VETERANS HEALTH CARE
Referral Coordination Initiative for Specialty Care Needs Improved Program Direction and Guidance
Report to Congressional Requesters
United States Government Accountability Office
View GAO‑25‑106678. For more information, contact Sharon M. Silas at (202) 512-7114 or SilasS@gao.gov.
Highlights of GAO‑25‑106678, a report to congressional requesters
Referral Coordination Initiative for Specialty Care Needs Improved Program Direction and Guidance
Why GAO Did This Study
VHA operates the largest health care delivery system in the U.S., providing health care to more than 6 million veterans. In the last decade, Congress has taken steps to expand the ability of eligible veterans to receive care from community health care providers. In fiscal year 2023, 2.9 million veterans received community care. GAO and others have identified challenges veterans have had in scheduling appointments both with VHA facility providers and community care providers.
GAO was asked to examine issues related to VHA appointment scheduling. This report 1) describes the status of the Referral Coordination Initiative’s implementation, and 2) assesses the initiative’s policy and guidance, among other objectives.
GAO reviewed VHA documentation for the Referral Coordination Initiative and surveyed 139 VHA medical facility officials responsible for implementing it, of which 133 responded. GAO also interviewed VHA central office officials and officials from four regional networks and conducted site visits to six VHA medical facilities.
What GAO Recommends
GAO is making five recommendations, including that VHA ensure the Referral Coordination Initiative’s strategic goals and other key aspects of program direction are documented in national policy, and guidance is evidence-based and aligned with policy. The Department of Veterans Affairs concurred with four recommendations and concurred in principle with one recommendation, as discussed in the report.
What GAO Found
In 2019, the Veterans Health Administration (VHA) updated its process for scheduling specialty care appointments. Under this process, called the Referral Coordination Initiative, referral coordination teams at VHA medical facilities review referrals for specialty care, such as cardiology, and discuss care options with veterans. The implementation of the initiative marked a significant change to the process previously followed for management of specialty care referrals.
GAO’s survey found that, as of March 2024, officials from nearly all VHA medical facilities reported using the new process to manage referrals for some specialties. Officials reported using the new process for 30 specialty services, on average. About a fourth reported implementing all planned services.
GAO’s survey of 133 VHA medical facility officials and VHA’s own studies found medical facilities experienced mixed results in implementing the initiative. For example, GAO found facilities experienced difficulties and inconsistencies in implementation. However, facilities also cited potential benefits such as reducing appointment scheduling time. In May 2024, VHA began a “refresh” of the initiative to improve consistency by increasing regional networks’ leadership and oversight of VHA medical facilities’ implementation of the initiative.
As of October 2024, VHA had not documented in policy key elements needed to guide the initiative’s implementation. These elements include strategic goals, standards for consistent implementation, roles and responsibilities, and oversight and accountability. Further, GAO found that VHA regional networks and medical facilities did not have evidence-based, timely, and consistent guidance that aligned with policy. Without national policy that defines program direction and quality guidance that aligns with policy, VHA networks and medical facilities may continue to experience inconsistencies in the initiative’s implementation and struggle to achieve its objectives, such as improving scheduling timeliness.
|
Abbreviations |
|
|
|
|
|
|
|
IVC |
Office of Integrated Veteran Care |
|
|
RCI |
Referral Coordination Initiative |
|
|
VA |
Department of Veterans Affairs |
|
|
VHA |
Veterans Health Administration |
|
|
VISN |
Veterans Integrated Service Network |
|
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
January 21, 2025
The Honorable Julia Brownley
Ranking Member
Subcommittee on Health
Committee on Veterans’ Affairs
House of Representatives
The Honorable Sheila Cherfilus-McCormick
House of Representatives
The Honorable Susie Lee
House of Representatives
The Honorable Chris Pappas
House of Representatives
The Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) operates the largest health care delivery system in the United States, providing health care to more than 6 million veterans.[1] Veterans may obtain health care from VHA providers or, in some cases, may be eligible to choose health care services from community providers through the Veterans Community Care Program.[2] According to VHA, in fiscal year 2023, 2.9 million veterans received community care and VA spent $26.7 billion on this care.
VHA has processes for making referrals and scheduling appointments for specialty care, such as cardiology, for veterans seeking to obtain care at VHA facilities and through community care. VHA’s Office of Integrated Veteran Care (IVC) is responsible for establishing policy and conducting oversight of appointment scheduling processes.[3] In 2019, VHA began implementing the Referral Coordination Initiative (RCI), a program aimed at streamlining scheduling for specialty care appointments at its medical facilities across the country.
Under the initiative, facility-based multidisciplinary referral coordination teams are charged with handling referrals for specialty care—including prioritizing a veteran’s care needs and scheduling appointments—rather than the referring provider, as was the prior practice. According to IVC officials, the COVID-19 pandemic slowed down implementation of the RCI, but implementation resumed in 2021. The VA Office of Inspector General reported in October 2022 that complete implementation—that is, implementation across all specialties at each facility—had not yet occurred for multiple reasons. The report cited reasons such as IVC’s lack of clear guidance on how to implement the initiative and insufficient communication with VHA medical facility officials.[4]
We and others have identified challenges VA has had ensuring that veterans’ health care appointments are scheduled and occur in a timely manner, both at VHA medical facilities and in the community, and have made several related recommendations.[5] In addition, VHA has acknowledged problems with its scheduling processes, citing variations in how scheduling is managed at its medical facilities and how complex scheduling processes at the facility level leads to inefficiencies, workarounds, delays in care, and inconsistent veteran experiences. Because of concerns with wait times and other issues, including the lack of clarity around VHA program offices’ and Veterans Integrated Service Networks’ (VISN) oversight responsibilities, VHA health care continues to be on our High Risk List.[6]
You asked us to examine issues related to VA appointment scheduling and wait times.[7] VHA has identified the RCI as a key effort to provide the soonest and best care to veterans and improve appointment scheduling timeliness for specialty care. Given this and the prior findings of the VA Office of the Inspector General, this report focuses on the RCI. Specifically, in this report, we
1. describe the status of the RCI’s implementation;
2. assess the extent to which RCI program direction is defined in policy and VISNs and VHA medical facilities have quality RCI guidance; and
3. assess the extent to which there are established metrics that provide VISNs and VHA medical facilities with the information needed to measure performance of the RCI.
To address these objectives, we reviewed VHA documents, including policies and guidance documents related to appointment scheduling and the RCI process. We also reviewed IVC documents regarding performance goals and metrics. To obtain a broad understanding of facilities’ experiences implementing the RCI, we conducted a survey of VHA medical facilities between January and March 2024 and analyzed information provided by 133 medical facility RCI officials (out of 139) who responded.[8] We also interviewed officials from IVC and from four VISNs and conducted a total of six site visits to VHA medical facilities—three in person and three virtually. The information we obtained from site visits is not generalizable to other VHA facilities. We evaluated information we collected against relevant VHA policies, including VHA’s directive for policy management and VHA’s directive for operating units.[9] We also evaluated this information against federal internal control standards related to using quality information and our key practices regarding evidence-building and performance management activities in the federal government.[10] See appendix I for additional details, including our survey methodology and site visit selection criteria.
We conducted this performance audit from March 2023 to January 2025 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
VHA Appointment Scheduling
There are three primary ways to initiate a request for health care once a veteran is enrolled in VHA: (1) a veteran-initiated appointment request, (2) a provider request for a follow-up appointment with the veteran, and (3) a provider referral of the veteran for a specialty care appointment.[11] For a veteran to receive a specialty care appointment, a VHA provider must initiate a request by submitting a referral, which VHA calls a consult.[12] Clinical staff (e.g., providers and nurses) and administrative staff (e.g., schedulers) at the VHA facility review the referral and consider eligibility for community care. Then, depending on whether the veteran is eligible for community care and the veteran’s scheduling preferences, facility staff will schedule an appointment either with a VHA provider at a VHA medical facility or with a non-VHA provider in the community.[13]
Community Care
Through the Veterans Community Care Program, which VHA implemented on June 6, 2019, in response to the VA MISSION Act of 2018 (VA MISSION Act), eligible veterans may choose to obtain health care services from community providers rather than from VHA providers in some circumstances.[14] There are six criteria that can qualify a veteran to receive care under the Veterans Community Care Program.[15] For example, veterans may qualify for community care when the needed services are not available at any VHA facility or if VHA cannot provide care within its designated access standards. VHA’s designated access standards specify that a veteran may be eligible for community care if
· the average drive time to a VHA provider is more than 30 minutes for primary care or more than 60 minutes for specialty care, or
· the first next available appointment with a VHA provider is not available within 20 days for primary care or 28 days for specialty care based on the date of the request for care unless a later date has been agreed upon.[16]
For additional details on community care eligibility determinations, see appendix II.
Roles and Responsibilities for Specialty Care Appointment Scheduling
VHA headquarters, its regional network of VISNs, and VHA medical facilities all play a role in managing referrals and scheduling veterans’ appointments for care in a timely manner at VHA medical facilities and in the community.[17]
· At the VHA headquarters level, IVC is responsible for establishing scheduling policy and conducting oversight of appointment scheduling processes for appointments at VHA medical facilities and through community care.[18] VHA’s scheduling and referral policy also sets the requirements for staff involved in the scheduling process.[19]
· Each VISN is responsible for overseeing policy implementation and the performance of the VHA facilities within its network.
· VHA medical facility directors are responsible for managing the facility’s implementation of scheduling and referral policy, processes, outcomes, and regular monitoring of performance on those outcomes.[20] Facility directors are also responsible for allocating sufficient resources to manage scheduling, including referrals, to ensure the timely delivery of care. At the VHA medical facility, clinics—including primary care, mental health, and specialty care—and the community care office have scheduling staff and supervisors who are responsible on a day-to-day basis for managing referrals and coordinating and scheduling veteran care.[21] Referring providers, who are typically VHA primary care providers, are responsible for entering referrals for specialty care into VHA’s electronic record system.[22]
RCI Program and Process
According to VHA, shortly after implementing the Veterans Community Care Program in response to the VA MISSION Act, it needed to update its referral processes. Accordingly, in November 2019, VHA issued memos to VISNs and VHA medical facilities announcing the RCI.[23]
According to IVC’s RCI Guidebook, the main guidance document for VISNs and VHA medical facilities, the RCI is intended to
· create dedicated referral coordination teams that are focused on sharing with veterans their health care options,
· empower veterans to make the health care choice that is right for them, and
· improve scheduling timeliness.
The RCI process is handled by facility referral coordination teams that include designated clinical and administrative staff who assist with scheduling and are trained to discuss veterans’ options for care at the time of scheduling. The process is intended to ensure that referrals are complete and include all pertinent clinical information before the coordination teams discuss care options and schedule appointments in VHA medical facilities or with community providers. See figure 1 for an overview of the RCI scheduling process. Prior to implementation of the RCI process in a particular specialty, if a veteran met community care eligibility criteria, the referral for specialty care could be sent directly to community care staff for scheduling. However, the veteran might not be informed of their options to obtain care in a VHA medical facility.
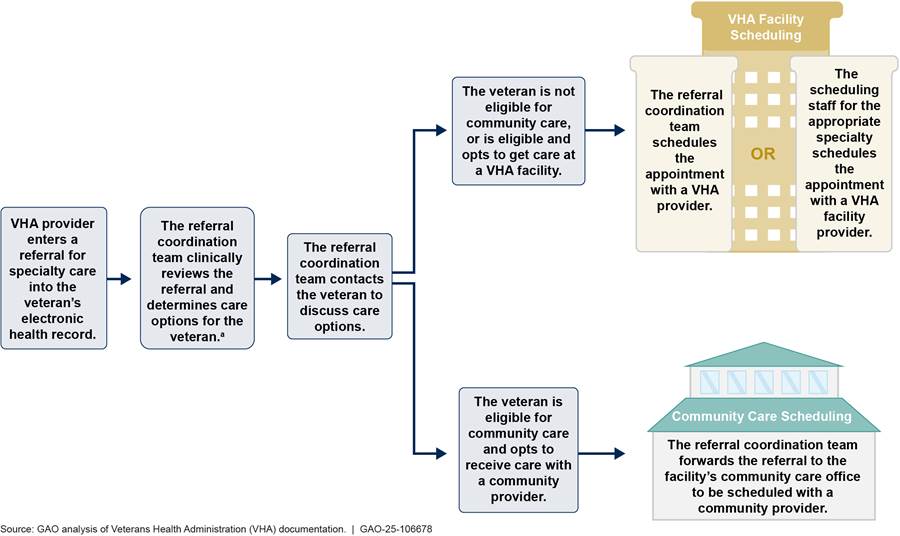
aThis step includes determining whether the veteran is eligible for community care. If the referral coordination team contacts the veteran to gather missing clinical information, they are to discuss care options with the veteran at that time.
VHA medical facilities can use different models to organize the staff of their referral coordination teams. In implementing the RCI, VHA provided facilities with guidance describing the different models—including factors to consider, such as availability of resources—but gave facilities flexibility in selecting a model. In a centralized staffing model, dedicated clinical and administrative team members work together to handle referrals for all specialties using the RCI process and report to a referral coordination team lead. In a decentralized model, clinical and administrative team members remain housed within their respective specialties, have other responsibilities, and report to leaders in their specialties. A hybrid staffing model combines elements of both models. VHA medical facilities were required to assign two key RCI positions: an executive sponsor and a champion. The individuals in these positions are responsible for leading the facility’s RCI implementation.
