Report to Congressional Requesters
United States Government Accountability Office
A report to congressional requesters
For more information, contact: Michelle B. Rosenberg at rosenbergm@gao.gov
What GAO Found
Assisted living facilities provide a residential alternative to in-home care and nursing homes for people who need assistance with activities of daily living such as eating and bathing.
GAO’s analysis of program data showed that federal Medicaid and Medicare spending for services provided in assisted living facilities totaled at least $12 billion in 2024. This amount is likely an undercount because of data limitations. For example, assisted living facilities are not a uniformly defined provider type and thus not consistently identified in the data.
· Federal Medicaid spending. GAO identified at least $3.5 billion in federal Medicaid spending for services provided in assisted living facilities in 2024. State Medicaid programs may cover assisted living services—that is, assistance with activities of daily living and other supportive services provided in assisted living facilities—as well as other services such as physical therapy.
· Medicare spending. GAO identified $8.5 billion in traditional Medicare spending for services provided in assisted living facilities in 2024. Medicare generally does not cover assisted living services but may cover other health care services such as hospice in assisted living facilities.
Other federal programs, such as Department of Housing and Urban Development and Department of Veterans Affairs programs, may be used by beneficiaries to help cover the costs of certain services, such as room and board, in assisted living facilities. The amount of spending by these programs for such services is unknown.
Forty-four states’ Medicaid programs covered assisted living services for older adults and people with disabilities as of March 2025. More than half of states—29 of the 44—covered these services under Medicaid home- and community-based services waivers. These waivers give states the flexibility to target enrollment to specific populations and to limit the number of participants.
State Medicaid Coverage of Assisted Living Services for Older Adults and People with Disabilities, as of March 2025
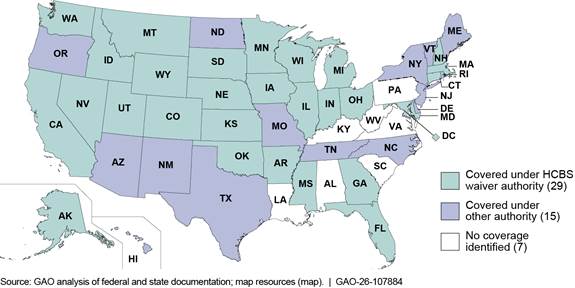
Note: HCBS refers to home- and community-based services. See fig. 3 in GAO-26-107884.
Why GAO Did This Study
Millions of older adults and people with disabilities need long-term care, which can be provided in a range of settings, including assisted living facilities. While most assisted living facility residents pay for their care using their own personal resources, federal programs including Medicaid cover certain services provided in assisted living facilities for those eligible.
GAO was asked to provide information on federal program coverage of and spending for services provided in assisted living facilities. Among other things, this report describes (1) federal spending for services provided in assisted living facilities and (2) state Medicaid coverage of assisted living services.
GAO analyzed Medicaid and Medicare claims data from 2024—the most recent year of data available, reviewed program documentation for other federal programs, and reviewed documents for state Medicaid programs covering assisted living services.
|
Abbreviations |
|
|
|
|
|
CMS |
Centers for Medicare & Medicaid Services |
|
HCBS |
home- and community-based services |
|
HHS |
Department of Health and Human Services |
|
HUD |
Department of Housing and Urban Development |
|
SSI |
Supplemental Security Income |
|
T-MSIS |
Transformed Medicaid Statistical Information System |
|
VA |
Department of Veterans Affairs |
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
June 2, 2026
Congressional Requesters
Millions of older adults and people with disabilities need long-term care, which includes services that assist individuals with activities of daily living such as eating and bathing. As the population ages, the need for long-term care in the United States is expected to grow rapidly and to lead to an increase in government spending for these services.[1] Long-term care can be provided in a range of settings, including institutions such as nursing homes, private homes, or other residential settings such as assisted living facilities.
There is no single definition of assisted living facilities, which are licensed and regulated at the state level.[2] States use varying terms for such facilities and may also have multiple licensing terms for facilities that provide similar services within a state.[3] For purposes of this report, we use the term “assisted living facility” to refer to a residential setting that primarily provides assistance with activities of daily living and other supportive services.[4] Other supportive services include assistance with, for example, meal preparation and medication management as well as recreational programming. We refer to assistance with activities of daily living and other supportive services provided in assisted living facilities as assisted living services.
While most assisted living facility residents pay for their care using their own personal resources, federal programs cover certain services provided in assisted living facilities for those who are eligible. For example, Medicaid programs can opt to cover assisted living services for certain program enrollees.[5] Medicaid programs are not allowed to cover the costs associated with room and board for beneficiaries receiving assisted living services.[6] Medicaid may also cover other health care services provided in assisted living facilities, such as physical therapy. Medicare generally does not cover assisted living services or room and board but may cover other health care services provided in these facilities, such as hospice services.[7] Residents of assisted living facilities may also leverage other federal programs to finance costs associated with assisted living. For example, residents eligible for federal disability benefits may use these benefits to pay for room and board costs.
You asked us to provide information on federal program coverage of and spending for services provided in assisted living facilities. This report describes
1. federal spending for services provided in assisted living facilities;
2. state Medicaid programs’ coverage of assisted living services for older adults and people with disabilities; and
3. stakeholder perspectives on factors affecting access to federally funded assisted living services.
To describe federal spending for services provided in assisted living facilities, we analyzed Medicaid and traditional, fee-for-service Medicare claims data for 2024, the most recent year of data available across both programs at the time of our analysis.[8] We analyzed total federal spending, average spending per beneficiary, and spending by type of service, to the extent the data were sufficient to do so. Assisted living facilities are not a uniformly defined provider category that can be consistently identified in Medicaid and Medicare claims. Thus, for purposes of our analysis, we included claims with a place of service code, procedure code, or provider code that specified “assisted living” as services provided in assisted living facilities. We also reviewed relevant regulations and documentation for other federal programs that may fund services provided in assisted living facilities—such as programs administered by the Social Security Administration, the Department of Veterans Affairs (VA), and the Department of Housing and Urban Development (HUD).[9] We interviewed officials and reviewed written responses from the Centers for Medicare & Medicaid Services (CMS)—the agency within the Department of Health and Human Services (HHS) responsible for overseeing Medicare and Medicaid—and from VA and HUD.
We assessed the reliability of the Medicaid and Medicare claims data by interviewing federal officials; reviewing related documentation, such as technical documentation from CMS describing the data and CMS’s assessment of its quality; comparing the results of our analysis to available published information; and testing the data for obvious errors. We determined that the data were sufficiently reliable for the purposes of our reporting objective. See appendix I for further details on our scope and methodology, including our data reliability assessment.
To describe state Medicaid program coverage of assisted living services for older adults and people with disabilities, we reviewed documents describing state coverage of assisted living services as approved by CMS as of March 2025, the most recent available at the time we began our review. We reviewed documents for all states to determine whether the state covered assisted living services for older adults and people with disabilities and under which Medicaid authorities.[10] For states that covered services for older adults and people with disabilities through what are referred to as home- and community-based services (HCBS) waivers, we reviewed additional information on the services covered, eligibility criteria, and estimated cost of services in waiver year 2024.[11] We also interviewed state Medicaid officials from five states—selected to achieve variation in the types of Medicaid authority used to cover assisted living services and geographic region—about assisted living services coverage considerations.[12]
To describe stakeholder perspectives on factors affecting access to federally funded assisted living services, we interviewed Medicaid officials from the five selected states and representatives from seven national stakeholder organizations. The seven national organizations were selected to include a range of perspectives and represent assisted living facilities, state aging and disability agencies, beneficiaries, and health plans. We also interviewed CMS officials.
We conducted this performance audit from October 2024 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
Assisted Living Facilities
Assisted living facilities provide a residential alternative to in-home care and nursing homes for people who need assistance with activities of daily living such as eating, bathing, and toileting. Assisted living facilities provide room and board, which includes housing, utilities, and meals, and typically provide access to round-the-clock staff. In contrast to nursing homes, assisted living facilities generally do not provide 24-hour skilled nursing services or rehabilitative services on an ongoing basis. See figure 1.
Figure 1: Examples of Services Provided in Assisted Living Facilities Compared to Other Long-Term Care Settings

Note: Assistance with activities of daily living includes help with personal care tasks such as eating, dressing, toileting, and bathing. Supportive services may include services such as meal preparation or medication management.
Unlike nursing homes, which are subject to extensive federal regulations, assisted living facilities are regulated at the state level. The regulatory approaches to assisted living facilities adopted by states vary.[13] For example, some states delineate the services that assisted living facilities may or may not provide—such as with multiple levels of licenses for more specialized care—while others grant more flexibility. Other differences in what state regulations address include facility size and whether facilities offer specified types of accommodations, such as private rooms. In a number of states, assisted living facility regulations emphasize residents’ independence, dignity, and privacy.
