Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
For more information, contact: Mary Denigan-Macauley at deniganmacauleym@gao.gov
What GAO Found
The U.S. Department of Health and Human Services (HHS) leads the federal public health and medical preparedness for, response to, and recovery from public health emergencies. HHS awarded almost $900 million in fiscal year 2024 to states and other jurisdictions to help them prepare for a range of public health threats and emergencies through two programs. First, the Public Health Emergency Preparedness (PHEP) program supports jurisdictions’ public health systems, which includes public health agencies at all government levels. Second, the Hospital Preparedness Program (HPP) supports health care systems, which include a community’s health care organizations such as hospitals. Jurisdictions distribute HPP funds to health care coalitions—made up of health care and other entities to support preparedness. HHS requires jurisdictions and health care coalitions to complete activities. These include exercises to help ensure that jurisdictions are prepared to respond to public health threats, such as infectious diseases and extreme weather events (e.g., hurricanes).

The two HHS agencies that administer these programs lack a formal mechanism, such as joint exercises, written agreements, or working groups, to coordinate them. Coordinating these preparedness programs could allow HHS to better manage them and support jurisdictions as they prepare both their public health and health care systems to respond to public health threats and emergencies. Lessons learned from the COVID-19 pandemic have demonstrated the importance of coordination between these systems, such as between state health departments and hospitals, if jurisdictions are to be effectively prepared. Additionally, officials from selected jurisdictions said that greater interagency coordination could help reduce resource inefficiencies associated with implementation of PHEP and HPP.
Further, HHS does not collect or analyze information on jurisdictions’ ability to meet the 15 public health and four health care preparedness capabilities and any related gaps. According to HHS documentation, it identified these capabilities to serve as national guidance. The capabilities describe skills and abilities jurisdictions need to effectively respond to, and recover from, public health threats and emergencies. For example, they include providing mass medical care and laboratory testing at scale for emerging pathogens. Collecting and analyzing such information would help HHS understand the extent to which jurisdictions are prepared to respond to public health threats and emergencies and whether any changes are needed.
Why GAO Did This Study
The United States faces ongoing risks from future public health threats, such as infectious diseases; extreme weather events; and biological, chemical, nuclear, and radiological events. In fiscal year 2024, HHS, through PHEP, provided $654 million, and through HPP, provided $240 million, to jurisdictions to aid preparedness for such threats.
The CARES Act includes a provision for GAO to examine public health preparedness and response efforts related to the COVID-19 pandemic. This report examines, among other objectives, the extent to which HHS agencies (1) coordinate PHEP and HPP and (2) collect and analyze information on jurisdictions’ capabilities.
GAO reviewed HHS documentation, including notices of funding opportunity, templates, and examples of documents submitted by eight selected jurisdictions. GAO also interviewed officials from HHS and the eight selected jurisdictions. GAO selected these jurisdictions to include variation among geographic location, percent of the population living in a rural setting, and public health governance structure.
What GAO Recommends
GAO is making five recommendations, including that HHS establish a mechanism to coordinate PHEP and HPP; and that it collect and analyze information on jurisdictions’ preparedness capabilities and any related gaps. HHS concurred with our recommendations.
Abbreviations
|
ASPR |
Administration for Strategic Preparedness and Response |
|
CDC |
Centers for Disease Control and Prevention |
|
FEMA |
Federal Emergency Management Agency |
|
HHS |
Department of Health and Human Services |
|
HPP |
Hospital Preparedness Program |
|
PHEP |
Public Health Emergency Preparedness |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
February 23, 2026
Congressional Committees
The United States faces risks from ongoing and future public health threats, which include infectious disease outbreaks, extreme weather events, radiological or nuclear incidents, and acts of terrorism.[1] We have previously reported on the importance of preparing for, and urgently responding to, public health threats, and on the need for significant improvements in how the federal government supports state and local governments during such times.[2] Not being sufficiently prepared for a public health threat or emergency can negatively affect the time and resources needed to achieve full recovery.[3]
The Department of Health and Human Services (HHS) leads the federal public health and medical preparedness for, response to, and recovery from public health emergencies. We have reported that a whole-of-nation approach is needed to effectively respond to nationally significant public health emergencies, including ensuring coordination between public health and health care systems.[4] A public health system includes public health agencies at all levels of government, and a health care system includes a community’s health care organizations such as hospitals. To that end, HHS has provided awards to public health department recipients in all states; territories; and freely associated states; as well as certain localities, to help them sustain and build their medical and public health emergency preparedness and response capabilities.[5] In this report we refer to these award recipients across levels of government as jurisdictions.
As of September 2025, HHS provided these awards through two cooperative agreements:
1. the Public Health Emergency Preparedness (PHEP) program administered by the Centers for Disease Control and Prevention (CDC), and
2. the Hospital Preparedness Program (HPP) administered by the Administration for Strategic Preparedness and Response (ASPR).[6]
PHEP is a primary source of federal funding for public health preparedness, while HPP is a primary source of federal funding for health care preparedness. Cooperative agreements are federal awards designed to carry out a public purpose. Cooperative agreements differ from grants in that they provide for substantial involvement between the federal awarding agency and non-federal entity. For example, the agency and entity work together to carry out activities covered by the award, which is not typical of a grant award.[7]
We have previously reported on how PHEP and HPP supported jurisdictions’ response to the COVID-19 pandemic.[8] For example, during the COVID-19 pandemic, we found that jurisdictions used PHEP funds to support public health laboratories, disease surveillance, and salaries for program staff, among other uses.[9] HPP funds were used by jurisdictions, for example, to help support medical surge response activities at hospitals during the COVID-19 pandemic.[10]
In fiscal year 2024, CDC awarded $654 million to jurisdictions through PHEP and ASPR awarded $240 million to jurisdictions through HPP. As a condition of these awards, jurisdictions must complete certain required activities. These include drafting preparedness plans, training staff, and conducting exercises. CDC and ASPR also release supplemental guidance that supports the completion of requirements by jurisdictions. They also provide additional information on the programs’ required activities, such as guidance on effectively conducting exercises to help ensure that jurisdictions are prepared and ready to respond to public health threats.
Separate from the required PHEP and HPP activities, HHS also developed 15 capabilities for public health emergency preparedness—referred to as the public health preparedness capabilities—and four capabilities for health care preparedness. These capabilities describe skills and abilities needed to effectively respond to, and recover from, public health threats and emergencies. For example, one capability is the ability to provide mass care, which involves public health agencies coordinating with and supporting partner agencies to provide medical care to hundreds or thousands (depending on the size of the jurisdiction) of individuals affected during a public health emergency.
The public health and health care preparedness capabilities serve as national guidance for jurisdictions’ preparedness activities, according to CDC and ASPR documentation. However, jurisdictions are not required to meet the capabilities. Jurisdictions may also vary in their ability to meet the capabilities.
