Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
Contact: Rashmi Agarwal at agarwalr@gao.gov
What GAO Found
The Department of Defense’s (DOD) decisions to partner with civilian medical facilities to train military medical personnel for the battlefield are influenced by various factors that can support or hinder the use of partnerships, according to officials. One type of partnership that DOD can establish through an external resource sharing agreement allows active-duty providers to provide medical care to beneficiaries in civilian medical facilities within DOD’s network. Using these partnerships can reduce costs by avoiding certain professional fees and by keeping patient care within the network. However, DOD has not fully explored the benefits of increasing the use of these partnerships. Developing strategies to identify opportunities for using such agreements could ultimately help reduce costs, increase clinical readiness, and improve access to care.

The Defense Health Agency (DHA)—the combat support agency responsible for providing the necessary clinical workload to meet the military departments’ medical readiness requirements—does not know the total number of partnerships department-wide. DHA has taken some steps to inventory partnerships with civilian entities consistent with DOD policy to do so. However, these steps have been ad hoc and have not resulted in a complete or updated inventory. Without a standardized process for collecting information on partnerships for such an inventory, DHA has limited visibility of partnerships with civilian entities that can be used to provide additional readiness opportunities for its military medical personnel.
DOD also has not fully assessed the contributions of partnerships to clinical readiness. The military departments have implemented some efforts to collect clinical activity data to assess the clinical readiness opportunities provided by partnerships they established. However, each military department maintains partnerships that have not been fully assessed. Similarly, DHA does not have complete data needed to fully assess partnerships department-wide because it has not issued guidance for collecting complete clinical activity data. Without such guidance, DOD risks having less information to evaluate partnership performance and trading off opportunities to send personnel to a partnership for skills sustainment in lieu of them working in a DOD medical facility to provide beneficiary care.
Why GAO Did This Study
DOD has had a longstanding concern that some military medical personnel may not be prepared to provide lifesaving medical care on the battlefield. To address this issue, DOD has, among other things, established partnerships with civilian trauma centers and other medical facilities to provide opportunities for training its military medical personnel.
Committee reports accompanying bills for the National Defense Authorization Act for Fiscal Year 2024 include provisions for GAO to assess DOD’s partnerships. This report examines (1) the factors influencing DOD’s decisions to use a partnership and efforts to reduce health care costs; (2) DHA’s inventory of partnerships; and (3) DOD’s assessment of partnership contributions to the readiness of its medical personnel.
GAO reviewed DOD guidance and documentation and analyzed timecard and readiness data, where available, from fiscal year 2020 through fiscal year 2024. GAO also interviewed DOD officials, including officials from seven medical facilities selected based on military department affiliation and size, as well as officials from civilian partners.
What GAO Recommends
GAO is making nine recommendations, including that DOD develop strategies to identify opportunities for reducing costs while increasing readiness through partnerships established by external resource sharing agreements; develop processes to inventory partnerships; and fully assess the readiness contributions of its partnerships. DOD concurred with seven recommendations and partially concurred with two recommendations. GAO believes all recommendations are sound and should be fully addressed.
|
Abbreviations |
|
|
|
|
|
BUMED |
Bureau of Medicine and Surgery |
|
DHA |
Defense Health Agency |
|
DOD |
Department of Defense |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
Congressional Committees
The Department of Defense’s (DOD) military health system exists to ensure that military medical personnel are prepared to provide medical care in support of missions that include operational, wartime, and mass casualty events, which is referred to as clinical readiness.[1] DOD relies on almost 107,000 active-duty personnel to provide both operational medical care in support of war and other contingencies and, with the help of DOD civilians and contractors, health care to eligible beneficiaries.[2] To that end, in peacetime and wartime, DOD’s military medical personnel deliver health care to service members and other beneficiaries entitled by law at DOD’s clinics, hospitals, and medical centers—referred to collectively as military medical treatment facilities (medical facilities).[3] These facilities are training venues for military medical personnel to develop, improve, and sustain their skills. Moreover, in wartime, the facilities provide health care to injured service members. DOD projected that the delivery of health care through its medical facilities in fiscal year 2026 will cost more than $10.7 billion.[4]
DOD, the Senate Armed Services Committee, and others have had a longstanding concern that DOD’s medical facilities may not be able to provide sufficient opportunities to sustain the skills of certain medical professionals—such as surgeons, emergency medicine physicians, combat medics, and those providing trauma and critical care services.[5] Specifically, there is concern that DOD medical facilities do not adequately expose such personnel to a high volume of critical injuries, leaving them unprepared to treat casualties and provide lifesaving medical care on the battlefield. To address these concerns, DOD has pursued additional skills sustainment opportunities for its military medical personnel, including providing care to civilian emergency patients at its medical facilities.[6] In addition, DOD has established partnerships with civilian trauma centers, civilian hospitals, and other civilian medical organizations (civilian partners) to care for patients, including patients with injuries resembling those treated through battlefield medicine.[7]
The annual National Defense Authorization Acts enacted throughout the past decade have mandated numerous military health system reforms. These reforms were intended to enhance access to health care, increase the operational readiness of military medical personnel, and lower the per capita costs of health care, according to a Senate Armed Services Committee report.[8] For example, section 707 of the National Defense Authorization Act for Fiscal Year 2017 directed the establishment of the Joint Trauma System to improve trauma care and outcomes.[9] This act also directed the Secretary of Defense to establish the Joint Trauma Education and Training Directorate to ensure that DOD’s traumatologists maintain readiness and are able to be rapidly deployed for future armed conflicts.[10] Additionally, the Secretary of Defense was authorized to partner with civilian academic medical centers and trauma centers.[11]
We have reported on DOD’s planning and implementation of some of these reforms. For example, in 2019 we reported that DOD’s methodology for assessing the clinical readiness of its providers was limited because DOD did not use complete, accurate, and consistent data that fully demonstrated results, and we made a recommendation to improve the methodology.[12] Moreover, in June 2021 we reported that the Defense Health Agency (DHA)—the combat support agency responsible for management of the TRICARE Program and oversight of DOD’s medical facilities—did not have a process to streamline or add new partnerships and recommended that the Secretary of Defense ensure that the DHA Director establish such a process.[13]
Committee reports accompanying bills for the National Defense Authorization Act for Fiscal Year 2024 included provisions for us to assess DOD’s partnerships with civilian partners and the extent to which they provide clinical readiness.[14] This report (1) describes the factors influencing DOD’s decisions to use partnerships and evaluates the extent to which it has identified opportunities to reduce health care costs; (2) evaluates the extent to which DHA maintains an inventory of partnerships and tracks the participation of its military medical facility personnel; and (3) evaluates the extent to which DOD assesses the contributions of its partnerships to the readiness of military medical personnel.
For each of our objectives, we interviewed officials from the Office of the Assistant Secretary of Defense for Health Affairs, DHA, and each of the military departments (Army, Navy, and Air Force). We also interviewed officials from a non-generalizable selection of seven DOD medical facilities that maintain one or more partnerships. We selected these medical facilities to provide variation across military department affiliation and size.[15] We also used data found in DHA’s readiness dashboards to make our selections.[16] Furthermore, we interviewed representatives from a non-generalizable selection of three civilian partners, each in a partnership that has been established by one of the military departments’ medical headquarters organizations or a training organization. We selected the civilian partners that provided the most readiness opportunities, according to DHA’s readiness dashboards.[17] Finally, we interviewed officials from five operational units or commands who participate in partnerships with civilian medical facilities.[18]
For our first objective, we identified factors DOD considers when deciding to partner with civilian medical facilities through our review of DOD documentation, such as relevant reports and studies conducted by DOD, which included information on factors influencing the use of partnerships. We identified DOD studies and reports through our interviews with knowledgeable DOD officials. We interviewed DOD officials to obtain their perspectives on factors influencing the use of partnerships. In addition, we reviewed DOD documentation and interviewed officials to identify ways DOD used partnerships to reduce health care costs. We compared DOD’s efforts to applicable law and DOD guidance.[19]
For our second objective, we reviewed DHA and military department documentation regarding their methods to identify and inventory partnerships. We reviewed department-wide inventories developed from October 2020 through June 2025, the most recent inventory established at the time of our review. We evaluated DOD’s efforts to inventory partnerships against DOD guidance and Standards for Internal Control in the Federal Government.[20] Specifically, we reviewed the internal control components of monitoring and control activities, along with the underlying principles that management should remediate identified internal control deficiencies on a timely basis and implement control activities through policies. We reviewed inventories for completeness by checking key fields for missing data and inclusion of known partnerships in the inventories. In addition, we interviewed DHA and military department officials to understand steps taken to maintain a complete and current inventory of partnerships. We determined that the data in the inventories were not complete and therefore not reliable to report on the total number of partnerships. As a result, we could not use the information to report on the total number of partnerships DOD has established, but we report on the number of partnerships DOD identified as of June 2025.
To examine the extent to which DHA tracks the use of its military medical personnel assigned to DOD medical facilities and participate in partnerships, we reviewed DOD documentation regarding approaches to track this information. We also interviewed officials from DHA and DOD medical facilities to identify approaches used to track the amount of time military medical personnel who are assigned to a DOD medical facility spend at partnerships. We reviewed data from DHA’s timecard system from fiscal year 2020 through fiscal year 2024—the last available full fiscal year of data at the time of our review—to identify the extent to which military medical personnel assigned to a DOD medical facility report their time at a partnership.[21] We met with DHA officials to discuss the accuracy and completeness of DHA’s timecard data. We determined the timecard data were sufficiently reliable to report on the number of military medical personnel who reported time at a partnership in DHA’s timecard system and the hours those individuals reported by type of occupation and partnership from fiscal year 2020 through fiscal year 2024 by conducting logic checks on the data and interviewing DHA officials.
To determine the completeness of timecard data in DHA’s timecard system for reporting participation at a partnership from May 2024 through April 2025, we compared DHA timecard data to clinical activity data in DHA’s readiness dashboards for clinical activities reported at a partnership for the same period. We used this comparison to identify the extent to which individuals had clinical activities from a partnership reported in DHA’s readiness dashboards but did not record hours spent at a partnership in DHA’s timecard data. We selected this time frame because it was the most recent 12-month period of data from both DHA’s timecard data and readiness dashboards available at the time of our review.
For our third objective, we reviewed documentation from the military departments regarding their efforts to collect clinical activity data for personnel participating in military-civilian partnerships.[22] We also interviewed officials from the military departments regarding these efforts. Furthermore, we reviewed DHA documentation regarding its processes to collect data on clinical activities completed in partnerships. To identify the extent to which DHA captured clinical activity data in its readiness dashboards for all personnel who recorded clinical activities performed in a partnership from December 2021 through April 2025, the most recent data available at the time of our review, we analyzed data from DHA’s readiness dashboards.[23] We determined that the clinical activity data were sufficiently reliable to report on the number of military medical personnel who had clinical activity data from a partnership captured in DHA’s readiness dashboards by occupation type from December 2021 through April 2025 by conducting logic checks on the data and interviewing DHA officials.
To determine the completeness of clinical activity data in DHA’s readiness dashboards, which present a 12-month period, we consolidated data for all personnel who recorded clinical activities performed in a partnership from May 2024 through April 2025. We selected this time frame because it was the most recent 12-month period of data available from both DHA’s timecard data and readiness dashboards available at the time of our review. We compared clinical activity data with self-reported DHA timecard data for individuals who reported participating in a partnership during the same period for 40 or more hours to identify personnel who reported working in a partnership in their timecard data but had no corresponding clinical activity data in DHA’s readiness dashboards.[24]
Furthermore, we reviewed DOD guidance to determine if it addresses the submission of complete clinical activity data to DHA for its readiness dashboards. To perform this analysis, an analyst reviewed DOD guidance to determine if submissions from various partnership types were addressed. Subsequently, another analyst reviewed these determinations to confirm them. We also reviewed military department and DHA documentation demonstrating their efforts to assess their partnerships. Finally, we interviewed military department and DHA officials regarding their efforts to assess their partnerships’ contributions to military medical personnel’s readiness. We compared the efforts of the military departments and DHA to assess the readiness contributions of partnerships with DOD guidance and Standards for Internal Control in the Federal Government.[25] Specifically, we reviewed the internal control component of monitoring along with the underlying principle that management should establish and operate monitoring activities to monitor its internal control system and evaluate the results.
We conducted this performance audit from July 2024 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
Roles and Responsibilities in Military Health System
According to DOD policy, the department will support the critical wartime medical readiness skills and core competencies of health care providers within the military services. To that end, the department will prioritize medical services provided at its medical facilities and establish partnerships when skills cannot be maintained within these facilities. Responsibility for ensuring the readiness of DOD’s medical personnel is shared among DHA and the military departments—Army, Navy, and Air Force—with the Office of the Secretary of Defense providing oversight.
· Under Secretary of Defense for Personnel and Readiness is the principal staff assistant and advisor to the Secretary of Defense for health-related matters. The Under Secretary is responsible for developing policies, plans, and programs for health and medical affairs to provide and maintain readiness.[26]
· Assistant Secretary of Defense for Health Affairs serves as the principal advisor to the Under Secretary of Defense for Personnel and Readiness for all DOD health-related policies, programs, and activities.[27] The Assistant Secretary has the authority to develop policies; conduct analyses; issue guidance; provide advice and make recommendations to the Secretary of Defense, the Under Secretary of Defense for Personnel and Readiness, and others; and provide oversight on matters concerning the military health system.[28] Furthermore, the Assistant Secretary, in coordination with the Secretaries of the military departments, is responsible for developing policy for DOD’s medical facilities to support the military departments in maintaining critical wartime medical skills.[29] The Assistant Secretary is also responsible for developing a unified medical program budget for the military health system.
