Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
Contact: Tatiana Winger at WingerT@gao.gov
What GAO Found
The Department of Veterans Affairs (VA) spends hundreds of millions of dollars annually to buy and maintain high-tech medical equipment (HTME)—such as magnetic resonance imaging equipment—to deliver health care to veterans. To maintain this equipment, and help ensure its safe use, medical centers can purchase maintenance services—often from equipment manufacturers—using agencywide or stand-alone contracts. Agencywide contracts help VA leverage its buying power to obtain quality medical equipment at the best prices possible.
VA’s approach to buying HTME, uses agencywide contracts that generally support equipment maintenance. But not all regional contracting officials use these contracts when buying maintenance services and some unknowingly duplicated other officials’ work by awarding their own contracts for the services.

GAO found VA procurement guidance contained inconsistent information about whether the agency-wide contracts for HTME are mandatory when purchasing maintenance services. Additionally, regional contracting officials found the national contracting office resources for purchasing maintenance services to be unclear. Clarifying these resources and guidance on whether agencywide HTME contracts are mandatory and how to appropriately use them would reduce administrative burden and could save the government time and money.
Selected medical centers generally reported satisfaction with maintenance services, and equipment was maintained per policy. These centers generally obtained similar prices as the agencywide contracts for selected equipment. However, GAO also found instances where regional contracting officials were not efficiently purchasing maintenance services. For example, in a few instances, officials did not clearly document the services purchased or verify that the prices paid matched the prices offered through the agencywide contracts. In one case, officials paid a higher price than the agencywide contract offered for the same service. Regional contracting officials responsible for purchasing maintenance attributed these instances in part to difficulty using resources for VA’s agencywide HTME contracts, and said they plan to seek a refund for the overpayment.
Why GAO Did This Study
In fiscal year 2024, VA obligated over $608 million for the purchase of HTME and related services, including maintenance. Since 2019, VA Acquisition Management has been on GAO’s High-Risk list, partially due to challenges with VA’s acquisition approach.
GAO was asked to review how VA uses contracts to maintain HTME and whether its approach provides the needed flexibility to meet the agency’s mission. This report examines the extent to which (1) VA’s acquisition approach for purchasing HTME supports HTME maintenance and (2) the selected medical centers’ approaches to maintenance result in satisfactory and cost-effective maintenance, among other objectives.
GAO analyzed VA’s HTME strategic sourcing contracts and data for federal procurement, contract performance, and equipment maintenance from fiscal years 2022 through 2024. GAO selected a nongeneralizable sample of eight medical centers and 16 maintenance orders and contracts based on diverse geographic regions, medical center characteristics, and contracting approaches. GAO conducted site visits and interviewed relevant regional and national contracting officials.
What GAO Recommends
GAO is making three recommendations to VA, including that VA clarify guidance and resources for using agencywide contracts to purchase HTME maintenance services. VA agreed with the recommendations and has plans to review and update its guidance and resources.
Abbreviations
CT computed tomography
DLA Defense Logistics Agency
FAR Federal Acquisition Regulation
FDA Food and Drug Administration
HTME high-tech medical equipment
IDIQ indefinite delivery, indefinite quantity
MRI magnetic resonance imaging
NAC National Acquisition Center
NCO Network Contracting Office
VA Department of Veterans Affairs
VHA Veterans Health Administration
VISN Veterans Integrated Service Network
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
May 6, 2026
The Honorable Jerry Moran
Chairman
The Honorable Richard Blumenthal
Ranking Member
Committee on Veterans’ Affairs
United States Senate
The Honorable Mike Bost
Chairman
The Honorable Mark Takano
Ranking Member
Committee on Veterans’ Affairs
House of Representatives
To provide advanced medical care to veterans, the Department of Veterans Affairs (VA) maintains high-tech medical equipment (HTME) worth billions of dollars. HTME include imaging and radiation therapy equipment, such as magnetic resonance imaging (MRI) equipment, as well as picture archiving and communication systems. Timely maintenance of HTME is critical to VA medical centers’ ability to safely diagnose and provide care to veterans. If equipment is not appropriately maintained, it can provide inaccurate results or break down, leading to delays in care or even cause harm to patients. To help keep HTME working properly, the Veterans Health Administration (VHA) employs biomedical engineers at its Veterans Integrated Services Networks (VISN) and medical centers.[1] VHA also awards contracts to equipment manufacturers or other service providers to maintain HTME in medical centers.
Since 2019 VA acquisition management has been on GAO’s High-Risk List, in part because of challenges VA has experienced in developing adequate acquisition strategies and policies. In February 2025, we reported that over the past 10 years VA’s total contract obligations increased substantially, rising over 150 percent.[2] In fiscal year 2024, VA obligated about $67 billion for goods and services, including over $608 million for HTME and related services. Our work continues to identify VA acquisition management challenges including (1) developing adequate strategies and policies, (2) managing its supply chain, (3) managing its acquisition workforce, and (4) providing consistent leadership and execution of management priorities.[3] VA has made some progress addressing these issues; however, substantial challenges remain.
You asked us to review VA’s use of contracts to maintain the agency’s HTME and whether VA’s contracting approach for purchasing and maintaining HTME provides the needed flexibility to meet the agency’s mission, among other things. This report examines (1) the extent to which VA’s approach to purchasing HTME supports VHA’s maintenance of the equipment, (2) how selected medical centers acquire services to maintain HTME, and (3) the extent to which these medical centers’ approaches to maintenance result in satisfactory and cost-effective maintenance.
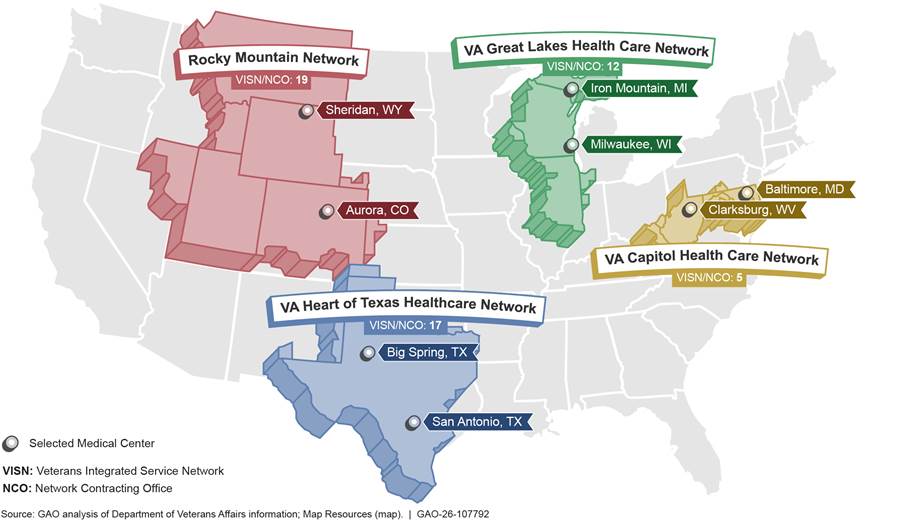
For our review, we included two types of HTME—imaging and radiology equipment (imaging) and radiation therapy equipment.[4] In addition, we selected a nongeneralizable sample of four VISNs and corresponding regional contracting offices, and eight medical centers within those VISNs. To inform our selections, we reviewed HTME inventory and biomedical engineering workforce data from November 2024 and September 2024, respectively.[5] We also reviewed VISN and medical center characteristics, such as complexity of care provided. In addition, we reviewed contract obligations during fiscal years 2022 through 2024, the last year of complete data when we initiated this review. Selection factors for the regions and medical centers included geography (rural and urban centers), workforce size, and types of HTME maintained, among others. We also selected a nongeneralizable sample of 16 HTME and their associated maintenance orders and contracts—two per selected medical center—using order and contract information that we obtained from the regional contracting offices. See figure 1 for the locations of the selected regions and medical centers and appendix I for more information about the selected centers’ orders and contracts for maintenance services.
Figure 1: Selected Veterans Integrated Service Networks, Regional Network Contracting Offices, and Selected Medical Centers Included in GAO’s Review
To assess the extent to which VA’s approach for purchasing HTME supports its maintenance, we analyzed the 48 HTME indefinite-delivery, indefinite-quantity (IDIQ) contracts that were active at some point during fiscal year 2022 through fiscal year 2024, according to VA. We refer to these contracts as base contracts in this report. VA purchases HTME by placing orders against these base contracts.[6] We reviewed acquisition planning documents, solicitations, and the base contracts to identify relevant terms that support VA’s maintenance of its HTME, such as requirements for equipment uptime—the time during which it is available for use—and whether maintenance services were available for purchase. We also reviewed available guidance and information for using the base contracts, as well as relevant sections of the Federal Acquisition Regulation (FAR).[7] We interviewed National Acquisition Center (NAC) officials about these contracts, how orders are placed, and pricing. We also interviewed leadership from selected regional contracting offices and contracting officials for the sample of 16 maintenance orders and contracts about their use of HTME base contracts and their understanding about how these contracts work. We assessed the documentary and testimonial evidence obtained against Standards for Internal Control in the Federal Government.[8]
To identify how selected medical centers acquire services to maintain HTME, we reviewed medical center information about the 16 selected HTME and their associated maintenance orders and contracts during fiscal years 2022 through 2024. Our sample allowed us to review contracts and orders for different types of equipment, services, and approaches to purchasing these services. It includes 10 orders placed on HTME base contracts, one General Services Administration Federal Supply Schedule order, and five stand-alone contracts.[9] We also reviewed VA’s policies for maintenance requirements. We conducted site visits at the eight selected medical centers. We interviewed officials from VHA health care technology management and selected VHA regional contracting offices; staff responsible for HTME at selected VISNs and medical centers; and other officials from the selected sites about policies, procedures, and oversight of HTME maintenance. We also discussed the factors that officials at selected medical centers considered when determining how they would maintain HTME.