The CARES Act includes a provision for us to examine public health preparedness and response efforts related to the COVID-19 pandemic.[11] This report is also part of our body of work on HHS’s leadership and coordination of public health emergencies, which we identified as an area of high risk in 2022.[12] This report examines the extent to which
1. CDC and ASPR coordinate PHEP and HPP;
2. CDC and ASPR have provided information on how their preparedness programs’ required activities support the development of jurisdictions’ preparedness capabilities; and
3. CDC and ASPR collect and analyze information on jurisdictions’ ability to meet the preparedness capabilities.
To address all three objectives, we
· reviewed relevant agency documentation, including PHEP and HPP notices of funding opportunity from 2012 through 2024, a time period starting after the release of the public health and health care preparedness capabilities through the most recent notices of funding opportunity available at the time of our review.[13] Each notice of funding opportunity specifies the program’s priorities and requirements, including information on activities jurisdictions must complete, over the 5-year PHEP and HPP award period. For example, the 2024 PHEP and HPP notices of funding of opportunity apply to the award period 2024 through 2029. We also reviewed associated supplemental guidance, program activity templates, and capability guidance.
· interviewed officials from ASPR and CDC to discuss PHEP and HPP coordination, goals, priorities, capabilities, reporting requirements, and changes made to each program as part of the 2024 notices of funding opportunity.
· interviewed selected jurisdiction officials in five states, two localities, and one territory to understand their experiences completing PHEP and HPP activities. We interviewed or received written responses from officials from the following eight selected jurisdictions: California, Kentucky, Los Angeles County, Missouri, New Mexico, New York (state), New York City, and Puerto Rico. We selected our five states to obtain variation in the following characteristics: population size, HHS region (i.e., geographic dispersion), percent of the population living in a rural setting, and public health governance structure (i.e., the relationship between state health agencies and local health departments). We selected two localities that received PHEP and HPP awards among each selected state. We selected Puerto Rico, because it is the U.S. territory with the largest population. The experiences of selected jurisdiction officials are not generalizable to other jurisdictions.
· reviewed PHEP and HPP documents submitted by each selected jurisdiction, including project narratives, work plans, risk assessments, multi-year integrated preparedness plans, capability self-assessments, and exercise after-action reports.[14]
To examine the extent to which CDC and ASPR coordinate PHEP and HPP, we reviewed the HPP and PHEP documentation described above and interviewed CDC and ASPR officials to specifically understand actions taken to coordinate PHEP and HPP. This includes gathering information on the rationale for changes to the 2024 notices of funding opportunity compared to coordination of the programs in previous notices of funding opportunity. We assessed actions taken by CDC and ASPR to coordinate PHEP and HPP activities against leading practices for interagency collaboration we identified in prior work.[15]
To examine the extent to which CDC and ASPR provided information on how their preparedness programs’ required activities support the development of jurisdictions’ preparedness capabilities, we reviewed the aforementioned PHEP and HPP documentation. We interviewed CDC and ASPR officials to gather information on the relationship between the PHEP activities and public health preparedness capabilities, and between the HPP activities and health care preparedness capabilities, in the programs’ respective 2024 notices of funding opportunity. We also gathered information on why this relationship changed from the programs’ prior notices of funding opportunity. We assessed any information provided about how the required activities support the development of the capabilities against guidance in the 2024 notices of funding opportunities and the public health and health care preparedness capability guidance documents.
To examine the extent to which CDC and ASPR collect and analyze information on jurisdictions’ public health and health care preparedness capabilities, we reviewed the agency documentation described above and interviewed CDC and ASPR officials, including to understand the rationale for changes to the 2024 notices of funding opportunity compared to information collected as part of previous notices of funding opportunity. We compared CDC’s and ASPR’s actions to collect information on jurisdictions’ public health and health care preparedness capabilities against the relevant component of the National Preparedness System and public health and health care preparedness capabilities guidance documents.[16]
We conducted this performance audit from April 2024 to February 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
National Preparedness Goal and National Preparedness System
Following Hurricane Katrina in 2005, the Post-Katrina Emergency Management Reform Act of 2006 required the President to develop a National Preparedness Goal and National Preparedness System for all levels of government, the private and nonprofit sectors, and the public.[17] In 2011, the White House released Presidential Policy Directive 8, which directed the Secretary of Homeland Security to develop a National Preparedness Goal and National Preparedness System, which the Secretary completed that year.[18] The National Preparedness Goal and National Preparedness System emphasize a capabilities-based approach to emergency preparedness.
· The National Preparedness Goal. The goal is a “secure and resilient nation with the capabilities required across the whole community to prevent, protect against, mitigate, respond to, and recover from the threats and hazards that pose the greatest risk.”
· The National Preparedness System. The system includes guidance that describes actions federal agencies, jurisdictions, and others need to take to achieve the National Preparedness Goal. The actions within the system include completing plans and providing training to ensure preparedness. The system also includes actions to collect and analyze information on capabilities to identify gaps to support preparedness efforts.
PHEP, HPP, and the public health and health care preparedness capabilities support the National Preparedness Goal and National Preparedness System, according to ASPR and CDC documentation.
PHEP Required Activities
The PHEP program’s purpose is to strengthen the public health system’s ability to prepare for, respond to, and recover from public health threats and emergencies.[19] To receive funding, jurisdictions are required to complete 34 activities, some multiple times, over the 5-year award period, according to the 2024 PHEP notice of funding opportunity.[20]
Examples of activities jurisdictions must complete to receive PHEP funding include the following:
· Conducting biological incident exercises: Such exercises provide opportunities for jurisdictions and others to test potential public health roles, functions, and countermeasures—such as vaccines, antiviral drugs, antibiotics, and masks and other protective equipment—when responding to a large-scale biological incident, such as pandemic influenza.[21] Jurisdictions are expected to use the Homeland Security Exercise and Evaluation Program methodology for such exercises.[22] That program provides guidance on the completion of an after-action report following an exercise to capture observations from the exercise, including summarizing and analyzing performance in the exercise, and making recommendations for post-exercise improvements. See figure 1 below for an example of a biological incident training exercise similar to the required PHEP biological incident exercise.

· Providing training to jurisdiction staff on public health preparedness requirements, such as incident management.[23] Incident management is a set of structured activities to respond to an incident, such as communication and coordination processes among all response personnel.
· Developing an administrative preparedness plan to enhance administrative operations—hire staff; execute contracts; and request, receive, and distribute federal funds—to be response ready.
· Completing a risk assessment to identify the top five risks the jurisdiction faces based on public health consequences.
Public Health Preparedness Capabilities
The 15 public health preparedness capabilities serve as national guidance for jurisdictions’ public health emergency preparedness activities. Although jurisdictions are not required to meet the capabilities, the capabilities are designed to support jurisdictions’ ability to prepare for, respond to, and recover from public health threats and emergencies. Each public health preparedness capability is categorized into one of six domains—areas of preparedness that state and local public health systems can use to better prepare for emergencies that impact the public’s health. CDC’s public health preparedness capabilities guidance document states that the capabilities also promote collaboration by establishing a common language among preparedness professionals. For an overview of the 15 public health preparedness capabilities, see figure 2. Appendix I contains a detailed list and description of each public health preparedness capability.

