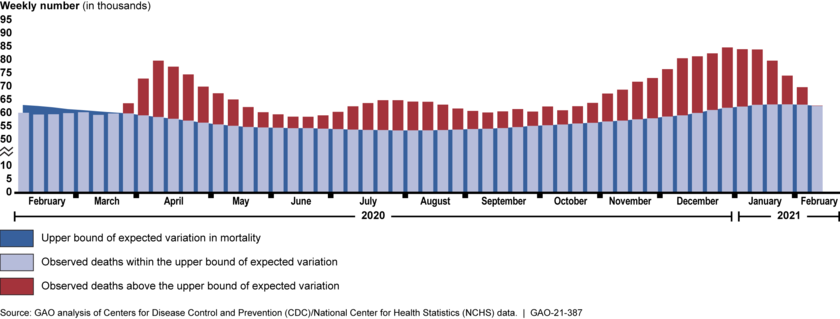
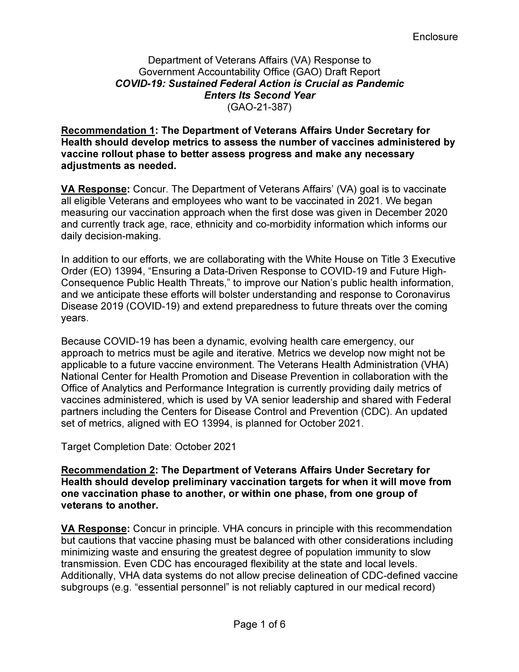
More than a year after the U.S. declared COVID-19 a public health emergency, the pandemic continues to result in catastrophic loss of life and substantial damage to the global economy, stability, and security. According to data from the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics, about 520,000 more deaths occurred from all causes (COVID-19 and other causes) than would be normally expected from February 2020 through mid-February 2021, highlighting the effect of the pandemic on U.S. mortality (see figure). The pandemic also continues to cause economic challenges, particularly for the labor market. As of February 2021, there were about 10 million unemployed individuals, compared to nearly 5.8 million at the beginning of 2020.
Higher-Than-Expected Weekly Mortality in the U.S., February 2020 through Mid-February 2021
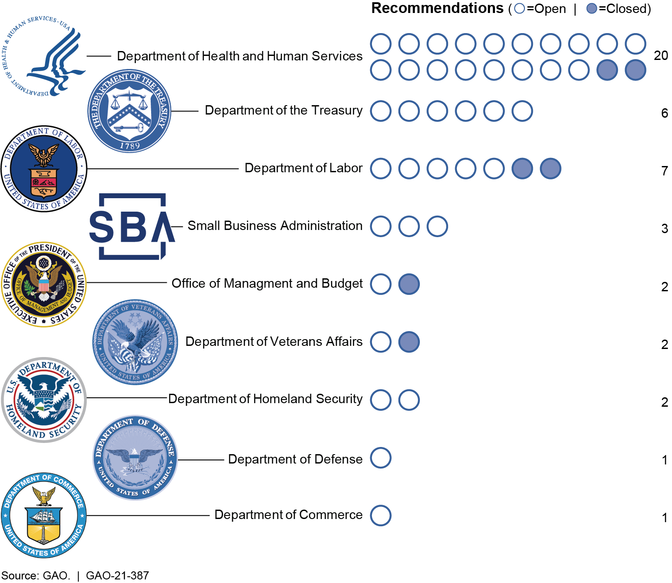
In the past year, GAO has made 44 recommendations for agency actions, 6 of which have been implemented. Since taking office, the new administration has taken some action consistent with GAO’s recommendations, such as issuing the National Strategy for the COVID-19 Response and Pandemic Preparedness and issuing executive orders calling for the development of a pandemic supply chain resilience strategy and providing emergency economic relief. GAO will continue to monitor the administration’s actions toward addressing GAO’s recommendations in future reporting.
In this report GAO is making 28 new recommendations in the areas of public health, the economy, and program integrity. Implementing these 28 recommendations, as well as 38 of GAO’s 44 prior recommendations that have not been fully implemented from CARES Act reports issued since June 2020, would improve the ongoing federal response to COVID-19.
GAO’s new recommendations are discussed below.
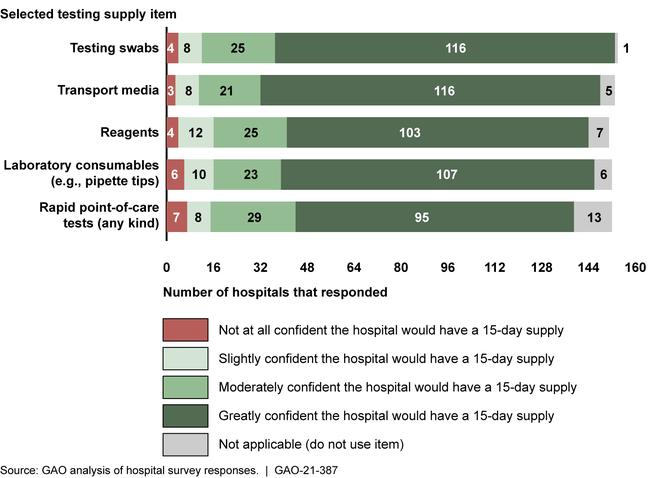
Hospital and Pharmacy Perspectives on COVID-19 Vaccine Administration and Medical Supply Availability
In February 2021, GAO surveyed hospitals and interviewed large retail pharmacy chains and an association of independent pharmacies to gain their perspectives on vaccine administration and medical supply availability. Providers expressed concerns about COVID-19 vaccine availability and limitations in the availability of certain key medical supplies for administering the vaccines—notably syringes and needles. For example, representatives from one retail pharmacy chain stated that the chain has the capacity to administer 25 million doses per month at 9,900 locations, but the chain’s initial allocation of vaccines from the federal government was expected to be only 230,000 doses at 250 locations. Several retail pharmacy chain representatives also indicated that limited vaccine availability has led to uncertainty regarding the amount of vaccines their pharmacies can expect to receive each week. The new administration has taken steps to increase certainty and vaccine availability. For example, the White House announced at the end of January 2021 that the federal government would begin notifying states earlier about availability and shipments of vaccines, to give greater certainty for planning vaccination efforts.
Of the 146 surveyed hospitals that plan to or have begun administering COVID-19 vaccines, 40 hospitals reported at the time of GAO’s survey being greatly concerned about having a sufficient quantity of syringes in the next 30 days for vaccine administration following the survey, and 43 hospitals were greatly concerned about having a sufficient quantity of needles. Additionally, shortages of personal protective equipment (PPE) and COVID-19 testing supplies also remain a challenge for some providers. GAO and other entities have documented persistent and evolving supply chain challenges throughout the pandemic, such as shortages of key supplies used for COVID-19 testing. GAO will continue to examine the medical supply chain, including the role of the Strategic National Stockpile, in future reporting, including actions to respond to GAO’s previous recommendations.
Emergency Use Authorizations
Emergency use authorizations (EUA)—which allow for the temporary use of unapproved medical products—have been instrumental in increasing needed supply of certain devices, such as PPE, during the COVID-19 pandemic response (see figure). However, there have been instances of inconsistencies between EUAs issued by the Food and Drug Administration (FDA) and device guidance from CDC and the Department of Labor (DOL), which led to confusion and hesitancy among providers about using such devices, according to provider associations. GAO recommends that FDA, CDC, and DOL work together to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with EUAs. The Department of Health and Human Services (HHS)—which includes FDA and CDC—and DOL agreed with this recommendation.
Examples of Medical Devices Other Than Tests with Emergency Use Authorizations for COVID-19
In addition, stakeholders—including associations representing manufacturers, distributors, and users of authorized devices, such as health care providers—raised concerns about what will happen to devices with EUAs after the declarations permitting their use for COVID-19 end. HHS has indicated that it intends to develop draft guidance for a transition plan for medical devices distributed under EUAs for COVID-19 by the end of fiscal year 2021. A plan for devices with EUAs that specifies a reasonable timeline and process for transitioning away from their use, taking into account stakeholder input, would help ensure a smooth transition. As HHS develops a transition plan for devices with EUAs, GAO recommends that the agencyspecify a reasonable timeline and process for transitioning authorized devices to clearance, approval, or appropriate disposition that takes into account input from stakeholders. HHS agreed with this recommendation.
COVID-19 Data for Health Care Indicators
Since June 2020, GAO has identified concerns with federal COVID-19 data and underscored that in the midst of a nationwide public health emergency, clear and consistent communication between the federal government and the public is critical given that effective response requires the public’s participation. As part of its efforts to communicate with the public and stakeholders about the pandemic, several experts suggested that the federal government should improve the accessibility of its COVID-19 data by making these data available from a central location on the internet. HHS publishes its data on COVID-19 health indicators across several websites. However, the data it makes publicly available are not all located on, or available from website links on, one online location. As a result, the public, including stakeholders, may not be able to fully understand the extent of the pandemic and use the data to best inform their decision-making.
To make the data more easily accessible, GAO recommends that HHS make its different sources of publicly available COVID-19 data accessible from a centralized location on the internet. HHS neither agreed nor disagreed with this recommendation, but agreed that COVID-19 data should be made accessible to support communication with the public about the pandemic.
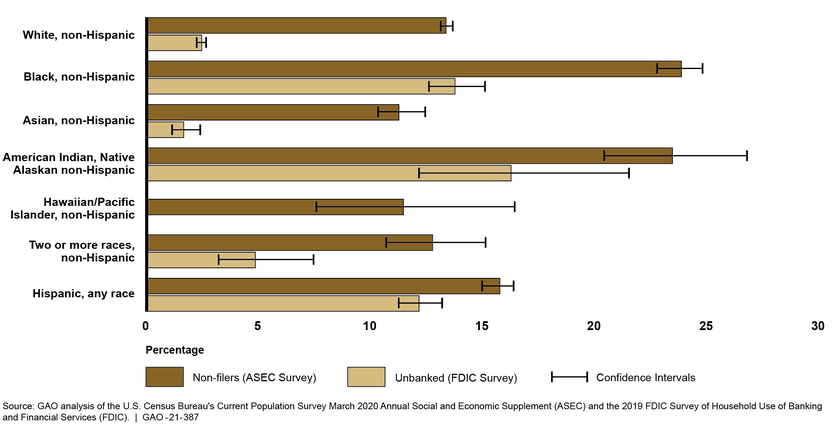
COVID-19 Health Disparities
GAO previously reported that communities of color have been disproportionately affected by the pandemic. According to HHS, as of February 8, 2021, data collected from states and jurisdictions on COVID-19 vaccine recipients were missing data on race and ethnicity for almost half of recipients. Without complete information on the race and ethnicity of those vaccinated, HHS may have difficulty determining whether vaccines are distributed equitably to communities of color. GAO recommends that HHS take steps to ensure the complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations. HHS neither agreed nor disagreed with this recommendation.
HHS’s July 2020 COVID-19 Response Health Equity Strategy has a goal to reduce health disparities by using data-driven approaches to attain the highest level of health possible for all individuals, including communities of color. However, the strategy lacks important elements of an effective national strategy. For example, HHS’s strategy does not provide specific actions that the agency will take to determine whether or where it needs to increase access to testing for populations at increased risk for COVID-19—an essential first step before taking steps to increase testing access. GAO recommends that HHS incorporate key elements of a national strategy to implement the agency’s COVID-19 Response Health Equity Strategy, including determining how intermediate outcomes should be prioritized. HHS agreed with this recommendation.
Nursing Homes
Collecting detailed information on vaccinations for nursing home populations is important for tracking and transparency, particularly because nursing homes have been an epicenter of the COVID-19 pandemic and HHS has recommended priority vaccinations for this group. HHS established a pharmacy partnership program for vaccinating staff and residents of long-term care facilities, and publicly reports the number of vaccination doses, by state, provided to residents and staff of all long-term care facilities participating in the program. However, HHS does not report data showing vaccination rates specifically for nursing homes and does not collect or report data for nursing homes not participating in the program. To improve the monitoring and transparency of nursing home vaccination efforts,GAO recommends that HHS collect data specific to COVID-19 vaccination rates in nursing homes and make these data publicly available. HHS neither agreed nor disagreed with this recommendation.
In addition, as of January 2021, HHS had not specified whether nursing homes would be required to offer COVID-19 vaccinations as they have with other vaccines and how these vaccinations would be incorporated into the agency’s nursing home quality strategy. Data on COVID-19 vaccinations in nursing homes will also be important for HHS’s ongoing efforts to monitor nursing home quality. GAO recommends that HHS require nursing homes to offer COVID-19 vaccinations to residents and staff and design and implement associated quality measures. HHS neither agreed nor disagreed with this recommendation.
Veterans Health Care
According to the Department of Veterans Affairs (VA), many veterans enrolled in VA’s health care system are at a higher risk of infection or severe disease from COVID-19 due to their age or underlying health conditions. GAO identified several areas where VA can improve its vaccination efforts:
VA does not have metrics related to staff and veterans who do not show (no-shows) for their vaccination appointments. Without data on no-shows, VA may be at risk for not being able to determine the extent to which staff and veterans are not showing up for appointments for their second vaccinations, and may miss opportunities to better target outreach to individuals not showing up for appointments.
VA lacks targets for when it will move from one vaccination phase to another or within one phase for when the agency will move from one group of veterans to another, making it difficult for the department to assess progress.
VA is utilizing a phased vaccine rollout; however, VA’s current metrics do not capture vaccine data by phases. As a result, VA is not able to determine which facilities may be at an earlier phase than others and direct resources or assistance to those facilities.
GAO recommends that VA (1) collect data on the number of staff and veterans who do not show up for a vaccination appointment to better monitor for completion of the second dose of the vaccine; (2) develop preliminary vaccination targets for when it will move from one vaccination phase to another; or within one phase, from one group of veterans to another; and (3) develop metrics to assess the number of vaccines administered by vaccine rollout phase to better assess progress and make any necessary adjustments. VA agreed with the first and third recommendations and agreed in principle with the second recommendation.
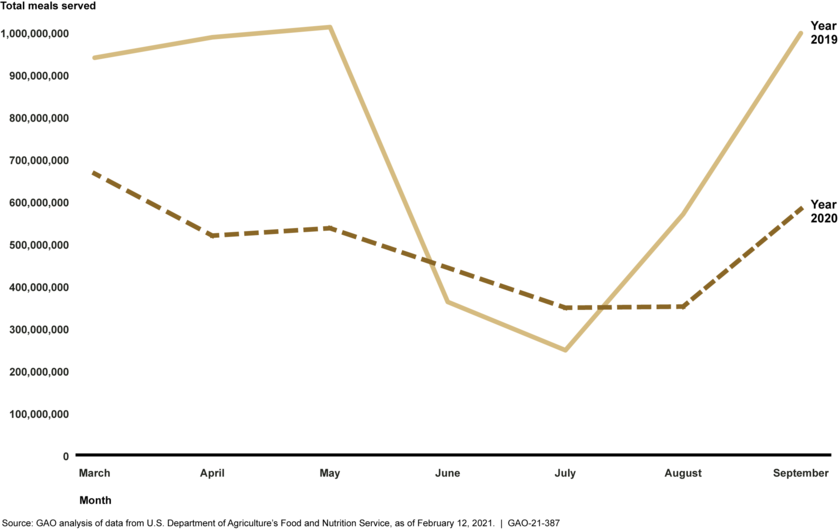
Nutrition Assistance
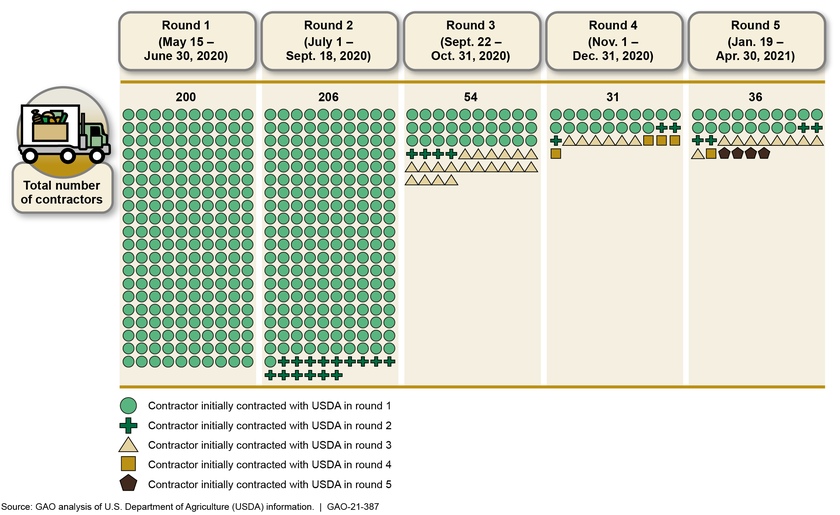
The U.S. Department of Agriculture (USDA) administers a number of federal nutrition assistance programs to vulnerable populations. Recent legislative and executive actions made several changes to these programs as the negative economic effects of the COVID-19 pandemic have continued. However, until recently, USDA had released minimal data about participation in these programs during the pandemic, and when the department released data in late January 2021, it did not publicly share sufficient information about data quality. In August 2020, USDA announced it had identified significant issues with the quality of state-reported data on two programs. As it worked to identify the root causes of the issues, USDA opted not to release participation data for any of its other nutrition assistance programs from July 2020 until late January 2021. When USDA released the data, the department did not explain how it resolved the data quality issues it previously disclosed, nor did it share necessary context to help stakeholders and the public understand and interpret the data.
As a result, stakeholders and the public lack sufficient information and appropriate context to interpret key program data and understand the effects of the pandemic on the programs. GAO recommends that USDA (1) provide sufficient context to help stakeholders and the public understand and interpret data on federal nutrition assistance programs during the pandemic and (2) disclose potential sources of error that may affect data quality during the pandemic, such as manual processing. USDA generally agreed with these recommendations.
Disaster Relief Fund and Assistance to Tribal Governments
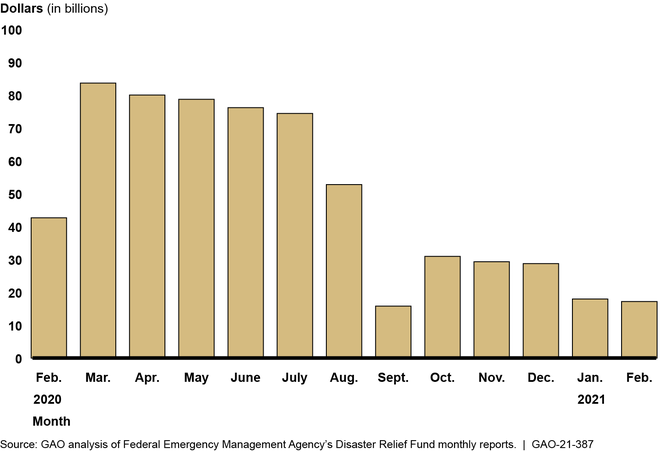
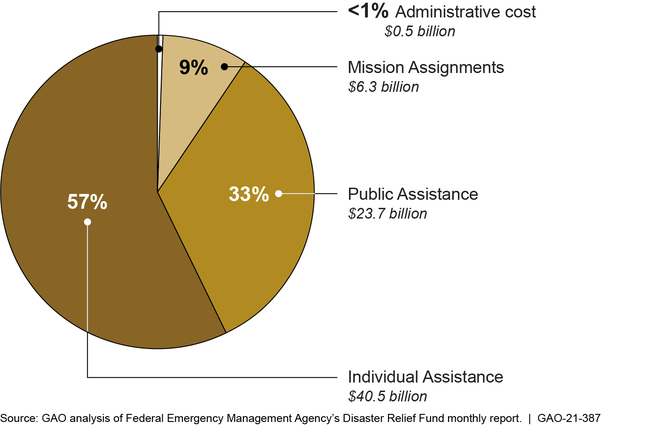
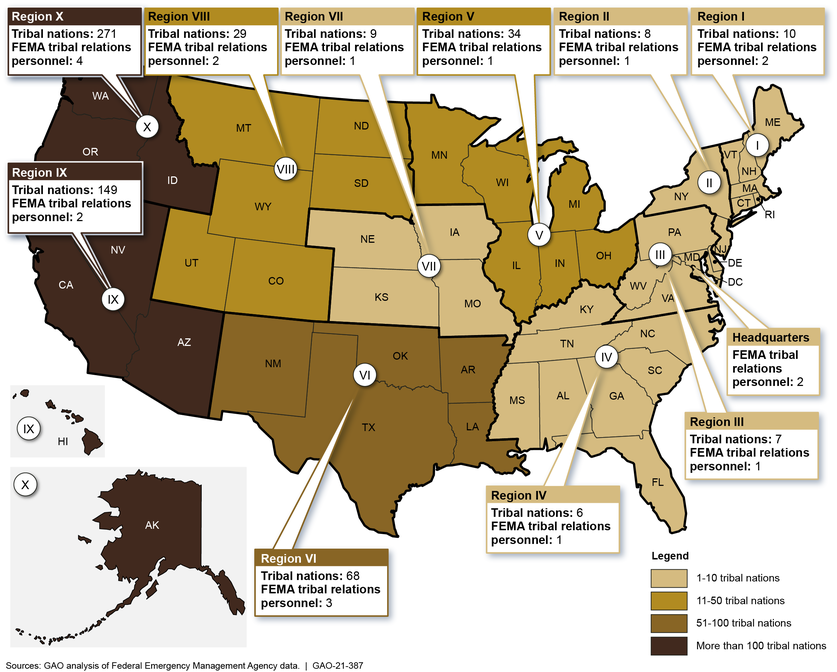
Available data from HHS indicate that tribes are among communities of color bearing a disproportionate burden of COVID-19 positive tests, cases, hospitalizations, and deaths. The Federal Emergency Management Agency (FEMA), within the Department of Homeland Security (DHS), plays a key role in the ongoing COVID-19 pandemic response effort, including using the Disaster Relief Fund to provide Public Assistance grants to reimburse tribal governments, among others, for pandemic costs, such as testing supplies, PPE, and vaccine distribution.
Several tribal organizations reported challenges related to completing administrative requirements to request and receive Public Assistance. For example, two tribal officials told GAO that when requesting technical assistance from FEMA to help with disaster activities such as developing a Public Assistance Administrative Plan, FEMA did not have staff to assist. FEMA’s initial assessment report of its response to the pandemic noted challenges and recommended that FEMA develop a tribal nation engagement strategy that includes providing the resources and personnel throughout each region required to support program delivery for all tribal nations. However, as of March 2021, FEMA had not developed this strategy.
GAO recommends that FEMA provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19. DHS agreed with this recommendation.
FEMA’s 2019 Tribal Consultation Policy specifies the process for consulting with tribes throughout the four phases that guide the agency in how to conduct regular and meaningful collaboration with tribes (see figure). However, GAO found that FEMA did not follow the tribal consultation process while developing an interim policy detailing eligible items for reimbursement under the Public Assistance program. If tribes had been formally consulted earlier in the process, they could have been in a better position to provide meaningful input to FEMA on how its policy might impact tribes. Further, there may have been less confusion on which items were considered eligible for reimbursement during the early months of the pandemic, and tribes could have made more informed decisions. GAO recommends that FEMA adhere to the agency’s protocols listed in the updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of the tribal consultation process when developing new policies and procedures related to COVID-19 assistance. DHS agreed with this recommendation.
Overview of FEMA’s Tribal Consultation Policy Process
K-12 Education
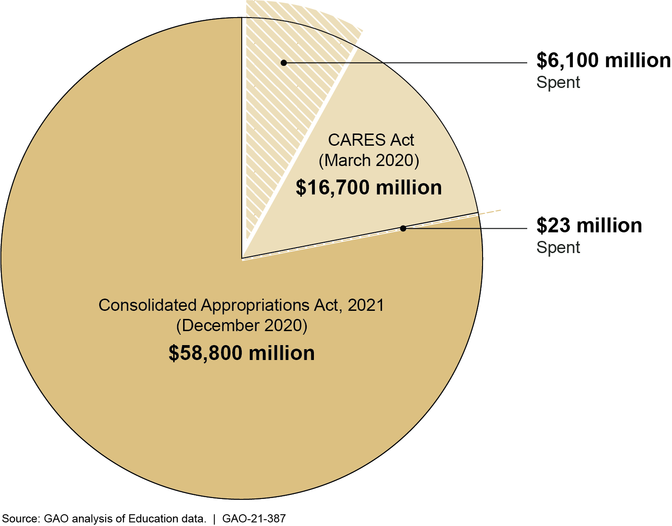
The Department of Education (Education) has taken steps to track state and school district spending of certain COVID-19 relief funds, but the data give an incomplete picture of the status of funds and understate the rate at which funds are being used. According to data collected by Education, as of February 28, 2021, states and territories have spent about $6.1 billion of the approximately $75 billion appropriated through the Education Stabilization Fund for states’ and territories’ education needs. However, federal spending data alone provide an incomplete picture of states’ and school districts’ spending, as there are several factors that influence the rate at which funds appear to be spent. For example, there is often a significant gap between when a district “uses” the funds (i.e., orders, contracts for, installs, and pays for goods or services, such as information technology equipment) and when those funds are reported as “spent” in state and federal reporting systems, as is common in federal grants management processes.
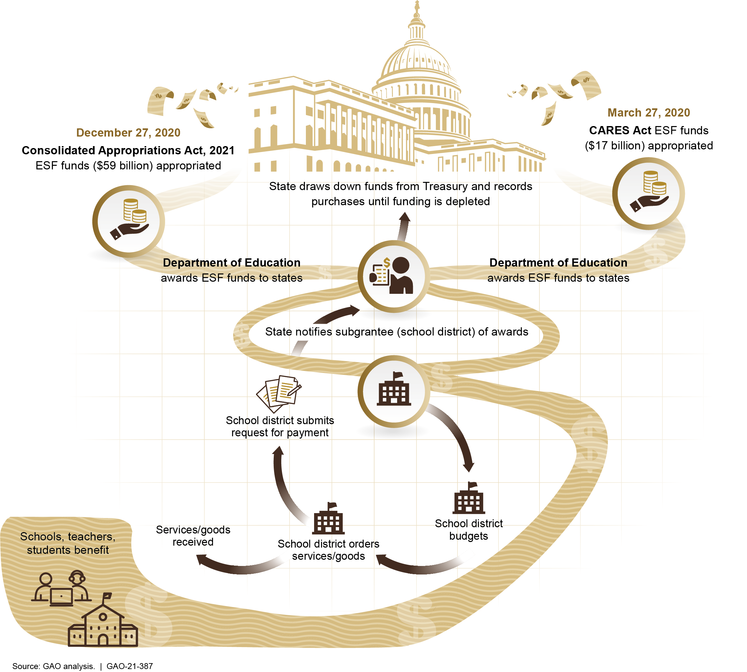
According to Education officials, states award applicable funds to school districts so that the school districts can obligate those funds for specific purposes. The state does not transfer funds to the district until the district requests payment for services or deliverables received. Education officials do not consider the funds spent until the state requests payment for expenses. Given this gap between when a district uses funds and funds are recorded as spent, absent information on obligations, policymakers will not have complete information on how these funds are being used to address the pandemic-related education needs of America’s schoolchildren. GAO recommends that Education regularly collect and publicly report information on school districts’ financial commitments (obligations), as well as outlays (expenditures) in order to more completely reflect the status of their use of federal COVID-19 relief funds. For example, Education could modify its annual report on state and school district spending data to include obligations data in subsequent reporting cycles. Education agreed with this recommendation.
Small Business Assistance Programs
The Consolidated Appropriations Act, 2021, appropriated additional funding for the creation of the Targeted Economic Injury Disaster Loan (EIDL) Advance program and authorized additional Paycheck Protection Program (PPP) loans, among other things, highlighting the continued need for ensuring program integrity. Since March 2020, the Department of Justice has publicly announced charges in numerous fraud-related cases associated with loans made through these programs. As a result of concerns about program integrity, GAO has added Small Business Administration (SBA) loans to GAO’s High Risk List. SBA has taken some steps to mitigate fraud risks to EIDL and PPP, but it has not taken a strategic approach to managing fraud risks to both programs. GAO recommends that SBA (1) implement a comprehensive oversight plan to identify and respond to risk in the EIDL program to ensure program integrity, achieve program effectiveness, and address potential fraud; (2) conduct and document a fraud risk assessment for the EIDL program and PPP; (3) develop a strategy that outlines specific actions to address assessed fraud risks in the EIDL program; and (4) outline specific actions to monitor and manage fraud risks in PPP on a continuous basis. SBA agreed with these recommendations.
Unemployment Insurance Programs
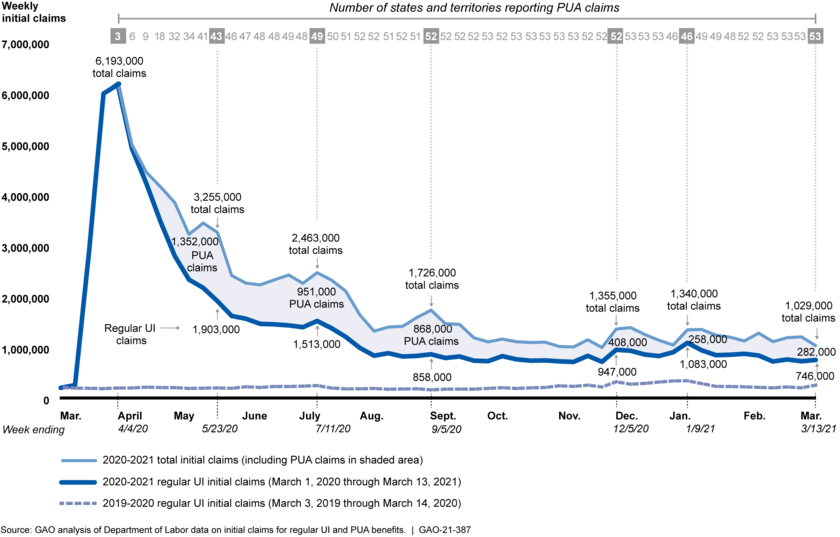
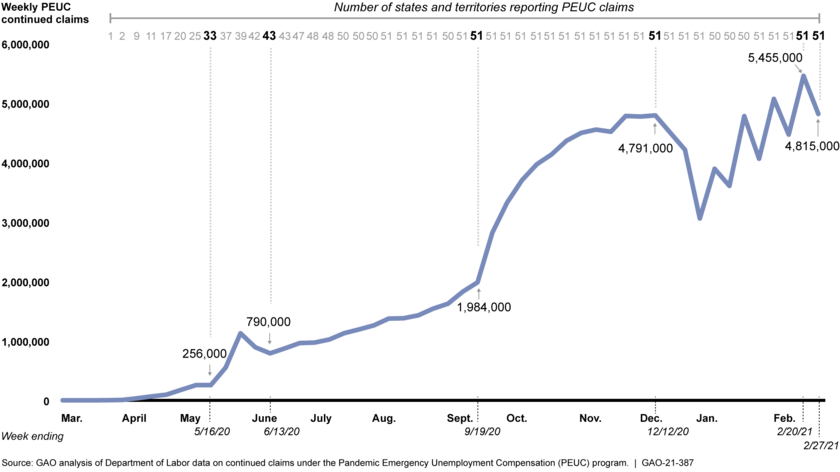
GAO continues to have concerns about overpayments and potential fraud in the unemployment insurance (UI) system, including the federally funded Pandemic Unemployment Assistance (PUA) program, which authorizes UI benefits to certain individuals not otherwise eligible for these benefits, such as self-employed and certain gig economy workers. As of March 15, 2021, DOL reported that states had identified more than $3.6 billion in PUA overpayments from March 2020 through February 2021. In response to a recommendation in GAO’s January 2021 report, DOL has taken steps to collect data on states’ recovery of PUA overpayments. However, the Consolidated Appropriations Act, 2021, enacted in December 2020, provided states with authority to waive certain PUA overpayments. Thus, additional data on the amounts of PUA overpayments states have waived are also needed to effectively monitor the recovery of overpayments. GAO recommends that DOL collect data from states on the amount of overpayments waived in the PUA program, similar to the regular UI program. DOL agreed with this recommendation.
This report contains additional recommendations related to transparency and accountability in the following areas: relief for health care providers, economic impact payments, federal contracts and agreements, audits of nonfederal entities receiving federal pandemic assistance, and employer tax relief and payroll tax deferrals.
GAO is also examining the federal government’s COVID-19 vaccine efforts, which will be the focus of an upcoming report. Finally, GAO will review actions federal agencies have taken in response to the American Rescue Plan of 2021 in future reporting.
Why GAO Did This Study
As of March 15, 2021, the U.S. had over 29 million reported cases of COVID-19 and more than 523,000 reported deaths, according to CDC. The country also continues to experience serious economic repercussions.
Five relief laws, including the CARES Act, were enacted as of January 31, 2021, to provide appropriations to address the public health and economic threats posed by COVID-19. As of January 31, 2021, of the $3.1 trillion appropriated by these five laws for COVID-19 relief, the federal government had obligated a total of $2.2 trillion and expended $1.9 trillion, as reported by federal agencies.
Most recently, in March 2021, a sixth relief law, the American Rescue Plan of 2021, was enacted and provides additional federal assistance for the ongoing response and recovery.
The CARES Act includes a provision for GAO to report on its ongoing monitoring and oversight efforts related to the COVID-19 pandemic. This report examines the federal government’s continued efforts to respond to and recover from the COVID-19 pandemic.
GAO reviewed data, documents, and guidance from federal agencies about their activities and interviewed federal and state officials, experts, and other stakeholders, including health care professionals.
What GAO Recommends
GAO is making 28 new recommendations for agencies that are detailed in this Highlights and in the report.
Recommendations
Recommendations for Executive Action
Recommendations for Executive Actions
We are making a total of 28 recommendations to federal agencies:
Number
Agency
Recommendation
1
Department of Health and Human Services
The Secretary of Health and Human Services should make the Department’s different sources of publicly available COVID-19 data accessible from a centralized location on the internet. This could improve the federal government’s communication with the public about the ongoing pandemic. See Health Care Indicators enclosure. (Recommendation 1)
2
Department of Health and Human Services
The Secretary of Health and Human Services should finalize and implement a post-payment review process to validate COVID-19 Uninsured Program claims and to help ensure timely identification of improper payments, including those resulting from potential fraudulent activity, and recovery of overpayments. See Relief for Health Care Providers enclosure. (Recommendation 2)
3
Department of Health and Human Services
The Secretary of Health and Human Services should ensure that the Director of the Centers for Disease Control and Prevention collects data specific to the COVID-19 vaccination rates in nursing homes and makes these data publicly available to better ensure transparency and that the necessary information is available to improve ongoing and future vaccination efforts for nursing home residents and staff. See Nursing Homes enclosure. (Recommendation 3)
4
Department of Health and Human Services
The Secretary of Health and Human Services should ensure that the Administrator of the Centers for Medicare & Medicaid Services, in consultation with the Centers for Disease Control and Prevention, requires nursing homes to offer COVID-19 vaccinations to residents and staff and design and implement associated quality measures. See Nursing Homes enclosure. (Recommendation 4)
5
Department of Veterans Affairs : Office of the Under Secretary for Health
The Department of Veterans Affairs Under Secretary for Health should develop metrics to assess the number of vaccines administered by vaccine rollout phase to better assess progress and make any necessary adjustments as needed. See Veterans Health Care enclosure. (Recommendation 5)
6
Department of Veterans Affairs : Office of the Under Secretary for Health
The Department of Veterans Affairs Under Secretary for Health should develop preliminary vaccination targets for when it will move from one vaccination phase to another; or within one phase, from one group of veterans to another. See Veterans Health Care enclosure. (Recommendation 6)
7
Department of Veterans Affairs : Office of the Under Secretary for Health
The Department of Veterans Affairs Under Secretary for Health should collect data on the number of staff and veterans who do not show up for a vaccination appointment to better monitor for completion of the second dose of the vaccine. See Veterans Health Care enclosure. (Recommendation 7)
8
Department of Health and Human Services
The Secretary of Health and Human Services should ensure that the Food and Drug Administration and the Centers for Disease Control and Prevention work with the Assistant Secretary of Labor for Occupational Safety and Health to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with emergency use authorization. See Emergency Use Authorizations for Medical Devices enclosure. (Recommendation 8)
9
Department of Labor : Occupational Safety and Health Administration
The Assistant Secretary of Labor for Occupational Safety and Health should work with the Food and Drug Administration and the Centers for Disease Control and Prevention to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with emergency use authorization. See Emergency Use Authorizations for Medical Devices enclosure. (Recommendation 9)
10
Department of Health and Human Services : Food and Drug Administration
As the Food and Drug Administration develops a transition plan for devices with emergency use authorizations, the Commissioner should specify a reasonable timeline and process for transitioning authorized devices to clearance, approval, or appropriate disposition that takes into account input from stakeholders. See Emergency Use Authorizations for Medical Devices enclosure. (Recommendation 10)
11
Department of Health and Human Services : Public Health Service : Centers for Disease Control and Prevention
The Director of the Centers for Disease Control and Prevention should incorporate key elements of a national strategy in the agency’s COVID-19 Response Health Equity Strategy. These elements include (1) specific actions to achieve intermediate outcomes, such as increased access to testing; (2) how intermediate outcomes should be prioritized within its four broad priority areas; (3) who will implement actions to achieve intermediate outcomes; and (4) how the strategy relates to other relevant strategies. See Health Disparities enclosure. (Recommendation 11)
12
Department of Health and Human Services : Public Health Service : Centers for Disease Control and Prevention
The Director of the Centers for Disease Control and Prevention should take steps to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations, such as working with states and jurisdictions to facilitate consistent collecting and reporting of this information. See Health Disparities enclosure. (Recommendation 12)
13
Department of Agriculture : Office of the Secretary
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to issue guidance—such as an acquisition alert or a reminder to contracting officials—on the use of the COVID-19 National Interest Action code for the Farmers to Families Food Box Program or successor food distribution program to ensure it accurately captures COVID-19-related contract obligations in support of the program. See Federal Contracts and Agreements for COVID-19 enclosure. (Recommendation 13)
14
Department of Agriculture : Office of the Secretary
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the Farmers to Families Food Box Program or successor future food distribution program, and take the necessary steps to ensure it has adequate contracting staff in place to award and administer any future contracts for the program. See Federal Contracts and Agreements for COVID-19 enclosure. (Recommendation 14)
15
Department of Labor
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments waived in the Pandemic Unemployment Assistance program, similar to the regular unemployment insurance program. See Unemployment Insurance Programs enclosure. (Recommendation 15)
16
Department of the Treasury : Internal Revenue Service
The Commissioner of Internal Revenue should periodically review control activities for issuing direct payments to individuals to determine that the activities are designed and implemented appropriately as IRS disburses a third round of Economic Impact Payments and prepares for advance payments on the Child Tax Credit. These control activities should include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients. See Economic Impact Payments enclosure. (Recommendation 16)
17
Department of Agriculture : Office of the Secretary
The Secretary of Agriculture should ensure that the Administrator of the Food and Nutrition Service (1) provides sufficient context to help stakeholders and the public understand and interpret data on federal nutrition assistance programs during the pandemic and (2) discloses potential sources of error that may affect data quality during the pandemic, such as manual processing. For example, the agency could publish key information from its internal communications plan that it developed for the January 2021 data release and include additional table notes in subsequent data releases to help explain these issues. See Nutrition Assistance enclosure. (Recommendation 17)
18
Department of the Treasury : Internal Revenue Service
The Commissioner of Internal Revenue should leverage employee counts from Form 941, Employer’s Quarterly Federal Tax Return, and Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees, to identify potentially ineligible COVID-19 related sick and family leave credit claims, and address discrepancies the Internal Revenue Service deems significant. See Employer Tax Relief and Payroll Tax Deferrals enclosure. (Recommendation 18)
19
Department of the Treasury : Internal Revenue Service
The Commissioner of Internal Revenue should conduct outreach to employment tax return filers to educate and promote accurate reporting of employee counts on Form 941, Employer’s Quarterly Federal Tax Return, and Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees. See See Employer Tax Relief and Payroll Tax Deferrals enclosure. (Recommendation 19)
20
Small Business Administration
The Administrator of the Small Business Administration should conduct and document a fraud risk assessment for the Economic Injury Disaster Loan program. See Economic Injury Disaster Loan Program enclosure. (Recommendation 20)
21
Small Business Administration
The Administrator of the Small Business Administration should develop a strategy that outlines specific actions to address assessed fraud risks in the Economic Injury Disaster Loan program on a continuous basis. See Economic Injury Disaster Loan Program enclosure. (Recommendation 21)
22
Small Business Administration
The Administrator of the Small Business Administration should implement a comprehensive oversight plan to identify and respond to risks in the Economic Injury Disaster Loan program to help ensure program integrity, achieve program effectiveness, and address potential fraud. See Economic Injury Disaster Loan Program enclosure. (Recommendation 22)
23
Small Business Administration
The Administrator of the Small Business Administration should conduct and document a fraud risk assessment for the Paycheck Protection Program. See Paycheck Protection Program enclosure. (Recommendation 23)
24
Small Business Administration
The Administrator of the Small Business Administration should develop a strategy that outlines specific actions to monitor and manage fraud risks in the Paycheck Protection Program on a continuous basis. See Paycheck Protection Program enclosure. (Recommendation 24)
25
Department of Homeland Security : Directorate of Emergency Preparedness and Response : Federal Emergency Management Agency
The Federal Emergency Management Agency Administrator should adhere to the agency’s protocols listed in its updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of the tribal consultation process when developing new policies and procedures related to COVID-19 assistance. See FEMA’s Disaster Relief Fund and Assistance to Tribal Governments enclosure. (Recommendation 25)
26
Department of Homeland Security : Directorate of Emergency Preparedness and Response : Federal Emergency Management Agency
The Federal Emergency Management Agency Administrator should provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19. See FEMA’s Disaster Relief Fund and Assistance to Tribal Governments enclosure. (Recommendation 26)
27
Department of Education : Office of the Secretary
The Secretary of Education should regularly collect and publicly report information on school districts’ financial commitments (obligations), as well as outlays (expenditures) in order to more completely reflect the status of their use of federal COVID-19 relief funds. For example, Education could modify its annual report on state and school district spending data to include obligations data in subsequent reporting cycles. See K-12 Education enclosure. (Recommendation 27)
28
Executive Office of the President : Office of Management and Budget
The Director of the Office of Management and Budget should work in consultation with federal agencies and the audit community (e.g., agency Offices of Inspector General; National Association of State Auditors, Comptrollers, and Treasurers; and American Institute of Certified Public Accountants), to the extent practicable, to incorporate appropriate measures in the Office of Management and Budget’s process for preparing single audit guidance, including the annual Single Audit Compliance Supplement, to better ensure that such guidance is issued in a timely manner and is responsive to users’ input and needs. See Single Audits enclosure. (Recommendation 28)
More than a year after the Secretary of Health and Human Services first declared a public health emergency for the U.S. and the World Health Organization characterized the Coronavirus Disease 2019 (COVID-19) as a pandemic, COVID-19 continues to result in catastrophic loss of life and substantial damage to the global economy, stability, and security.[1] Worldwide, as of March 15, 2021, there were more than 119,452,000 reported cases and about 2,648,000 reported deaths due to COVID-19; within the U.S., there were about 29,270,000 reported cases and more than 523,000 reported deaths.[2]
The country also continues to experience serious economic repercussions and turmoil as a result of the pandemic. As of February 2021, there were about 10 million unemployed individuals, compared to nearly 5.8 million individuals at the beginning of 2020.[3]
In March 2020, Congress took action in response to this unprecedented global crisis to protect the health and well-being of Americans. Notably, Congress passed, and the President signed into law, the CARES Act, which provided over $2 trillion in emergency assistance and health care response for individuals, families, and businesses affected by COVID-19.[4] Over the past year, agencies from across the federal government have demonstrated extraordinary dedication and commitment to responding to the unprecedented COVID-19 pandemic, including those serving on the front lines to establish and sustain services for those infected with the virus.
Since the enactment of the CARES Act—which includes a provision for GAO to report bimonthly on its ongoing efforts related to the pandemic—we have continued to monitor and oversee the federal government’s efforts to prepare for, respond to, and recover from the COVID-19 pandemic.[5] To date, we have issued six reports in response to this provision, made 44 recommendations to federal agencies, and raised four matters for congressional consideration to improve the federal government’s response efforts.[6]
Since taking office, the new administration has taken some action consistent with our recommendations, such as issuing the National Strategy for the COVID-19 Response and Pandemic Preparedness and issuing executive orders calling for the development of a pandemic supply chain resilience strategy and providing emergency economic relief. We will continue to monitor the administration’s actions towards addressing our recommendations in future reporting. Agencies should swiftly take action on the 38 prior recommendations that have not been fully implemented from our CARES Act reports issued since June 2020, including those on topics such as addressing potential fraud, developing national testing and vaccine strategies, and providing clear and consistent communication.
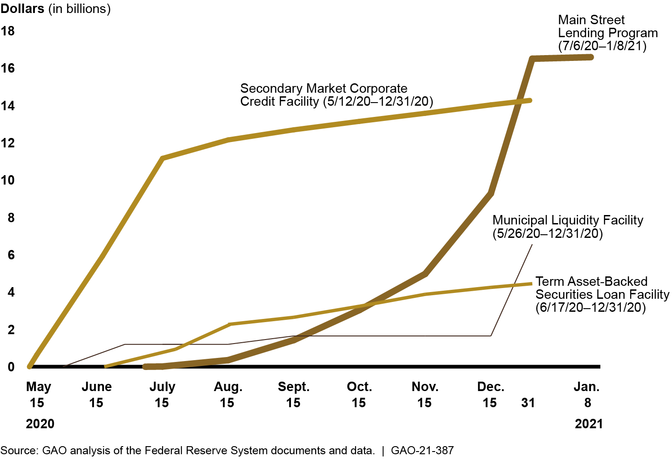
We are also examining the federal government’s COVID-19 vaccine efforts, which will be the focus of an upcoming report. In addition, we have issued other targeted COVID-19-related report in areas such as Federal Reserve lending programs supported by CARES Act funds, the Defense Production Act, and the CARES Act loan program for aviation and other eligible businesses, and we have reviews ongoing in these and other areas.[7] Additionally, we will review actions federal agencies have taken in response to the American Rescue Plan of 2021 in future reporting.
This report examines the federal government’s continued efforts to respond to and recover from the COVID-19 pandemic. We make 28 new recommendations to federal agencies in areas including relief for health care providers, veterans’ health care, nursing homes, federal contracts and agreements for the COVID-19 response, the Paycheck Protection Program, and unemployment insurance programs.
This report also includes 46 enclosures about a range of federal programs and activities across the government concerning public health and the economy. (See Appendix I) Figure 1 lists these enclosures by topic area and highlights those with new recommendations.
Figure 1: Report Enclosures by Topic Area
Given the government-wide scope of this report, we undertook a variety of methodologies to complete our work, including examining a wide range of data sources and conducting interviews with federal and state officials and representatives from stakeholder groups including health care professionals and other entities. Among other things, we examined federal laws, agency documents, and guidance. In each enclosure, we include a summary of the methodology specific to the work conducted.
See Appendix II for a list of ongoing GAO work related to COVID-19 and Appendix III for the status of matters for congressional consideration and recommendations for executive action made in our June, September, November 2020, and January 2021 CARES Act reports and in our November 2020 report on vaccines and therapeutics.
We conducted this performance audit from October 2020 to March 2021 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
The number of new reported COVID-19 cases reached a high in January 2021 and decreased considerably in February. Between February 25 and March 10, 2021, new reported COVID-19 cases averaged about 65,000 per day, which was about a quarter of the peak that occurred during the winter of 2021 and similar to the peak that occurred during the summer of 2020 (see fig. 2).[8] During this same 2-week period, reported new COVID-19 cases per day, on average, increased in 5 jurisdictions, held steady in 18 jurisdictions, and decreased in 28 jurisdictions.[9]
The need to remain vigilant in efforts to contain the spread of the virus is underscored by the emergence of new variants of the virus, the fragmented nature of our public health sector, the fragility of our medical supply chain, and longstanding disparities in health care access, treatment, and outcomes. The virus also continues to be an obstacle to a more robust economic recovery.
Figure 2: Reported COVID-19 Cases per Day in the U.S., through March 10, 2021
Note: Reported COVID-19 cases include confirmed and probable cases. Beginning April 14, 2020, states could include probable as well as confirmed COVID-19 cases in their reports to CDC. Prior to that time, counts only included confirmed cases. According to CDC, the actual number of cases is unknown for a variety of reasons, including that people who have been infected may not have been tested or may have not sought medical care. The data were accessed on March 15, 2021.
According to data from the Centers for Disease Control and Prevention’s (CDC) National Center for Health Statistics, about 520,000 more deaths occurred from all causes (COVID-19 and other causes) than would be normally expected from February 2020 through mid-February 2021, highlighting the effect of the pandemic on U.S. mortality (see fig. 3).
Figure 3: Higher-Than-Expected Weekly Mortality, February 2020 through mid-February 2021
Note: The figure shows the number of deaths from all causes in a given week through February 13, 2021, reported in the U.S. that exceeded the upper bound threshold of expected deaths calculated by CDC’s National Center for Health Statistics on the basis of variation in mortality experienced in prior years. See CDC’s National Center for Health Statistics webpage on excess deaths for further details on how CDC estimates this upper bound threshold: https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm, accessed on March 15, 2021. The number of deaths in recent weeks should be interpreted cautiously as this figure relies on provisional data that are generally less complete.
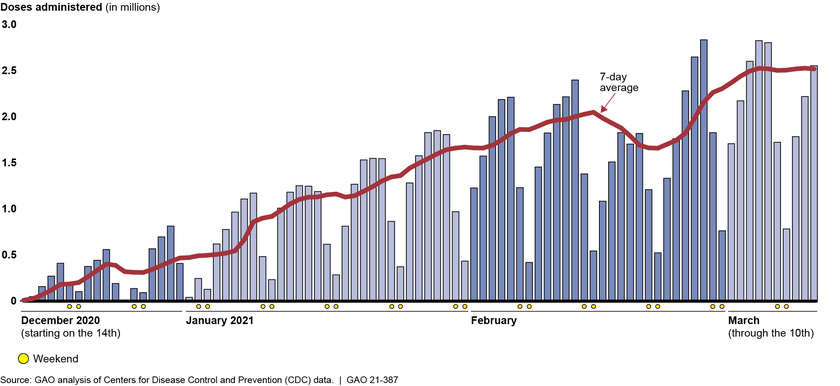
Providing the public with safe and effective vaccines to protect people from getting sick with COVID-19 is crucial to mitigating the public health and economic impacts of the virus and ending the pandemic. It is also a time-sensitive undertaking, with over 6 million cases of COVID-19 and 95,704 deaths reported in the United States in the month of January 2021 alone. Two, two-dose COVID-19 vaccines were authorized for emergency use in December 2020 and a third, one-dose vaccine was authorized in February 2021.[10] Doses of COVID-19 vaccine administered each day have steadily increased from December 14, 2020 through March 10, 2021, with a temporary dip in February due to severe weather across the country (see fig. 4). As of March 15, 2021, about 109,082,000 doses had been administered, according to CDC.
Figure 4: Daily Count of Doses of COVID-19 Vaccine Administered and Reported to CDC, through March 10 2021
Note: Data show the number of COVID-19 vaccine doses administered in the U.S. as reported to CDC by state, territorial, and local public health agencies, and federal entities, since the national vaccine program began on December 14, 2020, and include doses administered through all vaccine partners including jurisdictional partner clinics, retail pharmacies, long-term care facilities, Federal Emergency Management Agency and Health Resources and Services Administration partner sites, and federal entity facilities. The data were accessed on March 15, 2021. As of March 15, 2021, three COVID-19 vaccines were authorized for emergency use; two of these vaccines are two-dose regimens and the third vaccine requires one dose. The number of doses administered on a given day may be affected by several factors, such as weekend days, holidays, weather, and vaccine availability. On February 19, 2021, officials from the White House COVID-19 Response Team said in a press briefing that severe weather across the country impacted vaccine distribution and administration in all 50 states. Further, officials said the shipment of 3 days’ worth—about 6 million doses—of vaccines was delayed due to weather.
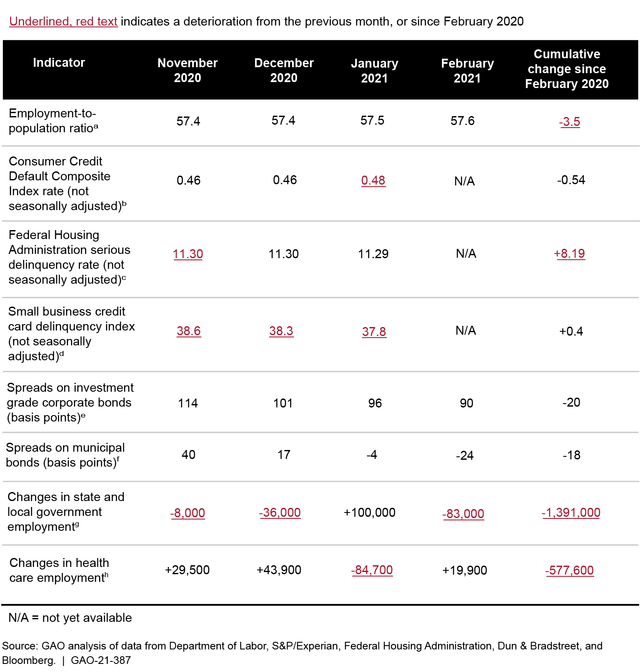
In addition to the public health effects, the pandemic continues to cause economic challenges, particularly for the labor market. For example, in February 2021, the employment-to-population ratio, which measures the share of the population employed, was 3.5 percentage points lower than in February 2020, indicating that labor market conditions remain worse than in the pre-pandemic period (see fig. 5).[11]
Figure 5: Employment Remains below Its Pre-pandemic Level, as of February 2021
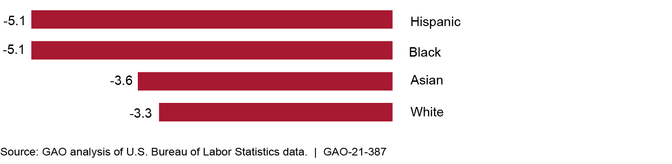
The pandemic has affected some sectors of the economy much more than others. In particular, sectors like leisure and hospitality, mining and logging, and education have seen the largest losses in employment during the pandemic. Importantly, individuals working in the leisure and hospitality sector historically have had the lowest average earnings among sectors and, moreover, during the pandemic have seen the most significant job losses, and many low-wage workers remained out of work as of February 2021 (see fig. 6).
Figure 6: Percentage Change in Employment by Sector, February 2020–February 2021
In response to the far-reaching public health and economic crises, Congress has passed, and the President has signed, legislation to fund recovery efforts for COVID-19 (COVID-19 relief laws). Figure 7 shows the COVID-19 relief laws enacted from March 2020 through March 11, 2021.
Figure 7: COVID-19 Relief Laws Enacted, as of March 11, 2021
Note: The figure shows selected COVID-19-related federal legislation. It does not show all of the COVID-19-related actions taken by Congress and the administration. Additional federal actions, such as the enactment of legislation providing limited and targeted relief to certain individuals and presidential actions authorizing federal support for states and individuals, also occurred during this time frame. Amounts for the first five COVID-19 relief laws are based on appropriation warrant information provided by the Department of the Treasury (Treasury) as of January 31, 2021. These amounts have increased over time and could increase in the future for programs with indefinite appropriations, which are appropriations that, at the time of enactment, are for an unspecified amount. The amount for the American Rescue Plan Act of 2021 is based on estimates made by the Congressional Budget Office.aThe Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, provided $7.8 billion to agencies for health emergency prevention, preparedness, and response activities related to COVID-19, with the Department of Health and Human Services receiving a majority of the funds. Pub. L. No. 116-123, 134 Stat. 146.bThe Families First Coronavirus Response Act provided supplemental appropriations for nutrition assistance programs and public health services and authorized the Internal Revenue Service to provide tax credits for paid emergency sick leave and expanded family medical leave that the act required certain employers to provide. In addition, the act provided states with flexibility to temporarily modify provisions of their unemployment insurance laws and policies related to certain eligibility requirements and provided additional federal financial support to the states. Pub. L. No. 116-127, 134 Stat. 178 (2020).cThe CARES Act provided supplemental appropriations for federal agencies to respond to COVID-19. In addition, it also funded various loans, grants, and other forms of assistance for businesses, industries, states, local governments, and hospitals; provided tax rebates for certain individuals; temporarily expanded unemployment benefits; and suspended payments and interest on federal student loans. Pub. L. No. 116-136, 134 Stat. 281 (2020). dThe Paycheck Protection Program and Health Care Enhancement Act provided additional appropriations for small business loans, grants to health care providers, and COVID-19 testing. Pub. L. No. 116-139, 134 Stat. 620 (2020).eThe Consolidated Appropriations Act, 2021, expanded or extended several CARES Act programs, including unemployment insurance programs, economic impact payments, and Paycheck Protection Program loans, and rescinded unobligated funds for certain programs. Pub. L. No. 116-260, 134 Stat. 1182 (2020). As of January 31, 2021, Treasury issued about $948.0 billion in warrants for appropriations for COVID-19 relief. In addition, approximately $478.8 billion from Treasury’s Economic Stabilization and Assistance to Distressed Sectors programs and $146.5 billion from the Small Business Administration’s Business Loans Program was rescinded, in response to the Consolidated Appropriations Act, 2021.fThe American Rescue Plan Act of 2021 provided additional relief to address the continued impact of COVID-19 on the economy, public health, state and local governments, individuals, and businesses. The Congressional Budget Office estimates the budgetary effects of the law to be $1.9 trillion. Pub. L. No. 117-2, 135 Stat. 4.
As of January 31, 2021, about $3.1 trillion had been appropriated to fund response and recovery efforts for—as well as to mitigate the public health, economic, and homeland security effects of—COVID-19.[12] As of January 31, 2021, the most recent date for which government-wide information was available at the time of our analysis, the federal government had obligated a total of $2.2 trillion and expended $1.9 trillion of the COVID-19 relief funds as reported by federal agencies to the Department of the Treasury’s (Treasury) Governmentwide Treasury Account Symbol Adjusted Trial Balance System (GTAS).[13]
Eight spending areas—the Business Loan Programs, unemployment insurance, economic impact payments, Public Health and Social Services Emergency Fund, Coronavirus Relief Fund, Education Stabilization Fund, Disaster Loans Programs, and Economic Stabilization and Assistance to Distressed Sectors programs—represent $2.6 trillion, or 84 percent, of the total amounts appropriated.[14] For these eight largest spending areas, agencies reported obligations totaling $2.0 trillion and expenditures totaling $1.7 trillion as of January 31, 2021. Table 1 provides additional details on appropriations, obligations, and expenditures of government-wide COVID-19 relief funds, including the eight largest spending areas.
Table 1: COVID-19 Relief Appropriations, Obligations, and Expenditures, as of January 31, 2021
Major spending area
Total appropriationsa ($ billions)
Total obligationsb ($ billions)
Total expendituresb ($ billions)
Business Loan Programs (Small Business Administration)
830.7c
611.3
538.1d
Unemployment Insurance (Department of Labor)
651.8
437.8
424.1
Economic Impact Payments (Department of the Treasury)
455.3
415.0
415.0
Public Health and Social Services Emergency Fund (Department of Health and Human Services)
280.0
195.0
133.9
Coronavirus Relief Fund (Department of the Treasury)
150.0
150.0
149.5
Education Stabilization Fund (Department of Education)
112.6
100.0
16.6
Disaster Loans Programs (Small Business Administration)
50.6
26.4
24.7d
Economic Stabilization and Assistance to Distressed Sectors (Department of the Treasury)
21.2e
21.1
19.5d
Other Areas
504.3
216.4
194.9
Totalf
3,056.6
2,172.9
1,916.2
Source: GAO analysis of data from the Department of the Treasury and applicable agencies. | GAO-21-387
aCOVID-19 relief appropriations reflect amounts appropriated under the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146. These amounts are based on appropriation warrant information provided by the Department of the Treasury as of January 31, 2021. These amounts have increased over time and could increase in the future for programs with indefinite appropriations, which are appropriations that, at the time of enactment, are for an unspecified amount. In addition, this table does not represent transfers of funds that federal agencies may make between appropriation accounts or transfers of funds they may make to other agencies. bObligation and expenditure data are based on data reported by applicable agencies. cThe Consolidated Appropriations Act, 2021, rescinded $146.5 billion from the Small Business Administration’s Business Loans Programs. dThese expenditures relate mostly to the loan subsidy costs (the loan’s estimated long-term costs to the U.S. government). eEconomic Stabilization and Assistance to Distressed Sectors programs received $500 billion in appropriations from the CARES Act, approximately $478.8 billion was rescinded in response to the Consolidated Appropriations Act, 2021. fThe sum of amounts may not agree due to rounding.
Throughout our reporting in response to the CARES Act, we have identified and continued to reinforce the importance of key principles that are essential for an effective federal response based on our prior work examining responses to public health and fiscal emergencies. Specifically, federal agencies should
coordinate, establish, and define roles and responsibilities among those responding to the crisis;
provide clear, consistent communication;
collect and analyze data to inform decision-making and future preparedness;
establish clear goals; and
establish mechanisms for accountability and transparency to help ensure program integrity and address fraud risks.
As the nation enters the second year of the COVID-19 pandemic, these principles remain important factors in the federal response to the crisis and a focus of our oversight. In our 2021 High-Risk report, we added Small Business Administration (SBA) loans to our High-Risk List because of concerns about program integrity.[15] In addition, in that report, we discuss other important challenges facing our nation that merit continuing close attention as emerging issues of concern, including Department of Health and Human Services’ (HHS) leadership and coordination of public health emergencies. We will determine whether the leadership and coordination issue should be added to the High-Risk List once we have completed ongoing and planned work in this area.
In this report we are making 28 new recommendations across the federal government in the areas of public health and the economy. As Congress and the administration carry out plans for the federal government’s ongoing COVID-19 response, we urge action on these 28 recommendations, as well as 38 of our 44 prior recommendations that have not been fully implemented from six CARES Act reports. For a summary and the status of all prior recommendations from these reports, see Appendix III.
Hospital and Pharmacy Perspectives on COVID-19 Vaccine Administration and Medical Supply Availability
In February 2021, we surveyed 383 hospitals and interviewed nine large retail pharmacy chains and an association of independent pharmacies to gain their perspectives on vaccine administration and medical supply availability. Providers expressed concerns about COVID-19 vaccine availability and limitations in certain key medical supplies for administering the vaccines—notably syringes and needles. Reported concerns included the following.
Vaccine availability. Of the 166 total hospitals that responded to our survey, 102 (61 percent) reported not having sufficient information to respond to questions from their staff, the public, and others about vaccine availability. In addition, 35 hospitals (21 percent) described concerns with general vaccine availability in open-ended survey responses. Similarly, our interviews with officials representing retail pharmacy chains and an association of independent pharmacies also revealed concerns about vaccine availability. For example, representatives from one retail pharmacy chain stated that the chain has the capacity to administer 25 million doses per month at 9,900 locations, but the chain’s initial allocation of vaccines from the federal government was expected to be only 230,000 doses at 250 locations.
Several retail pharmacy chain representatives also indicated that limited vaccine availability has led to uncertainty regarding the amount of vaccines their pharmacies can expect to receive each week. The new administration has taken steps to increase certainty and vaccine availability. For example, the White House announced at the end of January 2021 that the federal government would begin notifying states earlier about availability and shipments of vaccines, to give greater certainty for planning vaccination efforts.
Availability of syringes and needles. Out of the 146 hospitals that reported they have either begun administering COVID-19 vaccines or plan to do so, 40 hospitals (27 percent) reported being greatly concerned about having a sufficient quantity of syringes in the next 30 days, and 43 hospitals (29 percent) were greatly concerned about having a sufficient quantity of needles.
Capacity to administer COVID-19 vaccines. In addition to supplies, administering vaccines requires managing vaccine orders as well as having additional storage, staff, and information technology system capacity. Some of the most commonly cited concerns include having the ability to track the expected arrival of vaccine orders, having a sufficient number of trained providers to administer vaccines, and storing vaccines in ultra-cold storage.
Shortages of personal protective equipment (PPE) and COVID-19 testing supplies also remain a challenge for some providers.
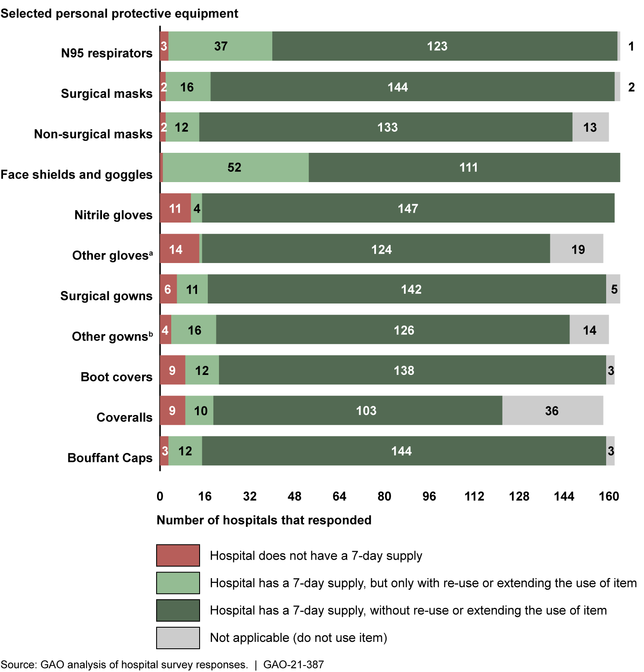
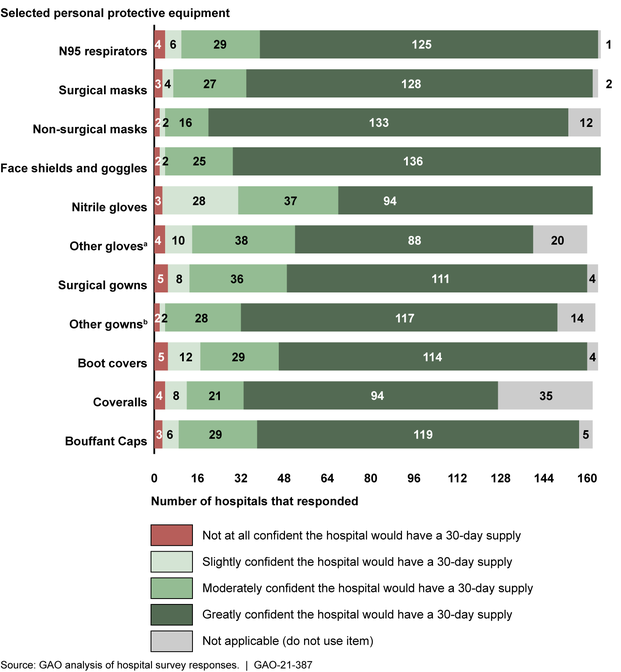
PPE supply. Most of the 166 hospitals that responded to our survey reported having an adequate 7-day supply of the 11 types of PPE we asked about in our survey. However, in some cases, hospitals reported avoiding shortages only with reuse or extending the use of the items. For example, 37 hospitals (23 percent) reported needing to reuse or extend the use of N95 respirators in order to have a 7-day supply. Representatives from all nine retail pharmacy chains reported being confident or very confident their pharmacies could access 30 days or more of PPE, and independent pharmacies generally reported sufficient access. See our enclosure on the Strategic National Stockpile and the Medical Supply Chain in appendix I for additional information and recommendations related to the medical supply chain.
Testing supplies. Most of the surveyed hospitals conducting COVID-19 diagnostic testing reported having at least a 7-day supply of testing supplies we asked about in our survey. However, hospitals were somewhat less confident about levels of those same supplies over the next 15 days. Representatives of the retail pharmacy chains and independent pharmacies that conduct COVID-19 testing did not report current problems accessing testing supplies. See our enclosure on Funding for COVID-19 Testing in appendix I for more information on testing issues.
Along with other entities, we have documented persistent and evolving supply chain challenges throughout the pandemic, such as shortages of key supplies used for COVID-19 testing. We will continue to examine the medical supply chain, including the role of the Strategic National Stockpile, in future reporting.
The Strategic National Stockpile (SNS), overseen by HHS, is a federal stockpile of vaccines, pharmaceuticals, and medical supplies and devices designed to be deployed to support the response to a public health emergency.[16] The near depletion of the SNS early in the COVID-19 response raised questions among the state officials and experts we interviewed about the role and expectations of the SNS during a nationwide pandemic. However, HHS officials told us that the SNS was not designed to provide states with supplies for a prolonged nationwide event such as the COVID-19 pandemic; it is primarily designed to respond to discrete and localized events.
Over the course of our CARES Act work, we have reported on efforts to modernize and restructure the SNS, including progress toward building a 90-day supply of certain key types of PPE, including eye protection or face shields, gowns, gloves, and N95 respirators, in order to respond to future surges in COVID-19 cases. According to HHS officials, they were aiming to meet their 90-day targets of certain PPE by the end of 2020; however, they also noted that they had to balance replenishing the stockpile with ensuring adequate commercial availability. As such, HHS reported delayed delivery of some items to the SNS to enable manufacturers to make them available in the commercial market to alleviate supply constraints. According to HHS data from February 2021, the SNS has reached, or almost reached, its 90-day targets for N95 respirators, surgical or procedural masks, and eye protection or face shields. However, supplies of gloves and gowns or coveralls remain far from their 90-day targets.
As we reported in January 2021, reexamining the role of the SNS in the U.S. response to pandemics will require difficult policy decisions and trade-offs about systems, budgets, and authorities. Stockpiling the SNS for the near term could help address the challenges faced at the beginning of the pandemic response, including the quality and quantity of supplies provided, and allow for more targeted allocation strategies. However, HHS officials were uncertain whether they would maintain the current 90-day target supply levels beyond the COVID-19 response.
In January 2021, the President signed an Executive Order calling for the development of a pandemic supply chain resilience strategy to design, build, and sustain a long-term capability to manufacture medical supplies for future pandemics and biological threats.[17] Per the order, this strategy is to include the role of the SNS in (1) providing and allocating supplies across state, local, tribal, and territorial governments, (2) sustaining supplies during a pandemic, and (3) contingency planning, among other things, within 180 days.[18] As we previously recommended, a process for regularly engaging with Congress and stakeholders in the development and implementation of a medical supply chain strategy to enhance pandemic response capabilities—to include the role of the SNS—would help guide this complex transformation.
Additionally, the Consolidated Appropriations Act, 2021, included a provision requiring the President to make publicly available a report containing a whole-of-government plan for effective response to subsequent COVID-19 outbreaks and for future global pandemic diseases.[19] The act stipulates that this pandemic plan should address how to improve the role of the federal government with respect to the regulation, acquisition, and disbursement of medical supplies necessary to respond to COVID-19 as well as the procurement and distribution of PPE, among other things. See the Strategic National Stockpile and the Medical Supply Chain enclosure in appendix I for additional information.
Funding for COVID-19 Testing
Diagnostic testing for COVID-19 is critical to controlling and understanding the spread of the virus, according to HHS. Overall, HHS reported total testing-specific obligations of about $42.9 billion as of February 28, 2021. A majority of this funding was obligated to states, localities, territories, and tribal organizations, but funding was also used by HHS agencies for testing-related activities, such as procurement of testing supplies and funding for testing for the uninsured.
Officials from all nine selected jurisdictions we spoke with in January 2021 told us that they had sufficient funding to meet their immediate testing goals.[20] While it appears as though a relatively small percentage (about 7 percent) of the federal testing funding obligated for state, local, and territorial jurisdictions has been expended, we found this is due, in part, to funding availability time frames. For example, officials from six of nine selected jurisdictions told us they or their members prioritized spending federal funds whose availability ended earliest. However, more than half of selected jurisdictions told us they had concerns about maintaining testing capacity and preparedness in the longer term. While the supplemental funding has helped jurisdictions address needs to respond to the pandemic in the short term, most jurisdictions interviewed for this report had concerns about future testing and related preparedness. The American Rescue Plan of 2021, enacted on March 11, 2021, includes funding for implementation of a national testing strategy, manufacturing and procurement of tests, and assistance to state, local, and territorial health departments.[21] The additional assistance may help ameliorate concerns about the sufficiency of funding for COVID-19 testing in the longer term. See the Funding for COVID-19 Testingenclosure in appendix I for additional information.
Emergency Use Authorizations
Generally, medical devices must be cleared or approved by the Food and Drug Administration (FDA) to be marketed in the U.S.; however, the Secretary of Health and Human Services may declare that circumstances exist justifying the authorization of emergency use of certain medical products, including devices.[22] Such emergency use authorizations (EUA) allow for the temporary use of unapproved medical products or unapproved uses of approved medical products, provided certain statutory criteria are met.[23] EUAs have been instrumental in increasing needed supply of certain devices, such as PPE, during the COVID-19 pandemic response. However, there have been instances of inconsistencies between EUAs issued by FDA and device guidance from CDC and the Department of Labor (DOL)—agencies that also have a role in ensuring proper use of respirators and other devices.[24] Such inconsistencies led to confusion and hesitancy among health care providers about using devices with EUAs, according to health care provider association officials, and may have undermined the use of these critical medical products early in the pandemic. We recommend that FDA, CDC, and DOL work together to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with EUAs. HHS—which includes FDA and CDC—and DOL agreed with this recommendation.
Additionally, officials representing health care providers, device manufacturers, and distributors raised a number of concerns about what will happen to authorized devices after the declarations permitting their use for COVID-19 end.[25] The Secretary of Health and Human Services is required to provide advance notice prior to the termination of the EUA declarations and consult with manufacturers about proper disposition of authorized devices. HHS has indicated that it intends to develop draft guidance for a transition plan for medical devices distributed under EUAs for COVID-19 by the end of the fiscal year 2021. As of March 15, 2021, the agency had not released a draft plan to provide a transition for the use of these devices. Specifying a reasonable timeline and process for transitioning away from use of authorized devices before the EUA declarations end, taking into account stakeholder input, would help ensure a smooth transition.
We also recommend that as HHS develops a transition plan for devices with EUAs, it should specify a reasonable timeline and process for transitioning authorized devices to clearance, approval, or appropriate disposition that takes into account input from stakeholders. HHS agreed with this recommendation. See the Emergency Use Authorizations for Medical Devices enclosure in appendix I for additional information.
COVID-19 Data for Health Care Indicators
Since June 2020, we have identified concerns with federal COVID-19 data, and we have underscored that in the midst of a nationwide public health emergency, clear and consistent communication between the federal government and the public is critical given that effective response requires the public’s participation.
As part of its efforts to communicate with the public and stakeholders about the pandemic, several experts suggested to us that the federal government should make federal COVID-19 data more accessible, such as by making them available from a central online location. HHS publishes its data on COVID-19 health indicators across several websites, but does not make all of the data accessible from a central online location. That is, all of its publicly available data are not located on, or available from website links on, one online location. As a result, the public, including stakeholders, may not be able to fully understand the extent of the pandemic and use the data to best inform their decision-making.
We are recommending that HHS make its different sources of publicly available COVID-19 data accessible from a centralized location on the internet. This could improve the federal government’s communication with the public about the ongoing pandemic. HHS neither agreed nor disagreed with our recommendation, but it agreed that COVID-19 data should be made accessible to support communication with the public about the pandemic.
We have previously reported that communities of color have been disproportionately affected by the pandemic. We continue to emphasize the need for HHS to implement our recommendation to improve data collection and work with stakeholders to identify and address COVID-19-related racial and ethnic disparities.
HHS released its COVID-19 Response Health Equity Strategy in July 2020 with a goal to reduce health disparities by using data-driven approaches to attain the highest level of health possible for all individuals, including communities of color. We found that HHS’s equity strategy does not include important elements of an effective national strategy, as defined by our prior work. For example, HHS’s strategy includes an intermediate outcome to increase access to testing for populations at increased risk for COVID-19. However, HHS’s strategy does not provide specific actions that the agency will take to determine whether or where it needs to increase access to testing for populations at increased risk for COVID-19—an essential first step before taking steps to increase testing access. By including these elements, HHS can better ensure the effective implementation of its equity strategy to help improve the health outcomes of populations disproportionately affected by COVID-19, including communities of color.
Improving completeness of race and ethnicity data for COVID-19 vaccinations is critical to federal efforts to advance equity. HHS plans to reach disproportionately affected communities through vaccination strategies, including plans to collect and report timely, complete, and representative data on COVID-19 vaccinations. However, according to HHS, as of February 8, 2021, data from states and jurisdictions on race and ethnicity were missing for almost half (45.6 percent) of COVID-19 vaccine recipients. HHS stated that this information is missing for a variety of reasons, including a lack of consistent data collection and reporting by physicians and pharmacists and challenges with transmitting data to HHS. Without complete information on the race and ethnicity of persons who have received COVID-19 vaccines, HHS may have difficulty determining whether vaccines are distributed equitably to communities of color who have been disproportionately affected by COVID-19.
We are recommending that HHS incorporate key elements of a national strategy in its COVID-19 Response Health Equity Strategy, including specific actions to achieve intermediate outcomes and determining how they should be prioritized. HHS agreed with this recommendation. In addition, we are recommending that HHS take steps to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations. HHS neither agreed nor disagreed with this recommendation. See the Health Disparities enclosure in appendix I for more information.
Relief for Health Care Providers
The Provider Relief Fund, which reimburses eligible providers for health-care-related expenses or lost revenues attributable to COVID-19, includes an allocation for the COVID-19 Uninsured Program.[26] Although HHS officials have not yet determined the total amount to be used for this program, as of March 1, 2021, approximately $2.2 billion from the Provider Relief Fund had been disbursed for COVID-19 treatment, testing, and vaccine administration of uninsured individuals. Providers who choose to participate in this program must attest to its terms and conditions, which include that the individual treated, tested, or administered a vaccine is uninsured, that the provider will accept reimbursement as payment in full, and that the provider will not bill the individual for the balance of the bill.
HHS’s risk assessment identified the potential for providers to falsify patients as being uninsured as a risk for the COVID-19 Uninsured Program.[27] HHS officials told us that HHS intends to perform post-payment reviews of claims to validate certain provider attestations. However, HHS did not have documentation describing how it plans to conduct these reviews. Without documented post-payment review policies and procedures and timely implementation of related control activities, HHS’s ability to consistently identify and recover improper payments will be limited, and the agency’s efforts to recover the payments identified as overpayments will be delayed, or the payments may not be recovered.
We are recommending that HHS finalize and implement a post-payment review process to validate COVID-19 Uninsured Program claims and to help ensure timely identification of improper payments, including those resulting from potential fraudulent activity, and recovery of overpayments. HHS agreed with the recommendation. See the Relief for Health Care Providers enclosure in appendix I for more information.
Nursing Homes
The health and safety of the 1.4 million elderly or disabled residents in the nation’s more than 15,000 Medicare- and Medicaid-certified nursing homes—who are often in frail health and living in close proximity to one another—has been of particular concern during the COVID-19 pandemic. According to HHS case-reporting data, as of February 7, 2021, more than 99 percent of Medicare- and Medicaid-certified U.S. nursing homes had reported at least one confirmed resident or staff case, and more than 80 percent had reported at least one resident or staff COVID-19 death.
Collecting detailed information on vaccinations for nursing home populations is important for tracking and transparency, particularly because nursing homes have been an epicenter of the pandemic and because HHS has recommended priority vaccinations for this group. The National Strategy for the COVID-19 Response and Pandemic Preparedness notes that agencies should share data on COVID-19 response and recovery efforts and that these data should be publicly available to support performance tracking and ensure transparency.
HHS collects data and publicly reports the number of vaccination doses, by state, provided to residents and staff of all long-term care providers participating in an HHS pharmacy partnership program for vaccinations in long-term care facilities. However, HHS does not publicly report data showing vaccination rates specifically for nursing homes and does not collect or report vaccination data for nursing homes not participating in this program. According to HHS, it does not report specifically for nursing homes because of concerns that such data would not accurately reflect vaccination rates in nursing homes—for example, some residents may have received their first dose before being admitted. Without public reporting of these data, it is unclear to what extent efforts to vaccinate nursing home residents have been successful, and it may be difficult to use these data to improve ongoing and future vaccination efforts for the nursing home population.
Further, since 2005, HHS has required nursing homes to offer influenza and pneumococcal vaccinations to nursing home residents. Data on these vaccinations are a key part of HHS’s oversight of nursing home infection prevention and control practices. However, as of January 2021, HHS had not specified whether nursing homes would be required to offer COVID-19 vaccinations or how these vaccinations would be incorporated into its requirements or quality measures for nursing homes. These data are important because they could help manage the risk of COVID-19 outbreaks in nursing homes and serve as an important source of information for consumers about quality of care, making the collection of complete vaccination rate data critical for any quality measures developed.
We are recommending that HHS (1) collect data specific to COVID-19 vaccination rates in nursing homes and make these data publicly available; and (2) require nursing homes to offer COVID-19 vaccinations to residents and staff and design and implement associated quality measures. HHS neither agreed nor disagreed with these recommendations. See the Nursing Homes enclosure in appendix I for more information.
Veterans Health Care
According to the Department of Veterans Affairs (VA), many veterans enrolled in VA’s health care system are at a higher risk of infection or severe disease from COVID-19 due to their age or underlying health conditions. VA developed and began executing a COVID-19 vaccination plan following the emergency use authorization of the Pfizer COVID-19 vaccine in December 2020. We identified several areas where VA can improve its vaccination efforts:
VA is utilizing a phased vaccine rollout; however, VA’s current metrics do not capture vaccine data by phases. Specifically, VA has metrics for vaccinations by veteran age and by high-risk condition, but these metrics do not provide information on vaccinations by phase, because phases may include veterans based on a combination of factors. For example, phase 1c includes veterans who are over the age of 65 and veterans under the age of 65 who have high-risk conditions. VA officials said that they only collect data required by CDC. Without the ability to review vaccination data by phase, VA is not able to determine which facilities may be at an earlier phase than others and direct resources or assistance to those facilities.
VA lacks targets for when it will move from one vaccination phase to another—or within one phase, from one group of veterans to another—making it difficult for the department to assess progress. According to VA, creating vaccination targets is challenging given that vaccine supply currently lags demand, and the amount of vaccine available to VA is unpredictable and fluctuates from week to week. As of March 10, 2021, VA had fully vaccinated—that is, administered two required doses of the Moderna or Pfizer vaccines, or one dose of the Janssen vaccine—to about 908,000 veterans out of the roughly 10 million currently enrolled in VA’s health care system and about 243,000 VA staff out of approximately 419,000. However, without preliminary targets, VA may not be able to assess the progress of its vaccination effort and signal to other groups when they might anticipate being vaccinated.
VA does not have metrics related to staff and veterans who do not show up for their vaccination appointments (no-shows), which is inconsistent with its own vaccination goal to track vaccine administration and completion of both doses of vaccine. Without data on no-shows, VA may be at an increased risk of not being able to determine the extent to which staff and veterans are not showing for appointments for their second vaccinations, and may miss opportunities to better target outreach to individuals not showing up for appointments. Officials told us that VA is collecting data required by CDC, which do not include no-show appointments.
Weare recommending that VA (1) develop metrics to assess the number of vaccines administered by vaccine rollout phase to better assess progress and make any necessary adjustments as needed; (2) develop preliminary vaccination targets for when it will move from one vaccination phase to another—or within one phase, from one group of veterans to another—and (3) collect data on the number of staff and veterans who do not show up for a vaccination appointment to better monitor for completion of the second dose of the vaccine. VA agreed with our first and third recommendations and agreed in principle with our second recommendation. See the Veterans Health Care enclosure in appendix I for more information.
Nutrition Assistance
The U.S. Department of Agriculture (USDA) administers a number of federal nutrition assistance programs to vulnerable populations. Recent legislative and executive actions made several changes to these programs as the negative economic effects of the COVID-19 pandemic have continued. For example, benefits for the largest of these programs—the Supplemental Nutrition Assistance Program (SNAP), administered by USDA’s Food and Nutrition Service (FNS)—were increased by 15 percent from January through September 2021 for all participants, according to USDA.[28] Additionally, eligibility was temporarily expanded to certain vulnerable populations.
Until recently, USDA had released minimal data about participation in these programs during the pandemic, and when the department released data in late January 2021, it did not publicly share sufficient information about data quality. In August 2020, USDA announced that it had identified significant issues with the quality of state-reported data on two programs, leading to larger-than-actual estimates for SNAP participation. As it worked to identify the root causes of the SNAP data issues, USDA opted not to release participation data for any of its other nutrition assistance programs from July 2020 until late January 2021. When USDA released the data, the department did not explain how it resolved the data quality issues it previously disclosed, nor did it share necessary context to help stakeholders and the public understand and interpret the data, such as the potential for error that manual adjustments to data may introduce.
Office of Management and Budget (OMB) guidelines direct agencies to consider the usefulness of information they disseminate to intended users, including the public, and state that the information should be presented in an accurate, clear, complete, and unbiased manner, and within a proper context, and that agencies should disclose any sources of error that affect data quality. Because the department has not published information on its efforts to address prior data quality issues or disclosed potential sources of error, stakeholders and the public lack sufficient information and appropriate context to interpret key program data and understand the effects of the pandemic on the programs. We are recommending that USDA (1) provide sufficient context to help stakeholders and the public understand and interpret data on federal nutrition assistance programs during the pandemic and (2) disclose potential sources of error that may affect data quality during the pandemic, such as manual processing. USDA generally agreed with our recommendations.
Disaster Relief Fund and Assistance to Tribal Governments
The Federal Emergency Management Agency (FEMA), within the Department of Homeland Security (DHS), continues to play a key role in the ongoing COVID-19 pandemic response effort, including using the Disaster Relief Fund to provide Public Assistance grants.[29] Public Assistance grants reimburse tribal governments, among others, for pandemic costs, such as testing supplies, PPE, and vaccine distribution.
Several tribal organizations reported challenges related to completing administrative requirements to request and receive Public Assistance as a direct recipient during the pandemic––requirements such as activating an emergency operations plan and submitting a tribal Public Assistance Administrative Plan.[30] While tribal representatives reported that some tribal nations received technical assistance, many other tribal nations were given little or no technical assistance when they requested support. For example, two tribal officials told us that when requesting technical assistance from FEMA to help with disaster activities, FEMA did not have staff available to assist. FEMA’s Tribal Pilot Guidance states that tribes may request technical assistance from FEMA to develop a disaster-specific Public Assistance Administrative Plan. Without the availability of consistent and timely technical assistance across regions, some tribal entities may be unable to request and receive Public Assistance directly from FEMA to help respond to the COVID-19 pandemic.
FEMA’s initial assessment report of its response to the pandemic noted challenges and recommended that FEMA develop a tribal nation engagement strategy that includes providing the resources and personnel throughout each region required to support program delivery for all tribal nations. However, as of March 2021, FEMA had not developed this strategy.
We are recommending that FEMA provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19. DHS agreed with our recommendation.
In addition, in May 2020, multiple tribal associations reported that DHS and FEMA did not formally consult with tribes for COVID-19 pandemic policies that have tribal implications.[31] In 2019, FEMA issued its Tribal Consultation Policy, which specifies the process for how FEMA engages with tribal governments in regular and meaningful consultation and collaboration on actions that have tribal implications.[32]
FEMA did not follow the tribal consultation process while developing an interim policy detailing eligible items for reimbursement under the Public Assistance program. FEMA officials agreed that this interim policy has tribal implications but the agency did not formally consult with tribes while developing the interim policy because they did not have the time due to the expedited nature of that policy and the immediate need to respond to questions from states, tribes, territories, and localities.
As a result, FEMA issued an interim policy clarifying the types of items and activities eligible for COVID-19 Public Assistance without tribal input. If tribes had been formally consulted earlier in the process, they could have been in a better position to provide meaningful input to FEMA on how its policy might impact tribes before FEMA issued the policy in September 2020. Further, there may have been less confusion on which items were considered eligible for reimbursement during the early months of the pandemic, and tribes could have made more informed decisions.
We are recommending that FEMA adhere to the agency’s protocols listed in its updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of its tribal consultation process when developing new policies and procedures related to COVID-19 assistance. DHS agreed with our recommendation.
The Department of Education (Education) has taken steps to track state and school district spending of certain COVID-19 relief funds, but the data give an incomplete picture of the status of funds.[33] According to data collected by Education, as of February 28, 2021, states and territories had spent about $6.1 billion of the approximately $75 billion appropriated for education. However, federal spending data alone provide an incomplete picture of states’ and school districts’ spending, as there are several factors that influence the rate at which funds appear to be spent.
For example, there is often a significant gap between when a district “uses” the funds (i.e., when the district orders, contracts for, installs, and pays for goods or services, such as information technology equipment) and when those funds are reported as “spent” in state and federal reporting systems, as is common in federal grants management processes. According to Education officials, states award applicable funds to school districts so that the school districts can obligate those funds to specific purposes. The state does not transfer funds to the district until the district requests payment for services or deliverables received. Education officials do not consider the funds to have been spent until the state requests payment for expenses.
Both Education and Congress have recognized the importance of accurately capturing the status of COVID-19 relief funds provided to states and school districts to inform the department’s monitoring and technical assistance, and to provide transparency to the public about uses of the funds. However, given the gap between when a district uses funds and funds are recorded as spent, without complete information on obligations, policymakers will not have information on how these funds are being used to address the pandemic-related education needs of America’s schoolchildren.
We are recommending that Education regularly collect and publicly report information on school districts’ financial commitments (obligations), as well as outlays (expenditures), in order to more completely reflect the status of their use of federal COVID-19 relief funds. For example, Education could modify its annual report on state and school district spending data to include obligations data in subsequent reporting cycles. Education agreed with our recommendation. See the K-12 Education enclosure in appendix I for more information.
Economic Impact Payments
The CARES Act and the Consolidated Appropriations Act, 2021, authorized Treasury and the Internal Revenue Service (IRS) to issue economic impact payments (EIP) as direct payments to help individuals address financial stress due to the pandemic.[34] Treasury and IRS quickly issued the second round of direct payments to most eligible individuals. As of February 28, 2021, Treasury and IRS had issued 168.2 million payments totaling $275.9 billion for the first round of payments (EIP 1) and 152.4 million payments totaling $147 billion for the second round of payments (EIP 2).
In December 2020, Treasury and IRS sent an estimated 13 to 19 million EIP 2 payments to temporary bank accounts. As a result, millions of individuals experienced a delay of up to a month to receive their EIP 2. Tax industry partners, such as tax preparers and tax financial services companies, had established these temporary accounts on behalf of their clients to receive tax refunds.
IRS officials said the EIP 2 payments were sent to the temporary bank accounts due to an error. These officials added that IRS attempted to address the issue of temporary bank accounts after EIP 1 but instead uploaded the wrong information for some accounts for EIP 2. IRS did not become aware of the error until December 31, 2020, when its tax industry partners notified it that EIP 2 payments had been sent to the temporary accounts. IRS officials said they did not perform a quality review of the revised records. According to officials, they were working under a compressed time frame, and preparing for the 2021 filing season.
IRS has documented quality review procedures for its operations. However, according to officials, they did not consistently follow these procedures for the second round of direct payments. With the enactment of the American Rescue Plan of 2021, which includes a third round of economic impact payments and advance payments of the Child Tax Credit, timely reviews of control activities for making direct payments to individuals could help IRS avoid costly or burdensome errors in the future.[35]
We are recommending that IRS periodically review control activities for issuing direct payments to individuals to determine that the activities are designed and implemented appropriately as IRS disburses a third round of EIPs and prepares for advance payments on the Child Tax Credit. These control activities should include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients. IRS disagreed with our recommendation. However, IRS acknowledged that it established additional procedures and reviews upon discovering that it had sent millions of payments to the wrong account. IRS stated it plans to assess the effectiveness of these new controls during the next round of Economic Impact Payments and will adjust them as warranted.
Economic Injury Disaster Loan Program and Paycheck Protection Program
The Consolidated Appropriations Act, 2021, appropriated additional funding for the creation of the Targeted Economic Injury Disaster Loan (EIDL) Advance program and authorized additional Paycheck Protection Program (PPP) loans, among other things, highlighting the continued need for ensuring program integrity.[36] On March 11, 2021, the American Rescue Plan Act of 2021 appropriated additional funding for entities that qualified for targeted EIDL advances under the Consolidated Appropriations Act, 2021, including setting aside a portion for smaller and more economically impacted businesses in low-income communities.[37] The American Rescue Plan Act of 2021 also appropriated additional funding for PPP loans.
Since March 2020, the Department of Justice (DOJ) has publicly announced charges in numerous fraud-related cases across the country, including charges of identity theft, wire and bank fraud, and money laundering. See the Federal Fraud-Related Cases enclosure in appendix I for more information. For example:
From May 2020 to February 2021, DOJ publicly announced charges in over 30 fraud-related cases associated with EIDL loans, charging over 50 defendants.
From May 2020 to February 2021, DOJ publicly announced charges in over 100 fraud-related cases associated with PPP loans, charging over 170 defendants.
As of February 2021, at least five defendants had pleaded guilty to federal charges of defrauding the EIDL program, and at least 30 defendants had pleaded guilty to federal charges of defrauding PPP.
Law enforcement officials we spoke with noted a large number of ongoing investigations and hotline complaints related to CARES Act loans, including loans made under the EIDL program and PPP. For example, according to a senior official at SBA’s Office of Inspector General (OIG), as of January 2021, the agency had opened more than 260 investigations related to CARES Act loans and received over 70,000 hotline complaints—both far exceeding numbers the office would typically receive in a year. Law enforcement officials also reported systemic patterns of fraud across EIDL and PPP investigations, including identity theft, false attestations on loan documents, misuse of proceeds, and fictitious and inflated employee counts. SBA officials told us that for EIDL, SBA is supporting many of the DOJ and SBA OIG investigations of EIDL through a team that researches case files, responds to inquiries from law enforcement agencies, and shares data on suspected fraud cases with the SBA OIG, DOJ, and U.S. Secret Service.
SBA has taken some steps to mitigate fraud risks to EIDL and PPP, such as identifying and addressing risks on a loan-level basis for both programs, but has not taken a strategic approach to managing fraud risks. We are recommending that SBA (1) conduct and document fraud risk assessments for the EIDL program and PPP, (2) develop a strategy that outlines specific actions to address assessed fraud risks in the EIDL program, and (3) outline specific actions to monitor and manage fraud risks in PPP on a continuous basis. SBA agreed with our recommendations.
In addition, in December 2020, SBA’s independent financial statement auditor stated that SBA was unable to provide adequate documentation to support a significant number of transactions and account balances related to EIDL due to inadequate processes and controls. The auditor noted discrepancies including more than one loan or advance approved and disbursed to the same borrower, and identified over 6,000 disbursed EIDL loans (over $212 million total) issued to potentially ineligible borrowers.[38] The auditor noted that SBA management did not properly design and implement overall effective management controls to account for new and expanded programs, such as EIDL, under the CARES Act and related legislation.[39] In response to the audit findings, SBA did recognize that documentation of its processes and controls was not sufficiently well developed to support the financial statement audit and stated that it is working diligently to correct any shortcomings for future audits. As a result of concerns about program integrity, we have added SBA loans to GAO’s High Risk List. We are recommending that SBA implement a comprehensive oversight plan to identify and respond to risks in the EIDL program to help ensure program integrity, achieve program effectiveness, and address potential fraud. SBA agreed with our recommendation.
We continue to have concerns about overpayments and potential fraud in the unemployment insurance (UI) system, including DOL’s federally funded Pandemic Unemployment Assistance (PUA) program, which authorizes benefits to certain individuals not otherwise eligible for other UI benefits, such as self-employed and certain gig economy workers.
For example, according to DOJ, from March 2020 through January 2021, DOJ filed federal charges against 92 individuals for defrauding the UI programs and an additional 11 individuals pleaded guilty to federal charges.[40] See the Federal Fraud-Related Cases enclosure in appendix I for more information.
In addition, as of March 15, 2021, DOL reported that states had identified more than $3.6 billion in PUA overpayments from March 2020 through February 2021.[41] As of March 15, 2021, DOL reported that states had identified about $2.6 billion in regular UI overpayments during the pandemic, in the final 3 quarters of 2020 combined. Overpayments are not necessarily a result of fraud, though some may be.
In response to the recommendation in our January 2021 report that DOL collect data from states on the amounts of overpayments recovered in the PUA program, DOL has taken steps to collect data on states’ recovery of PUA overpayments. As of March 15, 2021, 14 states had begun reporting some overpayment recovery data to DOL. However, the Consolidated Appropriations Act, 2021, enacted on December 27, 2020, provided states authority to waive certain PUA overpayments.[42] Therefore, additional data on the amounts of PUA overpayments states have waived are also needed to effectively monitor the recovery of overpayments. The large amount of already-reported PUA overpayments (about $3.6 billion as of March 15, 2021) indicates the need for timely data to monitor and support states’ use of overpayment waivers. According to DOL, states are able to retroactively waive PUA overpayments from the beginning of the program onward; waived overpayments do not have to be recovered. However, DOL did not include PUA overpayments waived in updated state reporting requirements issued in early 2021 because, according to officials, the agency needed to quickly issue guidance on new PUA provisions in the Consolidated Appropriations Act, 2021. In early February, DOL officials told us they did not have plans to collect data on which states are utilizing the authority to waive PUA overpayments or the amount of overpayments that states have waived. In a subsequent meeting in late February, DOL officials responded that they were developing requirements for states to report these data, which would be included in a future round of guidance.
We are recommending that DOL collect data from states on the amount of overpayments waived in the PUA program, similar to the regular UI program. DOL agreed with our recommendation. See the Unemployment Insurance Programs enclosure in appendix I for more information.
Federal Contracts and Agreements for the COVID-19 Response
Federal contracting activity continues to play a critical role in response to the pandemic. As of February 28, 2020, agencies obligated more than $55 billion on contracts to support the COVID-19 response, including $5.2 billion obligated by USDA. Nearly all of USDA’s obligations supported the Farmers to Families Food Box Program—a program implemented in May 2020 to assist commodity suppliers impacted by the pandemic and to provide food assistance to the public. However, USDA faced some data reporting challenges for its Farmers to Families Food Box Program. For example, in February 2021, we found that over $1.2 billion in obligations for the program were not reported with the COVID-19 National Interest Action (NIA) code. The COVID-19 NIA code was established on March 13, 2020, to enable the consistent tracking of COVID-19 contracting actions in the Federal Procurement Data System-Next Generation. USDA has since corrected the data reporting issues we identified, but has not established guidance for its contracting officials to ensure these challenges do not persist. USDA also experienced challenges compiling complete contract documentation for its contract awards. According to USDA officials, the hundreds of contract actions for the program have largely been executed by a small staff of one contracting officer and seven contracting specialists. A contracting official told us the speed with which the contracts were executed and the sheer volume of awards may have affected officials’ ability to ensure accurate contract reporting and the compilation of complete contract files.
Without guidance reinforcing the need to use the NIA code to track Farmers to Families Food Box contract actions, USDA may continue to face challenges reporting quality information on billions of dollars in contract activity to the public—including congressional decision makers, entities with oversight responsibilities, and taxpayers. Further, without assessing the workforce needed to manage existing contracts that underpin the program and any future food distribution contracts, USDA cannot ensure that the challenges the department has encountered with contract reporting and management of contract documentation are addressed, particularly given that additional funding continues to be provided to support pandemic-related food distribution efforts. USDA has taken some steps to mitigate these issues, including using a different contracting approach and completing a workforce reorganization. However, the challenges we found related to inaccurate contract reporting and incomplete contract files have persisted even after the change in contracting strategy. USDA has not assessed whether additional contracting officers will be assigned to support the program as of February 2021.
We are recommending that USDA (1) issue guidance—such as an acquisition alert or a reminder to contracting officials–on the use of the NIA code for the Farmers to Families Food Box Program or successor food distribution program to ensure it accurately captures COVID-19-related contract obligations in support of the program and (2) assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the program or successor food distribution program, and take the necessary steps to ensure it has adequate contracting staff in place to award and administer any future contract awards for the program. USDA neither agreed nor disagreed with our recommendations. See the Federal Contracts and Agreements for COVID-19 enclosure in appendix I for more information.
Single Audits
Single audits—required for non-federal entities that receive federal awards when their award expenditures meet a certain dollar threshold amount in a fiscal year—help identify deficiencies in the award recipients’ compliance with applicable laws and regulations, help ensure the appropriate use of federal funds, and reduce the likelihood of federal improper payments.[43]
Through provisions enacted in the COVID-19 relief laws, the federal government has provided billions of dollars to non-federal entities that must undergo these single audits when their award expenditures meet the threshold.[44] Each year, OMB, after consultation with federal agencies, issues a tool that auditors rely on that consolidates applicable legal requirements for numerous programs into one central place, called a Compliance Supplement.[45] OMB’s 2020 Compliance Supplement—issued in August 2020—was incomplete despite numerous audits already being underway. OMB released an addendum to the supplement in December 2020.
The lag between the distribution of COVID-19 relief funds to recipients and OMB’s issuance of single audit guidance contributed to delays in auditors conducting single audits and reporting the results, which may lead to inconsistent reporting and affect award recipients’ development of corrective actions. A process for timely preparing and providing the guidance contained in OMB’s annual Compliance Supplements to auditors is essential to help ensure that single audits can be performed timely and enhance the federal government’s ability to help safeguard billions of dollars in federal funds, including those provided under COVID-19 relief laws.
In addition to providing timely guidance, it is also essential that OMB establish and maintain a clear process that provides adequate time to work with stakeholders—including federal agencies and the audit community—to determine needed changes to more fully address their input and concerns, which in turn could help ensure the quality of the guidance. This is especially critical going forward given the magnitude of COVID-19 relief funding. OMB stated that it solicits comments from members of the audit community, and makes revisions as appropriate, prior to issuing its final annual Compliance Supplement. However, it is unclear to members of the audit community what OMB’s decision-making process is for resolving concerns raised during the comment period.
We are recommending that OMB work in consultation with federal agencies and the audit community (e.g., agency OIGs; National Association of State Auditors, Comptrollers and Treasurers; and American Institute of Certified Public Accountants), to the extent practicable, to incorporate appropriate measures in OMB’s process for preparing single audit guidance, including the annual Single Audit Compliance Supplement, to better ensure that such guidance is issued in a timely manner and is responsive to users’ input and needs. OMB neither agreed nor disagreed with our recommendation.
See the Single Audits enclosure in appendix I for more information.
Employer Tax Relief and Payroll Tax Deferrals
The Families First Coronavirus Response Act and the CARES Act provided tax credits to covered employers to mitigate the cost of paid sick and family leave for employees affected by COVID-19, among other tax relief, and the Consolidated Appropriations Act, 2021, amended and extended some of these credits.[46] Our analysis of IRS data showed that 3,379 employers that claimed a Families First Coronavirus Response Act leave tax credit may be ineligible for the credit, based on our review of employee counts reported on tax forms employers submit to IRS.[47]
Because the employee counts on these employer tax forms only account for one pay period during each quarter, they are therefore imperfect determinants of eligibility for the tax credit. However, they could serve as a screening tool. For example, because only employers with fewer than 500 employees are eligible for these credits, employers that report 500 or more employees on these forms could be contacted and asked to resolve the discrepancy or return any credit claims for which they were not eligible.
While IRS conducts compliance examinations for these tax forms, resource constraints at the agency allow for only a small number of examinations (0.1 percent of employment tax filings per fiscal year 2019); as a result, IRS risks not identifying and addressing a large percentage of potentially ineligible claims.
We are recommending that IRS leverage employee counts from its tax forms to identify potentially ineligible COVID-19-related sick and family leave credit claims and address discrepancies IRS deems significant. This approach could be less resource intensive than the examinations that IRS currently conducts. We are also recommending that IRS conduct outreach to employment tax return filers to educate and promote accurate reporting of employee counts on its tax forms. IRS agreed with both of our recommendations.
With the issuance of this report, we have now made 72 recommendations to federal agencies and four matters for congressional consideration to improve the federal response to COVID-19. These recommendations are tailored to specific federal programs and initiatives, and, if implemented, will strengthen the efficiency, effectiveness, and accountability of federal efforts. We will continue to monitor the status of these recommendations as part of our ongoing oversight of the federal government’s COVID-19 response and recovery efforts.
We are sending copies of this report to the appropriate congressional committees, the Office of Management and Budget, and other relevant agencies. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at (202) 512-5500 or dodarog@gao.gov. Questions can also be directed to Kate Siggerud, Chief Operating Officer, at (202) 512-5600; A. Nicole Clowers, Managing Director, Health Care, at (202) 512-7114 or clowersa@gao.gov; or Orice Williams Brown, Managing Director, Congressional Relations, at (202) 512-4400 or williamso@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report.
Gene L. Dodaro
Comptroller General of the United States
Congressional Addressees
The Honorable Patrick Leahy Chairman The Honorable Richard Shelby Vice Chairman Committee on Appropriations United States Senate
The Honorable Ron Wyden Chairman The Honorable Mike Crapo Ranking Member Committee on Finance United States Senate
The Honorable Patty Murray Chair The Honorable Richard Burr Ranking Member Committee on Health, Education, Labor, and Pensions United States Senate
The Honorable Gary C. Peters Chair The Honorable Rob Portman Ranking Member Committee on Homeland Security and Governmental Affairs United States Senate
The Honorable Rosa L. DeLauro Chairwoman The Honorable Kay Granger Ranking Member Committee on Appropriations House of Representatives
The Honorable Frank Pallone, Jr. Chair The Honorable Cathy McMorris Rodgers Republican Leader Committee on Energy and Commerce House of Representatives
The Honorable Bennie G. Thompson Chair The Honorable John Katko Ranking Member Committee on Homeland Security House of Representatives
The Honorable Carolyn B. Maloney Chairwoman The Honorable James Comer Ranking Member Committee on Oversight and Reform House of Representatives
The Honorable Richard Neal Chair The Honorable Kevin Brady Republican Leader Committee on Ways and Means House of Representatives
The federal government’s communication of data and COVID-19 indicators to the public and stakeholders could be improved.
Entity involved: Department of Health and Human Services
Recommendation for Executive Action
The Secretary of Health and Human Services should make the Department’s different sources of publicly available COVID-19 data accessible from a centralized location on the internet. This could improve the federal government’s communication with the public about the ongoing pandemic.
The Department of Health and Human Services neither agreed nor disagreed with our recommendation, but it agreed that COVID-19 data should be made accessible to support communication with the public about the pandemic.
Key Considerations and Future GAO Work
In January 2021, we reported on the need for more complete and consistent COVID-19 data to inform health care indicators. As we previously reported, the lack of complete and consistent data limits the Department of Health and Human Services’ (HHS) and others’ ability to monitor trends in the burden of the pandemic across states and regions, such as COVID-19 cases and hospitalizations; make informed comparisons between such areas; and assess the impact of public health actions to prevent and mitigate the spread of COVID-19. Additionally, incomplete and inconsistent data have limited HHS’s and others’ ability to prioritize the allocation of health resources in specific geographic areas or among certain populations most affected by the pandemic.
We recommended that HHS immediately establish an expert committee comprised of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. HHS agreed with our recommendation but said because of resource constraints and the ongoing response to the pandemic, it could not commit to immediately doing so. We plan to continue to monitor HHS’s progress in meeting this recommendation.
In addition to our January 2021 report, throughout this report and our other past bimonthly reports, we have identified continued concerns with federal COVID-19 data. For example, in this report we identified concerns with the quality of federal data related to
COVID-19 cases, deaths, and vaccinations in nursing homes—see our Nursing Homes enclosure; and
race and ethnicity for several COVID-19 health indicators, including testing, cases, hospitalizations, deaths, and vaccinations—see our Health Disparities enclosure.
Background
The rapid spread and evolving nature of the COVID-19 pandemic have underscored the importance of effectively communicating information about the current status of the pandemic with the public on a regular basis. In June 2020, we reported that, in the midst of a nationwide public health emergency, clear and consistent communication between the federal government and the public is critical given that effective response requires the public’s participation and that the lack of such communication can lead to a loss of credibility with the public.
Further, effectively communicating information about the incidence, spread, and containment of an outbreak can help ensure that the public complies with public health measures. For example, in our 2011 report on the H1N1 influenza pandemic, we found that uncoordinated communication between the federal government and the public contributed to confusion and in some cases, individuals’ failure to seek or receive public health interventions, such as influenza vaccinations.
The federal government has provided the public and other stakeholders with data on COVID-19 health indicators. For example, HHS has published data on COVID-19 cases, deaths, testing, hospitalizations, and vaccines on the Centers for Disease Control and Prevention’s (CDC) COVID Data Tracker.[48] Additionally, the Data Strategy and Execution Workgroup (under the White House COVID-19 Response Team) has published COVID-19 Community Profile Reports in another online location and the reports focus on trends in COVID-19 indicators in the last 7 days and changes relative to the week prior.[49] CDC also provides access to these reports through a web link on its COVID Data Tracker.
The COVID-19 Community Profile Reports also highlight selected “hotspot” areas that have a high case burden and thus have a potentially higher risk for experiencing health care resource limitations. For example, the March 10, 2021 Community Profile Report stated that in the last 7 days the Miami, Florida area reported 254 COVID-19 cases per 100,000 persons and a test positivity rate of 9.8 percent.[50] In comparison, in the last 7 days, the national rate of COVID-19 cases was 144 cases per 100,000 persons and the test positivity rate was 4.2 percent. In addition, Miami, Florida had a higher rate of confirmed COVID-19 hospital admissions (9 admissions per 100 beds) than the national rate of 5 admissions per 100 beds, in the last 7 days.[51] The report also noted some decreases from the previous week (e.g., the rate of confirmed COVID-19 hospital admissions decreased by 13 percent nationally and by 10 percent in Miami, Florida).
Additionally, on January 21, 2021, the White House released its National Strategy for the COVID-19 Response and Pandemic Preparedness (National Strategy) which states that the federal government will regularly communicate information to the public on the status of the pandemic through expert-led, science-based public briefings. On January 27, 2021, the federal government began regularly conducting these briefings which describe recent national trends in several COVID-19 indicators including cases, hospitalizations, and deaths.
Overview of Key Issues
All 10 of the National Academies experts we interviewed told us the federal government’s communication of COVID-19 health indicators to the public and stakeholders could be improved. Several of these experts highlighted the importance of the federal government making data on the allocation of vaccines available and ensuring the public and stakeholders are aware of, understand how to use, and are able to easily obtain the COVID-19 data most relevant to them. In addition, several experts also suggested the federal government improve the accessibility of the data by centralizing access to it.
Communicating data on populations receiving COVID-19 vaccinations. Several experts highlighted the importance of the federal government providing information about those receiving COVID-19 vaccinations to the public and stakeholders. Specifically, these experts suggested the federal government share data on the race and ethnicity of those being vaccinated, as well as other high-risk populations (e.g., such as those age 75 and older) to help ensure public confidence in the distribution of the vaccine.
Race and ethnicity. Several experts told us it was important to report information on the race and ethnicity of those being vaccinated to help ensure the vaccine is being equitably provided to different populations. In our November 2020 report, we found that racial and ethnic minority groups are disproportionately affected by the virus. Further, population immunity is not likely to be reached without high vaccination rates across all racial and ethnic groups.
On February 8, 2021, CDC began publishing data on the demographic characteristics of those who received vaccines on its COVID Data Tracker. Specifically, CDC is reporting data on the race and ethnicity, gender, and age of those vaccinated at the national level. However, the reporting of race and ethnicity is less complete compared to gender and age. For example, as of March 11, 2021, CDC found that reporting of race and ethnicity was 53.1 percent complete for recipients who received at least one dose while the same reporting on vaccine recipients’ age and gender were 92.0 percent and 91.1 percent complete, respectively. For further information on CDC data on the race and ethnicity of recipients of COVID-19 vaccinations, see our Health Disparities enclosure, which includes a recommendation for CDC to ensure the complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations.
One expert suggested using community-level data on vaccination use and the social characteristics of communities to assess the equity of vaccine distribution. For example, the Social Vulnerability Index (SVI) is CDC’s index to measure the relative vulnerability of every county by ranking each on 15 social factors, including unemployment, minority status, and disability.[52] According to CDC, these data might be used to help emergency response and public health officials identify and plan support for communities most likely to need support with a public health emergency. Currently, CDC does not make available county-level data on vaccination use, but does provide access to SVI data on its COVID Data Tracker.[53] However, CDC officials stated that the agency plans to provide county-level data on vaccination use on its COVID Data Tracker in March 2021.[54]
Other high-risk populations. Several experts said that it is important to make available to the public vaccination data that corresponds to individuals at higher risk of infection, which includes health care personnel, residents of long-term care facilities (e.g., nursing homes), persons age 75 or older, essential workers, and others, according to CDC recommendations.[55] Data on who is being vaccinated would inform the public of whether the goal of vaccinating those at higher risk per CDC recommendations (such as those age 75 and older) is being met. (For information on the need for additional data related to COVID-19 vaccinations of nursing home residents and staff, see our Nursing Home enclosure, which includes a recommendation for CDC to collect data specific to the COVID-19 vaccination rates in nursing homes.)
Several of these experts told us sharing vaccination data on high-risk populations with the public is also important because it can help ensure public confidence in the distribution of the vaccine. However, it may be challenging to report on certain groups who are at higher risk of infection, such as health care personnel, as information about vaccine recipients’ occupations are not reported to CDC by vaccine providers.
Key considerations for communicating federal COVID-19 data. In addition to emphasizing the importance of consistently communicating COVID-19 information, several experts emphasized the importance of the federal government ensuring that the public and stakeholders are aware of, understand how to use, and are able to easily obtain the COVID-19 data that are most relevant to them. Some of these experts noted that, in general, the public may be more aware of non-federal sources of data on COVID-19 indicators (e.g., the COVID Tracking Project, Johns Hopkins) than sources from the federal government.[56] Experts explained that at the beginning of the pandemic, the public and other stakeholders may have turned to non-federal sources for COVID-19 data because these sources provided more data than the federal government. For example, Johns Hopkins began publishing data on COVID-19 in January 2020, while CDC officials told us that its COVID Data Tracker began publishing data in April 2020. Further, because of their greater familiarity with non-federal sources of data, the public and stakeholders may have continued to use them—even as the federal government has continued to expand the COVID-19 data that it makes available to the public, including as part of CDC’s COVID Data Tracker and the Community Profile Report. For example, some of the experts told us they continue to use other non-federal sources of COVID-19 data and also that they were unaware of the Community Profile Reports.
Several experts also told us that it is important that the federal government help the public and stakeholders understand how to use its COVID-19 data. This could be done by explaining how to interpret community-level COVID-19 data it makes available, for example, to help inform the decisions of the public and other stakeholders (e.g. business owners deciding whether to open). For example, while CDC makes data available on case numbers for the variants of the virus that cause COVID-19, one expert told us that CDC does not explain how to interpret these numbers nor does the agency describe how stakeholders, including state and local public health officials, could use these data to inform their efforts to respond to the pandemic.[57] According to this expert, this information is important because different variants could increase the number of COVID-19 cases and deaths and reduce health care systems’ ability to care for patients. Our 2014 work on health care transparency states that tools for sharing health care information such as websites are most effective if they explain the purpose and value of the data reported to guide users in their interpretation of the data.
Several experts also commented on the importance of the federal government ensuring that users can readily obtain information that is most relevant to them, such as information about the status of the pandemic in their local area. For example, some of these experts stated that it is important to give users the ability to “drill down” to the level of data they need. Further, one expert stated that the federal government should allow data users to create a customized report that includes COVID-19 data that are of most relevance to them. Our 2014 work on health care transparency states that tools for sharing health care information such as websites are most effective if the information is structured in a way that enables users to obtain information that they consider most relevant to their personal circumstances (e.g., information about their communities) and if they allow users to easily adjust how those data are presented.
CDC has taken steps to ensure the public and stakeholders are aware of, understand how to use, and can easily obtain the COVID-19 data most relevant to them. For example:
On February 5, 2021, CDC published a communications tool kit for its COVID Data Tracker that, according to CDC, is updated weekly and includes social media graphics, videos, and media resources. CDC officials also told us that CDC shares information about its COVID Data Tracker on multiple social media platforms, including by promoting enhancements to the Data Tracker and featuring five COVID Data Tracker posts a week.
On February 12, 2021, CDC launched the COVID Data Tracker Weekly Review. According to CDC officials, this newsletter highlights key data from the COVID Data Tracker along with data trends, narrative interpretations of the data, and visualizations from the week.[58] As an example, the February 19, 2021 Weekly Review featured information about the variants of the virus that cause COVID-19, including the number of variants that are of concern to global public health leaders to date, and how to stop new variants of the virus from emerging.
CDC’s COVID Data Tracker provides tools to help users obtain the data most relevant to them. This includes the COVID-19 Integrated County View, which allows users to simultaneously view multiple types of information about the status of the pandemic in their county. As of February 22, 2021, county-level data across several COVID-19 indicators (e.g., cases, deaths, hospitalizations) were available from CDC’s COVID-19 Integrated County View tool.
Centralizing access to federal COVID-19 data. As part of its efforts to communicate with the public and stakeholders about the pandemic, several experts suggested that the federal government should improve the accessibility of its COVID-19 data by making these data available from a central location on the internet. CDC officials told us they were unaware of a single location on the internet where the public and stakeholders could access all of HHS’s COVID-19 data.
Further, in our review of selected HHS websites and COVID-19 data elements we found examples in which HHS published data for COVID-19 health indicators across several locations but did not make all the data accessible from a central online location (e.g., through website links). For example, we visited CDC’s COVID Data Tracker on March 12, 2021, and were unable to identify and access other publicly available HHS COVID-19 data from that website. While CDC’s COVID Data Tracker provided access to data on cases, testing, deaths, hospitalizations, and vaccinations, among other data, it did not provide users access to other HHS COVID-19 data such as higher-than-expected deaths and vaccine adverse events. That is, these data were not available on the COVID Data Tracker or accessible through links to the other websites where these data were located.
Several experts told us that taking steps to make it easier for members of the public to locate data on COVID-19 indicators, such as by making them accessible from one website, would help facilitate the use of those data by the public. These experts told us it is important to make data on COVID-19 health indicators more accessible because the information may help inform individuals’ decision-making. For example, one expert cited the importance of communicating data on vaccine adverse events in promoting public confidence in the vaccines. In our November 2020 report on COVID-19 vaccines and therapeutics development, we noted that timely, clear, and consistent communication about vaccine availability, efficacy, and safety can help ensure public confidence and trust, which in turn could encourage vaccine use.
As part of its Outbreak Communication Planning Guide, the World Health Organization highlights the importance of ensuring information is accessible to the public. Specifically, this guide states that information needed by at-risk parties to adopt behaviors that could minimize risk must be proactively released by authorities in a timely and accessible manner. The guide further states that information relevant to decisions and decision-making associated with the management of a serious public health event should be made available to interested parties so as to maintain trust in authorities, public support for control efforts and coordination among partners.
The National Strategy emphasizes the importance of the federal government ensuring its data for COVID-19 health indicators are accessible to the public and stakeholders. It states CDC will maintain public dashboard data on key COVID-19 related metrics and the federal government will ensure that Americans can simply and easily find information relevant to them on everything from testing, vaccines, testimonials, and all available public health guidance. Further, an executive order signed on January 21, 2021, directs federal agencies, including HHS, to take steps to make federal COVID-19 data publicly available and accessible.[59] The order states these efforts will assist federal, state, Tribal, territorial, and local authorities and further the public’s understanding of the pandemic and the response.
CDC officials told us that CDC’s COVID Data Tracker will serve as the public dashboard as stated in the National Strategy and that they coordinate with other HHS agencies by providing COVID-19 data through the COVID Data Tracker. However, CDC officials emphasized that each HHS agency is responsible for making its own COVID-19 data more accessible to the public and stakeholders and were unaware of other coordinated efforts at HHS to do so. The absence of a centralized online location for publicly accessible HHS COVID-19 data is reflective of how HHS agencies generally communicate other data to the public and other stakeholders; that is, they generally report data that they collect for their own purposes on separate agency-specific websites. Without a centralized online location in which individuals can identify and access all publicly available HHS COVID-19 data and easily obtain the information most relevant to them, the public, including stakeholders, may not be able to fully understand the extent of the pandemic and use the data to best inform their decision-making.
Agency Comments
We provided HHS and the Office of Management and Budget with a draft of this enclosure. HHS provided general comments, which are reproduced in appendix VI . In its comments, HHS neither agreed nor disagreed with our recommendation to make its different sources of publicly available COVID-19 data accessible from a centralized location on the internet. HHS officials agreed that data should be made publicly accessible where possible to support communication with the public about the COVID-19 pandemic. They also stated that increased transparency of data remains a key priority and indicated that HHS will continue to assess opportunities to streamline and provide transparency to the public and other government stakeholders. Given the importance of effectively communicating information about the status of the pandemic with the public, we maintain that HHS should make its publicly available COVID-19 data accessible from a centralized online location. Centralizing access to these data in a way that allows individuals to easily locate and obtain the information most relevant to them would improve the ability of the public to fully understand the extent of the pandemic and use the data to best inform their ongoing decision-making.
HHS also provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To conduct this work, we obtained input from 10 experts with knowledge in public health, health systems, and health economics in January 2021.[60] We obtained assistance from the National Academies in identifying these experts to better ensure a breadth of expertise was brought to bear in its preparation; however, all final decisions on the selection of experts for this work are the sole responsibility of GAO. We asked these experts a core set of questions to obtain their input on federal efforts to communicate COVID-19 health indicators. In addition, we reviewed relevant HHS documents and also obtained input from CDC officials about communicating COVID-19 health indicators to the public.
Influenza Pandemic: Lessons from the H1N1 Pandemic Should Be Incorporatedinto Future Planning. GAO-11-632. Washington, D.C.: June 27, 2011.
COVID-19: Federal Efforts Accelerate Vaccine and Therapeutic Development, but More Transparency Needed on Emergency Use Authorizations. GAO-21-207. Washington, D.C.: November 17, 2020.
Health Care Transparency: Actions Needed to Improve Cost and Quality Information to Consumers, GAO-15-11. Washington, D.C.: October 20, 2014.
Since the onset of the COVID-19 pandemic, mandated public health-related restrictions on economic activity, precautions by consumers, and adjustments by the private sector combined to create an extraordinary shock to the economy. In response, the federal government adopted a range of measures designed to support different areas of the economy, including labor markets, households, small business finances, corporate credit markets, and state and local government finances. These areas of the economy have recovered to greatly varying degrees over the last year (see table). Going forward, the strength of the economic recovery will continue to depend on the success of public health measures against the COVID-19 pandemic.
As of February 2021, indicators for some areas of the economy supported by the federal pandemic response had returned to pre-pandemic levels while other areas remained far from their pre-pandemic conditions.[61] Improvements in bond market indicators, for example, suggest that corporate borrowers and state and local governments had access to credit that was somewhat improved compared to before the pandemic. In contrast, the share of the population employed remained significantly below pre-pandemic levels, and the share of borrowers seriously delinquent on mortgage payments remained well above pre-pandemic levels. Moreover, our analysis of job losses and small business delinquencies identified sectors hard hit by the pandemic that have yet to fully recover, in particular the leisure and hospitality and mining and logging sectors.
Indicators for Areas of the Economy Supported by the Federal COVID-19 Pandemic Response, November 2020 through February 2021, Cumulative Changes since February 2020
aThe employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population 16 years and over. The ratio is subject to misclassification errors with respect to consistently identifying workers as employed and absent from work or unemployed on temporary layoff.bHigher levels in the Consumer Credit Default Composite Index rate indicate more defaults on consumer loans, including auto loans, bank cards, and mortgages. The Consumer Credit Default Composite Index could be subject to seasonal variation but is not seasonally adjusted.cSeriously delinquent loans are 3 months or more past due or in foreclosure, based on mortgages insured by the Federal Housing Administration (FHA). Increases in serious delinquency rates on FHA loans could to some extent reflect borrowers taking advantage of mortgage forbearance provisions of the CARES Act, but may also indicate financial challenges facing the minority and low-to-moderate income households that disproportionately take out mortgages insured by FHA.dLower levels of the small business credit card delinquency index indicate more delayed payments on credit. The small business credit card delinquency index is published under license and with permission from Dun & Bradstreet, and no commercial use can be made of these data.eCorporate bond spreads are option-adjusted spreads on dollar-denominated investment grade corporate bonds from Bloomberg and are measured in basis points or 1/100th of a percentage point. Higher spreads reflect higher perceived risk among corporate borrowers by investors.fSpreads on municipal bonds are calculated relative to interest rates on Treasury securities based on the Bloomberg-Barclays Municipal Bond Index and are measured in basis points or 1/100th of a percentage point. Higher spreads reflect higher perceived risk among municipal borrowers by investors.gState and local government employment data from January 2021 and February 2021 are preliminary.hHealth care employment data from January 2021 and February 2021 are preliminary.
