CHILD WELFARE
HHS Should Clarify Guidance on State Spending for Congregate Care
Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
For more information, contact: Kathryn A. Larin at larink@gao.gov.
What GAO Found
Twenty-six of 49 states have not decreased the use of congregate care for youth in foster care despite provisions in the Family First Prevention Services Act (Family First) that limit funding for such placements. Family First limits the time states can claim federal Title IV-E foster care funds for certain congregate care placements to 14 days, as of October 1, 2021. Given these limitations, many states increased the use of state, county, or local funds to support these placements.

All 49 states that responded to GAO’s survey of child welfare agencies reported challenges securing appropriate foster care placements for youth. Capacity challenges in non-congregate care settings, such as foster homes, can result in greater reliance on congregate care. A smaller number of states (20) reported benefits from Family First’s congregate care provisions.
Some youth are involved in both the child welfare and juvenile justice systems (known as dually involved). Twenty-five state child welfare and 26 state juvenile justice agencies did not know if the percentage of these youth in juvenile justice placements had increased since Family First, according to GAO’s surveys. Among states with this information, 10 of 20 states reported an increase in the percentage of dually involved youth in detention (i.e., in a facility where a youth is housed while they await the outcome of their delinquency case) since October 1, 2021. During that same time, 12 of 26 states reported an increase in youth placed in secure placements (i.e., in a locked facility where a youth is housed after the disposition of their case). Family First requires states to certify that they will not enact or advance policies or practices that significantly increase their state’s juvenile justice population in response to the limitation on the use of Title IV-E funds for congregate care. According to Department of Health and Human Services (HHS) officials, all states submitted this certification, and it is the state’s responsibility to ensure it does not violate the certification.
HHS monitors state spending under Title IV-E including whether states adhere to Family First’s 14-day limit on congregate care. One exemption to the 14-day limit is for facilities serving youth who have been found to be, or are at risk of becoming, sex trafficking victims. However, there is not detailed guidance regarding when to apply this exemption, and states have interpreted the exemption differently. These different interpretations may result in some states claiming less funds than they are eligible for, while other states claim all funds for which they are eligible. Without additional clarification of its guidance on using this exemption, states may continue to interpret these rules differently. This could result in a disparity in the amount of Title IV-E funding that states receive.
Why GAO Did This Study
Research has found that youth in foster care congregate settings (e.g., group homes and institutions) may have worse outcomes across a range of measures—such as emotional well-being and educational achievement— than youth placed in foster family homes. Over the last 20 years, states have taken steps to reduce the use of congregate care.
Congress included a provision in Family First for GAO to evaluate the impact of limiting the use of Title IV-E foster care maintenance payments to support congregate care. This report addresses: (1) how congregate care use by states has changed since Family First implementation, (2) challenges states faced and benefits states experienced related to Family First's congregate care provisions, (3) how these provisions affected dually involved youth, and (4) HHS monitoring of the use of federal funds for youth in congregate care.
GAO conducted surveys of the child welfare and juvenile justice agencies in the 50 states and Washington, D.C. We received responses from 49 child welfare agencies and 50 juvenile justice agencies. GAO also conducted an anonymous, non-generalizable survey of young adults with lived experience in congregate care. GAO conducted site visits to four states, selected on a variety of criteria, including that the state’s percentage of youth in congregate care was above the national average. GAO also reviewed relevant HHS documentation and interviewed HHS officials.
What GAO Recommends
GAO is making one recommendation to HHS to clarify its guidance on the appropriate use of Title IV-E funds for certain congregate care settings. HHS did not concur with the recommendation. GAO maintains that clarification of its guidance is needed.
|
Abbreviations |
|
|
|
|
|
ACF |
Administration for Children and Families |
|
AFCARS |
Adoption and Foster Care Analysis and Reporting System |
|
CFSR |
Child and Family Services Reviews |
|
CJRP |
Census of Juveniles in Residential Placement |
|
HHS |
Department of Health and Human Services |
|
IV-E Review |
Title IV-E Foster Care Eligibility Review |
|
Family First |
Family First Prevention Services Act |
|
PRTF |
Psychiatric Residential Treatment Facility |
|
QRTP |
Qualified Residential Treatment Program |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
March 3, 2026
Congressional Committees
Research has found that youth in foster care congregate settings, such as group homes and institutions, may have worse outcomes across a range of measures, such as emotional well-being and educational achievement, than youth placed in foster homes.[1] This has led to a decades-long effort to reduce the use of congregate care.[2] At the end of fiscal year 2002, there were nearly 101,000 youth in congregate care.[3] By the end of fiscal year 2023, the number had dropped to about 36,000.[4] In that same year, nearly $350 million in foster care maintenance payments under Title IV-E of the Social Security Act (Title IV-E) were made to support youth in congregate care.[5]
The Department of Health and Human Services’ (HHS) Administration for Children and Families (ACF) administers Title IV-E funds. The Family First Prevention Services Act (Family First) changed how Title IV-E foster care maintenance funds can be used. Among other things, the act limits the use of these funds for congregate care to 14 days, except under certain circumstances.[6] Family First also requires states to certify that they will not enact or advance any policies or practices that would result in a significant increase in the population of youth in their juvenile justice system as a result of the law’s funding limitations to support youth in congregate care.
Family First includes a provision for GAO to evaluate the impact of limiting the use of Title IV-E foster care maintenance payments to support youth in congregate care.[7] This report examines (1) how congregate care use by states has changed since Family First implementation, (2) challenges states faced and benefits states experienced related to Family First’s congregate care provisions, (3) what is known about how these provisions have affected youth involved in both the child welfare and juvenile justice systems; and (4) the extent HHS is monitoring the use of federal funds for youth in congregate care.
To address our objectives, we conducted two national surveys: one of state child welfare agencies, and one of state juvenile justice agencies.[8] These surveys covered a number of topics, including the percentage of youth placed in congregate care or juvenile justice facilities and the time youth remained in those placements; state spending on congregate care; challenges and benefits states experienced due to Family First’s congregate care provisions; and state experiences with ACF guidance. We administered these surveys from February to May 2025 and asked respondents to provide information about their experiences since October 2021.[9]
In addition to our surveys, we conducted site visits to four states and interviewed state child welfare and juvenile justice officials.[10] We selected states using a variety of criteria, including states with a higher percentage of youth in congregate care placements than the national average and states with different types of congregate care. To obtain the views of individuals with experience in the child welfare system, we conducted an anonymous, nongeneralizable survey of young adults aged 18 to 25 who had been placed in foster care congregate settings. The survey asked about their care and placements, among other topics. We received responses from 26 individuals who met our inclusion criteria.
To determine the extent HHS is monitoring the use of federal funds for youth in congregate care, we interviewed HHS officials and asked our selected states about their experiences with related federal monitoring and guidance.[11] We also reviewed relevant ACF guidance and assessed it using internal controls for use of quality information. Additional details about each of these methodologies can be found in appendix I.
We conducted this performance audit from June 2024 to March 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
State and local governments are the primary administrators of child welfare programs. Youth enter foster care when they have been removed from their parents or guardians and placed under the responsibility of a state child welfare agency.[12] Removal from the home most often occurs because of abuse or neglect. When youth are removed from their homes, the child welfare agency may place them in a foster home of a relative or nonrelative, or in a congregate care setting, depending on the needs of the youth and available placement options.
Trends in Congregate Care Placement
States have made efforts to reduce the use of foster care congregate settings. As shown in figures 1 and 2, the use of such placements has declined over the last two decades.
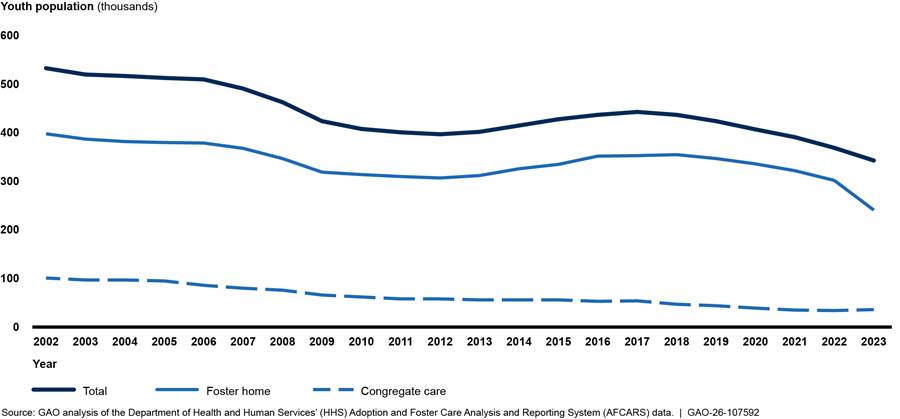
Note: Foster care congregate settings include group homes (a licensed or approved home providing 24-hour care, generally to seven to 12 youth) and institutions (a child care facility providing 24-hour care to more than 12 youth).
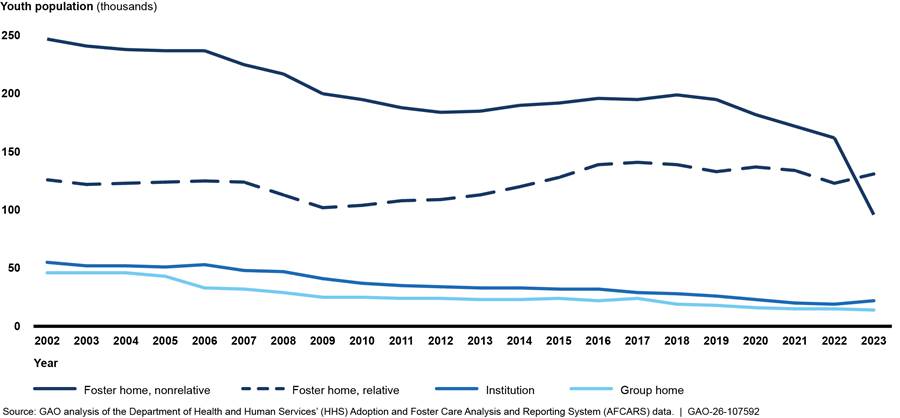
Note: Foster care group homes are licensed or approved homes providing 24-hour care, generally to seven to 12 youth. Foster care institutions are child care facilities providing 24-hour care to more than 12 youth.
Some youth are involved in both the child welfare and juvenile justice systems. These youth are known as dually involved youth and may be placed in foster care or juvenile justice settings, depending on the state and the youth’s individual circumstances. Like trends in the use of foster care congregate settings, the number of youth in juvenile justice placements has also decreased over time (see fig. 3).
