Report to the Ranking Member Committee on Veterans’ Affairs
House of Representatives
United States Government Accountability Office
A report to the Ranking Member, Committee on Veterans’ Affairs, House of Representatives
For more information, contact: Sharon M. Silas at silass@gao.gov
What GAO Found
Veterans Health Administration (VHA) medical facility officials are responsible for reviewing the clinical care delivered by their providers when concerns arise. GAO identified 104 providers with clinical care concerns (such as practicing in a manner that is unsafe or inconsistent with industry standards of care) at five selected VHA medical facilities between January 2020 and July 2024. GAO found these facilities did not consistently adhere to VHA policy when conducting quality reviews, or reporting providers to state licensing boards or the National Practitioner Data Bank. All five facilities also had missing or incomplete review documentation. As of March 2026, VHA has developed some mandatory training for facility staff related to credentialing providers, but not any on quality review and reporting processes. By failing to follow VHA policy, facilities increase the risk that these processes are conducted incorrectly and that these providers may continue to provide unsafe care to veterans.
Related to reporting, GAO also found these five facilities did not initiate processes to determine whether seven providers should have been reported to state licensing boards or the National Practitioner Data Bank. Completing the review process for these providers will provide VHA assurance that any identified quality concerns will be properly assessed and that the providers who should be reported are reported. Timely reporting helps reduce the risk that other VHA facilities or community hospitals and clinics hire providers with unreported clinical care issues, thereby potentially putting patients at risk.
In addition, GAO found that VHA oversight of review and reporting processes at medical facilities was limited in ensuring adherence to VHA policy requirements. Specifically, VHA’s oversight methods—which include a tracking tool and an annual facility self-assessment and audit—are not designed to assess adherence with all timeliness and documentation requirements. These limitations prevent VHA from comprehensively and consistently overseeing processes for monitoring provider clinical performance and ensuring safe, quality health care for veterans.
Why GAO Did This Study
VHA is responsible for ensuring providers deliver safe care to veterans at its more than 170 medical facilities. However, VHA has faced challenges ensuring providers with clinical care concerns undergo timely and documented reviews, and are reported to external entities when appropriate.
GAO was asked to examine VHA processes for reviewing concerns about providers’ clinical care. This report assesses (1) selected VHA medical facilities’ adherence to VHA policies for reviewing and reporting providers with clinical care concerns; and (2) VHA’s oversight of quality review and reporting processes for providers with clinical care concerns.
GAO reviewed VHA policy documents and interviewed VHA officials. GAO also selected a non-generalizable sample of five VHA medical facilities (based on factors such as facility complexity) and identified providers with clinical care concerns from January 2020 through July 2024. This time frame included the most recent facility meeting minutes and allowed for reviews and reporting to be completed. For each provider, GAO reviewed available documentation and interviewed local and regional VHA officials.
What GAO Recommends
GAO is making seven recommendations to VHA, including developing training, completing the reporting process for certain providers, and ensuring that oversight methods assess compliance with VHA’s review and documentation requirements. VA concurred or concurred in principle with GAO’s seven recommendations and identified steps it plans to take.
Abbreviations
|
FPPE Focused Professional Practice Evaluation |
|
NPDB National Practitioner Data Bank |
|
SLB state licensing board |
|
VA Department of Veterans Affairs |
|
VHA Veterans Health Administration |
|
VISN Veterans Integrated Service Network |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
May 12, 2026
The Honorable Mark Takano
Ranking Member
Committee on Veterans’ Affairs
House of Representatives
Dear Mr. Takano:
The Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) operates one of the largest health care systems in the nation, with more than 53,000 licensed independent providers across its more than 170 medical facilities.[1] Leadership at VHA medical facilities are responsible for ensuring that these providers deliver safe care to veterans. As part of this responsibility, medical facility leadership are to follow VHA processes when monitoring providers’ clinical care and conducting reviews after a potential clinical care concern arises.[2] Depending on the nature of the concern and findings from the review, facility leadership may take action to limit some, or revoke all, of the types of care the provider is allowed to deliver at the VHA medical facility—known as an adverse privileging action.[3]
VHA medical facility leadership are required to report any adverse privileging actions they take against physicians and dentists to the National Practitioner Data Bank (NPDB), which is used by health care entities, such as VHA medical facilities and community hospitals, to obtain information about providers with a history of substandard care.[4] Facility leadership are also required to report providers to relevant state licensing boards (SLB) when there are substantiated concerns about the quality of a provider’s clinical practice.[5] The SLB can then investigate and determine if any action against the provider’s license to practice should be taken, such as suspension, restriction, or revocation.
In recent years, we, along with the VA Office of Inspector General, have reported deficiencies with VHA’s oversight processes for reviewing and reporting medical facility providers for clinical care concerns. For example, in 2017, we found that five VHA medical facilities’ processes for overseeing provider quality reviews sometimes resulted in untimely or undocumented reviews, and that their respective Veterans Integrated Service Networks (VISN) lacked proper oversight of these facilities’ review and reporting processes.[6] The VA Office of Inspector General also found areas for improvement regarding monitoring, reviewing, and reporting quality of care concerns.[7] VHA has since taken action to address the deficiencies identified in these reviews.
In 2022, Congress passed and the President signed the Joseph Maxwell Cleland and Robert Joseph Dole Memorial Veterans Benefits and Health Care Improvement Act of 2022 (Cleland-Dole Act). The act called for VHA to ensure medical facility compliance with existing requirements regarding credentialing providers and reviewing and reporting quality of care concerns found in VHA policy.[8] The Cleland-Dole Act also contained a new requirement for VHA to provide mandatory training for medical facility staff responsible for reviewing the quality of clinical care provided by VHA providers and taking adverse privileging actions.[9]
You asked us to examine VHA medical facilities’ review and reporting processes for providers with clinical care concerns and VHA’s oversight of these processes. In this report, we assess
1. selected VHA medical facilities’ adherence to VHA policies for reviewing and reporting providers with clinical care concerns; and
2. VHA’s oversight of quality review and reporting processes for providers with clinical care concerns.
To address these objectives, we reviewed applicable VHA policy documents outlining requirements for (1) review and reporting processes, and (2) oversight responsibilities for VHA medical facility, VISN, and VHA central office officials.[10] We also reviewed requirements related to review and reporting processes outlined in the Cleland-Dole Act. We interviewed relevant VHA medical facility, VISN, and VHA central office officials about VHA’s review and reporting processes and their oversight responsibilities.
To assess selected medical facilities’ adherence to VHA policies for reviewing and reporting providers with clinical care concerns, we reviewed documentation for 104 providers that underwent a quality review or reporting to the NPDB or SLBs between January 2020 and July 2024 from a non-generalizable sample of five VHA medical facilities.[11] We selected these five facilities based on varying facility complexity, locations in different VISNs, and facility-reported provider data to VHA central office.[12]
We identified the 104 providers using two methods. First, we requested that the five facilities provide us with a list of providers that had quality reviews conducted or were reported to the NPDB or SLBs by their facility for our selected time frame. Second, we reviewed meeting minutes from each of the five facility’s credentialing committees during our time frame to identify any providers that underwent quality reviews or reporting to the NPDB or SLBs.[13] We compared the two lists of names and compiled a list of providers to review at each of the five selected VHA medical facilities.
We then conducted in-person sites visits at three facilities and virtual site visits at two facilities from September 2024 to February 2025. During the site visits we reviewed facility and VISN documentation of the quality reviews of the selected providers’ clinical care and any relevant reporting to the NPDB or SLBs. We interviewed officials at each of the five selected facilities—including facility directors, chiefs of staff, credentialing and privileging managers, and risk managers—and relevant VISN officials about the quality reviews and any reporting of these providers.[14] Based on the documentation and interviews, we assessed the extent to which the selected VHA medical facilities’ review and reporting processes adhered to VHA policy requirements for quality reviews and reporting to the NPDB and SLBs and against federal internal control standards related to control environment and risk assessment for these providers.[15]
To assess VHA’s oversight of quality review and reporting processes for providers with clinical care concerns, we reviewed VHA documentation on oversight processes conducted between January 2020 and July 2024, including assessments and audit results. We assessed the VHA oversight tools the selected medical facilities and related VISNs used for oversight of review and reporting processes against federal internal control standards related to monitoring.[16] We reviewed the provider data we received from VHA central office and the five selected VHA medical facilities to identify any obvious errors and omissions, and interviewed relevant VHA officials about the provider data. We identified potential limitations with the provider data and discuss these limitations later in this report.
We conducted this performance audit from April 2024 to May 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
VHA monitors the performance of providers who work at VHA medical facilities to ensure safe and quality medical care for veterans. VHA policies outline processes, and central office, VISN, and medical facility staff responsibilities for routinely monitoring provider performance and how to report providers to the NPDB and SLBs when quality of care concerns are substantiated.[17]
VHA central office staff establish policies for provider quality reviews and reporting, and provide guidance on these policies to VISN and medical facility officials. According to VHA policy, the medical facility director is ultimately responsible for oversight of provider quality review and reporting processes at the VHA medical facility. VISNs also oversee provider quality reviews and reporting of network facilities, including through providing guidance and consultation, and conducting annual audits of facility credentialing and privileging adherence to VHA policy.
Reviewing VHA Providers’ Clinical Care Concerns and Taking Adverse Privileging Actions When Necessary
According to VHA policy, when a concern about a provider’s clinical care is raised, medical facility leadership are required to review the concern and determine whether an adverse action should be taken against the provider’s privileges.[18] Facility leadership should first determine if allowing the provider to continue delivering care could result in imminent danger to veterans. If so, the provider should be removed from care through a summary suspension, which may include suspending some or all of a provider’s privileges, and should continue for the duration of the review of the provider’s clinical care, according to VHA policy.[19]
Next, facility leadership must determine the most appropriate quality review process to use to review a provider’s clinical care depending on the specific concerns and the situation. According to VHA policy, these quality review processes can include the following:
· Focused Professional Practice Evaluation (FPPE) for cause. During a FPPE for cause, a provider’s clinical care is monitored over a specified period, during which the provider can demonstrate improvement in a specific area of concern. This type of review is to be used when facility leadership determines that the provider’s clinical care concern is addressable without risk to patient safety.