To implement the RCI, VHA medical facilities needed to take a number of steps, including establishing a team, conducting analysis of workload to determine supply and demand for specific services, and determining staffing. Facilities also needed to develop service agreements for individual specialties to delineate the process for how referrals would be managed for those specialties, including any clinical triage (patient prioritization) unique to the service. IVC identified 57 specialty care services where the RCI was required to be implemented and tasked VHA medical facilities with prioritizing their RCI rollout to these specialties.
VHA Officials at Most Facilities Reported Implementing the RCI for Some Specialty Care; IVC Plans Changes to Increase Standardization
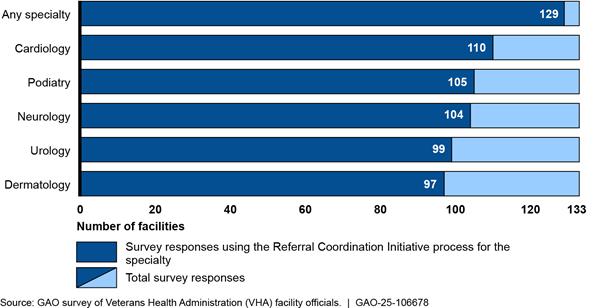
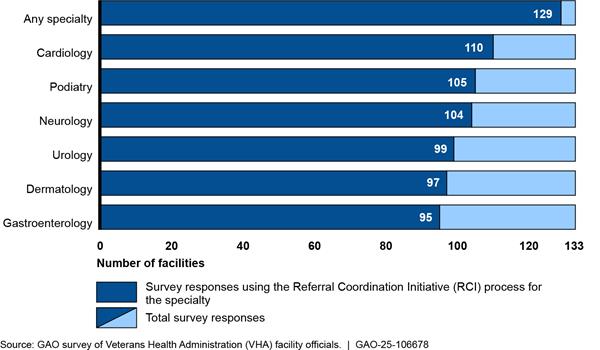
In early 2024, most VHA facility RCI officials responding to our survey reported using the RCI process (i.e., using referral coordination teams to review specialty care referrals and discuss care options with veterans) for some specialty care at their facilities.[24] In total, 129 out of 133 VHA facility RCI officials responding to our survey (97 percent) reported using the RCI process to manage any specialty. See figure 2. These officials reported using the RCI for an average of 30 specialty services. The most common specialty for which VHA facility RCI officials reported using the RCI process was cardiology (110 responses).
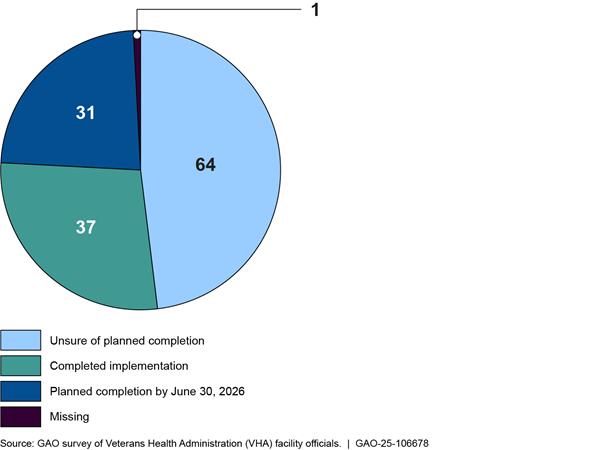
However, only about a fourth of VHA facility RCI officials reported completing their implementation of the RCI (37 of 133 responses), and about half (64 of 133 responses) said that they were unsure how long it would take to do so (see fig. 3).[25] Some VHA facility RCI officials who were unsure about how long it would take to fully implement the RCI said continued implementation would be dependent on their ability to acquire additional staff.
In our survey, facility RCI officials reported that they had difficulties in establishing the RCI. Specifically, 80 percent (103 of 129 responses) of officials from RCI-implementing facilities somewhat or strongly agreed that the process had been challenging to implement.[26] These officials identified several specific difficulties they encountered during implementation, including the following:
· Insufficient resources to implement the RCI (89 responses, 69 percent); only about a third of facility officials somewhat or strongly agreed that they had the clinical staff or administrative staff (43 responses, 33 percent) necessary to implement the RCI[27]
· Complex workflows for scheduling in the RCI process (61 responses, 47 percent)[28]
· Lack of standardized triage tools for referrals (59 responses, 46 percent)[29]
Only about a third of these officials somewhat or strongly agreed that training was high quality for clinical RCI staff (37 percent, 48 responses) and for administrative RCI staff (33 percent, 42 responses).[30] In addition, some officials from RCI-implementing facilities mentioned physician buy-in as a difficulty they encountered when implementing the RCI process in new specialties at their facilities. For example, in some cases, providers were wary of entrusting referral coordination teams with appointment triage responsibilities, such as ensuring that veterans had completed the right pre-appointment testing (e.g., lab tests and radiology exams).
Despite early challenges with implementation, over half of officials from RCI-implementing facilities somewhat or strongly agreed that using the RCI process had provided some benefits at their facility, including some of the intended benefits of the RCI. For example, 76 percent (98 of 129 responses) of VHA facility RCI officials somewhat or strongly agreed that the RCI helped scheduling staff to provide information to veterans about their options for care, and 51 percent (66 of 129 responses) somewhat or strongly agreed that it had reduced the average time to schedule appointments. Additionally, an RCI official from one site said that although provider buy-in was a significant challenge initially, the RCI has shown benefits at the facility, and leadership from additional specialties have requested that the RCI team manage referrals in their clinics.
Similar to our survey findings, VHA has found mixed results about the effect of the RCI in several studies it has conducted since 2021. For example, studies of implementation of the RCI process for a single specialty or a selection of specialties have shown potential for the RCI to provide benefits, such as increasing the percentage of veterans choosing VHA care or reducing wait times for appointments.[31] Another broader study found that the RCI did not measurably affect community care referral rates or appointment wait times for most specialties.[32] In addition to these studies, IVC has ongoing collaboration with the VA Collaborative Evaluation Center to evaluate the RCI.[33] The 2023 annual report from this collaboration found inconsistent practices among facilities and that facility-level RCI use was not consistently associated with appointment timeliness or use of community care.[34] This report also noted varied understanding among VHA facility staff about the RCI’s purpose and goals and recommended that VHA define and measure RCI goals.
Partly in response to these evaluation findings and feedback from VHA medical facilities, IVC began a “refresh” of the RCI to increase oversight and overall RCI adoption in May 2024. According to VHA documentation, data analysis and feedback from VHA medical facilities indicated that medical facilities had inconsistent adoption, processes, prioritization, and resourcing to support the RCI. Our survey results also identified inconsistencies. For example, an RCI official from one facility said their RCI team worked well, and the facility had implemented the RCI in all feasible areas. However, another respondent said their facility’s nursing leadership was unable to dedicate nurse staff for the clinical side of their team because nursing vacancies in positions providing direct patient care took higher priority. Facilities were also required to create their own triage tools specific to individual specialties to help RCI nurses determine the appropriate type of appointment for the veteran.[35] According to the VA Office of Inspector General, this was a time-consuming and inefficient process. According to the Inspector General’s October 2022 report, VISN and facility leaders said they would benefit from having standardized triage tools provided by IVC.
According to VHA documentation, such inconsistencies in adoption, process, prioritization, and resourcing may lead to underuse of care in VHA medical facilities and to some veterans not understanding all their options for care. The refresh effort is designed to address these inconsistencies by emphasizing a standard approach to referral review with nationally provided triage tools for selected specialties, providing scripts for VHA facility staff discussions with veterans regarding their care options, and encouraging resource sharing among VHA medical facilities in each VISN.
One key aspect of the refresh effort is that the VISNs, rather than VHA facilities, will be responsible for leading the implementation of the new RCI practices in selected specialties and responsible for providing RCI oversight, according to VHA documentation.[36] This “VISN-led” approach to the RCI is intended to enable VHA to streamline and standardize the referral process across VHA medical facilities, prioritize the offering of care within VHA medical facilities, and promote resource sharing within the VISN, according to IVC documentation. Specifically, in lieu of each VHA medical facility creating its own processes, VISNs will be tasked with identifying and standardizing RCI processes across their respective networks for as many high-cost or high-volume specialties as possible.[37]
According to VHA guidance introduced in May 2024, VISNs are now responsible for standardizing RCI processes in, at a minimum, three to five specialties by the end of fiscal year 2024.[38] IVC officials said they believe a VISN-based or similar approach is best for resource sharing, because the VISNs are best able to reinforce and strengthen adoption among VHA facilities given their oversight role. IVC officials said that, as of the transition to the RCI refresh, they are no longer communicating a separate list of required specialty services to VHA medical facilities. Instead, VISNs are responsible for selecting and communicating required services. IVC officials said their ongoing evaluation of the RCI will provide information about the new approach’s effectiveness, such as effects on cost and timeliness. According to draft IVC documentation, this evaluation is expected to continue through the second quarter of fiscal year 2026.
VISNs and VHA Medical Facilities Lack National Policy and Quality Guidance for the RCI
We found that IVC has not provided program direction—specifically, strategic goals, standards for consistent implementation, roles and responsibilities, and oversight and accountability—for the RCI in a VHA national policy. Additionally, we found that VHA facilities and VISNs have not had quality—that is, policy-aligned, evidence-based, timely, and consistent—guidance for RCI implementation.
VISNs and VHA Medical Facilities Do Not Have Program Direction in National Policy for RCI Implementation
|
Strategic Goals and Performance Management According to GAO’s prior work, setting goals is an important step in an effective performance management process. Organizations need strategic goals, which are long-term outcome-oriented statements of aim or purpose. These goals articulate the outcomes or impacts the organization intends to achieve to advance its mission and address relevant problems, needs, challenges, and opportunities. Source: GAO‑23‑105460. | GAO-25-106678 |
We found that, as of October 2024, IVC had not included the RCI in a VHA national policy with program direction to guide VISNs’ and VHA medical facilities’ RCI implementation. According to VHA policy, VHA policy owners like IVC are responsible for determining key program elements and incorporating these elements into VHA national policy.[39] Specifically, IVC has not defined in national policy these four elements to guide RCI implementation: (1) strategic goals, (2) standards for consistent implementation, (3) roles and responsibilities, and (4) oversight and accountability.
Strategic goals. According to VHA’s policy management directive, as the policy owner for issues related to scheduling and referrals, IVC is responsible for incorporating desired outcomes for RCI program success into national policy.[40] In particular, our prior work has shown that programs should have long-term strategic goals to which short-term performance goals or metrics can be aligned.[41] Clearly aligned goals help decision-makers, staff, and stakeholders assess performance by comparing planned and actual results.
While lacking strategic goals for the RCI in national policy, IVC has identified purposes for the RCI in operational memos and its main guidance document, the RCI Guidebook. However, these purposes are subject to change over the short term. For example, IVC’s May 2024 operational memo for the new VISN-led RCI identified two additional purposes for the RCI—(1) optimizing the use of all care resources, including in-person care, virtual care modalities, and community care and (2) standardizing the veteran experience—that are not included in the RCI Guidebook. Further, as noted previously, the 2023 annual report of a VHA evaluation found that facility officials did not have a consistent understanding of the intended purpose of the RCI.[42] For example, officials from one facility were unaware of the RCI’s purpose, and officials from another facility most frequently identified a previous purpose—reducing administrative burden for providers—as the main purpose of the RCI, even though it was no longer included in the RCI Guidebook.[43] Including strategic goals in national policy for the RCI would clarify such goals for facilities and VISNs and help ensure understanding across the enterprise.
Standards for consistent implementation. According to VHA’s policy and referral management directives, IVC is the policy owner and responsible for incorporating criteria for oversight and consistent implementation of its programs, such as the RCI, into national policy.[44] In particular, the policy management directive states VHA national policy should establish mandatory, minimum standards that eliminate the need for local policy at the VISN or medical facility level. In our survey, some facility RCI officials indicated a need for more standardization and less flexibility—or room for interpretation—in RCI implementation. For example, one respondent said that, in their experience, each VHA medical facility interpreted the RCI Guidebook differently. Another respondent said it would be beneficial if there were stricter guidelines and less flexibility. A third respondent said IVC tends to make suggestions but leave decisions open at the facility level. This respondent said their facility was later told their implementation decisions were incorrect. Outside of our survey, officials from one VISN similarly said they would prefer for IVC to provide more direction for the RCI. While IVC has provided guidance, defining standards to assist with consistent implementation and including such standards in national policy would help IVC better oversee and ensure consistency in future RCI implementation efforts.
