Report to Congressional Addressees
United States Government Accountability Office
A report to congressional addressees
Contact: Sharon Silas at silass@gao.gov
What GAO Found
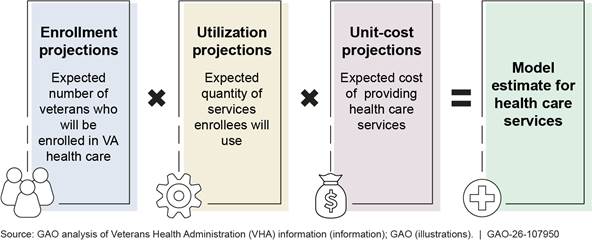
To support its health care budget projection each year, the Veterans Health Administration (VHA) contracts with an actuarial consultant to assist VHA with the annual Enrollee Health Care Projection Model update. The model produces three basic outputs: enrollment, utilization, and unit cost. Each output is subject to several complex adjustments to account for the characteristics of VHA health care and the veterans who access VHA’s health care services.
Basic Outputs of VHA’s Enrollee Health Care Projection Model
GAO found VHA’s processes for developing the model’s estimates align with most but not all relevant standards. For example, VHA’s Office of Enrollment and Forecasting (E&F) does not have a formalized process requiring VHA’s actuarial consultant to incorporate newly emerging data into the model after initial model delivery. According to VHA officials, incorporating newly emerging data after the delivery of its initial model scenario is not required because it depends on factors such as data availability, the timing of the President’s budget, and requests from the VHA Office of Finance. However, incorporating newly emerging data, when possible, could ensure that VHA’s health care cost estimates reflect the most current data, improve the accuracy and completeness of the model estimates, and potentially support a more informed budget request.
VHA uses performance measures to assess its actuarial consultant, but VHA’s standard operating procedure does not specify what E&F staff should be doing to ensure that the consultant adequately performs the tasks outlined in the performance work statement. According to VHA documents, VHA conducts a monthly review of the actuarial consultant’s invoices to ensure it is producing the deliverables laid out in the contract. However, because the invoices only indicate when the work was done, this review does not allow VHA to assess the quality of the consultant’s work. By not including specific oversight tasks in its standard operating procedures, such as establishing a formalized process for assessing the quality of specific tasks in the performance work statement, VHA may miss opportunities to improve the accuracy of its budgetary support provided by its actuarial consultant.
Why GAO Did This Study
VHA, within the Department of Veterans Affairs, serves about 9.1 million enrollees. In its budget request, VHA estimated the fiscal year 2025 medical care total obligational level to be $149.5 billion. Determining needed funding to ensure veterans have access to quality health care involves accurately projecting potential costs.
VHA and its actuarial consultant use a model to project cost estimates for health care services. These estimates are used to inform VA’s budget projection included in the President’s budget request. For fiscal year 2025, VA requested $6 billion in additional funding, beyond the level included in the President’s budget. Given this and that VHA has underestimated its funding needs for health care services in prior years, Congress has raised questions about VHA’s process for developing its budget estimates.
In this report, GAO (1) describes VHA’s current process for updating the actuarial model used to estimate its health care funding needs; (2) examines the extent to which VHA’s processes for developing VA’s health care model estimates align with relevant professional standards; and (3) examines VHA’s oversight of the performance of its actuarial consultant.
GAO reviewed documents from VHA and its actuarial consultant on the processes used to develop health care model estimates, as well as documents for assessing contractor performance. GAO also interviewed VHA officials and VHA's actuarial consultant.
What GAO Recommends
GAO is making five recommendations on VA’s development and oversight of its budget estimate. VA did not provide comments on the report.
Abbreviations
E&F Office of Enrollment and Forecasting
EHCPM Enrollee Health Care Projection Model
OMB Office of Management and Budget
VA Department of Veterans Affairs
VHA Veterans Health Administration
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
June 4, 2026
Congressional Addressees
The Department of Veterans Affairs’ (VA) Veterans Health Administration (VHA) operates one of the largest health care delivery systems in the nation, serving about 9.1 million enrollees through its VHA-operated (i.e., direct care) medical facilities and community health care providers.[1] Determining how much funding the agency needs to ensure veterans have access to quality health care involves projecting potential costs as accurately as possible. Each year, VHA and its actuarial consultant produce an actuarial model, the Enrollee Health Care Projection Model (EHCPM), that VHA uses in its budgeting and planning processes for health care services.[2] VHA uses these model estimates to inform its budget projection for health care services included in the President’s annual budget request.[3]
In July 2024, 4 months after the President submitted the fiscal year 2025 budget request wherein VHA estimated the 2025 medical care total obligation level to be $149.5 billion, VHA informed Congress that it needed additional funding of nearly $12 billion for fiscal year 2025. According to VHA, this increased amount was for health care services, driven by higher-than-expected costs for community care, staffing, medicines, and prosthetics for fiscal years 2024 and 2025. In November 2024, VHA reduced its projected need for fiscal year 2025 to roughly $6.6 billion. As part of the reason for this decrease in additional funding needs, VA reported to Congress that VHA had finished fiscal year 2024 with an additional $2.5 billion in unobligated balances.[4] In mid-March 2025, Congress appropriated to VHA an additional $6 billion using funds from the Cost of War Toxic Exposures Fund.[5] In response to VHA’s projected funding gap in fiscal years 2024 and 2025, along with projected funding gaps in certain fiscal years prior to fiscal year 2024, Congress has raised questions about VHA’s process for developing its budget projection.[6]
Along with the VA Office of Inspector General, we have reported on challenges VA has faced regarding the reliability and accuracy of its budget projection for health care services, as well as its supplemental funding requests.[7] For example, in February 2024, we reported that VA was not prepared to estimate the amount of supplemental funding needed during a catastrophic event, such as the COVID-19 pandemic, because it did not have the modeling capacity to do so.[8]
We performed our work at the initiative of the Comptroller General. In this report, we
1. describe VHA’s current process for updating the actuarial model used to estimate its health care funding needs;
2. examine the extent to which VHA’s processes for developing VA’s health care model estimates align with relevant standards, including actuarial standards of practice and federal internal control standards; and
3. examine VHA’s oversight of the performance of its actuarial consultant.
To describe VHA’s current process for updating the actuarial model used to estimate its health care funding needs, we reviewed documentation provided by VHA and its actuarial consultant, Milliman, describing the actuarial model update process, including procedures such as adjusting for discrepancies between actual workload (i.e., utilization of services) and model estimates. We also interviewed and reviewed written responses from VHA’s Office of Enrollment and Forecasting (E&F) and VHA’s Office of Finance.[9]
To examine the extent to which VHA’s processes for developing VA’s health care cost model estimates align with relevant standards, including actuarial standards of practice and federal internal control standards, we reviewed documentation from VHA and its actuarial consultant on the methods and processes used to develop health care model estimates produced by the EHCPM. For example, we reviewed the annual EHCPM documentation and analysis report, and a model risk assessment report that identifies sources of risk and describes the degree of uncertainty for the projection supporting the VA health care budget. We also reviewed budget impact analyses for fiscal years 2022 through 2025 that examine the drivers responsible for cost increases from the previous year. We interviewed VHA officials from E&F about their processes for communicating data quality and limitations. We also interviewed or received written responses from officials in VA’s Office of Actuarial Services, as well as key program offices including the Office of Integrated Veteran Care; Office of Productivity, Efficiency and Staffing; Pharmacy Benefits Management Services; Prosthetics and Sensory Aids Service; and officials from the Veterans Benefit Administration regarding their involvement in VHA’s budget development process.[10] We assessed these processes against eight relevant actuarial standards of practice.[11] We also identified five federal internal control standards that were relevant to our work.[12]
We examined VA’s actuarial consultant’s role in the actuarial modeling processes in the context of actuarial standards of practice. Our actuarial work on this engagement was conducted by a GAO Assistant Director and Actuary and GAO’s Chief Actuary (identified in the Staff Acknowledgment section of this report) who meet the qualification standards of the American Academy of Actuaries to conduct the actuarial aspects of our work for this report. While we conducted actuarial reviews of VHA’s models and processes, we did not evaluate the accuracy of VHA’s EHCPM model output or their underlying assumptions, as that type of analysis was outside the scope of this report.
To examine VHA’s oversight of the performance of its actuarial consultant, we reviewed VA documentation, including VHA’s standard operating procedure and quality assurance surveillance plan for assessing contractor performance, and the Actuarial Support Services contract and performance work statement that were in effect as of March 31, 2025. We also reviewed documentation related to VHA’s oversight activities, including contractor performance reviews, reviews of invoices, and contractor performance assessment reports for fiscal years 2019 through 2024. To understand the processes in place to monitor and assess contractor performance, we interviewed or received written responses from officials in VHA’s E&F and Office of Finance, and VA’s Office of Management, Office of Actuarial Services, and the Strategic Acquisition Center.[13] We also reviewed documentation and information from VHA officials regarding how oversight responsibilities are defined and executed in relation to tasks and deliverables outlined in the consultant’s performance work statement. We assessed these oversight practices against the Federal Acquisition Regulation, and VA Acquisition Regulation in the context of federal internal control standards for information and communication.[14]
Additional information about our scope and methodology is described in appendix I.
We conducted this performance audit from November 2024 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
Developing VHA’s Health Care Budget Projection Using the EHCPM
In preparation for the annual appropriations process, VHA develops an estimate of the resources needed to provide health care services—known as its health care budget projection—for two fiscal years.[15] For fiscal year 2025, VHA used the EHCPM estimates—known as model estimates—to develop approximately 89 percent of its health care budget projection and uses other methods for the remainder of the projection.[16] For example, the EHCPM projects cost estimates for outpatient and inpatient health care services provided at VHA facilities (i.e., direct care) and available through community providers (i.e., community care).[17] VA uses the health care budget projection to develop its budget request that is included in the President’s budget request for federal agencies.
The EHCPM projects 20 years into the future for health care services. VA uses the model estimates from EHCPM to make projections 3 and 4 years into the future for budget purposes based on data from the most recently completed fiscal year. For example, in 2023, VHA used data from fiscal year 2022 to develop its health care budget projection for the President’s fiscal year 2025 budget request and advance appropriation request for fiscal year 2026.
The EHCPM incorporates assumptions that affect the model estimate over time. The EHCPM produces three basic outputs: enrollment, utilization, and unit cost. Each output is subject to several complex adjustments to account for the characteristics of VHA health care and the veterans who access VHA’s health care services. (See fig. 1.)
