Report to Congressional Requesters
United States Government Accountability Office
A report to congressional requesters
For more information, contact: Alyssa M. Hundrup, HundrupA@gao.gov
What GAO Found
The Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) offers menopause care—treatments to manage symptoms of menopause—at its medical facilities through a wide array of treatment options, including medications and medical services. Primary care and gynecology providers are the key clinicians for veterans seeking to address menopause symptoms and can refer to other specialists such as mental health and physical therapy as needed.

To assist those providing menopause care, VHA is developing a clinical practice guideline. It is intended to provide evidence-based recommendations for providers on how to assess, diagnose, and treat menopause. However, the guideline was not complete at the time of GAO’s review. As part of the guideline development process, VHA plans to identify related performance measures. However, officials from the Office of Women’s Health, the sponsoring office for the guideline, could not confirm whether or how they plan to monitor the performance measures. Officials said it is difficult to make plans for monitoring before the recommendations and measures have been identified. Using performance measures to monitor implementation of the guideline’s recommendations could help VHA better achieve the objective of providing equitable, high-quality, and comprehensive health care services at all VHA facilities.
VHA has developed patient education about menopause care, which include brochures and a website to help educate women veterans on menopause care. However, this information may not be reaching many women veterans. More than half (60 percent) of the 348 women veterans who responded to GAO’s questionnaire reported that they had not encountered any VHA menopause resources. VHA facility officials reported challenges finding time to discuss menopause education and print brochures. VHA does not have a strategy to ensure that menopause education is regularly communicated to veterans. This information would help women become more knowledgeable about the changes occurring in their bodies and would help them be more empowered to approach their providers about their symptoms. Furthermore, this could help VHA better meet its goal of providing women veterans with comprehensive health care.
Why GAO Did This Study
Almost half of women veterans served by VHA are aged 45-64, the age range most likely to experience menopause, or the permanent cessation of menstruation. According to VHA research, veterans may experience worse menopause symptoms compared to non-veterans due to aspects of their service.
GAO was asked to review VA’s provision of menopause care. This report examines how VHA offers menopause care and educates veterans about menopause, among other topics.
GAO analyzed VHA data on menopause care from fiscal years 2019 through 2024. GAO interviewed VHA officials with roles related to menopause care and officials from six VHA medical facilities, selected to represent variation in geographic area, among other criteria. GAO also administered an online questionnaire and conducted discussion groups with women veterans about their experiences with VHA menopause care. Their responses are not generalizable to all women veterans but provide perspectives about VHA’s menopause education efforts and care offerings.
What GAO Recommends
GAO is making two recommendations to VA: (1) use identified performance measures to monitor implementation of menopause guideline recommendations, and (2) develop and implement a strategy to ensure women veterans approaching and experiencing menopause are provided education on menopause. VA did not provide comments on the report.
|
Abbreviations |
|
VA Department of Veterans Affairs |
|
VHA Veterans Health Administration |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
June 12, 2026
The Honorable Kirsten Gillibrand
Ranking Member
Special Committee on Aging
United States Senate
The Honorable Julia Brownley
Ranking Member
Subcommittee on Health
Committee on Veterans Affairs
House of Representatives
The Honorable Kelly Morrison
House of Representatives
The Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) provides health care services to over 9 million veterans through its medical facilities.[1] According to VA, women are the fastest growing group of veterans receiving VHA health care services. From fiscal years 2019 through 2024, VA data show the number of women veterans receiving care from VHA medical facilities grew 31 percent, from approximately 524,300 veterans to almost 687,000 veterans.
Almost half of women veterans served by VHA are aged 45 to 64. This is the age range most likely to experience menopause, the permanent cessation of menstruation, which is defined as occurring one year after the last menstrual period.[2] Women of this age are most likely to be affected by hormonal, biological, and psychosocial changes of menopause, which is characterized by changing health risks and unique health care needs. Common symptoms of menopause include hot flashes, mood changes, and problems with sleep. Some veterans may experience worse menopause symptoms compared to non-veterans due to aspects of their military service. In particular, mental health challenges such as post-traumatic stress disorder and military sexual trauma, which affect some veterans, can exacerbate menopause symptoms, highlighting the importance of VHA’s provision of menopause care.[3]
For the purposes of this report, we have defined “menopause care” to include treatment options to manage the common symptoms of menopause. For example, menopause care can include medications, including both hormonal and non-hormonal options. Women may also manage symptoms through counseling, exercise, acupuncture, and lifestyle changes.
A VHA policy directive requires that each VHA medical facility ensure that all eligible and enrolled women veterans have access to high-quality, equitable, and comprehensive medical care.[4] This medical care includes all medically necessary services, including menopause care.
You asked us to review various aspects of how VHA provides menopause care to veterans. In this report, we
1. examine how VHA offers menopause care for veterans at VHA medical facilities;
2. describe VHA’s education and training for its providers on menopause and menopause care; and
3. examine the extent to which VHA provides education to veterans about menopause and the menopause care available at VHA medical facilities.
To address these objectives, we undertook multiple methodologies. A summary of each is provided below. For additional information on our methods, see appendix I.
We reviewed documentation from and interviewed officials from VHA’s Office of Women’s Health, Office of Mental Health, Office of Quality and Patient Safety, and Pharmacy Benefits Management. We also reviewed VHA system-wide data for fiscal years 2019 through 2024, the most recent data at the time of our request, on (1) the number and types of VHA providers who offer menopause care and (2) the number of veterans who were diagnosed with menopause and received menopause care at each VHA medical facility. We interviewed officials about the limitations of the data and analyzed the data for any obvious errors and omissions. We determined these data were sufficiently reliable for the purposes of our audit objectives.
We also interviewed officials from a non-generalizable selection of six VHA medical facilities about the menopause care they offer. We selected these facilities to achieve variation in facility characteristics, such as geographic location and the number of women veterans served.[5] We also interviewed officials from the selected facilities’ associated Veterans Integrated Service Networks about their role in monitoring menopause care.[6] We also interviewed representatives from two organizations specializing in menopause—The Menopause Society and the American College of Obstetricians and Gynecologists.[7]
We evaluated information VHA provided about how it offers menopause care against VHA’s 2023 directive governing women’s health care and VHA’s policy for developing clinical practice guidelines for providers.[8] We also evaluated how VHA provides education to veterans on menopause and menopause care against VHA’s directive governing women’s health care and the Office of Women’s Health strategic plan.[9]
We also developed and distributed an online questionnaire to obtain information from women veterans aged 35 to 64 about their experiences with VHA menopause care. We worked with four national Veterans Service Organizations to advertise the questionnaire and solicit participation from women veterans. We received 348 completed questionnaires from women veterans across 48 states, Washington, D.C., and Puerto Rico.[10] For more information on the online questionnaire methodology and to see responses, see appendix II. We also conducted four discussion groups with 24 of the respondents to our online questionnaire to obtain further details about their experience with VHA’s menopause education and care provision. These veterans were randomly selected from questionnaire respondents who said they would be interested in participating in a discussion group. The information from the questionnaire and discussion groups cannot be generalized to all women veterans who receive VHA menopause care.
We conducted this performance audit from October 2024 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
Common Symptoms and Treatment of Menopause
Menopause is a normal part of aging for women, although each woman’s experience with menopause is unique. Symptoms can last between 2 and 8 years, and there may be wide variation in the symptoms a woman may experience and their severity. (See fig. 1.) It can be challenging to connect some symptoms to menopause; for example, joint pain may be due to hormonal changes or arthritis.

Veterans may face different risks during menopause compared to non-veterans due to aspects of their military service. For example:
· VHA research found that greater post-traumatic stress disorder symptoms among women veterans was linked with urinary and vasomotor symptoms (e.g., hot flashes and night sweats).[11]
· Military sexual trauma disproportionately affects women veterans and has been associated with a wide range of medical concerns. VHA research found strong associations between military sexual trauma and menopause symptoms, including increased risk of experiencing vasomotor and vaginal symptoms during menopause.[12]
· Women veterans are more likely than their male peers to have chronic pain and be prescribed an opioid. VHA research shows that among women veterans with chronic pain, having menopause symptoms was associated with potentially risky long-term opioid prescribing patterns.[13]
|
VHA Research on Menopause Care among Minority Veterans
VHA research has identified potential variations in the diagnosis and treatment of menopause symptoms in minority veterans. For example, Black women were less likely to have documented menopause symptoms than White women, despite evidence suggesting higher menopause symptom burden among Black women. Additionally, Black women and Hispanic women were less likely to be prescribed systemic hormone therapy than White women, according to the research. For a list of VHA menopause-related research publications see appendix III. Source: GAO analysis of Veterans Health Administration (VHA) research; fizkes/stock.adobe.com (photo). | GAO‑26‑107853 |

Menopause care aims to help women manage bothersome symptoms. Providers and patients make decisions about which treatment is best based on symptoms, a patient’s medical history, and comfort with risks of potential side effects.
Hormone therapy—also known as menopausal hormone therapy or hormone replacement therapy—involves medications that contain an estrogen and/or progesterone component dependent on the needs of the veteran. According to the American College of Obstetricians and Gynecologists, hormone therapy is the most effective treatment for vasomotor symptoms related to menopause.[14]
However, recommendations for treating vasomotor symptoms with hormone therapy have changed over time. In 2002, the Women’s Health Initiative found that hormone therapy increased health risks for women participating in its study.[15] According to VHA, following the release of the Women’s Health Initiative study, clinicians became reluctant to prescribe hormone therapy to treat menopause symptoms. Further studies that analyzed data from the Women’s Health Initiative found that, among younger women aged 50 to 59, hormone therapy did not significantly increase health risks and had a possibly favorable effect on mortality for women in this age range.[16] In November 2025, the Food and Drug Administration removed “black box” warnings about the risks associated with hormone therapy, noting that women may be under-utilizing approved therapies that can alleviate menopause symptoms and improve women’s health.[17]
Women’s VHA Health Care
VHA primary care providers include a subset of providers that VHA has designated “women’s health primary care providers.” According to VHA data, each VHA health care system has at least one primary care provider with this designation. To obtain this designation, these providers must have training in providing primary care to women veterans, including specialized knowledge about women’s health issues.[18] They must offer basic gynecology care, such as contraceptive care, as well as breast and cervical cancer screenings and menopause management.[19]
Women’s health primary care providers must maintain clinical competency through ongoing education and training and by having a certain percentage of women veterans on their patient panel. VHA policy requires that women be offered the opportunity to receive care from a women’s health primary care provider. According to VHA data, as of March 2026, 88 percent of women veterans were assigned to women’s health primary care providers.
