By late March 2022, daily COVID-19 cases in the U.S. had fallen substantially since the Omicron-related peak in January 2022. Though COVID-19-associated hospitalizations and deaths have also decreased, the effects of the Omicron variant—and the rising prevalence of its new BA.2 sublineage—underscore enduring challenges and the importance of a continued, agile federal response.
This response has included a focus on COVID-19 vaccinations. As of March 26, 2022, about 70 percent of the eligible U.S. population had been fully vaccinated. According to the Centers for Disease Control and Prevention (CDC), getting vaccinated and staying up to date with vaccines—including a booster dose—is the best way to protect against COVID-19. Data show that vaccinated adults experienced lower COVID-19-associated hospitalization rates (see figure).
Age-Adjusted Rates of COVID-19-Associated Hospitalizations by Vaccination Status in Adults Aged 18 Years and Older, Oct. 2021–Feb. 2022
Since June 2020, GAO has made 279 total recommendations for improving federal pandemic operations. These recommendations include improvements in such areas as publicly reporting COVID-19 nursing home vaccination data and targeting vaccine outreach to veterans. Agencies have fully or partially addressed 39 percent of these recommendations as of March 2022, fully addressing 22 percent (61 recommendations) and partially addressing another 17 percent (48 recommendations). Fully addressing GAO’s recommendations will enhance federal COVID-19 pandemic response and recovery efforts, and help prepare for future public health emergencies.
In this report, GAO makes 15 new recommendations and raises one matter for congressional consideration in the areas of COVID-19 payment oversight, public health data collection, and critical manufacturing, among others.
Payment Integrity: COVID-19 Spending
The Payment Integrity Information Act of 2019 defines improper payments as any payment that should not have been made or that was made in an incorrect amount (including overpayments and underpayments) under statutory, contractual, administrative, or other legally applicable requirements. Improper payments are a pervasive and growing problem in regular programs across the federal government. They also have been a significant concern in pandemic spending, especially among the largest programs such as unemployment insurance.
Under guidance from the Office of Management and Budget (OMB), agencies are to complete a risk assessment to determine a new program’s susceptibility to significant improper payments after the first 12 months of program operations and, if susceptible, develop corrective actions and report on improper payments the following fiscal year. This means that improper payment information for new COVID-19 programs may not be reported until November 2022. By that time, agencies may have disbursed most or even all COVID-19 funds before assessing risk or developing corrective actions to address potential improper payment issues.
GAO therefore suggested in its November 2020 report that Congress consider in any future legislation appropriating COVID-19 relief funds designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payment.”
GAO continues to believe that expeditiously estimating and reporting improper payments and developing corrective actions to reduce such payments is critical to agency accountability, particularly for new programs that receive large outlays in a given year. GAO reiterates the November 2020 matter, as well as a matter GAO made in a March 2022 testimony suggesting that Congress consider amending the Payment Integrity Information Act of 2019 to designate all new executive agency programs—such as those created specifically to respond to the COVID-19 pandemic—making more than $100 million annually in payments as “susceptible to significant improper payments” for their initial years of operation.
GAO also recommends that OMB require agencies to certify the reliability of submitted improper payment data. OMB neither agreed nor disagreed with this recommendation.
FEMA’s COVID-19 Funeral Assistance and Public Assistance Program
As of February 28, 2022, the Federal Emergency Management Agency (FEMA) had received and was processing more than 444,000 applications for funeral assistance since April 2021—when it began accepting applications—and awarded more than $1.92 billion for more than 296,000 approved applications. (See figure for obligations made for COVID-19 Funeral Assistance from May 10, 2021, through February 22, 2022.)
Cumulative Obligations for FEMA Funeral Assistance over Time, May 10, 2021–Feb. 22, 2022
However, GAO identified several gaps in FEMA’s internal controls meant to prevent improper or potentially fraudulent payments, such as cases in which these controls did not prevent duplicate applications for funeral assistance or assistance issued to ineligible recipients. For example, GAO identified 374 deceased individuals that were listed on more than one award-receiving application; in total, these applications received about $4.8 million in assistance. Without adequate controls in place, COVID-19 Funeral Assistance is at risk of improper payments and potential fraud.
GAO recommends that the FEMA Administrator take action to identify the causes of the gaps in internal control in COVID-19 Funeral Assistance and design and implement additional control activities, where needed, to prevent and detect improper payments and potential fraud.
GAO recommends that the FEMA Administrator address deficiencies in the COVID-19 Funeral Assistance data by updating data records as data are verified, and adding data fields where necessary, to ensure that consistent and accurate data are available for monitoring of potential fraud trends and identifying control deficiencies. The Department of Homeland Security (DHS) agreed with both recommendations.
COVID-19 Surveillance
CDC could be better positioned to lead and coordinate the national efforts to detect and monitor COVID-19 by including in the agency’s existing surveillance approach specific objectives for how it will achieve its goals and a description of how it will assess progress toward meeting them.
CDC’s COVID-19 surveillance approach outlines goals and activities for what the agency wants to achieve, but it does not detail how it will achieve its stated goals or how it will measure its progress—two components of an effective strategy GAO has noted in its past work. By including specific objectives that detail how CDC’s actions will allow it to meet its goals and describing measures to assess its progress towards reaching its goals, CDC could better ensure it is able to effectively monitor COVID-19 nationwide.
GAO recommends that the Director of CDC, in coordination with state, tribal, local, and territorial jurisdictions and public health partner organizations, ensure the agency builds upon its existing COVID-19 surveillance approach by detailing specific objectives for how it will achieve its COVID-19 surveillance goals and describing how it will assess progress toward meeting them. HHS agreed with our recommendation.
Public Health Data Collection and Standardization
CDC has made progress in modernizing the U.S. public health data collection and surveillance infrastructure through its Data Modernization Initiative, which aims to improve data collection and sharing, strengthen data reporting and analytics, and advance surveillance of future public health threats, among other goals.
However, CDC’s strategic implementation plan for the Data Modernization Initiative does not articulate the specific actions, time frames, and allocation of roles and responsibilities needed to achieve its objectives. In addition, CDC has not fully developed plans for how it will allocate certain funds for data modernization. Without more specific, actionable plans, CDC may not be able to gauge its progress on the initiative or achieve key results in a timely manner. In addition, such lack of progress to implement enhanced surveillance systems could affect the quality and timeliness of data needed to respond to future public health emergencies.
GAO recommends that the Director of CDC define specific action steps and time frames for the agency’s data modernization efforts. HHS agreed with this recommendation.
Critical Manufacturing Sector
The pandemic has impacted the Critical Manufacturing Sector by causing worker shortages, delays in shipments of goods, and increased cybersecurity vulnerability in critical infrastructure systems and assets. The Cybersecurity and Infrastructure Security Agency (CISA)—in its role as the lead federal agency for coordinating security and resilience efforts with the Critical Manufacturing Sector on behalf of DHS—took steps to respond to the pandemic’s impacts in the sector. For example, CISA developed voluntary guidance to help jurisdictions and critical infrastructure owners and operators identify essential work functions and ensure that the workers who performed those functions could continue to access their workplaces when restrictions, such as stay-at-home orders, were in place in their communities.
Members of the Critical Manufacturing Sector have identified a lessons-learned analysis as a high-priority need, and CISA has collected some information on the impact of the pandemic in the sector that could be leveraged in a lessons-learned analysis. However, as of February 2022, CISA had not finalized a plan for developing the analysis.
GAO recommends that the Director of CISA assess and document lessons learned from the COVID-19 pandemic’s impacts on the Critical Manufacturing Sector. DHS agreed with this recommendation and stated it plans to issue a lessons-learned report by December 2022.
Advance Child Tax Credit and Economic Impact Payments
During 2021, the Internal Revenue Service (IRS) and the Department of Treasury issued advance payments of the child tax credit (CTC) and a third round of Economic Impact Payments (EIP 3) to eligible individuals, totaling over $500 billion. Both payments could have had implications for individuals as they filed their 2021 taxes.
Information on Advance Child Tax Credit Payments, July 2021–Dec. 2021, as of April 6, 2022
To help individuals file accurate 2021 tax returns during the 2022 filing season, Treasury and IRS took several steps to reach out to individuals that received the advance CTC payments and EIP 3. However, Treasury and IRS missed opportunities to collaborate on these outreach efforts.
Relatedly, the communications plans and strategies IRS developed for several programs, including the advance CTC and EIP, do not include metrics for assessing the usefulness and accessibility of these outreach efforts. Such metrics would inform management of these efforts and help focus resources on what works. Without sufficient, relevant, timely, and comparable data on its outreach efforts, IRS is missing information it could use to develop performance metrics and to assess which aspects of their communications and outreach strategy were effective in reaching different audiences.
GAO is making three recommendations for Treasury and IRS to enhance communication and outreach efforts concerning the refundable tax credit. These recommendations focus on improving collaboration between the agencies and within IRS and on using data to assess the effectiveness of their efforts. Treasury and IRS neither agreed nor disagreed with the recommendations.
This report contains additional recommendations related to the Single Audit Compliance Supplement, the Capital Projects Fund, the Homeowner Assistance Fund, and Public Health Industrial Base Expansion. For example, GAO recommends that the Assistant Secretary for Preparedness and Response within HHS conduct a workforce assessment of its Innovation and Industrial Base Expansion Program Office to determine the critical skills and competencies needed to support and sustain the office, and develop corresponding workforce strategies to address those needs. HHS agreed with this recommendation.
Why GAO Did This Study
By the end of March 2022, the U.S. had about 80 million reported cases of COVID-19 and over 980,000 reported deaths, according to CDC. The country also experiences lingering economic repercussions related to the pandemic, including rising inflation and ongoing supply chain disruptions.
As of February 28, 2022 (the most recent date for which data were available), the federal government had obligated $4.2 trillion and expended $3.6 trillion for pandemic relief. These amounts reflect 91 and 79 percent, respectively, of the total amount of COVID-19 relief funds provided by the CARES Act and five other relief laws.
The CARES Act includes a provision for GAO to report on its ongoing monitoring and oversight efforts related to the COVID-19 pandemic. This report—GAO’s 10th comprehensive report—examines the federal government’s continued efforts to respond to, and recover from, the COVID-19 pandemic. In addition, GAO’s March 17, 2022 testimony included 10 new legislative suggestions to enhance the transparency and accountability of federal spending, which we reiterate here.
GAO reviewed federal data and documents and interviewed federal and state officials and other stakeholders.
What GAO Recommends
GAO is making 15 new recommendations for agencies and one matter for consideration by Congress that are detailed in this Highlights and in the report.
Recommendations
Matters for Congressional Consideration
Number
Matter
1
Congress should consider providing the Department of Health and Human Services the authority to require states to report the data necessary for the Secretary to estimate and report on improper payments for the Temporary Assistance for Needy Families program in accordance with 31 U.S.C. § 3352. See the Payment Integrity: COVID-19 Spending enclosure.
Recommendations for Executive Action
Recommendations for Executive Action
We are making a total of 15 recommendations to federal agencies:
Number
Agency
Recommendation
1
Executive Office of the President : Office of Management and Budget
The Director of the Office of Management and Budget should require agencies to certify the reliability of data submitted to PaymentAccuracy.gov. See the Payment Integrity: COVID-19 Spending enclosure. (Recommendation 1)
2
Department of Homeland Security : Directorate of Emergency Preparedness and Response : Federal Emergency Management Agency
The Federal Emergency Management Agency Administrator should take action to identify the causes of the gaps in internal control in COVID-19 Funeral Assistance and design and implement additional control activities, where needed, to prevent and detect improper payments and potential fraud. See FEMA’s COVID-19 Funeral Assistance and Public Assistance Program enclosure. (Recommendation 2)
3
Department of Homeland Security : Directorate of Emergency Preparedness and Response : Federal Emergency Management Agency
The Federal Emergency Management Agency Administrator should address deficiencies in the COVID-19 Funeral Assistance data by updating data records as data are verified, and adding data fields where necessary, to ensure that consistent and accurate data are available for monitoring of potential fraud trends and identifying control deficiencies. See FEMA’s COVID-19 Funeral Assistance and Public Assistance Program enclosure. (Recommendation 3)
4
Department of Education
The Secretary of Education should document policies and procedures for providing information to the Office of Management and Budget to better enable it to annually update the Compliance Supplement that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training, and (2) agency officials proactively involving internal stakeholders (e.g., the inspector general, general counsel and chief financial officer) and external stakeholders (e.g., the audit community) when developing audit procedures, prior to submitting drafts to the Office of Management and Budget, in order to ensure the guidance meets users’ needs. See the Single Audit Compliance Supplement enclosure. (Recommendation 4)
5
Department of Health and Human Services
The Secretary of Health and Human Services should document policies and procedures for providing information to the Office of Management and Budget to better enable it to annually update the Compliance Supplement, that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training, and (2) agency officials proactively involving internal stakeholders (e.g., the inspector general, general counsel and chief financial officer) and external stakeholders (e.g., the audit community) when developing audit procedures, prior to submitting drafts to the Office of Management and Budget, in order to ensure the guidance meets users’ needs. See the Single Audit Compliance Supplement enclosure. (Recommendation 5)
6
Department of the Treasury
The Secretary of the Treasury should document policies and procedures for providing information to the Office of Management and Budget to better enable it to annually update the Compliance Supplement, that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training, and (2) agency officials proactively involving internal stakeholders (e.g., the inspector general, general counsel and chief financial officer) and external stakeholders (e.g., the audit community) when developing audit procedures, prior to submitting drafts to the Office of Management and Budget, in order to ensure the guidance meets users’ needs. See the Single Audit Compliance Supplement enclosure. (Recommendation 6)
7
Department of the Treasury
The Secretary of the Treasury should document a comprehensive plan that includes timely and sufficient policies and procedures for monitoring recipients of the CPF to provide assurance that funds are being used in compliance with laws, regulations, agency guidance, and award terms and conditions, including ensuring that funds are being used for allowable purposes. See the Capital Projects Fund enclosure . (Recommendation 7)
8
Department of the Treasury
The Secretary of the Treasury should develop and implement written procedures to monitor Homeowner Assistance Fund participants’ programs and uses of funds for compliance with program requirements and improper payments. See the Homeowner Assistance Fund enclosure. (Recommendation 8)
9
Department of Health and Human Services : Public Health Service : Centers for Disease Control and Prevention
The Director of the Centers for Disease Control and Prevention should define specific action steps and time frames for the agency’s data modernization efforts. See the Public Health Data Collection and Standardization enclosure. (Recommendation 9)
10
Department of Health and Human Services : Public Health Service : Centers for Disease Control and Prevention
The Director of the Centers for Disease Control and Prevention, in coordination with state, tribal, local, and territorial jurisdiction and public health organization partners, should ensure the agency builds upon its existing surveillance approach by detailing specific objectives for how it will achieve its COVID-19 surveillance goals and describing how it will assess progress toward meeting them. See the COVID-19 Surveillance enclosure. (Recommendation 10)
11
Department of Homeland Security : Cybersecurity and Infrastructure Security Agency
The Director of the Cybersecurity and Infrastructure Security Agency should assess and document lessons learned from the COVID-19 pandemic’s impacts on the Critical Manufacturing Sector. See the Critical Manufacturing Sector enclosure. (Recommendation 11)
12
Department of Health and Human Services : Office of the Assistant Secretary for Preparedness and Response
The Assistant Secretary for Preparedness and Response within the Department of Health and Human Services should conduct a workforce assessment of its Innovation and Industrial Base Expansion Program Office to determine the critical skills and competencies needed to support and sustain the office, and develop corresponding workforce strategies to address those needs. See the Public Health Industrial Base Expansion enclosure. (Recommendation 12)
13
Department of the Treasury : Office of the Secretary
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should enhance collaboration among departmental components for refundable tax credit communication and outreach efforts by including relevant participants and clearly defining participant outcomes, roles, and responsibilities. See the Advance Child Tax Credit and Economic Impact Payments enclosure. (Recommendation 13)
14
Department of the Treasury : Internal Revenue Service : Office of the Commissioner
The Commissioner of Internal Revenue should enhance internal collaboration among its stakeholder outreach and education offices for refundable tax credit communications and outreach efforts by clearly establishing outcomes, roles and responsibilities, and developing resources to facilitate joint interactions and methods to document information sharing. See the Advance Child Tax Credit and Economic Impact Payments enclosure. (Recommendation 14)
15
Department of the Treasury : Internal Revenue Service : Office of the Commissioner
The Commissioner of Internal Revenue should collect sufficient, relevant, and comparable data on the usefulness and accessibility of its communications and outreach efforts for refundable tax credits and use these data to develop performance metrics to assess the effectiveness of ongoing efforts. See the Advance Child Tax Credit and Economic Impact Payments enclosure. (Recommendation 15)
As of March 24, 2022, nearly 80 million cases of COVID-19 have been reported in the U.S. since COVID-19 was first identified in January 2020. As of the week ending March 26, 2022, over 980,000 deaths attributed to COVID-19 have been reported in the U.S. According to estimates from the Centers for Disease Control and Prevention (CDC), as of March 26, 2022, the virus’s Omicron variant was the dominant strain circulating in the U.S.[1] New daily reported cases surged across the U.S. in January 2022, followed by increases in COVID-19-associated hospitalizations and deaths, as well as strain on hospital capacity and operations.
By late March 2022, the number of daily cases had fallen substantially since the January peak, according to CDC data. Hospitalizations and deaths of patients with COVID-19 have also decreased as of March 2022. The recent surge associated with the Omicron variant and the rising prevalence of its new sublineage, BA.2, highlight both the pandemic’s enduring challenges, as well as the importance of continued monitoring and an agile response to the COVID-19 pandemic.
Over the past year, the nation’s public health response has focused on making COVID-19 vaccines, testing, and therapeutics more widely available to the U.S. population. In March 2022, the White House released its National COVID-19 Preparedness Plan—an update to its January 2021 National Strategy for the COVID-19 Response and Pandemic Preparedness—that announced efforts to increase the availability of COVID-19 treatments to the public, among other federal activities to respond to COVID-19.[2] However, on March 15, 2022, the White House noted that additional funding was needed to implement several initiatives in the plan, including to secure sufficient booster doses, variant-specific vaccines, monoclonal antibody treatments, and antiviral treatments.[3] Additionally, the COVID-19 Uninsured Program, which covered treatment, testing, and vaccination for uninsured individuals, stopped accepting claims for testing and treatment on March 22, 2022, and for vaccinations on April 5, 2022, due to insufficient funding.[4]
Providing the public with safe and effective vaccines to protect against critical illness is crucial to mitigating the public health and economic impacts of the virus and ending the pandemic. As of March 26, 2022, about 70 percent of the eligible U.S. population—over 217 million individuals aged 5 years and older—had been fully vaccinated, and approximately 46 percent of fully vaccinated individuals aged 12 years and older had received a booster dose.[5]
The federal government has taken several steps to increase access to at-home, rapid tests for COVID-19, including providing tests to health centers and Medicare-certified rural health clinics, as well as directly to households.[6] According to the White House, over 260 million free tests had been delivered to households as of March 2, 2022. In January 2022, the Departments of Health and Human Services (HHS), Labor, and the Treasury released detailed guidance on the requirements for private health insurance companies and group health plans to cover over-the-counter COVID-19 tests, and in April 2022 the Centers for Medicare & Medicaid Services expanded access to free over-the-counter COVID-19 tests for Medicare beneficiaries.[7] Additionally, the federal government increased the number of rapid tests, as well as molecular tests, available to schools and added free federal testing sites across the country in January 2022.[8]
According to a recent study, self-reported at-home rapid test use generally increased between August 2021 and March 2022, and peaked in January 2022 during the Omicron-related surge in cases.[9] Increased at-home testing is a positive step, but rapid testing is not always reported to health officials. As a result, health officials may have an incomplete picture of testing results across the country.[10]
In addition to COVID-19’s devastating health effects, the pandemic has also had far reaching effects on the U.S. economy. The U.S. has continued to experience both lower levels of employment relative to the prepandemic period and, amid supply chain disruptions, rising U.S. consumer prices.[11] While inflation indicators suggest that inflation could be somewhat higher and persist for somewhat longer than previously expected, labor and employment indicators reflect general improvement from November 2021 through March 2022. Supply chain disruptions have resulted in shortages in multiple sectors, including for certain critical products such as computer chips—which are used in a wide range of consumer goods—as well as testing materials and other medical supplies for the COVID-19 response.
The federal government has taken some steps to help address such shortages. For example, the White House issued a report in June 2021 providing a framework for closing certain supply chain vulnerabilities.[12] Similarly, HHS—with the input of federal partners—released its National Strategy for a Resilient Public Health Supply Chain in September 2021.[13] See the Public Health Supply Chain Resilience enclosure in appendix I for more information on recent efforts to implement this strategy. In February 2022, HHS released a report describing progress made over the past year to strengthen the public health and medical supply chain and industrial base.[14]
Since March 2020, Congress has provided about $4.6 trillion through the CARES Act and other laws that were enacted to fund federal efforts to help the nation respond to and recover from the COVID-19 pandemic (COVID-19 relief laws).[15] Ongoing implementation of the provisions in the COVID-19 relief laws, as well as the size and scope of these efforts—from distributing funding to implementing new programs—continue to demand strong accountability and oversight. Furthermore, the government must remain vigilant and agile to address additional potential challenges while it continues to respond to the evolving COVID-19 pandemic.
The CARES Act includes a provision for us to report regularly on the federal response to the pandemic. Specifically, the act requires us to monitor and oversee the federal government’s efforts to prepare for, respond to, and recover from the COVID-19 pandemic.[16] This comprehensive report is our 10th recurring oversight report in response to this provision.[17]
This report includes 33 enclosures addressing a range of federal programs and activities across the government concerning public health and the economy (see appendix I). In these enclosures, we are making 15 new recommendations to federal agencies in areas including public health data modernization and industrial base expansion, as well as one matter for congressional consideration related to payment integrity for COVID-19 spending. Figure 1 lists these enclosures by topic area and highlights those with new recommendations.
Figure 1: Report Enclosures by Topic Area
In addition to the nine previously issued recurring oversight reports, as of April 1, 2022, we have issued 145 targeted COVID-19-related reports, testimonies, and science and technology spotlights in areas such as economic disaster loans, aviation operations, veterans nursing homes, and Medicaid telehealth use during the pandemic. On March 17, 2022, we testified on federal agencies’ oversight of COVID-19 relief funds, including improper payments and fraud risk management.[18] We also have reviews ongoing in other areas. See appendix II for highlights pages from our recently issued work on COVID-19 and appendix III for a list of our ongoing work related to COVID-19.
Across our body of COVID-19-related work, we have made 279 recommendations to federal agencies and have raised 15 matters for congressional consideration to improve the federal government’s response efforts as of March 2022. This includes 10 new matters intended to enhance the transparency and accountability of federal spending that we raised in our March 2022 testimony; see appendix IV for additional information on these matters. In addition, in January 2022 we designated HHS’s leadership and coordination of a range of public health emergencies as high risk.[19] As of March 2022, agencies had fully or partially addressed 109 of our COVID-19-related recommendations (39 percent); of these, agencies had fully addressed 61 and partially addressed 48 recommendations.[20] For example, in response to one of our recommendations, HHS required nursing homes to report the COVID-19 vaccination status of residents and staff. This information is now publicly available online for over 15,000 Medicare and Medicaid certified nursing homes, aiding in transparency and identifying facilities that may be in need of additional assistance and resources.[21]
See figure 2 for an overview of the status of our COVID-19-related recommendations by department. For a complete list of our COVID-related products, see https://www.gao.gov/coronavirus.
Figure 2: Status of Prior GAO Recommendations from COVID-19-Related Work, by Federal Department or Agency, as of Mar. 2022
Note: For this figure, recommendations made to the Internal Revenue Service are counted toward the total of recommendations made to the Department of the Treasury.
Given the government-wide scope of this report, we undertook a variety of methodologies to complete our work, including examining a wide range of data sources and conducting interviews and obtaining information from federal and state officials and related stakeholders, such as state and local health officials and airline industry representatives. We also examined federal laws, agency documents, and guidance, among other information. In each enclosure, we include a summary of the methodology specific to the work conducted.
We conducted this performance audit from August 2021 to April 2022 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
The COVID-19 pandemic continues to have devastating effects on public health following the circulation of the Omicron variant, which was associated with record levels of COVID-19 cases and hospitalizations, strain on hospital capacity and operations, and increased deaths in early 2022.
Cases. COVID-19 cases surged nationwide in December 2021 and January 2022, coinciding with the Omicron variant’s rise as the dominant COVID-19 strain, according to CDC estimates. The number of new reported COVID-19 cases peaked in mid-January 2022 at over 800,000 cases per day—more than three times the January 2021 peak. New reported COVID-19 cases then began to fall, averaging under 30,000 cases per day between March 11, 2022, and March 24, 2022. See figure 3 for 7-day U.S. case averages since March 2020. Between March 18, 2022, and March 24, 2022, the number of reported new COVID-19 cases per day, on average, increased in nine of 52 jurisdictions, held steady in three jurisdictions, and decreased in 40 jurisdictions, compared to the previous 7 days.[22]
Figure 3: 7-Day Averages of Reported COVID-19 Cases in the U.S., Mar. 1, 2020–Mar. 24, 2022
Note: COVID-19 cases reported from states and territories include confirmed and probable cases. Beginning April 14, 2020, states could include probable as well as confirmed COVID-19 cases in their reports to CDC. Previously, counts included only confirmed cases. According to CDC, the actual number of cases is unknown for a variety of reasons, including that people who have been infected may not have been tested or may not have sought medical care. See CDC, “COVID Data Tracker: Trends in Number of COVID-19 Cases and Deaths in the U.S. Reported to CDC, by State or Territory,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#trends_dailycases
Hospitalizations. HHS data show that COVID-19-associated hospitalizations sharply increased in late December 2021 and January 2022, following the surge in cases as described above. Hospitalizations then decreased through March 2022 (see fig. 4).[23] Similarly, the proportion of emergency department visits with an accompanying COVID-19 diagnosis had fallen to less than 1 percent by late March 2022, a decrease from the record proportion of COVID-19-related patient visits in January 2022, according to CDC data.[24]
Figure 4: Reported Daily Hospitalizations and 7-Day Averages of Patients with Confirmed COVID-19 in the U.S., Aug. 1, 2020–Mar. 27, 2022
Note: We included only hospitalizations with confirmed COVID-19 cases (rather than confirmed and suspected COVID-19) to be consistent with the Centers for Disease Control and Prevention’s COVID Data Tracker page on hospitalizations. Confirmation of the COVID-19 diagnosis is based on laboratory test results; counts in this figure may include patients with additional diagnoses. August 2020 was the first full month following HHS’s transition to its current hospital data collection process. We calculated the 7-day average as the average number of the adult and pediatric hospitalizations on a given date and each of the six previous days. See HHS, “COVID-19 Reported Patient Impact and Hospital Capacity by State Timeseries,” accessed March 28, 2022, https://healthdata.gov/Hospital/COVID-19-Reported-Patient-Impact-and-Hospital-Capa/g62h-syeh.
Surges in COVID-19 cases have stressed hospital systems and negatively affected health care and public health infrastructure, according to CDC. Increased COVID-19 infection rates among hospitalized patients have required hospitals to expand the use of resource-intensive infection prevention protocols, treat patients whose underlying medical conditions have experienced increased disease severity because of COVID-19, and adapt to hospital staffing shortages due to personnel infection and burnout.[25]
Coinciding with the Omicron-related surge in cases, the percentage of hospitalized patients with suspected or confirmed COVID-19 rose to nearly 27 percent in January 2022, according to HHS reporting, compared to 10 percent at the end of November 2021, before the Omicron variant was identified in the U.S.[26] This increase in COVID-19 infection rates among patients in January 2022, similar to that associated with the Delta variant in 2021, highlights how new COVID-19 variants have affected hospital and public health systems over the last 2 years, and how future variants may pose similar risks.
Deaths. Although CDC has reported that the Omicron variant generally causes less severe disease than prior variants, the rapid spread and large volume of cases in December 2021 and January 2022 coincided with increased COVID-19-associated deaths in January and February 2022, according to provisional data from CDC’s National Center for Health Statistics.[27] In late January 2022, the number of new reported COVID-19-associated deaths averaged about 20,000 per week—the highest since December 2020 and January 2021. COVID-19 deaths then decreased through March 2022, following similar trends in cases and hospitalizations.
The number of deaths in the U.S. has been higher during the pandemic than the expected number of deaths based on data from 2019 and earlier, according to provisional data from CDC’s National Center for Health Statistics. From early February 2020 through March 5, 2022, it was estimated that at least 900,000 more deaths occurred from COVID-19 and other causes than would normally be expected.[28]
The federal government continues to expand the availability of COVID-19 vaccines and therapeutics to the U.S. population to mitigate the pandemic’s effects on public health.
As of April 1, 2022, three COVID-19 vaccines—developed by Janssen, Moderna, and Pfizer—were available in the U.S. The Pfizer vaccine was licensed by the Food and Drug Administration (FDA) for individuals aged 16 and older (Comirnaty) and was also available for individuals aged 5 years and older under an emergency use authorization.[29] The Moderna vaccine was licensed for individuals aged 18 years and older (Spikevax), and the Janssen vaccine was authorized for individuals aged 18 and older.[30]
FDA has also authorized booster doses for all three available COVID-19 vaccines. Specifically, as of April 1, 2022, FDA had authorized a booster dose of the Pfizer vaccine for individuals aged 12 and older and booster doses of the Janssen and Moderna vaccines for individuals aged 18 and older.[31] Additionally, on March 29, 2022, FDA authorized a second booster dose of the Pfizer and Moderna vaccines for individuals aged 50 and older, as well as a second booster dose of the Pfizer and Moderna vaccines for certain immunocompromised individuals aged 12 and older and aged 18 and older, respectively.[32] See table 1 for estimated U.S. COVID-19 vaccinations by age group.
Table 1: Reported COVID-19 Vaccinations by Age Group in the U.S., as of Mar. 26, 2022
Percentage of population
Percentage of fully vaccinated population
Fully vaccinateda
Booster doseb
5 years of age and older
69.6
Not applicablec
12 years of age and older
73.9
46.4
18 years of age and older
75.4
48.2
65 years of age and older
89.0
67.2
Total
65.5
44.7c
Source: Centers for Disease Control and Prevention (CDC). | GAO-22-105397
aAs of April 1, 2022, CDC counts individuals as being fully vaccinated if they received two doses on different days (regardless of time interval) of the two-dose vaccines or received one dose of the single-dose vaccine. According to CDC, the number of people who are fully vaccinated may be under-estimated because CDC is not always able to link information on subsequent vaccine doses.
bThe count of people who received a booster dose includes anyone who is fully vaccinated and has received another dose of COVID-19 vaccine since August 13, 2021, including those who received booster doses and those who received additional doses. According to CDC, the number of people who have received a booster dose may be under-estimated because CDC is not always able to link information on subsequent vaccine doses.
cAs of April 1, 2022, children aged 5 to 11 were not eligible to receive a booster dose.
According to CDC, getting vaccinated and staying up to date with COVID-19 vaccines—including getting a booster dose when eligible—is the best way to protect against COVID-19, including the Omicron variant, and reduce the likelihood of new variants emerging.[33] CDC surveillance data suggest that rates of COVID-19 cases, COVID-19-associated hospitalizations, and COVID-19-associated deaths are higher among unvaccinated people than vaccinated people.[34] However, CDC has reported that the effectiveness of COVID-19 vaccines may decrease over time, particularly among people aged 65 or older.
Booster doses can increase the immune response to COVID-19. According to CDC, people who were fully vaccinated and had received boosters experienced lower COVID-19 case rates compared to vaccinated people who had not received boosters.[35] Additionally, between October 2021 and February 2022, adults in the U.S. who were fully vaccinated and boosted experienced lower COVID-19 hospitalization rates compared to both unvaccinated adults and fully vaccinated adults who had not received booster doses, particularly during the Omicron-related surge (see fig. 5). Similarly, a CDC analysis found that those who had received booster doses had a lower probability of COVID-19-associated emergency department and urgent care visits, compared to unvaccinated individuals and those who had received the vaccine but had not received boosters.[36] The pace of booster administration has slowed over time, and uptake across the U.S. has varied. See the Vaccine Distribution and Administration enclosure for more information on COVID-19 vaccination efforts, including the administration of booster doses.
Figure 5: Age-Adjusted Rates of COVID-19-Associated Hospitalizations by Vaccination Status in Adults Aged 18 Years and Older, Oct. 2021–Feb. 2022
Note: Hospitalization data are from CDC’s COVID-19-Associated Hospitalization Surveillance Network (COVID-NET), which generally includes data from 99 counties in 14 states, representing 10 percent of the U.S. population, and thus should not be generalized nationally. Additional data on vaccination status for individual cases are collected and available from COVID-NET areas in 13 of the 14 states. For fully vaccinated persons with an additional or booster dose, rates reflect COVID-19-associated hospitalizations among fully vaccinated persons with a positive SARS-CoV-2 test collected 14 or more days after receipt of an additional or booster dose. For fully vaccinated persons without a booster dose, rates reflect COVID-19-associated hospitalizations among fully vaccinated persons with a positive SARS-CoV-2 test collected 14 or more days after either the second dose of a two-dose vaccine series or after one dose of a single dose vaccine, who have not received an additional or booster dose. For unvaccinated persons, rates reflect COVID-19-associated hospitalizations among persons with a positive SARS-CoV-2 test who have no record of receiving any COVID-19 vaccine. According to CDC, these data are preliminary and subject to change as more data become available. See CDC, “Rates of laboratory-confirmed COVID-19 hospitalizations by vaccination status,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#covidnet-hospitalizations-vaccination.
In addition to vaccines, FDA has also authorized new COVID-19 antiviral drugs to combat the virus. In late December 2021, FDA authorized two oral antiviral drugs—Molnupiravir, developed by Merck and Ridgeback Biotherapeutics, and Paxlovid, developed by Pfizer—for use in individuals aged 18 and older at high risk of disease progression, such as those with certain underlying medical conditions like diabetes or cancer. Both drugs have been shown to reduce the risk of hospitalization and death in high-risk adults with COVID-19, and according to CDC, are expected to be active against all circulating variants, including Omicron. On February 11, 2022, FDA also authorized a new monoclonal antibody treatment—bebtelovimab, developed by Eli Lilly and Company—that works against the Omicron variant; the federal government purchased 600,000 courses of this treatment to prevent severe outcomes from COVID-19.[37]
In March 2022, the White House announced efforts to improve access to and availability of COVID-19 treatments. For example, beginning in March 2022, “One-Stop Test to Treat” locations test people for COVID-19 and—if they test positive and are eligible for treatment—provide and fill a prescription for free antiviral pills on the spot. Participating Test to Treat sites include pharmacy-based clinics, community health centers, long-term care facilities, and Veterans Health Administration and Department of Defense facilities across the country.[38] Also in March 2022, the White House launched COVID.gov, a website that allows individuals to locate COVID-19 vaccines, tests, high-quality masks, and treatment—including Test to Treat sites—near them.
The overall national economy has continued to recover from the economic downturn in early 2020 sparked by the COVID-19 pandemic, based on data available in early April 2022. The labor market improved in early 2022, but remained weaker than in the prepandemic period. Weekly initial claims for regular unemployment insurance benefits remained generally similar to prepandemic levels in January through mid-March 2022. See the Unemployment Insurance Programs enclosure in appendix I for more information. Moreover, in March 2022 the employment-to-population ratio, which measures the share of the population employed, increased 0.2 percentage points from the previous month, to 60.1 percent—nearing, but still slightly below, pre-pandemic levels (see fig. 6).[39] See the Economic Indicators enclosure in appendix I for more information.
However, the pandemic continues to present lingering economic challenges that complicate long-term recovery efforts, such as disruptions in global supply chains, as demand for goods has increased rapidly during the economic recovery. Increased demand and limited supply have, in turn, contributed to higher inflation. Indicators of inflation have generally increased across most of our inflation indicators since spring 2021, suggesting that inflation could be somewhat higher, and last for somewhat longer, than previously expected. The extent to which higher inflation will persist for a longer period of time is uncertain and depends on many factors, such as global supply chain issues or how the pandemic influences consumer demand.
In response to elevated inflation levels, the Federal Reserve raised interest rates on March 16, 2022, and noted that it anticipates making additional adjustments to U.S. monetary policy.[40] On March 31, 2022, the White House announced a plan to decrease gas prices by increasing domestic production of oil and releasing oil reserves.
As of February 28, 2022, about $4.6 trillion in relief funds had been provided to fund response and recovery efforts for—as well as to mitigate the public health, economic, and homeland security effects of—the COVID-19 pandemic from the six COVID-19 relief laws.[41]
As of February 28, 2022, the most recent date for which government-wide information was available at the time of our analysis, the federal government had obligated a total of $4.2 trillion and expended $3.6 trillion of those funds, as reported by federal agencies to the Department of the Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System.[42] Obligations and expenditures relative to the amounts provided through COVID-19 relief laws have varied over time, as new relief laws have provided additional relief funds and as the federal government has obligated and expended those funds (see fig. 7).
Figure 7: Percentage of COVID-19 Relief Funding Obligated and Expended, July 31, 2020–Feb. 28, 2022
Notes: Funding and spending amounts shown are based on trial balance information reported to the Department of the Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System. The percentages shown represent the portions of funds available as of each date shown that had been obligated and expended. Data as of October 31, 2021, were not available because agencies are not required to report October trial balance information. Funding has generally increased over time and could increase in the future for programs with indefinite appropriations (i.e., appropriations that, at the time of enactment, are for an unspecified amount). Prior to September 30, 2021, we reported funding based on appropriation warrant information provided by Treasury. The total amount we reported as of September 30, 2021, decreased from the amount we reported as of August 31, 2021, mostly due to the return of unused indefinite appropriations to the Treasury at the end of fiscal year 2021 by the Internal Revenue Service and the Department of Labor. To account for this and other actions affecting funding amounts for each activity, we used total budgetary resources reported to Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System starting with September 2021. Total budgetary resources, as opposed to the previously reported appropriation warrant information provided by Treasury, reflect appropriations, as well as transfers, adjustments, recoveries, rescissions, and returns of unused indefinite appropriations. Therefore, amounts can fluctuate from month to month.
An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of another party that are beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures reflected in the percentages shown include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. Increased spending in Medicaid and Medicare is not accounted for in the funding provided by the COVID-19 relief laws. Under Office of Management and Budget guidance, federal agencies were not directed to report COVID-19 related obligations and expenditures until July 2020.
The nine major spending areas shown in table 2 represent $3.8 trillion, or 83 percent, of the total amounts provided. For these nine spending areas, agencies reported obligations totaling $3.5 trillion and expenditures totaling $3.1 trillion as of February 28, 2022. Table 2 provides additional details on budgetary resources, obligations, and expenditures of government-wide COVID-19 relief funds, including the nine major spending areas as of February 28, 2022.
Table 2: COVID-19 Relief Funding and Spending as of Feb. 28, 2022
Major spending area
Total budgetary resources ($ in billions)
Total obligations ($ in billions)
Total expenditures ($ in billions)
Economic Impact Payments (Department of the Treasury)
871.5
850.3
850.3
Business Loan Programs (Small Business Administration)
838.0
828.2
827.8a
Unemployment Insurance (Department of Labor)
725.3
723.4
673.2
Coronavirus State and Local Fiscal Recovery Funds (Department of the Treasury)
350.0
245.4
245.4
Public Health and Social Services Emergency Fund (Department of Health and Human Services)
345.7
301.0
226.1
Education Stabilization Fundb (Department of Education)
278.1
259.9
59.8
Coronavirus Relief Fund (Department of the Treasury)
150.0
150.0
149.9
Supplemental Nutrition Assistance Programs (Department of Agriculture)
117.1
80.8
79.5
Disaster Relief Fundc (Department of Homeland Security)
97.0
80.7
27.5
Other areasd
802.1
638.4
487.9
Totale
4,574.4
4,158.1
3,627.5
Source: GAO analysis of data from the Department of the Treasury and applicable agencies. | GAO-22-105397
Notes: Total budgetary resources, obligations, and expenditure data shown for the major spending areas are based on data reported by applicable agencies to Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System. Each spending area may include multiple programs. Total budgetary resources reflect the amount of funding made available for the COVID-19 response under the American Rescue Plan Act of 2021 (ARPA), Pub. L. No. 117-2, 135 Stat. 4; Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M and N, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146. Total budgetary resources reflect appropriations, as well as transfers, adjustments, recoveries, rescissions, and returns of unused indefinite appropriations.
An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of another party that are beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures shown include some estimates, such as estimated subsidy costs for direct loans and loan guarantees.
aThe Small Business Administration’s Business Loan Program account includes activity for the Paycheck Protection Program loan guarantees and certain other loan subsidies. These expenditures relate mostly to the loan subsidy costs (i.e., the loan’s estimated long-term costs to the U.S. government).
bDepartment of Education officials told us that the Education Stabilization Fund amounts reported to the Department of the Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System for February 2022 did not include all COVID-19 related activity. Total obligations were $276.9 billion and expenditures were $93.2 billion as of February 28, 2022. Education told us that they will correct these amounts with the March 2022 submission.
cFunding provided to the Disaster Relief Fund is generally not specific to individual disasters. Therefore, Treasury’s methodology for determining COVID-19-related obligations and expenditures does not capture obligations and expenditures for the COVID-19 response based on funding other than what was provided in the COVID-19 relief laws. Further, Treasury’s methodology includes all obligations and expenditures based on funding in the COVID-19 relief laws, including those for other disasters. In its Disaster Relief Fund Monthly Report dated March 8, 2022, the Department of Homeland Security reported COVID-19-related obligations totaling $95.7 billion and expenditures totaling $71.2 billion as of February 28, 2022.
dSeveral provisions in the Families First Coronavirus Response Act and ARPA authorized increases in Medicaid payments to states and U.S. territories. The Congressional Budget Office estimated that federal expenditures from these provisions would be approximately $76.9 billion through fiscal year 2030. The largest increase to federal Medicaid spending is based on a temporary formula change rather than a specific appropriated amount. Some of the estimated costs in this total are for the Children’s Health Insurance Program, permanent changes to Medicaid, and changes not specifically related to COVID-19. This increased spending is not accounted for in the funding provided by the COVID-19 relief laws and therefore not included in this table.
eBecause of rounding, amounts shown in columns may not sum to the totals.
The COVID-19 relief laws provided more than $1 trillion to federal agencies to provide assistance related to the COVID-19 pandemic to states, the District of Columbia, localities, U.S. territories, and tribes through existing and newly created programs and funds.[43] Table 3 lists programs and funds that each received $10 billion or more—exclusively or primarily for states, the District of Columbia, localities, U.S. territories, and tribes—in at least one of the six laws. It also provides obligations and expenditures for these programs and funds as of February 28, 2022.
Table 3: COVID-19 Relief Funding for Federal Programs and Funds Receiving $10 Billion or More in Aid for States, the District of Columbia, Localities, U.S. Territories, and Tribes, as of Feb. 28, 2022
Program fund/description
Appropriations ($ in billions)
Obligations ($ in billions)
Expenditures ($ in billions)
Coronavirus State and Local Fiscal Recovery Funds Administered by the Department of the Treasury, these funds provide payments to states, the District of Columbia (D.C.), U.S. territories, tribal governments, and localities to mitigate the fiscal effects stemming from the COVID-19 pandemic.
350
245.4
245.4
Elementary and Secondary School Emergency Relief Fund Administered by the Department of Education, this fund generally provides formula grants to states (including D.C. and Puerto Rico) for education-related needs to address the impact of the COVID-19 pandemic.
190.3
189.5
36.3
Coronavirus Relief Fund Administered by Treasury, this fund provides payments to states, D.C., localities, U.S. territories, and tribal governments to help offset costs of their response to the COVID-19 pandemic.
150
150
149.9
Disaster Relief Fund Administered by the Federal Emergency Management Agency, this fund provides federal disaster recovery assistance for state, local, tribal, and territorial governments when a major disaster occurs.
95a
42.7b
26.3b
Medicaid Administered by states and U.S. territories according to plans approved by the Centers for Medicare & Medicaid Services, which oversees Medicaid at the federal level. This program finances health care for certain low-income and medically needy individuals through federal matching of states’ and U.S. territories’ health care expenditures. The Families First Coronavirus Response Act and American Rescue Plan Act of 2021 temporarily increased federal Medicaid matching rates under specified circumstances, among other changes.
76.9c
70.0d
70.0d
Transit Grants Administered by the Federal Transit Administration, these funds are distributed through existing grant programs to provide assistance to states, localities, U.S. territories, and tribes to prevent, prepare for, and respond to the COVID-19 pandemic.
69.5
59.9
34.8
Child Care and Development Fund Administered by the Department of Health and Human Services (HHS), this program provides funds to states, D.C., territories, and tribes to subsidize the cost of child care for low-income families. COVID-19 relief funds have supported assistance to health care and other essential workers without regard to income eligibility requirements. Additional child care stabilization funding was provided for subgrants to eligible child care providers to support the stability of the child care sector during and after the COVID-19 pandemic.e
52.5
52.5
15.1
Emergency Rental Assistance Administered by Treasury, this program provides assistance to states, D.C., U.S. territories, localities, and tribes to assist eligible households with rent, utilities and home energy costs, and other expenses related to housing and housing stability.f
46.6
39.3
39.3g
Public Health and Social Services Emergency Fund Administered by HHS, this fund provides for grants to states, U.S. territories, localities, and tribal governments to support COVID-19 testing, surveillance, and contact tracing, among other uses.
33.4
32.9
11.2
Airport Grants Administered by the Federal Aviation Administration, these grants provide funds for eligible airports to prevent, prepare for, and respond to the effects of the COVID-19 pandemic.h
20
19.6
10.7
Highway Infrastructure Administered by the Federal Highway Administration, these programs provide funds to states, D.C., U.S. territories, and tribes for highway construction and authorize the use of these funds for maintenance, personnel, and other purposes to prevent, prepare for, and respond to the COVID-19 pandemic.
10
5.4
2.9
Coronavirus Capital Projects Fund Administered by Treasury, this fund provides payments to states, D.C., U.S. territories, freely associated states, and tribal governments for critical capital projects that directly enable work, education, and health monitoring, in response to the COVID-19 pandemic.i
10
0j
0j
State Small Business Credit Initiative Administered by Treasury, this program provides funds to states, D.C., U.S. territories, tribal governments, and eligible municipalities to fund small business credit support and investment programs.k
10
0
0
Source: GAO analysis of federal laws, data from the Congressional Budget Office, and obligations and expenditures data from the Department of the Treasury and applicable agencies. | GAO-22-105397
Notes: The COVID-19 relief laws providing the appropriations shown are the American Rescue Plan Act of 2021 (ARPA), Pub. L. No. 117-2, 135 Stat. 4 (2021), the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M and N, 134 Stat. 1182 (2020), the Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020), the CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020), and the Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020). The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146, did not provide any specified amounts for these programs or funds for states, D.C., localities, territories, or tribes. The amounts shown are the cumulative amounts for each program or fund under the other five laws. Some appropriation amounts include an amount available for administration expenses or for the relevant inspectors general. Numbers are rounded to the nearest hundred million.
We did not independently verify obligations and expenditures amounts.
aAppropriations for the Disaster Relief Fund generally are not specific to individual disasters and may be used for various disaster assistance programs, including the Public Assistance program, which provides assistance to state, local, territorial, and tribal governments.
bThe obligations and expenditures listed in the table are for the Public Assistance program for the COVID-19 response.
cSeveral provisions in the Families First Coronavirus Response Act and ARPA authorized increases in Medicaid payments to states and U.S. territories. The Congressional Budget Office estimated that federal expenditures from these provisions would be approximately $76.9 billion through fiscal year 2030. The largest increase to federal Medicaid spending is based on a temporary funding formula change rather than a specific appropriated amount. Some of the estimated costs in this total are for the Children’s Health Insurance Program, permanent changes to Medicaid, and changes not specifically related to the COVID-19 pandemic.
dMedicaid obligations and expenditures are as of December 31, 2021. COVID-19 related obligation and expenditure amounts for Medicaid only reflect provisions in the Families First Coronavirus Response Act. Complete obligation and expenditure amounts for COVID-19 related Medicaid provisions in ARPA are not currently available from the Centers for Medicare & Medicaid Services.
eThe Child Care and Development Fund is made up of two funding streams: mandatory and matching funding authorized under section 418 of the Social Security Act, and discretionary funding authorized under the Child Care and Development Block Grant Act of 1990, as amended. See 42 U.S.C. §§ 618 and 9858m.
fWe refer to ERA1 and ERA2 as the ERA program for convenience. While Treasury uses this approach, it clarified that it considers them to be two separate programs managed by the same office.
gExpenditures represent funding disbursed to grantees by Treasury for distribution to renters, landlords, and utility providers, as well as associated administrative costs and certain housing stability services.
hFunds are available to eligible sponsors of airports. Nearly all of these airports are under city, state, county, or public-authority ownership.
iTreasury issued implementing guidance in September 2021 that provides that the application deadline for requesting allocations of the Coronavirus Capital Projects Fund from Treasury was (1) December 27, 2021, for states, D.C., and U.S. territories; and is (2) June 1, 2022, for tribal governments.
jCoronavirus Capital Projects Fund (CPF) recorded obligations and expenditures of $1.2 million as of February 28, 2022. In addition, Treasury reported significant obligations in March 2022, and as of March 18, 2022, a total of $9.9 billion has been obligated.
kStates, D.C., and territories were required to submit completed applications by February 11, 2022. Tribal governments must submit their applications by May 11, 2022.
The nation’s COVID-19 response and recovery efforts continue following a surge of cases, hospitalizations, and deaths from the Omicron variant in January 2022. Challenges to these efforts remain, including supply chain disruptions and higher inflation, while future variants continue to pose a risk for hospital and public health systems. This report identifies key issues for the federal government to consider as it addresses the ongoing public health and lingering economic challenges facing the nation. We are making 15 new recommendations and one matter for congressional consideration aimed at improving the integrity and effectiveness of the federal response.
In our prior CARES Act reports and other targeted COVID-19-related reports, we have made a total of 279 recommendations to federal agencies, which have addressed or partially addressed 109 (39 percent).[44] As of March 2022, agencies had addressed 61 of these recommendations, resulting in improvements such as publicly reporting COVID-19 vaccination data for nursing home residents and staff, and targeting outreach to veterans to improve completion of vaccine regimens. Agencies have also partially addressed an additional 48 recommendations. Fully addressing our previous recommendations as well as the new recommendations we are making in this report will enhance the quality, value, and accountability of the federal government’s investments in the response to and recovery from the COVID-19 pandemic.
Payment Integrity: COVID-19 Spending
Improper payments are those that should not have been made or were made in an incorrect amount, including overpayments and underpayments under statutory, contractual, administrative, or other legally applicable requirements.[45] Under Office of Management and Budget (OMB) guidance, agencies are to complete a risk assessment to determine a new program’s susceptibility to significant improper payments after the first 12 months of program operations, and, if susceptible, develop corrective actions and report on improper payments the following fiscal year.
Given the rapid timeline of COVID-19 program-related spending, such time lags in assessing risk and developing corrective actions may result in improper payment issues in COVID-19 programs, including those resulting from fraudulent activities, not being identified or addressed until after most or even all funds are disbursed. We therefore suggested in our November 2020 report that Congress consider in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments.”
We continue to believe that expeditiously estimating and reporting improper payments and developing corrective actions to reduce such payments is critical to agency accountability—particularly for new programs that receive large outlays in a given year. Therefore, in our March 2022 testimony on federal oversight of emergency relief funds, we suggestedthat Congress should consider amending the Payment Integrity Information Act of 2019 to designate all new executive agency programs—such as those that were created specifically to respond to the COVID-19 pandemic—making more than $100 million annually in payments as “susceptible to significant improper payments” for their initial years of operation. We reiterate here the importance of both matters for congressional consideration that we raised in November 2020 and March 2022.
Further, HHS reported it does not have the authority to obtain the information it needs to estimate or report improper payment information for its Temporary Assistance for Needy Families (TANF) program.[46] According to HHS’s 2021 agency financial report, TANF spent about $17 billion in fiscal year 2021 and is a risk susceptible program. ARPA provided $1 billion for TANF Pandemic Emergency Assistance for fiscal year 2021. HHS’s 2021 agency financial report identifies two statutory provisions in the Social Security Act that render HHS unable to require states to provide it with the data needed to develop a TANF improper payment estimate.[47] Consistent with recommendations made by HHS’s Office of Inspector General, HHS has in previous budget proposals requested, but not received, such authority from Congress.
To ensure that Congress and other external stakeholders will have key payment integrity information for monitoring improper payments, we are suggesting that Congress consider providing HHS the authority to require states to report the data necessary for the Secretary to estimate and report on improper payments for the TANF program. Providing such statutory authority would also help ensure accountability over TANF payments and enable HHS to collect the required information to implement and report on the effectiveness of corrective actions to address improper payments for the program.
OMB guidance does not require agencies to formally review or certify the reliability of their PaymentAccuracy.gov data submissions. To prepare the annual datasets for publication on PaymentAccuracy.gov, OMB sends a request (or “data call”) to agencies for submissions of agency and program-level improper payment data. Yet, in direct contrast to OMB’s guidance for agency financial reports, OMB does not require agencies to have any formal review or certification by agency management prior to submission.[48] Had a management-level review requirement been in place, it may have detected, for example, a roughly $1.4 billion error we identified in our review of PaymentAccuracy.gov.[49]
To help ensure users of the website obtain complete and reliable government-wide improper payment information, we are recommending that the Director of OMB require agencies to certify the reliability of data submitted to PaymentAccuracy.gov. OMB neither agreed nor disagreed with this recommendation.
FEMA’s COVID-19 Funeral Assistance and Public Assistance Program
The scope of the Federal Emergency Management Agency’s (FEMA) COVID-19 Funeral Assistance is unprecedented. According to FEMA data, as of February 28, 2022, it had received and was processing over 444,000 applications since April 2021—when it began accepting applications—and awarded over $1.92 billion for over 296,000 approved applications. In the decade before the COVID-19 pandemic, FEMA had processed approximately 6,000 applications for funeral assistance after other disasters, according to FEMA officials.
We identified several gaps in FEMA’s internal controls meant to prevent improper or potentially fraudulent payments. Specifically, we identified cases in which FEMA’s controls did not prevent funeral assistance provided (1) in response to duplicate applications listing the same decedents; (2) above the maximum of $9,000 allowed per decedent; and (3) in response to applications listing incorrect applicant identifying information. For example, GAO identified 374 deceased individuals that were listed on more than one award-receiving application; in total, these applications received about $4.8 million in assistance. Without adequate controls that, for example, prevent funeral assistance payments in response to duplicate applications, COVID-19 Funeral Assistance is at risk of improper payments and potential fraud.
We are recommending that the Federal Emergency Management Agency Administrator take action to identify the causes of the gaps in internal control in COVID-19 Funeral Assistance and design and implement additional control activities, where needed, to prevent and detect improper payments and potential fraud.
In addition, our review also determined that FEMA does not sufficiently maintain the quality of the application data for its COVID-19 Funeral Assistance in a way that would facilitate oversight of COVID-19 Funeral Assistance and prevent and detect potential fraud. Our Framework for Managing Fraud Risks in Federal Programs calls for agencies to follow leading practices, such as designing and implementing data analytics and other control activities to prevent and detect fraud. However, we determined that FEMA lacked consistent data on whether applications were paid, decedent death dates, the amount of funeral assistance awarded for specific decedents on an application listing multiple decedents, and applicant Social Security numbers.
While FEMA officials stated that they are able to obtain accurate data on each application by manually checking its history, FEMA would be unable to efficiently identify which applications merited manual review if automated checks first did not detect the relevant discrepancies. This information—in particular, information on whether an award that appears in FEMA’s data was truly paid—would be a key factor in implementing data analytics and managing fraud risk. Without consistent data, FEMA lacks assurance that it can use data analytics to prevent and detect potential fraud as part of its oversight of the COVID-19 Funeral Assistance.
We are recommending that the FEMA Administrator address deficiencies in the COVID-19 Funeral Assistance data by updating data records as data are verified, and adding data fields where necessary, to ensure that consistent and accurate data are available for monitoring of potential fraud trends and identifying control deficiencies.
The Department of Homeland Security agreed with both recommendations and stated that it agreed with the need for internal controls and the importance of maintaining accurate, current data.
OMB annually issues the single audit Compliance Supplement, which provides guidance to auditors performing audits of certain entities that receive funding from federal assistance programs when expenditures meet or exceed $750,000.[50] Auditors generally follow the implementing guidance in the annual Compliance Supplement and agency guidance specific to their programs to determine whether the recipient has complied with federal statutes, regulations, and award terms that may have a direct and material effect on each of the recipient’s major programs.
Each year, OMB requires federal awarding agencies to provide it with proposed updates for their respective program sections for inclusion in the Supplement. Annual updates to the Supplement are necessary for many reasons, including to add additional requirements resulting from changes in statutory or regulatory requirements, such as those in the COVID-19 relief laws. However, we found that three agencies we selected for review—the Departments of Education, Health and Human Services, and Treasury, which together received over $2 trillion in COVID-19 funding—have not developed comprehensive policies and procedures for providing this information to OMB. Establishing written policies and procedures could help expedite OMB’s final issuance of the Supplement, ensure agencies and OMB have adequate time to fully resolve concerns from stakeholders prior to issuance, and strengthen the quality of single audit guidance.
We are making three total recommendations, one each to the Secretary of Education, the Secretary of Health and Human Services, and the Secretary of the Treasury, to document policies and procedures for providing information to OMB to better enable OMB to update the Compliance Supplement, that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training; and (2) agency officials proactively involving internal and external audit stakeholders when developing audit procedures, prior to submitting drafts to OMB, in order to ensure the guidance meets users’ needs. The Departments of Education, Health and Human Services, and the Treasury each agreed with the recommendation.
The Coronavirus Capital Projects Fund (CPF), administered by Treasury, was established in March 2021. The fund may provide up to $10 billion to state, territorial, and tribal governments to support critical capital projects directly enabling work, education, and health monitoring, in response to the COVID-19 public health emergency. Although Treasury has documented application and grant review procedures for CPF, it has not yet begun recipient monitoring and has not documented a comprehensive plan and process that includes the design and documentation of procedures to monitor recipients’ use of funds for allowable purposes once funds have been disbursed.
We are recommending that the Secretary of the Treasury document a comprehensive plan that includes timely and sufficient policies and procedures for monitoring recipients of the CPF to provide assurance that funds are being used in compliance with laws, regulations, agency guidance, and award terms and conditions, including ensuring that funds are being used for allowable purposes. Treasury agreed with this recommendation.
The Homeowner Assistance Fund (HAF), created on March 11, 2021, under ARPA provided about $10 billion to mitigate financial hardships associated with the pandemic and prevent mortgage delinquencies and defaults, foreclosures, loss of utilities or home energy services, and displacement of homeowners. Treasury administers the HAF and disburses allocations to participants—states, territories, tribal entities, and the Department of Hawaiian Home Lands—to develop local programs and provide assistance to homeowners. HAF participants can use the funds to assist homeowners with mortgage and utility payments, delinquent property taxes and insurance, and other eligible uses.
As of March 20, 2022, Treasury had disbursed over $9 billion to participants and approved HAF plans for 50 of the 56 state and territorial participants (89 percent). The agency was in the process of reviewing HAF plans from three participants, and expects the three participants that had not submitted HAF plans to do so in the coming months, according to an agency official. While Treasury has disbursed most of the funds appropriated for the program, state and territorial participants have only spent about $121 million—about 1 percent of their allocations, based on participant-reported data provided by Treasury.
Treasury has not developed and implemented written procedures that describe how it will monitor the compliance of HAF participants’ uses of funds with program requirements and efforts to prevent improper payments.
According to a Treasury official, the Office of Recovery Programs, which oversees HAF and Treasury’s other pandemic relief programs, was developing a post-award compliance monitoring process that will apply to all of its programs. Treasury was also developing monitoring procedures specific to the HAF program. In addition, Treasury plans to monitor compliance through single audits and was developing guidance for OMB’s 2022 compliance supplement. However, Treasury had not finished and implemented any of these monitoring efforts as of late March 2022. Without written and implemented procedures for monitoring compliance, Treasury cannot have reasonable assurances that participants are meeting program requirements and managing improper payment risks.
We are recommending that the Secretary of the Treasury develop and implement written procedures to monitor Homeowner Assistance Fund participants’ programs and uses of funds for compliance with program requirements and improper payments. Treasury agreed with our recommendation and said it was developing a monitoring framework for its pandemic recovery programs to identify potential areas of noncompliance for remediation.
CDC could be better positioned to lead the nation’s efforts to detect and monitor COVID-19, in coordination with state, tribal, local, and territorial partners (collectively referred to as jurisdictions) and public health partner organizations. This could be accomplished by including in the agency’s existing surveillance approach specific objectives for how it will achieve its goals and a description of how it will assess progress toward meeting them.
Surveillance—the ongoing, systematic collection, analysis, and interpretation of health-related data—is intended to guide efforts to detect and monitor disease and assist in the management of, and recovery from, large-scale public health incidents, according to CDC. In the U.S., public health surveillance is a shared effort between CDC and thousands of agencies at the federal, state, local, tribal, and territorial levels, along with health care providers, laboratories, and others.
The COVID-19 pandemic prompted new funding to support public health activities at all levels of government. Specifically, the CARES Act, ARPA, and annual appropriation acts for fiscal years 2020 and 2021 together provided CDC with $1.1 billion to support data modernization and COVID-19 surveillance activities.[51]
CDC’s COVID-19 surveillance approach outlines goals and activities for what the agency wants to achieve, but it does not detail how it will achieve its stated goals or how it will measure its progress—two components of an effective strategy we have noted in our past work. By including specific objectives that detail how CDC’s actions will allow it to meet its goals and describing measures to assess its progress towards reaching its goals, CDC could better ensure it is able to effectively monitor COVID-19 nationwide.
We are recommending that the Director of CDC, in coordination with state, tribal, local, and territorial jurisdictions and public health partner organizations, ensure the agency builds upon its existing COVID-19 surveillance approach by detailing specific objectives for how it will achieve its COVID-19 surveillance goals and describing how it will assess progress toward meeting them. HHS agreed with our recommendation, and CDC noted that it will continue efforts to develop a document summarizing its COVID-19 surveillance goals and how it will assess progress towards meeting them.
The pandemic highlighted limitations in both the data that CDC collects and in the public health surveillance systems CDC uses to collect and share these data. Both the CARES Act and ARPA provided funding to CDC to support modernizing the nation’s public health surveillance infrastructure. CDC’s Data Modernization Initiative, launched in 2020, aims to improve data collection and sharing, strengthen data reporting and analytics, and advance surveillance of future public health threats, among other goals. CDC faces several challenges to collecting accurate and timely data and conducting surveillance across the U.S., such as outdated methods to collect and transmit data and lack of interoperability among key surveillance systems. CDC officials also noted that, among these challenges, the agency generally lacks authority to require reporting of public health data.
CDC has made progress in modernizing the U.S. public health data collection and surveillance infrastructure through its Data Modernization Initiative. However, CDC’s Data Modernization Initiative strategic implementation plan does not articulate the specific actions, time frames, and allocation of roles and responsibilities needed to achieve its objectives. In addition, CDC has not fully developed plans for how it will allocate ARPA funds for data modernization. While the agency’s draft spend plan includes estimates for how it will spend the $500 million from ARPA—such as $200 million for a data forecasting center—the draft spend plan lacks specific actions and associated time frames for such spending.
Without more specific, actionable plans, including time frames for achieving data modernization objectives, spending plans, and the entities that are responsible for taking actions, CDC may not be able to gauge its progress on the initiative or achieve key results in a timely manner. In addition, such lack of progress to implement enhanced surveillance systems could affect the quality and timeliness of data needed to respond to future public health emergencies.
We are recommending that the Director of CDC define specific action steps and time frames for the agency’s data modernization efforts. HHS agreed with this recommendation.
As with other infrastructure sectors that provide essential services to American society, the COVID-19 pandemic has impacted the Critical Manufacturing Sector, such as by causing delays in shipments of goods, worker shortages, and increased cybersecurity vulnerability in critical infrastructure systems and assets.[52] The Cybersecurity and Infrastructure Security Agency (CISA)—in its role as the lead federal agency for coordinating security and resilience efforts with the Critical Manufacturing Sector on behalf of the Department of Homeland Security (DHS)—took steps to respond to the pandemic’s impacts in the sector.[53] For example, CISA developed voluntary guidance to help jurisdictions and critical infrastructure owners and operators identify essential work functions and ensure that the workers who performed those functions could continue to access their workplaces during community restrictions, such as stay-at-home orders.[54]
CISA has not performed a lessons-learned analysis of the pandemic’s impacts in the Critical Manufacturing Sector, although sector members identified this analysis as a high-priority need. CISA officials said that they plan to pursue a lessons-learned analysis of the pandemic’s impacts in the Critical Manufacturing Sector beginning in March 2022. However, as of February 2022, the agency had not finalized a plan for developing the analysis.
DHS’s National Infrastructure Protection Plan says that leveraging lessons learned and applying corrective actions from incidents can help reduce vulnerabilities in critical infrastructure.[55] Additionally, the plan says DHS is responsible for documenting lessons learned from actual incidents and applying them to its security and resilience activities. A documented lessons-learned assessment that examines the impact of the pandemic in the Critical Manufacturing Sector, including strengths and weaknesses in the sector’s response, would allow CISA to identify how it could better support the sector to reduce the consequences of the pandemic and future incidents. It could also help identify strategies to strengthen the sector’s resilience.
We are recommending that the Director of CISA assess and document lessons learned from the COVID-19 pandemic’s impacts on the Critical Manufacturing Sector. DHS agreed with this recommendation and stated that CISA is working with Critical Manufacturing Sector stakeholders to identify pandemic impacts in the sector as well as mitigation actions, and plans to issue a lessons-learned report by December 2022.
As part of its role to lead the nation in medical and public health preparedness for, response to, and recovery from emergencies and disasters, HHS’s Office of the Assistant Secretary for Preparedness and Response (ASPR) is responsible for actively restoring and strengthening supply capabilities depleted during the pandemic and securing the public health supply chain going forward. ASPR’s efforts to address these needs include forming a new Innovation and Industrial Base Expansion Program (IBx) Office, beginning in September 2020. According to ASPR’s website, the mission of the IBx Office is to strengthen and expand the U.S. public health industrial base and deliver innovative solutions to counter health security threats.
ASPR has been primarily using detailees from other federal agencies to support the IBx Office, but it has begun hiring its own staff. However, the agency has not yet assessed the critical workforce skills and competencies needed to support and sustain the mission and goals of the office, nor has it developed strategies to achieve those workforce needs. Such an assessment would be consistent with key principles of strategic workforce planning we have previously identified, including (1) determining the critical skills and competencies needed to achieve current and future programmatic results; and (2) developing strategies to address gaps in the number of staff and their skills and competencies, in order to meet those results.
We are recommending that the Assistant Secretary for Preparedness and Response within HHS conduct a workforce assessment of its Innovation and Industrial Base Expansion Program Office to determine the critical skills and competencies needed to support and sustain the office, and develop corresponding workforce strategies to address those needs. HHS agreed with our recommendation, and stated that the agency will conduct a workforce assessment in the future.
Advance Child Tax Credit and Economic Impact Payments
During 2021, the Internal Revenue (IRS) and the Department of Treasury issued advance payments of the child tax credit (CTC) and a third round of Economic Impact Payments (EIP 3) to eligible individuals, totaling over $500 billion. Both advanced child tax credits and EIPs could have implications for individuals’ 2021 taxes filed in 2022. In general, to determine advance CTC payments, IRS used the reported information on an individual’s most recent tax return to estimate the total amount of the CTC that an individual qualified for under the law. Treasury and IRS issued EIP 3 to most eligible individuals. Eligible individuals who did not receive EIP 3—or their maximum applicable EIP 3 amounts—could claim a recovery rebate credit on their 2021 tax return.
To help individuals file accurate 2021 tax returns during the 2022 filing season, IRS and Treasury took several steps. For example, starting in December 2021, IRS began mailing millions of letters to advance CTC and EIP 3 recipients. IRS and Treasury also worked with federal, state, and local partners to encourage individuals to file taxes to claim credits they were eligible to receive. However, Treasury and IRS missed opportunities to collaborate on these outreach efforts.
According to Treasury officials, Treasury and IRS meet weekly to coordinate outreach and to ensure they are sharing consistent information. However, some key IRS officials said they were not always aware of Treasury’s efforts. The lack of collaboration and transparent communication between Treasury and IRS resulted in a missed opportunity to leverage resources and expertise on communication and outreach efforts.
Relatedly, IRS has developed communications plans and strategies for several programs, including the advance CTC and EIP. However, these plans and strategies do not include metrics for assessing the usefulness and accessibility of these outreach efforts. Such metrics would inform management of these efforts and help focus resources on what works.
Although the EIP and advance CTC outreach efforts are now complete, IRS plays a key role in and devotes considerable resources to educating taxpayers, as well as those who are not in contact with the tax system, about other refundable tax credits and eligibility. Collecting information on the usefulness and accessibility of the various outreach efforts from the past 2 years could help inform future IRS efforts to educate individuals about refundable tax credits and more reliably measure the success of such efforts.
We are recommending that the Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, enhance collaboration among departmental components for refundable tax credit communication and outreach efforts by including relevant participants and clearly defining participant outcomes, roles, and responsibilities. Treasury neither agreed nor disagreed with this recommendation, stating that it supports the goal of the recommendation and continues to work with IRS to raise awareness on current and future communication and outreach efforts. We maintain that without additional actions, such as including relevant participants and clearly defining outcomes, roles and responsibilities, Treasury and IRS will continue to miss opportunities to leverage their resources and expertise on communication and outreach efforts.
We are recommending that the Commissioner of Internal Revenue enhance internal collaboration among its stakeholder outreach and education offices for refundable tax credit communications and outreach efforts by clearly establishing outcomes, roles, and responsibilities, and by developing resources to facilitate joint interactions and methods to document information sharing. IRS neither agreed nor disagreed with this recommendation, stating that it has clearly established roles and responsibilities for its communication and outreach functions, which coordinate with each other regularly and look for ways to improve their joint efforts. We maintain that IRS offices overseeing stakeholder outreach and education do not consistently document and share key information. Without additional actions, such as developing resources to facilitate joint interactions and methods to document information sharing, IRS will continue to miss opportunities to fully leverage the knowledge and expertise that resides among its staff.
We are recommending that the Commissioner of Internal Revenue collect sufficient, relevant, and comparable data on the usefulness and accessibility of its communications and outreach efforts for refundable tax credits and use these data to develop performance metrics to assess the effectiveness of ongoing efforts. IRS neither agreed nor disagreed with this recommendation, stating that it obtains feedback, but these efforts are not easily captured or translated into performance metrics. We maintain that IRS is not collecting or using other types of information to assess what aspects of their communications and outreach efforts were effective in reaching different audiences. This data could help inform future IRS efforts to educate individuals about refundable tax credits and more reliably measure the success of such efforts.
The federal government’s efforts to respond to and recover from the COVID-19 pandemic continue. The current decrease in the number of daily cases is part of a cycle of increases and decreases the nation has faced over the previous 2 years, due in part to the emergence of new variants of the virus. Though labor conditions have improved recently, other lingering economic effects, in addition to the potential for new variants, illustrate the challenges to the nation’s response and recovery efforts and the work that remains. We are pleased that agencies have addressed 61 and partially addressed 48 of our 279 recommendations as of March 2022. Fully addressing our recommendations, including the new recommendations we are making in this report, and the new matters we raised in March 2022, can help improve the federal response and recovery efforts. Ensuring accountability and transparency in federal programs remains critical to respond to the COVID-19 pandemic, and in preparing the nation for potential future emergencies.
We are sending copies of this report to the appropriate congressional committees, the Office of Management and Budget, and other relevant agencies. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at (202) 512-5500 or dodarog@gao.gov. Questions can also be directed to Orice Williams Brown, Chief Operating Officer, at (202) 512-5600; Jessica Farb, Managing Director, Health Care, at (202) 512-7114 or farbj@gao.gov; or A. Nicole Clowers, Managing Director, Congressional Relations, at (202) 512-4400 or clowersa@gao.gov. Contact points for our Office of Public Affairs may be found on the last page of this report.
Gene L. Dodaro Comptroller General of the United States
Congressional Addressees
The Honorable Patrick Leahy Chairman The Honorable Richard Shelby Vice Chairman Committee on Appropriations United States Senate
The Honorable Ron Wyden Chairman The Honorable Mike Crapo Ranking Member Committee on Finance United States Senate
The Honorable Patty Murray Chair The Honorable Richard Burr Ranking Member Committee on Health, Education, Labor, and Pensions United States Senate
The Honorable Gary C. Peters Chairman The Honorable Rob Portman Ranking Member Committee on Homeland Security and Governmental Affairs United States Senate
The Honorable Rosa L. DeLauro Chair The Honorable Kay Granger Ranking Member Committee on Appropriations House of Representatives
The Honorable Frank Pallone, Jr. Chairman The Honorable Cathy McMorris Rodgers Republican Leader Committee on Energy and Commerce House of Representatives
The Honorable Bennie G. Thompson Chairman The Honorable John Katko Ranking Member Committee on Homeland Security House of Representatives
The Honorable Carolyn B. Maloney Chairwoman The Honorable James Comer Ranking Member Committee on Oversight and Reform House of Representatives
The Honorable Richard Neal Chairman The Honorable Kevin Brady Republican Leader Committee on Ways and Means House of Representatives
Based on data available in the beginning of April 2022, the overall national economy has continued to recover from the COVID-19 pandemic, while specific areas of the economy we are monitoring saw mixed performance in recent months. Indicators of inflation have generally increased, suggesting that inflation could be somewhat higher, and persist for somewhat longer than previously expected. Indicators for labor markets and state and local government employment generally improved from November 2021 through March 2022 (see table).[56]
Indicators for Areas of the Economy Supported by the Federal COVID-19 Pandemic Response, Nov. 2021–Mar. 2022, Cumulative Changes since Feb. 2020
aThe employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population 16 years and over. The ratio is subject to a misclassification error with respect to identifying workers as employed and absent from work who are likely unemployed on temporary layoff.
bState and local government and leisure and hospitality employment data from February 2022 and March 2022 are preliminary. These data reflect revisions to 2020-2021 data by Bureau of Labor Statistics as presented in the January 2022 Employment Situation and thus may differ from what we reported in previous CARES Act reports.
cHigher levels in the Consumer Credit Default Composite Index rate indicate more defaults on consumer loans, including auto loans, bank cards, and mortgages. The Consumer Credit Default Composite Index could be subject to seasonal variation but is not seasonally adjusted.
dSeriously delinquent loans are 3 months or more past due or in foreclosure, based on mortgages insured by the Federal Housing Administration (FHA). Decrease in serious delinquency rates on FHA loans may indicate improvement in the finances of the minority and low- to moderate-income households that disproportionately take out mortgages insured by FHA.
eLower levels of the small business credit card delinquency index indicate more delayed payments on credit. The small business credit card delinquency index is published under license and with permission from Dun & Bradstreet, and no commercial use can be made of these data.
Real gross domestic product (GDP) grew at a 6.9 percent annual rate in the fourth quarter of 2021, increasing from its third quarter growth rate of 2.3 percent, according to the Bureau of Economic Analysis.[57] Private inventory investment, including investment in motor vehicle dealer inventories, was notably higher in the fourth quarter, as were exports and consumer spending, especially spending on health care, financial services and insurance, and recreation. Faster GDP growth suggests that private sector demand growth more than offset the waning fiscal effects of the federal pandemic response.
Key trends in economic indicators. Based on monthly and weekly data from the Department of Labor, the labor market generally improved in January, February, and March 2022 but remained weaker than in the prepandemic period. Initial unemployment insurance claims remained similar to prepandemic levels from January through mid-March 2022 (see the Unemployment Insurance Programs enclosure in app. I). The overall labor market continued to improve, as the employment-to-population ratio in March 2022 increased 0.2 percentage points from the previous month, to 60.1 percent. The employment-to-population ratio in March 2022 was 1.1 percentage points lower than in the prepandemic period (see figure).
Changes in employment across sectors continue to reflect the differential impact of the pandemic on various sectors of the economy. For example, the leisure and hospitality sector experienced strong job growth in January, February, and March 2022, but employment in the leisure and hospitality sector was still 8.7 percent lower than it was in February 2020. State and local government employment also increased in January, February, and March 2022, but employment in these sectors remained 3.6 percent lower than in the prepandemic period.
Serious delinquency rates—loans that are 90 or more days past due or in foreclosure—for single-family mortgage loans insured by the Federal Housing Administration (FHA) decreased from March 2021 through February 2022, to 5.93 percent of loans, but still remained much higher than rates prior to the pandemic. FHA loans disproportionately serve minority and low- to moderate-income borrowers, and therefore falling delinquencies may indicate improvement in the finances of some of those households in recent months, including fewer borrowers relying on FHA mortgage forbearance.[58]
Key trends in inflation. Indicators of inflation have generally increased since Spring 2021, suggesting that inflation could be somewhat higher, and persist for somewhat longer than previously expected.[59] Specifically, higher inflation has been evident across most of our inflation indicators. Some level of inflation on average can help promote stable economic conditions, but persistently high levels of inflation can cause financial challenges that are experienced more acutely by low-income households.
If demand grows considerably faster than supply for an extended period of time, for example, then consumer price inflation could meaningfully increase. The extent to which higher inflation will persist for a longer period of time will depend on many factors that remain uncertain, for example, how the current state of global supply chain issues constrain production or how the pandemic influences consumer demand across the economy.
The Federal Reserve System’s Federal Open Market Committee (FOMC) aims for inflation of 2 percent on average over time and aims to achieve rates of inflation that are above 2 percent for some time after periods in which inflation is persistently below 2 percent.[60]
In previous work, we identified a number of indicators of inflation to facilitate ongoing and consistent monitoring of the inflation experience of consumers to help assess the extent to which higher inflation would persist over time, including indicators of current consumer price inflation, as well as expectations of future inflation.[61] Based on data available in March 2022 covering price trends through February 2022, inflation has generally increased in recent months (see table).
Indicators of Inflation, Feb. 2021–Feb. 2022, and Average Inflation Rates, 2000–2019
Note: Underlined, red text indicates a higher rate of inflation than the previous month while black text indicates a lower rate of inflation than the previous month but with prices still rising overall. Deflation, or falling prices, would be indicated with a negative sign. All indicators of inflation are rounded to two decimal places. As a result, indicators may appear equal across months in the table but are actually different when not rounded.
aPCE is based on the PCE price index, which reflects changes in the prices of goods and services purchased by or on behalf of consumers in the U.S. The Federal Open Market Committee states its longer-run inflation goal in terms of PCE inflation and typically aims for inflation of 2 percent on average over time, including by aiming to achieve inflation rates above 2 percent for some time after periods in which inflation is persistently below 2 percent.
bCPI is based on data from the Consumer Price Index for all urban consumers (CPI-U), in which year-over-year change is computed from the not-seasonally-adjusted series, and the month-over-month change is computed from the seasonally adjusted series.
cMedian CPI is based on the 1-month inflation rate of the component whose expenditure weight is in the 50th percentile of price changes. By omitting outliers (small and large price changes) and focusing on the interior of the distribution of price changes, the median CPI may provide a better signal of the underlying inflation trend than the all-items CPI.
dThe 16 percent trimmed-mean CPI is based on a weighted average of 1-month inflation rates of components whose expenditure weights fall below the 92nd percentile and above the 8th percentile of price changes. By omitting outliers (small and large price changes) and focusing on the interior of the distribution of price changes, the 16 percent trimmed-mean CPI may provide a better signal of the underlying inflation trend than the all-items CPI.
eThe 10-year expected inflation rate comes from a model that decomposes the TIPS to nominal Treasury spread into three components: inflation expectations, the inflation risk premium, and a third component that may capture the TIPS liquidity premium or other factors that influence the relative demand for TIPS. See S. D'Amico, D. H. Kim, and M. Wei, "Tips from TIPS: The Informational Content of Treasury Inflation-Protected Security Prices," Journal of Financial and Quantitative Analysis, vol. 53, no. 1 (2018): pp. 395–436.
fProfessional forecast of inflation is an average forecast of expected CPI inflation in 2023 (annualized) from forecasts collected by Bloomberg. Absent data for January 2021, we have used black text for February 2021 data based on the data for 10-year expected CPI inflation from TIPS.
Inflation remains higher than averages in recent decades and headline indicators of more recent price pressures (measured relative to the previous month) increased in January and February 2022. However, the median and trimmed mean CPIs, which omit outliers and focus on underlying inflation trends, decreased in February 2022 compared to the previous month (see figure). These trends suggest that price pressures in February 2022 may have been driven by a relatively small group of goods and services. All measures of inflation that we monitor relative to the previous year increased in January and February 2022, while the measures of inflation expectations are more mixed.
Percentage Change in Inflation Indicators from the Previous Month, Jan. 2020–Feb. 2022
Methodology
To identify indicators for monitoring areas of the economy supported by the federal response to the COVID-19 pandemic, in particular by the six COVID-19 relief laws, we reviewed a number of sources. Specifically, we used prior GAO work, data from federal statistical agencies, information from the Board of Governors of the Federal Reserve System (Federal Reserve) and relevant federal agencies responsible for the pandemic response and oversight of the health care system, data available on the Bloomberg Terminal, and input from internal GAO experts. We reviewed the most recent data from these sources as of March and the beginning of April 2022, depending on availability.
To identify indicators for monitoring inflation, we reviewed data from federal statistical agencies, academic and other research literature, information from the Federal Reserve, the Federal Open Market Committee, written responses to our questions provided by the Bureau of Labor Statistics and the Federal Reserve, data available on the Bloomberg Terminal, and input from internal GAO experts.
We assessed the reliability of the economic indicators we used through a number of steps, including reviewing relevant documentation, reviewing prior GAO work, and interviewing data providers. Collectively, we determined the indicators were sufficiently reliable to provide a general sense of (1) how the areas of the economy supported by the federal pandemic response were performing and (2) trends in the inflation experience of consumers.
Agency Comments
We provided the Department of Housing and Urban Development (HUD), the Department of Labor (DOL), the Department of the Treasury (Treasury), the Federal Reserve, and the Office of Management and Budget (OMB) with a draft of this enclosure. DOL, Treasury, and the Federal Reserve provided technical comments, which we incorporated as appropriate. HUD and OMB did not provide comments on this enclosure.
Contact information: Michael Hoffman, (202) 512-6445, hoffmanme@gao.gov
The Centers for Disease Control and Prevention could be better positioned to lead the nation’s efforts to detect and monitor COVID-19, in coordination with state, tribal, local, and territorial partners (collectively, jurisdictions) and public health partner organizations. This could be accomplished by including in the agency’s existing surveillance approach specific objectives for how it will achieve its goals and a description of how it will assess progress towards meeting them.
Entities involved: The Centers for Disease Control and Prevention, within the Department of Health and Human Services
Recommendation for Executive Action
The Director of the Centers for Disease Control and Prevention, in coordination with state, tribal, local, and territorial jurisdictions and public health partner organizations, should ensure the agency builds upon its existing COVID-19 surveillance approach by detailing specific objectives for how it will achieve its COVID-19 surveillance goals and describing how it will assess progress toward meeting them. The Department of Health and Human Services agreed with our recommendation, and the Centers for Disease Control and Prevention noted that it will continue efforts to develop a document summarizing its COVID-19 surveillance goals and how it will assess progress towards meeting them.
Background
According to the Centers for Disease Control and Prevention (CDC), public health surveillance is the ongoing, systematic collection, analysis, and interpretation of health-related data essential for planning, implementation, and evaluation of public health practice.[62] Surveillance is intended to guide efforts to detect and monitor disease and injuries, assess the impact of interventions and assist in the management of, and recovery from, large-scale public health incidents.[63] In the U.S., public health surveillance is a shared effort between CDC and thousands of agencies at the federal, state, local, tribal, and territorial levels (which we refer to collectively as “jurisdictions”), along with health care providers, laboratories, and others.
For surveillance of COVID-19, CDC’s approach is to collect multiple types of data, including data on cases, testing, hospitalizations, emergency department visits, hospital capacities, and variants. CDC uses this COVID-19 surveillance data in several ways, including to track the spread of the virus, identify geographic or other areas of concern, and inform decision-makers accordingly. These data contribute to CDC’s development of guidance for the public, at-risk groups, and health care providers. In addition, CDC provides information to the Department of Health and Human Services’ (HHS) leadership and to the White House to help direct the federal government’s pandemic response.
In our May 2018 report, we found that routine federal public health funding to jurisdictions had generally decreased over the years. The COVID-19 pandemic prompted new funding to support public health activities at all levels of government. Specifically, the CARES Act, American Rescue Plan Act of 2021 (ARPA), and annual appropriations acts for fiscal years 2020 and 2021 together provided CDC with $1.1 billion to support data modernization and COVID-19 surveillance activities.[64]
Overview of Key Issues
CDC’s COVID-19 surveillance approach outlines goals and activities for what the agency wants to achieve, but it does not detail how it will achieve its stated goals or how it will measure its progress—two components of an effective strategy we have noted in our past work. By including specific objectives that detail how CDC’s actions will allow it to meet its goals and describing measures to assess its progress towards reaching its goals, CDC could better ensure it is able to effectively monitor COVID-19 nationwide.
Given the many entities and numerous sources of data used, surveillance is a complex interagency and intergovernmental effort. (See our related Public Health Data Collection and Standardization and Public Health Situational Awareness Network Capabilities enclosures.) In our prior work, we found that such efforts can benefit from a strategy that clearly defines what the agency is aiming to achieve (goals), how goals will be achieved (objectives), and metrics for assessing progress (measures), among other things. Over time, some public health officials, researchers, and other infectious disease preparedness and response experts have emphasized the need for updated COVID-19 surveillance-related strategies, particularly as the pandemic shows signs of beginning to move from a period of crisis to a period of control. For example, in a January 2022 paper in the Journal of the American Medical Association, three experts noted that updated strategies for COVID-19 response and preparedness—including addressing data-related issues for improving and updating surveillance approaches—were needed going forward for moving from pandemic crisis to control.[65]
CDC‘s COVID-19 surveillance approach includes a framework that is based on eight COVID-19 surveillance goals and several broader initiatives, according to agency officials (see table).
Goals and Selected Initiatives in CDC’s Framework for COVID-19 Surveillance
Goals and Initiatives
Description
CDC’s eight COVID-19 surveillance goals
Monitor trends and intensity of COVID-19 transmission, identify outbreaks, and provide data to initiate case and contact investigations.
Understand disease severity and the spectrum of illness.
Monitor and track vaccine distribution, uptake, and effectiveness.
Describe risk factors for severe disease and transmission.
Monitor for variants.
Assess impact on health care systems.
Estimate disease burden, and forecast trends, impact, and clinical and public health needs.
Monitor impact of disease and interventions on health equity.
2014 Surveillance Strategy for improving capabilitiesa
Describes a number of efforts to improve CDC’s and the public health system’s overall surveillance capabilities by improving the timeliness and quality of surveillance data.
Public Health Science Agenda for COVID-19, last updated January 5, 2022b
Describes priority public health science questions organized around topic areas, including surveillance-related ones, such as testing or health equity. The priority questions outline critical scientific gaps identified by CDC or its public health partners that, if addressed, could provide improvements in public health outcomes.
Individual surveillance activity strategies
Strategies that are specific to 10 individual surveillance activities such as those for monitoring cases, deaths, hospitalizations, and other types of COVID-19 data.
Data Modernization Initiative, launched in 2020
An initiative launched in 2020 to modernize public health surveillance infrastructure with the goal of improving data integration to prevent or reduce problems. For more information on CDC’s Data Modernization Initiative, see the Public Health Data Collection and Standardization enclosure in this report.
COVID Data Tracker, updated dailyc
Online dashboard for CDC’s public reporting of COVID-19 surveillance data including maps and charts tracking cases, deaths, and trends of COVID-19.
Source: GAO summary of information from the Centers for Disease Control and Prevention (CDC). | GAO-22-105397.
aSee Centers for Disease Control and Prevention, Public Health Surveillance: Preparing for the Future (Atlanta, Ga.: 2014).
To meet the eight COVID-19 surveillance goals, CDC officials told us the agency uses data collected for COVID-19 through existing systems that also collect data for other pathogens (e.g., by adding COVID-19 case reporting to CDC’s case surveillance system) or by modifying existing systems to collect new types of information. CDC officials noted they work with jurisdictions to scale up existing surveillance activities and stand up new ones to monitor for COVID-19, based on longstanding shared work during both routine and emergency disease surveillance activities with these partners.
While CDC’s COVID-19 surveillance approach includes goals and activities conducted for each goal, which we have noted in our prior work as being desirable of an effective strategy, it lacks specific objectives for how the activities will help it achieve these surveillance goals, and measures to assess its progress meeting the goals. Specifically, in our prior work we noted that a desirable characteristic of an effective strategy includes a description of what the strategy is trying to achieve, steps to achieve those results, and performance measures to gauge results.[66]
One example of how CDC could include objectives and measures to build on its approach and ensure it best meets its goals for COVID-19 surveillance is in wastewater testing. CDC officials told us that part of the agency’s COVID-19 surveillance approach is to conduct wastewater testing, a form of testing that can be used in communities where timely clinical testing is unavailable. Wastewater surveillance is an activity that contributes to two of CDC’s COVID-19 surveillance goals: monitoring trends and identifying outbreaks (goal 1 in the table above); and estimating disease burden, and forecasting trends, impact, and clinical and public health needs (goal 7 in the table above), according to agency officials. However, CDC has not detailed the specific objectives that describe how wastewater surveillance contributes to achieving these goals. CDC also has not developed measures that would allow it to understand how well current wastewater surveillance contributes to progress in meeting these goals.
One potential objective that CDC could set, for example, could be the use of wastewater surveillance where clinical testing is limited in order to help the agency achieve its goal of monitoring and identifying outbreaks nationwide.[67] CDC could then set targets for the percentage of communities with wastewater being tested that would allow it to measure how well its wastewater surveillance is contributing to CDC’s larger COVID-19 surveillance efforts, such as filling gaps in communities where other types of testing is more limited. A defined measure for the level of wastewater surveillance needed to ensure effective monitoring of COVID-19 could also help CDC coordinate and align surveillance activities with jurisdictions and public health partner organizations.[68]
CDC officials told us that its approach to COVID-19 surveillance must change over time, and that a strategy, once written down, could become static and may not be as useful. However, a strategy that includes defining how the agency’s activities will help it to achieve its goals and how it will gauge progress would not limit CDC’s ability to adapt to changing circumstances. An effective national strategy that includes both objectives and measures would allow CDC to better adapt to changing circumstances, such as when new variants arise, and better ensure that public health partners are able to adapt and move in the same direction for a nationwide approach.
CDC officials told us they are thinking about the future of COVID-19 surveillance, as did all three public health partner organizations we interviewed.[69] One of the partner organizations further noted they are looking for leadership from CDC to help with this transition and to better ensure that surveillance approaches nationally align with their members’ approaches at the jurisdictional level. This moment—as CDC and partners think about the future of COVID-19 surveillance and the need to shift with changing circumstances—offers an ideal opportunity for CDC to incorporate objectives and measures into its COVID-19 surveillance approach.
According to CDC officials, they have discussed the use of different surveillance approaches, such as sentinel surveillance, and the amount of case data required to monitor trends.[70] Officials told us that they had these discussions in the summer of 2021, and that while they continued those and other discussions related to strategies for the future of COVID-19 surveillance, they had to shift their focus temporarily to respond to the rising COVID-19 cases from the Delta and Omicron variants.
CDC’s approach for surveillance going forward may be most effective by being adaptable to the changing nature of the pandemic and aligned with the White House’s COVID-19 and larger public health emergency planning and priorities. For example, the latest White House pandemic plan, released March 2, 2022, lays out a role for CDC surveillance leadership and includes preparing for new variants as one of four key goals in COVID-19 preparedness.[71] Having specific objectives and measures related to variant surveillance, also one of CDC’s eight goals, would better ensure that CDC is able to meet its own surveillance goal on variants, align with the White House plan, and better ensure that jurisdictions and public health partner organizations are aligned with this surveillance approach as well.
At this critical time, the U.S. needs a forward-looking approach to its surveillance strategy. We recognize the challenges of adapting a COVID-19 surveillance strategy to plan for the future while simultaneously responding to the present pandemic. We also recognize that a strategy that is flexible and adaptable to new information as it becomes available is only a starting point. Nevertheless, whether the nation enters a period of recovery or surge, CDC could be better positioned to lead the nation and coordinate with jurisdictions and public health partner organizations to detect and monitor COVID-19 by including in its existing surveillance approach specific objectives for how it will achieve its goals and a description of how it will assess progress towards meeting them.
Methodology
To understand CDC’s COVID-19 surveillance approach, we reviewed relevant CDC documents and agency webpages related to its COVID-19 surveillance and key initiatives that support the framework for surveillance, such as CDC’s Science Agenda webpage.[72] We also interviewed officials from CDC, as well as HHS, and obtained written information. We assessed CDC’s efforts against characteristics of an effective national strategy that we identified in previous work. Specifically, we compared CDC’s approach against a characteristic that effective strategies include goals, objectives, activities, and performance measures.
To gather perspectives from CDC’s public health partners involved in COVID-19 surveillance, we interviewed representatives from the three national organizations that support public health surveillance activities and that collectively represent local, state, and territorial public health agencies, and state epidemiologists: the Association of State and Territorial Health Officials, the National Association of County and City Health Officials, and the Council of State and Territorial Epidemiologists.
Agency Comments
We provided a draft of this enclosure to HHS and the Office of Management and Budget (OMB). HHS agreed with our recommendation, and its comments are reproduced in appendix VII. CDC noted that it will continue efforts to develop a document summarizing its COVID-19 surveillance goals and describe how it will assess progress towards meeting them. The document will describe surveillance goals, objectives, core surveillance approaches used to address the surveillance objectives, and additional layered surveillance approaches that provide additional situational awareness. CDC also noted that progress towards meeting surveillance goals is affected by agency efforts as well as jurisdictional activities, funding, data use agreements, and reporting authorities that are outside of its control.
CDC also provided technical comments, which we incorporated as appropriate. OMB did not provide comments.
GAO’s Ongoing Work
We will continue to review federal efforts related to COVID-19 surveillance.
GAO’s Prior Recommendations
The table below presents our recommendations on testing from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to COVID-19 Testing
Recommendation
Status
The Director of the Centers for Disease Control and Prevention should work with appropriate stakeholders—including public health and private laboratories—to develop a plan to enhance laboratory surge testing capacity. This plan should include timelines, define agency and stakeholder roles and responsibilities, and address any identified gaps from preparedness exercises (July 2021 report).
Open— partially addressed. The Department of Health and Human Services (HHS) agreed with our recommendation and has begun to implement it. CDC informed us in January 2022, that the agency has, in collaboration with internal and external partners, drafted a plan to enhance laboratory surge testing capacity outside of CDC and public health laboratories. This is a positive step forward and we will review the plan once it is finalized. In March 2022, CDC informed us they expect to finalize their plan and provide it to us for review in May.
The Director of the Centers for Disease Control and Prevention should assess the agency's needs for goods and services for the manufacturing and deployment of diagnostic test kits in public health emergencies. This assessment should evaluate how establishing contracts in advance of an emergency could help the Centers for Disease Control and Prevention quickly and cost-effectively acquire these capabilities when responding to future public health emergencies, including those caused by novel pathogens, and should incorporate lessons learned from the COVID-19 emergency (July 2021 report).
Closed— addressed. The Department of Health and Human Services (HHS) agreed with our recommendation that the Director of CDC assess the agency’s needs for goods and services for the manufacturing and deployment of test kits in public health emergencies. CDC informed us in March 2022, that the agency had assessed its existing contract mechanisms, flexibilities, and contract options and their ability to address COVID-19 response needs. CDC informed us that lessons learned from the COVID-19 response led the agency to institute additional flexibilities and contract options for existing, new, and future contracts mechanisms. CDC informed us that these changes could support the emergency production of goods and services during an emergency. As a result, we believe CDC’s actions address our recommendation.
The Secretary of Health and Human Services (HHS) should develop and make publicly available a comprehensive national COVID-19 testing strategy that incorporates all six characteristics of an effective national strategy. Such a strategy could build upon existing strategy documents that HHS has produced for the public and Congress to allow for a more coordinated pandemic testing approach (January 2021 report).
Open—partially addressed. HHS partially agreed with our recommendation. In January 2021, HHS agreed that the department should take steps to more directly incorporate some of the elements of an effective national strategy, but expressed concern that producing such a strategy at this time could be overly burdensome on the federal, state, and local entities that are responding to the pandemic, and that a plan would be outdated by the time it was finalized or potentially rendered obsolete by the rate of technological advancement. In March 2022, the White House updated its general COVID-19 strategy, which provided new strategic elements related to testing, but does not contain all of the elements of an effective national strategy, such as clearly defined performance metrics and benchmarks. As of March 2022, HHS had not fully addressed this recommendation.
To improve the federal government’s response to COVID-19 and preparedness for future pandemics, the Secretary of Health and Human Services should immediately establish an expert committee or use an existing one to systematically review and inform the alignment of ongoing data collection and reporting standards for key health indicators. This committee should include a broad representation of knowledgeable health care professionals from the public and private sectors, academia, and nonprofits (January 2021 report).
Open—not addressed. HHS partially agreed with our recommendation. As of July 2021, HHS stated that it planned to consider ways to establish more permanent work groups to incorporate best practices for ongoing interagency data needs and to scale up as necessary during future public health emergencies. We maintain that immediately establishing an expert committee—not limited to federal agency officials—that includes knowledgeable health care professionals from the public and private sectors, academia, and nonprofits is an important and worthwhile effort to help improve the federal government's response to the COVID-19 pandemic and its preparedness for future pandemics. As of March 2022, we were awaiting updates from the agency.
The Secretary of Health and Human Services should ensure that the Director of the Centers for Disease Control and Prevention (CDC) clearly discloses the scientific rationale for any change to testing guidelines at the time the change is made (November 2020 report).
Open—partially addressed. HHS agreed with our recommendation and has begun to implement it. Specifically, in April 2022, CDC outlined for GAO steps the agency plans to take to ensure that future updates to testing guidance include clear links to the underlying scientific rationale. For instance, agency officials plan to include on the agency’s testing guidance a hyperlink to the science brief page with underlying scientific rationale supporting the guidance. We will continue to monitor the implementation of these planned steps.
Infectious Disease Threats: Funding and Performance of Key Preparedness and Capacity-Building Programs. GAO-18-362. Washington, D.C.: May 24, 2018.
Biosurveillance: Efforts to Develop a National Biosurveillance Capability Need a National Strategy and a Designated Leader. GAO-10-645. Washington, D.C.: June 30, 2010.
Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism. GAO-04-408T. Washington, D.C.: February 3, 2004.
The Department of Health and Human Services was appropriated approximately $484 billion in COVID-19 relief funds. It reported that it had obligated about $418 billion and expended about $269 billion of this amount—about 86 percent and 55 percent, respectively—as of February 28, 2022.
Entity involved: Department of Health and Human Services
Background
The Department of Health and Human Services (HHS) received approximately $484 billion in COVID-19 relief appropriations from six COVID-19 relief laws enacted as of February 28, 2022. HHS COVID-19 relief funds may be used for a range of purposes, such as assistance to health care or child care providers; testing, therapeutic, or vaccine-related activities; or procurement of critical supplies. Many HHS COVID-19 relief funds are available for a multiyear period or until expended.
Overview of Key Issues
As of February 28, 2022, HHS reported that it had obligated about $418 billion (86 percent) and expended about $269 billion (55 percent) of the approximately $484 billion in COVID-19 relief funds appropriated (see figure below).
HHS-Reported COVID-19 Relief Appropriations, Obligations, and Expenditures from COVID-19 Relief Laws, as of Feb. 28, 2022
aThese amounts reflect appropriations provided in Divisions M and N of the Consolidated Appropriations Act, 2021, that are specifically designated for COVID-19 relief.
The table below shows HHS appropriations, obligations, and expenditures by COVID-19 relief law that HHS reported as of February 28, 2022.