The size, type, and cost of assisted living facilities vary widely. According to a nationwide study, in 2022, facilities ranged in size from a few beds to fifty or more, with 41 beds on average. The majority of facilities—57 percent—were chain-affiliated, while others were independently owned. About 82 percent of facilities were for-profit while 17 percent were nonprofit.[14] Facilities may specialize in serving particular populations, such as individuals with dementia. Some facilities may offer assisted living services as part of a broader continuum of care that could also include independent living or nursing home care. The cost for assisted living varies widely across and within states depending on factors such as the facility’s size, services, and location. For example, median monthly costs ranged from about $4,200 in Alabama to over $12,000 in Hawaii in 2025, according to a 2025 industry survey.[15]
Federal Program Coverage of Services Provided in Assisted Living Facilities
Most assisted living residents pay out-of-pocket, but eligible individuals may use Medicaid and other federal programs to help finance their care. State Medicaid programs may cover assisted living services and other health care services that beneficiaries receive in assisted living facilities, but programs are not allowed to cover room and board costs. Medicare generally does not cover assisted living services but covers other health care services that can be provided in an assisted living facility. Several other federal programs may be used by eligible individuals to finance room and board costs.
Medicaid
Medicaid is jointly financed by the federal government and states, with the federal government matching most state spending on coverage for Medicaid beneficiaries based on a statutory formula, known as the federal medical assistance percentage.[16] Medicaid is the nation’s primary payer for long-term care, with federal and state Medicaid spending of about $229 billion in 2023, according to CMS.[17] State Medicaid programs have the option to cover long-term care provided in people’s homes or in noninstitutional community settings—known as home- and community-based services (HCBS). This includes the option to provide coverage of assisted living services.
States that opt to provide coverage for assisted living services have considerable flexibility in doing so under various Medicaid authorities for covering HCBS. Certain authorities allow states to target services to specific populations or conditions, to limit the availability of those services geographically, and to limit the number of individuals served through the use of enrollment caps. These flexibilities are generally not otherwise allowed under Medicaid but may enable states to control costs. Some HCBS authorities are limited to serving beneficiaries who are eligible for an institutional level of care; that is, beneficiaries must have needs that rise to the level of care usually provided in a nursing home or other institution.[18] See table 1.
Table 1: Selected Medicaid Authorities That States Can Use to Cover Home- and Community-Based Services, Including Assisted Living Services
|
Authority |
Authorizing statutea |
Allows targeting to specific populations |
Allows capped enrollment |
Limited to individuals who would otherwise need an institutional level of careb |
|
Home- and community-based services waiver |
1915(c) |
ü |
ü |
ü |
|
Medicaid demonstration |
1115 |
ü |
ü |
— |
|
State plan personal care servicesc |
1905(a)(24) |
— |
— |
— |
|
State plan home- and community-based services |
1915(i) |
ü |
— |
— |
|
Community First Choice state plan option |
1915(k) |
— |
— |
ü |
Legend: ü = applicable to the authority; — = not applicable to the authority
Source: Social Security Act and Centers for Medicare & Medicaid Services. | GAO‑26‑107884
aAuthorizing statute refers to sections of the Social Security Act.
bIndividuals who need an institutional level of care are those who meet the state’s eligibility requirements for services in an institutional setting, such as a nursing home. For example, individuals may qualify for an institutional level of care if they require substantial assistance or supervision with multiple activities of daily living such as bathing, eating, and toilet use.
cPersonal care services include assistance with activities of daily living such as eating, bathing, dressing, and toileting, and may include other supportive services such as medication management.
The most common authority used to cover HCBS, which may include assisted living services, are HCBS waiver programs. These programs serve beneficiaries who are eligible for an institutional level of care but elect to receive services in noninstitutional settings. For example, individuals may qualify for an institutional level of care if they require substantial assistance or supervision with multiple activities of daily living such as bathing, eating, and toilet use. Beneficiaries must also meet financial eligibility criteria, which vary for different populations in Medicaid.[19] HCBS waivers can be used to cover people who would typically not be financially eligible for Medicaid services unless they resided in an institution. States’ HCBS waiver programs must be cost neutral; that is, the state must spend equal to or less per beneficiary on average than what would have been spent to serve the same population in an institution, such as a nursing home.
Medicare
Most assisted living facility residents are eligible for Medicare.[20] Medicare, however, generally does not cover assisted living services or assisted living facility room and board charges. However, Medicare may cover other health care services provided in assisted living facilities similar to how these services could otherwise be provided in a private residence. For example, Medicare-certified hospices and home health agencies may provide services in assisted living facilities.[21] Hospice is a program of care and support for people who are terminally ill. Services typically include physical care, counseling, drugs, equipment, and supplies for the terminal illness and related conditions. Home health agency services include skilled nursing care, such as giving certain drugs or injections, and skilled therapy services, such as physical therapy or speech therapy, that are required to restore, improve, or maintain functions affected by an illness or injury. Hospice and home health services may be provided concurrently with assisted living services that residents receive from assisted living facilities. These services could potentially allow beneficiaries with a need for skilled care to remain in the assisted living facility instead of moving to an institutional setting that provides a higher level of care, such as a nursing home. Medicare may also cover services such as in-home health evaluation visits that may be provided on-site in assisted living facilities.
Other Federal Programs
Some assisted living facility residents may be eligible for benefits from other federal programs, which they may use to help pay for room and board costs or cover certain services provided in the facility. For example:
· The Social Security Administration administers Supplemental Security Income (SSI), a federal assistance program that provides cash benefits for eligible individuals who are elderly, blind, or have a disability; and have little or no income and resources. The maximum SSI federal benefit amount is known as the SSI federal benefit rate.[22]
· HUD offers programs that help eligible low-income individuals, including older adults and people with disabilities, afford housing.
· VA provides benefits, health care, and other services to qualifying military veterans and their families, including veterans who need long-term care.
Federal Spending for Services Provided in Assisted Living Facilities Was at Least $12 Billion in 2024
Our analysis of claims data showed that federal Medicaid and traditional Medicare spending for services provided in assisted living facilities totaled at least $12 billion in 2024. Additional federal programs may help certain eligible beneficiaries cover the cost of room and board in assisted living facilities, but the amount of federal funds beneficiaries use for this purpose is unknown.
Federal Medicaid Spending Totaled over
$3 Billion in 2024 for Assisted Living and Other Services
Based on our analysis of Medicaid data, federal spending totaled at least $3.5 billion in 2024 for assisted living services and other health care services that were provided in assisted living facilities for approximately 300,000 beneficiaries.[23] (In total, combined federal and state Medicaid spending for services provided in assisted living facilities was at least $6.2 billion.) The amount of federal Medicaid spending we identified for services provided in assisted living facilities—and the number of beneficiaries receiving such services—is likely an undercount because the facilities are not a uniformly defined provider type that can be consistently identified in the data. For example, states may vary in terms used for assisted living facilities. We identified eight states where our analysis likely only captured a portion of spending for these reasons.[24]
The majority of the total federal and state Medicaid spending identified in our analysis was for assisted living services. Specifically, at least 56 percent of federal and state spending identified in our analysis was for assisted living services.[25] We did not categorize services in the remaining 44 percent due to data complexity such as variation in procedure codes used for such services. However, examples of other Medicaid-covered services included in the spending were psychotherapy, adult day services, respite care, and residential habilitation.
Federal-state Medicaid spending on services provided in assisted living facilities averaged about $23,000 per beneficiary. However, spending per beneficiary can vary substantially based, for example, on the extent and nature of services covered by state Medicaid programs, the length of time beneficiaries spent in the assisted living facility, and regional variation in costs.
Most Medicaid beneficiaries we identified as receiving services in assisted living facilities in 2024 were dually eligible for Medicare and Medicaid. The beneficiaries were younger, on average, than assisted living residents overall. Our analysis found that about 21 percent of Medicaid beneficiaries receiving services in assisted living facilities were aged 85 or older. In comparison, over half of assisted living residents were estimated to be aged 85 or older in 2022, according to a federal study.[26] About one-fourth of Medicaid beneficiaries who received services in assisted living facilities were eligible for Medicaid on the basis of receipt of SSI benefits.[27] See figure 2.
Figure 2: Characteristics of Medicaid Beneficiaries Who Received Services Provided in Assisted Living Facilities, 2024
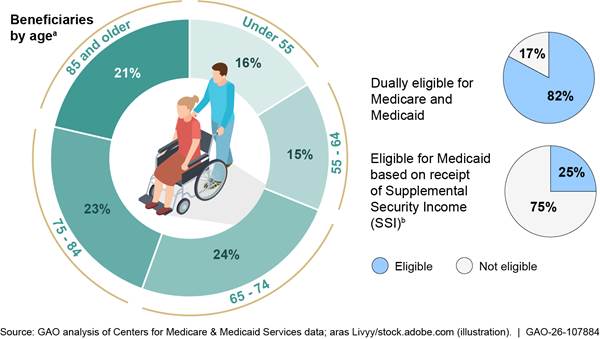
Notes: We identified Medicaid beneficiaries who received services in assisted living facilities based on claims information in the Transformed Medicaid Statistical Information System. We defined services provided in assisted living facilities as those with an assisted living provider code, place of service code, or procedure code. We included claims with a start date during calendar year 2024. We identified about 300,000 beneficiaries who received services in an assisted living facility in 2024. Percentages may not sum to 100 due to rounding.
aAge refers to the beneficiaries’ age as of the end of calendar year 2024.
bSSI is a federal program that provides cash benefits for eligible individuals who are elderly, blind, or have a disability, and have little or no income and resources.
