HEARING DETECTION AND INTERVENTION
Program Connects Deaf or Hard of Hearing Infants
and Children to Services, but Actions Needed
to Improve Access
Report to Congressional Committees
United States Government Accountability Office
Highlights of GAO-25-106978, report to congressional committees.
HEARING DETECTION AND INTERVENTION
Program Connects Deaf or Hard of Hearing Infants and Children to Services, but Actions Needed to Improve Access
Why GAO Did This Study
About one in every 500 infants is identified as deaf or hard of hearing. Receiving early intervention services can help children meet speech, language, social, and emotional development milestones. For example, with appropriate services, children can develop the comprehension and use of language, known as language acquisition. HRSA provides grants to 59 states and territories (states) to support their data tracking and referral efforts. For the current grant cycle, HRSA awarded $235,000 per year to each state. In addition, HRSA has provided additional funding through competitive grant opportunities to state EHDI programs for targeted purposes.
The Early Hearing Detection and Intervention Act of 2022 includes a provision for GAO to review the EHDI program. This report (1) describes how HRSA measures EHDI program performance; (2) describes HRSA and CDC efforts to address state programs’ reported challenges meeting EHDI benchmarks; (3) describes what HRSA and CDC have done to support state efforts to improve language acquisition and any challenges states may face in improving language acquisition; (4) examines HHS agencies’ actions to identify and address disparities in EHDI program access; and (5) describes HRSA’s efforts to help ensure support is available to parents of children with a hearing loss diagnosis.
To do this work, GAO analyzed HHS program documentation and relevant data from 2008 (the first year almost all states reported the same data since the creation of the program in 2000) to 2021 (most currently available at the time of GAO’s review).
GAO also interviewed HHS officials and six state EHDI program grantees, selected to vary by factors such as geography and whether they received additional funding to support enhanced data collection. The six selected states were Alaska, Connecticut, Georgia, Minnesota, Ohio, and Puerto Rico.
GAO also reviewed documentation and interviewed officials from the Department of Education (Education) on their interactions with the EHDI program and data-sharing at the state level between state EHDI program offices and Education-funded offices that administer early intervention programs.
GAO reviewed diversity and inclusion plans from all 59 states’ EHDI program offices. In addition to interviews with the four technical assistance centers HRSA funded in the last two funding cycles, GAO also interviewed three selected advocacy organizations. These organizations were the National Association of the Deaf, the Alexander Graham Bell Association for the Deaf and Hard of Hearing, and the American Society for Deaf Children.
What GAO Recommends
GAO is making two recommendations to HRSA: (1) require state EHDI programs to set performance goals that can be used to measure progress in addressing any identified disparities in access for underserved populations; and (2) assess the results of state EHDI programs’ access disparities performance and use it to inform future plans. HHS agreed with these recommendations.
View GAO-25-106978. For more information, contact Mary Denigan-Macauley at (202) 512-7114 or deniganmacauleym@gao.gov.
What GAO Found
The Early Hearing Detection and Intervention (EHDI) program, administered by the Department of Health and Human Services (HHS), tracks the screening and diagnosis of infants for hearing loss and refers them for appropriate intervention services. Within HHS, the Health Resources and Services Administration (HRSA) uses data the Centers for Disease Control and Prevention (CDC) collects to measure EHDI program performance. HRSA and CDC have adopted age-defined care standards, known as the 1-3-6 benchmarks, to measure program performance on a national level. According to the 1-3-6 benchmarks, all infants should be screened for hearing loss before 1 month of age, and those that do not pass the screening should see a specialist to diagnose any hearing loss, as well as the cause, before 3 months of age. By 6 months of age, infants who are identified as deaf or hard of hearing should be enrolled in early intervention services for support in developing communication skills.

Starting with 2021 data, CDC and HRSA agreed to change the measure the agencies use to assess state EHDI program progress against the 1-3-6 benchmarks. Previously, HRSA used a measure that did not count all infants who were eligible for follow-up care. For example, infants would not have been counted if their families could not be contacted by the state EHDI program to confirm whether the infants received follow-up care. HRSA plans to use a different performance measure to assess state progress starting with the 2024-2029 grant cycle that includes all infants with possible hearing loss as they progress through diagnostic and intervention services, according to HRSA officials. Officials from both agencies told GAO they are aware that the new measure will show a lower percentage of infants receiving timely access to services, but they agree it is a more accurate way to measure such access.
HRSA and CDC have taken steps to help address state challenges meeting EHDI benchmarks. For example, a 2023 program-wide survey and interviews with five of the six states GAO selected have found that shortages in experienced pediatric audiologists pose a challenge to improving access to timely diagnosis. HHS has taken steps to help states address this challenge by directing its technical assistance centers to focus on promising practices, such as the use of telehealth services, to overcome provider shortages.
In fiscal year 2024, HRSA set a new program requirement for state EHDI programs to measure language acquisition outcomes—that is, developing the comprehension and use of language. To help states begin collecting and measuring language acquisition outcomes, HHS agencies have taken actions such as conducting a pilot program and providing additional funding to strengthen state infrastructure to collect outcomes information. HHS also has efforts underway to address states’ reported challenges, such as providing technical assistance to increase states’ capacity for data collection.
HHS agencies took several actions to improve the EHDI program’s ability to identify and address disparities in access to services for children who are deaf or hard of hearing. HRSA required state EHDI programs to submit diversity and inclusion plans in 2021 to identify and address disparities in EHDI service access—differences in availability of services between groups defined by characteristics such as ethnicity or economic resources. However, GAO found that HRSA is unable to determine whether individual state EHDI programs’ efforts have been successful in addressing disparities in access because HRSA did not require states to set performance goals as part of their diversity and inclusion plans.
Further, GAO found that HRSA did not assess the results of the plans to understand how the plans might be updated or used to better address disparities in access in the 2024-2029 funding cycle. With a requirement in place for state EHDI programs to set and report on performance goals, states can demonstrate their progress in addressing access disparities for their identified underserved populations. In addition, HRSA’s assessment of states’ progress can inform future plans to support state EHDI programs. Doing so would better ensure children in underserved populations receive the care they need.
State EHDI programs have a variety of ongoing efforts to meet HRSA’s requirement to support families with a child who has hearing loss. Those efforts include: (1) parent-to-parent support through specially-trained parent guides who have a child who is deaf or hard of hearing; (2) adult deaf mentors who can help parents better understand what their child’s life might be like as a deaf or hard of hearing person; and (3) automatic referral processes to connect families with newly-diagnosed children to family support services to eliminate barriers to participation.
|
Abbreviations |
|
|
|
|
|
CDC |
Centers for Disease Control and Prevention |
|
HHS |
Department of Health and Human Services |
|
EHDI |
Early Hearing Detection and Intervention |
|
FL3 |
Family Leadership in Language and Learning |
|
HRSA |
Health Resources and Services Administration |
|
IDEA |
Individuals with Disabilities Education Act |
|
NIH |
National Institutes of Health |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
January 2, 2025
The Honorable Bernard Sanders
Chair
The Honorable Bill Cassidy, M.D.
Ranking Member
Committee on Health, Education, Labor and Pensions
United States Senate
The Honorable Cathy McMorris Rodgers
Chair
The Honorable Frank Pallone, Jr.
Ranking Member
Committee on Energy and Commerce
House of Representatives
About one in every 500 infants is identified as deaf or hard of hearing, according to the Centers for Disease Control and Prevention (CDC). In 2021, 6,518 babies were identified as deaf or hard of hearing, according to the most recently available CDC data. When left undetected, hearing loss can affect children through delays in their speech, language, social, and emotional development. Early intervention—such as speech therapy, American Sign Language, or other services based on the needs of the child and family—can help these children meet age-appropriate developmental milestones.
One way the federal government supports children who are deaf or hard of hearing is through the Early Hearing Detection and Intervention (EHDI) program. This program awards grants to states and territories to track screening and diagnosis for infants with hearing loss and refer them for appropriate interventions. The Health Resources and Services Administration (HRSA), within the Department of Health and Human Services (HHS), has made annual grant awards to a total of 59 states for their EHDI programs since the creation of the program in 2000.[1]
In fiscal year 2023, Congress appropriated approximately $18.8 million to HRSA for the EHDI program and has cumulatively appropriated approximately $90 million to HRSA for the program over the 5-year period from fiscal year 2019 through fiscal year 2023, according to HRSA officials. States administer their own EHDI programs and may receive additional funding from their state government or other federal programs. In 2024, HRSA announced a new program requirement to focus on improving language acquisition outcomes for the current 5-year grant period for state EHDI programs, which began in April 2024.
Along with HRSA, other HHS agencies support efforts to address hearing loss in infants and children. CDC provides cooperative agreements and technical assistance to states to develop, monitor, and collect data on early hearing screening, evaluation, and intervention programs and systems. The National Institutes of Health (NIH) has a role in the EHDI program in funding research related to the program. Finally, the U.S. Department of Education (Education) oversees and provides funds to state early intervention programs that assist children with disabilities, including those with hearing loss.
The Early Hearing Detection and Intervention Act of 2022 includes a provision for us to review the status of the EHDI program, including information on disparities in health care access to EHDI services and support to families of children who are deaf or hard of hearing.[2] Disparities generally refers to differences in access to or availability of services between population groups defined by socioeconomic characteristics such as ethnicity, economic resources, or geographic populations, according to HHS.[3]
This report
1. describes how HRSA measures EHDI program performance;
2. describes HRSA and CDC’s efforts to address state programs’ reported challenges meeting EHDI benchmarks;
3. describes what HRSA and CDC have done to support state efforts to improve language acquisition and any challenges states may face in improving language acquisition;
4. examines HHS agencies’ actions to identify and address disparities in EHDI program access; and
5. describes HRSA efforts to help ensure support is available to parents of children with a hearing loss diagnosis.
To address these five objectives, we reviewed EHDI program grant documentation and documentation from HRSA’s technical assistance centers that provided support and training to state EHDI programs from 2020 to 2024. We interviewed HHS officials from HRSA, CDC, and the NIH about their roles in the EHDI program. We also interviewed officials from each of the four EHDI technical assistance centers and officials from a non-generalizable sample of six state EHDI programs. Technical assistance centers for the EHDI program are funded through HRSA grants and provide support or training to specific groups, such as providing support for state EHDI programs. The six selected states were Alaska, Connecticut, Georgia, Minnesota, Ohio, and Puerto Rico. We selected these states for variation in factors such as geographic location and whether they received additional funding to support enhanced data collection, to learn about their implementation of the EHDI program at the state level, including their efforts in data collection, addressing disparities in access, and available support for parents and families.
· To further describe how HRSA measures EHDI program performance, we analyzed available annual aggregate summary data from CDC on the EHDI program, from the Hearing Screening and Follow-up Survey, for 2008 (the first year almost all states reported the same data since the creation of the program in 2000) through 2021 (most current available at the time of our review).[4] We assessed the reliability of these data by reviewing CDC documentation on the data and interviewing agency officials knowledgeable about the data, and determined that these data were sufficiently reliable for the purposes of our reporting objectives.
· To further describe HRSA and CDC’s efforts to address state programs’ reported challenges meeting EHDI benchmarks, we reviewed documentation summarizing 59 state EHDI program annual progress reports and survey results from an EHDI technical assistance center.
· To further describe what HRSA and CDC have done to support state efforts to improve language acquisition, we reviewed documentation and interviewed officials from Education on their interactions with the EHDI program and data-sharing at the state level between state EHDI program offices and Education-funded state programs that administer early intervention programs.
· To further examine HHS agencies’ actions to identify and address disparities in EHDI program access, we reviewed diversity and inclusion plans from all 59 states’ EHDI program offices. We assessed the content of the plans against the HHS’s strategic objective in effect at the time of the plans’ development, which was to improve Americans’ access to health care, including by reducing disparities in access.[5] We also assessed the instructions for, and HRSA’s actions to follow up on, the plans against leading practices for performance management. We also reviewed published literature from 2018 to 2023 to identify any promising practices in improving access to services for infants and toddlers who may be deaf or hard of hearing.