HHS-Reported COVID-19 Relief Appropriations, Obligations, and Expenditures, by Relief Law, as of Feb. 28, 2022
Legislation
Date of enactment
Appropriations $ in millions
Obligations $ in millions (% obligated)
Expenditures $ in millions (% expended)
Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 (Pub. L. No. 116-123)
March 6, 2020
6,497
5,830 (90)
4,491 (69)
Families First Coronavirus Response Act (Pub. L. No. 116-127)
March 18, 2020
1,314
1,309 (100)c
1,276 (97)
CARES Act (Pub. L. No. 116-136)a
March 27, 2020
142,833
139,386 (98)
127,470 (89)
Paycheck Protection Program and Health Care Enhancement Act (Pub. L. No. 116-139)
April 24, 2020
100,000
80,927 (81)
70,027 (70)
Consolidated Appropriations Act, 2021 (Pub. L. No. 116-260) b
December 27, 2020
73,175
68,138 (93)
26,296 (36)
American Rescue Plan Act of 2021 (Pub. L. No. 117-2)
March 11, 2021
160,494
122,073 (76)
39,166 (24)
Total
484,313
417,843 (86)
268,725 (55)
Source: Department of Health and Human Services (HHS) data. | GAO-22-105397
aHHS reported that it transferred $289 million from CARES Act appropriations to the Department of Homeland Security; this amount is not included in HHS’s reported obligations or expenditures.
bThese amounts reflect appropriations provided in Divisions M and N of the Consolidated Appropriations Act, 2021 that are specifically designated for COVID-19 relief. An additional $638 million in COVID-19 relief funds were appropriated under Division H to the Administration for Children and Families, an agency within HHS, to prevent, prepare for, and respond to the coronavirus, for necessary expenses for grants to carry out a low-income household drinking water and wastewater emergency assistance program. These funds were not included in the HHS-reported data on HHS COVID-19 relief appropriations, obligations, and expenditures, as HHS noted that the funds were not considered COVID-19 relief funding for USAspending.gov reporting purposes.
cThe percent obligated was 99.6 percent, which we show as 100 percent due to rounding.
The table below shows allocations, obligations, and expenditures of COVID-19 relief appropriations made to HHS under the six relief laws by agency or key fund as of February 28, 2022.
HHS-Reported Allocations, Obligations, and Expenditures of COVID-19 Relief Funding, by Agency or Key Fund, as of Feb. 28, 2022
Agency or key fund
Allocations ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
Administration for Children and Families
65,257.5
65,093.0
21,204.3
Administration for Community Living
3,200.0
2,995.8
1,216.9
Agency for Toxic Substances and Disease Registry
12.5
12.5
11.0
Centers for Disease Control and Prevention
27,225.9
20,041.1
7,878.4
Centers for Medicare & Medicaid Servicesa
935.0
719.3
107.2
Enhanced Use of Defense Production Act
10,000.0
1,473.3
142.2
Food and Drug Administration
718.0
270.1
112.2
Health Resources and Services Administration
11,729.8
10,542.2
4,515.5
Indian Health Service
7,980.0
5,458.8
4,991.4
National Institutes of Health
3,001.3
2,587.8
1,615.8
Office of Inspector General
17.0
7.9
6.7
Public Health and Social Services Emergency Fund (PHSSEF)b
346,001.4
301,032.2
226,114.7
Office of the Assistant Secretary for Healthc
5,267.8
4,992.9
4,313.6
Office of the Assistant Secretary for Preparedness and Responsec
32,723.8
25,922.6
15,168.9
Biomedical Advanced Research and Development Authorityc
45,994.2
44,419.2
22,023.5
Provider Relief Fundc, d
178,000.0
159,066.0
154,415.7
Other PHSSEFc
84,015.6
66,631.5
30,193.0
Substance Abuse and Mental Health Services Administration
8,235.0
7,608.5
808.7
Grand total
484,313.4
417,842.5
268,725.0
Source: Department of Health and Human Services (HHS) data. | GAO-22-105397
Note: For the purpose of this table, the term allocation includes both direct appropriations and transfers between HHS agencies. For example, according to HHS, the agency transferred $1,063.5 million to the Administration for Children and Families’ Unaccompanied Children Program from National Institutes of Health appropriations provided in the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, 134 Stat. 1182, 1913 (2020), citing the Secretary’s authorities under that act. HHS reported that it transferred $289 million to the Department of Homeland Security that is not included in the reported obligations or expenditures. With respect to the Consolidated Appropriations Act, 2021, the amounts reflect appropriations specifically designated for COVID-19 in Divisions M and N of the act.
aThese amounts do not reflect Medicaid and Medicare expenditures that resulted from statutory changes to these programs under the COVID-19 relief laws.
bPHSSEF is an account through which funding is provided to certain HHS offices, such as the Office of the Assistant Secretary for Preparedness and Response. Amounts have been appropriated to this fund for the COVID-19 response to support certain HHS agencies and response activities. The PHSSEF allocation amount includes $289 million that HHS reported it transferred to the Department of Homeland Security and is not included in the reported obligations or expenditures. Amounts appropriated to the PHSSEF and transferred to agencies within HHS listed in the table are included in the allocation amounts for the specified receiving agencies. For example, the National Institutes of Health received transfers from the PHSSEF and these amounts are included in the agency allocation rather than in the PHSSEF total.
cThe italicized amounts are subtotals of the PHSSEF and are already reflected in amounts listed for the PHSSEF.
dThe Provider Relief Fund reimburses eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19. Provider Relief Fund expenditures also may be referred to as disbursements. For additional information about Provider Relief Fund allocations and disbursements, see the Relief for Health Care Providers enclosure.
HHS reported allocations, obligations, and expenditures of appropriations from the six COVID-19 relief laws for a variety of COVID-19 response activity categories (see the table below). When response activities had spending related to multiple categories, they were only assigned to one. For example, certain funds for testing and vaccine distribution were included in the response activity category for support to states, localities, territories, and tribal organizations rather than in the testing or vaccine activity categories.
HHS officials noted that allocations for COVID-19 response activities are determined by appropriations made by Congress in combination with approved spend plan decisions. The timing of obligations and expenditures of allocations for response activities can vary due to a variety of factors, including the timing of the appropriations and the planned uses of funds. For example, some research programs are planned in phases, which affects the timing of the release of the funds.
HHS-Reported Allocations, Obligations, and Expenditures by Selected COVID-19 Response Activity, as of Feb. 28, 2022
COVID-19 response activity
Description
Allocations ($ in millions)
Obligations ($ in millions)
Expenditures ($ in millions)
Provider Relief Fund
Includes reimbursements to eligible health care providers for health care-related expenses or lost revenues that are attributable to COVID-19.
178,000.0
159,066.0
154,415.7
Testing
Includes procurement and distribution of testing supplies, community-based testing programs, testing in high-risk and underserved populations and in Indian Health Services’ programs, screening in schools, Centers for Disease Control and Prevention (CDC) testing-related activities such as technical assistance, and other activities.
57,582.1
43,685.9
19,865.7
Child Care and Development Funda
Includes funding for states and other governments for child care subsidies for eligible families and quality improvement activities, sub-grants to child care providers to stabilize the child care market, and payments for child care assistance.
52,450.0
52,449.7
15,143.2
Vaccines
Includes Biomedical Advanced Research and Development Authority (BARDA) funding for vaccine development and procurement; National Institutes of Health (NIH) research activities; and CDC vaccine distribution, administration, and technical assistance related activities.
41,508.2
37,346.7
17,721.1
Support to state, local, territorial, and tribal organizations’ preparedness
Includes funding for states and other governments to support testing, contact tracing, and surveillance; vaccine distribution; and other activities.
40,116.6
39,572.9
14,244.0
Drugs and therapeutics
Includes BARDA funding for development and procurement of therapeutics and NIH research activities.
17,546.8
15,932.8
7,168.5
Strategic National Stockpile
Includes funds for acquiring, storing, and maintaining ventilators, testing supplies, and personal protective equipment (PPE) and increasing manufacturing capacity for certain PPE.
13,919.9
10,512.5
8,449.4
Health centers
Includes support for COVID-19-related activities—such as testing—at health centers, which provide health care services to individuals regardless of their ability to pay.
9,620.0
9,487.4
4,073.4
Rural provider payments
Includes assistance for rural providers and suppliers, administered using the same mechanism as the Provider Relief Fund.
8,500.0
7,245.9
7,246.6
Mental health and substance use–related services
Includes substance abuse prevention and treatment, community-based mental health services, and other activities.
8,315.0
7,623.6
811.4
Diagnostics research and development
Includes BARDA diagnostic development programs and NIH projects, such as the Rapid Acceleration of Diagnostics Initiative.
2,411.4
1,958.8
1,298.5
Head Start
Includes grants to local programs for high-quality learning experiences and to respond to other immediate and ongoing consequences of COVID-19.
2,000.0
1,998.9
862.5
Testing for uninsuredb
Includes reimbursements to eligible providers for COVID-19 testing for individuals who are uninsured.
2,000.0
1,998.7
1,983.1
Global disease detection and emergency response
Includes support to governments and other organizations to rapidly diagnose cases and to ensure readiness to implement vaccines and therapeutics.
1,550.0
732.1
336.1
Telehealth
Includes efforts to support safety-net health care providers transitioning to telehealth, telehealth access—especially for vulnerable maternal and child health populations—and a telehealth website.
284.2
176.6
154.3
Other response activitiesc
Includes additional activities such as activities conducted by the Administration for Community Living, certain CDC-wide activities and program support, and activities conducted by the Food and Drug Administration.
48,509.2
28,054.0
14,951.5
Total
484,313.4
417,842.5
268,725.0
Source: Department of Health and Human Services (HHS) data, written HHS responses, and GAO analysis of HHS spend plans. | GAO-22-105397
Notes: The selected response activities represent examples of certain targeted activities that fall within particular HHS agencies, such as funding for health centers or Head Start, as well as broader categories of response activities that may span HHS agencies, such as testing-, vaccine-, and therapeutics-related response activities.
HHS reported allocations, obligations, and expenditures for these activities based on the primary programmatic recipient organization of the funds, although some activities apply to multiple categories. For example, certain funds in the “support to state, local, territorial, and tribal organizations for preparedness” category were provided for testing but are not reflected in the “testing” category. However, HHS also noted that testing-related funding awarded to states or localities that was appropriated under the American Rescue Plan Act of 2021 (ARPA) was included in the “testing” category. HHS officials explained that the activity names align with how funds were appropriated under different COVID-19 relief laws.
According to HHS officials, the allocations reported for the key activities above are based on amounts appropriated for these activities in the COVID-19 relief laws, HHS transfers of funds, and approved spend plan decisions made by HHS in coordination with the Office of Management and Budget. According to HHS, the agency used about $1.7 billion in appropriations provided under ARPA, including $1.2 billion appropriated for COVID-19 testing, contact tracing, and mitigation activities, for the Administration for Children and Families’ Unaccompanied Children Program, citing the Secretary’s authorities under the Public Health Service Act and the Consolidated Appropriations Act, 2021. See Pub. L. No. 116-260, div. H, tit. II, § 204, 134 Stat. 1182, 1589 (2020); 42 U.S.C. 238j(a). With respect to the Consolidated Appropriations Act, 2021, the amounts reflect appropriations specifically designated for COVID-19 in Divisions M and N of the act. HHS reported that it transferred $289 million to the Department of Homeland Security that is not included in the reported obligations or expenditures.
aThe Child Care and Development Fund is made up of two funding streams: mandatory and matching funding authorized under section 418 of the Social Security Act, and discretionary funding authorized under the Child Care and Development Block Grant Act of 1990, as amended. See 42 U.S.C. §§ 618 and 9858m.
bAccording to HHS officials, HHS has allocated an additional $4.8 billion to the testing for the uninsured program from section 2401 of ARPA, which HHS included in the “testing” response activity category.
cAccording to HHS officials, the agency transferred $1,063.5 million from NIH appropriations for research and clinical trials related to long-term studies of COVID-19 and $850 million from the Public Health and Social Services Emergency Fund, Strategic National Stockpile, to the Administration for Children and Families’ Unaccompanied Children Program citing authority provided in section 304 of the Consolidated Appropriations Act, 2021 for both transfers. See Pub. L. No. 116-260, div. M, tit. III, § 304, 134 Stat. at 1913, 1916, 1923 (2020).
Methodology
We obtained HHS data on appropriations, allocations, obligations, and expenditures of COVID-19 relief funds by HHS agency and by selected response activity, as of February 28, 2022. We reviewed the six COVID-19 relief laws and also reviewed appropriation warrant information provided by the Department of the Treasury as of February 28, 2022. To assess the reliability of the data reported by HHS, we reviewed HHS documentation, Department of the Treasury appropriation warrant information, and other available information on HHS’s use of COVID-19 relief funds. We did not independently validate the data provided by HHS. We determined that the HHS-reported data were sufficiently reliable for the purposes of our reporting objective.
Agency Comments
We provided HHS and the Office of Management and Budget with a draft of this enclosure. Neither agency provided comments on this enclosure.
GAO’s Ongoing Work
We will continue to examine HHS’s use of COVID-19 relief appropriations contained in COVID-19 relief laws and HHS’s oversight of these funds.
GAO’s Prior Recommendation
The table below presents our recommendation related to HHS COVID-19 funding from a prior quarterly CARES Act report.
Prior GAO Recommendation Related to Department of Health and Human Services (HHS) COVID-19 Funding
Recommendation
Status
To communicate information about and facilitate oversight of the agency’s use of COVID-19 relief funds, the Secretary of Health and Human Services should provide projected time frames for the planned spending of COVID-19 relief funds in the Department of Health and Human Services’ spend plans submitted to Congress. (July 2021 report).
Open-partially addressed. As of January, 2022, HHS reported that it had incorporated projected time frames of planned spending for certain activities, such as select grants and cooperative agreements. HHS stated that the department is unable to provide specific time frames for all relief funds due to the evolving environment of the COVID-19 response and the need to remain flexible in responding to incoming requests for response activities.
As of February 28, 2022, the Department of Health and Human Services had disbursed payments to providers totaling about $154.4 billion (about 87 percent) of the $178 billion appropriated by COVID-19 relief laws to the Provider Relief Fund. Moreover, HHS announced recently that all of the Provider Relief Fund has been allocated. The Health Resources and Services Administration has begun Provider Relief Fund payment integrity oversight by identifying payment integrity risks and conducting efforts to respond to and mitigate the risks, such as post-payment reviews of relief payments it has made, recovery of overpayments, and audits of providers’ use of payments.
Entities involved: Department of Health and Human Services, including its Health Resources and Services Administration
Background
Relief funds to health care providers have been allocated and disbursed by the Department of Health and Human Services (HHS) through the following programs:[73]
Provider Relief Fund. To respond to the pandemic, three of the six COVID-19 relief laws appropriated a total of $178 billion to the Provider Relief Fund (PRF) to reimburse eligible providers for health care-related expenses or lost revenues attributable to COVID-19:
the CARES Act appropriated $100 billion,
the Paycheck Protection Program and Health Care Enhancement Act appropriated $75 billion, and
the Consolidated Appropriations Act, 2021, appropriated $3 billion for this purpose.[74]
HHS’s Health Resources and Services Administration (HRSA) administers payments from the PRF, including allocations to the COVID-19 Uninsured Program and to the COVID-19 Coverage Assistance Fund.[75] In addition to the PRF, the American Rescue Plan Act of 2021 appropriated $8.5 billion for payments to eligible rural health care providers for health-care-related expenses and lost revenues attributable to COVID-19.[76]
HRSA oversees the PRF and the American Rescue Plan Rural Distribution and established the Provider Relief Bureau Program and Payment Integrity Branch to increase payment integrity through recovery of overpayments.[77] Some of HRSA’s post-payment oversight activities include (1) risk analysis and post-payment reviews of payment discrepancy types to determine whether HRSA made PRF overpayments (i.e., payments made to ineligible providers or made in incorrect amounts), (2) recovery efforts seeking repayment of overpayments, and (3) post-payment audits to determine whether PRF funds were used by providers in accordance with laws and terms and conditions of the program.[78]
The HHS Office of Inspector General (OIG) has identified concerns related to fraud schemes that divert PRF payments based on misrepresentation, among other things. For example, HHS OIG is currently investigating several cases where providers may have falsely attested that they were eligible to receive PRF payments or otherwise received PRF payments despite being ineligible, resulting in overpayments.
Accelerated and Advance Payments. HHS’s Centers for Medicare & Medicaid Services’ (CMS) Accelerated and Advance Payments Program provides loans to active Medicare providers and suppliers. Section 3719 of the CARES Act authorized the expansion of this program due to the COVID-19 pandemic, though no new loans have been made since January 2021.[79] Of the $107.3 billion in COVID-19-related loans disbursed under the program as of February 28, 2022, $63.3 billion in repayments have been made by providers and suppliers, and the current outstanding loan balance for the program is $43.9 billion.
Overview of Key Issues
Provider Relief Fund allocations, disbursements, and returned funds. As of February 28, 2022, HHS had allocated all of the $178 billion appropriated to the PRF, and disbursed about $154.4 billion. HHS allocated PRF funds as follows:
$86.3 billion for general distributions, for general relief to health care providers,
$55.8 billion for targeted distributions, for certain types of providers and facilities; and
Allocated and undisbursed funds. In March 2022, HHS officials told us that the remaining funds we previously reported as unallocated were being reserved to meet future demands of the ongoing COVID-19 pandemic—specifically, claims reimbursement programs, through the COVID-19 Uninsured Program and the COVID-19 Coverage Assistance Fund. Officials also told us that the timing of these remaining distributions will depend on several factors, including when claims are submitted by providers to HHS for reimbursement of COVID-19 testing, treatment, and vaccine administration.[81]
Fund disbursements. According to our analysis of information provided by HRSA, as of February 28, 2022, HRSA had disbursed about $74.8 billion from general distribution allocations, about $55.1 billion from the targeted allocations, and $24.5 billion for other distributions.[82] As of February 28, 2022, 439,304 providers had received 753,625 payments made from the PRF.
HRSA’s general distributions to providers have been distributed in phases, beginning April 10, 2020, with Phase I distributions to providers billing Medicare fee-for-service, to its recent Phase IV distributions, beginning December 16, 2021, of $17 billion in general distributions to a broad range of providers who could document COVID-related revenue loss and expenses from July 1, 2020, through March 31, 2021. HRSA officials told us that as of February 28, 2022, HRSA had disbursed about $10.7 billion of this $17 billion to providers who had successfully set up payment accounts to receive the disbursed funds.[83]
See table below for a summary of PRF allocations and disbursements as of February 28, 2022.
Provider Relief Fund: Summary of Allocations and Disbursements, as of February 28, 2022
Description
Allocation ($ in billions)
Disbursement ($ in billions)a
Date of initial disbursement
General distributions
Phase I: Medicare
42.816
41.907
April 10, 2020
Phase II: Medicaid and Children’s Health Insurance Program (CHIP) providers
3.678
3.159
July 3, 2020
Phase II: dental providers
1.002
0.995
July 28, 2020
Phase II: assisted living facilities
0.405
0.381
September 25, 2020
Phase III: general distribution
21.361
17.706
November 14, 2020
Phase IV: general distributionb
17.000
10.671
December 16, 2021
Subtotal of general distributions
86.262
74.819
n/a
Targeted distributions
Rural health care facilities
10.990
10.726
May 6, 2020
High-impact hospitalsc
20.685
20.655
May 7, 2020
Skilled nursing facilities
4.785
4.750
May 22, 2020
Indian health care providers
0.520
0.499
May 29, 2020
Safety net hospitals
13.074
12.838
June 12, 2020
Children’s hospitals
1.063
1.061
August 20, 2020
Nursing home infection control, quality, and performance
4.650
4.528
August 27, 2020
Subtotal of targeted distributions
55.767
55.057
n/a
Subtotal of general and targeted distributions
142.029
129.876
n/a
Other distributions
Treatment, testing, and vaccine administration for the uninsured and underinsuredd
18.300
12.375
May 15, 2020
Vaccine and therapeutic development and procurement activities
16.691
12.030
November 25, 2020
Administration
0.980
0.136
n/a
Subtotal other distributions
35.971
24.541
n/a
Unallocated fundse
0.000
0.000
n/a
Total Provider Relief Fund
178.000
154.417
n/a
Legend: n/a = not applicable
Source: Summary of Department of Health and Human Services (HHS) funding data. | GAO-22-105397
aProvider Relief Fund disbursements may also be referred to as expenditures.
bOn March 22, 2022, Health Resources and Services Administration (HRSA) announced that it had released for disbursement an additional $413 million to providers, bringing the total to nearly $12 billion released for disbursement to 82,000 providers, out of the $17 billion allocated for Phase IV general distributions. HRSA also announced, as of March 22, 2022, that 89 percent of applications from providers for Phase IV general distributions had been processed, and HRSA officials told us they expected to process the remaining Phase IV applications by the end of spring 2022.
cHigh-impact hospitals are hospitals that have a high number of confirmed COVID-19 inpatient admissions.
dHRSA covers treatment, testing, and administering the vaccine for the uninsured through its COVID-19 Uninsured Program, and covers the cost of administering the vaccine for the underinsured through its COVID-19 Coverage Assistance Fund.
eAccording to HRSA, all funding for the Provider Relief Fund had been allocated as of February 28, 2022.
Returned funds. Providers can return funds at any time and do so on a regular basis.[84] According to HRSA, providers had returned $9.8 billion from previous disbursements from the general and targeted distributions, as of February 28, 2022, an increase of $1 billion from the $8.8 billion in returned funds we previously reported, as of August 31, 2021.[85] According to HRSA, most of the returned funds were linked to payments automatically issued to providers based on HRSA’s determination of provider eligibility and payment calculation, rather than on providers’ applying for the funds.[86]
Provider Relief Fund payment integrity. HRSA has begun PRF payment integrity oversight by identifying payment integrity risks and taking actions such as post-payment reviews, recovery of overpayments, and audits.[87]
Post-payment reviews of relief payments made by HRSA. As of March 2022, HRSA was conducting or planning post-payment reviews of all payment discrepancy types, which HRSA designed for reviews to identify potential overpayments due to computation errors and ineligible providers, among other things. For example, a computation error could be due to incorrect data used to pay providers, and an ineligible provider could be a deceased provider or a provider with a Medicare or Medicaid fraud conviction.[88] HRSA conducts post-payment reviews of PRF general and targeted distributions to identify overpayments—payments made in incorrect amounts or to ineligible providers. As of February 2022, about $27.4 million had been identified for recovery from ineligible providers.
HRSA officials told us they plan to conduct post-payment reviews of all 753,625 PRF general and targeted distribution payments made to 439,304 providers, which total over $129 billion.[89] In preparation for this undertaking, the agency has conducted assessments to evaluate and mitigate the risks to payment integrity and planned to use these assessments to prioritize its post-payment reviews.[90]
Agency officials have also developed a post-payment manual and matrix. HRSA’s post-payment manual specifies that it will prioritize post-payment reviews according to the following criteria: high visibility cases, total dollar amount, number of providers impacted, suspected fraud, and complexity required to investigate. HRSA officials told us that they track reviews of payment discrepancy types in a post-payment matrix, which they regularly adjust to reflect current priorities based on the criteria above.
For final resolution of post-payment reviews, HRSA’s manual also specifies that a final discrepancy memo will be used to establish the decision for repayment by documenting the analysis and evidence of overpayments. This final discrepancy memo may be reviewed by HRSA’s Office of General Counsel and other stakeholders prior to HRSA taking action to recover funds from providers. According to agency officials, key elements of a final repayment memorandum include a definition of the payment discrepancy type, targeting criteria, relevant data sources, factors considered, and procedures for conducting the post-payment reviews. The post-payment matrix supplements the manual and lists all identified payment discrepancy types for conducting post-payment reviews and the status of completion—open or closed—based on each of the types.
As of February 2022, one final discrepancy memo—for the pilot post-payment review of renal dialysis payments—had been issued.[91] Final discrepancy memos had not been issued for the additional nine payment discrepancy types that had funds identified for repayment and for which HRSA was seeking repayment. In addition, another nine payment discrepancy types, which did not identify funds for repayment, were closed without a final memo. Agency officials told us that they do not issue memos for all closed discrepancy types, but they plan to begin producing final discrepancy memos to document repayment decisions for reviews that identify overpayments for recovery.
As of January 2022, there were a total of 57 payment discrepancy types for review, with 10 closed and 47 remaining open. The status of payment discrepancy types for review as of October 2021 was similar; there were a total of 55 payment discrepancy types for review, with 10 closed and 45 open (see table below).[92]
Status and Total of Payment Discrepancy Types for Post-payment Review
Status of Payment Discrepancy Types for Post-payment Review
Total as of
October 2021
January 2022
Open payment discrepancy types for post-payment reviewa
45
47
Open payment discrepancy types scheduled for review
9
10
Open payment discrepancy types to be scheduled for review in 2022
36
37
Closed payment discrepancy types for post-payment reviewb
10
10
Total payment discrepancy types for post-payment review
55
57c
Source: GAO analysis of Health Resources and Services Administration (HRSA) data. | GAO-22-105397
aHRSA officials noted that the post-payment matrix shows when reviews are scheduled to begin, but it does not show an anticipated completion date since distributions are continuing. Officials noted that reviews must remain open until no future payments are determined to be at risk or a control is put in place to prevent the discrepancy from occurring.
bAccording to the post-payment manual, final resolution of post-payment reviews that are closed are to be documented with a final discrepancy memo. At the time of our review, 10 payment discrepancy types were closed, but only one memo was available. As of March 2022, officials told us that they had completed four additional final discrepancy memos, but did not provide supporting documentation.
cHRSA designed payment discrepancy types for post-payment reviews to identify potential overpayments due to computation errors and ineligible providers, among other things. For example, a computation error could be due to incorrect data used to pay providers, and an ineligible provider could be a deceased provider or a provider with a Medicare or Medicaid fraud conviction. As of January 2022, HRSA had identified 57 payment discrepancy types, and at least 15 were related to ineligible providers. In March 2022, HRSA officials told us that they had identified 58 payment discrepancy types as of March 2022, of which 21 remain open, 4 are closed, 8 are closed due to consolidation, nine are scheduled to close pending a final discrepancy memo, and 16 are scheduled for review but not yet open for analysis. HRSA did not provide supporting documentation.
HRSA officials told us that the agency will continue to conduct post-payment reviews of payment discrepancy types until those types will have no more PRF payments. At that point, HRSA noted, it will consider the payment status final for all providers and then all post-payment reviews will be finalized and closed. As part of this process, HRSA also plans to issue final discrepancy memos for payment discrepancy types where the agency has identified funds for recovery but has not taken action to seek repayment.
As of March 2022, HRSA was in the process of addressing our recommendation from October 2021 to finalize post-payment oversight through actions such as establishing time frames for completing post-payment reviews to promptly address identified risks and identifying all overpayments made from the PRF.[93] Agency officials told us that HRSA and its contractor meet weekly to determine which payment discrepancy types will be reviewed in the upcoming week, and that they are continuously evaluating the prioritization order. HRSA provided the following reasons why it prioritizes post-payment reviews this way:
Officials said that reviews of different discrepancy types often run parallel to one another, since HRSA does not wait for one discrepancy review to be completed before starting a review of a different discrepancy.
Officials added that reviews of a particular discrepancy type may be temporarily suspended or delayed while another discrepancy type review moves forward, due to factors such as resource limitations, policy decisions, and case study investigations.
According to HRSA officials, their plan is to schedule, conduct, and close reviews in 2022, but the agency has not indicated when in 2022 all of its reviews of payments will be scheduled or completed. They also noted that continuous evaluations of priorities for post-payment reviews may result in processing payment discrepancy types in a concurrent manner. We maintain that establishing time frames for completing post-payment reviews of all payment discrepancy types and implementing recovery efforts expeditiously will help the agency succeed in recovering overpayments, particularly since disbursement of PRF funds began in April 2020.
HRSA recovery of overpayments. In October 2021, we recommended that HRSA finalize and implement post-payment recovery efforts to recoup overpayments. HRSA partially concurred and stated that payment recovery efforts will occur in the future. HRSA’s post-payment review process identifies potential overpayments for recovery, but not all will result in actions to seek repayment as not all will ultimately be determined to be overpayments, officials noted. For example, HRSA officials told us that it will not seek repayment of all potential overpayments identified from post-payment reviews because
Some potential overpayments have been offset by subsequent PRF distributions and resulted in a net correct payment amount, or
Some potential overpayments are below the minimum threshold under HRSA’s policy.
In addition, officials noted that some potential overpayments due to miscalculations may later be found (during the course of HRSA audits) to have been used appropriately by providers, and therefore would not be subject to repayment. For example, in the case of duplicate overpayments, HRSA’s notice to providers gives them the option of using the overpayment on expenses due to coronavirus or lost revenue, instead of submitting a repayment to HRSA.
Challenges to prompt action to review and recover have been further exacerbated by recent events.
As of March 2022, HRSA had suspended its recovery efforts for overpayments in order to establish a dispute process for providers to challenge HRSA’s repayment decisions. Officials told us that there are two instances of providers that are challenging the need to return funds (about $551,000 in disputed overpayments of the $187.3 million in identified overpayments that HRSA will seek for repayment), and therefore the agency is developing a dispute process.
Additionally, officials told us that they had encountered technical issues in seeking funds from providers with identified overpayments due to missing bank trace numbers that are used to seek repayment.[94] The agency is trying to resolve the issue which may continue in the future, since officials told us that bank practice is to delete and reuse trace numbers after 12 months.
Officials told us the agency will resume recovery efforts once the dispute process is established, however, it is unclear why HRSA is suspending its recovery efforts, since recovery efforts could continue while a dispute process is developed. There may be recovery steps HRSA can continue to take, such as sending notification letters to those providers with identified overpayments or continuing to identify potential overpayments.
Prior to its suspension of recovery efforts, as of August 2021, HRSA had taken actions to seek repayment of about 9 percent (about $15.1 of $167 million) of funds identified as overpayments in its post-payment reviews. In contrast, as of December 2021, HRSA had taken actions to seek repayment of about 14 percent (about $26.3 million of $187.3 million) of funds identified as overpayments in its post-payment reviews. Of the overpayments sought by HRSA, the agency had recovered about $2.9 million of $15.1 million as of August 2021 and about $14.1 million of $26.3 million as of December 2021. See table below.
Provider Relief Funds (PRF) Identified as Potential Overpayments and Overpayments Sought by Health Resources and Service Administration (HRSA) for Repayment
Agency Efforts Regarding Recovery of PRF Overpayments
Amount as of August 2021 (millions)
Amount as of December 2021 (millions)
Amount as of February 2022 (millions)
Potential overpayments HRSA identified through post-payment reviews
$305.0
$313.2
$313.2
HRSA will not seek repaymenta
$138.0
$125.9
$125.9
HRSA efforts to seek repayment
$167.0
$187.3
$187.3
HRSA has taken action to seek repaymentb
$15.1
$26.3
$26.3
HRSA has recovered overpayments
$2.9
$14.1
$22.8
HRSA plans to seek repayment but has not yet taken action
Note: Based on HRSA summary reports for total funds identified for recovery for August 2021 and December 2021, the potential overpayments went to about 3,000 providers.
aHRSA will not seek repayment of these potential overpayments because (1) some have been offset by subsequent PRF distributions and resulted in a net correct PRF payment, or (2) some potential overpayments are below the minimum threshold under HRSA’s policy.
bHRSA takes action to seek repayment by sending notification letters to providers requesting return of overpayment funds.
Post-payment audits of providers’ use of payments. HRSA has finalized its audit strategy manual expected to guide the agency’s audits on provider compliance with requirements for the use of PRF funds, and plans to begin audits later this year.[95]
According to officials, HRSA has initiated four pilot audits, involving four randomly selected providers and their 30 subsidiaries totaling $32.8 million from the first round of provider reports.[96] These pilot audits are being conducted to test audit procedures and plans and are estimated to be completed by July 2022.
In March 2022, according to officials, HRSA plans to audit a risk-based selection of providers that received funds. The selection of providers will be based on risk factors such as payment amount, prior single audit, and eligibility to receive payments, and on the risk score assigned to each provider based on these risk factors. In spring 2022, HRSA will begin the risk-based audit selection of all providers who reported in the first and second phases. According to officials, the audits will begin within a few weeks after selection of providers.
Methodology
To conduct our work, we examined publicly released HHS information, federal laws and agency guidance, and obtained information from CMS and HRSA in the form of written responses to questions, documents (including payment integrity oversight materials), and a data set. Our review of the data sources provides reasonable assurance of the data’s reliability. The Provider Relief Fund dataset, which includes disbursements as of February 28, 2022, came from HRSA, which is the only available source for the disbursement data. The allocation amounts and categories that were provided by HRSA were consistent with publicly available information. CMS provided data on the current status for loans and repayments under the Accelerated and Advance Payments program, as of February 28, 2022. Our review and analysis of HRSA’s payment integrity oversight efforts includes data received through February 18, 2022. Where appropriate we also included updated information provided by HRSA in late March 2022; however, we were not able to verify that data.
Agency Comments
We provided HHS and the Office of Management and Budget (OMB) with a draft of this enclosure. OMB did not provide comments on this enclosure. HHS provided technical comments on this enclosure, which we incorporated as appropriate. In its technical comments, HRSA provided updated data as of March 2022 on its payment integrity oversight efforts, specifically related to the post-payment reviews of payment discrepancy types and recovery of overpayments, but did not provide supporting documentation. We were not able to verify these data.
GAO’s Ongoing Work
As HHS works to distribute funds for COVID-19 relief activities and to eligible providers, it will continue to be important that HHS officials ensure funds are appropriately distributed and used. We plan to conduct additional work examining HHS’s COVID-19 relief funds, including payment oversight and funds returned by providers to HRSA.
GAO’s Prior Recommendations
The table below presents our recommendations from prior reports related to a post-payment review process for the PRF, and the Uninsured Program, funded from the PRF.
Prior GAO Recommendations Related to Department of Health and Human Services (HHS) Relief for Health Care Providers
Recommendation
Status
The Secretary of Health and Human Services should finalize and implement a post-payment review process to validate COVID-19 Uninsured Program claims and to help ensure timely identification of improper payments, including those resulting from potential fraudulent activity, and recovery of overpayments. (March 2021 report)
Closed—Addressed. HHS agreed with our recommendation to finalize and implement a post-payment review process. In July 2021, HHS stated it was developing the post-payment review audit strategy for the Uninsured Program, which includes detailed protocol and procedures for the assessments of the Uninsured Program to be executed by audit contractors. In March 2022, HHS provided us a copy of its COVID-19 Uninsured Program Assessment Strategy Manual. The manual provides detailed protocols and procedures for assessing the Uninsured Program claims to identify overpayments for recovery. As such, we believe this manual addresses our recommendation.
The Administrator of the Health Resources and Services Administration should establish time frames for completing post-payment reviews to promptly address identified risks and identify overpayments made from the Provider Relief Fund, such as payments made in incorrect amounts or payments to ineligible providers.
(October 2021 report)
Open—not addressed. HRSA partially concurred with this recommendation. HRSA has a broad schedule of plans to conduct post-payment reviews. According to HRSA officials, they plan to schedule reviews in 2022, but the agency has not indicated when all of its reviews of payments will be scheduled or completed. In March 2022, HRSA reported that it started performing post-payment reviews in October 2020. HRSA also stated that it has identified 58 types of reviews, each of which is currently either open, closed, scheduled for review, or to be scheduled for review. HRSA stated that it tracks the status and schedule of reviews, and the schedule is regularly revised to reflect emerging priorities. HRSA stated that it will continue reviews until no future payments are at risk or HRSA puts a control in place to prevent the risk. Absent time frames for conducting and completing reviews, however, it is unclear how promptly the agency is identifying risks and overpayments and may delay the agency in expeditiously identifying and recovering overpayments. We will continue to monitor HRSA’s progress towards completion of its post payment review process.
The Administrator of the Health Resources and Services Administration should finalize procedures and implement post-payment recovery of any Provider Relief Fund overpayments, unused payments, or payments not properly used.
(October 2021 report)
Open—not addressed. HRSA partially concurred with this recommendation. Despite initial actions to address this recommendation, HRSA has suspended its post-payment recovery efforts. In March 2022, HRSA provided updated data for the total funds identified for recovery or potential repayment. HRSA has two categories of unused funds for which the agency will seek repayment. HRSA stated that it will seek repayment for all PRF payments reported as unused. For providers who HRSA required to report and failed to do so, they may submit a request to report late or may submit repayment of unreported payment amounts. However, HRSA told us that it has suspended its recovery efforts in order to establish a dispute process for providers to challenge HRSA’s repayment decisions. In addition, HRSA has encountered technical challenges in seeking funds from providers with identified overpayments due to missing bank trace numbers that are used to seek repayment. The agency is trying to resolve the issue which may continue in the future. We will continue to monitor HRSA’s progress towards recovery of overpayment, unused payments, or payments not properly used.
The federal government lacks an interoperable network of systems for near real-time public health situational awareness 15 years after federal law first mandated that the Department of Health and Human Services establish such a network. Across our body of work in this area, we have made a total of six recommendations to help ensure the department has made progress in establishing network capabilities—four of which remain unaddressed as of March 2022.
Entities involved: Department of Health and Human Services, including the Centers for Disease Control and Prevention, the Office of the Assistant Secretary for Preparedness and Response, and the Office of the Chief Information Officer
Background
Public health officials across the U.S. and its territories rely on a variety of information from a number of sources to create the situational awareness they need to prepare for and respond to a disease outbreak, environmental threat, or other public health emergency. The rapid spread of COVID-19 and the ensuing COVID-19 pandemic have underscored the importance of having access to real-time, high-quality data. Access to timely and accurate data can help the federal government understand the effects of diseases on public health throughout the U.S. and its territories. Timely and accurate data can also help to inform agencies’ allocation of resources and help them make timely and responsive decisions related to public health and safety. We have described challenges related to public health data for nearly two decades, including challenges related to sharing and standardizing data and the coordination needed to do so. (See also our related COVID-19 Surveillance and the Public Health Data Collection and Standardization enclosures in this report.)
To address such challenges, Congress and the President have enacted three laws since 2006 aimed at establishing a near real-time electronic nationwide public health situational awareness capability through an interoperable network of systems.[97] This network would incorporate data from different sources and be used to enhance early detection of and rapid response to potentially catastrophic infectious disease outbreaks and other public health emergencies that originate domestically or abroad. The most recent act—the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019—reiterated that the Department of Health and Human Services (HHS) is to establish the network. In addition, this network is to be built on existing U.S. state and territory situational awareness systems or enhanced systems that enable interoperability. The 2019 act also required us to conduct a review of the progress HHS has made in implementing the legal requirements.
Overview of Key Issues
HHS has yet to establish an interoperable network of systems for public health situational awareness and biosurveillance, as required by law.[98] As a result, the federal government still lacks this capability. Our prior work in December 2010 and September 2017 noted that HHS had made little progress in planning and establishing the network, respectively. Across both reports, we made a total of six recommendations to assist HHS in ensuring progress in establishing network capabilities—four of which remain unaddressed as of March 2022. For example, in September 2017, we recommended that HHS task an integrated project team with including specific actions in the implementation plan for conducting all activities needed to establish and operate the network. We also recommended that the team be tasked with developing a project management plan that includes measurable steps. HHS has not taken action on these recommendations.
HHS developed a platform, called HHS Protect, to help integrate COVID-19 data and other types of health information collected by various federal, state, and local public health and commercial entities. However, we have previously reported that some public health and state organizations have raised questions about the completeness and accuracy of some of the COVID-19 data included in HHS Protect that are intended to support the federal government’s response to the pandemic. In our August 2021 report on HHS’s efforts to collect hospital capacity data, we noted that HHS identified the need for timely, complete, and high-quality data to support the federal government’s response to pandemics was a key lesson learned.
The limited progress made by HHS in establishing the network capabilities required by the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 could negatively affect the timeliness and accuracy of data utilized by federal and state governments for public health. This limited progress, coupled with concerns regarding the completeness and accuracy of some of the COVID-19 data in HHS Protect, could reduce the ability of public health officials to comprehensively monitor and effectively respond to COVID-19 and future pandemics.
Methodology
To conduct our ongoing work related to the establishment of network capabilities required by Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, we analyzed available documentation, such as descriptions of systems that are key to public health situational awareness and biosurveillance. We also followed up on related recommendations we have made in previous reports and administered a survey to public health officials from the 50 states, the District of Columbia, and five U.S. territories to obtain information on lessons learned and challenges from the COVID-19 pandemic. We also interviewed relevant officials from HHS, including the Centers for Disease Control and Prevention, the Office of the Assistant Secretary for Preparedness and Response, the Office of the Chief Information Officer, and the Office of the National Coordinator for Health Information Technology.
Agency Comments
We provided HHS and the Office of Management and Budget with a draft of this enclosure. Neither agency provided comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor HHS’s progress toward implementing our prior recommendations and establishing an electronic nationwide public health situational awareness capability through an interoperable network of systems. Such work will also include any challenges and lessons learned from COVID-19 that HHS, states, and territories could incorporate in the planning and implementation of the capability.
Related GAO Products
COVID-19: HHS’s Collection of Hospital Capacity Data.GAO-21-600. Washington, D.C.: August 5, 2021.
Public Health Information Technology: HHS Has Made Little Progress toward Implementing Enhanced Situational Awareness Network Capabilities. GAO-17-377. Washington, D.C.: September 6, 2017.
Public Health Information Technology: Additional Strategic Planning Needed to Guide HHS’s Efforts to Establish Electronic Situational Awareness Capabilities. GAO-11-99. Washington, D.C.: December 17, 2010.
Contact information: Jennifer R. Franks, (404) 679-1831, franksj@gao.gov
The Centers for Disease Control and Prevention needs to define specific action steps and time frames to ensure that its Data Modernization Initiative reaches its full potential. Through the Data Modernization Initiative, the agency intends to improve data collection and sharing, strengthen data reporting and analytics, and advance surveillance to monitor the spread of infection of COVID-19 and other public health threats, among other goals. In fiscal years 2020 and 2021, the Centers for Disease Control and Prevention received $1.1 billion in funds for public health data modernization.
Entity involved: Centers for Disease Control and Prevention, within the Department of Health and Human Services
Recommendation for Executive Action
The Director of the Centers for Disease Control and Prevention should define specific action steps and time frames for the agency’s data modernization efforts. The Department of Health and Human Services agreed with this recommendation.
Background
The evolving nature of the COVID-19 pandemic has underscored the importance of accurate and timely data and a robust public health surveillance infrastructure for monitoring the spread of infection and disease progression across the population.[99] As the nation’s lead public health agency, the Centers for Disease Control and Prevention (CDC), within the Department of Health and Human Services (HHS), maintains over 100 surveillance systems for uses which include tracking infectious diseases, noninfectious health conditions (e.g., lead poisoning), and risk factors and exposures (e.g., tobacco use). (See also our related COVID-19 Surveillance and Public Health Situational Awareness Network Capabilities enclosures in this report.)
CDC’s COVID-19 surveillance approach includes existing and new surveillance systems to collect, analyze, and publish data on COVID-19 cases, deaths, testing, hospitalizations, and vaccinations. Two such systems are the National Vital Statistics System (which includes information about events such as births and deaths) and the National Notifiable Diseases Surveillance System (which collects individual case data on approximately 120 notifiable diseases—including COVID-19—from hospitals, health care providers, laboratories, and other sources, through state, territorial, and local health departments).[100]
CDC relies on state and local public health departments and health care facilities to collect and voluntarily report needed data. CDC also provides technical assistance, guidance, and grants to these health departments to support activities related to collecting and reporting data.
The pandemic highlighted limitations in both the data that CDC collects, including COVID-19 data, such as test results and case reports from state and local public health departments, and in the public health surveillance systems CDC uses to collect and share these data. Specifically, since June 2020, we and others have identified concerns with federal COVID-19 data. For example, we reported in January 2021 that the federal government generally lacks consistent and complete COVID-19 data due, in part, to inconsistently reported state data, which complicates comparisons of COVID-19 case counts and rates across geographic areas and populations. Further, according to CDC officials, the pandemic highlighted limitations of the agency’s reliance on voluntary reporting from health departments and health care facilities.
CDC also has noted that the COVID-19 pandemic has underscored the need to improve how it collects, uses, and shares data. Further, stakeholders, such as the Association of Public Health Laboratories and the Association of State and Territorial Health Officials, have noted that public health surveillance systems lack timely and reliable data to protect against health threats.
Both the CARES Act and the American Rescue Plan Act of 2021 (ARPA) provided funding to CDC to support modernizing the nation’s public health surveillance infrastructure.[101] CDC’s Data Modernization Initiative, launched in 2020, aims to improve data collection and sharing, strengthen data reporting and analytics, and advance surveillance of future public health threats, among other goals. More specifically, CDC’s initiative includes modernizing existing public health surveillance systems, such as the National Notifiable Diseases Surveillance System. CDC reported that its surveillance systems will require continued updating and maintenance, and noted that efforts to modernize the data collection infrastructure will evolve with innovations in information technology.
Overview of Key Issues
Several challenges hinder CDC public health data collection and surveillance. CDC faces several challenges to collecting accurate and timely data and conducting surveillance across the U.S. We identified four key challenges that affect CDC’s public health data collection and surveillance infrastructure.
Manual collection and transmission of data. Outdated methods to collect and transmit data—such as manual entry or fax transmission—require more time for input and may increase the risk for errors, and in turn, the timeliness and usefulness of the data. CDC officials said that state and local health departments, the primary source of data for case surveillance, have varying capabilities to send and receive data. According to CDC officials, most state and local health departments transmit data electronically, but some departments, especially smaller ones, still send data manually, such as by fax.
Outdated methods to transmit data are also burdensome to health departments and health care providers. CDC estimated that thousands of providers began submitting data for integration into health departments’ public health surveillance systems during the COVID-19 pandemic. Accordingly, this led to a substantial increase in the volume of data submitted to public health departments.
Inconsistent and incomplete data. Currently, CDC and state, territorial, local, and tribal health departments lack common data standards across surveillance systems, which leads to inconsistencies in the data reported to CDC.[102] State, local, and territorial public health departments’ surveillance systems are the primary sources of data that states send to CDC. CDC has established voluntary data standards for state and territorial health department reporting; jurisdictions often apply different standards for information they obtain from their local health departments and share with CDC. Applying different standards leads to inconsistent data reporting, which could ultimately limit some of the data’s usefulness for comparing across jurisdictions and other analyses. Although CDC has attempted to facilitate the collection of more consistent and complete data by creating and making available data applications that incorporate uniform data standards, such as the National Electronic Disease Surveillance System Base System, many state and local health departments have not adopted this application.[103]
In addition, some public health surveillance systems do not capture data for the entirety of the U.S. For example, according to CDC, the National Syndromic Surveillance Program—which includes data on symptoms that could indicate a COVID-19 diagnosis—does not include data from 29 percent of the nation’s emergency departments as of February 2022.[104]
Lack of interoperability among key public health data collection and surveillance systems. The lack of interoperability—the ability of data collection systems to exchange information with and process information from other systems—creates barriers to data sharing and places additional burden on stakeholder entities that collect and transmit data. For state health departments that collect data from systems that cannot directly exchange information with CDC, it takes longer for CDC to receive data.
Furthermore, funding from CDC that local public health departments receive to support surveillance activities is often tied to programs focused on specific conditions and diseases. According to CDC officials, this traditional approach to funding data collection and surveillance systems has resulted in multiple public health surveillance systems. Accordingly, multiple stand-alone public health surveillance systems hinder interoperability.
Lack of sufficient workforce, particularly staff with information technology skills. Public health departments struggle to maintain their workforces generally.[105] In addition, CDC officials and stakeholders noted concerns with developing and maintaining workforces with the requisite skills to steward and use advanced information technology systems and CDC data proficiently. Specifically, CDC and stakeholders noted that sustained funding for state and local health departments for public health agencies’ workforce development is critical to improve the broader information technology capabilities of the public health data collection and surveillance infrastructure generally and over the long-term.
CDC officials also noted that, among these challenges, the agency generally lacks authority to require reporting of public health data.
CDC has made some progress in modernizing the public health data collection and surveillance infrastructure. CDC has made progress in modernizing the U.S. public health data collection and surveillance infrastructure through its Data Modernization Initiative. For example, CDC, in coordination with the Association of Public Health Laboratories and other public health organizations, implemented the COVID-19 Electronic Laboratory Reporting system in spring 2020. According to CDC, state and territorial public health departments use this system to electronically submit COVID-19 laboratory testing data to CDC. This new system facilitates electronic reporting of large volumes of COVID-19 testing data from laboratories that were equipped to submit data using the applicable standards. By April 2021, all 56 state and territorial health departments were reporting de-identified COVID-19 testing results data for their jurisdictions electronically to CDC.
The COVID-19 Electronic Laboratory Reporting system reflected CDC’s efforts to facilitate the implementation of a new requirement enacted under the CARES Act for laboratories to report standardized data on the COVID-19 tests that they were processing.[106] Under the act, laboratories are required to submit testing data directly to state or local public health departments, which then submit de-identified data to CDC on a daily basis. While laboratories are able to report electronically when possible, they are not required to do so. To implement the law, HHS established requirements for the data that the laboratories were obligated to report that detailed the specific data elements and how they should be formatted. Unlike other data systems CDC created in the past, which were dependent on data collected from the state health departments in the format of the state’s choosing, this new system helped to ensure that the data submitted would be comparable across jurisdictions.
CDC also reports that it has expanded electronic case reporting and begun modernizing other public health surveillance systems, including the National Syndromic Surveillance Program, the National Notifiable Diseases Surveillance System, and the National Vital Statistics System. For example, according to CDC, the National Notifiable Diseases Surveillance System implemented a COVID-19 Message Mapping Guide at the start of the pandemic, which standardized the data elements that states provide to CDC.[107] In addition, CDC reports it has made improvements to increase cloud-based capabilities and building platforms for a scalable emergency response.[108]
CDC’s Data Modernization Initiative’s strategic implementation plan lacks specific actions and time frames for achieving its goals. According to CDC officials, the agency’s data modernization plans include bolstering existing surveillance systems; automating data collection among state, territorial, tribal, and local public health entities; building a highly-skilled public health workforce; enhancing CDC’s data sharing and analysis; and improving access to data. CDC officials indicated a time frame of 4 years to spend the funds for data modernization it received from the CARES Act and ARPA. See the table below for the Data Modernization Initiative’s strategic implementation plan’s priorities and objectives.
Centers for Disease Control and Prevention’s (CDC) Priorities and Objectives for Its Data Modernization Initiative
Priorities
Objectives
1.
Build the right foundation: strengthen and unify critical infrastructure for a response-ready public health ecosystem
Provide a secure and scalable foundation with appropriate automated data sources to enable timely, complete data sharing for public health action; break down silos that keep critical data disconnected; and reduce the burden on state, tribal, local, and territorial partners for collecting and reporting data
1a. Develop a shared vision
1b. Expand foundational infrastructure
1c. Modernize and connect key surveillance systems and sources
1d. Transform legacy systems, processes, and activities
1e. Store, discover, analyze, and visualize data
2.
Accelerate data into action to improve decision-making and protect health
Faster, more interoperable data provides high-quality information that, in turn, leads to knowledge and provides a more real-time, comprehensive picture to improve decision-making and protect health
2a. Increase interoperability through data standards
2b. Increase data linkages
2c. Advance forecasting and predictive analytics
2d. Implement tools for scalable response
2e. Promote health equity
3.
Develop a state-of-the-art workforce
Identify, recruit, and retain critical workforce in Health Information Technology, Data Science, and Cybersecurity Specialists to be stewards of larger quantities of data and tools – better and faster – to generate meaningful public health insights
3a. Identify CDC workforce needs
3b. Increase CDC data science capacity
3c. Facilitate state, tribal, local, and territorial data science upskilling
4.
Support and extend partnerships
Engage with state, territorial, local, and tribal partners to ensure transparency, address policy challenges, and create new strategic partnerships to solve problems
4a. Ensure partner alignment and collaboration
4b. Support policies for data exchange
5.
Manage change and governance to support new ways of thinking and working
Provide the necessary structure to support modernization and aid adoption of unified technology, data, and data products
5a. Govern policies, planning, and resources
5b. Manage culture change
5c. Create a culture of innovation
5d. Streamline acquisition processes
5e. Evaluate Data Modernization Initiative activities and projects
Although CDC has plans to improve its data collection and infrastructure through the Data Modernization Initiative, its strategic implementation plan for this initiative does not articulate the specific actions needed to achieve its objectives, roles and responsibilities for actions or objectives, or time frames for achieving these objectives.
In addition, CDC has not fully developed plans for how it will allocate ARPA funds for data modernization. While the agency’s draft spend plan includes estimates for how it will spend the $500 million from ARPA—such as $200 million for a data forecasting center—the draft spend plan lacks specific actions and associated time frames for such spending.
According to CDC officials, the agency is currently gathering its subject matter experts to further build out the initiative’s framework with more detailed activities necessary to achieve key results. CDC officials told us the initiative largely remains in the planning phase due to the complexity of modernization projects that require agency-wide effort as well as state and local stakeholder participation. CDC officials also noted that its activities for the COVID-19 response are a competing priority.
Federal internal control standards state that management should define objectives and risk tolerances for federal programs. As part of this standard, management defines objectives in specific terms so they are understood at all levels of the entity, which involves clearly defining what is to be achieved, who is to achieve it, how it will be achieved, and the time frames for achievement.
Without more specific, actionable plans, including time frames for achieving data modernization objectives, spending plans, and the entities that are responsible for taking actions, CDC may not be able to gauge its progress on the initiative or achieve key results in a timely manner. In addition, such lack of progress to implement enhanced surveillance systems could affect the quality and timeliness of data needed to respond to future public health emergencies.
Methodology
To identify key challenges that affect CDC’s ability to improve its public health data collection infrastructure, we reviewed relevant CDC documents and written responses from agency officials. We also spoke with public health stakeholders who represent entities involved in collecting and transmitting data to CDC, such as laboratories and state and local health departments. Specifically, we spoke with representatives from the Association of State and Territorial Health Officials, the Council of State and Territorial Epidemiologists, the National Association of County and City Health Officials, and the Association of Public Health Laboratories.
To determine what progress CDC has made to improve its public health data collection systems and what is known about this progress, we reviewed relevant laws and CDC documents. We also obtained written information from and interviewed agency officials about these efforts. We also interviewed the stakeholders named above to obtain their perspectives on CDC’s data modernization efforts.
Agency Comments
We provided a draft of this enclosure to HHS and the Office of Management and Budget (OMB) for review and comment. HHS agreed with our recommendation and its comments are reproduced in appendix VII. In these comments, CDC noted that the Data Modernization Initiative will initially focus on developing objectives and key results that are measurable and associated with time frames for items critical for data modernization.
CDC also provided technical comments, which we incorporated as appropriate. OMB did not provide comments.
GAO's Ongoing Work
GAO will continue to monitor federal health care data surveillance and sharing efforts.
Contact information: Leslie V. Gordon, (202) 512-7114, GordonLV@gao.gov
The Department of Health and Human Services and its interagency partners are using planning documents that have the potential to be effective tools for implementing the National Strategy for a Resilient Public Health Supply Chain. The Department also plans to publicly release an annual implementation progress report. Releasing such information will help ensure Congress and other stakeholders have clear and consistent information on the complex, whole-of-nation actions needed to achieve the vision of the National Strategy—the creation of a resilient public health supply chain that can withstand future public health emergencies.
Entities involved: Department of Health and Human Services, Department of Defense, Department of Homeland Security, and Department of Veterans Affairs.
Background
As we have reported throughout the COVID-19 pandemic, this public health emergency triggered a significant increase in worldwide demand for medical supplies (including personal protective equipment and supplies for testing and vaccine administration) and disrupted global supply chains, limiting availability of critical supplies for U.S. health care providers.
In January 2021, Executive Order 14001 directed the Department of Defense, Department of Health and Human Services (HHS), and Department of Homeland Security, among others, to develop a supply chain resilience strategy to include an approach to design, build, and sustain long-term capability in the U.S. to manufacture medical supplies for future pandemics and biological threats.[109]
In September 2021, the National Strategy for a Resilient Public Health Supply Chain (National Strategy), signed by the Secretaries of Defense, Health and Human Services, Homeland Security, and Veterans Affairs, was publicly released. The National Strategy designates HHS as the lead agency for overseeing its implementation. Within HHS, the Office of the Assistant Secretary for Preparedness and Response (ASPR) is charged with this lead role, according to officials.
ASPR officials stated that they see the office’s lead role as one of coordinating implementation across all interagency partners involved, given the whole-of-nation approach needed to achieve the vision of the National Strategy.[110] According to the National Strategy, this whole-of-nation approach involves gathering supply chain intelligence, making investments in domestic medical countermeasure manufacturing, identifying gaps and shortages, addressing vulnerabilities proactively, and incentivizing pandemic preparedness at the federal level; at the state, local, tribal, and territorial levels; and across the U.S. health care system.
The National Strategy has three main goals:
building a diverse public health supply chain and sustaining domestic manufacturing capacity;
transforming governments’ ability to monitor and manage the public health supply chain through stockpiles, visibility, and engagement; and
establishing standards, systems, and governance to manage the supply chain.
To support these goals, the National Strategy includes objectives and recommendations. For example, to support the first goal, there is an objective to “safeguard supply chain diversity through policy, incentive, regulation, and other tools to reduce dependence on a single region, source, or product” and a recommendation for “bold investments and incentives for the American industrial base,” including “support for American-made supplies in the U.S. health care sector.”
We have previously identified six desirable characteristics—and individual elements that comprise those characteristics—that national strategies should contain in order to serve as effective, comprehensive management tools. (See figure below.)
Six Desirable Characteristics of Effective National Strategies
Overview of Key Issues
HHS and its interagency partners are developing plans to implement the National Strategy. As an initial step to implementing the National Strategy, HHS, its interagency partners, and the White House created “action items” stemming from the objectives and recommendations in the National Strategy. While they could still evolve, there are currently 22 action items identified to implement the National Strategy, according to ASPR officials in February 2022. These action items include, for example, creating an operational industrial base expansion plan, leveraging partnerships to strengthen regional and global public health supply chains, and strengthening the U.S. public health supply chain workforce.
Workgroups were also established to implement each action item and include a lead agency and support agencies. For example, HHS is designated the lead agency for 17 of these 22 action items, though each action item also involves a number of support agencies.[111] During the fall of 2021 through February 2022, the workgroups have been developing for each action item a separate Plan of Action and Milestones (POAM) to facilitate implementation, according to ASPR officials. To do so, the workgroups have followed a template developed by the White House that outlines specific sections of information to include in each POAM and related guidance.
Given ASPR’s lead role coordinating the implementation of the National Strategy, ASPR is consolidating the POAMs into a master implementation schedule for the National Strategy overall. ASPR officials said that because many of the action items are inter-related, they need all of the POAMs to design an implementation schedule that ensures interdependencies between action items are effectively coordinated. As of February 2022, ASPR officials told us they were waiting on POAMs for two action items before they could complete the master schedule. Officials expected to receive the remaining POAMs soon but could not provide an anticipated date.
The National Strategy and related plans provide reasonable assurance that an effective national supply strategy is being developed. Our review of the National Strategy along with POAM documentation—the POAM template, as well as draft POAMs for seven selected action items—indicates that ASPR and its interagency partners are in the process of developing an effective national strategy for making the public health supply chain more resilient, if they continue to develop and implement the POAMs as planned.[112]
Specifically, we found that the POAM template complements the National Strategy by outlining many of the characteristics we have identified that national strategies should contain in order to serve as effective, comprehensive management tools. For example, the POAM template directs workgroups to provide details on the tasks, milestones, and schedules needed for implementation of the action item. It also directs them to communicate resources and capabilities needed, risks to implementation, and the responsible entities for each task.
Our review of seven draft POAMs indicates that the template is being utilized by the workgroups, though at varying levels of completion. For example, one of the POAMs we reviewed was not specific about resources required, but instead stated that ASPR will conduct an initial review to identify resource and capability needs, among other actions.
ASPR officials stated that the POAMs are still evolving and that the intention is that they will all align with the details outlined in the template. As a result, if the template is fully utilized for each of the 22 action items, the POAMs have the potential to be effective implementation tools to achieve the vision of the complex National Strategy. (See figure below.)
How the National Strategy and Plan of Action and Milestones Template, if Fully Implemented, Align with Six Desirable Characteristics of an Effective National Strategy
aOfficials from the Office of the Assistant Secretary for Preparedness and Response told us that workgroups are in the preliminary stages of determining performance metrics, and that language is reflected in the template. The plan is to develop performance metrics more thoroughly as the workgroups move forward.
ASPR plans to report implementation progress. ASPR is in charge of submitting an annual “progress report” on the National Strategy by the end of July each year to the White House. According to ASPR officials, the annual “progress report” will serve as a summary of implementation progress on the National Strategy and will be a consolidation of the performance metrics information from each of the action items’ POAMs. In March 2022, ASPR officials stated they were on track to submit the first progress report to the White House in July 2022. ASPR officials also told us that, subsequent to White House review, the progress report would become publicly available.[113]
Creating a resilient public health product supply chain will be a complex effort and require significant, continued efforts across the U.S. government; state, local, tribal and territorial entities; and other stakeholders, such as the private sector and U.S. health care system. Reporting information on National Strategy implementation progress to Congress and other external stakeholders, will help ensure all involved have clear and consistent information on the complex and coordinated actions needed to achieve the vision of the National Strategy.
Reporting on implementation progress to external stakeholders could also help ASPR ensure it has the resources and capacity needed to coordinate implementation of the National Strategy while also leading 13 of the 17 action items assigned to HHS. In January 2022, we reported concerns about ASPR’s workforce capacity to take on the leadership of the development, manufacturing, and distribution of COVID-19 vaccines transferring to the agency and made related recommendations. Additionally, in our Public Health Industrial Base Expansion enclosure in this report, we cite concerns and make a related recommendation about ASPR’s lack of workforce planning for its new office, which is providing leadership of several action items in the National Strategy. ASPR’s capacity and related workforce planning to address its many responsibilities, including new responsibilities stemming from COVID-19, is a concern we recently cited when we raised HHS’s leadership and coordination of public health emergencies to our high risk-list in January 2022. We continue to monitor HHS efforts to address this new high-risk area, including ASPR’s capacity and workforce planning.
Methodology
We assessed the National Strategy for a Resilient Public Health Supply Chain and the POAM template against GAO’s six characteristics of an effective national strategy. Specifically, we looked at the elements that comprise each characteristic and assessed the extent to which the National Strategy or POAM template contained information related to the element, such as whether they contained adequate specificity and detail to identify the elements of the characteristics.
We also reviewed seven draft POAMs to see if they followed the POAM template. The seven included six from HHS that were most readily available for the agency to provide to us, according to ASPR officials (of the 17 the HHS is the lead for), and one from DHS—the only action item it leads.
We interviewed officials from HHS, as well as the Departments of Defense, Homeland Security and Veterans Affairs, to obtain information on their role in developing the National Strategy and related implementation planning—the leadership of all four departments were signers of the National Strategy. Within HHS, we interviewed ASPR officials charged with coordinating the National Strategy implementation effort.
Agency Comments
We provided HHS, DOD, DHS, VA, and the Office of Management and Budget with a draft of this enclosure. These agencies did not have any comments related to this enclosure.
GAO’s Ongoing Work
We continue to conduct work examining federal efforts related to the resilience of the public health supply chain, including work on the Strategic National Stockpile and advanced manufacturing.
GAO’s Prior Recommendations
See table below for our past related recommendations on public health supply chain resilience from prior CARES Act reports.
Prior GAO Recommendations Related to Public Health Supply Chain Resilience during COVID-19
Recommendation
Status
The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency—who head agencies leading the COVID-19 response through the Unified Coordination Group—should immediately document roles and responsibilities for supply chain management functions transitioning to the Department of Health and Human Services (HHS), including continued support from other federal partners, to ensure sufficient resources exist to sustain and make the necessary progress in stabilizing the supply chain, and address emergent supply issues for the duration of the COVID-19 pandemic (September 2020).
Open—not addressed. HHS disagreed with our recommendation. In a May 2021 update, the Office of the Assistant Secretary for Preparedness and Response (ASPR) noted that since March 2020, supply chain responsibility, coordination, and execution have been incorporated and integrated into ASPR. However, HHS has yet to document roles and responsibilities for supply chain management that are transitioning. As of March 2022, HHS had not provided any updated information.
The Secretary of Health and Human Services in coordination with the Administrator of the Federal Emergency Management Agency—who head agencies leading the COVID-19 response through the Unified Coordination Group—should further develop and communicate to stakeholders plans outlining specific actions the federal government will take to help mitigate remaining medical supply gaps necessary to respond to the remainder of the pandemic, including through the use of Defense Production Act of 1950 authorities. (September 2020 report).
Open—partially addressed. HHS disagreed with our recommendation. However, HHS has taken action to help mitigate medical supply gaps. HHS offered several examples of HHS and ASPR's supply chain work, including restocking the SNS. While HHS did not provide an update in March 2022, we believe these are good steps. We will continue to monitor HHS's efforts.
The Secretary of Health and Human Services and the Administrator of the Federal Emergency Management Agency —who head two of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response (September 2020 report).
Open—partially addressed. In September 2020, both HHS and the Department of Homeland Security (DHS) disagreed with our recommendation, noting, among other things, the work that the departments had done to manage the medical supply chain and increase supply availability, such as restocking the SNS (as noted above). HHS and DHS have reported separate actions taken as part of supply management efforts within their separate purviews; however, HHS has not articulated how they have worked with DHS and other relevant federal, state, territorial, and tribal stakeholders to devise interim solutions to help states better track, manage, and plan for supply needs for the remainder of the COVID-19 pandemic. HHS did not provide an update in March 2022.
The Assistant Secretary for Preparedness and Response should establish a process for regularly engaging with Congress and nonfederal stakeholders, including state, local, tribal, and territorial governments and private industry, as HHS refines and implements a supply chain strategy for pandemic preparedness, to include the role of the SNS (January 2021 report).
Open—not addressed. HHS generally agreed with our recommendation, while noting that the term "engage" is vague and unclear, and that they regularly engage with Congress and nonfederal stakeholders. HHS added that improving the pandemic response capabilities of state, local, tribal, and territorial governments is a priority. As of March 2022, HHS had not provided any updated information.
COVID-19: HHS and DOD Transitioned Vaccine Responsibilities to HHS, but Need to Address Outstanding Issues. GAO-22-104453. Washington, D.C.: January 19, 2022.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
Combating Terrorism: Evaluation of Selected Characteristics in National Strategies Related to Terrorism, GAO-04-408T. Washington, D.C.: February 3, 2004.
The Department of Health and Human Services created the Innovation and Industrial Base Expansion Program Office to address medical product supply vulnerabilities highlighted during the pandemic so that the nation is better prepared for future public health emergencies. However, the department has not fully assessed the workforce skills and competencies needed to support the mission and goals of the office, nor has it developed strategies to address those needs. Critical workforce planning is needed to ensure sustainment and success of the office.
Entities involved: The Department of Health and Human Services, Department of Homeland Security, and General Services Administration.
Recommendations for Executive Action
We recommend that the Assistant Secretary for Preparedness and Response within the Department of Health and Human Services conduct a workforce assessment of its Innovation and Industrial Base Expansion Program Office to determine the critical skills and competencies needed to support and sustain the office, and develop corresponding workforce strategies to address those needs. HHS agreed with our recommendation, and stated that the agency will conduct a workforce assessment in the future.
Background
The COVID-19 pandemic made it abundantly clear how important it is to the health and security of the nation to maintain and ensure a robust and resilient public health industrial base—goods and services needed to overcome a health emergency, such as personal protective equipment (PPE), diagnostics, therapeutics, vaccines, and related supplies. As we have previously reported, the pandemic response has highlighted our dependence on foreign suppliers for certain types of medical products, as well as limitations in our own domestic production of medical supplies.
The Department of Health and Human Services’ (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR) leads the nation’s medical and public health preparedness for, response to, and recovery from disasters and public health emergencies, including the COVID-19 pandemic. As part of this role and to address supply challenges that have plagued the nation’s pandemic response, ASPR is responsible for actively restoring and strengthening supply capabilities depleted during the pandemic, such as the Strategic National Stockpile, and securing the public health supply chain going forward, according to the agency’s website.
ASPR’s efforts to address these needs include forming a new Innovation and Industrial Base Expansion Program (IBx) Office, beginning in September 2020. According to ASPR’s website, the mission of the IBx Office is to strengthen and expand the U.S. public health industrial base and deliver innovative solutions to counter health security threats. To meet this mission, the office has been chiefly set up to
focus on expanding, securing, and building resilience across the U.S. public health industrial base to address vulnerabilities highlighted during the pandemic, such as critical deficiencies in certain medical supplies needed to respond, and
coordinate strategic public health industrial base expansion and innovation efforts across ASPR, federal partners, academia, and the private sector to facilitate the development and implementation of novel solutions and practices for response and recovery operations.
Overview of Key Issues
ASPR has been primarily using detailees from other federal agencies to support the IBx Office, and has begun hiring some staff; however, the agency has not yet assessed the critical workforce skills and competencies needed to support and sustain the mission and goals of the office, nor has it developed strategies to achieve those workforce needs. Such an assessment would be consistent with key principles of strategic workforce planning we have previously identified, including (1) determining the critical skills and competencies needed to achieve current and future programmatic results, and (2) developing strategies to address gaps in the number of staff and their skills and competencies, in order to meet those results.
As of February 2022, 12 detailees from the General Services Administration (GSA) and Department of Homeland Security (DHS) have supported the IBx Office. ASPR officials told us that to determine the need for detailees, ASPR officials held a series of meetings, including with White House officials in March 2021 to identify the staffing resources required to quickly implement the American Rescue Plan Act of 2021 (ARPA). This law appropriated $10 billion to support use of the Defense Production Act of 1950 (DPA) for medical supplies, including industrial base expansion projects.
The IBx Office was initially tasked with implementing efforts to plan for, and obligate, this $10 billion, according to ASPR officials. ASPR identified a baseline need of 20 full-time staff for the IBx Office to address this task, but officials said they were unable to get all 20 needed employees due to limited resource availability in GSA and DHS. Instead,
since June 2021, eight detailees from GSA have been supporting the IBx Office. ASPR and GSA officials expect the details to end in June 2022.
since September 2021, four detailees from DHS have supported the office. Three ended their details in January 2022 and the fourth may continue their detail until September 2022, according to ASPR officials.
The GSA and DHS detailees have expertise in project management, acquisitions, contracting, and data analytics, among other skills sought by ASPR to help rebuild its public health industrial base, according to GSA and DHS officials.
Additionally, since October 2021, ASPR has begun taking actions to hire 25 staff for the IBx Office under “term positions”—positions for defined amounts of time. ASPR officials stated that they were using term positions for two reasons. First, the positions are being funded with ARPA appropriations for DPA activities, which are available through fiscal year 2025. Second, ASPR officials cannot yet support permanent positions without annual appropriations for the IBx Office. Officials stated that they have submitted a baseline budget request to fund the IBx Office to inform the President’s fiscal year 2023 budget. ASPR officials also stated that term-position employees could be easily transitioned to permanent positions, if and when funding is available.
The term positions are for an initial period of up to 13 months, with the potential to extend to up to 4 years. As of February 2022,
ASPR had posted positions to hire a total of 20 staff and had hired and brought on board two of those 20, according to officials. Positions posted included management and program analysts, and acquisitions management professionals.
ASPR officials indicated that they were actively working on posting additional term positions to hire five more staff, including program analysts and contract specialists.
Although it has started hiring, in January 2022, ASPR officials told us they had not yet conducted a workforce needs assessment for the IBx Office for several reasons, including the following:
Competing demands have required ASPR staff to take immediate actions in other areas to address the needs of ongoing COVID-19 pandemic response, including recent efforts to coordinate acquisition and distribution of over-the-counter COVID-19 tests and masks for the American public, as well as supporting testing programs at schools, long term care facilities, and federally qualified health centers.
The roll-out of various COVID-19-related strategies, plans and laws, including the National Strategy for a Resilient Public Health Supply Chain and the Infrastructure Investment and Jobs Act have had implications for the scope of the IBx Office that need to be considered before conducting such an assessment. For example, the National Strategy for a Resilient Public Health Supply Chain, which was publicly released in September 2021, includes action items that the IBx Office is to lead, such as enhancing and maintaining supply chain visibility capabilities, and leveraging advanced manufacturing technology, according to officials. More recently, in a report released in February 2022, HHS announced plans for adding DPA related activities to the IBx office. Additionally, the Infrastructure Investment and Jobs Act (IIJA) includes provisions related to investments in manufacturing capacity, which could affect the scope of the office, according to officials. For example, the IIJA has a requirement for government contracts for personal protective equipment to be longer-term to incentivize production of these medical products in the U.S.
Potential realignment of ASPR by the Assistant Secretary for Preparedness and Response to better position the office to support its expanded responsibilities over the past several years, including from the COVID-19 response, may affect the role of the IBx Office and the workforce it requires.
The lack of baseline non-emergency funding makes it difficult to plan within budget constraints, according to ASPR officials.
In her January 11, 2022, statement to Congress, the Assistant Secretary for Preparedness and Response explained the importance of dedicated and persistent management and engagement in the expansion of the public health industrial base by ASPR. She also noted her efforts to institutionalize this mission in ASPR.
Because of the ongoing response to the ever-evolving COVID-19 pandemic and related changing circumstances, it may take some time for ASPR to define the long-term scope of the IBx Office, as well as to determine related resource needs. However, without conducting a workforce assessment in the near term based on current goals, ASPR risks not knowing if it is hiring and prioritizing the most appropriate positions. This includes the 27 term position hires that ASPR is currently hiring or planning to hire, which could become permanent hires. Furthermore, taking these critical workforce planning steps will help ensure ASPR is able to develop reliable budget estimates for the resources they need, target the right number of people with the right skills, and make well-informed hiring decisions, as well as any future decisions to extend details.
Until ASPR conducts a workforce capacity assessment to determine the critical skills and competencies needed to support and sustain the newly created IBx Office, and develops corresponding workforce strategies to address those needs, ASPR risks not being able to achieve the management and engagement that the Assistant Secretary described as essential for expanding and building resilience in the public health industrial base. Further, it places the current mission and goals of the IBx Office at risk—an office that was established to help secure the public health supply chain going forward so that the nation is better prepared for future public health emergencies. Lastly, the IBx Office is providing leadership for several action items from the National Strategy for a Resilient Public Health Supply Chain. (For more information see the Public Health Supply Chain Resilience enclosure.) A workforce with capabilities to provide such leadership will be critical to successful implementation of this important strategy.
Methodology
To conduct our review, we reviewed documentation related to the staffing of ASPR’s IBx Office, such as memorandums of understanding between GSA and ASPR and between DHS and ASPR regarding detailees assigned to the IBx Office. We interviewed officials in the ASPR Office of Strategy Policy, Planning, and Requirements, which provides leadership of the IBx Office. We received written responses from officials in ASPR’s Human Capital Office to obtain information about hiring for the IBx Office, and interviewed officials from HHS’s Staffing Recruitment Operations Center (the agency within HHS that conducts some hiring actions on behalf of ASPR). Lastly, we received written responses from GSA and DHS officials to collect information on detailees assigned to ASPR for the IBx Office. We assessed ASPR’s workforce planning against key principles of strategic workforce planning that we have identified in previous work, focusing our analysis on those principles that are related to determining current and future workforce needs and establishing strategies to fulfill those needs.
Agency Comments
We provided HHS, DHS, GSA, and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS agreed with our recommendation, in comments noted in Appendix VII. ASPR officials noted that a workforce assessment is an important component for supporting and sustaining the Innovation and Industrial Base Expansion Office, and agreed to conduct an assessment in the future. HHS did not provide any technical comments. DHS, GSA and OMB did not have any comments related to this enclosure.
GAO’s Ongoing Work
We continue to conduct work examining federal efforts to support medical product supply chain resilience and industrial base expansion, such as work examining federal efforts to support advanced manufacturing.
Related GAO Product
Human Capital: Key Principles for Effective Strategic Workforce Planning, GAO-04-39. Washington, D.C.: December 13, 2003.
When COVID-19 vaccines first became available in December 2020, the federal government used a population-based methodology, with some adjustments, to allocate the limited supply of vaccines to states, other jurisdictions, and some federal agencies. The government stopped using this methodology in June 2021 when sufficient vaccine supply was available to meet demand.
Entities involved: The Department of Defense and the Department of Health and Human Services
Background
In 2020—early in the pandemic—federal officials anticipated that COVID-19 vaccines would be available in limited supplies following authorization, so they developed a means for allocating available doses. Specifically, Operation Warp Speed—a partnership between the Department of Health and Human Services (HHS) and the Department of Defense (DOD)[114]—created a methodology to allocate the available supply of COVID-19 vaccine doses directly to jurisdictions (50 states, eight territories, and four cities) as well as five federal agencies.[115] Federal officials referred to these 67 entities collectively as “awardees.”[116]
Operation Warp Speed officials said they began evaluating approaches for allocating available vaccines in June 2020, with input from federal agencies such as HHS’s Centers for Disease Control and Prevention (CDC) and its Office of the Assistant Secretary for Preparedness and Response (ASPR). Officials told us they considered approaches that would take into account priority populations (i.e., individuals with high occupational exposure, advanced age, or multiple comorbidities). Ultimately, they proposed basing allocation amounts primarily on each awardee’s population of adults, aged 18 and older, in an attempt to increase simplicity and transparency in communicating the methodology to the awardees. The Secretary of Health and Human Services and the Secretary of Defense approved the methodology on November 6, 2020.[117]
In December 2020, HHS’s Food and Drug Administration (FDA) authorized the first COVID-19 vaccines for use, and Operation Warp Speed began implementing its vaccine allocation methodology.[118] FDA authorized Pfizer’s two-dose vaccine for emergency use on December 11, 2020, and a week later on December 18, 2020, it authorized Moderna’s two-dose vaccine.[119] Allocation efforts also included Janssen’s single-dose vaccine after it was authorized by FDA on February 27, 2021.[120]
Overview of Key Issues
The federal government used a population-based methodology to allocate available vaccine doses across 67 awardees, generally on a weekly basis, from December 2020 through late-June 2021. Awardees could order up to their allocated amount for distribution to their populations. Operation Warp Speed officials applied the methodology separately for the doses available from each vaccine company, which initially involved two sets of weekly calculations—one each for the Pfizer and Moderna vaccines—and then grew to three sets of weekly calculations after FDA authorized Janssen’s vaccine in February 2021. Because the Pfizer and Moderna vaccines each required two doses, officials allocated the entire two-dose regimen at the same time but usually shipped doses separately, with the second dose arriving 2 or 3 weeks after the first dose.
On June 24, 2021, the federal government stopped using its allocation methodology because vaccine supply had increased to sufficient levels to meet the needs of jurisdictions and federal agencies, according to federal officials. Officials told us that because sufficient vaccine doses were available after this date, awardees could order as many doses as they needed.[121]
The methodology involved a complex, iterative process, in which officials would go through calculations multiple times to ensure all available vaccine doses were allocated according to population, while also making three key adjustments. To start the allocation methodology, Operation Warp Speed officials totaled the adult populations for all awardees, and calculated each awardee’s proportion of that total.[122] Officials then divided the amount of available vaccine doses based on each awardee’s proportion and made the three adjustments. For these adjustments, officials
allocated vaccine doses to geographically isolated awardees on a monthly basis, rather than weekly;
rounded allocations up to minimum order quantities based on the size of company vaccine trays (the containers holding vials of vaccine doses used for shipping); and
adjusted allocations for jurisdictions with tribal populations that received vaccine doses through their jurisdictions rather than through the Indian Health Service (IHS).
Officials allocated vaccine doses to geographically isolated awardees on a monthly basis, rather than weekly. Operation Warp Speed officials made this adjustment for eight awardees to account for challenges with shipping or other logistical issues. Therefore, these eight awardees would receive a larger allocation during the first week of each month, and then not be allocated additional vaccine doses in the following weeks of the month. These geographically isolated awardees were Alaska, American Samoa, the Federated States of Micronesia, Guam, Northern Mariana Islands, the Republic of the Marshall Islands, the Republic of Palau, and the Department of State—due to the location of its employees around the world.[123]
Officials rounded up to minimum order quantities based on the size of company vaccine trays. The minimum order quantity for each available vaccine varied depending on the vaccine company’s product shipment configurations—that is, the tray sizes and how many vials and subsequent doses a tray could hold. In December 2020, at the beginning of vaccine allocation, Pfizer’s vaccine was shipped in trays that held 975 doses each, so its minimum order quantity was 1,950 doses—one tray of first doses and one tray of second doses. Moderna’s vaccine was shipped in trays of 100 doses, so its minimum order quantity was 200 doses. When Janssen’s vaccine became available in February 2021, it was shipped in trays of 100 doses. Because Janssen’s vaccine only required one dose, its minimum order quantity was also 100 doses.[124]
Operation Warp Speed officials said they rounded up to the next minimum order quantity each week when calculating allocations for each awardee. To allow for this rounding up, early in the weekly allocation process, officials set aside a small portion of the available vaccine doses for calculation purposes (about 3 percent in the first week) to ensure they had enough doses to align with minimum order quantities. If officials found that they set aside more doses than needed, they allocated the remaining amount to awardees according to the methodology.
The minimum order quantity adjustment generally resulted in a larger percentage increase for small states. For example, before adjusting for minimum order quantities, a state with a small population (Montana) and a state with a large population (California) would have each been allocated vaccine doses in proportion to their adult populations. However, Montana’s first week of Pfizer’s allocation increased by about 10 percent to factor in the minimum order quantity adjustment. California’s allocation also increased based on the minimum order quantity, but this increase was a much smaller percentage—about 0.2 percent—due to California’s larger population size. See the figure below.
Example of Allocation Calculations before and after Minimum Order Quantity Adjustments for Two States with Different Population Sizes
Note: The numbers in this figure are based on the first week of the Pfizer vaccine allocation, and the populations are adults aged 18 and older from the 2018 American Community Survey.
Officials adjusted allocations for jurisdictions with tribal populations that received vaccine doses through jurisdictions rather than through IHS. In the fall of 2020, the IHS polled its tribal health programs and Urban Indian Organizations nationwide, asking each one to decide whether to receive vaccine doses through IHS or from their state or local jurisdiction.[125] Operation Warp Speed based its allocation of vaccine doses to IHS—one of the 67 awardees—on the population served by federally-operated IHS facilities, as well as the populations served by tribal health program and Urban Indian Organizations that would receive vaccine doses from IHS. Tribal health programs and Urban Indian Organizations in 18 states and 1 city chose not to receive vaccine doses from IHS and therefore received vaccine doses from their respective states or city, according to documentation we reviewed. Because these awardees—the 18 states and one city—supplied vaccine doses for the populations served by tribal health programs or Urban Indian Organizations in their jurisdictions, Operation Warp Speed created a “sovereign nation supplement.” When the sovereign nation population adjustment was large enough to result in allocation of additional vaccine shipping trays, these states and city received increased allocations of vaccine doses.
For example, after adjusting for the sovereign nation supplement, New Mexico received about 6 percent more doses in the first week of the Pfizer vaccine allocation compared to before the adjustment, with similar effects in subsequent weeks. See the figure below.
Example of Allocation before and after the Sovereign Nation Supplement for One State
Note: The numbers in this figure are based on the first week of the Pfizer vaccine allocation, and the populations are adults aged 18 and older from the 2018 American Community Survey.
The three adjustments combined to affect vaccine allocations for states with more than one of the characteristics described above—geographically isolated, small populations, or large sovereign nation populations. For example, due to its location, Alaska received its entire month’s allocation of the Pfizer vaccine on December 14, 2020, when Operation Warp Speed made the first weekly allocation. Alaska also has a small population, so the effect of the minimum order quantity adjustment was greater, and it additionally received a large sovereign nation supplement. Therefore, in the first week of the Pfizer vaccine allocation, Alaska received about 57,880 (or nearly 6 times) more vaccine doses compared to its allocated amount before these adjustments were calculated.
Methodology
To conduct this work, we reviewed HHS and DOD documentation about the COVID-19 vaccine allocation methodology developed by Operation Warp Speed and interviewed Operation Warp Speed officials on how they created and implemented the methodology. We reviewed population data by comparing the data Operation Warp Speed used in its allocation methodology to the population data for the 50 states, four cities, and Puerto Rico, based on data published in the 2018 American Community Survey, a yearly survey conducted by the U.S. Census Bureau. We determined the data were sufficiently reliable for the purposes of our reporting objective.
Agency Comments
We provided DOD, HHS, and the Office of Management and Budget with a draft of this enclosure. None of the agencies provided comments on this enclosure.
GAO’s Ongoing Work
As the pandemic continues, the federal government continues to play a role in distributing and administering vaccines to help prevent the spread of COVID-19. We will continue to monitor the federal government’s vaccine response.
Related GAO Products
COVID-19: Federal Efforts to Provide Vaccines to Racial and Ethnic Groups.GAO-22-105079. Washington, D.C.: February 7, 2022.
COVID-19: HHS Agencies’ Planned Reviews Of Vaccine Distribution and Communication Efforts Should Include Stakeholder Perspectives. GAO-22-104457. Washington, D.C.: November 4, 2021.
Contact information: Alyssa M. Hundrup, (202)-512-7114, hundrupa@gao.gov
Federal, state, and local efforts have led to an estimated 70 percent of the eligible U.S. population being fully vaccinated against COVID-19. As vaccination efforts continue, stakeholders—including those representing state, territorial, and local health officials and health care providers—have reported ongoing challenges vaccinating children and administering booster doses.
Entities involved: Department of Health and Human Services, including the Office of the Assistant Secretary for Preparedness and Response, the Centers for Disease Control and Prevention, and the Food and Drug Administration
Background
COVID-19 vaccination, including the administration of booster doses, remains a high priority for the federal government. As of March 26, 2022, about 70 percent of the U.S. population eligible for vaccination (i.e., individuals aged 5 years and older) were fully vaccinated, according to estimates from the Centers for Disease Control and Prevention (CDC).[126] Vaccination coverage varied, however, among population groups. For example, a higher proportion of adults aged 65 years and older were fully vaccinated compared to younger adults. Additionally, about 46 percent of fully vaccinated individuals eligible to receive a booster dose (i.e., individuals aged 12 years and older) had received one, according to CDC estimates.[127]
In response to the pandemic, the federal government has provided substantial funding for COVID-19 vaccine-related activities. As of February 28, 2022, the Department of Health and Human Services (HHS) reported that $41.5 billion of its COVID-19 relief funding was for vaccine-related activities, such as vaccine development, procurement, and distribution. Of this amount, HHS reported that about $37.3 billion had been obligated, and over $17.7 billion had been expended as of the same date.[128]
As of April 1, 2022, three COVID-19 vaccines were available in the U.S. The Pfizer vaccine was available for individuals aged 5 years and older, and the Moderna and Janssen vaccines were available for individuals aged 18 years and older.[129] As of April 1, 2022, the primary vaccination series for individuals in the general population included two doses of the Pfizer or Moderna vaccines or a single dose of the Janssen vaccine. For certain immunocompromised individuals, a third dose of the Pfizer vaccine (for individuals aged 5 years and older) or Moderna vaccine (for individuals aged 18 years and older) was authorized for their primary vaccination series.[130] For certain immunocompromised individuals who received a single dose of the Janssen vaccine, a second dose of the Pfizer or Moderna vaccine was authorized for their primary vaccination series.
In addition, booster doses were authorized for individuals aged 12 years and older after completion of their primary vaccination series. In March 2022, a second booster dose was authorized to be administered to certain populations, including individuals aged 50 years and older.
State and local health officials have played a key role in federal efforts to distribute, administer, and communicate about COVID-19 vaccines. In November 2021, we recommended that HHS agencies obtain input from state and local health officials when identifying lessons learned from federal COVID-19 vaccination efforts. Specifically, we recommended that HHS agencies, including CDC, obtain feedback from, and incorporate perspectives of, state and local health officials and other key stakeholders as the agencies conduct their after action reviews. CDC concurred with this recommendation.[131]
Overview of Key Issues
COVID-19 vaccine for children. The Food and Drug Administration (FDA) authorized the Pfizer vaccine for children aged 5–11 years at the end of October 2021, and CDC recommended its use for this age group a few days later in early November 2021.[132] Before then, FDA had authorized and CDC recommended the Pfizer COVID-19 vaccine for those aged 16–17 years and older in December 2020.[133] Then, in May 2021, FDA also authorized and CDC recommended that vaccine for children aged 12–15 years.
Child Receiving COVID-19 Vaccination
As of March 26, 2022, CDC estimates showed that about one-third of children aged 5–11 years had received the first dose of the Pfizer vaccine, and over one-quarter had been fully vaccinated. In comparison, a larger proportion of older children (who had been eligible longer) were vaccinated, although at lower rates than for the adult population. (See table.)
Estimated COVID-19 Vaccination by Age Group, as of Mar. 26, 2022
Age group
When age group was recommended by CDC for vaccinationa
First dose
Fully vaccinatedb
Percentage of age group
Number (in millions)
Percentage of age group
Number (in millions)
5-11 years
November 2021
34.3
9.9
27.6
7.9
12-15 years
May 2021
66.7
11.3
56.8
9.6
16-17 years
December 2020
72.0
6.0
61.7
5.2
18 years and older
December 2020
88.3
228.0
75.4
194.7
Source: GAO analysis of Centers for Disease Control and Prevention (CDC) data and information. | GAO-22-105397
Notes: See CDC, “COVID Data Tracker: Demographic Characteristics of People Receiving COVID-19 Vaccinations in the United States,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#vaccination-demographic and “COVID Data Tracker: COVID-19 Vaccinations in the United States,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-total-admin-rate-total. As of April 1, 2022, the only vaccine authorized or licensed for children under age 18 years was the Pfizer vaccine, which was developed in collaboration with BioNTech. No COVID-19 vaccines had been authorized or licensed for children under 5 years as of April 1, 2022.
aAfter the Food and Drug Administration authorizes or licenses a vaccine, CDC’s Advisory Committee on Immunization Practices, a panel of medical and public health experts, typically meets to review available data and make recommendations on vaccines. The advisory committee’s recommendations become official CDC recommendations if they are approved by the CDC Director.
bAs of April 1, 2022, CDC counts individuals as being “fully vaccinated” if they received two doses on different days (regardless of time interval) of the two-dose vaccines or received one dose of the single-dose vaccine.
Additionally, the pace of vaccinations has varied over time for children eligible for COVID-19 vaccination. In mid-November 2021, children aged 5–11 years were receiving their first doses of vaccine at an average of more than 250,000 a day, according to CDC data. By mid-March 2022, the daily average had declined to fewer than 10,000 doses.[134]
A number of factors could be contributing to the declining pace of vaccinations for children, according to health care providers and others. For example, it was anticipated that a number of parents would be eager to get their children vaccinated soon after they became eligible, while other parents might defer their decisions because of questions they have about vaccinating young children against COVID-19.[135]
Some stakeholders representing state, territorial, and local health officials we interviewed characterized the rollout of COVID-19 vaccine for children aged 5–11 years as fairly successful but some also noted challenges. They said CDC had released helpful planning materials and held listening sessions with stakeholders, such as local health departments, prior to the rollout. However, these stakeholders and a stakeholder representing health care providers noted challenges, including the following:
Provider capacity and enrollment. Some providers’ capacity to administer COVID-19 pediatric vaccine was challenged by competing limited staff, according to some stakeholders. For example, one stakeholder said that pediatricians had widely reported that vaccines for younger children became available at one of the hardest stages of the pandemic when parents were seeking COVID-19 testing and provider practices were experiencing ongoing staff limitations. In addition, some stakeholders noted that some providers were having difficulties registering for or receiving vaccine in their clinics.
Limited use of local expertise. One stakeholder representing local health departments noted that the federal government did not seem to take into account the expertise of local health departments when planning the rollout of vaccines for children aged 5–11 years. The stakeholder said the federal government’s vaccination plans centered on using pharmacies and health care providers to administer vaccine and did not take into account local health departments’ relationships with schools, community centers, libraries, and other organizations that can target hard-to-reach families and children.
COVID-19 vaccine booster doses. Beginning in September 2021, FDA authorized, and CDC recommended, booster doses of COVID-19 vaccine because of waning protection from COVID-19 infection or severe illness over time after initial vaccination.[136] Over the next several months, FDA and CDC expanded the populations eligible for receiving a booster dose. This was in part because data had shown that booster doses can help broaden and strengthen protection against the Omicron variant and other COVID-19 variants, according to CDC.
As of April 1, 2022, FDA authorized, and CDC recommended, that individuals aged 12 years or older receive a booster dose after completing their primary vaccination series. For the general population, a booster dose is recommended at least 2 months after the single primary dose of the Janssen vaccine or at least 5 months after completion of the primary vaccination series of the Pfizer or Moderna vaccines. In addition, a second booster dose may be administered to individuals aged 50 years and older and to certain immunocompromised individuals aged 12 years and older, at least 4 months after receipt of a first booster dose.[137] (See table.) FDA also authorized the use of vaccine booster doses on a “mix and match” basis—that is, any available COVID-19 vaccine may be used as a booster dose regardless of which COVID-19 vaccine was used for the primary vaccination series.[138]
CDC Guidance on COVID-19 Booster Doses as of April 2022
Booster
Who may get a booster
When booster dose may be administered
Which vaccine may be administered as booster dose
First booster dose
Individuals aged 12 years and older
At least 5 months after the primary vaccination series of either the Pfizer or Moderna vaccines.a
At least 2 months after the single primary dose of the Janssen vaccine.b
Pfizer or Moderna vaccines are preferred in most cases. However, individuals aged 12-17 years may only receive the Pfizer vaccine.
Certain immunocompromised individuals aged 12 years and olderc
At least 3 months after the third dose in the primary vaccination series of either the Pfizer or Moderna vaccines.
At least 2 months after the second dose in a primary vaccination series of the Janssen vaccine
Pfizer or Moderna vaccines are preferred in most cases. However, individuals aged 12-17 years may only receive the Pfizer vaccine.
Second booster dose
Individuals aged 50 years and older
At least 4 months after the first booster dose of any COVID-19 vaccine
Pfizer or Moderna vaccines
Certain immunocompromised individuals aged 12 years and olderc
At least 4 months after the first booster dose of the Pfizer or Moderna vaccines
Pfizer or Moderna vaccines for individuals aged 18 years and older. However, individuals aged 12-17 years may only receive the Pfizer vaccine.
Adults who received a primary vaccine and booster dose of the Janssen vaccine
At least 4 months after the Janssen booster dose
Pfizer or Moderna vaccines
Source: Information from the Centers for Disease Control and Prevention (CDC). | GAO-22-105397
aPfizer developed its COVID-19 vaccine in collaboration with BioNTech.
bJanssen Pharmaceutical Companies are a part of Johnson & Johnson.
cThese are individuals considered to be moderately or severely immunocompromised who have a weakened immune system because of certain conditions or treatments, such as people who have undergone solid organ transplantation and are taking medicine to suppress the immune system, according to CDC.
As of March 26, 2022, about 97 million people had received a booster dose, or about 46 percent of the 209 million people aged 12 years and older who had been fully vaccinated, according to CDC estimates.[139] The extent to which different age groups had received a booster dose, however, has varied. For example, CDC estimated that about 67 percent of individuals aged 65 years or older who were fully vaccinated had received a booster dose.
Some stakeholders we interviewed acknowledged the tremendous public health accomplishment of administering hundreds of millions of COVID-19 vaccine doses, but all said they faced ongoing challenges administering booster doses. As we previously recommended, obtaining feedback from stakeholders, including state and local health officials, is critical as HHS identifies lessons learned from federal COVID-19 vaccination efforts. The challenges stakeholders identified related to booster doses included the following:
Competing public health priorities and staffing issues. Similar to what we reported in April 2021, some stakeholders reported competing public health priorities and staffing issues as challenges. When the federal government began rolling out booster doses, state and local health officials and providers were already busy with other pandemic-related activities, including continued outreach to unvaccinated individuals, administering pediatric COVID-19 vaccines, and managing testing, according to some stakeholders. In addition, health officials were also addressing other public health priorities at the time. For example, local health departments were busy providing routine childhood vaccinations, including those missed during the pandemic, and preparing for seasonal influenza vaccinations, while also dealing with limited health staff, according to one stakeholder. Pharmacies were also reporting staffing shortages at this time, which one stakeholder said had affected the availability of vaccination appointments.
Administrative procedures for ordering COVID-19 vaccine. Some stakeholders representing state, territorial, and local health officials said requirements for ordering vaccine doses, including booster doses, above federally set thresholds were burdensome and frustrating for some states. Since September 2021, each time states wanted to order more doses than their threshold, they were required to notify HHS, submit a justification request for additional doses, and wait for HHS’s evaluation and response, according to HHS officials.[140] The stakeholders said the extra work required by this process placed a heavy burden on already exhausted public health staff. It also resulted in delays or cancellations of provider orders, according to one stakeholder representing state immunization managers. In addition, these stakeholders said that it was frustrating for states to face these additional requirements to meet increased demand for vaccine, including booster doses, when the federal government was promoting booster doses and saying there was plenty of vaccine.
Communication related to complex and changing federal recommendations. Some stakeholders representing state, territorial, and local officials said communications regarding the complex and changing authorizations and recommendations for booster doses led to confusion among the public and health care providers. The challenges noted by one or more stakeholders included: (1) multiple changes in the populations eligible for booster doses, (2) differences in when to get booster doses depending on the vaccine, and subsequent changes to these time frames, (3) the different dosage for the Moderna vaccine booster (half the size of a full dose used for primary vaccination), (4) the difference between CDC recommendations on those who “should” get a booster dose and those who “may” get a booster dose, and (5) the difference between a third primary series dose recommended for certain immunocompromised individuals and a booster dose.[141]
Between September 22, 2021 (when booster doses were first authorized), and April 1, 2022, FDA amended COVID-19 vaccine EUAs regarding booster doses ten times, including the age groups for whom booster doses were authorized. CDC similarly updated its recommendations on booster doses and also made additional recommendations for individuals who are moderately or severely immunocompromised. One stakeholder representing local health departments said the more nuances there are in the recommendations, the harder it is to implement booster dose vaccinations on the ground, and that different caveats for different shots and language like “may” versus “should” make it very complicated to communicate to the public on booster doses.
Not receiving advance notice of changes. Some stakeholders we interviewed expressed frustration with learning about the changes to booster dose recommendations only when they were announced to the public and the media and not receiving advance notice from the federal government. They said advance notice is important to help state and local health officials prepare for potential questions from the public and to prepare communication materials for their communities.
One stakeholder also noted that when multiple changes occurred within a few days, without advance notification, states had to conduct the same work—including outreach to providers—multiple times in a short period. For example, after FDA and CDC changed the time frame for receiving a booster dose of the Pfizer vaccine from at least 6 months to at least 5 months after individuals were fully vaccinated, states revised their educational and outreach materials, including in various languages, noting that the time frame before getting a booster for Pfizer had changed but the time frame for the Moderna vaccine was still 6 months. A few days later, when FDA and CDC also reduced this time frame to at least 5 months for the Moderna vaccine, state health officials had to repeat their work to update all their materials again.
Limited information on vaccine shipments. Some stakeholders representing state, territorial, and local officials said some states and local health departments continued to have limited information on the locations where vaccine doses were being sent within their communities—for example to pharmacies and federally supported health centers. In November 2021, we reported that the lack of information on where doses were going made it challenging for states to optimally and equitably distribute the supplies of vaccine they had received from the federal government.
Minimum order sizes and vial sizes. Some stakeholders we interviewed also noted that minimum order sizes posed challenges for providing COVID-19 vaccine—both for primary series and booster doses—in manageable quantities to providers with smaller patient loads, including pediatricians and health care providers in rural areas. As of February 2022, the minimum order sizes for COVID-19 vaccines ranged from 100 to 300 doses, depending on the vaccine, according to HHS officials. In January 2021, we reported that a lesson learned from the 2009 H1N1 influenza pandemic was that a 100-dose minimum order was problematic because states had to break down the shipments into smaller sizes to be shipped to health care providers, which reportedly required significant staff time and delayed when providers received vaccine. We noted the minimum order sizes for COVID-19 vaccines (which at that time were 975 doses for Pfizer vaccine and 100 doses for Moderna vaccine) could pose similar or even greater challenges.
