Report to the Ranking Member, Committee on Veterans’ Affairs, House of Representatives
United States Government Accountability Office
For more information, contact Alyssa M. Hundrup at HundrupA@gao.gov.
Highlights of GAO-25-107497, a report to Ranking Member, Committee on Veterans’ Affairs, House of Representatives
Agreements to Share Services and Other Resources Should Be Evaluated
Why GAO Did This Study
VA and DOD operate two of the nation’s largest health care systems. Together, these systems serve over 18 million beneficiaries. VA’s health care system includes approximately 170 medical centers and 1,200 clinics, while DOD’s health care system includes more than 700 medical facilities worldwide. VA and DOD have entered into agreements to share health care services to improve access to and cost effectiveness of care.
GAO was asked to review the departments’ use of sharing agreements. This report describes the number and types of sharing agreements; examines the extent to which VA and DOD assess them; and examines how VA and DOD identify opportunities for new or expanded sharing agreements, among other topics.
GAO reviewed VA and DOD documents and data, including active sharing agreements as of April 2025; conducted site visits to 12 VA and DOD facilities with active agreements, selected to represent diversity in geography and the type of sharing taking place; and interviewed VA and DOD officials.
What GAO Recommends
GAO is making five recommendations, including that VA and DOD should evaluate the effectiveness of sharing agreements and make changes as needed, and that VA and DOD should develop a systematic process to identify and implement opportunities for new or expanded sharing agreements. The departments concurred with GAO’s recommendations.
What GAO Found
The Department of Veterans Affairs (VA) and Department of Defense (DOD) have shared mutually beneficial medical and other services through 185 sharing agreements, as of April 2025. For example, veterans may receive care at DOD facilities for services including surgery, orthopedics, and mental health. These agreements can result in greater access to care for veterans and cost savings for the federal government, in part because of the discounted rate that VA and DOD pay each other for health care delivered under such sharing agreements.

VA and DOD collect information on the characteristics of all sharing agreements as well as referrals of veterans to DOD facilities made through sharing agreements; however, the departments do not evaluate the effectiveness of sharing agreements. Officials told GAO that they use the number of sharing agreements and the continuation of agreements as measures of the agreements’ value. However, VA and DOD could maximize the benefits of these agreements by developing a performance management process, including establishing performance goals for the agreements, evaluating progress towards the goals, and making changes as appropriate.
VA and DOD have taken some steps to identify new or expanded sharing opportunities, including tracking space-sharing projects through a committee. However, the departments largely rely on local officials to identify potential areas for new and expanded sharing, which may result in missed opportunities for sharing. Developing a systematic, department-level process to identify and implement opportunities for new and expanded sharing agreements could help ensure the departments maximize sharing, which could in turn help improve patients’ access to care as well as reducing costs.
Abbreviations
DOD Department of Defense
VA Department of Veterans Affairs
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
June 30, 2025
The Honorable Mark Takano
Ranking Member
Committee on Veterans’ Affairs
House of Representatives
Dear Representative Takano:
The Department of Veterans Affairs (VA) and the Department of Defense (DOD) operate two of the nation’s largest health care systems. Together, VA and DOD provide health care to more than 18 million veterans, servicemembers, military retirees, and other beneficiaries with budgets of approximately $120 billion and $60 billion, respectively, for fiscal year 2024.[1] VA and DOD are authorized to enter into sharing agreements to share health care services and other resources to improve access to, and to enhance the quality and cost-effectiveness of, health care provided by the two departments.[2] For example, a VA facility may have an agreement with DOD to refer veterans to a DOD facility for specialized cardiology services related to the diagnosis or treatment of certain heart conditions.
Sharing agreements can benefit both departments and their beneficiaries. These agreements enable expanded access to specialty care for both veterans and servicemembers at a cost typically 20 percent lower than what the departments would pay for comparable care from civilian or community providers.[3] In addition, benefits of such sharing agreements for DOD can include opportunities for DOD providers to treat VA patients who may have greater clinical needs than servicemembers, which can help these providers maintain clinical readiness.[4]
Cost savings to the federal government resulting from sharing agreements are particularly important given the increasing costs of providing care to beneficiaries at both departments.[5] Specifically, between fiscal year 2020 and 2024, VA’s health care budget increased by approximately 50 percent and DOD’s health care budget increased by approximately 17 percent. Our prior work has found that identifying cost-saving opportunities, such as those resulting from sharing agreements, can help inform decisionmakers as they seek ways to address escalating fiscal pressures facing the federal government.[6]
We have previously reported on VA and DOD collaborative efforts, including sharing agreements. In 2012, we found the departments faced a number of barriers that hindered their implementation of sharing agreements, such as incompatible data systems and different billing practices.[7] Based on recommendations we made at that time, VA and DOD took several actions to address identified barriers, including taking steps to better exchange information between the departments’ two data systems and resolving issues with business and billing processes.
You raised questions about how VA and DOD are currently utilizing sharing agreements, as well as how those agreements are meeting the goal of improving access to care for veterans.
In this report, we:
· describe VA and DOD health care sharing agreements, including the number of active agreements and the types of services covered;
· examine the steps VA and DOD are taking to address key barriers in implementing health care sharing agreements;
· examine the extent to which VA and DOD evaluate the effectiveness of health care sharing agreements; and
· examine how VA and DOD identify opportunities for new or amended health care sharing agreements.
To describe VA and DOD health care sharing agreements, we reviewed associated documentation and data, including data maintained by VA headquarters on the total number, type, and locations of sharing agreements, as of April 2025. We also conducted site visits to a nongeneralizable sample of 12 facilities (six VA and six DOD) and interviewed VA and DOD officials at these locations about their sharing agreements and types of services covered through them.[8] We selected these sites to represent diversity in geography as well as in the level and type of sharing taking place through the agreements. We also interviewed VA and DOD headquarters officials about the sharing agreements.
To examine the steps VA and DOD are taking to address key barriers in implementing health care sharing agreements, we asked officials at the 12 facilities we visited to identify and describe any barriers they experienced related to their respective agreements. From these interviews, we identified key barriers by determining the most frequently cited barriers and reviewed relevant documentation on these barriers and efforts local officials took to address them. We also interviewed officials from veterans service organizations.[9] Furthermore, we interviewed VA and DOD headquarters officials about the steps they have taken to address key barriers across all facilities. We evaluated these efforts against a DOD instruction and federal internal control standards.[10]
To examine the extent to which VA and DOD evaluate the effectiveness of sharing agreements, we reviewed referral data provided by VA from fiscal years 2022 to 2024 (the years of complete data provided by most VA sites we visited, which we used for corroboration purposes) associated with sharing agreements. We also reviewed documentation and interviewed VA and DOD headquarters officials and local officials on our site visits about their processes for evaluating the effectiveness of sharing agreements. We compared these efforts against performance management leading practices identified in our prior work.[11]
To examine how VA and DOD identify opportunities for new or amended health care sharing agreements, we reviewed VA and DOD reports and documentation, such as documentation of a regional summit held to evaluate opportunities for sharing between the departments and Joint Executive Committee’s Joint Strategic Plan for VA and DOD for fiscal years 2022 to 2027.[12] We also interviewed VA and DOD headquarters officials and local officials on our site visits about their processes for identifying opportunities for new or amended health care sharing agreements. We compared these efforts to a VA directive and a DOD instruction on sharing agreements.
To assess the reliability of each data source above, we examined the data for errors, outliers, and omissions by reviewing available documentation on the data and, where applicable, compared data we obtained from VA and DOD headquarters with data from the medical facilities we visited. Additionally, we interviewed VA officials who are knowledgeable about these data to identify any limitations. As a result of these steps, we determined that all data were sufficiently reliable for the purposes of our reporting objectives.
We conducted this performance audit from April 2024 to June 2025 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
VA and DOD each have distinct missions. VA’s is to serve America’s veterans, and DOD’s is to provide the military forces needed to deter war and protect the country’s security. Correspondingly, they have separate health care systems to provide services to their respective beneficiaries. In 2025, VA’s health care system serves over 9 million veterans with a network of approximately 170 VA medical centers and 1,200 clinics. Most of these facilities offer primary, and in some cases, specialty care. These VA facilities report to 18 VA regional networks, called Veterans Integrated Service Networks.[13] DOD’s health care system included nine medical centers, 36 hospitals, 525 clinics, and 138 dental facilities worldwide as of fiscal year 2024. These facilities are organized into nine Defense Health Networks, serving a population of over 9 million servicemembers and other beneficiaries.[14]
VA and DOD are authorized to share services and resources in situations that are mutually beneficial. The departments have established an organizational structure to plan and carry out joint initiatives and projects, including sharing agreements, to provide services to their beneficiaries and share resources.[15] (See figure 1)
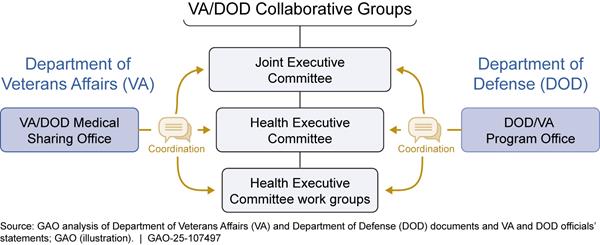
The Joint Executive Committee was established to provide broad strategic direction for collaboration between the two departments and to provide annual reports to Congress on its efforts. Subordinate to the Joint Executive Committee is the Health Executive Committee, which is to provide oversight for the specific cooperative efforts of each department’s health care organizations.
As a part of its duties, the Health Executive Committee oversees several work groups, some of which are responsible for identifying and facilitating sharing agreements, including the following:
· Shared Resources Work Group, a group the Health Executive Committee established in 2012 made up of membership from both departments. Its purpose is to monitor and assess sharing activities and explore, identify, and support additional opportunities for collaboration between the two departments.
· Operations Integrated Project Team, a group established in 2023, also made up of membership from both departments. This group’s purposes include identifying and evaluating DOD and VA facilities with unused space, facilitating partnership discussions, and making recommendations to the Health Executive Committee on potential sharing activities between the departments.
In addition to these committees and work groups, the departments have distinct program offices charged with providing guidance to facilities related to sharing agreements. Specifically, the director of the Veterans Health Administration’s VA/DOD Medical Sharing Office is responsible for providing guidance and assistance in facilitating, identifying, developing, and sustaining sharing opportunities at the VA regional network and VA facility levels. For DOD, the DOD/VA Program Office serves as the principal advisor to the Assistant Secretary of Defense (Health Affairs) for all DOD/VA health care related policies, programs, and activities and is responsible for enhancing medical resource sharing across the Military Health System.