Roles and responsibilities. According to VHA’s policy management directive, national policy should establish a mandatory course of action and assign execution responsibilities to identifiable individuals or groups.[45] Without national policy for the RCI, roles and responsibilities have been documented in guidance documents. Such guidance documents inconsistently outline VISN roles and responsibilities. For example, IVC’s RCI Guidebook identifies a VISN champion role. The person in this role is responsible for identifying and leading the RCI implementation team and providing feedback to facility RCI leadership and the VISN RCI steering committee, among other things.[46] However, IVC has a supplementary guidance document dedicated to roles and responsibilities that does not mention the VISN champion role.[47] Similarly, the RCI Guidebook assigns the VISN RCI steering committee the responsibilities of developing the RCI implementation timeline and identifying barriers and solutions. But these responsibilities are not present in the supplementary guidance document. Additionally, in our survey, 19 percent of officials from RCI-implementing facilities indicated that IVC had not clearly defined roles for RCI team members (25 of 129 responses).[48] Defining specific RCI roles and responsibilities for VISNs and medical facilities in VHA national policy would help provide consistent expectations to facilities and VISNs about their RCI duties.
Oversight and accountability. VHA policy defines oversight as actions to guide, control, monitor, and evaluate the organization to, for example, help ensure policies are implemented as intended and programs achieve expected results.[49] VHA requires oversight responsibilities for medical facilities, VISNs, and other leadership positions to be included in national policy.[50] VHA directives for policy management, operating units, and consult management envision IVC having a role in RCI oversight as part of its responsibilities. We found, however, that IVC’s oversight responsibilities for the RCI are not documented in policy, and officials’ understanding of their oversight role differs from requirements established in these VHA national directives.
Specifically, as the relevant VHA policy owner, IVC has responsibility for developing policy and providing oversight of referral management, including the RCI.[51] IVC is additionally responsible for overseeing consistent implementation of the RCI in coordination with VISNs.[52] However, IVC officials said their oversight role is focused only on program development and providing guidance, and VISNs are responsible for oversight of VHA medical facilities’ RCI implementation. The RCI Guidebook outlines oversight responsibilities for VISNs, such as developing implementation timelines, and monitoring and holding facilities accountable to RCI metrics. IVC officials told us that VISNs will be responsible for facility oversight as part of the VISN-led RCI under the RCI refresh. IVC officials said they plan to monitor the new VISN-led RCI effort through VISNs’ self-reporting and VISN-level performance metrics. However, these responsibilities for IVC are not explicitly established in the RCI Guidebook or VHA national policy. Defining RCI oversight responsibilities for VISNs and IVC in VHA national policy would help clearly define oversight and promote accountability for VHA medical facilities, VISNs, and IVC.
Some VHA medical facility and VISN officials noted challenges they experienced due to the lack of clear policy for the RCI from IVC. For example, RCI officials from one medical facility said their “biggest ask” of IVC would be for a clear policy that mandates RCI because their medical facility leadership questions the validity of RCI guidance. Officials from one VISN said that the lack of a “national mandate” such as a policy directive for the RCI has been challenging, in part because the RCI is a large effort but is only one priority among many others.
Rather than define program direction for the RCI through a national policy, IVC has communicated guidance through VHA operational memos and the RCI Guidebook.[53] Operational memos and guidebooks do not have the same level of authority as VHA national policy. According to VHA’s policy management directive, operational memos and the RCI Guidebook are guidance documents, which are meant to provide information to help VHA entities implement policy, such as uniform instructions or guidelines.[54] Such documents are not VHA policy and are not subject to the same process for development and review as national policy.
IVC officials told us that VHA Directive 1232 on processes and procedures for appointment referrals is the most applicable policy for the RCI. As of October 2024, however, this VHA directive did not include the four elements we identified to guide RCI implementation.[55] Officials from IVC, the policy owner, told us that planned updates to VHA Directive 1232 would include information on some elements of RCI program direction that are missing. Specifically, the updated VHA Directive 1232 will include high-level requirements for the RCI, including oversight responsibilities. Officials said the directive updates would not include RCI strategic goals, standards for consistent implementation, or detailed roles and responsibilities. Instead, the directive would refer to the RCI Guidebook for this information. Officials said RCI goals and standards for implementation are likely to change more frequently than the directive can be updated. As of October 2024, officials told us that updates to this directive were in the final stages of the policy update process, which they expected to complete by December 2024.
As IVC officials have acknowledged, RCI implementation has been inconsistent and has not had a finalized national policy that defines strategic goals, standards for consistent implementation, roles and responsibilities, and oversight and accountability. While the VISN-led RCI changes as part of the RCI refresh may help improve standardization within VISNs, the ongoing lack of RCI policy at the national level may lead to continued inconsistencies and challenges in RCI implementation across VISNs. This may lead to the RCI not fully achieving its intentions of providing veterans with a full understanding of their available care options, including all available VHA medical facility care.
VHA Facilities and VISNs Have Not Had Policy-Aligned, Evidence-Based, Timely, and Consistent Guidance for RCI Implementation
We found that VHA facilities and VISNs lacked guidance that was aligned with policy, evidence-based, timely, and consistent throughout RCI implementation, including the most recent change to a VISN-led approach. VHA policy and federal internal control standards support using guidance that is aligned with policy and provides quality information. Specifically, VHA policy requires that, when policy owners develop implementation guidance, they ensure the guidance is aligned with national policy.[56] VHA policy further states that office leadership should adopt evidence-based strategies for their programs.[57] Such strategies might include successful approaches identified in studies or best practices identified from high-performing VHA medical facilities and VISNs. Additionally, according to federal internal control standards, management should internally communicate quality information to enable personnel to achieve objectives.[58] One such method of communication would be through written guidance. According to these standards, quality information should be appropriate, complete, and provided on a timely basis. Further, our prior work has emphasized the benefit of using evidence to inform management decisions, such as guidance management provides.[59]
Regarding RCI implementation, we found shortfalls in complying with these standards.
Aligned with policy. As of October 2024, the RCI was not included in VHA national policy. As noted previously, IVC officials told us that planned updates to VHA’s policy for referral management (VHA Directive 1232) would include the RCI and references to the RCI Guidebook. When these updates are complete, it will be important for IVC to review RCI guidance, determine whether it is still needed, and ensure that it is aligned with the policy updates.
Evidence-based. We found that IVC used limited evidence to develop the initial RCI implementation guidance due to an expedited program rollout following implementation of VA MISSION Act requirements in June 2019. According to November 2019 operational memos, VA identified the need for the RCI and conducted the initial rollout within 6 months. When these memos were issued, VHA was conducting a pilot of the RCI process in one specialty—sleep medicine—at one VHA health care system.[60] IVC officials we spoke with could not identify other pilots or studies that informed the VHA-wide RCI implementation and said that officials who would have this information were no longer with IVC or the agency.
Such studies may have helped IVC provide more detailed guidance, which some VHA facility RCI officials expressed a need for in survey responses and during our site visits. For example, VHA facility RCI officials we interviewed at one site said they had to “build the plane while flying it” as they implemented the RCI. These officials said the RCI should have had a more comprehensive pilot because, from a clinical perspective, standardized clinical support tools from IVC, such as triage guidance for individual specialties, were missing. According to these officials, pilots at multiple sites could have helped IVC determine needed tools to provide to facilities.
Since the RCI was introduced, IVC has developed evidence about RCI implementation, such as the VA Collaborative Evaluation Center evaluation and a series of site visits IVC conducted to identify best practices from high performing sites. IVC has an opportunity to use this evidence to improve its guidance and provide information to VISNs and VHA medical facilities that could help them consistently and efficiently implement the RCI. For example, IVC could update the RCI Guidebook, its main guidance document, to include recommendations from the 2023 annual report of the evaluation, which was finalized after the most recent guidebook update. This evaluation found, for example, that it is important for RCI team members to be embedded in the specialty clinics for which they triage referrals.
Timely. We found that IVC did not provide timely guidance materials for the new VISN-led RCI when it was introduced in May 2024. Further, as of October 2024, IVC had not updated its RCI Guidebook to include the VISN-led RCI changes.
The VISN-led RCI was introduced in an operational memo and a new accompanying guidance document in May 2024. As part of this effort, VISNs were required to develop and begin using VISN-led standardized processes in three to five specialties by August 2024, giving VISNs just 4 months to make this change. We found that the guidance document IVC provided to VISNs and VHA medical facilities outlines seven tasks due in May 2024. However, resources—such as “how to” guidance and details about new metrics—for four of the tasks due in May 2024 were still pending updates in the guidance document at that time. Additionally, according to officials from one VISN, delays in one type of guidance—standardized triage tools for recommended specialties—were likely to cause rework. VISNs would need to create their own triage tools for the specialties and then replace the tools they created when standardized tools became available. Further, as of October 2024, while IVC had distributed some guidance for the new VISN-led RCI through memoranda and a guidance document, IVC had not updated the RCI Guidebook to reflect the recent change of converting the RCI to a VISN-led effort.
Since the RCI was introduced, IVC has continued to make changes to the initiative and its guidance. IVC officials told us they were prioritizing guidance for the VISN-led RCI and RCI refresh over, for example, updating existing guidance to ensure it remained up-to-date. IVC officials also acknowledged that introductory VISN-led RCI guidance resources were delayed. Officials said the formal concurrence process for these resources required extensive efforts from their small core RCI project team, and unexpected team absences further contributed to delays. Officials said they expected the delays to have minimal effect on VISNs’ ability to implement the VISN-led RCI.
Consistent. The May 2024 guidance document introducing the VISN-led RCI is inconsistent about the types of specialty care required to participate in the initiative. In one place, the guidance document tasks VISNs with standardizing RCI processes for high-cost, high-volume specialties and lists four specialties that VISNs must include in their referral coordination plans. Later, however, the same guidance document says VISNs can select a specialty outside of their high-cost or high-volume specialties, and that the four listed specialties are “recommended.” IVC officials did not agree with our assessment that the guidance document was inconsistent and said they have made concerted efforts to engage with stakeholders from VHA leadership, program offices, and VISNs and update guidance based on their feedback. The officials acknowledged that the plan for implementing specialties had changed since the guidance document was distributed to VISNs and said current expectations had been communicated in multiple venues.
These issues reflect overall challenges IVC has had providing quality guidance to VHA facilities. VHA facility RCI officials we surveyed reported that they lacked helpful, high-quality guidance for the RCI during initial implementation. Specifically, in response to our survey, less than half of VHA facility officials from RCI-implementing facilities either somewhat or strongly agreed that IVC guidance for the RCI was helpful for implementation (50 of 129 responses, 39 percent), accurate (56 of 129 responses, 43 percent), or timely (58 of 129 responses, 45 percent).[61] Almost one-third of these officials said that insufficient guidance from IVC was a challenge in implementation of the RCI process (40 of 129 responses, 31 percent).
IVC has continued to make changes to the RCI and its guidance since it was introduced in 2019, and officials anticipate that the RCI may continue to change. As IVC updates its referral management national policy, it will be important for IVC to review RCI guidance and ensure that it is aligned with such policy updates. By establishing a process to review and update key guidance like the RCI Guidebook when changes to RCI policy or requirements go into effect, IVC can better ensure that VHA and VISNs have the timely, consistent information they need to implement those changes. In the first years of RCI implementation, VISNs and facilities did not have the quality guidance they needed to implement the RCI effectively and achieve the RCI’s intended benefits, which led to inconsistent RCI adoption. Without quality guidance that is informed by evidence, IVC may continue to provide VISNs and facilities insufficient guidance to effectively implement the RCI’s objectives to improve scheduling timeliness and ensure veterans are aware of all their care options.
Existing RCI Metrics are Not Effective for Measuring RCI Performance and Outcomes
IVC developed metrics for VISNs and VHA facilities to use to monitor their RCI performance, but these metrics are not effective for measuring performance toward desired outcomes for the RCI. Our past work has found that performance management activities help an organization measure how well it is performing.[62] As part of these activities, organizations collect performance information to measure progress toward specific goals—such as performance metrics for the RCI—and use that information to assess results and inform decisions to ensure further progress toward achieving those goals. According to VHA policy, as policy owner, IVC is responsible for setting performance metrics related to activities within its purview, which would include referrals and scheduling.[63]
|
Performance goals or metrics According to GAO’s prior work, performance goals allow agencies to assess the desired near-term results for a given activity or program. Performance goals or metrics have quantitative targets and time frames against which performance can be measured. Performance goals must be clearly aligned to an organization’s strategic goals to help it illustrate and assess progress on broader outcomes. Source: GAO‑23‑105460. | GAO-25-106678 |
According to its RCI guidance, IVC is responsible for establishing RCI performance metrics and providing guidance to VISNs and VHA medical facilities on how to use the metrics. Also, according to RCI guidance, VISNs and VHA medical facilities are responsible for monitoring RCI performance metrics to identify facilities that may be underperforming or to identify issues or challenges with the RCI. In addition, they are responsible for monitoring, on an ongoing basis, how data on the metrics compare with baseline data from when the RCI was first established. VISNs and VHA facilities can review data on performance metrics through a dashboard that IVC developed for this purpose, according to IVC officials.[64]
When RCI implementation began in 2019, IVC communicated five RCI performance metrics for VISNs and facilities to use to monitor certain aspects of the RCI.[65] (See app. IV for the full set of RCI metrics and standards from IVC.) IVC established standards for three of the five performance metrics that VHA facilities should aim to meet. For example, one of the original metrics was related to scheduling timeliness, measured by the average number of days from the date an appointment is requested to the date an appointment is scheduled. The standard—the desired target for performance—for this metric was 3 business days for VHA facility appointments and 7 calendar days for community care appointments.