In January 2022, some stakeholders noted these challenges related to minimum order sizes. Stakeholders noted that although the minimum order size for Pfizer vaccine was smaller than earlier, some states still had to break down vaccine shipments to send to smaller providers.
Some stakeholders also said the vial sizes—that is, the amount of vaccine included in each multi-dose vial of COVID-19 vaccine—are a challenge because all of the vaccine in the vial must be used within hours of opening the vial and administering the first dose. (See table.) These stakeholders said some health care providers, such as those in rural areas, may not be able to administer all doses in a vial in a single day due to their small patient populations and have to discard any unused doses in the vial. As a result, vaccinators in such circumstances need a much larger supply of vaccine on hand, according to one stakeholder representing state immunization managers. Additionally, in some places, the concern about the potential for wasting vaccine doses coupled with the burden of enrolling led some pediatricians not to enroll or defer enrolling as COVID-19 vaccine providers, according to another stakeholder.
Minimum Order Sizes, Number of Hours in Which Doses in Opened Vials Must Be Used, and Vial Sizes for Available COVID-19 Vaccines, as of February 2022
Pfizera (12 years and older)
Pfizera (5–11 years)
Moderna (18 years and older)
Janssenb (18 years and older)
Minimum order size (in doses)
300
100
100
100
How long vaccine can be used after vial is opened
12 hoursc
12 hours
12 hours
6 hours refrigerated; 2 hours at room temperature
Number of doses per vial
6 doses
10 doses
10–11 dosesd
5 doses
Sources: GAO analysis of Food and Drug Administration (FDA) and Department of Health and Human Services (HHS) information. | GAO-22-105397
aPfizer developed its COVID-19 vaccine in collaboration with BioNTech.
bJanssen Pharmaceutical Companies are a part of Johnson & Johnson.
cThe Pfizer vaccine available for individuals aged 12 years and older comes in two formulations. The formulation that does not require dilution must be used within 12 hours of puncturing the vial. In February 2022, the U.S. government was only ordering the formulation that does not require dilution, and as of December 23, 2021, only this formulation was available for jurisdictions to order for individuals aged 12 years and older, according to HHS officials. The other authorized formulation, which must be diluted before administration, must be used within 6 hours of dilution.
dFor Moderna’s vaccine, the number of doses per vial reflects the number of doses available for primary series vaccinations; a larger number of doses may be extracted if used for booster doses. The number of doses is shown as a range because the type of syringe used may affect the number of doses that can be extracted from a vial. The Moderna vaccine is available in two different vial sizes for primary vaccination—one with 10-11 doses per vial and one with 13-15 doses per vial. Since November 10, 2021, the smaller vial containing 10-11 doses vial replaced the larger vial as the product available for ordering, according to HHS officials.
Methodology
To conduct this work, we reviewed CDC data on COVID-19 vaccines administered as of March 26, 2022. We determined the data were sufficiently reliable for the purposes of presenting CDC vaccination estimates. We also reviewed agency information from CDC, FDA, and HHS. In addition, we reviewed information and interviewed officials from stakeholders representing state officials, health officials—including state, territorial and local health officials—and health care providers.[142]
Agency Comments
We provided HHS, including CDC, and the Office of Management and Budget a draft of this enclosure. CDC provided technical comments, which we incorporated as appropriate. The Office of Management and Budget did not provide comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor HHS agencies’ efforts to gather information for and conduct after action reviews.
GAO’s Prior Recommendations
The table below presents our recommendation on vaccine distribution and administration from a prior bimonthly CARES Act report.
Prior GAO Recommendation Related to COVID-19 Vaccine Distribution and Administration
Recommendation
Status
The Secretary of Health and Human Services, with support from the Secretary of Defense, should establish a time frame for documenting and sharing a national plan for distributing and administering COVID-19 vaccine, and in developing such a plan ensure that it is consistent with best practices for project planning and scheduling and outlines an approach of how efforts will be coordinated across federal agencies and nonfederal entities. (September 2020 report)
Closed—not addressed. Since September 2020, the Centers for Disease Control and Prevention (CDC) and the White House issued vaccine planning documents, including a National Strategy for the COVID-19 Response and Pandemic Preparedness that broadly outline various programs for vaccine distribution. These documents contained general information on federally supported vaccine distribution activities, but did not provide details related to how the federal government was coordinating its efforts or information on the specific roles of the federal agencies and non-federal entities. We closed this recommendation in April 2022 because the time frame for its implementation had passed, due to widespread distribution and administration of COVID-19 vaccines.
COVID 19: HHS Agencies’ Planned Reviews of Vaccine Distribution and Communication Efforts Should Include Stakeholder Perspectives.GAO-22-104457. Washington, D.C.: November 4, 2021.
COVID-19: Efforts to Increase Vaccine Availability and Perspectives on Initial Implementation. GAO-21-443. Washington, D.C.: April 14, 2021.
Contact information: Alyssa M. Hundrup, (202) 512-7114, hundrupa@gao.gov
Employer-sponsored health insurance rates declined in 2020, but federal surveys estimated uninsurance rates did not increase significantly because of the pandemic, due in part to increased Medicaid and health insurance exchange enrollment. Some policy researchers we interviewed suggested options to help mitigate disruptions in health insurance coverage during economic downturns.
Entity involved: The Centers for Medicare & Medicaid Services, within the Department of Health and Human Services
Background
COVID-19 and the associated economic downturn caused massive job loss in the U.S., raising concerns about associated loss of health insurance provided by an individual’s employer, called employer-sponsored insurance (ESI). Congress included provisions in COVID relief laws supporting enrollment in health coverage alternatives to ESI, including in the following areas:[143]
Medicaid. Medicaid is a joint federal-state health financing program for certain low-income and medically needy individuals. States and territories administer their Medicaid programs within broad federal rules and according to state plans approved by the Centers for Medicare & Medicaid Services (CMS).[144]
Through the Families First Coronavirus Response Act, Congress temporarily increased the Federal Medical Assistance Percentage (FMAP), the percentage of expenditures for most Medicaid services that the federal government pays, by 6.2 percentage points.[145] To receive this increase during each quarter in which it is effect, states have to meet certain conditions, including not disenrolling Medicaid beneficiaries who were enrolled on or after March 18, 2020, through the end of the month in which the public health emergency ends (referred to as the continuous coverage requirement). On April 12, 2022, the Secretary of the Department of Health and Human Services extended the public health emergency for 90 days or through the duration of the emergency.[146]
Health insurance exchanges. Through federal and state health insurance exchanges (exchanges), individuals can compare and select among plans offered by participating private insurers that meet certain federal standards.[147] The American Rescue Plan Act of 2021 expanded eligibility for tax credits that help cover exchange premiums to those making above 400 percent of the poverty level and also increased premium tax credits for those making between 100 and 400 percent of the poverty level for 2021 and 2022.[148] The Act also provided additional premium tax credits to consumers from households in which a tax filer received or was approved to receive unemployment compensation for any week beginning in 2021.
Overview of Key Issues
Trends in health insurance coverage in 2020. Federal survey data as of February 2022 suggested that the overall rate of non-elderly American adults without health insurance did not increase significantly in 2020 (see figure below), even with the COVID-19 economic downturn and associated job loss.[149] Uninsurance rates were likely relatively stable because ESI loss was less than originally expected and also because some ESI loss was offset by increases in enrollment in Medicaid and the exchanges.[150]
Federal Survey Estimates of Uninsurance Rates among Non-Elderly Adults, 2018-2020
Notes: For more information about the survey data presented, including 2020 sources, collection methods, associated error rates, and other limitations, see the U.S. Department of Commerce, U.S. Census Bureau, Health Insurance Coverage in the United States: 2020 (Washington, D.C.: September 2021), available at https://www.census.gov/library/publications/2021/demo/p60-274.html, last accessed March 2, 2022 and its “2020 ACS 1-Year Experimental Data Tables,” available at https://www.census.gov/programs-surveys/acs/data/experimental-data/1-year.html, last accessed March 2, 2022 and the U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, Demographic Variation in Health Insurance Coverage: United States, 2020 (Hyattsville, Md..: February 2022), available at https://www.cdc.gov/nchs/data/nhsr/nhsr168.pdf, last accessed March 2, 2022. We also used 2018 and 2019 data from these surveys to compile the figure presented.
The Annual Social and Economic Supplement of the US Census Bureau’s Current Population Survey and the American Community Survey consider non-elderly adults to be respondents ages 19-64, while the National Center for Health Statistics’ National Health Interview Survey considers non-elderly adults to be respondents age 18-64. Further, the Annual Social and Economic Supplement of the Current Population Survey considers individuals to be uninsured if they do not have health insurance coverage for the entire calendar year. Therefore, if the respondent had insurance at some point in the year but subsequently became uninsured, they would not be counted as uninsured for that year by that survey. In contrast, the National Health Interview Survey and American Community Survey asked survey respondents if they were uninsured at the time of the survey.
COVID-19 may have affected federal survey collection efforts and therefore the accuracy of 2020 estimates. The U.S. Census Bureau reported that due to data collection challenges during COVID-19, the 2020 American Community Survey results were released as experimental estimates, which the U.S. Census Bureau defines as innovative statistical products created using new data sources or methodologies in the absence of other relevant products, but which may not meet all of the U.S. Census Bureau’s quality standards.
Racial and ethnic disparities. Disparities in uninsurance rates among racial and ethnic groups persisted during the COVID-19 pandemic. According to the National Center for Health Statistics’s National Health Interview Survey, Hispanics of all races and non-Hispanic Blacks had higher uninsurance rates than non-Hispanic Whites and Asians prior to the pandemic. These disparities persisted in 2020 (see figure below).
National Health Interview Survey’s Estimated Non-Elderly Adult Uninsurance Rate by Race and Hispanic Origin, 2018-2020
Notes: The National Health Interview Survey asked survey respondents if they were uninsured at the time of the survey. For more information about the survey data presented, including 2020 sources, collection methods, associated error rates, and other limitations, see U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics, Demographic Variation in Health Insurance Coverage: United States, 2020 (Washington, D.C.: February 2022), available at https://www.cdc.gov/nchs/data/nhsr/nhsr168.pdf, last accessed March 2, 2022. We also used 2018 and 2019 data from this survey to compile the figure presented.
COVID-19 may have affected federal survey collection efforts and therefore the accuracy of 2020 estimates. Non-elderly adults were those aged 18-64.
Trends in employer-sponsored insurance. Data from federal surveys found modest decreases in rates of health insurance coverage provided by an individual’s employer, called ESI, during the pandemic in 2020.[151] According to the Annual Social and Economic Supplement of the U.S. Census Bureau’s Current Population Survey, the estimated rate of Americans with ESI at the time of the survey declined 1.1 percentage points, from 54 percent in early 2019 to 52.9 percent in early 2021, a difference which was not statistically significant.[152] Further, data from the Agency for Healthcare Research and Quality’s Medical Expenditure Panel Survey found that the decline in the estimated number of private-sector workers enrolled in ESI between 2019 and 2020—a decrease from 62.5 million to 60.8 million—was not statistically significant.[153]
There are several reasons ESI loss during the COVID-19 pandemic was lower than originally anticipated, including the following:
Many people who lost their jobs during the COVID-19 pandemic had never been enrolled in ESI through their jobs. According to the Congressional Budget Office, the highest COVID-19-related job loss was in small companies and lower-wage industries less likely to offer health insurance, such as retail and food service.[154]
Some job loss and any associated ESI loss may have been temporary. A policy researcher noted that COVID-19 and the associated economic downturn differed from previous downturns, such as the financial crisis of 2008, because employers saw it as a temporary issue and were less likely to make permanent employment changes.[155] Similarly, a Bureau of Labor Statistics survey estimated that of the 13.5 million people who reported not working in June 2020, 10.6 million (or 79 percent) expected to be recalled to work at some point.[156]
Many individuals were able to retain their ESI while furloughed as the pandemic continued through 2020. According to another Bureau of Labor Statistics survey, 42 percent of establishments surveyed paid a portion or all health insurance premiums for some or all furloughed employees while they were not working in calendar year 2020.[157]
Medicaid. Medicaid total enrollment increased 14.9 million, or about 23 percent, between February 2020 and November 2021. CMS attributes the increased enrollment primarily to a larger share of individuals retaining their Medicaid coverage due to the continuous coverage requirement under the Families First Coronavirus Response Act rather than to an increase in new Medicaid enrollees.[158] According to CMS, the number of new applications for Medicaid and the Children’s Health Insurance Program, a public coverage program for eligible low-income children, was more than 30 percent higher in April 2020 than in 2018 and 2019 due to COVID-19 and the associated economic downturn, but dropped to normal or below normal levels after May 2020.[159]
In addition to implementing the continuous coverage requirement, many states took steps to expand Medicaid coverage for their populations during the COVID-19 pandemic through waivers and state plan amendments, which allow states flexibility in operating their Medicaid programs within federal parameters. In March 2020, CMS created a Medicaid state plan amendment template and instructions to assist states in responding to the COVID-19 national emergency. In December 2020, CMS reported that it had approved more than 600 waivers or other flexibilities aimed at addressing obstacles to beneficiary care and program enrollment through the COVID-19 public health emergency. The Kaiser Family Foundation reported that as of July 2021, 18 states had used Medicaid waivers and state plan amendments to relax eligibility documentation requirements and allow individuals to attest to the information they provide on Medicaid applications.[160]
Some policy researchers we interviewed said COVID-19 relief provisions related to Medicaid were effective in stabilizing the health insurance system and preventing large increases in the uninsured population due to COVID-19 and the associated economic downturn. Further, in our January 2022 report on the CARES Act, Medicaid officials in eight selected states said that the 6.2 percentage point FMAP increase was critical in enabling them to maintain program operations while they faced increased enrollment and decreased tax revenue. For example, New Hampshire officials noted their Medicaid enrollment increased 25 percent during the COVID-19 pandemic, and they said they would have faced serious financial challenges without the FMAP increase.
The continuous coverage requirement and FMAP increase will end following the end of the public health emergency.[161] Specifically, as authorized by section 6008 of the Families First Coronavirus Response Act, the continuous coverage requirement is in effect through the end of the month in which the public health emergency ends, and the FMAP increase is available through the end of the calendar quarter in which the public health emergency ends. In October 2021, some policy researchers we interviewed raised concerns about disruptions in coverage for current Medicaid enrollees when these eligibility re-determinations resume, including inappropriate disenrollment of those who are actually eligible. However, under new guidance released in March 2022, states will have up to 12 months to initiate eligibility assessments for all individuals enrolled in Medicaid and Children’s Health Insurance Program and two additional months to complete all renewals and other pending actions initiated during the 12-month unwinding period. As a part of this guidance, CMS identified five strategies states may use to promote continuity of coverage and prevent inappropriate disenrollment of those who are actually eligible during the unwinding period, including renewal for individuals based on Supplemental Nutrition Assistance Program eligibility and partnering with managed care plans to update beneficiary contact information.[162]
Exchange coverage. Enrollment in federal and state exchanges increased during the COVID-19 pandemic, supported by increased availability of premium tax credits and special enrollment periods. Based on the most recent data available at the time of this report, plan selection during the 2022 open enrollment period in federal and state exchanges was higher than in any previous open enrollment period.[163] CMS data show that there were about 3.1 million (27 percent) more individual plan selections during the 2022 open enrollment period than during the 2020 open enrollment period, which occurred before the COVID-19 pandemic.[164]
Further, CMS reported that more than 2.1 million people obtained coverage through a federally-facilitated exchange during a special enrollment period held in 2021, exceeding total special enrollment plan selections during the same time period in plan years 2019 and 2020.[165] On January 28, 2021, the administration announced this new special enrollment period for the federally-facilitated exchange in response to the 2021 COVID-19 public health emergency; the exchange was available for enrollment from February 15, 2021, through August 15, 2021.[166] It was open to all individuals and, unlike previous special enrollment periods, no qualifying life event was required to obtain coverage.[167] According to CMS, the special enrollment period was accompanied by an outreach campaign to raise awareness among the uninsured about the availability of financial assistance to pay for premiums for those who qualified.
Some policy researchers said the special enrollment periods made available during the COVID-19 pandemic helped increase enrollment in the exchanges. The ability to access a special enrollment period without needing a qualifying event may have increased enrollment because documenting a qualifying event may delay or prevent some consumers from enrolling.[168] However, other policy researchers said the COVID-19 special enrollment period was not necessary because consumers could have qualified for a special enrollment period if they experienced a qualifying event, such as losing ESI.
Some policy researchers said that the expanded exchange premium tax credits may have temporarily mitigated certain impediments to enrollment in the exchanges, but said that the issues will re-emerge if the credits end. Specifically, some policy researchers raised concerns about exchange coverage being unaffordable for some families because of the “family glitch.” The family glitch refers to the policy that bases eligibility for premium tax credits on whether ESI is considered affordable for the employee only, not whether ESI is considered affordable for their whole family. In other words, the employee’s family is not eligible for premium tax credit assistance as long as the cost of coverage for the employee only is considered affordable under the current policy. Some researchers suggested that Congress address this issue by making the expanded premium tax credits under the American Rescue Plan Act permanent. However, on April 7, 2022, the Biden Administration proposed a new rule to eliminate the family glitch.[169] According to the Administration, if finalized, the rule would allow family members of workers who are offered affordable self-only exchange coverage but unaffordable family coverage to qualify for premium tax credits to buy exchange coverage.
Policy options for future economic downturns. Despite relatively modest changes in the rate of uninsurance due to the COVID-19 pandemic, some policy researchers suggested that opportunities remain to strengthen access to health insurance for individuals during economic downturns. We spoke with policy researchers about a range of policy options related to access to health insurance, including those related to ESI, Medicaid, and federal and state health insurance exchanges:
Consumer outreach for health insurance exchanges. Some policy researchers emphasized that consumers would benefit from additional outreach to understand their exchange coverage options and premium tax credit availability.[170] A survey by the Urban Institute found that, in April 2021, fewer than half (48.2 percent) of uninsured nonelderly adults reported having heard “a lot” or “some” about the exchanges, and fewer than a third (32.2 percent) reported having heard a lot or some about the expanded premium tax credits; the remainder of both groups had heard only a little or nothing at all.[171]
CMS funds consumer outreach for the federal exchange partially through user fees paid by insurers who list a health insurance plan on the federal exchange. Currently, these outreach activities include television advertising and the use of navigators, community-based customer service representatives or groups who help consumers understand their exchange options and complete their application for coverage.[172] Some policy researchers said navigators are crucial to reaching underserved communities that may have been disproportionally affected by COVID-19 and the associated economic downturn. However, the executive director of a state-based exchange said while navigator programs, which all exchanges are required to establish, have an important role in enrolling consumers in exchange coverage, insurance agents and self-service options were more effective than navigators at enrolling consumers during the state’s COVID-19 special enrollment period.
CMS officials told us that the agency has obligated more than $300 million dollars in federal exchange user fees for marketing and outreach activities for the federal exchange in fiscal year 2021. However, CMS also told us that it has more than $1.1 billion in unspent exchange user fees as of December 2021.[173] According to CMS officials, the agency significantly increased spending on consumer information and outreach activities, including funding for navigators. Specifically, CMS reported $80 million in funding for 60 navigator programs serving consumers for the 2022 plan year, significantly higher than the $10 million in annual funding awarded in plan years 2019 through 2021. Further, CMS reported that outreach will be targeted to communities with lower access to health care and will be conducted in partnership with cultural marketing experts, for example, to target campaigns to African Americans, Spanish and English-speaking Latinos, and Asian American and Pacific Islander communities in multiple languages.
Automatic Medicaid FMAP increase. Some researchers said the FMAP should be automatically increased during future economic downturns to support states’ Medicaid programs, which could be faced with absorbing a large number of individuals experiencing disruptions in their ESI. Other researchers said the 2020 FMAP increase was not necessarily effective at addressing the effects of COVID-19 because the funding did not specifically target populations vulnerable to losing their ESI.
In our June 2020 CARES Act report, we reported that using a different formula that we had previously recommended could help make any future changes to the FMAP during COVID-19 and any future economic downturns more timely and targeted. The formula’s automatic trigger would improve timely targeted assistance using readily available economic data based on (1) increases in state unemployment and (2) reductions in total wages and salaries.
Automatic enrollment. Some policy researchers said that to prevent health insurance disruptions during economic downturns, Congress should examine options to make enrollment in Medicaid or the exchanges more automatic for those most vulnerable to the effects of the downturn, including low-income and uninsured individuals. One of these researchers noted that millions of uninsured Americans are eligible for either Medicaid or subsidized coverage through an exchange.
According to a policy researcher we interviewed, in an automatic enrollment system, individuals might indicate their health insurance status and desire for coverage on their federal tax forms. Then the uninsured could be automatically placed on Medicaid or in a low-premium exchange plan through a federal-state partnership and given the option to opt out if they did not want to be enrolled. This would provide coverage to consumers who otherwise would not enroll because of cost concerns or difficulty navigating the application process.
According to a 2018 Health Affairs article, health programs that use automatic enrollment with opt-out options—such as Medicare Part B—have achieved high take-up levels. [174] However, according to a 2021 research article and CMS officials, implementation of an automatic enrollment option would require systemic changes, such as aligning the timing of eligibility checks for exchange tax credits and Medicaid, determining ways to share complete and accurate consumer eligibility information between federal and state governments, policy decisions on the verification of consumer data, and ensuring inclusion of insurance information on federal tax forms.[175] Additionally, the author of a 2017 research article on automatic enrollment proposals suggested that even if an automatic enrollment system could be implemented, it would be complex and difficult to administer. Further, the author noted that many policy proposals for automatic enrollment assume that the necessary data would come largely from the information that the Internal Revenue Service already collects. This means that states would automatically enroll people in a health insurance coverage for the coming year based on their income, coverage, and family status from two years earlier, which could be out of date in many cases.[176]
Methodology
For this work, we spoke with federal officials, reviewed federal publications and documentation, reviewed the results of a literature search, and conducted Internet searches to identify federal survey and administrative data sources for information on health insurance market composition. We reviewed documentation for the data sources and spoke with officials to better understand their methodologies and processes for gathering these data. We also conducted a literature search to identify policy options to mitigate the loss of ESI or provide coverage through an alternative. We reviewed CMS data and reports on enrollment in exchanges from 2014 to 2022 and on enrollment in Medicaid from February 2020 to June 2021. We assessed the reliability of these data using manual checks and discussions with CMS officials and determined they were sufficiently reliable for our purposes. Through our literature search, we identified policy researchers who had published work on policy options related to health coverage options, such as federal and state exchanges and Medicaid, and we made a judgmental selection of 12 individuals to achieve variation across the group with respect to educational training, organizational affiliation, and policy perspective.
Agency Comments
We provided the Department of Health and Human Services (HHS) and the Office of Management and Budget (OMB) with a draft of this enclosure. HHS provided technical comments, which we incorporated as appropriate. OMB did not provide us with comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor trends in health insurance.
Contact information: John Dicken, (202) 512-7114, dickenj@gao.gov
From January through mid-March 2022, weekly claims for regular unemployment insurance benefits generally remained similar to prepandemic levels, as they had since late 2021. Even so, states continued to address challenges resulting from historic numbers of claims during the COVID-19 pandemic—such as delayed benefit payments, increased amounts of overpayments, and potential fraud—that have future implications.
Entity involved: Department of Labor
Background
The unemployment insurance (UI) system is a federal-state partnership that provides temporary financial assistance to eligible workers who become unemployed through no fault of their own. States design and administer their own UI programs within federal parameters. The Department of Labor (DOL) oversees states’ compliance with federal requirements, such as by reviewing state laws to confirm they are designed to ensure payment of benefits when due. Regular UI benefits are funded primarily through state taxes levied on employers.[177] These benefits are intended to replace a portion of a claimant’s previous employment earnings, according to DOL.
The CARES Act created three federally funded temporary UI programs that expanded benefit eligibility and enhanced benefits during the COVID-19 pandemic. These programs, which were amended by the Consolidated Appropriations Act, 2021 and the American Rescue Plan Act of 2021, expired in September 2021. About half of the states, however, ended their participation in at least one of these programs in June or July 2021, according to DOL. These temporary UI programs were:
Pandemic Unemployment Assistance (PUA), which authorized UI benefits for individuals not otherwise eligible for UI benefits, such as self-employed and certain gig economy workers, who were unable to work as a result of specified COVID-19-related reasons.[178]
Federal Pandemic Unemployment Compensation (FPUC), which generally authorized an additional weekly benefit for individuals who were eligible for weekly benefits under the regular UI or CARES Act UI programs.[179]
Pandemic Emergency Unemployment Compensation (PEUC), which generally authorized additional weeks of UI benefits for those who had exhausted their regular UI benefits.[180]
In addition, the Consolidated Appropriations Act, 2021 created the Mixed Earner Unemployment Compensation (MEUC) program, which was extended by the American Rescue Plan Act of 2021 and expired in September 2021.[181] According to DOL, the MEUC program was intended to cover regular UI claimants whose benefits did not account for significant self-employment income and who thus may have received a lower regular UI benefit than they would have received had they been eligible for PUA.[182]
DOL required participating states to process and pay PUA, FPUC, PEUC, and MEUC benefits to eligible claimants for all weeks of unemployment before the programs ended due to early termination or expiration. In August 2021, the Secretary of the Treasury and the Secretary of Labor issued a joint letter to Congress affirming that states and territories also had the option to use Coronavirus State and Local Fiscal Recovery Funds from the American Rescue Plan Act of 2021 to provide additional weeks of income support to workers whose benefits had expired in September 2021 and to workers who were not covered by the regular UI program. As of late March 2022, the Department of the Treasury noted it was reviewing reports it had received and was not yet able to provide complete information about particular uses of funds.
UI claimants who exhausted their regular UI and PEUC benefits in certain states also had access to the Extended Benefits program. The program, which existed before the pandemic and provides up to an additional 13 or 20 weeks of benefits, is activated in states during periods of high unemployment, according to DOL.[183]
Because of high numbers of regular UI claims during the pandemic, some states have held substantial federal loans to pay UI benefits.[184] As of March 31, 2022, nine states and one territory held federal loans totaling about $37.6 billion, approximately $2.3 billion less than the total held at the end of 2021, which we reported in January 2022. Following guidance from Treasury, some states used Coronavirus Relief Fund payments to reduce or prevent federal loan balances.[185] In addition, states may use Coronavirus State and Local Fiscal Recovery Funds from the American Rescue Plan Act of 2021 to restore their UI trust funds or to repay federal loan balances.[186] While interim reports for some states indicated that they planned to contribute some of these funds to their UI trust funds, as of late March 2022, Treasury noted it was still reviewing reports on use of funds.
Overview of Key Issues
From January through mid-March 2022, claims for regular UI benefits generally remained similar to prepandemic levels. Initial and continued claims for regular UI benefits have generally been similar to prepandemic levels since November 2021.[187] Although the numbers fluctuated somewhat week-to-week, from January through March 2022, the average number of regular UI initial claims submitted each week was about 5 percent higher than the average number submitted during the corresponding weeks in 2019. During the week ending on March 26, 2022, DOL reported that 195,460 initial claims for regular UI benefits were submitted nationwide.[188]
According to DOL officials, the number of continued claims may be a better measure of continuing demand for benefits than the number of initial claims. From January through mid-March 2022, the average number of regular UI continued claims submitted each week was about 8 percent lower than the average number submitted during the corresponding weeks in 2019.[189] During the week ending on March 12, 2022, DOL reported that about 1.7 million continued claims for regular UI benefits were submitted nationwide.[190]
During the pandemic, the number of regular UI continued claims submitted each week declined overall after the peak in late April and early May 2020 through mid-March 2022, though the number has remained relatively consistent since mid-October 2021 (see figure). Some of the decline in regular UI claims was due to claimants finding employment. However, some of the decline was also likely due to other factors, such as claimants exhausting regular UI benefits and beginning to claim other benefits. For example, eligible individuals who exhausted their regular UI benefits could then claim PEUC benefits instead, prior to that program’s expiration in September 2021.[191] Thus, some of the decline in regular UI claims during the period when PEUC and PUA were in effect likely represents claimants switching between programs.
Weekly Continued Claims Submitted Nationwide for Regular UI, PEUC, and Extended Benefits, Mar. 1, 2020–Mar. 12, 2022
Note: After exhausting regular UI benefits—generally available for up to 26 weeks in most states, according to the Department of Labor (DOL)—eligible individuals were generally able to apply for (1) PEUC; then (2) the Extended Benefits program, if activated in a state; and then (3) Pandemic Unemployment Assistance (PUA) benefits, in certain circumstances. PEUC and PUA expired on September 6, 2021. The weekly counts of continued claims shown are not seasonally adjusted. Counts are from DOL data we obtained on April 4, 2022, and include any adjustments submitted by states as of then. All 53 states and territories reported regular UI claims in each week shown. The number of states and territories reporting PEUC claims varied by week; for example, fewer than half of the states and territories reported data before mid-May 2020 and at least 50 states and territories reported data each week from mid-July 2020 through mid-June 2021, when certain states began terminating their PEUC programs. The number of states reporting Extended Benefits claims each week varied, partly on the basis of the number of states with the program activated each week. The Extended Benefits program, which existed before the pandemic, is activated in states during periods of high unemployment, according to DOL.
As we have regularly noted in our CARES Act reports, because of backlogs in processing historic numbers of claims in many states and other data issues, the number of continued claims did not approximate the number of individuals claiming benefits during the pandemic. For example, backlogs in claims processing led to individuals submitting claims for multiple weeks of benefits in a single reporting period, which states counted as multiple claims for that reporting period, particularly in the PUA program. As a result, reliable conclusions about trends in the number of individuals claiming benefits throughout the pandemic cannot be drawn from data on continued claims.
Timeliness of regular UI first payments improved in late 2021 and in January 2022, but declined again in February 2022 and remained below DOL’s acceptable level of performance. As we have previously reported, the percentage of regular UI first payments made within 3 weeks of a claimant’s initial eligibility has fluctuated during the pandemic.[192] Nationwide, regular UI first-payment timeliness dropped precipitously early in the pandemic, had improved by April 2021, and then generally declined again through October 2021 (see figure). First payment timeliness improved again in November and December 2021 and rose to 75.5 percent in January 2022, before declining again to 63.4 percent in February 2022, which was 23.6 percentage points below DOL’s acceptable level of performance of 87 percent.[193] In February 2022, DOL officials reiterated that first-payment timeliness levels may be due to enhanced fraud prevention efforts and to the time it took states to resolve and pay eligible claims that were initially identified as potentially fraudulent. We have previously reported in October 2021 and January 2022 other reasons DOL identified, such as the additional time and effort needed for states to process backlogs of claims requiring adjudication and appeals.
Timeliness of Nationwide First Payments of Regular Unemployment Insurance (UI) Benefits, Jan. 2020–Feb. 2022
Note: We analyzed regular UI first-payment timeliness data that states had reported to the Department of Labor (DOL) as of March 28, 2022. At that point, all 53 states and territories had reported data for February 2022 and prior months. One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible, depending on whether the state requires that eligible claimants serve a waiting period before receiving benefits. DOL considers 87 percent to be an acceptable level of performance. We focus on payments made within 21 days because in guidance released at the start of the pandemic DOL recommended that states consider temporarily waiving their waiting week requirements.
In some states, many regular UI claimants continue to face delays before receiving their first payments. For example, in 13 states, at least half of regular UI claimants who received their first benefits in February 2022 had been waiting longer than 3 weeks. In addition, nationwide, about 18 percent of regular UI claimants who received their first benefits in February 2022 had been waiting longer than 10 weeks. By comparison, of the regular UI claimants nationwide who received their first benefits in March 2020, less than 3 percent had been waiting longer than 3 weeks and less than 1 percent had been waiting longer than 10 weeks.
States and territories have continued to identify overpayments in UI programs, and more have begun submitting data to DOL on recovered and waived PUA overpayments since we last reported. DOL reported that as of March 28, 2022, states and territories had identified approximately $35.1 billion in overpayments made in UI programs during the first 7 quarters of the pandemic combined (April 2020 through December 2021). These reported overpayments are not necessarily a result of fraud, though states have reported that some are, and the amount that is due to fraud is not yet fully known.[194] This $35.1 billion in reported overpayments includes
States and territories reported recovering about $0.7 billion in overpayments in the PEUC and FPUC programs combined from April 2020 through December 2021 (i.e., during the 7 quarters since these programs were created).[198] In response to a recommendation in our January 2021 CARES Act report, DOL updated its state reporting requirements for the PUA program to include the collection of data on recovered PUA overpayments. As of March 28, 2022, 39 states and territories had reported some data on recovered PUA overpayments, reporting a combined total of about $1.3 billion recovered from April 2020 through December 2021.[199]
When overpayments are not due to fraud or the fault of the claimant, states and territories may waive the recovery of the overpayment in certain circumstances.[200] States and territories reported waiving about $1.6 billion of regular UI, Extended Benefits, PEUC, and FPUC overpayments from April 2020 through December 2021.[201] In response to a recommendation in our March 2021 CARES Act report, DOL updated state reporting requirements for the PUA program in September 2021 to include the collection of data on waived PUA overpayments.[202] As of March 28, 2022, 24 states had reported some data on waived PUA overpayments, reporting a combined total of about $0.4 billion waived from April 2020 through December 2021.[203]
Because of the limited number of states and territories that had reported data to DOL on recovered and waived PUA overpayments as of March 28, 2022, our related recommendations from our January and March 2021 CARES Act reports remain open. Sustained reporting by more states is needed to help inform DOL, policymakers, and the public about the amount of PUA overpayments that states have waived and recovered and about the amount that remains outstanding.
States and territories also report the amounts of overpayments that are due to fraud—a subset of the total overpayment amounts.[204] During the first 7 quarters of the pandemic (April 2020 through December 2021), states and territories reported that about $2.9 billion in overpayments they had identified resulted from fraud across the UI programs, including about $1.2 billion from PUA, $0.9 billion from FPUC, $0.6 billion from the regular UI and Extended Benefits programs, and $0.1 billion from PEUC.[205] However, according to DOL, states do not report such overpayments as fraud-related until investigations are complete and fraud has been confirmed, which may take a long time to accomplish. As a result of ongoing investigations, additional amounts of overpayments due to fraud could be reported in the coming months.
In addition to reporting overpayments, states conduct independent assessments of representative samples of paid and denied claims in permanent UI programs to determine the accuracy of UI benefit payments and estimate the amount and rate of improper payments, including overpayments and underpayments.[206] According to the Office of Management and Budget’s (OMB) paymentacccuracy.gov, DOL reported an estimated improper payment amount of $78.1 billion with an estimated improper payment rate of 18.92 percent for fiscal year 2021.[207] According to DOL officials, the estimated improper payment amount includes the regular UI, Extended Benefits, PEUC, and FPUC programs, and excludes PUA.
According to DOL officials, because PUA has unique and distinct eligibility requirements, applying the improper payment methodology used for the regular UI program and reported on paymentaccuracy.gov is not appropriate. Officials said they are exploring methods to estimate improper payments for PUA that will not be overly burdensome for states. At the end of February 2022, DOL reiterated its plans to submit the improper payment estimation methodology to OMB by June 2022 and to include the estimates in its fiscal year 2022 reporting.[208]
We have previously reported that the identification of improper payments could suggest that a program is vulnerable to fraud; however, it is important to note that fraudulent overpayments are a specific type of improper payment and that improper payment estimates are not intended to measure fraud in a particular program.
DOL continues to address potential fraud in the UI programs, equitable access to UI benefits, and timely payment of those benefits. In early 2022, DOL continued implementing its plan for using $2 billion in funding provided by the American Rescue Plan Act of 2021 to combat potential UI fraud, promote equitable access to UI benefits, and ensure timely payment of those benefits.[209] As we reported in January 2022, DOL deployed teams of experts to states to provide assistance and make recommendations related to payment timeliness, equity, technology, and fraud; solicited grant applications from states to address equity issues; awarded grants to help states address potential fraud and recover overpayments; awarded purchase agreements to vendors that states can use to combat identity-related fraud; and worked with the Social Security Administration to establish a secure incarceration data exchange, among other efforts.
Agency officials said that DOL had taken the following additional actions since our last report to address potential fraud, equitable access, and timely payments.
Began work to deploy expert teams to six additional states, for a total of 18 states. According to DOL officials, as of March 2022, 12 states—Alabama, Colorado, Connecticut, Iowa, Kansas, Kentucky, Nebraska, Nevada, Pennsylvania, Virginia, Washington, and Wisconsin—had received assistance from teams of experts in fraud, benefit payment timeliness, technology, and equity. Officials said expert teams began working with six more states between January and March 2022: Arizona, Delaware, Illinois, Michigan, New Hampshire, and Oregon. For the status of the expert teams’ activities in each of these states as of March 2022, see the figure below.
Status of DOL’s Expert Team Activities in 18 States as of March 2022, By Cohort of Participating States
DOL officials said expert teams have found that states face similar challenges related to adjudication, backlogs, call center operations, and balancing fraud prevention with expedient and equitable payment of benefits. However, they noted that expert teams’ recommendations may need to be contextualized to acknowledge differences between states, including differences in business process workflows, technological capabilities, staff training, and state UI laws. According to officials, examples of expert teams’ recommendations include simplifying communication with claimants, standardizing translation services, streamlining adjudication processes, implementing fraud risk scoring capabilities, and ensuring that states are following guidance from DOL. Officials said they are currently in the process of using the expert teams’ findings to identify best practices and solutions for common challenges, which they plan to make available as a resource for all states.
Reviewed and provided feedback on grant applications from 49 states and territories to address equity issues, and awarded the first two rounds of grants to seven states and the District of Columbia. As we reported in January 2022, DOL solicited grant applications from states for efforts to address equity issues, such as improving access to the regular UI program for individuals with disabilities or for those who have limited or no internet access, and improving parity across all demographic groups and underserved populations.[210] At the end of January 2022, DOL officials said they were in the process of reviewing the grant applications they had received from 49 of 53 states and territories. Officials noted that they were providing feedback and technical assistance to states on a rolling basis to help them meet the requirements for approval. On March 1, 2022, DOL announced it had awarded an initial round of grants totaling $20.5 million to three states—Oregon, Pennsylvania, Virginia—and the District of Columbia. On March 29, DOL announced it had awarded a second round of grants totaling $15.9 million to four states—Alabama, Idaho, Missouri, and New Mexico.
Announced a competitive grant opportunity for states to improve access to the UI program. In January 2022, DOL announced the availability of up to $15 million for selected states to participate in the American Rescue Plan Act UI Navigator Program. According to DOL, the purpose of the program is to help workers learn about, apply for, and, if eligible, receive UI benefits and related services, as well as to support state agencies in delivering timely benefits to workers, especially those who have faced obstacles to accessing UI benefits in the past. Specifically, selected states will partner with community-based organizations experienced in assisting UI claimants or unemployed job seekers to engage in activities that include outreach, training, education, and general assistance with completing applications for unemployment benefits, especially for individuals in groups that are historically underserved, marginalized, and adversely affected by persistent poverty and inequality.[211]
Initiated work to form partnerships with several selected states to analyze UI benefit equity on a limited scale. In early February 2022, DOL noted that it had begun working with several selected states to establish partnerships for sharing UI claims records and wage data with DOL’s Chief Evaluation Office to analyze equity-related indicators, including UI applications and denials by demographic characteristics. According to DOL, though the effort is in its early stages, the analysis is intended to test for demographic differences within and across states, including by race and ethnicity, which can inform efforts to improve program administration and outreach.
Continued to develop modular technology solutions. As we reported in January 2022, DOL officials said they have been working with OMB’s U.S. Digital Service to develop modular technology solutions that can be integrated with state IT systems. In January 2022, officials said they planned to begin pilot testing the first module, which is focused on the claimant experience, with Arkansas and New Jersey in late March 2022. In addition, officials said they held a town hall meeting with states in January 2022 to update them on the claimant experience pilot and share ideas for future pilot projects.
Methodology
To conduct this work, we analyzed regularly reported DOL data for calendar years 2019 through early 2022, having obtained the most recent data on April 4, 2022. We reviewed relevant federal laws and DOL guidance. We interviewed DOL officials about program data and agency actions, and we also interviewed DOL Office of Inspector General officials. In addition, we reviewed data file documentation and written responses from DOL officials. Further, we interviewed DOL officials about the UI database, PUA claims data files, and data on outstanding federal loans to pay UI benefits, specifically related to state-reported data on claims counts, overpayments, payment timeliness, and loan balance amounts. We examined the data for outliers, missing values, and errors. We determined that the DOL data we used were sufficiently reliable for the purposes of this report.
Agency Comments
We provided DOL, OMB, and Treasury with a draft of this enclosure. DOL and Treasury provided technical comments on this enclosure, which we incorporated as appropriate. OMB did not provide any comments.
GAO’s Ongoing Work
In our ongoing work on the UI program, we will soon be issuing three reports that address, among other issues, (1) implementation and administration of CARES Act UI programs; (2) implementation of the PUA program and the experiences of contingent workers during the pandemic; and (3) broad challenges facing the UI system, which includes UI programs that were established prior to and during the COVID-19 pandemic (e.g., the regular UI program, Extended Benefits, PUA, and others). As part of this body of work, we are assessing whether the challenges we and others have identified place the UI system at significant risk of impaired service delivery and financial loss. This ongoing work, once complete, may lead us to designate the UI system as an issue on GAO’s High-Risk List, which highlights federal programs and operations that we have determined are in need of transformation or vulnerable to fraud, waste, abuse, and mismanagement. We also have ongoing work examining (1) measures of the extent of fraud in the UI program and the status of DOL’s fraud risk management efforts; and (2) UI IT systems modernization.
GAO’s Prior Recommendations
The table below presents our recommendations on UI programs from prior CARES Act reports.
Prior GAO Recommendations Related to Unemployment Insurance (UI) Programs
Recommendation
Status
The Secretary of Labor should designate a dedicated entity and document its responsibilities for managing the process of assessing fraud risks to the unemployment insurance program, consistent with leading practices as provided in our Fraud Risk Framework. This entity should have, among other things, clearly defined and documented responsibilities and authority for managing fraud risk assessments and for facilitating communication among stakeholders regarding fraud-related issues (October 2021 report).
Open–not addressed. The Department of Labor (DOL) neither agreed nor disagreed with our recommendation. In late February 2022, DOL clarified that its Employment and Training Administration, in partnership with DOL’s Office of Chief Financial Officer, is responsible for fraud risk management in the UI program. We maintain that, consistent with our Fraud Risk Framework, it is important for DOL to clearly document this designation and these officials’ antifraud responsibilities in policies and procedures.
The Secretary of Labor should identify inherent fraud risks facing the unemployment insurance program (October 2021 report).
Open–not addressed. DOL neither agreed nor disagreed with our recommendation. In late February 2022, DOL reiterated that its current process allows it to identify, evaluate, and manage risks and identify mitigation strategies for such risks. However, DOL also said that it will use our Fraud Risk Framework in its risk assessment activities for the UI program, and that work on developing the assessment in the UI program using the framework will occur in fiscal year (FY) 2022. We will continue to monitor DOL’s fraud risk assessment activities.
The Secretary of Labor should assess the likelihood and impact of inherent fraud risks facing the unemployment insurance program (October 2021 report).
Open–not addressed. DOL neither agreed nor disagreed with our recommendation. In late February 2022, DOL reiterated that its current process allows it to identify, evaluate, and manage risks and identify mitigation strategies for such risks. However, DOL also said that it will use our Fraud Risk Framework to assess the likelihood and impact of inherent fraud risks facing the UI program, and that work on developing the assessment in the UI program using the framework will occur in FY 2022. We will continue to monitor DOL’s fraud risk assessment activities.
The Secretary of Labor should determine fraud risk tolerance for the unemployment insurance program (October 2021 report).
Open–not addressed. DOL neither agreed nor disagreed with our recommendation. In late February 2022, DOL reiterated that its current process allows it to identify, evaluate, and manage risks and identify mitigation strategies for such risks. However, DOL also said that it will use our Fraud Risk Framework to determine fraud risk tolerance for the UI program, and that work on developing the assessment in the UI program using the framework will occur in FY 2022. We will continue to monitor DOL’s fraud risk assessment activities.
The Secretary of Labor should examine the suitability of existing fraud controls in the unemployment insurance program and prioritize residual fraud risks (October 2021 report).
Open–not addressed. DOL neither agreed nor disagreed with our recommendation. In late February 2022, DOL reiterated that its current process allows it to identify, evaluate, and manage risks and identify mitigation strategies for such risks. However, DOL also said that it will use our Fraud Risk Framework to examine the suitability of existing fraud controls for the UI program and prioritize residual fraud risks, and that work on developing the assessment in the UI program using the framework will occur in FY 2022. We will continue to monitor DOL’s fraud risk assessment activities.
The Secretary of Labor should document the fraud risk profile for the unemployment insurance program (October 2021 report).
Open–not addressed. DOL neither agreed nor disagreed with our recommendation. In late February 2022, DOL reiterated that its current process allows it to identify, evaluate, and manage risks and identify mitigation strategies for such risks. However, DOL also said that it will use our Fraud Risk Framework to document the fraud risk profile for the UI program, and that work on developing the assessment in the UI program using the framework will occur in FY 2022. We will continue to monitor DOL’s fraud risk assessment activities.
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments waived in the Pandemic Unemployment Assistance (PUA) program, similar to the regular UI program (March 2021 report).
Open—partially addressed. DOL agreed with our recommendation and on September 3, 2021, issued PUA program guidance and updated instructions for states to report PUA overpayments waived. As of March 28, 2022, 24 states had reported some data on PUA overpayments waived. Sustained reporting by more states is needed to help inform DOL, policymakers, and the public about the amount of PUA overpayments states and territories have waived. We will continue to monitor state reporting of PUA overpayments waived.
The Secretary of Labor should ensure the Office of Unemployment Insurance collects data from states on the amount of overpayments recovered in the PUA program, similar to the regular UI program (January 2021 report).
Open—partially addressed. DOL agreed with our recommendation and on January 8, 2021, issued PUA program guidance and updated instructions for states to report PUA overpayments recovered. As of March 28, 2022, 39 states and territories had begun reporting some data on the amount of PUA overpayments recovered. Sustained reporting by more states is needed to help inform DOL, policymakers, and the public about the amount of PUA overpayments states and territories have recovered. We will continue to monitor state reporting of PUA overpayment recovery data.
The Secretary of Labor should ensure the Office of Unemployment Insurance pursues options to report the actual number of distinct individuals claiming benefits, such as by collecting these already available data from states, starting from January 2020 onward (November 2020 report).
Open—partially addressed. DOL partially agreed with our recommendation. Specifically, DOL agreed to pursue options to report the actual number of distinct individuals claiming UI benefits. However, DOL did not agree with the recommended retroactive effective date of the reporting. In a letter dated March 30, 2021, DOL stated that it had begun developing a new state report that would capture data related to distinct individuals claiming regular UI benefits; DOL estimated that this data collection might begin in early 2022.
In November 2021, DOL officials said their work on the new state report that would capture data related to distinct individuals claiming regular UI benefits had not yet been completed, due to other competing priorities. In late February 2022, officials said they plan to have the new data collection instrument ready to submit for public notice and comment early in 2022.
DOL expressed concerns about the feasibility of states’ reporting this information retroactively, including for the pandemic UI programs, without detracting from their primary obligation for timely and accurate claims processing.
We maintain that DOL should pursue options to report the actual number of distinct individuals claiming UI benefits, retroactive to January 2020. Even if the information is unavailable for some time, these data are vital to understanding how many individuals received UI benefits as well as the size of the population supported by the UI system during the pandemic. Given the substantial investment in UI programs during the pandemic, an accurate accounting of the size of the population supported by this funding may be critical to understanding the efficiency and effectiveness of the nation’s response to unemployment during the pandemic. An accurate accounting may also be critical to helping DOL and policy makers identify lessons learned about the administration and use of regular and expanded UI benefit programs.
The Secretary of Labor should ensure the Office of Unemployment Insurance revises its weekly news releases to clarify that in the current unemployment environment, the numbers it reports for weeks of unemployment claimed do not accurately estimate the number of unique individuals claiming benefits (November 2020 report).
Closed—addressed. DOL’s weekly news release of December 10, 2020, clarified that the numbers reported for weeks of UI benefits claimed do not represent the number of unique individuals claiming benefits.
The Secretary of Labor should, in consultation with the Small Business Administration (SBA) and the Department of the Treasury, immediately provide information to state unemployment agencies that specifically addresses SBA's Paycheck Protection Program (PPP) loans, and the risk of improper payments associated with these loans (June 2020 report).
Closed—addressed. DOL issued guidance on August 12, 2020, clarifying that individuals working full time and being paid through PPP are not eligible for UI. The guidance also clarified that individuals working part time and being paid through PPP would be subject to certain state policies, including state policies on partial unemployment, to determine their eligibility for UI benefits. Further, the guidance clarified that individuals being paid through PPP but not performing any services would similarly be subject to certain provisions of state law. Finally, the guidance noted that an individual receiving full compensation would be ineligible for UI.
Treasury has disbursed about $9.1 billion from the Homeowner Assistance Fund and approved program plans for most states and territories that received an award. However, states and territories have only spent about 1 percent of their allocations. In addition, Treasury has not developed monitoring procedures for the program, which are needed to ensure program compliance and deter improper payments.
Entities involved: Department of the Treasury
Recommendation for Executive Action
The Secretary of the Treasury should develop and implement written procedures to monitor Homeowner Assistance Fund participants’ programs and uses of funds for compliance with program requirements and improper payments. Treasury agreed with our recommendation and said it was developing a monitoring framework for its pandemic recovery programs to identify potential areas of noncompliance for remediation.
Background
The Homeowner Assistance Fund (HAF), created on March 11, 2021, under the American Rescue Plan Act of 2021, provides about $10 billion to mitigate financial hardships associated with the pandemic and prevent mortgage delinquencies and defaults, foreclosures, loss of utilities or home energy services, and displacement of homeowners.[212] Treasury administers the HAF program and disburses allocations to participants—states, territories, tribal entities, and the Department of Hawaiian Home Lands—to develop local programs that provide assistance to homeowners. Treasury calculated HAF allocations for states, Washington, D.C., and Puerto Rico based on their numbers of unemployed individuals and delinquent mortgages (with a minimum allocation of $50 million).[213]
HAF participants can use the funds to assist homeowners with mortgage and utility payments, delinquent property taxes and insurance, and other eligible uses.[214] HAF participants may also commit up to 15 percent of their total award for administrative expenses, planning, community engagement, and needs assessment.[215] Homeowners are eligible to receive HAF assistance if they experienced financial hardship after January 21, 2020, and have income at or below 150 percent of their area median or below 100 percent of the national median (whichever is greater).[216] Participants may also waive, or rely on self-attestations from households that they meet, the program’s income and financial hardship requirements. In addition, HAF participants are required to target at least 60 percent of their funds to assist homeowners with incomes at or below 100 percent of the area median or 100 percent of the national median (whichever is greater). Participants must also prioritize remaining funds to socially disadvantaged individuals.[217]
Participants are required to receive Treasury’s approval of their program plans to receive their full allocation. Treasury provided initial payments to HAF participants equal to 10 percent of their allocation. To receive the remaining 90 percent, participants must submit a HAF program plan for Treasury’s review and approval. HAF plans were required to describe several components, including the needs of local homeowners, program design, performance goals, readiness, and budget. Treasury encouraged participants to use their initial allocations to develop and test pilot programs while it reviewed their HAF plans.
Prior to the HAF program, the federal government took steps to limit mortgage defaults and foreclosures during the pandemic. The CARES Act, enacted in March 2020, temporarily prohibited most foreclosures of federally backed properties and required mortgage servicers to provide borrowers with federally backed mortgages the option to suspend or reduce their mortgage payments, known as forbearance.[218] Federal agencies that guarantee and insure mortgages and the government-sponsored enterprises (which securitize mortgages) extended those provisions and introduced new loss mitigation options to help borrowers modify their loans, repay missed payments, and avoid foreclosure. In addition, the Consumer Financial Protection Bureau amended its regulations for mortgage servicers in June 2021 to establish temporary procedural safeguards intended to limit avoidable foreclosures until January 1, 2022.[219]
Overview of Key Issues
Many borrowers may need assistance from the HAF program as foreclosures resume and borrowers exit forbearances. New foreclosure starts increased by 702 percent (from about 4,100 to 32,900) in one month from December 2021 to January 2022, according to the mortgage data provider Black Knight.[220] According to Black Knight, nearly half of the new foreclosure starts in January 2022 were among borrowers who became delinquent during the pandemic (March 2020 or later). New foreclosure starts increased significantly from December 2021 to January 2022 because the Consumer Financial Protection Bureau’s foreclosure rule limiting new foreclosures expired at the end of December 2021. The agency’s rule went into effect in August 2021 after the federal foreclosure moratorium expired in July 2021. According to Treasury, these foreclosure protections informed its timeline for approving and funding HAF programs. The spike in new foreclosures starts generally reflects the backlog of foreclosures and a return to prepandemic levels (about 43,000 in January 2020).
At the same time, the rate of mortgages that were delinquent for 30 or more days declined to 3.3 percent in January 2022—near the prepandemic rate of 3.2 percent in January 2020—as borrowers exited forbearances and returned to making payments, according to Black Knight. However, available data suggest that some borrowers exiting forbearance may need additional assistance. As of January 2022, about 11 percent of the nearly 8 million borrowers that entered forbearance during the pandemic had not yet exited and repaid their missed payments. An additional 379,000 borrowers had exited forbearance and finished loss mitigation (such as a loan modification or payment deferral) but not resolved their delinquency.
We previously reported that borrowers who were in forbearance or delinquent for extended periods during the pandemic had accrued large arrearages and generally had higher-risk financial characteristics, including lower credit scores and higher ratios of mortgage debt to income. Given that some of these borrowers may need additional assistance to reinstate their mortgage and mitigate other housing-related financial challenges in the coming months, it is critical that HAF participants begin disbursing funds.
Treasury has approved plans for and disbursed full payments to most HAF participants, but most have spent little of their allocation. As of March 2022, Treasury had approved HAF plans for and made second payments to 50 of the 56 state and territorial participants (or 89 percent) and was in the process of reviewing HAF plans for three participants (Iowa, Mississippi, and Virgin Islands). Three participants had not submitted HAF plans (Delaware, Washington, and American Samoa). In addition, Treasury had disbursed about $9.1 billion to all participants through March 20, 2022, including payments to state, territorial, and tribal participants, and the Department of Hawaiian Home Lands.
At the same time, state and territorial participants had spent about $121 million (or about 1 percent) of the nearly $9.4 billion allocated to them, according to interim reporting data provided by Treasury (see figure).[221] Participants had obligated about $331 million (or about 4 percent of their allocations), according to the data.
Status of Homeowner Assistance Fund (HAF) Programs and Percentage of Allocation Spent by State and Territory, as of March 2022
Note: Spending data were unavailable for some participants because they had not submitted interim reports to Treasury by the March 3, 2021 deadline.
Treasury officials we interviewed were in communication with participants that have not submitted HAF plans and expected them to submit plans in the coming months. In addition, Treasury officials said they had provided feedback to the participants that submitted plans but not received approval and were generally waiting for these participants to submit updated HAF plans. According to Treasury officials, the process for developing, reviewing, and approving HAF plans is iterative and occurs in stages. Treasury officials said they introduced the HAF plan requirement to ensure participants develop programs that are compliant and consistent with agency guidance. In addition, the planning requirement encourages participants to consider how they can maximize the benefit of HAF funds and not replace other homeowner protections and loss mitigation options. In general, Treasury provides participants with feedback on their initial HAF plan submissions, which participants are encouraged to incorporate before resubmitting an updated plan for final review and approval.
Monitoring procedures are needed to ensure program compliance. Treasury has not developed and implemented written procedures that describe how it will monitor HAF participants’ compliance with program requirements and efforts to prevent improper payments. Federal internal control standards highlight the importance of designing control activities to achieve objectives and of implementing control activities through policies. According to its interim reporting guidance, Treasury plans to use participant-reported data to monitor compliance with program requirements.[222] The Office of Recovery Programs, which oversees HAF and Treasury’s other pandemic relief programs, is in the process of developing a post-award compliance monitoring process that would apply to all of its programs, according to a Treasury official. In addition, Treasury is in the process of developing monitoring procedures specific to the HAF program. Treasury also plans to monitor compliance through single audits and is developing guidance for external auditors on evaluating participants’ HAF programs for the Office of Management and Budget’s 2022 compliance supplement.
However, Treasury had not finished and implemented any of these monitoring efforts as of late March 2022 and did not provide documentation we could evaluate to assess progress. Treasury required HAF participants to describe in their program plans the staffing, systems, contracts, and partners they planned to use to ensure effective program compliance. Yet, without written and implemented procedures to monitor compliance, Treasury cannot have reasonable assurances that participants have implemented these plans and are meeting program requirements and managing improper payment risks.
It is critical that Treasury clarify its monitoring procedures now as HAF participants begin initiating full programs. We reported in February 2022 that use of self-attestation of eligibility in another Treasury housing assistance program—Emergency Rental Assistance Program—increased improper payment risks, and a lack of timely monitoring procedures limited the agency’s ability to manage those risks and conduct required oversight. As we reported in our framework for managing fraud risks, preventive controls designed to deter improper payments are generally preferable and more cost-effective than managing improper payment risks after agencies have made payments. Written and implemented monitoring procedures will help clarify Treasury’s expectations around such controls.
Agency Comments
We provided Treasury and OMB with a draft of this enclosure. Treasury provided written comments, which are reproduced in appendix X, and technical comments, which we incorporated as appropriate. OMB did not provide comments.
Treasury agreed with our recommendation and stated that it is in the process of establishing a risk-based, data-driven framework for providing accountability and stewardship of recovery programs to achieve program goals and objectives. According to Treasury, this framework will include procedures to analyze participant-reported and single audit data to identify potential areas of noncompliance for remediation. We will continue to monitor how Treasury applies this framework to the HAF program.
Methodology
To conduct this work, we interviewed Treasury officials and reviewed agency data and documentation on HAF program implementation, payments to participants (disbursements), participant expenditures, and oversight. We assessed the reliability of Treasury’s data and found them to be sufficiently reliable for describing HAF payments and expenditures. We evaluated Treasury’s oversight efforts against federal internal controls standards for control activities. We also reviewed data on mortgage delinquencies and foreclosures from Black Knight, a leading provider of mortgage servicing data and analytics. We assessed the reliability of Black Knight’s data and found them to be sufficiently reliable for describing mortgage delinquencies and foreclosures.
GAO’s Ongoing Work
We will continue to monitor HAF participants’ expenditures and Treasury’s oversight efforts in future reports.
Related GAO Products
COVID-19 Housing Protections: Mortgage Forbearance and Other Federal Efforts Have Reduced Default and Foreclosure Risks. GAO-21-554. Washington, D.C.: July 12, 2021
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014
Emergency Rental Assistance: Additional Grantee Monitoring Needed to Manage Known Risks. GAO-22-105490. Washington, D.C.: February 10, 2022
A Framework for Managing Fraud Risks in Federal Programs.GAO-15-593SP, Washington, D.C.: July 28, 2015
Contact Information: Daniel Garcia-Diaz, (202) 512-8678, GarciaDiazD@gao.gov
Advance Child Tax Credit and Economic Impact Payments
Treasury and the Internal Revenue Service took steps to facilitate accurate tax reporting and address likely errors on 2021 tax returns, however, millions of taxpayers may still experience refund delays. Enhanced collaboration and performance measures would strengthen Treasury’s and the Internal Revenue Service’s abilities to clearly communicate key information to individuals eligible for the child tax credit.
Entities involved: Internal Revenue Service and the Department of the Treasury
Recommendations for Executive Action
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should enhance collaboration among departmental components for refundable tax credit communication and outreach efforts by including relevant participants and clearly defining participant outcomes, roles, and responsibilities. Treasury neither agreed nor disagreed with this recommendation, stating that it supports the goal of the recommendation and continues to work with IRS to raise awareness on current and future communication and outreach efforts. We maintain that without additional actions, such as including relevant participants and clearly defining outcomes, roles, and responsibilities, Treasury and IRS will continue to miss opportunities to leverage their resources and expertise on communication and outreach efforts.
The Commissioner of Internal Revenue should enhance internal collaboration among its stakeholder outreach and education offices for refundable tax credit communications and outreach efforts by clearly establishing outcomes, roles, and responsibilities, and by developing resources to facilitate joint interactions and methods to document information sharing. IRS neither agreed nor disagreed with this recommendation, stating that it has clearly established roles and responsibilities for its communication and outreach functions, which coordinate with each other regularly and look for ways to improve their joint efforts. We maintain that IRS offices overseeing stakeholder outreach and education do not consistently document and share key information. Without additional actions, such as developing resources to facilitate joint interactions and methods to document information sharing, IRS will continue to miss opportunities to fully leverage the knowledge and expertise that resides among its staff.
The Commissioner of Internal Revenue should collect sufficient, relevant, and comparable data on the usefulness and accessibility of its communications and outreach efforts for refundable tax credits and use these data to develop performance metrics to assess the effectiveness of ongoing efforts. IRS neither agreed nor disagreed with this recommendation, stating that it obtains feedback, but its efforts are not easily captured or translated into performance metrics. We maintain that IRS is not collecting or using other types of information to assess what aspects of their communications and outreach efforts were effective in reaching different audiences. This data could help inform future IRS efforts to educate individuals about refundable tax credits and more reliably measure the success of such efforts.
Background
The American Rescue Plan Act of 2021 (ARPA) authorized the Internal Revenue Service (IRS) and the Department of the Treasury to issue advance payments of the child tax credit (CTC).[223] As required by ARPA, IRS and Treasury were responsible for issuing half of the CTC through periodic advance payments (advance CTC). Eligible individuals received monthly advance CTC payments from July 2021 through December 2021, unless they elected not to receive the payments.[224] IRS reported that as of April 6, 2022, it had disbursed more than 216.8 million advance payments totaling nearly $93.5 billion—an average payment of $431 (see figure).
Information on Advance Child Tax Credit Payments, July 2021–Dec. 2021, as of April 6, 2022
aAverage number of monthly payments is the average volume of advance child tax credit payments IRS disbursed electronically or by paper check on a monthly basis between July and December 2021.
bTotal number of advance payment opt-outs is the cumulative volume of taxpayers who elected not to receive advance payments.
cAverage number of monthly children beneficiaries is the average volume of qualifying children for whom eligible individuals received advance child tax credit payments on a monthly basis between July and December 2021.
In August 2021, the U.S. Census Bureau’s Household Pulse Survey found that individuals who received the July 2021 advance CTC payment reported less financial hardship and food insufficiency after receiving the payment.[225] Survey results collected after the advance CTC payments ended found that more households with children had difficulty paying for usual household expenses.[226]
Advance CTC payments. In general, to determine advance CTC payments, IRS used the reported information on an individual’s most recent tax return to estimate the total amount of the CTC that an individual qualified for under the law.[227] Beginning in July 2021, IRS sent 50 percent of that amount divided across 6 monthly payments to recipients. In 2022, individuals were required to file a 2021 tax return to receive the remaining portion of the credit. At that time, individuals were responsible for reporting the total amount of advance CTC payments they received in 2021.
When IRS processes an individual’s 2021 tax return it determines whether the individual claimed the correct amount of the 2021 CTC based on the individual’s filing status, modified adjusted gross income, and number of qualifying children. IRS then calculates the difference between the total 2021 CTC and the amount received in advance payments. Based on these calculations, individuals may receive a higher amount of CTC as a federal tax refund or a reduction in federal income taxes owed. In other circumstances, some individuals may owe a balance in excess of their refund.[228]
Economic Impact Payments. Treasury and IRS also issued a third round of Economic Impact Payments (EIP 3) to most eligible individuals.[229] IRS reported that as of December 31, 2021, it had disbursed more than 175 million EIP 3 payments totaling over $409 billion.[230] Eligible individuals who did not receive EIP 3—or their maximum applicable EIP 3 amounts—could claim a recovery rebate credit (RRC) on their 2021 tax return.[231]
IRS began accepting and processing 2021 tax returns on January 24, 2022.[232] Additionally, IRS issued a revenue procedure for individuals who were not otherwise required to file 2021 federal income tax returns.[233] The procedure provided instructions for individuals to file simplified returns to receive the CTC, the RRC, and the earned income tax credit (EITC). The procedure also provided instructions for individuals to file electronic returns if they have zero adjusted gross income.
Overview of Key Issues
IRS is working to address return errors, but some refund delays are likely. IRS has taken several steps since the 2021 filing season to facilitate accurate tax reporting and address likely errors on returns filed in 2022. However, millions of taxpayers may still experience refund delays during the 2022 filing season.
As we reported, IRS experienced multiple challenges during the 2021 filing season as it struggled to respond to an unprecedented workload that included delivering COVID-19 relief. In late January 2022, IRS began the 2022 filing season with about 4 million unprocessed 2021 individual tax returns. As of early April 2022, this volume had decreased to about 2.4 million individual returns. IRS is processing the remaining backlogged 2021 returns and incoming 2022 returns simultaneously.
To help individuals file accurate 2021 tax returns during the 2022 filing season, IRS took several steps. Starting in December 2021, IRS began mailing millions of letters to advance CTC and EIP 3 recipients. The letters contained information on the total amount of advance CTC and EIP 3 payments individuals received in 2021. Through notices, alerts, and press releases, IRS also encouraged recipients to access the “Your Online Account” webpage to retrieve information on the total amount of payments received in 2021. IRS also continuously revised its FAQ for both the advance CTC and the RRC.
IRS officials said IRS is trying to answer most advance CTC and EIP 3 questions through automated phone services. Callers may use an interactive voice program to receive answers to some frequently asked questions or may speak with a live assistor who can help with general advance CTC or EIP 3 questions.[234] Callers who still have questions may then be redirected to an IRS customer service representative, who has access to taxpayer accounts. However, callers may have a difficult time reaching IRS representatives due to high call volumes. In November 2021, IRS estimated that customer service representatives would be able to answer about 35 percent of incoming calls during the 2022 filing season.[235] From January to late March 2022, IRS representatives answered almost 16 percent of taxpayers’ calls seeking live assistance.
IRS could still face challenges to quickly reconcile the advance CTC payments and issue refunds. From January to November 2021, IRS held for review about 35 million individual and business 2020 tax returns in its Error Resolution System.[236] In mid-2021, IRS projected that about 20 million 2021 tax returns could have advance CTC errors and 6 million returns could have EIP 3 errors.
IRS officials said they created an automated tool to use during the 2022 filing season to identify electronically filed tax returns with specific errors related to advance CTC and EIP reconciliation. IRS officials said the tool would save processing time by automatically addressing these errors. IRS staff must manually review individual tax returns suspended due to errors that cannot be automatically addressed by the tool. As we have previously reported, the need to manually review and correct errors during the 2021 filing season led to refund delays of up to several months for millions of taxpayers.[237] As of February 28, 2022, IRS had processed over 11 million 2021 individual tax returns claiming the CTC and over 2 million returns claiming the RRC. As of March 30, 2022, IRS officials said that IRS has resolved 7.2 million returns with errors using the automated tool.
Taxpayer Advocate Service officials and some of IRS’s tax industry partners raised concerns about CTC-related mistakes that cannot be automatically addressed. They said the advance CTC notification letter that IRS sent may be confusing to married couples who file their taxes jointly. Couples may be confused because IRS sent separate letters to each spouse. Each letter reported half the total payment amount received but the total number of reported children. The letter instructs couples to add the two amounts when they file. However, if the letters have identical amounts, individuals and their preparers may not realize they need to add the two amounts. IRS officials said it sent separate letters because they cannot know an individual’s 2021 filing status until the return is filed. There is also the risk that taxpayers may throw away the letters, not realizing the letters contain tax information. IRS officials said to mitigate these risks, IRS placed “Important Tax Document Enclosed” on the advance CTC notification envelope and formatted the letter to look like a tax statement. Additionally, IRS issued FAQs and press releases.
Tax industry partners and Low Income Taxpayer Clinic officials said they were also concerned about situations when a child custody agreement is not clear. To help address this challenge, IRS officials said it issued FAQs to include commonly asked shared custody questions. As we have previously reported, child custody issues are an ongoing challenge for IRS’s administration of refundable tax credits that have child residency and relationship requirements.
IRS efforts to authenticate the identity of online account users raise security, privacy, and access concerns. As we reported in October 2021, IRS contracted with a third-party vendor for ID.me licenses for identity proofing and authentication for the CTC Update Portal.[238] In November 2021, IRS stated that several IRS online services, including Your Online Account, would require individuals to establish a new account with ID.me by summer 2022 to access their tax records.
In January 2022, the Information Technology Acquisition Advisory Council (IT-AAC)—a nonprofit, public-private partnership that works with federal agencies to identify and meet IT modernization and cybersecurity challenges—sent an initial letter to IRS expressing concerns about privacy, security, and access issues that were disproportionately affecting lower-income individuals related to IRS’s use of ID.me licenses. Additionally, numerous members of Congress expressed their concerns with IRS’s use of facial recognition technology to verify individuals’ identities to access IRS’s online services.
Treasury and IRS took several steps to respond to these concerns. On February 21, 2022, IRS announced a temporary solution for individuals to access IRS online services during the 2022 filing season. IRS stated that individuals could choose to verify their identity virtually with an ID.me agent without the need to provide a selfie. ID.me officials said that as of March 13, 2022, the wait time to see an ID.me virtual agent was approximately 20 minutes. Individuals still had the option to authenticate their identities using biometric information, and IRS stated that new requirements were in place to ensure that the images were deleted. On March 15, 2022, ID.me officials told IRS that between March 4 and March 11, 2022, ID.me deleted the biometric data for approximately 11 million existing account holders. However, IRS officials said that affected individuals were not notified that their biometric information had been deleted.
According to IRS officials, IRS has also been working with the General Services Administration to provide a second option—Login.gov—that the public can use to sign in to access IRS online services.[239] IRS officials said that Login.gov will not be available until it meets federal standards for fraud and security. Officials anticipate Login.gov will be available for IRS users in November or December 2022. In the meantime, individuals will have to authenticate their identity using the revised ID.me processes.
As we reported in June 2018, designing authentication programs involves a balancing act—IRS needs to prevent fraudsters from using stolen taxpayer information to authenticate, but it must balance that against the burden of authentication on legitimate taxpayers. If IRS makes the authentication process too stringent, legitimate taxpayers may not be able to successfully authenticate.
IRS and Treasury missed opportunities to collaborate on outreach efforts related to the child tax credit. IRS and Treasury worked with federal, state, and local partners to encourage individuals to file taxes to claim credits they were eligible to receive, but missed opportunities to collaborate.
IRS led efforts to educate individuals about refundable tax credits, including the advance CTC, and available resources to file a 2021 tax return. IRS provided multilingual outreach resources, both online and in printed notices. IRS leveraged its partnerships with tax professionals to disseminate information to their clients and coordinated with the Federation of Tax Administrators to share information with state and local governments. These governments may use Coronavirus State and Local Fiscal Recovery Funds to conduct outreach efforts to increase individual uptake of federal tax credits.[240] During the 2022 filing season, IRS conducted in-person events to help individuals file a tax return.[241] IRS identified 89 Taxpayer Assistance Centers to conduct “Taxpayer Experience Days” that provided individuals more opportunities for in-person assistance while filing a return. As of March 12, 2022, IRS officials said over 5,000 individuals attended these events.[242]
Treasury also engaged in outreach activities focused on educating individuals about the CTC. According to Treasury officials, they worked with community-based organizations to train “navigators”—community-based guides—to help enroll individuals for the CTC. On January 24, 2022, Treasury and White House officials announced a new website, ChildTaxCredit.gov to help individuals file their taxes and access the remainder of the CTC or the full amount of the CTC. The website also provides resources and tools for partners to help reach families about the CTC and the EITC (a separate refundable tax credit for which many low-income workers are eligible). Treasury and the White House also conducted a Day of Action on February 8, 2022, to encourage state, local, and nonprofit organizations to assist individuals in filing taxes to receive the CTC and other refundable credits.
However, Treasury and IRS missed opportunities to collaborate on these outreach efforts. For example, some key IRS officials responsible for stakeholder partnerships, education, and communications, said they were not involved in the planning of the Day of Action event. The officials said they were first notified of the event 4 days prior when Treasury officials requested that IRS review the materials Treasury had developed, and IRS provided Treasury with its contact list. IRS officials also said they were not involved in the development or launch of the Treasury and White House website. Treasury officials said their intent with the ChildTaxCredit.gov website was to create a plain-language resource on a trusted government domain for new or infrequent tax filers. As of April 11, 2022, IRS.gov did not include a link to ChildTaxCredit.gov on its website.
According to federal standards on internal control, management should internally communicate the necessary quality information to enable personnel to perform and achieve agency objectives. Moreover, we have previously identified leading practices that agencies can use to enhance and sustain their collaborative efforts that include clearly defining outcomes, roles, and responsibilities. According to Treasury officials, Treasury and IRS meet weekly to coordinate outreach and to ensure they are sharing consistent information. Regularly-scheduled meetings with relevant participants are one helpful tool for collaboration. Developing materials aimed at different audiences can also be helpful. Even so, some key IRS officials said they were not always aware of Treasury’s efforts. The lack of collaboration and transparent communication between Treasury and IRS resulted in a missed opportunity to leverage resources and expertise on communication and outreach efforts.
IRS missed opportunities to coordinate internally on child tax credit outreach. Various IRS offices overseeing stakeholder outreach and education—such as Communications & Liaison and Stakeholder Partnerships, Education and Communication—missed opportunities to collaborate internally and leverage their expertise and resources to establish new community partnerships. According to IRS officials, each of these offices independently maintain contact lists of stakeholders and community partners, but there are no formal mechanisms for sharing this information. IRS officials also said that staff from these offices conduct informal discussions on their outreach efforts, but the results of these meetings are not documented and thus are not disseminated among offices. We have previously reported that practices such as developing resources to facilitate joint interactions and methods to document information sharing can also enhance collaboration.
In January 2021, IRS issued the Taxpayer First Act Report to Congress, which included a new Taxpayer Experience Strategy.[243] According to IRS, the report included input and feedback from taxpayers, tax professionals, and the tax community on how to improve the taxpayer experience. Among other things, the Strategy described the need to reorganize outreach and education functions to eliminate redundant activities, better leverage best practices, realize economies of scale, and amplify its reach and effectiveness with messaging spanning across its service and compliance programs. On March 4, 2022, IRS announced the establishment of the new Taxpayer Experience Office to help drive the agency’s strategic direction for improving the taxpayer experience. Establishing the new office could provide a timely opportunity to implement the Taxpayer Experience Strategy and by doing so, address the internal collaboration challenges we observed. In the meantime, IRS will continue to miss opportunities to fully leverage the knowledge and expertise that resides among its staff.
IRS lacks performance data and measures to evaluate the effectiveness of refundable tax credit outreach efforts. IRS has developed communications plans and strategies for each of the following: EIP, RRC, the advance CTC, refundable tax credits, and the 2021 and 2022 filing seasons. However, these plans and strategies do not include metrics for assessing the usefulness and accessibility of these outreach efforts. Such metrics would inform management of these efforts and help focus resources on what works. According to federal standards on internal controls, management should establish and operate monitoring activities and evaluate the results. Moreover, management should use information that is sufficient, relevant, timely, and comparable to make informed decisions and evaluate the agency’s performance in achieving key objectives.
According to IRS officials, IRS has an informal process for collecting and responding to partners’ and stakeholders’ feedback in real time. IRS officials said this allows them to adjust their messaging through press releases, social media updates, and changes to their FAQ page to address taxpayer questions and other issues as they learn about them. However, they are not collecting or using other types of information that could be helpful for assessing the usefulness or accessibility of their communications and outreach efforts. For example, in the Taxpayer Experience Strategy, IRS described plans to conduct three to five case studies in fiscal year 2021 to assess whether improved and increased social media presence influences taxpayer behavior. IRS officials said that they had not completed this survey because the office responsible for this review had not yet been established. In a March 4, 2022, press release, IRS announced the establishment of the new Taxpayer Experience Office, with plans to add staff in the coming months.
Although the EIP and advance CTC outreach efforts are now complete, IRS plays a key role and devotes considerable resources to educating taxpayers as well as those who are not in contact with the tax system about other refundable tax credits and eligibility. These include the EITC, the Child Tax Credit, and Additional Child Tax Credit, which provide tax benefits to millions of taxpayers—many of whom are low-income—who are working and raising children. For the past 2 years, through three rounds of economic impact payments and 6 months of advance CTC payments, IRS expanded its outreach and communication efforts to a larger and diverse audience. IRS’s outreach efforts included first-time filers as well as individuals who do not have a filing requirement and do not generally interact with the IRS. IRS’s communication efforts informed individuals about their eligibility for these payments and the claims process. Without sufficient, relevant, timely, and comparable data on its outreach efforts, IRS is missing information it could use to develop performance metrics and assess which aspects of their communications and outreach strategy were effective in reaching different audiences. Collecting information on the usefulness and accessibility of the various outreach efforts from the past 2 years could help inform future IRS efforts to educate individuals about refundable tax credits and more reliably measure the success of such efforts.
Methodology
To conduct this work, we examined Treasury and IRS data as of April 2022, in addition to federal laws and agency guidance. We interviewed Treasury and IRS officials to determine whether the data were sufficiently reliable to describe the number and amount of payments disbursed, and we determined that the data were sufficiently reliable for this purpose. We also interviewed Social Security Administration officials to learn about their coordination with Treasury and IRS to inform and respond to the public about the advance CTC. We also interviewed several IRS industry partners such as external organizations, for-profit businesses, and software developers. We conducted two discussion groups with 11 IRS Relationship Managers representing a mix of regions and urban and rural areas to receive examples of IRS’s community outreach efforts. Their views cannot be generalized to all Relationship Managers.
Agency Comments
We provided Treasury, IRS, and the Office of Management and Budget with a draft of this enclosure. Treasury and IRS provided comments, which are reproduced in appendix IX and X, respectively. The Office of Management and Budget did not provide comments on this enclosure.
In its comments, reproduced in appendix X, Treasury neither agreed nor disagreed with our first recommendation. Treasury stated that it supports the goal of our recommendation and continues to work with IRS to help ensure that all eligible families receive the remaining amount of the CTC on their 2021 tax return. Additionally, Treasury stated it continues to work with IRS on other credits such as the EITC and will coordinate with IRS regarding future outreach efforts. As we reported, Treasury and IRS have taken actions to inform individuals to file their taxes to claim credits they were eligible to receive. Still, some key IRS officials responsible for stakeholder partnerships, education, and communications said they were not always aware of Treasury’s efforts. The lack of collaboration and transparent communication between Treasury and IRS resulted in a missed opportunity to leverage resources and expertise on communication and outreach efforts.
In its comments, reproduced in appendix IX, IRS neither agreed nor disagreed with our other recommendations. In regard to our recommendation to enhance internal collaboration, IRS stated it has established roles and responsibilities for its communication and outreach functions. IRS also stated that all relevant functions continue to be involved in a coordinated communication, education, and outreach effort designed to inform and educate taxpayers about the availability of tax benefits under the American Rescue Plan—including eligibility requirements—and steps required to claim those benefits.
As we reported, IRS has expanded its outreach and communication efforts to reach a larger and more diverse audience. However, IRS also missed opportunities to collaborate internally and leverage employee expertise and resources to establish new community partnerships. For example, IRS offices overseeing stakeholder outreach and education independently maintain contact lists of stakeholders and community partners, but there are no formal mechanisms for documenting or disseminating this information. IRS’s new Taxpayer Experience Strategy includes plans to reorganize its outreach and education functions to eliminate redundant activities, better leverage best practices, realize economies of scale, and amplify its reach and effectiveness with messaging spanning across its service and compliance programs. Until IRS completes these efforts, it will continue to miss opportunities to fully leverage the knowledge and expertise that resides among its staff.
In regard to our recommendation to collect relevant data and develop performance metrics to assess the effectiveness of outreach and communications efforts, IRS stated that it obtains feedback through activities such as conducting surveys and monitoring social media trends. IRS further stated that during crisis periods like the pandemic, this ad hoc feedback is critical for communications and outreach leadership to quickly adapt and adjust efforts to address emerging issues. IRS also stated that in many situations, spending the time solving and addressing emerging issues can be a much more efficient use of limited staffing resources than simply logging data.
We recognize and have reported on the value of IRS’s informal processes for collecting and responding to partners’ and stakeholders’ feedback. However, as we have also reported, IRS is not collecting or using other types of information that could be helpful for assessing the usefulness or accessibility of their communications and outreach efforts. As the country moves beyond the crisis of the pandemic, IRS has an opportunity to assess what aspects of their communications and outreach efforts were effective in reaching different audiences, including individuals experiencing poverty or financial hardship and in need of economic assistance. Collecting information on the usefulness and accessibility of the various outreach efforts from the past 2 years requires a more comprehensive process than simply relying on anecdotal feedback. IRS should initiate steps to collect sufficient, relevant, and comparable data on the usefulness of its communications and outreach efforts for refundable tax credits and use these data to develop performance metrics to assess the effectiveness of future and ongoing efforts.
GAO’s Ongoing Work
We continue to monitor IRS’s and Treasury’s progress to reconcile the advance CTC and EIP 3 payments as part of our 2022 filing season audit. We will continue to monitor IRS’s and Treasury's efforts to improve communication and outreach to those without a filing requirement.
GAO’s Prior Recommendations Related to Economic Impact Payments and Advance Child Tax Credit
The table below presents our recommendations on the advance child tax credit and economic impact payments from our prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to Advance Child Tax Credit and Economic Impact Payments
Recommendation
Status
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should estimate the number of individuals, including nonfilers, who are eligible for advance child tax credit payments, measure the 2021 participation rate based on that estimate, and use that estimate to develop targeted outreach and communications efforts for the 2022 filing season; the participation rate could include individuals who opt in and out of the advance payments (October 2021 report).
Open-Not addressed. The Department of the Treasury neither agreed nor disagreed with this recommendation, stating that while it supports the goal of the recommendation, it has not estimated the eligible population for the advance child tax credit. Treasury also stated that it and the Internal Revenue Service (IRS) continue to undertake advance child tax credit outreach, education, and media campaign efforts.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should release interim findings on the effectiveness of the notices it sent in September 2020 to nonfilers who are potentially eligible for economic impact payments; incorporate that analysis into IRS outreach efforts as appropriate; and then, if necessary, release an update based on new analysis after the 2021 filing season (July 2021 report).
Open—not addressed. The Department of the Treasury neither agreed nor disagreed with this recommendation and stated that it shares the underlying goal of reaching as many nonfilers as possible to encourage them to claim Economic Impact Payment (EIP) online. However, Treasury does not plan to release any interim findings until it completes its analysis. According to Treasury officials, they needed additional time to process and analyze data as the 2021 filing season was extended to October 15, 2021. Treasury officials also said outreach efforts for the advance Child Tax Credit (CTC) included reminders that individuals who had not filed a 2020 federal income tax return could be eligible to receive EIP and recovery rebate credits (RRC).
According to Treasury officials, in December 2021, they started to analyze the income tax filing responses of individuals who were mailed the first-round EIP outreach letters in September 2020. They said that preliminary results—which could change as more data become available—suggest that the letters to non-filers modestly increased take-up of the first-round EIP.
The Commissioner of Internal Revenue should periodically review control activities for issuing direct payments to individuals to determine that the activities are designed and implemented appropriately as IRS disburses a third round of economic impact payments (EIP 3) and prepares for advance payments on the child tax credit. These control activities should include appropriate testing procedures, quality assurance reviews, and processes that ensure payments distributed by tax partners reach the intended recipients (March 2021 report).
Closed—addressed. IRS took steps to implement our recommendations, such as updating control procedures for issuing direct payments to individuals. Additionally, individuals had the opportunity to update their bank account information during the 2021 filing season, which ran from February 12 through May 17, 2021.
IRS officials said that the updated procedures resulted in the transmission of a small number of EIP 3 payments to incorrect bank accounts. The officials said they anticipated the same for July 2021 advance CTC payments.
The number of direct payments that were rejected was over 5.3 million for the second round of EIP and close to 2.5 million for EIP 3. Additionally, over 500,000 direct payments were rejected for the July 2021 advance CTC payments.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should begin tracking and publicly reporting the number of individuals who were mailed EIP notification letter and subsequently filed for and received an EIP and should use that information to inform ongoing outreach and communications efforts (November 2020 report).
Open—partially addressed. Treasury and IRS agreed with this recommendation. According to Treasury officials, Treasury began analyzing data in January 2021 on those individuals who received a notice and subsequently filed for, and received, a first-round EIP (EIP 1). According to Treasury officials, they needed additional time to process and analyze data, because the 2021 filing season had been extended to October 15, 2021. Treasury officials also said that outreach efforts for the advance CTC included reminders to individuals who had not filed a 2020 federal income tax return that they could be eligible to receive EIPs and RRC.
According to Treasury officials, in December 2021, they started to analyze the income tax filing responses of individuals who were mailed the first-round EIP outreach letters in September 2020. They said that preliminary results—which could change as more data become available—suggest that the letters to non-filers modestly increased take-up of the first-round EIP.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should make estimates of eligible recipients who have yet to file for an EIP, and other relevant information, available to outreach partners to raise awareness about how and when to file for EIPs (September 2020 report).
Open—partially addressed. Treasury and IRS neither agreed nor disagreed with this recommendation, but they took some actions that were consistent with it. For example, in September 2020, the agencies used tax return information to identify nearly 9 million individuals who had not received an EIP 1 and then notified these individuals that they may be eligible for a payment. The letters also provided instructions for requesting a payment. In addition, IRS publicly released detailed zip code data from the notices to help community outreach partners with their own outreach efforts.
Treasury officials said they needed additional time to process and analyze the data to determine who did or did not claim an EIP or RRC, because the 2021 filing season had been extended to October 15, 2021. Officials also said that a challenge to conduct this analysis is the information tax returns used in developing the September 2020 notices do not contain enough information to determine eligibility, limiting Treasury’s ability to make a determination.
Treasury officials said that because of resource constraints, Treasury and IRS focused on delivering the advance CTC. In June 2021, Treasury published a file containing, by zip code, the number of children who may be eligible to be claimed for the advance CTC but who had not been claimed on a recent tax return.
The Secretary of the Treasury, in coordination with the Commissioner of Internal Revenue, should update and refine the estimate of eligible recipients who have yet to file for an EIP to help target outreach and communications efforts (September 2020 report).
Open—partially addressed. Treasury and IRS neither agreed nor disagreed with this recommendation, but they took some actions that were consistent with it. For example, in January 2021, Treasury revised its estimate of eligible recipients who had not yet filed for an EIP 1 to 8 million. According to Treasury officials, this estimate is based on the 9 million notices IRS sent in September 2020. Treasury officials stated that some of the 9 million recipients likely have since claimed the EIP, but Treasury did not provide data supporting this claim.
Treasury officials said they needed additional time to process and analyze the data to determine who did or did not claim an EIP or RRC because the 2021 filing season was extended to October 15, 2021. Officials also said that a challenge to conducting this analysis is that the information tax returns used in developing the September 2020 notices do not contain enough information to determine eligibility, limiting Treasury’s ability to make these determinations.
Treasury officials said that because of resource constraints, Treasury and IRS focused on delivering the advance CTC. In June 2021, Treasury published a file containing, by zip code, the number of children who may be eligible to be claimed for the advance CTC but who had not been claimed on a recent tax return.
According to Treasury officials in December 2021, they started to analyze the income tax filing responses of individuals who were mailed the first-round EIP outreach letters in September 2020. They said that preliminary results—which could change as more data become available—suggest that the letters to non-filers modestly increased take-up of the first-round EIP.
The Commissioner of Internal Revenue should consider cost-effective options for notifying ineligible recipients on how to return payments (June 2020 report).
Closed—addressed. Treasury and IRS took steps to implement our recommendation, such as requesting on the IRS website that individuals voluntarily mail the appropriate EIP amount sent to decedents back to IRS, for both electronic and paper check payments. Treasury has also held and canceled payments made to decedents, along with payments that have been returned. As of April 30, 2021, around 57 percent (just over $704 million) of the $1.2 billion in EIP 1 sent to deceased individuals had been recovered.
As of March 2021, Treasury and IRS had not taken any further action to recoup unreturned payments to decedents. IRS officials determined that further actions, such as initiating erroneous refund cases against decedents’ estates that had not returned payments, could be burdensome to taxpayers, the federal court system, and IRS. As a result, IRS officials concluded that doing so was not prudent at that time.
Tax Filing: 2021 Performance Underscores Need for IRS to Address Persistent Challenges.GAO-22-104938. Washington, D.C.: April 11, 2022.
Tax Filing: Preliminary Observations on IRS’s Efforts to Address Persistent Challenges. GAO-22-105802. Washington, D.C: February 17, 2022.
Refundable Tax Credits: Comprehensive Compliance Strategy and Expanded Use of Data Could Strengthen IRS's Efforts to Address Noncompliance. GAO-16-475. Washington, D.C.: May 27, 2016.
Identity Theft: IRS Needs to Strengthen Taxpayer Authentication Efforts. GAO-18-418. Washington, D.C.: June 22, 2018.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
Managing For Results: Key Considerations for Implementing Interagency Collaborative Mechanisms.GAO-12-1022. Washington, D.C: September 27, 2012.
Contact information: James R. McTigue, Jr., (202) 512-6806, mctiguej@gao.gov
The Small Business Administration has partially addressed the four prior recommendations we made for the Economic Injury Disaster Loan program for COVID-19, to assess and manage fraud risks, develop an oversight plan, and develop and implement portfolio-level data analytics. In December 2021, the agency provided a fraud risk assessment that had been prepared by its contractor, and in February 2022, it designated an antifraud entity that will be responsible for developing a comprehensive antifraud action plan. In March 2022, agency officials said they were working with a vendor to develop portfolio-level analytics. Looking forward, lessons learned from the program—which include the importance of incorporating strong internal controls from the beginning of the program, taking steps to assess and manage fraud risks, and ensuring clear communication with small businesses—could be applied to future emergency lending and grant programs.
Entities involved: Small Business Administration
Background
Since March 2020, the Small Business Administration (SBA) has provided over $348 billion in loans and $7.6 billion in grants (called advances) through the Economic Injury Disaster Loan (EIDL) program to assist small businesses and nonprofits experiencing economic injury caused by COVID-19.[244] SBA provided these funds as a result of legislative actions and changes to certain EIDL program application requirements that were in place under the Small Business Act (see table).
For example, in the Paycheck Protection Program and Health Care Enhancement (PPPHCE) Act, enacted on April 24, 2020, Congress appropriated $50 billion in loan credit subsidies for SBA to cover the cost of making EIDL loans.[245] Additionally, in the CARES Act and the PPPHCE Act, Congress appropriated $20 billion for EIDL advances, a new component of the program that provided direct payments of up to $10,000 to qualifying small businesses that did not have to be repaid.[246] On July 11, 2020, SBA announced that it had fully allocated the $20 billion in funding for EIDL advances.
On December 27, 2020, under the Consolidated Appropriations Act, 2021, Congress appropriated an additional $20 billion for targeted EIDL advances to eligible entities with 300 or fewer employees that are located in low-income communities and experienced an economic loss of greater than 30 percent.[247] Qualifying entities may receive up to $10,000 in targeted advances.[248]
On March 11, 2021, under the American Rescue Plan Act of 2021 (ARPA), Congress appropriated additional funding for entities that qualified for targeted EIDL advances under the Consolidated Appropriations Act, 2021. Congress appropriated an additional $10 billion for eligible entities that have not received the full amount of $10,000 in targeted EIDL advances. Congress also appropriated $5 billion to provide an additional $5,000 in supplemental targeted advances for eligible entities in low-income communities that suffered an economic loss greater than 50 percent and employed not more than 10 employees. The $5,000 is available in addition to advances obtained under the CARES Act or targeted advances under the Consolidated Appropriations Act, 2021.
ARPA also appropriated $70 million for EIDL loans and additional funding for SBA administrative expenses for several programs, including the targeted advance programs and the EIDL loan program. The Infrastructure Investment and Jobs Act, signed into law on November 15, 2021, rescinded $13.5 billion of the EIDL loan appropriations and approximately $17.6 billion from the targeted EIDL advance appropriations.[249]
Key Legislation Affecting the Economic Injury Disaster Loan (EIDL) Program in Response to COVID-19
Legislation and date enacted
Appropriation amount
Key provisions and changes
Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 March 6, 2020
None
Deemed COVID-19 a disaster under the Small Business Act, making economic injury caused by COVID-19 eligible for EIDL loans
CARES Act
March 27, 2020
$10 billion for EIDL advances
Authorized the Small Business Administration (SBA) to provide eligible applicants with EIDL advances of up to $10,000 that do not need to be repaid
Removed the requirement that applicants must not be able to obtain credit elsewhere
Expanded eligibility for the EIDL program
Restricted SBA from obtaining federal tax transcripts as part of the EIDL application process
Paycheck Protection Program and Health Care Enhancement Act
April 24, 2020
$10 billion for EIDL advances and $50 billion for loan subsidies
Expanded EIDL eligibility to agricultural enterprises previously ineligible
Consolidated Appropriations Act, 2021
December 27, 2020
$20 billion for targeted EIDL advances
Removed restriction that SBA cannot obtain federal tax transcripts as part of the EIDL application process
Extended deadline to apply for EIDL loans and advances by 1 year, from December 31, 2020, to December 31, 2021
Provided targeted advances up to the full amount of $10,000 to certain eligible businesses and nonprofits that have fewer than 300 employees, are located in low-income areas, and have experienced at least a 30 percent loss in income
American Rescue Plan Act of 2021
March 11, 2021
$10 billion for targeted EIDL advances and $5 billion for supplemental targeted EIDL advances
Provided additional funding for targeted advances of up to $10,000 for the same entities eligible under the Consolidated Appropriations Act, 2021
Provided an additional $5,000 in supplemental targeted advances for eligible entities in low-income communities that suffered economic loss of greater than 50 percent and employed not more than 10 employees
The Infrastructure Investment and Jobs Act
November 15, 2021
None
Rescinded the unobligated amount up to about $17.6 billion for the targeted EIDL advances provided under the Consolidated Appropriations Act, 2021
Source: GAO analysis of legislation. | GAO-22-105397
Overview of Key Issues
Recent changes and current status of EIDL. On December 31, 2021, SBA stopped accepting both new loan and targeted advance applications. However, already approved borrowers can still request increases up to their maximum eligible loan amount for up to 2 years after their loan origination date, or until the funds are exhausted. Similarly, SBA stopped accepting new reconsideration and appeal requests for EIDL applications after December 31, 2021. It will continue to review requests received on or before that date if the reconsideration or appeal was received within the time frames in the regulation—6 months from the date of decline for reconsiderations and 30 days from the date of reconsideration decline for appeals, unless funding is no longer available.
As of March 3, 2022, SBA had approved more than 3.9 million EIDL loans totaling about $349 billion. According to SBA, the agency has approved more EIDL loans for COVID-19 than for all previous disasters combined. It has assisted more than 3.8 million businesses employing more than 20 million people. SBA has also funded 603,953 targeted advances totaling about $5.3 billion and 455,229 supplemental targeted advances totaling about $2.3 billion as of March 3, 2022.
On March 15, 2022, SBA granted an additional 6-month deferment of principle and interest payments to SBA’s existing COVID EIDL borrowers. Thus, borrowers approved for COVID EIDL loans in calendar years 2020, 2021, and 2022 have a total deferment of 30 months.
Recent data and trends in processing. SBA had a backlog of millions of applications for both loan modifications and for targeted and supplemental targeted advances, according to our analysis of data from the last 6 months of the program, June 1, 2021 through December 31, 2021. (See figure.) Both of these backlogs largely resolved by September 2021. Specifically, applications for loan modifications “in processing” (those SBA had received but not yet made loan decisions for) peaked in June 2021 and remained at more than one million applications until mid-August 2021. Similarly, the backlog of applications for targeted and supplemental targeted advances peaked and remained at more than one million until September 2021.
Number of EIDL Applications in Processing by Type and Week, June 1, 2021 through Dec. 31, 2021
Our analysis for the same 6-month period also showed the following:
SBA approved only 6 percent of new EIDL loan applications, while automatically declining 60 percent of new applications because of reasons including poor credit.[250]
SBA approved 22 percent of the applications for targeted and supplemental targeted advances.[251]
SBA approved 59 percent of applications for loan modifications for existing EIDL borrowers, providing about $140 billion in additional proceeds to borrowers.[252]
Of applicants who had their original application denied by SBA, 60 percent also had their requests for reconsideration or application to appeal denied by SBA.[253]
Lessons learned for future pandemic-related EIDL programs. In response to the adverse effects of the pandemic on small businesses, Congress expanded existing SBA programs, including the EIDL program, and appropriated additional funding to help affected businesses. To help these businesses, SBA rapidly processed loans and advances to millions of small businesses affected by COVID-19. Our evaluation of SBA’s implementation of EIDL in response to COVID-19, along with challenges highlighted by small business industry group representatives and officials from the SBA Office of Inspector General (OIG), offer potential lessons learned for future emergency lending and grant programs.
Incorporate strong internal controls from the beginning of the program. In part to help small businesses quickly, the EIDL program in response to COVID-19 was implemented with fewer safeguards than the traditional EIDL program. For example, SBA normally uses applicants’ federal tax returns to validate elements in an EIDL application, but the CARES Act prohibited SBA from obtaining these returns from applicants.[254] Although SBA stated that its internal controls at the time were robust, officials acknowledged that it was challenging to verify applicant eligibility for EIDL without the ability to obtain tax records.
Our work as well as the work of the SBA OIG indicated potential gaps in internal control that may have led to fraud and the provision of EIDL funding to ineligible entities. As we reported in January 2021, SBA had provided about $182 million in loans and advances to potentially ineligible businesses as of September 30, 2020.[255] Similarly, the SBA OIG reported in October 2020 that its preliminary review revealed strong indicators of widespread potential fraud in the program and that there were indications of deficiencies in internal control.
SBA has begun taking steps to address the recommendation we made in January 2021 to help mitigate the likelihood and impact of fraud. Specifically, in response to our recommendation to develop and implement portfolio-level data analytics across EIDL program loans and advances, SBA has started implementing fraud indicators for EIDL application data. In addition, when SBA transitioned the COVID EIDL program from the Office of Disaster Assistance to the Office of Capital Access (OCA) in July 2021, officials told us that OCA implemented additional controls, such as making the log-in process more secure, to help detect potential fraud. However, by incorporating stronger controls from the beginning of the program, SBA could have prevented additional fraudulent applications from getting approved.
Conduct a risk assessment when designing and implementing a new EIDL program. SBA has a process to identify and address potential risks in programs, but the process was not followed for EIDL in response to COVID-19.[256] Within SBA, two offices are responsible for working with program offices to identify and respond to potential risks. More specifically, the Office of Continuous Operations and Risk Management is responsible for, among other things, agency-wide recovery response for disasters and the evaluation and assessment of SBA’s critical risks and nonfinancial internal controls. In addition, according to an SBA official, when SBA implements a new program, the Office of Internal Controls coordinates with the program office to plan proper internal controls and ensure they are implemented. However, neither office was involved in the design or initial implementation of program controls for EIDL in response to COVID-19.
In addition, according to SBA officials, formal risk assessments for EIDL did not occur, as they usually do, during program planning. As part of its responsibilities, the Office of Continuous Operations and Risk Management oversees SBA’s Enterprise Risk Management program.[257] According to SBA guidance, program offices should identify and assess potential risks to a program, both initially and on an ongoing basis, to identify new, emerging, or changing risks. Potential risks include fraud, improper payments, infrastructure (such as information technology) problems, funding that is insufficient to address program need, or issues with external audits.[258] Once risks have been identified and assessed, SBA guidance states that a program office should strategize its response to minimize the risks and then implement and monitor those plans.
Due to the emergency nature of the program, the EIDL risk assessment did not follow SBA guidance, but rather, according to SBA officials, was conducted informally. Officials also acknowledged that the program faced some nonfraud risks, such as repayment deferment. By including expertise across SBA and following its standard practices regarding risk assessments, SBA could have identified and potentially minimized some risks and challenges, such as the risk that available funding would not be sufficient to meet the needs of small businesses that sought assistance (discussed below). Similarly, completing a risk assessment that included a risk tolerance could have helped SBA better determine what controls needed to be in place, given the need to take action rapidly under the circumstances.