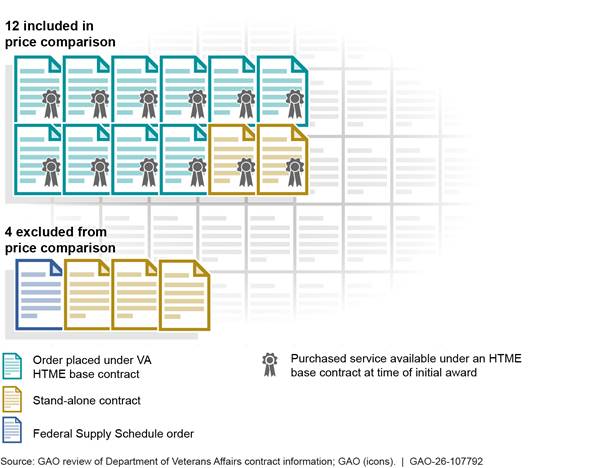
To assess the extent to which selected medical centers’ approaches to maintaining HTME result in satisfactory and cost-effective maintenance, we obtained and reviewed equipment and contractor performance information, and prices paid for the 16 HTME in our sample during fiscal years 2022 through 2024. We compared equipment performance information with VHA performance goals, policies, and procedures. We also compared evaluations of contractor past performance in available reports from the Contractor Performance Assessment Reporting System and contract files for the 16 orders and contracts with the relevant sections of the FAR.[10] We interviewed VHA officials responsible for HTME oversight nationally and officials from selected VISNs, contracting offices, and medical centers about the selected equipment and orders and contracts. We discussed the effectiveness of the centers’ approaches for maintaining HTME with the aforementioned officials and clinical users of the selected equipment, including availability to provide patient care and their satisfaction with the services received. For 12 of the selected 16 maintenance orders and contracts, we compared prices paid for the selected equipment’s service with prices for the same service that were available at the time under the HTME base contracts. We excluded the other four because the purchased services were not available from these vendors under a VA HTME base contract at the time of purchase (see fig. 2).
Figure 2: Sample of 16 High-Tech Medical Equipment (HTME) Maintenance Orders and Contracts Reviewed by GAO
We conducted this performance audit from September 2024 to May 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
High-Tech Medical Equipment and Its Maintenance
HTME, in this report, refers to imaging and radiation therapy equipment.[11] This includes their systems, subsystems, and components along with maintenance services, training, and incidental services related to the purchase of the imaging and radiology and radiation therapy equipment. This equipment is regulated by the U.S. Food and Drug Administration (FDA).[12] Some of the equipment can be technologically sophisticated.
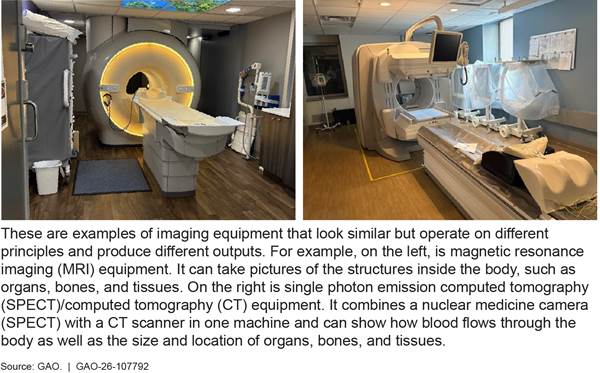
Imaging equipment allow medical staff to view the human body to diagnose, monitor, or treat medical conditions. Each type of technology gives different information about the area of the body being studied or treated, related to possible disease, injury, or the effectiveness of medical treatment, according to FDA.[13] Examples of imaging equipment include but are not limited to computed tomography (CT) scanners and MRI systems, as well as X-ray systems and related systems such as those used with cardiac catheterization and mammography, as well as repair parts, software, and accessories (see fig. 3).
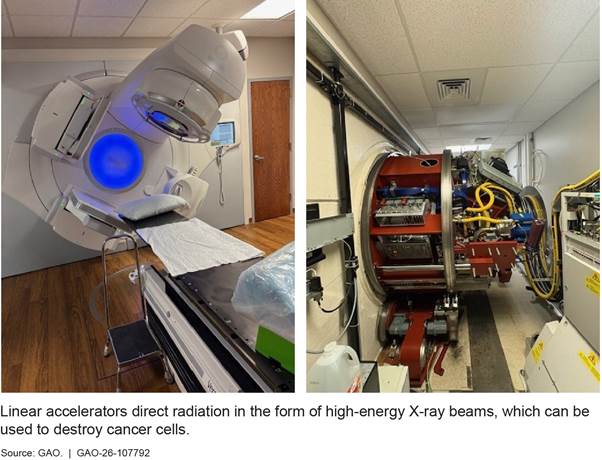
Radiation therapy equipment allows medical staff to safely and effectively treat cancer and other diseases. Examples of radiation therapy equipment include computer-controlled and imaging-guided linear accelerators, robotic linear accelerator systems, 3-D simulators, and therapy planning systems. Figure 4 includes two views of a linear accelerator.
To help ensure patient safety, a VHA directive establishes that VA manages oversight of medical technology across VHA consistent with relevant regulations and The Joint Commission standards.[14] The Joint Commission is a national standards-setting and accrediting body for quality care and patient safety. The standards generally state that hospitals must perform HTME maintenance according to the equipment manufacturer’s recommendations.[15]
Maintenance of this medical equipment helps to ensure that HTME consistently perform within certain parameters. Each manufacturer identifies equipment maintenance procedures and intervals in its manuals; these vary by type of equipment and model. Generally, maintenance includes two types—preventive and corrective.
· Preventive maintenance refers to activities performed to ensure equipment functionality, extend the life of a device, and prevent failure. These activities may include calibrating and lubricating equipment, running diagnostics, and visual examinations for wear. Preventive maintenance typically takes place at set intervals.
· Corrective maintenance, or repair, returns equipment to its original functionality after a failure. Failures requiring repairs are generally unplanned.
VA Offices Involved in the Purchase and Maintenance of HTME
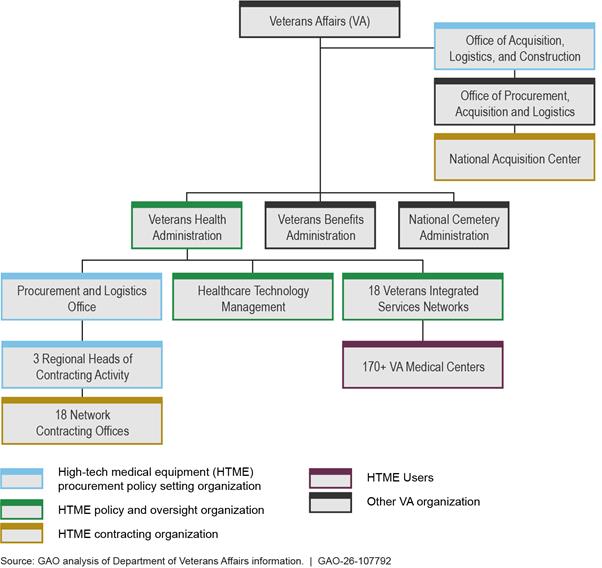
VA has established specific processes for purchase and maintenance of HTME that involve multiple offices within VA. At the time we conducted our audit, the location and leadership of the offices within VA differed (see fig. 5). For example, officials in the regional Network Contracting Offices that purchase maintenance services on behalf of the medical centers reported to different leadership than NAC—the office responsible for awarding and administering the agencywide HTME base contracts and ordering equipment on behalf of the medical centers. However, as of April 2026, VA reported it is in the process of reorganizing all contracting organizations under the Office of Acquisition, Logistics, and Construction.
Figure 5: Overview of the Offices Involved in the Purchase of High-Tech Medical Equipment and Its Maintenance Services (Prior to March 2026)
Generally, biomedical engineering or health care technology management departments are responsible for HTME maintenance either directly or by overseeing purchased maintenance services.[16] To help oversee a given maintenance contract, a contracting officer designates an individual at the medical center as the contracting officer’s representative. This person is typically a member of the medical center’s health care technology management team.
Contracting for HTME
In July 2003 VA and the Defense Logistics Agency (DLA), a Department of Defense agency, established a memorandum of agreement that aimed to combine the agencies’ buying power to achieve lower costs and to eliminate redundancies in contracting.[17] This effort included the agencies entering into joint VA/DLA national contracts for HTME—both equipment and maintenance.
