SEXUAL HEALTH EDUCATION
HHS Could Improve Efforts to Assess Grantee Performance
Report to the Ranking Member, Committee on Education and Workforce, House of Representatives
United States Government Accountability Office
A report to the Ranking Member, Committee on Education and Workforce, House of Representatives
For more information, contact: Mary Denigan-Macauley at DeniganMacauleyM@gao.gov.
What GAO Found
The Department of Health and Human Services (HHS) administers sexual risk avoidance education (SRAE) grants to states and other entities, such as community organizations. SRAE is a type of sexual health education that focuses on abstaining from non-marital sexual activity and other risky behaviors, such as alcohol use. SRAE programs are typically provided to youths aged 10 to 19 in schools during the day. Stakeholders, such as sexual health educators GAO interviewed, had various perspectives on whether SRAE was effective, medically accurate and complete, or culturally appropriate. GAO identified one peer-reviewed study on SRAE, which concluded it was effective for some outcomes.
HHS collects and reviews information of sufficient coverage and quality to assess SRAE grantees’ adherence to medical accuracy and cultural appropriateness program requirements. For example, HHS has a contractor-led process in place to review the medical accuracy of proposed program curricula. HHS also reviews information in grant applications that describe how grantees plan to serve certain populations and ensure program materials are culturally and linguistically appropriate.
HHS has assessed SRAE program results through a number of studies. For example, one study examined if implementation features—such as a non-school setting—were associated with intentions to delay sexual initiation. HHS also uses performance measures to assess whether grantees are meeting program objectives. However, HHS only has near-term goals for three of its performance measures. These are related to program reach and implementation. For example, its near-term goal for measuring the number of youth who attend a program session is to maintain the previous year’s number.
HHS does not have near-term goals related to measuring youth outcomes and program experiences, such as the percent of participants that plan to abstain from sex. According to HHS officials, it is piloting additional near-term goals for another pregnancy prevention program it manages and intends to adapt them for SRAE programs. However, the early results of this effort had not identified any near-term goals for performance measures related to youth outcomes and experiences. Setting near-term goals for these measures will help HHS more effectively assess the performance of SRAE grantees in influencing participants’ behavior intentions and their experiences in the programs over time.
Why GAO Did This Study
Preventing unintended pregnancies and sexually transmitted infections among youth is an important public health goal. Although the overall U.S. birth rate for youth aged 15 to 19 years has steadily declined since the early 1990s, it has remained higher than that of comparable high-income countries. Youth pregnancy can have high health and economic costs for the parents, their children, and society more generally. Sexual health education aims to provide youth with the knowledge and skills they need to protect themselves from these potential health and economic risks.
GAO was asked to examine issues related to SRAE. This report examines perspectives on the effectiveness, medical accuracy, and cultural appropriateness of SRAE; HHS’s use of information to assess grantee adherence to statutory and HHS requirements regarding medical accuracy and cultural appropriateness; and how HHS assesses the results of its SRAE programs.
GAO reviewed relevant published literature and HHS documentation, including procedures, grant applications, and performance measure documentation. GAO also interviewed HHS officials, and non-generalizable samples of 14 SRAE grantees in five states and eight stakeholders, including national advocacy organizations, professional medical or health associations, sexual health educators, and an academic researcher.
What GAO Recommends
GAO is making one recommendation to HHS to identify and implement appropriate near-term goals for performance measures related to youth outcomes and program experiences in SRAE programs. HHS concurred with the recommendation.
|
Abbreviations |
|
|
ACF |
Administration for Children and Families |
|
HIV |
human immunodeficiency virus |
|
HHS |
Department of Health and Human Services |
|
SRAE |
sexual risk avoidance education |
|
STI |
sexually transmitted infection |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
February 2, 2026
The Honorable Robert C. “Bobby” Scott
Ranking Member
Committee on Education and Workforce
House of Representatives
Dear Ranking Member Scott:
Preventing unintended pregnancies and sexually transmitted infections (STI) among youth is an important public health goal, given the potential long-term effects these could have on their health and well-being. Although the overall U.S. birth rate for youth aged 15 to 19 years has steadily declined since the early 1990s, it has remained higher than that of comparable high-income countries.[1] Youth pregnancy can have high costs for the parents, their children, and society more generally. For example, youth who are parents tend to have less education and are more likely to have lower incomes than their peers who are not parents, reducing their potential for economic self-sufficiency.
Sexually active youth are also more likely to experience STIs, such as chlamydia and gonorrhea, compared to adults, according to the Department of Health and Human Services (HHS). For example, in 2023, about half of reported cases for chlamydia, gonorrhea, and syphilis in the United States were among individuals aged 15 to 24 years. When left untreated, STIs can lead to health problems such as chronic pelvic pain, infertility, and poor birth outcomes.
Sexual health education provides youth with the knowledge and skills they need to protect themselves from pregnancy and STIs. One type of sexual health education is sexual risk avoidance education (SRAE). SRAE is an approach that targets youth aged 10 through 19 and focuses on abstaining from non-marital sexual activity and other risky behaviors, such as alcohol and illicit drug use. It also seeks to develop in youth life skills related to healthy relationships, decision making, goal setting, and self-regulation, according to HHS. The Administration for Children and Families (ACF), within HHS, administers the federal SRAE grant programs, which began in fiscal year 2016. Under these programs, SRAE grantees must provide information that is medically accurate and complete, as well as culturally appropriate. ACF works to promote the economic and social well-being of families, children, youth, individuals, and communities, according to its website.
Our prior work identified deficiencies in HHS and state efforts to assess the medical accuracy of materials used in ACF’s abstinence-only education programs—a type of sexual health education with similarities to SRAE.[2] In our 2006 report, we recommended that HHS develop procedures to help ensure the accuracy of materials used in abstinence-only education programs. HHS agreed with our recommendation and in response began requiring grantees to attest in their grant applications that their materials are accurate. We also found that while HHS, states, and researchers made efforts to assess the effectiveness of these programs, conclusions were difficult to arrive at due to, for example, limitations in study design.
You asked us to review issues related to sexual risk avoidance education. This report
1. describes the perspectives of selected stakeholders and published literature on the effectiveness, medical accuracy and completeness, and cultural appropriateness of sexual risk avoidance education;
2. examines the extent to which ACF uses quality information to assess how SRAE grantees meet medical accuracy and completeness, and cultural appropriateness requirements; and
3. examines how ACF assesses the results of its SRAE grant programs.
To identify and summarize the perspectives of selected stakeholders and any published literature on the medical accuracy, cultural appropriateness, and effectiveness of sexual risk avoidance education, we conducted a literature review of relevant U.S.-based research published from January 2015 through December 2024. We limited our search to literature published in the last 10 years to account for the beginning of ACF’s SRAE program, which began in fiscal year 2016. We identified studies through a search of multiple bibliographic databases. We examined the full text of 117 studies and identified nine peer-reviewed articles that met our inclusion criteria: one on sexual risk avoidance education and eight on abstinence-only sex education.[3] (See app. I for more information on our methods and the selected studies, including relevant findings and limitations.) We also interviewed a non-generalizable sample of stakeholders for their perspectives on these topics. We selected stakeholders representing a range of perspectives on sexual health education: two national advocacy organizations (Ascend, Advocates for Youth), two national professional medical or health organizations (American Academy of Pediatrics, Medical Institute for Sexual Health), three sexual health educators, and four academic researchers knowledgeable about sexual health education. We selected the educators and academic researchers through our attendance at the 2024 National Sex Education Conference, where they presented relevant sessions related to our objectives. Eight stakeholders were interviewed; three academic researchers did not respond to our request.
To examine the extent to which ACF uses quality information to assess how SRAE grantees meet medical accuracy and completeness, and cultural appropriateness requirements, we reviewed relevant ACF documentation, such as procedures or guidance, to identify the steps ACF takes to assess grantee adherence to these requirements. We reviewed relevant statutes and ACF’s notices of funding opportunity to identify relevant requirements.[4] We also obtained and examined grant application materials from a non-generalizable sample of SRAE grantees in five states—Arizona, Minnesota, Pennsylvania, South Carolina, and Texas—to understand the types of information ACF collects to assess grantee adherence to requirements.[5] States were chosen based upon the following factors: (1) the state had both Title V and General Departmental SRAE grantees; (2) the states represented a range of grant funding awarded; and (3) geographic variation. The Title V program awards funds to states and territories to implement SRAE programs, while the General Departmental program awards funds to organizations nationwide to implement SRAE programs. For each state, we interviewed or obtained written responses from state officials responsible for managing their Title V funding, as well as representatives from one randomly selected sub-grantee within each state.[6] We also interviewed or obtained written responses from a randomly selected General Departmental grantee from each of our selected states. We selected 14 SRAE grantees in total.
We interviewed and obtained written responses from ACF officials on the information they collect and how they use such information to assess grantee adherence to these requirements. We evaluated ACF’s efforts against our prior work on evidence-based policy making that emphasizes the collection of information of sufficient coverage and quality to inform decision making.[7]
To examine how ACF assesses the results of its SRAE grant programs, we reviewed ACF documentation, including program evaluations and performance measure documentation. We focused our analysis on 31 performance measures ACF uses related to youth outcomes—such as intentions to abstain from sex, avoid risky behaviors, practice healthy emotions—and program experiences.[8] We also interviewed and obtained written responses from ACF officials on how they assess the results of the SRAE grant programs. We assessed the extent to which ACF’s efforts followed key management practices identified in our prior work to effectively assess the results of their SRAE efforts.[9] These practices include collecting and analyzing evidence that can consist of quantitative and qualitative information, and may be derived from a variety of sources. Those sources include performance measurement, policy analysis, and program evaluation. As a part of these efforts, establishing near-term goals with specific targets and time frames can help the agency assess progress toward its goals. We also interviewed or obtained written responses from representatives from the 14 selected SRAE grantees to obtain their perspectives on ACF’s efforts to assess the results of the SRAE programs and grantee performance.