VHA Offers Menopause Care through a Variety of Providers and Services and an Upcoming Guideline Could Help Improve Quality of Care
|
Veteran Experiences with Veterans Health Administration (VHA) Menopause Care
Women veterans who responded to our online questionnaire reported that they were most likely to see a primary care provider or gynecologist for menopause care through VHA. Of the 108 respondents who reported they had received menopause care in the past 5 years from a VHA provider, 68 percent (73 respondents) said they had seen their primary care provider and 55 percent (59 respondents) said they had seen a gynecologist. For more information on our online questionnaire, see appendix II. Source: GAO analysis of veteran questionnaire responses; BuyOutFelix05/peopleimages.com/stock.adobe.com (photo). | GAO‑26‑107853 |

VHA Primary Care and Gynecology Providers Serve as Key Clinicians for Menopause Care
Primary care and gynecology providers are the key clinicians for veterans obtaining menopause care or related information through VHA medical facilities, according to Office of Women’s Health officials. Providers of primary care include doctors, physician assistants, and nurse practitioners. Gynecology providers include doctors, physician assistants and advance practice registered nurses. These providers may discuss symptoms, the effect of menopause on other diseases, treatment options, and potential lifestyle changes to help manage each individual veteran’s symptoms, according to Office of Women’s Health officials. Additionally, primary care providers and gynecologists can refer veterans to other specialists depending on their needs. (See fig. 2.)
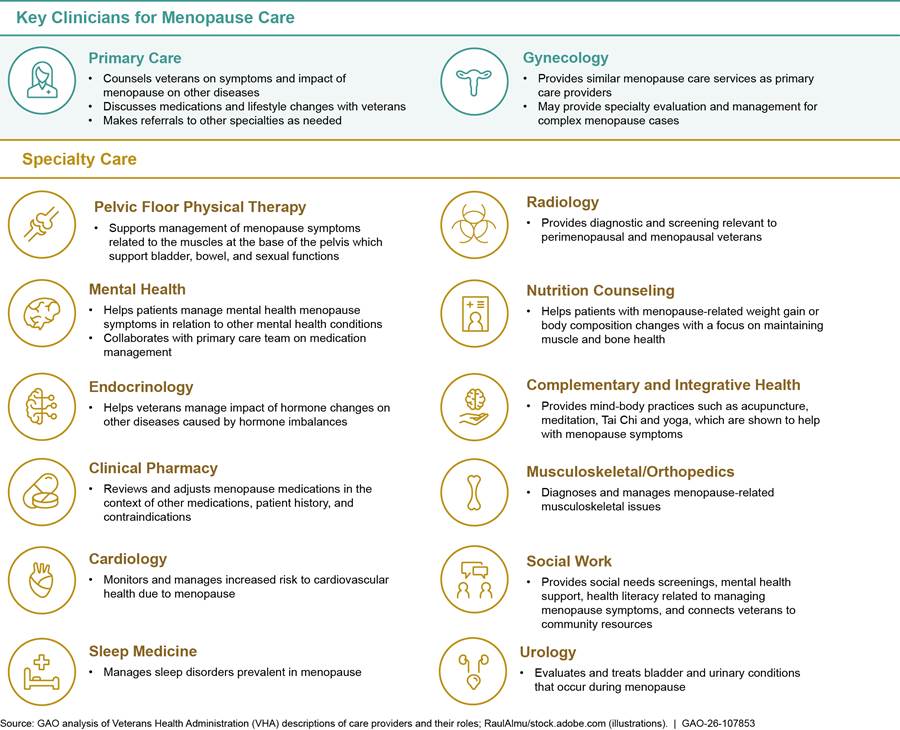
Note: Menopause is defined as occurring one year after the last menstrual period. The time leading up to menopause is called the menopause transition or perimenopause. In this figure, we use the term “menopause” to refer to both perimenopause and menopause.
For most veterans, a women’s health primary care provider will be the first line of menopause care, according to Office of Women’s Health officials. From fiscal years 2019 through 2024, VHA data show the number of full-time equivalent VHA women’s health primary care providers at VHA increased by 43 percent, from 2,688 to 3,832.[20] VHA medical facilities can increase the number of women’s health primary care providers by hiring new providers with women’s health experience or having primary care providers employed at their facilities trained in women’s health. Officials from five of the six VHA medical facilities in our review said they encourage all new primary care providers to become designated as a women’s health primary care provider.
Some women, often those who have a complex medical history or require specialty evaluation, may go to their gynecology provider for menopause care. From fiscal years 2019 through 2024, the number of full-time equivalent VHA gynecology providers increased by 56 percent, from 142 to 220, according to VHA data.[21]
|
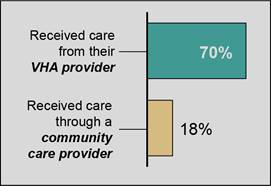
Veteran Experiences with Veterans Health Administration (VHA) Menopause Care
Of the 155 women veterans who responded to our questionnaire saying they received menopause care from any provider in the last 5 years, 70 percent (108 respondents) received care from their VHA provider and 18 percent (28 respondents) received care through a community care provider. Some respondents reported receiving care from both a VHA provider and a community care provider. Source: GAO analysis of veteran questionnaire responses. | GAO‑26‑107853 |
Officials from all six of the VHA medical facilities in our review noted they do not often refer women to providers in the community for menopause care. Officials at two of these facilities explained that wait times are often longer for care in the community. For example, officials from one facility told us the wait time for a veteran to see a community care gynecologist could be as long as 97 days, but veterans could receive gynecological care from a VHA women’s health primary care provider in as little as 5 days.
Additionally, officials from two of the facilities in our review noted that community care providers can lack an understanding of issues specific to female veterans, such as experiences with military sexual trauma or post-traumatic stress disorder, which may affect menopause care.
VHA Offers Medical Treatment Options and Other Services to Help Veterans Manage Menopause Symptoms
To help veterans manage menopause symptoms, VHA offers veterans multiple medical treatment options—including medications and medical services—as well as complementary and integrative health service options.
|
Menopause Diagnosis Rates across VHA Medical Facilities We found that the percent of female veterans aged 45 to 64 with a diagnosis of “menopausal and other perimenopausal disorders” in their patient charts ranged from 6 to 20 percent across VHA medical facilities in fiscal year 2024. This diagnosis is used to classify symptoms that occur during or around menopause including hot flashes, night sweats, and vaginal dryness. Office of Women’s Health officials said there could be many reasons for differences in menopause diagnosis across medical facilities including variations in patient awareness of and comfort with discussing symptoms or provider knowledge or comfort level in addressing menopause. Source: GAO analysis of Veterans Health Administration (VHA) data. | GAO‑26‑107853 |
Medications and Prescribing Support
VHA providers can prescribe all Food and Drug Administration-approved medications for the treatment of menopause symptoms, including both hormonal and non-hormonal medications. Providers from all six VHA
medical facilities in our review said they had access to the medications they needed to treat common menopause symptoms.[22]
|
Hormone Therapy Prescribing Rates across VHA Medical Facilities We found that the percent of female veterans aged 45 to 64 who filled a prescription for hormone therapy ranged from 3 percent to 35 percent across VHA medical facilities in fiscal year 2024. Office of Women’s Health officials said that, while they have not investigated it, reasons for the range could include either the provider or the patient. For example, there may be regional differences in patient comfort or desire for hormone therapy. Source: GAO analysis of Veterans Health Administration (VHA) data. | GAO‑26‑107853 |
Given the wide range of medication options, some VHA medical facilities provide additional supports for prescribing medications to treat menopause symptoms, including the use of clinical pharmacy practitioners and women’s health order sets (lists of common medications for women).
Clinical pharmacy practitioners. To help with the prescribing of medications, VHA medical facilities may employ a clinical pharmacy practitioner. Choosing the best medication to treat menopause symptoms depends on a patient’s medical history, other medications, and comfort with risks and potential side effects. A clinical pharmacy practitioner’s role is to take a holistic view of medications, prescribing or adjusting medications based on patients’ other conditions and medical history. VHA clinical pharmacy practitioners may have specialized women’s health training or experience, including for medications that treat menopause symptoms.[23]
VHA data show that VHA clinical pharmacy practitioners are increasingly seeing women of menopausal age. According to VHA data, the number of these providers who have had at least one encounter with women veterans aged 45 to 64 increased by 23 percent, from 6,083 in fiscal year 2019 to 7,453 in fiscal year 2024.[24] While some of this increase may be due to a higher number of women veterans aged 45 to 64 being referred to a clinical pharmacy practitioner, it may also be due to an increase in the number of clinical pharmacy practitioners at VHA medical facilities. Officials from two of the six facilities in our review noted they had recently hired a clinical pharmacy practitioner with women’s health experience.
Women’s health order set. Additionally, to assist providers with prescribing decisions, the Office of Women’s Health maintains a women’s health order set—a list of common medications for women’s health conditions, including menopause. The women’s health order set is housed on a centrally accessible Office of Women’s Health intranet page and each VHA medical facility can opt to include it as part of its electronic health records system. A gynecologist at one VHA medical facility in our review noted that the order set improved confidence in prescribing medications for the treatment of menopause symptoms.
Medical Services
Veterans also have access to a wide range of medical services to manage menopause symptoms through VHA. As mentioned previously, VHA research shows veterans may experience menopause differently than non-veterans due to higher rates of mental health disorders and chronic pain.[25] As such, VHA has services tailored to meet those unique needs. (For additional information on VHA’s menopause-related research, see appendix III.)
Mental health services. According to Office of Mental Health officials, menopause can exacerbate certain mental health conditions prevalent in veterans, such as post-traumatic stress disorder. To address this, veterans can receive counseling, psychotherapy, and mental health medications from mental health providers who specialize in reproductive mental health care, including menopause. According to Office of Mental Health officials, 91 percent (127 of 139) of VHA medical facilities have at least one reproductive mental health provider on staff. Additionally, the Office of Mental Health has a Reproductive Mental Health Consultation Program, in which a team of subject matter experts provide consultation to providers on menopause-related mental health issues, among other reproductive mental health concerns.
Pelvic floor physical therapy. Veterans may experience urinary or sexual dysfunction during menopause, which pelvic floor physical therapy can help in managing. This type of therapy can improve vaginal and urinary symptoms of menopause by strengthening pelvic muscle tone. However, research suggests that pelvic floor physical therapy can make certain mental health conditions, such as post-traumatic stress disorder, worse.[26] Providers can receive education about mental health conditions affecting veterans through VHA’s online training platform. Additionally, VHA pelvic floor physical therapy includes consideration of veterans’ mental health conditions related to past traumas, according to providers at two sites in our review. For example, for these veterans, providers may modify the way they conduct their evaluations, such as by doing an ultrasound instead of an internal exam.