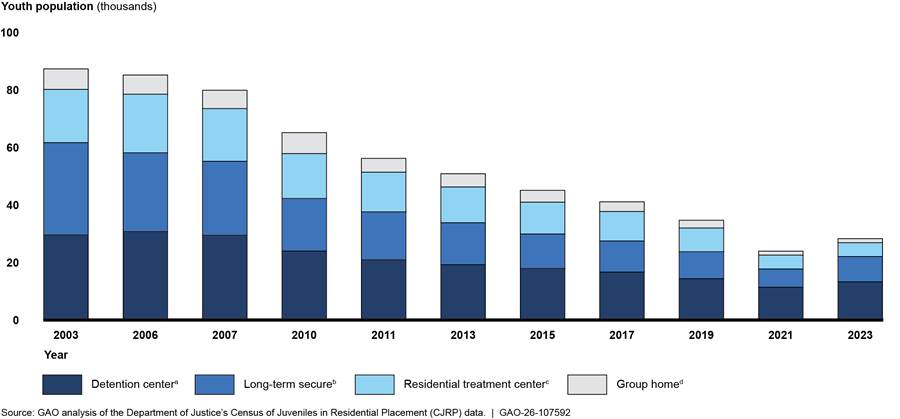
Note: According to the Department of Justice, Census of Juveniles in Residential Placement (CJRP) data are collected biennially and include a one-day count of youth populations in juvenile residential placement facilities. CJRP includes youth in residential placements charged with or court adjudicated for an offense and does not include youth on probation, in adult prisons or jails, or those placed in facilities used exclusively for mental health or substance use treatment or for dependent children. The figure excludes youth who were in residential placement facilities identified in CJRP as boot camps, ranch or wilderness camps, shelters, and reception or diagnostic centers. Data were only available for the specific years shown.
aA short-term facility that provides temporary care in a physically restricting environment for juveniles in custody pending court disposition and, often, for juveniles who are adjudicated delinquent and awaiting disposition or placement elsewhere, or are awaiting transfer to another jurisdiction.
bA specialized type of facility that provides strict confinement and long-term treatment generally for post-adjudication committed youth charged with or adjudicated for delinquency or status offenses.
cA facility that focuses on providing some type of individually planned treatment program for youth (substance abuse, sex offender, mental health, etc.) in conjunction with residential care.
dThese facilities are generally non-secure and typically intended for post-adjudication commitments in which young persons are allowed extensive contact with the community, such as attending school or holding a job.
Title IV-E Foster Care Program
Title IV-E pays a portion of state costs for the care of children in foster care (including congregate care), known as maintenance payments.[13] These payments are a regular monetary contribution provided to caregivers or congregate care providers, such as group homes or residential facilities. To be eligible for Title IV-E, youth must have been removed from their homes, come from families that meet income eligibility requirements, and be placed in an approved family foster home or congregate care setting, among other requirements.
Family First Prevention Services Act
Prior to Family First, Title IV-E funds could be used to support youth in foster homes or congregate care with no specific time limitation.[14] With Family First’s enactment, state use of Title IV-E funds for youth in congregate care is now limited. As of October 1, 2021, Title IV-E funds can only be used for congregate care for 14 days, with some exceptions.[15] For example, states may use Title IV-E for youth in congregate care for more than 14 days if the facility:
· specializes in providing prenatal, postpartum, or parenting supports for youth,
· provides high-quality residential care and supportive services to youth who have been found to be victims of sex trafficking or at risk of becoming such victims; or
· is a qualified residential treatment program (QRTP)[16] with a treatment model that is designed to address the needs of children with severe emotional or behavioral disorders.[17]
Family First also gave states the ability to use Title IV-E funds for certain evidence-based services to help prevent the need to place children in foster care. To use Title IV-E funds for prevention, states must submit a Title IV-E prevention services plan to HHS for approval. Prevention services include mental health treatment, substance use treatment, and parenting programs for youth and their parents.[18] It is possible that Title IV-E prevention services may reduce the number of youth entering foster care in the future, and thereby, further reduce the use of congregate care.[19]
Federal Monitoring
HHS’s ACF is responsible for administering federal foster care funds and monitoring states’ implementation of programs under Title IV-E. To monitor state child welfare programs and ensure the appropriate use of Title IV-E funds, ACF, in conjunction with states, conducts Child and Family Services Reviews (CFSR) and Title IV-E Foster Care Eligibility Reviews (IV-E Reviews):
· CFSR. CFSRs seek to (1) ensure conformity with certain federal child welfare requirements, (2) determine what is happening to children and families as they use child welfare services, and (3) assist states in enhancing their capacity to help children and families achieve positive outcomes. These reviews include an analysis of quantitative and qualitative information to evaluate state child welfare programs, practices, and systems.
· IV-E Reviews. IV-E Reviews help determine whether federal funds are spent on behalf of eligible children and in accordance with federal statute, regulation, and policy. These reviews also help identify improper payments, including overpayments and underpayments, among other things. ACF samples case records to validate program compliance and claims for reimbursement of foster care maintenance payments and to identify improper payments.
States Continue to Use Congregate Care and Increasingly Use State Funds to Support Youth in These Facilities
The Majority of States Have Not Reduced the Use of Congregate Care in Recent Years
States continue to rely on congregate care for youth in foster care despite Family First’s limitations on the use of Title IV-E funds for these placements. Twenty-six of the 49 state child welfare agencies that responded to our survey reported that the percentage of their youth in congregate care had either increased or remained the same since October 2021. Similarly, 26 child welfare agencies reported that the average number of days that youth remained in congregate care increased or remained the same since October 2021 (see fig. 4).[20]

Notes: In our surveys, we did not provide an end date for states to reflect on their experiences. As such, states could provide information on their experiences up to the date the state submitted their survey. In the figure, we excluded “don’t know” responses. As a result, the total frequencies of state responses vary.
States also continue to place youth in stopgap and out-of-state congregate care, according to our survey of child welfare agencies:
· Stopgap placements. Child welfare agencies continue to rely on transitional or stopgap placements, such as hotel rooms, office buildings, and hospital emergency rooms, because other placements are unavailable. Forty-two child welfare agencies reported that they used stopgap placements. Eighteen agencies reported they increased the use of stopgap placements since October 2021. Further, more state child welfare agencies reported an increase than a decrease in the length of time youth remained in emergency shelters and stopgap placements since October 2021.[21] Five states said that Title IV-E funding limitations contributed to the use of stopgap placements.
· Out-of-state placements. Most child welfare agencies (43) reported using out-of-state congregate care placements since October 2021.[22] Of these, 29 states reported that out-of-state congregate care placements had either increased (11) or remained the same (18). The most common reasons states provided for using out-of-state placements included the following:
· Non-QRTP congregate care providers were unwilling to serve certain populations of youth—for example, youth with significant behavioral challenges, autism, or intellectual disabilities (35 states).[23]
· There was a lack of psychiatric residential treatment facility (PRTF) beds in the state (32 states).[24]
· To place youth with relatives, fictive kin, or in preadoption placements in another state (29).[25]
· There was a lack of available non-PRTF behavioral health services or placements (27 states).
The Majority of States Have Adopted Qualified Residential Treatment Programs (QRTP)
According to our survey of state child welfare agencies, more than two-thirds of responding states (34) had at least some QRTPs—a type of congregate care program under Family First that is designed to address the needs of youth with significant emotional or behavioral disorders. Family First permits states to use Title IV-E funds for eligible youth in QRTPs beyond 14 days.
|
Qualified Residential Treatment Program (QRTP) Requirements To qualify as a QRTP, congregate care facilities must: · have a trauma-informed treatment model · have registered or licensed nursing staff and other licensed clinical staff available at all times · facilitate and document the participation of family members in the youth’s treatment · provide post-discharge planning and at least 6 months of family-based aftercare · be accredited and licensed Source: 42 U.S.C. § 672(k)(4). | GAO‑26‑107592 |
The extent that states reported using QRTPs varied, according to our survey. Four states reported that 100 percent of their congregate care facilities were QRTPs. Ten of 34 states with QRTPs reported that between 1 and 25 percent of their congregate care facilities were QRTPs (see fig. 5).[26] States that had not converted all their congregate care facilities to QRTPs reported that their remaining facilities continued to operate as other specialized or non-specialized congregate care facilities, other types of facilities, or shifted to providing community-based or other non-congregate care services. Ten states reported that at least some congregate care facilities closed because they could not or did not want to meet QRTP requirements.
Figure 5: Number of States with Qualified Residential Treatment Programs (QRTP) and Percentage of Congregate Care Facilities in Those States That Are QRTPs
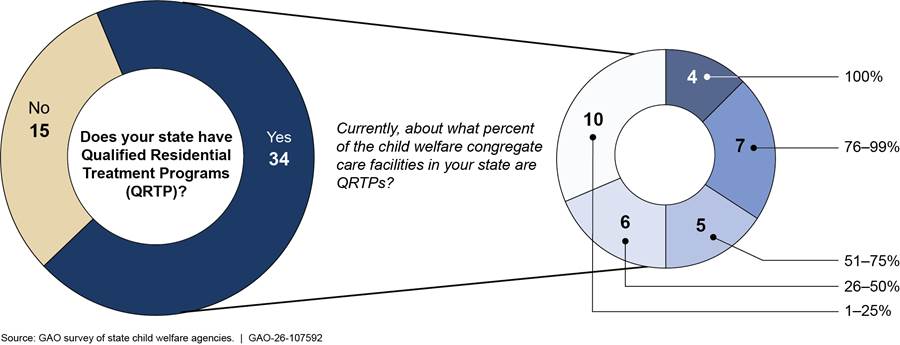
Notes: Forty-eight states and the District of Columbia responded to our child welfare agency survey. Two of the 34 states with QRTPs did not know what percent of their congregate care facilities were QRTPs.
States with QRTPs cited several reasons for their decision to implement this type of congregate care. The most common reason was to improve the quality of services for youth in congregate care, such as through the use of trauma-informed treatment models. The second most common reason was to remain eligible for Title IV-E funds beyond 14 days, followed by a belief that this model would help the state focus on reducing the use of congregate care or the time youth spent in such placements.
Though the majority of states have implemented QRTPs, 30 states reported that meeting QRTP requirements was challenging.[27] Among these states, the requirement reported most often as moderately, very, or extremely challenging was providing family-based aftercare support for at least 6 months post-discharge (see fig. 6). Family-based aftercare may include services to help with the transition home, such as counseling or educational or parenting support. Officials in two of three states with QRTPs that we visited said that the state was unable to claim Title IV-E funds for some youth because the QRTPs did not provide post-discharge services to all youth, although the facilities met other QRTP requirements.
Figure 6: State-Reported Challenges Meeting Family First Requirements for Qualified Residential Treatment Programs (QRTP)
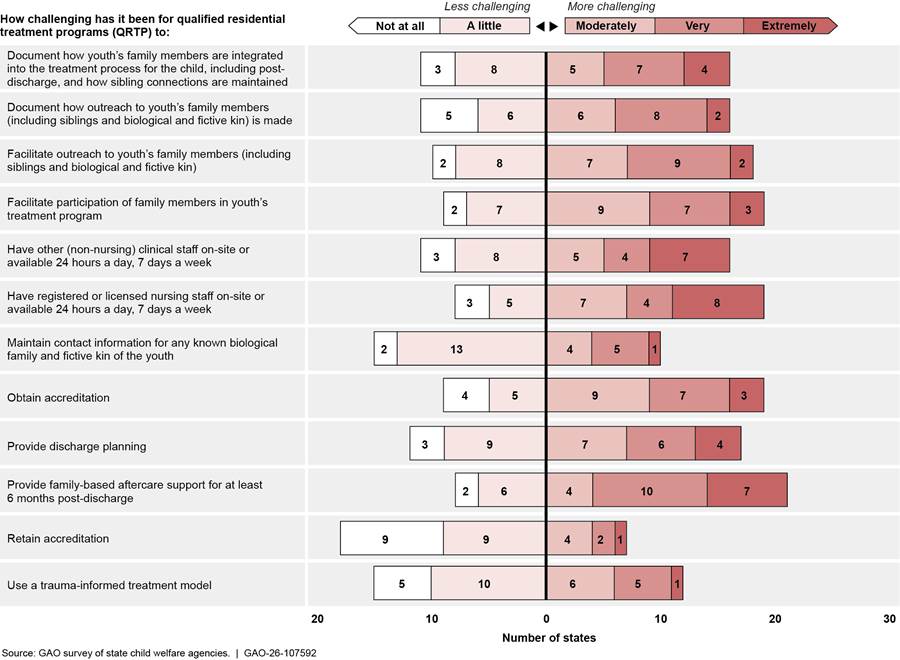
Notes: Figure includes responses from the 30 states that reported meeting QRTP requirements in the Family First Prevention Services Act has been challenging. In the figure, we excluded “don’t know” responses. As a result, the total frequencies of state responses vary.