· Director of DHA functions under the authority, direction, and control of the Assistant Secretary of Defense for Health Affairs. The Director’s responsibilities include management of the TRICARE Program and DOD’s medical facilities, as well as management and execution of the Defense Health Program appropriation.[30] In managing DOD’s medical facilities, the Director is responsible for providing the necessary clinical workload to meet the military departments’ medical readiness requirements. Moreover, in December 2016, Congress expanded the role of DHA by transferring responsibility for the administration of each DOD medical facility from the military departments to DHA.[31] When necessary and appropriate, the Director is responsible for establishing partnerships to provide venues and opportunities for military medical personnel staffed at DOD medical facilities to maintain clinical readiness.[32] Finally, the Director is responsible for maintaining a registry of partnerships and, in conjunction with the military departments, for establishing performance metrics to assess them.[33] The Director delegates responsibilities to DOD medical facility directors to execute and approve these partnerships.[34]
· Secretaries of the military departments have the authority and responsibility under title 10 of the United States Code to organize, train, and equip military forces.[35] The military departments seek to develop and maintain readiness for medical personnel through placement—primarily by assignment—of medical personnel at DOD’s medical facilities, where they deliver care to service members and their beneficiaries. The military departments also assign personnel to positions at partnerships to maintain their clinical readiness.
Each military department maintains one or more medical headquarters organizations, which are responsible for developing and maintaining the readiness of medical personnel. These organizations include the U.S. Army Medical Command, Navy Bureau of Medicine and Surgery (BUMED), and Air Force Medical Command. The Surgeon General of each respective military department leads its medical organization and serves as the principal advisor to the Secretary of the military department concerning all health and medical matters of the military department.
DOD Medical Facilities
DOD estimated that it would maintain 725 medical facilities—570 medical clinics, 109 dental clinics, and 46 inpatient hospitals and medical centers—in fiscal year 2026.[36] Based on data provided by DHA officials, DOD maintains one Level I, four Level II, six Level III, and one Level IV trauma centers as of December 2025.[37] According to DOD Instruction 6000.19, the primary purpose of DOD’s medical facilities is to support the readiness of the military services. In particular, the instruction states that the size, type, and location of DOD’s facilities must further this readiness objective. Moreover, each DOD medical facility must spend most of its resources supporting wartime skills, development and maintenance for military medical personnel, or the medical evaluation and treatment of service members.
DOD medical facilities serve as training and readiness platforms for active-duty medical personnel. For example, multiple DOD medical facilities host graduate medical and dental education programs for physicians and dentists and other training and education programs for DOD medical personnel, including those that train physician assistants, nurses, and enlisted technicians. Moreover, day-to-day patient care at DOD medical facilities helps maintain the clinical skills and readiness of DOD medical personnel.
In fiscal year 2023, of DOD’s approximately 107,000 active-duty medical personnel, over 50,000 were assigned to DOD’s medical facilities.[38] Within DOD’s medical facilities, DOD’s medical personnel provide health care to eligible beneficiaries, including active-duty personnel and their dependents (i.e., spouses and children); certain Reserve and National Guard personnel and their dependents; and retirees and their dependents and survivors. DOD Instruction 6000.19 states that medical services provided at medical facilities should be prioritized to sustain the medical skills of its personnel. However, when skills cannot be maintained within its facilities, the instruction states that it will establish partnerships that provide venues and opportunities for military medical personnel to sustain skills associated with their medical specialty or community.
Types of Partnerships
In general, DOD maintains two types of partnerships with civilian organizations that can provide skills sustainment for medical personnel:[39]
· Military-civilian partnerships enable military personnel to go to civilian medical facilities to care for civilian patients for purposes of skills sustainment. They are developed through training agreements, such as training affiliation agreements, memorandums of understanding, and medical training agreements. Per DOD policy, military-civilian partnerships are established when skills cannot be maintained within its medical facilities.[40] Moreover, these partnerships provide venues and opportunities for military medical personnel to obtain and maintain currency in clinical knowledge, skills, and abilities. Civilian partners range from university hospital systems with Level I trauma centers, which expose DOD’s emergency medicine physicians and trauma surgeons to complex cases, to local ambulance services that provide DOD’s medics with experiences providing pre-hospital care. The military departments have established these partnerships through their medical headquarters organizations or other organizations, such as the Office of the Army Surgeon General and the Air Force’s 711th Human Performance Wing’s U.S. Air Force School of Aerospace Medicine.[41] Additionally, operational units and commands have established partnerships for their assigned personnel, while DOD medical facilities have also established such partnerships.
· External resource sharing agreements establish partnerships that enable medical personnel to go to TRICARE network facilities to care for TRICARE beneficiaries. DOD is authorized to enter into external resource sharing agreements with TRICARE network facilities—including hospitals, clinics, and other facilities.[42] External resource sharing agreements are established on an ad hoc basis by DOD medical facility leadership in coordination with TRICARE and local civilian medical facilities to deliver health care.
Per DOD guidance, the purpose of external resource sharing agreements is to enable military medical personnel to provide covered medical services to active-duty and TRICARE beneficiaries in a facility within the TRICARE network.[43] According to DOD officials, while primarily supporting timely beneficiary care, these types of partnerships also provide opportunities for clinical readiness as a secondary benefit. According to DOD officials, participation in partnerships established by external resource sharing agreements is typically limited to physicians, although support staff, such as nurses and enlisted medical personnel, may participate in limited circumstances.
DOD medical personnel participating in a partnership are working on either a full-time, part-time, or rotating basis:[44]
· Full-time personnel (i.e., embedded personnel) are stationed at a civilian medical facility on a full-time basis per permanent change of station orders. This arrangement is ideal for DOD medical personnel with a significant requirement for trauma/critical care expertise (e.g., operational surgical teams).
· Part-time personnel are stationed at a DOD medical facility and spend part of their time at a civilian medical facility.
· Rotating personnel (i.e., rotators) rotate through civilian trauma centers on short temporary duty training assignments generally lasting 2 to 3 weeks. These programs are often referred to as “just-in-time” arrangements because personnel generally rotate through the trauma centers in preparation for a coming deployment to refresh, or in some cases, demonstrate specific skills.
Mission Zero Act Program
The Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 authorized establishment of a program—commonly referred to as the Mission Zero Act Program—to award grants to civilian trauma centers with the goal of enabling military trauma providers to provide trauma care and related acute care at such trauma centers.[45] Through this program, the Secretary of the Department of Health and Human Services, acting through the Assistant Secretary for Preparedness and Response and in consultation with the Secretary of Defense, awards Mission Zero Act Program grants subject to the availability of funds.[46] This integration involves sending military medical personnel to gain experience in civilian trauma centers with the purposes of maintaining their skills for deployment and improving the nation’s response to public health and medical emergencies.
Grantees may use funds to train and incorporate military trauma care providers into their trauma centers, including incorporation into operational exercises and training drills related to public health emergencies, expenditures for malpractice insurance, office space, information technology, specialty education and supervision, trauma programs, research, and applicable license fees for providers. To be eligible for a grant, civilian trauma centers must have a preexisting agreement with DOD.
Starting in fiscal year 2022, 25 military-civilian partnerships—many of which were established by the military departments—began receiving Mission Zero Act Program funding. For fiscal years 2022 through 2025, grant funding for these partnerships totaled approximately $13.6 million. Starting in fiscal year 2023, grantees received funding amounts that differed, based on the nature of the training. For example, in fiscal year 2025, 11 team-based partnerships were awarded about $204,300 each; eight individual-based partnerships with more than five military medical providers were awarded about $117,900 each; and six partnerships that had less than five military medical providers were awarded about $68,400 each.
DOD Considers Various Factors for Using Partnerships but Has Not Fully Identified Opportunities to Reduce Health Care Costs Through Them
DOD Cites Clinical Sustainment and Staffing Needs Among Influential Factors
Several factors influence whether DOD sends its personnel to military-civilian partnerships and partnerships established by external resource sharing agreements, according to DOD documentation and officials we interviewed. Specifically, officials stated that factors such as clinical sustainment needs of military medical personnel and beneficiary care needs support their decision for using a partnership. However, other factors such as staffing needs of the DOD medical facility and administrative and financial barriers may hinder DOD from entering into or sending personnel to a partnership (see fig. 1).

Note: For purposes of this report, “partnerships” refers to (1) partnerships at civilian medical facilities established through training agreements, training affiliation agreements, memorandums of understanding, or medical training agreements that are used for maintaining and sustaining the clinical skills and readiness of DOD medical personnel; and (2) partnerships at TRICARE facilities established by external resource sharing agreements that are used to provide additional opportunities for military medical personnel to care for beneficiaries.
Supporting Factors
|
Partnerships Can Increase Medical Personnel Satisfaction and Improve Recruitment and Retention According to Department of Defense (DOD) officials, military-civilian partnerships provide opportunities for increased satisfaction for its military medical personnel. Officials noted that this increased satisfaction is a result of providing opportunities for personnel to fully practice what they have trained for as well as to contribute to journal articles and research at academic civilian centers. For example, officials noted that the partnership opportunity has reenergized medical professionals and recommitted them to continue practicing military medicine. However, several DOD officials noted that while exposure to practicing at a civilian facility often provides a positive experience, it can make it easier to transition to the private sector once an individual’s active-duty commitment obligation has been met. Officials also noted that partnerships can help with recruitment, noting that partnerships exposed civilians working at a civilian hospital to military medicine. Source: GAO analysis of DOD interviews. | GAO‑26‑107677 |
Clinical sustainment. According to DOD documentation and DHA and DOD medical facility officials, DOD’s medical facilities do not always provide the clinical opportunities needed by certain medical specialties to meet clinical readiness metrics.[47] DOD officials stated that civilian partners play a critical role in providing opportunities that help meet these metrics. Moreover, according to DHA, military department, and DOD medical facility officials, partnerships enable military medical personnel to have opportunities to treat a high volume of high-acuity patients.
Furthermore, DOD officials noted that military-civilian partnerships with civilian trauma centers provide their workforce exposure to penetrating trauma (such as gunshot or stab wounds) and burn cases, which typically are not seen at DOD’s medical facilities. Such cases are particularly useful for training purposes as they more closely approximate battlefield injuries, according to DOD officials. Some military-civilian partnerships provide training opportunities for military members to train as a team at a trauma center. For example, one civilian partner we reviewed noted that while participants are not always working together at the civilian facility, there are set times for them to work as a team. Officials noted that caring for trauma patients as a team ideally allows for the surgeon, nurse, medic, and others to train together in complex and diverse cases they would not normally encounter at a DOD medical facility.
In addition, according to DOD and civilian partner officials, military-civilian partnerships benefit both the military and civilian medical communities and better position DOD to respond when emergencies, natural disasters, or pandemics require military and civilian medical personnel to work together. For one of the military-civilian partnerships we reviewed, military medical personnel worked with the civilian trauma staff responding to a 2017 mass casualty shooting that occurred in Las Vegas, Nevada.
Moreover, DOD medical facility officials noted that partnerships provide the opportunities needed by certain licensed medical specialties—such as surgical specialties—to maintain their professional qualifications, retain clinical licensure, and fulfill board certification requirements. For example, one DOD medical facility was exploring ways to send its pediatric intensive care unit nurse to a civilian facility to maintain her license since the facility did not have such a unit. The official noted that it would be more practical to send her to a local civilian partner rather than another DOD medical facility because the civilian facility is physically closer.
Officials noted that partnerships provide opportunities for increased satisfaction for military medical personnel and improve recruitment and retention. A 2024 study sponsored by DOD noted that partnerships could improve retention by reducing the concern over degradation of skills and improve recruitment by presenting an attractive set of possible places to work.[48]
Beneficiary care needs. DOD uses external resource sharing agreements to improve health care access for its beneficiaries. External resource sharing agreements allow active-duty physicians and, to a limited extent, support staff such as nurses to provide care to DOD beneficiaries at civilian hospitals when resources are not available at a DOD medical facility. These types of partnerships with civilian medical facilities minimize disruption for patients and provide a continuity of care. DOD medical facility officials noted that prompt care is especially important for service members as it minimizes their time away from duty. Based on our review of DHA’s timecard data from fiscal year 2020 through fiscal year 2024, family practice, obstetrics/gynecology, orthopedic surgery, general surgery, and otorhinolaryngology were among the top five physician specialties reporting hours spent at partnerships established through an external resource sharing agreement.[49]
Hindering Factors
Staffing needs. In July 2025, we reported on staffing at DOD’s medical facilities and noted that DOD faces staffing challenges at its medical facilities.[50] Accordingly, staffing needs of DOD’s medical facilities may hinder the department’s ability to use partnerships to sustain military medical personnel’s clinical skills. According to DOD medical facility officials, military medical personnel assigned to a DOD medical facility will not typically be sent to a partnership if it adversely affects staffing at the medical facility, particularly when a facility is already operating at low staffing numbers. For example, officials from one medical facility we spoke with noted that they have not used their partnership with a local civilian hospital for the past 7 months because their medical facility was not fully staffed. Officials noted that careful planning is needed to minimize adverse effects on the medical facility due to personnel participating in the partnership.
Administrative and financial barriers. According to DOD officials, establishing partnership agreements, meeting state licensure requirements, and identifying funding for expenses are hindering factors that can delay or prevent partnerships from forming.