· Focused clinical care review. These reviews, which occur when facility staff identify significant concerns with a provider’s care, examine care delivered during a specific period in the past. According to VHA policy, three external providers, usually of the same practice specialty (peer reviewers) to ensure fairness and objectivity, review the medical records of patients cared for by a provider to determine if the care met generally accepted standards of care.[20] Facility leadership are required by VHA policy to complete focused clinical care reviews after placing a provider under summary suspension, but also may complete this type of review independent of a summary suspension to review concerns that do not pose imminent danger to veterans.[21]
Once a review of the provider’s care is completed, facility leadership make decisions about next steps, which could include
· return the provider to regular ongoing monitoring if the review did not substantiate the clinical care concern;
· conduct additional reviews if the concern is substantiated and more information is needed (such as a FPPE for cause or a focused clinical care review to further investigate); or
· recommend an action against a provider’s privileges—known as an adverse privileging action—including limiting one or more privileges (such as prescribing medication or performing a certain procedure) or revoking all the provider’s privileges at the medical facility.
According to VHA policy, recommendations for adverse privileging actions are sent to the medical facility director who makes the final determination on the action.
Reporting VHA Providers to the NPDB and SLBs After Clinical Care Concerns are Substantiated
VHA policy requires its medical facilities to report a provider to the NPDB or relevant SLBs if a quality review substantiates serious concerns with the provider’s clinical performance. Specifically:
National Practitioner Data Bank. Under VHA policy, medical facility directors must report physicians and dentists to the NPDB (1) if the facility takes final action against the provider’s clinical privileges that adversely affects the provider’s privileges for a period longer than 30 days due to professional incompetence or misconduct, or (2) if the provider resigns or retires while under investigation for a clinical care concern.[22] To avoid any errors in the facts of the report, the facility director must notify any provider who is about to be reported to the NPDB and give the provider an opportunity to discuss the content of the report before it is submitted. See figure 1 for an overview of VHA’s NPDB reporting process after a clinical concern has been substantiated and an adverse privileging action has been recommended.
Figure 1: VHA Process for Determining NPDB Reporting for Adverse Privileging Actions, January 2020-July 2024
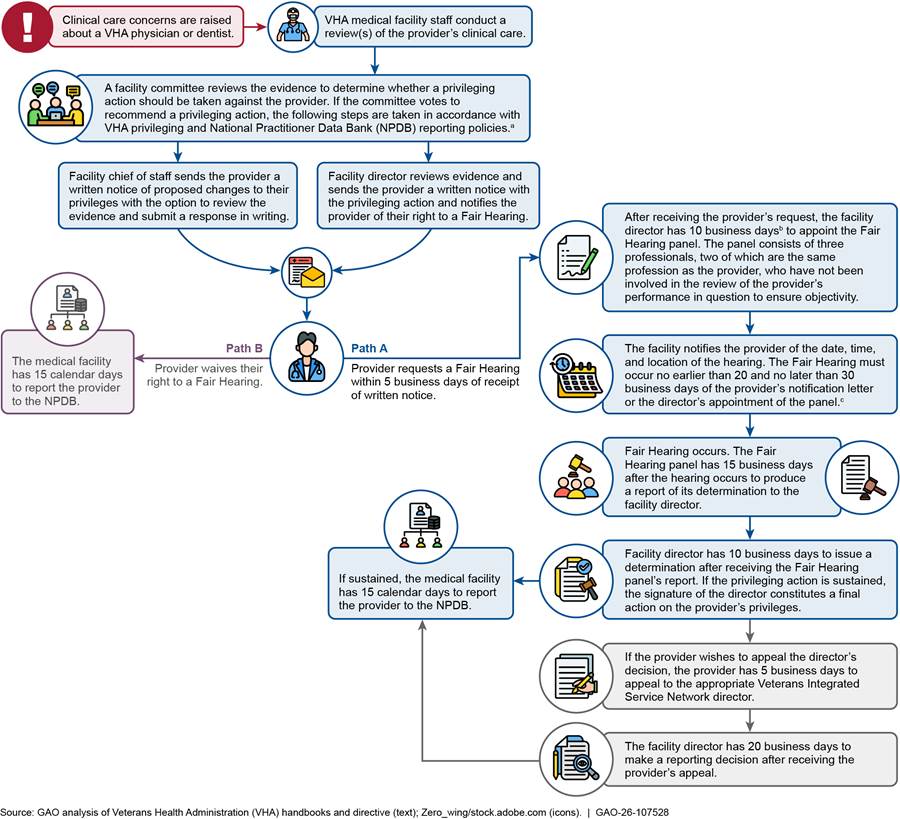
aNPDB reporting policies include Veterans Health Administration, National Practitioner Data Bank (NPDB) Reports, VHA Handbook 1100.17 (Washington, D.C.: Dec. 28, 2009); Veterans Health Administration, Credentialing and Privileging, VHA Handbook 1100.19 (Washington, D.C.: Oct. 2, 2007); and Veterans Health Administration, Privileging, VHA Directive 1100.21(1) (Washington, D.C.: Mar. 2, 2023).
bPrior to the new VHA Fair Hearing policy released in December 2023, VHA medical facility directors had 5 business days to appoint the Fair Hearing panel after the provider’s request for the hearing, whereas directors now have 10 business days.
cPrior to the new VHA Fair Hearing policy released in December 2023, Fair Hearing scheduling was based on the date of the provider’s notification letter, whereas currently it is based on the date of the panel appointment letter.
In addition to the two circumstances noted above, facility leadership are required by VHA policy to report to the NPDB any payment for the benefit of a physician, dentist, or other licensed provider made as the result of a settlement or judgment of a medical malpractice claim that was determined to include substandard care, professional incompetence, or professional misconduct during the episode of care.[23]
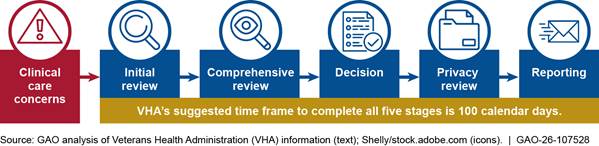
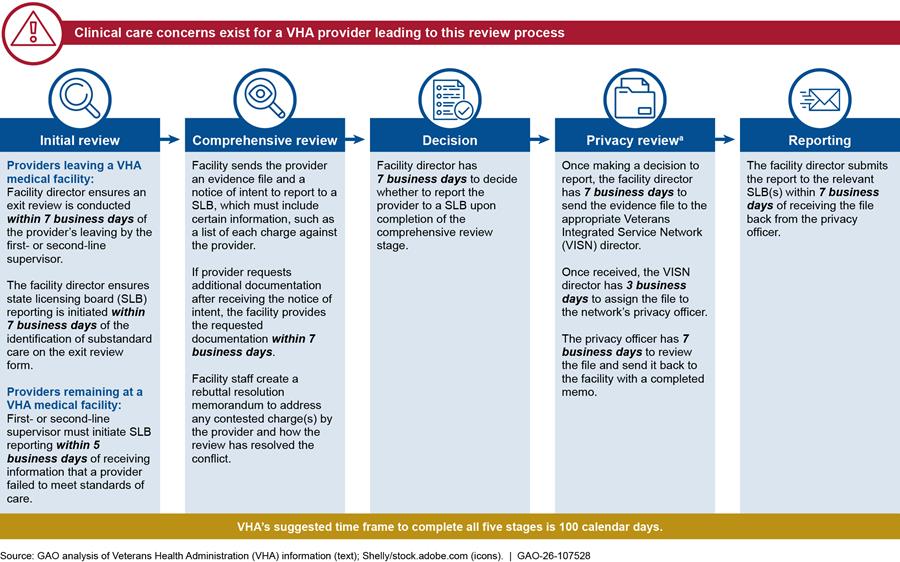
State licensing boards. According to VHA policy, facility officials are required to report providers—both current and former employees—to SLBs when they have determined that the provider’s behavior or clinical practice substantially failed to meet generally accepted standards of clinical care as to raise reasonable concerns for the safety of patients.[24] Facility directors are to report providers to all SLBs where the provider holds an active medical license, as well as the respective SLB in the state in which the provider is practicing, if not licensed in that state. VHA policy outlines a time frame for each step of the SLB reporting process to be completed by facility and VISN staff and an overall time frame of no more than 100 calendar days from start to finish. See figure 2 for an overview of the SLB reporting process that is initiated after a VHA provider’s behavior or clinical practice fails to meet accepted standards.
aDuring our review time frame, VHA updated its SLB guidance in January 2021. Under the earlier guidance, the privacy review stage was called the concurrence stage. In this stage, review of the evidence file could be completed by a facility privacy officer located in a different facility within the VISN if the case was deemed non-sensitive, or completed by VHA’s Office of General Counsel if the case was deemed sensitive.
Selected Facilities Did Not Consistently Adhere to VHA Review and Reporting Policies, Limited Training Reported as Factor
Selected VHA medical facilities did not consistently adhere to VHA policy requirements for conducting quality reviews or reporting providers to SLBs or the NPDB during our time frame. Specifically we found (1) selected facilities adhered to some but not all required review and reporting requirements; (2) some selected facilities did not initiate either the SLB or NPDB reporting processes to determine if reporting was necessary after a clinical care concern was identified for all providers; and (3) selected facilities were unable to produce required documentation or they produced required documentation that had missing key elements, such as dates. Facility staff cited a number of challenges to adhering to VHA review and reporting policies including limited training.
Selected Medical Facilities Did Not Consistently Adhere to VHA Policy When Conducting Quality Reviews and Reporting Providers with Clinical Care Concerns
Quality Reviews
We identified 104 providers with potential clinical care concerns and reviewed documentation for 91 of the providers that underwent quality reviews across the selected facilities during our time frame of January 2020 through July 2024.[25] For these providers, we found that selected facilities generally adhered to VHA policy requirements for conducting FPPEs for cause and initiating summary suspensions and focused clinical care reviews.[26] For example, we reviewed available documentation for 71 FPPEs for cause (completed for 64 unique providers) and found that the facilities generally adhered to VHA policy when conducting these reviews.[27] Specifically, we found that the facilities generally defined these reviews in advance, such as the time frame of the review and expectations for improvement, as required in VHA policy.[28]
However, we also found that two facilities did not carry out summary suspensions for one of their providers as required in VHA policy. One facility placed the provider with clinical care concerns under administrative suspension, discussed later in this report. This type of suspension is used for non-clinical performance reasons, such as extended leave due to a chronic illness. Another facility allowed the provider under summary suspension, with all privileges suspended due to clinical care concerns and patient welfare, to continue to provide care to patients.