Several states without QRTPs said the time or cost of meeting QRTP requirements was too burdensome, and some stated that providers could not meet QRTP requirements. Two of these states reported that they had implemented QRTPs, but that these facilities had since closed, or they paused implementation due to challenges meeting requirements. One of these two states reported that meeting QRTP paperwork requirements and court hearing timelines was too difficult for local child welfare agencies. Officials in one of the states we visited said there was little interest among congregate care providers in converting to QRTPs because of the challenges in meeting the requirements.
The Majority of States Have Increased Their Own Spending on Congregate Care as Federal Funds Have Diminished, Shifting Child Welfare Spending Priorities
Twenty-nine of 49 states that responded to our survey reported that the amount of Title IV-E funds supporting youth in congregate care had decreased since implementing Family First’s congregate care provisions. Twenty-one of the 29 states attributed the decrease in Title IV-E funds a lot or completely to Family First’s congregate care provisions. At the same time, 33 states reported increasing the amount of state, county, or local funds used to support youth in congregate care, according to our survey. Of these 33 states, 20 reported that Family First contributed to this change a lot or completely.[28] ACF officials told us that some states had significantly reduced or stopped claiming Title IV-E for nonspecialized congregate care placements because it was too complicated for them to claim for 14 days and then stop.
On our survey, 35 states reported that they were currently experiencing challenges related to congregate care funding. The most common funding challenges states reported were insufficient federal funds for congregate care, the inability to claim Title IV-E funding to support youth in non-QRTP congregate care for more than 14 days, and the increasing cost of congregate care for reasons unrelated to Family First.[29]
Officials in three of four states we visited reported they were using state funds to support youth in congregate care to make up for lost federal funds. An official in one of these states told us that the goal of reducing the use of congregate care was well intended, but noted that in practice, some youth still required congregate care. Officials in another of these states said that in many cases the state must now pay for the same services that it previously paid for with Title IV-E funds to prevent youth from sleeping in offices or other inappropriate settings. Officials also said that a lack of foster homes and youths’ challenging behaviors made placing youth with families difficult. This leaves the state few options but to continue to place youth in congregate care and pay for those placements with state funds.
Officials in three of four states we visited said that Family First shifted congregate care costs to states. State officials noted that the decline in the percent of federal funds for congregate care since the passage of Family First has been quite large. For example, one state provided data showing that from 2018 to 2024, the percent of Title IV-E funds supporting youth in congregate care dropped from 17.9 percent to 1.6 percent. Another state reported a drop from 22.3 percent to 3.3 percent over that same period. Officials from one state we visited with a Title IV-E prevention program said that it has not been able to claim enough Title IV-E funds to make up for lost congregate care funds.[30]
In open-ended survey responses, several states said that the need to use more state, county, or local funds to support youth in congregate care had resulted in a strain on state budgets and in fewer resources available for other child welfare priorities. For example, one state reported a decrease of available funding to support community-based and prevention services. A second state reported that the loss of federal funds for congregate care had led to a higher share of county funding needed to support congregate care placements, and that this had reduced the resources available to support other non-placement activities, such as workforce support and training.
Other states reported that increased reliance on state, county, or local funds for congregate care placements had reduced funding available for the child welfare workforce, family interventions, or other services. To address these funding challenges, some states reported requesting additional funding from the state or using other federal funding sources. For example, several states reported increasing the use of Medicaid, Title IV-B, and Temporary Assistance for Needy Families (TANF) dollars to fill gaps left by less Title IV-E.[31]
Almost All States Experienced Capacity, Service, and Staffing Challenges, but Many Reported Benefits from Family First’s Congregate Care Provisions
All States Reported Challenges Obtaining Enough Foster Care Placements
All 49 state child welfare agencies that responded to our survey reported challenges securing appropriate foster care placements for youth.[32] Many states reported difficulty placing youth because they lacked capacity across all types of foster care settings (see table 1). Capacity challenges in non-congregate care settings, such as foster homes, can result in greater reliance on congregate care, emergency shelters, or stopgap placements.
|
Placement type |
Yes |
No |
Don’t know |
Not applicable |
|
Therapeutic foster homesa |
4 |
38 |
2 |
4 |
|
Family foster homes (relative and nonrelative) |
10 |
36 |
3 |
0 |
|
Psychiatric Residential Treatment Facilities (PRTF)b |
7 |
27 |
9 |
6 |
|
Congregate care institution (non-QRTP)c |
16 |
22 |
5 |
6 |
|
Qualified Residential Treatment Programs (QRTP)d |
15 |
21 |
3 |
10 |
|
Specialized settings for sex trafficking victims/risk |
10 |
20 |
6 |
13 |
|
Congregate care group home (non-QRTP)e |
15 |
18 |
6 |
10 |
|
Specialized setting providing services to prenatal, postpartum, or parenting youth |
17 |
12 |
8 |
12 |
Source: GAO survey of state child welfare agencies. | GAO‑26‑107592
Note: Forty-nine states responded to our survey, but not all states answered each survey question. Not applicable responses indicate states do not use the placement type.
aA specialized type of family-based foster care designed to provide a supportive and therapeutic environment for children with serious emotional, behavioral, or medical needs.
bA nonhospital facility that provides psychiatric services to individuals under the age of 21 in an inpatient setting.
cA child care facility providing 24-hour care or treatment for youth. These facilities may include: child care institutions, residential treatment facilities, or maternity homes. An institution is larger than a group home, caring for more than 12 children.
dA program with a trauma-informed treatment model that is designed to address the needs of children with severe emotional or behavioral disorders and meet other statutory criteria.
eA licensed or approved home providing 24-hour care for children in a small group setting that generally has from seven to 12 children.
Limited foster homes can result in the increased use of congregate care for youth, which may be a more restrictive setting. A state child welfare consultant told us that there were not enough foster homes in the state, and it had become increasingly difficult to find families to foster youth. She noted that many foster parents chose not to foster after their first experience, because they were not prepared for the behavioral challenges and needs of the youth. Child welfare officials in another state told us that although they had worked to increase the number of therapeutic and family foster homes, many foster homes would not take older youth.
Child welfare agencies also reported challenges placing youth in congregate care specifically. For example, child welfare agencies reported that a lack of non-QRTP beds (26 agencies) and QRTP beds (22 agencies) was at least moderately challenging.[33] A child welfare case worker in one state said that there were not enough congregate care beds for youth with higher-level needs. This led to youth increasingly staying in stopgap placements (e.g., hotels and short-term rentals) until a congregate care bed could be found. This case worker said the state needed more and bigger congregate care facilities. Another case worker in this state said that there were not enough step-down beds (i.e., beds for youth with lower-level needs), which had resulted in youth remaining in higher-level care facilities longer than needed. As figure 7 shows, a lack of step-down beds was reported as a significant challenge in our survey.
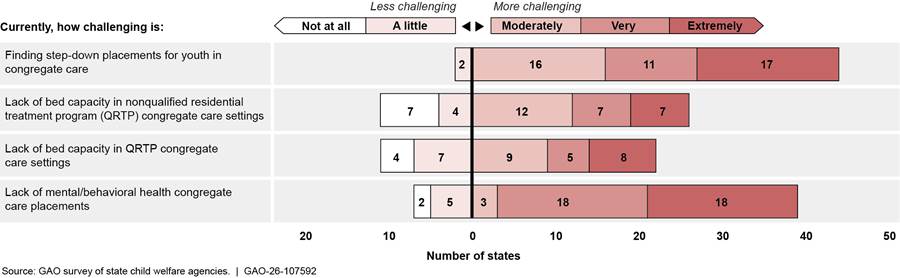
Note: In the figure, we excluded “don’t know” responses. As a result, the total frequencies of state responses vary.
Officials in all four states we visited told us that the severity of the needs of youth entering foster care had increased. One state official said this could make family foster care an inappropriate placement option for these youth. Survey respondents confirmed that the intensity of youths’ behavioral health needs could make finding placements difficult. Forty-one state child welfare agencies reported that finding placements for youth with significant behavioral challenges, autism, or intellectual disabilities was very or extremely challenging. This was due to some congregate care facilities’ unwillingness to serve these youth populations, according to our survey.
|
Intensity of Youth Behavioral Challenges and Needs State officials told us the intensity of the behavioral challenges and needs of youth entering foster care has increased in recent years. Officials reported seeing more youth with complex needs, such as: · Serious and complex behavioral challenges, · Violent behaviors, · Problematic sexual behaviors, · Low IQ, · Complex medical needs, · Substance use, and · Juvenile justice involvement. The causes of the increase in challenging behaviors and complex needs are not clear. Some officials said they believed that the COVID-19 pandemic contributed. Others said efforts to reduce the number of youth entering the system had resulted in a shift in the makeup of the child welfare population toward those with more significant needs. Source: GAO interviews. | GAO‑26‑107592 |
Child welfare officials in one state we visited said there were times when dually involved youth remained in a juvenile detention facility for an extended time, sometimes months, because there was no child welfare congregate care placement available. This could be because there were no congregate care beds available, or no congregate care facility was willing to accept the youth because of their behavioral needs.
Case workers in one state told us they relied on shelters when family foster care or congregate care placements were unavailable in order to keep youth out of hotels and office buildings. Youth are supposed to remain in these shelters no more than 30 days but often remain longer because no other placement is available, according to the case workers.
In addition to capacity challenges in various foster settings, child welfare agencies also reported placement challenges for specific populations of youth, though some of these challenges were more acute than others (see fig. 8).
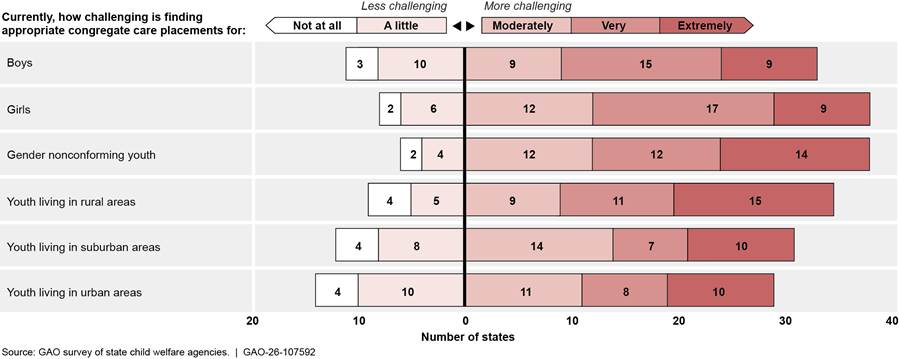
Note: In the figure, we excluded “don’t know” responses. As a result, the total frequencies of state responses vary.