· To further describe HRSA’s efforts to help ensure support is available to parents of children with a hearing loss diagnosis, we reviewed program documentation from technical assistance centers related to support provided to families of children who are deaf or hard of hearing. We also reviewed published literature to identify any background concepts related to family support for parents of children who are deaf or hard of hearing. We interviewed a non-generalizable selection of three advocacy organizations for people who are deaf or hard of hearing. Our three selected advocacy organizations were the National Association of the Deaf, the Alexander Graham Bell Association for the Deaf and Hard of Hearing, and the American Society for Deaf Children. We also interviewed four parents of children who are deaf or hard of hearing.
Appendix I provides more information on our scope and methodology.
We conducted this performance audit from July 2023 to January 2025 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
The EHDI Program was established by statute in 1999 and was most recently updated by the Early Hearing Detection and Intervention Act of 2022.[6] State EHDI programs use their grants from HRSA to track and refer infants with potential hearing loss to care. Three HHS agencies–HRSA, CDC, and NIH—have roles in the EHDI program.
EHDI Program Role in the Screening, Diagnosis, and Referral Process for Hearing Loss
HRSA provides grants to state EHDI programs to maintain and support a coordinated statewide screening, data-tracking, and referral system for infant hearing loss. Each state EHDI program tracks infants with possible hearing loss after newborn screening, encourages families to obtain a diagnosis, and refers infants and their families to early intervention service enrollment. The EHDI program is not responsible for the cost of actual clinical services such as the screening and diagnosis by medical providers.
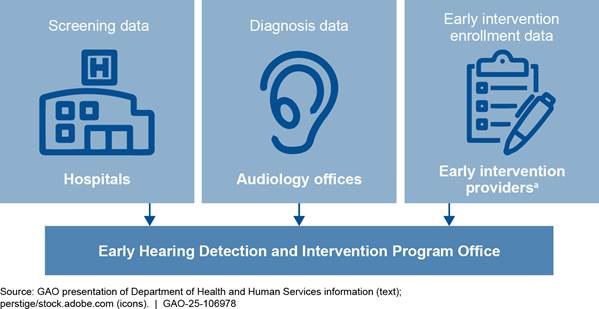
Each state EHDI program establishes data-sharing agreements with entities in its state such as hospitals, birthing centers, state offices of vital statistics, audiologists’ practices, and state early intervention providers to track and refer infants with hearing loss. (See figure 1.)
aEarly intervention is a system of services to help children under the age of 3, including children who are deaf or hard of hearing, with learning language and other important skills. For example, early intervention services may include assistive technology, speech and language therapy, or family training, such as training in American Sign Language. The recommended Early Hearing Detection and Intervention program benchmark is that all infants with hearing loss should begin intervention services before 6 months of age.
Hearing screening. Infants usually have their hearing screened while still in the hospital or birthing center after birth. An infant’s hearing can be screened using special equipment that measures the brain’s response to sound. Hearing screening is easy and is not painful. It takes a few minutes and infants are often asleep while being screened, according to CDC. (See figure 2.)

Note: Hearing screening is the first service provided to determine if an infant may have hearing loss. The Department of Health and Human Services recommends that all infants are screened for hearing loss before 1 month of age.
Diagnosis. Infants who do not pass the hearing screening should be evaluated by a health care provider called an audiologist. An audiologist is trained to test and diagnose hearing loss. The audiologist will do additional diagnostic testing to find out the extent of any hearing loss. There are many kinds of diagnostic tests for hearing loss, including determining how much hearing loss there is, and what type it is.
Early intervention. Enrollment into an early intervention program helps children with hearing loss to better communicate with others, do well in school, and get along with other children. Intervention services can include: (1) working with a professional or team who can help a family and child learn to communicate using various approaches; (2) fitting an infant with a hearing device, such as a hearing aid; and (3) joining family support groups. State EHDI programs generally refer children with hearing loss to early intervention programs funded through grants from Education under Part C of the Individuals with Disabilities Education Act (IDEA).[7] Part C programs serve children with (1) developmental delays, or (2) a diagnosed condition that has a high probability of resulting in developmental delay, such as hearing loss. State EHDI programs may partner with state Part C programs to obtain information on early intervention enrollment for infants with hearing loss.[8]
State EHDI programs are also responsible for providing family support. State EHDI programs are expected to engage families with children who are deaf or hard of hearing. For example, state EHDI programs provide peer support to parents of children with a hearing loss diagnosis to help guide them. State EHDI programs may also partner with nonprofit organizations in their states to provide parent and family support to equip parents to make decisions on behalf of their children.
HHS Agency Roles in the EHDI Program
Federal law specifies distinct roles for the EHDI program’s three implementing HHS agencies—HRSA, CDC, and NIH—and requires these agencies to coordinate with one another and with Education’s IDEA Part C program, among others.[9] EHDI program scope and focus areas have been changed over time to reflect changes in HHS’s overall strategic goals and the program’s authorizing legislation, according to HRSA. Specifically, in 2017, the EHDI program expanded to include young children, in addition to newborns and infants.[10] HRSA added a requirement in fiscal year 2020 for state EHDI programs to develop diversity and inclusion plans to ensure states address the needs of the various populations they serve. This addition was made to align with HRSA’s mission, which includes improving health outcomes and achieving health equity through access to quality services, according to HRSA. HRSA is the primary federal agency for improving access to health services for people who are geographically isolated, economically vulnerable, or medically vulnerable.
HRSA
HRSA funds and supports the 59 state EHDI program grantees in their efforts to track and refer children who are deaf or hard of hearing. HRSA awards grants, subject to annual appropriations, through a competitive process every 5 years. Multiple organizations or state offices can apply to be the grantee for a given state. HRSA communicates its requirements and goals through an announcement called a Notice of Funding Opportunity. For the current grant cycle from April 2024 through March 2029, HRSA awarded 59, $235,000 per year EHDI grants to fund infrastructure goals for the program, such as increasing data tracking capacity. In addition, HRSA has provided additional funding through competitive grant opportunities for up to 20 state EHDI programs for targeted purposes, such as a 2024 opportunity to apply for an optional Innovation Project to improve data collection. See Appendix II for a table of HHS EHDI grants.
HRSA also funds a network of technical assistance centers that support EHDI state programs in their work, including:
· The Family Leadership in Language and Learning Center, referred to as the FL3 Center, supports parents and families after a child has been identified as deaf or hard of hearing. The FL3 Center is led by the national chapter of Hands & Voices, a nonprofit dedicated to serving families with children who are deaf or hard of hearing.
· The Implementation and Change Center supports states and territories to improve the EHDI system of services by providing training on quality improvement and disseminating evidence-based practices. Prior to the current grant cycle that began in April 2024, this technical assistance center was called the National Technical Resource Center and was led by the National Center for Hearing Assessment and Management at Utah State University. Beginning in April 2024, the National Beacon Center at Gallaudet University leads the Implementation and Change Center.
· The Provider Education Center is new as of April 2024, and will provide training for health care professionals involved with the EHDI system. The American Academy of Pediatrics leads the Provider Education Center.
CDC
CDC awards cooperative agreements and provides technical assistance to state EHDI programs to enhance state programs’ data collection, tracking, and analysis capabilities. In 2020, CDC awarded cooperative agreements to 39 state EHDI programs.
CDC also supports EHDI program efforts by collecting aggregate data from state EHDI programs. This is done through an annual survey called the Hearing Screening and Follow-up Survey. The survey requests hearing screening, diagnostic, and intervention data on infants born in a specified calendar year.[11] The survey also asks states to report demographic information, such as the race and ethnicity of infants and their mothers, and the type and severity of hearing loss if an infant is diagnosed. The survey helps to assess EHDI efforts to identify infants with permanent hearing loss across the United States. CDC produces summary data reports and publishes them on the CDC’s EHDI website.
NIH
NIH is responsible for funding research on technology, interventions, and outcomes (e.g., language and other) for deaf and hard of hearing infants and toddlers, as well as older children and adolescents. This work is focused on both detection of and interventions for hearing loss, and includes research exploring outcomes such as speech, language, and literacy. NIH’s National Institute on Deafness and Other Communication Disorders leads NIH’s efforts to promote research on children who are deaf and hard of hearing. NIH-funded research in this area is mainly investigator-initiated, meaning the researchers bring NIH the most compelling questions and needs that can be addressed through research and that undergo peer review. NIH-funded research related to EHDI may include, but is not limited to, high- and low-risk clinical trials, implementation studies, and specific applications to address health disparities, according to NIH.
Disparities in Access to EHDI Services
According to CDC’s 2021 national Hearing Screening and Follow-up Survey data, certain demographic populations may not be able to access EHDI services as well as others. According to this 2021 survey, infant hearing screening rates are generally equivalent regardless of reported demographic factors. However, differences among certain demographic groups emerge around access to diagnostic evaluation. For example, a lower percentage of infants born to mothers younger than 25, mothers without a college education, or mothers identified as belonging to certain racial or ethnic groups received a diagnostic evaluation than infants born to older mothers or mothers with a college education. While 28.8 percent of infants born to mothers identified as Native Hawaiian or Pacific Islander received a diagnostic evaluation after not passing their hearing screening, 59.5 percent of infants born to mothers identified as White received the diagnostic evaluation.
Similar demographic patterns are seen for enrollment in early intervention services. Specifically, a lower percentage of infants born to mothers younger than 25, mothers without a college education, and mothers identified as belonging to certain racial or ethnic groups were enrolled in early intervention services after being diagnosed with permanent hearing loss as compared to infants born to older mothers, mothers with a college education, or mothers identified as White.
HRSA Measures EHDI Program Performance Primarily through Benchmark Data
HRSA Assesses State EHDI Programs Based on the Percentage of Infants Meeting Benchmark Targets for Hearing Screening, Diagnoses, and Enrollment in Early Intervention Services
HRSA assesses state EHDI program performance based on data collected from states by CDC on the percentage of infants who are screened for hearing loss before 1 month of age, diagnosed before 3 months of age, and enrolled in early intervention services before 6 months of age.[12] These data indicate performance on age-defined care standards known as the 1-3-6 benchmarks, which are considered best practice for early hearing detection and intervention. (See figure 3.)
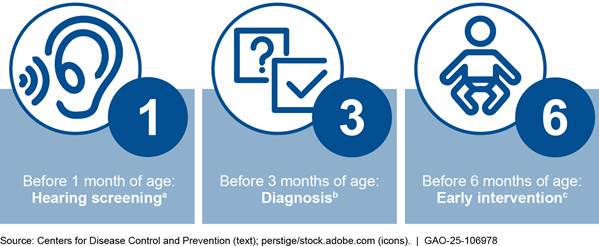
aHearing screening is the first service provided to determine if an infant may have hearing loss. The recommended EHDI benchmark is that all infants are screened for hearing loss before 1 month of age.
bDiagnosis involves a comprehensive test to determine if an infant has hearing loss, and the severity and type of hearing loss. The recommended EHDI benchmark is that all infants who do not pass the first screening should have a complete diagnostic hearing test by a hearing specialist before 3 months of age.
cEarly intervention is a system of services to help children under the age of 3, including children who are deaf or hard of hearing, with learning language and other important skills. For example, early intervention services may include assistive technology, speech and language therapy, or family training, such as training in American Sign Language. The recommended EHDI benchmark is that all infants with hearing loss should begin intervention services before 6 months of age.
HRSA sets performance targets for each of the 1-3-6 benchmarks and measures each state EHDI program’s progress against these targets. Targets are based on a state’s previous performance. For example, to meet HRSA’s 2024-2029 EHDI grant program targets, by March 2029, each state EHDI program should:
· Increase by 1 percent per year the number of infants who receive a newborn hearing screening before 1 month of age, or achieve at least a 95 percent screening rate;
· Increase by 10 percent the number of infants who receive a diagnostic audiological evaluation before 3 months of age, or achieve a minimum diagnosis rate of 85 percent; and
· Increase by 15 percent the number of infants identified as deaf or hard of hearing who are enrolled in early intervention services before 6 months of age, or achieve a minimum enrollment rate of 80 percent.