The national economy experienced a substantial contraction in the second quarter of 2020 but grew in the third and fourth quarters of 2020 based on the growth of Gross Domestic Product (GDP). The Federal Reserve Bank of New York’s Weekly Economic Index, which combines high-frequency economic data from a wide range of sources, also indicated a substantial contraction in March and April 2020, followed by a gradual recovery (see figure).[62] However, both GDP and the Weekly Economic Index suggest that, as of February 2021, the economic recovery has slowed and that the economy is smaller than it was a year ago.
Weekly Economic Index, January 2019 through February 2021
Note: The index value of the Weekly Economic Index corresponds to a year-over-year growth rate in gross domestic product were conditions to remain at that value for a full quarter.
As we noted in our June 2020 report, the impact of the COVID-19 pandemic on the economy will reduce federal tax revenues, while the fiscal response from the COVID-19 relief laws and heightened demands on federal social programs will increase expenditures.[63] Federal debt held by the public increased from $17.4 trillion in February 2020 to $21.8 trillion in February 2021. As a share of GDP, debt held by the public increased from 79.0 percent in the fourth quarter of 2019 to 100.7 percent in the fourth quarter of 2020. Interest rates on 3-month Treasury securities were 1.54 percent in February 2020 and fell to 0.14 percent in April 2020 as the Federal Reserve reduced its target interest rates. As of February 2021, 3-month interest rates were 0.04 percent.[64] While interest rates on Treasury securities are low at the moment, reducing the cost of newly issued debt, the long-term fiscal challenges facing the U.S. have been exacerbated by the pandemic and will require attention once the economy has returned to consistent growth and public health goals have been attained.[65]
Labor market conditions. In February 2021, the employment-to-population ratio, which measures the share of the population employed, was 3.5 percentage points lower than in February 2020, suggesting that labor market conditions remain worse than in the pre-pandemic period. The pandemic has affected some sectors of the economy much more than others. In particular, industries like leisure and hospitality and mining and logging have seen the largest percentage losses in employment during the pandemic (see figure). Importantly, individuals working in the leisure and hospitality sector historically have had the lowest average earnings among sectors and, moreover, during the pandemic have seen the most significant job losses, indicating that many low wage workers remained out of work as of February 2021.
Percentage Change in Employment by Sector, February 2020 through February 2021
Note: Other services include repair and maintenance, personal and laundry services, and membership associations and organizations. Data from February 2021 are preliminary.
Moreover, labor market conditions have weakened more for Hispanic, Black, and Asian Americans relative to White Americans since the pandemic began (see figure). In recent months, the number of initial claims for unemployment benefits have remained historically high, indicating ongoing instability in the labor market.
Change in Employment-to-Population Ratio by Race and Ethnicity, February 2020 through February 2021
Household financial conditions. While trends in consumer credit defaults suggest an overall improvement in household financial conditions over the last year, trends in mortgage delinquencies suggest ongoing financial challenges facing some households. Specifically, as of January 2021 the Consumer Credit Default Composite Index—a broad measure of households’ ability to make scheduled payments—improved somewhat over the course of the pandemic. In addition, subindexes for bank cards, first mortgages, and auto loans improved during the same time period.[66] Although changes in these indexes over time should provide a general indication of changes in the financial condition of households, forbearance arrangements could affect the measurement of consumer credit defaults.[67]
In contrast to measured consumer credit defaults, serious delinquency rates for single family mortgage loans—loans that are 90 or more days past due or in foreclosure—increased dramatically in May 2020, decreased slightly in more recent months, but remain much higher than in February 2020, as of January 2021 (see figure).
Serious Delinquency Rates on Single-Family Residential Mortgages, January 2019 through January 2021
Note: The serious delinquency rate on conventional loans is calculated based on a weighted average of serious delinquency rates of conventional loans guaranteed by Fannie Mae and Freddie Mac based on loan counts as of October 2020. Single-family seriously delinquent loans are 3 months or more past due or in the foreclosure process.
Increases in delinquencies to some extent reflect borrowers taking advantage of mortgage forbearance provisions of the CARES Act but may also indicate financial challenges facing households that may not be captured by indicators of default. Moreover, while serious delinquency rates on conventional loans, specifically those guaranteed by Fannie Mae and Freddie Mac, improved slightly in recent months, delinquency rates on loans insured by the Federal Housing Administration (FHA) still remain at near historically high levels. Increases in delinquency rates on FHA loans in particular could indicate that minority and low-to-moderate income households have experienced more financial hardship since the onset of the pandemic as FHA loans disproportionately serve minority and low-to-moderate income borrowers.[68]
Small business financial and credit conditions. Trends in the Small Business Health Index over the last year suggests that some aspects of the financial condition of small business have returned to pre-pandemic levels. However, small businesses also have earned less income and experienced significantly greater difficulty accessing credit than before the pandemic. In addition, small businesses in some sectors continue to make late payments on credit cards.[69]
The small business credit card delinquency index—a measure from Dun & Bradstreet of the timeliness of credit payments of small businesses—weakened for 3 consecutive months beginning in April 2020, but since then has returned to pre-pandemic levels. While the overall ability of small businesses to make timely payments on credit cards improved compared to February 2020, small businesses in some sectors, for example retail and mining and logging, had more late payment compared to pre-pandemic levels (see figure). In addition, small business income—measured by non-farm proprietors’ income from the Bureau of Economic Analysis—has been increasing gradually since June 2020 but as of January 2021 remained lower than in February 2020.[70]
Changes in the Small Business Credit Card Delinquency Index by Sector, February 2020 through January 2021
Note: Other services include repair and maintenance, personal and laundry services, and membership associations and organizations. The small business credit card delinquency index is published under license and with permission from Dun & Bradstreet, and no commercial use can be made of these data.
While some aspects of the financial condition of small businesses have improved compared with a year ago, more banks have tightened rather than loosened underwriting standards on the credit they have extended to small businesses for 4 consecutive quarters, beginning the first quarter of 2020, according to data collected by the Federal Reserve.[71] In addition, more banks have been raising rather than lowering the interest premiums they have charged on loans to small businesses over the same period. These changes indicate that banks anticipated greater risk associated with making these loans going forward.
Corporate credit market conditions. Trends in corporate bond market risk over the last year suggest that perceived risk among investment grade corporate borrowers and access to credit for investment grade corporations have returned to pre-pandemic levels. Specifically, spreads on investment grade corporate bonds increased dramatically starting in early March 2020, then fell rapidly starting in late March 2020 (see figure), and since August of 2020 have returned to levels that were typical during the past few years, prior to the pandemic.[72]
Spreads on Investment Grade Corporate Bonds, January 2019 through February 2021
Note: Corporate bond spreads are measured in basis points or 1/100th of a percentage point.
State and local government finances. State and local government fiscal conditions deteriorated significantly in the spring of 2020 as the national economy weakened and most states delayed income tax filing deadlines. Since this initial shock, total state and local government tax revenues and access to credit via municipal bond markets have significantly improved. In the aggregate, state and local government expenditures remained steady during the pandemic while state and local government employment is substantially lower than before the pandemic.
Based on Census Bureau data, tax revenue collected by state and local governments rose by $130 billion, on a seasonally adjusted basis, in the third quarter of 2020 after falling by over $69 billion in the second quarter (see figure).[73] With the increase in the third quarter revenues, over the first three quarters of 2020 state and local tax revenues were similar to the same period in 2019. Future tax revenues to state and local governments are likely to be sensitive to the strength of the economic recovery.
State and Local Government Tax Revenue, First Quarter 2019 through Third Quarter 2020
Note: State and local tax revenues are seasonally adjusted.
Spreads on municipal bonds increased dramatically in March 2020, peaking on March 23, and decreased gradually over the last year.[74] As of February 2021, municipal bond spreads were somewhat lower than their level as of February 2020, suggesting that perceived risk among municipal borrowers and access to credit for state and local governments were somewhat improved compared to pre-pandemic levels. In contrast, state and local government employment, another timely indicator of state and local fiscal conditions, fell dramatically in the spring of 2020 and remains 1.4 million below levels in February 2020 as of February 2021 (see figure). In the aggregate, state and local government expenditures remained steady during the pandemic, reflecting higher spending on social benefit payments but lower spending in other areas.[75]
State and Local Government Employment, January 2019 through February 2021
Agency Comments
We provided the Department of Housing and Urban Development (HUD), the Department of Labor (Labor), the Department of Treasury (Treasury), the Board of Governors of the Federal Reserve System (Federal Reserve), the Federal Housing Finance Agency (FHFA), the Office of Management and Budget (OMB), and the Small Business Administration (SBA) with a draft of this enclosure. Labor and Treasury provided technical comments, which we incorporated as appropriate. HUD, the Federal Reserve, FHFA, OMB, and SBA did not provide comments on this enclosure.
Methodology
To identify indicators for monitoring areas of the economy supported by the federal response to the COVID-19 pandemic, in particular by the six COVID-19 relief laws, we reviewed prior GAO work, data from federal statistical agencies, data from Fannie Mae and Freddie Mac, information from the Federal Reserve and relevant federal agencies responsible for the pandemic response and oversight of the health care system, data available on the Bloomberg Terminal, and input from internal GAO experts. We reviewed the most recent data from these sources as of January or February 2021, depending on availability.
We assessed the reliability of the economic indicators we used through a number of steps, including reviewing relevant documentation, reviewing prior GAO work, and interviewing data providers. Collectively, we determined the indicators were sufficiently reliable to provide a general sense of how the areas of the economy supported by the federal pandemic response were performing.
Contact information: Lawrance L. Evans, Jr., (202) 512-8678, evansl@gao.gov
The Department of Health and Human Services has not finalized and implemented a post-payment review process to validate claims for the HRSA COVID-19 Claims Reimbursement to Health Care Providers and Facilities for Testing, Treatment, and Vaccine Administration for the Uninsured (COVID-19 Uninsured Program). As of March 1, 2021, it had disbursed a total of about $120 billion (about 67 percent) of the $178 billion appropriated by COVID-19 relief laws for the Provider Relief Fund to help support health care providers and finance care for COVID-19 patients and underserved populations. The department also lent about $106.5 billion to health care providers through a program expanded by the CARES Act.
Entities involved: Department of Health and Human Services, including its Centers for Medicare & Medicaid Services and Health Resources and Services Administration
Recommendation for Executive Action
The Secretary of Health and Human Services should finalize and implement a post-payment review process to validate COVID-19 Uninsured Program claims and to help ensure timely identification of improper payments, including those resulting from potential fraudulent activity, and recovery of overpayments. HHS concurred with the recommendation and stated that it anticipates, among other things, finalizing the audit review strategy with contractor support to help ensure timely identification of improper payments and recovery of overpayments.
Key Considerations and Future GAO Work
As the Department of Health and Human Services (HHS) works to get funds to eligible providers, it will continue to be important that HHS officials remain attentive to establishing robust internal controls to help ensure funds are appropriately disbursed and used. We plan to conduct additional work to examine HHS’s efforts to provide assistance to providers.
Background
Provider Relief Fund. To respond to the pandemic, three of the five COVID-19 relief laws enacted as of March 1, 2021, appropriated $178 billion to reimburse eligible providers for health-care-related expenses or lost revenues attributable to COVID-19, known as the Provider Relief Fund. Specifically, the CARES Act appropriated $100 billion, the Paycheck Protection Program and Health Care Enhancement Act appropriated $75 billion, and the Consolidated Appropriations Act, 2021, appropriated $3 billion for this purpose.[76] The Health Resources and Services Administration (HRSA), within HHS, administers payments from the Provider Relief Fund, including allocations to the COVID-19 Uninsured Program.
Accelerated and Advance Payments Program. HHS’s Centers for Medicare & Medicaid Services’ (CMS) Accelerated and Advance Payments Program provides loans to providers and suppliers when there is a disruption in claims submission or processing, including during a public health emergency or a presidentially declared disaster.[77] Section 3719 of the CARES Act authorized the expansion of this program due to the COVID-19 pandemic. Under the expanded program, active Medicare providers and suppliers could apply for loans of up to 100 percent or 125 percent of the Medicare payments they received for a prior 3-month or 6-month period, depending on the type of provider or supplier. On April 26, 2020, CMS announced that provider applications for the Advance Payments Program were discontinued in light of grant payments made available for similar purposes through the Provider Relief Fund. As of October 8, 2020, CMS stopped accepting applications for accelerated or advance payments as they relate to the COVID-19 Public Health Emergency, although CMS will continue to monitor the ongoing impacts of COVID-19 on the Medicare provider and supplier community.
Overview of Key Issues
Provider Relief Fund. As of March 1, 2021, HHS had allocated about $154 billion from the Provider Relief Fund, with about $24 billion not yet allocated.[78] Of the total $154 billion allocated, about $120 billion had been disbursed and about $34 billion was yet to be disbursed. According to HHS officials, the agency allocated about $77 billion for general relief for health care providers and about $57 billion for targeted areas. See table below for a summary of Provider Relief Fund allocations and disbursements.
Summary of the Provider Relief Fund ($178 billion) Allocations and Disbursements, as of March 1, 2021
Description
Allocation ($ billions)
Date of initial disbursement
Disbursement ($ billions)
General distributions
Phase I: Medicare
46.016
April 10, 2020
41.971
Phase II: Medicaid and Children’s Health
Insurance Program (CHIP) providers
4.067
July 3, 2020
3.143
Phase II: dental providers
1.290
July 28, 2020
0.978
Phase III: assisted living facilities
0.627
September 25, 2020
0.299
Phase III: general distribution
24.500
November 14, 2020
14.393
Subtotal of general distributions
76.500
60.784
Targeted distributions
Rural health care facilities
11.092
May 6, 2020
10.963
High-impact hospitals
20.750
May 7, 2020
20.668
Skilled nursing facilities
5.000
May 22, 2020
4.761
Indian health care providers
0.520
May 29, 2020
0.509
Safety net hospitals
13.074
June 12, 2020
12.907
Children’s hospitals
1.063
August 20, 2020
1.062
Nursing home infection control, quality, and performance
5.000
August 27, 2020
4.405
Subtotal of targeted distributions
56.499
55.275
Subtotal of general and targeted distributions
132.999
116.059
Other
Treatment and testing of the uninsured/vaccine administration
10.000
May 15, 2020
2.165
Vaccine and therapeutic development
and procurement activities
9.970
November 25, 2020
1.664
Administration
0.980
n/a
0.036
Unallocated fundsa
24.051
n/a
0.000
Total
178.000
119.924
Legend: n/a = not applicable
Source: Summary of Health and Human Services funding data. | GAO-21-387
aHealth Resources and Services Administration (HRSA) officials told us that the amount of unallocated funds/uninsured treatment/vaccine administration is available for treatment of the COVID-19 Uninsured Program and for other Provider Relief Fund allocations.
Summary of fund disbursements. As of March 1, 2021, about $120 billion of the approximately $154 billion allocated from the Provider Relief Fund had been disbursed. The amount disbursed was less than the amount allocated because some of the disbursements were in progress and some of the funds were returned. HRSA officials told us that the returned funds are reflected in the above table. According to our analysis of information provided by HRSA, as of March 1, 2021, HHS had disbursed about $61 billion from general distribution allocations and about $55 billion from the targeted allocations.
From April 10, 2020, the date of the initial disbursement, to May 31, 2020, about $65 billion was disbursed. Funds were disbursed at a slower pace in the subsequent nine months through March 1, 2021. An additional $9.5 billion was disbursed during those months at an average monthly disbursement of $4.8 billion. HRSA officials told us that this slowdown reflected in part the fact that funds allocated through the General Distribution during that time required providers to submit applications that HRSA reviewed.
Payments returned to Provider Relief Fund. According to HRSA, providers had declined about $8 billion from previous disbursements as of February 26, 2021. HRSA officials told us that those funds are available for subsequent allocations.[79] According to our analysis of information provided by HRSA, 74 percent of the returned funds were from general distributions and 26 percent are from targeted distributions. About $4.4 billion was returned to HRSA after being disbursed as part of the first general allocation, Phase 1–Medicare. This amount is approximately 73 percent of all returned funds. About $1.2 billion was returned after being disbursed as part of the targeted allocation for High-Impact Hospitals. This amount is approximately 19 percent of all returned funds. Some providers returned funds because they were not needed. For example, a large health system headquartered in California returned all but one small disbursement, including funds from the Medicare, High-Impact, Skilled Nursing, and Nursing Home Infection Control allocations totaling to about $771 million. The health system stated in a press release that it was able to return the majority of funds due to actions taken to manage expenses.
COVID-19 treatment of uninsured. The Provider Relief Fund includes an allocation for the COVID-19 Uninsured Program, although the total amount to be used for this program has not yet been determined by HHS officials.[80] As of March 1, 2021, approximately $2.2 billion from the Provider Relief Fund had been disbursed for COVID-19 treatment, testing, and vaccine administration of uninsured individuals. As of March 1, 2021, over 25 million claims have been paid. HRSA officials reported that future disbursements for this purpose will come out of the approximately $24 billion remaining in unallocated funds in the Provider Relief Fund.
Providers who choose to participate in this program must attest to its terms and conditions, which include that the individual treated, tested, or administered a vaccine is uninsured, the provider will accept reimbursement as payment in full, and the provider will not bill the individual for the balance of the bill. Reimbursement is generally available at Medicare rates for treating uninsured individuals with a COVID-19 diagnosis as well as the testing and administration of a licensed or authorized COVID-19 vaccine to uninsured individuals.
HRSA has not yet finalized and implemented a post-payment review process to validate COVID-19 Uninsured Program provider claims. HRSA’s risk assessment identified a risk that COVID-19 Uninsured Program providers may falsify patient rosters.[81] In response to this risk, HRSA stated that providers must attest services were rendered to an uninsured patient. Under the COVID-19 Uninsured Program terms and conditions, HRSA can recover overpayments made for instances of provider non-compliance. HRSA intends to perform post-payment reviews of claims to validate certain provider attestations, according to agency officials. However, HRSA did not have documentation describing how it plans to conduct these reviews, such as review plans, standard operating procedures, or staff manuals, and the factors and criteria to be used for selecting and assessing the validity of selected provider claims.
Agency officials stated that the agency has been focused on prepayment processes and launching the Provider Relief Fund reporting portal. According to HRSA officials, the agency is working with a contractor to develop and recommend a post-payment audit strategy with phased implementation to begin in late calendar year 2021. Although we acknowledge that in emergency situations, such as the COVID-19 pandemic, agencies must implement programs and disburse certain relief funds quickly, strong internal controls help ensure that relief funds are used for only authorized purposes. Additionally, it is important for agencies to recover overpayments as quickly as possible.
Federal internal control standards state that management should design control activities to achieve objectives and respond to risks and implement control activities through policies.[82] As part of these standards, management designs specific actions to respond to the analyzed program risks on a timely basis, including the potential for fraud, and clearly documents internal controls in a manner that allows the documentation to be readily available for examination.
Without documented post-payment review policies and procedures and timely implementation of related control activities, HRSA’s ability to consistently identify and recover improper payments, including those resulting from potential fraudulent activity, will be limited. As a result, for those payments identified as an overpayment, HRSA’s efforts to recover them will be delayed, if they are recovered at all.
Single Audit Requirements. The Single Audit Act establishes requirements for states, the District of Columbia, local governments, U.S. territories, tribal governments, and nonprofit organizations that receive federal awards to undergo single audits of those awards annually (unless a specific exception applies), when their expenditures of the award meet a certain dollar threshold.[83] In its single audit implementing regulations, HHS further requires commercial (for-profit) organizations that meet a certain dollar threshold to undergo: (1) an audit in conformance with single audit requirements or (2) a financial related audit of the applicable award(s) in accordance with Generally Accepted Government Auditing Standards.[84] These audits are critical to helping to identify deficiencies in the award recipient’s compliance with applicable provisions of laws, regulations, contracts, or grant agreements and in its financial management and internal control systems. Correcting such deficiencies can help ensure the appropriate use of federal funds and reduce the likelihood of federal improper payments.
Auditors who conduct single audits follow guidance in the Office of Management and Budget’s (OMB) Compliance Supplement and agency guidance (e.g., FAQs) specific to their programs. The Provider Relief Fund reimburses health care providers for health-care-related expenses or lost revenues attributable to COVID-19. An auditor’s review of such reported health care expenditures and lost revenues may be a critical component of a Provider Relief Fund recipient’s single audit.[85]
Per the December 2020 Compliance Supplement Addendum, Provider Relief Fund expenditures (including lost revenues) will first be reported in the Schedule of Expenditures of Federal Awards (SEFA) and audited under OMB’s single audit guidance in fiscal years ending on or after December 31, 2020. However, for those entities with fiscal years ending on or after June 30, 2021, SEFA reporting guidance will be in the 2021 Compliance Supplement. As we previously reported, delays in issuing guidance could adversely affect auditors and the results and timing of their work, and may lead to inconsistent reporting. (See Single Audit enclosure for recommendation to OMB.)
Accelerated and Advance Payments Program. Under the expanded Accelerated and Advance Payments Program, amended by the CARES Act, CMS made accelerated and advance payments totaling about $107.3 billion as of January 12, 2021. Initially, recoupment of the accelerated and advance payments, through the offsetting of new Medicare claims, was to begin not more than 120 days after the funds were disbursed. Thus, recoupment was scheduled to begin in late July 2020.
However, the Continuing Appropriations Act, 2021 included a provision that delayed repayment until 1 year after the accelerated or advance payment was made, with recoupment of Medicare payments owed to providers beginning at 25 percent for the first 11 months, and at 50 percent for the following 6 months.[86] Accordingly, the provision allows 29 months from the date of the first payment to a provider or a supplier before requiring that the outstanding balance be paid in full. As of January 12, 2021, providers had voluntarily repaid about $8.4 billion and the outstanding loan balance in the Accelerated and Advance Payments Program was about $98.9 billion.
Agency Comments
We provided HHS and OMB with the draft of this enclosure. HHS provided technical comments on this enclosure, which we incorporated as appropriate. HHS provided written comments, reproduced in Appendix VI and technical comments, which we incorporated as appropriate. OMB did not provide any comments on this enclosure.
HHS agreed with our recommendation to finalize and implement a post-payment review process. As part of implementing this process, HHS stated that it will, with contractor support, finalize the audit review, pilot and test the post-payment audit review process, and validate COVID-19 Uninsured Program claims to help ensure timely identification of improper payments and recovery of overpayments. We urge HHS to implement this post-payment review process as expeditiously as possible.
Methodology
To conduct our work, we examined publicly released HHS information, federal laws and regulations, OMB’s single audit guidance, and obtained information from CMS and HRSA in the form of written responses to questions, documents, and datasets. Our review of the data sources provides reasonable assurance of the data’s reliability. The Provider Relief Fund dataset came from HRSA, which is the only available source for the disbursement data. The allocation amounts and categories that were provided by HRSA match publicly available information.
Contact information: Carolyn L. Yocom, (202) 512-7114, yocomc@gao.gov
After peaking in December 2020, rates of new COVID-19 cases and deaths in nursing homes have declined; however, additional data related to COVID-19 vaccinations in nursing homes is needed. Staffing in nursing homes also continues to be a concern.
Entities involved: Centers for Disease Control and Prevention and Centers for Medicare & Medicaid Services, both within the Department of Health and Human Services.
Recommendations for Executive Action
The Secretary of Health and Human Services should ensure that the Director of the Centers for Disease Control and Prevention collects data specific to the COVID-19 vaccination rates in nursing homes and makes these data publicly available to better ensure transparency and that the necessary information is available to improve ongoing and future vaccination efforts for nursing home residents and staff. HHS neither agreed nor disagreed with this recommendation.
The Secretary of Health and Human Services should ensure that the Administrator of the Centers for Medicare & Medicaid Services, in consultation with the Centers for Disease Control and Prevention, requires nursing homes to offer COVID-19 vaccinations to residents and staff and design and implement associated quality measures. HHS neither agreed nor disagreed with this recommendation.
Key Considerations and Future GAO Work
We have previously made two recommendations related to COVID-19 outbreaks in nursing homes:
In September 2020, we recommended that the Secretary of Health and Human Services, in consultation with the Centers for Medicare & Medicaid Services (CMS) and the Centers for Disease Control and Prevention (CDC), develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively back to January 1, 2020, and clarify the extent to which nursing homes had reported data before May 8, 2020.
Although the Department of Health and Human Services (HHS) partially agreed with this recommendation, as of February 2021, this recommendation had not been implemented.
In November 2020, we recommended that the Administrator of CMS quickly develop a plan that further detailed how the agency intended to respond to and implement, as appropriate, the 27 recommendations in the final report of the Coronavirus Commission on Safety and Quality in Nursing Homes, which CMS released on September 16, 2020.[87]
HHS neither agreed nor disagreed with our recommendation; instead, it highlighted actions that CMS has taken related to Commission recommendations and indicated that it would refer to and act upon the Commission’s recommendations as appropriate. As of February 2021, CMS had no additional updates.
We maintain the importance of our recommendations. Specifically, we maintain that collecting data on COVID-19 cases and deaths from nursing homes retroactively would better inform the government’s continued response and recovery, and we maintain that HHS could ease the burden by incorporating data previously reported to CDC or to state or local public health offices. Additionally, we maintain that developing a plan for whether and how CMS will proceed with the Commission’s recommendations would improve the agency’s ability to systematically consider the Commission’s recommendations going forward.
In this enclosure, we note additional concerns particularly around the availability of nursing home vaccination data. Further, we have ongoing work on the oversight of infection prevention and control and emergency preparedness in nursing homes.
Background
The health and safety of the 1.4 million elderly or disabled residents in the nation’s more than 15,000 Medicare- and Medicaid-certified nursing homes—who are often in frail health and living in close proximity to one another—has been a particular concern during the COVID-19 pandemic.[88] CMS, an agency within HHS, is responsible for ensuring that nursing homes meet federal quality standards to participate in the Medicare and Medicaid programs. To monitor compliance with these standards, CMS enters into agreements with state survey agencies within each state to conduct inspections, including recurring comprehensive standard surveys and as-needed investigations.
The CARES Act appropriated $100 million for this oversight, and it directed CMS to prioritize the use of funds for nursing home facilities in localities with community transmission of COVID-19.[89] According to CMS, of this amount, the agency plans to provide state survey agencies approximately $81 million through September 30, 2023, to be used to ensure that all nursing homes receive targeted infection control surveys, among other things.[90] CMS has set aside the remaining $19 million to enhance survey system technology, to fund PPE for federal surveyors, and to implement improvements recommended by the Nursing Home Commission, according to the agency.[91]
In addition, HHS announced in May 2020 that it would contribute $4.9 billion from the Provider Relief Fund, established with funds provided under COVID-19 relief laws to reimburse eligible providers for health care-related expenses or lost revenues attributable to COVID-19, as direct payments to assist nursing homes with responding to COVID-19.[92] In July, HHS announced that it would provide an additional $5 billion from the fund. HHS later announced that $2.25 billion from the fund would be dedicated to establishing an incentive-based program—the Quality Incentive Payment Program—to reward nursing homes that create and maintain safe environments for their residents. Payments would be made to nursing homes for their efforts to reduce COVID-19 infection and mortality rates among residents, based on CDC data. According to HHS, as of March 1, 2021, it awarded approximately $1.9 billion in four rounds.
In response to the pandemic, HHS, primarily through CMS and CDC, has taken a range of actions to address infection prevention and control in nursing homes, which we reported on in our previous reports from June, September, and November 2020 and January 2021. One recent action in October 2020 was to establish the Pharmacy Partnership for Long-Term Care Program, an agreement with pharmacy partners to conduct COVID-19 vaccination clinics for residents and staff of long-term care facilities, including nursing homes, to minimize the burden on facilities and jurisdictional health departments.[93]
Overview of Key Issues
COVID-19 cases and deaths in nursing homes. According to CDC case-reporting data, as of February 7, 2021, more than 99 percent of Medicare- and Medicaid-certified U.S. nursing homes had reported at least one confirmed resident or staff case, and more than 80 percent had reported at least one resident or staff COVID-19 death.[94] New weekly confirmed cases of COVID-19 in nursing homes fluctuated but generally remained under 12,000 new cases until late 2020 when weekly cases increased considerably reaching over 25,000. (See figure.) Specifically, new weekly resident cases peaked the week ending December 20, 2020, at more than 33,600 resident cases—178 percent higher than the previous peak for the week ending July 26, 2020. New weekly staff cases peaked one week prior with over 28,600 staff cases for the week ending December 13, 2020—141 percent higher than the week ending July 26, 2020. Since then cases have again been declining.[95]
New weekly resident deaths also saw an increase in late November, eventually reaching a new peak of 6,019 for the week ending December 20, 2020—about 72 percent higher than the previous peak the week ending May 31, 2020. Combined nursing home resident and staff deaths from COVID-19, as a percentage of total COVID-19 deaths in the U.S., remained largely unchanged throughout this time period (consistently making up about 30 percent of all COVID-19 deaths in the U.S.). The changing weekly COVID-19 death counts in nursing homes generally paralleled changes in the country as a whole.
New Weekly Confirmed COVID-19 Cases and Deaths among U.S. Nursing Home Residents and Staff, as Reported by Medicare- and Medicaid-Certified Nursing Homes, Weeks Ending May 31, 2020, through February 7, 2021
Notes: Dates refer to the end of a week (e.g., May 31 refers to the entire week from May 25 through May 31). According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time. Data presented in this enclosure reflect the data downloaded as of February 18, 2021, which includes data through the week ending February 7, 2021. We excluded data for the week ending May 24, 2020, because it is the first week for which data are available from the Centers for Disease Control and Prevention (CDC) and could include cases and deaths from multiple weeks dating back to January 1, 2020. Weekly and cumulative case and death counts are likely underreported because they do not include data for the nursing homes that did not report COVID-19 data to CDC for that week or from nursing homes that submitted data that failed data quality assurance checks. Additionally, as we previously reported, the Centers for Medicare & Medicaid Services (CMS) does not require nursing homes to report data prior to May 2020, although nursing homes may do so voluntarily. We recommended that the Secretary of Health and Human Services—in consultation with CMS and CDC—develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively to January 1, 2020.Weekly staff deaths reported for the weeks ending May 31, 2020, through February 7, 2021, ranged from 13 (week ending September 20) to 61 (week ending May 31).
Vaccination clinics for nursing home residents and staff offered through the pharmacy partnership near completion. The first vaccinations were administered to nursing home residents beginning in mid-December 2020, and CDC announced that the first round of on-site vaccine clinics, conducted through the Pharmacy Partnership for Long-Term Care Program, were completed in 99 percent of nursing homes by late January. The pharmacy partnership program, announced in October 2020, was responsible for much of the administration of vaccinations in nursing homes, as well as in other long-term care facilities. (See table below for a timeline of key dates.)
Key Dates in Roll Out of Vaccinations for Nursing Homes
Date
Milestone
October 2020
October 16: Pharmacy Partnership for Long-Term Care Program announced by HHS
Agreement with CVS, Walgreens, and Managed Health Care Associates to provide and administer COVID-19 vaccines to residents of long-term care facilities, including nursing homes
Manages the COVID-19 vaccination process, including storage, administration, and reporting, to minimize the burden on facilities and jurisdictional health departmentsa
December 2020
December 1: CDC’s Advisory Committee on Immunization Practices recommended prioritizing nursing home residents for vaccinations, in addition to health care personnel and other residents of long-term care facilities
December 3: CDC Director accepted the advisory committee’s recommendation for priority groups for the initial phase of the COVID-19 vaccination program
December 11: Food and Drug Administration authorized the emergency use of the Pfizer-BioNTech vaccine
December 18: Food and Drug Administration authorized the emergency use of the Moderna vaccine
December 18: First vaccine doses were administered to nursing home residents and staff members in two trial states—Connecticut and Ohio
December 21: Vaccinations through the Pharmacy Partnership for Long-Term Care Program begin
January 2021
January 4: All 54 jurisdictions that elected to participate in the Pharmacy Partnership for Long-Term Care Program had started the vaccination process
January 25: 99 percent of nursing homes participating in the Pharmacy Partnership for Long-Term Care Program completed their first clinics by the end of the week
February 2021
Early February: Continued third, and final, on-site vaccination clinics at nursing homes participating in the Pharmacy Partnership for Long-Term Care Program
Source: GAO analysis of information from the Department of Health and Human Services. | GAO-21-387
aThere are 64 jurisdictions which include all U.S. states and territories and some local health programs.
According to CDC and nursing home association officials, the Pharmacy Partnership for Long-Term Care Program is making progress towards its intended goals, specifically its goal to vaccinate the long-term care populations, including nursing home residents. According to CDC, the pharmacy partnership aimed to complete first vaccination clinics within 4 weeks of starting clinics in a jurisdiction.[96] Vaccination clinics began the week of December 21, 2020, and CDC reports that, as of January 25, 2021, first vaccination clinics were completed in 99 percent of nursing homes. Additionally, the nursing home associations we interviewed were pleased that nursing homes were prioritized and acknowledged that vaccinating the entire nursing home population was a massive undertaking that was generally successful.
Another goal of the partnership was to reduce the burden on facility staff. The two nursing home associations we interviewed indicated satisfaction with the pharmacy partnership on this goal as well. Officials from one of the associations noted that the burden on their member facilities was lessened by having the pharmacy partnership responsible for some of the administrative tasks associated with administering the vaccines.
According to nursing home association and state and local health department officials, the Pharmacy Partnership for Long-Term Care Program faced some challenges during the initial launch of the program. Key challenges have included a shift from federal to state control of the program, resident vaccination consent issues, and staff members’ reluctance to be vaccinated, among others.[97]
Decentralization of the Pharmacy Partnership for Long-Term Care. The two nursing home associations we interviewed said that some of the difficulties implementing the partnership program stemmed from the fact that the program is a state-controlled program, though it was originally designed to be a federal program. The federal government entered into agreements with the pharmacy partners and required facilities to sign up to participate in the partnership. However, each state is responsible for activating the partnership and allocating doses from the state’s overall allocation from the federal government.[98] Thus, vaccinations by the pharmacy partners cannot begin until the state activates the agreement and allocates doses to the pharmacy partners. According to state and nursing home association officials, this resulted in more than 50 different plans for implementation, which caused confusion among jurisdictions’ health departments, nursing homes, and pharmacy partners and hampered communication and vaccine education efforts. The officials said a more centralized distribution model may have created a more efficient approach to vaccinating the nursing home population.
Obtaining resident consent. The state and nursing home association officials noted confusion and difficulties obtaining consent from nursing home residents and their families to administer the vaccine, indicating that pharmacy partners in some cases wanted to gather written consent from residents before administering the vaccines. According to the CDC, written consent is not required by federal law for COVID-19 vaccination, but pharmacy partners that are administering the vaccine in long-term care facilities have the discretion to require verbal, email, or written consent from recipients.[99] Initial attempts to gather written consent may have delayed the start of vaccination clinics at some locations, though association officials said that once the pharmacies accepted informed consent, this was no longer an issue.
Staff reluctance to be vaccinated. The state and nursing home association officials indicated that, while vaccine take-up rates among residents were high, take-up rates for staff vaccinations were much lower, making it difficult for facilities to predict how many vaccine doses were needed.[100] The officials attributed staff reluctance to be vaccinated to several factors, including the challenge of convincing people to be the first to take a quickly developed vaccine, underlying issues of government mistrust, myths spread on social media, and the initial lack of information resources on vaccine safety. CDC responded to concerns about vaccination hesitancy by increasing the availability of materials to better inform and empower health care providers, including a communications toolkit with messages and strategies to combat hesitancy.
Detailed data for nursing home resident and staff vaccinations is not publicly reported, making it difficult to monitor ongoing vaccination efforts and nursing home quality. According to CDC, approximately 4.25 million vaccine doses were administered to residents and staff in nursing homes through the Pharmacy Partnership for Long-Term Care Program, as of February 11, 2021—79 percent of all doses administered through the partnership.[101] See table below. According to detailed data that we obtained from CDC, as of February 11, 2021, the program has completed 13,433 first vaccination clinics, 11,975 second vaccination clinics, and 2,340 third vaccination clinics in nursing homes.[102]
COVID-19 Vaccinations Conducted in Nursing Homes through the Pharmacy Partnership for Long-Term Care Program by Recipient Type, as of February 11, 2021
Recipient
Number receiving a first dose
Number receiving a second dose
Residents
1,788,470
712,646
Staff members
1,251,087
497,276
Total
3,039,557
1,209,922
Source: GAO analysis of information from the Centers for Disease Control and Prevention. | GAO-21-387
CDC does not have complete data on vaccines administered to residents and staff members of nursing homes outside of the Pharmacy Partnership for Long-Term Care Program, so it does not have insight into vaccination rates for individual nursing homes that chose not to participate in the program or for states that opted out of the program.[103] For example, while West Virginia—the only state that opted not to participate in the program—completed its first round of nursing home vaccination clinics before the end of December 2020, administration information for long-term care facilities was not reported to CDC.[104] As a result, these data are not included in CDC tracking data on nursing home vaccinations.[105] According to CDC officials, data on vaccines administered to residents and staff members of nursing homes that did not enroll in the federal program can be voluntarily reported by the facilities through the National Healthcare Safety Network, but it is unclear how many of those that are reporting are receiving vaccinations outside of the pharmacy partnership.[106]
Further, while CDC collects data on the number of vaccinations administered to nursing home residents and staff through the Pharmacy Partnership for Long-Term Care Program, it does not publicly report this information for nursing homes specifically. Instead, CDC reports the number of vaccination doses, by state, provided to residents and staff of all long-term care facilities vaccinated through the pharmacy partnership, which includes other types of long-term care providers.[107] According to CDC, it is not reporting nursing home specific data because of concerns it would not accurately reflect the vaccination rates in nursing homes due to turnover within facilities. For example, some residents may have received only a second dose through the pharmacy partnership, as they may have received the first dose prior to being admitted into the nursing home. However, any considerations for interpreting the data could be noted when presenting the data publicly and does not negate the value of reporting information on the number of first and second doses administered to both staff and residents at the state level for nursing homes for tracking purposes.
With nursing homes having long been an epicenter of the COVID-19 pandemic, and with CDC’s Advisory Committee on Immunization Practices recommending that residents be among the first to be vaccinated, detailed information on vaccinations for this population—similar to what is provided for long term-care facilities overall—is important for tracking and transparency. The National Strategy for the COVID-19 Response and Pandemic Preparedness notes that agencies should be sharing data on COVID-19 response and recovery efforts and that these data should be publicly available to support performance tracking and ensure transparency. Without publicly providing detailed vaccination data that shows vaccination rates for the different long-term care facilities, including nursing homes, it is unclear how successful efforts have been to vaccinate nursing home residents and may make it difficult to use these data to improve ongoing and future vaccination efforts for the nursing home population.
Further, data on COVID-19 vaccinations in nursing homes will also be important for CMS’s ongoing efforts to monitor nursing home quality. In January 2021, CMS had not specified whether nursing homes would be required to offer COVID-19 vaccinations or how these vaccinations would be incorporated into its requirements or quality measures for nursing homes. CMS also had not provided a time frame for making these decisions. The agency said that it continues to evaluate when and whether changes regarding the COVID-19 vaccine need to be incorporated into its infection control requirements for nursing homes. It also noted that it is collaborating with CDC to develop quality measures for COVID-19 vaccinations for appropriate staff and patients.
Vaccination data are a key part of CMS’s oversight of nursing home infection prevention and control practices—practices critical for managing outbreaks such as COVID-19. Since 2005, CMS has required nursing homes to offer influenza and pneumococcal vaccinations to nursing home residents, given the risk of complications, hospitalizations, and death caused by influenza and pneumococcal disease, particularly among the elderly.[108] These vaccination rates are publicly reported as part of CMS’s Nursing Home Quality Initiative and provide information on the potential risk of influenza and pneumococcal outbreaks in facilities. Furthermore, making this data transparent through public reporting provides consumers with insight into how well nursing homes are caring for their residents' physical and clinical needs, and we have previously reported (October 2014) that timely information on provider quality are characteristics of effective transparency tools.
COVID-19 has a mortality rate far exceeding that of influenza and, according to CDC, spreads more easily than influenza, making it a significant threat to nursing home residents. Like data on influenza and pneumococcal vaccination rates, data on COVID-19 vaccination rates could help manage the risk of COVID-19 outbreaks in nursing homes and serve as an important source of information for consumers about quality of care, making the collection of complete vaccination rate data critical for any quality measures developed.
Staffing challenges continue. The percentage of nursing homes experiencing staffing shortages improved slightly from when we reported in January.[109] According to data nursing homes self-reported to CDC, as of February 7, 2021, approximately
17 percent of nursing homes had a shortage of aides (a decrease of about 3 percentage points),
16 percent had a shortage of nursing staff (a decrease of about 2 percentage points),
9 percent had a shortage of other staff (a decrease of about 2 percentage points), and
2 percent had a shortage of clinical staff (a decrease of less than 1 percentage point).[110]
Nursing home association officials we interviewed noted that the workforce situation has not improved since we reported in January. These association officials said that staff in nursing homes are exhausted, face burn out from emotional trauma, may be required to quarantine due to exposure to the virus, or must stay home to take care of family members who become sick, all of which may further strain resources.[111] According to one nursing home association we interviewed, the employment of temporary nurse aides has been an important tool to avoid larger staffing shortages, reinforcing information we heard and reported on earlier in the pandemic. During the public health emergency, nursing homes have relied on nurse aides hired or retained under a CMS flexibility that waived or reduced certain training and certification requirements for nurse aides to allow nursing homes greater flexibility to address staffing shortages during the pandemic.[112]
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided general comments, which are reproduced in Appendix VI. In its comments, HHS neither agreed nor disagreed with our recommendations.
In response to our recommendation to collect and publicly report COVID-19 vaccination data for nursing homes, HHS said it is working towards better data transparency and noted that nursing homes have an opportunity to voluntarily report data through the National Healthcare Safety Network tracking system. However, our focus was on reporting data that is already collected through the Pharmacy Partnership for Long-Term Care and was provided to us for this report. Specifically, HHS should publicly report the first and second dose data for residents and staff of nursing homes—as it does for long-term care facilities on the whole—when the pharmacy partnership ends in order to provide insight into how successful the pharmacy partnership was in vaccinating nursing home residents and staff.
In response to our recommendation to require nursing homes to offer COVID-19 vaccinations to residents and staff and to design and implement associated quality measures, HHS said it agrees that access to vaccines is essential for nursing home residents. The department indicated that CMS is “actively evaluating” whether changes need to be made to its infection control requirements regarding the COVID-19 vaccine and that CMS and CDC “have made progress in developing quality measures related to COVID-19 vaccination.” We maintain the importance of these recommendations for providing insight into nursing home quality of care and protecting the vulnerable nursing home population.
HHS also provided technical comments, which we incorporated as appropriate. OMB did not have comments on this enclosure.
Methodology
To conduct this work, we reviewed CMS and CDC data, agency guidance, and other relevant information on HHS’s response to the COVID-19 pandemic. We also reviewed written responses from CMS and CDC and spoke to CMS and CDC officials. In addition, we interviewed representatives from two national nursing home associations and officials from associations representing various state and local officials.
In addition, we analyzed CDC data on COVID-19 reported by nursing homes for the week ending February 7, 2021.[113] We analyzed the CDC data as they were reported by nursing homes to CDC and publicly posted by CMS.
We did not otherwise independently verify the accuracy of the information with these nursing homes. We assessed the reliability of the data sets used in our analyses by checking for missing values and obvious errors and reviewing relevant CMS and CDC documents. We determined the data were sufficiently reliable for the purposes of our reporting objective.
Contact information: John E. Dicken, (202) 512-7114, dickenj@gao.gov
Related GAO Products
Infection Control Deficiencies Were Widespread and Persistent in Nursing Homes Prior to COVID-19 Pandemic. GAO-20-576R. Washington, D.C.: May 20, 2020.
While the Office of Assistant Secretary for Preparedness and Response has taken some steps to address immediate supply needs, the COVID-19 pandemic has highlighted long-standing challenges related to the Strategic National Stockpile’s role and capabilities; these will take time to address.
Entities involved: The Office of the Assistant Secretary for Preparedness and Response, within the Department of Health and Human Services.
Key Considerations and Future GAO Work
Over the course of our CARES Act work, we have reported on efforts to modernize and restructure the Strategic National Stockpile (SNS) including progress towards building a 90-day supply of certain key items to respond to future surges in COVID-19 cases, as well as federal and state efforts to address medical supply gaps. We made recommendations in our September and January reports.
In September 2020, we recommended that the Department of Health and Human Services (HHS), in coordination with the Federal Emergency Management Agency (FEMA) within the Department of Homeland Security, develop and communicate to stakeholders plans outlining specific federal government actions that will be taken to help mitigate supply gaps for the remainder of the COVID-19 pandemic, which could contribute to ensuring a more effective response.[114] HHS and the Department of Homeland Security disagreed with this recommendation.
In January 2021, we reported on HHS’s draft strategy to improve the medical supply chain to enhance pandemic preparedness by monitoring supply information, increasing domestic production, and re-thinking supply management.[115] We recommended that HHS develop a process for regularly engaging with Congress and nonfederal stakeholders as the agency refines and implements its supply chain strategy, to include the role of the SNS. HHS generally agreed with this recommendation.
We will continue to monitor federal actions to mitigate supply gaps through federal planning and SNS modernization efforts, as well as progress toward SNS 90-day inventory goals, in response to provisions in the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 and the CARES Act.[116]
Background
The SNS, overseen by HHS’s Office of the Assistant Secretary for Preparedness and Response (ASPR), is a federal stockpile of vaccines, pharmaceuticals, and medical supplies and devices designed to be deployed to support the response to a public health emergency.[117] At the outset of the COVID-19 pandemic, the SNS was a critical resource to states for needed and scarce medical supplies. However, the nationwide need for personal protective equipment (PPE) to protect responders and to treat Americans sickened with COVID-19 quickly exceeded quantities contained in the SNS.
On January 31, 2020 the Secretary of Health and Human Services declared a public health emergency and began to take actions to respond to the pandemic including distributing medical supplies through the SNS to states, localities, territories, and tribes beginning in March 2020. The U.S. Government COVID-19 Response Plan (PanCAP Adapted) identifies HHS as the lead federal agency for the COVID-19 response, with support from FEMA for coordination.[118] However, in March 2020, leadership for the overall response shifted to FEMA, including responsibility for the acquisition and distribution of supplies in conjunction with HHS.[119]
As of March 11, 2021, six relief laws had been enacted to assist the COVID-19 response.[120] These laws appropriated funding for HHS activities, and, in some cases, specifically authorized their use for the SNS. As of February 28, 2021, HHS reported it obligated about $8.9 billion of the $13.9 billion it planned to use for the SNS to purchase PPE and ventilators for immediate use as well as to replenish SNS inventory, among other purposes, and had expended about $5.2 billion.
Overview of Key Issues
Pandemic highlighted long-standing challenges related to SNS role and capabilities. The COVID-19 pandemic has been unprecedented in scale and has stressed the resources and capabilities of federal, state, and local governments, as well as the private and non-profit sectors. Over the course of the past year, as part of our CARES Act reports, we have discussed the SNS and its role in the pandemic response with officials from federal and state governments, public health associations, and experts on public health preparedness. From these interviews, a consistent set of long standing challenges emerged regarding the role, funding, and supply allocation of the SNS as well as challenges related to federal response coordination.
Determining the appropriate role of the SNS in a pandemic. The near depletion of the SNS early in the pandemic response raised questions among the state officials and experts we interviewed about the role, expectations and transparency of the SNS during a nationwide pandemic. For example, all eight states we interviewed in July and August 2020 reported that certain supplies they received from the SNS were not sufficient to meet their needs and most added that the SNS should be more transparent in the future about its contents to set realistic expectations about the availability of supplies.
ASPR officials, however, told us that the SNS was not designed to provide states with supplies for a prolonged nationwide event such as the COVID-19 pandemic; it is primarily designed to respond to discrete and localized events. The SNS was originally created to provide for the emergency health security of the United States in the event of a bioterrorist attack or other public health emergency.[121] Over time the SNS has been used to respond to a growing variety of threats including radiological and nuclear, influenza and other emerging infectious diseases, and natural disasters. In its fiscal year 2018-2022 budget plan for medical countermeasure development, HHS noted that building an inventory of supplies to address all types of threats has been a challenge.
Additionally, several of the experts we interviewed noted that a re-examination of the role of the SNS during a pandemic is needed so that there is clarity about what resources and capabilities would be made available to state, local, tribal, and territorial governments from the stockpile.
HHS has been discussing the proper role of the SNS for many years. For example, in 2016, HHS convened a National Academy of Sciences workshop to, among other things, reevaluate the SNS’s emphasis on potential chemical, biological, radiological, and nuclear attacks on the United States.[122] Participants noted that the role of the SNS was already broad and intended to support all types of hazardous events. As one participant noted, without better focus the SNS would not be able to fulfill the greatest amount of life saving potential.
Aligning SNS role and funding. Several of the experts we interviewed mentioned that it is important to ensure that SNS funding is adequate and flexible enough to match its role. The issue of aligning the SNS’s role with its funding was highlighted during the COVID-19 response as officials from all states and most public health associations we interviewed noted that certain types of PPE from the SNS were not sufficient in terms of quantity, and in some cases, quality. For example, one state and most public health associations reported that some supplies, such as masks, distributed by the SNS were past their expiration dates and could not be used.
ASPR officials told us that HHS did not replenish PPE to previous levels following the H1N1 influenza pandemic of 2009. According to an HHS budget document, in April 2009, at the start of the H1N1 pandemic, the SNS contained approximately 106 million N95 respirators. In December 2019, prior to the start of the COVID-19 pandemic, the SNS contained 12.6 million N95 respirators, which were remaining from the H1N1 pandemic. As of January 27, 2021, the federal response has supplied about 100 million N95 respirators to state, tribal, and territorial governments in response to COVID-19, according to federal data provided in a senior leadership brief.
ASPR officials told us that HHS did not replenish PPE to previous levels following the H1N1 influenza pandemic of 2009 because of a lack of funding. ASPR officials noted that requested funding has not always fully reflected SNS funding needs. They explained that this is because there are competing priorities and tradeoffs and the budget process involves aligning SNS budgetary needs with broader HHS needs and the President’s budget priorities.
Funding concerns were also identified in a 2013 working group report compiled by two HHS advisory bodies.[123] The working group concluded that the SNS was increasingly confronted with unfunded requirements as its responsibilities expanded and, without action, anticipated a widening gap between the responsibilities of the SNS and the resources available to fulfill them.
Allocating scarce SNS supplies. Some experts and all public health association officials told us that it was challenging to understand how the SNS allocated scarce medical supplies. For example, one expert—a state public health official—noted that it was difficult to understand what supplies were being sent out of the SNS and how they were being allocated, and all states noted that they did not receive the quantity of supplies requested.
As we reported in our June 2020 CARES Act report, ASPR officials told us they distributed SNS supplies to states in March and April 2020 primarily using a pro-rata allocation strategy, which provided supplies to every state based on population.[124] ASPR officials noted that this approach was used to distribute materials to states in previous public health emergencies, including the H1N1 influenza pandemic of 2009 when the SNS distributed 85 million N95 respirators, among other supplies. Given the finite amount of supplies contained in the SNS and the widespread demand, ASPR officials told us that this allocation strategy was the most equitable approach.
We also reported that HHS and FEMA officials believed that states may have requested more supplies than they needed. ASPR officials added that many of the processes the SNS and the states had put into place for supply request and distribution were not applicable to a nationwide response where the volume of supplies was not adequate. ASPR officials told us that another allocation approach—directing supplies to the areas of greatest need—was simply not an option at the beginning of the COVID-19 response due to the lack of reliable data and modeling uncertainty needed to target supplies. As such, they determined that pro-rata allocation was a reasonable approach for distributing the finite amount of supplies contained in the SNS at the start of the pandemic.
While the SNS had never faced a response of this scale or duration prior to the COVID-19 pandemic, ASPR has attempted to understand what supply allocation models might be appropriate in a large scale event. For example, the 2016 Public Health Emergency Medical Countermeasure Enterprise (PHEMCE) Strategy and Implementation Plan noted that PHEMCE was working to identify approaches to address medical countermeasure resource allocation when stockpile inventory was inadequate to meet the needs of a large-scale public health emergency.[125] ASPR officials were unable to recall or provide further information specific to this effort, but noted certain actions taken around determining the allocation of medical countermeasures and vaccines for an anthrax event. ASPR officials added that resource allocation approaches have been part of the planning discussions for influenza or other emerging infectious diseases for many years.
Clarifying roles and responsibilities among response partners. States, experts, and public health association officials noted challenges with requesting supplies when the responsibility shifted from HHS to FEMA in March 2020. For example, one expert noted that supply request confusion was compounded by the fact that states had processes to request and receive supplies from the SNS, but during the response there were additional agencies involved in the process. We identified similar issues in our September 2020 CARES Act report and made recommendations about the need to document roles and responsibilities for supply management functions transitioning to HHS from other federal partners, such as the Department of Defense, and devising interim solutions to help states track supply requests and plan for supply needs.
HHS officials told us that they have had extensive coordination and communication with states during the response, including holding calls with state governors, delivering trainings, providing briefings, and disseminating guidance. HHS officials noted that improving the pandemic response capabilities, practices, processes, and capacity of state, local, tribal, and territorial governments is a priority. ASPR officials added that there is always some confusion and lack of clarity related to supplies during an emergency and they are always looking for ways to improve and refine.
After-action reports of actual events and pandemic exercises have also identified issues with federal coordination. For example:
FEMA’s initial assessment report of its COVID-19 response issued in January 2021 noted that not all response members understood who led the resource allocation mission and how it fit into the overall response.[126] The report noted that differences between FEMA and HHS component agencies, including ASPR, created significant issues with coordination and service delivery to state, local, tribal, and territorial partners.
The after-action report of a large-scale avian influenza pandemic exercise conducted in August 2019 (“Crimson Contagion”) noted confusion among exercise participants around the process for requesting supplies from multiple federal entities.[127] For example, the after-action report noted that the resource request process was not transparent to the range of state, local, tribal, territorial, and federal response partners.
Finally, coordination issues among multiple federal response partners were also noted in the Centers for Disease Control and Prevention’s after-action report for the 2014 Ebola response. That report noted that agencies and organizations were often unaware of the mission and responsibilities of other response partners and a deeper understanding of capabilities, roles, and responsibilities will likely be needed in the future.
Both the FEMA COVID-19 assessment and Crimson Contagion after-action report made recommendations about conducting training and exercises focused on how federal agencies coordinate and communicate with state, local, tribal and territorial partners. ASPR officials noted in February 2021 that they have not yet had a chance to address the recommendations in the Crimson Contagion after action report due to the pandemic response. ASPR officials told us that they are collecting data to inform their COVID-19 after-action report as the response is ongoing and will analyze the data and prepare the report after the response has ended.
ASPR has taken steps to help address immediate COVID-19 supply needs. In the short term, ASPR, in conjunction with its federal partners, determined a key action would be to stockpile a 90-day supply of certain PPE, which could help address the scarcity of these supplies for the immediate pandemic and could help address allocation issues by having adequate supply. According to HHS officials, this effort was funded with COVID-19 relief funds, such as those made available through the CARES Act.
According to ASPR officials they were aiming to meet their 90-day targets of PPE by the end of 2020; however, as we previously reported, ASPR has to balance replenishing the stockpile with ensuring adequate commercial availability. As such, ASPR officials reported that they have delayed delivery of some contracted items to the SNS to enable manufacturers to make them available in the commercial market to alleviate supply constraints. For example, ASPR contract information shows that the SNS deferred delivery of 10.1 million N95 respirators from October 2020 to April 2022. Additionally, HHS also reported distributing supplies from the stockpile to address immediate supply needs. Both of these activities may continue to affect progress towards 90-day targets; although ASPR officials noted in February 2021 that they were not planning any additional deferrals.
According to ASPR data, as of February 2021, the SNS has reached, or almost reached, its 90-day targets for N95 respirators, surgical or procedural masks, and eye protection or face shields. However, supplies of gloves and gowns or coveralls remain far from their 90-day targets. According to ASPR officials, ensuring adequate supplies of nitrile gloves continues to be a problem due to the issues with the global supply chain. See table below for more on the SNS inventory of PPE. (For more information on medical supply availability and efforts to expand domestic medical product manufacturing, please see our enclosures on Hospital and Pharmacy Perspectives on COVID-19 Vaccine Administration and Medical Supply Availability and Domestic Medical Product Manufacturing.
Strategic National Stockpile Personal Protective Equipment Inventory
Personal protective equipment
Feb. 26, 2021 inventory on hand
Planned 90-day Inventory
Gloves – surgical/exam
227 milliona
4.5 billion
N95 respirators
307 million
300 million
Surgical or procedural Masks
411 million
400 million
Gowns or coveralls
65.8 million
265 million
Eye protection or face shields
17.6 million
18 million
Source: Data from the Office of the Assistant Secretary for Preparedness and Response (ASPR) within the Department of Health and Human Services. | GAO-21-387
Note: The SNS continues to deploy supplies in response to requests and these deployments may affect the ability to reach the SNS inventory targets and could also result in some fluctuation in inventory quantities over time, according to ASPR officials. aAccording to ASPR officials, the SNS contains a mix of glove types in its inventory including latex, vinyl, nitrile, and a blend of vinyl and nitrile. Of these types, the vinyl-nitrile blend makes up most of the glove inventory.
Stockpiling for the near term could help address challenges the SNS had with the quality and quantity of supplies they were able to provide at the beginning of the COVID-19 response and allow for more targeted allocation strategies. However, ASPR officials were uncertain whether they would maintain these target supply levels beyond the COVID-19 response. Additionally, ASPR officials noted that they have limited ability to rotate expiring PPE stock but have requested the use of COVID-19 relief funds to replace depleted or expiring PPE.
ASPR has also taken steps to improve efficiency in the distribution of certain pandemic supplies through a vendor managed inventory approach. Under this approach, ASPR has contracted with vendors to hold and distribute products that the SNS has purchased in response to the COVID-19 pandemic. ASPR officials told us that this model has advantages in a pandemic since it utilizes multiple distribution centers that are geographically diverse and can deliver directly to points of care.
Plans to address longer-term challenges facing SNS will take time to address. Efforts to address longer-term challenges that we and others have identified—such as the role of the SNS in future pandemics, budget planning for that role, and sustainment of current PPE inventory—will take longer to address. ASPR officials told us these issues are tied to developing a broader supply chain capability that includes the ability to monitor the commercial supply chain for disruptions to it and supporting domestic manufacturing capabilities for PPE and other medical countermeasures. To that end, HHS developed a national supply chain strategy that outlines the capabilities that they must acquire—including, but not limited to, the SNS—to address the challenges identified by the pandemic.[128] The draft strategy discusses many of the longer-term challenges we raise above.
However, the federal government is in a period of transition when it comes to developing and implementing a longer-term supply chain strategy to address both the specific SNS challenges we and others identified and broader supply chain issues. ASPR officials told us in late January 2021 that their draft supply chain strategy was on hold as the agency examines how it aligns with the new administration’s priorities.
As we reported in January 2021, reexamining the role of the SNS in the U.S. response to pandemics will require difficult policy decisions and tradeoffs about systems, budgets, and authorities. Further, the COVID-19 pandemic has shown how complex and difficult a coordinated response across numerous federal and state, local, tribal, and territorial entities can be. Our prior work (see Related Product section for our 2004 work on national strategies, for example) and that of others has shown that implementing significant organizational change requires a comprehensive, integrated strategic plan with desirable characteristics that provide additional guidance to responsible parties for developing and implementing national strategies. Such a plan can set a clear direction for transformation efforts, help decision makers more effectively guide and assess progress, and do so in a clear and transparent manner. Additionally, such planning can provide the government with a sound basis for making investment decisions and help assure that it is developing and maintaining the optimal set of capabilities to achieve its transformational goals. ASPR officials stated that they remain committed to following stated guidance and best practices regarding strategic planning and implementation, consistent with previous ASPR efforts.
In January 2021, the President signed an Executive Order calling for the development of a pandemic supply chain resilience strategy to design, build, and sustain a long-term capability to manufacture medical supplies for future pandemics and biological threats.[129] Per the order, this strategy is to include the role of the SNS in (1) providing and allocating supplies across state, local, tribal and territorial governments, (2) sustaining supplies during a pandemic, and (3) contingency planning, among other things, within 180 days. Implementing the recommendation we made in January 2021 to develop a process for regularly engaging with Congress and nonfederal stakeholders in the development and implementation of a medical supply chain strategy to enhance pandemic response capabilities—to include the role of the SNS—would help guide this complex transformation.
To address more immediate supply needs, the President has also called for action that is consistent with our September 2020 recommendation that HHS—in coordination with FEMA—develop and communicate to stakeholders plans outlining specific federal government actions that will be taken to help mitigate supply gaps. Specifically, the Executive Order also directed the Secretaries of State, Defense, Health and Human Services, and Homeland Security among other federal agencies to immediately review the availability of pandemic response supplies, including PPE, and take appropriate action to fill any identified shortfalls in consultation with state, local, tribal, and territorial governments and other critical entities, as appropriate.
Additionally, the Consolidated Appropriations Act, 2021—enacted in December of 2020—included a provision requiring the President to make publicly available a report containing a whole-of-government plan for effective response to subsequent COVID-19 outbreaks and for future global pandemic diseases.[130] The act stipulates that this pandemic plan should address how to improve the role of the federal government with respect to the regulation, acquisition, and disbursement of medical supplies necessary to respond to COVID-19 as well as the procurement and distribution of PPE, among other things.
We will continue to monitor efforts to develop plans and strategies to address challenges raised by the COVID-19 pandemic regarding the SNS’s capabilities and other efforts to create resiliency in the medical supply chain, as part of our future CARES Act and SNS work.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To understand and categorize SNS COVID-19 challenges, we reviewed interviews we conducted and documents we received over the course of our CARES Act reporting. This included (1) interviews, written responses, and documentation from ASPR, FEMA, the Department of Defense and other interagency groups about actions related to increasing supply, making distribution decisions, and modernizing the SNS; (2) interviews with eight states (in July and August 2020) that were selected based on a variety of criteria including a range of COVID-19 case counts per capita, regional diversity, and participation in Crimson Contagion, among other things; (3) interviews with 9 individuals (in September, October, November, and December 2020) with expertise on the operations or activities of the SNS, and an understanding of public health funding, preparedness, and COVID-19 response actions (referred to as “experts” in this enclosure); and (4) interviews with public health, private industry, laboratory and health care associations throughout the course of our work. To understand ASPR efforts to address challenges, as well as current efforts to develop COVID-19 supply chain strategies, we held interviews with ASPR officials in the current and former administrations and reviewed executive orders related to pandemic response. Finally, to assess the reliability of the SNS inventory data reported in this enclosure, we discussed inventory controls with agency officials and conducted comparisons to other sources to check for consistency. We determined the data were sufficiently reliable for the purposes of our reporting objectives.
Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism. GAO-04-408T. Washington, D.C.: February 3, 2004.
Selected jurisdictions told us that federal funding for testing has been generally sufficient for the short term, but concerns about longer-term sustainability remain.
Entities involved: Centers for Disease Control and Prevention, within the Department of Health and Human Services, and the Department of the Treasury
Key Considerations and Future GAO Work
We recently and repeatedly reported on concerns with the federal response to COVID-19 testing. For example:
In September 2020, we reported on challenges with testing supply availability, and recommended that HHS develop plans outlining specific actions the federal government could take to help mitigate remaining medical supply gaps—including testing supply shortages. As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability. We acknowledge those efforts, but continue to maintain that our recommendations are warranted. For more information on the availability of testing supplies, see the Hospital and Pharmacy Perspectives on Administering Vaccines and Medical Supply Availability enclosure.
In November 2020, we reported on issues with the transparency of Centers for Disease Control and Prevention (CDC) testing guidelines and recommended that the Department of Health and Human Services (HHS) ensure that the scientific rationale for any changes is included when such changes are made. HHS concurred with our recommendation and has begun to implement it. For example, on February 16, 2021, CDC issued Interim Guidance on Testing Healthcare Personnel and provided links to studies that explained the scientific rationale for the changes in guidance. We will continue to monitor implementation of this recommendation to ensure that these efforts continue.
In January 2021, we reported on the HHS COVID-19 testing strategy at that time and recommended that HHS produce and make publicly available a consolidated and comprehensive national strategy document that incorporated all six characteristics of an effective national strategy.[131] The new administration issued its National Strategy for the COVID-19 Response and Pandemic Preparedness (National Strategy) on January 21, 2021 that includes increasing testing capacity among its seven goals.[132] To meet this goal, the National Strategy describes several actions, including the issuance of an Executive Order establishing the COVID-19 Pandemic Testing Board (Testing Board). The Testing Board is tasked with implementation of a clear, unified approach to testing and coordinating federal government efforts to promote COVID-19 testing, among other things. We will continue to monitor Testing Board efforts and the development of any comprehensive plans to implement testing goals outlined in the National Strategy.
The Paycheck Protection Program and Health Care Enhancement Act requires HHS to submit Testing Strategy reports to Congress every 90 days until funds provided under the act are expended.[133] As of March 16, 2021, HHS had not submitted the report due in February to Congress or released it to the public. HHS officials told us that they do not have plans to make the report public and will defer to Congress on whether they will share the report broadly. Until a comprehensive national testing strategy is publicly available, HHS is at risk of key stakeholders and the public lacking crucial information to support an informed and coordinated testing response.
Since we last reported in January, officials from eight states and one territory (hereafter referred to as jurisdictions) we interviewed in January 2021 reported that federal funding available for testing has been generally sufficient for the short run. While about 7 percent of the $30 billion in CDC funding awarded to states, localities, and territories for testing has been expended as of February 28, 2021, officials told us they prioritized spending down general use funds with a shorter period of availability before using money that is more specifically targeted for testing, provided through CDC, and available for longer periods. At the same time, these selected jurisdictions shared concerns about maintaining testing capacity and preparedness in the longer term. While recent funding appropriated after we interviewed jurisdictions will likely bolster response efforts for COVID-19 testing, it is too soon to know whether this new funding will meet longer term needs. We will continue to monitor the use of federal funding for testing.
Background
Diagnostic testing for COVID-19 is critical to controlling and understanding the spread of the virus, according to the CDC. As the coordinating agency for the federal response to public health and medical emergencies, HHS leads the development and implementation of the national COVID-19 testing strategy. Under the testing strategy from the previous administration, states managed their own COVID-19 testing programs with federal support.
According to the new administration’s National Strategy, issued on January 21, 2021, the federal government will partner with jurisdictional leaders to implement a cohesive response strategy that will include the goal of mitigating the spread of COVID-19 by expanding testing, among other things.[134] To meet this goal, the National Strategy describes several actions, including the issuance of an Executive Order establishing the Testing Board and directing agencies to facilitate testing free of charge for those who do not have insurance coverage.
Additionally, the Consolidated Appropriations Act, 2021, requires the President to make publicly available a report containing a whole-of-government plan for an effective response to subsequent major outbreaks of COVID-19 by late March 2021.[135]
Overall, HHS reported total obligations of about $42.9 billion as of February 28, 2021 with expenditures of about $8.5 billion, for testing-related activities.[136] About $35.5 billion of this funding was obligated for awards to states, localities, territories and tribal organizations, but funding was also obligated and expended by HHS agencies for testing-related activities, such as procurement of testing supplies and funding for testing for the uninsured.[137]
For certain funds appropriated specifically to be made available to states, localities, and territories for testing and related purposes, HHS awarded funding through the CDC’s longstanding Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases (ELC) Cooperative Agreement. The ELC program is intended to enhance the capacity of state public health departments to cohesively and comprehensively address infectious disease needs.[138] According to CDC guidance, allowable costs for COVID-19 testing funding through the ELC program include personnel, laboratory equipment and necessary maintenance contracts, collection supplies, courier service contracts, and hardware and software necessary for robust implementation of electronic laboratory and surveillance data, among others. As a condition of funding, ELC recipients were required, within 30 or 60 days of receiving an award, to submit a work plan and budget describing proposed activities.[139]
In addition to the testing-specific funds distributed through the ELC, jurisdictions received other funding to support response activities. For example, the CARES Act appropriated $150 billion to the Coronavirus Relief Fund (CRF) for payments to states, localities, territories, and tribal organizations for necessary expenses incurred due to the COVID-19 public health emergency. Jurisdictions could use these funds to further support testing. In addition, the American Rescue Plan of 2021, enacted on March 11, 2021 appropriated $47.8 billion to HHS to carry out activities to detect, diagnose, trace, and monitor SARS-CoV-2 and COVID-19 infections and mitigate the spread of COVID-19.[140] These activities include implementation of a national testing strategy, manufacturing and procurement of tests, and assistance to state, local, and territorial health departments. The appropriation is available until expended.
Overview of Key Issues
Selected jurisdictions told us that funding for testing was generally sufficient for the short term. Officials from all nine selected jurisdictions told us in January 2021 that they had sufficient funding for testing in the immediate future. Some officials told us this was in part due to the availability of an additional $19.11 billion in ELC funding from the Consolidated Appropriations Act, 2021 enacted in late 2020. These officials told us that federal funding allowed them to meet their immediate testing needs by increasing laboratory capacity and public health infrastructure. For example, these officials said they used ELC funds to support testing through various activities including
funding local health departments,
contracting with laboratories for testing services,
purchasing testing equipment and supplies,
purchasing information technology to manage testing data, and
hiring additional staff, such as laboratory technicians and case investigators.
HHS reported that $35.5 billion of COVID-19 relief funding had been made available for testing activities by jurisdictions—of which about $30 billion had been obligated through ELC awards—as of February 28, 2021. (See table below.)
Obligations and Expenditures of Federal Funding for Testing-Related COVID-19 Response Activities Provided to States, Localities, and Territories through the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases (ELC) program, as of February 28, 2021
Key activity
Obligations ($ billions)
Expenditures ($ billions)
Percentage of obligated amounts expended, as of February 28, 2021
CARES Act ELC funding (March 27, 2020)
0.6
0.1
16.67
Paycheck Protection Program and Health Care Enhancement Act ELC funding (April 24, 2020)
Total support to state, local, and territorial preparedness through ELC
30.0
2.0
6.67
Source: GAO analysis of information provided by the Department of Health and Human Services. | GAO-21-387
Note: These amounts do not include funds appropriated and obligated for tribal organizations as those funds are not awarded through the ELC program. For example, the Indian Health Service (IHS) will provide $750 million in funds appropriated by the Paycheck Protection Program and Health Care Enhancement Act to IHS, tribal, and urban Indian Health programs to expand testing capacity and testing-related activities. In addition, these laws may have appropriated additional amounts that were available, but not required to be used, for testing-related COVID-19 response activities for states, localities, and territories. This table reflects only those amounts with availability limited to this purpose.
While it appears as though a relatively small percentage (about 7 percent) of the $30 billion in federal testing funding obligated for jurisdictions has been expended, we found this is due, in part, to funding availability time frames. First, much of the $30 billion was awarded relatively recently in January, 2021. Second, officials from six of nine selected jurisdictions, as well as three of four selected state and local public health stakeholder groups we interviewed, told us they or their members prioritized spending federal funds whose availability ended earliest. For example, some of these jurisdiction officials told us they began using ELC funds, which CDC made available until late 2022, to support testing largely after exhausting payments from the Coronavirus Relief Fund, which originally covered costs incurred only through the end of 2020.[141] (See figure below). Additionally, officials told us they have used ELC funds to hire staff and contract with laboratories, and that these jurisdiction-level obligations will be paid out over the full life of the ELC award.
Timeline of Selected Federal Funding Availability to States, Localities, Territories, and Tribal Organizations Used to Support Coronavirus Testing
Note: The CARES Act allows recipients to use CRF funds for eligible costs incurred beginning on March 1, 2020. ELC recipients may have applied awards to costs incurred up to 90 days prior to receiving awards and some reimbursed costs may have predated enactment of applicable appropriations. See 45 C.F.R. § 308(d)(1) (2019).aELC awards are funds awarded through the Centers for Disease Control and Prevention’s (CDC) Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases (ELC) Cooperative Agreement.
More than half of selected jurisdictions told us they had concerns about maintaining testing capacity and preparedness in the longer term. Our prior work on ELC and other HHS programs that provide funding to jurisdictions for preparedness activities has found that funding to jurisdictions had generally decreased over time before the pandemic.[142] Such decreases have limited state and local preparedness capacity—such as being able to maintain preparedness staff—and have increased the importance of supplemental appropriations to respond to infectious disease threats.[143]
While the supplemental funding has helped jurisdictions address needs to respond to the pandemic in the short term, most jurisdictions interviewed for this report had concerns about future testing and related preparedness. Officials from five of nine jurisdictions told us they were concerned about their ability to maintain current testing efforts over the long run. For example:
Officials from one jurisdiction told us they did not have a sufficient public health workforce to support widespread virus testing prior to the pandemic. These officials told us they are concerned that without ongoing supplemental federal funds they will be unable to keep the trained epidemic and laboratory workforce they developed using federal funds for Coronavirus response.
Officials from another jurisdiction told us its public health funding had declined by almost 50 percent over the last decade. These officials told us that, as a result, their jurisdiction had reduced its epidemiology staff and their office was only able to employ one epidemiologist on a part-time basis prior to the pandemic, leaving the jurisdiction with no capacity to respond to new infectious diseases. While officials said the temporary funding available from the COVID-19 relief laws helped them respond to COVID-19, they added that when the next pandemic occurs, they will face the same challenges building a workforce to support testing if additional funds for public heath are not provided beforehand.
New funding available for testing appropriated by the American Rescue Plan Act of 2021 may help ameliorate concerns about the sufficiency of funding for COVID-19 testing in the longer term. Specifically, $47.8 billion—to remain available until expended—was appropriated to HHS to carry out activities to detect, diagnose, and monitor COVID-19 infections and to mitigate the spread of COVID-19, including through support to states, localities, and territories.[144] While this will likely bolster response efforts for COVID-19 testing, it is too soon to know whether this new funding will meet longer term needs. We will continue to monitor the use of federal funding for testing.
Agency Comments
A copy of this enclosure was sent to the Department of Health and Human Services and the Office of Management and Budget. CDC provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To conduct this work, we examined federal law and agency guidance related to federal funding for COVID-19 testing. We also obtained HHS data on obligations and expenditures for COVID-19 testing as of February 28, 2021, as well as written responses to questions from relevant agency officials. To assess the reliability of the data reported by HHS, we reviewed HHS documentation, obligation data published by CDC, and information from the federal spending database, USAspending.gov, as well as from HHS’s spending database, taggs.hhs.gov, and we determined that the HHS reported data were sufficiently reliable for the purposes of our reporting objective.
Furthermore, we selected a nongeneralizable sample of nine jurisdictions (eight states and one territory) and interviewed officials from those departments of health to obtain information on their experiences using federal funding for COVID-19 testing. We selected these jurisdictions to achieve variation in geographic region, testing volume, and case counts, among other things. In doing so, we spoke with officials from Arizona, Louisiana, Michigan, Pennsylvania, Puerto Rico, South Dakota, Texas, Vermont, and Washington.
Additionally, we obtained perspectives from a set of four stakeholder groups representing state and local public health officials, including groups that represent over 100,000 state and local public health officials and epidemiologists, as well as other individuals knowledgeable about funding for COVID-19 testing.
Infectious Disease Threats: Funding and Performance of Key Preparedness and Capacity-Building Programs. GAO-18-362. Washington, D.C.: May 24, 2018.
Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism. GAO-04-408T. Washington, D.C.: February 3, 2004.
While waivers and other flexibilities, as well as increased federal Medicaid funding, have helped states respond to the public health emergency, they are not permanent. States will face challenges in resuming normal Medicaid activities, including backlogs for redetermining beneficiary eligibility for Medicaid coverage.
Entity involved: Centers for Medicare & Medicaid Services, within the Department of Health and Human Services
Key Considerations and Future GAO Work
Since the beginning of the public health emergency, states have implemented various flexibilities and put certain eligibility renewals and redeterminations on hold in their Medicaid programs. States have also received additional federal funds to manage the increased number of individuals enrolled in Medicaid. These funds are set to be reduced to pre-public health emergency levels at the end of the quarter in which the public health emergency ends.
While the public health emergency is in effect at least through April 20, 2021, and according to the Acting Secretary of Health and Human Services, it will likely continue at least through the end of 2021, the Centers for Medicare & Medicaid Services (CMS) began issuing guidance and tools to states in December 2020 on resuming normal activities once the public health emergency has ended, including redetermining beneficiaries’ eligibility for Medicaid enrollment. The agency also plans to issue guidance on resuming Medicaid program integrity activities.
Medicaid officials we interviewed from eight selected states expressed concerns about various aspects of resuming operations post-public health emergency.[145] For example, most states expressed concerns about resuming normal activities at the same time additional federal funding is ending. State Medicaid officials’ concerns included resolving eligibility redetermination backlogs and enrolling beneficiaries ineligible for Medicaid coverage into new health insurance coverage. We will continue to monitor CMS guidance and states’ responses to the end of public health emergency going forward.
Background
Medicaid is one of the nation’s largest sources of funding for health care services for low-income and medically needy individuals, covering an estimated 77 million people and spending an estimated $673 billion in total federal and state spending in fiscal year 2020.[146] The federal government matches states’ spending for Medicaid services according to a statutory formula known as the Federal Medical Assistance Percentage (FMAP).[147]
The Families First Coronavirus Response Act (FFCRA) provided a temporary increase in the FMAP for all qualifying states and territories through the end of the quarter in which the public health emergency, including any extensions, ends.[148] To receive the increased FMAP, states and territories were required to meet certain conditions, such as maintaining Medicaid enrollment for certain beneficiaries through the end of the month in which the public health emergency ends. FFCRA also created an option for states to provide Medicaid coverage of COVID-19 diagnostic testing and related services to uninsured individuals.[149]
States and territories administer their Medicaid programs within broad federal rules and according to state plans approved by CMS, the agency within the Department of Health and Human Services which oversees Medicaid at the federal level. In addition to its normal authority to approve state waiver applications, CMS has additional authorities in certain emergency circumstances to waive Medicaid requirements to help ensure the availability of care. The temporary authorities CMS has approved will terminate based on the conclusion of the public health emergency unless the states make certain temporary changes permanent, for example, by submitting a state plan amendment for CMS’s review and approval.
Overview of Key Issues
Medicaid enrollment. In the months since the beginning of the public health emergency, the number of people covered under Medicaid increased, due in part to increased applications for Medicaid coverage and requirements under FFCRA for states to maintain Medicaid enrollment for certain beneficiaries regardless of their eligibility. To receive the temporary increased FMAP, states must provide continuous coverage to Medicaid beneficiaries who were enrolled in Medicaid on or after March 18, 2020, regardless of any changes in circumstances or redeterminations at scheduled renewals that otherwise would result in termination, through the end of the month in which the public health emergency ends, among other requirements. States may terminate coverage for individuals who request a voluntary termination of eligibility, or who are no longer considered to be residents of the state. As shown in the figure below, from February 2020 through August 2020—the last month for which updated data were available at the time of our reporting—Medicaid enrollment increased by 5.6 million, or 9 percent. Preliminary data for September 2020 suggest this trend continued, with almost 780,000 individuals added to the Medicaid rolls over comparable data in August.
Medicaid Enrollment from October 2019 through September 2020, Preliminary and Updated Data
Notes: Enrollment counts presented in this figure generally represent the total unduplicated number of individuals enrolled in comprehensive benefits as of the last day of the reporting period. Some states reported their data differently. States report preliminary data soon after the close of the reporting month; the preliminary enrollment counts generally do not include individuals with retroactive eligibility or individuals whose applications were not fully processed before the end of the month. States report updated data about one month later; these data are considered more complete because they account for individuals in both of these groups.
Medicaid operations. According to CMS, during the public health emergency all states have delayed processing eligibility and enrollment actions.[150] In December 2020, CMS issued guidance to states on resuming normal eligibility and enrollment operations after the end of the public health emergency. These operations include processing applications received during the public health emergency, redetermining Medicaid eligibility and terminating coverage, as appropriate; for example, terminating coverage for beneficiaries who no longer meet eligibility requirements, but remained enrolled during the public health emergency due to FFCRA requirements. As shown in the figure below, CMS expects states to resume timely processing of all eligibility and enrollment actions within 6 months of the end of the public health emergency.
Centers for Medicare & Medicaid Services Guideline for States Resuming Timely Medicaid Eligibility and Enrollment Actions
Medicaid officials we interviewed in selected states said that CMS has taken helpful actions throughout the public health emergency, such as issuing guidance and being responsive to states’ questions, but also expressed concerns about returning to normal operations. For example, officials in all eight states we interviewed reported that they were concerned about resuming timely processing of eligibility and enrollment actions. According to CMS’s December 2020 guidance, CMS expects this to be completed within 6 months of the end of the public health emergency. Officials in one of the states we interviewed noted that it would be challenging to resume normal operations by this date, since the state will need to resolve the backlog of eligibility redeterminations that have developed since the public health emergency began. Officials in one of the states we interviewed expressed concerns about smoothly enrolling beneficiaries who are no longer eligible for Medicaid into other health insurance coverage, and noted that a health insurance exchange open enrollment period during the transition would be helpful.
In January 2021, the Acting Secretary Health and Human Services issued a letter to state governors indicating that the public health emergency will likely continue through the end of 2021, and that the department will provide states with 60 days’ notice prior to ending the public health emergency. Medicaid officials in one of the states we interviewed had said that sufficient notice of the end of the public health emergency was important for a timely return to normal operations.
Medicaid spending. As of February 28, 2021, COVID-19-related federal Medicaid expenditures totaled approximately $33 billion, or 7 percent of total federal spending on Medicaid services for this time period.[151] The majority of the COVID-19-related spending is for the 6.2 percentage point FMAP increase. The temporary FMAP increase will extend through the end of the quarter in which the public health emergency ends. Medicaid officials in seven of the eight selected states said that the increased FMAP was among the most important Medicaid program changes, for example, to increase provider payments and provide services to an increasing number of beneficiaries. Officials in one of the states we interviewed suggested extending the increased FMAP an additional quarter following the end of the public health emergency. These Medicaid officials anticipated the state budget would fall short of Medicaid program needs in the months following the end of the public health emergency.
Our prior work has shown that state budget challenges can persist well beyond the end of a recession. In June 2020, we urged Congress to use GAO’s FMAP formula to determine the timing and increase in FMAP for any future changes to the current or any future economic downturn. The increased FMAP formula targets variable state Medicaid needs and provides assistance that is automatic, timely (both when to begin and to gradually end assistance), and temporary in response to national economic downturns. Improving the responsiveness of federal assistance to states during economic downturns would facilitate state budget planning, provide states with greater fiscal stability, and better align federal assistance with the magnitude of the economic downturn’s effects on individual states. In January 2021, the Medicaid and CHIP Payment and Access Commission approved a recommendation that Congress should adopt a statutory mechanism to amend the Social Security Act to provide an automatic Medicaid countercyclical financing model, using the prototype we developed as a basis.
The remainder of COVID-19-related spending—about $20 million—was reported by 13 of the 19 states and territories approved to cover COVID-19 diagnostic testing and related services for uninsured individuals with a 100 percent federal match.[152]
The table below summarizes federal Medicaid spending related to the 6.2 percentage point FMAP increase, COVID-19 expenditures in Medicaid programs approved to cover testing for uninsured individuals, and total Medicaid spending for services as of February 28, 2021.
Federal Medicaid COVID-19 and Total Expenditures, by State and Territory, as of February 28, 2021
State or territory
COVID-19-related federal Medicaid expenditures from the 6.2-percentage-point-increased FMAP ($ millions)
COVID-19-related federal Medicaid expenditures for uninsured testing ($ millions)
Total federal Medicaid services expenditures ($ millions)
Alabama
378
N/A
4,819
Alaska
65
N/A
1,498
Arizona
629
N/A
12,366
Arkansasa
337
N/A
5,900
California
4,015
19
65,432
Colorado
465
< 1 million
5,970
Connecticutb
297
< 1 million
4,096
Delawareb
120
N/A
1,689
District of Columbia
167
N/A
2,509
Florida
1,667
N/A
17,962
Georgia
692
N/A
8,323
Hawaiia
110
N/A
1,684
Idaho
129
N/A
2,053
Illinoisa
1,226
< 1 million
16,234
Indiana
744
N/A
11,276
Iowa
283
< 1 million
3,988
Kansas
242
N/A
2,552
Kentuckya
520
N/A
10,203
Louisiana
565
< 1 million
10,055
Maine
178
< 1 million
2,342
Maryland
566
N/A
7,854
Massachusetts
985
N/A
11,266
Michigan
937
N/A
14,543
Minnesotab
692
< 1 million
7,092
Mississippi
351
N/A
4,728
Missouri
663
N/A
8,017
Montana
67
0
1,612
Nebraska
144
N/A
1,495
Nevada
173
0
3,200
New Hampshire
109
< 1 million
1,411
New Jersey
804
N/A
10,725
New Mexico
278
< 1 million
5,453
New Yorkb
3,634
N/A
46,602
North Carolina
904
< 1 million
11,001
North Dakota
62
N/A
836
Ohiob
1,283
N/A
19,333
Oklahoma
308
N/A
3,745
Oregon
460
N/A
8,263
Pennsylvania
1,788
N/A
21,875
Rhode Island
132
N/A
1,809
South Carolina
416
< 1 million
5,142
South Dakota
54
N/A
639
Tennessee
681
N/A
7,741
Texas
2,607
N/A
29,114
Utah
153
< 1 million
2,530
Vermont
87
N/A
1,069
Virginiac
473
N/A
6,676
Washingtonb
541
N/A
9,598
West Virginia
201
0
3,486
Wisconsin
600
N/A
6,413
Wyominga
35
N/A
365
States totald
33,018
20
454,585
American Samoa
3
N/A
40
Guam
4
N/A
105
Northern Mariana Islands
3
0
42
Puerto Rico
100
0
2,456
Virgin Islands
3
0
73
Territories totald
113
0
2,715
Legend: FMAP = federal medical assistance percentage N/A = Not applicable. States that are not approved to provide COVID-19 testing for uninsured individuals as of February 28, 2021.
Source: GAO analysis of Centers for Medicare & Medicaid Services’ data accessed on March 1, 2021. | GAO-21-387
Note: COVID-19 related and total federal Medicaid expenditure data were available for the second, third, and fourth quarters of fiscal year 2020 (January 1, 2020, through September 30, 2020), and for the first quarter of fiscal year 2021 (October 1, 2020, through December 31, 2020). Some preliminary expenditure data were also available for the first two months of the second quarter of fiscal year 2021 (January 1, 2021, through February 28, 2021). States are not required to report expenditures for the second quarter of fiscal year 2021 until April 30, 2021, 30 days after the end of the quarter. Expenditures do not include expenses for program administration. State expenditures are reviewed by states and certified as being Medicaid allowable expenditures. Both certified and uncertified state expenditures are preliminary, as they are subject to further review and are likely to be updated as states continue to report their expenditures and receive federal matching funds. States can report payments and adjustments to payments up to 2 years after a quarter ends. Expenditure data are certified unless otherwise noted. aFive states reported preliminary expenditures for the first two months of the second quarter of fiscal year 2021 (January 1, 2021, through February 28, 2021), with only Hawaii having certified its expenditures thus far. bSix states reported uncertified expenditures for the first quarter of fiscal year 2021 (October 1, 2020, through December 31, 2020). cOne state reported uncertified expenditures for the fourth quarter of fiscal year 2020. dTotals may not sum exactly due to rounding.
State waivers and flexibilities. As of December 17, 2020, CMS reported that the agency had approved more than 600 different waivers, state plan amendments, and other flexibilities to provide states with flexibility to respond to the public health emergency. Common types of flexibilities that states sought and CMS approved are shown in the table below.
Common Types of State Flexibilities Approved by Centers for Medicare & Medicaid Services since March 16, 2020
Purpose of flexibility
Specific state flexibilities approved
Maintain beneficiary eligibility for services
Suspended fee-for-service prior authorizations, which are used to demonstrate compliance with coverage and payment rules before beneficiaries can obtain certain services, rather than after the services have been provided.a
Extended the dates for reassessing and reevaluating beneficiaries’ needs, which are normally required for beneficiaries to retain eligibility for some home- and community-based services.b
Expand beneficiary eligibility
Permitted virtual evaluations, assessments, and person-centered planning normally conducted in person.b
Expanded coverage to uninsured individuals for COVID-19 testing.c
Remove obstacles to beneficiary access to care
Allowed telehealth to continue to provide some services that were previously provided in person.c
Allowed early refills of certain medications to avoid interruption in care.c
Increase the availability of providers
Waived some requirements to allow licensed out-of-state providers to enroll in their programs to maintain provider capacity.a,d
Authorized payments changed or added for telehealth services.c
Source: GAO analysis of Centers for Medicare & Medicaid Services approval documentation for states and District of Columbia. | GAO-21-387
aStates received approval under section 1135 of the Social Security Act, which authorizes the Secretary of Health and Human Services to temporarily waive or modify certain federal health care program requirements, including Medicaid requirements, to ensure that sufficient health care items and services are available to meet the needs of enrollees during an emergency. bStates received approval to make changes to their section 1915(c) home- and community-based services waivers under an Appendix K amendment in order to respond to the emergency. cStates received approval to revise policies in their Medicaid state plan related to eligibility, enrollment, benefits, premiums and cost sharing, and payments. To make these changes, states must submit a State Plan Amendment to the Centers for Medicare & Medicaid Services for approval. dStates approved to temporarily enroll licensed out-of-state providers must follow certain requirements, which include screening providers to ensure they are enrolled in the Medicaid program and licensed in the state relating to their Medicaid enrollment. Waiver of these federal requirements does not affect state or local licensure requirements.
Medicaid officials from the selected states we interviewed reported that these flexibilities were important for fulfilling their states’ Medicaid program mission. For example, Medicaid officials from all eight states noted that flexibilities to remove obstacles to beneficiary access to care, such as the use of telehealth, have been among the most important during the public health emergency. A Medicaid official in one of the states we interviewed said flexibilities permitting virtual evaluations, for example, provided Medicaid beneficiaries with an added sense of security and safety, while providing needed care.
Officials from all eight states we interviewed reported considering making certain flexibilities approved during the public health emergency permanent after the public health emergency has ended, in particular regarding telehealth. We will continue to monitor the use of services through telehealth, given the oversight challenges presented by the size, growth, and diversity of the Medicaid program.
Oversight of state Medicaid waivers and flexibilities. In our June 2020 report, we raised concerns about the potential effects of state flexibilities, including improper Medicaid payments. In December 2020, CMS reported that the agency plans to release guidance specific to COVID-19 program integrity issues, including beneficiary eligibility. According to CMS, the guidance will outline expectations for states to establish regular Medicaid program integrity operations both during and after the public health emergency, taking into account new changes to state programs as a result of implementing COVID-19 flexibilities. CMS officials have also reported that the agency is conducting and updating risk assessments for all Medicaid waivers and flexibilities issued as a result of the public health emergency. As of January 2021, CMS still plans to release the aforementioned guidance, which will include a discussion of CMS’ Medicaid risk assessment, so that states appropriately account for the risks and vulnerabilities associated with the Medicaid waivers and flexibilities. CMS has not specified when program integrity guidance will be released. We will continue to monitor CMS’s guidance and state efforts and report on our findings going forward.
Single audit requirements. The Single Audit Act establishes a requirement for federal award recipients (e.g., states, the District of Columbia, local governments, U.S. territories, Indian tribes, and nonprofit organizations) to undergo a single audit when federal award expenditures meet a certain dollar threshold in a fiscal year. The Office of Management and Budget (OMB) issued new guidance as to the applicability of the single audit to COVID-19 relief funding, including how to conduct such audits. Likewise, many federal awarding agencies issued new guidance to award recipients on how those funds should be reported and spent. CMS released several Frequently Asked Questions (FAQs) to provide guidance to state Medicaid agencies in their response to COVID-19 and implementation of the FFCRA and the CARES Act.
Single audits are essential in identifying deficiencies in the award recipient’s compliance with applicable provisions of laws, regulations, contracts, or grant agreements and in its financial management and internal control systems. Correcting such deficiencies can help ensure the appropriate use of federal funds and reduce the likelihood of federal improper payments. Medicaid is on GAO’s 2019 High-Risk list and has the largest reported amount of estimated improper payments out of all federal government programs determined to be susceptible to significant improper payment. For fiscal year 2020, HHS reported that Medicaid’s total estimated improper payments was about $86.5 billion, representing about 42 percent of the total $206.4 billion government-wide estimated improper payments reported for that fiscal year. Auditors who conduct single audits follow guidance in the Single Audit Act’s Compliance Supplement, which OMB updates and issues annually in coordination with federal agencies. Refer to the Single Audits enclosure for more information on single audits.
Agency Comments
We provided a draft of this enclosure to HHS and the Office of Management and Budget for review and comment. HHS provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed federal laws and CMS data from both its Medicaid expenditure reporting system and Medicaid and CHIP performance indicators project. We also reviewed CMS Medicaid guidance, including requirements for administering the optional COVID-19 testing for the uninsured and resuming normal state eligibility and enrollment operations after the end of the public health emergency; and our prior work related to Medicaid. We also reviewed CMS guidance to states on reporting COVID-19 expenditures through the Medicaid expenditure reporting system and conducted data reliability checks on both the state reported-expenditure data and performance indicators. We determined that the CMS data were sufficiently reliable for the purpose of this enclosure.
We also interviewed Medicaid officials from eight selected states regarding flexibilities they requested during the public health emergency, CMS assistance in obtaining and implementing these flexibilities, and plans for resuming normal operations after the public health emergency has ended. We selected states based on geographic diversity, size of the state Medicaid program, and approved Medicaid flexibilities.
Contact information: Carolyn L. Yocom, (202) 512-7114, yocomc@gao.gov
The Veterans Health Administration, within the Department of Veterans Affairs, began executing its COVID-19 vaccination plan following the Food and Drug Administration’s emergency use authorization of the Pfizer-BioNTech COVID-19 vaccine in December 2020. Its vaccination effort could benefit from performance targets and improved metrics for vaccine administration.
Entities involved: Veterans Health Administration, within the Department of Veterans Affairs
Recommendations for Executive Action
The Department of Veterans Affairs Under Secretary for Health should develop metrics to assess the number of vaccines administered by vaccine rollout phase to better assess progress and make any necessary adjustments as needed. VA agreed with our recommendation.
The Department of Veterans Affairs Under Secretary for Health should develop preliminary vaccination targets for when it will move from one vaccination phase to another; or within one phase, from one group of veterans to another. VA agreed in principle with our recommendation.
The Department of Veterans Affairs Under Secretary for Health should collect data on the number of staff and veterans who do not show up for a vaccination appointment to better monitor for completion of the second dose of the vaccine. VA agreed with our recommendation.
Key Considerations and Future GAO Work
The Department of Veterans Affairs (VA) has used COVID-19 relief funds to vaccinate veterans and Veterans Health Administration (VHA) staff. As of March 10, 2021, about 908,000 veterans and 243,000 staff have been fully vaccinated (i.e. received required two doses of the Moderna or Pfizer vaccines, or one dose of the Janssen (Johnson & Johnson) vaccine) by VHA.
We will continue to examine VA’s vaccination efforts, including ongoing work, reviewing how the department used COVID-19 relief funds to distribute and administer vaccines. In addition, we have ongoing work focusing on the vaccination of veterans and staff at VA community living centers.
Background
VA, through VHA, provides health care services to approximately 10 million enrolled veterans. Veterans can access services at one of VHA’s 1,294 sites of care, which includes 170 VA medical centers and about 1,000 outpatient sites. VHA is leading VA’s efforts for the distribution of COVID-19 vaccines.
In September 2020, VHA began planning for the availability of a COVID-19 vaccine, and developed the COVID-19 Vaccination Plan for the Veterans Health Administration, which was most recently updated on December 14, 2020.[153] The document describes several aspects of VHA’s vaccination plan, which include
the guiding principles and priorities of VHA’s vaccination effort, such as the safety of veterans and staff;
how VHA will operationalize these principles, for example by developing and implementing a plan to distribute the vaccines to facilities, and for administering vaccinations to veterans and staff;
roles and responsibilities of national leadership, Veterans Integrated Service Network leadership, and VA medical center leadership;[154]
development of an integrated project team to review feedback from VHA staff and recommend revisions to plans and products about the COVID-19 vaccines;[155] and
the creation of workgroups to develop vaccine communication, vaccine distribution plans, and vaccination metrics among other things.
Starting in December 2020, the Food and Drug Administration (FDA) took several steps to pave the way for vaccine distribution and administration nationally. Specifically, on December 11, 2020, FDA issued an emergency use authorization (EUA) for the Pfizer-BioNTech (Pfizer) COVID-19 vaccine.[156] A week later, on December 18, 2020, FDA issued an EUA for the Moderna vaccine. More recently on February 27, 2021, FDA issued an EUA for the Janssen vaccine.[157]
After the first EUA was in place, on December 16, 2020, VA released guidance through a memo to Veterans Integrated Service Network and VA medical center leadership detailing how vaccines would be distributed to sites, how to schedule vaccination appointments, how to document administering the vaccine, and information on training and data reporting requirements.[158] VA updated this guidance on December 23, 2020.[159] In addition, beginning on December 29, 2020, VA published vaccine information in Spanish and on January 26, 2021 began publishing the information in Tagalog.
VHA received approximately $17.2 billion in supplemental appropriations from the CARES Act to assist its response to COVID-19. According to VHA officials, they expect staffing to be the primary cost associated with vaccine distribution.[160] As part of the American Rescue Plan Act of 2021, VA will receive an additional $14.482 billion of funding for COVID-19 related health care.[161]
Overview of Key Issues
As of March 11, 2021, VA has recorded 236,176 COVID cases, including about 4,600 active cases among veterans and 130 active cases among staff. In addition, VA has recorded more than 10,000 known COVID-19 deaths among its patient population and 134 COVID-19 deaths among its staff.
The primary goal of VA’s vaccination effort is to lower the COVID-19 risk of infection and severe disease. To achieve this goal, VA plans to offer vaccines to the roughly 10 million eligible veterans currently enrolled in VHA’s health care system and its approximately 419,000 staff. According to VHA, many enrolled veterans are at a higher risk of infection or severe disease from COVID-19. For example, more than half of the veteran population enrolled in VHA services are over the age of 65 and a large proportion have at least one high-risk medical condition, such as cardiovascular disease. VHA also acknowledges that many staff are at risk for COVID-19, and can potentially transmit the virus to high-risk veterans. According to VHA, its staff are not required to receive the vaccine. However, VHA has provided education to its staff on vaccine safety and education and they are encouraged to become vaccinated.
VHA’s vaccination approach. VHA has a phased approach for its vaccination effort. Veterans and staff are prioritized based on their risk for either COVID-19 transmission, morbidity, or mortality, with higher risk individuals included in earlier phases. According to VHA, a risk-based phased approach is necessary as demand for the vaccine continues to outpace supply. VHA’s approach follows a risk stratification framework based on the Centers for Disease Control and Prevention (CDC) guidance, and VHA’s previous vaccination efforts.[162] See table below for details on VHA’s vaccination prioritization and phases.
Veterans Health Administration (VHA) COVID-19 Vaccination Phases and Prioritization, December 14, 2020
Phasea
Types of VHA staff who will receive vaccines
Groups of veterans who will receive vaccine
1a
All health care personnel
Veterans in VHA long term care facilities and inpatients at VHA Spinal Cord Injuries and Disorders Centers
1b
Veterans 75 and older receiving VHA care
Veterans under the age of 75 who are in high risk groups, such as veterans experiencing homelessnessb
Veterans who are frontline essential workers as defined by CDCc
1c
Other VHA personnel, non-health care staff
Veterans 65-74 years of age receiving VHA care
Veterans with a high-risk condition, such as cancer or obesity
Other essential workers as defined by CDC
Source: Department of Veterans Affairs, COVID-19 Vaccination Plan for the Veterans Health Administration. | GAO-21-387
Notes: VHA’s vaccination prioritization is for eligible veterans enrolled in its health care system. aVHA’s risk stratification is based on Centers for Disease Control and Prevention (CDC) guidance and VHA’s previous vaccination efforts. CDC’s guidance includes recommendations for prioritizing high-risk groups, such as health care personnel and long-term care residents, to receive vaccine doses first. CDC’s guidance allows for flexibility. For example, agencies can decide to further prioritize within a particular group. bVHA considers veterans in these groups high risk because they have either an increased risk of COVID-19 transmission and mortality. cCDC defines essential workers as those individuals who conduct a range of operations and services in industries that are essential to ensure the continuity of critical functions in the United States. Examples of Phase 1b essential workers include grocery store workers, postal workers, and public transit workers.
In addition, VHA developed a tool for facilities to help identify high-risk veterans. The tool identifies veterans by conditions such as age and comorbidities, which are known to elevate risk associated with COVID-19. According to officials from several VA medical centers in our review, the tool has been helpful in determining which staff and veterans to vaccinate first.
VHA’s top priorities are staff and veterans who are most at risk of contracting COVID-19 and of having the most severe symptoms. In particular, VA has prioritized:
Community living centers. According to CDC data, 21 percent of COVID-19 deaths have occurred in nursing home facilities, including community living centers (CLC)—which are owned and operated by VHA.[163] According to VHA’s risk stratification framework, staff working in CLCs were the first group of staff to be vaccinated because they interact with a greater number of residents and can more easily spread the virus. Veterans residing in CLCs were the first veterans to be vaccinated. According to VHA data we reviewed, 95 percent of CLC residents have received at least one dose of vaccine, and 86 percent have been fully vaccinated as of March 14, 2021.
Homeless veterans. Homeless veterans are also among the first groups of veterans eligible to receive a vaccine in VHA’s stratification framework. According to VHA, homeless veterans are a priority because they are at an increased risk of needing to be in congregate living settings where there is increased risk of infection, particularly during the winter months. Further, according to VHA, homeless veterans are more likely to have high-risk health conditions and be older, elevating the risk of morbidity and mortality from COVID-19. According to VHA officials, outreach efforts include bringing vaccine to homeless veterans in VA-funded congregate living environments, and a laminated pocket card with information about COVID-19 vaccination at VHA.
VHA estimates that as of December 14, 2020, there were about 242,000 homeless veterans. As of March 14, 2021, VHA data show that 41,253 homeless veterans have received at least one dose of vaccine, and 21,574 have been fully vaccinated.
VHA’s progress in distributing and administering vaccines. On December 14, 2020, VHA began distributing the initial doses of the Pfizer vaccine to 37 facilities. VHA reported that these facilities were selected because they had the ultra-cold storage capacity necessary for storage of the vaccine.[164] On December 21, 2020, VHA began distributing initial doses of the Moderna vaccines to 113 facilities that were identified based on factors such as their ability to appropriately store the vaccine. According to VHA, the Moderna vaccine is more suitable for smaller facilities due to less stringent cold storage requirements and smaller minimum order size, and it plans to focus distribution of those vaccines to rural and remote areas.[165] On March 3, 2021, VA received its first doses of the Janssen (Johnson & Johnson) vaccine. According to VA, the Janssen vaccine will help VA more effectively reach rural veterans as it only requires one dose. As of March 18, 2021, 868 of VHA’s 1,294 sites of care had received vaccine doses. VHA reported that it will distribute vaccines to additional facilities as vaccination supply increases.
As of March 10, 2021, VHA facilities had administered about 2.5 million vaccine doses to veterans and about 518,000 vaccine doses to staff. See figure below for details on the number of doses VHA has received, and administered.
Department of Veterans Affairs COVID-19 Vaccine Administration, as of March 10, 2021
Note: Both the Pfizer and Moderna vaccines require two doses separated by 3 weeks and 1 month, respectively. The Janssen vaccine requires one dose. Fully vaccinated individuals have either had two doses of the Pfizer or Moderna vaccines, or one dose of the Janssen vaccine.
VHA facilities noted challenges in planning due to vaccine allocation changes and uncertainty. Staff at VHA facilities in our review—12 facilities that received the Pfizer vaccine and 12 facilities that received the Moderna vaccine—told us that predictable vaccine allocation, or specified doses of vaccines to be made available, would improve their ability to plan for administration of the vaccine.
Facilities plan based on their assigned allocations of vaccines, which are based on the number of staff and veterans receiving care at a facility who are in specific risk categories (see above table showing COVID-19 vaccination phases and prioritization for details).
Staff from 18 of the 24 facilities in our review told us the vaccine supply chain was a challenge for several reasons, including the timeline for vaccine delivery changing and not receiving the quantity of vaccine they ordered. For example, staff at one facility reported to us receiving three times the amount of vaccine they initially planned for and noted that the facility had to make last-minute staffing changes to accommodate the increase. Further, staff from several of these 18 facilities told us that the uncertainties created challenges in scheduling appointments, staffing clinics, and accurately communicating with veterans and staff about what to expect.
Staff from some facilities in our review told us that uncertainty is challenging to manage because vaccination efforts are labor intensive to plan for and coordinate with staff. For example, vaccination clinics require coordination across a multidisciplinary team, such as staff from pharmacy, public affairs, scheduling, and information technology (IT) management. In addition, staff from some facilities told us the high volume of veterans to call and schedule for vaccination appointments, and the number of staff necessary to operate vaccination clinics is challenging.
Although VHA has received most of the vaccine doses it has ordered, VHA officials said planning at the facility level is challenging because VA learns its allocation of vaccine approximately one week in advance. Specifically, VA learns its weekly allocation of vaccine each Tuesday—it then uses its risk stratification framework to determine how these vaccines will be distributed across the country—and doses arrive on site between Monday and Thursday the following week.
VHA may face difficulties in assessing vaccination progress. Although VHA has outlined a phased vaccination approach, it has not developed metrics for tracking vaccines by phase, has not created vaccination targets for each phase, and does not track no-show appointments.
Phase-specific data. VHA is utilizing a phased vaccine rollout; however, VHA’s current metrics do not capture vaccine data by phases. VHA’s vaccination phases may include veterans based on a combination of factors. For example, Phase 1c includes veterans who are 65 and older and veterans under the age of 65 who have high-risk conditions or are essential workers.[166] According to VHA officials, VHA does not have data on all factors that define a particular phase, such as employment data to identify essential workers. However, VHA officials stated they are able to track age and health condition data, which includes the majority of some phases, such as 1b. Using data VHA currently has access to, VHA may be able to create metrics for some vaccination phases. VHA’s lack of data by vaccination phase is inconsistent with our Standards for Internal Control in the Federal Government, which states that management should use quality information to achieve objectives. Without the ability to review vaccination data by phase, VHA is not able to determine which facilities may be at an earlier phase than others and direct resources or assistance to those facilities.
Vaccination targets. VHA does not have targets as to when it will move from one vaccination phase to another; or within one phase, from one group of veterans to another. This lack of vaccination targets is inconsistent with effective management practices. We have previously reported that developing measurable targets is an effective practice to assess progress in meeting program goals.
VHA stated that creating vaccination targets is currently challenging given that vaccine supply currently lags demand that and the amount of vaccine available to VHA is unpredictable and fluctuates from week to week. Although the unpredictable supply of vaccine doses may prevent VHA from developing absolute targets, our previous work has shown that setting preliminary targets is an effective strategy when an agency cannot develop absolute targets. Without preliminary vaccination targets, VHA may not be able to determine its progress in vaccinating staff and veterans who have the highest risk, and signal to those lower risk groups when they might anticipate being vaccinated.
Appointment no-show data. VHA does not have metrics related to staff and veterans who do not show (no-shows) for their vaccination appointments, which is inconsistent with its own vaccination goal to track vaccine administration and completion of both doses of vaccine. [167] In addition, Standards for Internal Controlin the Federal Government state that management should use quality information to achieve objectives. Without data on no-shows, VHA may be at an increased risk for not being able to determine the extent to which staff and veterans are not showing for appointments for their second vaccinations, and may miss opportunities to better target outreach to individuals not showing up for appointments. Officials told us that VHA is collecting data required by the CDC, which does not include no-show appointments.[168]
VHA’s outreach to minority and rural veterans. We have previously reported—including in our December 2019 report on opportunities for VA to address racial and ethnic disparities—that racial and ethnic minority veterans have had worse health outcomes for some diseases. Further, members of specific racial and ethnic minority populations, including Black, Hispanic, American Indian, or Alaska Native, have borne a disproportionate share of COVID illness and death in the United States, according to CDC data. (See our related Health Disparities enclosure for more information. VHA’s vaccination plan acknowledges the importance of equitably administering the vaccine, and describes steps taken by the agency to develop communication products targeted at minority and rural veterans. (See tables below for information on vaccines delivered to certain veteran groups, by race and ethnicity, as of March 11, 2021.)
Since beginning vaccinations in mid-December 2020, VHA reported that its COVID-19 Communications Team meets regularly with a variety of stakeholders, including veterans groups representing different racial and ethnic populations and minority outreach coordinators.[169] These efforts led VHA to take several actions, including developing videos to address vaccine hesitancy. For example, according to VHA officials, one video features clinicians discussing vaccine hesitancy and why they chose to be vaccinated. According to VHA officials, these videos are played at VHA facilities, and shared on multiple platforms, including VA’s social media platforms.
Administration of vaccine to veterans aged 65 and older by race as of March 11, 2021
Race
Number of veterans that are fully vaccinated
White
634,240
Black or African American
111,901
Multiple
4,830
Asian
6,225
American Indian or Alaskan Native
3,961
Native Hawaiian or Other Pacific Island
5,584
Unknown
37,541
Declined to answer
21,418
Total
825,701
Source: GAO analysis of Department of Veterans Affairs data. | GAO-21-387
Administration of vaccine to veterans aged 65 and older by ethnicity as of March 11, 2021
Ethnicity
Number of veterans that are fully vaccinated
Non-Hispanic or Latino
739,233
Hispanic or Latino
41,230
Unknown
32,292
Declined to answer
12,946
Total
825,701
Source: GAO analysis of Department of Veterans Affairs data. | GAO-21-387
VHA officials told us that they anticipated it would be a challenge to deliver vaccine doses to rural areas because of constraints around storage and handling of the vaccine. Staff from several facilities in our review said it was challenging to distribute doses of vaccine from VA medical centers to community-based outpatient clinics due to storage and handling requirements. Specifically, VHA officials said both the Pfizer and Moderna vaccines—which must be stored -70 and -20 degrees, respectively—require 24/7 temperature monitoring and staff availability to address any temperature deviations. According to VHA, smaller facilities may not have staff available 24/7 to address potential deviations. Further, according to VHA officials, the requirements for transporting vaccine make doing so challenging.
Since beginning vaccinations, VHA has made adjustments to address these challenges and get more vaccine into rural communities. For example, VHA initially required facilities to have backup power in place to ensure continuous maintenance and monitoring of vaccine temperature. According to VHA officials, this requirement was waived to increase the number of locations eligible to receive vaccine because backup power was not available at smaller community-based outpatient clinics.
Agency Comments
We provided a draft of this enclosure to VA for review and comment. VA provided technical and general comments on this enclosure, which we incorporated as appropriate. VA’s general comments are reproduced in appendix XII.
VA agreed with our recommendation to develop metrics to assess the number of vaccines administered by vaccine rollout phase in order to better assess progress, and provided a target completion date of October 2021. VA is using a phased approach to provide vaccines because vaccine demand currently outpaces supply. Without data by phase, VA is not able to determine which facilities are at an earlier phase and may require additional resources or assistance to vaccinate veterans and staff who are at the highest risk.
VA agreed in principle with our recommendation to develop vaccination targets for when it will move from one vaccination phase to another; or within one phase, from one group of veterans to another. Although VA acknowledged there are many factors to consider when moving from one phase to another, and the importance of flexibility for local conditions, VA did not provide dates for when it would develop targets. We reiterate the importance of developing preliminary targets to determine vaccination progress and signal to veterans and employees when they may expect to be vaccinated.
VA agreed with our recommendation to collect data on the number of staff and veterans who do not show up for a vaccination appointment to better monitor for completion of second dose of the vaccine. VA indicated that it is collecting data that can track the completion of first and second doses; however, these data do not indicate if staff or veterans missed their second dose because they did not show for their appointment. A missed second dose, for example, could be due to delays in shipment or other supply issues. Without no-show data, VA may miss opportunities to better target outreach to individuals not showing up for appointments.
Methodology
To conduct this work, we reviewed VHA’s vaccination plan and related guidance for facilities administering the vaccines. In addition, we analyzed VHA data on the number of COVID-19 vaccines VHA facilities administered from mid-December through March 18, 2021. We assessed the reliability of the data used in our analyses by conducting manual checks and obtaining written responses from agency officials about the data. We determined the data were sufficiently reliable for the purpose of this enclosure. We also collected information from 24 VHA facilities—12 facilities that received the Pfizer vaccine and 12 facilities that received the Moderna vaccine—to understand their vaccination experiences. We selected these facilities to reflect a range of geography and complexity level.[170] Information from these facilities is not generalizable across all VHA facilities. We also spoke to representatives from two veteran service organizations, the American Legion and Paralyzed Veterans of America, to gain additional context.
COVID-19: Federal Efforts Accelerate Vaccine and Therapeutic Development, but More Transparency Needed on Emergency Use Authorizations. GAO-21-207. Washington, D.C: November 17, 2020.
VA Health Care: Opportunities Exist for VA to Better Identify and Address Racial and Ethnic Disparities.GAO-20-83. Washington, D.C.: December 11, 2019.
Managing for Results: Strengthening Regulatory Agencies’ Performance Management Practices. GAO/GGD-00-10. Washington, D.C.: October 28, 1999.
The Department of Defense reported 255,716 cumulative, confirmed cases of COVID-19 as of March 10, 2021; has a phased approach for vaccinating 11.3 million DOD personnel and other eligible beneficiaries; and began administering vaccines in December 2020.
Entities involved: Department of Defense, including the Defense Health Agency, Defense Logistics Agency, geographic combatant commands, and military departments.
Key Considerations and Future GAO Work
We have ongoing work examining the Department of Defense’s (DOD) vaccination efforts and broader efforts to protect personnel against COVID-19. We plan to report the results of this work in spring 2021. We will also continue to monitor DOD’s vaccination progress.
Background
DOD, through its Defense Health Program, provides worldwide medical services to military personnel and other eligible beneficiaries (approximately 9.6 million individuals total) through 475 military medical treatment facilities and the delivery of TRICARE benefits.[171] The Defense Health Agency (DHA) manages and oversees DOD’s immunization programs and leads efforts to plan for the distribution of COVID-19 vaccines.
Geographic combatant commands, the three military departments, other DOD components, and the U.S. Coast Guard are responsible for planning distribution of COVID-19 vaccines within their specific areas of responsibility. Logistics personnel consolidate requests from medical treatment facilities or other vaccination sites and send them to the U.S. Army Medical Materiel Agency Distribution Operations Center, which enters the orders into the Department of Health and Human Services’ vaccine ordering system.
Overview of Key Issues
Prevalence of COVID-19 among DOD personnel and dependents. As of March 10, 2021, DOD reported 255,716 cumulative, confirmed cases of COVID-19 among its workforce personnel and dependents of military servicemembers. See the table below for more detailed information by personnel category, including for dependents of military servicemembers.
Number of Cumulative, Confirmed Cases of COVID-19, Hospitalizations, and Deaths Reported by the Department of Defense (DOD), as of March 10, 2021
Cumulative cases
Hospitalizations
Deaths
Military servicemembers (active and reserve components)
166,357
1,424
24
Dependents
25,272
364
10
Civilians
47,070
1,349
202
Contractors
17,017
491
69
Total
255,716
3,628
305
Source: DOD data from defense.gov/explore/spotlight/coronavirus/, accessed March 10, 2021. I GAO-21-387
Note: DOD defines a “COVID-19 case” as one confirmed by a positive molecular laboratory test and “dependents” as family members (according to specified criteria) of military servicemembers.
DOD vaccination approach. In light of the limited supply of COVID-19 vaccines, DOD has planned and implemented a phased approach to vaccinating up to approximately 11.3 million eligible personnel, including military servicemembers and their dependents, other beneficiaries (e.g., retired military servicemembers and their dependents), civilian employees, and selected contractor personnel.[172] DOD established a priority framework for determining which groups of eligible personnel should be vaccinated based on guidance from the Centers for Disease Control and Prevention (table).
Department of Defense (DOD) COVID-19 Vaccine Prioritization for Military Servicemembers, Other Beneficiaries, Civilian Employees, and Contractors
Vaccination phase
Population group
1a
All health care providers, health care support, and emergency services and public safety personnel
1b
Personnel providing critical national capabilities, personnel forward deployed to austere environments and those preparing to deploy to locations outside the U.S., DOD beneficiaries ages 75 years and older, and frontline essential workers
1c
DOD beneficiaries ages 65–74 and those ages 16–64 with increased risk for severe illness as defined by the Centers for Disease Control and Prevention, personnel deployed or serving temporary duty for more than 30 days outside the U.S., and essential workers not previously included in phases 1a or 1b
aAs of February 24, 2021, only the Pfizer-BioNTech COVID-19 vaccine is authorized for individuals ages 16 and 17 years.
DHA’s immunization plan includes distributing the first available vaccines developed and authorized through the federal response effort. DOD distributed the first two vaccines authorized for emergency use within days after each authorization was made. Specifically:
On December 11, 2020, the Food and Drug Administration (FDA) issued an emergency use authorization for the Pfizer-BioNTech vaccine.[173] The same day, the U.S. Army Medical Materiel Agency Distribution Operations Center—responsible for managing vaccine shipments, to include tracking them through their delivery to states and territories—initiated shipments to the first of 14 initial vaccination sites within the U.S., selected because of their cold storage capabilities, proximity to substantial numbers of high-priority personnel, and access to sufficient medical personnel to administer the vaccines and monitor recipients after vaccination.
On December 18, 2020, the FDA issued an emergency use authorization for the Moderna vaccine and, within 2 days, the Army Medical Materiel Agency Distribution Operations Center initiated vaccine shipments to the first of 61 vaccination sites in the U.S. for that week. Within 4 days, the Defense Logistics Agency—responsible for shipments to foreign countries, deployed locations, and ships—began shipping Moderna doses to locations outside the U.S.
On February 27, 2021, the FDA issued an emergency use authorization for the Janssen (Johnson & Johnson) single-dose vaccine. DOD began administering the Janssen vaccine on March 2, 2021. DHA officials stated that the immunization plan may incorporate other new vaccines as they are authorized for emergency use by the FDA, including vaccines that DOD is developing.
Vaccination progress. From December 2020 through February 2021, DOD expanded its number of vaccination sites in the U.S. and overseas to more than 500 locations, according to briefing reports to the DHA Director. The percentage of vaccines DOD has administered at these sites relative to its on-hand supply has increased almost every week since vaccinations began in December 2020. As shown in the figure below, as of March 10, 2021, DOD had administered 1,412,016 vaccine doses, or about 87 percent of the doses delivered to its vaccination sites. A total of 875,707 individuals, or about 13 percent of DOD’s target population of 6.9 million in all vaccination phases, had received at least one dose, and 536,309 of these individuals had been fully vaccinated.
Vaccine Doses Received by Department of Defense Vaccination Sites and Administered to Individuals as of March 10, 2021
Notes: The 6.9 million eligible individuals targeted include those in all phases of DOD’s vaccination plan as of February 2021––phases 1a, 1b, 1c, and 2—who DHA estimates to be most likely to receive their vaccine from DOD rather than from a state-run facility or private provider. The target population includes eligible military servicemembers (those on active duty, members of the Selected Reserve including the National Guard, and members of the Coast Guard), military servicemembers who have retired and their dependent family members, dependent family members of active-duty servicemembers and of certain reserve component members, civilians, and contractors.aThe number of doses administered is not equal to the total number of individuals fully and partially vaccinated because the Pfizer-BioNTech and Moderna vaccines for COVID-19 both require two doses for full vaccination, while the Janssen (Johnson & Johnson) vaccine requires a single dose.
Of the 875,707 individuals at least partially vaccinated, 489,703 were military servicemembers, comprising about 23 percent of the eligible military servicemembers in all phases. DHA officials stated that the winter holidays and weather temporarily slowed administration efforts in the first month after vaccinations began (mid-December 2020 through mid-January 2021). The pace has generally improved through March 2021.
Each DOD vaccination site may begin vaccinating individuals in lower tier phases at a different date due to differences in the proportion of individuals who are available within each phase at each location, according to DHA officials.
The DHA Director monitors vaccine plan implementation on a daily basis, including allotment, distribution, and administration, broken out by vaccine manufacturer, dose (initial and second), category of eligibility (e.g., service component, contractors, civilian employees, and other beneficiaries), and location. The Director also receives updates on public affairs activities, new information from the Centers for Disease Control and Prevention, and relevant clinical considerations, such as any adverse effects in DOD vaccine recipients reported to the Vaccine Adverse Event Reporting System (a national vaccine safety surveillance system overseen by the Centers for Disease Control and Prevention and FDA).
Challenges and lessons learned. DOD officials have identified a number of challenges to the efficient and timely vaccination of workforce personnel and dependents of servicemembers, and have taken corresponding corrective actions to address them.
Predictability of supply levels. According to DHA officials, during the first weeks of distribution in December 2020, some vaccine shipments arrived at receiving facilities unexpectedly and without tracking numbers from the Army Medical Materiel Agency. As a result, DHA officials stated that staff at vaccination sites became concerned about supply levels and initially held back doses from the initial shipments to conserve supply for second doses, rather than using them to administer first doses to other eligible personnel. Army officials stated that Pfizer had shipped vaccines to some locations during those initial weeks before providing tracking numbers, resulting in deliveries occurring before the Army Medical Materiel Agency could notify those sites. DHA officials communicated the concerns to the Army Medical Materiel Agency to improve distribution and they continue to monitor progress as shipments increase. For example, according to officials from the Army Medical Materiel Agency, they have since participated in DHA’s Operational Planning Team for vaccine distribution and administration, and have briefed the DHA Director on a daily basis. They stated that all vaccines have been delivered on time and without any losses.
Vaccine confidence. DOD encourages but does not require military servicemembers to receive a COVID-19 vaccine authorized for emergency use.[174] Senior DOD leaders and DHA officials emphasized to us that communication and transparency with their eligible population are paramount to increasing vaccine confidence. In particular, they stated that education about the benefits and low risk of the FDA-authorized COVID-19 vaccines is critical to expanding the vaccination campaign and thereby protecting the health of individuals. To these ends, DOD has implemented a public affairs campaign with approaches such as public service announcement videos to address topics of concern, a video message from the Secretary of Defense, updates to websites, social media, press releases and briefings, and media round tables. Senior DOD leaders and military health professionals were among the first to receive the vaccines after their FDA authorizations, which they promoted with media events.
According to senior DOD leaders, they believe that continuing to promote confidence in the FDA-authorized COVID-19 vaccines will help address some degree of hesitancy that may exist among military servicemembers just as with the general population. To that end, DOD leaders have used the term “vaccine acceptance” to categorize the proportion of the military servicemembers who received a vaccine compared with those eligible to receive it. However, “acceptance” suggests that individuals not counted in the ratio have actively declined or resisted vaccination, while there could be other reasons that they have not yet received a vaccine, such as insufficient supply in a certain location or because they were traveling or were on leave at the time they could have been vaccinated.
DOD officials stated that as long as the demand for vaccines exceeds available supply (projected to be the case through late spring or summer of 2021), they cannot reliably determine how many military servicemembers or others may have delayed vaccination or do not plan to be vaccinated. Individuals who show up for an appointment at a DOD vaccination site and decide not to request the vaccine after reviewing educational material are asked to record their decision on DHA Form 207–“COVID-19 Screening and Immunization Document.” However, DHA officials noted that this decision reflects a single point in time, and the individual may choose to receive the vaccine at a later date. Meanwhile, DHA officials stated that they are monitoring demographic trends among DOD vaccine recipients, and when supplies increase to meet or exceed demand, they expect to learn more about personnel who may have postponed or declined COVID-19 vaccination.
DOD officials involved in the vaccine distribution and administration process have been documenting lessons learned and sharing them among DOD vaccination sites, other federal agencies, and select foreign collaborators. For example, according to DHA officials, on the basis of lessons learned, they expedited procedures by having staff prepare paperwork and fill vaccine syringes from vials prior to the arrival of the individuals to be vaccinated. In addition, officials have found that using large facilities, such as gymnasiums and warehouses, makes it possible to administer vaccines to large numbers of individuals and observe them post-vaccination while adhering to social distancing requirements.
Agency Comments
We provided a draft of this enclosure to DOD and the Office of Management and Budget for review and comment. DOD provided technical comments on this enclosure, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed DOD guidance and the most recent DOD data available as of March 2021 on COVID-19 cases and vaccines. We obtained COVID-19 case data from defense.gov/explore/spotlight/coronavirus and vaccine data from DHA. To assess the reliability of the data, we discussed them with agency officials, reviewed them for outliers or obvious errors, and reviewed relevant DOD documents. We determined that they were sufficiently reliable for the purposes of this enclosure but did not independently review them for accuracy.
We also interviewed DOD officials knowledgeable about COVID-19 vaccination efforts and reviewed publicly available DOD media reports, statements, and documents.
