, the Consolidated Appropriations Act, 2021 added new program integrity requirements for the CARES Act UI programs. For all of the CARES Act UI programs, this Act requires that states have a method in place to address circumstances in which UI claimants refuse to return to work or to accept an offer of suitable work without good cause.[199]
For the PUA program specifically, the Act requires claimants to provide documentation substantiating their employment to be eligible for benefits.[200] In addition, states are now required to have procedures for identity verification and for timely payment of PUA benefits, to the extent reasonable and practicable.[201] Also, as a condition of continued PUA eligibility, individuals will now generally be required to recertify with their state each week that they continue to meet the eligibility requirement related to not being able to work as a result of COVID-19.[202] Further, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount, but the state can waive that requirement under certain conditions.[203]
During the pandemic, regular UI claimants in certain states have also had access to the Extended Benefits program. The program, which existed prior to the pandemic and provides up to an additional 13 or 20 weeks of benefits, is activated in states during periods of high unemployment, according to DOL.[204] As of January 10, 2021, DOL reported that the Extended Benefits program was activated in 23 states due to high levels of unemployment.[205] If unemployment is not high enough to activate the Extended Benefits program in a state, or if regular UI claimants exhaust their Extended Benefits, they may be eligible for PUA benefits—provided they also meet certain PUA eligibility requirements.[206]
Overview of Key Issues
With the extension of CARES Act UI programs, millions of Americans claiming PUA and PEUC benefits will continue to rely on the financial support these programs provide, amid the continuing pandemic. The number of weekly initial claims for UI benefits remains persistently high, though at a lower level than early in the pandemic. DOL reported that 1,151,015 initial claims for regular UI benefits and 284,470 initial claims for PUA benefits were submitted nationwide during the week ending January 9, 2021.[207] The number of regular UI initial claims submitted in recent weeks is considerably lower than the peak of about 6.2 million submitted in the week ending April 4 (see figure).
The general decline in initial claims suggests that workers are losing jobs at a slower rate nationwide than in the early weeks of the pandemic. However, the number of regular UI initial claims submitted each week has remained considerably higher than pre-pandemic levels. For example, the 1,151,015 regular UI initial claims submitted during the week ending January 9, 2021—which does not include the 284,470 PUA initial claims also submitted—is about 3.5 times as high as the 337,798 submitted during the corresponding week in 2020, prior to the pandemic.
Weekly Initial Claims Submitted Nationwide for Regular Unemployment Insurance (UI) and Pandemic Unemployment Assistance (PUA) Benefits, March 1, 2020 through January 9, 2021
Notes: The weekly counts of initial claims shown in the figure are not seasonally adjusted. Counts for weeks through December 26, 2020, are from Department of Labor (DOL) data files that include any adjustments submitted by states as of January 14, 2021. Counts for the weeks ending January 2 and 9, 2021, are from DOL’s weekly report released on January 14, 2021, and the January 9 numbers reflect advance initial claims, which are preliminary and subject to revision. The number of states reporting PUA data is out of a potential total of 53 states and territories.
The number of initial claims is not intended to measure how many claimants were determined eligible to receive benefits or how many who filed for benefits earlier in the pandemic are still unemployed. DOL officials have stated that continued claims may be a better barometer than initial claims for determining whether demand for benefits remains high. Each week, DOL publishes the number of continued claims submitted by states (i.e., weeks of unemployment claimed by individuals during a reporting period). For example, for the week ending December 26, 2020, states reported about 18.4 million continued claims in all programs—about 5.3 million in the regular UI program, about 7.4 million in the PUA program, and about 5.6 million in other programs, such as the PEUC program. The high number of claims suggests continued high demand for benefits.
However, as we reported in November, the number of continued claims has not approximated the number of individuals claiming benefits during the pandemic due to backlogs in processing historic numbers of claims in many states and other data issues. For example, inconsistency in the number of states reporting PUA claims resulted in flawed week-to-week comparisons of total claims numbers; potential fraud in the UI system may have inflated some states’ claims numbers; and backlogs in claims processing led to individuals claiming multiple weeks of benefits in single reporting periods and thus being counted as multiple claims for that reporting period, particularly in the PUA program. As a result, reliable conclusions about trends in the number of individuals claiming benefits cannot be drawn from data on continued claims.
As the pandemic continues, some claimants have exhausted certain UI benefits. Eligible individuals in most states may receive up to 26 weeks of regular UI benefits, though benefit duration varies somewhat by state, according to DOL.[208] After exhausting regular UI benefits, eligible individuals are generally able to apply for (1) PEUC; then, (2) the Extended Benefits program, which was activated in 23 states as of January 10, 2021, according to DOL; and then, in certain circumstances, (3) PUA benefits.[209] PUA claimants who exhaust their weeks of benefits are generally not eligible to receive other forms of unemployment compensation, according to DOL officials.
The number of continued claims submitted nationwide (i.e., weeks of unemployment claimed by individuals during a reporting period) under PEUC and the Extended Benefits programs increased in the fall of 2020, likely due to individuals exhausting their regular UI benefits as the pandemic continued. For example, DOL reported that about 2 million PEUC continued claims were submitted for the week ending September 19, 2020. The number of PEUC continued claims submitted nationwide had grown to about 4.2 million for the week ending December 26, 2020 (see figure). Similarly, the number of continued claims submitted under the Extended Benefits program increased from about 352,000 during the week ending September 19 to about 1.3 million the week ending December 26, 2020.
Weekly Continued Claims Submitted Nationwide for Pandemic Emergency Unemployment Compensation (PEUC) Benefits, March 1, 2020 through December 26, 2020
Notes: The weekly counts of continued claims shown in the figure are not seasonally adjusted. Counts for weeks through December 19, 2020, are from Department of Labor (DOL) data that include any adjustments submitted by states as of January 14, 2021. The count for the week ending December 26, 2020, is from DOL’s weekly report released on January 14, 2021. The number of states reporting PEUC data is out of a potential total of 53 states and territories.
The large number of continued claims under PEUC and the Extended Benefits program suggests that many individuals who lost employment during the pandemic may be part of the growing population of individuals who are experiencing long-term unemployment; for example, those whose employers closed their businesses permanently or restructured during the pandemic. As we discussed in our November report, the number of unemployed individuals experiencing long-term unemployment has increased during the pandemic, from 2.0 million in April 2020 to 3.7 million in October 2020.
Backlogs in processing historic numbers of claims in many states have led to delays in eligible claimants receiving their benefits. DOL monitors timeliness of benefit payments in the regular UI program.[210] Prior to the pandemic, in November 2019, DOL reported that about 92 percent of regular UI claims were paid within 21 days of a claimant’s first week of eligibility, and payment took more than 70 days for about 1 percent of claims.[211] The timeliness of payments has declined substantially during the pandemic. According to data reported for November 2020, nationwide about 66 percent of regular UI claims were paid within 21 days—a drop of about 26 percentage points since November 2019. Similarly, payment took more than 70 days for about 21 percent of claims, an approximately 20 percentage point increase since November 2019. Timeliness of regular UI payments also varies by state. For example, according to data reported for November 2020, 10 states reported that fewer than half of their claims were paid within 21 days, and 19 states reported that it took more than 70 days to make payments for at least 25 percent of claims.
Although DOL has not tracked the timeliness of payments in the temporary PUA program, DOL officials told us that states have struggled with PUA payment timeliness. For example, they said regional officials had observed a number of implementation challenges at the state level that likely contributed to claims processing backlogs and payment delays.
In addition, as we reported in November, DOL officials told us that to facilitate implementation of the new program, most states decided to initially pay PUA claimants the minimum allowable benefit, and then recalculate benefits at a later point based on claimants’ documentation of their prior earnings, as set by DOL guidance.[212] States have previously used this approach to pay benefits more expediently under the Disaster Unemployment Assistance program, according to DOL officials. As of January 7, 2021, DOL officials said they did not know how many states had begun recalculating individuals’ benefits and making these back-payments. Officials told us that if PUA claimants submit documentation of prior earnings before the program expires, states must recalculate the claimants’ PUA benefits and provide back-payments of any differences.
As of January 11, 2021, 27 of the 43 states and territories that had submitted PUA payment data for November reported average weekly PUA benefits paid that were within 25 percent of the state’s minimum PUA benefit amount; 9 of these states and territories reported average benefits within 10 percent of the minimum.[213] This suggests that many individuals in these states and territories were receiving the minimum benefit in November—because the average is close to the minimum.
States are continuing to take out substantial federal loans to pay UI benefits. As the number of regular UI continued claims remains historically high, states continue to face financial strain, and some have sought loans from the federal government to pay UI benefits.[214] As of January 8, 2021, about 10 months since the March 2020 spike in UI claims, 18 states and the U.S. Virgin Islands held federal loans totaling about $46.3 billion (see figure).[215] This total loan balance is greater than the approximately $40.2 billion held by 30 states and territories at the end of 2010, the height of borrowing after the 18-month long 2007-2009 recession and early recovery.[216] If unemployment remains high, additional states may have to take out loans to pay UI benefits, and states with existing loans may need to borrow more. As we reported in November, states may take years to pay off the large loan balances and reestablish financial solvency in their UI programs.
Total Federal Loan Balance Held by States and Territories to Pay Unemployment Insurance (UI) Benefits, January 3, 2020 through January 8, 2021
Notes: The 19 states and territories with outstanding federal loans to pay UI benefits as of January 8, 2021, were California, Colorado, Connecticut, Georgia, Hawaii, Illinois, Kentucky, Louisiana, Massachusetts, Minnesota, Nevada, New Jersey, New Mexico, New York, Ohio, Pennsylvania, Texas, U.S. Virgin Islands, and West Virginia. The loan amounts shown in the figure represent the total balance held by all of these states and territories as of the end of each week. According to the Department of Labor, the U.S. Virgin Islands had a residual loan balance of about $0.06 billion at the beginning of 2020 left from the 2007-2009 recession.
DOL continues to stress the importance of addressing potential fraud in the UI programs. In November 2020, DOL officials told us that DOL continues to monitor states’ claims numbers to help states detect cases of potential fraud. DOL officials said they have also increased conversations with banking institutions, which are identifying potential fraud through data analytics and working with states to recover UI overpayments. In September 2020, DOL provided states with $100 million in administrative funding targeted specifically at addressing potential fraud and identity theft in the PUA and PEUC programs. DOL is requiring that states report quarterly on their progress in addressing potential fraud in the PUA and PEUC programs with these funds. The first report is due in February 2021 and will cover October 1 through December 31, 2020.
Officials from the National Association of State Workforce Agencies (NASWA) and its UI Integrity Center, funded by and operated in partnership with DOL, said that identity theft remains the biggest challenge for states in addressing potential UI fraud. According to officials, states have recently experienced increases in instances of criminals taking over legitimate claimants’ UI accounts and rerouting benefits to other bank accounts.[217] States are working to address these account takeovers through communication campaigns that raise public awareness about phishing attempts to steal account information, as well as coordinating with law enforcement and banking institutions.
According to the Department of Justice (DOJ), from March through November 2020, DOJ filed federal charges against 81 individuals for defrauding the UI programs.[218] In that same time frame, eight individuals pleaded guilty to federal charges of defrauding the UI programs. For example, one individual in Texas pleaded guilty to misappropriating personally identifiable information, such as Social Security numbers and dates of birth, to file multiple false and fraudulent claims for PUA and regular UI benefits between May and July 2020. In addition to these federal charges, investigations and prosecutions of potential fraud related to the UI programs during the pandemic have occurred at the state level.
DOL monitors overpayments and their recovery in the regular UI program, but additional efforts to track the recovery of PUA overpayments are needed. DOL data show that the dollar amount of reported overpayments in the regular UI program increased substantially during the pandemic. Overpayments could suggest that a program may also be vulnerable to fraud, though overpayments are not necessarily a result of fraud.[219] As of January 11, 2021, DOL reported that states had identified about $215 million in regular UI overpayments in the first quarter of 2020.[220] Overpayments identified in the second and third quarters of 2020 totaled approximately $728 million and $805 million, respectively.[221] Overall from January through September 2020, DOL reported that states had identified about $1.7 billion in regular UI overpayments. According to DOL officials, the increase in UI overpayments primarily corresponds with the spike in UI claims during the pandemic.[222]
DOL continues to emphasize and track the recovery of regular UI overpayments. For example, from January 2019 through the end of the first quarter of 2020, DOL reported that states recovered dollar amounts representing about 85 percent of the total of new overpayments during the period. Because states work continuously to recover overpayments, amounts recovered in a given period could be for overpayments made during any prior period. Over time, state data collected by DOL may indicate whether regular UI overpayments during the pandemic are recovered at similar rates.
Although DOL has also required states to report data on overpayments in the federally funded PUA program, as of the beginning of 2021, the agency was not tracking the extent to which these overpayments had been recovered. States are required to report PUA overpayments, including the number of cases, weeks, and dollar amounts of overpayments, and how many of these are due to fraud. However, DOL officials told us that states have been focused on processing the large volume of claims in the new PUA program, rather than on identifying and reporting overpayments. As a result, PUA overpayments data remain incomplete, according to DOL officials. As of January 11, 2021, states that had submitted data to DOL reported more than $1.1 billion in PUA overpayments from March through December, 2020.[223] This amount is likely to increase significantly as states shift their focus to identifying overpayments, according to DOL officials.
States are required to recover PUA overpayments that have not been waived, but as of the beginning of 2021, were not required to report the amount recovered.[224] According to DOL officials, PUA reporting requirements generally adhere to those for the Disaster Unemployment Assistance (DUA) program, which does not require states to report data on overpayments recovered.[225] However, the scale of overpayments in the PUA program is unprecedented in comparison to the DUA program. The DUA program provides benefits for individuals who become unemployed due to a presidentially declared disaster, and thus usually applies to individuals in one state or region at a time. In the 20 years prior to the pandemic (2000-2019), states reported a total of about $17 million in DUA overpayments. This 20-year total is far less than the over $1.1 billion in PUA overpayments already reported by states in the 10 months from March through December 2020.
Although the PUA program is temporary and generally follows DUA procedures, which according to DOL officials do not require certain reporting, DOL’s regular UI program goals and federal standards for internal control reinforce the importance of tracking the recovery of overpayments. For the regular UI program, overpayment recovery is one of DOL’s program integrity core performance measures. DOL establishes an annual goal for state overpayment recovery rates, and also tracks the recovery of overpayments nationally.[226]
In addition, federal internal control standards state that management should use quality information to achieve the entity’s objectives. As part of these standards, management should obtain data on a timely basis to use for effective monitoring. Although according to DOL officials certain requirements may not apply to the temporary PUA program, the large amount of already-reported PUA overpayments indicate the need for timely data to monitor and support states’ efforts to recover improperly expended federal funds. Additional data would help DOL, policymakers, and the public better understand how much federal funding states have been able to recoup from PUA overpayments and how much remains outstanding.
DOL agreed with our recommendation to collect data from states on the amount of overpayments recovered in the PUA program. In its comments, DOL noted that the Consolidated Appropriations Act, 2021 added an explicit provision that states must require claimants who received PUA benefits to which they were not entitled to repay the amount of those benefits, and that it provided authority for states to waive repayments in certain circumstances. DOL stated that it intends to issue guidance on the new provisions for the PUA program and will include revised reporting requirements and instructions for states to provide information on the amount of overpayments recovered.
On January 8, 2021, DOL took the first step toward implementing our recommendation by issuing new guidance and updated instructions for reporting PUA program activities. Specifically, DOL stated that it has revised its PUA reporting instrument to collect PUA overpayment recovery data from states, which will inform policymakers about the program, determine the effectiveness of identity theft prevention efforts, and assess additional program integrity needs.
Methodology
To conduct this work, we analyzed regularly reported DOL data for calendar years 2019, 2020, and 2021, with the most recent data being obtained on January 14, 2021. We also reviewed relevant federal laws, DOL guidance, and DOL Office of Inspector General reports; and interviewed DOL officials about program data and agency actions. We reviewed data file documentation and written responses from DOL officials, and interviewed DOL officials about the UI database, PUA claims data files, and data on outstanding loans to pay UI benefits, specifically related to state-reported data on claims counts, overpayments, payment timeliness, and loan balance amounts by state. We also examined the data for outliers, missing values, and errors. We determined the DOL data we used were sufficiently reliable for the purposes of this report.
Contact information: Thomas M. Costa, (202) 512-7215, costat@gao.gov
Related GAO Product
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: Sept. 10, 2014.
The Internal Revenue Service quickly issued a second round of more than 147 million economic impact payments, but some payments were sent to incorrect bank accounts and some eligible individuals will have to wait to receive their full payment until they file their 2020 tax return during the 2021 filing season, which begins February 12, 2021.
Entities involved: Internal Revenue Service and Bureau of the Fiscal Service, within the Department of the Treasury
Key Considerations and Future GAO Work
The CARES Act included direct payments to eligible individuals to address financial stress due to the pandemic. For this first round of economic impact payments (EIP 1) the Department of the Treasury (Treasury) and Internal Revenue Service (IRS) disbursed 168.2 million payments to individuals, totaling $275.9 billion.[227] Most of the payments went to individuals who filed a tax return in 2019 or 2018 and met the eligibility requirements, although individuals who do not normally file a tax return (non-filers) also received payments. Of the 168.2 million payments made, more than 27.7 million non-filers received a payment, including 21.2 million federal benefit recipients who received an automatic payment and just under 6.5 million non-filers who used IRS’s online tool known as the Non-Filers Tool to provide the necessary information in order to receive an EIP 1.
During the course of our work evaluating Treasury and IRS’s administration of the EIP 1, we made four recommendations to Treasury and IRS:
In June 2020, we reported that Treasury and IRS had sent $1.2 billion in EIP 1 to deceased individuals and we recommended that the Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments. Treasury and IRS have taken steps to implement our recommendation and are considering further actions. Currently, IRS has instructions on its website requesting that individuals voluntarily mail the appropriate economic impact payment amount sent to the decedent back to IRS, for both electronic and paper check payments. The envelopes in which paper checks were sent also had a checkbox to help an unintended recipient indicate that the intended recipient was deceased. After checking the box, the envelope could then be mailed back to the Bureau of the Fiscal Service (BFS). Treasury has also held and canceled payments made to decedents, along with those that have been returned. As of December 31, 2020, around 57 percent (just over $700 million) of the $1.2 billion in EIP 1 sent to deceased individuals had been recovered.
In our September 2020 report, we made two recommendations to help IRS better target its outreach and communications efforts to reach those individuals who may be eligible for a payment but have not received one. Specifically, we recommended that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP 1 to help target outreach and communications efforts. In addition, we recommended that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should make estimates of eligible recipients who have yet to file for an EIP 1, and other relevant information, available to outreach partners to raise awareness about how and when to file for an EIP 1. Treasury and IRS neither agreed nor disagreed with our recommendations.
In November 2020, we recommended that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed an economic impact payment notification letter and subsequently filed for and received an economic impact payment, and use that information to inform ongoing outreach and communications efforts. Treasury and IRS agreed to this recommendation. According to Treasury officials, Treasury began analyzing data in January on those who received a notice and subsequently filed for and received an EIP 1, but Treasury had not reported the results by the time of this report.
Our work on direct payments to individuals is ongoing. We will continue to examine Treasury and IRS efforts to identify and notify individuals about their eligibility for the EIP 1 and the second round of payments (EIP 2), and the agencies’ efforts to recoup payments sent to ineligible individuals. We will also review how many taxpayers claim the payment as a tax credit on their 2020 income tax return and examine challenges eligible recipients faced filing for an EIP 1 and EIP 2.
Background
On December 21, 2020, Congress passed the Consolidated Appropriations Act, 2021, which the President signed on December 27, 2020. The statute authorized a second round of direct payments to individuals to help address financial stress due to the pandemic.[228] To make this second round of payments (EIP 2), IRS used 2019 tax return information and information for those who receive certain federal benefits. The Joint Committee on Taxation estimates that in fiscal year 2021, this second round of payments will total over $164 billion. The act generally prohibits Treasury and IRS from making or allowing any EIP 2 after January 15, 2021.[229] According to IRS, eligible individuals who did not receive EIP 1 or EIP 2—or their maximum applicable EIP 1 and EIP 2 amounts—can claim a Recovery Rebate Credit (RRC) on their tax year 2020 income tax return equal to the amount of the credit for which they are eligible, as reduced by their EIP 1 and EIP 2 amounts.
The second round of payments shares some of the same eligibility requirements as the first round, but there are differences in several aspects, including the amount per individual and the eligibility of households with mixed-immigration status as shown in the table below.
Selected Features of Economic Impact Payments (EIP), Rounds One and Two
Features
EIP 1
EIP 2
Amount
Up to $1,200 per individual ($2,400 for married couples filing jointly)
Up to $600 per individual ($1,200 for married couples filing jointly)
Amount for qualifying children (under age 17)
$500 per qualifying child
$600 per qualifying child.
Payment phase outs
For single or married individuals filing separately, a 5 percent phase out begins at $75,000 adjusted gross income (AGI).
For individuals filing as head of household, the phase out begins at $112,500. For married couples filing jointly, the phase out begins at $150,000 AGI. In December 2020, the phase out for surviving spouses was amended to be the same as married couples filing jointly.a
For taxpayers with no qualifying children, the payment is fully phased out if AGI is at or above
$99,000 for single and married individuals filing separately,
$136,500 for heads of household, and
$198,000 for married couples filing jointly.
Same phase out threshold and rate, but because the amount of the credit is smaller for eligible individuals without qualifying children, it is completely phased out at
$87,000 AGI for single or married individuals filing separately,
$124,500 AGI for individuals filing as heads of household, or
$174,000 AGI for married couples filing jointly.
Offsets
The payments can be offset by the federal government only to collect delinquent child support obligations. The payments are not protected from garnishment or levy while held in accounts at financial institutions.
The payments are not subject to offset by the federal government for past due federal or state debts or child support obligations. The payments are also generally protected from garnishment or levy while held in accounts at financial institutions.
Ineligible individuals
Those ineligible for the payment include (1) nonresident aliens, (2) individuals who can be claimed as a dependent by another taxpayer, and (3) an estate or trust. In addition, otherwise eligible individuals cannot claim the credit if they do not include on their tax return a Social Security number (SSN) that is valid for employment.
Same eligibility requirements
Treatment of deceased individuals
The Department of the Treasury and Internal Revenue Service initially sent EIP 1 to eligible recipients who had filed a 2019 tax return, even if they were deceased at the time of payment, based on the agency’s interpretation of the CARES Act. Treasury and IRS subsequently adopted an interpretation of the statutory provision under which a person was not entitled to an advance payment if they were deceased as of the date the payment was to be paid.
Individuals deceased prior to January 1, 2020, will not receive a payment.
Mixed-immigration status households
Under the CARES Act, as originally enacted, married taxpayers filing jointly where one spouse has a valid SSN and one spouse does not are not eligible for a payment unless either spouse is a member of the U.S. armed forces at any time during the taxable year. In that case, only one spouse needs to have an SSN valid for employment.
This restriction was amended in December 2020. As amended, if married taxpayers file jointly and one spouse has an SSN and one spouse does not, they are eligible for a payment of $600, in addition to $500 per child with a valid SSN. However, IRS does not have plans to issue EIP 1 for individuals who are now eligible. These individuals will need to file their 2020 taxes in 2021 and claim a recovery rebate credit, if eligible.
Same as EIP 1 as amended, adjusted for the amounts of the EIP 2 credits. If married taxpayers file jointly and one spouse has an SSN and one spouse does not, they are eligible for a payment of $600, in addition to $600 per child with an SSN or Adoption Taxpayer Identification Number.
Source: GAO analysis of the CARES Act and Consolidated Appropriations Act, 2021. | GAO-21-265
aThe Internal Revenue Service (IRS) issued EIP 1 to surviving spouses based on the starting phase out amount prior to amendment—$75,000. According to IRS, it issued EIP 2 to surviving spouses also based on a $75,000 starting phase out amount because of time and resource constraints.
Overview of Key Issues
Treasury and IRS worked together to quickly disburse the second round of payments (EIP 2) using information from 2019 tax returns and certain federal beneficiaries, ensuring that millions of individuals received immediate relief as intended by the law. According to Treasury and IRS officials, they started preparing for a potential second round of payments prior to Congress passing the Consolidated Appropriations Act, 2021. The preparations positioned them to complete programming requirements to release payments just days after the new law was signed. Treasury and IRS officials said on December 29, 2020, two days after the Consolidated Appropriations Act, 2021 was signed, IRS provided BFS a single payment file containing all 147.2 million EIP 2 totaling $142.1 billion. After providing the single payment file, IRS did not provide additional payment files to BFS to disburse.
Starting on December 29, 2020, BFS disbursed the majority of these payments (113 million) directly into individuals’ bank accounts. On December 30, 2020, BFS began sending 34 million payments via paper checks and debit cards to individuals for whom bank account information was unavailable. BFS officials stated the agency started sending the first batch of 5 million paper check payments on December 30, 2020, and began sending debit card payments on January 4, 2021. BFS redesigned the envelopes in which debit cards were sent to help individuals identify them in the mail. BFS estimated it would disburse 5 to 7 million paper checks per week and 2.5 to 3.5 million debit cards per week. As of January 15, 2021, BFS had disbursed over 133 million payments, and it plans to issue the remaining payments by February 1, 2021.
According to IRS, some EIP 2 recipients’ payments were disbursed to temporary bank accounts, which had been established when the recipients filed their tax returns but were inactive when EIP 2 was disbursed. These temporary bank accounts receive the tax refund by direct deposit and are closed after the refund is disbursed to the taxpayer, tax return provider, and others. IRS officials said they requested tax industry partners to return all payments that were sent to temporary bank accounts. According to IRS, some tax industry partners did return the payments, and IRS will reissue those payments as a check or direct deposit by the end of January. Some tax industry partners did not return the payments and instead redirected the payments to taxpayers’ correct accounts.
As of January 15, 2021, IRS did not have available data on the number of taxpayers who were impacted by this issue or the number of taxpayers who have now received their payment. IRS officials said they expect to have these data available by the end of January 2021. We will continue to work with Treasury and IRS to determine how many taxpayers were impacted, and how many have since received their payment; how this happened; and the steps Treasury and IRS are taking to ensure future payments are delivered to the correct account.
According to IRS, some eligible recipients will have to wait to receive their full payment until they file their tax return for 2020 during the 2021 filing season, which begins February 12, 2021.
Eligible individuals who did not receive an EIP 1 or EIP 2, or who received less than they are eligible for because they experienced changes in circumstances between 2019 (or 2018) and 2020 can claim the additional amount as a Recovery Rebate Credit (RRC) on their 2020 tax Forms 1040 and 1040-SR. However, IRS officials raised concerns about their ability to provide sufficient telephone assistance to answer taxpayers’ questions about how to claim the correct amount due to limited staff.
A number of population groups did not receive timely payments during the first round of payments. For example, in June 2020 we reported that individuals who used the Non-Filers Tool between April 10 and May 17 for the first round of payments did not receive a payment that included additional money for qualifying children.[230] IRS corrected this error and mailed the remaining portion of individuals’ payment for qualifying children in August 2020. However, according to IRS officials, these individuals will have to file a 2020 tax return to claim the RRC for these same qualifying children instead of receiving the payment automatically. In addition, according to IRS, some spouses of deceased individuals did not receive automatic payments.
EIP 2 also will not be automatically sent to some eligible individuals who filed a 2018 tax return but did not file a 2019 tax return. The CARES Act directed IRS to use the 2019 tax return to calculate EIP 1, and if the individual had not filed a tax year 2019 return, to use information from the individual’s 2018 return, if such a return had been filed.[231] In contrast, the Consolidated Appropriations Act directs IRS to only use the 2019 tax return to calculate EIP 2.[232] Also, as of December 25, 2020, IRS was still processing 6.9 million 2019 tax returns. Some of these 2019 tax filers may be eligible for an EIP 2 but will not automatically receive one. Both 2018 and 2019 tax filers will have to file a 2020 return to claim the RRC if eligible.
IRS officials said they are working to determine how many eligible individuals did not yet receive their EIP 2, or how many received an incorrect amount because the payment did not include additional money for qualifying children. However, according to IRS officials, key data systems were down for maintenance in preparation for the tax filing season. IRS officials said that starting the week of January 25, 2021, these data systems will be back online and IRS will then have the data it needs to determine how many people were affected.
On January 4, 2021, IRS re-launched the Get My Payment on-line tool (https://www.irs.gov/coronavirus/get-my-payment), which allows individuals to check their eligibility and the status of their first and second round of payments. IRS officials also said they plan to send notification letters to those who received an EIP 2 by April 2021. IRS did not reopen the Non-Filers Tool for non-filers to register for an EIP 2, because Treasury and IRS had a short time frame for making payments before the start of the 2021 filing season.
Agency Comments
We provided a draft of this enclosure to Treasury, IRS, and the Office of Management and Budget. Treasury and IRS provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To review how Treasury and IRS administered EIP 1 and EIP 2 payments, we reviewed Treasury and IRS data as of January 15, 2021, examined federal laws and agency guidance, and interviewed Treasury and IRS officials. We assessed the reliability of the data by reviewing relevant Treasury and IRS documents, reviewing GAO’s prior use of the data sources, and interviewing agency officials. We determined the data were sufficiently reliable to describe the number and amount of payments disbursed.
Contact information: James R. McTigue Jr., (202) 512-9110, mctiguej@gao.gov
The Occupational Safety and Health Administration’s oversight and tracking of its COVID-19-adapted enforcement methods contain gaps, and employer-reported data do not capture all work-related COVID-19 cases.
Entity involved: Occupational Safety and Health Administration, within the Department of Labor
Recommendations for Executive Action
We are making the following three recommendations to the Occupational Safety and Health Administration, within the Department of Labor:
The Assistant Secretary of Labor for Occupational Safety and Health should develop a plan, with time frames, to implement the agency’s oversight processes for COVID-19-adapted enforcement methods, as described in its pandemic enforcement policies.
The Assistant Secretary of Labor for Occupational Safety and Health should ensure that the Occupational Safety and Health Administration Information System includes comprehensive information on use of the agency’s COVID-19-adapted enforcement methods sufficient to inform its oversight processes for these methods.
The Assistant Secretary of Labor for Occupational Safety and Health should determine what additional data may be needed from employers or other sources to better target the agency’s COVID-19 enforcement efforts.
Key Considerations and Future GAO Work
We reported in September 2020 that worker safety and health complaints have increased since February 2020 and that the Occupational Safety and Health Administration (OSHA) has adapted its enforcement methods in response to the COVID-19 pandemic, such as by permitting remote inspections in place of on-site inspections of workplaces.
Since September 2020, we have identified gaps in OSHA’s oversight and tracking of its adapted enforcement methods—specifically, OSHA does not have plans to implement the oversight outlined in its enforcement policy and is not tracking certain data related to its adapted enforcement methods. These gaps in oversight and tracking prevent OSHA from assessing the effectiveness of its enforcement methods during the pandemic, ensuring that its adapted enforcement methods do not miss violations, and ensuring that employers are addressing certain identified violations. We have also identified limitations in OSHA’s data on workplace COVID-19 exposure; more information would help the agency to target its enforcement efforts related to COVID-19 workplace safety.
Our review of OSHA’s efforts during the COVID-19 pandemic is ongoing. In addition, in 2021, we plan to begin work on the safety and health of workers at meat and poultry processing plants during the pandemic.
Background
The Department of Labor’s (DOL) OSHA helps ensure safe and healthful conditions for workers by setting mandatory workplace safety and health standards; conducting inspections; investigating complaints and reports of injuries, illnesses, and fatalities at worksites; and offering training, guidance, and outreach; among other efforts.[233] OSHA has 10 regional offices and 89 area offices that implement and oversee enforcement in the field.[234] OSHA is responsible for setting and enforcing workplace safety and health standards for the private sector in 29 states, the District of Columbia, and four territories.[235] Twenty-one states and Puerto Rico set and enforce their own workplace safety and health standards, under state plans approved by OSHA.[236] In response to the COVID-19 pandemic, OSHA is enforcing existing applicable standards, such as those related to personal protective equipment, and has issued industry-specific voluntary guidance for employers on COVID-19-related precautions.
OSHA has almost 1,900 employees, and its appropriation for fiscal year 2021 is approximately $592 million. Additionally, the CARES Act appropriated $15 million to DOL for “Departmental Management,” to remain available through September 30, 2022, to prevent, prepare for, and respond to the COVID-19 pandemic, including to enforce worker protection laws and regulations, among other things.[237] DOL officials said the department transferred $5.5 million of this amount to OSHA, and the Office of Management and Budget (OMB) apportioned the funds in June 2020. As of October 31, 2020, according to OSHA, about $3.4 million has been obligated and $1 million has been expended.
Overview of Key Issues
OSHA enforcement activity during the COVID-19 pandemic. From February through December 2020, related to COVID-19, OSHA received 12,769 complaints and referrals, 1,225 employer reports of severe injuries or illnesses, and 884 reports of fatalities.[238] In response, during the same time period, OSHA conducted 13,073 informal inquiries, 738 on-site inspections, and 689 remote inspections related to COVID-19.[239] As a result of these inspections, OSHA had cited 452 violations and issued about $3.4 million in penalties, as of January 2021.[240] (See table.)
COVID-19-Related Reports to OSHA and OSHA Enforcement Actions, February through December 2020
Feb.
Mar.
Apr.
May
June
Julya
Aug.a
Sept.a
Oct.a
Nov.a
Dec.a
Totala
Reports to OSHA
Complaints
13
1,361
1,983
1,482
1,315
1,457
973
605
771
1,151
1,034
12,145
Referrals
1
8
79
61
37
66
31
29
15
32
265
624
Employer reports of severe injury or illnessb
0
20
288
198
166
116
102
47
62
106
120
1,225
Reports of fatalitiesb
0
8
180
180
97
100
125
33
24
58
79
884
OSHA enforcement actions
Violations citedc
0
1
97
125
83
30
99
14
2
1
0
452
Penalties ($ thousands)c
0
0
776
922
657
210
725
119
15
2
0
3,427
Source: Occupational Safety and Health Administration (OSHA) analysis of OSHA Information System data. | GAO-21-265
Note: OSHA uses the term “referrals” to encompass reports of severe injuries and illnesses from employers and reports of potential workplace hazards from several other entities, such as a government agency. In this report, we use “referrals” to describe those reports from non-employer sources, and “employer reports” to describe those reports from employers. Employers are required to report all work-related in-patient hospitalizations, amputations, and losses of an eye within 24 hours, and all work-related fatalities within 8 hours. 29 C.F.R. § 1904.39. According to OSHA officials, most reports of fatalities come from employers. However, officials noted that they do receive reports of fatalities from other sources, such as the media or emergency medical personnel. In this report we refer to all reported fatalities as “reports of fatalities.” Data in this table include enforcement activity performed by OSHA only, and not by state agencies that operate under OSHA-approved state plans. aSince OSHA has 6 months from the occurrence of a violation to issue a citation and any related penalties, monthly totals for the number of violations cited and penalties issued from July through December 2020 may not reflect the total that will eventually be cited or issued related to inspections initiated during those months. These data are current as of January 4, 2021. bData reliability issues regarding COVID-19-related employer reports are discussed below in this report. cSome of these cases are still open and may have been contested or appealed by the employers, which could ultimately result in changes to the violations cited or penalties issued. Penalties do not sum to total because of rounding.
Comparing February through December 2020 to the same time period in 2019, OSHA received more complaints and referrals in 2020 (31,031) than in 2019 (27,766), even as many businesses were temporarily or permanently closed and more people collected unemployment benefits. OSHA also received more reports of fatalities in 2020 (2,681) than in 2019 (2,099). However, the agency received fewer employer reports of severe injuries or illnesses during this time period in 2020 (10,209) than in 2019 (11,166); this may be due, in part, to the time frame for OSHA’s reporting requirements for in-patient hospitalizations, which are described more fully in the section below on limited information on workplace COVID-19 exposure.
OSHA enforcement methods adapted for COVID-19. As we reported in September 2020, in response to the COVID-19 pandemic, OSHA temporarily granted area offices increased discretion to decide when and how to conduct inspections or informal inquiries, to help protect OSHA employees from the virus and address resource constraints. They also were given flexibility to determine whether to issue citations when they identify certain workplace violations. OSHA’s pandemic-related enforcement policy includes the following:
Remote inspections and informal inquiries. OSHA may use remote inspections or informal inquiries to conduct enforcement in place of on-site inspections, in an effort to assure the agency’s effective and efficient use of resources during the COVID-19 pandemic.[241] In areas with elevated levels of COVID-19, OSHA’s Area Directors are to prioritize for inspection workplaces with reported fatalities and potential imminent danger exposures related to COVID-19, but may conduct remote inspections or informal inquiries, in place of on-site inspections, based on resource constraints. OSHA refers to the informal inquiries as phone/fax investigations or rapid response investigations, as inspectors obtain information about an incident from employers by phone, fax, or email.[242]
Citation discretion for recurring requirements. OSHA area offices are to “take into strong consideration” employers’ good faith efforts to comply with certain annual or other recurring requirements when determining whether to cite violations.[243] OSHA enforcement policy provides area offices with examples of situations in which they may decide not to issue citations, and requires area offices to provide supporting documentation in the related case files for those decisions.[244]
Citation discretion for other requirements. OSHA area offices also have discretion to consider employer good faith efforts when determining whether to issue citations if they observe violations of certain personal protective equipment or recordkeeping requirements. This discretion takes into account potential personal protective equipment shortages and challenges in determining whether a COVID-19 case is work-related.[245]
Data from the OSHA Information System (OIS), which tracks the agency’s enforcement activities, indicate that inspectors have used the adapted enforcement methods described in OSHA policy.[246] For example, although OSHA did not conduct inspections remotely prior to the pandemic, from February through December 2020, according to OIS data, the agency conducted 715 inspections remotely, 689 of which were coded as related to COVID-19.[247] These 689 remote, COVID-19-related inspections represent about 48 percent of all COVID-19-related inspections. Data also show that area offices have used their discretion to not cite violations of recurring or annual requirements in seven inspections during that time period.[248] In addition, OIS data show that OSHA enforcement activities shifted substantially from inspections to informal inquiries during the pandemic months (see figure).[249]
OSHA Enforcement Activities Based on Report Type, February through December of 2019 and 2020
Note: OSHA uses the term “referrals” to encompass reports of severe injuries and illnesses from employers and reports of potential workplace hazards from several other entities, such as a government agency. In this report, we use “referrals” to describe those reports from non-employer sources, and “employer reports” to describe those reports from employers. Employers are required to report all work-related in-patient hospitalizations, amputations, and losses of an eye within 24 hours, and all work-related fatalities within 8 hours. 29 C.F.R. § 1904.39. According to OSHA officials, informal inquiries conducted in response to an employer-reported severe injury or illness, such as an in-patient hospitalization or amputation, are called rapid response investigations, and informal inquiries conducted in response to complaints from employees or referrals from entities other than employers are called phone/fax investigations. According to OSHA’s Field Operations Manual, if Area Directors consider employers’ responses to these informal inquiries to be inadequate, they may decide to initiate a related inspection.aCOVID-19-related enforcement activities are a subset of all enforcement activities from February through December 2020. The related bars represent the percentages of all COVID-19-related enforcement activities that were informal inquiries or inspections.
OSHA’s COVID-19-adapted enforcement methods contain gaps in oversight and tracking. OSHA’s pandemic-related enforcement policy describes oversight procedures that the agency will perform to ensure that its adapted enforcement methods are effective.[250] However, these procedures have yet to be implemented. These oversight procedures include follow-up steps that area offices and inspectors should implement when they have used enforcement methods adapted for COVID-19. For example:
Oversight of remote inspections. Area offices are expected to perform an on-site component for those inspections in response to COVID-19 fatalities and imminent danger exposures that were conducted remotely due to COVID-19-related resource constraints, if and when resources are available to do so.[251]
Oversight of informal inquiries. OSHA plans to develop a program to conduct monitoring inspections of a random sample of the prior fatality or imminent danger cases in which OSHA had conducted informal inquiries in place of inspections due to resource limitations.[252]
Oversight of citation discretion for recurring requirements. To ensure that employers have taken corrective actions for violations once normal activities resume, OSHA plans to conduct monitoring inspections of a random sample of cases in which inspectors had observed employer violations of certain OSHA standards but had exercised discretion to not cite these violations.[253]
Although OSHA’s pandemic-related enforcement policy describing this oversight was published in April and May 2020, OSHA has yet to implement it and officials said that the agency did not have specific plans or time frames for how and when to conduct the oversight.
For oversight of remote inspections and informal inquiries, in December 2020, OSHA officials told us that this oversight is contingent on resource availability, and that currently the agency is focusing only on immediate issues because of resource constraints. However, without this oversight outlined in OSHA’s pandemic enforcement policies, the agency lacks information on workplace hazards that may have been missed when using adapted enforcement methods, and on how effective these adapted methods have been overall in identifying hazards.[254]
For oversight of citation discretion for recurring requirements, in December 2020, OSHA officials told us that they will not make plans for this oversight until OSHA’s activities return to normal, in accordance with the related enforcement policy.[255] Since it is unclear when the pandemic will end and when OSHA’s activities will return to normal, developing a plan for this oversight will help OSHA ensure it is prepared to implement oversight when normal activities resume. For example, a plan will help the agency identify any data that need to be reliably collected now, in order to randomly select cases and conduct follow-up inspections later. Until OSHA has a plan and conducts this oversight outlined in its pandemic enforcement policies, OSHA lacks information on whether employers have taken corrective action on certain violations that were observed but not cited, potentially leaving workers at continued risk.
Once OSHA develops plans to conduct the oversight outlined in its enforcement policy, the agency may still face challenges conducting meaningful oversight because it cannot reliably track some types of adapted enforcement methods in OIS. For example:
Tracking remote inspections. In November 2020, OSHA started tracking in OIS which inspections were conducted remotely, and directed area offices to identify remote inspections in OIS going forward and retroactively to February 2020.[256] OSHA officials told us they believe all area offices are using the remote inspection code and have retroactively coded all such inspections conducted since February 2020. However, they said they are still working on a method to ensure reliability of the use of this code, and they do not have documentation from area offices to confirm that all data are complete. Until OSHA can assure that data on remote inspections are complete, OSHA cannot effectively rely on those data to identify worksites where the agency will perform on-site follow-up for its oversight of remote inspections.
Tracking informal inquiries in place of inspections. Although OSHA can identify the universe of informal inquiries, OSHA does not have a method to identify which informal inquiries—that is, which phone/fax investigations or rapid response investigations—were conducted in place of inspections.[257] For example, for agency responses to complaints and referrals, OSHA does not have a way to identify phone/fax investigations that occurred in place of inspections. Similarly, for agency responses to employer reports of severe injuries or illnesses and fatalities, OSHA does not have a way to systematically identify rapid response investigations that occurred in place of inspections.[258] OSHA officials told us that, especially in the early months of the pandemic, informal inquiries were used in place of some inspections, but they did not know how many. Without knowledge of which informal inquiries were conducted in place of inspections, OSHA will not be able to conduct its oversight of informal inquiries outlined in OSHA’s pandemic-related enforcement policy.[259] In addition, without such knowledge, the agency does not have a complete picture of the extent to which informal inquiries were conducted in place of inspections—to determine whether additional oversight is necessary.
Tracking citation discretion for recurring requirements. OSHA does not have a method to ensure that inspectors are consistently using the designated code to identify cases where inspectors observed, but did not cite, violations of recurring or annual requirements, according to OSHA officials. Without this method, if and when OSHA creates and implements a plan to conduct monitoring inspections of a random sample of these cases, the agency will not know if its sample is based on complete and reliable data.
Tracking citation discretion for other requirements. For violations of other requirements, such as those related to personal protective equipment, OIS does not have a code to identify when inspectors observed violations but did not cite them, according to OSHA officials. OSHA, therefore, does not know whether any such violations were identified and not cited. Knowing this information would help the agency determine whether any oversight is needed and, if so, conduct it.
Federal standards for internal control state that management should use quality information to achieve its objectives, such as data that are current and complete. Until OIS contains comprehensive information on OSHA’s use of adapted enforcement methods, the agency cannot fully oversee and assess the effectiveness of these methods, including conducting the oversight of remote inspections, informal inquiries, and citation discretion for recurring requirements outlined in OSHA’s enforcement policy.
OSHA has limited information on workplace COVID-19 exposure. From February through December 2020, related to COVID-19, OSHA received reports of 921 fatalities and employer reports of 1,716 hospitalizations. Over the same time period, OSHA received reports of 2,750 total fatalities and employer reports of 9,937 total hospitalizations, which reflects an increase in reported fatalities compared to the same time period in 2019 (2,145), but a small decrease in reported hospitalizations compared to the same time period in 2019 (10,259). This may be due, in part, to OSHA’s reporting requirement for hospitalizations that makes it unlikely that employers would report hospitalizations related to COVID-19, which the agency clarified in a September 2020 update to its COVID-19 Frequently Asked Questions (FAQ) webpage.
