COVID-19
Federal Efforts to Support Behavioral Health Programs During the Pandemic
Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
For more information, contact: Alyssa M. Hundrup at HundrupA@gao.gov.
What GAO Found
The Substance Abuse and Mental Health Services Administration (SAMHSA) leads federal efforts to advance behavioral health. This includes providing grant funding and technical assistance to states and behavioral health providers to implement behavioral health prevention and treatment programs. Selected SAMHSA state and provider awardees said they made various changes to continue delivering behavioral health services during the COVID-19 pandemic.
SAMHSA also provided technical assistance and flexibilities to assist awardees with grant administration and program implementation during the COVID-19 pandemic, according to agency documentation, as well as agency officials, selected state and provider awardees, and national associations. For example:
· SAMHSA provided one-on-one assistance, connected awardees with one another and with partners, and disseminated resources including webinars and published documents; nearly all selected awardees found this support helpful during the COVID-19 pandemic.
· SAMHSA provided grant administration flexibilities to help awardees meet pandemic needs. For example, SAMHSA extended COVID-19 supplemental funding project periods for its mental health and substance use block grants to allow awardees additional time to complete grant-funded activities.
· SAMHSA, in partnership with other federal agencies, provided program flexibilities to help awardees deliver services during the COVID-19 pandemic. Such flexibilities included allowing clinicians to prescribe certain medication to treat opioid use disorder via telehealth.
Why GAO Did This Study
Behavioral health conditions, which include mental and substance use disorders, affect millions of people in the U.S. and these numbers continue to grow. The COVID-19 pandemic exacerbated needs for behavioral health services and affected service availability and delivery.
In fiscal years 2020 through 2023, SAMHSA awarded over $32 billion in grant funding to support behavioral health services. This included approximately $8.3 billion in COVID-19 supplemental funding that SAMHSA awarded to help grant awardees address behavioral health needs due to the pandemic.
The Consolidated Appropriations Act, 2023, includes a provision for GAO to review SAMHSA programs and activities to support the continued provision of behavioral health services during the COVID-19 pandemic. Among other topics, this report describes how selected SAMHSA awardees provided services during the COVID-19 pandemic and how SAMHSA assisted awardees to support their response to the pandemic.
GAO reviewed documentation and interviewed officials from seven states and one territory (which we refer to collectively as selected states) and 16 behavioral health providers about experiences during the COVID-19 pandemic from January 2020 through May 2023. GAO selected states to obtain a mix of geographic regions, among other criteria, and selected two providers from each state to reflect receipt of certain SAMHSA grants. GAO also reviewed agency documentation, interviewed SAMHSA officials, and interviewed representatives from four national associations with behavioral health expertise.
|
Abbreviations |
|
|
|
|
|
HHS |
Department of Health and Human Services |
|
MHBG |
Community Mental Health Services Block Grant |
|
Policy Lab |
National Mental Health and Substance Use Policy Laboratory |
|
SAMHSA |
Substance Abuse and Mental Health Services Administration |
|
SUBG |
Substance Use Prevention, Treatment, and Recovery Services Block Grant |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
February 25, 2026
The Honorable Bill Cassidy, M.D.
Chair
The Honorable Bernard Sanders
Ranking Member
Committee on Health, Education, Labor, and Pensions
United States Senate
The Honorable Brett Guthrie
Chairman
The Honorable Frank Pallone, Jr.
Ranking Member
Committee on Energy and Commerce
House of Representatives
Behavioral health conditions, which include mental health conditions and substance use disorders, affect millions of people in the United States.[1] During the COVID-19 pandemic, the number of drug overdoses and the prevalence of mental health conditions both increased, amplifying the need for behavioral health services.[2] For example, in 2023, an estimated 85 million adults (33 percent) and 6 million adolescents (23 percent) had a behavioral health condition, an increase from 74 million adults (29 percent) and 5 million adolescents (21 percent) in 2020, according to the Substance Abuse and Mental Health Services Administration (SAMHSA).[3]
The COVID-19 pandemic exacerbated longstanding concerns about the availability of substance use treatment and mental health services and affected the modes of service delivery, according to SAMHSA. For example, SAMHSA reported that more than half of adults who received mental health services in late 2020 had appointments moved from in person to telehealth, and more than a third experienced appointment delays or cancellations.[4] The pandemic also increased concerns about behavioral health workforce shortages, as some providers laid off behavioral health staff and other providers closed because they did not have the financial reserves to survive financial losses and increased operating expenses, according to SAMHSA.
SAMHSA, an agency within the Department of Health and Human Services (HHS), leads federal efforts to advance the behavioral health of the nation.[5] To do so, the agency provides grant funding and technical assistance to states and behavioral health providers, among others, to implement mental health and substance use treatment and prevention programs. SAMHSA contributes to national behavioral health policy efforts through its National Mental Health and Substance Use Policy Laboratory (Policy Lab) and can draw on advice from the public and behavioral health professionals through its advisory councils to advance its goals.
In fiscal years 2020 through 2023, SAMHSA awarded over $32 billion through its annual budget authority to support programs that provided substance use treatment, substance use prevention, or mental health services, according to agency data. This included approximately $8.3 billion in COVID-19 supplemental funding that SAMHSA awarded to help address behavioral health needs that resulted from the pandemic.[6]
The Consolidated Appropriations Act, 2023, includes a provision for us to review SAMHSA programs and activities to support the continued provision of mental health and substance use disorder services and related activities during the COVID-19 pandemic.[7] In this report, we describe
1. how SAMHSA’s advisory councils and Policy Lab supported the agency’s COVID-19 response;
2. how selected SAMHSA awardees provided services during the COVID-19 pandemic and what challenges they experienced; and
3. how SAMHSA provided assistance to awardees to support their response to the COVID-19 pandemic.
To address our first objective, we reviewed documentation and interviewed SAMHSA officials. Specifically, we reviewed reports and meeting minutes and interviewed officials about SAMHSA’s advisory councils and committees—which we refer to as advisory councils for the purposes of this report—and the Policy Lab. We reviewed activities that took place from January 2020 through May 2023, the timeframe of the COVID-19 public health emergency, which we refer to as the COVID-19 pandemic for the purposes of this report. (See app. I for additional details on the scope and methodology.)
To address our second and third objectives, we reviewed documentation from and interviewed officials and representatives from SAMHSA, four national associations, and a nongeneralizable sample of SAMHSA awardees. Selected awardees included seven states and one territory—which we refer to collectively as selected states—and 16 behavioral health providers in the selected states. The eight selected states are Michigan, Mississippi, Montana, Oregon, Pennsylvania, Puerto Rico, Texas, and Vermont.[8] We use the following modifiers to quantify awardees’ responses:
· “Nearly all” represents seven states when we are referring to just the states we interviewed, 12 to 15 providers when we are referring to just the providers we interviewed, or 18 to 22 awardees (i.e., the total across states and providers we interviewed).
· “Many” represents five to six states, eight to 11 providers, or eight to 17 awardees.
· “Some” represents two to four states, three to seven providers, or three to seven awardees.
The experiences of the selected awardees are not generalizable across all SAMHSA awardees. However, the information we obtained from them illustrates a variety of experiences with SAMHSA grants and assistance during the COVID-19 pandemic. We selected states and providers that received funding through a selection of SAMHSA grants, including block grants and others, to obtain variation in rurality and geographic region, among other factors.[9] Together, these selected grant programs represent over three-quarters (approximately 78 percent) of SAMHSA’s total funding awarded to support behavioral health services from fiscal years 2020 through 2023. (See app. I for additional details on our scope and methodology, including how we selected SAMHSA grant programs and awardees for this review; app. II contains summary information on the selected SAMHSA grant programs.)
We conducted this performance audit from July 2024 to February 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
SAMHSA Programs and Activities
SAMHSA leads federal public health efforts to advance the behavioral health of the nation. SAMHSA is responsible for, among other things, providing federal funding through grants to states, local communities, and private entities to support community-based mental health and substance use treatment and prevention services. SAMHSA also provides technical assistance to help states, territories, Tribes, and other behavioral health providers develop and strengthen behavioral health services.
Several SAMHSA offices—including four centers, nine advisory councils, and the Policy Lab—supported and coordinated the work of the agency during the COVID-19 pandemic from January 2020 through May 2023.
· Centers. SAMHSA carries out most of its programs and activities through four centers—the Center for Behavioral Health Statistics and Quality, the Center for Mental Health Services, the Center for Substance Abuse Prevention, and the Center for Substance Abuse Treatment—and its other offices. The centers support state and local efforts through funding and technical assistance; they do not directly deliver treatment services. The centers administer SAMHSA’s major block grant programs and most of SAMHSA’s other grant programs.
· Advisory councils. SAMHSA’s advisory councils provide advice to SAMHSA on various topics such as women’s services, tribal health, and the coordination of behavioral health activities across the federal government.[10] Advisory councils are made up of members of the public and behavioral health professionals. Some of SAMHSA’s advisory councils may also review applications submitted for certain SAMHSA grants and recommend projects for approval.[11]
· Policy Lab. The Policy Lab supports SAMHSA’s efforts to implement policy changes, coordinate its programs, and disseminate information regarding evidence-based practices.[12] The Policy Lab collaborates with entities within and outside of SAMHSA on various activities, including efforts to develop evidence-based practice written products and implementing legislation. The Policy Lab also manages SAMHSA’s Evidence-Based Practices Resource Center, a searchable online database of mental health and substance use information supported by scientific research. These resources provide communities, clinicians, policymakers, and others with information and tools to incorporate evidence-based practices into communities or clinical settings.
Selected SAMHSA Grant Programs
SAMHSA funds various grant programs that support the direct provision of behavioral health services, including during the COVID-19 pandemic. For example, two of SAMHSA’s largest grant programs—the Community Mental Health Services Block Grant (MHBG) and the Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG)—awarded funds to states, territories, and the District of Columbia, which, in turn, may have distributed funds through subawards to local government entities and behavioral health service providers, among others.[13]
The MHBG supports the development, implementation, and maintenance of community mental health services for both adults with serious mental illness and children and adolescents with serious emotional disturbance.[14] The SUBG supports the planning, implementation, and evaluation of activities for prevention, treatment, and recovery from substance use disorders. Both block grants allow flexibility for recipients to address the mental health and substance use disorder needs of their populations, according to SAMHSA. In addition to its two block grant programs, SAMHSA also funds prevention, treatment, and recovery support services for opioid use disorder through its State Opioid Response grant program.[15]
SAMHSA also awarded grant funding directly to community behavioral health systems and provider organizations, referred to as behavioral health providers for the purposes of this report, during the COVID-19 pandemic. For example, SAMHSA awarded funding through its Certified Community Behavioral Health Clinic Expansion grants to clinics that have met or can meet certification criteria and provide coordinated comprehensive mental health and substance use services regardless of an individual’s ability to pay. These grants supported behavioral health providers in establishing new community clinics that comply with certification criteria, such as providing crisis management services 24 hours a day, 7 days a week. The grants also supported existing certified community behavioral health clinics in expanding and improving services.[16] (See app. II for summary information on selected SAMHSA grant programs that supported the direct provision of behavioral health services during the COVID-19 pandemic.)
Additionally, SAMHSA funds various training and technical assistance centers that offer free support to those working in behavioral health, including SAMHSA awardees. Some of these centers provide support specific to SAMHSA grant programs, such as a national training and technical assistance center for certified community behavioral health clinic awardees, while others provide general support on a specific topic or population, such as disaster behavioral health. SAMHSA’s training and technical assistance centers serve national audiences through webinars and written resources; specific groups through topic-based virtual learning collaboratives, communities of practice, or short-term training; and communities, states, and Tribes through intensive individualized technical assistance.
In addition to these grant programs that predated the COVID-19 pandemic, SAMHSA also funded various grant programs specifically to address pandemic needs. Some of these programs are discussed below.
SAMHSA’s Role During the COVID-19 Pandemic
During an emergency such as the COVID-19 pandemic, SAMHSA is responsible for providing technical assistance, training, consultation, and operational support to federal, state, territorial, and tribal authorities to address behavioral health needs.[17] These needs can include addressing the effect of disasters and emergencies on behavioral health critical infrastructure and supporting population-level interventions to promote coping with stresses, among others. SAMHSA is also responsible for providing timely public health messaging to the general public to mitigate stress caused by an emergency. According to SAMHSA, it is common for people to experience behavioral health effects associated with disease outbreaks such as COVID-19, natural disasters (e.g., hurricanes), and other types of disasters or emergencies. For example, people may experience symptoms such as anxiety or sadness after such disasters.[18] Not everyone with symptoms will go on to have a diagnosed condition.
Additionally, SAMHSA is responsible for supporting locally led recovery activities to restore and enhance behavioral health supports and systems, including populations experiencing post-disaster trauma.[19] While some people’s behavioral health symptoms resolve soon after a crisis, others may experience longer-term effects.[20] In addition, some people who have no symptoms right after a crisis may develop delayed symptoms later on.[21]
To help address the effects of the COVID-19 pandemic on behavioral health, SAMHSA awarded approximately $8.3 billion in COVID-19 supplemental funding in grants to recipients that included states, territories, the District of Columbia, Tribes, and nongovernmental organizations.[22] For example, SAMHSA awarded $3.1 billion to SUBG awardees and $2.3 billion to MHBG awardees with supplemental funding from the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021.[23]
Additionally, SAMHSA used $1.3 billion in COVID-19 supplemental funding for grants to support certified community behavioral health clinics and used $823 million to create the new Community Mental Health Centers grant program to enable community mental health centers to support and restore delivery of clinical services affected by the COVID-19 pandemic.[24] SAMHSA also used about $345 million in COVID-19 supplemental funding for the new Emergency Grants to Address Mental and Substance Use Disorders During COVID-19 (Emergency COVID-19 grants) to help states, territories, and Tribes provide crisis intervention services, mental and substance use disorder treatment, and other related recovery supports for people affected by the pandemic.[25] (See app. II for more information on SAMHSA’s use of COVID-19 supplemental funding to support selected grant programs during the pandemic.)