Complementary and Integrative Health Services
VHA medical facilities also offer complementary and integrative health services, which research suggests may help veterans manage some menopause symptoms.[27] As of fiscal year 2024, VHA data show that 97 percent or more of all VHA medical facilities offered acupuncture, yoga or Tai Chi, and meditation or mindfulness classes.[28] For sites that do not offer these services, veterans who meet certain requirements may receive these services through the community or via telehealth.
VHA Is Developing a Clinical Practice Guideline for Menopause Care but It Is Unclear Whether Officials Will Monitor the Guideline’s Implementation
To help guide the provision of its care, VHA (in collaboration with the Department of Defense) in February 2025 began developing a joint clinical practice guideline specific to menopause.[29] The process of developing the clinical practice guideline includes developing recommendations for providers and identifying performance measures associated with the recommendations.[30]
· Developing recommendations for providers. According to one VHA Office of Quality and Patient Safety official leading the workgroup responsible for developing the clinical practice guideline for menopause, the guideline will provide evidence-based recommendations to providers on how to assess, diagnose, and treat menopause. The recommendations are designed to address clinical ambiguity around treatment for menopause—such as in the diagnosis of menopause disorders and prescribing of hormone therapy, according to the official. The recommendations are intended to help providers deliver high-quality menopause care and reduce any unnecessary variations in care, according to VHA officials. As of April 2026, a draft guideline was undergoing review by the workgroup, with completion anticipated by mid-August 2026, according to the official.
· Identifying performance measures. The Office of Quality and Patient Safety official said that the workgroup intends to identify performance measures for the menopause guideline once the draft is further along in the review process. According to VHA policy, the clinical practice guideline development process should include identifying performance measures to monitor implementation of guideline recommendations. To begin this part of the guideline development process, the VHA official said the workgroup will first look to see if any currently published quality measures may align with potential menopause measures. As of April 2026, the VHA official said the workgroup had not yet begun the process, but anticipated beginning to draft potential performance measures in late May 2026.
While the workgroup is responsible for developing the performance measures, the Office of Quality and Patient Safety official said that the sponsoring office is responsible for monitoring the performance measures once the guideline is published. Officials from the Office of Women’s Health, the sponsoring office for the menopause guideline, could not yet confirm whether or how they plan to monitor performance measures. Officials said it is difficult to make plans for monitoring before the recommendations and measures have been identified. Office of Women’s Health officials told us monitoring menopause care is challenging as diagnosis and treatment decisions are based on many factors including type and severity of symptoms, and the individual’s medical history and comfort level. Office of Women’s Health officials told us they do plan to disseminate the guideline via multiple channels, including a webinar for clinicians and women’s health and gynecology communities of practice.
Monitoring implementation of the recommendations through performance measures would help VHA determine the extent to which providers are adhering to the guideline’s recommendations. VHA policy states that each medical facility provides all eligible and enrolled women veterans access to high-quality, equitable, and comprehensive medical care.[31] Monitoring the guideline’s implementation would help VHA ensure it is meeting its goals. Additionally, monitoring implementation of the guideline recommendations via established performance measures could help VHA identify and address any unnecessary variations in care.
VHA Offers Menopause-Related Education and Is Taking Steps to Address Providers’ Need for Additional Training
VHA Offers Menopause-Related Training Courses and Other Educational Support for Providers
VHA offers training courses on a variety of menopause-related topics as well as other educational support for VHA providers. According to the Office of Women’s Health, as of March 2026, VHA offered 36 menopause-related trainings providers could access throughout the year.
Two such trainings—one for providers and one for nurses—are the Women’s Health Mini Residency, an in-person training hosted by the Office of Women’s Health.[32] The mini residency covers 14 women’s health-related topics, including a 1.5-hour module on menopause. The menopause module includes topics on menopause symptoms and treatment, risks and benefits of hormone therapy, and bone health. The Office of Women’s Health recommends this mini residency to any primary care provider who treats women veterans, and it is one method by which primary care providers can become designated as women’s health providers.
VHA also offers 34 online trainings that encompass a variety of topics about menopause, including vasomotor symptoms and menopause-related mood changes. For example, the Office of Women’s Health offers an annual update on women’s health care topics. One previous update included information on prescribing hormone therapy to treat menopause symptoms. The online training courses are available for providers to view at any time in VA’s Talent Management System.[33]
In addition to training courses, VHA offers other educational support for providers. Specifically, VHA offers consult services for providers seeking additional information on providing menopause care, including:
· Reproductive mental health consult. VHA provides a reproductive mental health consultation program where a multidisciplinary team—two psychiatrists, a clinical pharmacy specialist, and a social worker—can offer guidance on comprehensive mental health care for veterans to all provider types. The team has both experience and training in reproductive mental health and can consult on questions related to menopausal mental health concerns.
· Interfacility consult. One medical facility in our review developed an online consult form to assist providers across its network in evaluating and treating menopause. Providers complete a form with information about a patient’s demographics, symptoms, history, current medications, recent tests, and treatment preferences. Providers then send the information to their facility’s gynecology department for treatment recommendations or direct provision of care.
The six medical facilities in our review generally rely on menopause training from the Office of Women’s Health, according to officials we interviewed. Officials from five facilities said they also regularly include menopause-related topics in monthly women’s health meetings or other events. Additionally, officials from one VHA regional network told us that clinical pharmacy practitioners in their network developed optional educational supports on menopause care for their providers. These supports include menopause quick reference guides that summarize available evidence for medication treatment options for menopause symptoms, including hormone therapy.
VHA Is Taking Steps to Address Identified Need for More Menopause Care Training for Its Providers
VHA officials said they are taking steps to address findings in two surveys the agency conducted that indicated its providers need more training and support for managing menopause symptoms.
In February 2023, the Office of Women’s Health surveyed 73 VHA medical facilities participating in the Women’s Health Practice-Based Research Network about providers’ needs related to menopause care.[34] Of the 60 facilities that responded to the survey, more than 70 percent reported needing more support for managing veterans’ menopause symptoms, such as vasomotor symptoms and sleep disorders, particularly citing the benefit of having primary care providers trained in menopause care.[35] VHA survey respondents cited barriers to providing menopause care, including a lack of knowledge about signs and symptoms of menopause and treatment options at the primary care level. Additionally, survey respondents noted that some primary care providers, including women’s health providers, do not feel comfortable managing veterans’ menopause symptoms.
In October 2024, the Office of Women’s Health conducted a national needs assessment survey of primary care providers and nurses to better understand priority areas for women’s health education. In total, 3,217 primary care providers, including physicians and nurses, responded to the survey.[36]
· Respondents to VHA’s survey selected menopause as the single most requested area for additional education. Respondents noted that primary care providers at their facilities were generally interested in learning more about managing veterans’ menopause symptoms during perimenopause, urinary and bladder infections in women, and osteoporosis in women.
· Respondents also indicated a preference for concentrated training—such as multi-day conferences or extended virtual trainings—over 1-hour webinars or online training.
Office of Women’s Health officials attributed primary care providers’ need for additional training and knowledge about managing menopause symptoms to several challenges, including a lack of menopause training during medical education. Another challenge officials noted was the long-term effects of the Women’s Health Initiative study and the subsequent hesitation to prescribe hormone therapy based on the initial results of the study.
In response to the findings from its 2023 and 2024 surveys, the Office of Women’s Health has begun taking steps to restructure trainings and increase its menopause training offerings. According to officials, among changes, the Office of Women’s Health
· is restructuring its education delivery model, transitioning from monthly webinars to quarterly 4-hour virtual updates. For example, it held a 4-hour training on menopause and hormone therapy in November 2025 that was attended by more than 1,100 VHA providers. According to VHA officials, providers prefer extended, dedicated training formats because this provides them protected time away from clinical responsibilities and reduces interruptions, enabling focused participation.
· focused its 360 Spotlight for the first quarter of fiscal year 2026 on menopause.[37] This included launching a VHA intranet page dedicated to menopause education and training, which contains clinical guidance, presentations, and videos, among other resources.
· has increased funding for external menopause training and is expanding the number of women’s health primary care providers at VA’s Clinical Resource Hubs.[38]
To monitor whether the changes to the training curricula address providers’ reported needs for additional training, Office of Women’s Health officials told us they conduct formal needs assessments as one of multiple tools to guide their training efforts. They said they plan to conduct assessments of priority areas for women’s health education every 5 years or more frequently if needed. Officials project the next survey to begin in fiscal year 2029. Officials said they also collect information from post-training evaluations for in-person and web-based training. Office of Women’s Health officials also told us that they regularly review and update training content to ensure it reflects the most up-to-date clinical information. Web-based trainings are to be reviewed at a minimum of every 3 years.
VHA Has Developed Patient Education about Menopause Care, but Information May Not Be Reaching Many Women Veterans
VHA Has Developed Menopause Patient Education Resources for Veterans
VHA’s Office of Women’s Health has developed brochures, a podcast, menopause campaign materials, and website information to help educate veterans on menopause care.
Brochures. The Office of Women’s Health had developed nine educational brochures as of March 2026 that cover topics relevant to menopause symptoms and the menopause care services provided at VHA. Three of the nine brochures are specific to menopause—one brochure gives an overview of menopause, one focuses on vaginal and urinary symptoms of menopause, and one is about healthy reproductive aging. The other six brochures cover topics related to menopause care, such as pelvic floor physical therapy. Officials from the Office of Women’s Health said they update educational brochures on a 3-year cycle and may update them more often when key information changes, such as VHA’s available services.
These brochures are available on VHA’s website for veterans to access and VHA medical facilities to download and provide directly to their patients.
Podcast. The Office of Women’s Health also published a weekly podcast called She Wears the Boots, targeted to women veterans about different health topics.[39] The first podcast on the topic of menopause was released in March 2021. As of March 2026, there were four episodes on topics related to menopause.[40] During the episodes, VHA providers, including gynecologists, provided information to veterans about symptoms of and treatment for menopause.