As a result, since May 2006, NAC and DLA have met HTME requirements using national, multiple award IDIQ contracts awarded to a group of qualified vendors that sell HTME—we refer to these as HTME base contracts. These vendors include equipment manufacturers and authorized sellers of equipment. NAC determines whether item prices are fair and reasonable before awarding the contract. The HTME base contracts allow VA to place orders for individual requirements such as the type of equipment and its maintenance. HTME base contracts are examples of category management or strategic sourcing contracts and are intended to obtain compatible, uniform, quality products, at the best prices possible.[18]
In fiscal years 2022 through 2024, VA used the base contracts to obligate over $1.1 billion for purchases of HTME and $504 million for related services, including an estimated $308 million for maintenance.[19] A total of 48 HTME base contracts were available for ordering imaging and radiation therapy equipment during this period, according to NAC officials. However, not all 48 were active at the same time.[20] According to NAC officials, 38 imaging and radiation therapy base contracts were available for ordering as of September 30, 2025. IDIQ contracts like the HTME base contracts provide flexibility in cases where the government cannot determine the exact quantities and required timing of a product or service. An order, which is placed when a specific need arises, obligates funds and authorizes work.[21] Under these multiple-award IDIQs, the requirement must be generally competed through “fair opportunity” among all of the IDIQ contract holders, unless an exception applies—such as when only one source is capable of providing the product or service at the level of quality required because the product or service is unique or highly specialized.[22] Justifications for exceptions to providing fair opportunity must be approved at various levels within the contracting organization, depending on the value.[23]
VA’s Contracts for Purchasing HTME Generally Support Maintenance, but Ineffective Guidance Undercuts Benefits
VA’s HTME base contracts for purchasing equipment generally support VHA’s maintenance of the equipment, but some of the base contracts do not offer maintenance services. Further, we found that the guidance for whether contracting officers should prioritize HTME base contracts when purchasing equipment and maintenance services is ineffective because it is unclear, expired, or inconsistent. Additionally, NAC has not provided sufficient guidance or training to contracting officers regarding the resources available to assist in using HTME contracts.
HTME Contracts Generally Support VA’s HTME Maintenance Efforts, but Only Some Streamline Its Acquisition
HTME base contracts that VA uses to purchase equipment help support VA’s HTME maintenance efforts. For example, the HTME contracts require a 1-year warranty during which equipment vendors maintain the equipment. The warranty period allows time for medical center staff to prepare for the approach they will use to maintain equipment after the warranty ends. There are generally a few approaches to maintenance, which we discuss later in this report, including: (1) medical center staff can receive training and maintain, or help maintain, the equipment or (2) the medical center can purchase a maintenance service plan.[24] The HTME base contracts also establish uptime standards, provide access to maintenance manuals, and establish the period for which vendors commit to supporting the equipment.[25] In addition, some imaging base contracts offer maintenance services for purchase at already-established prices, which can speed up the acquisition process.[26] Radiation therapy contracts active during our review generally did not offer maintenance services for purchase.
Imaging base contracts. The primary base contracts for imaging equipment include preventive and corrective maintenance services for purchase, according to NAC.[27] The imaging contracts that include maintenance services offer contracting officials a faster acquisition process because NAC determined pricing for the available HTME and maintenance services as fair and reasonable when establishing the contracts.
In general, maintenance services are available for purchase from the original equipment manufacturers as an order under the HTME base contract or through awarding a new contract. According to a May 2020 analysis of the HTME service maintenance market, VHA determined that the manufacturers are best positioned to complete preventive maintenance for their equipment, in part, because third-party service providers have limited access to software and need to subcontract with the manufacturers.[28] VHA’s analysis also identified circumstances in which contracting with a third-party service provider is reasonable, such as inspections and corrective maintenance.[29]
Following its analysis, in January 2021, VHA determined that four imaging equipment manufacturers that hold HTME base contracts were best positioned to provide preventative maintenance services for their equipment. Based on this analysis, VHA, together with NAC, prepared “class justifications” for use of an exception to the “fair opportunity” process under which an order typically must be competed among all holders of a multiple award IDIQ contract.[30] VHA invoked the exception for instances where only one contractor is capable of providing products or services at the level of quality required because the supplies or services ordered are unique or highly specialized.[31] The class justifications applied to all orders for maintenance services placed under the four manufacturers’ HTME base contracts, meaning those four vendors were considered the only acceptable sources from which VA could purchase maintenance services for this imaging equipment. During fiscal years 2022 through 2024, these four vendors accounted for about 82 percent of obligations for imaging HTME overall and about 97 percent of obligations for services on imaging HTME contracts.
The class justifications allow regional contracting officials to place orders for maintenance more quickly than through the typical fair opportunity process, according to VHA. Further, officials from NAC and four regional contracting offices stated that these class justifications for exceptions to the fair opportunity process allow contracting officials to quickly and easily place orders for maintenance from the equipment manufacturers, resulting in a streamlined acquisition process that reduces their administrative burden. One of these officials stated that the streamlined process can save them about a month of time.
Radiation therapy base contracts. In contrast, radiation therapy base contracts generally do not include maintenance services for purchase, according to VA officials.[32] As a result, contracting officials must take additional steps as they cannot use a preexisting contract to obtain maintenance services. Specifically, regional contracting officials need to individually obtain pricing and purchase these services from original equipment manufacturers using separate contracts instead of placing orders off already established HTME base contracts, which could save the officials time and leverage VA’s buying power.
Further, even though NAC’s acquisition plan for radiation therapy equipment identified the need for both equipment and maintenance services after the equipment’s warranty period, NAC did not include, nor did it pursue, maintenance services on all radiation therapy base contracts. Additionally, the July 2003 memorandum of agreement between VA and DLA states that joint contracts should include equipment and maintenance. When asked why radiation therapy maintenance services (after the warranty period) were not included in most of the 2019 base contracts, current NAC officials noted that they were not involved with award of these base contracts. Nonetheless, these officials cited a few potential reasons for the omission, such as a lack of adequate HTME acquisition planning, limited clinical demand for radiation therapy maintenance services, or medical centers’ infrastructure limiting the installation of radiation therapy machines.
Subsequently, while the March 2025 solicitation for radiation therapy base contracts referenced maintenance services as among VA’s general needs, NAC officials said that they did not require vendors to offer maintenance services or submit pricing for such services. Only one of the six contracts awarded in September 2025 included maintenance service for purchase, according to NAC officials.
Our review shows a need to assess the advantages and disadvantages of VA’s approach to purchasing maintenance services for radiation therapy equipment at an agencywide level. The current approach, as mentioned earlier, results in contracting officials needing to individually obtain pricing and purchase these services across VHA because maintenance services are not generally available under these base contracts. For example, when purchasing maintenance services for two pieces of radiation therapy equipment in our sample of 16 HTME, officials individually determined that the equipment manufacturers were the only source for the maintenance. However, this determination was limited to each of the two HTME that we reviewed.
Further, internal VHA analysis found that an agencywide approach is needed. VHA’s May 2020 analysis found that manufacturers are best positioned to complete preventive maintenance for their equipment, including for radiation therapy equipment, and an agencywide approach would be more efficient in terms of contracting and reduce equipment maintenance risks. Implementing an agencywide approach to purchasing radiation therapy maintenance services could streamline the acquisition process and leverage VA’s buying power. Doing so could help VA save the agency time and potentially money.
VHA Guidance Is Unclear on Whether HTME Base Contracts Are Mandatory
VHA guidance to contracting officials does not clearly and consistently identify whether HTME base contracts are mandatory for purchasing maintenance services, meaning that they must first be considered before using other vehicles.[33] VHA guidance focuses on the initial purchase of the HTME and does not directly address the purchase of maintenance services. For example, the 2024 update to the VHA procurement manual states that the VHA Heads of Contracting Activity made medical strategic sourcing contracts, including HTME base contracts, mandatory for contracting officers’ use.[34] However, the procurement manual states that the contracts were put in place for purchasing medical equipment, and does not refer to the purchase of maintenance services.
Similarly, an outdated 2009 VHA Directive for the initial purchase of HTME does not address maintenance services or if the HTME base contracts must be considered.[35] VHA procurement officials said that the directive was still active even though it expired in 2014 and the procedures described no longer reflect current practice. An official said that they have tried to update it multiple times, but that has not happened because of other priorities competing for leadership’s attention.
In addition, there have been inconsistencies within VHA guidance. For example, the VHA customer reference guide’s supply section, applicable when purchasing equipment, identifies the HTME contracts under the required sources of supplies and services section. However, until recently, the guide’s section for services did not. In January 2026, VHA updated the service section to include information about the availability of HTME contracts for maintenance services.[36]
We also found inconsistent understanding among officials. According to VHA procurement policy officials and NAC HTME officials, HTME base contracts are considered mandatory only for purchasing equipment but not for purchasing services.[37] However, we found varying understanding among the regional contracting officials responsible for our selected HTME orders and contracts. Two regional contracting officials said that the HTME base contracts are mandatory for maintenance services and have placed orders for these services under the HTME contracts. In contrast, a contracting official responsible for awarding a stand-alone contract said that they did not know that they could order maintenance services using the HTME base contracts. Accordingly, the official would not know whether the contracts are mandatory.
VHA’s guidance also lacks information to support a key acquisition step for purchasing HTME maintenance. For instance, a first step in an acquisition at VA is consideration of the VA Rule of Two. Under the VA Rule of Two, a VA contracting officer must set aside contracts for veteran-owned small businesses if, based on market research, the contracting officer has a reasonable expectation that two or more veteran-owned small businesses will submit offers at a fair and reasonable price that offers the best value to the government.[38] NAC officials said that the Rule of Two was considered before NAC awarded the HTME base contracts and competition was not limited to veteran owned small businesses. They also told us that the determination not to set aside the contracts applies to orders placed under those contracts. VA’s acquisition plans for the HTME awards show that the solicitations would not be limited to small businesses and DLA documented the decision not to set aside HTME contracts for small businesses in a memorandum for the record. However, acquisition planning documents and the DLA memorandum do not explicitly reference the VA Rule of Two, and are not available on the HTME website or in guidance, according to officials.