Grant Flexibilities Available During COVID-19
During a public health emergency such as the COVID-19 pandemic, SAMHSA is permitted to extend or waive certain block grant requirements for SUBG and MHBG recipients. For example, the Public Health Service Act allows SAMHSA to provide extensions, waive application deadlines, and waive compliance with other grant requirements as the circumstances of the public health emergency reasonably require.[26] Additionally, the Consolidated Appropriations Act, 2021, allowed SAMHSA to waive grant requirements related to allowable activities, timelines, or reporting for SUBG and MHBG COVID-19 supplemental funding awards to help awardees respond to COVID-19.[27]
Starting in March 2020, the Office of Management and Budget also allowed federal awarding agencies, including SAMHSA, to implement certain exceptions to government-wide grant requirements.[28] These exceptions—referred to as grant administration flexibilities for the purposes of this report—were intended to provide awardees with the administrative and financial relief necessary to complete grant-related activities during the COVID-19 pandemic, according to Office of Management and Budget guidance. The Office of Management and Budget authorized agencies to provide 16 flexibilities during the COVID-19 pandemic.[29] For example, agencies could extend awardees’ grant project periods by up to 1 year—referred to as a no-cost extension—to allow them to continue implementing program activities. Agencies could also allow awardees to spend grant funds on normally unallowable costs to meet pandemic needs. Federal agencies, including SAMHSA, could decide to make these flexibilities available to awardees as they deemed appropriate and to the extent they were permitted by law.
Additionally, certain federal agencies—including SAMHSA, the Drug Enforcement Administration, and HHS’s Office for Civil Rights—issued guidance allowing flexibilities in behavioral health program implementation during the COVID-19 pandemic. These changes, referred to as program flexibilities for the purposes of this report, were intended to help SAMHSA awardees and others deliver behavioral health services during the COVID-19 pandemic to meet pandemic needs.
Advisory Councils and Policy Lab Provided Advice and Resources to Support SAMHSA’s COVID-19 Response
Advisory Council Advice Related to COVID-19
Each of SAMHSA’s nine advisory councils that were active during the COVID-19 pandemic contributed to the agency’s COVID-19 response, including by providing advice, according to SAMHSA documentation and officials.[30] (See fig. 1 for a description of these councils.) SAMHSA officials told us the agency took some steps to address councils’ advice, though it is not required to do so under the federal act that governs the advisory councils.[31]
Figure 1: SAMHSA Advisory Councils and Focus Areas During the COVID-19 Pandemic, January 2020–May 2023
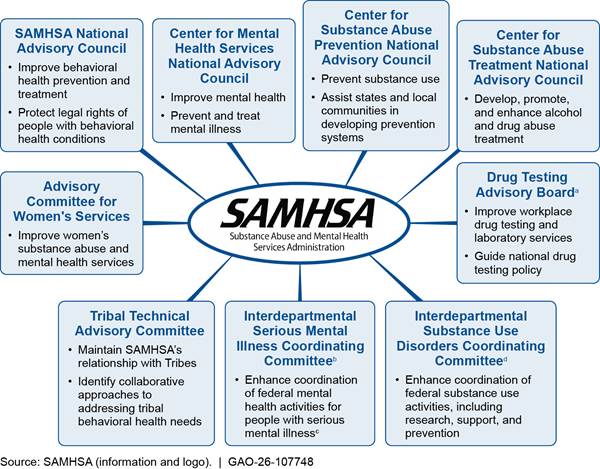
aThe Drug Testing Advisory Board was terminated effective March 31, 2025, according to SAMHSA’s website.
bThe Interdepartmental Serious Mental Illness Coordinating Committee was terminated effective April 9, 2025, according to SAMHSA’s website.
cAdults with serious mental illness are ages 18 and older with a diagnosable mental, behavioral, or emotional disorder—such as bipolar disorder, major depressive disorder, or schizophrenia—that substantially interferes with their life and ability to function, according to SAMHSA. Individuals with serious emotional disturbance are those under age 18 with a diagnosable mental, behavioral, or emotional disorder that substantially interferes with or limits the child’s role or functioning in family, school, or community activities, according to SAMHSA.
dThe Interdepartmental Substance Use Disorders Coordinating Committee was terminated effective May 6, 2025, as stipulated in the SUPPORT for Patients and Communities Act, according to SAMHSA’s website. Pub. L. No. 115-271, § 7022, 132 Stat. 3894, 4010–12 (2018). In December 2025, the law was reauthorized and set September 30, 2030, as the new termination date for the committee. SUPPORT for Patients and Communities Reauthorization Act of 2025, Pub. L. No. 119-44, § 110(b), 139 Stat. 669, 677–78. See also 42 U.S.C. § 290aa note.
|
Federal Advisory Councils Federal advisory councils and committees are to inform public policy and government regulations by advising the President and federal agencies on national issues. Federal advisory councils may be composed of subject matter experts, representative members, and federal government employees who provide advice and recommendations to help inform and improve executive branch operations and programs. Some of these councils—including eight of the nine councils that advised the Substance Abuse and Mental Health Services Administration (SAMHSA) during the COVID-19 pandemic—are governed by the Federal Advisory Committee Act. This act requires federal agencies to ensure that federal advisory councils make decisions that are independent and transparent to the public. For example, councils can only deliberate and decide on advice and recommendations to agencies during meetings that are open to the public, and they must make meeting minutes publicly available. Absent any statutory requirements, advisory councils are advisory only. The act does not require agencies to respond to or implement advisory council recommendations, or to publish information on any agency response to recommendations. Source: Information from U.S. General Services Administration and SAMHSA; 5 U.S.C. ch. 10. | GAO‑26‑107748 |
We found that all nine advisory councils discussed and advised SAMHSA on the use of telehealth during the COVID-19 pandemic. We found that all but one advisory council discussed and advised SAMHSA on specific populations’ experiences during the COVID-19 pandemic, grant implementation during the pandemic or program sustainability after the end of the pandemic, and future agency priorities to recover from COVID-19.[32] Members discussed these topics during public meetings and published meeting minutes and reports with advice related to COVID-19, for example.
Telehealth. Advisory council members discussed and advised the use of telehealth for mental health and substance use services during the COVID-19 pandemic. For example, one advisory council published a report to Congress in April 2022 that discussed the use of telehealth for people with serious mental illness and serious emotional disturbance.[33] The council reported that telehealth—including both video and telephone appointments—improved access to care for these individuals. In this report, the council advised federal agencies, including SAMHSA, to promote the use of evidence-based telehealth and publish guidelines for providing telehealth services.
Advisory council members also discussed the benefits and limitations of telehealth. For example, some advisory council members said that telehealth can reduce childcare and transportation barriers as well as stigma related to receiving behavioral health care. However, some advisory council members noted that telehealth may not work for all clients, including those with limited internet access, computer literacy skills, or privacy for appointments.
One council advised that SAMHSA continue research on benefits and drawbacks of telehealth, as well as its effectiveness in different socioeconomic and demographic populations. One council member emphasized the importance of studying telehealth practices and gathering population-level data to better understand how different communities benefit from telehealth or experience barriers to its use. A member of another council advised that SAMHSA research and evaluate telehealth services and support compared to in-person services provided during the COVID-19 pandemic. The member said that this research could help inform the use of telehealth in future emergencies.
According to officials, SAMHSA responded to this advice by sharing information with providers on using telehealth for behavioral health services, supporting increased use of telehealth during the COVID-19 pandemic, and working to identify telehealth best practices and ways to address limitations. For example, SAMHSA implemented a national training and technical assistance program on telehealth with over 300,000 behavioral health provider participants, according to officials.[34] Additionally, SAMHSA officials said the agency advocated for increased access to telehealth through telephone-based behavioral health appointments, rather than restricting services to video calls, to serve households with limited internet access or technology. According to SAMHSA, the agency partnered with the Federal Communications Commission to inform the public about extended cell phone minutes for individuals with severe mental illness who may need telephone-based mental health services.
Specific populations. Advisory council members discussed and advised SAMHSA on how the COVID-19 pandemic affected specific populations, such as women, tribal communities, youth, and health care providers. For example, some council members discussed factors that might have contributed to increased alcohol use among women, such as parenting-related stress. One council advised that SAMHSA collect data on women’s behavioral health during the COVID-19 pandemic to help explain why women were disproportionately affected. According to SAMHSA officials, the agency added questions to the National Survey on Drug Use and Health related to the receipt of telehealth services and the effect of COVID-19 on behavioral health to allow for an improved understanding of substance use and mental health patterns during the COVID-19 pandemic.[35]
In 2021, another council advised that SAMHSA update its National Tribal Behavioral Health Agenda to reflect the long-term effects of the COVID-19 pandemic on tribal entities and incorporate post-pandemic needs.[36] SAMHSA began updating the agenda in August 2022, according to officials, by gathering agency and tribal leaders and citizens to explore updates related to tribal behavioral health and COVID-19. In April 2023, SAMHSA officials solicited feedback from the advisory council on whether the agency should add a chapter to the agenda on the effects of COVID-19 on tribal communities, including stress to the health care system and workforce as well as a decline in life expectancy. Following multiple listening sessions and consultation with this advisory council, SAMHSA determined that the foundational elements of the agenda remained relevant and continued to address ongoing needs without the addition of information specifically addressing COVID-19, according to SAMHSA officials.
Grant implementation and program sustainability. Advisory councils discussed SAMHSA grants, including grant implementation, grant requirements, and program sustainability after the end of the COVID-19 pandemic.[37] For example, given the rise of mental illness during the COVID-19 pandemic, one council advised that SAMHSA consider increasing grant funding flexibility to allow awardees to serve individuals with less severe mental health diagnoses.[38] In response, SAMHSA included requests in its proposed budgets for fiscal years 2023 through 2025 that Congress designate a subset of MHBG funding to support evidence-based programs that address early intervention and prevention of mental disorders for at-risk youth and adults, according to SAMHSA officials. One council member also described some awardees’ difficulty meeting the Emergency COVID-19 grant requirement to spend 10 percent of funds to support health professionals with mental health concerns and suggested this population may be reluctant to seek help.
Members of four advisory councils expressed concern about program sustainability after the COVID-19 pandemic, including ensuring that awardees maintain program quality. One council advised that SAMHSA create a plan for states to continue and sustain behavioral health services after COVID-19 supplemental funding ended. Another council member advised that SAMHSA allow state and local awardees to use grant funding to invest in behavioral health systems to prepare for the future and long-term needs following the COVID-19 pandemic. SAMHSA officials said that awardees could contact agency officials as needed to discuss allowable expenses to support program sustainability.
Future priorities. Councils also advised SAMHSA on future priorities and considerations for the agency to promote recovery from the COVID-19 pandemic. For example, several advisory councils discussed the long-term effects of COVID-19 on behavioral health. During one meeting, a member advised SAMHSA to prepare for a long process of behavioral health recovery from the COVID-19 pandemic, given that people experience delayed emotional responses, such as grief and psychological stress, following a disaster.
SAMHSA officials also asked advisory council members for advice on addressing long COVID—a chronic condition that can occur after COVID-19 infection and may affect behavioral health—and received several suggestions.[39] One council member suggested that SAMHSA formalize and disseminate protocols for diagnosing and treating long COVID. Another member advised using existing knowledge about treating mental health conditions such as depression, anxiety, and posttraumatic stress disorder to treat long COVID.
Advisory councils also discussed lessons learned from the COVID-19 pandemic and made suggestions to improve future emergency response. In April 2023, SAMHSA jointly convened members from six advisory councils to discuss a range of topics, including lessons learned from the COVID-19 pandemic to help prepare for the next public health emergency. During this meeting, one council advised SAMHSA to clearly document activities during emergencies, such as the COVID-19 pandemic, to help the agency mobilize quickly during future disasters. In a report to Congress, another council advised that lessons learned from the COVID-19 pandemic—including those related to mental health, physical health, and health care delivery—should inform federal policies and programs.[40]
SAMHSA engaged in various activities to address the long-term effects of COVID-19 on behavioral health. For example, SAMHSA commissioned an external national association to publish a series of 10 technical assistance papers on mental health response during and beyond the COVID-19 pandemic, including a post-COVID-19 vision for mental health services.[41] Topics covered included disaster behavioral health, suicide prevention, and mental health system development in rural and remote areas, among others. HHS, including SAMHSA, published a report summarizing services and supports for longer-term effects of COVID-19, including those related to mental health, substance use, and long COVID.[42] SAMHSA also published various resources about long COVID, including a literature review summary of the effects of long COVID on behavioral health and an advisory resource with evidence-based resources for treatment.[43]
Policy Lab Support During the COVID-19 Pandemic
We found the Policy Lab supported SAMHSA’s COVID-19 response by publishing resources, providing information to Congress, coordinating activities within SAMHSA and across the federal government, and in some cases, deploying staff to assist with local COVID-19 response efforts.
Publishing resources. The Policy Lab published resources on evidence-based practices and service delivery models to help communities, clinicians, policymakers, and others incorporate evidence-based practices into their communities or clinical settings in response to COVID-19. For example, in June 2021, the Policy Lab issued an evidence-based resource guide on using telehealth to treat serious mental illness and substance use disorders, including during the COVID-19 pandemic.[44] This guide included an overview of telehealth, a summary of research findings on its effectiveness for mental health and substance use treatment, guidance for implementing evidence-based practices, and resources for evaluation and quality improvement. (See fig. 2 for telehealth implementation considerations and strategies to facilitate effective implementation on multiple, interrelated levels, as described in the Policy Lab resource.) This guide referenced COVID-19 because of the increased need for and expansion of telehealth during the pandemic, according to SAMHSA officials.
Figure 2: SAMHSA Policy Lab Considerations for Using Telehealth to Treat Serious Mental Illness and Substance Use Disorder
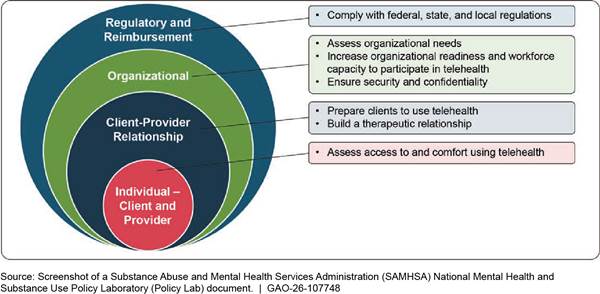
Notes: See Substance Abuse and Mental Health Services Administration, National Mental Health and Substance Use Policy Laboratory, Evidence-Based Resource Guide Series: Telehealth for the Treatment of Serious Mental Illness and Substance Use Disorders (Rockville, Md.: 2021).