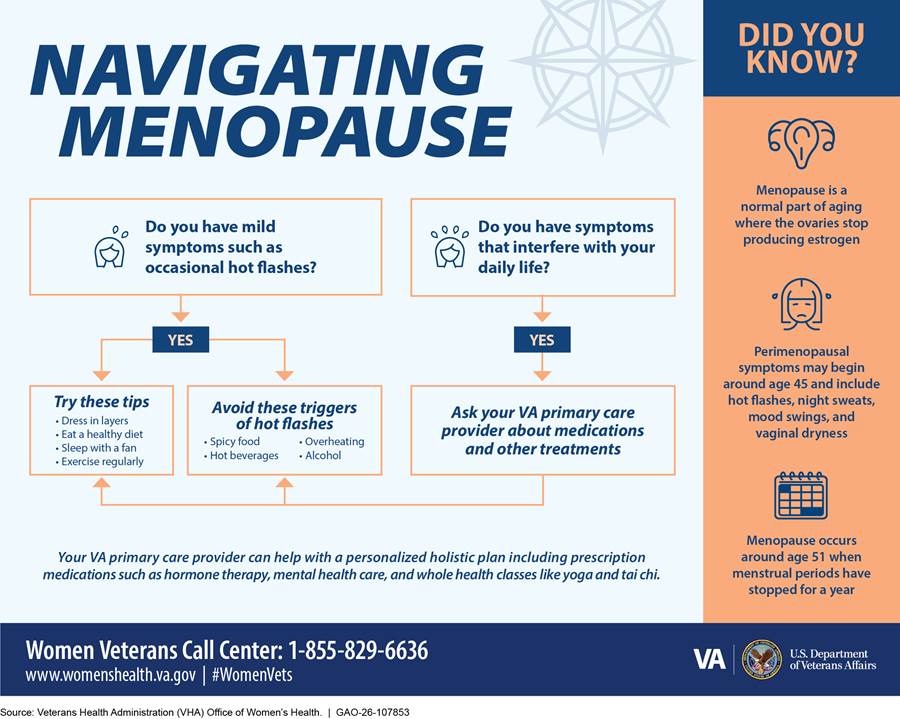
Menopause campaign materials. The Office of Women’s Health sponsored a national campaign focused on menopause in 2022.[41] The menopause campaign materials are available online and include information on VHA menopause care, such as hormone therapy and complementary and integrative health services, like yoga and meditation. Although the campaign has ended, according to VHA officials, the materials remain available for VHA medical facilities to download and use in local facility educational initiatives. See figure 3 for a graphic from one of the menopause campaign materials.
Website. VHA has a Women Veterans Health Care website with a page about menopause care for veterans. The website provides information on common menopause symptoms and care offered at VHA facilities to treat such symptoms such as hormone therapy. For example, the page provides information on changes veterans may notice at the onset of menopause, such as irregular menstrual periods and vaginal dryness.
VHA medical facilities can also create their own educational resources, but officials from four of the six facilities in our review said that they have not developed additional menopause educational materials. They said they rely on the materials from the Office of Women’s Health because those materials are comprehensive. One facility developed its own version of the Office of Women’s Health brochure with information specific to services offered at the individual facility, including information about menopause care and available treatments such as hormone therapy.[42]
Officials from each of the six VHA medical facilities also described sharing menopause information with veterans in other ways. For example, one facility included menopause topics in a quarterly town hall meeting for veterans, which included a presentation on pelvic health.
Additionally, officials from another medical facility told us that in August 2025 they started a perimenopause and menopause interdisciplinary group, which includes mental health experts, a pelvic floor physical therapist, and other providers. The purpose of this group is to offer support and educate women who are approaching menopause.
Providers from all six facilities in our review said they play a key role in educating veterans on menopause care and answering questions about available treatments to address menopause symptoms. For example, a clinical pharmacist at one facility reported talking to veterans about the risks and benefits of hormonal and non-hormonal treatments for their most bothersome symptoms. Of the veterans responding to our questionnaire who had encountered menopause information through VHA, 74 percent (103 veterans) reported that they were most likely to get information from their VHA health care provider.[43] Seventy six percent of these respondents (78 veterans) reported that they found it very or somewhat useful.
VHA’s Menopause Educational Materials May Not Be Reaching Many Women Veterans
Based on our survey results, discussions with veterans who participated in our survey, and interviews with officials from VHA medical facilities in our review, we found that menopause information may not be reaching many women veterans. For example, veterans reported that they were not always aware of VHA’s educational materials. Specifically, 60 percent of veterans (208 of 348) who responded to our online questionnaire reported that they had not encountered any VHA menopause resources.[44] The most frequent reason women veteran respondents who had not received menopause care reported for not receiving care was they were not aware they could receive care for menopause symptoms through VHA.[45] See text box for perspectives on VHA’s menopause education from selected veterans who participated in our discussion groups.
|
Selected Veterans’ Perspectives on VHA Menopause Education We conducted discussion groups with 24 of the veterans who responded to our online questionnaire. The following includes a summary of some of their responses about their expectations and experiences with VHA’s menopause education for veterans. One veteran said she follows VA social media accounts and has seen through these accounts that VHA provides menopause care. She said the monthly health campaigns have been helpful to get a sense of the breadth of services offered to women veterans. One veteran who receives her primary care and gynecology care through VHA said that in her experience, providers are not addressing perimenopause. She also said that having information on menopause, such as a pamphlet in the lobby or clinic waiting room, would be helpful. One veteran said that at her Women’s Clinic, there are usually a couple pamphlets and flyers about health services. Some of these are specific to women. She said it would be nice if there were more flyers about menopause care because she can pick them up and use them to start a conversation with her provider. One veteran said that veterans need information about menopause. She said it makes a difference in their lives to know what is going on with their bodies. Source: GAO analysis of discussion group responses. | GAO‑26‑107853 |
VHA Office of Women’s Health officials said they view their role as being a resource for frontline providers because trust in VA begins with conversations between veterans and their providers. Officials said providers play a key role in educating veterans about available menopause care, including providing them with educational materials. However, providers may not be discussing menopause with veterans. For example, according to officials, providers have challenges discussing menopause with veterans, including time constraints or lack of comfort with managing menopause. Further, as noted in VHA’s surveys of providers’ education needs, providers do not always feel comfortable managing veterans’ menopause symptoms.
Additionally, providers may not be consistently providing VHA menopause information to veterans. VHA officials from the six medical facilities in our review noted challenges in sharing menopause educational materials with veterans. For example, they told us providers may not have time to discuss menopause information with veterans or to print out the brochures, as it takes away time they spend with veterans. They also reported challenges finding space to store printed materials.
Officials from three medical facilities also noted that some providers may not initiate menopause conversations either because they do not have time during the appointment, or they lack guidelines for treating symptoms. Officials also noted that patients are not always aware of when they should seek care or may feel uncomfortable discussing symptoms and thus may expect their provider to bring up menopause. Veterans who participated in our discussion groups said that their providers did not always bring up menopause during appointments as these veterans expected. See text box.
|
Selected Veterans’ Perspectives on Who They Expect to Initiate Menopause Conversations We conducted discussion groups with 24 of the veterans who responded to our online questionnaire. The following includes a summary of some of their responses about their expectations for receiving menopause information and care from their VHA provider. One veteran said she expected to get menopause information from her provider. The doctor is the one she depends on for this information because she has a good relationship with her doctor. One veteran thinks providers should ask about menopause symptoms. She said she is asked about suicide risk at every appointment, why couldn’t they ask about menopause symptoms in the same way? One veteran felt comfortable bringing up menopause symptoms but did not always know that her symptoms were connected to menopause. She did not feel educated enough about menopause to know what was happening was related to menopause. One veteran said one of her physical therapists was very helpful and enlightening. The physical therapist talked to her about perimenopause and how it affects the body, including skin changes. She said no one had talked to her about these topics previously. The physical therapist suggested that she see a gynecologist or urogynecologist for help with her symptoms and suggested that she look into using estradiol cream. She said it was the first time she had heard of these options, despite having symptoms for many years. Source: GAO analysis of discussion group responses. | GAO‑26‑107853 |
According to officials from the Office of Women’s Health, VHA does not have a formal strategy to ensure that information on menopause and VHA menopause care is communicated to veterans approaching and experiencing menopause. This is inconsistent with the Office of Women’s Health’s goal of maintaining an overarching women’s health communications plan to include improving outreach to women veterans through enhanced communication across multiple platforms and methods.[46]
Implementing a strategy, such as through the development of guidance for providers to initiate conversations around menopause, would help ensure that women veterans are knowledgeable about the changes potentially occurring in their bodies. It would also empower them to approach their providers with questions about sensitive topics and allow providers to address medical misinformation around menopause. This in turn would help VHA meet its goal of providing women veterans with high-quality, equitable, comprehensive health care as outlined in VHA policy.[47]
Conclusions
VHA medical facilities’ wide array of menopause care offerings are instrumental in helping to address the unique health needs of the growing population of women veterans receiving VHA care. With nearly half of women veterans receiving VHA care in the age range most likely to be experiencing menopause and its accompanying symptoms, it is essential that VHA continues to focus on its mission of providing equitable and high-quality care for the large proportion of those women experiencing menopause.
VHA is taking an important step in developing a clinical practice guideline for its provision of menopause care, which is intended to provide evidence-based recommendations for providers to use in diagnosing and treating menopause. Monitoring performance measures associated with the recommendations would help VHA understand the extent to which providers are adhering to guideline recommendations across its facilities. VHA would then be in a better position to assess the extent to which variations across its facilities are appropriate and address any unnecessary variations. This would, in turn, support VHA in achieving its goal of providing equitable, high-quality, and comprehensive menopause care.
Additionally, VHA providers play a key role in educating veterans about menopause and menopause care through their interactions with veterans, which are key opportunities to discuss symptoms and treatments and share educational materials. However, information on menopause may not be reaching many veterans who could benefit from it. Implementing a strategy to help better ensure veterans are educated on menopause would help veterans be more knowledgeable about menopause. Having this information would help veterans address the often-sensitive topics associated with menopause with their VHA providers.
Recommendations for Executive Action
We are making the following two recommendations to VA:
The Undersecretary for Health should use the performance measures related to its clinical practice guideline for menopause to monitor implementation of the guideline recommendations across VHA medical facilities. (Recommendation 1)
The Undersecretary for Health should develop and implement a strategy to better ensure women approaching and experiencing menopause are provided educational information on menopause and VHA’s menopause care. (Recommendation 2)
Agency Comments
We provided a copy of this report to VA for review and comment. VA did not provide comments on the report.
We are sending copies to the appropriate congressional committees, the Secretary of Veterans Affairs, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at HundrupA@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix IV.

Alyssa M. Hundrup
Director, Health Care
In this report we (1) examine how the Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) offers menopause care for veterans at VHA medical facilities; (2) describe VHA’s education and training for its providers on menopause and menopause care and (3) examine the extent to which VHA provides education to veterans about menopause and the menopause care available within the VHA system.
Interviews with VHA officials. We interviewed VHA officials who have roles and responsibilities relating to menopause care from the Office of Women’s Health, Office of Mental Health, Pharmacy Benefits Management, and Office of Quality and Patient Safety. We interviewed Office of Women’s Health officials about which specialties are involved in menopause care and the services they offer, their efforts to provide menopause-related education and trainings to VHA providers, the extent to which they monitor quality of and access to menopause care, and their efforts to educate women veterans on menopause symptoms and services provided by VHA. We interviewed Office of Mental Health officials on the interaction between mental health issues common in the veteran population and menopause as well as resources for reproductive mental health. We interviewed Pharmacy Benefits Management officials about available drugs for the management of menopause symptoms as well as how VHA makes formulary decisions. We interviewed officials from the Office of Quality and Patient Safety about the development of a clinical practice guideline for menopause care and the extent to which they monitor measures related to veterans receiving menopause care through VHA.