Sharing Agreements
Since the 1980s, VA and DOD have entered into various types of sharing agreements to provide medical and nonmedical services, such as specialty, inpatient, and outpatient care. Sharing agreements provide a framework for the exchange of medical and nonmedical resources between the departments and are established to support increased patient access to medical care services, enhance cost savings, and enable the sharing of VA facility and DOD facility space. Sharing agreements can enable veterans to access select medical care services at DOD facilities, such as when these services are not available at their VA facility or cannot be provided in a timely manner. Some sharing agreements may also be set up to allow DOD servicemembers to access select medical care services at a VA facility.
VA and DOD typically develop sharing agreements when a VA facility or DOD facility has excess resources or services available that are not fully utilized, such as excess space or capacity to provide medical care, according to the departments’ documentation. These agreements are often between VA facilities and DOD facilities located in the same geographic area but may also be established between VA regional networks or VA program offices and DOD facilities. For example, a VA regional network may establish a sharing agreement for all VA facilities in its network to share services with a particular DOD facility. A single VA facility may also enter into sharing agreements with multiple DOD facilities.
VA and DOD are to document and approve sharing agreements through a standardized sharing agreement form. This form documents information about the sharing agreement, such as the participating VA regional network or VA facility and DOD facility, the medical care services, administrative services, or facility space shared, and the reimbursement methodology for these services. Each sharing agreement form must include a local operating procedure that outlines facility-specific procedures related to the sharing agreement as an addendum.
According to a VA directive, sharing agreements are to be reviewed and approved by VA regional networks and the VA/DOD Medical Sharing Office, within the Veterans Health Administration.[16] They must also be reviewed by officials from the DOD/VA Program Office. VA and DOD facilities may establish sharing agreements for up to 5 years, after which renewal is required. According to VA guidance, each sharing agreement must be assigned a VA regional network and VA facility-level resource sharing coordinator. According to DOD officials, each sharing agreement must also be assigned a local DOD point of contact to facilitate the implementation of the sharing agreement.
VA and DOD’s 185 Health Care Sharing Agreements Varied in the Scope and Types of Services Covered
VA and DOD had 185 sharing agreements in place nationwide, as of April 2025, according to departmental data. We found these sharing agreements varied in the scope and types of medical and nonmedical services facilities could share across the two departments. The sharing agreements included 77 VA facilities and 98 DOD facilities. The total number of agreements grew approximately 14 percent between October 2022, when 162 active agreements were in place, and April 2025, when 185 agreements were in place.[17] (See appendix I for a list of the active sharing agreements and types of shared services, as of April 2025.)
We found the departments’ sharing agreements varied in scope and the types of services covered, including sharing in the following areas: referrals for medical services, staff, facility space, and nonmedical services.
Referrals for medical services. Some sharing agreements allow VA facilities to refer veterans to DOD facilities to obtain certain medical services, such as specialty care.[18] For example, under a sharing agreement, a veteran whose local VA facility does not offer orthopedic surgery could be referred to a partnering DOD facility to obtain that care. Some sharing agreements also allow DOD facilities to refer military servicemembers to VA facilities for medical services.
When veterans or servicemembers are referred to the other department’s medical facility for care delivered under sharing agreements, the departments typically reimburse each other at the established reimbursement rate for civilian or community providers minus 20 percent.[19] As a result, such referrals contribute to cost-saving benefits for both VA and DOD. For example, an official at one VA facility we visited estimated the care provided at the DOD facility, with which VA has a sharing agreement, saves them 40 to 60 percent per veteran compared to care in the community. This is due to the 20 percent discounted reimbursement rate along with additional discounts outlined in the sharing agreement related to VA staff providing inpatient and outpatient cardiology care at the DOD facility.
In addition to sharing agreements that allow referrals for medical services, VA and DOD have used sharing agreements to explore ways to expand access to medical services provided through telehealth.[20] For example, at one site we visited, VA and DOD have implemented tele-intensive care services to treat veterans and DOD servicemembers remotely.[21]
Staff sharing. Some sharing agreements enable VA facilities and DOD facilities to share medical and administrative personnel. Under certain sharing agreements, staff may work at both VA and DOD facilities without being permanently stationed at the sharing partner’s medical facility (referred to as non-embedded staff). For example, officials at one site told us their cardiothoracic surgery sharing agreement allowed DOD surgeons from the DOD facility to use the VA facility’s operating room once a week, to treat veterans. Working at the VA facility’s operating room and with veterans gave DOD surgeons the opportunity to treat patients with greater needs, thus increasing their knowledge, skills, and abilities, officials said.
Other sharing agreements allow for personnel to be permanently assigned to the sharing partner’s medical facility (referred to as embedded staff). For example, at one VA facility we visited, officials told us there were 120 VA staff embedded at the partnering DOD facility including registered nurses, medical technicians, and administrative staff. These staff provided care to both servicemembers and veterans at the DOD facility.
The methodology for paying for shared staff varies, as it is negotiated between the sharing partners. For example, officials explained that DOD reimburses VA for the 120 VA staff who are embedded at the DOD facility. Officials at another VA facility said VA and DOD both pay part of the salaries for eight non-embedded medical technicians who work at the DOD sharing partner’s cardiology clinic multiple times a week.
Facility space sharing. Sharing agreements may also include sharing facility space through a permit. For example, at one site we visited, VA is permitted to occupy space at a DOD dental clinic on the military base. A VA official explained that the department pays less than $8,000 a year to utilize the permitted space at the DOD dental clinic. This is significantly lower than leasing space at a private dental clinic in the community, which the official said would be about $50,000 a year.
At another site we visited, VA established an outpatient clinic on the military base where veterans could receive medical care services. According to a DOD official, the reimbursement method for facility space sharing such as this is generally payment for operating costs. The official also told us that the costs to VA using DOD-owned buildings are minimal and reduce costs for VA.
Sharing of nonmedical services. Services such as physician training, patient administration, or laundry services are also shared under some sharing agreements. The reimbursement method for sharing nonmedical services varies. At one site we visited, officials told us the departments shared nonmedical services for housekeeping. VA paid DOD for the actual costs it incurred to provide these services, according to VA officials.
Per VA procedures, VA and DOD sharing agreements are categorized into five distinct levels of collaboration, based on the extent of sharing that occurs between a VA and DOD facility.[22] (See figure 2.) Elements of sharing considered for level determination include whether a patient is referred to a sharing partner to obtain medical care services, whether personnel—both clinical and administrative—are shared between facilities, and whether facility space is shared. A sharing agreement including nonmedical services, such as physician training, or administrative or laundry services, is also a factor when determining categorization levels for a sharing agreement.
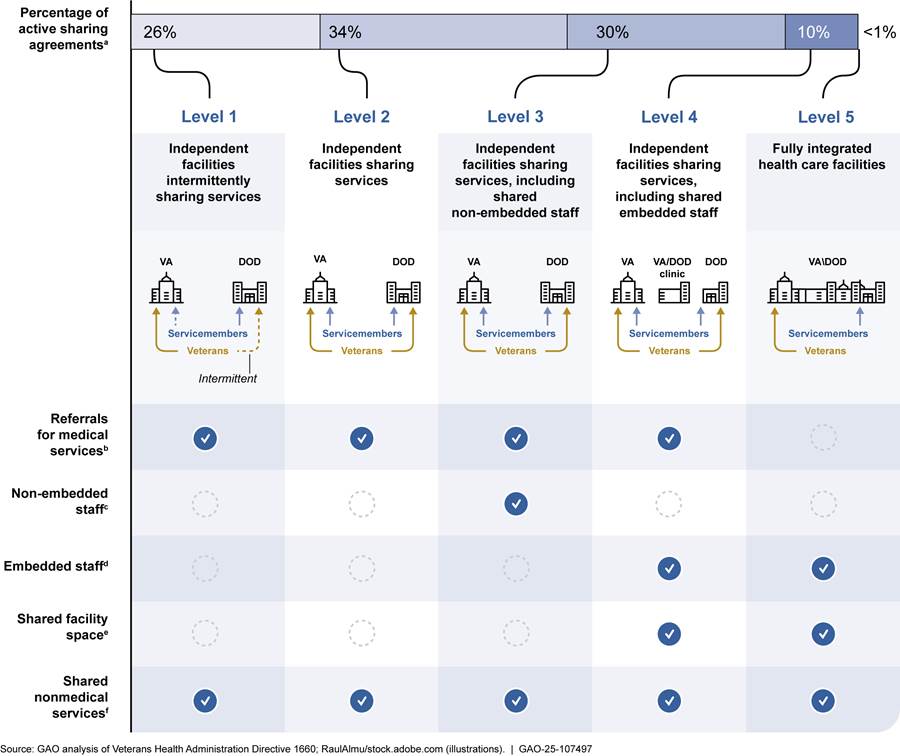
Note: The percentages do not equal 100 percent due to rounding.
aThis represents percentages of the 185 Department of Veterans Affairs (VA) and Department of Defense (DOD) sharing agreements as of April 2025, according to VA data. Most of the VA and DOD sharing agreements allow veteran patients to obtain medical care services from a DOD facility. However, some agreements allow DOD servicemembers to obtain medical care services from a VA facility.
bMedical services are obtained by referral from a VA facility or DOD facility. Medical care services may include ambulatory services, such as emergency medical care and psychiatric and mental health care; ancillary services, such as pharmacy or radiology; and inpatient care, such as internal medicine and general surgery. Demand for these services can be intermittent, as is the case with Level 1 sharing agreements, or continuous as is the case with Levels 2-4. For Level 5 sharing agreements, the medical facility is totally integrated, and a referral is not necessary to obtain care.
cNon-embedded includes five or more administrative or clinical staff who work in either sharing partners’ facility specialty clinics, inpatient wards, intensive care units, or surgical clinics, but are not assigned or attached to their partners’ medical facility.
dEmbedded staff includes ten or more administrative or clinical staff who are assigned or attached to work full time with either sharing partner’s facility specialty clinics, inpatient wards, intensive care units, or surgical clinics.
eShared facility space refers to sites located on the same federal property, or co-located sites where resources, such as clinical space or infrastructure, are utilized jointly by VA and DOD.
fNonmedical services may include clinical professional skills development and maintenance, patient administration or laundry services.
In addition to the varying scope of sharing offered under these agreements, we found the specific types of medical services shared differ. Medical services can be shared through referrals or staff sharing. Some sharing agreements delineate that a particular type of medical care service can be shared, while other sharing agreements allow for multiple medical services to be shared. As of April 2025, the most frequently shared medical services included internal medicine—which included services such as diabetes care and hypertension care—hematology and oncology, cardiology, physical medicine—which included rehabilitative services—and pulmonary medicine.[23]
While a specific medical service may be listed as one that can be shared under an agreement, determining whether such a medical service is available at any point in time is a collaborative effort between local VA facilities and DOD facilities, according to VA and DOD officials. To accommodate sharing information on availability, we found at four of the six partnering sites we visited, DOD facility medical staff generate a capability report. [24] Capability reports describe available medical care services and indicate whether the DOD facility has capacity to provide those services to veterans for particular dates. We found that the frequency with which DOD facilities provided these reports to VA facilities varied, such as weekly or monthly. VA and DOD officials told us that capacity to provide medical care services at a DOD facility can fluctuate based on a number of factors, including providers’ availability, variation related to deployment, and the number of servicemembers being treated. Capability reports are an efficient and real-time way for VA facilities to determine how many veterans they can refer to an DOD facility for medical services, according to VA officials.