HRSA’s most recently available target results are based on 2020 birth year data and reflect targets set to meet HRSA’s 2020-2024 grant period, according to HRSA officials. These data show that more than half of state EHDI programs (34 of 59) had met their 2020 - 2024 grant period performance targets for the 1-month screening benchmark. Fewer state EHDI programs had met 2020-2024 grant period targets for the 3-month benchmark for diagnosis and the 6-month benchmark for enrollment in early intervention services. (See figure 4.) The 2020 target results are low because of complications in data collection brought on by the COVID-19 pandemic, according to HRSA officials. Officials added that the data reflect state EHDI programs’ efforts to meet performance targets during the first year of the 4-year grant period that was affected by the COVID-19 pandemic.
Figure 4: Number and Percentage of States Meeting Early Hearing Detection and Intervention 2020-2024 Grant Period Performance Targets, 2020 Birth Year Data
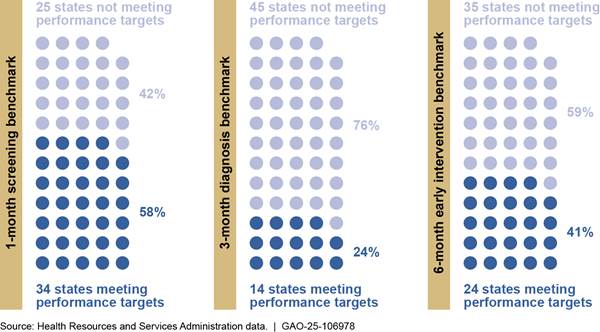
Note: The Health Resources and Services Administration provides Early Hearing Detection and Intervention grants to 59 states and territories (states).
At a national level, benchmark data show near-universal access to timely newborn hearing screening, with 96 percent of infants born in 2021 meeting the first benchmark by being screened before 1 month of age.[13] However, EHDI benchmark data show that national 3-month diagnosis and 6-month enrollment benchmark rates are significantly lower. In 2021, only 43 percent of infants not passing the initial hearing screen received a diagnostic evaluation before 3 months of age; only 42 percent of infants with confirmed permanent hearing loss received early intervention services by 6 months of age in 2021.[14]
Performance Measure Change for EHDI Benchmarks Should Allow HRSA to More Accurately Track State Progress
CDC collects and analyzes 1-3-6 benchmark data and creates annual summary reports used by HRSA to track and assess EHDI state and national performance. Prior to 2021, CDC included two different measures of performance for each of the benchmarks in its summary reports—the “Population in Services” measure and the “Eligible Population” measure.[15] HRSA used the Population in Services measure to assess state EHDI program progress for each benchmark, according to HRSA officials. Starting with its analyses of 2021 data, CDC began reporting only the Eligible Population measure for each benchmark. CDC and HRSA agreed the Eligible Population measure more accurately aligns with the public health goal to monitor state and national progress by tracking all infants who may have hearing loss, according to CDC officials. CDC officials said the Eligible Population measure allows the agencies to track infants and families more accurately as they progress through EHDI services by including those infants who are lost to follow-up in the performance calculations.
|
Lost to follow-up is the term the U.S. Department of Health and Human Services uses to describe infants who are identified by the Early Hearing Detection and Intervention (EHDI) program as needing further care, such as diagnostic evaluation or early intervention services, but the EHDI program does not know whether they receive that care for a variety of reasons. For example, the status of infant care may not be known because the infants’ families cannot be contacted, are unresponsive to EHDI outreach, or the infants’ receipt of follow-up care is otherwise unknown to the program. Source: Centers for Disease Control and Prevention and Health Resources and Services Administration documentation. | GAO‑25‑106978 |
The Eligible Population measure represents how many infants obtained services at each of the 1-3-6 benchmarks among a larger, more inclusive population than the Population in Services measure HRSA had been using to assess progress, according to our analysis of CDC summary reports. (See table 1.)
Table 1: Comparison of Two Early Hearing Detection and Intervention (EHDI) Program Performance Measures for the 1-3-6 Month Benchmarks
|
Benchmark |
Performance Measure |
|
|
|
Population in Services |
Eligible Population |
|
Percent screened before 1 month of agea |
Of infants screened, how many were screened before 1 month of age. |
Of all infants born, how many were screened before 1 month of age. |
|
Percent diagnosed before 3 months of ageb |
Of infants diagnosed, how many were diagnosed before 3 months of age. |
Of infants who did not pass their screening, how many were diagnosed before 3 months of age.d |
|
Percent enrolled in early intervention services before 6 months of agec |
Of infants enrolled in early intervention services, how many were enrolled before 6 months of age. |
Of infants diagnosed with permanent hearing loss, how many were enrolled in early intervention services before 6 months of age. |
Source: GAO analysis of Centers for Disease Control and Prevention information. | GAO‑25‑106978
Note: The Population in Services measure is being used by the Health Resources and Services Administration (HRSA) to assess EHDI program progress through the end of the 2020-2024 grant cycle, according to HRSA officials. The Eligible Population measure will be used to assess progress starting with the 2024-2029 grant cycle.
aHearing screening is the first service provided to determine if an infant may have hearing loss. The recommended Early Hearing Detection and Intervention (EHDI) benchmark is that all infants are screened for hearing loss before 1 month of age.
bDiagnosis involves a comprehensive test to determine if an infant has hearing loss, and the severity and type of hearing loss. The recommended EHDI benchmark is that all infants who do not pass the first screening should have a complete diagnostic hearing test by a hearing specialist before 3 months of age.
cEarly intervention is a system of services to help children under the age of 3, including children who are deaf or hard of hearing, with learning language and other important skills. For example, early intervention services may include assistive technology, speech and language therapy, or family training, such as training in American Sign Language. The recommended EHDI benchmark is that all infants with hearing loss should begin intervention services before 6 months of age.
dSome infants were referred directly to diagnosis without first being screened.
HRSA plans to use the Eligible Population measure to more accurately monitor state EHDI program progress, starting with the 2024-2029 grant cycle for all three benchmarks, according to HRSA officials. CDC changed its summary reports in coordination with HRSA, and officials from both agencies told us they are aware that the Eligible Population measure will ultimately show a lower percentage of infants receiving timely access to services than the prior measure.
Our analysis comparing the two sets of measures using state-submitted survey data from 2008 to 2020 confirms the officials’ observation.[16] For example, according to the Population in Services measure, of the 3.52 million infants screened for hearing loss in 2020, 97.2 percent were screened before 1 month of age. According to the Eligible Population measure, of the 3.59 million infants born in 2020, 95.4 percent were screened before 1 month of age. (See figure 5.)
Figure 5: Comparison of Two Measures for the Percentage of Infants Screened for Hearing Loss before 1 Month of Age, 2008-2020
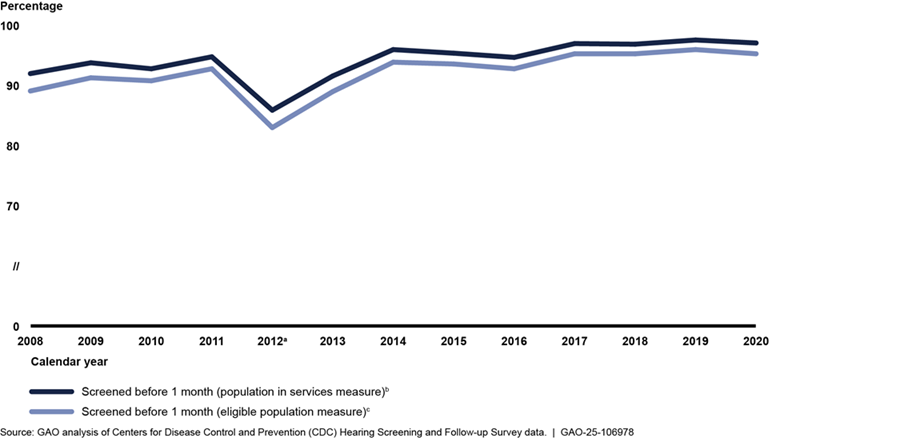
Notes: Hearing screening is the first service provided to determine if an infant may have hearing loss. The recommended Early Hearing Detection and Intervention (EHDI) benchmark is that all infants are screened for hearing loss before 1 month of age. Data include information about any services that infants born in the specified calendar year received through the next year, until time of survey reporting.
Some state EHDI programs did not report all data in all years. For newborn screening data, the number of reporting state EHDI programs ranged from 50 to 57 between 2008 and 2020.
Information reflects data that states have documented and reported to CDC without any estimation.
The COVID-19 pandemic interrupted the delivery of health care services in 2020, including newborn hearing screening and follow-up diagnostic and intervention services. As a result, infants born in 2020 and needing hearing screening and follow-up services may have experienced delays or had difficulties obtaining these services.
aIn 2012, a large state EHDI program reported issues with its screening data, which contributed to a noticeable decline in national percentages of infants screened before 1 month of age, according to CDC officials.
bThe Population in Services measure calculated the percentage of infants screened before 1 month of age among all infants screened for hearing loss, in a given year.
cThe Eligible Population measure calculates the percentage of infants screened before 1 month of age among all infants born, in a given year.
The difference in performance measures is more apparent for the 3-month diagnosis and 6-month enrollment benchmarks. According to the Population in Services measure, in 2020, of the 42,330 infants diagnosed, 60.6 percent of infants were diagnosed before 3 months of age. According to the Eligible Population measure, of the 68,741 infants who did not pass their hearing screening, 36.4 percent were diagnosed before 3 months of age in 2020. (See figure 6.)
Figure 6: Comparison of Two Measures for the Percentage of Infants Diagnosed with Hearing Loss before 3 Months of Age, 2008-2020
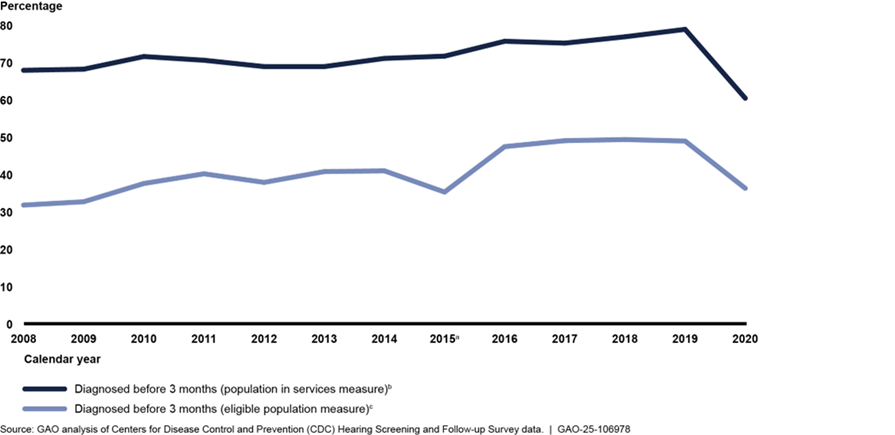
Notes: Diagnosis involves a comprehensive test to determine if an infant has hearing loss, and the severity and type of hearing loss. The recommended Early Hearing Detection and Intervention (EHDI) benchmark is that all infants who do not pass the first screening should have a complete diagnostic hearing test by a hearing specialist before 3 months of age. Data include information about any services that infants born in the specified calendar year received through the next year, until time of survey reporting.
Some state EHDI programs did not report all data in all years. For diagnosis data, the number of reporting state EHDI programs ranged from 48 to 57 between 2008 and 2020.
Information reflects data that states have documented and reported to CDC without any estimation.
The COVID-19 pandemic interrupted the delivery of health care services in 2020, including newborn hearing screening and follow-up diagnostic and intervention services. As a result, infants born in 2020 and needing hearing screening and follow-up services may have experienced delays or had difficulties obtaining these services.
aIn 2015, one state EHDI program submitted overall diagnoses data, but did not submit data on infants diagnosed before 3 months of age. According to CDC officials, this created a noticeable decline in the percentage of infants diagnosed before 3 months of age if calculated using the Eligible Population measure.
bThe Population in Services measure calculated the percentage of infants diagnosed before 3 months of age among all infants that received a diagnostic evaluation, in a given year.
cThe Eligible Population measure calculates the percentage of infants diagnosed before 3 months of age among all infants who did not pass their hearing screening, in a given year.
According to the Population in Services measure, in 2020, of the 3,883 infants who were enrolled in early intervention services, such as speech language therapy, 72.4 percent of infants were enrolled before 6 months of age. According to the Eligible Population measure, of the 6,321 infants diagnosed with permanent hearing loss, 44.5 percent were enrolled in early intervention services before 6 months of age in 2020. (See figure 7.)