Interviews with officials and providers at selected VHA medical facilities. We also interviewed officials from six selected VHA medical facilities about the menopause care they offer. We selected facilities to include in our review based on variation in several factors including geographic variation based on Veterans Integrated Service Network, the number of women veterans served, rural and urban designation, facilities with and without a Comprehensive Women’s Health Center, and facilities that do and do not participate in the VHA Women’s Health Practice-Based Research Network.[48] The selected facilities are (1) James J. Peters Department of Veterans Affairs Medical Center, Bronx, New York; (2) Washington VA Medical Center, Washington, DC; (3) Carl T. Hayden Veterans’ Administration Medical Center, Phoenix, AZ; (4) Carl Vinson Veterans’ Administration Medical Center, Dublin, GA; (5) Marion VA Medical Center, Marion IN; and (6) Sacramento VA Medical Center, Mather, CA. At each facility, we interviewed women’s health leadership; providers in primary care, gynecology, reproductive mental health, and Complementary and Integrative Health Services; and pharmacy officials. We interviewed officials about which specialties were involved in menopause care, where menopause care was typically provided, how they provided menopause education to providers, the extent to which they monitor menopause care, and any efforts to educate veterans about menopause. We interviewed primary care and specialty care providers about how they provide menopause care, the extent to which they have received training on menopause care, patient awareness of menopause, and any barriers they have faced to providing menopause care.
Online questionnaire and discussion groups with women veterans. To obtain veterans’ perspectives on VHA’s menopause education efforts and care offerings, we administered an online questionnaire from April 29 through June 15, 2025. We requested responses from women veterans aged 35 to 64 who had used a VHA medical facility in the last 24 months. We received 348 completed questionnaires from women veterans across 48 states, Washington, D.C. and Puerto Rico. As questionnaire respondents represent a self-selected group of women veterans receiving care through VHA, the information they provided is not generalizable to all women veterans receiving menopause care through VHA. For more information on the online questionnaire methodology and veterans’ responses, see appendix II.
We selected 24 of the respondents to our online questionnaire to participate in one of four discussion groups to obtain further details about their experience with VHA’s menopause education and care provision. We randomly selected respondents to be invited to the discussion groups from questionnaire respondents who said they would be interested in participating in a discussion group. Once invited, discussion groups were filled on a first come, first served basis. We conducted four discussion groups from July 24 through July 30, 2025. Two of the groups were with respondents who had received menopause care through VHA. The other two groups were with respondents who had received menopause care outside VHA or had not received any menopause care in the last 5 years. As participants were selected from online questionnaire respondents, their experiences are not generalizable to all women veterans receiving menopause care through VHA.
VHA menopause care offerings. We analyzed VHA data to describe how VHA offers menopause care. Specifically, we reviewed the number of full-time equivalent women’s health primary care and gynecology providers, and the number of clinical pharmacy practitioners who had an encounter with a woman aged 45 to 64 for each fiscal year from 2019 to 2024.[49] We interviewed officials from the two VHA offices responsible for providing the data—the Women’s Health Evaluation Initiative and Pharmacy Benefits Management—about the reliability of the data and any potential limitations. One limitation to the data is that full-time equivalent does not equate to the number of hours spent providing care for patients, but the number of hours spent in their role at VHA. Additionally, the database housing full-time equivalent data does not include residents, students, contract providers, or community care providers. Therefore, the number of full-time equivalent providers providing menopause care within the VHA system based on these data is an undercount. From fiscal years 2019 through 2024, six VHA medical facilities deployed the new Federal Electronic Health Record system from their legacy health record system.[50] In the fiscal year the medical facilities transitioned systems, clinical pharmacy practitioners may have been counted twice, once in the legacy system and once in the Federal Electronic Health Record System. This may overcount clinical pharmacy practitioners by a maximum of 1 percent for a given fiscal year. We also reviewed the data to identify any obvious errors and omissions. On this basis, we determined these data were sufficiently reliable for the purpose of our audit objective.
Additionally, we reviewed VHA data to determine the number of VHA medical facilities offering complementary and integrative health services, which may help in the management of menopause symptoms.[51] We interviewed officials from VHA’s Office of Patient Centered Care and Cultural Transformation about the reliability of the data and any potential limitations. We also reviewed the data to identify any obvious errors and omissions. On this basis, we determined these data were sufficiently reliable for the purpose of our audit objective.
To examine the extent to which VHA offers menopause care, we reviewed VHA data on the number of women veterans who received care through VHA providers. Specifically, for each fiscal year from 2019 to 2024, we examined the percent of women veterans between 45 and 64 with a diagnosis of “menopausal and other perimenopausal disorders” in their patient charts at each medical facility. We interviewed officials from the office responsible for providing the data, Women’s Health Evaluation Initiative, about the reliability of the data and any potential limitations. Limitations include removal of data from outputs that represented less than 11 veterans to maintain patient privacy. Additionally, an individual woman may be counted in more than one medical facility if she received care at multiple medical facilities within the fiscal year.
We also reviewed VHA data on the number of veterans within each VHA medical facility on hormone therapy. We interviewed officials from Pharmacy Benefits Management, the office responsible for providing the data, about the reliability of the data and any potential limitations.
In fiscal year 2020, the Canandaigua and Bath health care systems merged to become Finger Lakes, New York health care system. Therefore, tracking is limited to fiscal year 2020 and beyond for this facility. We also reviewed the data to identify any obvious errors and omissions. On this basis, we determined these data were sufficiently reliable for the purpose of our audit objective.
Finally, we assessed VHA’s provision of menopause care against VHA’s directive for delivering care to female veterans and its policy for developing clinical practice guidelines.[52]
VHA provider education on menopause. We requested a list of all menopause-related trainings offered by VHA. VHA officials provided us with a list of 36 trainings that they determined were related to menopause. We reviewed these trainings, including the training slides or presentations to ensure they were related to menopause care. We also reviewed VHA information on the frequency with which the training is offered and when the training was last updated. We also interviewed officials and reviewed documentation related to VHA’s assessments of provider training needs, which they conducted in February 2023 and October 2024.
VHA patient education on menopause. To examine the extent to which VHA provides education to veterans about menopause and the menopause care available within the VHA system, we reviewed veteran-facing educational materials developed by VHA’s Office of Women’s Health on menopause care. We also interviewed representatives from The Menopause Society and the American College of Obstetricians and Gynecologists about any best practices for menopause patient education. We assessed VHA’s efforts to educate veterans on menopause and menopause care against the Office of Women’s Health strategic plan, which has a goal of maintaining an overarching women’s health communication plan to include improving outreach to women veterans through enhanced communication across multiple platforms and methods.[53]
To collect information from veterans about their experiences with menopause care from the Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA), we developed and administered an online questionnaire for women veterans. The questionnaire asked respondents about VHA’s patient education on the topic of menopause and their experiences, if any, receiving VHA menopause care. It also included two open-ended questions where respondents could provide additional information about ways VHA could better provide them with menopause information or menopause care.
We also developed outreach materials—a flyer and social media blurb—to use to solicit veteran participation. These materials described the purpose of the questionnaire and ensured veterans that their responses would be kept confidential. We pre-tested the questionnaire and outreach materials with four veterans employed at GAO and updated the materials as appropriate.
To solicit veteran participation from women veterans, we reached out to several Veterans Service Organizations that are national, congressionally chartered, and have a documented interest in women’s health issues. The following four organizations responded and agreed to work with us: Disabled American Veterans, Military Officers Association of America, Paralyzed Veterans of America, and Veterans of Foreign Wars of the United States. These organizations posted the outreach flyer and social media blurb for the questionnaire, which was open from April 29 to June 15, 2025, through a variety of methods, including weekly newsletters, emails, and social media, such as a LinkedIn page. We received 348 completed questionnaires from respondents across 48 states, Washington, D.C. and Puerto Rico. Respondents reported that they were women veterans and aged 35 to 64.[54]
In this appendix we present summary information from the categorical questions in the questionnaire. We do not include respondents’ narrative responses to open-ended questions or questions with fewer than 10 responses to protect respondents’ identities. As our respondents were not randomly selected, results are not generalizable to all women veterans aged 35 to 64.
Table 1: In Your Interactions with VA, Have You Encountered Any of the Following Resources about Menopausal Symptoms and/or Menopausal Care Available through the VA? (Check All that Apply)
|
VA menopause education resources |
Number (percentage) of respondents |
|
VA brochures |
25 (7.2) |
|
VA bulletin boards or information booths |
14 (4.0) |
|
VA emails |
36 (10.3) |
|
VA’s podcast ‘She Wears the Boots’ |
9 (2.6) |
|
VA website |
27 (7.8) |
|
VA health care provider |
103 (29.6) |
|
VA social media |
14 (4.0) |
|
VA town halls |
10 (2.9) |
|
Other, please specify |
7 (2.0) |
|
I saw/heard information, but I do not recall the source |
21 (6.0) |
|
I did not see/hear any resources from VA about menopausal symptoms or menopausal care |
208 (59.8) |
|
Total respondents |
348 (100.0) |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could select more than one response. Therefore, the sum of the respondents for each response is larger than the total number of respondents. Further, respondents could provide additional responses in a text box field labeled “other.” The “other” responses have been incorporated into this list of providers where applicable.