The lack of documentation in VHA’s guidance for purchasing HTME maintenance has contributed to regional contracting officials unknowingly duplicating NAC’s efforts. Some regional contracting officials said that, when awarding orders for maintenance services off the HTME base contracts, they must first apply the VA Rule of Two by searching for veteran-owned businesses that could possibly perform this work.[39] These officials are separately conducting and documenting market research.
VHA has not documented the determination that made HTME contracts mandatory for equipment. As of May 2025, VHA officials stated that they are working with regional procurement offices and Heads of Contracting Activity on developing instructions for how a contract may be deemed mandatory and if the HTME base contracts should be deemed mandatory for maintenance services.[40]
Standards for Internal Control in the Federal Government states that management should internally communicate the necessary quality information to achieve entity objectives, such as through guidance.[41] Without determining whether the HTME base contracts are mandatory for maintenance services or updating its guidance on ordering procedures for purchasing HTME to include its maintenance, contracting officials may continue to miss opportunities to more effectively use these HTME base contracts.
Awarding new contracts for maintenance services, instead of using strategic sourcing contracts—such as these base contracts—takes more time and can cost more. Further, conducting additional market research leaves contracting officials with less time for other contracting work. Updating VHA guidance for the HTME base contracts could help regional contracting officials avoid duplication of effort that is a poor use of their time and extends the contracting process.
Insufficient NAC Guidance and Training Contribute to VHA’s Ineffective Use of HTME Base Contracts
NAC has several resources to assist regional contracting officers in using HTME base contracts, including an internal website, associated price books with vendors’ equipment and maintenance offerings and pricing, and a pricing tool. However, in interviews with contracting officials, we heard of several instances where these officials had difficulty effectively using those resources. We found NAC has not provided sufficient guidance to regional contracting officials regarding the NAC HTME resources and how to use them when purchasing maintenance services.
NAC website on HTME base contracts. NAC maintains an internal website that lists the HTME base contracts, the corresponding price books, recent modifications, and general points of contact, but VHA officials had mixed experiences using the website. Most health care technology management staff at the VISNs and medical centers, and regional contracting officials we spoke with were aware of the website. Further, some officials thought the website was helpful as it provided the contracts, equipment ordering procedures, and NAC points of contact. However, other officials said that the website was hard to use, were not aware of it, or accessed the HTME base contracts through other VA procurement sites. A few contracting officials also said that it was easy to overlook the HTME base contracts when purchasing maintenance services because NAC’s website was one of a number of sources they must check for information about existing contracts.
Additionally, NAC provides limited support to regional contracting officials using the HTME base contracts. NAC officials said that they are available to answer questions from regional contracting officials, but do not proactively engage with them regarding maintenance purchases using the HTME base contracts. NAC officials also said that they have not provided training to regional contracting officials on using the HTME base contracts when purchasing maintenance services, nor developed guidance to share about the base contracts.
Improving the resources about the contracts, such as developing guidance for how the contracts work or how to use them when ordering maintenance services (the type of information and guidance users in the field may be looking for) and providing training could lead to more consistent use. For instance, we found that contracting officials did not order from the imaging HTME base contracts for two of the purchases in our sample when they could have. Instead, they awarded stand-alone contracts. As a result, these officials did not take advantage of the time savings offered by the HTME base contracts.[42]
HTME price books. Contracting officials experienced challenges when using the vendor price books. Generally, each vendor’s price book includes the catalog number, short and long descriptions of the item, list price, minimum and maximum prices, and various discounts.[43] The internal HTME website lists the NAC contact’s name and email for each vendor. Some vendor price books contain large amounts of data, including pricing for tens of thousands of rows with medical equipment and services. One item in the price book may have 20 or more data fields associated with it. Officials from each of the four regional contracting offices we met with said that the price book files were difficult to access or navigate.
To facilitate use of HTME base contract pricing information, NAC officials created a tool that summarizes several price book fields. This tool is intended to allow contracting officials to quickly compare pricing across the HTME base contracts, but the information provided to do this in the tool is incomplete (see fig. 6).
Figure 6: Comparison of Notional High-Tech Medical Equipment (HTME) Price Book and Pricing Information Tool
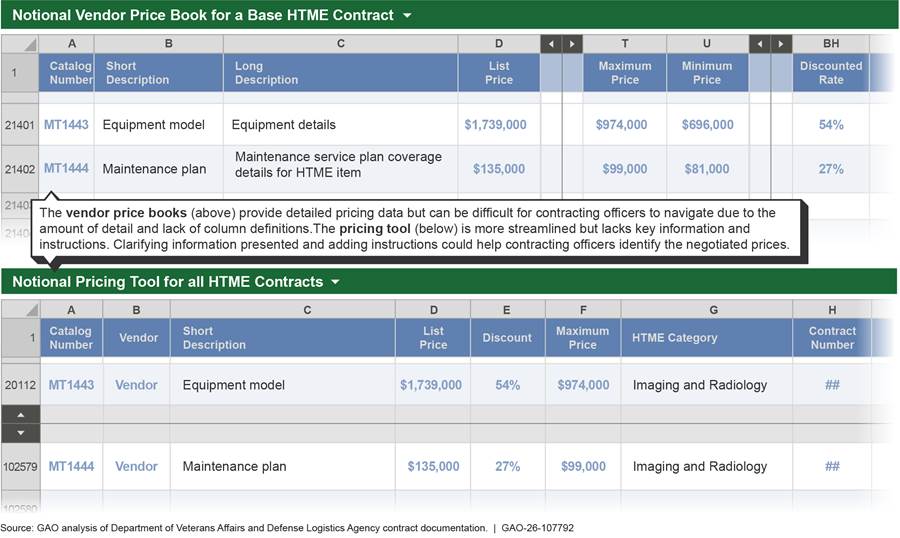
Some contracting officials said that the tool is helpful as it allows for quick searches using key words to identify items available on the HTME base contracts. As demonstrated in figure 6 above, it includes the catalog number, vendor, short description of the item, list and maximum prices, and discount percent. It also includes the first name of a NAC point of contact for each vendor. However, the tool does not include all HTME vendors or information needed to differentiate among maintenance service plans. For example, the short description may designate the item generally as a maintenance plan, but the long description would provide the details of the type of maintenance and the medical equipment. NAC officials said that including the long description in the tool would make it too text heavy and unwieldy, and contracting officials would need to refer to the original price books to access the long description. They said that no formal instructions exist for using the tool as it is meant to be intuitive and user friendly.
Limitations in the price books and other information available to regional contracting officials result in reliance on separate pricing and service information provided by vendors. Officials from three of four regional contracting offices said that they had trouble independently finding prices for specific maintenance services on the HTME base contracts. Our analysis of the 12 sample orders and contracts identified several challenges:
· Unspecified manufacturer item numbers for the maintenance services in the orders and contracts. For example, one order simply listed the equipment name and “Protection Service Plan,” which was not sufficient to identify it in the price book.
· Proposals submitted by vendors for purchases that did not clearly identify the prices of individual services included. For example, one vendor proposal listed the “Silver service agreement” with a total price. However, upon further communication, the vendor disclosed that the amount included other items beyond the “Silver service,” such as additional part coverage that represent an additional cost and are listed separately in the price book.
· Key information not included in price book documentation, such as effective dates and column explanations. For example, there are multiple columns that reflect the different pricing and discounts, but the price book does not explain what the price represents or which price to use when evaluating the vendor’s proposal.[44] When we asked a NAC official in what situation the minimum price would apply over the maximum price, they said that it depends on various factors such as the services being offered but this information is not documented.
NAC officials said that the price books and tool are self-explanatory and did not provide training on these resources to the regional contracting offices, which order maintenance services. However, the officials said that they provided training to NAC contracting officials. In addition, while it is not explicitly stated in the price book and there is no guidance, NAC officials said that contracting officials issuing the order know that they should not pay more than the maximum price. However, as we stated earlier, contracting officials had trouble finding prices for specific maintenance services on the HTME base contracts. As we discuss later in this report, one medical center paid more than the HTME base contract price for the same HTME maintenance service.
NAC officials also described internal procedures they use to obtain information for each HTME purchase that helps officials compare prices of equipment and avoid some of the challenges we identified. Prior to issuing an order, NAC officials said that they require HTME vendors to submit detailed proposals that include each item, its list price, discounted price, and catalog number. They said that those details are provided by the vendor for the explicit purpose of NAC comparing the vendor’s proposed prices to the prices listed in the HTME price books. NAC officials also said that regional contracting officials should be reviewing the price books to compare prices. As we discuss later in this report, we found that not to be the case—regional contracting officials did not verify whether the price they paid was at or below the HTME base contract maximum price for selected maintenances services at three of eight medical centers.
The Standards for Internal Control in the Federal Government states that management should internally communicate the necessary quality information to achieve entity objectives, such as through guidance and training.[45] Revising NAC resources, including developing guidance, and providing training to VHA contracting officials about the NAC resources on the HTME base contracts could help VA realize the benefits of these contracts by (1) increasing use of these strategic sourcing contracts and (2) enabling officials’ more effective use of these resources. Further, additional guidance for contracting officials on how to consistently compare prices in the vendor’s proposal with prices in the HTME price books would also help ensure that medical centers do not pay more than the maximum amount already established with the vendor.