Under OSHA’s regulations, employers are required to report all work-related in-patient hospitalizations within 24 hours, and all work-related fatalities within 8 hours.[260] Although OSHA has received reports of COVID-19-related hospitalizations, the regulations state that “for an in-patient hospitalization… you must only report the event to OSHA if it occurs within twenty-four (24) hours of the work-related incident.”[261] For COVID-19, according to OSHA, the work-related incident referred to in the regulation is exposure to the virus in the workplace.[262] Therefore, a COVID-19-related hospitalization is only to be reported to OSHA if the hospitalization occurs within 24 hours of the workplace exposure to COVID-19. Symptoms of COVID-19 may appear in as few as 2 days (48 hours) or up to 14 days after exposure, according to OSHA’s Guidance on Preparing Workplaces for COVID-19, which cites Centers for Disease Control and Prevention information. Consequently, a worker exposed to COVID-19 at a workplace would not show symptoms or be hospitalized within 24 hours, and the employer would therefore not be required to report the hospitalization to OSHA.
Federal standards for internal control state that agencies should use quality information to achieve their objectives, such as information that is complete. OSHA obtains such information in part through its requirement for employers to report work-related in-patient hospitalizations and fatalities, and uses these reports to help determine where to conduct inspections and other inquiries. OSHA may also be notified of COVID-19-related hazards through complaints and referrals, and OSHA officials told us they expect to learn about the majority of such hazards even without COVID-19-related hospitalization reports. However, because OSHA does not receive employer reports of all work-related hospitalizations related to COVID-19, as disease symptoms do not appear within the required reporting time frames, the agency does not have the same level of information to target its enforcement as it does in other cases; for instance, for severe injuries, which are likely immediately evident to the employer.[263]
Employers may also face challenges determining whether COVID-19 hospitalizations or fatalities are work-related because of COVID-19’s incubation period and the difficulties in tracking the source of exposure. Thus, it is difficult for OSHA to obtain meaningful data on COVID-19 worker exposures, hospitalizations, and fatalities that point to a workplace spread of the virus requiring OSHA intervention. More assessment on how to obtain such data is needed. For example, OSHA could explore the availability and quality of existing public health data that could help OSHA target its enforcement toward certain industries or locations that may warrant OSHA intervention. As another example of COVID-19 data, the state of Virginia obtains certain information on COVID-19 exposures at workplaces under an emergency temporary standard, which among other things, requires employers to report to the Virginia Department of Labor and Industry when three or more employees test positive for COVID-19 within a 14-day period.[264]
OSHA relies, in part, on employer reports to learn of potential safety and health issues for workers. Without comprehensive information on hospitalizations and fatalities associated with workplace exposure to COVID-19—based on scientific knowledge of how the virus spreads—or alternate data on workplace spread of the virus, OSHA is missing critical information on COVID-19 risks to workers to inform its enforcement activities. Moreover, without further assessment of what data would be most beneficial to OSHA’s mission of ensuring workplace safety and health, OSHA cannot determine the best way to obtain that data, such as by seeking other available data sources or by updating its reporting requirements.
Agency Comments
We provided DOL and OMB with a draft of this enclosure. OMB did not provide comments on this enclosure. DOL provided written comments, reproduced in Appendix VI: Comments from the Department of Labor on the Worker Safety Enclosure, and technical comments, which we incorporated as appropriate. In DOL’s comments, the agency neither agreed nor disagreed with our three recommendations.
On our recommendation to develop a plan, with time frames, to implement OSHA’s oversight processes for its COVID-19-adapted enforcement methods, DOL stated that OSHA developed an enforcement triage plan and has been reviewing available data and updating the plan as circumstances change. In this report, we refer to the enforcement triage plan as OSHA’s adapted enforcement methods that are described in its pandemic enforcement policies. Our recommendation, however, relates to OSHA’s specific oversight processes for these adapted enforcement methods, which are also outlined in OSHA’s pandemic enforcement policies. OSHA has not yet implemented its oversight processes and does not have specific plans for how to do so. It is these oversight processes that we continue to recommend that OSHA plan for. DOL also stated that OSHA will implement its oversight processes in its pandemic enforcement policies during fiscal year 2021, as operations return to normal. However, since it is unclear when the pandemic will end and when OSHA’s activities will return to normal, we continue to recommend that OSHA develop a plan now for this oversight, with time frames, to ensure the agency is prepared to implement its oversight processes as soon as it is safe to do so.[265]
On our recommendation to ensure that OIS includes comprehensive information on the use of OSHA’s adapted enforcement methods sufficient to inform its oversight processes, DOL stated that OSHA disagrees that the agency is unable to reliably track actions related to its adapted enforcement methods. DOL stated that OSHA updated OIS to track various COVID-19-related enforcement data, such as inspections related to COVID-19, inspections conducted remotely, and inspections where inspectors observed but did not cite violations—referred to as citation discretion in this report. We agree that this was an important step toward capturing key information on COVID-19 enforcement efforts.
However, as described in this report, citation discretion is only tracked in OIS for violations of recurring requirements, not for violations of other requirements for which this discretion is allowed. Moreover, we determined that OIS does not track which informal inquiries OSHA conducted in place of inspections. Further, the agency does not have reliability measures in place for at least two of the new OIS codes—remote inspections and citation discretion for recurring requirements. We therefore continue to recommend that OSHA ensure that OIS includes comprehensive information on the use of the agency’s adapted enforcement methods in order to fully oversee and assess the effectiveness of these methods.
On our recommendation to determine what additional data may be needed from employers or other sources to better target OSHA’s COVID-19 enforcement efforts, DOL stated that OSHA receives data from several sources. Based on the volume of complaints, referrals, and employer reports OSHA has received, the agency believes its efforts to obtain data have been effective. However, a large volume of data does not necessarily indicate that OSHA is receiving the most useful data to target its COVID-19 enforcement efforts.
As we describe in this report, OSHA does not receive employer reports of all work-related hospitalizations related to COVID-19. Because disease symptoms do not appear within the required reporting time frames, the agency does not have the same level of information to target its enforcement as it does in other cases. As we note in this report, other sources of meaningful data may be available, and in its comments, DOL stated that OSHA will continue to seek additional data and information—beyond employer reports—where available. OSHA should carefully assess whether the agency needs to intentionally seek out and obtain additional data on worker safety and health related to COVID-19, from employers or other sources, in light of the impact that COVID-19’s incubation period and employers’ difficulties in identifying work-related COVID-19 hospitalizations and fatalities have on employers’ mandated reporting.
We provided the Department of Veterans Affairs (VA) with a draft of this report’s Executive Summary, but we did not provide VA with a draft of this enclosure, because our findings in this enclosure do not specifically relate to VA activity. VA provided comments, reproduced in Appendix X: Comments from the Department of Veterans Affairs, on our recommendation that OSHA determine what additional data may be needed from employers or other sources to better target OSHA’s COVID-19 enforcement efforts. VA stated that this report’s Executive Summary does not consider that OSHA may receive information from data sources other than employers, that employers and other agencies will bear an additional record-keeping burden if this recommendation is implemented, and that there are difficulties in assessing whether COVID-19 exposure is work-related.
We acknowledge in this enclosure that OSHA has multiple sources of data and that there are difficulties in determining whether COVID-19 exposures are work-related. However, VA mischaracterizes our recommendation and we encourage the agency to read this full enclosure to better understand it. Our recommendation is not limited to employer data and fulfilling our recommendation does not necessarily require that OSHA revise its policies or procedures. Rather, it calls for OSHA to determine what additional data may be needed from employers or other sources in order to have the best available data to ensure workplace safety and health during the pandemic. In this enclosure, we describe examples of potential data sources, other than employers. As OSHA determines what additional data it might need, and how it might go about collecting it in response to our recommendation, we would expect OSHA to consider any potential burden on employers or other agencies. Finally, in this enclosure we describe the potential challenges employers may face in determining whether COVID-19 cases are work-related, noting that this is partly why it is difficult for OSHA to obtain meaningful data on COVID-19 worker exposures, hospitalizations, and fatalities that point to a workplace spread of the virus requiring OSHA intervention.
Methodology
To conduct this work, we reviewed OSHA guidance and enforcement policy, relevant federal laws and regulations, and the most recent OSHA data through December 2020.[266] To assess the reliability of OSHA’s data, we reviewed technical documentation and interviewed OSHA officials. We determined that OSHA’s data were sufficiently reliable for the purposes of our reporting objectives. We also interviewed OSHA headquarters officials.
Contact information: Thomas M. Costa, 202-512-7215, costat@gao.gov
Related GAO Product
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
The Administration for Community Living has provided guidance and support to help states and local agencies meet increased demand for nutrition assistance and provide other services for older adults, but challenges remain as the pandemic continues.
Entities involved: Administration for Community Living, within the Department of Health and Human Services; and Employment and Training Administration, within the Department of Labor
Key Considerations and Future GAO Work
In November 2019, we issued a report that examined the nutrition requirements in federal nutrition assistance programs serving older adults, and found that meal providers faced challenges meeting increased demand and addressing certain dietary needs, such as for diabetic or pureed meals. We recommended, among other things, that the Department of Health and Human Services (HHS) centralize information on promising approaches for making meal accommodations to help meal providers meet older adults’ nutritional needs, which is now of even greater concern during the pandemic.
Also, in May 2019, we reviewed services provided to older adults living in rural areas under the Older Americans Act of 1965, as amended (OAA), and found that rural older adults may have less access to OAA services compared to urban older adults.[267] We recommended that HHS take steps to better centralize access to information on promising practices or other useful information pertinent to serving more isolated rural older adults—information that may be relevant to urban older adults now, as they, too, are more isolated due to the pandemic.
HHS agreed with our recommendations in both these reports and has initiated actions, but as of January 2021, had not taken action to fully address them.
We have additional work under way to review the extent to which states have made use of the added funding and program flexibilities provided by the COVID-19 relief laws for OAA Title III services, which include nutrition assistance, home and community-based supportive services, and family caregiver supports. As part of this work, we will identify strategies that federal, state, and local agencies and service providers have implemented to address the challenges that older adults are facing during the pandemic.
Background
The Older Americans Act of 1965 (OAA), as amended, provides support for a broad array of programs to help meet the needs of older adults and help them continue to live in their homes and communities. Given the disproportionate impact of COVID-19 on the older adult population, more older adults are staying in their homes to avoid the virus.[268] As a result, OAA services are increasingly important to ensuring that older adults are able to meet their basic nutrition and other routine needs of daily living, to stay safe from abuse, and for certain older adults to have opportunities for employment, as appropriate, during the pandemic. To help address this increased demand, in fiscal year 2020, the Families First Coronavirus Response Act (FFCRA) and the CARES Act provided $1.12 billion in additional funding for select OAA programs.[269] In fiscal year 2021, an additional $175 million in COVID-19 relief funding for nutrition services was included in the Consolidated Appropriations Act, 2021 (CAA-21).[270]
The Administration for Community Living (ACL), within HHS, administers programs under OAA Title III that help provide older adults with meals, in-home services, and supports for their family caregivers. Generally, adults age 60 and older, and informal caregivers, are eligible to receive these services.[271] ACL provides guidance and support for the implementation of these programs, and distributes separate allotments of OAA Title III funding to states and territories for different types of services based on statutory funding formulas. The states, in turn, typically distribute their funds to Area Agencies on Aging (AAAs), which provide and coordinate OAA services on the local and regional level. States also have the ability to transfer certain portions of funds among Title III programs, such as from in-home care supportive services to home-delivered meals.
ACL administers several other programs for older adults under other titles of OAA, such as programs to help prevent elder abuse.[272] In addition, one OAA program, an employment services program for older adults, is authorized under OAA Title V, and is administered by the Employment and Training Administration (ETA), within the Department of Labor (DOL). Adults age 55 and older who are considered to have low employment prospects, and are living at or under 125 percent of the federal poverty level are eligible to receive these services.
In fiscal year 2020, the FFCRA and CARES Act provided $1.12 billion in additional funding for select OAA programs, expanding the total budget for those programs by more than 70 percent. For fiscal year 2021, the CAA-21 provided $175 million in COVID-19 relief funding specifically for nutrition services. The CARES Act also provided certain flexibilities to two OAA programs: nutrition assistance (Title III) and employment services (Title V).[273] (See table.) The states will report their use of the added funding and flexibilities during their normal annual and semi-annual reporting processes to ACL and ETA. ACL officials told us that they may have preliminary data in March 2021 to reflect this for the programs ACL administers, but the data will not be publicly released until ACL has completed its quality review. ETA officials told us that their annual reports for program year 2019 would cover grantee participation through June 2020, but as of mid-January 2021, these reports had not yet been released.
Overview of COVID-19 Relief Funding and Flexibilities for Select OAA Programs
Department/ administration responsible for the select OAA programs
OAA program
COVID-19 relief funding ($ millions)
How additional funding and flexibilities to be used
Programs administered by the Department of Health and Human Services (HHS), Administration for Community Living (ACL)a
Aging and Disability Resource Centers (ADRC) (Title II)
$50 (CARES Act)
Funding for programs that connect people at greatest risk to COVID-19 to community-based services to avoid unnecessary institutionalization, as well as mitigate the negative psychosocial impact of social isolation. ADRCs across the country are reporting unprecedented demand for in-person and virtual assistance with applications for services, care coordination, services that support people in returning home following hospitalization, among other things.
Home and Community-based Supportive Services (Title III-B)
$200 (CARES Act)
Funding to help greater numbers of older adults shelter in place to minimize their exposure to COVID-19. These services include personal care assistance; help with household chores and grocery shopping; transportation to essential services (such as grocery stores, banks, or doctors) when necessary; and case management.
Nutrition programs (Title III-C)
$240 (FFCRA)
$480 (CARES Act)
$168 (CAA-21)
Funding for more home-delivered meals, and also to expand "drive-through" or "grab-and-go" meals for older adults who typically would participate in meal programs at community centers and other locations that have been closed due to social distancing measures.
Flexibilities added:
Allows the Secretary of HHS to waive nutrition requirements for congregate and home-delivered meal programs.
Home-delivered meal eligibility criteria broadened to include individuals unable to obtain nutrition services because of social distancing.
Allows state agencies and area agencies on aging (AAAs), without prior approval, to transfer up to 100 percent of funds received for congregate and home-delivered meal programs between the two programs.
National Family Caregiver Support Program (Title III-E)
$100 (CARES Act)
Funding to expand a range of services that help family and informal caregivers provide support for their loved ones at home. These include counseling, respite care, training, and connecting people to information.
Nutrition and related services for Native American Programs (Title VI)
$10 (FFCRA)
$20 (CARES Act)
$7 (CAA-21)
Funding for nutrition and related services for Native American Programs to help tribes and tribal organizations provide meals and supportive services directly to Native American elders.
Long-term Care Ombudsman Program (Title VII)b
$ 20 (CARES Act)
Funding to support consumer advocacy services for residents of long-term care facilities across the country. Restrictions on visitation have significantly increased demand for ombudsman services, as families seek assistance in ensuring the well-being of their loved ones. Ombudsman programs will seek to expand their virtual presence to residents and their families, and continue to promote the health, safety welfare, and rights of residents in the context of COVID-19. This funding will give Ombudsman programs the flexibility to hire additional staff and purchase additional technology, associated hardware, and personal protective equipment once in-person visits resume.
Program administered by the Department of Labor (DOL), Employment & Training Administration (ETA)c
Senior Community Service Employment Program (SCSEP) (Title V)
--
No added funding, but flexibility added that allows the Secretary of Labor to extend individual participant duration limits and average duration limits for a grantee in situations where such an extension is appropriate due to the effects of the COVID-19 public health emergency.
Totals
$260 (FFCRA)
$860 (CARES Act)
$175 (CAA-21)
Source: GAO analysis of COVID-19 relief funding from Families First Coronavirus Response Act (FFCRA), the CARES Act, and the Consolidated Appropriations Act, 2021 (CAA-21), and agency documents. | GAO-21-265
aSee Administration for Community Living, ACL Announces Nearly $1 Billion in CARES Act Grants to Support Older Adults and People with Disabilities in the Community During the COVID-19 Emergency (press release, April 21, 2020, updated as of May 7, 2020). bUnder the CAA-21, ACL also received $100 million for elder justice programs, including no less than $50 million to be awarded for formula grants for state adult protective services programs. cSee the Department of Labor, Employment and Training website, COVID-19 Frequently Asked Questions, accessed November 12, 2020.
Overview of Key Issues
Key Issues Identified by Agency Officials for Serving Older Adults during the Pandemic
Note: FFCRA=Families First Coronavirus Response Act; OAA=Older Americans Act of 1965, as amended; PPE=personal protective equipment.
OAA nutrition services. During the pandemic, providers of OAA nutrition services have experienced an increased demand for home-delivered meals and have modified the delivery of nutrition services to prevent the transmission of COVID-19. HHS officials and provider representatives reported that OAA nutrition programs’ delivery of meals and food was one of the most needed services as a result of the COVID-19 pandemic, which increased demand and the need to avoid large gatherings. For example, according to a survey conducted in May 2020 by the National Association of Area Agencies on Aging (N4A), 98 percent of AAAs, which serve as local and regional providers of OAA nutrition services, reported increased demand for home-delivered meals as a result of the COVID-19 pandemic.[274] Also, a survey conducted by Meals on Wheels America (MOWA), a national organization that coordinates meal deliveries through a network of local providers using OAA funding, reported that their providers were serving 77 percent more meals, and 47 percent more older adults in July 2020 compared to March 1, 2020 (before the COVID-19 pandemic began in the U.S.).[275] In addition, MOWA reported that their waiting lists for home delivered meals grew by 26 percent in April 2020 compared to the last week of February 2020.[276]
During fiscal year 2020, the FFCRA and CARES Act provided $720 million in additional funding for OAA Title III nutrition services, which was allotted by ACL to the states using OAA’s established funding formula. This funding was in addition to the over $936 million in total funding for OAA Title III nutrition services previously provided in fiscal year 2020 to the states.[277] In addition, the CARES Act provided states the flexibility to transfer 100 percent of funds between Title III-C congregate and home-delivered meal nutrition programs.[278] However, according to ACL officials, states were granted even broader flexibility under OAA’s disaster relief provisions.[279]
Under the disaster relief provisions, states are allowed to use any portion of the funds made available under any and all sections of the OAA to provide disaster relief for older individuals. For example, under the disaster relief provisions, funds made available under OAA Titles III-B (home and community-based services), and III-E (caregiver services) could be used to provide more services under III-C (nutrition). The states will report their use of such authorities during the annual reporting process to ACL. As noted earlier, according to ACL officials, the first preliminary data reflecting the use of the additional funding under the FFCRA and the CARES Act, and use of funds under OAA’s disaster relief provisions, may be available in March 2021, but will not be released until ACL’s quality review of the data is complete.
The CARES Act also granted states added flexibilities to help provide continuity of service and to adapt to the pandemic. For example, ACL was allowed to waive any nutritional requirements for meals. Officials said this flexibility helped providers when they were initially experiencing food supply chain issues during the beginning of the COVID-19 pandemic, as the providers’ first priority was getting food to older adults as fast and as safely as they could. Also, the CARES Act makes the population of individuals unable to obtain nutrition services because of social distancing eligible to receive home-delivered meals regardless of current state policy. Providers were also allowed to provide groceries to older adults in addition to meals, or in limited cases, instead of meals.
Organizations we spoke with told us that some providers adapted to increased demand by delivering frozen and shelf-stable meals as an alternative to traditional hot meals, with the purpose of providing multiple days’ worth of prepared meals during a single delivery. MOWA reported changing their protocol for meal deliveries and modifying their delivery routes to limit human contact for the benefit of the safety of their workers. In addition, providers reported the need to train their staff and volunteers on personal safety and effective use of personal protective equipment to incorporate into their work routines. Going forward, organizations such as MOWA, AARP, and N4A told us that nutrition service providers will need additional funding to address their increased demand and strained resources as the pandemic continues. N4A anticipates that if the current demand continues without additional funding, people will get less food or will be removed from the rolls. The additional $168 million provided by CAA-21 for OAA Title III nutrition services could help mitigate these concerns, at least for the immediate future.[280]
OAA supports for daily living, safety, and well-being. Beyond nutrition assistance, OAA provides support for a comprehensive array of community-based, long-term care services to sustain older people in their communities and in their homes, including support to family members and other persons providing voluntary care to older individuals needing long-term care services. During the pandemic, many family members have reported experiencing greater stress with the decline in availability of support services and concern about protecting their older adult family members and themselves from the virus.[281]
While protecting against the risk of contracting the virus, the increase in isolation and drop off in support services may jeopardize older adults’ well-being in other ways, as many older adults rely on such supports to help them perform routine activities of daily living, such as eating, bathing, dressing, paying bills, and preparing meals. According to the N4A survey conducted in May 2020, 33 percent of AAAs were experiencing increased demand for home care services, and 52 percent of AAAs were experiencing increased demand for caregiver supports due to the pandemic.
Also, with fewer face-to-face contacts with extended family and other caregivers, doctors, and others, older adults may be more isolated and vulnerable to depression, self-neglect, exploitation, or abuse. State Adult Protective Service (APS) officials we contacted in eight states told us that conducting investigations in response to reports of abuse is more difficult due to the pandemic, as they have more limited ability to meet face-to-face with potential victims in their homes or in facilities.[282]
Some officials noted that while reports of abuse have declined, older adults actually may be at greater risk during the pandemic because they may be more reliant on the assistance of potential perpetrators of abuse, and may have less contact with individuals who typically report abuse on an older adults’ behalf, such as doctors and caregivers. For example, one state APS caseworker we spoke with described a situation where a son was allegedly financially abusing his mother, but the mother was dependent on the son to do shopping for her during the pandemic. During fiscal year 2020, the CARES Act provided $20 million of additional funding for the Title VII Long-Term Care Ombudsman program to help older adults in residential and long-term care facilities resolve problems related to their health and well-being, but no additional funding was provided for state APS programs to help address the challenges of investigating reports of abuse and ensure the safety and well-being of older adults more isolated in their homes during the pandemic.[283] For fiscal year 2021, however, the CAA-21 provided ACL $100 million for elder justice programs, including no less than $50 million to be awarded as formula grants for state APS programs.[284]
During fiscal year 2020, the CARES Act also provided additional funding for certain other OAA support programs. Specifically, it provided $200 million of additional funding for Title III-B home and community-based supportive services, and $100 million of additional funding for Title III-E services to help family and informal caregivers provide support for older adults and other eligible populations in their homes.[285] For fiscal year 2021, however, the CAA-21 did not provide additional COVID-19 relief funding for these programs. In addition, as noted above, the OAA disaster relief provisions allow states to use all available OAA funds, including those for home and community-based services and family caregiver supports, for whatever services are needed most to help older individuals.
OAA Senior Community Service Employment Program (SCSEP). According to DOL officials, participation in SCSEP—a program that helps certain adults age 55 and older find employment—fell due to the COVID-19 outbreak in Spring 2020. DOL officials told us that grantee offices that receive SCSEP funds closed across the U.S., and community service locations where participants worked also closed, reducing the availability of SCSEP community service assignments. While DOL officials told us they have not collected separate new data on the impact of the pandemic on SCSEP, they expect the extent of the reduced participation to be reflected in the next annual reports that they use to track program participation and performance.[286]
Neither the FFCRA nor the CARES Act provided any additional funding to SCSEP beyond its fiscal year 2020 funding of over $403 million. Funding for SCSEP for fiscal year 2021 remains at a similar amount. However, the CARES Act provided the following flexibilities to support SCSEP operations during the COVID-19 pandemic:
An extension of individual participant duration limits past the current 48-month maximum duration. (DOL has provided for up to an additional 12 months, resulting in a total of up to 60 months maximum duration per participant).
A change in the average participation cap for individuals (in the aggregate) by an amount that accounts for the individual durational limit extensions. According to officials, this is being implemented with the intention of keeping grantees from exceeding their average participation caps.
An increase in the amount of grant funds that can be used for administrative costs, allowing for up to 20 percent of the total grant amount to be applied towards administrative costs.[287]
DOL officials stated their main challenge with implementing the CARES Act flexibilities was updating their case management system to increase each participant’s 48-month limit to 60-months under the program. In order to assist grantees’ understanding of the CARES Act provisions, ETA issued a Training and Employment Guidance Letter (TEGL 22-19), and hosted teleconferences with grantees to discuss the provisions. According to officials, few grantees have exercised the option to increase the cap of their administrative costs, as the pandemic environment did not produce the additional need for administrative monies.
Officials told us that SCSEP participants often face barriers to employment, so it was important to ensure the continuity of the program during the COVID-19 pandemic. ETA took steps to inform grantees of the CARES Act flexibilities for SCSEP and implemented additional strategies to provide program continuity. For example, DOL officials said they provided technical assistance regarding existing flexibilities under SCSEP regulations that allow grantees to use paid sick leave for participants as a means to maintain payments of wages to participants and continue participants’ engagement in the program until services are available. DOL reported that grantees have successfully used this strategy as a means to continue providing services and wages.
DOL officials said they also encouraged grantees to provide remote and virtual community service options. Officials said that this strategy has been more challenging to implement, as SCSEP participants may require increased supervision for their work, and some participants may lack access to the appropriate technology. One example of an effort to address this challenge is a work program developed by the National Council on Aging (NCOA), a SCSEP grantee. NCOA launched an initiative to match COVID-19 contact tracing employers with SCSEP participants to work remotely as contact tracers. According to a NCOA official, many SCSEP participants received training and certification, but they have not had success being placed in contact tracing positions as of November 2020, because localities had looked to specific sources (such as medical students) to conduct this work. The official said NCOA was continuing to monitor the situation in case demand for their services changed.
Agency Comments
We provided the Department of Health and Human Services (HHS), the Department of Labor (DOL), and Office of Management and Budget with a draft of this enclosure. HHS and DOL provided technical comments that we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To conduct this work, we interviewed agency officials and national organizations involved in providing OAA services. In addition, we reviewed available data on the funding of OAA programs and various surveys and studies of OAA services provided during the first 6 months of the pandemic. We also asked state and local APS officials in eight selected states about the challenges they faced responding to reports of elder abuse during the pandemic, as part of the work conducted for GAO-21-90.
Elder Justice: HHS Could Do More to Encourage State Reporting on the Costs of Financial Exploitation. GAO-21-90. Washington, D.C.: December 18, 2020.
COVID-19: Urgent Actions Needed to Better Ensure an Effective Federal Response. GAO-21-191. Washington, D.C.: November 30, 2020.
Nutrition Assistance Programs: Agencies Could Do More to Help Address the Nutritional Needs of Older Adults. GAO-20-18. Washington, D.C.: November 21, 2019.
Older Americans Act: HHS Could Help Rural Service Providers by Centralizing Information on Promising Practices. GAO-19-330. Washington, D.C.: May 23, 2019.
The Department of Veterans Affairs suspended in-person disability medical exams in April 2020 and relied on other means such as telehealth to conduct some exams prior to resuming in-person exams in June 2020, when contractors could better address the resulting backlog of disability medical exams that occurred.
Entity involved: Department of Veterans Affairs, including the Veterans Benefits Administration and Veterans Health Administration
Key Considerations and Future GAO Work
In fiscal year 2019, the Veterans Benefits Administration (VBA) used contractors to conduct about two-thirds of the medical exams it uses to determine eligibility for benefits, while examiners who work for the Veterans Health Administration (VHA) conducted about a third.[288] We have previously reported on issues with VBA’s oversight of contracted disability medical examiners. In October 2018, we recommended that VBA improve its oversight of contracted examiners to ensure they offer high-quality, timely exams to veterans and to ensure that examiner training is completed and effective. While VBA has taken some steps to address these issues, as of January 2021, VBA has not fully implemented our recommendations.
As part of our ongoing work examining VBA’s use of contracted disability medical examiners, we will continue to monitor the pandemic’s effects on the Department of Veterans Affairs’ (VA) provision of disability medical exams.
Background
As one of the largest disability programs administered by the federal government, VA provides monthly disability compensation to veterans for a current disability resulting from an injury or disease that was caused by—or got worse because of—the veteran’s active military service. In fiscal year 2019, VA paid about $85 billion in disability compensation benefits to nearly 5 million veterans.
VA’s management of veterans’ disability compensation has been on GAO’s high-risk list since 2003, in part because veterans were experiencing lengthy wait times for decisions on their disability claims.[289] By the end of 2019, over 362,000 claims were awaiting a decision. Of those, over 19 percent had been awaiting a decision for over 125 days. By the end of 2020, that number had grown to over 471,000 claims with over 43 percent awaiting a decision for over 125 days.
Before a decision can be made on a claim, veterans who apply for disability compensation benefits may have to undergo a medical exam that VA claims processors use to help determine the connection to their military service and severity of the disability. Any delays in completing the disability exams, which are requested by VA claims processors, can contribute to delays in claim decisions. Prior to the COVID-19 pandemic, claims processors would send the exam request to either a VHA medical facility or a VBA contractor for completion.
VA received approximately $19.6 billion in supplemental funding to support its efforts to address COVID-19.[290] According to VBA officials, of this amount, the agency obligated $4.8 million to address the disability claims awaiting a decision. VBA used this funding to pay overtime for staff at the National Call Center and the Veterans Service Center.[291]
Overview of Key Issues
In response to the pandemic and to prevent the spread of COVID-19, VA took a number of steps that affected the ability of disability medical examiners to conduct medical exams for veterans seeking benefits. Specifically, in April 2020, VHA notified VBA that it would transition disability exams to VBA contractors to the fullest extent possible so that VHA could prioritize its response to the COVID-19 pandemic (see figure). VHA medical centers were to maintain minimal disability medical exam workloads and facilitate exams through such means as telehealth and Acceptable Clinical Evidence (ACE). [292] VBA subsequently suspended in-person disability medical exams and also instructed contractors to conduct exams using ACE or telehealth, when possible, to ensure the safety of veterans during the COVID-19 pandemic, according to VBA officials. Also according to VBA officials, that same month, VBA began to work with contractors to develop plans to conduct in-person exams using federal guidelines for a phased reopening approach.[293] Once VBA approved the plans, contractors could resume in-person exams, where possible. As of September, VBA officials told us the administration resumed in-person exams in all areas of the United States.
Department of Veterans Affairs’ Key Decisions during the COVID-19 Pandemic That Affected Disability Medical Exams
a The ACE process allows the medical examiner to complete exam reports using the medical evidence in a veteran’s claims file or medical records, supplemented by a telephone interview if necessary. Telehealth allows the medical examiner to conduct face-to-face medical exams using video technologies.
Contractors’ use of ACE and telehealth peaked in May 2020, when they reported completing roughly 22,000 ACE and 18,000 telehealth appointments (see figure).[294] According to VBA officials, contractors using telehealth should follow updated guidance from VHA. This guidance allows for contractors, when appropriate, to conduct telehealth exams without an attendant present and allows veterans to be examined from their homes.[295] VBA officials said these telehealth exams are primarily used for mental health and interview based assessments.
Reported Number of Acceptable Clinical Evidence, Telehealth, and In-person Disability Medical Exam Appointments Completed by Contract Examiners, April–December, 2020
Note: According to VBA officials, contractors began reporting the number of Acceptable Clinical Evidence, telehealth, and in-person disability medical exam appointments completed in April 2020. The data provided by VBA may be an underestimate as contractors provide periodic manual updates to VBA.
Contractors resumed in-person disability medical exams in June with VBA’s permission and in conjunction with the use of ACE and telehealth. Contractors reported completing over 26,000 in-person appointments in June 2020 and, after peaking in August, contractors reported completing over 59,000 appointments in December 2020.[296] VBA officials said the administration followed VHA’s criteria and risk assessment to identify when and where contractors could resume conducting in-person exams.[297] If VHA resumed in-person non-urgent appointments in an area, VBA used this as the trigger to resume in-person disability medical exams in that area. The agency instructed contractors to continue the use of ACE and telehealth during the COVID-19 pandemic, but the number of these completed appointments declined starting in June. According to VBA officials, this is because the contract examiners—all of whom conduct ACE, telehealth, and in-person exams—focused on completing the oldest pending exam requests, most of which required in-person exams.
The total number of pending disability medical exams remains above the pre-COVID-19 totals.[298] Almost 129,000 disability medical exams were pending when VBA suspended in-person exams in April 2020 and there were almost 348,000 exams pending as of December 2020, according to VBA (see figure). Further, the average number of days pending exams have awaited completion by a medical examiner has grown from almost 22 days in March 2020 to 89 days in December 2020.
Number of Pending Disability Medical Exams and Average Days for Pending Exam Completion, January–December 2020
VBA instructed contractors to not cancel exam requests when a veteran is unwilling to attend or fails to show up for an exam during COVID-19. If a contractor cancels the exam, the claim could be denied because of a lack of medical evidence.[299] VBA officials said the agency will place the claim on hold (i.e., not make a decision on the claim) until the exam can be completed.[300] According to VBA data, the number of claims on hold because of pending exams peaked in July at over 152,000 claims (see figure). [301] VBA instructed contractors to routinely follow up with veterans to assess their willingness to attend an in-person exam.
Number of Claims on Hold Because of an Incomplete Exam Request, January–December 2020
Agency Comments
We provided a draft of this enclosure to VA and the Office of Management and Budget. VA provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To conduct this work, we interviewed VBA officials and obtained their written responses to questions; analyzed exam request data from VBA’s Veterans Benefit Management System and Enterprise Data Warehouse as well as self-reported contractor data; and analyzed agency documents. We assessed the reliability of the data by examining written responses from VBA and accompanying agency documentation. We found the data are reliable for our purposes and we reported any limitations in this enclosure.
Contact information: Elizabeth Curda, (202) 512-7215, curdae@gao.gov
Related GAO Products
VA Disability Exams: Opportunities Remain to Improve Oversight of Contracted Examiners. GAO-19-715T. Washington D.C.: September 19, 2019.
High-Risk Series: Substantial Efforts Needed to Achieve Greater Progress on High-Risk Areas. GAO-19-157SP. Washington D.C.: March 6, 2019.
VA Disability Exams: Improved Oversight of Contracted Examiners Needed. GAO-19-213T. Washington D.C.: November 15, 2018.
VA Disability Exams: Improved Performance Analysis and Training Oversight Needed for Contracted Exams. GAO-19-13. Washington D.C.: October 12, 2018.
Congress has extended the Economic Injury Disaster Loans program related to COVID-19 to December 31, 2021. We remain concerned about the agency’s management of internal controls and fraud risks in the program.
Entity involved: Small Business Administration
Recommendation for Executive Action
The Administrator of the Small Business Administration should develop and implement portfolio-level data analytics across Economic Injury Disaster Loan program loans and advances made in response to COVID-19 as a means to detect potentially ineligible and fraudulent applications.
Key Considerations and Future GAO Work
In our November 2020 report, we identified concerns related to the potential for fraud in the Economic Injury Disaster Loan (EIDL) program. We remain concerned about these challenges and have ongoing work related to internal controls and fraud risk management in the EIDL program.
Background
To assist small businesses adversely affected by COVID-19, the Coronavirus Preparedness and Response Supplemental Appropriations Act made qualifying small businesses and nonprofit organizations experiencing economic injury caused by COVID-19 eligible for financial assistance from the EIDL program. In the Paycheck Protection Program and Health Care Enhancement (PPPHCE) Act, Congress appropriated $50 billion in loan credit subsidies for the Small Business Administration (SBA) to cover the cost of making these loans.[302] These funds supplemented the $1.1 billion in loan credit subsidy SBA already had to support EIDL loans.[303] Additionally, in the CARES Act and the PPPHCE Act, Congress appropriated $20 billion for EIDL advances, a new component of the program that provided direct payments of up to $10,000 to small businesses after they submitted their loan applications. On July 11, 2020, SBA announced that it had fully allocated the $20 billion in funding for EIDL advances and had stopped accepting requests for them.
In December 2020, under the Consolidated Appropriations Act, 2021 (the Act), Congress appropriated additional funding for certain EIDL advances, and amended CARES Act requirements related to EIDL loans and advances, including advances targeted at certain businesses in low-income communities.
The Act provided an additional $20 billion for targeted EIDL advances to eligible entities with 300 or fewer employees in low-income communities that have suffered an economic loss of greater than 30 percent.[304] In contrast to the advances made available in the CARES Act, these eligible entities qualify for the full amount of $10,000 in targeted advances regardless of their number of employees. Previously, SBA calculated the advance amount up to $10,000, based on the applicant’s number of employees. Eligible entities that previously received advances of less than $10,000 will receive the difference in funding after being approved for a targeted advance. Additionally, the Act requires SBA to verify eligibility for the targeted advances by requesting information the agency deems necessary for this purpose, such as tax records.
The Act extended the deadline to apply for EIDL loans under the relaxed requirements of the CARES Act from December 31, 2020, to December 31, 2021. These relaxed requirements include that applicants do not have to demonstrate that they cannot obtain credit elsewhere. However, the Act removed the CARES Act provision that prohibited SBA from requiring tax records as part of its eligibility determination.
Overview of Key Issues
EIDL loans related to COVID-19 continue through December 31, 2021. As mandated by the Act, SBA announced that it has extended the deadline to apply for EIDL loans related to COVID-19 to December 31, 2021. However, as of January 14, 2021, SBA has not announced how it will implement the targeted advances and other changes made under the Act.[305]
As of December 31, 2020, SBA had approved about 3.7 million loans related to COVID-19, totaling about $200 billion. SBA officials said that as of November 30, 2020, the agency had $24.5 billion of the $50 billion in loan credit subsidy appropriated specifically for COVID-19 remaining, which would allow the agency to make about $275.1 billion in new loans.
EIDL program faces fraud and contains loans to ineligible entities. SBA rapidly processed loans and advances to millions of small businesses affected by COVID-19 and, as permitted by the CARES Act, loosened application requirements, such as prohibiting requiring tax returns from applicants.[306] SBA has stated that its internal controls were robust. For example, SBA stated that it enhanced system controls and validation in processing loans and advances through an automated review of applications, such as by validating identification information and bank accounts. In processing loans, SBA loan officers also reviewed applications flagged by the automated review system.
However, our work as well as the work of SBA’s Office of Inspector General (OIG) and the Department of Justice indicates potential gaps in internal controls that may have led to fraud and the provision of EIDL funding to ineligible entities. Additionally, as we reported in our September and October 2020 reports, efforts to expedite processing may have contributed to increased fraud risk within the program. For example, to expedite processing of advances, applicants self-certified their eligibility and SBA did not flag ineligible business activities as part of its checks.
GAO’s Fraud Risk Framework cites data analytics as a leading practice in developing specific control activities to prevent and detect fraud—in particular, to mitigate the likelihood and impact of fraud. Additionally, internal control standards encourage ongoing monitoring of operations and internal controls. Data analytics can be used to detect potential fraud and can include a variety of techniques, such as data mining, data matching, and predictive analytics, to identity particular types of behavior. SBA has not provided evidence that it has conducted portfolio-level data analytics.
While the use of data analytics does not by itself necessarily confirm the existence of fraud, it could help SBA determine indicators of potential fraud and potential improper payments. Without conducting data analytics across EIDL loan and advance portfolios to identify patterns or anomalies, SBA may miss opportunities to detect potentially ineligible and fraudulent funding to recipients.
Our analysis of SBA data shows potential gaps in internal controls. Our analysis of SBA data on businesses’ self-reported industries shows that the agency approved EIDL loans and advances for potentially ineligible businesses.[307] Specifically, as of July 14, 2020, SBA provided about 5,000 advances totaling about $26 million to three types of potentially ineligible businesses—adult entertainment, casino gambling, and marijuana retail. Additionally, SBA approved at least 3,000 loans totaling about $156 million to potentially ineligible businesses in industries that SBA policies state were ineligible for the EIDL program, as of September 30, 2020. These industries include adult entertainment, casino gambling, multi-level marketing, insurance, and real estate development. SBA officials said that the CARES Act permitted businesses to self-certify their eligibility.[308] Additionally, they said that businesses self-reporting that they were in adult entertainment and gambling did not necessarily indicate ineligibility—for example, if those activities represented less than one-third of their revenues.
We also identified inconsistencies in EIDL advances disbursed compared to the number of employees. SBA policies at the time stated that businesses could receive $1,000 per employee up to $10,000 in EIDL advances, but SBA provided $3.2 million to 589 businesses in excess of what the businesses could receive based on their number of employees. For example, 194 of the 589 businesses reported having no employees or one employee but received $10,000 when they should have received $1,000. SBA also provided advances to 1,060 businesses that were a total of $3 million less than what the businesses could receive based on their number of employees.
Law enforcement agencies are investigating cases of potential fraud related to EIDL. The Department of Justice has filed fraud-related charges and the SBA OIG has conducted investigations associated with the EIDL program. The Department of Justice has filed charges in at least 20 cases related to the EIDL program based on law enforcement investigations. The charges—filed across the U.S. and investigated by a range of law enforcement agencies—include allegations of making false statements and engaging in identity theft, wire and bank fraud, and money laundering. In addition, as of October 1, 2020, SBA OIG representatives said the agency had received tens of thousands of complaints of wrongdoing on its hotline and initiated hundreds of investigations involving complaints of fraud associated with SBA loan programs, including EIDL. In October 2020, the SBA OIG reported that its preliminary review revealed strong indicators of widespread potential fraud in the EIDL program.[309] According to the report, the SBA OIG and other law enforcement agencies had seized over $450 million from over 15,000 fraudulent EIDL loans. According to SBA officials, they are working with law enforcement to support data requests and make referrals for potential investigation. We did not corroborate this coordination with law enforcement agencies nor evaluate the extent or effectiveness of SBA’s coordination with those agencies.
Concerns remain related to suspicious activity and potential fraud associated with the EIDL program. Between May and October 2020, over 900 U.S. financial institutions filed more than 20,000 suspicious activity reports related to the EIDL program with the Financial Crimes Enforcement Network (FinCEN).[310] Although the filing of a suspicious activity report does not necessarily mean that fraud has occurred, law enforcement agencies query these reports and use them to support investigations, such as those related to EIDL fraud. According to FinCEN officials, the financial transactions associated with suspicious activity involved potential fraud by EIDL recipients.[311] Financial institutions identified several instances of suspicious activity, including rapid movement of funds, identity theft, and forgeries, among others. The number of reports filed per month generally increased from May through October 2020 and ranged from 14 to 6,661 (see figure).
Suspicious Activity Reports Related to the Economic Injury Disaster Loan (EIDL) Program by Month, May through October 2020
Note: Although the EIDL program was available to assist small businesses suffering economic injury due to COVID-19 as early as March 2020, financial institutions did not file EIDL-related suspicious activity reports in March or April 2020.
Filings of suspicious activity reports and cases of alleged fraud indicate vulnerabilities to fraud and abuse within the loan program. Although these emerging fraud risk indicators are small in number compared to the total overall number of disbursed EIDL loans, they point to vulnerabilities typically managed through a fraud risk management approach, including a determination of fraud risk tolerance. To date, SBA has not provided us with a documented fraud risk assessment to include fraud risk tolerance for EIDL.
U.S. financial institutions filed EIDL-related suspicious activity reports in all 50 states (see figure).
Suspicious Activity Reports Related to the Economic Injury Disaster Loan (EIDL) Program as a Share of Total Number of EIDL Loans by State, May through September 2020
Note: We compared the number of suspicious activity reports filed per state to the number of EIDL loans, not including advances, to avoid double counting recipients that received both an EIDL loan and advance. We used the location of suspicious activity cited in report filings for this analysis.
Most EIDL advances and loans were made for businesses with few or no employees. Most businesses that received EIDL advances and loans had either no employees or fewer than 10 employees, as of January 31, 2020.[312] Further, as of September 30, 2020, about half of the 5.8 million EIDL advances disbursed and about half of the 3.6 million loans approved had gone to businesses that reported having no employees or one employee, according to SBA data (see figure).[313]
Number of Economic Injury Disaster Loan Advances and Approved Loans by Recipients’ Employees, as of September 30, 2020
In contrast, for both advances and loans, larger businesses (those with 10 or more employees) accounted for a larger share of the total dollar amount than their share of recipients (see figure).
Total Dollar Amount of Economic Injury Disaster Loan Advances and Approved Loans by Recipients’ Employees, as of September 30, 2020
Note: Percentages may not add up to 100 due to rounding.
In addition, most advance and loan amounts were on the smaller end of the size range. Of the advances, about 51 percent were for $1,000, while 16 percent were for the maximum amount of $10,000.[314] Although the maximum loan amount a business could receive was generally $150,000, most loans (about 65 percent) were for $50,000 or less, while about 34 percent were between $50,000 and $150,000. Less than 1 percent of the loans were larger than $150,000.[315]
Certain industries accounted for more advances and loans than others. As of September 30, 2020, the top five industries in which businesses both received advances and were approved for loans, based on recipients’ self-reported data, were
Across these industries, the EIDL program reached a relatively small proportion of all small businesses. Specifically, our analysis of Census Bureau and SBA data estimated that 14.1 percent of all small businesses in the accommodation and food services industry, 7.4 percent of those in the real estate industry, and 7.1 percent of those in the construction industry received EIDL advances and were approved for loans.[317]
Within those industries, a higher share of businesses with employees received assistance than those without employees: 21 percent versus 3 percent in the accommodation and food services industry, 41.1 percent versus 3 percent in the real estate industry, and 27 percent versus 1.6 percent in the construction industry.
Agency Comments
We provided SBA, the Department of the Treasury (Treasury), and the Office of Management and Budget (OMB) with a draft of this enclosure. SBA and Treasury provided technical comments that we incorporated as appropriate. OMB did not provide comments on this enclosure.