Medicare Spending Totaled over $8 Billion in 2024, Largely for Hospice
Our analysis of 2024 claims data identified $8.5 billion in traditional Medicare spending for hospice, home health, and other services provided in assisted living facilities for approximately 829,000 beneficiaries. The $8.5 billion in spending we identified is likely an undercount of all Medicare spending for services provided in assisted living facilities. For example, it does not include services paid through Medicare Advantage.[28] The largest category of spending—spending for hospice services—is likely more complete because hospice services are generally paid under traditional Medicare.[29] However, the identified spending for other services is incomplete because those services can be paid for through Medicare Advantage, which is not included in our analysis.[30]
About 89 percent of the identified traditional Medicare spending for services provided in assisted living facilities in 2024 was for Medicare hospice and home health services. See table 2. As described previously, Medicare-certified hospices and home health agencies may provide services in assisted living facilities in addition to the assisted living services residents receive from the facility. The remainder of the identified Medicare spending was for a broader range of other services such as home evaluation visits or durable medical equipment.
|
Type of service |
Spending |
Number of beneficiariesa |
Average spending per beneficiary |
|
Hospice |
$6.1 |
294,147 |
$20,735 |
|
Home health |
1.4 |
218,741 |
6,555 |
|
Other |
0.9 |
601,663 |
1,525 |
|
Total |
$8.5 |
829,327 |
$10,190 |
Source: GAO analysis of Centers for Medicare & Medicaid Services data. | GAO‑26‑107884
Notes: Spending by type of service does not sum to the total due to rounding. The analysis is limited to traditional Medicare and does not include services paid for under Medicare Advantage, a private health plan alternative to traditional Medicare. Additionally, the analysis is limited to claims for which an assisted living facility was the sole site of service. Overall Medicare paid approximately $261 million for claims that included services provided both in assisted living facilities and other sites of service under traditional Medicare during calendar year 2024. “Other” services include, for example, home visits or psychotherapy services.
aThe number of beneficiaries refers to the number of unique beneficiaries with paid traditional Medicare claims by type of service and in total across all types of services. The number of beneficiaries by type of service does not sum to the total as beneficiaries may utilize more than one type of service during the year.
The average spending per beneficiary in traditional Medicare varied according to the type of service.
· Hospice services. Across service types, average spending per beneficiary was highest for hospice services, at nearly $21,000 per beneficiary on average in 2024. Per-beneficiary spending generally ranged from about $400 to $72,000.[31] The most common services provided by hospices in assisted living facilities included hospice aide services, which can include personal care services to assist with activities of daily living; direct skilled nursing services by a registered nurse; and clinical social worker services.
· Home health services. Medicare spending per beneficiary for home health services provided in assisted living facilities was about $6,500 on average in 2024, and generally ranged from about $289 per beneficiary to $27,000 per beneficiary.[32] The most common home health services provided in assisted living facilities included direct skilled nursing services from a registered nurse, physical therapy services, occupational therapy services, and speech-language pathology services.
· Other services. On average, spending for other services delivered through traditional Medicare in assisted living facilities was about $1,500 per beneficiary in 2024. However, the services provided and associated spending per beneficiary in this category ranged widely, generally from about $18 per beneficiary to over $9,900 per beneficiary.[33] The most common examples of these other services included home visits to evaluate the patient’s health condition and manage their care; therapeutic procedures; debridement of nails; and psychotherapy services.
Other Federal Programs May Help Beneficiaries Pay for Room and Board, but Spending Amounts Are Unknown
While there are other federal programs that individuals can leverage to help pay for services in assisted living facilities—in particular, room and board—those programs are generally not targeted for that purpose. The amount of funding from these programs being used for services in assisted living facilities is unknown. For example, relevant HUD and VA programs do not have available data to indicate the amount of program funding being used in assisted living facilities, according to program officials we spoke with.
Key federal programs that individuals may use to help pay for services in assisted living facilities include the following:
·
SSI. SSI beneficiaries may use SSI payments to help cover
the cost of care in assisted living facilities. For example, SSI may be used to
complement Medicaid benefits to cover the cost of room and board at assisted
living facilities. Individuals who are eligible for SSI are usually also
eligible for Medicaid.[34]
· HUD. HUD operates rental assistance programs for low-income people, including older adults and people with disabilities, such as Housing Choice Vouchers which may be used to subsidize room costs in assisted living facilities. For example, HUD guidance specifies that Housing Choice Vouchers may be used in assisted living facilities and notes that this use could supplement Medicaid-covered services.[35] For additional information about how HUD funding may be used for services provided in assisted living facilities, see appendix II.
· VA. VA funds multiple benefits and services that may support veterans who are residents of assisted living facilities, although it did not directly cover costs associated with assisted living facilities as of March 2026.[36] For example, VA’s Aid and Attendance benefits provide eligible veterans an increased monthly payment that could offset the cost of room and board or services in assisted living facilities.[37] VA may also provide extra home- and community-based health care services to eligible veterans, including those residing in assisted living facilities. For additional information about how VA funding may be used for services provided in assisted living facilities, see appendix III.
Most State Medicaid Programs Covered Assisted Living Services; States Varied in Coverage Aspects
|
Assisted Living Services Medicaid authorities states use to cover assisted living services include · home- and community-based services waivers; · Medicaid demonstrations; and · state plan authorities, such as the Community First Choice state plan option or state plan personal care services. Source: GAO. | GAO‑26‑107884 |
Forty-Four States Covered Assisted Living Services for Older Adults and People with Disabilities; Most Used Authorities That Allowed Limits on Enrollment
Forty-four states’ Medicaid programs covered assisted living services for older adults and people with disabilities as of March 2025, according to our review of CMS and state documentation.[38] We use the term assisted living services to refer to assistance with activities of daily living and other supportive services provided in assisted living facilities.[39] More than half of these states—29 of the 44—covered these services under HCBS waivers, which give states the flexibility to target program enrollment to specific populations and limit the number of participants the program serves.[40]
The remaining 15 states covered these services through other Medicaid authorities. See figure 3.
Figure 3: State Medicaid Coverage of Assisted Living Services for Older Adults and People with Disabilities as of March 2025
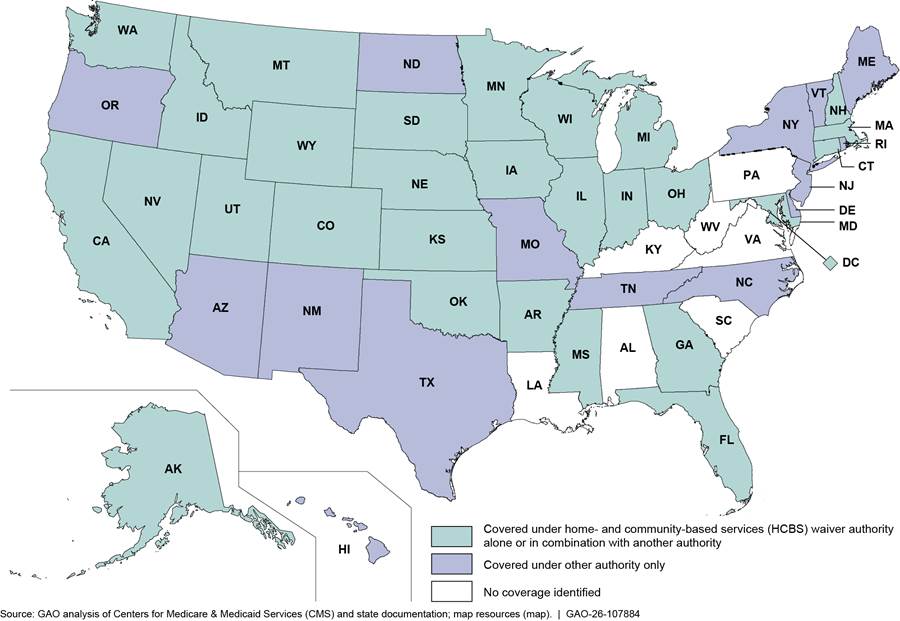
Notes: Assisted living services refer to assistance with activities of daily living—such as eating, bathing, and toileting—and other supportive services provided in an assisted living facility. We use the term assisted living facility to refer to a residential setting that primarily provides assistance with activities of daily living and other supportive services. States’ coverage approval documents may use different terms for assisted living services and facilities, such as supportive living or residential care. Therefore, we identified coverage of these services based on service descriptions consistent with CMS’s definition of assisted living services. We included coverage of personal care and attendant care services with an assisted living facility provider. States where we did not identify coverage of assisted living services may cover services, such as personal care services provided by outside providers, or other services, such as residential habilitation, for individuals who live in assisted living facilities. The term “older adults and people with disabilities” generally refers to adults aged 65 and over and individuals with disabilities aged 64 and under. However, a state may specify different age ranges to reflect state practice. One state—Connecticut—covered assisted living services for older adults but not for people with disabilities who were 64 and under.
HCBS waiver authority refers to waivers authorized under section 1915(c) of the Social Security Act. Other authorities include: (1) Medicaid demonstrations authorized under section 1115 of the Social Security Act, which waive certain federal Medicaid requirements for the purpose of testing and evaluating alternative approaches to service delivery; (2) the Community First Choice state plan option authorized under 1915(k) of the Social Security Act, which allows states to provide home- and community-based attendant services and supports; (3) state plan HCBS authorized under 1915(i) of the Social Security Act; and (4) state plan personal care services, authorized under section 1905(a)(24) of the Social Security Act. Not all coverage of assisted living services must be provided statewide.