We found that these metrics are insufficient for performance management because they are not directly aligned to strategic goals, which IVC doesn’t have for the RCI in policy, and they do not measure progress on all intended benefits of the RCI. Further, users of these metrics—VISNs and VHA facilities—found the metrics not useful or difficult to understand.
Metrics are not aligned to strategic goals. IVC does not have strategic goals outlined in policy, as noted previously. The RCI has three main intended benefits outlined in guidance, two of which are reflected in the original performance metrics. However, empowering veterans to make the health care choice that is right for them is the third intended benefit of the RCI, but RCI does not have a performance metric VISNs and VHA facilities should use to measure performance toward achieving that purpose. As a result, VHA lacks information on the extent to which the RCI is helping veterans make informed decisions about their health care.
Users do not find metrics useful or easy to understand. In response to our survey, 48 percent (62 of 129) of facility RCI officials said the metrics provided by IVC are either not useful or difficult to understand. Similarly, in our site visit interviews, VISN and VHA facility officials said the original RCI metrics did not accurately measure performance of the RCI and cited some challenges they experienced as a result. Specifically, officials from one facility said performance on the metric for engagement by the referral coordination team was not capturing performance of the RCI as intended.[66] As of the time of our review, VHA facilities were not required to implement the RCI in all specialty care services, but the metric does not exclude referrals for facility services where the RCI has not been implemented. As a result, the facility’s performance on the metric does not accurately reflect the performance for those services using the RCI. Additionally, officials we interviewed from four VISNs cited the lack of performance metrics that directly measure outcomes of the RCI as a challenge. For example, if scheduling timeliness has improved since RCI implementation, the current metric does not show that the RCI is the reason for the improvement because other efforts can affect scheduling timeliness.
There is no documentation of the steps IVC took to develop the original RCI metrics, including how they align with the goals of the RCI. IVC officials told us that the metrics were developed through a series of collaborative meetings that included staff from various facilities and disciplines, but they did not document the decision-making process. Consequently, it is unclear how IVC determined the original RCI metrics were designed to measure performance of the RCI. For example, IVC did not create a new scheduling timeliness metric that is specific to the RCI. Rather, officials told us they repurposed an existing metric intended to monitor whether facilities are meeting specialty care scheduling standards, regardless of participation in the RCI. As a result, the metric does not directly measure if the RCI improves scheduling timeliness, which is a goal of the RCI.
As part of the new VISN-led RCI implemented in spring 2024, IVC developed three additional RCI performance metrics and standards that IVC had VISNs begin monitoring in May 2024 (see app. IV).[67] However, these metrics and standards are not directly aligned to IVC’s intended benefits of the RCI. IVC officials told us they plan to keep the five original RCI performance metrics along with the new VISN-led metrics and would like VISNs and VHA facilities to prioritize the three new VISN-led RCI metrics going forward.
Because IVC does not have strategic goals in policy and metrics that directly align with those goals, IVC lacks assurance that its metrics are effective for measuring performance of the RCI. Accordingly, IVC cannot provide decision-makers within VA or the Congress with accurate information regarding the effectiveness of its efforts to streamline scheduling processes via the RCI. In addition, facilities and VISNs may struggle to understand their own RCI performance and to communicate how the RCI can improve the process for specialty care referrals. For example, referral coordination team officials from one facility we spoke to said that during RCI implementation, they experienced challenges with the lack of buy-in from specialty care providers. Officials from the same facility said that data from IVC on RCI successes would have helped persuade staff at the facility to use the RCI. Reviewing RCI performance metrics—and revising them as needed—to ensure alignment with strategic goals is an important step to provide VISNs and facilities with data to identify benefits and challenges of the RCI and provide IVC with data to help determine whether the RCI is achieving its intended outcomes.
Additionally, IVC officials said they have verbally communicated with VISNs about the extent to which they and their facilities should continue to monitor the original metrics while also prioritizing the new metrics. But, given facilities’ prior experiences with the original RCI metrics, IVC cannot be assured of VISN and medical facility understanding of either the original metrics or the new ones and how to use them.
Federal internal control standards state that management should internally communicate quality information to enable personnel to achieve objectives.[68] One such form of quality information could include clear performance metrics and standards. Clearly communicating the metrics and how VISNs and facilities should prioritize their efforts related to the original and the new VISN-led RCI metrics could help ensure consistent understanding of how to use the metrics.
Conclusions
VHA has faced longstanding challenges with scheduling VHA facility and community care appointments as well as ensuring veterans’ timely access to care. In recent years, VHA has updated its appointment scheduling process for specialty care referrals through the RCI, which focuses on both streamlining the referral process and providing veterans with more information about their options for care, so they are empowered to make the choice that is right for them. These efforts have drawn scrutiny as the agency faces continued difficulties in ensuring veterans have timely access to care, given continuing demand for care and the reliance on care in the community.
By ensuring that the program direction for the RCI—that is, the program’s strategic goals, standards for consistent implementation, roles and responsibilities, and oversight and accountability—is documented in national policy and that related guidance is updated accordingly, VHA can help facilities provide veterans with a consistent appointment scheduling experience across the VHA health care system. Further, ensuring that updates to the guidance are based on sound evidence will provide VISNs, VHA medical facilities, and frontline VHA staff with confidence that their efforts to carry out the RCI process are helping them serve veterans effectively.
Moreover, having clear strategic goals and aligned performance metrics would help IVC communicate its progress toward the outcomes the RCI is intended to achieve. By assessing its performance metrics to ensure they align with the initiative’s strategic goals, and revising or replacing them as needed, IVC will be better positioned to provide decision-makers, including VA leadership and the Congress, with information on the agency’s efforts to improve the scheduling process for specialty care. Further, if IVC clearly communicates with VISNs and VHA facilities regarding how the performance metrics measure progress toward the RCI goals, VISN and VHA facility staff will be better positioned to understand how their actions help to achieve those goals.
Taking such actions would further support VISNs and VHA medical facilities in serving veterans on a day-to-day basis and assist VHA in responding to ongoing challenges related to ensuring timely access to care and ultimately ensuring maximization of VHA resources, by getting veterans the right care at the right time.
Recommendations for Executive Action
We are making the following five recommendations to VA:
The Under Secretary for Health should ensure that IVC defines RCI program direction—strategic goals, roles and responsibilities, standards for consistent implementation, and oversight and accountability—in appropriate VHA national policy. (Recommendation 1)
The Under Secretary for Health, upon inclusion of the RCI in the appropriate VHA national policy, should ensure that IVC aligns RCI guidance with VHA national policy and updates it as needed to reflect available evidence, such as findings from studies, best practices, and other elements that promote consistent implementation. (Recommendation 2)
The Under Secretary for Health, following initial alignment of RCI guidance and national policy, should ensure that IVC establishes a process to ensure that any guidance remains current and accurate when IVC makes changes to RCI policy or program requirements. (Recommendation 3)
The Under Secretary for Health should ensure that IVC reviews the RCI performance metrics, and updates them as needed, to ensure that the metrics align with and assess progress toward all aspects of RCI’s strategic goals. (Recommendation 4)
The Under Secretary for Health should ensure that IVC communicates with VISNs and VHA facilities regarding how to use its metrics to measure performance toward the RCI goals. (Recommendation 5)
Agency Comments and Our Evaluation
We provided a draft of this report to VA for review and comment. VA provided written comments, which are reproduced in appendix V. In its written comments, VA concurred in principle with our first recommendation. VA acknowledged the importance of clear program direction and stated that the RCI was created to improve the referral coordination process, which is one piece of the overarching consult and referral management process. VA also said that the RCI should not be interpreted as a stand-alone process. We maintain that the RCI marks a significant change from how referrals have historically been managed within VA, and as such, our recommendation that program direction be fully defined in national policy would increase accountability mechanisms and help ensure veterans receive timely and effective care. VHA published a new national referral management policy on November 22, 2024. We will consider this new policy as part of our recommendation follow-up process.
VA concurred with our four other recommendations and described actions it would take to address them. VA estimated that their actions to address the five recommendations would be completed by November 2025. VA also provided technical comments, which we incorporated as appropriate.
As agreed with your offices, unless you publicly announce the contents of this report earlier, we plan no further distribution until 30 days from the report date. At that time, we will send copies of this report to the appropriate congressional committees, the Secretary of Veterans Affairs, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at (202) 512-7114 or SilasS@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix VI.
Sharon M. Silas
Director, Health Care
The objectives of our report are to (1) describe the status of the Referral Coordination Initiative (RCI) program’s implementation; (2) assess the extent to which RCI program direction is defined in policy and Veterans Integrated Service Networks (VISN) and Veterans Health Administration (VHA) medical facilities have quality RCI guidance; and (3) assess the extent to which there are established metrics that provide VISNs and VHA medical facilities with the information needed to measure performance of the RCI.
To describe the status of the RCI program’s implementation, we reviewed VHA documents, including policies and procedures related to appointment scheduling. We also reviewed VHA’s Office of Integrated Veteran Care (IVC) documents and data related to the RCI and interviewed IVC officials. In addition, we reviewed public and internal VHA studies related to RCI implementation. To obtain information on the experiences of officials at VHA facilities regarding the RCI, we conducted a survey of VHA medical facility officials and interviewed officials during site visits with selected VHA facilities and VISNs.
Survey of VHA medical facility officials. To examine the experiences of VHA officials during implementation of the RCI at their medical facilities, we conducted a survey of VHA facility officials who could speak to these experiences. To do so, we received a list of 139 VHA medical facilities from IVC and conducted outreach to these facilities to identify appropriate contacts, to whom we deployed the survey.[69] We received survey responses from officials from 133 of these 139 VHA facilities and analyzed those responses. Our survey, administered between January 2024 and March 2024, contained multiple choice questions covering topics including plans to implement the RCI, perspectives on the benefits and challenges of the RCI, and experiences with support for implementation from VISNs and IVC. The survey also included open-ended questions, such as requests for comments about challenges facility officials experienced during their implementations and about RCI oversight from IVC and VISNs. While the survey represents 96 percent of VHA facilities, results may not be generalizable to facilities that did not respond to the survey. Further, survey results only represent the point in time the survey was completed. See appendix III for the results of our survey analysis.
Site visits. To learn about the scheduling process for both VHA facility care and community care and facility staff experiences with scheduling, including the RCI, we conducted a total of six VHA medical facility site visits. These site visits included three exploratory in-person site visits and three virtual site visits. The in-person sites were selected based on variation in facility complexity and geographic location and ease of access and travel. We selected an additional three VHA facilities for virtual site visits using early survey response data to select sites based on whether the site had implemented the RCI, variation in facility complexity, geographic location, and RCI model. The information we obtained from site visits is not generalizable to other VHA facilities. See table 1 for the list of our in-person and virtual site visits. In addition to these site visits with VHA facilities, the team interviewed officials from four of the associated VISNs to learn more about VISN officials’ perspectives on the RCI implementation and oversight. During our site visits with VHA facilities and interviews with VISN officials, we asked about their experiences with the RCI, including challenges during implementation and any perceived benefits.
|
Facility location (visit type) |
VISN |
Complexity level |
Census region |
RCI model |
|
Orlando, FL (in-person) |
8 |
High (1a) |
South |
Decentralized |
|
Cleveland, OH (in-person) |
10* |
High (1a) |
Midwest |
Centralized |
|
Wilmington, DE (in-person) |
4* |
Medium (2) |
Northeast |
Decentralized |
|
White City, OR (virtual) |
20* |
Low (3) |
West |
Decentralized |
|
Las Vegas, NV (virtual) |
21* |
High (1b) |
West |
Hybrid |
|
San Antonio, TX (virtual) |
17 |
High (1a) |
South |
Hybrid |
Legend: * Indicates Veterans Integrated Service Network (VISN) selected for interviews with officials regarding VISN-wide Referral Coordination Initiative (RCI) practices and oversight.