Additionally, the Policy Lab published an advisory resource on long COVID that defines the condition, describes associated mental health symptoms, and provides evidence-based tools for diagnosis and treatment.[45] For example, this resource describes treatment approaches such as therapy to address new or relapsed psychiatric conditions related to long COVID; peer support groups to build connections with others with similar experiences; and physical rehabilitation to support recovery from chronic fatigue.
Providing information to Congress. The Policy Lab’s Office of Legislative Affairs provided technical assistance to Congress related to COVID-19 legislation and supplemental funding, according to SAMHSA officials. For example, SAMHSA officials said congressional staff consulted Policy Lab officials when developing legislation such as the CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021.[46] We previously reported that the Policy Lab responded to 298 inquiries from Congress, HHS, the Congressional Research Service, and the Congressional Budget Office in fiscal year 2022, according to SAMHSA officials.[47] The Policy Lab responded to 914 such inquiries in fiscal year 2023, according to officials.
Coordinating federal activities. The Policy Lab coordinated activities within SAMHSA and across the federal government to support the agency’s COVID-19 response. For example, beginning in 2022, the Policy Lab coordinated cross-cutting activities between the agency’s training and technical assistance programs, including assistance related to COVID-19, according to SAMHSA officials.[48] SAMHSA officials said that the Policy Lab hosted bimonthly meetings with SAMHSA’s training and technical assistance center program directors to discuss collaboration between programs and the dissemination of evidence-based practices. Officials from the Policy Lab also participated in a cross-governmental body that coordinated collaborative work on long COVID across 14 federal government agencies.[49] Additionally, the Policy Lab continued to coordinate SAMHSA’s nine advisory councils during the COVID-19 pandemic and supported their discussions and advice related to the pandemic, according to SAMHSA officials. For example, Policy Lab officials coordinated advisory council meeting agendas, speakers, and participants; ensured public access to meetings and oversaw completion of accurate meeting minutes; and modified advisory council meetings from in person to virtual during the COVID-19 pandemic, according to officials.
Deploying staff. SAMHSA deployed Policy Lab officials to Tribal Nations and the U.S. Public Health Service Commissioned Corps Headquarters Command Center to assist with the COVID-19 response.[50] For example, officials provided behavioral health support and mental health crisis response to staff at the Navajo Nation hospital and outpatient clinics in New Mexico and Arizona in August 2020, according to SAMHSA officials. Two Policy Lab officials supported the Headquarters Command Center, including by leading efforts to identify and safely deploy U.S. Public Health Service officers to support various local COVID-19 response efforts, according to SAMHSA officials.
Selected SAMHSA Awardees Made Various Changes to Service Delivery During the COVID-19 Pandemic Amid Challenges Such as Workforce Hiring and Retention
Selected Awardees Increased Telehealth to Maintain Services and Expanded Some Services to Address COVID-19 Needs
We found the 23 selected state and behavioral health provider awardees included in our review implemented a range of changes to their SAMHSA-funded behavioral health services to be able to continue providing services during the COVID-19 pandemic. These changes included using telehealth to deliver services, implementing COVID-19 safety measures for in-person services, expanding services to meet client needs, and developing new community and agency partnerships. (See fig. 3.)
Figure 3: Examples of Selected State and Provider Awardees’ Changes to Behavioral Health Services During the COVID-19 Pandemic
Increased use of telehealth. All 23 selected awardees reported using telehealth to maintain behavioral health services during the COVID-19 pandemic. Some awardees said they used telehealth prior to COVID-19, but on a more limited basis.[51] When the COVID-19 pandemic began in 2020, nearly all awardees said they increased telehealth capacity so they could continue to provide services while it was unsafe to provide them in person.
Nearly all awardees said they used video platforms such as Zoom, audio-only phone calls, and text messaging to provide services. Some awardees said they used SAMHSA funding to purchase equipment for providers to administer telehealth services. For example, one state used SAMHSA funding to supply providers with laptops, tablets, computer monitors, and videoconferencing equipment, according to a progress report submitted to SAMHSA.
Selected awardees used telehealth to provide behavioral health services such as counseling, peer support, case management, and crisis response to clients during the COVID-19 pandemic.[52] For example, one state installed telehealth kiosks in local emergency rooms to facilitate crisis screening and assessment and to allow for virtual face-to-face contact between the clinician and client, according to the state’s progress report submitted to SAMHSA. Another state’s residential treatment programs used telehealth to connect clients to off-site medical and psychiatric services, including medication-assisted treatment for substance use disorder, according to its progress report.[53] One provider said they provided coaching through telehealth to clients recovering from substance use disorders to help meet client needs when clients were unable to attend appointments in health care facilities due to COVID-19 restrictions.
Selected awardees used telehealth in a variety of locations. Some behavioral health staff delivered services from their homes, while others delivered telehealth services from clinics, according to providers. Clients received telehealth services at home, at clinics that were more accessible than those where behavioral health staff were located, or in private community locations with internet access, according to awardees. (See fig. 4.) For example, one provider said they set up telehealth infrastructure in rural clinics to connect clients to behavioral health staff at clinics in metropolitan areas. Some of these rural clinics were located hours away from metropolitan areas where providers were located, so this “hub-and-spoke” model helped clients in more remote areas receive care.
Figure 4: Examples of Locations for Behavioral Health Staff and Clients to Connect Through Telehealth
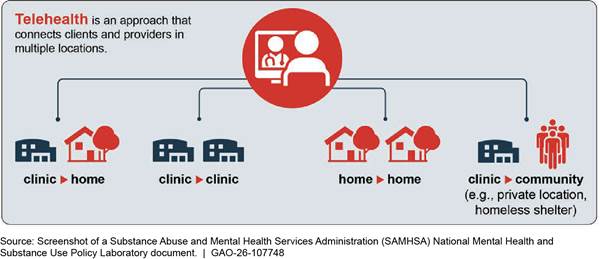
Notes: Telehealth can connect clients and providers in multiple locations such as at a home, private space in a clinical setting, or another location in the community, according to SAMHSA. Some telehealth appointments may connect a client in their home to behavioral health staff working from a clinic or from their own home. In other cases, clients may connect to behavioral health staff from a clinic site or private community location equipped with telehealth infrastructure, which can help address connectivity barriers. For example, clients and behavioral health staff can connect from separate rooms in the same clinic site to reduce COVID-19 spread, or from different clinic sites closer to each party’s home to reduce geographic barriers to care. See Substance Abuse and Mental Health Services Administration, National Mental Health and Substance Use Policy Laboratory, Evidence-Based Resource Guide Series: Telehealth for the Treatment of Serious Mental Illness and Substance Use Disorders (Rockville, Md.: 2021).
Many selected awardees said that clients benefitted from the increased use of telehealth to deliver services during the COVID-19 pandemic. Some awardees said that telehealth allowed them to serve more clients compared to before the COVID-19 pandemic began in 2020. Specifically, some awardees said client engagement and attendance improved as telehealth reduced some previous barriers to accessing services. Many awardees said telehealth helped clients in rural communities and areas with limited transportation who no longer had to travel long distances to access services. Some awardees also said that telehealth was particularly useful for adults who were technologically savvy and adjusted easily to virtual services.
Some selected awardees said that text messaging and audio-only telehealth helped clients with limited access to computers, internet, or smartphones to receive services during the COVID-19 pandemic. For example, one provider said they used SAMHSA funding to purchase work cell phones for behavioral health staff so that they could deliver services and conduct client outreach via text message. This provider said text messaging was useful for engaging with younger people, including young parents, who were comfortable with texting but did not always return phone calls.
Some selected awardees said behavioral health staff also benefitted from the use of telehealth, for example, because it allowed them to deliver services to clients while limiting their exposure to COVID-19. Some awardees said that behavioral health staff appreciated the convenience of telehealth, including the opportunity for remote or hybrid work. Telehealth also increased staff efficiency, according to representatives from one national association.[54] For example, one provider said that telehealth made it easier for clinicians to communicate with staff at other agencies, which allowed them to more efficiently coordinate their clients’ care.[55]
Implemented safety measures for in-person services. Nearly all selected awardees said they provided at least some services in person in addition to telehealth during the COVID-19 pandemic, and adjusted service delivery protocols to limit COVID-19 spread. Many awardees said that telehealth was not always the best option to provide certain types of services. For example, one provider said they met in person with clients who benefitted from face-to-face appointments, including clients receiving substance use treatment, to help ensure their safety. Additionally, some awardees said they generally continued to provide community-based services, such as assertive community treatment, in person to reach clients and maintain their connection to care while using safety measures to protect behavioral health staff and clients.[56]
Nearly all selected awardees increased use of safety and infection prevention measures, including personal protective equipment such as masks, to limit COVID-19 spread, according to state officials and providers. For example, one state used SAMHSA funding to purchase air purifiers and replacement filters for use by behavioral health staff to improve air quality and decrease COVID-19 risk, according to a progress report submitted to SAMHSA. This state also used SAMHSA funding to buy masks, COVID-19 testing kits, and cleaning and disinfecting supplies for staff delivering behavioral health services. In addition, some awardees said they reconfigured their clinics and waiting rooms to promote social distancing, including by installing clear plastic barriers.[57]
Additionally, many selected awardees said behavioral health staff met with clients in outdoor settings, such as pavilions, parks, and client yards, which allowed staff to safely check on clients and ensure they continued to receive services and support in convenient locations. For example, one state used SAMHSA funding to set up covered outdoor areas where behavioral health staff could meet with clients with reduced risk of COVID-19 spread, according to officials. Officials from this state said staff used these spaces to host youth and other mental health support groups that otherwise would not have had a safe space to meet and interact. Officials from one state said behavioral health staff worked out of their cars to reach clients in more rural areas and met with clients on the street. They delivered supplies and necessities, including sack lunches, to clients to maintain relationships and keep them connected to care. Many awardees said behavioral health staff met outdoors with clients at their homes for one-on-one or group meetings. For example, one provider said they delivered peer support, individual and group therapy, and counseling services in clients’ backyards.
Expanded services. Nearly all selected awardees said they expanded some of their behavioral health services during the COVID-19 pandemic, for example, by offering new services, increasing the reach of existing services, or targeting specific populations to address new or increased needs. Many awardees said they expanded peer support services during the COVID-19 pandemic. For example, one state expanded their peer support program to serve 26 of the state’s 36 counties, an increase from only a few counties served prior to COVID-19, according to officials. During the COVID-19 pandemic, this state’s peer support specialists served clients in community locations such as homeless encampments and laundromats, rather than only within hospital facilities, because fewer clients went into hospitals to receive services during the pandemic. Many awardees also expanded their crisis support services during the COVID-19 pandemic, such as crisis center hotlines, mobile crisis response teams, and walk-in crisis services located in clinics. For example, one state used SAMHSA funding to add a second staff member to each of their mobile crisis teams, which allowed them to provide services in people’s homes rather than solely in public settings such as schools and emergency departments.
Many selected awardees provided targeted services to certain populations that experienced increased needs during the COVID-19 pandemic, such as youth, people with co-occurring mental health and substance use disorders, tribal populations, health care professionals, and individuals experiencing homelessness. For example, one provider said they used SAMHSA funding to support a trauma-focused therapy program for children and adolescents to address trauma and disruption experienced during the COVID-19 pandemic. Another provider said they enhanced group programming and other services for clients with co-occurring mental health and substance use disorders to serve clients with more severe conditions, as they found this was increasingly common during the COVID-19 pandemic. Additionally, one provider said they enhanced culturally appropriate wellness services for tribal populations and worked closely with tribal leadership to coordinate behavioral health care for these clients. Some selected awardees said they provided services targeted to health care professionals, who experienced emotional strain due to the pandemic. For example, officials from one state said they hired clinical professionals to provide therapy and coaching for health care workers.
Developed or expanded partnerships. Nearly all selected awardees said they developed or expanded partnerships with community and faith groups, universities, or state and local governmental agencies to improve outreach during the COVID-19 pandemic. For example, one state partnered with faith-based organizations to educate congregants on addiction and mental illness and connect them to services and resources, according to officials. The state developed this partnership to reach the many residents who were already seeking support from faith leaders during the COVID-19 pandemic, officials said.
Many selected awardees said they developed or expanded partnerships with state and local government agencies, including public health and law enforcement agencies. For example, officials from one state and one provider said they partnered with other stakeholders, including law enforcement, to distribute the opioid overdose-reversal drug naloxone during the COVID-19 pandemic.[58] The state also worked with nonprofit organizations to help distribute naloxone, according to officials, to address COVID-19-related disruptions to the state’s original distribution plan. Some awardees also said they partnered with local law enforcement agencies to help de-escalate and intervene in situations involving people with severe mental illness and connect them to mental health services. For example, one state supplied police officers with internet-connected tablets they could use to connect people to crisis screening and intervention staff while responding to 911 calls, according to its progress report submitted to SAMHSA. Additionally, one provider said they delivered a crisis intervention training program to teach law enforcement officers about mental illness and proper intervention techniques during mental health emergencies.
Selected Awardees Experienced Workforce Hiring and Retention and Telehealth Implementation Challenges That Affected Service Delivery
The 23 selected state and behavioral health provider awardees in our review identified various challenges in providing behavioral health services during the COVID-19 pandemic. Awardees said they experienced challenges with workforce hiring and retention and the use of telehealth, among others, and that challenges affected service delivery.
Workforce hiring and retention. All 23 selected awardees experienced challenges hiring and retaining behavioral health provider staff during the COVID-19 pandemic, according to state officials and providers. Behavioral health provider workforce shortages existed prior to the start of the COVID-19 pandemic in 2020, and many awardees said that the pandemic exacerbated these challenges.[59] For example, some awardees said that state agency and provider staff were overwhelmed by having to take on additional responsibilities; struggled with burnout and fear of COVID-19 infection; and in some cases, left to work in other sectors that paid more, allowed remote work, or were less emotionally challenging. Additionally, one provider said that they experienced difficulties hiring community-based positions, such as case managers, that did not have a remote work option. Another awardee cited challenges hiring staff who were required to work in person, such as nurses and counselors. Officials from one state also said that some state behavioral health officials were reassigned to support the state’s pandemic response, causing staffing shortages at their agency.