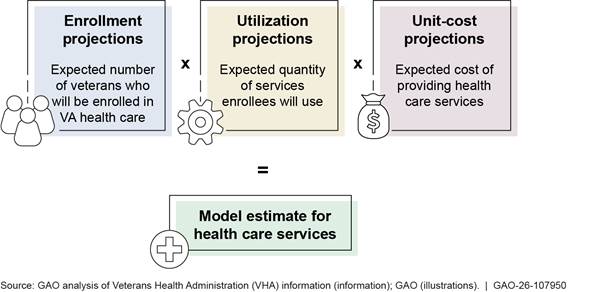
Notes: The EHCPM makes several complex adjustments to projections for VHA health care services to account for the characteristics of VHA health care and enrolled veterans. For example, the EHCPM includes adjustments to account for reliance on the Department of Veterans Affairs (VA) health care—that is, the extent to which enrolled veterans will choose to access health care services through VHA as opposed to other health care programs. Unit costs are the costs to VHA for providing a unit of service, such as a 30-day supply of a prescription or a day of care at a medical facility. The EHCPM produces model estimates to inform its budget projection for health care services that may be revised by the Office of the Under Secretary of Health.
Role of VHA and Its Actuarial Consultant in Developing Health Care Model Estimates
VHA’s E&F is responsible for (1) overseeing work performed by VHA’s actuarial consultant; (2) acting as the liaison between the actuarial consultant and VHA’s finance, leadership, and program offices; (3) gathering VA data and creating various files that are submitted to the actuarial consultant to update the EHCPM; and (4) at the request of VHA’s Office of Finance, VA and VHA leadership, and the Office of Management and Budget (OMB), working with the actuarial consultant to run different scenarios with changes in assumptions—estimates about uncertain future events used to assess risk and make informed decisions—several times a year.
According to VHA’s contract with its actuarial consultant, the consultant provides VHA with EHCPM estimates of VHA health care costs that are used to inform VHA’s budget projection.[18] The consultant’s contracted services include
· annually updating the EHCPM throughout the modeling cycle with VHA health care data, such as workload and cost of health care services, from the most recently completed fiscal year and other newly available data;
· using a variety of tools and methods for conducting technical reviews during the development of the EHCPM for testing and assessing the EHCPM and ensuring that the EHCPM is functioning as intended;
· responding to requests for comparisons of actual to projected enrollment, patients, utilization, and costs;
· providing VA staff and stakeholders, such as OMB and Congress, with trainings, briefings, tools, and databases to provide information about EHCPM methodology, assumptions, and projections; and
· assisting stakeholders, such as OMB and Congress, in understanding the EHCPM and the key drivers of projected veteran demand for VA health care.[19]
VHA’s Budget Projection for Inclusion in the President’s Budget Request
VHA’s annual budget projection—which includes the health care model estimates—is reviewed within VHA, by the Secretary of Veterans Affairs, and finally within OMB to inform the President’s budget request.[20] VHA generally starts to develop a health care budget projection in April of each year, approximately 10 months before the President submits the fiscal year budget request to Congress, which, by law, should occur no later than the first Monday in February.[21]
The VHA budget projection changes during the 10-month budget development process, in part, due to the various levels of review at VA and OMB before the President’s budget request is submitted to Congress. The Secretary of Veterans Affairs considers the health care budget projection developed by VHA when assessing resource requirements among competing interests within VA. OMB considers overall resource needs and competing priorities of other federal agencies to inform decisions on the level of funding to request for VHA’s health care services. OMB passes back decisions, known as a “passback,” to VA and other agencies on their budget projection, along with funding and policy proposals to be included in the President’s budget request.[22] (See fig. 2.)
Figure 2: Timeline for Developing the Budget Projection for VA Health Care Services Included in the President’s Budget Request
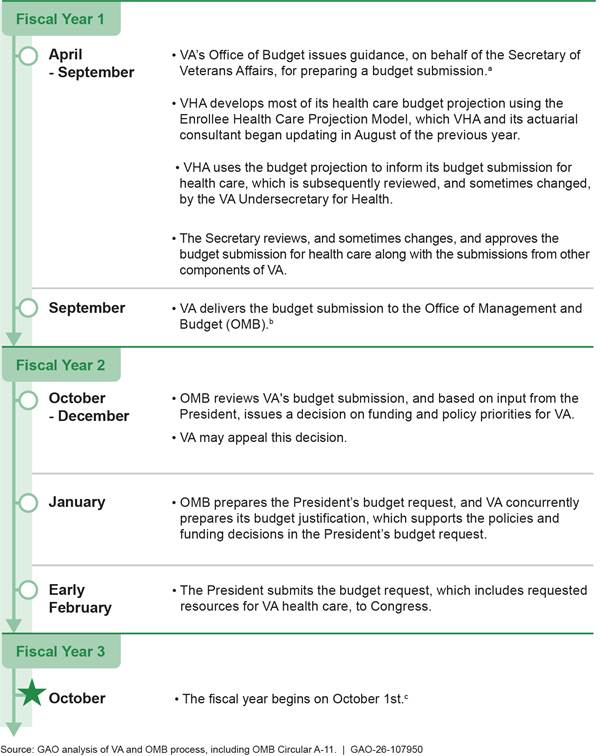
Notes: Under 31 U.S.C. § 1105, the President’s budget submission should be submitted by the first Monday in February. In practice, however, the President’s budget request is sometimes delivered later than early February.
aOMB coordinates the development of the President’s budget proposal by issuing circulars, memoranda, and guidance documents to the heads of executive agencies throughout the federal government. Executive agencies, including the Department of Veterans Affairs (VA), may then prepare their budget requests in accordance with the instructions and guidance provided by OMB. OMB’s Circular A-11, which is updated annually, is an extensive document that contains instructions and schedules for agency submission of budget requests and justification materials to OMB.
bThe VA budget submission includes the Veterans Health Administration’s (VHA) health care budget projection, as well as budget information from other VA components such as the Veterans Benefits Administration and the Office of Information and Technology.
cThis is the fiscal year in which VA is appropriated funds developed in fiscal year one.
Concurrent with OMB’s preparation of the President’s budget request, VA develops its congressional budget justification. The congressional budget justification contains actual obligations for the most recently completed fiscal year at the time of the release, and estimated obligations for the current fiscal year, as well as the 2 years for which appropriations are requested. For example, the VA’s congressional budget justification related to the President’s fiscal year 2025 budget request, which was released in March 2024, contains actual obligations for fiscal year 2023 and estimated obligations for fiscal years 2024 through 2026.
VHA’s Process for Updating its Actuarial Model Estimates Includes Gathering Data and Meeting with Program Offices
To develop its actuarial model estimates to support its health care budget projection each year, at the direction of E&F, VHA’s actuarial consultant conducts an EHCPM update. (See fig. 3.) At the beginning of the EHCPM update, E&F and VHA’s actuarial consultant hold a planning meeting with various VHA program offices, VHA stakeholders, and VHA officials. Each year, E&F and VHA’s actuarial consultant update the EHCPM to account for the most recently completed fiscal year’s actual data, including data on enrollment and health care costs, known as the base year. For example, the base year for the 2023 EHCPM uses fiscal year 2022 actual data to develop cost projections for fiscal years 2025 and 2026 to inform the health care budget request.
Figure 3: VHA Process for Updating the Enrollee Health Care Projection Model (EHCPM) and Model Delivery
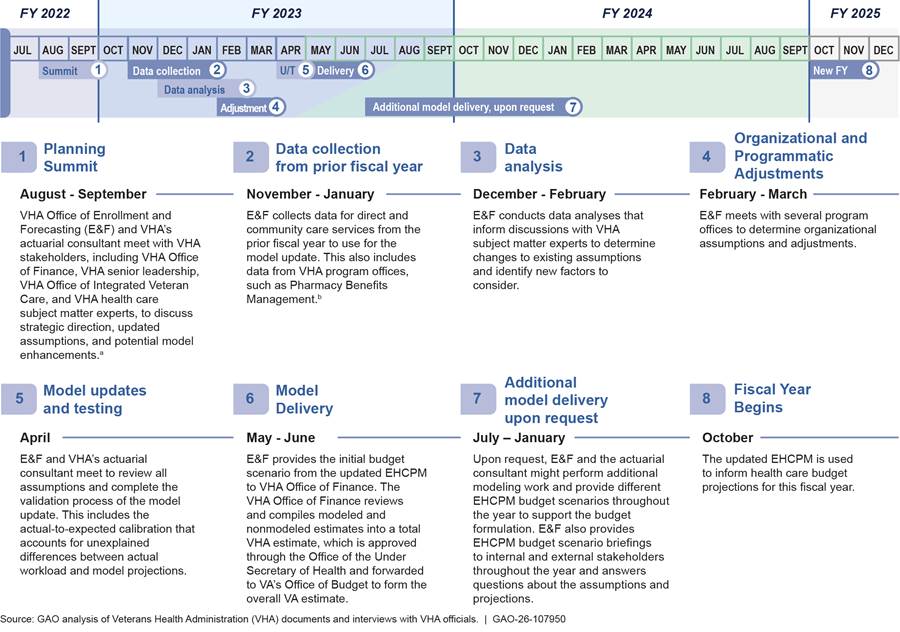
Note: The EHCPM provides health care model estimates for the budget year and the following year’s advance appropriation. For example, the 2023 EHCPM provides estimates for fiscal year 2025 budget and fiscal year 2026 advance appropriation.
aAccording to VHA officials, E&F meets with program offices such as Pharmacy Benefits Management Services; Primary Care; Geriatrics and Extended Care Services; and the Office of Productivity, Efficiency and Staffing.
bThe initial budget scenario includes a budget impact workbook, a report of the model data that includes projected costs for each service category broken out by direct and community care, and a projection supplement workbook that has projections for populations not modeled in the EHCPM.
E&F and VHA’s actuarial consultant update model assumptions—such as projected changes in relative morbidity, and veteran reliance on VHA health care estimates about uncertain future events used to assess risk and make informed decisions. For example, using actual data on currently enrolled and previously enrolled veterans from multiple years, VHA and the consultant might develop assumptions about the impact of a legislative change on enrollment eligibility. The Honoring our PACT Act of 2022 expanded benefits for veterans exposed to certain toxins in the course of their military service, which led to changes in the modeled assumptions for new enrollment and priority transitions.[23] There are three outputs of the EHCPM: enrollment, workload, and costs. The outputs are the projections that change based on assumptions such as enrollee demographic mix, reliance, geographic migration, and impacts of legislative initiatives. These assumptions may be updated or other assumptions added during the EHCPM update.