SLB and NPDB Reporting
Of the 104 providers with potential clinical care concerns during our time frame, we reviewed documentation for 28 SLB reports (submitted for 27 providers), and nine proposed adverse privileging actions (for eight physicians and dentists).[29]
We found selected facilities did not consistently meet all VHA reporting requirements.[30] (See app. III for details on the five facilities’ adherence to VHA policies related to SLB and NPDB reporting requirements.) For example, facilities generally met VHA’s SLB policy requirement to conduct an exit review of the provider’s care within 7 days of the provider’s departure, and to include required information in the Notice of Intent to Report letter sent to providers to inform them of potential SLB reporting. For NPDB reporting, we found the facilities generally met policy requirements for receiving the Fair Hearing panel’s report after the hearing occurred.[31]
However, the facilities did not fully meet other VHA policy requirements. For example:
· The SLB reporting process was initiated within the required 7 days of identifying substandard care on an exit review for three of 23 providers.[32]
· As previously noted, we found that one facility placed a provider on the incorrect type of suspension for a clinical care concern. The provider resigned while the facility was conducting the investigation. Because the provider was in the incorrect type of suspension, the facility did not initiate the NPDB reporting process to determine whether to report the provider for resigning while under investigation, as required in VHA policy.[33]
· We also found another facility may have reported a provider to the NPDB without allowing for due process. Specifically, the provider was reported for retiring while under investigation, but we found no evidence that the facility provided a limited hearing, as required in VHA policy, to determine whether reporting was necessary.[34]
Further, we identified seven providers with documented clinical care concerns for whom facility officials did not initiate either the SLB or NPDB reporting process to determine if reporting was necessary.[35] For example, two facilities each terminated a provider for clinical care concerns and noted on each provider’s exit review form that SLB reporting should be immediately initiated, which aligns with VHA policy.[36] However, the two facilities were unable to provide any documentation to show that the SLB reporting process was initiated for either provider. (For more information on these seven providers, see app. IV.)
Missing Documentation or Incomplete Information
In addition to varied adherence to VHA policy, we found the selected facilities had missing or incomplete documentation for the providers we reviewed that underwent quality reviews or reporting. The facilities were either unable to produce required documentation to allow us to determine if VHA policy requirements were met, or the facilities produced documentation with incomplete elements, such as missing dates, needed to determine policy adherence.[37]
· Missing documentation. Our review found the selected facilities were unable to produce some required documentation for quality reviews and SLB and NPDB reporting. For example, VHA requires certain documents to be maintained in a provider’s credentialing and privileging folder.[38] Specifically, we found the following:
· For 71 FPPEs for cause conducted (for 64 providers), facilities could not provide any documentation for four reviews (for four providers).
· For the 33 focused clinical care reviews (for 30 providers) completed during our time frame, facilities were unable to locate any documentation for seven reviews (for seven providers).[39]
· For SLB reporting, missing documentation was especially prevalent in the SLB review stage that required VISN involvement. For example, once the VISN completes its review of the SLB evidence file, the file must be returned to the medical facility director with a completed memo that stated the SLB evidence file was reviewed for protected information and is appropriate for submission to an SLB.[40] We did not receive a copy of that memo for 20 of 28 SLB reports.
· Selected facilities that reported a provider to the NPDB for adverse privileging actions were unable to produce required documentation for four of the seven reports.[41]
· Incomplete or inaccurate information. Our review also found the selected facilities provided quality review documentation with information that was incomplete or inaccurate. For example:
· Incomplete FPPE for cause information. We did not receive signed copies of 15 FPPE for cause memos (for nine providers) as required in VHA policy.[42]
· Incomplete focused clinical care review information. We found documentation for 25 focused clinical care reviews (for 23 providers) did not contain all information as required in VHA guidance, such as the review’s scope, data source, and conclusions.[43]
· Inaccurate information. We found inaccurate quality review documentation for seven providers. Specifically, the documentation for the FPPEs for cause for these providers stated that the clinical care concerns under review had been identified through a focused clinical care review. However, in these cases, we either confirmed with the facilities the review completed had instead been an informal management review or the facility could not confirm a review occurred.
Officials from the five selected facilities gave varying reasons for not meeting VHA policy requirements, including missing or incomplete documentation, when conducting quality reviews and reporting of providers with clinical care concerns. These reasons included documents needing to be reviewed by multiple individuals, differing methods of saving review and reporting documentation, staff turnover, inaccurate guidance from the VISN, and limited training. Officials from two of the five facilities stated that they want more training related to provider reporting requirements, and officials from one facility found the current training to be limited.
The Cleland-Dole Act required VHA to provide mandatory training on the following duties to employees responsible for them: (1) credentialing, (2) conducting quality reviews, (3) taking adverse privileging actions against providers that do not meet the standard of care, and (4) making notifications regarding clinical care concerns.[44] To meet these requirements, VHA officials stated that they have developed four required trainings related to credentialing and reviewing new provider privileges at a facility. However, VHA officials told us that VHA has not developed any training for relevant staff related to quality reviews or taking adverse actions against providers with substantiated quality care concerns. Effective training on these topics is important to help address the deficiencies we noted with review and reporting adherence above, and is consistent with federal internal controls.[45] Specifically, training can help ensure VHA medical facility staff understand the review and reporting requirements and time frames in VHA policy, and that required documentation about provider clinical care concerns is retained appropriately if needed for future staff reference. By failing to develop trainings related to quality review topics, VHA increases the risk that (1) medical facilities complete reviews and reporting in an incorrect or undocumented manner, and (2) allows providers with clinical care concerns to continue to treat veterans.
For the seven providers where facilities did not initiate SLB or NPDB reporting, facility officials stated they either misinterpreted VHA policy or were unable to provide a reason why the facility did not follow VHA policy. Not initiating the process to determine whether these providers should have been reported violates VHA policy and creates potential risks for veterans and patients outside of VHA facilities. Specifically, in any instance where a provider with substantiated clinical care concerns should have been reported to the SLB or NPDB, but was not, that provider may obtain privileges at another VHA medical facility or a community hospital because there would be no indication on their record that an adverse privileging action was taken against them, or that they resigned or retired while under investigation. Initiating the reporting process for the seven providers we identified would be consistent with VHA policy and help ensure that all providers who should be reported are reported.
Selected Medical Facilities Faced Challenges Meeting VHA’s Suggested Time Frames for Review and Reporting Processes of Providers with Clinical Care Concerns
Our review found the selected VHA medical facilities did not always complete certain quality reviews and SLB reporting processes within suggested time frames. Specifically, we found the following:
Untimely focused clinical care reviews. VHA guidance suggests that facilities complete summary suspensions and focused clinical care reviews within 30 days.[46] Of the 36 summary suspensions (for 31 providers) the facilities initiated during the period of our review, eight (for seven providers) resulted in a provider suspended for 30 days or less, while 25 suspensions (for 21 providers) exceeded 30 days.[47] For three suspensions (for three providers), available documentation did not allow us to determine the duration of the suspension. For the 23 focused clinical care reviews that followed a summary suspension at four facilities, we found that two reviews were completed within the suggested 30 days.[48]
Most of the selected VHA facility and VISN officials in our review reported resource challenges to completing these reviews within the suggested time frame. Namely, they cited challenges identifying multiple external reviewers with the clinical expertise and available time required to complete these reviews.[49] For example, officials at two VHA facilities and three VISNs told us that providers who serve as reviewers complete these reviews in addition to their clinical workload or at the cost of time spent with patients. Further, officials told us that time spent reviewing focused clinical care reviews do not count toward VHA provider productivity workloads, so providers may be hesitant to take part in activities that do not help them meet productivity goals.
Untimely SLB reporting. We found the selected facilities were unable to meet the 100-day time frame suggested in VHA policy to complete SLB reporting for most of the SLB reports—18 of 28—in our review.[50] For these 18 reports, overall reporting time frames ranged from 104 to 763 days. Further, we were unable to determine the overall time frames for five of the 28 SLB reports due to missing or undated documentation. For example, one facility was unable to provide us with the reporting letter sent to the SLB, and at another facility we received undated copies of the reporting letter sent to SLBs. We previously identified issues with untimely SLB reporting. Specifically, in November 2017, we reported that SLB reporting took significantly longer than the 100-day time frame for the two reports submitted from two selected VHA medical facilities.[51] Facility staff reiterated challenges discussed previously regarding nonadherence with VHA policy requirements including differing methods of saving review and reporting documentation, staff turnover, inaccurate guidance from the VISN, and limited training.
Although VHA policy suggests, but does not require, VHA facility officials to meet the time frames for conducting clinical care reviews and SLB reporting, not meeting these time frames creates risks. Reviews that exceed suggested time frames in policy limit veteran’s access to these providers, or to a provider covering their patient workload while they are removed from care during the review, for needed care and may increase wait times. Specifically, providers under summary suspension are unable to provide care to veterans and deserve to have quality reviews completed as timely as possible. Untimely reporting to SLBs increases the risk that information about a provider’s substantiated clinical care concern is unavailable to other VHA medical facilities or community clinics or hospitals.
Federal internal control standards state that entities analyze identified risks, estimate their significance, and respond to those risks.[52] In addition, the Cleland-Dole Act states that medical facilities must conduct timely reviews of providers that fail to meet standards and notify SLBs in a timely manner of substantiated clinical care concerns.[53]
Although our findings are specific to the selected facilities, the extent of the timeliness issues we identified, and the various challenges facility staff have reported related to meeting suggested time frames raise questions about the extent to which other VHA facilities may be encountering the same challenges meeting VHA’s suggested time frames. VHA officials stated they plan to pull monthly reports to review timeliness using a tracking tool discussed later in this report. Assessing the risks associated with the untimeliness—including the extent to which they occur in other facilities—and addressing the risks as appropriate would be consistent with federal internal control standards. This should include assessing the extent to which VA medical facilities are meeting the suggested time frames for conducting focused clinical care reviews and SLB reporting, and addressing any identified risks. By doing this, VHA can help ensure that all of its medical facilities are effectively responding to concerns about providers’ delivery of care while at the same time ensuring that review and reporting processes are timely.
Further, officials from one facility told us that they sometimes wait until after a Fair Hearing to determine whether SLB reporting should be initiated. This practice is consistent with our findings from 2017, where we previously found that two VHA medical facilities in the selected sample would also wait to start SLB reporting once all appeals had been exhausted.[54] It is unclear whether this is allowed or not. On the one hand, this practice is inconsistent with VHA’s policy that states the SLB reporting process is to be initiated immediately once a clinical care concern is identified.[55] However, VHA central office officials told us that waiting until after a Fair Hearing is allowed. VHA officials’ communication of practices is inconsistent with written policy and may lead to untimeliness in SLB reporting and nonadherence to VHA policy. Reviewing and clarifying its policy requirements would help VHA ensure that facilities are consistent in their SLB reporting processes and reduce any untimely related reporting.