Some selected awardees specifically struggled to hire staff to work in rural areas, according to state officials and providers. For example, officials from one state said that rural behavioral health clinics experienced challenges attracting qualified applicants, and one rural provider said they struggled to compete with providers in urban areas that could offer higher salaries. Some tribal communities also struggled to find licensed behavioral health staff willing to commute to isolated areas, because they tended to prefer living in larger cities and could find jobs closer to home, according to representatives from one national association.
Many selected awardees said that workforce shortages delayed grant implementation or interrupted service provision during the COVID-19 pandemic. For example, officials from one state said some of their subawardees took longer to begin implementing SAMHSA-funded behavioral health activities because they were understaffed and had to hire, train, and retain staff to administer services.[60] Officials from another state said that some clinics had to suspend enrollment in medication-assisted treatment services because they did not have enough staff to sustain services. Additionally, one provider said they delayed implementation of their peer support program due to staffing shortages. Another provider experienced challenges sustaining sufficient behavioral health staff—including those with a master’s degree—to provide mobile crisis services in a rural area for 24 hours a day, 7 days a week.
Selected awardees said they responded to workforce hiring and retention challenges in various ways, for example, by using SAMHSA grant funding to pay for new positions, increase salaries and provide bonuses, and implement staff wellness programs to improve morale. One provider said they used SAMHSA funding to hire 50 additional employees, including nurses, therapists, and prescribers such as physician assistants, which allowed the provider to serve more clients and meet the demand for services during the COVID-19 pandemic. In addition, this provider said they increased nurse and physician salaries to match market rates, gave sign-on bonuses to new hires, and gave referral bonuses to staff who helped with recruitment. One state also used SAMHSA funding to increase salaries for certain clinical staff that were difficult to hire and provided staff incentive payments, such as 6-month retention bonuses and tuition reimbursement, according to its progress report submitted to SAMHSA. Also, some awardees said they used SAMHSA funding to support workforce wellness efforts such as mindfulness coaching to address staff burnout, anxiety, and trauma that contributed to turnover during the COVID-19 pandemic.
Telehealth implementation. Many selected awardees said they experienced challenges using telehealth to provide behavioral health services during the COVID-19 pandemic, including issues with clients’ telehealth equipment and connectivity. For example, awardees said that some clients did not have access to telehealth devices, such as personal computers or smartphones, and some did not have consistent internet connection to join appointments. These challenges were more common in rural areas and among individuals with lower incomes or experiencing homelessness, according to some awardees. In rural areas, inconsistent broadband internet connectivity and cell phone service prevented some clients from receiving care; for example, one provider said that some rural clients experienced video call interruptions during telehealth sessions due to poor internet connection. Some awardees also said that behavioral health staff, especially those in rural areas, did not initially have access to devices to accommodate telehealth at the start of the COVID-19 pandemic in early 2020 but were generally able to quickly get the needed technology and equipment to provide services.
Selected awardees said they addressed clients’ telehealth equipment and connectivity challenges, for example, by setting up spaces in clinics or community locations where clients could access internet-connected telehealth devices. As a result, clients experiencing barriers to participating in telehealth from home could travel to a clinic or other facility and join telehealth appointments from that location. One state equipped rural mobile crisis response units with internet-connected tablets so behavioral health staff located in other areas could screen and assess rural clients, according to officials. Some awardees said behavioral health staff used audio-only phone calls to deliver services to clients who could not join video calls.
Many selected awardees also said that some clients, such as children and older adults, experienced challenges navigating telehealth platforms or participating in appointments outside of private settings. For example, some awardees said that clients sometimes joined telehealth appointments from public spaces or while family members were present. One provider said that the lack of privacy could affect certain clients’ ability to discuss confidential behavioral health issues as well as their safety, for example, from domestic violence. In response to challenges, some awardees said they taught clients how to use telehealth platforms and emphasized the importance of maintaining privacy and confidentiality during telehealth sessions. Some awardees said they resumed in-person services for clients who struggled to use telehealth when it was safe to do so.
Other challenges. Some selected awardees cited various other challenges to providing behavioral health services during the COVID-19 pandemic. These awardees said they experienced challenges meeting the increased demand for behavioral health services, including serving clients with more severe behavioral health needs that worsened during the COVID-19 pandemic. For example, officials from one state said they saw an increase in youth and college students with anxiety and depression, and two providers said that clients experienced increased trauma during the COVID-19 pandemic. Additionally, officials in one state said some clients who had been in long-term recovery relapsed during the COVID-19 pandemic. The increased demand for services strained awardee resources; for example, one provider said they had to waitlist clients.
Some selected awardees also expressed concern about the sustainability of services after the end of the grant project period. For example, officials from one state said local behavioral health clinics were reluctant to apply for subaward funding due to sustainability concerns, such as having to lay off staff when the state’s SAMHSA award ended.
Officials from one selected state and one selected provider said they experienced supply chain challenges during the COVID-19 pandemic that affected delivery of behavioral health services. For example, officials from one state said they experienced challenges in acquiring air purifiers, hand sanitizer, and masks for residential treatment facilities to protect clients and staff from COVID-19 infection. Additionally, one provider said they experienced difficulties securing computers, laptops, and cellphones, which delayed onboarding new staff and preparing them to deliver behavioral health services.
SAMHSA Provided Technical Assistance and Grant Administration and Program Flexibilities to Support Awardees During the COVID-19 Pandemic
Technical Assistance
SAMHSA provided one-on-one technical assistance, connected awardees with one another or with partners, and disseminated resources such as webinars and published documents to assist awardees during the COVID-19 pandemic, according to SAMHSA officials, selected state and behavioral health provider awardees, and representatives from national associations.[61] Officials from all states and nearly all providers said SAMHSA technical assistance and resources were generally helpful during the COVID-19 pandemic.[62]
Providing one-on-one technical assistance. SAMHSA officials said they continued to hold monthly video calls with each awardee during the COVID-19 pandemic and provided one-on-one awardee assistance on various topics through these meetings and in response to ad hoc inquiries. For example, SAMHSA officials advised awardees and answered questions on using COVID-19 grant flexibilities, determining allowable grant expenditures, building telehealth capacity, and enhancing mobile support services, according to agency officials. SAMHSA also established an electronic resource mailbox for recipients to submit COVID-19-related grants management questions, according to agency officials.
Among selected awardees, officials from all states and nearly all providers said they found one-on-one technical assistance helpful during the COVID-19 pandemic, and nearly all awardees said that SAMHSA officials were responsive and available to address their questions. For example, one provider said that SAMHSA officials helped them revise degree requirements for a grant-funded position, which helped them successfully hire staff. Officials from one state said SAMHSA officials shared strategies other states used to keep patients engaged in services during the COVID-19 pandemic.
SAMHSA provided individualized assistance to each awardee that was tailored to their unique circumstances or community needs, according to agency officials. Officials said that SAMHSA hired additional staff to help manage the increased number of awards the agency was administering because of the COVID-19 supplemental funding.
However, some selected awardees shared that they experienced challenges related to staff turnover with their assigned SAMHSA points of contact, and many selected awardees identified topics for which they would have liked more robust, clearer, or additional technical assistance from SAMHSA during the COVID-19 pandemic. For example, one provider said that SAMHSA staff turnover made it difficult to identify the correct SAMHSA point of contact to answer questions. Additionally, one provider located in a rural area said they could have benefitted from resources that were tailored to rural settings, such as resources on addressing transportation barriers for clients, and another provider said they would have appreciated additional technical assistance on clinical topics, such as delivering therapeutic interventions using telehealth. SAMHSA officials acknowledged that awardees likely experienced challenges during the COVID-19 pandemic, including related to SAMHSA staff turnover. To address these challenges, SAMHSA ensured grantees had consistent access to SAMHSA staff through the agency’s resource mailboxes; provided direct technical assistance support to awardees, including through SAMHSA-funded training and technical assistance centers; and produced specialized technical assistance products and resources, according to agency officials.
Facilitating awardee connections. SAMHSA and the training and technical assistance centers it funds connected awardees with other awardees or behavioral health partners for networking and support during the COVID-19 pandemic, according to officials from SAMHSA, representatives from national associations, and selected state and provider awardees.[63] Agency officials said SAMHSA provided peer learning opportunities and monthly meetings during the COVID-19 pandemic where state awardees presented best practices. For example, the SAMHSA-funded Certified Community Behavioral Health Clinic Expansion Grantee National Training and Technical Assistance Center hosted awardee learning communities for certified community behavioral health clinic awardees during the COVID-19 pandemic, according to representatives from one national association. This center also facilitated a mentorship program between newer clinics and more experienced certified community behavioral health clinics during the COVID-19 pandemic, according to representatives from one national association and some selected providers that participated in the program.
Officials from nearly all selected states and many provider awardees said that these connections were helpful, including in helping them address common challenges and figure out how best to provide services during the COVID-19 pandemic. For example, officials from one state said that awardees shared ideas for how to manage COVID-19 outbreaks in residential treatment facilities during one awardee meeting. Officials from another state said they discussed topics such as transportation barriers for patients and workforce shortages during SAMHSA-organized meetings with other state officials. Additionally, one provider said they used meetings to exchange ideas with other providers on topics such as best practices for providing medication-assisted treatment through telehealth during the COVID-19 pandemic. One provider said their connections with other awardees turned into ongoing relationships that continued after the COVID-19 pandemic ended.
Disseminating information and other resources. SAMHSA disseminated information to awardees and the public through webinars, published resources, and technical assistance centers during the COVID-19 pandemic, according to officials from SAMHSA, selected awardees, and representatives from national associations. SAMHSA’s COVID-19 webpage provided guidance and resources to assist individuals, communities, states, and behavioral health staff, including our selected state and provider awardees. For example, SAMHSA provided resources to assist awardees with grant administration, such as a sample COVID-19 revised budget document and a list of COVID-19 Frequently Asked Questions on grants management. In addition, SAMHSA published a range of resources to help awardees better deliver behavioral health services during the COVID-19 pandemic. For example, SAMHSA published guidance on using telehealth to treat serious mental illness and substance use disorders, and the SAMHSA-funded Disaster Technical Assistance Center published information on adaptations and innovations in behavioral health services during the COVID-19 pandemic.[64] (See fig. 5 for an example of a SAMHSA resource provided during the COVID-19 pandemic.)
Figure 5: Example SAMHSA Resource—Wallet Card on Managing Stress During the COVID-19 Pandemic, Published July 2020
Officials from all selected states and nearly all provider awardees said they benefitted from these resources. For example, awardees said they used SAMHSA resources on topics such as grant flexibilities; data collection, analysis, and reporting; COVID-19 updates; and clinical topics such as worker burnout and providing services safely in person or via telehealth during the COVID-19 pandemic. Officials from one state said SAMHSA’s webinars on co-occurring disorders helped them address increased needs among people with these conditions during the COVID-19 pandemic. One provider said SAMHSA compiled information and guidance from different federal agencies during COVID-19 and shared these resources with awardees, which helped the provider save time by not having to track changing federal guidance during the COVID-19 pandemic.
Grant Administration and Program Flexibilities
SAMHSA provided a range of flexibilities to assist awardees in grant administration and program implementation during the COVID-19 pandemic, according to SAMHSA documentation and agency officials. Some flexibilities—including those authorized in statute and those permitted by the Office of Management and Budget—helped awardees meet grant administration requirements, including managing grant funding, during the COVID-19 pandemic. Additionally, SAMHSA and other federal agencies provided some flexibilities to help awardees carry out program functions, such as delivering behavioral health services, during the COVID-19 pandemic. Selected awardees used grant administration and program flexibilities to varying degrees and cited some flexibilities, such as project period extensions and budget revisions, as particularly useful in adjusting their programs to address COVID-19-related needs. (See app. III for selected grant administration flexibilities allowed by SAMHSA during the COVID-19 pandemic.)
Grant Administration Flexibilities
SAMHSA provided a variety of grant administration flexibilities, upon request, to support awardees during the COVID-19 pandemic, including several that helped awardees manage grant funding to meet COVID-19 needs.[65] Specifically:
Project period extensions. SAMHSA provided a flexibility known as a no-cost extension—which allows awardees to extend the project period for an expiring grant without receiving additional grant funding from SAMHSA—for COVID-19 supplemental funding awards to nearly all SUBG and MHBG awardees, according to agency officials.[66] (See fig. 6.)
Figure 6: Number of SAMHSA Awardees That Received Project Period Extensions for Block Grant COVID-19 Supplemental Funding
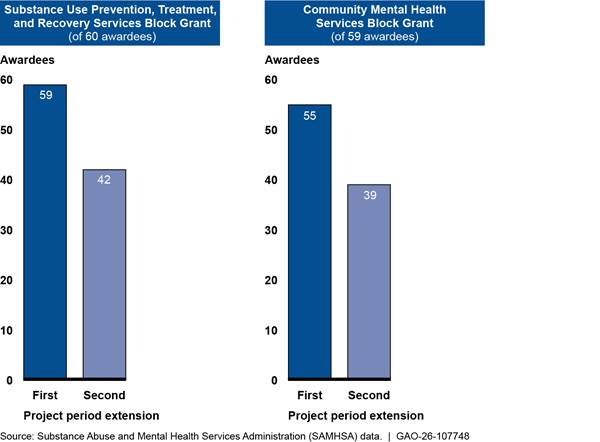
Notes: SAMHSA awarded $5.4 billion of COVID-19 supplemental funding to Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG) and Community Mental Health Services Block Grant (MHBG) awardees as authorized by the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021. Awardees initially had until March 14, 2023, to expend supplemental block grant funds from the Consolidated Appropriations Act, 2021, and were eligible to receive up to two project period extensions, known as no-cost extensions, each for up to 12 months, from SAMHSA to extend this deadline. American Rescue Plan Act of 2021 funds were not eligible for an extension, according to SAMHSA officials.
Of the eight selected state awardees we interviewed, all requested and received one or more no-cost extensions for SUBG COVID-19 supplemental funding, State Opioid Response, and Emergency COVID-19 grant awards during the COVID-19 pandemic, according to SAMHSA officials. Seven selected states received one or more no-cost extensions for MHBG COVID-19 supplemental funding, according to officials. Additionally, many selected providers we interviewed said they received no-cost extensions for SAMHSA awards during the COVID-19 pandemic.