According to documentation and VHA officials, as part of the EHCPM update and development process, VHA’s actuarial consultant uses tools and methods for conducting technical reviews that test and update the model during the development of the EHCPM. According to VHA officials, this ensures that the EHCPM is functioning as intended. For example:
· Enrollment key driver review. According to VHA documentation, this analysis measures the impact of updates to key drivers using all available years of enrollment data. Each key driver contributes to the change in enrollment from one period to the next, and each is reviewed for material changes over time. If material changes occur, then an explanation is sought through further analysis or engagement with VHA experts. For example, key drivers such as new enrollment, mortality, suspension, reinstatement, ineligibility, priority transitions, and geographic migration are measured on a monthly and annual basis.
· Unit costs and budget reconciliation. According to VHA documentation, as part of each annual update, unit costs—expected costs of providing health care services—are reviewed in relation to unit costs from prior years. As part of the annual update, any services where unit cost levels changed by what VHA considers a moderate amount are reviewed in more detail. Once detailed base year unit costs are calculated, they are loaded into the EHCPM. VHA’s actuarial consultant then conducts a budget reconciliation process by comparing the projected costs (resulting from applying the base year unit costs to the modeled base year utilization) to actual obligations.[24] For example, there are 31 budget reconciliation categories, split between community care and VA direct care, and each year the actuarial consultant validates that actual base year cost projections tie to the actual base year budget obligations.
· Actual to expected adjustment. According to VHA documents and officials, the base year projection in the EHCPM attempts to appropriately capture major impacts of veteran demand for health care services. That is, the EHCPM projection of the base year attempts to approximately align with actual workload experience. However, according to VHA documents and officials, there will always be unexplained differences between actual workload experience and what is projected in the base year prior to model calibration. This adjustment allows E&F and its actuarial consultant to identify and quantify areas of unexplained differences in utilization for further review and refinement. This adjustment may then be used to account for unexplained differences in utilization by calibrating what is estimated in the base year to what VA actually experienced. For example, if the EHCPM estimates 1,000 visits for a given health care service in the base year, but there were actually 500 visits, then a review would be conducted as to why the base year projections deviated significantly from actuals prior to the model being finalized.
·
Budget impact analysis. According to VHA documentation,
during model development, within the budget impact analysis, each key driver
that contributes to a change in projected utilization and costs is specifically
identified and quantified. As most of these drivers are present from one year
to the next, these outcomes are compared to the outcomes from the previous
model and against external sources, such as policy impact estimates developed
outside of the model. For example, the budget impact analysis reveals (1) the
drivers that are responsible for the majority of the cost increases from the
prior year; (2) if the drivers are population driven, program driven, or policy
driven; and (3) the projected cost bounds for certain drivers (i.e., the amount
of money saved by removing or changing a policy).
According to VHA officials, once the EHCPM update is complete, VHA’s E&F provides the initial budget scenario, which includes the model estimates for health care services, to VHA’s Office of Finance.[25] This includes a budget impact analysis, a report with projected costs for each service category broken out by direct and community care, and a projection supplement workbook that has projections for populations not modeled in the EHCPM.
The Office of Finance reviews, calculates, and combines both modeled and nonmodeled estimates into an overall VHA budget projection for review and approval by the Office of the Under Secretary for Health. The projection is sent to VA’s Office of Budget for approval before it is presented to VA’s Assistant Secretary for Management. The Secretary of Veterans Affairs approves and submits the overall budget request to OMB around September of each year.
According to VHA officials, E&F provides several EHCPM budget scenario briefings to internal and external stakeholders, such as Congress, as well as answers questions about the assumptions and projections. Additionally, E&F may produce additional budget scenarios based on other factors that arise between the delivery of the initial budget scenario and the publication of the President’s budget.[26]
VHA’s Processes for Developing its Health Care Cost Model Align with Most but Not All Relevant Standards
VHA’s Processes Largely Align with Relevant Standards
VHA’s processes for having its actuarial consultant develop EHCPM estimates align with most aspects of relevant actuarial standards of practice.[27] The following are examples of areas for which VHA’s processes align with these standards:
· Incurred Health and Disability Claims. According to VHA, its actuarial consultant adjusts utilization projections for changing economic conditions and includes unit cost reconciliation adjustments to account for administrative components of claim costs, which aligns with the Actuarial Standards of Practice No. 5.
· Risk Classification. According to VHA, its actuarial consultant classifies veteran enrollees based on their risks in terms of the expected cost of providing VA health care coverage or services. As a result, the EHCPM projects enrollment, utilization, and unit costs for VHA health care services based on veteran enrollee characteristics, including age, gender, priority group, period of service, and geographic location, which aligns with the Actuarial Standards of Practice No. 12.
· Expert Testimony by Actuaries. In April 2019, VHA’s actuarial consultant provided testimony before the Senate Committee on Veterans’ Affairs on implementing the Veterans Community Care Program. During the testimony, the consultant provided the description of EHCPM and disclosed some of the assumptions used in the model, which aligns with the Actuarial Standards of Practice No. 17.
See appendix II for more information on actuarial standards of practice relevant to VHA’s processes for developing EHCPM estimates, including other aspects of standards that VHA’s processes align with, and examples of VHA’s actuarial consultant’s work.
VHA is also taking steps to improve its processes for involving program offices and subject matter experts in assisting E&F and VHA’s actuarial consultant in developing the EHCPM inputs for specific areas such as community care, pharmacy services, and prosthetics services. In March 2025, the VA Office of Inspector General recommended that VHA establish and implement a plan to review current processes and procedures for involving program offices and pertinent subject matter experts in developing the EHCPM inputs and formalize the expectations of their involvement in this process through guidance or protocols.[28] VHA agreed with the recommendation and, in response, stated that it is developing standardized guidance documents on VHA program office engagement protocols for the EHCPM update.
VHA’s Processes Do Not Fully Align with Certain Aspects of Relevant Standards
While our review found that VHA’s processes align with most aspects of the actuarial standards of practice we reviewed for the purpose of this report, we also found that VHA’s processes do not fully align with certain aspects of relevant actuarial standards of practice and internal control standards in areas related to (1) data quality, (2) incorporation of newly emerging data, and (3) model estimate variability.[29] By following the practices and standards we discuss below, VHA will be better positioned to ensure its actuarial consultant maintains integrity and reliability in determining VHA’s estimates for health care funding.
Data quality. According to relevant actuarial standards of practice, when actuaries use data provided to them by others, ensuring the accuracy and completeness of data is the responsibility of those who supply the data.[30] Furthermore, relevant federal internal control standards state that agencies should obtain relevant data from reliable internal and external sources and process the data into quality information.[31]
We found that E&F obtains recent data and provides it to the consultant. According to VHA officials and documents, E&F is responsible for providing its actuarial consultant with data, including utilization and cost data, for use in the EHCPM when projecting potential future costs. At the beginning of a new fiscal year, according to E&F officials, E&F obtains data from the prior fiscal year either from VHA’s corporate data warehouse or from program offices and transmits it to its actuarial consultant. E&F also obtains data from relevant program offices in response to emerging needs such as legislative changes. Further, VHA’s actuarial consultant relies on E&F to communicate to it the quality of the data provided for use in the actuarial model.[32]
In prior work, we found VHA did not communicate all relevant information on the quality of its community care utilization and cost data, including any limitations affecting these data, to its actuarial consultant and recommended VHA take steps to do this.[33] VHA has implemented this recommendation by establishing a formalized process for E&F to communicate information on the quality of the community care data it provides to the actuarial consultant.[34] However, E&F does not have a similar process to communicate information on the quality of direct care data. Rather, it does so on an ad hoc basis, according to E&F officials. These direct care data include utilization and cost data E&F obtains from program offices such as the Office of Productivity, Efficiency and Staffing; Pharmacy Benefits Management Services; Prosthetics and Sensory Aids Service; and Veterans Benefits Administration. Given that veterans receive the majority of their health care services through direct care, it is important that the actuarial consultant is aware of any data limitations that could inform cost estimates for these services.
E&F officials explained to us why they do not document information on any limitations of the direct care data and communicate this information to the consultant. According to E&F officials, the data come from various VHA offices and databases that all have quality assurance practices. E&F officials added that they are users, not owners, of the data and they take steps to try to ensure the data they provide are complete. However, E&F could establish a formalized process for communicating to the actuarial consultant information on the quality of the direct care data it provides, including any limitations of those data, similar to the process E&F already has to communicate such information on a monthly basis for the community care data it provides to its actuarial consultant. Without doing so, there is a risk that this information may not be communicated to the consultant and subsequently not taken into account as the actuarial consultant develops the health care model estimate. Having a formalized process to communicate all relevant information to the actuarial consultant on the quality of the direct care data used in the EHCPM, including any limitations, would help the consultant address any such limitations as part of the actuarial modeling, thus improving the actuarial modeling that informs VHA’s health care budget projection.
Incorporation of newly emerging data. The actuarial standards of practice we reviewed state that actuaries should use data that is sufficiently current and consider the availability of additional or alternative data and the potential benefits of such data.[35] Further, federal internal control standards state that management should design control activities to achieve objectives and respond to risks; implement such activities through policies; and use quality information that is appropriate, current, complete, accessible, and provided on a timely basis to make informed decisions.[36]
VHA has the opportunity to incorporate newly emerging data in its annual EHCPM update after the initial model for the budget scenario is delivered during the President’s budget request cycle.[37] For example, E&F and VHA’s actuarial consultant updated the 2023 EHCPM model estimates in fiscal year 2024 by incorporating newly emerging fiscal year 2023 data. However, according to E&F officials, E&F does not have a formalized process requiring VHA’s actuarial consultant to incorporate newly emerging data into the model after initial model delivery when possible. According to VHA officials, incorporating newly emerging data after the delivery of its initial model scenario is not required because it depends on factors such as data availability and appropriateness of the data for use in the EHCPM update, the timing of the President’s budget, and requests from the VHA Office of Finance. However, given that in recent years the President’s budget has often been released later than the first Monday in February, VHA has had opportunities to incorporate newly emerging data. According to VHA officials, in 4 of the past 5 years, VHA’s actuarial consultant has incorporated newly emerging data in the model after initial delivery. However, incorporating newly emerging data after the initial model delivery is currently dependent on a request from the VHA Office of Finance. In addition, without a formal process for incorporating newly emerging data, there is a risk that this effort will not be sustained in light of any organizational or leadership changes that may occur. Therefore, formalizing this process would support consistent and timely incorporation of newly emerging data when possible.