VA and DOD Have Taken Steps to Address Key Sharing Barriers, but DOD Has Not Addressed the Barrier to Non-Reimbursable Sharing
VA and DOD have taken steps to address key barriers to care delivered through sharing agreements. However, we identified a new barrier related to sharing for non-reimbursable agreements, in which one party offers medical or nonmedical services deemed equivalent in value to what they would otherwise pay in the form of reimbursement to the other party. Specifically, DOD has not issued guidance on how to develop non-reimbursable sharing agreements.
VA and DOD Have Taken Steps to Address Key Barriers to Implementing Sharing Agreements
Officials at VA and DOD headquarters, our 12 site visits, and veterans service organizations identified key barriers that can affect care delivered through sharing agreements. Specifically, we found that veterans’ access to military bases, the interoperability of VA and DODs electronic health records systems, inconsistent relationships between VA and DOD staff, and billing and reimbursement issues were key barriers that can affect the effective implementation of sharing agreements.[25] We found the departments, along with the individual facilities in our review, have taken steps to address these issues, as described below.
Access to military bases. Accessing military bases to obtain medical care can add time and complexity for veterans visiting a DOD facility serving as a sharing site for VA, according to officials at DOD headquarters.[26] Officials from seven of the 12 VA and DOD sites we visited also identified access to military bases as a barrier to veterans obtaining care through the health care sharing agreements.
For example, to obtain base access, a veteran needs to present identification to the base visitor’s center, establish that they are suitable to access the base through a background check, and establish the purpose for the visit. Once a veteran has completed these steps, the visitor center enrolls the veteran, and the veteran is able to access the base with their identification card for up to 1 year. However, veterans with a felony criminal record are generally not granted base access, according to staff at four of the VA and DOD facilities we visited.
To address base access barriers, in 2019 DOD issued a manual that clarified the department’s policy regarding access to military bases.[27] The departmental guidance stated that the forms of identification acceptable for base access include veteran health identification cards. This policy allows veterans to use their veteran health identification cards when accessing military bases for health care services on military bases.
Similarly, officials at four of the sites we visited told us that they implemented additional solutions to facilitate base access including the following:
· One DOD facility developed a process in which a DOD official sponsored veterans requiring frequent care at the hospital on the military base, so that the veterans could receive a 6-month base access pass, allowing them to avoid having to obtain a visitor pass each time they need to access the base for care.
· VA officials, staffed at another DOD facility with a VA outpatient clinic located on the military base, told us they provided educational materials to veterans about how to register for base access.
· Furthermore, officials at two VA facilities told us they work closely with DOD facility officials to ensure that veterans who are eligible to receive care can access the base. For example, officials at one site said that VA staff contact the DOD facility with information about a veteran’s scheduled appointment. The DOD staff then communicate this information to the base’s visitor center in advance of the appointment to make the process of the veteran getting on base easier.
Interoperability of electronic health records systems. VA and DOD lack electronic health record systems that permit the electronic exchange of comprehensive patient health information, which has been a longstanding barrier to collaboration. To help mitigate this barrier, in 2013, VA and DOD developed the Joint Longitudinal Viewer, a web-based application that provides a near real-time and chronological view of health data contained in the departments’ separate electronic health records systems. Ten of the 12 VA and DOD facilities we visited use the Joint Longitudinal Viewer to transfer veterans’ and servicemembers’ medical information, including referrals, authorizations, and medical information, from DOD, VA, and provider organizations outside the federal health care systems.[28]
In June 2017, VA initiated the Electronic Health Records Modernization program to replace its electronic health record system.[29] This system, once in place across VA, will allow for the exchange of information with DOD’s health record system. After a multi-year pause in the deployment of the new electronic health record system to prioritize needed improvements, VA announced in March 2025 that system deployment would resume in 2026.
Officials at VA and DOD headquarters, seven of the 12 VA and DOD sites we visited, and veterans service organizations we interviewed confirmed that the lack of interoperable VA and DOD electronic health records systems remains a barrier to providing efficient and effective care. For example, officials at one site told us staff often have to document patients’ medical records separately in the two departments’ systems, increasing the risk of errors and frustrations for clinical staff. Despite the use of the Joint Longitudinal Viewer, officials at three sites also stated that the application is limited because it only allows a provider to read a patient’s medical records. For example, officials at one site said the Joint Longitudinal Viewer can only share radiology reports, and not radiology images, which providers may need to access. As a result, providers may need to request the patient repeat radiological imaging, or provide images separately to the provider, which may result in increased costs, delays, and patient burden. Issues related to the interoperability of the departments’ electronic health records will not be fully resolved until VA implements its new electronic health records system at all VA facilities. VA announced in March 2025 that it expects to achieve full implementation as early as 2031.
Relationships between VA and DOD staff. Frequent leadership changes at VA and DOD facilities can affect existing relationships between the staff at these facilities, according to officials at six of the 12 facilities we visited. Local officials from two of the sites said they spend a lot of time explaining the purpose of existing sharing agreements or rebuilding relationships whenever a leadership change occurs.
According to officials at one VA facility, rebuilding relationships can delay or possibly prevent health care sharing between VA and DOD facilities. For example, these officials told us it took 15 months to reestablish a relationship with the new DOD commander when a leadership change occurred at the DOD facility where it had a sharing agreement. In particular, VA facility officials had to explain the benefits of the sharing agreement with DOD officials before they could begin the process of expanding the sharing agreement to include opening a VA clinic on the military base.
In addition to leadership changes, we found that a poor relationship between VA and DOD staff who manage the sharing agreements can limit the sharing that occurs between a VA and a DOD facility. An official at one DOD site explained that not having an effective relationship with the VA staff responsible for managing the sharing agreement resulted in few veterans being referred to the DOD facility for care even though the facility had capacity to provide care to veterans.
According to VA and DOD officials, the departments established a new resource sharing agreement coordinator staff position at each VA and DOD facility with a sharing agreement. The departments created this position to help manage all joint VA and DOD efforts, including sharing agreements. Leadership officials at two of the sites we visited said these coordinators play a pivotal role in ensuring the sharing agreements are being implemented and that relationships between VA and DOD are maintained by sharing information and ensuring issues are addressed. We also found that the resource sharing agreement coordinators at a few sites we visited mitigated frequent changes in leadership by ensuring that officials were informed about the existing sharing agreement when they arrived at the VA or DOD facility.
In addition, officials from five sites said that they have developed work groups consisting of VA and DOD staff to discuss barriers with the sharing agreements. Some of these officials explained that recognizing personnel changes and maintaining communication is crucial, adding that they communicate regularly to address any issues. For example, officials at one of these sites recalled an occasion when they noticed a decrease in the number of veterans referred to the DOD facility for care and raised this issue at a work group meeting to determine why there was a decrease.
Billing and reimbursement. Billing and receiving reimbursement for medical care shared between VA and DOD continues to be a barrier, according to officials at both VA and DOD headquarters and nine of 12 VA and DOD sites we visited. Specifically, we found that payment delays for DOD medical claims and difficulties with appropriately registering patients could delay delivery of care. For example, officials at one DOD facility told us that DOD limited the number of VA referrals it accepted because they were not getting reimbursed for a medical service they provided.
The departments have taken action to reduce billing and reimbursement barriers, including the following:
· Delayed VA payments for DOD medical claims. The DOD national billing office found VA had not paid DOD more than $87 million for medical care services provided by DOD from fiscal years 2018 through 2022.[30] In September 2023, DOD submitted a letter to VA requesting that the departments agree to settle all unpaid claims for medical care services provided during this period. VA subsequently paid DOD the requested settlement of more than $76 million in August 2024, according to a DOD official.
A DOD official also told us that in August 2022 the department made changes to its billing system, RevCycle, which officials say will enable DOD facilities to transmit medical claims electronically to VA’s electronic claims adjudication management system and extract monthly reports on claim status. According to these officials, going forward, this change will allow DOD facilities to determine why claims are not being paid and act more quickly to seek payment.
· Difficulties with patient administration. Difficulties with patient administration sometimes resulted in billing and reimbursement issues, according to officials at five sites. Difficulties officials mentioned included needing to create retroactive referrals for emergency medical services received, which cause reimbursement delays, as well as difficulties determining whether to use VA or DOD benefits when registering a veteran with dual eligibility, potentially leading to double counting of individuals in billing.[31]
DOD officials told us that relevant staff at DOD facilities have to be trained on registering veteran patients using the new billing system, which may address barriers related to patient administration. Officials added that supervisors at each DOD facility are responsible for ensuring training has been completed. Furthermore, officials at one DOD facility told us that having VA staff embedded at the hospital significantly streamlines the registration process, especially for dual-eligible patients, as it allows direct assistance for veterans navigating VA and DOD benefits.
To continue to identify and address barriers related to billing and reimbursements, VA and DOD officials at both departments and at four of the VA and DOD sites we visited have also established joint VA and DOD work groups. For example, the Joint Reimbursement Work Group, established by the Health Executive Committee, serves as a forum for VA and DOD headquarters officials to discuss billing and reimbursement, including in sharing agreements. The group meets weekly and has discussed billing issues, including discussing why certain DOD medical claims to VA have not been paid and determining ways to address the issue, according to a DOD officials in the group.
Officials from VA and DOD facilities also established local reimbursement and billing work groups, including at four sites we visited. In one such local work group, VA and DOD staff have collaborative face-to-face meetings to review and confirm coding and billing procedures, resulting in thousands of paid claims, some of which may have otherwise been rejected, according to DOD officials.
DOD’s Lack of Guidance on Non-Reimbursable Agreements Has Created a Barrier to Sharing
Within some VA and DOD sharing agreements, facilities have established non-reimbursable agreements, in which one party offers medical or nonmedical services in exchange for benefits deemed equivalent in value to what they would otherwise pay in the form of monetary reimbursement. However, in 2020, DOD limited the development or renewal of such agreements after it found DOD facilities were entering into them without assurance that the agreements were mutually beneficial for both departments. Specifically, the Secretary of Defense issued a memorandum in June 2020 stating that DOD facilities could no longer provide non-reimbursable services to VA without first submitting a written justification. Such a justification is to articulate why providing the requested support on a non-reimbursable basis, or why waiving the requirement for reimbursement if a waiver is authorized by statute, supports the national defense strategy.