Take early steps to assess and manage fraud risks. While the program began making loans and advances in March 2020, it did not begin to formally assess the potential fraud risks to the program until May 2021. In March 2021, we reported growing concerns about fraud risk management in the EIDL program. Specifically, we noted that the Department of Justice and law enforcement agencies had reported ongoing efforts related to potential fraud. Law enforcement officials we spoke with for that report noted a large number of ongoing investigations and hotline complaints related to loans made under the EIDL program and reported systemic patterns of fraud across EIDL investigations.
Specifically we reported in March 2021 that SBA had not conducted a comprehensive fraud risk assessment in alignment with leading practices, nor documented its antifraud strategy outlining a strategic approach to managing fraud risks to EIDL. Consequently, we recommended in March 2021 that SBA (1) conduct and document a fraud risk assessment for the EIDL program and (2) develop a strategy that outlines specific actions to address assessed fraud risks in the EIDL program on a continuous basis.
SBA has begun taking steps to implement these recommendations. For example, an SBA contractor conducted a fraud risk assessment for EIDL in October 2021. The assessment found that even though SBA implemented controls to minimize fraud over the course of the program—such as implementing potential fraud flags that require manual review and approval prior to the disbursement of EIDL loans and verifying the identity of businesses through public records—EIDL continued to be susceptible to fraud risks that require mitigation and management. The contractor identified 21 active fraud risks in EIDL and made four recommendations to SBA to aid the agency in establishing a fraud governance process and inform its fraud tolerance approach.[259]
If SBA had conducted a fraud assessment earlier in the program, it could have targeted its controls to further minimize risks. Although the timing of the assessment limited its usefulness for managing the program, SBA could use the results of this fraud assessment to inform future emergency lending and grant programs. Based on our initial review of the assessment, SBA adhered to many fraud risk management leading practices, but missed key steps such as determining its fraud risk tolerance.
In addition, we found in March 2021 that one factor that contributed to the lack of a timely fraud risk assessment was that while SBA’s Office of Continuous Operations and Risk Management oversees risk management for the full spectrum of program risks, SBA did not have a dedicated entity to lead fraud risk management activities. As discussed in GAO’s Fraud Risk Framework, it is a leading practice to designate an entity to design and oversee fraud risk management activities. In carrying out its role, the antifraud entity, among other things, manages the fraud risk assessment process. According to documentation provided by SBA, the agency designated such an entity in February 2022 that is responsible for the oversight and coordination of SBA’s fraud risk prevention, detection, and response activities.
Make informed decisions on program design to meet borrower needs. SBA implemented EIDL for COVID-19 based on legislative actions that changed traditional EIDL program requirements in place under the Small Business Act. SBA was faced with making decisions about the design of the program, primarily regarding how to maximize the extent that loans would meet borrower needs. For example, SBA changed the limits on the caps for EIDL loans several times as it attempted to assist as many borrowers as possible but may have hampered some borrowers from obtaining sufficient funds for their economic losses. SBA’s standard operating procedures for EIDL state that the legislative limit of $2 million applies to EIDLs, depending on the financial effect of the disaster.[260] According to SBA officials, when SBA first began to provide EIDLs related to COVID-19, it limited the loans to 6 months of working capital up to a maximum of $500,000. As SBA began to process thousands of applications, the agency lowered the cap to $15,000 for several days as it monitored available funding before restoring the maximum to $500,000. When SBA reopened its EIDL application portal on May 4, 2020, it established the maximum loan amount at $150,000, and on April 6, 2021, SBA increased the loan limit back to $500,000. In September 2021, SBA announced an increase in the limit to $2 million.
SBA officials said they provided assistance to as many small businesses as possible with the funds available, and the program began allowing requests for increases in the original loan amounts. However, for some small businesses, in particular larger small businesses, loan caps were insufficient to cover operating expenses. We reported in July 2021 that for the initial $500,000 loan limit in place from March 16, 2020, through May 3, 2020, SBA approved about 7,000 EIDL loans in the amount of $500,000 for applicants with an economic injury greater than $500,000. The changes in loan limits may have placed these businesses at risk of shuttering because they did not obtain timely funding to cover a better part of their economic losses.
By the deadline for accepting new applications for the EIDL program in response to COVID-19, as discussed above, $13.5 billion of EIDL loan appropriations were unused and had been rescinded. Implementing an approach that maximized meeting the loan demands earlier in the program could have afforded more funding to small businesses and avoided the billions in appropriations that were rescinded.[261]
Ensure clear communication with small businesses. Although SBA moved quickly under challenging circumstances to provide EIDL funding to applicants, we reported in July 2021 that lack of important program information and application status put pressure on SBA’s resources and negatively affected applicants’ experiences. Despite distributing information about the EIDL program through various channels including media, its website, and resource partners, like Small Business Development Centers (SBDCs), SBA did not communicate key information (such as processing times and loan limits) and loan status to potential and actual applicants in an effective, consistent, or timely manner. For example, as discussed above, SBA lowered the loan maximum to $150,000 in May 2020, but did not provide this information on its website, in its press releases, or within the EIDL application. The first time SBA broadly announced the $150,000 loan maximum was in February 2021 when it updated its FAQ document. Consequently, we recommended that SBA develop a comprehensive strategy for communicating with potential and actual program applicants in the event of a disaster.
While SBA had not completed this strategy as of December 2021, it has taken steps and communication has improved over time, albeit to varying degrees, according to industry groups we met with that represent small businesses. For example, industry group representatives noted that SBA did a good job providing information related to program and policy changes in September 2021. However, based on our discussions with these groups in January 2022, borrowers continued to face challenges with customer service, including the inability to communicate with an SBA representative about their specific applications. By providing clear communication, SBA could prevent confusion among applicants and lessen the burden on its Customer Service Center, which was often overwhelmed with calls. Similarly, SBA could better leverage SBDCs to facilitate communication on the program to participants, given their role to partner with the agency in providing support to small businesses.
Methodology
To conduct this work, we reviewed our prior reports on EIDL and reports issued by the SBA OIG. In addition, we analyzed SBA’s data on the processing of loans, targeted advances, and supplemental targeted advances from June 1, 2021 through December 31, 2021. We assessed the reliability of SBA data by interviewing SBA officials. We determined that the data were sufficiently reliable for reporting the status of EIDL loans and targeted advances. We also interviewed small business industry group representatives and SBA officials.
Agency Comments
We provided SBA and the Office of Management and Budget (OMB) with a draft of this enclosure. SBA provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
Our work on the EIDL program is ongoing. We continue to examine the fraud risks in the program. We will also continue to monitor SBA’s progress toward developing and implementing corrective actions to address the material weaknesses identified in December 2020 and November 2021 by its independent financial statement auditor.
GAO’s Prior Recommendations
The table below presents our recommendations on the EIDL program from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to the Economic Injury Disaster Loan Program
Recommendation
Status
The Administrator of the Small Business Administration (SBA) should conduct and document a fraud risk assessment for the Economic Injury Disaster Loan (EIDL) program. (March 2021 report)
Open—partially addressed. SBA agreed with the recommendation, stating that it would work to ensure that a fraud risk assessment for the EIDL program is completed. In December 2021, SBA provided a fraud risk assessment that had been prepared by its contractor. Based on our initial review of the assessment, it adhered to many fraud risk management leading practices, but for example, SBA did not determine its fraud risk tolerance as called for by leading practices. In February 2022, SBA designated an antifraud entity that, according to SBA officials, would be responsible for determining a risk tolerance and implementing the fraud risk assessment’s recommendations. We will continue to monitor the agency's actions to address this recommendation.
The Administrator of SBA should develop a strategy that outlines specific actions to address assessed fraud risks in the EIDL program on a continuous basis. (March 2021 report)
Open—partially addressed. SBA agreed with the recommendation, stating that it would work to ensure that fraud risks are monitored on a continuous basis. In December 2021, SBA provided a fraud risk assessment, which would inform an antifraud strategy. In February 2022, SBA designated an antifraud entity that is responsible for oversight and coordination of SBA’s fraud risk prevention, detection, and response activities. SBA officials previously told us that once designated, the entity would work to develop an agency-wide comprehensive antifraud action plan. We will continue to monitor the agency's actions to address this recommendation.
The Administrator of SBA should implement a comprehensive oversight plan to identify and respond to risks in the EIDL program to help ensure program integrity, achieve program effectiveness, and address potential fraud. (March 2021 report)
Open—partially addressed. SBA agreed with the recommendation, stating that it will implement a comprehensive oversight plan. In February 2022, SBA designated an antifraud entity that is responsible for oversight and coordination of SBA’s fraud risk prevention, detection, and response activities We will continue to monitor the agency's actions to address this recommendation.
The Administrator of SBA should develop and implement portfolio-level data analytics across EIDL program loans and advances made in response to COVID-19 as a means to detect potentially ineligible and fraudulent applications. (January 2021 report)
Open—partially addressed. At the time of our report, SBA neither agreed nor disagreed with this recommendation. In December 2021, SBA stated that the agency had implemented fraud indicators for EIDL application data. SBA also stated that the agency shared these indicators with the Pandemic Response Accountability Committee for review. In March 2022, SBA stated that it was working with a vendor to develop portfolio-level analytics. We will continue to monitor the agency's actions to address this recommendation.
Economic Injury Disaster Loan Program: Additional Actions Needed to Improve Communication with Applicants and Address Fraud Risks. GAO-21-589. Washington, D.C.: July 30, 2021.
Small Business Administration: Disaster Loan Processing Was Timelier, but Planning Improvements and Pilot Program Evaluation Needed. GAO-20-168. Washington, D.C.: February 7, 2020.
Small Business Administration: Leadership Attention Needed to Overcome Management Challenges. GAO-15-347. Washington, D.C.: September 22, 2015.
A Framework for Managing Fraud Risks in Federal Programs, GAO-15-593SP. Washington, D.C.: July 28, 2015.
Contact information: William B. Shear, (202) 512-8678, shearw@gao.gov
As of March 31, 2022, the Federal Reserve’s lending programs (also known as facilities) supported by CARES Act funds had about $16.9 billion in outstanding assets and about $18.8 billion in outstanding loans borrowed from the Federal Reserve Banks. As of the same date, only the Main Street Lending Program’s facilities had reported losses—a total of about $23 million—but these and any future losses are covered by the funding that the Department of the Treasury invested in the Main Street facilities pursuant to the CARES Act. The Federal Reserve’s oversight of the facilities is ongoing and focuses on previously identified risk areas.
Entities involved: Department of the Treasury, Federal Reserve System
Background
In response to the economic effects of COVID-19, the CARES Act authorized at least $454 billion for Treasury to support the Board of Governors of the Federal Reserve System (Federal Reserve) in establishing facilities to provide liquidity to the financial system. With the Secretary of the Treasury’s approval, the Federal Reserve established nine facilities supported by CARES Act funding.[262] These programs were established to provide liquidity to the financial system that supports lending to states, tribes, municipalities, eligible businesses, and nonprofit organizations by purchasing assets (such as qualifying corporate bonds) from, or initiating lending to, eligible entities. In accordance with the Consolidated Appropriations Act, 2021, all nine facilities stopped purchasing assets or extending credit by January 2021. The facilities conducted a total of about $41 billion in transactions.
The Federal Reserve also established four facilities with the Treasury Secretary’s approval that did not receive CARES Act-appropriated funds.[263] These non-CARES Act facilities conducted a total of $403 billion in transactions. They were designed to provide liquidity to the financial sector and businesses. The last of these facilities stopped extending credit on July 30, 2021.
Overview of Key Issues
Status of facilities. As of March 31, 2022, the nine CARES Act facilities had about $16.9 billion in outstanding assets, of which about $12.7 billion were held by the Main Street Lending Program. The facilities also had about $18.8 billion in outstanding loans borrowed from the Federal Reserve Banks managing the facilities. For the non-CARES Act facilities, as of March 31, 2022, a total of about $23.5 billion remained outstanding in loans that eligible lenders borrowed through the Paycheck Protection Program Liquidity Facility—the facility established to encourage use of the Paycheck Protection Program.[264] The other three non-CARES Act facilities have repaid all of their loans to the Federal Reserve Banks.
CARES Act facilities. For the facilities that received CARES Act funds, outstanding assets—that is, assets (for example, corporate and municipal bonds) the facilities purchased and had not disposed of through sale or other means—peaked between November 2020 and January 2021.[265] These outstanding assets have since declined, and as of August 31, 2021, all of the Secondary Market Corporate Credit Facility’s holdings in exchange-traded funds and corporate bond assets had either matured or been sold.[266] Additionally, of the two entities that borrowed from (sold eligible notes to) the Municipal Liquidity Facility, one has repaid all of its borrowings.[267] See the figure below for outstanding assets held by the facilities as of March 2022.
Outstanding Assets of Federal Reserve Lending Facilities Supported by CARES Act Funding, June 2020–Mar. 2022
Note: Beginning on Feb. 24, 2021, the amount of the Main Street Lending Program’s outstanding assets is reported net of an allowance for loan losses, which is updated quarterly. The Main Street lending facilities purchased a participation interest in newly issued eligible loans that eligible lenders made to eligible small and midsized for-profit borrowers and nonprofit organizations.
The Federal Reserve analyzes all of the CARES Act facilities on a quarterly basis to determine if it is necessary to set aside an allowance for potential loan losses in accordance with generally accepted accounting principles. As of December 31, 2021, the most recent data available, only the Main Street Lending Program reflected a loan loss allowance, in the amount of approximately $2 billion.[268] Of this amount, a specific allowance of $1.1 billion is for loans for which it has been determined to be probable that the program will be unable to collect all of the contractual interest and principal payments as scheduled in the loan agreement. The remaining $905 million is a general allowance for all other outstanding loans under the program.
As of March 31, 2022, the most recent data available, the Main Street facilities had reported about $23 million in actual losses. According to Federal Reserve officials, the losses were recognized for a small number of loans due to credit events, such as a bankruptcy filing or other adverse business-related event that led to the acceleration of the loan by the lender or made liquidation or bankruptcy appear imminent. These, and any future losses, are covered by the funding Treasury invested in the Main Street facilities pursuant to the CARES Act. As of January 2022, a total of about $21.3 billion of Treasury’s investment was available to cover losses incurred by the CARES Act facilities. In its most recent report to Congress in April 2022, the Federal Reserve said it continued to expect that none of the facilities will result in a loss to the Federal Reserve.
Non-CARES Act facilities. As of October 14, 2020, the Commercial Paper Funding Facility had fully repaid all loans used to purchase commercial paper (short-term debt issued primarily by corporations). As of May 9, 2021, the Primary Dealer Credit Facility and the Money Market Mutual Fund Liquidity Facility had also fully repaid all loans to Federal Reserve Banks. None of the three facilities resulted in a loss to the Federal Reserve. According to the Federal Reserve’s combined annual financial statement, as of December 31, 2021, the Paycheck Protection Program Liquidity Facility did not require an allowance for loan losses. As of March 31, 2022, a total of about $23.5 billion remained outstanding in loans that eligible lenders borrowed through the facility.
Oversight of facilities. The Federal Reserve’s Division of Reserve Bank Operations and Payment Systems is in its third phase of oversight reviews. The division leveraged findings from previous oversight activities to identify risk areas for continued oversight, including collateral and asset management, conflicts of interest, risk management, and internal controls.[269]
Through its phase two oversight reviews, the division identified opportunities to enhance processes and controls across several facilities. For example, the division noted opportunities to improve a facility’s credit evaluation model and to document facilities’ comprehensive risk assessments. Based on our review of Federal Reserve documents, the facilities have either addressed or continue to make progress in addressing these enhancement opportunities. Federal Reserve officials told us that the division is planning additional oversight reviews and will continue to use previous findings to inform these reviews.
Methodology
To conduct this work, we reviewed Federal Reserve documentation on the facilities, including reports to Congress, and the most recent Federal Reserve data available on the facilities’ outstanding loans and assets, as of March 2022. We assessed the reliability of the data on outstanding asset purchases and loans by reviewing published data on the facilities and obtaining information from Federal Reserve officials on the collection, maintenance, and compilation of the data. We found these data to be reliable for our purposes. We also interviewed Federal Reserve officials.
Agency Comments
We provided a copy of this enclosure to the Federal Reserve, Treasury, and the Office of Management and Budget (OMB) for review. The Federal Reserve and Treasury provided technical comments, which we incorporated where appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
In our ongoing work on the Federal Reserve facilities, we will continue to monitor outstanding assets and loans and the Federal Reserve’s oversight of the facilities.
Related GAO Products
Federal Reserve Lending Programs: Credit Markets Served by the Programs Have Stabilized, but Vulnerabilities Remain. GAO-22-104640. Washington, D.C.: October 19, 2021.
Federal Reserve Lending Programs: Use of CARES Act-Supported Programs Has Been Limited and Flow of Credit Has Generally Improved. GAO-21-180. Washington, D.C.: December 10, 2020.
Contact information: Michael E. Clements, (202) 512-8678, clementsm@gao.gov
The Federal Aviation Administration has obligated nearly all funds and expended nearly $11 billion of the $20 billion made available for grants to help the nation’s airports respond to and recover from the economic effects of the COVID-19 pandemic.
Entity involved: Federal Aviation Administration, within the Department of Transportation
Background
Historic decreases in passenger demand for air travel due to the COVID-19 pandemic significantly affected U.S. airports’ abilities to generate the revenue needed for operating and infrastructure costs. According to data filed with the Department of Transportation (DOT), U.S. airlines carried about 27 percent fewer passengers in calendar year 2021 than in 2019, before the onset of the COVID-19 pandemic. However, according to airport associations, changes in passenger traffic have not been evenly distributed among airports, as some airports have seen stronger rebounds in passenger traffic than others. Airport associations reported that U.S. airports continue to experience an uneven recovery as domestic leisure traffic has begun to recover while international and business travel continues to lag.
The CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021 (ARPA) provided a combined total of $20 billion in federal funding for U.S. airports to respond to the COVID-19 pandemic, although funding allocation and certain allowable uses differ under each act.
Obligations and expenditures. Of the $20 billion combined total in federal COVID-19 relief funding for U.S. airports provided by the CARES Act, Consolidated Appropriations Act, 2021, and ARPA, nearly all has been obligated and nearly $11 billion expended by the Federal Aviation Administration (FAA) as of February 28, 2022, according to FAA officials.[270]
CARES Act. The CARES Act, signed into law on March 27, 2020, provided $10 billion to support U.S. airports of all sizes to prevent, prepare for, and respond to the COVID-19 pandemic. Airport owners—also known as airport sponsors—may use CARES Act grant funds for any purpose for which airport revenues may be lawfully used, including for airport operating expenses, capital improvements, and debt service directly related to the airport.
As of February 28, 2022, FAA had processed CARES Act grant applications for 3,215 U.S. airports and obligated nearly $10 billion in grant funding. As of the same date, FAA had expended over $8 billion to reimburse airports for eligible costs and to increase the federal share for the fiscal year 2020 Airport Improvement Program (AIP) and supplemental discretionary grants, according to FAA officials (see table).
Federal Aviation Administration (FAA) Obligations and Expenditures for CARES Act Airport Grants, as of Feb. 28, 2022
Funding group
Obligations ($ thousands)
Expenditures ($ thousands)
Increase federal share for 2020 Airport Improvement Program (AIP) grantsa
$548,672
$446,272
Commercial service airportsb
$7,195,771
$6,313,085
Primary airportsc
$1,630,750
$1,069,639
General aviation airportsd
$100,459
$81,179
Reallocated CARES Act fundse
$290,775
$232,497
Total
$9,766,427
$8,142,673
Source: GAO analysis of CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020) and data from the FAA. | GAO-22-105397
Note: The CARES Act directed FAA to allocate funding to these groups through various formulas. In addition, the CARES Act provides FAA the authority to retain up to 0.1 percent of the $10 billion (up to $10 million) provided for Grants-in-Aid for Airports to fund the award and oversight by FAA of grants made under the CARES Act. Pub. L. No. 116-136, div. B, tit. XII, 134 Stat 281, 597.
aApproximately 3,300 U.S. airports are part of the National Plan of Integrated Airport Systems and are eligible to receive federal AIP grants to fund the planning and development of eligible infrastructure projects. The CARES Act appropriated at least $500 million to increase the federal share to 100 percent for AIP grants awarded for airport infrastructure projects under fiscal year 2020 and supplemental discretionary grants.
bCommercial service airports are publicly owned airports with at least 2,500 passenger boardings per year and scheduled air service.
cPrimary airports are large, medium, and small hub and non-hub airports with more than 10,000 passenger boardings per year.
dGeneral aviation airports are public-use airports with fewer than 2,500 passenger boardings per year or no scheduled air service.
eUnder the Consolidated Appropriations Act, 2021, unallocated CARES funds as of December 27, 2020 were to be allocated under the Consolidated Appropriations Act, 2021 using the primary commercial service and certain cargo airports allocation formula. According to FAA officials, FAA calculated that $290,774,557 in CARES Act funds were available for reallocation under the Consolidated Appropriations Act, 2021.
Consolidated Appropriations Act, 2021. The Consolidated Appropriations Act, 2021, enacted on December 27, 2020, provided $2 billion in additional federal grants to help eligible airports and certain airport concessions prevent, prepare for, and respond to COVID-19.[271] Airports must use Consolidated Appropriations Act, 2021 grant funding for costs related to operations, personnel, cleaning, sanitization, janitorial services, combating the spread of pathogens at the airport, and debt service payments.[272] Certain amounts are also available to provide relief from rent and minimum annual guarantees to eligible airport concessions.
As of February 28, 2022, FAA had processed Consolidated Appropriations Act, 2021 grant applications for 2,966 U.S. airports and had obligated about $2 billion in grant funds. As of the same date, FAA had expended over $1 billion to reimburse airports for eligible costs, according to FAA officials (see table).
Federal Aviation Administration (FAA) Obligations and Expenditures for the Consolidated Appropriations Act, 2021 Airport Grants, as of Feb. 28, 2022
Funding group
Obligations ($ thousands)
Expenditures ($ thousands)
Primary commercial service airports and certain cargo airportsa
$1,751,347
$1,085,049
Non-primary commercial service and general aviation airportsb
$38,854
$16,258
Non-primary airports participating in the FAA Contract Tower programc
$4,782
$1,137
Concessions relief for primary commercial service airports
$199,416
$65,674
Small Community Air Service Development Programd
$4,000
$4,000
Total
$1,998,400
$1,172,119
Source: GAO analysis of the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1939-41 (2020), and data from the FAA. | GAO-22-105397
Note: The Consolidated Appropriations Act, 2021 directed FAA to allocate funding to these groups through various formulas. In addition, the Consolidated Appropriations Act, 2021, provides FAA the authority to retain up to 0.1 percent of the $2 billion (up to $2 million) provided for Grants-in-Aid for Airports to fund the award and oversight by FAA of grants made under the Consolidated Appropriations Act, 2021. Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1941 (2020).
aPrimary commercial service airports are publicly owned airports with more than 10,000 passenger boardings per year and scheduled air service. Cargo airports are airports that, in addition to any other air transportation services that may be available, are served by aircraft providing air transportation of only cargo with a total annual landed weight of more than 100 million pounds.
bNon-primary commercial service airports have at least 2,500 and no more than 10,000 passenger boardings each year. General aviation airports are public-use airports with fewer than 2,500 passenger boardings per year or no scheduled air service.
cNon-primary airports are the same as non-primary commercial service airports, and have at least 2,500 and no more than 10,000 passenger boardings each year. The Federal Contract Tower Program, established in 1982, allows the agency to contract out the operation of certain towers.
dThe Small Community Air Service Development Program is a grant program designed to help small communities address air service and airfare issues.
American Rescue Plan Act of 2021. ARPA, enacted on March 11, 2021, provided an additional $8 billion for airport assistance.[273] The allowable uses of grant funds are similar to those for the Consolidated Appropriations Act, 2021.[274] Certain amounts are available to increase the federal share for AIP grants and to provide relief from rent and minimum annual guarantees to eligible airport concessions.
As of February 28, 2022, FAA had processed ARPA grant applications for 2,982 U.S. airports and obligated about $8 billion in grant funds. As of that same date, it had expended over $1 billion to reimburse airports for eligible costs, according to FAA officials (see table).
Federal Aviation Administration (FAA) Obligations and Expenditures for the American Rescue Plan Act of 2021 (ARPA) Airport Grants, as of Feb. 28, 2022
Funding group
Obligations ($ thousands)
Expenditures ($ thousands)
Primary commercial service airports and certain cargo airportsa
$6,486,987
$1,193,186
Increase federal share for 2021 and select 2020 Airport Improvement Program (AIP) grants
$490,590
$219,854
Non-primary commercial service and general aviation airportsb
$95,244
$13,534
Concessions relief for primary commercial service airportsc
$782,828
$1,007
Total
$7,855,649
$1,427,580
Source: GAO analysis of the American Rescue Plan Act of 2021, Pub. L. No. 117-2, § 7102, 135 Stat. 4, 96-98, and data from the FAA. | GAO-22-105397
Note: ARPA directed FAA to allocate funding to these groups through various formulas. In addition, ARPA provides FAA the authority to retain up to 0.1 percent of the $8 billion (up to $8 million) provided for Relief for Airports to fund the award and oversight by FAA of grants made under ARPA. Pub. L. No. 117-2, § 7102, 135 Stat. 4, 98.
aPrimary commercial service airports are publicly owned airports with more than 10,000 passenger boardings per year and scheduled air service. Cargo airports are airports that, in addition to any other air transportation services that may be available, are served by aircraft providing air transportation of only cargo with a total annual landed weight of more than 100 million pounds.
bNon-primary commercial service airports have at least 2,500 and no more than 10,000 passenger boardings each year. General aviation airports are public-use airports with fewer than 2,500 passenger boardings per year or no scheduled air service.
cPrimary commercial airport sponsors may only use these funds to provide relief from rent and minimum annual guarantees to in-terminal airport concessions, subject to additional conditions. An eligible large airport concession is one that is in-terminal and has maximum gross receipts, averaged over the previous 3 fiscal years, of more than $56,420,000. An eligible small airport concession is one that is in-terminal and is a small business with maximum gross receipts, averaged over the previous 3 fiscal years, of less than $56,420,000, or is a joint venture. In general, a joint venture as defined in 49 C.F.R. § 23.3 is an association of an airport concession disadvantaged business enterprise firm and one or more other firms to carry out a single business enterprise.
Overview of Key Issues
Airport grant administration. Under the three COVID-19 relief laws, FAA has administered three new airport grant programs, developed program guidance, determined funding allocations, processed grant applications, and reimbursed thousands of U.S. airports and, in some cases, completed close-out reports, which we discuss in more detail below. As previously stated, while nearly all of the COVID-19 relief funding available for airports under the CARES Act, Consolidated Appropriations Act, 2021, and ARPA has been obligated, a smaller portion of the ARPA grant funds for airports has been expended. More specifically, as of February 28, 2022, FAA had expended less than $1.5 billion of $8 billion in total ARPA grant funding.
In October 2021, we reported airport association representatives’ perspective that FAA had been slow to administer and implement ARPA in the spring and summer of 2021, in part because FAA was administering multiple airport grant programs at the same time. According to airport association representatives, since we last reported, FAA’s implementation of the ARPA grant program had progressed in the fall and winter of 2021, as airports began to receive funds from FAA. These representatives also identified challenges related to administering the airport concessions relief portions of ARPA and the Consolidated Appropriations Act, 2021, which we discuss below under airport concessions relief.
As we reported in October 2021, FAA had identified ongoing challenges to administering these COVID-19 airport grant programs as well as taken some steps to help address those challenges. The need to process thousands of grants under expedited timeframes, with expanded eligible uses for these funds, were among the challenges FAA identified. As of August 2021, FAA had established a dedicated payment request processing team to help address these challenges, which included two full-time employees and three annuitants with prior airport grant management experience, and detailed additional personnel to assist in reviewing concessions relief plans.
As of March 2022, in order to address an increasing workload, FAA stated it had hired four additional employees to assist in all aspects of the COVID-19 grant programs. FAA officials noted that the grant application process is only one aspect of the COVID-19 airport grant programs and that FAA’s workload continues to be substantial. For example, FAA officials stated that FAA’s review team is currently processing three times as many reimbursement requests as before the Consolidated Appropriations Act, 2021, and will continue to do so until the ARPA airport grant program concludes in 2025. FAA further stated that it has been reviewing and approving general ARPA reimbursement requests with a two-week turnaround time, which they said is consistent with all grant payment requests.
Use of airport grant funds. FAA has continued to collect and consolidate data from airports on general spending categories for CARES Act funding through grant close-out reports, which are completed once all allocated airport funds for a grant agreement have been expended. Specifically, as of February 28, 2022, FAA officials reported that 918 CARES Act airport grants have been closed out, totaling over $3 billion. According to FAA officials, the majority of CARES Act airport grant funds have been used for payroll and debt servicing.
As of March 2022, FAA officials reported that they have not yet begun to close out Consolidated Appropriations Act, 2021 or ARPA grants. Airport association representatives said that airport sponsors are likewise generally using Consolidated Appropriations Act, 2021 and ARPA grants to pay down debt and pay for operating expenses such as payroll. Representatives from one airport association noted that using grant funds for any purpose, such as paying down debt, gives airport sponsors flexibility to manage other funds for other purposes, such as hiring staff.
Airport association representatives told us that the federal funding provided has been critical in helping airports maintain operations as revenues declined and fluctuated over the past 2 years. For example, by using federal funds to help maintain operations, airports were able to avoid some of the challenges of adjusting to steep declines and subsequent increases in passenger traffic and revenues. Airport association representatives also said that U.S. airports are continuing to work to manage increased costs as they seek to retain and hire employees to meet increasing travel demand.
Airport grant monitoring and oversight. Since we last reported in October 2021, an FAA contractor completed its review of FAA’s reimbursement processes for CARES Act airport grants and found that the program was not susceptible to significant improper payments, and therefore did not recommend any corrective actions.[275] According to officials, FAA hired the same contractor to conduct reviews of Consolidated Appropriations Act, 2021 and ARPA grant funds. For both programs, FAA expects the contractor to sample and test airport payment requests, including payments for concessions relief, with testing for the Consolidated Appropriations Act, 2021 funds to begin within the next few months. In addition, DOT’s Office of Inspector General is currently conducting an audit of FAA’s award and oversight of CARES Act funds, and FAA officials stated that if the agency takes actions in response to that audit, then FAA will also consider whether those actions are appropriate for the Consolidated Appropriations Act, 2021 and ARPA airport grant programs.
As we reported in October 2021, as non-federal entities, public airport sponsors that receive federal grants are also subject to the Single Audit Act, requiring the sponsors to undergo a single audit of those awards annually when their expenditures meet a certain dollar threshold—currently $750,000 or more in a fiscal year.[276] Single audits of an entity’s financial statements and federal awards can help identify deficiencies in an award recipients’ compliance with applicable laws and regulations, help ensure the appropriate use of federal funds, and reduce the likelihood of federal improper payments.
FAA officials stated that, in accordance with Single Audit Act requirements, the agency notifies airport sponsors if the amount of their expenditures triggers the $750,000 threshold. The airport sponsor must then confirm annually that the audit was completed and uploaded to the Federal Audit Clearinghouse. FAA officials explained that airport sponsors’ independent auditors conduct the Single Audits and that FAA often provides them with technical assistance about grant expenditures. The DOT Office of Inspector General may check compliance and review single audit reports for DOT fund recipients, and recently reviewed DOT’s processes for verifying that these audits have been submitted, among other things.[277] The Office of Inspector General made recommendations to ensure that FAA and other DOT operating administrations verify the complete and timely submission of their recipients’ single audits and follow up on findings to ensure that recipients have taken corrective actions. According to the Office of Inspector General, DOT concurred with these recommendations, and the Inspector General considers them resolved but open pending completion of planned actions.
Airport concessions relief. As part of the Consolidated Appropriations Act, 2021 and ARPA requirements, airport sponsors that accept concessions relief funds are to waive for eligible airport concessions some rent and minimum annual guarantee obligations due after December 27, 2020 and March 11, 2021, respectively, until the relief equals the total concessions relief allocation amount and to the extent permissible under state and local laws.[278] Eligible airport concessions under both acts include in-terminal concessions, with the Consolidated Appropriations Act, 2021 also including on-airport car rental and on-airport parking concessions. The concessions relief funds are intended to help provide airport concessionaires with support during the pandemic, including small airport concessions businesses.[279]
Since we last reported in October 2021, FAA has continued to process airport’s concessions relief applications under the Consolidated Appropriations Act, 2021, which were due to FAA by September 30, 2021. FAA also began processing applications for ARPA concessions relief but has not yet finalized a due date for these applications.[280] FAA is requesting that airport sponsors provide concessions relief plans with their payment requests when they are ready to accept their concessions-relief funding. For both Consolidated Appropriations Act, 2021 and ARPA concessions relief funds, FAA officials said they are reviewing these plans to ensure that airport sponsors are providing relief according to the law and FAA guidance prior to approving payment.[281]
According to FAA officials, as of February 28, 2022, FAA had obligated $199 million and expended $66 million of the $200 million provided by the Consolidated Appropriations Act, 2021 for concessions relief, and had obligated $783 million and expended $1 million of the $800 million provided by ARPA.[282] FAA stated that these totals reflect the agency’s prioritization of reviewing airport concessions rent relief plans and reimbursement under Consolidated Appropriations Act, 2021 concessions grants. According to FAA officials, the agency has recently used additional staff to accelerate its review of ARPA airport concessions relief plans and expects an increase in related ARPA expenditures, which we discuss in more detail below.
As we reported in October 2021, airport representatives noted that varying concessions agreements made it complex to determine concessions eligibility and to provide concessions relief proportionately under the Consolidated Appropriations Act, 2021. Airport association representatives stated that this variability has again presented challenges for some airports in allocating ARPA concessions relief funds. For example, they noted that ARPA distinguishes between funding for large and small airport concessions as well as between business models. They also said that many airport sponsors have had to work one-on-one with FAA to resolve questions unique to their airport’s circumstances.
Airport association representatives also stated that implementation of ARPA concessions relief have been slow overall—sometimes requiring months of correspondence before FAA approves an airport’s application—and attributed this in part to FAA’s new responsibilities and workload. Monitoring concessions relief funding and understanding the various airport-concessionaire contractual structures are new scopes of work for FAA’s Office of Airports. While time-consuming for both the airport sponsor and FAA staff, FAA officials stated that the development of concessions relief plans is necessary to ensure that the appropriate concessions are obtaining relief. Officials said that it is not unusual for FAA to contact airport sponsors at least once to obtain additional information about their plans, and FAA meets with sponsors in some cases. FAA officials added that they have encouraged concessionaires concerned about the timing of funding allocations to contact their airport sponsor to understand the concessions relief plan process.
As discussed above, FAA has hired additional staff to help address some of these challenges, including an employee who has experience with airport concessions and their contract relationships with airport sponsors. FAA officials told us that they also collaborated with staff from the Office of Civil Rights, who have subject matter expertise in the relationship between airports and concessionaires, to publish guidance for airports on how to develop a plan for providing concessions relief proportionally, as required. FAA officials further stated that the agency published additional guidance on airport concessions relief grants in November 2021 that incorporated lessons learned from reviewing airports’ concessions relief plans and addressed common questions from airport sponsors. Following release of that guidance, FAA’s approval of concessions relief plans and reimbursement under payment requests accelerated, according to FAA officials.
For both concessions relief programs, FAA also provided presentations, posted sample forms online, and conducted webinars, such as a February 2022 webinar for airport sponsors to explain how to complete their concessions relief plans and discuss updated guidance. FAA stated they are currently prioritizing approval and reimbursement under Consolidated Appropriations Act, 2021 concessions rent relief grants; however, with additional staff and the recent webinar, FAA expects a quicker disbursement of funds of both Consolidated Appropriations Act, 2021 and ARPA concessions funding.
A representative of an airport concessionaires association told us that dedicated concessions relief continues to be important to help airport businesses respond to the impacts of COVID-19. However, echoing what we heard from airport association representatives, the concessionaires’ representative said that FAA’s work to clarify these types of issues with airports has been time consuming, and that disbursements from FAA to airport sponsors have been slow as a result. The representative noted that airport concessionaires continue to face challenges due to the uncertainty of passenger traffic, difficulty recruiting and hiring staff, and increased costs. An airport concessions employee union told us that while many businesses in airports have reopened, there are no employee retention requirements associated with the concessions relief funds that they are aware of, and not all businesses are hiring enough workers to meet increasing demand. The employee union representatives stated that employment levels for their members had not increased since the summer of 2021 and remain at about 40 percent of pre-pandemic levels.
Methodology
To conduct this work, we analyzed FAA data on airport funding as of February 28, 2022. We determined the data were sufficiently reliable for the purposes of our reporting by performing interviews with agency officials and reviewing relevant documentation. We also reviewed the CARES Act, the Consolidated Appropriations Act, 2021, and American Rescue Plan Act of 2021 and related agency guidance, and conducted interviews with agency officials and representatives from two airport associations, an airport concessions association, and an airport concessions employee union, selected to represent a wide variety of industry and airport types.
Agency Comments
We provided FAA and the Office of Management and Budget (OMB) with a draft of this enclosure. FAA provided technical comments that we incorporated as appropriate. OMB did not have any comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor aviation operations, impacts, and lessons from the COVID-19 pandemic through other ongoing work.
Contact information: Heather Krause, (202) 512-2834 or krauseh@gao.gov
The Department of Transportation offered $717 million to 596 eligible applicants in the aviation manufacturing industry and has developed a plan to monitor recipients’ compliance with the terms and conditions of their Aviation Manufacturing Jobs Protection Program agreements.
Entity involved: Department of Transportation
Background
In March 2021, the American Rescue Plan Act of 2021 (ARPA) was enacted, establishing the Aviation Manufacturing Jobs Protection (AMJP) Program.[283] Through this program, the Department of Transportation (DOT) is to provide up to $3 billion in funding to eligible aviation manufacturing companies to pay up to half of the companies’ compensation costs for certain categories of employees, for up to 6 months.[284]
While some aviation manufacturing companies were eligible for other federal COVID-19 relief programs such as the three rounds of the Payroll Support Program (PSP) and the Paycheck Protection Program, others were not eligible due to their size, among other reasons.[285] In response to reduced commercial passenger demand during the COVID-19 pandemic, airlines parked or retired a substantial portion of their aircraft fleet, which in turn reduced demand for new commercial airplanes, engines, and spare parts, and also affected companies that provide aircraft maintenance services.
Eligible applicants can use AMJP program funds to help cover employee wages, salaries, and benefits and to facilitate the retention, rehire, or recall of employees.[286] For a company to be eligible, it must have involuntarily furloughed or laid off at least 10 percent of its workforce in 2020 as compared to 2019 or experienced a 15 percent decline in 2020 revenues compared to 2019.[287] Companies that received financial assistance from the first round of the Payroll Support Program (PSP1) or that were still expending Paycheck Protection Program assistance as of the date of their application to the AMJP program were ineligible for the program.[288]
When applying to the AMJP program, a company was required to identify a group of employees eligible for payroll support through the program.[289] Employees in the eligible employee group have to meet certain criteria, including that they: (1) do not exceed 25 percent of a company’s U.S. workforce as of April 1, 2020, (2) do not have a total compensation level greater than $200,000 per year, and (3) must be engaged in aviation manufacturing or maintenance, repair, and overhaul activities or services.
In order to receive AMJP funding, companies also had to make several commitments regarding the eligible employee group, including—but not limited to—a commitment not to involuntarily furlough or lay off employees in their eligible employee group for the duration of the agreement and receipt of public contributions under the AMJP program.[290]
DOT accepted applications for the program in three separate periods and recently completed executing the last round of agreements. The first application period was from June 15, 2021 through July 13, 2021, the second period was from August 4, 2021 through September 1, 2021, and the final period was from November 8, 2021 through December 13, 2021. DOT officials told us they entered into the first AMJP agreements on September 13, 2021 with companies that applied during the first application period. By statute, DOT must enter into all AMJP agreements within 6 months of the first agreement being executed; DOT officials told us they entered into all agreements by March 8, 2022.
Overview of Key Issues
DOT offered over $717 million to 596 eligible AMJP applicants.[291] DOT offered funding to 313 companies that applied in the first application period, 156 companies that applied in the second application period, and 127 companies that applied in the third application period. The average AMJP contribution offered to these applicants was $1.2 million; funding offers ranged in size from $2,500 to $75.5 million.[292]
Companies were offered funding for eligible employee groups as small as one employee and as large as 3,214 employees. On average, companies had 55 employees in their eligible employee group, and DOT approved award amounts that resulted in an average of approximately $22,000 per eligible employee. As of March 8, 2022, DOT disbursed $337 million to the eligible companies that entered into AMJP agreements.
Aviation Manufacturing Jobs Protection (AMJP) Program Eligible Recipients, by Funding Offer Amount, as of Mar. 8, 2022
DOT officials told us that 86 percent of applicants across all three application periods were offered funding; the remaining 14 percent were determined to be ineligible or disqualified.[293] According to officials, common reasons applications were ineligible or disqualified included missed submission deadlines, incomplete supporting documentation, and not meeting the eligibility criteria, such as not holding the required certifications. Additionally, officials told us that three applicants declined their funding offers after DOT made announcements of the award offers and a fourth applicant did not respond to DOT about their award offer.[294] DOT officials said that two of the applicants did not provide a reason for declining the AMJP offer, and the third told officials the program’s reporting requirements would be too complicated for the company because it was a temporary staffing company and therefore the employees on its payroll changed on a weekly basis.
DOT re-opened the AMJP program applications for a third time due to a correction regarding program eligibility. DOT guidance for the first and second application periods stated that DOT could not enter into an AMJP agreement with a company that was allowed the Employee Retention Credit for the quarter immediately prior to the one in which an AMJP agreement was to be entered into.[295] However, DOT officials later realized the restriction on allowing the Employee Retention Credit only applied if a company was allowed the credit for a calendar quarter occurring prior to July 1, 2021 because of the way applicable legal provisions were structured.[296]
During the first and second application periods, DOT provided a space in the AMJP application where companies could indicate if they accrued the Employee Retention Credit in the quarter prior to the quarter in which they anticipated receiving an AMJP award, and they could ask DOT officials to defer award of the AMJP agreement with the company.[297] However, according to DOT officials, some companies told them they did not apply to the AMJP program because of the program’s restriction on the Employee Retention Credit.
Therefore, upon determining the Employee Retention Credit restriction did not apply for credits taken after July 1, 2021, DOT reopened the application process for a third period from November 8, 2021 through December 13, 2021. DOT updated its application and guidance materials to clarify that Employee Retention Credits accrued after July 1, 2021, did not affect DOT’s ability to award an AMJP agreement to an otherwise eligible applicant. All other requirements for the program remained the same.
DOT officials have developed a plan to monitor recipients’ compliance with the terms and conditions of the AMJP agreements. DOT officials told us that all AMJP recipients are subject to post-award reporting requirements, performance assessment, and compliance reviews. Standard reporting will occur at three points:
Eligible employee group composition report. Within 10 days of a company entering into an AMJP agreement, the company is required to submit an eligible employee group composition report to DOT. According to DOT officials, this report provides DOT with validated or updated baseline information on which employees are in the recipient’s eligible employee group that DOT can use for evaluating any changes to the group over the course of the award period and the company’s adherence to its commitments made in the AMJP agreement.[298]
Interim financial reports. These reports are required from companies that DOT designated as higher risk.[299] DOT officials told us they review interim reports to check the validity of allowable costs and consistency with the eligible employee group reporting. DOT determines whether a company is higher risk at the time of award, and the additional interim reporting requirements are included in the company’s AMJP agreement.
Officials told us they use a number of criteria to determine if a company is higher risk. For example, companies that disclosed in their application that they were engaged in legal or business proceedings such as mergers, acquisitions, or bankruptcy proceedings are designated as higher risk. Officials also classify companies that told DOT that they were delinquent on a debt or companies that received more than $1.25 million in AMJP funding as higher risk. According to officials, as of March 8, 2022, 209 recipients had been designated as higher risk.[300]
Final report. DOT requires a final report from recipients before the final payment request is made. According to DOT officials, this allows them to monitor expenses incurred and compare the final eligible employee group to the original eligible employee group composition report. It also allows DOT to identify any claimed costs that do not correspond with the designated members of the eligible employee group.
DOT officials told us they hired a financial support contractor to assist in initial evaluation of applications and to conduct the initial review of the post-award reports and payment requests, as well as to follow-up with recipients on any identified discrepancies. The contractor can elevate any unresolved issues to the cross-organizational DOT team that manages the AMJP program. The DOT team authorizes awards and disbursements and is responsible for making determinations about post-award compliance.
DOT officials told us they are also examining approaches for post-award compliance reviews of certain eligibility criteria. For example, DOT officials are comparing AMJP recipients to the public list of Paycheck Protection Program recipients and asking any recipients of both programs to provide documentation to DOT that shows when the recipient finished expending or repaying their Paycheck Protection Program loans.[301] Additionally, officials are exploring whether companies’ tax filings will sufficiently identify if they were allowed Employee Retention Credits for the calendar quarter prior to July 1, 2021 for those recipients for which it is relevant. Officials told us this could potentially allow them to conduct post-award reviews of Employee Retention Credit eligibility restrictions.[302]
Finally, DOT has added information on the AMJP website to make it easy for the public to learn about how to report concerns about the use of AMJP funds, whistleblower protections, and information on how to contact the DOT Office of Inspector General.
Methodology
To conduct this work, we reviewed the CARES Act, the Consolidated Appropriations Act, 2021, the American Rescue Plan Act of 2021, and DOT’s Federal Register notices related to the AMJP program. We also reviewed DOT guidance, documents, and webinars, and interviewed DOT officials. We reviewed AMJP data as of March 8, 2022. We reviewed these data for consistency and completeness, and we determined that DOT’s data were sufficiently reliable for the purposes of our enclosure.
Agency Comments
We provided DOT and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
The Department of the Treasury has nearly completed making payroll support payments to the aviation industry and continues to monitor recipients’ compliance with the terms and conditions of the Payroll Support Program agreements.
Entity involved: Department of the Treasury
Background
In March 2020, Congress passed the CARES Act, which established the Payroll Support Program (PSP1). PSP1 provided $32 billion for passenger air carriers, cargo air carriers, and aviation contractors.[303] In December 2020, the Consolidated Appropriations Act, 2021 established the Payroll Support Program Extension (PSP2), which provided up to $16 billion for passenger air carriers and contractors.[304] In March 2021, the American Rescue Plan Act of 2021 (ARPA) created another round of the program (PSP3), which provided up to $15 billion in financial assistance for passenger air carriers and aviation contractors.[305]
As required by statute, payments from PSP1, PSP2, and PSP3 were to be used exclusively for the continuation of payment of wages, salaries, and benefits to employees of the recipient air carrier or eligible contractor. Eligible contractors may include those who perform catering functions or functions on airport property directly related to air transportation, such as security or airport ticketing. Recipients who receive payments agree to abide by the terms and conditions of the Payroll Support Program agreement, including statutory requirements such as refraining from conducting involuntary furloughs or terminations for specified amounts of time.
Treasury evaluates recipients’ compliance with statutory requirements and the applicable Payroll Support Program agreement through its compliance monitoring process, which consists of two levels of review—a set of automated testing rules that all recipients are assessed against, and for certain recipients, a more in-depth review by a Treasury analyst. Additionally, as allowed by statute to protect taxpayer interests, Treasury required that certain recipients provide notes, warrants, or both as appropriate compensation for the provision of financial assistance.[306] Passenger air carriers that received payments of more than $100 million and contractors that received more than $37.5 million were required to provide notes. In addition, cargo carriers that received payments through PSP1 were required to provide notes equal to 56 percent of the payroll support over $50 million. Payroll Support Program recipients that received payroll support over the dollar amounts listed above were also required to provide warrants, if they are publicly traded companies.
Overview of Key Issues
Treasury has made $59 billion in payments out of $63 billion available for PSP1, PSP2, and PSP3. Treasury has nearly completed making Payroll Support Program payments, and Treasury officials said that, as of March 2022, one PSP3 agreement is still awaiting Treasury’s approval. Based on data available in March 2022, across PSP1, PSP2, and PSP3, Treasury has made payments totaling $50.1 billion to the 10 largest air carriers. The remaining passenger air carriers received $3.4 billion, and aviation contractors received $4.6 billion, across PSP1, PSP2, and PSP3. Through PSP1, cargo air carriers received $827.4 million.[307] In total, according to Treasury officials, Treasury provided payments to 699 companies through PSP1, PSP2, and PSP3. This included 405 passenger air carriers, 256 contractors, and 38 cargo air carriers.
Treasury required some Payroll Support Program recipients to provide notes, warrants, or both as taxpayer protection. According to information provided by Treasury officials, as of January 2022, for PSP1, 36 recipients were required to provide notes, 12 of which have repaid their notes. For PSP2, 20 recipients were required to provide notes, two of which have repaid their notes. For PSP3, 19 recipients were required to provide notes, two of which have repaid their notes. All of the notes have a duration of 10 years.
As previously noted, passenger air carriers that received payroll support over $100 million, contractors receiving payroll support over $37.5 million, and cargo carriers receiving payroll support over $50 million were required to provide warrants, if they are publicly traded companies. In total, as of the most recent data available in March 2022, across PSP1, PSP2, and PSP3, 14 recipients met the criteria and provided warrants, according to Treasury data. These warrants will start to expire in 2025.
Treasury’s compliance monitoring continues for PSP1, PSP2, and PSP3 recipients. To ensure compliance with the applicable Payroll Support Program agreement, Treasury has developed a compliance monitoring approach that involves two levels of compliance testing.[308] The first level of compliance testing is based on quarterly compliance reports, which recipients must submit to Treasury at the end of each quarter via an online portal.[309] If a recipient does not submit a quarterly compliance report, Treasury follows up with the recipient to try to ensure it is submitted and may levy penalties for non-compliance.
According to Treasury officials, recipients who fail to submit their quarterly compliance report may be required to return to Treasury all Payroll Support Program payments made to date, and Treasury may withhold any additional payroll support payments. Treasury officials said that since the start of the Payroll Support Program, 99 percent of quarterly compliance reports have been submitted as required. According to these officials, for the most recent quarter of compliance testing, 682 recipients submitted quarterly compliance reports.[310]
All recipients then undergo Level 1 compliance testing, which consists of a set of automated business rules that are applied to each recipients’ quarterly compliance report. For example, according to Treasury documentation, one of Treasury’s business rules relates to salaries and wages, and allows Treasury to ensure recipient’s compliance with the prohibition to reduce employee salaries and wages during certain time periods. Treasury officials said that discrepancies identified in Level 1 testing are considered potential indicators of risk of non-compliance. Across all recipients and all rounds of testing, according to Treasury, about 2 percent of the critical business rules that Treasury assesses for Level 1 testing are flagged for additional follow-up.
If a discrepancy is identified in Level 1 testing, the recipient is elevated to Level 2 testing.[311] Level 2 testing involves a more in-depth review by a Treasury analyst, who can follow-up with recipients for additional information. During this review, a Treasury analyst conducts an in-depth review of information the recipient submitted in the online portal and other information provided by the recipient to determine compliance with the terms of the Payroll Support Program agreement. Upon the conclusion of Level 2 testing, according to Treasury officials, many of the Level 1 flags across all rounds of testing were instances where, for example, a recipient did not understand the question to which they were responding to in its quarterly compliance report.
A limited number of recipients have been found to be noncompliant with the Payroll Support Program agreement. If a recipient fails to submit a quarterly compliance report after Treasury follows up with the recipient or is found noncompliant through Level 2 testing, Treasury will issue a finding of noncompliance. As of January 2022, according to Treasury officials, 23 recipients, or about 3 percent of all recipients, over the duration of the program have been issued a finding of noncompliance. Of the 23 recipients that were issued a finding of noncompliance:
11 recipients were issued a finding of noncompliance because of failure to submit quarterly compliance reports,
10 recipients were issued a finding of noncompliance because of unallowable involuntary terminations, and
two recipients were issued a finding of noncompliance because payroll support funds were spent in an unallowable period.
Recipients that are found to be noncompliant with the terms of their Payroll Support Program agreements may be subject to remedial action or penalties. In accordance with the remedies set out in those agreements, Treasury may take action it deems appropriate. According to Treasury officials, as of January 2022, seven of the 23 recipients that were issued a finding of noncompliance were subjected to monetary penalties, and the remaining recipients have been notified of noncompliance and the proposed remedy. Other penalties may extend the length of time a prohibition imposed by the Payroll Support Program agreement is applied to a recipient. For example, Treasury officials said that in at least one case, they have extended the end date of the requirement that prohibits involuntary terminations. Treasury officials said that all penalties must be approved by senior officials and the penalty that a recipient may face varies depending on severity of noncompliance.
For most recipients, Treasury expects that Payroll Support Program compliance monitoring will end in early 2023. Treasury officials said that for most recipients the last quarterly compliance report will be due to Treasury in the second quarter of 2023.[312] However, if the recipient has a note, warrant, or other financial instrument associated with its Payroll Support Program payment, the recipient must continue to submit a quarterly report until the note, warrant, or other financial instrument is no longer outstanding or held by the federal government, which could be up to 10 years. In these cases, Treasury would continue to conduct compliance testing for as long as the note, warrant, or other financial instrument is held.
Treasury has not yet developed policies and procedures to guide action on the warrants. In October 2021, we recommended that the Secretary of the Treasury should develop policies and procedures to determine when to act on warrants obtained as part of the Payroll Support Program to provide appropriate compensation to the federal government. According to Treasury officials, they are developing these policies and procedures but told us in February 2022 that they do not have a time frame as to when these plans will be completed and implemented.
Through the Payroll Support Program, Treasury holds warrants that give it the option to purchase shares of stock in 14 recipients.[313] These warrants will start to expire in 2025, after which Treasury cannot exercise them. As we and others have noted, air carriers’ earnings and share prices have historically been volatile due to their sensitivity to economic, political, and health-related conditions that affect the cost of doing business and the demand for passenger travel. Further, as we and others have reported, the pandemic has had and continues to have an effect on air carriers’ financial conditions and by extension on their share prices. This volatility has a direct effect on the amount of money for which Treasury can expect to redeem the warrants. We maintain that developing policies and procedures immediately will help ensure that Treasury has the information needed for informed decision-making that helps maximize the value of exercised warrants.
Methodology
To conduct this work, we reviewed the CARES Act, the Consolidated Appropriations Act, 2021, and ARPA. We also reviewed agency documentation and interviewed Treasury officials to understand Treasury’s implementation and oversight processes for PSP1, PSP2, and PSP3. We reviewed PSP1 data as of March 25, 2022, PSP2 data as of March 23, 2022, and PSP3 data as of February 10, 2022. We reviewed these data for outliers and missing information, and we determined that Treasury’s data were sufficiently reliable for the purposes of summarizing the number, value, and timing of Payroll Support Program payments.
Agency Comments
We provided Treasury and the Office of Management and Budget (OMB) with a draft of this enclosure. Treasury provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor Treasury’s response to our prior recommendation.
GAO’s Prior Recommendations
The table below presents our recommendations on payroll support assistance for aviation businesses from prior quarterly CARES Act reports.
Prior GAO Recommendations Related to Payroll Support Assistance for Aviation Businesses
Recommendation
Status
The Secretary of the Treasury should finish developing and implement a compliance monitoring plan that identifies and responds to risks in the Payroll Support Program (PSP) to ensure program integrity and address potential fraud, including the use of funds for purposes other than for the continuation of employee wages, salaries, and benefits. (November 2020 report)
Closed-implemented. In April 2021, GAO confirmed that the Department of the Treasury (Treasury) had developed, documented, and implemented a risk-based approach to monitor PSP recipients’ compliance with the terms of the assistance. Treasury’s risk-based approach entails a two level compliance review. In the first level review, automated testing is conducted on all recipients’ quarterly reports using factors/thresholds that can trigger recipients being moved to the next review. In the second level review, Treasury analysts conduct a more detailed review of recipients that failed the first level review or were selected for other reasons. Treasury has also developed penalties and a process for remediating noncompliance with PSP agreement terms through Payroll Support Program agreements. As of April 2021, Treasury has identified noncompliance by recipients and applied penalties, as appropriate.
The Secretary of the Treasury should develop policies and procedures to determine when to act on warrants obtained as part of the Payroll Support Program to provide appropriate compensation to the federal government. (October 2021 report)
Partially addressed. Treasury agreed with our recommendation and said the agency is in the process of creating a policy to dispose of the warrants obtained as part of the Payroll Support Program. As of February 2022, Treasury is developing these policies and procedures but it does not have a time frame as to when these plans will be completed and implemented.
The Department of the Treasury continues to monitor 23 borrowers for risk of non-payment of their outstanding loans and all 35 original borrowers’ compliance with loan terms and conditions, which remain effective for 1 year after loans have been fully repaid.
Entity involved: Department of the Treasury
Background
The CARES Act authorized the Department of the Treasury to provide up to $46 billion in loans and loan guarantees to certain aviation businesses and other businesses deemed critical to maintaining national security (national security businesses).[314] This loan program was intended to provide liquidity to these sectors. Treasury executed 35 loan agreements with businesses in these targeted sectors, totaling about $22 billion, of which $2.7 billion was disbursed.[315]
Of these 35 loans, as of April 1, 2022, 12 loans have been fully repaid and the total value of outstanding loans is about $1 billion, as shown in the table below.[316] Consistent with the CARES Act, the executed loans have a duration of 5 years or less. No more loans will be executed through this program.
Executed and Outstanding Loans for the CARES Act Loan Program for Aviation and Other Eligible Businesses as of Apr. 1, 2022
Loan category
Number of loans executed
Total loan amount approved by Treasury ($ millions)
Total loan amount disbursed by Treasury ($ millions)
Number of loans outstanding
Total outstanding loan amount ($ millions)a
Passenger and cargo air carrier
17
21,116
1,903
8
237
Repair station operator
5
19
19
5
20
Ticket agent
2
21
21
1
0.6
National security business
11
736
736
9
745
Total
35
21,891
2,678
23
1,002
Source: GAO analysis of Department of the Treasury data. |GAO-22-105397
Note: Section 4003 of the CARES Act authorized maximum assistance available through loans in three categories: passenger air carrier, repair station operator, and ticket agent ($25 billion); cargo air carrier ($4 billion); and businesses critical to maintaining national security ($17 billion). CARES Act, Pub. L. No. 116-136, § 4003, 134 Stat. 281, 470 (2020). To match the Department of the Treasury’s reporting on these loans, and because air carriers that received loans could provide both passenger and cargo air services, we combined all air carriers into a single category.
aIncludes all loan disbursements and increases in loan principal amount arising from payment-in-kind interest, less any repayments of principal.
The CARES Act set out conditions for this loan program, including that borrowers, among other things, (1) not reduce employment levels by more than 10 percent from levels as of March 24, 2020, through September 30, 2020, (2) refrain from share buybacks and dividend payments, and (3) limit compensation to employees with salaries over certain amounts until 1 year after the date the loan or loan guarantee is no longer outstanding. Additionally, the CARES Act permitted Treasury to make loans to publicly traded companies only if those businesses provided a warrant—an option to buy shares of stock at a predetermined price before a specified date—or an equity interest in the company to Treasury.[317] This enclosure satisfies a provision in the CARES Act that directs us to submit annual reports regarding the loan program.[318]
Overview of Key Issues
Treasury continues to assess borrowers’ risk. According to officials, Treasury has developed and applies a rating system to gauge the riskiness of a borrower and the likelihood the borrower may not be able to pay off its loan balance. Treasury takes other steps to ensure borrowers are able to meet the financial terms of their loan agreements, including requiring submission of financial reports; reviewing recipient financial statements; and meeting with recipients’ management to discuss areas of concern. The Bank of New York Mellon, which serves as the financial agent for Treasury, also monitors the principal and interest payments from borrowers.
According to Treasury officials, all outstanding loan principal and interest are due on the loan’s maturity date, which ranges from September 2024 to November 2025. Before that date, borrowers may pay down the principal of their loan and, pay all, some, or none of the interest. Accrued interest left unpaid is added to their outstanding loan balance. As of April 2022, 12 of the 35 borrowers have fully repaid the principal and any interest accrued on their loans. Of the remaining 23 borrowers with outstanding loan balances:
two have repaid some of the loan principal, while 21 have not paid any loan principal; and
three have consistently paid off the accrued loan interest as it became due, while six have paid off some of the accrued interest, and 14 have not paid off any of the accrued interest.
According to Treasury officials, there is a possibility that some of the higher risk borrowers may default on their loans. If a default were to occur, there are two paths. A company may have to liquidate its assets in order to repay its debt. Alternatively, a company may have to restructure its debt.
Treasury continues to monitor loan recipients’ compliance with agreement terms and conditions. Each quarter, recipients answer questions, through an online portal, about their compliance with loan agreement terms. These questions focus on employee headcount, internal controls, and other loan agreement requirements.
First level review. Treasury uses an automated process to verify that the answers submitted by the recipient indicate compliance with loan agreement terms and conditions.
Second level review. If a potential compliance issue is identified through the first level review, then a Treasury analyst conducts a second, more detailed review of the answers and related documents submitted by the recipient. In this second review, a Treasury analyst will also contact the recipient to discuss the issue, if needed. During this review, potential compliance issues are cleared or determined to be an actual compliance issue that requires remediation.
As required by statute, certain terms and conditions of the loan agreements, including restrictions on paying dividends to shareholders and compensation for employees with salaries over certain thresholds, are in effect for 1 year after loans have been repaid in full. Once the 1-year anniversary of repayment passes, borrowers are no longer subject to Treasury’s loan program compliance monitoring. With the repayment of 10 loans in 2021, Treasury expects to continue monitoring all loan recipients’ compliance with loan agreement terms and conditions through at least the first quarter of 2022. For example, Ovation Travel Group, Inc. paid in full all outstanding principal and interest on January 21, 2021. Therefore, this company would submit its final compliance report in the first quarter of 2022. Since the loans can have a duration of up to 5 years, depending on the repayment status, Treasury may keep this compliance monitoring process in place through 2026.
Treasury addresses noncompliance issues as they arise. According to Treasury officials, as of January 2022, Treasury has found one borrower to be materially noncompliant with loan agreement terms and conditions. However, the borrower remedied the noncompliance, and Treasury does not plan to take further action.[319] Treasury officials expect that additional compliance issues, if any, will be found through the compliance monitoring process detailed above. If Treasury determines that a borrower is noncompliant, these cases may be referred to the Treasury Office of Inspector General for investigation.
Most of the penalties for noncompliance are laid out in the terms and conditions of each loan agreement; however, according to Treasury officials, they have the authority to negotiate amendments to agreements and address compliance violations as appropriate. Under the terms of the loan agreements, in certain circumstances Treasury has the ability to accelerate the loan—require payment of the loan before the terms of the loan agreement specify—in whole or in part.
Treasury has not yet developed policies and procedures to determine when it will act on warrants. In October 2021, we recommended that the Secretary of the Treasury should develop policies and procedures to determine when to act on warrants obtained as part of the loan program for aviation and other eligible businesses to benefit the taxpayers. According to Treasury officials as of February 2022, they are developing these policies and procedures but do not have a time frame as to when these plans will be completed and implemented.
Through the loan program, Treasury holds warrants that give it the option to purchase shares of stock in nine passenger air carriers.[320] These warrants expire in 2025, after which Treasury cannot exercise them. As we and others have noted, air carriers’ earnings and share prices have historically been volatile due to their sensitivity to economic, political, and health-related conditions that affect the cost of doing business and the demand for passenger travel. Further, as we and others have reported, the pandemic has had and continues to have an effect on air carriers’ financial conditions, and by extension on their share prices. This volatility has a direct effect on the amount of money for which Treasury can expect to redeem the warrants. We maintain that developing policies and procedures immediately will help ensure that Treasury has the information needed for informed decision-making that helps maximize the value of exercised warrants.
Methodology
To conduct this work, we reviewed the most recent Treasury data on the status of executed loans as of April 1, 2022; reviewed the CARES Act; and interviewed Treasury officials. We are continuing to use the data on loans that we have found reliable through interviews with agency officials on the data’s consistency and completeness during prior reviews. We determined the data were sufficiently reliable for the purposes of our enclosure.
Agency Comments
We provided Treasury and the Office of Management and Budget (OMB) with a draft of this enclosure. Treasury provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor Treasury’s response to our prior recommendation.
GAO’s Prior Recommendations
The table below presents our recommendation on loans for aviation and other eligible businesses from a prior quarterly CARES Act report.
Prior GAO Recommendation Related to Loans for Aviation and Other Eligible Businesses
Recommendation
Status
The Secretary of the Treasury should develop policies and procedures to determine when to act on warrants obtained as part of the loan program for aviation and other eligible businesses to benefit the taxpayers. (October 2021)
Partially addressed. Treasury agreed with our recommendation and said the agency is in the process of creating a policy to dispose of the warrants obtained as part of the loan program. As of February 2022, Treasury is developing these policies and procedures but it does not have a time frame as to when these plans will be completed and implemented.
Financial Assistance: Lessons Learned from CARES Act Loan Program for Aviation and Other Eligible Businesses.GAO-21-198. Washington, D.C.: December 10, 2020.
Sponsors of Capital Investment Grants projects for new transit systems or extensions of existing transit services are using American Rescue Plan Act of 2021 funds to mitigate increased project costs and shortfalls in local funding and in some cases to prevent project delays.
Entity involved: Federal Transit Administration, within the Department of Transportation
Background
Millions of Americans rely on public transportation systems for mobility and access to jobs, education, and essential services, such as medical care and grocery shopping. Within the Department of Transportation (DOT), the Federal Transit Administration (FTA) provides grants to state departments of transportation, local public transit systems, and tribes to support and expand transit services. These services may be provided by various public transportation modes, including buses, subways, light rail, commuter rail, trolleys, and ferries in urban, rural, and tribal areas.
The CARES Act appropriated about $25 billion to FTA to support the transit industry through two formula programs—the Urbanized Area Formula program ($22.7 billion) and the Formula Grants for Rural Areas program ($2.2 billion).[321] CARES Act grant funds were made available to transit agencies for COVID-19-related expenses incurred on or after January 20, 2020; FTA allocated the $25 billion to urbanized areas, states, and tribes on April 2, 2020.[322] These funds must now be directed, to the maximum extent possible, to payroll and operating expenses.[323] There is no limit on the amount of funds that recipients may use for operating expenses, and the funds are available until expended.[324]
On December 27, 2020, the Consolidated Appropriations Act, 2021 appropriated an additional $14 billion to FTA for the transit industry to prevent, prepare for, and respond to COVID-19.[325] Further, on March 11, 2021, the American Rescue Plan Act of 2021 (ARPA) appropriated approximately $30.5 billion to FTA for the same purpose.[326] ARPA funds are available for obligation until the end of fiscal year 2024.
Of the funding ARPA provided to FTA, $1.7 billion is allocated to the Capital Investment Grants program, a discretionary grant program that helps fund new transit systems or expansion of existing services.[327] This enclosure is primarily focused on Capital Investment Grants project sponsors’ use of ARPA funding, as well as FTA’s administration of that funding.
There are three categories of projects within the Capital Investment Grants program: New Starts; Core Capacity Improvement; and Small Starts.[328] Projects are designed and implemented by sponsors—usually local transit agencies, but also states’ departments of transportation or local governments. If selected for a grant award, project sponsors enter into a grant agreement with FTA, which specifies the maximum amount of federal funding a project may receive.[329]
FTA distributed ARPA funding for the Capital Investment Grants program among 45 eligible projects not yet open for service. To be eligible for ARPA funding, New Starts and Core Capacity Improvement projects must have an existing grant agreement and received an allocation prior to or for fiscal year 2020. However, certain Small Starts projects may be eligible for ARPA funding without a grant agreement. ARPA funding is additional to the federal funding provided through grant agreements and is not subject to the maximum amount of federal funding specified in these agreements. ARPA funding supplements projects’ non-federal funding, and project sponsors are not required to provide any matching funds for ARPA funds. ARPA allocates funds to Capital Investment Grants projects based on the percentage of project funding from sources other than the Capital Investment Grants program, which are specified in the grant agreement. Project sponsors are not required to provide additional justifications to FTA for use of these funds.
Overview of Key Issues
Transit agencies have obligated the majority of COVID-19 relief funds, and have expended the majority of CARES Act and Consolidated Appropriations Act, 2021 funding. According to FTA data, as of February 28, 2022, transit agencies had obligated 99 percent of allocated CARES Act funds and had expended 88 percent of the funds (see table). In addition, transit agencies had obligated about 91 percent of allocated funds from the Consolidated Appropriations Act, 2021 and about 80 percent of allocated formula funds from ARPA. FTA officials reported that as of February 28, 2022, 96 applications for new grants are in process for Consolidated Appropriations Act, 2021 funds and 193 applications are in process for ARPA formula funds.[330]
FTA Allocations and Transit Agency Obligations and Expenditures of COVID-19 Relief Formula Funds, as of Feb. 28, 2022
Funding source
Allocationse ($ millions)
Obligations ($ millions)
Expenditures ($ millions)
CARES Acta
24,925
24,580
21,628
Consolidated Appropriations, 2021b
13,990
12,720
9,217
American Rescue Plan Act of 2021c
28,222
22,613
3,848
Totald
67,137
59,913
34,693
Source: GAO analysis of Federal Transit Administration (FTA) data. | GAO-22-105397
aThe CARES Act appropriated $25 billion for transit industry grants.
cThe American Rescue Plan Act of 2021 appropriated about $30.5 billion, approximately $28.2 billion of which was formula funding.
dNumbers and percentages may not sum to totals because of rounding.
eAllocations do not include funding set aside for FTA administration and oversight.
Most Capital Investment Grant projects experienced increased costs during the pandemic, and seven projects used ARPA funding to mitigate shortfalls in local funding. Most of the 15 project sponsors we interviewed—responsible for 21 Capital Investment Grants projects—told us they experienced increased costs during the COVID-19 pandemic. Specifically, 12 sponsors—responsible for 14 projects—told us they experienced or anticipated experiencing at least one type of cost increase for at least one of their projects.
According to sponsors, these project cost increases were primarily caused by rising material and labor costs. For example, 11 projects reportedly experienced increased costs for raw materials, such as steel and lumber, and for manufactured items, such as spare parts. In addition, five projects reportedly experienced increased labor costs, such as increased wages, and five projects experienced increased costs related to COVID-19 restrictions and requirements, such as for additional cleaning and sanitation.
Sponsors of seven projects reported using the ARPA funds to offset shortfalls in their projects’ non-federal sources of funding, primarily local taxes and fare revenue. For example, one project sponsor initially planned to rely heavily on fare revenue to fund the non-federal share of its project. As a result of the pandemic, the project sponsor saw ridership drop to about 6 percent of pre-pandemic levels, and it has since increased to only about 20 to 25 percent of pre-pandemic levels. The ARPA funds helped the project sponsor offset the dramatic reduction in ridership and associated fare revenue to keep the project moving forward, according to the project sponsor. Similarly, another sponsor told us ARPA funding mitigated the shortfall in revenue from sales tax its project experienced due to the pandemic. Three project sponsors told us that because they could use ARPA funds as their local match, they were able to fund other capital projects with their non-federal funds. According to one sponsor, these investments, such as purchasing additional buses, will help delay or prevent future service or operating cuts.
While projects may experience construction delays, sponsors generally did not expect these delays to affect service dates, and about half said ARPA funding helped projects stay on schedule. Sponsors reported construction delays due to a variety of factors during the pandemic, but sponsors of 14 out of the 21 projects said these delays would not affect their planned dates to begin passenger service. For example, officials from one transit agency told us that while they had experienced delays in construction, they had built extra contingency time into their project schedule in anticipation of delays, allowing them to remain on schedule to begin service on the scheduled date. When projects experienced construction delays, sponsors we interviewed attributed them to multiple factors:
Supply chain issues. Eight projects experienced delays related to supply chain issues, such as increased delivery times for and shortages of materials.
COVID-19—related requirements. Four projects experienced extended timeframes due to COVID-19—related restrictions that affected construction. For example, one sponsor told us social distancing requirements had caused construction delays and inefficiencies.
Labor availability. Four projects experienced delays due to a lack of available labor. For example, one sponsor experienced extended timeframes due to operational shutdowns at its vehicle manufacturer. The vehicle manufacturer cited COVID-19 staff illnesses and labor availability among the reasons for its manufacturing delays.
Sponsors of 11 projects told us that ARPA funds have helped their projects stay on track to meet their scheduled service dates, even with shortfalls in fare revenue and local taxes. For instance, one project sponsor told us that ARPA funds ensured full funding was available for its two projects, which enabled the sponsor to continue awarding contracts and avoid critical project delays. Another project sponsor told us that the ARPA funds allowed it to absorb cost increases due to the pandemic, and stay on track awarding contracts. Lastly, another project sponsor said that the ARPA funds allowed it to proceed with material procurements and mitigate potential delays given the shortfall of local funds it had experienced.
FTA uses existing procedures to distribute and oversee the use of ARPA funds by Capital Investment Grant project sponsors. All project sponsors we interviewed said they had not experienced challenges related to the allocation, obligation, or expenditure of the ARPA funds. According to some sponsors, this was partly because FTA used existing Capital Investment Grants program procedures to distribute these funds. For example, officials from one transit agency told us that FTA’s use of existing procedures enabled them to draw on their prior funding experience with FTA and avoid any challenges accessing or obligating ARPA funding.
Similarly, FTA officials told us their oversight process for ARPA funds that sponsors obligate for Capital Investment Grants projects is identical to that used for Capital Investment Grants funding. According to officials, this oversight is primarily conducted by FTA’s regional offices and contractors, as well as FTA’s Office of Safety and Oversight. We previously reported on FTA’s implementation and oversight of the Capital Investment Grants program in July 2020.
Both FTA and project management oversight contractors play a role in oversight. Specifically, FTA officials said that prior to entering into a grant agreement, FTA reviews several factors, including a project’s cost and schedule and risks associated with the project. Officials told us that after a grant agreement is in place, FTA relies on project management oversight contractors to monitor projects to determine whether they are on schedule, within scope, and in compliance with federal regulations. According to officials, these contractors review reports from project sponsors on a quarterly basis, though they may do so on a monthly basis in cases where issues have been identified. These reports update project management oversight contractors on the status of the project, including progress on construction and negotiating contracts, and how the project aligns with the cost, scope, and schedule set out in the project’s grant agreement. Additionally, FTA officials said FTA regional administrators meet with project sponsors on a quarterly basis to discuss any areas of concern.
Methodology
To conduct this work, we analyzed COVID-19 relief laws, other applicable statutes and regulations, and FTA data on transit industry grant funding, as of February 28, 2022. To assess the reliability of these data, we reviewed a 2020 audit of DOT’s financial system, reviewed previous GAO reviews of FTA’s internal controls, and interviewed DOT officials. We found these data to be reliable for the purposes of describing federal allocations and transit agency obligations and expenditures.
We interviewed and reviewed written responses from FTA officials about how they were implementing provisions of the CARES Act; the Consolidated Appropriations Act, 2021; and ARPA. In addition, we conducted semi-structured interviews with officials from 15 Capital Investment Grants project sponsors. We interviewed officials, either by phone or through written questions and responses, to gather information on how project costs and timeframes have changed, if at all, due to the COVID-19 pandemic, and how project sponsors are using ARPA funding to support their projects. We also spoke with these officials to identify any challenges they faced using ARPA relief funding and steps FTA had taken to address these challenges. We identified these project sponsors as being the sponsors for the 20 Capital Investment Grants projects that had obligated ARPA funds as of January 19, 2022. In some cases, sponsors were responsible for multiple Capital Investment Grants projects that received ARPA funding, including one additional project which the sponsor began obligating funding for after January 19, 2022. This addition yielded a total of 21 projects in our analysis.
Agency Comments
We provided DOT and the Office of Management and Budget (OMB) with a draft of this enclosure. DOT provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
Our work on transit industry COVID-19 relief funds is ongoing.
Related GAO Products
Capital Investment Grants Program: FTA Should Improve the Effectiveness and Transparency of Its Reviews. GAO-20-512. Washington D.C.: July 16, 2020.
Contact information: Andrew Von Ah, (213) 830-1011, vonaha@gao.gov
The Small Business Administration has addressed one recommendation we previously made for the Paycheck Protection Program by developing and implementing an oversight plan for the program. It has partially addressed the three other recommendations we made. In December 2021, the agency provided a fraud risk assessment that had been prepared by its contractor, and in February 2022, it designated an antifraud entity that will be responsible for completing the assessment and developing a comprehensive antifraud action plan. The agency has developed a sampling plan and intends to report the program’s improper payment rate in its Fiscal Year 2022 Agency Financial Report.
Going forward, there are several lessons learned from the Paycheck Protection Program that could be applied to future emergency lending programs, including conducting a risk assessment when designing the program, incorporating strong oversight from the beginning of the program, and maintaining central documentation of program changes.
Entities involved: Small Business Administration, Department of the Treasury
Background
Since March 2020, Congress has provided commitment authority of about $814 billion for the Paycheck Protection Program (PPP) under the Small Business Administration’s (SBA) largest guaranteed loan program, its 7(a) small business lending program.[331] PPP loans, made by lenders but guaranteed 100 percent by SBA, are low interest (1 percent) and fully forgivable if certain conditions are met.[332]
PPP closed in May 2021, and as of March 27, 2022, lenders had made about 11.4 million PPP loans, totaling about $789 billion.[333] Of those, lenders made about 5.1 million loans (totaling about $518 billion) during Round 1 (April through August 2020). SBA relaunched the program (Round 2) on January 11, 2021, following enactment of the Consolidated Appropriations Act, 2021, which authorized additional PPP loans and made changes to the program. Among other things, the act expanded the categories of forgivable nonpayroll costs and allowed PPP borrowers to receive a second PPP loan (second draw loans) of up to $2 million, provided that they met certain criteria.[334] In Round 2, lenders made about 6.3 million loans totaling about $271 billion.
SBA implemented the program rapidly, and millions of small businesses have benefited from PPP.[335] However, the speed with which SBA implemented the program left it with limited safeguards to identify and respond to program risks, including susceptibility to improper payments and fraud. Consequently, we have made four recommendations in our prior bimonthly and quarterly CARES Act reports to help ensure program integrity, achieve program effectiveness, and address potential fraud. As discussed below, SBA has addressed one of the recommendations and partially addressed the other three.
Overview of Key Issues
Status of SBA’s loan forgiveness determinations. Based on our analysis of loan-level SBA data as of January 2, 2022, of the approximately 11.5 million PPP loans, SBA had received forgiveness decisions from lenders for about 9.3 million loans (about 81 percent).[336] The number of lender forgiveness decisions submitted to SBA peaked in August 2021 at around 1.3 million and has decreased each subsequent month, to about 390,000 in December 2021. SBA made forgiveness determinations on 9.2 million of the submitted forgiveness decisions, resulting in the vast majority, about 97 percent (9.0 million loans totaling more than $643 billion), receiving full forgiveness (see figure). About 104,000 lender forgiveness decisions were still being reviewed by SBA.[337]
Status of SBA Loan Forgiveness Determinations on Paycheck Protection Program Loans, as of Jan. 2, 2022
Note: As of January 2, 2022, lenders had not submitted loan forgiveness decisions for 2,172,874 PPP loans. Borrowers may not have submitted loan forgiveness applications to their lenders for these outstanding loans, as they typically have between 2 and 5 years, depending on when the loan was made, to apply for forgiveness.
In general, Community Development Financial Institutions (CDFI), Minority Depository Institutions (MDI), and nonbanks were the least likely to have submitted loan forgiveness decisions to SBA for their borrowers, as of January 2, 2022.[338] This pattern is more pronounced for loans made in 2021, as less than two-thirds of borrowers from CDFIs and MDIs (57 percent) and nonbanks (64 percent) had their loan forgiveness decisions submitted to SBA (see figure).[339] In contrast, smaller banks and credit unions had submitted loan forgiveness decisions for 81 percent of their borrowers who received loans in 2021. According to SBA officials, small banks, as compared to CDFIs and MDIs, have been working more effectively with their borrowers to collect forgiveness applications and submit decisions.[340]
Percentage of Paycheck Protection Program Loans with Loan Forgiveness Decisions Submitted to SBA by Lender Type and Year, as of Jan. 2, 2022
Note: For this analysis, “banks and credit unions” include banks, credit unions, and savings and loan associations. All nondepository lenders are categorized as “nonbanks,” including SBA Small Business Lending Companies, SBA Certified Development Companies, SBA Microlenders, Business and Industrial Development Corporations, Farm Credit System lenders, and state-regulated financial companies. We excluded 780 loans made in 2020 and 1,797 loans made in 2021 from our analysis because SBA’s data did not have an asset size for the lender.
Status of program oversight. In January 2022, SBA finalized an updated Master Review Plan for the review of loans made under the program and loan forgiveness decisions. The updated plan builds upon the one SBA provided us in December 2020 and includes an overview of the three types of reviews that SBA and its contractor conduct: an automated screening of all loans at both the individual loan and aggregate levels, a manual review of selected loans, and a quality control review of a sample of loans.[341] The updated plan includes additional information and incorporates changes to some of the reviews.
Automated review of loans made in 2021. Unlike the 2020 loans where SBA used an automated system to review loans after they were made, the plan describes additional screening performed for 2021 first and second draw loan applications before the loans were originated. To screen these loans, the contractor used a subset of the automated screening rules it used to review the 2020 loans for potential indicators of eligibility or fraud risks. The plan describes some of the elements included in these reviews and how lenders could resolve identified issues.
Contractor manual review of loans. In its updated plan, SBA revised some aspects of its manual review process. For example, it no longer requires all loans of $2 million or more to receive a manual review. Rather, they, like loans of less than $2 million, could receive a manual review if they were identified by the automated screening process or separately flagged for manual reviews. The updated plan also eliminated the loan necessity questionnaires that certain borrowers previously had to complete (discussed more below). In addition, the updated plan describes the following steps SBA has taken that affected the number and timing of manual reviews to be conducted. Specifically, SBA:
cleared (without performing a manual review) batches of loans that were identified as being in specific categories that present minimal risk of noncompliance with eligibility requirements, fraud, or abuse;
prioritized manual reviews based on their perceived risk and not the forgiveness request date; and
applied machine learning to identify alerts that indicated minimal risk of noncompliance with eligibility requirements, fraud, or abuse and could be cleared without manual reviews.[342]
By implementing the updated plan and the more detailed procedures referenced in it, SBA has, at least in part, addressed our concerns about the initial lack of upfront controls in the PPP loan approval process.[343] Through the backend screening of Round 1 loans, the upfront screening of Round 2 loans, and more detailed reviews of loans with potential problems, SBA has improved its oversight of the program.
Lessons learned for future emergency small business lending programs. The negative effects of the pandemic on small businesses led Congress to create a variety of programs to help affected businesses. PPP was the largest of these programs. Our evaluation of SBA’s implementation of the program, along with challenges highlighted by lenders and the SBA Office of Inspector General (OIG), offer possible lessons learned for future emergency-lending programs.
Provide clear legislative direction. Although Congress substantially outlined the structure for PPP in the CARES Act and subsequent legislation, it left key policy decisions to SBA and Treasury. The agencies’ implementation decisions affected both borrowers and lenders, and Congress passed subsequent legislation to provide more specific direction for the program.
While Congress did not put requirements into statute, it did express its views in a Sense of the Senate statement in the CARES Act that SBA should encourage lenders and agents to prioritize small business concerns and entities in underserved and rural markets, including veterans and members of the military community, small business concerns owned and controlled by socially and economically disadvantaged individuals, and businesses in operation for less than 2 years.[344] However, SBA stated in its initial interim final rule that PPP was “first-come, first-served.”[345] In addition, SBA did not ask for demographic information on the PPP loan application used in 2020, and few applicants provided this information.[346]
Subsequently, when Congress appropriated additional funding for PPP in April 2020, it allocated a total of $60 billion for PPP loans made by certain small insured depository institutions, certain small credit unions, and community financial institutions that are recognized as more likely to serve minority, underserved, veteran, and women-owned small businesses than other lending institutions.[347] In addition, the Consolidated Appropriations Act, 2021 included a provision that all future PPP applications include a means by which applicants may, at their discretion, submit demographic information including sex, race, ethnicity, and veteran status of the owner.[348] In January 2021, SBA revised its PPP loan application to request optional demographic data.
There was also a lack of clarity on the relevance of a business’s need for a PPP loan. When it created PPP, Congress eliminated the 7(a) program’s requirement that applicants demonstrate they cannot obtain credit through a conventional lender at reasonable terms—commonly referred to as the “credit elsewhere” requirement.[349] Instead, the CARES Act required applicants to make a good faith certification “that the uncertainty of current economic conditions makes necessary the loan request to support the ongoing operations of the eligible recipient,” among other things.
However, neither Congress nor SBA elaborated on this “economic necessity” requirement until after concerns were raised about some publicly traded companies receiving PPP loans. On April 23, 2020, SBA provided general information in a response to a frequently asked question (FAQ) published on its website that borrowers should carefully review the required certification to ensure that they qualify.[350] In the same response, SBA reiterated that borrowers must self-certify that their PPP loan was necessary, and stated that it was unlikely that a publicly traded company with substantial market value and access to capital markets would be able to make this certification in good faith. However, by then, more than 1.6 million businesses had received a PPP loan, including some publicly traded companies that potentially had access to alternative forms of credit.[351]
SBA announced in October 2020 that it would use questionnaires to inform its assessment of a business’s good faith certification of economic necessity. Released in December 2020, these questionnaires required for-profit and nonprofit businesses that, together with their affiliates, received PPP loans with an original principal amount of $2 million or greater to complete the questionnaire. However, in July 2021, SBA announced that it would no longer use the questionnaires, explaining that the reviews were resource intensive and had caused delays beyond the 90-day statutory timeline for forgiveness and that the results of the reviews it had completed showed that audit resources would be more efficiently deployed across all loans.[352] While SBA’s updated Master Review Plan discusses the questionnaires’ discontinuance, it does not mention whether SBA intends to use other means to evaluate an applicant’s economic necessity certification.
Finally, there has been confusion over eligibility for PPP loans. The CARES Act provided that in addition to small businesses, certain nonprofits, veterans’ organizations, and Tribal business concerns were eligible for PPP loans, but did not specify whether SBA should apply its existing loan eligibility restrictions or use different criteria. In its initial interim final rule, SBA determined that existing eligibility restrictions applicable to SBA business loans would also apply to PPP loans.[353] In addition, the CARES Act did not address whether businesses in bankruptcy were eligible for PPP loans. SBA determined that an applicant that was the debtor in a bankruptcy proceeding, either when it submitted the application or at any time before the loan was disbursed, was ineligible to receive a PPP loan. These eligibility criteria have been the subject of litigation.[354]
For second draw PPP loans, Congress expressly excluded several categories of businesses by incorporating certain eligibility restrictions contained in SBA regulation and excluding businesses primarily engaged in lobbying or political activities.[355] The statutory exclusion of specific categories of borrowers from eligibility for PPP loans could help limit future controversy involving eligibility.
Consider available resources and adjust where needed. SBA was able to launch PPP quickly in part because Congress created it under the 7(a) program. Under the CARES Act, lenders already approved for the 7(a) program were automatically approved to make PPP loans on a delegated basis, and SBA and Treasury could approve additional lenders to participate in the program.[356] However, nonbanks were largely unable to participate in the initial phase of the program.[357] As PPP continued, the proportion of loans made by nonbanks, CDFIs, and MDIs increased significantly, suggesting the need for their services.
SBA also relied on its existing 7(a) loan processing system when it launched PPP. However, the system was not built to process the volume of loans SBA received. For example, the SBA OIG reported in January 2021 that some PPP lenders had challenges accessing the system or experienced slow loan application processing times at the beginning of the program, which most likely delayed loan funds to some borrowers.[358] To address these problems, SBA officials told us that they increased the processing system’s memory, expanded the number of telecommunication lines, established a pacing mechanism to limit the number of loans any one lender can enter into the system per hour, and established batch file processing for lenders. However, SBA officials noted they could not implement these improvements as quickly as they wanted because of delays due to COVID-19, such as supply chain issues.
When SBA relaunched PPP in January 2021, it also launched a revised application portal tailored to PPP. Among other things, this system could support higher volume submissions and incorporated additional validations to prevent fraud that were not in place in the previous system, such as cross-referencing applicant information with Treasury’s Do Not Pay List.[359]
Conduct a risk assessment when designing and implementing a new program. For PPP, SBA did not follow its established process to identify and address potential risks in programs.[360] Within SBA, two offices are responsible for working with program offices to identify and respond to potential risks. More specifically, the Office of Continuous Operations and Risk Management is responsible for, among other things, agency-wide recovery response for disasters and the evaluation and assessment of SBA’s critical risks and nonfinancial internal controls. The office also oversees SBA’s Enterprise Risk Management program.[361] In addition, according to an SBA official, when SBA implements a new program, the Office of Internal Controls coordinates with the program office to plan proper internal controls and ensure they are implemented. However, neither office was involved in the design or initial implementation of program controls for PPP.
SBA officials stated that while risk assessments usually occur during program planning, such assessments did not occur until PPP was implemented, and then only informally. According to SBA’s Enterprise Risk Management guidance, program offices should identify and assess potential risks to a program, both initially and on an ongoing basis, to identify new, emerging, or changing risks. Potential risks include fraud, improper payments, infrastructure (such as information technology) problems, or misstatements in SBA’s consolidated financial statements.[362] Once risks have been identified and assessed, a program office should strategize its response to minimize the risks and then implement and monitor those plans. Officials acknowledged that the guidance was not followed, noting that PPP was atypical, as it was an emergency program that SBA was mandated to launch in less than 2 weeks.
Incorporate strong oversight from the beginning of the program. In an effort to launch PPP quickly and help small businesses, SBA officials said they put limited initial safeguards in place to help expedite the loan approval process, consistent with a mandate from Congress to provide rapid support for small businesses that was reinforced by Treasury. SBA’s initial interim final rule for PPP allowed lenders to rely on borrower self-certifications to determine borrowers’ eligibility and use of loan proceeds—which we noted in our March 2020 report can leave a program vulnerable to exploitation. The interim final rule also required limited lender review of documents provided by borrowers to determine the qualifying loan amount and eligibility for loan forgiveness. In addition, SBA did not conduct any review of loan or borrower information beyond looking for duplicate applications before agreeing to guarantee the loan.[363]
In June 2020, we found that while SBA and Treasury announced SBA would review loans of more than $2 million, SBA had not provided details on how it would conduct these reviews. SBA also had not described any reviews planned for loans of less than $2 million. Therefore, we recommended that SBA develop and implement plans to identify and respond to risks in PPP to ensure program integrity, achieve program effectiveness, and address potential fraud.
Consistent with our recommendation, SBA put in place additional oversight. As noted previously, SBA developed and began to implement a Master Review Plan for the loan review process, which outlined the three types of reviews it would conduct. To help implement this process, SBA hired a contractor with expertise in fraud detection. The contractor implemented an automated rules-based tool to screen all PPP loans to identify anomalies or attributes that may indicate noncompliance with eligibility requirements, fraud, or abuse, such as whether the borrower used the tax identification number of a deceased person. The contractor conducted the automated screenings for the approximately 5.1 million Round 1 PPP loans in August and early September 2020, and applied a version of the screening when SBA relaunched PPP in January 2021. Loans with identified potential issues were delayed from being closed until the issue was resolved.[364]
However, SBA and its contractor only began reviewing loans after Round 1 had finished and some businesses had begun applying for forgiveness.[365] In addition, as noted previously, SBA made revisions to its Master Review Plan after all PPP loans were made and the majority had been forgiven.[366] Although SBA could still attempt to recover funds from ineligible and fraudulent borrowers, we have previously reported that a leading practice in designing and implementing an antifraud strategy is to focus on fraud prevention over detection and response to avoid a “pay-and-chase” model, to the extent possible.[367]
Take early steps to estimate improper payments and determine fraud risks. The lack of initial safeguards for PPP contributed to the increased risk of improper payments, including fraud that we and others have reported.[368] Because SBA had not yet taken steps to address this risk, we recommended in November 2020 that SBA expeditiously estimate improper payments and report estimates and error rates for PPP. SBA noted in March 2022 that it would officially report the improper payment rate for PPP in its Fiscal Year 2022 Agency Financial Report. However, because SBA will have forgiven most loans by the time SBA reports on its improper payment testing, the testing will have limited usefulness in preventing improper payments.
Similarly, because SBA had not yet done so, we recommended in March 2021 that it conduct a comprehensive fraud risk assessment for PPP in alignment with leading practices and document an antifraud strategy (a strategic approach to managing fraud risks). According to SBA officials, because of the rapid response required to execute the program, SBA conducted an informal fraud risk assessment in late spring and early summer of 2020. This assessment included an identification of potential weaknesses in internal control processes by subject matter experts in the program office. The agency did not document findings from the assessment.
An SBA contractor ultimately conducted a fraud risk assessment for PPP in October 2021. The assessment found that SBA implemented additional fraud prevention controls over the course of the program—such as cross-referencing applicant information with Treasury’s Do Not Pay List and introducing a set of automated screening rules prior to the release of the SBA loan guarantee number. However, it noted that PPP continued to be susceptible to fraud risks that required enhancements to the current mitigation strategies. The contractor identified 25 active fraud risks in PPP and made four recommendations to SBA to aid the agency in establishing a fraud governance process and inform the agency’s fraud tolerance approach. If SBA had conducted a fraud assessment earlier in the program, it could have targeted its controls to further minimize risks. Although the timing of the assessment limited its usefulness for PPP, SBA could use the results of this fraud assessment to inform future programs.
In addition, we found in March 2021 that one factor that contributed to the lack of a timely fraud risk assessment of PPP was that SBA had not designated a dedicated entity to lead fraud risk management activities. As discussed in GAO’s Fraud Risk Framework, it is a leading practice to designate an entity to design and oversee fraud risk management activities. In carrying out its role, the antifraud entity, among other things, manages the fraud risk-assessment process. According to documentation provided by SBA, the agency designated such an entity in February 2022 that is responsible for the oversight and coordination of SBA’s fraud risk prevention, detection, and response activities.
Maintain central documentation of program changes. Throughout its implementation of PPP, SBA issued rolling guidance. According to SBA officials, SBA and Treasury continued to develop and issue rules and guidance in an effort to be responsive to lenders and borrowers and to implement statutory changes to the program. However, this guidance was often piecemeal and created confusion among lenders and borrowers.
Because PPP was an emergency program, SBA officials told us the agency did not issue a consolidated guidance document (such as a standard operating procedure) when PPP was launched. Instead, SBA relied on interim final rules, updates to FAQs, and procedural notices to expedite program implementation. As of January 1, 2022, SBA had issued 32 interim final rules and 28 updates to its PPP FAQs. Of these, roughly two-thirds were made from March 31, 2020, when SBA issued the initial program guidance, through August 8, 2020 (the end of the first round).
As we reported in July 2021, our survey of PPP lenders indicated that the changing guidance, presented in various document types, created challenges during Round 1.[369] We estimated that about 87 percent of PPP lenders thought changes in program rules and guidance were either very or moderately challenging when approving loan applications.[370] One survey respondent noted that it was particularly challenging when the bank was receiving many PPP applications at the same time and had to simultaneously read dozens of pages of new guidance. Similarly, we estimated that 75 percent of lenders thought the lack of a central document containing the program’s rules and guidance was either very or moderately challenging.[371]
By contrast, SBA released a more comprehensive interim final rule when it relaunched PPP in January 2021 and one for the loan forgiveness process a month later.[372] While SBA had to provide subsequent guidance to clarify other aspects of the program, these more comprehensive documents provided borrowers and lenders easier access to the program’s rules.
Ensure clear communication with key constituencies. SBA also could have lessened the impact of program changes by improving its communication with key constituencies. For example, as we reported in June 2020, representatives of two lender associations and a small business association told us that their members found it difficult to reach anyone at SBA district offices to get clarification on guidance; when someone did answer, members noted that the person did not always know the answer or provided incorrect information.
Similarly, SBA did not communicate clearly prior to implementing the additional program controls when it relaunched PPP in January 2021. Representatives of the four lender associations we interviewed told us the additional controls created confusion among lenders and delays in closing loans, in part, because lenders did not know of the additional controls in advance. In addition, the representatives told us their members were unable to get responses from SBA when they had questions related to the hold codes SBA placed on some Round 1 loan applications, which affected borrowers’ ability to receive a second draw loan until the issue was resolved.
Because of these communication challenges, we recommended in July 2021 that SBA develop and implement a process to help ensure it responds in a timely manner to PPP lender inquiries on loan reviews. SBA agreed with the recommendation, and SBA officials told us in October 2021 that they had taken steps to improve communication with lenders, such as having a customer service team handle all the lender inquiries from the lender platform and communicate to lenders reasons for delays or issues with loan reviews.
In March 2022, SBA provided us with documentation on procedures its customer service staff are to follow and templates for responses to questions. The procedures describe how SBA staff are to respond and track lender inquiries SBA receives through the platform lenders use to submit loan forgiveness decisions to SBA. In the sample templates created following our recommendation, SBA provided its staff with draft responses for communicating with lenders. For example, one template provides draft language to help lenders submit additional documentation when there is an identified problem but the platform does not accept the submission, allowing the process to continue.
The more extensive outreach that SBA conducted to lenders prior to launching its direct forgiveness portal, which provides certain PPP borrowers a streamlined process to submit their forgiveness application to their lender, demonstrates the benefits of early and effective communication.[373] SBA conducted a series of webinars and created a PPP customer service team to answer questions and directly assist borrowers with their forgiveness applications. Representatives from one lender association we spoke with noted that their members who were using the portal reported that the system was working very well, and that SBA and its vendor had been very accommodating when asked to make adjustments to improve process operations.
Methodology
To conduct this work, we analyzed SBA loan-level forgiveness data as of January 2, 2022. We assessed the reliability of the SBA data by performing electronic testing, reviewing documentation, and interviewing SBA officials. We determined that the data were sufficiently reliable for reporting the status of loan forgiveness determinations. We also reviewed SBA’s most recent oversight plan for PPP to identify changes, and our prior reports on PPP and reports issued by the SBA OIG to identify lessons learned.
Agency Comments
We provided SBA, Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. Treasury provided technical comments, which we incorporated as appropriate. SBA and OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
Our work on PPP is ongoing. We continue to examine the fraud risks in the program. We also continue to monitor SBA’s progress toward developing and implementing corrective actions to address the material weaknesses identified in December 2020 and 2021 by its independent financial statement auditor.
GAO’s Prior Recommendations
The table below presents our PPP recommendations from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to the Paycheck Protection Program
Recommendation
Status
The Administrator of the Small Business Administration (SBA) should conduct and document a fraud risk assessment for the Paycheck Protection Program (PPP). (March 2021 report)
Open—partially addressed. SBA agreed with the recommendation. In December 2021, SBA provided a fraud risk assessment that had been prepared by its contractor. Based on our initial review of the assessment, it adhered to many but not all fraud risk management leading practices. For example, SBA did not determine its fraud risk tolerance as called for by leading practices. In February 2022, SBA designated an antifraud entity that, according to SBA officials, would be responsible for determining a risk tolerance and implementing the fraud risk assessment’s recommendations.
The Administrator of SBA should develop a strategy that outlines specific actions to monitor and manage fraud risks in the Paycheck Protection Program on a continuous basis. (March 2021 report)
Open—partially addressed. SBA agreed with the recommendation, stating that it would work to ensure that fraud risks are monitored on a continuous basis. In December 2021, SBA provided a fraud risk assessment, which would inform an antifraud strategy. In February 2022, SBA designated an antifraud entity that is responsible for oversight and coordination of SBA’s fraud risk prevention, detection, and response activities. They had told us previously that once designated, the entity would work to develop an agency-wide comprehensive antifraud action plan.
The Administrator of SBA should expeditiously estimate improper payments and report estimates and error rates for PPP due to concerns about the possibility that improper payments, including those resulting from fraudulent activity, could be widespread. (November 2020 report)
Open—partially addressed. SBA neither agreed nor disagreed with our recommendation at the time of our report. In response to our recommendation, SBA stated that it was planning to conduct improper payment testing for PPP and that it takes improper payments seriously. In July 2021, SBA officials said that SBA would estimate both improper payments and error rates for PPP in the fourth quarter of fiscal year 2021. In February 2022, SBA provided a copy of its sampling plan dated July 2021. They noted in March 2022 that SBA would officially report the improper payment rate in its Fiscal Year 2022 Agency Financial Report. We will continue to monitor SBA’s progress in implementing our recommendation.