We conducted this performance audit from June 2024 to February 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
Sexual Health Education in the United States
Decisions about what is taught in K-12 education in the United States, including whether sexual health education is provided, are typically made at the state and local levels. Sexual health education, including what topics should be covered, is not universally required for students.
As of July 2025, 29 states and the District of Columbia require the provision of sexual health education in schools.[10] Additionally, although many states do not require the provision of sexual health education, when such education is provided, 41 states and the District of Columbia require that abstinence at least be discussed. Similarly, the majority of states (29 states and the District of Columbia) requires parental notice that sexual health education is being offered in schools or allows families to opt students out of sexual health education altogether (38 states and the District of Columbia).
ACF’s SRAE Programs
HHS, through ACF, administers two SRAE grant programs that focus on youth pregnancy prevention: the Title V program and General Departmental program.[11] Through these programs, ACF awards the following grants:
· Title V State. All states and U.S. territories are eligible for this funding;[12]
· Title V Competitive. Entities and organizations located in states or territories that do not receive Title V funds are eligible to apply for these competitive grants;[13] and
· General Departmental. Several types of entities and organizations may apply for this funding.[14]
For fiscal year 2025, the Title V program received $75 million and the General Departmental program received $35 million.[15] The Title V and General Departmental programs have funding periods of 2 and 3 years, respectively.
In fiscal year 2025, ACF had 158 active grantees across the grant programs, with a total of approximately $98 million in funding awarded. (See fig. 1.)
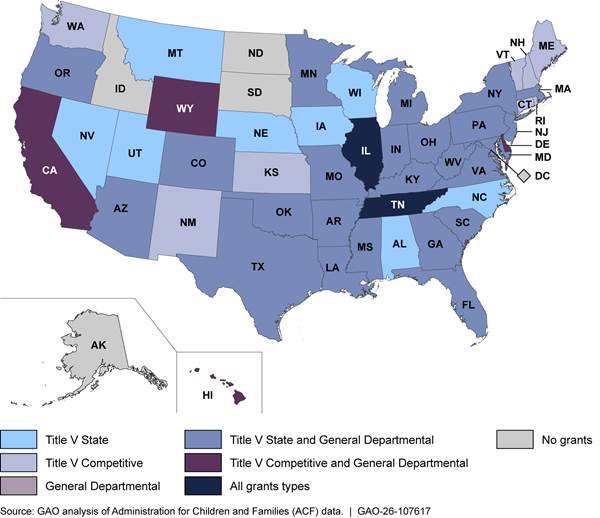
Note: In fiscal year 2025, Illinois and Tennessee received funding for all three grant types. According to ACF officials, Title V Competitive grants in these states ended in September 2025.
SRAE grantees served almost 325,000 youth in fiscal year 2024, according to ACF data. These data show that SRAE programs were most typically provided in schools during the day (approximately 90 percent of youth served). While less common, SRAE programs were also provided outside of school hours through, for example, community-based organizations or clinics. Middle school aged youth comprised most of the youth served by SRAE programs (approximately 62 percent).
While SRAE grantees have flexibility in their curriculum choice, selected curricula must, at a minimum, (1) teach the benefits associated with healthy decision making and a focus on the future; (2) discourage sexual coercion, dating violence, and other youth risk behaviors; and (3) normalize avoiding non-marital sexual activity, among other requirements, according to ACF’s notices of funding opportunity. According to a SRAE curriculum developer’s website, one commonly used SRAE curriculum approaches these requirements by focusing on topics such as
· knowing oneself (examining family origins and understanding personality styles);
· understanding the differences between healthy and unhealthy relationships (how to assess relationships, red flags, and how drugs and alcohol affect relationships);
· effective communication and conflict management (how to regulate strong emotions and discuss sensitive issues); and
· the success sequence (how the order of certain milestones affects the future).[16]
These teachings help contribute toward positive youth development and provide youth the knowledge and skills to refrain from non-marital sexual activity, according to the developer’s website.
Selected SRAE Program Requirements
Under the Title V program, grantees are required by statute to provide “medically accurate and complete” information.[17] In addition, educational materials specifically designed to address sexually transmitted diseases must contain medically accurate information about the effectiveness of condoms and disease prevention.[18]
Additionally, by statute, Title V grant programs must be “culturally appropriate, recognizing the experiences of youth from diverse communities, backgrounds, and experiences.”[19] The program’s fiscal year 2024 notice of funding opportunity expanded upon this requirement, indicating that grantees must provide culturally and linguistically appropriate interventions with the population served, and be inclusive of youth who identify as lesbian, gay, bisexual, transgender, questioning, intersex, asexual, and two-spirit.[20]
Under the General Departmental program, grantees are required to use “medically accurate information referenced to peer-reviewed publications by educational, scientific, governmental, or health organizations.”[21] ACF expanded on this requirement, stating in the fiscal year 2024 notice of funding opportunity that program materials should be reviewed in comparison to current medical statements of fact and in accordance with the most up-to-date scientifically supported information.
Additionally, programs are required to be culturally appropriate, incorporating the norms, beliefs, and values of the target population into the intervention, according to the fiscal year 2024 notice of funding opportunity. These programs must also be linguistically appropriate, trauma informed, and inclusive of youth who have been historically underserved, marginalized, and adversely affected by persistent inequities.
Stakeholder Perspectives Varied on Sexual Risk Avoidance Education; Study Suggests Effectiveness for Some Outcomes
The eight selected stakeholders we interviewed had various perspectives on whether SRAE in general, including federally funded SRAE, is effective, medically accurate and complete, or culturally appropriate. See figure 2 for statements stakeholders made on SRAE.
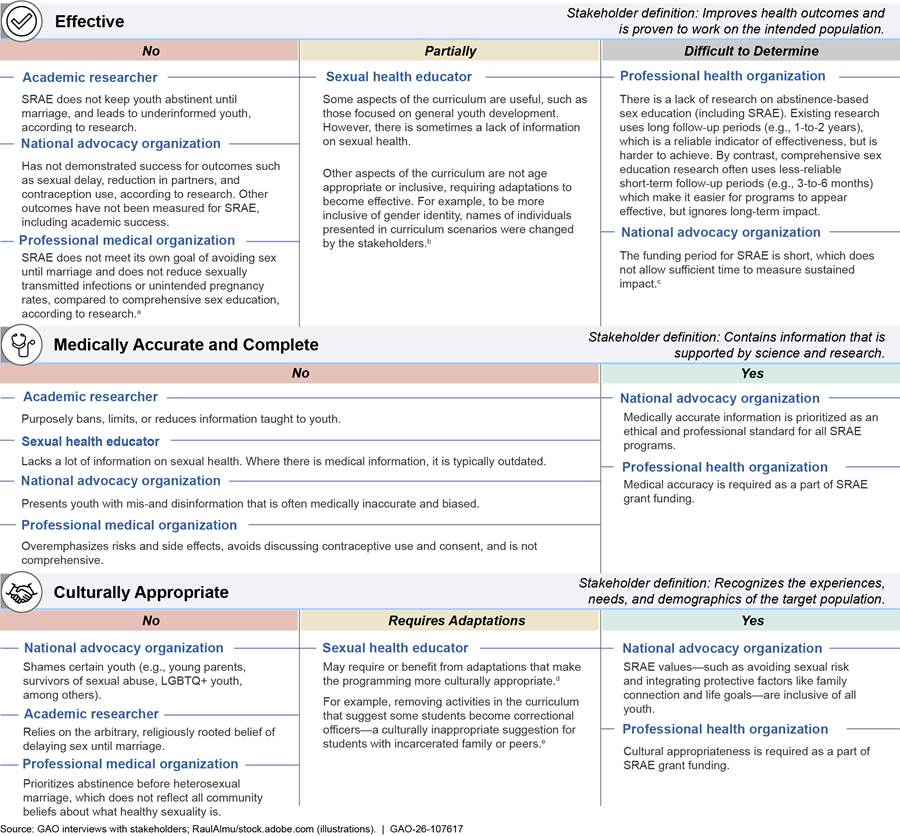
Notes: We interviewed a non-generalizable sample of eight stakeholders including national sexual health advocacy organizations, national professional medical or health organizations, sexual health educators, and academic researchers knowledgeable about sexual health education. Stakeholders commented on SRAE in general, including federally funded SRAE. As a result, some stakeholders provided perspectives that went beyond SRAE statutory requirements. Not all eight stakeholders we interviewed had perspectives on each topic. LGBTQ+ is the abbreviation for lesbian, gay, bisexual, transgender, or questioning.
aComprehensive sex education provides information on a range of topics related to reproductive and sexual health, according to the World Health Organization. For example, topics may include safer sex practices, including through the use of contraception.
bThis stakeholder referenced the following curricula: Making a Difference, Making Proud Choices, and Project Adult Identity Mentoring (AIM).
cThe Title V State SRAE and General Departmental SRAE programs have funding periods of 2 and 3 years, respectively.
dThis stakeholder referenced the following curricula: Making a Difference, Making Proud Choices, and Project AIM.
eThe stakeholder specifically referenced Project AIM curriculum when providing this example.