Table 2: For Each Resource that You Encountered from VA, Please Indicate How Useful You Found that Information. (Select One Response per Row)
|
VA menopause education resources |
|
Number (percentage) of respondents |
||||||
|
Not at all useful |
Not very useful |
Somewhat useful |
Very useful |
Extremely useful |
I do not know |
Missing |
Total Respondents |
|
|
VA brochures |
3 (12.0) |
2 (8.0) |
10 (40.0) |
6 (24.0) |
3(12.0) |
1 (4.0) |
0 (0.0) |
25 (100.0) |
|
VA bulletin boards or information booths |
2 (14.3) |
1 (7.1) |
7 (50.0) |
3 (21.4) |
1 (7.1) |
0 (0.0) |
0 (0.0) |
14 (100.0) |
|
VA emails |
1 (2.8) |
4 (11.1) |
16 (44.4) |
10 (27.8) |
3 (8.3) |
2 (5.6) |
0 (0.0) |
36 (100.0) |
|
VA’s podcast ‘She Wears the Boots’ |
0 (0.0) |
1 (11.1) |
3 (33.3) |
3 (33.3) |
0 (0.0) |
2 (22.2) |
0 (0.0) |
9 (100.0) |
|
VA website |
0 (0.0) |
3 (11.1) |
11 (40.7) |
8 (29.6) |
5 (18.5) |
0 (0.0) |
0 (0.0) |
27 (100.0) |
|
VA health care provider |
7 (6.8) |
16 (15.5) |
27 (26.2) |
22 (21.4) |
29 (28.2) |
0 (0.0) |
2 (1.9) |
103 (100.0) |
|
VA social media |
0 (0.0) |
0 (0.0) |
6 (42.9) |
4 (28.6) |
3 (21.4) |
0 (0.0) |
1 (7.1) |
14 (100.0) |
|
VA town halls |
0 (0.0) |
2 (20.0) |
3 (30.0) |
2 (20.0) |
2 (20.0) |
1 (10.0) |
0 (0.0) |
10 (100.0) |
|
Other |
1 (14.3) |
1 (14.3) |
0 (0.0) |
2 (28.6) |
1 (14.3) |
2 (28.6) |
0 (0.0) |
7 (100.0) |
|
I saw/heard information, but do not recall the source |
1 (4.8) |
6 (28.6) |
7 (33.3) |
0 (0.0) |
2 (9.5) |
5 (23.8) |
0 (0.0) |
21 (100.0) |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only select answers for resources they indicated they encountered earlier in the questionnaire.
Table 3: In the Past 5 years, Have You Received Menopausal Care from Any of the Following? (Check All that Apply)
|
Provider location |
Number (percentage) of respondents |
|
|
VA provider |
108 (31.0) |
|
|
VA referral to a community care provider |
28 (8.0) |
|
|
Other provider not associated with VA |
57 (16.4) |
|
|
I did not receive menopausal care from any |
189 (54.3) |
|
|
I do not know |
4 (1.1) |
|
|
Total respondents |
348 (100.0) |
|
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could select more than one response of options “VA provider,” “VA referral to a community care provider,” and “other provider not associated with VA.” Therefore, the sum of the respondents for each response is larger than the total number of respondents.
Table 4: Which of the Following Best Describes Why You Did Not Receive Care from Your VA Provider(s) or via a VA Referral to a Community Care Provider(s) to Address Menopausal Symptoms in the Last 5 Years? (Check All that Apply)
|
Reasons for not receiving care from a VA provider |
Number (percentage) of respondents |
|
|
Received menopause care only from provider not associated with VA |
Did not receive menopause care from any health care provider in the last 5 years |
|
|
I did not experience any menopausal symptoms in the last 5 years which prompted me to seek medical care |
N/Aa |
30 (27.8) |
|
I did not feel that my VA provider had the skill or expertise to address my menopause symptoms |
7 (19.4) |
24 (22.2) |
|
I could not get an appointment within the timeframe I wanted to get care |
6 (16.7) |
0 (0.0) |
|
I did not feel my VA provider was open to discussing all treatment options |
6 (16.7) |
20 (18.5) |
|
I did not feel comfortable talking to my VA provider about my menopausal symptoms |
3 (8.3) |
5 (4.6) |
|
I did not know I could receive care for my menopausal symptoms through my VA provider |
14 (38.9) |
44 (40.7) |
|
I felt more comfortable going to a provider outside the VA system |
13 (36.1) |
3 (2.8) |
|
I could not get adequate transportation to receive care from my VA provider |
1 (2.8) |
1 (0.9) |
|
Other, please explain |
12 (33.3) |
25 (23.1) |
|
I do not know |
1 (2.8) |
5 (4.6) |
|
Total respondents |
36 (100.0)b |
108 (100.0)c |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only fill out this question if they indicated earlier in the questionnaire that (1) they only received menopause care from a provider not associated with VA or (2) they did not receive menopause care from any health care provider in the last 5 years. Respondents could select more than one response. Therefore, the sum of the respondents for each response is larger than the total number of respondents. Further, respondents could provide additional responses in a text box field labeled “other.” The “other” responses have been incorporated into this list of providers where applicable.
aThis answer option was not shown to respondents who selected they had received care from a provider outside VA.
bWhile 57 respondents indicated that they had received menopause care from a provider not associated with VA, 21 of those indicated that they had also received care from a VA provider or a VA referral to a community care provider and therefore did not have an opportunity to answer this question.
cAn error in survey logic was discovered on May 12, 2025, which resulted in 81 respondents, who should have seen this question (based on earlier responses) not seeing it.
Table 5: Which of the Following VA Provider(s), If Any, Have You Seen Regarding Menopausal Care? (Check All that Apply)
|
Provider types |
Number (percentage) of respondents |
|
Primary care provider |
73 (67.6) |
|
Endocrinologist |
5 (4.6) |
|
Gynecologist |
59 (54.6) |
|
Pelvic floor physical therapist |
20 (18.5) |
|
Mental health provider |
20 (18.5) |
|
Clinical pharmacy practitioner (does not include pharmacists who primarily dispense medication) |
1 (0.9) |
|
Other, please specify |
15 (13.9) |
|
I do not know |
0 (0.0) |
|
Total respondents |
108 (100.0) |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only fill out this question if
they indicated earlier in the questionnaire that they had received care from a
VA provider. Respondents could select more than one response. Therefore, the
sum of the respondents for each response is larger than the total number of
respondents. Further, respondents could provide additional responses in a text
box field labeled “other.” The “other” responses have been incorporated into
this list of providers when applicable.
Table 6: Which of the Following Community Care Provider(s), If Any, Have You Seen via a VA Referral Regarding Menopausal Care? (Check All that Apply)
|
Provider types |
Number (percentage) of respondents |
|
Primary care provider |
4 (14.3) |
|
Endocrinologist |
0 (0.0) |
|
Gynecologist |
19 (67.9) |
|
Pelvic floor physical therapist |
6 (21.4) |
|
Mental health provider |
2 (7.1) |
|
Clinical pharmacy practitioner (does not include pharmacists who primarily dispense medication) |
1 (3.6) |
|
Other, please specify |
5 (17.9) |
|
I do not know |
0 (0.0) |
|
Total respondents |
28 (100.0) |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only fill out this question if they indicated earlier in the questionnaire that they had received care from a community care provider. Respondents could select more than one response. Therefore, the sum of the respondents for each response is larger than the total number of respondents. Further, respondents could provide additional responses in a text box field labeled “other.” The “other” responses have been incorporated into this list of providers where applicable.
Table 7: Overall, How Satisfied Were You with the Following Aspects of the Care You Received from Your VA Provider(s)? (Select One Response per Row)
|
Level of satisfaction |
Number (percentage) of respondents |
|||
|
Timeliness of care |
Quality of care |
|||
|
Extremely dissatisfied |
18 (16.7) |
20 (18.5) |
||
|
Slightly dissatisfied |
12 (11.1) |
10 (9.3) |
||
|
Neither satisfied nor dissatisfied |
15 (13.9) |
8 (7.4) |
||
|
Slightly satisfied |
20 (18.5) |
23 (21.3) |
||
|
Extremely satisfied |
42 (38.9) |
45 (41.7) |
||
|
I do not know |
1 (0.9) |
1 (0.9) |
||
|
Missing |
0 (0.0) |
1 (0.9) |
||
|
Total respondents |
108 (100.0) |
108 (100.0) |
||
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only fill out this question if they indicated earlier in the questionnaire that they had received care from a VA provider.
Table 8: Overall, How Satisfied Were You with the Following Aspects of the Care You Received from Your Community Care Provider(s)? (Select One Response per Row)
|
Level of satisfaction |
Number (percentage) of respondents |
|||
|
Timeliness of care |
Quality of care |
|||
|
Extremely dissatisfied |
2 (7.1) |
2 (7.1) |
||
|
Slightly dissatisfied |
3 (10.7) |
0 (0.0) |
||
|
Neither satisfied nor dissatisfied |
0 (0.0) |
0 (0.0) |
||
|
Slightly satisfied |
9 (32.1) |
7 (25.0) |
||
|
Extremely satisfied |
14 (50.0) |
18 (64.3) |
||
|
I do not know |
0 (0.0) |
0 (0.0) |
||
|
Missing |
0 (0.0) |
1 (3.6) |
||
|
Total respondents |
28 (100.0) |
28 (100.0) |
||
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only fill out this question if they indicated earlier in the questionnaire that they had received care from a community care provider.
Table 9: Please Indicate Which of the Following Describes Why You Were Not Satisfied with the Quality of Care You Received from Your VA Provider(s) to Address Your Menopausal Symptoms. (Check All that Apply)
|
Reasons for dissatisfaction |
Number (percentage) of respondents |
|
I did not feel my VA provider was open to discussing all treatment options |
18 (60.0) |
|
I did not feel my VA provider took my symptoms seriously |
21 (70.0) |
|
I did not feel my VA provider took my concerns about treatment options seriously |
21 (70.0) |
|
I could not get the treatment option I was looking for through VA |
14 (46.7) |
|
I did not feel my VA provider could effectively treat all my symptoms |
13 (43.3) |
|
I did not feel my VA provider had the skills or expertise to address my symptoms |
15 (50.0) |
|
Other, please explain |
6 (20.0) |
|
I do not know |
0 (0.0) |
|
Total respondents |
30 (100.0) |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
Note: Respondents could only fill out this question if they indicated earlier in the questionnaire that they were extremely or very dissatisfied with the quality of the care they received from their VA provider. Respondents could select more than one response. Therefore, the sum of the respondents for each response is larger than the total number of respondents. Further, respondents could provide additional responses in a text box field labeled “other.” The “other” responses have been incorporated into this list of reasons where applicable.
Table 10: Please Indicate Which of the Following Describes Why You Were Not Satisfied with the Quality of Care You Received from Your Community Care provider(s) to Address Your Menopausal Symptoms. (Check All that Apply)
|
Question received less than 10 responses |
Source: GAO analysis of questionnaire of women veterans administered between April and June 2025. | GAO‑26‑107853
The Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) conducts research with the stated goal of helping improve veterans’ health and well-being, with a focus on health issues that affect veterans. In April 2024, the VA Women’s Health Research Network, in partnership with the Office of Women’s Health, launched a national work group. The work group focused on gaining a better understanding of women veterans’ menopause-related symptoms and their impacts, these veterans’ access to and use of appropriate menopause-related health services, and the quality of menopause-related care through VHA.
We requested a list of studies that VHA conducted or had underway on perimenopause, menopause, or menopause care, as of March 2026, and present them as shared by VHA, below. We excluded oral presentations that presented other study findings.