By identifying an approach to help ensure that the actuarial consultant establishes a formalized process to incorporate newly emerging data in the model after initial model delivery—unless there is insufficient time due to the scheduling of the President’s budget request or data availability—VHA could ensure that its health care cost estimates reflect the most current data, improve the accuracy and completeness of the model estimates, and potentially support a more informed budget request.[38]
Model estimate variability. According to the actuarial standards of practice we reviewed, actuaries should communicate uncertainties in the model output, including identifying possible variability of model output such as variability around expected health care cost estimates.[39] Furthermore, federal internal control standards state that management should communicate relevant quality information to achieve the agency’s objectives, and identify, analyze, and respond to risks related to achieving an agency’s defined objectives.[40]
While E&F produces the EHCPM risk assessment report, based on the actuarial consultant’s work, to communicate model uncertainty associated with some of the key drivers, the report does not provide sufficient clarity about the extent to which the overall model estimate might vary due to the combination of all the key drivers identified.[41] According to VHA documentation, the EHCPM risk assessment report identifies sources of risk, such as economic conditions; enrollee and veteran preferences; and legislative, regulatory, and judicial policy. (See fig. 4.) However, the report does not include information on potential model output variability of health care cost estimates—that is, the extent to which the model estimate might vary. According to VHA officials, this is because VHA does not require its actuarial consultant to determine, document, and communicate the extent to which the model estimates might vary.
Figure 4: Sources of Risk Contributing to the Enrollee Health Care Projection Model (EHCPM) Estimate Used to Support the Veterans Health Administration’s (VHA) Fiscal Year 2025 Budget Projection
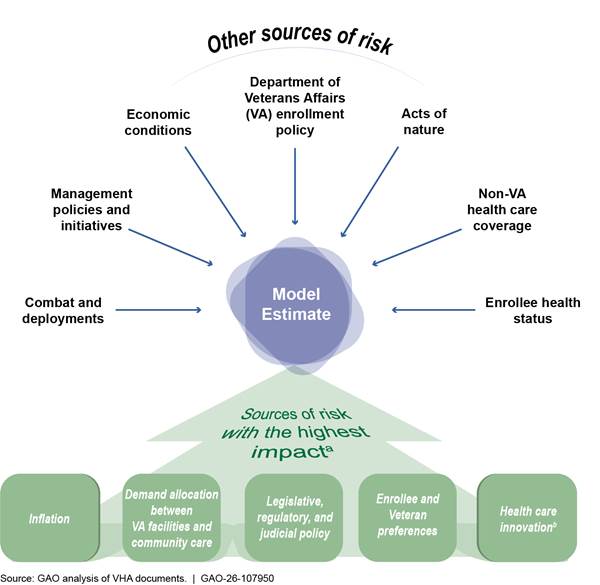
aSources of risk identified by VA as having the highest impact on the EHCPM budget scenario for fiscal year 2025.
bHealth care innovation refers to advancements in medical technology and pharmaceuticals such as the advancements in prosthetics for lost limbs. It is one of the highest impact sources of risk because its timing is difficult to predict, and it can change treatment utilization and costs.
VHA officials told us they do not require the actuarial consultant to provide certain information on the extent to which the model estimate might vary in the EHCPM risk assessment report due to concerns that sources of uncertainty cannot be statistically measured or assigned probabilities. However, according to actuarial literature on uncertainty, providing variability estimates is feasible.[42] For example, VHA’s actuarial consultant can use techniques such as scenario analysis and stress testing to provide information on potential output variability of health care model estimates.[43]
By having information on potential output variability of health care model estimates in the EHCPM risk assessment report, VHA can be better informed on how the model estimates might vary from actual obligations when using the EHCPM to make decisions and to develop budget requests. This lack of information could affect VHA’s decision-making as it uses the EHCPM to develop budget requests, potentially leading to underestimations of required funding and, as a result, the need for unexpected requests for supplemental funds as occurred in fiscal year 2025, for example. By identifying an approach to help ensure that the actuarial consultant better documents and more effectively communicates information on potential output variability of health care model estimates, VHA could ensure VA stakeholders, such as VA leadership, understand how to best use model estimates to support the formulation of VHA’s budget projection. Additionally, if this model estimate variability information were included and clearly communicated in the consultant’s risk assessment report, it could help VHA justify the need for additional funding if required.
VHA Uses Performance Measures to Assess Consultant, but Lacks Specific Oversight Responsibilities in its Standard Operating Procedure
In order to oversee the performance of its actuarial consultant, VHA’s E&F office conducts reviews of its actuarial consultant using performance metrics, defined in the quality assurance surveillance plan as outlined in VHA’s standard operating procedure.[44] E&F uses these performance metrics to ensure that the consultant is performing the services required by this performance work statement in an acceptable manner.[45] For example, according to VHA documentation, E&F can conduct periodic inspections, often reviewing a random sample of the actuarial consultant’s database and statistical output, actuarial analyses and briefing materials, and the EHCPM analysis report for accuracy and completeness. Additionally, VHA staff, who regularly work with VHA’s actuarial consultant and E&F, provide input and feedback to E&F to help ensure that the consultant is available for VHA staff and is meeting their needs. (See app. IV for a full list of quality assurance surveillance plan performance metrics used to assess VHA’s actuarial consultant.)
However, we found that VHA’s standard operating procedure does not specify what E&F staff should be doing to ensure that the consultant adequately performs the tasks outlined in the performance work statement. According to the Federal Acquisition Regulation, quality assurance is necessary to ensure the contractor complies with the work laid out in the contract’s requirements.[46] In contrast, VHA’s standard operating procedure only provides a broad overview of what E&F’s oversight responsibilities should be. For example, according to the VHA’s standard operating procedures, E&F is responsible for conducting (1) a monthly review of the consulting hours and deliverables of the actuarial consultant, and feedback that the deliverables met or did not meet the performance standards identified in the quality assurance surveillance plan; and (2) performance review meetings with the actuarial consultant and other VA staff, if necessary, to ensure that the consultant is providing the appropriate expertise and staffing level to successfully complete assigned tasks within required deadlines and discuss any performance issues.
According to VHA documents and officials, E&F conducts a monthly review of the actuarial consultant’s invoices to ensure it produces the deliverables laid out in the performance work statement and holds performance review meetings when needed with the consultant. However, because the invoices only indicate when the work was done, reviewing them does not allow E&F to assess the quality of the work. Additionally, according to VHA officials, E&F does review all deliverables produced by the actuarial consultant and will notify the consultant via email if there is an issue. However, there is no formal assessment of the quality of the documents. According to VHA documents and officials, E&F works closely and meets on an ad hoc basis at various times throughout the year with its actuarial consultant and does not believe there to be any concerns about the performance of the consultant. These officials also stated that they rely on the consultant’s internal review process to assess quality control for the consulting, modeling, and analytical services it provides to VHA. While VHA’s actuarial consultant may share aspects of the internal review, E&F does not formally review information pertaining to this process.
Given that for fiscal year 2025, VHA used the EHCPM estimates to develop approximately 89 percent of its health care budget projection, it would be beneficial to update the standard operating procedure to include responsibilities that require E&F to assess the quality of the consultant’s tasks and deliverables that are included in the performance work statement. For example, the standard operating procedure could include that E&F conduct a formal review process to assess the quality of the actual-to-expected analysis, the consultant’s model validation procedures, and the EHCPM analysis report, among other things. Additionally, the standard operating procedure could include that E&F conduct a formal review of the consultant’s internal review so it can ensure it was completed and is aware of any issues identified in this review. VHA officials told us that because E&F does not have actuaries on staff, it is unable to assess the actuarial merits of the consultant’s deliverables.
However, according to VHA officials, VA has set a goal for VA’s Office of Actuarial Services to be involved in VHA’s actuarial consultant’s development of model estimates for health care. According to VHA officials, this would include conducting an independent review of the reasonableness of these estimates.[47] As of September 2025, VHA officials told us that VA’s Office of Management was still in the process of operationalizing the Office of Actuarial Services’ oversight role in overseeing the consultant’s work and could not provide us with a formalized plan for this oversight role. Our body of work has shown that by setting implementation goals, an organization builds momentum and can show progress from day one, thereby helping ensure an initiative’s successful completion.[48] Furthermore, relevant federal internal control standards state that agencies should internally communicate relevant quality information—including objectives and responsibilities—down, across, and up the organization to achieve entity objectives.[49]
VA officials told us that the Office of Actuarial Services executive director is still learning more about VHA’s actuarial consultant’s process of developing model estimates for VHA’s budget projections. As of October 2025, VHA officials told us that the Office of Actuarial Services had started its involvement with the VHA budget process to provide comments on the fiscal year 2028 budget. As of January 2026, VHA officials told us that E&F and its actuarial consultants have had two meetings with the Office of Actuarial Services related to data inputs for the EHCPM. As of that time, there was no formal process, such as a Memorandum of Agreement, to ensure that the Office of Actuarial Services would provide assistance with oversight of the consultant’s work.
Effective contract management and oversight are essential to ensuring the government receives the goods and services it has contracted for. By not updating its standard operating procedure to specify in more detail how E&F should oversee the quality of the work produced by the actuarial consultant, VHA may not be able to reasonably ensure that its actuarial consultant is fulfilling the work requirements agreed upon in the performance work statement. Additionally, by not including specific oversight tasks, such as developing formal processes for reviewing the quality of the actuarial consultant’s work, VHA may miss opportunities to improve the accuracy of its budgetary support provided by the actuarial consultant. Additionally, by having a formalized process, such as a Memorandum of Agreement, for implementing VA’s goal for the Office of Actuarial Services to be involved in VHA’s actuarial consultant’s development of model estimates for health care, VA could help improve the efficiency and effectiveness of its efforts to oversee the quality of the work produced by its actuarial consultant.
Conclusions
While the amount of VHA’s budget projections are determined by several factors, including VA policy decisions and the President’s priorities, the EHCPM plays a critical role in projecting VA’s budgetary needs. Given that VHA has underestimated its funding needs for health care services in prior years, it is especially important that VHA takes steps to accurately project its funding needs for future health care services. Otherwise, VHA may run the risk of underestimating or overestimating the resources needed to provide health care services to veterans.