Selected Medical Centers Generally Acquire Services from HTME Manufacturers to Ensure Availability for Patient Care
Officials at the eight selected medical centers said that they generally acquire manufacturer-provided maintenance services to help ensure HTME are available for patients and to address medical center-specific circumstances. Purchasing manufacturer-provided services reduces their operational risks related to providing patient care, such as equipment downtime and reduced functionality, according to regional and medical center healthcare technology management officials we interviewed.[46] According to these officials, manufacturer technicians build expertise and frequently perform maintenance for specific equipment, whereas a medical center biomedical engineer typically supports a wide range of equipment—not only HTME—and may only perform a maintenance task on a given piece of HTME once a year. Several officials said that reducing downtime is especially important for more complex HTME, such as MRI, CT, and radiation therapy equipment where medical centers have little redundancy. For example, one official said that when there is an outage of a key piece of HTME, which they said is not often, it results in an “all-hands on deck” approach to restore the equipment to be functional. Downtime can negatively affect multiple clinical departments in the medical center because this equipment is used in preparation for, during, and after procedures.
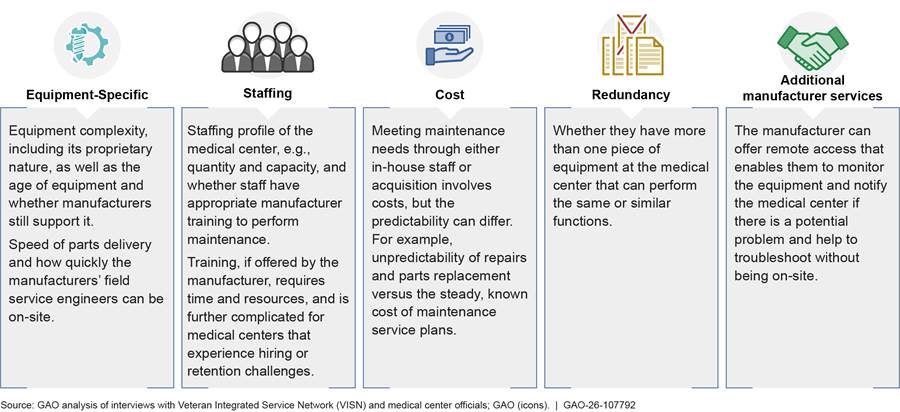
VHA policy provides medical centers flexibility in their approach to using staff, service contracts, or a combination thereof because it does not specify who must perform the maintenance. The policy requires that VA medical centers maintain HTME per manufacturer recommendations and that VA biomedical engineering staff oversee maintenance.[47] When determining a medical center’s approach to maintaining HTME, regional and medical center officials said that they generally consider numerous factors, such as equipment complexity, staff availability, cost, and how many pieces of that equipment the medical center owns, among others (see fig. 7). For example, the more complex the equipment is, the more technical knowledge is needed and the more likely a medical center is to purchase the manufacturer’s services. Relatedly, if equipment uses proprietary software or information, the manufacturer might not train VHA staff or other vendors to maintain the equipment. In this situation, the medical center must purchase maintenance from the manufacturer.
Figure 7: Factors That Biomedical Engineers at Selected Medical Centers and VISNs Consider When Determining Their Approach to Maintaining High-Tech Medical Equipment
To help maintain HTME during fiscal years 2022 through 2024, the eight medical centers reported a total of 87 orders and contracts (see appendix I). Obligations for these orders and contracts totaled about $32 million dollars during that time.[48] Orders under the HTME base contracts accounted for approximately $23 million or about 71 percent of these obligations.
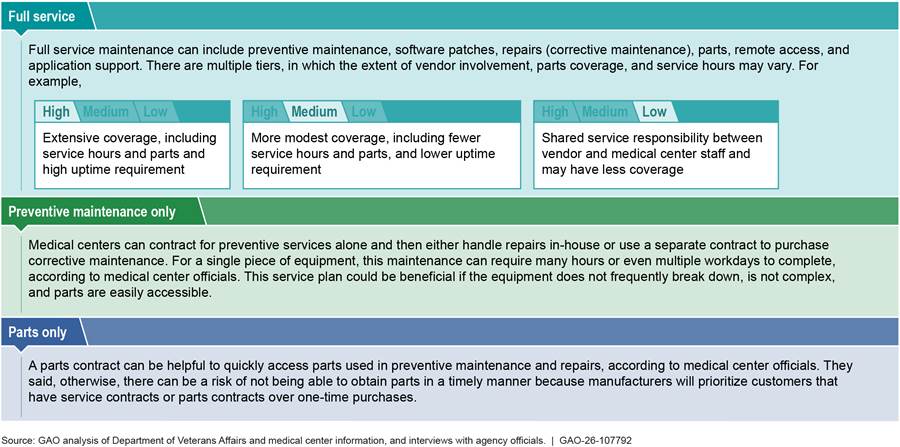
Medical centers typically purchase full-service plans from the manufacturers that include HTME preventive and corrective maintenance, especially for complex HTME, according to officials from the eight medical centers in our sample. A medical center can choose from various levels of maintenance service plans and vendor involvement once it has determined that it will purchase maintenance services. In addition, some service plans include more than on-site maintenance, such as remote monitoring of the equipment and application support to the clinical users. Alternatively, medical centers may choose to purchase maintenance services on a one-time basis. For example, a biomedical engineering staff may generally maintain X-ray equipment, but if that staff is not available, the medical center may choose to award a contract for an emergency repair to replace a broken X-ray tube or to purchase preventive maintenance. Figure 8 includes examples of services medical centers can purchase.
Figure 8: Examples of Service Plans That Selected Medical Centers Can Use to Maintain High-Tech Medical Equipment
Officials at three of the medical centers expressed interest in taking on a larger role maintaining less complex HTME, such as ultrasound and X-ray equipment. However, officials acknowledged that it may not be realistic given their current resources and the advantages of using manufacturers’ services previously mentioned.
Selected Medical Centers Are Satisfied with Maintenance Services, but the Contracting Process Is Not Working Efficiently
Medical center officials we interviewed were satisfied with the services provided by HTME manufacturers. We found, however, that regional contracting officials did not efficiently leverage existing HTME base contracts for five of the eight medical centers.
HTME Maintenance Was Generally Timely and Performed Satisfactorily
Medical center officials we interviewed were satisfied with the maintenance services received and reported that preventive maintenance was generally performed on-time.
Preventive maintenance. VHA policy requires that medical centers complete all preventive maintenance on-time and that biomedical engineering staff regularly document all maintenance performed.[49] The eight medical centers reported that preventive maintenance was generally completed on-time during fiscal years 2022 through 2024 for all 16 HTME that we selected for further review.[50] For one of the 16 HTME, staff said that a portion the maintenance was not completed. Staff at the medical center said that they learned upon switching to the manufacturer for maintenance service that the equipment’s software was not fully updated when working with the prior third-party service provider. They explained that this provider did not have direct access to software updates and typically subcontracted to the original equipment manufacturer. The contract with the third-party service provider ended as of September 2022. Staff said that the equipment manufacturer has since updated the software.
Officials at three selected medical centers brought up past examples in which they used third-party services (non-original equipment manufacturers) for maintenance. These officials said that they generally no longer use such firms for HTME preventive maintenance. The officials said that working with the third parties delayed maintenance because the third parties had to subcontract with the manufacturers to provide the updates and in some cases make repairs. They said that they had contracted with the third parties as part of an effort to work with veteran-owned businesses. In May 2020, VHA found that, generally, third-party service providers are not authorized by the manufacturer to install software updates and might not be able to timely repair equipment.[51] However, we found examples of contracting officials taking time in their market research to explore whether there were third-party providers of maintenance services beyond the HTME contracts.
A few medical center officials said that there are circumstances in which they must work with third-party service providers. For example, in our sample, one HTME was nearing the end of its service life and needed repair before the new, replacement equipment was ready for patient use. Officials reported that the manufacturer no longer supported the equipment due to its age. The medical center worked with the manufacturer to identify a third-party that had the necessary experience and knowledge to complete one-off repairs. This helped the medical center continue providing care until the medical center could begin using the new equipment.
Corrective maintenance. Corrective maintenance sometimes took longer than VHA’s 7-day goal. For 14 of the 16 HTME, corrective maintenance exceeded the goal at least once during fiscal years 2022 through 2024, according to medical center records. For the remaining two, maintenance was completed the same day on one HTME, and the other did not require any corrective maintenance during the period. In some cases, the issue requiring repair did not prevent equipment from being used. In others, it was inoperable. While VHA’s goal of 7 days was not consistently met, clinical staff we spoke with at each of the selected medical centers said that they have been generally satisfied with maintenance services and that service providers made a good faith effort to respond and address issues in a timely manner.
These staff said that they generally have been able to accommodate downtime without causing significant delays in patient care. For example, one medical center reported canceling 12 appointments after a power issue affected the CT scanner. An internal uninterruptable power supply was installed the next day to avoid future occurrences, and all affected patients were rescheduled for appointments the following week. If HTME downtime results in delays to patient care, medical centers file an “Issue Brief,” according to a VISN Chief Biomedical Engineer. The brief notifies medical center and VISN leadership about the issue and effects on patient care, such as rescheduling or sending the patient to a community health provider.
Health care technology management officials use information about the timely completion of maintenance to help support their oversight of medical equipment more broadly. This information contributes to key performance indicators—“Non-High Risk Medical Device PM Completion” that includes the timely completion of preventive maintenance, and “CM Completion Turn Around Time” that includes number of days required to complete corrective maintenance. While important equipment for patient care, HTME are considered non-high-risk compared with, for example, ventilators.[52] The non-high risk performance indicator includes HTME as well as other medical equipment such as patient lifts.