VHA Oversight of Reviews and Reporting of Providers with Clinical Care Concerns Is Limited
VHA has two oversight methods for medical facility and VISN staff to use to oversee providers: (1) a tracking tool of providers undergoing quality reviews and reporting, and (2) facility credentialing and privileging self-assessments and VISN audits.[56] As designed, however, we found that these methods do not allow VHA to comprehensively monitor adherence to all quality review and reporting requirements.
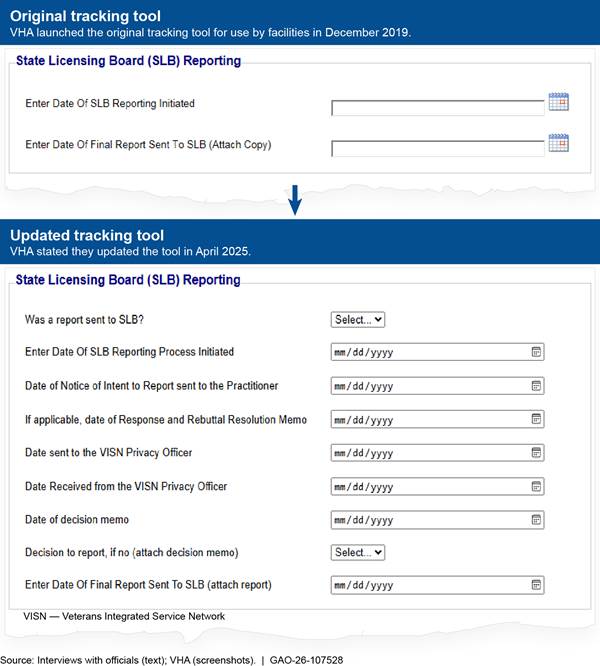
Provider quality review and reporting tracking tool. In 2019, VHA central office implemented a tool that medical facilities and VISNs are required to use to track completion of requirements for performing quality reviews and reporting providers to SLBs and the NPDB.
Specifically, the tracking tool allows facility staff to input dates of major quality review and reporting steps—such as initiation and completion of a focused clinical care review or final reporting—to monitor timeliness. VHA central office officials told us medical facility and VISN officials can use the tool’s timeliness data to investigate provider cases that are taking longer than VHA policy time frames suggest (e.g., 100 days for SLB reporting). Staff at our five selected medical facilities and officials at the five associated VISNs confirmed use of the tool.
However, we found the tool in place at the time of our review was not comprehensive, as it did not allow a facility to track all requirements included in VHA policy for completing provider quality reviews and for SLB and NPDB reporting. For example, it did not allow facilities to track the initiation and completion of FPPEs for cause or SLB reporting steps between initiation and submission of the final report.
In April 2025, VHA central office updated the tracking tool to include additional data fields, according to VHA central office officials. Officials told us the updated tool is intended to be more inclusive of all SLB and NPDB reporting timeliness requirements. New fields in the updated tool include dates for initiation and completion of FPPEs for cause, and completion of additional steps for SLB and NPDB reporting. (See fig. 3.)
Figure 3: Example of Updated Veterans Health Administration (VHA) Tracker Data Fields for Reporting to State Licensing Boards
Further, in September 2025, VHA officials told us additional efforts are underway to better ensure policy requirements around timeliness are being met through use of the tracking tool. For example, VHA officials plan to instruct VISN officials to pull weekly reports from the tool to ensure medical facilities are meeting timeliness requirements and to expand the tool’s reporting capabilities so that additional information may be monitored.
However, even with the updates and planned improvements, the tool remains limited for ensuring medical facilities adhere to all VHA policy requirements—particularly those related to maintenance of required documentation. Specifically, the tool does not allow medical facilities to confirm that documentation is complete and saved in the appropriate location.[57]
Without a comprehensive tool in place, we found that officials at all selected medical facilities and at two VISNs reported relying on separate tracking mechanisms (such as spreadsheets) to track provider quality reviews, as well as other VHA reporting requirements, in addition to those included in the tracking tool. We also found that, as a result of multiple tracking mechanisms, medical facilities could not accurately account for which providers underwent quality reviews, and which providers were reported due to substantiated clinical care concerns.
Specifically, we found that none of our selected facilities were able to provide complete or accurate lists of providers who had undergone reviews or reporting during our time frame. Through our review of medical facility meeting minutes, we identified an additional 16 providers across the five facilities who had not been included in the lists provided by the facilities. In addition, four of our selected facilities did not accurately report to us which types of reviews or reporting had been done for the providers they identified. We identified additional review and reporting actions for five providers through our review of facility documentation. Lastly, as noted above, we found that medical facilities did not initiate reporting of some providers to SLBs and the NPDB, and did not always have complete documentation for quality reviews and reporting.
Facility self-assessments and VISN audits. In addition to the use of a tracking tool, since 2020, VHA has required (1) medical facility staff to complete annual credentialing and privileging self-assessments, and (2) VISN officials to complete audits at each facility to monitor medical facility adherence with VHA policies. The facility self-assessment is intended to help identify any areas of credentialing and privileging policy nonadherence, including those related to conducting quality reviews and reporting providers with substantiated clinical care concerns. Medical facility staff first self-assess facility adherence to credentialing and privileging policies through completion of a set of questions, which VHA updates annually.[58] Once an area of non-adherence is identified, the facility should create a corrective action plan. VISN officials are to review the facility’s self-assessment results and any required corrective action plan and then conduct an audit. To conduct the audit, VISN officials select a random sample of providers and review provider documentation to validate that the facility adhered to the policy requirements included in that year’s self-assessment.
|
VHA Medical Facility Self-Assessments Related to Provider Quality Reviews and Reporting VHA medical facilities assessed their adherence to policies on provider quality reviews and reporting through a series of questions. These questions assess whether · there is a process for reporting provider clinical care concerns to the appropriate medical facility official to initiate a focused clinical care review to substantiate the concern and determine the next course of action; · the medical facility documented Focused Professional Practice Evaluations for cause with the appropriate template; · the National Practitioner Data Bank and state licensing board tracking tool was utilized to enter and monitor reporting to completion. |
|
Source: GAO review of Veterans Health Administration (VHA) information. | GAO‑26‑107528 |
However, we found that as currently designed and implemented, VHA medical facility self-assessments and VISN audits do not comprehensively and consistently monitor all documentation and timeliness requirements for facility quality reviews and reporting. As a result, the extent to which a facility’s self-assessment included quality reviews and reporting processes varied each year. For example, the 2020 self-assessment included multiple questions about initiating summary suspensions, but subsequent self-assessments did not include any questions related to summary suspensions.
Facility self-assessments primarily focus on policies related to credentialing and privileging processes, and while they include some questions on quality reviews and reporting, we found that they are not comprehensive. The self-assessments conducted during our time frame included questions on processes such as implementation of FPPEs for cause, initiation of focused clinical care reviews in response to provider care concerns, use of the tracking tool, and the timeliness of the privacy officer review stage for SLB reporting.[59] However, the assessments did not include questions that would assess adherence to all timeliness and documentation requirements for conducting focused clinical care reviews and determining whether reporting to the SLB and NPDB are warranted.
Similarly, we found the VISN audits may not consistently assess quality review and reporting processes and providers who have undergone these processes. Specifically, the VISN audits might not include (1) all relevant requirements in that year’s self-assessment, and (2) a sample of providers who have been through the quality review and reporting processes. We reviewed results of the VISN audits at our selected facilities and found that some VISNs made recommendations related to the quality reviews and reporting processes included in the self-assessments. For example, one VISN found their respective facility was not reporting FPPEs for cause appropriately at facility credentialing committee meetings and recommended reporting reviews at each meeting until review completion. However, we also found that the VISN may not assess any quality reviews or reporting documentation due to the selected sample of providers.[60] For example, the 2022 facility self-assessment included a question on use of the FPPE for cause template. Because the sample of providers for one facility did not include any providers that underwent an FPPE for cause, the VISN did not review any FPPE for cause documentation in that audit.
We found that VHA has not developed its facility self-assessments to fully include quality reviews and reporting. VHA intends for the facility self-assessments and VISN audits to evaluate facility credentialing and privileging programs, and monitor adherence to VHA policies for reviewing and reporting providers when quality concerns are raised. However, as we have previously noted, we found facilities did not consistently adhere to these quality review and reporting requirements. VHA officials told us that though quality reviews and reporting are important, the main purpose of the self-assessment is to focus on policies and procedures that directly relate to how the facility credentials and privileges its providers.
VHA policy requires VISN officials to oversee provider privileging processes at each facility in their network and oversee the internal monitoring system for privileging and clinical performance reviews.[61] Privileging processes, according to VHA policy, include those related to quality reviews and SLB and NPDB reporting. VHA’s limited oversight of these processes is inconsistent with federal internal control standards for monitoring, which state that entities should perform ongoing monitoring.[62]
Limitations identified in VHA’s facility self-assessments and VISN audits suggest VHA may not be identifying non-adherence to provider quality reviews and reporting. Modifying these two tools so that they allow VHA to comprehensively monitor adherence to review and reporting requirements will strengthen VHA’s oversight and help ensure that facilities address providers with quality concerns. In addition, leveraging these existing tools could better enable VISN monitoring and medical facility adherence to policy requirements and potentially help to identify deficiencies in the processes.
Conclusions
VHA has a responsibility to deliver safe health care to veterans. To do this, VHA has established responsibilities and processes for ensuring that providers at its medical facilities deliver safe care to veterans, which includes reviewing and addressing any concerns identified with a provider’s clinical care. However, we found that these processes are not followed consistently. Specifically, at selected VHA medical facilities, reviews and reporting of clinical care concerns were not always conducted or documented in adherence with VHA policy. In addition, we found facilities did not follow all requirements to determine if SLB or NPDB reporting is necessary for a provider. This nonadherence to VHA policy requirements is concerning for several reasons. First, carrying out quality review and reporting processes in an incorrect or untimely manner risks patient safety and quality of care. Second, without complete documentation, VHA lacks reasonable assurance that facilities are investigating concerns appropriately or limiting or revoking providers’ privileges when necessary. Finally, facilities’ failure to consistently initiate processes to determine if SLB or NPDB reporting is necessary for a provider undermines VHA policy. This also makes it possible for providers with performance issues to practice at other VHA medical facilities or in other health care systems. In effect, not consistently and comprehensively carrying out the review and reporting processes can shield providers from professional accountability inside and outside of VA’s health care system.