List of Menopause Studies Conducted or Underway by VHA, March 2026
Blanken, A., C.J. Gibson, Y. Li, et al. “Racial/Ethnic Disparities in the Diagnosis and Management of Menopause Symptoms among Midlife Women Veterans.” Menopause (July 2022): p. 877-882.
Cordasco, Kristina M., Anita H. Yuan, Marjorie J. Danz, et al. “Veterans Health Administration Primary Care Provider Adherence to Prescribing Guidelines for Systemic Hormone Therapy in Menopausal Women.” Journal for Healthcare Quality vol. 41, (March/April 2019): p. 99-109.
Diem, S.J., H. Miles-Mclean, D. Carney, et al. “Menopause-Related Service Needs in Veterans Health Administration Medical Centers: Findings from the Women’s Health Practice-Based Research Network Menopause Practice Scan.” Women’s Health Issues (July-August 2025): p. 283-291.
Fu. P., C.J. Gibson, W.B. Mendes, M. Schembri, and A.J. Huang. “Anxiety, Depressive Symptoms, and Cardiac Autonomic Function in Perimenopausal and Postmenopausal Women with Hot Flashes: A Brief Report.” Menopause (December 2018): p. 1470-1475.
Gerber M.R., et al. “Hormone Therapy Use in Women Veterans Accessing Veterans Health Administration Care: A National Cross-Sectional Study.” J Gen Int Med vol. 30, no. 2 (2014): p. 169-175.
Gibson, C.J., “Do Current Treatment Options Fall Short for Persistent Vasomotor Symptom Bother in Women over 60?” Menopause vol. 25, no.10 (2018): p. 1063-1064.
Gibson, C.J., et al. “Patient-Centered Change in the Day-to-Day Impact of Postmenopausal Vaginal Symptoms: Results from a Multicenter Randomized Trial.” Am J Obstet Gynecol (July 2020): p. 99.e1-99.
Gibson, C.J., et al. “Associations of Intimate Partner Violence, Sexual Assault, and Posttraumatic Stress Disorder With Menopause Symptoms among Midlife and Older Women.” JAMA Internal Medicine vol. 179, no. 1 (2019): p. 80-87.
Gibson, C.J., et al. “Interpersonal Trauma and Aging-Related Genitourinary Dysfunction in a National Sample of Older Women.” Am J Obstet Gynecol vol. 220, no. 94 (January 2019): p. 1-7.
Gibson, C.J., Y. Li, G.K. Jasuja, K.J. Self, K.H. Seal, A.L. Byers. “Menopausal Hormone Therapy and Suicide in a National Sample of Midlife and Older Women Veterans.” Medical Care vol. 59, no. 2 suppl 1 (February 2021): p. S70-S76.
Gibson, C.J., Y. Li, A.J. Huang, T. Rife, and K.H. Seal. “Menopausal Symptoms and Higher Risk Opioid Prescribing in a National Sample of Women Veterans with Chronic Pain.” J Gen Intern Med vol. 34, no. 10 (2019): p. 2159-2166.
Gibson, C.J., Y. Li, D. Bertenthal, A. Huang, and K.H. Seal “Menopause Symptoms and Chronic Pain in a National Sample of Midlife Women Veterans.” Menopause vol. 26, no. 7 (2019): p. 708-713.
Goldstein, L.A., K.P. Jakubowski, A.J. Huang, et al. “Lifetime History of Interpersonal Partner Violence Is Associated with Insomnia among Midlife Women Veterans.” Menopause vol. 30, no. 4 (2023): p. 370-375.
Haskell, S.G., B. Bean-Mayberry, J.L.Goulet, M. Skanderson, C.B. Good, and A.C. Justice. “Determinants of Hormone Therapy Discontinuation among Female Veterans Nationally.” Mil Med vol. 173, no. 1 (2008): p. 91-96.
Katon J.G., et al. “Vasomotor Symptoms and Quality of Life among Veteran and Non‑Veteran Postmenopausal Women.” Gerontologist vol. 56, no. S1 (2016): p. S40-S53.
Schapira, M.M., M.A. Gilligan, T.L. McAuliffe, and A.B. Nattinger. “Menopausal Hormone Therapy Decisions: Insights from a Multi‑Attribute Model.” Patient Education and Counseling vol. 52 (2004): p. 89-95.
Thomas, J.L., et al. “Dimensions of Posttraumatic Stress Disorder and Menopause-Related Health in Midlife Women Veterans.” Menopause vol. 31, no. 10 (2024): p. 842-852.
Travis, K.J., et al. “Military Sexual Trauma and Menopause Symptoms among Midlife Women Veterans.” J Gen Intern Med vol. 39, no. 3 (2023): p. 411-417.
GAO Contact
Alyssa M. Hundrup, HundrupA@gao.gov
Staff Acknowledgments
In addition to the contact named above, Janina Austin (Assistant Director), Emily Binek (Analyst-in-Charge), Lily Besel, and Samantha Flom made key contributions to this report. Also contributing were Jennie Apter, Julie Flowers, Jeanne Murphy-Stone, Monica Perez-Nelson, and Ethiene Salgado-Rodriguez.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]VHA medical facilities include both VHA medical centers and VHA health care systems. The health care systems comprise multiple medical centers. The medical centers operate VHA community-based outpatient clinics that provide basic primary care services on site. Other services provided by these clinics vary by facility. VHA also allows eligible veterans to obtain care from community providers when they face certain challenges accessing care at VHA medical facilities, such as when a facility does not offer the care needed.
[2]The time leading up to menopause is called the menopause transition or perimenopause. For the purposes of this report, we use the term “menopause” to refer to both perimenopause and menopause.
[3]Military sexual trauma is associated with prolonged menopause symptoms. See K.J. Travis et al., “Military Sexual Trauma and Menopause Symptoms among Midlife Women Veterans.” J Gen Intern Med, 39(3) 2023:411-417.
VA defines military sexual trauma as unwanted sexual behavior experienced during military service, including sexual harassment, physical assault of a sexual nature, and battery of a sexual nature. We previously reported that more than 350,000 veterans and service members screened positive for trauma related to experiences with unwanted sexual behavior from fiscal years 2015 to 2021, according to VHA data. See GAO, Unwanted Sexual Behavior: Improved Guidance, Access to Care, and Training Needed to Better Address Victims’ Behavioral Health Needs, GAO‑23‑105381 (Washington, D.C.: Aug. 2, 2023).
[4]Department of Veterans Affairs, Veterans Health Administration, VHA Directive 1330.01 (7) Health Care Services for Women Veterans, (Washington, D.C.: May 2023).
[5]Our review focused on the menopause care provided at VHA medical facilities and not through community care providers, who may also provide menopause care to eligible women veterans.
[6]VHA has 18 Veterans Integrated Service Networks, regional networks responsible for managing and overseeing VHA medical facilities.
[7]The Menopause Society is a nonprofit organization that provides tools and resources to providers and women in order to improve menopause care. The American College of Obstetricians and Gynecologists is a professional membership organization for obstetricians-gynecologists that provides comprehensive, expert-reviewed practice guidelines, management tools, and other learning opportunities.
[8]Department of Veterans Affairs, Veterans Health Administration, VHA Directive 1330.01 (7) Health Care Services for Women Veterans.
Department of Veterans Affairs, Veterans Health Administration and Department of Defense, U.S. Army Medical Command, Guideline for Guidelines (Feb. 1, 2011).
[9]Department of Veterans Affairs, Office of Women’s Health 2024 Strategic Plan.
[10]This was an online questionnaire without a defined study population. Veterans who met certain criteria were eligible to provide a questionnaire response. These criteria included being a woman, aged 35 to 64, and enrolled at a VHA medical facility. Respondents attested to meeting these criteria in their questionnaire responses.
[11]Jordan L. Thomas et al., “Dimensions of Posttraumatic Stress Disorder and Menopause-Related Health in Midlife Women Veterans,” Menopause, Journal of The Menopause Society, Vol. 31, No. 10, 2024: pp. 842-852.
[12]See K.J. Travis et al., “Military Sexual Trauma and Menopause Symptoms among Midlife Women Veterans.” J Gen Int Med, 39(3), 2023:411-417.
[13]Gibson, Carolyn J., Yongmei Li, Alison J. Huang, Tessa Rife, and Karen Seal. “Menopausal Symptoms and Higher Risk Opioid Prescribing in a National Sample of Women Veterans with Chronic Pain.” J Gen Intern Med 34(10):2159-66.
[14]American College of Obstetricians and Gynecologists. “Management of Menopausal Symptoms.” Practice Bulletin: Clinical Management Guidelines for Obstetrician-Gynecologists. No. 141 (January 2014).
[15]Writing Group for the Women’s Health Initiative Investigators. “Risks and Benefits of Estrogen Plus Progestin in Healthy Postmenopausal Women: Principal Results from the Women’s Health Initiative Randomized Controlled Trial,” Journal of the American Medical Association, 2002; 288(3):321-333.
The Women’s Health Initiative is a long-term national health study funded by the National Heart, Lung, and Blood Institute. The original study began in the early 1990s and concluded in 2005. Since 2005, the Women’s Health Initiative has continued as Extension Studies, which are annual collections of health updates and outcomes in active participants. The second Extension Study enrolled 93,500 women in 2010 and follow-up of these women continues annually.
[16]See, for example, Rossouw, J.E., et al., “Menopausal Hormone Therapy and Cardiovascular Diseases in Women with Vasomotor Symptoms: A Secondary Analysis of the Women’s Health Initiative Randomized Clinical Trials,” JAMA Intern Med, 2025, 185(11):1330-1339. See also Salpeter, S.R., et al., “Mortality Associated with Hormone Replacement Therapy in Younger and Older Women.” J Gen Int Med, 19 (2004): 791-804.
[17]According to the National Institutes of Health, boxed warnings (formerly known as “black box” warnings) are the highest safety-related warnings that medications can have assigned by the Food and Drug Administration. These warnings are intended to bring the consumer’s attention to the major risks of the drug. Medications can have a boxed warning added, taken away, or updated throughout their tenure on the market. Over 400 different medications currently have boxed warnings.
[18]Providers can be designated a women’s health primary care provider with one of the following: documentation of attendance at a Women’s Health Mini-Residency within the previous 3 years; documentation of at least 20 hours of women’s health continuing medical education or continuing education unit within the previous 3 years; documentation of at least 3 years in a practice with at least 50 percent women patients within the previous 5 years; evidence of completion of an internal medicine or family practice residency, women’s health fellowship, or women’s health, adult, or family practice nurse practitioner or physician assistant training within the previous 3 years; documentation of a current preceptorship arrangement with an experienced women’s health primary care provider such as weekly meetings for at least 6 months; or evidence of being recognized as a known women’s health leader and subject matter expert with experience practicing, teaching, and/or precepting women’s health.
