Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
Contact: Triana McNeil at Mcneilt@gao.gov or Jamila Jones Kennedy at Kennedyjj@gao.gov
What GAO Found
The Office of National Drug Control Policy’s (ONDCP) Drug-Free Communities (DFC) Support Program provides grants for community-based coalitions focused on drug use prevention efforts for youth 18 and under. In the 2025 evaluation report, it is claimed that the DFC program is meeting its strategic goal of reducing substance use among youth. However, that report states that it is not possible to establish a causal relationship between substance use changes in communities and the DFC program.
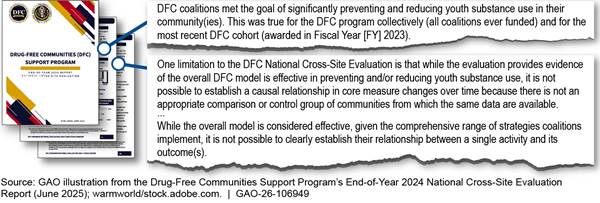
Selected statements on the Effectiveness of the Drug-Free Communities Support Program from the June 2025 National Cross-Site Evaluation Report
GAO found significant limitations in the program data—inconsistencies and unclear data sources. By law, coalitions have certain flexibility in how they collect data. Moreover, ONDCP’s cross-site evaluations have not transparently described its methodologies. Including the complete methodology would allow one to better understand and assess the results of the evaluation. Researchers have long reported on the challenges for documenting causality for community-based programs. However, available data provides insights on coalitions’ efforts to reduce substance use among youth.
ONDCP has taken some steps to effectively administer the DFC program, including working to ensure new coalitions meet program requirements and have access to mandatory training. In addition, ONDCP has established an internal controls framework to help ensure grantee compliance. However, ONDCP has not consistently enforced compliance with the statutory requirement that DFC coalitions maintain the involvement of all community sectors. Establishing and maintaining community drug prevention partnerships is a critical factor to the success of the DFC program. Further, ONDCP lacks transparency in its budget process. Enhanced budget disclosures would allow appropriators and program decision-makers to develop a more comprehensive understanding of the DFC program’s financial position.
Why GAO Did This Study
The U.S. faces multiple challenges related to illicit drugs and declared the opioid epidemic as a national public health emergency since 2017. The Centers for Disease Control and Prevention data indicated 1,413 drug overdose deaths occurred among those age 18 and under in 2023. The DFC program focuses on preventing and reducing youth substance use. In 2020, GAO designated drug misuse a high-risk issue and added it to the 2021 High-Risk Series.
The SUPPORT Act includes a provision for GAO to review ONDCP’s programs and operations, including the DFC program, every 4 years. This report examines the extent to which (1) the DFC program has met key program goals; and (2) ONDCP has effectively managed the DFC program.
For this report, GAO conducted a survey and site visits selected by geography and size, and analyzed annual evaluations of the DFC program, management protocols, and budget data for fiscal years 2018 through 2025. GAO also interviewed agency officials and contractors responsible for program evaluations.
What GAO Recommends
GAO is making six recommendations to ONDCP to develop a strategy to identify relevant data to better understand program impact, explore ways to standardize coalition data collection, document and report the methodology in its annual evaluations, enforce the community sectors involvement requirement, and increase transparency in its budget process. ONDCP concurred with each of the recommendations.
|
Abbreviations |
|
|
|
|
|
CDC |
Centers for Disease Control and Prevention |
|
DEA |
Drug Enforcement Administration |
|
DFC |
Drug-Free Communities Support Program |
|
FFR |
Federal Financial Reporting |
|
HHS |
U.S. Department of Health and Human Services |
|
OMB |
Office of Management and Budget |
|
ONDCP |
Office of National Drug Control Policy |
|
SUPPORT Act |
Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act |
|
SAMHSA |
Substance Abuse and Mental Health Services Administration |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
June 16, 2026
Congressional Committees
Youth substance use is one of multiple challenges the U.S. faces related to illicit drugs that can lead to tragic results. Data from the U.S. Department of Health and Human Services’ (HHS) Centers for Disease Control and Prevention (CDC) showed 1,413 drug overdose deaths occurred among those age 18 and under in 2023.[1]
In March 2019, we named drug misuse as an emerging issue requiring close attention. In March 2020, we determined that national efforts to prevent, respond to, and recover from drug misuse were high risk—and subsequently added drug misuse to our high-risk report issued on March 2, 2021.[2] Although federal agencies have made progress in addressing drug misuse,[3] more progress is needed to fully address all of GAO’s five criteria for removal from our high-risk list.[4] As such, we continue to designate drug misuse as high-risk and it is included in our recent 2025 High-Risk report.[5]
To help curb youth substance use, the Drug-Free Communities Act of 1997 established the Drug-Free Communities (DFC) Support Program— a federal program providing grants for the establishment of community-based coalitions, youth-focused, and drug abuse prevention efforts.[6] The DFC program grants funding to community-based coalitions that focus on preventing and reducing youth substance use—which generally include (1) the illegal use or misuse of controlled substances under the Controlled Substances Act,[7] (2) the misuse of over-the-counter drugs, or (3) the use of alcohol, tobacco, or other related products.[8] The Office of National Drug Control Policy (ONDCP),[9] a component of the Executive Office of the President, administers and partners with CDC to manage the DFC program[10]—including the day-to-day grant management services.[11] ONDCP reported about 546 coalitions across the United States received DFC funding in fiscal year 2025—with each coalition eligible to receive up to $125,000 per year for up to a 10-year period.[12]
According to its officials, each year, ONDCP releases a national cross-site evaluation, which measure the effectiveness of the DFC program in achieving its goals.[13] Generally, as part of this evaluation, it reviews, analyzes, and presents information provided by the coalitions, including data related to four core measures.
The Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act (SUPPORT Act) includes a provision for GAO to review ONDCP’s programs and operations, including the DFC program, every 4 years.[14] This report examines the extent to which (1) the DFC program has met key program goals; and (2) examines the extent to which ONDCP has effectively managed the DFC program.
To address both objectives, we administered a census survey to 750 DFC-funded coalitions to gain their perspectives on the DFC program’s benefits and challenges.[15] The survey was available for respondents from July 2024 to late-August 2024.[16] Additionally, we conducted 13 site visits to meet with knowledgeable representatives at selected DFC coalitions located throughout the U.S.—representing a wide range of communities (e.g., rural/frontier areas, suburban, and urban)—to obtain detailed information on the selected coalitions’ operations (including challenges experienced) and inform the development of our survey instrument.[17]
To address our first objective, we conducted comprehensive quality reviews of ONDCP’s national cross-site evaluation reports published in 2024 and 2023.[18] We also assessed whether they followed the Office of Management and Budget’s (OMB) standards for conducting program evaluations.[19] We interviewed ONDCP’s contractor, ICF, to better understand the reliability and validity of data used and analyses performed to support reported DFC program outcomes. We also conducted statistical analyses to assess the four core measures’ associations with (1) Youth Risk Behavior Survey[20] and U.S. Census Bureau data, including demographic characteristics; and (2) data collected from our survey, including DFC coalition activities and program tenure.[21] We obtained and reviewed DFC program evaluation plans, DFC coalitions data collected by the evaluator, and national evaluation reports. Finally, we conducted a literature review and examined pertinent research studies to identify evidence-based practices for youth drug misuse prevention.
To address our second objective, we obtained and analyzed the DFC program’s national cross-site evaluations and interagency agreements to understand how ONDCP and CDC manage the program.[22] We reviewed DFC program guidance and interviewed officials from ONDCP and CDC to describe their program administration, management, and oversight efforts—including mechanisms in place to manage grantee compliance.[23] We also reviewed documentation of ONDCP’s efforts to track its progress.
Additionally, we interviewed ONDCP and CDC officials to identify how they conduct program oversight and assess the efficiency and effectiveness of the DFC program. We obtained and analyzed ONDCP’s budget data and Congressional Budget Submissions to identify the DFC program’s annual appropriations, grant awards, administrative costs, and carryover balances. We also interviewed ONDCP officials to identify the extent to which the DFC program’s administrative related carryover balances are disclosed (including ONDCP’s planned use for the available carryover funds) to Congress during its annual budget process for each fiscal year 2018 through 2025. For a more detailed discussion on our scope and methodology, see appendix XI.
We conducted this performance audit from July 2023 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
DFC Program Goals
According to ONDCP, the DFC program’s two major goals are to:[24]
1. establish and strengthen collaboration among communities, public and private non-profit agencies, and federal, state, local, and tribal governments to support the efforts of community coalitions working to prevent and reduce substance use among youth; and
2. reduce substance use over time among youth and adults by addressing the factors in a community that increase the risk of substance use and promoting the factors that minimize the risk of substance use.[25]
Based on ONDCP guidance, coalitions receiving grant funds through the program aim to make annual progress on four core outcome measures. These relate to the prevalence of drug use among youth in their communities over the past 30 days, youth’s perceptions of the risk, and the separate perceptions of parental and peer disapproval of drug use. Table 1 describes each of the four core outcome measures.
|
Core Measures |
Description |
|
Past 30-Day Prevalence of Use |
Percentage of youth who reported misusing prescription drugs or using alcohol, marijuana, or tobacco, at least once in the past 30 days. |
|
Perception of Risk |
Percentage of youth who reported they perceived people who misuse prescription drugs or use alcohol (binge use), marijuana, or tobacco risk harming themselves to a moderate or great extent. |
|
Perception of Parental Disapproval |
Percentage of youth who reported they perceived their parent, guardian, or caregiver would feel the misuse of prescription drugs or regular use of alcohol, marijuana, or tobacco is wrong. |
|
Perception of Peer Disapproval |
Percentage of youth who reported they perceived their peers would feel the misuse of prescription drugs or regular use of alcohol, marijuana, or tobacco is wrong. |
Source: GAO analysis of DFC program information. | GAO‑26‑106949
Community-Based Coalitions
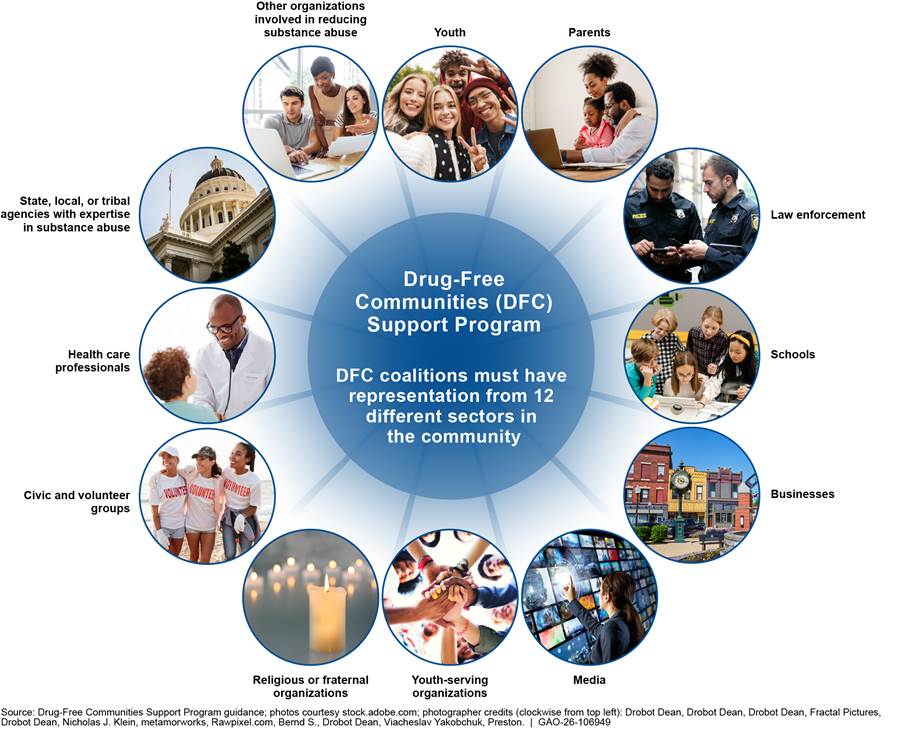
The DFC program awards grants to community-based coalitions that aim to prevent youth substance use and misuse. The program seeks to mobilize community leaders to identify and respond to the drug problems unique to their community and change local community conditions tied to substance use. As shown in figure 1 below, each DFC coalition is required to have a volunteer representative from each of 12 community sectors.[26] Some of these sectors include, but are not limited to youth; parents; schools; law enforcement; health care professionals; and state, local, or tribal governmental agencies with expertise in the field of substance use and misuse.[27] DFC grants are intended to support community-based coalitions and the activities they carry out.
Figure 1: Required Composition of Coalitions Receiving Grants through the Drug-Free Communities (DFC) Support Program
In fiscal year 2024, the DFC program awarded grants to 751 coalitions located throughout the U.S.—including the District of Columbia, Puerto Rico, and other U.S. territories (Guam and Virgin Islands)—that serve broad geographical areas (i.e., urban, suburban, and rural/frontier) and culturally diverse communities. According to ONDCP’s national cross-site evaluation, coalitions are present in diverse geographical areas throughout the U.S., they can build the local capacity (e.g., leverage the expertise and knowledge of community representatives) needed to prevent and reduce youth substance use. According to ONDCP’s 2025 Congressional Budget Submission, an estimated 77 million Americans (23 percent of the U.S. population) lived in communities served by DFC coalitions receiving funding in fiscal year 2022. This included approximately 3.1 million middle school students ages 12 to 14 and 4 million high school students ages 15 to 18—about 23 percent of all youth for each grade level.[28] Figure 2 shows the 2024 locations of the DFC coalitions throughout the United States, along with each state’s drug overdose rate (from October 2023 to September 2024), and coalitions we visited.
Figure 2: Locations of Drug-Free Communities (DFC) Support Program Coalitions in the United States, Drug Overdose Death Rate (by State), and Coalitions Visited
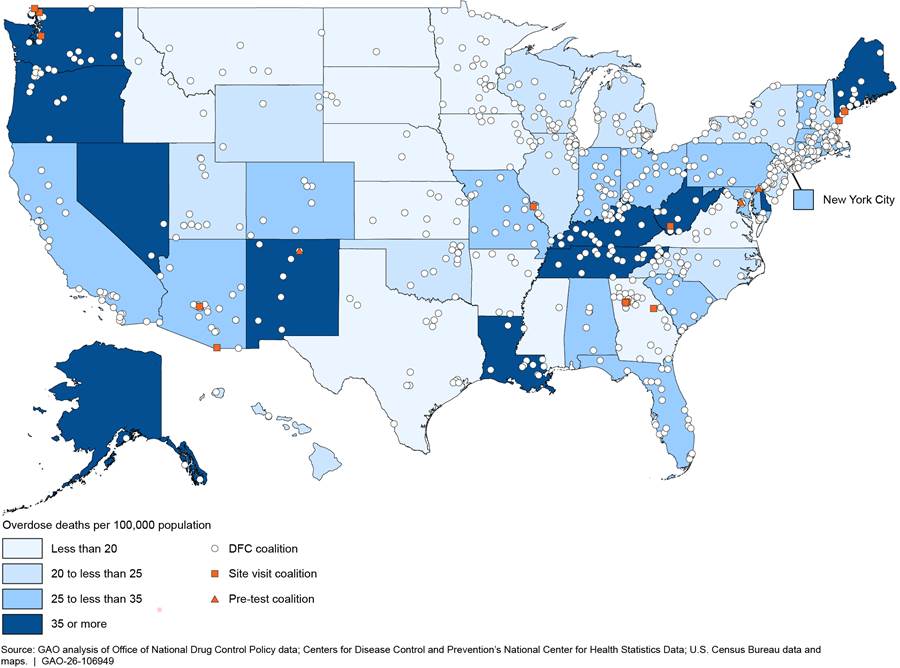
Note: The drug overdose death rate was calculated by dividing the predicted number of drug overdose deaths between October 2023 through September 2024 by the 2024 state population totals. The values are reported as overdose deaths per 100,000 population. The data on drug overdose deaths are from the Centers for Disease Control and Prevention’s National Center for Health Statistics Vital Statistics Rapid Release downloaded on March 18, 2025; they are provisional data and subject to change. The state population totals are from the U.S. Census Bureau’s State Population Totals: 2020-2024 vintage 2024. There are 10 DFC coalitions in U.S. territories, including 8 in Puerto Rico, 1 in Guam, and 1 in the U.S. Virgin Islands. Provisional drug overdose death count data were not available for these areas as of the download date and are therefore not shown. We visited the coalitions indicated in the map during fiscal year 2024.
Grant Awards and Funding
According to ONDCP officials, since its inception in 1997, the DFC program has been appropriated approximately $2.3 billion to support its mission to date. In fiscal year 2025, ONDCP allocated about $96.2 million for DFC grants and awarded DFC grants to 546 coalitions across the U.S.[29] ONDCP was appropriated approximately $835 million to manage and administer the DFC program over an 8-year period—fiscal years 2018 through 2025. DFC program funds are “no year funds” meaning the funds remain available until fully expended irrespective of the fiscal year. As shown in figure 3, ONDCP funded 5,718 DFC grant awards (an annual average of 715 coalitions with ONDCP allocating about $94 million for grant awards) over that 8-year period.
Figure 3: Drug-Free Communities (DFC) Support Program’s Number of Grant Awards and Available Appropriated Amount for Grant Awards—Fiscal Years 2018 Through 2025
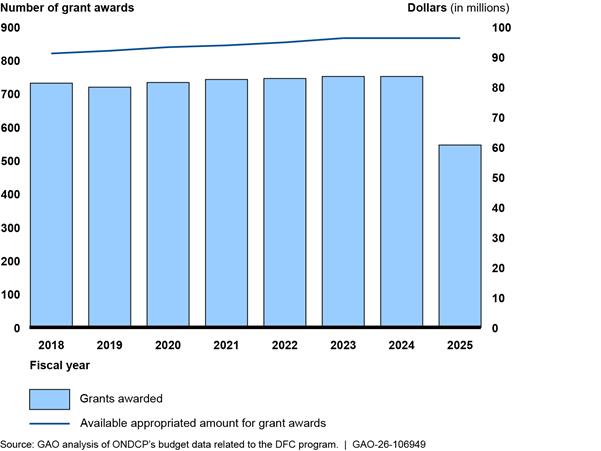
Note: For each fiscal year identified, the number of DFC grants awarded includes the four types of grants available to coalitions through the DFC program:(1) new; (2) continuation; (3) mentoring; and (4) mentoring continuation. ONDCP officials stated that the new and continuation grants represent a majority of the DFC grants awarded. See Appendix VI for additional information on the types of DFC grants. The available appropriated amount for grant awards represents the annual appropriated amount available for the DFC Support Program in the given fiscal year after ONDCP’s allocation of funds for administrative expenses. According to ONDCP officials, the mentoring grant has not been funded since the management of the DFC Program transitioned to CDC in 2020.
During this period, ONDCP allocated about $82 million to the DFC program for administrative costs (i.e., grant management and oversight efforts). Pursuant to 21 U.S.C. § 1524(b), not more than 8 percent of the funds appropriated for carrying out the DFC program may be used by ONDCP to pay for administrative expenses associated with its responsibilities. However, in recent years, ONDCP’s annual appropriations have specified the maximum amount of the appropriation that could be used for administrative expenses which exceeded the statutory limitation of 8 percent of the funds appropriated in 21 U.S.C. § 1524(b). For example, in fiscal year 2025, ONDCP was appropriated $109 million to operate the DFC program—which included up to nearly $12.8 million available for administrative expenses—almost 12 percent of the program appropriation.[30]
Grants Management Structure and Processes
Since 2020, ONDCP and CDC have operated the grant program through an interagency agreement that they update annually.[31] Specifically, ONDCP oversees the strategic planning and funding of the DFC program, while CDC conducts day-to-day management, such as interacting with grantees on a regular basis and reviewing their activities. ONDCP officials told us their staff are actively involved in all stages of the grant making process from Notice of Funding Opportunity development to grant closeout and/or termination. The DFC program operates on a yearly grant cycle. Appendix VII provides an overview of the DFC grant life cycle.
ONDCP’s Oversight and Evaluation of DFC Program
ONDCP seeks to assess the effectiveness of the DFC program through an annual national cross-site evaluation, which measures how the program performed in achieving its goals. As discussed earlier in this report, ICF evaluates the DFC program’s performance by using a mixed method approach, involving both qualitative and quantitative data collection and analysis. In its role managing day-to-day operations of the program, CDC reviews all CDC-managed grants, which include DFC awards, to ensure compliance with fiscal and grant management policies.
ONDCP monitors the performance of DFC coalitions through regular grantee reporting, such as annual progress reports and through weekly meetings with CDC. The DFC program does not formally assess efficiency, but requirements for grantees to match federal funds with additional funding from non-federal sources helps to improve grantees’ efficiency,[32] according to ONDCP officials. For a summary of ONDCP’s activities for overseeing the DFC program, see table 2 below.
Table 2: Office of National Drug Control Policy (ONDCP) Oversight of the Drug-Free Communities (DFC) Support Program
|
Oversight Activity |
Description |
|
National Evaluation |
Each year, ONDCP releases a national cross-site evaluation, which aims to measure the effectiveness of the DFC program in achieving its goals. The purpose of the national evaluation is to monitor data to demonstrate the progress of the DFC program and its grantees. ONDCP uses the evaluation to compile data reported by grantees and interpret them to give federal managers and policymakers a clear vision of what is working at the local level. |
|
Application Review |
ONDCP, in coordination with CDC, oversees DFC coalitions through its review of the documentation applicants submit in their applications. These materials, for example, enable the DFC program to ensure applicants have the personnel for overseeing the financial aspects of the grant (such as bookkeeping or accounting services), have an adequate financial management system, and comply with statutory funding requirements. |
|
Performance Reporting |
DFC grantees are required to submit annual progress reports to ONDCP that describe their community and coalition members, coalition accomplishments and challenges, and assessment activities. Progress reports typically describe coalition efforts (such as target substances), key efforts to prevent drug misuse (such as protective school factors), and key risks that could lead to drug misuse (such as family trauma or stress). Progress reports are to also identify measures of short-term, intermediate, and long-term outcomes, which can serve as benchmarks for measuring progress. |
Source: GAO analysis of ONDCP and CDC information. | GAO‑26‑106949
In 2017, we reported on the grantees’ compliance with the DFC program’s statutory requirements and need to strengthen the monitoring of grantee activities.[33] We recommended that HHS’s Substance Abuse and Mental Health Services Administration (SAMHSA), which managed the program for ONDCP at the time, (1) develop an action plan with time frames for addressing any deficiencies it finds through its reviews and making systemic changes to mitigate deficiencies on a prospective basis to strengthen the grant monitoring process, and (2) develop and implement a method for ensuring that the grantee status reports it provides to ONDCP are complete and accurate. SAMHSA agreed and implemented both recommendations—which resulted in the development of ONDCP’s web-based grant monitoring system.
Previously, in 2008, we reported on the DFC program and found weaknesses in grant program administration.[34] We recommended that ONDCP (1) strengthen internal controls; (2) ensure that funded grant applicants satisfy statutory eligibility criteria; and (3) more clearly define its own and SAMHSA’s roles and responsibilities. ONDCP implemented the three recommendations.
Data Limitations and Undefined Performance Targets Hinder Assessments of Progress on the DFC Program’s Two Key Goals
Our review of the DFC program data found significant limitations that make it challenging to determine the program’s impact in reducing youth substance use. These data limitations include inconsistencies in how coalitions collect data and report out on the program’s four core measures. In addition, ONDCP’s annual national cross-site evaluation includes analyses that were not described in sufficient detail for stakeholders to understand how the evaluation was conducted and how it reached its conclusions. Further, most coalitions we surveyed reported meeting the DFC program’s other key goal of engaging community sector members in their substance use prevention efforts among youth. However, ONDCP has not defined and documented similar performance goals or measures to assess the DFC program’s efforts to establish drug prevention partnerships in their respective communities.[35]
Data Limitations Present Challenges to Determining DFC Program’s Effect on Reducing Youth Substance Use, Although Some Data Provide Helpful Insights
Significant Data Issues Limit Evaluations of DFC Program’s Impact on Youth Substance Use
Our review of the DFC program data found significant limitations that make it challenging to determine the effects of the DFC program on preventing or reducing youth substance use.[36] These data limitations include inconsistencies in how coalitions collect data on the program’s four core measures and how these data are reported in the annual evaluations. Specifically, we found that the four core measures data reported in the annual evaluations were not always comparable and the sources of these data were not clearly identified. See table 3 below for further description of examples of these limitations.
|
Limitation |
Description |
|
Limited data availability |
Measures and format are standardized; however, there is variability in the cadence of grantee reporting as well as sample size, according to the Office of National Drug Control Policy officials. |
|
Limited data comparability |
Grantees submit data collection instruments for review and approval to ensure consistency, according to ONDCP officials. For example, core measures whose wording on the survey instrument does not align with the required DFC core measure wording, or is missing, may not be submitted by the grant recipient during their progress report submission. These are then excluded from the cross-site evaluations, according to ONDCP officials. |
|
Unidentified sources of data |
The data sources used to generate results are not clearly identified in the annual evaluation. According to the evaluation, for example, coalitions submit annual progress reports that include information such as descriptions of the community where coalitions perform substance use prevention activities and with whom they collaborate with, and details and descriptions of drug prevention activities implemented during the reporting period, among other required data. |
Source: GAO analysis of ONDCP’s DFC national cross-site evaluation reports and interviews with officials from ONDCP and the national cross-site evaluation contractor. | GAO‑26‑106949
Note: Pursuant to 21 U.S.C. § 1532(a)(6)(B)(ii), coalitions are required to conduct biennial surveys (or incorporate local surveys in existence at the time of the evaluation) to measure the progress and effectiveness of the coalition. As noted in the evaluation, another challenge related to core measures is that each DFC coalition makes local decisions regarding how to collect core measure data, such as where to administer the survey, what grades to collect data from, the length of the survey used, and the order in which survey items are presented.
ONDCP’s contractor acknowledged the limitations with the data they have available for conducting the annual cross-site evaluations. For example, in written responses to GAO, ONDCP’s contractor noted that school personnel may have concerns with certain survey items for youth, the amount of time required for youth to participate in surveys, or whether they are tracking parental consent properly. Coalitions may also obtain data from sources such as state health surveys or Youth Risk Behavior Survey data that may not include all outcome measures that the DFC program monitors. Finally, based on our assessment of evaluation reports, the evaluations do not clearly identify the different data sources that the evaluation team uses to derive its results.