· Establishing partnership agreements. DOD medical facility officials noted that the process for establishing a partnership can be burdensome. For example, DHA guidance states that when establishing military-civilian partnership agreements, DOD medical facilities must make every effort for military health care providers to be covered under the civilian facilities’ medical professional liability coverage (i.e., malpractice insurance).[51] However, if the civilian partner will not provide such coverage, DHA’s training agreement template states that the agreement should instead reference the Federal Tort Claims Act[52] and specify that military health care providers will be fully under the supervision of the training institution.[53] Additionally, these agreements must be sent to DHA to approve the waiving of malpractice insurance, which can delay the establishment of the partnership for several months, according to DOD officials.[54] Moreover, according to DOD officials, failure to successfully negotiate these terms may prevent a partnership from being established. Unlike partnerships established by DOD medical facilities, partnerships established by the military departments are not subject to these restrictions.[55] Military department officials noted that coordination with the universities and hospitals takes time to successfully navigate.
· Meeting state licensure and other requirements. Federal law allows military medical personnel to practice their profession in any state or territory, regardless of location, if it is within the scope of their authorized federal duties at a DOD medical facility.[56] However, this authority does not apply when military medical personnel participate in a partnership at a civilian facility. DOD officials noted that licensing requirements vary by state and can delay individual military medical personnel from being able to participate in a partnership. Similarly, officials noted that careful planning is needed to ensure that individuals are privileged to work at the facility in order to fully participate.[57] For example, one facility noted that during the first rotation at one partnership, the surgeons were unable to provide hands-on care and instead observed the care that was provided due to not having the proper privileges.
· Identifying funding for expenses. According to DOD officials, the cost of sending its medical workforce to a partnership can vary. Beyond the loss of personnel who would otherwise be working in the medical facility, some partnerships have minimal cost to DOD, according to DOD medical facility officials. For example, medical facility officials at an Army clinic noted that their partnership with a local civilian hospital did not incur additional costs for DOD because the civilian hospital is in proximity and parking is free. However, some partnerships do incur costs for DOD, such as travel to the partnership, parking, lodging, and administrative support, according to DOD officials. DOD officials noted that high costs due to the high cost of living can be a barrier.[58]
According to DOD officials, funding for partnership expenses is not always planned for or prioritized, making it difficult to identify funding. In these instances, officials stated that lack of funding can delay sending military medical personnel to the partnership and cause service members to pay out of pocket for certain expenses incurred, such as parking. Three civilian partners we spoke to who received a Mission Zero Act Program grant noted that the funding has helped offset the cost of the partnership as well as provided funding for additional training opportunities and administrative support. According to DOD officials, having administrative support for collecting data and navigating licensure requirements, among other things, has helped with the success of the partnerships.
DOD Has Not Fully Identified Opportunities to Reduce Overall Health Care Costs
DOD has not fully identified how some partnerships—specifically partnerships established by external resource sharing agreements—can reduce health care costs while also providing increased readiness opportunities. External resource sharing agreements are used by DOD medical facilities to allow active-duty providers to treat beneficiaries in TRICARE network facilities. Officials noted that these agreements are used when the needed resources are not available at a DOD medical facility. According to DOD officials, the local DOD medical facility leadership typically decides whether to use an external resource sharing agreement.
As noted earlier, while the purpose of partnerships established by external resource sharing agreements is to provide patient care to beneficiaries, these partnerships can provide military medical personnel readiness opportunities. For example, if a military surgeon determines that a patient needs surgery but does not have an operating room available at the DOD medical facility, then an external resource sharing agreement with a TRICARE network facility would allow the military surgeon to perform the surgery at the local hospital in lieu of referring the patient to a civilian surgeon at a TRICARE network facility. External resource sharing agreements do not typically provide any direct readiness training opportunities for support staff (registered nurses, medics, enlisted technicians, etc.) because the TRICARE network facility typically relies on their own support staff, according to DOD officials. However, according to DOD officials, using external resource sharing agreements keeps patient care within DOD’s network, which means that outpatient follow-up care is administered at DOD medical facilities, thus providing the potential for additional readiness opportunities for support staff for post-surgery care.
Moreover, using external resource sharing agreements has the potential to reduce health care costs for DOD, allowing its providers to perform procedures that they otherwise would be unable to perform at DOD medical facilities.[59] In a September 2022 DOD report, DOD stated that external resource sharing agreements allow DOD medical facility personnel to care for TRICARE beneficiaries at TRICARE network facilities and reduce total costs through the arrangement with the TRICARE network facility.[60] For example, in such an arrangement, DOD would pay for the TRICARE network facilities’ space, support staff, and supplies, but the department would not have to pay for the provider’s work time. As a result, by leveraging the external resource sharing agreement, the total billed to TRICARE for each procedure is reduced. Furthermore, officials noted that once beneficiaries are referred to the TRICARE network, it can be challenging to return them to a DOD medical facility (e.g., for post-surgery care), which ultimately leads to increased TRICARE costs.
DOD recognizes that using partnerships established by external resource sharing agreements has associated cost savings and cost avoidance, but actual cost savings and cost avoidance obtained through these agreements are not routinely tracked, according to officials. Instead, according to DHA officials, the DOD medical facility is expected to complete a business case analysis for each external resource sharing agreement. The business case analysis will identify the expected costs that will be saved (or avoided) at the time the agreement is established. For example, according to a business case analysis for an external resource sharing agreement that was provided by one of the DOD medical facilities we selected, the facility estimated cost avoidance of about $1.2 million per year in professional fees (provider work time) being charged.
DOD is authorized to enter into agreements to establish military-civilian integrated health delivery systems.[61] Specifically, section 706 of the National Defense Authorization Act for Fiscal Year 2017 requires DOD to establish partnerships in order to improve access to health care for covered beneficiaries; to enhance the experience of covered beneficiaries in receiving health care; to improve health outcomes for covered beneficiaries; to maintain services within DOD medical facilities; and to provide military medical personnel with additional training opportunities to maintain readiness skills, among other reasons. Moreover, according to DOD Instruction 6000.19, partnerships should be used when skills cannot be maintained within DOD’s medical facilities. Furthermore, according to DOD Instruction 6000.19, DHA should identify to the military departments opportunities for streamlining and adding partnerships as needed. In its September 2022 report, DOD further noted the need for an integrated, learning health care system that balances the requirement for accessible, high-quality care for TRICARE beneficiaries with hospital-based readiness training platforms for its military medical personnel.[62] Moreover, the report asserted that an integrated military-civilian health care delivery system can leverage bidirectional resource sharing that achieves the goals of improved readiness, better health for patients, a better care experience for both patients and providers, and reduced per capita cost.
DHA officials told us that they have made efforts to look for viable ways to use partnerships established by external resource sharing agreements. In accordance with their most recent TRICARE contracts (which started health care delivery in 2025), TRICARE network facilities can support the readiness mission by partnering with DOD medical facilities to enhance the clinical expertise of providers, according to DHA officials. DHA officials noted another effort includes medical residents—in addition to fully trained physicians—in external resource sharing agreements. DHA officials noted that including medical residents in external resource sharing agreements has reduced health care costs, promoted continuity of care, provided training on vital equipment not available at the DOD medical facilities, and helped medical residents complete mandatory surgical training.
Partnerships established by external resource sharing agreements have the potential to provide opportunities for additional readiness training. However, DHA officials noted that they have not fully developed or implemented department-wide strategies for identifying opportunities to lower health care costs and increase readiness through these agreements. Such a strategy could include reviewing where beneficiaries are being most frequently referred to the TRICARE network and using external resource sharing agreements to avoid loss of care to the network and increase readiness where it is needed, while also ensuring military medical personnel are available to participate in partnerships established by external resource sharing agreements. According to a senior Military-Civilian Partnership Working Group official, instead of exploring how to leverage external resource sharing agreements for readiness opportunities, the working group prioritized efforts on military-civilian partnerships for readiness opportunities and has no visibility of or involvement with partnerships established by external resource sharing agreements.[63] The official said there are limitations with external resource sharing agreements, such as lack of opportunity for certain specialties (e.g., emergency medicine physicians) to participate.
According to DHA officials, external resource sharing agreements have traditionally been used to improve continuity of care by allowing military providers to perform needed medical procedures on their existing patients, to maintain military medical personnel skill sets on equipment not available at the DOD medical facility, or to provide workarounds for shortages of staff or equipment at DOD medical facilities. For example, according to DOD medical facility officials from a DOD clinic that we met with, the clinic uses an external resource sharing agreement to allow its assigned orthopedic surgeons to perform procedures at the civilian facility since the DOD medical facility downsized from a hospital to a clinic and does not have the resources needed to provide surgery to active-duty patients.
The Congressional Budget Office projects that military health system costs will grow from $60 billion in 2025 to $74 billion in 2039.[64] Developing strategies to systematically identify additional opportunities to use partnerships established by external resource sharing agreements would help ensure that sharing opportunities are identified and optimized. Implementing such strategies could ultimately improve patients’ access to care, reduce costs, and increase readiness.
DHA Has Not Fully Inventoried DOD’s Partnerships or Tracked Its Medical Facility Personnel Participation
DHA Has Not Completed and Regularly Updated Its Inventory of DOD’s Partnerships
DHA has taken some steps to inventory partnerships, but it does not have a complete inventory or a process to ensure that a departmentwide inventory is complete and regularly updated. In June 2021, we found that DHA had not yet fully developed an inventory of partnerships in which enlisted medical personnel participate.[65] We recommended that DHA establish such an inventory. DOD concurred with this recommendation and has taken some steps toward addressing it. However, these efforts have been ad hoc and varied in the types of partnerships included in the inventory. For example, DHA’s 2022 inventory of partnerships was limited to DOD medical facility partnerships, and DHA’s most recent two efforts in 2024 and 2025 were based on partnerships identified by the military departments (see fig. 2).
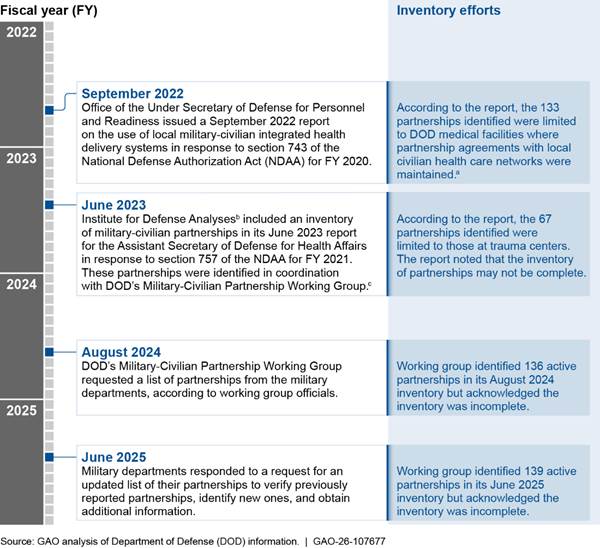
Note: DOD Instruction 6000.19 directs the Defense Health Agency (DHA) to maintain a comprehensive registry of partnerships and directs the military departments to report to DHA on their established partnerships. This figure includes department-wide efforts and does not include individual efforts made by military departments or other organizations. A civilian partner may have more than one military partner, and there may be multiple agreements between a military and civilian partner. For example, there may be agreements for each specialty participating in the partnership. For purposes of our analysis of the department-wide inventory, we defined a partnership as having a military and civilian partner with one or more partnership agreements.
aThe report includes partnerships for both clinical skills and readiness and/or graduate medical education. We were unable to determine the number of partnerships that were used solely for clinical skills and readiness.
bThe Institute for Defense Analyses is a federally funded research and development center sponsored by DOD. According to the institute, its mission is to answer the most challenging U.S. security and science policy questions with objective analysis by leveraging extraordinary scientific, technical, and analytic expertise.
cThe Military-Civilian Partnership Working Group was formed to, according to its charter, provide opportunities among the military departments, DHA, and other key supporting entities in and outside of the military health system to facilitate communications and develop recommendations for identifying, selecting, maintaining, and enabling partnerships. One responsibility includes maintaining the partnership registry.
In 2023 the Military-Civilian Partnership Working Group took the initiative to create an inventory of partnerships, according to working group officials. As part of this initiative, the working group requested a list of partnerships from the military departments and collated these submissions into a consolidated list, according to working group officials. This inventory was updated in 2024 and 2025 by requesting updated information from the military departments, according to working group officials. According to these officials, partnership information was requested from the military departments as part of their outreach, and they did not request such information from DOD medical facility directors and others who may have individually established a partnership. As a result, based on our review of the working group’s 2024 and 2025 inventories, none have resulted in a complete or current inventory of partnerships. According to a Military-Civilian Partnership Working Group official, as of December 2025, its inventory of partnerships has not been updated since June 2025.
According to military department officials, the military departments have not routinely and accurately inventoried all partnerships within their respective military departments. Instead, organizations within each military department track the partnerships they establish, according to military department officials. Moreover, changes in the administration and management of DOD’s medical facilities have resulted in shifting responsibilities for overseeing partnerships established by DOD medical facilities. Specifically, prior to transferring responsibility for the administration of medical facilities from the military departments to DHA, the military departments oversaw the partnerships established by DOD medical facilities. However, DHA is now responsible for the administration of each DOD medical facility, which includes overseeing each associated partnership.[66] As a result, the military departments’ oversight is now focused on the partnerships they participate in, and they do not maintain a current inventory or provide oversight of partnerships involving DOD medical facilities.
According to DOD officials, at the local level, the medical facility directors identify and establish partnerships with civilian medical facilities when needed. According to DHA officials, communicating the establishment of a partnership to DHA was typically prompted when the DOD medical facility needed a waiver approved for deviating from the DHA training agreement template. Otherwise, newly established partnerships were not routinely communicated to DHA. However, in June 2025 DHA’s Agreements and Partnerships Management Division sent a request to each DOD medical facility to add partnership agreements into an electronic repository, according to DHA officials. Specifically, DHA instructed the DOD medical facilities to upload agreements into the repository and complete metadata—such as agreement number, number of projected personnel participating in the partnership, and category (e.g., skills sustainment, graduate medical education (residency), and clinical phase I)—for each agreement in the repository. DHA also instructed DHA medical facilities to upload new training agreements and amendments as they are established on an ongoing basis. DHA’s request was submitted to the DOD medical facilities. According to DHA and Air Force officials, the Air Force plans to use the repository as their single source for all agreements. As of February 2026, according to a DHA official, there are no plans for the Army and Navy agreements to be included in the repository.