Source: GAO. | GAO‑25‑106678
To assess the extent to which RCI program direction is defined in policy and VISNs and VHA facilities have quality guidance, we reviewed RCI memoranda and guidance documents, including operational memos for the RCI, the RCI Guidebook, and available guidance materials for the VISN-led RCI, which VHA introduced in 2024. Additionally, we interviewed officials from IVC about their roles in policy development, oversight, and guidance. We also asked VISN and VHA facility officials about their perspectives on RCI oversight and guidance during our site visits, and we asked questions about oversight and guidance in our survey of facility RCI officials. We evaluated this information against relevant VHA policies, including VHA’s directive for policy management and VHA’s directive for operating units.[70] We also evaluated this information against federal internal control standards related to using quality information and our prior work on evidence-based policy making.[71]
To assess the extent to which there are established metrics that provide VISNs and VHA facilities with the information needed to measure performance of the RCI, we reviewed IVC documents regarding performance goals and metrics. We obtained and reviewed IVC data on the RCI performance metrics as of March 2024. We also interviewed IVC officials about the development of performance metrics for the RCI and data sources for metrics. We asked VISN and VHA medical facility officials about their perspectives on RCI performance metrics during our site visits, and we asked questions about performance metrics in our survey of facility RCI officials. We evaluated this information against relevant VHA policy, including VHA’s directive for policy management.[72] We also evaluated this information against federal internal control standards related to using quality information and key practices we developed regarding performance management activities in the federal government.[73]
We conducted this performance audit from March 2023 to January 2025 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Appendix II: Key Questions and Answers on the Process for Assessing Veterans’ Community Care Eligibility during Scheduling
To answer the key questions that follow, we reviewed guidance documents from the Veterans Health Administration (VHA) and interviewed officials from VHA’s Office of Integrated Veterans Care (IVC) about veterans’ eligibility determinations, appointment scheduling audits, and veteran experience surveys. We reviewed data VHA provided on the number of referrals that were eligible for community care and when the veteran chose community care, by eligibility criterion. To assess reliability of the eligibility data, we manually reviewed the data for errors and spoke with knowledgeable IVC officials about the sources of the data. Based on our review, we found the data sufficiently reliable for the purposes of reporting the number of referrals eligible for community care by criterion. We also gathered information on the veteran perspective regarding community care eligibility determinations by collecting data from sources such as VHA’s Survey of Healthcare Experiences of Patients and from interviews with selected veterans service organizations.
1. How is eligibility for community care assessed during the scheduling process?
There are several criteria used during the appointment scheduling process to assess whether a veteran may be eligible for community care.[74] When a VHA provider decides a veteran needs specialty care, such as an appointment with a cardiologist, the VHA provider enters a referral into the veteran’s electronic health record.[75] Next, a clinical reviewer reviews the referral to ensure it is complete and ready for scheduling. Once the referral is ready to be scheduled, the scheduler uses a scheduling tool to check community care eligibility status. The veteran may have already been determined eligible for community care prior to scheduling.[76] For example, if a provider determines that it is in the veteran’s best medical interest to see a community provider because it would be a significant burden for the veteran to travel to a VHA facility for care, that decision is already documented in the referral when the scheduler receives it. Similarly, a veteran may already have established eligibility if they live in a state without a full-service VHA medical facility.[77]
During scheduling, the scheduler also assesses whether the veteran is eligible based on the community care access standards and whether the service is available at VHA facilities. There are two access standards—wait time and drive time—that are used to assess community care eligibility.[78]
Wait time. Potential eligibility based on the wait time standard must be assessed for each referral. Specifically, VHA staff use the scheduling system to calculate the number of days between the day the appointment is requested and the first available appointment date to assess if a veteran is eligible for community care based on the wait time standard. Veterans are eligible for community care if an appointment is not available at a VHA medical facility within 20 days for primary care and certain mental health services and 28 days for specialty care.[79]
Drive time. Drive time eligibility is assessed at the same time as wait time eligibility, according to IVC officials. VHA staff use the scheduling system—which includes geographic information—to calculate drive time based on distance and the time it would take to travel from the veteran’s home address on file to the VHA facility. Veterans are eligible for community care if the drive time is more than 30 minutes for primary care and 60 minutes for specialty care.
Service not available. A veteran may be found eligible for community care based on a service not being available at any VHA facility. For example, VHA facilities do not provide maternity care, and a veteran referred for such care would be eligible to obtain that care in the community.
Once the scheduler has reviewed the referral for community care eligibility, the scheduler contacts the veteran to discuss care options, including whether the veteran is eligible for community care. If the veteran is eligible for community care, the veteran is given the choice to receive care with a community provider or schedule an appointment at a VHA facility that may be outside of the wait time or drive time standards. If the veteran chooses to receive community care, the scheduler documents the veteran’s decision in the referral and forwards the referral to the appropriate staff to begin scheduling.
2. Which eligibility criteria are most commonly used for veterans choosing to receive community care?
According to VHA data on the number of referrals where veterans chose to receive community care in fiscal year 2023, most veterans were determined eligible based on the drive time criterion, followed by wait time and service not available at VHA facility.[80] (See table 2.)
Table 2: Percentage and Number of Referrals Eligible for Community Care by Criterion for Veterans Choosing to Receive Community Care in Fiscal Year 2023a
|
Community care eligibility criterion |
Percent of referrals eligible |
Number of referrals |
|
Access standards (totals) Drive time Wait time |
73 59 14 |
4,644,408 3,773,905 870,503 |
|
Service not available at a VHA facility |
11 |
683,646 |
|
Best medical interest |
7 |
476,361 |
|
Full-service facility not available |
3 |
177,252 |
|
Grandfathered-in under the Veterans Choice Program |
2 |
118,401 |
|
Eligibility not documentedb |
4 |
256,908 |
|
Total |
|
6,356,976 |
Source: GAO analysis of Department of Veterans Affairs, Veterans Health Administration (VHA) data. | GAO‑25‑106678
aAccording to VHA officials, the data capture eligibility for veterans who decide to receive community care. Veterans who were eligible to see a community provider but decided to receive care at a VHA medical facility instead are not included in this data set.
bAccording to VHA officials, eligibility not documented reflects referrals for which data reliability of the eligibility field is insufficient for reporting.
3. How does VHA ensure community care eligibility determinations are made accurately?
VHA has taken some steps to ensure scheduling staff are properly trained in assessing for community care eligibility, are only using approved scheduling tools to assess for wait time eligibility and are following VHA scheduling policy for documenting eligibility.
Training. Scheduling staff receive training on how to correctly assess for community care eligibility when they are onboarded and then are retrained annually, according to VHA officials. VHA provides resources for additional training on specific community care eligibility criteria, such as assessing for wait time and drive time eligibility.
Approved scheduling tools. In January 2023, VHA released guidance that only approved scheduling tools should be used to assess for wait time eligibility and Veteran Integrated Service Network (VISN) and VHA facility officials were required to attest that they were only using the approved tools. An example of an approved tool would be a calculator IVC provided for schedulers to use to calculate wait time eligibility.
Scheduling audits. VHA uses its National Standardized Scheduling Audits to ensure VHA schedulers are following national scheduling policy. During the audits, an auditor reviews a sample of 10 appointments per scheduler, and the auditor provides feedback to the scheduler on the audit results.[81] The auditor reviews details about each appointment, such as whether the date the scheduler entered matches the date of the appointment request in the referral. According to VHA officials, the audits are designed to determine if schedulers properly document scheduling decisions and to provide feedback or additional training to schedulers when needed. For example, an auditor might also assess whether a scheduler properly documented that an eligible veteran chose to receive community care instead of VHA care. If the auditor finds errors, a scheduler may receive additional training as a result. According to VHA audit data for October 2023 through March 2024, approximately 8 percent of appointments audited had findings. VISNs are responsible for overseeing the audits, and VHA facilities are responsible for conducting the audits, according to VHA documentation.
VHA does not currently have a mechanism to audit whether schedulers correctly assessed for wait time eligibility. According to VHA officials, the agency is developing a report that will provide the ability to look back at previous wait time determinations. Specifically, the report will allow supervisors or other reviewers to retroactively see what appointments were available when a scheduler assessed a veteran’s community care eligibility based on wait time. According to VHA officials, the impetus for this report was to have the ability to retroactively see if community care wait time eligibility was assessed correctly at the time of scheduling.[82] IVC officials told us the report will be available after future updates to the scheduling system but did not provide information about the timing of the updates.
4. How does VHA monitor veterans’ experience with community care eligibility determinations?
VHA collects data on veterans’ experience with community care eligibility determinations through its Office of Quality and Patient Safety’s Survey of Health Experience of Patients. The survey includes two questions related to community care eligibility that make up an overall rating of the veteran’s experience with community care eligibility: 1) the eligibility requirements for VHA community care are clear and 2) the information available about eligibility for VHA community care is helpful. Veterans are asked to rate whether they agree or disagree with each statement. According to VHA survey data from the last quarter of fiscal year 2023, 63 percent of veterans either strongly agreed or agreed that eligibility requirements are clear, and the information about community care eligibility is helpful; 24 percent of veterans neither agreed nor disagreed; and 13 percent of veterans strongly disagreed or disagreed.
In 2019, the Veterans Health Administration (VHA) introduced the Referral Coordination Initiative (RCI) to streamline the specialty care referral process and allow it to provide timely, patient-centric care to veterans, according to VHA. Since then, the VHA Office of Integrated Veteran Care (IVC) and the Department of Veterans Affairs (VA) Office of Inspector General have both found substantial variation in the extent to which VHA medical facilities have implemented the initiative. The VA Office of Inspector General additionally found that facilities experienced challenges such as insufficient staffing in their efforts to implement the RCI.
To examine the status of the RCI and obtain information about VHA medical facilities’ staff experiences establishing referral coordination teams and using the RCI process at their facilities, we developed and deployed a survey to RCI officials at 139 VHA medical facilities. We pretested the survey with RCI staff at five different VHA facilities and revised the questions based on their feedback. We administered the survey from January through March 2024 and received responses from officials at 133 facilities for a survey response rate of 96 percent. The survey asked respondents about staff experiences implementing the RCI process and covered topics including plans to implement the RCI, perspectives on the benefits and challenges of the RCI, and experiences with support for implementation from their Veterans Integrated Service Network (VISN) and IVC.
To provide a more complete understanding of VHA medical facilities’ staff experiences in implementing the RCI, in this appendix we present summary information on multiple choice responses from officials at 133 VHA medical facilities to questions about their plans to complete RCI implementation and their experiences implementing the RCI. We do not include respondents’ narrative responses to open-ended questions in this appendix. We also do not include detailed responses from facilities about which services they are implementing or responses to some questions about specific resources. While the survey represents 96 percent of the VHA medical facilities we identified, results may not be generalizable to facilities that did not respond to the survey. Further, survey results represent only one point in time.
While this appendix contains responses from 133 VHA medical facility officials, our survey targeted some questions to specific subsets of facilities. For example, we asked several questions only of those facilities that indicated they were using the RCI process. Additionally, some respondents did not answer all questions, so the numbers and percentages for missing responses are also displayed.
Survey Responses from 133 VHA Medical Facilities
The following tables are based on survey responses to questions for 133 VHA medical facilities, including those where officials did not indicate they were currently using the RCI process to manage referrals.
Table 3: VHA Medical Facilities Using the Referral Coordination Initiative (RCI) Process to Manage Referrals
|
|
Number of facilities |
Percentage of facilities |
|
Using the RCI process |
129 |
96.99 |
|
Not using the RCI process |
3 |
2.26 |
|
Not sure if using the RCI process |
1 |
0.75 |
|
Total |
133 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from VHA medical facilities, administered between January and March 2024.
Table 4: VHA Facilities’ Plans to Complete Referral Coordination Initiative (RCI) Implementation for All Planned Specialty Care
|
Planned RCI completion |
Number of facilities |
Percentage of facilities |
|
The facility has completed implementation of all planned services as of March 2024 |
37 |
27.82 |
|
On or before June 30, 2024 |
12 |
9.02 |
|
On or before June 30, 2025 |
12 |
9.02 |
|
On or before June 30, 2026 |
7 |
5.26 |
|
The facility has started implementation but officials are unsure how long it will take to complete RCI implementation for all planned services |
62 |
46.62 |
|
The facility has not started implementation and officials are unsure how long it will take to complete RCI implementation for all planned services |
2 |
1.5 |
|
Missing |
1 |
0.75 |
|
Total |
133 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from VHA medical facilities, administered between January and March 2024. As of the time of our survey, the Office of Integrated Veteran Care (IVC) required VHA medical facilities to implement the RCI in 57 specialty services.
Table 5: Facility Referral Coordination Initiative (RCI) Officials Reporting That Their Facility or Veterans Integrated Service Network (VISN) Created Training to Supplement National RCI Training
|
|
Number of facilities |
Percentage of facilities |
|
Facility or VISN created additional training |
62 |
46.62 |
|
Facility or VISN did not create additional training |
38 |
28.57 |
|
Not aware of additional training |
33 |
24.81 |
|
Total |
133 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from VHA medical facilities, administered between January and March 2024.
The following table shows levels of agreement by RCI officials at facilities with statements regarding staff experiences with the RCI.
Table 6: Facility Staff Experiences with Referral Coordination Initiative (RCI) Support from their Veterans Integrated Service Network (VISN)
|
Statement |
Strongly disagree |
Somewhat disagree |
Neither agree nor disagree |
Somewhat agree |
Strongly agree |
|
|
Percent of facilities indicating level of agreement |
||||
|
Support from the VISN over the past 2 years has significantly helped our facility’s efforts to implement and manage the RCI. |
14.29 |
11.28 |
24.81 |
30.83 |
18.8 |
|
The VISN has communicated clear and reasonable expectations for our facility’s RCI implementation and performance. |
11.28 |
9.02 |
21.05 |
34.59 |
24.06 |
|
Our facility has received individualized support from the VISN that met our needs, such as responses to questions about RCI requirements or models, when requested. |
12.78 |
13.53 |
19.55 |
30.08 |
24.06 |
|
Our facility receives communication and support from the VISN RCI lead (RCI champion) that meets our facility’s needs. |
11.28 |
12.03 |
20.3 |
31.58 |
24.81 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 133 VHA medical facilities, administered between January and March 2024.