The contractor also acknowledged in the cross-site evaluation report that “it is not possible to establish a causal relationship” between substance use prevention activities in communities and the program’s core measures data.[37] As such, the claim—included in the executive summary of the cross-site evaluation report—that the DFC program is meeting its strategic goal of reducing substance use among youth may be overstated. Figure 4 is an extract taken from the June 2025 cross-site evaluation stating the DFC program’s impact on its efforts to reduce substance use among youth.
Figure 4: Selected Statements on the Effectiveness of the Drug-Free Communities (DFC) Support Program from the June 2025 National Cross-Site Evaluation
Claims about the impact of the DFC program are not supported given the significant limitations in the data that ONDCP’s contractor used in its evaluations of the DFC program.[38] When interviewed about the data they used to support the statement that the DFC program met its goal of preventing and reducing youth substance use, the contractor described comparing recent outcomes within each community on the four core measures to those from previous years to observe whether youth served by DFC coalitions have significantly lower rates of drug use over time (within coalition longitudinal trend analysis). Where possible, DFC data are also compared to national estimates.[39] According to the evaluation, this monitoring of trends suggests the DFC program was successful in helping to reduce substance use among youth.[40]
Researchers have long noted the challenges of documenting causality for community-based programs such as the DFC. They include, but are not limited to:
· small sample sizes and lack of suitable comparison groups to compare outcomes;
· inability to parse out the program’s influence from other trends and interventions happening at the same time;
· wide variability among communities on what strategies are used; and most notably, the
· length of time it takes for longer term outcomes to show up.
To address challenges like these, federal agencies can undertake several strategies: (1) collaborating with others on a common reporting format to ensure that the data they collect are sufficiently consistent; (2) supporting a special data collection that abstracts data from state systems and recodes them into a common format that would permit cross-state and national analyses; or (3) conducting periodic sample surveys or one-time studies to collect new data that supplements data from existing performance reporting systems.
According to ONDCP officials, the DFC program’s 8 percent administrative spending cap poses limitations on the kinds of administrative support they can provide, including funding more robust data collection efforts. The officials added that having more administrative funds for the program could help expand its data collection efforts and strengthen the grant’s oversight system. However, for FY 2022, the Consolidated Appropriations Act, 2022, appropriated $106 million for the DFC program, of which not more than $11.25 million (which represented nearly 11 percent of the appropriated amount for the program) was available for administrative expenses.[41] This set amount in the appropriations act was an increase from the program’s administrative cap of 8 percent of the funds appropriated pursuant to 21 U.S.C. § 1524(b). ONDCP officials told us they did not use the additional funding to improve the program data.
According to the officials, they do not require coalitions to use a single data collection instrument because they want to build in as much flexibility as possible for coalitions’ required annual reporting. As noted above, the program’s authorizing statute allows coalitions to conduct their own surveys or to incorporate existing local surveys to measure the progress and effectiveness of the coalition. The committee report accompanying the Drug-Free Communities Act of 1997 noted that the committee was sensitive to comments from the field that requiring surveys can be costly and that collecting existing data can be as effective and more cost-efficient.[42] As such, the committee included language giving coalitions the flexibility to use such existing data. As Congress recognized, quality data collection can be time and resource intensive, which is an important factor to be weighed in considering options for improved data collection. However, some of the issues with the program data we and the contractor observed were not related to coalitions’ use of a single data collection instrument and there may be opportunities to identify other relevant data to help better understand the program’s impact.[43]
According to the Standards for Internal Control in the Federal Government, management should use quality information to make informed decisions and evaluate the entity’s performance in achieving key objectives. Specifically, management processes the obtained data into quality information that supports the internal control system. Quality information meets the identified information requirements when relevant data from reliable sources are used and is appropriate, current, complete, accurate, accessible, and provided on a timely basis. Management uses the quality information to make informed decisions and evaluate the entity’s performance in achieving key objectives and addressing risks.[44]
Additionally, we previously found that many federal programs can find it challenging to assess the program’s effectiveness in achieving its key goals due to difficulties with obtaining data on those goals.[45] For example, this can occur because a federal program has limited control over how service providers collect and store information.
Having quality data could better enable ONDCP and CDC to better determine the DFC program’s impact—specifically, whether the DFC program caused reduction in substance use among youth. Data quality gives confidence that analyses and insights drawn from that data are sound and defensible. More reliable data would also help prevent risks associated with incomplete data, such as flawed analyses, wasted resources, and making faulty programmatic choices. Finally, reliable data could increase congressional and public confidence that the projected outcomes are worth the DFC program’s costs. However, quality data collection can be time and resource intensive, which is an important factor to be weighed in considering options for improved data collection.
ONDCP Does Not Fully Document the Methodology Used to Develop its National Cross-Site Evaluation Reports
ONDCP’s cross-site evaluation does not include a full discussion of the methodology it used to arrive at its findings and conclusions. A federal evaluation must be transparent in the planning, implementation and reporting phases to enable accountability and help ensure that aspects of an evaluation are not tailored to generate specific findings, according to OMB’s program evaluation guidance.[46]
ONDCP’s annual national cross-site evaluation includes analyses that were not described in sufficient detail for stakeholders to understand how the evaluation was conducted and how it reached its conclusions. As part of our review, we requested information on the methodology used for the analyses in the evaluation report. In response, the contractor described comparing recent outcomes on the four core measures to those from previous years to observe whether youth served by DFC coalitions have significantly lower rates of drug use than national estimates.[47]
According to ONDCP’s contractor, ONDCP does not require full documentation and reporting of the methodology in the cross-site evaluation reports in an effort to keep the reports understandable to its intended audiences. The contract officials said the evaluation reports included more methodological details in the past, including a lengthy technical analysis. However, ONDCP officials requested that the reports be shortened and less technical to improve the likelihood that stakeholders would read the reports.
While publishing evaluation reports that are understandable to a lay audience is important, a complete description of the evaluations’ methodologies could be discussed in the appendix of the reports. In doing so, the evaluator’s methods and resulting conclusions are transparent to all interested parties that may want to replicate the analysis. This approach would also help ONDCP and the program’s stakeholders better understand and appropriately assess the results and conclusions of the evaluation.
By not requiring that the contractor include the complete methodology used to develop the DFC program’s annual cross-site evaluations, it is unclear how the evaluators reached their conclusions about whether the program is achieving its goal of reducing substance use and misuse among youth.
Available Data Provide Some Useful Insights on Relationships Between Aspects of the DFC Program and Reported Outcomes
Available data shed light on coalitions’ efforts to reduce substance use among youth. These analyses provide valuable information about coalitions’ efforts to implement the DFC program and their perceptions of program results. However, findings from these analyses may be a result of several factors—including those unrelated to the beneficial impacts of the program—and should not be used to draw conclusions about the impact of the program. ONDCP’s national cross site evaluation explored the extent to which DFC coalitions implemented the DFC program as intended. We also conducted analyses that allow one to explore activities associated with the DFC program and DFC coalitions’ reported perceptions of outcomes on core measures.[48] Specifically, we analyzed data from the Youth Risk Behavior Survey to assess drug use, reported data from our survey of DFC coalition program officers, and conducted regressions to highlight any associations between the DFC program characteristics and outcomes on the four core measures.[49]
ONDCP’s National Cross-Site Evaluation. ONDCP’s contractor assessed the extent to which DFC coalitions followed the national program logic model when carrying out its substance use prevention activities.[50] ONDCP encourages DFC coalitions to follow the logic model framework, as successful implementation of a well-designed model may likely produce desired long-term outcomes. The contractor analyzed progress report data on coalitions’ resource investments, coalition activities, and staff perceptions of changes in awareness and behavior, among other things. The contractor found: high community sector representation; strong use of evidence-based practices for preventing substance use; and a keen focus on addressing risk factors present in DFC communities, among other things. According to the evaluation, DFC coalitions bring together a diverse range of community members who identify and work to prevent and reduce youth substance use through building capacity of those engaged with the coalition and through implementation of a wide range of prevention activities. In the evaluation, these findings indicate that the majority of coalitions are implementing the program as intended. Further, these prevention activities have the potential to directly impact current participants but may also bring about long-term change, according to the evaluation.
ONDCP officials told us they use the information from the evaluation reports for different purposes. For example, ONDCP used information gleaned from the evaluation reports to improve existing technical assistance support to coalitions. This information also facilitated information-sharing among coalition leaders on evidence-based practices, performance measure improvement, and best practices on program administration, according to ONDCP officials.
DFC Coverage Areas. We analyzed data on 30-day drug use from the Youth Risk Behavior Survey to assess whether there was a difference between high school youth that lived in zip codes served by a DFC coalition and those that were not served by a coalition.[51] We did not find statistically significant differences in substance use (e.g., tobacco, alcohol, marijuana, and prescription drugs) among high school youth in DFC and non-DFC areas. See appendix I for more details on this analysis.
DFC Program Tenure. We analyzed our survey data to explore whether DFC grantees who had been in the program longer differed on self-reported performance when compared to those coalitions with a shorter tenure. Using our survey data, we found a statistically significant association in our survey data between coalitions’ tenure in the DFC program and positive outcomes for all core measures as reported in our survey data.[52] For example, from analysis of our survey data, coalitions in years 4-7 of the grant were 5.8 times more likely to report greater reductions in 30-day drug use compared to coalitions in years 1-3 of the grant. According to ICF officials, coalitions with longer tenures in the DFC program may demonstrate greater positive benefits because they have experience, refined strategies, established community relationships, and gained valuable insights on implementing substance use prevention efforts. While this is plausible, analysis of our survey data does not support a causal link between program tenure and reduction in drug use because our analyses assess associations between these factors, not causality. In addition, threats associated with self-reported data and factors outside of the DFC program, such as a desire for DFC coalitions to present themselves favorably, may have influenced any actual positive outcomes. See appendix I for more details on this analysis.
DFC Coalitions’ Reported Outcomes. According to our survey of DFC coalitions, we found that an estimated 56 percent reported a reduction in 30-day drug use due to youth’s participation in the coalition’s programs and activities.[53] However, an estimated one-third of the coalitions surveyed were unsure or reported no change. Results were similar for the other core measures, as shown in table 4.
Table 4: Estimated Percentage of Survey Respondents Reporting Changes in the Four Core Measures Due to Drug-Free Communities (DFC) Support Program Participation
|
Core Measure |
Yes |
No |
Unsure |
|
Reduction in 30-Day Drug Use |
56.2% |
7.7% |
26.8% |
|
Perception of Risk |
59.5% |
9.2% |
22.0% |
|
Perception of Parent Disapproval |
51.8% |
12.7% |
26.2% |
|
Perception of Peer Disapproval |
57.0% |
9.7% |
24.1% |
Source: GAO analysis of its survey responses from DFC Coalitions. | GAO‑26‑106949
Note: The table does not include the percentage of survey respondents that did not respond to the question; therefore, percentages for each of the core measures do not sum to 100 percent. Approximately 9 percent of coalitions did not respond to the survey item for each core measure. Estimates account for the survey design and nonresponse based on DFC demographic region but may not fully account for all potential unmeasured response bias that may have influenced survey respondents. See appendix IX, table 16, which also includes the confidence intervals for each core measure.
As shown in figure 5, of those who reported they were unsure whether there was a change in 30-day drug use, an estimated 51 percent reported that lack of data or inability to obtain data directly from youth prevented them from determining whether there was a change. For example, coalitions reported that they were waiting on sources such as the Youth Risk Behavior Survey 2023 data to be released to collect information on that outcome measure. An estimated 13 percent of this group indicated that they could not be sure that the coalition directly affected the change because of reliance on secondary data sources (e.g., school district, or state or local government reports) for behavioral and attitudinal information. An estimated 12 percent did not have enough information to make comparisons because they were a new coalition.[54]
Figure 5: Estimated Percentage of Drug-Free Communities (DFC) Support Program Coalition Members Reported Reasons for Being Unsure About Coalitions Association with Changes in 30-Day Drug Use
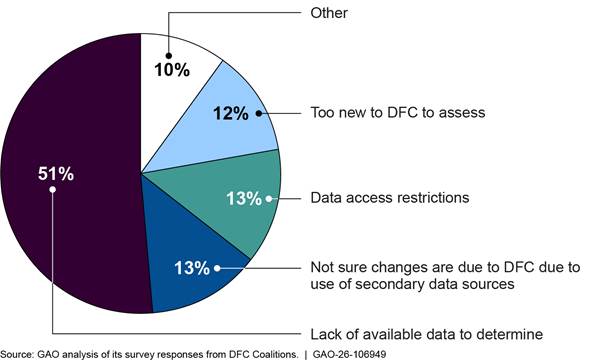
Note: Those respondents who indicated in Question 10 (see appendix IX, table 16) that they were unsure whether their coalition’s activities contributed to substance use reduction in their communities provided open-ended responses to explain their uncertainty. We coded these responses into five categories. Figure 5 shows the percentage of responses in each of those categories.
We conducted multivariate regression analyses to estimate the association between certain DFC survey responses, including the reported outcomes on the four core measures.[55] Figure 6 below presents the variables from our survey responses that were significantly associated with the outcome measure on 30-day drug use.[56] For example, we found that coalitions that sponsored a youth coalition within the last two years were over three times more likely to report a reduction in 30-day drug use.[57] See appendix II for associations between certain DFC survey responses and coalitions’ reported outcomes on the remaining three core measures.
Figure 6: Survey Responses Associated with Coalitions’ Reported Decrease in 30-Day Substance Use, by Odds Ratio
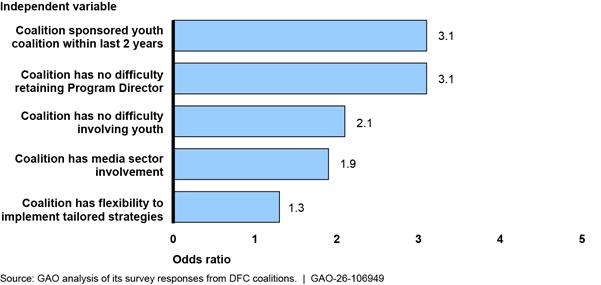
Note: Graph depicts the top five odds ratios greater than 1 for 30-day core measure that were significant at the 95 percent confidence level. Odds ratios were estimated from multivariate logistic regressions that accounted for the survey design and nonresponse based on DFC demographic region and controlled for Census Bureau demographic variables (ethnicity/race, population size, U.S. geographic region). We performed a nonresponse bias analysis and implemented weights to account for nonresponse and generate estimates that better generalize to the population of DFCs, based on characteristics of DFC regional demographics. Uncertainty is quantified through 95% confidence intervals. These adjustments may not fully account for all potential unmeasured response bias that may have influenced survey respondents.
Coalitions Report Meeting the Community Collaboration Goal, but ONDCP Does Not Have Clearly Defined Performance Targets for These Efforts
Most Coalitions Reported Meeting the Community Collaboration Goal but Some Reported Challenges Sustaining the Involvement of All Sectors
Most coalitions we surveyed reported meeting the DFC program’s other key goal of engaging community sector members in their substance use prevention efforts among youth. Our survey respondents reported experiencing some success in establishing involvement in their communities from the DFC program’s 12 required community sectors. For example, as part of our survey, an estimated 86 percent of the coalitions reported having representation in all twelve sectors.[58] However, an estimated 54 percent of coalitions reported they experienced challenges with retaining members from each of the 12 community sectors.[59] Further, though an estimated 68 percent of coalitions reported that retaining sector members did not have an impact on implementing the program in a sustainable manner, an estimated 21 percent reported that retention of sector members did affect sustainable program implementation.[60]
For example, in our survey, coalitions that reported closer engagement with the media sector were almost two times more likely to report reductions in 30-day drug use than those that reported lesser engagement.[61] Moreover, regression analysis of the survey data indicates that respondents who perceived challenges in securing sector involvement are associated with less favorable reported outcomes on the four core measures, which serve as the primary indicators of the DFC program’s drug prevention efforts.[62] However, analysis of our survey data does not support a causal link between sector involvement and outcomes on core measures, as factors outside of the DFC program may have influenced any positive outcomes.[63]
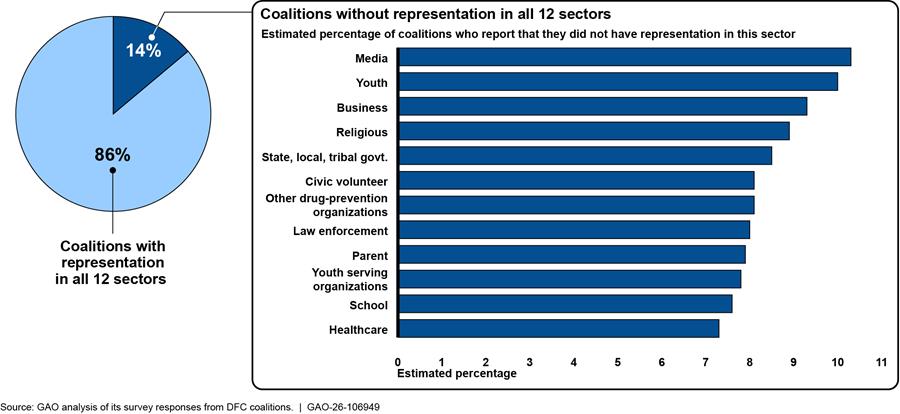
Overall, over half of the coalitions (7 of the 13) that we interviewed reported experiencing some challenges in sustaining the involvement of the 12 community sector representatives. Specifically, our survey indicated that an estimated 14 percent of the DFC coalitions reported that they did not have representation for all 12 sectors—primarily because these positions are voluntary in nature and it can be challenging to maintain participation.[64] Officials from seven of the 13 coalitions we visited reported experiencing challenges with recruiting and retaining—mainly in the religious-based or law enforcement sectors—at least one of the required 12 sector representatives. Officials from five of the 13 coalitions we visited said the challenges they experienced with recruiting and retaining certain sector representatives are due to the voluntary nature of the positions, historical secular traditions in the respective region or state, and some communities’ distrust of law enforcement. Figure 7 shows the results of DFC coalitions we surveyed and asked if all 12 community sectors were represented.
Figure 7: GAO Survey of Drug-Free Communities (DFC) Support Program’s Coalitions Representation in Community Sectors, August 2024
ONDCP Does Not Have Clearly Defined Performance Targets for Community Collaboration Goal
ONDCP has not defined and documented performance goals or measures to assess the DFC program’s efforts to establish drug prevention partnerships in their respective communities.
We previously found that results-oriented organizations set performance goals to clearly define desired program outcomes and develop performance measures that are clearly linked to the performance goals.[65] Further, we identified additional actions that can be leveraged by federal leaders and employees, or others, to help develop and implement these different performance goals.[66] Program performance goals and measures communicate what results the agency seeks and allow agencies to assess or demonstrate the degree to which those desired results are achieved. Performance measures also show the progress the agency is making toward achieving program goals.
Consistent with the DFC program’s key goal of establishing and strengthening collaboration among communities, an estimated 90 percent of coalitions we surveyed reported that they engaged with community sector members in their substance use prevention efforts. According to DFC program’s Notice of Funding Opportunity, coalitions are required to engage their respective communities in their drug prevention efforts. For example, coalitions are expected to work with their sector members to select and implement evidence-based and prevention-based practices to reduce substance use based on community needs.
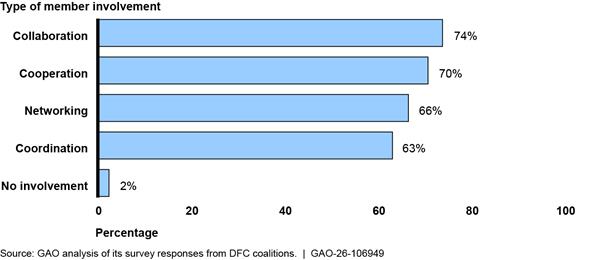
CDC encourages coalitions to use the SAMHSA Strategic Prevention Framework that provides information on engaging community sector members in their substance use prevention efforts to better address the needs of their community.[67] As shown in table 5, the framework identifies four ways in which sector members may involve themselves in those efforts.
Table 5: Types of Involvement Community Sector Members Use to Support Drug-Free Communities (DFC) Support Program Coalitions’ Prevention Efforts
|
Type of Involvement |
Description |
Example |
|
Collaboration |
Members create formal agreements (e.g., memoranda of understanding or contracts). They develop common data collection systems; partner on joint fundraising efforts; pool fiscal or human resources; and create common workforce training systems. |
“Let’s work together on a comprehensive plan to address the issue. After all, our missions overlap.” |
|
Cooperation |
Members publicize one another’s programs in newsletters, write letters of support of one another’s grant applications, co-sponsor trainings or professional development activities and/or exchange such resources as technology expertise or meeting space. |
“I’ll support your program, and you’ll support mine.” |
|
Coordination |
Stakeholders serve together on event planning committees and community boards or implement programs and services together. |
“Let’s partner on an event.” |
|
Networking |
Members share what they are doing during coalition meetings. They talk about community issues in which they all have a stake or communicate about existing programs, activities, or services. |
“Let’s talk and share information.” |
Source: A Guide to SAMHSA’s Strategic Prevention Framework. | GAO‑26‑106949
Most coalitions we surveyed reported that community sector members supported their coalitions’ efforts through all four types of involvement. Specifically, an estimated 74 percent of coalitions we surveyed reported that sector members engage in their prevention efforts through collaboration, as shown in figure 8.[68]
Coalitions we surveyed reported the various types of prevention activities they engage in with their communities. For example, coalitions reported that the business sector was involved in coalition work through cooperation, where they may publicize the coalition’s programs or exchange resources such as meeting spaces. During our site visits, coalition officials we interviewed also told us about their involvement with community sectors. For example, officials from one of the 13 coalitions we visited told us that their youth partner with local law enforcement to monitor the sale of alcohol beverages to individuals under the age of 21 years.
The DFC program uses various channels to communicate its performance toward one of its two chief performance goals—to reduce substance use among youth—including through the 2024 National Drug Control Strategy (Strategy), as well as the DFC program’s annual national cross-site evaluation.[69] For example, in the Strategy, ONDCP reports positive outcomes on the DFC program, including addressing alcohol and tobacco use among middle and high school students. These measures support one of the program’s two chief strategic goals—to reduce substance use among youth. Monitoring these performance targets over time provides ONDCP and CDC valuable insights into the potential impact of their youth drug prevention efforts.
However, ONDCP has not defined and documented similar performance goals or measures to assess the DFC program’s efforts to establish drug prevention partnerships in coalitions’ respective communities. According to ONDCP officials, annual performance goals and measures aimed at establishing collaboration in drug prevention efforts are not standardized but are determined by each coalition in accordance with its unique local circumstances. The officials said this approach recognizes that DFC-funded coalitions are at different stages of capacity development and are engaged in ongoing efforts to recruit and retain coalition members.
While establishing performance goals and measures at the local level remains essential, this does not fully capture its assessment of progress toward the DFC program’s overarching objective of establishing and strengthening community collaboration by incorporating program-wide performance measures. Such a measure, for example, could include tracking the number of communities that successfully establish drug prevention partnerships comprising representatives from all twelve required sectors over the course of the DFC recipients’ potential 10-year grant period. Having clearly defined goals related to building drug prevention partnerships in communities would better ensure that ONDCP can determine what type of evaluative information it needs to monitor and track the progress of the DFC program. Further, documenting or defining performance measurements—with specific annual targets or goals to establish and strengthen drug prevention collaboration within communities—would ensure that ONDCP can demonstrate its progress in achieving them.
ONDCP Has Not Consistently Enforced Grantee Compliance with Community Involvement Requirement or Provided Transparency in Budget Submissions
ONDCP has taken some steps to effectively administer the DFC program—including working to ensure new coalitions meet program requirements and have access to mandatory training. In addition, ONDCP has established an internal controls framework to help ensure grantee compliance. However, ONDCP has not consistently enforced compliance with the statutory requirement that DFC coalitions maintain the involvement of all community sectors.[70] Further, ONDCP has not been fully transparent in its budget submissions.
ONDCP Ensures New DFC Coalitions Meet Program Requirements and Provides Them Ongoing Training
ONDCP has taken steps to ensure that new coalitions meet DFC program requirements and to provide mandatory training. With respect to the program, by law, the Director of ONDCP is to establish a program to support communities in the development and implementation of comprehensive, long-term plans and programs to prevent and treat substance use and misuse among youth.[71] In carrying out the program, the Director of ONDCP is required to:
· make and track grants to grant recipients;
· provide for technical assistance and training, data collection, and dissemination of information on state-of-the-art practices that the Director of ONDCP determines to be effective in reducing substance use and misuse; and
· provide for the general administration of the program.[72]
The roles and responsibilities of ONDCP and CDC are outlined in a MOU. The MOU includes ONDCP’s program implementation and compliance guidance and CDC’s pre- and post-grant processes for new and continuing DFC grant awards. Our review assessed the program’s pre- and post-award activities, training and other technical supports, and general administration.
DFC Pre-award Activities
ONDCP and CDC initiate pre-award management activities before disbursing funds to new grantees. Pre-award activities begin when the agency plans for solicitation through the Notice of Funding Opportunity, and ends after applications have been reviewed and scored. According to CDC officials, CDC conducts a risk review to evaluate risks posed by applicants prior to receiving a federal award, as required by regulation.[73] This risk review for compliance and assessing risk is to be performed prior to issuing new, continuation, and competing continuation awards.
Specifically, according to CDC officials, CDC’s Office of Grants Services assesses an applicant’s compliance using information from public data sources including: SAM.gov, USASpending.gov, and the Tracking Accountability in Government Grants System.[74] For example, during one of our site visits, a DFC coalition official described this pre-award review process their organization underwent with CDC as exhaustive, including assessments of staff familiarity with the program’s administrative and reporting requirements.
CDC provides this program management through a total of 19 full-time staff, including 13 project officers and 6 grants management specialists.
DFC Post-award Activities
According to CDC officials, post-award activities for the DFC program begin when a successful applicant expends awarded funds and starts work on achieving the outcomes of the grant. According to CDC officials, post-award activities encompass ongoing monitoring of the funded project and conclude after the period of performance ends and closeout activities are completed.