Contact information: Brenda S. Farrell, (202) 512-3604, farrellb@gao.gov
As COVID-19 cases have surged across the country in late 2020 and into early 2021, requests for the Department of Defense to provide personnel to support civil authorities have increased and focused on specialties, such as critical care nurses.
Entities involved: Department of Defense; Federal Emergency Management Agency, within the Department of Homeland Security; and Department of Health and Human Services
Key Considerations and Future GAO Work
We plan to continue to monitor how the Department of Defense (DOD) will support vaccine distribution and administration efforts as part of its Defense Support of Civil Authorities mission and the government-wide pandemic response.
Background
While DOD’s primary mission is to defend the nation, the department is often asked to play a prominent role supporting civil authorities and must be prepared to provide rapid response when called upon during disasters and declared emergencies (natural or man-made). DOD provides such support through its Defense Support of Civil Authorities mission, and is authorized to do so when requested by another federal agency, with approval from the Secretary of Defense, or when directed by the President.[175] DOD provides such support using federal military forces; DOD civilians and contract personnel; and DOD component assets, to include the National Guard, the U.S. Army Corps of Engineers, and the Defense Logistics Agency.
National Guard forces may provide support to civil authorities when ordered to active duty—commonly referred to as Title 10 duty status. When ordered to active duty, National Guard forces are funded and commanded by DOD. National Guard personnel may also be ordered to a duty status pursuant to Title 32 U.S.C. § 502(f)—commonly referred to as Title 32 duty status—by the President or Secretary of Defense and with the consent of the Governor. When operating in a Title 32 duty status, National Guard forces are funded by DOD and commanded by the state. The following figure shows the state and federal command relationship based on the National Guard’s or other forces’ status in supporting civil authorities.
State and Federal Command Relationship Regarding Defense Support of Civil Authorities
Congress appropriated approximately $1.5 billion through the CARES Act for Army and Air National Guard personnel and operations expenses incurred to prevent, prepare for, and respond to the coronavirus, domestically or internationally.[176] The approximately $1.5 billion was required to be obligated by September 30, 2020. According to USAspending.gov, as of November 30, 2020, the National Guard had obligated about $153.0 million and spent about $91.7 million of that appropriation from the Army and Air National Guards’ Personnel and Operation and Maintenance accounts.[177]
Section 13001 of the CARES Act provided DOD with the authority to transfer amounts appropriated to the department by the act to other applicable DOD appropriations for expenses incurred in preventing, preparing for, or responding to COVID-19, including in support of other federal departments and agencies, and state, local, and tribal governments.[178] As we noted in our September 2020 report, DOD officials stated that the total amounts appropriated to the National Guard in the CARES Act could not be fully obligated before they expired on September 30, 2020.
Amounts appropriated to the National Guard are not available to support state-level response activities. Moreover, National Guard support to the states for the COVID-19 response was reimbursed by FEMA and the states. Specifically, the initial mission assignments for Title 32 National Guard support were issued with 100 percent of the cost of support reimbursed by the federal government and no cost to the states. On August 3, 2020, the President issued memorandums extending the authorization of Title 32 status for National Guard troops supporting the COVID-19 pandemic through December 31, 2020.[179]
Consequently, amounts appropriated in the CARES Act to the National Guard in support of the states’ COVID-19 response for fiscal year 2020 were identified as available for transfer to other DOD appropriations for COVID-19-related priority activities. By September 30, 2020, DOD had transferred approximately $1.28 billion of the amounts appropriated to the Army and Air National Guard through the CARES Act to other DOD appropriations for COVID-related expenses (see fig.).
CARES Act Appropriations to the National Guard and Subsequent Transfers from the National Guard to Other DOD Accounts, Fiscal Year 2020
aCoronavirus Aid, Relief, and Economic Security (CARES) Act, Pub. L. No. 116-136, div. B, title III, 134 Stat. 281, 518 and 520 (March 27, 2020).
According to a DOD Comptroller official, the CARES Act amounts were transferred out of the four National Guard accounts to other DOD appropriation accounts as part of the department’s CARES Act reprogramming actions. The official further stated that the National Guard amounts were combined with other amounts identified for reprogramming and transferred to other DOD appropriations for use on COVID-19 expenses. Our analysis of DOD reprogramming documentation found that the department transferred amounts initially appropriated to Army and Air National Guard accounts in the CARES Act to a number of other DOD appropriation accounts (see table).
Department of Defense (DOD) Accounts That Received CARES Act Appropriations Transferred from National Guard Accounts
National Guard account with CARES Act amounts available for transfer
DOD appropriation receiving CARES Act amounts transferred from National Guard accounts
Army National Guard
National Guard Personnel, Army
Operation and Maintenance, Army National Guard
Military Personnel, Army
Military Personnel, Navy
Military Personnel, Marine Corps
Operation and Maintenance, Army
Operation and Maintenance, Navy
Other Procurement, Army
Reserve Personnel, Marine Corps
Research, Development, Test, and Evaluation, Army
Air National Guard
National Guard Personnel, Air Force
Operation and Maintenance, Air National Guard
Military Personnel, Air Force
Operation and Maintenance, Air Force
Operation and Maintenance, Navy
Operation and Maintenance, Navy Reserve
Operation and Maintenance, Marine Corps
Defense Working Capital Fund
Source: GAO analysis of Department of Defense (DOD) budget documents. I GAO-21-387
We reported on DOD’s reprograming actions in November 2020. According to a September 2020 DOD internal reprogramming action, $24.4 million was available for transfer from the Army National Guard Personnel account to the Army Research, Development, Test, and Evaluation account. The reprogramming action stated that the funds were needed to assess COVID-19 testing capability for the Army force and would be used to evaluate the viability and reliability of two COVID-19 testing systems in operational settings.
As another example, approximately $254.6 million of CARES Act amounts appropriated to the Air National Guard Personnel account were transferred to three other accounts, specifically Air Force Personnel ($157.8 million), Marine Corps Operation and Maintenance ($90.5 million), and Navy Reserve Operation and Maintenance ($6.3 million) in July 2020. According to the department’s internal reprogramming action document, the amounts transferred to the Marine Corps were needed to support temporary camps and contract lodging to ensure social distancing and a safe training environment for new recruits and officer candidates, among other things.[180]
Overview of Key Issues
DOD has faced increased demand for personnel to support civil authorities. According to DOD officials, demand for the department’s support of civil authorities has continued to increase as large portions of the country experienced surges in COVID-19 cases and the department began supporting new missions, as discussed in more detail below. On January 22, 2021, the new Secretary of Defense released a statement affirming the department’s continued commitment to aid the nation’s health care professionals.
DOD officials stated that from March 2020 through January 2021 the department received over 400 Federal Emergency Management Agency (FEMA) mission assignments and other requests for DOD support. According to DOD officials, as of late February 2021, the department had active mission assignments for active-duty personnel in 26 states and territories. For example, DOD personnel were supporting civilian health care providers at medical facilities in California, Arizona, Texas, and the Navajo Nation through February 2021.[181] Subsequently, officials from DOD and FEMA reported in February 2021 that additional assignments to support federally run vaccination centers using DOD active-duty forces were underway.
In late January 2021, DOD officials told us that 391 DOD medical personnel were providing support under FEMA mission assignments. However, that number increased significantly in February 2021 as the department began deploying personnel for the vaccination center missions. As of February 28, 2021, approximately 3,700 DOD active-duty personnel were providing assistance to the states under the COVID-19 response.[182]
In addition, the number of National Guard personnel supporting the COVID-19 pandemic response has also increased, following a period of decreased need in the fall of 2020.[183] Specifically, as of February 28, 2021, approximately 29,000 National Guard members were activated to support the COVID-19 response in all 50 states, 3 territories, and the District of Columbia. This total represents an increase of approximately 12,000 National Guard members put on orders to support the response since fall 2020; however, this is still below the peak of National Guard support provided in spring 2020, when approximately 40,000 members were on orders. According to FEMA’s January 2021 COVID-19 Initial Assessment Report, the response to COVID-19 is the first time Title 32 has been authorized for National Guard support at this scale and is the largest number of mission assignments ever issued for Title 32 support.[184]
The figure below shows DOD personnel totals supporting civil authorities by month from March 2020 through February 2021.
Department of Defense (DOD) Personnel Supporting Civil Authorities’ COVID-19 Response, March 2020 through February 2021
Note: Personnel totals are as of the end of each month.
DOD has received increased requests for specialized medical support. According to DOD officials, as more has become known about COVID-19, the types of support requested of and provided by DOD have changed and become more targeted. Officials stated that, as of January 2021, the states’ primary needs were for nurses, especially critical care nurses for intensive care units.[185] According to those officials, the need for more specialized medical support underscores a notable shift away from the requests for more general medical capabilities in the spring of 2020 when little was known about the virus or its treatment and the requests for assistance were not being evaluated all together.[186] DOD officials also stated that the department had to balance requests for critical care nurses to help ensure that sufficient numbers of this type of nurse was available at its own medical treatment facilities to handle trauma cases, among other things.
Subsequently, in February 2021, DOD officials stated that the department’s COVID-19 support efforts was shifting from augmentation of local medical capabilities to establishing and supporting federal vaccination sites in states, using both nonmedical and medical active-duty personnel. As part of this new line of effort, FEMA requested as many as 50 Type 1 teams and as many as 50 Type 2 teams from DOD to support the vaccination sites.[187]
As of March 2, 2021, more than 2,200 military medical and support personnel were deployed in teams to support the federal vaccine response to the COVID-19 pandemic.[188] More specifically, on February 16, 2021, the first team of 222 U.S. military personnel began supporting a Type 1 vaccination site at California State University, Los Angeles.[189] The team—consisting of active-duty Army personnel—was tasked with administering vaccinations and providing supervisory and pharmacy support for the site through March 26, 2021 (see fig.). According to a DOD official, the site is capable of administering up to 6,000 vaccinations a day. The department subsequently deployed additional teams ranging in size from 25 servicemembers to 222 servicemembers to locations in Florida, Georgia, Illinois, Michigan, New York, New Jersey, North Carolina, Ohio, Pennsylvania, Texas, and the U.S. Virgin Islands in late February and March.[190]
Department of Defense Personnel Provide COVID-19 Vaccination Support in Los Angeles, California (March 2021)
According to DOD officials, a number of factors—such as access to and training on state-level vaccination tracking systems and the overall supply of vaccine doses—had to be addressed before DOD’s involvement in the vaccination efforts could expand.
National Guard support has shifted to align with the evolving vaccination-related needs of the states, but members have continued to support broader COVID-19 missions.
According to the National Guard Bureau, demand for National Guard assistance is likely to continue due to vaccine distribution, the strain on the health care system, and continued unemployment. Throughout the surge in COVID-19 cases in late 2020 and early 2021, National Guard members continued to provide support to a range of broad missions. However, with the rollout and prioritization of vaccinations, National Guard members also began assisting civil authorities in the distribution and administration of vaccines throughout the states. As of January 2021, 30 states were utilizing National Guard personnel to administer vaccines to the civilian population.
National Guard members have continued to support the broader COVID-19 missions listed below.
Testing and screening. National Guard members in 42 states have continued to support state and local government testing and screening for COVID-19 cases, as of January 2021. For example, in December 2020, the Mississippi National Guard administered COVID-19 testing in communities and at long-term care and correctional facilities. This included staffing more than 34 drive-through testing sites per day in addition to providing personnel to serve as members of outbreak response teams.
Mississippi National Guard Members Supporting COVID-19 Testing throughout the State in 2020
Medical planning. National Guard members in 37 states have conducted medical planning, as of January 2021. For example, in December 2020, Rhode Island National Guard members worked with state agency partners to provide assistance in planning and coordination for the distribution of the COVID-19 vaccine.
Warehouse operations. National Guard members in 35 states have continued to perform tasks related to storing and distributing supplies and equipment in warehouses, as of January 2021. For example, in December 2020, Maine National Guard members conducted warehousing, inventory, and distribution efforts at Centers for Disease Control and Prevention receiving, staging, and storage facilities, while Kansas National Guard members conducted coordination efforts with the state health department at a Topeka warehouse facility.
Other missions. Throughout the COVID-19 pandemic response, National Guard members in a range of states have supported local long-term care facilities; assisted health departments with contact tracing and mapping; distributed personal protective equipment; collected COVID-19 specimens; and supported food banks by collecting and distributing food and supplies, among other things.
Agency Comments
We provided a draft of this enclosure to DOD and the Office of Management and Budget for review and comment. DOD provided technical comments on this enclosure, which we incorporated as appropriate. The Office of Management and Budget did not provide any comments on this enclosure.
Methodology
To conduct this work, we reviewed DOD documentation and the most recent information available as of March 2, 2021. We also interviewed DOD officials knowledgeable about COVID-19 response efforts. The data were provided to us by the DOD COVID-19 Task Force, which maintains the COVID-19 data of record for the department and reports them to senior DOD leaders. While we did not independently verify the accuracy of the data, we assessed the reliability of the data provided to us by checking for obvious errors or outliers, discussing the ongoing levels of DOD personnel support with knowledgeable DOD officials, and reviewing relevant documentation. We determined that the data were sufficiently reliable for the purposes of reporting the levels of personnel support provided by DOD. We also reviewed spending data from USAspending.gov through November 30, 2020.
As of February 28, 2021, the Department of Health and Human Services reported that it had obligated about $232 billion and expended about $148 billion of the approximately $324 billion in COVID-19 relief funds appropriated in the five COVID-19 relief laws enacted as of January 1, 2021—about 72 percent and 46 percent, respectively.
Entity involved: Department of Health and Human Services
Key Considerations and Future GAO Work
We will continue to examine the Department of Health and Human Services’ (HHS) use of COVID-19 relief appropriations contained in COVID-19 relief laws enacted to help fund the COVID-19 response, including appropriations in the American Rescue Plan Act of 2021, a sixth COVID-19 relief law enacted on March 11, 2021.
Background
HHS received approximately $324 billion in COVID-19 relief appropriations from the five COVID-19 relief laws enacted as of January 1, 2021, to assist the response to COVID-19 (see table below).[191]
Appropriations to HHS for COVID-19 Response from the Five COVID-19 Relief Laws Enacted as of January 1, 2021
Legislation
Appropriations ($ millions)
Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 (Pub. L. No. 116-123)
6,497.0
Families First Coronavirus Response Act (Pub. L. No. 116-127)
1,314.0
CARES Act (Pub. L. No. 116-136)
142,833.4
Paycheck Protection Program and Health Care Enhancement Act (Pub. L. No. 116-139)
100,000.0
Consolidated Appropriations Act, 2021 (Pub. L. No. 116-260) a
73,175.0
Total
323,819.4
Source: Department of Health and Human Services (HHS) data. | GAO-21-387
Note: The Department of Health and Human Services (HHS) reported that, of its total appropriations for COVID-19 relief, the agency transferred $289 million to the Department of Homeland Security, and $300 million are not available until HHS has taken certain actions. aThis amount reflects appropriations provided in Divisions M and N of the Consolidated Appropriations Act, 2021 that are specifically designated for COVID-19 relief. An additional $638 million in COVID-19 relief funds were appropriated under Division H to the Administration for Children and Families, an agency within HHS, to prevent, prepare for, and respond to the coronavirus, for necessary expenses for grants to carry out a Low-Income Household Drinking Water and Wastewater Emergency Assistance Program. However, these funds were not included in the HHS-reported data on HHS COVID-19 relief appropriations, obligations, and expenditures, as HHS noted that it is not considered COVID-19 relief funding for USAspending.gov reporting purposes.
Overview of Key Issues
As of February 28, 2021, of the approximately $324 billion in COVID-19 relief funds appropriated, HHS reported that it had obligated about $232 billion and expended about $148 billion—about 72 percent and 46 percent, respectively (see figure below).
HHS’s Reported COVID-19 Relief Appropriations, Obligations, and Expenditures from COVID-19 Relief Laws, as of February 28, 2021
Note: These amounts reflect appropriations provided in Divisions M and N of the Consolidated Appropriations Act, 2021 that are specifically designated for COVID-19 relief.
In the following table, we list HHS appropriations, obligations, and expenditures by HHS agency that HHS reported as of February 28, 2021, from the five COVID-19 relief laws enacted as of January 1, 2021.
Department of Health and Human Services-Reported COVID-19 Relief Appropriations, Obligations, and Expenditures from Five COVID-19 Relief Laws, by Agency or Key Fund, as of February 28, 2021
Agency or key fund
Appropriations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Administration for Children and Families
16,524.0
16,117.5
3,517.7
Administration for Community Living
1,480.0
1,380.0
801.3
Agency for Toxic Substances and Disease Registry
12.5
12.4
4.1
Centers for Disease Control and Prevention (CDC)
15,250.0
7,175.1
1,682.4
Centers for Medicare & Medicaid Servicesa
200.0
119.9
35.1
Food and Drug Administration (FDA)
196.0
45.5
20.8
Health Resources and Services Administration (HSRA)
1,320.0
1,319.4
998.3
Indian Health Service (IHS)
1,096.0
779.3
690.7
National Institutes of Health (NIH)
3,031.4
981.7
335.5
Public Health and Social Services Emergency Fund (PHSSEF)b
280,034.5
203,086.0
139,564.6
Office of the Assistant Secretary for Preparedness and Responsec
15,695.1
10,507.8
6,436.4
Biomedical Advanced Research and Development Authority c
37,470.4
24,131.8
4,242.0
Provider Relief Fundc
178,000.0
128,601.4
120,151.7
Testing for uninsuredc
2,000.0
1,968.8
1,967.2
CDC c
1,000.0
393.2
181.4
FDAc
22.0
0.4
0.3
HRSAc
979.8
971.4
617.4
IHSc
790.0
18.7
0.0
NIHc
1,806.0
1,011.6
351.0
Office of Inspector Generalc
12.0
2.7
2.4
Other PHSSEFc
42,259.2
35,478.2
5,614.8
Substance Abuse and Mental Health Services Administration
4,675.0
1,109.0
85.6
Grand Total
323,819.4
232,125.8
147,736.1
Source: Department of Health and Human Service (HHS) data. | GAO-21-387
Note: HHS reported that of the total COVID-19 relief appropriations the agency transferred $289 million to the Department of Homeland Security, and that $300 million in appropriations are not available until HHS takes certain actions. HHS’s reported appropriations specifically designated for COVID-19 relief in the Consolidated Appropriations Act, 2021 (Pub. L. No. 116-260) reflect only appropriations provided under Divisions M and N. aThese amounts do not reflect Medicaid and Medicare expenditures. As of February 28, 2021, COVID-19-related federal Medicaid expenditures totaled approximately $33 billion, or 7 percent of total federal spending on Medicaid services for January 2020 through February 2021. In addition, the Congressional Budget Office estimated that some provisions of COVID-19 relief laws would affect Medicare payments. For example, the Congressional Budget Office estimated that provisions in Division N of the Consolidated Appropriations Act, 2021 will increase Medicare payments to providers by about $6 billion in 2021 through 2022. bPHSSEF is an account though which funding is provided to certain HHS offices, such as the Office of the Assistant Secretary for Preparedness and Response. Amounts have been appropriated to this fund for the COVID-19 response to support certain HHS agencies and response activities. For example, NIH received about $1.8 billion in transfers from the PHSSEF, and this amount is not included in the approximately $3 billion appropriated directly to NIH. cThe italicized amounts are subtotals of the PHSSEF and are already reflected in the total 280,034.5 billion listed for the PHSSEF. Italicized amounts listed under the PHSSEF appropriations column are HHS allocations based on appropriations made in the COVID-19 relief laws, and approved allotment decisions made by HHS in coordination with the Office of Management and Budget. Some amounts were appropriated to the PHSSEF for transfer to specified HHS agencies. The Provider Relief Fund reimburses eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19. Provider Relief Fund expenditures also may be referred to as disbursements.
HHS reported allocations, obligations, and expenditures of appropriations from the five COVID-19 relief laws for a variety of COVID-19 response activities, including activities to support testing, the development of vaccines or therapeutics, and the acquisition of critical supplies. Across these activities, the percentage of allocated funds that had been expended as of February 28, 2021, ranged from about 98 percent for testing for the uninsured to about 9 percent for support to state, local, territorial, and tribal organizations, which includes, in part, recent allocations from the fifth COVID-19 relief law, enacted on December 27, 2020.
The following table provides HHS’s reported allocations, obligations, and expenditures by selected key response activity.
Department of Health and Human Services-Reported Allocations, Obligations, and Expenditures of COVID-19 Relief Funds from five COVID-19 Relief Laws, by Selected Key Response Activity, as of February 28, 2021
Key response activity
Allocations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Health centersa
2,020.0
2,018.1
1,439.7
Head Start
1,000.0
744.5
352.6
Provider Relief Fundb
178,000.0
128,601.4
120,151.7
Testing for uninsured
2,000.0
1,968.8
1,967.2
Support to state, local, territorial, and tribal organizations for preparedness
37,392.1
35,529.5
3,442.3
Strategic National Stockpile
13,919.9
8,986.4
5,232.2
Telehealth
167.5
48.2
16.2
Testing
12,084.0
5,396.5
3,095.1
Vaccines
23,410.1
16,973.2
2,932.3
Drugs and therapeutics
7,628.4
7,014.2
1,246.0
Diagnostics research and development
3,100.6
1,569.9
474.2
Global disease detection and emergency response
800.0
306.3
84.3
Other response activitiesc
42,296.8
22,968.8
7,302.3
Total
323,819.4
232,125.8
147,736.1
Source: Department of Health and Human Services (HHS) data. | GAO-21-387
Notes: The selected response activities represent examples of certain targeted activities that fall within particular HHS agencies, such as funding for health centers or Head Start, as well as broader categories of response activities that may span HHS agencies, such as testing-, vaccine-, and therapeutics-related response activities. HHS reported allocations, obligations, and expenditures for these activities based on the primary programmatic recipient organization of the funds, although some activities apply to multiple categories. For example, certain funds in the “support to state, local, territorial, and tribal organizations for preparedness” category were provided for testing but are not reflected in the “testing” category. According to HHS officials, the allocations reported for the key activities above are based on amounts appropriated for these activities in the COVID-19 relief laws, and on approved allotment decisions made by HHS in coordination with the Office of Management and Budget. With respect to the Consolidated Appropriations Act, 2021, the amounts reflect only appropriations specifically designated for COVID-19 in Divisions M and N of the act. aHealth centers provide a comprehensive set of primary and preventative health care services to individuals regardless of their ability to pay. Approximately $17 million of this funding is for Health Center Program look-alikes, which are centers that do not receive Health Center Program funding but meet program requirements. bThe Provider Relief Fund reimburses eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19. Provider Relief Fund expenditures may also be referred to as disbursements. cAccording to HHS, other response activities include Centers for Disease Control and Prevention agency-wide activities and program support; health care preparedness and response activities; and certain activities conducted by the National Institutes of Health, among other activities.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS and OMB provided technical comments on this enclosure, which we incorporated as appropriate.
Methodology
We requested, and HHS provided, data on appropriations, allocations, obligations, and expenditures of COVID-19 relief funds by HHS agency and by key response activity, as of February 28, 2021. We also reviewed appropriation warrant information provided by the Department of the Treasury as of January 31, 2021. To assess the reliability of the data reported by HHS, we reviewed HHS documentation, Treasury appropriation warrant information, and information from the federal spending database, USAspending.gov, as well as HHS’s spending database, taggs.hhs.gov, and we determined that the HHS reported data were sufficiently reliable for the purposes of our reporting objective.[192] We also reviewed the five COVID-19 relief laws enacted as of January 1, 2021, to assist the response to COVID-19.
Contact information: Carolyn L. Yocom, (202) 512-7114, yocomc@gao.gov
Multiple federal agencies have efforts to enhance domestic manufacturing of medical products in response to the COVID-19 pandemic, and the federal government has recently initiated key steps to coordinate these efforts.
Entities involved: Department of Commerce, including the Bureau of Industry and Security and National Institute of Standards and Technology; Department of Defense; Department of Health and Human Services, including the Food and Drug Administration and the Office of the Assistant Secretary for Preparedness and Response; Department of Homeland Security, including the Federal Emergency Management Agency; Office of Management and Budget; U.S. International Development Finance Corporation
Key Considerations and Future GAO Work
The COVID-19 pandemic has highlighted the need to ensure a resilient U.S. supply chain for all medical products—drugs, biologics, and medical devices. One strategy to do so is to manufacture more medical products in the U.S. Enhancing domestic manufacturing of medical products is complex though, involving many different types of supplies and coordination of multiple federal agencies and the private sector.
In January 2021, we reported that the federal government had taken steps intended to create resilient domestic drug supply chains. However, we found that federal agencies did not have complete and accessible information to identify drug supply chain vulnerabilities or the manufacturing sources of drugs and their components. We recommended that the Food and Drug Administration (FDA) should obtain such information, including by working with manufacturers and other federal agencies and, if needed, seek authority to do so. FDA said that it would consider our recommendation as it continues efforts to enhance relevant authorities and close data gaps.
The federal government instituted many efforts to expand domestic production to respond to the COVID-19 pandemic. However, the dynamic environment and the shifting of responsibilities, raises questions about the federal government’s longer term plan for coordination and leadership.
The new administration took initial actions beginning in January 2021 to coordinate federal efforts to enhance domestic manufacturing, including directing federal agencies to develop a strategy for a resilient medical product supply chain by July 2021. We will continue to monitor these and other efforts to create a more resilient supply chain.
Background
The manufacturing of medical products has become an increasingly global enterprise over the past 30 years due in part to lower costs and fewer environmental regulations associated with overseas production, and other incentives. In particular, manufacturers of certain medical products, such as personal protective equipment (PPE) and generic drugs, have derived significant cost savings by manufacturing their products outside the U.S, which may also benefit consumers through lower prices for products.[193]
The COVID-19 pandemic has further increased interest in enhancing domestic manufacturing, also known as industrial base expansion, as demand and supply chain disruptions severely affected the availability of certain medical products, particularly PPE, that were coming from overseas. By increasing the availability of medical products manufactured in the U.S., the federal government hopes to strengthen national security by decreasing U.S. dependence on foreign sources, to respond more quickly and efficiently during current and future emergencies, and ultimately enhance the resiliency of the U.S. medical product supply chain.
However, the federal government faces many challenges with enhancing domestic manufacturing capacity. For example:
Industry associations have indicated that stringent environmental regulations, the cost and time needed to build facilities, and acquiring knowledgeable staff may serve as challenges to medical product manufacturing in the U.S.
Although federal purchasers are generally required to prioritize domestically manufactured products, federal purchasing alone is not a sufficient incentive for manufacturers to increase domestic production. Federal purchasers, such as the Department of Defense (DOD) and Department of Veterans Affairs (VA), make up about five percent of the U.S. commercial market, according to officials from DOD and the Office of the Assistant Secretary of Preparedness and Response (ASPR), within the Department of Health and Human Services (HHS).
Overview of Key Issues
Federal efforts to expand domestic production of medical products have increased in response to the COVID-19 pandemic. Multiple federal agencies have efforts, which include funding domestic manufacturing capacity, procuring domestically manufactured medical products, and promoting advanced manufacturing technology.
Funding domestic manufacturing capacity. The federal government has utilized CARES Act funding and Defense Production Act (DPA) authorities to directly fund manufacturers to increase production of PPE, drugs, and other medical supplies during the COVID-19 pandemic.[194] For example:
DOD and HHS awarded about $2.3 billion to domestic manufacturers to increase production of medical products, including PPE, drugs, and vaccine, ventilator, and testing materials, as of February 2021. (See the Defense Production Act enclosure for more detailed information about these awards.)
The U.S. International Development Finance Corporation, under DPA authority delegated to it, announced that it would award loans to U.S. private sector projects that supply resources or strengthen relevant supply chains needed to respond to the COVID-19 pandemic.[195] In November 2020, for example, this agency conditionally approved a $590 million loan to ApiJect to help build out infrastructure in North Carolina to package drugs and vaccines.
ASPR, through the Biomedical Advanced Research and Development Authority (BARDA), also made several awards to increase domestic production of medical products, including a May 2020 contract to Phlow Corporation for up to $812 million to manufacture drug ingredients needed during the COVID-19 response and future public health emergencies.
Federal procurement of domestically produced medical supplies. Recent Executive Orders, which are interrelated with existing federal acquisition requirements that preference U.S. made products, have further directed federal agencies to maximize the purchase of domestically manufactured goods.[196]
In August 2020, the Executive Order on Combating Public Health Emergencies and Strengthening National Security by Ensuring Essential Medicines, Medical Countermeasures, and Critical Inputs Are Made in the United States directed federal agencies to develop procurement strategies to purchase domestically sourced medical supplies and drugs.[197] This Order encourages agencies to take advantage of existing procurement authorities to limit competition, when permitted, to maximize the procurement of essential medicines, medical countermeasures, and critical inputs produced in the U.S.[198]
In January 2021, the Executive Order on Ensuring the Future Is Made in All of America by All of America’s Workers directed the federal government to consider amendments to the Federal Acquisition Regulation that would, among other things, increase the numerical threshold for domestic content requirements, under the implementation of the Buy American Act.[199] It also directed federal agencies to report on implementation of and compliance with domestic preference laws governing federal procurement, including the Buy American Act, and make recommendations on maximizing the use of products made in the U.S.
Federal agencies’ promotion of advanced manufacturing in the U.S. Several federal agencies have longstanding programs to promote technological advances in the domestic manufacturing of drugs and medical countermeasures, including PPE. In some cases, these programs have also assisted in the COVID-19 response.
In 2012, HHS established the Centers for Innovation in Advanced Development and Manufacturing to develop and manufacture medical countermeasures in the U.S.[200] In January 2021, one of these centers announced that production had begun for two separate COVID-19 vaccine candidates in Texas.[201]
Established in 2014, Manufacturing USA is a network of manufacturing institutes working with participating federal agencies, including the Department of Commerce (Commerce), DOD, and the Department of Energy. According to Commerce officials, each institute is a unique public-private partnership jointly funded by government and private industry that promotes U.S. advanced manufacturing through collaboration with private industry and academia. For example, in May 2020, Commerce awarded $8.9 million to the National Institute for Innovation in Manufacturing Biopharmaceuticals to, in part, identify reliable domestic supply chains for the production of respirators and PPE, and build flexible manufacturing capabilities that allow for the quick scale-up in production of biologic therapies and essential medical products.
Additionally, America Makes, which is a DOD-sponsored Manufacturing USA institute, partnered with FDA, VA, and the National Institutes of Health (NIH) to create an online forum of manufacturers with 3D printing capabilities, designers willing to share 3D print designs, and health care providers in need of PPE, according to the National Institute of Standards and Technology (NIST), within Commerce. NIST officials explained that VA helps to test the designs, which then may be reviewed by FDA. According to NIST, the manufacturing community used validated models posted on the NIH 3D Print Exchange, with an estimated production of millions of facemasks, face shields, and parts aligned to the needs of the supply chain crises.
Also established in 2014, FDA’s Emerging Technology Program seeks to promote innovation in drug manufacturing, such as through advanced manufacturing and continuous manufacturing. In January 2021, FDA and NIST signed a memorandum of understanding to collaborate on increasing resilience in the U.S. medical supply chain and advancing domestic manufacturing of drugs and medical devices.
Recent federal actions aim to increase coordination of efforts to enhance domestic medical product manufacturing. In response to the COVID-19 pandemic, multiple federal actions were initiated to coordinate efforts to enhance domestic medical product manufacturing. (See figure below.)
Selected Federal Entities Involved in the Coordination of Domestic Manufacturing Capacity Efforts in Response to the COVID-19 Pandemic
In March 2020, HHS established the Supply Chain Task Force, later renamed the Supply Chain Advisory Group, which includes detailees from the Federal Emergency Management Agency (FEMA) and DOD, according to Supply Chain Advisory Group officials.[202] The Advisory Group was established to maximize the nationwide availability of supplies needed for the COVID-19 response. Supply Chain Advisory Group officials said the Advisory Group assists ASPR with identifying targets for domestic production capacity for various medical supplies. Since the Supply Chain Advisory Group does not have procurement authority, the Defense Assisted Acquisition Cell, within DOD, awards funding to domestic manufacturers to increase their production capacity, according to FEMA and ASPR officials.[203] The Supply Chain Advisory Group transitioned its responsibilities, including those related to enhancing domestic manufacturing, to ASPR in late January 2021, according to ASPR and DOD officials. Supply Chain Advisory Group officials said that they are continuing to assist ASPR with these responsibilities and anticipate doing so through mid-March 2021.
In our September 2020 CARES Act report, we noted that DOD planned to transition their contract management responsibilities, including awarding domestic production expansion projects, to ASPR, within HHS, that month. In this report, we recommended that HHS, in coordination with FEMA, should immediately document roles and responsibilities for supply chain management functions transitioning to HHS. HHS disagreed, noting, among other things, the work that the departments had done to manage the medical supply chain and increase supply availability. We maintain the importance of this recommendation.
Separately, beginning in June 2020, ASPR led another work group, which was focused on modernizing the Strategic National Stockpile (SNS) and addressing supply chain vulnerabilities for critical drugs and medical supplies, called the Logistics, Supply Chain, Next Generation SNS Workgroup. This workgroup ended in September 2020, but ASPR’s work to expand domestic manufacturing work stream continued, according to ASPR officials. (See our Strategic National Stockpile and Medical Supply Chain enclosure for more details about the SNS).
In Fall 2020 ASPR drafted a national supply chain strategy that includes the goal of increasing domestic manufacturing capabilities of medical countermeasures and PPE, referred to as the “SNS 2.0 Strategy – Modernize the SNS.” ASPR officials acknowledged that some aspects of the strategy are beyond its mission and that the agency would need to involve other HHS components to implement it fully. Due to the change in administration in 2021, issuance of the SNS 2.0 Strategy had been paused, according to officials, who noted that any ASPR strategy or other coordination efforts will align with the priorities outlined by the new administration.
In December 2020, the Supply Chain and Industrial Base Assurance Steering Committee formed to continue ASPR’s work to expand domestic manufacturing. In particular, the Steering Committee will establish ASPR’s long-term strategy for a resilient supply chain for medical countermeasures, including by promoting domestic manufacturing. Additionally, ASPR plans to combine these responsibilities with those that were transferred from the Supply Chain Advisory Group. According to ASPR officials, ASPR also created an office focused on industrial base expansion in January 2021.
In September 2020, a White House task force on medical onshoring, which was led by the Office of Trade and Manufacturing Policy, started to coordinate the federal government approach to enhance domestic manufacturing, according to ASPR officials. The task force focused on implementation of the provisions of the Executive Order on Combating Public Health Emergencies and Strengthening National Security by Ensuring Essential Medicines, Medical Countermeasures, and Critical Inputs Are Made in the U.S. across the federal government, which included directing federal agencies to develop procurement strategies to increase U.S. manufacturing of medical supplies, among other things. Officials said that the efforts included the key federal agencies mentioned in the Executive Order, including FDA, DOD, and Commerce, but were unable to provide us with any additional details about the task force’s activities. According to ASPR officials, this task force was disbanded in November 2020 due to the change in administration.
Federal Coordination of Advanced Manufacturing
Federal coordination of advanced manufacturing was occurring prior to the COVID-19 pandemic. The America COMPETES Reauthorization Act of 2010, as amended, mandates the coordination of federal programs and activities that focus on advanced manufacturing programs, including those that pertain to enhancing domestic manufacturing. Specifically, the Committee on Technology under the National Science and Technology Council within the Executive Office of the President is responsible for planning and coordinating efforts to expand advanced manufacturing in the U.S., including for medical products. Members of the Council include the Department of Health and Human Services, the Department of Defense, and the Department of Commerce, among others. In 2018, the Council released a strategic plan, which included an objective to assure access to medical products through domestic manufacturing as part of its efforts to advance the technologies around medical product manufacturing.
Source: GAO analysis of 2018 report by the National Science and Technology Council and Pub. L. No. 111-358, 124 Stat. 3982 (2011) (codified in pertinent part, as amended, at 42 U.S.C. § 6622).| GAO-21-387
The new administration proposed additional actions to coordinate domestic manufacturing efforts for both the COVID-19 pandemic response and the longer term that may enhance federal coordination efforts beginning in late January 2021. Specifically, the White House
created the position of COVID-19 Response Supply Coordinator who is tasked with coordinating federal agencies involved in acquisition, supply, and expansion of domestic manufacturing to ensure a sustainable pandemic supply chain.
issued an Executive Order on A Sustainable Public Health Supply Chain directing federal agencies to present to the President a Pandemic Supply Chain Resilience Strategy.[204] The Order directs DOD, HHS, and the Department of Homeland Security (DHS), among others, to develop a strategy to design, build, and sustain a long-term capability in the U.S. to manufacture supplies for future pandemics and biological threats. According to ASPR officials, they have begun to coordinate with HHS, DOD, and DHS to develop the strategy. The strategy is to be completed by July 2021.
issued an Executive Order on America’s Supply Chains directing specified federal agencies to complete reports, including: (1) by June 2021, a review of supply chain risks and policy recommendations addressing them, including for HHS to report on the risks for drugs and active pharmaceutical ingredients; and (2) by February 2022, a report on the specified aspects of the supply chain, including for HHS to report on the supply chains for the public health and biological preparedness industrial base, such as by identifying the manufacturing or other capabilities needed to produce critical medical products, and assessing U.S. manufacturing capacity and gaps in domestic manufacturing capabilities.[205] These reports are to complement the ongoing work occurring for the A Sustainable Public Health Supply Chain Executive Order. The Assistant to the President for National Security Affairs and the Assistant to the President for Economic Policy are to coordinate the various federal agencies’ response to this Executive Order.
issued an Executive Order on Ensuring the Future Is Made in All of America by All of America’s Workers, which established the Made in America Office within the Office of Management and Budget (OMB) to further the Administration’s policy to use federal awards and procurements to maximize domestic manufacturing.[206] OMB officials indicated that efforts to implement the Executive Order are underway, but the Made in America Director had not yet been appointed as of February 2021. The office will assist the Director of OMB in reviewing and approving the waivers that federal agencies use to purchase products based on exemptions from federal acquisition regulations establishing a preference for domestic purchasing, including the Buy American Act provisions.
Enhancing domestic manufacturing is a complex endeavor involving multiple federal agencies and efforts. Since the COVID-19 pandemic, the number of actions to enhance domestic manufacturing has increased and some agency officials were unclear what entity, if any, was coordinating these efforts. In situations such as these, our key practices for interagency coordination, such as clarifying leadership roles and responsibilities and outlining how leadership will be sustained over the long term, may help ensure effective implementation and reduce the potential for duplication, overlap, and fragmentation. Several of the recent initial actions federal agencies are taking have the potential to enhance coordination and align with our best practices, but these efforts are all still in the early stages of development and we will continue to monitor them in our future work.
Agency Comments
We provided a draft of this enclosure to HHS, DOD, DHS, Commerce, and OMB; none of the agencies provided comments on this enclosure.
Methodology
To identify federal efforts to enhance domestic manufacturing of medical products and the coordination of such efforts, we reviewed federal agency documents and plans. We also received written responses and interviewed officials from ASPR, Commerce (Bureau of Industry and Security and NIST), DOD, FEMA, FDA, OMB, and the U.S. International Development Finance Corporation about their coordination of domestic manufacturing efforts in response to the COVID-19 pandemic and for advanced manufacturing.
During the COVID-19 pandemic, the Food and Drug Administration issued emergency use authorizations to temporarily increase supply of certain medical devices, such as personal protective equipment. Stakeholders—e.g., manufacturers and users of products with emergency use authorization—have raised concerns about inconsistent guidance from agencies that outline permissible use of these devices, and the timeline and process for transitioning away from such devices as the pandemic ends.
Entities involved: Centers for Disease Control and Prevention and Food and Drug Administration, within the Department of Health and Human Services; Occupational Safety and Health Administration, within the Department of Labor
Recommendations for Executive Action
The Secretary of Health and Human Services should ensure that the Food and Drug Administration and the Centers for Disease Control and Prevention work with the Assistant Secretary of Labor for Occupational Safety and Health to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with emergency use authorization. The Department of Health and Human Services concurred with this recommendation.
The Assistant Secretary of Labor for Occupational Safety and Health should work with the Food and Drug Administration and the Centers for Disease Control and Prevention to develop a process for sharing information to facilitate decision-making and guidance consistency related to devices with emergency use authorization. The Department of Labor concurred with this recommendation.
As the Food and Drug Administration develops a transition plan for devices with emergency use authorizations, the Commissioner should specify a reasonable timeline and process for transitioning authorized devices to clearance, approval, or appropriate disposition that takes into account input from stakeholders. The Department of Health and Human Services concurred with this recommendation.
Key Considerations and Future GAO Work
Emergency use authorizations (EUA) allow for the temporary use of unapproved medical products when the Secretary of Health and Human Services declares circumstances exist to justify their emergency use.[207] These authorized medical products have been instrumental in increasing needed supply of certain devices—such as personal protective equipment (PPE)—during the COVID-19 pandemic response, according to Food and Drug Administration (FDA) officials and stakeholder associations we interviewed. However, we identified instances of inconsistencies between device use permitted by certain FDA EUAs and device guidance from the Centers for Disease Control and Prevention (CDC) and the Occupational Safety and Health Administration (OSHA). Such inconsistencies led to confusion and hesitancy among providers about using devices with EUAs, according to provider association officials, and may have undermined the use of these critical medical products early in the pandemic. Developing an interagency process for sharing information would help to facilitate decision-making and guidance consistency.
Officials representing health care providers, device manufacturers, and distributors also raised a number of concerns about what will happen to authorized devices after the declarations permitting their use for COVID-19 end. A plan for devices with EUAs that specifies a reasonable timeline and process for transitioning away from their use, taking into account stakeholder concerns, will help ensure a smooth transition.
In November 2020, we reported on FDA’s use of EUAs for other types of products for COVID-19—specifically, EUAs for therapeutics to treat COVID-19 and vaccines to prevent the disease. We recommended that FDA increase the transparency of its decisions related to EUAs for these products. Since our report, FDA has taken action to address our recommendation and we consider the recommendation closed.
We have additional ongoing work examining EUAs for COVID-19 diagnostic and antibody tests. Therefore, this enclosure focuses on medical devices other than tests, including PPE, decontamination systems, ventilators, infusion pumps, respiratory assistance devices, and remote patient monitoring devices, among others.
Background
Medical devices used for COVID-19. Medical devices, such as PPE and ventilators, may be necessary to provide medical care to patients during a pandemic such as COVID-19. See figure below for examples of certain devices used during the COVID-19 pandemic.
Examples of Medical Devices Used for COVID-19
Note: Tests are also devices used for detecting and diagnosing COVID-19; however, tests are outside the scope of this review.
Device marketing and EUA process. Generally, before a medical device can be marketed in the U.S., it must be approved or cleared by FDA.[208] While the amount of evidence required to meet the applicable FDA standard varies by the level of risk the device poses to patients or users, high-risk devices generally require FDA premarket review and approval to determine whether the device meets the statutory standard of reasonable assurance of safety and effectiveness for its intended use. Moderate-risk and some lower-risk devices may require premarket notification—also known as 510(k) clearance.[209]
The Secretary of Health and Human Services may declare that circumstances, prescribed by statute, exist justifying the authorization of emergency use of certain medical products, including devices.[210] For COVID-19, the Secretary issued three declarations in February and March 2020 permitting FDA to authorize the emergency use of different medical devices.[211] Once an EUA declaration has been made, FDA may temporarily authorize the emergency use of unapproved medical products or unapproved uses of approved medical products through EUAs, provided certain statutory criteria are met.[212] Prior to the COVID-19 pandemic, FDA had issued EUAs for certain respirators during the H1N1 pandemic.
Reissuing and revoking EUAs. FDA is required to periodically review the circumstances and appropriateness of EUAs it has issued.[213] FDA may revise an EUA—e.g., by reissuing the EUA with changes—or revoke an EUA if the circumstances that led to the EUA declaration no longer exist, the criteria for issuance are no longer met, or reissuance or revocation is appropriate to protect public health or safety. For example, FDA may reissue an EUA if there is a material change in the risk-benefit assessment based on evolving understanding of the disease or condition or availability of authorized devices. In general, an EUA will remain in effect for the duration of the EUA declaration unless revoked at an earlier date.
EUA declarations advanced notice. The Secretary of Health and Human Services is required to provide advance notice that EUA declarations will be terminated and must consult with the manufacturers of any authorized products regarding appropriate disposition of the products if authorizations cease to be effective due to termination of the declarations.[214]
Other agencies also responsible for ensuring safe and effective use of certain devices, such as PPE. CDC’s National Institute for Occupational Safety and Health (NIOSH) studies and makes recommendations focused on worker safety and health. As part of this effort, the agency provides a testing, approval, and certification program, assuring respirators used in the workplace meet certain standards. For example, NIOSH-approved “N95” respirators are proven to filter at least 95 percent of airborne particles.[215] In response to the COVID-19 pandemic, CDC released crisis capacity strategies with recommendations for optimizing supplies of PPE, such as limited re-use of respirators or use of non-NIOSH approved respirators when alternatives are not available.
The Department of Labor’s (DOL) OSHA helps ensure safe and healthy conditions for workers by setting mandatory workplace safety and health standards and conducting inspections to enforce those standards.[216] One such standard requires that employers provide respirators to employees exposed to certain respiratory hazards, and take steps to ensure their proper use, including by using NIOSH approved respirators. In response to the COVID-19 pandemic, OSHA has issued industry-specific voluntary guidance for employers on COVID-19-related precautions, as well as other actions.
Overview of Key Issues
EUAs issued, reissued, and revoked for medical devices during COVID-19. FDA has issued 55 EUAs for medical devices since March 2020, as of March 10, 2021. These include 46 EUAs for individual devices as well as nine umbrella EUAs—a new EUA approach FDA developed for COVID-19 that authorizes certain classes of devices for emergency use rather than individual models.[217] As part of FDA’s periodic reviews of EUAs, the agency has reissued 16 of these 55 EUAs issued since March 2020 and revoked three of them.
EUAs for individual devices. As of March 10, 2021 FDA has issued 46 EUAs for COVID-19 for individual devices, each covering a specific product. It has revoked one EUA for these devices and reissued 12 of them. See table for the number of EUAs issued and reissued by individual medical device type.
Number of Emergency Use Authorizations (EUA) Issued and Reissued for Individual Devices by Device Category for COVID-19, as of March 10, 2021
Device category
Number of EUAs
Number of EUAs reissueda
Number of EUAs revoked
Personal protective equipment (PPE)
6
1
0
Decontamination systems for PPE
15
10
1
Remote patient monitoringb
5
0
0
Respiratory assistance
5
0
0
Blood purification
4
0
0
Continuous renal replacement therapy and hemodialysis
3
0
0
Infusion pumps
1
0
0
Other devicesc
7
1
0
Total
46
12
1
Source: GAO analysis of data from the Food and Drug Administration’s (FDA) website and information obtained from agency officials. | GAO-21-387
Note: We reviewed documentation made publicly available by FDA, including authorization and reissuance letters and information on FDA’s website, to determine the information in this table. aSome EUAs were reissued multiple times while others were reissued once. The count in this column reflects the number of EUAs FDA reissued at least once. bFDA’s website lists six EUAs under this category. However, one Patient Isolation Treatment Unit EUA is identical to an EUA found under the PPE category. To avoid duplication, this EUA is only counted once under the PPE category due to its primary use as a protective barrier. cOther medical devices consist of devices that provide life support to severely ill patients through external oxygenation (e.g., artificial lung and heart devices), conduct predictive screening for providers to anticipate which patients in intensive care units will be likely to experience low blood pressure or breathing difficulty, assist patients’ heart function through ventricular support systems, and help reduce COVID-19 transmission (e.g., non-surgical face masks).
Our review of FDA’s EUA documentation indicates that the majority of reissued individual EUAs were for decontamination units. This was primarily due to new information FDA received regarding respirators rather than due to issues surrounding the decontamination units themselves, according to FDA documentation. Specifically, FDA reissued certain decontamination unit EUAs to identify the types of respirators these units can decontaminate and to reduce the number of times a respirator could be decontaminated, among other things.
Umbrella EUAs. Since March 2020, FDA has issued nine umbrella EUAs for PPE and other medical devices.[218] FDA first used umbrella EUAs during the COVID-19 pandemic, allowing the agency to authorize certain types of devices rather than individual products, according to FDA officials. These nine umbrella EUAs covered at least 534 device models across at least 299 different manufacturers as of March 10, 2021, demonstrating how one umbrella EUA can expand access to many devices (see table). FDA has reissued four of these umbrella EUAs at least once and revoked two since March 2020.
Umbrella Emergency Use Authorizations (EUA), Reissuances, Revocations, and Number of Authorized Manufacturers and Device Models for COVID-19, as of March 10, 2021
Device category for EUA
Number of authorizedmanufacturers per each umbrella EUA
Number of authorized models per each umbrella EUA
Number of times EUA reissued
EUA revocations
Non-NIOSH approved KN95 respirators, manufactured in China
167
256
3
0
Non-NIOSH approved N95 respirators, manufactured outside of China
35
81
2
0
Surgical masks
17
34
0
0
Ventilators and ventilator accessories
84
163
0
0
NIOSH approved N95 respiratorsa
Not available
Not available
2
0
Surgical gowns and other apparela
Not available
Not available
0
0
Face shieldsa
Not available
Not available
1
0
Infusion pumpsb
0
0
0
1
Protective barrier enclosuresa
Not Available
Not Available
0
1
All devicesc
299
534
8
2
Source: GAO analysis of data from the Food and Drug Administration’s (FDA) website and information obtained from agency officials. | GAO-21-387
Note: We reviewed documentation made publicly available by FDA, including authorization, reissuance, and revocation letters and information on FDA’s website. Each row in the table represents a single umbrella EUA. aFDA did not require manufacturers to submit separate requests for models under these umbrella EUAs. Therefore, we cannot determine the total number of authorized manufacturers and models. bFDA authorized no manufacturers or infusion pump models prior to the EUA revocation. cNumbers per EUA device category may not add up to the “all devices” total, as some manufacturers were authorized to produce devices for several EUAs and would not have been counted more than once.
According to FDA, the agency revoked two umbrella EUAs—one for infusion pumps and one for protective barrier enclosures—determining, among other things, that individualized consideration of each EUA request for these devices would better protect the public health. In the case of the umbrella EUA for infusion pumps, FDA authorized no manufacturers or infusion pump models prior to the EUA revocation. FDA officials said they have learned several lessons about the umbrella EUA process during the pandemic, which have included gaining a better understanding of what device types are suited for umbrella EUAs.
FDA reissued four umbrella EUAs at least once, three of which were umbrella EUAs for filtering facepiece respirators (respirators):
The umbrella EUA for NIOSH approved respirators was reissued to expand the scope of authorization beyond filtering facepiece respirators to include other types of respirators, as well as to include respirators that undergo decontamination with an FDA authorized decontamination system.
The umbrella EUA for non-NIOSH approved KN95 respirators manufactured in China was reissued three times between April and October 2020 due to safety concerns, among other reasons. According to FDA documents, FDA limited the scope of authorization for these devices at several points in time based on new data that these respirators were not meeting FDA standards. The final reissuance in October 2020 was due to decreased demand in KN95 respirators within health care settings, resulting in FDA’s decision not to review any additional EUA requests for this type of device.
The umbrella EUA for non-NIOSH approved N95 respirators manufactured outside of China was reissued twice to improve availability, as well as to address safety concerns. For example, one reissuance allowed for the reuse of these respirators once decontaminated with an authorized decontamination unit, according to FDA documents.
Benefits of EUAs for devices during COVID-19. FDA officials and most stakeholder associations we interviewed stated that the use of EUAs helped address critical medical device shortages. According to FDA officials, EUAs are one of the key pathways to allow providers to gain access to critical medical devices that have not received premarket approval or 510(k) clearance.
Officials from some health care provider associations told us that medical device EUAs—in particular, those related to respirators—enabled providers to provide better care for COVID-19 patients and to protect themselves from infection. Association comments included:
Respirator EUAs opened up a new supply that mitigated shortages seen at the beginning of the pandemic, officials from one provider association told us. According to these officials, hospitals would have been unable to respond to the pandemic without such EUAs.
Remote patient monitoring devices authorized under EUAs allowed clinics to monitor patients with chronic diseases who were unable to meet with providers in-person during the pandemic, according to officials at another association.
In addition, officials from a device manufacturer association said that device EUAs enabled the medical technology industry to mobilize quickly to support health care providers and their patients. For example, FDA authorized the use of a decontamination system that could result in 750,000 masks per day being decontaminated for re-use, if fully utilized, according to these officials.
Coordination across FDA, CDC, and OSHA during current and future pandemics. FDA, CDC, and OSHA each have a role in ensuring the proper use of respirators and systems used to decontaminate them. However, we identified some inconsistencies between device use permitted by FDA’s EUAs for respirators and systems for their decontamination, and CDC and OSHA guidance for such devices. For example
FDA issued an EUA on March 2, 2020, to authorize use of NIOSH approved respirators past the manufacturer’s recommended shelf life; however, OSHA did not issue guidance permitting this until roughly a month later.[219] Similarly, FDA reissued the EUA on March 28, 2020, to permit the decontamination and reuse of certain respirators; however, OHSA did not release guidance on this topic until April 24, 2020, nearly a month later.
In October 2020, CDC recommended that respirators be reused no more than five times. However, between March 2020 and January 2021, FDA guidance for certain EUAs for decontamination systems authorized respirator decontamination and reuse up to 10 or 20 times. In January 2021, FDA reissued many decontamination system EUAs to limit the number of cycles to no more than four, consistent with CDC’s recommendations.
FDA and CDC officials explained that guidance inconsistencies for decontamination arose in part due to differing perspectives on the number of times a respirator can safely be reused. For example, while both agencies relied on scientific evidence to support their decisions, FDA’s EUA decisions also took into account the agency’s goal to increase the available supply as much as possible to meet demand. Both agencies said that inconsistencies could be minimized by better information sharing.
According to some association officials we interviewed, the inconsistent guidance caused confusion and hesitancy among providers about how these devices could be used. For example, providers were reluctant to use devices with EUAs out of concern that doing so would conflict with another agency’s standards. This potentially undermined the use of these critical devices in the early stages of the pandemic.
FDA initiated webinars with CDC and OSHA in June 2020 to help address stakeholder questions; however, officials from all three agencies acknowledged the importance of coordination and information sharing to help address conflicts between EUAs and related guidance sooner. Although officials from all three agencies noted that they have good informal relationships, there is no documented process for sharing information.[220] Such a lack of sharing between agencies increases the risk of inconsistent decision-making and guidance related to devices with EUAs during this pandemic or future emergencies. Our key practices for enhancing and sustaining collaboration among federal agencies recommend that agencies should establish compatible policies, procedures, and other means to operate across agency boundaries.
Developing a process for FDA, CDC, and OSHA to share EUA device information to facilitate decision-making and guidance consistency, would help to mitigate confusion and hesitancy among providers about using devices with EUAs. In turn, this would facilitate the realization of a key goal of EUAs—to mitigate device shortages by expanding access to and use of such critical medical supplies.
Transition from use of authorized devices after the relevant EUA declarations have been terminated. Officials from manufacturer and distributor associations we spoke with said that, to ensure a smooth transition after the EUA declarations have been terminated, it will be important for FDA to specify a reasonable timeline and process for transitioning devices authorized for use during the emergency to clearance, approval, or appropriate disposition.[221] Association officials made the following points:
Manufacturers with authorized devices will require time to obtain FDA clearance or approval to continue offering their devices after the EUA declarations end, according to officials from two associations. Depending on the level of risk associated with the devices, manufacturers generally need to obtain 510(k) clearance or premarket approval to continue to market authorized products after EUAs are no longer in effect. However, lengthy delays in FDA’s review of 510(k) submissions and lack of responsiveness about the status of submissions have been reported by medical device manufacturer association officials. FDA officials stated that 510(k) review times were within their goals for devices used in response to the pandemic, but explained that they have received a record number of EUA requests for COVID-19 and non-COVID-19 related 510(k) submissions.
Medical device distributors and manufacturers require a transition period to adjust supply chain purchasing, such as overseas material purchasing, and distribution, according to officials from two associations we interviewed. Distributors would be unlikely to be able to return—or recoup losses associated with—previously authorized devices. Similarly, manufacturers are not sure if they would need to immediately stop making and remove devices with EUAs from the market, or if there were any circumstances in which FDA might permit use of authorized devices after the EUA declarations end, according to association officials representing these stakeholders. Manufacturer association officials said that a member manufacturer did not pursue an EUA for a new device it had developed due to uncertainty about how the device could be used after the EUA declaration ends.
Frontline health care staff lack confidence in using some medical devices with EUAs because such usage is not standard care, and are concerned that employers will continue to use crisis capacity standards after the EUA declarations end, according to some provider associations. FDA, OSHA, and CDC will play a role in ensuring that providers return to conventional standards of care, for example, using only NIOSH approved respirators.
In addition to these association concerns, the Department of Health and Human Services (HHS) purchased for the Strategic National Stockpile certain ventilator models and respirators with EUAs, according to the agency responsible for the federal stockpile. Further, some states have stockpiled devices with EUAs, according to association officials representing states. As stockpiles are designed to provide for the security of the nation during public health emergencies, it is important to know how, and for how long, certain authorized devices may continue to be used after the EUA declarations end.
The ECRI Institute—an organization that conducts independent medical device evaluations—has similarly cautioned providers about the status of authorized products after the EUA declarations end.[222] For example, in an April 2020 alert, the ECRI Institute cautioned that hospitals should seek clarity on the post-EUA declaration status of ventilators before purchasing them, and in a May 2020 alert, it recommended that healthcare facilities consider the financial implications of purchasing devices with EUAs given that an EUA generally remains in effect only during the EUA declaration.[223]
The Secretary of Health and Human Services is required to provide notice prior to the termination of the EUA declarations and consult with manufacturers about proper disposition of authorized devices.[224] In addition, FDA has indicated that it intends to develop draft guidance for a transition plan for medical devices distributed under EUAs for COVID-19 by the end of the fiscal year 2021. FDA officials told us the agency would publish the transition plan as draft guidance to receive feedback from stakeholders and provide sufficient time before the EUA declarations end for stakeholders to provide comments. FDA officials also noted that they intend for the transition plan to describe a timeframe for manufacturers to obtain clearance or approval of their devices before the EUA declarations terminate. Further, FDA officials stated the transition plan will include a policy addressing authorized devices that have a pending premarket review submission but have not yet been approved or cleared by the time the EUA declarations terminate.
However, in light of the ongoing pandemic, as of March 15, 2021, the agency had not released a draft transition plan. As a result, important aspects of the transition plan for devices with EUAs are unknown and remain to be determined, including the timeline and process for transitioning authorized devices to full clearance, approval, or appropriate disposition and the extent to which stakeholder feedback, including from CDC and OSHA, will be incorporated.
Specifying a reasonable timeline and process for transitioning authorized devices to clearance, approval, or appropriate disposition that incorporates stakeholder input, before the EUA declarations end, would be consistent with the PanCAP Adapted. The PanCAP Adapted is the general operative plan for the federal response to COVID-19; it highlights the importance of clear communication during a crisis.[225] Further, it would be consistent with federal standards for control activities, which emphasize that agencies should design and implement policies and procedures to achieve their objectives—in this case, ensuring a smooth transition from use of authorized devices.[226]
Further, taking such action would help to provide a smooth transition for manufacturers, purchasers, and users of devices with EUAs. This is the agency’s opportunity to mitigate concerns about approval or clearance time, use of stockpiled devices with EUAs, and efforts by other federal agencies to return to conventional standards of care, prior to the end of the EUA declarations.
Agency Comments
We provided HHS, DOL, and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided general comments, which are reproduced in Appendix VI: Comments from the Department of Health and Human Services . HHS concurred with both of our recommendations. Regarding our recommendation for FDA and CDC to work with OSHA to develop a process for sharing information related to devices with EUAs, FDA commented that there is an opportunity to build on prior collaboration and lessons learned during the pandemic to assure there is a process in place that yields timely and consistent information for stakeholders using and purchasing authorized devices. Regarding our recommendation for FDA to specify a reasonable timeline and process for transitioning authorized devices that takes into account stakeholder feedback, FDA stated that it believes it is important to provide such a transition period to allow sponsors to meet any additional requirements. In addition, FDA stated it will provide the transition plan in the form of draft guidance for public comment so the agency can work to incorporate suggestions from those impacted by the transition.
DOL also concurred with the recommendation for OSHA to work with FDA and CDC to develop a process for information sharing related to devices with EUAs. HHS and DOL provided technical comments on this enclosure, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed relevant agency documents, including FDA’s guidance for EUAs and transcripts from webinars for medical device EUAs that FDA began hosting in June 2020. For each device EUA, we reviewed publicly available documentation on FDA’s website as of March 10, 2021, including authorization letters for each EUA.[227] We also reviewed relevant CDC and OSHA documents related to safe use of devices during the COVID-19 pandemic. We received written responses to questions from FDA, CDC, and OSHA officials.
We also interviewed or received written responses from 15 stakeholder associations—2 associations representing device manufacturers, 1 association representing device distributors, and 12 associations representing a variety of medical device purchasers, including 3 associations representing state or local public health or emergency management departments, 8 associations representing a variety of provider types, and 1 public health association. We selected these national associations based on their involvement in representing stakeholders that manufacture or purchase devices for use on the front lines of responding to the COVID-19 pandemic.
COVID-19: Federal Efforts Accelerate Vaccine and Therapeutic Development, but More Transparency Needed on Emergency Use Authorizations.GAO-21-207. Washington, D.C.: November 17, 2020.
Managing for Results: Key Considerations for Implementing Interagency Collaborative Mechanisms. GAO-12-1022. Washington, D.C.: September 27, 2012.
Results-Oriented Government: Practices That Can Help Enhance and Sustain Collaboration among Federal Agencies. GAO-06-15. Washington, D.C.: October 21, 2005.
The Department of Health and Human Services has continued collaboration and coordination efforts to mitigate cyber threats against assets and organizations targeted during the federal response to COVID-19. In addition, the department continues to make progress implementing our prior recommendations regarding cybersecurity weaknesses at its component agencies. We encourage the Department of Health and Human Services’ component agencies to implement the remaining open recommendations to bolster its cybersecurity posture.
Entities involved: Department of Health and Human Services; Cybersecurity and Infrastructure Security Agency, within the Department of Homeland Security; and Federal Bureau of Investigation, within the Department of Justice
Key Considerations and Future GAO Work
In our September 2020 report, we recommended that the Department of Health and Human Services (HHS) expedite implementation of our prior 434 recommendations regarding cybersecurity weaknesses at its component agencies. As of February 2021, HHS officials reported actions the department is taking to implement the recommendation, to include leveraging its monthly Chief Information Security Officer Council meetings to discuss recommendations made across the HHS component agencies.
Additionally, HHS’s relevant component agencies—the Food and Drug Administration (FDA), Centers for Medicare & Medicaid Services, and Centers for Disease Control and Prevention—have addressed additional cybersecurity weaknesses since we reported in November 2020.[228] Specifically, the three component agencies implemented an additional 17 of our previous cybersecurity recommendations, bringing the total number of implemented recommendations to 421 of the 434 we made to these agencies.[229] This amount reflects a 4 percent increase in corrective actions these component agencies have taken to bolster their cybersecurity.[230]
In addition to monitoring the department’s efforts to expedite implementation of our prior cybersecurity-related recommendations at its component agencies, we are conducting an ongoing review of HHS’s roles and responsibilities for assisting with cybersecurity in the health care and public health critical infrastructure sector.[231] This review includes an evaluation of the department’s efforts to collaborate and coordinate as part of its response to COVID-19-related cyberattacks.
Background
The federal response to COVID-19 has highlighted the need for additional focus on the security of information systems that are used by health care organizations involved in vaccine and therapeutic development and distribution, and that provide telehealth medical services. The prior administration initiated Operation Warp Speed in May 2020 to accelerate the development, manufacturing, and distribution of COVID-19 vaccines and therapeutics. In addition, health care organizations began offering health care services through telehealth appointments to slow the spread of the virus. All of these efforts rely heavily on the support of information systems.
During the nation’s response to COVID-19, systems operated by the health care and public health sector have been the target of malicious cyber activity. The actors behind this activity were attempting to obtain, among other things, patient information, intellectual property, public health data, and intelligence. Therefore, it is imperative that safeguards are implemented on the systems supporting the health care and public health sector. As the designated sector-specific agency for the health care and public health critical infrastructure sector, HHS is responsible for collaborating with sector partners and coordinating activities to mitigate the harm caused by cyber threats to the sector’s systems.[232]
Overview of Key Issues
In our November 2020 report, we described HHS’s collaboration with health care organizations and coordination with other federal agencies to address cybersecurity concerns associated with COVID-19 in the health care and public health sector between March 2020 and August 2020. Since that time, HHS has continued to collaborate with its sector partners through the various cybersecurity-focused working groups it leads. During the cybersecurity-focused working groups’ meetings, HHS and its partners shared information about efforts managed by Operation Warp Speed and ongoing efforts to secure telehealth medical services, as described here.
During an August 2020 meeting for the Joint Healthcare and Public Health Sector Cyber Working Group, the government and industry participants discussed chief information security officers’ concerns with Operation Warp Speed due to perceived cyber threats to potential COVID-19 therapeutic and vaccine supply chains.[233]
During a September 2020 biweekly meeting, the Government Coordinating Council’s (GCC) Cybersecurity Working Group Telehealth Task Group shared information on challenges to protecting the security and privacy of health information and personal data as telehealth medical services were expanded and information was transferred across networks.[234] The task group highlighted the importance of considering vulnerabilities in the system architecture supporting telehealth medical services as a way to mitigate security and privacy challenges.
During the October 2020 meeting for the GCC Cybersecurity Working Group, HHS’s Office of the Assistant Secretary for Preparedness and Response (ASPR) informed the meeting participants that its Telehealth Task Group would serve as the entity through which federal entities involved in providing telehealth medical services will collaborate to identify, prioritize, and develop resources for federal agencies and their stakeholders to mitigate the major cybersecurity, compliance, and privacy risks.
During a December 2020 meeting with the Joint Healthcare and Public Health Sector Cyber Working Group, the participants (1) discussed cybersecurity concerns related to Operation Warp Speed’s vaccine distribution process; and based on these concerns, (2) planned to document the cybersecurity risks and develop considerations for custodial checklists on cold storage that may help mitigate those risks.
Moreover, officials in HHS’s Office of the Chief Information Officer informed us that the department’s Chief Information Security Officer (CISO) attends weekly meetings with a limited group of key stakeholders to collaborate around the implementation of Operation Warp Speed. According to the officials, these meetings are held in addition to HHS CISO Council meetings and are classified.[235]
HHS has also continued to coordinate with the Cybersecurity and Infrastructure Security Agency (CISA) and Federal Bureau of Investigation (FBI). Specifically, HHS’s ASPR has continued to host weekly meetings with the HHS Health Sector Cybersecurity Coordination Center, CISA, and FBI as part of the Cyber Watch Project.[236] Since August 2020, these federal agencies have coordinated on:
identifying additional entities involved in the development of vaccines and therapeutics that the federal agencies plan to engage with as part of the project;
resolving redundancies in the list of entities covered by Operation Warp Speed and the Cyber Watch Project;
determining how best to accurately advertise cybersecurity webinars and briefings so that they reach the intended audiences;
informing critical entities about recent ransomware attacks that occurred within the health care and public health critical infrastructure sector; and
ensuring that all federal agencies leading cyber engagement activities with the entities involved in vaccine and therapeutic development have the latest information on all those activities.
Agency Comments
We provided HHS and the Office of Management and Budget a draft of this enclosure for review and comment. HHS and the Office of Management and Budget did not provide any comments on this enclosure.
Methodology
To conduct this work, we obtained documentation demonstrating recent efforts of HHS’s cybersecurity-focused working groups to collaborate and coordinate with other entities on cybersecurity issues related to COVID-19. Specific documentation we reviewed included meeting presentations, summaries, and notes describing the information shared and discussed during those working group meetings. In addition, we interviewed officials in HHS’s Office of the Chief Information Officer and ASPR to obtain information and documentation on any new collaboration or coordination efforts to respond to the increased cyberattacks associated with COVID-19. Further, to update the status of the recommendations made to the HHS component agencies, we obtained and assessed evidence to determine whether the agency took appropriate corrective action to resolve the cybersecurity weaknesses identified in our prior reports.
Contact information: Jennifer R. Franks, (404) 679-1831, franksj@gao.gov
Between April and July 2020, the Federal Communications Commission obligated the full $200 million appropriated by the CARES Act to prevent, prepare for, and respond to COVID-19, domestically or internationally, including for telehealth support through 539 awards to 532 health care providers to fund, among other things, telehealth visits and remote patient monitoring during the pandemic. According to Federal Communications Commission officials, as of February 18, 2021, $143.2 million of the $200 million had been disbursed.
Entity involved: Federal Communications Commission
Key Considerations and Future GAO Work
As of February 18, 2021, of the $200 million appropriated by the CARES Act, Federal Communications Commission (FCC) officials told us that $143.2 million had been disbursed to eligible health care providers (providers). FCC officials told us FCC expects the remaining $56.8 million to be disbursed shortly after FCC’s July 31, 2021, invoicing deadline. Additionally, in legislation enacted in December 2020, Congress appropriated approximately $250 million to FCC for the COVID-19 Telehealth Program, which FCC has used to provide additional funding to providers for telecommunications, information services, and connected devices.[237] As of February 2021, FCC officials told us that FCC was continuing to review comments received in the public record related to awarding this additional funding. We will continue to monitor FCC’s efforts to distribute funding appropriated through the COVID relief laws.
Background
Telehealth, or the provision of health care services through a range of telecommunications technologies, has increasingly assumed a critical role in health care delivery throughout the U.S. The ability to diagnose, monitor, and treat patients remotely allows providers to offer critical services to patients in their homes or in other physically distanced locations, which can reduce the spread of communicable diseases such as COVID-19.
Demand for telehealth services dramatically increased because the COVID-19 pandemic limited providers’ ability to treat patients in person.[238] However, providers faced challenges offering telehealth services, including high implementation costs and limited patient access to broadband internet. Such barriers particularly affect the public and nonprofit providers that serve low-income patients.
In March 2020, FCC established the $200 million COVID-19 Telehealth Program in response to the CARES Act to support eligible public and nonprofit providers’ provision of telehealth services by funding eligible telecommunications services, information services, and connected devices on a temporary basis.[239] Examples of eligible services and devices include costs for mobile hot spots, subscription costs for telehealth applications or platforms, and purchase costs for connected monitoring devices such as wifi, Bluetooth, or internet-connected blood pressure monitors.[240]
FCC obligated the $200 million to health care providers on a rolling basis between April 2020 and July 2020. As of February 18, 2021, approximately $143.2 million had been disbursed to awardees. In December 2020, FCC established a July 31, 2021 invoicing deadline for awardees to submit their requests for reimbursement to FCC.
Overview of Key Issues
FCC application and reimbursement processes. FCC required providers seeking CARES Act funding to submit applications that included information such as the medical services to be provided, conditions and types of patients to be treated, and supporting cost documentation. Providers were also required to complete additional steps, including obtaining an eligibility determination and registering with FCC and the System for Award Management.[241] FCC used a review process in which multiple teams at escalating levels of seniority iteratively reviewed applications. FCC officials considered a number of factors when reviewing and approving applications which, according to FCC officials, were consistent with the guidance in the Report and Order establishing the program. For example, FCC gave priority to providers that were located in areas hardest hit by COVID-19, including those that would have the greatest impact based on the amount of funding requested, the number of patients to be served, or whether a provider would serve tribal communities.[242]
Once FCC obligated funding to awardees, they purchased eligible goods and services and submitted requests to FCC for reimbursement, including invoice documentation, using the U.S. Department of the Treasury’s Invoice Processing Platform. FCC officials told us that, as with applications, these requests undergo a multilevel review process to verify that the goods and services purchased are eligible and that the invoice documentation supports the amount being requested for reimbursement.
FCC oversight and performance management. According to FCC officials, the multilevel application and reimbursement process provides FCC with oversight of the program and mitigates identified risks to program integrity. For example, awardees must submit detailed invoices substantiating reimbursement requests, which FCC reviews to ensure compliance with program rules. FCC officials explained that this process guards against the risk of, and helps FCC identify, improper payments. FCC officials told us that as of February 2021, they had identified seven improper payments totaling just under $160,000 through their invoice review processes or notification by awardees, and had recovered about $112,000.[243]
In addition, FCC is leveraging audits conducted under the Single Audit Act to oversee the program.[244] One FCC official told us that FCC estimates that about 66 percent of the funding disbursed through the program is subject to Single Audit Act requirements. As of February 2021, this official said that auditors had completed 22 audits under the Single Audit Act that contained the FCC compliance supplement for the COVID-19 Telehealth Program, and these audits did not contain any findings. FCC officials said that while FCC had not yet conducted any additional compliance audits, FCC continues to monitor the coverage of the Single Audit Act and other factors to determine the need for such audits. Further, FCC stated that all awardees should submit post-program feedback by January 2022 that includes, among other information, a description of the funding outcomes.
Program challenges. FCC officials, selected providers, and telehealth associations we spoke to identified some challenges with the application and reimbursement processes, such as the following:
Information technology system difficulties. FCC, both selected providers, and both telehealth associations we spoke to reported complicated application and reimbursement systems or systems that were not user-friendly or did not always work as planned. To address this challenge, FCC intends to update its application system before accepting applications for the additional funding appropriated in December 2020.[245]
Site-specific eligibility determinations. Both selected providers we spoke to told us that because eligibility is determined on a site-by-site rather than provider basis, it was more difficult for providers with multiple sites to apply for awards and seek reimbursement. FCC also noted that this site-specific requirement delayed its ability to move quickly on many applications. To address this challenge, in January 2021 FCC sought comment on using a different approach to determine whether a site is eligible for future funding.[246]
Lack of in-person assistance or unclear guidance from FCC. One selected provider and both telehealth associations told us that FCC guidance was confusing. For example, one provider said that email assistance from FCC did not help to clarify guidance on eligible goods and services, so the provider did not understand what was and was not eligible until the invoicing process, after completing purchases. As a result, the provider did not expect to receive reimbursement for its full award amount. In January 2021, FCC proposed providing additional outreach and guidance to applicants by, for example, publishing a list of eligible and ineligible equipment and services for future funding.[247]
Additionally, both selected providers and telehealth associations told us that FCC did not cover providers’ costs for support services and non-connected devices required to make eligible goods and services work properly, such as training costs or costs for things like power cords. As a result, according to one association, some providers were deterred from applying to the program, and some that received funding struggled to cover these costs.
Distribution of funding. FCC made 539 awards to 532 health care providers in 49 U.S. states, territories, and the District of Columbia.[248] According to our analysis of FCC data, the number of awardees and amount of funding varied across states (see figure). FCC awarded more than half of the $200 million to health care providers in 10 states: New York, Ohio, California, Pennsylvania, New Jersey, Texas, Florida, Massachusetts, Washington, and Louisiana. The awards generally aligned with FCC’s prioritization of the hardest-hit geographic areas.[249]
Total COVID-19 Telehealth Funding Awarded by the Federal Communications Commission and Number of Awardees, by State
Note: Funds for the awards came from CARES Act, Pub. L. No 116-136, 134 Stat. 281, 531 (2020).
According to our analysis of FCC public notices, most awards included funding to support telemedicine visits and to purchase connected devices, and were targeted toward continued patient care (see table).[250]
Purposes for the 539 COVID-19 Telehealth Awards Issued by the Federal Communications Commission
Award purpose
Number and percentage of awards that included funding for this purpose
Examples of award purposes
Type of health care service supported
Telemedicine visits and care
480 (89%)
Includes funding to support phone or video visits, consultations, or other remote care conducted over the phone or internet.
Remote monitoring
177 (33%)
Includes funding for a program in which a medical professional uses connected devices or telecommunications services to monitor vital signs, conditions, or other patient health statistics remotely.
Type of telecommunications service supported
Connected devices
471 (87%)
Includes devices such as laptops, tablets, telehealth carts, video equipment, or remote monitoring devices that are connected to and transmit health information using telecommunications services or that facilitate telehealth visits.
Telehealth software
297 (55%)
Includes applications, software licenses, subscriptions, or platforms that facilitate telehealth visits or remote monitoring.
Internet or telecommunications service
195 (36%)
Includes phone or internet services or plans, including mobile hotspots, as well as network upgrades that typically increase the overall speed, capacity, or capability of phone or internet services.
Target population
High-risk or vulnerable patients
251 (47%)
Includes funding specifically for patients that are at higher risk for adverse health outcomes, such as elderly or pediatric patients, patients with chronic conditions, and low-income, underserved, un- or under-insured, rural, and tribal populations.
Patients with suspected or confirmed COVID-19
173 (32%)
Includes funding for diagnosis or treatment of patients with suspected or confirmed COVID-19.
Continued care of patients without COVID-19
488 (91%)
Includes funding to support continued care of patients generally, such as primary or routine care, preventative care, or specialty care, or to treat patients with chronic conditions.
Source: GAO analysis of Federal Communications Commission public notices on COVID-19 telehealth awards from April to July 2020. | GAO-21-387
Note: Funds for the awards came from the CARES Act, Pub. L. No 116-136, 134 Stat. 281, 531 (2020). A single award can include all or some of the purposes listed here. As a result, the number of awards listed for each purpose does not add up to the total awards issued. Health care providers may seek reimbursement for different items or service than those upon which FCC based its awards, as long as they comply with program rules.
Agency Comments
We provided a draft of this enclosure to FCC and the Office of Management and Budget for comment. In its comments, reproduced in appendix V, FCC agreed with our findings. FCC also provided technical comments which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
Methodology
We analyzed FCC data on COVID-19 telehealth funding obligated between April and July 2020, including FCC’s public notices issued during that time. We conducted manual reviews, cross-checked these data with corroborating sources, and interviewed FCC officials and found these data to be reliable for the purposes of describing the obligation and purpose of the funding. We also interviewed FCC officials responsible for overseeing the program. To obtain nongeneralizable perspectives on the application and reimbursement processes, we interviewed two health care providers that received funding, which we selected for a variety of funding amounts and locations, and two telehealth associations that represent health care providers.
Contact information: Andrew Von Ah, (202) 512-2834, vonaha@gao.gov
Hospital and Pharmacy Perspectives on COVID-19 Vaccine Administration and Medical Supply Availability
Our February 2021 hospital survey and interviews with large retail pharmacy chains and an association of independent pharmacies revealed concerns about COVID-19 vaccine availability and limitations in certain key medical supplies for administering the vaccines—notably, syringes and needles. Personal protective equipment and COVID-19 testing supplies also remain a challenge for some.
Entities Involved: The Department of Health and Human Services and the Federal Emergency Management Agency.
Key Considerations and Future GAO Work
Our CARES Act work has highlighted persistent constraints with the availability of certain types of personal protective equipment (PPE) and testing supplies due to a supply chain with limited domestic production and high global demand. Specifically:
In September 2020, we found that the Food and Drug Administration (FDA) and the Federal Emergency Management Agency (FEMA) had both identified shortages of certain supplies. We also reported that an American Nurses Association survey indicated widespread reuse of single-use N95 respirators, and that the majority of nurses who were required or encouraged to do so were concerned about their safety as a result.
In November 2020, we published the results of a nationwide survey of state and territorial public health and emergency management officials, which indicated continued limitations in the availability of certain medical supplies, such as nitrile gloves and reagents used for COVID-19 testing.
In January 2021, we reported that FEMA issued an extension through June 30, 2021, of its temporary final rule that generally prohibits the export of critical PPE, including N95 respirators, surgical masks, nitrile gloves, and surgical gowns. In issuing the rule on December 31, 2020, the agency noted that “domestic supply of the allocated PPE has not kept pace with demand and is not anticipated to do so.”[251] Similarly, as vaccination efforts ramp up, FEMA has identified projected shortages in certain medical supplies necessary for vaccination, such as specific types of syringes and needles. The temporary final rule added these items to the list of supplies that may not be exported.
To address issues of supply shortages, we recommended in September 2020 that the Department of Health and Human Services (HHS)—the lead agency in charge of the federal public health response to the pandemic—in coordination with FEMA
further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate supply chain shortages for the remainder of the pandemic.
immediately document roles and responsibilities for supply chain management functions transitioning to HHS, including continued support from other federal partners, to ensure sufficient resources exist to sustain and make the necessary progress in stabilizing the supply chain.
HHS disagreed with these recommendations, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability.
We recognize the efforts of federal agencies in improving the supply chain. However, our February 2021 survey of officials from selected hospitals and our interviews with representatives from retail pharmacy chains and an association of independent pharmacies, described below, underscore the critical imperative that HHS and FEMA implement our recommendations. For example, communicating with stakeholders, as we recommended, would help the agencies to determine further steps needed to address concerns for the remainder of the pandemic. In our February review, we found that some hospital officials and retail pharmacy chain representatives raised concerns that the amount of vaccine doses they could administer were limited by the types of syringes they were receiving. Taking the actions we previously recommended would help address current medical supply chain challenges, as well as help to mitigate any future challenges.
The Consolidated Appropriations Act, 2021—passed in December of 2020—requires the President to make publicly available a report containing a whole-of-government plan for effective response to subsequent COVID-19 outbreaks and for future global pandemic diseases. The act stipulates that this pandemic plan should address how to improve the role of the federal government with respect to the regulation, acquisition, and disbursement of medical supplies necessary to respond to COVID-19, including the procurement and distribution of PPE, among other things. Developing and making publicly available a pandemic plan that addresses medical supply needs for the remainder of the current pandemic would be consistent with our September recommendation.
We recognize that the new administration has taken initial actions beginning in January 2021 to create a more resilient supply chain and increase vaccine availability. For example, the administration has directed certain federal agencies to develop a strategy by July 2021 to design, build, and sustain medical supply manufacturing capabilities in the U.S. long-term.[252] Further, the President has announced increased vaccine production, stating that the administration anticipates enough vaccine supply for every adult in the U.S. by the end of May 2021. We will continue to monitor these efforts, as well as progress on our recommendations regarding the medical supply chain.[253]
Background
Administering vaccines. Administering vaccines requires the ability of providers, such as hospitals and pharmacies, to manage orders as well as additional storage, staff, and IT system capacity.
Order management. Providers must be able to monitor the expected arrival of vaccine and ancillary supply kits.
Storage. Providers administering the vaccine need space for vaccines that may require varying levels of cold storage.
Staff. Providing COVID-19 vaccines requires a sufficient number of trained staff to handle the vaccines, manage vaccine inventory, and administer vaccines.
IT systems. Providers need to use information technology (IT) systems capable of managing the various processes involved in tracking COVID-19 vaccines.
Vaccine supplies. The quantity of supplies needed to administer COVID-19 vaccines to the U.S. population is so large that the federal government has contracted for the production and assembly of vaccine-related supplies into ancillary kits that it is distributing to facilities administering the vaccine. The ancillary supply kits contain surgical masks, face shields, syringes, needles, alcohol prep pads, vaccination cards, and—if applicable—diluent, a liquid for reconstituting a vaccine.[254] The kits do not include other supplies such as sharps disposal containers or bandages. (See figure below.) Our previous survey of state and territorial public health and emergency management officials in October 2020 generally indicated there were concerns about whether providers would have sufficient supplies to administer vaccines when available.
Examples of COVID-19 Vaccine Administration Supplies
Notes: The exact content of the kits may vary depending on the specific vaccine. A vaccination card shows an individual has received a vaccine (and how many doses) and documents relevant information such as vaccine manufacturer, lot number, and date of administration for each dose. Diluent is used to reconstitute Pfizer-BioNTech’s COVID-19 vaccine.
PPE and testing supplies. The demands of the global COVID-19 pandemic overwhelmed the medical supply chain, causing constraints in the availability of PPE supplies, including N95 respirators, surgical gowns, and gloves, as well as supplies needed to test patients for COVID-19 (see figures below). Testing supplies include nasal swabs used to collect viral specimens from patients, transport media that keep samples viable for testing, reagents and laboratory consumables—such as pipette tips—used to process tests, and rapid point-of-care tests.
Examples of Personal Protective Equipment
Examples of COVID-19 Testing Supplies
Overview of Key Issues
Our February 2021 survey of hospitals and interviews with large retail pharmacy chains and an association of independent pharmacies indicate these providers are concerned about COVID-19 vaccine availability and limitations in certain key medical supplies for administering the vaccines—notably, syringes and needles.[255] PPE and COVID-19 testing supplies also remain a challenge for some.
Providers expressed concerns about COVID-19 vaccine availability. Of the 166 total hospitals responding to our survey, 102 (61 percent) reported not having sufficient information to respond to questions from their staff, the public and others about vaccine availability.[256] Among the subset of rural hospitals responding to our survey (68 of 166 hospitals), 42 were concerned about responding to questions about vaccine availability.[257]
In addition, 35 of the 166 hospitals (21 percent) described concerns with general vaccine availability in open-ended survey responses.[258] For example, three hospitals reported concerns about having enough vaccine to administer a second dose to vaccine recipients. Another hospital’s staff responded that they had to cancel more than 1,000 planned vaccine doses to their most vulnerable populations due to lack of vaccines.
Similarly, our interviews with representatives from retail pharmacy chains and an association of independent pharmacies also revealed concerns about vaccine availability. Representatives from all nine retail pharmacy chains we interviewed stated that although their pharmacies have begun administering vaccines, their potential to administer vaccines is far greater than the current amount of vaccines available.
For example, representatives from one retail pharmacy chain that is participating in the Federal Retail Pharmacy Partnership Program—a federal program for administering vaccines—stated that the chain has the capacity to administer 25 million doses per month at their 9,900 locations.[259] However, the chain’s initial allocation of vaccines via the program was expected to be only 230,000 doses at 250 locations.
Representatives from an association of independent pharmacies expressed similar concerns about the quantity of vaccines available.
In addition to underutilization, several retail pharmacy chain representatives indicated that limited vaccine availability has led to uncertainty regarding the amount of vaccines their pharmacies can expect to receive each week. Without sufficient information on vaccine allocation, it is difficult to determine how many vaccine appointments they can schedule or the number of staff needed to fulfill those appointments. For example, representatives from one retail pharmacy chain said that due to uncertainty over the amount of vaccines they may receive in a given week, they can only schedule appointments on a week-to-week basis, which makes it difficult to address customers’ questions about when they will be able to schedule their vaccinations.
The new administration has taken steps to increase certainty and vaccine availability. For example, the White House announced at the end of January 2021 that the federal government would begin notifying states earlier about availability and shipments of vaccines, to give greater certainty for planning vaccination efforts.[260] Further, the President stated on March 2, 2021, that the administration expects to have produced enough vaccine for every adult in the U.S. by the end of May 2021.
Providers expressed concerns about availability of syringes and needles. In our survey, hospitals expressed concerns about the syringes and needles provided in the ancillary supply kits. Out of the 146 hospitals that reported they have either begun administering COVID-19 vaccines or plan to do so, 40 hospitals (27 percent) reported being greatly concerned about having a sufficient quantity of syringes in the next 30 days, and 43 hospitals (29 percent) were greatly concerned about having a sufficient quantity of needles.[261]
Among the 146 hospitals that had either begun administering COVID-19 vaccines or planned to do so, a subset of 56 were rural hospitals. Of these 56 rural hospitals, 10 hospitals were greatly concerned about quantities of syringes in the next 30 days, and 14 hospitals were greatly concerned about needles.
According to FDA, certain types of syringes and needles may allow health care providers to extract more doses of the COVID-19 vaccines than others.[262] Maximizing the number of doses is crucial during a time of constrained vaccine supply. Four hospitals specifically noted this issue in open-ended responses.[263]
Representatives from retail pharmacy chains also discussed this issue. Specifically, representatives from five of the nine retail pharmacy chains expressed concerns that the provided ancillary supply kits do not always contain the most efficient syringes needed to obtain the maximum doses of vaccines from each vial. Representatives from one retail pharmacy chain that had administered more than 200,000 doses at the time of our interview indicated that optimal syringes were only included in the ancillary supply kits about 50 percent of the time. Representatives from two retail pharmacy chains also noted that these syringes are in short supply on the open market.
The lack of more efficient syringes limits the ability to maximize the number of doses per vial, which further constrains the supply of vaccine. In January 2021, HHS and Department of Defense officials managing vaccine implementation told us they have recognized this issue and are working toward ensuring the majority of syringes included in the ancillary supply kits are the more efficient type of syringes. We will continue to monitor HHS’s vaccination efforts moving forward, including whether they have addressed this issue.
Providers cited several areas of concern about their capacity to administer the COVID-19 vaccine. In addition to supplies, administering vaccines requires managing vaccine orders as well as having additional storage, staff, and IT system capacity. See table below for the most commonly cited concerns among the 146 hospitals that plan to or have begun administering vaccines at the time of our survey. The subset of 56 rural hospitals generally cited the same concerns.[264]
Surveyed Hospitals’ Most Commonly Cited Concerns about Capacity to Administer Vaccines in February 2021
Number of hospitals
Hospitals that plan to or have begun administering COVID-19 vaccines
146
Orderingaconcerns
Being able to track the expected arrival of vaccine orders
40
Being able to track the expected arrival of kits with ancillary vaccination supplies to the hospital
22
Storageb concerns
Storing vaccine in ultra-cold storagec
32
Staffdconcerns
Having sufficient number of trained providers to administer vaccine
33
IT systemseconcerns
Interfacing with state or other external IT systems to document vaccine administration
31
Meeting federal reporting requirements for vaccine administration (e.g., reporting all required elements, reporting within required time frames)
24
Source: GAO analysis of hospital survey responses. | GAO-21-387
Notes: The results in this table are based on our non-generalizable survey sent to 383 short-term and critical access hospitals across the country. We fielded the survey from February 5, 2021 through February 25, 2021, and received responses from 166 hospitals. Twenty-one of the survey responses we received were on behalf of a larger health system or multiple facility group representing multiple hospitals. For the purposes of this enclosure, we reported each health system’s response as a single hospital response rather than as the number of hospitals represented by the system. For this survey question, we asked the 146 hospitals that reported they plan to, or have begun, administering COVID-19 vaccines to report whether they were greatly concerned about their capacity to handle specific aspects of the vaccine, as of the date they were answering the survey. Survey respondents also had an open-response option to report any other concerns not listed in the survey response options. The concerns in the table above were cited by at least 15 percent of the 146 hospitals. aOrdering vaccine concerns response options were: using required IT systems to order vaccine; being able to monitor the expected arrival of vaccine orders to the hospital; being able to monitor the expected arrival of kits with ancillary vaccination supplies to the hospital; other (fill-in); and no great concerns about ordering vaccines. 146 hospitals responded to the questions in the ordering category. bStoring vaccine concerns response options were: storing refrigerated (2°C to 8°C) vaccine; storing frozen(-15° C to -25°C) vaccine; storing ultra-cold (-60°C to -80°C) vaccine; other (fill-in); and no great concerns about vaccine storage. 145 hospitals responded to questions in the storing category. cPfizer-BioNTech’s COVID-19 vaccine requires ultra-cold storage between -80°C and -60°C (-112°F and -76°F) when storing for longer periods of time. dStaff to manage and administer vaccine concerns response options were: having sufficient number of trained staff to handle and manage vaccine inventory; having sufficient number of trained providers to administer vaccine; other (fill-in); and no great concerns about staff. 144 hospitals responded to questions in the staff category. eHaving/using IT systems to track/report administered doses concerns response options were: having IT systems to track the first dose of vaccine administered to patients; having IT systems to remind patients of need for a second dose, if needed; interfacing with state or other external IT systems to document vaccine administration; meeting federal reporting requirements for vaccine administration (e.g. reporting all data elements required, reporting administrations within required time frames); other (fill-in); and no great concerns about IT systems. 144 hospitals responded to questions in the IT systems category.
Representatives from all nine retail pharmacy chains and an association of independent pharmacies named data reporting requirements as a concern. Commonly cited concerns included
different local, state, and federal requirements. Representatives from eight retail pharmacy chains and an association of independent pharmacies noted challenges in meeting data requirements that differ across local, state, and federal governments. For instance, according to representatives from one retail pharmacy chain, one locality requires documenting recipients’ professions, while others do not. These unique elements are not always included in existing data systems, making it difficult to determine how to report them.
interoperability limitations. Representatives from seven retail pharmacy chains and a representative from an independent pharmacy also stated that interoperability limitations of some state data reporting systems have resulted in challenges, such as pharmacy staff having to manually transfer required information. As one retail pharmacy chain’s representative noted, this process is complicated, especially for chains that must coordinate across hundreds of locations.
time frames for reporting. The deadlines for submitting reports present some challenges. The federal government requires pharmacies to report data within 72 hours. However, representatives from five retail pharmacy chains and one independent pharmacy said that some states require reports within 24 hours. A representative from an independent pharmacy said such daily reporting has been a learning curve.
Representatives from three retail pharmacy chains and two independent pharmacies reported taking various actions to address identified challenges, including investing in new software, hiring additional administrative support, or modifying staff responsibilities, such as diverting pharmacists from administering vaccines. Representatives from two independent pharmacies mentioned the increased expenses pharmacies have incurred to address COVID-19 but noted that they have not received federal funding to pay for the additional staff and supplies they need.
We have previously reported on data challenges related to COVID-19. For example, in September 2020 we described state and local public health officials’ concerns regarding the cost and effort associated with providing data to federal entities to be integrated and shared on a nationwide basis. Also, in January 2021, we reported that the federal government does not have a process to help systematically define and ensure the collection of standardized data across the relevant federal agencies and related stakeholders to help respond to COVID-19. We recommended that HHS immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. In its comments, HHS partially concurred that it should establish such a body, but said because of resource constraints and the ongoing response to the pandemic, it could not commit to immediately doing so. We reiterate the importance of immediately establishing an expert committee and maintain that HHS could use an existing committee, which would help streamline the process and leverage existing resources, to help inform the federal government’s response to the pandemic with more complete and consistent COVID-19 data.
Providers generally reported sufficient PPE at current levels with some reuse, but were less confident of future availability for certain items. Most of the 166 hospitals that responded to our survey reported having an adequate 7-day supply of the 11 types of PPE we asked about in our survey. (See figure below.) However, in some cases, hospitals reported avoiding shortages only with reuse or extending the use of the items.[265]
For example, 37 out of 166 hospitals (23 percent) reported needing to reuse or extend the use of N95 respirators in order to have a 7-day supply.
Among the 68 rural hospitals that responded to our survey, 17 reported having to reuse N95 respirators in order to ensure a 7-day supply.
While CDC guidance allows for the reuse or extended use of certain PPE when there are supply shortages, once supply availability returns to normal, CDC recommends health care facilities promptly resume conventional practices. Our previous audit work has identified concerns among health care providers about the reuse or extended use of PPE. For example, in September 2020 we reported that an American Nurses Association survey indicated widespread reuse of single-use N95 respirators, and that the majority of nurses who were required or encouraged to do so were concerned about their safety as a result. The association’s latest survey, issued in March 2021, indicated this practice may still be prevalent—82 percent of nurses surveyed reported their facility or practice site had guidance allowing N95 respirators to be reused multiple times.[266]
Surveyed Hospitals’ 7-Day Supply Levels of Selected Personal Protective Equipment (PPE)
Notes: The results are based on our non-generalizable survey sent to 383 short-term and critical access hospitals across the country. We fielded the survey from February 5, 2021 through February 25, 2021, and received responses from 166 hospitals. Twenty-one of the survey responses we received were on behalf of a larger health system or multiple facility group representing multiple hospitals. For the purposes of this enclosure, we reported each health system’s response as a single hospital response rather than as the number of hospitals represented by the system. For this survey question, we asked—for each PPE item—if the hospital had at least a 7-day supply of the items listed above based on current operations: (1) without reusing or extending the use of the PPE item, or (2) with reusing or extending the use of the item. In addition to the four response categories shown above, respondents could answer “do not know” and one respondent did so for each PPE item above except for non-surgical masks and other gowns (2); nitrile gloves, other gloves, boot covers, and bouffant caps (3); and coveralls (6). Further, not all 166 hospitals responded to each PPE item in the question; there was one non-response for each PPE type listed above except for non-surgical masks (4), other gloves (5), other gowns (4), and coveralls (2).aOther gloves include those made of latex and vinyl. bOther gowns include non-surgical gowns and isolation gowns.
Like hospitals, pharmacies use PPE—primarily masks, gloves, and face shields—to protect their staff and to limit transmission of the virus. Representatives from all nine retail pharmacy chains and one independent pharmacy said their pharmacies had at least 7 days of PPE available, including masks and gloves. Representatives from five of the nine retail pharmacy chains and representatives from two independent pharmacies mentioned reuse of face shields after appropriate cleaning, but representatives from four other retail pharmacy chains indicated they had enough supply that staff did not need to reuse or extend the use of any PPE.
The extent to which hospitals expressed confidence in their future supply of PPE supplies (defined as expected PPE for the 30 days following the survey) varied by PPE type. (See figure below.) For example:
Of the 166 hospitals, 136 (82 percent) were greatly confident in having sufficient supplies for face shields and goggles.
In contrast, for nitrile gloves, 94 out of 166 surveyed hospitals (57 percent) were greatly confident they would have sufficient supplies over the next 30 days, while 31 hospitals (19 percent) responded that they were only slightly confident or not at all confident they would have sufficient supplies of these gloves.
Twelve of the sixty-eight rural hospitals reported they were slightly or not at all confident in having an adequate 30-day supply of nitrile gloves.
Surveyed Hospitals’ Levels of Confidence in Having Adequate Personal Protective Equipment (PPE) Supplies for the Next 30 Days
Notes: The results are based on our non-generalizable survey sent to 383 short-term and critical access hospitals across the country. We fielded the survey from February 5, 2021 through February 25, 2021, and received responses from 166 hospitals. Twenty-one of the survey responses we received were on behalf of a larger health system or multiple facility group representing multiple hospitals. For the purposes of this enclosure, we reported each health system’s response as a single hospital response rather than as the number of hospitals represented by the system. For this survey question, we asked—for each PPE item—the extent to which respondents were confident they would have sufficient supplies over the next 30 days following the survey. In addition to the five response categories shown above, respondents could answer “do not know,” and one respondent did so for each of the PPE items except for boot covers (2); nitrile gloves, other gowns, coveralls, and bouffant caps (3); and other gloves (5). Not all 166 hospitals responded to each PPE item in this question. The following PPE items each had one non-response: surgical masks, nitrile gloves, other gloves, surgical gowns, coveralls, and bouffant caps.aOther gloves include those made of latex and vinyl. bOther gowns include non-surgical gowns and isolation gowns.
In our interviews with retail pharmacy chains, all representatives explained that they maintained their supplies using a centralized procurement system, with four representatives saying they anticipated and ordered additional supplies in early 2020. Representatives from all nine retail pharmacy chains reported being confident or very confident their pharmacies could access 30 days or more of PPE. Representatives from three independent pharmacies also had no concerns about meeting their needs for PPE over the next month, although a representative from a fourth independent pharmacy reported challenges securing N95 respirators. While there was confidence over the next 30 days, representatives from three retail pharmacy chains and two independent pharmacies expressed concern regarding the future availability of gloves.
Hospitals reported some concerns about future availability of testing supplies, while pharmacies generally reported sufficient access. Of the surveyed hospitals conducting COVID-19 diagnostic testing (158 out of 166), most reported having at least a 7-day supply for each of the five testing items we asked about in our survey (ranging from 84 to 95 percent).[267] However, hospitals were somewhat less confident about levels of those same supplies over the next 15 days. (See figure.) In addition, rural hospitals conducting COVID-19 diagnostic testing generally reported having at least a 7-day supply for each testing item but were somewhat less confident about supplies over the next 15 days. For example, nine of the 66 rural hospitals conducting testing were not at all or only slightly confident in supplies of rapid point-of-care tests for the next 15 days following the survey.
Surveyed Hospitals’ Levels of Confidence in Having Adequate Testing Supplies for the Next 15 Days
Notes: The results are based on our non-generalizable survey sent to 383 short-term and critical access hospitals across the country. We fielded the survey from February 5, 2021 through February 25, 2021, and received responses from 166 hospitals. Twenty-one of the survey responses we received were on behalf of a larger health system or multiple facility group representing multiple hospitals. For the purposes of this enclosure, we reported each health system’s response as a single hospital response rather than as the number of hospitals represented by the system. For this survey question, we asked—for each testing item—the extent to which the 158 respondents conducting diagnostic tests for COVID-19 were confident they would have sufficient supplies over the next 15 days following the survey. In addition to the five response categories shown above, respondents could answer “do not know,” and five respondents did so for each of the above testing items, except for testing swabs (3). Not all of the 158 hospitals conducting COVID-19 diagnostic testing responded to each testing item in the question; the testing swabs, laboratory consumables, and rapid point-of-care tests items each had one non-response, and reagents had two.
Representatives from four of the nine retail pharmacy chains and the four independent pharmacies we interviewed conduct COVID-19 testing. These representatives did not report current problems accessing testing supplies. However, representatives from the association of independent pharmacies mentioned challenges obtaining the testing instruments needed to analyze rapid point-of-care tests. A representative from one independent pharmacy noted that there are “testing deserts” in his state due to the lack of this equipment.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS and OMB did not provide any comments.
Methodology
To conduct this work, we designed and fielded a survey to hospitals. The survey asked about hospital officials’ perspectives on the availability of supplies to administer vaccines as well as their capacity for, or concerns regarding, administering COVID-19 vaccines. The survey also contained questions designed to obtain hospital officials’ perspectives on the availability of PPE for hospital staff and COVID-19 testing supplies.
We fielded this survey from February 5 through February 25, 2021. Officials completing the survey included those knowledgeable of these issues such as chief executive officers and supply chain directors. We pretested a draft of the survey with officials from two hospitals to help ensure that the questions were understandable and answerable.
We obtained 383 hospital official email addresses for short-term and critical access hospitals in several states, to which we sent a personalized survey link.[268] From this, we received 166 responses from hospitals located in 40 states for a response rate of 43 percent. See table below for more information on our non-generalizable sample and response rates by hospital characteristic. In 21 instances, officials responded on behalf of multiple hospitals in a health system rather than on behalf of an individual hospital. (Therefore, we had 145 individual hospital respondents.) For the purposes of this enclosure, we reported each health system’s response as a single hospital response rather than as the number of hospitals represented by the system.[269]
Hospital Survey Sample Size, Characteristics, and Response Rates
Hospital characteristic
Populationa
Survey sampleb
Total number of survey responses receivedc
Number of survey responses received on behalf of individual hospitals
Survey response rate for individual hospitals (percent)d
Total
4,682
383
166
145
38
Type of hospital
Short-terme
3,328
281
N/A
92
33
Critical accessf
1,354
101
N/A
53
52
Intensive care services availability
Intensive care unit
3,177
258
N/A
87
34
Urban and rural settingsg
Urban
2,832
238
N/A
77
32
Rural
1,850
144
N/A
68
47
Legend: N/A = not applicable
Source: GAO analysis of survey data and the Centers for Medicare & Medicaid Services’ 2020 Provider of Services file. | GAO-21-387
Notes: We fielded our survey from February 5 through February 25, 2021. aThe population values represent the number of short-term and critical access hospitals in the Centers for Medicare & Medicaid Services’ 2020 Provider of Services file. bThe sample values represent the number of hospitals sent an email with a personalized survey link. Numbers for a particular characteristic may not sum to 383 because a health system was substituted for one hospital prior to sending the survey. cIn 21 instances, officials responded on behalf of multiple hospitals in a health system rather than on behalf of an individual hospital. For the purposes of this enclosure, we reported each health system’s response as a single hospital response rather than as the number of hospitals represented by the system. The 21 responses on behalf of multiple hospitals represented 300 hospitals. We could not categorize these responses by hospital characteristics (e.g., urban or rural) due to the multiple locations. dThe total response rate (166 out of 383) was 43 percent. eShort-term hospitals are hospitals that provide acute inpatient care. For this report, short-term hospitals refer to acute care hospitals that are not critical access hospitals. fCritical access hospitals are small, rural hospitals with no more than 25 inpatient beds. gCenters for Medicare & Medicaid Services’ Provider of Services file categorizes hospitals as urban if they are located in a county that contains a core urban area of 50,000 or more population. Hospitals are categorized as rural if they are located in a county not designated as such.
We checked for missing values and survey response errors such as inconsistencies—for example, responding to COVID-19 testing-specific questions after indicating the hospital does not conduct such testing—and followed up with hospital officials on survey responses as appropriate.
We also conducted semi-structured interviews with nine of the top 10 national retail pharmacy chains based on 2019 prescription drug revenue.[270] These retail pharmacy chains provide for a mix of size, as well as of urban and rural pharmacies. In addition to chain pharmacies, more than 21,000 (35 percent) of retail pharmacies nationwide were independently owned in 2019. We interviewed representatives from four independent pharmacies and from the National Community Pharmacists Association, which represents independent pharmacies.
The results of our survey and interviews are not generalizable beyond those we surveyed or interviewed, though they can provide important insights into hospitals’ and pharmacies’ experiences with vaccine administration and medical supplies.
The Centers for Disease Control and Prevention’s COVID-19 Response Health Equity Strategy aims to address health disparities and inequities related to COVID-19, but lacks key elements of a national strategy, and the agency does not have complete data on the race and ethnicity of recipients of COVID-19 vaccinations.
Entities involved: Department of Health and Human Services, including the Centers for Disease Control and Prevention.
Recommendations for Executive Action
The Director of the Centers for Disease Control and Prevention should incorporate key elements of a national strategy in the agency’s COVID-19 Response Health Equity Strategy. These elements include 1) specific actions to achieve intermediate outcomes, such as increased access to testing; 2) how intermediate outcomes should be prioritized within its four broad priority areas; 3) who will implement actions to achieve intermediate outcomes; and 4) how the strategy relates to other relevant strategies. The Centers for Disease Control and Prevention agreed with our recommendation.
The Director of the Centers for Disease Control and Prevention should take steps to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations, such as working with states and jurisdictions to facilitate consistent collecting and reporting of this information. The Centers for Disease Control and Prevention neither agreed nor disagreed with our recommendation. The Centers for Disease Control and Prevention stated that it is working to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations, such as by requiring providers that participate in CDC’s COVID-19 Vaccination Program to report the race and ethnicity of vaccine recipients.
Key Considerations and Future GAO Work
In September 2020, to help address gaps in race and ethnicity data on COVID-19 indicators, we recommended that the Director of the Centers for Disease Control and Prevention (CDC)
determine whether having the authority to require states and jurisdictions to report race and ethnicity information for COVID-19 cases, hospitalizations, and deaths is necessary for ensuring more complete data, and if so, seek such authority from Congress;
involve key stakeholders to help ensure the complete and consistent collection of demographic data; and
take steps to help ensure its ability to comprehensively assess the long-term health outcomes of persons with COVID-19, including by race and ethnicity.
CDC agreed with our recommendations. In response, in February 2021, CDC stated that it is working with stakeholders from across the agency and state and local health departments to review the quality of demographic data, including the completeness of race and ethnicity information, across CDC’s core surveillance systems. CDC added that the information derived from this review will be discussed with the CDC Director and used to assess potential opportunities and needs to enhance the collection of race and ethnicity data, including policy changes or legislative authorities and whether that would potentially advance this work. In addition, CDC said that the agency has various efforts underway with external partners to assess long-term health outcomes.
Since September 2020, we also have identified concerns related to CDC’s health equity strategy and its lack of data on the race and ethnicity of recipients of COVID-19 vaccinations. In addition, in November 2020, we continued to find gaps in data on indicators of COVID-19 burden by race and ethnicity. We continue to conduct work examining the Department of Health and Human Services (HHS), CDC, and other component agencies’ ongoing work regarding indicators of COVID-19, disparities that may exist for various populations, and actions the federal government is taking to help address such disparities.
Background
CDC has recognized the need to improve data collection and work with stakeholders to identify and address COVID-19 related racial and ethnic disparities. In July 2020, CDC released its COVID-19 Response Health Equity Strategy, which aims to reduce health disparities by using data-driven approaches to attain the highest level of health possible for all individuals, including communities of color.[271] CDC updated this strategy on August 21, 2020, and continues to use it to guide its efforts to improve the health outcomes of populations disproportionately affected by COVID-19.
In October 2020, CDC released guidance to states and jurisdictions on how to plan and operationalize vaccine distribution through an update to its COVID-19 Vaccination Program Interim Playbook.[272] The playbook specifies that within 24 hours of administering a vaccine, vaccine providers—such as medical doctors and pharmacists—are required to report information, including recipient race and ethnicity, to the relevant state, local, or territorial public health authority. According to the playbook, this information must be transmitted by jurisdictional immunization information systems to the CDC on a regular basis. Provider records on vaccinations also must be made available to federal, state, local, or territorial public health departments, to the extent required by law.
In addition, the Consolidated Appropriations Act, 2021, enacted in December 2020, requires CDC to submit a comprehensive COVID-19 vaccine distribution strategy to Congress that includes how the agency will focus efforts on high-risk and underserved populations, including communities of color.[273]
On January 21, 2021, the White House released its National Strategy for the COVID-19 Response and Pandemic Preparedness that directed HHS to increase the collection and reporting of health data to identify high-risk communities, and to establish a system for monitoring long-term health outcomes and understanding treatment needs, including for people of color.[274] The strategy includes a goal of protecting those most at risk for COVID-19 and advancing equity, including across racial, ethnic and rural/urban communities.
In addition, President Biden signed two executive orders on January 21, 2021 focusing on ensuring an equitable pandemic response by establishing a COVID-19 Health Equity Task Force, among other things, and directing federal agencies responding to the COVID-19 pandemic to strengthen equity-related data collection, reporting, and use.[275]
Overview of Key Issues
CDC data on race and ethnicity continue to be limited. We have previously reported, including in our September and November 2020 reports on the federal response to COVID-19, that gaps exist in data on indicators of COVID-19 by race and ethnicity. Available data on COVID-19 indicators by race and ethnicity continue to be limited.
Cases. As of March 8, 2021, race and ethnicity information was missing for 47.2 percent of COVID-19 cases with case report forms received by CDC, or 59.9 percent of total cases reported.[276]
Hospitalizations. CDC’s hospitalization data for COVID-19 are limited to select counties in 14 states, and race and ethnicity information are not complete in the reported data.[277]
Deaths. Race and ethnicity data were missing for 25.3 percent of COVID-19-related deaths with case report forms received by CDC, or 45.6 percent of total deaths reported through case reporting, as of March 8, 2021.[278]
Testing. Data on race and ethnicity were missing for 76 percent of COVID-19 laboratory tests as of January 7, 2021.[279]
Vaccinations. With the authorization of three vaccines for emergency use as of February 2021, CDC is also collecting information on the race and ethnicity of individuals being vaccinated. As of March 8, 2021, data collected from states and jurisdictions on race and ethnicity for COVID-19 vaccine recipients were missing for almost half (46.7 percent) of recipients who received at least one dose.
CDC data, though incomplete, continue to show disparities by race and ethnicity. We have previously reported that communities of color have been disproportionately affected by the pandemic. Though limited, available data from CDC continues to demonstrate racial and ethnic disparities in COVID-19 indicators.
Cases. CDC race and ethnicity data on COVID-19 cases, while incomplete, demonstrate that communities of color have been disproportionately affected. Among cases with known race and ethnicity reported to CDC as of March 8, 2021, 20.7 percent of cases were for persons who were Hispanic or Latino (compared to 18.5 percent of the U.S. population), and 0.4 percent were Native Hawaiian or Other Pacific Islander (compared to 0.2 percent of the U.S. population).[280]
Hospitalizations. CDC data indicate that communities of color are disproportionately hospitalized with COVID-19 in select counties in 14 states included in CDC’s COVID-NET. According to CDC’s analysis of this data, between March 1, 2020, and January 30, 2021 American Indian/Alaska Native persons were hospitalized with COVID-19 at a rate 3.6 times that of non-Hispanic White persons. Hispanic or Latino persons were hospitalized at a rate 3.2 times that of non-Hispanic White persons, and non-Hispanic Black persons were hospitalized at a rate 2.9 times that of non-Hispanic White persons when adjusting for age.
Deaths. As of January 6, 2021, CDC’s National Center for Health Statistics (NCHS) data show that non-Hispanic American Indian/Alaska Native persons died of COVID-19 at a rate 1.6 times higher than non-Hispanic White persons. Non-Hispanic Black persons died of COVID-19 at a rate 1.4 times higher than non-Hispanic White persons.[281]
Testing. Among COVID-19 diagnostic test results reported to CDC from laboratories from 48 jurisdictions as of January 7, 2021, with race and ethnicity information, the percent of tests that were positive by each racial and ethnic group was: 17.9 percent for Hispanic or Latino persons, 13.2 percent for non-Hispanic Native Hawaiian or Other Pacific Islander persons, 12.4 percent for non-Hispanic American Indian/Alaska Native, and 11.2 percent for non-Hispanic Black persons, compared to 9.5 percent for non-Hispanic White persons.[282]
Vaccinations. Although limited, existing data showed disparities by race and ethnicity in vaccine recipients who received at least one dose whose race and ethnicity was known as of March 8, 2021: 65.4 percent of those receiving at least one vaccine dose were non-Hispanic White (compared to 60.1 percent of the U.S. population), 8.5 percent were Hispanic or Latino (compared to 18.5 percent of the U.S. population), 7.1 percent were non-Hispanic Black (compared to 13.4 percent of the U.S. population), and 4.7 percent were non-Hispanic Asian (compared to 5.9 percent of the U.S. population).[283]
CDC equity strategy lacks key elements of an effective national strategy. On July 22, 2020, CDC released a COVID-19 Response Health Equity Strategy to accelerate progress toward reducing disparities in indicators of COVID-19 burden, among other efforts to achieve health equity, including intermediate outcomes. In the strategy, CDC provides intermediate outcomes within four broad priority areas that it plans to achieve within 3-12 months.[284] For example, related to expanding programs and practices for testing, one intermediate outcome consists of increasing access to testing for populations at increased risk of COVID-19.
We found that CDC’s equity strategy does not include several key elements of a national strategy, as defined by our prior work, including the following:
specific actions to achieve intermediate outcomes;
how intermediate outcomes should be prioritized within its four broad priority areas;
who will implement actions to achieve intermediate outcomes; and
how the strategy relates to other relevant strategies.[285]
For example, CDC’s strategy includes an intermediate outcome to increase access to testing for populations at increased risk for COVID-19. However, CDC’s strategy does not provide specific actions that the agency will take to determine whether or where it needs to increase access to testing for populations at increased risk for COVID-19—an essential first step before taking steps to increase testing access. Further, CDC does not specify how its intermediate outcomes should be prioritized amongst the other intermediate outcomes. In addition, the strategy does not specify who will implement actions to achieve these intermediate outcomes, such as specific program offices within CDC. Lastly, the strategy does not specify how it relates to other relevant strategies, such as HHS’s Testing Strategy Report and the National Strategy for the COVID-19 Response and Pandemic Preparedness.[286]
Our prior work sets forth several key elements of strategies that can guide agencies in planning and implementing an effective national strategy. As noted in our prior work, these elements include identifying specific actions, specifying how such actions should be prioritized, designating who will be implementing these actions, and indicating how a strategy relates to other strategies, such as those noted above.[287] These elements can be used to gauge progress when implementing programs and to determine whether adjustments need to be made in order to maintain progress within given time frames.
CDC stated that its equity strategy does not include these elements because they intended the strategy to be a broad and high-level framework of the activities necessary to improve the health outcomes of populations disproportionately affected by COVID-19. CDC officials added that because there was still so much to learn about COVID-19 when the strategy was developed, it was important to keep the strategy high level to allow room to pivot and adapt activities based on science and relevant data. CDC maintains an internal document to track progress on achieving the outcomes within CDC’s health equity strategy.
As CDC moves forward with implementing its equity strategy, it will be important for the agency to include several key elements of a national strategy, including the following actions:
Develop specific actions and priorities to facilitate the measurement of progress towards its intermediate outcomes. For example, by taking specific actions to determine the extent to which it needs to expand testing access, CDC may be better positioned to target its efforts to specific communities of color that lack access to testing.
Designate who will be implementing these actions, such as specific program offices within CDC. This will help CDC clarify roles and responsibilities and coordinate efforts across the agency.
Take steps to identify how CDC’s strategy is relevant to other strategies. By doing so, CDC can determine how the strategy’s scope complements, expands upon, or overlaps with other strategies.
By including the key elements we identified, CDC can better ensure the effective implementation of its equity strategy to help it improve the health outcomes of populations disproportionately affected by COVID-19, including communities of color. Additionally, as the federal government releases additional strategies to improve its response to the COVID-19 pandemic, it will be imperative for CDC to consider these strategies in relation to CDC’s equity strategy to facilitate a coordinated federal response.
Improving completeness of race and ethnicity data for COVID-19 vaccinations critical to federal efforts to advance equity. CDC requires providers administering COVID-19 vaccines to report the race and ethnicity of vaccine recipients, among other things, to relevant state, local, or territorial public health authorities, and must be transferred by jurisdictions to CDC. However, as noted, according to CDC, data collected from states and jurisdictions on race and ethnicity for COVID-19 vaccine recipients who received at least one dose was missing for almost half (46.7 percent) of recipients as of March 8, 2021.[288]
In its COVID-19 Response Health Equity Strategy, CDC reported that it aims to reach disproportionately affected communities through effective vaccination strategies and plans to collect and report timely, complete, and representative data on COVID-19 vaccinations. Similarly, the January 2021 National Strategy for the COVID-19 Response and Pandemic Preparedness states the importance of collecting and reporting data by race and ethnicity to inform COVID-19 response efforts, including equitable vaccine distribution.[289]
CDC stated that information on race and ethnicity for COVID-19 vaccine recipients is missing for a variety of reasons, including a lack of consistent collection and reporting of this information by physicians and pharmacists and challenges with transmitting data to CDC. Officials from two of the three selected states we interviewed said that it can be challenging to collect this information when administering COVID-19 vaccinations because recipients may refuse to provide their race and ethnicity at the time of vaccination, among other things. Stakeholders indicated that challenges with collecting race and ethnicity for indicators of COVID-19 burden, such as cases, can also affect the collection of race and ethnicity for COVID-19 vaccination recipients, such as the lack of reporting race and ethnicity information by providers and the use of broad race and ethnicity categories.[290] The lack of consistent collection and reporting of information on race and ethnicity is a persistent problem, as we previously reported. CDC officials stated that ongoing support for health care providers will be needed to help ensure the complete and consistent collection and reporting of race and ethnicity information.
Without complete information on the race and ethnicity of persons who have received COVID-19 vaccines, CDC may have difficulty determining whether vaccines are distributed equitably to communities of color who have been disproportionately affected by COVID-19. As noted, recent data from CDC, while limited, suggest disparities exist by race and ethnicity in COVID-19 vaccine recipients. Further, in the absence of more complete data, CDC does not know whether it is effectively meeting its aim to reach disproportionately affected populations with vaccination strategies.
Obtaining more complete information on the race and ethnicity of COVID-19 vaccine recipients would help inform CDC’s efforts to develop strategies to ensure the equitable distribution of vaccinations, such as initiating culturally and linguistically tailored programs. These strategies may be particularly important for communities of color, as several studies have shown that persons in various racial and ethnic groups may be more hesitant about receiving COVID-19 vaccinations.[291]
Agency Comments
We provided HHS, CDC, and the Office of Management and Budget (OMB) with a draft of this enclosure. CDC provided technical comments on this enclosure, which we incorporated as appropriate. HHS also provided general comments which are reproduced in Appendix VI: Comments from the Department of Health and Human Services. OMB did not provide comments on this enclosure.
CDC agreed with our recommendation to incorporate key elements of a national strategy in its COVID-19 Response Health Equity Strategy. CDC neither agreed nor disagreed with our recommendation to take steps to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations. In response to our recommendations, CDC stated that it will take steps to include key elements of a national strategy in an internal version of its COVID-19 Response Health Equity Strategy to help with coordination and tracking, among other actions to coordinate health equity activities across various task forces and with federal, state, and local partners. In addition, CDC stated that it is working to ensure more complete reporting of race and ethnicity information for recipients of COVID-19 vaccinations, such as by requiring providers that participate in CDC’s COVID-19 Vaccination Program to report the race and ethnicity of vaccine recipients.
Methodology
To conduct this work, we reviewed CDC’s reported data on COVID-19, reviewed federal laws, agency guidance and documentation, and interviewed or obtained written responses from HHS and CDC officials.
To assess HHS’s efforts, including CDC’s, related to CDC’s equity strategy and COVID-19 vaccine distribution for communities of color, we reviewed HHS and CDC documentation, including reports to Congress and strategic planning documents, and interviewed or obtained written responses from HHS and CDC officials. We also conducted interviews and reviewed written responses provided by organizations that represent entities involved in COVID-19 testing and vaccination efforts and from state public health officials from three selected states—Alabama, Nevada, and South Dakota—to obtain their perspectives on federal agency actions and challenges.[292] We compared HHS’s efforts to our prior work on key elements of strategies for effective government programs and standards for data collection within CDC’s COVID-19 Vaccination Program Interim Playbook.
To assess the reliability of the data on COVID-19 indicators we analyzed, we obtained written responses from CDC and HHS; reviewed related documentation; and reviewed the data to identify obvious errors or omissions. On the basis of these steps, we determined that the data were sufficiently reliable for the purpose of analyzing COVID-19 data.
Contact information: Alyssa M. Hundrup, (202) 512-7114, hundrupa@gao.gov
Related GAO Products
COVID-19: Federal Efforts Accelerate Vaccine and Therapeutic Development, but More Transparency Needed on Emergency Use Authorizations. GAO-21-207. Washington, D.C.: November 17, 2020.
COVID-19Data Quality and Considerations for Modeling and Analysis. GAO-20-635SP. Washington, D.C.: July 30, 2020.
Federal agencies continue to use the Defense Production Act, among other actions, to prioritize contracts, expand domestic production for medical supplies and COVID-19 vaccines, and collaborate with industry.
Entities involved: Department of Health and Human Services, Department of Defense, and Federal Emergency Management Agency
Key Considerations and Future GAO Work
The President issued an executive order in January 2021 that requires federal agencies to conduct assessments of domestic supply and demand for medical supplies, address any identified shortfalls through the Defense Production Act (DPA) and other actions, and develop a longer term strategy for the domestic production of medical supplies.[293] In March 2021 the American Rescue Plan Act appropriated $10 billion in support of the use of the DPA for medical supplies.[294]
We believe the DPA can be a powerful tool for federal agencies to mitigate medical supply chain issues and previously made recommendations to the Secretary of Health and Human Services (HHS) and the Office of Management and Budget related to the use of DPA and other actions to increase domestic production of medical supplies. Specifically:
In September 2020, we recommended that the Secretary of HHS—in coordination with the Federal Emergency Management Agency (FEMA)—should further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic, including through the use of DPA authorities. HHS disagreed with this recommendation, but we continue to believe this action is necessary to improve the federal government’s response to COVID-19.
In November 2020, we recommended that HHS identify how the DPA and other actions will be used to increase production of domestic medical supplies. HHS agreed, but has not yet taken steps to implement the recommendation.
In November 2020, we recommended that the Office of Management and Budget develop reporting guidance to provide more transparency on the use of DPA Title I authorities to place priority ratings on contracts. The Office of Management and Budget concurred with this recommendation, but has not yet taken actions to implement it.
We will monitor agency actions with regard to domestic production of medical supplies in future work, including a review of the personal protective equipment (PPE) supply chain.
Background
During the Korean War, Congress enacted the Defense Production Act of 1950 to ensure the availability of industrial resources to meet the Department of Defense’s (DOD) needs.[295] There are three major DPA authorities currently in effect: Titles I, III, and VII.
Title I: Priorities and Allocation Authority authorizes the President to require priority performance on contracts or orders and allocate materials, services, and facilities as necessary or appropriate to promote the national defense. This authority allows priority-rated contracts or orders to take preference over any other unrated contracts or orders if a contractor cannot meet all required delivery dates.[296]
Title III:Expansion of Domestic Capacity and Supply authorizes the President to provide various financial incentives to firms to meet a variety of national defense goals, including maintaining, restoring, and expanding the domestic industrial base. The financial incentives may be used only when certain conditions are met.
Title VII: General Provisions provides for a range of authorities, including antitrust protections for activities carried out under voluntary agreements for preparedness programs and protecting individuals and companies who carry out the voluntary agreement from certain lawsuits brought by other customers.
We reported in November 2020 that HHS and FEMA had placed priority ratings on 25 contracts for ventilators, N95 respirators, and other medical supplies to respond to COVID-19. In January 2021, we reported that HHS and DOD had awarded 32 domestic production expansion projects totaling approximately $1.4 billion through DPA and other actions for medical supplies.[297] FEMA also created a voluntary agreement in August 2020 focused on the manufacturing and distribution of medical supplies to respond to COVID-19 and future pandemics. FEMA began holding meetings with industry in October 2020 to solicit feedback on the next steps under the agreement.
This enclosure provides an update on federal agencies’ use of DPA authorities for medical supplies, and also includes data on vaccines and therapeutics.