Further, VHA is missing out on an opportunity to fully leverage its tracking tool and facility self-assessments and VISN audits to ensure facilities adhere to quality review and reporting policies. These oversight methods, as currently designed, do not allow VHA to assess facility adherence to all quality review and reporting requirements. By updating these methods to be more comprehensive of the quality review and reporting processes, VHA will be better able to ensure facility adherence to policy and the quality of care and patient safety for veterans throughout its health care system.
Recommendations for Executive Action
We are making a total of seven recommendations to VHA:
The Under Secretary for Health should develop training materials related to quality reviews, the NPDB adverse privileging process, and the SLB reporting process. As appropriate, these trainings should include reporting requirements; documentation requirements and preferred storage location; time frames; and provider scenarios. The trainings should be required for relevant VHA medical facility staff. (Recommendation 1)
The Under Secretary for Health should initiate the SLB or NPDB reporting process for the seven providers we identified to determine if SLB or NPDB reporting is warranted for those providers. (Recommendation 2)
The Under Secretary for Health should (1) assess the extent to which VHA medical facilities are meeting the suggested time frame in VHA policy when conducting external reviews, such as focused clinical care reviews; (2) assess the risk exceeding the suggested time frame poses to addressing clinical care concerns and to patient care; and (3) make changes to address identified risks as appropriate. (Recommendation 3)
The Under Secretary for Health should (1) assess the extent to which VHA medical facilities are meeting the suggested time frame in VHA policy when conducting the SLB reporting process; (2) assess the risk exceeding the suggested time frame poses to reporting substantiated clinical care concerns and to patient care; and (3) make changes to address identified risks as appropriate. (Recommendation 4)
The Under Secretary for Health should review and clarify its policy requirements as to when to begin the SLB reporting process when a clinical care concern is identified. (Recommendation 5)
The Under Secretary for Health should ensure that the facility tracking tool for reviewing and reporting providers with clinical care concerns be updated to include confirmation that required quality review and reporting documentation is complete and saved in the appropriate location at the facilities. (Recommendation 6)
The Under Secretary for Health should ensure that the annual facility self-assessment and VISN audit includes (1) an assessment of facility adherence to all VHA policy requirements for timeliness and maintenance of required documentation; and (2) a sample of providers who underwent quality reviews and SLB or NPDB reporting. (Recommendation 7)
Agency Comments
We provided a draft of this report to VA for review and comment. In its comments, reproduced in appendix V, VA concurred with our first, third, fourth, fifth, and sixth recommendations, and concurred in principle with our second and seventh recommendations. VA also provided technical comments, which we incorporated as appropriate.
Regarding our first recommendation, VA stated that it will create training materials related to quality reviews and reporting processes by May 2027.
For our second recommendation, VA stated that once it is provided with information on the providers we identified in our review, it will work with VHA medical facilities to determine whether reporting to the NPDB or SLB(s) is warranted. VA estimates it will complete this action by December 2026.
For our third and fourth recommendations, VA stated it will take action to evaluate the risks associated with (1) the external review process and (2) timely SLB reporting and address any identified risks accordingly. VA estimates it will complete these actions by October 2026.
For our fifth recommendation, VA stated it will revise policy documentation regarding the timing of initiating SLB reporting based on operational needs and any risks identified from the assessments completed to meet the intent of our third and fourth recommendations. VA estimates it will complete these actions by May 2027.
For our sixth recommendation, VA stated it will take action to ensure required information is added to the existing facility tracking tool and verify that quality review documentation is complete and stored appropriately at VHA medical facilities. VA estimates it will complete these actions by September 2026.
For our seventh recommendation, VA stated it will take action to evaluate facility self-assessments in correlation with VHA’s future determination of facility-based self-inspections as part of VHA’s restructuring plan. VA estimates it will complete this action by May 2028.
As agreed with your office, unless you publicly announce the contents of this report earlier, we plan no further distribution until 30 days from the report date. At that time, we will send copies to the appropriate congressional committees, the Secretary of Veterans Affairs, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact Sharon M. Silas at silass@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix VI.

Sharon M. Silas
Director, Health Care
To assess selected medical facilities’ adherence to Veterans Health Administration (VHA) policies for reviewing and reporting providers with clinical care concerns, we reviewed documentation for 104 providers that underwent a quality review, such as a Focused Professional Practice Evaluation for cause, or reporting to the National Practitioner Data Bank (NPDB) or state licensing boards (SLB) between January 2020 and July 2024 from a non-generalizable sample of five VHA medical facilities.[63] See table 1 for the number of VHA providers reviewed during our time frame.
Table 1: Number of VHA Providers with a Potential Clinical Care Concern from January 2020-July 2024 that GAO Reviewed at Five Selected VHA Medical Facilities
|
Number of VHA providers identified with a potential clinical care concern |
104 |
|
|
Reviews and suspensions |
|
|
|
Number of providers undergoing quality reviews |
91 |
|
|
Focused Professional Practice Evaluation for cause |
64 |
|
|
Focused clinical care reviews |
26 |
|
|
Number of providers undergoing summary suspension |
30 |
|
|
Reporting |
|
|
|
Number of providers reported to state licensing boards |
27 |
|
|
Number of providers with a proposed adverse privileging action |
9 |
|
|
Number of providers reported to the National Practitioner Data Bank |
8 |
|
Source: GAO review of Veterans Health Administration (VHA) information. | GAO‑26‑107528
Appendix II: Selected VHA Medical Facility Adherence to NPDB Reporting Requirements in VHA Policy for Malpractice Claims
To assess Veterans Health Administration (VHA) medical facility adherence to VHA policy requirements for National Practitioner Data Bank (NDPB) reporting for malpractice claims, we first selected a non-generalizable sample of five VHA medical facilities.[64] We selected these five facilities based on varying facility complexity, different related Veterans Integrated Service Networks, and facility-reported provider data to VHA central office.[65] Next, we requested a list of licensed independent providers that were involved in a malpractice claim from January 2020 through July 2024 from each of the five facilities. We reviewed the lists and randomly selected a sample of 67 providers across the five facilities.[66] Last, we requested and reviewed underlying documentation related to the malpractice claims’ process and compared that documentation to requirements in VHA’s NPDB reporting policy.[67] We also interviewed VHA medical facility staff about the malpractice claims’ reporting process.
Our review found that the five selected VHA medical facilities generally met VHA requirements and time frames for the malpractice claims’ reporting process. (See table 2.) In some instances, however, medical facility officials were unable to produce documentation for us to determine if they met VHA policy.
Table 2: Five Selected Medical Facilities’ Adherence to VHA Policy for Malpractice Claims for a Sample of 67 VHA Providers, January 2020-July 2024
|
VHA policy requirementa |
For the provider, selected VHA medical facility: |
||
|
Met requirement |
Did not meet requirement |
Documentation unavailable |
|
|
Providers named in a malpractice claim (67 providers) |
|||
|
VHA medical facility director has 30 calendar days to notify involved providers that a malpractice claim has been filed.b |
46 |
17 |
4 |
|
Providers in malpractice claims that were paid (14 providers) |
|||
|
VHA medical facility director must notify involved providers in writing of the opportunity to submit a written statement concerning the care that led to a paid claim. |
14 |
0 |
0 |
|
VHA medical facility director notification includes certain language, such as a statement that VHA is considering whether to report them to the National Practitioner Data Bank (NPDB). |
13 |
0 |
1 |
|
VHA medical facility has 75 calendar days to submit required materials after receiving a request from VHA’s Office of Medical-Legal Affairs.c |
8 |
5 |
1 |
|
Providers determined to need NPDB reporting (6 providers) |
|||
|
VHA medical facility director has 30 calendar days to report a provider to the NPDB once a determination has been made by VHA’s Office of Medical-Legal Affairs. |
5 |
1 |
0 |
|
VHA medical facility director has 30 calendar days to send a copy of the NPDB report to VHA’s Office of Medical-Legal Affairs. |
2 |
3 |
1 |
Source: GAO analysis of Veterans Health Administration (VHA) medical facility provider documentation. | GAO‑26‑107528
aSee Veterans Health Administration, National Practitioner Data Bank (NPDB) Reports, VHA Handbook 1100.17 (Washington, D.C.: Dec. 28, 2009).
bThere were two providers in our review that VHA’s Office of General Counsel told the VHA medical facility not to notify the providers as the statute of limitations had passed. We are counting those two cases as “met.”
cVHA’s Office of Medical-Legal Affairs, now known as Medical-Legal Risk Management, is responsible for coordinating the paid malpractice claim review process.
Appendix III: Selected VHA Medical Facility Adherence to SLB and NPDB Reporting Requirements in VHA Policy
We reviewed five Veterans Health Administration (VHA) medical facilities’ adherence to VHA policy requirements when reporting licensed independent providers with quality care concerns to state licensing boards (SLB) and the National Practitioner Data Bank (NDPB) between January 2020 and July 2024.[68]
SLB reporting. We reviewed documentation for 28 reports submitted to SLBs across our five selected sites for 27 providers and compared that documentation and facility actions against requirements and time frames in VHA policies to determine facility adherence.[69] During our review time frame, VHA updated its SLB guidance in January 2021.[70] Three of the 28 SLB reports fell under the previous VHA guidance, with the rest falling under the current VHA guidance. (See tables 3 and 4.)