HPP Required Activities
HPP’s purpose is to support health care systems within jurisdictions to plan for, respond to, and recover from public health threats and emergencies.[24] For example, HPP awards funds to jurisdictions’ public health departments which, in turn, distribute funding, resources, and other support to health care coalitions. A health care coalition is a collaborative network of health care, public health, and response organizations in a defined geographic location that conduct preparedness activities to ensure that each member has what it needs to respond to disasters and emergencies. Health care coalition members include, for example, acute care hospitals, public health agencies, emergency medical services, and emergency management agencies.[25] According to ASPR, HPP prepares the health care system within jurisdictions to save lives during emergencies that exceed the day-to-day capacity of health care and emergency response systems.
To receive funding, jurisdictions, or their health care coalitions, must complete 29 required activities, some multiple times, over the 5-year award period, according to the 2024 HPP notice of funding opportunity.[26] Examples of required HPP activities include the following:
· Conducting a patient movement exercise to improve coordination of patient movement, access to care, and to support equity during emergencies and disasters.
· Completing a readiness assessment to document health care coalitions’ ability to carry out required HPP activities and address health care readiness gaps.
· Developing a cybersecurity support plan to describe implementation of cybersecurity practices and steps to address cybersecurity gaps.
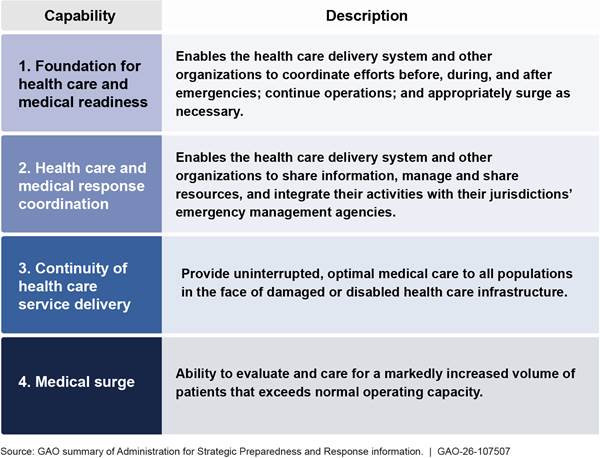
Health Care Preparedness Capabilities
Although jurisdictions are not required to meet the capabilities, the four health care preparedness capabilities serve as guidance for jurisdictions along with health care system members—such as hospitals, long term care facilities, primary care clinics, and pharmacies—to prepare for, respond to, and recover from public health threats and emergencies. For an overview of the four health care preparedness capabilities, see figure 3.
CDC and ASPR Lack a Mechanism to Coordinate Their Preparedness Programs
CDC and ASPR lack a formal mechanism, such as formal written agreements, working groups, or joint exercises, to coordinate PHEP and HPP. Rather, officials told us they rely on monthly meetings to discuss, for example, program due dates, updates on supplemental guidance, and information sharing events.[27] These informal meetings do not have documentation, such as agendas, according to ASPR officials.
In contrast, the agencies previously relied on several more formal mechanisms to coordinate PHEP and HPP. These mechanisms, which are no longer in effect, included the following:
· Interagency work group. CDC and ASPR participated in an interagency work group with other federal emergency management agencies, such as the U.S. Department of Homeland Security’s Federal Emergency Management Agency (FEMA), according to the 2012 PHEP and HPP notices of funding opportunity. This work group aimed to co-develop goals, strategies, and action plans among federal emergency management partners to better align grants with public health and health care preparedness components, such as PHEP and HPP, according to the notices of funding opportunity.
· Joint PHEP and HPP grant management. From 2012 through 2018, CDC and ASPR jointly managed PHEP and HPP. Specifically, CDC and ASPR jointly wrote and released the PHEP and HPP notices of funding opportunity. The notices of funding opportunity emphasized the importance of PHEP and HPP coordination to improve community preparedness and response nationwide, reduce awardee burden, and increase federal efficiency. However, joint administration of these programs ended in 2019 when ASPR became the sole grant manager for HPP, according to CDC officials.
· Joint CDC and ASPR site visits. From 2012 through 2018, CDC and ASPR conducted joint jurisdictional site visits to assess the activities, progress, and challenges of awardees. Additionally, according to the 2017 PHEP and HPP notices of funding opportunity, jurisdictions were encouraged to invite PHEP and HPP project officers and senior CDC and ASPR staff to attend or observe events such as scheduled exercises, regional meetings, jurisdictional conferences, senior advisory committee meetings, and coalition meetings supported by PHEP and HPP funding to gain insight on strengths and challenges in preparedness planning.
· Required joint PHEP and HPP activities. In the 2012 through 2019 PHEP and HPP notices of funding opportunity, CDC and ASPR required jurisdictions to jointly conduct and submit many program activities, such as plans, assessments, exercises, and trainings. For example, jurisdictions were required to complete state-wide exercises to test for example, a surge of patients into the health care system during a public health emergency. However, CDC and ASPR no longer require many joint activities for PHEP and HPP recipients. In the 2024 notices of funding opportunity, jurisdictions are required to complete 34 PHEP and 29 HPP activities during the 5-year award period and coordinate when completing a risk assessment.[28] Additionally, the 2024 PHEP notice of funding opportunity suggests that jurisdictions include health care coalitions as participants in PHEP exercises; however, this is not a requirement.
· Formal written agreements. In 2014, ASPR and CDC signed a memorandum of understanding—a formal agreement between two or more federal agencies to help monitor, evaluate, and update interagency collaboration.[29] Although no longer in effect, the memorandum stated that the coordination of PHEP and HPP supports national preparedness strategies for jurisdictions and the programs’ activities should be coordinated in the most cost-effective manner as possible. Additionally, the memorandum of understanding established a formal framework to support joint federal preparedness planning and outcomes, according to CDC officials.
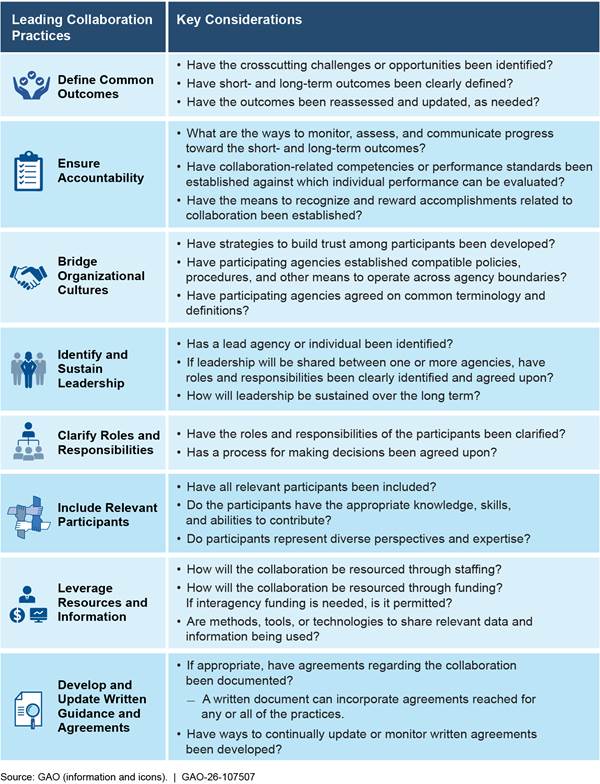
The use of such formal coordination mechanisms is consistent with leading practices for enhancing interagency collaboration, defined as any joint activity intended to produce more public value than could be produced when the entities act alone (see fig. 4). These leading practices state that coordination among agencies can help federal entities improve management of federal efforts—in this instance, CDC’s and ASPR’s respective management of PHEP and HPP. When utilized, these leading practices could leverage agency-wide skills, knowledge, and resources to improve the federal government’s overall capacity to support jurisdictions’ coordination of public health and health care systems, vital for responding to public health emergencies to ensure timely and appropriate responses that prevent harm.[30]
CDC and ASPR officials told us they no longer coordinate PHEP and HPP as they once did because the programs have distinct outcomes and requirements. ASPR officials also stated that they aimed to provide jurisdictions the flexibility to coordinate PHEP and HPP based on their respective preparedness needs. However, CDC and ASPR officials acknowledged that PHEP and HPP share the goal of strengthening the nation’s preparedness for public health threats. This shared goal aligns with lessons learned from the COVID-19 pandemic that we reported on in 2023, including that public health and health care systems cannot work independently to effectively prepare for, respond to, and recover from an emergency.[31] For example, we reported that regularly exercising preparedness plans with all response partners is imperative to identifying gaps in procedures, rectifying barriers to plan implementation, and supporting a whole-of-nation preparedness approach.[32]
Additionally, officials we spoke with from selected jurisdictions said greater interagency coordination between CDC and ASPR could help reduce resource inefficiencies associated with their implementation of PHEP and HPP. For example, officials at six of eight jurisdictions said CDC and ASPR could work together to better coordinate the PHEP and HPP required activities. This would reduce jurisdictions’ administrative burdens associated with determining how PHEP and HPP activities could be completed to meet similar requirements of both programs.