According to the metadata collected, the repository includes agreements used for skills sustainment as well as other types of agreements, such as those used for graduate medical education and initial training for enlisted medical personnel. Based on our review of the repository as of December 2025, there were 3,257 agreements listed, including 134 identified in the repository as agreements used for skills sustainment.[67] According to DHA officials, they have reviewed the repository and noticed errors in some of the metadata collected, such as missing or incorrect data entered into several fields, and are planning on providing additional training to those responsible for entering agreements into the repository in order to improve data collection of agreements. Based on our review of the repository, it does not include all partnership agreements.
DOD Instruction 6000.19 directs DHA to maintain a comprehensive registry of partnerships and directs the military departments to report to DHA on their established partnerships. Further, DOD Instruction 6040.47 directs DHA to develop and maintain a registry that tracks all partnerships for trauma. Moreover, DOD Instruction 6040.47 directs the military departments to (1) inform DHA of partnerships with civilian trauma centers that provide trauma teams and individual personnel with maximum exposure to a high volume of patients with trauma injuries and (2) coordinate with combatant commands when exploring opportunities to develop similar partnerships with military or civilian trauma centers in partner nations. Standards for Internal Control in the Federal Government require that management establish and operate monitoring activities and remediate identified deficiencies on a timely basis.[68] Moreover, these standards state that these activities should be performed routinely.
DHA’s inventory of partnerships has not been maintained because DHA has relied on ad hoc information requests and has not established a standardized process for routinely and accurately identifying and updating a complete inventory of partnerships. Moreover, according to DHA officials, DHA has not established a standardized process that includes the types of partnerships that should be included (e.g., partnerships established by the military departments, by DOD medical facilities, or through external resource sharing agreements). While the working group’s initiatives to identify partnerships and DHA’s more recent efforts to create a repository of agreements are promising, the prior efforts have been ad hoc and are incomplete, and there is no effort in place to ensure that a department-wide inventory of all partnerships is maintained, according to DHA officials. Such an effort would include having all entities that established a partnership routinely and accurately report on the type and status of established partnerships. Moreover, the military departments do not have a complete inventory of their partnerships because they also do not have a standardized process for routinely and accurately inventorying their partnerships.
DHA, in conjunction with the military departments, are expected to establish partnerships to provide training venues and opportunities for military medical personnel to obtain and maintain currency in clinical knowledge, skills, and abilities associated with their medical specialty or community at or above minimum established thresholds.[69] A comprehensive inventory of such partnerships would inform DOD decision-makers of additional clinical sustainment opportunities for their military medical personnel and for supporting their efforts to streamline, assess, and add partnerships as needed. Moreover, such an inventory would enable them to benefit from the factors identified earlier and to inform leadership of the partnerships to where DOD medical facilities are sending their military medical personnel. Until DHA establishes a standardized process for updating its inventory of partnerships, it will have limited visibility of partnerships across the department. Moreover, the military departments would be better positioned to ensure that all their partnerships are identified and communicated to DHA by establishing a process to maintain an inventory of their partnerships.
DHA Does Not Fully Track Military Medical Facility Personnel Participation in Its Partnerships
DHA does not fully track the number of and time spent by military medical facility personnel participating in partnerships. Specifically, DHA faces challenges in using its existing timecard system to collect complete and accurate information on the number of clinical hours its military medical personnel assigned to a medical facility spend at partnerships.
According to DOD officials, accurate and reliable timecard data are important for managing military medical personnel staffing at DOD medical facilities, which includes tracking clinical hours at partnerships. DHA’s guidance notes that sending military medical personnel to partnerships to sustain clinical readiness is an investment and that obtaining the cost of the investment by capturing all associated labor hours is critical.[70]
However, DOD officials expressed concern that DHA’s timecard system data may be incomplete and inaccurate due to issues such as personnel not properly recording their time spent at a partnership. DOD medical facility officials noted that they have instead relied on locally established scheduling tools to track and allocate personnel hours between DOD’s medical facilities and civilian partners. Based on our comparison of DHA timecard data with clinical activity data from DHA’s readiness dashboards, we found that of the 396 military medical personnel who were assigned to a DOD medical facility from May 2024 through April 2025 that reported clinical activity from a partnership in DHA’s readiness dashboards, 39 percent (155) did not report any hours spent at a partnership in the DHA timecard system for the same period.
We were unable to determine the total hours medical facility personnel spent at a partnership because of this underreporting of time spent at a partnership in DHA’s timecard system. Based on our review of DHA’s timecard data from fiscal year 2020 through fiscal year 2024, of those approximately 2,300 military medical facility personnel that did report hours at a partnership, we found they reported spending approximately 723,800 hours there—about 37 percent of hours at a partnership established by an external resource sharing agreement and the remaining 63 percent of hours at a military-civilian partnership (see fig. 3).
Figure 3: DHA Timecard Data for Military Medical Facility Personnel Participating in Partnerships, Fiscal Years 2020–2024
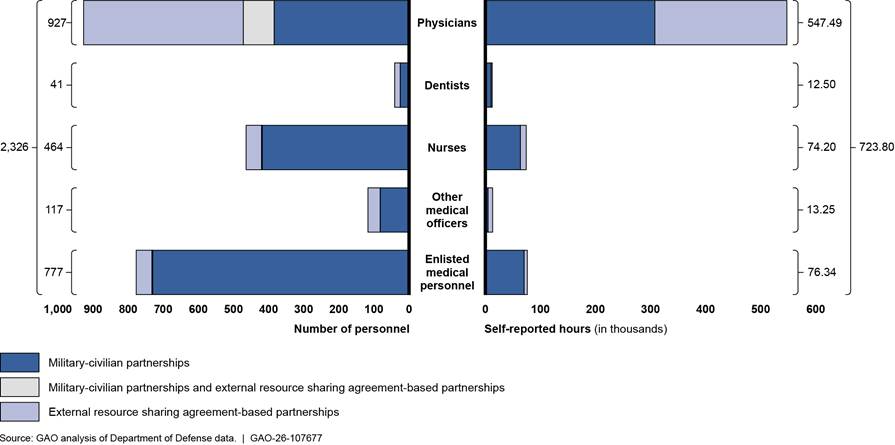
Notes: For purposes of this report, “partnerships” refers to (1) partnerships at civilian medical facilities established through training agreements, training affiliation agreements, memorandums of understanding, or medical training agreements that are used for maintaining and sustaining the clinical skills and readiness of DOD medical personnel (also referred to as military-civilian partnerships); and (2) partnerships at TRICARE facilities established by external resource sharing agreements that are used to provide additional opportunities for military medical personnel to care for beneficiaries.
Physicians include officers in the Medical Corps. We use the term “Other medical officers” to capture the Medical Service Corps, Army Medical Specialist Corps, Biomedical Sciences Corps, Veterinary Corps, and Warrant Officers. Enlisted medical personnel serve in occupations such as behavioral health specialists, operating room specialists, surgical technologists, and respiratory specialists.
We determined that the Defense Health Agency’s (DHA) timecard data were not sufficiently reliable to describe the total number of military medical personnel who participated in a partnership due to potential underreporting of time spent at a partnership. Instead, the information presented in this figure represents the number of military medical personnel whose time spent at a partnership was captured in DHA’s timecard system.
In July 2025, we reported that the number of military medical positions and assigned personnel in DOD medical facilities has declined over time and that DOD medical facilities face staffing challenges.[71] We found that DOD planned to use timecard data to monitor the available work time of military medical personnel to help mitigate facility staffing challenges. However, we also found that timecard data were not fully accurate or complete for DOD medical personnel serving at DOD medical facilities. We noted that this issue was longstanding, and prior DOD reports have identified concerns with the reliability of the timecard data, citing limitations in their accuracy and completeness.
We made five recommendations aimed at improving timecard data, including that DOD develop and disseminate a clear and consistent communication strategy to increase military medical personnel’s understanding of the importance of timecard data and how they are used; and analyze and address root causes of data quality issues with timecard data and implement any findings. DHA concurred with our recommendations and stated that it has been actively working to improve the data quality of its timecard data. We believe these recommendations will also improve the tracking of hours that medical facility personnel spend at partnerships and provide the information necessary to determine the use of partnerships. Moreover, reliable timecard data could help leadership to determine staffing needs of DOD medical facilities and inform their decision on whether to send military medical personnel to partnerships for additional readiness opportunities. We will continue to monitor the status of DHA’s activities to address these recommendations, including having personnel record their time spent at partnerships.
DOD Has Not Fully Assessed Partnerships’ Contributions to Readiness
Military Departments Have Not Fully Assessed Readiness Contributions of Their Military-Civilian Partnerships
Organizations within each military department have established mechanisms to capture data on clinical activities performed at military-civilian partnerships. For example, the military departments have developed digital tools to collect clinical activity data:[72]
· Army Medical Command maintains an online tool that its medical personnel are instructed to use to collect data on clinical activities that meet training requirements when participating in a partnership.[73]
· Navy BUMED maintains an online tool that its medical personnel are instructed to use to collect data on clinical activities that meet training requirements when participating in a partnership.[74]
· The Air Force’s 711th Human Performance Wing helped to develop an electronic data collection tool that medical personnel can use to record the completion of clinical activities that meet training requirements. In addition to this tool, the U.S. Air Force School of Aerospace Medicine’s Centers for Sustainment of Trauma and Readiness Skills has worked with an official from the Uniformed Services University of the Health Sciences to implement processes for collecting clinical activity data.[75]
Beyond digital data collection tools, we found that Navy BUMED’s four Hospital Corpsman Trauma Training military-civilian partnerships record clinical activities in manual logs. For examples of clinical activity data collected by the military departments’ medical headquarters and training organizations on their military-civilian partnerships to facilitate their assessment, see table 1.
Table 1: Examples of Clinical Activity Data Collected by Military Departments’ Medical Headquarters and Training Organizations on Their Military-Civilian Partnerships
|
U.S. Army Medical Command |
|
· Specialty-specific training requirements: U.S. Army Medical Command collects data on clinical activities meeting specialty-specific training requirements known as individual critical tasks. · Surgical case logs: U.S. Army Medical Command collects data on surgical procedures performed by credentialed providers. · Data from Mission Zero Act Programa partners: According to U.S. Army Medical Command officials, they collect clinical activity data and transmit these data to the Defense Health Agency to be scored as a part of its clinical readiness metrics. Officials stated that they review the data for accuracy and completeness. |
|
Navy Bureau of Medicine and Surgery (BUMED) |
|
· Specialty-specific training requirements: BUMED collects data on clinical activities meeting specialty-specific training requirements known as Navy Knowledge, Skills, and Abilities. · Clinical activities of Hospital Corpsman: BUMED collects clinical activity data for Hospital Corpsmen participating in its Hospital Corpsman Trauma Training military-civilian partnerships. |
|
U.S. Air Force School of Aerospace Medicineb |
|
· Specialty-specific training requirements: The U.S. Air Force School of Aerospace Medicine collects data on clinical activities meeting specialty-specific training requirements as a part of the Air Force’s Comprehensive Medical Readiness Program. · Clinical activities related to expeditionary casualty care: To complement data on clinical activities meeting specialty-specific training requirements, the U.S. Air Force School of Aerospace Medicine collects data on clinical activities that require skills needed in expeditionary casualty care. |
Source: GAO analysis of Department of Defense information. | GAO‑26‑107677
aThe Mission Zero Act Program awards grants to civilian trauma centers participating in military-civilian partnerships with the goal of enabling military trauma providers to provide trauma care and related acute care at such trauma centers.
bU.S. Air Force School of Aerospace Medicine is a part of the U.S. Air Force’s 711th Human Performance Wing.
We identified current and planned efforts by the military departments to use data they collect to assess their military-civilian partnerships’ contributions to the readiness of their military medical personnel. For example:
· Army Medical Command processes the data it collects into a dashboard by which it assesses the completion of training requirements for medical personnel participating in its partnerships.[76]
· Navy BUMED maintains a dashboard that consolidates data from its collection tool regarding medical personnel’s completion of clinical activities that meet training requirements when participating in its partnerships.[77]
· The Air Force’s Centers for Sustainment of Trauma and Readiness Skills have worked with a Uniformed Services University of the Health Sciences official to develop dashboards that aggregate clinical activities.
We also identified efforts by operational units to assess the readiness contributions of their military-civilian partnerships. For example, an Air Force special operations surgical team we met with submits quarterly reports to the Air Force Surgeon General detailing the status of training requirements for personnel embedded in its partnership. Similarly, an official overseeing a Navy fleet surgical team described efforts to enhance evaluation of the unit’s existing military-civilian partnership, including providing routine assessments of partnership outcomes to superiors.[78]
Despite the efforts described above, we found that the military departments are not fully assessing the readiness contributions of their military-civilian partnerships. For example:
· U.S. Army Special Operations Command officials overseeing 10 military-civilian partnerships stated that although participants record and report their clinical activities to their superiors, these data have not been consolidated and assessed in a meaningful way.