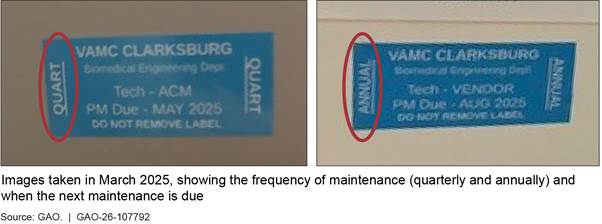
One way that VHA supports its oversight is by requiring that regional health care technology management officials regularly assess how well medical centers are sustaining medical equipment.[53] VHA guidance for assessments includes reviewing whether medical centers are completing preventive maintenance and repairs on-time for a sample of all medical equipment. While not specific to HTME, these assessments can help medical centers and VISNs identify and address maintenance delays. For example, one July 2024 assessment identified that 19 of 770 preventive maintenance labels—stickers affixed to the equipment—were out of date. By November 2024, medical center health care technology management officials reported that all stickers had been updated, and manufacturer maintenance procedures were performed. Medical centers use this visual method to cue users and biomedical engineers when maintenance is due (see fig. 9).
Contractor performance. We reviewed the Contractor Performance Assessment Reporting System for each of the 16 selected orders and contracts and did not identify any negative performance evaluation reports. For nine of the 16, VHA rated contractors as performing satisfactory or better, meaning that the contractor met the terms of the contract. For the other seven, three orders and one contract did not meet the dollar threshold for reporting performance during our review period, and ratings were not entered in the system for the remaining three orders. However, our review of contract files and interviews with contracting officers indicated that staff were satisfied with performance on these three orders, and our review of the associated base contracts in the system also identified satisfactory performance.
Medical center satisfaction with maintenance services. Health care technology management officials at each of the eight medical centers we visited said that they are generally satisfied with the HTME manufacturers’ maintenance services that they have received. Several officials said that numerous factors influence the timely completion of preventive and corrective maintenance. For example, officials at one medical center said that issues with the equipment can emerge during preventive maintenance that then require repair. Officials at several medical centers said that there can be parts delays due to supply chain challenges or vendors prioritizing customers with service contracts over one-off parts purchases. Further, they also said that manufacturers may have staffing issues such as turnover or limited availability that affects their response time. As mentioned previously, clinical staff we spoke with that use the equipment to deliver patient care also generally agreed that manufacturers and third-party service providers made good faith efforts.
Five of Eight Medical Centers Did Not Leverage HTME Base Contracts to Gain Efficiencies When Purchasing Maintenance Services
For five of the eight medical centers, we identified inefficiencies in the acquisition process for purchasing HTME maintenance services, such as contracting officials duplicating work. These inefficiencies reflect confusion in the contracting process—similar to the issues we raise above. For one of those medical centers, VHA paid more than the HTME base contract price for the same service.
We compared the prices paid on maintenance service orders and contracts for 12 selected HTME with the prices that were available in the price books at the time under VA and DLA HTME base contracts for the same services.[54] For 11 of the 12, prices for the selected HTME maintenance service were at or less than the maximum price and of these, eight were either less than the minimum prices or within about 1 percent—getting those medical centers the most value.[55] For the 12th, the regional contracting official overpaid.[56]
Through our analysis, however, we found that several contracting officials did not efficiently leverage the streamlined contracting process offered by the HTME base contracts. We found that challenges with officials’ understanding of when and how to use the HTME base contracts, as discussed in an earlier section of this report, contributed to their inefficient use and increased the risk of overpaying.
· For two medical centers, regional contracting officials awarded separate, stand-alone contracts for the same services and at the same prices available through HTME base contracts. As previously mentioned, orders placed under base contracts offer a faster process. In addition, awarding stand-alone contracts to purchase the same services at the same prices available for order under the HTME base contract unnecessarily duplicates NAC’s work on behalf of the agency.
· For three medical centers, regional contracting officials who issued the orders or awarded the contract (including one who awarded a separate, stand-alone contract) did not clearly document the services the medical centers expected to buy. The lack of clear documentation makes it difficult for contracting officials to confirm whether VHA is paying the correct price when issuing a new order or awarding a contract. Officials did not verify that pricing for the services purchased aligned with the pricing available through the HTME base contracts or could not confirm that pricing had been verified. As a result, officials missed an opportunity to leverage NAC’s prior work when awarding the base contracts. The officials we spoke with said that the price books were not readily available or were not aware of the HTME base contract. Additionally, clear documentation helps to ensure VHA is obtaining all services it paid for when overseeing the work of the contractor.
· For one medical center, as mentioned previously, a contracting official overpaid. Regional contracting officials attributed the overpayment to the contracting officer not having information about prices available on the base contract and said that they plan to seek a refund for amount paid above the base contract price.
The overpayment or lack of clarity about services for four out of 12 selected HTME and the fact that it occurred in each of the four selected regional contracting offices raises concerns about whether medical centers are getting services they intend to buy and at the base contract prices across VHA. Further, VA spent over $138 million on separate contracts with vendors that have HTME base contracts during fiscal years 2022 through 2024. While this amount likely includes some services not available for ordering under the base contracts, such as maintenance for radiation therapy equipment, VA has an opportunity to use the base contracts’ prices for a larger portion of HTME maintenance purchases.
Conclusions
Every year, VA spends hundreds of millions of dollars to purchase and maintain HTME as part of its mission to provide health care to veterans. VA has established agencywide contracts to efficiently purchase this equipment. Many imaging base contracts also include maintenance services, but most radiation therapy contracts do not. VA has an opportunity to leverage the agency’s buying power and reduce contracting redundancies when purchasing maintenance services for radiation therapy equipment.
In addition, VA’s purchasing of maintenance services for all types of HTME requires numerous offices across the department to work together. However, there is no clear guidance that these offices can reference to ensure a consistent and efficient approach to acquiring maintenance services. In some cases, this took contracting office resources away from other priorities. VHA has an opportunity to ensure guidance for HTME base contacts is clear, current, and consistent for its contracting officials to increase use of these strategic sourcing contracts. Doing so could also help VHA avoid duplicating work when buying maintenance services.
Further, NAC, as the office responsible for establishing and administering HTME base contracts, has opportunities to provide resources and training that are clear and address regional contracting officials’ needs. Doing so would help ensure that contracting officials have the tools and knowledge necessary to efficiently purchase HTME maintenance services at the discounted prices afforded to the government. Additional guidance is particularly important, as we identified instances where contracting officers did not have the information that they needed on maintenance prices to ensure they received the contract prices. As VA strives to provide essential care to veterans, it is important that it pursues all opportunities to avoid potential overpayment and administrative duplication that contributes to monetary waste.
Recommendations for Executive Action
We are making the following three recommendations to VA:
The Secretary of Veterans Affairs should ensure the Associate Executive Director of the National Acquisition Center evaluates how best to purchase maintenance services for radiation therapy equipment, including considering whether to modify the HTME base contracts to include these services. (Recommendation 1)
The Secretary of Veterans Affairs should ensure that the Veterans Health Administration Heads of Contracting Activity determine whether HTME base contracts are designated as mandatory for purchasing HTME maintenance services and reflect this decision across agency procurement guidance to contracting officials, including updating expired HTME guidance. (Recommendation 2)
The Secretary of Veterans Affairs should ensure the Associate Executive Director of the National Acquisition Center provides guidance and training to Veterans Health Administration contracting officials to facilitate effective use of the HTME base contracts, including updating its resources and identifying relevant information that regional officials should use when comparing prices and explaining how to use the center’s HTME resources. (Recommendation 3)
Agency Comments
We provided a draft of this report to VA for review and comment. In its comments, reproduced in appendix II, VA agreed with our three recommendations. For recommendation 1, VA stated that NAC will work with VHA’s National Radiation and Oncology Program to evaluate the current process for purchasing maintenance services for radiation therapy equipment, including whether those services should be standardized as part of equipment purchases. For recommendation 2, VA stated that the VA Senior Procurement Executive and Heads of Contracting Activity will determine whether to designate the HTME contracts as mandatory and will make changes across agency procurement guidance, as needed. For recommendation 3, VA stated that NAC will enhance guidance and training available to VHA acquisition personnel for the use of HTME contracts. VA also provided technical comments, which we incorporated as appropriate.
We are sending copies of this report to the Secretary of Veterans Affairs and the appropriate congressional committees. In addition, the report is available at no charge on the GAO website at https://www.gao.gov.
If you or your staff have any questions about this report, please contact me at WingerT@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations are on the last page of this report. GAO staff who made contributions to this report are listed in appendix III.

Tatiana Winger
Director, Contracting and National Security Acquisitions
Appendix I: Summary of Maintenance-Related Orders and Contracts at Eight Selected Medical Centers Reviewed by GAO
The 16 selected maintenance orders and contracts that we reviewed represented almost $11 million in obligations in fiscal years 2022 through 2024, or 34 percent of the obligations associated with the eight medical centers’ HTME maintenance orders and contracts during the period. Medical centers purchased service maintenance agreements with 15 of the 16 orders and contracts—14 of these included services purchased directly from the original equipment manufacturer and the 15th purchased the services from a third party service provider. With the 16th contract, the medical center purchased one-time repairs from a third party service provider.