We acknowledge that, as PHEP and HPP have evolved over time, the specific coordination mechanisms implemented previously, such as in 2012 and 2019, may no longer be effective and may also need to evolve. However, various mechanisms that could facilitate interagency collaboration include developing memoranda of understanding, working groups, or joint exercises; clearly defining common outcomes; and jointly identifying data, funding, and resource needs. Developing a mechanism, or mechanisms, to coordinate PHEP and HPP, for example, by taking into consideration leading practices we identified for effective interagency collaboration, could help CDC and ASPR better manage these preparedness programs and their activities. They could also better support jurisdictions as they prepare both their public health and health care systems to respond to public health threats and emergencies. Ultimately, such action could help support a whole-of-community preparedness approach.
CDC and ASPR Have Not Provided Information on How the Required Activities Support the Development of the Preparedness Capabilities
CDC’s and ASPR’s PHEP and HPP documentation state that those programs’ capabilities are to guide jurisdictions nationwide in effectively preparing for, responding to, and recovering from public health threats and emergencies. However, CDC and ASPR do not specify how their programs’ required activities support the development of these capabilities.
CDC and ASPR previously provided information on how the required activities supported the development of public health and health care preparedness capabilities:
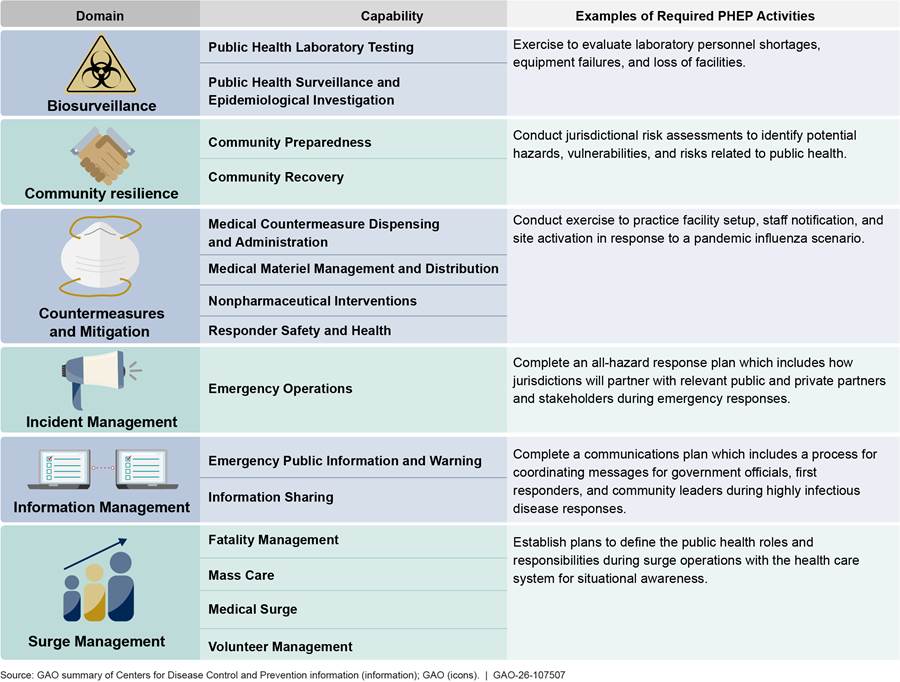
· CDC previously provided information on how required activities supported the public health preparedness capabilities. Specifically, in the 2019 PHEP notice of funding opportunity, which covered activities through 2024, CDC provided information on how required activities supported the public health preparedness capabilities.[33] For example, jurisdictions were required to complete a communications plan, which included a process for coordinating messages among government officials, first responders, and community leaders during highly infectious disease responses, and CDC explained this activity supported the “information sharing” public health preparedness capability. See figure 5 below for more examples of the required PHEP activities that previously supported the development of the public health preparedness capabilities in the 2019 PHEP notice of funding opportunity.
Figure 5: Examples of Public Health Emergency Preparedness (PHEP) Program Required Activities and Associated Program Capabilities in the 2019 Notice of Funding Opportunity
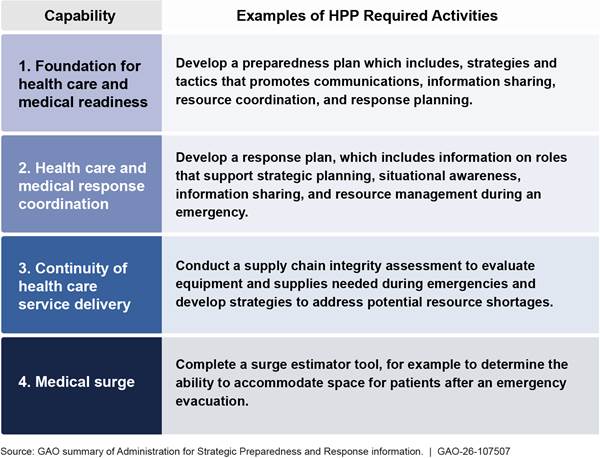
· ASPR previously provided information linking required activities to the health care preparedness capabilities. Similarly, in the 2019 HPP notice of funding opportunity which covered activities through 2024, ASPR previously provided information on how the required HPP activities supported the development of the health care preparedness capabilities.[34] Jurisdictions, including their health care coalitions, were expected to develop and strengthen the four health care preparedness capabilities through the implementation of certain activities. For example, they were required to complete a surge estimator tool, and ASPR explained that this supported the “medical surge” health care preparedness capability. See figure 6 below for more examples of the required HPP activities that previously supported the development of the health care preparedness capabilities in the 2019 HPP notice of funding opportunity.