· Navy officials stated that efforts to assess the four Hospital Corpsman Trauma Training military-civilian partnerships are limited to examining clinical activity data for personnel rotating through the partnerships and do not include embedded instructors. In September 2025, the Navy maintained 42 embedded instructors across the four partnership locations. Additionally, a Navy official overseeing a partnership between an operational unit and a nearby civilian trauma center stated that the unit has not assessed the partnership using information that participants have collected on clinical activities and instead monitors if participants spent adequate time at the partnership.
· The Air Force’s Centers for Sustainment of Trauma and Readiness Skills have taken steps to collect and assess clinical activity data for their military-civilian partnerships, but gaps in their efforts remain. Specifically, we found that five of the six centers have implemented a dashboard for physicians with the Uniformed Services University of the Health Sciences official.[79] Additionally, all six centers have implemented a dashboard for nonphysician personnel, such as nurses and enlisted medical personnel, with the Uniformed Services University of the Health Sciences official. However, as of January 2026, officials affiliated with four of the centers stated that they are not collecting clinical activity data for all nonphysician participants to populate their dashboards. Furthermore, an official overseeing the program stated that the data collected for nonphysician personnel have not been used to assess the readiness contributions of the partnerships. Rather, the official stated that it is possible to assess embedded personnel’s completion of specialty-specific training requirements as documented in the Air Force’s training system. However, the official stated that this ability is limited to embedded personnel and does not include rotators.
DOD has established principles to guide the sustainment of wartime medical skills among its military medical personnel. Specifically, DOD Instruction 6000.19 directs the military departments to develop and maintain readiness for military medical personnel primarily through their assignment to military medical facilities. However, when workload is insufficient at such facilities, the military departments must identify alternative training, such as participation in military-civilian partnerships. DOD Instruction 6000.19 also directs the military departments to assess care provided by the partnerships they establish with respect to clinical readiness support. Furthermore, Standards for Internal Control in the Federal Government state that management should establish and operate monitoring activities for its internal control system and assess the results by, for example, performing ongoing monitoring and separate evaluations.[80]
The military departments have not fully assessed their military-civilian partnerships because they have not established processes to assess partnerships’ readiness contributions by collecting and assessing complete clinical activity data from all partnerships. For example:
· U.S. Army Special Operations Command officials stated that they are exploring options for data collection and assessment to improve their understanding of their partnerships’ value but were unable to provide a time frame for doing so.
· A Navy official stated that the Navy’s process for collecting data does not include embedded staff at its Hospital Corpsman Trauma Training military-civilian partnerships because they are present to serve as guides to the students. However, the official confirmed the instructors perform clinical activities when students are not present. Additionally, a Navy official overseeing the unassessed partnership between the operational unit and the civilian partner described above stated that the unit requires personnel to record their clinical activities but has not used this information to assess the partnership. Instead, the official stated that the unit has focused on assessing a separate partnership that serves as its primary skills sustainment platform.[81]
· A program official overseeing the Air Force’s Centers for Sustainment of Trauma and Readiness Skills stated that the centers have not been required to implement the dashboard methodology for nonphysician personnel described above. According to this official, the methodology is being piloted to evaluate its effectiveness in assessing clinical activities performed in partnerships. Furthermore, although the tool developed by the 711th Human Performance Wing captures information on where clinical activities meeting training requirements are performed, Air Force officials stated that use of the tool is voluntary since it requires a personal device. Moreover, officials stated that once the data are aggregated into the Air Force’s readiness system, information on where training requirements are met is not recorded. Therefore, the readiness system does not allow users to assess the contributions made from individual partnerships.
DOD leadership has recognized the challenges faced by the military health system in providing enough personnel to support its medical facilities.[82] In sending their military medical personnel to participate in military-civilian partnerships to improve their readiness, the military departments are reducing the availability of personnel to work in DOD’s medical facilities. Until the military departments develop processes to fully assess the readiness contributions of their partnerships, they are not well positioned to evaluate their use of such partnerships in light of available military medical personnel resources and to identify the extent to which partnerships are contributing to achieving readiness objectives.
DHA Has Not Fully Assessed Readiness Contributions Within and Across Partnerships
DHA has also taken steps to assess the contributions of partnerships to the readiness of DOD’s military medical personnel. Efforts to assess partnerships’ readiness contributions are based on clinical readiness metrics managed by DHA’s Joint Knowledge, Skills, and Abilities Program Management Office (management office).[83] In 2018, DOD began testing these metrics, which now apply to 14 physician specialties. In addition to collecting clinical activity data on physicians’ activities at DOD’s medical facilities, the management office collects available clinical activity data from partnerships for these metrics.[84] For the latter, the management office relies on various parties to consolidate and transmit clinical activity data to an organizational email address periodically.[85]
Efforts to collect data. The management office uses its clinical readiness metrics and activity data to determine the overall readiness of physicians to deploy. To do so, the management office computes a point score based on physicians’ clinical activities from the prior 12 months and assesses the score against minimum thresholds.[86] The management office maintains specialty-specific readiness dashboards that present these scores and details on physicians’ clinical activities. Based on our review of the management office’s clinical readiness metric data collected as of August 2025, the office processed and scored clinical activity data for 649 active-duty military medical personnel who participated in a partnership from December 2021 through April 2025 within one of the 14 physician specialties (see table 2).[87]
Table 2: Number of Military Medical Personnel Participating in a Partnership with Clinical Activity Data According to DHA’s Readiness Dashboards, by Specialty, December 2021–April 2025
|
Specialty |
Number of personnel |
|
Cardiac/thoracic surgery |
16 |
|
Critical care/trauma medicine |
26 |
|
Critical care/trauma surgery |
70 |
|
Emergency medicine |
77 |
|
General surgery |
118 |
|
Neurological surgery |
11 |
|
Obstetrics/gynecology |
57 |
|
Ophthalmology |
4 |
|
Oral maxillofacial surgery |
9 |
|
Orthopedic surgery |
161 |
|
Otorhinolaryngology |
45 |
|
Peripheral vascular surgery |
22 |
|
Plastic surgery |
10 |
|
Urology |
23 |
|
Total |
649 |
Source: GAO analysis of Department of Defense (DOD) information. | GAO‑26‑107677
Note: For purposes of this report, “partnerships” refers to (1) partnerships at civilian medical facilities established through training agreements, training affiliation agreements, memorandums of understanding, or medical training agreements that are used for maintaining and sustaining the clinical skills and readiness of DOD medical personnel; and (2) partnerships at TRICARE facilities established by external resource sharing agreements that are used to provide additional opportunities for military medical personnel to care for beneficiaries. We determined the Defense Health Agency’s (DHA) clinical activity data were not sufficiently complete to describe the total number of military medical personnel who participated in a partnership due to underreporting of clinical activity data. Given the limitation of DOD’s clinical activity data, we were unable to report on the total number of medical personnel who participated in partnerships. Instead, this table represents the number of military medical personnel for whom clinical activity data from a partnership were captured in DHA’s system.
Beyond assessing physicians’ readiness, the management office’s readiness dashboards facilitate the assessment of partnerships. Specifically, they demonstrate readiness gained from DOD’s medical facilities and partnerships. We also found that the management office uses the data to conduct monthly briefings. For example, in briefing Defense Health Networks on opportunities to reduce the number of referrals sent to TRICARE network providers and increase physician readiness in September 2025, the management office used clinical activity data to provide information on the amount of readiness gained through procedures performed in partnerships relative to DOD’s medical facilities. The management office also provided information on the significance of specific military-civilian partnerships for ensuring the readiness of physicians from a select Defense Health Network.
Efforts to improve data collection. To improve its ability to assess physicians’ readiness and the readiness contributions of partnerships, the management office has implemented internal controls to ensure that it collects complete data. For example, the management office has developed dashboard metrics to identify the number of physicians embedded in a partnership who have not submitted data, as well as information regarding partnership locations not reporting clinical activities, by specialty.[88] Furthermore, officials stated that they are reviewing patient referrals to civilian medical facilities to identify physicians participating in partnerships established by external resource sharing agreements who are missing clinical activity data.
Additionally, the management office coordinates with internal and external stakeholders to improve data collection. For example, the management office has worked with Defense Health Networks to identify partnerships for which it was not receiving clinical activity data. Additionally, management office officials stated that they work with individual partnerships when submissions appear to be incomplete, noting that these efforts help them determine if data are missing or if physicians are no longer participating in the partnership. Finally, management office leadership has encouraged DOD medical facilities to coordinate with them regarding the medical facilities’ existing partnerships, which is intended to help the management office to ensure that it receives data from these local partnerships.
Beyond the management office’s efforts, other officials have worked to improve the completeness of the clinical readiness data. For example, three Air Force officials developed an intervention to improve collection of physician clinical activity data by, among other things, establishing a physician at each partnership who is responsible for organizing data collection and collaborating with civilian partnership facilities to access and report clinical activity data from their electronic health records.[89] Furthermore, one of these officials developed recommended practices to improve data quality from Mission Zero Act Program sites. These practices include being flexible in data collection and prioritizing passive data collection over self-reported data. Finally, Army Medical Command has worked with the management office to improve data quality by auditing data from its partnerships before submitting them for processing into the readiness dashboards.
While these efforts are positive, we found that DHA has not fully assessed the readiness contributions of partnerships. First, the management office’s clinical readiness metrics are limited to 14 physician specialties. As a result, its assessments of partnerships do not include any readiness gained from clinical activities performed by other physician specialties, nurses, or enlisted medical personnel. In February 2019, we reported DOD was, at that time, testing its metric for two specialties (general surgeons and orthopedic surgeons) but had not yet decided which other medical specialties to which it would apply a clinical readiness metric.[90] We also reported that DOD planned to assess the feasibility of expanding the clinical readiness metric to noncombat casualty care specialties. However, DOD officials stated that a clinical readiness metric may not be as beneficial for other types of provider specialties as it would be for assessing and improving combat casualty care providers’ wartime readiness. As a result, we recommended that the Assistant Secretary of Defense for Health Affairs, in coordination with the Surgeons General of the military departments and the Director of DHA, determine which critical wartime specialties perform high-risk, high-acuity procedures and rely upon perishable skill sets, and use this information to prioritize specialties to which the clinical readiness metric could be expanded.[91]
As of September 2025, management office officials stated that they are looking to implement additional readiness metrics for select nurse specialties and respiratory technicians. However, management office officials described challenges in collecting clinical activity data for nonphysician specialties. Specifically, they stated that data captured by DOD’s electronic health record are typically limited to physician specialties and other select providers. Furthermore, they stated that nonphysician specialties do not typically generate billing data in civilian billing systems. In response to these challenges, management office officials stated that they have identified a methodology for capturing clinical activity data from DOD’s electronic health record for select nurse specialties and respiratory technicians. Officials added that they are exploring options for using this methodology to capture clinical activity data from partnerships that use similar electronic health records.
Furthermore, we found that the management office has not assessed the readiness contributions of partnerships for all personnel from the 14 physician specialties with a clinical readiness metric. For example, officials overseeing two partnerships stated that the billing data they submit to the management office is limited to embedded personnel and does not include clinical activity data for personnel who rotate through the partnerships. We examined the management office’s dashboards for clinical activity data for three personnel who rotated through one of these partnerships from January through April 2025 and confirmed that they did not include any clinical activity data from a military-civilian partnership for these personnel.[92]
Similarly, we used DHA’s timecard data to identify military medical personnel from the 14 physician specialties who were assigned to a DOD medical facility and reported working in a partnership. We then compared this list of physicians with the management office’s dashboards to identify those who lacked clinical activity data from partnerships.[93] Based on our analysis, the dashboards contained clinical activity data for 53 of 128 physicians who reported working in a military-civilian partnership for 40 hours or more from May 2024 through April 2025.[94] Furthermore, the dashboards contained clinical activity data for 87 of 105 physicians who reported working in a partnership established by an external resource sharing agreement for 40 hours or more from May 2024 through April 2025.
DOD Instruction 6000.19 directs DHA to assess care provided by DHA-established partnerships with respect to clinical readiness support. It also directs DHA to establish performance metrics in conjunction with the military departments to assess partnerships.[95] Furthermore, Standards for Internal Control in the Federal Government state that agency management should establish and operate monitoring activities to monitor the internal control system and assess the results.[96]
We identified two reasons why DHA has not fully assessed the contributions of partnerships. First, DHA does not maintain a complete inventory of partnerships, as we discussed earlier. DHA officials stated it is likely there are additional partnerships managed by DOD medical facilities of which they are unaware, thereby restricting their ability to work with these partnerships to obtain complete data. Once DOD develops a process for inventorying its partnerships, it should have a more complete inventory that it can use to ensure that it receives complete data.
Second, we found that although DHA has provided some guidance and templates for collecting clinical activity data from partnerships, it has not issued guidance for collecting complete clinical activity data to support its clinical readiness metrics. DHA’s standardized agreement template for external resource sharing agreements requires DOD medical facility directors to ensure that data on care provided by DOD medical personnel are recorded in DOD’s electronic health record. Management office officials stated that they retrieve this data on relevant procedures and/or diagnoses along with all other relevant clinical activity data to generate physicians’ point scores. Officials stated that these steps are different from how the management office receives military-civilian partnership data.
Additionally, DHA’s management office has issued guidance and created a data collection template for civilian partners that receive grant funding as a part of the Mission Zero Act Program. However, the Mission Zero Act Program guidance and data collection template do not address the submission of clinical activity data for physicians who do not generate billing data when participating in a military-civilian partnership receiving Mission Zero Act Program funding, nor do they address the submission of data for physicians participating in military-civilian partnerships that do not receive Mission Zero Act Program funding (see table 3).