The Administrator of SBA should develop and implement plans to identify and respond to risks in PPP to ensure program integrity, achieve program effectiveness, and address potential fraud, including in loans of $2 million or less. (June 2020 report)
Closed—addressed. At the time of our report, SBA neither agreed nor disagreed with our recommendation. In late December 2020, SBA provided a Master Review Plan outlining steps it planned to take to review the PPP loans made in 2020. The document described three steps in the process: automated screenings of all loans, manual reviews of selected loans, and quality control reviews to ensure the quality, completeness, and consistency of the review process. Most of the loan reviews were to be conducted by contractors with SBA oversight. SBA later updated the plan in January 2022 to incorporate changes to its oversight, including the screening performed of 2021 loan applications before the loans were originated.
To implement the plan, SBA’s loan review contractor conducted automated screenings for all of the PPP loans made in 2020 in August and early September 2020. Specifically, the contractor used an automated rules-based tool to compare PPP loan data against publicly available information and apply eligibility and fraud detection rules to identify anomalies or attributes that may indicate noncompliance with eligibility requirements, fraud, or abuse. For example, the tool would flag loans made to a borrower in active bankruptcy or one who used the tax identification number of a deceased person. SBA and its contractor began conducting manual reviews of flagged loans of less than $2 million in early November 2020, and of loans of $2 million or more in January 2021. Starting in January 2021, SBA screened all PPP loans before the lender approved the loan. To screen these loans, the contractor used a subset of the automated screening rules it used to review the 2020 loans for potential indicators of non-eligibility or fraud risks. According to SBA officials, contractor staff had completed about 78,000 manual reviews and referred about 8,900 loans to SBA for further review, as of November 15, 2021. SBA will continue to conduct manual reviews of flagged loans.
Paycheck Protection Program: SBA Added Program Safeguards, but Additional Actions Are Needed. GAO-21-577. Washington, D.C.: July 29, 2021.
Aviation: FAA Needs to Better Prevent, Detect, and Respond to Fraud and Abuse Risks in Aircraft Registration. GAO-20-164. Washington, D.C.: March 25, 2020.
Small Business Administration: Leadership Attention Needed to Overcome Management Challenges. GAO-15-347. Washington, D.C.: September 22, 2015.
A Framework for Managing Fraud Risks in Federal Programs.GAO-15-593SP. Washington, D.C.: July 18, 2015.
Contact information: William B. Shear, (202) 512-8678, shearw@gao.gov
The Department of the Treasury has taken actions to collect and analyze planning information and spending data from states, territories, tribal governments, and local governments. The Department continues to develop policies and procedures for monitoring recipients of Coronavirus State and Local Fiscal Recovery Funds.
Entities involved: Department of the Treasury
Background
The Coronavirus State and Local Fiscal Recovery Funds (CSLFRF), established under the American Rescue Plan Act of 2021 (ARPA) and administered by the Department of the Treasury, allocated $350 billion to states, the District of Columbia, local governments, tribal governments, and U.S. territories to help cover a broad range of costs stemming from the fiscal effects of the COVID-19 pandemic.[374] Local governments consist of metropolitan cities, counties, and smaller local governments—those typically serving populations of less than 50,000— referred to as non-entitlement units of local government (NEU).[375]
Treasury had distributed more than $245 billion in CSLFRF allocations to recipients as of March 2, 2022, according to Treasury. The figure below shows the amounts of funding the CSLFRF allocates to various recipient types as well as the amount of funding Treasury distributed to each recipient type as of March 2, 2022. CSLFRF recipients have until December 31, 2024, to incur obligations with their CSLFRF awards and, according to Treasury, until December 31, 2026, to liquidate those obligations, in accordance with allowable uses established in ARPA.[376]
Coronavirus State and Local Fiscal Recovery Funds Allocations and Treasury Distributions as of Mar. 2, 2022, by Recipient Type
aNon-entitlement units of local government (NEU), are local governments typically serving populations of less than 50,000. 42 U.S.C. §§ 803(g)(5), 5302(a)(5). NEUs include cities, villages, towns, townships, or other types of local governments.
bA metropolitan city is defined as the central city within a metropolitan area (i.e., a standard metropolitan statistical area as established by the Office of Management and Budget) or any other city within a metropolitan area that has a population of 50,000 or more. 42 U.S.C. §§ 803(g)(4), 5302(a)(3)-(4). A metropolitan city includes cities that relinquish or defer their status as a metropolitan city for purposes of receiving allocations under section 5306 of title 42, United States Code, for fiscal year 2021.
cARPA provides that to receive their Coronavirus State and Local Fiscal Recovery Funds award, states, the District of Columbia, and U.S. territories must first provide Treasury with a signed certification stating that they require their award to carry out allowable activities and will comply with relevant requirements when they use their award. According to Treasury, states that had experienced a net increase of more than 2 percentage points in their unemployment rate from February 2020 to the date of the latest available data at the time the state certified for their payment received their full award in a single payment; other states receive award funds in two equal tranches, with the second tranche provided within 12 months after certification. Governments of U.S. territories will receive an award in a single payment. Treasury is required to distribute awards to metropolitan cities, states (for distribution to NEUs), and counties in two equal tranches, providing the first payment within 60 days after ARPA’s enactment, or May 10, 2021, to the extent practicable, and providing the second payment no earlier than 12 months after the first. After receiving award funds for distribution to NEUs, states have 30 days to make those distributions, unless Treasury grants an extension. According to Treasury, tribal governments received their award funds in two distributions: the first distribution in May 2021 and the second distribution, based on employment data, in August 2021.
On May 10, 2021, Treasury released an interim final rule for implementing the CSLFRF that identified reporting requirements for recipients:[377]
All recipients—except NEUs—were required to submit an interim report that provided an initial overview of the status and use of their funding.
States, U.S. territories, and metropolitan cities and counties with a population that exceeds 250,000 residents are also required to submit to Treasury annually, and post on their public websites, a recovery plan performance report (recovery plan). These recovery plans are to discuss planned uses of spending and include, among other things, descriptions of the projects funded.
All recipients are required to submit project and expenditure reports on a quarterly or annual basis—depending on the type of recipient—that provide information on their use of the funding and projects undertaken with the funding, among other things. Treasury extended the deadlines to all CSLFRF recipients for submitting the first project and expenditure reports.
Treasury released subsequent guidance that provides additional detail and clarification on the compliance and reporting responsibilities for each recipient type, including reporting deadlines, as shown in the figure below.[378] CSLFRF recipients must submit all required reports through Treasury’s online reporting portal.
Treasury’s Reporting Requirements for the Coronavirus State and Local Fiscal Recovery Funds, by Recipient Type, as of Feb. 28, 2022
Under ARPA, Treasury makes payments to states in two tranches (approximately 12 months apart) for NEUs, and states are required to allocate and distribute those payments to each NEU within their state.[379] According to Treasury, over 26,000 NEUs are receiving CSLFRF awards through their state governments.[380]
Treasury has issued guidance that includes steps states should follow for allocating and distributing funds to NEUs.[381] Among other things, these steps include identifying eligible NEUs, calculating initial allocation amounts, and establishing a process for NEUs to submit requests for their award.[382] Consistent with ARPA, states must also ensure an NEU’s total CSLFRF award (i.e., the sum of both tranches) does not exceed 75 percent of the NEU’s most recent budget.[383] According to Treasury guidance, states have some discretion in calculating the initial allocation of funds. For example, the guidance explains that states may divide any overlapping population between NEUs in a number of ways for the purpose of allocating funds.[384]
Overview of Key Issues
Treasury’s review of CSLFRF interim reports and recovery plan performance reports. According to Treasury officials, as of February 28, 2022, Treasury had received an interim report from 4,467 of the 4,792 recipients required to submit one, representing a 93 percent submission rate.[385] Treasury officials also told us that Treasury received a recovery plan performance report (recovery plan) from 379 of the 392 recipients required to submit one, representing a 97 percent submission rate.[386] Treasury has posted to its public website the individual interim reports and recovery plans that recipients submitted on or after August 31, 2021.[387]
Treasury officials told us that, for CSLFRF recipients that did not submit an interim report and recovery plan, Treasury sent follow-up emails notifying those recipients that they were out of compliance with the program’s requirements. Officials also told us that, for the recipients that remain non-compliant with the reporting requirements, Treasury is developing a remediation process to enforce compliance, which Treasury has not yet finalized. According to officials, the process will be consistent with the remedial actions described in the award terms and conditions that all recipients enter into prior to receiving CSLFRF funds.[388] Treasury officials also told us they are in the process of developing interim procedures to govern recipient non-compliance issues, including monitoring, remediation, penalty, and potential recoupment of funds. However, Treasury has not yet provided requested documentation regarding how and when they expect to finalize the details of their process.
In our October 2021 report, we recommended that Treasury design and document timely and sufficient policies and procedures for monitoring recipients of CSLFRF. Treasury agreed with the recommendation, which it has not yet fully implemented. Having timely and sufficient policies and procedures for monitoring CSLFRF recipients—including compliance with reporting requirements—is critical for providing assurance that recipients are managing their allocations in compliance with laws, regulations, agency guidance, and award terms and conditions, including ensuring that expenditures are made for allowable purposes.
Treasury officials told us that the agency’s review of the interim reports is complete, except for the portion of the reports related to NEU distributions, due to the additional time states needed to distribute CSLFRF funds to NEUs and report the data to Treasury. According to officials, while Treasury conducted a high-level review for completeness, it is not requiring recipients to correct or update incorrect data in the interim reports or to submit updated interim reports. Rather, Treasury has allowed recipients to provide corrected data as part of the recipient’s first project and expenditure report submission, due by either January 31, 2022, or April 30, 2022, depending on the type of recipient.
Treasury is in the process of reviewing recipients’ recovery plan submissions by performing “high-level” reviews of the data and contacting recipients to address missing information and to correct data errors. Further, Treasury officials told us that, as part of their reviews of the recovery plans, they are identifying data that may signal financial and other compliance risks, such as descriptions of potentially prohibited uses of the funds; ensuring the reports establish a baseline for future reporting; and identifying the extent to which recipients plan to use their funds to support eligible capital expenditures.[389]
Treasury officials said the agency plans to eventually cross-reference data and qualitative information across recipients’ project and expenditure reports and recovery plans. For example, Treasury may compare a recipient’s year-over-year spending and identify spending trends across certain states or other recipients with similar attributes. We asked Treasury officials about their plans for analyzing the data—including the agency’s intended uses of the data. Officials told us that, given that Treasury is in initial reporting cycles and will not receive the reports to cross-reference until sometime mid-year, Treasury views any discussion of the intended uses of the data as premature.
Treasury’s review of CSLFRF project and expenditure reports. According to Treasury officials, as of February 28, 2022, Treasury had received a project and expenditure report from 1,874 of the 1,910 recipients required to submit one by January 31, 2022, representing a 98 percent submission rate.[390] Treasury officials told us that they are currently following up with recipients who had not submitted a project and expenditure report by January 31, 2022. They also told us that, for those that have been submitted, Treasury plans to review the reports’ completeness, whether recipients addressed the requirements established in Treasury guidance and user guides, and any potential prohibited uses of funds. According to officials, Treasury is still finalizing these plans and could not provide an estimated target date for completing their review.
Further, as part of their review process, Treasury has developed steps—in the form of a flow chart—that Treasury program staff are to follow in reviewing the reports. Treasury officials told us that they expect the quality of the data submissions to improve over time as recipients complete multiple reporting cycles, particularly with Treasury’s recipient engagement and outreach efforts. Treasury officials also told us Treasury is developing a remediation process for enforcing compliance—similar to the one officials described for the interim reports and recovery plans—which Treasury has not yet finalized. According to the officials, this process will be consistent with the remedial actions described in the award terms and conditions that all recipients enter into prior to receiving CSLFRF funds.[391] However, Treasury did not provide requested documentation regarding how and when they expect to finalize the details of their process.
As we discussed above, our October 2021 report recommended that Treasury should design and document timely and sufficient policies and procedures for monitoring recipients of CSLFRF. We continue to believe that fully developing and finalizing these processes—including policies and procedures—is critical for ensuring that recipients are managing their allocations in compliance with laws, regulations, agency guidance, and award terms and conditions.
According to Treasury officials, Treasury is also in the process of hiring and training additional program staff in its Office of Recovery Programs, which oversees the CSLFRF program, to review the report submissions. Treasury officials also told us they anticipate that these staff will be trained to review other CSLFRF reports.
Treasury officials told us that they are in the early stages of determining how and when to make project and expenditure report data publicly available, including the types of data they plan to post on Treasury’s website or another public-facing platform and the timeframes for doing so. Treasury officials told us that once they have had an opportunity to review the submissions they expect to have a better understanding of how the data could be made publicly available.
Treasury’s NEU validation efforts. Treasury officials told us that after states collect the required information from NEUs for determining their eligibility for receiving CSLFRF allocations, Treasury will verify and validate the information to create accounts for NEUs in Treasury’s online reporting portal. According to Treasury officials, Treasury validated 26,092 eligible NEUs and had created accounts in its reporting portal for nearly all of them (26,064), as of March 17, 2022.
Treasury continues to create portal accounts for all eligible NEUs, pending accurate NEU information. Treasury relies on state-provided NEU information to create a portal account for each NEU. This information includes relevant NEU contact information for individuals responsible for managing the CSLFRF payments. We reported in January 2022 that Treasury had concerns with the quality and completeness of NEU contact information. According to Treasury officials, if states cannot provide Treasury with accurate NEU contact information, Treasury may be unable to create a portal account for every NEU in advance of the April 30, 2022, project and expenditure report submission due date. Treasury officials told us they are working closely with states to conduct data quality checks to help ensure that NEUs that received CSLFRF payments have an account in Treasury’s portal in advance of the first project and expenditure report due date.
In addition, Treasury officials told us they are checking the state-provided NEU data to ensure that states have not distributed payments to NEUs that exceed 75 percent of the NEU’s most recent budget that was in effect as of January 27, 2020.[392] As of March 17, 2022, five states provided one or more NEUs a payment that exceeded the 75 percent budget cap, according to Treasury officials. Treasury officials told us they are coordinating with those states to correct these payments. According to Treasury’s CSLFRF award terms and conditions, a recipient will owe a debt to the federal government if the recipient’s CSLFRF payments exceed its authorized funding amount.[393] Treasury can take any actions available to it to collect this debt; however, according to Treasury officials, they have not yet determined whether and which actions are needed.
Once an NEU’s account is established in Treasury’s reporting portal and prior to the April 30, 2022, due date, an NEU must provide Treasury copies of three documents: (1) an actual budget document validating the top-line budget total provided to the state as part of the request for funding, (2) a signed award terms and conditions agreement, and (3) a signed assurance of compliance with Title VI of the Civil Rights Act of 1964. NEUs that have a formal budget document must upload it into the reporting portal. Those without a formal budget document must upload the certification they provided to the state that affirmed their top-line budget, according to Treasury officials. Treasury officials said NEUs will not be able to submit a project and expenditure report without the required documentation.
Treasury officials told us they are reaching out to individual NEUs after creating their portal accounts to initiate contact and facilitate future communication. They also told us that in the spring of 2022 they plan to send NEUs reminders about uploading the required documentation for the project and expenditure report submissions. In addition, Treasury officials said they established a call center to provide NEUs and other CSLFRF recipients with individualized support.
Methodology
We reviewed federal laws and Treasury regulations, guidance, and documentation regarding the CSLFRF. We also interviewed Treasury officials and analyzed Treasury’s written responses to questions that we posed.
Agency Comments
We provided Treasury and OMB with a draft of this enclosure. Treasury provided technical comments, which we incorporated as appropriate. OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
Our work on the CSLFRF is ongoing. We will continue to review how CSLFRF recipients use their awards, address challenges they face in managing the funds, and evaluate outcomes of their funded projects. We will continue to monitor Treasury’s efforts to provide CSLFRF guidance and monitor funds. We will also continue to follow up on open recommendations.
GAO’s Prior Recommendations
The table below presents our recommendation on the CSLFRF from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to Coronavirus State and Local Fiscal Recovery Funds (CSLFRF)
Recommendation
Status
The Secretary of the Treasury should design and document timely and sufficient policies and procedures for monitoring recipients of Coronavirus State and Local Fiscal Recovery Funds to provide assurance that recipients are managing their allocations in compliance with laws, regulations, agency guidance, and award terms and conditions, including ensuring that expenditures are made for allowable purposes. (October 2021 report)
Open—partially addressed. Treasury agreed with the recommendation. In December 2021, Treasury officials stated the agency expected to have drafts of internal control policies and procedures for CSLFRF finalized in the coming weeks. As of February 2022, Treasury had not provided those draft policies and procedures. Treasury officials also stated they are taking steps towards developing processes for monitoring CSLFRF recipients, but had not yet finalized those processes. We will continue to monitor the actions Treasury takes in response to our recommendation.
As states and localities make progress spending the more than $1 trillion provided to federal agencies for COVID-19 assistance, some challenges emerged that warrant ongoing attention as implementation continues in the coming years. These challenges included differences in states’ and localities’ experiences implementing new versus existing programs and funds, confusion about which programs and funds should be used for specific purposes when allowable uses are similar, and managing different reporting requirements.
Background
The coronavirus relief laws enacted between March 2020 and March 2021 provided more than $1 trillion to federal agencies to provide assistance related to the COVID-19 pandemic to states, the District of Columbia, localities, U.S. territories, and Indian tribes through existing and newly created programs and funds.[394]
The table below lists 13 programs and funds that each received $10 billion or more—exclusively or primarily for states, the District of Columbia, localities, U.S. territories, and tribes—in at least one of the six COVID-19 relief laws.
COVID-19 Relief Funding for Federal Programs and Funds That Received $10 billion or More in Aid for States, the District of Columbia, Localities, U.S. Territories, and Tribes
Programs and funds
Descriptions
Appropriations ($ in billions)
Coronavirus State and Local Fiscal Recovery Funds
Administered by the Department of the Treasury, these funds provide payments to states, the District of Columbia (D.C.), U.S. territories, tribal governments, and localities to mitigate the fiscal effects stemming from the COVID-19 pandemic.
350
Elementary and Secondary School Emergency Relief Fund
Administered by the Department of Education, this fund generally provides formula grants to states (including D.C. and Puerto Rico) for education-related needs to address the impact of the COVID-19 pandemic.
190.3
Coronavirus Relief Fund
Administered by Treasury, this fund provides payments to states, D.C., localities, U.S. territories, and tribal governments to help offset costs of their response to the COVID-19 pandemic.
150
Disaster Relief Fund
Administered by the Federal Emergency Management Agency, this fund provides federal disaster recovery assistance for state, local, tribal, and territorial governments when a major disaster occurs.
95a
Medicaid
Administered by states and U.S. territories according to plans approved by the Centers for Medicare & Medicaid Services, which oversees Medicaid at the federal level. This program finances health care for certain low-income and medically needy individuals through federal matching of states’ and U.S. territories’ health care expenditures. The Families First Coronavirus Response Act and the American Rescue Plan Act of 2021 temporarily increased federal Medicaid matching rates under specified circumstances, among other changes.
76.9b
Transit Grants
Administered by the Federal Transit Administration, these funds are distributed through existing grant programs to provide assistance to states, localities, U.S. territories, and tribes to prevent, prepare for, and respond to the COVID-19 pandemic.
69.5
Child Care and Development Fundc
Administered by the Department of Health and Human Services (HHS), this program provides funds to states, D.C., territories, and tribes to subsidize the cost of child care for low-income families. COVID-19 relief funds have supported assistance to health care and other essential workers without regard to income eligibility requirements. Additional child care stabilization funding was provided for sub-grants to eligible child care providers to support the stability of the child care sector during and after the COVID-19 pandemic.
52.5
Emergency Rental Assistance
Administered by Treasury, this program provides assistance to states, D.C., U.S. territories, localities, and tribes to assist eligible households with rent, utilities and home energy costs, and other expenses related to housing and housing stability.d
46.6
Public Health and Social Services Emergency Fund
Administered by HHS, this fund provides for grants to states, U.S. territories, localities, and tribal governments to support COVID-19 testing, surveillance, and contact tracing, among other uses.
33.4
Airport Grantse
Administered by the Federal Aviation Administration, these grants provide funds for eligible airports to prevent, prepare for, and respond to the effects of the COVID-19 pandemic.
20
Highway Infrastructure
Administered by the Federal Highway Administration, these programs provide funds to states, D.C., U.S. territories, and tribes for highway construction and authorize the use of these funds for maintenance, personnel, and other purposes to prevent, prepare for, and respond to the COVID-19 pandemic.
10
Coronavirus Capital Projects Fund
Administered by Treasury, this fund provides payments to states, D.C., U.S. territories, freely associated states, and tribal governments for critical capital projects that directly enable work, education, and health monitoring, in response to the COVID-19 pandemic.
10
State Small Business Credit Initiative
Administered by Treasury, this program provides funds to states, D.C., U.S. territories, tribal governments, and eligible municipalities to fund small business credit support and investment programs.
10
Source: GAO analysis of federal laws and data from the Congressional Budget Office. | GAO-22-105397
Note: The COVID-19 relief laws providing the appropriations shown are the American Rescue Plan Act of 2021 (ARPA), Pub. L. No. 117-2, 135 Stat. 4 (2021), the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M and N, 134 Stat. 1182 (2020), the Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020), the CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020), and the Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020). The Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146, did not provide any specified amounts for these programs or funds for states, D.C., localities, territories, or tribes. The amounts shown are the cumulative amounts for each program or fund under the other five laws. Some appropriation amounts include an amount available for administration expenses or for the relevant inspectors general. Numbers are rounded to the nearest hundred million.
aAppropriations for the Disaster Relief Fund generally are not specific to individual disasters and may be used for various disaster assistance programs, including the Public Assistance program, which provides assistance to state, local, territorial, and tribal governments.
bSeveral provisions in the Families First Coronavirus Response Act and ARPA authorized increases in Medicaid payments to states and U.S. territories. The Congressional Budget Office estimated that federal expenditures from these provisions would be approximately $76.9 billion through fiscal year 2030. The largest increase to federal Medicaid spending is based on a temporary funding formula change rather than a specific appropriated amount. Some of the estimated costs in this total are for the Children’s Health Insurance Program, permanent changes to Medicaid, and changes not specifically related to COVID-19.
cThe Child Care and Development Fund is made up of two funding streams: mandatory and matching funding authorized under section 418 of the Social Security Act, and discretionary funding authorized under the Child Care and Development Block Grant Act of 1990, as amended. See 42 U.S.C. §§ 618 and 9858m.
dWe refer to ERA1 and ERA2 as the ERA program for convenience. While Treasury uses this approach, it clarified that it considers them to be two separate programs managed by the same office.
eFunds are available to eligible sponsors of airports. Nearly all of these airports are under city, state, county, or public-authority ownership.
Overview of Key Issues
States and localities generally experienced more challenges implementing COVID-19 relief under new versus existing programs, although existing programs also faced challenges such as managing expedited time frames. Some state and local COVID-19 relief programs and funds were newly created under the COVID-19 relief laws. For example, the Coronavirus Relief Fund (CRF) and the Coronavirus State and Local Fiscal Recovery Funds (CSLFRF) were newly created under the CARES Act and American Rescue Plan Act (ARPA), respectively.[395] Conversely, existing programs generally received funding—and in many cases were expanded—under the relief laws.
For example, Highway Infrastructure programs received additional funding and expanded allowable uses for recipients, including for costs related to preventative maintenance, routine maintenance, operations, and personnel, including salaries of employees (including for those on administrative leave), among others.[396] Similarly, Federal Transit grant programs received additional funding and expanded allowable uses, including reimbursement for operating costs to maintain service and lost revenue due to the coronavirus public health emergency, among others.[397] In addition, the Child Care and Development Fund received additional appropriations and expanded eligibility for the program.[398] Medicaid, the nation’s largest source of funding for health care services for low-income and medically needy individuals, received authority to provide enhanced funding to states under the relief laws.[399]
Officials from associations representing state and local governments and the three states we spoke with told us it is more challenging for states and localities to manage newly created programs than programs that already existed and received additional funding under the COVID relief laws. States and localities may experience a range of challenges in administering and managing new programs and funds. Some of these challenges include:
Capacity. Officials from the three states and several associations told us that with new programs, states may face challenges in developing the infrastructure to manage them and the cognizant federal agencies have less experience administering them. For example, officials from one association said it can be difficult for states to hire staff and train them to manage new programs.
Officials from another association said it can take states time to develop the capacity to manage new programs, including having sufficient staff with the knowledge and technical skills needed to manage new programs and the ability to employ technology for grant oversight and reporting. Officials from two states we spoke with also said they experienced challenges obtaining responses to their questions from federal agencies about implementing new programs. For example, officials from one state said they are generally able to reach Treasury officials for responses to questions about existing programs, but have experienced delays in obtaining responses to questions about new programs.
In October 2021, we reported lags in grantee spending of Emergency Rental Assistance (ERA) funding distributed by Treasury. According to Treasury officials, most grantees could not deploy funds immediately because they needed additional time to enhance existing rental assistance programs or develop new programs in order to accommodate the increased scale of operations made possible through the funding. Specifically, grantees had to develop new policies and procedures, hire additional staff, and develop electronic application and data collection systems.
Guidance. Treasury has provided guidance for new programs, but in some cases the guidance was unclear or untimely. In October 2021 we reported from the results of a survey we conducted from July through August 2021 that the majority of states (29 of 48) and localities (29 of 45) that responded to our survey reported needing additional information in the guidance about allowable uses of CSLFRF funds. In addition, 32 states and 17 localities that responded to our survey reported needing additional information about CSLFRF reporting requirements. [400]
Treasury is leveraging lessons learned from the roll-out of CRF guidance when implementing the CSLFRF. In July 2021 we reported that CRF recipients found Treasury’s guidance on eligible uses of the funds to be unclear. Treasury took steps intended to ensure the clarity of its CSLFRF guidance for recipients. For example, Treasury officials told us they consulted with eligible recipients, including tribes, on various aspects of CSLFRF implementation.
In addition, officials from one association told us that Treasury was slow to issue guidance on eligible expenses for the Coronavirus Capital Projects Fund. The officials said that although states anticipated the funds could be used for broadband projects, states were slow in planning for spending on such projects in the absence of clear guidance. Treasury issued general guidance detailing allowable uses for the program in September 2021. However, it has not yet issued detailed guidance on reporting requirements.
Similarly, we noted that in October 2021 Treasury updated its ERA program grantee guidance (known as frequently asked questions) several times to assist grantees in delivering ERA funds more efficiently. However, officials from one association told us that Treasury’s iterative guidance did not address states’ questions in a timely manner.
Existing programs also faced challenges, particularly in areas where these programs were already experiencing challenges prior to the pandemic or in expanding programs under expedited time frames. For example, we reported in July 2021 that FEMA’s available workforce was already overwhelmed by responding to natural disasters and could be further stretched by COVID-19. In October 2021 we reported that FEMA then experienced delays in processing applications for COVID-19 Public Assistance, and it inconsistently interpreted and applied its policies within and across its regions. Similarly, in January 2022, we reported on challenges that the Centers for Medicare & Medicaid Services (CMS) faced in implementing enhanced Medicaid funding for certain services under abbreviated timelines. Specifically, ARPA increased the federal Medicaid funding available for Home and Community Based Services to begin 3 weeks after its enactment. Officials from CMS said this time frame created challenges for CMS to quickly develop related guidance and system changes.
Similar allowable uses and varying time frames and availability of COVID-19 relief funds may affect how states and localities manage them. According to association officials, there may be some confusion among states and localities about which streams of funding should be used for specific purposes when allowable uses are similar. For example, officials from states and associations we met with noted that allowable uses for the CSLFRF funding are broad and may overlap with other programs. Association officials said both the CSLFRF and Coronavirus Capital Projects Fund can be used for broadband investment, and the recently passed Infrastructure Investment and Jobs Act provides additional broadband funding.[401] Similarly, officials from one association said some states experienced challenges understanding what allowable uses were for the CSLFRF relative to the Elementary and Secondary School Emergency Relief Fund (ESSER), and expressed concern about whether to use CSLFRF or ESSER funding for COVID-19 testing in schools.
Officials from two states we spoke with said they have been considering the period in which funds must be spent and the requirements associated with different programs when determining how to use the funding. For example, officials from one state said they made strategic decisions about the use of Disaster Relief Fund (DRF) and CRF funding in order to maximize the use and impact of both programs before the deadline to obligate CRF funds.[402] Officials from another association said states and localities were concerned about “moving goal posts” for the various streams of COVID-19 relief funding. Specifically, when new programs were introduced, jurisdictions were forced to reassess decisions they had already made. In addition, officials from one state said they were carefully considering how to sequence the various streams of funding available for broadband in order to achieve the state’s infrastructure goals. In October 2021, we reported that when deciding to use CARES Act funds or annually appropriated Child Care and Development Funds for providing assistance to child care providers, state administrators we interviewed said they considered various factors, such as when funding was available, allowable uses, and the period in which funds must be spent.[403]
Officials from states and associations we met with told us the timing of availability of funds and clarity on eligible uses has affected states’ and localities’ ability to use and manage it. For example, officials from some associations said it can be challenging when federal and state fiscal years do not align, and told us that it is important that federal agencies finalize programs’ eligible uses as quickly as possible because states may have their own appropriations processes that determine how to spend the funds.[404] The officials said if federal agencies are delayed in finalizing eligible uses, it may hinder states’ ability to make appropriations decisions about how they use federal funds and delay when funds reach intended recipients.
States faced challenges in managing different reporting requirements and transparency over use of funds. Officials from states and associations we met with told us states and localities may face challenges managing and meeting the various reporting requirements for multiple programs. Officials from one association told us there were concerns that some reporting requirements were duplicative, and that it would be helpful to have more alignment among reporting requirements for different programs. For example, officials from two associations suggested that requested data for reporting on COVID-19 relief programs and funds could be better aligned with those for the Community Development Block Grants (CDBG), which many recipients are already familiar with.[405]
We also previously reported on challenges in recipient reporting and oversight of program data. For example, in January 2022 we reported that Treasury extended the deadlines to all CSLFRF recipients for submitting their first project and expenditure reports.[406] Treasury officials told us that the deadline extensions were due, in part, to technological issues with the online reporting portal. Similarly, an association representing state housing agencies identified technical challenges states are facing using Treasury’s reporting portal to submit quarterly reports for the ERA program, which it asserted could negatively affect the quality of data on the program.
We also reported issues with transparency of grantee or sub-grantee funding. For example, in March 2021 we reported a gap between when school districts used COVID-19 relief funds and when the Department of Education recorded the funds as spent. We recommended that Education regularly collect and publicly report information on school districts’ obligations as well as expenditures in order to more completely reflect the status of their use of federal COVID-19 relief funds. We noted the importance of accurately capturing the status of COVID-19 relief funds provided to states and school districts to inform the department’s monitoring and technical assistance, and to provide transparency to the public about uses of the funds. Education agreed with our recommendation and implemented it by taking a number of steps to work with states to provide greater clarity on state and school district spending. For example, as of January 2022 Education updated its data collection instrument on the status of COVID-19 relief funding to more closely track recipient obligations and expenditures.
Methodology
To conduct this work, we reviewed our prior reports on specific COVID-19 relief programs and funds to states and localities and we included relevant prior findings, such as results from a survey of states and localities we conducted in summer 2021. To gather additional perspectives about states’ and localities’ use and management of COVID-19 relief funding across programs and funds receiving $10 billion or more in appropriations in at least one of the COVID-19 relief laws, we interviewed representatives from 10 organizations that collectively represent state and local governments: the Council of State Governments; the Government Finance Officers Association; the International City/County Management Association; the National Association of Counties; the National Association of State Auditors, Comptrollers and Treasurers; the National Association of State Budget Officers; the National Conference of State Legislatures; the National Governors Association; the National League of Cities; and the United States Conference of Mayors. We also interviewed officials from three states—Hawaii, North Carolina, and Rhode Island—about their experiences using and managing COVID-19 relief funding. These interviews were designed to provide illustrative examples of states’ and localities’ experiences with the use and management of COVID-19 relief funding, as of the time of our interviews in February 2022. We identified these states because they were mentioned by the associations we interviewed as having approaches they were applying across the programs and funds, such as centralized strategies for managing the funding and publishing data across programs and funds on their websites.
Agency Comments
We provided the Departments of Education, Health and Human Services, Homeland Security, Transportation, the Treasury, and the Office of Management and Budget (OMB) with a draft of this enclosure. The Departments of Education, Health and Human Services, Transportation, and the Treasury provided technical comments, which we incorporated as appropriate. The Department of Homeland Security and OMB had no comments.
GAO’s Ongoing Work
We currently have multiple ongoing or planned reviews of the funding that federal COVID-19 relief laws appropriated for agencies across the federal government to provide payments to states, the District of Columbia, localities, territories, and tribes for responding to, and recovering from, the COVID-19 pandemic.
Contact information: Jeff Arkin, (202) 512-6806, arkinj@gao.gov
The Department of the Treasury has documented application and grant review procedures for the Coronavirus Capital Projects Fund. However, Treasury has not yet begun recipient monitoring and has not yet documented a comprehensive plan and process that includes the design and documentation of procedures to monitor recipients’ use of funds for allowable purposes once funds have been disbursed.
Entity involved: Department of the Treasury
Recommendation for Executive Action
The Secretary of the Treasury should document a comprehensive plan that includes timely and sufficient policies and procedures for monitoring recipients of the Coronavirus Capital Projects Fund to provide assurance that funds are being used in compliance with laws, regulations, agency guidance, and award terms and conditions, including ensuring that funds are being used for allowable purposes. Treasury agreed with this recommendation.
Background
The Coronavirus Capital Projects Fund (CPF) was established in March 2021 under section 9901 of the American Rescue Plan Act of 2021 (ARPA). The fund may provide up to $10 billion to state, territorial, and tribal governments to support critical capital projects directly enabling work, education, and health monitoring, in response to the COVID-19 public health emergency.
Under ARPA, Congress allocated the $10 billion as follows: $9.8 billion to states, the District of Columbia, and Puerto Rico; $100 million to other territories and freely associated states;[407] and $100 million to tribal governments and the state of Hawaii (for Native Hawaiian Programs). Pursuant to implementing Treasury guidance, these funds are required to be expended by December 31, 2026, and recipients must return to Treasury any funds that are not used by that date.[408] As of February 28, 2022, $1.2 million in obligations and $1.2 million in expenditures of CPF were reported by Treasury for this program.[409] In addition, Treasury reported significant obligations in March 2022, and as of March 18, 2022, a total of $9.9 billion has been obligated.
In April 2021, Treasury established the Office of Recovery Programs (ORP) to oversee programs authorized through the COVID-19 relief laws (primarily the CARES Act, the Consolidated Appropriations Act, 2021, and ARPA). The CPF is administered by officials in a program office located within ORP. The program office is staffed with personnel specifically assigned to CPF, including one grants specialist. CPF officials also stated that some CPF program functions are handled centrally through ORP.
Overview of Key Issues
Treasury’s development of internal controls over CPF. Treasury officials told us in January 2022 that they were in the early stage of the program and were working on assessing internal control needs and were planning to establish a risk-based approach to monitoring CPF recipients’ use of funds. In March 2022, Treasury officials further stated that they are in the process of establishing monitoring procedures to include review of recipient-reported data, including single audit data, and data analysis to identify potential areas of non-compliance for remediation.
Treasury issued application and eligibility guidance. In September 2021, Treasury issued two guidance documents on CPF to provide information on project eligibility and terms and conditions, as well as the application process for grants under the CPF program. For states, territories, and freely associated states, applications were due by December 27, 2021, and grant plans are due by September 24, 2022.[410] For tribal governments, the application and grant plan deadline is June 1, 2022.[411] One guidance document was directed at states, territories, and freely associated states, and the other was directed at tribal governments. Both guidance documents explained the process for (1) submitting an initial application for CPF funds through Treasury’s automated Capital Projects Fund Portal; (2) executing a grant agreement with Treasury; and (3) submitting a grant plan providing information on the recipient’s intended uses of CPF funds. The guidance documents provide information to CPF applicants on the application process and on eligible uses of funds.
Treasury developed application and grant plan review procedures. ORP officials described Treasury’s current process for reviewing CPF applications as consisting of both automated reviews of applicant data in the CPF portal system, and additional manual reviews. Treasury officials said red flags identified in the automated review of an applicant’s submission would prompt further review and follow-up with the applicant. In the initial application review process, Treasury checks to see that (1) application entries are not duplicates; (2) an applicant is an authorized representative of the recipient government; and (3) applicants have requested allowable amounts for administrative expenses, among other matters.
Treasury has documented review procedures for applications from states, territories, and freely associated states in its “State Review Checklist.” However, grant plans for state, territorial, and freely associated state recipients are not due until September 24, 2022. In March 2022, Treasury officials stated that they have started receiving grant plans and are reviewing the grant plans on a rolling basis. Treasury officials stated they are in the process of documenting the review procedures established for these grant plans.
Treasury’s review procedures for tribal applications and grant plans are documented in procedural checklists used by the CPF program team staff. The tribal review procedures specify that the completed review is to be documented in a Tribal Government Application Review Checklist and an Action Memo. These documents reflect the programmatic review of the application, the administrative record for application-specific decisions, and Treasury’s approval of the application.
Treasury plans to develop further monitoring procedures. In addition to the application and grant plan reviews, Treasury’s plans for monitoring recipients’ use of funds include reviews of recipients’ detailed program plans,[412] as applicable, recipients’ quarterly project and expenditure reports and annual performance reports, and CPF-related findings in recipients’ single audit reports.[413] As of January 2022, Treasury had provided high-level requirements for recipient reporting in its guidance documents, but specific details for the reporting process had not been issued.
In developing its monitoring procedures, Treasury officials noted that they are considering both the lifecycle of the CPF and lessons learned from other pandemic relief efforts:
Lifecycle of the CPF. Although CPF recipients are permitted to use program funds for eligible purposes through December 31, 2026, Treasury may have recipient monitoring responsibility well beyond this expenditure deadline, in part due to the long-term nature of construction projects and permissible uses of CPF funds. Specifically, construction of capital assets may be multiyear projects and CPF recipients are required to commit that eligible projects will provide services or activities for at least 5 years from the completion of the project. As a result, Treasury’s monitoring responsibility of recipients to provide assurance over the allowable use of CPF funds could extend to several years after 2026. As of March 2022, Treasury officials stated that Treasury will publish recipient guidance setting forth the reporting obligations in advance of the first reporting deadlines, and that they are in the process of establishing a risk-based, data-driven framework for providing accountability and stewardship to achieve program goals and objectives. This framework will include procedures to review recipient-reported data, including single audit data, and data analysis to identify potential areas of non-compliance for remediation. Treasury expects to have these procedures in place when monitoring begins. Treasury officials noted they are still considering how they will monitor recipients’ use of CPF funds beyond December 31, 2026.
Lessons learned from other pandemic relief efforts. Treasury officials told us that in developing the CPF program they plan to take advantage of lessons learned from the agency’s experience with other pandemic relief programs. Since the start of the COVID-19 public health emergency, Treasury has been charged with administering multiple pandemic relief programs benefitting state, territorial, local, and tribal governments—among them the $150 billion Coronavirus Relief Fund enacted in the March 2020 CARES Act, and the $350 billion Coronavirus State and Local Fiscal Recovery Funds (CSLFRF) enacted in the March 2021 ARPA.[414]
Beginning with its mandate to administer the Coronavirus Relief Fund in March 2020, Treasury has faced increasing responsibilities in managing new programs such as CSLFRF and CPF. For example, Treasury’s role in the Coronavirus Relief Fund included disbursing funds to recipients and issuing program guidance, while Treasury’s Office of Inspector General performed oversight and monitoring of that program, as provided for in the CARES Act. By contrast, Treasury has been more actively involved in administering CSLFRF and CPF, including determining recipients’ program eligibility and developing periodic recipient reporting requirements.
We have previously reported on the challenges Treasury faced in responding to its new and expansive program management responsibilities under the CARES Act and ARPA. For example, we noted that recipients of the Coronavirus Relief Fund found Treasury’s guidance on eligible uses of the funds was unclear before Treasury published final guidance on that program in January 2021, approximately 11 months after the start of the period when recipients could use funds. In addition, we reported in October 2021 that Treasury had not finalized its design and documentation of key internal processes and control activities related to monitoring CSLFRF recipients’ use of the funds, although it had disbursed approximately $240 billion of those funds to recipients as of August 31, 2021.
Treasury officials indicated that they plan to leverage their experience with other programs such as CSLFRF when determining how to monitor CPF recipients. For example, they stated they are being more patient on developing reporting requirements and plan on getting the data collection design right before they issue guidance. In addition, Treasury officials agreed with our October 2021 recommendation related to the design and documentation of internal controls related to CSLFRF recipient monitoring and stated as of December 2021 that they have taken steps to address this recommendation.
Standards for Internal Control in the Federal Government states that management should design control activities to achieve objectives and respond to risks and should implement control activities through policies. As part of this process, management designs control activities in response to the entity’s objectives and risks to achieve an effective internal control system. Management then documents the internal control responsibilities in policies at an appropriate level of detail to allow management to effectively monitor the control activity.
Treasury has developed and documented application and grant review procedures for tribal CPF recipients and an application review checklist for states, territories, and freely associated states. However, the agency has not yet completed documentation of its procedures for recipient monitoring to help ensure that recipients are maintaining effective controls over the funds and that funds are expended in accordance with federal requirements (e.g., applicable legal provisions and internal control standards). As a result, development of key procedures is needed to help ensure program management fulfills its recipient monitoring and oversight responsibilities. For example, Treasury will also need to plan and document procedures for monitoring recipients’ use of funds for allowable purposes once CPF funds have been disbursed, and before the recipient monitoring phase begins.
Methodology
To conduct this work, we interviewed Treasury’s Office of Recovery Programs officials to obtain an understanding of their processes for monitoring CPF recipients’ internal controls to help ensure allowable use of CPF funding. In addition, we examined Treasury’s review procedures for evaluating CPF recipient applications and grant plans, as applicable.
Agency Comments
We provided Treasury and the Office of Management and Budget (OMB) with a draft of this enclosure. Treasury provided written comments, which are reproduced in appendix X, and technical comments, which we incorporated as appropriate. OMB did not provide comments.
Treasury agreed with our recommendation, and stated that the Office of Recovery Programs — the office that administers many pandemic-era economic recovery programs, including CPF — solicited stakeholder input in developing CPF reporting guidance, and it is in the process of establishing a risk-based, data-driven framework for providing accountability and stewardship to achieve program goals and objectives. This framework will include procedures to review recipient-reported data, including single audit data, and data analysis to identify potential areas of non-compliance for remediation. Treasury expects to have these procedures in place when monitoring begins. Treasury has stated that it is committed to administering CPF in an effective and timely manner while also mitigating risks of waste, fraud, and abuse.
GAO’s Ongoing Work
We will continue to monitor the status of Treasury’s management of the CPF program and its process to oversee CPF recipients.
Related GAO Products
Standards for Internal Control in the Federal Government.GAO-14-704G. Washington, D.C.: September 2014.
As of March 31, 2022, federal agencies continued to obligate billions of dollars monthly in support of COVID-19 response efforts through contracts.
Entities involved: Department of Defense, Department of Health and Human Services, Department of Homeland Security, and the Office of Management and Budget, among others
Background
Federal agencies have used a variety of contracting mechanisms to provide vital goods and services in support of federal, state, and local COVID-19 response efforts.[415] For example, federal agencies have reported billions of dollars in obligations on contracts subject to the Federal Acquisition Regulation—which provides uniform policies and procedures for acquisitions by all executive agencies.[416] Our prior work on disaster contracting has found that contracts play a key role in federal emergency response efforts, and that contracting during an emergency can present a unique set of challenges as officials can face significant pressure to provide critical goods and services as expeditiously and efficiently as possible.
The January 2021 National Strategy for the COVID-19 Response and Pandemic Preparedness emphasizes the important role contracts will continue to play during the response. The strategy states that the federal government will fully leverage contract authorities to strengthen the vaccine supply chain; staff vaccination sites; and fill supply shortages for personal protective equipment, drugs, and therapeutics.
As federal contracting activity through contracts and agreements continues to play a critical role in response to the pandemic, it is important to ensure that these contracts and agreements in response to COVID-19 are accurately reported and visible to congressional decision makers, entities with oversight responsibilities, and taxpayers. National Interest Action (NIA) codes were established in 2005 following Hurricane Katrina to enable the consistent tracking of emergency or contingency-related contracting actions in the Federal Procurement Data System (FPDS). The COVID-19 NIA code was established on March 13, 2020, to track contract actions and associated obligations in response to the pandemic in FPDS. The Department of Homeland Security (DHS) and DOD have subsequently extended the code five times—generally in 6-month increments, and most recently until September 30, 2022.[417]
Overview of Key Issues
Agencies obligated more than $115 billion on federal contracts, with DOD and HHS accounting for over three-quarters of obligationsas of March 31, 2022. At the beginning of the response, HHS accounted for the most federal contract obligations. However, as the response has progressed, DOD’s contract obligations exceeded HHS’s. The increase in DOD’s contract obligations is due, in part, to DOD’s support of interagency acquisition needs, which has included awarding contracts on behalf of HHS for vaccine and therapeutic production and medical supplies. As of March 31, 2022, DOD accounted for about 57 percent and HHS for about 20 percent of the total obligations made by federal agencies in response to the COVID-19 pandemic. See figure for obligation amounts by federal agency.
Contract Obligations in Response to COVID-19 by Federal Agency, as of Mar. 31, 2022
In our January 2022 report, we reported that government-wide contract obligations related to COVID-19 totaled $101.6 billion through December 15, 2021; by March 31, 2022, those obligations had increased by about $16.4 billion—to $118 billion. DOD accounted for about $11.1 billion, or about 68 percent of the increase in total contract obligations since December 15, 2021.
Significant increases in obligations early in the pandemic were due to large purchases of medical equipment and supplies—such as ventilators and personal protective equipment. Large vaccine and therapeutic purchases have continued to contribute to more recent spikes in obligations. For example, following purchases of about $4 billion in Pfizer and Moderna vaccines in December 2020, multi-billion dollar vaccine purchases by DOD in February, June, and July 2021 as well as in January 2022 contributed to monthly increases in reported contract obligations. Additionally, multi-billion dollar purchases of therapeutics from Pfizer and Regeneron contributed to monthly increases in September and November 2021. See figure for government-wide obligations and confirmed COVID-19 cases by month.
Government-wide COVID-19-Related Contract Obligations and Confirmed COVID-19 Cases by Month, Feb. 2020–Mar. 31, 2022
Types of goods and services purchased and competition rate changed over the course of the pandemic. As the response to the pandemic has progressed, the types of goods and services purchased have shifted from primarily medical equipment and supplies—such as ventilators and personal protective equipment—to drugs and treatments, such as COVID-19 vaccines and therapeutics. Drugs and treatments have become the largest area of government-wide obligations, accounting for 40 percent of total obligations over the course of the pandemic. These obligations increased almost fifteen fold from $3 billion as of November 2020, prior to the Food and Drug Administration’s emergency use authorizations for the Pfizer, Moderna, and Janssen vaccines, to about $47.3 billion as of March 31, 2022.[418]
Since the start of the pandemic, increases in obligations for drugs and treatments have included $32 billion in obligations for COVID-19 vaccines and therapeutics to Pfizer and Moderna, with recent increases in obligations due to purchases to support booster shots, pediatric vaccinations, international vaccine donations, and therapeutics to treat COVID-19. Further, the federal government’s efforts to distribute rapid antigen tests to U.S. households starting in January 2022 have also contributed to recent increases in monthly obligations for medical equipment and supplies. For example, as of March 31, 2022, DOD had obligated about $4.7 billion in 2022 for rapid antigen COVID-19 tests.
See figure for obligation amounts for the most-procured goods and services over time.
Contract Obligation Amounts for Top Five Goods and Services Procured in Response to COVID-19 by month, Feb. 2020–Mar. 31, 2022
Note: In addition to what is reflected in the figure, agencies canceled, or deobligated, $176.5 million and $335.8 million for drugs and treatments in July 2020 and April 2021, respectively. Obligations for fruits and vegetables were made primarily in support of the U.S. Department of Agriculture’s Farmers to Families Food Box Program.
As of March 31, 2022, COVID-19-related contracts for goods continued to be competed less frequently than contracts for services, but competition rates for goods have increased. For example, we reported in July 2021 that about 97 percent of obligations on drugs and therapeutics and 85 percent of obligations on medical equipment and supplies were not competed. As of March 31, 2022, about 74 percent of the $47.3 billion in obligations for drugs and treatments and about 60 percent of the $14.2 billion in obligations for medical and surgical equipment were on contracts awarded noncompetitively.
Overall, the proportion of COVID-19 related contracts identified as having been awarded noncompetitively was about 54 percent, or $63.7 billion, as of March 31, 2022.[419] Throughout the course of the pandemic, the percentage of obligations on these noncompetitive contracts has fluctuated from a high of 93 percent of obligations in July 2021 to a low of 21 percent of obligations in November 2021. The higher rate of obligations on noncompetitively awarded contracts in July 2021 was driven in part by large noncompetitive awards for vaccine production.
Agencies must provide for full and open competition when awarding contracts, unless one of several limited exceptions applies, such as when there is an unusual and compelling urgency for a needed supply or service. Agencies cited an urgent need for awarding contracts noncompetitively for about 85 percent, or about $53.9 billion, of the contract obligations associated with noncompetitive awards.[420]
Federal agencies’ use of undefinitized contracts increased. Undefinitized contracts are one technique that agencies have reported using to respond to COVID-19. Undefinitized contracts can enable the government to quickly fulfill requirements that are urgent or need to be met quickly by allowing contractors to begin work before reaching a final agreement with the government on all contract terms and conditions.[421] Undefinitized contract obligations for COVID-19 increased from about $6.2 billion as of December 15, 2021, to $6.7 billion as of March 31, 2022, continuing to total about 6 percent of government-wide obligations on contracts awarded in response to COVID-19. A majority of the increase was driven by undefinitized contracts awarded by HHS for the purposes of increasing community access to COVID-19 testing at pharmacy and retail locations. DOD continued to report the highest amount of undefinitized contract obligations, identifying about $4.3 billion, or about 6 percent of its overall COVID-19-related contract obligations, as being on undefinitized contracts.
Our prior work reviewed DOD’s, HHS’s, and the Department of Homeland Security’s (DHS) use of undefinitized contracts in response to COVID-19, including the use of CARES Act flexibilities for such contracts. We found that the timing of definitization and amount obligated prior to definitization varied across our selected contracts, and that officials at DOD—which accounted for the majority of undefinitized contract obligations—cited the ability to quickly award undefinitized contracts as a major benefit during the pandemic.
Opportunities exist to collect and share contracting lessons learned to improve future emergency response efforts. During the course of the pandemic, agencies identified a variety of challenges and positive practices with contracting in response to COVID-19. For example, in July 2021 we reported that contracting officials from selected agencies identified challenges with a lack of contracting personnel, working with vendors that were new to federal contracting or vendors supplying products they had not previously provided, and contracting for supplies and services the agency does not typically buy, among others. We also reported that officials identified positive contracting practices—such as establishing centralized email inboxes for vendors to communicate with agencies about available goods and services, and relying on pre-existing contract vehicles to more quickly provide some goods and services—that helped them during the response to the pandemic.
While certain agencies were collecting and sharing lessons learned from the COVID-19 response, we found that HHS and the Federal Emergency Management Agency (FEMA) within DHS were not including contracting lessons learned even though they had identified contracting challenges. We recommended that HHS and FEMA ensure that contracting lessons learned from COVID-19 and future emergency response efforts are collected and shared as part of ongoing lessons learned processes. HHS agreed with the recommendation and said it would use its existing lessons learned processes to collect, analyze, and share contracting lessons learned. FEMA also agreed and in December 2021, said it is developing an annual survey for contracting staff that will include a question asking contracting officials to identify any lessons learned and areas for improvement in future emergency response efforts.
We also found that while interagency coordination was critical to the contracting response, contracting officials from DOD, HHS, and DHS were not always aware of or involved in government-wide efforts to collect and share interagency lessons learned. We recommended that DOD, HHS, and DHS ensure that input from contracting officials on interagency contracting lessons learned in response to COVID-19 is collected and shared as part of government-wide efforts to report on lessons learned. All three agencies agreed and said they will collect, analyze, and report on interagency contracting lessons learned to share with the other departments and government-wide reporting efforts.
Further, we identified variations in how agencies used new contracting authorities provided by the CARES Act. Specifically, section 3610 of the CARES Act generally authorized federal agencies to reimburse contractors for paid leave provided to their employees and subcontractors who were unable to access work sites due to facility closures or other restrictions, and whose duties could not be performed remotely during the pandemic. We reported in July 2021, that due to the urgency of the pandemic, agencies prioritized quick implementation of section 3610 over a more deliberative process, resulting in variations in how the authority was tracked and used.
We found that selected agencies using the authority had captured or planned to capture lessons learned from implementing section 3610. However, the Office of Management and Budget (OMB)—which coordinates government-wide contracting policy—had not collected and shared lessons learned. We recommended that after the COVID-19 national emergency, OMB collect and share lessons learned from federal agencies’ implementation of COVID-19 paid leave reimbursement. OMB agreed with the recommendation and said they would collect and share individual agencies’ lessons learned to promote knowledge management, but has not yet provided an update on its progress.
Methodology
To identify agencies’ federal contract obligations and competition rate on contracts in response to COVID-19, we reviewed data reported in FPDS through March 31, 2022.[422] We primarily identified contract obligations related to COVID-19 using the NIA code. We supplemented the use of the NIA code by searching for “COVID-19” and “coronavirus” in the contract description field to identify a limited number of additional contract obligations.[423] For contract actions over $1 million, we removed obligations that were identified in the contract description as not related to COVID-19.
We assessed the reliability of federal procurement data by reviewing existing information about FPDS and the data it collects—specifically, the data dictionary and data validation rules—and by performing electronic testing. We supplemented our FPDS analysis with analysis of agency-provided data and interviews with agency officials. We determined that the data were sufficiently reliable for the purposes of describing agencies’ reported contract obligations in response to COVID-19.
Agency Comments
We provided DOD, HHS, DHS, and OMB with a draft of this enclosure. The agencies did not provide comments on this enclosure.
GAO’s Prior Recommendations
The table below presents our recommendations on federal contracts and agreements for COVID-19 from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to Federal Contracts and Agreements for COVID-19
Recommendation
Status
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to issue guidance—such as an acquisition alert or a reminder to contracting officials—on the use of the COVID-19 National Interest Action code for the Farmers to Families Food Box Program or successor food distribution program to ensure it accurately captures COVID-19-related contract obligations in support of the program (March 2021 report).
Closed-Addressed. The U.S. Department of Agriculture (USDA) neither agreed nor disagreed with our recommendation. In February 2021, following our identification of contract data reporting challenges using the COVID-19 National Interest Action code for the Farmers to Families Food Box Program, Agricultural Marketing Service officials said they conducted training with staff to review National Interest Action code data entry protocols. At that time, a senior Agricultural Marketing Service official also sent an email reminder to procurement division personnel about OMB’s guidance on the use of the COVID-19 National Interest Action code. Following this training and email, officials took action to retroactively report contract actions for the program with the National Interest Action code. In May 2021, the Agricultural Marketing Service updated its instructions for entering contract actions into the Federal Procurement Data System to include a reminder to utilize the proper National Interest Action code, if applicable.
The Secretary of Agriculture should direct the Administrator of the Agricultural Marketing Service to assess the contracting personnel needed to fully execute the award and administration of existing contracts in support of the Farmers to Families Food Box Program or successor future food distribution program, and take the necessary steps to ensure it has adequate contracting staff in place to award and administer any future contracts for the program (March 2021 report).
Closed-Addressed. USDA neither agreed nor disagreed with our recommendation, and according to Agricultural Marketing Service officials, they have discontinued the program, and are using other methods of hunger relief, so they do not anticipate needing additional permanent staff. However, in December 2021 the Agricultural Marketing Service placed an order on an existing USDA contract vehicle to obtain additional staff support for contract closeout services and other administrative needs for the awards that have been made under the Farmers to Families Food Box Program and other food purchasing efforts. The statement of work for the order estimates the number of contracts the Agricultural Marketing Service needs contract support services for, and required the contractor to deliver a staffing plan, identifying how it will meet USDA’s requirements. The contractor’s April 2022 staffing plan identifies a total of three additional staff to lead and support Agricultural and Marketing Services contract closeout needs for the Farmers to Families Food Box Program. The plan also states that staffing needs will be reassessed and additional resources acquired as needed, which will help to ensure that Agricultural and Marketing Services has the needed staff support to finalize the closeout of the contracts.
The Assistant Secretary for Preparedness and Response (ASPR), in coordination with the appropriate offices within the Department of Health and Human Services (HHS), should accurately report data in the federal procurement database system and provide information that would allow the public to distinguish between spending on other transaction agreements and procurement contracts (January 2021 report).
Open-Partially Addressed. ASPR agreed with our recommendation, and as of April 2021, ASPR officials stated that they have discussed within ASPR the need to consistently identify other transaction agreements in the Federal Procurement Data System (FPDS) and explored how their contract writing system may interface with the FPDS other transaction agreement module in the future. In December 2021, ASPR officials added that in the meantime, they have issued guidance to their contracting teams to manually track other transaction agreements in their contract writing system. We will continue to monitor ASPR’s efforts to implement our recommendation.
The Secretary of Homeland Security, in coordination with the Secretary of Defense, should (1) revise the criteria in the 2019 National Interest Action (NIA) code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Closed-Addressed. The Department of Homeland Security (DHS) did not agree with our recommendation. However, in March 2021, DHS, in coordination with the Department of Defense (DOD), issued a revised memorandum of agreement. The revised agreement establishes a process and timelines for communicating and evaluating NIA code extensions by requiring the General Services Administration to notify other federal agencies no less than seven days before a NIA code is set to expire so that agencies can request an extension as needed. The revised agreement also more clearly defines what constitutes a consistent decrease in contract actions to ensure criteria for extending or closing a NIA code is consistently applied.
The Secretary of Defense, in coordination with the Secretary of Homeland Security, should (1) revise the criteria in the 2019 National Interest Action code memorandum of agreement to clearly identify steps they will take to obtain input from key federal agencies prior to extending or closing a National Interest Action code, (2) establish timelines for evaluating the need to extend a National Interest Action code, and (3) define what constitutes a consistent decrease in contract actions and routine contract activity to ensure the criteria for extending or closing the National Interest Action code reflect government-wide needs for tracking contract actions in longer term emergencies, such as a pandemic (September 2020 report).
Closed-Addressed. DOD did not agree with our recommendation. However, in March 2021 DOD, in coordination with DHS, issued a revised memorandum of agreement. The revised agreement establishes a process and timelines for communicating and evaluating NIA code extensions by requiring the General Services Administration to notify other federal agencies no less than seven days before a NIA code is set to expire so that agencies can request an extension as needed. The revised agreement also more clearly defines what constitutes a consistent decrease in contract actions to ensure criteria for extending or closing a NIA code is consistently applied.
COVID-19 Contracting: Opportunities to Improve Practices to Assess Prospective Vendors and Capture Lessons Learned. GAO-21-528. Washington, D.C.: July 29, 2021.
COVID-19 Contracting: Contractor Paid Lead Reimbursements Could Provide Lessons Learned for Future Emergencies.GAO-21-475. Washington, D.C.: July 28, 2021.
COVID-19 Contracting: Actions Needed to Enhance Transparency and Oversight of Selected Awards. GAO-21-501. Washington, D.C.: July 26, 2021.
COVID-19 Contracting: Observations on Federal Contracting in Response to the Pandemic.GAO-20-632. Washington, D.C.: July 29, 2020.
DATA Act: Quality of Data Submissions Has Improved but Further Action Is Needed to Disclose Known Data Limitations. GAO-20-75. Washington, D.C.: November 8, 2019.
Disaster Contracting: FEMA Continues to Face Challenges with Its Use of Contracts to Support Response and Recovery. GAO-19-518T. Washington, D.C.: May 9, 2019.
2017 Disaster Contracting: Actions Needed to Improve the Use of Post-Disaster Contracts to Support Response and Recovery. GAO-19-281. Washington, D.C.: April 24, 2019.
2017 Disaster Contracting: Action Needed to Better Ensure More Effective Use and Management of Advance Contracts. GAO-19-93. Washington, D.C.: December 6, 2018.
Contact information: Marie A. Mak, (202) 512-4841, makm@gao.gov
The costs for importing goods into the U.S. have significantly increased since the beginning of the pandemic. U.S. import values of COVID-19-related products, such as face masks, ventilators, gloves, and hand sanitizer, have continued to fluctuate, while U.S. exports of COVID-19 vaccines have increased in recent months.
Background
Global trade has rebounded from the initial decline at the beginning of the COVID-19 pandemic, but international supply chains continue to experience disruptions. According to United Nations trade statistics, annual trade in world merchandise was forecasted to grow by 22 percent from the end of December 2020 through the end of December 2021, after declining by 7 percent from end of 2019 through the end of 2020.[424] An analysis by the World Trade Organization (WTO) suggests that this trend was driven by a surge in global demand for imported goods after the initial months of the pandemic.
According to the United Nations, increasing imbalances between global demand and supply of merchandise during COVID-19 have contributed to congestion at ports around the globe. According to a 2021 United Nations review of maritime trade, the rebound in trade combined with pandemic induced restrictions has led to port congestion, shortages in equipment and containers, less reliable services, and longer dwell times for ships and increased business uncertainty for importers and exporters. In addition, according to a report from the World Trade Organization (WTO), the surge in demand for imported items in many countries has led to gridlock at ports of entry.
The annual trade deficit of goods and services in the United States increased by 49 percent from $526 billion in 2019, the year before the pandemic started, to $859 billion in 2021. The annual trade deficit of goods increased by 27 percent from $862 billion in 2019 to over $1 trillion in 2021. The annual trade surplus of services decreased by 19 percent from $285 billion in 2019 to $232 billion in 2021.
Overview of Key Issues
Increasing shipping costs and port congestion. Import charges, including the cost of shipping goods across country borders has significantly increased in 2021 (see figure). Throughout 2019 and before the pandemic started in 2020, U.S. importers paid an average of about $283 in import charges, which includes freight cost, per $10,000 of merchandise imported.[425] After March 2020, the cost relative to dollar imported increased. In December 2021, U.S. importers paid almost $410 per $10,000 of merchandise imported.
Monthly Trends in U.S. Import Charges Relative to Value Imported, from Jan. 2018–Dec. 2021
Note: U.S. Census import data contains information on total monthly import charges paid on all imported shipments into the U.S. Census cannot reliabily account for shipments valued below $2,000. Therefore, Census implements statistical methodologies to account for imported shipments below $2,000 to account for coverage, timeliness, and relevance of the international merchandise trade statistics. Import charges include cost of freight; insurance; and other charges, excluding duties. December 2021 was the latest month of trade data available at the time of our analysis.
Cost of ocean freight has increased during the pandemic. According to Freightos, a digital booking platform for international shipping, the price of shipping a container of merchandise across the Pacific Ocean has stabilized in the beginning of 2022, but remains eight to nine times higher than pre-pandemic levels. According to the Federal Reserve of St. Louis, the average global market price of shipping a 40-foot container increased from an average of $1,331 in the first week of February 2020 to $11,109 in the second week of September 2021. Since shipping costs are often passed onto buyers of the imported product, increasing costs for ocean freight could lead to increased prices for U.S. importers and consumers. According to the Bureau of Labor Statistics, U.S. import prices increased by 10.9 percent from February 2021 through February 2022.
There are a number of factors that contributed to the increase in shipping prices after the initial months of the pandemic. According to an analysis by the United States International Trade Commission (USITC), in June 2020, shipping costs for ocean freight began to increase due to recovering consumer demand for goods as well as container shortages among other factors. Specifically, as noted in the same report, container shipping firms struggled to keep up with the resurgence in demand after reducing capacity in response to a decrease in consumer demand in the first months of the pandemic.[426] According to the same analysis, increased demand for certain types of products in 2020, most notably personal protective equipment (PPE), contributed to increased air freight shipping costs relative to 2019. In addition, COVID-19 outbreaks, more stringent health protocols, less flexible working conditions at U.S. ports and labor shortages led to bottlenecks, which further led to decreases in available containers to transport merchandise and further increased shipping costs.
The ports of Los Angeles and Long Beach have implemented some changes to their operations to reduce backlog. According to NASA satellite imagery, dozens of ships were waiting their turn to unload products at the ports of Los Angeles and Long Beach on October 10, 2021. Using data from the Marine Exchange of Southern California, NASA concluded that 60 ships were at anchor or in holding areas waiting to unload containers at the ports of Los Angeles and Long Beach on that day.[427] Using the same data, NASA found a large number of ships in holding areas or at anchor in June 2020. Before June 2020, cargo ships rarely had to wait to unload their goods. In January 2022, we reported that the number of shipping containers flowing through the ports of Los Angeles and Long Beach, which account for around 40 percent of U.S. containerized freight, had increased to record levels. On October 13, 2021, after a meeting between port leadership and the President, the U.S. administration announced that the Port of Los Angeles agreed to operate 24/7 in order to clear the backlog of ships waiting to unload their containers in the U.S.
As of March 22, 2022, most terminals were operating between 17 and 20 hours a day for at least 4 days a week, but none of the 6 Port of Los Angeles terminals had extended operations to 24 hours a day for 7 days a week.[428] At the port of Long Beach, one terminal announced a pilot program to extend operations closer to 24 hours a day for 4 days a week. However, truckers have rarely set appointments with the terminals at the port to pick up shipments during the extended hours of operation according to two news reports.
Fluctuations in U.S. trade of COVID-19-related products. U.S. import values of COVID-19-related products (e.g., face masks, ventilators, gloves, and hand sanitizer) have continued to fluctuate. According to U.S. Census Bureau trade statistics, U.S. import values of products in categories related to the COVID-19 response increased 13 percent from May through August 2021 before declining by 2 percent from August 2021 through December 2021.[429] Import values of these products in December 2021 were 31 percent higher than in February 2020, the last month before the declaration of the COVID-19 pandemic by the World Health Organization (see figure). Throughout 2021, monthly trends in COVID-related imports remained relatively stable with an average month-to-month growth of lower than 1 percent.
Monthly U.S. Import Values of COVID-19-Related Products, by Product Type, Jan. 2019–Dec. 2021
Note: U.S. Census Bureau trade statistics—a widely used source analyzing U.S. international trade—do not contain precise data on import values of COVID-19-related products. As a result, we estimated the import value of all product types and categories within those types using Harmonized Tariff Schedule of the United States (HTS) statistical reporting numbers and associated product groupings listed by the U.S. International Trade Commission (USITC). Examples of products included in the “Other” category of product type include hospital beds and wheelchairs. See U.S. International Trade Commission, COVID-19 Related Goods: U.S. Imports and Tariffs, Investigation No. 332-576, USITC Publication 5073 (Washington, D.C.: June 2020). Some HTS categories represent more than one product, and some categories contain products that are not directly relevant to COVID-19 response. Product categories that USITC identified as COVID-19-related refer only to the subset of goods considered to be COVID-19-related in each HTS-10 statistical reporting number. Furthermore, revisions to the HTS on July 1, 2020; January 1, 2021; and July 1, 2021, provided several new HTS-10 statistical reporting numbers that more narrowly defined some COVID-19-related product categories. In order to study import values of these products throughout and before the COVID-19 pandemic, we identified product categories that changed since June 2020 and mapped them to back to their original statistical reporting number in the USITC report mentioned above to provide a consistent time-series of monthly trade in these products. Therefore, the values shown overestimate the imports of products directly relevant to COVID-19 response. Nevertheless, the values shown are useful in tracking import value trends for such products throughout and before the start of the COVID-19 pandemic. For more information about factors influencing import trends in various types of COVID-19-related products, see U.S. International Trade Commission, COVID-19 Related Goods: The U.S. Industry, Market, Trade and Supply Chain Challenges, Investigation No. 332-580 (December 2020). December 2021 was the latest month of trade data available at the time of our analysis.
A rise in import values of personal protective equipment (PPE) and testing equipment has been driving the increase in import value of COVID-19-related products. Import values of PPE increased more than 500 percent from February 2020 through June 2020. Import values of PPE in December 2021 remained nearly 55 percent greater than in February 2020, before the pandemic, although import values of PPE declined by 37 percent from August 2021 through December 2021.
Import values of medical testing equipment doubled from February 2020 through August 2021 and further increased by 2 percent from August 2021 through December 2021. In addition, the monthly average value of medical testing equipment imports in 2021 was 80 percent higher than in February 2020. This includes a 24 percent increase in import value from November 2021 through December 2021, during which time WHO announced the Omicron variant as a variant of concern.
Demand for imported N-95 masks and swabs, key products needed to protect from and test for the COVID-19 virus, declined in the past year. Import quantities of N-95 masks declined by 91 percent and the unit value of N-95 masks declined by 82 percent from December 2020 through December 2021. Import quantity of swabs declined by 27 percent and the unit value declined by 5 percent from December 2020 through December 2021.[430] Declines in the import quantity and price suggest that U.S. buyers’ demand for these products from foreign suppliers has decreased. One possible explanation for this trend is an increased domestic production of these products.
There are many factors that could contribute to fluctuations in import values of COVID-19-related products. First, changes in import values are related to changes in both the quantity and price of the imported products. For instance, import values for a specific product can decrease even if the number of units imported increases if the decrease in price is large enough.[431] In addition, changes in the number of COVID-19 cases may shift the demand for some COVID-19-related products, such as pharmaceuticals and diagnostic equipment, over time.
Increased U.S. exports of COVID-19 vaccines. The U.S. has increased exports of COVID-19 vaccines in recent months. According to the World Trade Organization, U.S. exports of vaccine doses have increased since September 2021. As of January 31, 2021, the U.S. had exported roughly 714.4 million doses of vaccines, accounting for 14 percent of global COVID-19 vaccine exports, according to the same data source.[432]
U.S. exports of vaccines significantly increased after the first COVID-19 vaccine was approved for emergency use authorization (EUA). According to U.S. Census Bureau trade statistics, the value of exports of vaccines for human use, which include COVID-19 vaccines, increased over 26-fold from $92 million in December 2020, when the first COVID-19 vaccine was granted EUA, to over $2.4 billion in December 2021 (see figure).
After December 2020, the majority of U.S. export value of vaccines shifted to countries outside of the European Union (EU) member countries and the United Kingdom (UK). The value of U.S. export of vaccines for human use averaged $131 million per month from May 2020 through December 2020, but averaged over $1.7 billion from May 2021 through December 2021. Generally, the majority of U.S. vaccine exports—by value—prior to December 2020 went to EU member countries and the United Kingdom (UK), averaging 52 percent per month in 2020. However, the share of vaccine exports going to EU member countries and the UK dropped to an average of 27 per month in 2021.
Value of U.S. Exports of Vaccines for Human Use, Overall and to EU Member Countries and the United Kingdom, Jan. 2019 – Dec. 2021
Note: Domestic export data for products described in Schedule B code 3002.20.0000 reported in the figure above contain exports on all vaccines for human use (See Schedule B code 3002.20.0000—Vaccines for Human Medicine), including authorized COVID-19 vaccines, to every country. Schedule B product categories are a systematic grouping of commodities used by the U.S. Census Bureau to track exports of different products, which is based on the headings and subheadings in the International Harmonized System used by WTO members. As of January 2022, Schedule B product categories do not contain sufficiently granular information required to identify exports of COVID-19 vaccines specifically. December 2021 was the latest month of trade data available at the time of our analysis.
Methodology
To conduct this work, we reviewed the most recent publicly available U.S. trade statistics from the U.S. Census Bureau as well as U.S. International Trade Commission data on product categories that contain COVID-19-related products.[433] We also analyzed trends in U.S export data of vaccines for human use to provide context behind U.S. efforts to supply COVID-19 vaccines to other countries. We determined that the trade data were sufficiently reliable to provide an overview of U.S. trade of COVID-19-related products and the costs related to importing goods into the U.S.
Agency comments
We provided a draft of this enclosure to the Office of Management and Budget, which had no comments on this enclosure.
GAO’s Ongoing Work
We will continue to monitor international supply chain issues and Customs and Border Protection’s trade facilitation during COVID-19.
The extent of fraud associated with the COVID-19 relief funds appropriated to date has not yet been determined. However, many individuals or entities have already pleaded guilty to federal charges of defrauding COVID-19 relief programs—including the Small Business Administration’s Paycheck Protection Program and Economic Injury Disaster Loan program, and the Department of Labor’s unemployment insurance programs—and several hundred individuals or entities are facing federal charges. We have made previous recommendations to the Small Business Administration and the Department of Labor to better manage fraud risks to COVID-19 relief programs, in accordance with GAO’s Fraud Risk Framework.
Entities involved: Government-wide
Background
The public health crisis, economic instability, and increased flow of federal funds associated with the COVID-19 pandemic present increased pressures and opportunities for fraud.[434] Since March 2020, Congress has provided about $4.6 trillion through the CARES Act and other laws that were enacted to fund federal efforts to help the nation respond to and recover from the COVID-19 pandemic. By proactively managing fraud risks, federal officials can help safeguard taxpayer dollars to ensure they serve their intended purposes.
According to GAO’s A Framework for Managing Fraud Risks in Federal Programs (Fraud Risk Framework), effective managers of fraud risks refer instances of potential fraud to Offices of Inspector General (OIG) or other appropriate parties, such as law enforcement entities or the Department of Justice (DOJ), for further investigation.
Due to the very nature of the government’s need to quickly provide funds and other assistance to those affected by COVID-19 and its economic effects, federal relief programs are vulnerable to significant risk of fraudulent activities. However, the extent of fraud associated with the COVID-19 relief funds appropriated to date has not yet been determined. One of the many challenges to that determination is that because of fraud’s deceptive nature, programs can incur financial losses related to fraud that are never identified, and such losses are difficult to reliably estimate.
However, many individuals have already pleaded guilty to federal charges of defrauding COVID-19 relief programs, including the Small Business Administration’s (SBA) Paycheck Protection Program (PPP) and Economic Injury Disaster Loan (EIDL) program, the Department of Labor’s (DOL) unemployment insurance (UI) programs, and economic impact payments (EIP) issued by the Department of the Treasury and the Internal Revenue Service (IRS).[435] Also, six individuals have been convicted at trial of PPP-related fraud, and five individuals have been convicted at trial of fraud related to both the PPP and the EIDL program.[436] In addition, numerous others faced related federal charges as of January 31, 2022.
Further, federal hotlines have received numerous complaints from the public, many of them alleging potential fraud involving COVID-19 relief funds. For example, from March 2020 through January 2022, our hotline—known as FraudNet—received about 3,350 complaints related to the CARES Act, about half of which involve SBA’s PPP and EIDL program, DOL’s UI programs, and EIPs (see text box).[437]
Report Fraud, Waste, and Abuse
GAO’s FraudNet supports accountability across the federal government. Allegations of fraud, waste, or abuse can be submitted via the FraudNet portal or by calling the hotline at 1-800-424-5454.
In addition to fraud against federal programs, scammers are also targeting consumers, which can result in financial losses and undermine health and safety. For example, the Federal Trade Commission (FTC) is tracking complaints related to COVID-19 fraud against consumers. According to FTC reporting, the agency had received over 292,000 reports about fraud and over 198,000 reports about identity theft as of January 29, 2022.[438] The agency also reported that about 45 percent of the reports about fraud indicated a financial loss and cost Americans about an estimated $676 million.
In a March 2022 hearing on transparency and accountability for COVID-19 funds, we noted that recognizing fraud risks and deliberately managing them in an emergency environment can help federal managers safeguard public resources while providing needed relief. We also reported that focusing on fraud prevention can help most effectively manage risks. However, across our COVID-19 work, we found that agencies did not consistently apply leading practices to manage fraud risks in COVID-19 spending. Further, we reported that agency OIGs have also raised concerns about the ability of agencies to strategically manage fraud risks. We reported that Congress can strengthen fraud risk management practices across the government by reinstating the requirement for agencies to report on their antifraud controls and agency fraud risk management efforts in agency financial reports.
In prior CARES Act reports, we made recommendations to SBA and DOL to better manage fraud risks to COVID-19 relief programs, in accordance with the Fraud Risk Framework.[439] For example, in our March 2021 report, we recommended that SBA conduct and document fraud risk assessments for the PPP and EIDL program. In our October 2021 report, we made several recommendations to DOL, including to identify and assess fraud risks facing the UI programs and to designate a dedicated entity for managing the process of assessing fraud risks. We are reviewing agency efforts to address these recommendations.
Overview of Key Issues
Since March 2020, DOJ has publicly announced charges in numerous fraud-related cases involving COVID-19 relief programs, COVID-19-related consumer fraud schemes, or other types of fraud related to COVID-19.[440] The charges—filed across the U.S. and investigated by a range of law enforcement agencies—include making false statements and engaging in identity theft, wire and bank fraud, and money laundering.[441] The number of individuals facing fraud-related charges has continued to grow in the past year and will likely increase, as these cases take time to develop.[442] Other federal entities also continue to investigate and report on high levels of potential fraud. For example, as of March 17, 2022, DOL OIG reported opening more than 38,000 investigative matters involving alleged UI fraud. In October 2021, SBA OIG reported that from March 2020 through August 2021, it received 215,000 hotline complaints that alleged fraudulent activity in the PPP and EIDL program and has launched numerous investigations into this fraudulent activity.
Fraud against federal programs. From March 2020 through January 2022, at least 435 individuals or entities pleaded guilty to federal charges of defrauding COVID-19 relief programs, including SBA’s PPP and EIDL program and DOL’s UI programs, among others.[443] See the figure below for the number of individuals or entities who have pleaded guilty to federal fraud-related charges against COVID-19 relief programs as of January 31, 2022.
Number of Individuals or Entities That Have Pleaded Guilty to Federal Fraud-Related Charges by COVID-19 Relief Program, as of Jan. 31, 2022
aOne of these individuals was initially charged related to PPP, EIDL, and UI but only pleaded guilty to a UI-related charge.
Of the 435 individuals or entities who pleaded guilty, 238 had been sentenced as of January 31, 2022. See the figure below for additional sentencing details.[444]
Number of Individuals Who Have Pleaded Guilty to Federal Fraud-Related Charges and Have Been Sentenced, as of Jan. 31, 2022
Note: Some of these individuals were sentenced for additional charges not related to COVID-19 relief programs. Also, sentences can include things in addition to prison time such as restitution or other fees.
For example:
One individual was sentenced to over 9 years in prison and ordered to pay over $1.6 million in restitution associated with a PPP loan scheme. This individual pleaded guilty to charges of wire fraud and money laundering after submitting fraudulent PPP loan applications on behalf of three entities. Among other things, this individual falsely represented the number of employees and payroll expenses and submitted fraudulent tax records to support the claims. Further, this individual submitted one application in the name of an individual who died shortly before the application was submitted. In total, this individual sought over $2.6 million and actually obtained over $1.6 million in PPP funds, which this individual spent on luxury goods and to pay off a loan on a residential property. See the enclosure on the Paycheck Protection Program in appendix I for more information on the program.
In another case, an individual was sentenced to 18 months in prison and ordered to pay nearly $150,000 in restitution after pleading guilty to one count of wire fraud associated with a scheme to defraud SBA’s EIDL program. This individual admitted to filing false and fraudulent applications for EIDL funds on behalf of multiple entities. Among other things, this individual misrepresented the companies’ gross revenues, cost of goods sold, and number of employees. In total, this individual sought approximately $473,000, and SBA disbursed approximately $144,000. See the enclosure on the Economic Injury Disaster Loan Program in appendix I for more information on the program.
One individual was sentenced to 10 years in prison after pleading guilty to conspiracy charges and aggravated identity theft associated with a scheme to defraud UI. This individual admitted to leading a conspiracy in which the individual, along with others, gathered personal identification information and then submitted unemployment claims for individuals, including inmates, who were known to be ineligible to receive pandemic unemployment benefits. This individual charged fees to co-conspirator clients for the service of filing their fraudulent claims. A co-conspirator, who pleaded guilty to two conspiracy charges associated with the scheme, was sentenced to 5 years in prison. In total, these individuals and co-conspirators defrauded the government of more than $1.5 million. For more information on the UI programs, including information on state and territory reporting of overpayments that are due to fraud and DOL’s efforts to address potential fraud in the UI programs, see the enclosure on Unemployment Insurance Programs in appendix I.
One individual was sentenced to 3 years of probation and ordered to pay $1,200 in restitution to the IRS after pleading guilty to theft of government funds associated with an EIP. After this individual’s mother passed away in 2016, the Social Security Administration—which was not informed of the death—continued to deposit Social Security benefits into the mother’s bank account for several years, and the U.S. Treasury deposited a $1,200 EIP into the account in 2020. This individual obtained a copy of the bank card for the account and accessed the funds, including the EIP funds, for personal use.[445]
As part of another case, one individual pleaded guilty to filing a false claim with the U.S. associated with a scheme to defraud the IRS. Specifically, this individual filed a fraudulent form with the IRS claiming advance payment of over $625,000 of employer credits under the Families First Coronavirus Response Act by claiming to have a business with 50 employees and to have paid over $450,000 in quarterly wages when the business was a sole proprietorship and the individual was not entitled to the advance payment of credits.[446]
As of January 31, 2022, eleven individuals had been convicted at trial for COVID-19 relief fraud.[447] For example, a federal jury convicted an individual of multiple counts of wire fraud, bank fraud, and money laundering associated with schemes to defraud the PPP and EIDL program. This individual submitted several fraudulent PPP and EIDL loan applications seeking over $3.5 million and received over $2.8 million in COVID-19 relief funds as a result of the fraud. Specifically, this individual falsified the number of employees and payroll expenses and submitted fake tax documents to support applications submitted in the names of businesses with no actual operations or that were otherwise ineligible. As of January 31, 2022, this individual had not yet been sentenced.
Federal charges were pending against at least 548 individuals or entities for attempting to defraud COVID-19 relief programs as of January 31, 2022.[448] The majority of these individuals were charged with attempting to defraud SBA’s PPP and EIDL program and DOL’s UI programs, or fraudulently accessing EIPs, while others were charged with attempting to defraud other COVID-19 relief programs.[449] For example, one individual was charged with aggravated identity theft and wire fraud associated with a scheme to allegedly defraud SBA’s EIDL program and the Restaurant Revitalization Fund. In another case, a city government official was charged with wire fraud, conspiracy to commit federal program theft, and federal program theft associated with a scheme to allegedly steal federal funds granted to the city through the Coronavirus Relief Fund. See the enclosure on COVID-19 Relief Funding to States and Localities in appendix I for more information on the program.
Consumer fraud. In addition to fraud against federal programs, fraud can result in financial losses to consumers and undermine health and safety. From March 2020 through January 2022, 20 individuals or entities pleaded guilty to federal charges related to consumer fraud and one individual was convicted of a consumer fraud-related charge.[450] For example, one individual pleaded guilty to conspiracy to commit wire fraud in connection with a scheme purporting to sell COVID-19 vaccines. This individual admitted to conspiring with others to obtain access to a bank account to be used in a fraud scheme. The fraud scheme involved the creation of a fake website designed to resemble the website for a legitimate vaccine company. In another case, an individual pleaded guilty to conspiracy to commit wire fraud. This individual engaged in a scheme to trick consumers into purchasing pets online that were never delivered and used the COVID-19 pandemic to extract higher fees from victims, for example by claiming that additional fees were required for delivery because the pets had been exposed to coronavirus. In another case, an individual was sentenced to one year of probation after pleading guilty to distribution and sale of an unregistered pesticide, conspiracy to distribute and sell an unregistered pesticide, and making false statements to a government agency. This individual sold cards to multiple vendors, purporting that the cards—which could be worn around the user’s neck—protected against viruses, among other things.
There were also federal charges pending against 46 individuals or entities related to consumer fraud as of January 31, 2022.
As of January 31, 2022, the majority of the 67 individuals or entities that had pleaded guilty, faced federal charges for, or were convicted of COVID-19-related consumer fraud schemes were allegedly involved in schemes related to prevention or treatment of COVID-19 or personal protective equipment (PPE) sales (see figure).
Number of Individuals or Entities That Have Pleaded Guilty to, Faced Federal Charges for, or Were Convicted for Consumer Fraud, as of Jan. 31, 2022
aThe “other” category can include individuals or entities that engaged in deceptive business practices, making COVID-19-related claims that caused consumers to suffer or potentially suffer financial or other losses unrelated to prevention or treatment, personal protective equipment, or testing. For example, one individual pleaded guilty and was sentenced to 63 months in prison for, among other things, creating a website to sell other goods that were sought after during the pandemic and not delivering those goods.
Other federal cases. The federal government is also pursuing charges including conspiracy, wire fraud, and theft that are related to COVID-19 but separate from consumer fraud and fraud against the federal programs discussed earlier. From March 2020 through January 2022, 30 individuals or entities pleaded guilty to these types of federal charges.[451]
For example, one individual pleaded guilty to mail fraud and money laundering associated with a scheme to defraud the company the individual worked for as a human resources manager. Specifically, this individual arranged for COVID-19 testing of the company’s employees and issued a fraudulent invoice to the company in the name of a business owned by the individual when, in fact, the testing was provided by another entity at a lower cost. This individual then used the proceeds from the fraud to purchase a speedboat and trailer. This individual was sentenced to 41 months in prison.
In another case, an individual pleaded guilty to making false statements to the Federal Emergency Management Agency (FEMA) in order to obtain a contract to provide PPE. Specifically, this individual offered, through a company, to sell 10 million surgical masks for a total of $56.3 million, falsely claiming the masks were available immediately when the individual knew that the company did not have any surgical masks available at the time. FEMA awarded a contract to the company based in part on these false representations and later terminated the contract when the company failed to deliver any masks.[452]
In addition to the individuals or entities who pleaded guilty to these other types of federal charges, there were also other federal charges pending against 37 individuals as of January 31, 2022. For instance, as COVID-19 vaccines have become increasingly available and government and private entities have begun implementing vaccination requirements, non-consumer fraud involving COVID-19 vaccines has emerged. DOJ has publicly announced charges against individuals for several such cases.[453] In one case, an individual was charged with mail fraud and obstruction of justice in connection with the alleged distribution of fraudulent COVID-19 vaccination record cards. In another case, an individual was charged with fraudulently producing identification documents—COVID-19 vaccination record cards—and one count of lying to federal investigators about this individual’s own alleged role in producing the cards.
Other federal efforts to address and prevent future fraud-related cases. While DOJ has filed fraud-related charges against individuals and entities for actions related to COVID-19, other federal agencies have undertaken additional efforts to address fraud-related cases and prevent such cases in the future.
Taking administrative and other enforcement actions. From late May to late December 2021, the FTC issued warning letters to more than 20 marketers ordering them to stop making unfounded claims that their products and therapies could treat or prevent COVID-19. In the letters, the FTC noted that violators could face monetary penalties under the COVID-19 Consumer Protection Act.[454] Also, the Department of Health and Human Services (HHS) OIG reported taking enforcement action through civil monetary penalties related to potential fraud in the Provider Relief Fund.[455] For example, in December 2021, one business and an individual entered into a settlement agreement with HHS OIG for almost $63,000 for allegedly violating the Civil Monetary Penalties Law by falsely certifying to their eligibility to receive a CARES Act Provider Relief Fund payment.
Pursuing rulemaking to enhance antifraud efforts. In December 2021, the FTC launched a rulemaking aimed at combatting government and business impersonation fraud by enabling the FTC to seek refunds for consumers, in addition to civil penalties. According to the December 2021 press release announcing the rulemaking, the COVID-19 pandemic has led to a sharp increase in impersonation fraud. Specifically, according to the FTC, COVID-specific scam reports since the pandemic began included over 12,000 complaints of government impersonation and nearly 8,800 complaints of business impersonation.
Providing information to the public about emerging fraud schemes. As a result of complaints from the public alleging potential fraud involving COVID-19 relief funds received through hotlines and other fraud detection efforts, federal agencies have warned the public about emerging fraud schemes; these warnings can help prevent future cases of fraud against federal programs and consumers. For example:
As part of the fourth annual “Money Mule Initiative,” in December 2021, federal agencies educated state agencies and the public about money mules—individuals who receive money from fraud victims and forward the illicit funds, often to overseas perpetrators. Specifically, members of the Attorney General’s Coronavirus Fraud Enforcement Task Force used outreach materials created by the Pandemic Response Accountability Committee (PRAC) to educate the public about the use of money mules to steal pandemic relief funds.[456]
In addition, the FBI released a public service announcement about money mules, noting that individuals recruited as part of scams—such as employment scams due to the COVID-19 pandemic—can become unwitting or unknowing mules. According to the announcement, in 2020 and 2021, the FBI’s Internet Crime Complaint Center received an increase in complaints relating to COVID-19 related fraud. The increase could be the result of several factors, such as increases in remote work, which allowed criminals to instruct money mules to provide copies of their personal information online.
As part of an Annual National Tax Security Awareness Week in November 2021, the IRS and partners warned that taxpayers and tax professionals face an increased risk of fraud as fraudsters use the COVID-19 pandemic to trick people into sharing sensitive personal information that can then be used by identity thieves to file tax returns and steal refunds. Further, in February 2022, the IRS issued a reminder to taxpayers to protect their personal and financial information and to be alert for IRS impersonation scams. Among other things, the IRS cited an increase in text messages to taxpayers’ smartphones citing COVID-19 or “stimulus payments” and often containing links to scam websites purporting to be legitimate IRS websites.
As part of the 2022 Identity Theft Awareness Week beginning in late January, the PRAC provided information on identity theft in pandemic benefits programs and efforts by federal, state, and local oversight entities to address the issue. The PRAC noted that criminals stole personal information by hacking into social media accounts or through email phishing schemes and impersonation scams and then used the information to obtain unemployment checks or business loans.
We previously reported on examples of agency warnings to the public about emerging fraud schemes in our July 2021, October 2021, and January 2022 CARES Act reports. In addition, in our October 2021 report, we reported on other federal efforts to address and prevent future fraud-related cases, such as taking administrative and other enforcement actions and establishing task forces and working groups.
Methodology
To conduct this work, we reviewed information from DOJ to identify federal fraud-related charges related to COVID-19 relief funding as of January 31, 2022. We also analyzed related federal court documents. In addition, we reviewed FTC reports on complaints related to fraud and identity theft and press releases from other federal entities, including the FTC, describing COVID-19 fraud-related efforts.
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget, which provided no comments.
GAO’s Ongoing Work
In our ongoing work, we are reviewing fraud risk management and potential fraud in the PPP, EIDL, and UI programs, among others.
Related GAO Products
Emergency Relief Funds: Significant Improvements Are Needed to Ensure Transparency and Accountability for COVID-19 and Beyond.GAO-22-105715. Washington, D.C.: March 17, 2022.
Economic Injury Disaster Loan Program: Additional Actions Needed to Improve Communication with Applicants and Address Fraud Risks. GAO-21-589. Washington, D.C.: July 30, 2021.
Paycheck Protection Program: SBA Added Program Safeguards, but Additional Actions Are Needed. GAO-21-577. Washington, D.C.: July 29, 2021.
A Framework for Managing Fraud Risks in Federal Programs. GAO-15-593SP. Washington, D.C.: July 28, 2015.
The Federal Emergency Management Agency could do more to minimize fraud risks to its COVID-19 Funeral Assistance, and continues to face challenges in providing timely assistance for its Public Assistance program.
Entity involved: Federal Emergency Management Agency, within the Department of Homeland Security
Recommendations for Executive Action
The Federal Emergency Management Agency Administrator should take action to identify the causes of the gaps in internal control in COVID-19 Funeral Assistance and design and implement additional control activities, where needed, to prevent and detect improper payments and potential fraud.
The Federal Emergency Management Agency Administrator should address deficiencies in the COVID-19 Funeral Assistance data by updating data records as data are verified, and adding data fields where necessary, to ensure that consistent and accurate data are available for monitoring of potential fraud trends and identifying control deficiencies.
The Department of Homeland Security agreed with both recommendations and stated that it agreed with the need for internal controls and the importance of maintaining accurate, current data.
Background
Before the COVID-19 pandemic, the Federal Emergency Management Agency’s (FEMA) Disaster Relief Fund—the primary source of federal disaster assistance for state, local, tribal, and territorial governments—had never been used during a nationwide public health emergency.[457] As of February 28, 2022, FEMA had obligated about $95.7 billion from the Disaster Relief Fund to respond to COVID-19. As of the same date, the Disaster Relief Fund’s balance was about $32.2 billion. See the figure below.
Federal Emergency Management Agency’s Disaster Relief Fund Balance, by Month, Feb. 2021–Feb. 2022
In response to the COVID-19 pandemic, FEMA has provided three primary types of disaster assistance, funded through the Disaster Relief Fund.
Individual Assistance. FEMA provides Individual Assistance to disaster survivors to address necessary expenses and serious needs directly caused by a declared disaster. For the COVID-19 response, FEMA has provided lost wages assistance, funeral assistance, and crisis counseling.
Mission assignments. FEMA issues mission assignments—work orders directing other federal agencies to provide direct assistance to state, local, tribal, and territorial governments—to support disaster response and recovery. For the COVID-19 response, for example, FEMA issued a mission assignment to the Department of Defense to fund National Guard deployments to support state and territorial response efforts.
Public Assistance. FEMA provides Public Assistance to state, local, tribal, and territorial governments, and certain types of private nonprofit organizations, so that communities can quickly respond to, and recover from, major disasters or emergencies. After natural disasters, Public Assistance tends to be used for emergency cleanup and for permanent reconstruction projects—for example, to rebuild damaged public infrastructure.
For all 59 major disaster declarations for COVID-19, FEMA has authorized Public Assistance for emergency protective measures only. This may include eligible medical care, purchase and distribution of food, noncongregate medical sheltering, operation of Emergency Operations Centers, and the purchase and distribution of personal protective equipment.
On February 2, 2021, the President issued a memorandum that directed FEMA to fully reimburse state, territorial, and tribal governments for all work eligible for emergency protective measures assistance through September 30, 2021.[458] The President has extended this full reimbursement multiple times, most recently on March 1, 2022, extending full reimbursement to July 1, 2022.[459] According to FEMA officials, FEMA’s Public Assistance workforce consists of approximately 2,600 employees, of which about 400 are supporting the COVID-19 effort as of February 25, 2022.
Overview of Key Issues
FEMA’s use of the Disaster Relief Fund to support COVID-19 activities. As of February 28, 2022, FEMA had obligated about $95.7 billion from the Disaster Relief Fund to respond to COVID-19 since the beginning of the incident period, January 20, 2020. The figure below shows FEMA’s obligations for COVID-19, by program and activity.[460]
FEMA’s Disaster Relief Fund Obligations for COVID-19 by Program and Activity through March 2022
Note: The amounts shown include Disaster Relief Fund obligations through February 28, 2022, and projections through March 31, 2022. Percentages are rounded to the nearest whole number.
Individual Assistance. On August 8, 2020, a presidential memorandum directed that up to $44 billion be made available from the Disaster Relief Fund to provide lost wages assistance to supplement unemployment insurance compensation.[461] According to FEMA officials, as of February 28, 2022, FEMA had obligated approximately $38 billion for the Lost Wages Assistance program.
Further, in December 2020, the Consolidated Appropriations Act, 2021, appropriated $2 billion to the Disaster Relief Fund for eligible funeral expenses for individuals or households with COVID-19-related funeral expenses.[462] The American Rescue Plan Act of 2021 subsequently provided that FEMA is to provide financial assistance for COVID-19-related funeral expenses and that the $50 billion appropriated to the Disaster Relief Fund for major disasters in the same act was available for such assistance.[463]
On April 12, 2021, FEMA began accepting and processing applications for COVID-19 Funeral Assistance via a dedicated call center number. As of February 28, 2022, the call center had received and was processing over 444,000 applications and had approved over 296,000 applications for over $1.92 billion. The figure below shows the obligations made for COVID-19 Funeral Assistance from May 10, 2021, through February 22, 2022.
Cumulative Obligations for Federal Emergency Management Agency’s COVID-19 Funeral Assistance over Time, May 10, 2021 – Feb. 22, 2022
FEMA Funeral Assistance for COVID-19-related deaths. COVID-19 Funeral Assistance provides up to $9,000 per deceased individual to applicants who incurred COVID-19-related funeral expenses on or after January 20, 2020, and meet eligibility requirements. For instance, either the death certificate or a signed statement or letter from the certifying official, including the medical examiner or coroner, must attribute the death to COVID-19.[464]
The maximum allowable assistance provided to an applicant who incurred expenses for multiple deaths per state or territory is $35,500. FEMA provides financial assistance for eligible funeral expenses including remains transfer, caskets and urns, burial plots and cremation niches, markers and headstones, and other itemized expenses from a funeral home considered necessary for the funeral service.[465]
FEMA has developed internal controls for its COVID-19 Funeral Assistance, but additional steps needed to minimize fraud risks. The scope of FEMA’s COVID-19 Funeral Assistance is unprecedented. In the decade before the COVID-19 pandemic, FEMA had processed approximately 6,000 applications for funeral assistance after other natural disasters, according to FEMA officials. As of December 15, 2021—the most recent date for which application-level data were available—FEMA had awarded about $1.5 billion in assistance in response to about 235,000 applications for nearly 237,000 individuals deceased due to COVID-19. See figure below for a map of COVID-19 Funeral Assistance awards by county.
COVID-19 Funeral Assistance Awards as of December 15, 2021, by U.S. County
Note: COVID-19 funeral assistance was also awarded to individuals in U.S. territories. Award location reflects the reported location of death for each deceased individual listed on an application. Less than 1 percent of addresses were missing zip code information required for mapping and are therefore excluded from this map.
Based on our review of the application data, we identified several gaps in FEMA’s controls, which were not sufficient in preventing improper or potentially fraudulent payments. Specifically, we identified cases in which FEMA’s controls did not prevent funeral assistance provided (1) in response to duplicate applications listing the same decedents; (2) above the maximum of $9,000 allowed per decedent; and (3) in response to applications listing incorrect applicant identifying information.[466]
Duplicate applications for funeral assistance. We found evidence that FEMA’s controls did not consistently prevent duplication in COVID-19 funeral assistance for the same deceased individuals, which can result in improper payments or allow for potential fraud. Specifically, we identified 374 deceased individuals that were listed on more than one award-receiving application; in total, these applications received about $4.8 million in assistance.[467]
FEMA’s 2021 standard operating procedures for COVID-19 funeral assistance state that FEMA will only award assistance for a deceased individual to a single applicant or co-applicant under the same application. To prevent such duplication, FEMA case workers follow a set of procedures including looking for matches in decedent identifiers and sending applications containing possible duplication for additional manual review.
Most of the 374 deceased individuals that we identified as listed on more than one application were listed by different applicants. We provided three example applications that identified different applicants but duplicative decedents to FEMA. According to FEMA officials, the duplicative applications were incorrectly awarded funeral assistance due to processing errors. The officials provided documentation showing that, following our review, they had initiated recoupment efforts where necessary for two of the example applications in January 2022.[468]
About 50 of the 374 deceased individuals were listed on multiple applications from the same applicant. Although the data FEMA provided indicated that each of these applications was awarded assistance, FEMA officials initially told us that the cases reflected applicant transfers to corrected disaster areas and that in each case only one of the applications was paid.[469]
However, when we provided examples of these applications to FEMA officials, they confirmed that in each case, the duplicative applications were paid. The officials provided documentation showing that they had initiated recoupment efforts for one of the example duplicative applications in July 2021 and for the remaining two in February 2022, following our review.
Awards above the $9,000 maximum. In addition, we found evidence that FEMA’s controls do not prevent case workers from authorizing awards that exceed FEMA’s stated maximum of $9,000 per deceased individual. This can result in applicants receiving more assistance than allowed by FEMA rules and allows for potential improper payments or fraud.
According to FEMA’s 2021 standard operating procedures for COVID-19 funeral assistance, FEMA caseworkers review evidence of funeral expenditures for each application and determine the appropriate amount to award, up to the maximum allowed. However, we identified approximately 400 applications that were awarded more than this maximum, receiving up to $19,995 for a single deceased individual and totaling about $4.7 million.