Some states used a combination of Medicaid authorities to cover assisted living services, sometimes through multiple programs each targeted to specific populations. For example:
· Combination of HCBS waiver and state plan. Washington used an HCBS waiver to cover assisted living services for older adults and people with disabilities who have increased mental health, cognitive impairment, or substance use treatment needs. The state also used state plan authority, including the Community First Choice state plan option, to cover assisted living services for individuals, including older adults and people with disabilities, who do not have these increased needs.
· Combination of HCBS waiver and Medicaid demonstration. Florida used an HCBS waiver in combination with a Medicaid demonstration to cover assisted living services for older adults and people with disabilities. The state used the Medicaid demonstration to cover certain individuals with higher assets than would otherwise be eligible under the state’s HCBS waiver.
State coverage of assisted living services for older adults and people with disabilities has remained generally stable over the last decade. We previously reported that 45 states covered assisted living services for older adults, and 43 states did so for people with physical disabilities in 2014.[41]
States’ Coverage of Assisted Living Services Under HCBS Waivers Varied
Among the 29 states that covered assisted living services under HCBS waiver authority, our review of waiver approval documents showed some state differences in approaches to coverage.
Number of beneficiaries served. The 29 states varied in the numbers of older adults and people with disabilities to whom the state expected to provide assisted living services annually, according to their waiver approvals.[42] For example, 12 states expected to provide assisted living services to less than 2,000 individuals each year. In contrast, four states—California, Florida, Indiana, and Wisconsin—expected to serve over 20,000 beneficiaries annually.[43]
Priority populations. States varied in which populations receive priority for coverage for HCBS services, which would include assisted living services, when the states reach the caps on enrollment for their waivers. While these caps are not specific to how many people can receive assisted living services, the way states choose to prioritize may affect access to assisted living services.
· At least two-thirds of the states (22 of 29) had a system for prioritizing waiver enrollment if caps were reached and waiting lists became necessary.[44] For example, 14 of the 22 states indicated they prioritize enrollment on a first-come, first-served basis in at least one waiver.[45] Under this approach, the longest waiting individual is placed at the top of the list and receives the next available waiver slot. The eight remaining states reported they would prioritize individuals based on factors such as place of residence or imminent need for HCBS waiver services. Under this approach, states may prioritize individuals who are transitioning out of nursing homes or are at risk of institutionalization, for example.
· More than one-third of states (13 of 29) reserved HCBS waiver slots for select populations.[46] For example, Utah set aside 540 of its 2,500 waiver slots for individuals wishing to transition out of an institutional setting, such as a nursing home, and into a community-based setting. Montana reserved 28 of its almost 2,800 annual waiver slots for residents of assisted living facilities who have depleted their financial resources and are at risk of eviction or nursing home placement.
Income eligibility criteria. The 29 states varied in the income eligibility limits they set in their HCBS waivers and whether certain income may be disregarded in meeting eligibility requirements.[47]
· Most of the states (27 of 29) provided eligibility for HCBS waiver services to individuals with incomes up to 300 percent of the SSI federal benefit rate, known as the special income level.[48]
· Most of the 29 states (26 of 29) allowed individuals with income above the state eligibility limit to become eligible for HCBS waiver services by disregarding certain income used for health care services or held in trust to pay for health care services.[49]
Maintenance allowances. States also varied in the amount of income they allowed beneficiaries to keep for personal needs, such as room and board, also known as maintenance allowances; the remainder of their income would be used to pay for the cost of their care.[50] For example, Arkansas allowed beneficiaries to retain income up to 200 percent of the SSI federal benefit rate, while Maryland allowed beneficiaries to retain income up to 300 percent of the SSI federal benefit rate.
Covered services. While all 29 states covered assistance with activities of daily living and supportive services as part of their assisted living services, some states covered enhanced services for higher need individuals. For example, Washington covered behavioral health supports, such as mental health provider coordination or crisis prevention planning, as part of its assisted living services. Its program targets older adults and people with disabilities who have increased mental health needs.
Service costs. State estimates of daily costs of providing assisted living services in waiver year 2024 generally ranged from $50 a day to more than $150 a day across the 27 states for which such estimates were available.[51] This variation may reflect differences in the types of services facilities provide in that state, and expected service needs of beneficiaries.[52] According to CMS officials, rate setting typically considers the acuity level of the covered population. For example, states serving beneficiaries with specialized dementia care or behavioral health needs may pay higher rates to assisted living facilities.[53]
Despite the variation, states expected annual costs per beneficiary for assisted living services to be generally lower than their estimated costs for nursing home care.[54] For example, New Hampshire estimated the average annual cost to the Medicaid program for nursing home care in waiver year 2025 at $55,697 per beneficiary, compared to an estimated annual cost to Medicaid for assisted living services per beneficiary of $11,340.
Selected States Took Steps to Increase Medicaid Beneficiaries’ Access to Assisted Living Services
Our four selected states that covered assisted living services for older adults and people with disabilities used various strategies to increase access to Medicaid-covered assisted living services.[55] These states’ efforts focused on helping beneficiaries afford room and board costs and increasing the number of assisted living facilities that participate in Medicaid.
Room and board. The four selected states used a variety of strategies to help Medicaid beneficiaries afford room and board costs not covered by their Medicaid programs. For example, Oregon officials said that their state uses state-only funds, that is, funds for which the state does not receive federal Medicaid matching funds, on a limited basis to help certain Medicaid beneficiaries with the costs of room and board. Illinois requires assisted living facilities participating in Medicaid to align their rate for room and board with the SSI federal benefit rate. According to Illinois officials, the state also provides assisted living services in buildings developed with low-income housing tax credits. Connecticut provides assisted living services in federally subsidized housing developments allowing for lower-cost housing options for Medicaid beneficiaries, according to state officials.
Assisted living facility participation. The four selected states used a variety of strategies to encourage assisted living facilities to participate in Medicaid. For example, Connecticut, Illinois, and Oregon used tiered payment rates, with higher rates paid for beneficiaries with higher needs or for different geographic locations. (See table 3.) Beyond tiered rates, New Mexico officials told us the state is taking steps to streamline facilities’ administrative requirements by simplifying their credentialing and licensing processes to encourage more facility participation.
|
State |
Description of tiered rates for 2025 |
|
Connecticut |
Rates are set according to the intensity of care required, from $30.60 per day to $91.35 per day. |
|
Illinois |
Rates are set based on geographic regions, from $130.55 per day to $220.68 per day. |
|
Oregon |
Rates are set according to five tiers of care ranging from $64.07 per day to $150.43 per day. |
Source: GAO analysis of state documents. | GAO‑26‑107884
Notes: Assisted living services refer to assistance with activities of daily living—such as eating, bathing, and toileting—and other supportive services provided in an assisted living facility. Rates reflect states rate setting documentation.
Stakeholders Cited Limits in Coverage and Provider Participation as Key Factors Affecting Access to Federally Funded Assisted Living Services
Officials from the five state Medicaid agencies and representatives of the seven national organizations we interviewed told us that coverage limits, including the lack of coverage outside of the Medicaid program as well as coverage limits within Medicaid; challenges with assisted living facility participation (i.e., limited provider participation); and a changing demographic and policy landscape may affect access to federally funded assisted living services.
Lack of coverage outside of Medicaid. Representatives of national organizations highlighted that the lack of coverage outside of Medicaid affects access to federally funded assisted living services. Representatives of two national organizations noted that the lack of coverage of assisted living services by federal programs other than Medicaid particularly affects “the forgotten middle”—individuals who cannot afford the high cost of private pay assisted living services but whose income is too high to qualify for Medicaid coverage. Representatives of one national organization noted that many consumers are unaware that Medicare generally does not cover assisted living services. A representative from another national organization noted that in some states, there is no pathway to obtain federally funded coverage of assisted living services as state Medicaid programs are not required to cover these services.[56]
Coverage limitations within Medicaid. Officials from selected states and representatives of national organizations told us that limits to Medicaid coverage for assisted living services affect access even in those states that cover these services under Medicaid.
· Officials from four states and representatives of five national organizations discussed room and board costs and the lack of Medicaid coverage to help pay for them as key factors limiting access to federally funded assisted living services.[57] Officials from two of these states highlighted that the room and board costs can be unaffordable for those eligible for Medicaid. Representatives of a national organization said that the lack of funding for room and board under Medicaid leads to the perception of access to assisted living services through the Medicaid program on paper, but not in practice. As previously noted, the four selected states that cover assisted living services under Medicaid reported taking steps to help beneficiaries pay for the cost of room and board.
· Officials from two states and representatives of three national organizations noted that state-set caps on the number of people the state will enroll in an HCBS waiver program—which is allowable under federal law—can prevent access to individuals who would otherwise qualify for assisted living services under Medicaid.
Provider participation challenges. Officials from selected states and representatives of national organizations cited limited participation in Medicaid by assisted living facilities as a key factor affecting access.
· Officials from two states and representatives of four national organizations said that low Medicaid payment rates limit assisted living facility participation. For example, officials from one state and representatives from one organization said that Medicaid payment rates for assisted living services are often about one-third the amount paid by private payers, which they indicated disincentivizes serving Medicaid beneficiaries. Representatives from one national organization said that because few assisted living facilities accept states’ Medicaid payment rates, eligible beneficiaries may be diverted to nursing homes.