Overview of Key Issues
Federal agencies continued to place priority ratings on contracts to respond to COVID- 19. HHS, FEMA, and DOD used DPA Title I authorities to place priority ratings on 44 medical supply-, therapeutics, and vaccine-related contracts as of February 28, 2021. As shown in the figure below, from March through August 2020, agencies generally placed priority ratings on contracts for medical supplies, such as N95 respirators. From August through February 2021 agencies reported placing priority ratings on vaccine contracts, as well as on contracts for therapeutics and vaccine supplies such as vials.
Priority-Rated Actions by Supply Type, March 2020–February 2021
aMedical supplies include N95 respirators, ventilators, air purifying respirators, and goggles.bVaccine supplies include syringes, vials, manufacturing equipment, and other items necessary to support the production and delivery of COVID-19 vaccines.cAll six vaccine manufacturers received priority ratings. As of February 2021 three of the vaccines have received emergency use authorization from the Food and Drug Administration. The remaining three are undergoing clinical trials. dTherapeutics being purchased include monoclonal antibodies, which are laboratory-made antibodies that may potentially be used to prevent or treat COVID-19 infection. According to officials, as of February 2021 five therapeutics manufacturers received priority ratings. As of February 2021, two of five therapeutics have received emergency use authorization from the Food and Drug Administration. The remaining three are undergoing clinical trials.
Federal agencies reported receiving a majority of the N95 respirators, ventilators, air purifying respirators, and goggles that were on priority-rated contracts. For example, federal agencies reported receiving 60 percent of the N95 respirators and 100 percent of the goggles that were on priority-rated contracts.
In addition, as of February 28, 2021, the Centers for Disease Control and Prevention reported distributing over 96 million doses of Pfizer and Moderna vaccines. The government announced the purchase of a total of 600 million doses from these two contractors, which are expected by the end of July 2021. Additional information on vaccines can be found in our forthcoming report.
We interviewed representatives from three medical supply companies and obtained written responses from six vaccine manufacturers that received DPA Title I rated contracts to obtain their observations about the benefits of priority ratings. Representatives from these organizations generally said that the priority rating gave them timely access to raw materials and supplies. For example, one company representative said that demand had increased significantly for meltblown material—a raw material for N95 respirators and ventilators—in the spring of 2020. The company was able to place priority-rated orders to its meltblown material manufacturer to ensure it could meet the contractual delivery date.
HHS and DOD are increasing the domestic production of medical supplies, but challenges remain in addressing national demand. Federal agencies have made approximately $2.3 billion of investments in domestic production expansion projects through DPA and other actions. As shown in the table below, as of February 28, 2021, agencies were executing 42 projects to address shortages of PPE and related material, testing material, and vaccine supplies.
Medical Supply Domestic Production Expansion Projects, through February 2021
Medical supply
Number of projects
Projected annual production increasea (items, millions)
Personal protective equipment
N95 respirators
4
690
Gloves
1
450
Surgical masks
2
532
Gowns
1
1.5
Materials for personal protective equipment and ventilators
Ventilator components
1
7.8
Filter mediab
4
for N95 respirators
1,457
for ventilators
330
for surgical masks
4,344
Testing materials
Swabsticks
1
1,200
Swabs
5
3,388.8
Test and test kits
9
Over 995
Pipette tips
2
1,164
Vaccine supplies
Syringes
4
1,417
Vials
2
284
Fill finish capacity (doses)
1
300
Pharmaceuticals and otherc
5
N/A
Source: GAO analysis of Department of Defense and Department of Health and Human Services data and interviews with agency officials. I GAO-21-387
aAnnual increase is the projected quantity a contractor will produce in 1 year once full rate of production is reached. bFilter media prevents virus particles from passing through the air and is designed specifically for N95 respirators, surgical masks, and ventilators. Some of the agreements stated that the filter media can be used either for surgical masks or respirators. cThree projects are supporting development of a manufacturing technology and do not have an associated full rate of production, and two others did not have a defined full rate of production.
Nine projects were expected to reach full-rate production—an increased rate achieved after domestic expansion projects are fully implemented —as of February 28, 2021. The remainder with defined full rates are expected to achieve full-rate production from March 2021 through September 2022.
However, the federal government has determined that some supply gaps still exist. In January 2021, the National Strategy for the COVID-19 Response and Pandemic Preparedness identified 12 medical supplies with immediate shortfalls, including N95 respirators, isolation gowns, nitrile gloves, sample collection swabs, pipette tips, rapid test kits, and low dead-space needles and syringes.
The federal government has since announced actions to address shortfalls for some of these items. On February 5, 2021, White House officials announced six investments to expand the domestic supply of test kits by approximately 60 million by the end of summer 2021 and additional projects to expand production of nitrile gloves to 1 billion per month by December 2021. According to a White House official, domestic suppliers will be able to meet about half of the U.S. demand for nitrile gloves once these expansion projects are completed. The official stated that the government was negotiating these contracts and that they would be finalized at a later date. As of February 28, 2021, these contracts had not been finalized.
Additional priority ratings and domestic production expansion projects may be forthcoming as agencies implement a January 2021 executive order pertaining to sustaining the public health supply chain.[298] The executive order requires federal agencies, including DOD and HHS, to immediately complete assessments of the availability of medical supplies and the capacity of domestic companies to produce those supplies. It requires agencies to address any supply shortfalls through the DPA or other legal authorities, and provide a report to the White House’s COVID-19 coordinator.
Representatives from the medical supply companies we interviewed told us the following about benefits they had obtained from receiving funding for a domestic production expansion project:
Representatives from five companies said the funding allowed their companies to expand production faster than they could have on their own. Three representatives further stated that their companies would not have made the investments to expand production without receiving government funding.
Some of the companies used the funding to expand their facilities or acquire additional machinery. For example, one company used government funding to acquire nearly 100,000 square feet of production space. Another company used the funding to acquire new machinery and double its domestic production capacity.
Five companies hired additional personnel as they expanded production. These companies reported hiring between 90 and 650 new employees.
A representative from one company said that DOD took actions to help them maintain the schedule. The representative told us that DOD helped the company identify a new supplier to provide a special type of equipment necessary for expanding production. Additionally, the representative told us that DOD coordinated with an embassy to expedite the delivery of machinery from a foreign supplier
Federal agencies are leveraging Title VII authorities to share information and coordinate the distribution of PPE. On December 8, 2020, FEMA published a plan through its Title VII agreement to bring together manufacturers and distributers of PPE and coordinate their efforts. This plan is expected to allow federal agencies, including FEMA, DOD, and HHS, to gather data from private-sector representatives to inform the government’s demand estimates for PPE, and coordinate actions to distribute supplies, among other things. Under Title VII of the DPA, antitrust protections are available for activities carried out under a voluntary agreement.
Under this plan, FEMA created five subcommittees that are focused on a specific issue or supply item. One subcommittee is focused on defining PPE requirements, including the domestic demand for PPE.[299] The remaining four subcommittees are focused on N95 and other medical respirators, gowns, eye and facial coverings, and gloves. According to FEMA officials, in December 2020, the PPE requirements subcommittee developed a 90-day action plan to begin addressing PPE supply concerns. This plan includes efforts to address the supply of raw materials needed for domestic production, and communicate decontamination strategies to extend the life of current PPE, among other things.[300]
At a recent public meeting, FEMA officials stated that FEMA expects to release another plan focused on testing in early 2021.
Federal agencies are taking action to address challenges in executing DPA authorities. HHS and FEMA officials, as well as medical supply company representatives we interviewed identified challenges that they had experienced while executing DPA authorities. HHS and FEMA have taken steps to address some challenges.
Agencies took steps to address company concerns about the complexity of the procurement process. All of the company representatives we spoke with said their companies experienced some problems navigating the federal government’s procurement process, such as developing and submitting white papers to propose a project, negotiating the final terms and conditions of their contracts or agreements, and submitting invoices for payment.[301] In addition, some representatives said their companies had little or no previous experience working with the government. They also indicated that agency officials have been responsive to their questions and were able to assist them or are working to address their problems.
Some commercial companies experienced challenges obtaining a priority rating. HHS’s DPA office developed documents in December 2020 to guide companies through the process of requesting a priority rating. Operation Warp Speed officials also provided training to companies that received priority ratings on how to apply those ratings to subcontracts with their suppliers.
Agencies are considering the effects of priority ratings on supply chains. Federal agencies recognized the importance of maintaining awareness of the effect of priority ratings on suppliers. An HHS official noted that this stemmed from actions taken by agencies early in the pandemic that resulted in priority ratings being placed on multiple ventilator and N95 respirator contracts. Ventilators and N95 respirators share a common raw material—meltblown fabric—that the official said more than ten companies with priority ratings were trying to obtain at the same time. HHS officials worked with the ventilator and N95 companies to identify alternative suppliers and methods for producing meltblown fabric to avoid material shortages. DOD also awarded domestic production expansion projects to increase the supply of this material.
The HHS Acting DPA Program Office supervisor stated that to avoid similar issues for other types of supplies, HHS, DOD, FEMA, the Department of Commerce, and other agencies have been meeting weekly since the spring of 2020 to discuss the potential effect of priority ratings on the supply chain. HHS’s DPA Program Office also developed a template to help employees assess the potential effect of priority rating requests, such as the impact to other contracts or subtier suppliers.
HHS and FEMA have identified gaps in DPA expertise. In June 2020, HHS officials said the department’s contracting workforce had limited experience with, and training on DPA authorities. According to HHS officials, HHS recently took steps to improve its ability to use DPA authorities or other actions to increase domestic production of medical supplies. For example, an HHS official told us that a DPA office was created within the office of the Assistant Secretary for Preparedness and Response in 2020. The office, which is expected to have four full-time staff, is responsible for coordinating the use of DPA authorities, sharing knowledge, and processing priority rating requests. According to an official in the office of the Assistant Secretary for Preparedness and Response, HHS also created an Industrial Base Expansion program office that will manage requirements for medical domestic production expansion projects.
FEMA also identified gaps in its DPA expertise. The agency published a self-assessment of its response to the COVID-19 pandemic in January 2021, which identified as a major operational gap the lack of trained, permanent personnel with expertise to address technical supply chain issues.[302] Specifically, it noted that the FEMA DPA Program Office consists of four full-time employees. The team was given 26 additional federal employees during the COVID response, but only some were familiar with DPA authorities and many required DPA training. FEMA’s assessment recommended taking steps to identify personnel to support the DPA office, such as developing a plan to recruit and train identified positions or formalize an interagency process to allow staff with DPA expertise from other federal agencies to support FEMA.
The federal government is evaluating its future role regarding the domestic production of medical supplies. The COVID-19 pandemic highlighted the shortcomings of U.S. dependence on foreign sources for many medical supplies, including gowns and nitrile gloves. It has also highlighted the benefits the federal government could achieve by using DPA and similar actions to expand domestic production of medical supplies to address some of these shortcomings.
The federal government is currently evaluating what actions it will take in the future with regard to domestic production of medical supplies. Specifically, the January 2021 executive order mentioned earlier also requires agencies to develop a strategy by July 2021 to design, build, and sustain a medical domestic production capability, and create a multiyear implementation plan for the domestic production of medical supplies.[303]
It is too early to assess what specific actions will be taken in response to this executive order. Agency officials we spoke with identified several examples of how the federal government could help sustain medical domestic production capacity, including establishing a dedicated budget line for industrial base investment, helping companies enter into new markets, or entering into long-term procurement contracts with manufacturers, similar to how DOD maintains production with key suppliers of some weapon systems.
We believe that as part of the response to this executive order, HHS should also implement our recommendation from November 2020 to identify how the DPA and similar actions will be used to increase production of domestic medical supplies.
Agency Comments
We provided a draft of this enclosure to DOD, FEMA, HHS, and the Office of Management and Budget (OMB) for review and comment. FEMA and HHS provided technical comments that we incorporated as appropriate. DOD and OMB did not provide comments on this enclosure.
Methodology
To identify agencies’ use of DPA Title I actions, we reviewed agency announcements and interviewed relevant officials. To identify agencies’ use of DPA Title III and similar actions, we reviewed Federal Procurement Data System-Next Generation (FPDS) data and DOD and HHS documentation. To assess DPA Title VII actions, we analyzed FEMA documentation and interviewed key FEMA and other relevant federal agency officials. We solicited contractor perspectives by conducting semistructured interviews with representatives from six companies that had received DPA Title I priority-rated contracts, were executing a domestic production expansion project, or both. We selected those companies because they vary in size, federal contracting experience, and the type of products they produce. We also solicited written responses from all six COVID-19 vaccine manufacturers that received priority-rated contracts. Contractor perspectives are not generalizable to all contractors. We cross-referenced FPDS and agency data against contract announcements and in interviews with various agency and private industry representatives and determined that the data were sufficiently reliable for the purposes of describing agencies’ use of the DPA in response to COVID-19.
Contact information: William Russell, (202) 512-4841, RussellW@gao.gov
Related GAO Product
Defense Production Act:Opportunities Exist to Increase Transparency and Identify Future Actions to Mitigate Supply Chain Issues.GAO-21-108. Washington, D.C.: November 19, 2020.
As of February 28, 2021, federal agencies had reported obligating billions of dollars in support of COVID-19 through contracts and other transaction agreements. The U.S. Department of Agriculture faced challenges reporting more than $1 billion in COVID-19 contract obligations and managing contract files for its Farmers to Families Food Box Program, raising concerns about its guidance and personnel resources for the program.
Entities involved: Agricultural Marketing Service, within the U.S. Department of Agriculture; Department of Defense; Department of Health and Human Services; and Department of Homeland Security, among others
Recommendations for Executive Action
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to issue guidance—such as an acquisition alert or a reminder to contracting officials—on the use of the COVID-19 National Interest Action code for the Farmers to Families Food Box Program or successor food distribution program to ensure it accurately captures COVID-19-related contract obligations in support of the program. The U.S. Department of Agriculture neither agreed nor disagreed with our recommendation.
In a draft of this report provided to U.S. Department of Agriculture for comment, this recommendation included a provision to retroactively report prior contract actions with the National Interest Action code. The U.S. Department of Agriculture agreed and took prompt action that addressed our concern about adequately capturing COVID-19-related contract obligations in support of the Farmers to Families Food Box Program. As a result, we have removed that part of this recommendation from the final report.
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the Farmers to Families Food Box Program or successor future food distribution program, and take the necessary steps to ensure it has adequate contracting staff in place to award and administer any future contracts for the program. The U.S. Department of Agriculture neither agreed nor disagreed with our recommendation.
Key Considerations and Future GAO Work
As federal contracting activity continues to play a critical role in response to the pandemic, ensuring that contract actions made in response to COVID-19 are accurately reported and visible to congressional decision makers, entities with oversight responsibilities, and taxpayers is critical. In January 2021, we recommended that the Assistant Secretary for Preparedness and Response (ASPR) accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts. The Department of Health and Human Services (HHS) concurred and stated that it has taken steps to manually identify other transaction agreements in its contract writing system. HHS also plans to update its contract writing system. HHS did not provide an update on its progress implementing the recommendation.
In September 2020, we recommended that the Secretaries of Homeland Security and Defense (1) revise the 2019 National Interest Action (NIA) code memorandum of agreement to identify steps they will take to obtain input from key federal agencies prior to extending or closing a NIA code; (2) establish timelines for evaluating the need to extend a NIA code; and (3) define certain criteria for extending or closing the NIA code to reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic.[304]
The Department of Homeland Security (DHS) and the Department of Defense (DOD) did not agree with our recommendations. However, as of February 2021, a DOD official said that DHS and DOD were in the process of updating the agreement to clarify the steps they would take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close a NIA code. We will review the updated agreement when finalized to determine whether it meets the intent of the recommendation.
We have work underway related to the federal government’s use of contracts to respond to COVID-19, including, among other things, assessing (1) contracts awarded by selected agencies in response to COVID-19, including agencies’ efforts to review prospective contractors in advance of awarding a contract, and (2) selected agencies’ use of contracting flexibilities, such as other transaction agreements and undefinitized contracts.
Background
To facilitate the U.S. response to COVID-19, federal agencies have used a variety of contracting mechanisms to provide vital goods and services in support of federal, state, and local COVID-19 response efforts. For example, federal agencies have reported billions of dollars in obligations on contracts subject to the Federal Acquisition Regulation.[305] Our prior work on disaster contracting has found that contracts play a key role in federal emergency response efforts, and that contracting during an emergency can present a unique set of challenges as officials can face significant pressure to provide critical goods and services as expeditiously and efficiently as possible. The January 2021 National Strategy for the COVID-19 Response and Pandemic Preparedness emphasizes the important role contracts will continue to play during the response. The strategy states that the federal government will fully leverage contract authorities to strengthen the vaccine supply chain; staff vaccination sites; and fill supply shortages for personal protective equipment, drugs, and therapeutics.
In addition, federal agencies like DOD and HHS have relied on the use of other transaction agreements to respond to COVID-19. Such agreements can enable them to negotiate terms and conditions specific to a project. The CARES Act relaxed certain limitations on the use of other transactions for HHS and DOD, such as congressional reporting requirements and requirements for who can approve certain transactions.[306]
NIA codes were established in 2005 following Hurricane Katrina to enable the consistent tracking of emergency or contingency-related contracting actions in the Federal Procurement Data System-Next Generation (FPDS-NG). Based on the memorandum of agreement guiding the management of the NIA code, DHS and DOD are responsible for making determinations about whether to establish or close a code, based on a variety of considerations. The General Services Administration (GSA)—the agency that operates and maintains FPDS-NG—is responsible for adding or updating the NIA code in the system based on DHS’s and DOD’s decisions. The COVID-19 NIA code—used to track contract actions and associated obligations in response to COVID-19 in FPDS-NG—was originally established on March 13, 2020, and set to expire on July 1, 2020. DHS and DOD subsequently extended the code three times—first to September 30, 2020, then to March 31, 2021, and more recently to September 30, 2021. The extensions of the code are consistent with our prior recommendations to DHS, DOD, and GSA related to the importance of ensuring federal agencies, the public, and Congress have visibility into contract actions and associated obligations related to emergency response efforts.
In May 2020, USDA implemented the Farmers to Families Food Box Program to assist commodity suppliers impacted by the pandemic and to provide food assistance to the public. To accomplish these goals, USDA contracted with hundreds of distributors to purchase billions of dollars in fresh fruits, vegetables, dairy, and meat products, and package these products into family-sized food boxes for delivery to food banks, community and faith-based organizations, and other non-profit entities across the country.
Overview of Key Issues
Agencies obligated $55.5 billion on federal contracts, with DOD and HHS accounting for most obligations. In response to the COVID-19 pandemic, contract obligations totaled about $55.5 billion as of February 28, 2021. DOD accounted for about 43 percent and HHS for about 28 percent of the total obligations made by federal agencies. USDA’s obligations, almost all of which were in support of the Farmers to Families Food Box Program, accounted for $5.2 billion, or 10 percent of total obligations made in response to COVID-19 (see figure).[307]
Contract Obligations in Response to COVID-19 by Federal Agency, as of February 28, 2021
In our January 2021 report, we reported that government-wide contract obligations related to COVID-19 totaled $41.4 billion through December 31, 2020; by February 28, 2021, those obligations had increased by about $14 billion—to $55.5 billion. DOD accounted for about $9.7 billion, or about 70 percent of the increase in total contract obligations since December 31, 2020. See figure for government-wide obligations by week.
Government-wide Contract Obligations Related to COVID-19 by Week, February 2020–February 2021
Obligations on drugs and biologicals surpassed medical equipment and supplies to be the largest area of government-wide contract obligations in response to COVID-19. As of February 28, 2021 obligations for drugs and biologicals almost tripled to $14.6 billion from $5.4 billion as of December 31, 2020, and represented about two-thirds of the overall increase in contract obligations. About $6.3 billion of the increase in obligations for drugs and biologicals is for the purchase of an additional 100 million vaccine doses each from Pfizer and Moderna, along with the purchase of 1.25 million doses of Regeneron’s therapeutic to treat COVID-19. Medical equipment and supplies—including ventilators and personal protective equipment—increased by about $227.4 million since December 31, 2020, and accounted for about $8.9 billion, or 16 percent of government-wide contract obligations. Obligations for fruits and vegetables—made primarily in support of the USDA’s Farmers to Families Food Box Program—increased by an additional $1.5 billion, to $3.9 billion. This increase was driven in part by USDA’s updates to data reporting in response to our draft report recommendation that the Agricultural Marketing Service (AMS) address inaccurate contract action reporting. See figure for obligation amounts for the most-procured goods and services.
Contract Obligation Amounts for Goods and Services Most Procured in Response to COVID-19, as of February 28, 2021
As of February 28, 2021, the proportion of contracts identified as having been awarded non-competitively increased to about 60 percent of government-wide contract obligations, or about $33.5 billion.[308] Officials at HHS, DOD, and DHS have identified supply chain shortages for goods like personal protective equipment and testing supplies which, according to a DOD official, contributed to the need to award some contracts noncompetitively. Agencies must provide for full and open competition when awarding contracts, unless one of several limited exceptions applies, such as when there is an unusual and compelling urgency for a needed supply or service. Agencies cited an urgent need for awarding contracts noncompetitively for about 81 percent, or about $27.2 billion, of the contract obligations associated with noncompetitive awards.[309] However, our prior work has noted that promoting competition—even in a limited form—increases the likelihood of acquiring quality goods and services at a lower price in urgent situations.
As of February 28, 2021, contracts for goods continued to be competed less frequently than contracts for services: About 72 percent of the obligations for goods were on contracts that were not awarded competitively, compared with about 40 percent of the obligations for services. For example, about $14.1 billion, or 97 percent, of the $14.6 billion in obligations for drugs and biologicals and about $7.6 billion, or 85 percent, of the $8.9 billion in obligations for medical and surgical equipment, were on contracts awarded noncompetitively.
Undefinitized contracts are one technique that agencies have reported using to respond to COVID-19. Undefinitized contracts can enable the government to quickly fulfill requirements that are urgent or need to be met quickly by allowing contractors to begin work before reaching a final agreement with the government on all contract terms and conditions.[310] As of February 28, 2021, undefinitized contract obligations were about $4.9 billion, and accounted for about 9 percent of government-wide contract obligations on contracts awarded in response to COVID-19. DOD reported the highest amount of undefinitized contract obligations, identifying about $4 billion, or about 17 percent of its COVID-19-related contract obligations as being undefinitized. Our prior work has shown that these types of contracts can pose risks to the government. For example, contractors may lack incentives to control costs before all contract terms and conditions are defined.
Federal agencies have obligated at least $12.2 billion through other transaction agreements. Three federal agencies—DOD, HHS, and DHS—have continued to report using other transaction agreements in response to COVID-19. From December 31, 2020, through February 28, 2021, obligations associated with other transaction agreements reported by DOD, HHS, and DHS increased from about $11.9 billion to $12.2 billion. Of the $12.2 billion, DOD reported obligating about $10.8 billion through other transaction agreements, including at least $8.7 billion for Operation Warp Speed, an effort to manufacture large-scale vaccines and therapeutics in response to COVID-19.
Our analysis of FPDS-NG data and agreement documents found at least four other transaction agreements with about $1.5 billion obligated in support of the Operation Warp Speed effort and other medical countermeasures, which can include therapeutic treatments and testing capabilities. In our January 2021 report, we found that ASPR had misreported these other transaction agreements as procurement contracts. Our prior work has noted that the use of other transaction agreements can help agencies attract companies that do not typically do business with the government. However, their use also carries a risk of reduced accountability and transparency.
USDA faced challenges reporting more than $1 billion in contract obligations and managing contract documentation for the Farmers to Families Food Box Program. AMS, the USDA agency implementing the Farmers to Families Food Box Program, has awarded hundreds of contracts for the Farmers to Families Food Box Program. Contractors received contracts to purchase, package, and distribute food to food banks and other non-profits across the country. As USDA received additional funding for the program throughout 2020, AMS continued to periodically solicit prospective contractors and award contracts to keep the program operational.
We identified contract data reporting challenges related to AMS’s early awards in support of the program. For example, in February 2021, we found over 300 contract actions totaling about $1.2 billion in obligations for the Farmers to Families Food Box Program that were not reported with the NIA code, even though the base contracts were coded as related to the COVID-19 response. AMS has corrected these data reporting issues, which addresses our draft report recommendation that AMS retroactively report the contract actions with the NIA code. We also found some of the program’s contracts—totaling up to $218 million in obligations—were incorrectly reported in FPDS-NG as competitively awarded instead of as non-competitively awarded, which AMS officials also corrected after we brought it to their attention.
In addition to contract data reporting issues, we found that AMS has experienced challenges compiling complete contract documentation for the approximately 200 contracts awarded in the spring and summer of 2020. A contracting official involved in the program noted that currently contract documentation associated with some awards—such as acquisition planning documents, source selection and pricing decisions, and correspondence with contractors—are stored in various contracting personnel email accounts and computers, rather than in AMS’s Web Based Supply Chain Management System, the AMS system of record for maintaining contract files. This is the case even though some of these contracts were awarded more than 9 months ago in May 2020. The Federal Acquisition Regulation requires the heads of contracting offices to establish files containing the records of all contract actions to provide a complete background of the basis for the decisions made in the acquisition process.[311] AMS officials noted that the contract documentation in question exists and that its organization has improved over time.
According to AMS officials, the Farmers to Families Food Box Program was a new program implemented in a matter of weeks to address the economic difficulties facing farmers and agricultural producers, food suppliers and distributors, and unemployed Americans in need of food assistance as a result of COVID-19. However, the contract data reporting and documentation challenges we identified raise questions about whether AMS has provided sufficient guidance or contracting resources to the program to ensure that the contracts awarded to support the Farmers to Families Food Box Program have been effectively reported and managed. When we spoke to AMS officials, we found that no additional direction was provided to the AMS personnel responsible for entering contract actions into FPDS-NG regarding coding all procurement actions made in response to COVID-19 with the NIA code.
Furthermore, according to AMS officials, one contracting officer and seven contracting specialists largely executed the contracts made in support of the program—totaling over 1,200 contract actions and $5.2 billion in contract obligations as of February 28, 2021. According to a contracting official involved in the program, the speed with which the contracts for the program have been executed and the sheer volume of awards that continue to be made have affected contracting officials’ ability to ensure accurate contract reporting and the compilation of complete contract files. According to AMS officials, they leveraged about 20 staff to assist with vendor reviews, invoice approval, domestic origin verification, and food safety audits related to the program. However, AMS officials said they did not consider adding additional contracting officers or specialists from within AMS or other USDA agencies to award or administer Farmers to Families Food Box Program contracts, even though the obligations for the program accounted for about 74 percent of AMS’s total reported contract obligations over the past year.
AMS officials noted that they used a different contracting approach starting in September 2020 for the program that has added some efficiencies to the contracting process.[312] However, the challenges we found related to inaccurate contract reporting and incomplete contract files have persisted even after the change in contracting strategy. AMS officials also stated that they recently completed a reorganization based on a workforce analysis completed several years ago. Under the reorganization, AMS said they have hired or plan to hire at least 20 staff, including contracting officers and specialists. However, as of February 2021, AMS officials said that they have not specifically assessed whether the additional contracting officers will be assigned to support the Farmers to Families Food Box Program since it is expected to be completed in April 2021, and they are uncertain what plans, if any, there will be to continue the program.
In September 2020, we reported that the need to quickly execute the program led to challenges, including limited time to implement the program and limited staff, and that USDA did not have plans to evaluate the program to identify successes, challenges, and lessons learned. At that time, USDA officials stated that because the Farmers to Families Food Box Program was developed as a temporary measure in response to the COVID-19 outbreak, the costs of conducting a programmatic evaluation seemed to outweigh the benefits, and that the program was expected to be completed by the end of October 2020. However, since then, the program has been extended, with the agency receiving an additional $2 billion and awarding numerous additional contracts. Under the American Rescue Plan Act of 2021, signed into law on March 11, 2021, USDA is to receive an additional $4 billion in funding for the pandemic response, which includes additional funds for purchasing and distributing food to individuals in need.[313] Additional funding to continue food distribution efforts makes an assessment of the contracting workforce needed to award and administer contracts in support of the Farmers to Families Food Box Program, or a successor food distribution program, all the more crucial.
Federal internal control standards state that an agency’s management should internally and externally communicate quality information to achieve the agency’s objectives. Moreover, key principles for strategic workforce management emphasize the importance of determining the critical skills and competencies needed to achieve future programmatic results and addressing gaps in critical skills and competencies to achieve mission success. Without guidance reinforcing the need to use the NIA code to track Farmers to Families Food Box contract actions, AMS may continue to face challenges reporting quality information on billions of dollars in contract activity to the public—including congressional decision makers, entities with oversight responsibilities, and taxpayers. The accurate reporting of Farmers to Families Food Box Program contract obligations is especially important given that fruits and vegetables is the federal government’s third largest area of contract obligations, after “drugs and biologicals” and “medical equipment and supplies”. Moreover, without assessing the workforce needed to manage existing contracts that underpin the program and any future food distribution contracts, AMS cannot ensure that the contract reporting and management of contract documentation challenges they have encountered are addressed, particularly as an additional $4 billion in funding is provided.
Agency Comments
We provided HHS, DOD, DHS, USDA, and the Office of Management and Budget with a draft of this enclosure. HHS, DOD, DHS, and the Office of Management and Budget did not provide comments. USDA provided comments, which we incorporated as appropriate and summarize below.
In its comments, USDA agreed with part of a draft recommendation stating that USDA should retroactively report contract actions with the NIA code to adequately capture COVID-19-related contract obligations in support of the program. Prior to the publication of this report, USDA took action and addressed that part of the recommendation. As a result, we have removed that part of the recommendation from the final report.
USDA neither agreed nor disagreed with our recommendation to issue internal guidance on the use of the COVID-19 NIA code to ensure USDA AMS accurately captures its COVID-19-related food distribution contract obligations. According to AMS officials, additional guidance related to using the NIA code is not needed because Office of Management and Budget memorandum M-20-21 already directs agencies to use the COVID-19 NIA code for all procurement actions reported in the FPDS-NG.[314] However, with OMB’s guidance in place, AMS officials still encountered challenges accurately coding over $1 billion in contract actions. Moreover, several agencies, including DOD, DHS, HHS, and the Department of Veterans Affairs, have issued supplemental guidance or alerts to communicate the Office of Management and Budget requirements to their personnel. Additional guidance, such as an acquisition alert or reminder to contracting officials, would help to ensure AMS’s coding challenges do not persist in the future.
USDA also neither agreed nor disagreed with our recommendation to assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the Farmers to Families Food Box Program or successor future food distribution program. AMS officials stated that they had the right amount of staff to successfully execute contracts for the Farmers to Families Food Box Program, and that the number of staff supporting the program had little to do with the issues we identified. However, as noted above, AMS officials we spoke with did attribute challenges with contract data reporting and management to the sheer volume of awards that continue to be made in support of the program. AMS officials noted in their comments that they are in the process of filling some positions and adding staff, which we also note above, but AMS has not determined how these or other contracting staff will support contract management and administration needs. Given the additional $4 billion in funding USDA will receive for the pandemic response, which includes additional funds for food distribution efforts, we maintain that guidance to ensure the accurate reporting of its COVID-19- related contract obligations and an assessment of the contracting workforce needed to effectively support the program are prudent steps to take.
Methodology
To identify agencies’ federal contract and other transaction agreement obligations and competition rate on contracts in response to COVID-19, we reviewed data reported in the FPDS-NG through February 28, 2021.[315] We identified contract obligations related to COVID-19 using the NIA code, as well as the contract description field.[316] For contract actions over $1 million, we removed obligations that were identified in the contract description as not related to COVID-19.
We assessed the reliability of federal procurement data by reviewing existing information about FPDS-NG and the data it collects—specifically, the data dictionary and data validation rules—and by performing electronic testing. For the four other transaction agreements that HHS misreported as contracts, we removed the $1.5 billion associated obligations from our reported contract obligations and reported them instead as other transaction agreement obligations. We determined that the data were sufficiently reliable for the purposes of describing agencies’ reported contract obligations in response to COVID-19.
To assess USDA’s contract reporting and management of the Farmers to Families Food Box Program, we reviewed program documentation and interviewed AMS officials.
Contact information: Marie A. Mak, (202) 512-4841, MakM@gao.gov
Related GAO Products
Agriculture Spending: Opportunities Exist for USDA to Identify Successes and Challenges of the Farmers to Families Food Box Program to Inform Future Efforts.GAO-20-711R. Washington, D.C.: September 16, 2020.
COVID-19 Contracting: Observations on Federal Contracting in Response to the Pandemic.GAO-20-632. Washington, D.C.: July 29, 2020.
Defense Acquisitions: DOD’s Use of Other Transactions for Prototype Projects Has Increased. GAO-20-84. Washington, D.C.: November 22, 2019.
DATA Act: Quality of Data Submissions Has Improved but Further Action Is Needed to Disclose Known Data Limitations. GAO-20-75. Washington, D.C.: November 8, 2019.
Disaster Contracting: FEMA Continues to Face Challenges with Its Use of Contracts to Support Response and Recovery. GAO-19-518T. Washington, D.C.: May 9, 2019.
2017 Disaster Contracting: Actions Needed to Improve the Use of Post-Disaster Contracts to Support Response and Recovery. GAO-19-281. Washington, D.C.: April 24, 2019.
2017 Disaster Contracting: Action Needed to Better Ensure More Effective Use and Management of Advance Contracts. GAO-19-93. Washington, D.C.: December 6, 2018.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 2014.
Federal Contracting: Noncompetitive Contracts Based on Urgency Need Additional Oversight.GAO-14-304. Washington, D.C.: March 26, 2014.
Department of Homeland Security: Further Action Needed to Improve Management of Special Acquisition Authority. GAO-12-557. Washington, D.C.: May 8, 2012.
Defense Contracting: DOD Has Enhanced Insight into Undefinitized Contract Action Use, but Management at Local Commands Needs Improvement. GAO-10-299. Washington, D.C.: January 28, 2010.
Department of Homeland Security: Improvements Could Further Enhance Ability to Acquire Innovative Technologies Using Other Transaction Authority. GAO-08-1088. Washington, D.C.: September 23, 2008.
Human Capital: Key Principles for Effective Strategic Workforce Planning. GAO-04-39. Washington, D.C.: December 11, 2003.
The number of claims for unemployment insurance benefits remained historically high through mid-March 2021, as CARES Act unemployment insurance programs were extended for another several months. Although states have improved their timeliness in making first payments for certain unemployment insurance benefits since fall 2020, some claimants continue to face substantial delays in receiving these payments. We continue to focus on the implications of the high number of claims, including program integrity concerns.
Entity involved: Department of Labor
Recommendation for Executive Action
We are making the following recommendation to the Department of Labor:
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments waived in the Pandemic Unemployment Assistance program, similar to the regular unemployment insurance program. The Department of Labor concurred with our recommendation.
Key Considerations and Future GAO Work
The unemployment insurance (UI) system provides a vital safety net for individuals who become unemployed through no fault of their own, and this support is essential during widespread economic downturns. In mid-March, as CARES Act UI programs were extended through September 6, 2021, the UI system continued to experience high numbers of claims, indicating that many Americans are still relying on the financial support these programs provide as the U.S. economy continues to respond to the COVID-19 pandemic.
However, as we previously reported, the Department of Labor (DOL) does not collect or report reliable counts of the number of individuals claiming benefits. In November 2020, we recommended that DOL address this issue by (1) revising its weekly news releases to clarify that the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits, and (2) pursuing options to report the actual number of distinct individuals claiming benefits from January 2020 onward. DOL fully agreed with our first recommendation and partially agreed with our second recommendation, taking issue with retroactive reporting.
Starting with the December 10, 2020 weekly UI news release, DOL has clarified that the numbers it reports for weeks of unemployment claimed do not represent the number of unique individuals claiming benefits, and we consider this recommendation closed. However, as of March 18, 2021, DOL had not begun reporting the actual number of unique individuals claiming UI benefits on a weekly basis in its UI news releases. We maintain that these data are vital to understanding the size of the population supported by the UI system during the pandemic. Even if the information is unavailable for some time, reporting numbers for calendar year 2020 and after will help DOL and policymakers identify lessons learned about the administration and utilization of regular and expanded UI benefit programs during the pandemic. We encourage DOL to pursue options to report the actual number of individuals claiming benefits in the most feasible and least burdensome way.
We continue to focus on the implications of persistently high numbers of claims for UI benefits. Backlogs in processing historic numbers of UI claims during the pandemic have led to delays in eligible claimants receiving their first benefits. Although the timeliness of certain UI payments has improved since fall 2020, some claimants continue to face substantial delays in receiving their first benefit payments. In addition, as the number of UI claims remains historically high, states continue to face financial strain, and some have sought loans from the federal government to pay UI benefits. As of March 12, 2021, 20 states and territories held about $52.1 billion in federal loans taken out to pay UI benefits.
We also remain concerned about program integrity throughout the UI system. DOL continues to stress the importance of addressing potential fraud in the UI system and support states to help ensure UI program integrity. For example, early in 2021, DOL continued to stress the importance of UI program integrity in its guidance documents and provided additional administrative funding to carry out program integrity efforts. The Department of Justice, DOL’s Office of Inspector General, and states continue to take actions to prevent, detect, and respond to potential UI fraud.
In addition, in January 2021, we recommended that DOL collect data from states on the amount of overpayments recovered in the Pandemic Unemployment Assistance program. DOL agreed with our recommendation and on January 8, 2021, took the first step toward implementing it by issuing instructions for states to report this overpayment recovery data. As of March 15, 2021, 14 states had begun reporting some overpayment recovery data to DOL.
Additional data on the amounts of overpayments states do not intend to recover are also needed for effective monitoring of federal funding. Legislation enacted at the end of 2020 authorized states to waive certain overpayments made at any time in the Pandemic Unemployment Assistance program—for example, if the individual who was overpaid was without fault and repayment would be contrary to equity and good conscience.[317] DOL is not yet collecting information from states about these waived overpayments. Sustained reporting by states would inform DOL, policymakers, and the public about the extent of overpaid federal funds states have recovered, how much remains outstanding, and how much states do not intend to recoup.
Since our last report in January, several developments have expanded access to CARES Act UI benefits or affected the program in other ways. On February 25, 2021, DOL issued guidance expanding eligibility for benefits under the Pandemic Unemployment Assistance program to include, among others, certain individuals who refuse to return to work or accept an offer of new work that is unsafe.[318]
The American Rescue Plan Act of 2021, enacted on March 11, 2021, extended CARES Act UI programs through September 6, 2021, and included other provisions related to UI, such as allowing $10,200 of unemployment insurance compensation to be tax free in 2020, if an individual’s adjusted gross income is less than $150,000.[319] The law also provides $2 billion for DOL to detect and prevent fraud, promote equitable access, and ensure the timely payment of UI benefits, and $8 million for administrative expenses related to UI programs.[320] We will monitor these developments and program integrity issues as we continue our oversight work.
Background
The UI program is a federal-state partnership that provides temporary financial assistance to eligible workers who become unemployed through no fault of their own. States design and administer their own UI programs within federal parameters, and DOL oversees states’ compliance with federal requirements, such as ensuring states pay benefits when they are due. Regular UI benefits—those provided under the state UI programs in place before the CARES Act was enacted—are funded primarily through state taxes levied on employers, and are intended to typically be lower than a claimant’s previous earnings, according to DOL.[321]
The CARES Act created, and the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021, amended, three federally funded temporary UI programs that expanded benefit eligibility and enhanced benefits.[322]
Pandemic Unemployment Assistance (PUA), generally available through September 6, 2021, generally authorizes up to 79 weeks of UI benefits to individuals not otherwise eligible for UI benefits, such as self-employed and certain gig economy workers, who are unable to work as a result of specified COVID-19 reasons.[323]
Federal Pandemic Unemployment Compensation (FPUC) generally authorized an additional $600 weekly benefit through July 2020, and authorizes a $300 benefit for weeks beginning after December 26, 2020 and ending on or before September 6, 2021, for individuals eligible for weekly benefits under the regular UI and CARES Act UI programs.[324]
Pandemic Emergency Unemployment Compensation (PEUC), generally available through September 6, 2021, generally authorizes an additional 53 weeks of UI benefits to those who exhaust their regular UI benefits.[325]
The Consolidated Appropriations Act, 2021 created, and the American Rescue Plan Act of 2021 extended, the Mixed Earner Unemployment Compensation (MEUC) program, which authorizes an additional $100 weekly benefit for certain individuals.[326] To be eligible, claimants must have received at least $5,000 of self-employment income in the most recent tax year prior to their application for UI benefits. The $100 weekly benefit is in addition to other UI benefits received by claimants; however, individuals receiving PUA benefits may not receive MEUC payments.[327]
In addition to the extensions and expansions of benefits, the Consolidated Appropriations Act, 2021 added new program integrity requirements for the CARES Act UI programs. For example, the act generally requires PUA claimants to provide documentation substantiating their prior employment or self-employment and to recertify with their state each week that they continue to meet the eligibility requirement of not being able to work as a result of COVID-19.[328] In addition, states are required to have procedures for identity verification or validation and for timely payment of PUA benefits, to the extent reasonable and practicable.[329] Further, states must generally require individuals who receive PUA benefits they were not entitled to, to repay the amount, but states can waive that requirement under certain conditions.[330]
During the pandemic, regular UI claimants in certain states have also had access to the Extended Benefits program. The program, which existed prior to the pandemic and provides up to an additional 13 or 20 weeks of benefits, is activated in states during periods of high unemployment, according to DOL. If unemployment is not high enough to activate the Extended Benefits program in a state, or if regular UI claimants exhaust their PEUC and Extended Benefits, they may be eligible for PUA benefits—provided they also meet PUA eligibility requirements.[331]
Overview of Key Issues
About a year after enactment of the CARES Act, the number of weekly initial claims for UI benefits remains persistently high. DOL reported that 746,496 initial claims for regular UI benefits and 282,394 initial claims for PUA benefits were submitted nationwide during the week ending March 13, 2021.[332] The number of regular UI initial claims submitted in recent weeks is considerably lower than the peak of about 6.2 million submitted in the week ending April 4, 2020 (see figure). However, the number of regular UI initial claims submitted each week has remained considerably higher than pre-pandemic levels. For example, the 746,496 regular UI initial claims submitted during the week ending March 13, 2021—which does not include the 282,394 PUA initial claims also submitted—is about 3 times as high as the 251,851 submitted during the corresponding week in 2020, prior to enactment of the CARES Act.
Weekly Initial Claims Submitted Nationwide for Regular Unemployment Insurance (UI) and Pandemic Unemployment Assistance (PUA) Benefits, March 1, 2020 through March 13, 2021
Notes: The weekly counts of initial claims shown in the figure are not seasonally adjusted. Counts for weeks through February 27, 2021, are from Department of Labor (DOL) data files that include any adjustments submitted by states as of March 18, 2021. Counts for the weeks ending March 6 and 13, 2021, are from DOL’s weekly report released on March 18, 2021, and the March 13 numbers reflect advance initial claims, which are preliminary and subject to revision. The number of states and territories reporting PUA data is out of a potential total of 53. All 53 states and territories reported regular UI claims in each week shown.
The number of initial claims is not intended to measure how many claimants were determined eligible to receive benefits or how many who filed for benefits earlier in the pandemic are still unemployed. DOL officials have stated that continued claims may be a better barometer than initial claims for determining whether demand for benefits remains high. Each week, DOL publishes the number of continued claims submitted by states (i.e., weeks of unemployment claimed by individuals during a reporting period). For example, for the week ending February 27, 2021, states reported about 18.2 million continued claims in all programs, including:
about 6.1 million in other programs, such as the PEUC program.[334]
The about 4.5 million regular UI continued claims is substantially lower than the peak of over 20 million submitted per week in late April and early May 2020. Some of this decline is due to claimants finding employment, though some of the decline is also likely due to other factors, such as claimants exhausting regular UI benefits and beginning to claim PEUC or other benefits. Even with the decline—regardless of the cause—the number of regular UI continued claims submitted during the week ending February 27, 2021 (about 4.5 million) remains more than double the approximately 2.1 million claims submitted for the corresponding week in 2020, prior to the pandemic. In addition, during the 2007-2009 recession, by comparison, regular UI continued claims peaked at about 6 million submitted each week from December 28, 2008 through August 22, 2009.[335]
The persistently high number of claims suggests continued high demand for benefits. However, as we have previously reported, the number of continued claims has not approximated the number of individuals claiming benefits during the pandemic due to backlogs in processing historic numbers of claims in many states and other data issues. For example, backlogs in claims processing led to individuals claiming multiple weeks of benefits in single reporting periods and thus being counted as multiple claims for that reporting period, particularly in the PUA program. As previously stated, while DOL partially agreed to take action to address our recommendation on this issue, it has not yet taken steps to do so. As such, reliable conclusions about trends in the number of individuals claiming benefits cannot be drawn from data on continued claims.
The large number of claims submitted for PEUC and the Extended Benefits program suggests that many individuals may be experiencing long-term unemployment.[336] After exhausting regular UI benefits—generally available for up to 26 weeks in most states—eligible individuals are generally able to apply for (1) PEUC; then, (2) the Extended Benefits program, if activated in a state; and then, in certain circumstances, (3) PUA benefits.[337]
As we reported in January, the number of continued claims submitted nationwide (i.e., weeks of unemployment claimed by individuals during a reporting period) under PEUC and the Extended Benefits programs increased substantially in the fall of 2020, likely due to individuals exhausting their regular UI benefits as the pandemic continued. Although the number of PEUC continued claims submitted nationwide each week declined at the end of 2020 and beginning of 2021, the number remains high—about 4.8 million submitted during the week ending February 27, 2021 (see figure). Similarly, the number of continued claims submitted under the Extended Benefits program increased from about 352,000 during the week ending September 19 to about 1.1 million the week ending February 27, 2021.
Weekly Continued Claims Submitted Nationwide for Pandemic Emergency Unemployment Compensation (PEUC) Benefits, March 1, 2020 through February 27, 2021
Notes: The weekly counts of continued claims shown in the figure are not seasonally adjusted. Counts for weeks through February 20, 2021, are from Department of Labor (DOL) data that include any adjustments submitted by states as of March 18, 2021. The count for the week ending February 27, 2021, is from DOL’s weekly report released on March 18, 2021. The number of states and territories reporting PEUC data is out of a potential total of 53.
Most states are participating in the new Mixed Earner Unemployment Compensation program, which authorizes an additional $100 weekly benefit for certain self-employed individuals who are ineligible for PUA.[338] State participation in the new MEUC program is voluntary.[339] According to DOL, as of March 3, 2021, 51 of 53 states and territories had elected to participate in the MEUC program, though just 2 had begun paying MEUC benefits.[340] As states implement the MEUC program, they will be reporting monthly data to DOL on MEUC claims, including the number of initial claims, the number determined eligible, and the number of weeks compensated.
The MEUC program is intended to cover individuals who have sufficient earnings to qualify for regular UI, but whose regular UI benefits do not account for significant self-employment income, according to DOL. Individuals who qualify for regular UI are not eligible for PUA, and self-employment earnings are not considered when determining their regular UI benefits. Thus, certain individuals may receive a lower regular UI benefit than the benefit they would have received under PUA based on their self-employment earnings, had they been eligible for PUA.
For example, individuals who work in the performing arts may earn a majority of their income from performance gigs as independent contractors or self-employed individuals, and then supplement this income by working part-time at a restaurant. These part-time wages may make the individual eligible for regular UI benefits, and thus ineligible for PUA benefits. In 44 of 53 states and territories, the minimum weekly benefit for the regular UI program is below $100.[341] If this individual instead qualified for the PUA benefit based on their self-employment income, they would be eligible for at least the PUA minimum benefit, which is generally above $100 per week, and might be eligible for more than the minimum benefit, depending on their prior earnings.[342] Under the MEUC program, certain claimants may now receive an additional $100 weekly to supplement their regular UI benefits.
Backlogs in processing historic numbers of claims have led to delays in eligible claimants receiving their first benefits, though payment timeliness has been improving. The timeliness of first payments of regular UI benefits declined substantially during the pandemic (see figure), as states received historically high numbers of claims, which resulted in extensive claims processing backlogs.[343] Among regular UI claimants nationwide who received their first benefit payments in June 2020, about half had been waiting longer than 21 days since their first week of eligibility, according to DOL’s state-reported data. This represents a precipitous drop from the first 3 months of 2020, which reflect UI eligibility prior to the pandemic, when overall more than 90 percent of first payments were made within 21 days. In addition, nationwide, in October 2020, about a quarter of claimants who received their first benefit payments that month had been waiting longer than 70 days; in the 3 months prior to the pandemic, less than 1 percent of first payments took this long.
First payment timeliness improved in late 2020 and early 2021 (see figure). Among regular UI claimants nationwide who received their first benefit payments in January 2021, about 78 percent were paid within 21 days of their first week of eligibility. However, the extension of the CARES Act UI programs at the end of 2020 could impact payment timeliness if states had to reassign staff or focus resources on implementing new program requirements, according to DOL officials. In addition, timeliness of regular UI first payments varies by state (see figure). For example, 11 states reported that at least 87 percent of their regular UI first payments in January 2021 were paid within 21 days—DOL’s general benchmark for acceptable performance.[344]
On the other hand, 4 states reported paying less than half of their claims within 21 days, suggesting that several states continue to struggle to reach their pre-pandemic levels for timely payments. Further, officials we interviewed in a couple states told us that as of late 2020 and early 2021, backlogs in claims processing still exist. As eligible claims among these backlogs are processed, first payment timeliness in these states may decline, depending on how long these claims had been waiting to be processed.
Timeliness of First Payments of Regular Unemployment Insurance (UI) Benefits, January 2020 through January 2021
Notes: We analyzed first payment timeliness data that include reporting and adjustments submitted by states as of March 15, 2021, at which point just 25 of the 53 states and territories had reported data for February 2021. Thus, we analyzed data through January 2021; 52 of 53 states and territories had reported data for January 2021. The line graph represents the percentage of regular UI first benefits paid within 21 days, nationwide. The pie charts depict how many of the 53 states and territories paid a given percentage of first benefits within 21 days. One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible, depending on whether the state has a waiting week requirement. We focus on payments made within 21 days because in guidance released at the start of the pandemic, DOL recommended that states consider temporarily waiving their waiting week requirements. Our pie charts include a category for states that paid at least 87 percent within 21 days because states must pay at least 87 percent of claims within 14 or 21 days to reach an acceptable level of performance, according to DOL.
As we have previously reported, although DOL has not tracked the timeliness of payments in the temporary PUA program, DOL officials told us that states have struggled with making PUA payments in a timely manner. For example, they said regional officials had observed a number of implementation challenges at the state level that likely contributed to claims processing backlogs and payment delays. In addition, according to DOL officials, the PUA program changes enacted in the Consolidated Appropriations Act, 2021 are likely to slow the payment of PUA benefits as states focus on implementing the new program integrity provisions, for example.
More than half of states submitting data continue to report average PUA benefits paid that are close to the minimum amount. As of March 15, 2021, 26 of the 43 states and territories that had submitted PUA payment data for January 2021 reported average weekly PUA benefits paid that were within 25 percent of the state’s minimum PUA benefit amount; 14 of these states and territories reported average benefits within 10 percent of the minimum.[345] This suggests that many individuals in these states and territories were receiving the minimum benefit in January 2021—because the average is close to the minimum.
As we reported in November 2020, DOL officials told us that to facilitate implementation of the new program, most states decided to initially pay PUA claimants the minimum allowable benefit, and then recalculate benefits at a later point based on claimants’ documentation of their prior earnings, as set by DOL guidance.[346] States have previously used this approach to pay benefits more expediently under the Disaster Unemployment Assistance program, according to DOL officials. As of March 16, 2021, officials told us that DOL’s regional offices were monitoring this issue closely, but because the monitoring is ongoing, they did not know how many states had begun recalculating individuals’ benefits and making these back-payments.
States have taken different approaches to calculate PUA benefits, according to officials in a couple states. For example:
Officials from Florida’s Department of Economic Opportunity said that they initially paid eligible PUA claimants the minimum weekly benefit. They said they have faced challenges in determining if claimants qualify for a higher benefit amount because claimants often submit varied documentation of prior earnings—in many cases showing gross income—that officials must piece together to determine net income, which is needed to recalculate benefits. Officials also said recalculating the weekly benefit amount for each claim in a timely manner is challenging due to the large number of claims that need to be manually reviewed.
Officials from Wyoming’s Department of Workforce Services said that they have used claimants’ estimates of their prior income to calculate initial PUA benefit payments. Wyoming officials stated that individuals have 21 days to provide sufficient documentation to verify their estimate of prior income, and if not provided, the state reduces PUA claimants’ benefits to the minimum amount. State officials said they often had to correspond back and forth with claimants to obtain sufficient documentation.
States are continuing to take out substantial federal loans to pay UI benefits. As the number of regular UI continued claims remains historically high, states continue to face financial strain, and some have sought loans from the federal government to pay UI benefits.[347] As of March 12, 2021, about a year since the March 2020 spike in UI claims, 20 states and territories held federal loans totaling about $52.1 billion (see figure).[348] This total loan balance is greater than the approximately $40.2 billion held by 30 states and territories at the end of 2010, the height of borrowing after the 18-month long 2007-2009 recession and early recovery.[349] If unemployment remains high, additional states may have to take out loans to pay UI benefits, and states with existing loans may need to borrow more.
Total Federal Loan Balance Held by States and Territories to Pay Unemployment Insurance (UI) Benefits, January 3, 2020 through March 12, 2021
Notes: The 20 states and territories with outstanding federal loans to pay UI benefits as of March 12, 2021 were California, Colorado, Connecticut, Hawaii, Illinois, Kentucky, Louisiana, Maryland, Massachusetts, Minnesota, Nevada, New Jersey, New Mexico, New York, Ohio, Pennsylvania, Texas, U.S. Virgin Islands, Virginia, and West Virginia. The loan amounts shown in the figure represent the total balance held by all of these states and territories as of the end of each week. According to the Department of Labor, the U.S. Virgin Islands had a residual loan balance of about $0.06 billion at the beginning of 2020 left from the 2007-2009 recession, and did not begin borrowing during the COVID-19 pandemic until August 2020.
Some states are using funding under the CARES Act to pay off or prevent large loan balances, as high balances can lead to federal tax increases for employers. The regular UI program is funded through state and federal taxes on employers.[350] Generally, if a state holds a federal loan balance to pay UI benefits for two or more years, the rate of the federal tax on employers used to fund the UI program will increase.[351] As we reported in November 2020, states may take years to pay off large loan balances.
Some states have been using CARES Act funding from the Coronavirus Relief Fund to pay for UI benefits to reduce their federal loan balance or avoid taking out loans, under guidance from the Department of the Treasury.[352] For example, in October 2020, the Georgia Department of Labor announced a plan to allocate up to $1.5 billion from its Coronavirus Relief Fund payment to the state’s UI program.[353] According to the Georgia Department of Labor, this plan aimed to repay federal funds that Georgia borrowed to pay UI benefits during the pandemic, which would prevent increases in federal unemployment taxes, resulting in an estimated savings of millions of dollars annually for Georgia employers. Similarly, as of March 15, 2021, West Virginia had planned to allocate $587 million of its $1.25 billion payment from the Coronavirus Relief Fund to pay UI benefits, according to the West Virginia State Auditor’s website.[354] Given the persistently high levels of regular UI continued claims, states may continue to use funding under the CARES Act to pay off or prevent large loan balances, and avoid possible future increases in employer tax rates.[355]
DOL continues to stress the importance of addressing potential fraud in the UI programs. As we have previously reported, in September 2020, DOL provided states with $100 million in administrative funding targeted specifically at addressing potential fraud and identity theft in the PUA and PEUC programs. In January 2021, DOL announced the availability of an additional $100 million in administrative funding to assist states with, among other things, carrying out a provision in the Consolidated Appropriations Act, 2021 that requires states to conduct identity verification or validation of PUA claimants.[356]
States can use this funding to cover administrative expenses for tools or services to verify or validate the identity of PUA claimants, assist with efforts to prevent and detect fraud and imposter claims resulting from identity theft in the PUA and PEUC programs, and recover fraud overpayments in the PUA and PEUC programs. DOL is monitoring states’ use of funds and progress in carrying out these efforts through quarterly reports from states. In addition to providing funding to states, DOL officials told us in February 2021 that DOL continues to emphasize the importance of UI program integrity through published guidance and webinar presentations.
DOL’s Office of Inspector General (OIG) and the Department of Justice (DOJ), also continue to investigate potential UI fraud and examine program integrity issues. In February 2021, the DOL OIG reported that its analysis of state UI claims data for 35 states or territories identified more than $5.4 billion in potentially fraudulent UI benefits paid to individuals from March 2020 through October 2020, based on four types of potential fraud.[357] These include: (1) multi-state claims, in which individuals use the same Social Security number to file claims in multiple states; (2) claims filed using the Social Security number of deceased individuals; (3) claims filed by federal prisoners; and (4) claims filed using suspicious email accounts. According to the DOL OIG, the $5.4 billion only represents a subset of potential fraudulent activities. The DOL OIG expects the total amount of potential UI fraud across all states and territories is much larger.
According to DOJ, from March 2020 through January 2021, DOJ filed federal charges against 92 individuals for defrauding the UI programs.[358] In that same time frame, an additional 11 individuals pleaded guilty to federal charges of defrauding the UI programs. See the enclosure on Federal Fraud-Related Cases in appendix I for more information on DOJ charges.
In response to the Consolidated Appropriations Act, 2021, states have been focused on implementing new UI program integrity provisions related to identifying and preventing potential UI fraud, according to officials from the National Association of State Workforce Agencies (NASWA) and its UI Integrity Center, funded by and operated in partnership with DOL. For example, NASWA officials told us that all states have some process for verifying claimant identities, which is one of the new PUA program integrity provisions. Some states have faced challenges related to identity and employment verification, according to officials, such as lacking the technology for claimants to upload documentation electronically and identifying potentially fraudulent documents.
States have increased their utilization of the Integrity Data Hub to identify potential fraud in the UI system, according to DOL and NASWA officials. DOL officials told us that as of February 19, 2021, 33 states were sending their UI claimant data to the Integrity Data Hub for cross-matching with other states’ claims data and 22 states were using the Integrity Data Hub’s third-party identity verification services. NASWA officials told us that cross-matching can identify potentially fraudulent UI claims, such as instances where a single bank account or email address is associated with multiple claims in multiple states, or when a deceased individual’s information is used to file a fraudulent claim for benefits.
States have also pursued investigations and prosecutions of potential fraud related to the UI programs during the pandemic. For example:
Officials we spoke with at the Arizona Attorney General’s Office said that the large volume of UI fraud cases has been a major challenge during the COVID-19 pandemic. Officials said that they are pursuing some UI fraud cases independently, some through a state task force in coordination with the Arizona Department of Economic Security, and some through a federal COVID-19 task force. Arizona officials expressed appreciation for the federal task force, which they said involves numerous federal, state, and local agencies, such as DOJ, the Social Security Administration, U.S. Postal Inspectors, state police, and local law enforcement.
An official with the Massachusetts Attorney General’s Office said that the state’s UI fraud investigations primarily focus on three categories: (1) imposter fraud, in which perpetrators use individuals’ personal information without authorization to collect benefits; (2) fraud involving perpetrators who "assist" individuals in opening UI claims and take a percentage of the benefits, which is a significant issue in communities where English is not the primary language; and (3) fraud involving perpetrators who organize vulnerable populations, such as the homeless, to file false UI claims and take a percentage of the benefits. The official also stated that conducting certain investigative work, such as interviews, in the midst of a pandemic has been a challenge for the Attorney General’s office.
DOL has taken steps to collect data on the recovery of PUA overpayments, but additional efforts are needed to track the amount of PUA overpayments states have waived. Overpayments are not necessarily a result of fraud, though some may be.[359] As we reported in January 2021, DOL data show that the dollar amount of reported overpayments in the regular UI program increased substantially during the pandemic, coinciding with historically high numbers of UI claims. As of March 15, 2021, DOL reported that states had identified about $2.6 billion in regular UI overpayments during the pandemic, in the final 3 quarters of 2020 combined.[360] As of March 15, 2021, states that had submitted data to DOL also reported about $3.6 billion in PUA overpayments from March 2020 through February 2021.[361] These amounts are likely to increase as states shift their focus from program implementation and clearing claims processing backlogs to identifying overpayments, according to DOL officials.
In response to the recommendation in our January report, DOL has taken steps to collect data on states’ recovery of PUA overpayments. DOL updated its state reporting requirements for the PUA program to include the collection of data on the amount of PUA overpayments states have recovered. As of March 15, 2021, 14 states had reported some data on PUA overpayments recovered in either December 2020 or January or February 2021. Sustained collection of these data will help inform policymakers about the program, determine the effectiveness of identity theft prevention efforts, and assess additional program integrity needs, according to DOL.
However, additional data on the amounts of PUA overpayments states have waived are also needed to effectively monitor the recovery of overpayments. DOL did not include PUA overpayments waived in the updated state reporting requirements issued in early 2021 because, according to officials, the agency needed to quickly issue guidance on new PUA provisions in the Consolidated Appropriations Act, 2021. In early February, DOL officials told us they did not have plans to collect data on which states are utilizing the authority to waive PUA overpayments or the amount of overpayments that states have waived.[362] In a subsequent meeting in late February, DOL officials responded that they were developing requirements for states to report these data, which would be included in a future round of guidance. Federal internal control standards state that management should use quality information to achieve the entity’s objectives. As part of these standards, management should obtain data on a timely basis to use for effective monitoring. For the regular UI program, the amount of overpayments waived is a key data element used to calculate the percent of overpayments recovered, which is one of DOL’s regular UI program integrity core performance measures.
The large amount of already-reported PUA overpayments (about $3.6 billion as of March 15, 2021) indicates the need for timely data to monitor and support states’ use of overpayment waivers. According to DOL, states are able to retroactively waive PUA overpayments from the beginning of the program onward. Waived overpayments do not have to be recovered. Thus, additional data on waived overpayments would enable DOL, policymakers, and the public to accurately determine the percent of PUA overpayments recovered, how much remains outstanding, and how much overpaid federal funding states do not intend to recoup.
Agency Comments
We provided DOL and the Office of Management and Budget (OMB) with a draft of this enclosure. OMB did not have any comments on this enclosure. DOL provided written comments, reproduced in appendix IX, and technical comments, which we incorporated as appropriate.
DOL agreed with our recommendation to collect data from states on the amount of PUA overpayments states have waived. In its comments, DOL noted that the agency has issued guidance to states regarding their authority to waive PUA overpayments. DOL intends to issue additional PUA program guidance in April 2021 that will include revised reporting requirements and instructions for states to provide information on the amount of overpayments waived.
Methodology
To conduct this work, we analyzed regularly reported DOL data for calendar years 2019, 2020, and 2021, with the most recent data being obtained on March 18, 2021. We reviewed relevant federal laws, DOL guidance, and DOL Office of Inspector General reports; and interviewed DOL officials about program data and agency actions. We also interviewed officials from a few states and worker advocacy organizations as part of our ongoing work on UI during the pandemic, including officials from Arizona, Florida, Massachusetts, and Wyoming. We used selected information from these interviews as illustrative examples. We reviewed data file documentation and written responses from DOL officials, and interviewed DOL officials about the UI database, PUA claims data files, and data on outstanding federal loans to pay UI benefits, specifically related to state-reported data on claims counts, overpayments, payment timeliness, and loan balance amounts by state. We also examined the data for outliers, missing values, and errors. We determined the DOL data we used were sufficiently reliable for the purposes of this report.
Contact information: Thomas M. Costa, (202) 512-7215, costat@gao.gov
Related GAO Product
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
The Department of the Treasury and the Internal Revenue Service quickly issued the second round of direct payments to most eligible individuals, but could do more to fully implement past GAO recommendations to reach the estimated 8 million who have yet to receive a payment and timely ensure that direct payment control activities are designed and implemented appropriately.
Entities involved: Internal Revenue Service and Bureau of the Fiscal Service, within the Department of the Treasury
Recommendation for Executive Action
The Commissioner of Internal Revenue should periodically review control activities for issuing direct payments to individuals to determine that the activities are designed and implemented appropriately as IRS disburses a third round of Economic Impact Payments and prepares for advance payments on the Child Tax Credit. These control activities should include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients. IRS disagreed with this recommendation. IRS also stated it plans to assess the effectiveness of these new controls during the next round of Economic Impact Payments and will adjust them as warranted.
Key Considerations and Future GAO Work
The Department of the Treasury (Treasury) and Internal Revenue Service (IRS) have taken actions to implement our four previous recommendations related to the economic impact payments (EIP):
In June 2020, we reported that Treasury and IRS had sent $1.2 billion in the first round of Economic Impact Payments (EIP 1) to deceased individuals. We recommended that the Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments. Treasury and IRS have taken steps to implement our recommendation. For example, IRS has instructions on its website requesting that individuals voluntarily mail the appropriate EIP amount sent to the decedent back to IRS, for both electronic and paper check payments. The envelopes in which paper checks were sent also had a checkbox so people could indicate that the intended recipient was deceased, and then mail the envelope back. Treasury has also held and cancelled payments made to decedents, along with those that have been returned. As of February 28, 2021, around 57 percent (just over $703 million) of the $1.2 billion in EIP 1 sent to deceased individuals had been recovered. The recovered amount has not changed since August 2020.
As of March 2021, Treasury and IRS have not taken any further action to recoup payments made to decedents that have not been returned. IRS officials determined that further actions, such as initiating erroneous refund cases against the estates of the decedents to which payments were made and not returned, could be burdensome to taxpayers, the federal court system and IRS. As such, IRS officials concluded that doing so is not prudent at this time.
In our September 2020 report, we made two recommendations to help IRS better target its outreach and communications efforts to reach the estimated millions of individuals who may be eligible for a payment but have not received one. Specifically, we recommended that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP 1 to help target outreach and communications efforts. We also recommended that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should then make this estimate along with other relevant information, available to outreach partners to raise awareness about how and when individuals can file for an EIP 1.
Treasury and IRS neither agreed nor disagreed with our recommendations, but did take some actions that are consistent with our recommendations. For example, in September 2020, the agencies used tax return information to identify nearly 9 million individuals who had not received an EIP 1 and then notified these individuals that they may be eligible for a payment. The letters also provided instructions on how to request a payment. In addition, IRS publicly released detailed ZIP Code data from the notices to help community outreach partners with their own outreach efforts.
In January 2021, Treasury revised its estimate of eligible recipients who have yet to file for an EIP 1 to 8 million. According to Treasury officials, this estimate is based on the 9 million notices IRS sent in September 2020. Treasury officials stated that it is likely that some of the 9 million recipients have since claimed the EIP, but Treasury did not provide data supporting this claim.
Treasury and IRS did not initially plan to monitor the effectiveness of the outreach notices that were sent in September until February or March 2021. In November 2020, we recommended that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed an EIP 1 notification letter and subsequently filed for and received an EIP 1, and use that information to inform ongoing outreach and communications efforts.
Treasury and IRS agreed with this recommendation. According to Treasury officials, Treasury began analyzing data in January 2021 on those individuals who received a notice and subsequently filed for and received an EIP 1. As of the time of this report, Treasury’s analysis of these data is ongoing. Treasury has not reported any results or provided a timeline for when it plans to complete the analysis.
On January 22, 2021, the President issued Executive Order on Economic Relief Related to the COVID-19 Pandemic to provide economic relief to the millions of Americans affected by COVID-19, which directs agencies to prioritize actions that provide relief to individuals and families, among others.[363] We discuss actions Treasury and IRS are taking to expand and improve delivery of EIPs further below.
On March 10, 2021, Congress passed the American Rescue Plan Act of 2021, which the President signed on March 11, 2021. The statute authorized a third round of direct payments to individuals to help address financial stress due to the pandemic.[364] Treasury and IRS begin dispersing EIP 3 payments on March 12, 2021. As of March 19, IRS reported that it had dispersed 127.3 million payments totaling over $325 billion.
The statute also increased the amount of the Child Tax Credit and authorized IRS to send advanced payments of the credit to eligible individuals.[365] We will continue to examine Treasury and IRS efforts to provide direct payments and advance payments of the Child Tax Credit to eligible individuals during the 2021 tax filing season. We will also review the effect of selected tax policies—including provisions in the CARES Act and Tax Cuts and Jobs Act—on households by sex, race, and ethnicity.
Background
The CARES Act and the Consolidated Appropriations Act, 2021, authorized Treasury and IRS to issue EIPs as direct payments to help individuals address financial stress due to the pandemic. [366] Treasury and IRS quickly issued the second round of direct payments to most eligible individuals. As of February 28, 2021, Treasury and IRS issued 168.2 million payments totaling $275.9 billion for the first round of payments (EIP 1) and 152.4 million payments totaling $147 billion for the second round of payments (EIP 2).[367] According to IRS data, the average amount of EIP 1 was $1,665 and the average amount of EIP 2 was $965. From April 2020 through February 2021, the Bureau of the Fiscal Service (BFS) disbursed the first and second payments in the form of direct deposits, paper checks, and debit cards (see figure).
Number of Economic Impact Payments (EIP) Disbursed by Payment Type, Rounds 1 and 2, as of February 5, 2021
In February 2021, IRS announced that all legally permitted first and second round of EIPs have been issued. Eligible individuals who did not receive EIP 1 or EIP 2—or their maximum applicable EIP 1 and EIP 2 amounts—can claim a recovery rebate credit (RRC) on their tax year 2020 income tax return equal to the amount of the credit for which they are eligible, as reduced by their EIP 1 and EIP 2 amounts.[368]
As we previously reported, a number of population groups did not receive timely payments during the first or second round of payments. These groups, which include those who filed a tax return in 2018 but not 2019, and as such, did not receive an EIP 2, can claim the RRC. However, unlike the EIP, the RRC can be reduced to pay debts owed to federal or state agencies. The National Taxpayer Advocate reported that this offset created an inconsistency between the treatment of EIPs and the treatment of RRCs claimed on 2020 tax returns where the RRC will be reduced by outstanding liabilities.
According to IRS data, there are an estimated 15 million individuals who filed a tax return in 2018, but did not file in 2019, and will have to file a 2020 tax return to receive their credit. As of March 8, about 600,000 of these individuals filed for and received an RRC. Other groups, such as some incarcerated individuals, some qualifying widows and widowers, and individuals whose qualifying children payments were not initially included in EIP 1 and who may not have received the payment as part of EIP 2, will also have to claim the RRC.
On March 15, 2021, the Taxpayer Advocate Service reported that IRS agreed to use its discretion to refrain from offsetting RRCs to satisfy federal tax debts. According to IRS, it will update programming as soon as possible to exercise this authority. IRS is also exploring if it can legally reverse offsets that have already occurred and refund those amounts to taxpayers. IRS reported it does not have the authority to bypass debts collected through the Treasury Offset Program.
Overview of Key Issues
Treasury and IRS efforts to expand and improve EIP delivery. As mentioned earlier, on January 22, 2021, the President issued Executive Order on Economic Relief Related to the COVID-19 Pandemic that called on federal agencies to (i) promptly identify actions to address the economic crisis resulting from the pandemic and (ii) specifically consider actions that facilitate better use of data and other means to improve access to, reduce unnecessary barriers to, and improve coordination among programs funded in whole or in part by the federal government. The order directed agencies to prioritize actions that provide the greatest relief to individuals, families, and small businesses; and to state, local, tribal and territorial governments.
In response to the order, Treasury released a fact sheet to outline efforts Treasury will take to help households who have not yet been able to access payments. The fact sheet states Treasury will take the following three actions, in coordination with IRS, to (1) establish online tools for people who have not filed an income tax return to be able to claim their payments; (2) reach individuals who were issued an EIP 1 via debit cards or paper checks and have yet to activate or cash them; and (3) analyze and better understand unserved populations to enhance outreach efforts.
Treasury officials described a number of actions they plan to take; however, some of these actions do not differ significantly from earlier research and outreach actions Treasury and IRS were taking for EIP 1 or EIP 2, or actions Treasury and IRS normally take as part of the tax filing season. For example, Treasury and IRS have not created new online tools for non-filers, rather they are promoting existing online options. IRS officials said that non-filers can submit a tax return through the Free File program.[369] Treasury officials also said the Get My Payment Tool on the IRS website will be available for future EIPs to allow individuals to update their direct deposit information and receive a status of their payment.
According to BFS officials, just over 744,500 EIP 1 checks and almost 200,000 EIP 1 debit cards, totaling around $1.3 billion have not been cashed or activated. Additionally, around 2.8 million EIP 2 checks and over 1.3 million EIP 2 debit cards have not been cashed or activated, totaling $3.3 billion. [370] Treasury and IRS officials said they are continuing their outreach efforts online and in coordination with community and government outreach partners to reach individuals who have received but not cashed EIP 1 checks or activated debit cards. In February 2021, the Bureau of the Fiscal Service sent approximately 200,000 reminder letters to individuals that were mailed an EIP card in the first round of payments but have not yet activated their card. BFS sent a similar reminder notice in July 2020. The letter reminds recipients to activate their EIP card or to call customer service for a free replacement card if they have lost or discarded their EIP card. BFS officials said it sent approximately 1.3 million reminder letters on March 4, 2021, to those who have not yet activated their EIP 2 debit cards.
According to Treasury officials, Treasury is currently analyzing data on individuals who received a notice in September 2020 and subsequently filed for and received an EIP 1. Treasury began this analysis prior to the executive order and fact sheet and following the recommendation we made in November 2020. However, Treasury and IRS have no plans to conduct further analysis to better understand traditionally underserved populations and to enhance outreach efforts to those populations. Fully implementing our September and November recommendations would provide Treasury and IRS more information on the estimated size of the population who have yet to file for an EIP and also potentially provide insights into the effectiveness of different targeted outreach efforts to reach these populations.
IRS officials have taken some actions to improve delivery of EIP to individuals who are incarcerated. In November 2020, we reported that approximately 977,000 incarcerated individuals could be eligible for an EIP. According to IRS officials, they provided information to the Federal Bureau of Prisons and state Department of Correctional agencies on how individuals who are incarcerated could file for an EIP. IRS also set up a dedicated mailbox to address questions or concerns relevant to incarcerated individuals.
However, there continue to be challenges delivering timely payments to this population. According to IRS data, around at least 10,000 incarcerated individuals filed a paper return, but did not receive their EIP. IRS was unable to process their return in time due to a backlog of paper returns. According to IRS, these individuals will need to wait until they file their 2020 tax return, at which time they can file for the RRC. IRS sent some incarcerated individuals a debit card, but the prisons were either unable to process the card or identify who it belonged to. IRS subsequently sent instructions to those prisons on how to return the debit card and how individuals could file a 1040 tax return to claim the RRC.
The second round of EIPs are generally protected from levy, attachment, or garnishment.[371] According to IRS officials, this prohibition on garnishments only applies to garnishment orders that would otherwise be honored and collected by a financial institutions and that prisons are not financial institutions. As part of IRS’s outreach, they did not provide information to the Federal Bureau of Prisons and state Departments of Corrections concerning the statutory protection against garnishment. According to IRS officials, what happens to the funds once the payment is made to the right individual is beyond IRS’s jurisdiction.
Temporary bank accounts. In December 2020, Treasury and IRS sent an estimated 13 to 19 million EIP 2 payments to temporary bank accounts.[372] Tax industry partners, such as tax preparers and tax financial services companies, may establish these temporary accounts on behalf of their clients to receive a tax refund. As a result, millions of individuals, who had used a tax preparer to file their 2019 tax returns experienced a delay of up to a month to receive their EIP 2 payment.
According to IRS, when taxpayers obtain third-party tax preparation services, the return preparer provides the temporary bank account it established on behalf of the taxpayer to IRS. IRS sends the refund to this account by direct deposit, the return preparer deducts fees for its tax preparation services and other products its clients may have purchased and sends the remaining balance of the refund to the taxpayer. For taxpayers who file electronically, IRS asks tax preparers to provide information about taxpayers’ temporary and ultimate bank accounts, the account controlled by the taxpayer to which the return preparer will deposit the residual refund.
According to IRS, with EIP 1, it found that tax preparers’ did not always provide the correct ultimate bank account information. In August, 2020, in anticipation of legislation authorizing EIP 2, IRS worked with several of its tax industry partners to obtain correct banking information for their clients so that future EIPs issued by direct deposit would not be sent to temporary accounts. IRS obtained corrected bank account information for approximately 20 million individuals. However, due to a data formatting issue, IRS uploaded the same account information for some taxpayers as had been originally provided by the tax preparers when they filed taxpayers’ returns, rather than the correct ultimate bank account.
IRS did not become aware of the error until December 31, 2020 when their tax industry partners notified them that EIP 2 payments had been sent to the temporary accounts. IRS officials said they did not perform a quality review of the revised records. According to officials, they were working under a compressed time frame, and preparing for the 2021 filing season.
IRS has documented quality review procedures for its operations. However, according to officials, they did not consistently follow these procedures for the second round of direct payments. According to federal standards on internal control, when there is a significant change in an entity’s objectives or process, management should review its policies, procedures, and related control activities in a timely manner to determine that the control activities are designed and implemented appropriately. With the enactment of the American Rescue Plan of 2021, which includes a third round of economic impact payments and advance payments of the Child Tax Credit, timely reviews of control activities for making direct payments to individuals could help IRS avoid costly or burdensome errors in the future. For example, control activities could include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients.
According to IRS, upon learning that the EIPs had been sent to the temporary accounts, officials asked their tax industry partners to reject the payments so that IRS could reissue them either to the correct bank account or as a paper check. However, according to IRS officials, some partners did not return the payments. Instead, two large tax industry partners announced they planned to redirect the payments to their clients. IRS officials said this then raised concerns among their other partners that returning the payments to the IRS instead of redirecting the payments to clients would put them at a competitive disadvantage.
At the time, IRS’s main processing system was down to prepare for the 2021 tax filing season. IRS would not be able to reissue payments for about a month until the system was back online on January 25, 2021. IRS officials said industry partners were also concerned that their clients would have to wait to claim the RRC on their 2020 taxes instead of immediately receiving an EIP 2, and unlike EIP 2, the RRC can be reduced to pay some debts. Ultimately, IRS officials concluded that it had no legal authority to demand tax industry partners return the payments as IRS had sent the payments to the bank accounts taxpayers identified on their income tax returns as being accounts owned and controlled by the taxpayers.
Officials from two tax industry partners that had the majority of affected clients said they worked with their clients’ financial institutions to redirect most of the EIP 2 payments by January 7, 2021. For example, one national tax preparer reported that IRS sent 2.8 million payments to temporary accounts; the company reported that it was able to redirect almost all of those payments to the correct accounts. The preparer only had to return around 20,000 payments to IRS because it was unable to verify the ultimate bank account for the recipient. One tax financial services company reported that IRS sent over 11 million payments to temporary accounts; of those payments, the company reported that they redirected 10.4 million payments to the correct accounts. It returned 545,000 payments to IRS because it was unable to verify the ultimate bank account for the recipient.[373]
Working with BFS, IRS has reissued 5.2 million payments as of January 31, 2021, including those returned from tax industry partners; this number includes all rejected payments, not just those sent to the temporary bank accounts. According to IRS officials, certain tax industry partners have not yet provided IRS with key information, particularly the number of redirected payments. As of March 2021, IRS officials said they do not know the total number of payments sent to temporary bank accounts; the number of affected recipients that have now received their payment; or the number that have not yet received a redirected or reissued payment.
To prevent a similar issue from happening in the future, IRS officials said they have worked with tax industry partners to provide the ultimate bank account information in a standard format. Additionally, IRS is working with industry partners to confirm that IRS has the correct bank account information and is performing tests to validate that information.
Disparities in EIP disbursement related to the sex, race, or ethnicity of households. Certain demographic groups may be overrepresented in those who have not received EIPs or received them late because they are overrepresented among populations who did not file tax returns, did not have bank accounts, or are incarcerated.[374] The figure below shows our analysis of Census data of tax non-filers and unbanked rates among certain racial and ethnic groups. Additionally, our analysis of Census data estimates the non-filing rate for female-headed households is 18.4 percent; higher than male headed-households at 11.6 percent.[375] The unbanked rate for individuals by sex also varied by type of household. According to Federal Deposit Insurance Corporation estimates, unmarried female households had higher unbanked rates at 11.1 percent, compared with unmarried male households at 7.6 percent.[376] In contrast, the estimated unbanked rate for male individuals was higher at 8.7 percent than for female individuals at 5.8 percent.[377]
Non-filer and Unbanked Rates by Race and Ethnicity in 2019
Note: We define a non-filer as the ASEC householder/reference person who indicates a non-filing status. This does not consider the filing status of any other household members of the householder, including those who might be part of the same or a different family or tax unit. We define the household race/ethnicity as the householder/reference person’s race/ethnicity. Unbanked data are unavailable for Hawaiian/Pacific Islander, non-Hispanic because the sample size is too small to produce a precise estimate. Within a survey, non-overlapping confidence intervals for two estimates indicate estimates are statistically different at the 95 percent confidence level.
In November 2020, we reported that individuals who were incarcerated were at risk of receiving payments late or not at all. As such, the financial impact on racial and ethnic groups could vary. Imprisonment rates are highest among male, Black, and Hispanic adults. In 2019, the national imprisonment rate was 539 per 100,000 U.S. adults. However, this varies across demographic groups—the rate was 77 per 100,000 for female adults, 1,025 for male adults, 263 for White adults, 1,446 for Black adults, and 757 for Hispanic adults.[378]
We have ongoing work to examine how or whether the administration of certain COVID-19 relief provisions affected households differentially based on the sex, race, and ethnicity of the householders.
Agency Comments
We provided a draft of this enclosure to Treasury, IRS, and the Office of Management and Budget. Treasury and IRS provided technical comments, which we incorporated as appropriate.
In its comments, reproduced in appendix VIII, IRS disagreed with the recommendation. However, IRS acknowledged that it established additional procedures and reviews upon discovering that it had sent millions of payments to the wrong account. IRS also stated it plans to assess the effectiveness of these new controls during the next round of Economic Impact Payments and will adjust them as warranted.
As we reported, when there is a significant change in an entity’s objectives or process, management should review its policies, procedures, and related control activities in a timely manner to determine that the control activities are designed and implemented appropriately. With the enactment of the American Rescue Plan of 2021, which includes a third round of economic impact payments and advance payments of the Child Tax Credit, timely reviews of control activities for making direct payments to individuals before their distribution could help IRS avoid costly or burdensome errors in the future especially because IRS sent more than 13 million EIP 2 to the incorrect bank accounts.
IRS also described the commitment on the part of its employees, the many hours they worked and the actions they took to help deliver two rounds of economic impact payments. IRS is also taking steps to remind people who did not initially qualify for a payment—or did not receive the full amount—to file for the RRC, based on their 2020 circumstances.
Methodology
To review how Treasury and IRS administered EIP 1 and EIP 2 payments, we reviewed Treasury and IRS data as of February 2021, examined federal laws and agency guidance, and interviewed Treasury and IRS officials. We assessed the reliability of this data by reviewing relevant Treasury and IRS documents, reviewing our prior use of the data sources, and interviewing agency officials. We determined the data were sufficiently reliable to describe the number and amount of payments disbursed. We also interviewed representatives from H&R Block, Green Dot Corporation, and the Council for Electronic Revenue Communication Advancement (CERCA) to understand steps the tax industry took to redirect EIP 2 payments. We obtained the amount of EIP 2 payments that were redirected by two tax industry companies. We did not assess the reliability of this data.
We also reviewed published data from the Bureau of Justice Statistics and the Federal Deposit Insurance Corporation. We analyzed Census data from the Current Population Survey March 2020 Annual Social and Economic Supplement (ASEC). We used these data to estimate the rates of incarcerated persons, non-filing householders, and unbanked householders by sex, race, and ethnicity.
Contact information: James R. McTigue Jr., (202) 512-6806, mctiguej@gao.gov
Demand for nutrition assistance surged during the pandemic, leading to increases in participation in and expenditures for key federal nutrition assistance programs, but the Department of Agriculture did not release data on these programs for 6 months, raising questions about data quality as the pandemic persists.
Entity involved: Food and Nutrition Service, within the Department of Agriculture
Recommendation for Executive Action
We are making the following recommendation to the Department of Agriculture:
The Secretary of Agriculture should ensure that the Administrator of the Food and Nutrition Service (1) provides sufficient context to help stakeholders and the public understand and interpret data on federal nutrition assistance programs during the pandemic and (2) discloses potential sources of error that may affect data quality during the pandemic, such as manual processing. For example, the agency could publish key information from its internal communications plan that it developed for the January 2021 data release and include additional table notes in subsequent data releases to help explain these issues. In its comments, the Food and Nutrition Service generally concurred with our recommendation.
Key Considerations and Future GAO work
In June 2020, we reported that states and local governments faced challenges operating federal nutrition assistance programs during the pandemic and that some vulnerable populations may not have access to assistance. In November 2020, we identified several additional challenges, including that the Food and Nutrition Service (FNS) within the Department of Agriculture (USDA) lacked reliable data on participation and expenditures for some of its nutrition assistance programs during the pandemic. We will continue to monitor FNS’s efforts to ensure its key program data are reliable, timely, and publicly available.
We will also continue to monitor FNS’s use of COVID-19 relief funds, as well as the agency’s efforts to ensure program integrity and the challenges states and local agencies face implementing these programs.
Background
Expenditures for federal nutrition assistance programs have increased as the negative economic effects of the COVID-19 pandemic on vulnerable populations have continued. The largest of these programs—the Supplemental Nutrition Assistance Program (SNAP)—provided approximately $74 billion in benefits in fiscal year 2020, nearly matching the historic high for the program.[379] Last fiscal year, SNAP participation rose to an average of about 40 million individuals per month, according to recently released FNS data.[380] The Consolidated Appropriations Act, 2021, enacted in December 2020, provided approximately $101.8 billion to FNS to cover SNAP benefits in fiscal year 2021.
FNS administers SNAP and other federal nutrition assistance programs, including the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), the Emergency Food Assistance Program (TEFAP), and the Pandemic Electronic Benefits Transfer (Pandemic EBT) program—a new program authorized in the Families First Coronavirus Response Act (FFCRA).[381] Eligibility criteria vary across FNS’s nutrition assistance programs, and individuals and households may receive assistance from multiple programs. See table for program descriptions and total COVID-19 funding provided for these programs, as of January 2021.
Key Information on Federal Nutrition Assistance Programs during the COVID-19 Pandemic, as of January 31, 2021
Program
Description
Total COVID-19 funding ($)a
COVID-19 expenditures as of January 31, 2021 ($)d
SNAP
Provides low-income individuals and households with benefits to purchase allowed food items and achieve a more nutritious diet.
15.6 billionb
15.5 billion
Pandemic EBT
Provides benefits to purchase food to households with children who would have received free or reduced-price school meals if not for school closures due to COVID-19, as well as to eligible children in childcare.
12.8 billionc
10.7 billion
WIC
Provides eligible low-income women, infants, and children up to age 5 who are at nutrition risk with nutritious foods to supplement diets, information on healthy eating, and referrals to health care.
500 million
174.3 million
TEFAP
Provides groceries to low-income individuals through food banks.
1.25 billion
537 million
Source: GAO analysis of relevant provisions of the Families First Coronavirus Response Act, the CARES Act, and the Consolidated Appropriations Act, 2021, and information from the Department of Agriculture’s Food and Nutrition Service. | GAO-21-387
Notes: Pandemic EBT = Pandemic Electronic Benefits Transfer, SNAP = the Supplemental Nutrition Assistance Program, TEFAP = the Emergency Food Assistance Program, and WIC = the Special Supplemental Nutrition Program for Women, Infants, and Children. This table provides information on a selection of programs and is not intended to provide comprehensive information on all federal nutrition assistance funding provided during the pandemic. For example, Puerto Rico, the Commonwealth of the Northern Mariana Islands, and American Samoa received $100 million in the Families First Coronavirus Response Act, $200 million in the CARES Act, and $614 million in the Consolidated Appropriations Act, 2021 for nutrition assistance programs, and we do not present that funding in this table. aWith respect to funding from the Consolidated Appropriations Act, 2021, the amounts in this column reflect amounts appropriated in Division N, pertaining to COVID-19 response and relief. bThe Consolidated Appropriations Act, 2021 also provided an indefinite appropriation for FNS to carry out certain COVID-19 relief provisions, including a provision that generally increased SNAP benefits from January through June 2021. The total here—$15.6 billion—reflects only provisions for which FNS received appropriations with specific dollar amounts. As of January 31, 2021, data were not yet available to determine the extent of additional SNAP funding provided through the indefinite appropriation. cPandemic EBT received an indefinite appropriation of necessary amounts. The amount shown here is the apportionment provided for Pandemic EBT as of January 31, 2021. This amount will increase as states continue to implement Pandemic EBT in fiscal year 2021 and begin to provide benefits to eligible children in childcare. dAs of January 31, 2021, FNS had not received any Treasury appropriation warrants for funds provided in the Consolidated Appropriations Act, 2021. Consequently, the data in this column reflect expenditures only from funds provided in the Families First Coronavirus Response Act and the CARES Act.
Recent legislative and executive actions made several changes to federal nutrition assistance programs. For example, the Consolidated Appropriations Act, 2021 increased SNAP benefits amounts by 15 percent from January through June 2021 for all participants, according to FNS, and temporarily expanded eligibility for the program to certain vulnerable populations.[382] The act also created a task force to explore, among other things, options for using WIC benefits online and provided an additional $400 million to TEFAP.[383] In addition, the act changed several aspects of administering the Pandemic EBT program, including how states should determine if children in childcare are eligible.[384] In January 2021, the President issued an executive order, which led to FNS increasing Pandemic EBT benefits by approximately 15 percent, among other things. In March 2021, the American Rescue Plan Act of 2021 made further changes to key federal nutrition assistance programs, including SNAP and Pandemic EBT, and we will monitor how FNS implements these changes moving forward.
Overview of Key Issues
FNS did not release key data about nutrition assistance programs until January 2021, and has not publicly shared sufficient information about data quality.
Until late January 2021, FNS had made minimal data available on participation in and expenditures for its nutrition assistance programs during the pandemic. In August 2020, FNS announced it had identified significant issues with the quality of state-reported data on SNAP and Pandemic EBT.[385] Specifically, FNS noted that SNAP participation data might erroneously include Pandemic EBT participants, leading to larger-than-actual estimates for SNAP participation. At that time, the most recent reliable data for SNAP were from March 2020 and there were no publicly available data on Pandemic EBT. Data for WIC and TEFAP were available through April 2020 (published in July 2020).[386] While FNS worked to identify the root cause of the issues, it opted not to release participation data on its typical schedule for any of its nutrition assistance programs from July 2020 until late January 2021.
On January 27, 2021, FNS published participation and expenditures data for its nutrition assistance programs through September 2020, including previous months for which the agency had not released data prior in the pandemic. However, as part of this release, FNS did not publicly explain how it resolved the data quality issues it previously disclosed in August 2020, nor did the agency share sufficient context to help stakeholders and the public understand and interpret the data.
In March 2021, FNS officials told us that SNAP and Pandemic EBT data quality issues stemmed primarily from limitations with FNS’s data system that conflated SNAP and Pandemic EBT data. To address this issue, FNS officials explained that the agency had to separate participation and expenditures manually. FNS did not provide information on or explain this manual process in its public data release, even though it was a departure from the process for developing prior reports and introduced some potential for error.
FNS officials said they have implemented steps to verify the accuracy of the data produced through this manual process, but we found one instance in which the agency released inaccurate data. As a result, multiple media outlets reported this inaccurate information, which overstated the SNAP expenditures in fiscal year 2020 by $10 billion. When we brought this to FNS officials’ attention, they corrected the data, but as of mid-March 2021, the files posted on FNS’s website do not include an erratum or note to disclose to users that the data had changed or explain the reason for the change.
In addition, FNS has not provided sufficient context to help stakeholders and the public understand and interpret the agency’s data for the new Pandemic EBT program. FNS officials told us about several important nuances that were necessary to understand the Pandemic EBT data the agency released in January 2021, but the agency did not include any table notes explaining those nuances publicly. For example, FNS officials said that the agency reports a child as a participant in Pandemic EBT only in the month the child received benefits, even if those benefits cover additional months retroactively. As a result, FNS’s Pandemic EBT participation data show considerable variation month-to-month that does not fully reflect the total number of eligible children who received benefits covering a given month. Though this context is necessary for stakeholders and the public to interpret participation and expenditures data for Pandemic EBT accurately, FNS did not include it in the January 2021 data release.
In March 2021, FNS provided us with the internal communication plan officials used to inform certain key stakeholders about the data it released in January 2021. The plan indicated that the agency intends to return to its typical schedule of releasing key program data regularly as the pandemic continues. The plan also outlined several of the data quality challenges described above and the agency’s efforts to address them. For example, the plan noted that FNS needed to work with states and adjust its process to separately report SNAP and Pandemic EBT benefits, and that the unusual circumstances of the COVID-19 pandemic may continue to result in more revisions to the data than usual. FNS officials said that they are not aware of any plans to release this information publicly—such as on the website where FNS posts its monthly program data—so that a broader group of stakeholders and users of FNS’s data understand the data quality issues and the steps the agency is taking to address them.
The Office of Management and Budget (OMB) has issued guidelines to federal agencies on ensuring and maximizing the quality, objectivity, utility, and integrity of information agencies disseminate.[387] Among other things, the guidelines direct agencies to consider the usefulness of information to intended users, including the public. The guidelines state that agencies should present information in an accurate, clear, complete, and unbiased manner, and within a proper context. Further, the guidelines state that agencies should identify and disclose sources of error that affect data quality. Because FNS has not published information on its efforts to address prior data quality issues or disclosed potential sources of error, stakeholders and the public lack sufficient information and appropriate context to interpret key program data and understand the effects of the pandemic on the programs.
Expenditures and participation in key federal nutrition assistance programs have increased during the pandemic, but varied by program.
SNAP. According to recently released data from FNS, SNAP expenditures and participation have increased during the pandemic, though expenditures have increased by a greater amount due to temporary increases in benefits for some households.[388] From March through September 2020, FNS provided approximately $51.6 billion in SNAP benefits—a more than 60 percent increase when compared to the same months in 2019. The increase in expenditures reflects both increases in participation as well as increases to the amount of certain households’ benefits, known as emergency allotments.
In terms of participation, the number of individuals receiving SNAP increased by about 15 percent from March 2020 to a high of 42.9 million participants in September 2020.
In terms of increased benefits amounts, through March 2021, nearly all states were providing emergency allotments to certain households, which increased monthly SNAP benefits to the maximum available amount for the households’ size. In fiscal year 2020, FNS had estimated that emergency allotments cost approximately $2 billion per month.
Pandemic EBT. According to recently released data from FNS, the agency issued approximately $10.7 billion in Pandemic EBT benefits from March through September 2020, and a high of nearly 13 million children received Pandemic EBT in June 2020.[389] Because Pandemic EBT was a new program during the pandemic, there are no historical data available for comparison. These data primarily reflect expenditures and participation from school year 2019-20, when all 50 states and the District of Columbia operated Pandemic EBT.
States are currently working with FNS to request and receive approval to issue Pandemic EBT benefits for school year 2020-21. As of mid-March 2021, FNS had approved 24 states and Puerto Rico to administer Pandemic EBT for the current school year. FNS guidance allows states to issue retroactive benefits to cover the multiple months of the school year that passed prior to FNS’s approval of the states’ plans.[390] Consequently, as FNS approves more states, and schools continue to operate online or hybrid models for the current school year, Pandemic EBT disbursements are likely to increase significantly in the first few months of calendar year 2021.[391] To the extent that states have not yet issued benefits for school year 2020-21 or issued benefits retroactively, eligible children would not have had access to Pandemic EBT benefits to meet their needs earlier in the school year.
WIC. In contrast to SNAP, total food costs for WIC have decreased during the pandemic, according to the most recent FNS data available. Specifically, from March through September 2020, WIC food costs totaled $1.6 billion—a 12 percent decrease when compared to the same months in 2019. In addition, FNS has allocated all $500 million provided for WIC in FFCRA.[392] According to FNS, in December 2020 the agency allocated approximately $330 million for WIC food funds and $170 million for Nutrition Services and Administration funds to state agencies.[393]
Though food costs have decreased, WIC participation increased slightly during the pandemic. Specifically, the number of individuals receiving WIC increased by nearly 2 percent between March and September 2020. About 6.3 million women, infants, and children accessed WIC in September 2020, according to FNS data. The increase in WIC participation was driven entirely by a greater number of children participating in the program; the number of women and infants participating decreased during this period, according to FNS data. FNS officials told us there are several reasons why WIC food costs decreased at the same time participation increased. For example, they noted that the children’s WIC food package is less costly than the infant food package and the pregnant and breastfeeding women’s food packages. They also noted that, among other factors, WIC food costs fluctuate and that costs were highest in March compared to subsequent months in fiscal year 2020.
TEFAP. Expenditures for TEFAP also increased during the pandemic, according to the most recent FNS data available. From March through September 2020, FNS provided about $353 million in TEFAP foods to emergency food providers, a 12 percent increase compared to the same months in 2019. As previously reported, FNS does not collect national data on the number of individuals or households that participate in TEFAP, but representatives from organizations whose members administer TEFAP told us that demand at food banks has increased significantly during the pandemic.
Legislative changes have helped states administer SNAP and Pandemic EBT during the pandemic, while potentially presenting new operational challenges in fiscal year 2021.
In November 2020, we highlighted several challenges implementing SNAP, including FNS’s approach to reviewing states’ requests for various SNAP adjustments. For example, representatives we interviewed from several national research and advocacy organizations noted that FNS’s month-to-month approach to reviewing and extending several SNAP adjustments caused uncertainty for states and made implementing the program difficult.
Provisions in the Continuing Appropriations Act, 2021 and Other Extensions Act, enacted in October 2020, have helped to address many of the challenges states faced working with FNS to implement SNAP earlier in the pandemic. The act granted states broader authority to adjust some SNAP operations into fiscal year 2021 without obtaining prior approval from FNS.[394] According to FNS data as of mid-March 2021, 36 states, the District of Columbia, and the U.S. Virgin Islands had used at least one adjustment to their certification processes (e.g., to determine participants’ eligibility and benefit levels for SNAP). For example, the majority of these states waived interviews for individuals or households applying for SNAP benefits and for SNAP households due for recertification. According to representatives from the American Public Human Services Association, the broader authority for adjusting SNAP operations granted in the act has allowed states to expeditiously modify their SNAP operations and better respond to the pandemic’s effects on the program, such as increased caseloads. For other SNAP adjustments, such as providing emergency allotments, states still must request approval from FNS each month.
More recently, the Consolidated Appropriations Act, 2021, enacted in December 2020, made several changes to SNAP operations, including temporary changes to SNAP benefits levels and eligibility requirements. For example, as previously noted, the act increased SNAP benefits for all participants by 15 percent through the end of June 2021, according to FNS.[395] Among other provisions, the act also temporarily extended SNAP eligibility to qualifying low-income college students and excluded federal pandemic unemployment compensation as income and resources for determining SNAP eligibility and benefits amounts for 9 months following the month of receipt.[396] Such provisions may help vulnerable populations that otherwise would have been ineligible to access SNAP benefits during the pandemic.
These temporary changes to SNAP operations might also raise new challenges for FNS and for states as they administer the program during the pandemic. For example, states may have benefited from receiving more complete guidance from FNS on how to implement provisions related to college student eligibility. The act required states to implement these provisions by January 16, 2021. FNS issued initial guidance on December 31, 2020 and more detailed guidance on February 2, 2021 after consulting with the Department of Education. As a result of the delay in receiving detailed guidance, states may have delayed implementation or began to implement these provisions without complete guidance. In addition to written guidance, FNS said the agency is in regular communication with states to provide targeted technical assistance as needed on these temporary changes to SNAP. Furthermore, FNS and states may need to consider strategies for helping SNAP recipients understand and prepare for when these temporary adjustments to benefits levels and eligibility requirements expire.
As previously noted, recent legislative and executive actions also made changes to Pandemic EBT—including increasing benefits and changing eligible populations—and in some cases, the timing of FNS’s guidance has caused program delays. For example, for school year 2020-21, FNS provided guidance to states on November 16, 2020, that included information on the standards the agency would use to review and approve states’ Pandemic EBT plans. Consequently, states did not begin submitting plans for FNS approval until several months into the school year. FNS officials said they have been working closely with states to develop and operationalize Pandemic EBT plans for school year 2020-21, and anticipate approving several more states’ plans soon. In addition, on January 29, 2021, FNS provided guidance to states on extending Pandemic EBT to children under age 6 in eligible childcare settings. States may now move forward with submitting plans to FNS to implement this provision.
FNS has extended WIC waivers for the duration of the public health emergency, but access challenges remain.
In November 2020, we highlighted how FNS generally provided states with multiple-month waivers for WIC operations during the pandemic, and extended certain waivers until 30 days after the COVID-19 public health emergency ends. For example, the agency has approved all states to allow individuals to apply for WIC without being physically present in a WIC office and allowed nearly all states to issue benefits remotely, among others. Representatives from the National WIC Association said that extending waivers through the end of the pandemic has helped states address the uncertainty related to WIC operations.
WIC participants are currently unable to use their benefits online, but recent legislative action may help expedite FNS’s response in this area. To help develop a plan for WIC online purchasing, FNS announced in November 2020 that it awarded a $2.5 million, 3-year competitive grant to develop and test a safe and secure model for online purchasing. In addition, the Consolidated Appropriations Act, 2021, enacted in December 2020, requires USDA to establish a task force that will, among other things, study online purchasing options for WIC. The task force must make recommendations to USDA no later than September 30, 2021. Representatives from the National WIC Association said this provision will help FNS offer online purchasing, which could improve overall participation in WIC and help address the current unequal shopping experience for WIC participants, relative to SNAP participants.[397] FNS officials said the work of the task force will complement its ongoing effort to develop a plan for WIC online purchasing. FNS officials also said they must establish the task force by March 27, 2021, and may not be able to invite all interested parties to be members given the short time frames and criteria regarding the number and composition of the task force members.
As noted above, FNS recently provided $170 million from FFCRA to state WIC agencies to help cover increased administrative costs incurred during the pandemic, such as to purchase personal protective equipment for staff who cannot work remotely. Representatives from the National WIC Association also said that states’ WIC program administration costs have increased to accommodate operational changes related to the pandemic, including technology costs related to issuing benefits electronically so participants do not have to visit a WIC agency in person to obtain their benefits.
Canceled orders remain a major challenge for states in administering TEFAP during the pandemic.
Canceled TEFAP food orders during the pandemic continue to affect states’ ability to supply local food banks and use funds appropriated for the program. According to representatives from the American Commodities Distribution Association and Feeding America—whose members distribute food to food banks for TEFAP and other FNS programs—TEFAP cancelations have led to shortages of certain products in food banks nationwide at a time of increased demand, and made it difficult for states to spend TEFAP funds provided through COVID-19 relief laws. As we reported in November 2020, FNS officials and representatives from organizations we interviewed said that FNS had to cancel orders for several reasons, including that no vendors bid on a given order, the food was unavailable due to supply chain issues, and increased costs for transportation and raw materials. According to FNS data, the magnitude of canceled TEFAP orders in terms of both the estimated value of the food and total truckloads was greater from October to December 2020 when compared to March to September 2020. To help states address the impact of canceled TEFAP orders in fiscal year 2021, FNS said it was in the process of developing new procurement methods and offering new product options.
Agency Comments
We provided a draft of this enclosure to FNS and OMB for review and comment. FNS generally concurred with our recommendation. FNS and OMB provided technical comments, which we incorporated as appropriate.
Methodology
To conduct our work, we reviewed FNS data on program participation as of September 30, 2020 (released in January 2021), and expenditures as of January 31, 2021, the most recent data available at the time of our analysis. We determined these data were sufficiently reliable for our purposes by reviewing program documentation, discussing the data with knowledgeable FNS officials, and conducting manual testing for outliers or other errors. We also reviewed relevant federal laws, agency guidance and documents, and FNS’s written responses to our questions. Additionally, we interviewed officials from several national organizations, including the American Commodities Distribution Association, the American Public Human Services Association, Feeding America, and the National WIC Association.
Contact information: Kathryn A. Larin, (202) 512-7215, larink@gao.gov
Related GAO Product
Food Insecurity: Better Information Could Help Eligible College Students Access Federal Food Assistance Benefits. GAO-19-95. Washington, D.C.: December 21, 2018.
The Department of Agriculture has extended key flexibilities for school, summer, and child care programs through the summer of 2021, but meal programs are generally serving fewer meals to children than they did pre-pandemic and many school district nutrition programs report ongoing financial challenges.
Entity involved: Food and Nutrition Service, within the Department of Agriculture
Key Considerations and Future GAO Work
In September 2020, we reported on the number of meals served to children early in the COVID-19 pandemic and potential challenges for school districts and other meal providers in the 2020-21 school year. We continue to monitor data on the number of meals served, the Food and Nutrition Service’s use of COVID-19 relief funding and its efforts to provide flexibilities to states and school districts to support child nutrition, and plan to review its monitoring and oversight of child nutrition programs in our future work.
Background
Child nutrition programs administered by the Department of Agriculture’s (USDA) Food and Nutrition Service (FNS) provide cash reimbursements for meals and snacks for eligible children in schools, or at other locations when schools are closed. In fiscal year 2019, the National School Lunch Program (NSLP), School Breakfast Program (SBP), Summer Food Service Program (SFSP), Child and Adult Care Food Program (CACFP), and other child nutrition programs received $23.1 billion in federal funds.[398] In general, the largest subsidies are provided for free or reduced-price meals and snacks served to children from low-income households.
As we reported in June and September 2020, FNS granted various nationwide waivers in response to the pandemic to facilitate meal provision while limiting potential COVID-19 exposure. For example, one waiver allows meals to be served in non-congregate settings. Starting in the spring of 2020, schools and other meal providers were able to operate under the Summer Food Service Program (SFSP) and the Seamless Summer Option (SSO).[399] These summer meal programs typically operate from May through September for children on school vacation but may also operate during unanticipated school closures. FNS also waived the requirement that summer meal sites providing free meals to all children must be located in areas in which at least half the children are from low-income households. This waiver expanded the population of children eligible for free meals, and eased the administrative burden of tracking and collecting payment for school meals while maintaining social distancing guidelines.
Various COVID-19 relief laws have provided funding or authority to USDA to support child nutrition programs during the pandemic. For example:
The CARES Act provided $8.8 billion in supplemental funds.[400] As of January 31, 2021, FNS had obligated most of these funds ($7 billion) to reimburse schools for the cost of meals, and disbursed $6.4 billion to states and other meal providers. Meal reimbursement costs include the provision of free meals to more children, under waivers described below, as well as weekend meal service, according to FNS. A small portion of this funding, $185 million, was used to operate Emergency Meals-to-You, a new partnership that delivered meals to address pandemic-related nutrition needs in rural areas throughout the spring and summer of 2020.[401]
The Families First Coronavirus Response Act granted FNS authority to issue nationwide waivers in certain programs for specific purposes, and the Continuing Appropriations Act, 2021 and Other Extensions Act, enacted in October 2020, extended this authority.[402]
The Consolidated Appropriations Act, 2021, enacted in December 2020, provided additional funding to support CACFP child care providers and school nutrition programs by replacing some of the decline in reimbursement funding in the spring of 2020.[403]
Overview of Key Issues
Key child nutrition waivers are in place through the summer of 2021, but uncertainty remains for the 2021-22 school year. After multiple shorter-term extensions, on October 9, 2020, FNS extended several key waivers for child nutrition programs, in particular, those for the summer meal programs, ensuring flexibilities in meal provision through the 2020-21 school year.[404] School district officials and stakeholders commented that these waiver extensions have allowed them to plan for the remainder of the school year and provide meals while operating under different learning models (hybrid, in-person, remote). On March 9, 2021, FNS announced a further extension of these waivers through the summer to allow all children to continue to receive meals while schools are out of session and to help programs plan for the summer. These waivers are now in place through September 30, 2021.
Prior to the October extension, these waivers were extended for the summer meal programs on August 31, 2020 through the end of calendar year 2020 or until available funding ran out. According to our interviews with district nutrition officials, these waiver extensions were welcomed because their districts had been operating under summer meal programs, which are generally more flexible than NSLP, since the start of the pandemic. However, the late date of the extensions caused challenges, particularly for districts whose school year started prior to August 31. Specifically, many school district nutrition officials we interviewed reported switching from a summer meal program to NSLP prior to the waiver extensions, or taking actions anticipating that they would be required to operate under NSLP. Some districts reported declines in participation as a result of switching from one program to the other.
District nutrition officials said that they are facing numerous challenges planning for the upcoming 2021-22 school year, and some said that extending the waiver flexibilities into the upcoming school year would assist with planning. Some officials noted that it would be beneficial to know if FNS plans to extend waivers before early spring of 2021, as that is when districts begin planning, including budgeting, menu planning, and ordering food, for the fall. We asked FNS about waiver extensions, and in March 2021, FNS stated it was committed to announcing plans for the upcoming school year as soon as possible so that district nutrition officials may begin planning and procurement.
While the number of meals served through child nutrition programs has decreased, the number of children participating in these programs during the pandemic is unknownand some families may be accessing nutrition assistance through other programs. According to the most recent available data from FNS, in March through September 2020, the NSLP, SBP, SFSP, and CACFP programs served nearly 1.7 billion fewer total meals—a decline of over 30 percent—compared to the same months in the previous year (see figure).[405] This drop in meals served occurred even as FNS waivers expanded eligibility for free meals.
Total Meals Served Per Month in Key Child Nutrition Programs, March through September 2019 and 2020
Notes: The monthly totals include the four following child nutrition programs: National School Lunch Program (NSLP), School Breakfast Program (SBP), Summer Food Service Program (SFSP), and Child and Adult Care Food Program (CACFP) (child meals only). The NSLP and SBP numbers include meals served through the Seamless Summer Option, a program which allows school districts operating NSLP and SBP to continue the same meal service rules and claiming procedures used during the regular school year throughout summer and during unanticipated school closures. According to Food and Nutrition Service, the number of meals reported for any given month is subject to marginal revisions over time for a variety of reasons, including late claims and changes that come as a result of routine monitoring activity.
School district nutrition officials we interviewed attributed the drop in the number of meals served during the pandemic to several factors. For instance, school closures kept children from receiving meals in school and fear of exposure to COVID-19 kept some families from venturing out to pick up meals. In addition, families in need may have accessed food through other assistance programs, such as Emergency Meals-to-You or Pandemic Electronic Benefit Transfer (Pandemic EBT).[406] Although there was a drop in the number of meals served, nutrition officials in multiple states suggested that the need for meals had not decreased. They indicated that more children would likely qualify for free and reduced price meals as a result of the economic downturn since the pandemic began.
While data from FNS provide a partial picture of the number of meals served during the pandemic, the total number of children participating in these programs during the pandemic is unknown. Estimates of the number of children participating in child nutrition programs are typically available monthly for NSLP and SBP, quarterly for CACFP, and once a year in July for SFSP. According to FNS, many school meal programs are operating under SFSP; therefore, the once a year estimates of SFSP participation are too infrequent to assess participation during the pandemic. Further, in May 2018, we found FNS data on SFSP participation to be an unreliable estimate of children’s participation.[407] In March 2021, FNS told us of additional steps it is taking to address this issue, including gathering data to evaluate participation across child nutrition programs during the pandemic. We recognize the challenges of assessing child participation across multiple child nutrition programs during the pandemic and we will continue to examine this as part of our ongoing work.
School nutrition programs report continued financial challenges and FNS’s use of CARES Act funds may not align with needs. Nutrition officials we interviewed in three of the four state nutrition offices and a majority of districts reported facing financial challenges. They said these challenges stemmed from a decline in revenue due to the drop in the number of meals served—and thus the amount of federal reimbursements their nutrition programs received—during the pandemic. For instance, one district nutrition official reported serving about half as many meals in the fall of 2020 compared to the prior year, causing the district nutrition program’s fall revenue to decline by about half a million dollars. To cover monthly expenses, the program drew from its reserves. Officials we interviewed told us that nutrition programs that depleted their reserves and had debt would have to draw from their districts’ general funds to cover their expenses.[408] A few district nutrition officials specifically reported that these losses were exacerbated by a decline in revenue from à la carte sales during the pandemic. Almost all the district nutrition officials we interviewed reported that the FNS waivers were helpful in allowing them flexibilities to continue providing meals so they could receive some reimbursements, but that the reimbursements did not offset their lost revenue.
District nutrition officials we interviewed also reported increased program expenses in areas such as labor, supplies, and storage. For example, officials described new or increased expenses associated with obtaining personal protective equipment (PPE), providing individually wrapped items and packaging, as well as purchasing or renting additional coolers and freezers. Officials in half the districts reported receiving COVID-19 relief funds, private grants, or both to help with these expenses. Most of the programs that did not receive COVID-19 relief funds were in districts that used these funds for other K-12 priorities, according to district nutrition officials
FNS’s guidance to use the $8.8 billion CARES Act funds primarily for meal reimbursements did not always align with the needs of nutrition programs, according to state nutrition officials we interviewed. FNS said that using these funds for direct meal reimbursement would help ensure that sufficient federal resources were available to cover costs associated with the waivers, such as expanded eligibility and higher reimbursement rates for programs operating under SFSP. However, officials in three of the four state nutrition offices selected for our review said that because school districts in their states served fewer meals during the pandemic—despite expanded eligibility—their revenue from federal reimbursements was lower than in a typical year. They indicated the funds would have had a greater effect if FNS had used them to supplement existing reimbursements, thereby enabling them to cover pandemic-related costs such as hazard or overtime pay for staff, the purchase of PPE, additional packaging, and other items.[409]
Officials from districts and national organizations we interviewed indicated that they were concerned that financial challenges would continue in the 2020-21 school year and beyond. Funds from the Consolidated Appropriations Act, 2021, mentioned above, may be used for meals, supplements, and certain administrative costs. FNS said that these relief funds are intended to help defray costs incurred and decreased revenue as a result of the pandemic. An official from one national organization we interviewed noted these relief funds would help offset some losses from the spring of 2020 but, because there was no funding to cover pandemic losses from the summer or fall, would not fully address ongoing financial challenges. The act specified that these relief funds are available for obligation until September 30, 2021 and we will continue to examine this as part of our ongoing work.
Agency Comments
We provided a draft of this enclosure to FNS and the Office of Management and Budget (OMB) for review and comment. They did not provide comments on this enclosure.
Methodology
To conduct our work, we reviewed the most recent data available from FNS on meals served, which we determined were sufficiently reliable for our purposes. To assess the reliability of these data, we reviewed existing information about the data and reporting processes, interviewed agency officials, and conducted manual testing of the data. We also reviewed relevant federal laws, agency guidance and documents, and written responses from FNS to our questions. Additionally, we interviewed state nutrition directors from four states, and within each of those states interviewed district nutrition officials from three school districts. We further interviewed officials from the School Nutrition Association, Urban School Food Alliance, and Association of School Business Officials International. The information gathered from these interviews is not intended to be representative, but provides examples of experiences of meal providers during the COVID-19 pandemic.
Contact information: Kathryn A. Larin, (202) 512-7215, larink@gao.gov
Related GAO Product
Summer Meals: Actions Needed to Improve Participation Estimates and Address Program Challenges. GAO-18-369. Washington, D.C.: May 31, 2018.
As of January 2021, $10.2 billion in employer tax credits had been claimed and their use by small businesses varies by industry; the Internal Revenue Service should use employee count data to aid in identifying potentially ineligible claims.
Entities involved: Department of Agriculture; Department of Commerce, including the U.S. Census Bureau; Department of the Treasury, including the Internal Revenue Service; and the Office of Management and Budget.
Recommendation for Executive Action
We are making the following two recommendations to the Internal Revenue Service:
The Commissioner of Internal Revenue should leverage employee counts from Form 941, Employer’s Quarterly Federal Tax Return and Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees, to identify potentially ineligible COVID-19 related sick and family leave credit claims, and address discrepancies the Internal Revenue Service deems significant.
The Commissioner of Internal Revenue should conduct outreach to employment tax return filers to educate and promote accurate reporting of employee counts on Form 941, Employer’s Quarterly Federal Tax Return and Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees.
The Internal Revenue Service agreed with both of our recommendations.
Key Considerations and Future GAO Work
Our analysis of Internal Revenue Service (IRS) data showed that 3,352 employers who claimed a Families First Coronavirus Response Act (FFCRA) tax credit for providing paid leave to employees may be ineligible for the credit based on the number of employees reported on their Form 941. IRS could leverage these data and Form 943 data to detect potentially ineligible credit claims and address discrepancies that IRS deems significant. IRS could also provide outreach to employment tax return filers to promote accurate reporting of employee counts. We will continue to monitor the development and implementation of IRS’s compliance plans for these provisions.
The Consolidated Appropriations Act, 2021 amended and extended the eligibility criteria for the tax credits and deferrals for employers. For example, Paycheck Protection Program (PPP) loan recipients are newly eligible for the Employee Retention Credit. The American Rescue Plan Act of 2021—enacted March 11, 2021—extends the Employee Retention Credit and modifies sick and family leave credits.[410] We will continue to monitor implementation of these provisions, including how IRS is adapting the administration of the credits and any taxpayer compliance risks. We also have ongoing work analyzing how the effects of tax policies, such as those in the COVID-19 relief legislation and the Tax Cuts and Jobs Act, differ based on the small business owner’s sex, race, or ethnicity.
Background
FFCRA and the CARES Act provide tax credits to covered employers to mitigate the cost of paid sick and family leave for employees affected by COVID-19, as well as provide an Employee Retention Credit for all eligible employers, among other tax relief. The Consolidated Appropriations Act, 2021, enacted in December 2020, amended and extended some aspects of these credits.
Tax credits and deferrals for employers. IRS is administering the tax credits authorized by these laws, among other tax relief. The Joint Committee on Taxation estimates that the COVID- related tax credit provisions in the three laws will result in about $194 billion in foregone revenue for the federal government for fiscal years 2021-2030.[411] The IRS’s capacity to implement new initiatives, such as the relief laws’ tax credits, is an ongoing challenge cited in our 2021 High-Risk Report.[412] The tax provisions include the following:
Paid leave credits. Businesses and tax-exempt organizations with fewer than 500 employees, as well as self-employed individuals, are eligible for refundable FFCRA credits.[413] The credits are equal to qualified leave wages paid to employees, plus the employer share of Medicare taxes paid with respect to qualified wages and allocable health plan expenses, for leave taken from April 1, 2020 through March 31, 2021.[414] Credit recipients who receive PPP loans cannot count the wages paid for by the credit as payroll costs toward loan forgiveness.[415]
Payroll tax credits may be claimed on the employer’s employment tax return, typically Form 941, Employer’s Quarterly Federal Tax Return. To receive immediate relief, employers may reduce their semiweekly or monthly payroll tax deposits by the amount of their credit.[416] If an anticipated credit amount remains after reducing deposits, the employer may receive an advance refund by filing Form 7200, Advance Payment of Employer Credits Due to COVID-19. Form 7200 must be submitted using electronic fax (e-fax).
Employee Retention Credit. Under the CARES Act as amended by the Consolidated Appropriations Act, 2021, eligible employers of any size—including tax-exempt entities and self-employed individuals with employees—can claim the refundable Employee Retention Credit.[417] The credit amount is based on qualified wages paid to employees, including certain health care expenses. Only small employers, that average 500 or fewer full-time employees in 2019, may request an advance for 2021. As shown in the table, the Consolidated Appropriations Act, 2021, extended the availability of the credit to wages paid before July 1, 2021, expanded eligible wages, and made several other adjustments.
Selected Changes to the Employee Retention Credit in the Consolidated Appropriations Act, 2021
Coronavirus Aid, Relief, and Economic Security (CARES) Act
Changes in the Consolidated Appropriations Act, 2021
Eligibility period for qualified wages paid
March 13 - December 31, 2020
Extended January 1- June 30, 2021
Eligible entities
Any employer operating a trade or business or a tax-exempt organization, except governments and their agencies and instrumentalities
Expanded to include:
public colleges or universities,
government entities whose principal purpose is medical or hospital care, and
certain tax exempt federal entities a
Eligibilityrequirements
Employers must experience either:
full or partial suspension of operations due to government orders during any quarter or
significant decline of more than 50 percent in gross receipts compared with same quarter in previous calendar yearb
Amended to require decline to 80 percent of gross receipts for the same quarter in 2019 or the previous calendar quarterc
Percent of wages eligible for creditd
50 percent of qualified wages (up to $10,000 per employee for the year), including certain health care expenses
Increased qualified wages maximum to 70 percent (up to $10,000 per calendar quarter per employee) for wages paid between January 1 and June 30, 2021
Credit maximums
Maximum credit of $5,000 per employee in 2020
Increased the credit maximum per employee to $7,000 per employee per quarter in 2021
Small eligible employer size (average fulltime in 2019)e
100 or fewer employees, all wages count toward qualified wages
500 or fewer employees, all wages count toward qualified wages
Source: GAO Analysis of the Coronavirus Aid, Relief, and Economic Security Act and the Consolidated Appropriations Act, 2021. | GAO-21-387
aAn organization described in section 501(c)(1) of the Internal Revenue Code can claim the credit. bEmployers are no longer eligible in the first quarter after the one in which gross receipts are more than 80 percent of the same quarter in the previous calendar year. cBusinesses formed in 2020 may use the same quarter in 2020 to establish eligibility. dPub. L. No. 116-136, § 2301, 134 Stat. at 347–351. For employers with more than 100 full-time employees in 2019, the credit is calculated on wages paid to employees for time they are not providing services. For smaller employers, all wages are countable. eSmall eligible employers may treat wages paid to employees for providing services and wages paid to employees for not providing services as qualified wages. Large eligible employers may only treat wages that are paid to employees who are not providing services as qualified wages.
Under the CARES Act as originally enacted, PPP recipients were not eligible for the Employee Retention Credit, except for certain employers that repaid their PPP loans by May 18, 2020.[418] The Consolidated Appropriations Act, 2021 amended the CARES Act to allow PPP loan recipients to claim the Employee Retention Credit for qualified wages, although qualified wages for which the credit is claimed cannot be used to support forgiveness of the PPP loan.[419]
Employers who include any qualified wages in the amount reported to the Small Business Administration as payroll costs when applying for PPP loan forgiveness are deemed to have elected to not take those qualified wages into account for purposes of the credit.[420] PPP recipients can claim the credit for prior 2020 calendar quarters by filing an adjusted employment tax return. There is also a special rule—the “fourth-quarter rule”—for employment tax returns for the fourth quarter of 2020 for claiming credits for the second or third quarter of 2020 for an employer whose PPP loan forgiveness application was denied.[421]
Qualified leave wages for which FFCRA credits are allowed are not included in qualified wages for which an employer may claim the Employee Retention Credit.[422] Employers can claim the Employee Retention Credit on their employment tax returns. Employers may file Form 7200 for advance refunds, but should first should reduce payroll tax deposits by the credit amounts.[423]
Deferred payroll tax payments for employer share of Social Security. The CARES Act granted all employers the option to defer deposits and payments of the employer share of Social Security tax that they would otherwise be required to make during the period beginning March 27 through December 31, 2020, and payments of the tax imposed on wages paid during that period.[424] Self-employed individuals could defer half of their Social Security taxes imposed on net earnings from self-employment during the period beginning March 27 through December 31, 2020.[425] Deferred deposits and payments are to be reported on their employment tax returns, typically on Form 941, Employer’s Quarterly Federal Tax Return.[426]
Employee payroll tax deferrals. On August 8, 2020, the President signed a Presidential Memorandum that, in part, directed the Secretary of the Treasury to exercise authority under section 7508A of the Internal Revenue Code.[427] In response, IRS issued Notice 2020-65, which allowed for deferral of the withholding, deposit, and payment of the employee share of certain employment taxes imposed on wages or compensation paid from September 1, 2020, through December 31, 2020, if an employee’s wages or compensation are below a certain amount in a pay period.[428] If an employee’s employment taxes are deferred, that employee’s take-home pay is increased by the amount of the deferred taxes, but under law, the amount deferred must be repaid. The Presidential Memorandum directed the Secretary of the Treasury to make this deferral available to an employer for employees whose earnings during any biweekly pay period generally are less than $4,000 on a pre-tax basis, or the equivalent amount with respect to other pay cycles. The Office of Management and Budget directed executive branch agencies to defer the applicable payroll taxes for all employees who earn less than the $4,000 biweekly threshold and to inform and educate employees on the deferral’s anticipated impact on their paychecks in the coming months.[429]
Employers could defer the withholding and payment of the employee share of Social Security payroll taxes or the railroad retirement tax equivalent on applicable wages or compensation paid to employees for the period covered in the Presidential Memorandum. Under the Consolidated Appropriations Act, 2021, and Notice 2021-11, repayments may be collected until December 31, 2021.[430] During this period, employees’ payroll taxes are withheld from their pay as they normally would be and are also subject to withholding to recoup the previously deferred taxes. This results in a reduction in take-home pay as compared to what would have occurred without the deferral. Employers are to report deferred taxes.
Overview of Key Issues
IRS implementation of changes to the tax credits. On January 28, 2021, IRS released updated frequently asked questions for the leave credits to include the extended availability of the credits. On January 26, 2021, IRS issued a news release to summarize legislative changes made to the Employee Retention Credit for 2021 by the Consolidated Appropriations Act, 2021—including changes that limit the use of Form 7200 for claiming advance refunds to small employers.[431] To claim the Employee Retention Credit for 2020, PPP recipients may claim the credit retroactively on an adjusted return for the calendar quarter(s) involved.[432] IRS officials said they are unsure how much effect the anticipated adjusted employment tax returns—which can only be filed on paper—could have on IRS’s mail backlog.