Related to our literature review, we found one peer-reviewed study on SRAE related to effectiveness, based on our review of 117 articles published since 2015.[22] We did not identify any relevant published literature on the medical accuracy and completeness or cultural appropriateness of SRAE.
The one study we identified related to effectiveness examined 12 primarily rural middle schools in one state and concluded that SRAE was effective at reducing sexual activity and pornography viewing for participants 3 months following program completion.[23] Specifically, a larger percentage of students who had received SRAE reported not having engaged in sexual intercourse 3 months after having received the education, compared to students who did not receive SRAE.[24] Additionally, students that participated in SRAE reported more favorable attitudes toward other sexual risk avoidance beliefs, such as beliefs related to STI risks, than control students at follow-up. The study did not find differences between the two groups of students with respect to sending nude or semi-nude pictures or past month substance use.
ACF Obtains and Reviews Information of Sufficient Coverage and Quality to Assess Grantee Adherence with Selected Requirements
ACF collects and reviews information from grantees about their efforts to meet program requirements on medical accuracy and completeness, and cultural appropriateness. To assess adherence to the medical accuracy and completeness requirements, ACF relies on contractor-led post-award reviews of curricula. To assess compliance with cultural appropriateness requirements, ACF reviews grant applications and conducts post-award monitoring activities, such as site visits.
Independent Reviewers Assess Grantee Curricula to Identify Medical Accuracy and Completeness Issues
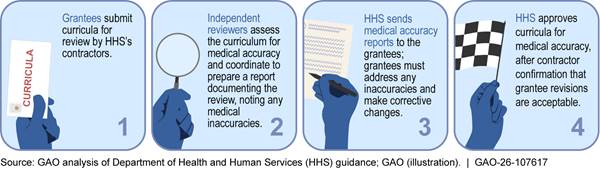
In 2011, ACF established a post-award contractor-led process to review the medical accuracy of grantees’ curricula, which includes all educational materials or information provided to participants, according to officials.[25] (See fig. 3.) As part of the process, the contractors maintain a list of approved curricula. Approved curricula retain that status for 5 years; therefore, the contractors typically review curricula only once every 5 years. However, all curricula not previously approved in the last 5 years will be reviewed by contractors. As of September 2025, there were 122 curricula on the approved list. However, ACF guidance encourages grantees to regularly review the curricula they use to update information as necessary.
Figure 3: Overview of the Medical Accuracy Review Process for ACF’s Sexual Risk Avoidance Education Grant Programs
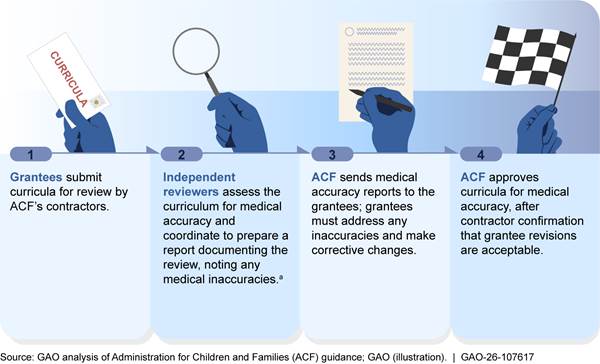
aThe types of issues ACF’s contractors look for include information that is inaccurate, incomplete, outdated, poorly referenced or supported by non-scientific studies, or confusing or misleading.
For fiscal year 2025, ACF’s contractors reviewed nine different SRAE curricula for medical accuracy and identified inaccuracies in four of them. (See table 1 for example issues.) According to ACF officials, they did not observe any patterns in the findings from the contractor reviews. Grantees addressed the inaccuracies in all instances, according to ACF.
Table 1: Examples of Medical Accuracy Issues in Grantee Sexual Risk Avoidance Education Curricula Identified by ACF’s Contractors
|
Issue |
Recommended solution |
Reference source |
|
A cited statistic about Human Papillomavirus infections is outdated and reflects data prior to vaccine introduction. |
Provide updated statistics regarding the incidence or prevalence of Human Papillomavirus infections. Also, Human Papillomavirus should be identified as the most common sexually transmitted infection (STI) in the country. |
Human Papillomavirus is the most common STI. The Centers for Disease Control and Prevention estimates there were 43 million Human Papillomavirus infections in 2018, many among people in their late teens and early 20s. In that same year, there were 13 million new infections. |
|
Incomplete (generalized) statements regarding condoms and their effectiveness. |
Specify type of condom and features as each type are not equally effective in STI prevention. |
According to the Centers for Disease Control and Prevention, latex condoms provide the best protection against HIV. Plastic condoms break more often than latex condoms. Natural membrane (such as lambskin) condoms have small holes in them and don’t block HIV and other STIs. These should not be used for HIV or STI prevention. |
|
The section [of the curricula] implies that HIV is a sexually transmitted disease. |
Provide correct information that HIV is a STI. |
Per the National Institutes of Health, STIs are infections that spread from person to person through sexual activity, including anal, vaginal, or oral sex. When left untreated, an STI can become a sexually transmitted disease. |
Source: Administration for Children and Families (ACF). | GAO‑26‑107617
Based on our review of the post-award process, we found that it provides ACF with information of sufficient coverage and quality to assess grantee adherence to the programs’ medical accuracy and completeness requirements. Having information of sufficient coverage and quality to inform decision making is a key practice to effectively managing and assessing the results of federal efforts.[26]
Program Staff Collect and Review Information Supplied by Grantees on Cultural Appropriateness, and Work with Grantees to Make Needed Adjustments
As of September 2025, ACF was collecting and reviewing information pre-award through grantees’ applications and through ongoing post-award monitoring to assess how grantees adhere to the programs’ cultural appropriateness requirements.
Pre-Award Activities
To determine how grant applicants plan to address the requirement that SRAE programs recognize the experiences of youth from different communities, backgrounds, and experiences, ACF reviews information required in grant applications, including information on the following:
· The types of participants by age groups or grade in school, race, ethnicity, and other descriptive factors;
· How the project will recruit and retain historically underrepresented and underserved populations within the targeted community;
· For example, according to its fiscal year 2024 notices of funding opportunity, ACF encouraged applicants to target youth populations that are historically and culturally underrepresented and underserved, including Hispanic, non-Hispanic Black, and American Indian/Alaska Native youth; youth from rural areas and territories; and youth who identify as lesbian, gay, bisexual, transgender, questioning, intersex, asexual, or two-spirit.
· How interventions will address the trauma needs of youth;
· How grantees will ensure that all curricula, services, and materials are culturally and linguistically appropriate, trauma informed, and inclusive of youth from diverse communities, backgrounds, and experiences.[27]
All of our selected General Departmental SRAE grantees targeted their programs toward (1) geographic areas that experience higher than average youth birth or pregnancy rates, or higher than average instances of youth STIs; or (2) racial and ethnic groups with elevated youth pregnancy rates, based on our review of the grantees’ applications. Additionally, four of the five Title V State grantees selected for our review articulated some combination of these populations as their targets in application materials submitted to ACF.[28] The remaining Title V State grantee noted that it would “target counties with health disparities due to either high rates of unplanned [youth] pregnancies, high rates of STIs, or high rates of other youth risk behaviors, such as drug and alcohol use. These counties represent a diverse demographic area of [the state], reaching urban, suburban, and rural populations.”
The populations targeted by our selected grantees are consistent with the top target populations across all grantees in fiscal year 2024. Specifically, of SRAE grantees’ programs, 85 percent targeted youth in high-need geographic areas, 58 percent targeted African American youth, and 54 percent targeted Hispanic/Latino youth, according to the most current ACF data available.[29]
|
Selected Grantees’ Steps to Ensure Sexual Risk Avoidance Education Programs Are Culturally Appropriate for the Populations Served Application materials we reviewed from three of our selected grantees articulated how they would ensure that their programs are culturally and linguistically appropriate, trauma informed, and are inclusive of youth from diverse communities, backgrounds, and experiences. For example: · One grantee works with additional community members to ensure that its lessons are relevant, affirming, appropriate, inclusive, and non-stigmatizing. This grantee has four cultural consultants and the grantee’s team is always in the process of making additional refinements based upon feedback received. · Another grantee maintains a workforce that is reflective of the populations it serves. Therefore, most staff speak more than one language, primarily Spanish, and program materials, publications, images and language reflect the populations they serve. Teachers are able to incorporate cultural experiences in programming instruction with the proposed curriculum. · A third grantee has selected a curriculum with embedded trauma-informed principles in its content and offers training to staff on the way trauma impacts youth. Additionally, all staff are required to attend an equity and inclusion training at the beginning of employment, and a cultural responsiveness training every semester, which involves identifying one’s own assumptions and privileges, being aware of bias, and identifying unique issues faced by [the] target population. |
Source: GAO review of three sexual risk avoidance education grantees’ application materials. | GAO‑26‑107617
Post-Award Activities
Through its post-award monitoring activities, such as monthly calls and site visits, ACF may identify opportunities to assist grantees with making updates to their programs to address any issues related to cultural appropriateness that may arise.[30]
· Monthly calls. During monthly calls between grantees and ACF project officers, grantees have requested technical assistance around serving special populations and ensuring cultural competency of curricula to specific populations, according to ACF officials. For example, ACF assisted a grantee with identifying curricula to serve a growing number of youth with special needs through its program.