According to CDC officials, CDC continuously monitors coalitions’ performance, activities, and progress through regular engagement. According to the MOU, another part of CDC’s role as the day-to-day manager of the DFC program is to notify ONDCP regarding recipients that are not compliant with the terms and conditions of the awards or are not meeting the expected grant requirements and performance goals.
According to CDC officials, if DFC grant recipients do not comply with the grant’s requirements, CDC Project Officer and Grants Management Office may consider enforcement actions as allowable under applicable grant regulations. CDC officials provided an example of when they terminated a grantee due to non-compliance, including failing to submit required progress reports and non-responsiveness. According to the MOU, the following are examples of non-compliant recipient actions:
· has a documented history of poor performance and/or non-responsiveness;
· is not financially stable;
· has a management system that does not meet applicable standards; or
· has not conformed to the terms and conditions of the award.
ONDCP officials stated that they have also developed a grants management and oversight system (DFC Management and Evaluation, or DFC-Me) to assist with the administration of the DFC program.[75] According to ONDCP officials, DFC-Me also functions as a portal for coalitions to submit their annual progress reports, core measure data, and sharing best practices. For example, some of the key findings from the annual progress reports include evidence of the program’s broad reach across a variety of community types (i.e., urban, rural, and suburban locations), diverse populations of youth, and extensive community sector partnerships.
In addition, ONDCP officials stated that DFC-Me enables program managers to collect and maintain real-time data on DFC grant recipients. For example, the system collects and maintains information on DFC coalitions’ status of compliance with program terms and conditions, its assigned CDC Project Officer, grant recipient contact information, upcoming events, and email notifications.
ONDCP officials also told us their offices meet weekly to discuss critical management issues and fiscal areas of the program’s implementation which includes debriefs of key program processes to determine program management efforts that are working effectively. The officials said additional topics during these meetings may include conducting necessary virtual or in-person site visits, identifying non-responsive grant recipients, reviewing and establishing the program’s grant funding process and timelines, planning upcoming trainings or webinars, and developing and streamlining the program’s Notice of Funding Opportunity.[76] ONDCP officials said these discussions then guide and inform future policies and procedures.
Training and Other Technical Supports
As part of its program management requirements, we found that ONDCP and CDC provide technical assistance and data collection support to DFC coalitions. According to CDC officials, CDC provides programmatic technical assistance related to the pre- and post-award processes for new and continuation DFC grant awards. According to ONDCP officials, ONDCP provides the DFC coalitions with monthly training that focuses on annual performance reporting, progress reporting, and the four core outcome measures. ONDCP officials noted that these training offerings have been well-attended and provide important opportunities for coalition officials to share among themselves and to ask questions.
ONDCP officials also noted the DFC-Me online portal provides grant managers with the ability to identify technical assistance needs. In addition, in 2021, ONDCP awarded a 5-year grant to CADCA to implement the National Community Anti-Drug Coalition Institute, which serves as a center for providing technical assistance, evaluation, research, and capacity building for community anti-drug coalitions throughout the U.S.[77]
According to ONDCP officials, the Institute allows the program to provide coalitions with program management support both in-person and through virtual platforms. Some of the programming offered throughout the year includes coalition training, sharing information on drug prevention evidence-based and practice-based strategies and activities, drug prevention principles and curriculum analysis, and the sharing of enhanced search tools for evidence-based interventions with coalitions.
General Administration of DFC Program
To assist in its oversight role, ONDCP entered into an interagency agreement with CDC’s National Center for Injury Prevention and Control in 2020 to help manage the program. Officials said working with CDC in this role provides more program oversight opportunities and coalitions receive a higher level of customer service to assist in implementing the grant’s goals and objectives.
In addition to its program administration and oversight structure, ONDCP provides required training through the National Coalition Institute to help coalitions mobilize their communities and to recruit and retain coalition members so that they are best positioned to implement their prevention interventions.
The DFC Program Uses an Internal Controls Framework to Help Manage Compliance-Related Risks
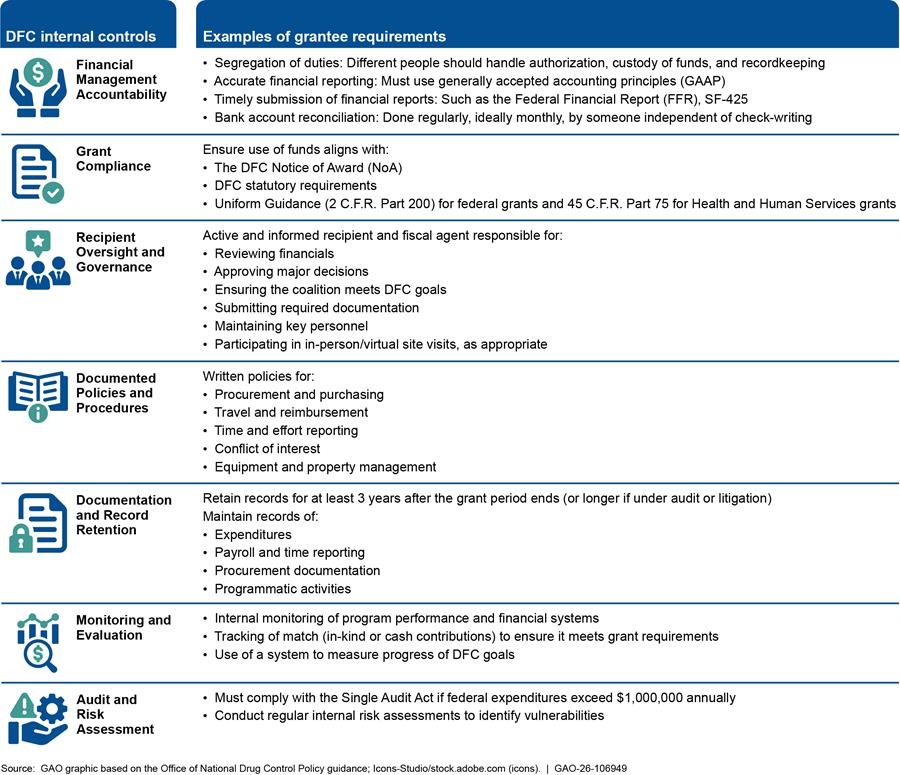
According to CDC officials, CDC establishes an internal controls environment at the application stage of the DFC program to help manage grantee compliance and other risks. Specifically, CDC’s internal controls framework begins by conducting pre-award assessments of DFC applicants to determine the risk an applicant poses to meeting federal programmatic and administrative requirements. Figure 9 identifies the DFC program’s internal controls framework, including examples of grantee requirements.
Figure 9: Drug-Free Communities (DFC) Support Program’s Internal Controls Framework and Examples of Grantee Requirements
According to ONDCP and CDC officials, the DFC program employs a multi-pronged strategy to oversee grantee program management throughout the grant lifecycle. CDC officials said this strategy includes: (a) conducting initial and ongoing program risk assessments; (b) requiring coalitions to use a designated payment management system; and (c) conducting oversight activities by Office of Grant Services specialists within CDC, in coordination with assigned project officers.
Risk Assessment Questionnaire. CDC’s Office of Grant Services uses a risk assessment tool which examines issues such as financial instability, insufficient management systems, non-compliance with award conditions, the charging of unallowable costs, and staff inexperience.[78] According to CDC’s guidance, the assessment also considers the applicant’s history in all available systems, including OMB-designated repositories of government-wide eligibility and financial integrity systems and other sources of historical information.[79]
Payment Management System. HHS also requires CDC to set up payment subaccounts within the Payment Management System for all new grant awards.[80] According to CDC guidance, the Payment Management System subaccounts provide recipients and CDC with a more detailed and accurate understanding of financial transactions at the grantee level. CDC guidance states that funds awarded to grantees in support of approved activities and draw down instructions are identified on the Notice of Award in an established Payment Management System subaccount. DFC grant recipients are required to draw down funds from award-specific accounts in the Payment Management System. The guidance states that DFC grantees are encouraged to demonstrate a record of fiscal responsibility and the ability to provide sufficient and effective oversight of its funds. Additionally, DFC grantees’ financial management systems must meet the requirements as described in 2 C.F.R. Part 200 which include, but are not limited to, the following:
· Effective control over, and accountability for, all funds, property, and other assets;
· Comparison of expenditures with budget amounts for each federal award;
· Written procedures for determining cost allowability; and
· Written procedures for financial reporting and monitoring.
According to CDC guidance, DFC grantees are also required to submit a completed Federal Financial Report (FFR) annually.[81] The guidance states that grantees’ FFRs must include only those funds authorized and disbursed during the timeframe covered by the report. The FFR must also indicate the exact balance of unobligated funds and may not reflect any unliquidated obligations. Finally, the guidance states that there can be no discrepancies between the final FFR expenditure data and the grantee’s Payment Management System cash transaction data. The guidance adds that failure to submit the required FFR in a timely manner could adversely affect future funding to the grantee.
Grant Management Reviews. CDC’s grants management specialists are to provide fiscal and management support to the DFC program. According to the DFC program’s handbook, CDC’s grants management specialists help ensure that federal funding guidelines and policies are followed, including assessing for fraud, waste, and abuse by conducting quarterly internal control reviews of grantee files overseen by the project officers. According to CDC officials, CDC’s project officers, in coordination with the grants management specialists, work to prevent fraud, waste, and abuse by conducting reviews of grantees’ program management practices in various ways, including:
· Identifying recipients or applicants that do not meet the statutory eligibility requirements;[82]
· Adding restrictions to recipients of concern (e.g. key personnel that are non-responsive, lack of key personnel, late submission of required documentation, and/or lack of progress);
· Ensuring percentage cap on the program’s evaluation costs;[83] and
· Scheduling site visits, where appropriate, to further investigate issues of concern.
According to statute and consistent with guidance in CDC’s handbook for program recipients, CDC may impose enforcement actions if a coalition is found to be out of compliance with program requirements.[84] These enforcement actions can include withholding payments, post-award grant suspension of award activities or termination, or initiate suspension or debarment proceedings.
According to CDC officials, since their agency started managing the DFC program in October 2020, CDC terminated five coalitions from the program. Reasons for these terminations varied, including failure to meet the goals and objectives of the program, including requirements related to action planning and providing budget submissions; cited for receiving more than 10 years of DFC funding,[85] in violation of the DFC program’s statutory eligibility requirements;[86] and insufficient organizational capacity to implement grant activities.
Project Officer Oversight. CDC’s project officers review all financial and programming reports for accuracy and adherence to program compliance. According to CDC guidance, each DFC grantee has a dedicated project officer who serves as their main point of contact related to the fiscal and programmatic requirements of the grant. The guidance states that CDC project officers are to conduct site visits and gauge the coalition’s progress toward planned activities and program requirements.
According to CDC officials, another aspect of the project officer’s responsibility in the day-to-day monitoring of DFC grant recipients includes assessing coalitions’ budgets to track for allowable and allocable costs and verifying that coalitions have appropriate key personnel in place to help establish internal controls, including mechanisms to detect and prevent fraud, waste, and abuse.[87]
ONDCP Did Not Consistently Enforce the Requirement for the Ongoing Involvement of All Community Sectors
Pursuant to 21 U.S.C. § 1532(a)(2), to be eligible to receive a DFC grant, an organization must consist of one or more representatives from each of 12 major sectors of its community.[88] In addition, if a grant recipient fails to continue to meet the statutory eligibility criteria, including the requirements for sector representation, the Administrator may suspend the grant, after providing written notice to the grant recipient and an opportunity to appeal.[89]
According to ONDCP program officials, CDC project officers review coalitions’ sector representation during the DFC program’s annual August Progress Report and systematically track and monitor coalitions’ compliance with this requirement in real-time. They said that while the project officers encourage coalition officials to regularly update the DFC-Me system to indicate when any sector is not participating, no DFC funded coalitions have had their grants terminated for failing to maintain the 12 sector representation requirement. However, we found no evidence that ONDCP officials had taken any enforcement action if coalitions do not complete the corrective action within the required 90 days. ONDCP has not established and implemented enforcement procedures for coalitions to formally document instances of non-participation by required sectors—during the course of the annual grant period with related disciplinary action—and collaborate with coalitions to promptly restore sector representation.
CDC also issued a DFC Handbook that includes all DFC statutory requirements, including maintaining a coalition made up of the 12 required sectors. Further, ONDCP officials told us their office, along with CDC, requires DFC coalitions to complete a checklist each year regarding the statutory eligibility requirements, including whether the coalition has one or more representatives and a signed Coalition Involvement Agreement form for each of the 12 required sectors of a community.[90]
According to ONDCP officials, if an item is checked “No,” on this checklist, the grantee must explain the reasons that the coalition does not currently meet this requirement and what corrective action the coalition will undertake to become fully compliant within the next 90 days. According to CDC officials, in fiscal year 2024, seven coalitions stated that they did not have the 12 required sectors.
ONDCP officials stated that they are aware of the challenges some coalitions are experiencing in maintaining community sector involvement in the DFC program. The officials said during the initial DFC application process, the applicant must identify the 12 sector community representatives—and that not having a representative for each sector is the primary reason many applicants are denied.[91] CDC officials said that their agency asks coalitions to document the specific barriers or challenges in their annual progress report.
CDC officials also stated that coalitions are provided with technical assistance and sector-building resources. ONDCP and CDC officials said while they generally work with coalitions to maintain the full complement of coalition members, coalition officials are generally able to identify a new sector representative quickly. However, we found this to be inconsistent with our site visits and survey results.
As discussed, officials from seven of the 13 site visits told us they experienced ongoing challenges retaining some sector members. Similarly, our survey found that over half of respondents who responded said they faced these challenges.[92] The officials also emphasized that DFC sector representatives are all community volunteers, and that coalition membership ebbs and flows throughout the year dependent on various local factors, especially in rural and frontier communities.
ONDCP officials told us that coalitions not having representatives from all 12 sectors will find it more difficult to mobilize their communities effectively around the issue of youth substance use. The officials also said coalition sector representatives play a critical role in community-based prevention efforts and without that community buy-in, coalitions would have a very difficult time implementing their prevention initiatives.
Establishing longstanding community drug prevention partnerships is a critical factor to the success of the DFC program. Without such collaboration and coordination at the grassroot level, DFC coalitions may not be best positioned to address the program’s chief goal of reducing substance use over time among youth in their communities. In addition, they are not in compliance with the requirement to consist of at least one representative from each of the 12 major sectors of their community.[93]
ONDCP’s Congressional Budget Submissions Do Not Provide Transparency on the DFC Program’s Administrative Carryover Funds
We have previously called attention to the importance of transparency in federal agencies’ budget presentations, including how much of an agency’s previous year’s funding remains available for obligations.[94] A thorough understanding of an agency’s processes for estimating and managing carryover balances offers critical insight into the agency’s ability to anticipate programmatic needs and optimize the use of available resources. Specifically, we have reported on the importance of transparency in budget presentations because the examination of all balances may assist decision makers in identifying opportunities to achieve budgetary savings or redirecting resources to other priorities.[95]
We analyzed ONDCP’s annual Congressional Budget Submissions for each fiscal year—2018 through 2025—and found that ONDCP did not disclose or identify the DFC program’s carryover balances available for the program’s administrative expenses.[96] Based on ONDCP’s budget data, ONDCP was appropriated about $835 million to manage and administer the DFC Program from fiscal years 2018 through 2025. During this period, ONDCP allocated about $82 million to the DFC program for administrative costs[97] (i.e., grant management and oversight efforts). At the same time, ONDCP requested additional funding from Congress for such expenses while consistently not disclosing its administrative costs carryover balances ranging from about $4.8 million to almost $11.9 million.[98] Further, ONDCP did not provide information on plans to use the available carryover funds to address new projects or potentially offset the program’s administrative costs related to projects to be funded in the year of the budget request.[99]
For example, in fiscal year 2024, ONDCP was appropriated up to about $12.8 million for the program’s administrative costs while having an available carryover balance of about $9 million for such costs—totaling about $21.8 million available for administrative costs.[100] According to ONDCP’s budget data, in fiscal year 2024, about $12.1 million was expended for the program’s administrative costs. Based on ONDCP’s budget submission in fiscal year 2024, Congress was not made aware of prior years’ carryover balances available for the program’s administrative costs nor an estimate of the preceding year’s carryover balance. Ordinarily the agency is subject to a statutory limitation in 21 U.S.C. § 1524(b) of 8 percent of the funds appropriated to carry out the program for administrative costs, but since 2022 ONDCP has requested and received appropriations that exceeded this statutory limitation.
Figure 10 provides an overview of ONDCP’s actual administrative expenses, carryover balances, and total budget authority available for the program’s administrative costs for fiscal years 2018 through 2025. Appendix XI provides detailed budget information on the DFC program—including the annual appropriations, grant awards, allocations for administrative costs, executed administrative costs, and carryover balances for fiscal years 2018 through 2025.
Figure 10: Drug-Free Communities (DFC) Support Program’s Administrative Costs and Carryover Balances—Fiscal Years 2018 through 2025
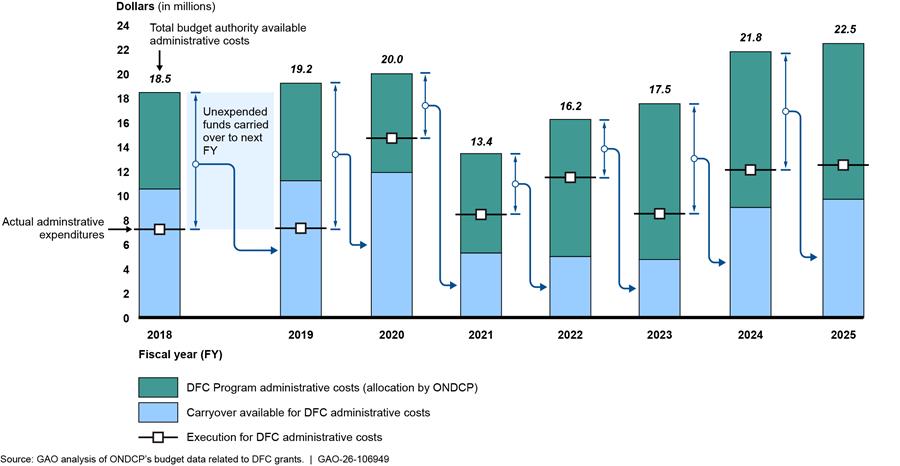
Note: In fiscal year 2020, ONDCP used some of these carryover funds and funds allocated for administrative expenses from its annual appropriation to pay for the administrative costs associated with SAMHSA and CDC providing day-to-day grant management and oversight services totaling around $14.7 million.
ONDCP officials told us its practice of carrying over funds from one fiscal year to the next is within its budget authority and allows for the flexible use of the funds based on program needs. For example, ONDCP officials said the administrative costs for the DFC program include a wide range of items, including grants management and program monitoring, support costs related to the DFC’s national cross-site evaluation, program administrator and policy analyst salaries, travel, printing, grantee trainings, grant application workshops, and grants oversight system development and maintenance. The officials said these costs fluctuate based on program requirements, particularly the cycles for the DFC technology and evaluation contracts.
According to ONDCP officials, the DFC program’s cumulative carryover balances from previous fiscal years—which are “no-year funds”—are added to its available budget authority and may be used for the program’s administrative costs beyond applicable statutory limitations.[101] The officials also stated that there is no policy or guidance that specifies the minimum amount of administrative carryover and they said ONDCP provides estimated and actual carryovers.
In addition, according to ONDCP officials, ONDCP reports the carryover balance in the President’s Budget Appendix. However, the carryover balance (or “unexpired unobligated balance, end of year”) reflected in the President’s Budget Appendix is the sum of all carryover funds appropriated within the “Other Federal Drug Control Programs” account. The Other Federal Drug Control Programs account includes several ONDCP programs, including the DFC program, Drug Court Training and Technical Assistance, Anti-Doping Activities, Model Acts Program, and other activities undertaken by ONDCP. As such, the President’s Budget Appendix does not specifically reflect the DFC program carryover balance for administrative expenses.
ONDCP officials indicated that because of the budget formulation cycle, ONDCP is unable to provide the carryover balance from the preceding year in its Congressional Budget Submission. However, ONDCP does have carryover balance information available from prior fiscal years. For example, ONDCP could have included in its Fiscal Year 2024 Congressional Budget Submission that about $4.8 million was the available carryover balance from fiscal year 2022, according to ONDCP’s budget data, even if fiscal year 2023 carryover was not final. In addition, ONDCP could provide an estimated carryover balance in its Congressional Budget Submissions.
While fluctuations in programmatic costs are to be expected, understanding an agency’s approach to estimating and managing carryover balances provides valuable insight into its capacity to anticipate program needs and allocate resources effectively. The lack of transparency in ONDCP’s budget process limits Congress’s visibility as to the full level of resources available for projects when making appropriations decisions, particularly as it considers appropriating amounts in excess of the statutory limitation in 21 U.S.C. § 1524(b).
Given the fiscal pressures facing the nation—and specifically programs like the DFC—examination of balances carried forward into future fiscal years provides an opportunity to identify areas where the federal government can improve and maximize the use of resources. Enhanced budget disclosures would allow appropriators and program decision-makers to develop a more comprehensive understanding of the DFC program’s financial position. Ensuring that all relevant information is considered during the budget process by providing Congress with comprehensive information on the carryover balance available for the DFC program’s administrative expenses—including how the carryover funds are expected to be expended on current or future projects and activities—would support this effort.
Conclusions
Assessing the impacts of programs like the DFC program is essential for identifying effective strategies for preventing and reducing youth substance use. Although ONDCP’s annual evaluations consistently suggest the DFC program meets its goal of significantly preventing and reducing substance use among youth, the program’s data limitations present challenges to drawing clear causal link between the DFC program’s prevention activities and changes in youth substance use. Identifying and collecting relevant data could help better assess the program’s impact. Once the program has determined the appropriate data to track—including its four core metrics—establishing consistent methods for collecting that information can further support efforts to assess how effectively the program is advancing toward its goals.
Additionally, fully documenting the methodology used to produce the evaluation reports would ensure that internal or external stakeholders can assess the quality and credibility of the evaluations. By doing so, ONDCP would be able to better ensure the credibility and quality of the evaluation’s results—and therefore, the impacts of the program—to internal and external stakeholders and decisionmakers.
Further, having clearly defined goals related to building drug prevention partnerships in communities would better ensure that ONDCP can determine what type of evaluative information it needs to monitor and track the progress of the DFC program. Documenting or defining performance measurements—with specific annual targets or goals to establish and strengthen drug prevention collaboration within communities—would ensure that ONDCP can demonstrate its progress in achieving them.
In addition, in its effort to provide flexibility to DFC coalitions, ONDCP does not consistently enforce accountability when coalitions fail to maintain participation from all 12 statutorily required community sectors. In the absence of full sector representation, the DFC program may compromise a fundamental aspect of its mission and strategic objectives—to build and strengthen collaborative drug prevention efforts within local communities. Establishing and implementing procedures to enforce full sector representation could provide ONDCP with better visibility over this statutory requirement and, in turn, ultimately strengthen DFC coalitions’ efforts to reduce substance use among youth in their communities.
Finally, ONDCP can enhance transparency in its budget formulation process by providing Congress with comprehensive information on the DFC program’s administrative expenditures. By providing Congress with comprehensive information on the carryover balance ONDCP has available for the DFC program’s administrative expenses—including how the carryover funds are expected to be expended on current or future projects and activities—ONDCP will enable appropriators and program decision-makers to obtain a more complete understanding of the program’s financial resources and funding strategies.
Recommendations for Executive Actions
We are making the following six recommendations to the Office of National Drug Control Policy:
· The Director of ONDCP, in consultation with the Director of the Centers for Disease Control and Prevention [or another federal statistical agency], should develop a strategy to identify relevant data to help better understand the DFC program’s impact. (Recommendation 1)
· The Director of ONDCP, in consultation with the Director of the Centers for Disease Control and Prevention [or another federal statistical agency], should explore ways to standardize its data collection methodology for its four core measures to help improve the quality of program performance data submitted to the DFC program. (Recommendation 2)
· The Director of ONDCP should ensure that its annual evaluation reports of the DFC program include complete documentation of the methodology used to develop the report’s findings and conclusions. (Recommendation 3)
· The Director of ONDCP should establish clearly defined performance goals and measures for the DFC program’s strategic goal of collaboration among communities to prevent and reduce substance use among youth. (Recommendation 4)
· The Director of ONDCP should establish and implement enforcement procedures for DFC coalitions that do not maintain all 12 sectors in accordance with statutory requirements, and work with the coalitions to reestablish these sectors in a timely manner. (Recommendation 5)
· The Director of ONDCP should provide Congress with information on the carryover balance available for the DFC program’s administrative expenses—including how any carryover funds are expected to be expended on current or future projects and activities. (Recommendation 6)
Agency Comments
We provided a draft of this report to the Department of Justice, HHS, and ONDCP for review and comment. ONDCP provided written comments, which are summarized below and reproduced in appendix XII. HHS and ONDCP provided technical comments, which we incorporated as appropriate. The Department of Justice did not provide any comments on the report.
ONDCP agreed with the recommendations. In response to our first recommendation that ONDCP develop a strategy to identify relevant data to help better understand the program’s impact, ONDCP noted that it will leverage internal expertise and engage both CDC and SAMHSA to develop such a strategy. In response to our second recommendation that ONDCP explore ways to standardize its data collection methodology, ONDCP said it has initiated a process to improve DFC grantee data collection. In response to our third recommendation that ONDCP ensure that its annual evaluation reports of the DFC program include complete documentation of the methodology used to develop the report’s findings and conclusions, ONDCP noted that the evaluator of the DFC program will include a methodology section in its annual evaluation reports moving forward. In response to our fourth recommendation that ONDCP establish clearly defined performance goals and measures for the DFC program’s strategic goal of collaboration among communities to prevent and reduce substance use among youth, ONDCP said it is working in collaboration with CDC and SAMHSA to establish innovative performance goals and measures to foster community collaboration. In response to our fifth recommendation that ONDCP establish and implement enforcement procedures for DFC coalitions that do not maintain all 12 sectors in accordance with statutory requirements, and work with the coalitions to reestablish these sectors in a timely manner, ONDCP noted that it will establish enforcement procedures. In response to our sixth recommendation that ONDCP provide Congress with information on the carryover balances available for the DFC program’s administrative expenses, ONDCP said it concurred with the recommendation and will provide Congress with information on the carryover balances for the program’s administrative expenses upon request. While providing information upon request may meet some congressional committee needs, Congress would be better informed if ONDCP provided supplemental budget materials on carryover balances as part of their regular reporting process. This would give congressional decision makers the opportunity to examine the necessary funding level to address administrative expenses associated with the program, determine whether to address the statutory limitation in 21 U.S.C. § 1524(b), and assist them in identifying opportunities to achieve budgetary savings or redirecting resources to other priorities. In addition, such transparency in ONDCP’s budget materials would help provide reasonable assurance that the DFC program is fully meeting congressional stakeholders’ needs.