Figure 7: Comparison of Two Measures for the Percentage of Infants with Hearing Loss Enrolled in Early Intervention by 6 Months of Age, 2008-2020
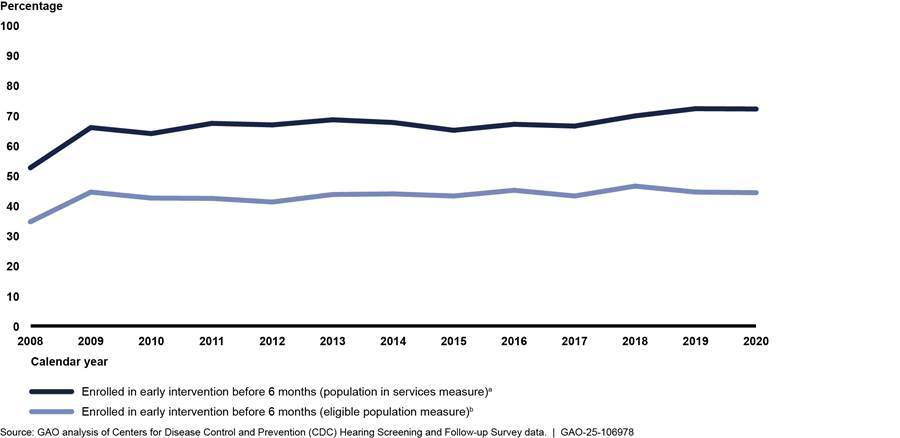
Notes: Early intervention is a system of services to help children under the age of 3, including deaf or hard of hearing children, with learning language and other important skills. For example, early intervention services may include assistive technology, speech and language therapy, or family training, such as training in American Sign Language. The recommended Early Hearing Detection and Intervention (EHDI) benchmark is that all infants with hearing loss should begin intervention services before 6 months of age. Data include information about any services that infants born in the specified calendar year received through the next year, until time of survey reporting.
Some state EHDI programs did not report all data in all years. For early intervention enrollment data, the number of reporting state EHDI programs ranged from 47 to 57 between 2008 and 2020.
Information reflects data that states have documented and reported to CDC without any estimation.
The COVID-19 pandemic interrupted the delivery of health care services in 2020, including newborn hearing screening and follow-up diagnostic and intervention services. As a result, infants born in 2020 and needing hearing screening and follow-up services may have experienced delays or had difficulties obtaining these services.
aThe Population in Services measure calculated the percentage of infants enrolled in early intervention services before 6 months of age among all infants enrolled in early intervention services, in a given year.
bThe Eligible Population measure calculates the percentage of infants enrolled in early intervention services before 6 months of age among all infants diagnosed with hearing loss, in a given year.
HRSA and CDC Provide Technical Assistance and Take Other Steps to Address States’ Challenges Meeting EHDI Benchmarks
HRSA and CDC have taken steps to help address state challenges meeting EHDI benchmarks. The EHDI program’s National Technical Resource Center fielded a program-wide survey in 2023 to gather information about state challenges operating their EHDI programs, including challenges related to meeting benchmarks. The survey found that the top three challenges states face in operating their EHDI programs were (1) shortages in experienced pediatric audiologists, (2) shifting federal priorities, and (3) low physician knowledge about how to support parents through the EHDI newborn hearing screening, diagnosis, and intervention process.[17] Officials from our six selected state EHDI programs echoed these challenges, emphasizing how these challenges relate to states’ efforts to meet the 3-month benchmark for diagnosis and 6-month benchmark for enrollment in early intervention services.[18] HRSA and CDC are working to address these program challenges by focusing technical assistance, providing new funding, and facilitating data sharing.
· Focusing technical assistance on provider shortages. According to the survey, 38 out of 58 responding state EHDI programs reported that a paucity of experienced pediatric audiologists is a moderate or substantial obstacle to their program’s success. Pediatric audiologists conduct the testing necessary to ensure that infants receive a diagnosis by 3 months of age to meet the EHDI 3-month benchmark. We heard from officials from five of six selected state programs that provider shortages, especially shortages in pediatric audiologists, pose a challenge to improving access to timely diagnosis.
HRSA directed its technical assistance centers to focus on disseminating promising practices that might address state program challenges, including provider shortages. In response, the program’s National Technical Resource Center provided guidance and training to state EHDI programs on the development of telehealth services that could help overcome the challenges of provider shortages as well as service interruptions during the COVID-19 pandemic. In 2018, the National Technical Resource Center also began enhancing a web-based national directory of facilities that offer pediatric audiology services for children under 5 years of age, to help encourage the directory’s use by EHDI state programs.[19]
· Developing data sharing strategies to help states meet federal priorities. According to the survey, 31 out of 58 responding state EHDI programs reported that shifting federal priorities is a moderate or substantial obstacle to their program’s success. Following the legislative changes made in 2017, HRSA expanded the EHDI program’s target population and scope, shifting the program’s focus and placing new pressure on state EHDI programs to obtain Education data to track children up to age 3. According to HRSA’s 2021 state EHDI program progress reports, one of the primary challenges state programs faced was establishing data sharing agreements and processes with Education’s state Part C programs. Officials from four selected state EHDI programs told us they face challenges tracking early intervention enrollment for young children up to age 3 because they are not notified when young children with hearing loss are identified by, or enroll in, Part C. Officials from three states told us that privacy concerns limit their state’s Part C program’s ability to share such data directly with EHDI.
HRSA, CDC, and Education issued a joint letter in August 2024 encouraging collaboration between state EHDI and Part C programs to address challenges obtaining state Part C data.[20] Specifically, the joint letter details: (1) requirements and expectations for interagency collaboration; (2) the importance of data sharing to support timely referral, service delivery, and monitoring of children’s outcomes; and (3) technical assistance resources available to state programs. The letter highlights existing avenues where data sharing between state EHDI and state Part C programs is possible, according to HRSA and Education officials. For example, the joint letter explains how state Part C programs may disclose limited personally identifiable information under current regulations when the state EHDI program serves as an authorized representative of the state Part C program and the information is shared to evaluate the state Part C program.[21] According to the joint letter, state EHDI programs may be able to access information within state Part C records to track the EHDI 6-month benchmark for early intervention enrollment.
· Providing funding for provider education efforts. According to the survey, 31 out of 57 responding state EHDI programs reported that low physician knowledge about how to support parents through the EHDI newborn hearing screening, diagnosis, and intervention process is a moderate or substantial obstacle to their program’s success. We also heard from officials from five of six selected state EHDI programs that low provider awareness of ways to encourage follow-up or to convey urgency to parents for timely diagnosis are challenges to meeting the 3-month diagnosis benchmark.
HRSA provided additional funding opportunities to help states address low provider awareness about recommended EHDI practices in 2020 and 2021; and funded a new technical assistance center for this purpose in 2024. In HRSA’s 2020 Notice of Funding Opportunity, HRSA announced the opportunity for state EHDI programs to apply for a 1-year $10,000 award to fund an optional project on the educational needs of health care professionals who interact with children who are deaf or hard of hearing and their families at the time of diagnosis. HRSA awarded the funding to 18 state EHDI programs, which states used to increase provider awareness and identify ways to navigate families through care and service options. In 2021, HRSA announced the opportunity for specialized education programs to apply for an award of up to $75,000 to train pediatric audiologists to work with infants and young children who are deaf or hard of hearing.[22] In 2024, HRSA also funded the American Academy of Pediatrics to lead the EHDI program’s first Provider Education Center to improve partnerships with providers and provider organizations serving EHDI children and families.
Other state EHDI program challenges are much larger issues well beyond the scope of the program, according to HRSA officials. For example, two selected states cited challenges with low provider payment rates from state Medicaid programs as a reason some audiologists limit their appointments for infant hearing evaluations. States generally set their own provider payment rates for health services covered by Medicaid, within certain federal guidelines.[23] Because state EHDI programs do not directly provide those services, funding decisions for those services are outside the scope of the EHDI program. HRSA officials said they work with state EHDI programs to support their partnerships with state Medicaid programs.
HHS Efforts to Promote Language Acquisition Include Seeking State Input, and Efforts Are Underway to Address States’ Challenges
Our review shows that two HHS agencies—HRSA and CDC—have taken steps to support state EHDI program efforts to promote language acquisition in children with hearing loss. In fiscal year 2024, HRSA included a new program requirement focusing on measuring language acquisition outcomes—that is, the development of the comprehension and use of language, which includes spoken, written, or other communication systems, such as American Sign Language. By 2029, HRSA expects state EHDI programs to identify, collect, and report baseline data on language acquisition outcomes for children up to 3 years of age. State EHDI programs are expected to determine how to measure language acquisition by the end of the 5-year performance period because HRSA is transitioning to a population health focus for the EHDI program, according to HRSA officials. This population health focus intends to improve the health and well-being of an entire group or subgroup, such as improving language outcomes in children who are deaf or hard of hearing, according to HRSA officials.
Prior to establishing this requirement, HRSA and CDC took several actions to assess and support state EHDI programs’ ability to begin collecting and measuring language acquisition outcomes. Specifically:
· Requesting input from state EHDI programs. In 2022, HRSA requested input from the public through a Request for Information to inform future EHDI program development, including promising practices that help children who are deaf or hard of hearing meet language development milestones. HRSA received 14 responses from state EHDI programs, with half (seven) providing suggestions to help children who are deaf or hard of hearing meet language-related milestones. For example, one state EHDI program response described implementing an annual assessment of language outcomes for children up to 9 years of age.
· Conducting a developmental outcomes pilot program. From 2020-2024, CDC funded a pilot program, called the Outcomes and Developmental Data Assistance Center for EHDI Programs, that supported participating sites in gathering, analyzing, and using intervention and developmental outcomes data, including language outcomes. CDC’s pilot program worked with 17 sites across the country, the majority of which were schools for the deaf, and required the sites to use certain assessment tools to measure developmental outcomes.[24] The purpose of the pilot program was to determine what CDC could feasibly ask state EHDI programs to collect in terms of outcomes data in future Notice of Funding Opportunities, according to CDC officials.
· Providing additional funding. In 2023 and 2024, HRSA provided additional financial support to state EHDI programs to strengthen their infrastructure and begin to collect and measure language acquisition. For example, in 2023, HRSA awarded 22 states $75,000 each through a competitive supplemental grant to assess and build state capacity to address language acquisition. Additionally, as part of the 2024 EHDI Notice of Funding Opportunity, state EHDI programs could apply for an optional 1-year EHDI Innovation Project grant. As part of these Innovation Project grants, HRSA planned to award an additional $75,000 each to up to 20 states to support innovative efforts to build states’ measurement capacity.
Officials from state EHDI programs we spoke with identified challenges in measuring language acquisition outcomes. These challenges include limited available data, low state capacity, and ineffective data sharing. HRSA, in coordination with other HHS agencies, has efforts underway that may help address these challenges.
Limited available data. Officials we interviewed from two state EHDI programs said that language acquisition data is limited because state Part C programs do not measure language acquisition in a way that may be useful for EHDI programs. Similarly, our review of Education documentation found that Education does not collect outcome measures that are specific to language acquisition or disaggregated by condition, such as hearing loss. Rather, state Part C programs report information on language development, which includes the combined percent of infants and toddlers who demonstrate improvement in the following areas: (1) positive social-emotional skills, (2) acquisition and use of knowledge and skills, including language and communication, and (3) use of appropriate behaviors to meet their needs.[25]
State Part C programs may choose to conduct other assessments that may include language acquisition, according to Education officials, but they said this is not uniform across the country, or even within states. Additionally, there is no other Education requirement for state Part C programs to collect data on language outcomes that are specific to language acquisition, according to Education officials. HRSA officials told us that not all children who are deaf or hard of hearing receive early intervention services through state Part C programs; some receive services through private entities whose information may not be available to EHDI programs. HRSA does not require state EHDI programs to use Part C data as the only source of language outcomes data, according to HRSA officials.