Notice 2021-20, issued in March 2021, addresses qualified wages for the Employee Retention Credit paid after March 12, 2020 and through the end of the year. Guidance applicable to 2021 for the credit is being developed, according to the notice. The notice summarizes the statutory provisions governing the credit and provides an overview of the options for employers to defer payment of employment taxes. The notice also addresses the interaction of the credit with PPP loans and incorporates information provided in frequently asked questions posted after the enactment of the CARES Act on the Employer Retention Credit, updated to reflect changes made by the Consolidated Appropriations Act, 2021.
Given legislative changes, IRS is revising plans and considering how to use PPP loan data for Employee Retention Credit compliance purposes. Specifically, IRS officials said they are communicating with the Small Business Administration to leverage the existing Memorandum of Understanding to request loan forgiveness data to help identify employers improperly claiming the credit.
IRS processing of tax credits and Social Security payroll tax deferrals. At the time of our analysis, for second and third quarter 2020, IRS had received employer tax return filings claiming about $2.7 billion in FFCRA leave tax credits and about $7.5 billion in Employee Retention Credits, according to our analysis (see table).[433] Of the 8.9 million second and third quarter employment tax return filings received, less than 1 percent of employers filed to claim the Employee Retention Credit.
Number and Amount of Families First Coronavirus Response Act Paid Leave Credits and Employee Retention Credits Claimed in Employers’ Tax Filings
Provision
Number of employers claiming
Dollars claimed a ($ billions)
Families First Coronavirus Response Act leave credits
382,727
2.7
Employee Retention Credit
79,330
7.5
Source: GAO analysis of Internal Revenue Service data. | GAO-21-387
Notes: The table includes second and third quarter electronically filed (e-file) returns and about 2.3 million paper filings. Paper return data are as of January 6, 2021 (main Form 941) and March 4, 2021 (Schedule R), and e-file data are as of January 12, 2021. The second quarter returns include amounts for the Employee Retention Credit from the end of the first quarter because legislation passed too late in the quarter to be reported then. Dollars claimed on Form 941 as credits include amounts also claimed as advance payments requested on Form 7200. These data do not include annual returns, and IRS continues to process a paper return backlog, which makes the data in the table above incomplete, particularly for small employers. aThe tax credit dollar figures we are reporting are as reported by taxpayers and are subject to taxpayer reporting error. These figures may differ from IRS’s reported figures because we are reporting what was filed on second and third quarter Form 941s without adjustments.
Of employers for whom the IRS collects data on closures, 436 employers claiming one of the tax credits or deferring payroll taxes (for either the employer or the employee share) reported their business would be closing or stopping payment of wages in the second or third quarter.[434] These employers claimed about $2.1 million in tax credits through the paid leave credits and Employee Retention Credits and deferred $3.3 million in employer or employee share of Social Security payroll tax payments. IRS officials said they have existing rules and procedures—such as through bankruptcy proceedings—to collect taxes from closed businesses.
IRS also continues to process Forms 7200 for tax credit advance refunds. As of February 25, 2021, IRS had issued $640.4 million in advance payments.[435] Of the $10.2 billion in claims for the Employee Retention Credit and leave credits on the second and third quarter Forms 941, we found about 6 percent were filed as advance refunds through a Form 7200 filing.[436]
IRS designated more than half (24,280 of 42,539 submissions) of Form 7200 claims it received as of February 25, 2021 as “rejected.”[437] According to IRS officials, the most common reasons for rejecting a Form 7200 claim were that the filer provided an unauthorized signature or filed a Form 7200 after submitting a Form 941 for the quarter or after the due date of the Form 941 for the quarter. IRS said as of February 25, 2021, it had mailed 21,764 letters to employers whose Form 7200 claims were rejected.
IRS officials said that, as of February 2021, it was taking approximately seven weeks to process Forms 7200, including four weeks to assign the forms to reviewers. A large influx of Forms 7200—more than 7,600—were received in January 2021, a 233 percent increase compared to December 2020. This increase was due to requests for advance payment of the Employee Retention Credit for PPP recipients, according to IRS officials.
IRS continues to process a paper return backlog, which makes the data in the table above incomplete, particularly for small employers. IRS officials said as of December 18, 2020 that they were caught up opening mail. However, as of March 2021, IRS officials said weather-related issues and the arrival of end of year returns caused another mail backlog. Additionally, officials said it is taking longer to process because IRS facilities that process paper Forms 941 continue to operate at reduced capacity to accommodate social distancing. In addition, annual employment tax return forms—generally due January 31, 2021—once processed, will include tax credit and deferral information for certain small employers and agricultural employers.
On February 8, 2021, the IRS announced the release of a new form for tax year 2020 for eligible self-employed individuals to determine their sick and family leave credits under the FFCRA. Calculations from the new Form 7202, Credits for Sick Leave and Family Leave for Certain Self-Employed Individuals, are included on the individual’s income tax return.
In our analysis of second and third quarter returns, we found a total of 256,321 employers deferred about $67 billion in Social Security taxes for the employer and employee share together.[438] Among the executive branch agencies for which the National Finance Center (NFC) provides payroll services, 369,000 eligible employees, or over half of all employees that NFC provides payroll services to, had the employee portion of their Social Security tax deferred during the deferral period.[439] According to IRS officials, employers are ultimately responsible for repaying the deferred taxes and the agency has no direct role in guiding employers on how to explain the deferral and repayment requirements. For employees that separated from their positions before or during the repayment period, NFC is implementing a process to collect deferred taxes, which includes established debt collection procedures.
IRS could leverage employee count data to identify potentially ineligible leave credit claims. Our analysis of IRS data showed that some employers who claimed a FFCRA leave tax credit may be ineligible for the credit based on the number of employees reported on their Form 941. We identified 3,352 employers who claimed a leave credit and reported—on their second or third quarter Form 941—500 or more employees.[440] Of these employers, 1,946 reported more than 700 employees, suggesting that fluctuations of employees within the quarter may not explain the apparent ineligibility. Further, 1,083 employers reported 10,000 or more employees, claiming a total of about $40.5 million of leave credits. Employers that report no employees are also a potential compliance risk. We found 4,244 employers reporting zero employees, claiming about $19 million in leave credits and 169 employee count lines that were blank, claiming about $81 million in leave credits.[441]
Form instructions for line 1 ask for the employee count as of a specific pay period in the quarter, while eligibility for leave credits is determined by employee counts on the dates that the employees took leave.[442] Form 943, Employer’s Annual Federal Tax Return for Agricultural Employees, has a similar line that asks for an employee count as of the pay period that includes March 12, 2020.[443] Because the employee counts on these forms only account for one pay period, they are imperfect determinants of eligibility, but could serve as a screening tool for compliance activities after refunds are issued.
IRS has a draft compliance plan for examining tax credits and officials said they are analyzing Form 941 data to aid in considering different compliance approaches. The draft plan mentions the possibility of using filters to identify leave credit claimants with 500 or more employees. February 2021 revisions to the plan did not mention using employee counts for compliance and IRS officials have not committed to use an employee count filter for compliance. IRS officials also said they have identified taxpayer errors in some employers’ entries. For Forms 941, IRS officials said they would ensure compliance with the law through examinations, which would include reviewing payroll and other records to confirm employee counts. IRS officials said they examine a small number of Forms 941 (0.1 percent for fiscal year 2019).
IRS’s Strategic Plan includes a strategic objective on resolving compliance issues, which includes activities to develop early-warning and notification systems to engage taxpayers to resolve compliance issues and errors faster. The employee count line on Forms 941 and 943, although not a perfect reflection of the tax credits’ requirements, is a possible tool that IRS could use to ensure compliance. IRS already uses employee count information from Form 7200 to validate eligibility for advance payments of tax credits. Specifically, IRS sends rejection letters to leave credits claimants who report 500 or more employees on Form 7200, line D. IRS has an opportunity to also use Form 941 and 943 employee count data, along with other information as needed. For example, employers that report 500 or more employees—or some other threshold value—on these forms could be contacted and asked to resolve the discrepancy or return any credit claims for which they were not eligible.
IRS could apply additional criteria to further target compliance efforts to employers the agency deems as potentially significant compliance risks. For example, IRS could identify and exclude from this effort any employers with a tax credit amount below a particular dollar threshold or employers who are included in other compliance efforts. This approach could be less resource intensive than examinations. Further, since IRS examines around 0.1 percent of Forms 941 per fiscal year, it risks not identifying and addressing a large percentage of potentially ineligible claims.
In advance of first and second quarter 2021 Form 941 filings, IRS could also conduct outreach—such as through an email, frequently asked questions, or other online tips—to inform employers about the importance of properly reporting employee counts. IRS previously issued other communication on COVID-19 related tax credits, such as a “tax tip” issued in April 2020 outlining common errors on Form 7200. Although in November 2020 IRS issued a tax tip on Form 941, it did not mention employee counts. Such communication to employment tax filers would contribute to the IRS strategic goal to help taxpayers understand their responsibilities for tax compliance. This action could also result in a decrease in leave credit claims with employee counts that are significantly inconsistent with FFCRA eligibility, beginning with first quarter Forms 941 that are due April 30, 2021.
Census survey data on small businesses’ use of paid leave credits and the Employee Retention Credit. Due to limitations of the employee counts on Form 941 and the limited data available in time for this report, we analyzed data from the U.S. Census Bureau’s Small Business Pulse Survey to identify characteristics of small businesses that reported receiving the paid leave credits and the Employee Retention Credit.
The 2020 Small Business Pulse Survey, an experimental data product, is a federal statistical rapid response survey conducted by the U.S. Census Bureau to measure small business experiences during the COVID-19 pandemic. The Census Bureau reports that nonresponse bias may be an issue, but states that precautionary steps were taken in the collection, processing, and tabulation of the data in an effort to minimize the influence of nonresponse bias.[444]
Due to nonresponse, we do not know whether estimates based on respondents to this survey would represent nonresponding businesses, including nonresponding business that recently closed or that differ in terms of the survey items being measured. In addition, the sampling frame for the survey was restricted to businesses with an active email and that were single location businesses, therefore this survey does not necessarily represent other types of businesses. All estimates we present based on this survey have the same potential limitation. Because of the limited data available on the characteristics of small businesses using the credits, we chose to use these data with the known limitations.
Among small businesses with fewer than 500 employees, estimated receipt of the credits was generally low and varied by industry, according to data from the Small Business Pulse Survey (see table).
According to the U.S. Census Bureau’s Small Business Pulse Survey, as of January 10, 2021, a significantly higher percentage of small businesses in the following industries reported receiving assistance from the paid leave credits compared to the national average across all sectors: manufacturing (9.6 percent) and health care and social assistance (8.3 percent).[445] Industries in which a significantly lower percentage of businesses reported receiving assistance from the paid leave credits, as compared to the national average, include finance and insurance (1.3 percent), information (2 percent), educational services (2.1 percent), real estate and rental and leasing (2.1 percent), transportation and warehousing (2.2 percent), wholesale trade (2.8 percent), other services except public administration (3.1 percent), and professional, scientific, and technical services (3.5 percent).
Small businesses in some industries reported greater receipt of the Employee Retention Credit, according to estimates from Census’ Small Business Pulse Survey. A significantly higher percentage of businesses in the following industries reported receiving assistance from the Employee Retention Credit, as compared to the national average across all sectors: arts, entertainment, and recreation (3.2 percent) and accommodation and food service (1.9 percent). A significantly lower percentage of small businesses in retail trade (0.2 percent) reported receiving assistance from the Employee Retention Credit as compared to the national average.
Small Business Pulse Survey’s Estimated Percentage of Small Businesses Receiving Paid Leave Credits and Employee Retention Credits, by Industry, as of January 10, 2021
Administrative and Support and Waste Management and Remediation Services
5.3
-
Construction
5.3
0.4
Arts, Entertainment, and Recreation
5.2
3.2*
Accommodation and Food Services
5.0
1.9*
Mining, Quarrying, Oil and Gas Extraction
3.9
-
Retail Trade
3.6
0.2*
Professional, Scientific, and Technical Services
3.5*
0.6
Other Services, except Public Administration
3.1*
0.4
Wholesale Trade
2.8*
0.5
Transportation and Warehousing
2.2*
0.3
Real Estate and Rental and Leasing
2.1*
0.4
Educational Services
2.1*
1.0
Information
2.0*
0.7
Finance and Insurance
1.3*
-
Average across all industries
4.5
0.6
Source: GAO analysis of U.S. Census Bureau’s Small Business Pulse Survey (week of January 4-10, 2021). | GAO-21-387
Note: An asterisk (*) indicates the estimate is statistically different at the 95 percent confidence level when compared to the national average across all industries for each credit. We compared the confidence intervals and determined the difference to be significant if the confidence intervals did not overlap. All Small Business Pulse Survey estimates in this table have a margin of error of ± 1.7 percentage points or less at the 95 percent confidence level, with two exceptions. The margins of error for the Utilities industry and Mining, Quarrying, Oil and Gas Extraction industry were ± 5.4 and 4.6 percentage points, respectively. In addition, Small Business Pulse Survey results are weekly data products and are subject to suppression based on overall response and disclosure avoidance thresholds set by the U.S. Census Bureau. As a result, some data in the table above have been suppressed, as indicated by a “-“. Due to nonresponse, we do not know whether estimates based on respondents to this survey would represent nonresponding businesses, including nonresponding business that recently closed or that differ in terms of the survey items being measured. The sampling frame for the survey was restricted to businesses with an active email and that were single location businesses.
Demographics of business owners. According to our analysis of 2018 estimates from the 2019 U.S. Census Bureau’s Annual Business Survey (ABS), the latest available estimates, a significantly higher percentage of businesses are male-owned rather than female-owned (63.6 percent compared to 20.8 percent, with 15.7 percent of firms classified as equally male-/female-owned).[446] An estimated 86.7 percent of businesses are White-owned, with significantly fewer businesses being Black-owned (2.3 percent) and Asian-owned (about 10.5 percent). A significantly higher percentage of firms are non-Hispanic-owned than Hispanic-owned as well (93.1 percent compared to 6.0 percent).[447]
We cannot draw any conclusions about the sex, race, or ethnicity of the business owners that reported receiving the paid leave credits and Employee Retention Credit because we do not have business-level demographic data for businesses that reported receiving the credits. In the absence of such business-level data, we compared industry-level data, and we did not find a clear relationship between the demographic makeup of business owners and small businesses’ receipt of the two tax credits by industry.[448]
Some industries with a higher percentage of businesses reporting receipt of one of the credits were industries that had higher percentages of businesses with owners classified as female, Black, Asian, or Hispanic.
The health care and social assistance industry had a higher percentage of small businesses that reported receiving assistance from the paid leave credits. This industry also had a higher percentage of businesses with owners classified as female, Black, and Asian.
The accommodation and food industry had a higher percentage of small businesses that reported receiving assistance from the Employee Retention Credit. This industry also had a higher percentage of businesses with owners classified as Asian or Hispanic.
Some industries with higher percentages of businesses reporting receipt of one of the credits were industries that had lower percentages of businesses with owners classified as female, Black, Asian, or Hispanic.
The manufacturing industry had a higher percentage of small businesses that reported receiving assistance from the paid leave credits. This industry also had a lower percentage of businesses with owners classified as female, Black, Asian, and Hispanic.
The arts, entertainment, and recreation industry had a higher percentage of small businesses that reported receiving assistance from the Employee Retention Credit. This industry also had a lower percentage of businesses with owners classified as Asian or Hispanic.
Agency Comments
We provided IRS, Treasury, the Department of Agriculture, including the NFC; Department of Commerce, including the U.S. Census Bureau; and the Office of Management and Budget with a draft of this enclosure. IRS’s written comments are reproduced in appendix VIII, and IRS and Treasury provided technical comments, which we incorporated as appropriate. The Department of Agriculture, the U.S. Census Bureau and the Office of Management and Budget did not have any comments on this enclosure.
In its written comments, IRS agreed with both recommendations. For the recommendation to leverage employee counts, IRS said its compliance plan states that IRS will identify employers with more than 499 employees to identify potentially ineligible COVID-19 related sick and family credit claims. The IRS compliance plan only states that using employee counts for identifying credit claim errors is one of several possibilities under consideration, but we are pleased that IRS is now planning to leverage employee count data.
Methodology
To conduct our work, we reviewed federal laws and agency documents; and interviewed officials at IRS. We also analyzed IRS data as of February 25, 2021 and the most recent Census data from the Small Business Pulse Survey and the Annual Business Survey (ABS).
We analyzed data on paid leave credits receipt, Employee Retention Credit receipt, and industry from the Small Business Pulse Survey for the week of January 4-10, 2021. All Small Business Pulse Survey estimates in this enclosure have a margin of error of ± 1.7 percentage points or less at the 95 percent confidence level, with two exceptions. For the estimated percentage of businesses receiving the paid leave credits, the margins of error for the Utilities industry and Mining, Quarrying, Oil and Gas Extraction industry were ± 5.4 and 4.6 percentage points, respectively, at the 95 percent confidence level.
The Census Bureau has not yet published its analysis of nonresponse bias for the Pulse Survey and reports that nonresponse bias may be an issue, but states that precautionary steps were taken in the collection, processing, and tabulation of the data in an effort to minimize the influence of nonresponse bias. Due to nonresponse, we do not know whether estimates would represent nonresponding businesses, including nonresponding businesses that recently closed or that differ in terms of the survey items being measured. In addition, the sampling frame for the survey was restricted to businesses with an active email and that were single location businesses, therefore this survey does not necessarily represent other types of businesses. Without a published nonresponse bias analysis, the reliability of the Pulse Survey data is undetermined. Because of the limited data available on the characteristics of small businesses using the credits of interest, we chose to use these data with the known limitations.
We also reviewed data on the percent of business owners with certain demographic traits, by industry, using the 2019 Annual Business Survey. In addition, some firms in the ABS data were classifiable by sex, race, and ethnicity, and some firms were not classifiable by sex, race, and ethnicity. The percentages presented in this section were calculated using the number of classifiable firms as the denominator. However, we also calculated percentages using the total number of firms in order to determine if it would impact our results. The change in denominator did not have a meaningful impact on our findings. There are practical difficulties in conducting any survey that may produce errors. There are two types of error associated with estimates based on data from sampled surveys: sampling error and nonsampling errors. We approximated sampling errors for all of the estimates we included in this report. However, the accuracy of the data depends on both measureable sampling errors and unmeasurable nonsampling errors. For particular estimates, the total error may considerably exceed the measured error. To assess the reliability of the ABS data, we reviewed Census technical documentation and reviewed written responses of Census officials to our questions. We determined that the data were sufficiently reliable for our purposes.
CARES Act funding for the Community Services Block Grant program assisted local agencies in meeting immediate community needs, such as emergency food and housing assistance, during the pandemic.
Entity involved: Administration for Children and Families, within the Department of Health and Human Services
Key Considerations and Future GAO Work
In November 2019, we reported on the Department of Health and Human Services’ (HHS) and states’ oversight of grant recipients’ activities under the Community Services Block Grant (CSBG) program. Among other matters, we found that HHS recently redesigned its performance management approach to improve its ability to assess whether the CSBG program is meeting the national program goals to reduce poverty, promote self-sufficiency, and revitalize low-income communities. However, several elements of the approach did not align with leading practices in federal performance management. We recommended that in developing a new performance management approach for the CSBG program, HHS should include information on how its national performance measure and state outcome measures align with national program goals and include a written plan for how it will assess data reliability. HHS officials agreed with our recommendations, and we will continue to monitor the agency’s progress in implementing them.
Background
In fiscal year 2020, the CSBG program, authorized by the Community Services Block Grant Act, as amended (CSBG Act), provided $740 million to states and over 1,000 local agencies to fight poverty in the U.S.[449] Local agencies, predominantly community action agencies, use CSBG funding to help provide services such as employment, education, financial management, housing, nutrition, and emergency services to help program participants achieve economic self-sufficiency; to revitalize communities; and to empower families.[450] In fiscal year 2018, CSBG served over 15.3 million low-income individuals in nearly 6.3 million families, according to the most recent data.
The Administration for Children and Families’ (ACF) Office of Community Services (OCS), within HHS, is primarily responsible for overseeing states that receive the block grant, and states are responsible for overseeing local agencies that receive the grant funding. States must prepare state plans for using the CSBG grant funds; distribute the funds to local agencies; report annually to OCS; and conduct a full onsite review of each local entity at least once every three years.[451]
The CSBG program was provided with $1 billion in additional funds under the March 2020 CARES Act to prevent, prepare for, and respond to COVID-19.[452] In May 2020, ACF awarded the supplemental CSBG CARES Act funds to states using the standard formula for regular annual appropriated funds. As of February 2021, ACF had allotted $985,000,000 of the CARES Act funds to states.[453] Given the CARES Act funds were a supplement to the annual CSBG appropriation for fiscal year 2020, ACF initially withheld about $43.5 million from 12 states that had already met their maximum allotment under the CSBG Act, but agency officials stated that, as of February 2021, these funds were released.[454] The Consolidated Appropriations Act, 2021 included a provision that excludes CARES Act funds from the maximum allotment provision.[455]
The CARES Act and ACF allowed flexibilities to help states provide supplemental funds to local agencies quickly and minimize administrative burden so agencies could focus on meeting immediate community needs during the pandemic (see figure).
Community Services Block Grant (CSBG) Flexibilities during the COVID-19 Pandemic, as of March 2021
Note: In addition to those mentioned in the table, ACF issued other guidance documents between March 2020 and March 2021.
Overview of Key Issues
CARES Act funding and related flexibilities assisted state and local CSBG agencies in meeting immediate community needs during the pandemic. For example, according to the National Association for State Community Services Programs (NASCSP), a majority of states used the flexibility to increase their income eligibility threshold to serve more households. NASCSP also reported that states and local agencies were able to quickly change to a remote environment to deliver services safely, including allowing potential recipients to submit online applications.
However, according to officials with NASCSP and three states we contacted, states initially faced challenges in obtaining adequate and timely guidance about federal requirements for developing plans, reporting, and monitoring the use of funds. According to NASCSP, in many cases, states received guidance after implementing contracts with local agencies and releasing funds. In particular, ACF issued guidance and supporting information on reporting and monitoring nearly a year into the public health emergency. The affected guidance covered the following:
Simplified procedures for state plans. According to NASCSP, states received the CARES Act funds from ACF in May 2020, and the majority of states were able to distribute the funds to local agencies within 30 days of receiving the funds. ACF also announced in May 2020 that states needed to amend their CSBG plans to address their use of CARES Act funds and submit them by September 1, 2020.
According to NASCSP and state officials we contacted, allowing states to prepare abbreviated plans for using CARES Act funds during the COVID-19 pandemic helped streamline states’ efforts, but ACF delayed issuing guidance about the modifications to federal requirements for state plans. Specifically, the agency did not issue guidance on these plans until July and August 2020.
The delay in issuing guidance limited the time states had to fully develop their state plans with input from their local agencies that would be providing the direct services to clients, according to NASCSP. Without local agency input, states may have missed obtaining information that could have been shared with federal stakeholders about the specific needs of their local communities and the agencies’ plans for how to use the funds to address these needs.
OMB flexibilities. According to NASCSP, states found the Office of Management and Budget (OMB) flexibilities to be helpful. However, NASCSP and state officials we contacted cited unclear guidance on what additional costs grantees could cover with CSBG funds and concern about the administrative burden of documentation regarding the requirement to exhaust other funding sources and reduce operational costs (such as initiating rent renegotiations) before charging CSBG during the public health emergency. ACF issued two documents in March 2020 acknowledging the OMB flexibilities. While these documents did not provide detailed guidance on using the OMB flexibilities, ACF officials told us that they responded with technical assistance to email requests from individual grantees.
Briefer reporting requirements. According to ACF guidance, during the pandemic, the required reports will be similar to the regular CSBG reports and will collect information on the number and characteristics of people served, services provided, and outcomes, but will have significant sections removed to avoid duplication of effort and minimize burden on agencies. The NASCSP official mentioned that states and local agencies had been serving households and collecting information on their use of funds from March to December 2020 without finalized reporting requirements and without training on ACF’s new briefer reporting forms.
ACF officials told us that the agency first discussed the reporting requirements for the CARES Act supplemental funds with states in a September 2020 conference presentation and emailed the state and local agencies regarding the revised reporting requirements and reporting forms in December 2020. As of February 2021, officials said that within several weeks, the agency would finalize the automated system for reporting and would provide training and technical assistance related to the reporting requirements (including how to use the forms and the automated data collection system) via webinar, quarterly calls, and individualized training and technical assistance.
Monitoring during COVID-19. Although the CSBG Act requires onsite visits, the NASCSP official said that states have been monitoring local agencies through desk reviews and virtual/remote processes to limit person-to-person contact, and have invested in online systems to share documents and interact safely with local agencies during the public health emergency.[456] NASCSP and officials in two states said that, as of December 2020, they faced challenges in obtaining adequate and timely guidance about monitoring fund use. At that time, ACF had not released any guidance on whether these revised state procedures would meet monitoring requirements.
ACF notified states in April 2020 that states may need to postpone onsite monitoring of local agencies during the COVID-19 pandemic; that this does not suspend statutory requirements for the onsite monitoring; and that ACF is exploring whether any flexibilities in monitoring can be provided during the pandemic. OCS officials reported in February 2021 that the agency has completed its research and consulted with the HHS Office of General Counsel in drafting guidance to allow states to conduct virtual instead of onsite monitoring. On March 10, 2021, ACF issued this monitoring guidance, and officials said the agency will provide detailed information to states in a subsequent webinar.
Beyond the above mentioned efforts, since CARES Act implementation, ACF has issued additional guidance and participated in virtual meetings and quarterly calls with states to provide information about the flexibilities for distributing and using CARES Act funds, among other things. ACF officials said the agency also has reached out to grantees through calls and emails to provide technical assistance, including targeting states that had been spending the supplemental funds at a slower rate than other states. Furthermore, an official in one state said the state was able to address its concerns about implementing the OMB flexibilities with technical assistance from NASCSP.[457]
Agency Comments
We provided a draft of this enclosure to ACF and OMB for review and comment. ACF provided technical comments that we incorporated when appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed the most recent HHS/ACF data as of February 24, 2021; reviewed federal laws and agency guidance; and obtained information from ACF officials on COVID-19 related efforts for the CSBG program. We also contacted officials from NASCSP and three states that were included in our November 2019 report on CSBG to obtain information on state and local officials’ experiences with administering CSBG programs during the pandemic. We assessed the reliability of data on individuals and families receiving program services by reviewing written statements from agency officials. We determined the data were sufficiently reliable for the purposes of our reporting objective.
Contact information: Kathryn A. Larin, (202) 512-7215 or larink@gao.gov
Related GAO Product
Community Services Block Grant: Better Alignment of Outcome Measures with Program Goals Could Help Assess National Effectiveness. GAO-20-25. Washington, D.C.: November 19, 2019.
The Small Business Administration has begun making targeted Economic Injury Disaster Loan program advances but has not adequately assessed program risks, including the risk of fraud, and needs to address accounting and control deficiencies.
Entity involved: Small Business Administration
Recommendations for Executive Action
We are making the following three recommendations to the Small Business Administration:
The Administrator of the Small Business Administration should conduct and document a fraud risk assessment for the Economic Injury Disaster Loan program.
The Administrator of the Small Business Administration should develop a strategy that outlines specific actions to address assessed fraud risks in the Economic Injury Disaster Loan program on a continuous basis.
The Administrator of the Small Business Administration should implement a comprehensive oversight plan to identify and respond to risks in the Economic Injury Disaster Loan program to help ensure program integrity, achieve program effectiveness, and address potential fraud.
The Small Business Administration agreed with these three recommendations.
Key Considerations and Future GAO Work
In January 2021, we recommended that the Administrator of the Small Business Administration (SBA) should develop and implement portfolio-level data analytics across Economic Injury Disaster Loan (EIDL) program loans and advances made in response to COVID-19 to detect potentially ineligible and fraudulent applications. SBA did not agree or disagree with our recommendation and has not taken steps to implement it.
In December 2020, SBA’s independent financial statement auditor issued a disclaimer of opinion on SBA’s consolidated financial statements as of and for the year ending September 30, 2020, meaning the auditor was unable to express an opinion due to insufficient evidence.[458] As part of the basis for the disclaimer, the auditor stated that SBA was unable to provide adequate documentation to support a significant number of transactions and account balances related to EIDL due to inadequate processes and controls. The auditor identified two material weaknesses and made seven recommendations to address controls related to accounting and reporting for EIDL and evaluation and monitoring of service organization (contractor) controls. In addition, the auditor identified one material weakness and made five recommendations to address entity-level controls that affect the operation of EIDL. SBA did not fully agree with the weaknesses and neither agreed nor disagreed with the recommendations.
SBA has begun to provide us with information on the oversight of the program and the role of its contractors. We have ongoing work to examine SBA’s actions to address internal control weaknesses and the integrity of the EIDL program. As part of our ongoing work, we will monitor SBA’s progress toward developing and implementing corrective actions to address the material weaknesses identified by its financial statement auditor. In addition, we remain concerned about fraud in the EIDL program, and have ongoing work related to fraud risk management.
Background
Since March 2020, SBA has provided millions of EIDL loans and advances to assist small businesses and nonprofits experiencing economic injury caused by COVID-19. In the Paycheck Protection Program and Health Care Enhancement (PPPHCE) Act, Congress appropriated $50 billion in loan credit subsidies for SBA to cover the cost of making EIDL loans. Additionally, in the CARES Act and the PPPHCE Act, Congress appropriated $20 billion for EIDL advances, a new component of the program that provided direct advance payments of up to $10,000 to small businesses after they submitted their loan applications. On July 11, 2020, SBA announced that it had fully allocated the $20 billion in funding for EIDL advances.
On December 27, 2020, under the Consolidated Appropriations Act, 2021, Congress appropriated an additional $20 billion for targeted EIDL advances to eligible entities with 300 or fewer employees that are located in low-income communities and experienced an economic loss of greater than 30 percent. Qualifying entities may receive up to $10,000 in targeted advances.[459] Previously, SBA calculated the advances provided under the CARES Act based on the applicant’s number of employees up to $10,000. These advances do not have to be repaid.
On March 11, 2021, under the American Rescue Plan Act of 2021, Congress appropriated additional funding for entities that qualified for targeted EIDL advances under the Consolidated Appropriations Act, 2021.[460] Congress appropriated an additional $10 billion for eligible entities that have not received the full amount of $10,000 in targeted EIDL advances. Congress also appropriated $5 billion to provide an additional $5,000 for eligible entities in low-income communities that suffered economic loss of greater than 50 percent and employ not more than 10 employees. The $5,000 is available in addition to advances obtained under the CARES Act or targeted advances under the Consolidated Appropriations Act, 2021. The act also appropriated $70 million for EIDL loans and additional funding for administrative expenses for several SBA programs including the targeted advance programs and the EIDL loan program.
In March 2021, we added a new area to our High-Risk List—Emergency Loans for Small Businesses—because of concerns regarding SBA’s administration of EIDL loans and advances and implementation of the Paycheck Protection Program following COVID-19. See the enclosure on the Paycheck Protection Program in appendix I for more information.
As of January 31, 2021, SBA officials stated that the agency had $24.2 billion remaining of the $50 billion in loan credit subsidy to facilitate lending related to COVID-19, which would allow the agency to make about $271.6 billion in new EIDL loans.
Overview of Key Issues
SBA has begun to implement targeted EIDL advances. The Consolidated Appropriations Act, 2021, prioritized targeted EIDL advances for applicants that received partial advances (less than $10,000) under the CARES Act. SBA data show that about 4.9 million out of the 5.8 million total advance recipients received partial advances. Of this group, SBA officials estimated that about 2.5 million are located in low-income communities. On February 1, 2021, SBA began contacting these applicants in phases. SBA officials said that the agency system is able to contact up to 200,000 applicants each day in the order in which they first submitted their EIDL applications. As required by statute, after processing applicants that have received partial advances, SBA plans to contact those that applied for EIDL assistance on or before December 27, 2020, but did not receive an EIDL advance due to the lack of program funding. Similarly, SBA plans to contact these applicants in the order in which they initially applied for EIDL. SBA officials said the agency anticipates announcing further changes for the targeted advances due to increased appropriations under the American Rescue Plan Act of 2021 and that pending funding availability, those that are eligible and applied for an EIDL loan after December 27, 2020 may be able to apply for targeted advances.
The Consolidated Appropriations Act, 2021, removed the CARES Act provision that prohibited SBA from requiring tax records as part of its eligibility determination. SBA is requesting that those applying for the targeted advances verify their eligibility requirements and provide monthly revenue information and permission for SBA to request 2019 tax transcripts from the Internal Revenue Service (IRS). The tax transcript will allow SBA to verify that the applicant business existed and filed taxes in 2019. The Consolidated Appropriations Act, 2021, also requires SBA to process targeted EIDL advances within 21 days of receiving a completed application. SBA begins measuring processing time on the day that the agency receives all requested documentation from the applicant. SBA officials anticipate the agency will meet the 21-day processing requirement.
SBA plans to require additional tax documentation for processing of loans. In addition to requesting tax transcripts for the targeted EIDL advances, SBA officials told us that the agency plans to revise its EIDL loan application to systematically request that all new loan applicants provide the agency authority to request tax transcripts from IRS. SBA officials have not provided details on when this change will go into effect, but said that SBA can now request tax transcripts as needed as part of the loan review process. Additionally, SBA officials said SBA has required IRS tax records since around May 2020 for applicants that request reconsideration or appeal of their loan applications, such as after being declined. SBA officials told us it was challenging to verify applicant eligibility for EIDL without the ability to obtain tax records.
While SBA is waiting to revise its EIDL loan application to systematically request tax transcripts, SBA has not issued interim guidance or updated a reference guide that loan officers use as part of loan review to detail when loan officers should request tax transcripts or what tax transcript information they should review. We are continuing to follow up on this issue in ongoing work.
Processing time for EIDL loan applications has largely remained consistent. As of February 13, 2021, SBA had approved about 3.7 million loan applications and declined about 6.0 million applications. Between August 1, 2020, and February 13, 2021, SBA’s cumulative average processing time for loans ranged between 29 and 31 days. The cumulative average processing time for approved loans ranged between 44 and 47 days, as compared to 16 and 22 days for declined loans during the same period. In contrast, the cumulative average processing time for declined applicants asking SBA to reconsider their applications increased and ranged from 14 to 47 days during the same period.
Concerns remain about SBA’s inability to support EIDL accounting and related controls. In December 2020, SBA’s independent financial statement auditor issued a disclaimer of opinion on SBA’s fiscal year 2020 consolidated financial statements, meaning the auditor was unable to express an opinion due to insufficient evidence. As the basis for the disclaimer, the auditor reported that SBA was unable to provide adequate documentation to support a significant number of transactions and account balances due to inadequate processes and controls related to its implementation of its programs authorized under the CARES Act and related legislation—specifically EIDL and the Paycheck Protection Program.
The auditor identified two material weaknesses in internal controls related to EIDL concerning approval of EIDL loans and advances and oversight of EIDL service organizations. To process EIDL loans and advances, SBA used a service organization’s system to first automatically validate applicants and then issue alerts, including fraud alerts, which SBA loan officers were to review and mitigate. In its discussion of these material weaknesses, the auditor noted discrepancies including more than one loan or advance approved and disbursed to the same borrower, and identified over 6,000 disbursed EIDL loans (over $212 million total) issued to potentially ineligible borrowers.[461] The auditor also noted that SBA did not adequately design and implement controls for the evaluation and monitoring of the service organization’s control environment, including the operating effectiveness of its validation controls for EIDL loans and advances.
In total, the auditor made seven recommendations to SBA to address these two material weaknesses related to EIDL. Among other things, the auditor recommended that SBA
review the EIDL portfolio and determine which transactions were made to ineligible recipients;
implement controls to detect or prevent loans from being approved for ineligible applicants;
train loan officers and supervisory loan officers to execute their responsibilities using established guidance and standard operating procedures; and
enhance its review and evaluation of service organization controls.
SBA’s financial statement auditor reported that deficiencies related to the majority of the identified material weaknesses related to EIDL were caused by an inadequate entity-level control environment at SBA—the agency’s overall management controls to establish an effective internal control system.[462] Specifically, the auditor reported a material weakness in SBA’s entity-level controls, citing that SBA management did not properly design and implement overall effective management controls to account for new and expanded programs, such as EIDL, under the CARES Act and related legislation. The auditor issued five recommendations to improve entity-level controls including, among other things, that SBA hold accountable individuals responsible for overseeing management’s design, implementation, and operation of SBA’s internal control system; developing and implementing monitoring controls; and documenting internal controls related to CARES Act implementation and related legislation.
The auditor noted that the deficiencies were primarily caused by SBA prioritizing the implementation of CARES Act provisions and related legislation as quickly and efficiently as possible over designing and implementing effective internal control processes. SBA moved quickly to set up new programs and expand existing programs in order to help small businesses facing adverse economic conditions as a result of COVID-19. In the case of EIDL, this included quickly distributing loans and advances without adequately designing and implementing controls to help ensure borrower eligibility and accurate recording.
SBA’s fiscal year 2020 agency financial report describes the unprecedented scale of this effort. For example, SBA reported that it approved more than 3.6 million EIDL loans totaling $194 billion in fiscal year 2020, which represented more than all of SBA’s prior disaster assistance lending combined in the agency’s history. As a result, SBA’s reported loans receivable increased from $9.5 billion in fiscal year 2019 to $183 billion in fiscal year 2020.
SBA disagreed with the material weaknesses related to approval of EIDL loans and advances and entity-level controls, partially agreed with the material weakness related to service organization oversight, and neither agreed nor disagreed with the recommendations. However, SBA did recognize that documentation of its processes and controls was not sufficiently well developed to support the financial statement audit and stated that it is working diligently to correct any shortcomings for future audits. We support the recommendations the auditor provided to address control weaknesses related to EIDL, and we encourage SBA to continue to work to improve its controls over the program, as well as to improve its documentation to support future financial statement audits.
Concerns remain about fraud risk management in the EIDL program. The Department of Justice (DOJ) and law enforcement agencies have reported ongoing efforts related to potential fraud in the EIDL program. From May 2020 to February 2021, DOJ publicly announced charges in over 30 fraud-related cases associated with EIDL loans and charged over 50 defendants. The charges—filed in federal courts across the U.S. and investigated by a range of law enforcement agencies—include allegations of making false statements and engaging in identity theft, wire and bank fraud, and money laundering, among other charges. As of February 2021, at least five defendants had pleaded guilty to federal charges of defrauding the EIDL program. For more information related to these guilty pleas, see the Federal Fraud-Related Cases enclosure in appendix I.
In addition to ongoing prosecutions, law enforcement officials we spoke with noted a large number of ongoing investigations and hotline complaints related to CARES Act loans, including loans made under the EIDL program and the Paycheck Protection Program. A senior official with SBA’s Office of Inspector General (OIG) told us that, as of January 2021, SBA OIG had opened over 260 investigations related to CARES Act loans, including EIDL loans—at least three times the number of investigations the office would typically open in a year. Similarly, SBA OIG reported receiving over 70,000 hotline complaints related to CARES Act programs, compared to the 700 to 800 it would receive in a typical year. SBA officials told us that the agency’s Office of Disaster Assistance is supporting many of the DOJ and SBA OIG investigations through a team that researches case files, responds to inquiries from law enforcement agencies, and shares data on suspected fraud cases with the SBA OIG, DOJ, and U.S. Secret Service.
Law enforcement officials also reported systemic patterns of fraud across EIDL investigations. Officials at SBA OIG and the Federal Bureau of Investigation told us that they have identified systemic patterns of potential fraud including identity theft, false attestations on loan documents, fictitious and inflated employee counts, falsified tax documentation, and misuse of proceeds. Similarly, we reported in January 2021 that we analyzed aggregate data on suspicious activity reports filed by financial institutions from May to October 2020. These reports identified multiple types of potentially suspicious activity related to EIDL, such as indicators of identity theft, the rapid movement of funds, and forgeries.
SBA has taken some steps to mitigate fraud risks in the EIDL program. According to SBA officials, SBA conducted an informal fraud risk assessment for EIDL that resulted in enhanced internal controls. Specifically, SBA officials told us they considered both fraud risks facing EIDL and the sources and likelihood of those risks, and residual risks. Further, SBA introduced new EIDL program controls, such as conducting eligibility checks through the Department of the Treasury’s Do Not Pay service and plans to obtain 2019 tax transcripts from IRS for the targeted advances.[463] Additionally, SBA officials told us SBA increased staffing for its OIG liaison team that reviews suspicious loans flagged by loan officers and forwards referrals to SBA OIG. According to SBA OIG, as of January 2021, it had received nearly 750,000 of these referrals related to identity theft and over 585,000 referrals related to other potentially fraudulent activities associated with the EIDL program.
Leading practices identified in GAO’s Fraud Risk Framework call for a strategic approach for assessing and managing fraud risks.[464] The Fraud Risk Framework notes that such an approach includes designating an entity to lead fraud risk management activities. According to SBA officials, the agency created the Fraud Risk Management Council, which has a direct reporting authority to SBA’s Administrator and its associated Enterprise Risk Management Board, to oversee and coordinate agency-wide management of fraud risk. In alignment with leading practices in the Fraud Risk Framework, this council has a direct reporting line to senior-level managers at SBA and is not located within SBA OIG. However, it is unclear at this time whether the council meets the leading practices as a dedicated antifraud entity, including (1) understanding the program and its operations, as well as the fraud risks and controls throughout the program, and (2) having defined responsibilities and the necessary authority across the program.
According to the Fraud Risk Framework, the dedicated antifraud entity should, among other activities, manage the fraud risk assessment process and coordinate antifraud initiatives across the program. The fraud risk assessment should (1) identify inherent fraud risks facing the program, (2) assess the likelihood and impact of inherent fraud risks facing the program, (3) determine fraud risk tolerance, (4) examine the suitability of existing fraud controls and prioritize residual fraud risks, and (5) document the program’s fraud risk profile.[465] Such an assessment helps program managers determine whether they have the right controls in place to combat the most likely and impactful risks facing the program. The fraud risk assessment is particularly informative when the volume and nature of fraud risk indicators signifies an evolving fraud risk landscape, as confirmed by law enforcement officials for EIDL-related fraud. Further, the risk profile serves as the basis for the antifraud strategy, which defines key elements, such as responsibilities, activities, and timelines for addressing residual risks and continuously identifying emerging fraud risks to the program.
Although SBA has taken steps to identify and address risks on a loan-level basis through an informal fraud risk assessment process, it has not conducted a comprehensive fraud risk assessment in alignment with leading practices, nor documented its antifraud strategy outlining a strategic approach to managing fraud risks to EIDL. According to SBA officials, given the rapid response required to execute the program, SBA conducted an informal fraud risk assessment and, as of February 2021, had not documented the results of its efforts.
Although SBA’s initial steps are important, a comprehensive assessment that considers the likelihood and impact of all inherent fraud risks, the suitability of existing controls, risk tolerance, and prioritization of residual risk is key to ensuring resources are appropriately allocated to the most pressing risks. Further, an antifraud strategy would help ensure that SBA takes a strategic, risk-based approach to prevent, detect, and respond to fraud risks. Although SBA implemented a number of preventive controls based on its informal fraud risk assessment, such as planning to verify businesses by requesting 2019 tax transcripts from IRS for targeted advances, there may be significant fraud risks unaddressed by these controls. For example, the tax transcript verification is intended to provide validation of business operations before the program start date, but it likely would be limited to detecting unsophisticated cases involving identity theft or synthetic identities.[466] In addition to preventive controls, a fraud risk management strategy would help SBA to continuously detect and respond to risks for loans and advances after they are made.
We recognize the importance of providing timely emergency loan assistance to small businesses. Conducting a fraud risk assessment need not hinder program delivery and can in fact facilitate program goals by ensuring that taxpayer dollars and government services serve their intended purposes. Further, SBA has existing resources it can leverage in such an effort. For example, SBA could build on its informal fraud risk assessment and leverage existing resources provided by the Office of Continuous Operations and Risk Management. This office can provide leadership and resources informed by its enterprise risk management efforts as well as insight into fraud risks across SBA’s loan portfolios.
In January 2021, we reported that SBA provided loans and advances to potentially ineligible entities. We recommended that SBA develop and implement portfolio-level data analytics across EIDL program loans and advances made in response to COVID-19 as a means to detect potentially ineligible and fraudulent applications. Although implementing this recommendation would help SBA further detect potential fraud after it occurs, conducting a comprehensive fraud risk assessment in alignment with leading practices, and using the resulting fraud risk profile to develop an antifraud strategy, would help SBA take a more strategic approach to managing fraud risks to the EIDL program. Such an approach could (1) more effectively safeguard billions of dollars of taxpayer funds, and (2) better ensure that SBA addresses the full portfolio of risks and strategically targets the most significant fraud risks facing the program as part of ongoing approvals for EIDL loans and targeted advances.
Identifying and managing risk in the EIDL program. As discussed above, we and others have identified gaps in controls that may have led to fraud and the provision of EIDL funding to ineligible entities. Federal internal control standards call for agency management officials to assess the internal and external risks their entities face as they seek to achieve their objectives. Management identifies risks throughout the entity to provide a basis for analyzing risks. Risk assessment is the identification and analysis of risks related to achieving the defined objectives to form a basis for designing risk responses.
SBA program offices are responsible for assessing controls and mitigating risks. However, SBA’s Office of Disaster Assistance, which administers the EIDL program, has not proactively assessed risks to the program. SBA officials from the Office of Disaster Assistance’s Processing and Disbursement Center, which reviews and processes loan applications, told us that SBA does not have documented risk assessments and that SBA has primarily identified problems through loan officer review of loan applications.
The lack of a comprehensive plan to proactively assess controls and mitigate risks in the EIDL program may hinder SBA from achieving the defined objectives of the program and identifying opportunities for improving preventive controls in a timely manner. For example, Processing and Disbursement Center officials told us that 4 months after SBA started using the service organization’s automated validation system to approve loan applications in batches, they realized that these applications contained alerts that should have been reviewed by loan officers. Additionally, some validation changes have not been systematically incorporated using the service organization’s automated system. For example, Processing and Disbursement Center officials told us that loan officers were instructed to closely scrutinize applications from agricultural enterprises and banks with only an online presence. However, SBA did not request automated alerts for agricultural enterprises or online banks as part of the automated system checks, which could have facilitated loan officers’ review. While the reference guide loan officers use as part of loan review instructs loan officers to review applications from agricultural enterprises, the reference guide did not contain similar instructions for online banks.
Agency Comments
We provided SBA, the Department of the Treasury (Treasury), and the Office of Management and Budget (OMB) with a draft of this enclosure. SBA provided technical comments that we incorporated as appropriate. OMB and Treasury did not provide comments on this enclosure.
In its comments, reproduced in appendix X , SBA agreed with all three recommendations. With respect to the two recommendations addressing fraud risk management, SBA noted that it would work to determine the appropriate resources and approach to implement the recommendations to ensure that a fraud risk assessment for EIDL is completed and that fraud risk is monitored on a continuous basis. In its technical comments, SBA asked us to make the recommendations solely to the SBA Administrator so that SBA could determine the best resources to implement the recommendations. Therefore, we revised our recommendations to direct them to the SBA Administrator to provide additional flexibility to SBA regarding who should conduct the fraud risk assessment and monitor fraud risks in the program and who should implement a comprehensive oversight plan.
Methodology
To conduct this work, we reviewed SBA documentation on implementation of targeted advances. Additionally, we interviewed officials from SBA, SBA OIG, and the Federal Bureau of Investigation. We monitored SBA’s fiscal year 2020 financial statement audit and reviewed its fiscal year 2020 agency financial report and the accompanying independent auditor’s report. We analyzed SBA’s summary data on the processing of loan applications and assessed the reliability of these data by interviewing SBA officials. We determined that the data were sufficiently reliable for reporting on the number and dollar amount of EIDL loans and processing times.
Contact information: William B. Shear, (202) 512-8678, shearw@gao.gov
Related GAO Products
High-Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas. GAO-21-119SP. Washington, D.C.: March 2, 2021.
A Framework for Managing Fraud Risks in Federal Programs.GAO-15-593SP. Washington, D.C.: July 28, 2015.
Standards for Internal Control in the Federal Government.GAO-14-704G. Washington, D.C.: September 10, 2014.
The Small Business Administration has begun making new Paycheck Protection Program loans and has implemented changes to its processes, but needs to address control and accounting deficiencies and has not adequately assessed the risk of fraud in the program.
Entities involved: Small Business Administration, Department of the Treasury
Recommendations for Executive Action
We are making the following two recommendations to the Small Business Administration:
The Administrator of the Small Business Administration should conduct and document a fraud risk assessment for the Paycheck Protection Program. SBA agreed with our recommendation.
The Administrator of the Small Business Administration should develop a strategy that outlines specific actions to monitor and manage fraud risks in the Paycheck Protection Program on a continuous basis. SBA agreed with our recommendation.
Key Considerations and Future GAO Work
In June 2020, we recommended that the Small Business Administration (SBA) develop and implement plans to identify and respond to risks in the Paycheck Protection Program (PPP) to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less. SBA neither agreed nor disagreed with our recommendation at that time. Consistent with our recommendation, in December 2020, SBA officials said the agency had completed oversight plans. In response to our request that SBA provide the policies and procedures detailing these plans, the agency provided a Loan Review Plan for the loan review process. Although the plan references detailed policies and procedures for some loan reviews and loan forgiveness reviews, they were not included in the document we received because these policies and procedures were being updated according to SBA officials. In February 2021, SBA provided all but one of the documents referenced in the plan and stated that it was still finalizing the last document. The documents SBA provided include additional details on how SBA and its contractors plan to conduct the various reviews. We continue to review these documents to determine the extent to which they address our recommendation.
In November 2020, we also recommended that SBA expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread. SBA neither agreed nor disagreed with our recommendation at that time. In response to our recommendation, SBA stated that it was planning to conduct improper payment testing for PPP and that it takes improper payments seriously. SBA officials stated that SBA has submitted the sampling plan for this testing to the Office of Management and Budget (OMB) and will use this sampling plan to estimate both improper payments and error rates for PPP. We will continue to monitor the agency's actions to address this recommendation.
In December 2020, SBA’s independent financial statement auditor issued a disclaimer of opinion on SBA’s consolidated financial statements as of and for the year that ended September 30, 2020, meaning the auditor was unable to express an opinion due to insufficient evidence.[467] As part of the basis for the disclaimer, the auditor stated that SBA was unable to provide adequate documentation to support a significant number of transactions and account balances related to PPP due to inadequate processes and controls. The auditor identified four material weaknesses and made 17 recommendations to address controls related to accounting and reporting for PPP and evaluation and monitoring of service organization (contractor) controls.[468] In addition, the auditor identified one material weakness and made five recommendations to address entity-level controls that affect the operation of PPP. SBA did not fully agree with the weaknesses and neither agreed nor disagreed with the recommendations.
In March 2021, we added Emergency Loans for Small Businesses, which includes PPP, as a new area in our High-Risk List because of the limited controls built into the PPP approval process, the related risk of hundreds of millions of dollars in improper payments, and the consequent need for greater program integrity and better management. These risks are exacerbated by SBA’s inability to support its accounting and related control deficiencies.
Our work on PPP is ongoing. We continue to examine the characteristics of borrowers that received PPP loans, the safeguards SBA implemented to help ensure that lenders and borrowers complied with program requirements, and the loan forgiveness process. We also continue to monitor SBA’s progress toward developing and implementing corrective actions to address the material weaknesses identified by its financial statement auditor.
Background
Since March 2020, Congress has provided commitment authority of about $814 billion for PPP (including lender fees) under SBA’s largest guaranteed loan program, its 7(a) small business lending program.[469] PPP loans, made by lenders but guaranteed 100 percent by SBA, are low interest (1 percent) and fully forgivable if certain conditions are met.[470]
According to SBA, as of February 21, 2021, lenders had made about 7.1 million PPP loans totaling about $663 billion. The majority of these loans (about 5.3 million loans totaling more than $521 billion according to SBA) were made during the initial phase of PPP, which ended August 8, 2020.[471] SBA relaunched the program (Round 2) on January 11, 2021, following enactment of the Consolidated Appropriations Act, 2021, which authorized additional PPP loans and made changes to the program. Among other things, the act expanded the list of allowable uses of proceeds and loan forgiveness and allowed PPP borrowers to receive a second PPP loan of up to $2 million provided that they meet certain criteria.[472]
In addition, the act simplified the loan forgiveness application process for loans of $150,000 or less.[473] In response to this legislation, SBA issued updated forms and guidance in January 2021. As of February 18, 2021, SBA had approved about 1.7 million loan forgiveness applications (about 32 percent of all loans) totaling about $152 billion, according to SBA.
In March 2021, the American Rescue Plan Act of 2021 appropriated an additional $7.3 billion for the program.
As of January 31, 2021, SBA had obligated about $603 billion across the two rounds of PPP, including lender fees, and expended about $530 billion, according to SBA.
Overview of Key Issues
Round 2 launched with more up-front controls. SBA made a number of changes to PPP as it implemented Round 2 of the program.
Priority for underserved small businesses. When SBA relaunched the program on January 11, 2021, it initially prioritized community financial institutions that specialize in serving underserved communities, including minority-, women- and veteran-owned small businesses.[474] SBA opened the application portal to smaller lenders on January 15, 2021.[475] According to SBA, SBA approved about 60,000 loan applications for more than $5 billion during this initial access period. SBA opened PPP to all participating lenders on January 19, 2021.
On February 22, 2021, the White House announced additional efforts to target PPP to the smallest businesses. For example, it instituted a 14-day period, starting February 24, 2021, during which only businesses with fewer than 20 employees could apply. In addition, the White House said it would revise the loan calculation formula for sole proprietors, independent contractors, and self-employed individuals to offer more relief and establish a $1 billion set-aside for these types of businesses without employees located in low- and moderate-income areas.
Second draw loans available. The Consolidated Appropriations Act, 2021, allowed eligible small businesses to get a second PPP loan.[476] According to SBA, as of February 21, 2021, about 1.3 million of the total loans made during Round 2 (or about 69 percent) were second draw loans.
Additional up-front controls. Unlike the initial round of PPP, in which SBA did not conduct any review of loan or borrower information prior to issuing a loan number, SBA is implementing front-end compliance checks of loan and borrower information prior to the loans being approved and closed by the lender. According to SBA officials and documentation, these reviews include comparisons of the loan applications against the Department of the Treasury’s Do Not Pay service and public records.[477] Among other things, these validation efforts include items such as determining whether the business was in operation as of February 15, 2020.
SBA oversight plans still being documented. As we have previously reported, SBA plans to review all PPP loans of $2 million or more and further stated that it may review any PPP loan it deems appropriate, including loans of less than $2 million. According to the Loan Review Plan SBA provided us, SBA’s oversight of PPP loans involves three types of reviews: an automated screening of all loans at both the individual loan and aggregate levels, a manual review of selected loans, and a quality control review of a sample of loans. As shown in the table below, most of the loan reviews are conducted by contractors with SBA oversight.
Small Business Administration (SBA) and Contractor Reviews of Paycheck Protection Program Loans
Description
Contractor role
SBA role
Status as of February 2021
Automated screenings
Individual loan level
All loans individually screened to identify certain anomalies and attributes that may indicate noncompliance with select eligibility requirements, fraud, or abuse.
Use proprietary automated tool to compare Paycheck Protection Program (PPP) loan data against publicly available information and apply eligibility and fraud detection rules.
Front-end system design.
Ongoing
Aggregated loan level
Following completion of a critical mass of individual loan screenings and manual loan reviews, all loans screened in the aggregate to identify and analyze relationships across loans, borrowers, and lenders to identify potentially suspicious relationships and activities.
Use proprietary, rules-based engine to analyze PPP loan portfolio.
Front-end system design.
Not yet started
Manual reviews
Required
Reviews of all loans of $2 million or greater for
eligibility, including loan necessity;
fraud or abuse; and
compliance with loan forgiveness rules when loan forgiveness decision is submitted.
Review loan data, conduct research, and request documentation from lenders, borrowers, or both as needed to determine compliance with eligibility requirements (including loan necessity) or indication of potential fraud or abuse.
Review all contractor reports, including those regarding loan necessity, and review all loan forgiveness applications.
Ongoing
Discretionary
Reviews of loans of less than $2 million that are identified by the automated screening process or separately flagged for manual review for
eligibility, excluding loan necessity;
fraud or abuse; and
compliance with loan forgiveness rules when loan forgiveness decision is submitted.
Review loan forgiveness decisions using automated tool and manually if necessary.
Review all contractor reports for loans where contractor recommended further action. Conduct quality assurance review of statistically valid sample of loans where the contractor recommends no further action.
Ongoing
Quality control reviews
Quality control reviews of a sample of loan review files to ensure that all steps of the loan review process as documented by SBA were completed and that the evidence in the loan review file is sufficient to support the decision.
Review sample of loan review files.
Front-end process design.
Just starteda
Source: GAO analysis of SBA documents. | GAO-21-387
aAccording to SBA officials, the contractor began conducting quality control reviews in early February 2021.
The Loan Review Plan references detailed policies and procedures for loan reviews and loan forgiveness reviews. In February 2021, SBA provided seven of the eight documents referenced in the plan and stated that it was still finalizing the last document. The documents SBA provided include additional details on how SBA and its contractors plan to conduct the various reviews, at least for those loans approved in 2020.[478]
Inability to support PPP accounting and related controls. In December 2020, SBA’s independent financial statement auditor issued a disclaimer of opinion on SBA’s fiscal year 2020 consolidated financial statements, meaning the auditor was unable to express an opinion due to insufficient evidence. As the basis for the disclaimer, the auditor reported that SBA was unable to provide adequate documentation to support a significant number of transactions and account balances due to inadequate processes and controls related to its implementation of its programs authorized under the CARES Act and related legislation—specifically PPP and the Economic Injury Disaster Loan (EIDL) program.[479] For more information on the auditor’s findings related to the Economic Injury Disaster Loan program, see the Economic Injury Disaster Loan Program enclosure in appendix I.
The auditor identified four material weaknesses in internal controls related to PPP concerning loan approvals, reporting, cost estimates, and oversight of service organizations integral to the servicing and reporting of SBA’s loan guarantee programs, including PPP. In its discussion of these material weaknesses, the auditor noted there were over 2 million approved PPP loans (with an approximate total value of $189 billion) flagged by management that were potentially not in conformance with the CARES Act and related legislation. The loans were flagged for one or more of 35 reasons (such as borrower with criminal record or inactive business).
In addition, the auditor found that SBA management did not have processes and controls in place to review the status of PPP loan guarantees and as a result reported approximately $6 billion of PPP loans that were approved but not disbursed due to unsubmitted or unprocessed reports from lenders. The auditor noted there were over 896,000 errors from lender reporting that were identified but not reviewed or processed by SBA. The auditor also found that SBA did not consider and document the effects of the $189 billion in flagged PPP loans or the errors from lender reporting on the PPP reestimate methodology. The auditor also reported that SBA did not conduct or properly document sufficient evaluations of internal control reports for service organizations integral to SBA’s loan guarantee programs, including PPP.
In total, the auditor made 17 recommendations to SBA to address these four material weaknesses related to PPP. Among other things, the auditor recommended that SBA
finalize its review plan and execute the loan review process for PPP;
implement adequate controls to prevent loans from being approved that are potentially not in conformance with legislative requirements and program terms;
review PPP loans with incomplete or inaccurate reporting and update records as appropriate;
enhance its review and evaluation of service organization controls; and
assess the accounting considerations and record any necessary adjustments for PPP loans determined to be not in conformance with the CARES Act and related legislation.
SBA’s financial statement auditor reported that deficiencies related to the majority of the identified material weaknesses related to PPP were caused by an inadequate entity-level control environment at SBA—the agency’s overall management controls to establish an effective internal control system.[480] Specifically, the auditor reported a material weakness in SBA’s entity-level controls, citing that SBA management did not properly design and implement overall effective management controls to account for new and expanded programs under the CARES Act and related legislation. The auditor issued five recommendations to improve entity-level controls, including recommending, among other things, that SBA hold accountable individuals responsible for overseeing management’s design, implementation, and operation of SBA’s internal control system; develop and implement monitoring controls; and document the internal controls related to implementation of the CARES Act and related legislation.
The auditor noted that the deficiencies were primarily caused by SBA prioritizing the implementation of CARES Act provisions and related legislation as quickly and efficiently as possible over designing and implementing effective internal control processes. In the case of PPP, the auditor found that SBA was faced with implementing a new program with the inherent challenges of not having historical precedent, evolving and complex guidance, inadequate systems for a program of such a large scale, and an insufficient number of personnel to assist with implementing the related statutory provisions. SBA’s fiscal year 2020 agency financial report describes the unprecedented scale of this effort. For example, the report states that SBA processed 14 years’ worth of loans in the first 14 days of PPP, and ultimately guaranteed 5.2 million PPP loans totaling $525 billion in fiscal year 2020. As a result, SBA’s reported liability for loan guarantees increased from $2 billion as of September 30, 2019, to $512.7 billion as of September 30, 2020, reflecting this dramatic increase in activity.
SBA disagreed with the material weaknesses related to PPP loan approvals, reporting, and cost estimates, as well as entity-level controls; partially agreed with the material weakness related to service organization oversight; and neither agreed nor disagreed with the related recommendations. However, SBA did recognize that documentation of the processes and controls was not sufficiently detailed to support the financial statement audit and stated that it is working diligently to correct any shortcomings for future audits. We support the recommendations the auditor provided to address control weaknesses related to PPP, and we encourage SBA to continue to work to improve its controls over the program, as well as to improve its documentation to support future financial statement audits.
Ongoing concerns about fraud risk management. The Department of Justice (DOJ) and law enforcement agencies have reported ongoing efforts related to potential fraud in PPP.[481] From May 2020 to February 2021, DOJ publicly announced charges in over 100 fraud-related cases associated with PPP loans, charging at least 170 defendants. The charges—filed in federal courts across the U.S. and investigated by a range of law enforcement agencies—include allegations of making false statements and engaging in identity theft, wire and bank fraud, and money laundering, among other charges. As of February 2021, over 30 defendants had pleaded guilty to federal charges of defrauding PPP. For more information related to these guilty pleas, see the Federal Fraud-Related Cases enclosure in appendix I.
In addition to ongoing prosecutions, law enforcement officials we spoke with noted a large number of ongoing investigations and hotline complaints related to CARES Act loans, including loans made under PPP and the EIDL program. A senior official with SBA’s Office of Inspector General (OIG) told us that, as of January 2021, the OIG had opened over 260 investigations related to CARES Act loans, at least three times the number of investigations the office would typically open in a year.[482] Similarly, the SBA OIG reported receiving over 70,000 hotline complaints related to CARES Act programs, compared to the 700 to 800 it would receive in a typical year.
Law enforcement officials also reported systemic patterns of fraud across PPP investigations. Officials at SBA OIG and the Federal Bureau of Investigation (FBI) told us that they have identified systemic patterns of potential fraud including identity theft, false attestations on loan documents, fictitious and inflated employee counts, falsified tax documentation, and misuse of proceeds. Additionally, the FBI reported in June 2020 that early investigations of PPP-related fraud involved bank insiders, previously convicted felons, the use of dormant or cash businesses, and identity theft. Similarly, we reported in January 2021 that we analyzed aggregate data on suspicious activity reports filed by financial institutions from April to October 2020. These reports identified multiple types of potentially suspicious activity related to PPP, such as indicators of identity theft, the rapid movement of funds, and forgeries.
SBA has taken some steps to mitigate fraud risks to PPP. According to SBA officials, they conducted an informal fraud risk assessment for PPP that resulted in reviews and addition of some upfront controls, as discussed above. For example, SBA brought together subject matter experts from SBA and the Department of the Treasury (Treasury), as well as contractors, to identify fraud risks and mitigating controls for the program. To identify fraud risks, SBA used information on vulnerabilities observed through existing loan reviews as well as information from external sources, such as SBA OIG reports.
Leading practices identified in GAO’s Fraud Risk Framework call for a strategic approach for assessing and managing fraud risks.[483] The Fraud Risk Framework notes that such an approach includes designating an entity to lead fraud risk management activities. According to SBA officials, the agency created the Fraud Risk Management Council, which has a direct reporting authority to SBA’s Administrator, and its associated Enterprise Risk Management Board to oversee and coordinate agency-wide management of fraud risk. In alignment with leading practices in the Fraud Risk Framework, this council has a direct reporting line to senior-level managers at SBA and is not located within the OIG. However, it is unclear at this time whether the council meets the leading practices as a dedicated antifraud entity, including (1) understanding the program and its operations, as well as the fraud risks and controls throughout the program, and (2) having defined responsibilities and the necessary authority across the program.
According to the Fraud Risk Framework, the dedicated antifraud entity should, among other activities, manage the fraud risk assessment process and coordinate antifraud initiatives across the program. The fraud risk assessment should (1) identify inherent fraud risks facing the program, (2) assess the likelihood and impact of inherent fraud risks facing the program, (3) determine fraud risk tolerance, (4) examine the suitability of existing fraud controls and prioritize residual fraud risks, and (5) document the program’s fraud risk profile.[484] Such an assessment helps program managers determine whether they have the right controls in place to combat the most likely and impactful risks facing the program. The fraud risk assessment is particularly informative when the volume and nature of fraud risk indicators signify an evolving fraud risk landscape, as confirmed by law enforcement officials for PPP-related fraud. Further, the risk profile serves as the basis for the antifraud strategy, which defines key elements, such as responsibilities, activities, and timelines for addressing residual risks and continuously identifying emerging fraud risks to the program.
Although SBA has taken steps to identify and address fraud risks on a loan-level basis through an informal fraud risk assessment process, it has not conducted a comprehensive fraud risk assessment in alignment with leading practices, nor documented its antifraud strategy outlining a strategic approach to managing fraud risks to PPP. According to SBA officials, given the rapid response required to execute the program, they conducted an informal fraud risk assessment. In February 2021, SBA officials told us the agency would complete a formal fraud risk assessment but did not provide a firm date for when they would complete such an assessment.
While SBA’s initial steps are important, a comprehensive assessment that considers the likelihood and impact of all inherent fraud risks, the suitability of existing controls, risk tolerance, and prioritization of residual risk is key to ensuring resources are appropriately allocated to the most pressing risks. Further, an antifraud strategy would help ensure that SBA takes a strategic, risk-based approach to prevent, detect, and respond to fraud risks. In addition to preventive controls, a fraud risk management strategy would help SBA continuously detect and respond to risks after loans are made.
In June 2020 and November 2020, respectively, we recommended that SBA (1) develop and implement plans to identify and respond to risks in the PPP to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less, and (2) expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility of improper payments, including those resulting from fraudulent activity. Although these recommendations note fraud risks, they are aimed at enhancing program integrity and estimating improper payments, activities that are broader than managing fraud risks. Implementing those recommendations may include establishing or enhancing different controls than those needed to address fraud risks. Addressing fraud risks effectively necessitates a fraud risk assessment.
We recognize the importance of providing timely emergency loan assistance to small businesses. Conducting a fraud risk assessment need not hinder program delivery and can in fact facilitate program goals by ensuring that taxpayer dollars and government services serve their intended purposes. Further, SBA has existing resources it can leverage in such an effort; for example, it could build on the informal fraud risk assessment and leverage existing resources provided by the Office of Continuous Operations and Risk Management. This office can provide leadership and resources informed by its enterprise risk management efforts as well as insight into fraud risks across SBA’s loan portfolios.
Conducting a comprehensive fraud risk assessment in alignment with leading practices, and using the resulting fraud risk profile to develop an antifraud strategy, would help SBA take a more strategic approach to managing fraud risks to PPP. Such an approach could (1) more effectively safeguard billions of dollars of taxpayer funds and (2) better ensure that SBA addresses the full portfolio of risks and strategically targets the most significant fraud risks facing the program as part of ongoing PPP approvals and forgiveness.
Agency Comments
We provided SBA, Treasury, and OMB with a draft of this enclosure. SBA provided comments in a letter, which is reproduced in appendix X . In its letter, SBA agreed with the recommendations and noted that it would work to determine the appropriate resources and approach to implement the recommendations to ensure that a fraud risk assessment for PPP is completed and that fraud risk is monitored on a continuous basis. SBA also provided technical comments that we incorporated as appropriate. In its technical comments, SBA asked us to direct the recommendations solely to the SBA Administrator so that SBA could determine the best resources to implement the recommendation. Therefore, we revised the two recommendations to direct them to the SBA Administrator to provide additional flexibility to SBA regarding who should conduct the fraud risk assessment and monitor fraud risks in the program.
Treasury provided technical comments that we incorporated as appropriate. OMB did not have any comments on this enclosure.
Methodology
To conduct this work, we reviewed SBA documentation and data on PPP loan approvals, loan forgiveness applications, and obligations and expenditures. We monitored SBA’s fiscal year 2020 financial statement audit and reviewed its fiscal year 2020 agency financial report and the accompanying independent auditor’s report. We interviewed officials from FBI, SBA, and the SBA OIG, and representatives of the three contractors involved in the loan review process. We assessed the reliability of the SBA data by interviewing SBA officials. We determined that the data were sufficiently reliable for reporting the number and dollar amount of PPP loans, the status of loan forgiveness applications, and the status of PPP expenditures.
Contact information: William B. Shear, (202) 512-8678, shearw@gao.gov
Related GAO Products
High-Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas. GAO-21-119SP. Washington, D.C.: March 2, 2021.
Small Business Administration: COVID-19 Loans Lack Controls and Are Susceptible to Fraud. GAO-21-117T. Washington, D.C.: October 1, 2020.
A Framework for Managing Fraud Risks in Federal Programs. GAO-15-593SP. Washington, D.C.: July 28, 2015.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
The CARES Act-supported lending programs (facilities) stopped purchasing assets or extending credit at the end of 2020, except for the Main Street lending facilities, which ended on January 8, 2021. Overall, the transaction volume and purchases of assets by the CARES Act-supported facilities totaled approximately $41 billion (or a little more than 2 percent) of their $1.95 trillion capacity. The Consolidated Appropriations Act, 2021, rescinded most of the CARES Act funding and generally prohibited the Department of the Treasury’s funding support for future facilities that would be the same as those implemented pursuant to Title IV of the CARES Act. Federal Reserve and Department of the Treasury officials told us they continue to monitor market conditions to assess the need for implementing new facilities.
Entities involved: Department of the Treasury, Federal Reserve System
Key Considerations and Future GAO Work
In July 2011, we made two recommendations regarding facilities that the Board of Governors of the Federal Reserve System (Federal Reserve) established in response to the 2007–2009 financial crisis. These two recommendations are for the Federal Reserve to (1) strengthen procedures related to high-risk borrowers and (2) estimate and track losses within and across all facilities. These recommendations are relevant because the Federal Reserve created similar facilities that were supported by CARES Act funds to respond to COVID-19.
In our December 2020 report on the Federal Reserve’s facilities and relevant market trends, we reported that the Federal Reserve took action to address the intent of the first recommendation and, therefore, we closed this recommendation in January 2021. We will continue to examine the status of the Federal Reserve’s actions in addressing our second recommendation.[485]
Background
The CARES Act appropriated $500 billion to the Department of the Treasury (Treasury) and authorized at least $454 billion of that total for Treasury to support the Federal Reserve in establishing programs—known as facilities—for the purpose of providing liquidity to the financial system that supports lending to states, tribes, municipalities, eligible businesses, and nonprofit organizations.[486] Of the $454 billion, Treasury committed $195 billion and, of that amount, disbursed $102.5 billion to support the facilities. The Federal Reserve also established four facilities that do not receive CARES Act-appropriated funds; these facilities aim to provide liquidity to the financial sector and businesses.
Overview of Key Issues
The Consolidated Appropriations Act, 2021, rescinded most of Treasury’s CARES Act funding and prohibited Treasury from funding future facilities that would be the same as those implemented under the CARES Act, except for the Term Asset-Backed Securities Loan Facility.[487] Additionally, in December 2020, the agreements governing the CARES Act facilities between Treasury and the Federal Reserve were amended to be consistent with the Consolidated Appropriations Act, 2021. The amendments included items such as cancelling commitments to make additional investments and adjusting Treasury’s contributed amounts, to be consistent with the act.
The transaction volume for the nine Federal Reserve lending facilities that received CARES Act funding was generally limited, relative to their capacity. In addition, the four non-CARES Act facilities, which the Federal Reserve and Treasury extended through March 31, 2021, have generally had limited transaction volumes since mid-May 2020. On March 8, 2021, the Federal Reserve and Treasury extended one of the non-CARES Act facilities—the Paycheck Protection Program Liquidity Facility—through June 30, 2021.
CARES Act facilities. The Federal Reserve established nine facilities supported by CARES Act funding:
Primary Market Corporate Credit Facility and Secondary Market Corporate Credit Facility. These two facilities were designed to support large businesses by purchasing qualifying corporate bonds and other eligible assets.
Main Street Lending Program. Under this program, a total of five facilities were designed to support small and mid-sized for-profit businesses and nonprofit organizations by purchasing participations in eligible loans.[488]
Municipal Liquidity Facility. This facility was designed to support states, certain counties, municipalities, multistate entities, and revenue bond issuers by purchasing eligible notes that these entities issued.
Term Asset-Backed Securities Loan Facility. This facility was designed to support consumers and businesses by providing nonrecourse loans to U.S. companies secured by qualifying asset-backed securities generally backed by recently originated consumer and business loans.
The Federal Reserve determined that these facilities combined could hold a maximum of $1.95 trillion in assets when they were purchasing eligible assets and extending credit. The nine facilities conducted about $41 billion in transactions—with the Main Street Lending Program accounting for more than $16.5 billion. In its most recent periodic report to Congress on the lending facilities, the Federal Reserve Board stated that it continued to expect that the facilities would not result in losses to the Federal Reserve.[489]
Although demand for the CARES Act facilities was generally limited relative to their capacity, the Main Street facilities experienced an increase in activity from mid-December through January 8, 2021. The Main Street facilities conducted a total of about $16.5 billion in transaction volume, with just over $7.3 billion in transactions from December 16, 2020, through January 8, 2021. The Municipal Liquidity Facility also conducted an additional $4.9 billion through two transactions in the last half of December 2020, bringing its total transaction volume to almost $6.6 billion.[490] See figure for the CARES Act-supported facilities’ transaction volumes.
Cumulative Transaction Volume of Federal Reserve Lending Facilities Supported by CARES Act Funding, May 2020–January 2021
Note: The Primary Market Corporate Credit Facility, Secondary Market Corporate Credit Facility, Term Asset-Backed Securities Loan Facility, and the Municipal Liquidity Facility ceased purchasing eligible assets or extending credit on December 31, 2020. The facilities in the Main Street Lending Program ceased purchasing participations in eligible loans on January 8, 2021. Moreover, two of the CARES Act-supported facilities did not conduct any transactions—the Primary Market Corporate Credit Facility and the Nonprofit Organization Expanded Loan Facility (a Main Street Lending Program facility).
Four of the CARES Act facilities stopped purchasing eligible assets or extending credit on December 31, 2020, and the five Main Street facilities stopped purchasing participating interests in loans that were still eligible on January 8, 2021. The Consolidated Appropriations Act, 2021, rescinded most of the CARES Act-appropriated funding for supporting the facilities, including (1) funding that Treasury had committed but not disbursed to support the facilities and (2) disbursed funds that exceeded the cost of assets held or principal of loans funded by the facilities. Of the $102.5 billion that Treasury disbursed to support the facilities, the Federal Reserve returned a little more than $62 billion in excess funding to Treasury, pursuant to the requirements of the Consolidated Appropriations Act, 2021.[491] According to Federal Reserve and Treasury officials, they continue to monitor market conditions to assess the need for implementing new facilities, which would be supported through non-CARES Act funds.
Non-CARES Act facilities. As of February 15, 2021, all four of the non-CARES Act facilities had conducted $313.5 billion in transactions—with the Paycheck Protection Program Liquidity Facility and the Primary Dealer Credit Facility accounting for about $118.9 billion and $132.3 billion, respectively (see table).
Federal Reserve Lending Facilities without CARES Act Funding
Name of facility
Purpose
Facility activity
Transaction volume, as of May 15, 2020 ($ in billions)
Transaction volume, as of Oct. 15, 2020 ($ in billions)
Transaction volume, as of Feb. 15, 2021 ($ in billions)
Commercial Paper Funding Facility
Serve as funding backstop to provide liquidity for U.S. issuers of commercial paper
Purchase commercial paper from eligible companies; eligible issuers include U.S. issuers of commercial paper, including municipal issuers and U.S. issuers with a foreign parent company
4.24
4.27
4.27
Money Market Mutual Fund Liquidity Facility
Assist money market mutual funds in meeting demands for redemption by households and other investors
Make nonrecourse loans available to eligible financial institutions that are secured by high-quality assets purchased by the financial institution from money market mutual funds
58.01
58.01
58.01
Paycheck Protection Program Liquidity Facility
Facilitate lending by eligible institutions that provide loans to small businesses under the Paycheck Protection Program (PPP)
Lend to institutions eligible for making PPP loans on a nonrecourse basis, taking PPP loans as collaterala
45.97
101.22
118.94
Primary Dealer Credit Facility
Provide support to primary dealers to facilitate the availability of credit to businesses and households
Provide loans to primary dealers in exchange for collateral
118.41
129.83
132.29
Source: GAO analysis of the Federal Reserve System documents and data. | GAO-21-387
aThe Federal Reserve established the PPP Liquidity Facility under its Section 13(3) authority to encourage participation in PPP, which was established under the CARES Act.
More than three-quarters of transactions in non-CARES Act facilities occurred before May 15, 2020. On November 30, 2020, the Federal Reserve and Treasury extended the non-CARES Act facilities through March 31, 2021. On March 8, 2021, the Federal Reserve and Treasury extended the Paycheck Protection Program Liquidity Facility through June 30, 2021. The Federal Reserve also announced that the remaining three non-CARES Act facilities would not be extended beyond March 31, 2021.[492]
Oversight of facilities. The Federal Reserve’s Division of Reserve Bank Operations and Payment Systems developed and documented a general framework for oversight of the facilities. The framework includes reviews of established governance structures, process workflows, and internal control design, among other things. The division had completed these reviews for all facilities by December 2020. According to Federal Reserve officials, as of March 2021, the division is finalizing its plans for the last phase of oversight reviews. This final phase is to build on the prior reviews by tailoring the reviews for each facility, taking into account each facility’s credit and other risks.
Agency Comments
We provided a copy of this enclosure to the Federal Reserve, Treasury, and the Office of Management and Budget for review. The Federal Reserve and Treasury provided technical comments that we incorporated, where appropriate.
Methodology
To conduct this work, we reviewed Federal Reserve documentation on each facility, including term sheets and related press releases, reports to Congress, and the most recent Federal Reserve transaction data available on the facilities, as of February 2021. We assessed the reliability of the transaction data by reviewing published data on the facilities and obtaining information from Federal Reserve officials on the collection, maintenance, and compilation of the data. We also interviewed Federal Reserve and Treasury officials.
Contact information: Michael E. Clements, (202) 512-8678, clementsm@gao.gov
Related GAO Products
Federal Reserve Lending Programs: Use of CARES Act-Supported Programs Has Been Limited and Flow of Credit Has Generally Improved. GAO-21-180. Washington, D.C.: December 10, 2020.
Federal Reserve System: Opportunities Exist to Strengthen Policies and Processes for Managing Emergency Assistance. GAO-11-696. Washington, D.C.: July 21, 2011.Loans for Aviation and Other Eligible Businesses
The Department of the Treasury provided loans for up to $22 billion to 35 aviation and national security businesses.
Entities involved: Department of Defense, Department of Transportation, and Department of the Treasury
Key Considerations and Future GAO Work
In December 2020, we reported on the Department of the Treasury’s (Treasury) implementation of the CARES Act loan program for aviation and other eligible businesses, and we identified lessons for designing and implementing this type of emergency lending program for Congress and Treasury for the future. As Treasury moves to monitoring borrowers’ compliance with loan terms and conditions, we continue to review the outcomes of loan applications and Treasury’s plans to monitor borrowers’ compliance with the terms and conditions of loan agreements.
Background
The CARES Act authorized Treasury to provide up to $46 billion in loans and loan guarantees to certain aviation businesses and other businesses deemed critical to maintaining national security (national security businesses).[493] This loan program was intended to provide liquidity to targeted sectors. Treasury executed 35 loans to businesses in these targeted sectors, totaling about $22 billion, as shown in the table below.[494]
Loans for the CARES Act Loan Program for Aviation and Other Eligible Businesses
Loan category
Number of loans executed
Assistance provided ($ millions)
Passenger and cargo air carrier
17
21,202
Repair station
5
20
Ticket agent
2
20
National security business
11
700
Total
35
21,942
Source: GAO Analysis of the Department of the Treasury data. | GAO-21-387
Note: Section 4003 authorized maximum assistance available through loans in three categories: passenger air carrier, repair station operator, and ticket agent ($25 billion); cargo air carrier ($4 billion); and businesses critical to national security ($17 billion). CARES Act, Pub. L. No. 116-136, § 4003, 134 Stat. 281, 470 (2020). To match Treasury’s reporting on these loans and because air carriers that received loans could provide both passenger and cargo air services, we combined all air carriers into a single category.
The loan agreements executed by Treasury ranged in size from nearly $295,000 to $7.5 billion, as amended.[495] Treasury prioritized applications from the largest passenger air carriers and executed loan agreements with seven of them totaling about $20.8 billion. Treasury’s authority to make new loans ended on December 31, 2020.
The CARES Act set out conditions for this loan program including, among other things, that borrowers not reduce employment levels by more than 10 percent from levels as of March 24, 2020, through September 30, 2020, and refrain from share buybacks and dividend payments until 12 months after the date the loan or loan guarantee is no longer outstanding.
Overview of Key Issues
Of the 35 loans executed, 26 were secured by business assets and 9 were unsecured. Loans to 16 air carriers, including seven major airlines, were secured by business assets including airline loyalty programs, aircraft, and aircraft parts. Five national security businesses, four repair station operators, and one ticket agent also had loans secured by business assets including equipment and accounts receivable.
The nine unsecured loans went to six national security businesses, one repair station operator, one air carrier, and one ticket agent. Treasury decided to offer unsecured loans for $20 million or less. As such, the size of unsecured loans ranged from $450,000 to $20 million.
Of the 35 loans executed, employment retention requirements for loans differed for aviation and national security businesses. The terms of the 24 loans made to air carriers, repair station operators, and ticket agents included the requirement to maintain employment levels as of March 24, 2020, to the extent practicable, and not reduce employment levels by more than 10 percent from March 24, 2020, levels through September 30, 2020—matching the requirement in the CARES Act. For 10 national security businesses, the employment requirement included in the loan terms does not expire until September 30, 2021. For the remaining national security business—Yellow Corp., formerly known as YRC Worldwide, Inc—the employment requirement does not expire until October 20, 2021.[496]
Other loan terms, including the interest rates and duration of loans were relatively uniform across the executed loan agreements. Specifically, all but two of the executed loans had a duration of 5 years or approximately 5 years.[497] Treasury officials said they worked with their financial advisors for the program to determine interest rates, and that Treasury set rates to reflect the risk of loans in accordance with the CARES Act. Interest rates for unsecured loans used a benchmark interest rate for short-term loans plus 5.5 percent and for secured loans added from 2.5 percent to 3.5 percent to this benchmark interest rate.[498] Treasury has allowed borrowers to defer interest for 1 year.
As of March 1, 2021, seven businesses still had funds available for use, and 28 had drawn down the entire loan amount or terminated access to remaining funds when they prepaid their loan. Depending on the size of the loan, Treasury generally required borrowers to draw down 10 percent or the entire amount of the loan when the loan agreement was executed. In nearly all cases, borrowers with loans over $300 million had to draw down 10 percent of the loan amount when the loan was executed, while borrowers with loans less than $300 million had to draw down the entire loan amount.
Eight companies—one national security business and seven passenger air carriers—had loans over $300 million, and all drew down at least the required 10 percent near the time the loan was executed.[499] The national security business has since drawn down more of its loan funds, with nearly 80 percent of that loan drawn down as of March 1, 2021. Initially, the seven air carriers had until March 26, 2021, to draw down additional loan funds. However, in January 2021, Treasury officials changed this date to May 28, 2021—allowing borrowers more time to decide if they need to use these funds and also giving borrowers more time to seek private financing.
As of March 1, 2021, two borrowers have repaid loans: Ovation Travel Group repaid its loan for $20 million in January 2021, and Hawaiian Airlines, Inc., repaid its loan of $45 million and terminated the commitment for undrawn funds in February 2021. Treasury’s loan agreements allow borrowers to repay loans early without penalty and terminate Treasury’s commitments, according to Treasury officials. Other borrowers may repay or replace Treasury loans in the near term. On March 8, 2021, American Airlines announced plans to raise financing in private markets, a portion of which it planned to use to repay the outstanding balance of its Treasury loan.
In their applications, loan recipients reported that they planned to use the proceeds of the loans for multiple purposes, including for payroll and other operating expenses and providing liquidity to ensure continued operations.
The most common reasons loan applicants were not approved for loans differed for aviation and national security business applicants. Most of the 193 businesses that applied as passenger or cargo air carriers, ticket agents, or repair station operators were withdrawn, and most of the 74 businesses that applied as businesses critical to national security were rejected, as shown in the table below. Aviation applications were withdrawn for reasons such as not responding to Treasury requests for more financial data (42 applicants), entering bankruptcy (24 applicants), or not meeting Treasury’s credit standards (8 applicants). National security business applications were most frequently rejected for not meeting Treasury’s criteria as a business critical to national security (25 applicants). Other reasons for rejection and withdrawal included missing deadlines or not responding to Treasury’s request for more information (11 applicants) and not meeting Treasury’s credit standards (9 applicants). We continue to review the effect of Treasury’s loan program in ongoing work.
Application Outcomes for the CARES Act Loan Program for Aviation and Other Eligible Businesses
Loan category
Number of applications
Number of applications approved
Number of applications rejected
Number of applications withdrawn
Passenger air carrier
93
15
0
61
Repair station operator
41
5
0
28
Ticket agent
50
2
0
34
Cargo air carriera
9
2
0
1
National security business
74
11
40
23
Totalb
267
35
40
147
Source: GAO Analysis of the Department of the Treasury data. | GAO-21-387
Note: CARES Act, Pub. L. No. 116-136, § 4003, 134 Stat. 281, 470 (2020). aOne of the loan recipients, Island Wings, operates as a passenger and cargo air carrier. However, this business applied and was approved for a Treasury loan as a cargo air carrier. bIn the data provided by Treasury, the status of 45 aviation applications was not indicated. That is, the applicants neither executed loan agreements with Treasury, nor was there any indication in the data that these applicants withdrew from the program or were asked by Treasury to withdraw.
Agency Comments
We provided DOT, Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT and Treasury provided technical comments, which we incorporated as appropriate. OMB did not have comments on the enclosure.
Methodology
To conduct this work, we reviewed the most recent Treasury data on the loan program applications as of February 18, 2021; reviewed agency reports and guidance; reviewed the Consolidated Appropriations Act, 2021 and the CARES Act; and interviewed Treasury officials. We reviewed data on applications and related data fields by interviewing agency officials about the data’s consistency and completeness. We determined the data were sufficiently reliable for the purposes of our enclosure.
Financial Assistance: Lessons Learned from CARES Act Loan Program for Aviation and Other Eligible Businesses.GAO-21-198. Washington, D.C.: December 10, 2020.
The Department of the Treasury continues to administer additional payroll assistance for the aviation industry, and has started but not completed a plan to monitor recipients’ compliance with the terms of this assistance.
Entities involved: The Department of Transportation and the Department of the Treasury
Key Considerations and Future GAO Work
In November 2020, we recommended that the Secretary of the Treasury should finish developing and implement a compliance monitoring plan that identifies and responds to risks in the first Payroll Support Program to ensure program integrity and address potential fraud, including the use of funds for purposes other than for the continuation of employee wages, salaries, and benefits. Consistent with our recommendation, Treasury has developed a compliance process document, but has not completed supporting documents detailing its procedures and how it will implement them. We will evaluate these documents, once provided, to determine whether they address our recommendation.
Passenger demand for air travel remains far below prior years’ demand, and, according to industry forecasts, faces a slow, uneven recovery over the next 3 or more years. While passenger demand for air travel is expected to eventually return—especially as COVID-19 vaccination rates increase—the strength and speed of the recovery is uncertain. As a result, many aviation sector businesses that depend on passenger travel, including airlines and those businesses that support passenger air travel, remain in a poor financial position.
In September and November 2020, we reported concerns with the rollout of the initial Payroll Support Program (PSP1), which was established in the CARES Act, and Treasury’s plans to monitor recipients’ compliance with agreement terms.[500] With a Payroll Support Program Extension (PSP2) in December 2020 and another extension in March 2021, we continue to monitor these and any new concerns, such as the timing of awards and the oversight of award amounts and use of funds.[501]
Background
The Consolidated Appropriations Act, 2021 appropriated $16 billion to Treasury to provide financial assistance to make additional payments to be used for employee wages, salaries, and benefits.[502] Under this act, PSP2 provides the financial assistance to two categories of applicants—up to $15 billion for passenger air carriers and up to $1 billion for certain aviation contractors. As was the case with PSP1, Treasury requires passenger air carriers receiving awards over $100 million and contractors receiving awards over $37.5 million to provide warrants or notes as taxpayer protection.[503] The amount of payroll support an applicant is eligible for depends on the business type, payroll, and participation in PSP1.
As required by statute, PSP2 recipients must agree to refrain from conducting involuntary furloughs or terminations and reducing pay rates and benefits of employees until March 31, 2021, among other requirements.[504] Within 72 hours after signing a PSP2 agreement, recipients must recall any employees who were involuntarily terminated or furloughed between October 1, 2020 (for recipients that received PSP1 financial assistance) or March 27, 2020 (for recipients that did not receive PSP1 financial assistance) and the date of the PSP2 agreement. In addition to recalling previously furloughed employees, PSP2 recipients must compensate returning employees for lost pay and benefits between December 1, 2020, (for passenger air carriers) or December 27, 2020, (for contractors) and when the applicant entered into the PSP2 agreement.
Overview of Key Issues
Treasury had awarded over $13.2 billion to 261 companies as of March 10, 2021. Treasury received 549 applications for PSP2, with 320 from passenger air carriers and 229 from aviation contractors.[505] Similar to the approach with PSP1, Treasury prioritized applications from businesses with the most employees. For example, Treasury signed PSP2 agreements with the 12 largest passenger airlines within 7 business days of their application to the program. As of March 10, 2021, 190 passenger air carriers and 71 aviation contractors had signed PSP2 agreements (see fig.). The average award amount was over $66 million for passenger air carriers and nearly $9 million for contractors, with 4 passenger air carriers receiving awards over $1 billion and 11 receiving awards over $100 million. Due to the high demand for the program and as authorized in statute, Treasury is prorating award amounts—with passenger air carriers expected to receive 40 percent and contractors expected to receive 30 percent of their total approved award amount.
Timing and Anticipated Award Amounts for Treasury’s Payroll Support Program Extension (PSP2), by Type of Recipient, as of March 10, 2020
Treasury built on lessons learned from PSP1 but has faced challenges rolling out PSP2. According to Treasury officials, the processes to review, approve, and distribute PSP2 payments are similar to those used with PSP1. Learning from issues that arose with PSP1, Treasury dedicated time and resources to redesigning the online application portal to ensure more complete responses and make it more user-friendly. Treasury is also using information from PSP1 compliance reports in its review of PSP2 applications. For example, if Treasury has concerns that a PSP2 applicant may not be in compliance with its PSP1 agreement terms, its PSP2 application will not advance through Treasury’s review process until the issues are resolved. If the issues cannot be resolved, the PSP2 application is not submitted for final review.
As was the case with PSP1, PSP2 is an emergency program with intense interest and high expectations from applicants. Treasury officials said they must balance the need to disburse funds quickly with the need to ensure all statutory requirements are met which, given the complexity of PSP2 requirements, has been a challenge.
Industry associations representing businesses eligible to apply to PSP2 said their members appreciated the extension of the program and noted improvements to the application process, notably in the application portal. However, these associations noted their members had concerns similar to those raised about PSP1, namely the length of time Treasury is taking to approve and disburse awards and the need for additional guidance.[506] Treasury officials said they would provide additional information or guidance if they observe a high frequency of the same issues on applications or they receive many questions from applicants or recipients on similar issues. On March 10, 2021, Treasury released a new question and answer document for PSP2 that covered recalling employees and PSP2 agreement terms, among other topics.
Treasury has started but not completed plans to monitor PSP1 recipients’ compliance with agreement terms. In February 2021, Treasury provided us a copy of its Process Overview for CARES Operations Compliance Testing. This document outlined the steps Treasury uses in its compliance process for PSP1 but did not include details on automated tests used on all recipients, factors or thresholds from testing that trigger additional review, or remedies and penalties for noncompliance. According to Treasury officials, the agency is using such tests, factors, and thresholds to conduct monitoring currently, but it is still developing and finalizing these details for PSP1, as well as for PSP2. We will more fully evaluate Treasury’s efforts to develop a compliance monitoring plan when we can review more detailed documents from Treasury; however, Treasury was not able to estimate when these documents will be completed.
While PSP2 had broad support from the aviation industry, most do not see a sustained recovery in 2021. There was broad aviation industry support for extending payroll support payments, including from airlines, unions representing airline employees, and industry associations representing smaller passenger air carriers and contractors. However, based on industry forecasts passenger demand for air travel is not expected to recover for several years.
In addition to the uncertainty around when the aviation industry will return to prepandemic levels of operation, how businesses have been affected by the pandemic has also differed, in some cases significantly. For example, air carriers that focus on transporting cargo have fared much better during the last year than those that depend on transporting passengers. Even among companies that focus on transporting passengers, the extent to which their business models rely on leisure or business travel, domestic or international travel, or scheduled or unscheduled air service may have resulted in different outlooks and levels of loss. As the year unfolds, trends in the pace or nature of recovery may be issues to consider in providing any future financial assistance to the aviation industry to ensure it is effective and efficient.
Agency Comments
We provided DOT, Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT provided technical comments; Treasury and OMB did not have comments on the enclosure.
Methodology
To conduct this work, we reviewed the most recent Treasury data on the Payroll Support Program extension (PSP2) as of March 10, 2021; reviewed agency guidance and policy; reviewed the Consolidated Appropriations Act, 2021; and interviewed Treasury officials. We reviewed PSP2 data for outliers and missing information and interviewed agency officials, and we determined that Treasury’s data were sufficiently reliable for the purposes of summarizing the number, value, and timing of PSP2 awards to recipients.
We also reviewed reports (8-Ks and 10-Ks) filed with the Securities and Exchange Commission from January 2021 through February 2021 by airlines that received payroll support awards of over $100 million. We reviewed these reports to understand these companies’ rationale for taking PSP2 funds and expected effects. We also interviewed industry associations representing passenger air carriers and contractors eligible for PSP2 funds to understand their experience so far with PSP2.
Amtrak used CARES Act funds and is using Consolidated Appropriations Act, 2021 funds to address shortfalls in ticket revenue, pay employee salaries, and cover other operating, debt, and capital expenses, but it faces immediate and longer-term challenges.
Entities involved: Amtrak; Federal Railroad Administration, within the Department of Transportation
Key Considerations and Future GAO Work
We will continue to monitor how the National Railroad Passenger Corporation (commonly known as Amtrak) uses Consolidated Appropriations Act, 2021 funds, as well as its rail service and workforce levels.
Background
Amtrak provides almost all intercity passenger rail service in the U.S. across an approximately 21,000-mile rail network. This system includes three lines of business: the Northeast Corridor, 28 state-supported short-distance (750 miles or less) routes funded in part by the 17 states they serve, and long-distance (greater than 750 miles) routes that connect rural areas with major cities.[507]
Amtrak depends on grants from the federal government to operate the national passenger rail system and reinvest in the underlying infrastructure. Amtrak has received annual federal funding through grants from the Federal Railroad Administration (FRA), which executes and oversees grant agreements with Amtrak. For example, the Consolidated Appropriations Act, 2021 provided $700 million for the Northeast Corridor Grants program and $1.3 billion for the National Network Grant program, which includes the state-supported and long-distance routes.[508]
Prior to the COVID-19 pandemic, Amtrak had seen steady increases in ridership and revenues on its network, with over 32 million trips taken in fiscal year 2019.[509] As a result of the pandemic, Amtrak experienced a significant drop in ridership and corresponding revenue from ticket sales across its network. Amtrak received $1.018 billion through the CARES Act to prevent, prepare for, and respond to COVID-19. This included $492 million through the Northeast Corridor Grants program and $526 million through the National Network Grants program, of which at least $239 million was to offset payments by states to Amtrak for operating its state-supported routes.[510] FRA has awarded all of these funds to Amtrak, and as of January 31, 2021, Amtrak had expended $995 million, or 98 percent of the funds. Amtrak officials said the remaining funds would be expended by the end of February 2021.
In December 2020, Congress passed the Consolidated Appropriations Act, 2021, which provided Amtrak with an additional $1 billion in emergency relief funds to support the Northeast Corridor, state-supported, and long-distance passenger rail services. This included $285 million to assist states and commuter rail providers in making required payments to Amtrak.[511] Officials from Amtrak said that the remaining $713 million in funds will be used to offset the loss in revenue from operations on the Northeast Corridor ($566.6 million) and the National Network ($146.7 million). According to Amtrak officials, they will administer and expend the Consolidated Appropriations Act, 2021 funds almost identically to how they administered and expended the CARES Act funds.[512] FRA awarded the Consolidated Appropriations Act, 2021 funds to Amtrak in February 2021.
In March 2021, the American Rescue Plan Act of 2021 provided Amtrak with an additional $1.7 billion to support the Northeast Corridor Grants program and National Network Grants program.[513]
Overview of Key Issues
Similar to what we reported in November 2020, Amtrak officials said they had not faced significant challenges expending the CARES Act funds. The Amtrak Office of Inspector General reported in August 2020 that Amtrak moved swiftly to develop a comprehensive plan for using, tracking, and reporting on CARES Act funds.[514] Furthermore, in December 2020, the Inspector General reported that Amtrak was effectively using, accounting for, and reporting on these funds, and that it had addressed the initial risks the Inspector General identified in August 2020.[515]
Immediate and long-term challenges. While Amtrak did not experience challenges expending the CARES Act funds and does not anticipate challenges administering the Consolidated Appropriations Act, 2021, funds, Amtrak continues to face both immediate and longer-term effects on its operations stemming from the pandemic, according to officials. As we previously reported, these challenges include reduced ridership and revenue and uncertainty over long-term financial sustainability. In addition, Amtrak officials identified potential challenges with training and staffing resulting from its workforce and service reductions.
Ridership and revenue. Amtrak continues to face reduced ridership, and ridership was 80 percent less in January 2021 than in January 2020 on all lines of business (see figure). In January 2021, Amtrak officials reiterated that they have not experienced, and are not forecasting in the near future, significant improvements in ridership. According to Amtrak officials, they reset their ridership forecasts at the start of the fiscal year and continue to base their assumptions on the availability of a vaccine, current rail and aviation travel trends, and customer survey data. Amtrak anticipates some increase in ridership in the third quarter of the fiscal year as the vaccine becomes more widely available. Amtrak officials expect that ridership will recover to 35 percent of pre-pandemic levels in the fourth quarter of fiscal year 2021, based on the capacity available and mix of markets served. This figure is likely to change as COVID-19 recovery trends continue to evolve and as Amtrak makes changes in future levels of train service provided through the end of fiscal year 2021.
Amtrak Ridership Actuals and Forecast, October 2018–September 2021
Note: The forecast for 2021 is tentative due to the uncertainty in the improvement in travel rates, the availability of a vaccine to the public, and the end of the seasonal flu, according to Amtrak officials.
Because revenue from ticket sales has fallen along with ridership, Amtrak has also dealt with reduced revenues and budget shortfalls. For example, Amtrak revenues were 80 percent lower in January 2021 than they were in January 2020.[516] According to Amtrak officials, they expect that revenue recovery will lag behind ridership recovery in the near term because business travelers—who tend to pay for higher-value seats or preferable travel times—appear less likely to resume travel. For example, ridership on the Acela line, which carries mostly business travelers on the Northeast Corridor, remained over 90 percent lower in January 2021 than it was in January 2020, while ridership on the long-distance routes was down about 67 percent in January 2021 compared to January 2020 ridership levels.
Amtrak has taken steps to mitigate and plan for the impact of low ridership and revenues by reducing its workforce and service levels. For example, Amtrak furloughed over 1,200 employees as of January 14, 2021. Furthermore, it reduced the frequency of service on most of its long-distance routes from daily to three times a week in October 2020, which it expects will reduce costs by $150 million.[517] However, according to Amtrak officials, the reductions in Amtrak’s workforce have led to potential staffing and training challenges. For instance, because Amtrak furloughed staff, it has less flexibility to backfill absenteeism in certain cases.[518] Amtrak told us it is monitoring staffing levels to minimize the impact on remaining service. Officials also noted that Amtrak is planning future training, particularly for high-skill positions with longer training cycles, to help ensure it has trained staff when it starts increasing service again as demand rises over the next few years. In addition, recently appropriated Consolidated Appropriations Act, 2021 funds are required to be used by Amtrak to prevent additional furloughs and reductions in long distance service.[519]
Long-term financial sustainability. There may also be uncertainties about Amtrak’s long-term financial sustainability stemming from the impact COVID-19 has had on ridership. Amtrak officials said it may take 3 to 5 years for ridership on its network to recover to 2019 levels. Amtrak has developed low, medium, and high plans for when it expects to achieve 100 percent of pre-pandemic ridership levels. Like the shorter-term forecasts, Amtrak anticipates revenue recovery to lag behind ridership recovery, although Amtrak does anticipate it will achieve profitability on the Northeast Corridor in 2023. However, as a whole, Amtrak officials said the company is not expected to become profitable until after fiscal year 2026.
In addition, Amtrak expects that, while there may be shifts in ridership demographics, such as a potential decline in business travelers that could impact revenues, some of these losses could be offset by Amtrak’s product modernization and capacity expansion plans, which could attract new riders. For example, Amtrak officials stated that they have continued with capital projects that had already been funded, such as the procurement of new Acela trainsets and the recently renovated Moynihan Train Hall in New York City. However, Amtrak officials said they may have to postpone new capital projects if they do not receive supplemental funding. Furthermore, Amtrak developed ventilation and cleaning measures to assure passengers of the safety of Amtrak travel in an attempt to increase ridership and protect staff, according to officials.
FRA support and oversight of funding. According to FRA officials, they have not experienced any challenges in overseeing Amtrak’s use of the CARES Act funds and do not anticipate any challenges with the Consolidated Appropriations Act, 2021 funds. According to FRA officials, they will use the same oversight structures used to oversee the CARES Act funds to monitor Amtrak’s use of the Consolidated Appropriations Act, 2021 funds. In addition, FRA plans to monitor the burn rates of Amtrak expenditures along different lines of accounting and will review new monthly reporting requirements to track expenditures of funds provided to assist commuter rail operators’ payments to Amtrak.
Amtrak officials said that the Consolidated Appropriations Act, 2021 funds will only cover expenses through April 2021. As a result, in January 2021, Amtrak submitted an updated funding request that included an additional $1.54 billion in supplemental funding. The request covered funding to operate and invest in Amtrak’s network, support its state and commuter partners, and addressed various congressional concerns, such as avoiding additional employee furloughs and restoring daily long-distance service. Amtrak’s immediate recovery will be affected by these funding decisions and the actions it takes to mitigate its near-term challenges. In March 2021, the America Rescue Plan, 2021 makes available $1.7 billion to Amtrak and requires Amtrak to use a portion of those funds to restore daily long-distance service and reinstate furloughed employees, among other things. Moreover, Amtrak’s authorization expires at the end of fiscal year 2021, and Amtrak has asked Congress to consider establishing an intercity passenger rail trust fund to provide a more stable funding source to help it improve and expand its network. Future decisions about Amtrak will also affect how it evolves to maintain long-term financial sustainability.
Agency Comments
We provided Amtrak, FRA, and the Office of Management and Budget (OMB) with a draft of this enclosure. OMB did not have comments on this enclosure. Amtrak and FRA provided technical comments that we incorporated, where appropriate.
Methodology
To conduct this work, we reviewed the most recent agency data Amtrak provided to FRA as of January 31, 2021, relevant laws, and agency guidance on the Northeast Corridor and National Network Grant programs. We also met with senior Amtrak officials to discuss Amtrak’s plans to recover from the pandemic-driven decline in ridership and revenue, and we obtained information from FRA about any challenges in overseeing Amtrak’s use of the CARES Act and Consolidated Appropriations Act, 2021 funds. To assess the reliability of the Amtrak data, we conducted interviews with knowledgeable officials and reviewed documentation on the assumptions underlying Amtrak’s ridership and revenue forecasts. We determined that the data were reliable for our purposes.
Contact information: Elizabeth Repko, (202) 512-2384, repkoe@gao.gov
By July 14, 2020, the Department of Commerce’s National Oceanic and Atmospheric Administration had obligated almost $297 million of the available $298 million in CARES Act funding for fishery participants, but as of February 1, 2021, fisheries commissions had disbursed $96.3 million to fishery participants.
Entity involved: National Oceanic and Atmospheric Administration, within the Department of Commerce.
Key Considerations and Future GAO Work
In January 2021, we recommended that the Assistant Administrator for the National Oceanic and Atmospheric Administration (NOAA) Fisheries develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner. NOAA concurred with this recommendation. As of February 1, 2021, the agency had developed an electronic tracking tool to track the disbursement of funds and had begun to input data into it.
We will continue to monitor CARES Act assistance to fishery participants in ongoing and planned work. In September 2020, the Department of Commerce’s Inspector General started an evaluation of the National Oceanic and Atmospheric Administration’s implementation of CARES Act funding, including examining the steps taken to implement the act, any challenges encountered, and the oversight of the funds obligated and disbursed under the act.
Background
Commercial and recreational marine fisheries are critical to the nation’s economy, contributing approximately $99.5 billion to the U.S. gross domestic product and supporting approximately 1.7 million jobs in 2016, according to NOAA.[520] Widespread restaurant closures in the spring of 2020 led to a decrease in demand for seafood, adversely affecting the fisheries industry.
The CARES Act authorizes the Department of Commerce to provide assistance to eligible tribal, subsistence, commercial, and charter fishery participants affected by COVID-19, which may include direct relief payments.[521] The act appropriated $300 million to the Department of Commerce to assist fishery participants.[522] After $2 million in administrative fees were assessed by NOAA, $298 million of the $300 million was obligated for fishery participants. These include tribes, persons, fishing communities, aquaculture businesses not otherwise eligible for certain assistance, processors, and other fishery-related businesses, who have incurred, as a direct or indirect result of COVID-19, certain specified economic revenue losses or other negative impacts.[523] Businesses such as vessel repair businesses, restaurants, and seafood retailers are not considered fishery-related businesses eligible to receive CARES Act funding, according to NOAA’s website.
Overview of Key Issues
Funding was allocated in May 2020. On May 7, 2020, the Secretary of Commerce announced the allocation of about $298 million of the $300 million in CARES Act funding for states, tribes, and territories with fishery participants, as shown in the table.[524]
Department of Commerce’s Allocation of CARES Act Funding for States, Tribes, and Territories with Fishery Participants on May 7, 2020
Interstate commissiona
State/tribe/territory
Allocationb ($ thousands)
Atlantic States Marine Fisheries Commission
Massachusetts
Florida
Maine
New Jersey
New York
North Carolina
Virginia
Maryland
Pennsylvania
Rhode Island
New Hampshire
Georgia
Connecticut
South Carolina
Delaware
27,808
23,471
20,166
11,259
6,703
5,422
4,489
4,096
3,345
3,271
2,713
1,908
1,823
1,515
993
Gulf States Marine Fisheries Commission
Louisiana
Texas
Alabama
Mississippi
14,682
9,173
3,277
1,524
Pacific States Marine Fisheries Commission
Alaska
Washington
California
Oregon
West Coast Tribes
Hawaii
American Samoa
Alaska Tribes
Guam
Commonwealth of the Northern Mariana Islands
49,650
49,650
18,222
15,871
5,062
4,307
2,535
993
993
993
Territory of Puerto Ricoc
993
Territory of the U.S. Virgin Islandsc
993
Total
297,902
Source: GAO analysis of Department of Commerce data. | GAO-21-387
Note: The CARES Act appropriated $300 million to the Department of Commerce to assist fishery participants. Pub. L. No. 116-136, § 12005(d), 134 Stat. at 518. aThese three commissions were established in the 1940s. The National Oceanic and Atmospheric Administration (NOAA) partners with them on cross-state issues related to managing shared fishery resources. According to NOAA officials, these commissions are also partnering with states in the process to disburse funds to fishery participants. bAccording to NOAA officials, allocations represent the maximum amount of total funding that fishery participants in a particular state, tribe, or territory can receive. These allocations are net of administrative fees that NOAA assessed. Additional administrative fees can be assessed by grantees, such as the interstate marine fisheries commissions, according to NOAA officials. cPuerto Rico and the U.S. Virgin Islands are not part of an interstate marine fisheries commission.
Most of the CARES Act funding was obligated in July 2020. NOAA used these allocations to obligate almost $297 million of the available $298 million in funding to the three interstate marine fisheries commissions from June 30 through July 2, 2020, and to Puerto Rico on July 14, 2020. NOAA also obligated $993,000 to the U.S. Virgin Islands on November 13, 2020. The commissions have played a role in distributing funds as part of NOAA’s fishery disaster assistance program, which provides funding to fishery participants experiencing economic losses from specific events, such as hurricanes or oil spills.[525] The commissions worked with states, tribes, and territories in their regions to develop spend plans for NOAA’s review and approval. These plans explain how states, tribes, and territories will verify whether fishery participants meet the requirements of the CARES Act to receive funds.
According to NOAA officials, the agency is in the process of reviewing and approving spend plans from states, tribes, and territories. NOAA officials said they expect to receive 30 spend plans from states and territories and 30 from tribes. As of February 1, 2021, NOAA had received 29 of the 30 plans it anticipated from the states and territories. Of these 29 plans, 27 had been approved, and 2 were under review.[526] As of February 1, 2021, 30 tribal spend plans had been submitted to NOAA; 23 of these had been approved and 7 were under review.
Once a spend plan has been approved by NOAA, the states, tribes, and territories solicit and review applications from fishery participants, determine whether participants meet the eligibility criteria, and determine the direct payment amount based on the methodology outlined in the spend plan.[527] The respective interstate marine fisheries commissions disburse the appropriate amount of funds directly to the fishery participant consistent with the approved spend plan, though some states and tribes may disburse funds themselves.[528]
Most CARES Act funding had not been disbursed to fishery participants as of February 1, 2021. As of February 1, 2021, three interstate marine fisheries commissions had disbursed about 32 percent of obligated funds ($96.3 million out of the $298 million) to fishery participants in 12 states and 1 tribe as shown in the table below.
Disbursement of CARES Act Funding, as of February 1, 2021
Interstate commission
State
Funds disbursed ($ thousands)
Atlantic States Marine Fisheries Commission
Massachusetts
Maine
Virginia
Rhode Island
Connecticut
Georgia
South Carolina
Maryland
27,774
15,786
4,477
3,107
1,687
1,525
1,201
547
Gulf States Marine Fisheries Commission
Louisiana
1,968
Pacific States Marine Fisheries Commission
California
Hawaii
Oregon
West Coast Tribesa
18,041
4,279
15,768
177
Total
96,307
Source: GAO analysis of Department of Commerce data. | GAO-21-387
Note: The CARES Act appropriated $300 million to the Department of Commerce to assist fishery participants. Pub. L. No. 116-136, § 12005(d), 134 Stat. at 518. aAccording to National Oceanic and Atmospheric Administration officials, one tribe from this group has received funding.
Across these three interstate commissions, we found that the percentage of funds they had disbursed varied from 47 percent for the Atlantic States Marine Fisheries Commission to 7 percent for the Gulf States Marine Fisheries Commission, as shown in the figure below.
Percentage of Obligated CARES Act Funds That Have Been Disbursed to Fishery Participants by the Interstate Fisheries Commissions, as of February 1, 2021
Note: The CARES Act appropriated $300 million to the Department of Commerce to assist fishery participants. Pub. L. No. 116-136, § 12005(d), 134 Stat. at 518.
States, territories, and tribes must still review and assess applications from fishery participants, and one state spend plan has not yet been submitted to NOAA for review. Office of Management and Budget guidance on the act discusses the importance of agencies awarding and distributing funds in an expedient manner.[529] NOAA officials reported using a more expedited process to review spend plans, which has resulted in getting funding out to fishery participants more quickly than in past fishery disasters. However, the officials acknowledged that there is not an overall schedule for disbursing funds to fishery participants since time frames are established in individual spend plans. NOAA officials said it takes time to review spend plans to ensure they are in compliance with the CARES Act and for states, tribes, and territories to implement these plans—noting that each spend plan has different time frames for submitting applications, making award decisions, and disbursing funds.
NOAA officials said they expect the vast majority of funds to be disbursed to fishery participants by May 2021, but until recently the agency did not have centralized information on the time frames established in individual spend plans to help ensure that funds are being disbursed expeditiously and efficiently. In January 2021, we recommended that NOAA develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner. NOAA concurred with this recommendation. As of February 1, 2021, the agency had developed an electronic tracking tool to track the disbursement of funds and had begun to input data into it based on approved spend plans and expects to update these data on a weekly basis as funds are disbursed. The agency anticipates that all current and relevant data will be input into the tracking tool by May 2021 and that data will continue to be added to it until all funding has been disbursed.
An additional $300 million in COVID-19 relief funds was appropriated in December 2020. An additional $300 million for certain COVID-19-related fisheries disaster assistance was appropriated under the Consolidated Appropriations Act, 2021, signed by the President into law on December 27, 2020.[530] The amount provided is only to be allocated to states bordering the Atlantic, Pacific, or Arctic Oceans, the Gulf of Mexico, or the Great Lakes, as well as to territories and certain tribes.[531] The act provides that of the $300 million, $30 million is for COVID-19-related fishing impacts for specified tribal fishery participants, and $15 million is for COVID-19-related fishing impacts to nontribal commercial, aquaculture, processor, and charter fishery participants in states bordering the Great Lakes.[532]
According to NOAA officials, as of February 2021, the agency was working with the Department of Commerce and the Office of Management and Budget on developing a plan to administer and distribute the additional funds. They said this plan could involve states and territories using their existing spend plans with some slight modifications. They noted that the additional funding includes funding for states in the Great Lakes region, which did not receive CARES Act funding, and that these states would need to submit plans for approval.
Agency Comments
We provided a copy of this enclosure to NOAA and the Office of Management and Budget (OMB) for review and comment. NOAA provided us with technical comments, which we have incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed NOAA data as of February 1, 2021; examined documents on the data system the data came from; and interviewed officials familiar with the data system. We determined that the data were sufficiently reliable for our purposes by reviewing agency documents and speaking with agency officials. We also reviewed the CARES Act, the Consolidated Appropriations Act, 2021, and agency documents, and interviewed NOAA officials.
The Internal Revenue Service cannot yet determine the full extent to which businesses are taking advantage of certain tax relief options—such as carrying additional losses back to prior tax years—but it has disbursed approximately $11 billion in tentative refunds so far and is continuing to process these refunds and all of the paper mail that was backlogged due to COVID-19 closures.
Entity involved: Department of the Treasury, including the Internal Revenue Service
Key Considerations and Future GAO Work
In November 2020, we recommended that the Internal Revenue Service (IRS) update the Form 1040-X instructions to include information for taxpayers on the electronic filing (e-file) capability for tax year 2019. IRS agreed with this recommendation. As of early December 2020, IRS officials said they planned to include this information in the next routine annual update of the instructions with a mid-2021 release, rather than updating them sooner, out of cycle. We are continuing to monitor this action.
IRS has made progress on reducing the backlog of paper returns that resulted from COVID-19 closures. However, we continue to have concerns and are monitoring the processing of backlogged paper refund requests. Despite the backlog, IRS had issued roughly $11 billion to businesses in tentative Net Operating Loss (NOL) carrybacks and Alternative Minimum Tax (AMT) credit refunds as of December 31, 2020.
Comprehensive data for all of the business provisions in the CARES Act will not begin to be available until tax year 2020 returns have been processed. We will continue to monitor the use of these provisions as data become available, as well as monitor IRS’s efforts to ensure taxpayers’ compliance with the CARES Act.
Background
To provide liquidity to businesses during the COVID-19 pandemic, the CARES Act includes tax measures to help businesses—including sole proprietors, estates, and trusts—reduce certain tax obligations, which, in some cases, led to cash refunds.[533] The IRS’s capacity to implement new initiatives, such as the CARES Act tax measures, is an ongoing challenge we cited in our 2021 High Risk Report. [534]
The CARES Act modified, among other provisions of the tax law, provisions enacted as part of the 2017 legislation known as the Tax Cuts and Jobs Act (TCJA).[535] The Consolidated Appropriations Act, 2021, amended and extended some of these provisions, and expanded on a tax deduction available prior to the CARES Act, among other things.[536] The Joint Committee on Taxation (JCT) estimates the following tax provisions will result in about $180 billion in foregone revenue for the federal government in fiscal years 2020-2030.[537] These tax provisions include the following:
NOL carrybacks. The CARES Act requires, unless waived, carrybacks for 5 years for NOLs arising in tax years beginning in 2018, 2019, and 2020, which may provide a cash refund for certain taxpayers.[538] Tax years prior to 2018 had a higher tax rate, so the ability of businesses to carryback post-2018 NOLs to earlier tax years with higher taxes increases the value of the carryback amounts. The carryback period can be waived and may affect other tax obligations.[539] For NOLs arising in tax years beginning after 2017, TCJA limited the deduction of NOL carrybacks and carryforwards to 80 percent of taxable income.[540] The CARES Act temporarily suspended the 80 percent limitation and those NOLs can reduce 100 percent of taxable income for tax years beginning before 2021.[541]
The Consolidated Appropriations Act, 2021, provides a special election for farmers who incurred an NOL composed of a farming loss in a taxable year beginning in 2018, 2019, or 2020. Such farmers may elect to not apply the CARES Act NOL amendments regarding the temporary suspension of the 80-percent NOL deduction limitation and the 5-year carryback period.[542] This allows farmers who deducted a 2-year net operating loss carryback prior to the CARES Act to elect to retain that 2-year carryback rather than claim the 5-year carryback provided in the CARES Act.[543]
Taxpayers who have amounts included in their income because of the transitional repatriation tax established in the TCJA (referred to as “section 965” tax), can elect to exclude those inclusion years from the carryback period to produce an NOL refund in other years.[544] NOL carryback refunds are typically claimed on Form 1120-X, an Amended U.S. Corporation Income Tax Return; paper Form 1139, Corporate Application for Tentative Refund; or paper Form 1045, Application for Tentative Refund (for individuals, including sole proprietors, estates and trusts). From April to December 31, 2020, IRS implemented temporary procedures to allow for e-fax of Forms 1139 and 1045 for a quick tentative refund during the period that IRS campuses were closed and mail was not being processed due to COVID-19.[545]
Acceleration of AMT Credit refunds. TCJA repealed the corporate AMT, but most corporations could claim their excess unused minimum tax credits as a refundable credit for tax years 2018 through 2021.[546] Under the CARES Act, corporations with AMT credits may claim a refund for tax years beginning in 2018 and 2019 and may either file Form 1139 or Form 1120-X to receive a refund for some or all of these credits.[547]
Increased limits on business interest. For tax years beginning in 2019 and 2020, taxpayers may generally deduct business interest expense in amounts not to exceed the sum of (1) the taxpayer’s business interest income, (2) 50 percent of their adjusted taxable income for the tax year, and (3) their floor plan financing interest for the tax year.[548] Taxpayers may also elect to use 2019 adjusted taxable income in computing their 2020 business interest expense deduction. Businesses may choose not to elect to use 2019 adjusted taxable income in 2020, to calculate their 2020 business interest expense deduction, as it may affect other credits or deductions.
Excess business losses. For taxpayers other than C corporations—such as partnerships and sole-proprietors—the limit that TCJA enacted on excess business losses is removed for tax years 2018-2020.[549] Taxpayers that applied the TCJA limits to any excess business loss that arose during the 2018 or 2019 tax year, or during both tax years, can file amended returns to claim refunds. The American Rescue Plan Act of 2021, enacted March 11, 2021, extends the limitation on excess business losses.[550] We will continue to monitor the implementation of this provision.
Business meal deduction. Before the Consolidated Appropriations Act, 2021 was enacted, taxpayers could generally deduct a maximum of 50 percent of the ordinary food and beverage expenses associated with operating a trade or business. The new law removed the 50 percent limitation, allowing taxpayers to deduct the full expenses for food or beverages provided by a restaurant that are incurred after December 31, 2020, and before January 1, 2023.[551]
Overview of Key Issues
Update on the status of tentative refunds. Complete data on the number of taxpayers taking advantage of these tax provisions will not be available until after tax year 2020 income tax returns are processed at the earliest in late in 2021. However, initial data are available on applications for and payments of tentative refunds related to NOL carrybacks and AMT credits. The table below shows information on tentative refund requests received via the temporary e-fax line, which closed on December 31, 2020. IRS has received more than 41,000 NOL carryback and AMT credit refund applications via e-fax. IRS had approved roughly $14 billion and dispersed roughly $11 billion of tentative refunds, as of December 31, 2020.
CARES Act Net Operating Loss (NOL) Carryback and Alternative Minimum Tax (AMT) Credit Tentative Refund E-fax Cases, as of December 31, 2020
Form and provision
Cases Received via E-faxa
Number of taxpayers filing
Number of cases in suspenseb
Form 1139, AMT only
1,134
907
30
Form 1139, NOL or AMT
18,124
15,842
229
Form 1045, NOL
22,051
18,750
53
Totals
41,309
35,499
312
Source: GAO analysis of Internal Revenue Service data. | GAO-21-387
Notes: The temporary procedures to e-fax these forms ended on December 31, 2020, and forms received through those lines are still being processed and approved. aA single case may include multiple e-fax submissions. Submissions for the same identification number, form, and tax period generally are one case. Submissions for the same number and form, but for different tax periods, are separate cases. bA case is in suspense because additional information is needed.
In late January, IRS officials said they had also received 12,135 NOL carryback and AMT credit refund applications on paper Forms 1139 and 1045, and 4,921 via amended returns. However, IRS officials said they are unable to determine whether the paper Forms 1139 and 1045 and amended returns are CARES Act specific.[552] As of December 31, 2020, 312 Forms 1045 and 1139 received via e-fax were still in suspense, which according to IRS officials, could be because IRS is awaiting a processed amended return, or because of other reasons.[553]
Size of received and approved refunds. As we reported in November, according to IRS officials, they are still extracting pertinent data from the tentative refund applications so that actual dollar amounts claimed may be reported. When a refund application is received via e-fax, IRS initially groups it by the total dollar amount of the claim, providing us with high level information on the ranges of refunds claims by dollar group. (See table.)
Number and Approval Rate of CARES Act Applications for Tentative Refunds Received on Forms 1139 and 1045 via E-fax, by Refund Amount, as of December 31, 2020
Size of Refund a
Form 1139 received b
Number of approved refunds from Form 1139
Form 1139 approval rate c
Form 1045 received
Number of approved refunds from Form 1045
Form 1045 approval rate
$0 to $4,999
3,642
2,782
76%
3,806
3,165
83%
$5,000 to $99,999
7,115
5,083
71%
11,716
7,126
61%
$100,000 to $999,999
4,118
2,542
62%
5,728
2,400
42%
> $1Million
2,115
1,000
47%
793
218
27%
Source: Internal Revenue Service data and GAO analysis. | GAO-21-387
Note: A single case may include multiple e-fax submissions. Submissions for the same identification number, form, and tax period generally are one case. Submissions for the same number and form, but for different tax periods, are separate cases. A business can submit more than one application. a In this table, the size of refund is determined by the dollar group it falls into when an application is received via e-fax. b Form 1139 is a Corporation Application for Tentative Refund and Form 1045 is an Application for Tentative Refund c To calculate this approval rate, we divided the number of approved refunds from Form 1139 by the number of Form 1139 applications received for each of the refund size categories. We did the same for Form 1045 in the last column of the table.
The table above shows that approval rates decrease as the size of refunds increase. About 48 percent of the Forms 1045 and 1139 received between March 27, 2020 and December 31, 2020 were for refunds between $5,000 and $99,999. Of the approved refunds over $1 million, about 82 percent were from Form 1139, which are filed by corporations as opposed to businesses such as sole proprietors and partnerships that file Form 1045.[554]
Refund claims in excess of $2 million must be reported to the Joint Committee on Taxation (JCT) for review. [555] According to IRS data, 426 refund applications have been subject to this review between April 6, 2020 and February 25, 2021. IRS officials said that these refund claims can take about 70 days for the IRS Joint Committee Specialists to review, and that IRS increased the staffing for the program that processes claims subject to JCT review in late 2020.[556] IRS officials said they moved to transmitting these cases electronically between IRS and JCT as of April 6, 2020, to help expedite the process.