We are sending copies of this report to the appropriate congressional committees, the Attorney General, the Secretary of Health and Human Services, Director of the Office of National Drug Control Policy, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact us at (202) 512-8777 or mcneilt@gao.gov or kennedyjj@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix XIII.

Triana McNeil,
Director, Homeland Security and Justice
Jamila Jones Kennedy,
Director, Applied Research and Methods
List of Committees
The Honorable Bill Cassidy, M.D.
Chair
The Honorable Bernard Sanders
Ranking Member
Committee on Health, Education, Labor and Pensions
United States Senate
The Honorable Rand Paul, M.D.
Chairman
The Honorable Gary C. Peters
Ranking Member
Committee on Homeland Security and Governmental Affairs
United States Senate
The Honorable Charles E. Grassley
Chairman
The Honorable Richard J. Durbin
Ranking Member
Committee on the Judiciary
United States Senate
The Honorable Bill Hagerty
Chair
The Honorable Jack Reed
Ranking Member
Subcommittee on Financial Services and General Government
Committee on Appropriations
United States Senate
The Honorable Brett Guthrie
Chairman
The Honorable Frank Pallone, Jr.
Ranking Member
Committee on Energy and Commerce
House of Representatives
The Honorable Jim Jordan
Chairman
The Honorable Jamie Raskin
Ranking Member
Committee on the Judiciary
House of Representatives
The Honorable James Comer
Chairman
The Honorable Robert Garcia
Ranking Member
Committee on Oversight and Government Reform
House of Representatives
The Honorable Dave Joyce
Chairman
The Honorable Steny Hoyer
Ranking Member
Subcommittee on Financial Services and General Government
Committee on Appropriations
House of Representatives
This report examines the extent: (1) the Drug-Free Communities (DFC) Support Program has met key program goals, and (2) the Office of National Drug Control Policy (ONDCP) has effectively managed the DFC program. To address both objectives, we reviewed relevant federal laws, regulations, agency policies and procedures, and past GAO, ONDCP, and Department of Health and Human Services’ (HHS) Centers for Disease Control and Prevention (CDC) documents related to the DFC program. We administered a census survey to 750 DFC-funded coalitions to gain their perspectives on the DFC program ‘s benefits and challenges. Additionally, we conducted 13 site visits—including three preliminary site visits—and met with knowledgeable representatives at selected DFC coalitions located throughout the U.S.—representing a wide range of communities (e.g., rural/frontier areas, suburban, and urban)—to obtain detailed information on the selected coalitions’ operations (including challenges experienced) and to inform the development of our survey instrument. We also interviewed cognizant officials from ONDCP, CDC, Department of Justice, and Drug Enforcement Administration (DEA) over the course of our review.
Survey Development and Administration
To collect information on DFC coalitions’ perspectives on the program’s benefits and challenges—including how well the DFC program works and how it could improve—we designed and administered a web-based survey.[102] We administered the survey from July 1, 2024, to August 28, 2024, to a census of 750 DFC-funded coalitions. We addressed the survey to the coalitions’ Project Coordinator, who manages the work of the coalition and program activities, including training, coalition communication, data collection and information dissemination. Other knowledgeable coalition representatives such as the Project Director responded to the survey if the Project Coordinator was not available. The survey covered topics under the following categories:
· Coalition Composition and Structure,
· Coalition Outcomes and Outcome Monitoring,
· Use of Evidence-Based Practices,
· Coalition Substance Focus and Strategies Used,
· Coalition Resource and Resource Needs,
· High Risk Groups, and
· Resources for Program Administration and Grant Compliance.
To develop the survey, we reviewed several sources of criteria in composing our questions, including the Substance Abuse and Mental Health Services Administration (SAMHSA) Strategic Prevention Framework, a comprehensive guide that provides DFC coalitions an approach for reducing substance use in their communities, and the DFC program’s Notice of Funding Opportunity. We pretested the survey via Zoom with key coalition staff from a judgmental sample of five coalitions. We selected those five coalitions from the sample of coalitions with whom we conducted preliminary and formal site visit interviews.[103] We also obtained an internal peer-review of our survey instrument and modified questions that were unclear or had multiple interpretations prior to sending the survey out to all coalitions. Appendix IX contains the survey questions and responses for survey items presented in this report. To encourage participation in the survey, we asked ONDCP to reach out to the coalitions announcing the survey’s release and encouraging their participation. We also sent automatic reminders and made follow-up phone calls to raise the response rate. The weighted survey response rate was 46 percent (359 respondents; Total =750).
Survey data presented in this report are subject to all the qualifiers associated with self-reported data. For example, participants may respond to survey questions in ways that present themselves favorably, rather than truthfully. Instead, the responses were based on the reports of key officials running the program. The self-report of these officials should be interpreted as attitudinal testimonial evidence and should be considered when reviewing the survey results.
Two types of errors arise in sample surveys: sampling errors and non-sampling errors. Surveys are subject to non-sampling errors due to the practical issue of conducting the survey. For example, differences in interpreting a particular question, sources of information available to respondents, or the type of people who do not respond can introduce variability in the survey results. We took steps to minimize these potential forms of survey bias. We conducted pre-tests of our survey instrument with key coalition staff. During that cognitive pretesting session, we asked participants to indicate which questions were subject to multiple interpretations. We changed the wording or eliminated those questions which were unclear or had multiple interpretations.
Threats to the validity of survey data grow from low survey response rates and concerns about response bias. Non-response bias occurs when people who do not complete a survey differ systematically from those who do, leading to results that are not representative of the larger population and potentially invalidating the results. To assess potential bias resulting from differences between those who responded to our survey and those who did not, we performed a nonresponse bias analysis to assess demographic differences between respondent and non-respondent DFC coalitions. We obtained demographic data from the Census Bureau on population size, gender, race, age, urbanicity, and U.S. geographic region and linked this data based on DFC zip code.
For the nonresponse bias analysis, we use a propensity model – i.e., a logistic regression model to estimate the probability that a DFC will respond to the survey, based on the following model and DFC demographic characteristics:
logit Pr(Responsej=1 | DFC Demographic Variables) ~ biAwardYeari + giPopulationSizei + eiGenderi + riRacei + wiAgei + kiRuralityj + niGeographicRegioni + si, for the ith DFC[104]
From this propensity model, we estimate a weight to account for nonresponse:
wi = 1/ji for the ith DFC
where ji = the predicted probability of the ith DFC responding to the survey
To sum, we assessed potential nonresponse bias based on DFC zip code population size, gender, race, age, urbanicity, and U.S. geographic region. We estimated weights to account for this nonresponse and generated estimates that better generalize to the population of DFC coalitions on census demographic data. Uncertainty due to this nonresponse was assessed through 95% confidence intervals around survey estimates. However, as with any survey and, more broadly, statistical analyses, we cannot account for unmeasured sources of potential bias (e.g., characteristics of a DFC office and school environment for students), which precludes complete certainty around estimates.
We performed an assessment of survey data reliability through checks of the time and source of survey responses, missing data, responses outside of designated ranges, outliers, skip patterns, and links to Census Bureau data using zip codes. Respondents that completed less than 10% of the survey only answered the first handful of questions and were counted as nonrespondents. Item nonresponse was not an issue for all other respondents.
We analyzed data in aggregate, with a coalition as a single case. We express the variability in results as a 95 percent confidence interval. The maximum margin of error was less than or equal to 5 percentage points for the coalition sample. We provide selected regression analyses and survey results in appendices II and IX, respectively.
Coalition Site Visits
We conducted 13 site visits with DFC coalitions. Our goals were to: 1) ascertain the coalitions’ program design, goals, evidence of effectiveness, and best practices and any innovative strategies; 2) inquire about the coalitions’ ability to address issues surrounding fraud, waste, and abuse; and 3) gain their perspectives on any challenges with complying with the DFC program requirements and adhering to the goals of the program. We conducted semi-structured interviews with project coordinators because they manage the work of the coalitions as well as program activities. Finally, we met with some available members of the twelve community sectors that make up the coalition.
We used purposeful sampling to identify 13 DFC coalition site visits based on several criteria. These included: CDC’s (2021) estimated overdose death rate data for counties served by coalitions; the coalition’s tenure as a grantee in the DFC program; and varying geography (e.g., rural/frontier areas, suburban, and urban) and demographics. The coalitions are located in Arizona (Santa Cruz County Drug Free Community Coalition, and Maricopa County Urban Indian Coalition); Georgia (Community Action Coalition, Family Connection of Warren County, Inc., and Power Through Prevention Community Coalition); Maine (Youth Resiliency Coalition of Southern Maine, SoPo Unite: All Ages, All In); Missouri (Alliance For Healthy Communities, and Iron County Health Coalition); Washington (Latinx King County Dream Coalition, Birch Bay-Blaine Thrives Coalition, and Mt. Baker Community Coalition); and West Virginia (Wyoming County Prevention Coalition). Appendix III provides information on the characteristics of each coalition that we visited, and the map shows the geographical location.
During the site visit interviews, we asked questions on the following topics: Purpose, Staffing, Composition, and Coalition Budget; Prevention Practices, Clients, and Coalition Effectiveness/Efficiency; Communications and Interactions with CDC/ONDCP and other DFC Coalitions; Coalition Sustainability; and DFC Strengths and Challenges. We also asked interview respondents about their willingness to complete a survey that was under development. We also conducted interviews with key officials from the DFC program offices (CDC and ONDCP) and the contractors who completed the annual national cross-site evaluation.
The information we gathered from the site visits helped us to identify a range of topics that might be included in the survey. These discussions also gave the team an in-depth look at some of the day-to-day issues that sector members face in implementing their prevention strategies. Data obtained from the site visits are not generalizable to the population of coalitions, but they provide context and illustrative examples of the kinds of issues coalitions may face.
Literature Review
We conducted a literature review to examine studies exploring the range of evidence-based practices for youth substance use and misuse prevention. We were interested in seeing whether the evidence-based practices presented in recent peer-reviewed research would align with the evidence-based practices reported by the coalitions from our survey. We also wanted to identify how many of the practices described in the literature review were culturally adapted to meet the needs of culturally diverse communities. We reviewed literature on community-based organizations engaging in evidence-based, promising substance use and misuse prevention practices/programming for youth.
During August 2023 and March 2024, we conducted a search that included different combinations of relevant terms: ONDCP, DFC program; federal drug control, evaluation, efficacy, efficiency, effectiveness, impact, outcome, impact, consequence. We expanded that search to include the additional search terms: substance use, substance misuse, drugs, alcohol, tobacco, marijuana, opioid, fentanyl, adolescent, youth, high school, middle school, child, teen, community, prevention, coordination, engagement, partnership, development, coalition, cost-effective.
Our initial search yielded 355 studies. We removed studies from our analysis based on the following exclusion criteria: 1) articles that did not address the 12–18-year age range; 2) studies that were not done on U.S. youth; and 3) articles that were not peer-reviewed. We were only reviewing research-based studies. This preliminary screen resulted in 146 total studies to review. As we undertook our review of these studies, we used a data collection instrument. We were not able to ascertain whether some of the strategies used based upon evidence-based practices were being carried out with the implementation requirements that were validated by research.
Meta-Evaluation of Past Annual Cross-Site Evaluations and Results and Interviews with Contractors Conducting the Evaluations
We reviewed the DFC National Cross-Site Evaluation Team’s (ICF) evaluation plan and end of year reports for 2022 and 2023 to determine whether the methodology and findings were sound and reasonable. The team held two sessions (September 19, 2024, and October 7, 2024) to discuss the following topics:
· Background and history of contractor’s work on the DFC cross-site evaluation plans;
· Purpose of the national cross-site evaluations;
· Data challenges; and
· Methodology
We also used a data collection instrument to independently review each of the evaluation reports and identify any insufficiencies in the evaluation reports’ methodology.[105] The data collection instrument covered questions about the following: (A) the Intervention, Evaluation Team, and Key Parameters of the Study, (B) Design, Data and Methods, and (C) Conclusions and Recommendations. Two evaluation analysts used the instrument to assess the quality of evidence presented in the reports. Each review consisted of two consecutive reviews by the analysts who were experienced in, and familiar with, research and evaluation methods. Their iterative review was followed by a meeting where the analysts discussed the evidence for coding decisions and reconciled any outstanding coding elements.
We assessed whether the reports followed the Office of Management and Budget’s (OMB) standards for conducting program evaluations.[106] We also interviewed ONDCP’s contractor, ICF, to better understand the reliability and validity of data used and analyses performed to support reported DFC program outcomes.
DFC Coverage Areas
To independently assess characteristics associated with DFC versus non-DFC zip codes, we obtained data directly from CDC that included non-publicly available zip code information for national 2017, 2019, 2021, and 2023 Youth Risk Behavior Survey data.[107] We merged these data with Census Bureau demographic data for these zip codes. We used the Youth Risk Behavior Survey, implementing its survey design (e.g., survey weights), to perform a multivariate logistic regression to estimate the association between drug use over the past 30 days and whether a student in the survey lives in a zip code where there is a DFC, after adjusting for student demographic variables and Census Bureau zip code demographic characteristics. For simplicity, the model specification for the logistic regression model without accounting the nonresponse weight follows:
logit Pr(30DayDrugUsej=1 | DFC Zip Code, Demographic Variables) ~
biDFCZipCodei + giSchoolGradei + tiStudentGenderi + jiZipCodeGenderi+ eiStudentRacei + riZipCodeRacei + wiStudentAgei + kiZipCodeAgei + kiRuralityj + niGeographicRegioni + si, for the ith Student[108]
Building on the regression model, the weighted estimates for regression coefficients are a function of likelihood function for weighted logistic regression expressed as follows:
l(DFC Zip Code, Demographic Variables, YRBS Survey Weight, Coefficients) =

Where:
wi = the
YRBS survey weight
pi = the
probability that the ith
Student reports substance use
We report the association between 30-day substance use and Key Independent Variables of interest as Odds Ratios where
Odds Ratio = eb
The purpose of this analysis was to assess the association between zip codes and the core measurements rather than the impact of DFC coalition activities on increased or decreased substance use among youth.
DFC Program Tenure Analysis
To examine whether tenure in the DFC program was associated with survey respondents’ reported program outcomes, we classified each coalition into one of the following categories based on the information reported by our survey respondents. We categorized early tenure for coalitions that had been operating for 1-3 years, intermediate tenure for coalitions that had been operating for 4-7 years, and mature tenure for coalitions that had been operating for 8-10 years. We estimated the association between four outcomes of core measurements, key independent variables of interest, and adjusted for DFC demographic variables, adjusting for nonresponse using wi from the nonresponse bias analysis. For simplicity, the model specification for the logistic regression model without accounting the nonresponse weight
logit Pr(DFCTenurej=1 | DFC Demographic Variables) ~
biKeyIndependentVariablei + tiAwardYeari + giPopulationSizei + eiGenderi + riRacei + wiAgei + kiRuralityj + niGeographicRegioni + si, for the ith DFC[109]
Building on the regression model, the weighted estimates for regression coefficients are a function of likelihood function for weighted logistic regression expressed as follows:
l(Key Independent Variable, DFC Demographic Variables, Nonresponse Weight, Coefficients) =

where:
· wi = the nonresponse bias weight
· pi = the probability that the ith DFC responds “Yes” to the Core Measurement
We report the association between DFC Tenure and Key Independent Variables of interest as Odds Ratios where:
Odds Ratio = eb
DFC Program’s Oversight, Management, and Compliance
To address our second objective, we reviewed ONDCP and CDC’s latest standard operating procedures for DFC program’s oversight and management, and evaluated their alignment with the statutory requirements for the DFC program. We collected and examined available performance and financial audit information and interagency agreements to identify program management findings. We also interviewed ONDCP officials to identify the extent to which the DFC program’s administrative related carryover balances are disclosed (including ONDCP’s planned use for the available carryover funds) to Congress during its annual budget process for each fiscal year—2018 through 2025. We also reviewed documentation of ONDCP’s efforts to track its progress in addressing any findings, if applicable. Furthermore, we assessed the DFC program’s compliance with its internally established management protocols, applicable federal grant oversight regulations, and relevant guidance issued by GAO pertaining to grants administration.
To help inform our assessment of the management of the DFC program, we selected a diverse sample of local coalitions from across the U.S. to capture a broad range of perspectives from coalition officials. Our coalition site visit selection criteria included (a) state-level youth overdose death rates; (b) geographic diversity—spanning urban, suburban, rural, and frontier areas; (c) demographic characteristics; and (d) tenure as a DFC grantee. While the findings from these interviews cannot be generalized, this approach enabled us to examine important variation in program implementation across different contexts. We supplemented our findings by conducting interviews with DEA’s community outreach specialists. These officials provided additional context on the environmental and drug-related conditions in the communities we visited, as well as the extent of their collaborative efforts with the DFC program. Additionally, we interviewed ONDCP and CDC officials to describe how they conduct program oversight and assess the efficiency and effectiveness of the DFC program.
We conducted this performance audit from July 2023 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
We conducted multivariate logistic regression analyses to estimate odds ratios that assess the association between certain Drug-Free Communities (DFC) survey responses from our survey and survey responses on the four core measure outcomes.[110] Results from these analyses do not provide evidence for causality between the implementation of the DFC program and outcomes on the core measures. Variation in outcomes associated with features under program control, such as the characteristics of service providers or their activities, may identify opportunities for managers to take action to improve performance. Variation associated with factors outside the control of the program, such as neighborhood characteristics, can help explain program results, but may not identify actions to improve program performance. Moreover, the responses were based on the reports of key officials running the program. However, participants may have responded to survey questions to present themselves favorably. Thus, the self-report of these officials should be interpreted as attitudinal testimonial evidence, and should be considered when reviewing the survey results. For a more detailed discussion of our survey methodology and limitations, see appendix I.
Figure 11 below presents the variables significantly associated with each of the four core measures and the corresponding odds ratios for each.[111] These odds-ratios quantify associations with the core measures. For example, the first bar under parental disapproval in Figure 11 can be interpreted as follows: DFCs that self-reported youth involvement in planning youth coalitions were 16.3 more likely to report increases in the parental disapproval core measure in our survey, compared to DFCs that did not self-report youth involvement. However, these odds ratios do not reflect causality.
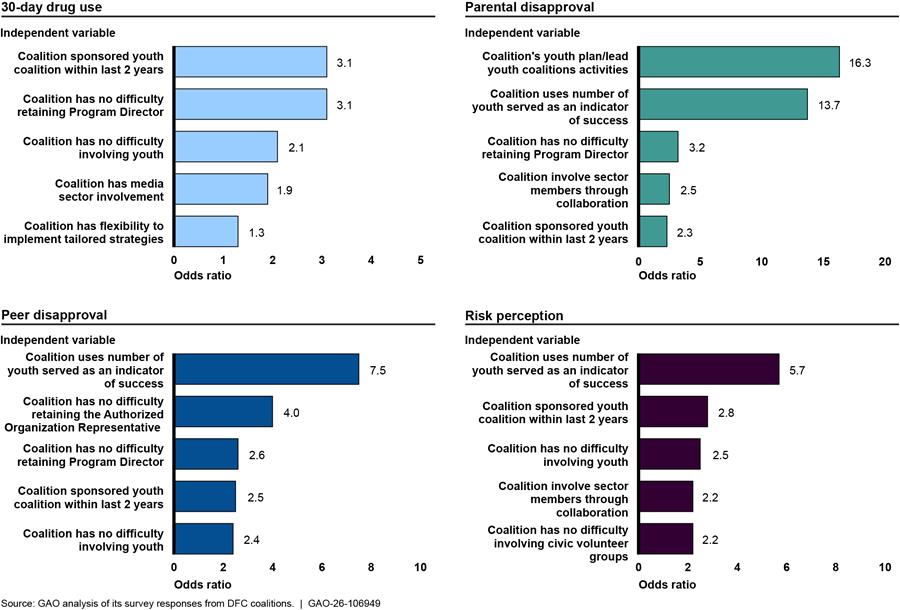
Notes: Graph depicts the top five odds ratios greater than one for each core measure that were significant at the 95 percent confidence level. Odds ratios were estimated from multivariate logistic regressions that accounted for the survey design and nonresponse based on Drug-Free Communities (DFC) demographic region and controlled for Census Bureau demographic variables (ethnicity/race, population size, U.S. geographic region). We performed a nonresponse bias analysis and implemented weights to account for nonresponse and generate estimates that better generalize to the population of DFCs, based on characteristics of DFC regional demographics.
The variables showing the strongest associations in the regression model were different for each of the four core measures.
· Reported decreases in thirty-day drug use were most strongly associated with youth involvement in planning youth coalitions, program director involvement, media sector involvement, the coalition’s ease of involving youth, and the perceived flexibility that the program office gave their coalitions to implement community-specific strategies.
· Reported increases in parental disapproval were most strongly associated with youth involvement in planning youth coalitions, a coalition’s use of youth served as a success marker, coalitions with no challenges in retaining a program director, community involvement through collaboration, and the sponsorship of a youth coalition.
· Reported increases in peer disapproval were most strongly associated with a coalition’s use of youth served as a success marker, the lack of difficulty in retaining an authorized organization representative, coalitions with no challenges in retaining a program director, and sponsorship of a youth coalition in the last two years.
· Reported increases in risk perception were most strongly associated with the coalition’s use of youth served as a success marker, sponsorship of a youth coalition in the last two years, ease of involving youth, collaboration as a form of community involvement, and ease with which a coalition involved civic volunteer groups.
In addition, coalitions reported that certain aspects of the DFC program or engaging in certain coalition activities were positively associated with outcomes on the four core measures. Specifically:
· Coalitions with active youth engagement reported stronger positive associations on all four core measures.
· Coalition program staff presence, especially program directors, was positively associated with most of the core measures.
· Sponsorship of a youth coalitions, a highly recommended evidence-based practice, was positively associated with all outcome measures.
· Collaboration as a form of sector involvement was positively associated with better outcomes on two core measures, with different sectors showing greater association with these outcomes.
Appendix III: Characteristics of the Drug-Free Communities (DFC) Support Program Coalitions GAO Visited in Fiscal 2024
The Office of National Drug Control Policy (ONDCP) administers and partners with the Centers for Disease Control and Prevention (CDC) to manage the Drug-Free Communities (DFC) Support Program—which provides grants to community coalitions to reduce local youth substance use. The DFC program aims to mobilize community leaders to identify and respond to the drug problems unique to their community and change local community environmental conditions tied to substance use.
According to ONDCP, in 2023, the DFC coalition population was comprised of diverse communities and they reported serving one or two of the five community types—frontier, rural, suburban, urban, and inner city. Most coalitions identified as working in rural (51 percent) or suburban (47 percent) communities, followed by urban (27 percent) inner-city (10 percent) or frontier (3 percent) communities.[112] In 2023, a national cross-site evaluation conducted by ONDCP reported that one in four Americans lived in communities served by DFC funded coalitions. Since 2005, 51 percent of the U.S. population has lived in a community with a DFC coalition, according to ONDCP.
In fiscal year 2024, ONDCP reported that 751 community coalitions across the U.S.—including the District of Columbia, Puerto Rico, and U.S. territories (Guam and Virgin Islands)—received funding (up to $125,000 per year) to strengthen collaboration among local partners and create an infrastructure that reduces youth substance use. As mentioned earlier in this report, we conducted 13 site visits and met with knowledgeable representatives at selected DFC program coalitions located throughout the U.S.[113]—representing a wide range of communities (e.g., rural/frontier areas, suburban, and urban)—in order to obtain their perspectives and detailed information on the selected coalitions’ operations (including successes and challenges experienced with participating in the program) and to assist with the development of our survey instrument.[114] Table 6 provides an overview of the selected characteristics (i.e., date organized and community served) of the 13 DFC coalitions that we visited as part of our review. In addition, we included CDC’s estimated overdose death rate for the county in which the selected coalition was located.
Table 6: Characteristics of 13 Drug-Free Communities (DFC) Support Program Coalitions that GAO Selected to Visit in Fiscal Year 2024
|
DFC Coalition and Location |
Date Organized |
Community Served |
Coalition Mission |
Year of DFC Fundinga |
Estimated Drug Overdose Death Rate, 2021b |
|
Alliance for Healthy Communities, Creve Coeur, Missouri |
2016 |
Suburban |
Aims to reduce youth substance misuse and suicide risk by raising awareness and changing community norms. |
9 |
40 |
|
Birch Bay-Blaine Thrives Coalition Blaine, Washington |
2020 |
Suburban |
Serves as a community hub for bringing people together to help foster resilience among youth, families, schools, and the community. Stakeholders explore ways to promote a thriving community by leveraging strengths and assets and enhancing healthy social environments in the Birch Bay, Blaine, and Point Roberts areas. |
5 |
22 |
|
Community Action Coalition Atlanta, Georgia |
2020 |
Urban |
Works to reduce drug use in the community by strengthening ties among key community members from parents, students, schools, and other partners. |
5 |
27 |
|
Family Connection of Warren County Incorporated Warrenton, Georgia |
2018 |
Rural |
Strives to strengthen children and their families through strong family, community, and school linkages. |
7 |
21 |
|
Iron County Health Coalition Ironton, Missouri |
2022 |
Rural |
Works with all members of the community to improve the physical and mental health of local youth and community members through prevention and treatment of substance misuse and other harmful conditions. |
3 |
46 |
|
Latinix King County Dream Coalition Seattle, Washington |
2022 |
Urban |
Provides culturally appropriate education and services to Latinx youth and families in King County, Washington. |
3 |
30 |
|
Maricopa County Urban Indian Coalition Phoenix, Arizona |
2019 |
Urban |
Creates a sustainable community coalition that addresses prevention of suicide, underage drinking and use of marijuana and prescription drugs through the foundation of cultures to improve the overall well-being of Urban American Indian youth and families. |
6 |
38 |
|
Mt. Baker Community Coalition Bellingham, Washington |
2020 |
Rural |
Builds a strong community that offers well-being to all by focusing on youth and families, through substance use/misuse prevention strategies and mental health promotion. This work provides education, resources, eliminates risk, increases protective factors, and leverages the community’s strengths and assets. |
5 |
22 |
|
Power Through Prevention Community Atlanta, Georgia |
2020 |
Urban |
Aims to mobilize community leaders to identify and respond to the drug problems unique to Atlanta, Georgia and change local community environmental conditions tied to substance use. |
5 |
27 |
|
Santa Cruz County DFC Nogales, Arizona |
2020 |
Frontier |
Works to reduce drug use in the community, strengthen community partnerships, and maintain healthy and drug-free lifestyles by helping to establish community health values. |
5 |
23 |
|
SoPo Unite: All Ages, All In South Portland, Maine |
2021 |
Suburban |
Helps to creates and sustain a safe, just, and healthy community to prevent youth substance use. |
4 |
37 |
|
West Virginia’s Wyoming County Prevention Matheny, West Virginia |
2023 |
Frontier |
Focuses on reducing substance use in Wyoming County, West Virginia by creating hope and awareness. |
2 |
150 |
|
Youth Resiliency Coalition of Southern Maine York, Maine |
2022 |
Rural |
Fosters community collaboration to help reduce and prevent the area’s pressing health challenges: youth substance use and poor mental health. |
3 |
40 |
Source: GAO’s analysis of background information obtained from each of the DFC coalitions we visited in fiscal year 2024. | GAO‑26‑106949
aAs mentioned earlier, based on DFC program requirements, each DFC coalition is eligible to receive up to $125,000 per year for up to a 10-year period. 21 U.S.C. § 1532(b).
bThe year 2021 data presented is the Centers for Disease Control and Prevention’s most recent model-based estimates of drug overdose death rates at the county level available based on final deaths. The model-based estimates were designed to produce stable estimates of drug overdose death rates at the county level. The death rate is deaths per 100,000 population.