A patient panel is a group of patients assigned to a given VHA provider, responsible for supervising those patients’ care. Women’s health primary care providers’ panels may include both men and women. To account for the unique needs of women veterans during appointments, VHA recommends that women’s health primary care providers’ panels be reduced by the number of unique patients equal to 20 percent of the total number of women veterans in the panel. Veterans Health Administration, VHA Directive 1330.01 (7) Health Care Services for Women Veterans.
[19]More specialized care for women is typically provided by a gynecology provider. Services provided by a VHA gynecologist include treatment of menstrual disorders, fertility assessments, treatment of gynecological malignancies, surgical management of gynecologic disorders, and performance of gynecological procedures such as colposcopies.
[20]Full-time equivalent represents a 40-hour work week. These data do not include women’s health primary care providers who are residents, students, contract providers, or community care providers and thus undercount the number of full-time equivalent women’s health primary care providers at VHA medical facilities. Additionally, these data reflect the total number of hours worked and not the number of hours spent providing care for women.
[21]These data do not include residents, students, contract providers, or community care providers and thus undercount the number of full-time equivalent gynecology providers providing care at VHA medical facilities. Additionally, these data reflect the total number of hours worked and not the number of hours spent providing care for women.
[22]These medications are included on VHA’s formulary or may be accessed via VHA’s non-formulary request process. VHA’s formulary includes those medications approved by VHA’s National Formulary Committee based on efficacy, safety, quality, and best value to the agency, according to Pharmacy Benefits Management officials. To prescribe medications not on the formulary, providers are to follow a process to document that patients meet specific criteria. For more information on the VHA formulary status for menopause medications, see Department of Veterans Affairs, Veterans Health Administration, Commonly Used Menopausal Agents and VA National Formulary Status.
[23]VHA does not collect data on how many clinical pharmacy practitioners have women’s health specific training or experience.
[24]From fiscal years 2019 through 2024, six VHA medical facilities (located in Spokane, Wash.; Walla Walla, Wash.; Columbus, Ohio; Roseburg, Ore.; White City, Ore.; and North Chicago, Ill.) deployed to the new Federal Electronic Health Record system from their legacy health record system. In the fiscal year the medical facilities transitioned systems, clinical pharmacy practitioners may have been counted twice, once in the legacy system and once in the Federal Electronic Health Record System. This may overcount clinical pharmacy practitioners by a maximum of 1 percent for a given fiscal year, according to VHA Pharmacy Benefits Management officials.
[25]See Thomas, J.L., et al., “Dimensions of Posttraumatic Stress Disorder and Menopause-Related Health in Midlife Women Veterans,” Menopause, vol 31, no. 10 (2024): p. 842-852. See also Gibson, C.J., et al., “Menopausal Symptoms and Higher Risk Opioid Use in a National Sample of Women Veterans with Chronic Pain,” J Gen Intern Med, vol 34, no. 10 (2019): p. 2159-2166.
[26]Karsten, Matty D. A., et al., “Sexual Function and Pelvic Floor Activity in Women: The Role of Traumatic Events and PTSD Symptoms.” European Journal of Psychotraumatology 11 (1), 2020: 1764246.
[27]See for example, Avis, Nancy E., Remy R. Coeytaux, Beverly Levine, Scott Isom, and Timothy Morgan, “Trajectories of Response to Acupuncture for Menopausal Vasomotor Symptoms: The Acupuncture in Menopause Study,” Menopause 24 (2): 171-79, 2017. Additionally, Cramer, Holger, Romy Lauche, Jost Langhorst, and Gustav Dobos, “Effectiveness of Yoga for Menopausal Symptoms: A Systematic Review and Meta-Analysis of Randomized Controlled Trials,” Evidence-based Complementary and Alternative Medicine, 2012. See also Carmody, James Francis, et al., “Mindfulness Training for Coping with Hot Flashes: Results of a Randomized Trial.” Menopause: The Journal of the North American Menopause Society 18 (6): 611-20, 2011.
[28]In fiscal year 2024, out of 139 total VHA medical facilities—health care systems and medical centers that are not part of larger health care systems—135 (97 percent) offered acupuncture, 136 (98 percent) offered yoga or Tai Chi, and 138 (99 percent) offered meditation or mindfulness classes.
[29]Clinical practice guidelines are systematically developed statements to assist providers in making informed decisions about patient care based on the best available research evidence. Guidelines help to provide consistent quality of care throughout VHA. The use of guidelines must always be in the context of a health care providers clinical judgement in the care of a particular patient.
[30]See Department of Veterans Affairs, Veterans Health Administration and Department of Defense, U.S. Army Medical Command, Guideline for Guidelines (Feb. 1, 2011).
[31]See Department of Veterans Affairs, Veterans Health Administration, VHA Directive 1330.01 (7) Health Care Services for Women Veterans, (Washington, D.C.: May 2023).
[32]In fiscal year 2025, the Office of Women’s Health hosted the Women’s Health Mini Residency 46 times. It was offered three times as a large national training with over 700 providers, including primary care providers and nurses, in attendance. The mini residency was delivered 43 times across 22 VHA medical facilities in rural areas with an additional 390 providers in attendance.
[33]The Talent Management System is a web-based enterprise application for managing education and training records within the VA workforce. It serves as the main access point to training for VHA providers.
[34]Diem et al., “Menopause-Related Service Needs in Veterans Health Administration Medical Centers: Findings from the Women’s Health Practice-Based Research Network Menopause Practice Scan,” Women’s Health Issues, 35(4): 283-291(2025). The Office of Women’s Health, in collaboration with the Women’s Health Research Network, surveyed site leads at VHA medical facilities within the national Women’s Health Practice-Based Research Network—a national network of 76 VHA facilities that voluntarily participate in ongoing VHA efforts to enhance women veterans’ health and health care. VHA excluded three sites from this survey because they did not have active site leads at the time the survey was fielded.
[35]Medical facilities responding to the survey reported the extent to which they agreed or strongly agreed with the need for more resources or support for managing specific menopause symptoms, including sexual function (90 percent agreed/strongly agreed), vasomotor symptoms (81 percent agreed/strongly agreed), urologic concerns (81 percent agreed/strongly agreed), sleep disorders (78 percent agreed/strongly agreed), vulvovaginal health (73 percent agreed/strongly agreed), bone health (72 percent agreed/strongly agreed), and mood disorders (71 percent agreed/strongly agreed).
[36]According to VHA officials, dissemination of this survey was managed locally at each facility and VHA did not track the response rate. At the close of fiscal year 2024, VHA employed 8,024 primary care providers.
[37]According to Office of Women’s Health officials, the 360 Spotlight is an opportunity to highlight a core health care theme over an entire quarter. The spotlight contains curated resources and customized content unique to the audience’s role. The Office of Women’s Health shares these resources across multiple forums including national calls with VHA facility’s Women Veteran Program Managers and Women’s Health Medical Directors, Women’s Health Community of Practice Calls, and the Office of Women’s Health Round Up newsletter. In past quarters, the 360 Spotlight has focused on topics such as musculoskeletal health, breast health, and trauma-informed care.
[38]Clinical Resource Hubs provide telehealth support to increase access to VHA clinical services for veterans when local facilities have gaps in care or service capabilities.
[39]As of March 2026, VHA officials told us that the podcast is on hold with no plans to start back up. The episodes, however, are still available on VHA’s website and other podcast platforms such as Spotify.
[40]These episodes included the following as of March 2026: She Wears the Boots, podcast “Healthy Aging,” August 1, 2024; “The Importance of Pelvic Health”, February 14, 2022; “Menopause Hormone Therapy Facts and Myths,” May 19, 2021; and “Menopause,” March 26, 2021.
[41]This was part of the Office of Women’s Health series of monthly campaigns on different women’s health topics.
[42]The brochure was last updated in April 2022.
[43]All 348 questionnaire respondents provided a response to whether they had encountered any VHA menopause education—141 reported that they had encountered VHA menopause information.
[44]All 348 questionnaire respondents provided a response as to whether they had encountered any VHA menopause education—140 (40 percent) reported that they had encountered VHA menopause information. The questionnaire asked if veterans had encountered any menopause care education through VHA which could include information directly from a provider at an appointment or through other sources such as on bulletin boards or through social media and emails.
[45]Of the women who stated they did not receive menopause care from any health care provider in the last 5 years in our online questionnaire, 41 percent (44 of 108 respondents) selected “I did not know I could receive care for my menopausal symptoms through my VA provider.” See appendix II, table 4, for a list of other reasons veterans reported not receiving menopause care from VHA.
[46]U.S. Department of Veterans Affairs, Office of Women’s Health 2024 Strategic Plan.
[47]Department of Veterans Affairs, Veterans Health Administration, Directive 1330.01 (7) Health Care Services for Women Veterans.
[48]Comprehensive Women’s Health Centers are clinics that have a separate entrance and waiting area and generally have women’s primary care, gynecological care, mental health care, and social work services co-located in the same space. The Women’s Health Practice-Based Research Network is a national network of 76 VHA facilities that voluntarily participate in ongoing VA efforts to enhance women veterans’ health and health care.
[49]We selected the age rage 45 to 64 to represent menopausal age to be consistent with how VHA defines menopausal age in its own research. See, for example, Gibson, C.J., et al., “Menopausal Symptoms and Higher Risk Opioid Use in a National Sample of Women Veterans with Chronic Pain,” J Gen Intern Med vol 34, no. 10 (2019): p. 2159-2166. Additionally, fiscal year 2024 was the most recent data available at the time of our review.
[50]These facilities are located in Spokane, Wash.; Walla Walla, Wash.; Columbus, Ohio; Roseburg, Ore.; White City, Ore.; and North Chicago, Ill.
[51]VHA medical facilities include both VHA medical centers and VHA health care systems. The health care systems comprise multiple medical centers.
[52]Department of Veterans Affairs, Veterans Health Administration, Health Care Services for Women Veterans, VHA Directive 1330.01 (7) (Washington, D.C.: May 2023).
[53]Department of Veterans Affairs, Office of Women’s Health 2024 Strategic Plan.
[54]VHA’s research uses the ages 45 to 64 to target those women most likely to be going through menopause. See, for example, Gibson, C.J., et al., “Menopausal Symptoms and Higher Risk Opioid Prescribing in a National Sample of Women Veterans with Chronic Pain,” J Gen Intern Med vol 34, no. 10 (2019): p. 2159-2166. We expanded this age range to 35, as we wanted to understand the extent to which VHA educational materials were reaching women before they might need them.
Respondents answered a series of screening questions to help us determine whether they met the criteria for inclusion such as their age and whether they received any care from a VHA medical facility in the previous 2 years.