Table 3: Defense Health Agency Guidance and Templates on Clinical Activity Data Collection from Partnerships for 14 Physician Specialties
|
Type of clinical activity data collection |
Information included in guidance or template |
|
Physicians participating in partnerships established by external resource sharing agreements |
✓ |
|
Physicians participating in Mission Zero Act Programa partnerships who generate billing data |
✓ |
|
Physicians participating in Mission Zero Act Programa partnerships who do not generate billing data |
✗ |
|
Physicians participating in military-civilian partnerships that do not receive Mission Zero Act Programa funds |
✗ |
Legend:
✓ = Yes
✗ = No
Source: GAO analysis of Department of Defense information. | GAO‑26‑107677
Note: For purposes of this report, “partnerships” refers to (1) partnerships at civilian medical facilities established through training agreements, training affiliation agreements, memorandums of understanding, or medical training agreements that are used for maintaining and sustaining the clinical skills and readiness of DOD medical personnel; and (2) partnerships at TRICARE facilities established by external resource sharing agreements that are used to provide additional opportunities for military medical personnel to care for beneficiaries
aThe Mission Zero Act Program awards grants to civilian trauma centers participating in military-civilian partnerships with the goal of enabling military trauma providers to provide trauma care and related acute care at such trauma centers
Beyond this guidance, the management office maintains online resources that address DOD’s development of the dashboards and how they are maintained. Specifically, the management office’s website includes responses to frequently asked questions regarding the clinical readiness metrics for each specialty. Furthermore, the management office’s website includes a document for each of the 14 specialties that outlines the methodology and data used to develop its corresponding dashboard. However, we found that these resources lack key information. For example, while the responses to frequently asked questions states that the dashboards include clinical activity data from partnerships submitted by medical personnel to the management office via email, they do not prescribe the process for doing so. Furthermore, management office officials stated that the methodology documents are not intended to prescribe the data collection process to medical personnel from the 14 specialties.
Having a more complete understanding of the readiness contributions that partnerships make would help inform DOD efforts as it works to balance the need for a predictable workforce that supports the direct care mission with the need to ensure a ready medical force. Issuing guidance to improve its collection of clinical activity data would help ensure that DOD collects complete information on the contributions that partnerships make to the medical force’s clinical readiness. Without such guidance, DOD risks having less information to evaluate partnership performance and trading off opportunities to send personnel to a partnership for skills sustainment in lieu of them working in a DOD medical facility to provide beneficiary care.
Conclusions
Military medical personnel perform key roles in the delivery of military health care and must be ready to provide lifesaving care to injured and ill service members in an expeditionary setting. DOD relies on its partnerships to provide clinical skills sustainment when its medical facilities are unable to do so. In some instances, partnerships established by external resource sharing agreements may not only provide readiness opportunities for military medical personnel but may also provide cost savings for the overall military health system budget. Developing strategies to systematically identify opportunities to use sharing agreements would help ensure that all sharing opportunities are identified and optimized.
DOD has taken steps toward inventorying its partnerships; however, it continues to have an incomplete inventory that is not regularly maintained. Without such an inventory, DHA and the military departments do not have the ability to assess all partnerships and develop a comprehensive understanding of how partnerships may support readiness. As a result, it is difficult to determine current and future training investments. Further, the absence of an inventory contributes to the lack of quality information to assess readiness contributions of partnerships by limiting DHA’s ability to identify partner facilities and initiate data collection efforts. While the military departments and DHA have made progress in tracking clinical activities of its medical workforce in their respective partnerships, both the military departments and DHA do not have quality information about clinical activities performed at partnerships. By developing standardized processes to inventory partnerships and assess partnerships’ contributions to clinical readiness to address these issues, DOD could better evaluate its use of partnerships in light of resource and readiness considerations.
Recommendations for Executive Action
We are making a total of nine recommendations, including three to the Secretary of Defense, two to the Secretary of the Army, two to the Secretary of the Navy, and two to the Secretary of the Air Force.
The Secretary of Defense should ensure that the Director of DHA develops and implements department-wide strategies to identify opportunities for reducing health care costs while increasing readiness through use of partnerships established by external resource sharing agreements. (Recommendation 1)
The Secretary of Defense should ensure that the Director of DHA, in coordination with the Secretaries of the military departments, develop a standardized process for routinely and accurately inventorying its partnerships, including identifying types of partnerships that should be included in its inventory. (Recommendation 2)
The Secretary of the Army should establish a standardized process for routinely and accurately inventorying its partnerships. (Recommendation 3)
The Secretary of the Navy should establish a standardized process for routinely and accurately inventorying its partnerships. (Recommendation 4)
The Secretary of the Air Force should establish a standardized process for routinely and accurately inventorying its partnerships. (Recommendation 5)
The Secretary of the Army should establish processes to fully assess the readiness contributions of its military-civilian partnerships. (Recommendation 6)
The Secretary of the Navy should establish processes to fully assess the readiness contributions of its military-civilian partnerships. (Recommendation 7)
The Secretary of the Air Force should establish processes to fully assess the readiness contributions of its military-civilian partnerships. (Recommendation 8)
The Secretary of Defense should ensure that the Director of DHA issues guidance for collecting complete clinical activity data from military-civilian partnerships for all personnel in specialties with clinical readiness metrics. (Recommendation 9)
Agency Comments and Our Evaluation
We provided a draft of this report to DOD and the Department of Health and Human Services for review and comment. DOD provided technical comments, which we incorporated as appropriate. In DOD’s written comments, reproduced in appendix II, DOD partially concurred with our first two recommendations and concurred with our remaining seven recommendations. The Department of Health and Human Services did not provide comments.
DOD partially concurred with our first recommendation to develop and implement department-wide strategies to identify opportunities for reducing health care costs while increasing readiness through resource sharing partnerships. In its comments, DOD stated that the terminology of “resource sharing partnerships” is incorrect. DOD also stated that the terminology is important, as an agreement and a partnership are different legal relationships, and imprecise use of terms leads to confusion within the direct care and private sector care environments. We agree with the department. In response, we clarified the terminology used in our recommendation as well as throughout our report, to distinguish between partnerships established by external resource sharing agreements and partnerships established by other types of agreements, such as training agreements, training affiliation agreements, medical training agreements, and memorandums of understanding.
DOD partially concurred with our second recommendation to develop a standardized process for routinely and accurately inventorying its partnerships, including identifying types of partnerships that should be included in its inventory. In its comments, DOD stated that DHA concurs with routinely and accurately inventorying its partnerships for skills sustainment. DOD also stated that providing a clear intent of skills sustainment partnerships will enable relevant stakeholders to identify the types of agreements and partnerships that should be included, and the individuals responsible for building the inventory. As we noted in our report, we believe DOD’s process should identify the types of partnerships that should be included in its inventory (e.g., partnerships established by the military departments, by DOD medical facilities, or through external resource sharing agreements). We are encouraged that DOD recognizes the need to routinely and accurately inventory its partnerships for skills sustainment.
We are sending copies of this report to the appropriate congressional committees; the Secretary of Defense; the Under Secretary of Defense for Personnel and Readiness; the Assistant Secretary of Defense for Health Affairs; the Director of DHA; the Secretaries of the Army, the Navy, and the Air Force; the Secretary of the Department of Health and Human Services; and the Principal Deputy Assistant Secretary for Preparedness and Response. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at agarwalr@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix III.

Rashmi Agarwal
Director, Defense Capabilities and Management
List of Committees
The Honorable Roger Wicker
Chairman
The Honorable Jack Reed
Ranking Member
Committee on Armed Services
United States Senate
The Honorable Mitch McConnell
Chair
The Honorable Christopher Coons
Ranking Member
Subcommittee on Defense
Committee on Appropriations
United States Senate
The Honorable Mike Rogers
Chairman
The Honorable Adam Smith
Ranking Member
Committee on Armed Services
House of Representatives
The Honorable Ken Calvert
Chairman
The Honorable Betty McCollum
Ranking Member
Subcommittee on Defense
Committee on Appropriations
House of Representatives
The military departments, who are responsible for organizing, training, and equipping military forces, have established a number of military-civilian partnerships through their medical headquarters organizations or other organizations. The Department of Defense does not have a complete inventory of partnerships and therefore tables 4 through 6 include examples of civilian partners that we identified by military department.
|
Civilian partner |
Location |
Army Medicine Military-Civilian Trauma Team Training sitea |
U.S. Army Special Operations Command Medical Proficiency Training siteb |
Mission Zero Act Program partnerc |
|
Atrium Health |
Charlotte, NC |
No |
Yes |
Yes |
|
Cooper University Hospital |
Camden, NJ |
Yes |
No |
Yes |
|
Grady Memorial Hospital |
Atlanta, GA |
Yes |
Yes |
Yes |
|
Harborview Medical Center |
Seattle, WA |
Yes |
Yes |
Yes |
|
Medical College of Wisconsin & Froedtert Hospital |
Milwaukee, WI |
Yes |
Yes |
Yes |
|
Oregon Health & Science University |
Portland, OR |
Yes |
No |
Yes |
|
University of Chicago Medicine |
Chicago, IL |
Yes |
No |
Yes |
|
Jackson Memorial Hospital |
Miami, FL |
No |
Yes |
Yes |
|
University of North Carolina Health System |
Chapel Hill, NC |
Yes |
Yes |
Yes |
|
Vanderbilt University Medical Center |
Nashville, TN |
Yes |
Yes |
Yes |
Source: GAO analysis of Department of Defense information. | GAO‑26‑107677
Note: We selected these military-civilian partnerships to reflect U.S. Army Medical Department Military-Civilian Trauma Team Training sites and U.S. Army Special Operations Command Medical Proficiency Training sites that receive Mission Zero Act Program funding.
aThe U.S. Army Medical Department Military-Civilian Trauma Team Training program is designed to provide Army medical personnel assigned to Forward Resuscitative Surgical Detachments with access to a high volume of trauma and critically ill patients to maintain and enhance skills proficiency for trauma readiness. All sites provide embedded and rotational opportunities except for the Medical College of Wisconsin & Froedtert Hospital, which only hosts embedded personnel.
bU.S. Army Special Operations Command Medical Proficiency Training sites provide medical proficiency training rotations for Combat Medics, Civil Affairs Medical Sergeants, and Special Forces Medical Sergeants.
cThe Mission Zero Act Program awards grants to civilian trauma centers participating in military-civilian partnerships with the goal of enabling military trauma providers to provide trauma care and related acute care at such trauma centers.
|
Civilian partner |
Location |
Hospital Corpsman Trauma Training sitea |
Mission Zero Act Program partnerb |
|
Cook County Health |
Cook County, IL |
Yes |
No |
|
Los Angeles General Medical Center |
Los Angeles, CA |
No |
Yes |
|
University of Florida Health Jacksonville |
Jacksonville, FL |
Yes |
Yes |
|
University Hospitals Health Systemc |
Cleveland, OH |
Yes |
Yesd |
|
University of Pennsylvania Health System |
Philadelphia, PA |
No |
Yes |
|
Wake Medical Center |
Raleigh, NC |
Yes |
No |
Source: GAO analysis of Department of Defense information. | GAO‑26‑107677
Note: We selected these military-civilian partnerships to reflect Navy Bureau of Medicine and Surgery partnerships, including those that receive Mission Zero Act Program funding.
aThe Hospital Corpsman Trauma Training program is designed to provide Hospital Corpsmen with a robust clinical experience in coordination with existing and future training partnerships with civilian trauma centers. Corpsmen will receive hands-on training and exposure to trauma patients, similar to those encountered on the battlefield and aboard ships.
bThe Mission Zero Act Program awards grants to civilian trauma centers participating in military-civilian partnerships with the goal of enabling military trauma providers to provide trauma care and related acute care at such trauma centers.
cUniversity Hospitals Health System’s flagship medical center—University Hospitals Cleveland Medical Center—is located in Cleveland, Ohio. Other participating locations are found throughout northern Ohio.
dUniversity Hospitals Cleveland Medical Center is the Mission Zero Act Program site.
|
Civilian partner |
Location |
Center for Sustainment of Trauma and Readiness Skills |
Mission Zero Act Program partnera |
|
Soin Medical Center |
Dayton, OH |
Yes |
No |
|
SSM St. Louis University Hospital |
St. Louis, MO |
Yesb |
No |
|
University of Cincinnati Medical Center |
Cincinnati, OH |
Yes |
Yes |
|
University of Maryland Medical Center, R Adams Cowley Shock Trauma Center |
Baltimore, MD |
Yes |
Yes |
|
University of Nebraska Medical Center |
Omaha, NE |
Yes |
Yes |
|
University Medical Center of Southern Nevada |
Las Vegas, NV |
Yes |
Yes |
|
Washington University School of Medicine– Barnes-Jewish Hospital |
St. Louis, MO |
Yesb |
Yes |
Source: GAO analysis of Department of Defense information. | GAO‑26‑107677
Note: We selected these military-civilian partnerships to reflect the Air Force’s 711th Human Performance Wing’s U.S. Air Force School of Aerospace Medicine’s Centers for Sustainment of Trauma and Readiness Skills, including those that receive Mission Zero Act Program funding.
aThe Mission Zero Act Program awards grants to civilian trauma centers participating in military-civilian partnerships with the goal of enabling military trauma providers to provide trauma care and related acute care at such trauma centers.
bSSM St. Louis University Hospital and Washington University School of Medicine–Barnes-Jewish Hospital are each a part of the Center for Sustainment of Trauma and Readiness Skills–St. Louis.