We found that VHA’s processes for developing EHCPM estimates align with most but not all relevant actuarial and internal control standards. These standards are important to ensuring that VHA’s contracted actuaries maintain integrity and reliability in determining VHA’s estimates for health care funding. We identified deficiencies in VHA’s budget development process related to relevant standards including (1) data quality, (2) incorporating newly emerging data, and (3) model estimate variability. Developing a formalized process to ensure limitations affecting direct care data are properly communicated to VHA’s actuarial consultant would help the agency ensure the reasonableness of the model estimates for the budget. Additionally, by including newly emerging data in the annual model update, VHA could ensure that the model reflects the most current data, improve the accuracy and completeness of the model estimates, and potentially support a more informed budget request. Further, reporting information on the extent to which the EHCPM estimates can vary could better inform VHA’s decision-making as it uses the EHCPM to develop its health care budget requests.
In addition, because VHA is reliant on an actuarial consultant to help develop budget estimates for veterans’ health care services, it is critical that VHA assess the performance of its consultant. However, VHA’s standard operating procedure does not outline specific responsibilities for overseeing the actuarial consultant’s tasks, such as formalized processes for reviewing the quality of the work produced by the consultant. This limits the agency’s ability to ensure the consultant properly carries out its work in estimating VHA’s needed resources for health care services. Establishing specific oversight responsibilities in the standard operating procedure would better enable VHA to reasonably ensure that its actuarial consultant is fulfilling its work requirements. Additionally, because E&F does not have actuaries on staff to assess the actuarial consultant’s technical code or calculations, it is important that VA have a formal process to ensure that VA implements its goal that the Office of Actuarial Services provide assistance with oversight of the consultant’s work. By having a formalized process, such as a Memorandum of Agreement, VA could help improve the efficiency and effectiveness of its efforts to oversee the quality of the work produced by its actuarial consultant.
Recommendations for Executive Action
We are making the following five recommendations to VA:
The VA Undersecretary for Health should establish formalized processes for communicating to its actuarial consultant during the annual model update process information on the data quality, including any limitations, of VA direct care data used in the actuarial modeling that informs VA’s health care budget projection. (Recommendation 1)
The VA Undersecretary for Health should identify an approach to help ensure that there is a formalized process for incorporating newly emerging data, when possible, in the model after initial model delivery and prior to submitting the health care budget projection for the President’s budget request. (Recommendation 2)
The VA Undersecretary for Health should identify an approach to help ensure that information on the extent to which the EHCPM estimates can vary are documented and reported, such as in the annual risk assessment report and take action to implement that approach. (Recommendation 3)
The VA Undersecretary for Health should update its standard operating procedure for assessing its actuarial consultant’s performance to include a formalized process for assessing the quality of the consultant’s deliverables to ensure the consultant complies with the work laid out in the performance work statement. (Recommendation 4)
The VA Undersecretary for Health should ensure it has a formalized process, such as a Memorandum of Agreement, for meeting its goal for VA’s Office of Actuarial Services to be involved in VHA’s development of model estimates for health care. (Recommendation 5)
Agency Comments
We are sending copies of this report to the appropriate congressional committees and the Secretary of Veterans Affairs. The report is also available at no charge on GAO’s website at http://www.gao.gov.
If you or your staff has any questions regarding this report, please contact me at silass@gao.gov. Contact points for our Offices of Congressional Relations and Media Relations may be found on the last page of this report. GAO staff who made key contributions to this report are listed in appendix V.

Sharon M. Silas
Director, Health Care
List of Addressees
The Honorable Jerry Moran
Chairman
Committee on Veterans’ Affairs
United States Senate
The Honorable John Boozman
Chairman
Subcommittee on Military Construction, Veterans Affairs, and Related Agencies
Committee on Appropriations
United States Senate
The Honorable Mike Bost
Chairman
The Honorable Mark Takano
Ranking Member
Committee on Veterans’ Affairs
House of Representatives
The Honorable John R. Carter
Chairman
Subcommittee on Military Construction, Veterans Affairs, and Related Agencies
Committee on Appropriations
House of Representatives
The Honorable Mariannette Miller-Meeks
Chairwoman
Subcommittee on Health
Committee on Veterans’ Affairs
House of Representatives
The Honorable Jen Kiggans
Chairwoman
Subcommittee on Oversight and Investigations
Committee on Veterans’ Affairs
House of Representatives
The Honorable Jack Bergman
House of Representatives
The Department of Veterans Affairs’ (VA) Enrollee Health Care Projection Model (EHCPM) projects enrollment, utilization, and costs for the enrolled veteran population in more than 140 categories of health care services 20 years into the future. In fiscal year 2025, the EHCPM supported approximately 89 percent of the VA medical care budget.
We performed our work at the initiative of the Comptroller General. In this report, we
1. describe Veterans Health Administration’s (VHA) current process for updating the actuarial model used to estimate its health care funding needs;
2. examine the extent to which VHA’s processes for developing VA’s health care model estimates align with relevant standards, including actuarial standards of practice and federal internal control standards; and
3.
examine VHA’s oversight of the performance of its actuarial consultant.
Data Used and Data Reliability
Our review uses the following information from VHA:
· VHA’s annual actuarial report for base years 2021 through 2023 that describes the methodology, supporting analyses, and assumptions for the EHCPM.
· VHA model risk assessment report that identifies sources of risk and uncertainty for the projections supporting the VA health care budget.
· Budget impact analyses for fiscal years 2022 through 2025 that presents the specific characteristics of the scenario used for that year’s EHCPM.
To assess the reliability of these data, we reviewed VHA documentation, conducted electronic and manual testing of the data, and interviewed VHA officials responsible for maintaining the data. We found the data sufficiently reliable for our purposes of examining the extent to which VHA’s processes for developing VA’s health care model estimates align with relevant standards.
Methodology
To describe VHA’s current process for updating the actuarial model used to estimate its health care funding needs, we reviewed documentation provided by VHA and its actuarial consultant, Milliman, describing the actuarial model update process, including procedures such as adjusting for discrepancies between actual workload (i.e., utilization of services) and model estimates. We also interviewed and reviewed written responses from VHA’s Office of Enrollment and Forecasting (E&F) and VHA’s Office of Finance.[50]
To examine the extent to which VHA’s processes for developing VA’s health care model estimates align with relevant standards, including actuarial standards of practice and federal internal control standards, we reviewed and analyzed the extent to which VHA’s modeling processes for projecting future health care demands follow selected key practices and standards.[51] Additionally, we reviewed actuarial documents and other modeling documents provided by E&F.[52] We also reviewed the cost projections for fiscal years 2022 through 2027 developed for E&F by its actuarial consultant. We reviewed data sources used for developing the cost projection.
To evaluate the actuarial modeling process, we reviewed E&F documents about the actuarial assumptions and methods E&F used to develop the 20-year projection of future health care service costs. We reviewed a model risk assessment report that identifies sources of risk and describes the degree of uncertainty for the projections supporting the VA health care budget. In addition, we reviewed the morbidity and reliance model adjustments for veteran reliance and utilization of VHA services. Further, we reviewed the E&F model’s use of external data including data from other government agencies, such as the Department of Defense and U.S. Census. We assessed these processes against eight relevant actuarial standards of practice.[53] We also identified five federal internal control standards that were relevant to our work.[54] We selected these standards because they describe the procedures an actuary should follow when performing actuarial services and identify what the actuary should disclose when communicating the results of those services. Finally, we interviewed VHA officials and VHA’s actuarial consultant on the development and validation of the model and how the model’s outputs are used to support VHA’s budget formulation for veteran health care.
We interviewed VHA officials from E&F about their processes for communicating data quality and limitations. We also interviewed or received written responses from officials in VA’s Office of Actuarial Services, as well as key program offices including the Office of Integrated Veteran Care; Office of Productivity, Efficiency and Staffing; Pharmacy Benefits Management Services; Prosthetics and Sensory Aids Service; and officials from the Veterans Benefit Administration regarding their involvement in VHA’s budget development process.[55]
We examined VA’s actuarial consultant’s role in the actuarial modeling processes in the context of actuarial standards of practice. Our actuarial work on this engagement was conducted by a GAO Assistant Director and Actuary and GAO’s Chief Actuary (identified in the Staff Acknowledgment section of this report), who meet the qualification standards of the American Academy of Actuaries to conduct the actuarial aspects of our work for this report. While we conducted actuarial reviews of models and processes, we did not evaluate the accuracy of VHA’s projections or their underlying assumptions, as that type of analysis was outside the scope of this report.
To examine VHA’s oversight of the performance of its actuarial consultant, we reviewed VA documentation, including VHA’s standard operating procedure and quality assurance surveillance plan for assessing contractor performance, the Actuarial Support Services contract and performance work statement, as well as documentation related to oversight activities including contractor performance reviews, reviews of the actuarial consultant’s invoices, and the contractor performance assessment report. To understand the processes in place to monitor and assess contractor performance, we interviewed or received written responses from officials in VHA’s E&F and Office of Finance, and VA’s Office of Management, Office of Actuarial Services, and the Strategic Acquisition Center.[56] We also reviewed documentation and information from VHA officials regarding how oversight responsibilities are defined and executed in relation to tasks and deliverables outlined in the performance work statement. We assessed these oversight practices against the Federal Acquisition Regulation, and VA Acquisition Regulation in the context of federal internal control standards for information and communication.[57]
Limitations
In performing this analysis, we relied on actuarial reports and documentation provided by E&F. We reviewed the documents for reasonableness, but did not audit them for accuracy. We performed all reviews in accordance with actuarial principles and relevant Actuarial Standards of Practice (Actuarial Standards Board), including Actuarial Standard of Practice No. 12, Risk Classification; Actuarial Standard of Practice No. 23, Data Quality; Actuarial Standard of Practice No. 25, Credibility Procedures; Actuarial Standard of Practice No. 41, Actuarial Communications; and Actuarial Standard of Practice No. 56, Modeling. To the extent that there are material deficiencies in completeness and accuracy in E&F’s actuarial reports, the cost estimates may be materially different from those shown in the report had these deficiencies not been present. This review is not a technical review, and we did not verify the accuracy of the calculations performed by the third-party actuaries.
We conducted this performance audit from November 2024 to June 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
We identified actuarial standards of practice relevant to the Enrollee Health Care Projection Model (EHCPM), the actuarial modeling that the Veterans Health Administration (VHA) uses to inform the Department of Veterans Affairs’ budget estimates for health care services. Table 1 lists relevant actuarial standards of practice we identified, along with examples from the actuarial consultant’s work.