As we reported in 2015, capacity is a longstanding challenge for child welfare systems, although Family First may have exacerbated this issue, according to some officials in the states we visited.[34] To address capacity challenges, child welfare agencies reported taking a variety of steps. For example, officials in one state we visited said that its contract with congregate care providers included a “no reject/no eject” policy. This means that facilities must accept almost all youth referred by the agency and cannot remove them from the facility due to behavior. According to child welfare officials in this state, this helped the state ensure there were placements for youth who were hard to place. This state also pays congregate care providers a reduced rate for unoccupied beds to help provide financial stability for providers and ensure beds are available when needed.
On our survey, states cited several efforts to manage capacity challenges. These efforts included increasing community-based services to families in need to prevent entry into foster care; increasing payment rates for congregate care providers; increasing recruitment efforts for foster homes; and developing new training for foster parents related to parenting youth who had experienced trauma and had maladaptive behaviors.
Almost All States Reported Challenges Related to Providing Services to Youth and Staffing Congregate Care Facilities
Almost all state child welfare agencies reported experiencing challenges related to providing services to youth in foster care. According to our survey, the most significant service-related challenges for child welfare agencies were the lack of community-based mental and behavioral health services, other specialized services for youth in child welfare, and substance use treatment services for youth (see fig. 9). When youth cannot obtain needed services while living with their birth or foster parent, it can sometimes lead to congregate care. Juvenile justice agencies we surveyed also reported insufficient behavioral health services as the primary service-related challenge for their systems, with 11 states citing a lack of these services in the community or available congregate care facilities in response to an open-ended question.
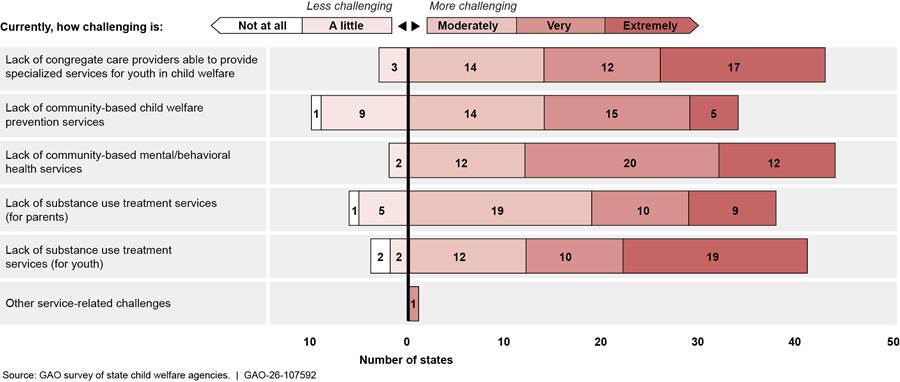
Notes: The figure includes the 48 states that reported having service-related challenges. In the figure, we excluded “don’t know” responses. As a result, the total frequencies of state responses vary.
Officials in the states we visited also discussed these challenges. One child welfare official said that a capacity crisis facing behavioral health providers in their state affected the child welfare system. They noted that psychiatric hospitals, mental and behavioral health systems, and the juvenile justice system were overwhelmed. Youth who were unable to obtain needed behavioral health services in the community often cycled between psychiatric hospitals and the foster care system. In a second state, a foster parent told us that there were limited resources for foster parents when their child was having a behavioral health emergency. She said that over a 2-year period, she spent more than 100 nights in hospital emergency rooms with her foster child because it was the only option for psychiatric services.
Young adults who responded to our anonymous survey generally rated their congregate care experiences negatively. The 26 respondents were about evenly split regarding whether they received all the services they needed while in care. Of the 15 young adults who reported that they did not receive needed services while in care, 12 indicated they did not receive regular contact with family or access to appropriate clothing and hygiene products. (For a selection of additional comments from youth, see app. II.)
In addition to service challenges, in our survey most state child welfare agencies reported staffing challenges, including hiring and retaining congregate care staff and caseworkers. During our site visits, agency officials and congregate care providers told us that other factors, such as COVID, exacerbated longstanding staffing issues. For example, officials in one state told us that providers were struggling to meet the needs of youth and facing challenges with staff turnover and that one of the main factors resulting in the loss of QRTP providers was staffing challenges.[35] Officials in another state said sometimes congregate care facilities had open beds but could not take additional youth because they could not hire or retain enough qualified staff to meet required staffing ratios.
Several young adults who responded to our survey reported that staff at some congregate care facilities did not provide a supportive environment, though others had more positive experiences (see fig. 10).
Figure 10: Examples of GAO Survey Responses About Young Adults’ Feelings on Staff in Congregate Care

To address these service-related challenges, child welfare agencies reported they had increased collaboration with state mental health, juvenile justice, education, and developmental disabilities departments to better address the needs of specific populations of youth. They also reported that they had increased community-based behavioral health and prevention services, among other actions. To address staffing shortages, states reported taking actions including increasing the salaries of frontline case workers, increasing pay rates for congregate care staff, and broadening the qualifications staff need to work at congregate care facilities.
Many States Reported Family First’s Congregate Care Provisions Helped Reduce the Use of Congregate Care or Had Other Benefits
On our survey, 20 state child welfare agencies reported experiencing benefits from Family First’s congregate care provisions (see fig. 11). These agencies agreed the following were at least moderate benefits:
· reducing the use of congregate care placements for youth who would be better served in a family setting (14 agencies);
· decreasing the use of congregate care overall and improving the use of trauma-informed care for youth in congregate care (12 agencies each); and
· reducing the average length of time youth spent in congregate care and improving family engagement for youth while in congregate care (11 agencies).
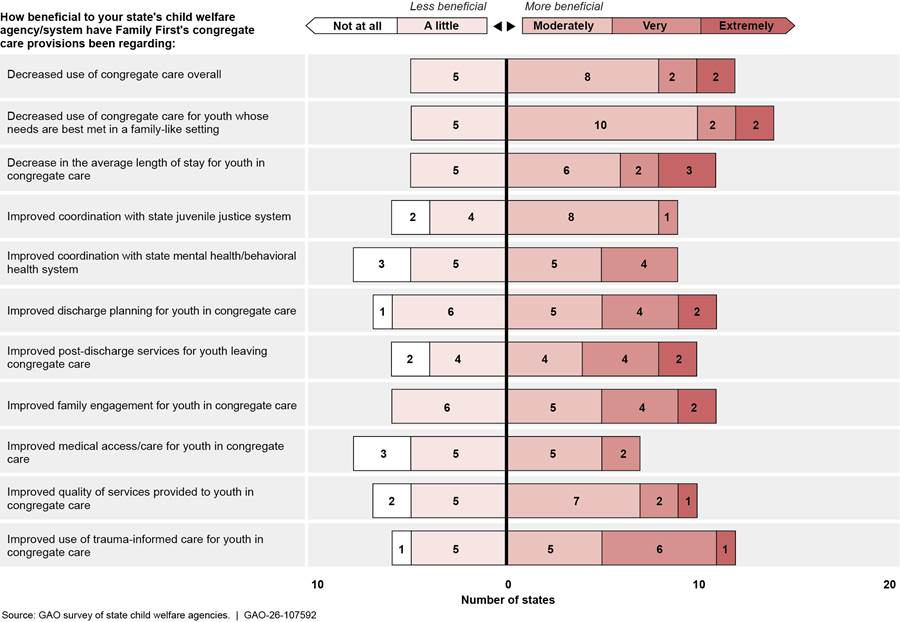
Notes: The figure includes the 20 states that reported benefits of the Family First Prevention Services Act’s congregate care provisions. In the figure, we excluded “don’t know” and “not applicable” responses. As a result, the total frequencies of state responses vary.
Several child welfare agency officials also said they generally believed in the goals of these provisions. Child welfare officials in all four states we visited said that they supported the effort to reduce the use of congregate care and keep more children with families. Similarly, respondents to our survey reported that they supported Family First’s emphasis on reducing the use of congregate care placements, promoting the use of trauma-informed care, enhancing services provided in congregate care, and increasing court oversight of non-family-like placements.
Our survey of state juvenile justice agencies asked respondents to describe any benefits of Family First’s congregate care provisions to their systems. Eight juvenile justice agencies reported that these provisions had increased collaboration with the child welfare agency. Two juvenile justice agencies reported reducing the use of congregate care facilities, and one agency reported reducing the length of time youth spent in congregate care. In addition, three juvenile justice agencies reported they had increased the use of evidence-based community services.
Many States Did Not Know Whether More Dually Involved Youth Had Been Placed in Juvenile Justice Placements Since Family First Implementation
Many states did not know if the percentage of dually involved youth in juvenile justice placements or the time youth spent in those placements had changed since October 1, 2021, according to our two national surveys.[36] Specifically, 25 of 49 responding state child welfare agencies did not know whether there had been any change in the percentage of dually involved youth placed in detention or secure juvenile justice facilities. A similar number of state child welfare agencies reported not knowing about changes in the length of time dually involved youth remained in those placements (see table 2).
|
Juvenile Justice Placement Types For the purposes of this report, GAO defined dually involved youth as those who simultaneously have an open case in the child welfare and juvenile justice systems. These youth may be placed in residential care by either system. Juvenile justice placement options can include · foster care congregate settings, such as group homes and qualified residential treatment programs. · detention, which is a facility where a youth is housed while they await the disposition of their delinquency case; and · secure facilities, such as a locked facility or prison, in which a juvenile is housed after the disposition of their delinquency case. Source: GAO analysis of information from the Medicaid and CHIP Payment and Access Commission, interviews with state officials and stakeholders, prior GAO work, the Family First Prevention Services Act, and the Juvenile Justice Delinquency and Prevention Act. | GAO-26-107592 |
Table 2: Number of State Child Welfare Agencies Reporting Placement and Length of Stay Changes for Dually Involved Youth Since October 1, 2021
|
|
Child welfare agencies |
||||
|
|
Increased |
Remained |
Decreased |
Don’t know |
Not applicable |
|
Pre-disposition detention placementsa |
3 |
3 |
5 |
25 |
13 |
|
Pre-disposition detention length of staya |
2 |
3 |
4 |
24 |
15 |
|
Post-disposition secure placementsb |
2 |
5 |
4 |
25 |
12 |
|
Post-disposition secure length of stayb |
2 |
4 |
4 |
25 |
14 |
Source: GAO survey of state child welfare agencies. | GAO‑26‑107592
Note: In our surveys, we did not provide an end date for states to reflect on their experiences. As such, states could provide information on their experiences up to the date the state submitted their survey. Total frequency of state responses varies because not all states responded to each survey question.
aPre-disposition detention refers to a facility where a youth is housed while they await the disposition of their delinquency case.
bPost-disposition secure placements refer to secure juvenile justice facilities, that is, a locked facility or prison for juveniles after the disposition of their delinquency case.