· Site visits. Each year, ACF conducts site visits for selected grantees to assess their performance across 11 core areas, including cultural appropriateness. As a part of grantee site visits, ACF assesses how effective grantees are in implementing a curriculum that addresses the age-related and culturally specific needs of the population served. For fiscal year 2025, ACF conducted 15 site visits out of 158 active grantees. From these 15 site visits, ACF identified issues with cultural appropriateness during one visit, according to officials. Specifically, during this site visit, ACF observed grantee staff using harmful language with youth related to ethnic identity and intellectual stereotypes. To address this issue, ACF provided technical assistance and resources to support the grantee’s ability to be more culturally aware and responsive to the needs of the population served.
Should grantees want to update their programs to make them more culturally appropriate to the population being served, ACF has a process for grantees to submit proposed updates for review, according to officials. Specifically, grantees first consult with their curriculum’s developer to determine if changes are allowable. If the adaptation is allowable by the developer, or the developer is not involved in that decision making process, the grantee will email their ACF project officer to inform them of the requested change. The grantee’s project officer will determine if the change is substantive, if it follows program guidelines, and is allowable under program statute. If the adaptation is non-substantive, the project officer will provide an email approval. If the change is substantive, the grantee is required to submit a grant amendment explaining the change requested.
Three of the selected grantees we interviewed highlighted ways they have adapted their programs to make them more culturally appropriate for the population they served. For example:
· One grantee said it adapted program materials to ensure it resonated culturally with its target population. The grantee told us it uses cultural consultants to help with these adaptations.
· Another grantee said when same-sex marriage was legalized, it updated the language in its materials from “husband/wife” to “spouse.”
· A third grantee said more Spanish-speaking facilitators were added to its program because the grantee began to realize a large portion of the youth served spoke Spanish as their primary or secondary language. The grantee informed its state grant officer and technical assistance team of this decision, and both entities were supportive of the decision.
Based on our review of ACF’s process in place at the time of this report, we found that it provides agency officials with information of sufficient coverage and quality to assess grantee adherence to the programs’ cultural appropriateness requirements. In January 2025, the White House issued Executive Orders calling for the termination of all federal diversity, equity, and inclusion efforts, and prohibiting federal funds from being used to promote “gender ideology”.[31] According to ACF documentation we reviewed, the agency has made changes in response to the orders. For example, ACF updated the fiscal year 2025 notice of funding opportunity for the Title V program to state that ACF does not allow funds to be used to support any costs related to diversity, equity, and inclusion activities. ACF also updated the Title V program terms and conditions to prohibit grantees from including content that teaches gender identity as being distinct from biological sex in any program or service funded with the award.[32] Additionally, ACF halted plans to seek additional information related to sexual identity and gender orientation from SRAE program participants. In September 2025, several states filed suit against HHS and ACF, challenging implementation of Executive Order 14168 with respect to the Title V program.[33] In October of that year, the district court issued a preliminary injunction preventing HHS from taking steps to implement the Executive Order with respect to the states that filed suit, including any requirement for the states to remove references to gender identity from their sexual health education curricula. At the time of reporting, this litigation was ongoing.[34] It is unclear how ACF assessment of grantees’ adherence to cultural appropriateness requirements may change in future grant years.
ACF Assesses the Results of Sexual Risk Avoidance Education Programs in Various Ways, but Most Performance Measures Lack Near-Term Goals
ACF has conducted a variety of studies and uses performance measures to assess the results of its SRAE grant programs. However, we found that most of the performance measures ACF uses do not have near-term goals, including measures related to youth outcomes and their experiences with SRAE programs.
ACF Has Conducted Studies to Assess the Results of its Programs
As part of its efforts to assess the results of the SRAE programs, ACF has conducted a variety of studies examining various aspects of the programs, including evaluations examining whether programs’ characteristics are associated with positive youth outcomes. ACF also plans to conduct a multi-site impact study to determine SRAE programs’ impact on short-term and longer-term behavioral outcomes. According to ACF, these efforts—referred to as the SRAE National Evaluation—are intended to meet the statutory requirement that ACF produce one or more rigorous evaluations of the Title V SRAE program.[35]
Completed Studies
Study on early grantee preparation. To better understand how grantees planned and implemented their programming and to inform future efforts related to improving the effectiveness of the SRAE programs, ACF surveyed grantees in 2020 and collected information related to topics such as the SRAE curricula used, intended youth population, and settings where programming took place.[36] The information from this study helped ACF develop a research question for a subsequent study that examined student and teacher experiences with SRAE content and what program characteristics are associated with positive youth outcomes, according to ACF.
Study on student and teacher experiences and positive youth outcomes. Based on data collected from SRAE grantees and youth in the 2022-2023 school year, ACF completed a nationwide implementation study that had two main goals: (1) to describe and understand students’ and teachers’ experiences with curricula and required SRAE topics; and (2) to determine if certain implementation features—such as setting, curriculum, or educator experience—were associated with youth outcomes, such as intentions to delay sexual initiation and skills for healthy relationships.[37] Key findings from this study included the following:
· Youth said that most of the SRAE content was relevant, but some wanted more information on relationships, sexually transmitted diseases, sexuality, setting healthy boundaries, the consequences of sexual activity, and deciding the right age to have sex.
|
Sexual Risk Avoidance Education Program Evaluations Conducted by Grantees ACF provides support to grantees who choose to conduct an optional evaluation of their own programming (local evaluation). These evaluations allow grantees to evaluate program practices that are customized to their unique context, according to ACF officials. For example, one of our selected grantees analyzed student survey data to assess the extent to which the program may have had an impact on outcomes—such as decision-making around sexual risk avoidance choices and behaviors—over time. The evaluation also examined student satisfaction with the program. ACF’s support is intended to improve the rigor and viability of the local evaluations, officials told us. For example, ACF may provide support on issues such as helping increase sample sizes or by providing suggestions for incentives to increase youth attendance—thereby ensuring higher quality data. Source: Administration for Children and Families (ACF) documentation and interviews. | GAO‑26‑107617 |
· Youth outcomes tended to be better when SRAE programs were provided outside of school time or in a non-school setting. Youth outcomes were also better, on average, when providers served both middle school- and high school-aged youth in the same program than when providers served only middle school-aged youth.
The study noted that these findings could help build the foundational pieces of a new evidence base for SRAE programs, as well as point the way toward potentially effective implementation approaches.
Evaluation of co-regulation facilitation strategies. In 2022 and 2023, ACF studied the effectiveness of training SRAE teachers on co-regulation facilitation strategies and how those strategies impacted youth outcomes.[38] Co-regulation is a process by which adults provide a warm, supportive environment to youth using methods such as specific coaching, modeling, and feedback activities, according to ACF.[39] As a part of the study, youth reported that co-regulation strategies supported the development of their self-regulation skills, a common theme in SRAE curriculum. For example, one student said that breathing exercises helped to create a quiet, calm environment by removing tension from the classroom. The study also found that teachers could consistently use co-regulation strategies if provided appropriate training and support. Based on this finding, ACF developed resources for grantees to train their teachers on co-regulation strategies.[40]
Planned Study
A multi-site impact evaluation. ACF plans to conduct an impact evaluation on short-term and longer-term youth outcomes for a small sample of grantees that meet certain criteria. According to ACF officials, these criteria could include grantees’ time remaining in their grant award period, experience participating in rigorous evaluations, consistent implementation fidelity, or enrollment targets, among others. ACF chose to focus on a smaller selection of grantees for this planned impact evaluation due to the substantial variability of grantees’ characteristics. This variability makes conducting a large-scale, nationally representative study of SRAE effectiveness infeasible, according to officials. Although still in the planning stages, ACF officials said they hope to examine the impact of grantee programming on student behavior intentions through this evaluation. As of September 2025, ACF had begun to examine potential sites for selection and the feasibility of the proposed work.
ACF has used the findings of the studies it has completed to identify areas for further examination, according to officials. For example, ACF has developed research questions as part of its ongoing evaluative work to examine how youth receiving SRAE in child welfare and juvenile justice systems experience SRAE content, and how grantees adapt the content and activities of their SRAE programs to the different populations they serve. Additionally, ACF has identified opportunities to simplify how it collects data, which will improve the efficiency of its efforts, according to officials. Specifically, ACF will attempt to collect data on a timeline that better aligns with the grantee reporting periods to account for the response burden of concurrent data collection requests.
ACF Uses Various Performance Measures to Assess Grantee Services, but Most Measures Do Not Have Near-Term Goals
|
Planned Updates to Sexual Risk Avoidance Education Student Surveys ACF requires grantees to survey students at the start and end of the program. These surveys include questions regarding student intentions to delay sex, avoid risky behaviors, improve life skills, and satisfaction with the program. Selected sexual risk avoidance education grantees with whom we spoke identified limitations with these surveys. For example: · Eight grantees said the questions are too difficult for students to understand. · Six grantees said the surveys take too long to complete. ACF received similar feedback from grantees about these limitations, including that youth found the survey language and skip patterns confusing, according to agency officials. To improve the quality of the data collected, ACF is working on revisions to the surveys; for example, rephrasing questions to remove double-negatives, simplifying responses, and removing long parenthetical examples, according to officials. As of September 2025, ACF was awaiting Office of Management and Budget approval to implement these changes, according to officials. Source: GAO interviews with Administration for Children and Families (ACF) officials and selected sexual risk avoidance education grantees. | GAO‑26‑107617 |
In addition to the studies, ACF uses performance measures to assess whether grantees are delivering the expected services and meeting program objectives.[41] The measures also highlight areas in which performance might be lagging, according to ACF. These performance measures are associated with the SRAE programs’ long-term goal of providing messages to youth that normalize avoiding non-marital sexual activity and other behaviors that increase the risk for youth sex, according to officials. An effective SRAE program, according to ACF officials, is one that complies with legislation and serves youth based on program objectives and requirements.