Update on processing of paper filings. COVID-19 caused IRS facilities to shut down and the subsequent large-scale staffing changes prevented the timely opening and processing of paper returns, including Form 1040-X. IRS processing centers re-opened in June 2020 and IRS officials said they have been processing mail in the order of receipt while operating at partial capacity to accommodate social distancing. IRS officials said that they had opened all of the backlogged paper mail as of December 18, 2020. However, as of March 2021, IRS officials said weather-related issues and the arrival of end of year returns on paper caused another mail backlog.[557] As of March 6, 2021, the backlog of unopened mail was 1.6 million returns, a decrease of 425,000 compared to the previous week, according to IRS officials.
Even when the paper mail is opened, it takes time to get those returns processed. In late January, IRS officials said 15.7 million individual and business tax returns were opened, but still waiting to be processed.[558] In some locations, IRS is still processing returns dated as early as July 15, 2020. IRS officials said they do not have a target date for processing all backlogged returns, but they continue to monitor available staffing. They expected that more employees would return to the office in February to help with the backlog
This processing backlog affects the processing of tentative refund applications as well. As we reported in November 2020, some taxpayers need to file an amended income tax return (generally a 1040-X for individual taxpayers, including sole proprietors) before using e-fax to file Forms 1139 and 1045. However, due to system limitations, if the taxpayer filed a paper Form 1040, that taxpayer would not be able to e-file Form 1040-X.[559]
The paper backlog is preventing IRS from processing paper-filed Forms 1040-X for tax year 2018 and 2019 in a timely manner, according to IRS officials. There were 1.3 million Forms 1040-X waiting to be processed as of February 11, 2021. Paper applications for tentative refunds may also be held up in this backlog, now that the temporary e-fax line for filing Forms 1139 and 1045 has closed, making applications for NOL carrybacks and AMT credits received by paper harder to obtain in a timely manner.
Agency Comments
We provided IRS, Treasury, and the Office of Management and Budget with a draft of this enclosure. IRS’s written comments are reproduced in appendix VIII. IRS also provided technical comments, which we incorporated as appropriate. The Office of Management and Budget and Treasury did not have any comments on this enclosure.
Methodology
We reviewed IRS data as of December 31, 2020, federal laws, and agency guidance; and interviewed IRS officials. To analyze IRS data, we obtained guidance from IRS and Treasury on the appropriate methodology to conduct the data analysis, extracted the relevant data sets from IRS databases, and processed our results. We determined that the data were sufficiently reliable for our purposes.
We are concerned about the Federal Emergency Management Agency’s lack of personnel needed to engage effectively with tribal governments, as well as the demands on the Disaster Relief Fund to effectively respond to the COVID-19 pandemic, considering the increasing amounts to be reimbursed to state, local, tribal, and territorial governments.
Entities involved: Federal Emergency Management Agency, within the Department of Homeland Security
Recommendations for Executive Action
The Federal Emergency Management Agency Administrator should adhere to the agency’s protocols listed in the updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of the tribal consultation process when developing new policies and procedures related to COVID-19 assistance.
The Federal Emergency Management Agency Administrator should provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19.
The Department of Homeland Security concurred with both of our recommendations.
Key Considerations and Future GAO Work
In November 2020, we reported that the Federal Emergency Management Agency’s (FEMA) Disaster Relief Fund—the primary source of federal disaster assistance for state, local, tribal, and territorial governments—had never before been used during a nationwide public health emergency on the scale of the COVID-19 pandemic. In March 2020, the CARES Act appropriated $45 billion to the Disaster Relief Fund, and in March 2021, the American Rescue Plan Act of 2021 appropriated $50 billion to the Disaster Relief Fund.[560] FEMA has used the Disaster Relief Fund to respond to the COVID-19 pandemic by providing lost wages assistance and crisis counseling services to individuals, and by awarding Public Assistance grants. Through Public Assistance grants, FEMA reimburses states, local, tribal, and territorial governments for pandemic-related costs, such as for testing supplies, personal protection equipment, National Guard activities, and vaccine distribution, among other things.
At that time, we noted that the number of concurrent demands on the Disaster Relief Fund and the unpredictability of any future response needs raise questions about funding availability for COVID-19 and a significant number of active disasters in different stages of recovery.[561]
For example, in 2020, in addition to providing COVID-19 assistance to respond to 58 major disaster declarations (in every U.S. state, the District of Columbia, territory, and two tribal nations), FEMA responded to assist with a record-setting number of hurricanes on the East Coast and with wildfires in the western U.S.[562]
We will continue to monitor the Disaster Relief Fund as part of our continued work on the nationwide pandemic, disaster response and recovery work, and the nation’s fiscal health.
Background
As of February 28, 2021, the Disaster Relief Fund balance was over $17 billion, which is an estimated 79 percent decrease from March 2020 at the start of COVID-19 (see figure), and FEMA projected at the time that the balance for the remainder of fiscal year 2021 would decrease to a deficit of over $22 billion.[563]
FEMA Disaster Relief Fund Balance by Month, February 2020 through February 2021
Note: In March 2021, the American Rescue Plan Act of 2021 appropriated $50 billion to the Disaster Relief Fund to support FEMA’s costs associated with major disaster declarations. American Rescue Plan Act of 2021, Pub. L. No. 117-2, § 4005, 135 Stat. 4, 79.
FEMA has used the Disaster Relief Fund to respond to the COVID-19 pandemic by providing three primary types of disaster assistance: (1) Public Assistance grants, (2) Individual Assistance, and (3) mission assignments. For natural disasters, Public Assistance grants tend to be used for emergency cleanup and for permanent reconstruction projects, for example, to rebuild damaged public infrastructure. FEMA typically provides 75 percent of the costs, while state, local, territorial and tribal entities cover 25 percent. FEMA’s Individual Assistance program provides assistance to disaster survivors to cover necessary expenses and serious needs—such as housing assistance, counseling, or child care—which cannot be met through insurance or low-interest loans. FEMA also issues mission assignments—work orders directing other federal agencies to provide direct assistance to state, local, tribal, and territorial governments—to support disaster response and recovery.
In addition, federally recognized Indian tribal governments have the option to request a presidential emergency or major disaster declaration and become a direct recipient of federal assistance or may elect to become a subrecipient under a state declaration.[564] Additional administrative requirements apply to direct recipients, such as developing a FEMA-approved administrative plan that describes how the tribal entity intends to administer Public Assistance funds.[565] FEMA policy states that FEMA personnel are available to provide technical assistance to tribal governments seeking Public Assistance as direct recipients to meet the administrative requirements, including for the COVID-19 response.[566] FEMA updated its tribal consultation policy in 2019 specifying steps that the agency should take in consulting with tribes when developing new policies or procedures.[567]
Overview of Key Issues
FEMA’s use of the Disaster Relief Fund to support COVID-19 activities increased in early 2021. FEMA currently uses the Disaster Relief Fund to fund the three programs mentioned above—(1) Public Assistance; (2) Individual Assistance; and (3) mission assignments, among others––as part of the agency’s COVID-19 response.[568] As of February 28, 2021, FEMA had obligated over $62 billion from the Disaster Relief Fund to respond to COVID-19. The figure below shows FEMA’s obligations for COVID-19 by program and activity.
Disaster Relief Fund Obligations and Projections for COVID-19 by Program and Activity through March 2021
Note: This figure includes estimated obligations that FEMA projected for March 2021.
Individual Assistance. The Crisis Counseling Assistance and Training program assists individuals and communities in recovering from the psychological effects of natural- and human-caused disasters through community-based outreach and educational services.[569] According to FEMA officials, FEMA had provided about $408 million in support of the Crisis Counseling and Training program for COVID-19, as of March 8, 2021. In addition, on August 8, 2020, President Trump issued a presidential memorandum that directed that up to $44 billion be made available from the Disaster Relief Fund to provide Lost Wages Assistance to supplement unemployment insurance compensation.[570] Further, in December 2020, Congress appropriated $2 billion to the Disaster Relief Fund for eligible funeral expenses for individuals or households with COVID-19-related funeral expenses.[571] As of February 2021, FEMA was developing its program to provide this assistance.
Public Assistance. For all 58 major disaster declarations for COVID-19, FEMA has authorized Public Assistance grants for emergency protective measures only. This may include eligible medical care, purchase and distribution of food, non-congregate medical sheltering, operation of Emergency Operations Centers, and the purchase and distribution of personal protective equipment. On February 2, 2021, the President issued a presidential memorandum that directed FEMA to fully reimburse states, territories, and tribes for all work eligible for assistance under Category B.[572]
FEMA officials stated that previous Public Assistance policy was limited to funding response activities and did not extend to operational costs at facilities. However, a January 21, 2021 Presidential memorandum expanded the definition of eligible goods and services under FEMA’s Public Assistance program to include the costs of opening and operating facilities such as schools, domestic violence shelters, transit systems, and others and may include the funding for the provision of personal protective equipment and disinfecting services and supplies.[573] According to FEMA officials, the memorandum will likely have a significant impact on their resources and operations. Specifically, FEMA officials stated that the eligibility of reopening and operating expenses for schools and other facilities is likely to significantly increase the number of applicants and cost of eligible claims under Public Assistance.
Mission assignments. The presidential memorandum issued on January 21, 2021 provided that FEMA would fully reimburse expenses for National Guard activities to respond to COVID-19, which may include vaccination distribution.[574] According to FEMA, the estimated cost is over $3 billion for National Guard assistance as of February 2021.
As of February 2021, FEMA, through its National Response Coordination Center and 10 regional offices across the nation, was coordinating with other federal agencies to meet state, tribal, and territory needs to support the distribution of COVID-19 vaccines. In addition, FEMA is deploying additional personnel to vaccination sites where they will assist people obtaining the vaccine. As of March 9, 2021, FEMA officials stated that it obligated almost $4 billion to states, tribes, and territories, and to Washington, D.C. for vaccine distribution.[575] According to FEMA officials, assistance for vaccine distribution may include but is not limited to:
Leasing facilities or equipment to administer and store the vaccine;
Staffing and training support;
Providing personal protective equipment and other administrative supplies; and
Using technology to register and track vaccine administration.
As of February 28, 2021, FEMA estimated that the obligation rate for COVID-19 will increase in March 2021 given the issuance of the presidential memorandum directing FEMA to retroactively reimburse states, locals, tribes, and territories at 100 percent of the costs for eligible emergency protective measures such as for masks, gloves, and emergency feeding actions.
FEMA did not consult with tribal entities in advance of issuing its policy on eligible Public Assistance costs early in the COVID-19 pandemic. In May 2020, multiple tribal associations reported that the Department of Homeland Security and FEMA did not formally consult with tribes for COVID-19 pandemic policies that have tribal implications.[576] Specifically, at the National Congress of American Indians in January 2021, tribal leaders voiced concerns over the continued lack of timely and consistent tribal consultation during the COVID-19 pandemic.
Further, representatives from two tribal entities we interviewed reported that they did not have the opportunity to provide input to FEMA’s policy on the types of COVID-19-related items or activities that would be considered eligible for reimbursement under the Public Assistance for COVID-19 and not having the opportunity to do so made it more difficult to make decisions on behalf of their tribe. For example, one tribal representative stated in the early months of the COVID-19 pandemic that tribal government employees were considered emergency workers and therefore were eligible to receive reimbursement for masks, but FEMA later restricted the reimbursement to first responders and health care workers only. As a result, the restriction meant that tribal government personnel who were performing critical functions to respond to COVID-19, such as monitoring incoming traffic at various tribal checkpoints, were no longer eligible to receive the reimbursement for masks under the revised policy.
In 2019, FEMA issued its Tribal Consultation Policy, which specifies the process for how FEMA engages with tribal governments in regular and meaningful consultation and collaboration on actions that have tribal implications (see figure below).[577]
Overview of FEMA’s Tribal Consultation Policy Process
Specifically, the policy states that FEMA commits to an inclusive and collaborative tribal consultation process that provides tribal governments’ sufficient time to submit input on actions that have tribal implications. This includes considering tribal input on actions that have tribal implications and following up with tribes on the final decision about how input was utilized. FEMA did not follow the tribal consultation process while developing an interim policy detailing eligible items for reimbursement under Category B of the Public Assistance program.
Although FEMA officials agreed that the interim policy clarifying eligible items under the Public Assistance program has tribal implications, the agency did not formally consult with tribes while developing the policy. Doing so would have allowed tribes the opportunity to provide meaningful input before FEMA issued the policy in September 2020. As a result, FEMA issued an interim policy clarifying the types of items and activities eligible for COVID-19 Public Assistance items without tribal input.
In December 2020, FEMA hosted a listening session for tribal entities seeking tribal input three months after the policy had already been issued. According to FEMA officials, they did not have the time to formally consult with tribes prior to issuing the interim policy due to the expedited nature of that policy and the immediate need to respond to questions from states, tribes, territories, and localities. Nevertheless, FEMA’s Tribal Consultation policy states that FEMA is committed to strengthening its nation-to-nation relationship and consultation efforts with tribal governments by collaborating and communicating early in the process to exchange information, receive input, and consider the views of tribes on actions that have tribal implications. If tribes had been formally consulted earlier in the process, they could have been in a better position to provide input to FEMA on how its policy might impact tribes. Further, there may have been less confusion on which items were considered eligible for reimbursement during the early months of the pandemic, and tribes could have made more informed decisions.
FEMA has not provided timely and consistent technical assistance to tribal governments, so tribes may be missing opportunities to receive Public Assistance as direct recipients for the COVID-19 pandemic. As of February 2021, FEMA reported that 60 percent of the 574 tribes were working with FEMA to receive Public Assistance for COVID-19, either as direct recipients or subrecipients. Tribal organization representatives told us that tribes may prefer to request Public Assistance as a direct recipient rather than as a subrecipient because (1) states do not always distribute assistance to tribes in a timely manner, (2) tribes may not have a positive relationship with the state, and (3) tribes may not want to sign a waiver that they believe could limit their rights as a sovereign entity. Conversely, tribes may decide to be a subrecipient through a state if they do not have the capacity or emergency management expertise to fulfill administrative requirements necessary to be direct recipients.
Several tribal organizations reported challenges related to completing administrative requirements to request and receive Public Assistance as a direct recipient during the pandemic––requirements such as activating an emergency operations plan and submitting a tribal Public Assistance Administrative Plan.[578] While some FEMA regions have not required the plan to be completed before distributing grant funding to tribal nations, other regions have not been as flexible with tribal needs. Moreover, some tribal nations have reported that certain FEMA regions have added region-specific requirements to their application process, thereby creating some inconsistency in how these requirements are administered throughout the FEMA regions.[579] While tribal representatives reported that some tribal nations received technical assistance, many other tribal nations were given little or no technical assistance when they requested support. Two tribal officials told us that when requesting technical assistance from FEMA to help with disaster activities, such as developing a Public Assistance Administrative Plan, FEMA did not have staff to assist.
In its 2020 report to the Administrator, FEMA’s National Advisory Council raised tribal capacity as a significant issue.[580] For example, the National Advisory Council recommended that in addition to increasing FEMA staff, FEMA should conduct a thorough survey of emergency management capabilities to gather specific information on the number of full-time emergency management staff in each tribal nation, their grant management capacity, their planning capacity, and other key resilience factors by January 2022.
FEMA stated that the agency has provided tribal relations personnel on an as-needed basis to provide technical assistance, but acknowledged that the number and expertise of tribal relations personnel varied throughout the regions and that the level of support was likely inconsistent. See figure below for the ratio of FEMA tribal relations personnel to tribal nations by FEMA region.
Ratio of FEMA Tribal Relations Personnel to Tribal Nations by FEMA Region as of February 2021
Note: Two tribes, the Seminole Tribe of Florida and the Navajo Nation, are direct recipients with a major disaster and an emergency declaration.
In its initial assessment report of its response to the pandemic, FEMA noted challenges and recommended that the agency develop a tribal nation engagement strategy. FEMA reported that the strategy should include providing the resources and personnel throughout each region required to support program delivery for all tribal nations, particularly to improve tribal emergency management programs related to low-frequency, high-impact events such as pandemics.[581] As of March 2021, FEMA had not developed this strategy, but planned to develop the strategy and implementation timeline by June 2021.
Given tribes’ limited capacity to fulfill administrative requirements related to the COVID-19 Public Assistance process, tribes are likely to benefit from technical assistance as they develop documents and other information related to their request for Public Assistance. FEMA’s Tribal Pilot Guidance states that tribes may request technical assistance from FEMA to develop a disaster-specific Public Assistance Administrative Plan. However, the guidance states technical assistance is subject to the availability of staff and disaster activity at the regional and national levels.[582] In addition, available data from the Centers for Disease Control and Prevention indicates that tribes are among the communities of color bearing a disproportionate burden of COVID-19 positive tests, cases, hospitalizations, and deaths. For example, the limited available data on COVID-19 hospitalizations shows that, as of February 12, 2021, the rate of COVID-19-associated hospitalizations for non-Hispanic American Indian/Alaska Native persons is 3.7 times the rate for non-Hispanic White persons, when adjusting for age. Without the availability of consistent and timely technical assistance across the FEMA regions, some tribal entities may be unable to request and receive Public Assistance directly from FEMA to help respond to the COVID-19 pandemic.
Agency Comments
We provided a draft of this enclosure to the Department of Homeland Security (DHS), FEMA, and the Office of Management and Budget (OMB). DHS concurred with both recommendations. Specifically, DHS stated that FEMA’s National Tribal Affairs Adviser, based in the Office of External Affairs, will coordinate with other FEMA offices and directorates, as appropriate, to review the agency’s adherence to protocols listed in the Tribal Consultation policy. For the second recommendation, DHS stated that FEMA’s Recovery Directorate will publish a memorandum that will contain direction to FEMA regions regarding the assignment of Public Assistance program delivery managers to promote equitable delivery of Public Assistance to tribal governments. The extent to which these steps will address our recommendation that FEMA provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients is not clear. We will continue to monitor DHS efforts to implement these efforts in the coming months. DHS comments are reproduced in appendix VII. FEMA provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed data from the Disaster Relief Fund and FEMA obligations data for March 2020 through February 2021. We reviewed federal laws, FEMA policies and guidance on how states, local, tribal, and territorial entities may apply for and receive assistance to respond to the COVID-19 pandemic.
We also reviewed May 2020 letters to Congress from eight tribal organizations; January 21, 2021, and January 26, 2021, presidential memorandums; FEMA’s February 3, 2021 fact sheet; and FEMA Advisories. Finally, we interviewed FEMA officials, representatives from four tribal nations residing in different parts of the country, and two tribal associations. One of the tribal associations is the oldest, largest, and most representative American Indian and Alaska Native organization serving the broad interests of tribal governments and communities, and the other’s focus is on emergency management. While the information from these interviews cannot be generalized to all tribal nations, it provides illustrative examples of the tribal nation experience in obtaining federal assistance to respond to the COVID-19 pandemic.
Contact information: Chris Currie, (404) 679-1875, curriec@gao.gov
Related GAO Products
The Nation's Fiscal Health: Action Is Needed to Address the Federal Government's Fiscal Future. GAO-20-403SP. Washington, D.C.: March 12, 2020.
Tribal Consultation: Additional Federal Actions Needed for Infrastructure Projects. GAO-19-22. Washington, D.C.: March 19, 2019.
Emergency Management: Implementation of the Major Disaster Declaration Process for Federally Recognized Tribes. GAO-18-443. Washington, D.C.: May 23, 2018.
Centers for Disease Control and Prevention guidance on reassessing schools’ operating status is more clear and consistent than prior guidance; the Department of Education has taken steps to track state and school district spending of certain COVID-19 relief funds, but the data gives an incomplete picture of the status of funds.
Entities involved: Department of Education and the Department of Health and Human Services, including the Centers for Disease Control and Prevention
Recommendation for Executive Action
The Secretary of Education should regularly collect and publicly report information on school districts’ financial commitments (obligations), as well as outlays (expenditures), in order to more completely reflect the status of their use of federal COVID-19 relief funds. For example, Education could modify its annual report on state and school district spending data to include obligations data in subsequent reporting cycles. Education agreed with our recommendation.
Key Considerations and Future GAO Work
We continue to monitor challenges related to educating children during the COVID-19 pandemic. In June and September 2020, we reviewed state and territory expenditure rates related to funds provided through the Education Stabilization Fund (ESF) that could be used for K-12 education needs. We also reviewed guidance from the Centers for Disease Control and Prevention (CDC) on returning to in-person education. We identified a lack of cogent, clear, and consistent federal guidance to help states and school districts reassess the operating status of K-12 schools.[583]
We recommended that the Director of the CDC ensure that, as CDC updates federal guidance related to reassessing schools’ operating status, the guidance is cogent, clear, and consistent. The administration announced a national strategy to respond to COVID-19 on January 21, and directed federal agencies to coordinate guidance to help schools safely return to in-person education.[584] CDC did so on February 12. The guidance focuses on considerations for returning to in-person learning, as well as mitigation strategies to help prevent and reduce the spread of COVID-19 in school settings. After reviewing the current guidance and CDC’s website, we determined that CDC’s February 12 guidance for school operating status during COVID-19 is more cogent, clear, and consistent and encourage CDC to continue with these efforts. As such, we closed our recommendation as implemented.
The Department of Education (Education) developed an annual reporting process and launched the first phase of a public website in November 2020 to track and provide information on, among other things, how states and territories are spending their ESF funds. According to data collected by Education, as of February 28, 2021, states and territories had spent about $6.1 billion on education. However, federal spending data alone provide an incomplete picture of the status of funds, as there are several factors that influence spending rates. For example, when school districts use available ESF funds, school district officials told us they have to budget for and obligate these funds before they are permitted to request payment from the state and the state draws down the funds—that is, requests funds to disburse to the school districts—which is when Education recognizes the funds as spent. This process can result in a significant gap in time between when a state reports it has spent the funds and the actual rate at which the funds are being obligated, or “used.”[585]
We will continue to monitor the administration’s plans to help schools safely return to in-person learning, as well as state and local efforts to use COVID-19 relief funding to support K-12 education during the pandemic. For example, we have ongoing work on issues related to disconnected students (that is, students who have difficulty accessing and staying engaged in virtual learning) and pandemic-related learning loss.
Background
Since spring 2020, CDC has provided information and guidance to help states and local school district officials fulfill their roles as key decision makers regarding how and when to safely reopen schools for in-person learning. For example, CDC’s guidance includes considerations on whether and how to screen students and staff for symptoms of COVID-19, considerations for school readiness and planning, and frequently asked questions for school administrators, teachers, parents, and child care providers.
The Consolidated Appropriations Act, 2021, enacted on December 27, 2020, appropriated approximately $59 billion for states’ and territories’ COVID-19-related education needs through the ESF.[586] This is in addition to the approximately $17 billion in the ESF for states and territories appropriated under the CARES Act on March 27, 2020.[587] Education awards these funds to the states and the states then award the majority of the funds to the school districts and other education-related entitles.[588] The American Rescue Plan Act, enacted on March 11, 2021, appropriated approximately $126 billion specifically for ESF programs previously authorized by the CARES Act and Consolidated Appropriations Act, 2021 for K-12 education-related purposes.[589]
Overview of Key Issues
Guidance for safely reopening K-12 school buildings. Since spring 2020, the federal government has offered information and guidance to help states and local school district officials make risk-based decisions regarding how and when to reopen schools for in-person learning. As part of a national strategy for safely reopening schools for in-person learning, in January 2021, the President issued an Executive Order directing Education and the Department of Health and Human Services, including CDC, to, among other things, work together to ensure that guidance for schools is evidence-based.
In addition to the Executive Order, the President directed Education to work with CDC to issue a school reopening handbook to help answer school administrators’ and educators’ questions about how to ensure safe operations. On February 12, 2021, CDC issued updated guidance on safely returning to in-person education.[590] As with the previous guidance, the update focuses on five mitigation strategies for safe school operations during COVID-19: (1) universal and correct wearing of masks; (2) physical distancing; (3) handwashing and respiratory etiquette; (4) cleaning and maintaining healthy facilities, including ventilation improvements; and (5) contact tracing in combination with isolation and quarantine, in collaboration with the state, local, territorial or tribal health departments. Simultaneously, Education released a handbook—the first of a series of volumes—which includes practical approaches for implementing CDC’s five mitigation strategies in elementary and secondary schools.[591]
We first reviewed federal guidance on reopening schools in June 2020 and in September 2020 we reported on weaknesses and CDC agreed with our recommendation to ensure its guidance was cogent, clear, and consistent. Since then, CDC reported that it continues to review COVID-19 guidance and has taken actions to make updates more consistently across guidance documents and across its website. After reviewing the current guidance and CDC’s website, we determined that CDC’s guidance for school operating status during COVID-19 is more cogent, clear, and consistent and encourage CDC to continue with these efforts.
ESF spending. Federal spending data alone provides an incomplete picture of states’ and school districts’ spending. According to data collected by Education, as of February 28, 2021, states and territories had spent about $6.1 billion on COVID-19-related education needs. (See figure).
Federal COVID-19 Relief for States and Territories Provided through Education Stabilization Funds and Amount Spent, as of February 28, 2021
Notes: Dollar figures are rounded to the nearest million.The Consolidated Appropriations Act, 2021, enacted on December 27, 2020, appropriated approximately $59 billion for states’ and territories’ COVID-19-related education needs through the ESF. This is in addition to the approximately $17 billion in the ESF for states and territories appropriated under the CARES Act on March 27, 2020.These funds provide aid to states, the District of Columbia, and Puerto Rico across two emergency relief funds, as well as through formula grants to other U.S. territories (referred to in the law as outlying areas). The CARES Act also provided aid for states through ESF discretionary grants. Pub. L. No. 116-260, div. M, tit. III, §§ 311(a)(1), 312, 313, 134 Stat. at 1924-1932 and Pub. L. No. 116-136, §§ 18001(a)(1), 18001(a)(3), 18002, 18003, 134 Stat.at 564-567. Funds were also provided through the ESF for institutions of higher education and for programs operated or funded by the Bureau of Indian Education; however, these components are outside of the scope of this enclosure and are not reflected in the figure.
The CARES Act allows states a year after they receive their grants to award (subgrant) certain ESF funds to school districts (subgrantee).[592] Once awarded, districts have until the end of fiscal year 2022 to obligate the CARES Act funds for specific purposes.[593] The Congressional Budget Office (CBO) estimated that more than half of the CARES Act ESF funds will be spent (outlayed or expended) by the end of fiscal year 2021—a target that states and school districts appear on track to meet. There are several factors that may contribute to the rate at which funds appear to be spent.
First, there is often a significant gap between when a district “uses” the funds (i.e., orders, contracts for, installs, and pays for goods or services, such as IT equipment) and when those funds are reported as “spent” in state and federal reporting systems, as is common in federal grants management processes. According to Education officials, states award applicable ESF funds to school districts so that the school districts can obligate those funds to specific purposes. The state does not transfer funds to the district until the district requests payment for services or deliverables received. According to Education officials, they do not consider the funds spent, and their public website does not show them as such, until the state requests payment for expenses.[594] School district officials told us that they budget for how they will use available ESF funds and may obligate them well before they request funds from states to make payments. (See figure below.)
Examples of Key Milestones in the Funding Stream for the Education Stabilization Fund
Note: This figure provides examples of key milestones. In some instances, additional or different steps may occur in the funding stream.
Second, some of the funds are used for services that occur and are paid for over time. For example, if a school district uses its ESF funds to hire additional custodial staff, substitute teachers, or other staff to address pandemic needs, the district would pay for these services as they are rendered (for example, via bi-weekly payroll) and would request the ESF funds from the state over time.
Third, some equipment, such as laptops and new heating, ventilation, and air conditioning (HVAC) systems, must be ordered well in advance, and some high demand items are reportedly significantly delayed. For example, in one case, district officials told us that the air filters needed for their HVAC system are not currently available in the U.S. due to high demand during the pandemic and they do not know when they will receive the parts. Officials from another school district told us that the laptops they ordered in October 2020 were backordered and not expected to arrive until April 2021.
Fourth, during its monitoring efforts, Education found that some states had drawn down CARES Act funds before they were needed to pay for a good or service. Education found that at least one state did not follow federal cash management requirements when it drew down funds and provided advance funding to school districts (subgrantees). Education has requested states redeposit those funds in the U.S. Treasury until they are needed. Some states have already returned these funds; however, total spending may appear inflated in those states that have not yet redeposited or spent their funds.
Education data sharing. In an effort to shed light on how CARES Act ESF funds are being spent, Education took an important step toward transparency by launching two efforts in November 2020—an annual reporting process and the ESF Transparency Portal website (https://covid-relief-data.ed.gov). The annual report collects information on, among other things, how states and subgrantees, such as school districts, have spent their ESF funds, whereas the portal will initially focus on state spending and the amounts awarded to subgrantees.[595] Neither focuses on the amount of ESF funds subgrantees have obligated but have not yet drawn down (known as unliquidated obligations). Education officials told us that they are still working out key details around the public interface with these data from both efforts, such as how much and what portions of the annual report data will be shared on the portal.
For the annual report, Education asked states to provide, by February 1, 2021, detailed information on how subgrantees, such as school districts, have spent the ESF funds that they received in fiscal year 2020—that is, through September 30, 2020; Education plans to publish data from the annual report via the ESF portal in April 2021. Education also asked states to report information on subgrantee activities that specifically target key student groups (for example, children from low-income families or children who are experiencing homelessness). Education plans to ask states to report annually on how subgrantees spent funds until all the funds have been drawn down from the ESF.
Education’s ESF Transparency Portal website launched on November 20, 2020. (See figure below for an image of the portal’s main page.) Its state profile pages provide information on how much money from the CARES Act ESF each state has been awarded and how much money each has spent.[596] Education obtains information on state awards and spending from a variety of federal sources that regularly capture financial transactions.[597] The state profile pages also include other details, such as breakdowns of a state’s awards to school districts.[598] Education plans to update the portal frequently, with some data updated on a weekly basis, according to Education officials.
Department of Education Transparency Portal Main Page, as of February 26, 2021
Although both efforts are a good first step toward insight into how states, school districts, and other subgrantees are using ESF funds, Education’s choices about the timeframes for which data are collected and the type of budget data requested present an incomplete picture of the rate at which school districts and states are using ESF funds for K-12 education purposes. Regarding school district subgrantee data, both the annual report and the portal report on “cash out the door” (i.e., outlays or expenditures) rather than information on financial commitments to purchase goods or services (i.e., obligations). Education officials told us that the national emergency required them to act quickly and the size of the ESF required a balanced approach to oversight. They said they chose to focus on outlays because this information could easily be corroborated and it was already in use in their other oversight activities.
We appreciate the challenges of quickly standing up oversight tools for a new, non-recurring, and large program while also developing another relief program. However, both Education and the Congress have recognized the importance of accurately capturing the status of COVID-19 relief funds provided to states and school districts to inform the department’s monitoring and technical assistance, and to provide transparency to the public about uses of the funds. While tracking obligations and outlays each serve a different purpose, obligations—not outlays—measure legal commitments to pay for goods and services ordered and received. Federal budgeting guidance states that both methods of tracking funds play an important part in ensuring the financial accountability of the government to the American people, and agencies cannot overlook either of them. Absent information on the degree to which school districts have obligated their COVID-19 relief funding, policymakers will not have an accurate, complete picture of the status of school district spending. Further, given the gap that often exists between when funds are obligated and when they are disbursed, absent information on obligations, policymakers will not have complete information on how these funds are being used to address the pandemic-related education needs of America’s schoolchildren.
Methodology
To conduct this work, we reviewed relevant federal laws, regulations, and Education and CDC guidance. We also interviewed Education officials regarding program implementation and analyzed Education spending data. To assess the reliability of Education’s spending data, we reviewed information on the sources of these data, and we followed up with knowledgeable individuals as needed to answer questions about the appropriate use and potential limitations of these data. We found these data to be sufficiently reliable for our purposes.
To collect the perspectives of a range of state and local stakeholders, we interviewed officials from the Council of Chief State School Officers, the School Superintendents Association, and National Governors Association. We also worked with the School Superintendents Association to conduct interviews with eight state and local school agency officials. Information from the interviews provided examples of how state and local agencies were using ESF funds, and does not reflect the views of all state and local agency officials. In addition, we conducted two interviews with state educational agency officials after reviewing ESF spending rates and information in states’ ESF applications. In addition, to obtain information on Education’s monitoring of grantees’ use of ESF funds, we reviewed about 575 correspondence related to the Elementary and Secondary School Emergency Relief or Governor’s Emergency Education Relief funds between Education and states, governors, and state educational agencies. Our review was limited to correspondence dated between December 1, 2020 and January 31, 2021.
Agency Comments
We provided CDC, Education, and the Office of Management and Budget (OMB) with a draft of this enclosure. Education provided general comments, which are summarized below and reproduced in appendix IV, and technical comments, which we incorporated as appropriate. OMB and CDC did not provide comments on this enclosure.
In its comments, Education agreed with GAO’s recommendation, stating that it is important to track obligations, outlays, and drawdowns to ensure accountability for state and school district spending. Education also committed to working collaboratively with states to develop reporting processes that provide greater clarity on state and school district spending. We will continue to monitor Education’s efforts to collect and report on state and school district outlays (expenditures) as well as their financial commitments (obligations).
Contact information: Jacqueline M. Nowicki, (617) 788-0580, nowickij@gao.gov
Related GAO Product
A Glossary of Terms Used in the Federal Budget Process. GAO-05-734SP, Washington D.C.: September 2005.
Transit agencies continue to use CARES Act funding, but anticipate long-term financial and operational challenges due to the COVID-19 pandemic.
Entity involved: Federal Transit Administration, within the Department of Transportation
Key Considerations and Future GAO Work
We will continue to monitor the status of CARES Act grants and other COVID-19 relief funding to transit agencies in ongoing and planned work.
Background
Millions of Americans rely on public transportation systems for mobility and access to jobs, education, and essential services, such as medical care and grocery shopping. Within the Department of Transportation (DOT), the Federal Transit Administration (FTA) provides grants to state departments of transportation, local public transit systems, and tribes to support and expand services. These services may include buses, subways, light rail, commuter rail, trolleys, and ferries in urban, rural, and tribal areas.
The CARES Act appropriated about $25 billion to FTA to support the transit industry through its Urbanized Area ($22.7 billion) and Rural Area ($2.2 billion) formula programs.[599] CARES Act grant funds were available to transit agencies for any expenses incurred related to COVID-19 on or after January 20, 2020, although now these funds must be directed, to the maximum extent possible, to payroll and operations expenses.[600] There is no limit on the amount of funds recipients may use for operating expenses.[601]
On December 27, 2020, the Consolidated Appropriations Act, 2021, appropriated an additional $14 billion to FTA to prevent, prepare for, and respond to coronavirus to support the transit industry.[602] Similar to the CARES Act, FTA is allocating these funds through its Urbanized Area and Rural Area formula programs. However, of the available funds, $50 million is for FTA’s program for the enhanced mobility of seniors and individuals with disabilities.[603] The Consolidated Appropriations Act, 2021, limited funding to 75 percent of an urbanized area’s 2018 operating expenses and 125 percent of a state’s 2018 rural operating expenses when combined with the area’s CARES Act funding.[604] As a result, urbanized areas and states whose CARES Act allocations already exceeded the applicable 2018 operating expenses threshold are not eligible to receive funding under the Consolidated Appropriations Act, 2021.
On March 11, 2021, the American Rescue Plan Act of 2021 appropriated approximately an additional $30 billion to FTA for grants to prevent, prepare for, and respond to coronavirus to support the transit industry.[605] We will continue to monitor those funds.
Overview of Key Issues
FTA continues to distribute CARES Act grant funds and support transit agencies. According to FTA officials, as of February 28, 2021, 97 percent of available CARES Act funding had been obligated. FTA officials reported that an additional 127 grants were in progress. FTA officials said that as of February 28, 2021, recipients had obligated 86.3 percent of CARES Act funds for operating expenses, though obligating funds for capital and planning expenses is also allowed (see table).
Transit Agency Obligations of CARES Act Grant Funds by Expense Category in Urban, Rural, and Tribal Areas, as of February 28, 2021
Expense
Urban ($ millions)
Rural ($ millions)
Tribal ($ millions)
Total ($ millions)
Operating
$20,304
$1,217
$7
$21,528
Capital
$1,685
$397
$15
$2,098
Othera
$16
$442
$0.3
$458
Totalb
$22,005
$2,056
$23
$24,084
Source: GAO analysis of Federal Transit Administration data. | GAO-21-387
Note: The law appropriating the amounts obligated here is the CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020). a”Other” includes expenses for project and program administration, intercity bus, planning, job access and reverse commute, and training expenses. bNumbers may not total due to rounding.
FTA continues to oversee CARES Act grants and will integrate CARES Act monitoring into its existing program review processes. Officials said that the status of CARES Act obligations is reported twice a week to the FTA Office of the Administrator, and is reported regularly to both the DOT Office of the Secretary and the Office of Management and Budget. In addition, FTA officials stated that the agency reinitiated its oversight review processes in October 2020, which will include updated review materials that integrate CARES Act oversight into the agency’s existing Triennial and State Management review processes.
A smaller portion of urbanized areas, states, and tribes received allocations under the Consolidated Appropriations Act, 2021, compared to the CARES Act. According to FTA officials, 360 of 500 urbanized areas had already received funds that cover at least 75 percent of their operating expenses under the CARES Act, and these areas will not receive funds under the Consolidated Appropriations Act, 2021. FTA allocated these funds on January 11, 2021, and as of February 28, recipients had obligated approximately 1 percent of available funds (see table). The act directs recipients, including those who have not obligated all of their CARES Act funds, to prioritize payroll and operational needs unless the recipient certifies that it has not furloughed any employees.
Transit Industry Allocations and Obligations by Program under the Consolidated Appropriations Act, 2021, as of February 28, 2021
Urban ($ millions)
Rural ($ millions)
Tribal ($ millions)
Enhanced Mobility ($ millions)
Obligations
$151
$12
$2
$0.7
Total allocated funds
$13,262
$648
$30
$50
Source: GAO analysis of Federal Transit Administration data. | GAO-21-387
Note: The law appropriating the amounts obligated here is the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182 (2020).
Transit agencies continue to report using CARES Act grants to mitigate the spread of COVID-19. As we reported in November 2020, transit agency officials we spoke to said they took steps to mitigate the spread of COVID-19, including general practices such as enhanced cleaning and sanitation, requiring the use of masks, and social distancing. According to officials from two transit industry groups, transit agencies generally continue to employ such measures. Additionally, one of these industry groups has identified these types of measures, among others, as best practices after a pandemic viral outbreak.[606]
In January 2021, FTA published the second version of its COVID-19 recovery practices document, which outlines practices implemented by transit systems worldwide in response to COVID-19. The document includes many of the aforementioned practices, such as cleaning and disinfecting vehicles and minimizing interactions between employees and passengers. In addition, it includes examples of how transit agencies can communicate with passengers and plan for future service changes.
Transit agencies anticipate long-term consequences from the COVID-19 pandemic. Officials from two transit industry groups we spoke to said transit agencies are reorienting their focus from immediate concerns about health and safety to mitigating the anticipated long-term consequences of the COVID-19 pandemic. According to officials, these anticipated consequences include reduced demand for transit services, increased operating costs, and the inability of state and local funding sources to match FTA funds. Industry group officials said while some transit agencies quickly used all allocated CARES Act funding, others are reserving as much as 50 percent of their funding to mitigate anticipated negative effects of the COVID-19 pandemic. According to officials from one industry group, transit agencies that primarily rely on income from ridership fares tended to use their CARES Act funding more rapidly than agencies that rely mostly on tax revenue. In November 2020, we reported that seven of the 22 transit agencies we spoke to said they did not expect to use all their CARES Act funding until a year or more to mitigate future uncertainty and the expectation of a slow economic recovery; the remaining 15 had either used all their funding or planned to do so within a year. FTA officials said that some smaller rural and tribal transit agencies found that they needed to purchase additional vehicles to maintain social distancing and needed levels of service. Purchasing additional vehicles under the CARES Act required these recipients to obtain Statewide Transportation Improvement Program approval, and the procurement process may extend the amount of time the agencies need to expend funds, according to FTA officials.
Officials from two industry groups said that FTA guidance has generally been clear and effective. However, officials from one of these groups stated that confusion can sometimes arise when state departments of transportation provide guidance that appears to contradict what is posted on FTA’s website. For example, officials said transit agencies sometimes receive conflicting information about the extent to which they can continue using transit assets for delivery services to persons who are homebound. According to FTA officials, FTA has issued guidance and provided technical assistance to provide clarity on these issues.
Agency Comments
We provided DOT and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we analyzed DOT and FTA data on transit industry grant funding as of February 28, 2021. Our analysis, as well as discussions with agency officials and a review of related documentation, found the data to be reliable for the purposes of describing federal allocations and transit agency obligations and expenditures. We reviewed written responses from DOT and FTA officials about how they were implementing applicable provisions of the CARES Act and the Consolidated Appropriations Act, 2021. In addition, we interviewed the Community Transportation Association of America and the American Public Transit Association to discuss the impact of the funds appropriated by CARES Act and the Consolidated Appropriations Act, 2021, on their members.
Contact information: Andrew Von Ah, (202) 512-2834, vonaha@gao.gov
The Federal Aviation Administration is administering funding for grants to help the nation’s airports respond to and recover from the economic effects of the COVID-19 pandemic.
Entity involved: Federal Aviation Administration, within the Department of Transportation
Key Considerations and Future GAO Work
Since we reported on airport grants in November 2020, we have identified airports’ continued concerns about declines in revenue and operations, and uncertainty about when airports will return to pre-pandemic activity levels. We will continue to monitor CARES Act grants and other COVID-19-related assistance to airports in future GAO work.
Background
U.S. airports are important contributors to the U.S. economy and fulfill a variety of vital roles, from supporting scheduled commercial air service to supporting freight transportation, emergency medical transportation, and disaster relief. Approximately 3,300 airports in the U.S. are part of the national airport system and are eligible to receive federal Airport Improvement Program (AIP) grants to fund infrastructure projects. As we reported in February 2020, from fiscal years 2013 through 2017, airports received an average of $3.2 billion annually in federal AIP grants.
Historic decreases in passenger demand for air travel due to the COVID-19 pandemic are significantly affecting U.S. airports’ abilities to generate the revenue needed for operating and infrastructure costs. According to data filed with Department of Transportation (DOT), U.S. airlines carried 61 percent fewer passengers in November 2020 than in November 2019. One airport association estimates that U.S. airports will face $40 billion in expected operating losses and additional costs related to COVID-19 from March 2020 to March 2022.
Federal funding for airports. The CARES Act and the Consolidated Appropriations Act, 2021, provide U.S. airports with a combined total of $12 billion in federal funding to respond to the COVID-19 pandemic, although funding allocation and allowable uses differ. The CARES Act, signed into law on March 27, 2020, provided $10 billion to support U.S. airports of all sizes experiencing severe economic disruption caused by the COVID-19 pandemic (see table).[607] Airport owners—also known as airport sponsors—may use CARES Act funds for any purpose for which airport revenues may be lawfully used, including for airport operating expenses and debt service.
CARES Act Airport Grants
Funding groups
Funds appropriated (in dollars)a
Formula applied
1) Increase federal share for 2020 Airport Improvement Program (AIP) grants
At least 500 million
Increase the federal share to 100 percent for grants awarded for airport infrastructure projects under fiscal year 2020 AIP and supplemental discretionary grantsb
2) Commercial service airports (i.e., publicly owned airports with at least 2,500 passenger boardings per year and scheduled air service)
At least 7.4 billion
Allocate based on a formula that considers an airport’s passenger boardings, the airport sponsor’s debt service, and the sponsor’s ratio of unrestricted reserves to debt servicec
3) Primary airports (i.e., large, medium, and small hub and non-hub airports with more than 10,000 passenger boardings per year)d
Up to 2 billion
Allocate based on statutory AIP entitlement formulas
4) General aviation airports (i.e., airports with fewer than 2,500 passenger boardings per year and no scheduled air service)
At least 100 million
Allocate based on the categories these airports are placed in given activity measures (e.g., volume and type of flights) and other factors in the most current National Plan of Integrated Airport Systems (NPIAS)
Source: GAO analysis of CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020). | GAO-21-387
aThe CARES Act gives the Federal Aviation Administration (FAA) the authority to retain up to 0.1 percent of the $10 billion (up to $10 million) provided for Grants-in-Aid for Airports to fund the award and oversight by FAA of grants made under the CARES Act. bNational system airports are eligible to receive federal funding from AIP grants for infrastructure development. The distribution of federal AIP grants is based on a combination of formula funds—also referred to as entitlement funds—that are available to national system airports, and discretionary funds that FAA awards for selected eligible projects. Entitlement funds are apportioned by formula to airports and may generally be used for any eligible airport improvement or planning project. Discretionary funds are approved by FAA based on FAA selection criteria and a priority system, which FAA uses to rank projects based on the extent to which they reflect FAA’s nationally identified priorities. The federal share for AIP grants generally ranges from 75 percent to 95 percent. cThe FAA used fiscal year 2018 Certification Activity Tracking System (CATS) data, reported as of March 14, 2020, to calculate allocations under the CARES Act formulas for commercial service airports. More specifically, the total allocation to a commercial service airport is determined by a formula that considers an airport’s passenger boardings for calendar year 2018 (50 percent), the airport sponsor’s debt service (25 percent), and the sponsor’s ratio of unrestricted reserves to debt service (25 percent), both for fiscal year 2018. dThis funding group may also include non-primary commercial service airports with 8,000 to 9,999 passenger boardings. CARES Act, div. B, tit. XII, para. (3), 134 Stat. at 597.
The Consolidated Appropriations Act, 2021, enacted on December 27, 2020, provides $2 billion in additional federal aid to help eligible airports and certain tenants to prevent, prepare for, and respond to COVID-19 (see table).[608] The funding groups and allocation formulas for the Consolidated Appropriations Act, 2021 grants differ from the CARES Act grant funding, as do the allowable uses of funds.[609] Airports must use Consolidated Appropriations Act, 2021 grant funding for costs related to operations, personnel, cleaning, sanitization, janitorial services, combating the spread of pathogens at the airport, and debt service payments. According to FAA guidance, examples of eligible development to combat the spread of pathogens at the airport include replacing or upgrading a heating, ventilation, and air conditioning system; and reconfiguring the terminal to accommodate increased social distancing or health screening.
1) Primary Commercial Service Airports and Certain Cargo Airportsb
Not less than 1.75 billion
Allocate first based on the statutory Airport Improvement Program (AIP) primary and cargo entitlement formulas. Allocate the remainder based on the number of enplanements the airport had in calendar year 2019, the most recent calendar year of available enplanement data, as a percentage of total 2019 enplanements for all primary airports.
2) Non-Primary Commercial Service and General Aviation Airportsc
Not less than 45 million
Allocate based on current National Plan of Integrated Airport Systems (NPIAS) categories, reflecting the percentage of the aggregate published eligible development costs for each such category, and then dividing the allocated funds evenly among the eligible airports in each category. Any remaining funds are to be allocated to primary commercial service airports and certain cargo airports described in Funding Group 1.
2a) Non-Primary Airports Participating in the Federal Aviation Administration (FAA) Contract Tower Programd
Not less than 5 million (of the 45 million above)
Allocate based on participating in the FAA contract tower program. Funds are divided equally among eligible airports.e
3) Tenant Relief for Primary Commercial Service Airportsf
At least 200 million
Allocate based on the number of airport enplanements in calendar year 2019 as a percentage of total calendar year 2019 enplanements for all primary airports.
4) Small Community Air Service Development Programg
Up to 5 million
Transfers funding to the Office of the Secretary, Salaries and Expenses. Gives priority to communities or consortia of communities that have had air carrier service reduced or suspended as a result of the coronavirus pandemic.
Source: GAO analysis of the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1939-41 (2020). | GAO-21-387
aThe Consolidated Appropriations Act, 2021 gives the Federal Aviation Administration (FAA) the authority to retain up to 0.1 percent of the $2 billion (up to $2 million) provided for Grants-in-Aid for Airports to fund the award and oversight by FAA of grants made under the Consolidated Appropriations Act, 2021. bPrimary commercial service airports are publicly owned airports with more than 10,000 passenger boardings per year and scheduled air service. Cargo airports are airports that, in addition to any other air transportation services that may be available, are served by aircraft providing air transportation of only cargo with a total annual landed weight of more than 100 million pounds. cNon-primary commercial service airports have at least 2,500 and no more than 10,000 passenger boardings each year. General aviation airports are public-use airports with fewer than 2,500 passenger boardings per year or no scheduled air service. dNon-primary airports are the same as non-primary commercial service airports, and have at least 2,500 and no more than 10,000 passenger boardings each year. The Federal Contract Tower Program, established in 1982, allows the agency to contract out the operation of certain towers. Contract towers are air traffic control towers that are staffed by employees of private companies rather than by FAA employees. There are currently 256 contract towers, for which the FAA pays for air traffic control services on a contract basis. eUnder the Consolidated Appropriations Act, 2021, airport sponsors of non-primary airports that participate in the FAA Contract Tower Program may use these funds to cover any lawful costs associated with supporting their FAA contract tower operations. FAA guidance states that these costs include payroll, utilities, service contracts, and items generally having a limited useful life, including personal protective equipment and cleaning supplies. The $5 million in funding to this group comes from the minimum of $45 million in funding appropriated for non-primary commercial service and general aviation airports in funding group 2 described above. fPrimary commercial airport sponsors may only use these funds to provide relief from rent and minimum annual guarantees to on-airport car rental, on-airport parking, and in-terminal airport tenants, subject to additional conditions. gThe Small Community Air Service Development Program is a grant program designed to help small communities address air service and airfare issues. The airport serving the community or consortium is not larger than a small hub airport, which is a primary commercial service airport that receives 0.05 to 0.25 percent of the annual U.S. commercial enplanements, as determined using the FAA’s most recently published classification effective on the date that the community or consortium files an application.
The American Rescue Plan Act of 2021, enacted on March 11, 2021, appropriates an additional $8 billion for assistance to sponsors of airports.[610] We will monitor this funding going forward.
Workforce retention requirements. Certain airport sponsors accepting CARES Act grant funds were required to continue to employ, through December 31, 2020, at least 90 percent of the number of individuals employed as of March 27, 2020.[611] Similarly, airports receiving funds from the Consolidated Appropriations Act, 2021 were required to employ at least 90 percent of the number of individuals employed as of March 27, 2020 through February 15, 2021.[612] According to FAA, the 130 largest U.S. airports, serving approximately 96 percent of U.S. commercial service passenger boardings in 2018, were subject to this requirement. However, airports with limited commercial service or that primarily serve general aviation flights were exempt from this requirement.[613]
Allocations, obligations and expenditures. Following the enactment of the CARES Act, FAA finalized grant allocation amounts totaling nearly $10 billion.[614] As of February 14, 2021, FAA had obligated about $9.4 billion and expended over $5.4 billion to reimburse airports for eligible costs and to increase the federal share for 2020 AIP grants, according to FAA officials (see table).
FAA Obligations and Expenditures for CARES Act Airport Grants by Funding Group, as of February 14, 2021
Funding group
Obligations ($ millions)
Expenditures ($ millions)
1) Increase federal share for 2020 Airport Improvement Program (AIP) grantsa
509
220
2) Commercial service airportsb
7,123
4,673
3) Primary airportsc
1,629
469
4) General aviation airportsd
100
53
Total
9,361
5,415
Source: GAO analysis of CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020) and data from the Federal Aviation Administration (FAA). | GAO-21-387
aNational system airports are eligible to receive federal funding from AIP grants for infrastructure development. The CARES Act appropriated at least $500 million to increase the federal share to 100 percent for grants awarded for airport infrastructure projects under fiscal year 2020 and supplemental discretionary grants. bCommercial service airports are publicly owned airports with at least 2,500 passenger boardings per year and scheduled air service. The CARES Act appropriated at least $7.4 billion in funding to airports in this funding group, and allocated funds based on a formula that considers an airport’s passenger boardings, the airport sponsor’s debt service, and the sponsor’s ratio of unrestricted reserves to debt service. cPrimary airports are large, medium, and small hub and non-hub airports with more than 10,000 passenger boardings per year. The CARES Act appropriated up to $2 billion in funding to airports in this funding group, and allocated funds based on statutory AIP entitlement formulas. This funding group may also include non-primary commercial service airports with 8,000 to 9,999 passenger boardings. CARES Act, div. B, tit. XII, para. (3), 134 Stat. at 597. dGeneral aviation airports are public-use airports with fewer than 2,500 passenger boardings per year and no scheduled air service. The CARES Act appropriated at least $100 million in funding to airports in this funding group, and allocated funds based on the categories these airports are placed in given activity measures (e.g., volume and type of flights) and other factors in the most current National Plan of Integrated Airport Systems.
Following the enactment of the Consolidated Appropriations Act, 2021, Federal Aviation Administration (FAA) officials determined individual airport allocations in February 2021, based on calendar year 2019 enplanement data—the most recent data available—and published updated guidance.[615] As of February 2021, FAA had not yet obligated or expended Consolidated Appropriations Act, 2021 funds for grants to airports.
Overview of Key Issues
Airport grant administration and monitoring. With regard to CARES Act funding, FAA has continued to process CARES Act airport grant applications, obligate funds, and review invoices to reimburse airport sponsors. As of February 14, 2021, FAA had processed CARES Act grant applications for 3,228 U.S. airports, including territories and tribes, totaling about $8.86 billion.
Since we last reported in November 2020, FAA had also taken additional actions to oversee and monitor compliance with workforce retention requirements for the 130 affected airports mentioned previously. FAA officials said that as of January 2021, all 130 airports complied with September and December reporting requirements, and FAA had not received any waiver requests. Officials also said they will continue to track workforce requirements for the Consolidated Appropriations Act, 2021, and will compare airport workforce numbers to those from March 2020 to ensure airports meet the 90 percent threshold.
As we previously reported, FAA has identified challenges to administering and monitoring CARES Act airport grants, including the need to process grants for over 3,000 airport sponsors under expedited time frames, with expanded eligible uses for these funds. To address the increased workload of processing and monitoring these grants, FAA rehired annuitants in September 2020, who are primarily responsible for reviewing CARES Act payment requests and quickly processing payments, according to FAA officials. FAA also revised and simplified requirements to allow airport sponsors to submit a detailed invoice summary with each payment request in lieu of individual invoices.[616] Additionally, FAA issued updated guidance on December 3, 2020 to provide consolidated information to airports about eligibility determinations. FAA officials also reported that the agency hired a contractor in the fall of 2020 to review FAA’s invoicing processes, develop a monitoring dashboard, develop auditing policies and procedures, and compare those procedures to other federal programs.
In January 2021, FAA established the Airport Coronavirus Response Grant Program to administer the $2 billion in funds from the Consolidated Appropriations Act, 2021, and in February, issued guidance for airports. FAA guidance states that airports will apply for the funds using the SF-424, Application for Federal Assistance form, similar to the CARES Act and AIP grant funding process, by June 30, 2021, and must use the funds within 4 years. As previously mentioned, as of February 2021, FAA officials have determined airport grant allocation amounts. Airports that received more than four times their operating budget from the CARES Act funds are not eligible for Consolidated Appropriations Act, 2021 funding.[617]
As part of the Consolidated Appropriations Act, 2021 requirements, airport sponsors that accept tenant relief funds will waive rent and minimum annual guarantee obligations for eligible airport tenants—which may include on-airport car rental and parking, and in-terminal concession tenants—beginning December 27, 2020, until the relief has equaled the total tenant relief allocation amount to the extent permissible under state and local laws. To administer the tenant relief portion of the funding, FAA officials have published additional guidance and a video presentation to instruct airport sponsors on how to claim and use airport tenant relief funds, and to ensure compliance.
Airport grant funding uses. Airport association representatives told us that the federal funding provided has been critical to the survival of the industry. FAA has begun to collect data from airports on general spending categories for CARES Act funding through grant close-out reports, but officials said that they have limited information until airport sponsors draw down all funds for reimbursed costs. While FAA collects these data, officials said airports are generally using CARES Act funds on payroll, utilities, minor maintenance, and debt service. Although FAA officials have not yet obligated or expended any Consolidated Appropriations Act, 2021 funding, airport associations said that airport sponsors generally plan to use these grants to pay for operational expenses and costs related to mitigating effects of the COVID-19 pandemic, such as cleaning and sanitation, social distancing measures, and upgrading heating and cooling systems.
Agency Comments
We provided DOT and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT and OMB did not provide comments on this enclosure.
Methodology
To conduct this work, we reviewed FAA data on airport funding as of February 14, 2021, which we found to be reliable for the purposes of describing allocations, obligations, and expenditures through interviews with agency officials and reviewing relevant documentation. We also reviewed federal laws and agency guidance related to the CARES Act and the Consolidated Appropriations Act, 2021 and conducted interviews with agency officials and representatives from airport associations, selected to represent a wide variety of industry and airport types.
Contact information: Heather Krause, (202) 512-2834 or krauseh@gao.gov
Related GAO Product
Airport Infrastructure: Information on Funding and Financing for Planned Projects.GAO-20-298. Washington, D.C.: February 13, 2020.
U.S. imports of COVID-19-related products in December 2020 remained higher than pre-pandemic levels, and over the course of the pandemic, U.S. Customs and Border Protection has taken actions to facilitate trade.
Entity involved: U.S. Customs and Border Protection, within the Department of Homeland Security.
Key Considerations and Future GAO Work
We plan to continue to monitor the effect of COVID-19 on international trade and the medical supply chain, potentially including challenges in facilitating trade of COVID-19-related products. For more information, see the Domestic Medical Product Manufacturing enclosure in appendix I.
Background
The COVID-19 pandemic has disrupted businesses around the world and international supply chains. According to the World Trade Organization (WTO), world merchandise exports decreased by 4 percent in the third quarter of 2020 over the previous year. This was a significant improvement from the 21 percent decline in the second quarter of 2020, as production resumed and lockdown measures were eased in major economies.[618] U.S. imports of COVID-19-related products, such as face masks, ventilators, gloves, and hand sanitizers, have fluctuated. U.S. Customs and Border Protection (CBP) is tasked with facilitating lawful trade, and has taken steps to address issues that affect U.S. imports and exports of such essential products.
Overview of Key Issues
Available data indicate that U.S. imports of product categories related to the COVID-19 response decreased by 4 percent from October to December 2020 (see figure).[619] However, even with a decline in recent months, as of December 2020, imports of these products were 27 percent higher compared to a year ago and had increased by 27 percent since February 2020. Many factors that affect product availability, such as supply chain constraints and export restrictions, and product demand could drive trends in imports of COVID-19 products. Additionally, total import value trends are related to changes in prices. For example, the unit value of N95 respirators fell by more than 60 percent from July to December 2020, according to the United States International Trade Commission (USITC), which could be linked to decline in personal protective equipment (PPE) import values. Overall, the need for medical supplies in response to the pandemic explains the increase in imports of these products since early 2020.
Monthly U.S. Imports of COVID-19-Related Products by Product Type, January 2018 to December 2020
Notes: Census trade statistics, a widely used source analyzing U.S. international trade, do not contain precise data on imports of COVID-19-related products. As a result, we estimated the import value of all product categories and types using Harmonized Tariff Schedule of the United States (HTS) statistical reporting numbers and associated product groupings listed by the U.S. International Trade Commission (USITC) in COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). A revision to the Harmonized Tariff Schedule on July 1, 2020, provided several new HTS-10 statistical reporting numbers for previously identified COVID-19-related product categories. We identified these product categories and included them in the analysis. Some HTS categories represent more than one product, and some categories contain products that are not directly relevant to COVID-19 responses. Product types only refer to the subset of goods considered COVID-19-related in each HTS-10 statistical reporting number. Therefore, the values presented may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, they are useful indicators for tracking import trends of such products. For more information on factors influencing import trends in different types of COVID-19-related products, see USITC, COVID-19 Related Goods: The U.S. Industry, Market, Trade and Supply Chain Challenges, Investigation No. 332-580 (December 2020).
Imports of COVID-19-related products from China, which accounted for close to 14 percent of such imported products in December 2020, continued to decline, and imports of the same products from the rest of the world declined after experiencing a month of growth.[620] Imports from China decreased by 8 percent (from roughly $2.7 billion to $2.4 billion) from October to December 2020, after declining by 27 percent from September 2020 to October 2020 (from roughly $3.7 billion to $2.6 billion).[621] Meanwhile, imports of COVID-19-related product categories from other countries declined by 3 percent (from $15.6 billion to $15.1 billion) from October 2020 to December 2020, after increasing by 7 percent (from $14.5 billion to $15.6 billion) from September to October 2020.
CBP has taken actions to address challenges related to the COVID-19 pandemic. CBP officials reported operational challenges during the pandemic. For instance, CBP has had to conduct virtually many of its trade-related activities that had previously been conducted in person, such as processing of shipments and visiting brokers and importers. In addition, due to access restrictions at ports, those in the importing and exporting community shifted to digitizing all documents—a process many of them needed to learn. CBP officials also reported challenges related to the surge in imports of COVID-19-related products. Specifically, CBP officials explained that there were challenges related to the increase of new importers, such as state and local governments that were importing COVID-19-related products for the first time and that were unfamiliar with the paperwork, procedures, and applicable duties.
Among other activities, CBP implemented the following actions to address these challenges and support importers experiencing financial hardships since the beginning of the pandemic:
Established COVID-19 Cargo Resolution Team (CCRT). Related to the increase of new importers, in April 2020, CBP created the CCRT to respond to questions about importing and exporting medical supplies and PPE. The CCRT is a multidisciplinary team that also coordinates with ports and other government agencies, such as the Food and Drug Administration (FDA) and Federal Emergency Management Agency (FEMA), to facilitate shipments of medical supplies, PPE, syringes and other vaccination supplies, and Pfizer’s COVID-19 vaccine. According to CBP officials, by late January 2021 the CCRT had responded to almost 3,000 questions and facilitated 373 Operation Warp Speed shipments valued at an estimated $69 million. CBP officials also reported that between April and June 2020 CBP facilitated clearance of more than 400 FEMA-arranged flights full of critical medical supplies.
Participated in FEMA’s Export Cargo Review Working Group. CBP is part of FEMA’s Export Cargo Review Working Group. The Export Cargo Review Working Group reviews shipments, provides advice to FEMA regarding implementation of the allocation order, and periodically evaluates the categories of health and medical resources included in the Temporary Final Rule for Prioritization and Allocation of Certain Scarce and Critical Health and Medical Resources for Domestic Use.[622]
Seized counterfeit, illicit, or prohibited materials. According to CBP officials, CBP has seized thousands of COVID-19-related products that are counterfeit, illicit, or prohibited, including test kits, face masks, hand sanitizers, and various medicines.[623]
Temporarily postponed certain duties, taxes, and fees for certain importers. According to CBP officials, upon instruction from the Secretary of the Treasury, CBP temporarily postponed certain duties, taxes, and fees for 2,921 importers experiencing a COVID-19-related financial hardship in March or April 2020.[624] In total, these importers paid over $575 million under extended deadlines.[625]
Agency Comments
We provided a draft of this enclosure to CBP and the Office of Management and Budget. They had no comments on this enclosure.
Methodology
To conduct this work, we reviewed the most recent trade statistics from the U.S. Census Bureau combined with USITC data on product categories that contain COVID-19 products.[626] In addition, we reviewed agency announcements and guidance from CBP and interviewed CBP officials. By reviewing agency documents and conducting consistency checks, we found the data to be sufficiently reliable to describe trade in COVID-19-related products.
The Department of State and U.S. Agency for International Development have obligated all $908 million of supplemental COVID-19 humanitarian assistance funding, but policy changes delayed USAID’s obligations, according to officials.
Entities involved: Department of State and U.S. Agency for International Development
Key Considerations and Future GAO Work
As part of our ongoing review of supplemental COVID-19 humanitarian assistance, we will review the challenges the pandemic crisis has presented to the Department of State (State) and U.S. Agency for International Development (USAID) in managing program monitoring.
Background
The COVID-19 pandemic has created new humanitarian needs and exacerbated existing vulnerabilities around the world. The United Nations (UN) estimated that 270 million people worldwide would be acutely food insecure by the end of 2020—an increase from 149 million before the COVID-19 pandemic. The UN also estimated that there were more than 79 million forcibly displaced people in July 2020, with those numbers expected to continue rising.
Congress appropriated $908 million in supplemental funding in fiscal year 2020 for international humanitarian assistance activities.[627] Specifically, the Coronavirus Preparedness and Response Supplemental Appropriations Act and the CARES Act provided a total of $350 million for Migration and Refugee Assistance programming, managed by State’s Bureau of Population, Refugees, and Migration (PRM), and $558 million for International Disaster Assistance programming, managed by USAID’s Bureau for Humanitarian Assistance (BHA).[628]
Overview of Key Issues
State had fully obligated its supplemental humanitarian assistance funding as of August 26, 2020, using a preexisting process. State approved its first award of $64 million from the 2020 supplemental Migration and Refugee Assistance funds on April 27, 2020. This approval constituted about 18 percent of its $350 million in supplemental Migration and Refugee Assistance funding. State had obligated nearly half of this supplemental funding by June 1, 2020. The figure below shows the timing of State’s approval and obligation of supplemental humanitarian funding.
Timing of State Approval and Obligation of Supplemental Humanitarian COVID-Response Funding
According to State data, State obligated the $350 million in supplemental Migration and Refugee Assistance funding through 21 awards spread across 68 countries. State data also show that the vast majority of PRM’s supplemental awards (totaling about $339 million, or 97 percent) were voluntary contributions to public international organizations.[629] In making funding decisions, PRM considered these organizations’ appeals for funding to support their worldwide COVID-19 responses. For example, PRM’s planning for its award of $64 million took into account emergent needs and priorities detailed in the UN High Commissioner for Refugees’ Coronavirus Emergency Appeal.[630] According to PRM, the remaining awards (totaling about $11 million, or 3 percent) went primarily to nongovernmental organizations with which PRM had preexisting programs.
Because voluntary contributions to public international organizations support multisectoral activities and are designed to provide flexibility to the organizations, PRM officials were unable to itemize the humanitarian assistance obligations by sector, according to the officials. However, according to PRM, its awards supported humanitarian partners as they pivoted to undertake COVID-19 prevention, mitigation, and response measures on behalf of PRM’s populations of concern: refugees, conflict victims, internally displaced persons, stateless populations, and vulnerable migrants. These populations can be highly vulnerable to COVID-19 because of their reduced access to health care and their location in congested areas, such as refugee camps, according to PRM officials. PRM funding also supported broader community and national public health systems’ pandemic responses.
State programmed its supplemental Migration and Refugee Assistance funding through PRM’s Policy and Program Review Committee process—a preexisting, PRM-specific process that seeks to engage bureau-level stakeholders in strategy and funding decisions. According to PRM, the process includes specific procedures for emergency response. For COVID-19 supplemental funding, the committee approved 11 funding memorandums, each detailing proposed implementers, programming, and monitoring approaches. According to PRM officials, because of the rapidly evolving pandemic situation, PRM made a policy decision to fund only current partners to undertake additional COVID-19-related programming in their current locations. PRM officials stated that this additional programming was discussed in PRM’s weekly internal COVID-19 programming meetings and coordinated with BHA in weekly program coordination meetings, and funding decisions were consolidated and shared with State’s Coronavirus Global Response Coordination Unit; however, the overall programming process was very similar to PRM’s existing emergency processes.
USAID had fully obligated its supplemental humanitarian assistance funding as of July 31, 2020, using a new process. USAID approved country-level allocations for its first tranche of $110 million—about 20 percent of the $558 million in supplemental International Disaster Assistance funding—on March 26, 2020. By June 1, 2020, it had obligated $27.9 million, or 5 percent of the total funding. The figure below shows the timing of USAID’s approval of tranched funding and obligation of supplemental humanitarian funding.[631]
Timing of USAID Approval and Obligation of Supplemental Humanitarian COVID-Response Funding
According to USAID data, USAID obligated the $558 million in supplemental International Disaster Assistance funding through 188 awards in 43 countries. According to USAID data and officials, initial programming primarily focused on augmenting ongoing health interventions and water, sanitation, and hygiene support to mitigate widespread transmission of COVID-19, address public health consequences, and maintain essential health services for crisis-affected populations. Subsequent programming aimed to address the longer-term food-security and economic impacts of COVID-19 in humanitarian settings to prevent a further deterioration of preexisting crises, according to USAID data and officials. The table below shows USAID’s total obligations for supplemental humanitarian assistance by programming sector.
USAID Supplemental International Disaster Assistance Obligations, by Programming Sector
Sector
Total obligated, in dollars
Nutrition and Food Assistance
189,342,490
Health
136,890,850
Water, Sanitation, and Hygiene
115,270,666
Logistics
59,863,966
Protectiona
23,568,653
Multipurpose Cash Assistance
13,734,813
Humanitarian Coordination and Information Management
8,719,255
Agriculture and Food Security
5,218,735
Humanitarian Policy, Studies, Analysis, or Applications
1,644,836
Shelter and Settlements
1,564,664
Economic Recovery and Market Systems
1,490,034
Risk Management Policy and Practice
691,038
Total
558,000,000
Source: U.S. Agency for International Development (USAID) data. | GAO-21-387
aUSAID defines protection programming as activities that support the needs of vulnerable populations such as women, children, persons with disabilities, and elderly-headed households.
USAID obligated its supplemental COVID-19 funding through a new process that required BHA to coordinate with a series of newly established entities at USAID and State prior to senior leadership approval of proposed funding plans.[632] According to BHA officials, USAID developed this centralized process to ensure that its awarding of supplemental COVID-19 funding was coordinated, approved, and publicly announced in discrete tranches in tandem with State. The process comprised the following steps:
BHA developed country prioritizations and preliminary funding plans through its regional teams on the basis of factors such as disease presence and implementing partner capacity.
BHA regional teams, in close coordination with technical teams and BHA’s newly established COVID-19 Response Management Team, reviewed and coordinated these preliminary plans with the USAID COVID-19 Task Force and other groups in USAID and State to ensure that the plans aligned with the joint USAID and State COVID-19 Response Strategy.[633]
On the basis of feedback from those groups, BHA and the Response Management Team revised the plans for further review and final leadership approval.
State and USAID publicly announced BHA’s and other bureaus’ funding plans by country as part of a specific funding tranche.
Once the tranche was approved, BHA reviewed potential partner applications, awarded grants and cooperative agreements, and obligated funding.
USAID disbanded the USAID COVID-19 Task Force on September 9, 2020, and the COVID-19 Response Management Team on October 31, 2020. According to BHA, USAID has integrated COVID-19 activities into regularly funded programming in fiscal year 2021.
Policy changes delayed USAID’s obligation of supplemental humanitarian funding. According to BHA officials, policy changes from the White House and USAID COVID-19 Task Force delayed the agency’s obligations of supplemental humanitarian assistance funding. These policy changes consisted of (1) restrictions on the procurement of personal protective equipment (PPE), (2) USAID leadership’s reevaluation of existing branding and marking waivers in high-threat environments, and (3) a government-wide restriction on funding for the World Health Organization (WHO).[634] In addition, BHA officials said that delays stemming from the policy changes were sometimes exacerbated by challenges related to the tranche approval process.[635]
Delays related to PPE funding restriction. On March 20, 2020, the USAID COVID-19 Task Force notified BHA that no USAID funds could be used to procure PPE.[636] According to BHA officials, this restriction not only jeopardized implementing partners’ ability to protect their staff and safely proceed with humanitarian programming but also created funding delays.
BHA encouraged partners to use alternative donor funding for PPE, and regional teams were encouraged to explore alternative programming that was not reliant on PPE. However, according to BHA officials, it was initially unclear how to handle applications that had already been submitted with PPE components, which constituted most applications. Specifically, the restriction notice did not specify which types of PPE were covered or whether USAID would make exceptions for emergency humanitarian programming. Furthermore, the Task Force did not allow BHA to ask partners to resubmit their applications to exclude programming requiring PPE, which delayed action on those applications for approximately 7 weeks, according to officials.[637] BHA officials estimated that such delays affected 49 awards in 21 countries, with a total value of over $100 million. For example, in Syria, awards for more than $18.5 million for five partners were delayed because PPE was necessary for program implementation, according to BHA.
On June 9, 2020, the USAID COVID-19 Task Force approved revised guidance on award language that loosened the restriction by allowing procurement of PPE without prior USAID authorization under specified conditions.[638] According to BHA officials, implementing partners indicated that they were able to operate without much difficulty once they were permitted to procure PPE under these conditions.[639]
Delays related to reevaluation of branding waivers. On March 24, 2020, the USAID COVID-19 Task Force informed BHA that USAID leadership wanted to reevaluate existing branding and marking waivers meant to ensure the safety of staff and beneficiaries in high-threat environments.[640] According to USAID documentation, this decision reflected USAID leadership’s intent to fully publicize U.S. contributions in response to the pandemic. However, after surveying its partners, BHA estimated on March 31, 2020, that this decision would prevent implementation of nearly half of the COVID-19 supplemental humanitarian programming that USAID had approved at that point ($52.3 million of $110 million) in at least 11 high-priority countries and would prevent all proposed activities in nine of the countries. For example, no partners were willing to proceed with award implementation in Syria without a branding and marking waiver because of the inherent risks to their staff.
The reevaluation of branding and marking waivers affected USAID’s obligations of COVID-19 supplemental humanitarian funding until April 27, 2020, when the USAID Acting Administrator approved the pre-existing waivers for selected countries and programs. According to BHA, until this reapproval, affected programming was fully paused.[641]
Delays related to government-wide pause on WHO funding. On April 14, 2020, President Trump instructed the administration to halt funding to WHO. As a result, five awards worth $31 million to WHO were paused pending further guidance, according to BHA. BHA officials noted that WHO is the primary organization for coordinating health-related humanitarian responses with local and national authorities. BHA officials also told us that some governments grant WHO exclusive authorities, largely because of WHO’s role as the UN Health Cluster lead agency.
Because of the restriction on WHO funding, BHA staff were required to identify new implementing partners and restart the application review process, which affected overall programming and further delayed obligation of funds, according to BHA officials. Ensuring that the new partners were capable of providing the needed interventions and soliciting new applications took additional time, the officials said.
However, USAID field teams for several countries—Afghanistan, Libya, the Democratic Republic of the Congo, Sudan, Ethiopia, Iraq, and Syria—reported being unable to identify implementing partners with capacity comparable to WHO’s. For example, before the restriction was announced, USAID was in conversation with WHO to supply medical equipment in northwest Syria. After the restriction was announced, BHA was able to find partners for alternative activities in the region, but these activities did not replace the proposed WHO projects, according to BHA officials. The officials stated that in certain settings, WHO operates as the provider of last resort—that is, as the sole provider of health care for some populations. BHA officials told us that although they were able to find alternative partners for most projects, no other organizations had the capacity, technical capability, and access required to conduct the needed programming for some projects.[642]
Challenges related to tranche approval process. According to BHA officials, challenges related to the new tranche approval process exacerbated delays stemming from the policy changes. Until funding was approved through the tranche process and BHA knew how much would be allocated for specific countries, it could not begin to receive and review applications from potential implementers, according to officials. In addition, BHA officials said that the public announcement of funding levels by country, combined with new restrictions on adjusting the announced funding levels after approval, eliminated BHA’s flexibility to revise its funding plans if needs or conditions changed.
Agency Comments
We provided a draft of this enclosure to State, USAID, and the Office of Management and Budget (OMB) for comment. State and USAID provided technical comments, which we incorporated as appropriate. In its comments, reproduced in appendix XI, USAID stated that it would build on the lessons learned over the past year and would continue to adapt program management and internal policies for the new operational context. State and OMB did not provide formal written comments on this enclosure.
Methodology
To conduct this work, we reviewed financial data from State’s State Assistance Management System and USAID’s Phoenix database. To assess the data’s reliability, we reviewed agency responses to data reliability questions, noting the specific tagging required for COVID-19 supplemental funding. We also compared the data we received with the data State and USAID reported to Congress and with original approval documentation. We found that the data we received were sufficiently reliable for describing obligation and programming information for COVID-19 supplemental programming. We also reviewed documentation and interviewed relevant officials at State and USAID.
Contact information: Chelsa Kenney, (202) 512-2964 or kenneyc@gao.gov.
About $775 million from a combination of sources has been either appropriated to or designated by the Federal Bureau of Prisons for COVID-19 response efforts.[643] This includes $100 million in CARES Act supplemental funds, which the Bureau has already expended.[644] The Bureau has periodically modified its operations and amended its plans for responding to the pandemic in response to evolving federal and other guidance.
Entity involved: Federal Bureau of Prisons, within the Department of Justice
Key Considerations and Future GAO Work
We are monitoring the Federal Bureau of Prisons’ (BOP) COVID-19 response and recovery efforts to address the pandemic, including its obligation and expenditure of funds. Specifically, our ongoing work will address the extent to which BOP’s response to the pandemic has evolved to incorporate changing guidance and best practices. We will also address the reported impact of the pandemic on BOP-managed and private prison facilities, inmates, and staff.[645]
Background
BOP, a component within the Department of Justice (DOJ), was responsible for the care and custody of approximately 152,000 inmates, as of February 25, 2021. Because inmates and approximately 37,000 BOP staff live and work in confined spaces and in close proximity to each other, the prison population has been particularly vulnerable to COVID-19. Further, about 12 percent of the federal prison population is over age 55, and many have underlying health conditions such as diabetes and chronic heart disease—two factors that further increase the risk for severe illness from the virus that causes COVID-19.
As of February 25, 2021, BOP reported that 47,860 inmates and 6,490 staff had contracted COVID-19. BOP also reported that 222 inmates and four staff had died from it.[646] BOP is implementing a phased action plan to reduce the spread and manage the virus's impact on inmates and staff.
About $775 million from a combination of sources has been either appropriated to or designated by the Federal Bureau of Prisons for COVID-19 response efforts.[647] Specifically, the CARES Act appropriated $100 million to BOP for preventing, preparing for, and responding to the COVID-19 pandemic. Additionally, the Consolidated Appropriations Act, 2021, appropriated $300 million to BOP for preventing, preparing for, and responding to COVID-19, domestically or internationally.[648] Further, according to BOP officials, BOP obligated about $375 million from its fiscal years 2020 and 2021 Salaries and Expenses appropriation for COVID-19 expenses. Officials from BOP explained that funds from all three sources are to be used for, among other things, personal protective equipment, cleaning supplies, and contracts for medical care provided outside BOP facilities. As our work continues, we plan to examine the specific obligations and expenditures from each source in detail.
Overview of Key Issues
BOP’s modified operations for the pandemic response and the impact on its inmates. BOP had a pandemic response plan in place before the onset of the COVID-19 pandemic. BOP officials told us that they developed the plan for responding to a flu pandemic specifically and as such, the plan did not address the unique challenges the COVID-19 pandemic presented, such as the rapidly spreading nature of the virus. BOP therefore supplemented the existing plan with additional guidance from the BOP Medical Director regarding identifying and screening for COVID-19, starting on January 31, 2020. Additionally, on February 29, 2020, the Bureau issued its phase 1 action plan. This plan was the first in a multiphased planning approach. According to BOP officials, the intent was to modify operations to adapt to evolving guidance from the Centers for Disease Control and Prevention (CDC) and others in direct response to the changing conditions of the pandemic.
In addition to guidance provided in the action plans, BOP modified operations at all 122 of its prison facilities in an effort to maximize social distancing. As of February 22, 2021, BOP was implementing its phase 9 action plan.[649] This plan includes restrictions or a suspension of inmates’ access to people, areas, and programs as the primary mechanism for social distancing and curbing spread of the virus. Specifically, BOP restricted inmates’ in-person access to legal counsel and social visitors such that access was to be granted based upon request and the availability of space to allow for adequate social distancing. BOP also completely restricted social visitations for inmates in isolation or quarantine. Similarly, BOP restricted inmates’ access to areas such as the commissary, laundry room, and showers to small groups of inmates at a time, and only if inmates practiced established guidelines for social distancing.
Lastly, while BOP continues to offer inmates access to certain programs, such as drug abuse, General Educational Development, and anger management classes, it has restricted the capacity of these programs, in some cases to no more than six participants at a time. It has also scheduled them in outdoor or otherwise unused spaces in an effort to maximize safety and social distancing.
Our ongoing study of BOP’s response to the pandemic will examine more fully how BOP modified its operations to incorporate evolving guidance from CDC and others. Our work will also describe the impact these modifications had on its inmates, staff, and institutions.
BOP’s policy and procedures for screening and testing inmates and staff. BOP’s COVID-19 testing strategy is contained in its COVID-19 phased action plans. BOP officials said that the strategy has changed multiple times since the beginning of the pandemic to adapt to changing CDC guidance and as BOP addressed challenges in obtaining testing supplies. On July 31, 2020, BOP awarded a contract to a national laboratory in an effort to help improve its COVID-19 testing capacity and strategy for inmates; however, BOP does not have a universal testing policy for inmates or staff. While some BOP facilities have conducted targeted or mass testing of their inmates when facing COVID-19 outbreaks, BOP’s policy is to test inmates only if they become symptomatic, if they have had contact or suspected contact with a COVID-19 positive individual, and before they are transferred in or out of a BOP institution. BOP does not test staff on site, but refers them to community testing resources and requires staff to report testing results if the results are positive. Our ongoing work on BOP’s response to the pandemic will examine the specific policies and procedures BOP has established for screening and testing staff for COVID-19.
BOP’s methods for tracking data on inmate and staff infections and deaths. BOP tracks information on inmates and staff who have tested positive, recovered from, and died of COVID-19 on a daily basis and per facility, and reports this information on its public website. We are assessing the methods BOP uses to track this information, including measures it has taken and continues to take, to ensure accuracy and reliability of the data. We also continue to examine the extent to which BOP’s data collection efforts include inmates housed in privately run, contracted facilities.
Agency Comments
We provided a draft of this enclosure to the Department of Justice and the Office of Management and Budget (OMB) for review and comment. Department of Justice officials provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
Methodology
To address our objectives, we conducted virtual site visits at six BOP facilities, which we selected based on criteria such as geographic location, facility security level, and COVID-19 infection rate. At these facilities we interviewed facility management officials as well as representatives of the BOP employees’ union. We also interviewed officials at BOP’s Central Office who oversee COVID-19 policies, reviewed BOP documents, and analyzed BOP data and written responses to our questions. We assessed the reliability of obligations data by interviewing knowledgeable officials about their financial management systems and how the data are used, and found the data sufficiently reliable for our purposes.
Contact information: Gretta L. Goodwin, (202) 512-8777, goodwing@gao.gov
In the year since the passage of the CARES Act, the number and features of federal websites that track and report on COVID-19 supplemental spending have grown considerably, including a new section of USAspending.gov and the launch of PandemicOversight.gov.[650] Progress has been made to align these sites with key practices for transparently reporting data. However, Treasury can take further action on our 2017 recommendation to disclose known data limitations on USAspending.gov by implementing a more systematic approach for identifying and disclosing them.
Entities involved: Department of Health and Human Services; Department of Labor; Office of Management and Budget; Pandemic Response Accountability Committee; Small Business Administration; Department of the Treasury
Key Considerations and Future GAO Work
Our work examining the quality and display of COVID-19-related and other spending data available on USAspending.gov is ongoing. We will continue to review the extent to which the spending data submitted and displayed on USAspending.gov are timely, complete, and accurate, including whether information regarding limitations is disclosed. We are also examining the use and usefulness of COVID-19 and other federal spending data available from USAspending.gov, PandemicOversight.gov, and the Department of the Treasury’s (Treasury) Data Lab website.
Background
The CARES Act contains several requirements for federal agencies and nonfederal entities receiving federal awards for the timely reporting of covered funds.[651] Office of Management and Budget (OMB) guidance issued in April 2020 made some modifications to the existing framework of reporting requirements for emergency or disaster relief spending already in place. These modifications allowed agencies to meet many CARES Act reporting requirements using USAspending.gov, which tracks federal contracts, financial assistance (which includes grants and loans), and other federal spending at the state, congressional district, and local levels.[652]
The CARES Act required the Pandemic Response Accountability Committee (PRAC) to create a website—PandemicOversight.gov—in part to foster greater accountability and transparency in COVID-19 spending.[653] The website displays COVID-19 spending data sourced from USAspending.gov, federal agencies, and Inspectors General offices.[654] Treasury’s Data Lab website supplements COVID-19 spending information on USAspending.gov by providing a broader view of COVID-19 spending across agencies. The website also includes information to explain how COVID-19 spending moves from appropriations to individuals and businesses.
In the year since the passage of the CARES Act, the number and features of federal websites that track and report on COVID-19 spending have grown considerably. Many agencies—such as the Department of Health and Human Services (HHS), the Department of Labor (DOL), and the Small Business Administration (SBA)—added spending data for individual COVID-19 programs to their websites.[655] Unlike USAspending.gov and PandemicOversight.gov, these websites sometimes do not include data analysis or visualization features besides lists or tables.
See the table below for more information on the characteristics of the three federal websites that provide government-wide COVID-19 spending data.
Federal Agency Websites Reporting Government-wide COVID-19 Spending Data
USAspending.gova
Official source of spending data for the U.S. government. Includes information on COVID-19 spending enacted under various acts.d
Displays total COVID-19 spending obligations and outlays by agency, federal account, and object class.
Displays COVID-19 award obligations, outlays, and loan face value by recipient, agency and sub-agency, and Catalog of Federal Domestic Assistance Program listing. Coverage includes contracts, grants, loans, direct payments, and other financial assistance.e
Data for individual prime awards include total and nonfederal funding, total and COVID-19 obligated amounts, and COVID-19 outlayed amounts.
Among the COVID-19 spending not specifically reported by agencies:
Provider Relief Fund payments to individual providersf
Federal Medical Assistance Percentage spending attributable to the Families First Coronavirus Response Actf
Subrecipient awards for Coronavirus Relief Fundf
COVID-19 spending by 14 small independent, legislative branch, and judicial branch entitiesg
PandemicOversight.govb
Data displayed are sourced from USAspending.gov, federal agencies, and Inspectors General offices.
Unlike USAspending.gov, the website includes Coronavirus Relief Fund subrecipient data originating from the Department of the Treasury Office of the Inspector General, including subaward amount and money spent to date. The website also identifies Paycheck Protection Program (PPP) recipients and visualizes PPP loan totals by state, county, industry, and business type.
Data Labc
In contrast to the two other websites, Data Lab only provides aggregated government-wide COVID-19 spending data. However, users can view the following information:
Breakdown of COVID-19 financial relief by statute.
Total estimated value of legislation, including new agency funding and tax relief.
Total estimated lending for credit, loans, and loan guarantee programs.
Diagram of the process used to move COVID-19 spending through the full budget lifecycle to the American people (including appropriations, obligations, and outlays).
How much of the COVID-19 funding has been spent. This includes outlays and obligated and unobligated amounts by appropriation.
Sources: USAspending.gov, PandemicOversight.gov, Data Lab website, and Congressional Research Service. | GAO-21-387
Note: Web links to identified URLs were active as of February 19, 2021. The table excludes agency websites that report spending for individual COVID-19 programs. aSee https://www.usaspending.gov/disaster/covid-19. bSee https://www.pandemicoversight.gov/. cSee https://datalab.usaspending.gov/federal-covid-funding. dCoronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); Coronavirus Aid, Relief, and Economic Security Act or the CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2021); and American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4 (2021). eOMB Memorandum M-20-21 requires agencies to provide a funding identifier—a Disaster Emergency Funding Code (DEFC)—in their financial file submissions to track and report contracts funded by COVID-19 supplemental spending. OMB M-10-21 also requires agencies to use a separate National Interest Action (NIA) code for all procurement actions (e.g. contracts) reported into the Federal Procurement Data System-Next Generation that are related to the COVID-19 response. However, use of the NIA code is not necessarily tied to COVID-19 supplemental appropriations. As a result, awards with the COVID-19 NIA value may not have a COVID-19 DEFC value, and vice versa. Because of this difference in how COVID-19 related contract awards are tagged with DEFC and NIA codes, it may be unclear to a user of USAspending.gov that the DEFC-based COVID-19 spending numbers presented on the site do not capture the entirety of federal spending on procurement actions for COVID-19 relief and response efforts. See the Federal Contracts and Agreements for COVID-19 enclosure in Appendix I for information on contract obligations in response to COVID-19 tracked in the Federal Procurement Data System-Next Generation. fAccording to Treasury officials, COVID-19 spending for the listed awards, payments, and Federal Medical Assistance Percentage spending attributable to the Families First Coronavirus Response Act was not covered because agencies adhered to Office of Management and Budget policy or otherwise declined to report such spending to USAspending.gov. gThe following 10 entities received COVID-19 funding but do not report any spending information under the Digital Accountability and Transparency Act of 2014 to USAspending.gov: the Architect of the Capitol; Capitol Police; Courts of Appeals, District Courts, and Other Judicial Services; Defender Services; House Office of the Attending Physician; House of Representatives; Library of Congress; Senate (miscellaneous); Sergeant at Arms and Doorkeeper of the Senate; and U.S. Supreme Court. The Department of the Treasury (Treasury) told us that COVID-19 spending for three other entities—the Corporation for Public Broadcasting, Federal Payment for Emergency Planning and Security Costs in the District of Columbia, and Legal Services Corporation—is coded as Treasury spending. Treasury also told us that COVID-19 spending for a fourth entity—Historically Black College and University Capital Financing—is coded as Department of Education spending. Therefore, it is not possible for a user to obtain specific information on COVID-19 spending for these four entities apart from overall spending reported by the Departments of the Treasury and Education.
Overview of Key Issues
Treasury and PRAC have taken steps to align COVID-19 spending data websites with key practices for transparently reporting data and identifying data limitations. In a December 2018 report, we identified several key practices to help ensure the transparent presentation of government data, including by presenting data in a way that helps users to easily explore them. Key actions to implement these practices include providing tools such as interactive maps and visualizations and search functions to help users find information or display search results using tables, charts, and maps. We also reported in December 2018 and November 2019 on the importance of being transparent about the quality of the information presented on USAspending.gov, including the value of clearly identifying data limitations.
Interactive maps, visualizations, and search. Since the CARES Act was enacted in March 2020, Treasury added new features enabling users to view and download COVID-19 spending data on USAspending.gov. For instance, users can view USAspending.gov’s COVID-19 Spending Profile Page for an overview of the federal funding response to the COVID-19 pandemic.[656] In addition, the COVID-19 Spending Profile Page uses an interactive map to display obligations and outlays through grants, contracts, loans, and other assistance by state, county, or congressional district.
Treasury enhanced USAspending.gov’s Advanced Search feature so that users can filter search results by Disaster Emergency Funding Code (DEFC) to show COVID-19 spending awards.[657] The search results table includes columns containing COVID-19 obligations and outlays for each award, and displays COVID-19 spending by state, locality, or congressional district. Treasury also enhanced its Data Lab website to allow users to explore how COVID-19 funding makes its way from Congress into the economy.[658]
In February 2021, PRAC added data transparency and completeness to its list of top management challenges facing federal agencies in responding to and providing relief for COVID-19.[659] In 2020, PRAC launched PandemicOversight.gov, which presents COVID-19 spending data through a variety of interactive visual displays. For example, the website’s funding overview page includes graphics showing funding totals by category—such as state, local, and tribal governments, higher education, and small businesses—and funding by category for the top 10 agencies receiving COVID-19 funding.[660] The website uses maps to visualize COVID-19 spending data from USAspending.gov, the Coronavirus Relief Fund, and the Paycheck Protection Program. Users may also access the website’s Pandemic Response Funding portal to view COVID-19 obligation and spending data in graphs and tables that answer several basic questions, including “Where is the money being spent?,” “Who is spending the money?,” and “How is the money being spent?”[661]
PandemicOversight.gov also allows users to filter data by agency, location, type of assistance, or key word. The website’s presentation of COVID-19 spending data and search functions enhance transparency and help ensure that Congress and the public can quickly and easily find, understand, and analyze the data.
Transparency regarding information quality and data limitations. Treasury has also taken steps to disclose known data quality issues and limitations on USAspending.gov, as we recommended in November 2017. Consistent with our recommendation, in August 2020, Treasury began disclosing some data limitations for COVID-19-related spending on USAspending.gov. At that time, Treasury reported data limitations for four COVID-19 programs administered by various agencies.
Treasury expanded this list over time. On January 8, 2021, the list was updated to include data limitations for six COVID-19 programs administered by federal agencies.[662] This includes information from specific federal agencies on reporting issues that may affect the accuracy or completeness of COVID-19 data displayed on the USAspending.gov, as well as web links to detailed information on COVID-19 programs that HHS did not make available on USAspending.gov.[663] These disclosures are an important step toward more fully identifying and disclosing known COVID-19 data limitations on USAspending.gov.
PandemicOversight.gov also provides information on COVID-19 spending data limitations in a list of frequently asked questions (FAQs). The website describes limitations regarding data obtained through USAspending.gov as well as other sources, such as SBA and Treasury’s Office of Inspector General (OIG). The website also discloses reasons why modifications to an award may result in the display of negative or zero amounts. A PRAC official told us that PRAC is planning to be more specific about limitations in data obtained from USAspending.gov in a forthcoming update to its FAQs.
Treasury has opportunities to further disclose COVID-19 spending data limitations. For example, USAspending.gov does not disclose that it does not publish or break out $272.6 million in COVID-19 spending by 14 entities—including for the U.S. Supreme Court, Architect of the Capitol, and Corporation for Public Broadcasting—which received COVID-19 funding.[664] In contrast, PandemicOversight.gov notes that USAspending.gov does not include COVID-19 spending data for these entities. Although COVID-19 spending by the 14 entities is small compared to total COVID-19 spending government-wide, users will not know about limitations in data by legislative and judicial branch agencies without Treasury’s clear identification of such limitations on USAspending.gov.
Treasury officials told us that the department has focused its efforts on identifying the most significant COVID-19 spending data limitations on USAspending.gov. However, Treasury has agreed to review data limitations that GAO and other sources have identified. Treasury can help users make better use of COVID-19 spending data on USAspending.gov or identify other sources of data, if necessary, by more fully communicating information about the completeness of data displayed on the website.
Treasury has taken some positive steps to further disclose limitations related to COVID-19 spending data. For example, Treasury demonstrated for us a planned page for inclusion in USAspending.gov that would automate updates related to certain data limitations. However, we believe that additional action can be taken to implement a more systematic approach to identifying and disclosing known data limitations, consistent with our 2017 recommendation. Such an approach could include procedures for addressing wide-ranging issues including communicating changes in reporting requirements or information about data that may be unreported or incomplete. This, in turn, would help users better understand potential data quality issues as well as how to appropriately interpret the data. We will continue to monitor Treasury’s efforts in this area to determine whether they are sufficient to address our previous recommendation.
Errors in tracking initial COVID-19 spending data caused discrepancies between outlays and obligations reported on USAspending.gov. The CARES Act requires federal agencies to report on the use of funds, and subsequently in April 2020, OMB directed agencies to change their reporting periods for covered funds and to begin reporting obligations and expenditures to USAspending.gov on a monthly basis.[665] Further, OMB directed agencies to expand their use of DEFCs to cover COVID-19 supplemental funding, while acknowledging that agencies may not be able to track some spending using an appropriate DEFC value. OMB directed that these reporting changes were effective for April, May, and June 2020 data, which were to be included with quarterly data submissions in August 2020.
Users of USAspending.gov identified issues affecting their use of the USAspending.gov website, including examples of COVID-19-related awards where reported award outlays were greater than obligations. We analyzed the USAspending.gov database in January 2021 and identified COVID-19-related awards in which outlays exceeded obligations at HHS, DOL, the Department of Education, and SBA.[666]
According to agency officials from Treasury, DOL, HHS, and SBA, these discrepancies resulted from errors in how data were DEFC-coded for initial award transactions prior to the OMB-mandated changes effective for April, May, and June 2020 data. For example, SBA officials told us that they tagged COVID-19 transactions prior to June 2020 with an incorrect DEFC, while DOL officials told us that they did not DEFC-tag obligations prior to June 2020. Additionally, HHS officials told us that they did not DEFC-tag obligations prior to the third quarter of fiscal year 2020. In all cases, these situations resulted in discrepancies between obligations and outlays for selected grants reported on USAspending.gov.
Agency spending data submissions are validated by the DATA Act Broker, an intermediary service that standardizes and formats agency-submitted data and assists reporting agencies in validating their data before submitting them to Treasury. Treasury officials told us that while the DATA Act Broker does not currently verify that outlays do not exceed obligations, they would consider adding such a rule.
Some agencies we identified as having inconsistencies in this area are in the process of correcting these errors and recertifying their data. For example, SBA officials told us that they have added a validation process to check for discrepancies between outlays and obligations before submission to USAspending.gov. DOL officials said that they are working with Treasury to address these errors. Both SBA and DOL told us that they plan to validate outlays in their data submissions prior to certification in the future.
Within HHS, officials at the Centers for Disease Control and Prevention and the Administration for Children and Families told us that they were working to internally address data issues. At the department level, HHS officials from the Office of the Assistant Secretary for Financial Resources (ASFR) told us that internal data for this period have since been correctly DEFC-tagged. Further, these officials told us that while the department has no plans to resubmit corrected data to USAspending.gov, corrected data are publically available through the HHS Tracking Accountability in Government Grants System website. According to ASFR officials, HHS has not been required or received a request from OMB to resubmit DEFC-tagged data.
If agencies implement these changes in correcting and recertifying data with discrepancies or add specific data limitation disclosures to USAspending.gov, and verify that future data submissions do not contain obligation and outlay discrepancies, users may be better able to understand the limitations in using these data. We will continue to work with affected agencies to ensure discrepancies in reported data are addressed.
Agency Comments
We provided a draft of this enclosure to DOL, HHS, OMB, PRAC, SBA, and Treasury for review and comment. HHS, OMB, PRAC, and Treasury provided technical comments, which we incorporated as appropriate. DOL and SBA did not comment on the draft enclosure.
Methodology
To conduct this work, in January 2021, we reviewed federal COVID-19 DEFC-tagged spending data available on USAspending.gov. We also reviewed federal COVID-19 spending data limitations identified by USAspending.gov and PandemicOversight.gov.
We compared award-level COVID-19 outlays to obligations for all awards from USAspending.gov tagged with COVID-19-related DEFC codes in fiscal years 2020 and 2021 until December 31, 2020. We identified those awards with higher outlays than obligations and summarized the number of awards and the total number of discrepancies by agency, DEFC, and object class. We found these data from USAspending.gov to be sufficiently reliable for our purposes of identifying awards with obligation and outlay discrepancies. We interviewed or received written responses from Treasury, HHS, DOL, and SBA to determine the source and reasons for the discrepancies.[667] We further interviewed or received written responses from PRAC officials and nongovernmental organizations using spending data from USAspending.gov and PandemicOversight.gov.
DATA Act: Quality of Data Submissions Has Improved but Further Action Is Needed to Disclose Known Data Limitations. GAO-20-75. Washington, D.C.: November 8, 2019.
Open Data: Treasury Could Better Align USAspending.gov with Key Practices and Search Requirements. GAO-19-72. Washington, D.C.: December 13, 2018.
DATA Act: OMB, Treasury, and Agencies Need to Improve Completeness and Accuracy of Spending Data and Disclose Limitations. GAO-18-138. Washington, D.C.: November 8, 2017.
Federal agencies’ enforcement actions on fraud-related charges help protect consumers and ensure that taxpayer dollars and government services related to COVID-19 serve their intended purposes.
Entities involved: Government-wide
Key Considerations and Future GAO Work
We will continue our oversight of government-wide fraud risk management efforts.
Background
The public health crisis, economic instability, and increased flow of federal funds associated with the COVID-19 pandemic present increased pressures and opportunities for fraud.[668] By proactively managing fraud risks, federal officials can help safeguard taxpayer dollars to ensure they serve their intended purpose, particularly given that Congress has appropriated about $3.1 trillion as of January 31, 2021, to fund COVID-19 response and recovery efforts.[669] According to GAO’s A Framework for Managing Fraud Risks in Federal Programs, among other things, effective managers of fraud risks refer instances of potential fraud to Offices of Inspector General (OIG) or other appropriate parties, such as law enforcement entities or the Department of Justice, for further investigation.
The extent of fraud associated with the COVID-19 relief funds appropriated to date has not yet been determined. One of the many challenges is that because of fraud’s deceptive nature, programs can incur financial losses related to fraud that are never identified, and such losses are difficult to reliably estimate. However, several individuals have already pleaded guilty to federal charges of defrauding COVID-19 relief programs—including the Small Business Administration’s (SBA) Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program and the Department of Labor’s (DOL) unemployment insurance (UI) program—and numerous others faced related federal charges as of January 31, 2021. In addition, federal hotlines have received numerous complaints from the public alleging potential fraud involving COVID-19 relief funds. For example, from March 13, 2020, through January 31, 2021, our hotline—known as FraudNet—received over an estimated 1,500 complaints related to the CARES Act, many of which involve SBA’s PPP and EIDL program and DOL’s UI program (see text box).
Report Fraud, Waste, and Abuse
GAO’s FraudNet supports accountability across the federal government. Allegations of fraud, waste, or abuse can be submitted via the FraudNet portal or by calling the hotline at 1-800-424-5454.
Overview of Key Issues
Because of the economic effects of COVID-19 and the government’s need to quickly provide funds and other assistance to those affected by it, federal relief programs are vulnerable to significant risk of fraudulent activities. The schemes used to defraud the government as well as private businesses and individuals are endless, and many have emerged during the COVID-19 pandemic. Since March 2020, the Department of Justice has publicly announced charges in numerous fraud-related cases.[670] The charges—filed across the U.S. and investigated by a range of law enforcement agencies—include making false statements and engaging in identity theft, wire and bank fraud, and money laundering. The number of individuals facing fraud-related charges continues to grow and will likely increase, as these cases take time to develop.[671]
Fraud against federal programs. Forty-six individuals pleaded guilty to federal charges of defrauding COVID-19 relief programs—including SBA’s PPP and EIDL program and DOL’s UI program—from March 2020 through January 2021.[672] For example:
In one case, an individual pleaded guilty to fraudulently obtaining two PPP loans for over $2.5 million. The individual created fraudulent payroll documentation for two businesses, falsely representing that the businesses had dozens of employees with millions of dollars in payroll expenses, when in fact they had few, if any, employees.[673] For more information on potential PPP fraud, see the enclosure on the Paycheck Protection Program in appendix I.
As part of another case, an individual pleaded guilty to wire fraud associated with a scheme to defraud SBA’s PPP and EIDL program by providing false information on nine loan applications. Six of the individual’s nine fraudulent loan applications were approved, and he fraudulently obtained more than $700,000 in relief funds. For more information on potential fraud in the EIDL program, see the enclosure on the Economic Injury Disaster Loan Program in appendix I.
In another guilty plea, an individual admitted to involvement in a scheme to obtain fraudulent UI program loans using stolen personal identity information. The individual obtained more than $189,912 in fraudulent UI benefits using approximately 70 stolen identities.[674] For more information on potential fraud in the UI programs, see the enclosure on Unemployment Insurance Programs in appendix I.
As of January 31, 2021, federal charges were pending against 238 individuals for attempting to defraud these programs. In addition, two individuals pleaded guilty to identity theft in connection with economic impact payments (EIP), and related federal charges are pending against four other individuals.[675] These cases each involved individuals unlawfully obtaining the personal identification information of other individuals, filing false tax returns, and obtaining EIPs.[676] See the figure below for the number of individuals who have pleaded guilty or faced federal charges for fraud against COVID-19 relief programs as of January 31, 2021.[677]
Number of Individuals Facing Federal Charges or Who Have Pleaded Guilty to Fraud-Related Charges by COVID-19 Relief Program, as of January 31, 2021
Note: The number of individuals presented in the figure exceeds the total number of individuals who faced federal charges or pleaded guilty because some faced charges or pleaded guilty to charges related to more than one federal program. Thirty individuals faced federal charges related to both PPP and EIDL, and one individual faced federal charges related to both UI and EIP as of January 31, 2021. Four individuals pleaded guilty to federal charges related to both PPP and EIDL as of January 31, 2021.
In February 2021, an individual pleaded guilty to making false statements to multiple federal agencies in order to fraudulently obtain COVID-19 emergency relief loans and multimillion-dollar federal contracts.[678] Specifically, this individual applied for PPP and EIDL loans on behalf of his company, falsely overstating the number of employees and the amount of the company’s payroll. This individual also used some of the loan proceeds for personal expenditures rather than to pay employees or for other appropriate business expenses. The loss to the federal government from this fraud is approximately $261,500.
In addition, this individual made false statements to the Department of Veterans Affairs (VA) and the Federal Emergency Management Agency (FEMA) in order to obtain lucrative contracts to provide COVID-19 personal protective equipment (PPE). Based on the individual’s false statements, VA and FEMA awarded his company contracts valued at $35,000,000 and $3,510,000, respectively. The company failed to supply any PPE to VA and FEMA. While the federal government suffered no financial loss because the contract called for payment upon delivery and inspection of the goods, according to the Acting U.S. Attorney for the Eastern District of Virginia, this individual’s “fraudulent conduct during a critical time in our Nation’s fight against COVID-19 undermined the government’s ability to provide much needed PPE to the community.”
Consumer fraud. In addition to fraud against federal programs, fraud can result in financial losses to consumers and undermine health and safety. Nine individuals or entities pleaded guilty to federal charges related to consumer fraud from March 2020 through January 2021.[679] For example:
In one case, an individual admitted to operating a website advertising the sale of PPE, including respirator masks and protective masks. However, the individual did not provide the PPE to the majority of customers, stealing at least $3,800. This individual pleaded guilty to wire fraud.[680]
In another case involving a fraud scheme related to the prevention or treatment of COVID-19, an individual listed for sale online an unregistered pesticide, falsely claiming the product would protect the buyer or wearer from viruses or bacteria.[681] The individual pleaded guilty to one count of distribution and sale of an unregistered pesticide.
As part of another case, the Department of Justice issued a permanent injunction to address a fraud scheme related to COVID-19 testing. In this case, a business advertised and offered to perform a COVID-19 test that was not approved by the Food and Drug Administration. There were also federal charges pending against 29 individuals or entities related to consumer fraud as of January 31, 2021. In addition, the Federal Trade Commission and the Food and Drug Administration have issued warning letters to companies for allegedly selling fraudulent COVID-19-related products, including those making deceptive or scientifically unsupported claims about their ability to treat or cure COVID-19.[682] As of January 31, 2021, 38 individuals and entities had pleaded guilty or faced federal charges for different types of consumer fraud, including schemes related to PPE sales, prevention or treatment, and testing (see figure).
Number of Individuals or Entities Who Have Pleaded Guilty to or Faced Federal Charges for Consumer Fraud, as of January 31, 2021
aThis category includes individuals or entities that offered or promoted products to prevent or treat COVID-19 prior to vaccines becoming available.
As COVID-19 vaccines become available, another type of potential consumer fraud has emerged. While the extent of vaccine-related fraud is unknown, U.S. Attorney’s Offices have warned of fraud schemes related to COVID-19 vaccines.[683] Also, according to a December 2020 press release from the Federal Bureau of Investigation (FBI), the FBI, Department of Health and Human Services OIG, and Centers for Medicare & Medicaid Services have received complaints of scammers using the public’s interest in COVID-19 vaccines to obtain personally identifiable information and money through various schemes. As a result, these agencies have warned the public about several emerging fraud schemes related to COVID-19 vaccines (see figure).[684]
Examples of Consumer Warnings about COVID-19 Vaccine Scams
Other federal cases. The federal government is also pursuing charges including conspiracy, wire fraud, and theft that are related to COVID-19 but separate from consumer fraud—including vaccine-related fraud—and fraud against the federal programs discussed earlier. Nine individuals pleaded guilty to these types of federal charges from March 2020 through January 2021.[685] For example, one individual—a hospital pharmacist—agreed to plead guilty to attempting to spoil hundreds of COVID-19 vaccine doses. Another individual pleaded guilty to wire fraud related to a scheme to defraud his employer by allegedly faking a positive COVID-19 medical excuse letter, causing the employer to stop business and sanitize the workplace. This individual later admitted that he did not have COVID-19. According to information presented in court, the closure of the facility for cleaning and the cost of paying employees during the shutdown resulted in a loss in excess of $100,000 to the corporation. There were also other federal charges pending against 22 individuals as of January 31, 2021. For example, two individuals were indicted on charges of conspiracy, possession of stolen goods being shipped interstate, and theft of government property for allegedly stealing 192 U.S. government-owned medical ventilators worth about $3 million.[686]
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget, which had no comments.
Methodology
To conduct this work, we reviewed information from the Department of Justice to identify federal fraud-related charges related to COVID-19 relief funding as of January 31, 2021.
In 2020, federal direct payments and federal crop insurance net payments to agricultural producers were projected to be about $52 billion ($46 billion in direct payments and $6 billion in net crop insurance payments) representing 43 percent of about $121 billion in net farm income, of which about $30 billion came from COVID-relief programs.
Entities involved: U.S. Department of Agriculture, including its Office of the Secretary
Key Considerations and Future GAO Work
We continue to examine the U.S. Department of Agriculture’s (USDA) spending and oversight of COVID-relief and Commodity Credit Corporation funding.
Background
COVID-19 has caused disruptions in the U.S. food supply chain, from the farms where raw agricultural commodities are produced to the food processing and distribution network that enables these commodities to be used by consumers.[687] Congress has appropriated billions of dollars for the agricultural sector through coronavirus relief and other legislation. Specifically, $19.7 billion was appropriated to USDA’s Office of the Secretary, and the Commodity Credit Corporation’s borrowing authority was replenished in the amount of $45.8 billion across three separate pieces of legislation.[688] The Commodity Credit Corporation is a wholly government-owned entity that finances a broad array of agriculture support programs. It has permanent authority to borrow up to $30 billion at any given time from the Treasury.[689] The specific amounts appropriated are as follows:
$8.5 billion to USDA’s Office of the Secretary through the CARES Act[690]
$14 billion to the Commodity Credit Corporation through the CARES Act[691]
$23.9 billion to the Commodity Credit Corporation through the Continuing Appropriations Act, 2021, and Other Extensions Act[692]
$11.2 billion to USDA’s Office of the Secretary through the Consolidated Appropriations Act, 2021[693]
$7.9 billion to the Commodity Credit Corporation through the Consolidated Appropriations Act, 2021[694]
In addition, USDA made available $6.5 billion for direct payments to agricultural producers from funding that was generally available to the agency through the Commodity Credit Corporation prior to the CARES Act reimbursement.[695]
See the table below for the funding amounts USDA made available to agricultural producers in the form of direct payments through the Coronavirus Food Assistance Program (CFAP) 1 and 2 and CFAP Consolidated Appropriations, 2021. These amounts are a subset of the amounts discussed above that Congress provided in COVID relief and Commodity Credit Corporation reimbursements, and the $6.5 billion USDA made available from previously available borrowing authority in the Commodity Credit Corporation.
Apportioned Amounts and Funding Sources for the Coronavirus Food Assistance Program (CFAP) Direct Payments to Agricultural Producers as of January 19, 2021
Program
Apportioned amounta ($ billions)
Monthb
Funding source
CFAP 1
Up to 6.5c
May 2020
CCC Charter Act authoritiesd
Up to 9.5e
May 2020
Appropriations under the CARES Act
CFAP 2
Up to 14.0f
September 2020
CCC Charter Act authorities
Up to 0.1g
September 2020
Appropriations under the CARES Act
CFAP Consolidated Appropriations, 2021
Up to 9.7h
January 2021
Consolidated Appropriations Act, 2021
Total
Up to 39.7
Source: GAO analysis of U.S. Department of Agriculture (USDA) data. | GAO-21-387
aThe apportioned amount column shows how much the Office of Management and Budget first apportioned for the programs. bThe month column shows when the Office of Management and Budget first apportioned funding for the programs. The table is dated as of January 19, 2021, because the apportionment for CFAP Consolidated Appropriations, 2021 was approved by the Office of Management and Budget on that date. cUSDA transferred $6.5 billion from the Commodity Credit Corporation (CCC) account to the Office of the Secretary account on May 1, 2020. dRecent laws that replenished the CCC include the CARES Act, Pub. L. No. 116-136, div. B, tit. I, § 11002, 134 Stat. at 509, which reimbursed $14 billion of the Commodity Credit Corporation’s net realized losses. eAccording to USDA officials, the previous administration reapportioned $0.5 billion of the $9.5 billion to the Farmers to Families Food Box Program. The Consolidated Appropriations Act, 2021, subsequently reduced the original $9.5 billion by repurposing $1 billion of that amount. fUSDA transferred $14.0 billion from the CCC account to the Office of the Secretary account on September 16, 2020. USDA received an early reimbursement of the CCC in the Continuing Appropriations Act, 2021 and Other Extensions Act, enacted on October 1, 2020, for the net realized losses as of September 17, 2020. Pub. L. No. 116-159, div. A, § 173, 134 Stat. at 725 . gThis $0.1 billion for CFAP 2 from the CARES Act is a subset of the $9.5 billion appropriation to USDA’s Office of the Secretary, Pub. L. No. 116-136, div. B, tit. I, 134 Stat. at 505, and, therefore, this column does not total. The $0.1 billion will be used for payments to tobacco producers. hThe Office of Management and Budget apportioned $9.7 billion for “COVID-19 CFAP Consolidated Approps, 2021” in January 2021 from the Consolidated Appropriations Act, 2021.
USDA estimates that in 2020 agricultural producers obtained $5.9 billion dollars in Paycheck Protection Program loans made available through the CARES Act. The agency forecasts that in 2021 agricultural producers will obtain $2.8 billion in Paycheck Protection Program loans made available through the Consolidated Appropriations Act, 2021. Overseen by the Small Business Administration, the Paycheck Protection Program provides forgivable loans to help businesses keep their workforce employed during the coronavirus crisis. The table below shows the potential amounts in forgiveness-eligible loans provided to agricultural producers through the Paycheck Protection Program.
Potential Amounts and Funding Sources for the Paycheck Protection Program (PPP) Loans to Agricultural Producers, as of February 5, 2021
Program
Amount of Loans ($ billions)
Year
Funding source
PPP
5.9a
2020
CARES Act
2.8b
2021
Consolidated Appropriations Act, 2021
Potential total
8.7
Source: GAO analysis of U.S. Department of Agriculture’s Economic Research Service Farm Income and Wealth Statistics. | GAO-21-387
Note: The Small Business Administration administers the PPP. aFor calendar year 2020, the Economic Research Service reported $5.9 billion in PPP loans to entities primarily engaged in production agriculture (North American Industry Classification System codes 111 and 112) based on Small Business Administration data released on November 24, 2020. bFor calendar year 2021, the Economic Research Service projects $2.8 billion in PPP loans to entities primarily engaged in production agriculture (North American Industry Classification System codes 111 and 112).
Overview of Key Issues
In 2020, federal direct payments and federal crop insurance net payments to agricultural producers were projected to be about $52 billion. This amount includes about $46 billion in direct payments and $6 billion in crop insurance indemnities minus producer-paid premium and represents 43 percent of $121 billion in net farm income, of which about $30 billion came from COVID-relief programs.[696] Accounting for about a fourth of net farm income, these COVID-relief payments contributed to making 2020 the third highest year for farm income since 2008. Without the COVID-relief payments, 2020 would have been the seventh highest farm income year since 2008.[697] The figure below shows the amount of federal direct payments (including forgiveness-eligible loans) and federal crop insurance net payments (indemnities minus producer-paid premium) to agricultural producers that contributed to net farm income from 2008 through 2021. The amounts for 2020 and 2021 are projections, which include estimates and forecasts.
Contribution of Federal Direct Payments and Net Crop Insurance Payments to Net Farm Income, 2008–2021, Adjusted for Inflation, as of February 5, 2021
Notes: Dollar amounts are adjusted for inflation using the chain-type Gross Domestic Product deflator, base year=2021, according to the U.S. Department of Agriculture’s (USDA) Economic Research Service (ERS). Years are calendar years. The years 2020 and 2021 include USDA forecasts for some categories as of February 5, 2021, according to ERS. ERS characterizes “Consolidated Appropriations Act, 2021 – COVID-related payments,” Coronavirus Food Assistance Program, Paycheck Protection Program, Market Facilitation Program, supplemental and ad hoc disaster, Farm Bill Title II – Conservation, Farm Bill Title I – Commodities, and Other payments as direct government payments. The ERS Farm Income and Wealth Statistics started reporting on federal crop insurance indemnities and premiums in 2008 and the agency accounts for crop insurance indemnities as farm-related income and accounts for producer-paid premiums as expenses. We accounted for crop insurance as the net amount a producer receives from the federal crop insurance program by subtracting producer-paid premium from indemnities. Private insurance companies share underwriting risk with the federal government, however, from crop year 2008 to 2019 (the latest crop year for which data is publicly available), the companies altogether had net underwriting gains in all years, except for crop year 2012. The “Consolidated Appropriations Act, 2021–COVID-related payments” is the ERS projection of COVID-related direct payments USDA will provide to farmers and ranchers from the Consolidated Appropriations Act, 2021. The “Other” category includes Cotton Ginning Cost Share Program, Tobacco Transition Payments Program, Biomass Crop Assistance Program, and miscellaneous programs.
Agency Comments
We provided a draft of this enclosure to USDA and the Office of Management and Budget for review and comment. USDA’s Office of the Secretary, Office of the Chief Economist, Farm Production and Conservation Business Center, Farm Service Agency, and Economic Research Service provided technical comments that we have incorporated into this enclosure, as appropriate. Comments from the Office of the Secretary, Farm Production and Conservation Business Center, Farm Service Agency, and Economic Research Service largely focused on providing context for our apportionments and ERS analysis. Comments from the Office of the Chief Economist focused on providing additional context for the crop insurance portion of our analysis. The Office of Management and Budget provided technical comments that we have incorporated into this enclosure, as appropriate.
Methodology
To conduct this work, we reviewed USDA officials’ written responses to our questions; USDA budgetary data as of February 1, 2021; and the USDA Economic Research Service’s (ERS) Farm Income and Wealth Statistics as of February 5, 2021. USDA noted in its description of the Farm Income and Wealth Statistics that the data include estimates that are subject to revision as new data become available. ERS develops the Farm Income and Wealth Statistics from administrative data, as well as the department’s Agricultural Census, Agricultural Resources Management Survey, and other survey data. We found the data to be reliable for our purposes of describing federal spending to assist farmers and the contribution of those payments to farm income.
For our figure on the contribution of federal direct payments and net crop insurance payments to farm income, we analyzed ERS’s Farm Income and Wealth Statistics, as of February 5, 2021. ERS characterizes the amounts in the following categories included in the figure as direct federal government payments: “Consolidated Appropriations Act, 2021 – COVID-related payments,” “Coronavirus Food Assistance Program,” “Paycheck Protection Program,” “Market Facilitation Program,” “supplemental and ad hoc disaster,” “Farm Bill Title II – Conservation,” “Farm Bill Title I – Commodities,” and “Other”. To create our figure, we created new categories using the data from the ERS analysis. Specifically, we created three distinct categories—Coronavirus Food Assistance Program, Paycheck Protection Program, and Consolidated Appropriations Act, 2021 – COVID-related payments—from ERS’s “supplemental and ad hoc disaster” category. We created the “Farm Bill Title I – Commodities” category by combining the eleven Farm Bill Title I program lines in the ERS data. We also created the “Crop insurance net payments (indemnities minus producer-paid premium)” category. We calculated the net payments to producers by subtracting producer-paid premium from indemnities. ERS accounts for federal crop insurance indemnities as farm-related income and accounts for producer-paid premiums as expenses. Private insurance companies share underwriting risk with the federal government; however, from crop year 2008 to 2019 (the latest year for which data are publicly available), the companies altogether had net underwriting gains in all years, except for in crop year 2012.
Contact information: Steve D. Morris, (202) 512-3841, morriss@gao.gov
According to the U.S. Department of Agriculture, contractors—a key component of the Farmers to Families Food Box Program—delivered 5.3 million food boxes in the first 30 days (January 19 through February 18, 2021) of the fifth round of the program. Across all five rounds of the program (or since May 15, 2020), contractors delivered 138 million food boxes across the country, spending $4 billion of the almost $5 billion obligated.
Entities involved: U.S. Department of Agriculture, including its Agricultural Marketing Service and Office of the Secretary
Key Considerations and Future GAO Work
We continue to examine the U.S. Department of Agriculture’s (USDA) spending and oversight of the Farmers to Families Food Box Program (Food Box Program).
In our September 2020 report identifying opportunities for USDA to identify successes and challenges, we recommended that USDA evaluate the Food Box Program after the third round of funding. USDA did not evaluate the program after the third round.
Background
As part of its response to the COVID-19 pandemic, USDA established the Food Box Program. Since May 2020, through local, regional, and national contractors, USDA has purchased fresh fruits and vegetables and meat and dairy products for distribution to food banks, community and faith-based organizations, and other nonprofits that serve persons in need.
In the figure below we describe the funding amounts, obligations, and expenditures for the five rounds of the Food Box Program.
Funding Amounts, Obligations and Purchases (Expenditures) for the Farmers to Families Food Box Program, as of January 31, 2021
Notes: According to USDA, the agency determines expenditures (or purchases) by the payments it makes on invoices it receives from contractors. As such, expenditures (or purchases) can be lower than obligations because of the time it takes for USDA to receive and process invoices. aFamilies First Coronavirus Response Act, Pub. L. No. 116-127, div. A, tit. I, §1101(g) and (i), 134 Stat. 178, 180 (2020)bThe CARES Act, Pub. L. No. 116-136, div. B, tit. I, 134 Stat. 281, 505 (2020)cConsolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182, 2105 (2020)
Overview of Key Issues
USDA continues to spend funds on food purchases through its Food Box Program. As the figure above shows, USDA had obligated about $5 billion in awards to contractors (as of January 31, 2021).[698] Contractors are a key component of the Food Box Program because they are responsible for packaging food into boxes and delivering those boxes to recipients (food banks, community and faith-based organizations, and other non-profits serving persons in need). Below we describe what the available USDA data say about contractors’ participation, awards, costs to the government, and delivery.
Contractor participation. As of February 2, 2021, 243 contractors had participated in the Food Box Program’s five rounds, according to our analysis of program data.[699] The figure below shows the contractors participating across all five rounds.
Contractors Participating in the Farmers to Families Food Box Program across the Rounds, as of February 2, 2021
Contract awards. According to our analysis, as of February 2, 2021, USDA had awarded more than 50 percent of the Food Box Program’s total obligations to 21 contractors. These contractors collectively delivered boxes in all 50 states, Puerto Rico, and the U.S. Virgin Islands. Across the five rounds, the largest award amount to a contractor was $278 million and the smallest was $7,700.[700] The average contract award increased in rounds 2 through 5 relative to round 1, as shown below.
Average Contract Award per Contractor for the Farmers to Families Food Box Program, by Round, as of February 2, 2021
Round 1
(May 15 – June 30, 2020)
Round 2
(July 1 – Sept. 18, 2020)
Round 3
(Sept. 22 – Oct. 31, 2020)
Round 4
(Nov. 1 – Dec. 31, 2020)
Round 5
(Jan. 19 – Apr. 30, 2021)
Average award amount per contractor
$5.6 m
$9.5 m
$16.9 m
$15.7 m
$9.8 m
Source: GAO analysis of U.S. Department of Agriculture data. | GAO-21-387
Cost of individual food boxes. USDA purchased five different types of food boxes for delivery to recipient organizations:
fresh fruit and vegetables,
milk,
dairy,
precooked meat, and
combination boxes (which include a mix of fruit and vegetables, milk, dairy, and precooked meat, eggs, or egg products).
The costs for individual food boxes varied widely among contractors, according to our analysis. For example, in rounds 1 and 2 boxes of milk varied from $1.35 to $35.05, fresh fruit and vegetables from $9.70 to $580.00, and precooked meat from $17.65 to $180.00.[701] Beginning in round 3, USDA issued consistent requirements for food boxes.[702] Based on our analysis of the data for rounds 3 through 5, the range in costs for individual food boxes was not as wide compared to rounds 1 and 2. Specifically, the range in costs (i.e., the difference between the maximum and minimum costs) for combination food boxes in rounds 1 and 2 was $139.70, but the range in rounds 3 through 5 were between $32.34 and $77.21. According to USDA officials, the differences in costs reflect the differences in what suppliers charge based on box content and size (weight), delivery locations, and other factors. For example, these officials noted in a written response that in rounds one and two, the cost of the food boxes was among other factors that USDA used in awarding contracts. However, according to USDA, beginning in round 3, the cost of the food boxes delivered to a particular state was the primary factor in awarding contracts. For example, USDA officials said that some states, such as Alaska, required higher transportation costs, which were included in the cost per food box. The table below shows the range in cost to the government for the combination food box, which contractors provided in all five rounds of the program.
Range in Cost for Combination Food Boxes for the Farmers to Families Food Box Program, by Round, as of February 2, 2021
Round 1
(May 15 – June 30, 2020) (In dollars)
Round 2
(July 1 – Sept. 18, 2020) (In dollars)
Round 3
(Sept. 22 – Oct. 31, 2020) (In dollars)
Round 4
(Nov. 1 – Dec. 31, 2020) (In dollars)
Round 5
(Jan. 19 – Apr. 30, 2021) (In dollars)
Combination Food Boxes
Max.