Table 3: Five Selected Medical Facilities’ Adherence to VHA Policy for Three State Licensing Board (SLB) Reports for Three VHA Providers, January 2020-January 27, 2021
|
|
For the SLB report, VHA medical facility: |
|
|||
|
VHA policy requirementa |
Met requirement |
Did not meet requirement |
Documentation unavailable |
||
|
Initial review stage requirements |
|
||||
|
Facility director ensures SLB reporting is initiated within 7 calendar days of the identification of substandard care on a provider’s exit review.b |
0 |
3 |
0 |
|
|
|
Comprehensive review stage requirementsc |
|
||||
|
Facility director must advise the provider of the purpose of the review and allow for provider comment. |
3 |
0 |
0 |
|
|
|
Notice of Intent to Report must include certain information, such as a list of each charge against the provider. |
3 |
0 |
0 |
|
|
|
Facility creates a Rebuttal Resolution Memorandum to address any contested charge by the provider and how the facility has resolved the conflict. |
3 |
0 |
0 |
|
|
|
VHA’s suggested time frame to complete this stage is 45 calendar days. |
0 |
3 |
0 |
|
|
|
Decision stage requirements |
|
||||
|
Facility director has 7 calendar days to decide whether to report the provider. |
1 |
2 |
0 |
|
|
|
Concurrence stage requirements |
|
||||
|
Facility director decides if provider case is sensitive within 5 calendar days of deciding to report.d |
0 |
0 |
3 |
|
|
|
VHA’s suggested time frame to complete this stage is 35 calendar days if review was completed by the VHA facility privacy officer (non-sensitive) and 60 calendar days if requiring General Counsel review (sensitive). |
0 |
0 |
3 |
|
|
|
Reporting stage requirements |
|
||||
|
Facility director submits report to relevant SLB within 7 calendar days of receiving concurring legal review opinion. |
0 |
2 |
1 |
|
|
|
VHA’s suggested time frame to complete all five stages is 100 calendar days. |
0 |
3 |
0 |
|
|
Source: GAO analysis of Veterans Health Administration (VHA) medical facility provider documentation. | GAO‑26‑107528
aSee Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Handbook 1100.18 (Washington, D.C.: Dec. 22, 2005). We determined these providers to be under VHA Handbook 1100.18 requirements if SLB reporting had progressed to the concurrence stage prior to January 27, 2021.
bThe three providers in our review during this time frame had SLB reporting initiated from an exit review. Providers can also remain at a VHA facility and be reported to an SLB.
cIn addition to the requirements in the table for this stage, there was one requirement dependent on a provider. VHA policy states that a provider has 14 calendar days to respond to the Notice of Intent to Report. Facilities met that requirement for all three providers. One provider in our review did not respond to the first Notice of Intent to Report. According to the handbook, the medical facility should have sent a second Notice of Intent to Report; however, we did not see evidence of that happening. See VHA Handbook 1100.18.
dA case could be determined sensitive if, for example, it involved the death of a patient or there was media attention associated with some aspect of the incident or review.
Table 4: Five Selected Medical Facilities’ Adherence to VHA Policy for 25 State Licensing Board (SLB) Reports for 24 VHA Providers, January 28, 2021-July 1, 2024
|
|
For the SLB report, VHA medical facility: |
||||
|
VHA policy requirementa |
Met requirement |
Did not meet requirement |
Documentation unavailable |
||
|
|
|
|
|
||
|
Initial review stage requirements |
|||||
|
Providers leaving a VHA medical facility – facility director ensures an exit review is conducted within 7 business days of the provider’s leaving. |
15 |
5 |
0 |
||
|
Providers leaving a VHA medical facility – facility director ensures SLB reporting is initiated within 7 business days of the identification of substandard care on the exit review. |
3 |
14 |
3 |
||
|
Providers remaining at a VHA facility – First- or second-line supervisor must initiate SLB reporting within 5 business days of receiving information that a provider failed to meet standards of care. |
1 |
4 |
0 |
||
|
Comprehensive review stage requirementb |
|||||
|
The Notice of Intent to Report must include certain information, such as a list of each charge against the provider. |
22 |
0 |
3 |
||
|
If provider requests documentation, facility provides within 7 business days. |
2 |
2 |
3 |
||
|
Facility creates a Rebuttal Resolution Memorandum to address any contested charge by the provider and how the review has resolved the conflict. |
18 |
0 |
7 |
||
|
Decision stage requirements |
|||||
|
Facility director has 7 business days to decide whether to report the provider. |
10 |
7 |
8 |
||
|
Privacy review stage requirementc |
|||||
|
Facility director has 7 business days to send the evidence file to the Veterans Integrated Service Network (VISN) director. |
2 |
3 |
20 |
||
|
VISN director has 3 business days to assign the file to a VISN privacy officer. |
0 |
0 |
25 |
||
|
VISN privacy officer has 7 business days to review the file. |
0 |
0 |
25 |
||
|
Reporting stage requirements |
|||||
|
Facility director submits report to relevant SLB within 7 business days of receiving the file back from the VISN privacy officer. |
2 |
5 |
18 |
||
|
VHA’s suggested time frame to complete all five stages is 100 calendar days. |
5 |
15 |
5 |
||
Source: GAO analysis of Veterans Health Administration (VHA) medical facility provider documentation. | GAO‑26‑107528
aSee Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Directive 1100.18 (Washington, D.C.: Jan. 28, 2021). We determined these providers to be under VHA Directive 1100.18 if SLB reporting had progressed to the concurrence stage after January 27, 2021. One provider was reported on two separate occasions to the SLB during our time frame.
bIn addition to the requirements in the table for this stage, there was one requirement dependent on a provider. VHA policy states that a provider has 7 business days to respond to the Notice of Intent to Report. Facilities met that requirement for 18 of the providers, did not meet the requirement for four of the providers, and we did not have enough information to determine if they met the requirement for three of the providers. VHA policy allows VHA medical facilities to consider late provider responses. See VHA Directive 1100.18.
cWe reviewed self-made data trackers from some Veterans Integrated Service Network privacy officers and one VHA medical facility credentialing and privileging manager that included some privacy review stage dates, but we did not receive underlying documentation to confirm these dates/trackers were accurate.
NPDB reporting. We reviewed documentation for eight providers (physicians or dentists) across four selected VHA medical facilities where the facility proposed nine adverse privileging actions and compared the documentation and actions against requirements and time frames in VHA policy to determine facility adherence.[71] (See table 5.)
Table 5: Four Selected Medical Facilities’ Adherence to VHA Policies for Nine Proposed Adverse Privileging Actions for Eight VHA Providers, January 2020-July 2024
|
|
For the proposed adverse privileging action, VHA medical facility: |
|||
|
VHA policy requirementa |
Met |
Did not meet requirement |
Documentation unavailable |
|
|
Number of proposed adverse privileging actions (9 in our time frame) |
||||
|
Providers requesting a Fair Hearing (4 providers in our time frame)b |
||||
|
Facility director has 5 or 10 business days to appoint the Fair Hearing panel after receiving the provider’s request for a hearing.c |
0 |
1 |
3 |
|
|
The Fair Hearing must occur between 20 and 30 business days of the panel appointment letter.d |
0 |
4 |
0 |
|
|
The Fair Hearing panel has 15 business days to produce a report of its determination after the hearing occurs. |
3 |
0 |
1 |
|
|
Director has 10 business days to issue a determination after receiving the Fair Hearing panel’s report. |
0 |
3 |
1 |
|
|
Facility has 15 calendar days to report the provider to the NPDB once the facility director issues the decision to reduce, revoke, or deny privileges.e |
1 |
1 |
0 |
|
|
Providers appealing the Fair Hearing panel decision (1 provider in our time frame) |
||||
|
Provider has 5 business days to appeal a medical facility director’s decision to report to the NPDB. |
0 |
1 |
0 |
|
|
Facility director has 20 business days to make a reporting decision after receiving the provider’s appeal. |
0 |
1 |
0 |
|
|
Providers declining a Fair Hearing (4 providers in our time frame)f |
||||
|
Facility has 15 calendar days to report the provider to the NPDB after they waive their right to a Fair Hearing. |
1 |
4 |
0 |
|
Source: GAO analysis of Veterans Health Administration (VHA) medical facility provider documentation. | GAO‑26‑107528
aSee Veterans Health Administration, National Practitioner Data Bank (NPDB) Reports, VHA Handbook 1100.17 (Washington, D.C.: Dec. 28, 2009); Veterans Health Administration, Credentialing and Privileging, VHA Handbook 1100.19 (Washington, D.C.: Oct. 2, 2007); and Veterans Health Administration, Privileging, VHA Directive 1100.21(1) (Washington, D.C.: Mar. 2, 2023).
bThere was one additional provider where we received documentation that they were reported to the NPDB for resigning while under investigation, but the VHA medical facility was unable to provide any additional documentation to be able to determine whether or not the provider was offered a Fair Hearing.
cPrior to the new Fair Hearing policy released in December 2023, VHA medical facility directors had 5 business days to appoint the Fair Hearing panel after the provider’s request for the hearing, whereas directors now have 10 business days.
dPrior to the new VHA Fair Hearing policy released in December 2023, Fair Hearing scheduling was based on the date of the provider’s notification letter, whereas currently it is based on the date of the panel appointment letter.
eNot all providers who have a Fair Hearing are reported to the NPDB.
fOne provider had two separate privileging actions proposed during our time frame and declined a Fair Hearing on both occasions.
Appendix IV: Seven Provider Cases from Selected VHA Medical Facilities Where SLB and NPDB Reporting Was Not Initiated
We reviewed five Veterans Health Administration (VHA) medical facilities’ adherence to VHA policy requirements when reporting licensed independent providers with quality care concerns to state licensing boards (SLB) and the National Practitioner Data Bank (NDPB) between January 2020 and July 2024.[72] We found facility staff did not initiate either the SLB or NPDB reporting processes for seven providers to determine if reporting was necessary after a clinical care concern was identified.[73] Specifically, we found the following:
· Two facilities each terminated one provider for clinical care concerns and noted on each provider’s exit review form that SLB reporting should be immediately initiated, which aligns with VHA policy.[74] However, we found no evidence that the SLB reporting process was initiated for either provider.
· One facility substantiated a concern for clinical performance and patient safety through a focused clinical care review and revoked the provider’s scope of practice. The provider remained at the facility working in a role overseen by a licensed independent provider, but the facility did not initiate the SLB reporting process. VHA policy includes SLB reporting requirements for a provider who remains at a facility, but has been identified as providing substandard care in one or more episodes of care to a patient.[75]
· One provider retired while under investigation for clinical care concerns, which is reportable to SLBs under VHA policy.[76] However, we found no evidence that the SLB reporting process was initiated.
· One facility terminated a contract provider for clinical care concerns, but we found no evidence a Fair Hearing was offered to the contractor to determine reporting to the NPDB. Specifically, we found the initial notice for a Fair Hearing was sent to the provider, but later rescinded by the facility staff. Staff stated they believed that a contractor was not eligible to receive a Fair Hearing. However, this is incorrect and not in alignment with VHA policy.[77]
· Two facilities each terminated one provider for clinical care concerns. VHA policy states NPDB reporting must occur when the facility director revokes a provider’s privileges.[78] For one provider, NPDB reporting was required after termination because of the due process steps at that time, but we did not find any evidence this provider was reported. For the other provider, we did not find evidence that a Fair Hearing was offered to determine reporting to the NPDB.
Sharon M. Silas, silass@gao.gov.