· An official from the selected state that did not cover Medicaid assisted living services, described concerns about the ability to attract sufficient participation from assisted living facilities should the state begin covering services in the future. This official noted that it is more difficult to sustain an assisted living facility in areas that are more rural and also noted that facilities require a sufficient volume and mix of Medicaid and private pay residents to do so. Officials from two additional states said that rural areas in their states may not have a sufficiently large or wealthy population to sustain assisted living facilities, as these facilities primarily rely on private rather than Medicaid payments.
· Officials from two states and representatives of two national organizations told us that long-term care workforce shortages may limit the pool of assisted living facilities that are appropriately staffed to serve Medicaid beneficiaries. Representatives from one national organization said some assisted living facilities may not have access to a sufficiently trained workforce to serve Medicaid beneficiaries who increasingly have higher, more complex care needs. Representatives of the national organization also told us that temporary enhanced federal Medicaid funding during the COVID-19 pandemic was used by states to invest in their HCBS workforce. CMS noted that all states used these funds to support workforce recruitment and retention, among other activities.[58]
Changing landscape. Officials from selected states and representatives of national organizations said that the landscape around assisted living services is changing, likely increasing the demand for assisted living services, even as states’ capacity to fund coverage for the services may decrease.
· Officials from four selected states and representatives of four national organizations indicated that the aging of the population will increase the need for assisted living services. Furthermore, according to representatives of two national organizations, a growing number of individuals will face affordability challenges in paying for these services. This will further increase the demand for Medicaid-covered assisted living services.
· Officials from one selected state and representatives of four national organizations said that federal legislation enacted in July 2025 may affect access to assisted living services under Medicaid in future years.[59] These state officials and representatives of national organizations expressed concerns that the legislation will result in reductions in federal Medicaid funds for states, which could affect states’ ability to cover optional Medicaid benefits, such as assisted living services. On the other hand, the legislation also expanded coverage options for assisted living services by creating a new HCBS waiver option under which states can provide services for individuals who do not require an institutional level of care, such as in nursing homes.[60]
CMS officials said that the factors identified by stakeholders described above were generally consistent with previous comments stakeholders submitted to CMS. Further, officials noted that access to assisted living services by Medicare beneficiaries is limited by the high cost of services, including room and board, and the lack of insurance coverage to offset these costs. They said that unless a Medicare beneficiary is also eligible for Medicaid, there is little pathway for these beneficiaries to access assisted living services unless the beneficiary is able to pay privately or has long-term care insurance that covers assisted living services. CMS officials also noted that they have heard anecdotally that there are long waiting lists for Medicaid waivers that cover assisted living services, which further reduces access. Officials said that changes in federally funded assisted living services would likely require congressional or individual state action.
Agency Comments
We provided a draft of this report to HHS, HUD, and VA for comment. HHS and VA provided technical comments, which we incorporated as appropriate. HUD did not have any comments on the report.
As agreed with your offices, unless you publicly announce the contents of this report earlier, we plan no further distribution until 30 days from the report date. At that time, we will send copies to the appropriate congressional committees, the Secretary of Health and Human Services, the Secretary of Housing and Urban Development, the Secretary of Veterans Affairs, and other interested parties. In addition, the report is available at no charge on the GAO website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at RosenbergM@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix IV.

Michelle B. Rosenberg
Director, Health Care
List of Requesters
The Honorable Kirsten Gillibrand
Ranking Member
Special Committee on Aging
United States Senate
The Honorable Richard Blumenthal
United States Senate
The Honorable John Fetterman
United States Senate
The Honorable Mark Kelly
United States Senate
The Honorable Raphael Warnock
United States Senate
The Honorable Elizabeth Warren
United States Senate
To describe federal spending for services provided in assisted living facilities, we analyzed Centers for Medicare & Medicaid Services (CMS) claims data for calendar year 2024. We conducted separate analyses for Medicaid and Medicare spending.
Medicaid Spending
To describe federal Medicaid spending for services provided in assisted living facilities, we analyzed claims data from CMS’s Transformed Medicaid Statistical Information System (T-MSIS) for calendar year 2024, the most recent year of data available.[61] We included claims with a start date during calendar year 2024.[62] We analyzed data for all states and the District of Columbia, including both fee-for-service claims and claims submitted by health plans (referred to as encounter claims).[63] However, we excluded eight states from certain analyses as described further below.
Identification of claims for services provided in assisted living facilities. Assisted living facilities are not a uniformly defined provider type that can be consistently identified in Medicaid claims data, and the definition of and terminology for assisted living facilities may vary across states.[64] We limited our analysis to claims that included codes that directly referenced assisted living facilities or services.[65] The claims for services provided in assisted living facilities could include any type of service provided in an assisted living facility, including services outside of home- and community-based services.
· Place of service code. We included claims with a place of service of “assisted living facility.”[66]
· Provider taxonomy code. We included claims with a billing provider or servicing provider taxonomy code that included the term “assisted living facility.”[67]
· Procedure code. We included claims with procedure codes for “assisted living; waiver” that did not have conflicting provider taxonomy information.[68]
We excluded claims from the analysis in instances where the procedure or provider codes indicated assisted living facility services or providers, but the place of service was coded as an institutional setting, such as a nursing home.[69]
Analysis of federal Medicaid spending. We identified total federal-state Medicaid spending reported in claims for services provided in assisted living facilities that we identified as described above. This spending included both fee-for-service payment amounts and payment amounts that health plans reported paying to providers on encounter claims.[70] We calculated the federal portion of the total federal-state Medicaid spending amount based on states’ fiscal year 2024 federal medical assistance percentages.[71] The results of the analysis are likely an undercount of federal spending because the analysis did not account for increased federal matching available for certain services or populations. In addition, it is also likely an undercount because assisted living facilities are not a uniformly defined provider type and states may refer to them using different terms. As such, states may vary in the extent to which assisted living place of service, provider type, and procedure codes identify assisted living facilities.[72] For example:
· We identified eight states where our analysis likely did not identify most spending for services provided in assisted living facilities. We identified these states because, for example, per-beneficiary spending was low and overall identified spending was lower than available information such as state cost estimates for Medicaid assisted living services. These states were Connecticut, Maryland, Massachusetts, New York, Tennessee, Vermont, Washington, and Wisconsin. We included the spending that we were able to identify from these states in the total amount of identified Medicaid spending for services provided in assisted living facilities. However, we excluded these states from our analysis of per-beneficiary spending.
· In the remaining states, the analysis may not have identified all spending for similar reasons. For example, we did not identify spending for services provided in assisted living facilities to the extent that providers used a different place of service code, such as “home,” and were not already included in the analysis based on provider or procedure codes.
Analysis of beneficiary characteristics. Among beneficiaries that our analysis identified who received services in assisted living facilities in 2024, we reviewed age, dual eligibility for Medicare and Medicaid, and whether beneficiaries were eligible for Medicaid on the basis of Supplemental Security Income (SSI). Individuals who were eligible for Medicaid on the basis of age or disability in states where Medicaid eligibility criteria are more restrictive than SSI eligibility criteria are included as eligible based on SSI.
Data reliability. To assess the reliability of T-MSIS data, we interviewed CMS officials and reviewed documentation, such as technical documentation from CMS describing the data and CMS’s assessment of its quality. We also tested the T-MSIS data for obvious errors and missing information. In addition, we compared the results of our analysis to available related documentation. This included state Medicaid program approval documents in certain states that provide cost estimates for assisted living services, and other state documentation, such as billing guidance for assisted living services. Based on our assessment, we determined the combination of data elements we used to identify claims for services provided in assisted living facilities—place of service codes, procedure codes, and provider taxonomy codes—were sufficiently reliable for the purposes of our analysis, and we accounted for data limitations in our reported results.
Medicare Spending
To describe Medicare spending for services provided in assisted living facilities, we analyzed claims data from CMS’s Integrated Data Repository for calendar year 2024. We included claims with a start date during calendar year 2024.[73] We excluded Medicare Advantage encounter claims due to previously identified data limitations.[74]
Identification of claims for services provided in assisted living facilities and analysis of spending. As noted previously, assisted living facilities are not a uniformly defined provider type that can be consistently identified. We limited our analysis to fee-for-service claims under traditional Medicare that included codes that directly referenced assisted living facilities or services.
· Hospice and home health claims. We included hospice and home health claims with a procedure code for “hospice or home health care provided in an assisted living facility.”
· Other fee-for-service claims. We included fee-for-service claims for other Medicare services with a place of service code for “assisted living facility.”
We excluded claims that did not have a Medicare payment amount greater than zero. We also excluded claims that included multiple sites of service on the same claim.
We totaled the payment amounts from the identified claims to determine Medicare spending for services provided in assisted living facilities and used claim types and procedure codes to assess spending by type of service. The results of the analysis are likely an undercount of total Medicare spending for services provided in assisted living facilities, due to the exclusion of Medicare Advantage encounter claims. (Approximately half of Medicare beneficiaries were enrolled in Medicare Advantage in 2024.) The largest category of spending—spending for hospice services—is likely more complete because hospice services are generally paid under traditional Medicare.[75] The identified spending for other services is less complete because those services can be paid for through Medicare Advantage. In addition to not capturing spending under Medicare Advantage, our analysis did not identify spending for services provided in an assisted living facility to the extent that providers may have identified a different place of service code, such as “home.”