According to an official from DOD’s Uniform Business Office, as of April 2025, the department is developing updated procedures on VA and DOD sharing agreements, which will include guidance on non-reimbursable agreements. According to this official, the guidance will include instructions on developing a written justification, such as a business case analysis plan for non-reimbursable agreements. However, the official said it was unknown when the procedures would be finalized and available for DOD facilities to use in developing sharing agreements with VA. In the meantime, the official said DOD plans to issue interim guidance on how to develop a business case analysis for non-reimbursable agreements in May 2025.
Without updated procedures that include guidance on non-reimbursable agreements, officials at some DOD facilities told us it is unclear whether they can establish or renew these types of agreements, resulting in a barrier to sharing some health care services. For example, officials at two DOD facilities we visited said it was unclear whether new non-reimbursable agreements would be allowable, or if existing agreements would be allowed to continue. Officials at one facility also noted the difficulties of determining the value of services included in a non-reimbursable sharing agreement to develop a business case to use such agreements. These officials said they needed guidance on how to develop a business case analysis plan to be able to clearly articulate mutual benefits that would result from the agreement.
The lack of guidance for developing non-reimbursable sharing agreements is inconsistent with DOD policy. DOD policy requires it to develop guidance, including reviewing and recommending approval of the Defense Health Agency’s billing methodologies for the DOD/VA Health Care Resource Sharing Program.[32] Additionally, federal standards for internal control state that management should use quality information and internally communicate the necessary quality information to achieve the entity’s objectives.[33]
Finalizing and providing procedures that include guidance on non-reimbursable sharing agreements, including instructions on how to develop a business case analysis plan, would align with DOD policy and enhance the departments’ ability to continue to share services that are mutually beneficial.
For example, at one site we visited, the DOD facility established a non-reimbursable sharing agreement allowing veterans to receive positron emission tomography scans at the facility, in exchange for the VA facility providing a technician to operate the scanner.[34] This, in turn, resulted in cost savings of more than $100,000 in fiscal year 2024 compared to referring veterans to the community for these services, according to a VA official. Officials at the DOD facility explained that without procedures on how to document this sharing agreement, including developing a business case analysis plan, they may not be able to continue sharing these mutually beneficial medical care services.
With appropriate procedures, VA and DOD facilities can better ensure they can continue existing non-reimbursable agreements as well as develop new ones with confidence, potentially resulting in cost savings and continued access to care for veterans and servicemembers.
VA and DOD Collect Information on Sharing Agreements, but Have Not Evaluated the Effectiveness of These Agreements
VA and DOD Collect Information to Oversee Sharing Agreements, Including Referrals VA Made to DOD Facilities
VA and DOD collect information on sharing agreements, including on data on referrals VA made to DOD facilities. Specifically, we found the VA/DOD Medical Sharing Office, the VA office responsible for providing guidance on sharing agreements, regularly collects the following information as a part of their general efforts to oversee sharing agreements:
Characteristics of each VA and DOD sharing agreement, including the VA and DOD facilities involved, the level of sharing collaboration, and the services shared through the agreement.[35] Additionally, officials from the VA/DOD Medical Sharing Office told us they collect information on new sharing agreements as they are created, the agreements that have been terminated and why, the number extended, and the number renewed.
Data on VA patient referrals made to DOD facilities through sharing agreements, when such information is relevant.[36] VA data on referrals show that the total number of completed veteran referrals to DOD facilities made through relevant agreements remained consistent for the past 3 fiscal years.[37] Specifically, VA data show 51,080 VA patient referrals to DOD facilities in fiscal year 2022, 48,445 such referrals in fiscal year 2023, and 50,005 in fiscal year 2024. Officials from the VA/DOD Medical Sharing Office stated that they occasionally pull referral data to share in meetings with senior leadership, but they do not regularly assess trends associated with these referral data.
VA and DOD Have Not Evaluated the Effectiveness of Sharing Agreements
We found VA and DOD have not evaluated the effectiveness of existing agreements, in part because they do not have a process for doing so. Specifically, we found that VA and DOD lack key performance management practices we have identified in prior work. Regularly assessing progress toward goals using performance measures is important to show the effectiveness of sharing agreements in improving access to care for beneficiaries of both departments and in providing cost savings.[38]
These performance management practices call for organizations to 1) establish goals that communicate the results an organization wants to achieve 2) establish performance measures, which are concrete conditions that allow the organization to assess progress made on each goal, and 3) use performance information to regularly assess results and inform decisions to ensure progress toward achieving goals.
Furthermore, we have reported that such performance measurement information can assist decision-makers in assessing progress and identifying areas for improvement. VA and DOD’s enabling statute for sharing agreements, as well as VA and DOD’s own health care goals, all emphasize access, and costs as important considerations in the delivery of health care.[39] VA and DOD’s lack of a process to evaluate the effectiveness of sharing agreements is inconsistent with these standards.
DOD officials told us they do not evaluate the effectiveness of sharing agreements because they have not been directed to do so by their leadership. For their part, VA officials said they use the number of sharing agreements in existence and lack of termination of these sharing agreements as a measure of their value. Officials from the VA/DOD Medical Sharing Office also told us the role of their office is to advise VA facilities and VA regional networks on sharing agreements rather than to manage each sharing agreement individually. They added that the VA/DOD Medical Sharing Office provides advice, technical assistance, and policy insight as part of its programmatic oversight responsibility.
We found the departments have taken steps towards evaluating one type of sharing agreement. Officials from the VA/DOD Medical Sharing Office said that in December 2024, they held an initial meeting to begin developing a process for evaluating sharing agreements specific to facility space—including joint leasing and construction proposals, following a request to do so from the Health Executive Committee. According to officials, the effort will involve VA and DOD headquarters collaborating to develop a tool that VA facilities, VA regional networks, and DOD facilities with space-sharing agreements will use to document performance goals associated with agreements, such as cost avoidance related to utility fees or enhancing providers’ clinical knowledge, skills, and abilities. VA officials said they will use this process for annual review and oversight of sharing agreements specific to facility space.
The VA/DOD Medical Sharing Office plans to complete an instructional document by September 30, 2025, to help sites develop self-assessments of their sharing agreements, officials said. This represents progress toward establishing a process to evaluate the effectiveness of facility space-related sharing agreements, but it does not include other types of agreements, such as those focused on referring veterans to DOD facilities or sharing staff.
By implementing a process to evaluate the effectiveness of all types of sharing agreements, including establishing performance goals and related performance measures, VA and DOD could maximize the benefits of these agreements to both departments.[40] Specifically, VA and DOD could develop performance goals in collaboration with facilities with sharing agreements, tailored to the specific expected benefits of particular agreements, including cost savings, expanded access to care for veterans, and enhanced DOD provider clinical readiness.
For example, the departments could establish a process to evaluate the effectiveness of sharing agreements related to cost savings. The VA and DOD headquarters, in collaboration with regional and local partners, could collect information about costs saved by referring veterans to DOD facilities through sharing agreements instead of referring them to community providers outside of the VA and DOD systems.[41] The departments could then use this information to establish performance goals for individual sharing agreements. To measure progress toward these goals, the departments could collect information such as the number and proportion of referrals made to DOD facilities versus the number or proportion of referrals made to care in the community over time at VA facilities with sharing agreements, and associated cost savings. Implementing a process to evaluate the effectiveness of sharing agreements could result in cost savings to the federal government. For example, if the process results in an increase of referrals to DOD instead of community care by 10 percent over a period of 5 years, it could amount to millions of dollars in savings.[42]
Developing a process to evaluate the effectiveness of sharing agreements would also allow the departments to identify agreements that may not be working as intended and offer support to facilities to help them improve the effectiveness of these agreements. Further, implementing changes based on the results of a process to evaluate the effectiveness of sharing agreements will help ensure the departments reap the full benefits of these agreements.
VA and DOD Have Taken Some Steps to Expand Sharing, but Do Not Have a Process to Systematically Identify New or Expanded Opportunities
VA and DOD have taken some steps to identify opportunities for new or expanded sharing between the departments, based on our review of the departments’ documentation. However, we found the departments do not have a systematic process at the regional or national level to identify opportunities for new or expanded sharing agreements.
VA and DOD’s efforts to identify opportunities for new or expanded sharing between the departments have included:
· Facility-space-sharing opportunities. The Joint Executive Committee established the Capital Asset Planning Committee in 2005 to facilitate an integrated approach to joint construction projects and sharing real property between the departments.[43] The committee reports to the Joint Executive Committee, and membership includes headquarters-level leaders from both departments. Documentation shows the local officials who propose the projects break them into action items, with information on their status and estimated costs for completing them. As of February 2025, the committee is tracking several opportunities identified by local officials, including four facility-space-sharing projects in progress and two potential project opportunities.
· Site-specific sharing opportunities. VA and DOD are tracking six site-specific sharing opportunities identified at the local level through the Operations Integrated Project Team as of August 2024.[44] For example, one initiative is to expand access for VA patients at DOD facilities in a particular region, with goal dates to 1) discuss opportunities for VA patients to be seen at a DOD facility’s emergency department, 2) have neurology services offered to VA patients at the DOD facility, and 3) conduct an ongoing review for expansion opportunities to rheumatology, infectious disease, and other services to be determined. According to DOD officials, local officials working at specific medical facilities identify these sharing opportunities.
· Regional summit. VA and DOD held a regional summit in May 2024, a conference attended by headquarters, regional, and local level officials from both departments to evaluate and plan for sharing in one region in the eastern U.S. Documentation from the regional summit showed 29 potential sharing opportunities in the region. According to VA officials, local officials identified the potential sharing opportunities. For example, officials from one facility that participated in the summit identified an opportunity to establish a dental clinic to serve both veterans and servicemembers using available DOD facility space. Additionally, according to documentation from the summit, VA and DOD leadership assigned each sharing opportunity a VA and DOD committee or work group, such as the Capital Asset Planning Committee or the Operations Integrated Project Team, to serve in a consultation role.
VA and DOD officials said they viewed the regional summit as a success but told us that the departments have no plans to hold additional regional summits in the future. Further, they said that pursuing similar efforts to expand sharing agreements are on hold while DOD fulfils obligations through the Military Health System Stabilization Initiative.[45]
While these efforts represent progress towards identifying expanded opportunities for sharing, these efforts rely on local officials to identify opportunities. As such, they are ad hoc, and do not represent a larger and more systematic process for periodically identifying potential sharing opportunities nationally. VA and DOD’s reliance on local officials and lack of a process to systematically identify opportunities for new or expanded sharing is inconsistent with VA’s charge to facilitate, develop, and sustain sharing agreements and DOD’s responsibility to identify opportunities to enhance mutually beneficial services and resources.[46]
According to VA and DOD officials, as of April 2025 the departments do not have a process to systematically identify new and expanded opportunities for sharing. VA officials told us this is because they believed officials from local facilities were best positioned to recognize and pursue these opportunities based on their operational needs. DOD officials told us they do not have such a process because they wanted to give as much authority as possible to their Defense Health Networks. VA and DOD headquarters officials also told us they do not have authority to oversee the implementation of the sharing opportunities; rather, the departments serve in an advisory and support function only. VA officials stated that these support functions include offering technical assistance, subject matter expertise, and programmatic support to local officials.