Survey Responses from VHA Medical Facilities Using the RCI Process to Manage Referrals
The following tables show facility RCI officials’ responses from the 129 VHA medical facilities using the RCI process to manage referrals regarding staff experiences with RCI implementation.
Table 7: Referral Coordination Initiative (RCI) Most Frequently Implemented Specialty Services Required by VHA’s Office of Integrated Veteran Care (IVC)
|
Specialty service using the RCI (stop code) |
Number of facilities |
Percentage of facilities |
|
Cardiology (303) |
110 |
85.27 |
|
Podiatry (411) |
105 |
81.40 |
|
Neurology (315) |
104 |
80.62 |
|
Urology (414) |
99 |
76.74 |
|
Dermatology (304) |
97 |
75.19 |
|
Gastroenterology (307) |
95 |
73.64 |
|
Orthopedics Joint Surgery (409) |
94 |
72.87 |
|
Pain Clinic (420) |
94 |
72.87 |
|
Physical Therapy (205) |
94 |
72.87 |
|
General Surgery (401) |
92 |
71.32 |
|
Pulmonary Chest (312) |
92 |
71.32 |
|
Gastrointestinal Endoscopy (321) |
91 |
70.54 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
This table includes specialty services if at least 70 percent of surveyed RCI officials reported that their facility had implemented the RCI process to manage referrals for the specialty service. VHA’s IVC tracks services using identifiers called stop codes. The stop code for each service is indicated in parenthesis after the service’s name. VHA’s IVC has a list of 57 required stop codes. GAO asked facilities about whether they had implemented each of these 57 stop codes.
Table 8: Referral Coordination Initiative (RCI) Models VHA Medical Facilities Are Implementing as of March 2024
|
RCI model |
Number of facilities |
Percentage of facilities |
|
Centralized model |
39 |
30.23 |
|
Decentralized model |
43 |
33.33 |
|
Hybrid model |
47 |
36.43 |
Source: GAO survey of Veterans Health Administration (VHA) facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of medical facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
This table includes responses from officials who indicated that their facilities use the RCI process to manage referrals. RCI model refers to the staffing model facilities use for their referral coordination teams. In a centralized staffing model, clinical and administrative team members are dedicated to processing referrals through the initiative and report to a referral coordination team lead. In a decentralized model, clinical and administrative team members have other responsibilities and report to leaders in their service lines. A hybrid staffing model combines elements of both types of models.
|
Has the facility changed RCI models since 2019? |
Number of facilities |
Percentage of facilities |
|
Yes |
49 |
37.98 |
|
No |
69 |
53.49 |
|
Not sure |
11 |
8.53 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of facility RCI officials from VHA medical facilities, administered between January and March 2024.
This table includes responses from officials who indicated that their facilities use the RCI process to manage referrals. RCI model refers to the staffing model facilities use for their referral coordination teams. In a centralized staffing model, clinical and administrative team members are dedicated to processing referrals through the initiative and report to a referral coordination team lead. In a decentralized model, clinical and administrative team members have other responsibilities and report to leaders in their service lines. A hybrid staffing model combines elements of both types of models.
Table 10: VHA Medical Facilities Use of Required Methods to Track Referral Coordination Initiative (RCI) Referrals
|
Method |
Number of facilities |
Percentage of facilities |
|
Staff use a previously required method to track referralsa |
33 |
25.58 |
|
Staff use the currently required method to track referralsb |
118 |
91.47 |
|
Staff use other tracking methods |
25 |
19.38 |
|
Missing |
1 |
0.78 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
VHA has required different methods for facilities to use to track specialty care referrals at different points in time. Officials could select multiple tracking options. As a result, the number of facilities in this table may total more than 129, and percentages in this table may total more than 100 percent.
aBeginning March 2021, VHA required facility staff to write #RCT# in comments for referrals that were processed through the RCI. IVC discontinued this method with updates to the Consult Toolbox, a tool RCI staff use to manage referrals.
bBeginning September 2023, the Office of Integrated Veteran Care (IVC) made updates to require RCI staff to identify themselves as referral coordination team members in the Consult Toolbox. The Consult Toolbox identifies a referral as an RCI referral if it was processed by a referral coordination team member who is identified as such in the toolbox. This method for identifying referrals is required to be in use at facilities as of December 2023.
Table 11: VHA Medical Facilities Where Referral Coordination (RCI) Staff Use Community Care Wait Time Information from the Required Decision Support Tool
|
|
Number of facilities |
Percentage of facilities |
|
Facilities that use community care wait time information from the decision support tool |
91 |
70.54 |
|
Facilities that do not use community care wait time information from the decision support tool |
25 |
19.38 |
|
Not sure |
11 |
8.53 |
|
Missing |
2 |
1.55 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of facility RCI officials from VHA medical facilities, administered between January and March 2024.
The decision support tool is meant to help staff determine whether a patient is eligible for community care. The tool is intended to provide data such as drive time projections based on the veteran’s home address, average wait times for the requested service at VHA facilities near the veteran’s home, and average wait times for community care appointments.
Table 12: VHA Medical Facilities’ Overall Experiences with the Referral Coordination Initiative (RCI)
|
Statement |
Strongly disagree |
Somewhat disagree |
Neither agree nor disagree |
Somewhat agree |
Strongly agree |
|
|
Percent of facilities indicating level of agreement |
||||
|
The RCI process has been challenging to implement at our facilities |
3.1 |
7.75 |
9.3 |
51.16 |
28.68 |
|
RCI members understand their role in the RCI process |
1.55 |
10.08 |
1.55 |
41.86 |
44.19 |
|
Providers understand how to request consults in the RCI process |
5.43 |
22.48 |
10.85 |
48.06 |
13.18 |
|
The RCI process has reduced the average time to schedule appointments |
6.2 |
14.73 |
27.91 |
20.16 |
31.01 |
|
The RCI process has reduced overall appointment wait times |
7.75 |
14.73 |
35.66 |
26.36 |
15.5 |
|
The RCI process has helped scheduling staff provide information about options for care |
3.38 |
6.2 |
13.95 |
40.31 |
35.66 |
|
The RCI process has reduced the administrative burden for clinicians |
10.08 |
15.5 |
15.5 |
33.33 |
25.38 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 13: Challenges VHA Medical Facilities Experienced during Referral Coordination Initiative (RCI) Implementation
|
Challenge |
Number of facilities indicating |
Percentage of facilities indicating |
|
Insufficient guidance documents from VHA Office of Integrated Veteran Care (IVC) |
40 |
31.01 |
|
Insufficient resources to implement the RCI |
89 |
68.99 |
|
RCI scheduling workflow complexities |
61 |
47.29 |
|
Lack of standardized triage tools for referrals |
59 |
45.74 |
|
Lack of common scheduling workflows for the RCI in individual specialties |
48 |
37.21 |
|
Lack of recruitment tools for new RCI staff |
38 |
29.46 |
|
Inability to centrally assign staff the referral coordination team user role for tracking referrals |
38 |
29.46 |
|
Challenges with reliable (complete and accurate) community care wait time estimates to share with veterans |
72 |
55.81 |
|
Challenges receiving answers from VHA IVC to RCI-related questions |
30 |
23.26 |
|
Challenges determining which RCI staffing model to implement at the facility |
42 |
32.56 |
|
Lack of VHA performance metrics or measures for the RCI |
37 |
28.68 |
|
Other |
43 |
33.33 |
|
No challenges |
3 |
2.33 |
|
Missing |
1 |
0.78 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Officials could select multiple challenges. As a result, facilities in this table may total more than 129, and percentages in this table total more than 100 percent.
Table 14: VHA Medical Facility Referral Coordination Initiative (RCI) Officials’ Assessment of Whether They Have Sufficient Staff to Implement the RCI as Recommended by VHA Office of Integrated Veteran Care Guidance
|
Statement about staffing |
Strongly disagree |
Somewhat disagree |
Neither agree |
Somewhat agree |
Strongly agree |
|
|
Percent of facilities indicating |
||||
|
Our facility has the administrative staff needed to fully implement the RCI as required/recommended by VHA guidance |
34.11 |
21.71 |
10.85 |
21.71 |
11.63 |
|
Our facility has the clinical staff needed to fully implement the RCI as required/recommended by VHA guidance |
33.33 |
24.81 |
8.53 |
22.48 |
10.85 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 15: VHA Medical Facilities’ Understanding of Specialty Services That are Part of the Referral Coordination Initiative (RCI)
|
Services required for the RCI |
Number of facilities |
Percentage of facilities |
|
VHA’s Office of Integrated Veteran Care requires facilities to implement the RCI for certain services if the facility offers those services |
82 |
63.57 |
|
VHA’s Office of Integrated Veteran Care recommends facilities implement the RCI for certain services if the facility offers those services |
29 |
22.48 |
|
Our facility is not aware of a list of services that are part of the RCI process |
7 |
5.43 |
|
Other |
10 |
7.75 |
|
Missing |
1 |
.78 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 16: Facility Staff Experiences with Referral Coordination Initiative (RCI) Support from VHA’s Office of Integrated Veteran Care (IVC)
|
Statement |
Strongly disagree |
Somewhat disagree |
Neither agree nor disagree |
Somewhat agree |
Strongly agree |
Unsure/no basis on which to judge |
|
|
Percent of facilities indicating level of agreement |
|||||
|
Guidance from VHA IVC about how to structure and implement the RCI process has been timely |
11.63 |
15.5 |
22.48 |
29.46 |
15.5 |
5.43 |
|
Guidance from VHA IVC about how to structure and implement the RCI process has been accurate |
10.08 |
16.28 |
26.36 |
26.36 |
17.05 |
3.88 |
|
Guidance from VHA IVC about how to structure and implement the RCI process has helped our facility staff make decisions about how to implement the RCI process at our facility. |
13.95 |
20.93 |
23.26 |
20.16 |
18.6 |
3.1 |
|
Our facility receives timely responses to inquiries about the RCI process from VHA IVC |
6.2 |
9.3 |
27.91 |
16.28 |
20.16 |
20.16 |
|
Our facility has a reliable way to contact VHA IVC |
6.98 |
10.08 |
16.28 |
24.03 |
30.23 |
12.4 |
|
Support for RCI implementation from VHA IVC has improved from the beginning of fiscal year 2023 to the present |
5.43 |
10.08 |
25.58 |
19.38 |
27.13 |
12.4 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 17: Facility Staff Experiences with Referral Coordination Initiative (RCI) Training from VHA’s Office of Integrated Veteran Care (IVC)
|
Statement |
Strongly disagree |
Somewhat disagree |
Neither agree nor disagree |
Somewhat agree |
Strongly agree |
Unsure/no basis on which to judge |
|
|
Percent of facilities indicating level of agreement |
|||||
|
Training from VHA IVC for RCI clinical staff has been of high quality |
10.85 |
14.73 |
25.58 |
24.03 |
13.18 |
11.63 |
|
Training from VHA IVC for RCI administrative staff has been of high quality |
10.85 |
12.4 |
27.91 |
21.71 |
10.85 |
16.28 |
|
Training from VHA IVC for RCI clinical staff has provided enough information for staff to perform their role |
9.3 |
17.83 |
21.71 |
21.71 |
19.38 |
10.08 |
|
Training from VHA IVC for RCI administrative staff has provided enough information for staff to perform their role |
10.85 |
10.85 |
25.58 |
22.48 |
14.73 |
15.5 |
|
Roles for RCI members have been clearly defined by IVC |
6.98 |
12.4 |
17.05 |
34.11 |
27.13 |
2.33 |
|
Training from for RCI staff has improved from the beginning of fiscal year 2023 to the present |
7.75 |
6.2 |
29.46 |
24.03 |
19.38 |
13.18 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 18: VHA Medical Facility Officials’ Perceptions of Referral Coordination Initiative (RCI) Performance Metrics from the Office of Integrated Veteran Care
|
Perception of performance metrics |
Number of facilities |
Percentage of facilities |
|
The metrics are clear and useful |
43 |
33.33 |
|
The metrics are clear but not useful |
34 |
26.36 |
|
The metrics are difficult to understand |
28 |
21.71 |
|
No opinion on the clarity or usefulness of the metrics |
24 |
18.6 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 19: VHA Medical Facility Officials’ Perceptions on the Extent to Which Feedback About Referral Coordination Team Performance Has Been Helpful
|
Feedback |
Not at all helpful |
Slightly helpful |
Somewhat helpful |
Very helpful |
Extremely helpful |
Not applicable (no feedback received) |
Not Sure |
Missing |
|
|
Percentage of Facilities |
|||||||
|
From Veterans Integrated Service Network |
11.63 |
13.18 |
28.68 |
20.16 |
10.85 |
10.08 |
3.1 |
2.33 |
|
From VHA’s Office of Integrated Veteran Care |
12.4 |
15.5 |
20.16 |
13.95 |
10.85 |
20.16 |
5.43 |
1.55 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility Referral Coordination Initiative officials from 129 VA medical facilities, administered between January and March 2024.