In its comments, reproduced in Appendix VII: Comments from the Small Business Administration on the Economic Injury Disaster Loan Program Enclosure, SBA neither agreed nor disagreed with our recommendation. SBA took issue with our finding that potentially ineligible businesses received EIDL advances and loans. SBA mentioned actions it takes to prevent payments to ineligible businesses for loans, such as conducting manual reviews of applications in prohibited categories and approving them upon further determination that they were eligible. According to SBA, it declined most applications in three prohibited business categories we identified (adult entertainment, casinos, and marijuana shops) following the manual reviews and approved some applications in these categories after manual reviews indicated that they were eligible. However, SBA did not provide any documentation that would enable us to verify the results of its manual reviews. In addition, we identified other prohibited business categories (multi-level marketing, insurance, and real estate development) where potentially ineligible businesses received EIDL loans. SBA did not address these other prohibited categories in its comments. Further, to date SBA has not provided us information we have requested on actions it and its contractors take to prevent payments to ineligible businesses. Therefore, we lack assurance that the actions SBA takes are effective in identifying ineligible businesses.
Our analysis was intended to provide an illustration of how fraud risk indicators can point to vulnerabilities typically managed through a fraud risk management approach. Such indicators are especially important in programs with heavy reliance on borrower certifications. We maintain that portfolio-level data analytics could help SBA manage its risk of providing funds to ineligible businesses.
Methodology
To conduct this work, we analyzed SBA data on approved EIDL loans related to COVID-19 through September 30, 2020, data on all EIDL advances obligated before the program ended in July 2020, and summary data on the processing of loan applications. We assessed the reliability of the data by identifying missing data and duplicate records, comparing data on the amount and number of loans and advances to information available from other sources, conducting logic checks for data fields, and interviewing SBA officials about the data. We determined that all data fields in the advance data were sufficiently reliable for our use in analyzing EIDL advances made to businesses. For the loan data, we determined that with the exception of the business activity field describing business industries, other fields were sufficiently reliable. Having determined that the industry field in the advance data was sufficiently reliable, we matched businesses that received both an advance and a loan based on the application number in order to analyze the industry field for those businesses.[318] We analyzed the Census Bureau’s County Business Patterns and Nonemployer Statistics data on the number of business establishments by size and by industry. We assessed the reliability of the data by reviewing relevant methodological documents and determined that they were sufficiently reliable for our use as a basis for estimating how many businesses exist by industry. We analyzed FinCEN data on suspicious activity reports and assessed the reliability of the data by reviewing relevant FinCEN documents, reviewing GAO’s prior use of the data sources, and interviewing agency officials. We determined the data were sufficiently reliable to describe the number of suspicious activity report filings. We also reviewed documents from the SBA OIG and news releases from the Department of Justice.
Contact information: William B. Shear, (202) 512-8678, shearw@gao.gov
Related GAO Product
Small Business Administration: COVID-19 Loans Lack Controls and Are Susceptible to Fraud. GAO-21-117T. Washington, D.C.: October 1, 2020.
A Framework for Managing Fraud Risks in Federal Programs.GAO-15-593SP. Washington, D.C.: July 28, 2015.
Standards for Internal Control in the Federal Government.GAO-14-704G. Washington, D.C.: September 10, 2014.
From April through October 2020, lenders filed more than 21,000 reports of potentially suspicious activity related to the Paycheck Protection Program, and law enforcement agencies have initiated investigations and filed charges related to fraud in the program.
Entities involved: Small Business Administration, Department of the Treasury
Key Considerations and Future GAO Work
In June 2020, we recommended that the Small Business Administration (SBA) develop and implement plans to identify and respond to risks in the Paycheck Protection Program (PPP) to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less. SBA neither agreed nor disagreed with our recommendation at that time. Consistent with our recommendation, in early December 2020, SBA officials said the agency had completed oversight plans and provided a document that SBA characterized as an overview of these plans. At that time, the agency told us it had not yet finalized more comprehensive documentation detailing its oversight plans and how it will implement them. SBA provided a draft Master Review Plan for the Loan Review Process at the end of December 2020. Although the draft plan references detailed policies and procedures for some loan reviews and loan forgiveness reviews, like those we had previously requested, they were not included in the document we received. According to SBA officials, these policies and procedures were being updated. Until SBA provides the policies and procedures, we will not be able to determine if they address our recommendation.
In November 2020, we also recommended that SBA expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread. SBA neither agreed nor disagreed with our recommendation at that time. In response to our recommendation, SBA stated that it was planning to conduct improper payment testing for PPP and that it takes improper payments seriously. SBA officials also stated that SBA works to prevent improper payments before they occur through its loan review process. However, the agency has not provided documentation of its plans for testing, including estimates of improper payments and error rates for PPP.
Our work on PPP is ongoing. We continue to examine the borrowers that received PPP loans, the safeguards SBA implemented to help ensure that lenders and borrowers complied with program requirements, and the loan forgiveness process.
Background
The CARES Act and the Paycheck Protection Program and Health Care Enhancement Act appropriated a total of $670 billion for PPP (including lender fees) under SBA’s largest guaranteed loan program, its 7(a) small business lending program.[319] PPP loans, made by lenders but guaranteed 100 percent by SBA, are low interest (1 percent) and fully forgivable if certain conditions are met.[320]
As of August 8, 2020 (the close of the program’s initial application period), lenders had made over 5.2 million PPP loans totaling more than $525 billion.[321] According to SBA officials, SBA had obligated about $532 billion for PPP, including lender fees, and expended about $528 billion, as of December 31, 2020.
In December 2020, the Consolidated Appropriations Act, 2021, authorized additional PPP loans through March 31, 2021, and made changes to PPP.[322] The Act increased the commitment authority for PPP loans from $659 billion to $806.45 billion. It also:
Allows additional businesses to receive PPP loans;
Expands the list of allowable uses of proceeds and loan forgiveness to include certain operations, property damage, supplier, and worker protection expenditures;[323] and
Allows PPP borrowers to receive a second PPP loan of up to $2 million provided that they meet certain criteria such as having not more than 300 employees, having used or intending to use the full amount of their PPP loan, and documenting quarterly revenue losses of at least 25 percent in a quarter of 2020 relative to the same quarter in 2019.
Overview of Key Issues
Improper payments, suspicious activity, and potential fraud associated with PPP. As we reported in November 2020, it is especially important for agencies with large appropriated amounts, like SBA, to expeditiously estimate their improper payments, identify root causes, and develop corrective actions when there are concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread. Moreover, financial institutions have filed more than 21,000 suspicious activity reports (SAR) related to PPP with the Financial Crimes Enforcement Network (FinCEN).[324] Although the filing of a SAR does not necessarily mean that fraud has occurred, law enforcement agencies use these reports to help support investigations, such as those related to PPP fraud.[325] Over 1,400 institutions have filed SARs related to PPP, and the number of SARs filed generally increased from April through October 2020.[326] The number of PPP-related SARs filed from April to October 2020 ranged from 25 to 6,462 (see figure below).
Paycheck Protection Program-Related Suspicious Activity Reports Filed from April 2020 to October 2020
According to FinCEN officials, these suspicious financial transactions involved questionable activity and potential fraud committed by PPP loan recipients, such as the rapid movement of funds, identity theft, and forgeries.[327] U.S. financial institutions filed PPP-related SARs across the country, and the number of SARs as a share of the number of PPP loans issued in each state varied (see figure below). The number of PPP-related SARs filed per state ranged from 13 to 3,850, and represented less than 1.5 percent of the PPP loans issued in each state.
Suspicious Activity Reports Related to the Paycheck Protection Program (PPP) as a Share of the Number of PPP Loans from April 2020 to October 2020, by State
Note: We used the location of the potentially suspicious activity cited in report filings for this analysis.
In addition to suspicious activity reported by financial institutions, law enforcement agencies reported receiving complaints and initiating investigations related to PPP. According to SBA’s Office of Inspector General (OIG), as of October 1, 2020, it had received tens of thousands of complaints of potential wrongdoing on its hotline and initiated hundreds of investigations into complaints of fraud associated with SBA loan programs, including PPP. Additionally, the U.S. Federal Bureau of Investigation (FBI) indicated that it is investigating several hundred suspected fraud cases involving PPP.
Based on the results of these investigations, the Department of Justice (DOJ) has filed charges in multiple cases related to PPP. From May 2020 to November 2020, DOJ publicly announced charges in at least 70 fraud-related cases associated with PPP loans. The charges—filed across the U.S. and investigated by a range of law enforcement agencies—include allegations of making false statements and engaging in identity theft, wire and bank fraud, and money laundering. As of November 2020, DOJ estimated that the defendants in these cases sought more than $260 million in PPP loans.
According to SBA officials, the agency is working closely with the SBA OIG, DOJ, and in some cases the FBI, to support data requests and make referrals for potential investigation. We did not corroborate this coordination with the law enforcement agencies nor evaluate the extent or effectiveness of SBA’s coordination with those agencies.
Filings of suspicious activity reports and cases of alleged fraud indicate vulnerabilities to fraud and abuse within the loan guarantee program. Although these emerging fraud risk indicators are small in number compared to the total overall number of disbursed PPP loans, they point to vulnerabilities typically managed through a fraud risk management approach, including a determination of fraud risk tolerance. SBA has stated that it is actively pursuing cases of fraud and has a robust loan review process. However, to date, SBA has not provided us with a documented fraud risk assessment to include fraud risk tolerance for PPP.
Loan forgiveness. As we reported in November 2020, SBA has begun receiving and processing loan forgiveness decisions from lenders.[328] According to SBA officials, SBA had received about 595,000 loan forgiveness decisions from lenders (about 11.4 percent of all PPP loans) as of November 22, 2020, and had begun remitting loan forgiveness payments for loans of less than $2 million that were not flagged by an automated review tool or otherwise identified for manual review.[329] According to SBA officials, as of November 22, 2020, SBA had made about 367,000 forgiveness payments totaling $38.4 billion. SBA officials told us SBA was still finalizing a document that presents its procedures for reviewing lenders’ loan forgiveness decisions as of December 1, 2020.
Representatives of the seven lenders we interviewed stated that they had begun receiving and processing loan forgiveness applications. Representatives of one lender said that it had already received applications from about two-thirds of its borrowers, as of November 10, 2020. In contrast, representatives of another lender said that it was encouraging its borrowers to wait to apply for loan forgiveness to see if any additional legislative changes were made to the process, such as automatic forgiveness for loans below a certain threshold.[330] In December 2020, the Consolidated Appropriations Act, 2021, created a simplified application process for loans up to $150,000.[331]
Unlike with the initial application process, lenders had approximately 2 months between the issuance of the first interim final rule on loan forgiveness and the beginning of the loan forgiveness process to develop a process to accept and review loan forgiveness applications.[332] However, the seven lenders noted that many of the loan forgiveness applications they had received were incomplete and that they had to work with borrowers to obtain any missing information.
In addition, representatives of some lenders cited the legislative requirement that any Economic Injury Disaster Loan (EIDL) advance be subtracted from the loan forgiveness amount as a challenge for borrowers, as some borrowers may not have been aware of this requirement.[333] In December 2020, Congress repealed this requirement.[334]
SBA oversight plans. As we reported in September 2020, SBA has said that it plans to review all PPP loans of $2 million or more and further stated that it may review any PPP loan it deems appropriate, including loans of less than $2 million. As part of its oversight of loans over $2 million, SBA announced on October 26, 2020, that it had developed two questionnaires—one for for-profit businesses that, together with their affiliates, received PPP loans with an original principal amount of $2 million or greater and one for nonprofit businesses that met the same criterion. According to SBA, the agency will use the information collected through these questionnaires to inform its assessment of whether a business’s certification that economic uncertainty made the loan request necessary to support the business’s ongoing operations was made in good faith.[335] Among other things, the questionnaires ask the borrower to provide documentation related to (1) the borrower’s business activities, such as whether its operations were shut down or altered in response to COVID-19, and (2) the business’s liquidity, including whether it paid dividends or prepaid debt during the loan forgiveness covered period. According to SBA, a request to complete the questionnaire does not mean that SBA is challenging the borrower’s certification, and SBA’s assessment of a borrower’s certification will be based on the totality of the borrower’s circumstances through a multi-factor analysis.
On November 17, 2020, a group of 80 national organizations that represent small business borrowers and lenders participating in PPP expressed concerns about these new questionnaires in letters to members of Congress, SBA, and the Department of the Treasury. Among other things, they stated that the new forms add a confusing and burdensome process for both lenders and borrowers that, as of the date of the letters, had not been described in any official regulations or SBA procedural notice. According to SBA officials, SBA issued responses to frequently asked questions in April and May that describe the loan review process. They also said that SBA did not widely publicize the questionnaire instructions to protect the integrity of the review from PPP borrowers who could use the information to avoid the requirements of the review. Treasury officials said that SBA sent a letter and user guide to lenders with additional information on the questionnaires and provided an overview of how SBA would use the questionnaires in a December 2020 response to a frequently asked question.
In their letter, the organizations also noted that the questionnaires (1) focus on the period after the business received the PPP award instead of the situation at the time it requested the loan, and (2) assess the good-faith certification based on information, such as the personal finances of small business owners, unrelated to what the borrower was asked to consider at the time of the loan. According to SBA officials, business activities in the period after the loan was received may be important in assessing the borrower’s need for the loan at time of loan application. In addition, they noted that assessment of need is based on the totality of the circumstances and that the personal finances of small business owners are relevant to the certification of need (for example, to the issue of liquidity).
As for the specifics of its reviews of PPP loans of over and under $2 million, in early December 2020, SBA provided us with a document that the agency characterized as an overview of the layers of review.[336] For example, the document describes three steps in the loan review process: automated screenings of all loans, manual reviews of selected loans, and quality control reviews to ensure the quality, completeness, and consistency of the review process.
A contractor will use a proprietary, automated tool to screen every disbursed PPP loan by applying eligibility and fraud detection rules to identify anomalies and attributes that may be indicative of noncompliance, fraud, or abuse.
A contractor will manually review loans for issues that triggered the manual review and provide SBA with an analysis and recommendation for either (1) further action, if the loan contains indications of noncompliance, fraud, or abuse (“unresolved”), or (2) no further action, if the loan following review does not contain indications of noncompliance, fraud, or abuse (“resolved”). SBA will manually review (1) all loans of $2 million or greater, (2) all unresolved loans of less than $2 million, and (3) a statistically valid sample of resolved loans of less than $2 million where the contractor recommended no further action.
A separate contractor will conduct quality control reviews of a sample of loan review files (including loans manually reviewed by SBA or contractor staff) after SBA has conducted its review and made its determination.
At the end of December 2020, SBA provided a draft Master Review Plan for the Loan Review Process. The document provided more details on the automated loan reviews, but did not contain detailed policies and procedures for the manual loan reviews or loan forgiveness reviews as we had previously requested. According to SBA officials, these were in the process of being updated. Until we receive detailed documentation and can review the policies and procedures being used in the review process, we cannot more fully evaluate SBA’s process.
The Consolidated Appropriations Act, 2021, requires SBA to submit to the Senate and House Small Business Committees an audit plan that details the policies and procedures for conducting forgiveness reviews and audits of PPP loans within 45 days of enactment and to provide monthly updates thereafter. The Act also requires SBA to respond to requests from GAO within 15 days (or such later date as the Comptroller General may specify) or report to Congress on the reasons for the delay.
Agency Comments
We provided SBA, Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. SBA provided comments in a letter, which is reproduced in Appendix VIII: Comments from the Small Business Administration on the Paycheck Protection Program Enclosure. In its letter, SBA reiterated that it takes improper payments very seriously and works to minimize them in its loan programs. In addition to testing for and estimating improper payments, SBA also told us that it works to prevent improper payments before they occur through its loan review process, and is committed to actively ensuring strong internal controls and guidelines regarding the loan review process. However, the agency has not provided documentation of its plans for improper payments testing.
SBA and Treasury provided technical comments that we incorporated as appropriate. OMB did not have any comments.
Methodology
To conduct this work, we analyzed aggregate SAR data related to PPP that financial institutions submitted to FinCEN between April and October 2020. We interviewed SBA officials and representatives of seven PPP lenders selected based on factors such as lender type, asset size, and geography. The views of the lenders we interviewed are not generalizable to other lenders but offered important perspectives. We assessed the reliability of FinCEN and SBA data by interviewing FinCEN and SBA officials. We determined that the data were sufficiently reliable for reporting on PPP-related SARs, the number and dollar amount of PPP loans, the status of PPP expenditures, and the status of loan forgiveness applications.
Contact information: William B. Shear, (202) 512-8678, shearw@gao.gov
Almost half of the CARES Act lending programs (facilities) stopped purchasing eligible assets or extending credit on December 31, 2020, and the rest—the five Main Street facilities—stopped purchasing a participating interest in still eligible loans on January 8, 2021. The Federal Reserve and Treasury extended the facilities not supported by CARES Act funds (non-CARES Act facilities) through March 31, 2021. Overall, the CARES Act facilities’ transaction volume and purchases of assets were relatively limited, but saw an increase of 39 percent from October 15, 2020, to December 15, 2020, mostly due to an increase of over $6 billion in lending through the Main Street facilities. The Main Street facilities conducted just over $7 billion in additional transactions from December 16 through December 31, 2020. The use of non-CARES Act facilities has diminished since May 2020. The Consolidated Appropriations Act, 2021, rescinded most of the CARES Act funding and generally prohibited Treasury’s funding support for future facilities identical to those implemented pursuant to Title IV of the CARES Act.
Entities involved: Department of the Treasury, Federal Reserve System
Key Considerations and Future GAO Work
In July 2011, we made two recommendations regarding facilities that the Board of Governors of the Federal Reserve System (Federal Reserve) established in response to the 2007–2009 financial crisis. These two recommendations are to (1) strengthen procedures related to high-risk borrowers and (2) estimate and track losses within and across all facilities. Because the Federal Reserve created similar facilities that are supported by CARES Act funds to respond to COVID-19, both recommendations are still relevant.
In our December 2020 report on the Federal Reserve’s design, implementation, and monitoring of the facilities and relevant market trends, we reported that the Federal Reserve had taken action to address the intent of the first recommendation.[337] We continue to examine the status of the Federal Reserve’s actions in addressing our second recommendation as part of our ongoing review of the Federal Reserve’s facilities.[338]
Background
The CARES Act appropriated $500 billion to the Department of the Treasury (Treasury) and authorized at least $454 billion of that total for Treasury to support the Federal Reserve in establishing programs or facilities for the purpose of providing liquidity to the financial system that supports lending to states, tribes, municipalities, and eligible businesses and nonprofit organizations.[339] Treasury committed $195 billion, or about 43 percent, of the $454 billion from the CARES Act available to support the facilities and disbursed $102.5 billion of that commitment.[340] The Federal Reserve also established four facilities that do not receive CARES Act-appropriated funds; these facilities aim to provide liquidity to the financial sector and businesses.
Overview of Key Issues
As of December 15, 2020, the transaction volume for the nine Federal Reserve lending facilities with CARES Act funding remained relatively limited. On November 19, 2020, Treasury announced that the CARES Act facilities would stop purchasing eligible assets or extending credit on December 31, 2020.[341] The Consolidated Appropriations Act, 2021, rescinded most of the CARES Act funding and, except for the Term Asset-Backed Securities Loan Facility, prohibited Treasury’s funding support for future facilities identical to those implemented pursuant to Title IV of the CARES Act.[342] Additionally, according to Treasury officials, Treasury and the Federal Reserve amended the agreements governing the CARES Act facilities to be consistent with the Consolidated Appropriations Act, 2021, and these agreements canceled all of Treasury’s additional investment commitments to these facilities. The four non-CARES Act facilities remain in operation, with limited transaction volumes since mid-May 2020. The Federal Reserve and Treasury extended all four non-CARES Act facilities through March 31, 2021.
CARES Act facilities. Overall, the Federal Reserve determined that all CARES Act facilities combined could hold a maximum of $1.95 trillion in assets when they were purchasing eligible assets and extending credit. As of December 15, 2020, the nine facilities in operation had conducted about $29 billion in transactions—with the Secondary Market Corporate Credit Facility accounting for more than $14 billion (see table). December’s cumulative transaction volume of $29 billion is a 39 percent increase from October’s volume of $21 billion (which we reported in November 2020). In its December periodic report to Congress on the lending facilities, the Federal Reserve Board stated that it continued to expect that the facilities will not result in losses to the Federal Reserve.[343]
Federal Reserve Lending Facilities with CARES Act Funding
Name of facility
Purpose
Facility activity
Transaction volume as of Oct. 15, 2020 ($ in billions)
Transaction volume as of Nov. 15, 2020 ($ in billions)
Transaction volume as of Dec. 15, 2020 ($ in billions)
Primary Primary market facility: purchase qualifying bonds, and purchase portions of qualifying syndicated loans or bonds at issuance.
Secondary Secondary market facility: purchase qualifying corporate bonds, certain bond portfolios, and U.S.-listed exchange-traded funds in the secondary market.
Primary 0
Secondary 13.15
Primary 0
Secondary 13.58
Primary 0
Secondary 14.03
Businesses Main Street New Loan Facility
Main Street Priority Loan Facility
Main Street Expanded Loan Facility
Nonprofits Nonprofit Organization New Loan Facility
Nonprofit Organization Expanded Loan Facility
Businesses Support small and mid-sized businesses
Nonprofits Support small and mid-sized nonprofit organizations
Businesses New loan and priority loan facilities: purchase 95 percent participation interest in newly issued eligible loans that eligible lenders make to eligible small and mid-sized for-profit borrowers.
Expanded loan facility: purchase 95 percent participation interest in a new extension of credit under an existing eligible loan made by an eligible lender to an eligible small or mid-sized for-profit borrower.
Nonprofits Nonprofit new loan facility: purchase 95 percent participation interest in newly issued eligible loans that eligible lenders make to eligible nonprofit organization borrowers.
Nonprofit expanded loan facility: purchase 95 percent participation interest in a new extension of credit under an existing eligible lender to eligible nonprofit organization borrowers.
3.04 total, for all Main Street facilities
4.97 total, for all Main Street facilities
9.28 total, for all Main Street facilities
Municipal Liquidity Facility
Support states and certain counties, cities, multistate entities, and revenue bond issuers
Purchase eligible notes directly from eligible issuers at time of issuance.
1.65
1.65
1.65
Term Asset-Backed Securities Loan Facility
Support consumers and businesses
Provide nonrecourse loans to U.S. companies secured by qualifying asset-backed securities generally backed by recently originated consumer and business loans.
3.24
3.88
4.25
Source: GAO analysis of Board of Governors of the Federal Reserve System (Federal Reserve) documents and data. | GAO-21-265
Although demand for the CARES Act facilities was generally limited relative to their capacity, the Main Street facilities experienced an increase in activity from October to December 2020.[344] Specifically, as of December 15, 2020, the Main Street facilities serving small and mid-sized for-profit businesses and nonprofit organizations had conducted $9.28 billion in transactions, an increase of 205 percent from $3.04 billion on October 15. The Main Street facilities also conducted just over $7 billion in additional transactions from December 16 through December 31, 2020.
On November 19, 2020, Treasury announced that the CARES Act facilities would stop purchasing eligible assets or extending credit, as applicable, by or on December 31, 2020.[345] In December 2020, the Consolidated Appropriations Act, 2021, affirmed the December 31, 2021, deadline for many of the facilities but extended the deadline for the Main Street Lending facilities to purchase participation in eligible loans to January 8, 2021, provided that purchases in January 2021 are limited to loans submitted to the lender portal on or before December 14, 2020. On December 29, 2020, the Federal Reserve issued term sheets for the Main Street Lending facilities to reflect this new requirement.
The Consolidated Appropriations Act, 2021, rescinded most of CARES Act-appropriated funding for supporting the facilities, including (i) funding that Treasury had committed, but not disbursed to support the facilities, and (ii) disbursed funds that the facilities did not use. Of the $102.5 billion that Treasury had disbursed to support the facilities, pursuant to the requirements of the Consolidated Appropriations Act, 2021, the Federal Reserve has returned a little more than $62 billion in unused facilities funding to Treasury.
Non-CARES Act facilities. As of December 15, 2020, all four of these facilities were operational and had conducted almost $300 billion in transactions—with the Paycheck Protection Program Liquidity Facility and the Primary Dealer Credit Facility accounting for about $106 billion and $130 billion, respectively (see table). More than three-quarters of transactions in non-CARES Act facilities occurred before May 15, 2020. On November 30, 2020, the Federal Reserve and Treasury extended the non-CARES Act facilities through March 31, 2021.[346]
Federal Reserve Lending Facilities without CARES Act Funding
Name of facility
Purpose
Facility activity
Transaction volume as of Oct. 15, 2020 ($ in billions)
Transaction volume as of Nov. 15, 2020 ($ in billions)
Transaction volume as of Dec. 15, 2020 ($ in billions)
Commercial Paper Funding Facility
Serve as funding backstop to provide liquidity for U.S. issuers of commercial paper
Purchase commercial paper from eligible companies; eligible issuers include U.S. issuers of commercial paper, including municipal issuers and U.S. issuers with a foreign parent company
4.27
4.27
4.27
Money Market Mutual Fund Liquidity Facility
Assist money market mutual funds in meeting demands for redemption by households and other investors
Make nonrecourse loans available to eligible financial institutions that are secured by high-quality assets purchased by the financial institution from money market mutual funds
58.01
58.01
58.01
Paycheck Protection Program Liquidity Facility
Facilitate lending by eligible institutions that provide loans to small businesses under the Paycheck Protection Program (PPP)
Lend to institutions eligible for making PPP loans on a nonrecourse basis, taking PPP loans as collaterala
101.22
105.18
106.03
Primary Dealer Credit Facility
Provide support to primary dealers to facilitate the availability of credit to businesses and households
Provide loans to primary dealers in exchange for collateral
129.83
130.23
130.78
Source: GAO analysis of Board of Governors of the Federal Reserve System (Federal Reserve) documents and data. | GAO-21-265
aThe Federal Reserve established the PPP Liquidity Facility under its Section 13(3) authority to encourage participation in the PPP established under the CARES Act.
Oversight of facilities. The Federal Reserve’s Division of Reserve Bank Operations and Payment Systems developed and documented a general framework for oversight of the facilities. The framework includes reviews of established governance structures, process workflows, and internal control design, among other things. As of the end of December 2020, the Division had completed reviews of these elements for all facilities.
Agency Comments
We provided a copy of this enclosure to the Federal Reserve, Treasury, and the Office of Management and Budget for review. The Federal Reserve and Treasury provided technical comments that we incorporated, where appropriate.
Methodology
To conduct this work, we reviewed Federal Reserve documentation on each facility, including term sheets and related press releases; reports to Congress on the facilities; and the most recent agency transaction data on the facilities available, as of December 2020. We also interviewed Federal Reserve officials and obtained updated information from Treasury.
Contact information: Michael E. Clements, (202) 512-8678, clementsm@gao.gov
Related GAO Product
Federal Reserve Lending Program: Use of CARES Act-Supported Programs Has Been Limited and Flow of Credit Has Generally Improved. GAO-21-180. Washington, D.C.: December 10, 2020.
Federal Reserve System: Opportunities Exist to Strengthen Policies and Processes for Managing Emergency Assistance. GAO-11-696. Washington, D.C.: July 21, 2011.
The CARES Act provided a direct appropriation of $9.5 billion to the U.S. Department of Agriculture’s Office of the Secretary and a reimbursement of $14 billion to the Commodity Credit Corporation. The department does not track the legislative source of Commodity Credit Corporation replenished borrowing authority with specific Commodity Credit Corporation spending; as a result, the department does not specify how it is spending the replenished borrowing authority provided by the CARES Act reimbursement.
Entities involved: U.S. Department of Agriculture, including its Agricultural Marketing Service, Farm Service Agency, and Office of the Secretary
Key Considerations and Future GAO Work
We continue to examine the U.S. Department of Agriculture’s (USDA) spending and oversight of CARES Act funding, including the extent to which USDA tracks the expenditure of CARES Act reimbursements to the Commodity Credit Corporation.
Background
COVID-19 has caused disruptions in the U.S. food supply chain, from the farms where raw agricultural commodities are produced, to the food processing and distribution network that enables these commodities to be used by consumers.[347] Congress provided the following amounts to USDA through coronavirus relief legislation, among other things:
$9.5 billion to USDA’s Office of the Secretary through the CARES Act,[348]
$14 billion to the Commodity Credit Corporation through the CARES Act,[349] and
$4 billion through the Families First Coronavirus Response Act.[350]
In addition, USDA has made available $6.5 billion for direct payments to agricultural producers from funding that was generally available to the agency through its Commodity Credit Corporation prior to the CARES Act reimbursement.[351] The Commodity Credit Corporation is a wholly government-owned entity that finances a broad array of agriculture support programs.[352] It has permanent authority to borrow up to $30 billion at any given time from the Treasury.[353]
See table below for the funding amounts USDA made available for three coronavirus relief programs from the CARES Act, the Families First Coronavirus Response Act, and available borrowing authority of the Commodity Credit Corporation:
Coronavirus Food Assistance Program 1 (CFAP 1) direct payments to agricultural producers,
Coronavirus Food Assistance Program 2 (CFAP 2) direct payments to agricultural producers, and
Farmers to Families Food Box Program (Food Box).
Funding Amounts and Funding Sources for the Coronavirus Food Assistance Program (CFAP) 1 and 2 Direct Payments to Agricultural Producers and the Families to Farmers Food Box Program (Food Box), as of November 30, 2020
Program
Funding amounta
Monthb
Funding source
CFAP 1
Up to $6.5 billionc
May 2020
CCC Charter Act authoritiesd
Up to $9.5 billion
May 2020
Appropriations under the CARES Act
CFAP 2
Up to $14.0 billione
September 2020
CCC Charter Act authorities
Up to $0.1 billionf
September 2020
Appropriations under the CARES Act
Food Box
Up to $3.0 billiong
May 2020
Families First Coronavirus Response Act
Food Box
Up to $1.0 billiong
September 2020
Families First Coronavirus Response Act
Food Box
Up to $0.5 billionh
October 2020
Appropriations under the CARES Act
Total
Up to $34.0 billion
Source: GAO analysis of U.S. Department of Agriculture (USDA) data. | GAO-21-265
aThe Funding amount column shows the amounts the Office of Management and Budget apportioned for the programs. bThe Month column shows the month in which the Office of Management and Budget apportioned the funding for the programs. cUSDA transferred $6.5 billion from the Commodity Credit Corporation account to the Office of the Secretary account on May 1, 2020. dRecent laws that replenished the Commodity Credit Corporation (CCC) include the CARES Act, Pub. L. No. 116-136, div. B, tit. I, § 11002, 134 Stat. at 509, which reimbursed $14 billion of the Commodity Credit Corporation’s net realized losses and the Further Consolidated Appropriations Act, 2020, Pub. L. No. 116-94, 133 Stat. 2534, 2625. eUSDA transferred $14 billion from the Commodity Credit Corporation account to the Office of the Secretary account on September 16, 2020. USDA received an early reimbursement of the Commodity Credit Corporation in the Continuing Appropriations Act, 2021 and Other Extensions Act, enacted on October 1, 2020, for the net realized losses as of September 17, 2020. Pub. L. No. 116-159, div. A, § 173, 134 Stat. 709, 725 (2020). fThis $.1 billion for CFAP 2 from the CARES Act is a subset of the $9.5 billion appropriation to USDA’s Office of the Secretary, Pub. L. No. 116-136, div. B, tit. I, 134 Stat. at 505, and, therefore, this column does not total. The $1 billion will be used for payments to tobacco producers. gThe Families First Coronavirus Response Act, Pub. L. No. 116-127, div. A, tit. I, §1101(g) and (i), 134 Stat. 178, 180 (2020), provided “such amounts as are necessary” for the Secretary of Agriculture to purchase commodities for emergency distribution in the United States during a public health emergency designation during fiscal year 2020. hThis $0.5 billion for the Farmers to Families Food Box Program from the CARES Act, Pub. L. No. 116-136, div. B, tit. I, 134 Stat. at 505, is a subset of the $9.5 billion appropriation to USDA’s Offices of the Secretary. Therefore, this column does not total.
Overview of Key Issues
In our November 2020 report, we discussed the difficulty in tracking whether the $14 billion replenished borrowing authority from the CARES Act reimbursement is the same $14 billion that USDA is using to fund CFAP 2 because USDA does not track this information.[354] In addition, we stated in the November 2020 report that a further difficulty in tracking the funding was that USDA made the following transfers from the Commodity Credit Corporation to the Office of the Secretary:
We reported this difficulty not because of an issue with the purpose of the spending but because we are interested in understanding how USDA is spending its CARES Act funds including any replenished borrowing authority to the Commodity Credit Corporation. The figure below shows the funding sources and transfers between the accounts that USDA is using to fund CFAP 1 and 2 direct payments to agricultural producers and food purchases under the Farmers to Families Food Box Program. The figure also includes funding sources and amounts of replenished borrowing authority associated with the Commodity Credit Corporation.
Funding Sources, Related Transfers between Treasury Accounts, and Related Account Balances for the Coronavirus Food Assistance Program 1 and 2 and Families to Farmers Food Box Program, from March 1, 2020, through November 30, 2020
Notes: Unless otherwise specified, amounts in the Treasury account rows are approximate account balances as of the beginning of the month. The Treasury accounts for the Commodity Credit Corporation and the Office of the Secretary have amounts coming in and out that are not shown in the figure. Dates associated with specific amounts generally indicate the effective date of an appropriations transfer or Treasury warrant. Box sizes are not precisely proportional to their dollar amounts. aThe Families First Coronavirus Response Act, Pub. L. No. 116-127, div. A, tit. I. §1101(g) and (i), 134 Stat. 178, 180 (2020), provided “such amounts as are necessary” for the Secretary of Agriculture to purchase commodities for emergency distribution in the United States during a public health emergency designation during fiscal year 2020. bUSDA received a reimbursement of the Commodity Credit Corporation in the Continuing Appropriations Act, 2021 and Other Extensions Act, enacted on October 1, 2020, for the net realized losses as of September 17, 2020. Pub. L. No. 116-159, div. A, § 173, 134 Stat. 709, 725 (2020). As of September 17, 2020, the corporation’s net realized losses were $23.9 billion. cOn May 1, 2020, the Commodity Credit Corporation account beginning balance was about $9.7 billion in borrowing authority. That day USDA transferred $6.5 billion from the Commodity Credit Corporation to the Office of the Secretary.dOn May 1, 2020, the Commodity Credit Corporation had about $3.2 billion remaining in borrowing authority after USDA transferred $6.5 billion from the Commodity Credit Corporation to the Office of the Secretary. eUSDA requested to transfer $14 billion from the Commodity Credit Corporation to the Office of the Secretary on September 16, 2020. The effective date of the transfer is September 11, 2020.fOn September 1, 2020, the Commodity Credit Corporation had $16.4 billion in borrowing authority. On September 11, 2020, USDA transferred $14 billion from the Commodity Credit Corporation to the Office of the Secretary.gThe Commodity Credit Corporation has a maximum borrowing authority of $30 billion. hThe Office of Management and Budget apportioned the following amounts for the Farmers to Families Food Box Program from the Families First Coronavirus Response Act: (1) $3 billion in May 2020, and (2) an additional $1 billion in September 2020. In October 2020, the Office of Management and Budget apportioned $0.5 billion for the Families to Food Box Program from the CARES Act $9.5 billion appropriation to the Office of the Secretary. iIn May 2020, the Office of Management and Budget apportioned $6.5 billion from the Commodity Credit Corporation and the $9.5 billion CARES Act appropriation for CFAP 1. jIn September 2020, the Office of Management and Budget apportioned $14 billion from the Commodity Credit Corporation for CFAP 2. The Office of Management and Budget also apportioned $0.1 billion from the CARES Act $9.5 billion appropriation to the Office of the Secretary for CFAP 2 payments to tobacco producers. This $0.1 billion is not depicted in the figure.kIn October 2020, the Office of Management and Budget apportioned $0.5 billion from the $9.5 billion CARES Act appropriation to the Office of the Secretary for the Families to Farmers Food Box Program.lThese boxes denote other amounts in the Office of the Secretary account.
USDA is tracking the expenditures of the CARES Act $9.5 billion and the Families First Coronavirus Response Act $4 billion direct appropriations to the Office of the Secretary as coming from specific sections of those laws. We confirmed this using USDA documents, and could also track and report the spending of direct appropriations from the CARES Act and the Families First Coronavirus Response Act back to the legislative funding sources. However, as the figure above shows and as we stated in November 2020, we cannot track spending of the $14 billion replenished borrowing authority from the CARES Act reimbursement to the Commodity Credit Corporation back to the legislative funding source (that is, the CARES Act).[356] USDA officials said that the department does not track the legislative funding source of replenished borrowing authority with spending as a general practice. Therefore, according to these same officials, USDA does not, for example, specify how much of the $14 billion replenished borrowing authority from the CARES Act to the Commodity Credit Corporation is being used for direct payments under CFAP 1 and 2.
In a year where the Commodity Credit Corporation only receives an annual replenishment, there may be one legislative funding source for the reimbursement of net realized losses. As of December 31, 2020, the Commodity Credit Corporation was replenished at least three times under three different legislative sources, according to USDA officials. USDA is using or plans to use these funds for a range of purposes. For fiscal year 2020, this amounts to about $45.8 billion in net realized loss reimbursements—$14 billion from the CARES Act, $23.9 billion from the Continuing Appropriations Act, 2021 and Other Extensions Act, and $7.9 billion from the Consolidated Appropriations Act, 2021.[357] This total reimbursement that the Commodity Credit Corporation received for net realized losses incurred in fiscal year 2020 is the highest reimbursement of net realized losses incurred in a fiscal year, since at least fiscal year 2005.
Consolidated Appropriations Act, 2021
The Consolidated Appropriations Act, 2021, was enacted on December 27, 2020. This omnibus spending bill includes all 12 fiscal year 2021 appropriations bills, coronavirus relief, and authorizations. Under coronavirus relief for agriculture, among other things, the bill provides $11.1875 billion to USDA’s Office of the Secretary to support agricultural producers, growers, and processors.[358] Of the $11.1875 billion to the Office of the Secretary, at least $1.5 billion is for purchasing food and agricultural products, including seafood,[359] and an unspecified amount is for supplemental Coronavirus Food Assistance Program (CFAP) payments,[360] among other things. Under fiscal year 2021 appropriations, the bill reimburses the Commodity Credit Corporation for its net realized losses as of the close of fiscal year 2020,[361] which were about $7.9 billion, according to USDA officials.
Agency Comments
We provided a draft of this enclosure to USDA and the Office of Management and Budget for review and comment. USDA and the Office of Management and Budget did not have any comments related to this enclosure.
Methodology
To conduct this work, we reviewed budgetary data provided to us by USDA as of November 30, 2020, and reviewed responses to our questions by USDA officials in writing. We found the data mentioned above to be reliable for our purposes of describing our efforts to track USDA spending.
Contact information: Steve D. Morris, (202) 512-3841, morriss@gao.gov
By July 14, 2020, the Department of Commerce’s National Oceanic and Atmospheric Administration had obligated almost $297 million of the available $298 million in CARES Act funding for fishery participants, but as of December 4, 2020, only $53.9 million of that funding had been disbursed.
Entity involved: National Oceanic and Atmospheric Administration, within the Department of Commerce.
Recommendation for Executive Action
The Assistant Administrator for the National Oceanic and Atmospheric Administration Fisheries should develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner.
Key Considerations and Future GAO Work
We will continue to monitor CARES Act assistance to fishery participants in ongoing and planned work. In September 2020, the Department of Commerce’s Inspector General started an evaluation of the National Oceanic and Atmospheric Administration’s implementation of CARES Act funding, including examining the steps taken to implement the act, any challenges encountered, and oversight of the funds obligated and disbursed under the act.
Background
Commercial and recreational marine fisheries are critical to the nation’s economy, contributing approximately $99.5 billion to the U.S. gross domestic product and supporting approximately 1.7 million jobs in 2016, according to the Department of Commerce’s National Oceanic and Atmospheric Administration (NOAA).[362] Widespread restaurant closures in the spring of 2020 led to a decrease in demand for seafood, adversely affecting the fisheries industry.
The CARES Act authorizes the Department of Commerce to provide assistance to eligible tribal, subsistence, commercial, and charter fishery participants affected by COVID-19, which may include direct relief payments.[363] The act appropriated $300 million to the Department of Commerce to assist fishery participants.[364] After $2 million in administrative fees were assessed by NOAA, $298 million of the $300 million was obligated for fishery participants. These include tribes, persons, fishing communities, aquaculture businesses not otherwise eligible for certain assistance, processors, and other fishery-related businesses, who have incurred, as a direct or indirect result of COVID-19, certain specified economic revenue losses or other negative impacts.[365] Businesses such as vessel repair businesses, restaurants, and seafood retailers are not considered fishery-related businesses eligible to receive CARES Act funding, according to NOAA’s website.
Overview of Key Issues
Funding was allocated in May 2020. On May 7, 2020, the Secretary of Commerce announced the allocation of about $298 million of the $300 million in CARES Act funding for states, tribes, and territories with fishery participants, as shown in the table.[366]
Department of Commerce’s Allocation of CARES Act Funding for States, Tribes, and Territories with Fishery Participants on May 7, 2020
Interstate commissiona
State/tribe/territory
Allocationb ($ thousands)
Atlantic States Marine Fisheries Commission
Massachusetts
Florida
Maine
New Jersey
New York
North Carolina
Virginia
Maryland
Pennsylvania
Rhode Island
New Hampshire
Georgia
Connecticut
South Carolina
Delaware
27,808
23,471
20,166
11,259
6,703
5,422
4,489
4,096
3,345
3,271
2,713
1,908
1,823
1,515
993
Gulf States Marine Fisheries Commission
Louisiana
Texas
Alabama
Mississippi
14,682
9,173
3,277
1,524
Pacific States Marine Fisheries Commission
Alaska
Washington
California
Oregon
West Coast Tribes
Hawaii
American Samoa
Alaska Tribes
Guam
Commonwealth of the Northern Mariana Islands
49,650
49,650
18,222
15,871
5,062
4,307
2,535
993
993
993
Territory of Puerto Ricoc
993
Territory of the U.S. Virgin Islandsc
993
Total
$297,902
Source: GAO analysis of Department of Commerce data. | GAO-21-265
Note: The CARES Act appropriated $300 million to the Department of Commerce to assist fishery participants. Pub. L. No. 116-136, § 12005(d), 134 Stat. at 518. aThese three commissions were established in the 1940s. The National Oceanic and Atmospheric Administration (NOAA) partners with them on cross-state issues related to managing shared fishery resources. According to NOAA officials, these commissions are also partnering with states in the process to disburse funds to fisheries participants. bAccording to the NOAA officials, allocations represent the maximum amount of total funding that fishery participants in a particular state, tribe, or territory can receive. These allocations are net of administrative fees that NOAA assessed. Additional administrative fees can be assessed by grantees, such as the interstate marine fisheries commissions, according to NOAA officials. cPuerto Rico and the U.S. Virgin Islands are not part of an interstate marine fisheries commission.
Most of the funding was obligated in July 2020. NOAA used these allocations to obligate almost $297 million of the available $298 million in funding to the three interstate marine fisheries commissions between June 30 and July 2, 2020, and to Puerto Rico on July 14, 2020. NOAA also obligated $993,000 to the U.S. Virgin Islands on November 13, 2020. The commissions have played a role in distributing funds as part of NOAA’s fishery disaster assistance program, which provides funding to fisheries participants experiencing economic losses from specific events, such as hurricanes or oil spills.[367] The commissions worked with states, tribes, and territories in their regions to develop spend plans for NOAA’s review and approval. These plans explain how states, tribes, and territories will verify whether fishery participants meet the requirements of the CARES Act to receive funds.
According to NOAA officials, the agency is in the process of reviewing and approving spend plans from states, tribes, and territories. NOAA officials said they expect to receive 29 spend plans from states and territories and 31 from tribes. As of November 25, 2020, NOAA had received 27 of the 29 plans it anticipated from the states and territories. Of these 27 plans, 23 had been approved, and 4 were under review.[368] As of November 25, 2020, 31 tribal spend plans had been submitted to NOAA; 7 of these had been approved and 24 were under review.
Once a spend plan has been approved by NOAA, the states, tribes, and territories will solicit and review applications from fishery participants, determine whether participants meet the eligibility criteria, and determine the direct payment amount based on the methodology outlined in the spend plan.[369] The respective interstate marine fisheries commissions will disburse the appropriate amount of funds directly to the fishery participant consistent with the approved spend plan, though some states and tribes may disburse funds themselves.[370]
Most funding had not been disbursed to fisheries participants as of December 4, 2020. As of December 4, 2020, two interstate marine fisheries commissions had disbursed only about $53.9 million to fishery participants in eight states as shown in the table below.
Disbursement of CARES Act Funding, as of December 4, 2020
Interstate commission
State
Funds disbursed ($ thousands)
Atlantic States Marine Fisheries Commission
Massachusetts
Virginia
Connecticut
Georgia
South Carolina
Maryland
27,760
3,855
1,675
1,525
875
165
Pacific States Marine Fisheries Commission
California
Oregon
18,044
36
Total
53,935
Source: GAO analysis of Department of Commerce data. | GAO-21-265
Note: The CARES Act appropriated $300 million to the Department of Commerce to assist fishery participants. Pub. L. No. 116-136, § 12005(d), 134 Stat. at 518.