Table 1: Actuarial Standards of Practice Relevant to Enrollee Health Care Projection Model (EHCPM) Modeling and Examples of How the VHA’s Work Addresses Those Standards
|
Actuarial standards of practice |
Examples from EHCPM work |
|
Incurred Health and Disability Claims (No. 5): Provides guidance for estimating health care claims. The standard states an actuary should make a reasonable effort to understand changes in plan provisions or business practices and consider how such changes are likely to affect projections of claims costs. This standard also states that an actuary should consider including economic influences, among other things, in projecting claims. |
According to the Veterans Health Administration (VHA), its actuarial consultant estimates the Department of Veterans Affairs’ (VA) community care claims and adjustments to utilization projections that reflect the effects of changing economic conditions over time. For example, during the unit cost and budget reconciliation process for community care services the unit cost reconciliation adjustment loads in certain administrative components of the unit costs. Unit costs for these services are developed using the claims costs on the baseline data, since source data lacks the administrative costs. As part of the model update, VHA’s actuarial consultant confirms the total claims cost on the baseline data is close to the actual obligations once the delivery operations billing and processing costs, care coordination costs, and the proportional distribution of national overhead are accounted for. |
|
Risk Classification (No. 12): Provides guidance for designing, reviewing, and changing risk classifications. This standard defines risk classification as a system used to assign the individuals into groups intended to reflect the relative likelihood of expected outcomes. The standard states that when selecting which risk characteristics to use in a risk classification system, the actuary should consider the relationship of risk characteristics and the expected outcomes. |
According to VHA, its actuarial consultant classifies veteran enrollees based on their risks in terms of the expected cost of providing VA health care coverage or services. As a result, the EHCPM projects enrollment, utilization, and unit costs for VHA health care services based on veteran enrollee characteristics, including age, gender, priority group, period of service, and geographic location. For example, Vietnam-era enrollees exhibit higher utilization patterns than non-Vietnam era enrollees for some health care services. |
|
Expert Testimony by Actuaries (No. 17): Provides guidance for giving expert testimonies (e.g., congressional testimony). In offering expert testimony, the actuary should comply with all rules of evidence and procedure, and any other rules applicable in the forum. In addition, the actuary should review and comply with any applicable actuarial standards of practice, the Qualification Standards for Actuaries Issuing Statements of Actuarial Opinion in the United States, and the Code of Professional Conduct. |
VHA’s actuarial consultant provides support to VHA for congressional hearings, as needed. An example was an April 2019 testimony before the Senate Committee on Veterans’ Affairs on implementing the Veterans Community Care Program. During the testimony, VHA’s actuarial consultant provided the description of EHCPM, disclosed some of the assumptions used in the model, and discussed how the VA Maintaining Internal Systems and Strengthening Integrated Outside Networks Act of 2018 might affect veterans’ reliance on VHA health care and projected obligations. |
|
Data Quality (No. 23): Provides guidance for (1) selecting the data that underlie the actuarial work product; (2) relying on data supplied by others; (3) reviewing data; (4) using data; (5) preparing data to be used by other actuaries in an actuarial work product; and (6) making appropriate disclosures with regard to data quality. |
According to VHA, its actuarial consultant reviews the reasonableness (e.g., consistency with past data) of data used for modeling, including both the VA data and other external data. |
|
Credibility Procedures (No. 25): Provides guidance for selecting or developing credibility procedures and the application of those procedures to sets of data. |
According to VHA, its actuarial consultant considers the credibility of data (i.e., the extent to which data can be relied on to predict trends and explain veterans’ behavior) when developing adjustments for enrollment rates, morbidity, reliance, unit costs, and other factors used in the actuarial modeling. For example, adjustments for veteran enrollment rates are developed based on priority rating, a 5-year age band (e.g., 30 to 34 years of age), and a geographic area, such as a sector—the smallest geographic location considered by the EHCPM, which consists of one or more contiguous counties. Because too few veterans may be within a particular priority group or 5-year age band living in a particular sector, VHA’s actuarial consultant develops enrollment rates using a blend of rates from the sector level, which has low credibility, and from larger geographic locations, including the area covered by a regional Veterans Integrated Service Network, to improve the data credibility. |
|
Actuarial Communications (No. 41): Provides guidance for preparing actuarial communications, including those that may be required by other actuarial standards of practice. The performance of a specific actuarial engagement or assignment typically requires significant and ongoing communications between the actuary and the intended users regarding the following: the scope of the requested work; the methods, procedures, assumptions, data, and other information required to complete the work; and the development of the communication of the actuarial findings. |
According to VHA, its actuarial consultant communicates the effects of model enhancements resulting from the annual update of the EHCPM. Briefings are provided for internal and external budget stakeholders, which include communicating the assumptions in the current budget scenario and enhancements to the newly updated EHCPM. These briefings include information on how updates and enhancements to the model and material changes to the assumptions between the current budget scenario and the previous budget scenario affected projected spending for a particular year or years in the future. In addition, the annual EHCPM report documents model updates, including enhancements and changes to assumptions. |
|
The Use of Health Status Based Risk Adjustment Methodologies (No. 45): Provides guidance for applying health status-based risk adjustment methodologies to quantify differences in relative health care resource use due to differences in health status. |
According to VHA, its actuarial consultant uses non-VA utilization benchmarks developed for commercial and Medicare markets when projecting utilization for many VA health care services. The actuarial consultant adjusts these benchmarks to account for differences in the morbidity, or health status, of the veteran enrollee population compared to the commercial and Medicare populations. |
|
Modeling (No. 56): Provides guidance to actuaries when performing actuarial services with respect to designing, developing, selecting, modifying, using, reviewing, or evaluating models. |
According to VHA, its actuarial consultant works with VHA in ensuring the EHCPM serves its intended purpose, selecting relevant data used for projections, setting assumptions, and developing projections of veteran health care costs. They also review the models including their inputs, calculations, and outputs to ensure the outputs are reasonable and consistent with program office expectations. |
Source: GAO review of VHA’s EHCPM against relevant actuarial standards of practice. | GAO‑26‑107950
Appendix III: VHA’s Actuarial Consultant’s Tasks, Deliverables, and Required Due Dates for the Deliverables
The Veterans Health Administration’s (VHA) actuarial consultant, Milliman, performs its work under an actuarial support services contract, which is managed by VHA’s Office of Enrollment and Forecasting (E&F). As part of the contract, the actuarial consultant is responsible for several tasks as outlined by the performance work statement. The consultant supports VHA in its development of budget estimates, including updating the Enrollee Health Care Projection Model (EHCPM), developing projections for workforce planning, and developing EHCPM briefings for stakeholders, among other things. (See table 2.)
Table 2: Full List of Project Tasks, Deliverables, and Required Delivery Dates for VHA’s Actuarial Consultant as Outlined in the Performance Work Statement, as of April 2025
|
Project task |
Deliverables |
Required delivery date |
|
Enrollee Health Care Projection Model (EHCPM) Project Plan Updates |
Actuarial consultant shall provide a Project Management Plan that lays out the consultant’s approach, timeline, and tools to be used in execution of the contract. |
Monthly |
|
Progress reports |
The actuarial consultant shall provide status reports to the contracting officer’s representative via a joint bi-weekly conference call with the actuarial consultant EHCPM Project Team and the Chief Strategy Office EHCPM Project Team. |
Bi-weekly |
|
Travel and other direct cost reports |
Report with cover sheet containing the actuarial consultant’s name, contract number, purchase order number, invoice number, date, and period of performance covered by the invoice, cost, and travel, and a list of deliverables for the month and cumulative year to date. |
Monthly |
|
Actuarial consulting, modeling, and analyses |
The actuarial consultant shall provide the Department of Veterans Affairs (VA) support to use the EHCPM to assess the impact of an evolving VA health care system and the broader environment, proposed polices, regulations, and legislation, as well as support for the VA medical care budget process, VA leadership, and stakeholders including the Office of Management and Budget (OMB), Congress, the GAO, Congressional Budget Office, and the Veteran Service Organizations. At the direction of the contracting officer’s representative, the actuarial consultant shall provide documentation that includes data summaries and documentation at a level of detail appropriate for stakeholders and identifies the data, assumptions, and methods used with sufficient clarity that another actuary qualified in the same practice area could evaluate the reasonableness of the actuary’s work. |
Ongoing |
|
Special analyses |
This task provides for consultation to meet VA’s needs for special analyses. Tasks will be defined and accomplished with internal or external workgroups led by VA staff. VA staff that have clinical and programmatic expertise in the task area provide insight into the VA health care system, data, policies, and programmatic guidance. The actuarial consultant shall provide technical and analytical expertise to the workgroup and serve as a member of the workgroup. The workgroup will assess the potential impact on VA and develop assumptions for input into the EHCPM. This consultation will be coordinated by the consultant’s project manager and the VA contracting officer’s representative to support VA staff, specific workgroups or external groups as authorized by VA. |
As requested |
|
VA medical care budget support |
Actuarial consultant shall provide consulting, analyses, modeling, and briefing support to educate VA leadership, the OMB, Congress, the GAO, Congressional Budget Office, Veteran Service Organizations, and other stakeholders regarding the enrollment, utilization, and cost projections supporting the VA medical care budget, including supporting analyses, assumptions, methodology, and key factors driving demand for VA health care. |
Ongoing |
|
EHCPM projection scenarios |
This task permits VA to use the EHCPM to assess the impact of adjusting various model assumptions to support the VA medical care budget; policy analysis; strategic, capital, and workforce planning; or to respond to stakeholder requests. The actuarial consultant shall project enrollment, utilization, and costs that reflect the assumptions specified by VA as directed by the VA contracting officer’s representative. At the direction of the VA contracting officer’s representative, the actuarial consultant shall provide a range of deliverables from each EHCPM scenario depending on the needs of the stakeholder requesting the scenario. |
As requested |
|
Maintain, enhance, and update the EHCPM |
VA requires actuarial consulting and modeling support to maintain, enhance, and annually update the EHCPM. The actuarial consultant shall assume responsibility for the EHCPM at the level of detail and functionality as currently structured. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the 2024 EHCPM (expected to be developed during the final option periods of the existing contract) to the actuarial consultant. The actuarial consultant shall use the current EHCPM as the starting point for updating and producing the 2025 EHCPM. |
April 30 |
|
Maintain, enhance, and update the EHCPM veteran, enrollment, and patient projection models |
The actuarial consultant shall assume responsibility for the EHCPM enrollment model at the level of detail and functionality as currently structured. |
April 30 |
|
Maintain, enhance, and update the EHCPM utilization, unit cost, and cost projection models |
The actuarial consultant shall assume responsibility for the EHCPM utilization, unit cost, and cost models at the level of detail and functionality. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the 2024 EHCPM to the actuarial consultant. The actuarial consultant shall use the current EHCPM as the starting point for updating, enhancing, and producing the EHCPM. The actuarial consultant shall need to propose a comparable methodology and/or benchmarks for the private sector-based utilization projection model in place of those used by the incumbent. |
April 1 |
|
EHCPM documentation and analysis report |
The actuarial consultant provides an accurate, complete report detailing methodology, analyses, assumptions, and data used to develop the updated EHCPM. |
October 30 |
|
Maintain and update the EHCPM global relative value units |