We provided three examples of applications with payments above the maximum allowed to FEMA; officials said that each application had experienced a case processing error in which the necessary amount was not deducted prior to award. The officials told us that they provided feedback to the caseworker involved in each case and provided documentation showing they had initiated recoupment efforts for one of the example applications in September 2021 and the remaining two example applications by February 2022, following our review.
Incorrect information on applications. We also found evidence that FEMA’s controls do not always prevent applicants with invalid identity documentation from being awarded funeral assistance, which can result in improper payments or allow for potential fraud. Specifically, we identified about 230 award-receiving applications in which the applicant’s or co-applicant’s listed Social Security Number (SSN) appeared to be incorrect.
FEMA’s 2021 standard operating procedures for COVID-19 funeral assistance state that applicants are required to provide an SSN and that the decedent’s SSN cannot be listed in the applicant SSN field.[470] FEMA officials stated that FEMA verifies applicant identity—including SSN—using the LexisNexis data service, which uses national data repositories to calculate fraud risk.[471] According to the officials, applicants that do not pass the LexisNexis identity verification must provide documentation to prove their identity before FEMA can process the application.
We identified about 80 applications, awarded a total of about $570,000, in which the applicant or co-applicant SSN was the same as the decedent SSN listed on the application. We also identified about 150 applications, awarded a total of about $1 million, in which the applicant or co-applicant SSN was listed on the Social Security Administration’s (SSA) December 2021 full death file with a death date prior to the application date and under a different name and date of birth.[472]
We provided examples of applications with potentially incorrect SSNs to FEMA. FEMA officials stated that based on their review of these applications’ documentation, in most cases, the correct SSN was obtained during the application review process but never updated in the SSN data field. However, in at least one case, officials said that the correct SSN documentation was never obtained and FEMA had initiated efforts to validate the applicant’s identity based on our review. FEMA officials provided documentation showing they had initiated recoupment efforts for this application in February 2022, following our review.
Data quality. Our review also determined that FEMA does not sufficiently maintain the quality of its application data in a way that would facilitate oversight of COVID-19 Funeral Assistance and prevent and detect potential fraud. Our July 2015 Framework for Managing Fraud Risks in Federal Programs calls for agencies to follow leading practices such as designing and implementing data analytics and other control activities to prevent and detect fraud. However, we determined that FEMA lacked consistent data on whether applications were paid, decedent death dates, the amount of funeral assistance awarded for specific decedents on an application listing multiple decedents, and applicant SSNs.
While FEMA officials stated that they are able to obtain accurate data on each application by manually checking its history, FEMA would be unable to efficiently identify which applications merited manual review if automated checks first did not detect the relevant discrepancies. This information—in particular, information on whether an award that appears in FEMA’s data was truly paid—would be a key factor in implementing data analytics and managing potential fraud risk.
For example, we found that FEMA does not maintain consistent data that would allow it to accurately determine and report on the total number of applications that were awarded or amount of assistance that was awarded. As described previously, FEMA officials told us that where application transfers occurred, the application is duplicated in the data even though the award was only paid once.[473] FEMA officials told us that they do not have a way to identify which awards were made or duplicated in the data without manually checking an application’s history.
In addition, FEMA does not maintain consistent data on death date, which is a key factor in eligibility for assistance.[474] We identified over 11,000 award-receiving applications that had a missing or invalid death date according to the data that FEMA provided. We provided examples of these applications to FEMA; officials told us that they manually checked each application’s history and it appeared that the correct dates were ultimately obtained during the application process.
However, the death date field itself was never updated in FEMA’s data. FEMA officials told us that while it has always been a requirement that case workers update this field, it was never reinforced. According to the officials, FEMA has reiterated the requirement to case workers based on our review.
FEMA officials also told us that the database containing the funeral assistance data does not contain a field identifying the amount of assistance awarded for each deceased individual on an application with multiple decedents.[475] Rather, the database is designed such that only the total amount of assistance awarded per application is maintained in a specific field.
FEMA officials told us that they must manually check an application’s history to obtain more detailed information for specific decedents. Unless FEMA performs a manual review, it is unable to determine whether an applicant listing multiple decedents received more than the maximum amount allowed for a given decedent.
As described previously, we identified about 230 award-receiving applications in which the applicant or co-applicant SSN appeared to be incorrect and provided examples to FEMA. Upon their review of each example’s history, officials stated that in most cases, the correct SSNs were obtained but the SSN data fields were never updated.
However, FEMA would be unable to perform a global analysis of the extent to which it is successfully verifying identities—for example, through post-award quality control checks—without manually checking each application’s history for correct SSNs. Further, without verifying the identities of applicants prior to awarding funeral assistance, FEMA is increasing the risk of improper payments and potential fraud and creating a potential “pay and chase” scenario for recovering these payments, which is costly and inefficient.
Without adequate controls and application data—for example, controls that prevent funeral assistance payments in response to duplicate applications, and consistent data on whether applications were paid—COVID-19 Funeral Assistance is at risk of improper payments and potential fraud.
In addition, without consistent data, FEMA lacks assurance that it can use data analytics to prevent and detect potential fraud as part of its oversight of COVID-19 Funeral Assistance. Of the about 235,000 award-receiving applications we reviewed, the proportion we identified as at-risk is relatively small. However, our findings are significant due to the possibility of improper payments and potential fraud in not only this disaster, but also future disasters.
FEMA’s Disaster Relief Fund continues to support a variety of activities. In addition to individual assistance and funeral assistance, FEMA has provided mission assignments, a separate effort to run mobile vaccination units, and Public Assistance.
Mission assignments. FEMA has issued mission assignments to multiple federal agencies—the Department of Agriculture, Department of Labor, Environmental Protection Agency, and Department of Defense, among others—to assist in the COVID-19 response.
The presidential memorandum issued on January 21, 2021, provided that FEMA would fully reimburse expenses to the Department of Defense for mission assignment activities performed by the National Guard to respond to COVID-19 such as vaccination distribution.[476] According to FEMA, the estimated cost for National Guard assistance totaled nearly $6.6 billion as of February 28, 2022.
Mobile Vaccination Units. FEMA runs mobile vaccination units that offer primary vaccinations, booster shots, and pediatric vaccines for children ages 5 and above. According to FEMA, these vaccination units are intended to operate in trusted settings and emphasize convenience and equity. All states, tribes, and territories may request mobile vaccination units.
Currently, FEMA has the capacity to run 10 mobile vaccination units, and all ten started operating between December 15, 2021, to January 18, 2022: two in Washington, four in New Mexico, three in Oregon, and one in Pennsylvania. FEMA reported that as of March 4, 2022, the 10 mobile vaccination units have administered 136,770 vaccinations.[477]
Public Assistance. FEMA officials stated that as of March 2, 2022, FEMA had received 29,238 applications for Public Assistance. With the emergence of the Delta and Omicron variants of COVID-19, FEMA officials stated that there has not been a significant increase in COVID-19-related Public Assistance projects, but costs increased per project.
From the beginning of the COVID-19 incident period (January 20, 2020) through February 28, 2022, FEMA obligated a total of approximately $41.9 billion for Public Assistance for about 14,300 projects.[478] The figure below shows the number of projects and award amount for each of FEMA’s 10 regions from the beginning of the COVID-19 declaration incident period through February 28, 2022.
Number of FEMA Projects and Amounts Obligated for Public Assistance for COVID-19, by Region, through Feb. 28, 2022
As noted above, the major disaster declarations for COVID-19 authorized emergency protective measures. A January 21, 2021, presidential memorandum provided that FEMA was to make available assistance for emergency protective measures that may be required to facilitate the safe opening and operation of all eligible facilities, including schools, domestic violence shelters, and transit systems, among others. Such assistance may include funding for the provision of personal protective equipment and disinfecting services and supplies.[479]
A Presidential Memorandum and a subsequent FEMA policy extended the eligibility retroactively for such assistance to the beginning of the incident period.[480] According to FEMA officials, the January 2021 memorandum did not have a significant impact on their resources and operations.
In addition to FEMA-run mobile vaccination units described above, work and associated costs to support the distribution and administration of COVID-19 vaccines may be eligible for Public Assistance. As such, FEMA is coordinating with other federal agencies to meet state, local, tribal, and territorial needs. Specifically, FEMA officials stated that as of March 2, 2022, the agency had obligated more than $6.6 billion to state, tribal, and territorial governments for vaccine distribution through Public Assistance.
According to FEMA officials, eligible work and costs under Public Assistance for vaccine distribution may include, but is not limited to:
leasing facilities or equipment to administer and store the vaccine,
providing staffing and training support,
providing personal protective equipment and other administrative supplies, and
using technology to register and track vaccine administration.[481]
States note positive relationships with FEMA’s regional management but challenges remain with processing and reimbursements with the Public Assistance Program. Our October 2021 CARES Act report includes our findings on FEMA’s Public Assistance to state governments. We found that, among other things, FEMA was inconsistently applying COVID-19 Public Assistance policies. We recommended that FEMA (1) ensure consistency of the agency’s interpretation and application of the COVID-19 Public Assistance policy within and across regions, and (2) require training to ensure that COVID-19 Public Assistance policy is applied consistently nationwide.
To follow up on the progress FEMA has made to address these recommendations, we solicited information from 11 state emergency management agencies, with 10 responding to our request in January and February 2022. State emergency managers indicated that there are some areas of positive development including good or improving relationships with FEMA’s regional management, but challenges remain with the Public Assistance program.
For instance, eight state emergency managers we interviewed stated that they have good or improving relationships with FEMA regional management. Five states indicated that there are good lines of communication with their FEMA counterparts as they work through COVID-19 issues and all disasters. Four states noted that these relationships have resulted in better support and technical assistance for issues as they rise. For instance, one state indicated that they have easier resolution of issues and questions with its regional management than when the COVID-19 declaration first started in 2020.
In addition, most states indicated improvement in FEMA’s guidance. Specifically, six states indicated that FEMA’s most recent guidance released in January 2021 was adequate, improved, or helpful. One state noted that the COVID-19 guidance is no longer continuously changing, so states better understand what expenses are eligible, or are able to talk to FEMA about expenses that are questionable. The stable guidance helps states better understand what is eligible for reimbursement.
However, seven states said that there are continued challenges with clarity concerning eligible reimbursements. For instance, one state emergency manager said that FEMA’s guidance on ventilators is a continuing challenge. The state asserted that it could clearly identify the needs and quantities, but FEMA continued to question the needs for the amount of ventilators that the state procured.
Further, the state officials said there was too much conversation back and forth with FEMA on whether ventilators are disposable or permanent equipment, which affects how used ventilators should be treated and how many ventilators the state should buy. They were still waiting and still being questioned on these expenditures. There had been no reimbursement on the ventilators as of January 2022, which cost approximately $30-$60 million.
In addition, seven states indicated that there were undue administrative burdens and tasks with some documentation requirements, affecting timeliness of getting reimbursed for items. Such problems reduce the states’ capacity to support their communities. One state emergency manager we spoke with stated that FEMA was still inconsistent with eligibility guidance at the regional level, and what qualifies or does not qualify was still unclear.
The state official said that the state has spent a lot of time trying to track down if something is eligible or not. Also, the state official stated that when new information such as circulars or advisories are published, it is not clear what has changed. FEMA has not told the states upfront what has changed in these publications, if anything, placing the burden on the state agencies to determine whether there is new information.
A state emergency manager from another state said that FEMA’s expedited processing for vaccines did not extend to other important projects. The emergency manager stated that separating out the different projects has hampered the state’s ability to procure services such as vaccine call centers, testing and lab services, and temporary morgue operations.
In another state, emergency managers stated that FEMA had requested the state’s assistance to quarantine in non-congregate shelters individuals arriving on cruise ships in March 2020. However, after quarantining the individuals, FEMA stated that it wanted proof that each individual had COVID, although the state understood the directive to apply to all the passengers on the cruise ships. According to the state, nearly 2 years later, FEMA was still questioning the authorization for the project and requesting the same data repeatedly. As of January 2022, the state is awaiting reimbursement for the expenses incurred for sheltering the passengers.
Further, another state that requested assistance through one of FEMA’s consolidated resource centers for project approval and reimbursement said that the centers are receptive to funding new projects but over-scrutinize projects for COVID-19 program eligibility.[482] For example, a locality purchased sterilization chambers for sterilizing PPE. The “Request for Information” from the consolidated resource center stated: “Please describe how the UV light sterilization chambers are an emergency protective measure that prevents the spread of COVID-19.” The state official asserted that this level of scrutiny poses a challenge to the state. FEMA stated that this was an example of the review process working as it was intended; however, the state believed that it is well known that UV lights can sterilize PPE.
FEMA Public Assistance officials acknowledged that they have heard complaints from states about inconsistent application of eligibility requirements, but they have not received specific information to explain what items were inconsistent. However, we were able to identify inconsistencies, which we share above and in our October 2021 CARES Act report. Because states are still experiencing challenges in working with the Public Assistance program, our recommendations will remain open until there is more reported consistency among the regions and states.
Tribal governments continue to struggle to obtain FEMA resources to combat the COVID-19 pandemic. In our March 2021 CARES Act report, we reviewed FEMA’s assistance to tribal governments and found that FEMA had not provided timely and consistent technical assistance and recommended that FEMA do so. To determine FEMA’s progress in addressing this recommendation, we met with two national tribal associations that represent tribes throughout the country.
According to one organization, tribes have been under duress because of COVID-19 outbreaks in their communities, so much so that it has impacted the ability of tribes to get resources from FEMA or from the states they work with. Further, some tribes lack the emergency management personnel to address the pandemic as it goes through its communities. The tribal association stated that while they have tried to reach out to FEMA at all levels of management, they are unable to communicate with FEMA to talk about how they should get access to needed PPE and other resources.
Another tribal organization stated timeliness in getting technical assistance has been difficult. For example, according to this organization, one tribe submitted to FEMA a number of Public Assistance projects. While the tribe initially had received positive feedback on the projects’ suitability to be funded, all the projects were rejected for funding without explanation or help to understand how they could be improved.
In addition, one of the tribal associations stated that FEMA had not provided meaningful data on how many tribal organizations were receiving funding through FEMA’s programs, which would help FEMA and tribal organizations assess FEMA’s ability to provide services to tribes. FEMA stated that such data is readily available from multiple sources and cited three sources. However, two of three sources cited were internal FEMA documents, and the one online source—titled OpenFEMA—did not focus on tribal declarations but on all declarations, making it difficult to navigate without knowing how to focus on tribal data for specific declarations.[483]
FEMA Public Assistance officials stated that they have resources dedicated to communicating to tribal nations in each region; these resources are meant to help individuals contact the right people, including being able to contact program delivery managers assigned to the tribes, with contact information in the tribes’ accounts in FEMA’s Grants Portal, the system by which Public Assistance projects are managed.
FEMA officials also stated that they hold question and answer sessions that tribal nations are encouraged to attend. However, tribal organization officials stated that the sessions are not held regularly and it is hard for nations to attend with little notice and little time to prepare. Moreover, a tribal association stated that FEMA spent most of some sessions explaining the policies and leaving little time for the tribal government to provide feedback or receive answers to their questions. Based on the information we received from the tribal organizations, our recommendation remains open until FEMA provides additional and timely assistance to tribal governments.
Methodology
To conduct this work, we reviewed FEMA’s monthly Disaster Relief Fund reports to obtain FEMA obligations data for Individual Assistance, Public Assistance, and mission assignments for February 2021 through February 2022. We reviewed federal laws and FEMA policies and guidance on how states, local, tribal, and territorial governments may apply for, and receive, assistance to respond to the COVID-19 pandemic. We also reviewed information on FEMA’s mobile vaccination units, Public Assistance, and funeral assistance related to COVID-19. In addition, we reviewed previous GAO reports on FEMA’s response to the COVID-19 pandemic. We found the funeral assistance data to be reliable to provide the number of claims and costs for the program. Although we present FEMA data on Public Assistance, we did not independently determine the reliability of the data.
In addition, to assess the extent to which FEMA has implemented controls to help prevent potential fraud in COVID-19 Funeral Assistance, we requested and reviewed application data from FEMA, reviewed relevant policies, and interviewed FEMA officials. FEMA provided data for all applications submitted from the onset of COVID-19 Funeral Assistance on April 12, 2021, through November 2021, the most current data available at the time of our request.[484] The data contained records for all applicants requesting COVID-19-related funeral assistance as well as the amount of payment received.
To identify indications of potentially improper payments or fraud, we performed testing of these data, including determining whether funeral assistance was provided more than once for the same deceased individual; whether more funeral assistance was provided than the maximum allowed by FEMA; and whether applicant and decedent SSNs appeared valid. As part of the latter analysis, we matched the FEMA application data to the SSA full death file to identify potentially problematic SSNs, such as applicant SSNs that appeared on the full death file under a different name and date of birth.[485] We used a copy of SSA’s full death file that was current as of December 2021, the most recent version available at the time we performed the analysis. We plan to share our findings with the Department of Homeland Security, Office of Inspector General for additional review and action, as appropriate.
To assess the accuracy and reliability of the FEMA application data, we interviewed and obtained written responses from FEMA officials and performed electronic testing of the data, including checks for missing, out of range, or logically inaccurate data. As part of our reliability checks, where we identified potential issues such as death dates that appeared invalid, we provided example application identification numbers to FEMA and obtained detailed information from FEMA officials on the history and status of those applications. We identified several reliability concerns that we describe in this report. Otherwise, we determined that the data were sufficiently reliable for the purposes of our report.
To obtain information on states’ perception of FEMA’s Public Assistance program, we interviewed or otherwise received information from state emergency officials from California, Idaho, Illinois, Iowa, Kansas, New Jersey, North Carolina, Pennsylvania, South Carolina, and Washington. Further, to obtain perceptions on FEMA’s progress working with tribal governments on Public Assistance, we met with two national tribal associations. Finally, we interviewed FEMA officials regarding their efforts to implement COVID-19 Funeral Assistance and the COVID-19 Public Assistance program for COVID-19.
Agency Comments
We provided a draft of this enclosure to the Office of Management and Budget (OMB), the Department of Homeland Security (DHS), and FEMA. OMB had no comments on the enclosure. In DHS’s comments, which are reproduced in appendix VIII, the department concurred with both recommendations and agreed with the need for internal controls and the importance of maintaining accurate, current data.
However, FEMA stated that its existing controls were sufficient in mitigating the risk of fraud in COVID-19 Funeral Assistance, citing as evidence the agency’s estimation of improper payments of less than 1 percent and specific internal controls currently in place. In addition, FEMA stated that its funeral assistance data system of record is designed to update all application data in real-time, and that data elements regarding applicant payments, decedent death dates, and applicant SSN are maintained at a sufficiently high quality such that no action is necessary to broadly update them.
We disagree that FEMA’s existing controls are sufficient. Regardless of an agency’s improper payment rate, agencies are required to assess and manage fraud risks. Our evidence illustrates that additional steps are needed to do so.
For example, despite FEMA’s existing controls, we identified cases in which FEMA provided funeral assistance above the maximum assistance allowed per decedent or to duplicate applications listing the same decedents. These examples demonstrate that applicants could defraud FEMA without additional internal controls in place. During the course of our audit, we provided 15 example applications to FEMA illustrating instances in which we identified possible gaps in FEMA’s controls. Of these 15 applications, FEMA officials stated that they had initiated recoupment efforts for 2 prior to our review, and confirmed the need to initiate recoupment efforts for at least an additional 8 applications. The examples we provided were emblematic of larger numbers of applications with issues, suggesting that additional applications may require recoupment efforts.
In addition, our evidence illustrates that FEMA does not maintain the quality of its application data in a way that would facilitate oversight and prevent and detect fraud. For example, despite FEMA’s existing data maintenance procedures, we identified award-receiving applications with missing or invalid death dates and incorrect applicant identifying information. When we provided example applications to FEMA, officials told us that in most cases, the correct information was obtained during the application process but never updated in the respective data elements. As a result, these applications may not be compared to accurate data for other applications. Further, without consistent data, FEMA is less able to perform accurate data analytics as part of its oversight of COVID-19 Funeral Assistance.
We continue to believe that FEMA should take action to identify the causes of the gaps in internal control we identified, design and implement additional control activities, where needed, and address deficiencies in the COVID-19 Funeral Assistance data. We will continue to monitor FEMA’s actions in these areas to determine if they address our recommendations.
GAO’s Ongoing Work
We will continue to monitor FEMA’s efforts to respond to COVID-19 and assistance provided to states, local, tribal, and territorial governments.
GAO’s Prior Recommendations
The table below presents our recommendations on FEMA’s response to COVID-19 from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to COVID-19
Recommendation
Status
The Federal Emergency Management Agency Administrator should improve the consistency of the agency’s interpretation and application of the COVID-19 Public Assistance policy within and across regions by further clarifying and communicating eligibility requirements nationwide. (October 2021)
Open-Partially Addressed. In October 2021, the Department of Homeland Security (DHS) concurred with the recommendation and provided a number of steps it has taken. For instance, the Federal Emergency Management Agency (FEMA) stated that the applicable time period of eligibility for reopening was extended retroactively to the beginning of the incident period of January 20, 2020, which FEMA stated will improve consistent interpretation and application of COVID-19 Public Assistance policy nationwide. Further, FEMA stated that it holds biweekly discussions with FEMA Regional Recovery Division Directors and FEMA Regional PA Branch Chiefs, which includes discussion on COVID-19 policy and needs being faced in localities across the nation. In December 2021, FEMA provided us with a number of training sessions it has held via a website that Public Assistance officials can access as they have questions about aspects of COVID-19 assistance. These all are consistent with the recommendation. However, FEMA has not explained how it intends to measure the success of its efforts to ensure that all regions are implementing policy the same throughout the country. In January and February 2022, we conducted outreach to 10 states to determine if the states had found that FEMA had improved the consistency of the agency’s interpretation and application the Public Assistance Policy. States told us that they were still facing challenges related to consistency on application of policy. Therefore, we will keep this recommendation open.
The Federal Emergency Management Agency Administrator should require the agency’s Public Assistance program employees in the regions and at its Consolidated Resource Centers to attend training on changes to COVID-19 Public Assistance policy to help ensure it is interpreted and applied consistently nationwide. (October 2021)
Open-Partially Addressed. In October 2021, FEMA concurred with the recommendation and stated that it took a number of actions to educate staff on changes to COVID-19 Public Assistance policy. For example, FEMA conducted a webinar with over 300 staff, which covered a number of issues. Further, FEMA set up a number of training sessions online so officials can access them when needed. However, FEMA has not indicated whether these training sessions are required, nor whether they are ensuring the staff understand the content and are applying it. In January and February 2022, we conducted outreach to 10 states to determine if the states had found that FEMA had improved the consistency of the agency’s interpretation and application the Public Assistance Policy. States told us that they were still facing challenges related to consistency on application of policy. Therefore, we will keep this recommendation open.
The Federal Emergency Management Agency Administrator should adhere to the agency’s protocols listed in the updated 2019 Tribal Consultation Policy by obtaining tribal input via the four phases of the tribal consultation process when developing new policies and procedures related to COVID-19 assistance. (March 2021).
Closed-Addressed. In March 2021, DHS concurred with our recommendation. DHS states that FEMA’s National Tribal Affairs Advisor, based in the Office of External Affairs, will coordinate with other FEMA offices and directorates, as appropriate, to review the agency’s adherence to protocols listed in the Tribal Consultation policy. According to FEMA officials, in March 2021, FEMA conducted formal consultation with Tribal Leaders on COVID-19 Funeral Assistance before finalizing the interim policy. In April 2021, FEMA sent letters to tribal leaders discussing (1) FEMA policy and procedure for financial assistance to individuals and households for COVID-19 related funeral expenses incurred after January 20, 2020; and (2) a framework, policy details and requirements for determining the eligibility of safe opening and operation work and costs under the Public Assistance program. According to FEMA officials, as of March 2022, no additional COVID-related policies or regulations are under development. As a result, we consider this recommendation as closed-addressed.
The Federal Emergency Management Agency Administrator should provide timely and consistent technical assistance to support tribal governments’ efforts to request and receive Public Assistance as direct recipients, including providing additional personnel, if necessary, to ensure that tribal nations are able to effectively respond to COVID-19. (March 2021).
Open-Partially Addressed. In March 2021, DHS concurred with our recommendation. DHS stated that FEMA’s Recovery Directorate will publish a memorandum that will contain direction to FEMA regions regarding the assignment of Public Assistance Program delivery managers to promote equitable delivery of Public Assistance to tribal governments. According to FEMA officials, in August 2021, FEMA sent a memorandum that provided updates on how FEMA would deliver assistance. This guidance provides FEMA’s regional staff the ability to work with all tribal applicants to understand their capacity to address issues through their assigned Public Assistance program delivery manager. FEMA also stated that in September 2021, it hosted a webinar to further enhance staff readiness to deliver direct technical assistance and support to tribes. Further FEMA stated that as of December 2021, 223 out of 355 of the tribal entities that are eligible Public Assistance applicants have requested and received a program delivery manager. During the winter of 2022, we reached out to representatives from the tribal governments to see if the assistance provided by these program delivery managers has been reliable and generally has addressed their needs and concerns. According to two organizations we met with, communication with FEMA has been unreliable, so they could not say that FEMA has improved its technical assistance in a timely or consistent manner. Therefore, we believe this recommendation should remain open.
The Federal Emergency Management Agency Administrator—who heads one of the agencies leading the COVID-19 response through the Unified Coordination Group—consistent with their roles and responsibilities, should work with relevant federal, state, territorial, and tribal stakeholders to devise interim solutions, such as systems and guidance and dissemination of best practices, to help states enhance their ability to track the status of supply requests and plan for supply needs for the remainder of the COVID-19 pandemic response. (September 2020)
Open- Partially Addressed. In September 2020, the Department of Homeland Security (DHS) disagreed with this recommendation, noting, among other things, work that FEMA had already done to manage the medical supply chain and increase supply availability. Although DHS disagreed with our recommendation, it began taking some actions in March 2021. As of May 2021, DHS had not demonstrated action to devise interim solutions that would systematically help states, tribes, and territories effectively track, manage, and plan for supplies to carry out the COVID-19 pandemic response in the absence of state-level end-to-end logistics capabilities that would track critical supplies required for a response of this scale. We note that we made this recommendation to both DHS and the Department of Health and Human Services (HHS) with the intent that they would work together under the Unified Coordination Group to address challenges reported by state officials with both public health and emergency management responsibilities. Moreover, we recommended they take actions that were consistent with the roles and responsibilities that were to be more clearly defined as HHS took a more central role in leading supply distribution. The recommendation to define those roles and responsibilities remains open. Both DHS and HHS have reported separate actions, taken as part of other efforts within each separate purview. For instance, FEMA has developed and released an updated distribution management plan guide that, according to FEMA, provides actionable guidance for state, local, tribal, and territorial agencies, among others, to effectively and efficiently distribute critical resources to disaster survivors in the community. In addition, FEMA published and put online a logistics technical assistance program, which assists in the development, readiness, and enhancement of logistics planning and operational capabilities for state, local, tribal and territorial agencies. Further, FEMA provided information about listening sessions conducted at the regional level. However, as of February 2022, neither FEMA nor HHS has articulated how it worked with the other at the headquarters level, nor how they assessed whether the actions changed the experiences of state officials who reported issues during our prior work. Without systematic and deliberate action to help states ensure they have the support they need to track, manage, and plan for supplies, states, tribes, and territories on the front lines of the whole-of-nation COVID-19 response may continue to face challenges that hamper their effectiveness.
A Framework for Managing Fraud Risks in Federal Programs. GAO-15-593SP. Washington, D.C.: July 2015.
Hurricane Sandy: FEMA Has Improved Disaster Aid Verification but Could Act to Further Limit Improper Assistance.GAO-15-15. Washington, D.C.: December 12, 2014.
Contact information: Chris Currie, (404) 679-1875, curriec@gao.gov and Rebecca Shea, (202) 512-6364, shear@gao.gov
The Cybersecurity and Infrastructure Security Agency took steps to respond to the COVID-19 pandemic’s impacts on the Critical Manufacturing Sector but has not assessed lessons learned.
Entity involved: Cybersecurity and Infrastructure Security Agency, within the Department of Homeland Security
Recommendation for Executive Action
The Director of the Cybersecurity and Infrastructure Security Agency should assess and document lessons learned from the COVID-19 pandemic’s impacts in the Critical Manufacturing Sector. The Department of Homeland Security agreed with this recommendation and stated that the Cybersecurity and Infrastructure Security Agency is working with Critical Manufacturing Sector stakeholders to identify pandemic impacts in the sector as well as mitigation actions, and plans to issue a lessons-learned report by December 2022.
Background
The nation’s critical infrastructure provides the essential services that underpin American society. Critical infrastructure consists of systems and assets so vital that their incapacity or destruction would have a debilitating impact on the nation’s security, economic security, or public health or safety.[486] The Critical Manufacturing Sector, one of 16 federally defined critical infrastructure sectors, processes raw materials and produces specialized parts and equipment that are essential to the operations of other industries and critical infrastructure sectors, such as defense, energy, and transportation.[487] As with other sectors, the COVID-19 pandemic has impacted the Critical Manufacturing Sector, such as by causing worker shortages, delays in shipments of goods, and increased cybersecurity vulnerability in critical infrastructure systems and assets.
The Critical Manufacturing Sector is composed of four broad manufacturing industries, as shown in the figure below: (1) primary metals manufacturing, (2) machinery manufacturing, (3) electrical equipment, appliance, and component manufacturing, and (4) transportation equipment manufacturing. Critical Manufacturing Sector assets are primarily privately owned and operated, and include manufacturing facilities, processing and distribution facilities, and sales offices. There were about 62,000 private critical manufacturing establishments, such as manufacturing and product storage facilities and sales offices—in the U.S., as of June 30, 2021.[488]
Federally Defined Categories within the Critical Manufacturing Sector
The Cybersecurity and Infrastructure Security Agency Act of 2018 established the Cybersecurity and Infrastructure Security Agency (CISA) as an agency within the Department of Homeland Security (DHS).[489] CISA leads the national effort to understand, manage, and reduce risk to our cyber and physical infrastructure. CISA—through its Critical Manufacturing Section—also acts on behalf of DHS as the lead federal agency, or sector risk management agency, for the Critical Manufacturing Sector and is responsible for coordinating efforts to protect and improve the sector’s security and resilience.[490] In addition to critical infrastructure, CISA is responsible for leading cybersecurity programs—such as securing the federal network—and ensuring the nation’s emergency communications capabilities.
CISA offers manufacturing owners and operators resources to manage risks, improve security (both physical and cyber), and respond to incidents in the form of training, guidance documents, cybersecurity services, access to sensitive information, and routine presentations.
DHS’s 2013 National Infrastructure Protection Plan (National Plan) established “partnership structures” between private sector infrastructure owners and operators and various levels of governments for each critical infrastructure sector.[491] Sector Coordinating Councils (SCC)—one type of partnership structure—are self-organized and self-governed councils composed of critical infrastructure owners and operators, their trade associations, and other industry representatives. The Critical Manufacturing SCC serves as the principal collaboration point between the federal government and the private sector owners and operators that make up the Critical Manufacturing Sector.
Overview of Key Issues
CISA took steps to respond to the pandemic’s impacts in the Critical Manufacturing Sector. According to officials, CISA focused its pandemic response efforts on supporting entities involved in the development and deployment of the COVID-19 vaccine—such as hospitals and pharmaceutical companies—by scanning their IT systems for vulnerabilities and providing other cybersecurity services, for example. However, CISA also took a variety of steps to respond to the pandemic’s impacts in the Critical Manufacturing Sector.
CISA shared federal pandemic response information with Critical Manufacturing Sector members. CISA officials said they shared information with, and addressed questions from, Critical Manufacturing Sector members during the pandemic. For example, CISA officials estimated they convened approximately 100 conference calls with private critical infrastructure sector members from March 2020 to May 2021 to align and support cross-sector operations among members and government partners. Officials said the primary purpose of the calls was to share information about the pandemic and the federal response with private sector stakeholders. According to officials, CISA organized calls twice per week at the start of the pandemic, with almost 10,000 attendees initially. CISA officials said they invited Critical Manufacturing Sector members to join the conference calls, and representatives we spoke with from two manufacturing associations said they participated in the calls.
Additionally, according to officials, CISA’s Critical Manufacturing Section also received thousands of phone calls and emails from private companies and stakeholders seeking guidance in the early days of the pandemic. Officials said they provided individualized responses on a variety of topics, such as workplace safety guidance from the Centers for Disease Control and Prevention. One CISA official said they similarly fielded hundreds of queries about CISA’s Essential Critical Infrastructure Workforce Guidance (discussed in more detail below), including from members of the Critical Manufacturing Sector.[492]
CISA participated in efforts to collect information about the impact of the pandemic on the sector. CISA initiated and responded to a variety of requests for information about the impact of the pandemic on critical infrastructure, including the Critical Manufacturing Sector. For example, from February through May 2020, CISA requested that the sector risk management agencies collect and submit information about the pandemic’s impact on their respective critical infrastructure sectors on a weekly basis. According to officials, CISA incorporated the collected information into briefings for senior leadership. Additionally, in April 2020, CISA responded to a request from the White House asking whether mining or mineral commodity industries—critical manufacturing industries—were experiencing personal protective equipment shortages.
Additionally, in September 2020, the Critical Manufacturing SCC Executive Committee requested that CISA administer a survey of SCC members to facilitate information sharing about the pandemic’s impacts on sector operations and the steps companies took to mitigate the spread of COVID-19.[493] According to CISA officials, they administered the survey and compiled anonymized responses for the SCC Executive Committee, but did not analyze or assess the responses. At the request of the SCC Executive Committee, CISA administered the survey again in August 2021, with additional questions about the vaccine rollout, and gave the anonymized results to the SCC Executive Committee.
CISA identified trends in the pandemic affecting critical infrastructure, including the Critical Manufacturing Sector. According to officials, in November 2020, CISA stood up a COVID Task Force to support the federal government’s COVID-19 response across sectors. While the COVID Task Force primarily focused on the Healthcare and Public Health Sector, it included the Critical Manufacturing Sector in its analyses when relevant, according to officials. For example, CISA’s COVID Task Force produced weekly Infrastructure Outlook Briefs during the pandemic, which on occasion included information on trends in the Critical Manufacturing Sector and related supply chains.
According to CISA officials, the COVID Task Force’s Infrastructure Outlook Briefs were intended to identify trends in the pandemic and forecast risks to critical infrastructure, and were shared with CISA leadership and other federal agencies. The Infrastructure Outlook Briefs prioritized information about vaccine development and delivery, cybersecurity, and misinformation circulated about the pandemic. CISA officials said the briefs helped CISA identify and address priorities for critical infrastructure, including the Critical Manufacturing Sector, such as issuing additional cybersecurity guidance for remote work. According to officials, the briefs included information about the Critical Manufacturing Sector when it was related to their main priorities. For example, CISA officials reported in a May 2020 that manufacturing was among the industries being targeted by cyber attackers, who were focusing attacks on industries heavily impacted by COVID-19.
Additionally, the COVID Task Force performed two analyses identifying risks to critical infrastructure that related to the Critical Manufacturing Sector, according to officials. Officials described one analysis in which they cross-checked counties across the U.S. with a high likelihood of vaccine hesitancy to counties with a high number of critical infrastructure workers, such as manufacturing workers, to identify locations likely to experience a degradation of critical infrastructure operations. Officials described a second analysis that concluded that the Critical Manufacturing Sector was likely to suffer from a lack of cybersecurity expertise in the future, due to an increase in demand for cybersecurity workers across sectors and low salaries for cybersecurity workers in manufacturing industries.[494]
CISA issued essential workforce guidance that included Critical Manufacturing Sector workers. In response to the pandemic, CISA developed the Essential Critical Infrastructure Workforce Guidance to help jurisdictions and critical infrastructure owners and operators identify essential critical infrastructure workers.[495] According to CISA officials, the agency took the initiative to develop the guidance in response to the White House’s March 16, 2020, statement about the important role of critical infrastructure workers during the pandemic.[496] CISA issued the first version of the guidance on March 19, 2020, and issued its sixth, most recent version on August 5, 2021.[497] The guidance includes critical manufacturing workers—such as those involved in manufacturing steel and semiconductors—among the pool of essential workers, such as physicians, emergency medical technicians, and grocery store workers. See the figure below for the critical infrastructure sectors represented in the guidance.
Critical Infrastructure Sectors Represented in the Essential Critical Infrastructure Workforce Guidance
The guidance was intended to help states, local jurisdictions, and critical infrastructure owners and operators identify essential work functions to ensure that the workers who performed those functions could continue to access their workplaces during community restrictions, such as stay-at-home orders. While the guidance was voluntary, CISA determined that, as of April 28, 2020, 33 states and the District of Columbia had adopted it exclusively or as part of their own essential worker guidance.[498] Additionally, according to officials, CISA shared the guidance with 24 countries and six international organizations to help inform the development of their essential workers lists.
According to officials, the first version of the guidance was developed using a variety of inputs, including:
Pandemic-related critical infrastructure plans prepared by DHS and the National Infrastructure Advisory Council;[499]
Ongoing decision-making around how to prioritize personal protective equipment across the country;
Feedback from federal agencies, such as sector risk management agencies; and
Vetting by private-sector partnership structures, such as the critical infrastructure SCCs.
Each version of the guidance included a solicitation for feedback from stakeholders—including the private sector, government agencies, and the public—and after the initial one, revisions to the subsequent five versions were primarily based on that feedback. According to officials, CISA expanded and added detail to the critical manufacturing category in subsequent versions as it received feedback and requests for clarification; in Version 3.0, for instance, CISA added manufacturing workers related to the aerospace industry because of industry feedback. Officials from automobile and electrical manufacturing associations we spoke with said they provided feedback on the guidance, including the need for more specificity on the types of industries included in the guidance. CISA subsequently revised the guidance to clarify what was included in certain industries, such as by adding vehicle sales to the list of included industries in Version 3.0.
According to CISA officials, the agency issued updated versions when it received a critical mass of feedback—a significant number of people or entities contacting them with similar comments—from the private sector or government agencies, and then when a new CISA Director was confirmed in July 2021. Additionally, CISA officials said updates reflected the evolving nature of the pandemic; teachers, for example, were not included in early versions of the list because schools had previously been closed.[500]
After issuing the guidance, CISA matched the essential worker categories to industry-based classification codes.[501] According to officials, this helped critical infrastructure owners and operators identify which of their workers fell into essential worker categories. CISA officials said they shared the coding analysis with the Federal Emergency Management Agency, the Department of Health and Human Services, and the Centers for Disease Control and Prevention for the purpose of assisting their efforts to prioritize personal protective equipment and vaccine distribution to essential workers.
CISA supported the Critical Manufacturing Sector’s application of the Essential Critical Infrastructure Workforce Guidance. CISA took steps to help sector members apply essential workforce guidance and continue operations during the pandemic. For example, CISA’s International Affairs Branch helped foreign essential workers, including those in the Critical Manufacturing Sector, enter the U.S. to continue critical infrastructure operations during the pandemic. Presidential Proclamation 10052, issued on June 22, 2020, had temporarily suspended the entry of certain nonimmigrants into the country.[502] CISA worked with U.S. Customs and Border Protection to facilitate National Interest Exceptions to the Proclamation.
Among those potentially eligible for National Interest Exceptions were certain applicants whose proposed job duties or position indicated the individual would provide significant and unique contributions to an employer meeting a critical infrastructure need. Officials said they provided companies with language related to essential workers and critical infrastructure to help justify the waiver requests, and worked with U.S. Customs and Border Protection to clarify the workers’ travel plans, for example. According to CISA’s records, in 2021, four companies related to critical manufacturing requested National Interest Exceptions for seven individual workers; six of the seven requests were granted.[503]
CISA’s International Affairs Branch also applied the guidance to help the federal government coordinate with Mexico to determine which critical manufacturing companies were essential during the pandemic. In March 2020, Mexico issued an emergency health decree that suspended all “non-essential” activities. The list of essential workers in Mexico’s decree, however, was narrower than CISA’s guidance, according to officials. As a result, Mexico’s decree significantly impacted U.S. manufacturing operations and disrupted key U.S. supply chains. For example, Mexican manufacturing plants that supplied ventilator components or air conditioning units for U.S. hospitals were ordered closed.
CISA officials said they worked with the U.S. Chamber of Commerce to facilitate conversations with the Mexican government and develop a survey of U.S. companies impacted by Mexico’s policy. CISA officials also said they used the survey results and the guidance to identify critical companies that reported having to stop operations because of Mexico’s shutdown, which included critical manufacturing-related companies. CISA officials said that, in May 2020, they provided a tiered list of critical U.S. companies to National Security Council staff, for the purpose of coordinating with the Mexican government to ensure those companies could continue operations.
While the guidance provided direction to states and local jurisdictions on which workers across critical infrastructure sectors should have access to their worksites during community restrictions, CISA also issued an access request letter on July 13, 2020, specific to the Critical Manufacturing Sector. The letter asks that, in the interest of homeland security, jurisdictions extend “any courtesy”—such as flexibility with local pandemic orders—to critical manufacturing essential workers during the pandemic. For example, according to officials, the letter was provided to the Critical Manufacturing Sector to facilitate essential workers’ travel across county and state borders to access their worksites.
CISA could benefit from assessing lessons learned from the pandemic specific to the Critical Manufacturing Sector. CISA has not performed a lessons-learned analysis from the pandemic’s impacts in the Critical Manufacturing Sector, although sector members identified this analysis as a high-priority need. CISA has collected some information on the pandemic’s impacts that could be leveraged in a lessons-learned analysis. As described earlier, CISA was involved in several efforts during the pandemic to collect information directly from sector members. For example, CISA collected information about supply chain issues and levels of absenteeism among the workforce.
Further, CISA was involved in a similar lessons-learned analysis for other critical infrastructure sectors. Specifically, CISA worked with the SCCs from the Information Technology Sector and Communications Sector to conduct a lessons-learned analysis on the impacts of the pandemic on those supply chains.[504] That assessment identified key issues from the pandemic’s impacts on information and communications technology supply chains and included recommendations to help companies increase the resilience of their supply chains.
In July 2021, CISA issued a report summarizing the findings from a strategic planning conference it organized with SCC members (private sector stakeholders representing manufacturing industries).[505] The report identified general security needs, including the need for sector-specific resources that incorporate lessons learned from the impacts of the COVID-19 pandemic on manufacturing facilities.
According to officials, CISA’s Critical Manufacturing Section has a team of four staff who are not equipped to perform in-depth analyses, such as a lessons-learned analysis. However, CISA has previously used partnerships with contractors and the National Laboratories to conduct analyses, such as with the strategic planning conference, and has analyst resources within its own National Risk Management Center to conduct such analyses.
DHS’s National Infrastructure Protection Plan identifies leveraging lessons learned and applying corrective actions from incidents as one step towards reducing vulnerabilities in critical infrastructure.[506] Additionally, it says DHS is responsible for documenting lessons learned from actual incidents and applying them to its security and resilience activities. The National Plan also directs agencies to take actions that enable timely and efficient response after an incident to reduce its consequences.[507] Further, CISA’s Critical Manufacturing Section identified after-action reporting as a method to identify key areas for improvements.[508]
In commenting on a draft of this enclosure, CISA officials said that, at the request of the Critical Manufacturing Sector SCC Executive Committee, they plan to pursue a lessons-learned review of the pandemic’s impacts in the Critical Manufacturing Sector beginning in March 2022. However, as of February 2022, CISA had not finalized a plan for developing this review. A documented lessons-learned assessment that examines the impacts of the pandemic in the Critical Manufacturing Sector, including strengths and weaknesses in the sector’s response, would allow CISA to identify how it could better support the sector to reduce the consequences of the pandemic and future incidents. It could also help identify strategies to strengthen the sector’s resilience.
Methodology
To conduct this work, we reviewed relevant federal statutes and regulations, DHS risk management guidance, DHS’s National Infrastructure Protection Plan, the Critical Manufacturing Sector-Specific Plan, and the Strategic Planning Initiative.[509] We also examined publicly available CISA information and guidance, such as the Critical Manufacturing Sector security guide; agency analyses, such as CISA analyses of pandemic impacts on critical infrastructure sectors; survey results from conferences or other activities, such as the SCC’s annual survey results; and internal CISA briefings on the pandemic.[510] In addition, we interviewed CISA officials regarding steps the agency has taken to address the pandemic’s impacts on the critical manufacturing sector and to assess lessons learned.
To obtain industry perspective on the pandemic’s impacts in the Critical Manufacturing Sector and CISA’s efforts to respond, we reached out to one association representing each of the four federally defined industry categories, two of which are members of the SCC and two of which are not, as of April 2021. Of these, two responded to our requests for an interview: the National Electrical Manufacturers Association and the Alliance for Automotive Innovation. According to these associations, each represents a large number of manufacturers in their respective industries.
Agency Comments
We provided DHS and OMB with a draft of this enclosure. DHS provided written comments, which are reproduced in appendix VIII. OMB did not provide comments.
In its comments, DHS agreed with our recommendation and stated that in March 2022 CISA officials conducted a lessons-learned workshop with members of the Critical Manufacturing SCC to identify pandemic impacts on the sector and responses partners have taken—or plan to take—to mitigate these impacts. DHS stated that CISA plans to compile input from the workshop, and subsequent stakeholder feedback, into an after-action report that includes recommendations for sector partners to consider when they address pandemic-related impacts on both daily and incident response operations. According to DHS, CISA plans to complete the report by December 30, 2022, and share it with Critical Manufacturing Sector partners through the SCC and other mechanisms. These actions, if fully implemented to include lessons learned, should address the intent of our recommendation.
GAO’s Ongoing Work
We have additional work underway related to the Critical Manufacturing Sector. We are currently examining the causes and extent of the current global semiconductor shortage along with the federal government’s and U.S. manufacturers’ response to the shortage. More broadly, we are also reviewing the effectiveness of the federal sector risk management agencies in carrying out certain specific responsibilities—such as assessing risk and supporting incident management—for the critical infrastructure sectors.[511]
Contact Information: Tina Won Sherman, (202) 512-8461 or shermant@gao.gov
Delays in agency reporting of improper payment information related to COVID-19 spending, as well as changes to processes for reporting improper payments, have impacted the transparency, timeliness, reliability, and completeness of available improper payments information. These delays also contributed to the federal government’s inability to identify the full extent to which improper payments occur and take appropriate actions to reduce them.
Entities involved: Government-wide
Matters for Congressional Consideration
Congress should consider providing the Department of Health and Human Services the authority to require states to report the data necessary for the Secretary to estimate and report on improper payments for the Temporary Assistance for Needy Families program in accordance with 31 U.S.C. § 3352.
Recommendations for Executive Action
The Director of the Office of Management and Budget should require agencies to certify the reliability of data submitted to PaymentAccuracy.gov. The Office of Management and Budget neither agreed nor disagreed with this recommendation.
Background
Agency-reported improper payment estimates for fiscal year 2021 totaled about $281 billion—an increase from the fiscal year 2020 total of $206 billion. An improper payment is defined as any payment that should not have been made or that was made in an incorrect amount (including overpayments and underpayments) under statutory, contractual, administrative, or other legally applicable requirements.[512] To help ensure that federal funds are appropriately monitored, executive branch agencies are required to take various steps regarding improper payments under the Payment Integrity Information Act of 2019 (PIIA) and as directed by Office of Management and Budget (OMB) guidance.[513]
PIIA requires agencies to conduct risk assessments of their programs at least once every 3 fiscal years, aimed at identifying those with annual outlays exceeding $10 million that may be susceptible to significant improper payments.[514] Agencies are then required to develop and report improper payment estimates, root causes, and corrective action plans for those programs identified as susceptible. Under OMB’s guidance, agencies are directed to complete an initial risk assessment for new programs after the first 12 months of a program’s operation.[515] For programs newly identified as susceptible to significant improper payments, OMB guidance instructs agencies to begin reporting estimates and other information in the fiscal year following the risk assessment. OMB directs agencies to submit their improper payment data to be compiled and published on PaymentAccuracy.gov, a public website containing current and historical improper payment information in dashboards and downloadable datasets.
COVID-19 relief laws provided about $4.6 trillion to fund response and recovery efforts. The extent and significance of improper payments associated with COVID-19 relief funds has not yet been determined. However, the impact of these improper payments, including those that are the result of fraud, could be substantial.[516] Even if improper payments are limited to one percent of the COVID-19 relief funds provided to date, this would equate to $46 billion.
Federal law enforcement agencies are actively investigating potential fraud. From March 2020 through January 2022, 435 individuals pleaded guilty to federal charges of defrauding COVID-19 relief programs. As of January 31, 2022, 11 individuals had been convicted at trial for COVID-19 relief fraud. Federal charges were pending against 548 individuals for attempting to defraud COVID-19 relief programs as of January 31, 2022. See the enclosure on Federal Fraud-Related Cases in appendix I for more information.
Overview of Key Issues
Agencies did not report improper payment estimates for key COVID-19 spending for fiscal year 2021. COVID-19 relief laws did not require agencies to deem all programs receiving COVID-19 relief funds that expended a significant amount in any one fiscal year as "susceptible to significant improper payments," as we suggested in our November 2020 report on the CARES Act. OMB staff informed us at that time that OMB would not direct agencies to designate new programs as susceptible to significant improper payments in order to expedite reporting an improper payment estimate for new COVID-19 programs. OMB staff stated that this decision was due in part to their assessment that it is unclear whether (1) the current controls and guidance in place to identify and report improper payments are insufficient and (2) the benefit of increased reporting would outweigh the added burden to do so. In our November 2020 report, we also reported that because of OMB’s guidance on the timing of risk assessments and improper payment reporting for new programs, improper payment estimates associated with new COVID-19 programs may not be reported until November 2022.
Six major spending areas received more than $100 billion in COVID-19 relief funding, but none of these areas reported an improper payment estimate for the risk-susceptible programs for fiscal year 2021 (see table). Three of the major spending areas included at least one program that was identified as susceptible to significant improper payments: the Small Business Administration’s Business Loan Programs, the Department of Labor’s Unemployment Insurance Programs, and the Department of Health and Human Services’ Public Health and Social Services Emergency Fund.
Fiscal Year 2021 Improper Payment Estimates Reporting for Major Spending Areas Receiving Over $100 Billion in COVID-19 Funding, as of February 28, 2022
Major Spending Area (Agency)
Programs Determined to be Susceptible to Significant Improper Paymentsa
Fiscal Year 2021 Estimated Improper Payments Reporting
Total COVID-19 Expenditures (billions)
Economic Impact Payments (Department of the Treasury)
The Department of the Treasury (Treasury) determined these payments are not susceptible to significant improper payments.
Not reported
$850.3
Business Loan Programs (Small Business Administration)
The Small Business Administration (SBA) reported that the Economic Injury Disaster Loan program was susceptible to significant improper payments.
SBA did not report on the susceptibility of the Paycheck Protection Program (PPP) to significant improper payments. However, SBA officials stated that PPP would report improper payment estimates in fiscal year 2022.
Not reported
$827.8
Unemployment Insurance (Department of Labor)
The Department of Labor (Labor) determined that the Pandemic Emergency Unemployment Compensation and Pandemic Unemployment Assistance programs were susceptible to significant improper payments.
Labor did not report on the susceptibility of the Federal Pandemic Unemployment Compensation and Mixed Earner Unemployment Compensation programs.
Partially reportedb
$673.2
Coronavirus State and Local Fiscal Recovery Funds (Treasury)
Treasury did not report on the susceptibility of Coronavirus State and Local Fiscal Recovery Funds to significant improper payments.
Not reported
$245.4
Public Health and Social Services Emergency Fund (Department of Health and Human Services)
The Department of Health and Human Services determined that two Provider Relief Fund programs were susceptible to significant improper payments.
Not reported
$226.1
Coronavirus Relief Fund (Treasury)
Treasury determined that the Coronavirus Relief Fund was not susceptible to significant improper payments.
Not reported
$149.9
Source: PaymentAccuracy.gov, Treasury, and Department of Labor Office of the Inspector General. | GAO-22-105397
aA program is considered to be susceptible to significant improper payments if, in the preceding fiscal year, the sum of the program’s improper payments and payments whose propriety cannot be determined due to lacking or insufficient documentation may have exceeded either (1) 1.5 percent of program outlays and $10 million or (2) $100 million (regardless of the improper payment rate). 31 U.S.C. § 3352(a).
bLabor did not separately report an estimate for the Unemployment Insurance pandemic programs, but instead the reported improper payment estimate for the Unemployment Insurance program of $78 billion included the Federal Pandemic Unemployment Compensation and Pandemic Emergency Unemployment Compensation programs. The UI estimate does not include the Federal Pandemic Unemployment Assistance and Mixed Earner Unemployment Compensation program.
While there may be additional burdens by the agencies that would be susceptible to significant improper payments, we do not believe that the cost of these activities outweigh the benefits of expediting the estimation and reporting of improper payments. Specifically, reporting improper payment estimates quickly for risk-susceptible programs helps hold agencies accountable and provides additional transparency for Congress and others in their oversight of government-wide improper payments. In addition, estimating improper payments and identifying root causes, including those that may contribute to potential fraud, would help ensure that agencies timely develop and implement corrective actions to help reduce them.
As we reported in November 2020, according to OMB staff, OMB guidance directs agencies to identify and recover overpayments for all programs regardless of whether a program formally reports an improper payment estimate or performs an improper payment risk assessment. Although we acknowledged at that time that agencies may take actions to identify and recover overpayments, we stated that quickly identifying programs that are susceptible to significant improper payments is critical. This identification process is an important step in establishing controls to prevent future improper payments.
Given that trillions of COVID-19 expenditures were not required to be considered in agencies’ fiscal year 2021 improper payment estimate methodologies, it’s not possible to completely estimate the government-wide total of improper payments for fiscal year 2021. In our November 2020 report, we suggested that Congress consider, in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments.” In March 2022, we expanded on our suggestion to include all new programs and activities by amending the PIIA. Specifically, we suggested that Congress amend the PIIA to designate all new executive agency programs and activities—such as those that were created specifically to respond to the COVID-19 pandemic—making more than $100 million in payments in any one fiscal year as “susceptible to significant improper payments” for their initial years of operation to help prevent such delays in estimating and reporting of improper payments from occurring in the future.
The Department of Health and Human Services does not report improper payment estimates for the Temporary Assistance for Needy Families program. According to the Department of Health and Human Services’ (HHS) 2021 agency financial report, the Temporary Assistance for Needy Families (TANF) program—which spent about $17 billion in fiscal year 2021—is a risk-susceptible program that has not estimated or reported improper payments.[517] The American Rescue Plan Act of 2021 provided $1 billion for TANF Pandemic Emergency Assistance for fiscal year 2021.
According to HHS’s fiscal year 2021 financial report, HHS does not have the authority to require states to participate in a TANF improper payment measurement.[518] Specifically, HHS indicated that it is unable to compel states to collect the necessary information required to conduct an improper payment measurement for TANF due to Section 411 of the Social Security Act, which specifies the data elements that HHS may require states to report, and Section 417 of the same Social Security Act, which dictates that the federal government may only regulate the conduct of states where Congress has given the express authority to do so. Accordingly, HHS states that it does not have the authority to collect data pertaining to case and payment accuracy for TANF since the information is not included under the Social Security Act. HHS has previously requested such authority in its budget proposals.
In its audit reports, HHS’s Office of Inspector General (OIG) has noted that HHS has not been able to produce an improper payment estimate for the TANF program and has made recommendations to pursue legislative authority.[519] Providing HHS with the legal authority to collect that data would help ensure accountability over TANF payments.
Federal internal control standards state that management should use quality information to achieve the entity’s objectives. Without statutory authorization for HHS to require states to participate in the measurement of improper payments, Congress and other external stakeholders will continue to lack key payment integrity information for monitoring improper payments in the TANF program. In addition, HHS will not be able to collect the required information to implement and report on the effectiveness of corrective actions on improper payments for the program.
Agencies reported various ways the pandemic negatively impacted improper payment estimation and reporting. In their fiscal year 2021 financial reports, agencies identified multiple pandemic-related factors that affected the quality and completeness of their improper payment estimation and reporting. For example:
HHS reported that it suspended reviews in the Foster Care program to protect the health and safety of state and federal reviewers and to ensure that state child welfare officials remain focused on mission-critical activities serving children and families. These reviews, which occur onsite, are conducted triennially on a rolling basis to generate a non-statistical estimate of improper payments. As a result, HHS did not estimate or report on improper payments in the Foster Care program for fiscal year 2021.
The Department of the Treasury reported that it delayed its plans for reporting improper payments for the Premium Tax Credit program. Treasury based its decision on a June 17, 2020, memorandum from OMB, which allowed agencies to give priority to audits that are associated with programs at higher risk due to COVID-19 and to delay work on programs that are lower risk.[520]
In their reviews of agencies’ fiscal year 2020 PIIA compliance, multiple OIGs noted some additional impacts on estimating improper payments due to the pandemic. For example, the department’s OIG reported that Labor permitted state workforce agencies to suspend improper payment sampling efforts for the final quarter of the Unemployment Insurance program year to reduce the burden on program resources responsible for processing Unemployment Insurance benefit claims and implementing new COVID-19 pandemic related programs.[521] This allowed 74 percent of program year expenditures to go untested for fiscal year 2020 reporting. As a result, those payments were not considered in Labor’s improper payments rate estimates for fiscal year 2020 reporting.[522] Labor applied the nine-month improper payment rate against the outlays for the 12-month period, which might have lead to an unreliable estimate of improper payment amounts for fiscal year 2020 reporting.
In addition, its OIG reported that the Department of Housing and Urban Development did not test the complete payment cycle, to include payments issued by state, local, or other agencies due to the impacts of COVID-19. This was the case for three of the department’s four programs that are susceptible to significant improper payments.[523] As a result, the department’s sampling and estimation methodology was not comprehensive and led to an incomplete estimate of improper payments.[524]
OMB guidance has reduced the visibility and quality of agency improper payment information. The COVID-19 relief laws have provided about $4.6 trillion to fund COVID-19 response and recovery efforts, therefore reporting of improper payment information for such programs is critical to accountability and transparency over whether appropriated funds were spent for their intended purposes. This is especially important because much of the funds had to be disbursed quickly, thereby increasing the risk of improper payments and fraud.
PIIA requires OMB to report annually, among other things, a government-wide improper payment estimate, recovery actions, improper payment reduction targets, and a discussion of progress made towards meeting those targets.[525] OMB reports the aggregated amount of improper payment estimates from all reporting programs and activities for the federal government in the dataset provided at PaymentAccuracy.gov.
OMB guidance shifts improper payment reporting from agency financial reports to PaymentAccuracy.gov. OMB’s Circular A-136 Financial Reporting Requirements provides guidance for agencies on preparing agency financial reports, including the reporting of improper payment information. Beginning with its 2020 update to the Circular, OMB did not direct agencies to include improper payment information in agency financial reports or performance and accountability reports as had been done in prior years. OMB instructed agencies to report only actions taken to address recovery auditor recommendations within their financial reports and direct readers to PaymentAccuracy.gov for all other improper payment information.
As shown in the table below, about two-thirds of the government-wide improper payment estimates were reported in agency financial reports for fiscal year 2021.
Fiscal Year 2021 Estimated Improper Payments Reported in Federal Agency Financial Reports
Amount of Estimated Improper Payments Reported in Agency Financial Reports
$189.2 billion
Amount of Government-wide Estimated Improper Payments Reported on PaymentAccuracy.gov
$281.2 billion
Percentage of Estimated Improper Payments Reported in Agency Financial Reports
67%
Source: Office of Management and Budget (data) and GAO (analysis). | GAO-22-105397
According to OMB officials, centralized reporting of agencies’ improper payment information on PaymentAccuracy.gov facilitates efficient analysis of government-wide improper payment information because data is presented in a more consistent manner. In addition, OMB staff stated that posting estimated improper payment information only on the website reduced the burden on agencies. OMB staff stated that they designed the fiscal year 2021 reporting format in a manner that they believe would ensure each program would fulfill the individual reporting requirements required under PIIA and also provide some additional context needed for the user to understand the payment integrity story associated with the requirements under PIIA.
While we agree that centralized reporting could facilitate analysis, financial reports are the principal means to convey to the President, Congress, and the American people each agency’s commitment to sound financial management and stewardship of public funds, including COVID-19 relief funds. By removing the requirements for agencies to report estimated improper payments, users of these reports may not be provided additional context in relation to agencies’ financial information, including whether appropriated funds are spent for their intended purposes. Further, reporting on websites where information can be easily edited raises concerns over the permanence of the reported information relative to published financial reports. In fact, OMB officials stated that they make changes to improper payment data on PaymentAccuracy.gov without notification to users. In addition, OMB’s shift to reporting on the website resulted in less timely information, as agency financial reports have generally been published in November, while PaymentAccuracy.gov did not publish fiscal year 2021 data until the end of December.
In March 2022, to improve the transparency of improper payment information, we suggested that Congress enact legislation to require that improper payment information be reported in the agencies’ annual financial reports.
OMB does not require agency certification of reliability for PaymentAccuracy.gov submissions. In order to prepare the annual datasets for publication on PaymentAccuracy.gov, OMB sends a request to agencies for submissions of agency- and program-level data, known as “data calls.” OMB then compiles the information in the data calls to create the final dataset and to populate the interactive program dashboards on PaymentAccuracy.gov. However, OMB does not require these agency data calls to have any formal review or certification by agency management prior to submission.[526] For example, officials from two agencies told us that when submitting their data calls for PaymentAccuracy.gov, there was no place in the submission tool to certify that the data was reviewed.
OMB staff stated that they did not see a need for data certification because no significant data quality issues have been found. However, when we reviewed PaymentAccuracy.gov we found one agency’s overpayments that had been identified and recaptured were overstated by nearly $1.4 billion compared to the information published in the agency’s financial report.[527] OMB requires agencies to review financial data in their agency financial reports. Specifically, OMB guidance requires that agency financial reports include an assessment by the agency head of the completeness and reliability of the performance and financial data used in the report.[528] A similar requirement for agency heads to both assess and attest to information reported to PaymentAccuracy.gov would help ensure complete and reliable data for users of the website.
Federal internal control standards state that management should use quality information to achieve the entity’s objectives. OMB’s guidance does not direct agencies to provide sufficient review and certification of their data submissions’ reliability to PaymentAccuracy.gov. Further, not requiring agency data calls to be subject to the same level of oversight as agency financial reports may increase risk of errors and omissions in data published to PaymentAccuracy.gov. Without sufficient direction from OMB for agencies’ management to review and certify the reliability of their data before submitting to OMB, improper payments information reported on PaymentAccuracy.gov may be incomplete and unreliable, reducing users’ ability to identify the full extent to which improper payments occur.
Methodology
To conduct this work, we reviewed relevant improper payment legislation and guidance, agency financial reports, OIG compliance reports, improper payment data requested directly from agencies, and data submitted for OMB’s PaymentAccuracy.gov website to obtain information on changes to improper payment reporting requirements and the pandemic’s impact on fiscal year 2021 improper payment estimates. We identified new program or major funding streams for existing programs and the agencies responsible and interviewed OMB staff to obtain information on changes to improper payment reporting requirements.
Agency Comments
We provided HHS, OMB, and Treasury with a draft of this enclosure. OMB and Treasury did not provide comments on this enclosure. HHS provided technical comments which we incorporated, as appropriate.
GAO’s Prior Recommendations
The table below presents our matter for congressional consideration and recommendation on payment integrity from the November 2020 CARES Act report.
Prior GAO Matters for Congressional Consideration and Recommendations Related to Payment Integrity
Matter for Congressional Consideration or Recommendation
Status
To hold agencies accountable and increase transparency, Congress should consider, in any future legislation appropriating COVID-19 relief funds, designating all executive agency programs and activities making more than $100 million in payments from COVID-19 relief funds as “susceptible to significant improper payments” for purposes of 31 U.S.C. § 3352. (November 2020)
Open – not addressed
The Director of the Office of Management and Budget should develop and issue guidance directing agencies to include COVID-19 relief funding with associated key risks, such as provisions contained in the CARES Act and other relief legislation that potentially increase the risk of improper payments or changes to existing program eligibility rules, as part of their improper payment estimation methodologies. This should especially be required for already existing federal programs that received COVID-19 relief funding. (November 2020)
Closed – addressed. The Office of Management and Budget (OMB) neither agreed nor disagreed with our recommendation. In March 2021, OMB issued new guidance on improper payments to implement the requirements from the Payment Integrity Information Act of 2019. In addition, in January 2022, OMB added further clarification in its platform's question and answer section for agencies and their Offices of lnspector General regarding their consideration of payment integrity risks. Specifically, it states that agencies are encouraged to ensure that significant payment integrity risks are part of the sampling methodology so that the estimates can be used to assist in the process of identifying the root causes of improper payments and developing corrective action plans to address them. We believe that OMB has taken sufficient corrective actions which addressed the recommendation.
Standards for Internal Control in the Federal Government. GAO-14-704G. Washington, D.C.: September 10, 2014.
Emergency Relief Funds: Significant Improvement Are Needed to Ensure Transparency and Accountability for COVID-19 and Beyond. GAO-22-105715. Washington, D.C.: March 17, 2022.
Contact information: Beryl H. Davis, (202) 512-2623, davisbh@gao.gov
The Office of Management and Budget annually issues the single audit Compliance Supplement, which provides guidance to auditors performing audits of certain entities that receive funding from federal assistance programs. The federal agencies we selected for our review have not developed comprehensive policies and procedures for providing information to the Office of Management and Budget to better enable it to update program information included in the Compliance Supplement.
Entities involved: The Department of Education; the Department of Health and Human Services; the Department of the Treasury, and the Office of Management and Budget.
Recommendations for Executive Action
The Secretary of Education should document policies and procedures for providing information to the Office of Management and Budget to better enable it to annually update the Compliance Supplement that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training, and (2) agency officials proactively involving internal stakeholders (e.g., the inspector general, general counsel, and chief financial officer) and external stakeholders (e.g., the audit community) when developing audit procedures, prior to submitting drafts to the Office of Management and Budget, in order to ensure the guidance meets users’ needs.
The Secretary of Health and Human Services should document policies and procedures for providing information to the Office of Management and Budget to better enable it to annually update the Compliance Supplement, that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training, and (2) agency officials proactively involving internal stakeholders (e.g., the inspector general, general counsel, and chief financial officer) and external stakeholders (e.g., the audit community) when developing audit procedures, prior to submitting drafts to the Office of Management and Budget, in order to ensure the guidance meets users’ needs.
The Secretary of the Treasury should document policies and procedures for providing information to the Office of Management and Budget to better enable it to annually update the Compliance Supplement, that include steps for (1) establishing management’s expectations of staff competence for key roles (e.g., relevant knowledge, skills and abilities) and providing ongoing training, and (2) agency officials proactively involving internal stakeholders (e.g., the inspector general, general counsel, and chief financial officer) and external stakeholders (e.g., the audit community) when developing audit procedures, prior to submitting drafts to the Office of Management and Budget, in order to ensure the guidance meets users’ needs.
The Departments of Education, Health and Human Services, and Treasury each agreed with the recommendation.
Background
Through provisions enacted in the COVID-19 relief laws, the federal government has provided billions of dollars in federal funding to state and local governments, U.S. territory and tribal governments, and nonprofit organizations. Many of these recipients will be required to complete a single audit, some for the first time. Under the Single Audit Act and implementing guidance from the Office of Management and Budget (OMB), states, the District of Columbia, localities, Indian tribes, U.S. territories, and nonprofit organizations that receive federal awards must undergo single audits (or, in limited circumstances, program-specific audits) of these awards annually (unless a specific exception applies) when federal award expenditures meet or exceed $750,000.[529]
Auditors who conduct single audits generally follow implementing guidance in OMB’s annual Compliance Supplement and agency guidance specific to their programs to determine whether the recipient has complied with federal statutes, regulations, and award terms that may have a direct and material effect on each of the recipient’s major programs. For programs included in the Supplement—which includes information about a program’s objectives, procedures, and compliance requirements— an auditor can rely on the program’s compliance requirements contained in the Supplement. Without the Supplement, which OMB says provides a more efficient and cost-effective research approach, auditors would need to research many statutes and regulations for each program under audit to identify compliance requirements that could have a direct and material effect on that program. For those programs whose compliance requirements are not contained in the 2021 Compliance Supplement, auditors are directed to its Part 7 guidance.[530]
OMB requires federal awarding agencies to provide updates to agency program information before publishing the Supplement each year. Annual updates to the Supplement are necessary for many reasons, including adding additional requirements as a result of changes in statutory or regulatory requirements, such as those in the COVID-19 relief laws. In March 2021, we reported that auditors who conduct single audits of entities with June 30 year-ends have expressed a need to obtain the Supplement by no later than April of each year in order to effectively plan their audits and conduct interim testing. OMB issued the 2021 Compliance Supplement and two related addendums between August 2021 and January 2022. OMB plans to issue the 2022 Compliance Supplement at the end of April 2022.
Overview of Key Issues
Three selected agencies, which together received over $2 trillion in COVID-19 relief funding, generally did not document policies and procedures for their Compliance Supplement activities. Each year, OMB requires agencies to provide OMB with proposed updates for their respective program sections for inclusion in the Supplement. OMB provides agencies with a Compliance Supplement Preparation Guide (Guide) to assist in preparing, providing updates for, and reviewing program sections for inclusion in the Supplement.
While the selected agencies—the Department of Education, the Department of Health and Human Services (HHS), and the Department of the Treasury—stated that their proposed Supplement updates are vetted by experienced staff, we found that the agencies’ documented policies and procedures were not comprehensive and lacked specific details on staff involvement for reviewing updates prior to submission to OMB for inclusion in the Supplement. For example, Treasury did not document procedures on how its Single Audit Management Liaison monitors or oversees the updates provided by the various program offices. According to Treasury officials, the Single Audit Management Liaison coordinates internally with individual program offices and directs these offices to follow OMB’s Guide to complete their respective proposed Supplement section updates.
While Education and HHS had documented policies on review processes in place for their lead offices or point of contact for the single audit process, neither agency had documented policies and procedures at the program-office level, which has primary responsibility for updating the sections submitted to OMB for inclusion in the Supplement.
HHS stated that standard operating procedures should be developed by OMB and then implemented by agencies instead of agencies attempting to design their own standard operating procedures. While OMB provides guidance to assist agencies in updating program sections for inclusion in the Supplement, it is the agencies’ responsibility to develop internal policies and procedures on their staff involvement and reviews prior to submission to OMB. The policies and procedures are needed at both the lead office and program-office level to ensure consistency across the agency.
Federal standards for internal control state that management should implement control activities through policies. Management documents the internal control responsibilities in policies at an appropriate level of detail to allow management to effectively implement and monitor the control activity and communicates to personnel the policies and procedures so that personnel can implement the control activities for their assigned responsibilities.
Staff competence and training. Officials from Education and Treasury stated they assign competent staff to submit updates for inclusion in the Supplement, and the procedures from Education noted that its general counsel and a senior program official should be involved in the Supplement updates. HHS stated that its senior leadership reviews drafts before submitting to OMB. However, none of the three agencies’ documented policies and procedures specified the level of competence expected for key roles, such as the minimum number of years’ experience.
These agencies also have not documented policies and procedures for training staff on the process for updating information for the Supplement. Education officials stated they rely on more senior staff to train newer staff through practical experience. Treasury officials stated that new staff are provided with OMB’s Guide and work with experienced staff who provide on-the-job training. HHS developed a foundational set of on-demand single audit training courses and is developing a new course in 2022. However, none of the agencies had documented policies that: (1) requires staff involved in updating information for the Supplement to either be provided on-the-job training—such as by more senior staff—or complete agency developed courses or external courses, or both and (2) establishes the frequency with which staff should either be trained or complete courses, or both.
HHS indicated that additional guidance materials and training from OMB could further enhance its own training courses. Specifically, HHS suggested that OMB provide guidance and training courses on topics such as understanding the basics of the Supplement and developing objectives for single audits. In March 2022, we met with OMB and representatives from the audit community (the National Association of State Auditors, Comptrollers, and Treasurers (NASACT) and the American Institute of Certified Public Accountants (AICPA)). During the meeting, an official from the AICPA stated that a comprehensive training session would be beneficial, especially for agency program staff that are responsible for working on the Supplement for the first time. According to an OMB official, training has been available through an OMB contractor at the request of agencies.
While additional OMB guidance or trainings about the overall process for updating the annual Supplement would be beneficial, training their staff is the agencies’ responsibility. Specifically, agencies can help assure that their staff are properly trained and knowledgeable of the programs that need to be updated in the Supplement. Training can include information that would be helpful for staff when tasked with creating submissions for new Supplement sections for programs created as a result of recent legislation.
Federal standards for internal control state that management establishes expectations of competence for key roles to help the entity achieve its objectives and evaluate the competence of personnel across the entity in relation to established policies. Competence includes having the relevant knowledge, skills, and abilities that staff gain largely from professional experience, training, and certifications. Federal standards for internal control also state that personnel need to possess and maintain a level of competence that allows them to accomplish their assigned responsibilities as well as understand the importance of effective internal control. Detailed policies and procedures about performing internal reviews and designating personnel can help ensure that staff with the requisite expertise and knowledge are involved in the process for updating information for the Supplement.
Internal and external audit stakeholders’ involvement. We found that HHS and Treasury did not document policies and procedures detailing the level of involvement and timing of the internal stakeholders’ review process—including the Offices of Inspectors General (OIG)—before submitting drafts to OMB for inclusion in the Supplement. Although Education’s standard operating procedures state that an OIG team member reviews updates and revisions, the procedures do not specify the level of OIG involvement at the program-office level. An Education OIG official stated the department did not have a consistent approach, and each program office determined the timing and extent of OIG involvement during the internal stakeholders’ review process.
HHS officials stated that in addition to a review by the HHS point of contact for the single audit process, its OIG also reviews drafts of all its Supplement sections to ensure compliance with auditing standards, statutes, regulations, and award terms and conditions, and to ensure audit objectives and suggested audit procedures are within the scope of the provisions of the Single Audit Act. However, HHS did not document that the OIG review is required in its policies and procedures.
HHS OIG officials also stated that OIG does not have written policies or procedures outlining its own responsibilities for the Supplement review process and that it provides technical assistance when requested by HHS program offices. HHS OIG officials stated that they review all audit community comments on HHS draft Supplement sections, identify fatal flaws, and advise the agency when it is not in its best interest to accept changes suggested by the audit community. However, HHS OIG officials stated that it is ultimately up to the HHS program officials to decide on the information to submit to OMB for inclusion in the Supplement.
Treasury officials stated Treasury engages with its OIG to understand emerging and ongoing risks and areas to prioritize for oversight across programs, but its OIG generally does not participate in the Supplement process and that OIG’s involvement depends on its statutory role in a particular program. Treasury OIG officials also stated that there are no policies and procedures requiring Treasury to request OIG input and for OIG to provide input. Other than the Coronavirus Relief Fund and the Emergency Rental Assistance programs, Treasury has not requested its OIG to review the Supplement update submissions for the other federal financial assistance programs it administers. Treasury requested its OIG’s input for the Coronavirus Relief Fund and the Emergency Rental Assistance programs due to its OIG’s responsibilities set forth by the COVID-19 relief laws.
Although there is no statutory requirement for OIGs to review their agencies’ proposed updates for inclusion in the Supplement, OMB recently issued a memorandum stressing the importance of agency and OIG collaboration, including proactive, front-end exchange of information to ensure expertise is applied.[531] Furthermore, OMB’s Controller Alert for the 2022 Compliance Supplement publication schedule encourages agencies to coordinate with their OIGs and the AICPA, as well as key recipient stakeholders and program officials, to obtain both program management and auditor feedback on the clarity of their proposed Supplement updates prior to submitting drafts to OMB.
Similarly, representatives from NASACT and the AICPA told us that more coordination with agency OIGs may improve audit guidance in the Supplement, since OIGs are more familiar with the auditing profession and more aware of information that should be audited.
Education, HHS, and Treasury also did not document policies and procedures detailing the involvement of external audit stakeholders (the audit community) in developing audit procedures, prior to submitting proposed Supplement updates to OMB. While these agencies stated they attend meetings with the audit community where single audit concerns are discussed, the agencies rely on OMB to coordinate with audit community members after submitting their agency updates to OMB. Specifically, OMB obtains feedback from the audit community during the final vetting of the draft Supplement and shares this feedback with the agencies. Treasury officials stated that they regularly engage with OMB to obtain additional feedback from external auditors and has worked to incorporate feedback in developing submission updates for new Supplement guidance. In addition, Education’s standard operating procedures state that consultations with OMB and the audit community are held as necessary.
As noted in our March 2021 CARES Act report, members of the audit community stated there is a need for more collaboration between the agencies and the audit community during the Supplement update process to identify the areas of highest risk and to ensure that suggested audit procedures are capable of consistent measurement against objective criteria. Further, the audit community continues to voice concerns that agencies and OMB did not address the comments they provided during the final vetting process. For example, the audit community stated there continue to be major concerns with the auditing requirements for Education’s Student Financial Assistance program in the Supplement despite comments from the audit community during the vetting process. An official from the AICPA also stated that there are situations where the same comments are made on various programs year after year with no action or response by the agencies or OMB.
Establishing procedures for agencies to work with the audit community, including proactive and front-end collaboration, could help expedite OMB’s final issuance of the Supplement and ensure agencies and OMB have adequate time to fully resolve concerns prior to issuance. In addition, it could help strengthen the quality of single audit guidance. For example, the audit community has suggested that agencies should collaborate with auditors to better ensure they include applicable and objective criteria when developing the Supplement’s audit requirements. The front-end collaboration between agency staff and auditors is especially important given that agency staff developing the Supplement are program experts, but may not have an auditing background.
Federal standards for internal control state that management considers the entity’s overall responsibilities to external stakeholders and establishes reporting lines that allow the entity to both communicate and receive information from external stakeholders. Without involving the audit community, agencies risk providing guidance for OMB’s inclusion in the Supplement that does not meet the needs of auditors conducting single audits.
Methodology
To conduct this work, we reviewed federal laws and guidance related to OMB’s Compliance Supplement. We selected for our audit three agencies that together received over $2 trillion of the total of $4 trillion in COVID-19 relief funding: Education ($1.7 trillion), HHS ($484 billion), and Treasury ($282 billion). Additionally, we selected Treasury because it is relatively new to developing submissions for inclusion in the Supplement; prior to the pandemic it was not a large grant-making agency with experience over awards. We provided questions to and interviewed officials from Education, HHS, and Treasury regarding their respective processes for developing the Supplement, including the agencies’ interactions with OMB and the audit community. We interviewed representatives from Education, HHS, and Treasury OIGs and officials from NASACT and the AICPA to obtain information on their experiences in working with agencies to resolve issues with single audit guidance in the Supplement. Findings from these three agencies are not generalizable to agencies that were not included in this review. We reviewed federal internal control standards to determine relevant guidance for documenting policies and procedures, commitment to competence, and organizational structures.
Agency Comments
We provided Education, HHS, Treasury, and OMB with a draft of this enclosure. Education provided written comments, which are reproduced in appendix VI. In its comments, Education agreed with our recommendation and stated that it has already established, and will continue to enhance, its policies and procedures for transmitting the draft Supplement to OMB. Education also stated that it will review and enhance, where necessary, its current methodology for training and establishing management expectations of staff competencies and its current engagement with internal and external stakeholders to ensure collaboration during the Supplement review process.
HHS provided written comments, which are reproduced in appendix VII. In its comments, HHS agreed with the recommendation and stated it will solidify policies and procedures for updating the Supplement. HHS also stated that its policies and procedures for updating the Supplement will include recommendations on staff competence for key roles and training and a description of internal stakeholders and how to best engage with them. However, as we noted in our recommendation, we continue to believe it is important for HHS to also include procedures for collaborating with external stakeholders.
Treasury provided written comments, which are reproduced in appendix X. In its comments, Treasury agreed with the recommendation and stated it will prepare documentation that includes steps for (1) establishing management’s expectations of staff competencies for key roles and providing ongoing training; and (2) involving internal and external audit stakeholders when developing audit procedures, as appropriate, prior to submitting draft Supplements to OMB. Treasury also provided technical comments, which we incorporated as appropriate.
OMB did not provide comments on this enclosure.
GAO’s Ongoing Work
Our work on single audits is ongoing. We will monitor the status of our open recommendations and continue our oversight of single audit efforts and OMB’s guidance for single audits.
GAO’s Prior Recommendations Related to Single Audits and Coronavirus State and Local Fiscal Recovery Funds
The table below presents our recommendations on the Office of Management and Budget’s (OMB) single audit Compliance Supplement from prior bimonthly and quarterly CARES Act reports.
Prior GAO Recommendations Related to Single Audits and Coronavirus State and Local Fiscal Recovery Funds
Recommendation
Status
The Director of OMB, in consultation with the Secretary of the Treasury, should issue timely and sufficient single audit guidance for auditing recipients' uses of payments from the Coronavirus State and Local Fiscal Recovery Funds. (July 2021 report).
Open—partially addressed. OMB neither agreed nor disagreed with our recommendation. In December 2021, OMB issued single audit guidance for the Coronavirus State and Local Fiscal Recovery Funds in Addendum 1 of the 2021 Compliance Supplement. We will review Addendum 1 and obtain feedback from members of the audit community (e.g., agency Offices of Inspector General; National Association of State Auditors, Comptrollers, and Treasurers; and American Institute of Certified Public Accountants) to determine if the guidance is sufficient.
The Director of OMB should work in consultation with federal agencies and the audit community (e.g., agency Offices of Inspector General; National Association of State Auditors, Comptrollers, and Treasurers; and American Institute of Certified Public Accountants), to the extent practicable, to incorporate appropriate measures in OMB’s process for preparing single audit guidance, including the annual Single Audit Compliance Supplement, to better ensure that such guidance is issued in a timely manner and is responsive to users’ input and needs (March 2021 report).
Open—partially addressed. OMB neither agreed nor disagreed with our recommendation. In its response to the March 2021 report, OMB stated that it was actively working, to the extent practicable, to update processes to better ensure that single audit guidance is issued in a timely manner, and is responsive to users' input and needs. OMB also stated that it continued to work with federal agencies and the audit communities to develop and publish single audit guidance for major programs in the Compliance Supplement.
As we previously reported, auditors who conduct single audits for entities with June 30 year-ends have expressed a need to obtain the Compliance Supplement by no later than April of each year in order to effectively plan their audits and conduct interim testing. OMB did not issue the 2021 Compliance Supplement until August 2021, and it lacked guidance for several American Rescue Plan Act of 2021 (ARPA) programs.
OMB issued single audit guidance for two ARPA programs in Addendum 1 of the 2021 Compliance Supplement in December 2021 and published Addendum 2 in January 2022. OMB also issued a Controller Alert in December 2021 that included a timeline for preparing the 2022 Compliance Supplement (in collaboration with federal agencies and the audit community), and estimated it will publish the Supplement by April 30, 2022. We continue to meet periodically with OMB and the audit community to discuss the audit community’s concerns and additional single audit guidance needed. We will continue to monitor the actions OMB takes in response to our recommendation.
Our review of economic studies provides consistent evidence that the Paycheck Protection Program strengthened labor markets and improved small businesses’ financial condition; however, challenges in receiving assistance at some businesses may have limited the economic impact of the program.
Background
The CARES Act, signed into law by the President on March 27, 2020, established the Paycheck Protection Program (PPP) under section 7(a) of the Small Business Act to provide loans to small businesses and other organizations—referred to collectively here as “small businesses”—that are fully forgivable if certain conditions are met. Under the law, qualifying businesses could obtain loans equal to 2.5 months of average total monthly payments for payroll costs up to $10 million and were required to self-certify their need for the loan. Qualifying businesses generally include businesses with 500 or fewer employees or that meet Small Business Administration’s (SBA) industry-based size standard. When loan approvals ended in June 2021, Congress authorized for commitment about $814 billion to PPP in three phases (see table). For more details on PPP implementation, see the Paycheck Protection Program enclosure in appendix I.
Paycheck Protection Program (PPP) Phases
Phase
Legislation
Date enacted
Commitment authority provided
Application period
1.
CARES Act
March 27, 2020
$349 billion
April 3, 2020–April 16, 2020
2.
Paycheck Protection Program and Health Care Enhancement Act
April 24, 2020
$310 billion
April 27, 2020–August 8, 2020
3.
Consolidated Appropriations Act, 2021
December 27, 2020
$147.45 billion
January 11, 2021–May 31, 2021a
American Rescue Plan Act of 2021
March 11, 2021
$7.25 billion
Source: GAO analysis of relevant laws. | GAO-22-105397
aThe PPP Extension Act of 2021 extended the application period for Phase 3 from March 31, 2021, to May 31, 2021, and allowed the Small Business Administration until June 30, 2021, to process those applications. On May 4, 2021, the PPP general fund was exhausted and closed to new applications, except those processed by a community financial institution lender.
Overview of Key Issues
To better understand the economic effects of PPP—one of the largest federal pandemic response programs—we conducted a review of relevant empirical research. We reviewed studies that examined the short-run effects of PPP on economic activity, including labor markets and small businesses’ financial conditions.[532] These studies collectively provide consistent evidence that PPP increased small businesses’ employment, especially for businesses with fewer employees, and improved their financial condition. Similarly, these studies also suggest that PPP strengthened local labor markets. However, some evidence suggests that some portion of PPP assistance did not initially go to the areas hit hardest by the pandemic and that smaller businesses faced challenges in obtaining PPP assistance, which may have limited the economic impact of the program.
Small business employment. Researchers consistently found that PPP increased small businesses’ employment, especially for businesses with fewer employees. For example, one study found that recipients’ employment increased by 8 percent within the first month of being approved for a PPP loan.[533] The effect decreased over time but remained statistically significant and positive 7 months after PPP loan approval. Two other studies found a positive, but smaller, effect of PPP on employment when the authors instead used the number of employees before the pandemic as an indicator of whether a business was eligible for PPP.[534] For example, one study found that employment at firms assumed to be eligible increased by 2 percent to 4.5 percent more than employment at presumed ineligible firms over the period from the end of March 2020 through the end of May 2020.[535]
Several studies we reviewed suggest that PPP had a greater effect on employment at smaller businesses than at larger businesses. For example, one study found the largest effects of PPP in small establishments and establishments that predominantly employed low-wage workers.[536] Another study found that PPP was most effective for relatively smaller firms.[537]
Small business financial conditions. Researchers found that PPP generally improved small businesses’ financial conditions but may have also encouraged small businesses to stay closed longer in the beginning of the pandemic. For example, one study found that an increase in the number of PPP loans per small business in a county was associated with fewer bankruptcy filings in the county.[538] A different study focused on the timing of PPP funding and found that businesses that received PPP loans earlier (at the end of the first round) were less likely to face financial distress, more likely to make timely payments to creditors, and less likely to close permanently than businesses that received PPP loans later (at the beginning of the second round).[539] A third study found that both small business revenue and the number of open small businesses were lower in counties with more PPP lending per dollar of assets in May and June 2020.[540] This suggests that while PPP kept employees on the payrolls, reducing unemployment, the program may have also encouraged small businesses to remain closed longer and therefore reduced their revenue.[541]
Local labor markets and program accessibility. Researchers found that greater PPP loan concentration likely strengthened local labor markets. For example, two studies we reviewed found that PPP loan concentration at the county level reduced unemployment rates.[542] Similarly, another study found that an increase in eligible payroll covered by PPP in counties led to a smaller jump in weekly initial and continuing unemployment insurance claims.[543]
While PPP likely improved local labor market conditions, funds may not have initially flowed to geographic areas hardest hit by the pandemic. For example, one study found that before the initial round of funding was exhausted, areas that had more business shutdowns in the week of March 22nd–March 28th received smaller PPP allocations.[544] Moreover, the study did not find a strong relationship between indicators of economic damages in the early part of the pandemic and the fraction of businesses in an area that received a PPP loan. Similarly, another study found that early PPP loans flowed to larger firms and to firms and counties less affected by the pandemic. The same study estimated that the second round of the program was much more effective than the first in increasing overall employment, as firms in the more affected counties at the baseline received more PPP loans in the second round.[545]
Studies we reviewed suggest that factors such as banks’ roles in allocating PPP loans and smaller businesses’ awareness of the program influenced where PPP funds flowed.[546] One study we reviewed noted that banks prioritized making PPP loans to businesses they already had a relationship with for two reasons: (1) the application process for existing customers was less costly for banks than the application process for new customers, and (2) banks had an economic interest in the long-term survival of their existing borrowers.[547] Another study found that firms that were larger, paid higher average wages, or had a pre-existing relationship with a bank that did more PPP lending were more like to apply for a PPP loan.[548] A third study found that the smallest businesses were less aware of PPP and less likely to apply for a PPP loan. When they did apply, the smallest businesses applied later, faced longer processing times, and were less likely to have their application approved, controlling for other factors.[549] Because PPP likely had a greater effect on employment at smaller businesses, challenges in receiving assistance at these businesses may have limited the initial economic impact of the program.[550]
Total jobs saved and cost per job saved. Researchers estimated the total number of jobs saved by PPP and the cost per job saved, but also identified additional factors that would be needed to provide a more comprehensive cost-benefit assessment of PPP. Studies we reviewed estimated that PPP likely saved millions of jobs overall.[551] However, these estimates are based on certain assumptions that may not be valid; for example, that relationships between PPP lending and employment in a limited context could be applied nationwide and over a longer period. In addition, these estimates varied depending on many factors, including the characteristics of the data used in the study (e.g., period covered, granularity of information, sample size, and the population the sample represented), the type of businesses studied (e.g., PPP recipients, PPP applicants, or PPP-eligible businesses), and how the number of employees working at PPP-participating firms was estimated.
Studies we reviewed also reported a wide range of estimates of the cost per job saved by PPP.[552] However, these estimates are based on the same assumptions as the estimates of total jobs saved—assumptions that, as we noted above, may not hold in practice. These estimates also varied depending on many factors, including assumptions about the duration of each job saved and all the factors that affected the estimates of total jobs saved.
While most cost-per-job saved estimates appear high relative to replacement salaries, researchers emphasized that a more complete assessment of the costs and benefits of PPP would include other factors. For example, by keeping workers on the payroll, PPP may have reduced use of social insurance programs, like unemployment insurance, and safety net programs, like the federal Supplemental Nutrition Assistance Program.[553] Moreover, PPP likely improved small business financial conditions, so metrics based solely on jobs saved are likely to paint a misleading picture of the program’s overall effect.[554]
In addition, a majority of the studies we reviewed estimated the total number of jobs and the cost per job saved by PPP based on their estimated short-term impacts of PPP on employment, but the ultimate impact of PPP will take longer to discern. For example, one study noted that it is too soon to assess the extent to which PPP preserved valuable firm-specific human capital, employer-employee matches, and networks.[555] Another study noted the long-run economic effect of PPP will depend in part on the evolution of employment at businesses that received PPP loans versus those that did not.[556] The study also noted that PPP may have preserved valuable intangible capital, which would have economic benefits in the long run that are not detectable this early in the recovery process. Finally, the study noted that a thorough evaluation of the effectiveness of PPP would need to consider the amount of time that PPP’s effects on employment and businesses last, as well as likely outcomes for workers and businesses in PPP’s absence and the extent to which new jobs and businesses would have replaced those lost without it.
Methodology
For our review of empirical research on the economic effects of PPP, we searched for peer reviewed journal articles and working papers in various databases including EconLit, Scopus, ProQuest Research Library, Social Science Research Network, Google Scholar, and IDEAS/RePEc. Our search was limited to publications with the program name in titles, abstracts, or subject keywords and that were published in 2020 and 2021. We conducted our literature search between December 2021 and early January 2022. After an initial screening for relevance, two economists independently reviewed the abstracts of 119 studies related to the effects of PPP. We identified 37 studies that used an empirical approach to estimate the impact or effectiveness of PPP for further review. Two economists then independently conducted in-depth reviews and identified papers that were retrospective in nature, based on sufficiently reliable data, and that used rigorous statistical methods. Ultimately, we included 22 studies in our literature review and recorded the studies’ data, methodology, assumptions, key findings, and limitations—we used this information to summarize relevant research findings.
Agency Comments
We provided the Department of the Treasury (Treasury), SBA, and the Office of Management and Budget (OMB) with a draft of this enclosure. Treasury provided technical comments, which we incorporated as appropriate. SBA and OMB did not provide comments on this enclosure.
Studies included in our literature review
Autor, D., D. Cho, L. D. Crane, M. Goldar, B. Lutz, J. Montes, W. B. Peterman, D. Ratner, D. Villar, and A. Yildirmaz. "An Evaluation of the Paycheck Protection Program Using Administrative Payroll Microdata." Working Paper (2020).
Barraza, S., M. A. Rossi, and T. J. Yeager. "The Short-Term Effect of the Paycheck Protection Program on Unemployment." SSRN Working Paper (2020).
Bartlett III, R. P., and A. Morse. "Small-Business Survival Capabilities and Fiscal Programs: Evidence from Oakland." Journal of Financial and Quantitative Analysis, vol. 56, no. 7 (2021): 2500-2544.
Berger, A. N., P. G. Freed, J. A. Scott, and S. Zhang. "The Paycheck Protection Program (PPP) from the Small Business Perspective: Did the PPP Help Alleviate Financial and Economic Constraints?" SSRN Working Paper (2021).
Chetty, R., J. N. Friedman, N. Hendren, M. Stepner, and The Opportunity Insights Team. “How Did COVID-19 and Stabilization Policies Affect Spending and Employment? A New Real-Time Economic Tracker Based on Private Sector Data.” NBER Working Paper No. 27431 (2020).
Cole, A. "The Impact of the Paycheck Protection Program on Small Businesses: Evidence from Administrative Payroll Data." SSRN Working Paper (2020).
Dalton, M. “Putting the Paycheck Protection Program into Perspective: An Analysis Using Administrative and Survey Data.” U.S. Bureau of Labor Statistics Working Paper 542 (2021).
Denes, M., S. Lagaras, and M. Tsoutsoura. "First Come, First Served: The Timing of Government Support and Its Impact on Firms." SSRN Working paper (2021).
Doniger, C., and B. Kay. "Ten Days Late and Billions of Dollars Short: The Employment Effects of Delays in Paycheck Protection Program Financing.” SSRN Working Paper (2021).
Faulkender, M., R. Jackman, and S. I. Miran. "The Job-Preservation Effects of Paycheck Protection Program Loans." Office of Economic Policy Working Paper 2020-01, Department of the Treasury (2020).
Gertler, M., C. Huckfeldt, and A. Trigari. "Temporary and Permanent Layoffs over the Business Cycle: Evidence, Theory, and an Application to the Covid-19 Crisis." Working Paper (2021).
Granja, J., C. Makridis, C. Yannelis, and E. Zwick. “Did the Paycheck Protection Program Hit the Target?” NBER Working Paper No. 27095 (2021).
Hubbard, R. G., and M. R. Strain. “Has the Paycheck Protection Program Succeeded?” NBER Working Paper No. 28032 (2020).
Humphries, J. E., C. A. Neilson, and G. Ulyssea. "Information Frictions and Access to the Paycheck Protection Program." Journal of Public Economics, vol. 190 (2020): 104244.
James, C., J. Lu, and Y. Sun. "Time is Money: Real Effects of Relationship Lending in a Crisis." Journal of Banking & Finance, vol. 133 (2021): 106283.
Joaquim, G., and F. Netto. "Bank Incentives and the Effect of the Paycheck Protection Program." Federal Reserve Bank of Boston Working Paper No. 21-15 (2021).
Kapinos, P. "Did the Paycheck Protection Program Have Negative Side Effects on Small-Business Activity?" Economics Letters, vol. 208 (2021): 110045.
Kapinos, P. "Paycheck Protection Program: County-Level Determinants and Effect on Unemployment." Federal Reserve Bank of Dallas Working Paper 2105 (2021).
Kim, P. H., and D. Stillerman. "Incentive Structures and Borrower Composition in the Paycheck Protection Program." Working Paper (2021).
Kurmann, A., E. Lalé, and L. Ta. "The Impact of COVID-19 on Small Business Dynamics and Employment: Real-Time Estimates with Homebase Data." Drexel Economics Working Paper Series WP 2021-15 (2021).
Li, L., and P. E. Strahan. "Who Supplies PPP Loans (and Does It Matter)? Banks, Relationships and the COVID Crisis." Journal of Financial and Quantitative Analysis, vol. 56, no. 7 (2021): 2411-2438.
Wheat, C. and C. Mac. "Did the Paycheck Protection Program Support Small Business Activity?" JPMorgan Chase Institute Research Brief (2021).
Contact information: Michael Hoffman, (202) 512-6445, hoffmanme@gao.gov
Appendix II: Highlights Pages from Recently Issued GAO COVID-19 Products
We issued Federal Prisons: Monitoring Efforts to Implement COVID-19 Recommendations and Examining First Step Act Implementation, GAO-22-105691, on January 21, 2022.
We issued Freedom of Information Act: Selected Agencies Adapted to the COVID-19 Pandemic but Face Ongoing Challenges and Backlogs, GAO-22-105040, on January 26, 2022.
We issued COVID-19: Federal Telework Increased during the Pandemic, but More Reliable Data Are Needed to Support Oversight, GAO-22-104282, on February 8, 2022.
We issued Defense Contracting: More Insight into Use of Financing Payments Could Benefit DOD in Future Emergencies, GAO-22-105007, on February 17, 2022.
We issued DHS Annual Assessment: Most Acquisition Programs Are Meeting Goals Even with Some Management Issues and COVID-19 Delays, GAO-22-104684, on March 8, 2022.
We issued Emergency Relief Funds: Significant Improvements Are Needed to Ensure Transparency and Accountability for COVID-19 and Beyond, GAO-22-105715, on March 17, 2022.
We issued K-12 Education: An Estimated 1.1 Million Teachers Nationwide Had At Least One Student Who Never Showed Up for Class in the 2020-21 School Year, GAO-22-104581, on March 23, 2022.
We issued Freedom of Information Act: Selected Agencies Adapted to COVID-19 Challenges but Actions Needed to Reduce Backlogs, GAO-22-105845, on March 29, 2022.
We issued Scientific Integrity: HHS Agencies Need to Develop Procedures and Train Staff on Reporting and Addressing Political Interference, GAO-22-104613, on April 20, 2022.
Appendix III: List of Ongoing GAO Work Related to COVID-19 as of April 27, 2022
When reviewing the federal government’s response to the COVID-19 pandemic, GAO found that agencies had significant shortcomings in their application of fundamental internal controls and financial and fraud risk management practices.[557] Such shortcomings—stemming in part from the need to distribute funds quickly—were exacerbated by existing financial management weaknesses. As a result, billions of dollars were at risk for improper payments, including those from fraud, providing limited assurance that programs effectively met their objectives.
To help address these shortcomings, GAO suggests Congress take the following 10 legislative actions:
Congress should pass legislation requiring the Office of Management and Budget (OMB) to provide guidance for agencies to develop plans for internal control that would then immediately be ready for use in, or adaptation for, future emergencies or crises and requiring agencies to report these internal control plans to OMB and Congress.
Congress should amend the Payment Integrity Information Act of 2019 to designate all new federal programs making more than $100 million in payments in any one fiscal year as “susceptible to significant improper payments” for their initial years of operation.
Congress should amend the Payment Integrity Information Act of 2019 to reinstate the requirement that agencies report on their antifraud controls and fraud risk management efforts in their annual financial reports.
Congress should establish a permanent analytics center of excellence to aid the oversight community in identifying improper payments and fraud.
Congress should clarify that (1) chief financial officers (CFO) at CFO Act agencies have oversight responsibility for internal controls over financial reporting and key financial management information that includes spending data and improper payment information; and (2) executive agency internal control assessment, reporting, and audit requirements for key financial management information, discussed in an existing matter for congressional consideration in our August 2020 report, include internal controls over spending data and improper payment information.
Congress should require agency CFOs to (1) submit a statement in agencies’ annual financial reports certifying the reliability of improper payments risk assessments and the validity of improper payment estimates, and describing the actions of the CFO to monitor the development and implementation of any corrective action plans; and (2) approve any methodology that is not designed to produce a statistically valid estimate.
Congress should consider legislation to require improper payment information required to be reported under the Payment Integrity Information Act of 2019 to be included in agencies’ annual financial reports.
Congress should amend the DATA Act to extend the previous requirement for agency inspectors general to review the completeness, timeliness, quality, and accuracy of their respective agency data submissions on a periodic basis.