Since enactment of the CARES Act in March 2020, about 80 percent of obligated funding has not been disbursed to fisheries participants. States, territories, and tribes must still review and assess applications from fishery participants, and other state spend plans have not yet been submitted to NOAA for review. Office of Management and Budget guidance on the act discusses the importance of agencies awarding and distributing funds in an expedient manner.[371] NOAA officials reported using a more expedited process to review spend plans, which has resulted in getting funding out to fishery participants more quickly than in past fishery disasters. However, the officials acknowledged that there is not an overall schedule for disbursing funds to fishery participants since time frames are established in individual spend plans. NOAA officials said it takes time to review spend plans to ensure they are in compliance with the CARES Act and for states, tribes, and territories to implement these plans—noting that each spend plan has different time frames for submitting applications, making award decisions, and disbursing funds. NOAA officials said they expect that the vast majority of funds to be disbursed to fisheries participants by early 2021, but the agency does not have centralized information on the time frames established in individual spend plans to help ensure that funds are being disbursed expeditiously and efficiently. Establishing a mechanism to track progress in disbursing funds could help NOAA determine whether states, tribes, and territories are encountering challenges in meeting time frames established in their spend plans and work with these entities to help identify how to address those challenges.
Agency Comments
We provided a copy of this enclosure to NOAA and the Office of Management and Budget (OMB) for review and comment. NOAA concurred with our recommendation and provided us with technical comments, which we have incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed data as of December 4, 2020, provided by NOAA. We examined documents on the data system from which these data came and interviewed officials familiar with the data system, and we determined that the data were sufficiently reliable for our purposes. We also reviewed the CARES Act and agency documents and interviewed NOAA officials.
As of December 31, 2020, federal agencies had reported billions of dollars in obligations in support of COVID-19 through contracts and agreements—such as technology investment agreements, cooperative agreements, and other transaction agreements—but the Department of Health and Human Services has misreported its use of other transaction agreements, raising accountability and transparency concerns.
Entities involved: Department of Health and Human Services; Department of Defense; and Department of Homeland Security, among others
Recommendation for Executive Action
The Assistant Secretary for Preparedness and Response, in coordination with the appropriate offices within the Department of Health and Human Services, should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts.
Key Considerations and Future GAO Work
As federal contracting activity continues to play a critical role in response to the pandemic, ensuring that criteria for tracking contract actions and associated obligations are consistently applied and account for the long-term needs of users—such as federal agencies and Congress—is critical. Doing so will help ensure consistent tracking and transparency into federal contracting activity related to the pandemic and future emergencies.
In September 2020, we recommended that the Secretaries of Homeland Security and Defense (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code; (2) establish timelines for evaluating the need to extend a National Interest Action code; and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic.[372]
The Department of Homeland Security (DHS) and the Department of Defense (DOD) did not agree with our recommendations in September 2020. However, as of January 2021, in response to our recommendations, a DOD official said that DOD and DHS met in December 2020 to discuss potential revisions to the 2019 National Interest Action code memorandum of agreement. Following that meeting, the official said that DHS and DOD were in the process of updating the agreement to clarify the steps they would take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close a National Interest Action code. We will review the updated agreement when finalized to determine whether it meets the intent of the recommendation.
In November 2020 we also recommended that the Department of Health and Human Services (HHS) identify how the Defense Production Act of 1950 (DPA) and similar actions will be used to increase production of domestic medical supplies. HHS concurred with this recommendation.
We have additional work underway related to the federal government’s use of contracts to respond to COVID-19, including, among other things, assessing (1) contracts awarded by selected agencies in response to COVID-19, including agencies’ efforts to review prospective contractors in advance of awarding a contract; (2) selected agencies’ use of contracting flexibilities, such as other transaction agreements and undefinitized contracts; (3) the use of the DPA and similar actions to increase domestic production of medical supplies; and (4) DOD’s defense industrial base risk mitigation.
Background
To facilitate the U.S. response to COVID-19, federal agencies have used a variety of contracting mechanisms to provide vital goods and services in support of federal, state, and local COVID-19 response efforts. For example, federal agencies have reported billions of dollars in obligations on contracts subject to the Federal Acquisition Regulation.[373] Our prior work has found that contracts play a key role in federal emergency response efforts, and that contracting during an emergency can present a unique set of challenges as officials can face a significant amount of pressure to provide critical goods and services as expeditiously and efficiently as possible.
Federal agencies have also relied on authorities provided through the DPA.[374] During the Korean War, Congress enacted the DPA to ensure the availability of industrial resources to meet DOD’s needs. The DPA facilitates the supply and timely delivery of products, materials, and services to military and civilian agencies in times of peace as well as in times of war. Title III of the DPA authorizes the President to provide a variety of financial incentives—often provided through contracts and agreements, among other means—to firms to meet a variety of national defense goals, including maintaining, restoring, and expanding the domestic industrial base. The financial incentives may be used only when certain conditions are met.
In addition, agencies like DOD and HHS have relied on the use of other transaction agreements to respond to COVID-19. Other transaction agreements can enable federal agencies to negotiate terms and conditions specific to a project. The CARES Act relaxed certain limitations on the use of other transactions for HHS and DOD, such as congressional reporting requirements and requirements for who can approve certain transactions.[375]
Overview of Key Issues
Agencies obligated $41.4 billion on federal contracts, with HHS and DOD accounting for most obligations. In response to the COVID-19 pandemic, contract obligations totaled about $41.4 billion as of December 31, 2020. HHS accounted for about 34 percent and DOD about 33 percent of the total obligations made by federal agencies (see figure).
Contract Obligations in Response to COVID-19 by Federal Agency, as of December 31, 2020
In our November 2020 report, we reported that government-wide contract obligations related to COVID-19 totaled $33.4 billion through October 15, 2020; by December 31, 2020, those obligations had increased by about $8 billion—to $41.4 billion. DOD accounted for about $4.9 billion, or about 61 percent of the increase in total contract obligations since October 15, 2020. See figure for government-wide obligations by week.
Government-wide Contract Obligations Related to COVID-19 by Week, February–December 2020
Consistent with what we have previously reported, medical equipment and supplies—including ventilators and personal protective equipment—continue to be the largest area of government-wide contract obligations in response to COVID-19. As of December 31, 2020, these obligations had increased by about $467.9 million since October 15, 2020, and accounted for about $8.7 billion, or 21 percent of government-wide contract obligations. Obligations for drugs and biologicals increased the most since October 15, 2020, from about $1.9 billion to $5.4 billion. Obligations for fruits and vegetables—made primarily in support of the U.S. Department of Agriculture’s Farmers to Families Food Box Program increased by an additional $521.1 million, to $2.4 billion. See figure for obligation amounts for the most-procured goods and services.
Contract Obligation Amounts for Goods and Services Most Procured in Response to COVID-19, as of December 31, 2020
As of December 31, 2020, the proportion of contracts identified as having been awarded non-competitively increased to about 55 percent of government-wide contract obligations, or about $22.7 billion. Officials at HHS, DOD, and DHS have identified supply chain shortages for goods like personal protective equipment and testing supplies, which according to a DOD official, contributed to the need to award some contracts noncompetitively. Agencies cited an urgent need for awarding contracts noncompetitively for about 74 percent, or about $16.8 billion, of the contract obligations associated with noncompetitive awards.[376] Awarding contracts under the unusual and compelling urgency exception to full and open competition can be necessary in certain circumstances. However, our prior work has noted that promoting competition—even in a limited form—increases the likelihood of acquiring quality goods and services at a lower price in urgent situations.
Contracts for goods continued to be competed less frequently than contracts for services: About 67 percent of the obligations for goods were on contracts that were not awarded competitively, compared with about 38 percent of the obligations for services. For example, about $7.5 billion, or 86 percent, of the $8.7 billion in obligations for medical and surgical equipment, and about $5.2 billion, or 97 percent, of the $5.4 billion in obligations for drugs and biologicals were on contracts awarded noncompetitively.
DOD and HHS are using the Defense Production Act and similar actions to mitigate industrial base issues. According to HHS and DOD officials, a total of about $2.2 billion in CARES Act funding will be used for DPA actions and similar actions to mitigate medical and defense industrial base issues.[377] Of this amount the CARES Act originally provided DOD $1 billion for DPA purchases to prevent, prepare for, and respond to COVID-19, domestically or internationally. According to HHS and DOD officials they plan to execute similar actions using HHS funding to expand the available pool of funds for industrial base risk mitigation to about $2.2 billion.
Specifically, HHS and DOD plan to use:
$1.5 billion for medical domestic production expansion projects using DPA Title III and similar actions;
$100 million to support domestic loans under the authority of section 4532, Title 50 of the U.S. Code, in collaboration with the United States International Development Finance Corporation to increase the domestic production of N95 respirators, other personal protective equipment, pharmaceuticals, ventilators, airway management consumables, and testing supplies;[378] and
$687 million for DPA Title III investments to offset financial distress in the defense industrial base.
As of December 31, 2020, HHS and DOD awarded over $2 billion for industrial base expansion and risk mitigation —about $1.36 billion for medical industrial base expansion projects and about $663.4 million for defense industrial base risk mitigation. See the figure below for the type of projects funded.
Medical and Defense Industrial Base Projects, as of December 2020
Medical industrial base expansion projects. DOD awarded 32 projects to expand domestic production for a range of medical supplies needed in the response to COVID-19. See the table below for a list of these efforts.
Medical Industrial Base Expansion Projects, as of December 2020
Medical supply
Projected annual production increasea (items, millions)
Personal protective equipment
N95 respirators
Gloves
Surgical masks
Gowns
834
450
532
1.5
Materials for personal protective equipment and ventilators
Ventilator components
7.8
Filter mediab
for N95 respirators
for ventilators
for surgical masks
1,457
330
4,344
Testing materials
Swabsticks
Swabs
Test and test kits
Pipette tips
1,200
988.8
Over 765
1,164
Vaccine supplies
Syringes
540
Source: GAO analysis of Department of Defense and Department of Health and Human Services data. I GAO-21-265
aAnnual increase is the projected quantity a contractor will produce in 1 year once full rate of production is reached. bFilter media prevents virus particles from passing through the air and is designed specifically for N95 respirators, surgical masks, and ventilators. According to the agreement language, the filter media will be used for either surgical masks or respirators.
Defense industrial base risk mitigation. DOD has awarded 37 projects to offset financial distress in the defense industrial base caused by COVID-19. According to the Under Secretary of Defense for Acquisition and Sustainment these efforts are primarily targeted in the electronics, aviation, and shipbuilding sectors, which DOD has identified as having fragile or at-risk supply chains. For example:
DOD awarded approximately $20 million to a forging manufacturer, which has a unique capability to produce heavy forged metal parts and components for multiple military aviation programs. The manufacturer plans to use this DPA investment to make efficiency improvements to its manufacturing systems and avoid the disruption of its business to prevent the loss of its skilled workforce.
DOD also awarded approximately $50 million to a critical supplier for multiple U.S. Navy nuclear powered ships. The company plans to use this DPA investment to expand its facilities and increase the on-site technical capabilities in material processing, welding, machining, and material handling to meet the demands of multiple U.S. Navy nuclear shipbuilding programs. The company also expects that this investment will add millions of man hours of capacity per year to the defense industrial base.
Federal agencies have obligated at least $11.9 billion on other transaction agreements, but HHS misreports agreements as procurement contracts when reporting data. Three federal agencies—DOD, HHS, and DHS—have continued to report using other transaction agreements in response to COVID-19, although we found that HHS has not accurately reported data in the federal procurement database system because it misreports agreements as procurement contracts. From October 15, 2020, through December 31, 2020, obligations associated with other transaction agreements reported by DOD, HHS, and DHS increased from about $10 billion to $11.9 billion. Of the $11.9 billion, DOD reported obligating about $10.4 billion on other transaction agreements, including at least $8.7 billion for Operation Warp Speed, an effort to manufacture large-scale vaccines and therapeutics in response to COVID-19.
However, HHS’s Office of the Assistant Secretary for Preparedness and Response (ASPR)—which leads the nation’s response to public health emergencies and is partnering with DOD on the Operation Warp Speed effort—misreports its other transaction agreements in support of COVID-19 efforts as procurement contracts when reporting data to the Federal Procurement Data System-Next Generation (FPDS-NG). Federal acquisition regulations generally require agencies to report data on its procurement contract actions in FPDS-NG, which is a comprehensive web-based reporting tool.[379] Federal agencies use FPDS-NG data to create reports for the President, Congress, GAO, executive branch agencies, and the general public. Our analysis of FPDS-NG data and agreement documents found at least four other transaction agreements with about $1.5 billion obligated in support of the Operation Warp Speed effort and other medical countermeasures that ASPR misreported as procurement contracts.
Unlike procurement contracts, other transaction agreements are generally not subject to federal acquisition regulations. Agencies can report other transaction agreements in a separate module of FPDS-NG under certain conditions.[380] Our prior work has noted that the use of other transaction agreements can help agencies attract companies that do not typically do business with the government. However, their use also carries a risk of reduced accountability and transparency.
DOD and DHS report their other transaction agreements into the separate FPDS-NG module from the procurement contracts module, but ASPR does not. ASPR officials told us that their contract writing system, which is an HHS-wide system managed by a separate office within HHS, currently does not allow them to report other transaction agreements separately from procurement contracts. ASPR officials also told us they were not aware of the module in FPDS-NG specific to other transaction agreements and would explore steps required to use it in the future, but provided no time frame for implementing a change. HHS’s approach of reporting other transactions in the contract module of FPDS-NG is inconsistent with federal acquisition regulations and does not provide a way for FPDS-NG users to systematically identify which actions are other transaction agreements.
Federal internal control standards state that an agency’s management should externally communicate quality information to achieve the agency’s objectives. Furthermore, the Digital Accountability and Transparency Act of 2014 (DATA Act) was enacted to, among other things, increase transparency and improve the quality of federal spending data submitted to USASpending.gov, which relies on data reported to FPDS-NG, by holding federal agencies accountable for the completeness and accuracy of the data submitted.[381] Without quality information on which ASPR actions are other transaction agreements rather than procurement contracts, the public, including congressional decision makers, entities with oversight responsibilities, and taxpayers, do not have insight into the extent to which ASPR is spending federal dollars on procurement contracts or other transaction agreements.
Agency Comments
We provided HHS, DOD, DHS, and the Office of Management and Budget with a draft of this enclosure. HHS provided comments, which are reproduced in Appendix IV: Comments from the Department of Health and Human Services. In its comments, HHS concurred with our recommendation and stated that it has taken steps to manually identify its other transaction agreements in its contract writing system to allow the public to distinguish between spending on agreements and procurement contracts in FPDS-NG. HHS also plans to update its contract writing system. DOD provided technical comments, which we incorporated as appropriate. DHS and the Office of Management and Budget did not provide comments on this enclosure.
Methodology
To identify agencies’ federal contract obligations and competition rate on contracts in response to COVID-19, we reviewed data reported by FPDS-NG through December 31, 2020.[382] We identified contract obligations related to COVID-19 using the National Interest Action code, as well as the contract description field.[383] For contract actions over $1 million, we removed obligations that were identified in the contract description as not related to COVID-19. We assessed the reliability of federal procurement data by reviewing existing information about FPDS-NG and the data it collects—specifically, the data dictionary and data validation rules—and by performing electronic testing. We determined that the data were sufficiently reliable for the purposes of describing agencies’ reported contract obligations in response to COVID-19.
To identify agencies’ use of DPA Title III and similar actions we reviewed FPDS-NG data and DOD and HHS documentation. To identify agencies’ use of other transaction agreements, we reviewed FPDS-NG data and agreements from DOD and HHS. For the four other transaction agreements that HHS misreported as contracts, we removed the $1.5 billion associated obligations from our reported contract obligations and are reporting them as other transaction agreement obligations.
Contact information: Marie A. Mak, (202) 512-4841, MakM@gao.gov, William Russell, (202) 512-4841, RussellW@gao.gov
Related GAO Products
Defense Production Act:Opportunities Exist to Increase Transparency and Identify Future Actions to Mitigate Supply Chain Issues.GAO-21-108. Washington, D.C.: November 19, 2020.
Covid-19 Contracting: Observations on Federal Contracting in Response to the Pandemic.GAO-20-632. Washington, D.C.: July 29, 2020.
Defense Acquisitions: DOD’s Use of Other Transactions for Prototype Projects Has Increased. GAO-20-84. Washington, D.C.: November 22, 2019.
Data Act: Quality of Data Submissions Has Improved but Further Action Is Needed to Disclose Known Data Limitations. GAO-20-75. Washington, D.C.: November 8, 2019.
Disaster Contracting: FEMA Continues to Face Challenges with Its Use of Contracts to Support Response and Recovery. GAO-19-518T. Washington, D.C.: May 9, 2019.
2017 Disaster Contracting: Actions Needed to Improve the Use of Post-Disaster Contracts to Support Response and Recovery. GAO-19-281. Washington, D.C.: April 24, 2019.
2017 Disaster Contracting: Action Needed to Better Ensure More Effective Use and Management of Advance Contracts. GAO-19-93. Washington, D.C: December 6, 2018.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 2014.
Federal Contracting: Noncompetitive Contracts Based on Urgency Need Additional Oversight.GAO-14-304. Washington, D.C.: March 26, 2014.
Department of Homeland Security: Further Action Needed to Improve Management of Special Acquisition Authority. GAO-12-557. Washington, D.C.: May 8, 2012.
Defense Contracting: DOD Has Enhanced Insight into Undefinitized Contract Action Use, but Management at Local Commands Needs Improvement. GAO-10-299. Washington, D.C.: January 28, 2010.
Department of Homeland Security: Improvements Could Further Enhance Ability to Acquire Innovative Technologies Using Other Transaction Authority. GAO-08-1088. Washington, D.C.: September 23, 2008.
Defense Acquisitions: DOD Has Implemented Section 845 Recommendations but Reporting Can Be Enhanced.GAO-03-150. Washington, D.C.: October 9, 2002.
U.S. imports of COVID-19-related products in October 2020 were lower than the peak level in June. Many factors, including an increase in domestic production and stockpiling, could have played a role in the changing demand for imports.
Key Considerations and Future GAO Work
We plan to continue to monitor the effect of COVID-19 on international trade and the medical supply chain.
Background
The COVID-19 pandemic has disrupted businesses around the world. The World Trade Organization reported on June 23, 2020, that international trade fell sharply as the pandemic upended the global economy, estimating a drop of almost 19 percent from 2019. In the face of disrupted international supply chains, U.S. imports of COVID-19-related products such as face masks, ventilators, gloves, and hand sanitizers have fluctuated.
Overview of Key Issues
Available data indicate that imports of product categories related to the COVID-19 response decreased by 9 percent from June to October 2020 (see figure).[384] However, despite this decline in recent months, as of October 2020, imports of these products were 21 percent higher compared to a year ago and had increased by 32 percent since February 2020. Imports of COVID-related products from China declined while imports of the same products from the rest of the world increased slightly. Imports from China decreased by 47 percent (from roughly $5.1 billion to $2.6 billion) from June to October 2020.[385] Meanwhile, imports of COVID-19-related product categories from other countries increased by 3 percent (from $15.1 billion to $15.6 billion) over the same period.[386] Imports from China accounted for close to 15 percent of overall COVID-19-related product categories imported in October 2020 compared to roughly 25 percent in June 2020.[387] Before the decline, imports of product categories related to the COVID-19 response increased by 46 percent from February 2020 to June 2020.
Monthly U.S. Imports of COVID-19-Related Products by Product Type, January 2018 to October 2020
Notes: Census trade statistics, a widely used source analyzing U.S. international trade, do not contain precise data on imports of COVID-19-related products. As a result, we estimated the import value of all product categories and types using Harmonized Tariff Schedule of the United States (HTS) statistical reporting numbers and associated product groupings listed by the U.S. International Trade Commission (USITC) in COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). USITC changed the HTS numbers for 12 of these product categories in its July 1, 2020, revision to the HTS. We identified the changes in the product categories that contained COVID-19-related products and used the revised HTS numbers in the July through October 2020 data for our analysis. Some HTS categories represent more than one product, and some categories contain products that are not directly relevant to COVID-19 responses. Product types only refer to the subset of goods considered COVID-19 related in each HTS-10 statistical reporting number. Therefore, the values presented may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, they are useful indicators for tracking import trends of such products.
The decline in COVID-related imports from June to October 2020 was largely driven by a decrease in the value of personal protective equipment (PPE) imports. During this period, imports of PPE declined by 50 percent. Imports of PPE fell by 29 percent from September to October 2020. This decline is a slight reversal from previous months, when imports of PPE increased 512 percent from February 2020 to June 2020.
Previous trends in imports of medicines (pharmaceuticals) and testing equipment also reversed after September 2020. From June to September 2020, imports of pharmaceuticals decreased by 20 percent, but increased by 29 percent from September to October 2020. Meanwhile, imports for testing equipment increased by 21 percent from June to September 2020 but declined by 19 percent from September to October 2020. Imports for swab and viral transport medium sets and reagents can partially explain the overall trends in imports of testing equipment.[388] Imports for reagents increased by 23 percent from June to September 2020 before declining by 20 percent from September to October 2020. Imports for the swab sets increased by 23 percent from June to September 2020 before declining by 9 percent from September to October 2020.
Many confounding factors could have played a role in the supply and demand of COVID-19-related products. These factors could influence fluctuations in both the import quantities and prices. Changes in either prices or quantities would drive the import trends of these products. On the supply side, the federal government has helped domestic companies to increase domestic production of key medical supplies. For instance, according to a Department of Defense official’s congressional testimony, the Department of Defense has awarded millions of dollars to U.S. companies to produce PPE and diagnostic equipment under the Defense Production Act since April 2020.[389] The increased domestic production may have led to less reliance on certain imports.
On the demand side, the initial surge in imports may be driven by stockpiling. For example, the Strategic National Stockpile (SNS) increased its inventory of N95 respirators, surgical masks, and face shields by several million units from July to October 2020.[390] Additionally, high global demand could have played a role in the amount the U.S. imported as countries competed for limited supply. GAO has reported that officials at the Department of Health and Human Services responsible for stocking the SNS stated that demand for certain testing equipment like nasal swabs and pipettes were outpacing supply and that one-third to one-half of states surveyed by GAO reported shortages for reagents needed to conduct diagnostic tests, testing instruments, and rapid point-of-care tests. Such shortages reflect the strain on supply chains and highlight challenges for sourcing some of these COVID-19-related products both domestically and internationally.
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget, which had no comments.
Methodology
To conduct this work, we reviewed the most recent trade statistics from the Census Bureau combined with U.S. International Trade Commission data on Harmonized Tariff Schedule codes associated with COVID-19 products. We found the data to be sufficiently reliable to describe trade in COVID-19-related products by reviewing agency documents and conducting consistency checks.
USAID provided 8,722 ventilators to 43 countries at a cost of about $200 million, and has initiated efforts to bolster the limited information it currently has on the location of the ventilators within recipient countries.
Entities involved: National Security Council, Department of State, U.S. Agency for International Development
Key Considerations and Future GAO Work
We continue to assess (1) the U.S. Agency for International Development’s (USAID) actions to locate all ventilators provided abroad and (2) U.S. agencies’ efforts to build other countries’ capacity to prevent, detect, and respond to infectious disease threats. We eliminated a recommendation from this enclosure that USAID develop a process to track the locations of the ventilators after dialogue with USAID facilitated the development of such a process, and USAID informed us that it had approved funding for an asset-management tracking platform to support oversight of the ventilators.
Background
COVID-19 has reached nearly every country around the globe, and the Department of State (State) and USAID warn that it could overwhelm health care institutions and reverse valuable economic and development gains made over many years. Two COVID-19 relief laws enacted in fiscal year 2020 appropriated $2.3 billion in supplemental funding for diplomatic and foreign assistance programming administered by State and USAID.[391] We previously reported in June and September 2020 on State and USAID’s use of this funding to provide health, humanitarian, and economic assistance to over 100 countries.
State and USAID developed a joint strategy and guidance on the use of these funds, including criteria to prioritize countries for assistance and to evaluate potential projects proposed for funding.[392] (See figure for State and USAID’s strategy.) The guidance outlines the process for programming new obligations of these supplemental foreign assistance resources.[393] The guidance also provides deadlines by which each regional and functional bureau may submit initial, priority-ranked proposals as part of the programming process.
March 2020 State and USAID Strategy for Using Supplemental Funding to Respond to COVID-19 Abroad
Note: The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, appropriated $435 million (reflected in Pillar 2 in the figure) for the Global Health Programs account and directed that not less than $200 million be transferred and merged with the Emergency Reserve Fund established pursuant to section 7058(c)(1) of the Department of State, Foreign Operations, and Related Programs Appropriations Act, 2017. Pub. L. No. 116-123, tit. IV, 134 Stat. 146, 152. The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, and the CARES Act also appropriated $95 million to USAID for operating expenses and $1 million to the USAID Office of Inspector General for COVID-19-related work. Pub. L. No. 116-123, tit. IV, 134 Stat. at 152; Pub. L. No. 116-136, div. B, tit. XI, 134 Stat. 281, 590. In addition, $7 million of the $250 million appropriated for the Economic Support Fund Account in Pillar 4 was transferred to USAID for operating expenses, according to USAID officials.
Overview of Key Issues
USAID reported obligating about $200 million in supplemental COVID-19 funding to provide 8,722 ventilators and related assistance to 43 countries, as of September 30, 2020.[394] According to USAID data, these funds were drawn from the Global Health Programs account and Emergency Reserve Fund, which State and USAID identified as the funding sources supporting Pillar 2 of their strategy on the use of supplemental funding to respond to COVID-19 abroad (see figure above). USAID also used the Economic Support Fund account to fund some of the ventilators provided under Pillar 4 of the strategy.[395]
USAID’s contractor began delivering the ventilators in May 2020, with the first three shipments going to South Africa, El Salvador, and Russia, according to USAID data. Almost all of the 8,722 ventilators had been delivered by September 30, 2020 (see figure).[396] According to data provided by USAID, the approximately $200 million it obligated to its contractor for ventilators, as of September 30, 2020, represented its single largest award of supplemental COVID-19 funding to an implementing partner.[397]
U.S. Agency for International Development (USAID)-Provided Ventilators Arrive in Uzbekistan and Bangladesh
The National Security Council (NSC) coordinated U.S. policy on USAID ventilator donations. According to USAID, NSC staff communicated to USAID the U.S. government decisions regarding ventilator donations, including the recipient countries, quantities, and manufacturers.[398] Additionally, USAID stated that the ventilator donation program was not part of its initial strategy for COVID-19 response. As a result, USAID further explained that it did not base the selection of recipient countries or the number of ventilators provided on its guidance on the use of funds or on its process for approving and programming new obligations of supplemental COVID-19 foreign assistance resources.
For some countries, obligations for ventilators represented a large share of USAID’s total COVID-19 assistance funding. For 21 of the 43 recipient countries, obligations for ventilators, as of September 30, 2020, represented more than half of the total supplemental COVID-19 response funding that USAID obligated to those countries, indicating a considerable financial commitment to ventilators over other potential forms of assistance.[399] For example, as shown in the table below, USAID provided 1,000 ventilators to Indonesia and Brazil, representing over 70 percent of total obligations for all COVID-19-related assistance to those countries, as of September 30, 2020. The obligations for 200 ventilators for Bolivia represented about 87 percent of total obligations for COVID-19-related assistance to that country.
Ventilators Provided by USAID Using Supplemental COVID-19 Funding, as of September 30, 2020, and Country COVID-19 Cases
Recipient
Number of ventilators provided
Date of USAID transfer letter to recipient
Number of new cases per day on date of transfer letter
Number of deaths per day on date of transfer letter
Total obligations for ventilators and related assistance, as of 9/30/20 (in dollars)
Total supplemental COVID-19 obligations, as of 9/30/20 (in dollars)
Total ventilator obligations as percentage of total supplemental obligations, as of 9/30/20
Brazil
1,000
06/23/20
33,322
1046
21,400,823
29,784,622
71.9
Indonesia
1,000
07/15/20
1,540
70
20,359,125
27,609,125
73.7
South Africa
1,000
05/22/20
1,010
24
21,879,350
27,043,701
80.9
El Salvador
600
05/20/20
74
1
12,001,892
11,924,334
100.7
Peru
500
06/17/20
4,229
193
7,702,564
20,042,100
38.4
Paraguay
280
06/25/20
50
0
5,013,738
4,716,832
106.3
Ecuador
250
06/29/20
573
31
5,550,000
18,549,089
29.9
Egypt
250
07/21/20
663
51
4,375,000
4,300,000
101.7
Ethiopia
250
06/04/20
124
2
5,145,326
29,349,197
17.5
Honduras
210
06/01/20
161
5
9,904,571
11,725,333
84.5
Bolivia
200
07/17/20
1,563
50
4,887,785
5,637,785
86.7
Colombia
200
06/29/20
3,468
133
4,181,826
16,847,500
24.8
India
200
06/12/20
10,830
341
4,052,728
12,450,000
32.6
Kenya
200
06/30/20
222
3
4,098,327
16,598,327
24.7
NATO
200
05/12/20
N/A
N/A
3,693,814
3,693,814
100.0
Nigeria
200
08/10/20
408
4
4,424,581
39,349,081
11.2
Pakistan
200
07/01/20
3,771
83
5,396,045
18,075,000
29.9
Russia
200
06/09/20
8,798
170
5,600,000
5,600,000
100.0
Sri Lanka
200
08/07/20
3
0
4,216,314
8,016,314
52.6
Uzbekistan
200
07/27/20
620
5
3,734,986
6,734,986
55.5
Afghanistan
100
07/29/20
96
5
3,064,938
21,464,938
14.3
Bangladesh
100
09/27/20
1,409
30
1,992,460
19,882,184
10.0
Italy
100
10/21/20
1,423
10
9,804,400
50,000,000
19.6
Nepal
100
10/22/20
3,704
16
2,106,885
7,046,609
29.9
Panama
100
08/07/20
1,038
23
1,774,478
2,299,885
77.2
Philippines
100
08/11/20
4,009
39
2,839,938
16,889,938
16.8
Rwanda
100
07/23/20
30
0
2,498,931
3,198,931
78.1
Vietnam
100
09/30/20
4
0
2,793,893
9,293,893
30.1
Maldives
60
06/29/20
17
0
1,778,234
2,378,234
74.8
Democratic Republic of Congo
50
09/25/20
14
0
1,719,969
25,078,668
6.9
Dominican Republic
50
08/03/20
1,354
14
1,598,769
3,598,769
44.4
Ghana
50
08/27/20
89
1
1,680,589
3,280,589
51.2
Guatemala
50
09/18/20
505
23
1,501,706
9,452,039
15.9
Kosovo
50
08/19/20
148
10
999,132
1,063,132
94.0
Mongolia
50
08/10/20
0
0
1,534,069
0
N/A
Mozambique
50
07/10/20
24
0
1,780,589
13,780,589
12.9
Papua New Guinea
40
06/09/20
0
0
1,411,997
3,586,997
39.4
Haiti
37
09/14/20
22
1
1,185,478
11,735,478
10.1
Fiji
30
06/29/20
0
0
972,447
822,447
118.2
Zimbabwe
20
07/21/20
109
1
857,078
16,021,525
5.3
Bhutan
15
08/13/20
4
0
825,517
1,353,582
61.0
Kiribati
10
08/07/20
0
0
440,499
365,499
120.5
Nauru
10
07/22/20
0
0
490,816
340,816
144.0
St. Kitts & Nevis
10
07/14/20
0
0
506,956
506,956
100.0
Total
8,722
203,778,563
541,488,838
37.6
Legend: NATO = North Atlantic Treaty Organization; N/A = not applicable
Source: GAO analysis of U.S. Agency for International Development (USAID) and World Health Organization data. | GAO-21-265
Notes: Transfer letters from USAID confirm USAID’s intention to deliver ventilators to recipient countries. In some instances in which USAID did not provide transfer letters, we relied on other correspondence between USAID and recipient countries to confirm the intent to deliver ventilators. The obligated funds were for costs of ventilators; related consumables, durables, service agreements, and freight; and assessments and technical assistance. Daily country COVID-19 cases and deaths were reported by the World Health Organization using a 7-day rolling average (see https://covid19.who.int/table). USAID’s total supplemental obligations were from the following foreign assistance accounts that received supplemental COVID-19 funding: Global Health Programs, Emergency Reserve Fund, Economic Support Fund, and International Disaster Assistance. The totals do not include obligations from the Migration and Refugee Assistance account, which also received supplemental funding but which the Department of State administers. According to USAID officials, some ventilator obligations amounted to more than 100 percent of total supplemental COVID-19 obligations because worldwide obligations were attributed to specific countries.
Some countries that received ventilators had few or no COVID-19 cases. Several recipient countries had few or no new COVID-19 cases per day, as of the dates USAID confirmed it would provide ventilators to those countries (see table).[400] According to the World Health Organization, as of December 7, 2020, two of these countries, Nauru and Kiribati, had never had a reported COVID-19 case. In addition, the relationship between the number of ventilators provided and the number of new COVID-19 cases varied widely within the same region. For example, in Latin America, El Salvador, which had 74 new cases per day as of the date of its transfer letter, received 600 ventilators, whereas Honduras, which had 161 new cases, received 210. Similarly, Sri Lanka, which had only three new cases, received 200 ventilators whereas Bangladesh, with 1,409 new cases, received 100.
USAID does not know the locations of the ventilators within all recipient countries but has initiated efforts to obtain this information. Although nearly all ventilators had been transferred to the recipient countries as of December 2020, USAID had limited information about the locations of the ventilators within these countries. USAID told us in December 2020 that it had begun implementing a process to identify the locations of the ventilators. According to a USAID official, this process involves soliciting and combining information from the ventilator manufacturers and service providers, recipient country ministries of health, and implementing partners.
USAID is working to obtain and compile information from these sources in order to track the location and functionality of each ventilator, as well as any related training provided. According to USAID officials, 12 of the 43 recipient countries have provided final distribution lists that indicate the locations of the ventilators within each country, and USAID is working with manufacturers and service providers to update and combine this information with other types of relevant data, such as serial numbers. USAID has received planned distribution lists from another 11 of the recipient countries, and does not have a status regarding the final or planned distribution within the remaining 20 countries. In its January 2021 comments on this enclosure, USAID noted that agency funding had been approved for an asset-management tracking platform to support and inform the long-term oversight, management, and reporting of the donated ventilators.[401]
USAID has indicated it may conduct some limited monitoring of countries’ use of the ventilators. USAID internal operational policies generally require officials to oversee implementation and understand progress toward measurable results.[402] This includes the development of performance indicators, including baseline data, for foreign assistance efforts.[403] Although the ventilators accounted for about 38 percent of total COVID-related obligations within the recipient countries, USAID stated that it considers the ventilator distribution activity to be exempt from some requirements related to monitoring, planning, and timing, such as those related to Performance Management Plans or Monitoring, Evaluation and Learning plans.[404] USAID stated that it has focused its monitoring and evaluation efforts on its assigned task—the procurement and delivery of ventilators.
According to USAID, given the limited focus and duration of the U.S. government’s ventilator donation program, as well as the limited role of USAID in the management of the donated equipment, USAID considers this level of monitoring and evaluation to be appropriate in scope. Nevertheless, in November 2020, USAID officials told us that they had discussed developing an assessment tool that could help USAID to understand how ventilators are being used.
Agency Comments
We provided a draft of this product to State, USAID, the NSC, and the Office of Management and Budget (OMB) for comment. State provided technical comments, which we incorporated. In its comments, reproduced in Appendix IX: Comments from the U.S. Agency for International Development, USAID questioned whether the number of cases of COVID-19 in each country as of the dates USAID confirmed it would provide ventilators is the most appropriate metric for judging the effectiveness of the ventilator effort. We included this case information for context to illustrate the reach of the pandemic in these countries at the time. We did not comment on the effectiveness of the ventilator effort or indicate that the number of cases would be an appropriate metric for determining its effectiveness. USAID did not provide us with the criteria used for the allocation decisions and as noted earlier in this enclosure, the NSC did not respond to our request for information regarding ventilator allocations. Additionally, the NSC did not provide any comments on this enclosure, and OMB did not comment on this enclosure.
Methodology
To conduct this work, we reviewed State and USAID’s strategy and guidance documents on the use of supplemental funding, and USAID’s operational guidance in its Automated Directives System, Chapter 201, Program Cycle Operational Policy. We also reviewed USAID’s congressional notifications related to funding for the ventilators, documents associated with the USAID contract to deliver the ventilators, and letters transferring ownership of the ventilators from USAID to recipient country governments. We also analyzed USAID data on the ventilators, including the number of ventilators provided to each country and the funding amounts obligated for this purpose. We analyzed the data and corrected discrepancies through discussions with USAID officials. We also incorporated World Health Organization data on the number of COVID-19 cases in each country that received ventilators. We found these data sufficiently reliable for the purposes of this report. In addition, we interviewed USAID officials and representatives of USAID’s contractor for the ventilator procurement and delivery effort. We submitted questions to the NSC, to which we did not receive a response.
Contact information: David Gootnick, (202) 512-3149, gootnickd@gao.gov
Federal agencies’ responses to the risk of fraud during the COVID-19 pandemic include enforcement actions and education. Such actions help protect consumers and ensure that taxpayer dollars and government services related to COVID-19 serve their intended purposes.
Entities involved: Government-wide
Key Considerations and Future GAO Work
In November 2020, we recommended that the Office of Management and Budget (OMB) develop and issue guidance directing agencies to include COVID-19 relief funding with associated key risks, such as provisions contained in the CARES Act and other relief legislation that potentially increase the risk of improper payments or changes to existing program eligibility rules, as part of their improper payment estimation methodologies. This action should especially be required for already-existing federal programs that received additional COVID-19 relief funding.
Given that the COVID-19 relief laws appropriated about $2.7 trillion as of November 30, 2020 to fund response and recovery efforts—as well as to mitigate the public health, economic, and homeland security effects of—COVID-19, developing reliable improper payment estimates is essential for understanding and addressing financial vulnerabilities.[405] Additionally, developing corrective action plans that respond to the root causes of payment errors, which can include failure to verify eligibility and identify fraud, is a key component in government-wide efforts to reduce improper payments.[406]
While OMB neither agreed nor disagreed with this recommendation in our November report, in January 2021, OMB staff stated that they believe current OMB guidance sufficiently addresses our recommendation and concerns. Additionally, OMB staff stated that OMB is actively coordinating and engaging with the Pandemic Response Accountability Committee and Inspectors General to share and discuss information relevant to COVID-19 spending risks and improper payment reduction strategies. We do not agree that current OMB guidance sufficiently addressed our recommendation and concerns. In November 2020, we reported that although OMB issued a memorandum providing agencies the option to incorporate new COVID-19 relief funding into their normal sampling processes, it did not specifically direct agencies to do so. In addition, the guidance did not direct agencies to consider associated key risks, such as changes to eligibility rules and different payment processes, as part of their improper payment estimation methodologies. Further, while coordination with the Inspectors General is important, federal agencies ultimately maintain the primary responsibility for payment integrity efforts. Therefore, we continue to maintain that without OMB guidance for agencies to include COVID-19 relief funding and associated key risks as part of their improper payment estimation methodologies, agencies are at increased risk that their processes may not result in reliable estimates, calling into question their usefulness for developing effective corrective actions.
We will monitor the status of our recommendation in future reports and continue our oversight of government-wide payment integrity and fraud risk management efforts.
Background
The public health crisis, economic instability, and increased flow of federal funds associated with the COVID-19 pandemic present increased pressures and opportunities for fraud.[407] The extent of fraud associated with the COVID-19 relief funds appropriated to date has not yet been determined. However, several individuals have already pleaded guilty to federal charges of defrauding COVID-19 relief programs—including the Small Business Administration’s (SBA) Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program, and the Department of Labor’s (DOL) unemployment insurance program—and numerous others faced related federal charges as of November 30, 2020. One of the many challenges, however, is that because of fraud’s deceptive nature, programs can incur financial losses related to fraud that are never identified, and such losses are difficult to reliably estimate. Fraud can also result in financial losses to consumers and undermine health and safety.
Overview of Key Issues
Due to the very nature of the government’s need to quickly provide funds and other assistance to those affected by COVID-19 and its economic effects, federal relief programs are vulnerable to significant risk of fraudulent activities. The schemes used to defraud the government as well as private businesses and individuals are endless, and many have already emerged during the COVID-19 pandemic. Since March 2020, the Department of Justice has publicly announced charges in numerous fraud-related cases. The charges—filed across the U.S. and investigated by a range of law enforcement agencies—include making false statements and engaging in identity theft, wire and bank fraud, and money laundering. The number of individuals facing fraud-related charges continues to grow and will likely increase, as these cases take time to develop.[408]
Fraud against federal programs. Twenty-three individuals pleaded guilty to federal charges of defrauding COVID-19 relief programs—including SBA’s PPP and EIDL program and DOL’s unemployment insurance program—from March through November 2020.[409] For example:
In one case, an individual pleaded guilty to bank fraud arising from an effort to defraud a financial institution by applying for a PPP loan, falsely claiming, among other things, that the business had 68 employees and, in 2019, paid wages, tips, and other compensation totaling $2.8 million. The business had no employees and no payroll expenses of any kind, and was not an operational business. This individual managed to withdraw $172,000 of the $590,000 loan obtained before the remainder was frozen.
In another case, an individual pleaded guilty to one count of wire fraud, admitting to carrying out a scheme to defraud several different government COVID-19 relief programs by creating fake payroll and tax records for fake entities. The individual submitted four fraudulent applications seeking a total of over $1.5 million from three different lenders for PPP loans and a fraudulent application to SBA for EIDL in the name of one of the fake entities. SBA provided this individual a $10,000 EIDL advance before the fraud was detected.[410]
As part of another guilty plea, an individual admitted to lying to SBA by fraudulently applying for and obtaining multiple loans and advances under the EIDL program. Specifically, this individual purchased more than 35 “aged, off-the-shelf” corporations, and then submitted approximately 68 fraudulent applications for loans and nonrefundable grant advances of up to $10,000 through SBA’s EIDL program.[411]
In a plea agreement for a fourth case, an individual admitted to falsely reporting his income to obtain an additional weekly payment, and fraudulently obtaining over $13,000 in unemployment benefits related to COVID-19 relief funds to which he was not entitled.
Federal charges are pending against 197 individuals for attempting to defraud these programs.[412] In addition, one individual pleaded guilty to identity theft in connection with economic impact payments, and related federal charges are pending against four other individuals.[413] These cases each involved individuals unlawfully obtaining the personal identification information of other individuals, filing false tax returns, and obtaining economic impact payments.[414]
Consumer fraud. In addition to fraud against federal programs, fraud can result in financial losses to consumers and undermine health and safety. For example, eight individuals or entities pleaded guilty to federal charges related to consumer fraud from March through November 2020.[415] In one case, an individual sold an unregistered pesticide online, claiming that it would help protect individuals from viruses. This individual pleaded guilty to violating the Federal Insecticide, Fungicide, and Rodenticide Act. In another case, an individual pleaded guilty to an internet-based loan scam that cheated victims out of more than $1 million. Specifically, this scam involved offering to assist individuals in preparing loan applications to obtain SBA-guaranteed loans in exchange for an advance fee, soliciting potential customers on the basis of false, fraudulent, and misleading statements and representations, but doing virtually nothing to even attempt to obtain loans for customers. There are also federal charges pending against 24 individuals or entities related to consumer fraud. In addition, the Federal Trade Commission and the Food and Drug Administration have issued warning letters to companies for allegedly selling fraudulent COVID-19-related products, including those making deceptive or scientifically unsupported claims about their ability to treat or cure COVID-19.
Other federal cases. The federal government is also pursuing charges including conspiracy, wire fraud, and theft that are related to COVID-19 but separate from consumer fraud and fraud against the federal programs discussed earlier. Six individuals pleaded guilty to these types of federal charges from March through November 2020. For example, one individual pleaded guilty and was sentenced to federal prison for causing more than $200,000 in damage to a former employer and delaying the shipment of personal protective equipment during the COVID-19 pandemic.[416] Also, an employee at a Department of Veterans Affairs Medical Center pleaded guilty to theft of government property and admitted stealing COVID-19-related medical supplies to sell for the employee’s own gain.[417] There are also other federal charges pending against 17 individuals. For example, two individuals were indicted on charges of conspiracy and wire fraud for attempting to fraudulently sell 50 million nonexistent N95 facemasks to a foreign government, allegedly attempting to bilk the foreign government out of more than $317 million.[418]
Federal investigations and reporting mechanisms. The federal response to COVID-19 fraud involves the standing up of task forces; investigations by offices of inspector general (OIG) and other law enforcement agencies; and other mechanisms to receive allegations and complaints.
Task forces. Federal agencies have organized task forces focused on COVID-related fraud. For example, the Department of Justice has established the National Unemployment Insurance Fraud Task Force to coordinate efforts across the federal government. To address the proliferation of fraudulent COVID-19-related products, the Food and Drug Administration set up a cross-agency task force.