Overall, the eight medical centers in our review reported a total of 87 HTME maintenance-related orders and contracts. These orders and contracts obligated about $32 million during that period. We identified obligation data for these specific orders and contracts in the Federal Procurement Data System from fiscal years 2022 through 2024 (see table 1).
Table 1: HTME Maintenance-Related Orders and Contracts at Selected Medical Centers During Fiscal Years 2022 through 2024
|
Veterans Integrated Service Network (VISN) |
Medical center location |
Contract vehicles |
Number of contracts and orders |
Obligations (millions) |
|
VISN 5 |
Baltimore, MD |
Federal Supply Schedule orders (3) HTME orders (10) Other order (1) Stand-alone contract (6) |
20 |
$6.11 |
|
VISN 5 |
Clarksburg, WV |
Federal Supply Schedule order (1) HTME orders (4) Stand-alone contract (2) |
7 |
$4.09 |
|
VISN 12 |
Iron Mountain, MI |
HTME orders (3) |
3 |
$0.97 |
|
VISN 12 |
Milwaukee, WI |
HTME orders (5) Stand-alone contract (24) |
29 |
$3.55 |
|
VISN 17 |
Big Spring, TX |
HTME orders (4) |
4 |
$0.48 |
|
VISN 17 |
San Antonio, TX |
HTME orders (9) Stand-alone contract (5) |
14 |
$12.11 |
|
VISN 19 |
Aurora, CO |
HTME orders (4) Stand-alone contract (2) |
6 |
$4.36 |
|
VISN 19 |
Sheridan, WY |
HTME orders (3) Stand-alone contract (1) |
4 |
$0.59 |
Source: GAO analysis of contract and order data for high-tech medical equipment (HTME) maintenance from selected regional contracting offices and the Federal Procurement Data System. | GAO‑26‑107792
GAO Contact
Tatiana Winger, Director, WingerT@gao.gov
Staff Acknowledgments
In addition to the contact named above, Timothy J. DiNapoli (Managing Director), Mona Sehgal (Director), Teague Lyons (Assistant Director), Leslie Ashton (Analyst-in-Charge), Matthew T. Crosby, Andrea Evans, Suellen Foth, Sylvia Kramer, Britt Morey, and Adam Wolfe made key contributions to this report.
Janina Austin, Hayden Huang, Jeffrey Knott, Jean McSween, Susan Murphy, Justin Snover, Anne Taylor, and Alyssa Weir also contributed to this report.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]VISNs are responsible for providing administrative and clinical oversight and help manage the day-to-day functions of the medical centers in their regions.
[2]GAO, High-Risk Series: Heightened Attention Could Save Billions More and Improve Government Efficiency and Effectiveness, GAO‑25‑107743 (Washington, D.C.: Feb. 25, 2025).
[3]In September 2025, we reported on VA’s implementation of its category management policies. VA assigned officials to manage 10 common spending categories, such as medical goods and services (e.g. HTME maintenance services). We reported that VA has an opportunity to better position itself to make informed procurement decisions and pursue opportunities by assessing prices paid and cost avoidance data. We made six recommendations to improve VA’s implementation of category management, including that VA establish category-specific savings goals. VA agreed with these recommendations. GAO, VA Acquisitions: Leadership Accountability and Savings Goals Needed to Improve Purchasing Efficiency, GAO‑25‑107398 (Washington, D.C.: Sept. 2, 2025).
[4]We excluded the third type of HTME—picture-archiving computer systems—because these generally do not require similar physical maintenance as imaging and radiation therapy equipment.
[5]We also reviewed HTME inventory and VHA workforce data from July 2025 to provide more up-to-date information in the background section.
[6]An IDIQ contract provides for an indefinite quantity, within stated limits, of supplies or services during a fixed period. The government places orders for individual requirements. See Federal Acquisition Regulation (FAR) § 16.504(a). HTME base contracts are multiple-award IDIQs, under which a group of prequalified contractors compete for future orders under streamlined ordering procedures once agencies determine their specific needs. FAR § 16.505(b).
[7]The FAR is currently undergoing a complete overhaul called the Revolutionary FAR Overhaul. This initiative began in April 2025 in response to Executive Order 14275. See 90 Fed. Reg. 16,447 (Apr. 15, 2025). The initiative involves rewriting the FAR in plain language and removing most text not required by statute or Executive Order, other than text essential to sound procurement. Through the initiative, rewritten FAR parts are issued as model deviation text for agencies to adopt until the FAR is formally revised through the rulemaking process. The modal deviation text for the rewritten FAR parts was issued incrementally between May 2 and October 28, 2025. During that time, VA adopted modal deviation text for the rewritten FAR parts. However, because legacy version of the FAR was in place when VA took the contracting actions reviewed in this report, we reference the legacy version of the FAR rather than the Revolutionary FAR Overhaul.
[8]GAO, Standards for Internal Control in the Federal Government, GAO‑14‑704G (Washington, D.C.: Sept. 10, 2014).
[9]The Federal Supply Schedules, managed by the General Services Administration, provides federal agencies a simplified method of purchasing commercial products and services at prices associated with volume buying. A schedule is a set of contracts awarded to multiple vendors that provide similar products and services. Stand-alone contracts, also called “definitive contracts,” are contracts other than an indefinite delivery vehicle that must be reported to the government-wide database used to report data on government procurements. FAR 4.601. Stand-alone contracts generally are not available for agencywide use.
[10]The Contractor Performance Assessment Reporting System is the official source for evaluations of contractor past performance. In general, evaluations are required annually and at the time the work under a contract or order is completed for those contracts and orders that exceed the simplified acquisition threshold. FAR 42.1502. As of October 1, 2025, the threshold is generally $350,000. FAR 2.101.
[11]HTME, as defined by VA, also includes picture-archiving and communication systems. However, we did not include these systems in the scope of this report.
[12]FDA regulates HTME and other radiation-emitting electronic products to help protect the public from hazardous and unnecessary exposure to radiation from electronic products. See 21 C.F.R. pts. 1000-1040.
[13]U.S. Food and Drug Administration, Medical Imaging, https://www.fda.gov/radiation-emitting-products/radiation-emitting-products-and-procedures/medical-imaging, accessed August 5, 2025.
[14]Department of Veterans Affairs, Veterans Health Administration, VHA Directive 1860, Healthcare Technology Management Continuous Performance Monitoring and Improvement (Washington, D.C.: Aug. 19, 2024).
[15]This applies to hospitals that use Joint Commission accreditation to participate in and receive federal payment from Medicare or Medicaid programs. The Joint Commission, Standards: EC.02.04.03 and EC.02.04.01, Chapter: Environment of Care (The Joint Commission Resources Edition: Aug. 1, 2024).
[16]In August 2024, the VA Inspector General reported that over 20 percent of medical centers (over 28 out of the 139 surveyed) reported a severe shortage of biomedical engineers in fiscal years 2022 through 2024. Department of Veterans Affairs, Office of Inspector General, OIG Determination of Veterans Health Administration’s Severe Occupational Staffing Shortages Fiscal Year 2024, Report #24-00803-222 (Washington, D.C.: Aug. 7, 2024). In August 2025, the Inspector General reported that, while some medical centers continued to report severe shortages, less than 20 percent of medical centers surveyed reported biomedical engineers as a severe staffing shortage in fiscal year 2025. Department of Veterans Affairs, Office of Inspector General, OIG Determination of Veterans Health Administration’s Severe Occupational Staffing Shortages Fiscal Year 2025, Report #25-01135-196 (Washington, D.C.: Aug. 12, 2025). As of July 2025, VHA reported it employs about 2,074 biomedical engineers and biomedical equipment support specialists overall, and about 177 of these staff specialize in supporting HTME.
[17]Memorandum of Agreement Between the Department of Defense and the Department of Veterans Affairs, Medical Equipment (July 24, 2003).
[18]Category management uses fewer, larger contracts that, among other things, secure better pricing for all federal buyers. It is a government-wide initiative led by the Office of Management and Budget, which reported that it saves the federal government billions of dollars by improving how agencies buy common goods and services. Medical is one of the 10 common spending categories and is managed jointly by the Department of Defense and VA. HTME base contracts are tier 3 contracts. According to the Office of Management and Budget, tier 3 contracts are intended to offer federal buyers access to pre-vetted government-wide contracts and to increase the prices-paid data available for agency and government-wide analysis of buying behavior for common products and services. For more information about VA’s implementation of category management, see GAO‑25‑107398.
[19]This includes obligations for orders placed on HTME base contracts per information VA reported in the Federal Procurement Data System. We could not reliably identify maintenance service obligations on other contract vehicles, so we limited the amount to the services ordered under HTME base contracts with related descriptions. While HTME has a unique product and service code to identify equipment, HTME maintenance service does not. As such, we took steps to identify maintenance-related obligations, but we cannot precisely report VA’s overall obligations for HTME maintenance services.
[20]VA awarded 18 and DLA awarded 17 imaging contracts that were active at some point during our review (35 total). However, three are no longer available for use according to NAC. VA also awarded a total of 13 radiation therapy contacts that were active in our review. Seven of these contracts were awarded in 2019. NAC terminated one of these in 2024 after the vendor declared bankruptcy. After the 2019 contracts expired, the remaining six vendors each received contract awards in 2024. NAC awarded the six contracts in 2024 as a bridge for 12 months to ensure there was no lapse in contractual coverage while they conducted a competitive follow-on acquisition, according to NAC’s June 2024 acquisition plan. In September 2025 NAC awarded six radiation therapy contracts to replace the expired bridge contracts.