Similarly, 26 of 50 responding state juvenile justice agencies did not know whether the percentage of dually involved youth placed in detention had increased. Twenty-eight agencies did not know whether there had been an increase in the length of time youth remained in those placements. Agencies also reported that they did not know whether there had been an increase in post-disposition secure placements (22 agencies) or in the length of time such youth remained in those types of placements (24 agencies) (see table 3).
Table 3: Number of State Juvenile Justice Agencies Reporting Increased Number of Placements or Length of Stay for Dually Involved Youth Since October 1, 2021
|
|
Juvenile justice agencies |
|||
|
|
Yes, |
No, |
Don’t |
Not |
|
Pre-disposition detention placementsa |
10 |
10 |
26 |
4 |
|
Pre-disposition detention length of staya |
11 |
8 |
28 |
3 |
|
Post-disposition secure placementsb |
12 |
14 |
22 |
2 |
|
Post-disposition secure length of stayb |
10 |
13 |
24 |
2 |
Source: GAO survey of state juvenile justice agencies. | GAO‑26‑107592
Note: In our surveys, we did not provide an end date for states to reflect on their experiences. As such, states could provide information on their experiences up to the date the state submitted their survey. Total frequency of state responses varies because not all states responded to each survey question.
aPre-disposition detention refers to a facility where a youth is housed while they await the disposition of their delinquency case.
bPost-disposition secure placements refer to secure juvenile justice facilities, that is, a locked facility or prison for juveniles after the disposition of their delinquency case.
Officials in two states we visited said it was difficult to track dually involved youth because of challenges sharing data between their child welfare and juvenile justice agencies. For example, juvenile justice officials in one state said that tracking dually involved youth across the child welfare and juvenile justice systems must be done manually. In another state, officials from the child welfare agency said they did not have the data to identify youth who cross between their child welfare and juvenile justice systems. Officials from the juvenile justice agency in that state said there was hardly any data sharing capability between the two agencies.
State juvenile justice agencies responding to our survey that could provide information on changes in the percentage of dually involved youth who were placed in a juvenile justice facilities reported the following:
· Ten (of 20 states) reported an increase in the percentage of dually involved youth placed in pre-disposition detention since October 2021.
· Twelve (of 26 states) reported an increase in the percentage of dually involved youth placed in post-disposition secure placements since October 2021.
Three state juvenile justice agencies attributed the increase in the percentage of dually involved youth placed in pre-disposition detention, at least in part, to Family First’s congregate care provisions. For example, one state juvenile justice agency reported that some of their state’s providers were unable to meet Family First’s QRTP requirements, resulting in fewer available congregate care placements for justice-involved youth. Officials in another state said their state was unable to increase its payment rate for QRTP providers enough to attract and retain qualified providers, particularly providers serving girls. The limited availability of residential treatment has resulted in youth remaining in detention longer while juvenile justice officials try to find appropriate services for those youth. Five state juvenile justice agencies attributed the increase in the percentage of dually involved youth placed in post-disposition secure facilities, at least in part, to Family First. For example, one agency reported that Family First’s restrictions on the use of congregate care led to fewer available congregate care providers.
State juvenile justice agencies responding to our survey that could provide information on changes in the length of time dually involved youth remained in juvenile justice placements reported the following:
· Eleven (of 19 states) reported an increase in the length of time dually involved youth remained in pre-disposition detention placements since October 2021.
· Ten (of 23 states) reported an increase in the length of time dually involved youth remained in post-disposition secure placements since October 2021.
Three state juvenile justice agencies attributed the increase in the length of time dually involved youth remained in pre-disposition detention, at least in part, to Family First. One state reported that youth remained in such placements longer due to their state’s child welfare agency’s limited resources, and no other child welfare placement options being available. Similarly, three state juvenile justice agencies attributed the increase in the length of time dually involved youth remained in post-disposition secure placements, at least in part, to Family First. For example, one state reported the increased length of time was due to an insufficient number of less restrictive placements such as QRTPs.
Child welfare and juvenile justice officials we interviewed during our site visits also reported an increase in the length of time dually involved youth remained in juvenile justice detention placements. For example, child welfare officials in one state said there were instances where a dually involved youth’s stay in a juvenile detention facility could last for months due to a lack of child welfare congregate care placements. They noted that this issue had worsened over the last several years. In another state, judges reported that dually involved youth were remaining in detention longer because child welfare congregate care facilities would not take these youth, leading to a lack of available placements.
ACF conducts Child and Family Services Reviews (CFSR) to monitor how well states are meeting Title IV-E requirements, including the appropriateness of placements for youth in foster care.[37] ACF officials said that dually involved youth in juvenile justice settings might be included in state CFSR case samples if the youth were in a foster care placement for more than 24 hours during the CFSR period under review. ACF officials said that CFSR final reports’ narrative sections might also discuss dually involved youth.
As previously noted, Family First requires states to certify that they will not enact or advance any policies or practices that significantly increase their state’s juvenile justice population in response to the limitation on the use of Title IV-E funds for congregate care. According to ACF officials, all states submitted this certification to HHS. Further, ACF officials told us that it is the state’s responsibility to ensure it does not violate the signed certification, and there is no mechanism for ACF to monitor this further.
ACF Monitors the Use of Federal Funds for Congregate Care, But Some States Interpret Title IV-E Claiming Rules Differently
ACF uses Title IV-E Foster Care Eligibility Reviews (IV-E Reviews) to monitor states to ensure they claim the funds appropriately, including funds to support youth in congregate care. ACF updated its IV-E Review instrument to reflect Family First’s 14-day limit on Title IV-E to support youth in certain foster care congregate settings. In addition, ACF updated the instrument to include settings exempt from the 14-day limit.
Since 2021, ACF has identified at least six states that improperly claimed Title IV-E for youth in congregate care. For example, in a 2024 review ACF found five cases where one state claimed Title IV-E beyond the 14-day timeframe for youth placed in congregate care settings that were not exempt from the limit. In another example, ACF found that a state claimed Title IV-E funds for a child who had been in a QRTP setting for more than 1 year without an approval letter from the director of the state child welfare agency to HHS, as required.[38]
Although HHS has monitored state compliance with Family First’s congregate care provisions, there is not detailed guidance for states regarding how to interpret the Family First exemption that allows states to claim Title IV-E funding beyond 14 days for placements in a setting that provides high-quality residential care and supportive services to youth who have been found to be, or are at risk of becoming, sex trafficking victims. Family First does not provide additional information on how this language is to be interpreted.
|
Determining Whether Youth Are Victims or at Risk of Sex Trafficking States use different criteria to determine whether a youth is a victim or at risk of sex trafficking. Neither the Family First Prevention Services Act nor the Administration for Children and Families defines youth found to be or at risk of becoming victims of sex trafficking. For example, one state has a decision matrix that includes three primary risk factors: · experiencing forms of sexual exploitation, including pornography or sexual performance (commercial or noncommercial); · connected to family members or other individuals who are or were sexually exploited, or who buy or sell sex; or · experiencing labor trafficking or exploitation, or wage theft. Additionally, this state identified 10 secondary risk factors including youth getting kicked out of their home, experiencing substance use disorder, having known or suspected gang affiliation, or engaging in truancy or running away. If a youth is determined to have one or more primary risk factors or two or more secondary risk factors, they are deemed at risk of sex trafficking or commercial sexual exploitation. By comparison, two states from our site visits and one state with more than 20 percent of youth in their child welfare system whose placements are funded through Title IV-E beyond 14 days because they are victims or at risk of sex trafficking, told us that they have no official definition of youth who are at risk of sex trafficking. |
Source: GAO interviews with state child welfare agencies. | GAO‑26‑107592
Although ACF recently updated its monitoring tool, its guidance offers no additional information on this exemption.[39] For example, ACF guidance provides no information on whether states should individually assess youth to determine whether they are a victim or at risk of sex trafficking.
States have interpreted the law and ACF guidance on the sex trafficking exemption differently. Specifically, some states interpret the exemption to mean that any youth placed in a congregate care facility that provides services to youth who have been or are at risk of sex trafficking is eligible for Title IV-E beyond 14 days. Other states interpret it to mean that each individual youth placed in such a facility must be assessed and found to be a victim or at risk of sex trafficking in order to claim Title IV-E for more than 14 days.
We followed up with eight states and found that officials in three states believed they could claim Title IV-E funding for more than 14 days for any youth otherwise eligible for Title IV-E and placed in a facility designated as serving youth who are victims or at risk of sex trafficking (see table 4).[40] At least one state has designated all its congregate care facilities as this type of setting and claims Title IV-E beyond 14 days for all youth in congregate care in the state. Officials from this state told us that they believed all youth in congregate care were at heightened risk of sex trafficking.[41] However, officials in five states said that youth placed in such facilities must be individually assessed and determined to be a victim of sex trafficking or at risk thereof to be eligible for Title IV-E funding beyond 14 days. These differing interpretations may impact the amount of Title IV-E funds that states receive, with states that believe youth must be individually assessed potentially receiving less Title IV-E funding than other states.
Table 4: Selected States’ Interpretations of Whether to Individually Assess Youth to Be Eligible for Title IV-E Funds for Congregate Care Beyond 14 Days
|
State |
Percent of youth whose placements are funded by Title IV-E who meet the definition of a victim of or at risk of sex trafficking |
State’s interpretation: Must individually assess each youth placed in settings for victims of or those at risk of sex trafficking to receive Title IV-E funds for more than 14 days (Yes/No) |
|
State 1a |
Unsure |
No |
|
State 2 |
21—40% |
No |
|
State 3a |
Unsure |
No |
|
State 4 |
81—95% |
Yes |
|
State 5 |
21—40% |
Yes |
|
State 6 |
21—40% |
Yes |
|
State 7a |
Unsure |
Yes |
|
State 8a |
Unsure |
Yes |
Source: GAO interviews with and survey of state child welfare agencies. | GAO‑26‑107592
Note: Four of the states included in this table are states that we did not visit. We selected these four states to follow up with because, in their responses to GAO’s survey of child welfare agencies, the states reported that more than 20 percent of the youth in their child welfare system whose placements were funded by Title IV-E met their definition of a victim of sex trafficking or at risk of sex trafficking.
aState was included in site visits.
ACF officials told us that it was permissible for a state to designate all their congregate care as settings providing services to youth who were victims or at risk of sex trafficking if the facilities met the requirements in Family First. Further, ACF officials confirmed that there was no requirement for states to individually assess youth placed in such settings, but this is not explicitly stated in ACF’s guidance. Officials said that because Family First does not include language requiring states to individually assess youth placed in facilities providing these services, ACF did not include discussion of individually assessing youth in its guidance.
Federal internal control standards require management to use quality information to achieve the entity’s objectives.[42] Without additional clarification on the use of settings providing care and supportive services for youth who have been found to be, or are at risk of becoming, sex- trafficking victims, states may continue to interpret this guidance differently. These differing interpretations may lead some states to forgo Title IV-E funds they are eligible for while other states claim all funds for which they are eligible, leading to disparities in the amount of Title IV-E funds that states receive. Forgoing these funds could result in youth in some states receiving fewer services than those in other states.