Ongoing investigations. OIGs and other law enforcement agencies have initiated numerous fraud-related investigations. The Department of Justice Offices of the United States Attorneys are also partnering with entities such as the Federal Bureau of Investigation, the Internal Revenue Service Criminal Investigation Division, the U.S. Postal Inspection Service, and OIGs at DOL, the Federal Deposit Insurance Corporation, and SBA to carry out investigations. Federal agencies are also working with states to detect and respond to unemployment insurance fraud. For example, potentially large fraud schemes have prompted several federal agencies to assist states with their investigations. The National Unemployment Insurance Fraud Task Force also warns that “fraudsters, some of which are transnational criminal organizations, are using the stolen identities of U.S. citizens to open accounts and file fraudulent claims for unemployment insurance benefits.” These investigations have already led to some states canceling claims and may eventually result in further fraud convictions. For example, Maine canceled almost 24,000 initial claims and 41,000 continued claims between late May and late June 2020 that it determined to be fraudulent, according to a state labor department news release.
Allegations and complaints. Federal hotlines have received numerous complaints from the public alleging potential fraud involving COVID-19 relief funds. For example, the Inspector General for SBA testified on October 1, 2020, that the hotline operated by his office has received tens of thousands of allegations of wrongdoing. Similarly, from March 13, 2020, through November 30, 2020, our hotline—known as FraudNet—received over an estimated 1,000 complaints related to the CARES Act, many of which involve SBA’s PPP and EIDL program. Additionally, the Pandemic Response Accountability Committee, established by the CARES Act to conduct oversight of the federal government's pandemic response and recovery effort, provides online reporting mechanisms (see text box).
Report Fraud, Waste, and Abuse
GAO’s FraudNet supports accountability across the federal government. Allegations of fraud, waste, or abuse can be submitted via the FraudNet portal or by calling the hotline at 1-800-424-5454.
Allegations of fraud, waste, abuse, or whistleblower reprisal can also be reported to the Pandemic Response Accountability Committee’s Hotline website.
The Federal Trade Commission is tracking complaint data related to COVID-19 and taking actions against scammers using the pandemic to deceive or defraud consumers. According to Federal Trade Commission reporting, the agency had received over 136,000 reports about fraud and over 37,000 reports about identity theft as of November 30, 2020.[419]
Another reporting mechanism law enforcement agencies use to support investigations is suspicious activity reports (SAR), which financial institutions file with the Financial Crimes Enforcement Network (FinCEN) in compliance with the Bank Secrecy Act.[420] From March through October 2020, 5,344 financial institutions filed 118,625 SARs associated with the CARES Act programs. Examples of suspicious activity identified by financial institutions included rapid movement of funds, identity theft, and forgeries. Although the filing of a SAR does not necessarily mean that fraud has occurred, law enforcement agencies use these reports to help support investigations. For more information on suspicious activity reports specifically associated with the PPP and EIDL program, see the enclosures on the Paycheck Protection Program and the Economic Injury Disaster Loan Program in appendix I.
Beginning in March 2020, FinCEN has issued seven notices or advisories to financial institutions related to potential illicit financial activity associated with COVID-19. FinCEN officials also told us that as of October 30, 2020, they had received 545 COVID-19-related inquiries. According to FinCEN officials, most inquiries were from financial institutions concerned about issues related to Bank Secrecy Act compliance in light of the COVID-19 pandemic. Additionally, according to FinCEN officials, as of December 2020, FinCEN has shared over 3,000 referrals with the Department of Justice SAR Review Team and other task forces.
Other federal response actions. In addition to the enforcement actions and reporting mechanisms described above, the federal government’s response to fraud includes warnings and public awareness. For example, on their websites, the Department of Justice and the OIG at the Department of Health and Human Services have issued warnings about fraud schemes and scams. The Federal Trade Commission also educates consumers on how to spot and avoid COVID-19 scams through various resources, such as its website, print publications, and videos (see figure).
Example of Information Provided by the Federal Trade Commission to Help Consumers Avoid COVID-19 Scams
Fraud risk management. Effective fraud risk management helps ensure that federal programs’ services fulfill their intended purpose, funds are spent effectively, and assets are safeguarded. The federal response to fraud—for example, through investigations and prosecutions—is one part of fraud risk management; however, efforts to prevent and detect fraud are also critical control activities for managing fraud risk. In 2015 we published A Framework for Managing Fraud Risks in Federal Programs (Fraud Risk Framework), which provides a comprehensive set of leading practices for agency managers to develop or enhance efforts to combat fraud in a strategic, risk-based manner.[421] In its Circular A-123 guidelines, OMB states that agencies should adhere to the Fraud Risk Framework’s leading practices as part of their efforts to effectively design, implement, and operate an internal control system that addresses fraud risks.[422]
OMB has acknowledged that the COVID-19 pandemic significantly expanded the risks of improper payments and fraud across multiple programs.[423] For example, OMB memorandum M-20-21 notes that in implementing new or modified activities provided for in COVID-19 relief legislation, agencies should prioritize, for example, balancing the need for expediency with steps to mitigate the risk of fraud, waste, abuse, and improper payments.[424] OMB officials also acknowledged that under the Fraud Risk Framework, assessing and managing fraud risk in the risk profile may include periodic changes and adjustments made upon new and emerging risks, impacts, and other factors, including the creation of new programs, a surge of funding, new statutory requirements, or the realization of a risk progressing to an issue or crisis such as a pandemic.[425]
In memorandum M-20-21, OMB notes that OIGs should be leveraging new resources to develop plans to prevent and detect waste, fraud, and abuse related to agency implementation of the relief legislation. Also according to OMB officials, the agency plans to review additional reports issued by GAO and the OIGs to gain more insight about where these audits and investigations have identified additional payment integrity risk factors and successful mitigation strategies that should be shared with federal agencies.
While coordination between OIGs and federal agencies is important, federal program managers maintain the primary responsibility for enhancing program integrity, including managing fraud risks. Our Fraud Risk Framework supplements OMB guidance by providing additional details on leading practices to aid federal program managers in managing fraud risks, particularly in emergency environments. These practices—including sharing information with relevant stakeholders and using data analytics to help prevent and detect fraud—are also discussed in greater detail in appendix V in our June 2020 report on the federal response to COVID-19.
Agency Comments
We provided OMB and the Department of the Treasury (Treasury) with a draft of this enclosure for comment. OMB and Treasury provided technical comments, which we incorporated as appropriate.
Methodology
To conduct this work, we reviewed information from the Department of Justice to identify federal fraud-related charges related to COVID-19 relief funding as of November 30, 2020. We also reviewed information from GAO’s A Framework for Managing Fraud Risks in Federal Programs and other measures to address fraud risk, such as OMB guidance. In addition, we reviewed OMB’s written responses to questions about its guidance and written responses from FinCEN about COVID-19-related concerns it has received from financial institutions.
In our June 2020 CARES Act report, we made three matters for Congress to consider and three recommendations for executive action; in our September 2020 CARES Act report, we made 16 recommendations; in our November 2020 CARES Act report, we made one matter for Congress and 11 recommendations; and in November 2020, we issued a report on COVID-19 vaccines and therapeutics and made one recommendation. Following are the matters for Congress, our recommendations, and their status.
Status of matters and recommendations made in our June 2020 CARES Act report
Matter 1.In the absence of efforts to develop a plan, we urge Congress to take legislative action to require the Secretary of Transportation to work with relevant agencies and stakeholders, such as the Departments of Health and Human Services (HHS) and Homeland Security (DHS), and members of the aviation and public health sectors, to develop a national aviation preparedness plan to ensure safeguards are in place to limit the spread of communicable disease threats from abroad while at the same time minimizing any unnecessary interference with travel and trade.
Status: Open
Comment: In May 2020, the House of Representatives passed H.R. 6800, referred to as the HEROES Act, which would require the Department of Transportation (DOT), in coordination with HHS, DHS, and other appropriate federal departments and agencies, to develop a national aviation preparedness plan. Most recently, in September 2020, the Senate passed S. 3681, Ensuring Health Safety in the Skies Act of 2020, which would require HHS, DHS, and DOT to form a joint task force on air travel during and after the COVID-19 public health emergency, among other provisions. Also, in October 2020, H.R. 8712, National Aviation Preparedness Plan Act of 2020, was introduced. If enacted, this bill would require DOT, in collaboration with DHS, HHS, and other aviation stakeholders, to develop a national plan to prepare the aviation industry for future communicable disease outbreaks.
We again urge Congress to take swift action to require a national aviation-preparedness plan, without which the U.S. will not be as prepared to minimize and quickly respond to ongoing and future communicable disease events.
Matter 2. To provide agencies access to Social Security Administration's (SSA) more complete set of death data, we urge Congress to provide the Department of the Treasury (Treasury) with access to SSA’s full set of death records, and to require that Treasury consistently use it.
Status: Closed
Comments: In December 2020, Congress passed and the President signed into law the Consolidated Appropriations Act, 2021, which requires SSA, to the extent feasible, to share its full death data with Treasury’s Do Not Pay working system for a 3-year period, effective on the date that is 3 years from enactment of this Act. Sharing this data will allow agencies to enhance their efforts to identify and prevent improper payments to deceased individuals. Therefore, it will be important for SSA and Treasury to work together to implement this legislation.
Matter 3. To help ensure that federal funding is targeted and timely, we urge Congress to use GAO's Federal Medical Assistance Percentage formula for any future changes to the Federal Medical Assistance Percentage during the current or any future economic downturn.
Status: Open
Comments: To help ensure that federal funding is targeted and timely, we urged Congress to use GAO’s Federal Medical Assistance Percentage formula to determine the timing and increase in Federal Medical Assistance Percentage—which determines the amount of federal Medicaid funding provided to states—for any future changes to the current or any future economic downturn. Our past work has found that during economic downturns—when Medicaid enrollment can rise and state economies weaken—the formula, which is based on each state’s per capita income, does not reflect current state economic conditions. No congressional action has been taken to date.
Recommendation 1. The Secretary of Labor should, in consultation with the Small Business Administration (SBA) and Treasury, immediately provide information to state unemployment agencies that specifically addresses SBA's Paycheck Protection Program (PPP) loans, and the risk of improper payments associated with these loans.
Status: Closed
Comment: The Department of Labor (DOL) neither agreed nor disagreed with our recommendation. Following our recommendation, DOL issued guidance on August 12, 2020, that clarified that individuals working full-time and being paid through PPP are not eligible for unemployment insurance (UI), and that individuals working part-time and being paid through PPP would be subject to certain state policies, including state policies on partial unemployment to determine their eligibility for UI benefits. Further, the guidance clarified that individuals being paid through PPP but not performing any services would similarly be subject to certain provisions of state law, and noted that an individual receiving full compensation would be ineligible for UI.
Recommendation 2. The Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments.
Status: Open
Comment: The Internal Revenue Service (IRS) agreed with our recommendation. Treasury and IRS have taken steps to implement this recommendation and are considering further actions. Currently, IRS has instructions on its website requesting that individuals voluntarily return by mail the appropriate economic impact payment (EIP) amount sent to a decedent, for both electronic and paper check payments. Also, the envelopes in which paper checks were sent have a checkbox to indicate if the recipient is deceased, and individuals could mail envelopes with that checkbox indicated to the Bureau of the Fiscal Service. Finally, Treasury has held and canceled EIPs to decedents in addition to the EIPs that have been returned.
Of the $1.2 billion in EIPs sent to decedents, as of December 31, 2020, around 57 percent (just over $700 million) had been recovered. There are likely more returned EIPs in unopened mail that IRS has yet to process. Treasury and IRS continue to review and monitor data on the number of EIPs that were sent to decedents and have since been recovered to determine whether further action may be warranted.
Treasury was considering sending letters to request the return of outstanding checks and the repayment of amounts already paid by direct deposit or by checks that have been cashed. However, according to Treasury, it has not moved forward with this effort because Congress is currently considering legislation that would clarify or change the eligibility requirements of the EIPs, including payments to deceased individuals.
Our work on EIPs is ongoing. We will continue to examine Treasury and IRS efforts to recoup payments sent to ineligible individuals.
Recommendation 3. The Administrator of SBA should develop and implement plans to identify and respond to risks in PPP to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less.
Status: Open
Comment: At the time of our report, SBA neither agreed nor disagreed with our recommendation. Since then, SBA officials have said the agency has completed oversight plans, but SBA has not provided documentation that fully details these plans. As we reported in September 2020, SBA has said that it plans to review all PPP loans of $2 million or more and further stated that it may review any PPP loan it deems appropriate, including loans of less than $2 million. In early December 2020, SBA provided us with a series of slides that contained an overview of the loan review process. For example, the document describes three steps in the process: automated screenings of all loans, manual reviews of selected loans, and quality control reviews to ensure the quality, completeness, and consistency of the review process. At the end of December 2020, SBA provided a draft Master Review Plan for the Loan Review Process, but the document did not contain detailed policies and procedures for some loan reviews or loan forgiveness reviews as we had previously requested. According to SBA officials, these were in the process of being updated.
Status of recommendations made in our September 2020 CARES Act report
Recommendation 1. The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency—who head agencies leading the COVID-19 response through the Unified Coordination Group—should immediately document roles and responsibilities for supply chain management functions transitioning to HHS, including continued support from other federal partners, to ensure sufficient resources exist to sustain and make the necessary progress in stabilizing the supply chain, and address emergent supply issues for the duration of the COVID-19 pandemic.
Status: Open
Comment: As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability.
Recommendation 2. The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency—who head agencies leading the COVID-19 response through the Unified Coordination Group—should further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic, including through the use of Defense Production Act authorities.
Status: Open
Comment: As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability.
Recommendation 3. The Secretary of Health and Human Services—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response.
Status: Open
Comment: As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability.
Recommendation 4. The Administrator of the Federal Emergency Management Agency—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with its roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response.
Status: Open
Comment: DHS disagreed with our recommendation, noting, among other things, the work that it had done to manage the medical supply chain and increase supply availability.
Recommendation 5. The Secretary of Health and Human Services, with support from the Secretary of Defense, should establish a time frame for documenting and sharing a national plan for distributing and administering a COVID-19 vaccine and, in developing such a plan, ensure that it is consistent with best practices for project planning and scheduling and outlines an approach for how efforts will be coordinated across federal agencies and nonfederal entities.
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. In November 2020, we reported that HHS and the Department of Defense (DOD) had released initial planning documents for the distribution and administration of potential COVID-19 vaccines, but also reported that stakeholders indicated that they would like to see additional information as planning continued. Since our November report, HHS and DOD have continued their efforts related to vaccine implementation. We will continue to monitor federal efforts to determine whether the actions taken address our recommendation.
Recommendation 6. As the Centers for Disease Control and Prevention (CDC) implements its COVID-19 Response Health Equity Strategy, the Director of CDC should determine whether having the authority to require states and jurisdictions to report race and ethnicity information for COVID-19 cases, hospitalizations, and deaths is necessary for ensuring more complete data and, if so, seek such authority from Congress.
Status: Open
Comment: CDC agreed with our recommendation. In response to our recommendation, CDC stated in December 2020 that the agency is committed to having discussions with stakeholders to assess whether having the authority to require states and jurisdictions to report race and ethnicity information for COVID-19 cases would result in improved reporting. We will continue to conduct work examining HHS, CDC, and other component agencies’ ongoing work regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation 7. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should involve key stakeholders to help ensure the complete and consistent collection of demographic data.
Status: Open
Comment: CDC agreed with our recommendation. In response to our recommendation, CDC stated in December 2020 that the agency is working with state and local health departments, in addition to other stakeholders, to accelerate the reporting of demographic data and improve data quality, including for information on race and ethnicity. We will continue to conduct work examining HHS, CDC, and other component agencies’ ongoing work regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation 8. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should take steps to help ensure CDC’s ability to comprehensively assess the long-term health outcomes of persons with COVID-19, including by race and ethnicity.
Status: Open
Comment: CDC agreed with our recommendation. In response to our recommendation, CDC noted in October 2020 that the agency is convening a team to develop a plan to monitor the long-term health outcomes of persons with COVID-19 by identifying health care surveillance systems that can electronically report health conditions to state and local health departments. As of December 2020, CDC stated it has various efforts underway such as partnering with clinicians to understand the clinical needs of patients after COVID-19 infection and establishing studies with external partners to assess long-term health outcomes. In addition, CDC stated the agency is analyzing electronic health record data to describe health outcomes after COVID-19 diagnosis as well as analyzing race and ethnicity in any data collected for long-term health effects. We will continue to conduct work examining HHS, CDC, and other component agencies’ ongoing work regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation 9.The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP to help target outreach and communications efforts.
Status: Open
Comment: Treasury neither agreed nor disagreed with our recommendation. In response to our recommendation, Treasury and IRS took actions that are consistent with our recommendation, such as using tax return information to identify and notify nearly 9 million individuals that they may be eligible for an EIP. However, Treasury and IRS did not update estimates of those who could be eligible, but have yet to file. Without an updated estimate, Treasury, IRS, other federal agencies, and IRS’s outreach partners are limited in their ability to appropriately scale and target outreach and communication efforts to individuals who may be eligible for a payment.
Our work on EIPs is ongoing. We will continue to examine Treasury and IRS efforts to identify and notify individuals about their eligibility for a payment and we will review how many taxpayers claim one as part of their 2020 tax filing.
Recommendation 10.The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should make estimates of eligible recipients who have yet to file for an EIP, and other relevant information, available to outreach partners to raise awareness about how and when to file for EIPs.
Status: Open
Comment: Treasury neither agreed nor disagreed with our recommendation. Treasury and IRS took actions that are consistent with our recommendation, such as using tax return information to identify and notify nearly 9 million individuals that they may be eligible for an EIP. Without an updated estimate, Treasury, IRS, other federal agencies, and IRS’s outreach partners are limited in their ability to appropriately scale and target outreach and communication efforts to individuals who may be eligible for an EIP.
In November, the IRS’s Non-Filers Tool closed, which had allowed individuals who do not normally file a tax return to claim an EIP. In September, Treasury and IRS sent nearly 9 million notices to nonfilers to raise awareness about EIPs. However, Treasury and IRS are not monitoring the effectiveness of the notices. If they knew how many nonfilers who had received notices ultimately received an EIP, they could then determine whether additional or targeted outreach is needed for the 2021 filing season.
Our work on EIPs is ongoing. We will continue to examine Treasury and IRS efforts to identify and notify individuals about their eligibility for an EIP, and we will review how many taxpayers claim an EIP as part of their 2020 tax filing.
Recommendation 11. The Director of the Office of Management and Budget (OMB), in consultation with Treasury, should issue the addendum to the 2020 Compliance Supplement as soon as possible to provide the necessary audit guidance.
Status: Closed
Comment: OMB neither agreed nor disagreed with the recommendation. OMB issued the 2020 Compliance Supplement Addendum on December 22, 2020.
Recommendation 12. The Director of CDC should ensure that, as it makes updates to its federal guidance related to reassessing schools’ operating status, the guidance is cogent, clear, and internally consistent.
Status: Open
Comment: CDC agreed with our recommendation, and in its December 2020 update, noted having taken steps to synchronize content across its website so that when information is updated, it will update not just in one place, but across the entire site. However, this recommendation remains open as of January 6, 2021, CDC’s guidance related to school operating status continues to contain contradictory statements across documents. We will continue to review guidance from CDC.
Recommendation 13. The Secretary of Homeland Security, in coordination with the Secretary of Defense, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic.
Status: Open
Comment: DHS disagreed with our recommendation. A DOD official said that DOD and DHS met in December 2020 to discuss potential revisions to the 2019 National Interest Action code memorandum of agreement. Following that meeting, the DOD official said that DHS and DOD have begun the process of updating the agreement to clarify the steps they take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close a National Interest Action code. When finalized, we will review the updated agreement to determine whether it meets the intent of our recommendation.
Recommendation 14. The Secretary of Defense, in coordination with the Secretary of Homeland Security, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic.
Status: Open
Comment: DOD disagreed with our recommendation. A DOD official said that DOD and DHS met in December 2020 to discuss potential revisions to the 2019 National Interest Action code memorandum of agreement. Following that meeting, the DOD official said that DHS and DOD have begun the process of updating the agreement to clarify the steps they take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close a National Interest Action code. When finalized, we will review the updated agreement to determine whether it meets the intent of our recommendation.
Recommendation 15. The Secretary of Health and Human Services, in consultation with the Centers for Medicare & Medicaid Services (CMS) and CDC, should develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively back to January 1, 2020, and to clarify the extent to which nursing homes have reported data before May 8, 2020. To the extent feasible, this strategy to capture more complete data should incorporate information nursing homes previously reported to CDC or to state or local public health offices.
Status: Open
Comment: HHS partially agreed with our recommendation. As of October 23, 2020, no specific action had been taken by HHS, although it HHS continues to consider how to implement our recommendation.
Recommendation 16. Based on the imminent cybersecurity threats, the Secretary of Health and Human Services should expedite implementation of our prior recommendations regarding cybersecurity weaknesses at its component agencies.
Status: Open
Comment: HHS agreed with our recommendation and is considering how to implement it. Although HHS has not taken action on this recommendation at the department-level, as of January 2021, the relevant component agencies—the Food and Drug Administration (FDA), CMS, and CDC—have addressed additional cybersecurity weaknesses since we reported in September 2020. Specifically, FDA, CMS, and CDC implemented an additional 54 of our cybersecurity recommendations, bringing the total number of implemented recommendations to 404 of the total 434 we made to these agencies. This reflects a 12-percent increase in corrective actions taken to bolster cybersecurity at the component agencies.
Status of matter and recommendations made in our November 2020 CARES Act report
Matter 1.In November 2020, we suggested that Congress consider, in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments.”
Status: Open
Comment: No new legislation designating executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” has been enacted to date.
Recommendation 1.The Secretary of Health and Human Services should ensure that the Director of CDC clearly discloses the scientific rationale for any change to testing guidelines at the time the change is made.
Status: Open
Comment: HHS concurred with our recommendation, noting that CDC officials typically consult with scientific stakeholders when issuing guidance and that HHS will continue to evaluate its processes in this area. In December 2020, CDC told us that that they continue outreach to scientific experts when considering scientific recommendations; however, CDC’s testing overview page, for example, has yet to include scientific rationale for previous changes to testing guidelines.
Recommendation 2.The Administrator of CMS should quickly develop a plan that further details how the agency intends to respond to and implement, as appropriate, the 27 recommendations in the final report of the Coronavirus Commission on Safety and Quality in Nursing Homes, which CMS released on September 16, 2020. Such a plan should include milestones that allow the agency to track and report on the status of each recommendation; identify actions taken and planned, including areas where CMS determined not to take action; and identify areas where the agency could coordinate with other federal and nonfederal entities.
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. HHS officials highlighted actions that CMS has taken related to Commission recommendations and said it would refer to and act upon the Commission’s recommendations, as appropriate. We maintain that developing a plan that details how CMS will proceed with remaining recommendations, includes milestones, and demonstrates that coordination with other federal and nonfederal stakeholders would improve CMS’s ability to systematically consider the Commission’s recommendations going forward.
Recommendation 3. The Department of Veterans Affairs Under Secretary for Health should develop a plan to ensure inspections of state veterans homes occur during the COVID-19 pandemic—which may include using in-person, a mix of virtual and in-person, or fully virtual inspections.
Status: Open
Comment: VA agreed with our recommendation to develop a plan and provided a targeted completion date of November 2021. We urge VA to move up its targeted completion date, because it cannot ensure the quality of nursing home care provided to veterans in these facilities until it develops a plan to resume these inspections (virtually, in person, or both). Without these inspections, veterans are at risk of receiving poor quality care.
Recommendation 4. VA Under Secretary for Health should collect timely data on COVID-19 cases and deaths in each state veterans home, which may include using data already collected by CMS.
Status: Open
Comment: VA concurred in principle with our recommendation. Consistent with our recommendation, in January 2021, Congress passed and the President signed into law the Johnny Isakson and David P. Roe, M.D. Veterans Health Care and Benefits Improvement Act of 2020, which requires state veterans homes during a covered public health emergency to submit weekly to VA data on the number of (1) suspected and confirmed COVID-19 infections and (2) total deaths and COVID-19 deaths among residents and staff. In addition, the act requires VA to make these data on the total number of residents and staff who are infected with or died from COVID–19 publically available on its website and to update at least weekly. We will monitor VA’s efforts to implement this requirement.
Recommendation 5. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed an economic impact payment notification letter and subsequently filed for and received an economic impact payment, and use that information to inform ongoing outreach and communications efforts.
Status: Open
Comment: Treasury agreed with our recommendation, noting that it intends to begin tracking and publicly reporting the number of individuals who received a notice and subsequently filed for an EIP in January 2021, sooner than it previously planned. Treasury also noted it will use this information to inform outreach and communication efforts.
Recommendation 6. The Commissioner of Internal Revenue should update the Form 1040-X instructions to include information on the electronic filing capability for tax year 2019.
Status: Open
Comment: IRS agreed with our recommendation and said that it would start to update the Form 1040-X instructions to include information on the electronic filing (e-file) capability for tax year 2019.
As of early December 2020, the IRS planned to include this information in the next routine annual update of the instructions with a mid-2021 release, rather than updating them sooner, out of cycle. According to the IRS, the normal revision process takes 10 months to complete properly, and would be difficult to do in a shorter time frame. IRS’s planned revision will occur after the deadline for submitting an application for a tentative refund via the temporary electronic fax procedures, which requires an accompanying Form 1040-X for some taxpayers. This means that taxpayers who filed their 1040-X before the December 31 deadline with the temporary procedures did not find the e-file capability in the form instructions. However, some taxpayers will use Form 1040-X for other CARES refunds after that deadline, so instructions that are updated in 2021 would still help ensure these taxpayers are aware of this option. A timelier update to the instructions would help taxpayers filing the 1040-X between now and when the annual update to the instructions occurs in mid-2021.
In the meantime, IRS previously posted information about the e-file availability on the Form 1040-X product page at IRS.gov, which is referenced in the first paragraph of the Form 1040-X instructions. We will continue to monitor any updates to this page and the instructions.
Recommendation 7. The Secretary of Labor should ensure the Office of Unemployment Insurance revises its weekly news releases to clarify that in the current unemployment environment, the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits.
Status: Closed
Comment: DOL’s weekly news release of December 10, 2020 clarified that the numbers reported for weeks of unemployment insurance (UI) benefits claimed do not represent the number of unique individuals claiming benefits.
Recommendation 8. The Secretary of Labor should ensure the Office of Unemployment Insurance pursues options to report the actual number of distinct individuals claiming benefits, such as by collecting these already available data from states, starting from January 2020 onward.
Status: Open
Comment: DOL partially agreed with our recommendation. Specifically, DOL agreed to pursue options to report the actual number of distinct individuals claiming UI benefits. However, DOL did not agree with the retroactive effective date of the reporting. DOL indicated that state UI programs may face challenges implementing any new reporting requirements, particularly retroactively. In addition, DOL stated that the CARES Act UI provisions are scheduled to expire in December 2020 and noted that requirements to provide notice and comment for the new data collection could take up to a year to complete, further reducing the utility of retroactive reporting.
We maintain that DOL should pursue options to report the actual number of distinct individuals claiming UI benefits, retroactive to January 2020. These data are vital to understanding how many individuals are receiving UI benefits, as well as the size of the population supported by the UI system during the pandemic. We acknowledge that certain provisions of the CARES Act were scheduled to expire in December 2020 and that the process to begin collecting new data may take months. However, our recommendation to pursue options to report on the number of distinct individuals claiming benefits applies to the CARES Act UI programs as well as the regular UI program, which has not expired.
Even if the information is unavailable for some time, reporting numbers retroactively, beginning with calendar year 2020, will help DOL and policy makers identify lessons learned about the administration and utilization of regular and expanded UI benefits programs during the pandemic. As of September 30, 2020, hundreds of billions of dollars have been obligated for UI programs as part of COVID-19 relief funds. Given this substantial investment, an accurate accounting of the size of the population supported by this funding, even retroactively, may be critical to understanding the efficiency and effectiveness of the nation’s response to unemployment during the pandemic.
DOL has reported flawed estimates of the number of individuals receiving benefits each week throughout the pandemic. This record should be corrected so that future analyses of the effects of expanded UI benefits rely on accurate information. Retroactive data collection and reporting would provide an opportunity for future analyses to identify lessons learned from the pandemic, which could be valuable in considering policy solutions to address any future economic disruptions of a similar magnitude. In addition, establishing a way of accurately reporting the number of individuals claiming benefits now would help ensure DOL is ready to report this information in real time in the future, especially in times of increased demand and if the expanded UI programs are reauthorized.
We encourage DOL to pursue options to report the actual number of individuals claiming benefits in the most feasible and least burdensome way. Collecting already available data from states is one way DOL can address the recommendation, but DOL could also develop other ways of gathering and reporting this information.
Recommendation 9. The Director of OMB should develop and issue guidance directing agencies to include COVID-19 relief funding with associated key risks, such as provisions contained in the CARES Act and other relief legislation that potentially increase the risk of improper payments or changes to existing program eligibility rules, as part of their improper payment estimation methodologies. This should especially be required for already existing federal programs that received COVID-19 relief funding.
Status: Open
Comment: As of January 2021, OMB has not issued new guidance to address our recommendation. In January 2021, OMB staff stated they believe current OMB guidance sufficiently addresses our recommendation and concerns. In November 2020, we reported that although OMB issued a memorandum providing agencies the option to incorporate new COVID-19 relief funding into their normal sampling processes, it did not specifically direct agencies to do so. In addition, the guidance did not direct agencies to consider associated risks, such as changes to eligibility rules and different payment processes, as part of their improper payment estimation methodologies. Further, OMB staff stated that OMB is actively coordinating and engaging with the Pandemic Response Accountability Committee and Inspectors General to share and discuss information relevant to COVID-19 spending risks and improper payment reduction strategies. We continue to maintain that without OMB guidance for agencies to include COVID-19 relief funding and associated key risks, as part of their improper payment estimation methodologies, agencies are at increased risk that their processes may not result in reliable estimates, calling into question their usefulness for developing effective corrective actions.
Recommendation 10. The Administrator of SBA should expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread.
Status: Open
Comment: SBA neither agreed nor disagreed with our recommendation, stating that it is planning to conduct improper payment testing for PPP. However, SBA has not finalized the plan for estimating improper payments for its PPP. Therefore, we maintain that our recommendation is important to help expedite the identification and reduction of improper payments. The Consolidated Appropriations Act, 2021, requires SBA to submit to the Senate and House Small Business Committees an audit plan that details the policies and procedures for conducting forgiveness reviews and audits of PPP loans within 45 days of enactment and to provide monthly updates thereafter. The act also requires SBA to respond to requests from GAO within 15 days (or such later date as the Comptroller General may specify) or report to Congress on the reasons for the delay.
Recommendation 11. The Secretary of the Treasury should finish developing and implement a compliance monitoring plan that identifies and responds to risks in the Payroll Support Program to ensure program integrity and address potential fraud, including the use of funds for purposes other than for the continuation of employee wages, salaries, and benefits.
Status: Open
Comment: Treasury neither agreed nor disagreed with our recommendation, but committed to reviewing additional measures that may further enhance its compliance monitoring and ensure that Payroll Support Program funds are used as intended.
Status of recommendation made in our November 2020 report on vaccines and therapeutics
Recommendation 1. The Secretary of Health and Human Services should direct the FDA Commissioner to identify ways to uniformly disclose to the public the information from FDA’s scientific review of safety and effectiveness data—similar to the public disclosure of the summary safety and effectiveness data supporting the approval of new drugs and biologics—when issuing emergency use authorizations (EUA) for therapeutics and vaccines, and, if necessary, seek the authority to publicly disclose such information.
Status: Closed.
Comment: In response to our recommendation, FDA said it would explore approaches to achieve the goal of transparency. On November 17, 2020, FDA made an announcement on the agency’s ongoing commitment to transparency for COVID-19 EUA. FDA also developed a process to disclose its scientific review documents for therapeutic EUAs and released such summaries for one previous therapeutic EUA and the two additional therapeutic EUAs issued since our recommendation. These summaries disclosed information similar to what FDA releases to support new drug approvals and biologic licensures. Additionally, for the two vaccine EUAs FDA issued since our recommendation, FDA released decision memos containing detailed information about FDA’s review of safety and effectiveness data. FDA’s actions meet the intent of our recommendation and will improve transparency.
Appendix IV: Comments from the Department of Health and Human Services
Governmentwide Treasury Account Symbol Adjusted Trial Balance System
HHS
Department of Health and Human Services
IRS
Internal Revenue Service
NIA
National Interest Action
NOAA
National Oceanic and Atmospheric Administration
OMB
Office of Management and Budget
OSHA
Occupational Safety and Health Administration
PPP
Paycheck Protection Program
PSP
Payroll Support Program
PUA
Pandemic Unemployment Assistance
SAR
suspicious activity report
SBA
Small Business Administration
SNS
Strategic National Stockpile
SSA
Social Security Administration
Treasury
Department of the Treasury
TSA
Transportation Security Administration
UI
unemployment insurance
VA
Department of Veterans Affairs
End Notes
[1]Worldwide data from the World Health Organization reflect laboratory-confirmed cases and deaths reported by countries and areas. Data on COVID-19 cases in the U.S. are based on aggregate case reporting to the Centers for Disease Control and Prevention (CDC) and include probable and confirmed cases as reported by states and jurisdictions. CDC COVID-19 counts are subject to change due to delays or updates in reported data from states and territories. According to CDC, the actual number of COVID-19 cases is unknown for a variety of reasons, including that people who have been infected may have not been tested or may have not sought medical care. CDC’s National Center for Health Statistics COVID-19 death counts in the U.S. are based on provisional counts from death certificate data, which do not distinguish between laboratory-confirmed and probable COVID-19 deaths. Provisional counts are incomplete due to an average delay of 2 weeks (a range of 1–8 weeks or longer) for death certificate processing.
[2]Bureau of Labor Statistics, Unemployment Level (UNEMPLOY), retrieved from FRED, Federal Reserve Bank of St. Louis, accessed January 12, 2021, https://fred.stlouisfed.org/series/UNEMPLOY.
[3]Pub. L. No. 116-136, 134 Stat. 281 (2020). As of January 1, 2021, four other relief laws were also enacted in response to the COVID-19 pandemic: the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146. In this report, we refer to these five laws, each of which was enacted as of January 1, 2021, and provides appropriations for the COVID-19 response, as “COVID-19 relief laws,” and the funding appropriated by these laws as “COVID-19 relief funds.”
[4]Pub. L. No. 116-136, § 19010, 134 Stat. at 579-81.
[5]GAO, COVID-19: Urgent Actions Needed to Better Ensure an Effective Federal Response, GAO-21-191 (Washington, D.C.: Nov. 30, 2020); COVID-19: Federal Efforts Accelerate Vaccine and Therapeutics Development, but More Clarity Needed, GAO-21-207 (Washington D.C.: Nov. 17, 2020); COVID-19: Federal Efforts Could Be Strengthened by Timely and Concerted Actions, GAO-20-701 (Washington, D.C.: Sept. 21, 2020); COVID-19: Brief Update on Initial Federal Response to the Pandemic, GAO-20-708 (Washington, D.C.: Aug. 31, 2020); and COVID-19: Opportunities to Improve Federal Response and Recovery Efforts, GAO-20-625 (Washington, D.C.: June 25, 2020).
[6]CDC COVID-19 counts are subject to change due to delays or updates in reported data from states and territories.
[7]The 52 states and jurisdictions include all 50 states, Washington, D.C., and New York City. COVID-19 case counts for New York City are reported separately from New York State. We defined states as holding steady if they had less than a 1 percent increase or decrease in average daily new cases over the time frame. The average percent change in daily new cases was calculated as the average of the daily rates of change of the 7-day moving average between December 31, 2020, and January 13, 2021. Centers for Disease Control and Prevention COVID Data Tracker data were accessed on January 14, 2021. COVID-19 case reporting was likely affected by reporting delays during the holidays and should be interpreted with caution.
[9]BLS conducts surveys of households and businesses that differ in scope, which may result in different measures of employment between the two surveys. For example, the household survey includes self-employed workers whose businesses are unincorporated, and unpaid family workers, agricultural workers, and private household workers, who are excluded by the survey of businesses, also known as the establishment survey. In addition, in the household survey, individuals are counted only once even if they have more than one job. In the survey of businesses, employees working at more than one job and thus appearing on more than one payroll are counted separately for each appearance.
[10]The employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population age 16 and over. The ratio is subject to misclassification errors with respect to consistently identifying workers as employed and absent from work or unemployed on temporary layoff.
[11]An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes. This amount does not include appropriations enacted in the Consolidated Appropriations Act, 2021, as appropriations warrant information issued by the Department of the Treasury was not available at the time of our analysis. The House Committee on Appropriations estimates that provisions of the Consolidated Appropriations Act, 2021 provide an additional $900 billion in appropriations for emergency coronavirus relief, and the Congressional Budget Office estimates that outlays for coronavirus response and relief provided in divisions M and N of the Act will total about $868 billion. An outlay refers to the issuance of checks, disbursement of cash, or electronic transfer of funds made to liquidate a federal obligation. We will examine and report appropriations enacted in the Consolidated Appropriations Act, 2021 in future reporting.
[12]An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of the other party beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. Increased spending in Medicaid is not accounted for in the appropriations provided by the COVID-19 relief laws. Federal agencies use GTAS to report proprietary financial reporting and budgetary execution information to Treasury.
[13]The Small Business Administration’s Business Loan Program account includes activity for the Paycheck Protection Program and certain loan subsidies.
[14]We requested the funding and spending information for the six largest areas as of December 31, 2020, from the applicable agencies. We did not receive all of the necessary information to include in this report; it will be incorporated into our March report. Therefore, we are reporting the amounts as of November 30, 2020.
[15]A. Nicole Clowers, Managing Director of GAO’s Health Care team, Roundtable: Are We Prepared? Protecting the U.S. from Global Pandemics, testimony before the Senate Committee on Homeland Security and Governmental Affairs. 116th Cong., 2nd sess., Feb. 12, 2020.
[16]Pub. L. No. 116-260, 134 Stat. 1182. In addition, the Johnny Isakson and David P. Roe, M.D. Veterans Health Care and Benefits Improvement Act of 2020—enacted in January 2021—requires action by the Department of Veterans Affairs (VA) that will address one of our prior recommendations to improve veteran health care during the pandemic. Pub. L. No. 116-315, § 3003, 134 Stat. 4932, 4990-91 (2021).
[17]The key components within DOD and HHS that provide support to Operation Warp Speed include DOD’s Joint Program Executive Office for Chemical, Biological, Radiological, and Nuclear Defense and HHS’s Biomedical Advanced Research and Development Authority, CDC, and the National Institutes of Health.
[18]There were no FDA-licensed COVID-19 vaccines as of January 8, 2021. Any COVID-19 vaccine that is authorized for emergency use is expected to ultimately be reviewed and receive licensure through a biologics license application, according to FDA guidance.
[19]The Secretary of Health and Human Services may declare that circumstances, prescribed by statute, exist justifying the emergency use of certain medical products. Once a declaration has been made, FDA may temporarily allow use of unapproved medical products or unapproved uses of approved medical products through an EUA. For FDA to issue an EUA, it must be reasonable to believe that the medical product may be effective and that the known and potential benefits of the product outweigh the known and potential risks, among other statutory criteria. See 21 U.S.C. § 360bbb-3.
[20]FDA approved remdesivir for the treatment of COVID-19 in adults and pediatric patients (12 years of age and over weighing at least 40 kg) requiring hospitalization. As of January 8, 2021, five therapeutics were authorized for emergency use by FDA for the treatment of COVID-19: remdesivir, COVID-19 convalescent plasma, bamlanivimab, baricitinib in combination with remdesivir, and casirivimab and imdevimab. The EUA for remdesivir remains in effect for other pediatric patients not covered by the approval.
[22]CDC’s Advisory Committee on Immunization Practices is comprised of medical and public health experts who make recommendations on the use of vaccines in the civilian population of the U.S. Its recommendations serve as public health guidance for safe use of vaccines and other related products and are not binding; jurisdictions can adopt different approaches.
[24]Pub. L. No. 116-260, div. M, tit. III, 134 Stat. at 1912.
[25]From October 10 through October 21, 2020, we fielded a survey to senior public health and emergency management officials in the 50 states; Washington, D.C.; and the five U.S. territories to gain their perspectives on the availability of personal protective equipment, testing, and vaccine administration supplies. We received 47 survey responses representing 41 states; Washington, D.C.; and all five territories.
[26]Office of the Assistant Secretary for Preparedness and Response officials informed us that the strategy would be finalized in January, but as of January 13, 2021, that had not occurred and our review is based on a draft of the strategy.
[28]Molecular viral tests detect the presence of genetic material from SARS-CoV-2, the virus that causes COVID-19. The antigen viral tests detects the presence of a protein that is part of SARS-CoV-2. Non-diagnostic COVID-19 serology tests, known as antibody tests, are used to detect antibodies produced in patients who have had COVID-19.
[29]The six desirable characteristics of an effective national strategy are clear purpose, scope, and methodology; problem definition and risk assessment; goals, subordinate objectives, activities, and performance measures; resources, investments, and risk management; organizational roles, responsibilities, and coordination; and integration and implementation. Each characteristic has several sub-elements. See GAO, Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism, GAO-04-408T (Washington, D.C.: Feb. 3, 2004).
[30]Pub. L. No. 116-260, div. W, tit. VI, § 621(b), 134 Stat. at 2403-04 (2020).
[31]The CARES Act relaxed certain limitations on the use of other transaction agreements for HHS and DOD—which can enable agencies to negotiate terms and conditions specific to a project—such as congressional reporting requirements and requirements for who can approve certain transactions. Pub. L. No. 116-136, §§ 3301, 13006, 134 Stat. at 383, 522.
[32]Pub. L. No. 116-136, § 12005(d), 135 Stat. at 518. An additional $300 million for certain COVID-19-related fisheries disaster assistance was appropriated under the Consolidated Appropriations Act, 2021, enacted on December 27, 2020. Pub. L. No. 116-260, div. M, tit. I, 134 Stat. at 1909-10. This report does not provide information on that additional funding.
[33]Office of Management and Budget, Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019 (COVID-19) (Washington D.C.: Apr. 10, 2020).
[34]The Consolidated Appropriations Act, 2021 appropriated additional funding for certain EIDL advances and amended the CARES Act requirements related to loans and advances, including advances targeted at businesses in low-income communities. Pub. L. No. 116-260, div. N, tit. III, §§ 331-32, 134 Stat. at 2043-46. The act also authorized additional PPP loans through March 31, 2021—increasing the commitment from $659 billion to $806.45 billion—allows additional businesses to receive the loans, expands the list of allowable uses of proceeds and loan forgiveness, and allows PPP borrowers to receive a second PPP loan of up to $2 million upon meeting certain criteria. Pub. L. No. 116-260, div. N, tit. III, §§ 304, 311, 316-18, 323, 134 Stat. at 1993-96, 2001-07, 2011-13, 2018-22.
[35]In November 2020, one of these individuals was sentenced to 12 months in prison and 2 years of supervised release. In December 2020, another individual was sentenced to 24 months in prison and 5 years of supervised release.
[36]A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[37]Certain financial institutions are required to file a suspicious activity report (SAR) when a transaction involves or aggregates at least a certain dollar amount in funds or other assets (generally $5,000), and the institution knows, suspects, or has reason to suspect that the transaction is designed to evade any Bank Secrecy Act requirements or involves funds derived from criminal activities. See e.g. 31 C.F.R. § 1020.320 (2019). Under the Bank Secrecy Act’s implementing regulations, banks are also required to file a SAR when a transaction meets certain other criteria, such as for known or suspected criminal violations involving insider abuse of any amount. See 12 C.F.R. §§ 21.11(c)(1), 163.180(d)(3)(i), 208.62(c)(1), and 353.3(a)(1) (2020).
[38]In November 2020, we reported that, to facilitate implementation of the PUA program, most states decided to initially pay PUA claimants the minimum allowable benefit, and then recalculate benefits at a later point based on claimants’ documentation of their prior earnings, as set by DOL guidance. Data reported by states as of January 11, 2021, suggest that many states were paying claimants minimum PUA benefits in November 2020.
[39]Under the Consolidated Appropriations Act, 2021, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount, but the state can waive that requirement if the individual was without fault and repayment would be contrary to equity and good conscience. Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. at 1952. On January 8, 2021, DOL issued new guidance and updated instructions for reporting PUA program activities.
[40]See Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, div. A, tit. II, 134 Stat. at 147; and CARES Act, Pub. L. No. 116-136, § 1110, 134 Stat. at 306-08.
[41]Pub. No. No. 116-260, div. N, tit. III, § 332(1), 134 Stat. at 2045.
[42]In December 2020, the Department of Health and Human Services began publishing a Community Profile Report with information on COVID-19 indicators at the county, state, and national levels. These reports are available online at: https://beta.healthdata.gov/National/COVID-19-Community-Profile-Report/gqxm-d9w9 (accessed Jan. 14, 2021). We plan to obtain input from our group of experts regarding HHS’s communication of COVID-19 information in this report and elsewhere.
[43]In our November 2020 report, we obtained input on COVID-19 health indicators and data that inform the indicators from five experts. In this report, we also obtained input on these issues from an additional five experts.
[44]Viral tests provide data on ongoing infections, while antibody tests provide data on prevalence of past infections. A higher positivity rate could indicate that not enough testing is being conducted to find and isolate infected individuals before they spread the disease further.