ACF uses its measures to biannually assess grantee performance in areas ranging from program execution and grant management to the effectiveness of SRAE messaging. These measures can be categorized into three groups.
· Youth outcomes and program experiences. Based on data collected from students through entry and exit surveys, these measures provide data on student intentions to delay sex, avoid risky behaviors, manage emotions and practice healthy relationship skills, as well as student satisfaction with the SRAE program.[42] For example, the percent of participants that
· plan to abstain from sex,
· plan to not drink alcohol,
· plan to manage their emotions in healthy ways, and
· felt respected as a person [in the program].
These measures, in particular, are most directly related to whether SRAE grantees are effectively influencing youth behavior intentions. As of September 2025, there were 31 measures in this category.
· Structure, cost, and support for program implementation. Based on data collected from grantees, this group includes measures on programming, such as the intended number of program hours, core curriculum, and SRAE topics covered. As of September 2025, there were 53 measures in this category.
· Attendance, reach, and dosage. Based on data collected from grantees, these measures include the number of youth served overall and by program setting; the extent to which youth attended most of the intended program hours; and whether the majority of youth served were in one of several identified vulnerable populations. As of September 2025, there were six measures in this category.
As of September 2025, ACF had near-term goals with specific targets and time frames for three performance measures. (See table 2.) However, ACF does not have near-term goals for the remaining performance measures, including 31 measures related to youth outcomes and program experiences.[43]
Table 2: Sexual Risk Avoidance Education Program Performance Measures with Near-Term Goals, as of September 2025
|
Category |
Performance measure |
Near-term goal |
|
Structure, Cost, and Support for Program Implementation |
The percentage of programs that addressed all eight of the required topics. |
Maintain the established baseline (68%). |
|
Attendance, Reach, and Dosage |
The number of youth who attended at least one program session. |
Maintain the previous year’s result. |
|
The percentage of youth who completed at least 75 percent of the scheduled program hours. |
Maintain the previous year’s result. |
Source: GAO review of Administration for Children and Families (ACF) performance measure documentation. | GAO‑26‑107617
In our prior work, we identified several practices for performance management that can help organizations and agencies measure progress toward achieving goals, including establishing near-term goals.[44] Our prior work has also found that it can be beneficial for near-term goals to have specific targets and time frames. For example, a near-term goal for the performance measures related to youth planning to abstain from sex could be for ACF to set a target of the percentage of youths they expect to plan to abstain from sex by the end of the grant year.
According to ACF officials, most of the performance measures do not have near-term goals because ACF efforts have been focused on developing the full set of performance measures and building the data systems that allow grantees to submit and analyze their performance measure data, a process that began in 2017. Officials said they are in the early stages of piloting near-term goals for the Personal Responsibility Education Program—another pregnancy prevention program managed by ACF—with the intention of later adapting them to the SRAE programs. However, ACF’s efforts to develop near-term goals are focused on the performance measures related to the attendance, reach, and dosage, as well as structure, cost, and support for program implementation—categories for which the SRAE programs already have near-term goals for some of the performance measures.[45] As of September 2025, the pilot had not identified any near-term goals for performance measures related to youth outcomes and program experiences. Without doing so, ACF will be unable to assess how effectively grantees are implementing SRAE programs that are influencing youth behavior intentions and providing positive experiences for youth.
Conclusions
Effective sexual health education can provide youth with the knowledge and skills to make informed decisions about their future relationships and potentially reduce rates of pregnancy and STIs. While ACF assesses the results of SRAE programs in some ways, most of its performance measures, including 31 that track youth outcomes and program experiences, do not have near-term goals. These measures are important for measuring how effectively grantees are implementing programs that are influencing youth behavior intentions and providing positive experiences for youth. Setting near-term goals for these measures would allow ACF to compare planned and actual results over time and help ACF more accurately assess grantee performance, including determining whether changes to how grantees provide SRAE messaging are needed. It would also help ACF better assess whether SRAE programs are contributing to their aim of working to promote the economic and social well-being of children, families, and communities.
Recommendation for Executive Action
The Administrator of ACF should identify and implement appropriate near-term goals with specific targets and time frames for the performance measures related to youth outcomes and program experiences for the SRAE programs. (Recommendation 1)
Agency Comments
We provided a draft of this report to HHS for review and comment. In its written response, reproduced in appendix II, HHS concurred with our recommendation. HHS officials said, upon receipt of a fiscal year 2026 budget, they plan to begin the planning process to develop appropriate near-term goals with specific targets and time frames for the performance measures related to youth outcomes and experiences for SRAE programs in spring 2026. We also acknowledged programmatic updates that HHS noted in its letter due to the change in administration since our work began. HHS also provided technical comments, which we incorporated as appropriate.
As agreed with your office, unless you publicly announce the contents of this report earlier, we plan no further distribution until 28 days from the report date. At that time, we will send copies of this report to the Secretary of Health and Human Services and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at DeniganMacauleyM@gao.gov. Contacts points for our Offices of Congressional Relations and Public Affairs may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix III.

Mary Denigan-Macauley
Director, Health Care
To identify and summarize what is known about the medical accuracy, cultural appropriateness, and effectiveness of sexual risk avoidance education (SRAE), we conducted a literature review of relevant research published from January 2015 through December 2024.[46]
Methodology
We conducted 12 searches through multiple bibliographic databases, including but not limited to, Scopus, APA PsychInfo, Embase, EMCare, ERIC, PAIS International, SciSearch, and Social SciSearch. We used the search term “sexual risk avoidance” because SRAE was the focus of our review. We also included the search term “abstinence only” because the goal of abstinence-only sex education is similar to that of SRAE: to abstain from sex until marriage.
Following our searches, we reviewed resulting study abstracts to determine which studies appeared relevant to our objective.[47] For the relevant abstracts, we analyzed the full-text of the studies to determine inclusion in our literature review.[48] While our searches captured literature that was not peer-reviewed, we chose to only include articles that were peer-reviewed and therefore published in journals.[49] Articles we chose that related to cultural appropriateness discussed, for example, gender and sexuality. Articles we chose that related to effectiveness discussed, for example, health outcomes and participant perceptions. We also reviewed the citations of selected studies to identify other potential studies for inclusion—a process known as waterfalling. In total, we reviewed 258 abstracts and examined 117 full-text studies.[50]
We excluded studies based on the following criteria:
· The study did not focus on the medical accuracy, cultural appropriateness, or effectiveness of SRAE or abstinence-only sex education.[51]
· The study analyzed data prior to 2015.[52]
· The study was not based in the United States.
· The study was not peer-reviewed (e.g., it was an opinion piece or dissertation).
· The study’s population of interest focused on individuals outside the age range of 10-19 years.[53] We excluded these studies because the target population of the Administration for Children and Families’ SRAE programs is 10-19 years.
Results
Based upon these steps, we selected nine studies for inclusion in our final review—one study on SRAE (discussed previously in the report), and eight studies on abstinence-only sex education.[54] (See table 3.) All nine studies reported methodological limitations.