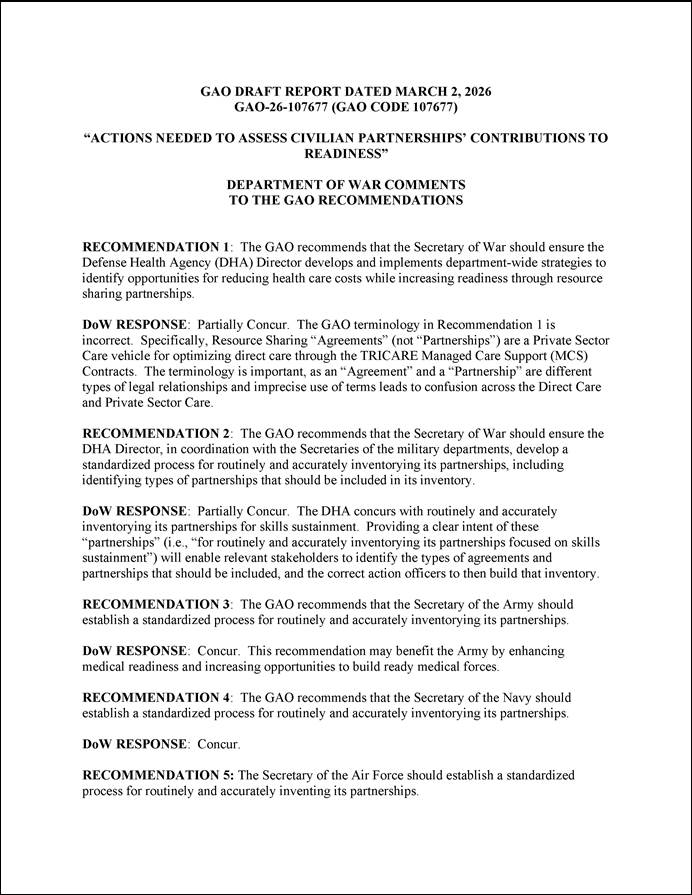
GAO Contact
Rashmi Agarwal, agarwalr@gao.gov
Staff Acknowledgments
In addition to the contact named above, Lori Atkinson (Assistant Director), Stephanie Santoso (Analyst in Charge), Brady Anderson, Nicole Ashby, Sharon Ballinger, Alexandra Gonzalez, Jesse Jordan, Alberto Leff, Michael Silver, and Norma-Jean Simon made key contributions to this report.
Defense Health Care: Information Needed to Improve Monitoring of Military Personnel Staffing at Medical Facilities. GAO‑25‑106988. Washington, D.C.: July 21, 2025.
Defense Health Care: Actions Needed to Address Long-Standing Management Challenges with Medical Facilities. GAO‑25‑107432. Washington, D.C.: April 10, 2025.
Defense Health Care: DOD Should Reevaluate Market Structure for Military Medical Treatment Facility Management. GAO‑23‑105441. Washington, D.C.: August 21, 2023.
Defense Health Care: Additional Assessments Needed to Determine Effects of Active Duty Medical Personnel Reductions. GAO‑23‑106094. Washington, D.C.: July 11, 2023.
Defense Health Care: Improved Monitoring Could Help Ensure Completion of Mandated Reforms. GAO‑23‑105710. Washington, D.C.: June 22, 2023.
Military Health Care: Improved Procedures and Monitoring Needed to Ensure Provider Qualifications and Competence. GAO‑22‑104668. Washington, D.C.: August 11, 2022.
Defense Health Care: Actions Needed to Improve Billing and Collection of Debt for Civilian Emergency Care. GAO‑22‑104770. Washington, D.C.: July 7, 2022.
Defense Health Care: Actions Needed to Define and Sustain Wartime Medical Skills for Enlisted Personnel. GAO‑21‑337. Washington, D.C.: June 17, 2021.
Defense Health Care: Additional Information and Monitoring Needed to Better Position DOD for Restructuring Medical Treatment Facilities. GAO‑20‑371. Washington, D.C.: May 29, 2020.
Defense Health Care: DOD Should Collect and Use Key Information to Make Decisions about Incentives for Physicians and Dentists. GAO‑20‑165. Washington, D.C.: January 15, 2020.
Defense Health Care: Actions Needed to Determine the Required Size and Readiness of Operational Medical and Dental Forces. GAO‑19‑206. Washington, D.C.: February 21, 2019.
Defense Health Care: Additional Assessments Needed to Better Ensure an Efficient Total Workforce. GAO‑19‑102. Washington, D.C.: November 27, 2018.
Military Personnel: Additional Actions Needed to Address Gaps in Military Physician Specialties. GAO‑18‑77. Washington, D.C.: February 28, 2018.
Defense Health Care Reform: DOD Needs Further Analysis of the Size, Readiness, and Efficiency of the Medical Force. GAO‑16‑820. Washington, D.C.: September 21, 2016.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]DOD defines clinical readiness as clinical practice that is relevant to a provider or provider team’s ability to perform their assigned deployed role. Department of Defense Instruction 6000.19, Military Medical Treatment Facility Support of Medical Readiness Skills of Health Care Providers (Feb. 7, 2020). For purposes of this report, “military medical personnel” refers to active-duty military medical personnel unless otherwise noted.
[2]To expand the capabilities of the active-duty forces in providing operational medical care, DOD also relies on approximately 63,000 military medical personnel of the Reserve and National Guard in the Selected Reserve. DOD’s more than 9 million eligible beneficiaries include service members and their families, retirees, dependent survivors, certain members of the Selected/Retired Reserve, and certain former spouses of service members or former service members.
[3]DOD’s medical facilities vary in size and capabilities. Clinics are the smallest of DOD’s medical facilities, offering no hospitalization services and a limited number of specialties. DOD’s hospitals offer hospitalization, outpatient, and specialty care services. With multiple specialties and subspecialties, medical centers are the largest of DOD’s medical facilities.
[4]More than $10.7 billion represents the Defense Health Program funding estimate for care delivered through DOD’s medical facilities, dental care, and pharmaceuticals. This estimate does not include the cost of the more than 50,000 military personnel estimated to be staffed at the medical facilities in fiscal year 2026.
[5]S. Rep No. 114-255, at 174 (2016); See To Receive Testimony on Stabilizing the Military Health System to Prepare for Large-Scale Combat Operations: Hearing Before the S. Comm. on Armed Services, 119th Cong. 2-5, 23 (2025) (statements of Sen. Roger Wicker and Col. (Dr.) Jeremy W. Cannon, USAFR (Ret.), Professor of Surgery, Perlman School of Medicine, University of Pennsylvania). See also Ensuring Medical Readiness in the Future: Hearing Before the Subcommittee on Military Personnel of the H. Comm. on Armed Services, 114th Cong. 23-24 (2016) (statement of LTC Jean-Claude G. D’Alleyrand, M.D., Chief, Orthopedic Traumatology Service, Walter Reed National Military Medical Center). See also DOD Inspector General, Evaluation of DOD Efforts to Assign Medical Personnel to Locations Where They Can Maintain Wartime Readiness Skills and Core Competencies (June 13, 2025).
[6]GAO, Defense Health Care: Actions Needed to Improve Billing and Collection of Debt for Civilian Emergency Care, GAO‑22‑104770 (Washington, D.C.: July 7, 2022). In this report, we recommended that DOD assess and monitor how providing civilian emergency care maintains clinical readiness. DOD concurred and has implemented this recommendation by performing assessments on the clinical readiness obtained from providing medical care to civilians at its medical facilities.
[7]For purposes of this report, “partnerships” refers to (1) partnerships at civilian medical facilities established through training agreements, training affiliation agreements, memorandums of understanding, or medical training agreements that are used for maintaining and sustaining the clinical skills and readiness of DOD medical personnel (also referred to as military-civilian partnerships); and (2) partnerships at TRICARE facilities established by external resource sharing agreements that are used to provide additional opportunities for military medical personnel to care for beneficiaries. We excluded partnerships used to train military medical personnel in graduate medical education and other initial training, such as initial training for enlisted medical personnel. We also excluded from our scope partnerships with Veterans Affairs, such as resource sharing agreements between DOD and the Department of Veterans Affairs. For more information on resource sharing agreements between DOD and the Department of Veterans Affairs, see GAO, VA AND DOD Health Care: Agreements to Share Services and Other Resources Should Be Evaluated, GAO‑25‑107497 (Washington, D.C.: June 30, 2025).
[8]S. Rep. No. 114-255, at 175-176 (2016). These objectives overlap with DOD’s goals for the military health system, referred to as the “Quadruple Aim”: better health, better care, lower costs, and increased readiness.
[9]Pub. L. No. 114-328, § 707 (2016).
[10]Pub. L. No. 114-328, § 708(a) (2016).
[11]Pub. L. No. 114-328, § 708(c) (2016), as amended by Pub. L. No. 115-232, § 719 (2018).
[12]GAO, Defense Health Care: Actions Needed to Determine the Required Size and Readiness of Operational Medical and Dental Forces, GAO‑19‑206 (Washington, D.C.: Feb. 21, 2019). DOD concurred and has taken some steps in response to our recommendation, including establishing an organization within the Defense Health Agency to oversee its clinical readiness metrics. To fully address our recommendation, DOD should use its clinical readiness data to assess its linkage to retention outcomes.
[13]GAO, Defense Health Care: Actions Needed to Define and Sustain Wartime Medical Skills for Enlisted Personnel, GAO‑21‑337 (Washington, D.C.: June 17, 2021). DOD concurred and implemented our recommendation. Specifically, in September 2025 DHA issued an interim procedures memorandum that established processes for entering into new partnership agreements. The interim procedures memorandum requires the use of standardized agreements and that formal agreements be in place before training under the partnership begins, among other things. Defense Health Agency Interim Procedures Memorandum 25-002, Training Agreements (Sept. 9, 2025).
[14]H.R. Rep. No. 118-125, at 200 (2023); S. Rep. No. 118-58, at 173-174 (2023).
[15]We selected four large medical facilities (i.e., hospitals and medical centers): Eisenhower Army Medical Center (Army), Naval Medical Center Portsmouth (Navy), David Grant U.S. Air Force Medical Center (Air Force), and Walter Reed National Military Medical Center (DHA). We also selected three small medical facilities (i.e., clinics), one affiliated with each military department, that serve a rural and medically underserved area. We selected Raymond W. Bliss Army Health Center at Fort Huachuca (Army), Naval Health Clinic Oak Harbor at Naval Air Station Whidbey Island (Navy), and the 509th Medical Group at Whiteman Air Force Base (Air Force).
[16]DHA’s readiness dashboards consolidate data on medical personnel’s clinical activities, such as diagnoses and procedures, to generate metrics that can be used by DOD to evaluate personnel’s readiness to deploy and to identify gaps in their peacetime medical practice. Currently, DHA maintains a dashboard with clinical readiness metrics for 14 physician specialties: cardiac/thoracic surgery; critical care/trauma medicine; critical care/trauma surgery; emergency medicine; general surgery; neurological surgery; obstetrics/gynecology; ophthalmology; oral maxillofacial surgery; orthopedic surgery; otorhinolaryngology; peripheral vascular surgery; plastic surgery; and urology. The medical centers we selected had the lowest percentage of providers that were above a clinical readiness metric threshold based on fiscal year 2024 data taken from DHA’s readiness dashboards. We selected fiscal year 2024 because this time frame included the most current and complete set of data available at the time of our selection. We excluded those medical facilities that had less than 10 providers reporting clinical activity data in DHA’s readiness dashboards.
[17]We selected a partnership established by the Office of the Army Surgeon General (Vanderbilt University Medical Center), a partnership established by the Navy’s Bureau of Medicine and Surgery (BUMED) (University of Pennsylvania Health System), and a partnership established by the Air Force School of Aerospace Medicine (University Medical Center of Southern Nevada). For partnerships executed by each military department, we selected the corresponding civilian partner that reported the highest clinical readiness score in DHA’s readiness dashboards.
[18]We interviewed officials from each military department. We selected three operational units that share a partner with a DOD medical facility we interviewed. These units include Navy Fleet Surgical Team 8 and Naval Special Warfare Group, which—like Naval Medical Center Portsmouth—partner with Virginia Commonwealth University Health, as well as the Air Force’s 60th Aeromedical Evacuation Squadron which—like David Grant U.S. Air Force Medical Center—partners with University of California Davis Health. We also interviewed U.S. Army Special Operations Command officials who maintain 10 partnerships, including five partnerships that are co-located with partnerships established by U.S. Army Medical Command. Finally, we interviewed officials from the Air Force’s 720th Special Tactics Group, which shares a partner with one of the Air Force’s Centers for Sustainment of Trauma and Readiness Skills.
[19]10 U.S.C. § 1096; DOD Instruction 6000.19.
[20]DOD Instruction 6000.19; Department of Defense Instruction 6040.47, Joint Trauma System (Sept. 28, 2016) (incorporating change 2, effective June 14, 2022); and GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.; Sept. 2014).
[21]DHA’s timecard system is called the Defense Medical Human Resources System–internet. Defense Health Agency Procedures Manual 6010.13 states that medical facility personnel must ensure their labor hours are distributed to the appropriate work center, which is accomplished in DHA’s timecard system. Defense Health Agency Procedures Manual 6010.13, vol. 1, Medical Expense and Performance Reporting System (MEPRS) for Fixed Military Medical and Dental Treatment Facilities (DTFs): Business Rules (Sept. 27, 2018).
[22]Clinical activity data refer to documentation of specific direct patient care action taken by medical personnel. Examples include performing surgery, conducting a biopsy, and delivering wound care.
[23]We received clinical activity data from DHA’s readiness dashboard as of August 2025. Data uploaded into DHA’s readiness dashboards have a 2-month lag.
[24]We applied a 40-hour threshold to eliminate individuals who may not have had adequate time in a partnership to generate clinical activity data.
[25]DOD Instruction 6000.19; GAO‑14‑704G.