[45]Antigen tests are a type of viral test that detect the presence of a protein that is part of the virus, while molecular diagnostic viral tests detect the presence of genetic material from the virus.
[47]See 85 Fed. Reg. 54,820 (Sept. 2, 2020) (requiring certain hospitals that participate in Medicare or Medicaid to report information in accordance with a frequency and format specified by the Secretary of Health and Human Services during the COVID-19 public health emergency).
[48]COVID-NET is a surveillance system that collects data on COVID-19 hospitalizations that are confirmed by laboratory testing.
[49]Resolve to Save Lives is a public health organization focused on preventing deaths from epidemics, and it is part of Vital Strategies, a global public health organization that works with governments to help address public health challenges such as epidemics.
[50]Centers for Disease Control and Prevention, “Updated Guidelines for Evaluating Public Health Surveillance Systems,” Morbidity and Mortality Weekly Report, vol. 50, no. RR-13 (2001).
[51]For our November report, we met with five other experts we identified with assistance from the National Academies. We obtained their input on the COVID-19 health indicators we previously reported on, suggestions for additional indicators, and on data that inform the indicators.Among others, the health indicators we reported on included higher than expected deaths, COVID-19 test positivity rate (as a measure of testing sufficiency), and ICU bed availability.
[52]The Weekly Economic Index combines high-frequency economic data from a wide range of sources. See Daniel J. Lewis, Karel Mertens, and Jim Stock, U.S. Economic Activity during the Early Weeks of the SARS-Cov-2 Outbreak, Federal Reserve Bank of New York Staff Report No. 920 (April 2020).
[53]We identified a number of economic indicators to facilitate ongoing and consistent monitoring of areas of the economy supported by the federal pandemic response. To the extent that federal pandemic responses are effective, we would expect to see improvements in outcomes related to these indicators. However, while trends in these indicators may be suggestive of the effect of provisions of the COVID-19 relief laws over time, those trends will not on their own provide definitive evidence of effectiveness. Division N of the Consolidated Appropriations Act, 2021, provides additional support for areas of the economy we have been monitoring, including labor markets, households, and small businesses, through, for example, direct payments to individuals and families, additional support for unemployed workers, and continuation of small business support.
[54]BLS conducts surveys of households and businesses that differ in scope, which may result in different measures of employment between the two surveys. For example, the household survey includes self-employed workers whose businesses are unincorporated, unpaid family workers, agricultural workers, and private household workers who are excluded by the survey of businesses, also known as the establishment survey. In addition, in the household survey, individuals are counted only once even if they have more than one job. In the survey of businesses, employees working at more than one job and thus appearing on more than one payroll are counted separately for each appearance.
[55]The CARES Act provides temporary protections for millions of households against foreclosure and eviction, as well as temporary forbearance on mortgage payments. In fiscal year 2020, for example, 34.2 percent of all FHA purchase and refinance borrowers were minorities, 50.4 percent of FHA forward mortgage borrowers were of low-to-moderate income, and 83.1 percent of home purchasers under the FHA forward mortgage insurance program were first-time homebuyers. See U.S. Department of Housing and Urban Development, FHA Annual Management Report Fiscal Year 2020. Although FHA includes loans under active consideration for loss mitigation foreclosure in its delinquency counts, the CARES Act includes a provision (Section 4021) to protect the credit of consumers who reach an agreement with their lender to delay or otherwise modify payments because of the COVID-19 pandemic.
[56]Spreads on corporate bonds relative to benchmark interest rates (e.g., Treasury interest rates) measure the premium corporate borrowers must pay to compensate lenders for taking on the risk of loss due to default (risk premium) and for foregoing investments in more liquid assets (liquidity premium).
[57]Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1920 (2020); Pub. L. No. 116-139, div. B, tit. I, 134 Stat. 620, 622 (2020); Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 563 (2020). The Consolidated Appropriations Act, 2021, also provided that not less than 85 percent of Provider Relief Fund funds unobligated as the date of enactment and funds recovered from providers after the date of enactment shall be for any successor to the Phase 3 General Distribution to reimburse health care providers based on applications that consider financial losses and changes in operating expenses attributable to COVID-19 occurring in the third and fourth quarters of 2020 and the first quarter of 2021.
[58]The Accelerated Payments Program provides loans to Part A providers and the Advance Payments Program provides loans to Part B suppliers.
[59]HHS uses the term “allocations” to describe the funding amounts it has set aside for particular purposes or for particular types of health care providers. The $145 billion includes $0.980 billion for administration.
[60]An additional estimated $8 billion was disbursed from December 1, 2020, through December 31, 2020.
[62]MITRE, Coronavirus Commission on Safety and Quality in Nursing Homes: Commission Final Report, PRS Release Number 20-2382, September 2020.
[63]COVID-19 has affected vulnerable populations in other settings beyond nursing homes, including assisted living facilities. However, as the federal role in oversight of nursing homes is more significant than in other settings such as assisted living facilities, the federal response has been more focused on nursing homes.
[65]According to CMS, as of September 30, 2020, it obligated almost $19 million. In fiscal year 2021, the agency indicated it plans to obligate about $28 million.
[66]As of November 2020, CDC defines a confirmed case as having a positive COVID-19 test resulting from a molecular test, a nucleic acid test, or an antigen test, including antigen point-of-care test results.
[67]These numbers are likely underreported because they do not include data for the 1,467 nursing homes (about 9.6 percent) that did not report COVID-19 data to CDC for the week ending December 6, 2020, or that submitted data that failed data quality assurance checks. Additionally, as we previously reported, CMS does not require nursing homes to report data prior to May 8, 2020; while some nursing homes may have reported such data, the data set does not currently identify which reported cases and deaths occurred prior to May 8. Further, according to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time. Data presented in this enclosure reflect the data downloaded as of December 17, 2020, which includes data through the week ending December 6, 2020.
[68]The week ending May 31 is the first single week of data reported to CDC. The only earlier week of data, for the week ending May 24, could potentially include cases and deaths for multiple weeks dating back to January 1, 2020, for those homes which voluntarily reported such data, and is therefore not comparable with data for other weeks.
[69]CMS guidance states that in-person ombudsmen access should be restricted if there are concerns about infection control and transmission of COVID-19, although the guidance also emphasizes that facilities must facilitate resident communication with ombudsmen (e.g., by phone) in cases where in-person access is restricted.
[70]The guidance allowed nursing homes to resume visitations depending on the degree of community spread and required that these visitations be conducted according to a nursing home’s structure and resident needs. For example, it notes that outdoor visits are preferred due to the reduced risk of transmission, recommends limits on the number of visitors, and recommends that visitors be tested for COVID-19 prior to visiting. Centers for Medicare & Medicaid Services, Nursing Home Visitation—COVID-19, QSO-20-39-NH (Baltimore, Md.: Sept. 17, 2020).
[71]Our November report covered data nursing homes self-reported to CDC as of October 4, 2020.
[72]As of December 6, 2020, about 3 percent of nursing homes (a decrease of 3 percentage points) reported that they had no remaining supplies of at least one of these types of PPE.
[73]CMS’s response to the Commission’s report notes that, among other things, the Federal Emergency Management Agency (FEMA) provided 14-day supply shipments to nursing homes beginning in April 2020 and that HHS shipped N95 respirators from the Strategic National Stockpile to nursing homes beginning in August 2020. This consisted of sending a 7-day supply of N95 respirators to about 3,336 nursing homes. However, one-time shipments of 1- to 2-week supplies of PPE do not meet the Nursing Home Commission’s recommendation that CMS help homes to sustain a 3-month supply of PPE on an ongoing basis. CMS told GAO that PPE acquisition is outside the agency’s purview.
[74]CMS released guidance on Prioritization of Survey Activities in March 2020 and updated the guidance in September 2020 that refers to CDC guidance for using PPE. See Centers for Medicare & Medicaid Services, Prioritization of Survey Activities, QSO-20-20-ALL (Baltimore, Md.: Mar. 20, 2020). CDC developed guidance for optimizing supplies of PPE and other equipment during shortages. The guidance offers different measures based on three tiers of surge capacity – conventional, contingency, and crisis capacity. This guidance can be used by health care providers to prioritize and conserve PPE supplies along the continuum of care. See Centers for Disease Control and Prevention, “Optimizing Supply of PPE and Other Equipment during Shortages,” accessed December 9, 2020, https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/general-optimization-strategies.html.
[75]Our November report covered data nursing homes self-reported to CDC as of October 4, 2020.
[76]According to CDC, aides include certified nursing assistants, nurse aides, medication aides, and medication technicians; nursing staff include registered nurses, licensed practical nurses, and vocational nurses; clinical staff include physicians, physician assistants, and advanced practice nurses; and other staff include any staff not included in the other three categories, such as cooks, pharmacists, and physical therapists.
[77]The Nursing Home Commission recommended that CMS increase wages for nursing home staff through Medicare and Medicaid payment reform.
[78]Medicare and Medicaid Programs, Clinical Laboratory Improvement Amendments (CLIA), and Patient Protection and Affordable Care Act; Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency; 85 Fed. Reg. 54,820 (Sept. 2, 2020) (to be codified at 42 C.F.R. § 483.80(h)). CMS later released guidance on these testing requirements, noting that nursing homes should prioritize testing staff and residents with symptoms of COVID-19 first; followed by performing testing of all staff and residents in the case of an outbreak; and, finally, routine staff testing based on the degree of community spread, ranging from testing staff once a month in counties with low community spread to twice a week in counties with high community spread. On September 29, 2020, CMS announced an update to the methodology for determining the level of community spread, adding consideration of the number of tests performed in a county to the existing consideration of a county’s positivity rate. Department of Health and Human Services, Centers for Medicare & Medicaid Services, CMS Updates COVID-19 Testing Methodology for Nursing Homes (Baltimore, Md.: Sept. 29, 2020), accessed October 1, 2020, https://www.cms.gov/newsroom/press-releases/cms-updates-covid-19-testing-methodology-nursing-homes.
[79]Data for the weeks ending November 29, 2020 and December 6, 2020 were incomplete for this data field.
[80]In the week ending August 16, about 7 percent of nursing homes (about 1,000) reported that they would be unable to test all staff within the next week, if needed, and about 6 percent (about 900) nursing homes reported that they would be unable to test all residents.
[81]Testing data are available from CDC beginning with the week ending August 16, 2020. Some nursing homes may have used POC testing prior to CDC beginning its collection of testing data.
[82]On October 19, 2020, HHS updated requirements for CMS certified long-term care facilities, including nursing homes to report all POC antigen test results through CDC’s National Healthcare Safety Network application (NHSN). NHSN routes the POC laboratory test data to the public health agency at the local or state level that has jurisdictional authority and responsibility to receive those data. Health agencies, in turn, will use the data to fulfill their public health functions, which include reporting to HHS, where the data will be used in the COVID-19 response. However, according to officials we interviewed from two nursing home associations, the test reporting system requires lengthy enrollment procedures and burdensome data requirements that have delayed adoption. Also, because of delayed implementation and questions of interoperability, some states still require all nursing homes to report testing results directly to state and local reporting systems. Therefore, nursing homes may face duplicate reporting requirements that, according to officials from two nursing home associations we interviewed, increase the burden on nursing home staff. CDC officials indicated that the agency is working on solutions to address these challenges. According to CDC, as of November 13, 2020, 1,574 facilities have reported POC records in the new NHSN POC reporting tool.
[83]Molecular tests detect the virus’s genetic material, while antigen tests detect certain proteins on the surface of the virus. The antigen tests provided by HHS can produce results within approximately 15 minutes, which can be significantly faster than waiting for results from molecular tests, most of which rely on polymerase-chain reaction technology and typically must be processed in a laboratory.
[84]As part of the program, vaccines will be provided with no out-of-pocket costs for residents or staff, or costs to the facilities. The pharmacy will schedule and coordinate on-site vaccination clinic dates; order vaccines and associated supplies; ensure cold chain management for the vaccine; provide on-site administration; report required vaccination data to local, state, and federal jurisdictions; and adhere to all applicable CMS COVID-19 testing requirements for facility staff.
[85]According to data presented at the December 1, 2020, advisory committee meeting, there are approximately 21 million health care personnel and an additional 1.3 million skilled nursing facility residents who are included in the initial prioritized group to receive the vaccinations. See Kathleen Dooling, “Phased Allocation of COVID-19 Vaccines” (presented at the Centers for Disease Control and Prevention Advisory Committee on Immunization Practices meeting, Dec. 1, 2020).
[86]The agreement with CVS and Walgreens covers nursing homes within 75 miles of a CVS or Walgreens store. According to one nursing home association, this covers about 85 percent of all nursing homes in the U.S.
[87]Nursing homes without policies and procedures in place to ensure that residents are offered vaccinations, such as the influenza and pneumococcal vaccination, can be cited as having an infection control deficiency during a state survey.See GAO, Infection Control Deficiencies Were Widespread and Persistent in Nursing Homes Prior to COVID-19 Pandemic. GAO-20-576R (Washington, D.C.: May 20, 2020). Officials from one nursing home association confirmed that CMS has not provided information on whether COVID-19 vaccinations would be treated the same way.
[88]We analyzed the most recent data available on December 17, 2020. The CDC data on COVID-19 in nursing homes were accessed on December 17, 2020, for the week ending December 6, 2020, from https://data.cms.gov/Covid19-nursing-home-data. For the data on COVID-19 in nursing homes, we analyzed and reported data that had been determined by CDC and CMS to pass quality assurance checks for data entry errors. According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time.
[89]We also recommended in September 2020 that (1) HHS and FEMA immediately document roles and responsibilities for supply chain management functions transitioning to HHS and (2) HHS and FEMA work with relevant stakeholders to devise interim solutions to help states enhance their ability to track the status of supply requests and plan for supply needs. HHS and the Department of Homeland Security disagreed with these recommendations.
[90]See 85 Fed. Reg. 86,835, 86,836 (Dec. 31, 2020). In this temporary final rule, FEMA also added specific types of syringes and hypodermic needles to the list of items that may not be exported because the projected domestic supply of them is not expected to meet demand.
[92]As of December 18, 2020, ASPR officials reported that the SNS contained 72 million gloves (inventory goal of 4.5 billion), 190 million N95 respirators (inventory goal of 300 million), 201 million surgical or procedural masks (inventory goal of 400 million), 108.7 million gown equivalents or coveralls (inventory goal of 265 million), and 19 million eye protection or face shields (inventory goal of 18 million).
[93]Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, Pub. L. No. 116-22, § 403(a)(5), 133 Stat. 905, 946-47; CARES Act, Pub. L. No. 116-136, § 19010, 134 Stat. 281, 579-81 (2020).
[94]This effort was sometimes referred to as the “National Pharmaceutical Stockpile” in annual appropriations acts. Since its inception, the stockpile has been the responsibility of HHS except for a brief period from 2002 to 2004 when it was transferred to the Department of Homeland Security (DHS). The Secretary of Health and Human Services transferred responsibility for the SNS from the Centers for Disease Control and Prevention to ASPR in 2018. Other agencies have had a role in coordinating with HHS on stockpiling activities, including DHS and the Department of Veterans Affairs.
[95]Pub. L. No. 107-188, § 121, 116 Stat. 594, 611-13 (2002) (codified, as amended, at 42 U.S.C. § 247d-6b).
[96]PHEMCE was established in 2006 and codified under the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019. Pub. L. No. 116-22, § 402, 133 Stat. at 942-43 (codified at 42 U.S.C. § 300hh-10a). PHEMCE is responsible for providing recommendations to the Secretary of Health and Human Services on medical countermeasure priorities, and coordinates the life cycle of medical countermeasure research beginning at basic research. PHEMCE includes certain HHS agencies, as well as the Departments of Defense, Veterans Affairs, Homeland Security, and Agriculture, and the Office of the Director of National Intelligence. Medical countermeasures are drugs, biologics, and devices, such as personal protective equipment, used to diagnose, treat, prevent, or mitigate harm from any chemical, biological, radiological, and nuclear agent.
[97]See National Biodefense Science Board and the Office of Public Health Preparedness and Response Board of Scientific Counselors, Anticipated Responsibilities of the SNS in the Year 2020: An Examination with Recommendations, April 3, 2013, accessed June 1, 2020, https://www.phe.gov/Preparedness/legal/boards/nbsb/recommendations/Documents/nbsb-bsc-sns-2020-final.pdf. Among other actions, the work group recommended actions for the SNS to meet its anticipated responsibilities.
[98]The SNS maintains an $8 billion supply of other materials, such as antibiotics, vaccines, antitoxins, and antivirals, according to HHS documents.
[99]In addition to staff within the HHS Office of the Secretary and ASPR, the work group also included officials from the Federal Emergency Management Agency, Department of Defense, Department of Commerce, Department of Veterans Affairs, Supply Chain Advisory Group, Office of Management and Budget, and the Office of Trade and Manufacturing Policy.
[100]As of January 01, 2021, the five relief laws enacted to assist the response to COVID-19 were the Consolidated Appropriations Act, 2021, Pub. L. No. 116-620, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[101]These obligations do not reflect obligations of amounts provided under the Consolidated Appropriations Act, 2021, enacted on December 27, 2020. That law appropriated $705 million specifically for the SNS, and authorizes the Secretary to use up to an additional $3.25 billion in appropriations provided under the law for the SNS.
[102]ASPR officials informed us that the strategy would be finalized in January, but as of January 13, 2021, that had not occurred and our review is based on a draft of the strategy.
[103]According to ASPR officials, a key aspect of this goal is the Supply Chain Control Tower. Developed by FEMA’s Supply Chain Advisory Group and later transitioned to HHS, the Supply Chain Control Tower was implemented at the beginning of the response to track commercial orders and the distribution of those medical supplies.
[104]The National Response Framework is part of the National Preparedness System established in Presidential Policy Directive 8, and is to be used to manage any type of disaster or emergency response, regardless of scale, scope, and complexity. Department of Homeland Security, National Response Framework, Fourth Edition, (Washington, D.C.: October 2019). It identifies 15 emergency support functions (ESF), including ESF-8: public health and medical services, led by ASPR.
[105]GAO, Government Reorganization: Key Questions to Assess Agency Reform Efforts, GAO-18-427 (Washington, D.C.: June 13, 2018).
[106]The six characteristics of an effective national strategy are: (1) clear purpose, scope, and methodology; (2) problem definition and risk assessment; (3) goals, subordinate objectives, activities, and performance measures; (4) resources, investments, and risk management; (5) organizational roles, responsibilities, and coordination; and (6) integration and implementation. Each characteristic has several sub-elements.
[108] Molecular viral tests detect the presence of genetic material from SARS-CoV-2, the virus that causes COVID-19. The antigen viral tests detect the presence of a protein that is part of SARS-CoV-2. Non-diagnostic COVID-19 serology tests, known as antibody tests, are used to detect antibodies produced in patients who have had COVID-19.
[109]FDA may issue an emergency use authorization if the agency determines that certain medical products, such as a test, “may be effective” at diagnosing, treating, or preventing a disease, among other criteria. See 21 U.S.C. § 360bbb-3. An emergency use authorization allows tests and other products to be made available in a much shorter time frame than typically would be necessary for approval or clearance, in part because it requires a lower level of evidence than, for example, the “reasonable assurance of effectiveness” standard, which is part of the requirements for FDA medical device approvals. To approve or clear tests outside of an emergency, FDA determines whether there is reasonable assurance that the tests are safe and effective for their intended clinical use or that they otherwise meet the applicable statutory standard.
[110]FDA has also issued EUAs for one molecular test and two antigen tests that can be performed entirely in an individual’s home, without laboratory involvement.
[111]According to this testing strategy document, the federal government’s roles and responsibilities for testing include providing a blueprint for state testing plans, publishing and updating procedural guidance for administering diagnostic tests, and providing strategic direction and technical assistance regarding the best use of available testing technologies. The testing strategy document defines state, local, and tribal government’s roles and responsibilities as developing testing plans and maximizing the use of all testing platforms and venues (e.g., private, public, hospital, and clinic-based laboratories), among others. See White House, Centers for Disease Control and Prevention, and Food and Drug Administration, Testing Blueprint: Opening Up America Again (Apr. 27, 2020).
[112]Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (May 24, 2020); Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (August 22, 2020); and Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (November 20, 2020). The Paycheck Protection Program and Health Care Enhancement Act requires HHS to update the plan every 90 days until funds provided under the act are expended. Pub. L. No. 116-139, div. B, tit. I, 134 Stat. at 626-27 (2020).
[113]Department of Health and Human Services, U.S. Government COVID-19 Response Plan (Mar. 13, 2020). The U.S. Government COVID-19 Response Plan, known as the PanCap Adapted, outlines plans for the COVID-19 response, including roles for key stakeholders.
[114]According to CDC officials, $10.25 billion in funds appropriated by the Paycheck Protection Program and Health Care Enhancement Act were obligated for awards to states, territories, and local jurisdictions through CDC’s Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases cooperative agreement to help them expand their testing and contact tracing capacity, among other things. In addition, the Indian Health Service (IHS) will provide $750 million in funds appropriated by the Paycheck Protection Program and Health Care Enhancement Act to IHS, tribal, and urban Indian Health programs to expand testing capacity and testing-related activities.
[115]Pub. L. No. 116-260, div. M., tit. 3, 134 Stat. at 1918-19.
[116]We previously reported that at times during the pandemic, laboratory capacity, where most molecular tests are processed, has been constrained due to shortages in supplies and equipment, as well as increased demand for tests associated with emerging hotspots in disease transmission, leading to delays in turnaround times for testing results. Because rapid antigen tests, described above, do not rely on laboratory processing in the same way as molecular tests and because results are provided at the point of care, they may help alleviate the burden on these facilities. However, some epidemiologists have expressed concerns with widespread use of such tests, citing the need for more validation data. We also previously reported that some states were reluctant to use antigen tests in nursing homes due to the concern surrounding false positive results, and that across the country, nursing homes were slow to make use of antigen tests. See our Nursing Homes enclosure for more information on the use of antigen tests in nursing homes.
[118]For example, HHS suggested states use the tests to reopen schools, for first responders, and for congregate living facilities. HHS also sent Abbott rapid antigen tests to historically Black colleges and universities, home health and hospice organizations, disaster relief operations in 8 states, and to the Indian Health Service. As we reported in November 2020, the development of clear guidance around the use of rapid antigen tests has proven challenging for federal agencies due to concerns surrounding the sensitivity of tests and use of tests in asymptomatic individuals, for example.
[119]In June 2020, we reported percent positivity as a key indicator of the sufficiency of viral testing for COVID-19. In addition, according to CDC, percent positivity has provided insights into transmission of infectious diseases. CDC’s formula for calculating percent positivity is the number of positive tests (numerator) divided by the total number of resulted reported tests (denominator). Additionally, CDC acknowledges that states may calculate percent positivity differently, including whether they include or exclude antigen test results. See Centers for Disease Control and Prevention, Coronavirus Disease 2019 (COVID-19), Calculating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Laboratory Test Percent Positivity: CDC Methods and Considerations for Comparisons and Interpretation, Updated Sept. 3, 2020. The President’s Opening Up America Again Guidelines suggest using percent positivity as a metric when considering phased reopening, and the indicator is also used as a threshold for testing requirements for nursing homes at the county level.
[120]As described earlier, HHS articulated the national testing strategy in the White House Testing Blueprint, following the release of the President’s Opening Up America Again Guidelines. As of the end of 2020, HHS had submitted three statutorily-required strategic testing plans (May, August, and November) to Congress—documents that outline the implementation of the federal testing strategy. White House, Centers for Disease Control and Prevention, and Food and Drug Administration, Testing Blueprint: Opening Up America Again (Apr. 27, 2020) and Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (May 24, 2020); Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (August 22, 2020); and Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (November 20, 2020). The Paycheck Protection Program and Health Care Enhancement Act required HHS to issue a testing plan following enactment of the law and to update the plan every 90 days until funds provided under the act are expended. Pub. L. No. 116-139, div. B, tit. I, 134 Stat. at 626-27.
[121]Each characteristic has several sub-elements. See our February 2004 work listed as a related product.
[122]Department of Health and Human Services, U.S. Government COVID-19 Response Plan (Mar. 13, 2020).
[123]Pub. L. No. 116-260, div. W, tit. VI, § 621(b), 134 Stat. at 2403-04.
[124]FDA approves chemically derived drugs through review of new drug applications; it licenses biologically derived products, such as vaccines, through review of biologics license applications. FDA is required to publish the approval package for new drugs and biologics on FDA’s website. An approval package includes a summary review memo that contains detailed information about the preclinical and clinical data reviewed to support effectiveness and safety for the product, including clinical statistical efficacy trials and conclusions about those trials.
[125]The agency also posted this commitment to transparency for both chemically derived drugs and biologically derived products, such as vaccines, on its Coronavirus Treatment Acceleration Program website.
[126]The two EUAs issued in late-November 2020 were for baricitinib in combination with remdesivir on November 19, 2020 and casirivimab and imdevimab, which are administered together, on November 21, 2020.
[127]On December 11, 2020, FDA issued an EUA for Pfizer-BioNTech’s vaccine for the prevention of COVID-19 in individuals 16 years of age and older. On December 18, 2020, FDA issued an EUA for Moderna’s vaccine for the prevention of COVID-19 in individuals 18 years of age and older. FDA issued these EUAs after holding public Vaccines and Related Biological Products Advisory Committee meetings on December 10, 2020, and December 17, 2020, to discuss the Pfizer and Moderna vaccines, respectively.
[128]There are 64 jurisdictions, including all U.S. states, territories, and local health programs in Chicago, the District of Columbia, Houston, New York City, Philadelphia, and San Antonio.
[129]For example, an Operation Warp Speed official and the Secretary of Health and Human Services made statements indicating that 40 million doses would be available by the end of 2020, enough to vaccinate about 20 million people.
[130]Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1912 (2020).
[131]There were no FDA-licensed COVID-19 vaccines, as of January 8, 2021. Any COVID-19 vaccine that initially receives an EUA from FDA is expected to ultimately be reviewed and receive licensure through a biologics license application, according to FDA guidance.
[132]The Secretary of Health and Human Services may declare that circumstances, prescribed by statute, exist justifying the emergency use of certain medical products. Once a declaration has been made, FDA may temporarily allow use of unapproved medical products or unapproved uses of approved medical products through an EUA. For FDA to issue an EUA, it must be reasonable to believe that the medical product may be effective and that the known and potential benefits of the product outweigh the known and potential risks, among other statutory criteria. See 21 U.S.C. § 360bbb-3.
[133]FDA approved remdesivir for the treatment of COVID-19 in adults and pediatric patients (12 years of age and older and weighing at least 40 kg) requiring hospitalization. As of January 8, 2021, five therapeutics were authorized for emergency use by FDA for the treatment of COVID-19: remdesivir, COVID-19 convalescent plasma, bamlanivimab, baricitinib in combination with remdesivir, and casirivimab and imdevimab. The EUA for remdesivir remains in effect for other pediatric patients not covered by the approval. We have forthcoming work on the federal government’s contributions to the development of remdesivir.
[134]The key components within DOD and HHS that provide support to Operation Warp Speed include DOD’s Joint Program Executive Office for Chemical, Biological, Radiological, and Nuclear Defense and HHS’s Biomedical Advanced Research and Development Authority, CDC, and the National Institutes of Health.
[135]The FPDS-NG.gov (now beta.Sam.gov) website includes information on DOD’s and HHS’s awards and obligations. HHS officials have stated that HHS is the original source of funding for all COVID-19 vaccine and therapeutics development and production. Outside of Operation Warp Speed, DOD is also pursuing medical research and development projects for COVID-19 vaccines, therapeutics, and diagnostics as part of its efforts to protect servicemembers from COVID-19.
[136]Updates from DOD officials and company representatives indicate there are at least one billion vaccine doses under contract as of January 2021. Moreover, the government may acquire additional doses through the exercise of options or execution of new agreements.
[137]Manufacturing includes instances where a company uses proprietary manufacturing technology and processes to produce a vaccine.
[138]At least one agreement did not specify pricing for the initial doses to be delivered.
[139]10 U.S.C. § 2371b.In the sixth case, DOD awarded a firm-fixed-price contract in accordance with the Federal Acquisition Regulation (FAR) and Defense FAR Supplement (DFARS). FAR subpart 16.2; DFARS subpart 216.2.
[140]GAO, COVID-19 Contracting: Observations on Federal Contracting in Response to the Pandemic, GAO-20-632 (Washington, D.C.: July 29, 2020).
[141]Under an OTA, the parties can tailor provisions to address concerns about intellectual property and unique government requirements and regulations. The parties are not necessarily bound by FAR-based contract requirements. For example the Bayh-Dole Act governs intellectual property rights in FAR-based contracts but not in OTAs. 35 U.S.C. §§ 200-212.
[142]The Defense Production Act, as delegated, generally provides federal agencies authority to, among other things, place priority ratings on contracts so that they receive priority treatment over any other unrated contracts or orders if necessary to meet the delivery or performance dates specified in the order. See Pub. L. No. 81-774, 64 Stat.798 (1950) (codified, as amended, at 50 U.S.C. § 4501, et seq.). Exec. Order No. 13,603, 77 Fed. Reg. 16651 (Mar. 22, 2012); 15 C.F.R. pt. 700, Sch. 1. Operation Warp Speed officials said that they have prioritized 18 supply contracts under the Defense Production Act, as of December 2020.
[143] On December 23, 2020, HHS and DOD jointly announced an agreement with Merck for its therapeutic as part of Operation Warp Speed, but had not provided GAO the related contract documents by the end of audit work to enable us to incorporate the relevant information.
[144]Monoclonal antibodies are laboratory-made antibodies that may potentially be used to prevent COVID-19 infection, treat early illness in outpatients, and late-stage illness in hospitalized patients.
[145]There are 64 jurisdictions, including all U.S. states, territories, and local health programs in Chicago, the District of Columbia, Houston, New York City, Philadelphia, and San Antonio. See Operation Warp Speed, “From the Factory to the Frontlines: The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine,” accessed Dec. 7, 2020, https://www.hhs.gov/sites/default/files/strategy-for-distributing-covid-19-vaccine.pdf; Operation Warp Speed, “Vaccine Delivery Milestones,” accessed December 11, 2020 https://media.defense.gov/2020/Nov/05/2002529911/-1/-1/0/201105-D-XT155-001.JPG; and Department of Health and Human Services, Centers for Disease Control and Prevention, COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations, Version 2.0 (Washington, D.C.: Oct. 29, 2020).
[147]CDC has a Vaccine Taskforce to support jurisdictional planning and implementation. According to CDC officials, the Vaccine Taskforce has provided remote and on-site technical assistance, trainings, communication materials and vaccine guidance and developed a clinical inquiries line and jurisdictional call center to respond to jurisdictions’ inquiries in real time.
[148]The total doses administered includes both first and second doses that have been administered. The two COVID-19 vaccines authorized as of January 14, 2021 were two-dose vaccine regimens. A second dose is required after about 21 days for the Pfizer vaccine and about 28 days for the Moderna vaccine. The data on COVID-19 vaccine distribution and administration in the U.S. are being updated each weekday (Monday-Friday) on CDC’s website. According to the CDC website, healthcare providers report doses to federal, state, territorial, and local agencies up to 72 hours after administration. There may be additional lag for data to be transmitted to CDC. See https://covid.cdc.gov/covid-data-tracker/#vaccinations (accessed Jan. 15, 2021).
[150]Pub. L. No. 116-260, div. M, tit. III, 134 Stat. at 1911.
[151]In 2020, CDC awarded jurisdictions a total of $340 million in CARES Act funds for COVID-19 vaccine preparedness in September 2020 ($200 million) and December 2020 ($140 million).
[152]Pub. L. No. 116-260, div. BB, § 311, 134 Stat. at. 2923-24. Other goals of the campaign are to include combating misinformation about vaccines, and disseminating scientific and evidence-based vaccine-related information, with the goal of increasing rates of vaccination across all ages, as applicable, particularly in communities with low rates of vaccination, to reduce and eliminate vaccine-preventable diseases.
[153]Certain documents, such as the Operation Warp Sheet fact sheet, are periodically updated with new information. For this enclosure, we reviewed the fact sheet as of December 2, 2020, which was the most current at the time of our work. For Operation Warp Speed’s strategy, see Operation Warp Speed, “From the Factory to the Frontlines: The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine,” accessed Dec. 7, 2020, https://www.hhs.gov/sites/default/files/strategy-for-distributing-covid-19-vaccine.pdf.
[154]FPDS-NG data from beta.SAM.gov accessed December 31, 2020. Advanced Technology International manages the Medical Chemical, Biological, Radiological and Nuclear Defense Consortium (MCDC), a partnership with industry, academic, and not-for-profit partners to support the DOD’s medical, pharmaceutical and diagnostic requirements.
[156]Department of Health and Human Services, Centers for Medicare and Medicaid Services, 2018Actuarial Report on the Financial Outlook on Medicaid (Baltimore, Md.).
[157]The FMAP is calculated based on each state’s per capita income relative to national per capita income. For the District of Columbia and U.S. territories, the FMAP is set by statute regardless of their per capita incomes. Additionally, federal law specifies a maximum amount, or allotment, for federal contributions to Medicaid spending in U.S. territories, in contrast to the states and the District of Columbia, for which federal Medicaid spending is open-ended.
[160]We excluded one state, Montana, because state officials told us they are not implementing coverage. CMS officials noted that Montana has not requested to rescind coverage as of December 31, 2020.
[161]FFCRA, div. A, tit. V, 134 Stat. at 182; Pub. L. No. 116-139, div. B., tit. I, 134 Stat. 620, 626 (2020).
[162]The most recent available payment information is for the second quarter of fiscal year 2020 (January 1, 2020, through March 31, 2020) through the first quarter of fiscal year 2021 (October 1, 2020, through December 31, 2020). States can report payments and adjustments to payments up to 2 years after a quarter ends. The increased federal medical assistance percentage (FMAP) is available for Medicaid medical assistance expenditures for which each state’s standard state-specific FMAP rate is used to determine federal funding.
[163]A veteran may have multiple episodes of care. According to VA, in the context of telehealth, the term “episode(s) of care” is used to express, for example, one real time video visit and one store and forward event.
[164]See VA Memorandum Guidance to Avoid All Routine or Non-urgent Face to Face Visits (March 31, 2020).
[166]VHA’s Office of Connected Care focuses on improving health care through technology by engaging veterans and care teams outside of traditional health care visits. For example, the use of telehealth improves convenience to veterans by providing access to care from their homes or local communities when they need it.
[167]VA’s Office of Information and Technology is responsible for providing strategy and technical direction, guidance, and policy related to how IT resources are to be acquired and managed for VA, and for working closely with its business partners—such as VHA—to identify and prioritize business needs and requirements for information technology systems.
[168]The percentage of specimens testing positive for COVID-19 is one indicator the Centers for Disease Control and Prevention (CDC) uses to monitor COVID-19 activity. According to CDC, percent positivity provides a strong indication of how widespread infection is in an area where testing is being conducted, but is dependent upon whether testing is keeping up with the level of disease transmission and the criteria used for testing.
[169]Some VA employees are also veterans and therefore captured in the veteran deceased data.
[170]VA pointed to several research studies on video telehealth effectiveness and use, including a study showing higher patient satisfaction with video visits than in-person visits during the COVID-19 response. See A. Ramaswamy et al., “Patient Satisfaction with Telemedicine during the COVID-19 Pandemic: Retrospective Cohort Study,” Journal of Medical Internet Research, vol. 22, no. 9,(2020): e20786.
[171]On March 31, 2020, VHA provided facilities guidance to convert all routine and non-urgent outpatient appointments to telehealth appointments, to the extent possible.
[172]According to VHA officials, as appointments are cancelled, rescheduled, and as visits occur each day, the numbers will fluctuate based on the time the data were pulled.
[173]Eligible veterans may choose to obtain health care services from community providers rather than from a VA provider when the veteran is enrolled in VA’s health care system, or is not enrolled but otherwise eligible to receive care under 38 U.S.C. § 1705(c)(2), and meet certain other conditions for community care.
[174]Department of Veterans Affairs, Office of Inspector General, Appointment Management During the COVID-19 Pandemic, Report #20-02794-218 (Washington, D.C.: September 2020).
[175]This amount does not include $73 billion in COVID-19 relief funds that were appropriated to HHS in a fifth relief law, the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020)—enacted on December 27, 2020.
[176]Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020).
[177]The data provided by HHS did not include appropriations, allocations, obligations, and expenditures from the Consolidated Appropriations Act, 2021, Pub. L. 116-260, 134 Stat. 1182 (2020).
[178]We searched HHS’s Tracking Accountability in Government Grants System website and USAspending.gov—a publicly available website developed and operated by the Department of the Treasury that includes detailed data on federal spending, including obligations, across the federal government. See https://taggs.hhs.gov/coronavirus, accessed 1/4/2021, and https://USAspending.gov, accessed 1/4/2021. We did not independently validate the data provided by HHS.
[180]Medical countermeasures include drugs, vaccines, and devices to diagnose, treat, prevent, or mitigate potential health effects of exposure to chemical, biological, radiological, and nuclear agents and emerging infectious diseases, pandemics or epidemics, as well as personal protective equipment. Critical inputs are API, API starting materials, and other drug ingredients and device components that FDA determines to be critical for assessing safety and effectiveness of essential medicines and countermeasures.
[181]The CARES Act requires manufacturers to annually report volume information to FDA starting in September 2020. See Pub. L. No. 116-136, § 3112, 134 Stat. 281, 362 (2020) (codified in pertinent parts at 21 U.S.C. §§ 356c and 360(j)). The agency noted that they would have preferred the additional required data to be more detailed and reported more frequently so FDA could determine how much product is manufactured at each establishment and how reliant manufacturers are on certain suppliers.
[182]In January 2021, Congress passed the National Defense Authorization Act, 2021, which directs DOD to report to congressional defense committees on restricting procurement of pharmaceuticals and API, among other goods and services, to U.S. suppliers. See Pub. L. No. 116-283, div. A, § 849, 134 Stat. 3388, 3770. The report is required by January 2022.
[183]The contracting officers are generally expected to take actions to verify incomplete or conflicting information when they have reason to believe that a company will be providing a non-compliant product. In December 2018 we found that VA and other agencies faced various levels of challenges in applying the Trade Agreements Act waivers and Buy American Act exceptions to acquire foreign made products, and that VA lacked training for how contracting officers are to determine compliance with Buy American Act requirements. In 2020, VA revised its guidance to address our recommendation that it should clarify existing guidance or provide training to help contracting officials identify sources of information available for determining products’ origins and the steps to be taken to verify information that is inconsistent.
[184]GAO, Standards for Internal Control in the Federal Government, GAO-14-704G (Washington, D.C.: September 2014).
[185]VA officials also expressed concerns that the Executive Order may make it difficult to access drugs if they are not available from domestic sources.
[186]Our work focuses on human drugs and not on most biologics, veterinary medicines, or other items or products for which FDA conducts inspections.
[187]FDA identifies mission critical inspections on a case-by-case basis by considering many factors related to the public health benefit of patients having access to the product subject to inspection as well as considering the safety of its inspection staff and employees of the establishment to be inspected.
[188]According to the Joint Explanatory Statement accompanying the Consolidated Appropriations Act, 2021, $3.5 million of FDA’s fiscal year 2021 appropriation is to be used for foreign unannounced human drug inspection pilots. See Explanatory Statement, 166 Cong. Rec. H7891 (daily ed. Dec. 21, 2020) (statement of Rep. Lowey); Pub. L. No. 16-260, § 4, 134 Stat. 1182, 1185 (2020) (clarifying that the explanatory statement regarding this act shall have the same effect as a joint explanatory statement with respect to the allocation of funds and implementation of certain divisions).
[189]For the purposes of this report, when we refer to European regulators, we are referring to the 28 European regulators that are part of the mutual recognition agreement with FDA, including the United Kingdom. A separate mutual recognition agreement between FDA and the United Kingdom will go into effect after the United Kingdom leaves the European Union.
[190]See 21 U.S.C. § 374(a)(4). Prior to the COVID-19 pandemic, FDA used this authority in a more limited capacity to oversee 10 establishments that the agency would not routinely inspect because of travel warnings. In fiscal year 2019, for example, this included establishments in Colombia, Egypt, Israel, Mexico, Pakistan, and Saudi Arabia, among others.
[191]We have previously reported on concerns about the accuracy of translations during foreign inspections. Specifically, FDA inspection staff said FDA’s reliance on translators provided by the establishment raised questions about the accuracy of information collected. We plan to examine this issue as part of our ongoing work.
[192]To be eligible for regular UI benefits, applicants generally must be able and available to work, and be actively seeking work. 42 U.S.C. § 503(a)(12). The regular UI program is also financed by a federal tax on employers, which according to DOL officials, primarily supports the administration of the program.
[193]The CARES Act also addressed other aspects of the UI system, such as authorizing certain flexibilities for states to hire additional staff and to participate in Short-Time Compensation programs. In addition to the CARES Act, the Families First Coronavirus Response Act provided up to $1 billion in emergency grant funding to states in fiscal year 2020 for UI administrative purposes. In addition, on August 8, 2020, the President signed a memorandum directing the Department of Homeland Security’s Federal Emergency Management Agency (FEMA) to provide up to $44 billion in lost wages assistance (LWA). Pursuant to the presidential memorandum, upon receiving a FEMA grant, states and territories could provide eligible claimants $300 or $400 per week—which included a $300 federal contribution—in addition to their UI benefits. The White House, Memorandum on Authorizing the Other Needs Assistance Program for Major Disaster Declarations Related to Coronavirus Disease 2019 (Aug. 8, 2020). FEMA approved 54 states and territories to provide LWA to eligible claimants for at most 6 weeks of unemployment experienced from the week ending August 1, 2020, through the week ending September 5, 2020.
[194]Pub. L. No. 116-260, div. N, tit. II, § 201(a), (b), 134 Stat. 1182, 1950-1951 (2020); Pub. L. No. 116-136, § 2102, 134 Stat. at 313. The Consolidated Appropriations Act, 2021 increased the maximum number of weeks of PUA benefits authorized from 39 to 50, and generally extended the expiration of the program from December 31, 2020 to March 14, 2021. That Act provided that individuals receiving PUA benefits as of March 14, 2021 who have not exhausted such benefits may continue to receive PUA benefits after that date, but that no PUA benefits are payable for any week beginning after April 5, 2021. In addition, claimants whose first application for PUA is filed after December 27, 2020, may only claim benefits retroactively to December 1, 2020. Under the CARES Act, PUA claimants could originally claim benefits retroactively to January 27, 2020. See also Department of Labor, Continued Assistance to Unemployed Workers Act of 2020 – Pandemic Unemployment Assistance (PUA) Program: Updated Operating Instructions and Reporting Changes, Unemployment Insurance Program Letter (UIPL) 16-20 Change 4 (Washington, D.C.: Jan. 8, 2021). The CARES Act also provided funding for up to an additional 7 weeks of PUA benefits in certain states with high rates of unemployment. Department of Labor, CARES Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Operating, Financial and Reporting Instructions, Unemployment Insurance Program Letter (UIPL) 16-20 (Washington, D.C.: Apr. 5, 2020).
[195]Pub. L. No. 116-260, div. N, tit. II, § 203, 134 Stat. 1182, 1953; Pub. L. No. 116-136, § 2104, 134 Stat. at 318. The Consolidated Appropriations Act, 2021 authorized the $300 benefit (and accompanying time period of potential eligibility).
[196]Pub. L. No. 116-260, div. N, tit. II, § 206(a), (b), 134 Stat. 1182, 1954; Pub. L. No. 116-136, § 2107, 134 Stat. at 323. The Consolidated Appropriations Act, 2021 increased the maximum number of weeks of PEUC benefits authorized from 13 to 24, and generally extended the expiration of the PEUC program from December 31, 2020 to March 14, 2021. That Act provides that individuals receiving PEUC benefits as of March 14, 2021 who have not exhausted such benefits may continue to receive PEUC benefits after that date, but that no PEUC benefits are payable for any week beginning after April 5, 2021.
[197]Pub. L. No. 116-260, div. N, tit. II, § 261(a)(1), 134 Stat. 1182, 1961.
[198]Department of Labor, Continued Assistance for Unemployed Workers (Continued Assistance) Act of 2020 – Federal Pandemic Unemployment Compensation (FPUC) Program Reauthorization and Modification and Mixed Earners Unemployment Compensation (MEUC) Program Operating, Reporting, and Financial Instructions, Unemployment Insurance Program Letter (UIPL) 15-20, Change 3 (Washington, D.C.: Jan. 5, 2021).
[199]Pub. L. No. 116-260, div. N, tit. II, § 251, 134 Stat. 1182, 1961. The method must include a reporting mechanism for employers to notify the state when a claimant refuses an offer of employment, and a plain-language notice provided to such claimants about state return to work laws and related rights and information.
[200]Pub. L. No. 116-260, div. N, tit. II, § 241(a), 134 Stat. 1182, 1959-1960.
[201]Pub. L. No. 116-260, div. N, tit. II, § 242(a), 134 Stat. 1182, 1960.
[202]Pub. L. No. 116-260, div. N, tit. II, § 263(a), 134 Stat. 1182, 1963.
[203]Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952.