Table 20: How Frequently VHA’s Office of Integrated Veteran Care (IVC) Requests Feedback from VHA Medical Facilities about Referral Coordination Initiative (RCI) Implementation
|
Frequency |
Number of facilities |
Percentage of facilities |
|
About once a month |
7 |
5.43 |
|
About quarterly |
6 |
4.65 |
|
About twice a year |
24 |
18.6 |
|
Once per year or less frequently |
29 |
22.48 |
|
IVC has not requested feedback from our facility about RCI implementation |
18 |
13.95 |
|
Not sure |
45 |
34.88 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 21: How Frequently VHA Medical Facility Referral Coordination Initiative (RCI) Leadership Internally Reviews RCI Performance
|
Frequency of RCI performance review |
Number of facilities |
Percentage of facilities |
|
At least once per month |
80 |
62.02 |
|
At least once per quarter |
13 |
10.08 |
|
Semi-annually or less frequently |
6 |
4.65 |
|
As needed |
15 |
11.63 |
|
Not sure |
15 |
11.63 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 22: VHA Medical Facility Referral Coordination Initiative (RCI) Officials’ Perceptions on Whether RCI Leadership Has the Information Needed to Understand the Facility’s RCI Performance
|
Facility official perspective |
Number of facilities |
Percentage of facilities |
|
Yes, RCI leadership has the information needed to understand the facility’s RCI performance |
102 |
79.07 |
|
No, RCI leadership does not have the information needed to understand the facility’s RCI performance |
10 |
7.75 |
|
Not sure |
16 |
12.4 |
|
Missing |
1 |
0.78 |
|
Total |
129 |
100 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Note: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Table 23: Additional Referral Coordination Initiative (RCI) Support VHA Medical Facility RCI Officials Would Like to Receive from Their Veterans Integrated Service Network (VISN)
|
Support |
Number of facilities |
Percentage of facilities |
|
Sharing of RCI best practices across the VISN |
76 |
58.91 |
|
VISN-wide presentations or training on RCI topics |
58 |
44.96 |
|
Individualized support |
47 |
36.43 |
|
Guidance on implementing the RCI within the VISN |
44 |
34.11 |
|
Other VISN support needed |
26 |
20.16 |
|
None |
17 |
13.18 |
|
Missing |
6 |
4.65 |
Source: GAO survey of Veterans Health Administration (VHA) medical facility officials. | GAO‑25‑106678
Notes: This table reports information from a GAO survey of facility RCI officials from 129 VHA medical facilities, administered between January and March 2024.
Officials could select multiple types of support. As a result, percentages in this table total more than 100 percent. Officials could select multiple types of support; as a result, facilities in this table may total more than 129, and percentages in this table total more than 100 percent.
Table 24: Original Referral Coordination Initiative Metrics Established by VHA’s Office of Integrated Veteran Care in 2019
|
Performance metric |
Definition |
Standard |
|
Scheduling timeliness |
Average number of days from the date an appointment is requested to the date an appointment is scheduled |
3 business days for VHA facility appointments 7 calendar days for community care appointments |
|
Engagement by the referral coordination teama |
Percentage of referrals that are reviewed by a referral coordination team member |
90 percent of referrals at all facilities |
|
Community care scheduling preferences |
Percentage of community care referrals that had scheduling preferences captured by the referral coordination team before the referral is sent to community care schedulers |
90 percent of referrals at all facilities |
|
Consult pattern trends |
Of the veterans eligible for community care, how many chose to receive care with a community care provider and how many chose to receive care at VHA |
No standard set |
|
Veteran satisfaction |
No definition available |
In developmentb |
Source: GAO analysis of Veterans Health Administration (VHA) documentation. | GAO‑25‑106678
aAccording to Office of Integrated Veteran Care (IVC) officials, the engagement metric is the only metric they regularly monitor for the Referral Coordination Initiative.
bAccording to IVC officials, the standard for this metric was still in development as of October 2024.
Table 25: Veterans Integrated Service Network-Led Referral Coordination Initiative (RCI) New Metrics Established by VHA’s Office of Integrated Veteran Care in 2024
|
Performance metric |
Definition |
Standard |
|
RCI deployment and engagement |
This metric has three components: 1. Implementing the RCI in as many high-cost or high-volume services as possible 2. Decrease in the number of community care referrals 3. Percentage of referrals that are eligible for community care with documentation of VHA care offered |
Each component has a separate standard: 1. Implementation in three to five specialties 2. Decrease in community care referral volume or community care to VHA facility referral ratio 3. 90 percent of referrals by the end of the first quarter of fiscal year 2025 |
|
Nurse first clinical review |
Percentage of referrals that are reviewed by a referral coordination team member with clinical experience, such as a nurse |
55 percent of referrals by the end of the first quarter of fiscal year 2025 |
|
Cross-facility sharing and modality options |
Increase in usage of sharing care across facilities and modality options, such as telehealtha |
25 percent increase by the end of the first quarter of fiscal year 2025 |
Source: GAO analysis of Veterans Health Administration (VHA) documentation. | GAO‑25‑106678
aAccording to VHA documentation, cross-facility sharing includes sending a referral to be scheduled at another facility within the Veterans Integrated Service Network.
GAO Contact
Sharon M. Silas, (202) 512-7114 or silass@gao.gov.
Staff Acknowledgments
In addition to the contact named above, Marcia A. Mann (Assistant Director), Julie T. Stewart (Analyst-in-Charge), Lauren Anderson-Boring, Brittaini Maul, and Ester Weir made key contributions to this report. Also contributing were Jacquelyn Hamilton, Ying Hu, and Cynthia Khan.
Veterans Community Care Program: VA Needs to Strengthen Contract Oversight. GAO‑24‑106390. Washington, D.C.: Aug. 21, 2024.
Veterans Health Care: Opportunities Exist to Improve Assessment of Network Adequacy for Mental Health. GAO‑24‑106410. Washington, D.C.: June 3, 2024.
Veterans Community Care Program: Additional Information on VA Statutory Appointment Timeliness Measurements Is Needed. GAO‑24‑105308. Washington, D.C.: Mar. 28, 2024.
Veterans Health Care: VA Actions Needed to Ensure Timely Scheduling of Specialty Care Appointments. GAO‑23‑105617. Washington, D.C.: Jan. 4, 2023.
Veterans Community Care Program: VA Needs to Strengthen Its Oversight and Improve Data on Its Community Care Network Providers. GAO‑23‑105290. Washington, D.C.: Nov. 10, 2022.
Veterans Community Care Program: VA Took Action on Veterans’ Access to Care, but COVID-19 Highlighted Continued Scheduling Challenges. GAO‑21‑476. Washington, D.C.: June 28, 2021.
Veterans Community Care Program: Improvements Needed to Help Ensure Timely Access to Care. GAO‑20‑643. Washington, D.C.: Sept. 28, 2020.
Veterans Choice Program: Improvements Needed to Address Access-Related Challenges as VA Plans Consolidation of its Community Care Programs. GAO‑18‑281. Washington, D.C.: June 4, 2018.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on Facebook, Flickr, X, and YouTube.
Subscribe to our RSS Feeds or Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454 or (202) 512-7700
Congressional Relations
A. Nicole Clowers, Managing Director, ClowersA@gao.gov, (202) 512-4400, U.S. Government Accountability Office, 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs
Sarah Kaczmarek, Managing Director, KaczmarekS@gao.gov, (202) 512-4800, U.S.
Government Accountability Office, 441 G Street NW, Room 7149
Washington, DC 20548
Strategic Planning and External Liaison
Stephen J. Sanford, Managing
Director, spel@gao.gov, (202) 512-4707
U.S. Government Accountability Office, 441 G Street NW, Room 7814, Washington,
DC 20548
[1]This includes both veterans treated by VHA providers and those whose health care by non-VHA providers in the community is reimbursed by VHA.
[2]Veterans may be eligible to obtain care from non-VHA providers if they face certain challenges accessing care at VHA medical facilities, such as long wait times or lengthy travel distances. VA implemented the Veterans Community Care Program on June 6, 2019, as required under the VA MISSION Act of 2018. The Veterans Community Care Program replaced the prior temporary program that had been in place since 2014—the Veterans Choice Program—and consolidated it with other existing community care programs. Pub. L. No. 115-182, tit. I, §101, 132 Stat. 1393, 1395 (2018).
In this report, we refer to care provided by community providers through the Veterans Community Care Program as “community care.”
[3]IVC was established in the spring of 2022 when portions of two prior offices within VHA—the Office of Veterans Access to Care and the Office of Community Care—were merged. IVC generally has taken on the responsibilities of those two offices, although some functions of the Office of Community Care went to other offices within VHA, including the Office of Finance.
[4]Department of Veterans Affairs, Office of Inspector General, Additional Actions Needed to Fully Implement and Assess the Impact of the Patient Referral Coordination Initiative, 21-03924-234 (October 2022). To help IVC with implementation and oversight of the RCI, the VA Office of Inspector General made seven recommendations. VHA concurred with all of the recommendations. One recommendation, that VHA assign specific RCI roles and responsibilities to IVC, was open as of November 2024. The other six recommendations have been closed.
[5]For a full list of related GAO products, see the end of this report.
[6]We maintain a high-risk program to focus attention on government operations identified as high risk due to their greater vulnerabilities to fraud, waste, abuse, and mismanagement or the need for transformation to address economy, efficiency, or effectiveness challenges. We added VA health care to the High Risk List in 2015. For the most recent high-risk report, see GAO, High-Risk Series: Efforts Made to Achieve Progress Need to Be Maintained and Expanded to Fully Address All Areas, GAO‑23‑106203 (Washington, D.C.: Apr. 20, 2023).
VHA’s health care system is divided into 18 areas called VISNs. Each VISN is responsible for managing and overseeing the VHA medical facilities within a defined geographic area.
[7]We also have ongoing work looking at the information technology systems VHA uses for scheduling appointments and the creation and implementation of VHA’s IVC.
[8]We contacted officials from 139 VHA medical facilities. Most of these facilities were VA medical centers or VA health care systems, which may contain multiple VA medical centers. Other facilities included a multi-specialty community-based outpatient center, three outpatient clinics, and one federal health care facility that combines VA and Department of Defense medical care in one facility. We refer to all these types of facilities as “VHA medical facilities” within the report.
[9]Department of Veterans Affairs, Veterans Health Administration Directive 0999(1): Policy Management (Washington D.C.: Mar. 29, 2022, amended Jan. 10, 2024) and Veterans Health Administration Directive 1217: VHA Operating Units (Washington D.C.: Aug. 14, 2024).
[10]Internal control is a process effected by an entity’s oversight body, management, and other personnel that provides reasonable assurance that the objectives of an entity will be achieved. GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.: Sept. 10, 2014).
See also GAO, Evidence-Based Policy Making: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington D.C.: July 2023).
[11]For purposes of this report, we are focusing on the scheduling process for specialty care referrals.
[12]VHA policy uses the terms “consult” and “referral” when describing requests placed by VHA providers. For the purposes of this report, we will use the term referral. For a limited number of outpatient specialty services, veterans can schedule an initial or follow-up appointment at VHA medical facilities without a referral from a provider. Veterans can use this option for audiology, optometry, and podiatry, among other services.
[13]In addition to VHA medical facility scheduling on behalf of veterans, as of March 2024, 33 of 139 facilities were receiving contractor support in scheduling community care appointments. In some limited cases, veterans may also directly schedule appointments with providers.
[14]Pub. L. No. 115-182, tit. I, § 101, 132 Stat. 1393, 1395 (2018) (codified, as amended, at 38 U.S.C. § 1703).
[15]38 C.F.R. §§ 17.4000 - 17.4040 (2024).
[16]In addition to the six criteria, veterans must either be enrolled in VA health care or be eligible for VA care without needing to enroll, and in most circumstances, veterans must receive approval from VHA prior to obtaining care from a community provider. See Pub. L. No. 115-182, tit. I, § 101, 132 Stat. at 1395-1404 (codified, as amended, at 38 U.S.C. § 1703(d), (e)) and implementing regulations at 38 C.F.R. §§ 17.4000 - 17.4040.
[17]VHA is headed by the Under Secretary for Health, who reports to the Secretary of Veterans Affairs.
[18]VHA Directive 1217 sets forth the roles, responsibilities, and decision rights for VHA operating units. VHA Directive 0999(1) establishes requirements for VHA policy development, distribution, communication, and management.
[19]See for example, Department of Veterans Affairs, Outpatient Scheduling Management, VHA Directive 1230 (Washington, D.C.: June 1, 2022) and Consult Processes and Procedures, VHA Directive 1232(5) (Washington, D.C.: Aug. 24, 2016, amended Dec. 5, 2022).
[20]VHA has established standards that facilities need to meet to ensure the timeliness of scheduling specialty care appointments for VHA facility and community care. For example, specialty care appointments at VHA facilities must be scheduled within 3 business days from the date of the referral.
[21]VHA facility staff have had key responsibilities in managing the appointment scheduling process and determining veterans’ eligibility for community care since the Veterans Choice Program, the predecessor to the current Veterans Community Care Program.
[22]According to VHA officials, in some cases, specialty providers may refer veterans to other specialty providers.