Conclusions
Some state child welfare officials said that Family First has reduced the use of congregate care and increased the use of family foster homes when children must enter foster care—a longstanding child welfare goal. Thus far, however, limiting the use of Title IV-E for certain congregate care placements has not eliminated the continuing challenges states have faced related to foster care capacity, service provision, or staffing, and may have exacerbated some challenges.
States have interpretated Family First’s exemption on the use of Title IV-E funds for facilities providing care to youth who are found to be, or are at risk of becoming, victims of sex trafficking differently. These differing interpretations can affect the amount of federal funds states claim, leading to potential disparities across states. Without additional clarification from ACF, some states may be foregoing federal funds for which they are eligible, which could negatively impact services available to youth in their child welfare systems.
Recommendations for Executive Action
The Secretary of Health and Human Services should direct the Administration for Children and Families to clarify its guidance on the appropriate use of Title IV-E funds for youth in facilities designated as settings “providing high-quality residential care and supportive services to children and youth who have been found to be, or are at risk of becoming, sex trafficking victims.” (Recommendation 1)
Agency Comments and Our Evaluation
We provided a draft of this report to HHS and DOJ for comment. We received written comments from HHS, which are reproduced in appendix III and summarized below. HHS and DOJ also provided technical comments, which we incorporated as appropriate.
HHS did not concur with our recommendation that ACF clarify guidance on the appropriate use of Title IV-E funds for youth in facilities designated as settings providing high-quality residential care and supportive services to children and youth who have been found to be, or are at risk of becoming, sex trafficking victims. HHS stated that our recommendation would require ACF to issue additional guidance and would restrict states’ ability to define settings and determine placement direction. HHS acknowledged that additional guidance to states is necessary to help them develop a federally reimbursable continuum of care and proposed collaborating with HHS’s Substance Abuse and Mental Health Services Administration and Centers for Medicare & Medicaid Services in this area. While we agree additional guidance and collaboration in this area could be helpful for states, we do not believe these actions address our recommendation.
ACF should provide clarification to states on claiming Title IV-E beyond 14 days for youth placed in facilities serving youth who have been found to be, or are at risk of becoming, sex trafficking victims. We do not believe that providing such clarification would require ACF to develop new guidance nor that clarifying its guidance would restrict states’ placement flexibilities. We found that states interpret ACF’s guidance about requirements for claiming Title IV-E funds for youth placed in these facilities differently. As such, some states are not claiming Title IV-E funds for which they may be eligible. ACF could address this issue through communication with states that is less formal than new guidance, such as an email or Dear Colleague letter to state child welfare agencies. In the absence of such clarification, some states may continue to forgo Title IV-E funds for which they are eligible, potentially negatively impacting services available to youth in those states.
We are sending copies of this report to the appropriate congressional committees, the Secretary of Health and Human Services, and other interested parties. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at LarinK@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix IV.

Kathryn A. Larin, Director
Education, Workforce, and Income Security Issues
List of Committees
The Honorable Mike Crapo
Chairman
The Honorable Ron Wyden
Ranking Member
Committee on Finance
United States Senate
The Honorable Charles E. Grassley
Chairman
The Honorable Richard J. Durbin
Ranking Member
Committee on the Judiciary
United States Senate
The Honorable Jason Smith
Chairman
The Honorable Richard E. Neal
Ranking Member
Committee on Ways and Means
House of Representatives
The Honorable Jim Jordan
Chairman
The Honorable Jamie Raskin
Ranking Member
Committee on the Judiciary
House of Representatives
This report examines (1) how congregate care use by states has changed since the implementation of the Family First Prevention Services Act, (2) challenges states have faced and benefits states have experienced related to Family First’s congregate care provisions, (3) what is known about how these provisions have affected youth dually involved in the child welfare and juvenile justice systems, and (4) the extent the Department of Health and Human Services (HHS) is monitoring the use of federal funds for youth in congregate care. To address these objectives, we surveyed state child welfare and juvenile justice agencies and youth with congregate care experience, conducted site visits to four states, and interviewed child welfare and juvenile justice experts. We also analyzed Adoption and Foster Care Analysis and Reporting System (AFCARS) and Census of Juveniles in Residential Placement (CJRP) data. We also interviewed HHS officials and reviewed the agency’s monitoring tools, reports, and guidance, which we assessed using internal controls for quality information. We also reviewed relevant federal laws and regulations.
Survey of State Child Welfare and Juvenile Justice Agencies
To learn about how Family First’s congregate care provisions affected states, we administered two web surveys, one to child welfare agencies and another to juvenile justice agencies in all 50 states and the District of Columbia. Forty-eight states and the District of Columbia responded to our child welfare agency survey; Alaska and Massachusetts did not respond. Forty-nine states and the District of Columbia responded to our juvenile justice agency survey; California did not respond.
The child welfare and juvenile justice surveys asked about similar topics but were not identical. The juvenile justice survey focused primarily on youth involved in the juvenile justice and child welfare systems (dually involved youth), while the child welfare survey included questions about this population but also questions about youth involved only in the child welfare system. Both surveys asked questions on a range of topics, including:
· available placements for youth involved in each system,
· changes in placement patterns and the length of time youth spent in various placement types since October 2021,[43]
· challenges each system faced,
· benefits the systems experienced due to Family First’s congregate care provisions, and
· federal guidance.
We administered the surveys from February to May 2025.
Because we surveyed all state child welfare and juvenile justice agencies, our surveys had no sampling error. We took several steps to minimize nonsampling error, including identifying the appropriate agency leadership to respond to the survey using lists from HHS and the Council of Juvenile Justice Administrators. We also conducted pretests with child welfare agency officials from three states and juvenile justice officials from four states to help ensure the survey questions were clear and understandable. We revised the surveys based on feedback from those pretests. We contacted all respondents who had not returned the questionnaire by the date requested by email or phone. We also followed up with respondents who submitted answers that required clarification and revised erroneous survey responses, as needed. Not all survey respondents answered all questions.
Survey of Young Adults
To obtain the perspectives of individuals who had experienced congregate care placements, we conducted an anonymous, nongeneralizable web survey of young adults ages 18 to 25. The survey was conducted from February 3 to March 5, 2025. It included questions about types of placements respondents had experienced, the care and services they received while in congregate care placements, and differences between the various placements they had experienced, among other topics. The survey was distributed by two organizations—Think of Us and FosterClub—to their network of youth and young adults who are or have been involved in the child welfare system. A link to the survey was also posted to GAO’s Facebook, LinkedIn, Instagram, and X social media pages. We received 112 responses to the survey. We eliminated 49 incomplete responses, 35 respondents that did not have congregate care experience at any time since 2021, one respondent that was outside of the 18- to 25-year-old age range, and one duplicate response. This resulted in 26 respondents that met all inclusion criteria. See appendix II for a selection of survey responses.
Site Visits
We conducted site visits to four states to obtain more detailed information than what can be collected through a survey. During site visit interviews, we discussed topics such as the implementation of Family First’s congregate care provisions, the use of congregate care and how it has changed over time, and challenges states and providers faced. We visited Iowa, Tennessee, and Texas in person and West Virginia virtually. We selected these states based on a variety of criteria, including states in which the percentage of youth in the child welfare system who were in congregate care placements was above the national average, according to AFCARS data.[44] We also considered each state’s Administration for Children and Families regional office and whether states had:
· qualified residential treatment programs (QRTPs),
· psychiatric residential treatment facilities (PRTFs), and
· an approved Title IV-E Prevention Plan.[45]
We selected states to include a mix of states with and without these characteristics.
During our site visits, we interviewed child welfare and juvenile justice agency leadership and child welfare case workers and juvenile justice probation officers. We also interviewed child welfare officials responsible for licensing and monitoring congregate care facilities, child welfare fiscal team officials, state Medicaid officials, and juvenile and family court judges. During these interviews, we discussed topics including: the implementation of Family First congregate care provisions within the state; the reasons why states had chosen to or not to implement QRTPs; challenges the states were facing in the child welfare and juvenile justice systems and how Family First’s congregate care provisions were impacting those challenges; the fiscal implications of Family First; coordination between the state child welfare and juvenile justice agencies; and federal monitoring and guidance, among others.
We also visited and spoke with officials from at least one congregate care facility in each state about how Family First’s congregate care provisions were affecting their operations and other issues. Additionally, in some states, we interviewed members of youth advisory councils or commissions and youth or adults with lived experience in the foster care system or as foster parents who consult for the state child welfare agency. Lastly, in three states we spoke to representatives from the state’s disability rights organization and/or Youth Law Center.
Additional Interviews
To inform the development of our surveys and address all research objectives, we conducted interviews with representatives from nine organizations with expertise in child welfare or juvenile justice issues and a researcher who has focused on issues affecting dually involved youth. In addition, we interviewed HHS and Department of Justice officials. We also obtained written responses from HHS, including from each regional office, to several sets of questions.
Data Analysis
To obtain information about trends in child welfare placements over time, we analyzed AFCARS data from fiscal years 2002-2023, the most recent data available. Similarly, we analyzed CJRP data maintained by the Department of Justice’s Office of Juvenile Justice and Delinquency Prevention for 2003 to 2023, the most recent data available.[46] We assessed the reliability of these data sources by reviewing relevant documentation, such as code books, user guides, program instructions, and data submission forms, and by testing the data electronically. We determined that these data were sufficiently reliable for the purposes of our reporting objectives.
We conducted this performance audit from June 2024 to March 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Appendix II: Online Questionnaire of Young Adults and Selected Responses About Experience in Congregate Care
We administered an anonymous web questionnaire to young adults with experience in foster care congregate settings. The questionnaire was disseminated through two national organizations, Think of Us and FosterClub, and through GAO social media from February 3 to March 5, 2025. Our inclusion criteria included that the respondent must be between ages 18 and 25 and have experienced at least one congregate care placement since 2021. Below are selected responses that indicate a range of experiences. We did not attempt to independently verify the responses. In addition, allegations of abuse do not constitute proof of actual abuse.
The first two survey questions asked respondents: (1) While in foster care, have you lived in a congregate care setting at any point since 2021? and (2) What is your current age? These questions were used to screen out respondents who did not meet our inclusion criteria. We received 26 responses that met our inclusion criteria. Although the questionnaire was anonymous, we asked respondents to identify their age, race and ethnicity, gender identity, sexual orientation, and the state in which they experienced their most recent congregate care placement.
Survey responses
Note: Some comments have been edited for readability, such as adding punctuation, correcting spelling, or removing the names of individuals and facilities.
Q. What additional information, if any, about your overall care would you like to share with us?
“…You try to just stay out of the way and get things done so they don’t pick on you or have a reason to put you in a higher level facility. There are some workers that are nice, but it’s distasteful that you can tell they have to “sneak” to be nice to you, they don’t want to get caught by the managers or other staff. You can’t be close with any staff it’s against the rules. You are not treated like a human being, rather an inmate. When you did nothing to get there.”
“The care I received was horribly negligent and left me with lasting trauma. I was being mistreated by staff after I had been grieving my mother, witnessed a developmentally disabled girl I was in the group home with get groomed by the male staff they appointed as an overnight in an all girls group home, and then harassed by the CEO once another girl and I expressed our experiences online after seeing that their agency was shut down by the state for the numerous incident reports against them.”