Figure 6: Examples of Hospital Preparedness Program (HPP) Required Activities and Associated Health Care Preparedness Capabilities in the 2019 Notice of Funding Opportunity
CDC and ASPR officials said they did not provide information on how the current required activities support the capabilities because they changed the focus of these programs, along with about half of the required activities, as part of the 2024 PHEP and HPP notices of funding opportunity. Specifically, they moved away from capability-based preparedness activities, which had been the focus of the prior notices of funding opportunity. However, officials from both agencies acknowledged that the programs’ capabilities are still important and foundational to their programs. See appendix I for information about the new PHEP and HPP focus areas—the Response Readiness Framework for PHEP and core functions for HPP—which do not reference the programs’ capabilities.
Officials from all eight jurisdictions in our review said the public health and health care preparedness capabilities remain relevant and important for guiding their preparedness efforts. In addition, officials from five of these jurisdictions elaborated that the public health and health care preparedness capabilities are foundational to their preparedness work and considered in their day-to-day operations. For example, officials from two of these jurisdictions commented that their departments are organized around the public health preparedness capabilities.
Officials from four of eight jurisdictions also reported challenges with the change in focus of the programs and movement away from the capabilities, including the following:
· Officials from one jurisdiction said they faced challenges understanding the Response Readiness Framework and alignment between the required activities and capabilities due to limited information provided by CDC. For example, the Response Readiness Framework is a 1-page document with one sentence descriptions of each priority area.
· Officials from three jurisdictions said they are trying to figure out how the new focus for activities fits within the HPP core functions as well as the health care preparedness capabilities. Officials from one of these jurisdictions said that because the core functions are new and ASPR has not provided additional guidance, individuals within that jurisdiction and health care coalition faced challenges understanding the relationship between the core functions, capabilities, and required activities.
· Officials from three jurisdictions commented that especially with scare resources, those resources will go to the activities required by the programs’ new focus areas, potentially leaving capabilities unaddressed.
Although CDC and ASPR explained that the PHEP and HPP required activities support the programs’ new focus areas, both the PHEP and HPP 2024 notices of funding opportunity maintain that the programs’ capabilities provide the framework to support jurisdictions to prepare for, respond to, and recover from public health threats and emergencies.[35] Similarly, CDC’s 2018 public health preparedness capabilities guidance document states that jurisdictions should plan activities that specifically relate to the capabilities, and the 2024 HPP notice of funding opportunity also states that jurisdictions are responsible for using the health care preparedness capabilities to inform planning their activities.[36]
By providing information to the jurisdictions on how PHEP and HPP required activities support the programs’ preparedness capabilities, CDC and ASPR would help ensure jurisdictions understand how their completion of these activities develop their preparedness capabilities. This information could also help CDC and ASPR ensure that the activities they are providing funds for are indeed helping to support the development of jurisdictions’ preparedness capabilities nationwide. Further, providing this information would be consistent with the PHEP and HPP 2024 notices of funding opportunity and capabilities guidance documents that emphasize the role of the capabilities in planning and guiding jurisdictions’ preparedness activities.
CDC and ASPR Do Not Collect Information on Jurisdictions’ Ability to Meet the Preparedness Capabilities
CDC and ASPR do not collect and analyze information on jurisdictions’ ability to meet the public health or health care preparedness capabilities or gaps in their ability to do so.
CDC and ASPR officials provided a few reasons for not collecting and analyzing information on jurisdictions’ ability to meet the 15 public health and four health care preparedness capabilities, respectively.
· CDC. CDC officials said their collection of information focuses on jurisdictions’ progress completing the required activities within the required time frames. Further, CDC officials said collecting information about jurisdictions’ capabilities is challenging to standardize because of the variety of threats faced by jurisdictions.
· ASPR. Similarly, ASPR officials said they collect information on jurisdictions’ achievements in completing the required HPP activities rather than the capabilities.[37]
Collecting information on jurisdictions’ ability to meet the capabilities and identifying any gaps would be consistent with the National Preparedness System. The public health and health care preparedness capabilities guidance documents link the programs’ capabilities to this System.[38] The National Preparedness System provides a framework for the nation to track progress on building and improving the capabilities necessary to prevent, protect against, mitigate the effects of, respond to, and recover from threats. An important component of the National Preparedness System is a mechanism to collect and analyze existing and needed capabilities to identify gaps.
CDC and ASPR previously collected some information on jurisdictions’ ability to meet the capabilities through an annual capability self-assessment. Through this self-assessment, required in the 2019 PHEP and HPP notices of funding opportunity, jurisdictions reported information on the importance, status, challenges, and barriers for each public health and health care preparedness capability to CDC and ASPR, respectively.
CDC and ASPR officials told us they retired the prior capability self-assessment as part of an effort to reduce reporting requirement burdens on jurisdictions for the 2024 PHEP and HPP notices of funding opportunity. However, instead of collecting no information, CDC and ASPR officials could use their past experiences with the capability self-assessments, along with feedback from jurisdictions, to develop a mechanism that allows them to collect and analyze information on jurisdictions’ ability to meet the capabilities and identify related gaps. CDC and ASPR could also use after-action reports submitted by jurisdictions following completion of an exercise or response to an incident as part of, or to help inform, such a mechanism (see sidebar).
|
Public Health Emergency Preparedness (PHEP) Program and Hospital Preparedness Program (HPP) After-Action Reports Exercises and after-action reports are important components of preparedness as they provide the opportunity to shape planning, assess and validate capabilities, and address areas for improvement. Jurisdictions are required to submit after-action reports to the Centers for Disease Control and Prevention (CDC) and the Administration for Strategic Preparedness and Response (ASPR) after completion of required PHEP or HPP exercises, respectively. CDC and ASPR also require jurisdictions to submit an after-action report following a response to an incident—an occurrence, natural or human-made, that necessitates a response to protect life or property, such as an emergency or disaster. When completing exercises and after-action reports, CDC
and ASPR require jurisdictions to follow the Homeland Security Exercise and
Evaluation Program methodology. This methodology provides a set of
fundamental principles for conducting exercises and completing after-action
reports. For example, the methodology suggests formatting of after-action
reports to indicate which capabilities were performed, if any, and any
ratings provided on their performance. Source: U.S Departments of Health and Human Services and Homeland Security information. | GAO‑26‑107507 |
CDC and ASPR could also consider how other agencies collect such information. See text box for an example of an agency that has a systematic approach to collecting and analyzing information on jurisdictions’ preparedness capabilities.
|
Example of a Federal Agency’s Collection of Preparedness Information from Jurisdictions Within the U.S. Department of Homeland Security, the Federal Emergency Management Agency (FEMA)—the agency that coordinates disaster preparedness, response, and recovery support at the national level—has a system to regularly collect and analyze information from jurisdictions on their preparedness capabilities. FEMA provides grants to jurisdictions to support emergency response preparedness activities, and jurisdictions are required to annually report to FEMA on their capacity or ability to meet each preparedness capability. These capabilities include, for example, mass search and rescue operations and fire management and suppression. FEMA uses the capability information reported by jurisdictions, in part, to produce its annual preparedness report which assesses the nation’s preparedness and provides information on risks and capabilities that support decisions about program priorities, resource allocations, and community actions. The 2024 National Preparedness Report summarizes progress made toward achieving the National Preparedness Goal and building and sustaining capabilities required to prevent, protect against, mitigate, respond to, and recover from threats and hazards that pose the greatest risk to our nation. |
Source: GAO summary of FEMA documentation. | GAO‑26‑107507
Collecting and analyzing information on jurisdictions’ ability to meet the public health and health care preparedness capabilities and related gaps, in partnership with jurisdictions, would help CDC and ASPR track the progress made by jurisdictions in building public health and health care preparedness capabilities—a foundational aspect of PHEP and HPP. In addition, collecting information on jurisdictions’ capabilities would help ASPR and CDC measure the extent to which federal government investments through PHEP and HPP contribute to building and sustaining capabilities nationwide and whether changes to improve preparedness are needed. They could also use the information on capability gaps to focus their resources in overseeing the two programs and thereby maximize their effectiveness in achieving the aims of the programs.