150.00
150.00
99.00
64.95
105.00
Min.
10.30
10.30
34.95
32.61
27.79
Mean
45.85
47.44
47.38
40.30
34.48
Median
39.20
39.00
46.44
38.96
31.85
Source: GAO analysis of U.S. Department of Agriculture data. | GAO-21-387
Note: According to USDA, the solicitation for round 3 of the program indicated a preference for combination boxes over individual box types. As noted above, starting with round 3, USDA provided more specifications for the contents of combination boxes. Prior to that, for rounds 1 and 2 there was less specificity but there had to be a dairy product, precooked meat, milk, and fruit and vegetables in the box.
Food delivery. According to USDA, as of February 18, 2021, contractors delivered about 138 million food boxes across the country across all five rounds of the program (or since May 15, 2020). In the first 30 days (January 19 through February 18, 2021) of the fifth round of the program contractors delivered 5.3 million food boxes.
The number of boxes delivered refers to those received and accepted by recipients and for which contractors will be paid by the government, according to USDA. USDA awards contracts based on the maximum number of boxes that the contractors indicated they could deliver during the contract’s performance period. The available data provide information on the delivery rate for the first four rounds of the program. The delivery rate is the percentage of boxes contractors delivered out of the maximum amount allowed by their contract award.
As of February 2, 2021, contractors participating in rounds 1 through 4 delivered 79 percent of the food boxes allowed by their contract with USDA. We found that deliveries improved over time. For rounds 1 and 2, contractors delivered about 75 percent of boxes allowed by their contracts as compared to about 96 percent of boxes in rounds 3 and 4. As of February 2, deliveries in round 5 had not yet been completed.
Agency Comments
We provided a draft of this enclosure to USDA and the Office of Management and Budget for review and comment. USDA provided technical comments that we have incorporated into this enclosure, as appropriate. The Office of Management and Budget did not have any comments related to this enclosure.
Methodology
To conduct this work, we analyzed the most recent USDA data as of February 2, 2021; reviewed applicable federal laws, agency reports, and other documents; and interviewed USDA officials. We reviewed data on this program by electronically testing them for missing elements, errors, and outliers; reviewing related documentation; and interviewing USDA officials about their data system as it relates to data quality. We determined the data were sufficiently reliable for the purposes of describing contractors participating in the program, as well as their award and food box delivery data.
Contact information: Steve D. Morris, (202) 512-3841, morriss@gao.gov
Related GAO Product
Agriculture Spending: Opportunities Exist for USDA to Identify Successes and Challenges of the Farmers to Families Food Box Program to Inform Future Efforts.GAO-20-711R. Washington, D.C.: September 16, 2020.
Auditors face challenges obtaining timely and useful guidance for performing single audits, a type of audit which could help identify and correct deficiencies to help ensure award recipients’ appropriate use of federal funds, including billions of dollars provided by COVID-19 relief laws, and reduce the likelihood of federal improper payments.
Entity involved: Office of Management and Budget
Recommendation for Executive Action
The Director of the Office of Management and Budget should work in consultation with federal agencies and the audit community (e.g., agency Offices of Inspector General; National Association of State Auditors, Comptrollers, and Treasurers; and American Institute of Certified Public Accountants), to the extent practicable, to incorporate appropriate measures in the Office of Management and Budget’s process for preparing single audit guidance, including the annual Single Audit Compliance Supplement, to better ensure that such guidance is issued in a timely manner and is responsive to users’ input and needs.
The Office of Management and Budget neither agreed nor disagreed with our recommendation.
Key Considerations and Future GAO Work
In September 2020, we reported on the Office of Management and Budget’s (OMB) efforts to issue an addendum to its annual Single Audit Compliance Supplement (Compliance Supplement) containing needed guidance specifically related to COVID-19 relief funds. As stated in our prior report, the addendum could help ensure the timeliness and efficiency of single audits conducted for recipients who received COVID-19 relief funds from programs such as the Coronavirus Relief Fund. We recommended that OMB issue the addendum as soon as possible, as many single audit efforts were underway.
OMB issued the addendum in December 2020. However, the addendum did not address some of the concerns raised by auditors who use the guidance to conduct single audits.[703] Timely and useful single audit guidance is needed to help ensure award recipients’ appropriate use of federal funds and reduce the likelihood of federal improper payments.
We plan to continue to monitor OMB’s process for issuing single audit guidance, in consultation with agencies and the audit community, and stay abreast of key issues and concerns experienced by the users of such guidance concerning its usefulness and timeliness.
Background
Through provisions enacted in the COVID-19 relief laws, the federal government has provided billions of dollars in federal funding to state and local governments, U.S. territory and tribal governments, and nonprofit organizations in such areas as health care and higher education. The Single Audit Act requires non-federal entities that receive federal awards to undergo a single audit of those awards annually (unless a specific exception applies), when their federal award expenditures meet a certain dollar threshold in a fiscal year.[704] Single audits help identify deficiencies in the award recipient’s compliance with applicable provisions of laws, regulations, contracts, or grant agreements and in its financial management and internal control systems. Correcting such deficiencies can help ensure the appropriate use of federal funds and reduce the likelihood of federal improper payments.
The Single Audit Act authorizes the Director of OMB to develop government-wide guidelines and policy on performing audits to comply with the act.[705] As part of this role, each year OMB, after consultation with federal agencies, issues a Compliance Supplement, a tool designed to help consolidate applicable legal requirements for numerous programs into one central place. Without the Compliance Supplement, auditors would need to research compliance requirements per program in numerous statutes and regulations. Auditors rely on the Compliance Supplement to understand a federal program’s objectives, procedures, and compliance requirements. In turn, this review helps auditors design their single audit objectives and audit procedures for determining award recipients’ compliance with applicable provisions of laws, regulations, contracts, or grant agreements.[706]
Overview of Key Issues
As noted in our September 2020 report, OMB’s 2020 Compliance Supplement, issued in August 2020, specified that OMB was still working with federal agencies to identify the need for additional guidance for auditing new COVID-19 relief funded programs and existing programs with compliance requirement changes. Recognizing that many audits were already underway, we recommended that OMB issue the addendum to its 2020 Compliance Supplement containing this additional audit guidance as soon as possible. The American Institute of Certified Public Accountants (AICPA) also issued a letter to OMB in September 2020 expressing its concern that some auditors were waiting for OMB’s addendum to be issued in order to begin testing the new COVID-19-related programs and other existing programs that were expected to be included. OMB subsequently issued the addendum in December 2020.[707]
In developing this Compliance Supplement and addendum, OMB consulted with federal agencies to identify the need for guidance and compliance requirements for auditing new and complex COVID-19-related programs, as well as existing programs, to address challenges across the federal government wrought by the COVID-19 pandemic. Specifically, OMB stated that it provides general guidelines to agencies on areas of focus for program guidance and verifies the formatting used by agencies.[708] OMB further explained that agencies are responsible for determining oversight requirements for the programs they administer and for selecting the areas subject to audit in the Compliance Supplement. OMB did not indicate whether its process includes established time frames for providing its general guidelines to agencies or for agencies to provide Compliance Supplement updates upon enactment of annual appropriations, supplemental appropriations, if any, and other newly enacted provisions of law for effective monitoring of federal funds.
The lag between the distribution of COVID-19 relief funds to recipients and OMB’s issuance of single audit guidance contributed to delays in auditors conducting single audits and reporting the results. These audits were also delayed because of deadline extensions for 2020 single audit report submissions.[709] While these deadline extensions might have provided helpful flexibilities to auditors and award recipients, delays in issuing guidance and completing audits could impact award recipients’ development of corrective action plans, management decisions, and resolution of findings identified during the audits.
OMB is currently working with federal agencies to identify compliance requirements for inclusion in the 2021 Compliance Supplement, including compliance requirements for new and existing programs that received funding under recent COVID-19 relief laws, such as the Consolidated Appropriations Act, 2021, enacted in December 2020.[710] This includes large COVID-19 relief programs; for example, the Provider Relief Fund (see our Relief for Health Care Providers enclosure in this report, programs susceptible to significant improper payments (see our Medicaid Enrollment, Spending, and Flexibilities enclosure in this report , and programs for meeting immediate community needs during the pandemic (see our Community Services Block Grant enclosure in this report. The American Rescue Plan Act of 2021 was enacted on March 11, 2021, and given the timing of such, we did not have an opportunity to determine OMB’s plans for providing guidance on the funding provided as a result of this recent act.[711]
Based on a single audit working group discussion with audit community stakeholders—state auditors; representatives from federal agency Offices of Inspector General (OIG); the AICPA; and the National Association of State Auditors, Comptrollers and Treasurers (NASACT);[712]—auditors who conduct single audits for entities with June 30 year-ends, have expressed a need to have the Compliance Supplement by no later than April of each year to effectively plan their audits and conduct interim testing.[713] However, for the past 3 years, OMB issued its annual Compliance Supplements later in the year. Specifically, the 2018-2020 annual Compliance Supplements were not issued until May 2018, August 2019, and August 2020, respectively, and the 2020 Addendum containing additional guidance related to COVID-19 relief funded programs and other existing programs was not issued until December 2020.
OMB did not provide an estimated timeline for issuing the 2021 Compliance Supplement, but stated that it believes there is currently an appropriate balance between the timeliness of issuing the annual Compliance Supplement and the consideration given to the inputs or comments by the stakeholders. Although OMB has an established process for issuing guidance, it is unclear whether OMB has a target timeframe and representatives from the audit community continue to express a need to have the Compliance Supplement earlier. In September 2010, GAO made a recommendation for OMB to issue the Compliance Supplement by no later than March 31 each year. Our 2010 recommendation to OMB was not implemented and we are making a similar recommendation in this enclosure to address the timeliness concerns noted by the audit community.
Our Standards for Internal Control in the Federal Government emphasize the need for providing timely information, such as the guidance in the Compliance Supplement, for effective monitoring. These standards also state that management should identify, analyze, and respond to significant changes, such as the establishment of new COVID-19-related programs, which would in turn require changes to the Compliance Supplement to specify compliance requirements. Management can anticipate and plan for significant changes by using a forward-looking process wherein it identifies on a timely basis, changes that have already occurred or are expected to occur.
This forward-looking process would include established timeframes to capture annual changes needed to the Compliance Supplement based on annual appropriations, supplemental appropriations, if any, and other newly enacted provisions of law for effective monitoring of federal funds. A process for timely preparing and providing the guidance contained in OMB’s annual Compliance Supplements to auditors is essential to help ensure that single audits can be performed timely and enhance the federal government’s ability to help safeguard billions of dollars in federal funds, including those provided under COVID-19 relief laws. As we previously reported, delays in issuing guidance could adversely affect auditors and the results and timing of their work, and may lead to inconsistent reporting.
In addition to providing timely guidance, it is also essential that OMB establish and maintain a clear process that provides adequate time to work with stakeholders—including federal agencies and the audit community—to determine needed changes to more fully address their input and concerns, which in turn could help ensure the quality of the guidance. This is especially critical going forward given the magnitude of COVID-19 relief funding. OMB stated that it solicits comments from members of the audit community, and makes revisions as appropriate, prior to issuing its final annual Compliance Supplement. However, it is unclear to members of the audit community what OMB’s decision-making process is for resolving concerns raised during the comment period.
According to the AICPA, there are ongoing enhancements needed to OMB’s process for annually updating the Compliance Supplement. These include a need for the Compliance Supplement to focus on areas of highest risk and ensure audit procedures are capable of consistent measurement against objective criteria. The AICPA has also suggested that greater transparency around OMB’s decision-making process for changes to the Compliance Supplement and enhanced collaboration among audit community stakeholders would be helpful.
The concerns raised by the AICPA are similar to those concerns identified in early fiscal year 2020 (over a year ago) by the single audit working group referenced earlier. Based on a survey conducted with members of the single audit working group, there is a need for the audit community to have a greater role in the updates/revisions to ensure that single audit requirements for auditors include applicable and objective criteria. We reached out to OMB to provide an overview of the working group’s findings and OMB stated that it planned to offer a listening session in April 2020. One of OMB’s stated goals of the listening session was to gain insights from the audit community of key challenges associated with single audits. However, OMB subsequently stated that the listening session was delayed due to the COVID-19 pandemic and has not yet been scheduled, as of March 10, 2021. OMB stated that it welcomes an overview of the working group’s findings and we will coordinate with OMB on scheduling a meeting.
In addition, OMB stated that in August 2020 it held two meetings—one with the AICPA and NASACT (on August 17, 2020) and another with the OIGs (on August 18, 2020)—to discuss the single audit challenges and the merit, value, and challenge of focusing on federal program performance review. Given the timing of these meetings, it is unlikely that concerns raised during these meetings were addressed in the 2020 Compliance Supplement as it was issued on August 14, 2020.
In the August 2020 Compliance Supplement, OMB stated that it would work with federal awarding agencies to identify the COVID-19 funding programs and the necessity for these programs to be added in an addendum to that Supplement. However, representatives from the AICPA and NASACT stated in February 2021 that the addendum issued in December 2020 did not address some of the concerns raised by auditors who use the guidance to conduct single audits.
GAO’s Standards for Internal Control in the Federal Government state that management should use quality information to achieve the entity’s objectives. This includes designing a process that uses objectives and related risks to identify the information requirements needed to achieve objectives and address the risks. Information requirements should consider the expectations of both internal and external users. A clear and transparent process for considering and incorporating, as appropriate, input received on the Compliance Supplement is an important aspect of OMB’s efforts to help ensure it provides useful and timely guidance.
Agency Comments and Our Evaluation
We provided OMB with a draft of this enclosure. OMB provided technical comments, which we incorporated as appropriate. In its technical comments, OMB stated that it has a formal process in place for preparing the annual Compliance Supplement, which includes a comprehensive vetting process and opportunities for the audit community stakeholders to review the draft and submit comments. OMB stated that it reviews and considers these comments and makes revisions as appropriate during the preparation of the final document. Additionally, OMB stated that stakeholders are invited to provide comments during the annual notice of availability of the Compliance Supplement published in the Federal Register and that any comments received are reviewed and considered as OMB develops the subsequent year’s Compliance Supplement. While we recognize OMB has a formal process in place, the need for earlier issuance has been a long-standing issue and key stakeholders from the audit community continue to express concerns with the timeliness and quality of the Compliance Supplement. Therefore, we continue to believe that OMB should implement appropriate measures to better ensure that the Compliance Supplement is responsive to users’ input and needs.
Methodology
To conduct this work, we reviewed federal laws and regulations, as well as single audit guidance issued by OMB. We also contacted officials at OMB to obtain information about its processes for issuing single audit guidance and met with representatives from the audit community (i.e., state auditors, officials from OIGs, and representatives from the AICPA and NASACT) to obtain information on their experiences with using OMB’s single audit guidance in the course of their audits. We reviewed the Standards for Internal Control in the Federal Government to determine relevant federal internal control standards for responding to change and issuing quality information in a timely manner.
COVID-19: Federal Efforts Could Be Strengthened by Timely and Consorted Actions. GAO-20-701. Washington, D.C.: September 21, 2020.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
Recovery Act: Opportunities to Improve Management and Strengthen Accountability over States’ and Localities’ Uses of Funds.GAO-10-999. Washington, D.C.: September 20, 2010.
Federal Food Safety Inspections and Inspectors’ Exposure to COVID-19
The U.S. Department of Agriculture is maintaining staffing and federal inspections at meat and poultry plants.
Entity involved: Food Safety and Inspection Service, within the U.S. Department of Agriculture
Key Considerations and Future GAO Work
Our work on the U.S. Department of Agriculture’s (USDA) implementation and oversight of a range of CARES Act funds,[714] including on any implementation challenges, is ongoing. We will continue to examine the department’s capacity to ensure the continuity of food safety inspections at meat and poultry plants and other establishments.
Background
COVID-19 has caused disruptions in the U.S. food supply chain, from the farms where raw agricultural commodities are produced, to the food-processing and distribution network that enables these commodities to be used by consumers.[715] The 7,799 inspectors and other frontline staff from the USDA’s Food Safety and Inspection Service (FSIS) work in 6,512 federally inspected meat and poultry plants and other establishments.[716] These inspectors help ensure the safety and wholesomeness of the meat and poultry that enter interstate commerce, and some have been exposed to COVID-19. According to April 2020 interim guidance from the Centers for Disease Control and Prevention and the Occupational Safety and Health Administration, working in close conditions may contribute to exposure to COVID-19. In response to the executive order on Protecting Worker Health and Safety, on January 29, 2021, the Occupational Safety and Health Administration published COVID-19 worker safety guidance, including recommendations for workplace COVID-19 prevention programs and policies.[717]
As of January 31, 2021, USDA had obligated $18 million and spent $16 million of the $33 million in CARES Act funds that Congress appropriated to FSIS in March 2020 to prevent, prepare for, and respond to COVID-19 with regard to food safety inspections.[718]
Overview of Key Issues
FSIS has spent over $6 million in CARES Act funds to protect inspection personnel and other staff. To mitigate risks associated with COVID-19, FSIS directs inspection personnel to wear face coverings or masks in conjunction with face shields—supplies provided by the agency. As of January 31, 2021, of the total $16 million USDA spent, $6 million was for FSIS employees’ personal protective equipment, including for supplies to combat heat stress, according to officials.[719] In November 2020, we reported that for the remaining funds USDA spent CARES Act funds to maintain staffing of FSIS inspectors including to cover costs for additional hours worked by part-time inspectors, bring in inspectors from other USDA offices, and pay for nonreimbursable overtime. USDA officials told us that the agency will also continue to use CARES Act funds to cover the expenses for inspectors’ equipment and funds may be needed to pay for those employees not working due to illness––that is, to pay for additional part-time inspectors; inspectors from other USDA offices and associated travel; and nonreimbursable overtime, as needed.[720] USDA officials said that as of January 31, 2021, there were no establishments that had to close because of a lack of available FSIS inspectors.
USDA has tracked FSIS inspectors’ and other staff’s COVID-19-related absences and followed agency protocols for contact tracing. According to USDA documentation, as of January 29, 2021, 1,405 inspectors and staff had reported a COVID-19 diagnosis confirmed by a test or medical professional, since the first reported case in March 2020. Of these employees, 1,295 had returned to work and 31 were self-quarantining.[721] In addition to the 1,405 diagnoses, there were 12 employee deaths due to COVID-19. FSIS employees deceased from COVID-19 are not included in the cumulative count of employees who had a COVID-19 diagnosis, according to USDA documentation. Although FSIS does not have a specific requirement for employees to report COVID-19 infections and relies on staff to self-report, FSIS employees are required to report an absence from work. According to USDA’s FSIS Human Pandemic Operations Plan, under the agency’s leave directive, FSIS employees are required to report to their supervisors if they will be absent from duty and, in the event of a human pandemic, supervisors and managers should initiate a follow-up for any unscheduled employee absence.[722]
Upon notification of a positive COVID-19 test result from an employee, FSIS follows USDA protocols for contact tracing, according to officials. This includes gathering pertinent information such as illness onset, testing date and result, last time in building, and contact with employees at the workplace. USDA uses the information to determine any necessary notifications to FSIS and meat and poultry plant personnel, according to officials. For notification of COVID-19 outbreaks at plants, FSIS relies on meat and poultry plants to notify local FSIS supervisors at facilities. According to officials, the agency does not have authority to require meat and poultry plants to make this notification, but exchange of information at the local level between FSIS and industry about COVID-19 positive cases has been effective.
FSIS has continued U.S. inspection activities throughout the COVID-19 pandemic. According to USDA officials, during the COVID-19 pandemic, FSIS has maintained required inspection services to ensure that establishments including meat and poultry plants can operate. In response to the COVID-19 pandemic, FSIS reduced testing for pathogens in meat and poultry products in the second quarter of fiscal year 2020, resumed normal testing by July 2020, and further increased testing and analysis to meet fiscal year 2020 goals. According to officials, FSIS is currently executing its fiscal year 2021 testing plan with no impact from the COVID-19 pandemic. In addition, agency officials told us that a similar percentage of plants that the agency inspected continued to meet the Salmonella performance standard—the maximum allowable number of poultry product samples testing positive for the pathogen—from the second quarter of fiscal year 2020 through the first quarter of fiscal year 2021.[723]
FSIS also has responsibility for inspecting meat and poultry products at U.S. ports and conducting on-site audits of foreign food safety inspection systems. According to agency officials, FSIS inspections of meat, poultry, catfish, and processed egg products imported into the U.S. continued throughout the pandemic at the same established rate and frequency as the previous year. However, since FSIS is currently unable to schedule on-site verification audits of foreign inspection systems, according to officials, the agency has developed an approach to conduct remote audits of foreign systems through electronic communication and information exchanges. This approach is similar to the one taken by some trading partners for auditing the U.S. inspection system during this time. It is in place as a temporary measure due to current limitations resulting from the COVID-19 pandemic, and on-site verification audits are expected to resume once conditions allow for them, according to officials. The agency continues to monitor the situation and will evaluate the feasibility of on-site audits as the situation evolves, including reviewing State Department guidance on foreign travel.
Agency Comments
We provided a draft of this enclosure to USDA and the Office of Management and Budget for review and comment. USDA and the Office of Management and Budget did not have any comments related to this enclosure.
Methodology
To conduct this work, we reviewed the most recent USDA data on COVID-19 illnesses and exposures among FSIS employees available as of January 29, 2021; the CARES Act; agency policy and other guidance; USDA expenditure data including purchases of personal protective equipment, as of January 31, 2021; and written responses to questions we emailed USDA officials in the FSIS. We assessed the reliability of agency data by reviewing relevant USDA FSIS documents, reviewing our prior use of the data sources, and reviewing written responses from the agency about the data. We determined the data were sufficiently reliable for estimating the number of FSIS staff that had become ill with COVID-19.
Contact information: Steve D. Morris, (202) 512-3841, morriss@gao.gov
Related GAO Product
Food Safety: USDA Should Take Further Action to Reduce Pathogens in Meat and Poultry Products.GAO-18-272. Washington, D.C.: March 19, 2018.
Appendix II: List of Ongoing GAO Work Related to COVID-19, as of March 17, 2021
In our June 2020 CARES Act report, we made three matters for congressional consideration and three recommendations for executive action. In our September 2020 CARES Act report, we made 16 recommendations. In our November 2020 CARES Act report, we made one matter for congressional consideration and 11 recommendations. Also, in November 2020, we issued a report on COVID-19 vaccines and therapeutics, and made one recommendation. In our January 2021 CARES report we made 13 recommendations. Following are the recommendations, and their status by department (see fig. 8).
Figure 8: Status of Prior GAO Recommendations by Department or Agency
Below we list by department or agency our four prior matters for congressional consideration and our 44 prior recommendations, and characterize their implementation status.
Status of matters for congressional consideration and recommendations made regarding the Department of Health and Human Services (HHS)
Matter. To help ensure that federal funding is targeted and timely, we urge Congress to use our Federal Medical Assistance Percentage formula for any future changes to the Federal Medical Assistance Percentage during the current or any future economic downturn (June 2020 report).
Status: Open
Comments: Our past work has found that during economic downturns—when Medicaid enrollment can increase and state economies weaken—the formula, which is based on each state’s per capita income, does not reflect current state economic conditions. No congressional action has been taken to date.
Recommendation. The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency (FEMA)—who head agencies leading the COVID-19 response through the Unified Coordination Group—should immediately document roles and responsibilities for supply chain management functions transitioning to HHS, including continued support from other federal partners, to ensure sufficient resources exist to sustain and make the necessary progress in stabilizing the supply chain, and address emergent supply issues for the duration of the COVID-19 pandemic (September 2020 report).
Status: Open
Comment: As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability. We acknowledge those efforts, but continue to maintain that our recommendations are warranted.
Recommendation. The Secretary of Health and Human Services in coordination with the Administrator of FEMA—who head agencies leading the COVID-19 response through the Unified Coordination Group—should further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic, including through the use of Defense Production Act authorities (September 2020 report).
Status: Open
Comment: As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability. We acknowledge those efforts, but continue to maintain that our recommendations are warranted.
Recommendation. The Secretary of Health and Human Services—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
Status: Open
Comment: As of January 2021, HHS disagreed with our recommendation, noting, among other things, the work that the department had done to manage the medical supply chain and increase supply availability. We acknowledge those efforts, but continue to maintain that our recommendations are warranted.
Recommendation. The Secretary of Health and Human Services, with support from the Secretary of Defense, should establish a time frame for documenting and sharing a national plan for distributing and administering a COVID-19 vaccine and, in developing such a plan, ensure that it is consistent with best practices for project planning and scheduling, and outlines an approach for how efforts will be coordinated across federal agencies and nonfederal entities (September 2020 report).
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. In November 2020, we reported that HHS and the Department of Defense (DOD) had released initial planning documents for the distribution and administration of potential COVID-19 vaccines, but also reported that stakeholders indicated that they would like to see additional information as planning continued. Since our November report, HHS and DOD have continued their efforts related to vaccine implementation. We will continue to monitor federal efforts to determine whether the actions taken address our recommendation.
Recommendation. Based on the imminent cybersecurity threats, the Secretary of Health and Human Services should expedite the implementation of our prior recommendations regarding cybersecurity weaknesses at its component agencies (September 2020 report).
Status: Open
Comment: HHS agreed with our recommendation and has reported actions the department is taking to implement it, such as leveraging its monthly Chief Information Security Officer Council meetings to discuss recommendations made across the HHS component agencies. Additionally, the relevant component agencies—the Food and Drug Administration (FDA), Centers for Medicare & Medicaid Services (CMS), and Centers for Disease Control and Prevention (CDC)—have addressed additional cybersecurity weaknesses since we reported in January 2021. Specifically, FDA, CMS, and CDC implemented an additional 17 of our cybersecurity recommendations, bringing the total number of implemented recommendations to 421 of the total 434 we made to these agencies. This reflects a 4-percent increase in corrective actions taken to bolster cybersecurity at the component agencies.
Recommendation. The Secretary of Health and Human Services should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that HHS has produced for the public and Congress to allow for a more coordinated pandemic testing approach (January 2021 report).
Status: Open
Comment: HHS partially agreed with our recommendation. HHS agreed that the department should take steps to more directly incorporate some of the elements of an effective national strategy, but expressed concern that producing such a strategy at this time could be overly burdensome on the federal, state, and local entities that are responding to the pandemic, and that a plan would be outdated by the time it was finalized or potentially rendered obsolete by the rate of technological advancement. Additionally, HHS stated that, to be of value to the whole of nation response to COVID-19, testing plans need to establish guidelines and use metrics that are operationally relevant, which necessitates strategic flexibility in testing plans to guide those managing the response in the use of available resources to address local and state conditions rather than a single static nationwide plan.
Recommendation. To improve the federal government’s response to COVID-19 and preparedness for future pandemics, the Secretary of Health and Human Services should immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. This committee should include a broad representation of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits (January 2021 report).
Status: Open
Comment: HHS partially agreed with our recommendation. HHS agreed that it should establish a dedicated working group or other mechanism with a focus on addressing COVID-19 data collection shortcomings. However, HHS said because of resource constraints and the ongoing response to the pandemic, it could not commit to immediately doing so.
HHS CDC
Recommendation. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should determine whether having the authority to require states and jurisdictions to report race and ethnicity information for COVID-19 cases, hospitalizations, and deaths is necessary for ensuring more complete data and, if so, seek such authority from Congress (September 2020 report).
Status: Open
Comment: CDC agreed with our recommendation. In response, in February 2021, CDC stated that it is reviewing race and ethnicity data completeness across its core surveillance systems and engaging stakeholders from across the agency and in state and local health departments to improve the collection of race and ethnicity data. CDC noted that stakeholders include CDC leadership, key taskforces from within CDC’s COVID-19 emergency response, and data and surveillance experts in CDC and state health agencies. CDC reported that the information derived from this review will be discussed with the CDC Director and used to assess potential opportunities to enhance the collection of race and ethnicity data, including policy changes or seeking legislative authorities. We will continue to conduct work examining HHS, CDC, and other component agencies’ ongoing work regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should involve key stakeholders to help ensure the complete and consistent collection of demographic data (September 2020 report).
Status: Open
Comment: CDC agreed with our recommendation. In response, in February 2021, CDC stated that it is reviewing the quality of demographic data, including the completeness of race and ethnicity data, across its core surveillance systems and engaging stakeholders from across the agency and in state and local health departments on the issue. CDC noted that stakeholders include CDC leadership, key taskforces from within CDC’s COVID-19 emergency response, and data and surveillance experts in CDC and state health agencies. CDC reported that the information derived from this review will be discussed with the CDC Director and used to assess potential opportunities to enhance the collection of race and ethnicity data, including seeking policy changes or legislative authorities. CDC also stated that it is working with public health partners to automate the generation and transmission to CDC of COVID-19 case reports that contain demographic information, including race and ethnicity. According to CDC, as of January 12, 2021, more than 6,500 facilities are sending COVID-19 electronic case reports to state and jurisdictional health departments. We will continue to conduct work examining HHS, CDC, and other component agencies’ ongoing work regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. As CDC implements its COVID-19 Response Health Equity Strategy, the Director of CDC should take steps to help ensure CDC’s ability to comprehensively assess the long-term health outcomes of persons with COVID-19, including by race and ethnicity (September 2020 report).
Status: Open
Comment: CDC agreed with our recommendation. In response to our recommendation, CDC noted in October 2020 that the agency is convening a team to develop a plan to monitor the long-term health outcomes of persons with COVID-19 by identifying health care surveillance systems that can electronically report health conditions to state and local health departments. CDC said that as of January 2021 the agency had various efforts underway with external partners to assess long-term health outcomes. For example, CDC is funding a number of prospective studies in partnership with universities to understand the long-term effects of COVID-19 illness, including a study examining the neurological health outcomes of a large cohort of Black and Hispanic or Latino persons who had COVID-19. In addition, CDC stated the agency is analyzing electronic health record data to describe health outcomes after COVID-19 diagnosis as well as analyzing race and ethnicity in any data collected for long-term health effects. We will continue to conduct work examining HHS, CDC, and other component agencies’ ongoing work regarding indicators of COVID-19 and disparities that exist for various populations.
Recommendation. The Director of CDC should ensure that, as it makes updates to its federal guidance related to reassessing schools’ operating status, the guidance is cogent, clear, and internally consistent (September 2020 report).
Status: Closed
Comment: This recommendation is closed as implemented. CDC’s guidance for school operating status during COVID-19 is more cogent, clear, and consistent. On February 12, 2021, CDC released revised guidance for returning to in-person learning, as well as mitigation strategies to help prevent and reduce the spread of COVID-19 in school settings. We found the guidance consolidated much of the earlier guidance into one document that clearly displays all five of CDC’s mitigation strategies and includes steps school officials should consider when deciding to reopen schools. In addition, we identified increased efforts to synchronize content across CDC’s website. We found that CDC had removed some and updated other information and had begun including summaries of changes made to the guidance at the top of some webpages.
Recommendation. The Secretary of Health and Human Services should ensure that the Director of CDC clearly discloses the scientific rationale for any change to testing guidelines at the time the change is made (November 2020 report).
Status: Open
Comment: HHS agreed with our recommendation and has begun to implement it. For example, on February 16, 2021, CDC issued Interim Guidance on Testing Healthcare Personnel that stated asymptomatic health care personnel who have recovered from COVID-19 may not need to undergo repeat testing or quarantine in the case of another exposure within 3 months of their initial diagnosis. To support this guidance, CDC’s website provided links to studies that explained the scientific rationale. Additionally, CDC told us that it continues to consult with scientific stakeholders when issuing or updating guidance documents. We will continue to monitor the implementation of this recommendation to ensure that these efforts continue.
HHS CMS
Recommendation. The Administrator of CMS should quickly develop a plan that further details how the agency intends to respond to and implement, as appropriate, the 27 recommendations in the final report of the Coronavirus Commission on Safety and Quality in Nursing Homes, which CMS released on September 16, 2020. Such a plan should include milestones that allow the agency to track and report on the status of each recommendation; identify actions taken and planned, including areas where CMS determined not to take action; and identify areas where the agency could coordinate with other federal and nonfederal entities (November 2020 report).
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. HHS officials highlighted actions that CMS has taken related to Commission recommendations and said it would refer to and act upon the Commission’s recommendations, as appropriate. As of February 2021, CMS had no additional updates. We maintain that developing a plan that details how CMS will proceed with remaining recommendations, includes milestones, and demonstrates that coordination with other federal and nonfederal stakeholders would improve CMS’s ability to systematically consider the Commission’s recommendations going forward.
Recommendation. The Secretary of Health and Human Services, in consultation with CMS and CDC, should develop a strategy to capture more complete data on confirmed COVID-19 cases and deaths in nursing homes retroactively back to January 1, 2020, and to clarify the extent to which nursing homes have reported data before May 8, 2020. To the extent feasible, this strategy to capture more complete data should incorporate information nursing homes previously reported to CDC or to state or local public health offices (September 2020 report).
Status: Open
Comment: HHS partially agreed with our recommendation. As of February 2021, no specific action had been taken by HHS, although according to HHS it continues to consider how to implement our recommendation.
HHS FDA
Recommendation. The Secretary of Health and Human Services should direct the FDA Commissioner to identify ways to uniformly disclose to the public the information from FDA’s scientific review of safety and effectiveness data—similar to the public disclosure of the summary safety and effectiveness data supporting the approval of new drugs and biologics—when issuing emergency use authorizations (EUA) for therapeutics and vaccines, and, if necessary, seek the authority to publicly disclose such information (November 2020 report on vaccine and therapeutics).
Status: Closed.
Comment: In response to our recommendation, FDA said it would explore approaches to achieve the goal of transparency. On November 17, 2020, FDA made an announcement on the agency’s ongoing commitment to transparency for COVID-19 EUAs. FDA also developed a process to disclose its scientific review documents for therapeutic EUAs and released such summaries for one previous therapeutic EUA and the two additional therapeutic EUAs issued since our recommendation. These summaries disclosed information similar to what FDA releases to support new drug approvals and biologic licensures. Additionally, for the two vaccine EUAs FDA issued since our recommendation, FDA released decision memorandums containing detailed information about FDA’s review of safety and effectiveness data. FDA’s actions meet the intent of our recommendation and will improve transparency.
Recommendation. The Commissioner of FDA should, as the agency makes changes to its collection of drug manufacturing data, ensure the information obtained is complete and accessible to help identify and mitigate supply chain vulnerabilities, including by working with manufacturers and other federal agencies (e.g., the DOD and the Department of Veterans Affairs (VA)) and, if necessary, seek authority to obtain complete and accessible information (January 2021 report).
Status: Open
Comment: HHS neither agreed nor disagreed with our recommendation. In HHS’s response, FDA said that as the agency continues efforts to enhance relevant authorities and close data gaps, it will consider our recommendation.
Recommendation. The Commissioner of FDA should, as inspection plans for future fiscal years are developed, ensure that such plans identify, analyze, and respond to the issues presented by the backlog of inspections that could jeopardize the goal of risk-driven inspections (January 2021 report).
Status: Open
Comment: FDA agreed with our recommendation and stated that it is actively tracking the list of sites that need to be inspected. FDA further noted that the size of the backlog will depend on the extent to which alternative inspection tools are used.
Recommendation. The Commissioner of FDA should fully assess the agency’s alternative inspection tools and consider whether these tools or others could provide the information needed to supplement regular inspection activities or help meet the agency’s drug oversight objectives when inspections are not possible in the future (January 2021 report).
Status: Open
Comment: FDA agreed with our recommendation and stated that it would continue to evaluate these alternative tools. FDA stated that the resulting information will help determine how they can be used to streamline and supplement regular inspection activities and to prioritize inspections when normal inspection operations are not possible.
HHS Office of the Assistant Secretary for Preparedness and Response
Recommendation. To improve the nation’s response to and preparedness for pandemics, the Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders—including state, local, tribal, and territorial governments and private industry—as HHS refines and implements a supply chain strategy for pandemic preparedness, to include the role of the Strategic National Stockpile (January 2021 report).
Status: Open
Comment: HHS generally agreed with our recommendation, while noting that the term “engage” is vague and unclear, and that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority.
Recommendation. The Assistant Secretary for Preparedness and Response, in coordination with the appropriate offices within HHS, should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts (January 2021 report).
Status: Open
Comment: HHS agreed with our recommendation and stated that it has taken steps to manually identify its other transaction agreements in its contract writing system to allow the public to distinguish between spending on agreements and procurement contracts in the Federal Procurement Data System-Next Generation. HHS also plans to update its contract writing system.
Status of recommendations made to the Department of the Treasury (Treasury)
Recommendation. The Secretary of the Treasury should finish developing and implement a compliance monitoring plan that identifies and responds to risks in the Payroll Support Program to ensure program integrity and address potential fraud, including the use of funds for purposes other than for the continuation of employee wages, salaries, and benefits (November 2020 report).
Status: Open
Comment: Treasury neither agreed nor disagreed with our recommendation. In February 2021, Treasury provided its Process Overview for CARES Operations Compliance Testing. This document outlined the steps in Treasury’s compliance monitoring process. However, it did not include details on how Treasury considers risks in this process, such as listing the automated tests it uses to review recipient quarterly reports or the thresholds for these tests that trigger additional review. The document also did not provide details on the penalties or remedies for noncompliance that Treasury would use. According to Treasury officials, the agency is still developing and finalizing these details. We will more fully evaluate Treasury’s efforts to develop a compliance monitoring plan when we can review more detailed documents from Treasury.
Recommendation. The Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments (June 2020 report).
Status: Open
Comment: Treasury and the Internal Revenue Service (IRS) have taken steps to implement our recommendation. For example, IRS has instructions on its website requesting that individuals voluntarily mail the appropriate economic impact payment (EIP) amount sent to the decedent back to IRS, for both electronic and paper check payments. The envelopes in which paper checks were sent also had a checkbox so people could indicate that the intended recipient was deceased, and then mail the envelope back. Treasury has also held and cancelled payments made to decedents, along with those that have been returned. As of January 29, 2021, around 57 percent (just over $703 million) of the $1.2 billion in the first round of economic impact payments (EIP 1) sent to deceased individuals had been recovered. The recovered amount has not changed since August 2020. As of February 2021, Treasury and IRS had not taken any further action to recoup payments made to decedents that had not been returned, but they are considering whether they will undertake further efforts.
Recommendation. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP to help target outreach and communications efforts (September 2020 report).
Status: Open
Comment: Treasury and IRS neither agreed nor disagreed with our recommendation, but did take some actions that are consistent with our recommendation. For example, in September 2020, the agencies used tax return information to identify nearly 9 million individuals who had not received an EIP 1 and then notified these individuals that they may be eligible for a payment. The letters also provided instructions on how to request a payment. In addition, IRS publicly released detailed zip code data from the notices to help community outreach partners with their own outreach efforts.
In January 2021, Treasury revised its estimate of eligible recipients who have yet to file for an EIP 1 to 8 million. According to Treasury officials, this estimate is based on the 9 million notices IRS sent in September 2020. Treasury officials stated that it is likely that some of the 9 million recipients have since claimed the EIP, but Treasury did not provide data supporting this claim.
Recommendation. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should make estimates of eligible recipients who have yet to file for an EIP, and other relevant information, available to outreach partners to raise awareness about how and when to file for EIPs (September 2020 report).
Status: Open
Comment: Treasury and IRS neither agreed nor disagreed with our recommendation, but did take some actions that are consistent with our recommendation. For example, in September 2020, the agencies used tax return information to identify nearly 9 million individuals who had not received an EIP 1 and then notified these individuals that they may be eligible for a payment. The letters also provided instructions on how to request a payment. In addition, IRS publicly released detailed zip code data from the notices to community outreach partners with their own outreach efforts.
In January 2021, Treasury revised its estimate of eligible recipients who have yet to file for an EIP 1 to 8 million. According to Treasury officials, this estimate is based on the 9 million notices IRS sent in September 2020. Treasury officials stated that it is likely that some of the 9 million recipients have since claimed the EIP, but Treasury did not provide data supporting this claim.
Recommendation. The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed an EIP notification letter and subsequently filed for and received an EIP, and use that information to inform ongoing outreach and communications efforts (November 2020 report).
Status: Open
Comment: Treasury and IRS agreed with this recommendation. According to Treasury officials, Treasury began analyzing data in January 2021 on those individuals who had received a notice and subsequently filed for and received an EIP 1. As of the time of this report, Treasury’s analysis of these data was ongoing. Treasury has not reported any results or provided a timeline for when it plans to complete the analysis.
Recommendation. The Commissioner of Internal Revenue should update the Form 1040-X instructions to include information on the electronic filing capability for tax year 2019 (November 2020 report).
Status: Open
Comment: IRS agreed with our recommendation and said that it would start to update the Form 1040-X instructions to include information on the electronic filing (e-file) capability for tax year 2019.
As of early December 2020, IRS planned to include this information in the next routine annual update of the instructions with a mid-2021 release, rather than updating them sooner, out of cycle. According to IRS, the normal revision process takes 10 months to complete properly, and would be difficult to complete in a shorter time frame. IRS’s planned revision will occur after the deadline for submitting an application for a tentative refund via the temporary electronic fax procedures, which for some taxpayers, may require an accompanying Form 1040-X. This means that taxpayers who filed their 1040-X before the December 31 deadline with the temporary procedures did not find the e-file capability in the form instructions. However, some taxpayers will use Form 1040-X for other CARES Act refunds after that deadline, so instructions that are updated in tax year 2021 would still help ensure these taxpayers are aware of this option. A timelier update to the instructions would help taxpayers filing the 1040-X between now and when the annual update to the instructions occurs in mid-2021.
In the meantime, IRS previously posted information about the e-file availability on the Form 1040-X product page at IRS.gov, which is referenced in the first paragraph of the Form 1040-X instructions. We will continue to monitor any updates to this page and the instructions.
Status of recommendations made to the Department of Labor (DOL)
Recommendation. The Secretary of Labor should, in consultation with the Small Business Administration (SBA) and Treasury, immediately provide information to state unemployment agencies that specifically addresses SBA's Paycheck Protection Program (PPP) loans, and the risk of improper payments associated with these loans (June 2020 report).
Status: Closed
Comment: DOL neither agreed nor disagreed with our recommendation. Following our recommendation, DOL issued guidance on August 12, 2020, that clarified that individuals working full-time and being paid through PPP are not eligible for unemployment insurance (UI), and that individuals working part-time and being paid through PPP would be subject to certain state policies, including state policies on partial unemployment to determine their eligibility for UI benefits. Further, the guidance clarified that individuals being paid through PPP but not performing any services would similarly be subject to certain provisions of state law, and noted that an individual receiving full compensation would be ineligible for UI.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance revises its weekly news releases to clarify that in the current unemployment environment, the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits (November 2020 report).
Status: Closed
Comment: DOL’s weekly news release of December 10, 2020, clarified that the numbers reported for weeks of UI benefits claimed do not represent the number of unique individuals claiming benefits.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance pursues options to report the actual number of distinct individuals claiming benefits, such as by collecting these already available data from states, starting from January 2020 onward (November 2020 report).
Status: Open
Comment: DOL partially agreed with our recommendation. Specifically, DOL agreed to pursue options to report the actual number of distinct individuals claiming UI benefits. However, DOL did not agree with the retroactive effective date of the reporting. DOL indicated that state UI programs may face challenges implementing any new reporting requirements, particularly retroactively. In addition, DOL stated that the requirements to provide notice and comment for the new data collection could take up to a year to complete.
We maintain that DOL should pursue options to report the actual number of distinct individuals claiming UI benefits, retroactive to January 2020. These data are vital to understanding how many individuals are receiving UI benefits, as well as the size of the population supported by the UI system during the pandemic, especially as Congress again expanded UI benefits in December 2020 and March 2021. Even if the information is unavailable for some time, reporting numbers retroactively, beginning with calendar year 2020, would help DOL and policy makers identify lessons learned about the administration and utilization of regular and expanded UI benefit programs during the pandemic. Given the substantial investment in UI programs during the pandemic, an accurate accounting of the size of the population supported by this funding, even retroactively, may be critical to understanding the efficiency and effectiveness of the nation’s response to unemployment during the pandemic.
As of March 18, 2021, this recommendation remained open, as DOL had not begun reporting the actual number of unique individuals claiming UI benefits on a weekly basis in its UI news releases. We encourage DOL to pursue options to report the actual number of individuals claiming benefits in the most feasible and least burdensome way. Collecting data from states is one way DOL can address the recommendation, but DOL could also develop other ways of gathering and reporting this information.
Recommendation. The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments recovered in the Pandemic Unemployment Assistance (PUA) program, similar to the regular UI program (January 2021 report).
Status: Open
Comment: DOL agreed with our recommendation to collect data from states on the amount of overpayments recovered in the PUA program. On January 8, 2021, DOL took the first step toward implementing our recommendation by issuing new guidance and updated instructions for reporting PUA program activities. Specifically, DOL revised its PUA reporting instrument to collect PUA overpayment recovery data from states. As of March 15, 2021, this recommendation remained open, as just 14 states had begun reporting some data on the amount of PUA overpayments recovered. We will continue to monitor state reporting of PUA overpayment recovery data.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should develop a plan, with time frames, to implement the agency’s oversight processes for COVID-19-adapted enforcement methods, as described in its pandemic enforcement policies (January 2021 report).
Status: Open
Comment: DOL neither agreed nor disagreed with our recommendation. In February 2021, the Occupational Safety and Health Administration (OSHA) provided an update on its plans to implement some oversight processes, but these plans did not include specific time frames or fully address the processes to oversee OSHA’s use of adapted enforcement methods, as outlined in the agency’s pandemic enforcement policies. For example, OSHA provided no plans to perform an on-site component for remote inspections, or to perform follow-up inspections specifically for informal inquiries conducted in place of inspections. As we reported in January 2021, without this monitoring, the agency lacks information on workplace hazards that may have been missed when using adapted enforcement methods and on how effective these methods have been overall in identifying hazards. Our review of Worker Safety and Health during the COVID-19 pandemic is ongoing. We will continue to examine OSHA’s efforts to implement its oversight processes for COVID-19-adapted enforcement methods.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should ensure that the OSHA Information System includes comprehensive information on use of the agency’s COVID-19-adapted enforcement methods sufficient to inform its oversight processes for these methods (January 2021 report).
Status: Open
Comment: DOL neither agreed nor disagreed with our recommendation. In February 2021, OSHA said that the agency believes its current OSHA Information System coding related to COVID-19 and adapted enforcement methods is sufficient to enable agency oversight, and it will add new coding if and when it is needed. We continue to believe that there are gaps in OSHA Information System coding that prevent reliable tracking of some of the agency’s adapted enforcement methods. Our review of Worker Safety and Health during the COVID-19 pandemic is ongoing. We will continue to examine OSHA’s efforts to ensure that the OSHA Information System includes sufficient information to inform its oversight processes.
Recommendation. The Assistant Secretary of Labor for Occupational Safety and Health should determine what additional data may be needed from employers or other sources to better target the agency’s COVID-19 enforcement efforts (January 2021 report).
Status: Open
Comment: DOL neither agreed nor disagreed with our recommendation. In February 2021, OSHA said that it had considered our recommendation and has determined that it does not need additional information from employers to identify where pandemic-related enforcement should be targeted. OSHA also said that, pursuant to the President’s January 21, 2021, executive order on Protecting Worker Health and Safety, OSHA is working to launch a national program to focus OSHA’s COVID-19-related enforcement efforts on violations that put the largest number of workers at serious risk or are contrary to anti-retaliation principles. Our review of Worker Safety and Health during the COVID-19 pandemic is ongoing. We will continue to examine OSHA’s efforts in order to determine whether actions taken, including the implementation of OSHA’s new national program, address our recommendation.
Status of recommendations made to the Small Business Administration (SBA)
Recommendation. The Administrator of SBA should develop and implement plans to identify and respond to risks in PPP to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less (June 2020 report).
Status: Open
Comment: At the time of our report, SBA neither agreed nor disagreed with our recommendation. Since then, SBA officials have said the agency has completed oversight plans, but SBA has not provided documentation that fully details these plans. As we reported in September 2020, SBA has said that it plans to review all PPP loans of $2 million or more and further stated that it may review any PPP loan it deems appropriate, including loans of less than $2 million. In late December 2020, SBA provided a Loan Review Plan for the loan review process. The document describes three steps in the process: automated screenings of all loans, manual reviews of selected loans, and quality control reviews to ensure the quality, completeness, and consistency of the review process. Although the draft plan references detailed policies and procedures for some loan reviews and loan forgiveness reviews, they were not included in the document we received. SBA officials told us these policies and procedures were being updated. In February 2021, SBA provided all but one of the documents referenced in the plan and stated that it was still finalizing the last document. The documents SBA provided include additional details on how SBA and its contractors will conduct the various reviews. We continue to review these documents to determine the extent to which they address our recommendation.
Recommendation. The Administrator of SBA should expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread (November 2020 report).
Status: Open
Comment: SBA neither agreed nor disagreed with our recommendation at that time. In response to our recommendation, SBA stated that it was planning to conduct improper payment testing for PPP and that it takes improper payments seriously. SBA officials stated that it has submitted the sampling plan to the Office of Management and Budget (OMB) and will use this sampling plan to estimate both improper payments and error rates for PPP. We will continue to monitor the agency's actions to address this recommendation.
Recommendation. The Administrator of SBA should develop and implement portfolio-level data analytics across Economic Injury Disaster Loan (EIDL) program loans and advances made in response to COVID-19 as a means to detect potentially ineligible and fraudulent applications (January 2021 report).
Status: Open
Comment: SBA neither agreed nor disagreed with our recommendation. SBA took issue with our finding that potentially ineligible businesses received EIDL advances and loans. SBA mentioned actions it takes to prevent payments to ineligible businesses for loans, such as conducting manual reviews of applications in prohibited categories and approving them upon further determination that they were eligible. According to SBA, it declined most applications in three prohibited business categories we identified (adult entertainment, casinos, and marijuana shops) following the manual reviews and approved some applications in these categories after manual reviews indicated that they were eligible. However, SBA did not provide any documentation that would enable us to verify the results of its manual reviews. In addition, we identified other prohibited business categories (multi-level marketing, insurance, and real estate development) where potentially ineligible businesses received EIDL loans. SBA did not address these other prohibited categories in its comments. Further, to date SBA has not provided us information we have requested on actions it and its contractors take to prevent payments to ineligible businesses. Therefore, we lack assurance that the actions SBA takes are effective in identifying ineligible businesses.
Our analysis was intended to provide an illustration of how fraud risk indicators can point to vulnerabilities typically managed through a fraud risk management approach. Such indicators are especially important in programs with heavy reliance on borrower certifications. We maintain that portfolio-level data analytics could help SBA manage its risk of providing funds to ineligible businesses.
Status of recommendations made to OMB
Recommendation. The Director of OMB should develop and issue guidance directing agencies to include COVID-19 relief funding with associated key risks, such as provisions contained in the CARES Act and other relief legislation that potentially increase the risk of improper payments or changes to existing program eligibility rules, as part of their improper payment estimation methodologies. This should especially be required for already existing federal programs that received COVID-19 relief funding (November 2020 report).
Status: Open
Comment: As of January 2021, OMB had not issued new guidance to address our recommendation. In January 2021, OMB staff stated they believe current OMB guidance sufficiently addresses our recommendation and concerns. In November 2020, we reported that although OMB issued a memorandum providing agencies the option to incorporate new COVID-19 relief funding into their normal sampling processes, it did not specifically direct agencies to do so. In addition, the guidance did not direct agencies to consider associated risks, such as changes to eligibility rules and different payment processes, as part of their improper payment estimation methodologies. Further, OMB staff stated that OMB is actively coordinating and engaging with the Pandemic Response Accountability Committee and Inspectors General to share and discuss information relevant to COVID-19 spending risks and improper payment reduction strategies. We continue to maintain that without OMB guidance for agencies to include COVID-19 relief funding and associated key risks, as part of their improper payment estimation methodologies, agencies are at increased risk that their processes may not result in reliable estimates, calling into question their usefulness for developing effective corrective actions.
Recommendation. The Director of OMB, in consultation with Treasury, should issue the addendum to the 2020 Compliance Supplement as soon as possible to provide the necessary audit guidance (September 2020 report).
Status: Closed
Comment: OMB neither agreed nor disagreed with the recommendation. OMB issued the 2020 Compliance Supplement Addendum on December 22, 2020.
Status of recommendations made to VA
Recommendation. The VA Under Secretary for Health should develop a plan to ensure inspections of state veterans homes occur during the COVID-19 pandemic—which may include using in-person, a mix of virtual and in-person, or fully virtual inspections. (November 2020 report)
Status: Closed
Comment: On December 7, 2020, VA developed an interim process for reviewing records from state veterans homes, such as evidence that previous corrective action plans were implemented and documentation of infection control assessments, to assess the state veterans homes’ compliance with federal regulations. VA reported it implemented this process until a new inspection contract could be awarded and completed 25 of these record reviews. VA awarded a contract in January 2021, to conduct full virtual, blended virtual, or on-site inspections, and reported that the contractor began conducting inspections on January 19, 2021, which are ongoing.
Recommendation. The VA Under Secretary for Health should collect timely data on COVID-19 cases and deaths in each state veterans home, which may include using data already collected by CMS (November 2020 report).
Status: Open
Comment: As of February 2021, VA is collecting data on COVID-19 cases and deaths at most state veterans homes in collaboration with CDC’s National Healthcare Safety Network.
On March 11, 2021, VA posted data on its website on COVID-19 cases and deaths among residents and staff at 130 out of 158 state veterans homes that reported weekly data to CDC. VA officials told us they have reached out to all state veterans homes that are not reporting data, and states it will continue to update the website weekly as required by Public Law 116-315.
We will continue to monitor their progress.
Status of recommendations made to the Department of Homeland Security (DHS)
Recommendation. The Secretary of Homeland Security, in coordination with the Secretary of Defense, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Status: Open
Comment: DHS disagreed with our recommendation. As of February 2021, a DOD official said that DHS and DOD were in the process of updating the agreement to clarify the steps they would take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close a NIA code. We will review the updated agreement when finalized to determine whether it meets the intent of the recommendation.
Recommendation. The Administrator of FEMA—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with its roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
Status: Open
Comment: DHS disagreed with our recommendation, noting, among other things, the work that it had done to manage the medical supply chain and increase supply availability.
As of February 2021, FEMA has not taken action to devise interim solutions that would systematically help states, tribes, and territories effectively track, manage, and plan for supplies to carry out the COVID-19 pandemic response in the absence of state-level end-to-end logistics capabilities that would track critical supplies required for a response of this scale . According to FEMA officials, the challenges states, territories, and tribes reported have continued to improve. These officials stated that FEMA has supported several states’ actions to enhance their logistics capabilities and warehouse capacities, for example, by assigning logisticians to provide technical assistance. In addition, on January 21, 2021, the President issued a memorandum that clarified and expanded the eligibility of certain supplies and announced that all supplies would be 100 percent federal cost share, which addresses some of the planning challenges we discussed in making this recommendation. FEMA officials also said that most states now have a 30-60 day PPE supply and many are using inventory management systems. However, without action across the board to help states ensure they have the support they need to track, manage, and plan for supplies, states, tribes, and territories on the front lines of the whole-of-nation COVID-19 response may continue to face challenges that hamper their effectiveness.
Status of recommendations made to DOD
Recommendation. The Secretary of Defense, in coordination with the Secretary of Homeland Security, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report)
Status: Open
Comment: DOD disagreed with our recommendation. As of February 2021, a DOD official said that DHS and DOD were in the process of updating the agreement to clarify the steps they would take to obtain input from other federal agencies and some of the factors considered when determining whether to extend or close a NIA code. We will review the updated agreement when finalized to determine whether it meets the intent of the recommendation
Status of recommendation made to the Department of Commerce
Recommendation. The Assistant Administrator for the National Oceanic and Atmospheric Administration Fisheries should develop a mechanism to track the progress of states, tribes, and territories in meeting timelines established in spend plans to disburse funds in an expedited and efficient manner (January 2021 report).
Status: Open
Comment: As of February 1, 2021, the agency had developed an electronic tracking tool to track the disbursement of funds and had begun to input data into it based on approved spend plans. The agency plans to update these data on a weekly basis as funds are disbursed. The agency anticipates that all current and relevant data will be input into the tracking tool by May 2021 and that data will continue to be added to it until all funding has been disbursed.
Status of matter for congressional consideration regarding the Social Security Administration
Matter. To provide agencies access to the Social Security Administration’s more complete set of death data, we urge Congress to provide Treasury with access to the Social Security Administration’s full set of death records, and to require that Treasury consistently use it (June 2020 report).
Status: Closed
Comments: In December 2020, Congress passed and the President signed into law the Consolidated Appropriations Act, 2021, which requires the Social Security Administration, to the extent feasible, to share its full death data with Treasury’s Do Not Pay working system for a 3-year period, effective the date that is 3 years from enactment of this Act. Sharing this data will allow agencies to enhance their efforts to identify and prevent improper payments to deceased individuals. Therefore, it will be important for the Social Security Administration and Treasury to work together to implement this legislation.
Status of matter for congressional consideration regarding to the Department of Transportation
Matter. We urge Congress to take legislative action to require the Secretary of Transportation to work with relevant agencies and stakeholders, such as HHS and DHS, and members of the aviation and public health sectors, to develop a national aviation preparedness plan to ensure safeguards are in place to limit the spread of communicable disease threats from abroad while at the same time minimizing any unnecessary interference with travel and trade (June 2020 report).
Status: Open
Comment: In May 2020, the House of Representatives passed H.R. 6800, referred to as the HEROES Act, which would require the Department of Transportation, in coordination with HHS, DHS, and other appropriate federal departments and agencies, to develop a national aviation preparedness plan. Most recently, in September 2020, the Senate passed S. 3681, Ensuring Health Safety in the Skies Act of 2020, which would require HHS, DHS, and the Department of Transportation to form a joint task force on air travel during and after the COVID-19 public health emergency, among other provisions. Also, in October 2020, H.R. 8712, National Aviation Preparedness Plan Act of 2020, was introduced. If enacted, this bill would require the Department of Transportation, in collaboration with DHS, HHS, and other aviation stakeholders, to develop a national plan to prepare the aviation industry for future communicable disease outbreaks. Members of the House and Senate announced that they would reintroduce similar bills in the new Congress. For example, in February 2021, H.R. 884 introduced the National Aviation Preparedness Plan of 2021.
We again urge Congress to take swift action to require a national aviation preparedness plan, without which the U.S. will not be as prepared to minimize and quickly respond to ongoing and future communicable disease events.
Status of matter for congressional consideration regarding future COVID-19 relief funds
Matter. In November 2020, we urged Congress to consider, in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” (November 2020 report).
Status: Open
Comment: No new legislation designating executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” has been enacted to date.
Appendix IV: Comments from the Department of Education
Governmentwide Treasury Account Symbol Adjusted Trial Balance System
HHS
Department of Health and Human Services
IRS
Internal Revenue Service
NIA
National Interest Action
OIG
Office of Inspector General
OMB
Office of Management and Budget
OSHA
Occupational Safety and Health Administration
PPE
personal protective equipment
PPP
Paycheck Protection Program
PRF
Provider Relief Fund
PUA
Pandemic Unemployment Assistance
SBA
Small Business Administration
SNAP
Supplemental Nutrition Assistance Program
SNS
Strategic National Stockpile
Treasury
Department of the Treasury
TSA
Transportation Security Administration
UI
unemployment insurance
USDA
U.S. Department of Agriculture
VA
Department of Veterans Affairs
End Notes
[1]On January 31, 2020, the Secretary of Health and Human Services declared a public health emergency for the U.S., retroactive to January 27. Subsequently, on March 13, 2020, the President declared COVID-19 a national emergency under the National Emergencies Act and a nationwide emergency under section 501(b) of the Robert T. Stafford Disaster Relief and Emergency Assistance Act (Stafford Act). The President has also approved major disaster declarations under the Stafford Act for all 50 states, the District of Columbia, and five territories.
[2]Worldwide data from the World Health Organization reflect laboratory-confirmed cases and deaths reported by countries and areas. Data on COVID-19 cases in the U.S. are based on aggregate case reporting to the Centers for Disease Control and Prevention (CDC) and include probable and confirmed cases as reported by states and jurisdictions. CDC COVID-19 counts are subject to change due to delays or updates in reported data from states and territories. According to CDC, the actual number of COVID-19 cases is unknown for a variety of reasons, including that people who have been infected may have not been tested or may have not sought medical care. CDC’s National Center for Health Statistics COVID-19 death counts in the U.S. are based on provisional counts from death certificate data, which do not distinguish between laboratory-confirmed and probable COVID-19 deaths. Provisional counts are incomplete due to an average delay of 2 weeks (a range of 1–8 weeks or longer) for death certificate processing. The data were accessed on March 23, 2021. Data include deaths occurring from January 2020 through the week ending on March 13, 2021.
[3]Bureau of Labor Statistics, Unemployment Level (UNEMPLOY), retrieved from FRED, Federal Reserve Bank of St. Louis, accessed March 17, 2021, https://fred.stlouisfed.org/series/UNEMPLOY.
[4]Pub. L. No. 116-136, 134 Stat. 281 (2020). As of March 11, 2021, five other relief laws were also enacted in response to the COVID-19 pandemic: the American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4; the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146. In this report, we refer to these six laws, each of which was enacted as of March 11, 2021, and provides appropriations for the COVID-19 response, as “COVID-19 relief laws,” and the funding appropriated by these laws as “COVID-19 relief funds.”
[5]Pub. L. No. 116-136, § 19010, 134 Stat. at 579-81.
[6]COVID-19:Critical Vaccine Distribution, Supply Chain, Program Integrity, and Other Challenges Require Focused Federal Attention, GAO-21-265 (Washington, D.C.: Jan. 28, 2021); COVID-19: Urgent Actions Needed to Better Ensure an Effective Federal Response, GAO-21-191 (Washington, D.C.: Nov. 30, 2020); COVID-19: Federal Efforts Accelerate Vaccine and Therapeutics Development, but More Clarity Needed, GAO-21-207 (Washington D.C.: Nov. 17, 2020); COVID-19: Federal Efforts Could Be Strengthened by Timely and Concerted Actions, GAO-20-701 (Washington, D.C.: Sept. 21, 2020); COVID-19: Brief Update on Initial Federal Response to the Pandemic, GAO-20-708 (Washington, D.C.: Aug. 31, 2020); and COVID-19: Opportunities to Improve Federal Response and Recovery Efforts, GAO-20-625 (Washington, D.C.: June 25, 2020).
[8]CDC COVID-19 counts are subject to change due to delays or updates in reported data from states and territories. We compared the relative difference between the average of new cases between February 25 and March 10, 2021 and the average number of new cases in the 14-day windows around the peaks in the summer of 2020 and the winter of 2021.
[9]The 52 states and jurisdictions include all 50 states, Washington, D.C., and New York City. COVID-19 case counts for New York City are reported separately from New York State. One state was then excluded due to unstable data. We defined states as holding steady if they had less than a 1 percent increase or decrease in average daily new cases over the time frame. The average percent change in daily new cases was calculated as the average of the daily rates of change of the 7-day moving average between February 25, 2021, and March 10, 2021. CDC COVID Data Tracker data were accessed on March 15, 2021. These COVID-19 case counts may change as new or updated data are reported by states.
[10]Pfizer’s two-dose COVID-19 vaccine was authorized for emergency use on December 11, 2020, and Moderna’s two-dose COVID-19 vaccine was authorized on December 18, 2020. Janssen’s (Johnson & Johnson) one-dose COVID-19 vaccine was authorized for emergency use on February 27, 2021.
[11]The employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population age 16 and over. The ratio is subject to misclassification errors with respect to consistently identifying workers as employed and absent from work or unemployed on temporary layoff.
[12]An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes.
[13]An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of the other party beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. Increased spending in Medicaid is not accounted for in the appropriations provided by the COVID-19 relief laws. Federal agencies use GTAS to report proprietary financial reporting and budgetary execution information to Treasury.
[14]The Small Business Administration’s Business Loan Program account includes activity for the Paycheck Protection Program and certain loan subsidies.
[15]GAO, High Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas, GAO-21-119SP (Washington, D.C.: Mar. 2, 2021). GAO’s High-Risk Series identifies government operations with vulnerabilities to fraud, waste, abuse, and mismanagement, or in need of transformation to address economy, efficiency, or effectiveness challenges.
[16]See 42 U.S.C. § 247d-6b. The U.S. Government COVID-19 Response Plan (PanCAP Adapted) identifies HHS as the lead federal agency for the COVID-19 response, with support from the Federal Emergency Management Agency (FEMA), within the Department of Homeland Security (DHS), for coordination. However, in March 2020, leadership for the overall federal response shifted to FEMA, including responsibility for the acquisition and distribution of supplies in conjunction with HHS. At the outset of the COVID-19 pandemic, the SNS was a critical resource to states for needed and scarce medical supplies.
[21]Pub. L. No. 117-2, tit. II, § 2401, 135 Stat. at 40.
[22]High-risk devices generally require FDA premarket review and approval to determine whether the device meets the statutory standard of reasonable assurance of safety and effectiveness for its intended use. Moderate-risk and some lower-risk devices may require premarket notification—also known as 510(k) clearance—whereby they demonstrate that the new device is substantially equivalent to a legally marketed predicate device. Certain low-risk devices are exempt from the 510(k) clearance process, but the manufacturer must still register with FDA. Novel devices that are low to moderate risk but are not substantially equivalent to a legally marketed predicate device must be authorized through the De Novo classification process.
[23]Among other statutory criteria, the threat must be capable of causing a serious or life-threatening disease or condition, and it must be reasonable to believe, based on the totality of scientific evidence available, that the product may be effective in diagnosing, treating, or preventing the disease or condition and that the known and potential benefits of the product outweigh the known and potential risks. In addition, there must be no adequate, approved, and available alternatives to the product. 21 U.S.C. § 360bbb-3(c).
[24]DOL’s Occupational Safety and Health Administration (OSHA) helps ensure safe and healthy conditions for workers by setting mandatory workplace safety and health standards and conducting inspections to enforce those standards. In response to the COVID-19 pandemic, OSHA has issued industry-specific voluntary guidance for employers on COVID-19-related precautions, as well as other actions.
[25]The Secretary of Health and Human Services issued three EUA declarations for medical devices for COVID-19—on February 4, 2020, regarding in-vitro diagnostic devices for detection or diagnosis of COVID-19; on March 2, 2020, related to personal respiratory protective devices for COVID-19; and on March 24, 2020, for medical devices including alternative products used as medical devices during the COVID-19 pandemic. EUAs remain in effect until the EUA declaration under which the EUA was issued terminates or the EUA is revoked, whichever is earlier. At the time of our review, the Secretary had not indicated when the relevant EUA declarations would terminate, according to FDA officials.
[26]In this report, we refer to the HHS’s Health Resources and Services Administration COVID-19 Claims Reimbursement to Health Care Providers and Facilities for Testing, Treatment, and Vaccine Administration for the Uninsured Program as the “COVID-19 Uninsured Program.”
[27]The Office of Management and Budget Circular No. A-123, Management’s Responsibility for Enterprise Risk Management and Internal Control, requires executive agencies to evaluate the risks to accomplishing their strategic, operations, reporting, and compliance objectives and provide an annual Statement of Assurance that represents the agency head’s informed judgment as to the overall adequacy and effectiveness of the agency’s internal control. Accordingly, HHS’s Health Resources and Services Administration developed an A-123 risk assessment to identify and assess COVID-19 Uninsured Program risks and identify internal control activities in response to such risks as of September 30, 2020.
[28]SNAP provides low-income individuals and households with benefits to purchase allowed food items and achieve a more nutritious diet.
[29]The Disaster Relief Fund receives an annual appropriation and has routinely received supplemental appropriations.
[30]We have previously reported on the administrative challenges tribal nations have faced in the past when requesting federal assistance for a major disaster or emergency.
[31]Letter to Senators Mitch McConnell and Chuck Schumer on COVID-19 recovery legislative proposals (phase 4), May 26, 2020. The following tribal associations signed the letter: the Association on American Indian Affairs, the Inter-Tribal Emergency Management Coalition of Oklahoma, National Congress of American Indians, National Tribal Emergency Management Coalition, North West Tribal Emergency Management Council, Montana Tribal Emergency Management Council, Tribal Emergency Management Association, and United South and Eastern Tribes Sovereignty Protection Fund.
[32]FEMA Policy Number 101-002-02, Tribal Consultation Policy, July 2019.
[33]In this report we refer to State Educational Agencies as states and Local Educational Agencies as school districts. These include the State Educational Agencies and Local Educational Agencies in the District of Columbia and Puerto Rico, as well as the U.S. Virgin Islands, Guam, the Commonwealth of the Northern Mariana Islands, and American Samoa.
[34]CARES Act, Pub. L. No. 116-136, § 2201, 134 Stat. at 335–40; Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, § 272, 134 Stat. at 1965–76.
[35]Pub. L. No. 117-2, § 9601, 135 Stat. at 138–44.
[36]The Consolidated Appropriations Act, 2021, appropriated additional funding for certain EIDL advances and amended the CARES Act requirements related to loans and advances, including advances targeted at businesses in low-income communities. Pub. L. No. 116-260, div. N, tit. III, §§ 331-32, 134 Stat. at 2043-46. The act also authorized additional PPP loans and allowed additional businesses to receive the loans, expanded the list of allowable uses of proceeds and for loan forgiveness, and allowed PPP borrowers to receive a second PPP loan of up to $2 million upon meeting certain criteria. Pub. L. No. 116-260, div. N, tit. III, §§ 301-23, 134 Stat. at 1993-2022.
[37]The American Rescue Plan Act of 2021 appropriated an additional $10 billion for eligible entities that have not received the full amount of $10,000 in targeted EIDL advances. The act also appropriated $5 billion to provide an additional $5,000 for eligible entities in low-income communities that suffered economic loss of greater than 50 percent and employ not more than 10 employees. The $5,000 is available in addition to advances obtained under the CARES Act or targeted advances under the Consolidated Appropriations Act, 2021. Pub. L. No. 117-2, § 5002, 135 Stat. at 85.
[38]Other discrepancies include loans and grants issued to borrowers with inaccurate or invalid tax identification numbers, employer identification numbers, or Social Security numbers; loans issued that SBA flagged as potentially fraudulent; and loans issued to borrowers that SBA flagged because the borrowers were excluded from doing business with the government.
[39]GAO’s Standards for Internal Control in the Federal Government provides the overall framework for establishing and maintaining an effective internal control system, and it lists five components of internal control representing the highest level of the hierarchy of standards for internal control in the federal government. The five components of internal control are (1) control environment, (2) risk assessment, (3) control activities, (4) information and communication, and (5) monitoring. The five components of internal control must be effectively designed, implemented, and operating, and operating together in an integrated manner, for an internal control system to be effective. GAO, Standards for Internal Control in the Federal Government, GAO-14-704G (Washington, D.C.: Sept. 10, 2014).
[40]Federal charges refer to criminal complaints and indictments. A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[41]We accessed the PUA overpayments data on March 15, 2021; these data are subject to change as more states report data and states revise previously reported data. The number of states that have reported PUA overpayments data varies by month; for example, 1 state reported overpayment amounts in March 2020, 15 states reported overpayment amounts in April 2020, 35 states reported overpayment amounts in January 2021, and 7 states reported overpayment amounts in February 2021. Among the states reporting data, we identified wide variation in the amount of PUA overpayments reported in any given month.
[42]According to the Consolidated Appropriations Act, 2021, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount, but the state can waive that requirement if the individual was without fault and repayment would be contrary to equity and good conscience. Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182 at 1952.
[43]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing OMB guidance is reprinted in 2 C.F.R. Part 200 (2020). Non-federal entities (states, U.S. territory and tribal governments, local governments, or nonprofit organizations) that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit, which is an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[44]For example, the CARES Act appropriated $100 billion to the fund to reimburse eligible providers (including for-profit providers) for health-care-related expenses or lost revenue attributable to the COVID-19 pandemic, known as the Provider Relief Fund. Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. at 563. The Paycheck Protection Program and Health Care Enhancement Act added an additional $75 billion to the fund, and the Consolidated Appropriations Act, 2021, added another $3 billion to the fund. Pub. L. No. 116-139, div. B, tit. I, 134 Stat. at 622-23; Pub. L. No. 116-260, div. M, tit. III, 134 Stat. at 1920-21. Pursuant to single audit regulations issued by HHS, which manages the Provider Relief Fund, for-profit recipients (which do not meet the statutory definition of non-federal entities and are thus not subject to the Single Audit Act) that receive $750,000 or more in annual aggregated HHS awards (including Provider Relief Fund payments) during their fiscal year must undergo (1) an audit in conformance with single audit requirements or (2) a financial related audit of the applicable award(s) in accordance with Generally Accepted Government Auditing Standards. 45 C.F.R. §§ 75.216, 75.501.
[45]The Compliance Supplement provides guidance for auditors that conduct single audits and identifies important compliance requirements.
[46]Families First Coronavirus Response Act, Pub. L. No. 116-127, § 7001-05, 134 Stat. at 210–19; CARES Act, Pub. L. No. 116-136, div. A, § 3606, 134 Stat. at 411–12; Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. N, § 286, 134 Stat. at 1989–91.
[47]Form 941—Employer’s Quarterly Federal Tax Return—asks for employee counts as of a specific pay period in the quarter, and Form 943—Employer’s Annual Federal Tax Return for Agricultural Employees—has a similar line that asks for employee counts as of the pay period that includes March 12, 2020. However, eligibility for leave credits is determined by employee counts on the dates that the employees took leave. For example, for the second quarter, employers are instructed to report as of June 12.
[49]The Data Strategy and Execution Workgroup began publishing the daily COVID-19 Community Profile Report in December 2020. These reports are available online at: https://beta.healthdata.gov/National/COVID-19-Community-Profile-Report/gqxm-d9w9 (accessed Mar. 12, 2021). This Workgroup, which is managed by an interagency team with representatives from several agencies and offices including HHS and CDC, also makes available similar information through its State Profile Reports, which HHS began publishing on January 27, 2021. These reports are available online at: https://beta.healthdata.gov/browse?tags=covid-19-spr (accessed Mar. 15, 2021).
[50]The test positivity rate, also known as the percentage of positive COVID-19 test results, is calculated as the number of positive tests divided by the number of tests performed and resulted.
[51]We have not assessed the reliability of these data. As stated in the Community Profile Report, test positivity rate is based on viral (RT--PCR) laboratory tests. Data on tests are reported by states as well as directly by clinical laboratories. Some states do not report on certain days, which may affect the total number of tests resulted and positivity rate values. Data on cases are aggregated by CDC from data reported by state and local health departments. Most states and localities report both confirmed and probable cases, although some report just confirmed cases. Hospital data are reported to HHS either directly from facilities or via a state submission. Due to inconsistent reporting and data errors, these data may not represent the true number of admissions.
[52]SVI further groups the 15 social factors into four related themes: socioeconomic status, household composition and disability, minority status and language, and housing type and transportation. Each county receives a ranking for each Census variable and for each of the four themes, as well as an overall ranking.
[54]In March 2021, CDC released a report based on its analysis of county-level COVID-19 vaccination rates by the SVI. CDC found that between December 14, 2020, and March 1, 2021, high social vulnerability counties had lower COVID-19 vaccination rates than did low social vulnerability counties. See Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, Vol. 70 (March 17, 2021).
[55]CDC’s Advisory Committee on Immunization Practices (ACIP) recommended priority groups for COVID-19 vaccination. The committee’s recommendations serve as public health guidance for safe use of vaccines and other related products and are not binding, as jurisdictions can adopt different approaches. See https://www.cdc.gov/vaccines/hcp/acip-recs/vacc-specific/covid-19.html (accessed Mar. 15, 2021) for ACIP’s current COVID-19 vaccine recommendations.
[56]As of March 7, 2021, the COVID Tracking Project no longer collects and publishes new COVID-19 data on its website. Representatives explained that they ended this work because they have more confidence in federal efforts to manage COVID-19 data.
[59]Ensuring a Data-Driven Response to COVID-19 and Future High-Consequence Public Health Threats, Exec. Order No. 13994, 86 Fed. Reg. 7,189 (January 21, 2021).
[60]We interviewed six experts and received written responses from four experts that we previously interviewed for our November and January reports. These experts included former leaders of federal agencies, including the Centers for Disease Control and Prevention, Food and Drug Administration, and Centers for Medicare & Medicaid Services.
[61]We identified a number of economic indicators to facilitate ongoing and consistent monitoring of areas of the economy supported by the federal pandemic response. To the extent that federal pandemic responses are effective, we would expect to see improvements in outcomes related to these indicators. However, while trends in these indicators may be suggestive of the effect of provisions of the COVID-19 relief laws over time, those trends will not on their own provide definitive evidence of their effectiveness.
[62]See Daniel J. Lewis, Karel Mertens, and Jim Stock, U.S. Economic Activity during the Early Weeks of the SARS-Cov-2 Outbreak, Federal Reserve Bank of New York Staff Report No. 920 (April 2020). The index value of the Weekly Economic Index corresponds to a year-over-year growth rate in gross domestic product were conditions to remain at that value for a full quarter.
[63]For Covid-19 relief provisions, see American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4; Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[64]The 3-month Treasury interest rate is the constant maturity rate from the Federal Reserve’s H.15 Selected Interest Rates release.
[65]See GAO, The Nation’s Fiscal Health: Action Is Needed to Address the Federal Government's Fiscal Future, GAO-20-403SP (Washington, D.C.: Mar. 12, 2020).
[66]The S&P/Experian Consumer Credit Default Composite Index measures the proportion of consumer credit account balances that enter default across auto loans, first and second mortgages, and bank cards each month.
[67]The CARES Act provided temporary protections for millions of households against foreclosure and eviction, as well as temporary forbearance, suspending mortgage payments for up to 360 days. In addition, the CARES Act includes a provision (section 4021) to protect the credit of consumers who reach an agreement with their lenders to delay or otherwise modify payments because of the COVID-19 pandemic.
[68]In fiscal year 2020, for example, 34.2 percent of all FHA purchase and refinance borrowers were minorities, 50.4 percent of FHA forward mortgage borrowers were of low-to-moderate income, and 83.1 percent of home purchasers under the FHA forward mortgage insurance program were first-time homebuyers. See U.S. Department of Housing and Urban Development, FHA Annual Management Report Fiscal Year 2020.
[69]The Small Business Health Index combines information on the timeliness of payments, failure rates, and utilization of credit for a sample of over 10 million active small businesses with fewer than 100 employees. The Small Business Health Index is published under license and permission from Dun & Bradstreet and no commercial use can be made of these data.
[70]We excluded Paycheck Protection Program (PPP) loans to businesses from non-farm proprietors’ income. When including PPP loans, small business income began increasing in May 2020, exceeded the pre-pandemic levels from August through October, fell rapidly in November and December 2020, and remained lower than pre-pandemic levels as of January 2021.
[71]Survey data from the Senior Loan Officer Opinion Survey, conducted by the Board of Governors of the Federal Reserve System quarterly.
[72]Spreads on corporate bonds relative to benchmark interest rates (e.g., Treasury interest rates) measure the premium corporate borrowers must pay to compensate lenders for taking on the risk of loss due to default (risk premium) and for foregoing investments in more liquid assets (liquidity premium).
[73] See Quarterly Summary of State and Local Tax Revenues, Census Bureau. We use seasonally adjusted data to compare changes in tax revenues from quarter to quarter. State and local governments also faced disruptions in the timing of revenue collections. For example, most states extended their individual income tax filing deadlines to match the federal government’s shift in the deadline for filing federal income tax returns from April 15 to July 15. It is not clear how much of the second quarter decline or third quarter increase can be attributed to the delayed tax filing deadline.
[74]Spreads on municipal bonds relative to benchmark interest rates (e.g., Treasury interest rates) incorporate thefavorable tax treatment received by municipal debt and may also reflect any premium state and local borrowers pay to compensate lenders for taking on the risk of loss due to default (risk premium) and for tying up their investment funds for a period of time (liquidity premium). We report spreads calculated based on the Bloomberg Barclays Municipal Bond Index. Spreads are calculated using yield to worst, which results in a conservative—that is, lower—estimate of potential returns on callable bonds.
[75]State and local government expenditure data are from the Bureau of Economic Analysis National Income and Product Accounts, Table 3.3.
[76]Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1920 (2020); Pub. L. No. 116-139, div. B, tit. I, 134 Stat. 620, 622 (2020); Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 563 (2020).Additionally, the American Rescue Plan Act of 2021, signed into law on March 11, 2021, appropriated $8.5 billion for payments to eligible rural health care providers for health care-related expenses and lost revenues that are attributable to COVID–19. Pub. L. No. 117-2, § 9911, 135 Stat. 4, 236-38.
[77]The Accelerated Payments Program provides loans to Part A providers and the Advance Payments Program provides loans to Part B suppliers.
[78]HHS uses the term “allocations” to describe the funding amounts it has set aside for particular purposes or for particular types of health care providers.
[79]The Consolidated Appropriations Act, 2021, provided that not less than 85 percent of Provider Relief Fund funds unobligated as of the date of enactment and funds recovered from providers after the date of enactment shall be for any successor to the Phase 3 General Distribution to reimburse health care providers based on applications that consider financial losses and changes in operating expenses attributable to COVID-19 occurring in the third and fourth quarters of 2020 and the first quarter of 2021.
[80]In addition to the allocation from the Provider Relief Fund for treatment and vaccine administration of uninsured individuals, the Families First Coronavirus Response Act and the Paycheck Protection Program and Health Care Enhancement Act each appropriated $1 billion to reimburse providers for the testing of uninsured individuals. Pub. L. No. 116-127, div. A, tit. V, 134 Stat.178, 182 (2020); Pub. L. No. 116-139, div. B., tit. I, 134 Stat.at 626 (2020). These funds are also administered by HRSA as part of the COVID-19 Uninsured Program. According to HRSA officials, these funds have been depleted; therefore, HRSA will continue to reimburse COVID-19 testing claims to the COVID-19 Uninsured Program using Provider Relief Fund funding.
[81]The Office of Management and Budget (OMB) Circular No. A-123, Management’s Responsibility for Enterprise Risk Management and Internal Control, requires executive agencies to evaluate the risks to accomplishing their strategic, operations, reporting, and compliance objectives and provide an annual Statement of Assurance that represents the agency head’s informed judgment as to the overall adequacy and effectiveness of the agency’s internal control. Accordingly, HRSA developed an A-123 risk assessment to identify and assess COVID-19 Uninsured Program risks and identify internal control activities in response to such risks as of September 30, 2020.
[82]GAO, Standards for Internal Control in the Federal Government, GAO-14-704G (Washington, D.C.: September 10, 2014).
[83]Single Audit Act, codified, as amended, at 31 U.S.C. §§ 7501 - 7506, and implementing OMB guidance reprinted in 2 C.F.R. part 200, Uniform Administrative Requirements, Cost Principles, and Audit Requirements for Federal Awards. Federal award recipients that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit, which is an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501. HHS has implemented OMB’s Single Audit Act guidance at 45 C.F.R. part 75, Uniform Administrative Requirements, Cost Principles, and Audit Requirements for HHS Awards.See, e.g., 45 C.F.R. § 75.501.
[84]For-Profit reporting entities that received $750,000 or more in annual aggregated HHS awards (including Provider Relief Fund payments) during their fiscal year are subject to audit requirements, as set forth in HHS’s single audit regulations at 45 C.F.R. §§ 75.216, 75.501.
[85]According to HHS guidance, HHS executed agreements with all Provider Relief Fund recipients (regardless of whether they are subject to the Single Audit Act) that included a set of terms and conditions that included special requirements regarding submitting reports related to the Provider Relief Fund to HHS consistent with applicable HHS reporting instructions. HHS most recently issued guidance providing instructions on these special reporting requirements in January 2021. That guidance stated that Provider Relief Fund recipients must report whether they are subject to single audit requirements during the current fiscal year, and, if yes, whether the auditors selected Provider Relief Fund payments to be within the scope of the single audit (if known at the time the recipient submits its report). According to OMB’s Compliance Supplement Addendum, auditors should test compliance with these special reporting requirements for audits of Provider Relief Fund recipients with fiscal years ending on or after December 31, 2020.
[87]MITRE, Coronavirus Commission on Safety and Quality in Nursing Homes: Commission Final Report, PRS Release Number 20-2382, September 2020.
[88]COVID-19 has affected vulnerable populations in other settings beyond nursing homes, including assisted living facilities. However, as the federal role in oversight of nursing homes is more significant than in other settings such as assisted living facilities, the federal response has been more focused on nursing homes.
[90]According to CMS, as of September 30, 2020, it obligated almost $19 million. In fiscal year 2021, the agency indicated it plans to obligate about $28 million.
[91]Additionally, the American Rescue Plan Act of 2021 appropriated $250 million for the creation of state strike teams that will be deployed to nursing facilities with diagnosed or suspected cases of COVID–19 among residents or staff for the purposes of assisting with clinical care, infection control, or staffing during the COVID-19 emergency period and the following year. Pub. L. No. 117-2, § 9818, 135 Stat. 4, 218.
[92]Specifically, the CARES Act appropriated $100 billion, the Paycheck Protection Program and Health Care Enhancement Act appropriated $75 billion, and the Consolidated Appropriations Act, 2021, appropriated $3 billion for this purpose. Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1920 (2020); Pub. L. No. 116-139, div. B, tit. I, 134 Stat. 620, 622 (2020); Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 563 (2020).
[93]As part of the program, vaccines will be provided with no out-of-pocket costs for residents or staff, or costs to the facilities. The pharmacy partners—including CVS, Walgreens, and Managed Health Care Associates Inc.—will schedule and coordinate on-site vaccination clinic dates; order vaccines and associated supplies; ensure cold chain management for the vaccine; provide on-site administration; report required vaccination data to local, state, and federal jurisdictions; and adhere to all applicable CMS COVID-19 testing requirements for facility staff.
[94]CDC defines a confirmed case as having a positive COVID-19 test resulting from a molecular test, a nucleic acid test, or an antigen test, including antigen point-of-care test results.
[95]These numbers are likely underreported because they do not include data for the 998 nursing homes (6.5 percent) that did not report COVID-19 data to CDC for the week ending February 7, 2021, or that submitted data that failed data quality assurance checks. The week ending May 31, 2020, is the first single week of data reported to CDC. The only earlier week of data, for the week ending May 24, could potentially include cases and deaths for multiple weeks dating back to January 1, 2020, for those homes which voluntarily reported such data, and is therefore not comparable with data for other weeks. According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time. Data presented in this enclosure reflect the data downloaded as of February 18, 2021, which includes data through the week ending February 7, 2021.
[96]Through the Pharmacy Partnership for Long-Term Care Program, partner pharmacies conduct three, temporary, on-site vaccination clinics per enrolled facility for nursing home residents and staff.
[97]Other challenges mentioned by officials from two nursing home associations include initial scheduling and coordination challenges between nursing home facilities and pharmacy partners, as well as shortages in pharmacy staff to conduct the vaccination clinics.
[98]Allocation of COVID-19 doses was originally done based in direct proportion to the nation's adult population 18 years and older. States and jurisdictions order against weekly allocations provided by CDC. States determine the number of doses to direct to the pharmacy partnership from their weekly allocations.
[99]CDC also notes that pharmacy partners will work with long-term care facilities to ensure that staff and residents who receive the vaccine also receive an emergency use authorization fact sheet. Under the terms of the COVID-19 vaccine emergency use authorizations issued as of January 31, 2021, vaccine providers must inform recipients or their caregivers that the vaccine is not approved by FDA but has been authorized for emergency use and that the recipient or their caregiver has the option to accept or refuse the vaccine, among other things.
[100]According to a recent CDC analysis, during the first month of the Pharmacy Partnership for Long-Term Care Program, an estimated median of 77.8 percent of residents and an estimated median of 37.5 percent of staff members per facility received a dose of COVID-19 vaccine at the first vaccination clinics. See R. Gharpure et al., “Early COVID-19 First-Dose Vaccination Coverage Among Residents and Staff Members of Skilled Nursing Facilities Participating in the Pharmacy Partnership for Long-Term Care Program—United States, December 2020-January 2021,” Centers for Disease Control and Prevention Morbidity and Mortality Weekly Report, vol. 70 (Feb. 1, 2021). Anecdotally, officials from one nursing home association said take-up rates for staff have improved for facilities that have completed their second clinics.
[101]The remaining doses were administered in other long-term care settings, such as assisted living facilities. According to CDC’s vaccine distribution and administration tracking website, doses administered refers to vaccine administered to long-term care facility residents and staff, as reported to CDC by the pharmacy partners participating in the Pharmacy Partnership for Long-Term Care Program. These data do not include doses administered to long-term care facility residents and staff outside this partnership. As of January 4, 2021, a total of 54 out of 64 jurisdictions have started the program. Program start dates varied based on the jurisdiction. The 64 jurisdictions include all U.S. states and territories and some local health programs.
[102]According to CDC, some jurisdictions have requested that pharmacy partners do not initiate first dose vaccinations to residents and staff at the third—and final—clinics, due to their future plans to vaccinate nursing home residents and staff using a different vaccine product. This may hinder vaccination take-up rates on the part of staff members who did not get the vaccine at previous clinics but are now wanting the vaccine after seeing colleagues and others get the vaccine without complications.
[103]Certain individual nursing homes are receiving their vaccinations outside of the Pharmacy Partnership for Long-Term Care Program. Facilities were not required to participate in the program and could opt to have vaccine supply and management services coordinated by a pharmacy provider of its choice. According to HHS, 2 percent (374 out of 15,727) of nursing homes chose not to enroll in the program.
[104]COVID-19 vaccine administrators are expected to report certain administration data to state information systems, which are subsequently submitted to CDC. As a result, CDC does report data on vaccines administered in West Virginia overall, but not for long-term care facilities specifically.
[105]According to a state press release, pharmacies in West Virginia administered about 28,000 first doses of the vaccine to residents and staff members in about 210 long-term care facilities.
[106]According to CDC, as of February 17, 2021, more than 2,200 nursing homes (around 14 percent) are voluntarily reporting staff vaccination data and over 2,800 nursing homes (around 18 percent) are voluntarily reporting resident vaccination data.
[107]In addition to nursing homes, long-term care facilities include assisted living facilities, continuing care retirement communities, adult family homes, intermediate care facilities for individuals with developmental disabilities, and other congregate living settings where most individuals receiving care or supervision are older than 65 years of age.
[109]Our January report covered data nursing homes self-reported to CDC as of December 6, 2020.
[110]According to CDC, aides include certified nursing assistants, nurse aides, medication aides, and medication technicians; nursing staff include registered nurses, licensed practical nurses, and vocational nurses; clinical staff include physicians, physician assistants, and advanced practice nurses; and other staff include any staff not included in the other three categories, such as cooks, pharmacists, and physical therapists.
[111]A report released in October 2020 by the HHS Assistant Secretary for Policy and Evaluation also found that nursing home staffing shortages and attrition have further strained nursing homes during the pandemic. The report found that in response to challenging working conditions, and the high risk of COVID-19 infection, some nurses and nurse aides are leaving the nursing home sector during this critical time when there is an increased demand for their skills and expertise.
[112]On March 30, 2020 CMS announced that the agency is waiving the requirements at 42 C.F.R. § 483.35(d) (with the exception of 42 C.F.R. § 483.35(d)(1)(i)), which require that a skilled nursing facility or nursing facility not employ anyone working as a nurse aide for longer than four months unless they met the training and certification requirements under section 483.35(d).
[113]We analyzed the most recent data available on February 18, 2021. The CDC data on COVID-19 in nursing homes were accessed on February 18, 2021, for the week ending February 7, 2021, from https://data.cms.gov/Covid19-nursing-home-data. For the data on COVID-19 in nursing homes, we analyzed and reported data that had been determined by CDC and CMS to pass quality assurance checks for data entry errors. According to CDC, data used in this analysis are part of a live data set, meaning that facilities can make corrections to the data at any time.
[114]We also recommended in September 2020 that (1) HHS and FEMA immediately document roles and responsibilities for supply chain management functions transitioning to HHS, and (2) HHS and FEMA work with relevant stakeholders to devise interim solutions to help states enhance their ability to track the status of supply requests and plan for supply needs. HHS and the Department of Homeland Security disagreed with these recommendations.
[115]Our review was based on a draft of the strategy, which the Office of the Assistant Secretary for Preparedness and Response had been in the process of finalizing, as of January 13, 2021.
[116]Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, Pub. L. No. 116-22, § 403(a)(5), 133 Stat. 905, 946-47; CARES Act, Pub. L. No. 116-136, § 19010, 134 Stat. 281, 579-81 (2020).
[118]See Department of Health and Human Services, U.S. Government COVID-19 Response Plan (PanCAP Adapted), March 13, 2020.
[119]Beginning in March 2020, state, tribal, and territorial governments unable to meet local PPE needs through the purchase of materials from the commercial market or other state-initiated efforts, could make a resource request to FEMA. According to ASPR and FEMA officials, responsibility for fulfilling the request for PPE first falls to FEMA and, if FEMA cannot provide the PPE, the request is assigned to others, such as to the SNS, to fulfill.
[120]As of March 11, 2021, the six relief laws enacted to assist the response to COVID-19 were the American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4; Consolidated Appropriations Act, 2021, Pub. L. No. 116-620, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[121]See Pub. L. No. 107-188, § 121, 116 Stat. 594, 611-13 (2002) (codified, as amended, at 42 U.S.C. § 247d-6b).
[122]See National Academies of Sciences, Engineering, and Medicine, The Nation’s Medical Countermeasures Stockpile: Opportunities to Improve the Efficiency, Effectiveness, and Sustainability of the CDC Strategic National Stockpile: Workshop Summary. Washington, D.C.: National Academies Press. 2016.
[124]ASPR distributed SNS supplies in three separate allocations. In each of the first and second allocations, ASPR distributed 25 percent of available SNS supplies to 62 areas across all 50 states, four large metropolitan areas, and the eight territories and freely associated states, according to ASPR officials. In the last substantial distribution of supplies from the SNS—based on a decision made by the Unified Coordination Group—ASPR provided most of the remaining SNS inventory to states, reserving 10 percent for federal health care and other responders.
[125]The PHEMCE—a federal interagency body led by ASPR—has made recommendations regarding research, development, procurement, stockpiling, deployment, distribution and utilization with respect to medical countermeasures. Medical countermeasures are drugs, biologics, and devices, such as personal protective equipment, used to diagnose, treat, prevent, or mitigate harm from any chemical, biological, radiological, and nuclear agent.
[126]Department of Homeland Security, Federal Emergency Management Agency, Pandemic Response to Coronavirus Disease 2019 (COVID-19): Initial Assessment Report (January 2021).
[127]Department of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response, Crimson Contagion 2019 Functional Exercise After-Action Report (January 2020). Crimson Contagion consisted of multiple meetings in 2019, which culminated in a four-day functional exercise held in August 2019.
[128] According to ASPR officials, the strategy—entitled “SNS 2.0 Strategy – Modernize the SNS”—was approved by the previous Assistant Secretary for Preparedness and Response in mid-January 2021, but has not been released publically. For more information on this strategy, please see our January 2021 CARES Act report.
[129]Exec. Order No.14,001, 86 Fed. Reg. 7,219 (Jan. 26, 2021).
[130]Consolidated Appropriations Act, 2021, Pub. L. No. 116-620, div. W, § 621(b), 134 Stat. at 2403-04.
[131]The six characteristics of an effective national strategy are: (1) clear purpose, scope, and methodology; (2) problem definition and risk assessment; (3) goals, subordinate objectives, activities, and performance measures; (4) resources, investments, and risk management; (5) organizational roles, responsibilities, and coordination; and (6) integration and implementation. Each characteristic has several sub-elements.
[132]See White House, National Strategy for the COVID-19 Response and Pandemic Preparedness, January 21, 2021.
[133]Pub. L. No. 116-139, div. B, tit. I, 134 Stat. at 626-27 (2020). For previous Testing Strategy reports, see Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (May 24, 2020); Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (August 22, 2020); and Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan (November 20, 2020).
[134]See White House, National Strategy for the COVID-19 Response and Pandemic Preparedness, January 21, 2021.
[136]In March 2020, Congress passed, and the President signed into law, the CARES Act, which provided over $2 trillion in emergency assistance and health care response for individuals, families, and businesses affected by COVID-19. Pub. L. No. 116-136, 134 Stat. 281 (2020). As of January 1, 2021, four other laws had been enacted that provide relief in response to the COVID-19 pandemic: Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[137]Specifically, as of February 28, 2021, HHS reported having obligated $5.4 billion (and having expended $3.1 billion) for general testing activities and having obligated $2.0 billion (and having expended roughly $2.0 billion) in funding for testing for the uninsured. Not included in the total obligated and expended amount for testing is funding for diagnostics research and development, of which $1.57 billion has been obligated (and $474 million has been expended), according to HHS.
[138]In addition to support for epidemiology, laboratory, and health information systems, ELC funding also supports disease-specific program areas. Established in 1995, the ELC program provides more than $200 million each year to 64 recipients, including all 50 states, six localities, and U.S. territories and affiliates. ELC-supported activities in each jurisdiction are overseen by an ELC Governance Team, with representation from epidemiology, laboratory, and health information systems. According to CDC, this structure has been successfully utilized by ELC recipients to manage activities and funding from special appropriations provided in response to a number of infectious disease emergencies, such as H1N1, Ebola, and Zika.
[139]To receive ELC funding made available under the CARES Act, ELC recipients were required, within 30 days of receiving a notice of award, to submit a work plan and budget describing proposed activities. To receive ELC funding made available under the Consolidated Appropriations Act, 2021, ELC recipients were required, within 60 days of receiving a notice of award, to submit and work plan and budget describing proposed activities. For more information on the ELC program and other funds for infectious disease preparedness, see GAO, Infectious Disease Threats: Funding and Performance of Key Preparedness and Capacity-Building Programs, GAO-18-362 (Washington, D.C.: May 24, 2018).
[140]American Rescue Plan Act of 2021, Pub. L. No. 117-2, tit. II, § 2401, 135 Stat. 4, 40.
[141]The Consolidated Appropriations Act, 2021, extended this period until the end of 2021. Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. at 2403 (2020).
[142]Furthermore, a public health stakeholder group has also identified preparedness concerns. For example, the National Association of County and City Health Officials published results from a 2019 survey of local health departments, indicating decreased workforce capacity, budget shortfalls, and decreased service provision before the pandemic. See National Association of County and City Health Officials, 2019 National Profile of Local Health Departments (Washington, D.C.: 2020), accessed February 11, 2021 from https://www.naccho.org/uploads/downloadable-resources/Programs/Public-Health-Infrastructure/NACCHO_2019_Profile_final.pdf.
[143]See our May 2018 work on Infectious Disease Threats. (See Related Products.) For this report, we reviewed ELC, CDC’s Hospital Preparedness Program, and the Assistant Secretary for Preparedness and Responses’ Public Health Emergency Preparedness cooperative agreement—HHS’s three key preparedness and capacity-building programs. While ELC is specific to infectious disease preparedness, the other two support “all-hazard” preparedness capacity, meaning they help build capacities to respond to a range of public health threats, including infectious diseases, natural disasters, or terrorist events. Our review found that combined awards from the three programs to jurisdictions decreased from about $1.4 billion in 2003 to about $1 billion in 2017; though awards through ELC—the smallest of the programs—increased from about $0.1 billion to $0.2 billion.
[144]American Rescue Plan Act of 2021, Pub. L. No. 117-2, tit. II, § 2401, 135 Stat. at 40. On March 17, 2021, HHS announced the availability of $10 billion in funds provided under the new law to states and territories to support COVID-19 testing for the reopening of schools.
[145]We interviewed state Medicaid officials in Georgia, Iowa, Louisiana, New Hampshire, New Jersey, New Mexico, Ohio, and Washington.
[146]Department of Health and Human Services, Centers for Medicare and Medicaid Services, 2018Actuarial Report on the Financial Outlook on Medicaid (Baltimore, Md.).
[147]The FMAP is calculated based on each state’s per capita income relative to national per capita income. For the District of Columbia and U.S. territories, the FMAP is set by statute regardless of their per capita incomes. Additionally, federal law specifies a maximum amount, or allotment, for federal contributions to Medicaid spending in U.S. territories, in contrast to the states and the District of Columbia, for which federal Medicaid spending is open-ended.
[150]Federal regulations provide states with an exception to meeting the timeliness standards for processing Medicaid applications and redeterminations caused by an administrative or other emergency beyond the agency’s control.
[151]The most recent available payment information is for the second quarter of fiscal year 2020 (January 1, 2020, through March 31, 2020) through the first two months of the second quarter of fiscal year 2021 (January 1, 2021, through February 28, 2021). States can report payments and adjustments to payments up to 2 years after a quarter ends. The increased FMAP is available for Medicaid medical assistance expenditures for which each state’s standard state-specific FMAP rate is used to determine federal funding.
[152]Three states and three territories that are approved to cover COVID-19 diagnostic testing and related services for uninsured individuals with a 100 percent federal match did not report COVID-19 expenditures for these individuals as of February 28, 2021.
[153]Department of Veterans Affairs, COVID-19 Vaccination Plan for the Veterans Health Administration, Version 2.0 (Washington, D.C.: Dec. 14, 2020).
[154]Veterans Integrated Service Networks are regional networks responsible for managing and overseeing VA medical centers.
[155]The integrated project team is a multi-disciplinary team comprised of stakeholders from across VHA, including those with clinical and operational expertise—e.g., representatives from pharmacy, nursing, office of community care, and labor and management relations.
[156]During an emergency, as declared by the Secretary of Health and Human Services under 21 U.S.C. § 360bbb-3(b), FDA may temporarily authorize unapproved medical products or unapproved uses of approved medical products through an emergency use authorization, provided certain statutory criteria are met. For example, an EUA request must include evidence that the vaccine may be effective and that the known and potential benefits outweigh the known and potential risks, among other requirements. (See our November 2020 report on vaccination EUAs. GAO-21-207)
[157]According to VA officials, it is updating its COVID-19 Vaccination Plan to reflect the EUA for the Janssen COVID-19 vaccine.
[158]Department of Veterans Affairs, Departmentof Veterans Affairs (VA) Guidance on COVID-19 Vaccine, (Washington, D.C.: Dec. 16, 2020).
[159]Department of Veterans Affairs, Updated: Departmentof Veterans Affairs Guidance on COVID-19 Vaccine, (Washington, D.C.: Dec. 23, 2020).
[160]VA primarily receives funding for all health care it provides or purchases through four separate accounts. The medical services account includes appropriations for health care services VA provides to eligible veterans, the medical community care account includes appropriations for services VA authorizes for veterans and other beneficiaries to receive in the community, the medical support and compliance account is used for medical and research activities, and the medical facilities account is used for operation and maintenance of VHA’s infrastructure.
[161]American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4.
[162]CDC’s guidance includes recommendations for prioritizing high-risk groups, such as health care personnel and individuals 75 and older, to receive vaccine doses first. CDC’s vaccine guidance allows for flexibility as a way to ensure equitable administration of vaccine doses. For example, agencies can decide to further prioritize within a particular phase.
[164]According to FDA, the Pfizer vaccine must be stored in ultra-cold conditions between -112 and -76 degrees Fahrenheit, and the two doses should be separated by three weeks.
[165]According to FDA, the Moderna vaccine must be stored frozen between -13 and 5 degrees Fahrenheit, and the two doses should be separated by 1 month.
[166]CDC defines essential workers as those individuals who conduct a range of operations and services in industries that are essential to ensure the continuity of critical functions in the United States. Examples of Phase 1b essential workers include grocery store workers, postal workers, and public transit workers.
[167]VA guidance requires that second dose appointments are scheduled at the time of the first dose administration.
[169]The VHA COVID-19 Vaccine Communications Workgroup is responsible for communications products that provide awareness and information about VHA’s COVID-19 vaccination program
[170]VHA categorizes VA medical centers according to complexity level, which is determined on the basis of the characteristics of the patient population, clinical services offered, educational and research missions, and administrative complexity.
[171]TRICARE is DOD’s regionally structured health care program that provides purchased care to beneficiaries through networks of civilian providers.
[172]DOD has included civilians and contractors in its vaccine-eligible population, although these personnel would not otherwise be eligible for DOD health care services unless they were also a dependent family member of a military servicemember or of one who has retired. Thus, DOD’s vaccine-eligible population (about 11.3 million) is wider in scope than its population eligible for health care services (about 9.6 million). DHA officials have estimated that their target vaccine-eligible population is actually about 6.9 million individuals because many eligible reservists and National Guard members, and eligible beneficiaries, civilians, and contractors will choose to receive their COVID-19 vaccine from a state-run facility or private provider.
[173]During an emergency, as declared by the Secretary of Health and Human Services under 21 U.S.C. § 360bbb-3(b), FDA may temporarily authorize unapproved medical products or unapproved uses of approved medical products through an emergency use authorization, provided certain statutory criteria are met. For example, an emergency use authorization request must include evidence that the vaccine may be effective and that the known and potential benefits outweigh the known and potential risks, among other requirements.
[174]Federal law states that a vaccine released under an emergency use authorization cannot be made mandatory. 21 U.S.C. § 360bbb-3(e)(1)(A)(ii)(III).
[175]Requesting agencies could include, for example, the Federal Emergency Management Agency (FEMA), the Department of Health and Human Services (HHS), and the U.S. Department of Agriculture.
[176]Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub. L. No. 116-136, div. B, title III, 134 Stat. 281, 518 and 520 (March 27, 2020). DOD received about $10.5 billion under the act which, in addition to the approximately $1.5 billion for the National Guard activities, included appropriations for the Defense Health Program, the defense working capital funds, and the Office of the Inspector General, among other things. We discuss the funding provided to the Defense Health Program for military health care in the Military Personnel Vaccinations enclosure.
[177]USAspending.gov, accessed on January 14, 2021.
[178]Coronavirus Aid, Relief, and Economic Security (CARES) Act, Pub. L. No. 116-136, div. B, title III, § 13001, 134 Stat. 281, 521 (March 27, 2020).
[179]The presidential memorandums extending authorization of Title 32 status also reduced the federal cost share from 100 percent to 75 percent from August 22, 2020, through December 31, 2020, with exceptions for a few states that maintained the 100-percent federal cost share. As part of the new administration’s policy to combat and respond to COVID-19 with the full capacity and capability of the federal government, a January 21, 2021, presidential memorandum restored the 100-percent federal cost share for Governors’ use of the National Guard to respond to COVID-19 through September 30, 2021.
[180]According to DOD, recruits and officer candidates are required to quarantine prior to starting and during training.
[181]In January 2021, the Department of Health and Human Services requested that DOD medical personnel support a medical facility in the Navajo Nation reservation. The DOD medical personnel worked alongside civilian and U.S. Public Health Service Commissioned Corps health care providers to treat COVID-19 patients. According to DOD, the addition of the DOD medical personnel allowed the medical facility to double the bed capacity in its intensive care unit.
[182]As of March 6, 2021, the department had identified more than 6,200 active-duty forces to support COVID-19 vaccination centers, although not all had been deployed as part of a team as of that date.
[183]In November 2020, we reported that as of September 30, 2020, more than 16,000 National Guard members remained on orders in 43 states and three territories in support of the COVID-19 response.
[184]FEMA, Pandemic Response to Coronavirus Disease 2019 (COVID-19): Initial Assessment Report, FEMA Operations January through September 2020 (January 2021).
[185]According to DOD officials, about 75 percent of requests for DOD medical personnel have been for nurses and, of those requests, 75 percent have been for critical care nurses.
[186]DOD officials stated that the Emergency Support Function #8 Council was established in the spring of 2020 to look across all of the requests for assistance and includes representatives from DOD and the Department of Health and Human Services, among other federal entities. Officials further stated that the council has managed the requests for assistance to meet critical high-priority needs, while preserving limited capabilities to respond to the next need.
[187]According to FEMA’s Community Vaccination Centers Playbook, vaccination centers are classified based on facility throughput over a 12-hour period. A Type 1 vaccination center has the approximate capacity to administer 6,000 doses per day, while a Type 2 vaccination center is about half that size and has the approximate capacity to administer 3,000 doses per day. Additionally, the FEMA playbook identifies Type 3 vaccination centers as having an approximate capacity to administer 1,000 doses per day, while Type 4 and 5 vaccination centers can administer 250 doses per day. See FEMA, Community Vaccination Centers Playbook (February 4, 2021).
[188]Type 1 teams consist of 222 personnel to support mega vaccination sites that can administer as many as 6,000 vaccinations per day, while the smaller Type 2 teams consist of 139 personnel to support smaller vaccination centers that can administer 3,000 vaccinations per day.
[189]According to the FEMA Task Order associated with the California mission assignment, the team includes 15 command and control personnel, 80 vaccinators, 15 registered nurses, 57 clinical staff, and 55 general purpose staff.
[191]Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146 (2020).
[192]We searched HHS’s Tracking Accountability in Government Grants System website and USAspending.gov—a publicly available website developed and operated by the Department of the Treasury that includes detailed data on federal spending, including obligations, across the federal government. See https://taggs.hhs.gov/coronavirus, accessed 3/1/2021, and https://USAspending.gov, accessed 3/4/2021. We did not independently validate the data provided by HHS.
[193]PPE are clothing and equipment worn to shield the wearer from injury or exposure to hazardous or infectious substances.
[194]CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Defense Production Act, Pub. L. No. 81-774, 64 Stat. 798 (1950) (codified, as amended, at 50 U.S.C. § 4501, et seq.). The Defense Production Act, as delegated, generally provides federal agencies authority to, among other things, prioritize certain contracts over others. See, Exec. Order No. 13603, 77 Fed. Reg. 16651 (Mar. 22, 2012); 15 C.F.R. pt. 700 (2020). For example, in times of national disasters, the President may invoke the DPA to facilitate the supply and timely delivery of products by providing incentives to expand domestic production. The DPA was authorized for use in response to the COVID-19 pandemic as early as March 2020.
[195]DPA authority was granted to the U.S. International Development Finance Corporation through a May 2020 Executive Order Delegating Authority Under the Defense Production Act of 1950 to the Chief Executive Officer of the United States International Development Finance Corporation to Respond to the COVID-19 Outbreak. Exec. Order No. 13922, 85 Fed. Reg. 30,583 (May 19, 2020). According to DOD, these loans will be supported through $100 million of DPA funding appropriated under the CARES Act.
[196]Federal acquisition requirements include the Buy American Act, enacted in 1933, which requires federal procurement of domestic products, including drugs, but permits federal agencies to procure foreign products under certain exceptions, such as in cases in which domestic products are not reasonably available in sufficient quantities of a satisfactory quality. Restrictions also may be waived under international trade agreements so that goods provided by designated countries can compete on an equal footing with domestic products.
[197]Exec. Order No. 13944, 85 Fed. Reg. 49,929 (Aug. 14, 2020). The Executive Order considers an essential medicine or medical countermeasure to be “produced in the U.S.” if the finished product and the critical inputs used to produce it were, in turn, produced in the U.S. Critical inputs are active pharmaceutical ingredients, active pharmaceutical ingredient starting materials, and other drug ingredients and device components that FDA determines to be critical for assessing safety and effectiveness of essential medicines and countermeasures.
[198]The Executive Order also directed Commerce to report on the status of the public health industrial base and provide recommendations for initiatives to strengthen it. This report is directed to be completed by February 2021. The Bureau of Industry and Security (BIS), within Commerce, expects to complete this report by March 31, 2021.
[200]Medical countermeasures are drugs, vaccines, and devices, such as personal protective equipment, used to diagnose, treat, prevent, or mitigate harm from any chemical, biological, radiological, and nuclear agent.
[202]Prior to June 2020, when it was renamed the Supply Chain Advisory Group, the Supply Chain Task Force was the primary federal body coordinating and managing supply chain responsibilities, according to DOD officials. In contrast to the Task Force, the Advisory Group has an advisory and assistance role, focused on transitioning responsibilities to other federal stakeholders. The Supply Chain Task Force was one of eight task forces under the Unified Coordination Group, which is led by the FEMA Administrator, the Assistant Secretary for Preparedness and Response, and a representative of the Centers for Disease Control and Prevention, and responsible for the operational command, leadership, and decision making for the COVID-19 pandemic response.
[203]In January 2021, FEMA released an initial assessment of their COVID-19 response from January through September 2020, which found that there was not a consistent strategy or established guidance for coordinating or communicating engagement with industry partners to expand domestic manufacturing. The lack of a strategic nationwide approach to engage industry led to duplicate contracts and missed opportunities to expand domestic manufacturing, according to the assessment. In response to this finding, FEMA recommended articulating a long-term strategy for engaging industry partners and coordinating across the field in future disaster responses. Department of Homeland Security, Federal Emergency Management Agency, Pandemic Response to Coronavirus Disease 2019(COVID-19): Initial Assessment Report (January 2021).
[204]Exec. Order No.14001, 86 Fed. Reg. 7219 (Jan. 26, 2021).
[208]Medical devices must also meet other requirements, such as establishment registration and device listing with FDA. See 21 C.F.R. Part 807 (2020).
[209]For devices FDA determines are high risk, device sponsors must generally receive premarket approval from FDA. For moderate- or some lower-risk devices, sponsors must generally receive 510(k) clearance from FDA, whereby they demonstrate that the new device is substantially equivalent to a legally marketed predicate device. Certain low-risk devices are exempt from the 510(k) clearance process, but the manufacturer must still register with FDA. See 21 U.S.C. §§ 360(k), 360c, and 360e. Novel devices that are low to moderate risk but are not substantially equivalent to a legally marketed predicate device may be authorized through the De Novo classification process. See 21 U.S.C. § 360c(f)(2).
[211]The Secretary of Health and Human Services issued three EUA declarations for medical devices for COVID-19—on February 4, 2020, regarding in-vitro diagnostic devices for detection or diagnosis of COVID-19; on March 2, 2020, related to personal respiratory protective devices for COVID-19; and on March 24, 2020, for medical devices including alternative products used as medical devices during the COVID-19 pandemic (such as systems to decontaminate N95 respirators for reuse by healthcare personnel).
[212]Among other statutory criteria, the threat must be capable of causing a serious or life-threatening disease or condition, and it must be reasonable to believe, based on the totality of scientific evidence available, that the product may be effective in diagnosing, treating, or preventing the disease or condition and that the known and potential benefits of the product outweigh the known and potential risks. In addition, there must be no adequate, approved, and available alternatives to the product. 21 U.S.C. § 360bbb-3(c).
[214]The period of advance notice must be sufficient to allow for disposition of authorized products or disposition of the product labeling (in the case of an unapproved use of an approved product). 21 U.S.C. § 360bbb-3(b). In addition, even if the EUA declaration is terminated or an EUA is revoked, an authorization will continue to be effective to provide for continued use of an unapproved product for patients to whom it was administered during the emergency period, if found necessary by the patient’s physician. 21 U.S.C. § 360bbb-3(f)(2).
[215]See 42 C.F.R. § 84.170(a)(3)(iii) (2019). Other countries also regulate and test masks and respirators. For example, “KN95” respirators are determined by the Chinese government to filter at least 95 percent of airborne particles.
[216]OSHA carries out these activities under the Occupational Safety and Health Act of 1970 (OSH Act), Pub. L. No. 91-596, 84 Stat. 1590 (codified, as amended, at 29 U.S.C. § 651 et seq.). Under the OSH Act, states, territories, and other jurisdictions can be approved by OSHA to set and enforce their own workplace safety and health standards, which must be at least as effective as the federal standards. There are currently 22 State Plans—programs through which jurisdictions set and enforce their own standards—covering both private sector and state and local government workers, and there are six State Plans covering only state and local government workers. Federal OSHA still enforces federal workplace safety and health standards for private employers in the six State Plans that cover only state and local government workers.
[217]FDA also issued EUAs for various COVID-19 tests. These EUAs are not included in this review; we have ongoing work to examine EUAs for tests.
[218]In addition to the nine umbrella EUAs, FDA also issued two umbrella EUAs for diagnostic tests for COVID-19. We will examine EUAs for tests in separate ongoing work.
[219]For COVID-19, OSHA released temporary guidance regarding enforcement of the respirator standard. OSHA released enforcement guidance on April 3, 2020, outlining enforcement discretion to permit the use of respirators beyond the manufacturer’s recommended shelf life. OSHA released guidance on April 24, 2020 outlining enforcement discretion related to reuse of respirators that have been decontaminated.
[220]FDA has a memorandum of understanding with CDC that is not specific to EUAs but does provide a framework for certain information sharing, according to FDA officials. There is no similar MOU between FDA, CDC, and OSHA, according to FDA officials.
[221]EUAs remain in effect until the EUA declaration under which the EUA was issued terminates or the EUA is revoked, whichever is earlier. 21 U.S.C. § 360bbb-3(f)(1). At the time of our review, the Secretary had not indicated when the relevant EUA declarations would terminate, according to FDA officials.
[222]The ECRI Institute is designated an Evidence-based Practice Center by HHS’s Agency for Healthcare Research and Quality and a federally certified HHS Patient Safety Organization. As part of its work, the ECRI Institute provides clinical evidence to inform and support decisions on the effectiveness of medical technologies and clinical practice guidelines.
[223]See ECRI Institute, Use of Unapproved Devices or New Applications for Existing Medical Devices to Address COVID-19 Shortages without an EUA May Jeopardize Patient or Staff Safety (Plymouth Meeting, Penn.: May 15, , 2020) and ECRI Institute, Ventilators on FDA Emergency Use Authorization List: Hospitals Should Seek Clarity on Post EUA Status Before Purchasing (Plymouth Meeting, Penn.: April 29, 2020).
[225]See Department of Health and Human Services, U.S. Government COVID-19 Response Plan (Mar. 13, 2020).
[226]According to federal internal control standards for control activities, management should design control activities to achieve objectives and implement those controls through policies. GAO-14-704G.
[227]We did not examine EUAs for COVID-19 tests as we have ongoing work examining EUAs for COVID-19 tests separately.
[228]In November, we reported that the component agencies made a 12 percent increase in the number of recommendations they implemented, bringing the total number of recommendations implemented from 350 to 404.
[229]As of January 2021, the Centers for Disease Control and Prevention had implemented all the prior cybersecurity recommendations we made to the agency.
[230]We issued two cybersecurity recommendations to FDA. FDA had previously issued a waiver for one and accepted the risk for the other; as a result, the recommendations were not implemented.
[231]Presidential Policy Directive 21 on critical infrastructure security and resilience identifies health care and public health as one of 16 critical infrastructure sectors. Critical infrastructure includes assets, networks, and systems that are vital to the nation’s safety, prosperity, and well-being.
[232]Sector-specific agencies are federal agencies with institutional knowledge and specialized expertise about a particular sector and have been designated to have a lead role in critical infrastructure protection efforts for that sector. With regard to critical infrastructure protection efforts going forward, the William M. (Mac) Thornberry National Defense Authorization Act for Fiscal Year 2021 states that the term “sector risk management agency” has the meaning that was given to the term “sector-specific agency”. Pub. L. No. 116-283, § 9002, 134 Stat. 3388, 4768 (Jan. 1, 2021).
[233]The Joint Healthcare and Public Health Sector Cyber Working Group is co-led by ASPR, the HHS Office of the Chief Information Officer, and FDA, along with industry partners. It is a forum of government and industry partners that facilitates discussion of issues and development of resources to enhance cybersecurity among health care sector stakeholders.
[234]The Government Coordinating Council’s Cybersecurity Working Group is an ASPR-led group of federal, state, local, tribal, and territorial health care partners that coordinates to enhance critical infrastructure resiliency and to reduce cyber risks across the public landscape of the health care sector. It established a Telehealth Task Group in August 2020 to develop a standard-based practice guide to mitigate the major cybersecurity, compliance, and privacy risks in the Telehealth ecosystem.
[235]The CISO Council is a collaborative effort led by the HHS department-level CISO and is intended to facilitate the sharing of information among the different HHS component-level CISOs.
[236]The Health Sector Cybersecurity Coordination Center is a component of HHS’s Office of the Chief Information Officer. It is intended to support the defense of the healthcare and public health sector’s information technology infrastructure by providing technical analysis and information sharing within the sector. The Cyber Watch Project is intended to execute and coordinate government-wide cyber engagements in support of health care sector entities that are developing and testing COVID-19 therapeutics and vaccines.
[237]Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. L, tit. IX, § 903, 134 Stat. 1182, 2128-29 (2020). Of the approximately $250 million, $50,000 is allocated for the FCC Inspector General for oversight of the COVID-19 Telehealth Program. In January 2021, FCC issued a request for public comments on matters identified in the authorizing legislation, including the criteria FCC will use to select awardees. See Federal Communications Commission, Public Notice: Wireline Competition Bureau Seeks Comment on COVID-19 Telehealth Program Application Evaluation Metrics (Washington, D.C.: Jan. 6, 2021).
[238]For the purposes of the COVID-19 Telehealth Program, FCC refers to “connected care services,” which it broadly defines as a subset of telehealth that uses broadband internet access service-enabled technologies to deliver remote medical, diagnostic, patient-centered, and treatment-related services directly to patients outside of traditional brick and mortar facilities—including specifically to patients at their mobile location or residence. See Federal Communications Commission, Promoting Telehealth for Low-Income Consumers, Report and Order, 35 FCC Rcd. 3366 (2020) ¶ 14.
[239]CARES Act, Pub. L. No 116-136, 134 Stat. 281, 531 (2020). FCC limited the program to public and nonprofit eligible health care providers that fall within 47 U.S.C. § 254(h)(7)(B). See 35 FCC Rcd. 3366 (2020) ¶ 19, 20.
[240]Connected devices must be integral to patient care. Eligible services and devices may be for provider or patient use. See 35 FCC Rcd. 3366 (2020) ¶¶ 19, 24.
[241]Federal Communications Commission, Public Notice: Wireline Competition Bureau Provides Guidance on the COVID-19 Telehealth Program Application Process (Washington, D.C.: Apr. 8, 2020). While applicants were required to have an eligibility determination in order to receive an award, FCC permitted applicants to file an application with the Commission while their request for eligibility determination was pending.
[242]FCC officials told us that they used Johns Hopkins University resource center data to identify the hardest hit areas. As part of their compliance review, FCC officials said they also verified that applicants were not on the Department of the Treasury’s “Do Not Pay” list.
[243]FCC officials said that they are in the process of recovering the remaining improper payments and expect to recover all funds.
[244]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing Office of Management and Budget (OMB) guidance is reprinted in 2 C.F.R. Part 200 (2020). Federal award recipients that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit, which is an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 31 C.F.R. § 200.501 (2020).
[245]In its January 2021 public notice, FCC sought comment on processes for the second round of funding appropriated in December 2020. FCC, Public Notice (2021).
[248]FCC officials noted that some providers may have facilities in multiple states that benefitted from the funding, which is not depicted in the award data. As a result, some states may have actually benefitted from more or less funding than described here. Six health care providers received two or more awards, which, according to FCC officials, were awarded for different locations, services, or connected devices. FCC officials also told us that FCC issued some awards to health care consortiums that included providers from different organizations.
[249]These determinations were based on the number of COVID-19 cases states reported to the Centers for Disease Control and Prevention as of June 30, 2020.
[250]Health care providers may use funding for different items and services than those for which FCC based its award upon, as long as they comply with program rules. As a result, while FCC based its awards on the items and services listed in the application, as described in our analysis, health care providers may seek reimbursement for different eligible items or services. However, the extent to which actual spending varied from the purposes identified in the awards above is unclear because FCC’s deadline for submitting requests for reimbursement is not until July 2021.
[254]The exact content of the kits may vary depending on the specific vaccine. A vaccination card shows an individual has received a vaccine (and how many doses) and documents relevant information such as vaccine manufacturer, lot number, and date of administration for each dose. Diluent is used to reconstitute Pfizer-BioNTech’s COVID-19 vaccine.
[255]Survey results are based on our survey fielded to 383 hospitals across the country from February 5 through February 25, 2021. We received responses from 166 hospitals. Not all hospitals responded to each survey question. Results of the survey cannot be generalized. We also interviewed nine large retail pharmacy chains (based on 2019 prescription drug revenue) and a pharmacy association representing independently owned pharmacies, along with four of its member pharmacies. Results of the interviews cannot be generalized. See “Methodology” section of this enclosure for more detail.
[256]For our non-generalizable survey, we asked all survey respondents which of the following items they would say their hospitals did not have sufficient information about to respond to COVID-19 vaccine inquiries from staff, the public, and others: vaccine availability; vaccine efficacy/effectiveness; how to respond to vaccine questions in languages other than English; how to increase an individual’s interest or address lack of interest or willingness to be vaccinated; other locations administering the vaccine, if the hospital does not plan to administer vaccine or does not have any vaccine (e.g., using tools such as VaccineFinder); other (with a space for respondents to fill in). Respondents were asked to select all options that applied as of the date they were answering the survey. 165 hospitals (out of 166) responded to this question, with 102 hospitals reporting “vaccine availability” as a concern. The second highest selected response to our question was, “how to increase an individual’s interest in vaccination or to address lack of interest or willingness to be vaccinated,” with 30 hospitals (18 percent) reporting this response. All other response options to this question were reported by less than 15 percent of survey respondents.