However, as we have previously reported, relying on local facility leadership to identify opportunities for collaboration can have limitations.[47] By depending on local leadership, the identification and implementation of sharing opportunities becomes dependent on local leaders’ personalities and willingness to collaborate, which may vary.
Further, local officials may not be aware of opportunities for sharing at other locations in their area for several reasons, including being primarily focused on the operations of their own facility, not having information about resources available in the partner department, leadership transitions, and a lack of relationships with counterparts at the partner department. For example, an official from one site we visited described resistance from their sharing partner to provide information on or fully utilize the existing agreement.
Developing a systematic process for identifying new or expanded sharing opportunities would be consistent with a broader recommendation we made to VA and DOD in 2012.[48] Specifically, we recommended that the departments further develop a systematic process for identifying and furthering collaboration opportunities, such as through sharing agreements and other means of collaboration. The departments agreed, and in response, the departments at the headquarters level conducted a pilot program that involved comparing the departments’ geo-spatial data with VA and DOD beneficiary data to identify market sharing opportunities. Documentation showed the pilot was successful in increasing the number of referrals from the VA facility pilot sites to DOD facilities, as well as reducing wait times.[49]
VA officials told us in January 2025 that they did not extend the pilot beyond the initial sites because of decreased referral volume due to the Veterans Choice Program, which allows veterans to select their location of care from federal providers, such as DOD, or other community providers if they meet certain criteria.[50] However, officials from six sites we visited told us they use strategies such as having local facility staff educate veterans on the benefits of selecting DOD care, like shorter wait times compared to care in the community, to help promote DOD as a care location choice.[51] VA officials also stated that the pilot was not continued because of issues reported by the sites involved in the pilot related to billing, including problems related to properly identifying and billing for patients who are dual-eligible for TRICARE and VA benefits. As discussed above, however, VA and DOD have taken steps to address this and other barriers related to billing.
To implement a systematic process for identifying new or expanded sharing opportunities, VA and DOD headquarters and regional partners could leverage department-level information and develop a data-driven approach to assess opportunities for sharing at a regional and national level. This approach could include the departments collaborating to develop an assessment of DOD capacity matched with VA needs.
In April 2025, VA and DOD officials told us they have held preliminary discussions within their respective departments about developing new strategies to identify sharing opportunities at a national level. Specifically, DOD officials said they are shifting towards a strategy of identifying sharing opportunities at the national level, rather than leaving the identification of such opportunities to local officials. For their part, VA officials said that VA at the headquarters level is planning to assess the department’s specific needs that align with DOD’s clinical readiness mission, which could include absorbing care teams into each other’s facilities. However, both DOD and VA officials emphasized that developing such strategies are in the early planning stages and no actions have yet been taken.
Developing a process for systematically identifying opportunities to expand sharing that involves national and regional level partners would help ensure that all sharing opportunities are identified and maximized. Additionally, this process could help enhance collaboration across the departments, and ultimately improve patients’ access to care and reduce costs. For example, if the departments implement a process, and newly identified opportunities result in an increase of referrals by even 10 percent over a period of 5 years, it could amount to millions of dollars in cost savings.[52]
Conclusions
Sharing agreements provide an important mechanism to help VA and DOD improve access to and provide quality care to beneficiaries, achieve cost savings for the departments, and assist with military readiness for DOD. The departments continue to take steps to address key barriers to implementing sharing agreements, such as establishing workgroups to address billing and reimbursement issues.
However, medical facilities lack information on developing non-reimbursable agreements, and although DOD is working on procedures to address this, it has yet to finalize them or establish a time frame for doing so. By finalizing the procedures, and providing them to its medical facilities, DOD can help ensure the departments’ ability to continue to share services that are mutually beneficial to both departments and ultimately veterans and servicemembers.
Further, VA and DOD collect information to oversee sharing agreements, but the departments have not taken steps to evaluate the effectiveness of their sharing agreements. By implementing a process to evaluate the effectiveness of sharing agreements—including establishing performance goals and measures and collecting data to assess progress towards these goals—the departments can use those results to make any needed improvements. This, in turn, will better ensure they reap the full benefits of sharing agreements, including cost savings for the federal government, and enhanced DOD provider clinical readiness.
Finally, VA and DOD have taken some steps to identify opportunities for new or expanded sharing, including using a long-standing committee to track facility-space-sharing projects. However, they do not have a department-level approach to identify potential areas for new and expanded sharing as of April 2025, potentially resulting in missed opportunities. Developing a process to systematically identify opportunities to expand sharing nationally can help ensure the departments identify and maximize sharing between the departments. By identifying these opportunities, the departments can maximize the use of resources and achieve cost savings, as well as enhance access to care for beneficiaries.
Recommendations for Executive Action
We are making the following five recommendations, including three to DOD and two to VA:
The Under Secretary of Defense for Personnel & Readiness should finalize procedures that include guidance on developing non-reimbursable sharing agreements, including instructions on how to develop a required justification through a business case analysis plan, and provide the procedures to its DOD facilities. (Recommendation 1).
The VA Under Secretary for Health should work with DOD to implement a process for evaluating the effectiveness of all its sharing agreements and use the results to make changes as appropriate. Such a process should include establishing performance goals, establishing performance measures, and collecting data to assess progress towards these goals. (Recommendation 2).
The Assistant Secretary of Defense for Health Affairs should work with VA to implement a process for evaluating the effectiveness of all its sharing agreements and use the results to make changes as appropriate. Such a process should include establishing performance goals, establishing performance measures, and collecting data to assess progress towards these goals. (Recommendation 3).
The VA Under Secretary for Health should work with DOD to develop and implement a systematic process for identifying opportunities for new and expanded sharing agreements (Recommendation 4).
The Assistant Secretary of Defense for Health Affairs should work with VA to develop a systematic process for identifying opportunities for new and expanded sharing agreements (Recommendation 5).
Agency Comments
We provided a draft of this report to DOD and VA for review and comment. The departments’ comments are reprinted in appendix II and III. In written comments, DOD and VA concurred with our recommendations and identified steps they plan to take. VA also provided technical comments, which we incorporated as appropriate.
We are sending copies to the appropriate congressional committees, the Secretary of Defense, and the Secretary of Veterans Affairs. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at hundrupa@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report. GAO staff who made key contributions to this report are listed in Appendix IV.

Alyssa M. Hundrup
Director, Health Care
This appendix provides information on each sharing agreement VA and DOD have in place, as of April 2025. Sharing agreements provide a structure to exchange medical and nonmedical services between the Department of Veterans Affairs (VA) and Department of Defense (DOD) health care facilities. VA and DOD establish such agreements to improve access to, and enhance the quality and cost-effectiveness of, health care the departments provide. A VA facility and DOD facility can have multiple sharing agreements between them, or a single sharing agreement may include multiple DOD facilities.
As of April 2025, VA and DOD data show that the departments had established 185 sharing agreements nationwide of varying types, through which a range of medical and nonmedical care services could be shared (see Table 1). These sharing agreements included 77 VA facilities and 98 DOD facilities.