The actuarial consultant shall maintain the proper functioning of the model to conduct analysis, updates, and validate the integrity of the system. The actuarial consultant shall also enhance the system via updates to SAS and SQL coding, etc., to ensure the proper functioning of the model to conduct proper maintenance, analysis, updates, and validate the integrity of the system. The actuarial consultant shall assume responsibility for the EHCPM at the level of detail and functionality as currently structured. |
June 30 |
|
EHCPM projections for strategic, capital, and workforce planning |
VA requires actuarial analysis, projections, and modeling support to enhance the EHCPM to support strategic, capital, workforce planning, and other applications of the EHCPM. VA requires documentation that meets varying stakeholder needs. The actuarial consultant shall provide documentation that includes data summaries and documentation at a level of detail appropriate for stakeholders and identifies the data, assumptions, and methods used with sufficient clarity that another actuary qualified in the same practice area could evaluate the reasonableness of the actuary’s work. |
June 30 |
|
Enhance the EHCPM to support strategic, capital, and workforce planning |
This task provides for consultation to assist VA in developing projections to support strategic, capital, and workforce planning, and other applications of the EHCPM. Tasks will be defined and accomplished with VA program offices and led by Chief Strategic Office staff. VA staff who have clinical and programmatic expertise in the task area provide insight into VA’s health care system, data, policies, and programmatic guidance. The actuarial consultant shall provide technical and analytical expertise to the workgroup and participate as a member of the workgroup. |
June 30 |
|
Health System Planning Category Projections |
The actuarial consultant shall produce Health System Planning Category Projections for an EHCPM scenario defined by VA from the newly updated EHCPM. Additional Health System Planning Category Projections may be required for alternative scenarios as directed by the VA contracting officer’s representative. |
June 30 |
|
Model validation |
VA requires actuarial consulting, analysis, and modeling support to assess the predictive power of the EHCPM, and to respond to requests for comparisons of actual enrollment; patients; utilization; and costs to project enrollment, patients, utilization, and costs. VA requires documentation that meets varying stakeholder needs. At the direction of the contracting officer’s representative, the actuarial consultant shall provide documentation that includes data summaries and documentation at a level of detail appropriate for stakeholders and identifies the data, assumptions, and methods used with sufficient clarity that another actuary qualified in the same practice area could evaluate the reasonableness of the actuary’s work. |
February 28 |
|
Comparisons of actual enrollment, patients, utilization, and costs |
VA requires actuarial consulting, analysis, and modeling support to report on the accuracy of the EHCPM, and to respond to requests for comparisons of actual enrollment; patients; utilization; and costs to projected enrollment, patients, utilization, and costs. The actuarial consultant shall produce summaries of actual-to-expected analyses and document known reasons for discrepancies. Specific analyses and the level of detail required will be directed by the contracting officer’s representative. |
February 28 |
|
Annual EHCPM validation study |
The purpose of a model validation study is to analyze the predictive power of the EHCPM at a very detailed level and provide recommendations for future model enhancements on the basis of this analysis. The actuarial consultant shall compare modeled projections with actual experience at a very detailed level, identify services or populations that require special analyses to identify reasons for discrepancies, and recommend whether improvements can be made to improve the predictive power of the EHCPM. Documentation shall identify the data, assumptions, and methods used with sufficient clarity that another actuary qualified in the same practice area could evaluate the reasonableness of the actuary’s work. |
February 28 |
|
Monthly comparisons of actual enrollment and patients to projected |
Periodic (more frequent than annual) actual-to-expected analyses provide up-to-date information on the model’s predictive accuracy, as well as trends in the VA health care system. The actuarial consultant shall conduct an actual-to-expected analysis on a monthly basis. This analysis shall compare VA actual enrollment with projected enrollment for 1- and 3-year projections. Currently, this comparison is performed at the submarket and Veterans Integrated Service Networks level by priority level, age band (under age 45, ages 45 to 64, and over age 65) and enrollee type. Level of detail required may change to meet stakeholder needs. Analysis shall also be performed on modeled patients as the data become available. |
Monthly |
|
Comparisons of actual utilization and costs to projected during the fiscal year |
VA desires the ability to compare actual utilization and costs to projected utilization and costs during the fiscal year. The actuarial consultant shall work with the Veterans Health Administration’s (VHA) Office of Finance to develop a methodology to align projected utilization and costs from the EHCPM with actual utilization and obligations from the Managerial Cost Accounting System to allow for a comparison during the fiscal year. |
June 30 |
|
Maintain, enhance, and update the Civilian Health and Medical Program Veterans Affairs projection model |
The actuarial consultant shall update the Civilian Health and Medical Program of the Department of Veterans Affairs model and supporting analyses with new data from the most recently completed fiscal year period and other newly available data, update supporting analyses, integrate new or updated assumptions, scenarios, and projections with enhanced methodology. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current Civilian Health and Medical Program Veterans Affairs model to the actuarial consultant. The actuarial consultant shall use the current Civilian Health and Medical Program Veterans Affairs model as the starting point for updating, enhancing, and producing the Civilian Health and Medical Program Veterans Affairs model. |
April 30 |
|
Maintain, enhance, and update the Program of Comprehensive Assistance for Family Caregivers projection model |
The actuarial consultant shall update the Program of Comprehensive Assistance for Family Caregivers model and supporting analyses with new data from the most recently completed fiscal year period and other newly available data, update supporting analyses, integrate new or updated assumptions, scenarios, and projections with enhanced methodology. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current Program of Comprehensive Assistance for Family Caregivers model to the actuarial consultant. The actuarial consultant shall use the current Program of Comprehensive Assistance for Family Caregivers model as the starting point for updating, enhancing, and producing the Program of Comprehensive Assistance for Family Caregivers model. |
April 30 |
|
Maintain, enhance, and update the expenditure projections to support the provision of newborn services |
The actuarial consultant shall update the Newborn Projection model and supporting analyses with new data from the most recently completed fiscal year period and other newly available data, update supporting analyses, integrate new or updated assumptions, scenarios, and projections with enhanced methodology, and produce projections for Women’s Health for an initial current policy scenario and other EHCPM scenarios as defined by VA. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current Newborn Care expenditure projections to the actuarial consultant. The actuarial consultant shall use the current Newborn Care expenditure projections as the starting point for updating, enhancing, and producing the Newborn Care expenditure projections. |
April 30 |
|
Maintain, enhance, and update the expenditure projections to support the provision of fertility services |
The actuarial consultant shall update the Fertility Services model and supporting analyses with new data from the most recently completed fiscal year period and other newly available data, update supporting analyses, integrate new or updated assumptions, scenarios, and projections with enhanced methodology, produce projections for the VHA Office of Women’s Health for an initial current policy scenario and other EHCPM scenarios as defined by VA, and report updated projections in the Budget Projection Supplement for the Office of Finance. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current fertility services expenditure projections to the actuarial consultant. The actuarial consultant shall use the current fertility services expenditure projections as the starting point for updating, enhancing, and producing the fertility services expenditure projections. |
April 30 |
|
Maintain, enhance, and update the expenditure projections to support other than honorable projections |
The actuarial consultant shall update the Non-Enrolled Registered Patient and Other Than Honorable Expenditure Projection models and supporting analyses with new data from the most recently completed fiscal year period and other newly available data, update supporting analyses, integrate new or updated assumptions, scenarios, and projections with enhanced methodology, produce projections, as requested, for the VHA Office of Mental Health and Suicide Prevention for an initial current policy scenario and other EHCPM scenarios as defined by VA, and report updated projections in the Budget Projection Supplement for the Office of Finance. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current Other Than Honorable Expenditure Projections to the actuarial consultant. The actuarial consultant shall use the current Other Than Honorable Expenditure Projections as the starting point for updating, enhancing, and producing the Other Than Honorable Expenditure Projections. |
April 30 |
|
Maintain, enhance, and update mental health residential rehab treatment program diagnosis and demographic-based demand model |
The actuarial consultant shall update the mental health residential rehab treatment program diagnosis and demographic-based demand model and supporting analyses with new data from the most recently completed fiscal year period and other newly available data, update supporting analyses, integrate new or updated assumptions, scenarios, and projections with enhanced methodology, and produce projections for the VHA Office of Mental Health and Suicide Prevention for an initial current policy scenario and other EHCPM scenarios as defined by VA. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current mental health residential rehab treatment program diagnosis and demographic-based demand model to the actuarial consultant. The actuarial consultant shall use the current mental health residential rehab treatment program diagnosis and demographic-based demand model as the starting point for updating, enhancing, and producing the mental health residential rehab treatment program diagnosis and demographic-based demand model projections. |
June 30 |
|
Maintain, enhance, and update readjustment counseling service projection model |
The actuarial consultant shall update the readjustment counseling service projection model and supporting analyses with new data from the most recently completed fiscal year period and other newly available data; update supporting analyses; integrate new or updated assumptions, scenarios, and projections with enhanced methodology; and produce projections for the VHA Office of Readjustment Counseling Services for an initial current policy scenario and other scenarios as defined by VA. VA will provide the necessary data, documentation of the methodology and assumptions, and the SAS or SQL code that constitutes the current readjustment counseling service projection model to the actuarial consultant. The actuarial consultant shall use the current readjustment counseling service projection model as the starting point for updating, enhancing, and producing the readjustment counseling service model projections. |
June 30 |
|
EHCPM training and transparency |
VA requires documentation that meets varying stakeholder needs. At the direction of the contracting officer’s representative, the actuarial consultant shall provide documentation that (1) includes data summaries and documentation at a level of detail appropriate for stakeholders; and (2) identifies the data, assumptions, and methods used with sufficient clarity that another actuary qualified in the same practice area could evaluate the reasonableness of the actuary’s work. |
As requested |
|
EHCPM training, briefings, and knowledge transfer |
The actuarial consultant shall develop trainings, briefings, and briefing materials for VA staff and stakeholders to increase the transparency of the EHCPM. This task will require extensive collaboration between VA and the actuarial consultant. The VA contracting officer’s representative will define and direct required training topic, duration, and location. The actuarial consultant may be required to conduct the trainings/briefings or prepare VA staff to conduct the trainings/briefings. |
As requested |
|
EHCPM transparency tools |
The actuarial consultant shall develop new tools and enhance the functionality of the current tools as directed by the VA contracting officer’s representative. At a minimum, the tools shall be produced for each annual EHCPM update based on a scenario defined by the VA contracting officer’s representative. However, VA may require that the tools be produced based on additional EHCPM scenarios. |
As requested |
Source: GAO review of VHA’s performance work statement. | GAO‑26‑107950
Note: According to Office of Enrollment and Forecasting officials, the delivery dates are added to clarify the general timeline and are dependent on VA processes outside the actuarial consultant’s control, such as acquiring VA data and leadership decisions.