Appendix IV: Historical Perspective of the Drug-Free Communities (DFC) Support Program’s Administration, Since 1997
The Drug-Free Communities Act of 1997 established the Drug-Free Communities (DFC) Support Program—a federal program to support communities in the development and implementation of comprehensive, long-term plans and programs to prevent and treat substance use and misuse among youth.[115] Since the DFC program’s inception in 1997, the Office of National Drug Control Policy (ONDCP), a component of the Executive Office of the President, has administered and partnered with other federal agencies to assist with managing the program. Most recently, in 2020, ONDCP entered into an agreement with the Centers for Disease Control and Prevention (CDC) to manage the program—providing the day-to-day grants management for the program.[116] Figure 12 identifies the federal agencies involved in administering and managing the program since 1997.
Figure 12: Federal Agencies Involved in the Administration and Management of the Drug-Free Communities (DFC) Support Program, Since Its Inception in 1997
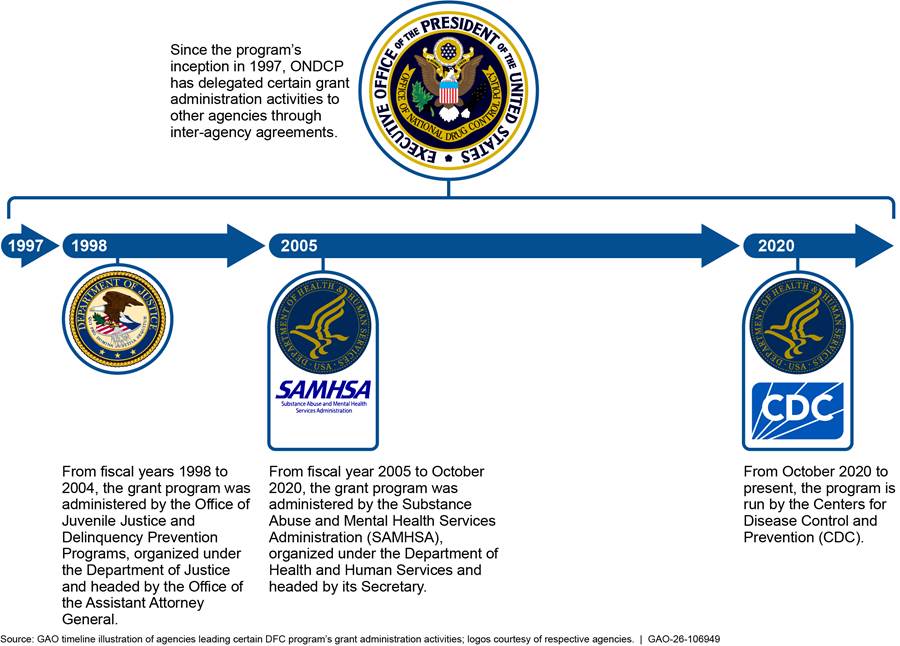
The Drug-Free Communities (DFC) Support Program’s coalitions engaged in a range of activities to reduce youth substance use and misuse, including drug prevention education campaigns, and they report on these activities in their annual progress reports to the Centers for Disease Control and Prevention (CDC). The Office of National Drug Control Policy (ONDCP), through its program manager (CDC),[117] routinely reviews the nature and scope of these activities to ensure they fit within one of the Seven Strategies for Community Change.[118] For example, according to ONDCP, one of these seven strategies is “providing information.” To execute this strategy, DFC coalitions held face-to-face information sessions on topics such as the consequences of youth substance use and the importance of drug abstinence. Figure 13 shows the DFC program’s overarching goal, its specific program goals, ONDCP’s seven strategies for goal attainment, and examples of coalitions’ activities aligned with each.
Figure 13: Drug-Free Communities (DFC) Support Program Goals, Strategies, and Examples of Coalition Activities
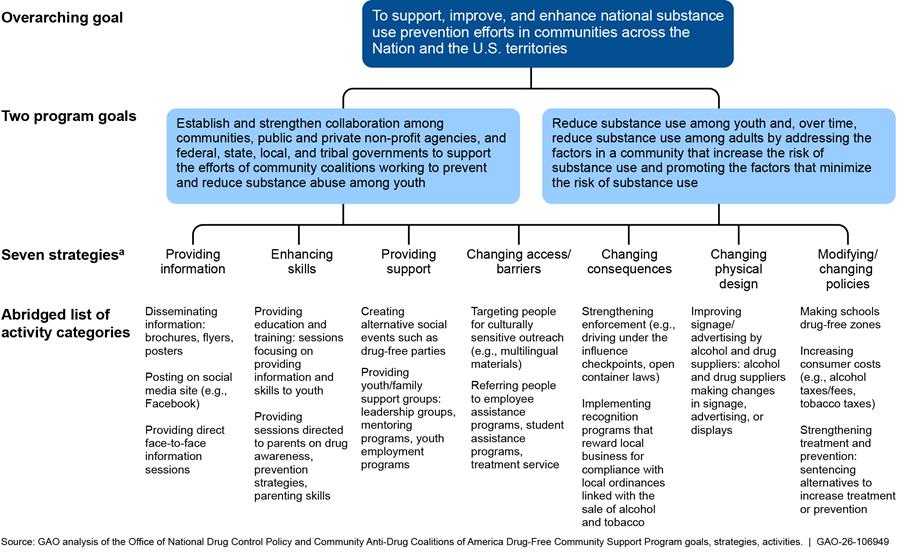
aThese are strategies that the DFC program associates with supporting community change.
To help curb youth substance use, the Drug-Free Communities Act of 1997 established the Drug-Free Communities (DFC) Support Program—a federal program to support communities in the development and implementation of comprehensive, long-term plans and programs to prevent and treat substance use and misuse among youth.[119] The DFC program focuses its efforts on the prevention and reduction of the use of substances. The Office of National Drug Control Policy (ONDCP) administers the DFC program, in coordination with the Centers for Disease Control and Prevention (CDC).[120] ONDCP awards four types of DFC program grants.[121] Specifically:
· New grants represent those grants openly competing for their 1st or 6th year of DFC funding.
· Continuation grants represent annual “in-cycle” grants for years 2 through 5, or 7 through 10 of DFC funding.[122]
· Mentoring grants are awarded to existing coalitions to support their work to create new DFC coalitions.
· Mentoring continuation grants represent the second year of the 2-year award.
According to ONDCP officials, the new and continuation grants represent the majority of grants awarded. For example, in fiscal year 2024, ONDCP awarded 192 new grants and 559 continuation grants but did not award any mentoring grants or mentoring continuation grants.[123] Each new and continuation grant awards up to $125,000 per fiscal year and mentoring grants limit awards to $75,000 per fiscal year.[124]
The Office of National Drug Control Policy (ONDCP) and Centers for Disease Control and Prevention (CDC) have operated the Drug-Free Communities (DFC) Support Program through an interagency agreement since 2020 that they update annually.[125] Specifically, ONDCP’s DFC Program Office oversees the strategic planning and funding of the DFC program, while CDC conducts day-to-day administration, such as interacting with grantees on a regular basis and reviewing their activities. ONDCP officials told us their staff are actively involved in all stages of the grant making process from Notice of Funding Opportunity development to grant closeout and/or termination.
ONDCP and CDC require grantees to submit annual progress reports through an ONDCP system called DFC Management and Evaluation (DFC-Me). These reports contain descriptions of the activities the grantees conducted in supporting the program’s two broad goals,[126] as well as their progress against the program’s four core measures:
1. Past 30-Day Prevalence of Use—youth who reported use of alcohol, tobacco, marijuana, or illicit use of prescription drugs at least once in the past 30 days.
2. Perception of Risk—youth who reported that the use of alcohol, tobacco, marijuana, or illicit use of prescription drugs is harmful.
3. Perception of Parental Disapproval—youth who reported their parents feel the regular use of alcohol, tobacco, and marijuana, or illicit use of prescription drugs is wrong or very wrong.
4. Perception of Peer Disapproval—youth who reported their friends thought it would be “wrong or very wrong” for them to drink alcohol, engage in any tobacco or marijuana use, or illicit prescription drug use.
The DFC program operates on a yearly grant cycle, working through a given calendar year. The DFC grant life cycle follows a typical federal grant life cycle, as shown in figure 14.
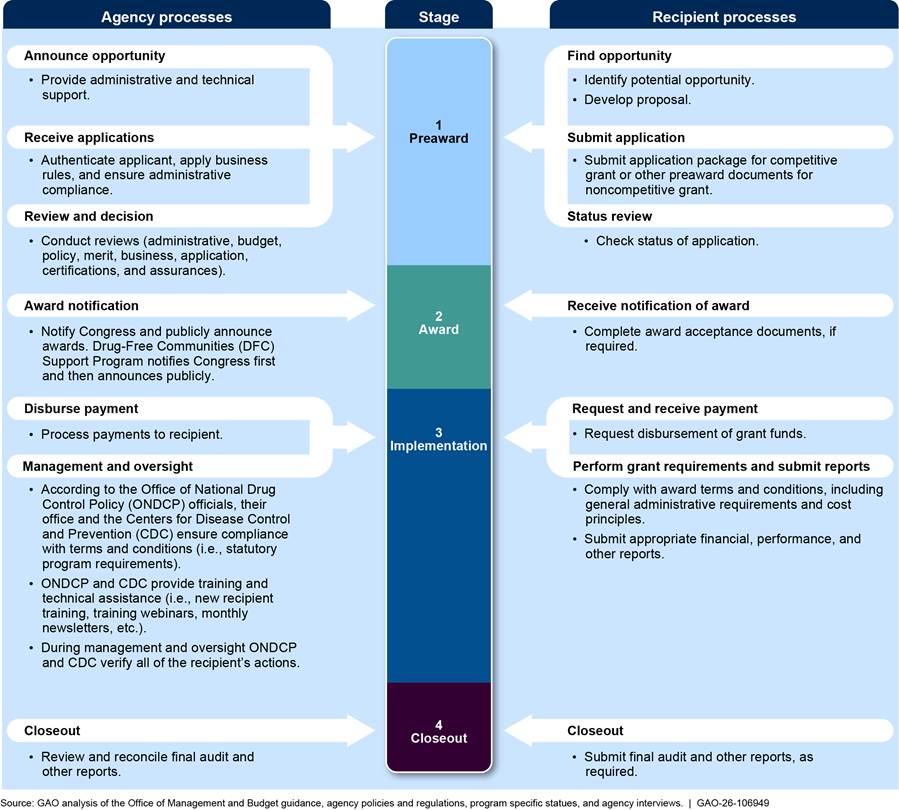
Note: ONDCP officials stated that the DFC-Me is also used to share the coalitions best practices and provides coalitions with the ability to identify their technical assistance needs. The following are additional examples of the type of data DFC-Me collects and maintains—status of compliance with requirements (coalition classification tool, survey reviews, core measures, data management plan, progress report, sector representatives, and sustainability plan); DFC grant recipient contact information; CDC project officer assignment; learning center (resources and success stories); DFC progress reports; upcoming events; and E-Blasts.
As we have previously reported, conducting grant management processes like those illustrated above, in accordance with internal control standards, statutory requirements, and leading practices for collaborating agencies is essential for achieving program outcomes.[127]
Methodological designs differ in their ability to make defensible causal claims about a program’s effectiveness. For example, the credibility of a claim that the Drug- Free Communities (DFC) Support Program caused reductions in substance use or misuse is critically dependent on the methods and measures employed to enhance the validity of the approach. The impact of a program can be demonstrated with an experimental design, in some cases, a well-designed quasi-experimental method or well-controlled non-experiment. Randomized experiments, under certain conditions, can provide the most credible evidence of effectiveness but even those have threats to validity and therefore must be designed carefully. Experimental studies used in program evaluations are typically conducted to measure impact.
Well-designed quasi-experimental studies can allow us to estimate impact by using comparison groups and using several statistical approaches that control for external factors.[128] Non-experimental designs, and in some cases, quasi-experimental designs, allow for description of observations or associations between variables that do not typically allow causal claims to be made based on those associations alone.
Experimental methods. An experimental method, such as a randomized controlled study, prospectively and randomly assigns participants to a treatment group that receives the intervention being examined and to a control group that does not receive the intervention. Any differences in these groups’ subsequent outcomes are believed to represent the program’s effect because the factors that influence outcomes other than the program should be evenly distributed between the two groups through the random assignment. Randomized experiments are best suited for assessing program impact when it is possible, ethical, and practical to conduct and maintain random assignment to minimize the influence of external factors on program outcomes.
In one study identified through our literature review, researchers aimed to identify barriers to the implementation of a particular strategy that could be used across many different Boys and Girls clubs.[129] The researchers examined 15 clusters of Boys & Girls Club sites implementing CHOICE (control group), a five-session evidence-based alcohol and drug prevention program. They compared these sites to 14 Boys & Girls Club sites implementing CHOICE and supported by a two-year implementation support intervention called Getting to Outcomes (intervention group). The researchers found that sites using the CHOICE program and supported by Getting to Outcomes performed better than the sites who had only been exposed to the CHOICE curriculum.
Economic impact studies use econometric methods to determine impact. Although econometric studies (i.e., cost-effectiveness, cost-benefit analysis) are not experiments, they are often classified with experimental methods because they provide a standardized calculation of program impact. For example, cost-benefit analyses are methods of identifying and comparing relevant quantitative and qualitative costs and benefits associated with a program or activity, usually expressed in monetary terms. Cost-effectiveness analyses are methods of identifying the cost of achieving a single goal, non-monetary outcome, or objective, which can be used to identify the least costly alternatives for meeting that goal.
One of the studies identified through our literature review examined the Helping to End Addiction Long Term intervention that has been implemented in response to the opioid and fentanyl crisis.[130] The HEAL Prevention Cooperative (HPC) includes ten research projects funded with the goal of developing effective prevention interventions across various settings (e.g., community, health care, juvenile justice, school) for older adolescent and young adults at risk for opioid misuse and opioid use disorder. These researchers are conducting an ongoing economic evaluation to provide information on the costs, cost-effectiveness, and sustainability of these interventions.
Quasi-experimental studies. Many impact evaluations employ a quasi-experimental comparison group design to estimate causal impact.[131] This design also uses a treatment group and one or more comparison groups; however, unlike the groups in a true experiment, membership in these groups is not randomly assigned. Because the groups were not formed through a random process, they may differ with regard to other factors that affect desired outcomes. Therefore, it is usually not possible to infer that the “raw” difference in outcomes between the groups has been caused by the treatment. Instead, statistical adjustments such as analysis of covariance should be applied to the raw difference to compensate for any initial lack of equivalence between the groups.
In one of the studies from our literature review, researchers conducted a real-world, quasi-experimental test of the effectiveness of a web-based videogame, smokeSCREEN, designed to promote knowledge that would reduce the likelihood of tobacco use, including vaping. Researchers compared before-after scores of a survey on beliefs about tobacco product use.[132] This study provides an example where a control group could not be completely achieved. Instead, researchers measured short-term knowledge changes before and after the intervention where each individual served as their own control. The researchers found statistically significant differences before and after the smokeSCREEN intervention. Their results suggest that a videogame intervention may have a promising effect on beliefs and knowledge about tobacco product use.
Non-experimental designs. Non-experimental methods involve obtaining measurement of variables as they naturally occur and testing the degree of association between or among those variables. Associations observed among variables in these studies typically do not allow for any defensible statement of causal impact.[133] One non-experimental approach is a cross-sectional study that measures the target population’s exposure to an intervention (rather than controls its exposure) and compares the outcomes of individuals receiving different levels of the intervention. Case studies can also be used to assess the effectiveness of complex interventions. In-depth case studies provide descriptive information on how an intervention operates and produces outcomes and, thus, may help generate hypotheses about program effects.
One cross-sectional study identified in our literature review examined community factors that may be associated with outcomes of a tobacco cessation program.[134] The researchers in this study gathered data from a cross-sectional sample of school districts and county offices of education administrators throughout the state of California. The sample included communities that had applied for state funding to reduce tobacco use and those that had not. Specifically, they studied population density, student ethnicity, the degree to which smoking cessation was a community priority, and perceptions of the gravity of youth tobacco use in the community. They found that several of the community characteristics measured were associated with the adoption of evidence-based tobacco cessation programs in schools.
According to studies from our literature review and scholars in the evaluation program field, community-based programs face considerable challenges in drawing conclusions about program impact. In figure 15, we illustrate some of the challenges that community-based programs, like the DFC program, face and potential solutions to those challenges.
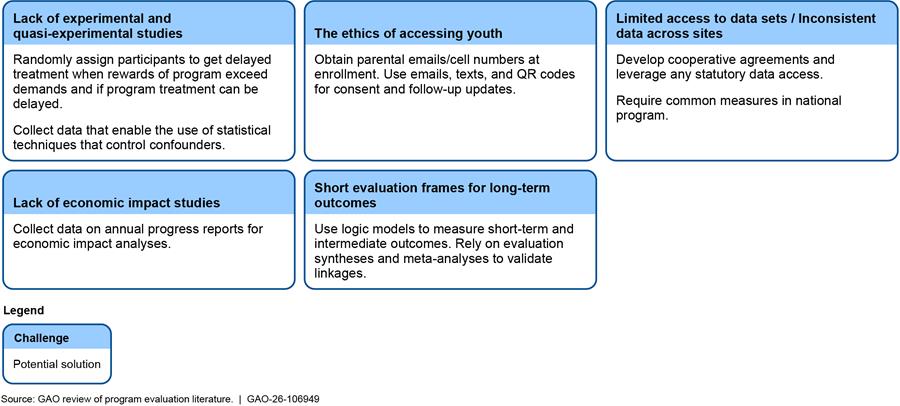
Appendix IX: Responses to Selected Questions on the Drug-Free Communities (DFC) Support Program Survey
We administered a web-based survey to 750 Drug-Free Communities (DFC) coalitions that have received funding from the DFC Support Program.[135] The survey aimed to gain coalition officials’ perspectives on how well the DFC program works and how it could improve. We administered the survey to the coalitions’ Project Coordinator, who manages the work of the coalition and program activities, including training, coalition communication, data collection and information dissemination. Other knowledgeable coalition representatives such as the Project Director responded to the survey if the Project Coordinator was not available. We administered the survey from July 2024 to late-August 2024. Our weighted response rate was 46 percent.
Survey data presented in this report are subject to all the qualifiers associated with self-reported data, and should be considered when reviewing the survey results, particularly for responses related to program effectiveness. Potential issues of concern include conflicts-of-interest, incentives, motivated reasoning or perception bias. Moreover, threats to the validity of survey data grow from low survey response rates and concerns about nonresponse bias. We took steps to adjust for nonresponse bias across DFC demographic characteristics obtained through Census Bureau data (ethnicity/race, population size, U.S. geographic region), and uncertainty is quantified through 95% confidence intervals.[136] These adjustments reduce, but may not eliminate, potential unmeasured bias resulting from non-response.
The responses to selected survey questions that underlie our reportable objectives are shown below. Our survey comprised closed- and open-ended questions. In this appendix, we do not provide information on responses provided to the open-ended questions. For a more detailed discussion of our survey methodology and limitations, see appendix I.
Table 7: Does your DFC coalition currently have a representative member from each of the 12 community sectors? (Question 1)
|
|
Yes |
No |
|||
|
Sector |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
|
Youth |
90% |
87-93% |
3% |
1-5% |
|
|
Parent |
92% |
89-95% |
1% |
0-2% |
|
|
Business |
91% |
88-94% |
2% |
1-4% |
|
|
Media |
90% |
87-93% |
3% |
2-5% |
|
|
School |
92% |
90-95% |
1% |
0-2% |
|
|
Youth-serving organization |
92% |
89-95% |
1% |
0-2% |
|
|
Law enforcement |
92% |
89-95% |
1% |
0-3% |
|
|
Civic/ volunteer group |
92% |
89-95% |
1% |
0-2% |
|
|
Religious/ fraternal organization |
91% |
88-94% |
3% |
1-4% |
|
|
Healthcare professional |
93% |
90-95% |
0% |
0-1% |
|
|
State, local, or tribal government agencies |
91% |
89-94% |
1% |
0-2% |
|
|
Other organization |
92% |
89-95% |
1% |
0-2% |
|
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have representation from the 12 sectors, which include: youth; parents; business; media; schools; youth-serving organizations; law enforcement; civic/ volunteer groups; religious/ fraternal organizations; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse; and other organizations involved in reducing substance use and misuse. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 8: Has your coalition experienced any challenges with retaining members from each of the 12 community sectors? (Question 3)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Yes |
54% |
49-59% |
|
No |
37% |
32-42% |
|
I am not sure |
2% |
1-3% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have representation from the 12 sectors, which include youth; parents; business; media; schools; youth-serving organizations; law enforcement; civic/ volunteer groups; religious/ fraternal organizations; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse; and other organizations involved in reducing substance use and misuse. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 9: Has your coalition’s ability to retain members from each of the 12 community sectors affected your capacity needed to effectively implement drug prevention and reduction initiatives for youth within your community in a sustainable manner? (Question 4)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Yes |
21% |
17-25% |
|
No |
68% |
63-73% |
|
I am not sure |
3% |
1-5% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have representation from the 12 sectors, which include: youth; parents; business; media; schools; youth-serving organizations; law enforcement; civic/ volunteer groups; religious/ fraternal organizations; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse; and other organizations involved in reducing substance use and misuse. We defined “sustainability” as the process of building an adaptive and effective system that achieves and maintains desired long-term results. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 10: Overall, how would you describe your DFC coalition member’s level of involvement in efforts to reduce substance use and misuse? (Question 6)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Collaborationa |
74% |
69-78% |
|
Cooperationb |
70% |
66-75% |
|
Coordinationc |
63% |
58-68% |
|
Networkingd |
66% |
62-71% |
|
No involvemente |
2% |
1-4% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have representation from the 12 sectors, which include: youth; parents; business; media; schools; youth-serving organizations; law enforcement; civic/ volunteer groups; religious/ fraternal organizations; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse; and other organizations involved in reducing substance use and misuse. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aCollaboration: members create formal agreements (e.g., memoranda of understanding or contracts). They develop common data collection systems; partner on joint fundraising efforts; pool fiscal or human resources; and create common workforce training systems.
bCooperation: members publicize one another’s programs in newsletters, write letters of support of one another’s grant applications, co-sponsor trainings or professional development activities and/or exchange such resources as technology expertise or meeting space.
cCoordination: stakeholders serve together on event planning committees and community boards or implement programs and services together.
dNetworking: members share what they are doing during coalition meetings. They talk about community issues in which they all have a stake or communicate about existing programs, activities, or services.
eNo involvement: members engage in separate activities, strategies, and policies.
Table 11: Overall, how would you describe each sector’s level of involvement in your coalition’s activities and efforts to reduce substance use and misuse? (Question 6a)
|
|
Collaborationa |
Cooperationb |
Coordinationc |
Networkingd |
||||
|
Sector |
Estimated % |
95% CI |
Estimated % |
95% CI |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
Youth |
42% |
37-47% |
20% |
16-24% |
15% |
11-18% |
11% |
8-14% |
|
Parent |
26% |
21-30% |
27% |
22-31% |
17% |
14-21% |
16% |
13-20% |
|
Business |
24% |
20-28% |
25% |
21-29% |
15% |
11-18% |
24% |
20-29% |
|
Media |
26% |
22-31% |
27% |
22-31% |
13% |
9-16% |
21% |
17-26% |
|
School |
59% |
54-64% |
12% |
9-15% |
15% |
11-19% |
3% |
1-5% |
|
Youth-serving organization |
54% |
49-59% |
15% |
11-18% |
17% |
13-21% |
4% |
2-6% |
|
Law enforcement |
47% |
42-52% |
17% |
13-21% |
17% |
14-21% |
7% |
4-9% |
|
Civic/ volunteer group |
33% |
28-37% |
20% |
16-24% |
20% |
16-24% |
15% |
11-18% |
|
Religious/ fraternal organization |
23% |
19-27% |
26% |
22-30% |
12% |
8-15% |
26% |
22-31% |
|
Healthcare professional |
40% |
35-45% |
20% |
16-24% |
17% |
13-21% |
13% |
10-17% |
|
State/ local/ tribal government agencies |
40% |
35-45% |
17% |
13-20% |
18% |
14-22% |
14% |
10-17% |
|
Other organization |
45% |
40-50% |
16% |
12-20% |
16% |
12-20% |
9% |
6-11% |
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have representation from the 12 sectors, which include: youth; parents; business; media; schools; youth-serving organizations; law enforcement; civic/ volunteer groups; religious/ fraternal organizations; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse; and other organizations involved in reducing substance use and misuse. The table does not include values for “no involvement,” which is defined as members that engage in separate activities, strategies, and policies. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aCollaboration: members create formal agreements (e.g., memoranda of understanding or contracts). They develop common data collection systems; partner on joint fundraising efforts; pool fiscal or human resources; and create common workforce training systems.
bCooperation: members publicize one another’s programs in newsletters, write letters of support of one another’s grant applications, co-sponsor trainings or professional development activities and/or exchange such resources as technology expertise or meeting space.
cCoordination: stakeholders serve together on event planning committees and community boards or implement programs and services together.
dNetworking: members share what they are doing during coalition meetings. They talk about community issues in which they all have a stake or communicate about existing programs, activities, or services.