Officials from selected states and providers described using no-cost extensions to spend remaining grant funding, serve additional clients, and complete data collection and reporting, for example. Additionally, officials from nearly all states and some providers said they used no-cost extensions to make up for COVID-19-related delays in grant implementation. For example, one state’s subawardees encountered behavioral health staff workforce shortages, which delayed implementation of grant projects, according to agency officials. One provider said they had reached about 90 percent of their goal for number of clients served at the end of their original grant project period, and receiving a no-cost extension allowed them to meet and eventually exceed this goal.
While SAMHSA provided these project period extensions, officials from many selected states said they nonetheless experienced challenges planning and implementing grant activities within the program project periods allowed by some COVID-19 supplemental funding awards.[67] For example, officials from one state said its subawardees experienced challenges with staff capacity, which made it difficult to implement grant programs and spend all grant funding within the allotted timeframe.
Budget revisions. SAMHSA allowed awardees to request re-budgeting of award funds due to COVID-19 circumstances.[68] For example, SAMHSA approved budget revisions for five selected states’ State Opioid Response grants during the COVID-19 pandemic, according to agency officials. In addition, some selected providers said SAMHSA approved budget revisions for their certified community behavioral health clinic and community mental health center awards. Awardees described revising budgets for various reasons, such as purchasing technology, increasing staff salaries, or limiting COVID-19 spread. For example, one provider said that because they were unable to hire staff for all of the positions originally included in their award budget, they worked with SAMHSA officials to reallocate funds from unfilled staff positions to other activities, such as training staff, purchasing medical equipment, and leasing a vehicle to conduct home visits or transport clients to services. Another provider said SAMHSA approved their revised budget to increase salaries to help recruit staff, and to renovate clinic space to facilitate social distancing.
Financial reporting extensions. SAMHSA allowed awardees to take up to 3 months beyond the original due date to reconcile financial expenditures and submit final financial reports as needed, according to agency officials.[69] Four selected states received an extension for SUBG financial reporting and five selected states received an extension for MHBG financial reporting, according to SAMHSA officials. Officials from one state said these extensions helped staff manage their workloads, particularly as staff were heavily involved in COVID-19 response. One provider also said they received a financial reporting extension.
Waivers of maintenance of effort requirements. During COVID-19, SAMHSA allowed some waivers of block grant “maintenance of effort” requirements, which required recipients to maintain a certain level of state expenditures for activities.[70] SAMHSA allowed for a waiver of this requirement if states provided documentation of the effects of COVID-19 on mental health or substance use disorder services expenditures, such as decreased service delivery due to challenges with in-person treatment, according to agency documentation. SAMHSA waived maintenance of effort requirements for three selected states’ MHBG awards and for four selected states’ SUBG awards from 2020 through 2023, according to SAMHSA officials. For example, SAMHSA waived these requirements for one state that cited reduced state spending due to its increase in telehealth and reduced staffing, according to SAMHSA officials.
Expansion of allowable costs. SAMHSA allowed awardees to spend grant funds on some activities that were normally not allowed under the grant, according to agency officials. Three selected states used this flexibility to continue providing behavioral health services through their State Opioid Response grants during the COVID-19 pandemic, according to SAMHSA officials. For example, states used this flexibility to support COVID-19 testing at mobile care units or to purchase personal protective equipment so behavioral health staff could safely continue to provide grant-funded services, according to agency officials.
Program Flexibilities
SAMHSA and other federal agencies such as the Drug Enforcement Agency made certain program flexibilities and modifications available to help states and behavioral health providers, including our selected awardees, deliver services during the COVID-19 pandemic. (See table 1 for an overview of selected program flexibilities available to SAMHSA awardees.)
Table 1: Selected Flexibilities Related to SAMHSA Awardees’ Program Implementation During and After the COVID-19 Pandemic
|
Flexibility |
Description |
Status |
|
Take-home methadone |
Prior to the COVID-19 pandemic, federal regulations required frequent patient visits to Opioid Treatment Programs to receive doses of methadone, a medication used to treat opioid use disorder.a During the COVID-19 pandemic, the Substance Abuse and Mental Health Services Administration (SAMHSA) issued guidance allowing states to request blanket exceptions for all stable patients in Opioid Treatment Programs to receive 28 days of take-home doses of the patient’s medication for opioid use disorder, such as methadone, and up to 14 days for patients who are less stable but who the program believes can safely handle this level of take-home medication. |
SAMHSA issued a final rule revising the Opioid Treatment Program regulations to allow patients to receive take-home doses of methadone under certain conditions, effective April 2024.b |
|
Telehealth initiation of buprenorphine |
Prior to the COVID-19 pandemic, prescribers—including Opioid Treatment Programs—were generally required to perform an in-person medical evaluation before prescribing buprenorphine via telehealth. During the COVID-19 pandemic, this requirement was waived, allowing prescription of buprenorphine via phone or video telehealth without a prior in-person visit in certain situations. SAMHSA issued similar telehealth buprenorphine prescribing guidelines specific to Opioid Treatment Programs. |
SAMHSA issued a final rule revising the Opioid Treatment Program regulations to allow initial prescribing of buprenorphine via phone or video telehealth, and initial prescribing of methadone via audiovisual telehealth in certain situations, which went into effect in April 2024.b The Drug Enforcement Administration and SAMHSA issued a joint final rule codifying the buprenorphine telehealth prescribing allowance in certain situations, effective December 31, 2025.c |
|
Virtual client data collection |
Prior to the COVID-19 pandemic, SAMHSA required certain awardees to collect some client data through in-person interviews. During the COVID-19 pandemic, SAMHSA allowed certain awardees to collect the required client data over the phone or electronically.d |
According to SAMHSA officials, awardees may continue to collect these data virtually, as of September 2025. |
|
Telehealth platforms |
The Department of Health and Human Services (HHS) Office for Civil Rights is responsible for enforcing the Health Insurance Portability and Accountability Act of 1996 and its implementing regulations, the Privacy and Security Rules, which set out privacy and security requirements for protected health information. The Office for Civil Rights can issue penalties for noncompliance with these rules.e |
Expired in May 2023, according to an HHS Office for Civil Rights Notice of Expiration issued in April 2023.g |
Source: GAO analysis of federal legislation and documentation from SAMHSA and HHS Office for Civil Rights, and interviews with SAMHSA officials. | GAO‑26‑107748
Notes: The Secretary of Health and Human Services declared a public health emergency in response to COVID-19 on January 31, 2020, under section 319 of the Public Health Service Act; it expired on May 11, 2023. This information pertains to flexibilities SAMHSA provided to awardees during the COVID-19 public health emergency. We refer to the COVID-19 public health emergency as the COVID-19 pandemic for the purposes of this table.
aOpioid Treatment Programs are certified by SAMHSA to prescribe medications for the treatment of opioid use disorder, such as methadone and buprenorphine.
bMedications for the Treatment of Opioid Use Disorder, 89 Fed. Reg. 7528 (Feb. 2, 2024) (to be codified at 42 C.F.R. pt. 8).
cExpansion of Buprenorphine Treatment via Telemedicine Encounter, 90 Fed. Reg. 6504 (Jan. 17, 2025); see also Expansion of Buprenorphine Treatment via Telemedicine Encounter and Continuity of Care via Telemedicine for Veterans Affairs Patients, 90 Fed. Reg. 13410 (Mar. 24, 2025).
dThis flexibility also waived consequences for awardees that were delayed in submitting their data or unable to collect these data during the COVID-19 pandemic.
eSee 45 C.F.R. pts. 160 and 164.
f85 Fed. Reg. 22,024 (Apr. 21, 2020).
g88 Fed. Reg. 22,380 (Apr. 13, 2023).
Selected SAMHSA awardees described their experiences using these program flexibilities during COVID-19, including how each flexibility benefitted their programs and services.
|
Opioid Treatment Programs Opioid Treatment Programs provide evidence-based medications to treat opioid use disorder, in combination with counseling and related services to support remission and recovery. All Opioid Treatment Programs dispense and administer methadone—which may generally only be administered or dispensed by an Opioid Treatment Program—and many also offer buprenorphine and naltrexone, the three types of medication approved by the Food and Drug Administration to treat opioid use disorder. Opioid Treatment Programs must be accredited, certified by the Substance Abuse and Mental Health Services Administration (SAMHSA), registered with the Drug Enforcement Administration, and licensed by the state in which they operate. As of May 2024, SAMHSA has certified over 2,100 Opioid Treatment Programs across most states and territories, and several operated by Tribal Nations. Source: SAMHSA documentation. | GAO‑26‑107748 |
Take-home doses of methadone to treat opioid use disorder. In March 2020, SAMHSA allowed states to request blanket exceptions for patients in Opioid Treatment Programs to receive up to 28 days of take-home methadone doses, rather than the daily in-person dose administration generally required prior to the exception.[71] This flexibility allowed clinicians to continue to treat opioid use disorder during the COVID-19 pandemic while reducing direct patient contact, according to SAMHSA. Clients, treatment programs, and states generally supported the methadone take-home flexibility, and research has shown that this flexibility eliminated requirements that promoted stigma and discouraged people from accessing treatment, according to SAMHSA.
Of the 52 states, territories, and the District of Columbia with SAMHSA-certified Opioid Treatment Programs, 43 states and the District of Columbia—including four of our selected states—opted into this flexibility to allow the Opioid Treatment Programs in their state to use this flexibility starting in March 2020, according to SAMHSA officials.[72] One selected provider said they used this flexibility to allow patients to take home methadone doses. Officials from one state said this flexibility was beneficial as it prevented interruptions in patients’ treatment and helped address transportation barriers to receiving care. Officials from another state said this flexibility reduced the number of clients who visited Opioid Treatment Programs in person, and as a result, the state’s Opioid Treatment Programs did not experience COVID-19 outbreaks.
Telehealth initiation of buprenorphine to treat opioid use disorder. SAMHSA worked with the Drug Enforcement Administration to allow clinicians to prescribe buprenorphine via telehealth starting in 2020, including audio-only telephone calls, to new clients who had not previously been evaluated in person.[73] Nearly all selected states and some provider awardees said they used this flexibility, although one of these providers said they preferred to complete initial medical evaluations in person before prescribing buprenorphine whenever possible. Awardees said that this flexibility was beneficial for a variety of reasons. For example, officials from one state said this flexibility helped them increase access to medication and expand the number of clinicians who could prescribe medication for opioid use disorder during the COVID-19 pandemic. One provider said this flexibility helped clients overcome barriers to treatment, such as finding childcare or coordinating in-person services with work schedules to attend in-person clinic visits.[74]
Virtual client data collection. SAMHSA allowed awardees to collect required grant data on clients served over the phone or electronically during the COVID-19 pandemic, rather than in person as required prior to the pandemic, according to agency documentation and officials. Officials from nearly all selected states and all providers said they used this flexibility. Officials from one state said this flexibility was useful because collecting data in person was not always possible during the COVID-19 pandemic. In addition, one provider said staff were able to collect these data much faster over the phone.
Nearly all awardees said they used the virtual client data collection flexibility; however, officials from some selected states and many selected providers said they experienced challenges meeting data collection and reporting requirements during the COVID-19 pandemic.[75] For example, officials from one state said that behavioral health staff struggled to collect required client data before the pandemic, but this challenge was exacerbated during the COVID-19 pandemic due to the increased number of clients. SAMHSA officials said they provided technical assistance and increased flexibility to awardees that reported data collection challenges, and the agency did not penalize awardees for unavoidable challenges with data collection.
Telehealth platforms. SAMHSA worked with the HHS Office for Civil Rights to allow health care providers to use telehealth platforms during the COVID-19 pandemic that were not compliant with the Health Insurance Portability and Accountability Act of 1996 rules for privacy and security of protected health information, according to agency officials.[76] Officials from many selected states and some providers said they used noncompliant telehealth platforms at some point during the COVID-19 pandemic. For example, one provider said they used platforms that were not compliant early in the COVID-19 pandemic to quickly deliver telehealth services before eventually transitioning to a compliant platform. Another provider said that this flexibility was particularly useful for the rural community they serve, because clients did not always have consistent internet connection and were more easily reached by Apple FaceTime or other communication tools that were not compliant with Health Insurance Portability and Accountability Act of 1996 rules.
Agency Comments
We provided a copy of this draft report to HHS. HHS provided technical comments, which we incorporated as appropriate.
We are sending copies of this report to the appropriate congressional committees, the Secretary of Health and Human Services, and other interested parties. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at HundrupA@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix IV.

Alyssa M. Hundrup
Director, Health Care
The Consolidated Appropriations Act, 2023, includes a provision for us to review Substance Abuse and Mental Health Services Administration (SAMHSA) programs and activities to support the continued provision of mental health and substance use disorder services and related activities during the COVID-19 pandemic.[77] In this report, we describe
1. how SAMHSA’s advisory councils and National Mental Health and Substance Use Policy Laboratory (Policy Lab) supported the agency’s COVID-19 response;
2. how selected SAMHSA awardees provided services during the COVID-19 pandemic and what challenges they experienced; and
3. how SAMHSA provided assistance to awardees to support their response to the COVID-19 pandemic.
To address our first objective, we reviewed documentation and interviewed SAMHSA officials about the agency’s advisory councils and committees—which we refer to as advisory councils for the purposes of this report—and the Policy Lab. We reviewed documentation and interviewed officials about activities from January 2020 through May 2023—the beginning and end of the public health emergency declaration for COVID-19, which we refer to as the COVID-19 pandemic for the purposes of this report. We reviewed documents from the advisory councils and the Policy Lab, such as reports, meeting minutes, and information from the General Services Administration’s Federal Advisory Committee Act database.[78] We also interviewed officials from SAMHSA and its Policy Lab to identify additional ways that these groups supported SAMHSA’s COVID-19 response, such as through discussions or informal advice.