Table 3: Selected Sexual Risk Avoidance Education and Abstinence-Only Education Literature, 2021 to 2024
|
Study citation |
Topics discussed |
Purpose |
Study design |
Study sample |
Relevant findings |
Reported limitations |
|
Sexual Risk Avoidance Education |
||||||
|
Ashley, O., S.R. Shamblen, A. Gluck, and C. Wood. “A Group Randomized Controlled Trial of Relationships Under Construction Sexual Risk Avoidance Education.” Journal of School Health, vol. 94, no. 8 (2024). DOI: 10.1111/josh.13441 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☒ Cultural appropriateness |
To evaluate effectiveness of Relationships Under Construction, a sexual risk avoidance education program that promotes positive youth development and healthy relationships. |
School-based randomized effectiveness trial with a wait-listed control design.a |
Sample: Age: Black 11% White 76% Hispanic 6% Native American 1% |
Findings suggest that Relationships Under Construction significantly reduced sexual activity and pornography viewing at 3-month follow-up. |
Low number of schools. Could not collect identifying information on individual student characteristics. |
|
Abstinence-Only Sex Education |
||||||
|
Burns, P.A., F. Teng, A.A. Omondi, E.T. Burton, and L. Ward. “Sex Education and Sexual Risk Behavior among Adolescents and Youth in the Deep South: Implications for Youth HIV Prevention.” The Southern Medical Association, (2022). DOI: 10.14423/SMJ.0 000000000001391 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☐ Cultural appropriateness
|
To investigate the impact of Abstinence Only Until Marriage education, compared with no sex education, among youth and young adults in Mississippi.b |
State-specific data from the 2015 Youth Risk Behavior Surveillance System were used to investigate the impact of sex education on adolescents and young adults.c |
Sample: 2,154 students in 45 public high schools in Mississippi during fall of 2015; 2,081 responses were included in analysis. Age: 12 – 18 years Sex/Gender: Female 53.4% Male 46.6% Race/Ethnicity: Black 47.9% White 35.1% Other 17.0% |
There were no statistically significant differences in early sexual debut (less than age 13), number of sex partners, and condom use between those who were enrolled in abstinence-only sex education compared with those who were not. |
Findings limited to sample in Mississippi. Survey limitations prohibit longitudinal analysis. Subject to recall bias. |
|
Caulfield, N.M., A.K Fergerson, M. Buerke, and D.W. Capron. “Considering the Impact of High School Sexual Education on Past Sexual Victimization and Rape Myth Acceptance in a College Sample.” Journal of Interpersonal Violence (2024): 1-17. DOI: 10.1177/ 08862605241257599 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☐ Cultural appropriateness |
To explore the impact of high school sexual education type and past sexual victimization. |
Survey administered online with college student participants who received course credit. |
Sample: 664 Sex/Gender: Female 82.4% Male 17.6% Race/Ethnicity: White 70.9% Nonwhite 29.1% |
Those who received comprehensive sex education were 2.5 times more likely to receive education about consent than those who received abstinence-based or no sex education. |
Non-generalizable. Mostly female. |
|
Chan, C.T., B.L. Olivieri-Mui, and K.H. Mayer. “Associations between State-Level High School HIV Education Policies and Adolescent HIV Risk Behaviors.” Journal of School Health, vol. 92, no. 3 (2022). DOI: 10.1111/josh.13130 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☐ Cultural appropriateness |
To evaluate associations between state-level high school HIV education policies and adolescent HIV risk behaviors. |
Cross-sectional analysis of Youth Risk Behavior Survey by the Centers for Disease Control and Prevention, and state level policy on HIV education from the Guttmacher Institute Sex and HIV Education Report.c |
Sample: Representative sample of high school students grades 9-12; 128,986 respondents representing 8,267,520 high school students from 33 states Age: Not reported Sex/Gender: Female 51.5% Male 48.9% Race/Ethnicity: Black 12.6% Hispanic 29.1% White 47.6% Other 10.7% |
State policies requiring HIV education to stress abstinence were associated with 20% higher odds of having at least four lifetime sexual partners and 19% higher odds of no condom use at last sex. There was no association between policies stressing abstinence and substance use before last sex. |
No causal inferences possible. Generalizability limited to the states represented in the survey. |
|
Grasso K.L., and L.A. Trumbull. “Hey, Have You Been Tested? The Influence of Comprehensive or Abstinence-Only Sexuality Education on Safer Sex Communication and Behavior.” American Journal of Sexuality Education, vol. 16, no. 2 (2021): 257-281. DOI: 10.1080/ 15546128.202 1.1880512 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☐ Cultural appropriateness |
To examine how sexuality education relates to sexual behavior and communication among U.S. adults through an online survey. |
Used Amazon MTurk to recruit participants for an online survey. |
Sample: 140 Age: 18-28 years Sex/Gender: Male 60% Female 40% Race/ethnicity: White 69.3% Other groups not reported |
Those who reported abstinence-only education reported sexual debut one year later than those who had comprehensive sexual education. |
Nonrandom sample. Subject to recall bias. Could have fraudulent responses. Unable to analyze by lesbian, gay, bisexual, transgender, queer or questioning (LGBTQ+) identity. Measurement of education and communication variables imperfect. |
|
Harris, S., C. Meier, J. Gast, L. Ward, and M. Ferguson. “Utah LGBQ + Youth Need Inclusive and Comprehensive Sex Education Opportunities: Results From the 2022 Utah College Retrospective Sexual Behavior Survey.” American Journal of Sexuality Education (2024). DOI: 10.1080/155 46128.2024.2336009 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☒ Cultural appropriateness |
To examine the perceptions of five core topics of sex education among young adults who attended high school in Utah, which taught abstinence as its primary source of pregnancy and sexually transmitted infection prevention at the time of the study. |
Cross-sectional emailed survey of sex education perspectives and sexual behaviors, with special attention to LGBTQ+ input. |
Sample: Surveyed 8,982 students at four Utah universities; final number of responses was 1,091. Age: 18-21 years Sex/Gender: Female 65.3% Male 28.8% Genderqueer/non-conforming 4.1% Different identity 1.0% More than one identity 1.0% Trans male 0.6% Trans female 0.2% Race/Ethnicity: Asian 1% Black/African American 0.5% Hispanic 3.2% White 91.2% Other 4.1% |
LGBTQ+ respondents reported higher levels of disagreement that they received sufficient sex education. Members of the Church of Latter-Day Saints reported they received sufficient sex education. |
Convenience sample. Subject to recall bias. Non-generalizable. Cross-section design. |
|
Mata, D., A. K. Korpak, B. L. Sorensen, B. Dodge, B. Mustanski, and B. A. Feinstein. “A Mixed Methods Study of Sexuality Education Experiences and Preferences Among Bisexual, Pansexual, and Queer (Bi+) Male Youth.” Sexuality Research and Social Policy, vol. 19 (2022): 806-821. DOI: 10.1007/s13178-021-00593-8 |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☒ Cultural appropriateness |
To examine experiences of LGBTQ+ male youth in learning about sex at school and from other sources, and their preferences for sexuality education programs. |
Online survey followed by semi-structured interview about preferences for sexual education and experiences learning about sex at school and from other source (e.g., parents or the internet). Data analysis included thematic analysis. |
Sample: 56 Age: 14 to 17 years Sex: Males 100% Cisgender 79% Transgender 21%. Race/ethnicity: Black 20% Latinx 32% White 39% Other 9% |
Most participants described receiving some type of sex education at school. Approximately one-quarter of participants specifically received abstinence-only education. Those who received this type of sex education commonly described the sex education as heteronormative. |
Not a probability sample. Subject to recall bias. Some respondents only received a subset of questions. |
|
McKay, E.A., M. Placencio-Castro, M.R. Fu, and H.B. Fontenot. “Associations Between Sex Education Types and Sexual Behaviors Among Female Adolescents: a Secondary Data Analysis of the National Survey of Family Growth 2011-2019.” Sexuality Research and Social Policy, vol. 19 (2022): 922-935. DOI: 10.1007/s13178-021-00664-w |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☒ Cultural appropriateness
|
To describe sex education content received; to assess the prevalence and impact of different sex education types, such as abstinence-only, on sexual intercourse and contraceptive behavior of adolescent females; and to examine differences by sexual identity. |
National Survey of Family Growth collected data about sexual health topics, including receipt of sex education and behavioral outcomes, from a nationally representative sample of men and women. |
Sample: 3,952 Age: 15 – 19 years Sex/Gender: Female 100% Race/ethnicity: Black 17.1% White 72.4% Other 10.5% |
Compared to no sex education, with a few exceptions, exposure to any type of sex education, including abstinence-only, reduced likelihood of sexual intercourse. However, it also increased the probability of not using contraception. |
Amount of exposure to each topic, specific messages communicated, accuracy of information, and quality of teaching not assessed. Based on retrospective self-reports. |
|
Mollen, D., E.M. Klann, M. Hinton, M. Vidican, A. and Romines. “Sex education among recent high school graduates.” Sexuality Research and Social Policy (2024). DOI: 10.1007/s13178-024-01041-z |
☒ Effectiveness ☐ Medical accuracy and/or completeness ☐ Cultural appropriateness
|
To examine associations between type of sex education, sexuality knowledge, and attitudes among recent high school graduates. |
Survey administered online with a convenience sample recruited through social media sites (e.g., Facebook, Reddit). |
Sample: 1,005 Age: >18 years Sex/Gender: Women 51.1% Men 46.3% Trans/Nonbinary 1.8% Race/ethnicity: Asian-American 5% Biracial/Multiracial 0.3% Hispanic 3.2% Native American 2.7% White 68.8% Black/African-American 19.9% |
Compared with those who received comprehensive sex education, those who reported receiving abstinence only education reported more beliefs emphasizing, among other things, abstinence until heterosexual marriage and fewer positive beliefs about sex.d |
No way to verify type of sex education received. |
Source: GAO review of published literature. | GAO‑26‑107617
Notes: Where it existed, we reviewed selected relevant literature related to the effectiveness, medical accuracy and completeness, and cultural appropriateness of sexual risk avoidance education and abstinence-only sex education, in response to congressional interest in these topics. Limitations were identified by the study authors.
aA wait-listed control design is where the control group does not receive the intervention until after the study ends.
bAt the time of the study, Mississippi only had abstinence-only-until-marriage education available in schools per a 1998 law, according to the study.
cThe Youth Risk Behavior Surveillance System measures health-related behaviors and experiences that can lead to death and disability among youth and adults. The system uses multiple surveys to collect this data, including the Youth Risk Behavior Survey, which is administered in every state every 2 years to monitor the prevalence of health-related behaviors, including sexual risk behaviors.
dPositive beliefs about sex were measured using the Sex Positivity Scale, a 26-item scale measuring behaviors and attitudes about sex, talking about sex and communication, and personal beliefs, knowledge, and experience.
Summary of Findings from Selected Abstinence-Only Sex Education Literature
The eight studies on abstinence-only sex education included in our review examined different aspects of effectiveness, when compared to other types of sexual health education, such as whether abstinence-only sex education delayed sexual activity and affected other youth outcomes. Selected literature also addressed whether abstinence-only sex education is inclusive of lesbian, gay, bisexual, transgender, queer, or questioning populations. We did not find any literature relating to the medical accuracy of abstinence-only sex education.