Table 12: Overall, how easy or difficult has it been to involve each of the sectors in your coalition’s activities and efforts to reduce substance use and misuse? (Question 6b)
|
Sector |
Mean Value |
95 percent confidence interval |
|
Youth |
2.5 |
2.4-2.6 |
|
Parent |
2.7 |
2.6-2.8 |
|
Business |
2.7 |
2.6-2.8 |
|
Media |
2.4 |
2.3-2.5 |
|
School |
2.0 |
1.9-2.1 |
|
Youth-serving organization |
1.7 |
1.6-1.8 |
|
Law Enforcement |
2.1 |
1.9-2.2 |
|
Civic/ volunteer group |
2.2 |
2.1-2.3 |
|
Religious/ fraternal organization |
2.6 |
2.5-2.8 |
|
Healthcare professional |
2.0 |
1.9-2.1 |
|
State/ local/ tribal government agencies |
2.1 |
2.0-2.3 |
|
Other organization |
1.9 |
1.8-2.0 |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have representation from the 12 sectors, which include: youth; parents; business; media; schools; youth-serving organizations; law enforcement; civic/ volunteer groups; religious/ fraternal organizations; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse; and other organizations involved in reducing substance use and misuse. The response options to this question were 1=extremely easy, 2=somewhat easy, 3=neither easy nor difficult, 4=somewhat difficult, or 5=extremely difficult. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 13: Has your coalition faced any challenges retaining key personnel that are responsible for implementing and managing the grant? (Question 7)
|
|
Yes |
No |
Unsure |
|||
|
Personnel |
Estimated % |
95% CI |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
Authorized organization representativea |
5% |
3-7% |
85% |
81-88% |
1% |
0-2% |
|
Project directorb |
8% |
5-11% |
82% |
78-86% |
1% |
0-1% |
|
Project coordinatorc |
19% |
15-23% |
70% |
66-75% |
1% |
0-2% |
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to have an Authorized Organization Representative, Project Director, and Project Coordinator. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aAuthorized Organization Representative is a representative of the recipient organization authorized to act on the organization’s behalf with awards and administration of grants. This person must be an employee of the recipient organization and not be the same person as the program director/principal investigator and project coordinator. In signing a grant application, this individual agrees that the organization will assume the obligations imposed by applicable federal statutes and regulations and other terms and conditions of the award. These responsibilities include overseeing the financial aspects of the grant and the performance of the grant-supported project or activities as specified in the approved application.
bProject Director provides programmatic oversight of the grant and is accountable to officials of the recipient organization. The program director/principal investigator must be an employee of the recipient organization and cannot be the same person as the authorized organization representative.
cProject Coordinator manages the work of the coalition and program activities, including training, coalition communication, data collection, and information dissemination. The program director/principal investigator and project coordinator can be the same person and must also be an employee of the recipient organization.
Table 14: Did the Office of National Drug Control Policy (ONDCP), Centers for Disease Control and Prevention (CDC), CADCA, or DFC National Cross-Site Evaluation Team provide your coalition with any of the types of information described below? (Question 9)
|
|
Yes |
No |
Unsure |
|||
|
Information Type |
Estimated % |
95% CI |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
Strategies your coalition can use to maximize collaboration and coordination across all community sectors |
77% |
73-82% |
5% |
3-8% |
8% |
5-11% |
|
Steps your coalition can take to identify which prevention activities are the most cost-effective and are reaching the largest number of youths |
63% |
58-68% |
14% |
11-18% |
14% |
10-17% |
|
Strategies that can be used to assess your coalition’s progress in reaching goals to reduce substance use and misuse |
77% |
73-82% |
5% |
2-7% |
9% |
6-12% |
|
Strategies that can be used to bolster effectiveness of your coalition’s programs and activities |
76% |
72-81% |
7% |
4-9% |
8% |
5-10% |
|
Best practices for efficiently managing costs/resources to support your coalition’s programs and activities |
60% |
56-65% |
15% |
12-19% |
15% |
11-18% |
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
|
Information Type |
Mean Value |
95 percent confidence interval |
|
Strategies your coalition can use to maximize collaboration and coordination across all community sectors |
3.9 |
3.8-4.0 |
|
Steps your coalition can take to identify which prevention activities are the most cost-effective and are reaching the largest number of youths |
3.9 |
3.8-4.0 |
|
Strategies that can be used to assess your coalition’s progress in reaching goals to reduce substance use and misuse |
4.0 |
3.9-4.1 |
|
Strategies that can be used to bolster effectiveness of your coalition’s programs and activities |
3.9 |
3.8-4.0 |
|
Best practices for efficiently managing costs/resources to support your coalition’s programs and activities |
3.9 |
3.8-4.0 |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The response options to this question were 1=not at all useful, 2=slightly useful, 3=moderately useful, 4=very useful, or 5=extremely useful. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 16: Have youth in your community reported changes in any of the four metrics listed below because of their participation in your coalition’s programs or activities? (Question 10)
|
|
Yes |
No |
Unsure |
|||
|
Core Measure |
Estimated % |
95% CI |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
Past 30-day drug usea |
56% |
51-61% |
8% |
5-10% |
27% |
22-31% |
|
Perception of riskb |
59% |
55-64% |
9% |
6-12% |
22% |
18-26% |
|
Perception of parental disapprovalc |
52% |
47-57% |
13% |
9-16% |
26% |
22-31% |
|
Perception of peer disapprovald |
57% |
52-62% |
10% |
7-13% |
24% |
20-28% |
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. The DFC program requires coalitions to report on four core measures—see definitions below. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aPast 30-day Prevalence of Use is the percentage of youth who reported misusing prescription drugs or using alcohol, marijuana, or tobacco, at least once in the past 30 days.
bPerception of Risk is the percentage of youth who reported they perceived people who misuse prescription drugs or use alcohol (binge use), marijuana, or tobacco risk harming themselves to a moderate or great extent.
cPerception of Parental Disapproval is the percentage of youth who reported they perceived their parent, guardian, or caregiver would feel the misuse of prescription drugs or regular use of alcohol, marijuana, or tobacco is wrong.
dPerception of Peer Disapproval is the percentage of youth who reported they perceived their peers would feel the misuse of prescription drugs or regular use of alcohol, marijuana, or tobacco is wrong.
|
|
Yes |
No |
||
|
Indicator |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
Number of programs conducted during each performance period |
78% |
74-82% |
11% |
8-15% |
|
Number of youth served |
86% |
83-90% |
4% |
2-6% |
|
Confidence in coalition capability |
59% |
54-64% |
31% |
27-36% |
|
An accounting of inter-sector collaboration |
44% |
39-49% |
47% |
42-52% |
|
Number of events implemented by the coalition |
85% |
81-88% |
5% |
3-8% |
|
Number of coalition members involved in sponsored activities |
75% |
71-79% |
15% |
11-18% |
|
The level of involvement of each sector in coalition activities |
66% |
61-71% |
24% |
20-29% |
|
Data on groups disproportionately affected by substance use |
60% |
55-65% |
30% |
26-35% |
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 18: If yes, how successful has your coalition been in reaching these markers since receiving DFC funding? (Question 11a)
|
Indicator |
Mean Value |
95 percent confidence interval |
|
Number of programs conducted during each performance period |
2.7 |
2.6-2.7 |
|
Number of youth served |
2.7 |
2.6-2.7 |
|
Confidence in coalition capability |
2.6 |
2.5-2.7 |
|
An accounting of inter-sector collaboration |
2.4 |
2.3-2.4 |
|
Number of events implemented by the coalition |
2.7 |
2.6-2.7 |
|
Number of coalition members involved in sponsored activities |
2.4 |
2.3-2.5 |
|
The level of involvement of each sector in coalition activities |
2.3 |
2.2-2.4 |
|
Data on groups disproportionately affected by substance use |
2.3 |
2.2-2.4 |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Survey respondents received this question if they answered “yes” to Question 11. The response options to this question were 1=not successful, 2=somewhat successful, or 3=very successful. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 19: In general, are the resources (e.g., grant funding, training, technical assistance, etc.) that the DFC Support Program provides sufficient for your coalition to carry out the programming that you feel is necessary to meet the program goals of preventing and reducing substance use and misuse in your community? (Question 12)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Yes |
68% |
64-73% |
|
No |
21% |
17-26% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 20: Has your DFC coalition sponsored a youth coalitiona within the last two years? (Question 14)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Yes |
67% |
62-72% |
|
No |
23% |
19-27% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aYouth coalition is a group of youth who work together to plan and implement activities related to the mission of the full coalition. An adult coalition member serves as a mentor or leader, but the youth have key leadership roles. The youth coalition is integral to the full coalition, but generally meets independently.
Table 21: Were youth involved in planning or leading your youth coalitiona activities? (Question 14a)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Yes |
64% |
59-69% |
|
No |
1% |
0-3% |
|
Unsure |
1% |
0-2% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aYouth coalition is a group of youth who work together to plan and implement activities related to the mission of the full coalition. An adult coalition member serves as a mentor or leader, but the youth have key leadership roles. The youth coalition is integral to the full coalition, but generally meets independently.
|
Frequency |
Estimated percentage |
95 percent confidence interval |
|
Weekly |
21% |
17-25% |
|
Monthly |
38% |
33-43% |
|
Quarterly |
5% |
3-8% |
|
Bi-annually |
1% |
0-1% |
|
Annually |
1% |
0-3% |
|
Not at all |
0% |
0-1% |
|
I am not sure |
0% |
0-1% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Survey respondents received this question if they answered “yes” to Question 14a. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aYouth coalition is a group of youth who work together to plan and implement activities related to the mission of the full coalition. An adult coalition member serves as a mentor or leader, but the youth have key leadership roles. The youth coalition is integral to the full coalition, but generally meets independently.
Table 23: Which of the four core measure substances are the focus of your coalition’s work? (Question 18)
|
Substance |
Estimated Percentage |
95 percent confidence interval |
|
Alcohol |
82% |
78-86% |
|
Marijuana |
75% |
70-79% |
|
Tobacco |
59% |
55-64% |
|
Prescription Drugs |
47% |
42-52% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 24: Has your coalition focused on addressing any of the following substances of emerging risk that go beyond the four key substances? (Question 20)
|
|
Yes |
No |
|||
|
Substance |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
|
Synthetic opioida |
66% |
62-71% |
21% |
17-25% |
|
|
Vaping |
86% |
82-89% |
3% |
1-4% |
|
|
Prescription opioidsb |
63% |
58-68% |
21% |
17-25% |
|
|
Heroin |
23% |
18-27% |
56% |
51-61% |
|
|
Methamphetamine |
21% |
17-25% |
59% |
54-64% |
|
|
Cocaine |
12% |
8-15% |
66% |
61-71% |
|
|
Ecstasy |
7% |
4-10% |
70% |
65-75% |
|
|
Other |
10% |
7-13% |
30% |
26-35% |
|
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aFentanyl is an example of a “synthetic opioid.”
bMethadone, oxycodone, or hydrocodone are examples of “prescription opioids.”
Table 25: If yes, has your coalition been effective in reducing use for this substance? (Question 21a)
|
|
Yes |
No |
||
|
Substance |
Estimated % |
95% CI |
Estimated % |
95% CI |
|
Synthetic opioida |
19% |
15-23% |
7% |
4-9% |
|
Vaping |
49% |
44-54% |
9% |
6-12% |
|
Prescription opioidsb |
30% |
25-35% |
4% |
2-6% |
|
Heroin |
6% |
4-8% |
2% |
0-3% |
|
Methamphetamine |
7% |
4-9% |
2% |
0-3% |
|
Cocaine |
4% |
2-7% |
1% |
0-2% |
|
Ecstasy |
2% |
1-3% |
1% |
0-2% |
|
Other |
2% |
1-4% |
1% |
0-2% |
Legend: Estimated % = estimated percentage; 95% CI = 95 percent confidence interval
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Survey respondents received this question if they answered “yes” to Question 20. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
aFentanyl is an example of a “synthetic opioid.”
bMethadone, oxycodone, or hydrocodone are examples of “prescription opioids.”
Table 26: Has your coalition done anything differently to address the emerging threat of fentanyl, opioids, and counterfeit pills? (Question 21b)
|
Responses |
Estimated percentage |
95 percent confidence interval |
|
Yes |
58% |
53-63% |
|
No |
31% |
27-36% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Table 27: How flexible or inflexible are ONDCP’s DFC Support Program requirements in allowing your coalition to develop and offer the specific kinds of prevention programs and activities needed to address drug use and misuse in your community? (Question 23)
|
Responses |
Estimated Percentage |
95 percent confidence interval |
|
Very flexible |
38% |
33-42% |
|
Slightly flexible |
29% |
24-33% |
|
Neither flexible nor inflexible |
10% |
7-13% |
|
Slightly inflexible |
6% |
3-8% |
|
Very inflexible |
1% |
0-1% |
Source: GAO. | GAO‑26‑106949
Notes: We conducted a census survey of 750 coalitions funded by the Drug-Free Communities (DFC) Support Program. Estimated percentages for each response do not sum to 100 percent because the table does not include percentages for “missing values” for those responses. Upper- and lower-bound 95 percent confidence intervals are provided for each estimate.
Appendix X: Drug-Free Communities (DFC) Support Program’s Applicant Eligibility Criteria and Program Requirements
The Drug-Free Communities (DFC) Support Program grants funding to community-based coalitions that focus on preventing and reducing youth substance use—which generally include the illegal use or misuse of controlled substances under the Controlled Substances Act,[137] the misuse of inhalants or other over-the-counter drugs, or the use of alcohol, tobacco, or other related products.[138] The Office of National Drug Control Policy (ONDCP), a component of the Executive Office of the President, administers and partners with the Centers for Disease Control and Prevention (CDC) to manage the DFC program—including the day-to-day grant management.
ONDCP reported that 751 coalitions across the United States received DFC funding in fiscal year 2025—with each coalition eligible to receive up to $125,000 per year for up to a 10-year period.[139] Each DFC coalition is required to have a volunteer representative from each of 12 community sectors.[140] Some of these sectors include, but are not limited to, youth; parents; schools; law enforcement; health care professionals; state, local, or tribal governmental agencies with expertise in the field of substance use and misuse.[141] Generally, to meet the statutory requirements of the DFC program, a coalition must:
· submit an application to the Administrator;[142]
· consist of one or more representatives from each of the 12 sectors—at least one representative per sector;[143]
· demonstrate that the representatives of the coalition have worked together on substance use and misuse reduction initiatives for at least 6 months (prior to applying);[144]
· demonstrate substantial participation from volunteer leaders in the community involved;[145]
· have as its principal mission the reduction of substance use and misuse in a comprehensive and long-term manner, with a primary focus on youth in the community;[146]
· describe and document the nature and extent of the substance use and misuse problem in the community;[147]
· provide a description of the substance use and misuse prevention and treatment programs and activities in existence at the time of the grant application and identify substance use and misuse programs and service gaps in the community;[148]
· develop a strategic plan to reduce substance use and misuse among youth in a comprehensive and long-term fashion;[149]
· work to develop a consensus regarding the priorities of the community to combat substance use and misuse among youth;[150]
· establish a system to measure and report outcomes;[151]
· conduct an initial benchmark survey of drug use among youth as well as biennial surveys to measure the progress and effectiveness of the coalition and provide assurances that the entity conducting the evaluation or from which the coalition receives information has experience in gathering data related to substance use and misuse among youth or in evaluating the effectiveness of community anti-drug coalitions;[152] and
· demonstrate that the coalition is an ongoing concern by demonstrating that it is a nonprofit organization, an entity that the Administrator determines to be appropriate, or part of, or is associated with, an established legal entity that receives financial support from non-federal sources and has a strategy to solicit substantial financial support from non-federal sources to ensure that the coalition and the programs operated by the coalition are self-sustaining.[153]
In addition to meeting statutory eligibility requirements, grantees must also comply with the DFC program’s terms and conditions. For example, along with setting up internal control procedures, the program requires that grantees develop a comprehensive 12-month action plan that includes an appropriate strategy for each drug (i.e., marijuana, alcohol, or tobacco) they will be addressing—as well as a mechanism for demonstrating their progress along the way. Further, two grantees may not serve the same zip code, unless both have clearly demonstrated a plan for collaboration.[154]
The Office of National Drug Control Policy (ONDCP) is responsible for overseeing the implementation of the nation’s drug control policy and leading the national drug control effort.[155] ONDCP also manages several programs (including the Drug-Free Communities (DFC) Support Program) that support the National Drug Control Program agencies.[156] The DFC program grants funding to community-based coalitions that focus on preventing youth substance use and misuse. Through a partnership with ONDCP, the Centers for Disease Control and Prevention (CDC) manages the DFC program—including day-to-day grant management.[157]
As mentioned earlier in this report, based on ONDCP’s budget data, over a 8-year period—fiscal years 2018 through 2025, ONDCP was appropriated about $835 million to manage and administer the DFC Program—and funded 5,718 DFC grant awards (averaging about 715 grant awards annually).[158] During this period, ONDCP allocated about $82 million to the DFC program for administrative costs[159] (i.e., grant management and oversight efforts), and requested additional funding from Congress for such expenses while consistently not disclosing its administrative carryover balances ranging from about $4.8 million to almost $11.9 million.[160]
According to ONDCP, by fiscal year 2018, it had accumulated nearly $10.5 million in carryover funds available for administrative expenses for the DFC program. By fiscal year 2020, ONDCP had accumulated nearly $11.9 million in carryover funds available for administrative expenses. In fiscal year 2020, ONDCP used some of these carryover funds and funds allocated for administrative expenses from its annual appropriation to pay for the administrative costs associated with SAMHSA and CDC providing day-to-day grant management and oversight services totaling around $14.7 million. According to ONDCP officials, in fiscal year 2021, CDC began to solely manage the program—providing more program oversight opportunities and coalitions received a higher level of customer service to assist in implementing the grant program’s goals and objectives. Subsequently, ONDCP’s carryover funds available for administrative expenses for the DFC program were reduced to nearly $5.3 million for fiscal year 2021. In that fiscal year, ONDCP allocated nearly $8.2 million from its annual appropriation of $102 million for the administration of the DFC program from the Consolidated Appropriations Act, 2021,[161] in accordance with the statutory limitation in 21 U.S.C. § 1524(b), and expended around $8.4 million for administrative expenses for the DFC program, resulting in a reduction of the carryover balance to nearly $5 million.
In ONDCP’s Congressional Budget Submission for fiscal year 2022, ONDCP requested $106 million for the DFC program. In addition, ONDCP “request[ed] up to 12 percent for administrative costs associated with the program. This is a change from the current 8 percent cap for administrative costs. The increase of $4 million is to provide for the additional 4 percent increase in administrative costs without reducing DFC grants.” The budget submission also stated:
In FY 2020, ONDCP collaborated with the CDC to transition the administration of the DFC grants from SAMHSA. Effectively managing the DFC Program, which currently funds over 700 community-based coalitions, requires a significant level of administrative support and program management oversight to ensure that recipients continue to be successful, while also practicing sound grants management policies and procedures. Invaluable lessons were learned during the FY 2020 transition, including the need for additional resources to support the management of the programs. In order to continue to lead the Nation’s effort to mobilize communities to prevent substance misuse among youth, ONDCP is requesting an administrative cap increase to 12%. The level of support and guidance given by ONDCP and the agency administering the grants is directly tied to the success of the coalitions. This increase would go towards ensuring that the coalitions have appropriate oversight, receive timely responses to their technical assistance needs and allows for stronger collaboration. Examples include conducting site visits on a more frequent, reoccurring basis and coordination and delivery of technical and subject matter expertise on multiple public health issues.
However, ONDCP’s budget submission did not disclose information related to ONDCP’s carryover balance of nearly $5 million from fiscal year 2021, an estimate of its fiscal year 2021 carryover balance, or any of the preceding years’ carryover balances. Subsequently, the Consolidated Appropriations Act, 2022, appropriated $106 million for the DFC program, of which not more than $11.25 million (which represented nearly 11 percent of the appropriated amount for the program) was available for administrative expenses.[162] Based on ONDCP’s data, it expended nearly $11.5 million for administrative expenses in fiscal year 2022, reducing its carryover balance for administrative expenses to nearly $4.8 million.
In ONDCP’s Congressional Budget Submission for fiscal year 2023, ONDCP requested $106 million for the DFC program and “request[ed] up to 12 percent for administrative costs associated with the program. This is a change from the current 8 percent for administrative costs. According to ONDCP officials, the DFC Program’s administrative cap has not been raised in over a decade and is necessary to sustain effective program management and proper oversight.” ONDCP, in its budget submission stated that:
Since October 2020, ONDCP partners with CDC’s National Center for Injury Prevention and Control (NCIPC) for the day-to-day management of the DFC Program. The DFC Program, which currently funds 745 community-based coalitions, requires a significant level of administrative support and program management oversight to ensure that recipients continue to be successful. This enhanced oversight with the CDC also ensures sound grants management policies and procedures are followed. Invaluable lessons were learned during the transition, including the need for additional resources to support the management of the programs. In order to continue to lead the Nation’s effort to mobilize communities to prevent substance misuse among youth, ONDCP is requesting an administrative cap increase up to 12%. The level of support and guidance given by ONDCP and the agency administering the grants (CDC) is directly tied to the success of the coalitions. This increase would go towards ensuring that the coalitions have appropriate oversight, receive timely responses to their technical assistance needs, while allowing for stronger collaboration. Examples include conducting site visits on a more frequent and reoccurring basis; strengthening coordination and delivery of technical/subject matter expertise on multiple public health issues; and ensure ratio of grant recipient to federal staff/subject matter expert allows for individualized support.
However, according to ONDCP officials, ONDCP’s budget submission did not disclose information related to ONDCP’s carryover balance of nearly $4.8 million from fiscal year 2022, an estimate of its fiscal year 2022 carryover balance, or any of the preceding years’ carryover balances. The Consolidated Appropriations Act, 2023, appropriated $109 million for the DFC program, of which not more than nearly $12.8 million (which represented nearly 12 percent of the appropriated amount for the program) was available for administrative expenses.[163] According to ONDCP data, ONDCP expended nearly $8.5 million for administrative expenses in fiscal year 2023, resulting in an increase of its carryover balance for administrative expenses by nearly $4.3 million to a total carryover balance for administrative expenses of around $9 million. According to ONDCP officials, administrative expenses may fluctuate based on program requirements, particularly the cycles for the DFC Technology and Evaluation contracts.
Similarly, in fiscal year 2024, ONDCP requested in its Congressional Budget Submission and was appropriated $109 million for the DFC program, of which not more than nearly $12.8 million (which represents nearly 12 percent of the appropriated amount for the program) was available for administrative expenses.[164] ONDCP officials stated that ONDCP’s congressional budget submission for fiscal year 2024 did not disclose a total carryover balance for administrative expenses of around $9 million, an estimate of its fiscal year 2023 carryover balance, or any of the preceding years’ carryover balances. According to ONDCP data, ONDCP expended around $12.1 million for administrative expenses in fiscal year 2024, resulting in an increase of its carryover balance for administrative expenses to a total carryover balance for administrative expenses of nearly $9.7 million for fiscal year 2025.
For fiscal year 2025, ONDCP requested $109 million for the DFC program, of which not more than nearly $12.8 million would be available for administrative expenses. The Full-Year Continuing Appropriations and Extensions Act, 2025, generally continued the funding levels from the fiscal year 2024 appropriations acts under the same authorities and limitations, unless otherwise specified.[165] Table 28 provides an overview of the DFC program’s appropriations, administrative costs, grant awards, and carryover balances for each fiscal year—2018 through 2025.
Table 28: Overview of Drug-Free Communities (DFC) Support Program’s Appropriations, Grant Awards, Administrative Costs, and Carryover Balances for Fiscal Years 2018 Through 2025
|
|
Fiscal Years |
|||||||
|
DFC Program’s Budget Components |
2018* |
2019* |
2020* |
2021* |
2022** |
2023** |
2024** |
2025** |
|
Annual appropriation |
$99,000,000 |
$100,000,000 |
$101,250,000 |
$102,000,000 |
$106,000,000 |
$109,000,000 |
$109,000,000 |
$109,000,000 |
|
Number of grant awards |
731 |
719 |
733 |
742 |
745 |
751 |
751 |
546 |
|
Grant award amounts |
$91,080,000 |
$92,000,000 |
$93,150,000 |
$93,840,000 |
$94,750,000 |
$96,220,000 |
$96,220,000 |
$96,220,000 |
|
Administrative costs (allocation by the Office National Drug Control Policy)a |
$7,920,000 |
$8,000,000 |
$8,100,000 |
$8,160,000 |
$11,250,000 |
$12,780,000 |
$12,780,000 |
$12,780,000 |
|
Carryover available for administrative costsb |
$10,530,504 |
$11,214,786 |
$11,893,051 |
$5,285,312 |
$4,998,283 |
$4,756,571 |
$9,021,245 |
$9,692,847 |
|
Total budget authority available for administrative costs |
$18,450,505 |
$19,214,786 |
$19,993,051 |
$13,445,312 |
$16,248,283 |
$17,536,571 |
$21,801,245 |
$22,472,847 |
|
Execution for administrative costs |
$7,235,719 |
$7,321,735 |
$14,707,739c |
$8,447,029 |
$11,491,712 |
$8,515,326 |
$12,108,398 |
$12,498,609 |
|
Balance available for administrative expenses (ending each fiscal year) |
$11,214,786 |
$11,893,051 |
$5,285,312 |
$4,998,283 |
$4,756,571 |
$9,021,245 |
$9,692,847 |
$9,974,238 |
Source: GAO Analysis of the Office of National Drug Control Policy’s (ONDCP) budget data related to the DFC program. | GAO‑26‑106949
Note: As mentioned earlier in this report, for each fiscal year identified, the number of DFC grants awarded includes the four types of grants available to coalitions through the DFC program—(1) new; (2) continuation; (3) mentoring; and (4) mentoring continuation. According to ONDCP officials, the new and continuation grants represent a majority of the DFC grants awarded. According to ONDCP officials, the mentoring grant has not been funded since the management of the DFC Program transitioned to CDC.
aThis represents ONDCP’s allocated funds for administrative expenses from annual appropriations in accordance with statutory or appropriations limitations for each of the respective fiscal years—2018 through 2025.
bAn agency’s obligational authority is the sum of budget authority enacted for a given fiscal year; and unobligated balances of amounts that have not expired brought forward from prior years. The balance of obligational authority is an amount carried over from one year to the next if the budget authority is available for obligation in the next fiscal year. Not all obligational authority that becomes available in a fiscal year is obligated and paid out in that same year. Balances are described as (1) obligated, (2) unobligated, or (3) unexpended.
cIn fiscal year 2020, ONDCP decided to transition the management of the DFC program from SAMHSA to CDC. While in this transition period, ONDCP incurred a total of approximately $14.7 million in administrative costs to retain SAMHSA and CDC’s management services, according to ONDCP officials. ONDCP officials stated that this is why the program’s administrative costs in fiscal year 2020 were larger when compared other fiscal years.