To address our second and third objectives, we reviewed documentation from and interviewed a nongeneralizable sample of SAMHSA awardees. Awardees included seven states and one territory—which we refer to collectively as selected states—and 16 behavioral health providers in the selected states. The selected states are Michigan, Mississippi, Montana, Oregon, Pennsylvania, Puerto Rico, Texas, and Vermont. Puerto Rico also operated a behavioral health provider organization, and state officials spoke to us about their experiences both as a state agency and as a behavioral health provider receiving SAMHSA grants during the COVID-19 pandemic. Therefore, Puerto Rico is counted both as a state awardee and a behavioral health provider awardee, and we interviewed a total of 23 selected awardees. We use the following modifiers to quantify awardees’ responses: “nearly all” represents seven states when we are referring to just the states we interviewed; 12 to 15 providers when we are referring to just the providers we interviewed; or 18 to 22 awardees (i.e., the total across states and providers we interviewed). Likewise, “many” represents five to six states, eight to 11 providers, or eight to 17 awardees; and “some” represents two to four states, three to seven providers, or three to seven awardees.
The experiences of selected awardees are not generalizable across all SAMHSA state or provider awardees. However, the information we obtained from them illustrates a variety of experiences with SAMHSA grants and assistance during the COVID-19 pandemic. We selected states
1. that received funding through four SAMHSA grants: Community Mental Health Services Block Grant (MHBG); Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG); State Opioid Response; and Emergency Grants to Address Mental and Substance Use Disorders During COVID-19 grant programs (Emergency COVID-19 grants);
2. with two or more providers that participated in SAMHSA’s Certified Community Behavioral Health Clinic Expansion grant program or Community Mental Health Centers grant program during the COVID-19 pandemic; and
3. to obtain variation in rurality, health department governance structure (i.e., the relationship between state and local health agencies), and geographic region, among other factors.
To select behavioral health providers, we selected two providers in each selected state to achieve variation in rurality, SAMHSA awards received (i.e., Certified Community Behavioral Health Clinic Expansion grant, Community Mental Health Centers grant, or both), and the timing of awardees’ first Certified Community Behavioral Health Clinic Expansion grant award relative to the COVID-19 pandemic (see below for more details about these grant programs).
We focused our review on six SAMHSA grant programs: MHBG, SUBG, State Opioid Response, Emergency COVID-19 grants, Certified Community Behavioral Health Clinic Expansion, and Community Mental Health Centers grant programs. We selected these six grant programs based on several criteria, including provision of direct behavioral health services to clients, total funding amount awarded from fiscal years 2019 through 2023, and a grant purpose to fund COVID-19 behavioral health response. Together, these selected grant programs represented over three-quarters (approximately 78 percent) of SAMHSA’s total funding awarded to support behavioral health services in fiscal years 2020 through 2023. The selected SAMHSA grant programs also provided variation in awardee type (i.e., inclusion of states, territories, and behavioral health providers), grant type (i.e., block grants—noncompetitive, formula grants mandated by Congress—and non-block grants), type of behavioral health services funded (i.e., mental health, substance use, or both), and grant program start date in relation to the COVID-19 pandemic. Two of these six grant programs—Emergency COVID-19 grants and Community Mental Health Centers grants—were created specifically to respond to the COVID-19 pandemic, while the other four grant programs predated the pandemic. (See app. II for summary information on selected SAMHSA grant programs that supported the direct provision of behavioral health services during the COVID-19 pandemic.)
To describe selected state and provider awardees’ provision of behavioral health services and challenges they experienced, we reviewed documentation and interviewed selected awardees on these topics regarding their experiences from January 2020 through May 2023. We reviewed progress reports state awardees submitted to SAMHSA that summarized awardees’ changes in services and challenges during the COVID-19 pandemic. We also interviewed selected awardees about how they provided services and any challenges they experienced during the COVID-19 pandemic. Additionally, we interviewed representatives from four national associations to gain a broader perspective on SAMSHA awardees’ experiences and challenges during the COVID-19 pandemic. Specifically, we interviewed representatives from the following four national associations: (1) National Association of State Mental Health Program Directors; (2) National Association of State Alcohol and Drug Agency Directors; (3) National Indian Health Board; and (4) National Council for Mental Wellbeing. SAMHSA contracts with the National Council for Mental Wellbeing to operate the Certified Community Behavioral Health Clinic Expansion Grantee National Training and Technical Assistance Center. These associations have expertise in areas relevant to our review, including mental health services and wellbeing, substance use disorders, and SAMHSA awardees’ experiences providing behavioral health services during the COVID-19 pandemic.
To describe the assistance SAMHSA offered to awardees during the COVID-19 pandemic, including any flexibilities the agency provided to awardees for grant administration and program implementation, we reviewed documentation and interviewed agency officials, selected state and behavioral health provider awardees, and national association representatives. For example, we reviewed progress reports and budget modification requests that state awardees submitted to SAMHSA, relevant federal statutes and regulations, and documentation from SAMHSA and other federal agencies to summarize the assistance and flexibilities that SAMHSA provided during the COVID-19 pandemic.
The Substance Abuse and Mental Health Services Administration (SAMHSA) awarded over $32 billion during the COVID-19 pandemic—fiscal years 2020 through 2023—to support programs that provided direct behavioral health services, according to agency data. This included approximately $8.3 billion in COVID-19 supplemental funding. Together, these selected grant programs represent over three-quarters (approximately 78 percent) of SAMHSA’s total funding awarded to support behavioral health services in fiscal years 2020 through 2023.
Our selection of grant programs was informed by several criteria, including provision of direct behavioral health services to clients, total funding amount awarded in fiscal years 2020 through 2023, and a purpose to fund the COVID-19 behavioral health response. We selected grant programs to provide variation in grant type (i.e., block grants—noncompetitive, formula grants mandated by Congress—and non-block grants), awardee type (i.e., inclusion of states, territories, and behavioral health providers), type of behavioral health services funded (i.e., mental health, substance use, or both), and program start date in relation to the COVID-19 pandemic. Two of these six programs—the Community Mental Health Centers grant program and the Emergency Grants to Address Mental and Substance Use Disorders During COVID-19—were created specifically to respond to the pandemic, while the other four programs predated the pandemic. (Table 2 provides information on the six grant programs included in the scope of this review, including the amount of funding SAMHSA awarded through each program during the COVID-19 pandemic.)
Table 2: Summary of Selected SAMHSA Grant Programs That Supported Behavioral Health Services During the COVID-19 Pandemic, Fiscal Years 2020–2023
|
Grant program |
Purpose |
Number and type |
Total funding awarded (COVID-19 supplemental funding awarded)a |
|
Substance Use Prevention, Treatment and Recovery Services Block Grant (SUBG) |
Plan, implement, and evaluate activities that prevent and treat substance use. Specifically targets pregnant women and women with dependent children; injection drug users; tuberculosis services; early intervention services for HIV/AIDS; and primary prevention services. |
60 states, territories,
Pacific jurisdictions, District of Columbia, |
$10.4 billion ($3.1 billion) |
|
Community Mental Health Services Block Grant (MHBG) |
Provide comprehensive, community-based mental health services to adults with serious mental illness and to children with serious emotional disturbance and to monitor progress in implementing a comprehensive, community-based mental health system. |
59 states, territories, Pacific jurisdictions, and District of Columbia |
$5.5 billion ($2.3 billion)b |
|
State Opioid Response |
Increase access to medication-assisted treatment for opioid use disorder, reduce unmet treatment need, and reduce opioid overdose deaths. |
58 states, territories, Pacific jurisdictions, and District of Columbia |
$5.8 billion ($0) |
|
Certified Community Behavioral Health Clinic Expansion |
Help community behavioral health systems and clinics meet the certification criteria and establish certified clinic programs, improve and enhance existing certified community behavioral health clinic programs, and provide support for uncompensated care. The certified community behavioral health clinic model includes 24 hours a day, 7 days a week crisis services, comprehensive behavioral health services, and care coordination.c |
525 certified community behavioral health clinics and clinics seeking certificationd |
$2.4 billion ($1.3 billion) |
|
Community Mental Health Centers |
Support and restore the delivery of clinical services that were impacted by the COVID-19 pandemic and effectively address the needs of individuals with serious emotional disturbance, serious mental illness, and co-occurring disorders. This grant program was created specifically to respond to the COVID-19 pandemic. |
230 community mental health centers, including centers operated by state and local government agencies |
$823 million |
|
Emergency Grants to Address Mental and Substance Use Disorders During COVID-19 |
Provide crisis intervention services, mental and substance use disorder treatment, and other related recovery supports for children and adults impacted by the COVID-19 pandemic. This grant program was created specifically to respond to the COVID-19 pandemic. |
125 states, territories, District of Columbia, Tribes, and tribal organizations |
$345 million |
Source: Substance Abuse and Mental Health Services Administration (SAMHSA) documentation and statements from officials. | GAO‑26‑107748
Notes: In fiscal years 2020 and 2021, SAMHSA received $8.5 billion in supplemental funding to help address behavioral health needs that resulted from the COVID-19 pandemic through appropriations in the CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021, and through interdepartmental funding, according to agency officials. SAMHSA awarded approximately $8.3 billion of this supplemental funding in grants to recipients that included states, territories, the District of Columbia, Tribes, and nongovernmental organizations.
aCOVID-19 supplemental funding awarded reflects the total amount of grant funding awarded to SAMHSA awardees as of July 28, 2025, and it excludes funds that have been relinquished by awardees, according to SAMHSA officials. For existing grant programs that predated the COVID-19 pandemic, the amount of COVID-19 supplemental funding awarded is displayed in this table as a subset of the total funding awarded. For new grant programs created during the COVID-19 pandemic using COVID-19 supplemental funding—including the Community Mental Health Centers grant program and the Emergency Grants to Address Mental and Substance Use Disorders During COVID-19 program—only one funding amount is displayed.
bAlthough the COVID-19 supplemental funding appropriated $3.1 billion to SAMHSA for the MHBG, the Consolidated Appropriations Act, 2021, required some of this funding to be used to support community mental health centers. See Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1913 (2020). As a result, SAMHSA awarded approximately $823 million to the Community Mental Health Centers grant program, according to officials.
cThis includes Certified Community Behavioral Health Clinic Planning, Development, and Implementation Grants to help establish new certified community behavioral health clinics, as well as Improvement and Advancement Grants to help existing certified community behavioral health clinics to expand.
dThis reflects the number of certified community behavioral health clinic awardees with active SAMHSA awards during the COVID-19 public health emergency (January 2020 through May 2023), according to SAMHSA data. Therefore, this does not include certified community behavioral health clinic awardees that received funds through SAMHSA’s 2023 Certified Community Behavioral Health Clinic Expansion Grants, which the agency awarded in September 2023, after the end of the COVID-19 public health emergency.
Appendix III: Selected Grant Administration Flexibilities Allowed by SAMHSA During the COVID-19 Pandemic
The Substance Abuse and Mental Health Services Administration (SAMHSA) allowed awardees to use a range of flexibilities related to grant administration during the COVID-19 pandemic from January 2020 through May 2023, according to agency documentation and officials. Although SAMHSA extended COVID-19 flexibilities to all grant recipients, there was variability in which programs allowed the use of certain flexibilities because some have different regulatory and statutory requirements, according to SAMHSA officials. Table 3 includes an overview of selected grant administration flexibilities generally available to SAMHSA awardees.
Table 3: Overview of Selected Grant Administration Flexibilities Allowed by SAMHSA During the COVID-19 Pandemic
|
Grant flexibility |
Description |
|
No-cost extensions on expiring awards |
Allowed awardees to extend project period of performance for expiring grants by up to 1 year. |
|
Extension of financial and other reporting |
Allowed awardees to delay submitting financial and other reporting up to 3 months beyond original due date. |
|
Extension of closeout |
Allowed awardees to delay submission of reporting required for grant closeout for up to 1 year after award expires. |
|
Waiver of maintenance of effort requirementa |
Allowed awardees to request waived maintenance of effort requirements for state expenditures for block grants. May be granted through a Public Health Emergency waiver or an economic circumstances waiver. |
|
Exceptions to compliance with Synar requirementsb |
Allowed Substance Use Prevention, Treatment, and Recovery Services Block Grant awardees to delay submission of Synar report in 2020, submit incomplete report without penalty, or request 1-year coverage study extension. |
|
Flexibility with applicant System for Award Management registrationc |
Relaxed requirements for active registration in the System for Award Management at the time of application, or extended deadlines for recertifications. |
|
Abbreviated non-competitive continuation requests |
Allowed awardees to request continuation of grant projects by providing a brief statement verifying ability to resume activities and accept further grant funding. |
|
Expenditure of awards for salaries and other project activities |
Allowed awardees to continue to charge salaries and benefits (consistent with awardee pay policies) and other costs necessary to resume grant activities. |
|
Expanded allowable costs |
Allowed awardees to charge normally unallowable costs, such as cancelling events or travel, necessary for pausing and restarting activities. |
|
Waivers from prior approval requirements |
Waived requirements for prior approval of special or unusual costs as necessary to effectively address the response. |
|
Extension of currently approved indirect cost rates |
Allowed awardees to use current indirect cost rates for 1 additional year without submitting a new proposal. |
|
Budget revisions or modifications |
Allowed awardees to re-budget funds to other activities because of COVID-19, as long as the activities are allowable under the Funding Opportunity Announcement and in line with other requirements. |
Source: GAO analysis of Substance Abuse and Mental Health Services Administration (SAMHSA) documents, information from the Office of Management and Budget, and statements from SAMHSA officials. | GAO‑26‑107748
Notes: This information pertains to flexibilities SAMHSA provided to awardees during the COVID-19 public health emergency (January 2020 through May 2023). Flexibilities available to SAMHSA awardees varied across grant programs.
aUnder the maintenance of effort requirement, a state must maintain its expenditures for relevant activities at a level that is not less than the average maintained by the state in the 2-year period before the fiscal year for which it is applying for the block grant. See 42 U.S.C. § 300x-4(b); 42 U.S.C. § 300x-30(a). SAMHSA may waive the maintenance of effort requirement for a state if it determines that “extraordinary economic conditions” justify such a waiver or in the case of a public health emergency such as COVID-19. See 42 U.S.C. § 300x-4(b)(3); 42 U.S.C. § 300x-30(c). Under the public health emergency waiver, SAMHSA can grant extensions and waive application deadlines or compliance with any other requirement for awardees of non-discretionary grants. 42 U.S.C.§ 300x-67.
bThe Synar program monitors the sale and distribution of tobacco products to minors. Synar inspections are carried out each year by youth inspectors, who visit retail establishments and attempt to purchase tobacco products. The coverage study inventories retail outlets in each state that sells tobacco products.
cThe System for Award Management is an online system that facilitates federal awards processes, including registering to do business with the federal government and viewing contract data.