Congress should amend the DATA Act to clarify the responsibilities and authorities of OMB and Department of the Treasury for ensuring the quality of data available on USAspending.gov.
Congress should amend the Social Security Act to accelerate and make permanent the requirement for the Social Security Administration to share its full death data with the Department of the Treasury’s Do Not Pay working system.
Appendix V: Comments from the Department of Defense
[1]According to CDC, viruses, such as COVID-19, constantly change through mutation, and new variants are expected to occur. Sometimes, new variants emerge and disappear, while at other times, new variants persist. First identified in the U.S. on December 1, 2021, the Omicron variant superseded the Delta variant to become the dominant COVID-19 strain circulating in the U.S. during the week ending December 25, 2021. As of April 5, 2022, CDC has reported the presence of multiple sublineages of the Omicron variant in the U.S., including BA.2; BA.2 became the dominant strain circulating in the U.S. during the week ending March 26, 2022. Both the Omicron and Delta variants spread faster than previous COVID-19 variants, though the Omicron variant generally causes less severe disease than the prior variants, according to CDC. As of March 29, 2022, CDC reported that current vaccines protect against severe illness, hospitalizations, and deaths due to the Omicron variant, and that some monoclonal antibody treatments are less effective against Omicron’s BA.2 lineage, though non-monoclonal antibody treatments remain effective against Omicron.
[2]The White House, National COVID-19 Preparedness Plan (Washington, D.C.: Mar. 2022). This document was issued as an update to the White House’s previous COVID-19 strategy document. The White House, National Strategy for the COVID-19 Response and Pandemic Preparedness (Washington, D.C.: Jan. 2021). The National COVID-19 Preparedness Plan focuses on four goals: protecting and treating COVID-19, preparing for new variants, preventing shutdowns, and global vaccination. Additionally, in April 2022, the White House issued a memorandum charging the Secretary of the Department of Health and Human Services with coordinating the federal response to the long-term effects of COVID-19. This includes developing a report on services and mechanisms of support across federal agencies to assist the public with the long-term effects, as well as developing a national research action plan on long COVID—new, returning, or ongoing health problems 4 or more weeks after an initial case of COVID-19, potentially affecting up to 23 million people in the U.S. For more information on long COVID, see GAO, Science & Tech Spotlight: Long COVID, GAO-22-105666 (Washington, D.C.: Mar. 2, 2022).
[3]The White House, Fact Sheet: Consequences of Lack of Funding for Efforts to Combat COVID-19 if Congress Does Not Act. (Washington, D.C.: Mar. 2022).
[4]The Department of Health and Human Services’ Health Resources and Services Administration covered treatment, testing, and administering the vaccine for the uninsured through its COVID-19 Uninsured Program. The agency covered the cost of administering the vaccine for the underinsured through its COVID-19 Coverage Assistance Fund, which also stopped accepting vaccination claims on April 5, 2022, due to a lack of sufficient funds.
[5]As of April 1, 2022, CDC counts individuals as being fully vaccinated if they received two doses on different days (regardless of time interval) of the two-dose vaccines or received one dose of a single-dose vaccine. CDC counts individuals as having received a booster dose if they are fully vaccinated and have received another dose of COVID-19 vaccine since August 13, 2021, including those who received booster doses and those who received additional doses. See CDC, “COVID Data Tracker: COVID-19 Vaccinations in the United States,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-total-admin-rate-total.
[6]In January 2022, the White House, in partnership with the U.S. Postal Service, began to distribute 1 billion at-home, rapid tests, with an initial four free tests—and an additional four tests announced in March 2022—available to each household.
[7]State Medicaid programs and the Children’s Health Insurance Program were required to cover at-home COVID-19 tests authorized by the Food and Drug Administration without cost-sharing under guidance issued by the Centers for Medicare & Medicaid Services in August 2021.
[8]As of April 1, 2022, the Food and Drug Administration has authorized two types of COVID-19 diagnostic and screening tests. Rapid antigen tests can be conducted in doctors’ offices, pharmacies, and other health care settings, as well as in homes or other non-health care settings, and typically provide results in 30 minutes or less. Molecular tests are considered the “gold standard” for diagnostic testing and typically provide results in 1 to 3 days.
[9]See B. Rader et al., “Use of At-Home COVID-19 Tests — United States, August 23, 2021–March 12, 2022,” Morbidity and Mortality Weekly Report, vol. 71, no. 13 (Apr. 1, 2022). This analysis relied on self-reported survey data from a nonprobability-based sample of U.S. adults.
[10]In October 2021, we reported that if rapid antigen testing continues to expand, especially with the increasing availability of over-the-counter tests, the ongoing limited reporting of antigen test results could reduce the ability of public health officials to more comprehensively monitor and effectively respond to the COVID-19 pandemic. These issues highlight the importance of HHS and CDC efforts aimed at improving reporting and exploring additional approaches for surveillance.
[11]According to the Department of Labor’s Consumer Price Index, which is one measure of the prices of consumer goods and services, prices increased 7.9 percent between February 2021 and February 2022, with larger increases recorded in the prices for certain items, such as gasoline. According to the Department of Labor, this represents the largest year-over-year increase since the period ending January 1982.
[12]The White House, Building Resilient Supply Chains, Revitalizing American Manufacturing, and Fostering Broad-Based Growth (Washington, D.C.: June 2021). This report specifically examined the supply chains of four critical products: semiconductor manufacturing and advanced packaging, large capacity batteries, critical minerals and materials, and pharmaceuticals and active pharmaceutical ingredients.
[13]HHS, National Strategy for a Resilient Public Health Supply Chain (Washington, D.C.: July 2021). This strategy was developed in response to Executive Order 14001, which directed the Department of Defense, Department of Homeland Security, and HHS, among others, to develop a supply chain resilience strategy to include an approach to design, build, and sustain long-term capability in the U.S. to manufacture supplies for future pandemics and biological threats. A Sustainable Public Health Supply Chain, Exec. Order No. 14001, § 4, 86 Fed. Reg. 7,219, 7,220-21 (Jan. 26, 2021).
[14]HHS, Public Health Supply Chain and Industrial Base One-Year Report In Response to Executive Order 14017 (Washington, D.C.: Feb. 2022). Among other things, the report outlines actions HHS has taken or plans to take to strengthen the public health supply chain and industrial base for personal protective equipment and durable medical equipment, testing and diagnostics, and pharmaceuticals—including therapeutics, vaccines, and active pharmaceutical ingredients.
[15]For the purposes of our review, the COVID-19 relief laws consist of the six laws providing comprehensive relief across federal agencies and programs that Treasury uses to report COVID-19 spending. These six laws are the American Rescue Plan Act of 2021 (ARPA), Pub. L. No. 117-2, 135 Stat. 4; Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M and N, 134 Stat. 1182 (2020); Paycheck Protection Program and Health Care Enhancement Act, Pub. L. No. 116-139, 134 Stat. 620 (2020); CARES Act, Pub. L. No. 116-136, 134 Stat. 281 (2020); Families First Coronavirus Response Act, Pub. L. No. 116-127, 134 Stat. 178 (2020); and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020, Pub. L. No. 116-123, 134 Stat. 146.
[16]Pub. L. No. 116-136, § 19010, 134 Stat. at 579–81.
[17]Our recurring oversight reports are GAO, COVID-19: Significant Improvements are Needed for Overseeing Relief Funds and Leading Responses to Public Health Emergencies, GAO-22-105291 (Washington, D.C.: Jan. 27, 2022); COVID-19: Additional Actions Needed to Improve Accountability and Program Effectiveness of Federal Response,GAO-22-105051 (Washington, D.C.: Oct. 27, 2021); COVID-19: Continued Attention Needed to Enhance Federal Preparedness, Response, Service Delivery, and Program Integrity, GAO-21-551 (Washington, D.C.: July 19, 2021); COVID-19:Sustained Federal Action Is Crucial as Pandemic Enters Its Second Year, GAO-21-387 (Washington, D.C.: Mar. 31, 2021); COVID-19:Critical Vaccine Distribution, Supply Chain, Program Integrity, and Other Challenges Require Focused Federal Attention, GAO-21-265 (Washington, D.C.: Jan. 28, 2021); COVID-19: Urgent Actions Needed to Better Ensure an Effective Federal Response, GAO-21-191 (Washington, D.C.: Nov. 30, 2020); COVID-19: Federal Efforts Could Be Strengthened by Timely and Concerted Actions, GAO-20-701 (Washington, D.C.: Sept. 21, 2020); COVID-19: Brief Update on Initial Federal Response to the Pandemic, GAO-20-708 (Washington, D.C.: Aug. 31, 2020); and COVID-19: Opportunities to Improve Federal Response and Recovery Efforts, GAO-20-625 (Washington, D.C.: June 25, 2020).
[18]The testimony focused on our assessment of (1) federal agencies' application of fundamental internal controls and financial and fraud risk management practices for COVID-19 spending, and (2) opportunities for Congress to improve these practices during emergencies and national crises. See GAO, Emergency Relief Funds: Significant Improvements Are Needed to Ensure Transparency and Accountability for COVID-19 and Beyond, GAO-22-105715 (Washington, D.C.: Mar. 17, 2022).
[19]We designate federal programs and operations as “high risk” due to their vulnerabilities to fraud, waste, abuse, and mismanagement, or because they need transformation. For more information on programs and operations on our High-Risk List, see https://www.gao.gov/high-risk-list.
[20]We consider a recommendation to be addressed when the target agency has completed the implementation of the recommendation. We consider a recommendation to be partially addressed when the agency is in the process of developing an action, has started but not yet completed or has partially implemented an action, or has taken steps toward implementation.
[21]In March 2021, we recommended that the Secretary of HHS ensure that the Director of CDC collects data specific to the COVID-19 vaccination rates in nursing homes and makes these data publicly available to better ensure transparency and that the necessary information is available to improve ongoing and future vaccination efforts for nursing home residents and staff.
[22]The 52 states and jurisdictions include all 50 states; Washington, D.C.; and New York, N.Y. COVID-19 case counts for New York, N.Y., are reported separately from the state of New York. We defined states as holding steady if they had less than a 5 percent increase or decrease in the average of the 7-day moving averages of new cases from March 18-24, 2022 compared to March 11-17, 2022. This is a change from our prior reports where we used a 1 percent threshold for comparing average daily percent changes in the 7-day moving averages—a change we made because of less frequent state reporting of case count data to CDC. See CDC, “United States COVID-19 Cases and Deaths by State Over Time,” accessed on April 1, 2022, https://data.cdc.gov/Case-Surveillance/United-States-COVID-19-Cases-and-Deaths-by-State-o/9mfq-cb36. These COVID-19 case counts may change as new or updated data are reported by states.
[24]CDC, “Percentage of Emergency Department visits with Diagnosed COVID-19 in United States, All Ages,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#ed-visits. Data are from the National Syndromic Surveillance Program. For insights into COVID-19 trends, CDC monitors a subset of emergency departments in 50 states to identify visits that have a COVID-19 diagnosis associated with them.
[25]Many people hospitalized with confirmed COVID-19 will have additional diagnoses, either related to COVID-19 or not, each of which may contribute to their need for hospitalization. Examples of resource-intensive protocols may include placing patients with COVID-19 in single-person rooms or designated units, providing personal protective equipment for healthcare personnel, and frequent cleaning and disinfection of facilities.
[27]CDC’s National Center for Health Statistics COVID-19 death counts in the U.S. are based on provisional counts from death certificate data, which do not distinguish between laboratory-confirmed and probable COVID-19 deaths. Data are provisional and subject to updates. In more recent weeks, the data are more likely to be incomplete due to an average delay of 2 weeks (a range of 1–8 weeks or longer) for death certificate processing. See CDC, National Center for Health Statistics, “Provisional Death Counts for Coronavirus Disease 2019 (COVID-19),” accessed April 4, 2022, https://www.cdc.gov/nchs/nvss/vsrr/covid19/index.htm.
[28]This number represents the number of deaths from all causes reported in the U.S. in a given week from February 2020 through March 5, 2022, that exceeded the upper-bound threshold of expected deaths calculated by CDC’s National Center for Health Statistics on the basis of variation in mortality in prior years. As in prior reports, we continue to report excess deaths based on the more conservative upper bound estimate of expected deaths. For further details of CDC’s methodology, see CDC, National Center for Health Statistics, “Excess Deaths Associated with COVID-19,” accessed April 1, 2022, https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm.
[29]Typically, FDA must license a vaccine before it can be marketed in the U.S. See 42 U.S.C. § 262. However, during an emergency, FDA may temporarily allow the use of unlicensed vaccines through an emergency use authorization, provided certain statutory criteria are met. See 21 U.S.C. § 260bbb-3. The Pfizer vaccine was developed in collaboration with BioNTech.
[30]Janssen Pharmaceutical Companies are a part of Johnson & Johnson.
[31]As of April 1, 2022, the Pfizer and Moderna booster doses were authorized to be administered at least 5 months after completion of the primary vaccination series (two doses for most individuals), and the Janssen booster dose was authorized to be administered at least 2 months after administration of the primary vaccination series (one dose). FDA also authorized a “mix and match” booster approach for eligible individuals following completion of the primary vaccination series with a different available COVID-19 vaccine. For additional information on vaccine distribution, see GAO, COVID-19: HHS Agencies’ Planned Reviews of Vaccine Distribution and Communication Efforts Should Include Stakeholder Perspectives, GAO-22-104457 (Washington, D.C.: Nov. 4, 2021).
[32]In March 2022, CDC also recommended that adults who received a primary and booster dose of the Janssen vaccine receive a second booster dose of the Pfizer or Moderna vaccine.
[33]As of April 1, 2022, CDC recommended that everyone 5 years and older remain up to date on their vaccinations by getting their primary series of COVID-19 vaccines and receiving a booster dose when eligible. As of the same date, getting a second booster dose was not necessary to be considered up to date on COVID-19 vaccines. See CDC, “Stay Up to Date with Your COVID-19 Vaccines,” accessed April 1, 2022, https://www.cdc.gov/coronavirus/2019-ncov/vaccines/stay-up-to-date.html
[34]Data on COVID-19 cases and COVID-19-associated deaths by vaccination status were from surveillance data from about half of U.S. states, representing over 60 percent of the U.S. population. See CDC, “Rates of COVID-19 Cases and Deaths by Vaccination Status,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status. Data on COVID-19-associated hospitalizations are from CDC’s COVID-19-Associated Hospitalization Surveillance Network (COVID-NET), a population-based surveillance system that includes 99 counties in 14 states; findings should not be generalized nationally. See CDC, “Rates of laboratory-confirmed COVID-19 hospitalizations by vaccination status,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#covidnet-hospitalizations-vaccination. Surveillance data are preliminary and subject to change as more data become available.
[35]For example, see CDC, “Rates of COVID-19 Cases and Deaths by Vaccination Status,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#rates-by-vaccine-status. Data on COVID-19 cases by booster status between September 19, 2021 and February 19, 2022, were from surveillance data from 26 U.S. jurisdictions, representing over 60 percent of the U.S. population.
[36]See M. G. Thompson et al., “Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance — VISION Network, 10 States, August 2021–January 2022,” Morbidity and Mortality Weekly Report, vol. 71, no. 4 (Jan. 28, 2022). This analysis only included people who had received Pfizer or Moderna vaccines.
[37]FDA has previously authorized monoclonal antibodies—laboratory-made proteins that mimic the immune system’s ability to fight off harmful pathogens such as viruses—to treat COVID-19, though variants can affect the effectiveness of certain treatments. In January 2022, FDA revised the authorizations for two of these treatments—bamlanivimab and etesevimab (administered together) and REGEN-COV (casirivimab and imdevimab)—to limit their use based on data showing these treatments are highly unlikely to be active against the Omicron variant. In April 2022, FDA revoked the authorization for a third treatment—sotrovimab—as data show this treatment is unlikely to be effective against the Omicron BA.2 variant.
[38]The American Medical Association has criticized the Test to Treat initiative, suggesting that pharmacy-based clinics may be unable to sufficiently consider patients’ medical history, evaluate drug interactions, and manage possible negative reactions when prescribing antivirals for COVID-19.
[39]The employment-to-population ratio represents the number of employed people as a percentage of the civilian noninstitutional population 16 years and older. The ratio is subject to misclassification errors with respect to consistently identifying workers as employed and absent from work or unemployed on temporary layoff.
[40]The Federal Reserve System’s Federal Open Market Committee aims for inflation of 2 percent on average over time and aims to achieve rates of inflation that are above 2 percent for some time after periods in which inflation is persistently below 2 percent.
[41]Total budgetary resources, reported to Treasury’s Governmentwide Treasury Account Symbol Adjusted Trial Balance System, reflect appropriations, as well as transfers, adjustments, recoveries, rescissions, and returns of unused indefinite appropriations.
[42]An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of another party that are beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. Expenditures include some estimates, such as estimated subsidy costs for direct loans and loan guarantees. Increased spending in Medicaid and Medicare is not accounted for in the funding provided by the COVID-19 relief laws. Federal agencies use the Governmentwide Treasury Account Symbol Adjusted Trial Balance System to report proprietary financial reporting and budgetary execution information to Treasury.
[43]This total is based on (1) an analysis of the appropriated amounts in ARPA, Divisions M and N of the Consolidated Appropriations Act, 2021, the Paycheck Protection Program and Health Care Enhancement Act, the CARES Act, the Families First Coronavirus Response Act, and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 that are available to agencies for assistance to states, the District of Columbia, localities, U.S. territories, and tribes; and (2) the Congressional Budget Office’s estimated outlays for Medicaid resulting from authorized increases in payments to states and U.S. territories under those laws.
[44]This number includes recommendations from our June 2020, September 2020, November 2020, January 2021, March 2021, July 2021, October 2021, and January 2022 CARES Act reports as well as other targeted COVID-19-related reports in areas such as emergency rental assistance and oversight of infection control and prevention in veteran nursing homes. For a complete list of our COVID-related products, see https://www.gao.gov/coronavirus.
[45]The Payment Integrity Information Act of 2019 (PIIA) further states that this definition includes any payment to an ineligible recipient, any payment for an ineligible good or service, any duplicate payment, any payment for a good or service not received (except for such payments where authorized by law), and any payment that does not account for credit for applicable discounts. See PIIA, Pub. L. No. 116-117, 134 Stat. 113, 114 (2020) (codified at 31 U.S.C. § 3351(4)). PIIA also provides that when an executive agency’s review is unable to discern whether a payment was proper as a result of insufficient or lack of documentation, this payment must also be included in the improper payment estimates. 31 U.S.C. § 3352(a), (c)(2).
[46]The TANF program serves as the nation’s major cash assistance program for low-income families with children.
[47]Department of Health and Human Services, FY 2021 Agency Financial Report (Washington, D.C.: November 2021), pg. 233. Specifically, HHS identified section 411 of the Social Security Act, which specifies the data elements that HHS may require states to report, and section 417 of that act, which dictates that the federal government may only regulate the conduct of states where Congress has given the express authority to do so.
[48]OMB A-123 Appendix C. OMB A-136 guidance requires that agency financial reports include an assessment by the agency head of the completeness and reliability of the performance and financial data used in the report.
[49]Specifically, we identified a $1.4 billion overstatement in one agency’s dataset for overpayments that had been identified and recaptured when compared to information provided in the agency financial report. According to OMB staff, the overstatement occurred because one agency failed to convert its recovery amount into millions of dollars prior to entering it into the OMB data call tool.
[50]The Single Audit Act is codified at 31 U.S.C. §§ 7501-06, and implementing OMB guidance is reprinted in 2 C.F.R. part 200. The Act requires a “single audit” of the entity’s financial statements and federal awards (or a program-specific audit, in limited circumstances) for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[51]CARES Act, Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 554 (2020); ARPA, Pub. L. No. 117-2, § 2404, 135 Stat. 4, 42. Committee reports accompanying the Further Consolidated Appropriations Act, 2020, Pub. L. No. 116-94, and the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, specified that $50 million from each law was to be used for data modernization. See H.R. Rep. No. 38-679 at 107 (2020); and H.R. Rep. No. 43-750, pt. 2, at 1608 (2021).
[52]The 16 critical infrastructure sectors are: chemical; commercial facilities; communications; critical manufacturing; dams; defense industrial base; emergency services; energy; financial services; food and agriculture; government facilities; healthcare and public health; information technology; nuclear reactors, materials and waste; transportation systems; and water and wastewater systems.
[53]In January 2021, the William M. (Mac) Thornberry National Defense Authorization Act for Fiscal Year 2021 established “sector risk management agency” responsibilities for federal departments or agencies designated as such for each critical infrastructure sector or subsector. Pub. L. No. 116-283, § 9002(c), 134 Stat. 3388, 4770. Prior to enactment of the act, a “sector risk management agency” was called a “sector-specific agency.” CISA is also the sector risk management agency for the Chemical, Commercial Facilities, Communications, Dams, Emergency Services, Information Technology, and Nuclear Reactors, Materials and Waste Sectors.
[54]Cybersecurity and Infrastructure Security Agency, Guidance on the Essential Critical Infrastructure Workforce: Ensuring Community and National Resilience in COVID-19 Response (Washington, D.C.: March 19, 2020).
[55]Department of Homeland Security, National Infrastructure Protection Plan 2013: Partnering for Critical Infrastructure Security and Resilience (Washington, D.C.: December 2013).
[56]In previous work, we identified a number of economic indicators to facilitate ongoing and consistent monitoring of areas of the economy supported by the federal pandemic response, including labor markets, household finances, and small business credit and financial conditions. To the extent that federal pandemic responses are effective, we would expect to see improvements in outcomes related to these indicators. However, while trends in these indicators may be suggestive of the effect of provisions of the COVID-19 relief laws over time, those trends will not on their own provide definitive evidence of effectiveness.
[57]Real GDP is a measure of the value of all goods and services produced in the economy in a given year, adjusted for changes in the price level.
[58]In fiscal year 2021, 32.8 percent of all FHA purchase and refinance borrowers were minorities, 52.6 percent of FHA forward mortgage borrowers were of low-to-moderate income, and 84.6 percent of home purchasers under the FHA forward mortgage insurance program were first-time homebuyers. See Department of Housing and Urban Development, FHA Annual Management Report Fiscal Year 2021. FHA forbearance have expired for borrowers who requested an initial forbearance before October 1, 2020. On the other hand, FHA allowed servicers to initiate new forbearance between October 1, 2021 and the end of the COVID-19 national emergency. This report also includes an enclosure on Homeowner Assistance Fund, designed to prevent mortgage delinquencies and defaults, foreclosures, loss of utilities or home energy services, and displacement of homeowners experiencing financial hardship associated with the coronavirus pandemic (see the Homeowner Assistance Fund enclosure in app. I).
[59]Inflation is the increase in the price of goods and services over time, and is typically measured as the percentage change in those prices over a set period, often 1 year. For example, an inflation rate of 2 percent would mean that the prices of goods and services, on average, increased 2 percent over the last year.
[60]See the FOMC’s 2020 Statement on Longer-Run Goals and Monetary Policy Strategy.
[61]Higher levels of inflation over short periods—described as transitory—are not unusual and are less cause for concern. The prices of goods and services regularly shift in response to economic changes, and any impact on household finances is more limited because prices increase more rapidly for only a short period of time. In contrast, high levels of inflation that persist for long periods are more cause for concern, and can reduce the pace of economic growth.
[62]Public health practice involves the application of proven methods to monitor the health status of the community, investigate unusual occurrences of diseases or other conditions, and implement preventive control measures based on current understanding within public health sciences. See https://www.cdc.gov/training/publichealth101/surveillance.html, accessed March 3, 2022, for more information about public health surveillance.
[64]CARES Act, Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 554 (2020); ARPA, Pub. L. No. 117-2, § 2404, 135 Stat. 4, 42. Committee reports accompanying the Further Consolidated Appropriations Act, 2020, Pub. L. No. 116-94, and the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, specified that $50 million from each law was to be used for data modernization. See H.R. Rep. No. 38-679, at 107 (2020); and H.R. Rep. No. 43-750, pt.2, at 1608 (2021).
[65]David Michaels, Ezekiel J. Emanuel, and RickA. Bright, “Viewpoint: A National Strategy for COVID-19: Testing, Surveillance, and Mitigation Strategies,” JAMA, vol. 327, no. 3, 213-214. See also Center for Infectious Disease Research and Policy (CIDRAP), University of Minnesota, COVID-19: CIDRAP Viewpoint: Part 5: SARS-CoV-2 Infection and COVID-19 Surveillance: A National Framework, July 9, 2020; and Mark McClellan, Scott Gottlieb, Farzad Mostashari, Caitlin Rivers, and Lauren Silvis, Duke University, Margolis Center for Health Policy, A National COVID-19 Surveillance System: Achieving Containment, Durham, N.C.: Apr. 7, 2020.
[66]Other characteristics relate to purpose, problem definition, risk management, coordination, and implementation.
[67]This objective and measure is intended to be illustrative only and not prescriptive of an actual objective we are proposing that the agency employ.
[68]Jurisdictional participation in wastewater surveillance is voluntary, according to CDC information.
[69]These three CDC public health partner organizations support COVID-19 surveillance activities and, collectively, represent state, local, and territorial public health agencies, and state epidemiologists.
[70]In sentinel surveillance, a network of health care providers or other relevant entities regularly report specified health events such as cases or hospitalizations. According to officials, sentinel surveillance has been used for monitoring influenza, where the goal of surveillance is information on trends rather than individual case investigation.
[73]Providers may have also received other assistance from several sources, including the Department of the Treasury, the Small Business Administration, the Federal Emergency Management Agency, the Paycheck Protection Program, and local, state, and tribal government assistance sources.
[74]Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1920 (2020); Pub. L. No. 116-139, div. B, tit. I, 134 Stat. 620, 622 (2020); Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 563 (2020).
[75]HRSA’s COVID-19 Uninsured Program covers treatment, testing, and administering the vaccine for the uninsured, and its COVID-19 Coverage Assistance Fund covers the cost of administering the vaccine for the underinsured.
[76]Pub. L. No. 117-2, § 9911, 135 Stat. 4, 236-38. According to HHS officials, these funds are administered using the same mechanism as the PRF. HRSA began disbursing these funds to rural providers in November 2021.
[77]According to HRSA’s post-payment standard operating procedures, the agency seeks repayment and recovery of inaccurate and improper payments, which it defines as any payment that should not have been made or that was made in an incorrect amount.
[78]In addition to audits, officials told us that they also conduct assessments to determine appropriate use of PRF funds in accordance with the terms and conditions of the program. According to officials, assessments are generally used to review the use of payments from the COVID-19 Uninsured Program distributions rather than payments from general and targeted distributions.
[79]Pub. L. No. 116-136, § 3719, 134 Stat. at 426.
[80]Other distributions also included funding for treatment, testing, and vaccine administration, as well as funding for administrative contracts and full-time equivalents to support PRF activities.
[81]According to the White House, as of March 2022, the COVID-19 Uninsured Program stopped accepting new claims for testing and treatment, and as of April 2022, the COVID-19 Uninsured Program and COVID-19 Coverage Assistance Fund stopped accepting claims for vaccinations for the uninsured and underinsured.
[82]The disbursement of $74.8 billion represents about 87 percent of allocations of the current general distributions, and $55.1 billion represents about 99 percent of allocations from the targeted distributions.
[83]HRSA officials told us that there may be a few weeks of lag time between when providers successfully set up a payment account and when the funds are transferred.
[84]HRSA officials explained that providers may return funds for a variety of reasons, including if they believe (1) the original payment calculation sent to them was too high or they expect a reissuance of a different amount from HRSA—possibly a corrected lower amount or a reissuance to a different entity in their health care system—or (2) the funds were not needed and they have no intention of receiving a new amount through a reissued payment.
[85]HRSA officials told us that payments returned to HRSA’s claims reimbursement programs, including those for the uninsured and underinsured, are used for future payments by those programs and not reallocated by HRSA. These returned payments include overpayment amounts returned by a provider and overpayment amounts that are subtracted from a provider’s subsequent claims submitted to the program. There were no returned funds for administrative expenditures.
[86]When funds are returned, the disbursement totals reported are calculated after deducting the returned funds. Officials said that returned funds are not included in the disbursement totals shown in the above table and are available for subsequent allocations. The Consolidated Appropriations Act, 2021, provided that not less than 85 percent of PRF funds unobligated as of the date of enactment and funds recovered from providers after the date of enactment shall be for any successor to the Phase III General Distribution to reimburse health care providers based on applications that consider financial losses and changes in operating expenses attributable to COVID-19 occurring in the third and fourth quarters of 2020 and the first quarter of 2021.
[87]Throughout the enclosure, the term “post-payment reviews” refers to HRSA’s post-payment quality control reviews.
[88]As of January 2022, HRSA had identified 57 payment discrepancy types, and at least 15 were related to ineligible providers. HRSA officials updated this information to 58 payment discrepancy types as of March 2022.
[89]The number of payments was 753,625 as of February 28, 2022; the number of payments will grow over time as HRSA continues to disburse PRF payments while the COVID-19 pandemic continues and funds are available. Officials noted that payments may be reviewed multiple times as the payments may fall under multiple payment discrepancies.
[90]The agency has conducted two PRF risk assessments—one as part of the OMB A-123 requirement and another as an internal programmatic evaluation. HRSA has also conducted post-payment analyses to identify risks of overpayments. HRSA officials told us in January 2022 that they planned to use the risk assessment implemented as part of its programmatic risk evaluation in order to prioritize internal controls.
[91]In March 2022, HRSA officials told us that they had completed four additional final discrepancy memos but did not provide supporting reporting documentation.
[92]HRSA officials told us that post-payment reviews may remain open (1) to allow for further analysis, (2) to allow offsets by future payments, or (3) for policy decisions that may determine that repayments will not be sought.
[93]GAO-22-105051: Additional Actions Needed to Improve Accountability and Program Effectiveness of Federal Response. Washington, D.C., October 27, 2021.
[94]HRSA officials told us that the bank that issues PRF payments uses trace numbers to process payments and repayments.
[95]The audits will determine whether providers used payments to cover only COVID-19 eligible expenses or related revenue losses not reimbursed from other sources in accordance with laws and HRSA guidance. Providers may have received other assistance from several sources, including the Department of the Treasury, the Small Business Administration, the Federal Emergency Management Agency, the Paycheck Protection Program, and local, state, and tribal governments.
[96]HRSA officials noted that they would schedule audits to follow the receipt of the first round of provider reports, which were due by September 30, 2021—this deadline was subsequently extended until November 30, 2021. For the first PRF payments disbursed from April 10 to June 30, 2020, providers were required to use the funds by June 30, 2021, and report on the use of these funds no later than September 30, 2021—which was subsequently extended to November 30, 2021.
[97]Pandemic and All-Hazards Preparedness Act, Pub. L. No. 109-417, 120 Stat. 2831 (2006); Pandemic and All-Hazards Preparedness Reauthorization Act of 2013, Pub. L. No. 113-5, 127 Stat. 161 (2013); Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019, Pub. L. No. 116-22, 133 Stat. 905 (2019).
[98]The Pandemic and All-Hazards Preparedness Reauthorization Act of 2013 added biosurveillance activities to the measurable steps that HHS was to include in the implementation plan required to develop the network.
[99]Public health surveillance refers to the ongoing, systematic collection, analysis, and interpretation of health-related data essential to planning, implementation, and evaluation of public health practice. Definition adapted from Stephen B. Thacker and Guthrie S. Birkhead, “Surveillance,” in Field Epidemiology, ed. Michael B. Gregg (Oxford: Oxford University Press, 2008), 38-66.
[100]The Council of State and Territorial Epidemiologists works with CDC to recommend which diseases should be included in the National Notifiable Diseases Surveillance System and the development of standardized case definitions for these diseases each year. Through this system, about 3,000 local health departments transmit data electronically to 60 state, territorial, and other health departments, which in turn share the data with CDC.
[101]CARES Act, Pub. L. No. 116-136, div. B, tit. VII, 134 Stat. 281, 554. In addition to public health data modernization, ARPA includes a provision to “establish, expand, and maintain efforts to modernize the United States disease warning system to forecast and track hotspots for COVID–19, its variants, and emerging biological threats, including academic and workforce support for analytics and informatics infrastructure and data collection systems.” Pub. L. No. 117-2, § 2404, 135 Stat. 4, 42. CDC has received additional appropriations that may be used for data modernization. For example, the Paycheck Protection Program and Health Care Enhancement Act appropriated money to CDC that can be used for a variety of purposes, including public health data surveillance and analytics infrastructure modernization. Pub. L. No. 116-139, div. B, tit. I, 134 Stat. 620, 624 (2020).
[102]Data standards, for the purposes of this enclosure, refer to specifications for discrete data elements to be collected by public health entities, such as patient characteristics (e.g., name, sex, and race) and clinical information (e.g., diagnosis and test results), that include definitions, inclusion criteria, and formatting.
[103]CDC’s National Electronic Disease Surveillance System Base System integrates and transmits electronic data on infectious diseases from multiple sources, including state health departments, laboratories, and health care organizations. Also, according to CDC, states have the option of procuring commercial systems that are based on National Electronic Disease Surveillance System standards.
[104]According to CDC officials, CDC’s National Syndromic Surveillance Program also includes, to a lesser extent, data from inpatient care facilities and outpatient care facilities, such as urgent care centers.
[105]For example, according to the National Association of County and City Health Officials, the number of full-time equivalent employees in local public health departments decreased from 5.2 per 10,000 people in 2008 to 4.1 per 10,000 in 2019.
[106]Pub. L. No. 116-136, § 18115, 132 Stat. at 574. This requirement is in effect for the duration of the COVID-19 public health emergency declaration.
[107]According to CDC, a disease-specific message mapping guide is similar to a data dictionary and indicates the data elements (generic or disease-specific) and the valid values for those data elements and how they should be packaged into a case notification. The case notification is the set of information sent on an individual case from the state or local health department for inclusion in the surveillance data systems at CDC.
[108]According to CDC, the agency monitors its progress on a growing number of modernization projects through the Data Modernization Monitoring and Evaluation Hub. Through the hub, CDC reports it can monitor how the agency is using initiative-related investments, impacts individual projects are making, and impacts of the initiative. According to CDC, it also hosts a Data Modernization Implementation Support website (at https://www.cdc.gov/csels/dmi-support/index.html) that provides resources and information outlining CDC’s priority efforts to support public health departments and partners in implementing data modernization activities.
[109]A Sustainable Public Health Supply Chain, Exec. Order No. 14001, § 4, 86 Fed. Reg. 7,219, 7220-21 (Jan. 26, 2021).
[110]HHS and its interagency partners are referred to as an Interagency Policy Committee, which was established through the White House Domestic Policy Council system. Interagency partners include the Departments of Commerce, Defense, Energy, Homeland Security, State, and Veterans Affairs and the Office of Management and Budget, among others.
[111]The other five action items are each led by a different agency: (1) Department of State, (2) Department of Energy, (3) Federal Emergency Management Agency within the Department of Homeland Security, (4) the Office of Management and Budget, and (5) Department of Labor.
[112]We reviewed six POAMs for which HHS is the lead, and one POAM for which the Federal Emergency Management Agency within the Department of Homeland Security is the lead.
[113]ASPR officials stated that a version of the progress report would be made publicly available. However, some information may be national-security sensitive information, for example, and not be publicly released.
[114]Operation Warp Speed was established in May 2020 to accelerate the development, manufacturing, and distribution of COVID-19 vaccines. The name of this partnership was changed to the HHS-DOD COVID-19 Countermeasures Acceleration Group in April 2021, but for the purposes of this enclosure, we will refer to both iterations of the partnership as Operation Warp Speed.
[115]The five federal agencies were the Bureau of Prisons, DOD, Department of State, Department of Veterans Affairs, and Indian Health Service (IHS). The Department of Homeland Security was initially an awardee but chose to receive its vaccine doses through the Department of Veterans Affairs.
[116]In addition to vaccine allocations to awardees—the focus of this enclosure—in February 2021, the federal government separately implemented additional vaccine distribution programs, such as to retail pharmacies, as we described in two GAO reports issued in November 2021 and February 2022.
[117]According to DOD officials, the Coordinator of the White House Coronavirus Response reviewed and reaffirmed the population-based allocation methodology on January 22, 2021 following the transition to the new administration.
[118]FDA generally licenses biologics, including vaccines, through review of a biologics license application. See 42 U.S.C. § 262. An emergency use authorization (EUA) allows for the temporary use of vaccines without FDA licensure, provided certain statutory criteria are met. For example, it must be reasonable to believe that the vaccine may be effective and that the known and potential benefits of the vaccine outweigh the known and potential risks. See 21 U.S.C. § 360bbb-3.
[119]Pfizer’s COVID-19 vaccine was developed in collaboration with BioNTech.
[120]Janssen Pharmaceutical Companies are a part of Johnson & Johnson.
[121]Separate from the population-based allocation methodology, federal officials explained that beginning in September 2021, they implemented thresholds for the number of doses that jurisdictions could order, to help decrease the potential for expired doses and vaccine wastage. According to officials, they set and adjusted the thresholds based on distribution and administration rates, and communicated to jurisdictions that they should maintain 4-6 weeks of supply. Jurisdictions could also submit requests and receive approval to order doses above the threshold when necessary.
[122]For the 50 states and four cities, Operation Warp Speed officials used population data from the 2018 American Community Survey. For Puerto Rico, officials used the 2018 Puerto Rico Community Survey. For the other seven territories, officials used the population data as of November 2020 provided by the Central Intelligence Agency’s “World Factbook.” With the exception of DOD, each federal agency provided an estimate of the population it served to Operation Warp Speed in November 2020. Operation Warp Speed, which included DOD officials, estimated a population number for DOD. According to Operation Warp Speed officials, populations served by each federal agency may also be represented in the populations of the states, territories, and cities. A DOD official told us that the federal agency populations were relatively small, and therefore any double counting did not significantly affect allocations to states or cities.
[123]According to Operation Warp Speed officials, the Republic of the Marshall Islands, the Federated States of Micronesia, and the Republic of Palau did not have ultra-cold freezer capacity or dry-ice-making capabilities necessary to store the Pfizer vaccine. Therefore, officials did not allocate Pfizer vaccine doses to those three awardees, but instead provided the equivalent amount of the other available vaccines. In addition, according to Operation Warp Speed officials, the monthly allocation of vaccine to the Department of State allowed for the efficient transportation of vaccines by plane to the department’s diplomatic locations worldwide.
[124]Pfizer’s minimum order quantity was originally 1,950 doses because each order was a minimum of two trays, each tray held 195 vials, and each vial held five doses. Then, in January 2021, FDA determined that up to 6 doses of Pfizer’s vaccine could be extracted from a vial instead of 5, so the minimum order quantity increased to 2,340. According to HHS officials, as of February 24, 2022, Pfizer’s vaccine was available in minimum dose orders of 300 (for individuals aged 12 years and older) and in minimum dose orders of 100 (for individuals aged 5 through 11); Moderna’s vaccine in minimum dose orders of 100; and Janssen’s vaccine in minimum dose orders of 100.
[125]IHS is an agency within HHS that provides health care for more than 2 million American Indians and Alaska Natives who are members or descendants of federally recognized tribes.
[126]As of April 1, 2022, CDC considered individuals to be fully vaccinated if they had received their primary series of COVID-19 vaccines—that is, for most people, that they had received either two doses of a two-dose vaccine or one dose of the single-dose vaccine. See CDC, “COVID Data Tracker: COVID-19 Vaccinations in the United States,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-total-admin-rate-total.
[127]A booster dose is a subsequent dose of vaccine administered to improve protection, which may have waned over time after primary series vaccination, according to CDC.
[128]This amount does not include all vaccine-related funding. HHS reported allocations, obligations, and expenditures for a variety of COVID-19 response activity categories, including vaccines. When funding was related to multiple response categories, it was only assigned to one. For example, certain funds for vaccine distribution were included in the response activity category for “support to states, localities, territories, and tribal organizations” rather than in the “vaccine activity” category.
[129]As of April 1, 2022, the Pfizer vaccine, which was developed in collaboration with BioNTech, was licensed for individuals aged 16 years and older (Comirnaty) and was also available under an emergency use authorization (EUA) for individuals aged 5 years and older. Typically, the Food and Drug Administration (FDA) must license a vaccine before it can be marketed in the U.S. See 42 U.S.C. § 262. However, during an emergency, FDA may temporarily allow the use of unlicensed vaccines through an EUA, provided certain statutory criteria are met. See 21 U.S.C. § 360bbb-3. The Moderna vaccine was licensed for individuals aged 18 years and older (Spikevax), and the Janssen vaccine was available under an EUA for individuals 18 years and older. Janssen Pharmaceutical Companies are a part of Johnson & Johnson.
[130]These are individuals considered to be moderately or severely immunocompromised who have a weakened immune system because of certain conditions or treatments, such as people who have undergone solid organ transplantation and are taking medicine to suppress the immune system, according to CDC.
[131]In November 2021, CDC said it had not established a timeline for an after action review, as the agency remained involved in the response to the pandemic. CDC said that in the meantime it continued to incorporate continuous feedback from stakeholders.
[132]On February 1, 2022, Pfizer requested FDA amend the EUA for its COVID-19 vaccine to include children aged 6 months through 4 years. Due to additional findings from an ongoing clinical trial, FDA postponed a decision and, as of April 1, 2022, had not authorized the Pfizer vaccine for children under 5 years.
[133]Although COVID-19 vaccine was available to individuals aged 16-17 years in December 2020, adults were prioritized for vaccination until May 2021, according to CDC officials.
[135]For example, in early 2022, an estimated 32 percent of parents with children aged 5–11 years said their child had received at least one dose of COVID-19 vaccine, 8 percent said their child will get vaccinated, 27 percent said their child would probably get vaccinated or were unsure, and 33 percent said their child probably or definitely will not get vaccinated, according to CDC. These estimates are from CDC’s National Immunization Survey Child COVID Module, data collection period January 30 through February 26, 2022, according to CDC. See https://covid.cdc.gov/covid-data-tracker/#vaccine-confidence, accessed April 1, 2022.
[136]After FDA authorizes or licenses a COVID-19 vaccine, CDC’s Advisory Committee on Immunization Practices, a panel of medical and public health experts, typically meets to review available data and make recommendations on vaccines. CDC’s vaccine recommendations are formulated by the advisory committee’s recommendations and approved by the CDC Director.
[137]In March 2022, CDC also recommended that adults who received a primary and booster dose of the Janssen vaccine receive a second booster dose of the Pfizer or Moderna vaccines.
[138]In December 2021, CDC recommended that in most situations, the Pfizer or Moderna vaccines are preferred over the Janssen vaccine for primary and booster vaccination due to the risk of a rare but serious adverse event with the Janssen vaccine. The Janssen vaccine may be considered in some situations, according to CDC, including for persons who (1) had a severe reaction after a dose of Pfizer or Moderna vaccine or have a severe allergy to an ingredient in the Pfizer or Moderna vaccines; (2) who would otherwise remain unvaccinated for COVID-19 due to limited access to Pfizer and Moderna vaccines; or (3) who want to get the Janssen vaccine despite the safety concerns.
[139]CDC counts people as having received a booster dose if they are fully vaccinated and received another dose of COVID-19 vaccine since August 13, 2021. CDC’s count does not distinguish if an individual is immunocompromised and received an additional dose as part of a primary series. According to CDC, these data may underestimate booster doses because of challenges in linking doses when an individual is vaccinated in different jurisdictions or by different providers. See CDC, “COVID Data Tracker: COVID-19 Vaccinations in the United States,” accessed April 1, 2022, https://covid.cdc.gov/covid-data-tracker/#vaccinations_vacc-total-admin-rate-total.
[140]According to HHS officials, the threshold system was implemented to help decrease the potential for expired doses and vaccine wastage. Thresholds were established to try to “right size” the inventory in the field based on how much vaccine was administered, how much vaccine remained in inventory, and how much vaccine was ordered, according to HHS officials.
[141]For example, in September 2021, CDC’s recommendation stated that some groups “should” receive a Pfizer vaccine booster dose, including individuals aged 50–64 years with underlying medical conditions who received the Pfizer vaccine as their primary series. At the same time, however, CDC’s recommendation stated that other groups “may” receive a Pfizer vaccine booster dose, including individuals aged 18–49 years with underlying medical conditions who received the Pfizer vaccine as their primary series.
[142]For perspectives of state, territorial, and local officials, including health officials, we interviewed representatives from the Association of Immunization Managers, the Association of State and Territorial Health Officials, the National Association of County and City Health Officials, and the National Governors Association. For perspectives of providers, we interviewed representatives from the American Academy of Pediatrics.
[143]Actions taken also included a 100 percent subsidy through September 30, 2021, for benefits under the Consolidated Omnibus Budget Reconciliation Act of 1985 (COBRA) and COBRA-like provisions for state and local employees. COBRA provides certain individuals who lose their employer-sponsored health coverage the option to continue it for limited periods of time under certain circumstances.
[144]States are responsible for determining applicants’ eligibility for Medicaid, including re-determining eligibility at regular intervals and disenrolling individuals who are no longer eligible. In assessing eligibility for Medicaid, states must determine whether applicants meet eligibility criteria, such as financial and citizenship requirements.
[145]See Families First Coronavirus Response Act, Pub. L. No. 116-127, div. F, § 6008, 134 Stat. 205 (2020) (“FFCRA”).
[146]The Department of Health and Human Services declared a public health emergency for COVID-19 on January 31, 2020. Since then, the public health emergency has been extended several times, most recently on April 12, 2022.
[147]According to CMS, for the 2022 plan year, 33 states are using the HealthCare.gov platform, including the federally-facilitated exchange and state-based exchanges, and 13 states and the District of Columbia operate their own state-based exchanges.
[148]Pub. L. No. 117-2, § 9661, 135 Stat. 4, 182 (codified as amended at 26 U.S.C. § 36B).
[149]According to officials responsible for federal surveys, COVID-19 may have affected federal survey collection efforts and therefore the accuracy of 2020 estimates. For example, the U.S. Census Bureau switched from its usual in-person data collection efforts to telephone data collection for the Annual Social and Economic Supplement of the Current Population Survey in March 2020. They reported that the March 2020 response rate was 10 points lower than prior years for this survey. Further, due to COVID-19 data collection challenges, the 2020 American Community Survey results were released as experimental estimates, which the U.S. Census Bureau defines as innovative statistical products created using new data sources or methodologies in the absence of other relevant products, but which may not meet all of the U.S. Census Bureau’s quality standards.
[150]An example of ESI loss expectations is detailed in an October 2020 issue brief by the Commonwealth Fund that predicted that COVID job losses would result in an 8 percent reduction in total ESI coverage in the United States. See Paul Fronstin and Stephen A. Woodbury, “How Many Americans Have Lost Jobs with Employer Health Coverage During the Pandemic,” Commonwealth Fund (October 2020).
[151]Like for federal survey data about uninsurance, some officials have raised concerns about the quality of federal survey data for ESI coverage in 2020. According to the Department of Health and Human Services, the COVID-19 pandemic created challenges in conducting government-administered surveys that provide the most robust measurement of insurance coverage. As a result, survey measurement of insurance may have more uncertainty than normal, though the magnitude of these impacts are not yet known.
[152]See U.S. Department of Commerce, U.S. Census Bureau, Health Insurance Coverage in the United States: 2020 (Washington, D.C.: September 2021).
[153]See Agency for Healthcare Research and Quality, Statistical Brief #536: Trends in Health Insurance at Private Employers, 2008-2020 (Rockville, Md..: September 2021).
[154]See Congressional Budget Office, Federal Subsidies for Health Insurance Coverage for People Under 65: 2020 to 2030 (September 2020).
[155]See U.S. Department of Labor, Bureau of Labor Statistics, As the COVID-19 pandemic affects the nation, hires and turnover reach record highs in 2020 (Washington, D.C.: June 2021).
[156]See U.S. Department of Labor, Bureau of Labor Statistics, The Employment Situation—June 2020, (Washington, D.C.: July 2, 2020).
[157]See U.S. Department of Labor, Bureau of Labor Statistics, Business Response Survey to the Coronavirus Pandemic, (Washington, D.C.: Dec. 7, 2020).
[158]See FFCRA § 6008(b)(3), 134 Stat. at 208 (continuous coverage requirement for temporary increase of Medicaid FMAP).
[159]See Department of Health and Human Services, Centers for Medicare & Medicaid Services, October and November 2021 Medicaid and CHIP Enrollment Trends Snapshot.
[161]On April 12, 2022, the Secretary of the Department of Health and Human Services extended the public health emergency for 90 days or through the duration of the emergency.
[162]See Department of Health and Human Services, Centers for Medicare & Medicaid Services, RE: Promoting Continuity of Coverage and Distributing Eligibility and Enrollment Workload in Medicaid, the Children’s Health Insurance Program (CHIP), and Basic Health Program (BHP) Upon Conclusion of the COVID-19 Public Health Emergency, SHO# 22-001 (Baltimore, Md.: March 2022). Prior guidance suggested all renewals and other actions must be completed within the 12-month unwinding period. See Department of Health and Human Services, Centers for Medicare & Medicaid Services, RE: Updated Guidance Related to Planning for the Resumption of Normal State Medicaid, Children’s Health Insurance Program (CHIP), and Basic Health Program (BHP) Operations Upon Conclusion of the COVID-19 Public Health Emergency, SHO #21-002 (Baltimore, Md.: August 2021).
[163]The 2022 open enrollment period extended from November 1, 2021, through January 15, 2022.
[164]See Centers for Medicare & Medicaid Services, Health Insurance Marketplaces 2022 Open Enrollment Report.
[165]See Centers for Medicare & Medicaid Services, 2021 Final Marketplace Special Enrollment Period Report.
[166]All of the states that operated their own exchanges also opened similar special enrollment periods in response to COVID-19, though timeframes varied.
[167]Qualifying life events include losing minimum essential health coverage, which may include ESI. Health insurance that meets the definition of “minimum essential coverage” includes certain types of government-sponsored coverage (such as Medicare Part A or most Medicaid coverage) as well as most types of private insurance plans that provide benefits consistent with the law, but does not include coverage that provides limited benefits.
[168]A 2016 study by the Urban Institute suggested that the special enrollment period verification process would probably reduce enrollment among eligible people because consumers are less likely to enroll when administrative requirements are added. See Stan Dorn, “Helping Special Enrollment Periods Work under the Affordable Care Act,” Urban Institute (June 2016).
[169]See 87 Fed. Reg. 20,354 (proposed April 7, 2022).
[170]A 2018 Health Affairs article reported that found that people living in counties with higher numbers of exchange ads sponsored by the federal government were significantly more likely to shop for and enroll in an exchange plan. See Sarah E. Gollust, et. al., “TV Advertising Volumes Were Associated With Insurance Marketplace Shopping And Enrollment In 2014,” Health Affairs (June 2018).
[171]See Jennifer M. Haley and Erik Wengle, “Uninsured Adults’ Marketplace Knowledge Gaps Persisted in April 2021,” Urban Institute (September 2021).
[172]According to CMS, navigators may also assist consumers in determining their eligibility for and enrolling in Medicaid.
[173]CMS officials told us that due to contracts that have grant award dates early in the fiscal year, CMS requires a reasonably substantial account balance to ensure sufficient funds are in place at time of the grant award.
[174]See Stan Dorn, James C. Capretta, Lanhee J. Chen, “Making Health Insurance Enrollment As Automatic As Possible (Part 1),” Health Affairs (May 2018)
[175] James C. Capretta, “Covering the Uninsured in the United States’ Multi-Payer Health System,” American Enterprise Institute (May 2021).
[176]See Paul N. Van De Water, “Automatic Enrollment in Health Insurance Would Be Complex and Difficult to Administer.” Center on Budget and Policy Priorities (June 2017).
[177]To be eligible for regular UI benefits, applicants generally must be able and available to work and actively seeking work. 42 U.S.C. § 503(a)(12). Administration of the regular UI program is financed by a federal tax on employers, according to DOL.
[178]Pub. L. No. 116-136, § 2102, 134 Stat. 281, 313 (2020), as amended.
[179]Pub. L. No. 116-136, § 2104, 134 Stat. at 318, as amended.
[180]Pub. L. No. 116-136, § 2107, 134 Stat. at 323, as amended.
[181]The MEUC program, which was voluntary for states, authorized an additional $100 weekly benefit for certain UI claimants who received at least $5,000 of self-employment income in the most recent tax year prior to their application for UI benefits. Pub. L. No. 117-2, § 9013(a), 135 Stat. 4, 119; Pub. L. No. 116-260, div. N, tit. II, § 261(a)(1), 134 Stat. 1182, 1961.
[182]According to DOL, 51 states and territories elected to participate in the MEUC program, with Idaho and South Dakota opting not to participate, but 23 states terminated their participation in June or July 2021. The remaining 28 states and territories continued participating in the MEUC program until it expired in September 2021, including Maryland, which intended to terminate participation but did not because of litigation at the state level, according to DOL. As of February 7, 2022, not all participating states and territories had begun paying MEUC benefits, according to DOL.
[183]After the PEUC program ended in September 2021, Extended Benefits were available to claimants who exhausted their regular UI benefits in certain states.DOL reported that as of April 10, 2022, the Extended Benefits program was not activated in any state. The Extended Benefits program was activated in all states and territories except South Dakota at some point during the pandemic, according to DOL.
[184]While the CARES Act UI programs were federally funded, regular UI is funded primarily through state and federal taxes on employers. When a state exhausts the funds available for regular UI benefits, it may borrow from the federal government. According to DOL data, even before the pandemic, many states were not collecting enough UI tax revenue to satisfy the solvency standard specified in DOL regulations providing for interest-free loans to states. See 20 C.F.R. § 606.32.
[185]The CARES Act established the $150 billion Coronavirus Relief Fund to provide payments to state, local, territorial, and tribal governments to cover the costs of necessary expenditures incurred because of the COVID-19 pandemic. Pub. L. No. 116-136, § 5001, 134 Stat. 281, 501-504. In its guidance on the Coronavirus Relief Fund, Treasury reported that states may use this funding to make payments to their state UI trust funds to prevent expenses related to the COVID-19 public health emergency from causing these UI trust funds to become insolvent. The Consolidated Appropriations Act, 2021 extended the period for states and other entities to use these funds through December 31, 2021. Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. 1182, 2145.
[186]Coronavirus State and Local Fiscal Recovery Funds, 86 Fed. Reg. 26,786, 26,822 (May 17, 2021). Funds may be used to restore a state’s unemployment trust fund to its balance on January 27, 2020, or to pay back advances received for the payment of benefits between January 27, 2020, and May 17, 2021. 31 C.F.R. § 35.6(b)(5).
[187]For this enclosure and prior enclosures, we used claims numbers that are not seasonally adjusted. Claims counts are from DOL data we obtained on April 4, 2022, and include any adjustments submitted by states and territories as of then. States and territories may revise and resubmit data for 3 years, according to DOL officials. An initial claim is the first claim filed by an individual to determine eligibility for UI benefits after separating from an employer. According to DOL, after filing an initial claim to establish eligibility for UI benefits, individuals then generally file a continued claim on a weekly basis to claim benefits for the preceding week of unemployment.
[188]Counts for the week ending on March 26, 2022, reflect advance initial claims, which are preliminary and subject to revision.
[189]The number of regular UI continued claims submitted each week from December 12, 2021, through March 12, 2022, was lower than the number submitted during each of the corresponding weeks in 2019.
[190]During the week ending on March 12, 2022, states also reported that 57,474 continued claims were submitted in other programs, including Extended Benefits, programs for federal employees and former service members, other state benefit programs, and Short-Time Compensation or work-sharing. In addition, states reported continued claims submitted that week for the PUA and PEUC programs, which expired on September 6, 2021. According to DOL, these continued claims were for weeks of unemployment before the programs expired.
[191]After exhausting regular UI benefits—generally available for up to 26 weeks in most states, according to DOL—eligible individuals were generally able to apply for (1) PEUC; then (2) the Extended Benefits program, if activated in a state; and then (3) PUA benefits, in certain circumstances.
[192]One of DOL’s core performance measures is the percentage of all regular UI first payments made within either 14 or 21 days of the first week of benefits for which claimants are eligible; DOL considers 87 percent to be an acceptable level of performance. For the purposes of this enclosure, we focus on payments made within 21 days.
[193]We analyzed first-payment timeliness data that states had reported to DOL as of March 28, 2022. At that point, all 53 states and territories had reported data for February 2022 and prior months.
[194]While some overpayments may be caused by unintentional error, fraud involves obtaining something of value through willful misrepresentation. Whether an act is fraudulent is determined through the judicial process or other adjudicative systems. According to DOL, in the case of these payments made by states, whether an act is fraudulent is defined by states and must be determined through the appropriate adjudication process.
[195]States and territories report PUA overpayments data to DOL on a monthly basis, and the total amount shown includes overpayments related to identity theft. We accessed the PUA overpayments data on March 28, 2022; these data are subject to change as more states report data and as states revise previously reported data. For consistency with the regular UI overpayment data, which states and territories report on a quarterly basis, the PUA overpayment amount shown is for April 2020 through December 2021. As of March 28, 2022, 43 states and territories had reported approximately $0.5 billion of additional PUA overpayments since December 2021. The number of states and territories that have reported PUA overpayments data varies by month; for example, 46 reported overpayment amounts in December 2021, and 26 reported overpayment amounts in February 2022.
[196]FPUC benefits were paid in addition to other UI benefits. About 92 percent of reported FPUC overpayment amounts were paid on regular UI or PUA claims.
[197]Due to rounding, the sum of these overpayment amounts by program differs from the total overpayment amount. States and territories report regular UI, Extended Benefits, PEUC, and FPUC overpayments data to DOL on a quarterly basis. We accessed the data on March 28, 2022. At that point, not all states and territories had reported overpayment amounts for all programs in all quarters. States and territories may revise the amount of overpayments they have identified for 3 years after the reporting quarter, according to DOL officials.
[198]We accessed the recovered overpayments data on March 28, 2022; these data are subject to change as more states and territories report data and as states and territories revise previously reported data.
[199]The total PUA amount shown also includes recovered overpayments related to identity theft. As of March 28, 2022, 35 states had reported about $13 million of additional PUA overpayments recovered since December 2021. As of March 28, 2022, states and territories had also reported recovering about $2.0 billion in the regular UI and Extended Benefits programs from April 2020 through December 2021. However, the amounts recovered for any quarter may be from overpayments established in many previous periods. Thus, the total amount does not measure the extent to which overpayments made during the pandemic have been recovered.
[200]According to DOL, states generally may waive a nonfraud overpayment, in accordance with state law and an established waiver policy, if the overpayment was not the fault of the claimant and if requiring repayment would be against equity and good conscience or would otherwise defeat the purpose of the UI law. States were authorized to waive PUA overpayments under the Consolidated Appropriations Act, 2021. According to this act, if an individual receives PUA benefits they were not entitled to, the state must generally require such individuals to repay the amount; however, the state can waive that requirement if the individual was without fault and repayment would be contrary to equity and good conscience. Pub. L. No. 116-260, div. N, tit. II, § 201(d), 134 Stat. 1182, 1952. According to DOL, states are able to retroactively waive PUA overpayments from the beginning of the program onward.
[201]We accessed the waived overpayments data on March 28, 2022; these data are subject to change as more states and territories report data and as states and territories revise previously reported data.
[203]As of March 28, 2022, 19 states had reported about $0.1 billion of additional PUA overpayments waived since December 2021.
[204]According to DOL guidance, an overpayment is established when a formal notice of determination has been issued. Whether an act is fraudulent is determined through the judicial or other adjudicative systems. According to DOL, because states may use different definitions for categorizing an overpayment as fraudulent, an overpayment that is classified as fraudulent in one state might not be classified as fraudulent in another state.
[205]Due to rounding, the sum of these fraud overpayment amounts by program differs from the total fraud overpayment amount. We accessed the fraud overpayments data on March 28, 2022; these data are subject to change as more states and territories report data and as states and territories revise previously reported data. The total PUA amount shown also includes fraud overpayments related to identity theft. As of March 28, 2022, 35 states and territories had reported about $26 million of additional PUA fraud overpayments since December 2021.
[206]An improper payment is defined as any payment that should not have been made or that was made in an incorrect amount (including overpayments and underpayments) under statutory, contractual, administrative, or other legally applicable requirements. 31 U.S.C. § 3351(4).
[207]The estimated improper payment amount and rate include unknown payments. For the purpose of producing an improper payment estimate, when the executive agency cannot determine, due to lacking or insufficient documentation, whether a payment is proper or not, the payment shall be treated as an improper payment. 31 U.S.C. § 3352(c)(2).
[208]According to OMB guidance, OMB does not formally approve improper payment estimation methodologies submitted by agencies prior to implementation. See Office of Management and Budget, Appendix C to OMBCircular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-21-19 (Washington, D.C.: Mar. 5, 2021).
[210]For more information about these grants, including other allowable uses of these funds, see Department of Labor, Grant Opportunity for Promoting Equitable Access to Unemployment Compensation (UC) Programs, UIPL 23-21 (Washington, D.C.: Aug. 17, 2021). State grant applications were due on December 31, 2021.
[211]For more information about these grants, see Department of Labor, Grant Opportunity for States to Participate in the American Rescue Plan Act (ARPA) Unemployment Insurance (UI) Navigator Program, UIPL 11-22 (Washington, D.C.: Jan. 31, 2022).
[212]The American Rescue Plan Act of 2021 appropriated $9.961 billion for the HAF and set aside up to $40 million for Treasury to administer and oversee the fund, and up to $2.6 million for the Treasury Office of Inspector General to oversee the fund. See Pub L. No. 117-2, tit. III, §§ 3206(a),(d), 135 Stat. 4, 63 (2021).
[213]Department of the Treasury, Data and Methodology for State and Territory Allocations (Washington, D.C.: April 14, 2021). The act also set aside a total of $30 million for territories (Guam, American Samoa, the U.S. Virgin Islands, and the Commonwealth of the Northern Mariana Islands), which were allocated based on population. Tribal allocations were based on the formulas used for the Emergency Rental Assistance Program under the Consolidated Appropriations Act, 2021. See American Rescue Plan Act of 2021 §§ 3206(d),(f) (to be codified at 15 U.S.C. 9058d(d),(f)); Consolidated Appropriations Act, Pub. L. No. 116-260, div. N, tit. V, § 501(b)(2)(A), 134 Stat. 1182, 2069-78 (2020) (to be codified at 15 U.S.C. § 9058a(b)(2)(A).
[214]American Rescue Plan Act of 2021 § 3206(c)(1) (to be codified at 15 U.S.C. § 9058d(c)(1)). Department of the Treasury, Homeowner Assistance Fund Guidance, (Washington, D.C.: Feb. 24, 2022).
[215]Treasury’s guidance does not specify how much of the 15 percent participants can spend on each allowable activity.
[216]Department of the Treasury, Homeowner Assistance Fund Guidance.
[217]American Rescue Plan Act of 2021 § 3206(c)(2) (to be codified at 15 U.S.C. § 9058d(c)(2)). Treasury defines socially disadvantaged individuals as those whose ability to purchase or own a home has been impaired due to diminished access to credit on reasonable terms as compared to others in comparable economic circumstances, based on disparities in homeownership rates in the HAF participant’s jurisdiction as documented by the U.S. Census. Department of the Treasury, Homeowner Assistance Fund Guidance.
[218]Pub. L. No. 116-136, div. A, § 4022, 134 Stat. 490 (2020). Federally backed mortgages are those that federal entities insure, guarantee, directly originate, purchase, or securitize.
[219]Consumer Financial Protection Bureau, Protections for Borrowers Affected by the COVID-19 Emergency Under the Real Estate Settlement Procedures Act (RESPA), Regulation X, 86 Fed. Reg. 34848 (June 30, 2021).
[220]Black Knight, Black Knight’s First Look At January 2022 Mortgage Data, February 24, 2022; Black Knight, Mortgage Monitor December 2021 Report, February 7, 2022.
[221]Illinois requested a reduced second payment because its HAF plan included some but not all of its planned program elements. Treasury officials said Illinois plans to submit another HAF plan in the future detailing the remaining use of its allocation.
[222]Department of the Treasury, Homeowner Assistance Fund Guidance on Required Interim Report (Washington, D.C.: Feb. 17, 2022).
[223]Pub. L. No. 117-2, § 9611, 135 Stat. 4, 144–150 (2021), codified at 26 U.S.C. §§ 24(i)-(j), 7527A. ARPA made several temporary changes that expanded eligibility for the CTC to additional qualified individuals and increased the amount of the credit. These changes included temporarily eliminating the earned income requirement for eligible individuals to receive the refundable CTC. ARPA also temporarily increased the maximum amount of the CTC—raising it from $2,000 per any qualifying child to $3,600 for a young qualifying child (0 to 5 years old) and $3,000 for an older qualifying child (6 to 17 years old).
[224]ARPA required Treasury to establish an online portal that allowed taxpayers to elect not to receive advance CTC payments, among other things. Pub. L. No. 117-2, § 9611, 135 Stat. at 147, codified at 26 U.S.C. § 7527A(c)(1). As of December, 31, 2021, 2.1 million individuals with eligible children had used the CTC Update Portal to make such an election. Individuals who elected not to receive the advance CTC payments were eligible for the total amount when they filed their 2021 taxes in 2022.
[226]United States Census Bureau, “Harder to Pay the Bills Now That Child Tax Credit Payments Have Ended” (Washington, D.C.: Feb. 28, 2022), accessed March 31, 2022, https://www.census.gov/library/stories/2022/02/harder-to-pay-bills-now-that-child-tax-credit-payments-have-ended.html. The Household Pulse Survey surveyed individuals from late January 2022 to early February 2022 after the last round of advance CTC payments. Individuals were randomly selected and may not have been the same individuals interviewed for the August 2021 survey.
[227]When IRS processed the advance CTC payments, IRS used individuals’ most recent 2020 tax return, or the 2019 return if the 2020 return was not available. Eligible individuals who used IRS’s Non-Filer Sign-up Tool in 2020 or 2021 also received advance CTC payments.
[228]Taxpayers who would otherwise be required to repay advance CTC payments to IRS as an additional income tax may be protected by a statutory safe harbor. Taxpayers will not qualify for any repayment protection if their modified adjusted gross income is at or above certain amounts based on the filing status on their 2021 tax return. These amounts are $120,000 for those who are married and filing a joint return or are filing as a qualifying widow or widower; $100,000 for those who are filing as a head of household; and $80,000 for single filers or for those who are married and filing a separate return. Pub. L. No. 117-2, § 9611(b)(2), 135 Stat. at 148–149, codified at 24 U.S.C. § 24(j).
[229]Pub. L. No. 117-2, § 9601, 135 Stat. at 138–144. The CARES Act (in March 2020) and the Consolidated Appropriations Act, 2021 (in December 2020) respectively authorized Treasury and IRS to issue EIP 1 and EIP 2 as direct payments to help individuals address financial stress due to the pandemic. Pub. L. No. 116-136, § 2201, 134 Stat. 281, 335–340 (2020); Pub. L. No. 116-260, § 272, 134 Stat. 1182, 1965–1976 (2020). IRS issued EIP 3 from March 17, 2021 to December 31, 2021. Pub. L. No. 117-2, § 9601(a), 135 Stat. at 140–141, codified at 26 U.S.C. § 6428B.
[230]The last day IRS issued EIP 3 payments was December 17, 2021.
[231]The amount of the RRC would equal the amount of the credit, as reduced by the amount of any EIP 3.
[232]The filing deadline for most individuals to complete a 2021 tax return was April 18, 2022. Individuals requesting an extension may have until October 17, 2022.
[234]IRS established a vendor hotline to address EIP phone calls to reduce the number of phone calls to IRS’s customer service. In the summer 2021, IRS established a similar hotline to address advance CTC questions. The customer service vendor does not have access to taxpayer accounts.
[235]IRS defines its telephone “level of service” as the percentage of taxpayers seeking and reaching live assistance. This estimated target is based on IRS’s projections for the volume of incoming calls and staffing levels.
[236]IRS’s Error Resolution System is a computer program that allows for review and correction to systemically identified errors on tax returns prior to completing the processing of the return. IRS has the authority to correct some types of errors; other errors require the taxpayer to provide additional information.
[237]IRS suspends returns that contain errors and prevent IRS’s systems from processing the returns automatically. Such errors include math errors or discrepancies in income amounts reported on the taxpayer’s return that do not match IRS records.
[238]The CTC Update Portal allowed qualified individuals to check their eligibility for the advance payments, opt out of receiving the payments, update their bank account information, and change their mailing address. Individuals could make changes from June to November 2021.
[239]Login.gov is a General Services Administration shared service that allows the public to use one common login to interact with participating agencies’ systems.
[240]The Coronavirus State and Local Fiscal Recovery Fund, established under the ARPA and administered by Treasury, allocated $350 billion to the states, the District of Columbia, local governments, tribal governments, and U.S. territories to help cover a broad range of costs stemming from the fiscal effects of the COVID-19 pandemic. Pub. L. No. Pub. L. No. 117-2, § 9901, 135 Stat. at 223, codified at 42 U.S.C. §§ 802-803; 87 Fed. Reg. 4338, 4362, 4369 (Jan. 27, 2022).
[241]Taxpayer Experience Days were conducted on February 12, March 12, April 9, and May 14, 2022.
[242]At the time of publication, IRS was unable to provide the attendance level of the April 9, 2022 event.
[243]Department of the Treasury Internal Revenue Service, Taxpayer First Act Report to Congress, Publication 5426 Catalog Number 74637F (Washington, D.C.: January 2021).
[244]All references to the EIDL program in this report refer to the program administered in response to the COVID-19 pandemic unless otherwise noted.
[245]EIDL loans are limited by statute to a maximum of $2 million. However, SBA set lower maximum amounts for periods in 2020 and 2021. From March 16, 2020 through May 3, 2020, SBA limited the maximum loan amount to $500,000, even if the calculated economic injury exceeded that amount. From May 4, 2020, through April 5, 2021, SBA limited the maximum loan amount to $150,000. Beginning on April 6, 2021, SBA increased the loan limit back to $500,000. In September 2021, SBA increased the loan limit to $2 million.
[246]When implementing the advances under the CARES Act, SBA provided advances in the amount of $1,000 per employee up to a maximum of $10,000.
[247]The Consolidated Appropriations Act, 2021 defines economic loss as the amount by which the gross receipts of the covered entity declined during an 8-week period between March 2, 2020, and December 31, 2021, relative to a comparable 8-week period immediately preceding March 2, 2020, or during 2019. For seasonal businesses SBA shall determine the economic loss as appropriate.
[248]These eligible entities qualify for the full amount of $10,000 in targeted advances—regardless of their number of employees—minus the amount they received under the CARES Act advances, which SBA based on employee numbers.
[249]The Infrastructure Investment and Jobs Act rescinded the unobligated amount up to $17.6 billion for the targeted EIDL advances provided under the Consolidated Appropriations Act, 2021, but according to SBA only approximately $15.8 billion was unobligated at the time of rescission.
[250]We excluded from this calculation the 70,936 withdrawn applications. Applications can also be automatically declined because of fraud alerts, the lack of an economic injury, or if the loans were to be used for a prohibited activity.
[251]We excluded from this calculation the 115,658 withdrawn applications.
[252]We excluded from this calculation the 141,934 withdrawn applications.
[253]We excluded from this calculation the 3,458 withdrawn applications. Declined applicants can request that SBA reconsider their applications. Applicants who have their reconsideration requests denied can appeal SBA’s decision. We reported in February 2020 that SBA received about 15,000 requests for reconsideration following the 2017 hurricanes. Of the requests SBA accepted, about half had their applications approved, about 30 percent were denied, and about 20 percent were withdrawn.
[254]The CARES Act restricted SBA from obtaining federal tax transcripts—typically a component of SBA’s review of a disaster loan application—as part of the EIDL application process. The Consolidated Appropriations Act, 2021 removed this restriction. SBA said they had other controls available, such as validations from secretaries of state to confirm that the borrowers were in business at the time they claimed they were.
[255]SBA had provided about 5,000 advances totaling about $26 million to potentially ineligible businesses in three types of industries—adult entertainment, casino gambling, and marijuana retail—as of July 14, 2020. In addition, SBA had approved at least 3,000 loans totaling about $156 million to businesses that SBA policies state were ineligible for the EIDL program, such as real estate developers and multilevel marketers, as of September 30, 2020.
[256]In September 2015, we recommended that SBA develop its enterprise risk management consistent with GAO's risk management framework and document the specific steps that the agency planned to take to implement its enterprise risk management process. In response to our recommendation, SBA developed additional guidance on its process in June 2016.
[257]Enterprise risk management is an agency-wide approach to addressing the full spectrum of the organization’s significant risks by understanding the combined impact of risks as an interrelated portfolio, rather than addressing risks only within silos.
[258]SBA’s fiscal year 2020 and 2021 consolidated financial statements received a disclaimer of opinion, meaning the auditor was unable to express an opinion due to insufficient evidence. As the basis for the disclaimers, the auditor reported that SBA was unable to provide adequate evidence to support a significant number of transactions and account balances due to inadequate processes and controls related to its implementation of its programs authorized under the CARES Act and related legislation, including EIDL.
[259]As noted below, SBA is taking steps to complete its fraud risk assessment including designating an antifraud entity.
[260]These standard operating procedures apply to the EIDL program broadly, not only in response to COVID-19.
[261]In addition, approximately $15.8 billion of appropriations for targeted and supplemental targeted EIDL advances were unused and had been rescinded by the deadline for accepting new applications for the EIDL program in response to COVID-19. By statute, these advances were limited to entities in low-income areas suffering economic losses greater than 30 percent and 50 percent, respectively. We reported in January 2022 that SBA officials said that demonstrating the requisite revenue decline was burdensome for borrowers.
[262]The facilities were authorized under Section 13(3) of the Federal Reserve Act, which permits the Federal Reserve to provide emergency lending, and were approved by the Secretary of the Treasury. The CARES Act-supported facilities were the Primary Market Corporate Credit Facility, Secondary Market Corporate Credit Facility, Municipal Liquidity Facility, Term Asset-Backed Securities Loan Facility, and five facilities under the Main Street Lending Program—the Main Street New Loan Facility, Main Street Priority Loan Facility, Main Street Expanded Loan Facility, Nonprofit Organization New Loan Facility, and Nonprofit Organization Expanded Loan Facility.
[263]The facilities not supported with CARES Act funds were the Commercial Paper Funding Facility, Money Market Mutual Fund Liquidity Facility, Primary Dealer Credit Facility, and the Paycheck Protection Program Liquidity Facility.
[264]The Federal Reserve established the Paycheck Protection Program Liquidity Facility under its Section 13(3) authority to encourage lender participation in the Paycheck Protection Program. Although the Paycheck Protection Program was established through the CARES Act, the Paycheck Protection Program Liquidity Facility did not receive support through CARES Act funds.
[265]The Term Asset-Backed Securities Loan Facility provided loans in exchange for eligible asset-backed securities.
[266]The Primary Market Corporate Credit Facility did not conduct any transactions.
[267]As of January 2022, the State of Illinois had repaid all of its borrowings from the Municipal Liquidity Facility.
[268]The allowance for loan losses is an estimate of potential losses based on the Main Street Lending Program’s holdings as of December 31, 2021, and does not indicate losses experienced by the program.
[269]We have previously reported on the Federal Reserve’s continued monitoring and oversight of the CARES Act lending facilities; see the October 2021 and December 2020 reports in Related GAO Products.
[270]This $20 billion amount includes up to 0.1 percent of the airport grant funding provided by the CARES Act, the Consolidated Appropriations Act, 2021, and ARPA that the FAA is authorized to retain to fund the award and oversight by FAA of grants made under these acts. Pub. L. No. 116-136, div. B, tit. XII, 134 Stat 281, 597; Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1941 (2020); Pub. L. No. 117-2, § 7102, 135 Stat. 4, 98.
[271]Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1939-41 (2020). Division M of the Consolidated Appropriations Act, 2021 is also referred to as the Coronavirus Response and Relief Supplemental Appropriations Act, 2021 (CRRSA). The Consolidated Appropriations Act, 2021, made up to $5 million of the $2 billion in funding available for the Small Community Air Service Development Program.
[272]The 31 airports that received CARES Act funds in excess of four times their annual operating expenses are excluded from receiving Consolidated Appropriations Act, 2021 funding. See Pub. L. No. 116-260, 134 Stat. at 1939. Specific amounts appropriated by the Consolidated Appropriations Act, 2021 are also available to cover lawful expenses to support FAA contract tower operations and to provide relief from rent and minimum annual guarantees to on-airport car rental, on-airport parking, and in-terminal concessions.
[274]As with the Consolidated Appropriations Act, 2021, the 31 airports that received CARES Act funds in excess of four times their annual operating expenses are excluded from receiving ARPA funding.
[275]More specifically, the contractor identified improper payment amounts within three sampled reimbursement claims made out of 102 samples tested. Based on these results, the contractor determined that the estimated improper payment rate was below the statutory threshold established by OMB Circular A-123, Appendix C.
[276]The Single Audit Act is codified, as amended, at 31 U.S.C. §§ 7501-06, and implementing Office of Management and Budget guidance is reprinted in 2 C.F.R. part 200. The Single Audit Act establishes requirements for nonfederal entities (defined as states, localities, and nonprofit organizations) that receive federal awards to undergo audits of those awards annually (unless a specific exception applies) when their expenditures meet a certain dollar threshold. More specifically, nonfederal entities that expend $750,000 or more in federal awards in a fiscal year are required to undergo a single audit—that is, an audit of an entity’s financial statements and federal awards, or a program-specific audit, for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501. If public airport sponsors do not meet this threshold in a fiscal year, then they are subject to applicable local and state audit requirements. Because private owners of public-use airports are not nonfederal entities as defined by the Single Audit Act, private owners of public-use airports are not subject to the Single Audit Act; however, they are still subject to grant assurances that they agree to when they accept federal airport grants. For example, under one grant assurance, a private owner of a public-use airport would agree to keep all project accounts and records which fully disclose the amount and disposition by the recipient of the proceeds of this grant, the total cost of the project in connection with which this grant is given or used, and the amount or nature of that portion of the cost of the project supplied by other sources, and such other financial records pertinent to the project. Additionally, private owners of public-use airports must make any documents pertinent to a grant available to the Comptroller General for the purpose of audit and examination. Finally, DOT may require that an appropriate audit be conducted by a recipient.
[277]Department of Transportation, Office of Inspector General, DOT Does Not Ensure Compliance With All Single Audit Provisions of OMB’s Uniform Guidance, FS2022024 (Washington, D.C.: March 2022).
[278]Both the Consolidated Appropriations Act, 2021, and ARPA direct airport sponsors to provide such relief to the extent permissible under state laws, local laws, and applicable trust indentures.
[279]167 Cong. Rec. H1196, H1283 (Mar. 10, 2021) (Explanatory Statement language accompanying selected provisions of bill H.R. 1319, enacted as the America Rescue Plan Act of 2021, drafted by the Committee on Financial Services).
[280]Airport concessions relief allocation amounts were calculated based on each airport’s passenger boardings compared to total passenger boardings of all airports eligible for concessions relief for calendar year 2019. ARPA appropriated a certain amount of funding for small airport concessions and a certain amount for large airport concessions.
[281]According to FAA guidance, FAA requires airport concessions to provide certifications of eligibility directly to airport sponsors, which then keep the documentation on file for possible audits.
[282]According to officials, 53 of the 379 eligible primary commercial service airports declined their Consolidated Appropriations Act, 2021 concessions relief funds by the time funding expired on September 30, 2021, and 64 of those airports had declined ARPA concessions relief funding as of February 28, 2022.
[283]Pub. L. No. 117-2, §§ 7201-02, 135 Stat. 4, 101-07.
[284]Under ARPA, DOT may use up to 1 percent of the funds appropriated ($30 million) for implementation costs and administrative expenses. Pub. L. No. 117-2 § 7202(a), 135 Stat. at 103.
[285]The Payroll Support Programs provided funds to be used by air carriers and aviation contractors for employee wages, salaries, and benefits. To be an eligible contractor for the Payroll Support Programs, the CARES Act and Treasury guidance defined a contractor as a person that, under contract with a passenger air carrier conducting operations under 14 C.F.R. pt. 121, performs catering functions or functions on airport property that are directly related to the air transportation of persons, property, or mail, such as ground-handling of aircraft, among other things. Eligibility for the Paycheck Protection Program was limited to small businesses (as defined by provisions authorizing the program).
[286]Funds cannot be used for back pay of returning rehired or recalled employees. Pub. L. No. 117-2, § 7202(b), 135 Stat. at 103.
[287]For a company to be eligible for AMJP funding, it must be a company that actively manufactures an aircraft, aircraft engine, propeller, or a component, part, or systems of an aircraft or aircraft engine under a Federal Aviation Administration production approval; hold specific certifications; or operate certain certified processes, among other requirements. The company must also be established, created, or organized under U.S. laws and have significant operations in and the majority of employees engaged in aviation manufacturing or maintenance, repair, and overhaul activities and services based in the U.S.
[288]See Pub. L. No. 117-2, §7202(c), 135 Stat. at 104.
[289]Each company has to identify its eligible employee group and the amount of the total compensation level for the eligible employee group, supported by sworn financial statements or other appropriate data.
[290]Specifically, entities with certain certificates related to passenger airplanes with a seating capacity of 50 or more, must agree to refrain from conducting involuntary layoffs or furloughs or reducing pay rates and benefits for the eligible employee group until September 30, 2021, or the duration of the agreement and receipt of funds, whichever period ends later. Entities that do not fall within this group must agree to refrain from these actions for the duration of the agreement and receipt of funds. If an approved company experiences natural attrition within the eligible employee group, or terminates any employee in the eligible employee group due to performance or conduct issues in accordance with employer policy, DOT will not require the company to backfill vacancies. However, the company will be required to disclose any reduction in the total compensation costs for the eligible employee group, and DOT may make comparable reductions in the actual disbursements to the company. For the duration of the agreement and receipt of funds, companies must provide DOT with immediate notice and justification of involuntary furloughs or layoffs that exceed 10 percent of the company’s workforce for whom they are not receiving AMJP funding. In addition, for the duration of the AMJP agreement, a company must also commit that it will fund all compensation costs for the eligible employee group that are not paid from AMJP funds. This company-provided funding must be at least 50 percent of the compensation costs for the eligible employee group. According to DOT guidance, financial benefits from any other federal or state financial assistance program that help the business cover its payroll costs during the term of the AMJP agreement will reduce DOT’s public contribution under the AMJP agreement.
[291]In certain cases, holding companies elected to submit separate applications for AMJP awards for their subsidiaries. According to DOT guidance for AMJP applications, if the subsidiary was a truly independent business, the subsidiary could apply separately and needed to ensure there was no overlap or redundancy in requested funding or covered costs. For reporting purposes, DOT treats each of these entities that applied as a separate company, and we have done the same. Additionally, two companies that applied in the second application period declined the AMJP offers and subsequently reapplied during the third application period and received new offers, which they accepted. For the purposes of calculating the number of eligible applicants, we counted each of these companies once. For the purposes of calculating program summary statistics throughout this report, such as the total amount offered to eligible applicants and average award offered, we excluded the data from these companies’ second application period offers.
[292]DOT offered companies AMJP funding based on what DOT determined to be the “maximum public contribution” based on the companies’ eligible employee group size, the maximum 6 month term of the agreement, and the statutory requirement to provide 50 percent of the cost of the eligible employee group’s total base compensation and benefits as they existed on April 1, 2020 (excluding overtime, premium pay, and payroll taxes). According to DOT officials, 58 companies from the three application periods requested an award that was less than they were entitled to by statute.
[293]DOT officials told us that they received 744 applications across all three application periods. However, 48 of those applications were either withdrawn or superseded by newer applications from the applicants; as a result, DOT evaluated a total of 696 applications. Of those, DOT determined 97 were either ineligible or disqualified and 598 were initially deemed eligible.
[294]According to DOT officials, after reaching out to the applicant that did not respond to DOT about their AMJP award offer, DOT received an automated response that the business had initiated Chapter 7 bankruptcy proceedings and ceased operations.
[295]As we reported in July 2021, eligible employers of any size—including tax-exempt entities, certain governmental entities, and self-employed individuals with employees—can claim the refundable Employee Retention Credit, as established under the CARES Act, extended by the Consolidated Appropriations Act, 2021, and as provided by ARPA. The credit amount is based on qualified wages paid to employees, including certain health care expenses. DOT officials refer to this as the Employee Retention Tax Credit. By statute, DOT cannot enter into an AMJP agreement with a company that was allowed the Employee Retention Credit under section 2301 CARES Act (Pub. L. No. 116-136 § 2301, 134 Stat. 281, 347 (2020) (codified at 26 U.S.C. § 3111 note)) for the immediately preceding calendar quarter from the quarter in which they enter the AMJP agreement. Pub. L. No. 117-2, § 7202(c), 135 Stat. at 104. The Consolidated Appropriations Act, 2021 extended section 2301 of the CARES Act; after that, ARPA created a new provision for Employee Retention Credits.
[296]DOT currently interprets the AMJP statute as not disqualifying an applicant that accrued an Employee Retention Credit after July 1, 2021 from receiving an AMJP award because the statute creating AMJP only cites to Section 2301 of the CARES Act, which was extended to wages paid before July 1, 2021 by the Consolidated Appropriations Act, 2021. Pub. L. No. 116-260, div. EE, tit. II § 207(a), 134 Stat. at 3062. Credits taken after July 1, 2021 were authorized by section 9651 of ARPA, which did not amend the CARES Act or extend the existing Employee Retention Credit, but instead created a new provision for Employee Retention Credits. Therefore, DOT officials told us they realized that this new provision did not pose a continued restriction under the AMJP statutory provisions, which is a change from information DOT conveyed about the program for the first two application periods.
[297]According to DOT officials, 46 eligible applicants from the first and second application periods requested delayed AMJP awards.
[298]The AMJP application required data on the eligible employee group to be based on corporate data as of April 1, 2020. DOT officials told us they recognized that most companies experienced some level of change in organizational structure, staffing, or both between April 1, 2020 and when a company entered into an AMJP agreement. According to DOT officials, the company is able to replace employees in their eligible employee group, but this must be documented and reported to DOT.
[299]DOT officials told us that companies that request an interim disbursement of award funds are also required to submit interim financial reports. Requesting an interim disbursement of award funds does not impact the company’s risk designation by DOT.
[300]DOT officials told us that they have separated the 209 higher risk companies into “moderate risk” and “elevated risk” groups. 203 of the companies fall in the “moderate risk” group and six companies fall into the “elevated risk” group. The six companies in the “elevated risk” group had to fulfill additional special conditions imposed by DOT before DOT authorized the initial disbursement of funds to those companies.
[301]As noted earlier, under ARPA, companies that received financial assistance from the first round of the Payroll Support Program (PSP1) established by section 4113 of the CARES Act or that are still expending Paycheck Protection Program assistance as of the date of application to the AMJP program are ineligible for the program. Similar to Employee Retention Credits taken after July 1, 2021, ARPA does not address employers that have received financial assistance under two programs similar to PSP1 established under new statutes, the Payroll Support Program Extension (PSP2) established by the Consolidated Appropriations Act, 2021, and the Payroll Support Program Extension (PSP3) established by ARPA. Prior to the first application deadline, DOT corrected its application to reflect that receiving PSP2 or PSP3 funds did not disqualify an applicant from receiving AMJP funding.
[302]This would apply to 280 recipients who signed their AMJP agreement prior to September 30, 2021.
[303]Pub. L. No. 116-136, § 4112, 134 Stat. 281, 498 (2020) (codified at 15 U.S.C. § 9072).
[304]Pub. L. No. 116-260, div. N, tit. IV, § 402, 134 Stat. 1182, 2053 (2020) (codified at 15 U.S.C. § 9092).
[305]Pub. L. No. 117-2, § 7301, 135 Stat. 4, 104-107.
[306]Notes are financial instruments whose value is a percentage of the payroll support provided over a certain threshold and must be repaid by recipients. Warrants represent the right to buy shares of a company’s stock at a predetermined price before a specified date.
[307]Cargo air carriers were only eligible to receive financial support through PSP1.
[308]The Treasury Inspector General also provides oversight of Payroll Support Program funds. The amount of payroll support that a recipient receives is based on its reported employee salaries and benefits. Some carriers report this information to the Department of Transportation. However, other carriers do not, and instead submit certified wage and salary documentation to Treasury. For some of these recipients, the Treasury Inspector General conducts certification audits. According to the Treasury Inspector General, the purpose of these audits is to evaluate the accuracy, completeness, and sufficiency of the documentation submitted, which is used to determine the amount of payroll support the recipient may receive.
[309]A recipient that receives financial assistance from multiple rounds of the Payroll Support Program generally submits a single quarterly report, according to Treasury officials.
[310]According to Treasury officials, the number of recipients that have submitted quarterly compliance monitoring reports fluctuates due to the timing of when Payroll Support Program agreements are fully executed. Across all quarters of compliance monitoring, between 490 and 682 recipients have been tested.
[311]According to Treasury officials, there are other reasons beyond a Level 1 discrepancy that may result in a recipient being elevated to Level 2 testing. For example, Treasury may receive information from a union or an inspector general that results in the recipient being elevated to Level 2 testing. Treasury also provides additional scrutiny to recipients who were required to provide taxpayer protections because of the size of their Payroll Support Program payment.
[312]The Payroll Support Program Agreement lays out the time period that recipients are required to undergo compliance monitoring. According to the PSP3 agreement, recipients are required to report to Treasury until the calendar quarter that begins after the later of January 1, 2023, or the date on which no taxpayer protection instrument is outstanding. PSP1 recipients were required to report to Treasury until the calendar quarter that begins after the later of March 24, 2022, or the date on which no taxpayer protection instrument is outstanding, and PSP2 recipients were required to report to Treasury until the calendar quarter that begins after the later of October 1, 2022, or the date on which no taxpayer protection instrument is outstanding.
[313]These 14 businesses include passenger air carriers and a cargo air carrier, specifically: Alaska Airlines, Allegiant Air, Atlas Air, American Airlines, Delta Air Lines, ExpressJet Airlines, Frontier Airlines, Hawaiian Airlines, JetBlue Airways, Republic Airlines, Southwest Airlines, SkyWest Airlines, Spirit Airlines, and United Airlines.
[314]CARES Act, Pub. L. No. 116-136, § 4003, 134 Stat. at 470 (codified at 15 U.S.C. § 9042). The CARES Act did not provide criteria for which businesses were “critical to maintaining national security.” Treasury established the following definition: (1) performing under a “DX”-priority-rated contract or order under the Defense Priorities and Allocations System regulations (15 C.F.R. pt. 700) or (2) operating under a valid top secret facility security clearance under the National Industrial Security Program regulations (32 C.F.R. pt. 2004). Treasury guidance further noted that applicants that did not meet either of these criteria may still be considered for loans, if based on the recommendation and certification by the Secretary of Defense or the Director of National Intelligence, the applicant’s business is critical to maintaining national security.
[315]Of the 35 executed loans, seven borrowers did not draw down the full authorized amount of their loan. These seven companies, all passenger air carriers, drew down about $1.6 billion of the $20.8 billion in loan funds Treasury made available to them. According to Treasury officials, the obligated but undisbursed loan amounts were obligated by the non-budgetary financing account, and amounts not disbursed by the loan draw date were deobligated within the financing account.
[316]As directed by the CARES Act, Treasury coordinated with the Department of Transportation (DOT) to determine the eligibility of certain applicants. DOT confirmed applicants held the appropriate air carrier certificates and the status of their operations, and reported this information to Treasury, according to DOT. Treasury also coordinated with the Department of Defense to determine the eligibility of applicants.
[317]For other businesses, Treasury had discretion to obtain a warrant or equity interest or senior debt instrument.
[318]Specifically, the CARES Act directs GAO to submit a report to specified committees on the Section 4003 loan program within 9 months of the enactment of the Act, and then annually thereafter through the year succeeding the last year for which the loans, loan guarantees, or other investments made from the loan program are outstanding. Pub. L. No. 116-136, § 4026(f), 134 Stat. at 496 (codified at 15 U.S.C. § 9060). Our report in December 2020 (GAO-21-198) satisfied the initial 9 month reporting requirement, our enclosure in our July 2021 recurring CARES Act oversight report (GAO-21-551) satisfied our first annual reporting requirement, and this enclosure satisfies our second annual reporting requirement as it pertains to the loans to passenger air carriers (and certain specified related businesses), cargo air carriers, and businesses critical to maintaining national security under sections 4003(b)(1)-(3).
[319]On August 3, 2021, Treasury issued a Notice of Non-Compliance to Caribbean Sun Airlines, Inc., a borrower through the Treasury loan program, because this borrower did not respond to a request from the Special Inspector General for Pandemic Recovery (SIGPR) to fill out a survey about its experience with the loan program. Pursuant to this Notice of Non-Compliance, if Caribbean Sun Airlines, Inc. did not respond to the survey by September 2, 2021, an event of default would occur, which would allow Treasury to pursue remedies including declaring the loan immediately due and payable. Caribbean Sun Airlines, Inc. did not respond by September 2, 2021, and therefore, an event of default occurred with the loan. Following the event of default, Treasury again communicated with Caribbean Sun Airlines, Inc. about the need to complete the survey. Caribbean Sun Airlines, Inc. responded to the survey on September 10, 2021, and responses were forwarded to SIGPR on September 13, 2021. Therefore, according to Treasury officials, Caribbean Sun Airlines is now in compliance with the loan terms and conditions, and Treasury does not plan to take further action on this matter. According to Treasury officials, Caribbean Sun Airlines, Inc. has not been found to be out of compliance with other terms and conditions of the loan agreement.
[320]These nine passenger air carriers are Alaska Airlines, American Airlines, Frontier Airlines, Hawaiian Airlines, JetBlue Airways, Mesa Airlines, Republic Airways, SkyWest Airlines, and United Airlines.
[321]Pub. L. No. 116-136, 134 Stat. 281, 599 (2020). Formula programs allocate funding to recipients using a distribution formula set by statute. At the time the CARES Act was enacted, $30 million was set aside for tribal transit programs from the Rural Area formula program appropriation. The CARES Act provided an additional $75 million set-aside for the administration and oversight of the appropriated funds.
[322]An urbanized area is an area that encompasses a population of 50,000 or more and has been defined and designated as such by the Secretary of Commerce. Designated recipients of FTA Urbanized Area formula funds can include entities designated by local officials, state governors, and local public transportation operators; alternatively, a state or regional authority responsible for public transportation may be the designated recipient. 49 U.S.C. § 5302.
[323]As of December 27, 2020, recipients were required to direct funds, to the maximum extent possible, to payroll and operations of public transit (including payroll and expenses of private providers of public transportation), unless the recipient certifies to the Secretary of Transportation that the recipient has not furloughed any employees. If the recipient has certified this, the agency may use relief funds for other uses such as capital or planning expenses. Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1947 (2020).
[324]These flexibilities are exceptions to the usual program requirements for FTA’s Urbanized Area and Rural Area formula programs. An additional exception is that there is no requirement for local matching funds for grants provided to large and small urban areas and rural areas. All other Urbanized Area and Rural Area program requirements apply to CARES Act funds, with the exception that operating expenses and certain capital expenses do not have to be included in a transportation improvement program, a long-range transportation or statewide transportation plan, or a statewide transportation improvement program.
[325]Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1945. Division M of the Consolidated Appropriations Act, 2021 is also referred to as the Coronavirus Response and Relief Supplemental Appropriations Act, 2021 (CRRSAA).
[326]Pub. L. No. 117-2, § 3401, 135 Stat. 4, 72. While Consolidated Appropriations Act, 2021 funds are available for obligation until expended, ARPA funds are available for obligation until the end of fiscal year 2024.
[328]See 49 U.S.C. § 5309. At the time ARPA was enacted, these projects were generally defined as follows: New Starts projects were projects for capital investments for which sponsors request $100 million or more in Capital Investment Grants funding or have an anticipated total project cost of $300 million or more. Core Capacity projects were substantial capital investments in existing fixed guideway systems that increase the capacity of a transit corridor by not less than 10 percent. Small Starts projects included certain types of projects, such as new fixed guideway capital projects, for which sponsors were provided, or would be provided, less than $100 million in Capital Investment Grants funding and have an anticipated total project cost of less than $300 million. The Infrastructure Investment and Jobs Act subsequently amended the monetary thresholds for New Starts and Small Starts projects. See Pub. L. No. 117-58, § 30005, 135 Stat. 429, 894 (2021) (codified as amended at 49 U.S.C. § 5309).
[329]According to FTA, a grant agreement defines the project, including its cost, scope, schedule, and level of service; commits to a maximum amount of annual and total Capital Investment Grants program financial assistance (subject to appropriations); establishes the terms and conditions of federal financial participation; defines the period of time for completion of the project; and helps FTA oversee and the project sponsor manage the project in accordance with applicable federal statutes and regulations. Upon completion of the payment schedule outlined in the agreement, the Capital Investment Grants funding commitment has been fulfilled.
[330]FTA officials review grant applications to ensure that a transit agency’s proposed expenditures are eligible for reimbursement by FTA. Only transit agencies whose applications are approved may obligate funding.
[331]See Pub. L. No. 116-136, § 1102(b), 134 Stat. 281, 293-94 (2020); Pub. L. No. 116-139, § 101(a), 134 Stat. 620, 620 (2020); Pub. L No. 116-260, div. N, tit. III, § 323(a) 134 Stat. 1182, 2018-19 (2020); Pub. L. No. 117-2, § 5001(d) 135 Stat. 4, 85 (2021). The program also paid fees to lenders for processing PPP loans.
[332]As originally implemented by SBA, at least 75 percent of the loan forgiveness amount must have been used for payroll costs. In addition, the CARES Act required loans to be used within an 8-week period in order for the loans to be fully forgiven. However, the Paycheck Protection Program Flexibility Act of 2020 modified this to at least 60 percent and allowed borrowers to pay or incur those expenses over a 24-week period. Pub. L. No. 116-142, § 3, 134 Stat. 641, 641-42 (2020). Under that act, the loan forgiveness covered period for PPP loans was to end the earlier of 24 weeks after origination or December 31, 2020. The Consolidated Appropriations Act, 2021 further modified the covered period for forgiveness to allow the borrower to choose a covered period ending on any date between 8 and 24 weeks after origination. Pub. L. No. 116-260, div. N, tit. III, § 306, 134 Stat. 1182, 1997 (2020).
[333]New applications were accepted through May 31, 2021, and SBA had until June 30, 2021, to process submitted applications.
[334]The Consolidated Appropriations Act, 2021 expanded the categories of forgivable nonpayroll costs to include certain operations, property damage, supplier, and worker protection expenditures. PPP borrowers were eligible to receive a second PPP loan of up to $2 million provided that they met certain criteria, such as having not more than 300 employees, having used the full amount of their initial PPP loan, and having experienced revenue reductions of at least 25 percent in a quarter of 2020 when compared to the same quarter in 2019. Pub. L No. 116-260, div. N, tit. III, § 311, 134 Stat. 1182, 2001-07 (2020); see also 86 Fed. Reg. 3712 (Jan. 14, 2021).
[336]Under SBA rules and guidance, the borrower submits the forgiveness application to the lender. The lender then has 60 days from receipt of the application to review and submit its forgiveness decision (approved in full, approved in part, or denied) to SBA. SBA reviews the lender decision, makes a final forgiveness determination, and remits the appropriate forgiveness amount to the lender. In general, SBA must remit the forgiveness amount to the lender within 90 days of that amount being determined. SBA and Treasury officials told us they interpreted the CARES Act requirement to remit funds within 90 days to be subject to SBA’s review of loans. The total number of PPP loans in our analysis is slightly different from the number publicly reported by SBA as of March 27, 2022, because of timing.
[337]According to SBA officials, lenders had recommended that 2,925 of the approximately 104,000 loans still under SBA review not receive any forgiveness, as of February 15, 2022. Lenders are responsible for reviewing that a borrower’s loan forgiveness application is complete and confirming the receipt of sufficient documentation to verify payroll and nonpayroll costs and the borrower’s calculations. A lender may deny forgiveness if it identifies errors in the borrower’s calculation or material lack of substantiation in the borrower’s supporting documents that cannot be remedied.