In addition to the contact named above, Marcia A. Mann (Assistant Director), Kate Tussey (Analyst-in-Charge), Maggie Devlin, and Emily O’Brien made key contributions to this report. Also contributing were Ann Marie Cortez, Jacquelyn Hamilton, David Jones, and Drew Long.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]A VHA licensed independent practitioner/provider is an individual permitted by law and a VHA medical facility to provide patient care services independently within the scope of the individual’s license and in accordance with privileges, or in some occupations, a scope of practice, granted by the facility. Privileges are the specific set of clinical services that a practitioner/provider is approved to perform independently at a specific medical facility, based on an assessment of the practitioner’s/provider’s professional performance, judgment, clinical competence, and skills. Scopes of practice allow certain VHA employees, such as clinical pharmacists and physician assistants, to function independently within a defined set of clinical duties. For the purposes of this report, we use the term “providers” to refer to licensed independent practitioners providing care at a VHA medical facility under privileges or scopes of practice.
[2]Examples of concerns about a provider’s clinical care can range from a provider not adequately documenting information about a patient visit to a provider practicing in a manner that is unsafe or inconsistent with industry standards of care. Such concerns may arise, for example, as the result of a facility’s routine performance monitoring or from patient complaints. In this report, we use “quality reviews” to refer to reviews conducted to investigate provider clinical care concerns.
[3]Facility leadership includes the medical facility director, medical facility chief of staff, and the provider’s clinical service chief.
[4]The NPDB is an electronic
repository administered by the Department of Health and Human Services that
collects and releases information on providers who either have been disciplined
by a state licensing board, professional society, or health care entity, such
as a hospital, or have been named in a medical malpractice settlement or
judgment. Industry standards call for health care entities to query the NPDB
and verify with the appropriate state licensing board that a provider’s medical
licenses are current and in good standing before appointing a provider to the
entity’s medical staff and when renewing clinical privileges. VHA policy
requires clinical privileges to be renewed every 3 years.
At the time of our review, VHA policy required the reporting of physicians and
dentists to the NPDB. In June 2025, VHA published a final rule, effective July
2025, which removed VHA’s own regulations governing NPDB reporting. Instead,
VHA relies on Department of Health and Human Services regulations that govern
the NPDB, a Memorandum of Understanding between VA and the Department of Health
and Human Services, and VA policy and procedures. Reporting to the National
Practitioner Data Bank, 90 Fed. Reg. 24,511 (June 11, 2025) (codified at 38
C.F.R. pt. 46). At this time, VHA has not
updated VHA Handbook 1100.17 to account for the change.
[5]An SLB is the agency of a state that is primarily responsible for the licensing of providers to furnish health care services.
[6]See GAO, VA Health Care: Improved Policies and Oversight Needed for
Reviewing and Reporting Providers for Quality and Safety Concerns, GAO‑18‑63 (Washington,
D.C.: Nov. 15, 2017). We made four recommendations to VHA to document reviews
of providers’ clinical care after concerns are raised, develop timeliness
requirements for these reviews, and ensure proper VISN oversight of such
reviews, as well as timely VHA medical facility reporting of providers to the
NPDB and SLBs. VHA has since implemented these recommendations.
VISNs are regional systems of care that oversee the day-to-day functions of VHA
medical facilities that are within their network. Each facility is assigned to
one of VHA’s 18 VISNs.
[7]For example, see Department of Veterans Affairs, Office of Inspector General, Noncompliant and Deficient Processes and Oversight of State Licensing Board and National Practitioner Data Bank Reporting Policies by VA Medical Facilities, 20-00827-126 (Washington, D.C.: Apr. 7, 2022). This inspection was initiated after a number of VA Office of Inspector General reports raised concerns about facility directors’ noncompliance with VHA’s SLB and NPDB reporting policies suggesting potential systemic failures. The VA Office of Inspector General made four recommendations in that report regarding compliance with VHA reporting policies and oversight of reporting, one of which has not yet been implemented. In addition, see Department of Veterans Affairs, Office of Inspector General, Deficiencies in Facility Leaders’ Summary Suspension of a Provider and Patient Safety Reporting Concerns at the VA Black Hills Health Care System in Fort Meade, South Dakota, 23-01502-234 (Washington, D.C.: Aug. 29, 2024). The VA Office of Inspector General made two recommendations regarding compliance with VHA policy for summary suspensions and focused clinical care reviews, both of which have been implemented.
[8]Pub. L. No. 117-328, div. U, § 112, 136 Stat. 4459, 5411 (codified at 38 U.S.C. § 7414).
[9]Pub. L. No. 117-328, div. U, § 112, 136 Stat. at 5411. In response, VA reported to Congress in April 2023 and December 2023 on adherence with Cleland-Dole Act requirements. Specifically, VHA reported ongoing efforts met the Cleland-Dole Act requirements including adding dedicated credentialing and privileging staff at VISNs and VHA medical facilities, updating relevant policies, and developing mandatory training for staff.
[10]For policies outlining requirements for quality reviews during our review time frame, see Veterans Health Administration, Credentialing and Privileging, VHA Handbook 1100.19 (Washington, D.C.: Oct. 2, 2007); Veterans Health Administration, Credentialing of Health Care Providers, VHA Directive 1100.20 (Washington, D.C.: Sept. 15, 2021); and Veterans Health Administration, Privileging, VHA Directive 1100.21(1) (Washington, D.C.: Mar. 2, 2023). For policies outlining requirements for NPDB and SLB reporting, see Veterans Health Administration, National Practitioner Data Bank (NPDB) Reports, VHA Handbook 1100.17 (Washington, D.C.: Dec. 28, 2009); Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Handbook 1100.18 (Washington, D.C.: Dec. 22, 2005); and Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Directive 1100.18 (Washington, D.C.: Jan. 28, 2021).
[11]We selected this time frame for our review to (1) ensure there was enough time for reviews and reporting to be completed, and to (2) review the most recently available VHA medical facility meeting minutes.
[12]VHA officials stated they maintain a tracking tool for all VHA medical facilities to self-report information on providers reported to the NPDB and SLBs.
[13]VHA medical facilities generally have a committee responsible for making recommendations to facility leadership on matters related to credentialing and privileging. Credentialing is the process of collecting and reviewing information—such as a provider’s professional training, malpractice history, peer references, and other components of professional background—to determine whether the provider has suitable abilities and experience to provide medical services at a VHA medical facility.
[14]A risk manager is responsible for developing and managing VHA’s risk management program at the facility, including developing and maintaining programs designed to reduce risk at all levels within the health care delivery system. This includes managing the malpractice claim process at the facility level.
[15]Internal control is a process effected by an entity’s oversight body, management, and other personnel that provides reasonable assurance that the objectives of an entity will be achieved. See GAO, Standards for Internal Control in the Federal Government, GAO‑25‑107721 (Washington, D.C.: May 15, 2025).
[16]See GAO‑25‑107721.
[17]See VHA Handbook 1100.19, VHA Directive 1100.20, VHA Directive 1100.21(1), VHA Handbook 1100.17, VHA Handbook 1100.18, and VHA Directive 1100.18.
[18]To identify clinical care concerns, facility officials monitor each provider’s performance on an ongoing basis in a variety of ways, including conducting ongoing performance evaluations and peer reviews, complaints, incident reports, and malpractice claims. These monitoring processes also apply to contract providers—those performing direct patient care at VHA medical facilities via a contract.
[19]Facility leadership may later place a privileged provider under summary suspension if at any point in the review process a determination is made that the provider should be removed from clinical care.
[20]According to VHA policy, focused clinical care reviews also may include methodologies such as interviews or direct observation. See VHA Directive 1100.21(1).
[21]If a provider is removed from care during a focused clinical care review, the applicable privileges should be summarily suspended while the review is conducted. If a review lasts longer than 30 days, the summary suspension is extended for the duration of the review.
[22]In VHA policy, a final action against a provider’s privileges occurs when all applicable internal due process procedures have been completed and the facility director has signed off on the action—including, a reduction, suspension, denial (other than initial), nonrenewal, or revocation of privileges for a period exceeding 30 calendar days.
In June 2025, VHA published a final rule, effective July 2025, which removed VHA’s own regulations governing NPDB reporting. Instead, VHA relies on Department of Health and Human Services regulations that govern the NPDB, a Memorandum of Understanding between VA and the Department of Health and Human Services, and VA policy and procedures. Reporting to the National Practitioner Data Bank, 90 Fed. Reg. 24,511 (June 11, 2025) (codified at 38 C.F.R. pt. 46). At this time, VHA has not updated VHA Handbook 1100.17 to account for the change.
[23]In VHA policy, a “malpractice payment” is defined as a payment, by way of settlement or judgment, by the United States on a claim of medical malpractice as defined in 38 C.F.R. § 46.1(b). See VHA Handbook 1100.17. As discussed above, in June 2025 VHA issued a final rule that removed VHA’s own regulations governing NPDB reporting, which included the definition of “malpractice payment.” 90 Fed. Reg. 24,511 (June 11, 2025). At this time, VHA has not updated VHA Handbook 1100.17 to account for the change.
[24]See VHA Handbook 1100.18 and VHA Directive 1100.18.
[25]Not all 104 providers we reviewed with potential clinical care concerns needed to have an FPPE for cause or focused clinical care review conducted. For example, one provider was reported to an SLB for impairment on the job, but resigned immediately following the incident, so no quality review was conducted at the time of the incident. See appendix I for the number of VHA providers we reviewed during our time frame at the selected facilities.
[26]By generally adhered, we mean these selected facilities met most, but not all, of VHA’s requirements related to quality reviews. Specifically, to initiate summary suspensions, VHA policy requires facilities to notify providers with a letter that includes information such as a summary of the event(s) that triggered the suspension immediately following identification of a clinical care concern. We reviewed documentation for 36 summary suspensions (for 31 providers). We found that facilities used the notification letter template for 35 summary suspensions (for 30 providers). For one provider’s suspension, the facility could not provide us with summary suspension documentation. For the 30 suspensions where we could determine the date the facility identified the provider’s clinical care concern, we found that the facility initiated the suspension within 30 days for 24 of these suspensions (for 22 providers).
VHA policy requires facilities to conduct a focused clinical care review upon initiation of a provider’s summary suspension to investigate significant clinical care concerns. Of the 36 summary suspensions we reviewed, we found facilities initiated appropriate reviews following 23 of the suspensions (for 20 providers).
[27]We found some providers underwent more than one FPPE for cause during our review. We also found that the selected facilities differed in the extent of use of FPPEs for cause. For example, one of our selected facilities did not complete an FPPE for cause during our time frame. A different facility conducted 27 FPPEs for cause for 25 providers at their facility.