Data reliability. To assess the reliability of the Medicare fee-for-service data, we reviewed documentation, such as technical documentation from CMS describing the claims, and tested the data for obvious errors and missing information. Based on our assessment, we determined that the fee-for-service Medicare claims data were sufficiently reliable for the purposes of our analysis, and we accounted for data limitations in our reported results.
HUD does not directly fund services provided in assisted living facilities. However, HUD operates rental assistance programs that may be used in assisted living facilities or that may be used in coordination with Medicaid coverage of assisted living services.[76] For example, the Housing Choice Voucher Program helps low-income people afford housing in the private market. Program participants may live in an eligible housing unit, including in an assisted living facility, with rent partially covered by a subsidy.[77] HUD officials noted that in practice, however, payment limits for the Housing Choice Vouchers often constrain their use for this purpose. See table 4 for additional information about use of HUD programs in assisted living facilities.
Table 4: Department of Housing and Urban Development (HUD) Rental Assistance Programs That May Fund Services in Assisted Living Facilities
|
Rental assistance program |
Description |
Use in assisted living facilities |
|
Housing Choice Voucher Program |
The Housing Choice Voucher Program provides subsidies for eligible low-income households to rent a unit in the private market. Additional “special purpose” vouchers are targeted to particular populations, such as veterans or people with disabilities. Project-based vouchers are also a component of the program, where public housing agencies receiving HUD program funds contract with housing owners to reserve units for voucher holders. The rental subsidy is connected to the property rather than the tenant. |
Program participants can use housing choice vouchers in an assisted living facility. The cost of meals and assisted living services cannot be included in the rent payment and must be paid through other sources. According to HUD officials, program data are not available to track use of these vouchers in assisted living facilities or to provide a complete count of assisted living facilities that contract with public housing agencies to provide project-based vouchers. |
|
Supportive housing programs |
The Section 202 Supportive Housing for the Elderly program provides capital advances and project-based rental assistance contracts to nonprofit organizations to help create affordable rental housing for eligible households with one or more persons aged 62 or older. This usually includes a service coordinator who links residents at Section 202 properties to supportive services in the community to allow them to live independently in an environment that provides supports such as cleaning, cooking and transportation. Additionally, owners can use up to $15 per unit per month for providing supportive services. The Section 811 Supportive Housing for People with Disabilities program provides capital advances and project-based rental assistance contracts to nonprofit organizations to help create affordable rental housing for eligible households with disabilities, among other activities. |
Supportive housing program funding may not be used in operating or developing an assisted living facility, according to HUD officials. However, these properties may partner with agencies that provide Medicaid assisted living services to residents. For example, Connecticut does not license and regulate assisted living facilities; instead, the state licenses and regulates “assisted living service agencies.” These agencies can provide services in HUD-subsidized housing. HUD officials did not have information on the number of properties that partner with agencies that provide Medicaid assisted living services. |
|
Public Housing program |
The Public Housing program provides government-owned housing for eligible low-income households. |
Medicaid programs may partner with public housing agencies to provide Medicaid assisted living services in public housing projects, according to HUD officials. HUD officials said that they understand that such partnerships exist but did not have a way to quantify their extent. |
Source: GAO analysis of HUD program documentation and written responses from HUD officials. | GAO‑26‑107884
Note: State and local public housing agencies administer the Housing Choice Voucher and Public Housing programs.
VA provides long-term care services for eligible veterans, but this does not include assisted living services. However, VA funds several programs that may support veterans who are residents of assisted living facilities. For example, VA provides an extra monthly payment for eligible veterans that can be used to offset the cost of long-term care, including in assisted living facilities. See table 5 for more information on VA programs that may fund services provided in assisted living facilities.
Table 5: Department of Veterans Affairs (VA) Programs That May Fund Services Provided in Assisted Living Facilities
|
Type of program |
Description |
Use in assisted living facilities |
|
Aid and Attendance benefits |
VA offers eligible veterans two types of Aid and Attendance benefits depending on their circumstances. One is part of the VA pension program, available to wartime veterans (or surviving spouses) with nonservice-connected disabilities who meet income and net worth limits and require help with daily living activities. The other is Special Monthly Compensation based on Aid and Attendance, which is available to certain veterans with service-connected disabilities who need daily assistance. According to agency officials, there are no specific requirements for how veterans spend the benefits, and thus their use may include offsetting the cost of assisted living services. |
According to VA officials, data on this benefit do not indicate whether the veteran is residing at an assisted living facility. Officials reported that about 50,000 veterans received Aid and Attendance benefits in fiscal year 2023. |
|
Health care services |
VA may provide extra home- and community-based health care services to eligible veterans, including those residing in assisted living facilities. The extra services include home-based primary care, skilled home health care, and homemaker or home health aide services. For veterans residing in assisted living facilities, VA only provides those services that are not already offered by the assisted living facility, according to agency officials. |
According to VA officials, agency data on provision of these services do not indicate whether they were provided at an assisted living facility. |
|
Community Residential Care Program |
Through this program, VA provides health care supervision to veterans who are unable to live independently due to medical or psychosocial health conditions and who have no available family to provide care and support. VA recruits, screens, and inspects facilities participating in the program, which could include assisted living facilities. VA program staff then refer veterans interested in assisted living services to participating facilities and may assist them in selecting a facility. VA then provides continued oversight of the facility as well as case management services to the veterans. Veterans are responsible for the cost of assisted living care. |
According to VA officials, data on this program do not indicate whether the veteran is residing at an assisted living facility. In fiscal year 2023, the program served 1,956 veterans in 378 facilities. |
|
Department of Housing and Urban Development-Veterans Affairs Supportive Housing (HUD-VASH) program |
This program provides assistance to homeless veterans in the form of VA case management and clinical services coupled with HUD housing choice rental vouchers, which may be used in assisted living facilities. |
VA officials said they were aware of a small number of veterans receiving these services in assisted living facilities in fiscal year 2023, but VA does not comprehensively track this number. |
Source: GAO analysis of VA documentation and interviews with VA officials. | GAO‑26‑107884
While VA did not directly cover assisted living services at the time of our review as of March 2026, legislation enacted in January 2025 included a provision for a new pilot program to assess the effectiveness and satisfaction of eligible veterans receiving assisted living services.[78] Under the legislation, the pilot program will operate in two of VA’s regional systems of care, will serve up to 60 veterans in each region, and must begin no later than two years after enactment. VA officials told us that they have begun work to identify sites to participate in the pilot and do not have a specific time frame for when the pilot will begin, apart from meeting the statutory deadline. According to VA officials, VA previously conducted an assisted living pilot program from 2002 to 2004. In its report for the pilot, VA found that assisted living services could be an important element of its long-term care services but noted barriers to implementing them, such as contracting challenges and the high cost of care.
GAO Contact
Michelle B. Rosenberg, RosenbergM@gao.gov
Staff Acknowledgments
In addition to the contact named above, Susan Barnidge (Assistant Director), Kate Nast Jones (Assistant Director), Emily Beller Holland (Analyst-in-Charge), and Elise Pressma made key contributions to this report. Other contributors included Laura Elsberg, Kaitlin Farquharson, Elizabeth Flow-Delwiche, Dan Lee, Sang Lee, Jeff Tamburello, Brienne Tierney, and Ethiene Salgado-Rodriguez.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]For example, the 85 and older population is projected to more than double from 6.5 million in 2022 to 13.7 million in 2040. See Administration for Community Living, 2023 Profile of Older Americans (Washington, D.C.: May 2024).
[2]In this report, references to states include the District of Columbia.
[3]For example, some states use the term assisted living for licensing certain facilities while using a different term for residential facilities that provide assistance with activities of daily living under Medicaid. Other states may use different terms for facilities based on other distinctions, such as whether they offer shared or private rooms.
[4]Our use of the term “assisted living facility” includes settings where agencies that provide assistance with activities of daily living and other supportive services may be licensed separately from the residential facility. For example, at least one state does not license assisted living facilities, but licenses assisted living service agencies to provide services in residential facilities that meet certain requirements.
[5]Medicaid is a joint federal-state program that finances health care for certain low-income and medically needy individuals. As of November 2025, Medicaid enrollment totaled about 68.8 million individuals.
[6]This restriction is codified in multiple regulatory provisions. See, e.g., 42 C.F.R. § 441.310(a)(2) (providing that federal financial participation is not available for the cost of room and board with certain exceptions, such as for respite care services).
[7]Medicare is the federally financed health coverage program for people 65 and older, certain individuals with disabilities, and people with end-stage renal disease. As of November 2025, there were 69.7 million Medicare beneficiaries.
[8]Medicare coverage options include traditional Medicare, where Medicare pays claims directly to providers under fee-for-service, and the Medicare Advantage program, a private health plan alternative to fee-for-service Medicare. We did not analyze Medicare encounter claims submitted by health plans due to data limitations. For purposes of this report, we use the term “traditional Medicare” to refer to services delivered on a fee-for-service basis.
[9]Our review focused on federal spending for services provided in assisted living facilities, including assisted living services, other health care services that may be provided in these facilities, and room and board. We did not include federal spending for development or construction of assisted living facilities.