GAO Contact
Alyssa M. Hundrup, HundrupA@gao.gov
Staff Acknowledgments
In addition to the contact named above, Karen Doran (Assistant Director), Rachel Weingart (Analyst-in-Charge), Matthew Curtis, Mal Kennedy, Jeff Mayhew, and Cynthia Turner made key contributions to this report. Also contributing were Sonia Chakrabarty, Laura Elsberg, David Jones, Ariel Landa-Seiersen, and Eric Peterson.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]We define behavioral health conditions as mental, emotional, and substance use disorders, which are often co-occurring. Examples of mental health conditions include anxiety disorders; mood disorders, such as depression; post-traumatic stress disorder; and schizophrenia. Examples of substance use disorders include alcohol use disorder and opioid use disorder.
[2]See GAO, Behavioral Health and COVID-19: Higher-Risk Populations and Related Federal Relief Funding, GAO‑22‑104437 (Washington, D.C.: Dec. 10, 2021). The Secretary of Health and Human Services declared a public health emergency in response to COVID-19 on January 31, 2020, under section 319 of the Public Health Service Act; it expired on May 11, 2023. We refer to this period as the COVID-19 pandemic for the purposes of this report.
[3]Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality, Key Substance Use and Mental Health Indicators in the United States: Results from the 2023 National Survey on Drug Use and Health (Rockville, Md.: July 2024) and Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality, Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey on Drug Use and Health (Rockville, Md.: Oct. 2021).
[4]Specifically, among adults aged 18 or older who received mental health services in the past year, 58.3 percent (26.6 million) had appointments moved from in person to telehealth and 38.7 percent (17.7 million) experienced delays or cancellations in appointments, according to SAMHSA data for quarter 4 of 2020 (October through December). About 10.7 percent (4.9 million) were unable to access needed care resulting in a perceived moderate to severe impact on health, according to these data. See Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality, Key Substance Use and Mental Health Indicators in the United States: Results from the 2020 National Survey.
[5]On March 27, 2025, HHS announced that it would be restructuring the department, including by consolidating SAMHSA into a new Administration for a Healthy America. See U.S. Department of Health and Human Services, Office of the Assistant Secretary for Public Affairs, HHS Announces Transformation to Make America Healthy Again (March 27, 2025). In May 2025, several states filed a lawsuit challenging the March 27 announcement; litigation is ongoing. See New York v. Kennedy, No. 25-cv-00196 (D.R.I. May 5, 2025). As of February 2026, the transition to a new structure had not occurred and accordingly, we refer to the agency as SAMHSA throughout this report.
[6]SAMHSA received $8.5 billion in COVID-19 supplemental funding in fiscal years 2020 and 2021, according to agency officials. Some of this funding was appropriated to SAMHSA from March 2020 through March 2021 through the CARES Act, Pub. L. No. 116-136, div. B, tit. VIII, 134 Stat. 281, 556 (2020); the Consolidated Appropriations Act, 2021, Pub. L. No. 116-260, div. M, tit. III, 134 Stat. 1182, 1913 (2020); and the American Rescue Plan Act of 2021, Pub. L. No. 117-2, tit. II, subtit. H, 135 Stat. 4, 45–48. Unless otherwise stated, references to the Consolidated Appropriations Act, 2021, in this report refer to the COVID-19 supplemental funding in Division M of that act (Coronavirus Response and Relief Supplemental Appropriations Act, 2021). See GAO‑22‑104437. SAMHSA also received supplemental funding through interdepartmental funding, according to agency officials.
[7]Pub. L. No. 117-328, § 2112(e), 136 Stat. 4459, 5722 (2022).
[8]Puerto Rico is counted both as a state awardee and a behavioral health provider awardee because officials spoke with us about their experiences both as a state agency and as an operator of a behavioral health provider organization receiving SAMHSA grants during the COVID-19 pandemic. Counting Puerto Rico as a single awardee, we interviewed a total of 23 selected awardees.
[9]We focused our review on six SAMHSA grant programs: Community Mental Health Services Block Grant (MHBG); Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG); State Opioid Response; Emergency Grants to Address Mental and Substance Use Disorders During COVID-19 (Emergency COVID-19 grants); Certified Community Behavioral Health Clinic Expansion; and Community Mental Health Center grant programs. Block grants are noncompetitive, formula grants mandated by Congress.
[10]SAMHSA’s advisory councils were authorized by the Public Health Service Act in accordance with the Federal Advisory Committee Act, according to the agency. See 42 U.S.C. § 290aa-1; 5 U.S.C. ch. 10. According to SAMHSA’s website, three of the nine advisory councils had been terminated by the agency as of September 2025.
[11]See 42 U.S.C. § 290aa-3.
[12]See GAO, Behavioral Health: Activities of the National Mental Health and Substance Use Policy Laboratory, GAO‑24‑106760 (Washington, D.C.: May 16, 2024). Evidence-based practices are interventions that promote individual-level or population-level outcomes and are guided by the best research evidence with practice-based expertise, cultural competence, and the values of the people receiving the services, according to SAMHSA.
[13]We refer to states, territories, and the District of Columbia as states for the purposes of this report. SAMHSA also awarded SUBG funding to one Tribe. SAMHSA awards block grant funding using a formula specified in statute that takes into account three factors: (1) population of the state, (2) costs of services in the state, and (3) fiscal capacity of the state. All states have minimum allotments. See 42 U.S.C. § 300x-7; 42 U.S.C. § 300x-33.
[14]Adults with serious mental illness are those aged 18 and older with a diagnosable mental, behavioral, or emotional disorder—such as bipolar disorder, major depressive disorder, or schizophrenia—that substantially interferes with their life and ability to function, according to SAMHSA. Individuals with serious emotional disturbance are those under age 18 with a diagnosable mental, behavioral, or emotional disorder that substantially interferes with or limits the child’s role or functioning in family, school, or community activities, according to SAMHSA.
[15]For more information on SAMHSA’s State Opioid Response grant program, see GAO, Opioid Use Disorder Grants: Opportunities Exist to Improve Data Collection, Share Information, and Ease Reporting Burden, GAO‑25‑106944 (Washington, D.C.: Dec. 17, 2024) and Opioid Use Disorder: Opportunities to Improve Assessments of State Opioid Response Grant Program, GAO‑22‑104520 (Washington, D.C.: Dec. 9, 2021).
[16]Substance Abuse and Mental Health Services Administration, Certified Community Behavioral Health Clinic Certification Criteria (Rockville, Md.: Feb. 2023). For more information on SAMHSA’s activities to support crisis response services, see GAO, Behavioral Health: Federal Activities to Support Crisis Response Services, GAO‑25‑107586 (Washington, D.C.: Sept. 4, 2025).
[17]See Department of Health and Human Services, All-Hazards Plan (Washington, D.C.: June 2024).
[18]See D.J. DeWolfe, Training Manual for Mental Health and Human Service Workers in Major Disasters, Department of Health and Human Services Publication no. ADM 90-538, (2nd ed.) (Rockville, Md.: Substance Abuse and Mental Health Services Administration, 2000); Substance Abuse and Mental Health Services Administration, Warning Signs and Risk Factors for Emotional Distress, accessed July 25, 2025; and Substance Abuse and Mental Health Services Administration, Survivors of Disasters Resource Portal, accessed July 25, 2025.
[19]According to HHS, behavioral health recovery may include support for those grieving losses, those with traumatic experiences, those with high levels of chronic stress, those with substance use issues related to the post-disaster environment, and those with pre-disaster clinical behavioral health needs.
[20]See D.J. DeWolfe, Training Manual for Mental Health; Substance Abuse and Mental Health Services Administration, Tips for Survivors of a Disaster or Other Traumatic Event: Managing Stress, Department of Health and Human Services Publication No. SMA-13-4776 (Rockville, Md.: January 2013); and Substance Abuse and Mental Health Services Administration, Warning Signs and Risk Factors.
[21]See E. Goldmann and S. Galea, “Mental Health Consequences of Disasters,” Annual Review of Public Health, vol. 35 (2014).
[22]SAMHSA received the supplemental funding through appropriations from Congress in the CARES Act, the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021, and through interdepartmental funding, according to agency officials.
[23]See Pub. L. No. 116-260, div. M., tit. III, 134 Stat. 1182, 1913 (2020); Pub. L. No. 117-2, §§ 2701–02, 135 Stat. 4, 45–46. Awardees had until March 14, 2023, to expend supplemental funding from the Consolidated Appropriations Act, 2021, and until September 30, 2025, to expend supplemental funding from the American Rescue Plan Act of 2021.
[24]The Consolidated Appropriations Act, 2021, specified that a certain portion of the supplemental appropriations had to be used for community mental health centers. See Pub. L. No. 116-260, 134 Stat. 1182, 1913 (2020). Eligible applicants for the grant funding included nonprofit community mental health centers, as defined in the Public Health Service Act, including those operated by state and local governments. See 42 U.S.C. § 300x-2(c). The centers may or may not also be certified community behavioral health clinics, according to SAMHSA officials.
[25]The CARES Act and the Consolidated Appropriations Act, 2021, specified that a certain part of the supplemental appropriations had to be used for emergency response activities. See 42 U.S.C. § 290aa(o).
[26]See 42 U.S.C. § 300x-67.
[27]See Pub. L. No. 116-260, div. M, tit. III, 134 Stat.1182, 1914 (2020). On May 18, 2021, SAMHSA provided guidance establishing its ability to waive these same requirements for MHBG and SUBG COVID-19 supplemental funding awards authorized by the American Rescue Plan Act of 2021. See Substance Abuse and Mental Health Services Administration, Letter to Single State Authority Directors and State Mental Health Commissioners (Rockville, Md.: May 18, 2021).
[28]For more information on COVID-19-related grant flexibilities, including their broader use within HHS, see GAO, Grants Management: OMB Should Collect and Share Lessons Learned from Use of COVID-19-Related Grant Flexibilities, GAO‑21‑318 (Washington, D.C.: Mar. 31, 2021).
[29]The Office of Management and Budget issued this guidance in a series of five memorandums. See Office of Management and Budget, Administrative Relief for Recipients and Applicants of Federal Financial Assistance Directly Impacted by the Novel Coronavirus (COVID-19), M-20-11 (Washington, D.C.: Mar. 9, 2020); Administrative Relief for Recipients and Applicants of Federal Financial Assistance Directly Impacted by the Novel Coronavirus (COVID-19) Due to Loss of Operations, M-20-17 (Washington, D.C.: Mar. 19, 2020); Repurposing Existing Federal Financial Assistance Programs and Awards to Support the Emergency Response to the Novel Coronavirus (COVID-19), M-20-20 (Washington, D.C.: Apr. 9, 2020); Extension of Administrative Relief for Recipients and Applicants of Federal Financial Assistance Directly Impacted by the Novel Coronavirus (COVID-19) due to Loss of Operations, M-20-26 (Washington, D.C.: June 18, 2020); and Promoting Public Trust in the Federal Government through Effective Implementation of the American Rescue Plan Act and Stewardship of the Taxpayer Resources, M-21-20 (Washington, D.C.: Mar. 19, 2021).
[30]Advisory council members vote on formal recommendations during meeting proceedings, according to SAMHSA officials. During a meeting, a member may propose a formal recommendation, and in the subsequent meeting, the chair will follow up on the formal recommendation for members to vote on, according to officials. For the purposes of this report, we define “advice” to include all other advisory activities beyond formal recommendations.
[31]The Federal Advisory Committee Act does not require agencies to respond to or implement advisory council recommendations, and advisory councils are not required to publish information on any agency response to recommendations. See 5 U.S.C. ch. 10. See also GAO, Federal Advisory Committees: Actions Needed to Enhance Decision-Making Transparency and Cost Data Accuracy, GAO‑20‑575 (Washington, D.C.: Sept. 10, 2020). Eight of SAMHSA’s nine advisory councils are governed by this act.
[32]The advisory council that did not discuss these topics—the Drug Testing Advisory Board—had a narrower scope focused on forensic workplace drug testing and other related topics.
[33]Interdepartmental Serious Mental Illness Coordinating Committee, Advances Through Collaboration: Federal Action for a System That Works for All People Living with SMI and SED and Their Families and Caregivers, Report to Congress (Rockville, Md.: Apr. 2022).
[34]Specifically, two SAMHSA-funded technical assistance centers—the Addiction Technology Transfer Center Network and the Center for Excellence for Protected Behavioral Health Information—and other organizations facilitated a learning series in 2020 that involved presentations, national online discussion, and resource sharing for substance use disorder treatment providers and peer support specialists transitioning their services to telehealth and videoconferencing during the COVID-19 pandemic, according to one center’s website.
[35]The National Survey on Drug Use and Health collects and provides nationally representative data on the use of tobacco, alcohol, and illicit drugs; substance use disorders; mental health conditions; and receipt of substance use and mental health treatment, according to SAMHSA.
[36]Substance Abuse and Mental Health Services Administration, The National Tribal Behavioral Health Agenda (Rockville, Md.: Dec. 2016). The agenda identifies priorities and strategies to improve behavioral health for American Indian and Alaska Native populations. SAMHSA’s Tribal Technical Advisory Committee devised the initial concept for the agenda and helped shape and guide its development, which was a collaborative effort among Tribes, leaders, organizations, and federal agencies.
[37]During the COVID-19 pandemic, three advisory councils continued to review grant proposals for certain SAMHSA grants and cooperative agreements; they also served in this role prior to COVID-19, according to SAMHSA officials. Specifically, peer reviewers first evaluate grant applications for SAMHSA funding opportunities, and then some grant programs are subject to a secondary review by an advisory council, according to the agency website.
[38]For example, MHBG awardees must use funds to provide community mental health services to adults with serious mental illness and children with serious emotional disturbance. See 42 U.S.C. § 300x(b). The Emergency COVID-19 grant required awardees to use 20 percent of funding to provide services to individuals with mental disorders less severe than serious mental illness.