|
|
|
Medical servicea |
Nonmedical serviceb |
|
||||||||||||||||||||||||||
|
VA facilityc |
DOD facilityd |
Collaboration level |
Ambulatory service |
Inpatient service |
Othere |
Administration and supportf |
Professional skills development and maintenance |
Facility space |
Otherg |
|
||||||||||||||||||||
|
Albuquerque Medical Center |
377th Medical Group-Kirtland Air Force Base |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Albuquerque Medical Center |
377th Medical Group-Kirtland Air Force Base |
1 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Albuquerque Medical Center |
377th Medical Group-Kirtland Air Force Base |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Albuquerque Medical Center |
377th Medical Group-Kirtland Air Force Base |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Albuquerque Medical Center |
377th Medical Group-Kirtland Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Alexandria Medical Center |
Bayne-Jones Army Community Hospital |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Alexandria Medical Center |
Louisiana Army National Guard |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Anchorage Medical Center |
Bassett Army Community Hospital |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Anchorage Medical Center |
673rd Medical Group-Joint Base Elmendorf-Richardson |
4 |
✓ |
✓ |
✓ |
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
Anchorage Medical Center |
673rd Medical Group-Joint Base Elmendorf-Richardson |
4 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Ann Arbor Medical Center |
180 Air Combat Command Medical Squadron |
3 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Augusta Medical Center |
Eisenhower Army Medical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Augusta Medical Center |
Eisenhower Army Medical Center |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Baltimore Medical Center |
Air Force Space Command |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Baltimore Medical Center |
The Joint Pathology Center |
2 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Baltimore Medical Center |
Walter Reed Army Institute of Research |
2 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
Bay Pines Medical Center |
Army Medical Department Professional Management Command |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Bayne-Jones Army Community Hospital |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
96th Medical Group-Eglin Air Force Base |
4 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
81st Medical Group-Keesler Air Force Base |
4 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
81st Medical Group-Keesler Air Force Base |
3 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
Biloxi Medical Center |
325th Medical Group-Tyndall Air Force Base |
3 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
325th Medical Group-Tyndall Air Force Base |
2 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Louisiana Army National Guard |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Naval Hospital Pensacola |
4 |
|
|
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Naval Hospital Pensacola |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Naval Hospital Pensacola |
3 |
|
|
|
|
|
✓ |
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Naval Hospital Pensacola |
4 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Biloxi Medical Center |
Naval Hospital Pensacola |
3 |
|
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Biloxi Medical Center |
Naval Hospital Pensacola |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Birmingham Medical Center |
Fox Army Health Center |
2 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Birmingham Medical Center |
Army Medical Department Professional Management Command |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Boise Medical Center |
124 Air Combat Command Medical Squadron |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Buffalo Medical Center |
107 Air Combat Command Medical Squadron |
2 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Buffalo Medical Center |
174 Air Combat Command Medical Squadron |
2 |
✓ |
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Buffalo Medical Center |
914 Aircraft Medical Squad 22 AF Air Medical Command |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Buffalo Medical Center |
Guthrie Ambulatory Health Care Clinic |
3 |
|
|
|
|
|
✓ |
|
|
||||||||||||||||||||
|
Charleston Medical Center |
628th Medical Group-Joint Base Charleston |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Charleston Medical Center |
628th Medical Group-Joint Base Charleston |
2 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Charleston Medical Center |
Naval Hospital Beaufort |
4 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Charleston Medical Center |
Naval Hospital Beaufort |
4 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
Charleston Medical Center |
Naval Health Clinic Charleston |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Charleston Medical Center |
Naval Health Clinic Charleston |
3 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Charleston Medical Center |
Naval Health Clinic Charleston |
2 |
✓ |
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Cheyenne Medical Center |
90th Medical Group-F.E. Warren Air Force Base |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Chillicothe Medical Center |
88th Medical Group-Wright-Patterson Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Cleveland Medical Center |
256th Combat Support Hospital |
1 |
|
|
|
|
|
|
✓ |
|
||||||||||||||||||||
|
Cleveland Medical Center |
88th Medical Group-Wright-Patterson Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Columbia Medical Center |
Eisenhower Army Medical Center |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Columbia Medical Center |
Eisenhower Army Medical Center |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Dallas Medical Center |
301 Medical Squadron 10 Air Force |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Dayton Medical Center |
88th Medical Group-Wright-Patterson Air Force Base |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Dayton Medical Center |
88th Medical Group-Wright-Patterson Air Force Base |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Dayton Medical Center |
88th Medical Group-Wright-Patterson Air Force Base |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Denver Medical Center |
Colorado Military Health Systemi |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Denver Medical Center |
Colorado Military Health Systemi |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Dublin Medical Center |
Eisenhower Army Medical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Dublin Medical Center |
Naval Hospital Jacksonville |
1 |
|
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Dublin Medical Center |
Naval Hospital Jacksonville |
3 |
✓ |
|
✓ |
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Durham Medical Center |
Naval Health Clinic Cherry Point |
2 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
El Paso Medical Center |
William Beaumont Army Medical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Erie Medical Center |
Keller Army Community Hospital |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Fargo Medical Center |
319th Medical Group-Grand Forks Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Fayetteville Medical Center |
4th Medical Group-Seymour Johnson Air Force Base |
2 |
|
|
|
|
|
✓ |
|
|
||||||||||||||||||||
|
Fayetteville Medical Center |
4th Medical Group-Seymour Johnson Air Force Base |
3 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Fayetteville Medical Center |
Naval Medical Center Camp Lejeune |
3 |
✓ |
✓ |
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Fayetteville Medical Center |
44th Medical Brigade - Ft. Liberty |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Fayetteville Medical Center |
Womack Army Medical Center |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Fayetteville Medical Center |
Womack Army Medical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Fort Meade Medical Center |
28th Medical Group- Ellsworth Air Force Base |
1 |
✓ |
|
|
|
|
|
|
|
||||||||||||||||||||
|
Fort Meade Medical Center |
Army Medical Department Professional Management Command |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Fort Meade Medical Center |
Army Medical Department Professional Management Command |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Fort Meade Medical Center |
Armed Forces Experimental Training Agency, Camp Peary |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Fort Meade Medical Center |
South Dakota Army National Guard |
2 |
|
|
|
|
|
✓ |
|
|
||||||||||||||||||||
|
Fresno Medical Center |
144 Air Combat Command Medical Squadron |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Fresno Medical Center |
Naval Health Clinic Lemoore |
4 |
✓ |
✓ |
✓ |
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Gainesville Medical Center |
Army Medical Department Professional Management Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Hampton Medical Center |
633rd Medical Group-Joint Base Langley-Eustis |
2 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Hampton Medical Center |
633rd Medical Group-Joint Base Langley-Eustis |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Hampton Medical Center |
633rd Medical Group-Joint Base Langley-Eustis |
3 |
|
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Hampton Medical Center |
Naval Medical Center Portsmouth |
4 |
✓ |
✓ |
|
|
|
|
|
|
||||||||||||||||||||
|
Harlingen Medical Center |
Brooke Army Medical Center and 59th Medical Wing-Wilford Hall Ambulatory Surgical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Harlingen Medical Center |
Naval Health Clinic Corpus Christi |
3 |
✓ |
|
|
|
|
|
|
|
||||||||||||||||||||
|
Honolulu Medical Center |
Naval Hospital Guam |
3 |
✓ |
✓ |
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Honolulu Medical Center |
Tripler Army Medical Center |
4 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Honolulu Medical Center |
Tripler Army Medical Center |
4 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Indianapolis Medical Center |
Naval Hospital Pensacola |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Kansas City Medical Center |
184th Wing Kansas Air Guard |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Kansas City Medical Center |
22nd Medical Group-McConnell Air Force Base |
2 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Kansas City Medical Center |
22nd Medical Group-McConnell Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Kansas City Medical Center |
Irwin Army Community Hospital |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Kansas City Medical Center |
Munson Army Health Center |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Kansas City Medical Center |
Army Medical Department Professional Management Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Las Vegas Medical Center |
99th Medical Group-Nellis Air Force Base |
2 |
✓ |
✓ |
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Lebanon Medical Center |
Army Medical Department Professional Management Command |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Little Rock Medical Center |
19th Medical Group-Little Rock Air Force Base |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Loma Linda Medical Center |
452nd Medical Group Air Force Reserve |
2 |
|
|
|
✓ |
✓ |
✓ |
|
|
||||||||||||||||||||
|
Madison Medical Center |
115 Air Combat Command Medical Squadron |
1 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Madison Medical Center |
115 Air Combat Command Medical Squadron |
1 |
✓ |
|
|
|
|
|
|
|
||||||||||||||||||||
|
Martinez Medical Center |
60th Medical Group-Travis Air Force Base |
4 |
✓ |
✓ |
|
|
|
|
|
|
||||||||||||||||||||
|
Martinez Medical Center |
60th Medical Group-Travis Air Force Base |
4 |
|
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Memphis Medical Center |
164 Air Medical Command Medical Squadron |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Miami Medical Center |
Naval Hospital Jacksonville |
3 |
✓ |
|
✓ |
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Miami Medical Center |
Naval Hospital Jacksonville |
3 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
Miami Medical Center |
Eisenhower Army Medical Center |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Montgomery Medical Center |
Martin Army Community Hospital |
2 |
✓ |
✓ |
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Montgomery Medical Center |
42 Medical Group-Maxwell Air Force Base |
2 |
✓ |
|
✓ |
|
|
✓ |
|
|
||||||||||||||||||||
|
Montgomery Medical Center |
Lyster Army Health Clinic |
2 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Montrose Medical Center |
Keller Army Community Hospital |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Montrose Medical Center |
Keller Army Community Hospital |
3 |
|
|
|
|
|
✓ |
|
|
||||||||||||||||||||
|
Montrose Medical Center |
Keller Army Community Hospital |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Montrose Medical Center |
Keller Army Community Hospital |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Nashville Medical Center |
Arnold Engineering Development Complex |
1 |
✓ |
|
|
|
|
|
|
|
||||||||||||||||||||
|
Nashville Medical Center |
Arnold Engineering Development Complex |
1 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Nashville Medical Center |
Blanchfield Army Community Hospital |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Nashville Medical Center |
Blanchfield Army Community Hospital |
2 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
New Orleans Medical Center |
Army Medical Department Professional Management Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
New Orleans Medical Center |
Army Medical Department Professional Management Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
New Orleans Medical Center |
Naval Hospital Pensacola |
3 |
|
|
|
|
✓ |
|
|
|||||||||||||||||||||
|
New Orleans Medical Center |
Naval Hospital Pensacola |
3 |
|
|
|
|
✓ |