Studies Examining Effectiveness
Abstinence-only education vs. comprehensive sex education (five studies). Literature suggested the following:
· abstinence-only sex education was more likely to delay sex (two studies);[55]
· comprehensive sex education was more effective at providing participants information and tools on how to manage sexual relationships (four studies); [56]
· no difference in participants’ use of birth control (one study).[57]
Abstinence-only education versus no sexual education (one study). There was little to no difference between youth who received abstinence-only education or no sexual education with respect to having multiple sexual partners, alcohol use, and engagement in sexual risk behaviors.[58]
No comparison group (one study). Participants who received abstinence-only education reported not receiving information on sexually transmitted infection (STI) prevention and expressed the opinion that abstinence did not make sense when most adolescents have already engaged in sexual activity.[59]
Studies Examining Cultural Appropriateness
Two studies we reviewed suggested abstinence-only sex education was not culturally appropriate because it focused exclusively on heterosexual relationships (e.g., sex or marriage between a man and a woman).
· One study found that abstinence-only sex education participants who identified as lesbian, gay, bisexual, transgender, queer, or questioning were more likely to feel they were not getting sufficient information about topics such as making the choice to have sex, healthy relationships, and exploring sexuality when compared to participants who did not identify as such.[60]
· The second study found those who received abstinence-only sex education commonly described that education as only focusing on sex between men and women, particularly cisgender men and women.[61]
GAO Contact
Mary Denigan-Macauley, DeniganMacauleyM@gao.gov.
Staff Acknowledgments
In addition to the individual named above, Stella Chiang (Assistant Director), Nick Bartine (Analyst-in-Charge), Mac Hoeve, Rayna Ketchum, Jeanne Murphy-Stone, and Caylin Rathburn-Smith made key contributions to this report. Also contributing were Andrea Dawson, Leia Dickerson, Kaitlin Farquharson, Janice Latimer, Drew Long, Eric Peterson, Steven Putansu, and Ethiene Salgado-Rodriguez.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
A. Nicole Clowers, Managing Director, CongRel@gao.gov
General Inquiries
[1]The U.S. birth rate for females aged 15 to 19 years declined 78 percent from 1991 to 2021, with the rate declining from 15 to 14 births per 1,000 females in 2020 and 2021, respectively. See Department of Health and Human Services, Centers for Disease Control and Prevention, About Teen Pregnancy (May 15, 2024).
As of 2023, births per 1,000 women aged 15 to 19 was five in Germany, eight in the United Kingdom, and 13 in the United States, according to the World Bank. See World Bank Group, United Nations Population Division, Adolescent fertility rate (births per 1,000 women ages 15-19) (2025).
[2]See GAO, Abstinence Education: Efforts to Assess the Accuracy and Effectiveness of Federally Funded Programs, GAO‑07‑87 (Washington, D.C.: Oct. 3, 2006). According to ACF officials, there are some similarities between the prior federally funded abstinence-only education programs and SRAE, such as the focus on abstaining from sex until marriage and requiring that programs be medically accurate. However, SRAE also has other goals such as teaching the benefits of self-regulation, success sequence for poverty prevention, healthy relationships, goal setting, and resisting youth risk behaviors, according to ACF officials.
[3]We define peer-reviewed articles as those published in peer-reviewed journals. These articles therefore have gone through an evaluation process in which journal editors and other expert scholars critically assess the quality and scientific merit of the article and its research methods.
We included abstinence-only sex education literature in our review because its goal is similar to that of SRAE: to abstain from sex until marriage. However, because the focus of our review was SRAE, we only discuss SRAE literature in the body of the report. For a discussion of abstinence-only sex education literature, see appendix I.
[4]See Department of Health and Human Services, Administration for Children and Families, Standing Notice of Funding Opportunity for Title V State Sexual Risk Avoidance Education, HHS-2024-ACF-ACYF-SRAE-0044 (2024); General Departmental Sexual Risk Avoidance Education (GD – SRAE), HHS-2024-ACF-ACYF-SR-0041 (2024); and Title V Competitive Sexual Risk Avoidance Education (SRAE), HHS-2024-ACF-ACYF-TS-0040 (2024).
[5]Other documentation reviewed included site visit reports and corrective action letters, as available.
[6]States that receive a Title V SRAE grant can award the funds to sub-grantees within the state. At the time of our review, South Carolina had not published a request for proposals for Title V SRAE sub-grants. As such, we did not interview a South Carolina Title V SRAE sub-grantee.
[7]See GAO, Evidence-Based Policymaking: Practices to Help Manage and Assess the Results of Federal Efforts, GAO‑23‑105460 (Washington, D.C.: July 12, 2023).
[8]ACF has 131 performance measures to assess grantees in areas ranging from program execution and grant management to the effectiveness of SRAE messaging.
[9]See GAO‑23‑105460.
[10]According to the website for the Guttmacher Institute, a research and policy organization committed to advancing sexual and reproductive health and rights.
[11]HHS also administers two other youth pregnancy prevention programs: the Teen Pregnancy Prevention program and the Personal Responsibility Education Program. These programs were outside the scope of our review.
[12]The amount of Title V funding allotted to each state or territory in a given fiscal year is equal to the product of (1) the total amount appropriated for the Title V program for the fiscal year minus any reservations (up to 20 percent) made by HHS for administering it, and (2) the state or territory’s relative proportion of low-income children nationally. 42 U.S.C. § 710(a)(1). States and territories that receive a Title V grant may award the funds to sub-grantees within the state or territory to implement SRAE programs. States and territories have primary oversight responsibility for their sub-grantees, according to ACF.
[13]42 U.S.C. § 710(a)(2). The funding available for these Title V Competitive grants depends on the amount remaining after allotments to states and territories have been made.
[14]Through the grant application process, HHS has identified multiple types of entities that are eligible for funding, including localities (county, city, township, and special districts); school districts; public and state-controlled institutions of higher education; federally recognized tribal governments; Native American tribal organizations; public and Indian housing authorities; nonprofit organizations other than institutions of higher education; private institutions of higher education; small business; and for-profit organizations other than small businesses.
[15]See 42 U.S.C. § 710(f)(1) (providing $75 million for the Title V program for fiscal year 2025). For the General Departmental program, see Full-Year Continuing Appropriations and Extensions Act, 2025, Pub. L. No. 119-4, § 1101(a)(8), 139 Stat. 9, 45. The President’s budget request for fiscal year 2026 recommends eliminating the General Departmental program.
[16]See The Dibble Institute, Love Notes 4.1 - Sexual Risk Avoidance Adaptation (Berkley, Calif.: 2025).
[17]42 U.S.C. § 710(b)(2)(B). The term “medically accurate and complete” is defined to mean verified or supported by the weight of research conducted in compliance with accepted scientific method and either (1) published in peer-reviewed journals; or (2) comprising information that leading professional organizations and agencies with relevant expertise in the field recognize as accurate, objective, and complete. 42 U.S.C. § 710(e)(2).
[18]Section 317P of the Public Health Service Act states that educational materials specifically designed to address sexually transmitted diseases must contain medically accurate information regarding the effectiveness or lack of effectiveness of condoms in preventing the disease the materials are designed to address. 42 U.S.C. § 247b-17(c)(2). We previously found that section 317P applies to abstinence education materials prepared by grant recipients, depending on the substantive content of those materials. ACF agreed, noting that if grantees’ educational materials are specifically designed to address sexually transmitted diseases, they must comply with section 317P. See GAO, Abstinence Education: Applicability of Section 317P of the Public Health Service Act, B-308128 (Washington, D.C.: Oct. 18, 2006).
[19]42 U.S.C. § 710(b)(2)(E).
[20]According to the Indian Health Service, traditionally Native American two-spirit people were male, female, and sometimes intersexed individuals who combined activities of both men and women with traits unique to their status as Two-Spirit people. In most tribes, they were considered neither men nor women; they occupied a distinct, alternative gender status.
[21]The General Departmental program was first established and funded by the Consolidated Appropriations Act, 2016, Pub. L. No. 114-113, div. H, tit. II, 129 Stat. 2242, 2617 (2015). Subsequent appropriations laws have provided authority and funding for the program. See, for example, Further Consolidated Appropriations Act, 2024, Pub. L. No. 118-47, div. D, tit. II, 138 Stat. 460, 671; Full-Year Continuing Appropriations and Extensions Act, 2025, Pub. L. No. 119-4, § 1101(a)(8), 139 Stat. 9, 45.
[22]See appendix I for a description of our literature review scope and methods. Our literature review also identified published literature addressing the effectiveness and cultural appropriateness of abstinence-only education, a type of sexual health education similar to SRAE. For more information about these articles’ findings, see appendix I.
[23]See O. Ashley, S.R. Shamblen, and A. Gluck, C. Wood, “A Group Randomized Controlled Trial of Relationships Under Construction Sexual Risk Avoidance Education,” Journal of School Health, vol. 94, no. 8 (2024).
This study had limitations related to sample size and study design. See appendix I for more information.
[24]Students who did not receive SRAE received health or science curriculum that included information about conception and contraception, but little to no relationship education.
[25]These materials could include, but are not limited to, teacher and student manuals, handouts, video links, and brochures. ACF folded the SRAE programs into this process upon their creation, according to ACF officials.
[26]See GAO‑23‑105460. Coverage involves having evidence that covers all aspects of the key questions, relevant goal(s), and contributing strategies. Quality affects the conclusions that can be drawn from the evidence, and ultimately, how useful it is to decision makers. Various attributes can affect quality, including whether the evidence is accurate, complete, consistent, credible, rigorous, and timely.
[27]These information requirements applied to applications for fiscal year 2024 grant funding.
[28]The target populations states described may not have been the populations served.