Additionally, language outcomes can be collected in a variety of ways, and CDC has yet to determine a uniform way to measure this information, according to CDC officials. For example, sites participating in CDC’s developmental outcomes pilot program found it difficult to collect outcomes data due to: (1) limited staffing of early interventionists and administrative personnel; (2) reduced family participation in intervention services; (3) limited access to early intervention services for families; and (4) variation among states in terms of collaboration between state EHDI personnel and early intervention personnel, according to program documentation. CDC officials told us replicating the pilot program across all state EHDI programs would be resource intensive and inefficient in accomplishing the goal of standardizing language outcomes data collection.
To address the challenge of limited available data, HRSA officials told us they are coordinating with CDC to work with state EHDI programs to determine how to measure language acquisition, including what language outcomes data are available for state EHDI programs to collect during the current 5-year funding period. CDC officials plan to examine state readiness to measure language outcomes and determine what outcomes data are currently available within state Part C program’s data systems that may be useful to state EHDI programs. CDC officials emphasized that in order to collect national outcomes data, they first must determine states’ ability to measure language acquisition, develop specific definitions for measuring language outcomes, and ensure such definitions are applicable across state EHDI programs.
Low state capacity. Most state EHDI programs reported to the National Technical Resource Center that they do not have the capacity to collect and interpret language acquisition data due to a lack of a standardized language measurement, trained staff to collect outcome measures, and funding to implement the necessary data systems, according to EHDI National Technical Resource Center officials. For example, officials from one state EHDI program we interviewed told us that an increase in medical provider turnover has required EHDI officials to continually educate new staff on EHDI functions and reporting requirements. Additionally, officials from four of our selected states told us their focus is on improving their 1-3-6 screening, diagnosis, and enrollment benchmark metrics. Officials from one state EHDI program reported feeling overwhelmed by HRSA’s program requirements, including measuring language acquisition and expressed concern that continuing to expand the program would negatively affect their ability to carry out basic EHDI functions like collecting newborn screening data.
Officials from the National Technical Resource Center told us they believe very few of the 59 state EHDI programs have the capacity to begin collecting language acquisition outcomes in the first year of the current grant cycle.
To address the challenge of low state capacity, HRSA established the Implementation and Change Center, operated by the National Beacon Center for Early Language System Accountability and Data, to support state EHDI programs in identifying evidence-based and promising practices for improving language acquisition outcomes. For example, Implementation and Change Center officials told us they are establishing a workgroup of experts in the field of early language acquisition and assessment to serve as a resource and guide for state EHDI programs. HRSA officials also told us this workgroup will inform the field about measurement of language acquisition outcomes. Additionally, Implementation and Change Center officials told us they are aware state EHDI programs are starting with limited expertise and data systems to collect and interpret language acquisition data. However, officials said they are launching two efforts to meet these state EHDI program challenges. One effort will provide individual and small group assistance across all state EHDI programs, and the second will work more intensively with a select group of five states each year.
Obstacles to Data Sharing. As previously discussed, state EHDI programs may experience challenges obtaining enrollment data from state Part C programs. For example, officials from one state EHDI program told us they rely on the altruism of state Part C officials to obtain enrollment data because the state Part C program is not required to share such data. Officials from another state EHDI program told us their understanding was that Part C’s privacy regulations limit the extent to which the two state programs can share data. Because effective collaboration between state EHDI and Part C programs varies by state, obtaining data from Part C programs on language acquisition may pose additional challenges for state EHDI programs.
To address the challenge of data sharing obstacles, as discussed previously, HRSA, CDC, and Education published the August 2024 joint letter to facilitate collaboration between state EHDI and Part C programs, including data sharing to support monitoring of children’s outcomes like language acquisition. The letter describes allowable strategies for navigating data privacy requirements and provides data sharing agreement templates to help state EHDI programs resolve data sharing challenges between Part C and EHDI programs.
While it is too early for GAO to determine how effective these efforts will be, these three efforts have the potential to help state EHDI programs measure language acquisition outcomes.
HHS Actions Include Requiring Plans for Reaching Underserved Populations, but States Are Not Required to Report Progress
HHS’s HRSA, CDC, and NIH have each taken actions during the past two EHDI grant program funding cycles to improve the EHDI program’s ability to identify and address disparities in access to the screening, diagnostic, and intervention services.[26] According to program documentation, addressing these disparities aligns with HHS’s Strategic Plan.[27] These actions include:
|
Disparities refer to differences in access to, or availability of, health care services between population groups defined by socioeconomic characteristics such as ethnicity, economic resources, or geography. Source: Department of Health and Human Services. | GAO-25‑106978 |
Supporting enhanced data collection. To enhance state EHDI programs’ ability to identify and track disparities in access, CDC provided funding to nine states in 2017 and 39 states in 2020 to collect and report individual-level data in states’ databases.[28] These data expand upon the Hearing Screening and Follow-up Survey data that most states collect and report to demonstrate program performance, to include more information about risk factors associated with hearing loss, and infant and family demographics, in addition to the hearing screening and evaluation results, and referral and enrollment status for early intervention services that state EHDI program submit in the survey. Collecting individual-level data in the states’ EHDI information systems, rather than summary survey data, allows CDC and state EHDI programs to conduct detailed analyses to better understand why some underserved populations are disproportionately lost to follow-up—meaning they require further care but do not have a record of receiving the needed care.[29] Because of this, individual-level data can also guide state efforts to improve access to services, according to CDC officials. CDC offers these 39 state EHDI programs assistance with data analyses to identify disparities, according to officials.
|
Underserved populations are populations sharing a particular characteristic, as well as geographic communitie, that have been systematically denied a full opportunity to participate in aspects of economic, social, and civic life. Source: Exec. Order No. 13985, 2(b), 86 Fed. Reg. 7009 (Jan. 20, 2021). | GAO 25 106978 |
Encouraging foundational research. To encourage research critical to identifying and addressing disparities in access to EHDI services, NIH’s National Institute on Deafness and Other Communication Disorders, which leads NIH’s efforts to promote research on children who are deaf and hard of hearing, set a goal in its 2023-2027 strategic plan to define the rates of hearing impairment by race and ethnicity by 2030. To date, there has been limited effort to systematically explore health disparities through research, including issues of racism and discrimination affecting people with hearing loss and other communication disorders, according to NIH officials. In July 2024, HHS released a first set of hearing health survey data for estimating these rates based on survey questions developed by NIH, according to NIH officials.[30] The National Institute on Deafness and Other Communication Disorders also set a goal to identify and develop interventions targeted to specific subpopulations within the deaf and hard of hearing community. Further, according to the NIH officials, the agency encourages research to advance the understanding of, or reduce the effect of, health disparities and inequities in communication disorders, including hearing loss. For example, NIH-supported researchers are examining sources of structural racism and discrimination for children with communication disorders, including hearing loss, within the Part C early intervention system.
Promoting promising practices. To give state EHDI programs tools for addressing disparities in access to EHDI services, HRSA promoted promising practices—practices supported by evidence—such as telehealth services. For example, the HRSA-funded National Technical Resource Center created two resource guides to support telehealth implementation for audiologists and early intervention service providers working with the EHDI program helping to expand their services to rural, underserved populations.[31] The National Technical Resource Center also launched the Journal of Early Hearing Detection and Intervention in 2016, which published numerous articles on access to EHDI services and health care disparities in EHDI programs.[32] (See appendix III for examples of promising practices states can leverage to address disparities in EHDI service access.)
Requiring plans to target the underserved. To systematically identify and address disparities in access to detection and intervention services at the state EHDI program level, HRSA required all state EHDI programs to submit diversity and inclusion plans in fiscal year 2021. HRSA asked that the plans include a description of the target population chosen, justification for why the target population was chosen, an action plan to reach the population, and an estimated timeline for activities, but allowed states flexibility in how they developed and implemented their plans. In response, all 59 state EHDI programs submitted plans targeting a variety of underserved populations. According to our analysis of the submitted plans, the most commonly targeted underserved populations include racial or ethnic groups (30 of 59 plans) and geographically rural populations (18 of 59 plans). (See table 2.)
Table 2: Underserved Populations Targeted by State Early Hearing Detection and Intervention Program (EHDI) Diversity and Inclusion Plans
|
Population |
Number of state plans targeting the population |
Percent of state plans targeting the population |
|
Racial or ethnic groups |
30 |
51 |
|
Living in rural geographic area |
18 |
31 |
|
Living in non-rural geographic area |
12 |
20 |
|
Socio-economically disadvantaged |
7 |
12 |
|
Foreign born or refugee |
4 |
7 |
|
Non-hospital births |
3 |
5 |
|
No specified target population |
9 |
15 |
Source: GAO analysis of fiscal year 2021 state EHDI program diversity and inclusion plans. | GAO‑25‑106978
Note: Some diversity and inclusion plans targeted specific EHDI benchmark phases in addition to specific populations. For example, three plans specifically targeted newborn screening; four plans targeted diagnostic evaluation; and one plan targeted early intervention enrollment.
Percents are rounded to the nearest whole number. Data reflect the analysis of 59 state submitted plans. The number and percentage of those plans targeting various populations exceed 59 state plans and 100 percent because individual state plans may target multiple populations.
State action plans for reaching target populations to address disparities in access to detection and intervention services varied according to the needs of individual state EHDI programs, according to HRSA officials and our review. For example, one state used the opportunity to map out a strategy for expanding tele-audiology services in order to reach rural, underserved communities. Another state planned for expanded partnerships with community organizations and providers serving a particular socio-economically disadvantaged region. Other states planned to conduct outreach efforts to midwives and tribal authorities to improve screening for non-hospital births and infants born within Native American populations.
However, we found that HRSA is unable to determine whether individual state EHDI programs’ efforts have been successful in addressing disparities in access because HRSA did not require states to set performance goals as part of their diversity and inclusion plans. As a result, state EHDI programs are not able to measure progress toward achieving any goals.
While HRSA’s instructions for the plans encouraged states to create timelines and actionable steps for reaching underserved populations, the agency did not instruct states to determine how they would measure the success of their planned actions. According to our analysis of fiscal year 2021 state diversity and inclusion plans, only seven of the 59 states included quantifiable methods for measuring progress in their submitted plans.[33] HRSA officials also told us the agency has met with each state program on a regular basis to discuss overall grant program progress, but did not follow up with states to specifically determine how the plans were implemented including the extent to which they were successful.[34]
Further, we found that HRSA did not assess the results of the plans to understand how the plans might be updated or used to better address disparities in access in the 2024-2029 funding cycle. The requirement to submit diversity and inclusion plans was intended as a first step for states to begin identifying disparities and making plans to address them and were not intended to collect information on progress, according to HRSA officials.
HRSA’s decision to not require performance goals or assess state EHDI program progress related to access disparities does not support efforts to implement HHS’s Strategic Plan, which includes an agencywide focus on reducing disparities in access to health care.[35] It is also inconsistent with leading practices for performance management. Our prior work identified leading practices for performance management, including three key steps to help organizations measure and assess programs: (1) setting performance goals to identify the results organizations seek to achieve; (2) collecting performance information to measure progress; and (3) using the information to assess results and inform decisions to ensure further progress toward achieving goals.[36]
If HRSA requires state EHDI programs to set performance goals that can be used to measure progress in addressing disparities in access for underserved populations and regularly report that information to HRSA, the agency will have information on whether, and to what extent, state EHDI programs are making progress addressing disparities in access to detection and intervention services. Further, if HRSA assesses the results of the state EHDI programs’ access disparities performance, the agency will have the information necessary to inform future plans for addressing access disparities.
Setting requirements for performance goals and regular reports of progress could be done in the next notice of funding opportunity, for example, which would provide state EHDI programs with several years to identify their performance goals. HRSA could require state programs to set their own performance goals that can be used measure progress in addressing any identified disparities in access for underserved populations. HRSA could then use those goals and associated targets to assess states’ progress and take actions that support HRSA’s role in implementing HHS’s Strategic Plan. With these steps in place, HRSA can be better positioned to ensure equitable access to detection and intervention services for children who are deaf or hard of hearing.
HRSA Sets Requirements for States to Support Families; Selected States Used Various Strategies to Provide Support
Families with children who are deaf or hard of hearing benefit from family-to-family support and family support services, according to HRSA. Family-to-family support refers to trained parents of children with hearing loss reaching out to families new to the EHDI program to provide emotional support and guidance. To that end, HRSA requires state EHDI programs to devote at least 20 percent of their funding to family support and engagement in its most recent Notice of Funding Opportunity.