[10]Medicaid coverage of assisted living services may be authorized under various sections of the Social Security Act. For example, under section 1915(c), the Secretary of Health and Human Services may waive certain Medicaid requirements, allowing states to target services to specific groups and limit the number of beneficiaries served. These waivers are known as HCBS waivers. Our review of state Medicaid program coverage of assisted living services did not include services that may be provided by Medicaid health plans or programs in lieu of, or in addition to, Medicaid-covered services.We identified that a state covered assisted living services based on service descriptions that aligned with the definition of assisted living services in CMS waiver guidance. This included services that states refer to by state-specific service names in their approval documents, such as supportive living programs. We included personal care or attendant care services with an assisted living facility provider. States may also use different terms for assisted living facilities. States where we did not identify coverage of assisted living services may cover services, such as personal care services provided by outside providers, or other services, such as residential habilitation, for individuals who live in assisted living facilities.
[11]Our analysis of HCBS waivers included waivers that (1) provide services for individuals who would otherwise require services at the level of a nursing home, (2) provide services in a residential setting other than the personal home of the individual, and (3) include the “aged or disabled, or both—general” target group, which generally includes adults aged 65 and older and individuals with physical or other disabilities age 64 and under. We refer to individuals in this general target group as older adults and people with disabilities.
[12]The five selected states were Connecticut, Illinois, New Mexico, Oregon, and South Carolina.
[13]States vary in the term they use for assisted living facilities. In addition to assisted living, states may refer instead to personal care homes, boarding homes, residential care facilities, adult homes, and homes for the aged, among others.
[14]See Centers for Disease Control and Prevention, National Center for Health Statistics, Table 1: Post-Acute and Long-Term Care Providers by Geographic and Organizational Characteristics, United States, 2022. Data tables are from the National Post-Acute and Long-Term Care Study. Residential facilities included in the study were those with at least four beds that serve a predominately adult population and were licensed or regulated by the state to provide room and board, around the clock on-site supervision, and help with activities of daily living or other health-related services such as medication management. Facilities that were licensed to exclusively serve individuals with severe mental illness or intellectual and developmental disabilities were not included in the study.
An estimated 1 million Americans were living in such facilities in 2022, according to the National Post-Acute and Long-Term Care Study. See Melekin A, Sengupta M, Caffrey C. Residential care community resident characteristics: United States, 2022. National Center for Health Statistics Data Brief, no. 506. (Hyattsville, Md: National Center for Health Statistics, 2024).
[15]The survey identified assisted living facilities according to the licensure requirements of the state, noting that terms may vary across states, and defined this setting as residential arrangements providing personal care and health services, in which the level of care may not be as extensive as that of a nursing home. The costs reflect rates for a one-bedroom, single occupancy unit. See CareScout, Cost of Care Survey, 2025, Ranked Median Costs by State Data Tables (CareScout Holdings, Inc. 2026).
[16]Federal and state Medicaid spending totaled $871.7 billion in 2023, according to estimates from CMS’s Office of the Actuary.
[17]In 2023, federal and state Medicaid spending for long-term care, also referred to as long-term services and supports in Medicaid, totaled $228.6 billion, with home- and community-based services accounting for $145.9 billion and institutional services accounting for $82.7 billion. See Carpenter, Alexandra, Cara Stepanczuk, Caitlin Murray, and Andrea Wysocki. Trends in Users and Expenditures for Home and Community-Based Services as a Share of Total Medicaid Long-Term Services and Supports Users and Expenditures, 2023. (Mathematica, Oct. 17, 2025). This research brief was prepared by Mathematica under contract with CMS.
[18]States define the criteria used to determine whether individuals need an institutional level of care.
[19]For example, there are different financial eligibility rules for older adults and people with disabilities, and people who need long-term care, compared to other adults and children. To meet the financial eligibility criteria applicable to HCBS waivers, individuals must have income and resources that fall below established levels, which may vary by state, but are within standards set by the federal government.
[20]Most assisted living facility residents are estimated to be age 65 or older, and therefore likely eligible for Medicare. See Melekin, Sengupta, and Caffrey. Residential care community resident characteristics: United States, 2022.
[21]Home health agencies and hospices must be separately certified and approved for Medicare participation.
[22]For 2025, the SSI federal benefit rate was $967 per month for an individual and $1,450 for a couple.
[23]We calculated the federal portion of identified federal and state Medicaid spending using fiscal year 2024 state federal medical assistance percentages. The calculation does not account for increased federal matching available for certain services or populations. Examples of other Medicaid-covered services that can be provided in assisted living facilities include physical therapy, home evaluation visits, or psychotherapy sessions.
[24]In one state, for example, we identified Medicaid billing guidance for assisted living services that instructed providers to code the place of service as a custodial care facility. Use of the “custodial care facility” place of service code identified $26 million in spending, compared to our analysis which identified $280,000. We did not determine whether this code may also be used for other types of facilities. The billing guidance also included state-specific procedure codes for assisted living services, which identified $27 million in spending, most of which was part of the $26 million in spending identified under the custodial care facility place of service code. Incorporating state-specific coding practices across states was beyond the scope of our analysis.
[25]For our analysis, the term assisted living services refers to assistance with activities of daily living and other supportive services provided in assisted living facilities. Thus, the amount of spending for assisted living services includes spending for assisted living or general personal care and attendant care services. This does not capture all potential spending for such services, because states may use different codes for such services.
[26]In addition, the study found that while 17 percent of all assisted living residents were Medicaid beneficiaries, the percentage of residents with Medicaid varied by age. Among all assisted living residents under age 75, 32 percent were Medicaid beneficiaries, compared to 19 percent of residents aged 75 to 84, and 12 percent of residents who were aged 85 and older. See Melekin, Sengupta, and Caffrey, Residential care community resident characteristics: United States, 2022.
[27]Receipt of SSI is one eligibility pathway for Medicaid in most states. This group does not necessarily account for all Medicaid beneficiaries who may be receiving SSI benefits.
[28]In addition to not capturing spending under Medicare Advantage, our analysis did not identify spending for services provided in an assisted living facility to the extent that providers may have identified a different place of service code, such as “home.” This amount also does not include payments for services provided in assisted living facilities when other sites of service were also included on the same claim.
[29]Identified spending from hospice claims is more complete because once a beneficiary enrolled in a Medicare Advantage or other health plan elects the hospice benefit, their hospice-related benefits are paid under traditional Medicare and thus are included in our analysis.
[30]Approximately half of Medicare beneficiaries were enrolled in Medicare Advantage in 2024. We did not analyze the Medicare Advantage data due to data limitations. We and others previously identified data limitations with Medicare Advantage encounter data. See Medicare Payment Advisory Commission, Report to the Congress: Medicare Payment Policy (Washington, D.C.: Mar. 2026); GAO, Medicare Advantage: Continued Monitoring and Implementing GAO Recommendations Could Improve Oversight, GAO‑22‑106026 (Washington, D.C.: June 28, 2022); and GAO, Medicare Advantage: CMS Should Fully Develop Plans for Encounter Data and Assess Data Quality before Use, GAO‑14‑571 (Washington, D.C.: July 31, 2014).
[31]This range reflects spending for 98 percent of Medicare beneficiaries who received hospice services in assisted living facilities.
[32]This range reflects spending for 98 percent of beneficiaries who received home health services in assisted living facilities under traditional Medicare.
[33]This range represents spending for 98 percent of beneficiaries who received services under traditional Medicare other than hospice or home health in assisted living facilities.
[34]In most states, SSI beneficiaries are automatically eligible for Medicaid. Eight states have Medicaid eligibility criteria that are more restrictive than SSI eligibility criteria, but most SSI beneficiaries are still eligible for Medicaid.
[35]The Housing Choice Voucher Program provides rent subsidies that help eligible low-income individuals afford housing in the private market.
[36]The Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act, enacted in January 2025, included a provision for a new pilot program, to begin no later than two years after enactment, to assess the effectiveness of providing and satisfaction of veterans receiving assisted living services. Pub. L. No. 118-210, § 127, 138 Stat. 2706, 2734-38 (2025) (codified at 38 U.S.C. § 1710B note).
[37]VA offers Aid and Attendance benefits through the VA pension program and offers Special Monthly Compensation based on the need for aid and attendance. The payments are in addition to the VA nonservice connected pension or standard disability compensation.
[38]One of the 44 states covered assisted living services for older adults; while this could include individuals with disabilities, the state did not cover assisted living services for the disabled population aged 64 and under.
[39]States and their coverage approval documents may use different terms for services that we refer to as assisted living services. Therefore, we identified coverage of these services based on service descriptions consistent with CMS’s definition. States that do not cover assisted living services may still cover other services, such as residential habilitation—assistance acquiring the self-help, socialization, and adaptive skills necessary to reside successfully in home- and community-based settings—that may be provided in assisted living facilities.
[40]Some states that used HCBS waiver authority also covered the services under state plan or other authorities.
[41]GAO, Medicaid Assisted Living Services: Improved Federal Oversight of Beneficiary Health and Welfare Is Needed, GAO‑18‑179 (Washington D.C.: Jan. 5, 2018).
[42]States’ waiver approvals include information on the annual expected number of users for each service covered by the waiver, including the number expected to use assisted living services.