[204]The Consolidated Appropriations Act, 2021 provides optional, time-limited, and temporary waiver authority on the 13-week mandatory “off” period for states that have triggered “off” of an Extended Benefits period and later trigger back “on” for weeks between November 1, 2020 and December 31, 2021, if state law permits. Department of Labor, Continued Assistance for Unemployed Workers Act of 2020 (Continued Assistance Act) – Summary of Key Unemployment Insurance (UI) Provisions, Unemployment Insurance Program Letter (UIPL) 9-21 (Washington, D.C.: Dec. 30, 2020), and Department of Labor, Continued Assistance for Unemployed Workers Act (Continued Assistance Act) of 2020 – Provisions Affecting the Federal-State Extended Benefits Program, Unemployment Insurance Program Letter (UIPL) 24-20, Change 1 (Washington, D.C.: Dec. 31, 2020).
[205]The Extended Benefits program was activated in all states except South Dakota at some point during the pandemic, according to DOL. For example, as of June 28, 2020, the Extended Benefits program was available in 49 states, the District of Columbia, Puerto Rico, and the Virgin Islands, according to DOL.
[206]If approved for PUA benefits, the number of weeks of regular UI and Extended Benefits a claimant already received is subtracted from the duration of PUA benefits. Department of Labor, CARES Act of 2020 – Summary of Key Unemployment Insurance (UI) Provisions and Guidance Regarding Temporary Emergency State Staffing Flexibility, Unemployment Insurance Program Letter (UIPL) 14-20 (Washington, D.C.: Apr. 2, 2020).
[207]An initial claim is the first claim filed by an individual to determine eligibility for UI benefits after separating from an employer. Initial claims counts presented are not seasonally adjusted, and counts for the week ending January 9, 2021 reflect advance initial claims, which are preliminary and subject to revision. In some cases, advance initial claims represent estimates submitted by states. For example, in late September, California paused its acceptance of initial claims to reduce its backlog of claims and to implement tools to help prevent fraud in the program. As a result, California submitted estimated numbers of initial claims to DOL for the weeks ending September 26, October 3, and October 10.
[208]According to DOL, as of July 2020, 45 of 53 states and territories generally provide up to a maximum of 26 weeks of regular UI benefits. Some states provide fewer than 26 weeks, though some of these states also provide additional weeks of benefits under limited circumstances, such as periods of high unemployment, according to DOL.
[209]The extension of PEUC benefits and increase in the number of weeks of PEUC benefits from 13 to 24, authorized in the Consolidated Appropriations Act, 2021, may result in some claimants being eligible for PEUC after initially exhausting PEUC and then receiving Extended Benefits or PUA benefits. For information about the coordination of benefits in these circumstances, see Department of Labor, Continued Assistance for Unemployed Workers Act of 2020 (Continued Assistance Act) – Summary of Key Unemployment Insurance (UI) Provisions, Unemployment Insurance Program Letter (UIPL) 9-21 (Washington, D.C.: Dec. 30, 2020).
[210]One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible. DOL uses 14 days as the timeliness goal for states with a waiting week requirement and 21 days for states without a waiting week requirement. According to DOL, some states require that individuals who are otherwise eligible for benefits, serve a waiting period—generally one week—before receiving benefits. In its guidance released at the start of the pandemic, DOL recommended that states consider temporarily waiving their waiting week requirements. Thus, we focus on payments made within 21 days.
[211]For its core performance measure, DOL determined that states must pay at least 87 percent of claims within 14-21 days to reach an acceptable level of performance.
[212]The minimum benefit for PUA aligns with the minimum benefit for the Disaster Unemployment Assistance program and is set in Unemployment Insurance Program Letter (UIPL) 3-20. Department of Labor, Minimum Disaster Unemployment Assistance (DUA) Weekly Benefit Amount: January 1 - March 31, 2020, UIPL 3-20 (Washington, D.C.: Dec. 12, 2019). DOL guidance notes that when individuals submit sufficient documentation of wages, states must immediately recalculate their weekly benefits and pay the full PUA benefit amount with the greatest promptness that is administratively feasible. Department of Labor, CARES Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Reporting Instructions and Questions and Answers, UIPL 16-20, Change 1 (Washington, D.C.: Apr. 27, 2020); see also 20 C.F.R. § 625.9(e). Under the CARES Act, the regulations for DUA generally apply to PUA. Pub. L. No. 116-136, § 2102(h), 134 Stat. 281, 317.
[213]We calculated PUA average benefit amounts by dividing the state-reported monthly amounts for total compensation paid by total weeks compensated. Benefit amounts are based on data reported by states as of January 11, 2021, at which point two states had reported PUA data for December. Thus, we analyzed benefit payment data for November. The following states and territories did not report PUA monthly data for November: Alaska, Florida, Massachusetts, Nevada, Oklahoma, Oregon, Puerto Rico, South Carolina, Vermont, and Washington.
[214]While the CARES Act UI programs were federally funded, regular UI is primarily funded through state and federal taxes on employers. When a state exhausts the funds available for regular UI benefits, it may borrow from the federal government. According to DOL data, even before the pandemic, many states were not taking in enough UI tax revenue to satisfy the solvency standard specified in DOL regulations providing for interest-free loans to states. See 20 C.F.R. § 606.32 (2019).
[215]According to DOL, the U.S. Virgin Islands had a residual loan balance of about $0.06 billion at the beginning of 2020 left from the 2007-2009 recession.
[216]DOL compiles and publishes historical data on outstanding federal loan balances in its ET Financial Data Handbook 394. According to the National Bureau of Economic Research, the 2007-2009 recession began in December 2007 and ended in June 2009.
[217]The UI Integrity Center assists states in their efforts to improve integrity in the UI program.
[218]Federal charges refer to criminal complaints and indictments. A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[219]Fraud involves obtaining something of value through willful misrepresentation. Some overpayments may be the result of fraud. However, whether an act is in fact fraud is a determination to be made through the judicial or other adjudicative system.
[220]According to DOL, overpayments include those in the regular UI, Extended Benefits, and emergency unemployment compensation programs (specifically, those programs enacted during the 2007-2009 recession, according to officials), and exclude overpayments that have been waived. According to DOL, states may waive a non-fraud overpayment, in accordance with state law, if the overpayment was not the fault of the claimant and requiring repayment would be against equity and good conscience or would otherwise defeat the purpose of the UI law.
[221]States may revise the amount of overpayments they have identified for 3 years after the reporting quarter, according to DOL.
[222]For example, the number of regular UI continued claims submitted during the week ending September 26, 2020, the last week of the third quarter, was more than 7 times the number submitted during the corresponding week in 2019.
[223]We accessed the PUA overpayments data on January 11, 2021; these data are subject to change as more states report data and states revise previously reported data. The number of states that have reported PUA overpayments data varies by month; for example, 1 state reported overpayment amounts in March 2020, 14 states reported overpayment amounts in April 2020, 32 states reported overpayment amounts in November 2020, and 2 states reported overpayment amounts in December 2020. Among the states reporting data, we identified wide variation in the amount of PUA overpayments reported (e.g., thousands of dollars or hundreds of millions of dollars reported in a given month). According to DOL officials, states are starting to shift their focus to identifying overpayments. States are generally expected to report overpayments in the month the cases were established, though states may also report or adjust data for prior months.
[224]According to the Consolidated Appropriations Act, 2021, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount, but the state can waive that requirement if the individual was without fault and repayment would be contrary to equity and good conscience. Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952.
[225]Under the CARES Act, the regulations for DUA generally apply to PUA. Pub. L. No. 116-136, § 2102(h), 134 Stat. 281, 317.
[226]For states to meet DOL’s acceptable level of performance for 2019, they needed an overpayment recovery rate of at least 68 percent.
[227]The volume of payments is taken from the IRS Master File and does not include reversals or payments to residents of territories. The amount of payments is taken from the Treasury general ledger and includes reversals and payments to the U.S. Territories.
[228]Pub. L. No. 116-260, div. N, § 272(a), 134 Stat. 1182, 1965–1971 (2020), classified at 26 U.S.C. § 6428A. These payments are an advance refund for a tax year 2020 tax credit. The act refers to this credit and the advance refund as the Recovery Rebate Credit. We refer to direct payments authorized by the Consolidated Appropriations Act, 2021, as EIP 2 and those authorized by the CARES Act as EIP 1. The Consolidated Appropriations Act, 2021 also amended the provision of the CARES Act authorizing EIP 1. Pub. L. No. 116-260, div. N, § 273, 134 Stat. at 1976–1978.
[232]26 U.S.C. § 6428A(f)(1). IRS is allowed to use information provided by certain other agencies (for example, the Social Security Administration and the Railroad Retirement Board) to calculate EIP 1 and EIP 2.
[233]OSHA carries out these activities under the Occupational Safety and Health Act of 1970, Pub. L. No. 91-596, 84 Stat. 1590 (codified as amended at 29 U.S.C. §§ 553, 651-678).
[234]OSHA also has four district offices that are subordinate to an area office.
[235]In five of these states and the U.S. Virgin Islands, the state or territory is responsible for setting and enforcing standards for state and local government employers, under a state plan approved by OSHA.
[236]These state plans cover both private sector and state and local government employers. State standards and their enforcement must be at least as effective as the federal standards in protecting workers and in preventing work-related injuries, illnesses, and fatalities. Federal agencies are generally responsible for maintaining their own occupational safety and health programs, consistent with OSHA’s regulations.
[237]Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 553-554 (2020). The CARES Act authorized the Secretary of Labor to transfer the amounts provided under this heading as necessary to OSHA and certain other administrations, to prevent, prepare for, and respond to COVID-19, including for enforcement, oversight, and coordination activities in those accounts.
[238]OSHA has tracked data related to COVID-19 in the workplace since February 2020. OSHA uses the term “referrals” to encompass reports of severe injuries and illnesses from employers and reports of potential workplace hazards from several other entities, such as a government agency. In this report, we use “referrals” to describe those reports from non-employer sources, and “employer reports” to describe those reports from employers. Employers are required to report all work-related in-patient hospitalizations, amputations, and losses of an eye within 24 hours, and all work-related fatalities within 8 hours. 29 C.F.R. § 1904.39. According to OSHA officials, most reports of fatalities come from employers. However, officials noted that they do receive reports of fatalities from other sources, such as the media or emergency medical personnel. In this report we refer to all reported fatalities as “reports of fatalities.” Data throughout this report include enforcement activity performed by OSHA only, and not by state agencies that operate under OSHA-approved state plans.
[239]OSHA started centrally tracking data on remote inspections in November 2020, and concerns about reliability are discussed below.
[240]OSHA assesses financial penalties for violations based on various factors outlined in statute and OSHA policy. For example, in 2020, violations determined to be serious were subject to penalties of up to $13,494 per violation, and violations determined to be willful or repeated were subject to penalties of up to $134,937 per violation. See 29 C.F.R. § 1903.15(d). Since under the Occupational Safety and Health Act of 1970, OSHA has 6 months from the occurrence of a violation to issue a citation and any related penalties, monthly totals for the number of violations cited and penalties issued from July through December 2020 may not reflect the total that will eventually be cited or issued related to inspections initiated during those months. In addition, some of these cases are still open and may have been contested or appealed by the employers, which could ultimately result in changes to the violations cited or penalties issued. These data are current as of January 4, 2021.
[241]Occupational Safety and Health Administration, Updated Interim Enforcement Response Plan for Coronavirus Disease 2019 (COVID-19) (May 19, 2020). OSHA’s enforcement policy related to COVID-19 is available at https://www.osha.gov/enforcementmemos.
[242]According to OSHA officials, informal inquiries conducted in response to an employer-reported severe injury or illness, such as an in-patient hospitalization or amputation, are called rapid response investigations, and informal inquiries conducted in response to complaints from employees or referrals from entities other than employers are called phone/fax investigations. According to OSHA’s Field Operations Manual, if Area Directors consider employers’ responses to these informal inquiries to be inadequate, they may decide to initiate a related inspection.
[243]For example, employers may not be able to conduct OSHA-mandated annual health and safety training, medical testing, or equipment inspections because of pandemic-related closures and other restrictions, and inspectors are to consider an employer’s “good faith” efforts when deciding whether to issue a related citation.
[244]Occupational Safety and Health Administration, Discretion in Enforcement when Considering an Employer's Good Faith Efforts During the Coronavirus Disease 2019 (COVID-19) Pandemic (Apr. 16, 2020).
[245]See, for example, Occupational Safety and Health Administration, Enforcement Guidance for Respiratory Protection and the N95 Shortage Due to the Coronavirus Disease 2019 (COVID-19) Pandemic (April 3, 2020); and Revised Enforcement Guidance for Recording Cases of Coronavirus Disease 2019 (COVID-19) (May 19, 2020).
[246]OIS does not provide a complete picture of OSHA’s use of adapted enforcement methods because of tracking gaps discussed below.
[247]OSHA started centrally tracking data on remote inspections in November 2020 and concerns about reliability are discussed below. For example, officials said that the remaining 26 of the 715 remote inspections were also COVID-19-related but were not coded correctly. In December 2020, OSHA officials told us they were working to resolve this issue.
[248]OSHA’s data do not track when inspectors use discretion to not cite violations of other requirements, such as personal protective equipment requirements, as discussed below.
[249]OIS documents when informal inquiries were used, but does not identify when they were used in place of inspections. That is, OIS does not specify when COVID-related constraints caused an area office to use an informal inquiry, in place of an inspection, to address the complaint, referral, or employer report. Therefore, as discussed below, the precise extent to which OSHA’s adapted enforcement methods affected the shift from inspections to informal inquiries is unclear.
[250]In this report, we use the term “oversight” to describe follow-up and monitoring activities for OSHA’s COVID-19-adapted enforcement methods. According to OSHA officials, OSHA uses the term “oversight” to describe a broader range of activities it uses to enforce workplace safety and health standards.
[251]Occupational Safety and Health Administration, Updated Interim Enforcement Response Plan for Coronavirus Disease 2019 (COVID-19) (May 19, 2020).
[252]Occupational Safety and Health Administration, Updated Interim Enforcement Response Plan for Coronavirus Disease 2019 (COVID-19) (May 19, 2020).
[253]Occupational Safety and Health Administration, Discretion in Enforcement when Considering an Employer's Good Faith Efforts During the Coronavirus Disease 2019 (COVID-19) Pandemic (Apr. 16, 2020). OSHA’s pandemic enforcement policies outline oversight for citation discretion for violations of recurring requirements, but not for violations of other requirements for which citation discretion is allowed.
[254]OSHA officials told us that there is no evidence that remote inspections are not identifying hazards, and based on their review of violations cited during remote inspections, such inspections are identifying the same number of violations as on-site inspections. However, officials agreed that until the agency conducts the on-site component for remote inspections, they will not know definitively whether additional violations would have been identified in an on-site inspection.
[255]OSHA officials said that it is possible that the new presidential administration in January 2021 may provide different direction.
[256]OIS did not document whether inspections were conducted on-site or remotely from February 2020 through October 2020. In October 2020, OSHA officials said that they had not requested an update to OIS to identify remote inspections, although OSHA officials who manage OIS told us that such an update would be easy to make. In response to our inquiry, OSHA officials told us that they made the OIS update and in November 2020, directed area offices to identify remote inspections in OIS.
[257]OIS documents when informal inquiries were used, as shown in the figure above, but does not identify when they were used in place of inspections. That is, OIS does not specify when COVID-related constraints caused an area office to use an informal inquiry, in place of an inspection, to address the complaint, referral, or employer report.
[258]For reports of fatalities from employers, OSHA officials stated that they were able to go through a several-step process and manually identify 11 rapid response investigations for COVID-19-related fatalities from February through December 2020. For employer reports of severe injuries or illnesses, the agency does not have a way to identify rapid response investigations that occurred in place of inspections.
[259]Although OSHA has a manual method to identify rapid response investigations conducted in response to employer reports of COVID-19-related fatalities, it does not have a method to identify imminent danger cases where a phone/fax investigation or rapid response investigation was conducted in place of an inspection.
[262]In a September 2020 update to its Frequently Asked Questions (FAQ) page regarding COVID-19, OSHA clarified that to be reportable under the regulation, “an in-patient hospitalization due to COVID-19 must occur within 24 hours of an exposure to SARS-CoV-2 at work.” According to OSHA officials, prior to updating its FAQ page, the agency had received reports of COVID-19 hospitalizations for which employers had considered the work-related incident to be a worker testing positive for COVID-19 (as opposed to exposure to the virus); this may account, in part, for the COVID-19-related hospitalizations employers have reported to OSHA.
[263]OSHA officials told us that other illnesses may also take several days to manifest symptoms serious enough to result in hospitalization, such as those resulting from chemical exposure at the workplace, so this situation is not unique to COVID-19. They noted that the reporting requirement does not work as well for reporting illnesses as it does for other severe injuries, such as amputations.
[264]16 Va. Admin. Code § 25-220-40. This standard took effect July 27, 2020, and will expire after 6 months, upon expiration of the Governor’s State of Emergency, or when superseded by a permanent standard, whichever occurs first.
[265]Additionally, DOL provided examples of OIS updates that OSHA made to collect data on its adapted enforcement methods. While these data can assist OSHA with its oversight processes, data collection is not the main substance of this recommendation. We discuss our data collection concerns below in our second recommendation about tracking adapted enforcement methods.
[266]These data are current as of January 4, 2021.
[267]HHS officials commented that although older adults living in rural areas may receive services less frequently, a higher percentage of the older adult rural population is served compared to their representation in the population. They stated that in fiscal year 2018, 34.5 percent of older adults served through OAA programs lived in rural areas while only 22.8 percent of all older adults live in rural areas.
[268]Though all populations are at risk of COVID-19, data indicate that older adults—those over age 65—are more likely to be hospitalized and to die from the virus. See Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, vol. 69, no. 15 (Apr. 17, 2020). In fact, according to the Centers for Disease Control and Prevention, 8 out of 10 COVID-19-related deaths reported in the U.S. have been among adults age 65 and older. See Centers for Disease Control and Prevention, Coronavirus Disease 2019 (COVID-19): Older Adults (Updated September 11, 2020).
[269]See FFCRA, Pub. L. No. 116-127, div. A, tit. V, 134 Stat. 178, 182 (2020) and CARES Act, Pub. L. No. 116-136, 134 Stat. 281, 559-60 (2020).
[270]See Pub. L. No. 116-260, div. N, tit. VII, § 731, 134 Stat. 1182, 2104 (2020).
[271]Eligible family caregivers include adult family members or other informal caregivers age 18 and older providing care to individuals 60 years of age and older, or individuals of any age with Alzheimer’s disease and related disorders; as well as older relatives (not parents) age 55 and older providing care to children under the age of 18, or to adults ages 18-59 with disabilities.
[272]For example, various aging resource centers are authorized under OAA Title II; nutrition and related services for Native Americans are authorized under OAA Title VI; and services to prevent the abuse, neglect, and exploitation of older adults is authorized under OAA Title VII.
[273]See Pub. L. No. 116-136, §§ 3222-3223, 134 Stat. at 379-80. The CAA-21 also provided these flexibilities to the OAA Title III nutrition assistance program. See Pub. L. No. 116-260, div. N, tit. VII, § 732, 134 Stat. at 2104-05.
[274]This figure comes from an internal N4A membership survey that was conducted among N4A members during the period of May 7 to May 15, 2020. N4A reported that AAAs’ response rate to the survey was 46 percent, and that survey respondents included a balanced representation of AAA structures (e.g., nonprofit, county-based) and service areas (e.g., rural, urban). National Association of Area Agencies on Aging, #AAAsAtWork for Older Adults, A Snapshot of Area Agency on Aging Responses to COVID-19 (July 2020).
[275]These figures come from a survey that was conducted for Meals on Wheels America by Trailblazer Research between July 9-16, 2020, among Meals on Wheels America’s membership. According to Meals on Wheels America, its membership is representative of the national senior nutrition provider network of more than 5,000 individual community-based programs.
[276]This figure comes from a survey that was conducted between April 22-28 among Meals on Wheels America’s membership, which according to Meals on Wheels America is representative of the national senior nutrition provider network of over 5,000 individual community-based programs. The survey has a +/- 4 percent margin of error.
[277]In fiscal year 2020, the FFCRA and CARES Act also provided $30 million in additional funding for OAA Title VI nutrition and related services for Native American programs. This was in addition to the $35 million previously provided in fiscal year 2020 to fund these programs.
[278]See Pub. L. No. 116-136, § 3222(b), 134 Stat. at 379-80 and Pub. L. No. 116-260, div. N, tit. VII, § 732, 134 Stat. at 2104-05.
[280]To help meet the demand for nutrition assistance for individuals of all ages, including older adults, CAA-21 also provided more than $101 billion in fiscal year 2021 appropriations for Supplemental Nutrition Assistance Program (SNAP) benefits—nearly double the prior year’s initial appropriation for benefits. Among other SNAP provisions, the act also generally increased the maximum household benefit through June 30, 2021, and provided $100 million for the cost of state administrative expenses related to carrying out these benefit increases and administering the program. For more information on SNAP funding during the pandemic, see GAO-21-191, 181-188.
[281]For example, see Rosalyn Carter Institute on Caregiving, Caregivers in Crisis: Caregiving in the Time of COVID-19 (October 2020).
[282]While conducting audit work for our report, GAO-21-90, we added questions about the effects of the pandemic on Adult Protective Services (APS) programs more generally in our interviews of APS officials conducted from March through June 2020 in eight states: California, Florida, Maine, Nevada, New York, Oregon, Pennsylvania, and Virginia.
[283]See Pub. L. No. 116-136, 134 Stat. at 559-60.
[284]See Pub. L. No. 116-260, div. M, tit. III, 134 Stat. at 1916.
[285]See Pub. L. No. 116-136, 134 Stat. at 559-60.
[286]The next annual reports for program year 2019 will describe grantee performance from July 2019 through June 2020. Officials said ETA is in the process of finalizing the data. As of mid-January 2021, the reports for program year 2019 had not yet been released.
[288]VBA contracts with three private firms to perform disability medical exams.
[289]GAO’s High-Risk program focuses attention on government operations with greater vulnerabilities to fraud, waste, abuse, and mismanagement, or that are in need of transformation to address economy, efficiency, or effectiveness challenges. To learn more about VA’s actions to improve and modernize federal disability programs, see our March 2019 High-Risk report.
[290]Families First Coronavirus Response Act, Pub. L. No. 116-127, div. A, tit. VI, 134 Stat. 178, 183 (2020) ($60M) and the CARES Act, Pub. L. No. 116-136, div. B, tit. X, 134 Stat. 281, 582-84 (2020) (approximately $19.6B). Funds appropriated to VA under the Families First Coronavirus Response Act are available until September 30, 2022. Funds appropriated for VA programs under the CARES Act are available until September 30, 2021, except those for the VA Office of the Inspector General (OIG). CARES Act funds for the VA OIG are available until September 30, 2022.
[291]The National Call Center provides information over the phone about the full range of federal veterans’ benefits, such as disability benefits, education, home loans, and insurance benefits and can assist with some claims-related processes. The Veterans Service Center can provide information on veterans’ health benefits and assistance with disability compensation benefits, among other services. Overall, most of the CARES Act funding that has been obligated by VA— about $7 billion of the almost $8.3 billion obligated as of January 5, 2021—was obligated by VHA. The Consolidated Appropriations Act, 2021 authorized the transfer of up to $140 million of certain funds from VHA to VBA to prevent, prepare for, and respond to coronavirus, to include expenses to address the backlog of disability claims. Pub. L. No. 116-260, div. J, tit. V, § 514, 134 Stat. 1182, 1689-1690 (2020). According to VBA officials, they plan to use the transferred funding to support overtime to address the disability claims backlog.
[292]According to VHA and VBA officials, some VHA facilities resumed exams starting in May using ACE or telehealth. The ACE process allows the medical examiner to complete exam reports using the medical evidence in a veteran’s claims file or medical records, supplemented by a telephone interview if necessary. Telehealth allows the medical examiner to conduct face-to-face medical exams using video technologies, when appropriate.
[293] White House and Centers for Disease Control and Prevention, Opening Up America Again (Washington, D.C.: Apr. 16, 2020) Office of Management and Budget and Office of Personnel Management, Aligning Federal Agency Operations with National Guidelines for Opening up America Again, Memorandum M-20-23 (Washington, D.C.: Apr. 20, 2020).
[294]According to VBA officials, contractors began reporting on the number of ACE, telehealth, and in-person disability medical exam appointments completed in April 2020. The data provided by VBA may be an underestimate as contractors provide periodic manual updates to VBA.
[295]According to VBA officials, prior to the updated guidance, attendants were usually required to be present during telehealth exams to conduct tests, such as obtaining vital signs, during the course of the exam. As such, veterans usually had to go to a community-based outpatient clinic or to a veterans service organization facility.
[296]According to VBA officials, the number of appointments typically drops in November and December due to the holidays.
[297]VHA criteria included state or regions with downward trajectories of influenza-like illnesses and COVID-like cases reported within a 14-day period as well as a downward trajectory in documented COVID-19 cases or positive COVID-19 tests as a percent of total COVID-19 tests within that same period. According to VBA, the agency decided to resume in-person disability exams outside the U.S. by using feedback from local health officials, local government health guidance, and weekly reports provided by the VBA vendor servicing the contract.
[298]Pending exams are VBA exam requests that have not been completed by a medical examiner.
[299] A claims processor can make a decision on a claim using evidence such as the veteran’s military service records, medical exams, and treatment records from VHA medical facilities and private medical service providers, but the disability exam might be needed to provide support to substantiate the claim. A claims decision without the full evidence could result in a decision that resulted in a lower disability payment for the veteran.
[300] VBA stated that claims processors were provided instructions not to deny a claim when a veteran is unable or unwilling to report to an exam during the COVID-19 pandemic. However, a recent VA Office of Inspector General (OIG) report found that VBA prematurely or improperly denied claims based on canceled exams or exams where the veteran failed to show during the pandemic. According to the report, delays in clear guidance for claims processors contributed to the cancelation of claims that should, otherwise, have been placed on hold. However, the OIG also found that the number of claims that were prematurely or improperly denied based on a canceled exam dropped after clear guidance was issued in May. Further, VBA had begun a review to identify denied claims with one or more canceled exams, potentially indicating premature or improper denial. See Department of Veterans Affairs Office of Inspector General, Enhanced Strategy Needed to Reduce Disability Exam Inventory Due to the Pandemic and Errors Related to Canceled Exams, Report #20-02826-07 (Washington D.C.: Nov. 19, 2020)
[301]Veterans may file a claim that includes multiple medical issues that the claims processor needs to assess. According to VBA officials, the agency will make a partial decision (i.e., decide on one or more of the medical issues) when it has sufficient evidence to decide part of the claim and will wait for completed disability medical exams to make decisions on other medical issues.
[302]The amount of loans SBA can make changes based on the EIDL program’s estimated subsidy rate, which changes each fiscal year. We estimate that with the $50 billion in appropriations, SBA could make a total of about $470 billion in EIDL loans.
[303]SBA supported between $7 billion and $8 billion loans with the existing $1.1 billion in loan credit subsidy.
[304]Eligible entities include those businesses eligible for EIDL loans under the CARES Act (including most businesses with 500 employees or less). The Act excluded certain agricultural entities that are eligible for loans under the CARES Act. A low-income community is defined as a census tract where the poverty rate is at least 20 percent, or in the case of a tract not located within a metropolitan area, the median family income does not exceed 80 percent of the statewide median family income. For census tracts in metropolitan areas, the median family income for the tract must not exceed 80 percent of the greater of the statewide median family income of the metropolitan area median family income. Economic loss is defined as the amount by which the gross receipts of the covered entity declined during an 8-week period between March 2, 2020, and December 31, 2021, relative to a comparable 8-week period immediately preceding March 2, 2020 or during 2019. For seasonal businesses, SBA shall determine the economic loss as appropriate. Of the $20 billion appropriated for targeted EIDL advances, the Act designated $20 million to be made available to SBA’s Office of Inspector General to prevent waste, fraud, and abuse in the targeted EIDL advances program.
[305]The information in the remainder of this report pertains to advances provided under the CARES Act, which did not have a targeted advances program.
[306]The Consolidated Appropriations Act, 2021, permits SBA to obtain tax records as part of its application verification process for loans and targeted advances going forward.
[307]SBA officials said that SBA’s eligibility requirements for loans and advances differed. For advances, SBA officials said that applicants certified that they did not derive revenue from or present live performances of a prurient sexual nature or derive more than one-third of their income from gambling. For loans, SBA policies state that industries including adult entertainment, casino gambling, multi-level marketing, insurance, and real estate development were not eligible. The Consolidated Appropriations Act, 2021 amended certain eligibility requirements for advances going forward.
[308]Under the Consolidated Appropriations Act, 2021, SBA is permitted to verify eligibility for loans and required to verify eligibility for advances.
[309]Small Business Administration, Office of Inspector General, Inspection of Small Business Administration’s Initial Disaster Assistance Response to the Coronavirus Pandemic, Report No. 21-02 (Washington, D.C.: Oct. 28, 2020).
[310]Institutions are required to electronically file a suspicious activity report when a transaction involves or aggregates at least $5,000 in funds or other assets, and the institution knows, suspects, or has reason to suspect that the transaction meets certain criteria qualifying as suspicious. Banks are also required to file a report for known or suspected criminal violations involving insider abuse of any amount, as well as violations aggregating $5,000 or more when a suspect can be identified, and $25,000 or more without a potential suspect. See, e.g., 31 C.F.R. § 1020.320. See also 12 C.F.R. §§ 21.11(c)(1)-(3), 163.180(d)(3)(i)-(iii) (OCC); 12 C.F.R. § 208.62(c)(1)-(3) (Federal Reserve); 12 C.F.R. § 353.3(a)(1)-(3) (FDIC).
[311]FinCEN officials also said that these SARs may include defensive filings—a practice in which a financial institution sometimes files SARs to avoid criticism during exams conducted by federal financial supervisors. Additionally, beginning in March 2020, FinCEN issued seven notices and advisories to financial institutions related to illicit financial activity associated with COVID-19. FinCEN officials also told us that as of October 30, 2020, they had responded to 545 COVID-19-related inquiries. According to FinCEN officials, the majority of the inquiries were from financial institutions concerned about issues related to Bank Secrecy Act compliance in light of the pandemic.
[312]According to the Census Bureau, businesses with no paid employees, or nonemployers, make up a majority of all business establishments.
[313]The EIDL loan data are for approved loans. SBA asked EIDL advance and loan applicants to provide the number of employees, as of January 31, 2020.
[314]SBA stated that for advances, each business could receive $1,000 per employee, up to the maximum of $10,000. Applicants that reported having no employees or one employee could receive $1,000.
[315]SBA placed a $150,000 limit on loans on May 4, 2020.
[316]Federal agencies use codes under the North American Industry Classification System (NAICS) to classify industries. EIDL program applicants did not provide NAICS codes, but could select from a range of industry categories SBA provided. Applicants’ self-reporting and interpretation of the industry categories SBA provided may affect the accuracy in describing their industries. We found that SBA’s industry categorization for construction, accommodation and food services, and real estate generally matched NAICS classifications and that retail approximated NAICS classifications for the same category but did not include all possible types of retail. SBA’s health services category did not match NAICS classification for health care and included non-health-care related services, such as spas and weight loss centers. We matched businesses that received both an advance and a loan based on the application number. Our analysis resulted in about 2.4 million matched records for businesses that both received an EIDL advance and were approved for a loan.
[317]The CARES Act generally defines small businesses as those with 500 or fewer employees. We identified the total number of businesses with fewer than 500 employees by industry, including those with no employees, using the Census Bureau’s County Business Patterns and Nonemployer Statistics data. We then calculated the percentage of businesses within an industry that both received an EIDL advance and were approved for a loan, according to SBA data.
[318]Our analysis resulted in about 2.4 million matched records for businesses that both received an EIDL advance and were approved for a loan, accounting for about two-thirds of the 3.6 million businesses approved for loans.
[320]As originally implemented by SBA, at least 75 percent of the loan forgiveness amount must have been for payroll costs. In addition, the CARES Act required loans to be used within an 8-week period in order for the loans to be fully forgiven. However, the Paycheck Protection Program Flexibility Act of 2020 modified this to at least 60 percent and allowed borrowers to pay or incur those expenses over a 24-week period. Pub. L. No. 116-142, § 3, 134 Stat. 641, 641-42 (2020). Under the Paycheck Protection Program Flexibility Act of 2020, the covered period for PPP loans was to end the earlier of 24 weeks after origination or December 31, 2020.
[321]Totals exclude canceled loans. According to SBA, canceled loans may include, but are not limited to, duplicative loans, loans not closed for any reason, and loans that were fully paid off. In our September 2020 report, we provided information on the types of borrowers that received PPP loans and the size of PPP loans.
[322]See Consolidated Appropriations Act, 2021, Pub. L No. 116-260, Div. N, Tit. III, 134 Stat. 1182, 1993 (2020).
[323]The Consolidated Appropriations Act, 2021, allows borrowers to select a PPP loan forgiveness covered period between 8 weeks and 24 weeks after the loan’s origination date. Pub. L. No. 116-260, Div. N, Tit. III, § 306, 134 Stat. 1997; see also 86 Fed. Reg. 3692, 3706 (Jan. 14, 2021).
[324]We analyzed aggregate SAR data across U.S. financial institutions from April to October 2020. These data did not include identifying information on financial institutions that filed SARs, such as PPP lender status.
[325]SARs are reports certain financial institutions are required to file if a transaction involves or aggregates at least a certain dollar amount in funds or other assets (generally $5,000), and the institution knows, suspects, or has reason to suspect that the transaction is designed to evade any Bank Secrecy Act requirements or involves money laundering, tax evasion, or other criminal activities. See e.g. 31 C.F.R. § 1020.320. Under the Bank Secrecy Act’s implementing regulations, banks are also required to file a SAR when a transaction meets certain other criteria, such as for known or suspected criminal violations involving insider abuse of any amount. See 12 C.F.R. §§ 21.11(c), 163.180(d)(3) (OCC); 12 C.F.R. § 208.62(c) (Federal Reserve); 12 C.F.R. § 353.3(a) (FDIC). Law enforcement agencies query FinCEN systems as part of their investigations of potential financial and other crimes.
[326]Banks and other financial institutions must file a SAR no later than 30 calendar days after the date of initial detection of facts that may constitute a basis for filing a SAR. If no suspect was identified on the date of detection of the incident requiring the filing, the financial institution may delay filing a SAR for an additional 30 calendar days to identify a suspect, but the report must be filed no more than 60 calendar days after the date of initial detection of a reportable transaction.
[327]FinCEN officials also said that SARs could be filed on denied loans or by financial institutions involved in defensive filings—a practice in which a financial institution sometimes files SARs to avoid criticism during exams conducted by federal financial supervisors. Beginning in March 2020, FinCEN has issued eight notices or advisories to financial institutions related to potential illicit financial activity associated with COVID-19, as well as Paycheck Protection Program Frequently Asked Questions. FinCEN officials also told us that as of October 30, 2020, they had received 545 COVID-19-related inquiries.
[328]Borrowers submit loan forgiveness applications to their lenders, and lenders submit their decisions on loan forgiveness to SBA.
[329]According to SBA officials, all loan forgiveness decisions from lenders are reviewed using an automated review tool to identify potential indicators of noncompliance with selected eligibility requirements, fraud, or abuse. Loans flagged by the tool are subject to additional review by contractor and SBA staff. These reviews are discussed in more detail later in this enclosure.
[330]On October 8, 2020, exercising their authority under the CARES Act to grant de minimis exemptions for certain PPP forgiveness requirements, SBA and the Department of the Treasury posted an interim final rule that simplified the forgiveness and loan review processes for PPP loans of $50,000 or less. In conjunction with the rule, SBA released a new form (Form 3508S) that requires fewer calculations and less documentation for eligible borrowers. SBA had previously released two other loan forgiveness applications—a long form (Form 3508) and an abbreviated form (Form 3508EZ). The 3508S is shorter than the 3508EZ. The form the borrower can use depends on factors such as the amount borrowed and whether the business reduced the number of employees or their salaries.
[331]Under the provisions of the Act, a borrower must sign and submit to the lender a certification that is not more than one page in length, that includes a description of the number of employees the borrower was able to retain because of the covered loan, the estimated total amount of the loan spent on payroll costs, and the total loan value. The borrower must also attest that the borrower accurately provided the required certification and complied with PPP loan requirements. SBA must establish this form within 24 days of enactment and may not require additional materials unless necessary to substantiate revenue loss requirements or satisfy relevant statutory or regulatory requirements. Additionally, borrowers are required to retain relevant records related to employment for four years and other records for three years.
[332]SBA posted the first interim final rule on the PPP program 1 day prior to accepting loan applications (6 days after passage of the CARES Act).
[333]The EIDL program provides low-interest loans of up to $2 million for expenses—such as operating expenses—that cannot be met because of a disaster. The CARES Act expanded EIDL program eligibility to include additional small business entities and appropriated $10 billion to create a program to provide small businesses up to $10,000 in advances toward payroll, sick leave, and other business obligations. In the Paycheck Protection Program and Health Care Enhancement Act, Congress appropriated another $10 billion for advances. The Consolidated Appropriations Act, 2021, included an additional $20 billion for targeted EIDL advances to eligible entities with 300 or fewer employees in low-income communities that have suffered an economic loss of greater than 30 percent. Borrowers do not have to repay these advances, even if they are subsequently denied the EIDL. However, Section 1110(e)(6) of the CARES Act stated that “the advance amount shall be reduced from the loan forgiveness amount” for any PPP loan received by the EIDL applicant.
[334]Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, Div. N, Tit. III, § 333, 134 Stat. 2046-47. The Act also required SBA to issue rules that ensure that borrowers who already applied for forgiveness and had their EIDL advance deducted from the forgiven amount be treated equally. Any EIDL advance amounts previously deducted from a borrower’s forgiveness amount will be remitted to the lender, together with interest to the remittance date. 86 Fed. Reg. 3692, 3707 (Jan. 14, 2021).
[335]As set forth in the CARES Act, borrowers had to certify in good faith that, among other things, (1) current economic uncertainty made the loan request necessary to support the applicant’s ongoing operations and (2) the funds would be used for allowed business-related purposes, such as to retain workers and maintain payroll or to make mortgage interest payments, lease payments, or utility payments.
[336]As we reported in September 2020, SBA officials said a contractor would use the automated review tool to flag potentially questionable loans, and contractor and SBA staff would conduct a manual review of loans flagged by the tool. According to SBA officials in October 2020, SBA was also flagging loans for manual review identified in a variety of ways, including DOJ or SBA Office of Inspector General referrals, fraud tips, media reports, or whistleblowers.
[337]For more information, see GAO, Federal Reserve Lending Program: Use of CARES Act-Supported Programs Has Been Limited and Flow of Credit Has Generally Improved, GAO-21-180 (Washington, D.C.: Dec. 10, 2020). Section 4026(f) of the CARES Act contains a provision for us to review the loans, loan guarantees, and other investments provided under section 4003 of the act and report no later than 9 months after the date of enactment of the act, and annually thereafter through the year succeeding the last year for which loans, loan guarantees, or other investments made under section 4003 are outstanding.
[338]The Federal Reserve has taken some actions to address the second recommendation. However, some documentation we need for a full assessment of the actions was not available at the time of our reporting.
[339]The facilities are authorized under Section 13(3) of the Federal Reserve Act, which permits the Federal Reserve to provide emergency lending, and are approved by the Secretary of the Treasury. Section 13(3) facilities must comply with requirements relating to loan collateralization and taxpayer protection, among others. Of the $500 billion appropriated under Section 4027 of the CARES Act, $25 million remains available to the Special Inspector General for Pandemic Recovery.
[340]To implement these facilities, the Federal Reserve used legal entities known as special purpose vehicles to purchase qualifying assets from, or initiate lending to, eligible entities. Treasury’s investments in these facilities took the form of equity investments in these special purpose vehicles using CARES Act funds. For Treasury loan program subsidies under Section 4003 of the CARES Act (Economic Stabilization Program), total obligations of budget authority are recorded on a net present value basis. As a result, and following the rescissions mandated by the Consolidated Appropriations Act, 2021, total Economic Stabilization Program outlays related to the Federal Reserve facilities are $19.07 billion.
[341]The December 31, 2020 end date was codified by the Consolidated Appropriations Act, 2021, for most facilities. However, under the act, loans submitted to the lender portal for the Main Street Lending facilities by December 14, 2020, may still participate in the program if the facility purchased a participation interest in the loan on or before January 8, 2021.
[342]The Consolidated Appropriations Act, 2021, rescinded at least $429 billion of the $500 billion previously appropriated to Treasury under Title IV of the CARES Act. Certain funds appropriated out of the $500 billion, including $25 million for the Special Inspector General for Pandemic Recovery, $5 million for the Congressional Oversight Committee and $100 million to pay costs and administrative expenses are not rescinded. Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, § 1003(a)(2)(C) (2020).
[343]According to Federal Reserve officials, the expectation of the facilities incurring no losses for the Federal Reserve takes into account Treasury’s support using funds appropriated under the CARES Act.
[344]On October 30, 2020, the Federal Reserve lowered the minimum loan amount for most Main Street facilities from $250,000 to $100,000. The Main Street Expanded Loan Facility and Nonprofit Organization Expanded Loan Facility continued to have a minimum loan requirement of $10 million.
[345]For most of the CARES Act and non-CARES Act facilities that include a special purpose vehicle, the responsible Federal Reserve Banks will continue to fund the vehicle after the facility’s termination date until the vehicle’s underlying assets mature or are sold.
[346]The Primary Dealer Credit Facility, the Commercial Paper Funding Facility, the Money Market Mutual Fund Liquidity Facility, and the Paycheck Protection Program Liquidity Facility will terminate on March 31, 2021, unless extended.
[347]COVID-19 affected consumer prices for food. In May 2020, the U.S. Bureau of Labor Statistics reported that April 2020 saw the sharpest increase in grocery store prices since 1974.
[348]The CARES Act, Pub. L. No. 116-136, div. B, tit. I, 134 Stat. 281, 505 (2020).
[349]Pub. L. No. 116-136, div. B, tit. I, § 11002, 134 Stat. at 509. Generally, appropriations acts enacted annually reimburse the Commodity Credit Corporation for its net realized losses.
[351]The Commodity Credit Corporation Charter Act is codified at 15 U.S.C. §§ 714-714p.
[352]The Commodity Credit Corporation’s debt to the Treasury can be described as net expenditures and net realized losses. “Net expenditures” are where the outlays (e.g., loans made, conservation program payments, commodity purchases, and disaster payments) are offset by receipts (e.g., loan repayment, sale of commodities, and fees). “Net realized losses” are expenditures that will never be recovered.
[353]“Borrowing authority” is authority that permits agencies to incur obligations and make payments to liquidate the obligations out of borrowed moneys. Borrowing from the Treasury is the most common form and is also known as “public debt financing.” GAO, Principles of Federal Appropriations Law, 4th ed., 2016 rev., ch. 2, GAO-16-464SP (Washington, D.C.: March 2016), 9.
[354]We continue to seek additional information from USDA regarding the $14 billion reimbursement to the Commodity Credit Corporation provided under the CARES Act, and the use of the Commodity Credit Corporation for CFAP 1 and CFAP 2 payments.
[355]According to USDA officials, the $14 billion transfer resulted in a corresponding net realized loss for the Commodity Credit Corporation. USDA received a reimbursement of the Commodity Credit Corporation in the Continuing Appropriations Act, 2021 and Other Extensions Act, enacted on October 1, 2020, for the net realized losses as of September 17, 2020. Pub. L. No. 116-159, div. A, § 173, 134 Stat. 709, 725.
[356]To track spending, we were looking for documentation on the use of Commodity Credit Corporation replenishments by legislative funding source as the agency has done, for example, in its Appropriations Weekly Covid Reports, which include the following by program: funding account, public law that provided the funding, the amount enacted, the amount allocated, the amount obligated, the date of the most recent update, and explanation and timing for the obligation of the remaining funding.
[357] The Consolidated Appropriations Act, 2021 provided a reimbursement of the Commodity Credit Corporation’s net realized losses as of the close of fiscal year 2020, which was $7.9 billion, according to USDA officials.
[358] Pub. L. No. 116-260, div. W, tit. VII, subtit. B, ch. 1, § 751, 134 Stat. at 2105.
[359] Pub. L. No. 116-260, div. W, tit. VII, subtit. B, ch. 1, § 751, 134 Stat. at 2107.
[360] Pub. L. No. 116-260, div. W, tit. VII, subtit. B, ch. 1, § 751, 134 Stat. at 2105-2106.
[361] Pub. L. No. 116-260, div. A, tit. I, 134 Stat. at 1199.
[362]U.S. Department of Commerce, National Oceanic and Atmospheric Administration, National Marine Fisheries Service, Fisheries Economics of the United States, 2016, Technical Memorandum NMFS-F/SPO-187a (Silver Spring, MD: December 2018). Information on gross domestic product and jobs includes data on commercial seafood harvesters, processors, dealers, wholesalers, distributors, importers, and retailers, as well as recreational fishing trips and fishing equipment. Data for 2016 were the most recent available at the time of our review.
[363]Pub. L. No. 116-136, § 12005(a), 134 Stat. at 518.
[364]Id. § 12005(d). An additional $300 million for certain COVID-19-related fisheries disaster assistance was appropriated under the Consolidated Appropriations Act, 2021, signed by the President into law on December 27, 2020. Pub. L. No. 116-260, div. M, tit. I, 134 Stat. 1182, 1909-1910 (2020). This enclosure does not provide information on that additional funding.