Information on jurisdictions’ capabilities is crucial to help understand how prepared jurisdictions are, as a whole-of-nation, to respond to public health emergencies and threats. Further, obtaining and understanding capability information is important for federal government planning, because when an effective emergency response is beyond the capabilities of jurisdictional governments, those governments can request federal assistance, including from CDC and ASPR.
Conclusions
Effectively preparing for public health threats, such as hurricanes and wildfires, is essential to saving lives during emergencies. CDC and ASPR play a key role by providing funding to jurisdictions to complete activities—plans, exercises, assessments, and trainings—to build and sustain jurisdictions’ preparedness capabilities through PHEP and HPP. These activities are crucial to support jurisdictions and their health care system partners to prepare for and respond to public health threats.
Coordinating PHEP and HPP—taking into consideration leading practices we have identified for effective interagency collaboration—could help CDC and ASPR better manage these preparedness programs and support jurisdictions as they prepare their public health and health care systems to coordinate during an emergency.
By providing information to the jurisdictions on how PHEP and HPP required activities support the programs’ preparedness capabilities, CDC and ASPR would help ensure jurisdictions understand how their completion of these activities develop their preparedness capabilities. This information would also help CDC and ASPR ensure that the activities they are providing funds for are indeed helping to support the development of jurisdictions’ preparedness capabilities nationwide.
Lastly, collecting and analyzing information specific to jurisdictions’ ability to meet the public health and health care preparedness capabilities and identifying any related gaps, would help CDC and ASPR track the progress made by jurisdictions in building the preparedness capabilities. Obtaining such information is crucial for CDC and ASPR, in part because when an effective emergency response is beyond the capabilities of jurisdictional governments, those governments can request federal assistance, including from CDC and ASPR. In addition, collecting information on jurisdictions’ capabilities would help ASPR and CDC measure the extent to which federal government investments through PHEP and HPP contribute to building and sustaining capabilities nationwide.
Recommendations for Executive Action
We are making the following five recommendations to HHS:
The Assistant Secretary for Preparedness and Response and the Director of CDC should develop a mechanism, or mechanisms, to coordinate PHEP and HPP by, for example, taking into consideration GAO’s Leading Practices to Enhance Interagency Collaboration and Address Crosscutting Challenges. (Recommendation 1)
The Director of CDC should provide information to jurisdictions on how the required PHEP activities support the development of the public health preparedness capabilities. (Recommendation 2)
The Assistant Secretary for Preparedness and Response should provide information to jurisdictions on how the required HPP activities support the development of the health care preparedness capabilities. (Recommendation 3)
The Director of CDC should collect and analyze information on jurisdictions’ ability meet the public health preparedness capabilities and identify any related gaps in partnership with jurisdictions. (Recommendation 4)
The Assistant Secretary for Preparedness and Response should collect and analyze information on jurisdictions’ ability to meet health care preparedness capabilities and identify any related gaps in partnership with jurisdictions. (Recommendation 5)
Agency Comments
We provided a draft of this report to the Department of Homeland Security and HHS for review and comment. HHS provided written comments, which are reproduced in appendix II. HHS concurred with our five recommendations. HHS also provided technical comments, which we incorporated as appropriate. The Department of Homeland Security did not provide any comments on the draft report.
We are sending copies of this report to the appropriate congressional committees, the Secretary of Health and Human Services, the Secretary of the Homeland Security, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at DeniganMacauleyM@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix III.

Mary Denigan-Macauley,
Director, Health Care
List of Committees
The Honorable Susan Collins
Chair
The Honorable Patty Murray
Vice Chair
Committee on Appropriations
United States Senate
The Honorable Mike Crapo
Chairman
The Honorable Ron Wyden
Ranking Member
Committee on Finance
United States Senate
The Honorable Bill Cassidy, M.D.
Chair
The Honorable Bernard Sanders
Ranking Member
Committee on Health, Education, Labor, and Pensions
United States Senate
The Honorable Rand Paul, M.D.
Chairman
The Honorable Gary C. Peters
Ranking Member
Committee on Homeland Security and Governmental Affairs
United States Senate
The Honorable Tom Cole
Chairman
The Honorable Rosa DeLauro
Ranking Member
Committee on Appropriations
House of Representatives
The Honorable Brett Guthrie
Chairman
The Honorable Frank Pallone, Jr.
Ranking Member
Committee on Energy and Commerce
House of Representatives
The Honorable Andrew Garbarino
Chairman
The Honorable Bennie G. Thompson
Ranking Member
Committee on Homeland Security
House of Representatives
The Honorable James R. Comer
Chairman
The Honorable Robert Garcia
Ranking Member
Committee on Oversight and Government Reform
House of Representatives
The Honorable Jason Smith
Chairman
The Honorable Richard E. Neal
Ranking Member
Committee on Ways and Means
House of Representatives
Appendix I: Additional Information on the Public Health Emergency Preparedness Program and Hospital Preparedness Program
Public Health Emergency Preparedness Program
According to the 2024 Public Health Emergency Preparedness (PHEP) Program notice of funding opportunity, capabilities provide the framework to support advancement of preparedness, response, and recovery operations.[39] The 15 public health preparedness capabilities are designed to support jurisdictions capacity or ability to prepare for, respond to, and recover from public health threats and emergencies. For an overview of the 15 public health preparedness capabilities, see table 1 below.