[23]See Department of Veterans Affairs, Veterans Health Administration Memorandum: Referral Coordination Initiative VISN and Facility Champion (Washington D.C.: Nov. 25, 2019) and Memorandum: Referral Coordination Initiative VISN and Facility Executive Sponsor (Washington D.C.: Nov. 29, 2019). According to these memos, VHA launched its efforts to implement the VA MISSION Act on June 6, 2019.
[24]We conducted our survey of VHA facility RCI officials from January through March 2024. At the time of our survey, IVC required facilities to implement the RCI process for a list of 57 specialty services, which IVC tracked based on clinical identifiers called stop codes. Some specialty care clinics were required to implement the RCI for multiple stop codes or services within their specialties. According to IVC officials, while the specialty services on this list were required, IVC had not set a deadline by which facilities were expected to complete implementation for all 57 specialty services. In our survey, we asked facilities about their implementation of these specialties. See table 7 in appendix III for more details about specialty services facilities have implemented. As of October 2024, IVC officials said that IVC was no longer reinforcing or communicating the requirement for VHA medical facilities to implement the RCI in these 57 specialty services.
[25]Prior to distributing our survey, we contacted VHA medical facilities to identify knowledgeable officials who could speak to RCI implementation at their facilities. We refer to confirmed survey contacts as “facility RCI officials” based on this outreach.
Our survey asked facility RCI officials when they anticipated completing implementation of the RCI process for all specialty services they planned to implement, including both the specialty services IVC required at the time of our survey in early 2024 and any additional specialty services.
[26]For more details about RCI staff experiences with the RCI, see appendix III.
[27]See table 14 in appendix III.
[28]See table 10 in appendix III for more information about how referral coordination teams manage referrals.
[29]According to VA, a clinical triage tool is a guideline used by referral coordination teams for referral review, triage, documentation, and scheduling. These tools are built collaboratively with specialty providers, referral coordination nurses, and the administrative team. They provide a clinical algorithm to aid in referral coordination team nurses’ decision-making.
[30]For more information, see table 17 in appendix III.
[31]Alice Cusick et al., “Michigan Market Referral Coordination Initiative: A Regional Market Approach to VA Specialty Care,” Journal of General Internal Medicine, vol. 38, no. S3 (2023): 871-877 and Lucas M. Donovan et al., “The Referral Coordination Team: A Redesign of Specialty Care to Enhance Service Delivery and Value in Sleep Medicine,” NEJM Catalyst: Innovations in Care Delivery, vol. 2. no. 2 (2021).
[32]Daniel A. Asfaw et al., “The Effects of the Veterans Health Administration’s Referral Coordination Initiative on Referral Patterns and Waiting Times for Specialty Care,” Health Services Research, vol. 59, no. 3 (2024).
[33]The VA Collaborative Evaluation Center is part of the VA Seattle-Denver Center of Innovation. It is a VA virtual center composed of quantitative, qualitative, and mixed methods evaluation experts who conduct evaluations of VA’s implementation of initiatives.
[34]Lucas M. Donovan et al., Referral Coordination Initiative Evaluation 2023 Annual Report: A Collaboration between the VA Collaborative Evaluation Center (VACE) and the Office of Integrated Veteran Care (IVC) (March 2024).
[35]For example, if triaging a referral for a gastroenterology appointment for a veteran to have a procedure such as a colonoscopy, an RCI nurse may use a triage tool to determine the appropriate level of sedation for the veteran, taking into consideration other health care concerns. The level of sedation required could affect scheduling for the appointment.
[36]For the remainder of the report, we refer to the revised approach to the RCI as the VISN-led RCI.
[37]This requirement for VISNs is distinct from the list of required specialty services for which IVC previously required VA medical facilities to use the RCI process.
[38]We discuss the implementation of this change in findings later in the report.
[39]VHA Directive 0999(1). This VHA directive establishes requirements for VHA policy development, distribution, communication, and management. According to the directive, VHA national policy—communicated through VHA directives or notices—sets minimum acceptable standards for which compliance is mandatory and accountability is absolute.
[40]VHA Directive 0999(1); VHA Directive 1232.
[41]See GAO, Evidence-Based Policy Making: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington D.C.: July 2023). We discuss IVC’s performance goals in more detail later in this report.
[42]Lucas M. Donovan et al., “Referral Coordination Initiative Evaluation 2023 Annual Report: A Collaboration between the VA Collaborative Evaluation Center (VACE) and the Office of Integrated Veteran Care (IVC).”
[43]IVC officials said an intended benefit of the standardized review process in the RCI refresh was for nurses to conduct most clinical triage, thereby removing administrative burden from VHA providers, who previously would have conducted these tasks. However, as of October 2024, this intended benefit was not an overall goal of the RCI.
[44]VHA Directive 0999(1).
[45]VHA Directive 0999(1).
[46]According to the RCI Guidebook, the VISN RCI Steering Committee is the VISN RCI governing body. This committee consists of facility and VISN officials who provide RCI oversight, guidance, and support.
[47]Veterans Health Administration, Office of Integrated Veteran Care, RCI Roles and Responsibilities Guidance (April 2022).
[48]See table 17 in appendix III for more information.
[49]VHA Directive 0999(1).
[50]VHA Directive 0999(1).
[51]VHA Directive 1232(5).
[52]VHA Directive 1217.
[53]VHA introduced the RCI in two memos published in November 2019, the “Referral Coordination Initiative VISN and Facility Executive Sponsor Memo” and the “Referral Coordination Initiative VISN and Facility Champion Operational Memo,” which required VISNs and facilities to identify key roles for the RCI. In March 2021, VHA set requirements for the RCI in the “Veterans Integrated Service Network (VISN) Referral Coordination Initiative (RCI) Standards and Expectations for Fiscal Year (FY) 21 Operational Memo” and provided an updated RCI Guidebook. IVC revised the RCI Guidebook in May 2022. According to officials, the RCI Guidebook is the main guidance document for the RCI. Finally, VHA provided requirements and guidance for the VISN-led RCI in the “VISN-Led Referral Coordination Initiative (RCI) Expansion” memo and accompanying RCI VISN Implementation Planning Guide.
[54]VHA Directive 0999(1).
[55]VHA Directive 1232(5).
[56]VHA Directive 0999(1). Per this policy, guidance is an inclusive term for documents used to convey uniform instructions, guidelines, and programmatic processes. These documents provide supplemental information that establishes a course of action or procedures.
[57]VHA Directive 1217.
[59]GAO‑23‑105460. As noted in our prior work, management should leverage knowledge learned from evidence to inform management decision-making, such as changes to existing strategies to achieve better results or reallocation of resources. Using evidence in decision-making helps ensure that an organization’s activities are targeted at addressing identified problems and achieving desired results.
[60]Donovan et al. “The Referral Coordination Team: a Redesign of Specialty Care to Enhance Service Delivery and Value in Sleep Medicine.” The pilot in this study was conducted in sleep medicine at the VA Puget Sound Health Care System, which contains two high-complexity facilities, from May 2018 through December 2019.
[61]For more details from our survey about facility RCI officials’ perspectives on staff experiences implementing the RCI, see appendix III.
[62]For the purposes of this report, we refer to performance goals as performance metrics. GAO‑23‑105460.
[63]VHA Directive 0999(1).
[64]This dashboard includes multiple reports and allows users to filter the data so they can review the performance metrics and other RCI data for their VISN or facility. For example, one report shows the volume of referrals that are reviewed by the referral coordination team at each medical facility.
[65]The performance metrics included 1) scheduling timeliness, with standards for appointments scheduled within 3 business days for VHA facility appointments and 7 calendar days for community care appointments; 2) engagement by the referral coordination team, with standards for 90 percent of referrals at all facilities to have such engagement; and 3) community care scheduling preferences, with standards to have preferences recorded for 90 percent of community care referrals at all facilities. Two additional metrics for consult pattern trends and veteran satisfaction did not have set standards. See appendix IV for more details.
[66]The standard for the engagement by the referral team metric—the percentage of referrals that should be reviewed by a referral coordination team member—is 90 percent.
[67]The additional performance metrics include 1) RCI deployment and engagement, with standards to implement in three to five specialties, show a decrease in community care referral volume or community care to VHA facility referral ratios and document VHA care offered for 90 percent of referrals in these specialties that are eligible for community care; 2) nurse first clinical review, with a standard to have 55 percent of referrals in selected specialties processed through a nurse first clinical review; and 3) cross-facility sharing and modality options, with requirements to have a 25 percent increase in these options for selected specialties. For more detail, see appendix IV.
[69]Of the 139 VHA medical facilities we contacted, most were VHA health care systems or VHA medical centers. Some VHA health care systems contain multiple medical centers. We confirmed with officials from these health care systems that they would respond on behalf of all the medical centers within the system. Other facilities included a multi-specialty community-based outpatient center, three outpatient clinics, and one federal health care facility that combines Department of Veterans Affairs and Department of Defense medical care in one facility. We refer to these types of facilities as “VHA medical facilities” within the report and to officials from all these types of facilities as “facility RCI officials.”
[70]Department of Veterans Affairs, Veterans Health Administration Directive 0999(1): Policy Management (Washington D.C.: Mar. 29, 2022, amended Jan. 10, 2024) and Veterans Health Administration Directive 1217: VHA Operating Units (Washington D.C.: Aug. 14, 2024).
[71]GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.: Sept. 10, 2014) and Evidence-Based Policy Making: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington D.C.: July 2023).
[72]See VHA Directive 0999(1).
[73]See GAO‑14‑704G and GAO‑23‑105460.
[74]Community care eligibility criteria were established under the VA MISSION Act of 2018. Five of the six criteria are mandatory: 1) the Department of Veterans Affairs (VA) is unable to furnish care in a manner that meets its access standards; 2) the veteran and their referring provider agree that furnishing care in the community is in the veteran’s best medical interest based upon VA’s criteria; 3) VA does not offer the care or services the veteran requires; 4) VA does not operate a full-service medical facility in the state in which the veteran resides; and 5) the veteran was grandfathered in due to prior eligibility under the Choice Act program and met other criteria. The sixth criterion is discretionary and occurs when VA determines that a medical service line where care is needed is not providing care that complies with the standards for quality established under 38 U.S.C. § 1703C. Under this quality standards criterion, VHA conducts ongoing assessments to determine when a health care service line is falling short of the agency’s standards for quality. When this occurs, the Secretary of Veterans Affairs may decide veterans are eligible to receive care from a community provider for those specific services while the agency works to remediate and improve the quality of those services. However, according to officials, VHA has not had to use this eligibility criterion.
If a veteran is eligible for and chooses to receive community care, the appointment request will be sent to the facility community care office to be scheduled with a community provider.
[75]For the purposes of this report, we focus on specialty care referrals. The process may differ for new patients requesting care and patients requesting follow-up appointments. For example, veterans who are not already receiving care through VHA must submit an application to enroll before they can schedule an appointment.
VHA uses the Veterans Health Information Systems and Technology Architecture to manage health care delivery to its patients, which includes the department’s electronic health record. Referral appointment requests are made through the computerized patient record system. VA has taken steps to replace the Veterans Health Information Systems and Technology Architecture with a new health information system. However, the program is currently paused after deploying at only six sites. It is not clear when deployment for the remainder of VHA medical facilities will resume.
[76]For certain referrals, a veteran may be automatically eligible for community care without an assessment by a scheduler. For example, if a veteran resides in Alaska, Hawaii, New Hampshire, Guam, American Samoa, Northern Mariana Islands, or the U.S. Virgin Islands where there are no full-service VHA facilities where veterans can receive care.
[77]In 2014, the Veterans Access, Choice, and Accountability Act of 2014, among other things, established a temporary program—called the Veterans Choice Program—and provided up to $10 billion in funding for veterans to obtain health care services from community providers when they faced long wait times, lengthy travel distances, or other challenges accessing care at VHA facilities. Pub. L. No. 113-146, §§ 101, 802(d), 128 Stat. 1754, 1755-1765, 1802-1803 (2014).
In 2019, the VA MISSION Act of 2018 (VA MISSION Act) aimed to strengthen and improve VA’s health care system for veterans and their caregivers, and required, among other things, VA to implement a permanent community care program. Pub. L. No. 115-182, tit. I, §101, 132 Stat. 1393, 1395 (2018).
[78]A scheduler can see if the veteran is eligible based on the drive time standard using a tool in the scheduling system. The system averages drive time on a Wednesday at 10:00 a.m. in the veteran’s local time. The system updates historical traffic data 2-3 times per year to reflect local travel patterns.
[79]VA considers certain types of mental health services, such as psychological testing and mental health vocational assistance, to be specialty care services. For these services, a veteran may be eligible for community care if the veteran’s average drive time to a VA provider exceeds 60 minutes; or the next available appointment with a VA provider is not available within 28 days based on the date of the request for care.
[80]According to VHA officials, the VHA data capture eligibility for veterans who decide to receive community care. Veterans who were eligible to see a community provider but decided to receive care at VA instead are not included in this data set.
[81]The number of audits each month may vary by facility, but there must be at least one audit per scheduler each month.
[82]As of June 2024, VA Office of Inspector General officials told us they are conducting a review of the accuracy of all community care eligibility criteria.