“They would hit us [and] not feed us.”
“Therapeutic restraints on kids.”
“The conditions were not appropriate for children. Congregate care felt confining, absent of love, and prison-like. Access to extracurriculars, family, friends, and education were limited.”
“Don’t know how to properly treat mental health.”
Q. How would you describe any differences between your experiences and/or
the services/programs you received while in different types of congregate care
or while in congregate care compared to other foster care placements?
(If comparing different placements, please try to specify which placements
you are comparing.)
“The group home was the best. However the eating disorder center provided better care for my specific needs.”
“Congregate care homes get used as foster homes when social workers can’t find placement for youth and sometimes these youth are “troubled” and then bring trouble with them to treatment facilities which impacts the treatment of everyone in the home. Sometimes this means introducing drugs or gang/ trafficking lifestyles to people who never knew what that was and are mentally ill.”
“I personally liked the group homes better just because they have one set of state rules they must follow, and can get in trouble if they don’t. So I would always know what to expect and what I was going into. The downside is there’s many more foster girls there with no limitations or boundaries to their background or behavior. I hated my foster home because the lady was so bipolar. One day you’d get a mom that wants to take you to go do fun stuff, the next day she’d be in bed and if you tried to talk to her she’d scream at you. You were supposed to know everything and how to get around [city] on a bus at the age of 17. It was mentally frightening, I did my best to emancipate myself even before I turned 18 because I couldn’t take it.”
“Transitional housing was more laidback, but you were expected to be independent while the staff did not do many things to help you transition into adulthood.”
“Every time we moved to a new foster home it would slowly get better. Like my 2nd foster home, they would physically abuse us, then my next foster home wouldn’t, but she would never feed us. Then the next would just say disrespectful things, and my last foster home she was the best.”
“The foster homes made me more comfortable and feel connected to my young adult self and not like I was completely singled out. Group homes made me rebellious and I felt unstable and unheard. There was always things occurring and not enough structure.”
“I felt like I was treated better in the juvenile detention center then I was treated at the [name] mental hospital for children. I felt more safe being in a group home or a residential facility than I did being in a foster home. Out in the community, some people don’t know how to clean, some people don’t know how to cook. Some people don’t know how to properly take care of youth that they are bringing into their homes. In the facilities, you know you’re getting three meals a day, you know you have a warm bed to sleep on and warm blankets. You know you have people to talk to, you know you have somebody in there.”
“I had eleven congregate care placements and three outside placements, two of which were foster homes. Congregate care was void of individual attention and care, overfilled, understaffed, and underqualified to serve as a “home” for a child. Being in a foster home versus a congregate facility pose vastly different experiences for youth. Congregate care felt like incarceration. We slept on mats on the floor, had our belongings taken away, got ten minute phone calls a day, timed showers, and lived by a schedule on the wall. While foster homes may not always be rosy, they are incomparable to congregate facilities.”
“There isn’t any really. Depends on who you are as [a] child which dictates how you’re treated there and by staff.”
Q. What impact, if any, did your foster care placement(s) in congregate
care settings have on you (emotionally, academically, socially, mentally,
etc.)?
(In other words, how did your placement in congregate settings affect you?
Reminder: congregate care includes group homes, institutions, or residential
treatment facilities.)
“It impacted my whole life. Going to school while constantly changing placements was hard. I will always have a special place in my heart for my old group home. It is where I learned so much and felt connected.”
“It has a terrible effect on me because I never felt like I belonged anywhere, and [it] made my mental health worse.”
“They definitely made me grow up quicker. I wanted to get out of there as quick as I could, so I learned how to make money (the legal way) and get my own place. They also exposed me to all the kinds of people there are in different cultures socially.”
“It taught me to build myself on my own because it felt like nobody understood me.”
“…I feel like my growth socially was stunted due to not being able to go outside with friends without the fear of being called AWOL, and people my age not understanding why I had to follow certain rules or why they couldn’t come over. I used to be pretty lively until the mistreatment started as well, and have become withdrawn as an adult. People think I’m unkind because I don’t know how to interact with people. Academically, the group home I was placed in during high school said I’d need to take myself to school while they transported other girls, and my commute was 2 hours each way via public transport, so I had difficulties with staying consistent in high school and with academics in general. I’m in college now taking my general education courses, and it is sort of hard to grasp subjects when I was supposed to learn this stuff in high school.”
“I was depressed and had anxiety throughout my foster homes. Also trauma, but my last foster home I would take therapy and it would help. I still take therapy till this day but [I’m] able to control my feelings and understand.”
“No impact.”
“Mentally draining on top of the things you have going on with your family situation…”
“It made [me] desensitized from life. I went into survival mode and shut off my emotions. I couldn’t focus on schools because of the constant moving, which contributed to a low GPA that has followed me even into adulthood. I isolate because I don’t feel safe completely opening up to anyone because everything feels temporary. I struggle a lot with dissociation.”
“It took me a long time to come to that realization however, it wasn’t [facility name] that was the issue, but the peers I had around me. I was roommates [with] this guy when I was 17 and I saw him 3 years ago at a Kroger in my college town. His life was totally different than mine but we came from the same background. I’ve asked the question why but the answer is that there aren’t many youth/young adult programs out there that might have lead him to a better lifestyle.”
“It honestly just depended on the facility in the juvenile detention center. The staff there were just so welcoming, and they were kind and they helped me overcome some mental obstacles. They had seen me at my worst in the middle of my addiction. …... I spent my whole senior year there and I went to high school pregnant and they took me to school every day. They supported me. They helped me raise a child in the midst of also going to high school. It was really nice. It was a good place to be.”
“Transitioning from one place to another made school really hard cause my transcripts rarely moved with me.”
“Congregate care had a strong impact on me in many aspects. Academically, I switched high schools five times. I had little to no help when I decided to apply to colleges. These facilities care that you are not failing in school, with little emphasis on excelling. Emotionally, these facilities changed my life. I entered my first congregate facilities because the state could not find anywhere for me to go. I vividly remember the doors clicking behind me and the fear that filled my chest. In these facilities, I saw abhorrent acts of violence, sexual assault, and suicidal behaviors. These memories still haunt me through adulthood.’
“I had PTSD from my living situation in my personal life at that time and it made it grow into C- PTSD due to more abusive and traumatizing things I saw and went through in those places.”
“My mental health is extremely worse. I have experienced so many traumas, paranoia from my stuff being stolen…. [and] excess anxiety because I never had my own personal space. More anger for people not listening to me when I really needed something. Socially awful. I have no friends now that I’ve been in the system. I’ve cried almost every day and when I come from school back to the house once I see the street. I literally break down in tears because the house feels like hell.”
Q. What additional comments either positive or negative do you have about your experiences related to your foster care placements in congregate care settings?
“The system needs to change for youth by imposing better standards and policies for youth in placement.”
“I’m thankful I was in foster care due to the resources I have received thru housing and education after aging out. I don’t know what I would have done without the resources. So, it was a blessing in disguise.”
“I had some good therapists in care that were some of the smartest and most empathic people I’ve met. There were some residential staff that were kind as well, and they acknowledged they wished they had the resources/authority to help us more. I learned how to become a little more self-reliant and to make sure to keep accounts of where I was/what I do to cover my bases, and I attribute that to having to check in with staff constantly so I wouldn’t get in trouble.”
“There’s hardly any good foster homes but I’m glad my last foster home was good. I just wish it was like that in every foster home.”
“I was severely neglected by the system.”
“There’s pros and cons to everything. It’s just they need to try and actually fix the cons by looking into different solutions when things aren’t working out.’
“Even though I had a rough upbringing, I learned a lot about myself and others. I’m beginning to build my life to what I want it to be now.”
“It really just depends on the facility. I personally feel from my experiences and all my placements and congregate settings that it really depends on the people that are running the place. It really depends on the workers’ attitude. Places could’ve been better, but I am also still alive and that’s all we can ever be thankful for.”
“Congregate care facilities should never be utilized for anything other than short-term care. There needs to be accountability in place to ensure these places remain safe and give children a safe and empowering experience.”
“It was more awful than losing my parents and that’s saying something. I don’t think I’ll be able to return in the same area as the congregate care home because it’s just too painful.”
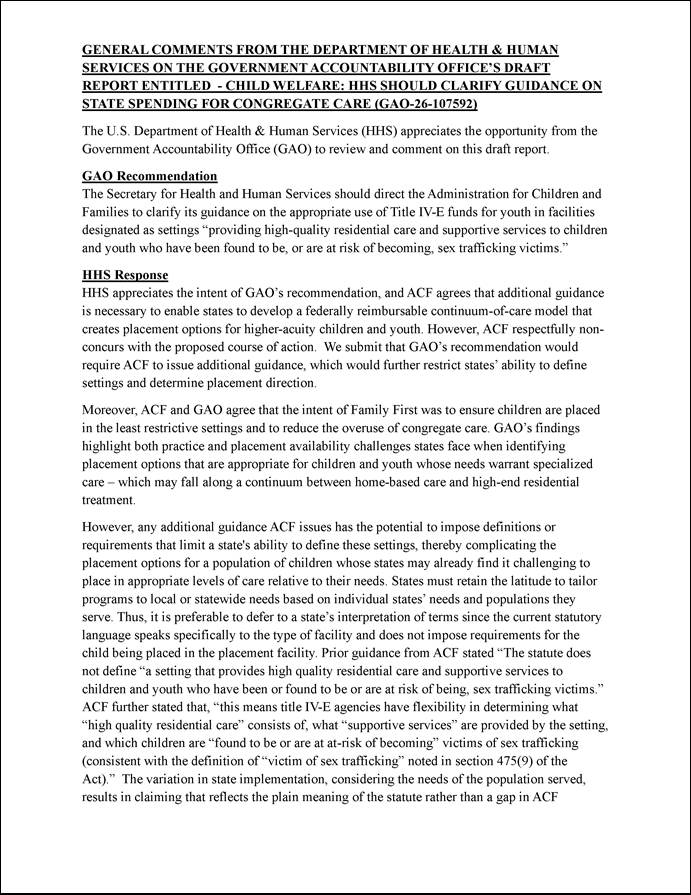

GAO Contact
Kathryn A. Larin, Director, LarinK@gao.gov
Staff Acknowledgments
In addition to the contact named above, Andrea Dawson (Assistant Director), David Barish (Analyst in Charge), Tangere Hoagland, and Adam Windram make key contributions to this report. Joanna Carroll, Youjin Chung, Melissa Jaynes, Jean McSween, James Rebbe, Jerry Sandau, Brian Schwartz, Joy Solmonson, Almeta Spencer, and Curtia Taylor provided additional support.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]Foster care congregate settings include group homes (a licensed or approved home providing 24-hour care, generally for seven to 12 youth) and institutions (a child care facility providing 24-hour care to more than 12 youth). For more information on outcomes for youth in foster care congregate settings, see, for example, Dongdong Li, Grace S. Ching, and Chi Meng Chu, “Comparing Long-Term Placement Outcomes of Residential and Family Foster Care: A Meta-Analysis,” Trauma, Violence, & Abuse, vol. 20 no. 5 (2019) and Wendy Wiegmann, Emily Putnam-Hornstein, Vanessa X. Barrat, Joseph Magruder, and Barbara Needell, The Invisible Achievement Gap, Part II: How the Foster Care Experience of California Public School Students Are Associated with Their Education Outcome, (2014).