*Pursuant to 21 U.S.C. § 1524(b), not more than 8 percent of the funds appropriated to carry out the DFC program may be used by ONDCP to pay administrative costs associated with the program.
**In these fiscal year appropriations, the annual appropriations specified the amount of the appropriation that could be used for administrative expenses (which was greater than the statutory limitation in 21 U.S.C. § 1524(b)).
GAO Contacts
Triana McNeil, McNeilT@gao.gov
Jamila Jones Kennedy, KennedyJJ@gao.gov.
Staff Acknowledgments
In addition to the contact named above, Frederick Lyles, Jr. (Assistant Director), Terell Lasane, (Assistant Director), Anthony Patterson (Analyst in Charge), Valerie Caracelli, Lawrence Crockett, Koffi Dogbevi, Eric Hauswirth, Nicole Hewitt, Michael Hoffman, Danny Lee, and Kevin Reeves also made key contributions to the report. Also contributing to the report were Gergana Danailova-Trainor, Jill Lacey, John Mingus, Pamela Snedden, Raquel Qualls-Hampton, and Sirin Yaemsiri.
High-Risk Series: Heightened Attention Could Save Billions More and Improve Government Efficiency and Effectiveness, GAO‑25‑107743. Washington, D.C.: Feb. 25, 2025.
Drug Policy: Preliminary Observations on the 2022 National Drug Control Strategy. GAO‑22‑106087. Washington, D.C.: June 15, 2022.
Drug Control Grants: ONDCP Should Document Its Process for Identifying Duplication, Overlap, and Fragmentation. GAO‑22‑104666. Washington, D.C.: December 8, 2021.
High-Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas. GAO‑21‑119SP. Washington, D.C.: March 2, 2021.
Substance Use Disorder: Reliable Data Needed for Substance Abuse Prevention and Treatment Block Grant Program. GAO‑21‑58. Washington, D.C.: December 14, 2020.
Drug Misuse: Agencies Have Not Fully Identified How Grants That Can Support Drug Prevention Education Programs Contribute to National Goals. GAO‑21‑96. Washington, D.C.: November 18, 2020.
Prescription Drug Monitoring Programs: Views on Usefulness and Challenges of Programs. GAO‑21‑22. Washington, D.C.: October 1, 2020.
Bureau of Prisons: Improved Planning Would Help BOP Evaluate and Manage Its Portfolio of Drug Education and Treatment Programs. GAO‑20‑423. Washington, D.C.: May 26, 2020.
Workforce Innovation and Opportunity Act: Additional DOL Actions Needed to Help States and Employers Address Substance Use Disorder. GAO‑20‑337. Washington, D.C.: May 21, 2020.
Drug Misuse: Sustained National Efforts Are Necessary for Prevention, Response, and Recovery. GAO‑20‑474. Washington, D.C.: March 26, 2020.
Drug Control: Actions Needed to Ensure Usefulness of Data on Suspicious Opioid Orders. GAO‑20‑118. Washington, D.C.: January 29, 2020.
Opioid Use Disorder: Barriers to Medicaid Beneficiaries’ Access to Treatment Medications. GAO‑20‑233. Washington, D.C.: January 24, 2020.
Drug Control: The Office of National Drug Control Policy Should Develop Key Planning Elements to Meet Statutory Requirements. GAO‑20‑124. Washington, D.C.: December 18, 2019.
Veterans Health Care: Services for Substance Use Disorders, and Efforts to Address Access Issues in Rural Areas. GAO‑20‑35. Washington, D.C.: December 2, 2019.
Drug Policy: Preliminary Observations on the 2019 National Drug Control Strategy. GAO‑19‑370T. Washington, D.C.: March 7, 2019.
Drug Control: DOD Should Improve Its Oversight of the National Guard Counterdrug Program. GAO‑19‑27. Washington, D.C.: January 17, 2019.
Colombia: U.S. Counternarcotics Assistance Achieved Some Positive Results but State Needs to Review the Overall U.S. Approach. GAO‑19‑106. Washington, D.C.: December 12, 2018.
Opioid Crisis: Status of Public Health Emergency Authorities. GAO‑18‑685R. Washington, D.C.: September 26, 2018.
Prescription Opioids: Medicare Needs Better Information to Reduce the Risk of Harm to Beneficiaries. GAO‑18‑585T. Washington, D.C.: May 29, 2018.
VA Health Care: Progress Made Towards Improving Opioid Safety, but Further Efforts to Assess Progress and Reduce Risk Are Needed. GAO‑18‑380. Washington, D.C.: May 29, 2018.
Illicit Opioids: Office of National Drug Control Policy and Other Agencies Need to Better Assess Strategic Efforts. GAO‑18‑569T. Washington, D.C.: May 17, 2018.
Illicit Opioids: While Greater Attention Given to Combating Synthetic Opioids, Agencies Need to Better Assess their Efforts. GAO‑18‑205. Washington, D.C.: March 29, 2018.
Substance Use Disorder: Information on Recovery Housing Prevalence, Selected States’ Oversight, and Funding. GAO‑18‑315. Washington, D.C.: March 22, 2018.
Opioid Use Disorders: HHS Needs Measures to Assess the Effectiveness of Efforts to Expand Access to Medication-Assisted Treatment. GAO‑18‑44. Washington, D.C.: October 31, 2017.
Counternarcotics: Overview of U.S. Efforts in the Western Hemisphere. GAO‑18‑10. Washington, D.C.: October 13, 2017.
Preventing Drug Abuse: Low Participation by Pharmacies and Other Entities as Voluntary Collectors of Unused Prescription Drugs. GAO‑18‑25. Washington, D.C.: October 12, 2017.
Prescription Opioids: Medicare Needs to Expand Oversight Efforts to Reduce the Risk of Harm. GAO‑18‑15. Washington, D.C.: October 6, 2017.
Drug Control Policy: Information on Status of Federal Efforts and Key Issues for Preventing Illicit Drug Use. GAO‑17‑766T. Washington, D.C.: July 26, 2017.
Drug-Free Communities Support Program: Agencies Have Strengthened Collaboration but Could Enhance Grantee Compliance and Performance Monitoring. GAO‑17‑120. Washington, D.C.: February 7, 2017.
Office of National Drug Control Policy: Office Could Better Identify Opportunities to Increase Program Coordination. GAO‑13‑333. Washington, D.C.: March 26, 2013.
ONDCP Media Campaign: Contractor’s National Evaluation Did Not Find That the Youth Anti-Drug Media Campaign Was Effective in Reducing Youth Drug Use. GAO‑06‑818. Washington, D.C.: August 25, 2006.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries

[1]Centers for Disease Control and Prevention, National Center for Health Statistics. National Vital Statistics System, Provisional Mortality on CDC WONDER Online Database. Data are from the final Multiple Cause of Death Files, 2023, as compiled from data provided by the 57 vital statistics jurisdictions through the Vital Statistics Cooperative Program. Accessed at http://wonder.cdc.gov/mcd‑icd10‑provisional.html on Dec 9, 2025. According to CDC, the widespread availability of illicit manufactured fentanyl, proliferation of counterfeit pills resembling prescription drugs but containing illicit manufactured fentanyl or other illicit drugs, and ease of purchasing pills through social media have increased fatal overdose risk among adolescents.
[2]GAO, High-Risk Series: Substantial Efforts Needed to Achieve Greater Progress on High-Risk Areas, GAO‑19‑157SP (Washington, D.C.: Mar. 6, 2019). GAO, Drug Misuse: Sustained National Efforts Are Necessary for Prevention, Response, and Recovery, GAO‑20‑474 (Washington, D.C.: Mar. 26, 2020). GAO, High-Risk Series: Dedicated Leadership Needed to Address Limited Progress in Most High-Risk Areas, GAO‑21‑119SP (Washington, D.C.: Mar 2, 2021).
[3]More than a dozen federal agencies—known as “National Drug Control Program agencies”—have responsibilities for drug prevention, treatment, and law enforcement activities. These agencies include the Office of National Drug Control Policy (ONDCP) and the departments of Agriculture, Defense, Education, HHS, Homeland Security, Housing and Urban Development, Interior, Justice, Labor, State, Transportation, Treasury, and Veterans Affairs, as well as AmeriCorps, U.S. Postal Inspection Service, the Court Services and Offender Supervision Agency for the District of Columbia, and the Federal Judiciary.
[4]GAO uses five criteria to assess progress in addressing high-risk areas: (1) leadership commitment; (2) agency capacity; (3) an action plan; (4) monitoring efforts; and (5) demonstrated progress.
[5]GAO, High-Risk Series: Heightened Attention Could Save Billions More and Improve Government Efficiency and Effectiveness, GAO‑25‑107743 (Washington, D.C.: Feb. 25, 2025).
[6]Pub. L. No. 105-20, 111 Stat. 224 (1997) (codified, in part, at 21 U.S.C. § 1531). Based on ONDCP DFC program requirements, the term “youth” is defined as individuals 18 years of age and younger. In carrying out the DFC program, the ONDCP is to (1) make and track grants to grant recipients; (2) provide for technical assistance and training, data collection, and dissemination of information on state-of-the art practices that the Director determines to be effective in reducing substance abuse; and (3) provide for the general administration of the program.
[7]See 21 U.S.C. § 812.
[8]21 U.S.C. §§ 1523(9), 1532(a)(3)(A), (a)(4)(A).
[9]ONDCP describes its primary functions to include: (1) developing and overseeing the implementation of the National Drug Control Strategy, (2) developing and overseeing the implementation of the National Drug Control Budget, and (3) administering programs to address overdoses, disrupt drug trafficking, and support community-led efforts to reducing youth substance abuse. 21 U.S.C. § 1702(a)(2), (3), and (6).
[10]In fiscal year 2020, ONDCP transitioned its management of the DFC program from HHS’s Substance Abuse and Mental Health Services Administration (SAMHSA) to CDC.
[11]See 21 U.S.C. §§ 1531(b)-(c), 1533(b).
[12]See 21 U.S.C. § 1532(b).
[13]Since 2009, ICF—an independent third-party evaluator—has served as the DFC National Evaluation Team, receiving an estimated $13 million from 2018-2025 to provide cross-site evaluation reports, training, and annual reports summarizing findings for ONDCP and participating coalitions. The cross-site evaluation reports summarize coalitions’ performance and provide an overall assessment of the program’s effectiveness.
[14]Pub. L. No. 115-271, § 8220, 132 Stat. 3894, 4134 (codified at 21 U.S.C. § 1715) (2018).
[15]The DFC program awarded grants to 751 coalitions in fiscal year 2024. At the time of our survey, ONDCP terminated 1 coalition due to non-compliance, which resulted in 750 coalitions. Our weighted response rate was 46 percent (359 respondents; Total = 750). For more information regarding our objectives, scope, and methodology, including information on our survey methodology and important limitations, see appendix I.
[16]To assess potential bias resulting from differences between those who responded to our survey and those who did not, we conducted nonresponse bias analysis and implemented weights to account for nonresponse and generate estimates that better generalize to the population of DFC coalitions, based on certain characteristics of DFC regional demographics. Uncertainty is quantified through 95% confidence intervals. These adjustments reduce, but may not eliminate, all potential unmeasured bias resulting from non-response. See appendix I for further discussion on the nonresponse bias analysis and other considerations about the survey methodology.
[17]We selected 13 DFC coalitions for site visits based on several criteria—including varying geography and demographics. The coalitions are located in Arizona (Santa Cruz County Drug-Free Community Coalition, and Maricopa County Urban Indian Coalition); Georgia (Community Action Coalition, Family Connection of Warren County, Inc., and Power Through Prevention Community Coalition); Maine (Youth Resiliency Coalition of Southern Maine, SoPo Unite: All Ages, All In); Missouri (Alliance For Healthy Communities, and Iron County Health Coalition); Washington (Latinx King County Dream Coalition, Birch Bay-Blaine Thrives Coalition, and Mt. Baker Community Coalition); and West Virginia (Wyoming County Prevention Coalition). Appendix III provides information on the characteristics of each coalition that we visited, and the map shows the geographical locations.
[18]See appendix I for details of our comprehensive quality reviews. In 2025, ONDCP’s contractor published its 2024 national cross-site evaluation. We did not comprehensively review that report. Therefore, we did not include that report in our analysis. However, we did review the 2025 report for updates on outcome measures. See ICF, Drug-Free Communities (DFC) Support Program National Cross-Site Evaluation: End-of-Year 2024 Report (Washington, DC: Office of National Drug Control Policy, June 2025).
[19]See OMB Memorandum M-20-12, Phase 4 Implementation of the Foundations for Evidence-Based Policymaking Act of 2018: Program Evaluation Standards and Practices. This guidance provides standards for federal agencies to conduct program evaluations, ensuring they are useful, relevant, and address important agency issues. The guidance also emphasizes the importance of stakeholder engagement, rigorous documentation of findings, and the use of evaluation results to improve programs.
[20]CDC conducts the Youth Risk Behavior Survey, a national survey, which monitors key health behaviors and experiences that contribute to leading causes of death and illness during adolescence and adulthood. The survey collects data from students in high school (grades 9-12) and middle school (grades 6-8). Data for students grades 9-12 cover 36 of 50 states. Data for students grades 6-8 cover 12 of 50 states.
[21]In this report, our quantitative analyses are based on a GAO survey of DFC coalition program staff. The results of these analyses do not suggest any causal relationships between any of the factors we measured and the outcomes of the program. Survey results are based on the self-reported perceptions of the key DFC coalition program staff. There are several potential unmeasured response biases that may have influenced their self-reports. Additionally, information on program outcomes are from DFC officials who may have drawn from aggregate numbers from national surveys. Our findings should be reviewed with these considerations in mind.
[22]See appendix IV for a timeline showing the various federal agencies involved in the administration and management of the DFC program since its inception in 1997.
[23]Our scope included a comparison of the DFC program’s compliance-related efforts against leading practices as outlined in GAO, A Framework for Managing Fraud Risks in Federal Programs, GAO‑15‑593SP (Washington, D.C: July 28, 2015), to help with the prevention and detection of fraud and abuse. We interviewed CDC officials due to their role in day-to-day management of the DFC program.
[24]Pursuant to 21 U.S.C. § 1522, the DFC program has eight statutory purposes: “(1) to reduce substance use and misuse among youth in communities throughout the United States, and over time, to reduce substance use and misuse among adults; (2) to strengthen collaboration among communities, the Federal Government, and State, local, and tribal governments; (3) to enhance intergovernmental cooperation and coordination on the issue of substance use and misuse among youth; (4) to serve as a catalyst for increased citizen participation and greater collaboration among all sectors and organizations of a community that first demonstrates a long-term commitment to reducing substance use and misuse among youth; (5) to rechannel resources from the fiscal year 1998 Federal drug control budget to provide technical assistance, guidance, and financial support to communities that demonstrate a long-term commitment in reducing substance use and misuse among youth; (6) to disseminate to communities timely information regarding the state-of-the-art practices and initiatives that have proven to be effective in reducing substance use and misuse among youth; (7) to enhance, not supplant, local community initiatives for reducing substance use and misuse among youth; and (8) to encourage the creation of and support for community anti-drug coalitions throughout the United States.”
[25]Appendix V provides information on how the coalitions—to support program goals—are implementing a range of community-based prevention activities and strategies that fit within one of the Seven Strategies for Community Change. The strategies include (1) provide information; (2) enhance skills; (3) provide support; (4) change access/barriers; (5) change consequences, incentives/disincentives; (6) change physical design; and (7) modify and change policies. CADCA derived the strategies from work by the University of Kansas Work Group on Health Promotion and Community Development, a World Health Organization Collaborating Center.
[26]Pursuant to 21 U.S.C. § 1532(a)(2)(C), an individual who is a member of the coalition may only serve on the coalition as a representative of one of the community sector categories.
[27]21 U.S.C. § 1532(a)(2)(A). In addition, pursuant to 21 U.S.C. § 1532(a)(2)(B), if feasible, in addition to the 12 community sectors, the coalition is required to have an elected official (or a representative of an elected official) from the Federal Government and the government of the appropriate State and political subdivision thereof or the governing body or an Indian tribe.
[28]These data were reported by ONDCP in its 2023 national cross-site evaluation. This evaluation was released in October 2024 and was based on program data from August 2022 to July 2023.
[29]According to ONDCP officials, the agency expects to award the 546 cohort (all non-competing continuation awards) in July 2026. The officials also noted that no new grants were awarded in fiscal year 2025 as the agency paused to ensure alignment of Notice of Funding Opportunities with the administration’s policy priorities and applicable executive orders. Each new and continuation grant awards up to $125,000 per fiscal year. ONDCP also previously awarded mentoring grants, which have not been funded since the management of the DFC Program transitioned to CDC in 2020, according to ONDCP officials.
[30]Further Consolidated Appropriations Act, 2024, Pub. L. No. 118-47, 138 Stat. 460, 536.
[31]In October 2020, ONDCP transitioned the management of the DFC program from SAMHSA to CDC. SAMHSA managed the DFC program from fiscal years 2005 to 2020.
[32]21 U.S.C. § 1532(b). In addition, pursuant to 21 U.S.C. § 1532(a)(5)(B)-(C), to be eligible to receive a DFC grant, the coalition must demonstrate that the coalition is an ongoing concern by demonstrating that the coalition receives financial support (including in the discretion of the Administrator of the program, in-kind contributions) from non-Federal sources and has a strategy to solicit substantial financial support from non-Federal sources to ensure that the coalition and the programs operated by the coalition are self-sustaining.
[33]GAO, Drug-Free Communities Support Program: Agencies Have Strengthened Collaboration but Could Enhance Grantee Compliance and Performance Monitoring, GAO‑17‑120 (Washington, D.C.: Feb. 7, 2017).
[34]GAO, Drug-Free Communities Support Program: Stronger Internal Controls and Other Actions Needed to Better Manage the Grant-Making Process, GAO‑08‑57 (Washington, D.C.: July 31, 2008).
[35]Pursuant to 21 U.S.C. § 1532(a)(2), to be eligible to receive a DFC grant, an organization must consist of one or more representatives from each of 12 major sectors of its community.
[36]There are methodological designs that can assess the causal link between the DFC program and outcomes on the four core measures. For example, these include implementing an experimental design, an economic impact study, or in some cases, a well-designed quasi-experimental method. These methodological designs vary in their ability to make defensible causal claims and can be costly and difficult to implement. See appendix VIII for detailed descriptions of these methodological options with illustrative examples from our literature review.
[37]In an interview with ONDCP’s contractor, we asked whether they had considered an experimental design to assess the DFC program’s impact. The contractor said they would need to randomly select a control group from applicants interested in the DFC program that would be willing to collect and submit core measure data as non-grant recipients. The contractor said they were unclear whether that was a feasible option.
[38]ICF, an independent third-party evaluator under contract with ONDCP, has produced the DFC program’s cross-site evaluation reports since 2009. These annual evaluations summarize coalitions’ performance and provide an overall assessment of the DFC program’s effectiveness.
[39]ICF, Drug-Free Communities (DFC) Support Program National Cross-Site Evaluation: End-of-Year 2023 Report. Data on outcomes are provided by DFC coalitions in their annual progress report submissions to ONDCP. ICF compares DFC coalition data on outcomes to the national sample from the Youth Risk Behavior Survey data. CDC conducts this national survey, which monitors key health behaviors and experiences that contribute to leading causes of death and illness during adolescence and adulthood. The survey collects data from students in high school (grades 9-12) and middle school (grades 6-8). Data for students grades 9-12 cover 36 of 50 states. Data for students grades 6-8 cover 12 of 50 states.
[40]In the published 2024 evaluation, ONDCP’s contractor monitored core measure data submitted by DFC coalitions in the progress reports from 2002 to 2023. Monitoring trends in the data can provide useful information about substance use among youth. In addition, certain analyses can explore associations between data to gain useful insights about the program, as we describe later in this report.
[41]Pub. L. No. 117-103, 136 Stat. 49, 254-55 (2022).
[42]See H.R. Rep. No. 105-105, the committee report accompanying the Drug-Free Communities Act of 1997, Pub. L. No. 105-20, 111 Stat. 224 (1997).
[43]To the extent ONDCP determines it requires additional authority to standardize or collect additional relevant data, ONDCP officials may develop a legislative proposal in accordance with OMB Circular No. A-19.
[44]GAO, Standards for Internal Control in the Federal Government, GAO‑25‑107721 (Washington, D.C.: May 15, 2025).
[45]GAO, Designing Evaluation 2012 Revision, GAO‑12‑208G (Washington, D.C.: January 31, 2012).
[46]OMB, Phase 4 Implementation of the Foundations for Evidence-Based Policymaking Act of 2018: Program Evaluation Standards and Practices, M-20-12 (Washington, D.C.: Mar.10, 2020).
[47]ICF, Drug-Free Communities (DFC) Support Program National Cross-Site Evaluation: End-of-Year 2023 Report. Data on outcomes are provided by DFC coalitions in their annual progress report submissions to ONDCP. ICF compares DFC coalition data on outcomes to the national sample from the Youth Risk Behavior Survey data. CDC conducts this national survey, which monitors key health behaviors and experiences that contribute to leading causes of death and illness during adolescence and adulthood. The survey collects data from students in high school (grades 9-12) and middle school (grades 6-8). Data for students grades 9-12 cover 36 of 50 states. Data for students grades 6-8 cover 12 of 50 states.
[48]In this report, our quantitative analyses are based on a GAO survey of DFC coalition program staff. The results of these analyses do not suggest any causal relationships between any of the factors we measured and the outcomes of the program. Survey results are based on the self-reported perceptions of the key DFC coalition program staff. There are several potential unmeasured response biases that may have influenced their self-reports. Additionally, information on program outcomes are from DFC officials who may have drawn from aggregate numbers from national surveys. Our findings should be reviewed with these considerations in mind.
[49]We provide selected regression analyses and results of our survey administered to DFC coalitions in appendices II and IX, respectively.
[50]A logic model is a systematic and visual tool used to explain and illustrate the theory and assumptions underlying how a program is expected to work. It acts as a roadmap, showing the connections between the resources invested, the activities undertaken, and the desired changes or results.
[51]We conducted a multivariate regression analysis using data from the Youth Risk Behavior Survey collected through CDC.
[52]We performed multivariate logistic regression analyses to assess associations among key DFC program elements. Regression analysis can adjust for measured difference between respondents, but that analysis cannot correct for systemic misreporting if that bias is not directly observed and correctly modeled. The survey data presented in this report are subject to all the qualifiers associated with self-reported data, and should be considered when reviewing the survey results, particularly for questions around program effectiveness. Potential issues here include conflicts-of-interest, incentives, motivated reasoning or perception bias. As a result, these analyses do not provide evidence of causality between the implementation of the DFC program and the reduction of drug use rates.
[53]See table 16 in appendix IX for further description of these survey results.
[54]Generally, pursuant to 21 U.S.C. § 1532(a)(4)(B), to be eligible for a DFC grant, coalitions must describe and document the nature and extent of the substance use and misuse problem, which, at a minimum, includes the use and abuse of drugs in the community and, pursuant to 21 U.S.C. § 1532(a)(6)(B)(i), for an initial grant, conduct an initial benchmark survey of drug use among youth (or use local surveys or performance measures available or accessible in the community at the time of the grant application). The DFC program does not require coalitions to collect and submit data on core measures until the second year of the grant. However, ONDCP’s contractor said they encourage coalitions to collect and submit core measure data before the two-year requirement to establish a baseline for measuring the coalitions’ progress.
[55]The odds ratio quantifies the association between dependent (outcome of interest) and independent variables (cause of changes in dependent variables). An odds ratio greater than 1 indicates that the odds of the dependent variable increases by that factor for every unit increase in the independent variable. Conversely, an odds ratio less than 1 indicates that the odds of the dependent variable decreases by that factor for every unit increase in the independent variable. We conducted multivariate regression analyses to estimate these odds ratios, accounting for the survey design and adjusting for demographic variables (ethnicity/race, population size, U.S. geographic region).
[56]See tables 7, 12, 13, 20, and 27 in appendix IX for further description of the results that underlie figure 6 and odds ratios quantifying associations with 30-day drug use.
[57]We performed multivariate logistic regression analyses to assess associations among key DFC program elements and the results should not be considered valid for inferring causality. As noted above, among other things, these results reflect perceived success, not verified outcomes.
[58]See table 7 in appendix IX for further description of these results for each of the 12 community sectors.
[59]See table 8 in appendix IX for further description of these results.
[60]See table 9 in appendix IX for further description of these results.
[61]See figure 11 in appendix II for odds ratios quantifying associations with 30-day drug use and the other core measures.