[43]The 29 states estimated that approximately 174,000 beneficiaries would receive assisted living services.
[44]States’ waiver approvals described policies for the selection of individuals for entrance to waiver coverage if waiting lists became necessary. However, five states specifically noted that they do not maintain waiting lists. Five states noted that they allow entrance to all eligible applicants.
[45]CMS provides high-level guidance on waiting list management through waiver instructions stating that if a waiting list is implemented, states must have policies in place to govern how individuals are selected for the waiver when a slot becomes available, and that these policies should be objective and applied consistently across the waiver’s service area.
[46]Reserving waiver slots means that some waiver openings are set aside for specific groups of applicants who will be admitted to the waiver on a priority basis.
[47]In assessing eligibility, states consider both income and resources. Resources—cash or real personal property that are owned and can be converted to cash—must be below specified standards that can vary by state.
[48]Under the special income level, states may provide Medicaid benefits to people who require institutional care and have incomes up to 300 percent of the SSI federal benefit rate (which was about 220 percent of the federal poverty level in 2025). In 2025, 300 percent of the highest SSI federal benefit rate amounted to a maximum income eligibility limit of $2,901 per month, or $34,812 per year for an individual.
[49]There are two primary ways states allowed certain income to be disregarded from the state financial eligibility limit. The first is through a medically needy program, which allows individuals with incomes higher than the eligibility limit to subtract the amount they spend on health care expenses from the income counted for Medicaid eligibility purposes. The second is through specialized trusts, sometimes known as “Miller Trusts,” which allow income in the trust to be excluded for Medicaid eligibility purposes. When a Miller Trust is established, the person’s income is deposited into an irrevocable trust which is used to pay for the cost of their care. Upon the person’s death, funds remaining in the Miller Trust are used to reimburse the state’s Medicaid program for the cost of the unreimbursed care.
[50]Individuals who qualify for assisted living services may be required to contribute available income toward the cost of their care.
[51]States’ waiver applications include information on expected costs per unit of service. Most states provided estimates of costs based on expected daily payment rates for the service. Kansas and Michigan were excluded from this analysis because they provided estimated rates per 15 minutes of service. The analysis is based on the lowest daily cost listed in each state’s waivers. Four states’ cost estimates exceeded $150 per day, with the highest estimated at over $350 per day.
[52]The CareScout 2025 Cost of Care Survey found the median private pay daily rate including room and board for a one-bedroom, single occupancy unit in an assisted living facility ranged from $138 to $397, depending on the state. See CareScout, Cost of Care Survey.
[53]For example, specialized dementia care—also called memory care—commands a higher payment rate in Ohio because individuals requiring memory care have a higher level of need for hands-on assistance, redirection, supervision, and cueing when receiving assisted living services.
[54]As part of their request for a HCBS waiver, states must provide an assurance that the estimated average per-capita expenditure for medical assistance under the waiver in any fiscal year does not exceed 100 percent of the average per-capita expenditure that the state reasonably estimates would have been made during the same year for expenditures under the state plan if the waiver not been granted. 42 U.S.C. § 1396n(c)(2)(D).
[55]The four states are Connecticut, Illinois, New Mexico, and Oregon. Our fifth selected state, South Carolina, does not cover assisted living services.
[56]While two stakeholders mentioned other federal programs that may fund assisted living or similar services, such as HUD programs that cover supported living in subsidized housing units or the Program of All-Inclusive Care for the Elderly that combines Medicaid and Medicare funding to serve some beneficiaries in assisted living facilities, they described these as small programs or limited by long waiting lists, and tangential compared to Medicaid-covered services.
[57]As noted earlier, when states choose to cover assisted living services under their Medicaid programs, they are not permitted to cover the cost of room and board.
[58]The American Rescue Plan Act of 2021 provided qualifying states with a temporary 10 percentage point increase to the federal medical assistance percentage for certain Medicaid expenditures for HCBS beginning April 1, 2021, and ending March 31, 2022. Pub. L. No. 117-2, § 9817, 135 Stat. 4, 216-17 (codified at 42 U.S.C. § 1396d note). The act provided approximately $37 billion to states for activities to enhance, expand, or strengthen HCBS. CMS officials said that states were able to spend these funds beyond 2022 and anticipated that most states will expend the funds by the end of federal fiscal year 2026.
[59]The officials and representatives referred to legislation enacted on July 4, 2025, commonly known as the One Big Beautiful Bill Act. They cited, for example, provisions that limit states’ ability to tax providers. These provisions will generally prevent increases to pre-existing health care-related taxes and the imposition of new health care-related taxes, effective October 1, 2026. Pub. L. No. 119-21, § 71115, 139 Stat. 72, 301-02 (2025) (codified at 42 U.S.C. § 1396b(w)(4)). States may use these taxes to finance the nonfederal share of Medicaid spending.
[60]The One Big Beautiful Bill Act allows states to establish a standalone HCBS waiver under section 1915(c) of the Social Security Act for individuals who do not need an institutional level of care, beginning in July 2028. Pub. L. No. 119-21, § 71121, 139 Stat. at 317-19 (codified at 42 U.S.C. § 1396n(c)(11)).
[61]Specifically, we reviewed data from CMS’s T-MSIS Analytic Files, a series of research-ready analytic files CMS created to support analysis, research, and data-driven decisions on key Medicaid topics, as well as program oversight. We reviewed data from the Other Services File, the Long-Term Care File, and the Annual Demographic and Eligibility File. For the purposes of our report, we refer to the T-MSIS Analytic Files as T-MSIS data. We used T-MSIS data as of March 6, 2026. T-MSIS data may change over time as states make updates and corrections to their data.
[62]Some of these claims may include services that occurred in 2025. Additionally, some claims for services that occurred in 2024 may not be included if the claim start date was during calendar year 2023.
[63]Hereafter, references to states include the District of Columbia.
[64]For purposes of this report, we defined assisted living facilities as residential settings that primarily provide assistance with activities of daily living and other supportive services.
[65]This approach relied on the term “assisted living.” We previously found that 48 states reported about $10 billion in federal-state Medicaid spending for assisted living services in 2014 based on a state survey. The survey defined assisted living facilities broadly to include a state or locally regulated and monitored residential care setting that provides or coordinates services to meet residents’ individualized needs. See GAO, Medicaid Assisted Living Services: Improved Federal Oversight of Beneficiary Health and Welfare Is Needed, GAO‑18‑179 (Washington D.C.: Jan. 5, 2018).
[66]Place of service codes are two-digit codes placed on health care professional claims to indicate the setting in which a service was provided. CMS maintains place of service codes used throughout the health care industry, according to the CMS website.
[67]See American Medical Association National Uniform Claim Committee provider taxonomy.
[68]States may use varying national or state-specific procedure codes for Medicaid billing. We identified procedure codes for “assisted living; waiver” as commonly used for services provided in assisted living facilities based on state documentation. We included these claims when the billing or servicing provider taxonomy code was missing or indicated a facility that provides assisted living services.
[69]These excluded claims represented approximately $11 million in identified federal-state spending. We also excluded certain claims that we identified as anomalies where the place of service code was an assisted living facility but the provider was an inpatient hospital.
[70]Our analysis of encounter claims did not include per-enrollee payments that states make to health plans. It included payments to providers for services that health plans reported on Medicaid encounter claims.
[71]The federal medical assistance percentage, which varies by state and is determined by a formula set in statute, is used to reimburse states for the federal share of most Medicaid expenditures.
[72]Incorporating state-specific coding practices across states was beyond the scope of our analysis.
[73]Some of these claims may include services that occurred in 2025. Additionally, some claims for services that occurred in 2024 may not be included if the claim start date was during calendar year 2023.
[74]Medicare coverage options include traditional Medicare, where Medicare pays claims directly to providers under fee-for-service, and the Medicare Advantage program, a private plan alternative to traditional, fee-for-service Medicare. Approximately half of Medicare beneficiaries were enrolled in Medicare Advantage in 2024. We and others previously identified data limitations with Medicare Advantage encounter data. See Medicare Payment Advisory Commission, Report to the Congress: Medicare Payment Policy (Washington, D.C.: Mar. 2026); GAO, Medicare Advantage: Continued Monitoring and Implementing GAO Recommendations Could Improve Oversight, GAO‑22‑106026 (Washington, D.C.: June 28, 2022); and GAO, Medicare Advantage: CMS Should Fully Develop Plans for Encounter Data and Assess Data Quality before Use, GAO‑14‑571 (Washington, D.C.: July 31, 2014).
[75]Once a beneficiary enrolled in a Medicare Advantage or other health plan elects the hospice benefit, their hospice-related benefits are paid under traditional Medicare and thus are included in the analysis.
[76]We refer to assistance with activities of daily living and other supportive services provided in assisted living facilities as assisted living services.
[77]The property owner receives a subsidy, and the household pays the difference between the actual rent charged by the property owner and the housing subsidy.
[78]Senator Elizabeth Dole 21st Century Veterans Healthcare and Benefits Improvement Act, Pub. L. No. 118-210, § 127, 138 Stat. 2706, 2734-38 (2025) (codified at 38 U.S.C. § 1710B note). Veterans eligible for the program are those who are receiving VA-funded nursing home care or requiring a higher level of domiciliary care than that provided by VA but not meeting the requirements for nursing home level of care, and eligible for assisted living services.