Some state EHDI programs contract with a family-focused organization to coordinate family support, while others hire an individual family member to lead parent support as a member of the state EHDI program staff, officials from the FL3 Center told us. Additionally, HRSA charged its technical assistance center for parents, the FL3 Center, to increase state capacity for family-to-family support by providing training for individuals to family leadership skills, and engaging adults who are deaf or hard of hearing as mentors to families in their state. The FL3 Center offers programs and information to states to support their family engagement efforts.
Officials from six selected state EHDI programs told us about the types of information and support provided to parents and families of children who are deaf or hard of hearing to satisfy HRSA’s grant requirement.
|
Early Hearing Detection and Intervention Support: Unbiased Information Unbiased information is educational, informative, available in multiple languages, and reflects the full continuum of family choice on communications options to families with children who are deaf or hard of hearing. Well-informed families are better able to make decisions to support their family and to lead the healthy development of their children who are deaf of hard of hearing, according to the Health Resources and Service Administration (HRSA). Source: HRSA Notices of Funding Opportunity and Documentation from the FL3 Center. | GAO‑25‑106978 |
Unbiased Information. All state EHDI program officials we spoke with said their states provide unbiased information about communication methods for children. Officials from the FL3 Center told us that families are not always given balanced, comprehensive information about all available early intervention options. This is sometimes because providers leave out information about resources that are locally unavailable, they lack knowledge about resources, or have a bias toward a particular early intervention option. State EHDI programs and their parent support partners fill that gap by providing more complete options so that parents can make informed choices for their families.
Officials from some of the state EHDI programs also said they provide culturally and linguistically appropriate resources to parents. For example, one state EHDI program provides print materials in several languages, including Spanish, Hmong, and Somali. This state EHDI program also sends each identified child’s family a binder of print materials upon receiving a diagnosis of hearing loss, to assist and inform parents. According to a parent leader we spoke with, having information in a person’s birth language allows families to navigate the EHDI system.
|
Early Hearing Detection and Intervention Support: Parent-to-Parent Specially trained parent guides who have a child who is deaf or hard of hearing can facilitate personal interaction and connection. Families with children who are deaf or hard of hearing report the most valuable source of support is other families that have children who are also deaf or hard of hearing, according to the Health Resources and Services Administration (HRSA). Source: FL3 Center documentation and HRSA Notice of Funding Opportunity. | GAO‑25‑106978. |
Parent-to-Parent Support. Officials from all six state EHDI programs we spoke with said they provide parent-to-parent support through a nonprofit organization. For example, in one state the EHDI program has a nonprofit partner that provides support to parents at the time of a child’s diagnosis with hearing loss. In another state, the EHDI program employs a family representative and has two family support nonprofit partners. There are various types of parent support services offered by the six states, including:
· Parent leadership training. Three state EHDI programs provide training to parents to become parent-leaders for either the state EHDI program’s nonprofit partner or in the EHDI program itself. After training, these parents in turn provide peer support to parents and families with children diagnosed with hearing loss. For example, one state EHDI program’s nonprofit partner provides training to parents to provide support to other families with children who are deaf or hard of hearing.
· Parent advocacy. Two states provide programs to support parent advocacy in schools on behalf of their child’s education. One of these states has such a program in place for parents to receive advocacy training. Parent advocates are important because they help ensure the success of children who are deaf or hard of hearing during their school years, according to FL3 Center officials.
· Deaf mentorship. Deaf or hard of hearing mentors are an important part of the EHDI program because most children are born to hearing parents who do not know what it is like to be deaf or hard of hearing, according to officials from the FL3 Center. Families with children who are deaf or hard of hearing benefit from access to support, mentorship, and guidance from adults who are deaf or hard of hearing because they can help parents better understand what their child’s life may be like, according to HRSA.
Four of our six selected state EHDI programs provide support to families through a deaf mentor program, according to documents and interviews with state EHDI officials. For example, officials from one state EHDI program told us that they have a contract with a nonprofit partner to connect families to deaf role models for support. These adult mentors have a variety of hearing loss conditions and use a variety of communication methods, including American Sign Language, cochlear implants, and hearing aids, and can speak to their lived experienced with families. Another state program noted that there is a shortage of willing and qualified mentors. Officials say their program’s mentors recently retired and the program has not been able to find new mentors.
|
Parent Perspective “I value relationship-building with parents within the Early Hearing Detection and Intervention (EHDI) system. Families are not just to be contacted for diagnosis and receipt of services. Rather, there is an emphasis to connect families with the deaf community and to build a support system. It is very important to build relationships with the families within the EHDI system to provide them with the support they need.” – EHDI parent leader |
Source. EHDI Parent Leader. | GAO‑25‑106978
|
Early Hearing Detection and Intervention Support: Automatic Referral A direct referral process can eliminate barriers to participation for families. For example, a database entry can automatically trigger referrals to other services. Then, family support partners may reach out to the family proactively to begin providing support. Source: FL3 Center officials and documentation. | GAO‑ |
Automatic referral. One state employs automatic notification processes to alert their partner parent support organization when a child receives a diagnosis of hearing loss to reach the family. This state EHDI program’s partner is automatically notified when a child is diagnosed as deaf or hard of hearing, to connect with the family. Automatic referral of parents to the state’s family support partner is a good practice that eliminates the need for parents to opt in to receive family-to-family support, according to the FL3 Center. Parents may therefore be more likely to obtain the support they need.
|
Early Hearing Detection and Intervention (EHDI) Support: Websites Websites can provide family-friendly information with an appropriate reading level and materials available in a variety of modalities, such as written, auditory, and video. The Health Resources and Service Administration (HRSA) requires state EHDI programs to develop and maintain a website with accurate, comprehensive, and culturally-appropriate information for families to use in making decisions about communication modalities. Source: National Technical Resource Center documentation and HRSA Notice of Funding Opportunity. | GAO-25-106978 |
Websites. Parents need timely information to make informed decisions regarding the early needs of their children with hearing loss, and the internet is increasingly a key source for health information, according to an article from our literature review. In past years, the EHDI National Technical Resource Center awarded “Best of EHDI” website awards to recognize state EHDI websites that excelled at providing accurate, timely, and visually-appealing information, among other factors. Criteria for websites includes ease of navigation, browser compatibility with multiple web browsers, and the inclusion of health information at an appropriate reading level, among many others. According to the chair of the EHDI website award committee, six states do not currently have a website; 39 states have websites that meet enough of the National Technical Resource Center’s website award criteria to be assessed for the competition; and 14 do not meet enough criteria to be assessed. The National Technical Resource Center also published a website resource guide that focused on key elements of effective websites, including content, design and layout, and accessibility.
State EHDI program officials we spoke with reported various levels of ability to update their websites and track the number of website visitors. Officials from two states we spoke with have experienced problems making updates to their websites. For example, one state official said the state is temporarily unable to make updates because of a security breach within the state’s Department of Health website. As a result, the department halted website updates as well as usage tracking. Officials from two of our six selected state EHDI programs told us they can track website utilization to help them identify which resources are being accessed online.
Other types of support. In addition, state EHDI programs may provide additional types of extended support for parents and families. For example, officials from one state we spoke with told us that the state government has chosen to fund American Sign Language instruction at no cost for 2 years to families who qualify, such as those with children who are deaf or hard of hearing.
Conclusions
The EHDI program plays an important role in identifying the thousands of infants each year diagnosed as deaf or hard of hearing, and connecting those infants to essential early intervention services that can prevent developmental delays. To address disparities in access to detection and intervention services, HRSA required states to submit diversity and inclusion plans that target underserved populations. However, HRSA has not asked programs to set performance goals and report on their progress to address access disparities. As a result, HRSA does not have the full information necessary to understand states’ progress. With a requirement in place for state EHDI programs to set and report on performance goals, states can demonstrate their progress in addressing access disparities for their identified underserved populations. In addition, HRSA’s assessment of states’ progress can inform future plans to support state EHDI programs. Doing so would better ensure infants and children in underserved populations receive the care they need.
Recommendations for Executive Action
We are making the following recommendations to the Department of Health and Human Services’ Health Resources and Services Administration:
The HRSA Administrator should require state EHDI programs to set performance goals that can be used to measure progress in addressing any identified disparities in access for underserved populations and regularly report that progress to HRSA. (Recommendation 1)
The HRSA Administrator should assess the results of the state EHDI programs’ access disparities performance and use the results to inform future plans for addressing access disparities. (Recommendation 2)
Agency Comments
We provided a draft of this report to Education and HHS for review and comment. We also provided excerpts of this report to technical assistance centers that we interviewed for their review and comment. Education did not provide comments. HHS’s written comments are reproduced in appendix IV. HHS and the technical assistance centers also provided technical comments, which we incorporated as appropriate. HHS concurred with our two recommendations and identified steps the department will take to address them.
With respect to our first recommendation, HHS stated that work is underway to require state EHDI programs to set performance goals related to addressing identified disparities. Specifically, in its fiscal year 2027 progress report instructions, HRSA plans to include a requirement for state EHDI programs to set performance goals that will allow them to measure progress in addressing any identified disparities in access for underserved populations. The fiscal year 2027 progress reports are expected beginning in December 2026.
With respect to our second recommendation that HRSA should assess the results of the state EHDI programs’ access disparities performance, HHS stated that HRSA plans to evaluate the results of state EHDI programs’ progress addressing access disparities as part of future planning.
We are sending copies of this report to the appropriate congressional committees, the Secretary of Health and Human Services, the Secretary of Education, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff members have any questions about this report, please contact me at (202) 512-7114 or DeniganMacauleyM@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix V.

Mary Denigan-Macauley
Director, Health Care
This report (1) describes how the Health Resources and Services Administration (HRSA) measures Early Hearing Detection and Intervention (EHDI) program performance; (2) HRSA and the Centers for Disease Control and Prevention’s (CDC’s) efforts to address state programs’ reported challenges meeting EHDI benchmarks; (3) describes what HRSA and CDC have done to support state efforts to improve language acquisition and any challenges states may face in improving language acquisition; (4) examines Health and Human Services (HHS) agencies’ actions to identify and address disparities in EHDI program access, and (5) describes HRSA’s efforts to help ensure support is available to parents of children with a hearing loss diagnosis.
To address these five objectives, we reviewed EHDI program grant documentation and documentation from HRSA’s 2020-2024 technical assistance centers that provided support and training to state EHDI programs. We interviewed HHS officials from HRSA’s Maternal and Child Health Bureau on their efforts to oversee the EHDI program and address disparities. We interviewed officials from the Centers for Disease Control and Prevention’s (CDC) National Center on Birth Defects and Developmental Disabilities about their efforts to measure program outcomes and collect data. We interviewed officials from the National Institutes of Health’s (NIH) National Institute on Deafness and Other Communications Disorders about their role in the EHDI program, including funding relevant research. We also interviewed officials from each of the EHDI technical assistance centers from the 2020-2024 and 2024-2029 grant cycles.[37]
We conducted interviews with officials from a non-generalizable sample of six state and territorial (state) EHDI program offices. We selected these states for variation in factors such as geographic location and whether the states received additional grant awards from CDC to support and enhance their EHDI information systems. We interviewed these states to learn about their implementation of the EHDI program at the state level, including their efforts in data collection, addressing disparities in access, and available support for parents and families. The six selected states were Alaska, Connecticut, Georgia, Minnesota, Ohio, and Puerto Rico.
To address the first objective, we analyzed available annual aggregate summary data from HHS on the EHDI program, from the Hearing Screening and Follow-up Survey. Specifically, we calculated the percentages of infants meeting HHS’s EHDI 1-month screening, 3-month diagnosis, and 6-month enrollment benchmarks for calendar years 2008 through 2021 based on two separate calculation methodologies employed by CDC to measure benchmarks—the “Population in Services” measure and the “Eligible Population” measure. We selected the years 2008-2020 for our analysis years because starting in 2008, almost all states—47 of 59—reported data on each of the 1-3-6 benchmarks used to make these calculations; and 2021 was the year CDC began reporting only the Eligible Population measure for each benchmark. We also drew comparisons to demonstrate how the two measures differ. We shared our analysis with HRSA and CDC officials to verify our calculations and comparisons.