Table 1: Centers for Disease Control and Prevention’s Public Health Preparedness and Response Capabilities
|
Capability |
Description |
|
Community preparedness |
Ability to prepare for, withstand, and recover from public health incidents in both the short and long term. |
|
Community recovery |
Ability to identify critical assets, facilities, and other services within public health, emergency management, health care, human services, mental and behavioral health, and environmental health sectors that can guide and prioritize recovery operations. |
|
Emergency operations coordination |
Ability to coordinate with emergency management and to direct and support an incident or event with public health or health care implications by establishing a standardized, scalable system of oversight, organization, and supervision. |
|
Emergency public information and warning |
Ability to develop, coordinate, and disseminate information, alerts, warnings, and notifications to the public and incident management personnel. |
|
Fatality management |
Ability to coordinate with organizations and agencies (e.g., medical examiner) to provide fatality management services, such as recovery and identification of human remains. |
|
Information sharing |
Ability to exchange health-related information and situational awareness data among federal, state, local, tribal, and territorial levels of government and the private sector. |
|
Mass care |
Ability to coordinate with and support partner agencies to address, within a congregate location, the public health, health care, mental and behavioral health, and human services needs of those impacted by an incident. |
|
Medical countermeasure dispensing and administration |
Ability to provide medical countermeasures (e.g., vaccines and antiviral drugs) to prevent, mitigate, or treat the adverse health effects of a public health incident. |
|
Medical materiel management and distribution |
Ability to acquire, manage, transport, and track medical materiel (e.g., pharmaceuticals and ventilators) during and after a public health incident. |
|
Medical surge |
Ability to provide adequate medical evaluation and care during events that exceed the limits of the normal medical infrastructure of an affected community. |
|
Nonpharmaceutical interventions |
Actions that people and communities can take to help slow the spread of illness or reduce the adverse impact of public health emergencies, such as restrictions on movement and travel advisories or warnings. |
|
Public health laboratory testing |
Ability to implement and perform methods to detect, characterize, and confirm public health threats. |
|
Public health surveillance and epidemiological investigation |
Ability to create, maintain, support, and strengthen routine surveillance and detection systems and epidemiological investigation processes. |
|
Responder safety and health |
Ability to protect public health and other emergency responders during pre-deployment, deployment, and post-deployment. |
|
Volunteer management |
Ability to coordinate with emergency management and partner agencies to identify, recruit, register, verify, train, and engage volunteers to support the jurisdictional public health agency’s preparedness, response, and recovery activities during pre-deployment, deployment, and post-deployment. |
Source: GAO summary of Centers for Disease Control and Prevention information. | GAO‑26‑107507
In 2023, the Centers for Disease Control and Prevention (CDC) established the Response Readiness Framework to serve as an organizing framework for response readiness activities and included the framework as part of the 2024 PHEP notice of funding opportunity. The Response Readiness Framework includes priority areas that define state, local, and territorial response readiness; identify essential components of response readiness; and serve as an organizing framework for response readiness activities, according to CDC documentation. See table 2 below for an overview of the 10 Response Readiness Framework priority areas.
|
Priority area |
Description |
|
Prioritize a risk-based approach |
All-hazards planning that addresses evolving threats and supports medical countermeasures logistics. |
|
Enhance partnerships |
To effectively support community preparedness efforts by enhancing partnerships with federal and nongovernmental organizations. |
|
Expand local support |
Improve jurisdictional readiness to effectively manage public health emergencies by expanding local support. |
|
Improve administrative and budget preparedness system |
Ensure timely access to resources for supporting jurisdictional responses. |
|
Build workforce capacity |
Meet jurisdictional surge management needs and support staff recruitment, retention, resilience, and mental health. |
|
Modernize data collection and systems |
Improve situational awareness and information sharing with health care systems and other partners. |
|
Strengthen risk communications activities |
Improve proficiency in disseminating critical public health information and warnings and address misinformation and disinformation. |
|
Incorporate health equity practices |
Enhance preparedness and response support for communities experiencing differences in health status due to structural barriers. |
|
Advance capacity and capability of public health laboratories |
Characterize emerging public health threats through testing and surveillance. |
|
Prioritize community recovery efforts |
Support health department reconstitution and incorporate lessons learned from public health emergency responses. |
Source: GAO summary of Centers for Disease Control and Prevention information. | GAO‑26‑107507
As part of the 2024 Hospital Preparedness Program (HPP) notice of funding opportunity, the Administration for Strategic Preparedness and Response (ASPR) established the nine core functions (see table 3 below).[40] Every jurisdiction and their health care coalitions must perform the core functions as part of the required activities in the HPP cooperative agreement according to the 2024 HPP notice of funding opportunity. According to ASPR, jurisdictions and health care coalitions will perform the core functions to support health care readiness.
|
Core function |
Description |
|
Assessment and risk mitigation |
Anticipate challenges and mitigate risks to support decision-making that meets community or jurisdiction health care needs during a disaster or emergency. |
|
Information sharing |
Collect and share near real-time information to provide multidirectional health care situational awareness during an emergency or disaster. |
|
Specialty care planning and coordination |
Incorporate necessary expertise to support health care readiness planning, disaster and incident management, including for specialty care delivery, and/or to address specific hazards or events. |
|
Respond |
Coordinate and support the implementation of plans, policies, and procedures among recipients, health care coalitions and their members, and their partners to address patient care needs during an emergency or disaster. |
|
Health care workforce support |
Equip, protect, and support the health care workforce by providing access to health care readiness resources, training, and exercises. |
|
Resource management |
Facilitate resource management and planning among recipients, health care coalitions and their members, and their partners to mitigate shortfalls, maintain operations, and sustain delivery of patient care services during an emergency or disaster. |
|
Training, exercise, and evaluation |
Conduct trainings, exercises, and evaluations that incorporate input from assessments, plans, policies, and previous trainings and exercises to evaluate, validate, and improve readiness and response processes. |
|
Continuity and recovery |
Support the improvement of processes and systems that promote continuity of health care operations and aid in recovery. |
|
Organizational development |
Create and carry out strategies to sustain and grow health care coalitions and their partnerships. |
Source: GAO summary of Administration for Strategic Preparedness and Response information. | GAO‑26‑107507
Mary Denigan-Macauley, Director, Health Care, DeniganMacauleyM@gao.gov
In addition to the contact named above, Deirdre Brown (Assistant Director), Danielle Blazek, Jenna Moody, and Carl Potenzieri made key contributions to this report. Also contributing were N. Rotimi Adebonojo, Jennie Apter, Kaitlin Farquharson, Eric Peterson, and Roxanna Sun.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]A public health threat is an event, disease, or disorder with significant potential to become a public health emergency.
[2]See, for example, GAO, Public Health Preparedness: Building and Maintaining Infrastructure beyond the COVID-19 Pandemic, GAO‑24‑105891 (Washington, D.C.: Nov. 7, 2023); Public Health Preparedness: HHS Should Address Strategic National Stockpile Requirements and Inventory Risks, GAO‑23‑106210 (Washington, D.C.: Oct. 17, 2022); and COVID-19: Significant Improvements Are Needed for Overseeing Relief Funds and Leading Responses to Public Health Emergencies, GAO‑22‑105291 (Washington, D.C.: Jan. 27, 2022).
[3]See GAO, Public Health Preparedness: HHS Reserve Funding for Emergencies, GAO‑23‑106102 (Washington, D.C.: Aug. 15, 2023).
[4]GAO, Public Health: Preparedness: Critical Need to Address Deficiencies in HHS’s Leadership and Coordination of Emergencies, GAO‑23‑106829 (Washington, D.C.: May 11, 2023).
[5]These localities are Chicago, Los Angeles County, New York City, and Washington, D.C..
[6]For purposes of this report, we refer to PHEP and HPP as HHS’s “preparedness programs”. In July 2022, the Secretary of Health and Human Services removed ASPR from the HHS Office of the Secretary and created a new operating division in the department, to be known as the Administration for Strategic Preparedness and Response. In this report, we refer to ASPR, the organizational name in place at the time we conducted our review.
[7]See 2 C.F.R. § 200.1 (2025).