[365]Id.§ 12005(b). Specifically, “fishery participants” are defined as belonging to these categories and as having incurred, as a direct or indirect result of the COVID-19 pandemic, economic revenue losses greater than 35 percent as compared with their prior 5-year average revenue or any negative impacts to subsistence, cultural, or ceremonial fisheries. Additionally, the CARES Act provided that the Department of Commerce may use up to 2 percent of the $300 million for administration and oversight activities.
[366]Puerto Rico and the U.S. Virgin Islands are not part of an interstate commission.
[367]The commissions, established in the 1940s, partner with NOAA on data collection and management of fisheries resources that are shared across states, such as striped bass.
[368]As of November 25, 2020, NOAA was reviewing the spend plans for Delaware, New Hampshire, Puerto Rico, and Washington.
[369]NOAA officials said that states, tribes, and territories can also use existing records, such as fishing permits, to identify eligible recipients.
[370]Puerto Rico and the U.S. Virgin Islands are not part of an interstate marine fisheries commission, so they will disburse funds directly to fishery participants.
[371]Office of Management and Budget, Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019 (COVID-19), (Washington D.C., Apr. 10, 2020).
[372]National Interest Action codes were established in 2005 after Hurricane Katrina with the purpose of tracking federal procurements for specific disasters, emergencies, or contingency events. The National Interest Action code for COVID-19 was established on March 13, 2020, and as of December 2020, is active until March 31, 2021. We continue to monitor the end date for the COVID-19 National Interest Action code.
[373]For the purposes of this report, “contract obligations” refers to obligations on procurement contracts that are subject to the Federal Acquisition Regulation and does not include, for example, grants, cooperative agreements, loans, other transactions for research, real property leases, or requisitions from federal stock.
[374]Pub. L. No. 81-774 (1950), codified at 50 U.S.C. §§ 4501 et seq., as amended.
[375]Pub. L. No. 116-136, §§ 3301, 13006, 134 Stat. at 383, 522.
[376]For the purposes of this report, obligations on contracts identified as using the unusual and compelling urgency exception include those associated with contracts subject to Federal Acquisition Regulation 6.302-2, as well as orders under multiple award contracts, which are subject to separate competition requirements under Federal Acquisition Regulation Part 16. Specifically, under Federal Acquisition Regulation 16.505(b)(2), orders on multiple award contracts require contracting officers to give every awardee a fair opportunity to be considered for a delivery order or task order exceeding $3,500, with exceptions, including if the agency need for the supplies or services is so urgent that providing a fair opportunity would result in unacceptable delays. When using the unusual and compelling urgency exception to full and open competition, agencies still must request offers from as many potential sources as is practicable under the circumstances.
[377]DPA actions refer to actions executed under DPA Title III authority. Similar actions refer to actions identified by DOD that have similar goals of industrial base expansion for medical supplies but are not executed under the DPA Title III authority.
[378]In November 2020 the International Development Finance Corporation announced that it planned to award one $590 million loan to expand domestic production of prefilled injectors to deliver a projected annual capacity of 3 billion vaccine doses at full rate of production of production, and another loan up to $1.1 billion to facilitate mass production of raw materials for vaccines and testing capacity. We have ongoing work evaluating the International Development Finance Corporation’s activities.
[379]The Federal Acquisition Regulation (FAR) requires agencies to report contract actions in FPDS-NG, which are generally any oral or written actions that result in the purchase, rent, or lease of goods or services over a certain dollar threshold and generally do not include non-FAR based transactions such as other transaction agreements. FAR 4.601 and 4.603(b).
[380]Other transaction agreements may be included in FPDS-NG only if they can be segregated from FAR-based actions and written approval from the FPDS program office is obtained. FAR 4.606(a), (b), and (c).
[381]Pub. L. No. 113-101, 128 Stat. 1146 (2014). The DATA Act amended the Federal Funding Accountability and Transparency Act of 2006. Pub. L. No. 109-282, 120 Stat. 1186 (2006), codified at 31 U.S.C. § 6101 note.
[382]FPDS-NG data from beta.SAM.gov accessed December 31, 2020. For purposes of this report, “competition rate” is the percentage of total obligations associated with contracts awarded competitively. We calculated competition rates as the percentages of obligations on competitive contracts and orders over all obligations on contracts and orders. Competitive contracts included contracts and orders coded in the FPDS-NG as “full and open competition,” “full and open after exclusion of sources,” and “competed under simplified acquisition procedures” as well as orders coded as “subject to fair opportunity,” “fair opportunity given” and “competitive set aside.” Noncompetitive contracts included contracts and orders coded in the FPDS-NG as “not competed,” “not available for competition,” and “not competed under simplified acquisition procedures,” as well as orders coded as an exception to “subject to fair opportunity,” including “urgency,” “only one source,” “minimum guarantee,” “follow-on action following competitive initial action,” “other statutory authority,” and “sole source.” Even for contracts identified as noncompetitive, agencies may have solicited more than one source.
[383]Our prior work has identified some inconsistencies in the information agencies report in the contract description field in the FPDS-NG. See GAO-20-75. Data on DOD contract obligations based on information in the description field were only available through October 15, 2020, due to differences in the time frames for which DOD data are made publicly available.
[384]These product categories were identified by the U.S. International Trade Commission (USITC) in its report, COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). USITC changed 12 of these product categories in its July 1, 2020 revision to the Harmonized Tariff Schedule. We identified these product categories and included them in the July through October 2020 data for our analysis.
[385]Some imports from China have been subject to tariffs imposed by the Office of the U.S. Trade Representative (USTR) at the direction of the President under Section 301 of the Trade Act of 1974 since 2018.
[386]Some Harmonized Tariff Schedule of the United States categories identified in USITC Publication 5073 represent more than one product, and some categories contain products that are not directly relevant to COVID-19 responses. Product types only refer to the subset of goods considered COVID-19 related in each HTS-10 statistical reporting number. Therefore, the values presented may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, they are useful indicators for tracking import trends of such products.
[387]Imports from China accounted for 5 percent of overall COVID-19-related product categories imported in March 2020.
[388]Swab and viral transport medium sets are described in HTS-10 statistical reporting number 3821.00.0000, according to USITC. Reagents are described in HTS-10 statistical reporting numbers 3002.15.0000, 3822.00.1090 and 3822.00.5090, according to USITC. Product types only refer to the subset of goods considered COVID-19 related in each HTS-10 statistical reporting number. Therefore, the values presented may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, they are useful indicators for tracking import trends of such products.
[389]Ellen M. Lord, Under Secretary for Defense for Acquisition & Sustainment, Supply Chain Integrity, testimony before the Senate Subcommittee on Readiness and Management Support, 116th Cong., 2nd sess., October 1, 2020. See https://www.businessdefense.gov/DPA-Title-III/Overview/ for an overview of the Defense Production Act, accessed on December 8, 2020.
[391]This funding was provided through two COVID-19 relief laws, the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, and the CARES Act, and directed to specific accounts. Pub. L. No. 116-123, tit. IV, 134 Stat. at 152-53; Pub. L. No. 116-136, div. B, tit. XI, 134 Stat. at 590. In fiscal year 2021, the Consolidated Appropriations Act, 2021, appropriated additional funding to respond to the coronavirus to the Global Health Programs Account and the Consular and Border Security Programs Account in Pub. L. No. 116-260, div. K, tit. IX, 134 Stat. at 1821-22. The funds appropriated in fiscal year 2021 are not included in our discussion about appropriations from COVID-19 relief laws.
[392]Criteria include countries’ caseload of COVID-19, fragility of health systems, and diplomatic considerations, among others.
[393]State and USAID Guidance on the Process for Investing Supplemental Foreign Assistance Resources to Respond to the Pandemic of COVID-19, effective April 1, 2020.
[394]In addition to providing ventilators directly to 43 countries, USAID provided 200 ventilators to the North Atlantic Treaty Organization. As of September 30, 2020, USAID had delivered 8,139 of the 8,722 ventilators ordered. According to USAID’s contractor for this effort, ventilators were generally delivered into the custody of recipient countries’ ministries of health.
[395]COVID-19 funding for humanitarian assistance under Pillar 3 was not a source for funding the ventilator procurements and deliveries.
[396]USAID used its existing “Global Health Supply Chain Program-Procurement and Supply Management” contract with Chemonics International to procure and deliver the ventilators. USAID’s Bureau for Global Health manages this contract.
[397]Implementing partners may include contractors, international organizations, and other awardees. After its award to Chemonics International, USAID’s next largest award amount of obligations to an implementing partner was about $53 million to the United Nations’ World Food Program for humanitarian assistance, primarily to support countries’ efforts to augment their national health systems and enable access to critical medical supplies, treatment, and training.
[398]Memoranda we obtained from Chemonics International note that the “absence of competition” was justified because the NSC had determined the ventilator quantities and destination countries, and communicated this to Chemonics via USAID task orders in an effort to share resources internationally and combat the COVID-19 pandemic. The NSC did not respond to our request for information regarding ventilator allocations.
[399]According to a USAID official, USAID is assessing what global health assistance to continue to provide in support of countries’ response to COVID-19 with funding it has available.
[400]New daily COVID-19 cases are reported by the World Health Organization based on a 7-day rolling average (see https://covid19.who.int/table). Transfer letters from USAID confirm USAID’s intention to deliver ventilators to recipient countries, according to a USAID official. In some instances in which USAID did not provide transfer letters, we relied on other correspondence between USAID and recipient countries to confirm the intent to deliver ventilators.
[401]USAID officials told us that such a platform would also potentially be used to manage the distribution of other COVID-related assistance, such as vaccine doses.
[402]USAID’s internal operational policies for monitoring and evaluation are contained in the Automated Directives System. U.S. Agency for International Development, Automated Directives System, 201.3.5.4 and 201.3.6 (Washington, D.C.: Oct. 28, 2020).
[404]According to USAID, the ventilation distribution activities are exempt under 201.3.5.1(d) of the Automated Directives System. USAID explained that this exempts activities targeted at preventing, mitigating, responding to, recovering from, and transitioning from crisis from monitoring requirements such as creating an activity monitoring, evaluation and learning plan.
[405]An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes. This amount does not include appropriations in the Consolidated Appropriations Act, 2021, as the specific Treasury appropriations warrants were not available at the time of our analysis. The House Appropriation Committee estimates that provisions of the Consolidated Appropriations Act, 2021 provide an additional $900 billion in appropriations for emergency coronavirus relief, and the Congressional Budget Office estimates that outlays for coronavirus response and relief provided in divisions M and N of the Act will total about $868 billion. An outlay refers to the issuance of checks, disbursement of cash, or electronic transfer of funds made to liquidate a federal obligation. We will examine and report appropriations enacted in the Consolidated Appropriations Act, 2021 in future reporting.
[406]Improper payments could suggest that a program may also be vulnerable to fraud, although it is important to note that fraud is one specific type of improper payment and that improper payment estimates are not intended to measure fraud in a particular program. An improper payment is defined as any payment that should not have been made or that was made in an incorrect amount (including overpayments and underpayments) under statutory, contractual, administrative, or other legally applicable requirements, and it includes any payment that is the result of fraud. Improper payment is defined at 31 U.S.C. § 3351(4). While an improper payment may be the result of fraudulent activity, not all improper payments are the result of fraud. Fraud involves obtaining something of value through willful misrepresentation. Whether an act is in fact fraud is a determination to be made through the judicial or other adjudicative system.
[407]Fraud and “fraud risk” are distinct concepts. Fraud—obtaining something of value through willful misrepresentation—is challenging to detect because of its deceptive nature. Fraud risk (which is a function of likelihood and impact) exists when individuals have an opportunity to engage in fraudulent activity, have an incentive or are under pressure to commit fraud, or are able to rationalize committing fraud. Fraud risk management is a process for ensuring program integrity by continuously and strategically mitigating the likelihood and impact of fraud. When fraud risks can be identified and mitigated, fraud may be less likely to occur. Although the occurrence of fraud indicates there is a fraud risk, a fraud risk can exist even if actual fraud has not yet been identified or occurred.
[408]The statute of limitations for mail fraud and wire fraud prosecutions is 5 years (18 U.S.C. § 3282), except for mail and wire fraud schemes that affect a financial institution, in which case the statute is 10 years (18 U.S.C. § 3293). Also, based on our analysis, these cases can take many years to resolve. For example, the Department of Housing and Urban Development Office of Inspector General closed cases in 2017–2020 resulting from Hurricane Sandy in 2012.
[409]In November 2020, one of these individuals was sentenced to 12 months in prison and 2 years of supervised release. In December 2020, another individual was sentenced to 24 months in prison and 5 years of supervised release.
[410]Unlike a loan, an advance does not have to be repaid.
[411]Aged off-the-shelf companies are shell companies—companies that have no active business and usually exist only in name as a vehicle for another company’s business operations—that had been created at an earlier date to give banks and regulatory authorities the impression the company has longevity.
[412]A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[413]There are 21 individuals facing other charges such as bank fraud related to counterfeit economic impact payments.
[414]In June 2018, we raised concerns about the Internal Revenue Service’s inability to securely authenticate taxpayers online. For example, we recommended that the Internal Revenue Service develop a plan for implementing changes to its online authentication programs consistent with new guidance and implement improvements to its systems to fully implement the new guidance. As of January 2020, the agency had taken steps on these recommendations but had not yet fully implemented them.
[415]Two of the eight individuals or entities have also pleaded guilty to federal charges of defrauding COVID-19 relief programs. In November 2020, one of the individuals was sentenced to 36 months of incarceration. Four individuals or entities in other cases had been sentenced to 2 to 3 years of probation and ordered to pay fines as of November 30, 2020.
[416]In October 2020, this individual was sentenced to 1 year and 1 day in prison, and ordered to pay restitution in the amount of $221,200. Two individuals in other cases had been sentenced to 2 to 3 years of probation and ordered to pay fines as of November 30, 2020.
[417]On January 11, 2021, this individual was sentenced to 3 months in prison and 9 months of home confinement, and ordered to pay restitution in the amount of $132,291.
[418]Authorities stopped the transaction before it could be completed.
[419]According to the Federal Trade Commission, these data reflect reports in the Consumer Sentinel Network that mention COVID, stimulus, N95, and related terms.
[420]SARs are reports certain financial institutions are required to file if a transaction involves or aggregates at least a certain dollar amount in funds or other assets (generally $5,000), and the institution knows, suspects, or has reason to suspect that the transaction is designed to evade any Bank Secrecy Act requirements or involves money laundering, tax evasion, or other criminal activities. Under the Bank Secrecy Act’s implementing regulations, banks are also required to file a SAR when a transaction meets certain other criteria, such as for known or suspected criminal violations involving insider abuse of any amount. See 12 C.F.R. §§ 21.11(c), 163.180(d)(3) (OCC); 12 C.F.R. § 208.62(c) (Federal Reserve); 12 C.F.R. § 353.3(a) (FDIC).
[421]The Fraud Risk Framework helps managers meet their responsibilities to assess and manage fraud risks, as required by federal internal control standards. The leading practices of the Fraud Risk Framework are also required to have been incorporated into OMB guidelines and agency controls under the Fraud Reduction and Data Analytics Act of 2015 (FRDAA) and its successor provisions in the Payment Integrity Information Act of 2019. FRDAA, Pub. L. No. 114-186, 130 Stat. 546 (2016), enacted in June 2016, required OMB to establish guidelines for federal agencies to create controls to identify and assess fraud risks and to design and implement antifraud control activities. The act further required OMB to incorporate the leading practices from the Fraud Risk Framework in the guidelines. Although FRDAA was repealed in March 2020, the Payment Integrity Information Act of 2019, Pub. L. No. 116-117, 134 Stat. 113 (2020), requires these guidelines to remain in effect, subject to modification by OMB as necessary and in consultation with GAO.
[422]Office of Management and Budget, Management’s Responsibility for Enterprise Risk Management and Internal Control, OMB Circular A-123 (Washington, D.C.: July 15, 2016).
[423]Office of Management and Budget, Risk-Based Financial Audits and Reporting Activities in Response to COVID-19 (June 17, 2020).
[424]Office of Management and Budget, Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019, M-20-21 (Apr. 10, 2020).
[425]Office of Management and Budget, Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-18-20 (Washington, D.C.: June 26, 2018). OMB officials identified multiple risk factors likely to alter the payment integrity risk during COVID-19, such as (1) the creation of new programs; (2) new legal provisions contained in the CARES Act and other legislation; (3) change to existing program eligibility rules; (4) program executing all or part of the payment process differently; (5) increased volume of program applications; (6) limited time to spend the full amount of funding; and (7) significant increase in funding. As outlined in OMB memorandum M-18-20, management is required to manage its payment integrity risk—including fraud risk— to an agency achieving its strategic, operations, reporting, or compliance objectives.
Contacts
A. Nicole Clowers
Managing Director, Health Care, clowersa@gao.gov, (202) 512-7114
Congressional Relations
Orice Williams Brown, Managing Director, williamso@gao.gov, (202)-512-4400 U.S. Government Accountability Office 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs
Chuck Young, Managing Director, youngc1@gao.gov, (202)-512-4800 U.S. Government Accountability Office 441 G Street NW, Room 7149, Washington, DC 20548
Strategic Planning and External Liaison
Stephen J. Sanford, Acting Managing Director, spel@gao.gov, (202)-512-4707 U.S. Government Accountability Office 441 G Street NW, Room 7814, Washington, DC 20548
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s cost of production and distribution. Pricing and ordering information is posted on our website.
To Report Fraud, Waste, and Abuse in Federal Programs
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Copyright
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.












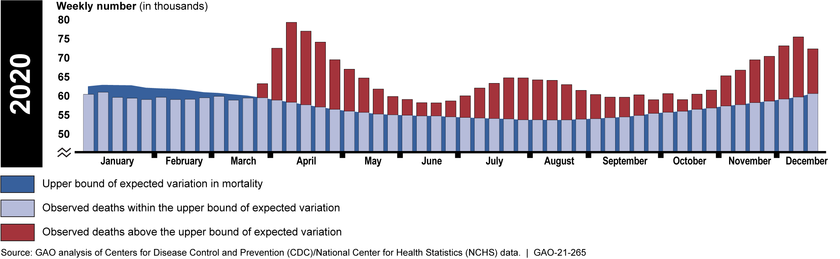




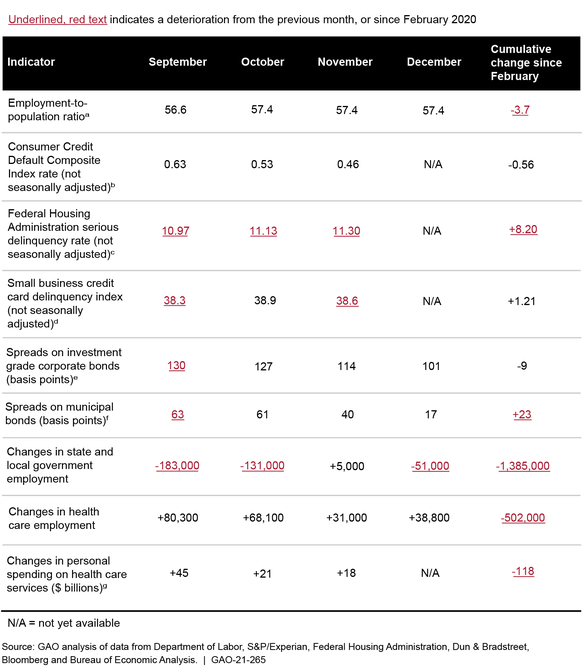
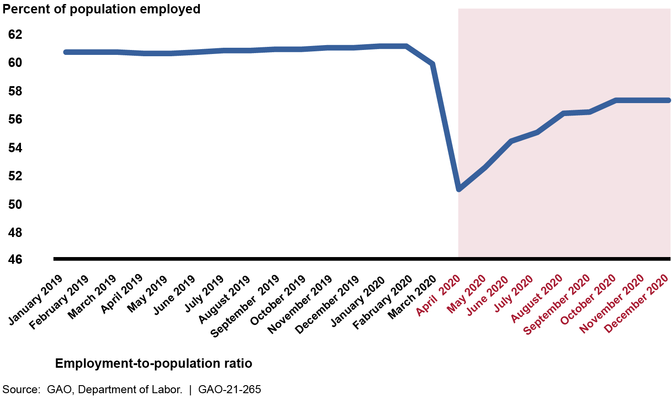
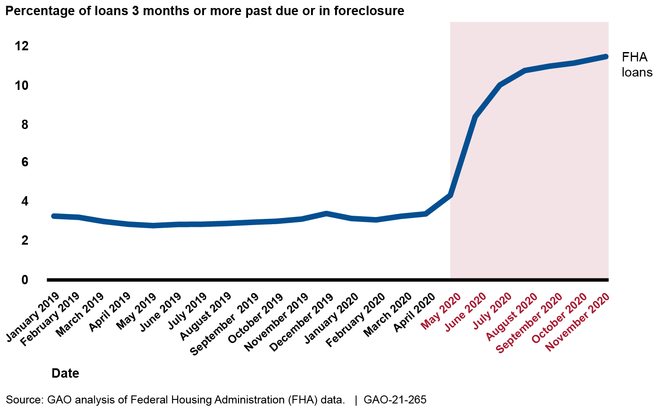


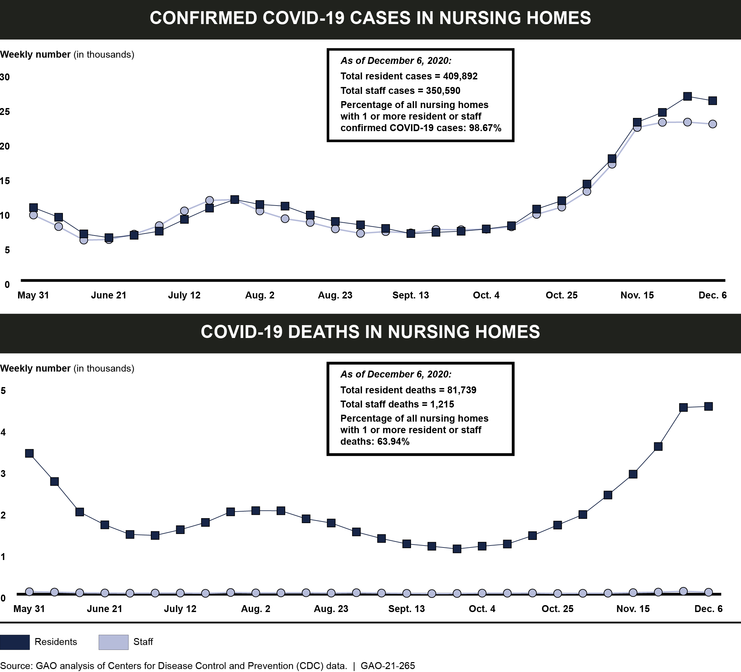
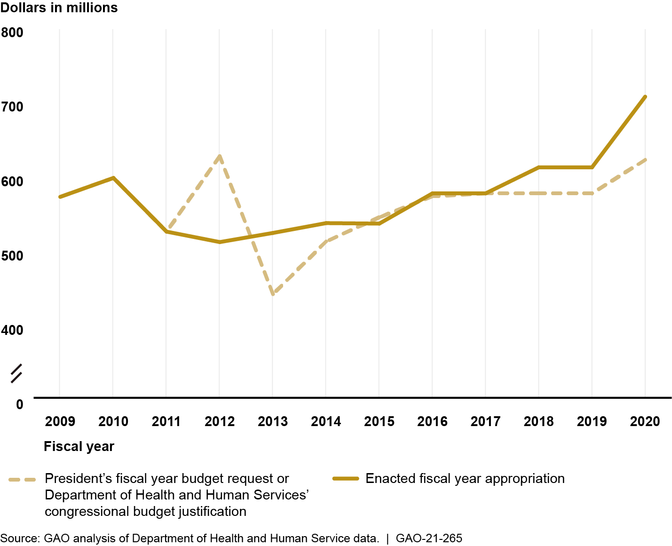


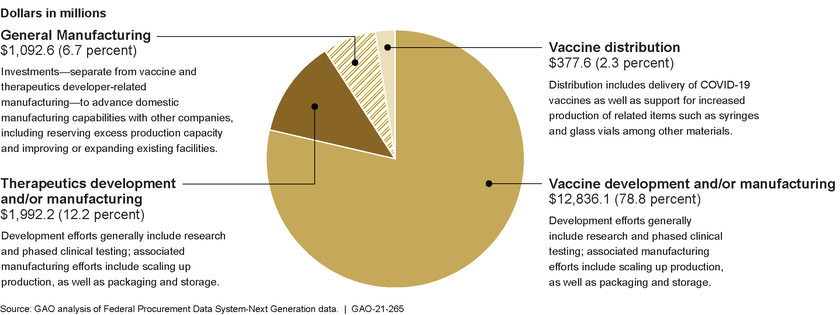
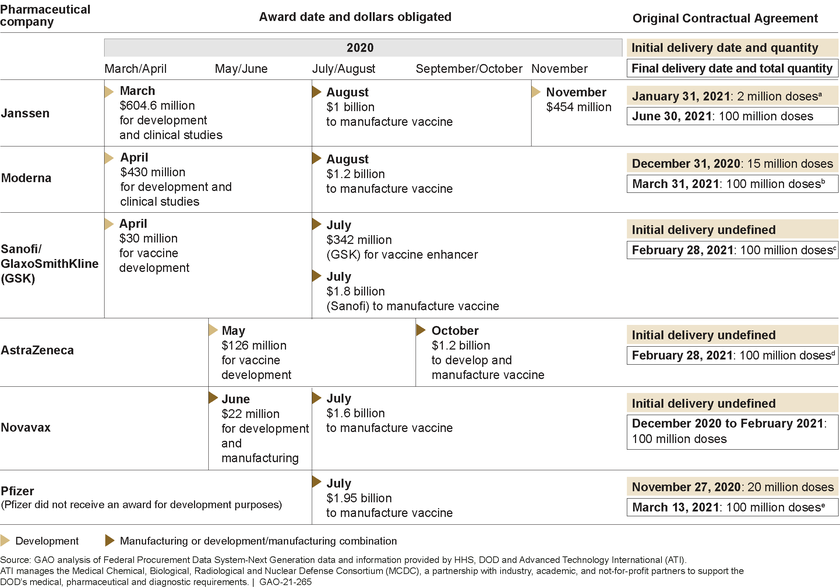
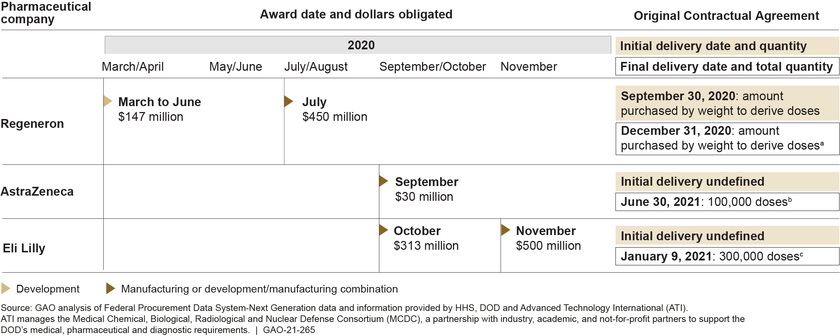




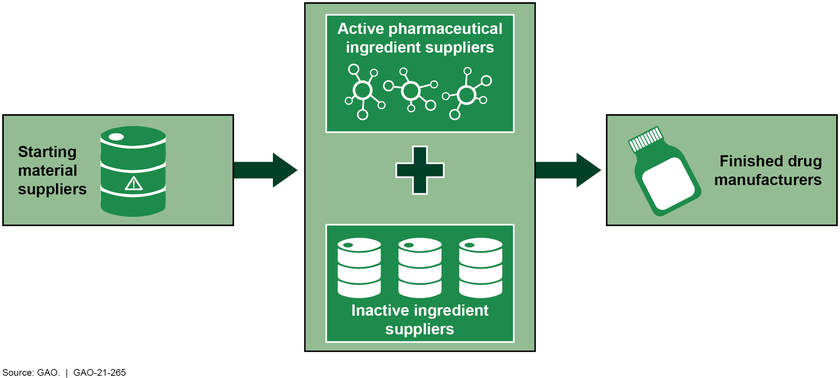

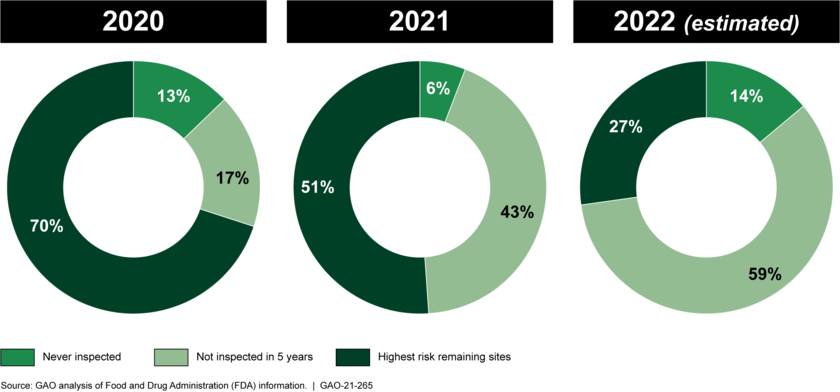
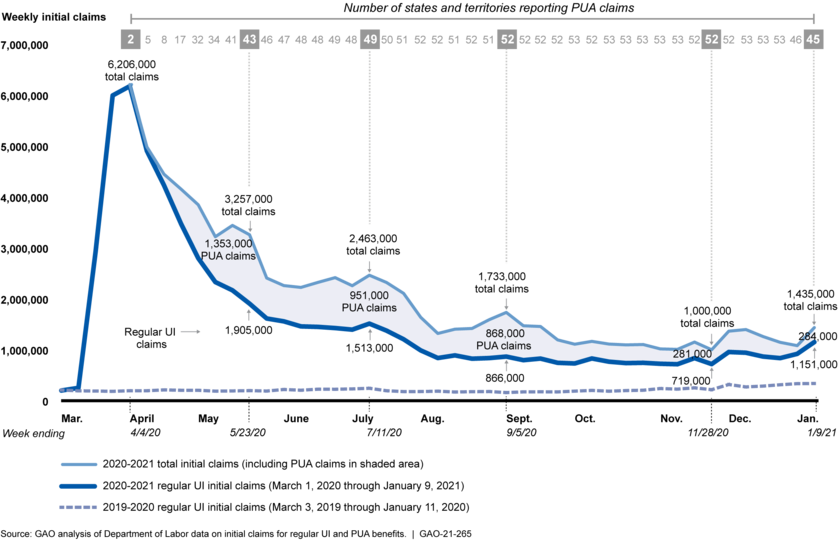
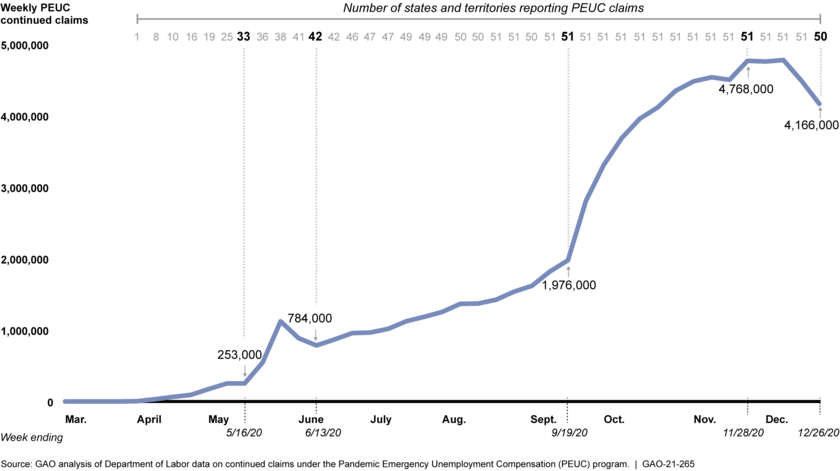
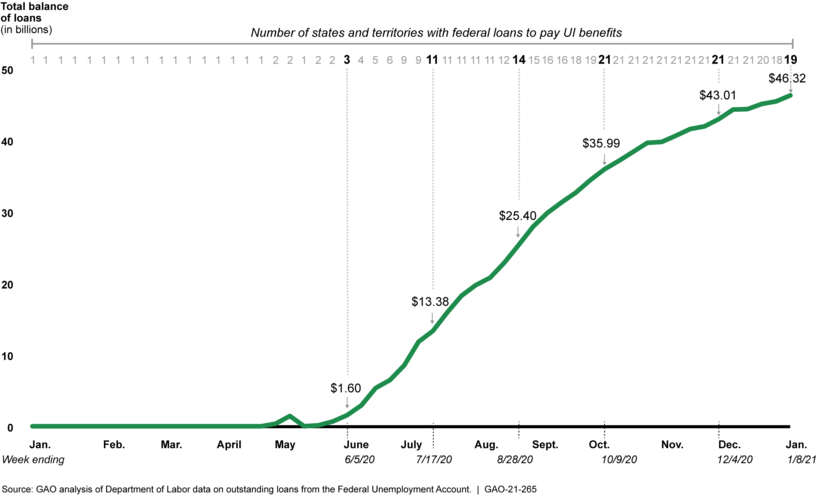



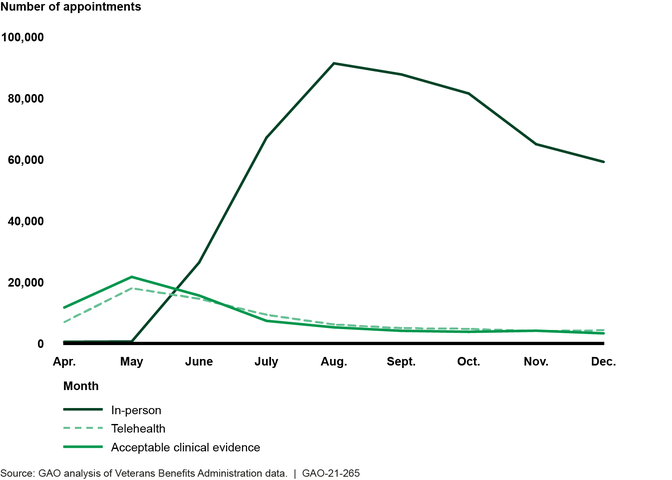
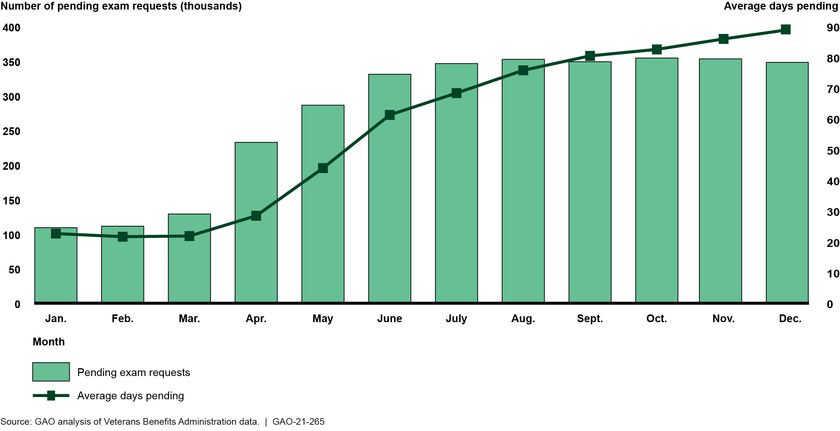

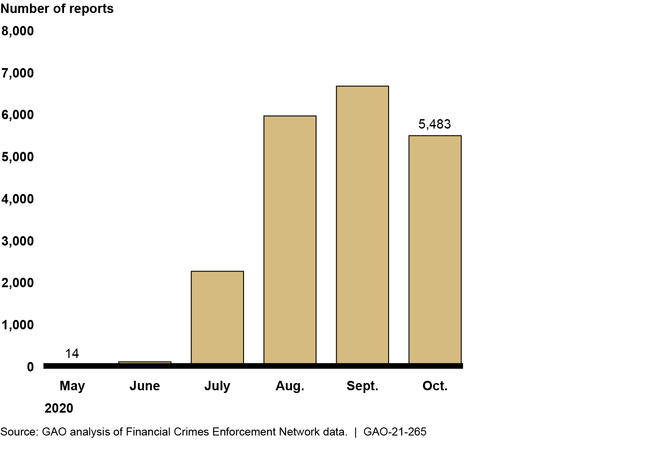

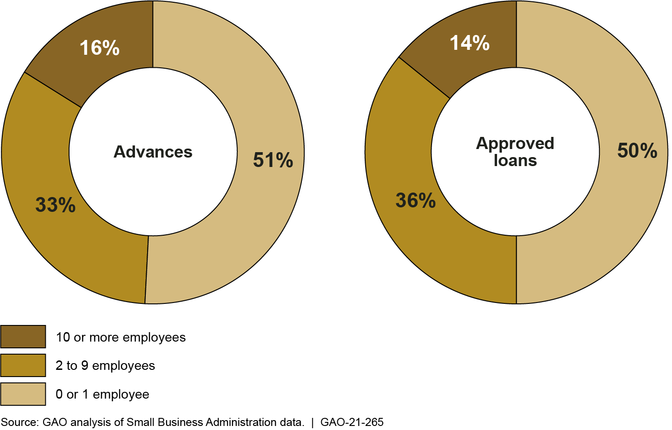

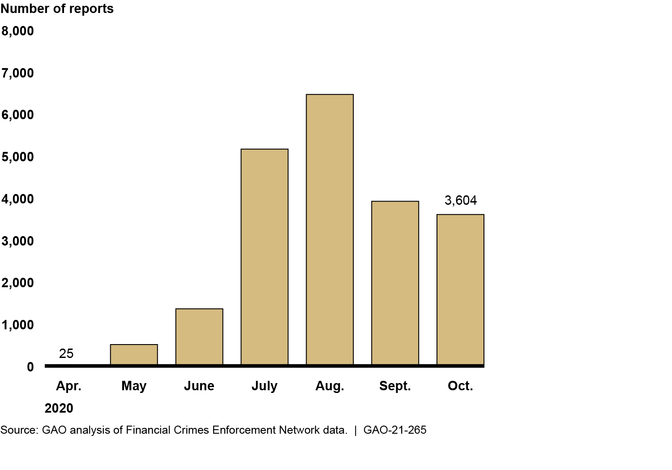
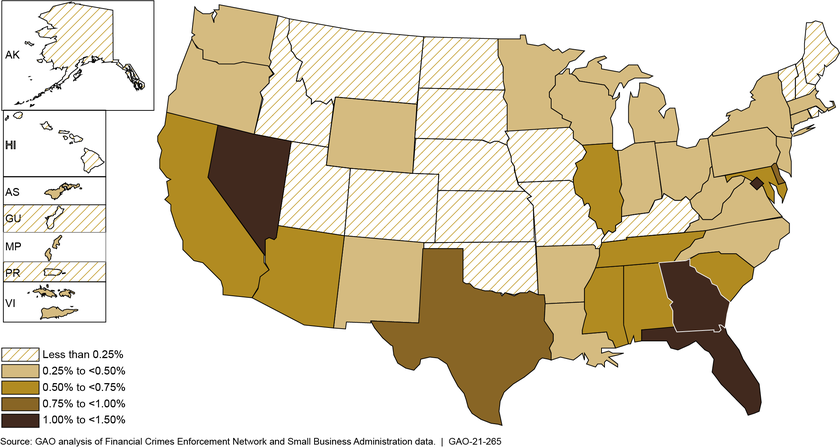
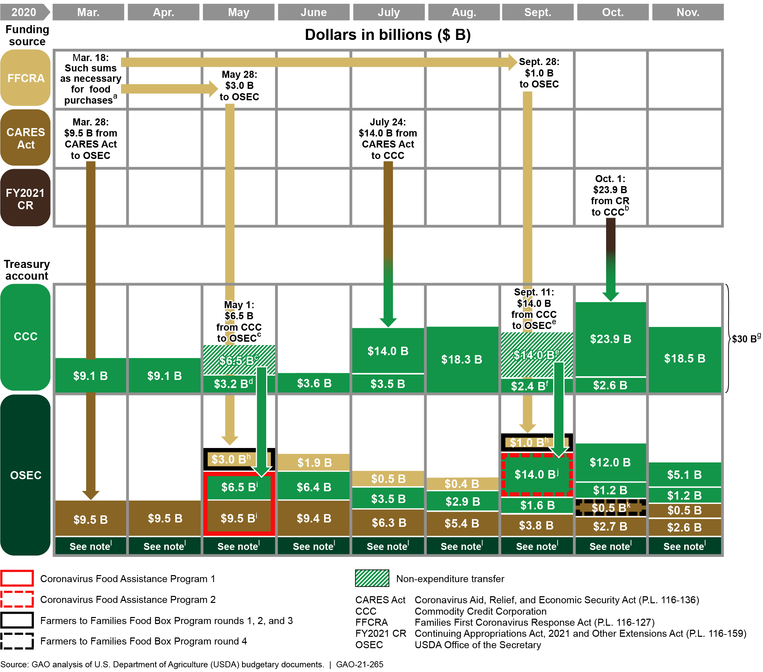


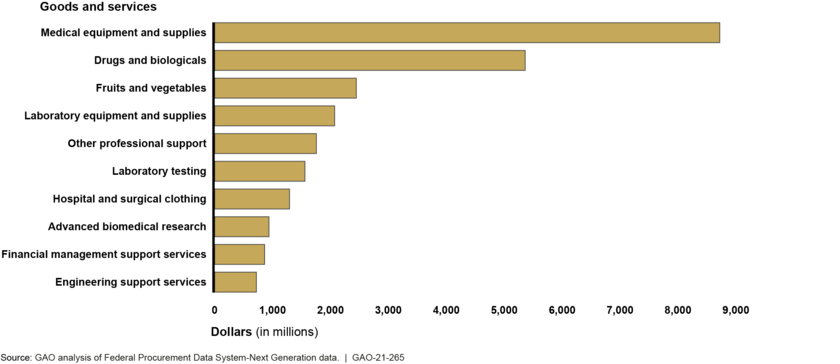
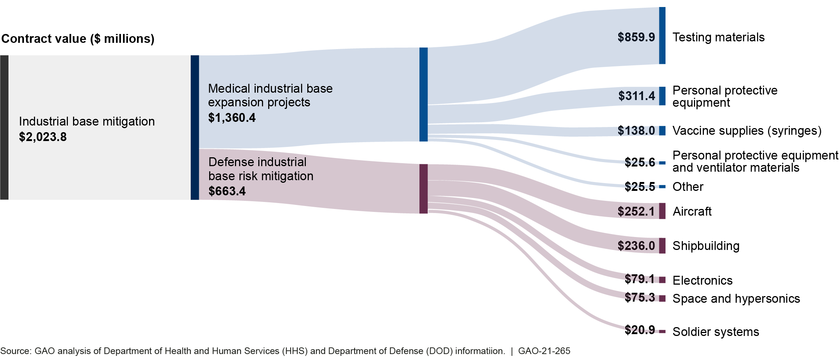

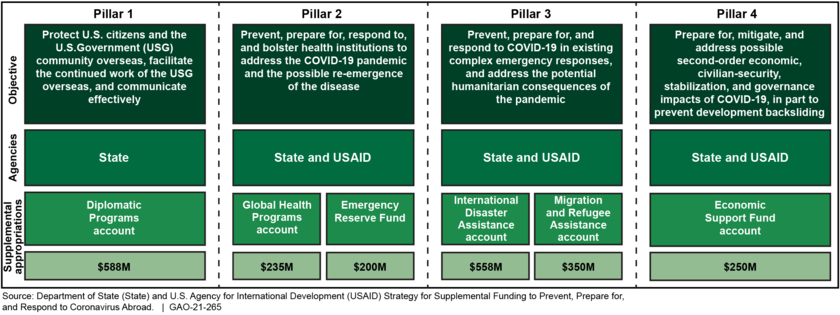


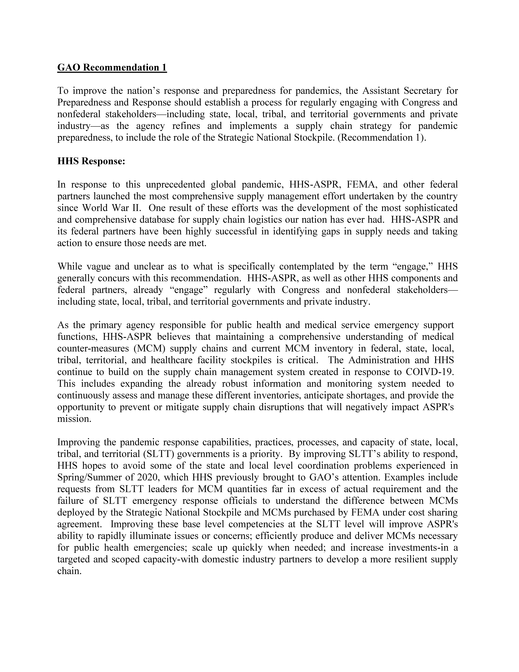








_Page_1-1611269321534.png)
_Page_2-1611269355672.png)