[21]Orders must be within the scope, period of performance, and maximum value and or quantities agreed to in the contract. Under an IDIQ contract, the government must order, and the contractor must provide, a minimum agreed-upon quantity of products or services, also known as a minimum guarantee. In addition, the contractor must provide any other quantities ordered by the government up to a stated maximum.
[22]FAR § 16.505(b)(2)(i). Competition is a cornerstone of the acquisition system, and promoting competition in federal contracting presents the opportunity for significant cost savings, among other benefits. Office of Management and Budget, Office of Federal Procurement Policy, Increasing Competition and Structuring Contracts for the Best Results (Washington, D.C.: Oct. 27, 2009).
[23]FAR § 16.505(b)(2)(ii)(C).
[24]HTME vendors include original equipment manufacturers and authorized sellers of HTME equipment. However, typically, only original equipment manufacturers are best positioned to offer maintenance service plans, according to VHA. For example, at least two radiation therapy equipment manufacturers do not authorize others to perform maintenance on their equipment.
[25]The imaging base contracts allow for equipment to be supported for at least 10 years and radiation therapy base contracts allow for at least 5 years.
[26]With the HTME base contracts, each vendor submits their discounted commercial prices and government discounts for equipment and services with their initial proposals to NAC and DLA. The agencies determine whether item prices are fair and reasonable before awarding their respective contracts and any items that are subsequently added must go through the same level of price analysis prior to inclusion in the base contract.
[27]NAC identified 19 imaging base contracts as offering some level of maintenance. According to the Federal Procurement Data System, the eight HTME base contracts for imaging that NAC reported as having full-service maintenance agreements available for purchase comprised over 80 percent of total contract obligations for imaging in fiscal years 2022 through 2024.
[28]The Office of Equipment Lifecycle Management, within VHA’s Procurement & Logistics Office, conducted an internal assessment of the HTME maintenance service market and in May 2020 summarized its draft findings, Streamlined Service Maintenance Agreements Business Case.
[29]In May 2018, the U.S. Food and Drug Administration reported that the continued availability of third-party entities to service and repair medical devices—including but not limited to HTME—is critical to the functioning of the U.S. health care system. U.S. Food and Drug Administration, FDA Report on the Quality, Safety, and Effectiveness of Servicing of Medical Devices: In accordance with Section 710 of the Food and Drug Administration Reauthorization Act of 2017 (FDARA) (May 2018).
[30]See FAR 16.505(b).
[31]FAR 16.505(b)(2)(i)(B).
[32]One of the seven radiation therapy vendors offered one maintenance service plan during the period of our review. However, NAC only placed one order for equipment under that vendor’s contract, and no regional contracting offices placed orders for services during fiscal years 2022 through 2024. Further, NAC terminated the contract early due to vendor bankruptcy.
[33]HTME base contracts being mandatory refers to a policy requirement, whereby, under certain circumstances, contracting officers consider these contract vehicles before using other existing contract vehicles or awarding new contracts. Specifically, the Veterans Affairs Acquisition Regulation (VAAR) states that if strategic sourcing contracts were subject to the VA Rule of Two, the head of the contracting activity may determine the contracts are mandatory, meaning that contracting officers must consider these priority contract vehicles before using other existing contract vehicles. VAAR 808.004-70(b). The VAAR defines the VA Rule of Two as the process by which a VA contracting officer must set aside contracts for veteran-owned small businesses if the contracting officer has a reasonable expectation that two or more such businesses will submit offers and the award can be made at a fair and reasonable price that offers best value to the United States. VAAR 802.101.
[34]VHA Procurement Manual, Part 808.004-70, Use of Other Priority Sources, effective April 15, 2024. This part of the VHA Procurement Manual implements the VAAR 808.004-70(b), which addresses strategic sourcing priorities and application of the VA Rule of Two.
[35]Department of Veterans Affairs, Veterans Health Administration, Acquisition of High-Cost, High-Technical Medical Equipment, VHA Directive 2009-017 (Washington, D.C.: March 20, 2009).
[36]Veterans Health Administration, Customer Reference Guide, Chapter 7: Detailed Customer Procedures, effective August 15, 2024. See also, Attachment 3, Equipment and Supply, August 1, 2024 and Attachment 15, Biomed Equipment Repair Service and/or Parts, effective December 15, 2022, and January 15, 2026.
[37]VHA officials stated that placing orders for HTME services under HTME base contracts is not mandatory, but the HTME base contracts are still preferred over going to the open market.
[38]VA is required by statute to give preference to veteran-owned small businesses when awarding contracts, which it does using the Veterans First Contracting Program. See 38 U.S.C. § 8127; VAAR subpart 819.70.
[39]According to NAC, one radiation therapy contract and 19 imaging HTME contracts offer some type of maintenance services, of which one was awarded to a veteran-owned small business.
[40]The integrated project team comprised of representatives from VHA, its regional contracting offices, and VA’s Office of Acquisition, Logistics, and Construction is examining contract requirements to determine which contracts can be consolidated. Officials stated that they are also conducting an analysis on obtaining HTME maintenance services. As mentioned previously, VHA’s Equipment Lifecycle Management team conducted similar analyses in 2020.
[42]VHA equipment life-cycle management officials have raised these and similar issues to NAC and VHA procurement policy officials since 2019.
[43]For some large vendors the price books can be split into two Excel workbooks: one for equipment and another for services.
[44]To understand what the multiple price columns in the price books represent, contracting officials must access the HTME base contract solicitation’s instructions. These instruct the vendor on what must be included in the price books and definitions for at least some of the fields. For example, the “list price” is not the price that the government should pay and instead represents the discounted commercial price. NAC and DLA generally obtained further discounted prices for the government’s use, i.e., the maximum price. In some cases, there is the potential for a “minimum price.” However, neither the base contract’s solicitation instructions nor the price book explains the circumstances in which those additional discounts would apply. The contracting officer would need to follow up with the vendor to request additional discounts and to learn when the minimum price is available.
[46]Downtime and reduced functionality mean that medical centers are not able to fully use HTME to diagnose or treat patients and could result in delays to patient care or increased costs resulting from sending patients out to non-VA hospitals for care. There may be additional burdens in rural areas because of the longer distances and fewer alternatives for care.
[47]Veterans Health Administration, Healthcare Technology Management Service Bulletins, Planned Maintenance Programs, SB2017-002 (April 2017); Documentation of Biomedical Engineering Services, SB2014-004 (May 22, 2014).
[48]The 16 maintenance orders and contracts in our sample represent about $11 million in obligations overall in fiscal years 2022 through 2024, or 34 percent of the obligations on HTME maintenance orders and contracts reported by the eight medical centers during the period.
[49]Time frames for completing preventive maintenance must align with manufacturers’ instructions and are outlined in VHA SB2017-002 and VHA SB2014-004. VHA recently updated its guidance for its preventive maintenance with Veterans Health Administration, Healthcare Technology Management Service Bulletin, VHA Planned Maintenance Program, SB2025-001 (December 2024). As mentioned previously, the frequency of preventive maintenance is determined by the equipment manufacturer. We observed variation in frequency in the maintenance completion reports for the selected HTME at the medical centers in our sample. For example, one manufacturer required annual maintenance for its CT scanner, whereas another manufacturer required semi-annual maintenance for its CT scanner.
[50]There are a couple caveats to the timely completion of the maintenance for this equipment. For example, in one instance maintenance was completed on-time but staff recorded it in the computerized maintenance management system late.
[51]Veterans Health Administration, The Office of Equipment Lifecycle Management, Streamlined Service Maintenance Agreements Business Case (May 2020).
[52]Maintenance of high risk devices is reported separately and include life-supporting medical equipment such as ventilators. VHA policy cites the Association for the Advancement of Medical Instrumentation definition of life support medical equipment as any device used for the purpose of sustaining life and whose failure to perform its primary function, when used according to manufacturer’s instructions and clinical protocol, will lead to patient death in the absence of immediate intervention. Association for the Advancement of Medical Instrumentation, American National Standards Institute/ Association for the Advancement of Medical Instrumentation EQ89: 2015 Guidance for the use of medical equipment maintenance strategies and procedures (2015); and Veterans Health Administration, Healthcare Technology Management Service Bulletin, High Risk Medical Equipment, SB2020-30 (July 27, 2020).
[53]Department of Veterans Affairs, VHA Directive 1860.
[54]We excluded services for four selected HTME from our price comparison analysis because the vendors from whom VHA purchased the services did not sell the same services via HTME base contracts or did not have an HTME base contract.
[55]Vendors’ HTME base contracts include a maximum price the government should pay and can offer a further discounted price (minimum price) for equipment and services. In some cases, a contract’s maximum and minimum prices are the same.
[56]Our initial analysis found that contracting officials in each of the four selected regions potentially paid more than the maximum prices for the same services that were available at the time under the HTME base contracts. When we asked contracting officials to explain why VHA paid more, the officials for one region provided additional supporting information and officials in the other three regions agreed with our analysis. However, following a detailed review by HTM officials, VHA identified additional services that accounted for the higher prices paid, thereby resulting in prices paid close to or at the minimum amount in the vendor’s price book. In two of these cases, regional contracting officials reviewed VHA’s analysis and confirmed the additional services were intended to be part of the purchase and have been received. For the third, regional contracting officials said that the medical center did not request or receive the additional services. They attributed the overpayment to the contracting officer not having information about prices available on the base contract and plan to seek a refund for amount paid above the established base contract price.