We assessed the reliability of the Hearing Screening and Follow-up Survey data by reviewing HHS documentation on the data and interviewing agency officials knowledgeable about the data. We determined that these data were sufficiently reliable for the purposes of our reporting objectives. We also reviewed and reported demographic data from the survey’s 2021 summary report, the most current summary data available.
To address the second objective, we reviewed summaries of state EHDI programs’ annual progress reports that detailed challenges states face with screening, diagnosing, and enrolling infants in early intervention services. We also reviewed the results of a program-wide survey conducted by the HRSA-funded National Technical Resource Center in 2023 asking state EHDI programs to report on their obstacles to effective program management.
To address the third objective, we reviewed documentation and interviewed officials from the U.S. Department of Education on their interactions with the EHDI program and data-sharing at the state level between state EHDI program offices and Education-funded agencies that administer early intervention programs. Early intervention is designed to ensure that all eligible infants and toddlers with a disability have an individualized plan developed to meet their developmental needs. Services are tailored to meet a child and family’s particular needs. These services may include speech therapy, physical therapy, counseling, or other services, depending on the child and the family’s needs. We also interviewed officials from the Outcomes and Developmental Data Assistance Center for EHDI Programs, a CDC-funded pilot program to measure language acquisition outcomes and reviewed documentation from the pilot program.
To address the fourth objective, we reviewed diversity and inclusion plans from all 59 state EHDI program offices. We reviewed the diversity and inclusion plans for target populations, action plans to reach the identified target population, and any outcome measures for the plan. We assessed the content of the plans against the HHS’s strategic objective in effect at the time of the plans’ development, which was to improve Americans’ access to health care, including by reducing disparities in access to health care.[38] We also assessed the instructions for and HRSA’s actions to follow up on the plans against leading practices for performance management, including the three key steps of: (1) setting performance goals to identify the results organizations seek to achieve; (2) collecting performance information to measure progress; and (3) using the information to assess results and inform decisions to ensure further progress toward achieving goals.[39] We also reviewed published peer-reviewed literature from 2018 to 2023 to identify any promising practices in improving access to screening, diagnosis, and early intervention enrollment for infants and toddlers who may be deaf of hard of hearing. Finally, we analyzed available individual-level and aggregate data associated with the EHDI program to assess its completeness and reliability.
To address the fifth objective, we reviewed program documentation from technical assistance centers for the EHDI program related to support provided to families of children who are deaf or hard of hearing. We also reviewed published, peer-reviewed literature from 2018 to 2023 to identify relevant research findings related to family support for parents of children who are deaf or hard of hearing. We also interviewed a non-generalizable sample of three advocacy organizations for people who are deaf or hard of hearing, ensuring we selected organizations that represented a variety of perspectives on communication methods for people who are deaf or hard of hearing. Our three selected advocacy organizations included the National Association of the Deaf, the Alexander Graham Bell Association for the Deaf and Hard of Hearing, and the American Society for Deaf Children.
We also interviewed four parents of children who are deaf or hard of hearing. We identified parents who attended either the 2023 or 2024 EHDI Annual Conference, and reached out through the National Technical Resource Center that organized the conference. We interviewed this selection of parents about their perspectives on the EHDI program and types of available support for parents and families of children who are deaf or hard of hearing, and thus their responses are not generalizable to all parents of children who are deaf or hard of hearing.
We conducted this performance audit from July 2023 to January 2025 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Appendix II: Early Hearing Detection and Intervention (EHDI) Grant and Cooperative Agreement Programs
Both the Health Resources and Services Administration (HRSA) and the U.S. Centers for Disease Control and Prevention (CDC) make grants or establish cooperative agreements with state EHDI programs and technical assistance centers on behalf of the EHDI program. See table 3 for a list of grants and cooperative agreements from 2020-2029 for the EHDI program. (See table 3.)
Table 3: Early Hearing Detection and Intervention (EHDI) Grant and Cooperative Agreement Programs, 2020-2029, by Awarding Agency and Period of Performance
|
Agency |
Short and full funding opportunity name |
Period of performance |
Description |
|
Health Resources and Services Administration (HRSA) |
EHDI National Network Cooperative Agreement |
2024-2029 |
Funds three EHDI national centers that provide system-wide technical assistance: (1) Implementation and Change Center (ICC); (2) Family Leadership in Language and Learning Center; and (3) Provider Education Center. |
|
HRSA |
EHDI State and Territory Program Grants |
2024-2029 |
Supports up to 59 state EHDI programs with the goal of ensuring families with children who are deaf or hard of hearing receive timely hearing screening, diagnosis, and early intervention. |
|
HRSA |
EHDI State and Territory Program Grants |
2020-2024 |
Supported up to 59 state EHDI programs with the goal of ensuring families with children who are deaf or hard of hearing receive timely hearing screening, diagnosis, and early intervention. |
|
HRSA |
EHDI National Technical Resource Center Cooperative Agreement |
2020-2024 |
Supported a resource center that provided technical assistance and disseminated best practices to state EHDI programs. |
|
HRSA |
Family Leadership in Language and Learning Center Cooperative Agreement |
2020-2024 |
Supported a resource center that provided technical assistance to state EHDI programs to increase family engagement and leadership and strengthen family support. |
|
U.S. Centers for Disease Control and Prevention (CDC) |
EHDI-Information Systems (IS) Cooperative Agreement |
2020-2025 |
Supports the capacity of state EHDI information systems used to track the screening, diagnostic, and intervention services that infants receive. The funding’s purpose is to improve state EHDI programs’ ability to report, analyze, and use individual-level data to direct decision making and program improvement. |
|
CDC |
Outcomes and Developmental Data Assistance Center for EHDI Programs Cooperative Agreement |
2020-2024 |
Established a research and data center to collect and analyze developmental outcomes in a standardized way. The center used data to assess the relationship between interventions and developmental outcomes, including those related to child language acquisition. |
Source: GAO analysis of Department of Health and Human Services (HHS) notices of funding opportunities. | GAO‑25‑106978
Appendix III: Promising Practices to Address Disparities in Access to Early Hearing Detection and Intervention (EHDI) Services
Promising Practices Literature Review Results
Results of our review of published, peer-reviewed articles on infant hearing loss and hearing disparities show limited evidence for promising practices to address disparities in access to Early Hearing Detection and Intervention (EHDI) services for underserved populations.[40] Of the 123 articles published between 2018 to 2023 that met our search criteria, only two articles had sufficient evidence based on their research designs and statistical analyses to show an association between an intervention and increased access to EHDI services for underserved populations (such as infants and families living in rural areas or out of hospital births; see Sapp et al., 2021 and Palmer et al. 2019, respectively). The National Institute on Deafness and Other Communication Disorders at the National Institutes of Health (NIH) identified further examples of evidence-based interventions to increase EHDI service access. (See table 4.)
Table 4: Examples of Promising Practices to Increase Access to Early Hearing Detection and Intervention Services for Underserved Populations
|
Practice |
Why it is promising |
Where it is used |
Source of evidence |
|
Use educational audiologists. Equip and train existing audiologists at regionally-based, public school special education centers to diagnose infants for hearing loss. |
Increases number of sites equipped to diagnose infants. Addresses shortages in pediatric audiologists by expanding the types of services educational audiologists can perform. Improves timeliness of first hearing evaluation, reduces travel burden, and increases likelihood of receiving on-guideline audiology care. |
Iowa |
Caitlin Sapp, et al., “Expanding the Role of Educational Audiologists After a Failed Newborn Hearing Screening: A Quality Improvement Study,” American Journal of Audiology, vol. 30 (Sept 2021): 631-641. |
|
Engage midwives. Equip and train midwives to provide newborn hearing screenings. |
Increases the likelihood that babies born at home receive a newborn hearing screening. |
Michigan |
Shannon B. Palmer, et al., “Newborn Hearing Screenings for Babies Born at Home: Report from an Initiative in Michigan,” Journal of Early Hearing Detection and Intervention 4, no. 1 (June 2019): 36-42. |
|
Assign patient navigators. Assign trained health care educators to support families of infants who fail their hearing screening to obtain diagnostic services. |
Increases likelihood of needed diagnostic follow-up. Improves timeliness of first hearing evaluation. Increases parental knowledge about recommended diagnosis procedures for infant hearing loss. |
Kentucky |
Matthew L. Bush, et al., “Promotion of Early Pediatric Hearing Detection Through Patient Navigation: A Randomized Controlled Clinical Trial,” Laryngoscope, 127, Suppl 7 (Nov 2017): S1-S13, Author manuscript.a |
|
Establish tele-audiology and tele-intervention services. Establish specialty referral protocols for hearing follow-up care via telemedicine. |
Addresses lack of access to specialty hearing care in low-resource settings, such as rural communities. Reduces the time to follow-up and increases the likelihood of obtaining needed follow-up care in rural communities. |
Alaska Kentucky |
Susan D. Emmett, et al., “Mobile Health School Screening and Telemedicine Referral to Improve Access to Specialty Care in Rural Alaska: A Cluster Randomized Controlled Trial,” Lancet Global Health, vol. 10 (July 2022).b |
Source: GAO analysis of peer-reviewed literature and National Institutes of Health documents. | GAO‑25‑106978
aA study of patient navigation program effectiveness was conducted from April 2019 through March 2024 in the state of Kentucky through support provided by the National Institutes of Health. For a further description, see: Matthew Bush, et al., “Communities Helping the Hearing of Infants by Reaching Parents (CHHIRP) through Patient Navigation: A Hybrid Implementation Effectiveness Stepped Wedge Trial Protocol,” BMJ Open (2022); 12:e054548. doi:10.1136/bmjopen-2021-054548.
bA study of specialty telemedicine referral program effectiveness is ongoing in the state of Kentucky through support provided by the National Institutes of Health. For example, see: Appalachian STAR Trial, https://reporter.nih.gov/project‑details/10831880.
Examples of Selected State EHDI Programs’ Use of Promising Practices
State EHDI program officials from our selected states described having implemented several of these promising practices to help address disparities in access.[41] For example, officials from three state EHDI programs said their state supports tele-audiology or mobile audiology services and three state programs train or equip midwives to provide screening access for out-of-hospital births. One state EHDI program adopted a care coordinator model that provides support and guidance to families, similar to a patient navigator model.
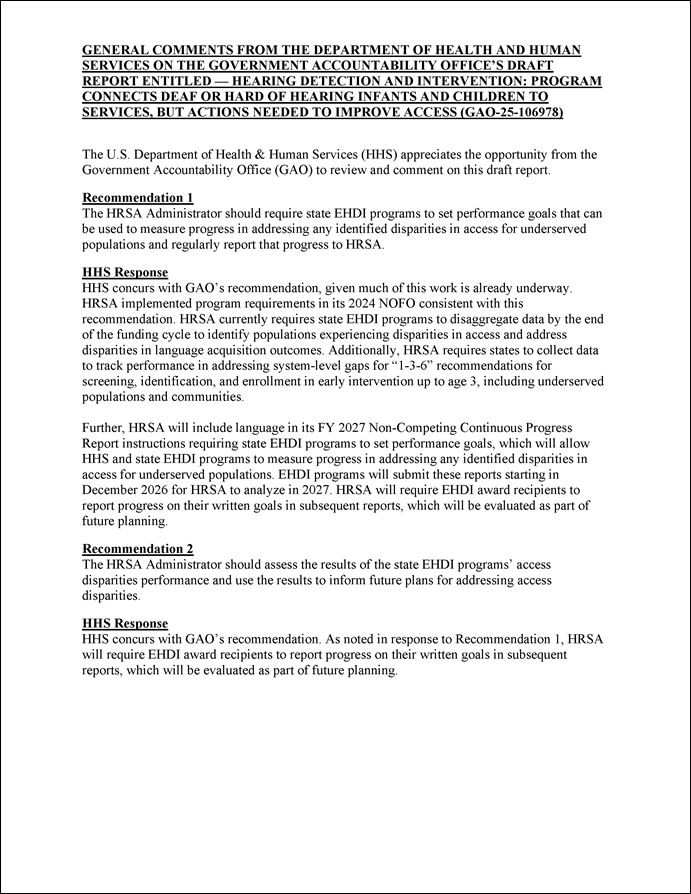
GAO Contact:
Mary Denigan-Macauley, (202) 512-7114 or DeniganMacauleyM@gao.gov
Staff Acknowledgments:
In addition to the contact named above, Malissa G. Winograd (Assistant Director), Margot Bolon (Analyst-in-Charge), Jenna Moody and Elise Pressma made key contributions to this report. Sam Amrhein, Joycelyn Cudjoe, Leia Dickerson, Cynthia Khan, Jennifer Rudisill, and Nicole Willis also made important contributions.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on Facebook, Flickr, X, and YouTube.