[29]This data includes grantees from the Title V State SRAE, Title V Competitive SRAE, and General Departmental SRAE grant programs. The target populations were not necessarily the populations programs actually served. Target population categories are not mutually exclusive. Programs could target more than one population, and many did, so percentages can sum to more than 100 percent. “High-need geographic areas” refer to areas that experience higher than average youth birth or pregnancy rates or higher than average instances of youth STIs, according to ACF.
[30]In addition to ACF’s post-award monitoring activities, the HHS Office for Civil Rights—responsible for enforcing federal civil rights law and investigating complaints about potential violations—had not received any complaints about ACF’s SRAE grant programs, as of May 2025, according to HHS officials.
[31]See White House, Ending Radical and Wasteful Government DEI Programs and Preferencing, Executive Order 14151 (Washington D.C.; Jan. 20, 2025); and White House, Defending Women from Gender Ideology Extremism and Restoring Biological Truth to the Federal Government, Executive Order 14168 Washington D.C.; Jan. 20, 2025). According to Executive Order 14168, “‘[g]ender ideology’ replaces the biological category of sex with an ever-shifting concept of self-assessed gender identity, permitting the false claim that males can identify as and thus become women and vice versa, and requiring all institutions of society to regard this false claim as true. Gender ideology includes the idea that there is a vast spectrum of genders that are disconnected from one’s sex. Gender ideology is internally inconsistent, in that it diminishes sex as an identifiable or useful category but nevertheless maintains that it is possible for a person to be born in the wrong sexed body.”
[32]Additionally, ACF updated its standard terms and conditions, which apply to all awards administered by the agency. Those updated terms and conditions state that, by accepting an award, grantees are certifying that they do not, and will not during the term of the award, operate any programs that advance or promote diversity, equity, and inclusion.
[33]The states also challenged implementation of the Executive Order with respect to the Personal Responsibility Education Program. Washington v. HHS, No. 25-cv-01748 (D. Or. Sept. 26, 2025).
[34]The states that filed suit are Colorado, Connecticut, Delaware, the District of Columbia, Hawaii, Illinois, Maine, Maryland, Massachusetts, Michigan, Minnesota, New Jersey, New York, Oregon, Rhode Island, Washington, and Wisconsin.
[35]See 42 U.S.C. § 710(c)(1).
[36]ACF produced three briefs and one data snapshot from this study. See T. Neelan, D. DeLisle, and S. Zief, Launching a National Sexual Risk Avoidance Education Program: Title V State SRAE Program Plans, OPRE report no. 2022-90 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2022); T. Neelan, D. DeLisle, and S. Zief, The Title V Competitive and General Departmental Grantees’ Sexual Risk Avoidance Education Program Plans, OPRE report no. 2022-91 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2022); T. Neelan, D. DeLisle, and S. Zief, Sexual Risk Avoidance Education Programs: Preparing for and Supporting Program Implementation, OPRE report no. 2022-92 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2022); and T. Neelan, D. DeLisle, and S. Zief, Sexual Risk Avoidance Education Programs: Serving Youth in Out-of-Home Settings, OPRE report no. 2022-93 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2022).
[37]ACF published two reports from this study. See T. Neelan, B. Keating, L. M. Bryant, K. Hunter, E. Boyle, B. Starks, and S. Zief. The Sexual Risk Avoidance Education National Evaluation: Understanding Program Implementation Experiences, OPRE report no.2023-307 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2023); and H. Inanc, C. Jones, and E. Sama-Miller. Which Sexual Risk Avoidance Education Implementation Features and Provider Characteristics are Associated with Youth Outcomes?, OPRE report no. 2023-335 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2023).
[38]ACF published one report and a brief from this study. See L. Tingey, R. Piatt, A. Hennigar, C. O’Callahan, S. Weaver, and H. Zaveri, The Sexual Risk Avoidance Education National Evaluation: Using Co-regulation in Youth Programs, OPRE report no. 2023-281 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2023); and C. O’Callahan, L. Tingey, and H. Zaveri. The Sexual Risk Avoidance National Evaluation: Co-Regulation from the Perspective of Youth, OPRE brief no. 2023-276 (Washington, D.C.: Administration for Children and Families, Office of Planning, Research, and Evaluation, 2023).
[39]ACF chose to study the effectiveness of program components, such as co-regulation strategies, to increase the pool of potential grantee participants in the study, according to officials. Specifically, studying program components allowed more grantees to participate in ACF studies as opposed to requiring grantees to reorganize their programs around an ACF study.
[40]See Administration for Children and Families, Office of Planning, Research and Evaluation, Co-regulation in Action Video Series Tip Sheets, OPRE report no. 2023-306 (Washington, D.C.: 2023).
[41]ACF refers to this as its SRAE Performance Analysis Study.
[42]In addition, these surveys collect demographic information from youth through 41 performance measures.
[43]Some performance measures in the structure, cost, and support for program implementation and attendance, reach, and dosage groups may not be suitable for near-term goals because they are intended for grant management, such as “percentage of total SRAE grant funding obligated for evaluation and/or research.”
[44]See GAO‑23‑105460.
[45]For example, ACF is piloting near-term goals for measures addressing the percentage of teachers trained in delivering the selected curriculum or the percentage of funding obligated for the provision of the program.
[46]We limited our search to literature published in the last 10 years—from January 2015 through December 2024—to account for the beginning of the Administration for Children and Families’ SRAE program, which began in fiscal year 2016. We included 2015 in our search to ensure no relevant literature was missed.
[47]Two analysts independently read the abstracts and indicated whether they thought an abstract seemed relevant to our objective and therefore should move on to full-text review. Where there was disagreement, a third analyst served as tiebreaker.
[48]Four analysts each reviewed a set of articles to determine whether the content of the articles was relevant for our purposes. If an analyst was unsure of an article’s relevance, the team discussed it as a group. For articles deemed relevant, a methodologist then assisted in analyzing the articles.
[49]We define peer-reviewed articles as those that have gone through an evaluation process in which journal editors and other expert scholars critically assess the quality and scientific merit of the article and its research methods. Articles that pass this process are published in peer-reviewed journals.
[50]Fifty-seven of the abstracts and 26 of the studies we reviewed were identified through waterfalling.
[51]For example, studies that focused on health textbooks or did not discuss the effects of the education on youth outcomes or behavior.
[52]If a study was published in 2015 or later, but analyzed data from before 2015, the article was excluded from our review. If an article used a mix of data from before and after 2015, we included the article if more than half of the data was from 2015 or later. Fifty articles were excluded because they analyzed data from before 2015.
[53]If a study focused on populations aged 20 or older, but asked them about their experiences with sex education while they were 19 years or younger that occurred during or after the year 2015, we did not exclude the study.
[54]We classified whether a study discussed SRAE or abstinence-only sex education based on the study author’s own designation of the education.
[55]See K.L. Grasso and L.A. Trumbull, “Hey, Have You Been Tested? The Influence of Comprehensive or Abstinence-Only Sexuality Education on Safer Sex Communication and Behavior,” American Journal of Sexuality Education, vol. 16, no. 2 (2021): 257-281; and E.A. McKay, M. Placencio-Castro, M.R. Fu, and H.B. Fontenot, “Associations Between Sex Education Types and Sexual Behaviors Among Female Adolescents: a Secondary Data Analysis of the National Survey of Family Growth 2011-2019,” Sexuality Research and Social Policy, vol. 19 (2022): 922-935.
[56]See K.L. Grasso and L.A. Trumbull, “Hey, Have You Been Tested?; D. Mollen, E.M. Klann, M. Hinton, M. Vidican, and A. Romines, “Sex education among recent high school graduates,” Sexuality Research and Social Policy (2024); N.M. Caulfield, A.K Fergerson, M. Buerke, and D.W. Capron, “Considering the Impact of High School Sexual Education on Past Sexual Victimization and Rape Myth Acceptance in a College Sample,” Journal of Interpersonal Violence (2024): 1-17; and C.T. Chan, B.L. Olivieri-Mui, and K.H. Mayer, “Associations between State-Level High School HIV Education Policies and Adolescent HIV Risk Behaviors,” Journal of School Health, vol. 92, no. 3 (2022).
[57]See K.L. Grasso and L.A. Trumbull, “Hey, Have You Been Tested?
[58]See P.A. Burns, F. Teng, A.A. Omondi, E.T. Burton, and L. Ward, “Sex Education and Sexual Risk Behavior among Adolescents and Youth in the Deep South: Implications for Youth HIV Prevention,” The Southern Medical Association (2022).
[59]See D. Mata, A.K. Korpak, B.L. Sorensen, B. Dodge, B. Mustanski, and B.A. Feinstein, “A Mixed Methods Study of Sexuality Education Experiences and Preferences Among Bisexual, Pansexual, and Queer (Bi+) Male Youth,” Sexuality Research and Social Policy, vol. 19 (2022): 806-821.
[60]See S. Harris, C. Meier, J. Gast, L. Ward, and M. Ferguson, “Utah LGBQ + Youth Need Inclusive and Comprehensive Sex Education Opportunities: Results From the 2022 Utah College Retrospective Sexual Behavior Survey,” American Journal of Sexuality Education (2024).
[61]See D. Mata, A.K. Korpak, B.L. Sorensen, B. Dodge, B. Mustanski, and B.A. Feinstein, “A Mixed Methods Study of Sexuality Education Experiences and Preferences Among Bisexual, Pansexual, and Queer (Bi+) Male Youth,” Sexuality Research and Social Policy, vol. 19 (2022): 806-821.
Cisgender describes someone whose internal sense of gender corresponds with the sex the person was identified as having at birth.