|
|
|||||||||||||||||||||
|
Oklahoma City Medical Center |
71st Medical Group-Vance Air Force Base |
3 |
|
|
✓ |
|
|
|
|
|||||||||||||||||||||
|
Oklahoma City Medical Center |
72nd Medical Group-Tinker Air Force Base |
1 |
|
|
|
✓ |
|
✓ |
|
|||||||||||||||||||||
|
Oklahoma City Medical Center |
72nd Medical Group-Tinker Air Force Base |
4 |
✓ |
|
✓ |
|
|
|
|
|||||||||||||||||||||
|
Oklahoma City Medical Center |
82nd Medical Group-Sheppard Air Force Base |
1 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Oklahoma City Medical Center |
82nd Medical Group-Sheppard Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Oklahoma City Medical Center |
Army Medical Department Professional Management Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Oklahoma City Medical Center |
Reynolds Army Health Clinic |
2 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Omaha Medical Center |
132 Air Combat Command Medical Squadron |
1 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Omaha Medical Center |
55th Medical Group-Offutt Air Force Base |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Omaha Medical Center |
55th Medical Group-Offutt Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Omaha Medical Center |
Iowa National Guard |
1 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Orlando Medical Center |
45th Medical Group-Patrick Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Palo Alto Medical Center |
60th Medical Group-Travis Air Force Base |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Palo Alto Medical Center |
Madigan Army Medical Center |
3 |
✓ |
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Palo Alto Medical Center |
Madigan Army Medical Center |
3 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Phoenix Medical Center |
56th Medical Group-Luke Air Force Base |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Providence Medical Center |
Naval Health Clinic New England |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Reno Medical Center |
Naval Health Clinic Lemoore |
4 |
✓ |
✓ |
✓ |
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Salem Medical Center |
Army Medical Department Professional Management Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Salt Lake City Medical Center |
419 Aircraft Medical Squad 22 AF Air Medical Command |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
San Antonio Medical Center |
Brooke Army Medical Center and 59th Medical Wing-Wilford Hall Ambulatory Surgical Center |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
San Antonio Medical Center |
Brooke Army Medical Center and 59th Medical Wing-Wilford Hall Ambulatory Surgical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
San Antonio Medical Center |
Brooke Army Medical Center |
4 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
San Antonio Medical Center |
59th Medical Wing-Wilford Hall Ambulatory Surgical Center |
3 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
San Antonio Medical Center |
59th Medical Wing-Wilford Hall Ambulatory Surgical Center |
3 |
✓ |
✓ |
✓ |
|
|
✓ |
|
|
||||||||||||||||||||
|
San Antonio Medical Center |
59th Medical Wing-Wilford Hall Ambulatory Surgical Center |
3 |
|
|
✓ |
|
|
✓ |
|
|
||||||||||||||||||||
|
San Diego Medical Center |
Naval Medical Center San Diego and Naval Hospital Camp Pendleton |
2 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
San Diego Medical Center |
Naval Medical Center San Diego and Naval Hospital Camp Pendleton |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
San Diego Medical Center |
Naval Medical Center San Diego and Naval Hospital Camp Pendleton |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Seattle Medical Center |
Madigan Army Medical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Seattle Medical Center |
Naval Health Clinic Oak Harbor |
2 |
|
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Seattle Medical Center |
Naval Health Clinic Oak Harbor |
3 |
✓ |
|
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Shreveport Medical Center |
2nd Medical Group-Barksdale Air Force Base |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Sioux Falls Medical Center |
114 Air Combat Command Medical Squadron |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Spokane Medical Center |
92nd Medical Group-Fairchild Air Force Base |
1 |
|
|
|
✓ |
|
|
✓ |
|
||||||||||||||||||||
|
Spokane Medical Center |
92nd Medical Group-Fairchild Air Force Base |
1 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Spokane Medical Center |
92nd Medical Group-Fairchild Air Force Base |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
St. Louis Medical Center |
375th Medical Group-Scott Air Force Base |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
St. Louis Medical Center |
375th Medical Group-Scott Air Force Base |
3 |
✓ |
|
|
|
|
✓ |
|
|
||||||||||||||||||||
|
Tampa Medical Center |
6th Medical Group-Macdill Air Force Base |
2 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Tampa Medical Center |
6th Medical Group-Macdill Air Force Base |
3 |
|
|
|
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Tampa Medical Center |
6th Medical Group-Macdill Air Force Base |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Temple Medical Center |
Carl R. Darnall Army Medical Center |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Temple Medical Center |
Carl R. Darnall Army Medical Center |
3 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Tucson Medical Center |
355th Medical Group-Davis Monthan Air Force Base |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Tucson Medical Center |
355th Medical Group-Davis Monthan Air Force Base |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
VA Central Office |
6th Medical Group-Macdill Air Force Base |
1 |
|
|
|
|
|
|
✓ |
|
||||||||||||||||||||
|
VA Central Office |
99th Medical Group-Nellis Air Force Base |
2 |
|
✓ |
|
|
|
|
|
|
||||||||||||||||||||
|
VA Central Office |
Defense Health Agency |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
VA Central Office |
The Joint Pathology Center |
1 |
|
|
✓ |
|
|
|
|
|
||||||||||||||||||||
|
VA Central Office |
The Joint Pathology Center |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
VA Central Office |
Vision Center of Excellence |
2 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 4 |
National Capital Region Network |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 5 |
National Capital Region Network |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 6 |
National Capital Region Network |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 7 |
National Capital Region Network |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 8 |
National Capital Region Network |
2 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 10 |
88th Medical Group-Wright-Patterson Air Force Base |
4 |
✓ |
✓ |
✓ |
✓ |
|
✓ |
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 10 |
National Capital Region Network |
2 |
|
✓ |
|
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 15 |
General Leonard Wood Army Community Hospital |
2 |
✓ |
✓ |
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 15 |
National Capital Region Network |
1 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 16 |
Naval Hospital Pensacola |
4 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Veterans Integrated Service Network 20 |
National Capital Region Network |
1 |
✓ |
✓ |
✓ |
|
|
|
|
|
||||||||||||||||||||
|
Washington DC Medical Center |
Alexander T. Augusta Military Medical Center |
2 |
✓ |
|
✓ |
✓ |
|
|
|
|
||||||||||||||||||||
|
Washington DC Medical Center |
Alexander T. Augusta Military Medical Center |
2 |
|
|
|
✓ |
|
✓ |
✓ |
|
||||||||||||||||||||
|
Washington DC Medical Center |
Walter Reed National Military Medical Center |
3 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
West Los Angeles Medical Center |
61st Medical Group-Los Angeles Air Force Base |
2 |
|
|
|
|
✓ |
|
|
|
||||||||||||||||||||
|
Wilmington Medical Center |
436th Medical Group-Dover Air Force Base |
1 |
|
|
|
✓ |
|
|
|
|
||||||||||||||||||||
Legend:
✓ = Shared service
Bolded text = GAO conducted site visits at the VA and DOD facility.
Source: GAO Analysis of Department of Veterans Affairs (VA) data. | GAO‑25‑107497
Notes: As of April 2025, the Department of Veterans Affairs (VA) and Department of Defense (DOD) had 185 active sharing agreements. VA and DOD facilities can have multiple sharing agreements. In addition, a single sharing agreement may include multiple DOD facilities.
VHA Directive 1660 categorizes VA and DOD sharing agreements into five distinct levels of sharing collaboration based on the extent of the collaboration. A Level 1 sharing agreement denotes VA and DOD facilities intermittently sharing independent medical or nonmedical services. A Level 2 sharing agreement represents VA and DOD facilities sharing independent medical or nonmedical services. A Level 3 sharing agreement also represents VA and DOD facilities sharing independent medical or nonmedical services and can include sharing clinical and non-clinical personnel. Level 4 sharing agreements represent VA and DOD sharing mutually dependent medical and nonmedical services and can include sharing clinical and non-clinical personnel.
aMedical care services are obtained by referral from a VA medical center or military treatment facility. Medical care services may include ambulatory services, such as emergency medical care and mental health care; and inpatient care, such as internal medicine and general surgery. Sharing of these services can be intermittent, as is the case with Level 1 sharing agreements, or continuous as is the case with Levels 2-4.
bNonmedical care services may include administration and support, such as providing transportation services or laundry services. In addition, VA and DOD consider sharing facility space through a space permit as a nonmedical care service.
cVA facilities that have established sharing agreements include VA medical centers, Veterans Integrated Service Networks and VA Central Office.
dDOD facilities that have established sharing agreements include military treatment facilities, DOD regional networks and medical facilities, such as the Vision Center of Excellence.
eOther medical services shared by VA and DOD facilities include dental services and ancillary services, such as pharmacy or radiology.
fAdministration and support services shared by VA and DOD facilities include ambulatory and inpatient administration and housekeeping and laundry services.
gOther nonmedical services shared by VA and DOD facilities include providing unique military services, such as base operations or decedent affairs.
hThe Colorado Military Health System includes four military treatment facilities—460th Medical Group at Buckley, 10th Medical Group at the US Air Force Academy, AF-21st Medical Group at Peterson and Evans Army Community Hospital, Fort Carson, Colo.
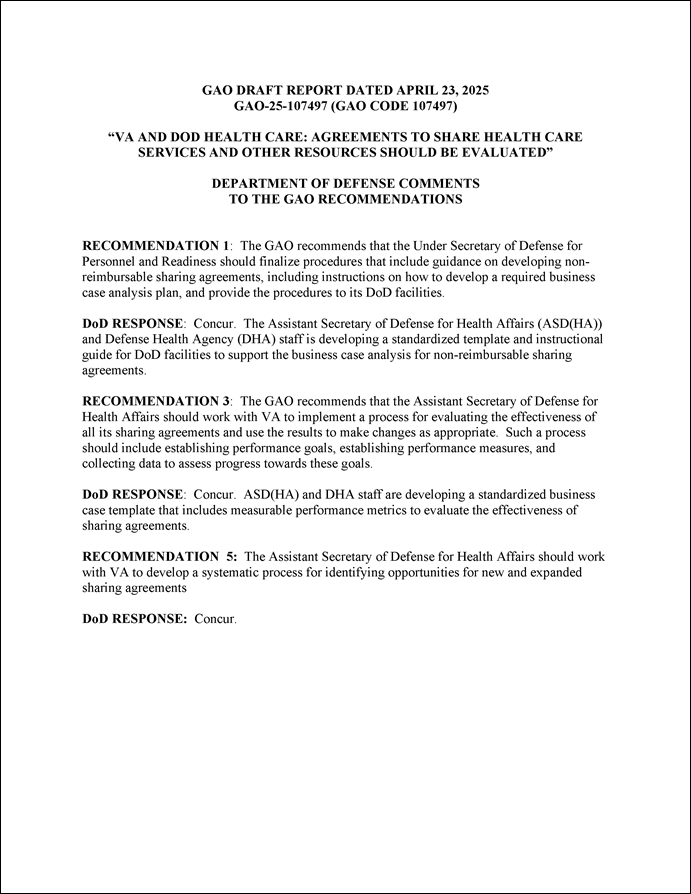
GAO Contact
Alyssa M. Hundrup at HundrupA@gao.gov.
Staff Acknowledgments
In addition to the contact named above, Michael Zose (Assistant Director), Deitra H. Lee (Analyst in Charge), Hiba Sassi, and Helen Sauer Young made key contributions to this report. Also contributing to this report were Jennie Apter, Jacquelyn Hamilton, and Ethiene Salgado-Rodriguez.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
A. Nicole Clowers, Managing Director, CongRel@gao.gov
General Inquiries
[1]VA beneficiaries include veterans of military service and certain dependents and survivors. DOD beneficiaries include active duty servicemembers and their dependents, medically eligible National Guard and Reserve servicemembers and their dependents, and military retirees and their dependents and survivors.
[2]See 38 U.S.C. § 8111. All resource sharing agreements are to be developed and implemented in accordance with the Memorandum of Understanding between the VA and the DOD, entitled “VA/DOD Health Care Resources Sharing Guidelines,” agreed to by both Departments on July 29, 1983. DOD also applies its DOD Memorandum, Subject: “VA/DOD Health Care Resources Sharing Reimbursement Guidelines,” dated May 17, 1989, also issued under 38 U.S.C. § 8111 authority. VA and DOD also have authority to enter into agreements with each other for the planning, design, and construction, or the leasing, of facilities to be operated as shared medical facilities. See 38 U.S.C. § 8111B and 10 U.S.C. § 1104a.
[3]Both VA and DOD’s private sector care programs (VA’s Veterans Community Care Program and TRICARE, respectively) generally base rates on the current Medicare rates. See 38 U.S.C. § 1703(i) and 10 U.S.C. §§ 1079(h), 1086(f). Under a health care sharing agreement with DOD, only veterans are referred to a DOD facility. When veterans are referred to a DOD facility for care or DOD beneficiaries are referred to VA for care, the departments typically reimburse each other at the established rate for civilian or community providers minus 20 percent.
[4]Clinical readiness refers to a DOD provider or provider team’s ability to perform their assigned deployed role, such as having the knowledge, skills, and abilities needed for combat casualty care.
[5]Sharing agreements can also result in cost savings beyond lower reimbursement payments, such as through VA using space at DOD facilities and reimbursing DOD at a rate lower than what VA would pay for non-federally owned space.
[6]See GAO, VA and DOD Health Care: Department-Level Actions Needed to Assess Collaboration Performance, Address Barriers, and Identify Opportunities, GAO 12-992 (Washington, D.C.: Sept. 28, 2012).
[7]See GAO 12-992. In this work, we also found that VA and DOD did not have a fully developed process for systematically identifying all opportunities for new or enhanced collaboration. We made five recommendations to both departments, including that VA and DOD require collaboration sites to develop performance measures related to access, quality, and costs; address barriers hindering collaboration; and develop a process to more systematically identify new or expanded collaboration opportunities. VA and DOD agreed with all of the recommendations and took steps to implement each of them.