Subscribe to our RSS Feeds or Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454 or (202) 512-7700
Congressional Relations
A. Nicole Clowers, Managing Director, ClowersA@gao.gov, (202) 512-4400, U.S. Government Accountability Office, 441 G Street NW, Room 7125, Washington, DC 20548
Public Affairs
Sarah Kaczmarek, Managing Director, KaczmarekS@gao.gov, (202) 512-4800, U.S.
Government Accountability Office, 441 G Street NW, Room 7149
Washington, DC 20548
Strategic Planning and External Liaison
Stephen J. Sanford, Managing
Director, spel@gao.gov, (202) 512-4707
U.S. Government Accountability Office, 441 G Street NW, Room 7814, Washington,
DC 20548
[1]This total includes all 50 states and the District of Columbia, American Samoa, Guam, Republic of the Marshall Islands, Micronesia, Northern Mariana Islands, Republic of Palau, Puerto Rico, and the U.S. Virgin Islands. For the purpose of this report, we include territories when discussing states.
[2]Early Hearing Detection and Intervention Act of 2022, Pub. L. No. 117-241, § 3, 136 Stat. 2332, 2332.
[3]According to the definition by HHS’s Agency for Healthcare Research and Quality.
[4]We later excluded 2021 from our analysis because in 2021 there was a change in the way these data were reported.
[5]See U.S. Department of Health and Human Services, HHS Strategic Plan, Fiscal Year 2018-2022 (2017).
[6]The EHDI law was first enacted as part of the Departments of Labor, Health and Human Services, and Education Fiscal Year 2000 Appropriations Act, Pub. L. No. 106-113, Appendix D, Title VI, 113 Stat. 1501, 1501A-276 (1999) and was subsequently added as amendment to the Public Health Service Act by section 702 of the Children’s Health Act of 2000, Pub. L. No. 106-310, Div. A, Title VII, 114 Stat. 1101, 1120. See also Pub. L. No. 117-241, 136 Stat. 2332 (codified as amended at 42 U.S.C. § 280g-1).
[7]See 20 U.S.C. §§ 1431-44. For purposes of this report, we refer to the Infants and Toddlers with Disabilities Program set forth in these sections of the U.S. Code as Part C.
[8]Under various federal laws, state Part C programs generally must limit disclosure of the personally identifiable information in children’s educational records. See, e.g., 20 U.S.C. § 1417(c). However, state Part C programs are permitted to share such information with state EHDI programs under certain circumstances, such as with the written consent of the child’s parents or to support state or federal program evaluations. See 34 C.F.R. § 99.35 (2024).
[9]See 42 U.S.C. § 280g–1(c)(1)(B).
[10]Early Hearing Detection and Intervention Act of 2017, Pub. L. No. 115-71, § 2(b), 131 Stat. 1218, 1218. HRSA subsequently specified that “young children” referred to children up to age 3 in the 2024 Early Hearing Detection and Intervention State/Territory Program Notice of Funding Opportunity.
[11]Submitting data to CDC from the Hearing Screening and Follow-up Survey is voluntary. However, most states submit at least partial data. For example, in 2021, 55 states submitted hearing screening data to CDC.
[12]CDC collects and analyzes infant 1 month screening, 3 month diagnosis, and 6 month enrollment data (1-3-6 benchmarks) reported by state EHDI programs in the annual Hearing Screening and Follow-up Survey.
[13]Data from 2021 are the most recent publicly available data.
[14]Centers for Disease Control and Prevention (CDC), Summary of 2021 National CDC Early Hearing Detection and Intervention (EHDI) Data (Nov. 2023).
[15]The Population in Services measure focuses on infants who receive the appropriate EHDI service by the age-defined benchmark. It counts only the infants who have progressed to the next stage in obtaining services. The Eligible Population measure focuses on infants who are eligible for the next phase of EHDI services. It counts all children, even if they have not progressed to the next stage.
[16]We used 2008 through 2020 survey data because 2008 was the first year almost all states reported data on each of the 1-3-6 benchmarks used to make the calculations; and 2020 was the last year the prior measure was in use in order to make a comparison.
[17]Results from the Early Hearing Detection and Intervention (EHDI) Program National Technical Resource Center, State of EHDI Survey, 2023.
[18]The six selected state EHDI programs are Alaska, Connecticut, Georgia, Minnesota, Ohio, and Puerto Rico.
[19]The web-based directory is called the Early Hearing Detection and Intervention Pediatric Audiology Links to Services.
[20]Health Resources and Services Administration, Centers for Disease Control and Prevention, and United States Department of Education, Joint Dear Colleague Letter on Early Hearing Detection and Intervention and Part C Programs, (August 5, 2024).
[21]See 34 C.F.R. §§ 99.35(a)(1) and 303.414(b)(2) (2024).
[22]The 2021 pediatric audiology competitive supplemental funding opportunity was open to HRSA’s Leadership Education in Neurodevelopmental and Related Disabilities program recipients to train an average of two long-term, pediatric audiology trainees each year, for a minimum total of 10 long-term, pediatric audiology trainees by the end of the program’s 5-year period of performance. HRSA has provided pediatric audiology supplements to Leadership Education in Neurodevelopmental and Related Disabilities programs since 2011. The first competitive supplemental funding opportunity was in 2016, according to HRSA officials.
[23]Federal law requires states to assure that Medicaid payment rates are, among other things, sufficient to enlist enough providers to the program so that care and services for Medicaid beneficiaries are available to at least the same extent as to the general population in the area.
[24]CDC’s pilot program required participating sites to use either the MacArthur-Bates Communicative Development Inventories, or the Developmental Assessment of Young Children-Second Edition. The MacArthur-Bates Inventories assess a child’s expressive vocabulary skills, including vocabulary comprehension, communicative and symbolic gestures, grammar, and cognitive-linguistic abilities. The Developmental Assessment of Young Children-Second Edition measures abilities in five developmental domains: cognition, communication, social emotional, physical, and adaptive behavior.
[25]Education’s IDEA program requires each state to submit a State Performance Plan/Annual Performance Report that includes indicators to measure child and family outcomes and other indicators that measure compliance with the requirements of IDEA. The language-related items listed here are part of Indicator 3.
[26]The two HRSA state grant program funding cycles cover the period from 2016 through 2024. The first funding cycle began in April 2016 and ended in March 2020. The second began in April 2020 and ended in March 2024.
[27]The HHS Strategic Plan includes an agencywide objective to improve Americans’ access to health care, including by implementing strategies for reducing disparities in access to health care. See U.S. Department of Health and Human Services, HHS Strategic Plan, Fiscal Year 2018-2022 (2017).
[28]According to CDC officials, CDC is focusing its limited resources on funding 39 states, rather than funding all 59 states. Officials from one state EHDI program told us that it collects individual-level data on its own without CDC assistance but may not be able to collect as much detailed data. In addition, other states are not eligible for the assistance because they have yet to build sufficient data infrastructure or have less than 5,000 resident annual births.
[29]The Hearing Screening and Follow-up Survey data collected by CDC and used by HRSA to assess EHDI program performance are summary data. As noted earlier, the survey requests non-estimated hearing screening, diagnostic, and intervention information on infants born in a specified calendar year. The numbers are collected in totals, rather than on individual infants.
[30]NIH’s National Institute on Deafness and Other Communication Disorders sponsored a set of new questions on hearing and balance in the 2023 National Health Interview Survey, including questions about hearing ability, most recent hearing exam, and use of hearing aids for a sample of participants that included children up to 17 years of age, according to NIH officials. The survey also includes detailed information on sociodemographic variables that can be used to examine the data by race or ethnic groups and other demographic categories, according to officials. Results of the Hearing and Balance questions to the 2023 National Health Interview Survey can be accessed at: https://www.cdc.gov/nchs/nhis/2023nhis.htm. The National Institute on Deafness and Other Communication Disorders also supported a pilot study of the Hearing Examination and Questionnaire Protocol for the National Health and Nutrition Examination Survey 2025-2026. The protocol, which collects data on hearing threshold exams, had been paused during the COVID-19 pandemic. The hearing threshold exams conducted and collected through the National Health and Nutrition Examination Survey have been used to establish national and international norms since collection of this information began in the 1960s for representative samples of the U.S. population, both children and adults, according to NIH officials.
[31]One of the goals included in both the current and prior funding agreement for HRSA’s technical assistance centers is to identify evidence-based and evidence-informed practices and increase their knowledge and use by the EHDI state programs and partners.
[32]Examples of recent publications related to disparities in EHDI services, include: Nannette Nicholson, et al., “Impact of Social Determinants of Health on Early Hearing Detection and Intervention Screening/Diagnosis Outcomes,” Journal of Early Hearing Detection and Intervention 7, no. 3 (November 2022): 16-34; Nicole Perez, et al., “Sociodemographic Factors Influencing Pandemic-Era EHDI Use and Access,” Journal of Early Hearing Detection and Intervention 8, no. 2 (November 2023): 26-33.
[33]For example, a quantifiable measure could be to reduce by 10 percent the number of children from an underserved population without follow-up testing after not passing an initial newborn screen.
[34]HRSA officials said they collect overall performance information, including possible information about the implementation of the diversity and inclusion plans, in required annual progress reports. States submitted their final progress reports in July 2024 which cover the grant cycle during which diversity and inclusion plans were required. HRSA is still reviewing these submissions to assess the extent to which states report any information about whether they were able to implement their diversity and inclusion plans.
[35]See U.S. Department of Health and Human Services, HHS Strategic Plan, Fiscal Year 2018-2022 (2017).
[36]See GAO‑23‑105460. The Government Performance and Results Act of 1993 (GPRA) created a federal performance planning and reporting framework. Pub. L. No. 103-62, 107 Stat. 285 (1993). The GPRA Modernization Act of 2010 (GPRAMA) amended and significantly expanded the framework to address a number of persistent federal performance challenges, including focusing attention on crosscutting issues and enhancing the use and usefulness of performance information. Pub. L. No. 111-352, 124 Stat. 3866 (2011). In addition, the Foundations for Evidence-Based Policymaking Act of 2018 (Evidence Act), created a framework for federal agencies to take a more comprehensive and integrated approach to evidence building, and to enhance the federal government’s capacity to undertake those activities. Pub. L. No. 115-435, 132 Stat. 5529 (2019). Several of the Evidence Act’s evidence-building requirements are directly tied to performance planning requirements in GPRAMA.
[37]These centers are located in Washington, D.C.; Itasca, IL; Boulder, CO; and Logan, UT.
[38]See U.S. Department of Health and Human Services, HHS Strategic Plan, Fiscal Year 2018-2022 (2017)
[39]GAO‑23‑105460. The Government Performance and Results Act of 1993 (GPRA) created a federal performance planning and reporting framework. Pub. L. No. 103-62, 107 Stat. 285 (1993). The GPRA Modernization Act of 2010 (GPRAMA) amended and significantly expanded the framework to address a number of persistent federal performance challenges, including focusing attention on crosscutting issues and enhancing the use and usefulness of performance information. Pub. L. No. 111-352, 124 Stat. 3866 (2011). In addition, the Foundations for Evidence-Based Policymaking Act of 2018 (Evidence Act), created a framework for federal agencies to take a more comprehensive and integrated approach to evidence building, and to enhance the federal government’s capacity to undertake those activities. Pub. L. No. 115-435, 132 Stat. 5529 (2019). Several of the Evidence Act’s evidence-building requirements are directly tied to performance planning requirements in GPRAMA.
[40]For the purpose of the literature review, promising practices are defined as practices to improve access to newborn, infant, and toddler hearing screening, diagnosis, or early intervention enrollment that are supported by evidence-based findings in peer-reviewed literature.
[41]The six selected state EHDI programs we spoke with are Alaska, Connecticut, Georgia, Minnesota, Ohio, and Puerto Rico.