[8]See GAO‑24‑105891 and GAO, Public Health Preparedness: COVID-19 Medical Surge Experiences and Related HHS Efforts, GAO‑22‑105461 (Washington, D.C.: Aug. 17, 2022).
[11]Specifically, the act includes a provision for us to monitor and oversee the federal government’s efforts to prepare for, respond to, and recover from the pandemic. Pub. L. No. 116-136, § 19010(b), 134 Stat. 281, 580 (2020). The American Rescue Plan Act of 2021 also includes a provision for us to conduct oversight of the COVID-19 response. Pub. L. No. 117-2, § 4002, 135 Stat. 4, 78. All of GAO’s reports related to the COVID-19 pandemic are available for no charge on GAO’s website at https://www.gao.gov/coronavirus.
[12]See GAO, High-Risk Series: Heightened Attention Could Save Billions More and Improve Government Efficiency and Effectiveness, GAO‑25‑107743 (Washington, D.C.: Feb. 25, 2025); High-Risk Series: Efforts Made to Achieve Progress Need to Be Maintained and Expanded to Fully Address All Areas, GAO‑23‑106203 (Washington, D.C.: Apr. 20, 2023); and appendix “New High-Risk Designation: HHS and Public Health Emergencies” in COVID-19: Significant Improvements Are Needed for Overseeing Relief Funds and Leading Responses to Public Health Emergencies, GAO‑22‑105291 (Washington, D.C.: Jan. 27, 2022).
[13]From 2012 through 2024, ASPR and CDC released six notices of funding opportunity for PHEP and HPP. The joint 2012 PHEP-HPP notice of funding covered 5 years starting in 2012 through 2017. The joint 2017 PHEP-HPP notice of funding opportunity covered 2 years starting in 2017 through 2019 when ASPR took over grant administration of HPP from CDC. The 2019 PHEP and HPP notices of funding opportunity covered 5 years starting in 2019 through 2024. The 2024 PHEP and HPP notices of funding opportunity will cover 5 years starting in 2024 through 2029.
[14]These documents were submitted by jurisdictions in response to the 2019 and 2024 PHEP and HPP notices of funding opportunity.
[15]See GAO, Government Performance Management: Leading Practices to Enhance Interagency Collaboration and Address Crosscutting Challenges, GAO‑23‑105520 (Washington, D.C.: May 24, 2023).
[16]The National Preparedness System is a document including a government-wide set of planning and policy guidance created in 2011 in accordance with the Post-Katrina Emergency Management Reform Act of 2006. Pub. L. No. 109-295, tit. VI, §§ 642, 644, 120 Stat. 1355, 1394, 1425 (codified at 6 U.S.C. §§ 742, 744). It is designed to strengthen national preparedness to ultimately enable the nation to meet the National Preparedness Goal of having a secure and resilient nation. See U.S. Department of Homeland Security, National Preparedness System (Nov. 2011).
[17]Pub. L. 109-295, tit. VI, §§ 642, 643, 644, 120 Stat. at 1425 (codified at 6 U.S.C. §§ 742-44).
[18]See White House, Presidential Policy Directive/PPD-8: National Preparedness (Mar. 30, 2011). See also U.S. Department of Homeland Security, National Preparedness Goal: First Edition (Sept. 2011), and National Preparedness System (Nov. 2011).
[19]According to CDC, a public health system is defined as public health agencies at all levels of government, such as state and local public health departments.
[20]Some of these activities must be completed multiple times over the 5-year award period; therefore, the total number of required activities jurisdictions must complete is 103.
[21]Jurisdictions are required to exercise public health risks and threats through a series of discussion-based and operations-based exercises. Discussion-based exercises are defined as seminars, workshops, tabletops, and games. Operations-based exercises are defined as drills, functional exercises, and full-scale exercises.
[22]See U.S. Department of Homeland Security, Homeland Security Exercise and Evaluation Program (Jan. 2020).
[23]An incident is an occurrence, natural or human-made, that necessitates a response to protect life or property which includes planned events as well as emergencies and disasters of all kinds and sizes.
[24]According to ASPR, a health care system is defined as a community’s health care organizations which include hospitals, long term care facilities, blood banks, and pharmacies, among others.
[25]The HPP 2024 notice of funding opportunity states that health care coalition membership must, at a minimum, include membership of leaders of organizations from the following categories: health care (e.g., hospitals, health systems, health care facilities), emergency management, health care response incident management, emergency medical services and patient transport services, and public health.
[26]Some of the 29 activities must be completed multiple times over the 5-year award period; therefore, the total number of required activities jurisdictions must complete is 80.
[27]Officials also said that CDC and ASPR jointly present information to provide updates on PHEP and HPP and hear concerns from jurisdictions at national annual meetings organized by the National Association of County and City Health Officials and Association of State and Territorial Health Officials.
[28]Some of the 34 PHEP and 29 HPP activities must be completed multiple times over the 5-year award period; therefore, the total number of required activities jurisdictions must complete is 103 for PHEP and 80 for HPP.
[29]This memorandum of understanding also included FEMA, HHS’s Health Resources and Services Administration, and the U.S. Department of Transportation.
[30]GAO, Public Health Preparedness: Critical Need to Address Deficiencies in HHS’s Leadership and Coordination of Emergencies, GAO‑23‑106829 (Washington, D.C.: May 11, 2023).
[31]GAO, Public Health Preparedness: Critical Need to Address Deficiencies in HHS’s Leadership and Coordination of Emergencies, GAO‑23‑106829 (Washington, D.C.: May 11, 2023).
[33]U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Public Health Emergency Preparedness (PHEP) Cooperative Agreement Notice of Funding Opportunity (Opportunity number: CDC-RFA-TP19-1901).
[34]U.S. Department of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response, Hospital Preparedness Program Cooperative Agreement Program (Opportunity number: EP-U3R-19-001).
[35]U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Public Health Emergency Preparedness (PHEP) Cooperative Agreement Notice of Funding Opportunity (Opportunity number: CDC-RFA-TU24-0137) and Administration for Strategic Preparedness and Response, Hospital Preparedness Program Cooperative Agreement Notice of Funding Opportunity (Opportunity number: EP-U3R-24-001).
[36]U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health (Oct. 2018) and Administration for Strategic Preparedness and Response, Hospital Preparedness Program Cooperative Agreement Notice of Funding Opportunity (Opportunity number: EP-U3R-24-001).
[37]According to ASPR officials, they collect performance measures from jurisdictions and health care coalitions organized by the activities and requirements laid out in the HPP notice of funding opportunity.
[38]See U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Public Health Emergency Preparedness and Response Capabilities: National Standards for State, Local, Tribal, and Territorial Public Health (Oct. 2018) and Assistant Secretary for Preparedness and Response, 2017-2022 Health Care Preparedness and Response Capabilities (Nov. 2016).
[39]U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Public Health Emergency Preparedness (PHEP) Cooperative Agreement Notice of Funding Opportunity (Opportunity number: CDC-RFA-TU24-0137).
[40]U.S. Department of Health and Human Services, Administration for Strategic Preparedness and Response, Hospital Preparedness Program Cooperative Agreement Notice of Funding Opportunity (Opportunity number: EP-U3R-24-001).