[39]Some of the most common behavioral health-related conditions associated with long COVID include depression, anxiety, psychosis, obsessive-compulsive disorder, and posttraumatic stress disorder, according to SAMHSA. Long COVID can also aggravate pre-existing conditions or contribute to new mental health or substance use disorders. For more information on long COVID, see GAO, Science & Tech Spotlight: Long COVID, GAO‑22‑105666 (Washington, D.C.: Mar. 2, 2022).
[40]Interdepartmental Serious Mental Illness Coordinating Committee, Advances Through Collaboration.
[41]National Association of State Mental Health Program Directors, Ready to Respond: Mental Health Beyond Crisis and COVID-19, Reimagining a Sustainable and Robust Continuum of Psychiatric Care (Alexandria, Va.: Sept. 2021).
[42]Department of Health and Human Services, Services and Supports for Longer-Term Impacts of COVID-19 (Washington, D.C.: Aug. 2022).
[43]Substance Abuse and Mental Health Services Administration, Overview of the Impacts of Long COVID on Behavioral Health (Rockville, Md.: Mar. 2023) and Substance Abuse and Mental Health Services Administration, National Mental Health and Substance Use Policy Laboratory, Identification and Management of Mental Health Symptoms and Conditions Associated with Long COVID (Rockville, Md.: June 2023).
[44]Substance Abuse and Mental Health Services Administration, National Mental Health and Substance Use Policy Laboratory, Evidence-Based Resource Guide Series: Telehealth for the Treatment of Serious Mental Illness and Substance Use Disorders (Rockville, Md.: 2021).
[45]Substance Abuse and Mental Health Services Administration, Mental Health Symptoms and Conditions Associated with Long COVID.
[46]These COVID-19 relief acts appropriated over $8 billion to SAMHSA in COVID-19 supplemental funding, which SAMHSA used to support various behavioral health programs and activities. See GAO‑22‑104437.
[47]See GAO‑24‑106760.
[48]The Policy Lab assumed this training and technical assistance coordination role starting in April 2022, when SAMHSA expanded the Policy Lab to better align with 21st Century Cures Act designated roles, according to SAMHSA officials. See GAO‑24‑106760.
[49]The Long COVID Coordination Council was chaired by the Assistant Secretary for Health and made up of representatives from 14 federal agencies, including SAMHSA. The council published various resources that incorporated mental health and substance use issues. See, for example, Department of Health and Human Services, Services and Supports for Longer-Term Impacts of COVID-19. The Policy Lab continued its work on long COVID after the end of the COVID-19 public health emergency, including by hosting a Policy to Action Initiative meeting in May 2024 with researchers, clinicians, representatives from national organizations, individuals with lived experience of long COVID, and federal agency colleagues. During this 2-day meeting, participants discussed challenges related to the behavioral health effects of long COVID and identified key messages and strategies to raise awareness.
[50]The U.S. Public Health Service Commissioned Corps is a uniformed service branch of public health professionals. Commissioned Corps emergency response teams are trained and equipped to respond to public health crises and national emergencies, according to HHS. Commissioned Corps Headquarters is responsible for the administration and response coordination of the U.S. Public Health Service Commissioned Corps.
[51]In reporting selected awardees’ responses, we use “nearly all” to represent 18 to 22 awardees, “many” to represent eight to 17 awardees, and “some” to represent three to seven awardees.
[52]According to SAMHSA, counseling may involve licensed professionals or peers working with and advising individuals, families, couples, or groups on a range of issues related to mental health and substance use. Peer support involves nonclinical activities provided by individuals with lived experience in recovery from a mental or substance use disorder. Case management is a coordinated approach to the delivery of health, substance abuse, mental health, and social services, linking clients with appropriate services to address specific needs and achieve stated goals. Behavioral health crisis response services provide access to behavioral health professionals for individuals experiencing mental health or substance use-related crises and offer an alternative to emergency departments and law enforcement intervention.
[53]Residential treatment programs allow clients to stay at a facility for a few weeks to a few months while receiving treatment for mental health conditions or substance use disorder, according to SAMHSA. Medication-assisted treatment combines behavioral therapy and the use of certain medications, such as buprenorphine, to reduce the misuse of or addiction to opioids and to increase treatment retention.
[54]According to SAMHSA, telehealth can make behavioral health visits more efficient by allowing staff to see more patients in a shorter period of time and by reducing costs associated with in-person care. See Substance Abuse and Mental Health Services Administration, Advisory: Using Technology-Based Therapeutic Tools in Behavioral Health Services (Rockville, Md.: 2021).
[55]Care coordination helps people navigate behavioral health care, physical health care, social services, and other systems they are involved in, according to SAMHSA. For example, care coordination might involve helping clients schedule appointments or helping them access or enroll in benefits. SAMHSA requires certified community behavioral health clinics to provide care coordination to clients. See Substance Abuse and Mental Health Services Administration, Certified Community Behavioral Health Clinic Certification Criteria.
[56]Assertive community treatment is designed to provide comprehensive community-based services to people with a serious mental illness. Assertive community treatment programs use a variety of treatment and rehabilitation practices, including medications; behaviorally oriented skill teaching; crisis intervention; support, education, and skill teaching for family members; supportive therapy; cognitive-behavioral therapy; group treatment; and supported employment. Under the assertive community treatment model, services are delivered by a mobile, multidisciplinary treatment team. These services are to be available 24 hours a day, 365 days a year. See GAO, Serious Mental Illness: HHS Assessments of Assisted Outpatient Treatment Have Yielded Inconclusive Results, GAO‑25‑107526 (Washington, D.C.: July 10, 2025).
[57]Social distancing, also known as physical distancing, is a way to keep people from interacting closely or frequently enough to spread an infectious disease such as COVID-19, according to SAMHSA. The Centers for Disease Control and Prevention defines physical distancing as putting physical distance between people to lower the risk of spreading a respiratory virus.
[58]Naloxone is a medication designed to quickly reverse the effects of opioid overdoses, according to SAMHSA. Overdose prevention services may involve distributing naloxone to individuals at risk of overdose, or to those who are likely to respond to an overdose of another individual.
[59]We previously reported on behavioral health workforce shortages and federal efforts to address them. See GAO, Behavioral Health: Available Workforce Information and Federal Actions to Help Recruit and Retain Providers, GAO‑23‑105250 (Washington, D.C.: Oct. 27, 2022).
[60]For some SAMHSA grants, state awardees distribute funding to subawardees, such as individual healthcare clinics providing behavioral health services directly to patients.
[61]We interviewed a nongeneralizable sample of SAMHSA awardees, including eight selected states and 16 behavioral health provider awardees in the selected states (Michigan, Mississippi, Montana, Oregon, Pennsylvania, Puerto Rico, Texas, and Vermont). Selected state awardees received MHBG, SUBG, State Opioid Response, and Emergency COVID-19 grants from SAMHSA. Selected provider awardees participated in SAMHSA’s Certified Community Behavioral Health Clinic Expansion or Community Mental Health Center grant programs, or both programs. We also interviewed representatives from four national associations.
[62]To characterize awardees’ responses throughout this report, “nearly all” represents seven states, 12 to 15 providers, or 18 to 22 awardees (i.e., the total across states and providers); “many” represents five to six states, eight to 11 providers, or eight to 17 awardees; and “some” represents two to four states, three to seven providers, or three to seven awardees.
[63]SAMHSA-funded training and technical assistance centers offer free support to those working in the behavioral health field—including SAMHSA awardees—on topics across the behavioral health spectrum, according to the agency. This includes assistance for states, Tribes, nonprofits, communities, health care professionals, and behavioral health specialties including licensed clinicians and peer support specialists.
[64]See Substance Abuse and Mental Health Services Administration, Telehealth for the Treatment of Serious Mental Illness and Substance Use Disorders; and Substance Abuse and Mental Health Services Administration, Disaster Technical Assistance Center Supplemental Research Bulletin: Adaptations and Innovations for Delivering Mental Health and Substance Use Disorder Treatment Services During the COVID-19 Pandemic (Rockville, Md.: Aug. 2022).
[65]SAMHSA provided grant administration flexibilities to awardees on a case-by-case basis upon awardee request. The Office of Management and Budget required awarding agencies to document certain grant flexibilities provided to award recipients during the COVID-19 pandemic, including project period extensions (i.e., no-cost extensions) and financial reporting extensions. We reviewed documentation for selected state awardees and interviewed SAMHSA officials to confirm that the agency tracked these flexibilities during COVID-19.
[66]SAMHSA awarded $5.4 billion to SUBG and MHBG awardees in COVID-19 supplemental funding as authorized by the Consolidated Appropriations Act, 2021, and the American Rescue Plan Act of 2021. Awardees initially had until March 14, 2023, to expend supplemental block grant funds from the Consolidated Appropriations Act, 2021, and were eligible to receive up to two project period extensions, known as no-cost extensions, each for up to 12 months, from SAMHSA to extend this deadline. American Rescue Plan Act of 2021 funds were not eligible for an extension, according to SAMHSA officials. Pub. L. 116-260, div. M, tit.II, 134 Stat. 1182, 1913 (2020); Pub. L. No. 117-2, tit. II, subtit. H, 135 Stat. 4, 45. Traditional (i.e., non-supplemental) block grant funds were also not eligible for extensions, according to SAMHSA officials.
[67]These challenges are similar to challenges identified in our prior work examining federal relief funding for behavioral health during the COVID-19 pandemic. See GAO‑22‑104437 for more information on behavioral health grantee challenges implementing programs within short project periods during the COVID-19 pandemic.
[68]Awardees submit a budget as part of their SAMHSA grant applications, which SAMHSA approves when it selects grant applications for funding, according to the agency. Awardees must submit a revised budget for SAMHSA approval to reallocate funds to address unexpected program changes. Revisions to the budget involve transferring funds that were not previously approved in the application. According to SAMHSA documentation, awardees had the flexibility to re-budget up to 25 percent of their budget (or up to $250,000, whichever was less) without submitting a formal budget modification request to the agency. If the awardee intended to re-budget more than this amount due to COVID-19 circumstances, SAMHSA required them to submit a COVID-19 post-award amendment for SAMHSA approval. This flexibility only applied to non-block grant awardees.
[69]SAMHSA requires awardees to submit federal financial reports detailing expenditures and other financial information annually and at the end of the program project period, according to agency documentation. Awardees must generally submit the final federal financial report 120 days after the project period end date.
[70]Under the maintenance of effort requirement, a state must maintain its expenditures for relevant activities at a level that is not less than the average maintained by the state in the 2-year period before the fiscal year for which it is applying for the MHBG or SUBG grant. See 42 U.S.C. § 300x-4(b); 42 U.S.C. § 300x-30(a). SAMHSA may waive the maintenance of effort requirement for a state if it determines that “extraordinary economic conditions” justify such a waiver or in the case of a public health emergency such as COVID-19. See 42 U.S.C. § 300x-4(b)(3); 42 U.S.C. § 300x-30(c); 42 U.S.C. § 300x-67.
[71]Methadone is a medication used to treat opioid use disorder that generally can only be dispensed through a SAMHSA-certified Opioid Treatment Program. According to SAMHSA, practitioners should consider whether therapeutic benefits of take-home doses outweigh the risks for each patient, such as the potential for overdose.
[72]SAMHSA initially provided this flexibility in March 2020 to simplify the process for Opioid Treatment Programs to request approval for providing take-home methadone doses, according to officials. According to SAMHSA officials, some states with few Opioid Treatment Programs opted to have the programs submit requests to use this flexibility directly to SAMHSA rather than through the state. SAMHSA issued additional guidance regarding this flexibility in November 2021 that extended the take-home flexibility to one year after the end of the COVID-19 public health emergency or until publication of revised Opioid Treatment Program regulations. At that time, 42 states and the District of Columbia—including five of our selected states—requested and received approval to use this flexibility, according to agency officials. SAMHSA revised its Opioid Treatment Program regulations in February 2024 to codify this flexibility. Medications for the Treatment of Opioid Use Disorder, 89 Fed. Reg. 7528 (Feb. 2, 2024) (to be codified at 42 C.F.R. pt. 8).
[73]Buprenorphine is a medication to treat opioid use disorder that can be prescribed or dispensed in physician offices, according to SAMHSA. SAMHSA made a similar flexibility available to Opioid Treatment Programs in April 2020 and issued additional guidance in November 2021, according to agency officials. At that time, 36 states—including five of our selected states—allowed Opioid Treatment Programs in their state to use this flexibility. According to SAMHSA officials, the agency did not allow telehealth initiation of methadone to treat opioid use disorder because differences in the medications required in-person assessment.
[74]In addition, in March 2020, the Drug Enforcement Administration announced that prescribers who were registered with the agency in one state and were authorized by another state’s laws to prescribe controlled substances for clients in that state, including via telehealth, did not have to obtain an additional registration from the Drug Enforcement Administration for that state. See Drug Enforcement Administration, Letter to Registrants (DEA067), (Springfield, Va.: Mar. 25, 2020). SAMHSA communicated with Opioid Treatment Programs and treatment providers about this flexibility and worked with the Drug Enforcement Administration to provide clarification as questions arose, according to SAMHSA officials.
[75]These challenges are similar to challenges identified in our prior work examining federal relief funding for behavioral health during the COVID-19 pandemic. See GAO‑22‑104437 for more information on behavioral health grantee challenges meeting client data reporting requirements during the COVID-19 pandemic.
[76]The Health Insurance Portability and Accountability Act of 1996 and its implementing regulations, the Privacy and Security Rules, establish standards to safeguard patients’ protected health information. To comply with these rules, health care providers must use certain technology platforms, including video and other remote communication technologies, that meet privacy and security requirements. See 45 C.F.R. pts. 160 and 164. During the COVID-19 pandemic, the Office for Civil Rights announced that it would not impose penalties against health care providers who used certain noncompliant telehealth platforms in good faith. See 85 Fed. Reg. 22,024 (Apr. 21, 2020).
[77]Pub. L. No. 117-328, § 2112(e), 136 Stat. 4459, 5722 (2022).
[78]Eight of SAMHSA’s nine advisory committees are subject to Federal Advisory Committee Act requirements. These committees are required to make committee records, such as meeting minutes, agendas, and reports, available to the public. See 5 U.S.C. § 1009. SAMHSA’s Tribal Technical Advisory Committee is not subject to Federal Advisory Committee Act requirements, according to SAMHSA officials.