[338]CFDIs and MDIs target loans to businesses and individuals in traditionally underserved areas, with the goal of expanding economic opportunity. CDFIs include both banks and nonbanks that are certified by Treasury as lenders that share a common goal of expanding economic opportunity in low-income communities by providing access to financial products and services for local residents and businesses. MDIs are generally defined as depositories that meet the following criteria: (1) if a privately owned institution, 51 percent is owned by socially and economically disadvantaged individuals; (2) if publicly owned, 51 percent of the stock is owned by socially and economically disadvantaged individuals; and (3) in the case of a mutual institution, the majority of the board of directors, account holders, and the community that the institution serves are predominantly minority. The term “minority” means any Black American, Native American, Hispanic American, or Asian American. 12 U.S.C. § 1463 note; 15 U.S.C. § 636(a)(36)(A)(xi)(II). We assigned to the CDFI/MDI group all lenders SBA flagged as CDFIs, MDIs, or both, and all remaining lenders to one of the other groups.
[339]Borrowers may not have submitted loan forgiveness applications to their lenders for these outstanding loans.
[340]About 78 percent of the PPP loans made by community financial institutions, which include CDFIs and MDIs, were for less than $150,000, compared to about 50 percent for the program as whole. On July 30, 2021, SBA published an interim final rule with changes meant to simplify the loan forgiveness process for borrowers with the smallest loans. 86 Fed. Reg. 40921 (July 30, 2021). The interim final rule gave borrowers with loans of $150,000 or less whose lenders have opted into using SBA’s direct borrower forgiveness platform the option to apply for forgiveness directly to SBA instead of their lender. Similar to loan forgiveness applications submitted directly to the lender, the lender would approve (or deny) the loan forgiveness request.
[341]As we reported in July 2021, an SBA contractor screens all PPP loans using an automated rules-based tool. The tool compares PPP loan data against publicly available information and applies eligibility and fraud detection rules to identify anomalies or attributes that may indicate noncompliance with eligibility requirements, fraud, or abuse. Loans that are identified by the automated screening process or separately flagged will be considered for manual review for eligibility, fraud or abuse, or compliance with applicable loan forgiveness rules. A separate contractor will conduct quality control reviews on a sample of loans to independently review whether the loan review process was executed as designed and whether the evidence in the loan review file sufficiently supported SBA’s loan review decision.
[342]Machine learning is a process through which systems begin with data—generally in large amounts—and infer rules or decision procedures that aim to predict specified outcomes. This inference happens when the system is able to train itself using data to increase the accuracy of its predictions.
[343]As discussed in more detail later, SBA has not yet developed a strategy to manage fraud risks in the program.
[344]Pub. L. No. 116-136, § 1102(a), 134 Stat. 281, 293 (2020). A “sense of” provision is a non-binding statement that expresses the opinion of Congress or the relevant chamber. The resolutions are not legally binding, have no formal effect on public policy, and have no force of law. See Congressional Research Service, “Sense of” Resolutions and Provisions, Report No. 98-825 (Washington, D.C.: Oct. 16, 2019).
[345]According to Treasury officials, this approach was adopted to get the money out as quickly as possible due to the economic emergency. They further noted that one issue that arose early in the program was that banks (especially big banks) placed restrictions on who they would serve, focusing primarily on their existing clients.
[346]Of the 5.1 million borrowers who received a PPP loan in 2020, 70 percent did not include information on the applicant’s gender, 84 percent did not provide information on the applicant’s race, and 77 percent did not provide information on the applicant’s veteran status. SBA did include an optional form for demographic information in the loan forgiveness application it first made available in May 2020.
[347]Among other things, community financial institutions include CDFIs and MDIs. Pub. L. No. 116-139, § 101(d), 134 Stat. 620, 621-22 (2020).
[348]Pub. L. No. 116-260, div. N, tit. III, § 309, 134 Stat. 1182, 2000 (2020).
[349]Reasonable terms and conditions take into consideration factors such as the business industry in which the loan applicant operates, whether the applicant is an enterprise that has been in operation for not more than 2 years, the adequacy of the collateral available, and the loan term necessary to assure the ability of the applicant to repay the debt from the cash flow of the business. 15 U.S.C. § 632(h). SBA also requires lenders to certify that 7(a) borrowers cannot obtain financing from personal resources or the resources of the business or its owners of 10 percent or more.
[350]In its response to the FAQ, SBA clarified that borrowers must make the economic necessity certification in good faith, taking into account their current business activity and their ability to access other sources of liquidity sufficient to support their ongoing operations in a manner that is not significantly detrimental to the business.
[351]In subsequent guidance, SBA announced that borrowers who had previously applied for a PPP loan could repay the loan in full by May 18, 2020, and would be considered to have made their certifications in “good faith.” Some publicly traded companies repaid their PPP loans under this option.
[352]The Associate General Contractors of America, Inc., filed a lawsuit in December 2020 alleging, among other things, that the necessity questionnaires and the process used to approve them violated the Administrative Procedure Act and the Paperwork Reduction Act. Among other things, the lawsuit filings noted that the questionnaires ask borrowers to describe their business success (or failure) after applying for the loan, not the status of their operations at the time they applied for the loan.
[353]85 Fed. Reg. 20811, 20812 (April 15, 2020). The initial interim final rule provided that businesses that are not eligible for PPP loans are identified in 13 C.F.R. § 120.110 and described further in SBA Standard Operating Procedure (SOP) 50 10, Subpart B, Chapter 2, with certain exceptions. SBA regulations generally restrict eligibility for 7(a) loans for certain businesses including those engaged in illegal activity; financial businesses primarily engaged in lending; and those that present live performances of a prurient sexual nature. Later issued SBA rules modified PPP loan eligibility criteria. See, e.g., 86 Fed. Reg. 3692, 3698 (January 14, 2021); 86 Fed. Reg. 3712, 3718 (January 14, 2021).
[354]Lawsuits have been brought by live adult entertainment businesses, lobbying firms, business owners with criminal histories, payday lenders, and companies in bankruptcy proceedings.
[355]Pub. L. No. 116-260, div. N, tit. III, § 311(a), 134 Stat. 1182, 2001-2002 (2020).
[357]In general, nonbanks provide lending services but do not accept deposits. The CARES Act permitted SBA and Treasury to approve additional lenders to process, close, disburse, and service PPP loans. The agencies provided the lender agreement for some lender types prior to the program’s launch, but they did not provide the agreement for nonbank lenders until 5 days after the program started. PPP was launched on April 3, 2020, and the initial appropriations were exhausted on April 16, 2020. Congress appropriated additional funding, and the program resumed lending on April 27, 2020.
[358]Small Business Administration, Office of Inspector General, Inspection of SBA’s Implementation of the Paycheck Protection Program, Report No. 21-07 (Washington, D.C.: Jan. 14, 2021).
[359]Treasury’s Do Not Pay service is an analytics tool that helps federal agencies detect and prevent improper payments made to vendors, grantees, loan recipients, and beneficiaries. Agencies can use the service to check multiple data sources to make payment eligibility decisions.
[360]In September 2015, we recommended that SBA develop its enterprise risk management consistent with GAO's risk management framework and document the specific steps that the agency planned to take to implement its enterprise risk management process. In response, SBA developed additional guidance on its process in June 2016.
[361]Enterprise risk management is an agency-wide approach to addressing the full spectrum of the organization’s significant risks by understanding the combined impact of risks as an interrelated portfolio, rather than addressing risks only within silos.
[362]SBA’s fiscal year 2020 and 2021 consolidated financial statements received a disclaimer of opinion, meaning the auditor was unable to express an opinion due to insufficient evidence. As the basis for the disclaimers, the auditor reported that SBA was unable to provide adequate evidence to support a significant number of transactions and account balances due to inadequate processes and controls related to its implementation of its programs authorized under the CARES Act and related legislation, including PPP.
[363]SBA issues a loan number when it agrees to guarantee the loan. According to SBA officials, this occurs after the lender approves the loan and submits certain information to SBA and there are no errors with the information. The lender makes the loan once it receives the loan number from SBA.
[364]Borrowers who had a hold code placed on their first draw loans would have their application for a second draw loan delayed until the issue was resolved. An application for a first draw loan would not receive a loan number until the issue was resolved.
[365]According to SBA officials, SBA did not start conducting reviews of loans of less than $2 million until early November 2020 and did not start conducting reviews of loans of $2 million or more until January 2021. According to SBA data, about 92,000 loans totaling about $2.7 billion received forgiveness in October 2020.
[366]For example, the Master Review Plan no longer requires all loans of $2 million or more to receive a manual review. Rather, they, like loans of less than $2 million, could receive a manual review if they were identified by the automated screening process or separately flagged for manual reviews.
[367]Similarly, the Office of Management and Budget has established that for executive offices to be effective, they should prioritize efforts toward preventing improper payments from occurring to avoid operating in a pay and chase environment.
[368]Improper payments are payments that should not have been made or were made in the incorrect amount, and may suggest that a program is vulnerable to fraud. While an improper payment may be the result of fraudulent activity, not all improper payments are the result of fraud. Fraud involves obtaining something of value through willful misrepresentation. The judicial or other adjudicative system determines whether an act is fraud.
[369]We surveyed a generalizable sample of 1,383 PPP lenders to obtain their perspectives on the loan approval and loan forgiveness processes and the program in general. The survey closed on April 15, 2021, and we received 781 responses. We obtained a weighted response rate of 57.3 percent.
[370]The 95 percent confidence interval for this estimate is (84, 89). Survey respondents were asked to rate challenges using the following scale: very challenging, moderately challenging, somewhat challenging, not at all challenging, and do not know. According to Treasury officials, most of these program changes were made at the request of banks or PPP participants to reduce program burdens or streamline processes.
[371]The 95 percent confidence interval for this estimate is (72, 78).
[372]In addition to incorporating regulations required by the Economic Aid Act, the January 2021 rule consolidated the interim final rules issued to date governing borrower eligibility, lender eligibility, and PPP application and origination requirements for new PPP loans, as well as providing general rules relating to loan increases and loan forgiveness. The February 2021 loan forgiveness interim final rule consolidated prior rules on the loan forgiveness process.
[373]Only PPP borrowers who have loans of $150,000 or less and whose lenders opted in to use the direct forgiveness portal can apply for forgiveness using the portal.
[374]Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 223 (2021) (codified at 42 U.S.C. §§ 802-803) (ARPA). Sections 602 and 603 of the Social Security Act as added by section 9901 of ARPA appropriated $350 billion in total funding for two funds—the Coronavirus State Fiscal Recovery Fund and the Coronavirus Local Fiscal Recovery Fund. For purposes of this report, we discuss these two funds as one—the Coronavirus State and Local Fiscal Recovery Funds (CSLFRF). 42 U.S.C. §§ 802-803. For purposes of the CSLFRF, ARPA establishes that the District of Columbia is considered to be a state. 42 U.S.C. §§ 802(g)(5), 803(g)(9).
[376]Coronavirus State and Local Fiscal Recovery Funds, 87 Fed. Reg. 4,338, 4,448 (Jan. 27, 2022) (codified at 31 C.F.R. § 35.5).
[377]Subsequently, on May 17, 2021, Treasury published the interim final rule in the Federal Register. See Coronavirus State and Local Fiscal Recovery Funds, 86 Fed. Reg. 26,786. Treasury provided initial guidance on reporting requirements for all recipients in the supplemental information section of the interim final rule. The text of the rule in the interim final rule did not contain specific reporting requirements, but rather implemented recipients’ obligation to provide regular detailed reporting and other information as Treasury requires. This general provision was retained in the final rule, which Treasury released on January 6, 2022. Treasury published the final rule in the Federal Register on January 27, 2022. See Department of Treasury, Coronavirus State and Local Fiscal Recovery Funds, 87 Fed. Reg. 4338 (codified at 31 C.F.R. pt. 35, subpt. A).
[379]42 U.S.C. § 803(b)(2), (7). Treasury considers state governments that request their own allocations also to have requested allocations for NEUs within their states. Treasury will make payments to states from the Coronavirus Local Fiscal Recovery Fund for distribution to NEUs in two tranches, with the second tranche payment to be made no earlier than 12 months after the date on which the first tranche payment is paid to the state.
[380]Territories also allocate and distribute payments to NEUs. For purposes of payments to NEUs, ARPA defines “states” to include territories (i.e., American Samoa, the Commonwealth of the Northern Mariana Islands, the Commonwealth of Puerto Rico, Guam, and the U.S. Virgin Islands). 42 U.S.C. § 803(g)(9). However, for purposes of this report we excluded territories from our analysis.
[382]ARPA requires states to distribute to NEUs an amount that is the same proportion to the amount of payment as the population in the NEU as a share of the total population of all NEUs in the state. 42 U.S.C. § 803(b)(2)(C)(i).
[383]ARPA provides that each NEU’s total distribution (i.e., the total of distributions under both the first and second tranche) is capped at 75 percent of its most recent budget, in effect as of January 27, 2020. 42 U.S.C. § 803(b)(2)(C)(iii). The supplemental information accompanying Treasury’s interim final rule that implements CSLFRF defined a NEU’s most recent budget for purposes of the cap to mean the NEU’s most recent annual total operating budget, including its general fund and other funds, as of January 27, 2020. Coronavirus State and Local Fiscal Recovery Funds, 86 Fed. Reg. 26,786, 26,814 (May 17, 2021). Treasury’s final rule specifies that the NEU’s total annual budget includes both operating and capital expenditure budgets, in effect as of January 27, 2020. 87 Fed. Reg. at 4453 (codified at 31 C.F.R. § 35.12(b)).
[384]In some states, the boundaries of some NEUs overlap with or encompass other NEUs within the state, typically resulting in overlapping populations between the larger “parent” NEU and the subsidiary NEU (e.g., a township that encompasses a city).
[385]Recipients that submitted these interim reports included states, U.S. territories, tribal governments, and certain local governments.
[386]Recipients that submitted these recovery plans included states, U.S. territories, and certain local governments.
[388]These remedies may include imposing additional conditions on award funds and, if that does not resolve the noncompliance, pursuing other remedies appropriate in the circumstances, as provided in OMB’s Uniform Administrative Requirements, Cost Principles, and Audit Requirements for Federal Awards. See, 2 C.F.R. § 200.339.
[389]Capital expenditures means expenditures to acquire capital assets or expenditures to, among other things, make additions, improvements, modifications, replacements, or rearrangements to capital assets that materially increase their value or useful life. 31 C.F.R. § 35.3; 2 C.F.R. § 200.1.
[390]Recipients that submitted these project and expenditure reports included states, U.S. territories, and certain local and tribal governments.
[391]These remedies may include imposing additional conditions on award funds and, if that does not resolve the noncompliance, pursuing other remedies appropriate in the circumstances, as provided in OMB’s Uniform Administrative Requirements, Cost Principles, and Audit Requirements for Federal Awards. See, 2 C.F.R. § 200.339.
[392]Treasury’s final rule defines an NEU’s budget for purposes of calculating the 75 percent budget cap as its total annual budget, including both operating and capital expenditure budgets, in effect as of January 27, 2020. See, 31 C.F.R. § 35.12(b).
[394]This total is based on (1) an analysis of the appropriated amounts in the American Rescue Plan Act of 2021 (ARPA), Divisions M and N of the Consolidated Appropriations Act, 2021, the Paycheck Protection Program and Health Care Enhancement Act, the CARES Act, the Families First Coronavirus Response Act, and the Coronavirus Preparedness and Response Supplemental Appropriations Act, 2020 that are available to agencies for assistance to states, the District of Columbia., localities, U.S. territories, and tribes; and (2) the Congressional Budget Office’s estimated outlays for Medicaid resulting from authorized increases in payments to states and U.S. territories under those laws.
[395]Pub. L. No. 116-136, div. A, tit. V, § 5001(a), 134 Stat. 281, 501, (2020) (codified as amended at 42 U.S.C. 801) (CRF); Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 223 (2021) (codified as amended at 42 U.S.C. §§ 802-803) (CSLFRF).
[396]Pub. L. No. 116-260, div. L, tit. IV, 134 Stat. 1182, 1941-42.
[397]Pub. L. No. 117-2, tit. III, subtit. D, § 3401, 135 Stat. 4, 72; Pub. L. No. 116-260, div. M, tit. IV, 134 Stat. 1182, 1945, 1947, and Pub. L. No. 116-136, Div. B. tit. XII, 134 Stat. 281, 599-600.
[398]Funds may be used to provide child care assistance to health care sector employees, emergency responders, sanitation workers, and other essential workers without regard to the income eligibility requirements. Pub. L. No. 117-2, tit. II, subtit. C, § 2201, 135 Stat. 4, 31; Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1914-15, and Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 557-558.
[399]Medicaid did not receive additional funding under the COVID-19 relief laws. As noted above, estimated increases in federal expenditures for Medicaid resulted from authorized increases in Medicaid payments to states and U.S. territories in several provisions in the Families First Coronavirus Response Act and ARPA. These two COVID-19 relief laws provided states with temporary increases to their Federal Medical Assistance Percentage (FMAP) rates in response to the COVID-19 public health emergency. See Pub. L. No. 116-127, div. F, §§ 6004(a)(3), 6008, 134 Stat. 178, 205, 208 Pub. L. No. 117-2, tit. IX, subtit. J, §§ 9811, 9817, 135 Stat 4, 208, 216.The FMAP is a statutory formula that the federal government uses to match states’ spending for Medicaid purposes.
[400]In January 2022, Treasury issued a final rule on the program which provided, among other things, clarification on eligible uses of the funds. Treasury also updated its Compliance and Reporting Guidance in November 2021 and February 2022 that provided additional detail and clarification on the compliance and reporting responsibilities for each recipient type, including reporting deadlines. See Department of the Treasury, Coronavirus State and Local Fiscal Recovery Funds, Final Rule, 87 Fed. Reg. 4338 (Jan. 27, 2022) (codified at 31 C.F.R. pt. 35, subpt. A) and Compliance and Reporting Guidance: State and Local Fiscal Recovery Funds, ver. 2.1 (Nov. 15, 2021) and ver. 3.0 (Feb. 28, 2022), https://home.treasury.gov/system/files/136/SLFRF-Compliance-and-Reporting-Guidance.pdf.
[401]Infrastructure Investment and Jobs Act, Pub. L. No. 117-58, div. F, 135 Stat. 429, 1182-1250 (2021).
[402]CRF recipients had to obligate their funds by December 31, 2021. CARES Act, Pub. L. No. 116-136, div. A, tit. V, § 5001(a), 134 Stat. 501 as amended by the Consolidated Appropriations Act, 2021, div. N, tit. X, § 1001, 134 Stat. 2146 (codified at 42 U.S.C. § 801(d)(3)). See also, Treasury guidance https://home.treasury.gov/system/files/136/CRF-Guidance_Revision-Regarding-Cost-Incurred.pdf.
[403]States have up to September 30, 2022, to obligate CARES Act funds appropriated for the Child Care and Development Block Grant program and must spend these funds by September 30, 2023.
[404]While the federal fiscal year runs from October 1 to September 30, most states have different fiscal years (e.g., 46 states have July 1 to June 30 fiscal years).
[405]The CDBG program provides annual grants on a formula basis to states, cities, and counties to develop viable urban communities by providing housing and a suitable living environment, and by expanding economic opportunities, principally for low- and moderate-income persons. Regulations require CDBG grantees to submit an Annual Performance Report to HUD within 90 days of the close of a grantee's program year.
[406]While prior Treasury guidance specified that such reports were originally due on October 31, 2021, states, territories, certain metropolitan cities and counties and tribal governments allocated more than $30 million were later required to submit their reports by January 31, 2022, with reports covering the period between March 3, 2021, and December 31, 2021. For Non-entitlement Units, other metropolitan cities and counties, and tribal governments allocated less than $30 million, the first reports are now due on April 30, 2022, and will cover the period between March 3, 2021 and March 31, 2022.
[407]Territories and freely associated states consist of the territories of the United States Virgin Islands, Guam, American Samoa, and the Commonwealth of the Northern Mariana Islands; and the freely associated states of the Republic of the Marshall Islands, the Federated States of Micronesia, and the Republic of Palau. Freely associated states refer to nations that are affiliated with the United States through a compact of free association. For the purposes of CPF allocations, Puerto Rico, a territory, is included with states and the District of Columbia.
[408]ARPA appropriated CPF funding without fiscal year limitation. 42 U.S.C. § 804(a). In September 2021, however, Treasury issued implementing guidance establishing December 31, 2026, as the end of the period of performance for CPF grants by which grants funds must be expended and unused funds returned to Treasury. In its guidance, Treasury noted that, at its sole discretion, it may extend the period of performance upon CPF recipient requests.
[409]An obligation is a definite commitment that creates a legal liability of the U.S. government for the payment of goods and services ordered or received, or a legal duty on the part of the U.S. government that could mature into a legal liability by virtue of actions on the part of another party that are beyond the control of the U.S. government. An expenditure is the actual spending of money, or an outlay. In the context of this enclosure, expenditures are amounts distributed by Treasury to prime recipients of CPF.
[410]For states, territories, and freely associated states, the grant plan is filed separately from the initial application. Grant plans for these recipients consist of an executive summary; an allocation table showing the broad categories of capital projects the recipient seeks to undertake using grant funds and how much the recipient intends to spend on each such category; and one or more program plans, which are intended to provide more detailed information on a particular type of capital project(s) the recipient intends to undertake. Treasury’s guidance includes a provision for a waiver of the grant plan deadline at the discretion of the agency.
[411]For tribal governments, the grant plan is included in the application, and consists of a short description of the proposed use for the grant funds, documented by either selection of one of the presumptively eligible uses in the application form, or by brief description of the otherwise eligible use.
[412]For states, territories, and freely associated states, a program plan included within the grant plan provides more detailed information on a particular type of capital project(s) the recipient intends to undertake, and constitutes an eligible applicant’s request for funding for those capital projects. There is no requirement for tribal governments to submit program plans in their grant plans to Treasury.
[413]The Single Audit Act is codified at 31 U.S.C. §§ 7501-06, and implementing Office of Management and Budget guidance is reprinted in 2 C.F.R. part 200. Nonfederal entities (states, U.S. territories, Indian tribes, local governments, and nonprofit organizations) that expend $750,000 or more in federal awards in their fiscal year are required to undergo a single audit—that is, an audit of the entity’s financial statements and federal awards for the fiscal year, or in limited circumstances, a program-specific audit. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[414]Coronavirus Relief Fund: CARES Act, Pub. L. No. 116-136, § 5001, 134 Stat. 281, 501-04 (2020), as amended by the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. N, tit. X, § 1001, 134 Stat. 1182, 2146 (2020) (codified at 42 U.S.C. § 801). CSLFRF: ARPA, Pub. L. No. 117-2, tit. IX, subtit. M, § 9901, 135 Stat. 4, 223 (2021) (codified at 42 U.S.C. §§ 802-803). Sections 602 and 603 of the Social Security Act as added by section 9901 of ARPA appropriated $350 billion in total funding for two funds—the Coronavirus State Fiscal Recovery Fund and the Coronavirus Local Fiscal Recovery Fund. For purposes of this report, we discuss these two funds as one—the Coronavirus State and Local Fiscal Recovery Funds (CSLFRF). 42 U.S.C. §§ 802-803.
[415]The CARES Act includes a provision for GAO to provide a comprehensive audit and review of federal contracting pursuant to the authorities provided in the Act. In addition to specific contracting reviews, we have reported on federal contracting in response to the pandemic as part of regularly issued government-wide reports on the federal response to COVID-19.
[416]For the purposes of this report, “contract obligations” refers to obligations on procurement contracts that are subject to the Federal Acquisition Regulation and does not include, for example, grants, cooperative agreements, loans, other transactions for research, real property leases, or requisitions from federal stock.
[417]According to the memorandum of agreement guiding the management of the NIA code, DHS and DOD are responsible for making determinations about whether to establish or close a code, based on a variety of considerations. The General Services Administration (GSA)—the agency that operates and maintains FPDS—is responsible for adding or updating the NIA code in the system based on DHS’s and DOD’s decisions. The extensions of the code are consistent with our prior recommendations to DHS, DOD, and GSA related to the importance of ensuring federal agencies, the public, and Congress have visibility into contract actions and associated obligations related to emergency response efforts.
[418]Emergency use authorizations allow for the temporary use of unapproved medical products. Janssen Pharmaceutical Companies are a part of Johnson & Johnson.
[419]Our methodology for identifying noncompetitive contracts is explained in detail at the end of this enclosure.
[420]For the purposes of this report, obligations on contracts identified as using the unusual and compelling urgency exception include those associated with contracts subject to Federal Acquisition Regulation 6.302-2, as well as orders under multiple award contracts, which are subject to separate requirements under Federal Acquisition Regulation subpart 16.5. Specifically, under Federal Acquisition Regulation 16.505(b)(2), orders on multiple award contracts require contracting officers to give every awardee a fair opportunity to be considered for a delivery order or task order exceeding $3,500, with exceptions, including if the agency need for the supplies or services is so urgent that providing a fair opportunity would result in unacceptable delays. When using the unusual and compelling urgency exception to full and open competition, agencies still must request offers from as many potential sources as is practicable under the circumstances.
[421]Undefinitized contracts include letter contracts, as well as other undefinitized actions. Letter contracts are a preliminary contract that authorizes the contractor to begin work immediately, and undefinitized contract actions include any contract action for which the contract terms, specifications, or price are not agreed upon before performance has begun under the action. Federal Acquisition Regulation 16.603 and Defense Federal Acquisition Regulation Supplement 217.74.
[422]FPDS data from SAM.gov accessed through March 31, 2022. For purposes of this report, “competition rate” is the percentage of total obligations associated with contracts awarded competitively. We calculated competition rates as the percentages of obligations on competitive contracts and orders over all obligations on contracts and orders. Competitive contracts included contracts and orders coded in the FPDS as “full and open competition,” “full and open after exclusion of sources,” and “competed under simplified acquisition procedures” as well as orders coded as “subject to fair opportunity,” “fair opportunity given,” and “competitive set aside.” Noncompetitive contracts included contracts and orders coded in the FPDS as “not competed,” “not available for competition,” and “not competed under simplified acquisition procedures,” as well as orders coded as an exception to “subject to fair opportunity,” including “urgency,” “only one source,” “minimum guarantee,” “follow-on action following competitive initial action,” “other statutory authority,” and “sole source.” Even for contracts identified as noncompetitive, agencies may have solicited more than one source.
[423]In November 2019 we identified some inconsistencies in the information agencies report in the contract description field in the FPDS. Data on DOD contract obligations based on information in the description field were available only through January 1, 2022, due to differences in the time frames for which DOD data are made publicly available.
[425]U.S. Census import data contains information on total monthly import charges paid on all imported shipments. Census cannot reliably account for shipments valued below $2,000. As such, Census implements statistical methodologies to account for imported shipments below $2,000 to account for coverage, timeliness and relevance of the international merchandise trade statistics. Import charges include cost of freight; insurance; and other charges, excluding duties.
[427]The Marine Exchange of Southern California is a non-profit organization dedicated to development and efficient flow of commerce through the 4 major ports in Southern California that include the ports of Los Angeles and Long Beach. The Marine Exchange maintains a continuous 24-hour service, and utilizes a state-of-the-art, comprehensive, computerized database system to provide vital statistics and information on ships calling into both ports.
[428]One of the six terminals at the Port of Los Angeles operated close to 20 hours each day of the week as of 3/21/2022.
[429]For the purposes of our analysis, U.S. import values refer to the value of imports for consumption, which is a measure of merchandise that has physically cleared through customs.
[430]Unit values equal the total import value of the product divided by the quantity imported. Trends in this measure serve as a proxy for understanding fluctuations in import price.
[431]For example, the number of imported N-95 respirators increased by 15 percent from June 2021 through August 2021 while the unit values of these products declined by 42 percent in the same time period. Overall, U.S. import values for N-95 respirators fell by 33 percent from June 2021 through August 2021.
[433]We compared COVID-19-related HTS-10 statistical reporting numbers before and after July 1, 2020, before and after January 1, 2021, and before and after July 2021. If no data existed for an HTS-10 statistical reporting number, we checked USITC guidance to determine whether the original reporting number had been annotated or discontinued. If it had been annotated or discontinued, we included import values of those codes after July 1, 2020; January 1, 2021; or July 1, 2021, in our analysis. For instance, on July 1, 2020, according to guidance provided by the USITC, the HTS statistical reporting number 4818.50.0000 split into two new HTS-10 statistical reporting numbers, 4818.50.0080 and 4818.50.0020. Therefore, we included imports for products contained in 4818.50.0080 and 4818.50.0020 after July 1, 2020, in our calculations. Therefore, we may overestimate the value of imports for COVID-19 related products. Nevertheless, the values shown are useful indicators for tracking import trends for such products. December 2021 was the latest month of trade data available at the time of our analysis.
[434]Fraud and “fraud risk” are distinct concepts. Fraud—obtaining something of value through willful misrepresentation—is challenging to detect because of its deceptive nature. Fraud risk (which is a function of likelihood and impact) exists when individuals have an opportunity to engage in fraudulent activity, have an incentive or are under pressure to commit fraud, or are able to rationalize committing fraud. Fraud risk management is a process for ensuring program integrity by continuously and strategically mitigating the likelihood and impact of fraud. When fraud risks can be identified and mitigated, fraud may be less likely to occur. Although the occurrence of fraud indicates there is a fraud risk, a fraud risk can exist even if actual fraud has not yet been identified or occurred.
[435]In July 2021, we reported that SBA’s initial implementation of PPP contributed to increased risk of improper payments and extensive fraud. Also in July 2021, we reported on efforts SBA has taken to address risks of fraud in the EIDL program and provision of funds to ineligible applicants. Further, in October 2021, we reported on fraud risks in UI programs and strategies DOL is implementing to address potential fraud in UI programs.
[436]We consider convictions to be cases where an individual was convicted of a fraud-related charge at trial.
[437]The remainder of the complaints relate to a variety of other programs and issues, including other federal programs, such as the Restaurant Revitalization Fund Grant program and Higher Education Emergency Relief fund; COVID-19-related mortgage fraud; grants; and testing and vaccines. While not all of the complaints received involve allegations of potential fraud, many of them do.
[438]According to the FTC, the fraud reports reflect complaints in the Consumer Sentinel Network that mention COVID, stimulus, N95, and related terms. The identity theft reports reflect complaints that mention COVID, stimulus, or related terms in the following identity theft subtypes: tax, employment and wage, government benefits, and government documents.
[439]For the status of recommendations related to the PPP, EIDL, and UI programs, see the PPP, EIDL, and UI enclosures in appendix I.
[440]A charge is merely an allegation, and all defendants are presumed innocent until proven guilty beyond a reasonable doubt in a court of law.
[441]The federal government may enforce laws through civil or criminal action. Such action may be resolved through a trial, a permanent injunction, a civil settlement, or a guilty plea. Since March 2020, DOJ has resolved an EIDL fraud-related case against one individual and PPP fraud-related cases against ten individuals or entities through civil settlements. For example, in one case, an individual agreed to pay over $280,000 to settle allegations brought by a former employee that this individual misappropriated PPP loan proceeds obtained on behalf of this individual’s company for personal expenses. In addition to the federal government, state governments have brought COVID-19-related unemployment insurance and PPP fraud charges.
[442]The statute of limitations for mail fraud and wire fraud prosecutions is 5 years (18 U.S.C. § 3282), except for mail and wire fraud schemes that affect a financial institution, in which case the statute is 10 years (18 U.S.C. § 3293). Also, based on our analysis, these cases can take many years to resolve. For example, the Department of Housing and Urban Development OIG closed cases in 2017–2020 resulting from Hurricane Sandy in 2012.
[443]Differences between the numbers reported here and those we reported in March 2022 reflect further analysis of publicly available information on the status of cases.
[444]In addition to the individuals who pleaded guilty and had been sentenced, six individuals who were convicted at trial were sentenced as of January 31, 2022, as discussed later in this enclosure.
[445]In addition to the $1,200 restitution to the IRS, this individual was also ordered to pay over $80,000 in restitution to the Social Security Administration.
[446]The Families First Coronavirus Response Act authorized the IRS to provide advance payment of tax credits to small and midsize employers to reimburse them for providing paid emergency sick leave and expanded family medical leave to their employees for leave related to COVID-19. Pub. L. No. 116-127, 134 Stat. 178 (2020).
[447]Six of these individuals had been sentenced as of January 31, 2022. Sentences ranged from 1 year and 1 day in prison and an order to pay restitution of over $10.7 million for PPP- and EIDL-related fraud to 17 years in prison and an order to pay over $1.5 million in restitution for an individual convicted of PPP-related fraud. As of January 31, 2022, there had not been any convictions at trial related to UI, EIP, or other federal COVID-19 relief programs.
[448]Some of these individuals also faced federal charges related to consumer fraud or other types of COVID-19-related fraud.
[449]Of the 548 individuals or entities, 83 faced charges related to more than one federal COVID-19 relief program. For example, 56 individuals faced federal charges related to both PPP and EIDL, 12 individuals faced federal charges related to both EIDL and UI, and one individual faced federal charges related to PPP, the Accelerated and Advance Payments Program, and the Provider Relief Fund as of January 31, 2022.
[450]One of the 20 individuals or entities also pleaded guilty to federal charges of defrauding a COVID-19 relief program. Also, 13 of the 20 individuals or entities had been sentenced as of January 31, 2022. Sentences for individuals ranged from 6 months of probation and almost $5,000 in restitution to more than 5 years in prison. In addition to these 20 individuals or entities, since March 2020, DOJ resolved a civil complaint of consumer fraud against one entity through a civil settlement.
[451]Nineteen individuals had been sentenced as of January 31, 2022. Sentences ranged from 1 year of probation and a $2,000 fine in the case of an individual who pleaded guilty to conspiracy associated with a COVID-19 vaccine-related healthcare fraud scheme to almost 7 years in prison and an order to pay over $61 million in restitution in the case of an individual who pleaded guilty to conspiracy associated with a Medicare healthcare fraud scheme that exploited the COVID-19 pandemic. In addition to these 19 individuals, since March 2020, DOJ resolved complaints against four individuals or entities for activities such as hoarding and price gouging through settlements.
[452]This individual also pleaded guilty to theft of government funds associated with a scheme to defraud the EIDL program.
[453]In addition to the federal government, state governments have brought fraud charges related to COVID-19 vaccinations. In prior CARES Act reports, we have reported that, while the extent of vaccine-related fraud is unknown, DOJ has publicly announced charges or other actions in consumer fraud cases involving individuals or entities that claimed to offer vaccines to prevent COVID-19.
[454]The COVID-19 Consumer Protection Act, which became law in December 2020 as part of the Consolidated Appropriations Act, 2021, gives the FTC authority to seek civil penalties on the first offense for scams and deceptive practices related to the COVID-19 pandemic. Pub. L. No. 116-260, div. FF, tit. XIV, § 1401, 134 Stat. 1182, 3275-3276 (2020).
[455]42 U.S.C. § 1320a-7a. According to HHS OIG, in each Civil Monetary Penalty case resolved through a settlement agreement, the settling party has contested OIG’s allegations and denied any liability. No Civil Monetary Penalty judgment or finding of liability has been made against the settling party.
[456]The Attorney General established this task force on May 17, 2021, to marshal the resources of DOJ in partnership with agencies across the government. The task force held its first meeting on May 27, 2021, where task force members discussed priority goals, including increased efforts to combat fraud related to COVID-19 relief programs.
[457]The Disaster Relief Fund receives an annual appropriation and has routinely received supplemental appropriations. In March 2020, the CARES Act was enacted, appropriating $45 billion for the Disaster Relief Fund. Pub. L. No. 116-136, div. B, tit. VI, 134 Stat. 281, 543 (2020). The Consolidated Appropriations Act, 2021 appropriated $17 billion to the Disaster Relief Fund for major disasters and an additional $2 billion to provide assistance for COVID-19-related funeral expenses. Pub. L. No. 116-260, div. F, tit. III, 134 Stat. 1182, 1462 (2020); Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910. In March 2021, the American Rescue Plan Act of 2021 appropriated $50 billion to the Disaster Relief Fund. Pub. L. No. 117-2, § 4005, 135 Stat. 4, 79.
[458]White House, Memorandum on Maximizing Assistance from the Federal Emergency Management Agency (Feb. 2, 2021).
[459]White House, Memorandum on Maximizing Assistance to Respond to COVID-19 (Aug. 17, 2021); White House, Memorandum for the Secretary of Homeland Security and the Administrator of the Federal Emergency Management Agency on Maximizing Assistance to Respond to COVID-19 (Nov. 9, 2021); White House, Memorandum on Maximizing Assistance to Respond to COVID-19, Memorandum for the Secretary of Homeland Security, the Administrator of the Federal Emergency Management Agency (Mar. 1, 2022).
[460]The amounts shown in the figure below include Disaster Relief Fund obligations through February 28, 2022, and projections through March 31, 2022.
[461]White House, Memorandum on Authorizing the Other Needs Assistance Program for Major Disaster Declarations Related to Coronavirus Disease 2019 (Aug. 8, 2020). Pursuant to the presidential memorandum, upon receiving a FEMA grant, states and territories may provide eligible claimants $300 or $400 per week—which includes a $300 federal contribution—in addition to their Unemployment Insurance benefits. The presidential memorandum directed that the program would end either when $44 billion had been obligated, the balance of the Disaster Relief Fund reached $25 billion, on December 27, 2020, or upon the enactment of legislation providing supplemental federal unemployment compensation, whichever comes first.
[462]Pub. L. No. 116-260, div. M, tit. II, 134 Stat. at 1910.
[463]Pub. L. No. 117-2, § 4006, 135 Stat. at 79. Appropriations to the Disaster Relief Fund are generally not specific to individual disasters and may be use for various disaster assistance programs.
[464]Specifically, for deaths that occurred between January 20, 2020, and May 16, 2020, applicants can submit a signed statement or letter from the certifying official on the death certificate, or from the medical examiner or coroner in the jurisdiction in which the death occurred, that attributes the death to COVID-19. For deaths occurring after May 16, 2020, applicants must include a copy of the death certificate that attributes the death to COVID-19.
[465]Eligible funeral service expenses include, but are not limited to, transportation for up to two individuals to identify decedent, transfer of remains, casket or urn, burial plot or cremation niche, marker or headstone, clergy or officiant services, arrangement of funeral ceremony, use of funeral home equipment or staff; interment, costs associated with producing and certifying multiple death certificates, and additional expenses mandated by any applicable state or local government laws or ordinances. Costs associated with travel to scatter ashes outside of a memorial service and clothing to attend a funeral service are among expenses not eligible for funeral assistance. Applicants must be U.S. citizens, noncitizen nationals, or qualified aliens who incurred funeral expenses that are not covered by other sources, such as burial insurance.
[466]In this enclosure, funeral assistance refers to COVID-19 Funeral Assistance.
[467]We identified duplicate decedents using decedent Social Security Number (SSN). The $4.8 million in assistance described above may include cases where assistance was also awarded for additional deceased individuals listed on an application, beyond those we identified here.
[468]According to FEMA officials, FEMA has various quality control measures in place for COVID-19 funeral assistance, including reviewing application files for quality and identifying areas for improvement. FEMA identifies improper payments in various ways including the quality control reviews and initiates recoupment efforts where necessary. According to the officials, the recoupment process consists of various phases, including identifying potential debt and notifying applicants of potential debt; not all applications undergoing the process will ultimately require recoupment. The officials stated that as of March 1, 2022, 929 applications were undergoing the recoupment process.
[469]Applicants are required to apply in the disaster area (i.e., state or territory) where the decedent died. According to FEMA officials, if it is discovered during the application process that an applicant applied in an incorrect disaster area, the original application will be canceled and a new application will be generated in the correct area.
[470]FEMA policy states that co-applicants are not required to provide SSN.
[471]In December 2014, we reported that FEMA’s internal controls for identifying invalid SSNs in assistance applications did not prevent payments to some potentially ineligible recipients, although FEMA had improved its ability to detect improper and potentially fraudulent payments since the mid-2000s. We recommended, among other things, that FEMA should collaborate with the Social Security Administration (SSA) to assess the cost and feasibility of checking recipient SSNs against the Enumeration Verification System and the full death file, and if determined to be cost-beneficial take steps to implement a partnership to use SSA data. In March 2018, FEMA reported that it had collaborated with SSA and, based on its analysis, had chosen to maintain its use of the LexisNexis data service, for several reasons including the costs associated with establishing a new data exchange with SSA.
[472]SSA does not guarantee the accuracy of the information in this file. SSA has historically collected death information about SSN-holders so it does not pay Social Security benefits to deceased individuals and to establish benefits for survivors. SSA receives death reports from a variety of sources, including states, family members, funeral directors, post offices, financial institutions, and other federal agencies. We refer to SSA’s complete file of death records as “the full death file.” A subset of the full death file that may not include death data received by the states, which SSA calls “the Death Master File,” is available to the public.
[473]As described previously, we identified evidence showing that in at least some cases, the awards were paid twice—both for the initial application and for the transferred application.
[474]To be eligible for assistance, applicants must have incurred funeral expenses on or after January 20, 2020, due to a death attributed to COVID-19. FEMA officials told us that while deaths could have occurred prior to this date, FEMA uses death date as an initial indicator of eligibility and performs additional manual review of applications with earlier death dates. We defined valid death dates as those occurring between December 1, 2019, and November 30, 2021, as FEMA officials stated that our data contained applications submitted through November 30, 2021.
[475]Approximately 2 percent of the award-receiving applications we reviewed listed more than one decedent.
[476]White House, Memorandum to Extend Federal Support to Governors’ Use of the National Guard to Respond to COVID-19 and to Increase other Federal Assistance Provided to States (Jan. 21, 2021). Eligible work under these mission assignments remains limited to those activities which constitute emergency protective measures, as authorized for and defined by Public Assistance policies for COVID-19.
[477]The mobile vaccination units were developed in December 2021 based on a Presidential Statement on December 2, 2021. Mobile vaccination units are independent of FEMA’s other previous vaccination efforts.
[478]The President issued an emergency declaration for COVID-19 on March 13, 2020, and subsequent major disaster declarations. However, funding for Public Assistance projects was made retroactive to the start of the incident period, which is January 20, 2020.
[479]White House, Memorandum to Extend Federal Support to Governors’ Use of the National Guard to Respond to COVID-19 and to Increase other Federal Assistance Provided to States (Jan. 21, 2021).
[480]A presidential memorandum, issued on February 2, 2021, required FEMA to provide 100 percent cost share reimbursement for work eligible under Public Assistance for emergency protective measures for work performed after January 20, 2020. This requirement did not include the operational expenses made eligible by the January 21, 2021, memorandum, which receive 100 percent cost share reimbursement for work performed after January 21, 2021. White House, Memorandum on Maximizing Assistance from the Federal Emergency Management Agency (Feb. 2, 2021). On August 17, 2021, the President extended this full reimbursement for all work eligible under Public Assistance retroactively to work performed after January 20, 2020. White House, Memorandum on Maximizing Assistance to Respond to COVID-19 (Aug. 17, 2021). White House, Memorandum on Maximizing Assistance to Respond to COVID-19 (Aug.17, 2021). FEMA, Coronavirus (COVID-19) Pandemic: Safe Opening and Operation Work Eligible for Public Assistance (Interim), FEMA Policy 104-21-0003, Version 2 (Sept. 8, 2021).
[481]See Section C.3.i of Coronavirus (COVID-19) Pandemic: Medical Care Eligible for Public Assistance (Interim) (Version 2) FEMA Policy #104-21-0004.
[482]Consolidated Resource Centers are FEMA entities to centralize and standardize the public assistance grant applications process used by some government state and territorial entities.
[487]The 16 critical infrastructure sectors are: chemical; commercial facilities; communications; critical manufacturing; dams; defense industrial base; emergency services; energy; financial services; food and agriculture; government facilities; healthcare and public health; information technology; nuclear reactors, materials and waste; transportation systems; and water and wastewater systems.
[488]U.S. Bureau of Labor Statistics. North American Industry Classification System 331 (Primary Metal Manufacturing), 333 (Machinery Manufacturing), 335 (Electrical Equipment, Appliance, and Component Manufacturing), and 336 (Transportation Equipment Manufacturing).
[489]Cybersecurity and Infrastructure Security Agency Act of 2018, Pub. L. No. 115-278, § 2(a), 132 Stat. 4168, 4169 (codified as amended at 6 U.S.C. § 652).
[490]In January 2021, the William M. (Mac) Thornberry National Defense Authorization Act for Fiscal Year 2021 established “sector risk management agency” responsibilities for federal departments or agencies designated as such for each critical infrastructure sector or subsector. Pub. L. No. 116-283, § 9002(c), 134 Stat. 3388, 4770. Prior to enactment of the act, a “sector risk management agency” was called a “sector-specific agency.” CISA is also the sector risk management agency for the Chemical; Commercial Facilities; Communications; Dams; Emergency Services; Information Technology; and Nuclear Reactors, Materials and Waste Sectors.
[491]Department of Homeland Security, National Infrastructure Protection Plan 2013: Partnering for Critical Infrastructure Security and Resilience (Washington, D.C.: December 2013). The National Plan outlines how government and private sector participants in the critical infrastructure community can work together to manage risks and achieve security and resilience outcomes for critical infrastructure. According to CISA officials, DHS plans to issue an updated version of the National Plan in fiscal year 2022.
[492]Cybersecurity and Infrastructure Security Agency, Guidance on the Essential Critical Infrastructure Workforce: Ensuring Community and National Resilience in COVID-19 Response (Washington, D.C.: March 19, 2020).
[493]As of April 2021, the Critical Manufacturing SCC had 96 members.
[494]CISA published CISA Insights: Cyber Threats to Critical Manufacturing Sector Industrial Control Systems, which further elaborated on this risk to the Critical Manufacturing Sector. CISA determined there is an increased risk of cyber threats in the sector because of expanded work-from-home during the pandemic—which increase the risks associated with authenticating accounts—and the use of remote-based control systems that manage industrial processes.
[495]Cybersecurity and Infrastructure Security Agency, Guidance on the Essential Critical Infrastructure Workforce: Ensuring Community and National Resilience in COVID-19 Response (Washington, D.C.: March 19, 2020).
[496]The White House, The President’s Coronavirus Guidelines for America (Washington, D.C.: March 16, 2020).
[497]As of February 2022, CISA has issued six versions of the Essential Critical Infrastructure Workforce Guidance: Version 1.0 on March 19, 2020; Version 2.0 on March 28, 2020; Version 3.0 on April 17, 2020; Version 3.1 on May 19, 2020; Version 4.0 on August 18, 2020; and Version 4.1 on August 5, 2021.
[498]The Essential Critical Infrastructure Workforce Guidance stated that the list was “advisory in nature,” and should not be considered a federal directive. State, local, tribal, and territorial governments were responsible for implementing COVID-19 pandemic response efforts in their jurisdictions.
[499]According to CISA officials, the most useful pandemic planning document they relied on to develop the Essential Critical Infrastructure Workforce Guidance was the National Infrastructure Advisory Council’s Chemical, Biological, and Radiological Events and the Critical Infrastructure Workforce, Final Report and Recommendations by the Council (January 8, 2008). Officials also cited Department of Homeland Security, U.S. Critical Infrastructure 2025: A Strategic Risk Assessment (Washington, D.C.: April 2016), and Department of Homeland Security, Pandemic Impacts to Lifeline Critical Infrastructure (Washington, D.C.: July 30, 2015).
[500]Version 4.0, issued on August 18, 2020, introduced an essential worker category for education, which included teachers.
[501]Classification codes group businesses into industries according to similarity. For example, the code for “machinery manufacturing” can be further narrowed into specific industry groups, such as “industrial machinery manufacturing,” of which “semiconductor machinery manufacturing” is a sub-industry.
[503]Workers from the four critical manufacturing-related companies that requested National Interest Exceptions were from countries that included France, South Africa, Germany, and Ireland.
[504]Cybersecurity and Infrastructure Security Agency, Building a More Resilient ICT Supply Chain: Lessons Learned During the COVID-19 Pandemic, An Analysis (Washington, D.C.: November 2020).
[505]Cybersecurity and Infrastructure Security Agency, Critical Manufacturing Sector Strategic Planning Initiative: Summary Report (Washington, D.C.: July 2021).
[506]Department of Homeland Security, National Infrastructure Protection Plan 2013: Partnering for Critical Infrastructure Security and Resilience (Washington, D.C.: December 2013).
[507]Department of Homeland Security, Supplemental Tool: Executing a Critical Infrastructure Risk Management Approach (Washington, D.C.).
[508]Department of Homeland Security, Critical Manufacturing Sector-Specific Plan, An Annex to the NIPP 2013 (Washington, D.C.: 2015).
[509]Cybersecurity and Infrastructure Security Agency, Critical Manufacturing Sector, Strategic Planning Initiative: Summary Report (Washington, D.C.: July 2021).
[510]Cybersecurity and Infrastructure Security Agency, Critical Manufacturing Sector: Security Guide (Washington, D.C.: July 2020).
[511]In January 2021, the William M. (Mac) Thornberry National Defense Authorization Act for Fiscal Year 2021 established “sector risk management agency” responsibilities for federal departments or agencies designated as such for each critical infrastructure sector or subsector. See Pub. L. No. 116-283, § 9002(c), 134 Stat. 3388, 4770.
[512]The Payment Integrity Information Act of 2019 (PIIA) further states that this definition includes any payment to an ineligible recipient, any payment for an ineligible good or service, any duplicate payment, any payment for a good or service not received (except for such payments where authorized by law), and any payment that does not account for credit for applicable discounts. See PIIA, Pub. L. No. 116-117, 134 Stat. 113, 114 (Mar. 2, 2020), codified at 31 U.S.C. § 3351(4). PIIA also provides that when an executive agency’s review is unable to discern whether a payment was proper as a result of insufficient or lack of documentation, this payment must also be included in the improper payment estimate. 31 U.S.C. § 3352(c)(2).
[513] PIIA repealed the prior statutes governing executive agency improper payment reporting, and enacted substantially similar provisions in a new subchapter of the U.S. Code. However, the core structure of executive branch agency assessment, estimation, analysis, and reporting of improper payments remains consistent with the prior statutory framework. See 31 U.S.C. §§ 3351-3352. See also Office of Management and Budget (OMB), Appendix C to OMB Circular A-123, Requirements for Payment Integrity Improvement, OMB Memorandum M-21-19 (Washington, D.C.: Mar. 5, 2021); Office of Management and Budget, Financial Reporting Requirements, Circular No. A-136, (Washington, D.C.: Aug. 10, 2021).
[514] A program is considered to be susceptible to significant improper payments if, in the preceding fiscal year, the sum of the program’s improper payments and payments whose propriety cannot be determined due to lacking or insufficient documentation may have exceeded either (1) 1.5 percent of program outlays and $10 million or (2) $100 million (regardless of the improper payment rate). 31 U.S.C. § 3352(a).
[516]While not all improper payments are the result of fraud, all payments made as a result of fraudulent activities are considered to be improper payments. In addition, improper payment estimates are not intended to measure fraud in a particular program.
[517] The TANF program serves as the nation’s major cash assistance program for low-income families with children.
[518]Department of Health and Human Services, FY 2021 Agency Financial Report (Washington, D.C.: November 2021), pg. 233.
[519]HHS Office of Inspector General, Office of Audit Services, U.S. Department of Health and Human Services Met Many Requirements, but It Did Not Fully Comply With the Payment Integrity Information Act of 2019 and Applicable Improper Payment Guidance for Fiscal Year 2020, A-17-21-52000 (Washington, D.C.: May 14, 2021), pg. 14.; U.S. Department of Health and Human Services Met Many Requirements of the Improper Payments Information Act of 2002 but Did Not Fully Comply for Fiscal Year 2019, A-17-20-52000 52000 (Washington, D.C.: May 8, 2020), pg. 14.
[520]Office of Management and Budget, Risk Based Financial Audits and Reporting Activities in Response to COVID-19 (Washington, D.C.: June 17, 2020).
[521]Labor’s improper payment rate estimates for fiscal year 2020 reporting covers July 1, 2019, through June 30, 2020.
[522]Department of Labor, Office of the Inspector General, The U.S. Department of Labor Complied with the Payment Integrity Information Act for FY 2020, But Reported Unemployment Insurance Information Did Not Represent Total Program Year Expenses, No. 22-21-007-13-001 (Washington, D.C.: Aug. 6, 2021).
[523]The three risk-susceptible programs are the Office of Public and Indian Housing’s Tenant-Based Rental Assistance Program, the Office of Multifamily Housing Programs’ Project-Based Rental Assistance Program, and the Office of Community Planning and Development’s Disaster Recovery Assistance – Hurricanes Harvey, Irma, Maria.
[524]Department of Housing and Urban Development Office of Inspector General, HUD Did Not Fully Comply With the Payment Integrity Information Act of 2019, 2021-AT-0002 (Atlanta, GA: May 17, 2021).
[527]According to OMB staff, this occurred because one agency failed to convert their recovery amount into millions of dollars prior to entering it into the OMB data call tool.
[529]The Single Audit Act is codified at 31 U.S.C. §§ 7501-06, and implementing OMB guidance is reprinted in 2 C.F.R. part 200. The Act requires a “single audit” of the entity’s financial statements and federal awards for the fiscal year. 31 U.S.C. § 7502; 2 C.F.R. § 200.501.
[530]See 2 C.F.R. § 200.514(d)(3). For any program not contained in the Supplement, auditors must follow the general guidance in Part 7 of the 2021 Compliance Supplement, which provides guidance in how to identify the compliance requirements to tests for compliance.
[531]Office of Management and Budget, Promoting Accountability through Cooperation among Agencies and Inspectors General, OMB Memorandum M-22-04 (Washington, D.C.: Dec. 3, 2021).
[532]We conducted an in-depth review of 22 studies that met our criteria for relevance and methodological rigor. We identified a number of data and methodological limitations in the studies we reviewed. For example, some studies used data from only the initial PPP rounds or data on PPP loans that could be combined with data from other sources and did not include information on all PPP loans. Moreover, studies used methods that may not have fully identified causal relationships or fully accounted for possible spillover effects of PPP. In addition, most of the studies had not yet been peer reviewed at the time of writing and are subject to revision. Nevertheless, collectively, the studies we reviewed provide useful information on economic effects of PPP during the beginning of the pandemic.
[533]M. Dalton, “Putting the Paycheck Protection Program into Perspective: An Analysis Using Administrative and Survey Data,” U.S. Bureau of Labor Statistics Working Paper 542 (2021).
[534]Qualifying businesses for PPP generally include businesses with 500 or fewer employees or that meet SBA’s industry-based size standard. To the extent that smaller businesses are more vulnerable to shocks (e.g., due to smaller cash reserves and poorer access to credit), these findings suggest that PPP helped small businesses achieve similar, or even better, employment outcomes compared to larger firms during the pandemic.
[535]D. Autor, D. Cho, L. D. Crane, M. Goldar, B. Lutz, J. Montes, W. B. Peterman, D. Ratner, D. Villar, and A. Yildirmaz, "An Evaluation of the Paycheck Protection Program Using Administrative Payroll Microdata," Working Paper (2020). Similarly, another study found that employment growth at eligible businesses was about two percentage points higher than employment growth at larger firms over the period from early April 2020 to mid-August 2020. R. Chetty, J. N. Friedman, N. Hendren, M. Stepner, and The Opportunity Insights Team, “How Did COVID-19 and Stabilization Policies Affect Spending and Employment? A New Real-Time Economic Tracker Based on Private Sector Data,” National Bureau of Economic Research (NBER) Working Paper No. 27431 (2020).
[536]Dalton, “Putting the Paycheck Protection Program into Perspective: An Analysis Using Administrative and Survey Data.” This study, which as discussed above found that recipients’ employment increased by 8 percent on average within the first month of being approved for a PPP loan, also examined PPP’s effects on employment by recipient’s size and wage class. The study measured size based on average monthly employment in 2019 and measured wage class based on the establishment-wide average wage paid in 2019.
[537]R. G. Hubbard and M. R. Strain, “Has the Paycheck Protection Program Succeeded?” NBER Working Paper No. 28032 (2020). The authors measured firm size based on employment in February 2020.
[538]C. James, J. Lu, and Y. Sun, "Time is Money: Real Effects of Relationship Lending in a Crisis," Journal of Banking & Finance vol. 133 (2021): 106283.
[539]M. Denes, S. Lagaras, and M. Tsoutsoura, "First Come, First Served: The Timing of Government Support and Its Impact on Firms," SSRN Working paper (2021). There was a 10-day delay between April 16 and 27 in the approval of PPP loans caused by insufficient initial funding. Therefore, the first round of PPP loans ended on April 16, and the second round started on April 27.
[540]P. Kapinos, “Did the Paycheck Protection Program Have Negative Side Effects on Small-Business Activity?" Economics Letters, vol. 208 (2021): 110045. Importantly, the decision for small businesses to remain closed longer may have helped mitigate public health risks associated with COVID-19 at the time.
[541]Other studies found that PPP loan concentration at county level reduced unemployment rates. For example, see P. Kapinos, "Paycheck Protection Program: County-Level Determinants and Effect on Unemployment," Federal Reserve Bank of Dallas Working Paper 2105 (2021).
[542]Kapinos, "Paycheck Protection Program: County-Level Determinants and Effect on Unemployment." The author measured PPP concentration using county level ratios of PPP loans per jobs lost. The study also suggested that PPP reduced unemployment the most in counties with smaller populations and with relatively educated labor forces. S. Barraza, M. Rossi, and T. J. Yeager, "The Short-Term Effect of the Paycheck Protection Program on Unemployment," SSRN Working Paper (2020). In some specifications, the study used the 2019 density of Small Business Administration member bank offices in a county as an instrument for PPP loans originated in that county during April 2020.
[543]M. Faulkender, R. Jackman, and S. I. Miran, "The Job Preservation Effects of Paycheck Protection Program Loans," Office of Economic Policy Working Paper 2020-01, Department of the Treasury (2020).
[544]J. Granja, C. Makridis, C. Yannelis, and E. Zwick, “Did the Paycheck Protection Program Hit the Target?” NBER Working Paper No. 27095 (2021). There was a lack of clarity on determining a business’s need for a PPP loan (see the Paycheck Protection Program enclosure in appendix I). Although PPP assistance may not have gone to the hardest hit areas, it may have gone to the hardest hit sectors. We previously reported that businesses in the hardest hit sectors received a higher share of loans than the share of small businesses in those sectors. See GAO, Paycheck Protection Program: Program Changes Increased Lending to the Smallest Businesses and in Underserved Locations, GAO-21-601 (Washington, D.C.: Sept. 21, 2021).
[545]G. Joaquim and F. Netto, "Bank Incentives and the Effect of the Paycheck Protection Program," Federal Reserve Bank of Boston Working Paper No. 21-15 (2021).
[546]We previous reported that banks collectively made more than 93 percent of all loans in Phase 1 (April 3-April16 2020). See GAO-21-601. In addition, nonbanks, which generally provide lending services but do not accept deposits, were largely unable to participate in the initial phase of the program (see the Paycheck Protection Program enclosure in appendix I).
[547]L. Li and P.E. Strahan, "Who Supplies PPP Loans (and Does It Matter)? Banks, Relationships and the COVID Crisis," Journal of Financial and Quantitative Analysis, vol. 56, no. 7 (2021): 2411-2438. In addition, we previously reported that minority-owned businesses were less likely to have a relationship with a bank. On the other hand, Community Development Financial Institutions and Minority Depository Institutions were more likely than other types of lenders to report that they accepted applications from borrowers with whom they had no prior relationship. See GAO-21-601.
[548]A. Cole, "The Impact of the Paycheck Protection Program on Small Businesses: Evidence from Administrative Payroll Data," SSRN Working Paper (2020).
[549]J. E. Humphries, C. A. Neilson, and G. Ulyssea, "Information Frictions and Access to the Paycheck Protection Program," Journal of Public Economics, vol. 190 (2020): 104244. In addition, we previously reported that larger businesses—small businesses with 10 to 499 employees—received a higher share of loans in Phase 1 (April 3-April 16, 2020) relative to their share of all small businesses. Specifically, 42 percent of loans in Phase 1 went to these larger businesses, despite accounting for only 4 percent of all small businesses in the U.S. See GAO-21-601.
[550]For examples of studies suggesting that PPP likely had a greater effect on employment at smaller businesses, see Dalton, “Putting the Paycheck Protection Program into Perspective: An Analysis Using Administrative and Survey Data” and Hubbard and Strain, “Has the Paycheck Protection Program Succeeded?”
[551]Jobs saved were generally defined as the number of jobs preserved because of PPP. Researchers generally calculated the numbers of jobs saved based on their estimates of the effect of PPP on employment and of numbers of employees working at firms eligible for PPP loans. For example, one study estimated that PPP saved 1.3 million jobs from April through August 15, 2020, while another study estimated that PPP had saved 7.5 million jobs as of the beginning of August 2020. Chetty, Friedman, Hendren, Stepner, and The Opportunity Insights Team, “How Did COVID-19 and Stabilization Policies Affect Spending and Employment? A New Real-Time Economic Tracker Based on Private Sector Data.” Joaquim and Netto, "Bank Incentives and the Effect of the Paycheck Protection Program."
[552]For example, one study we reviewed estimated an average cost of between $20,000 and $34,000 for each month that PPP kept an employee on the payroll, and another study estimated the average cost at between $26,000 and $62,000. Dalton, “Putting the Paycheck Protection Program into Perspective: An Analysis Using Administrative and Survey Data.” Cole, "The Impact of the Paycheck Protection Program on Small Businesses: Evidence from Administrative Payroll Data."
[553]Hubbard and Strain, “Has the Paycheck Protection Program Succeeded?”
[554]As originally implemented by SBA, at least 75 percent of the loan forgiveness amount must have been for payroll costs, while the rest of loan forgiveness could also cover mortgage interest, rent, and utility payments, for example. In addition, the Paycheck Protection Program Flexibility Act of 2020 modified this to at least 60 percent. The Consolidated Appropriations Act, 2021 expanded the categories of forgivable non-payroll costs to include certain operations, property damage, supplier, and worker protection expenditures.
[555]Hubbard and Strain, “Has the Paycheck Protection Program Succeeded?”
[556]Autor, Cho, Crane, Goldar, Lutz, Montes, Peterman, Ratner, Villar, and Yildirmaz, "An Evaluation of the Paycheck Protection Program Using Administrative Payroll Microdata."
[557]GAO, Emergency Relief Funds: Significant Improvements Are Needed to Ensure Transparency and Accountability for COVID-19 and Beyond, GAO-22-105715 (Washington, D.C.: Mar. 17, 2022).
Contacts
Jessica Farb
Managing Director, Health Care, farbj@gao.gov, (202) 512-7114
Congressional Relations
A. Nicole Clowers, Managing Director, clowersa@gao.gov, (202) 512-4400 U.S. Government Accountability Office 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs
Chuck Young, Managing Director, youngc1@gao.gov, (202) 512-4800 U.S. Government Accountability Office 441 G Street NW, Room 7149, Washington, DC 20548
Strategic Planning and External Liaison
Stephen J. Sanford, Managing Director, spel@gao.gov, (202) 512-4707 U.S. Government Accountability Office 441 G Street NW, Room 7814, Washington, DC 20548
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s cost of production and distribution. Pricing and ordering information is posted on our website.
To Report Fraud, Waste, and Abuse in Federal Programs
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Copyright
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.






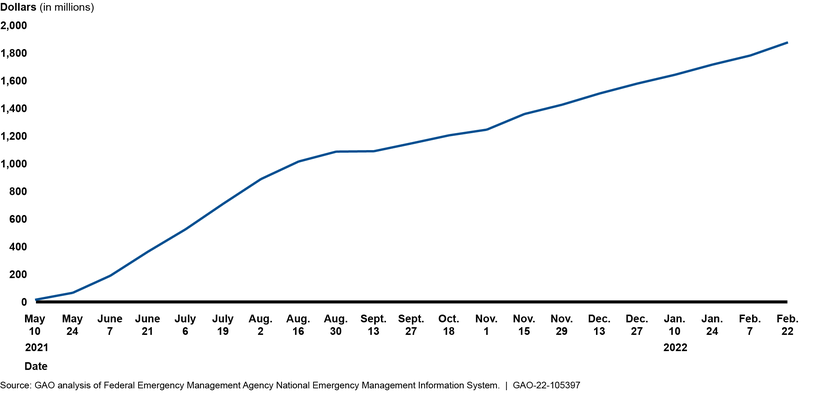


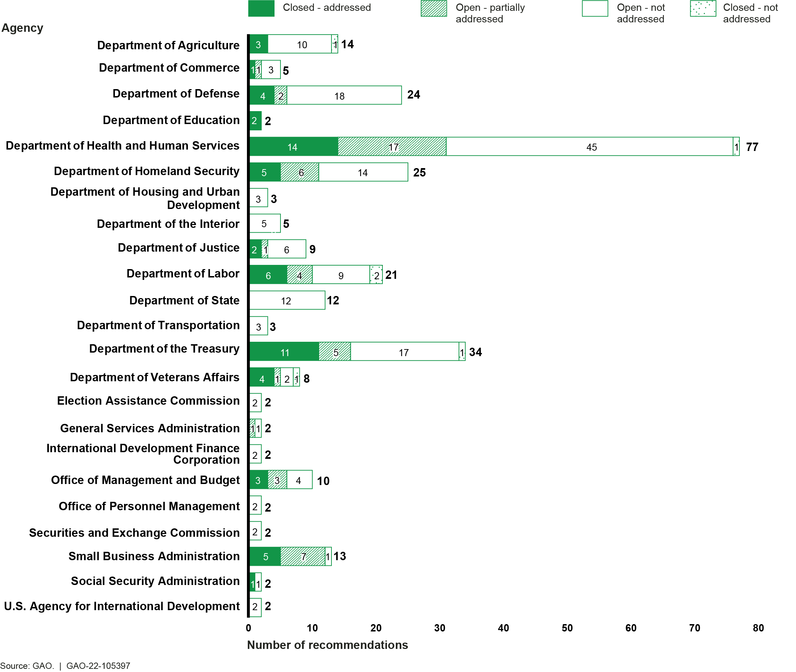




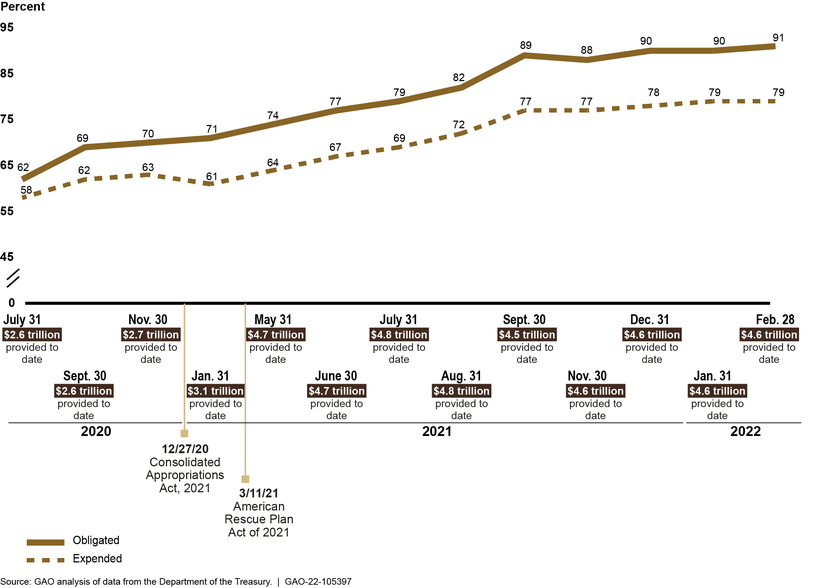



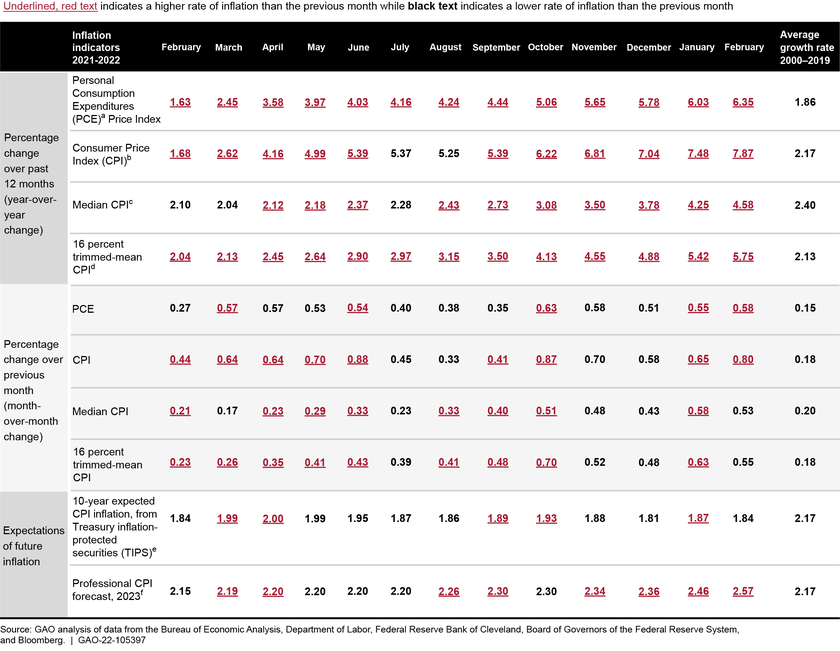
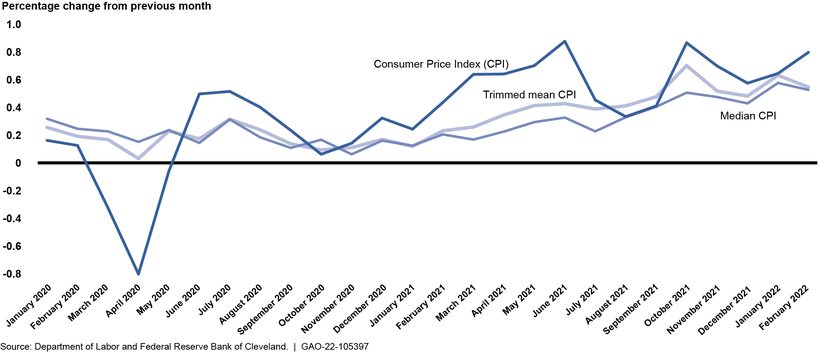

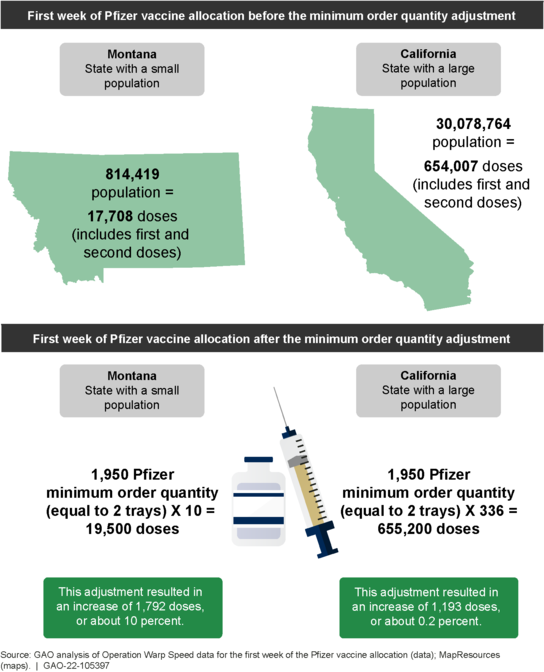
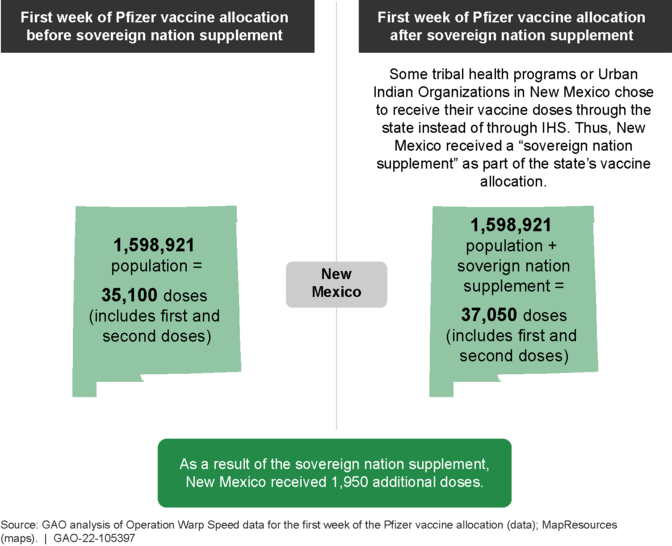

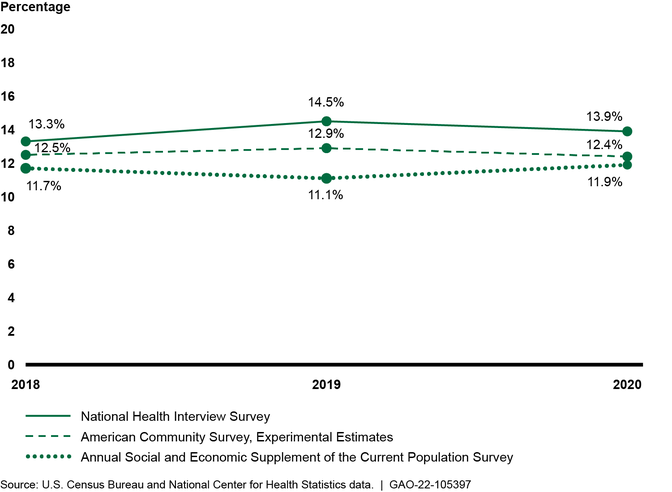
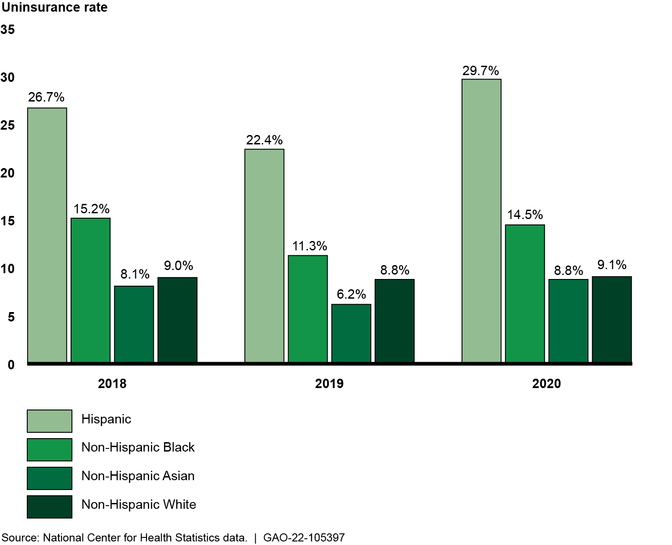
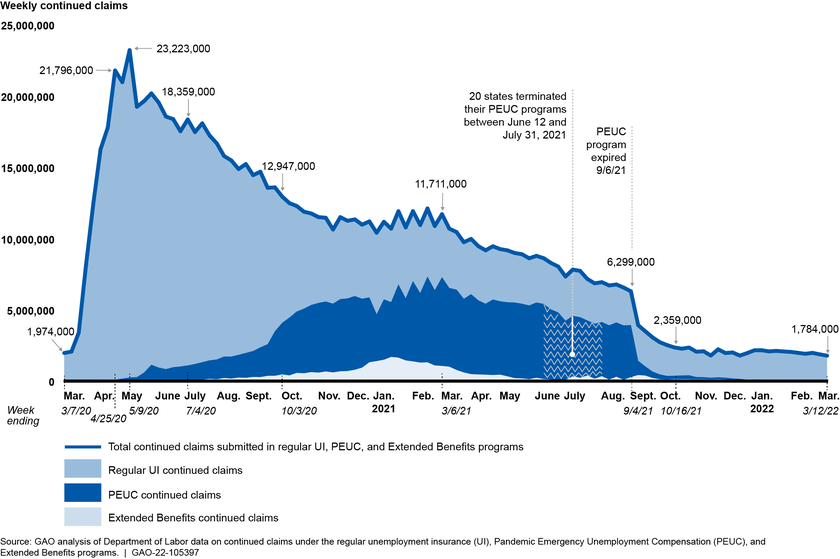
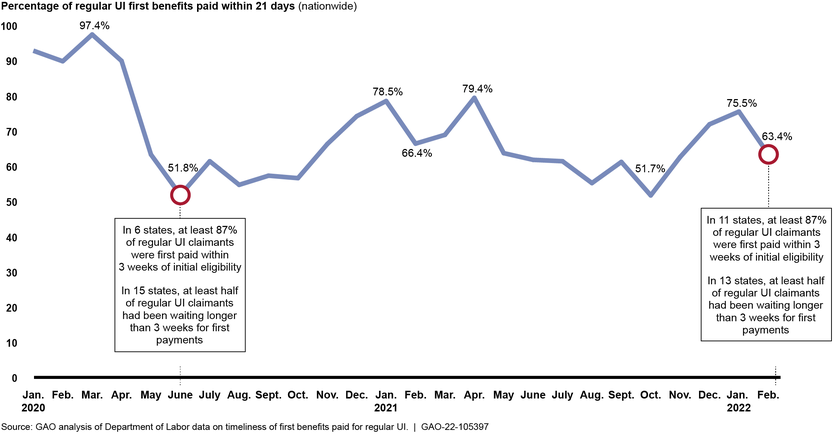

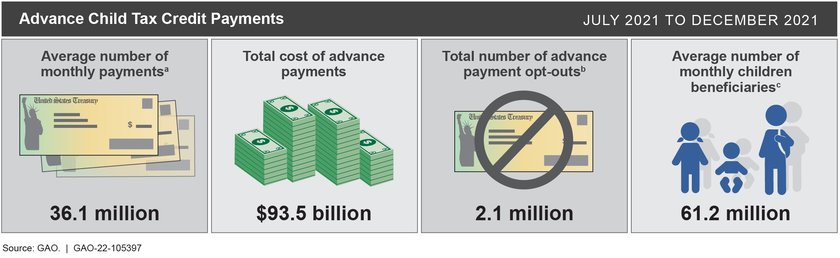
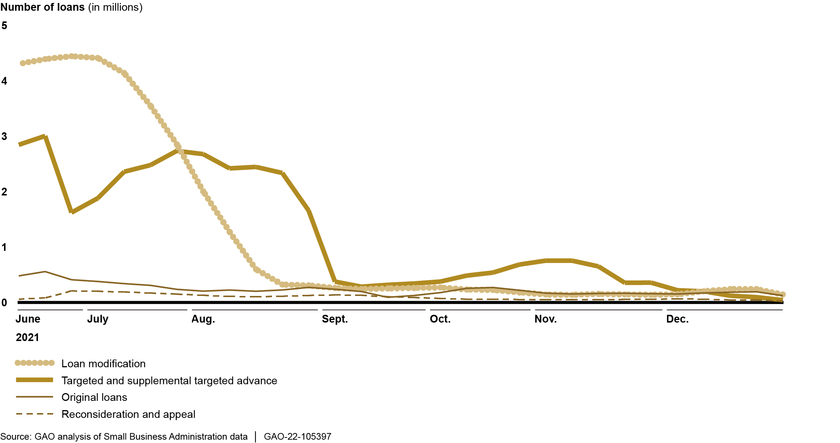
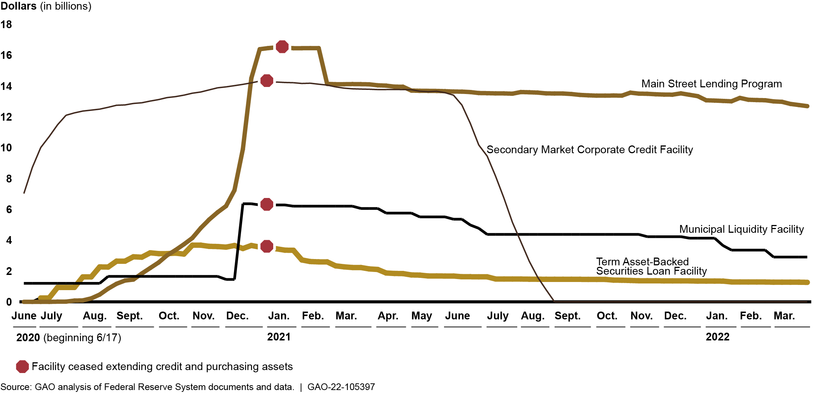
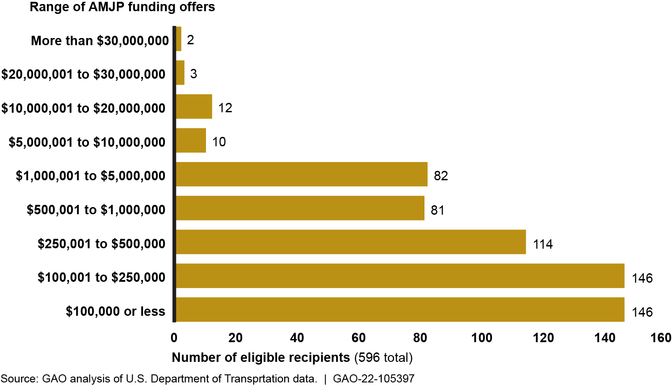
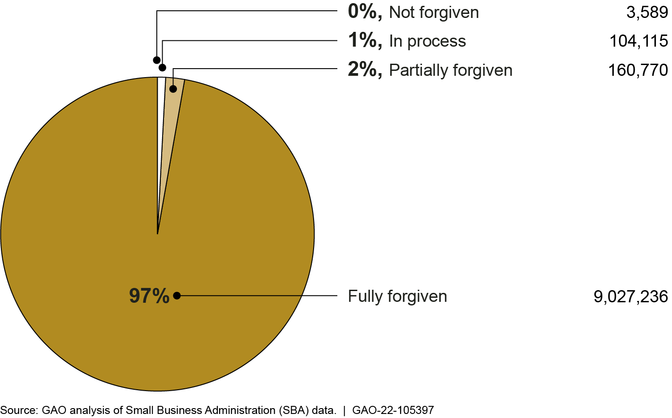
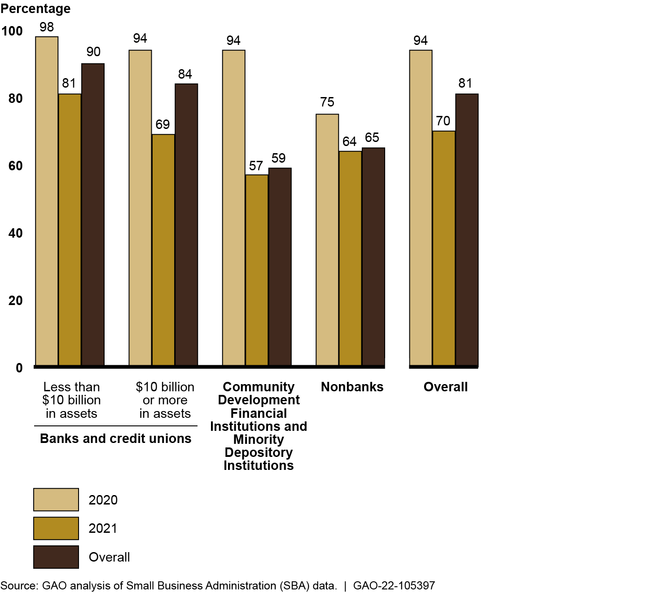
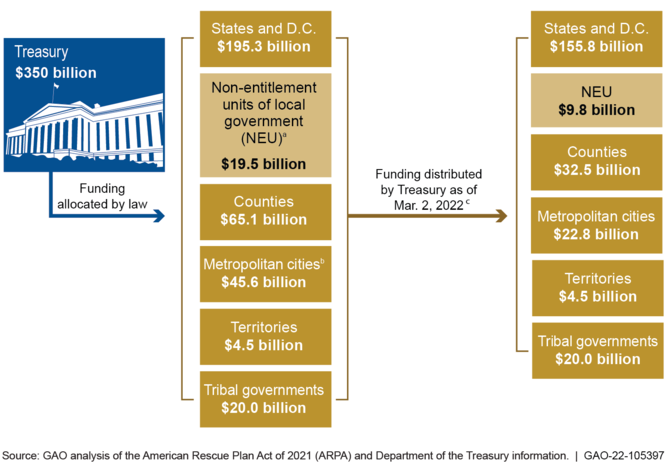
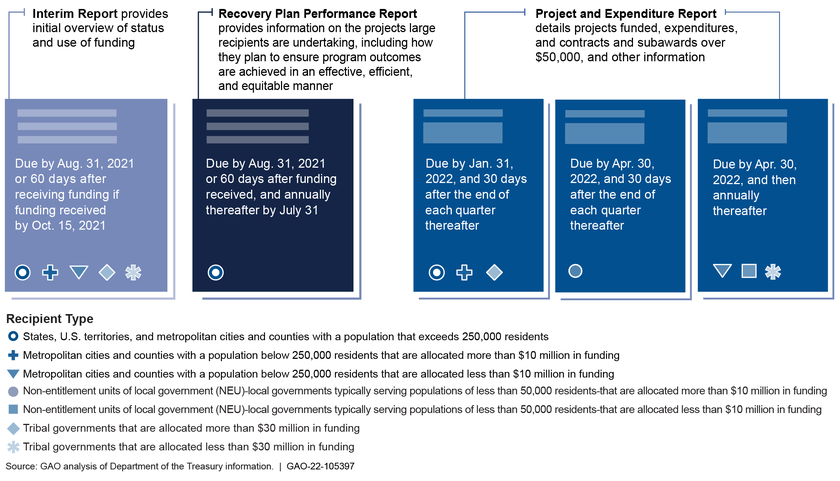
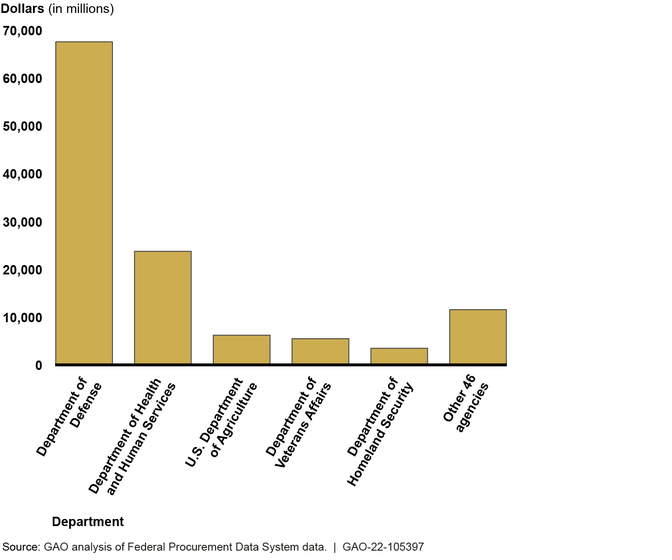

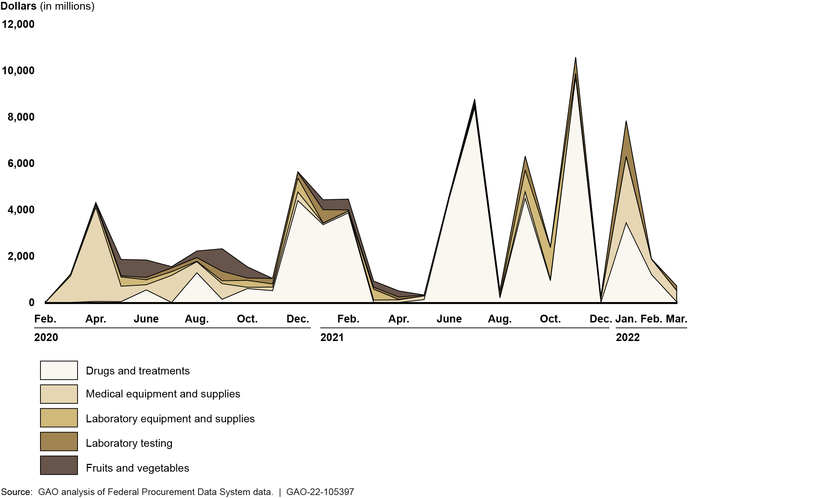
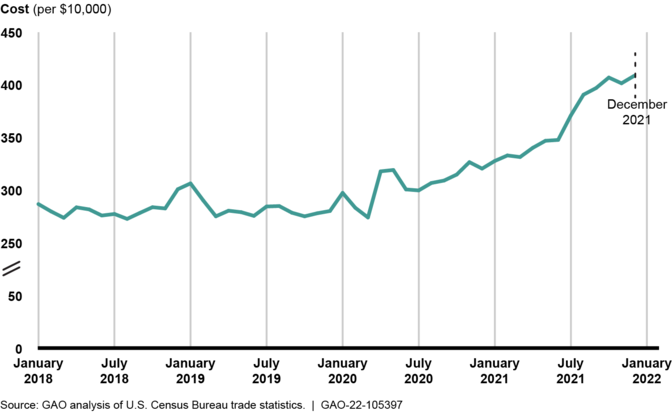
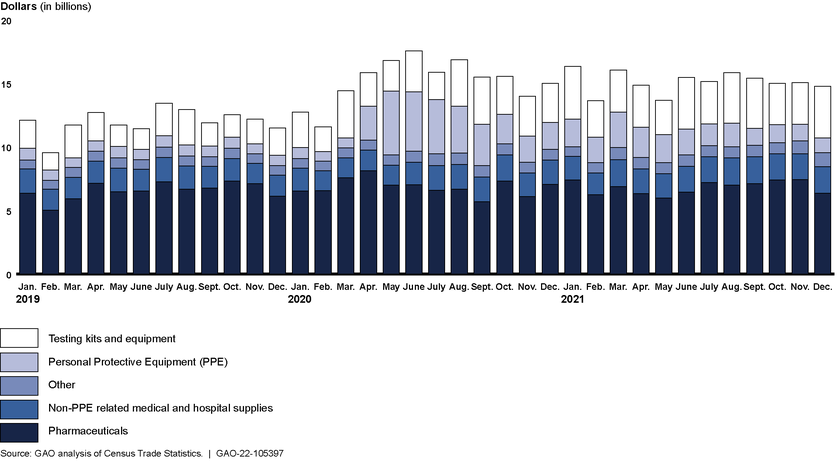

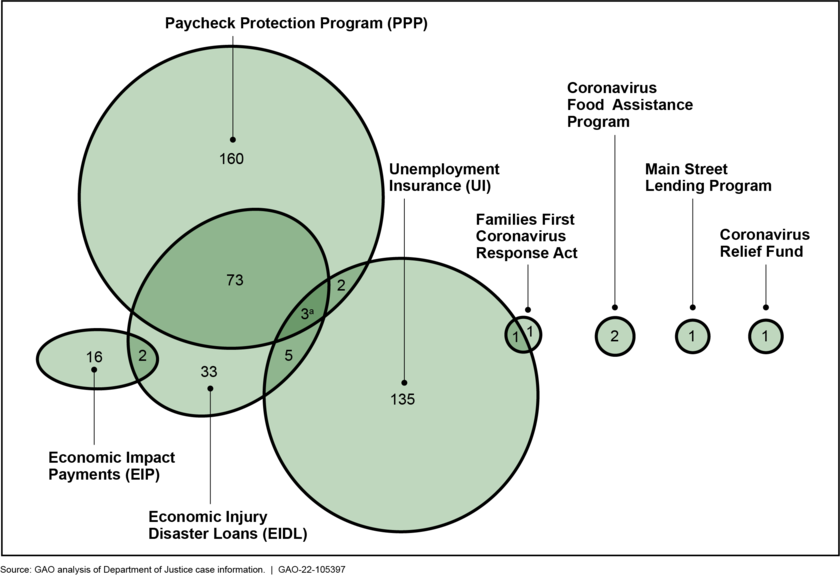

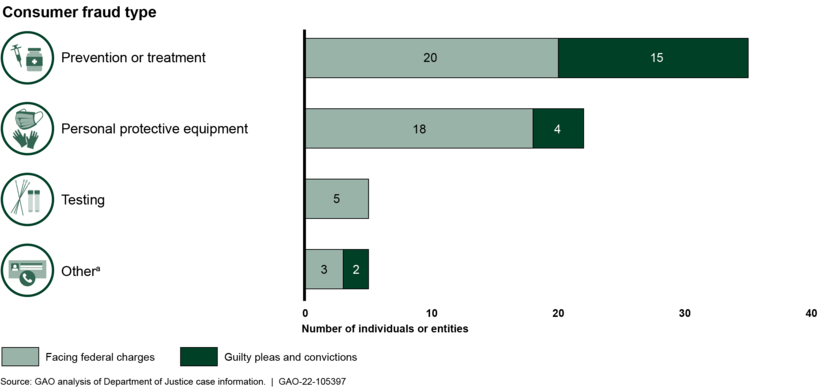
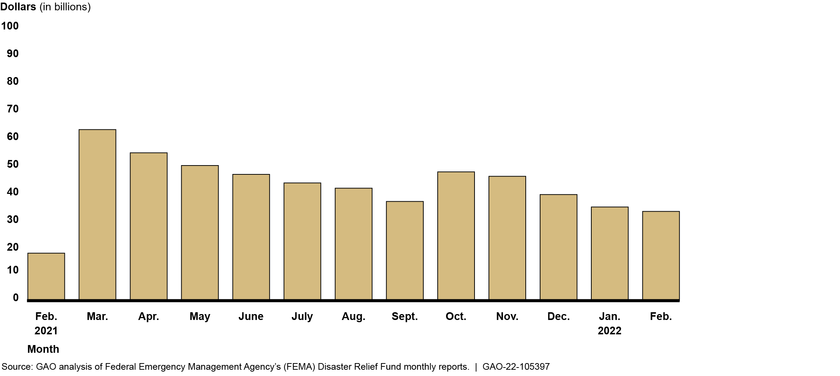
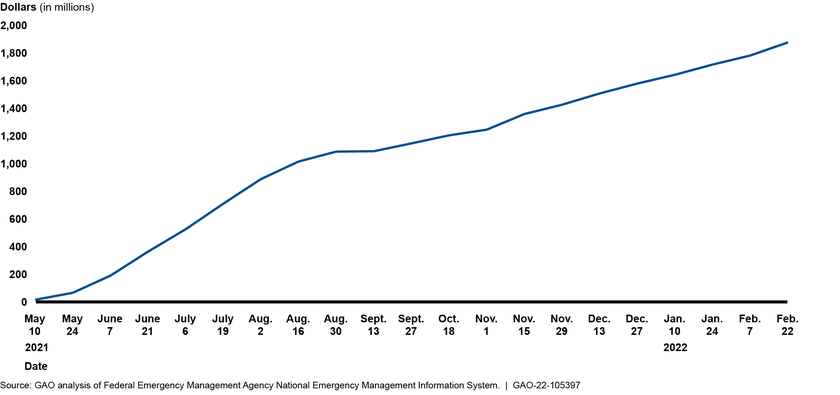

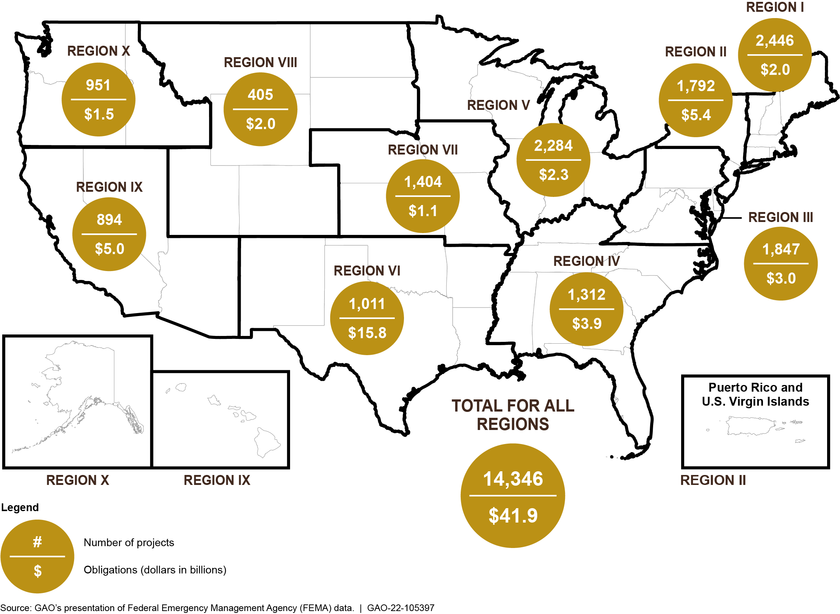
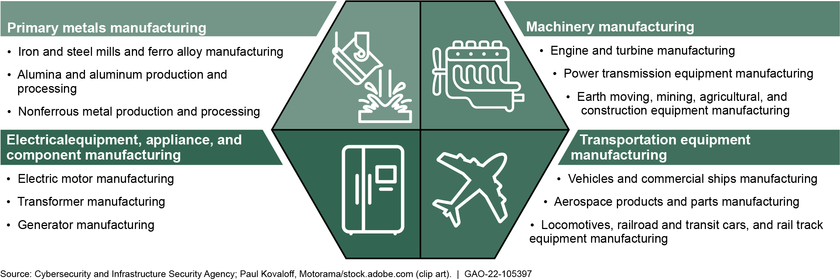


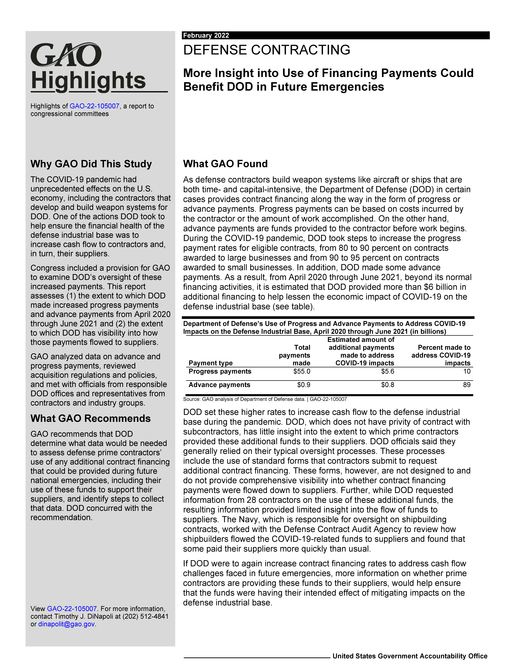
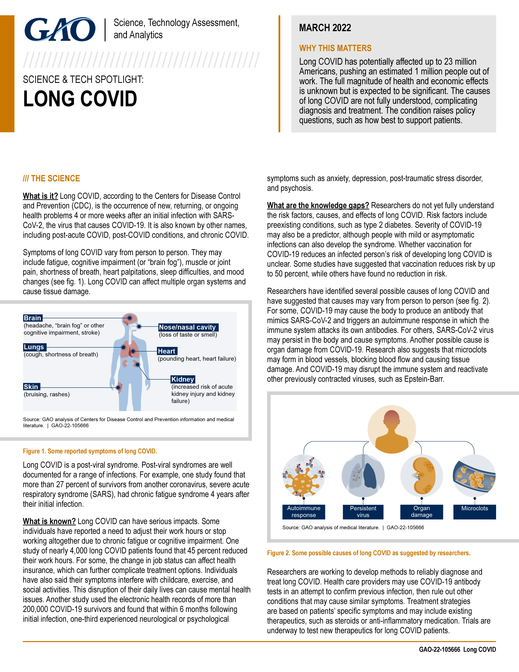


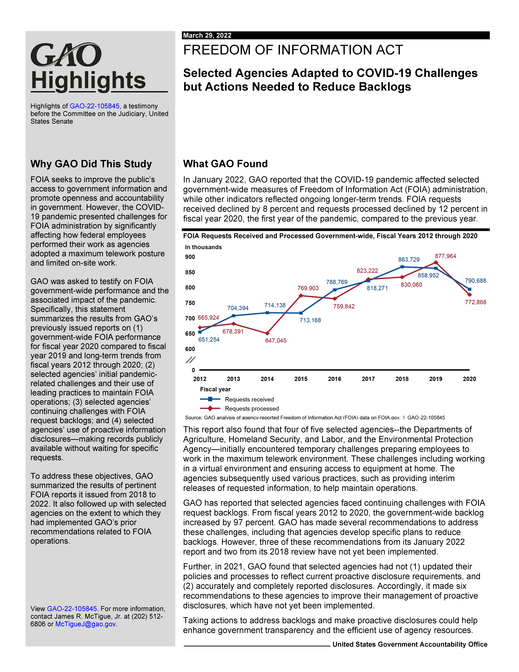



-1650404448776.png)