[62]We performed multivariate logistic regression analyses to measure correlations among key DFC program elements. Correlational analyses do not provide evidence for causal connections between the implementation of the DFC program and the reduction of drug use rates. Additionally, survey data presented in this report are subject to all the qualifiers associated with self-reported data and should be considered when reviewing the survey results. For example, threats to the validity of survey data grow from low survey response rates and concerns about response bias. We took steps to adjust for nonresponse bias across DFC demographic characteristics obtained through Census Bureau data (ethnicity/race, population size, U.S. geographic region), and uncertainty is quantified through 95% confidence intervals. These adjustments reduce, but may not eliminate, potential unmeasured bias resulting from non-response.
[63]There are significant threats to validity of any causal claims about the impact of the DFC program on core outcomes.
[64]This finding is consistent with the results from ONDCP’s Drug-Free Communities Support Program, End-of-Year 2023 National Cross-Site Evaluation Report, which showed that about 24 percent of DFC coalitions reported not having at least one active member in all 12 sectors. The Drug-Free Communities Support Program, End-of-Year 2022 National Cross-Site Evaluation Report, indicated about 27 percent of DFC coalitions reported not having at least one active member in all 12 sectors. See table 7 in appendix IX for further description of these results for each of the 12 community sectors.
[65]GAO, Executive Guide: Effectively Implementing the Government Performance and Results Act, GAO/GGD‑96‑118 (Washington, D.C.: June 1996); Veterans Justice Outreach Program: VA Could Improve Management by Establishing Performance Measures and Fully Assessing Risks, GAO‑16‑393 (Washington, D.C.: Apr. 28, 2016); Performance Measurement and Evaluation: Definitions and Relationships, GAO‑11‑646SP (Washington, D.C.: May 2, 2011); and Managing for Results: Enhancing Agency Use of Performance Information for Management Decision Making, GAO‑05‑927 (Washington, D.C.: Sept. 9, 2005).
[66]GAO, Evidence-Based Policymaking: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington, D.C.: July 12, 2023).
[67]SAMHSA’s strategic prevention framework is a comprehensive guide to plan, implement, and evaluate prevention practices and programs. See Substance Abuse and Mental Health Services Administration (SAMHSA): A Guide to SAMHSA’s Strategic Prevention Framework (Rockville, MD: Center for Substance Abuse Prevention, June 2019).
[68]See table 10 in appendix IX for further description of these survey results. See also tables 11 for further context on community sector involvement in coalition activities.
[69]Pursuant to 21 U.S.C. § 1705(b)(1), the Director of ONDCP is required to promulgate a National Drug Control Strategy, which is required to set forth a comprehensive plan to reduce illicit drug use and the consequences of such illicit drug use in the U.S. by limiting the availability of and reducing the demand for illegal drugs and promoting prevention, early intervention, treatment, and recovery support for individuals with substance use disorders.
[70]21 U.S.C. § 1532(a)(2).
[71]21 U.S.C. § 1531(a).
[72]21 U.S.C. § 1531(b).
[73]45 C.F.R. § 75.205(b). 45 C.F.R. Part 75 was removed and reserved, effective October 1, 2025. Pursuant to 2 C.F.R. § 300.106, HHS adopts the Office of Management and Budget guidance in 2 C.F.R. parts 200 and 376, with the additional HHS provisions. See also 2 C.F.R. § 200.206(b).
[74]SAM.gov, or System for Award Management, is the official website of the federal government used to register and manage entities that intend to do business with the federal government. USASpending.gov serves as the federal government’s official website for tracking federal spending. The Tracking Accountability in Government Grants System is a centralized database managed by HHS. TAGGS provides detailed information on federal grants awarded by HHS, offering transparency into how taxpayer dollars are allocated.
[75]ONDCP officials said the chief motive for the development and the continual enhancements of this web-based system was GAO’s review of the program in 2017, GAO‑17‑120. According to ONDCP officials, DFC-Me also serves as the DFC program’s online system to improve communication and help coalitions better manage the federal grants.
[76]The criteria for determining site visits are outlined in the interagency agreement with CDC. These site visits are based on several conditions, including: (1) a recipient has exhibited areas of concern related to programmatic and/or grants management requirements (e.g. lack of responsiveness, out of compliance with requirements, inadequate spend-down of funds); (2) recipient is in compliance with the programmatic and statutory requirements of the DFC grant, but has issues with programmatic progress and/or new key personnel who could benefit from an one-on-one site visit; or (3) recipient has specific successes/achievements to share that would benefit other DFC coalitions. CDC prioritizes recipients in year 3 and year 8 but may also include recipients from other funding years, as appropriate.
[77]According to its website, CADCA provides training and coalition development support, including an annual National Coalition Academy, to strengthen the capacity of DFC coalitions on core competencies and the essential processes to establish or maintain a highly effective anti-drug coalition.
[78]45 C.F.R. § 75.205(a), establishes requirements for any HHS awarding agency to conduct a review of risk posed by applicants prior to making a federal award, including a review of OMB-designated repositories of governmentwide data. 45 C.F.R. Part 75 was removed and reserved, effective October 1, 2025. Pursuant to 2 C.F.R. § 300.106, HHS adopts the Office of Management and Budget guidance in 2 C.F.R. parts 200 and 376, with the additional HHS provisions. See also 2 C.F.R. § 200.206(a).
[79]These systems include but are not limited to the Federal Awardee Performance and Integrity Information System, including past performance on federal contracts as per Duncan Hunter National Defense Authorization Act of 2009, Pub. L. No. 110-417, 122 Stat. 4356 (2008); the Do Not Pay list; and System for Award Management exclusions.
[80]Based on HHS guidance, the Payment Management System is a shared service provider in processing grant payments for the federal government. The Payment Management System offers awarding agency and grant recipients with cash management services, centralized payment services, personal grant accounting support, and financial reporting support. The Payment Management System also promotes financial integrity and operational efficiencies within the federal government through leading accounting practices.
[81]SF-425. The Federal Financial Report form is used by federal grant recipients to submit reports on their grant’s financial progress.
[82]See appendix X for an overview of DFC program applicants’ eligibility criteria and requirements.
[83]According to the program’s Notice of Funding Opportunity, no more than 10 percent of the total grant funds may be allocated for evaluation purposes, unless approved by the project officer and grants management specialist.
[84]21 U.S.C. § 1532(b)(1)(A)(ii), (2)(A)(iii), and (3)(E); 45 C.F.R. § 75.371 (45 C.F.R. Part 75 was removed and reserved, effective October 1, 2025. Pursuant to 2 C.F.R. § 300.106, HHS adopts the Office of Management and Budget guidance in 2 C.F.R. parts 200 and 376, with the additional HHS provisions. See also 2 C.F.R. § 200.339).
[85]21 U.S.C. § 1532(b).
[86]21 U.S.C. § 1532(b)(1)(A)(ii), (2)(A)(iii), and (3)(E).
[87]Requirements for coalitions’ internal controls are outlined in 45 C.F.R. § 75.303. HHS also addresses internal controls requirements in the HHS Grants Policy Statement. Adherence to the HHS Grants Policy Statement. is required in CDC’s General Terms and Conditions. A recipient must also meet the standards and requirements for financial management systems as outlined in 45 C.F.R. § 75.302. 45 C.F.R. Part 75 was removed and reserved, effective October 1, 2025. Pursuant to 2 C.F.R. § 300.106, HHS adopts the Office of Management and Budget guidance in 2 C.F.R. parts 200 and 376, with the additional HHS provisions. See also 2 C.F.R. §§ 200.303 and 200.302, respectively.
[88]According to the DFC program’s Request for Applications, the responsibilities of the community sector representatives can include, but are not limited to—being a community leader amongst the represented sector and acting as a positive role model for youth, families, and peers; attending coalition meetings, participating on committees, and engaging in coalition-sponsored training, town hall meetings, and other community events; ensuring clear communication between the sector represented and the coalition, contributing to the strategic action planning process and participating in sustaining the coalition’s capacity, involvement, and goals; promoting evidence-based and practiced-based environmental strategies; and using his/her activities as match (or in-kind), if applicable.
[89]21 U.S.C. § 1532(b)(1)(A)(ii). Pursuant to 21 U.S.C. § 1532(b)(2)(A), for rural coalitions (a coalition that represents a county with a population that does not exceed 30,000 individuals), the Administrator may waive any statutory eligibility requirement, if the Administrator considers that waiver to be appropriate. However, the Administrator may suspend the grant, after providing written notice to the grant recipient and an opportunity to appeal, if the grant recipient fails to continue to meet any statutory eligibility criteria that has not been waived by the Administrator.
[90]Based on the DFC program’s 2023 national cross-site evaluation report, about 90 percent of coalitions reported having at least one member from each of the 12 sectors, although fewer, about 73 percent reported active members from all sectors. ONDCP implemented the signed Coalition Involvement Agreement to address this issue.
[91]H.R. Rep. No. 105-105, the committee report accompanying the Drug-Free Communities Act of 1997, Pub. L. No. 105-20, 111 Stat. 224 (1997), noted the importance of community sector involvement, stating that “[c]ommunity coalitions seem to be one of the most effective demand-side tools to reduce youth drug abuse. By fostering cooperation among all sectors of a community and tailoring solutions to local problems, community coalitions have made substantial progress in selected locales. In addition, the report noted that “[i]n order to receive Federal support, a community must first demonstrate a comprehensive, long-term commitment to address teenage drug abuse through major sector involvement (substantial volunteer participation from youth, parents, business, the media, schools, law enforcement, faith leaders, health care professionals and others), a focused mission, and the implementation of strategies to reduce drug abuse.” GAO, Drug Control: Observations on Elements of the Federal Drug Control Strategy, GAO/GGD‑97‑42 (Washington, D.C.: Mar. 1997).
[92]See table 8 in appendix IX for further description of these results.
[93]See 21 U.S.C. § 1532(a)(2), (b)(1)(A)(ii), and (b)(2)(A)(iii).
[94]GAO, Army Corps Of Engineers: Budget Formulation Process Emphasizes Agencywide Priorities, but Transparency of Budget Presentation Could be Improved, GAO‑10‑453 (Washington, D.C.: April 2, 2010).
[95]GAO, Budget Issues: Key Questions to Consider When Evaluating Balances in Federal Accounts, GAO‑13‑798 (Washington, D.C.: Sept. 30, 2013).
[96]An agency’s obligational authority is the sum of budget authority enacted for a given fiscal year; and unobligated balances of amounts that have not expired brought forward from prior years. The balance of obligational authority is an amount carried over from one year to the next if the budget authority is available for obligation in the next fiscal year. Not all obligational authority that becomes available in a fiscal year is obligated and paid out in that same year. Balances are described as (1) obligated, (2) unobligated, or (3) unexpended.
[97]Pursuant to 21 U.S.C. § 1524(b), not more than 8 percent of the funds appropriated for carrying out the DFC program may be used by ONDCP to pay for administrative expenses associated with its responsibilities. For fiscal years 2022 through 2025, the annual appropriations specified the maximum amount of the appropriation that could be used for administrative expenses (which exceeded the statutory limitation in 21 U.S.C. § 1524(b)).
[98]According to ONDCP officials, carryover funds are added to the budget authority available for that year and used for administrative costs. All DFC funds are “no year funds” meaning the funds remain available until fully expended irrespective of the fiscal year. Carryover depends on the level of funding appropriated and the administrative costs of the prior year. Costs fluctuate based on program requirements, particularly the cycles for the DFC Technology and Evaluation contracts.
[99]Pursuant to 21 U.S.C. § 1524(b), not more than 8 percent of the funds appropriated for carrying out the DFC program may be used by ONDCP to pay for administrative expenses associated with the responsibilities of ONDCP.
[100]Further Consolidated Appropriations Act, 2024, Pub. L. No. 118-47, 138 Stat. 460, 536.
[101]No-year funds represent budget authority available for obligation indefinitely until expended, regardless of fiscal year.
[102]Appendix IX contains the survey questions and responses for survey items presented in this report.
[103]We conducted three preliminary site visit interviews with DFC coalitions that had 5 to 10 years of experience as grantees in the DFC program or served youth in a tribal community. These coalitions also participated in our survey pretest.
[104]AwardYear (First year DFC received funding); PopulationSize (Proportion of DFC zip code that has population size at least 20,000); Gender (Proportion of DFC zip code that is Female); Race (Proportion of DFC zip code that is White); Age (Proportion of DFC zip code that is older than 25); Rurality (Proportion of DFC zip code that is at least 50% Rural); GeographicRegion (East North Central, East South Central, Middle Atlantic, Mountain, New England, Pacific, Puerto Rico, South Atlantic, West North Central, West South Central); s = the residual error that is not accounted for by model variables.
[105]GAO, Foreign Assistance: Agencies Can Improve the Quality and Dissemination of Program Evaluations, GAO‑17‑316 (Washington, D.C.: March 3, 2017). GAO developed the data collection instrument for this report and has tailored it for use in this report other GAO reports.
[106]See OMB Memorandum M-20-12, Phase 4 Implementation of the Foundations for Evidence-Based Policymaking Act of 2018: Program Evaluation Standards and Practices. This guidance provides standards for federal agencies to conduct program evaluations, ensuring they are useful, relevant, and address important agency issues. The guidance also emphasizes the importance of stakeholder engagement, rigorous documentation of findings, and the use of evaluation results to improve programs.
[107]The Youth Risk Behavior Survey is a national survey conducted by CDC that is part of the Youth Risk Behavior Surveillance System.
[108]30DayDrugUse (at least one day a week over the past 30 days = 1, no use = 0); DFCZipCode (1 = a Student is in a zip code with a DFC, 0 = a Student is NOT in a zip code with a DFC); StudentGender (Gender of Student); ZipCodeGender (Proportion of zip code that is Female); StudentRace (Race of Student); ZipCodeRace (Proportion of zip code that is White); StudentAge (Age of Student); ZipCodeAge Proportion of zip code that is older than 25); Rurality (Proportion of zip code that is at least 50% Rural); GeographicRegion (East North Central, East South Central, Middle Atlantic, Mountain, New England, Pacific, Puerto Rico, South Atlantic, West North Central, West South Central); s = the residual error that is not accounted for by model variables.
[109]AwardYear (First year DFC received funding); PopulationSize (Proportion of DFC zip code that has population size at least 20,000); Gender (Proportion of DFC zip code that is Female); Race (Proportion of DFC zip code that is White); Age (Proportion of DFC zip code that is older than 25); Rurality (Proportion of DFC zip code that is at least 50% Rural); GeographicRegion (East North Central, East South Central, Middle Atlantic, Mountain, New England, Pacific, Puerto Rico, South Atlantic, West North Central, West South Central); s = the residual error that is not accounted for by model variables.
[110]Multivariate regression analyses were performed to estimate odds ratios. The odds ratio quantifies the association between dependent and independent variables. An odds ratio greater than 1 indicates that the odds of the dependent variable increases by that factor for every unit increase in the independent variable. Conversely, an odds ratio less than 1 indicates that the odds of the dependent variable decreases by that factor for every unit increase in the independent variable.
[111]See tables 7, 11, 12, 13, 17, 20, 21, and 27 in appendix IX for further description of the results that underlie figure 11 and odds ratios quantifying associations with the four core measures.
[112]Percentages do not add to 100 percent because some DFC coalitions serve more than one community type.
[113]We selected 13 DFC coalitions for site visits based on several criteria—including varying geography and demographics. The coalitions are located in Arizona (Santa Cruz County Drug Free Community Coalition, and Maricopa County Urban Indian Coalition); Georgia (Community Action Coalition, Family Connection of Warren County, Inc., and Power Through Prevention Community Coalition); Maine (Youth Resiliency Coalition of Southern Maine, SoPo Unite: All Ages, All In); Missouri (Alliance For Healthy Communities, and Iron County Health Coalition); and Washington (Latinx King County Dream Coalition, Birch Bay-Blaine Thrives Coalition, and Mt. Baker Community Coalition).
[114]We administered a census survey to 750 DFC-funded coalitions to gain their perspectives on how well the DFC program works and how it could improve. The survey was available for respondents from July 2024 to late-August 2024. Specifically, we administered the survey to the coalitions’ project coordinator or project director, who manages the work of the coalition and program activities, including training, coalition communication, data collection and information dissemination. Our weighted response rate was 46 percent (359 respondents; Total = 750).
[115]Pub. L. No. 105-20, 111 Stat. 224 (1997).
[116]21 U.S.C. §§ 1531(c), 1533(b).
[117]See 21 U.S.C. §§ 1523(1) and 1531(c).
[118]ONDCP administers and partners with CDC to manage the DFC program. Specifically, CDC provides day-to-day grant management services for the program and evaluates it. See 21 U.S.C. § 1533(b).
[119]Pub. L. No. 105-20, 111 Stat. 224 (1997). Based on ONDCP DFC program requirements, the term “youth” is defined as individuals 18 years of age and younger.
[120]In addition, ONDCP is responsible for, among other things, overseeing and coordinating the implementation of the Administration’s national drug control strategy.
[121]According to ONDCP officials, the mentoring grant has not been funded since the management of the DFC program transitioned to CDC. However, ONDCP officials stated that ONDCP funds the National Coalition Institute which is the primary training and technical assistance resource for community anti-drug coalitions, operated by the Community Anti-Drug Coalitions of America.
[122]Based on DFC program guidance, DFC grantees must provide matching non-federal funds, including in-kind contributions, equivalent to or greater than the amount of requested federal funds. DFC match requirements include—100 percent match for funding years 1 through 6, 125 percent match for funding years 7 and 8, and 150 percent match for funding years 9 and 10. See 21 U.S.C. § 1532(b)(1)(A).
[123]According to ONDCP officials, in fiscal year 2025, ONDCP awarded DFC grants to 546 coalitions across the U.S.
[124]21 U.S.C. §§ 1532(b)(1)(A)(iv), 1535(g)(2)-(3). According to ONDCP officials, the mentoring grant has not been funded since the management of the DFC Program transitioned to CDC.
[125]In fiscal year 2020, ONDCP transitioned the management of the DFC program from the Substance Abuse and Mental Health Services Administration (SAMHSA) to CDC. SAMHSA managed the DFC program from 2005 through 2020.
[126]According to ONDCP officials, the DFC program’s two broad goals are to—(1) establish and strengthen collaboration among communities, private non-profit agencies, and federal, state, local, and tribal governments to support the efforts of community coalitions to prevent and reduce substance use among youth; and (2) reduce substance use over time among youth and adults by addressing the factors in a community that increase the risk of substance use and promoting the factors that minimize the risk of substance use.
[127]GAO, Drug-Free Communities Support Program: Agencies Have Strengthened Collaboration but Could Enhance Grantee Compliance and Performance Monitoring, GAO‑17‑120 (Washington, D.C., Feb. 7, 2017), GAO, Grants Management: Actions Needed to Address Persistent Grant Closeout Timeliness and Undisbursed Balance Issues, and GAO‑16‑362 (Washington D.C., Apr. 14, 2016), GAO, Results Oriented Government: Practices That Can Help Enhance and Sustain Collaboration among Federal Agencies, GAO‑06‑15 (Washington, D.C.: Oct. 21, 2005).
[128]Methods such as cost-benefit analysis and cost-effectiveness studies are methods also used to determine impact. We intended to use advanced statistics to model causality, using contractor data collected from progress reports over the last five years. We did not pursue this analysis due to missing data that did not meet our reliability quality standards.
[129]J. S. Cannon, M. Gilbert, P. Ebener, P. S. Malone, C. M. Reardon, J. Acosta, and M. Chinman. “Influence of an Implementation Support Intervention on Barriers and Facilitators to Delivery of a Substance use Prevention Program.” Prevention Science, vol. 20, no. 8 (2019): 1200–1210.
[130]Laura J. Dunlap, Margaret R. Kulinski, Alexander Crowell, Kathryn E. McCollister, Diana M. Bowser, Mark Campbell, Claudia-Santi F. Fernandes, Pranav, Kemburu, Bethany J. Livingston, Lisa A. Prosser, Vinod Rao, Rosanna Smart, Tansel Yilmazer. “Economic Evaluation Design within HEAL Prevention Cooperative.” Prevention Science, vol. 24, Supplement 1(2023): 550-560.
[131]GAO, Designing Evaluation 2012 Revision, GAO‑12‑208G (Washington, D.C.: January 31, 2012).
[132]Kimberly D. Hieftje, Claudia-Santi F. Fernandes, I-Hsin Lin, and Lynn E. Fiellin. “Effectiveness of a Web-Based Tobacco Product Use Prevention Videogame Intervention on Young Adolescents’ Beliefs and Knowledge.” Substance Abuse, vol. 42, no. 1 (2021): 47–53.
[133]A causal claim can be made from a non-experimental design when the analysis convincingly shows that observed differences in outcomes are attributable to the intervention and not to other factors. In practice this is difficult to achieve because it requires a credible counterfactual, plausible exogenous treatment, correct timing and robustness to alternative explanations – conditions that are difficult to satisfy outside of well-designed experiment.
[134]Melissa A. Little, Pallav Pokhrel, Steve Sussman, Karen J. Derefinko, Zoran Bursac and Louise Ann Rohrbach. “Factors Associated with the Adoption of Tobacco Cessation Programmes in Schools.” Journal of Smoking Cessation, vol. 12, no. 1 (2017):55-62.
[135]The Drug-Free Communities Act of 1997, Pub. L. No. 105-20, 111 Stat. 224, established the Drug-Free Communities (DFC) Support Program—a federal program to support communities in the development and implementation of comprehensive, long-term plans and programs to prevent and treat substance use and misuse among youth. The DFC program grants funding to community-based coalitions that focus on preventing and reducing youth substance use—which generally include the illegal use or misuse of controlled substances under the Controlled Substances Act, the misuse of inhalants or other over-the-counter drugs, or the use of alcohol, tobacco, or other related products.
[136]We performed a nonresponse bias analysis to assess whether there were demographic differences between respondent and non-respondent DFCs. Demographic data were obtained from the Census Bureau on population size, gender, race, age, urbanicity, and U.S. geographic region and linked this data based on DFC zip code. We estimated weights to account for nonresponse and generate estimates that better generalize to the population of DFCs, based on characteristics of DFC regional demographics. Uncertainty due to this nonresponse was assessed through 95% confidence intervals around survey estimates. However, as with any survey and, more broadly, statistical analyses, we cannot account for unmeasured sources of potential bias (e.g., characteristics of a DFC office, school environment for students), which precludes complete certainty around estimates.
[137]See 21 U.S.C. § 812.
[138]21 U.S.C. §§ 1523(9), 1532(a)(3)(A), (a)(4)(A).
[139]21 U.S.C. § 1532(b).
[140]Pursuant to 21 U.S.C. § 1532(a)(2)(C), an individual who is a member of the coalition may only serve on the coalition as a representative of one of the community sector categories.
[141]21 U.S.C. § 1532(a)(2)(A). In addition, pursuant to 21 U.S.C. § 1532(a)(2)(B), if feasible, in addition to the 12 community sectors, the coalition is required to have an elected official (or a representative of an elected official) from the Federal Government and the government of the appropriate State and political subdivision thereof or the governing body or an Indian tribe.
[142]21 U.S.C. § 1532(a)(1).
[143]21 U.S.C. § 1532(a)(2)(A). Pursuant to 21 U.S.C. § 1532(a)(2)(C), an individual who is a member of the coalition may serve on a coalition as a representative of not more than 1 of the sectors. Also, Pursuant to 21 U.S.C. § 1532(a)(2), to be eligible to receive a DFC grant, an organization must consist of one or more representatives from each of 12 major sectors of its community.
[144]21 U.S.C. § 1532(a)(3).
[145]21 U.S.C. § 1532(a)(3)(B).
[146]21 U.S.C. § 1532(a)(4)(A).
[147]21 U.S.C. § 1532(a)(4)(B).
[148]21 U.S.C. § 1532(a)(4)(C). According to ONDCP officials, their agency does not fund or perform treatment programming.
[149]21 U.S.C. § 1532(a)(4)(D).
[150]21 U.S.C. § 1532(a)(4)(E).
[151]21 U.S.C. § 1532(a)(6)(A).
[152]21 U.S.C. § 1532(a)(6)(B)-(C). According to CDC officials, the benchmark survey is a key tool used to assess the effectiveness of local coalitions in reducing youth substance use. The survey collects baseline and ongoing data on youth drug, alcohol, and tobacco use, attitudes, and perceptions in communities receiving DFC grants.
[153]21 U.S.C. § 1532(a)(5).
[154]See 21 U.S.C. § 1532(b)(1)(B).
[155]21 U.S.C. § 1702(a)(1)-(2).
[156]Under 21 U.S.C. § 1701(11), “the term ‘National Drug Control Program agency’ means any agency (or bureau, office, independent agency, board, division, commission, subdivision, unit, or other component thereof) that is responsible for implementing any aspect of the National Drug Control Strategy, including any agency that receives federal funds to implement any aspect of the National Drug Control Strategy, but does not include any agency that receives funds for drug control activity solely under the National Intelligence Program or Joint Military Intelligence Program.”
[157]21 U.S.C. § 1531(c).
[158]The number of DFC grants awarded includes the four types of grants available to coalitions through the DFC program—(1) new; (2) continuation; (3) mentoring; and (4) mentoring continuation. According to ONDCP officials, the new and continuation grants represent a majority of the DFC grants awarded. According to ONDCP officials, the mentoring grant has not been funded since the management of the DFC Program transitioned to CDC.
[159]Pursuant to 21 U.S.C. § 1524(b), not more than 8 percent of the funds appropriated for carrying out the DFC program may be used by ONDCP to pay for administrative expenses associated with its responsibilities. For fiscal years 2022 through 2024, the annual appropriations specified the maximum amount of the appropriation that could be used for administrative expenses (which exceeded the statutory limitation in 21 U.S.C. § 1524(b)).
[160]According to ONDCP officials, carryover funds are added to the budget authority available for that year and used for administrative costs. All DFC funds are “no year funds” meaning the funds remain available until fully expended irrespective of the fiscal year. Carryover depends on the level of funding appropriated and the administrative costs of the prior year. Costs fluctuate based on program requirements, particularly the cycles for the DFC Technology and Evaluation contracts.
[161]Pub. L. No. 116-260, 134 Stat. 1182, 1395.
[162]Pub. L. No. 117-103, 136 Stat. 49, 254-55.
[163]Pub. L. No. 117-328, 136 Stat. 4459, 4665.
[164]Further Consolidated Appropriations Act, 2024, Pub. L. No. 118-47, 138 Stat. 460, 536.
[165] Pub. L. No. 119-4, 139 Stat. 9.