[28]VHA policy requires facilities to define the review through use of an FPPE for cause template. The template outlines required information for the review, such as the provider’s identified clinical care concerns, monitoring processes for each identified concern, benchmarks to define expectations for improvement, and period of review. Specifically, we found that the facilities used the required template for 58 FPPEs for cause (for 54 providers). For the 13 FPPEs for cause (for 10 providers) where we could not confirm that the FPPE for cause template was used (six of which were at one facility), the documentation for nine reviews defined how the review would be conducted with monitoring processes stated for each identified clinical care concern. FPPE for cause documentation was unavailable for four reviews. See VHA Directive 1100.21(1).
[29]One provider during our time frame was both reported to a SLB and had a proposed privileging action on two separate occasions during our time frame. One of our selected facilities did not propose an adverse privileging action for a physician or dentist provider during our selected review time frame.
[30]There were two VHA policies covering SLB reporting in effect during our review; see VHA Handbook 1100.18 and VHA Directive 1100.18. During our review time frame, VHA updated its SLB guidance in January 2021 by adopting VHA Directive 1100.18, which rescinded VHA Handbook 1100.18.
In addition to reporting certain providers to the NPDB for actions taken against a provider’s privileges, VHA medical facilities are responsible for reporting providers with paid malpractice claims resulting from the provision of substandard care to the NPDB. See appendix II for our analysis of malpractice reporting for providers at these selected medical facilities between January 2020 and July 2024.
[31]The Fair Hearing process includes steps and time frames to determine if a physician or dentist should be reported to the NPDB as the result of an adverse privileging action.
[32]See VHA Directive 1100.18.
[33]See VHA Handbook 1100.17.
[34]We did not receive any documents from the facility to be able to determine that this limited hearing was offered to the provider prior to reporting. See VHA Handbook 1100.19.
[35]VHA policies state VHA medical facility directors are required to report providers—both current and former—to SLBs when there are serious concerns about the provider’s clinical care. See VHA Handbook 1100.18 and VHA Directive 1100.18. In addition, VHA medical facility directors are required to report physician and dentist providers to the NPDB when (1) the facility takes action that affects the provider’s privileges for a period longer than 30 days and is related to professional incompetence or misconduct, or (2) the provider resigns or retires while under investigation for clinical care concerns. See VHA Handbook 1100.17.
We previously reported on this topic in 2017 and found five selected VHA medical facilities did not report the majority of providers who should have been reported to SLBs or the NPDB in accordance with VHA policy. See GAO‑18‑63.
[36]VHA policy states a provider can be reported to an SLB if they are fired following the completion of a disciplinary action relating to the provider’s clinical competence. See VHA Handbook 1100.18 and VHA Directive 1100.18.
[37]In addition to VHA policy requirements, the Cleland-Dole Act states that VHA medical facilities must conduct documented reviews of providers that fail to meet standards. Pub. L. No. 117-328, div. U, § 112, 136 Stat. at 5412.
We similarly found in 2017 that five selected VHA medical facilities were unable to provide documentation for almost half of the reviews conducted, and that all five facilities lacked at least some documentation of the reviews they told us they conducted. See GAO‑18‑63.
[38]For example, VHA policy on NPDB reporting states that copies of reports to the NPDB and related documentation must be filed in the provider’s credentialing and privileging folder. See VHA Handbook 1100.17.
[39]In addition to the 23 focused clinical care reviews (for 20 providers) completed following a summary suspension, we identified 10 reviews (for 10 providers) completed independently of a summary suspension.
[40]See VHA Directive 1100.18.
[41]For example, we received an NPDB report for an additional provider—outside of the eight providers previously discussed—who resigned while under investigation. However, the VHA medical facility was unable to provide any additional documentation for us to be able to determine whether the facility offered that provider due process through a Fair Hearing, and to determine adherence to VHA policy. See figure 1 for the steps in the NPDB reporting process.
[42]VHA policy requires FPPEs for cause documentation to be shared with the provider in advance for agreement and understanding and to be signed by the provider. See VHA Directive 1100.21(1).
[43]VHA guidance states that focused clinical care reviews should, at a minimum, contain the following elements: purpose or charge, scope, information/data source, findings/results, and conclusions. This documentation allows medical facility officials to evaluate the review and determine next steps for the provider.
[44]Pub. L. No. 117-328, div. U, § 112, 136 Stat. at 5413 (codified at 38 U.S.C. § 7414(f)).
[45]Federal internal control standards state that entities enable individuals to develop competencies appropriate for key roles and tailor training based on the needs of the role. See GAO‑25‑107721.
[46]See Veterans Health Administration, Provider Competency And Clinical Care Concerns Including: Focused Clinical Care Review and FPPE for Cause Guidance (Washington, D.C.: January 2018).
[47]We found some providers underwent more than one summary suspension during our review.
[48]Facilities did not always conduct a focused clinical care review following a summary suspension, as discussed above.
[49]VHA guidance states that a facility should contact the VISN or VHA program director for assistance with identifying qualified external reviewers for focused clinical care reviews.
[50]See VHA Handbook 1100.18 and VHA Directive 1100.18.
[52]See GAO‑25‑107721.
[53]Pub. L. No. 117-328, div. U, § 112, 136 Stat. at 5412 (codified at 38 U.S.C. § 7414(c)-(d)). The act provides that, where the medical facilities substantiate a clinical care concern, the appropriate medical center shall timely notify, as appropriate, the appropriate licensing, registration or certification body in each State in which the health care professional is licensed, registered or certified; the Drug Enforcement Administration; the NPDB; and any other relevant entity. Pub. L. No. 117-328, div. U, § 112, 136 Stat. at 5412-3.
[55]See VHA Handbook 1100.18 and VHA Directive 1100.18.
[56]In 2017, we recommended that VHA require VISN officials to (1) oversee medical facility quality reviews, and (2) establish a process for overseeing that medical facilities report providers to the NPDB and SLB. In response, VHA implemented two new oversight processes in December 2019. See GAO‑18‑63.
[57]Currently, the tracking tool allows facilities to attach certain documents associated with a provider, such as the SLB reporting letter; however, in September 2025, officials told us that they plan to eliminate the requirement to upload documents to the tracking tool. According to officials, this change focuses the tool on tracking facility actions to ensure adherence with VHA policy rather than enabling review of documents specific to providers, which better aligns with the oversight role of the central office.
[58]The self-assessment is standardized across medical facilities. VHA officials told us that central office staff develop the self-assessment questions in consultation with an advisory panel of VISN staff. VHA officials told us the assessment questions, which change annually, are based on agency priorities, concerns raised by external oversight bodies, and risk area findings from previous assessments.
[59]VHA policy requires VISN privacy officers to review SLB evidence files within 7 business days of receipt to ensure information such as patient records are appropriately redacted prior to release. See VHA Directive 1100.18.
[60]VHA requires medical facilities to sample licensed independent providers to include certain specialties and occupations. For example, the sample should include medical doctors, dentists, advanced practice registered nurses, and specialties such as pathology, gastroenterology, and radiation oncology.
[61]See VHA Directive 1100.21(1).
[62]See GAO‑14‑704G.
[63]Not all 104 providers we reviewed with potential clinical care concerns needed both a quality review and reporting. In addition, we found some providers underwent multiple quality reviews, suspensions, or reporting during our time frame.
[64]The NPDB is an electronic repository administered by the Department of Health and Human Services that collects and releases information on providers who either have been disciplined by a state licensing board, professional society, or health care entity, such as a hospital, or have been named in a medical malpractice settlement or judgment. Industry standards call for health care entities to query the NPDB and verify with the appropriate state licensing board that a provider’s medical licenses are current and in good standing before appointing a provider to the entity’s medical staff and when renewing clinical privileges.
[65]VHA central office maintains a tracking tool for VHA medical facilities to self-report information on providers reported to the NPDB and state licensing boards.
[66]The team started with a sample of 75 providers (15 from each of the five sites). As of December 2025, there were three providers involved in malpractice claims that were still pending a decision of denial or payment, and five providers in which the claims were paid, but the NPDB determination process has not been completed. We removed those providers from our analysis as final determinations are pending.
[67]See Veterans Health Administration, National Practitioner Data Bank (NPDB) Reports, VHA Handbook 1100.17 (Washington, D.C.: Dec. 28, 2009).
[68]We selected a non-generalizable sample of five VHA medical facilities based on varying facility complexity, different related Veterans Integrated Service Networks, and facility-reported provider data to VHA central office.
[69]One provider was reported on two separate occasions to the SLB during our time frame.
[70]See Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Handbook 1100.18 (Washington, D.C.: Dec. 22, 2005); and Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Directive 1100.18 (Washington, D.C.: Jan. 28, 2021). The major difference between the two policies was in the concurrence stage. Under the handbook, this stage of review could be completed by a facility privacy officer located in a different facility within the Veterans Integrated Service Network if the case was deemed non-sensitive, or completed by VHA’s Office of General Counsel if the case was deemed sensitive. Under the directive, this stage is now called the privacy review stage and is completed by the Veterans Integrated Service Network director and privacy officer.
[71]One of our selected facilities did not propose an adverse privileging action for a physician or dentist during our review time frame. One provider had two separate privileging actions proposed during our time frame.
[72]We selected a non-generalizable sample of five VHA medical facilities based on varying facility complexity, different related Veterans Integrated Service Networks, and facility-reported provider data to VHA central office.
[73]VHA policies state VHA medical facility directors are required to report providers—both current and former—to SLBs when there are serious concerns about the provider’s clinical care. See Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Handbook 1100.18 (Washington, D.C.: Dec. 22, 2005); and Veterans Health Administration, Reporting and Responding to State Licensing Boards, VHA Directive 1100.18 (Washington, D.C.: Jan. 28, 2021). In addition, VHA medical facility directors are required to report physician and dentist providers to the NPDB when (1) the facility takes action that affects the provider’s privileges for a period longer than 30 days and is related to professional incompetence or misconduct, or (2) the provider resigns or retires while under investigation for clinical care concerns. See Veterans Health Administration, National Practitioner Data Bank (NPDB) Reports, VHA Handbook 1100.17 (Washington, D.C.: Dec. 28, 2009).
[74]VHA policy states a provider can be reported to an SLB if they are fired following the completion of a disciplinary action relating to the provider’s clinical competence. See VHA Handbook 1100.18 and VHA Directive 1100.18.
[75]See VHA Directive 1100.18.
[76]VHA policy states a provider can be reported to an SLB if they resigned after serious concerns about their clinical competence had been raised, but not resolved. See VHA Directive 1100.18.
[77]VHA policy states that contractors are subject to VHA policies and NPDB reporting, including when VHA terminates the services (and associated medical staff appointment and clinical privileges) of a contractor employee under a continuing contract for possible incompetence or improper professional conduct. See VHA Handbook 1100.17.
[78]See VHA Handbook 1100.17.