[2]In our 2024 report, we summarized GAO’s work over a more than 20-year period on youth in the foster care system who are placed in congregate care, including concerns with the physical, emotional, and sexual abuse of these youth. GAO, Child Welfare: Abuse of Youth Placed in Residential Facilities, GAO‑24‑107625 (Washington, D.C.: June 12, 2024).
[3]The 100,913 youth in congregate care on September 30, 2002 represented about 19 percent of the 533,000 youth in foster care at the end of fiscal year 2002. In this report, the word “youth” includes children (under age 18) and youth (up to age 21). As of June 2024, at least 34 states and the District of Columbia offered federally funded extended foster care. Extended foster care allows individuals to remain in care up to age 21, provided they meet certain requirements, such as attending school.
[4]The 35,894 youth in congregate care on September 30, 2023, represented about 10 percent of the 343,077 youth in foster care at the end of fiscal year 2023. Department of Health and Human Services, Children’s Bureau, Adoption and Foster Care Analysis and Reporting System (AFCARS) fiscal year 2023 data, May 1, 2025. AFCARS fiscal year 2023 data do not include Washington or Wyoming.
[5]Title IV-E of the Social Security Act is the largest source of federal child welfare funding. In fiscal year 2023, federal Title IV-E expenditures totaled about $9.5 billion. Title IV-E supports youth in foster care and youth who leave foster care for new permanent families (via adoption or legal kinship guardianship). Under Title IV-E, the federal government reimburses state child welfare agencies between 50 and 83 percent of eligible foster care maintenance payments, including payments for congregate care. Title IV-E may also be used to support certain prevention services for states with approved prevention plans. Participating Tribes may also receive Title IV-E funding. Tribes were excluded from our analysis for the purposes of this report.
[6]42 U.S.C. § 672(k)(1). Exceptions to Family First’s limitations on using Title IV-E funds for congregate care are discussed later in this report.
[7]In this report, we refer to “Title IV-E foster care maintenance funds” as “Title IV-E funds.”
[8]The surveys were sent to child welfare and juvenile justice agencies in the 50 states and the District of Columbia. Forty-eight states and the District of Columbia responded to our child welfare agency survey, and 49 states and the District of Columbia responded to our juvenile justice agency survey. We include the District of Columbia when we refer to states in this report.
[9]The Family First provisions concerning the 14-day time limit on Title IV-E support for children placed in certain child care institutions were effective as of October 1, 2019. States could take up to 2 years to implement this provision and many states opted to do so. However, these provisions were in effect in all states as of October 1, 2021. In our surveys, we did not provide an end date for states to reflect on their experiences. As such, states could provide information on their experiences up to the date the state submitted their survey.
[10]We conducted in-person site visits in Iowa, Tennessee, and Texas and a virtual site visit in West Virginia.
[11]We also interviewed Department of Justice officials to obtain information about youth in juvenile justice congregate care placements, including those dually involved in the child welfare system.
[12]When a Tribe operates its own Title IV-E foster care program, youth may be placed under the responsibility of a tribal child welfare agency.
[13]Title IV-E is also used for payments for children who have left foster care for adoption or guardianship, administrative and other costs associated with providing child welfare services and maintenance payments, and certain evidence-based child welfare prevention services. For more information on the Title IV-E program, see GAO, Child Welfare: States’ Use of TANF and Other Major Federal Funding Sources, GAO‑25‑107467 (Washington, D.C.: April 8, 2025).
[14]To be eligible for Title IV-E, placements settings must meet other requirements. For example, the placement must be licensed or approved by the state.
[15]Limitations on Title IV-E funds for congregate care went into effect on October 1, 2019. However, states had the option to delay implementation for up to 2 years. Many states chose to delay implementation for some or all of that time. States that delayed implementation of Family First’s congregate care provisions could not claim Title IV-E for prevention services until they had implemented the congregate care provisions. Limitations on the use of Title IV-E to support youth in congregate care were effective in all states as of October 1, 2021. Title IV-E funds can also be used to support licensed residential family-based treatment facilities for substance use treatment and supervised independent living placements. For the purposes of this report, we excluded family-based treatment facilities and supervised independent living placements.
[16]42 U.S.C. § 672(k)(2). Family First created QRTPs as a new category of congregate care setting under Title IV-E. To qualify as a QRTP and be eligible to receive Title IV-E for more than 14 days, a facility must meet several criteria, which are outlined in Family First.
[17]In this report, we refer to these three types of excepted congregate care facilities as “specified settings” or “specialized placements.”
[18]Title IV-E funds can be used to provide prevention services listed on ACF’s Title IV-E Prevention Services Clearinghouse to eligible children and their parents or kin caregivers if the programs and service are found to be "promising," "supported," or "well-supported" through an independent systematic review.
[19]State implementation of the Title IV-E Prevention Program was outside the scope of this review.
[20]Placements and time in care showed similar patterns for non-specialized congregate care placements (i.e., congregate care facilities that are not QRTPs or facilities providing services to youth who have been or are at risk of sex trafficking or to pregnant and parenting youth) as for congregate care placements overall, even though Family First prohibits states from claiming Title IV-E funds after 14 days for youth in these settings. Twenty-six states reported the percentage of youth in non-specialized congregate care placements had increased or remained the same, and 24 reported the length of time youth remained in those settings had increased or remained the same since October 1, 2021.
[21]Some states we visited use emergency shelters in addition to, or instead of, stopgap placements to house youth when no other placement is available. For example, officials in two states said they used these shelters in a variety of ways, but according to state officials, they are typically supposed to be used for a limited time, such as overnight or for 30 days or less.
[22]In this report, “several” indicates 6—15 survey respondents, “many” indicates 16—25, “the majority” indicates 26—35, “most” indicates 36—45, and “almost all” indicates 45 or more.
[23]While less commonly reported, 23 states said that they sent youth to out-of-state congregate care placements because QRTPs in the state would not serve youth with significant behavioral challenges, autism, or intellectual disabilities.
[24]A psychiatric residential treatment facility (PRTF) is a nonhospital facility that provides psychiatric services to individuals under the age of 21 in an inpatient setting. PRTFs are a state Medicaid option, and not all states have them.
[25]Fictive kin are individuals who are unrelated to the youth but have such a close emotional relationship that they are considered like family.
[26]Two of the 34 states with QRTPs did not know what percent of their congregate care facilities were QRTPs.
[27]Nine additional states reported this was not applicable because they did not have any QRTPs.
[28]Six additional states said that Family First contributed moderately to the increase in the use of state, county, or local funds, and three more said that it contributed moderately to the decrease in Title IV-E funds.
[29]These challenges were cited as extremely or very challenging by 22, 20, and 20 states, respectively. The other challenges most frequently cited as extremely or very challenging were the increasing costs of congregate care due to Family First provisions (19) and insufficient state, county, or local funds (14). At least one state reported losing contracted congregate care beds because state funds were not available to replace lost federal funds.
[30]Officials told us that Family First funding limitations were not the only factor reducing their use of Title IV-E. They also said that income eligibility requirements for Title IV-E are part of the reason that states are drawing down less Title IV-E funds. The number of children eligible for Title IV-E has declined over time because the maximum income for a Title IV-E—eligible family is based on guidelines from the 1996 public assistance program and has not been adjusted for inflation.
[31]Title IV-B of the Social Security Act funds a variety of services to prevent and address child abuse and neglect. TANF funds a wide range of benefits and services for low-income families, including child welfare payments and services. For more information on using Title IV-B and TANF for child welfare purposes, see GAO‑25‑107467.
[32]Several state juvenile justice agencies noted a lack of available placements as a challenge in response to an open-ended survey question. Two states said that this lack of placements was especially challenging for girls.
[33]Thirteen child welfare agencies said that the QRTP bed question was not applicable because they did not have QRTPs.
[34]GAO, Foster Care: HHS Could Do More to Support States’ Efforts to Keep Children in Family-Based Care, GAO‑16‑85 (Washington, D.C.: Oct. 9, 2015).
[35]The other two issues most frequently cited by providers in this state, according to child welfare officials, were the increased severity of the needs of youth and their challenging behaviors and the reduction in youth being placed from out of state, which generally garnered significantly higher daily rates.
[36]For the purposes of this report, we defined “dually involved youth” as youth with an open case in both the state’s child welfare and juvenile justice systems. In our surveys, we did not provide an end date for states to reflect on their experiences. As such, states could provide information on their experiences up to the date the state submitted their survey.
[37]CFSR's also monitor compliance with Title IV-B requirements.
[38]Family First requires that if a youth is placed in a QRTP for more than 12 consecutive months or 18 nonconsecutive months, the head of the state child welfare agency must submit signed approval to HHS for the continued placement of the child in that setting. In addition, the state agency must submit, among other things, evidence that demonstrates that ongoing assessment of the youth continues to support the determination that the youth’s needs cannot be met through placement in a foster family home, that the placement in a qualified residential treatment program provides the most effective and appropriate level of care for the youth in the least-restrictive environment, and that the placement is consistent with the short- and long-term goals for the youth.
[39]See ACFY-CB-PI-18-07, Public Law 115-123, the Family First Prevention Services Act: Implementation of Title IV-E Plan Requirements, July 9, 2018.
[40]We followed up with our four site visit states as well as the four states that reported on our survey that more than 20 percent of youth in their child welfare system whose placements were funded through Title IV-E were victims of or at risk of sex trafficking.
[41]ACF guidance states that Family First does not define a setting that provides high quality residential care and supportive services to children and youth who have been or found to be or are at risk of being, sex trafficking victims and that ACF is not defining it further. According to ACF guidance, Title IV-E agencies have flexibility in determining what “high quality residential care” consists of, what “supportive services” are provided by the setting, and which children are “found to be or are at-risk of becoming” victims of sex trafficking (consistent with the definition of “sex trafficking victim” in 42 U.S.C. § 475(9)).
[42]GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.: September 2014).
[43]In our surveys, we did not provide an end date for states to reflect on their experiences. As such, states could provide information on their experiences up to the date the state submitted their survey.
[44]Based on fiscal year 2022 data from the Adoption and Foster Care Analysis and Reporting System (AFCARS), the most recently available data at the time we made our site visit selection.
[45]Family First authorized new optional Title IV-E funding for time-limited prevention services for mental health, substance abuse, and in-home parent skill-based programs for children or youth who are candidates for foster care, pregnant or parenting youth in foster care, and the parents or kin caregivers of those children and youth. Title IV-E agencies that elect to provide the Title IV-E prevention program must submit a 5-year plan for their Title IV-E prevention program to the Children’s Bureau for review and approval.
[46]According to the Department of Justice, CJRP data reflect a one-day count of youth populations held for an offense in juvenile residential placement facilities, typically on the fourth Wednesday in October. CJRP data are from “Easy Access to the Census of Juveniles in Residential Placement,” available at: https://www.ojjdp.gov/ojstatbb/ezacjrp/.