[26]Department of Defense Directive 5124.02, Under Secretary of Defense for Personnel and Readiness (USD(P&R)) (June 23, 2008) (incorporating change 2, July 23, 2025).
[27]Department of Defense Directive 5136.01, Assistant Secretary of Defense for Health Affairs (ASD(HA)) (Sept. 30, 2013) (incorporating change 1, Aug. 10, 2017).
[28]DOD Directive 5136.01.
[29]DOD Instruction 6000.19.
[30]Department of Defense Directive 5136.13, Defense Health Agency (Sept. 30, 2013) (incorporating change 2, effective Sept. 12, 2023). TRICARE is DOD’s worldwide health care program serving 9.4 million eligible beneficiaries. It comprises DOD’s medical facilities worldwide (collectively called the direct care system) with network and non-network TRICARE-authorized civilian health care professionals, institutions, pharmacies, and suppliers.
[31]Initially, DOD was expected to transfer responsibility for administration of its medical facilities to DHA by October 1, 2018. Pub. L. No. 114-328, § 702 (2016), codified as amended at 10 U.S.C. § 1073c. However, section 711 of the John S. McCain National Defense Authorization Act for Fiscal Year 2019 amended the law to allow DOD to complete the transfer by September 30, 2021. In November 2022, DOD completed its multiyear transition of medical facilities from the military departments, making DHA responsible for the management of all DOD medical facilities.
[32]DOD Instruction 6000.19.
[33]DOD Instruction 6000.19 directs the Director to maintain a registry of all partnerships established by the Director, DHA, or the Secretaries of the military departments that are intended to provide venues and opportunities for military medical personnel to obtain and sustain clinical knowledge, skills, and abilities associated with their medical specialty or community.
[34]Defense Health Agency Administrative Instruction 5136.03, Delegation of Authority and Assignment of Responsibility for Administration and Management of Direct Care (Nov. 2022). Each DOD medical facility is commanded by a dual-hatted military officer who serves as facility director and service commander. As facility directors, they exercise authority, direction, and control of all facility operations, and control of all personnel assigned or performing work duties at the facility, among other things. As service commanders for military medical personnel assigned to DOD medical facilities, they exercise administrative control in the facilities and command and control over such personnel executing military service duties.
[35]Sections 7013, 8013, and 9013 of title 10, United States Code, grant authority to the Secretaries of the Army, the Navy, and the Air Force, respectively, to conduct all affairs of their departments, including recruiting, organizing, supplying, equipping, training, servicing, mobilizing, demobilizing, administering, maintaining, and military construction and maintenance.
[36]DOD, Defense Health Program: Fiscal Year (FY) 2026 Budget Estimates–Operation and Maintenance, Procurement, and Research, Development, Test and Evaluation (June 2025).
[37]A Level I trauma center has the highest designation and must meet annually minimum volume requirements for evaluating and treating severely injured patients, including the most complex trauma patients. A Level II trauma center has clinical standards identical to Level I trauma centers, although a Level II trauma center either supports a Level I center or is the lead trauma center in the absence of a Level I center. Level III and Level IV trauma centers provide emergency assessment, resuscitation, and stabilization before possible transfer to a higher-level trauma center.
[38]For more information on staffing of DOD’s medical facilities, see GAO, Defense Health Care: Information Needed to Improve Monitoring of Military Personnel Staffing at Medical Facilities, GAO‑25‑106988 (Washington, D.C.: July 21, 2025).
[39]Military medical personnel (active and reserve), civilians, and contractors may participate in a partnership.
[40]DOD Instruction 6000.19.
[41]See appendix I for more information about selected military department programs and their civilian partners.
[42]10 U.S.C. § 1096.
[43]TRICARE Operations Manual 6010.62-M, ch. 15, sec. 2, Resource Sharing (Apr. 2021, incorporating change 56, May 7, 2026).
[44]Institute for Defense Analyses, Independent Study of Force Mix Options and Service Models to Enhance Readiness of the Medical Force (Alexandria, Va.: June 2023).
[45]Pub. L. No. 116-22, § 204 (2019) (codified at 42 U.S.C. § 300d-91).
[46]The Department of Health and Human Service’s Administration for Strategic Preparedness and Response leads the nation’s medical and public health preparedness for, response to, and recovery from disasters and other public health emergencies. The administration collaborates with hospitals; health care coalitions; biotech firms; community members; state, local, tribal, and territorial governments; and other partners across the country to improve readiness and response capabilities. The program was authorized $11.5 million for each of fiscal years 2019 through 2023. Appropriations for this program were initially provided in fiscal year 2022, with $2 million appropriated in fiscal year 2022 and $4 million appropriated for each of fiscal years 2023, 2024, and 2025.
[47]DHA and the military departments have developed clinical readiness metrics to ensure that military medical personnel are proficient and clinically ready to deploy and provide care in an operational setting. More information about DHA and the military departments’ assessments of partnerships’ contributions to clinical readiness is covered later in this report.
[48]RAND, Reimagining the Army Medical Corps: Five Ideas for Raising Recruitment, Restoring Retention, and Restructuring Requirements (Sept. 2024).
[49]Physicians who specialize in otorhinolaryngology have special training in diagnosing and treating diseases of the ear, nose, and throat. These physicians are also known as ENTs.
[50]GAO‑25‑106988. In that report, we examined trends in staffing of military medical personnel at DOD medical facilities and reviewed DOD’s staffing process at the facilities.
[51]Defense Health Agency Interim Procedures Memorandum 25-002, Training Agreements (Sept. 9, 2025).
[52]The Federal Tort Claims Act permits individuals injured by the wrongful or negligent acts or omissions of federal employees, including medical malpractice in certain situations, to seek and receive compensation from the federal government through an administrative process and, ultimately, through the federal courts. 28 U.S.C. §§ 2671-2680.
[53]These agreement provisions fulfill requirements agreed on by the Department of Justice and the military departments to ensure that the United States can assert applicable legal defenses in malpractice lawsuits.
[54]DHA officials stated that they implemented these review and waiver processes to ensure that agreements comply with the Department of Justice’s legal requirements.
[55]Partnerships can be established by DOD medical facilities, military departments, and others.
[56]10 U.S.C. § 1094.
[57]A provider’s privileges define the scope and limits of their practice based on factors such as the health care setting they are serving in and their relevant training and experience. For more information on credentialing and privileging at DOD medical facilities, see, for example, GAO, Military Health Care: Improved Procedures and Monitoring Needed to Ensure Provider Qualifications and Competence, GAO‑22‑104668 (Washington, D.C.: Aug. 11, 2022).
[58]Military medical personnel participating in a partnership continue to receive their military compensation, which consists of basic pay, housing allowance, subsistence allowances, special pays, and other pays and allowances to which they are entitled.
[59]DOD cost savings are reduced for Medicare-eligible beneficiaries because the associated health care costs are primarily reimbursed by Medicare. DOD’s liability is financed through its Medicare Eligible Retiree Health Care Fund rather than through annual DOD appropriations. Of the 9.4 million eligible beneficiaries, approximately 2.4 million are Medicare-eligible, including military retirees, survivors, and other special eligibility groups who qualify and receive benefits from Medicare by law.
[60]DOD, Study and Plan on the Use of Military-Civilian Integrated Health Delivery Systems (Sept. 2022).
[61]Pub. L. No. 114-328, § 706 (2016). See also 10 U.S.C. § 1096.
[62]DOD, Study and Plan on the Use of Military-Civilian Integrated Health Delivery Systems (Sept. 2022).
[63]According to its charter, the purpose of the Military-Civilian Partnership Working Group is to provide opportunities among the military departments, the DHA, and other key supporting entities in and outside of the Military Health System to facilitate communications and develop recommendations for identifying, selecting, maintaining, and enabling civilian partnerships.
[64]Congressional Budget Office, Long-Term Implications of the 2025 Future Years Defense Program (Nov. 2024). Amounts reported by the Congressional Budget Office include Defense Health Program operation and maintenance costs, military compensation, civilian compensation, and accrual payments for retirees.
[66]10 U.S.C. §1073c; DOD Instruction 6000.19. The Director of DHA manages, among other things, the execution of policies issued by the Assistant Secretary of Defense for Health Affairs and manages and executes the Defense Health Program appropriation. DOD Directive 5136.13.
[67]We did not independently review the contents of each of the agreements to verify this information.
[69]DOD Instruction 6000.19.
[70]Defense Health Agency, DCFM Financial Management Guide, Annex-E: Medical Expense & Performance Reporting System (MEPRS) Cost Accounting (Feb. 6, 2025).
[72]The use of digital tools maintained by Army Medical Command, Navy BUMED, and the Air Force’s 711th Human Performance Wing are not limited to personnel participating in partnerships.
[73]U.S. Army Medical Command Operation Order 24-15, Readiness Reporting Decision Dashboard and MyEvaluations Implementation–USAMEDCOM (Mar. 2024).
[74]BUMED currently instructs personnel assigned to one of its expeditionary medical platforms to use its tool. We found that personnel embedded in BUMED’s military-civilian partnerships with Cook County Health Hospital System and the University of Pennsylvania Health System use this tool. We also found that personnel embedded in the Navy Trauma Training Center at the Los Angeles General Medical Center use this tool, although officials noted that they are not assigned to one of BUMED’s expeditionary medical platforms. Furthermore, Los Angeles General Medical Center hosts rotating Navy medical personnel. According to this partnership’s director, rotators include personnel assigned to a BUMED expeditionary medical platform and other Navy medical personnel who are not. To ensure data on clinical activities are captured for all rotators, the director of the partnership stated that it recently implemented a process by which rotators submit their clinical activities to a data coordinator who consolidates and enters the data into BUMED’s data collection tool. According to a BUMED official, BUMED is developing a policy to expand the use of this tool to all BUMED personnel. Finally, Navy officials stated that Navy medical personnel participating in its Hospital Corpsman Trauma Training military-civilian partnerships do not use this tool to record clinical activities and instead rely on an alternative data collection method, as described later in this report.
[75]Uniformed Services University of the Health Sciences trains and educates health professionals. Uniformed Services University of the Health Sciences is responsible for providing subject matter expertise to DHA’s clinical readiness program, which is described in greater detail later in this report.
[76]The Army Medical Command’s dashboard demonstrates the completion of training requirements only for embedded personnel in its partnerships, according to an Army Medical Command official. However, Army Medical Command maintains data on the completion of training requirements by personnel rotating through its partnerships.
[77]According to a BUMED official, data in its dashboard for personnel rotating through Los Angeles General Medical Center are limited to those assigned to one of BUMED’s expeditionary medical platforms. However, BUMED collects and maintains data on personnel rotating through this partnership who are not assigned to one of BUMED’s expeditionary medical platforms.
[78]According to this official, the unit temporarily paused rotations at the civilian facility to provide unit leadership with time to evaluate and enhance the partnership.
[79]The remaining center hosts a critical care course for enlisted medical personnel within a civilian medical center. According to an official overseeing this center, only one physician is assigned as an instructor and works within the civilian medical center.
[81]According to this official, the unassessed partnership serves as an alternative location when the unit’s medical personnel cannot participate in its primary military-civilian partnership.
[82]Deputy Secretary of Defense Memorandum, Stabilizing and Improving the Military Health System (Dec. 6, 2023).
[83]The management office was established within DHA in April 2022.
[84]DHA management office officials stated that they collect data on clinical activities performed in partnerships established by external resource sharing agreements from DOD’s electronic health record, whereas procedural and diagnostic codes from billing data are provided to DHA’s management office for activities performed in military-civilian partnerships. According to management office officials, they began collecting clinical activity data from military-civilian partnerships in 2022.
[85]Mission Zero Act Program civilian partners are required to submit clinical activity data to the management office on behalf of military medical personnel participating in the partnerships. However, Army Medical Command officials stated that they submit data to the management office on behalf of their civilian partners that receive grant funding under the program.
[86]The management office assigns a point score to each clinical activity based on factors such as complexity.
[87]Given the limitations of the management office’s data, we are unable to determine the total number of medical personnel within these specialties who participated in a partnership but did not submit readiness data.
[88]Management office officials explained that the presence of a partnership on this list does not necessarily indicate that it has failed to submit clinical activity data for physicians, as it is possible that no physicians of that specialty are participating in the partnership.
[89]Lieutenant Colonel Justin Fox, Colonel Ryan Earnest, and Colonel Valerie Sams, “The Military-Civilian Partnerships Quality Improvement Program Concept: A Process to Improve Data Collection and Outcomes Assessment,” Military Medicine, vol. 189, no. 11-12 (2024). Officials tested their data-quality improvement process at two locations—a DOD medical facility’s partnership program and an embedded partnership program not associated with a DOD medical facility. The study concluded that further examination of the data-quality improvement process is needed at other institutions to validate its effectiveness.
[90]GAO‑19‑206. At the time we issued this report, DOD had piloted its metric for two specialties: general surgeons and orthopedic surgeons.
[91]In 2023, DOD determined that 17 medical specialties meet the conditions in this recommendation. Consequently, we closed this recommendation as implemented.
[92]These personnel consisted of two emergency medicine physicians and one orthopedic surgeon.
[93]We limited our analysis to those physicians who reported working 40 hours or more in a partnership. Only medical personnel working in a fixed DOD medical facility are required to complete a timecard. Therefore, personnel who have not worked in a DOD medical facility—such as those embedded full time in a partnership—were not examined in our analysis. Furthermore, some personnel who are required to complete a timecard are not permitted to record time spent in a partnership, such as personnel assigned to operational units who intermittently work in a DOD medical facility.
[94]Given the limitation of DHA’s data, we are unable to determine the total number of medical personnel within the 14 specialties who participated in a partnership but did not submit readiness data.
[95]DOD Instruction 6000.19.