[8]We conducted in-person site visits to the Nashville (Tenn.) VA medical center; Blanchfield Army Community Hospital (Fort Campbell, Ky.); Sacramento VA medical center (Mather, Calif.); David Grant Medical Center (Fairfield, Calif.); Audie L. Murphy Memorial Veterans’ Hospital (San Antonio, Texas); and Brooke Army Medical Center (at Fort Sam Houston, Texas). We conducted virtual site visits with the Denver (Colo.) VA medical center; Colorado Military Health System (includes four military treatment facilities—460th Medical Group at Buckley, 10th Medical Group at the US Air Force Academy, 21st Medical Group at Peterson and Evans Army Community Hospital, Fort Carson, Colo); the Biloxi (Miss.) VA medical center; Keesler Medical Center (Biloxi, Miss.); and the Mike O’Callaghan Military Medical Center (Nellis Air Force Base, Nevada). Additionally, we interviewed officials with the VA TeleCritical Care Program, located at a VA facility, which is involved in a sharing agreement with the Mike O’Callaghan Military Medical Center.
[9]We interviewed two veterans service organizations. Where possible, we also interviewed members of the local veterans service organizations where we conducted our site visits to identify barriers that they may have experienced accessing care at locations using sharing agreements.
[10]See, for example, DOD Instruction 6010.23, which requires DOD to develop policy and guidance, including reviewing and recommending approval of Defense Health Agency’s billing methodologies for the DOD/VA Health Care Resource Sharing Program.
Internal control is a process effected by an entity’s oversight body, management, and other personnel that provides reasonable assurance that the objectives of an entity will be achieved. GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.: Sept. 2014). Federal internal control standards state that agencies should use quality information to achieve the entity’s objectives (Principle 13) and internally communicate the necessary quality information to achieve the entity’s objectives (Principle 14).
[11]GAO, Evidence-Based Policymaking: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington, D.C.: July 12, 2023).
[12]See VA-DOD Joint Executive Committee, Joint Strategic Plan, Fiscal Years 2022-2027 (Washington, D.C.). The Joint Executive Committee—co-chaired by the Deputy Secretary of VA and the Under Secretary of Defense for Personnel and Readiness—is made up of senior VA and DOD officials and provides strategic direction for interagency collaboration between the two departments.
[13]The Veterans Health Administration’s 18 regional Veterans Integrated Service Networks are responsible for managing the day-to-day functions of medical centers in their regions and providing administrative and clinical oversight of individual medical centers.
[14]Defense Health Networks are groups of military medical and dental facilities in the same region with a goal of coordinating and improving the delivery and continuity of health services, according to DOD documentation.
[15]In addition to sharing agreements, another type of collaborative effort the departments can pursue includes the Joint Incentive Fund, which provides funding for pilot projects that may result in new sharing agreements.
[16]See Veterans Health Administration Directive 1660, Department of Veterans Affairs-Department of Defense Health Care Resources Sharing Agreements (November 30, 2022).
[17]VA facilities that have sharing agreements include VA medical centers, VA regional networks, VA program offices and VA Central Office. DOD facilities that have sharing agreements include military medical treatment facilities, DOD regional networks and other medical facilities, such as the Vision Center of Excellence. A VA facility and DOD facility can have multiple sharing agreements, and a single sharing agreement may include multiple DOD facilities.
[18]Typically, primary care providers refer veterans to specialty care, such as cardiology, neurology, and dermatology. Staff at the VA facility are to review referrals, determine a veteran’s eligibility to receive care from other providers outside of the VA facility, and discuss options with the veteran. The VA MISSION Act of 2018 allows eligible veterans to choose the provider, including DOD providers available through sharing agreements. After a VA facility establishes a referral, an appointment is scheduled, and the veteran can obtain the medical care services from the chosen provider.
[19]See Veterans Health Administration Directive 1660, Department of Veterans Affairs-Department of Defense Health Care Resources Sharing Agreements (Nov. 30, 2022).
[20]For most sharing agreements, individuals receive referred medical services with a provider, according to the sharing agreement data.
[21]Tele-intensive care services involve the use of telecommunication technology to provide critical care remotely. These services typically include real-time monitoring of patients in intensive care units at the DOD facility and allows off-site VA critical care specialists to assist the DOD medical team in real-time.
[22]VHA Directive 1660 defines separate health care facilities in different locations that do not have a sharing agreement for shared medical care or non-medical care services as Level 0 facilities. In contrast, level 5 is a single integrated health care facility with integrated governance and full sharing of clinical, ancillary, administrative and facility operations. As of April 2025, there was one Level 5 sharing agreement, the Captain James A. Lovell Federal Health Care Center in North Chicago. For work we have done specific to this sharing agreement, see VA Health Care Facilities: Leveraging Partnerships to Address Capital Investment Needs GAO‑22‑106017 (Washington, D.C.: May 12, 2022).
[23]The list of most frequently shared services was compiled based on GAO analysis of information provided by VA and may not be representative of all services shared through sharing agreements.
[24]The VA procedures do not require DOD facilities to provide capability reports to VA facilities.
[25]We previously reported about similar barriers in our 2012 report. See GAO‑12‑992.
[26]Base access requirements apply to veterans as well as approved caregivers accompanying them.
[27]See DOD Manual 5200.08, Volume 3. Physical Security Program: Access to DOD Installation (Jan. 2019).
[28]Under the sharing agreement between the VA facility and the DOD facility that use telecommunication technology to provide critical care remotely, the Joint Longitudinal Viewer is not used.
[29]See GAO, Electronic Health Records: VA Making Incremental Improvements in New System but Needs Updated Cost Estimate and Schedule, GAO‑25‑106874 (Washington, D.C.: Mar. 12, 2025). GAO has previously made 15 recommendations on the electronic health record modernization in issued reports; 14 of the 15 have not been implemented. In our 2025 report, GAO made three additional recommendations on cost estimating, schedule, and system metrics. VA agreed with each of the recommendations made in these reports.
[30]DOD identified four root causes for the backlog in VA paying DOD for services provided including, (1) DOD facilities provided care to VA patients without obtaining a VA authorization, (2) DOD facilities exceeded the scope of care authorized by VA, (3) VA’s Health Sharing Referral Manager system erroneously overwrote authorizations issued by VA to DOD causing VA to deny payment to DOD and (4) VA sent patients to DOD facilities without issuing an authorization to DOD for the care requested.
[31]Veterans and servicemembers that are eligible for both VA and TRICARE benefits are considered dual-eligible. According to VA policy, it is the dual-eligible beneficiary’s responsibility, at each episode of care, to identify which benefit (VA or TRICARE) they intend to use.
[32]DOD, DOD and Department of Veterans Affairs Health Care Resource Sharing Program, DOD Instruction 6010.23 (Feb.3, 2022).
[33]GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.: Sept. 10, 2014). Federal internal control standards state that agencies should use quality information to achieve the entity’s objectives (Principle 13) and internally communicate the necessary quality information to achieve the entity’s objectives (Principle 14).
[34]In general, positron emission tomography scans may be used to evaluate organs or tissues for the presence of disease or other conditions such as cancer.
[35]VA officials stated that they use information on the levels of collaboration identified by sites with sharing agreements as a general gauge of the overall level of collaboration between VA and DOD.
[36]Sharing agreements that do not produce referral data include agreements to share clinical and non-clinical staff or facility space and agreements of a non-medical nature, such as agreements to share housekeeping or laundry services.
[37]Officials with the VA/DOD Medical Sharing Office told us that data on the number of referrals of veterans to DOD facilities made through sharing agreements are available through a data repository populated by VA facilities. In fiscal year 2024, 35 of the approximately 77 facilities with sharing agreements reported referral data, according to data from the VA/DOD Medical Sharing Office.
[38]See GAO, Evidence-Based Policymaking: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington, D.C.: July 12, 2023).
[39]See 38 U.S.C. § 8111, which cites improving access and cost effectiveness as health care collaboration goals.
[41]When veterans or servicemembers are referred to the other department for care, VA and DOD will typically reimburse the other department at their established rate for civilian or community providers minus 20 percent.
[42]GAO cannot precisely estimate the amount of cost savings that would result from implementing this evaluation process, because it would depend on whether, when, and how such an evaluation process is implemented.
[43]According to its charter, the Capital Asset Planning Committee provides a formalized structure to facilitate cooperation and collaboration in achieving an integrated approach to planning, design, construction, leasing, and other real property initiatives for medical facilities that are mutually beneficial to both VA and DOD.
[44]The Operations Integrated Project Team is a group established in 2023 with membership from both VA and DOD that meets monthly, according to DOD officials. This group’s purposes include identifying and evaluating DOD and VA facilities with unused space, facilitating partnership discussions, and making recommendations to the Health Executive Committee on potential sharing activities between the departments.
[45]On December 6, 2023, the Deputy Secretary of Defense signed a memo directing the stabilization of the Military Health System. The memo requires that the Military Health System add capacity to reattract patients and beneficiaries, improve access to care in military hospitals and clinics, and increase opportunities to sustain military clinical readiness for medical forces.
[46]See Department of Veterans Affairs, Veterans Health Administration Directive 1660, Department of Veterans Affairs-Department of Defense Health Care Resources Sharing Agreements (Nov. 30, 2022) and DOD Instruction 6010.23, DOD and Department of Veterans Affairs Health Care Resource Sharing Program. (Feb. 3, 2022).
[49]For this pilot program, the departments compared data on VA enrollees with a drive time greater than 60 minutes to the nearest VA medical center and enrollees that are within 60 minutes of a DOD hospital. The analysis focused on where VA and DOD had the most purchased care, and where the departments could bring care back within the VA and DOD systems.
[50]The Veterans Access, Choice, and Accountability Act of 2014 established the temporary Veterans Choice Program to help address problems with veterans’ timely access to care at VA medical facilities. Pub. L. No. 113-146, §§ 101, 802, 128 Stat. 1754, 1755-1765, 1802-1803 (2014). Under the Choice Program, when eligible veterans faced long wait times, lengthy travel distances, or other challenges accessing care at VA medical facilities, they could obtain health care services from providers in the community. On June 6, 2019, VA implemented the Veterans Community Care Program, as required under the VA MISSION Act of 2018. Pub. L. No. 115-182, tit. I, § 101, 132 Stat. 1393, 1395-1404 (2018). The Veterans Community Care Program is a permanent program that consolidated or replaced VA’s previous community care programs, including the Choice Program.
[51]Additionally, officials from two facilities we visited stated that embedding DOD providers at VA facilities can help familiarize veterans with DOD providers, and therefore promote DOD as a care location choice.
[52]GAO cannot precisely estimate the amount of cost savings that would result from implementing this process, because it would depend on whether, when, and how it is implemented.