[257]166 hospitals responded to our non-generalizable survey. Of these, 68 hospitals (41 percent) were categorized as rural and 77 hospitals (46 percent) were categorized as urban. Hospitals categorized as urban are located in a county that contains a core urban area of 50,000 or more population, and those categorized as rural are located in a county not designated as such. Twenty-one of the survey responses we received were on behalf of a larger health system or multiple facility group representing multiple hospitals and therefore could not be categorized as urban or rural due to their multiple locations.
[258]For our non-generalizable survey, we asked all survey respondents to elaborate on their survey responses or share any additional information or thoughts concerning their hospital’s recent experiences during the COVID-19 pandemic. 55 hospitals (out of 166) responded to this question. Our survey did not specifically ask whether hospitals were concerned about the supply of vaccines.
[259]The Federal Retail Pharmacy Partnership Program is a collaboration between the federal government, states and territories, and 21 national pharmacy partners and independent pharmacy networks to increase access to COVID-19 vaccines across the United States.
[261]Of the 166 hospitals that responded to our non-generalizable survey, 146 hospitals (88 percent) have begun administering COVID-19 vaccines or plan to. Of these 146 hospitals, 140 (96 percent) had begun administering the vaccines at the time of our survey. We asked the 146 survey respondents that reported that they have either begun administering COVID-19 vaccines or plan to do so whether they were greatly concerned about having sufficient quantity of certain items—alcohol prep pads; bandages; diluent, if needed; needles; syringes; sharps containers; vaccination cards; other (fill-in)—in order to successfully handle and administer any COVID-19 vaccine in the next 30 days. Respondents were asked to select all options that applied. 144 hospitals (out of the 146) responded to this question. The next highest selected response to our question was “sharps containers,” with 23 (16 percent) of the 146 respondents reporting this concern. Hospitals must procure these containers themselves—they are not provided in the ancillary supply kits. All other response options to this question were reported by less than 15 percent of survey respondents.
[262]The vials of COVID-19 vaccine manufactured by Pfizer were initially labeled for five doses of vaccine each, and the Moderna vaccine vials were labeled for 10 doses each. Depending, in part, on the type of syringes and needles used to withdraw doses from the vials, providers may be able to obtain a sixth dose from each vial of Pfizer vaccine and an eleventh dose for the Moderna vaccine. As of February 25, 2021, FDA has instructed providers that Pfizer vials have enough vaccine for six doses with the use of low dead-volume syringes and needles, which minimize waste by reducing dead space between the syringe hub and the needle.
[263]We were unable to determine whether the 40 hospitals reporting they were greatly concerned about having a sufficient quantity of syringes and the 43 hospitals reporting such concerns for needles, did so because of this issue or because of other general concerns about having enough supplies.
[264]The exception among rural hospitals was “being able to track the expected arrival of kits with ancillary vaccination supplies to the hospital” with five of the 56 rural hospitals responding that they had great concerns about this issue.
[266]The American Nurses Foundation conducted a survey of 22,316 nurses across the country. American Nurses Foundation, Pulse on the Nation’s Nurses COVID-19 Survey Series: Year One COVID-19 Impact Assessment (Feb. 2021). Further, representatives from the American Association of Critical-Care Nurses told us that a March 2021 survey of 295 of their members found that among the 180 respondents who described their worksites as “fully equipped with N95 respirators,” 125 (69 percent) were still required or encouraged to reuse them despite the adequate supply, suggesting such policies are becoming entrenched.
[267]Of the 166 hospitals that responded to our survey, 158 hospitals reported that they conduct diagnostic tests for COVID-19. Our survey did not address antibody tests, which do not diagnose a current infection, but rather indicate an infection in the past. Those hospitals that do not conduct diagnostic testing did not respond to the testing supplies questions. See our enclosure Funding for COVID-19 Testing for more information on testing issues.
[268]To obtain these 383 email addresses, we randomly selected and then contacted 600 short-term and critical access hospitals from 4,682 of these types of hospitals in the Centers for Medicare & Medicaid Services’ 2020 Provider of Services file. We selected these types of facilities because they are most likely to be on the front lines of treating COVID-19 patients, since they provide acute care.
[269]The 21 responses on behalf of multiple hospitals represented 300 hospitals.
[270]We attempted to interview all of the top 10 national retail pharmacy chains. We interviewed representatives from Ahold Delhaize; Albertsons Companies; Costco Wholesale; CVS Pharmacy; H-E-B; Publix; Rite Aid Corporation; Walgreens; and Walmart U.S. One retail pharmacy chain (The Kroger Co.) declined to participate.
[271]Centers for Disease Control and Prevention, CDC COVID-19 Response Health Equity Strategy: Accelerating Progress Towards Reducing COVID-19 Disparities and Achieving Health Equity (July 22, 2020, updated August 21, 2020).
[272]Department of Health and Human Services, Centers for Disease Control and Prevention, COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations, version 2.0 (Washington, D.C.: Oct. 29, 2020).
[273]Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1912.
[274]The White House, National Strategy for the COVID-19 Response and Pandemic Preparedness (January 21, 2021).
[276]CDC officials reported that the number of cases with case report forms received by CDC is less than the total number of reported cases because there is generally a 2-week lag from when total cases are reported by state and jurisdictional health departments to when CDC receives the case report forms. Total cases reported by CDC include both probable and confirmed cases as reported by states or jurisdictions. A probable case does not have confirmatory laboratory evidence, but meets certain other criteria.
[277]COVID-NET collects data on COVID-19 hospitalizations that are confirmed by laboratory testing from select counties in 14 states, representing 10 percent of the U.S. population. It includes data from hospitals in select counties in California, Colorado, Connecticut, Georgia, Iowa, Maryland, Michigan, Minnesota, New Mexico, New York, Ohio, Oregon, Tennessee, and Utah. As of January 30, 2021, race and ethnicity were missing for 2.3 percent of COVID-19-associated hospitalizations included in CDC’s COVID-19-Associated Hospitalization Surveillance Network (COVID-NET). In addition to COVID-NET, HHS also collects national hospitalization data through its HHS Protect Public Data Hub, https://protect-public.hhs.gov/, accessed February 23, 2021; however, HHS does not make available data on COVID-19 hospitalizations by race and ethnicity through this website.
[278]CDC officials noted that the number of deaths with case report forms it has received is less than the total number of reported deaths through case reporting because there is generally a 2-week lag from when total deaths are reported by state and jurisdictional health departments to when CDC receives case report forms noting deaths. CDC also makes data available on COVID-19 deaths from death certificate data through its National Vital Statistics System (NVSS). CDC stated that over 99 percent of deaths in NVSS have race and ethnicity information.
[279]CDC data represent viral COVID-19 laboratory test results from laboratories in the U.S., including commercial laboratories, public health laboratories, and other testing locations from 48 jurisdictions. The data represent total laboratory tests, not individual people, and exclude antibody and antigen tests.
[280]Additionally, among cases with known race and ethnicity reported to CDC as of March 8, 2021, 12.2 percent were non-Hispanic Black (compared to 13.4 percent of the U.S. population), 3.6 percent were non-Hispanic Asian (compared to 5.9 percent of the U.S. population), 1.2 percent were American Indian/Alaska Native (compared to 1.3 percent of the U.S. population), and 56.0 percent were non-Hispanic White persons (compared to 60.1 percent of the U.S. population).
[281]Department of Health and Human Services, Centers for Disease Control and Prevention. Report to Congress on Paycheck Protection Program and Health Care Enhancement Act Disaggregated Data on U.S. Coronavirus Disease 2019 (COVID-19) Testing, 8th 30-Day Update (January 2021).
[282]Department of Health and Human Services, Centers for Disease Control and Prevention. Report to Congress on Paycheck Protection Program and Health Care Enhancement Act Disaggregated Data on U.S. Coronavirus Disease 2019 (COVID-19) Testing, 8th 30-Day Update (January 2021). CDC data represent viral COVID-19 laboratory test results from laboratories in the U.S., including commercial laboratories, public health laboratories, and other testing locations from 48 jurisdictions. The data represent total laboratory tests, not individual people, and exclude antibody and antigen tests. (See our related Funding for COVID-19 Testing enclosure for additional information.)
[283]CDC COVID Data Tracker, https://covid.cdc.gov/covid-data-tracker/#vaccination-demographic, accessed March 9, 2021. Data from CDC’s COVID Data Tracker also indicated that 1.7 percent of COVID-19 vaccine recipients who received at least one dose whose race and ethnicity was known as of March 8, 2021 were non-Hispanic American Indian/Alaska Native (compared to 1.3 percent of the U.S. population), 0.3 percent were non-Hispanic Native Hawaiian or Other Pacific Islander (compared to 0.2 percent of the U.S. population), and 12.3 percent were non-Hispanic Multiple/Other races (compared to 2.8 percent of the U.S. population). In addition, in February 2021, CDC released a report assessing the demographic characteristics of persons who received the COVID-19 vaccine from December 14, 2020 through January 14, 2021, and found that it is critical to ensure efficient and equitable administration of the vaccine to persons at highest risk for infection and severe health outcomes. See Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, Vol. 70, No. 5 (February 5, 2021).
[284]The four broad priority areas of CDC’s equity strategy are (1) expand the evidence base; (2) expand programs and practices for testing, contact tracing, isolation, healthcare, and recovery from the impact of unintended negative consequences of mitigation strategies in order to reach populations that have been put at increased risk; (3) expand program and practice activities to support essential and frontline workers to prevent transmission of COVID-19; and (4) expand an inclusive workforce equipped to assess and address the needs of an increasingly diverse U.S. population.
[285]GAO, Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism, GAO-04-408T (Washington, D.C.: Feb. 3, 2004). This report identifies the key elements of a national strategy.
[286]See Department of Health and Human Services, Report to Congress: COVID-19 Strategic Testing Plan Second Update (November, 2020). As part of this plan, HHS reported that it aims to protect and improve health outcomes among populations at higher risk for COVID-19. In January 2021, we recommended that HHS should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that HHS has produced for the public and Congress to allow for a more coordinated pandemic testing approach. See GAO-21-265.
[289]In addition, the January 2021 executive order on equitable pandemic response directed federal agencies to assess plans and policies to determine whether resources, including vaccines, have been or will be allocated equitably. Exec. Order No. 13995, 86 Fed. Reg. 7,193 (Jan. 21, 2021).
[290]We interviewed or received written responses from stakeholders including the American Hospital Association, the American Medical Association, the American Public Health Association, American Pharmacists Association, the Association of State and Territorial Health Officials, and the National Association of County and City Health Officials. These stakeholders were selected for a variety of reasons including their representation of entities involved in COVID-19 testing and vaccination efforts. We previously reported challenges with collecting race and ethnicity for indicators of COVID-19 burden, such as providers not collecting demographic information from patients at the point of care and state and jurisdictional health departments combining certain racial and ethnic groups into an “Other” category. See GAO-20-701.
[291]For example, see Langer Research Associates, COVID Collaborative Survey: Coronavirus Vaccination Hesitancy in the Black and Latinx Communities (November 2020).
[292]We interviewed or received written responses from stakeholders including the American Hospital Association, the American Medical Association, the American Public Health Association, American Pharmacists Association, the Association of State and Territorial Health Officials, and the National Association of County and City Health Officials. These stakeholders were selected for a variety of reasons including their representation of entities involved in COVID-19 testing and vaccination efforts. We selected three states—Alabama, Nevada, and South Dakota—based on the relative percentage of persons in racial and ethnic groups residing in the states compared to the national distribution, the COVID-19 case rate per 100,000 people in the last 7 days as of December 9, 2020, and variation in geographic region.
[293]A Sustainable Public Health Supply Chain, Exec. Order No. 14001, 86 Fed. Reg. 7219 (Jan. 26, 2021).
[294]American Rescue Plan Act of 2021, Pub. L. No. 117-2, § 3101, 135 Stat. 4, 53-54.
[295]Pub. L. No. 81-774 (1950), codified at 50 U.S.C. §§ 4501 et seq., as amended.
[296]Title I of the DPA also enables agencies to issue three types of allocation orders that require a person or corporation to (1) reserve resource capacity in anticipation of a rated order; (2) take or refrain from taking certain actions or divert the use of materials, services, or facilities from one purpose to another; or (3) limit the amount of a resource to be used for a specific purpose.
[297]“Other” actions refer to those identified by DOD that have similar goals of industrial base expansion for medical supplies but are not executed under the DPA Title III authority.
[298]Exec. Order No. 14001, 86 Fed. Reg. 7219 (Jan. 26, 2021). Another executive order, Organizing and Mobilizing the United States Government to Provide a Unified and Effective Response to Combat COVID-19 and to Provide United States Leadership on Global Health and Security, established the position of Coordinator of the COVID-19 Response to report directly to the President and coordinate federal efforts to produce, supply, and distribute medical supplies, including through the use of the DPA, among other things. Exec. Order No. 13987, 86 Fed. Reg. 7019 (Jan. 25, 2021).
[299]The subcommittees are led by FEMA officials and staffed with federal agency and private-sector representatives. According to the plan, FEMA can add additional subcommittees if they (1) cover a specific, well-defined PPE area and (2) are recommended to be added by the subcommittee in charge of defining requirements.
[300]FDA has authorized decontamination units, which use ultraviolet germicidal irradiation, hydrogen peroxide vapor, or steam cleaning, to decontaminate N95 respirators to allow health workers to reuse them in clinical environments.
[301]The Department of Defense can authorize contractors to begin work and incur costs before reaching final agreement on contract terms, specifications, or price, using an undefinitized contract action or agreement. The contract or agreement is definitized once the final terms and conditions are agreed to by all parties. The contracts or agreements our selected companies received were generally awarded undefinitized.
[303]Exec. Order No.14001, 86 Fed. Reg. 7219 (Jan. 26, 2021).
[304]NIA codes were established in 2005 after Hurricane Katrina to track federal procurements for specific disasters, emergencies, or contingency events. The Department of Defense, the Department of Homeland Security, and the General Services Administration established the NIA code for COVID-19 on March 13, 2020, and as of February 2021, it was to remain active until September 30, 2021.
[305]For the purposes of this report, “contract obligations” refers to obligations on procurement contracts that are subject to the Federal Acquisition Regulation and does not include, for example, grants, cooperative agreements, loans, other transactions for research, real property leases, or requisitions from federal stock.
[306]Pub. L. No. 116-136, §§ 3301, 13006, 134 Stat. at 383, 522.
[308]Our methodology for identifying noncompetitive contracts is explained in detail at the end of this enclosure.
[309]For the purposes of this report, obligations on contracts identified as using the unusual and compelling urgency exception include those associated with contracts subject to Federal Acquisition Regulation 6.302-2, as well as orders under multiple award contracts, which are subject to separate competition requirements under Federal Acquisition Regulation Part 16. Specifically, under Federal Acquisition Regulation 16.505(b)(2), orders on multiple award contracts require contracting officers to give every awardee a fair opportunity to be considered for a delivery order or task order exceeding $3,500, with exceptions, including if the agency need for the supplies or services is so urgent that providing a fair opportunity would result in unacceptable delays. When using the unusual and compelling urgency exception to full and open competition, agencies still must request offers from as many potential sources as is practicable under the circumstances.
[310]Undefinitized contracts include letter contracts, as well as other undefinitized actions.
[312]For rounds 3, 4, and 5 of the Farmers to Families Food Box Program, AMS officials established basic ordering agreements with vendors, who then competed amongst themselves to fulfill specific requirements for the program.
[313]American Rescue Plan Act of 2021, Pub. L. No. 117-2, § 1001, 135 Stat. 4.
[314]Office of Management and Budget M-20-21, Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019 (COVID-19), April 10, 2020.
[315]FPDS-NG data from beta.SAM.gov accessed February 28, 2021. For purposes of this report, “competition rate” is the percentage of total obligations associated with contracts awarded competitively. We calculated competition rates as the percentages of obligations on competitive contracts and orders over all obligations on contracts and orders. Competitive contracts included contracts and orders coded in the FPDS-NG as “full and open competition,” “full and open after exclusion of sources,” and “competed under simplified acquisition procedures” as well as orders coded as “subject to fair opportunity,” “fair opportunity given,” and “competitive set aside.” Noncompetitive contracts included contracts and orders coded in the FPDS-NG as “not competed,” “not available for competition,” and “not competed under simplified acquisition procedures,” as well as orders coded as an exception to “subject to fair opportunity,” including “urgency,” “only one source,” “minimum guarantee,” “follow-on action following competitive initial action,” “other statutory authority,” and “sole source.” Even for contracts identified as noncompetitive, agencies may have solicited more than one source.
[316]In November 2019 we identified some inconsistencies in the information agencies report in the contract description field in the FPDS-NG. Data on DOD contract obligations based on information in the description field were available only through December 1, 2020, due to differences in the time frames for which DOD data are made publicly available.
[317]Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952.
[318]The DOL guidance defines unsafe worksites as those not in compliance with local, state, or national health and safety standards related to COVID-19, such as standards related to facial mask wearing, physical distancing measures, or the provision of personal protective equipment consistent with public health guidelines. Department of Labor, Expanded Eligibility Provisions for the Pandemic Unemployment Assistance (PUA) Program, Unemployment Insurance Program Letter (UIPL) 16-20 Change 5 (Washington, D.C.: Feb. 25, 2021).
[321]To be eligible for regular UI benefits, applicants generally must be able and available to work, and be actively seeking work. 42 U.S.C. § 503(a)(12). The regular UI program is also financed by a federal tax on employers, which according to DOL officials, primarily supports the administration of the program.
[322]The CARES Act also addressed other aspects of the UI system, such as authorizing certain flexibilities for states to hire additional staff and to participate in Short-Time Compensation programs. In addition to the CARES Act, the Families First Coronavirus Response Act provided up to $1 billion in emergency grant funding to states in fiscal year 2020 for UI administrative purposes. In addition, on August 8, 2020, the President signed a memorandum directing the Department of Homeland Security’s Federal Emergency Management Agency (FEMA) to provide up to $44 billion in lost wages assistance (LWA). Pursuant to the presidential memorandum, upon receiving a FEMA grant, states and territories could provide eligible claimants $300 or $400 per week—which included a $300 federal contribution—in addition to their UI benefits. The White House, Memorandum on Authorizing the Other Needs Assistance Program for Major Disaster Declarations Related to Coronavirus Disease 2019 (Aug. 8, 2020). FEMA approved 54 states and territories to provide LWA to eligible claimants for at most 6 weeks of unemployment experienced from the week ending August 1, 2020, through the week ending September 5, 2020.
[323]Pub. L. No. 117-2, § 9011(a), (b), 135 Stat. 4, 118; Pub. L. No. 116-260, div. N, tit. II, § 201(a), (b), 134 Stat. 1182, 1950-1951 (2020); Pub. L. No. 116-136, § 2102, 134 Stat. at 313. The Consolidated Appropriations Act, 2021 increased the maximum number of weeks of PUA benefits authorized from 39 to 50, and generally extended the expiration of the program from December 31, 2020 to March 14, 2021. The American Rescue Plan Act of 2021 further increased the maximum number of weeks of PUA benefits to 79, and generally extended the expiration of the program to September 6, 2021. The CARES Act also provided funding for up to an additional 7 weeks of PUA benefits in certain states with high rates of unemployment. Department of Labor, CARES Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Operating, Financial and Reporting Instructions, Unemployment Insurance Program Letter (UIPL) 16-20 (Washington, D.C.: Apr. 5, 2020).
[324]Pub. L. No. 117-2, § 9013, 135 Stat. 4, 119; Pub. L. No. 116-260, div. N, tit. II, § 203, 134 Stat. 1182, 1953; Pub. L. No. 116-136, § 2104, 134 Stat. at 318. The Consolidated Appropriations Act, 2021 authorized the $300 benefit initially through March 14, 2021, and the American Rescue Plan Act of 2021 extended that benefit through September 6, 2021.
[325]Pub. L. No. 117-2, § 9016(a), (b), 135 Stat. 4, 119-120; Pub. L. No. 116-260, div. N, tit. II, § 206(a), (b), 134 Stat. 1182, 1954; Pub. L. No. 116-136, § 2107, 134 Stat. at 323. The Consolidated Appropriations Act, 2021 increased the maximum amount of PEUC benefits from 13 to 24 times the individual’s average weekly benefit amount, and generally extended the expiration of the PEUC program from December 31, 2020 to March 14, 2021. The American Rescue Plan Act of 2021 further increased the maximum amount to 53 times the individual’s average weekly benefit amount, and generally extended the expiration of the program to September 6, 2021. Consistent with the CARES Act and program extension in the Consolidated Appropriations Act, 2021, the increased maximum amount of PEUC benefits translates to 53 weeks of benefits for individuals who are totally unemployed. However, individuals may receive more weeks of benefits if they are receiving a reduced weekly benefit amount for weeks of partial unemployment. See Department of Labor, Continued Assistance for Unemployed Workers Act of 2020—Pandemic Emergency Unemployment Compensation (PEUC) Program: Extension, Transition Rule, Increase in Total Benefits, and Coordination Rules, Unemployment Insurance Program Letter (UIPL) 17-20, Change 2 (Washington, D.C.: Dec. 31, 2020).
[326]Pub. L. No. 117-2, § 9013(a), 135 Stat. 4, 119; Pub. L. No. 116-260, div. N, tit. II, § 261(a)(1), 134 Stat. 1182, 1961. The American Rescue Plan Act of 2021 generally extended MEUC through September 6, 2021.
[327]Department of Labor, Continued Assistance for Unemployed Workers (Continued Assistance) Act of 2020 – Federal Pandemic Unemployment Compensation (FPUC) Program Reauthorization and Modification and Mixed Earners Unemployment Compensation (MEUC) Program Operating, Reporting, and Financial Instructions, Unemployment Insurance Program Letter (UIPL) 15-20, Change 3 (Washington, D.C.: Jan. 5, 2021).
[328]Pub. L. No. 116-260, div. N, tit. II, §§ 241(a), 263(a), 134 Stat. 1182, 1959-1960, 1963.
[329]Pub. L. No. 116-260, div. N, tit. II, § 242(a), 134 Stat. 1182, 1960.
[330]Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952. According to the Consolidated Appropriations Act, 2021, states can waive the requirement if the individual was without fault and repayment would be contrary to equity and good conscience.
[331]If approved for PUA benefits, the number of weeks of regular UI and Extended Benefits a claimant already received is subtracted from the duration of PUA benefits. Department of Labor, CARES Act of 2020 – Summary of Key Unemployment Insurance (UI) Provisions and Guidance Regarding Temporary Emergency State Staffing Flexibility, Unemployment Insurance Program Letter (UIPL) 14-20 (Washington, D.C.: Apr. 2, 2020).
[332]An initial claim is the first claim filed by an individual to determine eligibility for UI benefits after separating from an employer. Initial claims counts presented are not seasonally adjusted, and counts for the week ending March 13, 2021 reflect advance initial claims, which are preliminary and subject to revision. In some cases, advance initial claims represent estimates submitted by states that are later revised.
[333]One state and one territory did not report PUA continued claims data for the week ending February 27, 2021; the continued claims count represents the total across the 51 of 53 states and territories reporting data.
[334]Two states did not report PEUC continued claims data for the week ending February 27, 2021.
[335]According to the National Bureau of Economic Research, the 2007-2009 recession began in December 2007 and ended in June 2009.
[336]In its Employment Situation news releases, the Bureau of Labor Statistics defines the long-term unemployed population as those who are jobless for 27 weeks or more.
[337]According to DOL, as of July 2020, 45 of 53 states and territories generally provide up to a maximum of 26 weeks of regular UI benefits. Some states provide fewer than 26 weeks, though some of these states also provide additional weeks of benefits under limited circumstances, such as periods of high unemployment, according to DOL. As of March 14, 2021, DOL reported that the Extended Benefits program was activated in 17 states and territories due to high levels of unemployment. However, 1 territory was scheduled to stop providing Extended Benefits on March 20, 2021. The Extended Benefits program was activated in all states except South Dakota at some point during the pandemic, according to DOL. For example, as of June 28, 2020, the Extended Benefits program was available in 49 states, the District of Columbia, Puerto Rico, and the Virgin Islands, according to DOL.
[338]The Consolidated Appropriations Act, 2021 created the MEUC program, and the American Rescue Plan Act of 2021 generally extended MEUC through September 6, 2021. Pub. L. No. 117-2, § 9013(a), 135 Stat. 4, 119; Pub. L. No. 116-260, div. N, tit. II, § 261(a)(1), 134 Stat. 1182, 1961.
[339]See Department of Labor, Continued Assistance for Unemployed Workers (Continued Assistance) Act of 2020 – Federal Pandemic Unemployment Compensation (FPUC) Program Reauthorization and Modification and Mixed Earners Unemployment Compensation (MEUC) Program Operating, Reporting, and Financial Instructions, Unemployment Insurance Program Letter (UIPL) 15-20, Change 3 (Washington, D.C.: Jan. 5, 2021).
[340]As of March 3, 2021, Idaho and South Dakota had opted not to participate in the MEUC program, according to DOL.
[341]Minimum weekly benefits are based on state laws and regulations as reported to DOL, effective July 2020. See Department of Labor, Significant Provisions of State Unemployment Insurance Laws Effective July 2020 (Washington, D.C.).
[342]Minimum weekly PUA benefits are greater than $100 in 52 of 53 states and territories. Department of Labor, Minimum Disaster Unemployment Assistance (DUA) Weekly Benefit Amount: January 1 - March 31, 2020, Unemployment Insurance Program Letter (UIPL) 3-20 (Washington, D.C.: Dec. 12, 2019). According to DOL, states must use the amounts set in UIPL 3-20 as the minimum weekly benefit amount for all PUA claims. See Department of Labor, Coronavirus Aid, Relief, and Economic Security (CARES) Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Reporting Instructions and Questions and Answers, Unemployment Insurance Program Letter (UIPL) 16-20, Change 1 (Washington, D.C.: Apr. 27, 2020).
[343]DOL monitors timeliness of benefit payments in the regular UI program. One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible. DOL uses 14 days as the timeliness goal for states with a waiting week requirement and 21 days for states without a waiting week requirement. According to DOL, some states require that individuals who are otherwise eligible for benefits, serve a waiting period—generally one week—before receiving benefits. In its guidance released at the start of the pandemic, DOL recommended that states consider temporarily waiving their waiting week requirements. Thus, we focus on payments made within 21 days. We analyzed first payment timeliness data reported by states to DOL as of March 15, 2021, at which point just 25 of the 53 states and territories had reported data for February 2021. Thus, we analyzed data through January 2021; 52 of 53 states and territories had reported data for January 2021.
[344]For its core performance measure, DOL determined that states must pay at least 87 percent of claims within 14 or 21 days to reach an acceptable level of performance.
[345]We calculated PUA average benefit amounts by dividing the state-reported monthly amounts for total compensation paid by total weeks compensated. Benefit amounts are based on data reported by states as of March 15, 2021, at which point 9 states had reported PUA data for February 2021. Thus, we analyzed benefit payment data for January 2021. The following states and territories did not report PUA monthly amount compensated data for January 2021: Alabama, Arizona, Colorado, Delaware, Florida, Kansas, Maryland, Puerto Rico, South Carolina, and Vermont. The minimum benefit for PUA aligns with the minimum benefit for the Disaster Unemployment Assistance program and is set in Unemployment Insurance Program Letter (UIPL) 3-20. Department of Labor, Minimum Disaster Unemployment Assistance (DUA) Weekly Benefit Amount: January 1 - March 31, 2020, Unemployment Insurance Program Letter (UIPL) 3-20 (Washington, D.C.: Dec. 12, 2019). According to DOL, states must use the amounts set in UIPL 3-20 as the minimum weekly benefit amount for all PUA claims. For this analysis, we compared the PUA minimum weekly benefit amounts in UIPL 3-20 to PUA average weekly benefit amounts, by state.
[346]DOL guidance notes that when individuals submit sufficient documentation of wages, states must immediately recalculate their weekly benefits and pay the full PUA benefit amount with the greatest promptness that is administratively feasible. Department of Labor, CARES Act of 2020 – Pandemic Unemployment Assistance (PUA) Program Reporting Instructions and Questions and Answers, Unemployment Insurance Program Letter (UIPL) 16-20, Change 1 (Washington, D.C.: Apr. 27, 2020); see also 20 C.F.R. § 625.9(e). Under the CARES Act, the regulations for DUA generally apply to PUA. Pub. L. No. 116-136, § 2102(h), 134 Stat. 281, 317.
[347]While the CARES Act UI programs were federally funded, regular UI is primarily funded through state and federal taxes on employers. When a state exhausts the funds available for regular UI benefits, it may borrow from the federal government. According to DOL data, even before the pandemic, many states were not taking in enough UI tax revenue to satisfy the solvency standard specified in DOL regulations providing for interest-free loans to states. See 20 C.F.R. § 606.32 (2019).
[348]According to DOL, the U.S. Virgin Islands had a residual loan balance of about $0.06 billion at the beginning of 2020 left from the 2007-2009 recession, and did not begin borrowing during the COVID-19 pandemic until August 2020.
[349]According to the National Bureau of Economic Research, the 2007-2009 recession began in December 2007 and ended in June 2009.
[350]According to DOL officials, the federal tax primarily supports the administration of the program, while the state taxes fund the benefits.
[351]Under the Federal Unemployment Tax Act (FUTA), employers are generally required to pay a federal unemployment tax at a rate of 6.0 percent on the first $7,000 of wages paid to an employee each year, which funds administrative costs associated with the regular UI program and the federal share of benefits paid under the Extended Benefits program, among other things. FUTA provides a credit of up to 5.4 percent against federal tax liability to employers who pay state taxes timely under an approved state UI program. If a state has outstanding loan balances on January 1 for two consecutive years, and does not repay the full amount of its loans by November 10 of the second year, the FUTA credit rate for employers in that state will be reduced. Thus, the federal taxes paid by employers will increase, all else equal.
[352]According to the Department of the Treasury, the CARES Act established the $150 billion Coronavirus Relief Fund to provide payments to state, local, territorial, and tribal governments to cover the costs of necessary expenditures incurred due to the COVID-19 pandemic. In its guidance on the Coronavirus Relief Fund, the Department of the Treasury reported that states may use this funding to make payments to their state UI trust funds to prevent expenses related to the COVID-19 public health emergency from causing these UI trust funds to become insolvent. On January 15, 2021, the Department of the Treasury re-published in a final form the guidance it had previously made available on its website regarding the Coronavirus Relief Fund. Prior to publication in the Federal Register, the last version of its guidance and frequently asked questions documents were dated September 2, 2020 and October 19, 2020, respectively. 86 Fed. Reg. 4,182 (Jan. 15, 2021).
[353]On December 11, 2020, Georgia held loans to pay UI benefits totaling almost $886 million. By the end of 2020, Georgia no longer held outstanding federal loans for UI benefits. Georgia again took out loans during the first couple months of 2021, and held about $103 million in federal loans to pay UI benefits as of March 5, 2021. However, as of March 12, 2021, Georgia had paid these loans and held no balance.
[354]The West Virginia State Auditor’s Office is monitoring coronavirus expenditures on its COVID-19 Transparency webpage. West Virginia State Auditor’s Office, “West Virginia COVID-19 Transparency,” accessed March 16, 2021, https://stories.opengov.com/westvirginia/published/mnOzKr2wB.
[355]As of December 31, 2020, the Department of the Treasury reported that it had obligated all of the $150 billion from the Coronavirus Relief Fund to state, local, territorial, and tribal governments. The Consolidated Appropriations Act, 2021 extended the period for states and other entities to use these funds through December 31, 2021. Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. 1182, 2145.
[356]Pub. L. No. 116-260, div. N, tit. II, § 242(a), 134 Stat. 1182, 1960.
[357]Department of Labor Office of Inspector General, Alert Memorandum: The Employment and Training Administration (ETA) Needs to Ensure State Workforce Agencies (SWA) Implement Effective Unemployment Insurance Program Fraud Controls for High Risk Areas, Report Number 19-21-002-03-315 (Washington, D.C.: Feb. 22, 2021).
[358]Federal charges refer to criminal complaints and indictments. A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[359]Fraud involves obtaining something of value through willful misrepresentation. Some overpayments may be the result of fraud. However, whether an act is in fact fraud is a determination to be made through the judicial or other adjudicative systems.
[360]States may revise the amount of overpayments they have identified for 3 years after the reporting quarter, according to DOL. According to DOL, overpayments include those in the regular UI, Extended Benefits, and emergency unemployment compensation programs (specifically, those programs enacted during the 2007-2009 recession, according to officials), and exclude overpayments that have been waived. According to DOL, states may waive a non-fraud overpayment, in accordance with state law, if the overpayment was not the fault of the claimant and requiring repayment would be against equity and good conscience or would otherwise defeat the purpose of the UI law.
[361]We accessed the PUA overpayments data on March 15, 2021; these data are subject to change as more states report data and states revise previously reported data. The number of states that have reported PUA overpayments data varies by month; for example, 1 state reported overpayment amounts in March 2020, 15 states reported overpayment amounts in April 2020, 35 states reported overpayment amounts in January 2021, and 7 states reported overpayment amounts in February 2021. Among the states reporting data, we identified wide variation in the amount of PUA overpayments reported in any given month.
[362]According to the Consolidated Appropriations Act, 2021, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount, but the state can waive that requirement if the individual was without fault and repayment would be contrary to equity and good conscience. Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952.
[363]Executive Order 14002, 86 Fed. Reg. 7229 (Jan. 27, 2021).
[364]Pub. L. No. 117-2, § 9601, 135 Stat. 4, 138–144.
[365] The statute makes the full Child Tax Credit available to children in families with low earnings or that lack earnings in a year, and it increases the credit’s maximum amount to $3,000 per child and $3,600 for children under age 6. It also extends the credit to 17-year-olds. Pub. L. No. 117-2, § 9611, 135 Stat. at 144–150.
[367]The number of payments is taken from the IRS Master File and includes reissued payments but does not include payments to residents of territories. The amount of payments is taken from the Treasury general ledger and includes reversals and payments to the U.S. territories.
[368]IRS sent over 1.2 million notices in December 2020 notifying individuals that they had not received their EIP 1 because IRS had not yet processed their 2019 tax return.
[369] Free File, Inc. is a public-private partnership between the IRS and a consortium of tax preparation companies that provide their products for free if a taxpayer’s adjusted gross income is below a certain level.
[370] Approximately 87,000 EIP 1 and 617,000 EIP 2 debit cards have been activated but not used, amounting to over $629 million.
[371]Pub. L. No. 116-260, § 272(d)(2)(A), 134 Stat. at 1972.
[372]IRS confirmed that it sent at least 13 million EIP 2 payments to temporary bank accounts. Tax industry partners provided us data that at least 5.6 million additional EIP 2 payments were sent to temporary accounts. We did not independently verify the data we received from tax industry partners.
[373] We did not independently verify these figures.
[374]We previously reported on challenges IRS had in delivering EIP payments to non-filers and unbanked households. In addition, we reported on steps IRS had been taking assist in the return of payments made to individuals who are incarcerated, which had been previously withheld. However, IRS does not does not collect demographic data indicating which households house received the EIP, and data we use do not have household-level demographic data indicating which households have and have not received EIPs, therefore based on our analyses, it is not conclusive whether there are disparities in the disbursement of EIP by sex, race, or ethnicity.
[375]GAO analysis of the U.S. Census Bureau's Current Population Survey March 2020 Annual Social and Economic Supplement (ASEC). The 95 percent margins of errors for these estimates are within +/- 0.54 percentage points.
[376]Federal Deposit Insurance Corporation, 2019 FDIC Survey of Household Use of Banking and Financial Services. The 95 percent margins of errors for these estimates are within +/- 1.79 percentage points.
[377]The 95 percent margins of errors for these estimates are within +/- 0.96 percentage points.
[378]E. Ann Carson, Prisoners in 2019, NCJ Bulletin 255115 (U.S. Department of Justice, Office of Justice Programs, Bureau of Justice Statistics, October 2020). The imprisonment rate is “the number of prisoners sentenced to more than 1 year under state or federal jurisdiction per 100,000 U.S. residents.”
[379]In nominal terms, SNAP expenditures peaked in fiscal year 2013, when benefits totaled $76.1 billion, according to FNS data. SNAP expenditures had declined since then, with benefits totaling $55.6 billion in fiscal year 2019.
[380]Data presented here are FNS’s preliminary data on SNAP participation and expenditures for fiscal year 2020, released on January 27, 2021. FNS noted that data are subject to significant revision. On March 12, 2021, FNS released additional data covering the first two months of fiscal year 2021 (October and November 2020). Those data show that, in November 2020, 41.4 million individuals participated in SNAP and monthly benefits totaled approximately $7.8 billion.
[382]Pub. L. No. 116-260, div. N, tit. VII, § 702(a), (e), (h), 134 Stat. 1182, 2092-2094. In March 2021, the American Rescue Plan Act of 2021 extended the increase in SNAP benefits amounts through September 2021 and provided $1.15 billion for SNAP administrative expenses to be available through September 2023, among other provisions. Pub. L. No. 117-2, § 1101(a), 135 Stat. 4, 15.
[383]The American Rescue Plan Act of 2021 generally authorized USDA to increase the WIC cash-value voucher—participants can use these vouchers to purchase fruits and vegetables—up to $35 through September 2021 and provided $490 million to carry out this temporary increase. The act also provided $390 million for WIC program outreach, innovation, and modernization efforts to increase participation and benefit redemption. Pub. L. No. 117-2, §§ 1105, 1106, 135 Stat. 4, 16-17.
[384]The American Rescue Plan Act of 2021 made additional changes to Pandemic EBT, including authorizing USDA to approve states to operate the program during the summer months and extending the authority of the program in the event of a future public health emergency. Pub. L. No. 117-2, § 1108(1), 135 Stat. 4, 18.
[385]Similarly, in its fiscal year 2020 Annual Financial Report, USDA acknowledged that data availability and quality, as well as antiquated reporting systems, presented challenges to FNS in monitoring nutrition assistance programs during the pandemic.
[386]Typically, FNS publishes new program data each month on a 3-month lag—that is, FNS published April 2020 data in July 2020.
[387]Office of Management and Budget, Guidelines for Ensuring and Maximizing the Quality, Objectivity, Utility, and Integrity of Information Disseminated by Federal Agencies (Washington, D.C.: Oct. 1, 2001).
[388]Data presented throughout this section are FNS’s preliminary data on participation in and expenditures for its nutrition assistance programs for fiscal year 2020, released on January 27, 2021. As mentioned above, FNS noted that data are subject to significant revision. On March 12, 2021, FNS released additional data covering the first two months of fiscal year 2021 (October and November 2020). Those data show that, in November 2020, 41.4 million individuals participated in SNAP and monthly benefits totaled approximately $7.8 billion.
[389]As noted above, according to FNS officials, the agency reports a child as a participant in Pandemic EBT only in the month the child received benefits, even if those benefits cover additional months retroactively. For example, a child that received Pandemic EBT benefits in June 2020 to cover the months of March, April, May, and June 2020 is only reported as a participant for June 2020. FNS officials said this is consistent with how the agency reports participation and benefits for SNAP.
[390]States not previously approved to issue benefits for the beginning of school year 2020-21 may include those months (generally August and September 2020) in their plans.
[391]The Continuing Appropriations Act, 2021 and Other Extensions Act also expanded Pandemic EBT to include certain children in childcare. Pub. L. No. 116-159, § 4601(6), 134 Stat. 709, 744. In December 2020, the Consolidated Appropriations Act, 2021 changed eligibility, and on January 29, 2021, FNS issued guidance to states on implementing this provision. Pandemic EBT disbursements are likely to increase significantly once states are able to issue benefits to certain children in childcare.
[392]As we reported in November 2020, FNS had not needed to disburse any of these funds for WIC in fiscal year 2020.
[393]FNS provides WIC state agencies with a food grant and the Nutrition Services and Administration grant. WIC state agencies can use the food grant to provide supplemental foods, such as WIC-approved eggs, milk, and infant formula. State agencies can use the Nutrition Services and Administration grant for administrative costs and certain WIC public health initiatives, including nutrition education and breastfeeding support services.
[394]Pub. L. No. 116-159, § 4603(a)(1), 134 Stat. 709, 745-746.
[395]According to USDA, the agency is reviewing its authority to permit states to provide additional SNAP benefits through emergency allotments for households already receiving the maximum benefit for their household size. USDA also noted that it will expedite its implementation of the provision of the Agriculture Improvement Act of 2018 requiring USDA to reevaluate the Thrifty Food Plan by 2022 and every 5 years thereafter. See Pub. L. No. 115-334, § 4002, 132 Stat. 4490, 4624. The Thrifty Food Plan is the basis for determining SNAP benefits amounts, and USDA’s review will determine if the plan adequately reflects the present costs of a nutritious diet.
[396]Pub. L. No. 116-260, div. N, tit. VII, § 702(d) and (e), 134 Stat. 1182, 2093. In June 2020, we reported that FNS denied requests from 31 states to suspend the requirement that college students work at least 20 hours per week or participate in federal work study to be eligible for SNAP. FNS officials explained at the time that they did not have authority to suspend the requirement in the FFCRA. Additionally, we recommended in December 2018 that FNS improve SNAP eligibility information for college students on its website and share information on how states may help eligible college students access SNAP.
[397]Households receiving SNAP benefits in most states had the option to use their benefits online during the COVID-19 pandemic. The SNAP Online Purchasing Pilot began in April 2019 in New York, followed by Washington in January 2020. As of mid-March 2021, FNS has approved 47 states, including the District of Columbia, to participate. In addition, the Consolidated Appropriations Act, 2021 includes $5 million for SNAP online purchasing technical assistance and related technology improvements, among other things.
[398]This review includes NSLP, SBP, SFSP, and CACFP. The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) program is not included in this review.
[399]The Seamless Summer Option is a program that allows school districts to operate a modified version of the National School Lunch Program and School Breakfast Program into the summer, or during unanticipated school closures. The program is reimbursed at the same rate as the National School Lunch Program. In contrast, the Summer Food Service Program has a higher reimbursement rate.
[400]Pub. L. No. 116-136, div. B, tit. I, 134 Stat. 281, 507.
[401]Emergency Meals-to-You was a public-private partnership between USDA, the Baylor University Collaborative on Hunger and Poverty, McLane Global, and PepsiCo. It began as a summer pilot project in 2019, but was expanded in response to the COVID-19 pandemic.
[403]Pub. L. No. 116-260, div. N, tit. VII, § 722, 134 Stat. 1182, 2097. This law provided an indefinite appropriation of funds based on a formula that generally takes into account the difference in reimbursements paid between March-June of 2019 and March-June of 2020.
[404]This action was taken following the Continuing Appropriations Act, 2021 and Other Extensions Act enacted on October 1, 2020, that extended USDA’s waiver authority under the Families First Coronavirus Response Act and provided an indefinite appropriation to carry out the extension.
[405]These updated data reported by FNS show a larger drop in meals served than previously reported data for March and April 2020. We previously reported in September 2020 that initial FNS data showed the number of meals served dropped by almost 400 million (21 percent) in March and April 2020 compared to March and April 2019. Updated FNS data showed more than 740 million fewer meals (39 percent) were served in March and April 2020 compared to the same months in 2019. According to FNS, state agencies submit monthly meal claim reports to FNS. Initial monthly tabulations reported 30 days following the end of the claim month include estimated data based on the previous year, and the uncertainty of meal service during the COVID-19 pandemic has made it difficult for states to utilize historical data to report estimates of meals served, according to FNS. Data reported by states to FNS 90 days following the end of the claim month are based on actual meal claims, rather than estimates. According to FNS, these data are subject to revision.
[406]During the spring and summer 2020, the Emergency Meals-to-You program mailed boxes of 10 breakfasts and 10 lunches to eligible students in participating school districts. The purpose of the program was to serve students who were no longer able to receive meals at school due to the pandemic-related school closures, and resided in rural school districts in which at least 50 percent of enrolled students were eligible for free or reduced-priced lunch. The Pandemic EBT program provides benefits to households with children who would have received free or reduced-priced school meals if not for school closures due to COVID-19.
[407]In our May 2018 report, we recommended FNS improve its estimate of participation by focusing on addressing data reliability issues caused by variations in the number of operating days of meal sites and in the months in which states see the greatest number of meals served. This recommendation remains open. FNS recently reported that it plans to use results from an upcoming study on summer meals to gather more information on how SFSP participation is captured.
[408]Per federal regulations, nutrition programs’ reserves are generally limited to no more than three months’ average expenditures. See 7 C.F.R. § 210.14(b).
[409]FNS did not explicitly designate CARES Act funds for pandemic-related expenses; instead, FNS guidance states that funds received through meal reimbursements may be used to pay for reasonable pandemic-related expenses. In one state, the nutrition official did not express concern about the manner in which FNS provided CARES Act funds.
[411]On December 21, 2020, the Joint Committee on Taxation updated estimates for forgone revenue to reflect changes in the Consolidated Appropriations Act, 2021.
[412]High-Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas. GAO-21-119SP. Washington, D.C.: March 02, 2021.
[413]Pub. L. No. 116-127, §§ 7001–7004, 134 Stat. 178, 210–219 (2020). A refundable tax credit reduces tax liability, dollar for dollar; if the credit exceeds tax liability, a refund is due. Full-time and part-time employees are counted. Both credits have maximum payouts. Self-employed individuals may not file for advances on their credit refunds.
[414]The Consolidated Appropriations Act, 2021 extended this credit to include qualified leave wages paid for periods of leave from December 31, 2020 to March 31, 2021. Pub. L. No. 116-260, div. N, § 286(a), 134 Stat. 1182, 1989 (2020). For 2020, the credit is available to eligible employers that paid qualified leave wages as required by FFCRA. The FFCRA requirement for paid leave expired on of December 31, 2021; thus, for 2021, the credit is available to employers that voluntarily pay leave wages if those wages would have met the FFCRA requirements for qualified leave wages.
[415]15 U.S.C. § 636(a)(36)(A)(viii)(II)(dd), (ee). PPP recipients must meet certain criteria for loan forgiveness.
[417]Pub. L. No. 116-136, § 2301, 134 Stat. at 281, 347–351 (2020); Pub. L. No. 116-260, div. N, § 206, 134 Stat. at 3059–3061. Some government entities, including tribal governments, tribal entities, state or locally-run colleges, universities, and organizations providing medical or hospital care, are also eligible for the Employee Retention Credit.
[418]Pub. L. No. 116-136, § 2301(j), 134 Stat. at 350; See also 85 Fed. Reg. 23450 (Apr. 28, 2020); 85 Fed. Reg. 29845 (May 19, 2020); 85 Fed. Reg. 31357 (May 26, 2020).
[419]Pub. L. No. 116-260, div. N, § 206(c)(2)(B)(i), 134 Stat. at 3061. This change was retroactive to March 27, 2020, the date of the enactment of the CARES Act
[420]IRS Notice 2021-20, 2021-11 I.R.B. 922 (Mar. 15, 2021), available online at: https://www.irs.gov/pub/irs-irbs/irb21-11.pdf (accessed Mar. 15, 2021). Eligible employers may elect not to take into account certain qualified wages for purposes of the credit. Pub. L. No. 116-260, div. N, § 206(c)(2)(A), 134 Stat. at 3060–3061.
[421]Pub. L. No. 116-260, § 206(e)(2), 134 Stat. at 3061. This rule can also apply to claiming the credit for health care expenses paid.
[422]There are other wages for which an employer may not claim the Employee Retention Credit. For example, for 2020, employees counted under a Work Opportunity Tax Credit (WOTC) are not counted for purposes of the Employee Retention Credit, and for 2021, the Employee Retention Credit cannot be claimed for wages for which the WOTC is claimed.
[423]Only employers with an average of 500 or fewer full-time employees in 2019 may receive advance payments of the Employee Retention Credit and the amount of any such advance is limited. Pub. L. No. 116-260, § 207(g), 134 Stat. at 3063–3064.
[424]Pub. L. No. 116-136, § 2302, 134 Stat. at 351–352, as amended by the Paycheck Protection Program Flexibility Act, Pub. L. No. 116-142, § 4, 134 Stat. 641, 643 (2020). To be considered timely, deferred payments of 50 percent of tax are to be made by December 31, 2021, with the remainder due December 31, 2022. The employer share of Social Security tax is 6.2 percent of taxable earnings up to the Social Security wage base cap on taxable income. The tax finances the Social Security trust funds.
[425]Self-employed individuals pay the employer and employee tax share, which is 12.4 percent of taxable earnings, up to the Social Security wage base cap on taxable income.
[426]Deferred payments for self-employment taxes are reported on Form 1040, Schedule SE and deferred payments for household employment taxes are reported on Form 1040, Schedule H.
[428]IRS Notice 2020-65, 2020-38 I.R.B. 567 (Sept. 14, 2020), available online at: https://www.irs.gov/irb/2020-38_IRB (accessed Oct. 20, 2020). We were asked to issue a legal decision regarding whether Notice 2020-65 is a rule under the Congressional Review Act. We determined that since IRS submitted Notice 2020-65 to us under the Congressional Review Act, there is no need for a legal decision from our office. See GAO, Request for a Congressional Review Act Opinion on IRS Notice 2020-65, B-332517 (Washington D.C.: September 2020). As noted in our correspondence, on September 4, 2020, Representative John Larson of Connecticut introduced House Joint Resolution 94 which is a resolution of disapproval of the Notice. H. R. J. Res. 94, 116th Cong. (2020).
[429]Office of Management and Budget, Guidance on Implementing Payroll Tax Deferral for Federal Employees (Sept. 11, 2020), accessed online March 1, 2021, https://www.whitehouse.gov/wp-content/uploads/2020/09/M-20-35.pdf. The memorandum does not cover legislative and judicial branch entities.
[430] Pub. L. No. 116-260, div. N, § 274, 134 Stat. at 1978 (2020); IRS Notice 2021-11, 2021-6 I.R.B 827 (Feb. 8, 2021). The guidance directs employers to ratably withhold and pay the deferred taxes, meaning, in general, equally apportioned across the period.
[431]Small employers are defined as those with an average of 500 or fewer full-time employees in 2019.
[432]On Jan. 22, 2021, IRS also released guidance implementing the legislation allowing PPP recipients who have had their request for loan forgiveness denied have the option to claim the credit with respect to second or third quarter qualified wages on their fourth quarter Form 941, acknowledging that this may be difficult before returns are due.
[433]The tax credit dollar figures we are reporting are as reported by taxpayers and are subject to taxpayer reporting error. These figures may differ from IRS’s reported figures because we are reporting what was filed without adjustments. These figures represent paper returns, as of January 6, 2021 (main Form 941) and March 4, 2021 (Schedule R) and e-file returns, as of January 12, 2021.
[434]This number is likely an undercount because it does not include employers who either file on paper returns (IRS does not capture this line), or who do not provide this information because it is not on Schedule R, Allocation Schedule for Aggregate Form 941 Filers. According to IRS officials, this may also include employers who have switched to a third-party filer or, in certain circumstances, who have been acquired, merged, or consolidated.
[435]Some of these advances are also included in the table above because employers are to report on Form 941 the advance credits they have received.
[436]This calculation is based on the amount of advance credits received reported by taxpayers on Form 941, which differs from the amount of advance credits IRS has issued.
[437]Multiple Forms 7200s may be included in each e-fax receipt, including duplicate submissions and aggregate submissions from the same employer.
[438]We could not separate employee and employer share of the deferrals because, according to IRS officials, data on the new Form 941 line with employee share of deferrals will not be available in their database until late March 2021.
[439] The Department of Agriculture’s National Finance Center provides payroll services for more than 600,000 federal employees.
[440]IRS officials said they have noted many employers who entered the same value for their employee count and their wages, tips and other compensation (line 2) on their Form 941. Our counts of potentially ineligible leave credit claimants include 643 employers who made this error. To ensure our employee counts were not inflated by aggregate reporting, we analyzed employee counts by client on Schedule R, rather than aggregated counts reported on the Form 941 for these employers.
[441]Although sole proprietors are eligible for the credit, they are instructed to file for the credit on their income tax return. Some of the employers reporting zero employees have closed, based on Form 941 information. Other employers may have had no employees during the pay period for which the Form 941 instructions request employee counts, but had employees at other times in the quarter. The returns with no value in line 1 were all paper returns, suggesting IRS error transcribing the returns. Regardless of the error source, IRS could follow up on these returns.
[442]For example, for the second quarter, employers are instructed to report as of the pay period that includes June 12.
[443]We have not analyzed Forms 943 for 2020 because data were not available in time for this report.
[444]U.S. Census Bureau officials stated that they plan to conduct a nonresponse bias analysis and expect to complete it by June 30, 2021. In addition, for the survey week covering January 4-10, 2021, response rates by state ranged from 16 to 30 percent.
[445]Data analyzed was for the week of January 4-10, 2021. Survey respondents self-reported whether they had received assistance from the included credits. All Small Business Pulse Survey estimates in this enclosure have a margin of error of ± 1.7 percentage points or less at the 95 percent confidence level, unless noted otherwise. Industry-specific percentages were calculated for each two-digit North American Industry Classification System (NAICS) code represented in the survey for that week.
[446]All estimates in this paragraph have a margin of error of ± 0.4 percentage points or less at the 95 percent confidence level.
[447]The U.S. Census Bureau classified firms by the sex, race, and ethnicity of firm owners. According to the U.S. Census Bureau, not all firms were classifiable by sex, race, and ethnicity. Firms not classifiable by sex, race, and ethnicity include firms that have no owners with a 10 percent or greater ownership of the stock or equity in the business. In addition, firms could be classified as more than one racial group. This might happen when the sole owner was reported to be of more than one race, when the majority owner was reported to be of more than one race, or when a majority combination of owners was reported to be of more than one race. Other race categories not described in this enclosure include American Indian and Alaska Native, Native Hawaiian and Other Pacific Islander, Minority, Nonminority, and Equally Minority/Nonminority. In the ethnicity grouping, firms could be also be classified as Equally Hispanic/non-Hispanic. All sex, race, and ethnicity percentages were calculated using the total number of classifiable firms as the denominator.
[448]We determined that estimates of owner’s race or ethnicity by business size and industry available through Census’ published tables of ABS estimates were not reliable for our purposes, as many of these estimates were suppressed. Census suppresses estimates when there are data quality concerns such as high sampling variability or poor response quality. Due to time constraints for this report, we were unable to examine alternative groupings of business size and race or ethnicity, such as through an analysis of ABS microdata, necessary to determine groupings of race or ethnicity and business size within industries that produce reliable estimates. Instead, we examined sex, race, and ethnicity by industry for all businesses, rather than by business size, since these estimates in Census’ ABS tables generally were not suppressed. Based on our analysis of ABS data, an estimated 99.7 percent of employer firms are small businesses (less than 500 employees). However, this may vary by industry. Among the industries in our analysis, the percent of firms that are small ranged from between 96.1 and 99.9 percent. We could not determine the percent of small firms for three industries in our analysis, due to data suppression issues.
[449]The CSBG Act is codified at 42 U.S.C. §§ 9901-9926. In this enclosure, we use “states” to refer to “states, territories, and tribes.”
[450]Community action agencies are private or public nonprofit organizations that were created to combat poverty in geographically designated areas. Other local recipients of CSBG funds include local governments, federal and state-recognized Indian tribes and tribal organizations, and organizations with migrant and seasonal farm worker programs.
[451]States must distribute no less than 90 percent of the CSBG grant funds to local agencies, and may reserve a portion of funds not to exceed 10 percent for administrative costs, training, technical assistance, and other activities, in accordance with the CSBG Act. 42 U.S.C. § 9907.
[452]Pub. L. No. 116-136, 134 Stat. 281, 558 (2020).
[453]As of February 24, 2021, ACF confirmed this was the final allotment. The total CSBG CARES Act appropriation included $971,398,810 for states, $5,000,000 for territories, and $8,601,190 for tribes.
[454]See CSBG Act Section 675B(b)(3) (42 U.S.C. § 9906(b)(3)). The 12 states subject to the maximum allotment were Alaska, Delaware, Hawaii, Idaho, Montana, Nevada, New Hampshire, North Dakota, South Dakota, Utah, Vermont, and Wyoming.
[455]Consolidated Appropriations Act, 2021, div. M, tit. III, § 306, 134 Stat. 1182, 1923.
[456]The CSBG Act requires states to conduct onsite monitoring as follows: (1) each local agency at least once within each three-year period, (2) each new local agency after the first year of receiving CSBG funds, and (3) follow-up reviews including return visits to local agencies that fail to meet goals, standards, and requirements established by the states. 42 U.S.C. § 9914(a).
[457]This state also received help from Community Action Program Legal Services (CAPLAW), a nonprofit membership corporation that is the national legal expert for community action agencies, and provides consultations, training, and resources to local agencies.
[458]Small Business Administration, Office of Performance Management and the Chief Financial Officer, Agency Financial Report for Fiscal Year 2020 (Washington, D.C.: Dec. 18, 2020).
[459]Pub. L. No. 116-260, div. N, tit. III, § 331, 134 Stat. 1182, 2043-45.
[461]Other discrepancies include loans and grants issued to borrowers with inaccurate or invalid tax identification numbers, employer identification numbers, or Social Security numbers; loans issued that SBA flagged as potentially fraudulent; and loans issued to borrowers that SBA flagged because the borrowers were excluded from doing business with the government.
[462]GAO’s Standards for Internal Control in the Federal Government provides the overall framework for establishing and maintaining an effective internal control system, and it lists five components of internal control representing the highest level of the hierarchy of standards for internal control in the federal government. The five components of internal control are (1) control environment, (2) risk assessment, (3) control activities, (4) information and communication, and (5) monitoring. The five components of internal control must be effectively designed, implemented, and operating, and operating together in an integrated manner, for an internal control system to be effective.
[463]Department of the Treasury’s Do Not Pay service is an analytics tool that helps federal agencies detect and prevent improper payments made to vendors, grantees, loan recipients, and beneficiaries. Agencies can check multiple data sources in order to make payment eligibility decisions.
[464]The Fraud Risk Framework helps managers meet their responsibilities to assess and manage fraud risks as required by federal internal control standards.
[465]According to federal internal control standards, inherent risk is the risk to an entity prior to considering management’s response to the risk. Residual risk is the risk that remains after inherent risks have been mitigated by existing control activities.
[466]Synthetic identity fraud is a crime in which perpetrators combine real or fictitious information, such as Social Security numbers and names, to create identities with which they may defraud financial institutions, government agencies, or individuals.
[467]Small Business Administration, Office of Performance Management and the Chief Financial Officer, Agency Financial Report Fiscal Year 2020 (Washington, D.C.: Dec. 18, 2020), 39–63.
[468]A material weakness is a deficiency, or combination of deficiencies, in internal control over financial reporting, such that there is a reasonable possibility that a material misstatement of the entity’s financial statements will not be prevented, or detected and corrected, on a timely basis. A deficiency in internal control exists when the design or operation of a control does not allow management or employees, in the normal course of performing their assigned functions, to prevent, or detect and correct, misstatements on a timely basis.
[469]See Pub. L. No. 116-136, §§ 1102(b), 1107(a)(1), 1112, 134 Stat. 281, 293, 301; Pub. L. No. 116-139, § 101(a), 134 Stat. 620, 620 (2020); Pub. L No. 116-260, div. N, tit. III, §323 134 Stat. 1182, 2018-22 (2020); Pub. L. No. 117-2, § 5001(d) 135 Stat. 4, 85 (2021).
[470]As originally implemented by SBA, at least 75 percent of the loan forgiveness amount must have been for payroll costs. In addition, the CARES Act required loans to be used within an 8-week period in order for the loans to be fully forgiven. However, the Paycheck Protection Program Flexibility Act of 2020 modified this to at least 60 percent and allowed borrowers to pay or incur those expenses over a 24-week period. Pub. L. No. 116-142, § 3, 134 Stat. 641, 641-42 (2020). Under the Paycheck Protection Program Flexibility Act of 2020, the covered period for PPP loans was to end the earlier of 24 weeks after origination or December 31, 2020. The Consolidated Appropriations Act, 2021, further modified the covered period to allow the borrower to choose a covered period ending any date between 8 and 24 weeks after origination. Pub. L. No. 116-260, div. N, tit. III, § 306, 134 Stat. 1182, 1997 (2020).
[471]Totals exclude canceled loans. According to SBA, canceled loans may include, but are not limited to, duplicative loans, loans not closed for any reason, and loans that were fully paid off. In our September 2020 report, we provided information on the types of borrowers that received PPP loans and the size of PPP loans.
[472]The Consolidated Appropriations Act, 2021, expanded the list of allowable uses of proceeds and loan forgiveness to include certain operations, property damage, supplier, and worker protection expenditures. PPP borrowers are eligible to receive a second PPP loan of up to $2 million provided that they meet certain criteria, such as having not more than 300 employees, having used or intending to use the full amount of their initial PPP loan, and documenting quarterly revenue losses of at least 25 percent in a quarter of 2020 when compared to the same quarter in 2019. Pub. L No. 116-260, div. N, tit. III, § 311, 134 Stat. 1182, 2001 (2020); see also 86 Fed. Reg. 3712 (Jan. 14, 2021).
[473]Under the Consolidated Appropriations Act, 2021, the loan forgiveness certification was required to be not more than one page in length and could only require borrowers to provide a description of the number of employees they were able to retain because of the loan, the estimated amount of the loan amount spent on payroll costs, and the total loan value. Borrowers must also attest that they complied with all PPP loan requirements. Borrowers must retain relevant employment records for 4 years following submission of the form and other relevant records for 3 years. SBA retains the right to review and audit these loans for fraud.
[474]The Consolidated Appropriations Act, 2021, set aside $15 billion for initial and second draw PPP loans issued by community financial institutions, including community development financial institutions and minority depository institutions, and an additional $15 billion for initial and second draw PPP loans issued by certain small depository institutions. Pub. L. No. 116-260, div. N, tit. III, § 323(d)(1)(A), 134 Stat. 1182, 2019-20 (2020).
[475]SBA considered smaller lenders to be those with $1 billion or less in assets.
[476]Eligible entities include businesses, certain nonprofit organizations, housing cooperatives, veterans’ organizations, tribal businesses, self-employed individuals, sole proprietors, independent contractors, and small agricultural co-operatives that received a PPP loan, employ not more than 300 employees, and meet certain other criteria. See Pub. L. No. 116-260, div. N, tit. III, § 311, 134 Stat. 1182, 2001 (2020); see also 86 Fed. Reg. 3712 (Jan. 14, 2021).
[477]The Department of the Treasury’s Do Not Pay service is an analytics tool that helps federal agencies detect and prevent improper payments made to vendors, grantees, loan recipients, and beneficiaries. Agencies can check multiple data sources in order to make payment eligibility decisions.
[478]According to the documents and SBA officials, SBA is in the process of updating its review policies to reflect changes made in implementing the Consolidated Appropriations Act, 2021.
[479]The Economic Injury Disaster Loan program provides low-interest loans of up to $2 million for expenses—such as operating expenses—that cannot be met because of a disaster. The CARES Act expanded EIDL program eligibility to include additional small business entities and appropriated $10 billion to create a program to provide small businesses up to $10,000 in advances toward payroll, sick leave, and other business obligations. In the Paycheck Protection Program and Health Care Enhancement Act, Congress appropriated another $10 billion for advances. The Consolidated Appropriations Act, 2021, included an additional $20 billion for targeted EIDL advances to eligible entities with 300 or fewer employees in low-income communities that have suffered an economic loss of greater than 30 percent.
[480]GAO’s Standards for Internal Control in the Federal Government provides the overall framework for establishing and maintaining an effective internal control system, and it lists five components of internal control representing the highest level of the hierarchy of standards for internal control in the federal government. The five components of internal control are (1) control environment, (2) risk assessment, (3) control activities, (4) information and communication, and (5) monitoring. The five components of internal control must be effectively designed, implemented, and operating, and operating together in an integrated manner, for an internal control system to be effective.
[481]We reported on the potential for fraud in PPP in October 2020.
[482]SBA officials noted that the number of PPP loans made also was significantly higher than the number made in a typical year.
[483]The Fraud Risk Framework helps managers meet their responsibilities to assess and manage fraud risks as required by federal internal control standards.
[484]According to federal internal control standards, inherent risk is the risk to an entity prior to considering management’s response to the risk. Residual risk is the risk that remains after management’s response to inherent risk. A fraud risk profile documents the findings from a fraud risk assessment, including the analysis of the types of fraud risks, their perceived likelihood and impact, risk tolerance, and the prioritization of risks.
[485]The Federal Reserve has taken some actions to address the second recommendation, such as conducting scenario-based analyses for the facilities established in 2020 to assess the extent of possible losses in a range of scenarios. However, some documentation needed for a full assessment of the agency’s actions was not available at the time of our reporting.
[486]The facilities were authorized under Section 13(3) of the Federal Reserve Act, which permits the Federal Reserve to provide emergency lending, and were approved by the Secretary of the Treasury. Section 13(3) facilities must comply with requirements relating to loan collateralization and taxpayer protection, among others.
[487]The Consolidated Appropriations Act, 2021, rescinded at least $429 billion of the $500 billion previously appropriated to Treasury under Title IV of the CARES Act. Certain funds appropriated out of the $500 billion were not rescinded, including $25 million for the Special Inspector General for Pandemic Recovery, $5 million for the Congressional Oversight Committee, and $100 million to pay costs and administrative expenses. Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. N, tit. X, § 1003(a)(2)(C), 134 Stat. 1182, 2145 (2020).
[488]The Main Street Lending Program comprises five facilities: the Main Street New Loan Facility, Main Street Priority Loan Facility, Main Street Expanded Loan Facility, Nonprofit Organization New Loan Facility, and Nonprofit Organization Expanded Loan Facility.
[489]The Federal Reserve’s expectation of the facilities incurring no losses for the agency takes into account Treasury’s support using funds appropriated under the CARES Act, according to Federal Reserve officials.
[490]These two transactions were with the same two entities that had previously participated in the facility.
[491]The CARES Act funds rescinded by the Consolidated Appropriations Act, 2021, were returned to the General Fund.
[492]The three non-CARES Act facilities that will terminate on March 31, 2021 are the Primary Dealer Credit Facility, the Commercial Paper Funding Facility, and the Money Market Mutual Fund Liquidity Facility.
[493]CARES Act, Pub. L. No. 116-136, 134 Stat. 281, 470 (2020). The CARES Act did not provide criteria for which businesses were “critical to maintaining national security.” Treasury established the following definition: (1) performing under a “DX”-priority-rated contract or order under the Defense Priorities and Allocations System regulations (15 C.F.R. part 700) or (2) operating under a valid top secret facility security clearance under the National Industrial Security Program regulations (32 C.F.R. part 2004). Treasury guidance further noted that applicants that did not meet either of these criteria may still be considered for loans, if, based on the recommendation and certification by the Secretary of Defense or the Director of National Intelligence that the applicant’s business is critical to maintaining national security, the Secretary of the Treasury determines that the applicant business is critical to maintaining national security.
[494]As directed by the CARES Act, Treasury coordinated with the Department of Transportation (DOT) to determine the eligibility of certain applicants. DOT confirmed the type of carrier applicants (passenger and cargo) and the status of their operations, and reported this information to Treasury, according to DOT. Treasury also coordinated with the Department of Defense to determine the eligibility of applicants.
[495]This figure includes amendments to loan commitments made to loan agreements after the initial closings. The amendments include increases in loan commitments that reallocated unused funds, according to Treasury.
[496]For Yellow Corp., the maintenance of employment requirement expires 12 months after the initial funding date for each tranche of its loan. Tranche A funding occurred on July 9, 2020, and tranche B initial funding occurred on October 20, 2020.
[497]Yellow Corp. and Hawaiian Airlines executed loans with a duration of approximately 4 years.
[498]The benchmark interest rate used in these loan agreements is the London Inter-Bank Offered Rate (LIBOR).
[499]The eight companies are Alaska Airlines, American Airlines, Frontier Airlines, Hawaiian Airlines, JetBlue Airways, SkyWest Airlines, United Airlines, and Yellow Corp. When Treasury increased loan commitments, Treasury did not require borrowers to make additional draws to reach 10 percent of the new total commitment.
[500]The CARES Act authorized Treasury to provide up to $32 billion in financial assistance through PSP1. Treasury signed PSP1 agreements with passenger air carriers, cargo air carriers, and certain aviation contractors from April 2020 through October 2020. CARES Act, Pub. L. No. 116-136, § 4112, 134 Stat 281, 498 (2020).
[501]The American Rescue Plan Act of 2021, enacted on March 11, 2021, appropriates an additional $15 billion for eligible air carriers and contractors to extend the Payroll Support Program. Pub. L. No. 117-2, § 7301, 135 Stat. 4, 104-07.
[502]Pub. L. No. 116-260, div. N, tit. IV, 134 Stat. 1182, 2052-61 (2020).
[503]Passenger air carriers, when applicable, are required to provide notes equal to 30 percent of the value of awards over $100 million with a 10-year term. Contractors, when applicable, must provide notes equal to 44 percent of the payroll support provided for over $37.5 million with a 10-year term. Cash interest on the notes is payable semiannually each year beginning on March 31, 2021. The warrants provide Treasury with the right to purchase shares of common stock or receive cash payment.
[504]Contractors must agree to refrain from involuntary furloughs or layoffs until March 31, 2021, or until the contractor has expended all of its PSP2 funds, whichever occurs later. The Consolidated Appropriations Act, 2021 authorized the Secretary of the Department of Transportation (DOT) to require, “to the extent reasonable and practicable,” an air carrier receiving financial assistance under the act to maintain scheduled air transportation service as the Secretary deems necessary to ensure services to any point served by that air carrier before March 1, 2020. Other requirements all applicants must follow include agreeing to not pay dividends or make any other capital distributions, with respect to the common stock of the applicant through at least March 31, 2022.
[505]According to Treasury guidance, applications received before 11:59 p.m. EDT on January 14, 2021, were to be processed as quickly as possible. Applications received after 11:59 p.m. EDT on January 25, 2021, may not have been considered.
[506]Seventy-eight percent of the 549 companies that applied to PSP2 also participated in PSP1. Eighty-three percent of passenger air carriers that applied to PSP2 received PSP1 awards and 69 percent of contractors that applied to PSP2 received PSP1 awards.
[507]Amtrak owns about 360 of the 457 miles of the Northeast Corridor, which generally runs from Boston, Massachusetts, to Washington, D.C. However, Amtrak provides the majority of its long-distance and state-supported service on infrastructure (tracks and other facilities) owned by others, such as freight railroads or public agencies.
[508]Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. L, tit. I, 134 Stat. 1182, 1849-50 (2020).
[509]In the years since it first began operations in 1971, Amtrak’s annual operating expenses exceeded its revenues. Amtrak operated at an overall loss of $881 million in fiscal year 2019, but Amtrak officials had thought that in 2020, on an adjusted operating loss basis, revenues would exceed these expenses for the first time in 50 years.
[510]The CARES Act limited the amount that Amtrak could invoice the states for their share of losses on routes that Amtrak operates on behalf of states in fiscal year 2020 to 80 percent of the amount each state paid for fiscal year 2019. For example, if a state paid the company $1 million for this service in fiscal year 2019, the state could not pay more than $800,000 in fiscal year 2020. To offset this reduction, the CARES Act provided $239 million in funds that Amtrak was to draw down each month to cover the difference between the full cost of providing state-supported services and the reduced amount the company can charge the states. The CARES Act also allowed FRA to transfer and merge the funds provided for the Northeast Corridor Grants and National Network Grants programs. CARES Act, Pub. L. No. 116-136, 134 Stat. 281, 598-599 (2020).
[511]Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1944-45 (2020). Specifically, $174.9 million is to be used toward state payments for partner cost-sharing under Sec. 209 of the Passenger Rail Investment and Improvement Act, and $109.8 million in lieu of capital payments from states and commuter rail passenger transportation providers subject to the cost allocation policy developed under 49 U.S.C. § 24905(c). Additionally, the law allows the Department of Transportation to retain up to $2.030 million to fund the costs of project management and oversight of certain activities authorized by the Fixing America’s Surface Transportation Act.
[512]As we reported in November 2020, the expenditure categories include operating labor, direct-COVID expenditures, protected pay, and other qualifying expenses, which Amtrak expanded to include eligible capital expenses and debt service payments, along with train-related expenses such as fuel, power, and commissary food.
[513]Pub. L. No. 117-2, § 3401, 135 Stat. 4, 94-96.
[514]Amtrak, Office of Inspector General, Governance: Observations on Amtrak’s Use of CARES Act Funds, OIG-MAR-2020-013 (Washington, D.C.: Aug. 5, 2020). In January 2021, the Amtrak Inspector General initiated an audit assessing Amtrak’s administration of the Consolidated Appropriations Act, 2021 funds to continue to help it respond to COVID-19.
[515]Amtrak, Office of Inspector General, Governance: Final Observations on Amtrak’s Use of CARES Act Funds, OIG-A-2021-005 (Washington, D.C.: Dec. 15, 2020). In August 2020, the Inspector General reported that while Amtrak was taking steps to provide transparency over how it was allocating the $239 million in CARES Act funds set aside for state-supported routes, the Inspector General had an ongoing audit assessing the cost-sharing and billing processes between Amtrak and its state partners.
[516]In November 2020, we reported that Amtrak also faced challenges due to the potential loss of financial support from states and commuter railroads that operate on Amtrak’s network. The Consolidated Appropriations Act, 2021 provided $284.7 million to assist states and commuter railroads with making required payments to Amtrak, which may alleviate this challenge to some degree.
[517]According to Amtrak, the reduction of long-distance service should provide $300 million in costs savings, which is offset by a $150 million loss in ticket revenues, for an expected overall savings of $150 million. Amtrak officials said they would consider resuming daily service on the long-distance routes using three metrics: 1) COVID-19 pandemic hospitalization rates, 2) the percentage of trips booked for 2021, and 3) actual ridership levels. With the passage of the American Rescue Plan, 2021, Amtrak plans to restore long-distance service using a phased approach starting in May 2021.
[518]According to Amtrak officials, staffing needs vary by location, and in most locations, they have had more than sufficient staffing. However, in a few cases, Amtrak has had to recall furloughed employees when several employees were suddenly absent.
[519]The Consolidated Appropriations Act, 2021 directs Amtrak to use funds made available under the act to prevent further furloughs or service cuts. Furthermore, with the passage of the American Rescue Plan, 2021, Amtrak plans to recall all of its employees furloughed on or after October 1, 2020, in response to COVID-19.
[520]U.S. Department of Commerce, National Oceanic and Atmospheric Administration, National Marine Fisheries Service, Fisheries Economics of the United States, 2016, Technical Memorandum NMFS-F/SPO-187a (Silver Spring, MD: December 2018). Information on gross domestic product and jobs includes data on commercial seafood harvesters, processors, dealers, wholesalers, distributors, importers, and retailers, as well as recreational fishing trips and fishing equipment. Data for 2016 were the most recent available at the time of our review.
[521]Pub. L. No. 116-136, § 12005(a), 134 Stat. at 518.
[523]Id. § 12005(b). Specifically, “fishery participants” are defined as belonging to these categories and as having incurred, as a direct or indirect result of the COVID-19 pandemic, economic revenue losses greater than 35 percent as compared with their prior 5-year average revenue or any negative impacts to subsistence, cultural, or ceremonial fisheries. Additionally, the CARES Act provided that the Department of Commerce may use up to 2 percent of the $300 million for administration and oversight activities.
[524]Puerto Rico and the U.S. Virgin Islands are not part of an interstate commission.
[525]The commissions, established in the 1940s, partner with NOAA on data collection and the management of fisheries resources that are shared across states, such as striped bass.
[526]As of February 1, 2021, NOAA was reviewing the spend plans for Alaska and Washington.
[527]NOAA officials said that states, tribes, and territories can also use existing records, such as fishing permits, to identify eligible recipients.
[528]Puerto Rico and the U.S. Virgin Islands are not part of an interstate marine fisheries commission, so they will disburse funds directly to fishery participants.
[529]Office of Management and Budget, Implementation Guidance for Supplemental Funding Provided in Response to the Coronavirus Disease 2019 (COVID-19), (Washington D.C.: Apr. 10, 2020).
[530]Pub. L. No. 116-260, div. M, tit. I, 134 Stat. 1182, 1909-10. Specifically, the act appropriated $300 million, to remain available until September 30, 2021, to prevent, prepare for, and respond to COVID-19, domestically or internationally, which is to be only for activities authorized under section 12005 of the CARES Act.
[531]With regard to tribes, the act specifies that tribes eligible for funding are federally recognized tribes in any of the nation’s coastal states and territories as well as federally recognized tribes in any of the nation’s Great Lakes states with fisheries on the tribe’s reservation or ceded or usual and accustomed territory.
[532]Additionally, the act provides that each eligible state and territory, other than those states bordering the Great Lakes, is to receive an amount equal to not less than 1 percent of the total $300 million, and not greater than, from amounts provided under the CARES Act or this appropriation, that state’s or territory’s total annual average revenue from commercial fishing operations, aquaculture firms, the seafood supply chain, and charter fishing businesses.
[534]High Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas. GAO-21-119SP. Washington, D.C.: March 02, 2021.
[536]Pub. L. No. 116-260, div. N, §§ 271–288, div. EE, §101–306, 134 Stat. 1182, 1964–1993, 3038–3082 (2020).
[537]This is an updated estimate to include the $6.3 billion for the meal deduction provision included in the Consolidated Appropriations Act, 2021.
[538]Pub. L. No. 116-136, § 2303, 134 Stat. at 352–356. An NOL occurs when a taxpayer's allowable deductions exceed its gross income for a tax year. During an NOL year, a taxpayer generally does not owe any income taxes. TCJA generally repealed NOL carrybacks and required NOLs to be carried over indefinitely. Pub. L. No. 115-97, § 13302(b), 131 Stat. at 2122. The NOL offsets the taxpayer's taxable income in other tax years. 26 U.S.C. § 172(a). For ease of reporting, we use the term taxpayer to refer to an entity that may use the CARES Act tax relief provisions described in this enclosure.
[539]NOLs must be carried back unless taxpayers make a valid election to waive the carryback. 26 U.S.C. § 172(b)(3).
[540]Pub. L. No. 115-97, § 13302(a)(1), 131 Stat. at 2121.
[541]Pub. L. No. 116-136, § 2303(b)(1), 134 Stat. at 353–354. Losses carried forward can reduce future taxable income and tax, but cannot reduce taxable income below zero.
[542]Pub. L. No. 116-260, div. N, § 281(a), 134 Stat. at 1983. Farmers that, prior to the date of enactment of the Consolidated Appropriations Act, 2021, had filed federal income tax returns that disregard the CARES Act NOL amendments are generally treated as having made that election. Farmers are also allowed to make an affirmative election to disregard the CARES Act NOL amendments.
[543]The CARES Act also allows farmers who previously waived an election to carry back a net operating loss to revoke the waiver.
[544]26 U.S.C. § 965. Corporations that elect to exclude the transition tax years from the carryback period may receive a higher refund. 26 U.S.C. § 172(b)(1)(D)(iv), (v).
[546]Pub. L. No. 115-97, § 12001(a), 131 Stat. at 2092. Prior to TCJA, corporations were required to calculate their tax liability under two sets of rules—they computed their regular tax liability and their tentative AMT liability and paid whichever was greater. If the tentative AMT was more than the regular tax, the difference between them was AMT. The purpose of the AMT was to prevent companies from eliminating their tax liability from overuse of certain corporate tax preferences. In general, AMT applied a lower tax rate to a broader tax base by limiting the use of tax preferences and disallowing credits and deductions.
[547]Pub. L. No. 116-136, § 2305, 134 Stat. at 357. Under the CARES Act, corporations with AMT credits in excess of the credit allowed to offset regular tax liability (excess credit) may claim 50 percent of the excess credit as a refundable credit for the first tax year beginning in 2018 and then claim any remaining excess credit as a refundable credit in 2019. Alternatively, a taxpayer may elect to claim the entire excess credit as a refundable credit in the tax year beginning in 2018. If a corporation elects to claim all of the excess credit as a refundable credit in 2018, the corporation may use Form 1139 to receive a refund for this credit. If a corporation does not file Form 1139 to make this election, it may file a Form 1120-X to make the election and obtain a refund.
[548]Pub. L. No. 116-136, § 2306, 134 Stat. at 358. TCJA limited the business interest expense deduction to the sum of interest income, 30 percent of adjusted taxable income and floor plan financing interest expense. Pub. L. No. 115-97, § 13301, 131 Stat. at 2117. Businesses may elect to be governed by the TCJA’s 30 percent limit instead, as it may affect other credits and deductions. The higher limitation does not apply to partnerships until tax year 2020, and special rules apply to partnerships for tax years beginning in 2019.
[549]CARES Act, § 2304, 134 Stat. at 356. An excess business loss is the amount by which the total deductions from all trades or businesses exceed a taxpayer’s total gross income and gains from those trades or businesses, plus $250,000 ($500,000 for a joint return). 26 U.S.C. § 461(I)(3)(A).
[551]Pub. L. No. 116-280, div. EE, § 210, 1182 Stat. at 3066.
[552]Tentative refunds are available for other reasons before the CARES Act was enacted, and IRS cannot distinguish whether paper forms were submitted for CARES Act claims or for other reasons.
[553]There may be additional Form 1045 and 1139 in suspense that were received via paper, but we were not able to collect data on this.
[554] We calculated this percentage by dividing the number of approved applications for tentative refund over $1 million for Form 1139 by the total number of approved applications for tentative refund over $1 million for both Forms 1139 and 1045.
[555]Generally, the IRS cannot issue refunds over $2 million ($5,000,000 in the case of a C corporation) until 30 days after reporting them to JCT. 26 U.S.C. § 6405(a). In the case of a refund for net operating loss carrybacks, IRS reports to the Joint Committee on Taxation after the refund is made. 26 U.S.C. § 6405(b).
[556] IRS officials said that most of the 70 days includes processing and review on the IRS side, which includes the IRS’s Joint Committee Specialists reviewing the examiner’s case files for procedural, computational, and technical accuracy, and preparing the report that is submitted to the JCT for their review. The JCT generally only takes a few days to review the refund once the IRS refers it to them.
[557] According to IRS officials, IRS processing centers see increases in returns around due dates every year, but the IRS did not track these backlogs prior to the pandemic and is unable to provide any prior year data for comparison.
[558]15.7 million is 2.6 million more returns than what IRS reported in December 2020 and what GAO reported in GAO-21-251, which discusses the IRS backlog in greater length and detail.
[559]The electronic file capability for the 1040-X is only for tax years 2019 and on. Taxpayers who needed to file an amended return for tax year 2018, would have had to do so on paper.
[560]CARES Act, Pub. L. No. 116-136, tit. VI, 134 Stat. 281, 543 (2020); American Rescue Plan Act of 2021, Pub. L. No. 117-2, § 4005, 135 Stat. 4, 79.
[561]The Disaster Relief Fund receives an annual appropriation and has routinely received supplemental appropriations. In March 2020, the CARES Act was enacted, appropriating $45 billion for the Disaster Relief Fund. Pub. L. No. 116-136, div. B, tit. VI, 134 Stat. 281, 543 (2020). The Consolidated Appropriations Act, 2021, appropriated $17 billion to the Disaster Relief Fund for major disasters and an additional $2 billion to provide assistance for COVID-19 related funeral expenses. Pub. L. No. 116-260, div. F, tit. III, 134 Stat. 1182, 1462 (2020); Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910. In March 2021, the American Rescue Plan Act of 2021 appropriated $50 billion to the Disaster Relief Fund. Pub. L. No. 117-2, § 4005, 135 Stat. at 79.
[562]Under the Robert T. Stafford Disaster Relief and Emergency Assistance Act (Stafford Act), the President may declare that a major disaster exists in response to a Governor’s or tribal chief executive’s request if the disaster is of such severity and magnitude that effective response is beyond the capabilities of a state, tribe, or local government and federal assistance is necessary. See 42 U.S.C. § 5170.
[563]The projected obligations for the remainder of fiscal year 2021 are primarily a result of increased estimates resulting from cost share adjustments, vaccine distribution initiatives, and additional National Guard needs, as well as continuing increases in other COVID-19 requirements, as of January 2021. Other initiatives such as the safe re-opening and operation of eligible schools, transit systems, and other facilities are not included in these estimates and would substantially increase obligations from the Disaster Relief Fund. We will continue to monitor and report on FEMA’s projections for the Disaster Relief Fund balance in the coming months.
[564]The Sandy Recovery Improvement Act of 2013 amended the Stafford Act to provide tribal governments the option to request a presidential emergency or major disaster declaration. 44 U.S.C. §§ 5170(b), 5191(c). A tribal government may also receive one type of assistance under a state or territorial declaration and another type of assistance under its own declaration, provided there is no duplication of benefits. The tribal government cannot receive the same type of assistance through both tribal and state declarations for the same incident.
[566]FEMA, Tribal Declarations Pilot Guidance, January 2017.
[567]FEMA Policy Number 101-002-02, Tribal Consultation Policy, July 2019.
[568]FEMA continues to play a key role in the ongoing COVID-19 pandemic response effort, including distributing personal protective equipment, supporting Defense Production Act activities, and providing incident management coordination and leadership.
[569]See 42 U.S.C. § 5183; 44 C.F.R. § 206.171. When states or tribal entities request major disaster declarations, they may request assistance under the Crisis Counseling Assistance and Training program. Likewise, when the President makes a major disaster declaration, the declaration may authorize FEMA’s Individual Assistance program, which may also include the Crisis Counseling Assistance and Training program. On April 28, 2020, President Trump delegated authority to approve the Crisis Counseling Assistance and Training program for COVID-19 pandemic-related disasters to the FEMA Administrator for disasters declared prior to that date.
[570]The White House, Memorandum on Authorizing the Other Needs Assistance Program for Major Disaster Declarations Related to Coronavirus Disease 2019 (Aug. 8, 2020). Pursuant to the presidential memorandum, upon receiving a FEMA grant, states and territories may provide eligible claimants $300 or $400 per week—which includes a $300 federal contribution—in addition to their Unemployment Insurance benefits. The presidential memorandum directed that the program would end when $44 billion had been obligated; the balance of the Disaster Relief Fund reached $25 billion; on December 27, 2020; or upon the enactment of legislation providing supplemental federal unemployment compensation, whichever comes first.
[571]Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910.
[572]White House, Memorandum on Maximizing Assistance from the Federal Emergency Management Agency, February 2, 2021.
[573]White House, Memorandum to Extend Federal Support to Governors’ Use of the National Guard to Respond to COVID-19 and to Increase other Federal Assistance Provided to States, January 21, 2021. The February 2, 2021 Presidential memorandum authorizes 100 percent cost share reimbursement for work eligible under Public Assistance Category B from January 20, 2020 through September 30, 2021, except for the operational expenses made eligible by the January 20, 2021 memorandum, discussed above, which receive 100 percent cost share reimbursement from January 21, 2021 through September 30, 2021.
[574]White House, Memorandum to Extend Federal Support to Governors’ Use of the National Guard to Respond to COVID-19 and to Increase other Federal Assistance Provided to States, January 21, 2021.
[575]FEMA officials stated that the almost $4 billion had been obligated through the Public Assistance program.
[576]Letter to Senators Mitch McConnell and Chuck Schumer on COVID-19 recovery legislative proposals (phase 4), May 26, 2020. The following tribal associations signed the letter: the Association on American Indian Affairs, the Inter-Tribal Emergency Management Coalition of Oklahoma, National Congress of American Indians, National Tribal Emergency Management Coalition, North West Tribal Emergency Management Council, Montana Tribal Emergency Management Council, Tribal Emergency Management Association, and United South and Eastern Tribes Sovereignty Protection Fund.
[577]FEMA Policy Number 101-002-02, Tribal Consultation Policy, July 2019.
[578]We have previously reported on the administrative challenges tribal nations have faced in the past when requesting federal assistance for a major disaster or emergency.
[579]Letter to Senators Mitch McConnell and Chuck Schumer on COVID-19 legislative recovery proposals (phase 4), May 26, 2020. The following tribal associations signed the letter: the Association on American Indian Affairs, the Inter-Tribal Emergency Management Coalition of Oklahoma, National Congress of American Indians, National Tribal Emergency Management Coalition, North West Tribal Emergency Management Council, Montana Tribal Emergency Management Council, Tribal Emergency Management Association, and United South and Eastern Tribes Sovereignty Protection Fund.
[580]FEMA, National Advisory Council November 2020 Report to the Administrator (Washington, D.C.: November 2020).
[581]Pandemic Response to Coronavirus Disease 2019 (COVID-19): Initial Assessment Report: FEMA Operations January through September 2020 (Washington, D.C.: January 2021). Developed by a research and analysis team consisting of FEMA personnel and emergency management, public health, and other subject matter experts, the report focuses on the period from January 2020 through September 2020.
[582]FEMA, Tribal Declarations Pilot Guidance, January 2017.
[583]In this enclosure we refer to state educational agencies (SEAs) as states and local educational agencies (LEAs) as school districts. This includes the SEAs and LEAs in the District of Columbia and Puerto Rico, as well as the U.S. Virgin Islands, Guam, the Commonwealth of the Northern Mariana Islands, and American Samoa.
[585]The timing of when obligations are made for these state-administered programs varies based on the kinds of goods and services for which obligations are made. See 34 C.F.R. § 76.707.
[586]These funds provide aid to states, the District of Columbia, and Puerto Rico across two emergency relief funds, as well as through formula grants to other U.S. territories (referred to in the law as outlying areas). Pub. L. No. 116-260, div. M, tit. III, §§ 311(a)(1), 312, 313, 134 Stat. 1182, 1924-1932 (2020). The ESF also allocated funds for institutions of higher education through the Higher Education Emergency Relief Fund and for programs operated or funded by the Bureau of Indian Education; however, these components are outside of the scope of this enclosure.
[587]These funds provide aid to states, the District of Columbia, and Puerto Rico across two emergency relief funds, as well as through the ESF discretionary grants and formula grants to other U.S. territories (referred to in the law as outlying areas). Pub. L. No. 116-136, §§ 18001(a)(1), 18001(a)(3), 18002, 18003, 134 Stat. 281, 564-567 (2020). The ESF also allocated funds for institutions of higher education through the Higher Education Emergency Relief Fund and for programs operated or funded by the Bureau of Indian Education; however, these components are outside of the scope of this enclosure.
[588]School districts are not the only subgrantees of ESF funds. For example, governors are awarded some of the ESF funds and can make subawards to school districts, institutes of higher education, or other education-related entities. This enclosure is focused on subawards to school districts.
[589]American Rescue Plan Act of 2021, Pub. L. No. 117-2, §§ 2001, 2002, 135 Stat. 4, 19-23.
[591]See Department of Education, Office of Planning, Evaluation and Policy Development, ED COVID-19 Handbook, Volume 1: Strategies for Safely Reopening Elementary and Secondary Schools, Washington, DC, 2021. This guidance is also available at: https://www2.ed.gov/documents/coronavirus/reopening.pdf.
[592]Pub. L. No. 116-136, §§ 18002(d), 18003(f), 134 Stat. at 565, 567. This requirement generally applies to governors and states receiving funding within the ESF funds.
[593]Similarly, districts have until the end of fiscal year 2023 to obligate the ESF funds awarded through the Consolidated Appropriations Act, 2021 to specific purposes.
[594]School districts request reimbursement from the state and the state requests a drawdown from the U.S. Treasury.
[595]The portal also tracks how institutions of higher education have spent their CARES Act ESF funds; however, this information is outside the scope of this enclosure. The portal does not track ESF discretionary grants or funds provided through the ESF for Bureau of Indian Education programs.
[596]Education officials told us that they would include ESF funds granted through the Consolidated Appropriations Act, 2021 in the portal, but had not yet determined whether they would be presented separately or combined with CARES Act funds.
[597]As part of the Digital Accountability and Transparency Act (DATA Act), the grantees are required to submit all contract, grant, loan, direct payment, and other award data on a frequent basis to be published on USAspending.gov. Pub. L. No. 113-101, 128 Stat. 1146 (2014). The DATA Act amended the Federal Funding Accountability and Transparency Act of 2006. Pub. L. No. 109-282, 120 Stat. 1186, codified at 31 U.S.C. § 6101 note. USASpending.gov is the official open data source of federal spending information and is operated by the Bureau of the Fiscal Service of the Department of the Treasury. Education draws information on the demographics of school districts that receive ESF funds from its Common Core of Data.
[598]The site also provides information on certain funds awarded by the department and used by states, territories, school districts, institutions of higher education, and other education-related entities to alleviate the impact of COVID-19.
[599]Pub. L. No. 116-136, 134 Stat. 281, 599 (2020). Within the funds appropriated to the Rural Area formula program, $30 million is set aside for tribal transit programs, and an additional $75 million is set aside for the administration and oversight of the funds. FTA allocated the $25 billion to urbanized areas, states, and tribes on April 2, 2020.
[600]As of December 27, 2020, recipients were required to direct funds, to the maximum extent possible, to payroll and operations of public transit (including payroll and expenses of private providers of public transportation), unless the recipient certifies to the Secretary of Transportation that the recipient has not furloughed any employees. Consolidated Appropriations Act, 2021, div. M, tit. IV, 134 Stat. 1182, 1947.
[601]These flexibilities are exceptions to the usual process for FTA’s Urbanized Area and Rural Area formula programs. An additional exception is that there is no requirement for local matching funds for grants provided to large and small urban areas and rural areas. All other Urbanized Area and Rural Area program requirements apply to CARES Act funds, with the exception that operating and certain capital expenses do not need to be included in a transportation improvement program, a long-range transportation or statewide transportation plan, or a statewide transportation improvement program.
[602]Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. at 1945-48. Division M of the Consolidated Appropriations Act, 2021, is also referred to as the Coronavirus Response and Relief Supplemental Appropriations Act, 2021 (CRRSAA).
[603]Consolidated Appropriations Act, 2021, funds are also provided at 100 percent federal share for FTA’s program for the enhanced mobility of seniors and individuals with disabilities, with no local match required.
[604]Operating expenses for 2018 were determined from data reported to FTA’s National Transit Database.
[605]Pub. L. No. 117-2, § 3401, 135 Stat. 4, 72-77.
[607]Pub. L. No. 116-136, 134 Stat. 281, 596-97. The CARES Act gives the Federal Aviation Administration (FAA) the authority to retain up to 0.1 percent of the $10 billion (up to $10 million) provided for Grants-in-Aid for Airports to fund the award and oversight by FAA of grants made under the CARES Act.
[608]Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1939-41 (2020). Division M of the Consolidated Appropriations Act, 2021 is also referred to as the Coronavirus Response and Relief Supplemental Appropriations Act, 2021 (CRRSA).
[609]As we previously reported in June 2020, the grant formula in the CARES Act and available data for calculating the awards for commercial service airports (i.e., passenger boardings, debt service, and the ratio of unrestricted reserves to debt service) resulted in some small airports being allocated large amounts relative to their passenger activity or annual operating budgets. In other cases, the formula and available data resulted in some airports with large annual passenger boardings being awarded less funding than airports with fewer annual passenger boardings.
[610]Pub. L. No. 117-2, § 7102, 135 Stat. 4, 96-98.
[611]Airports were required to retain 90 percent of full-time equivalent employees working at the airport as of March 27, 2020, as the baseline comparison. According to FAA guidance, airport sponsors did not need to count contractors providing services other than airport management, tenants, or concessionaires. Airport sponsors may make adjustments for retirements or voluntary employee separations when calculating the workforce retention percentage. Nonhub and non-primary airports were excluded from the workforce retention requirement.
[612]As with the CARES Act, DOT could waive the workforce retention requirement under the Consolidated Appropriations Act, 2021, if DOT determined that the airport was experiencing economic hardship as a direct result of the requirement, or the requirement reduces aviation safety or security. Additionally, nonhub and non-primary airports were also excluded from the workforce retention requirement, as with the CARES Act. The American Rescue Plan Act of 2021 extended workforce retention requirements through September 30, 2021.
[613]Specifically, nonhub and non-primary airports are excluded from the workforce retention requirement. As a result, nonhub primary commercial service airports (airports with more than 10,000 annual passenger boardings, but less than .05 percent of total annual passenger boardings); non-primary commercial service airports (airports with at least 2,500 and no more than 10,000 passenger boardings each year); general aviation airports (public-use airports that do not have scheduled service or have scheduled service with fewer than 2,500 passenger boardings each year); and reliever airports (airports designated by FAA to relieve congestion at commercial service airports) are all exempt from the workforce retention requirement.
[614]Specifically, FAA allocated $500 million to increase the federal share for grants awarded for airport infrastructure projects under fiscal year 2020 AIP and supplemental discretionary grants, and allocated $9.1 billion to the remaining grant funding groups. FAA has not yet allocated $350 million of the up to $2 billion in grant funding available to primary airports. FAA officials stated that this funding may be used to increase the federal share to 100 percent for grants awarded for airport infrastructure projects, or distributed to commercial service airports.
[615]The Consolidated Appropriations Act, 2021 directed FAA to allocate the unallocated CARES funds under the Consolidated Appropriations Act, 2021 allocation formula and conditions for primary airports. In February 2021, FAA allocated $290,774,557 of unallocated CARES Act funding to primary airports’ Consolidated Appropriations Act, 2021 awards based on each airport’s proportional share of 2019 enplanements. The 31 airports that received CARES Act allocations in excess of four times their annual operating expenses are excluded from receiving this funding.
[616]However, FAA officials said that they may still request individual invoices from airport sponsors if there are outstanding questions from the information provided on the invoice summary.
[617]As we reported in June 2020, the grant formula in the CARES Act and available data for calculating the awards for commercial service airports (i.e., passenger boardings, debt service, and the ratio of unrestricted reserves to debt service) resulted in some small airports being allocated large amounts relative to their passenger activity or annual operating budgets. For example, some airports that reported unrestricted reserves but no debt service, and relatively few annual passenger boardings in 2018, were allocated nearly $17 million; amounts that greatly exceeded annual operating budgets. FAA then limited each airport’s initial CARES Act airport grant to no more than four times its annual operating expenses, unless the remaining amount would be less than $1 million.
[619]These product categories were identified by the U.S. International Trade Commission (USITC) in its report, COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). A revision to the Harmonized Tariff Schedule on July 1, 2020, provided several new HTS-10 statistical reporting numbers for previously identified COVID-19-related product categories. We identified these product categories and included them in the analysis.
[620]Some Harmonized Tariff Schedule of the United States categories identified in USITC Publication 5073 represent more than one product, and some categories contain products that are not directly relevant to COVID-19 responses. Product types only refer to the subset of goods considered COVID-19-related in each HTS-10 statistical reporting number. Therefore, the values presented may overestimate the imports of products directly relevant to COVID-19 responses. Nevertheless, they are useful indicators for tracking import trends of such products.
[621]Some imports from China have been subject to tariffs imposed by the Office of the U.S. Trade Representative at the direction of the President under Section 301 of the Trade Act of 1974 since 2018.
[622]Prioritization and Allocation of Certain Scarce and Critical Health and Medical Resources for Domestic Use, Temporary Final Rule, 85 Fed. Reg. 86,835 (Dec. 31, 2020).
[623]As of December 31, 2020, CBP officials reported seizures of 177,579 COVID-19 test kits prohibited by FDA; about 14.7 million counterfeit face masks; 36,839 antivirus lanyards prohibited by the Environmental Protection Agency; 6,379 tablets of antibiotics, such as azithromycin; and 37,884 tablets of chloroquine or hydroxychloroquine; as well as 299,778 seizures of counterfeit and illicit hand sanitizers.
[624]Specifically, in April 2020, the Secretary of the Treasury, in consultation with CBP, temporarily postponed the deadline for importers of record with a significant financial hardship to deposit certain estimated duties, taxes, and fees that they would ordinarily be obligated to pay as of the date of entry, or withdrawal from warehouse for consumption, for merchandise entered in March or April 2020, for a period of 90 days from the date that the deposit would otherwise have been due but for the emergency action. See 85 Fed. Reg. 22,349 (Apr. 22, 2020).
[625]According to CBP officials, as of early February 2021, approximately $1.7 million of the $575 million postponed had not been paid, and CBP followed existing procedures to follow up on these unpaid duties, taxes, and fees. The temporary postponement applies to federal excise taxes on imported products. The temporary postponement does not apply to merchandise subject to antidumping duties, countervailing duties, or duties assessed pursuant to Section 232 of the Trade Expansion Act of 1962 or Sections 201 or 301 of the Trade Act of 1974.
[626]We compared COVID-19-related HTS-10 codes both prior to and after July 1, 2020. If no match was found, we checked USITC guidance to determine if the original code had been annotated or discontinued. If annotated or discontinued, we included imports of those codes after July 1, 2020, in our analysis. For instance, according to guidance provided by the USITC, products under 4818.50.0000 were to be split into two new HTS-10 product categories: 4818.50.0080 and 4818.50.0020. Therefore, we included imports for products contained in 4818.50.0080 and 4818.50.0020 after July 1, 2020, in our calculations.
[627]The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, and the CARES Act appropriated about $2.3 billion for diplomatic and foreign assistance programming administered by State and USAID, to respond to COVID-19 abroad. This supplemental funding included $908 million appropriated to the International Disaster Assistance account and the Migration and Refugee Assistance account. See Pub. L. No. 116-123, tit. IV, 134 Stat. at 153; Pub. L. No. 116-136, div. B, tit. XI, 134 Stat. at 590. In March 2021, the American Rescue Plan Act of 2021 appropriated funds for Global Response and Humanitarian Response. See Pub. L. No. 117-2, tit. X, §§ 10003-04, 135 Stat. at 239. According to State officials, all $500 million appropriated for Humanitarian Response will go to the MRA account. According to USAID officials, they anticipate programming the $3.09 billion appropriated for Global Response through the Act for international disaster relief, rehabilitation, and reconstruction, for health activities, and to meet emergency food security needs. Discussion about funding in this enclosure does not include the funds appropriated by the American Rescue Plan Act of 2021.
[628]USAID established BHA in 2020, consolidating the former Office of U.S. Foreign Disaster Assistance and Office of Food for Peace.
[629]According to State guidance, voluntary contributions are discretionary financial assistance provided to public international organizations, among other institutions, which are meant to directly support the activities of the organization or to sustain its general budget and operations. While the funds may be used to advance specific activities and goals of the U.S. government, the central purpose of the funds is to enable the recipient to carry out its activities. According to State officials, this means that generally U.S. voluntary contributions cannot be traced to specific activities within a given country, since the funding is pooled with resources from other donor countries.
[630]This funding appeal fell under the umbrella of theUN’s consolidated Global Humanitarian Response Plan: COVID-19. The UN plan and its subsequent updates consolidated the COVID-19 response needs of various UN humanitarian agencies into a single funding appeal.
[631]The USAID funding approval date was determined by the date the USAID Administrator or Acting Administrator signed the USAID Action Memo approving the transmittal of funds.
[632]BHA officials noted that the process for COVID-19 funding differed from processes used in other emergencies. For example, during the Syria crisis, the USAID Disaster Assistance Response Team coordinated with field teams throughout the region on funding decisions without waiting for external approvals.
[633]These groups included other USAID operating units, USAID’s Technical Working Group, and State’s Coronavirus Global Response Coordination Unit and Office of Foreign Assistance.
[634]According to PRM officials, these issues did not affect State’s obligation of supplemental humanitarian assistance.
[635]USAID’s Office of Inspector General noted delays in obligating supplemental humanitarian assistance and questioned whether this response aligned with the typical approach of moving funds for humanitarian assistance quickly to places in need. U.S. Agency for International Development, Office of Inspector General, Top Management Challenges Facing USAID in Fiscal Year 2021 (Nov. 13, 2020).
[636]According to USAID’s Office of Inspector General, USAID officials said this decision was made under the advisement of the USAID COVID-19 Task Force based on direction from the White House Coronavirus Task Force to offset the shortage of PPE for domestic health care workers. U.S. Agency for International Development, Office of Inspector General, TopManagement Challenges 2021.
[637]On May 8, 2020, the USAID COVID-19 Task Force approved guidance on award language that, among other things, specified the types of equipment covered by the restriction and confirmed zero exception for humanitarian funding.
[638]The guidance stated that implementing partners must generally seek prior written approval from USAID to procure listed commodities, which included some types of PPE. However, the guidance also explained that partners could procure PPE without prior USAID authorization in the following two situations: (1) for their staff, from any source; and (2) for the protection of beneficiaries of USAID programs, from PPE manufactured locally or in the same region where USAID is providing assistance, as long as the PPE is not, and could not reasonably be, intended for the U.S.
[639]On February 22, 2021, BHA officials told us that the Bureau for Management had approved a limited waiver for local and regional PPE procurement that will remain in place through April 30, 2021. The officials also stated that the new administration was reviewing the policy on PPE procurement.
[640]USAID policy mandates that all agency assistance be identified as American aid, except in rare circumstances. USAID policy states that branding refers to the naming and communication of USAID’s sponsorship of the program, project, or activity and that marking refers to affixing USAID identity or other approved logos to the deliverables associated with a program, project, or activity. See U.S. Agency for International Development, Automated Directives System, section 320.1. According to USAID policy, principal officers may grant a waiver on determining that USAID-required markings would pose compelling political, safety, or security concerns or that marking would have an adverse impact in the host country. In truly exceptional circumstances, the principal officer may approve a blanket waiver by region or country. See U.S. Agency for International Development, Automated Directives System, section 320.3.2.6.
[641]BHA officials reported that as of February 22, 2021, current branding regulations and policy continue to apply to USAID awards, and partners must continue to follow the branding requirements in their awards.
[642]On January 20, 2021, President Biden reversed the decision to withdraw from the WHO.
[643]According to Department of Justice officials, as of January 2021, the Bureau of Prisons deobligated $24.34 million in fiscal year 2020 obligations that the Bureau had previously reported for COVID-19 obligations, reducing the total amount to approximately $750 million.
[644]Pub. L. No. 116-136, 134 Stat. 281, 513 (2020).
[645]Approximately 80 percent of federal inmates are confined in a BOP-managed facility. Depending on their circumstances, such as required security level or length of time remaining on their sentence, others are living in home confinement; confined in a contracted, privately operated prison; or living in a Residential Reentry Center designed to help facilitate their return to the community.
[646]BOP uses different methods for tracking and reporting infection and death rates among inmates and staff. We are examining its methods as part of our ongoing work.
[647]According to Department of Justice officials, as of January 2021, BOP deobligated $24.34 million in fiscal year 2020 obligations that BOP had previously reported for COVID-19 obligations, reducing the total amount to approximately $750 million.
[648]Pub. L. No. 116-260 (Section 543 of Division B of the Consolidated Appropriations Act, 2021)(Dec. 27, 2020).
[649]BOP updated its phase 9 action plan for the COVID-19 pandemic response on November 25, 2020.
[651]Pub. L. No. 116-136, §§ 15010, 15011, 134 Stat. at 533–42.
[652]OMB memorandum M-20-21 notes that some provisions may be excluded from this requirement, and in these instances, agencies should work with their OMB representative to identify an alternative reporting approach to provide transparency on how the funds are spent.
[653]Pub. L. No. 116-136, § 15010(g)(1)(A), 134 Stat. at 539.
[654]For this enclosure, we define “COVID-19 spending” as supplemental spending addressing COVID-19 from the following statutes: Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); Coronavirus Aid, Relief, and Economic Security Act or the CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182 (2021); and American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4 (2021).
[655]The Congressional Research Service provides a list of agency websites with COVID-19 spending data. See Jennifer Teefy and Maria Kreiser, Resources for Tracking Federal COVID-19 Spending, accessed February 18, 2021, https://www.crs.gov/Reports/R46491?source=search.
[656]See https://www.usaspending.gov/disaster/covid-19, accessed February 19, 2021. The COVID-19 Spending Profile Page includes details on total obligations and outlays by agency, federal accounts, and object classes. Users can see obligations and outlays through different award types by agency and by Catalog of Federal Domestic Assistance program.
[663]HHS provided links to public use files for its Provider Relief Fund and COVID-19 Uninsured Program. The data HHS submitted to USAspending.gov only reflects obligations to a single entity that is processing payments and claims reimbursements on behalf of HHS.
[664]Treasury told us that COVID-19 spending for three of the 14 entities—the Corporation for Public Broadcasting, Federal Payment for Emergency Planning and Security Costs in the District of Columbia, and Legal Services Corporation—is coded as Treasury spending. Treasury also told us that COVID-19 spending for a fourth entity—Historically Black College and University Capital Financing—is coded as Department of Education spending. Therefore, it is not possible for a user to obtain specific information on COVID-19 spending for these four entities apart from overall spending reported by the Departments of the Treasury and Education. According to Treasury, the other 10 entities do not meet the definition of “agency” used in the Federal Funding Accountability and Transparency Act.
[665]Pub. L. No. 116-136, § 15011(b)(1)(A), 134 Stat. at 541.
[666]We identified 257 HHS awards, nine DOL awards, eight SBA awards, and one Education award where outlays exceeded obligations.
[667]We did not reach out to Education because we only found one award where outlays exceeded obligations.
[668]Fraud and “fraud risk” are distinct concepts. Fraud—obtaining something of value through willful misrepresentation—is challenging to detect because of its deceptive nature. Fraud risk (which is a function of likelihood and impact) exists when individuals have an opportunity to engage in fraudulent activity, have an incentive or are under pressure to commit fraud, or are able to rationalize committing fraud. Fraud risk management is a process for ensuring program integrity by continuously and strategically mitigating the likelihood and impact of fraud. When fraud risks can be identified and mitigated, fraud may be less likely to occur. Although the occurrence of fraud indicates there is a fraud risk, a fraud risk can exist even if actual fraud has not yet been identified or occurred.
[669]An appropriation provides legal authority for federal agencies to incur obligations and make payments out of the U.S. Treasury for specified purposes. The American Rescue Plan Act of 2021 provides additional relief to address the continued impact of COVID-19 on the economy, public health, state and local governments, individuals, and businesses. The Congressional Budget Office estimates the budgetary effects of the law to be $1.9 trillion. Pub. L. No. 117-2, 135 Stat. 4.
[670]A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[671]The statute of limitations for mail fraud and wire fraud prosecutions is 5 years (18 U.S.C. § 3282), except for mail and wire fraud schemes that affect a financial institution, in which case the statute is 10 years (18 U.S.C. § 3293). Also, based on our analysis, these cases can take many years to resolve. For example, the Department of Housing and Urban Development OIG closed cases in 2017–2020 resulting from Hurricane Sandy in 2012.
[672]In November 2020, one of these individuals was sentenced to 12 months in prison and 2 years of supervised release. In December 2020, another individual was sentenced to 24 months in prison and 5 years of supervised release. In January 2021, a third individual was sentenced to 3 months in federal prison.
[673]The individual obtained approximately $2,501,753 in loan proceeds, and used these funds to pay for items unrelated to any legitimate PPP-related expense, including an automobile, an aircraft, personal taxes, the down-payment on a luxury residence, day-to-day living expenses, and various purchases of jewelry, clothing, accessories, and shoes.
[674]Officials from the National Association of State Workforce and its UI Integrity Center, funded by and operated in partnership with DOL, said that identity theft remains the biggest challenge for states in addressing potential UI fraud. According to officials, states have recently experienced increases in instances of criminals taking over legitimate claimants’ UI accounts and rerouting benefits to other bank accounts. In January 2021, we reported that states are working to address these account takeovers through communication campaigns that raise public awareness about phishing attempts to steal account information, as well as coordinating with law enforcement and banking institutions.
[675]There are 23 individuals facing other charges, such as bank fraud related to counterfeit EIPs.
[676]In June 2018, we raised concerns about the Internal Revenue Service’s inability to securely authenticate taxpayers online. For example, we recommended that the Internal Revenue Service develop a plan for implementing changes to its online authentication programs consistent with new guidance and implement improvements to its systems to fully implement the new guidance. As of January 2020, the agency had taken steps on these recommendations but had not yet fully implemented them.
[677]The federal government may enforce laws through civil or criminal action. Such action may be resolved through a trial, a permanent injunction, a civil settlement, or a guilty plea. For example, in January 2021, the Department of Justice obtained a civil settlement for fraud against PPP. In this case, a company and its president and Chief Executive Officer agreed to pay a combined $100,000 in damages and penalties to resolve allegations.
[678]Separate from COVID-19-related fraud, this individual also defrauded the Department of Veterans Affairs by falsely claiming to be entitled to veteran’s benefits for serving in the U.S. Marine Corps when, in fact, he never served.
[679]Two of the nine individuals or entities have also pleaded guilty to federal charges of defrauding COVID-19 relief programs. In November 2020, one of the individuals was sentenced to 36 months of incarceration. Four individuals or entities in other cases had been sentenced to 2 to 3 years of probation and ordered to pay fines as of January 31, 2021.
[680]This individual also pleaded guilty to mail fraud for a separate fraud scheme unrelated to COVID-19 relief funds. Sentencing was consolidated into one proceeding and in November 2020, the individual was sentenced to 36 months of incarceration.
[681]In January 2021, we reported on a case with similar circumstances where an individual pleaded guilty to violating the Federal Insecticide, Fungicide, and Rodenticide Act.
[682]The COVID-19 Consumer Protection Act, which became law in December 2020 as part of the Consolidated Appropriations Act, 2021, gives the Federal Trade Commission authority to seek civil penalties on the first offense for scams and deceptive practices related to the COVID-19 pandemic. Pub. L. No. 116-260, div. FF, tit. XIV, § 1401, 134 Stat. 1182, 3275-3276 (2020).
[683]From March 2020 through January 2021, the Department of Justice publicly announced charges or other actions in consumer fraud cases involving individuals who had claimed to offer products or services to prevent COVID-19.
[684]In addition to these warnings, in December 2020, the Federal Trade Commission, together with the National Association of Attorneys General, issued a blog post warning consumers about these types of scams.
[685]In October 2020, one individual was sentenced to 1 year and 1 day in prison, and ordered to pay restitution in the amount of $221,200 for causing damage to a former employer and delaying the shipment of PPE during the COVID-19 pandemic. In January 2021, an individual was sentenced to 3 months in prison and 9 months of home confinement, and ordered to pay restitution in the amount of $132,291, for stealing COVID-19-related medical supplies to sell for the individual’s own gain. Two individuals in other cases had been sentenced to 2 to 3 years of probation and ordered to pay fines as of January 31, 2021.
[686]Following an investigation, law enforcement found most of the stolen ventilators.
[687]COVID-19 affected consumer prices for food. In May 2020, the U.S. Bureau of Labor Statistics reported that April 2020 saw the sharpest increase in grocery store prices since 1974.
[688]“Borrowing authority” is authority that permits agencies to incur obligations and make payments to liquidate the obligations out of borrowed moneys. Borrowing from the Treasury is the most common form and is also known as “public debt financing.” GAO, Principles of Federal Appropriations Law, 4th ed., 2016 rev., ch. 2, p. 2-6, GAO-16-464SP (Washington, D.C.: March 2016).
[689]The Commodity Credit Corporation Charter Act is codified at 15 U.S.C. §§ 714-714p. Many Commodity Credit Corporation activities are authorized through omnibus farm bills—most recently the Agriculture Improvement Act of 2018 (2018 farm bill), Pub. L. No. 115-334, 132 Stat. 4490. Farm bills direct programs (including commodity and conservation programs) to utilize the Commodity Credit Corporation’s borrowing authority, thereby dispensing with the need for an annual appropriation for individual programs.
[690]The CARES Act, Pub. L. No. 116-136, div. B, tit. I, 134 Stat. 281, 505 (2020), appropriated $9.5 billion to the Office of the Secretary. The Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. A, tit. VII, § 799C(b), 134 Stat. 1182, 1234, made $1 billion of the $9.5 billion available for other purposes. This reduced the amount available to prevent, prepare for, and respond to coronavirus to $8.5 billion.
[691]Pub. L. No. 116-136, div. B, tit. I, § 11002, 134 Stat. at 509. Generally, appropriations acts enacted annually reimburse the Commodity Credit Corporation for its net realized losses.
[692] Pub. L. No. 116-159, div. A, § 173, 134 Stat. 709, 725 (2020).
[693] Pub. L. No. 116-260, div. M, tit. VII, subtit. B, ch. 1, § 751, 134 Stat. 1182, 2105. Section 751 provides $11.2 billion to USDA’s Office of the Secretary to prevent, prepare for, and respond to coronavirus by providing support for agricultural producers, growers, and processors impacted by coronavirus. Among other things, section 751 provides that at least $1.5 billion of the $11.2 billion be used to purchase food and agricultural products, including seafood, to distribute to individuals in need.
[694] Pub. L. No. 116-260, div. A, Tit II, 134 Stat. at 1199.
[695]The Commodity Credit Corporation Charter Act is codified as amended at 15 U.S.C. §§ 714-714p.
[696]Dollar amounts are nominal. The Funding Amounts and Funding Sources for the Coronavirus Food Assistance Program (CFAP) Direct Payments to Agricultural Producers table above provides the amounts the Office of Management and Budget apportioned for different rounds of CFAP. The apportioned amounts differ from the USDA Economic Research Service projections of actual payments. The Economic Research Service projects $29.6 billion to agricultural producers from COVID-relief programs ($23.7 billion in Coronavirus Food Assistance Program payments and $5.9 billion in Paycheck Protection Program forgiveness-eligible loans) in calendar year 2020. The agency estimates a total of $46.3 billion in federal direct payments, including the $29.6 billion from COVID-relief programs. We calculated $52 billion in federal direct payments and net crop insurance payments by adding $46.3 billion in direct payments to $5.7 billion in crop insurance indemnities minus producer-paid premiums. The Economic Research Service accounted for federal crop insurance indemnities as farm-related income and accounted for producer-paid premiums as expenses.
[697]According to USDA’s Economic Research Service, net farm income reflects income after expenses from production in the current year and is calculated by subtracting farm expenses from gross farm income. Gross farm income reflects the total value of agricultural output plus government farm program payments.
[699]The data we received from USDA and analyzed include one contractor to which USDA did not intend to award a contract to deliver food boxes, but mistakenly did so due to the contractor being miscoded in USDA’s internal tracking mechanism for the program. According to USDA officials, the contractor delivered some food boxes before USDA recognized the mistake and terminated the contract for convenience of the government. The number of food boxes this vendor delivered does not appear in the data.
[700]To calculate the total award amount we summed the contract awards, by contractor, across the rounds in which that contractor participated. For example, the largest contract was the total award amount across the first three rounds of the program because the contractor only participated in the first three rounds.
[701]The maximum food box cost of $580.00 applied to 31 of 9,601 food boxes delivered by one contractor across rounds 1 and 2 (for a total of $17,980), according to our analysis. According to USDA documentation, each of these 31 food boxes weighed 570 pounds. A USDA official clarified that each of these food boxes were containers with 570 pounds of apples.
[702]In its solicitations for rounds 1 and 2, USDA provided examples of products permitted in the food boxes, but did not require specific contents. Starting in round 3, USDA indicated that it would purchase only combination boxes that weighed between 30 and 40 pounds and contained: (1) 10-12 pounds of fresh fruit and vegetables, including 2-4 pounds of root vegetables (e.g., potatoes, yams, carrots), 2-4 pounds of fruits with longer storage life (e.g., citrus, apples, and melons), and 1 or 2 locally grown fruit or vegetable items, as available; (2) 5-6 pounds at least two dairy items, such as cheese, butter, and sour cream; (3) 5-6 pounds of at least two pre-cooked meat items but not more than 1 pound of lunch meat; and (4) at least 10 pounds of meat and dairy combined.
[703]Auditors raised concerns that the addendum lacked objective and measurable criteria for auditing certain programs.
[704]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing OMB guidance is reprinted in 2 C.F.R. part 200. Non-federal entities (states, U.S. territory and tribal governments, local governments, or nonprofit organizations) that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit, which is an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[705]To help administer the new COVID-19 relief funding, many federal awarding agencies also issued new guidance to award recipients on how those funds should be reported and spent.
[706]When there have been changes in the compliance requirements and those changes are not reflected in the annual Compliance Supplement, the auditor must determine the current compliance requirements and modify the audit procedures accordingly. 2 C.F.R. § 200.514(d)(3).
[707]OMB, in consultation with federal agencies, annually issues an updated Single Audit Compliance Supplement. The Compliance Supplement provides guidance for auditors that conduct single audits and identifies important compliance requirements. Issuing a Compliance Supplement addendum, however, is not typical.
[708] General guidelines may be related to Cross Agency Priority Goals or the President’s Management Agenda.
[709]The Addendum directs federal awarding agencies, in their capacity as cognizant or oversight agencies for audit, to provide audit submission extensions of up to 3 months for certain award recipients with original 2020 single audit reporting package due dates of October 1, 2020, through June 30, 2021. In earlier single audit guidance, OMB had directed such federal agencies to provide audit reporting package submission extensions of up to 6 months for award recipients with original reporting due dates of March 30, 2020, through June 30, 2020, and up to 3 months for award recipients with original reporting due dates of July 31, 2020, through September 30, 2020. See OMB M-20-26, Extension of Administrative Relief for Recipients and Applicants of Federal Financial Assistance Directly Impacted by the Novel Coronavirus (COVID-19) Due to Loss of Operations (June 18, 2020).
[711]American Rescue Plan Act of 2021, Pub. L. No. 117-2, 135 Stat. 4.
[712]The single audit working group was an initiative convened by the Comptroller General to determine the extent of issues, if any, related to single audits and to identify areas, if any, where the Compliance Supplement could be enhanced. The working group consisted of representatives from the AIPCA and NASACT, as well as state auditors from nine states and OIGs from four agencies as identified by the NASACT and Council of the Inspectors General on Integrity and Efficiency, respectively, and GAO.
[713]Entities may also have fiscal year-ends at other times of the year, such as of March 31, September 30, or December 31.
[714]Pub. L. No. 116-136, div. B, tit. I, 134 Stat. 281, 506 (2020).
[715]COVID-19 affected consumer prices for food. In May 2020, the U.S. Bureau of Labor Statistics reported that April 2020 saw the sharpest increase in grocery store prices since 1974.
[716]FSIS also has responsibility for inspecting meat and poultry products at U.S. ports and conducting audits of foreign food safety inspection systems overseas. The Food and Drug Administration (FDA) covers food safety activities for other types of food production. FDA did not receive CARES Act funds for food safety-related activities. We plan to examine FDA’s response to COVID-19 with respect to food safety inspections and related activities.
[717]Exec. Order No. 13999, 86 Fed. Reg. 7211 (Jan. 26, 2021). U.S. Department of Labor, Occupational Safety and Health Administration. Protecting Workers: Guidance on Mitigating and Preventing the Spread of COVID-19 in the Workplace, January 29, 2021. https://www.osha.gov/coronavirus/safework (last accessed on Feb. 12, 2021). This report does not cover worker safety. In January 2021, we reported on the Department of Labor Occupational Safety and Health Administration’s efforts to protect worker safety and health and plan to conduct future work.
[719]According to USDA officials, this includes personal protective equipment purchased for in-plant personnel in the field and personal protective equipment for FSIS employees based in laboratories and office locations. The additional protective gear, such as face shields, that FSIS inspection personnel are wearing to protect against COVID-19 can trap heat close to the body and may contribute to heat stress. To combat heat stress, the agency purchased electrolyte fluids, neck cooling scarves, cooling vests, cooling hat liners, evaporative cooling hard hat pads, evaporative cooling bandanas, and cooling hat ties.
[720]According to a USDA FSIS official, nonreimbursable overtime is paid when an inspector has already worked a full shift and needs to work additional hours at another establishment that is not in an overtime status and subject to paying FSIS an overtime fee.
[721]The total number of FSIS employees with a confirmed diagnosis of COVID-19 does not equal the total number of employees who have returned to work or self-quarantined because the status of some employees is not indicated in USDA documentation provided to us. According to USDA documentation, the number of employees who had a COVID-19 diagnosis is cumulative and this cumulative number includes employees who have returned to work (i.e., recovered from the disease). This number combines inspectors and staff whose occupational exposures may vary.
[722]See U.S. Department of Agriculture, Office of the Administrator, The Food Safety and Inspection Service Human Pandemic Operations Plan, March 2020, U.S. Department of Agriculture, Food Safety and Inspection Service, Leave, FSIS Directive 4630.2 (Washington, D.C.: Sept. 15, 2010).
[723]We have not independently verified whether a similar percentage of plants met the Salmonella standard during this time period. In March 2018, we reported that FSIS developed standards limiting the amount of Salmonella and Campylobacter—pathogens that can cause foodborne illness in humans—permitted in certain meat (beef and pork) and poultry (chicken and turkey) products, such as ground beef, pork carcasses, and chicken breasts. However, the agency had not developed standards for other products that are widely available, such as turkey breasts and pork chops. We recommended that the agency document its process for deciding which products to consider for new standards.
Contacts
A. Nicole Clowers
Managing Director, Health Care, clowersa@gao.gov, (202) 512-7114
Congressional Relations
Orice Williams Brown, Managing Director, williamso@gao.gov, (202)-512-4400 U.S. Government Accountability Office 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs
Chuck Young, Managing Director, youngc1@gao.gov, (202)-512-4800 U.S. Government Accountability Office 441 G Street NW, Room 7149, Washington, DC 20548
Strategic Planning and External Liaison
Stephen J. Sanford, Acting Managing Director, spel@gao.gov, (202)-512-4707 U.S. Government Accountability Office 441 G Street NW, Room 7814, Washington, DC 20548
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s cost of production and distribution. Pricing and ordering information is posted on our website.
To Report Fraud, Waste, and Abuse in Federal Programs
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Copyright
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.