Appendix IV: Quality Assurance Surveillance Plan Performance Metrics Used to Assess VHA’s Actuarial Consultant
The Veterans Health Administration (VHA) is responsible for assessing the performance of its actuarial consultant’s tasks as described in the consultant’s performance work statement. According to VHA officials and documents, VHA assesses the quality of the consultant’s tasks in the performance work statement using the surveillance methods and measures, as defined in the quality assurance surveillance plan. (See table 3.)
Table 3: Quality Assurance Surveillance Plan Performance Metrics Used to Assess the VHA’s Actuarial Consultant, as of April 2025
|
Description of deliverables provided by actuarial consultant to fulfill tasks defined in VHA’s performance work statement |
Performance standard and |
Surveillance |
|
Analyses, briefing materials, reports, and documentation |
Deliverables are accurate, understandable to a non-actuarial audience, and usable. Draft provided to the Department of Veterans Affairs (VA) for comments and delivered on the schedule agreed upon by VA and the actuarial consultant. Final report is accurate and complete with the final report 90% acceptable on first submission to government, and 100% acceptable on subsequent submission. |
100% inspection, random sampling, periodic inspection, and customer input. |
|
Consulting |
Appropriate expertise and staffing are available to meet stakeholder needs and deadlines. |
Periodic inspection and customer input. |
|
Database, tools, and SAS code |
The data team and contracting officer’s representative shall review a random sampling of the actuarial consultant’s database and SAS and SQL deliverables. |
Random sampling and periodic inspection. |
|
VA Enrollee Health Care Projection Model documentation and analysis report |
Draft report sections created by the actuarial consultant are provided to VA for comments at least 4 weeks before the final due date. Actuarial consultant provides comments to VA on draft report sections created by VA within 2 weeks from submission. Final report is accurate and complete with the final report 90% acceptable on first submission to government, and 100% acceptable on subsequent submission. |
100% inspection and customer input. |
|
Stakeholder satisfaction |
The contracting officer’s representative shall review the actuarial consultant’s performance corresponding to a validated stakeholder complaint or validated inability to perform in accordance with the performance standard in a specific area and document the results. More than three complaints per contract staff will be reviewed for appropriate action. |
Complaints from |
Source: GAO review of the Veterans Health Administration’s (VHA) quality assurance surveillance plan. | GAO‑26‑107950
GAO Contact
Sharon M. Silas, Silass@gao.gov.
Staff Acknowledgments
In addition to the contact named above, Michael Zose (Assistant Director), Courtney Liesener (Analyst-in-Charge), Shidi Dai, Lijia Guo (Assistant Director and Actuary), Ravi Sharma, and Frank Todisco (Chief Actuary) made key contributions to this report. Also contributing were Ann Marie Cortez, Jacquelyn Hamilton, Drew Long, and Ethiene Salgado-Rodriguez.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]The Veterans Community Care Program allows eligible veterans to receive care from community providers when they face certain challenges accessing care at VA medical facilities.
[2]In 1998, VHA began contracting for actuarial services including modeling of enrollment and health care demand projections. The contract continues to be competitively awarded. VA’s actuarial consultant shall provide actuarial consulting, modeling, and analytical services to assess the impact of an evolving VA health care system and broader environment on veteran enrollment and demand for VA health care.
[3]While the EHCPM estimates inform most of VA’s budget projection, the amount of the budget projection is determined by several factors, including VA policy decisions and the President’s priorities, and will not necessarily match the EHCPM estimates in any given year.
[4]Since VA receives multi-year appropriations, it is possible to have unobligated balances from prior years. According to VA, the $6.6 billion shortfall estimate was less than the original estimate provided to Congress earlier that year as VHA’s actual spending more closely aligned with the fiscal year 2025 President’s budget than anticipated at the time of the original request. According to VA, this was a result of VHA’s efforts to mitigate the projected need for additional funding by delaying hiring and limiting the purchase of new medical equipment.
[5]The Cost of War Toxic Exposures Fund is a VA fund established by the Honoring our PACT Act of 2022 to provide dedicated funding for health care and benefits to veterans exposed to environmental hazards during their military service. Pub. L. No. 117-168, § 805, 136 Stat. 1759, 1804.
[6]VHA has previously reported projected funding gaps for fiscal years 2005, 2006, and 2015. The 2015 projected funding gap of around $2.75 billion was driven by higher-than-expected care in the community costs and costs related to Hepatitis C treatments. The 2005 projected funding gap of $975 million and the 2006 funding gap of $1.977 billion was driven by higher-than-expected demand for VHA services.
[7]See Department of Veterans Affairs, Office of Inspector General, Veterans Health Administration: The Causes and Conditions that Led to a $12 Billion Supplemental Funding Request, VA OIG 24-03127-66 (Washington, D.C: Mar. 27, 2025).
[8]In this report, modeling capacity included data collection and the ability to run budget simulations on a continual basis to systematically assess and manage the risk of catastrophic events. In this report, we made two recommendations, including that VA enhance its modeling capacity to prepare estimates of the funding needed to meet the needs of veterans in the event of another pandemic or catastrophe. VA agreed with our recommendations and is taking steps to implement them. See GAO, Veterans Affairs: Improvements Needed in Estimating Funding for Potential Future Health Emergencies, GAO‑24‑106359 (Washington, D.C.: Feb. 8, 2024).
[9]E&F and VHA’s actuarial consultant are responsible for the actuarial model used to develop estimates for VA’s health care funding needs for modeled services, based on feedback and assumptions provided by VHA subject matter experts and leadership. VHA’s Office of Finance reviews, adjusts, and combines both the modeled and nonmodeled estimates into an overall VHA estimate for review and approval by the Office of the Under Secretary for Health.
[10]The Office of Actuarial Services provides coordination and oversight in the development of actuarial estimates, polices, and services for the department. The Office of Integrated Veteran Care is a national program office that manages and advocates for veterans’ and beneficiaries’ access to health care in both VA and community facilities. The Office of Productivity, Efficiency, and Staffing is responsible for developing VA’s clinical productivity metrics and efficiency models. The Pharmacy Benefits Management Services provides leadership for pharmacy activities in VHA. The Prosthetics and Sensory Aids Service provides prosthetic devices and sensory aids service to veterans. The Veterans Benefit Administration provides financial and other forms of assistance to veterans and their dependents.
[11]Actuarial standards of practice are promulgated by the Actuarial Standards Board. These 58 standards describe the procedures an actuary should follow when performing actuarial services and identify what the actuary should disclose when communicating the results of those services. We selected eight as the most relevant to VHA’s processes for developing EHCPM model estimates. For more information, see Incurred Health and Disability Claims (No. 5), Risk Classification (No. 12), Expert Testimony by Actuaries (No. 17), Data Quality (No. 23), Credibility Procedures (No. 25), Actuarial Communications (No. 41), The Use of Health Status Based Risk Adjustment Methodologies (No. 45), and Modeling (No. 56).
[12]Internal control is a process effected by an entity’s oversight body, management, and other personnel that provides reasonable assurance that the objectives of an entity will be achieved. In this review, we relied specifically on internal control Principle 7, 10, 12, 13, and 15. See GAO, Standards for Internal Control in the Federal Government, GAO‑25‑107721 (Washington, D.C.: May 15, 2025).
[13]The Office of Management enables VA to provide a full range of benefits and services to veterans by providing strategic and operational leadership in budget, asset enterprise management, financial management, financial management business transformation service, actuarial services and business oversight. The Strategic Acquisition Center provides dedicated acquisition and program management expertise and support for life cycle management of non-IT enterprise-wide solutions for VA’s highly complex requirements. Contracting officer’s representatives play a critical role in ensuring that contractors meet the commitment of their contracts. They ensure proper development of requirements and assist contracting officers in managing their contracts.
[14]Under the Federal Acquisition Regulation contracting officers are responsible for ensuring performance of all necessary actions for effective contracting, ensuring compliance with the terms of the contract, and safeguarding the interests of the United States in its contractual relationships. 48 C.F.R. § 1602-2. The Veterans Affairs Acquisition Regulations state that contract administration means government actions taken after contract award to obtain compliance with such contract requirements as timely delivery of supplies or services, acceptance, payment, and closing of the contract. These actions include, but are not limited to, technical, financial, audit, legal, administrative, and managerial services in support of the contracting officer. 48 C.F.R. § 842.070. Internal controls include Principle 14.
[15]An appropriation provides budget authority for federal agencies to incur obligations and to make payments out of the Department of the Treasury for specified purposes. Supplemental appropriations are provided in an act appropriating funds in addition to those already enacted in an annual appropriation act. An obligation is a definite commitment that creates a legal liability of the government for the payment of goods and services ordered or received, or a legal duty on the part of the United States that could mature into a legal liability by virtue of actions on the part of the other party beyond the control of the United States. See GAO, A Glossary of Terms Used in the Federal Budget Process, GAO‑05‑734SP (Washington, D.C.: Sept. 1, 2005). VA’s annual appropriations for health care include advance appropriations, which are appropriations that become available one or more fiscal years after the fiscal year for which the appropriations act was enacted.
[16]In addition to the EHCPM, VHA uses two other actuarial models, the Civilian Health and Medical Program Veterans Affairs Model and the Program of Comprehensive Assistance for Family Caregivers Projection Model, and “non-modeled” cost estimates, such as non-recurring maintenance at VA medical facilities and state-based long-term services and supports programs, to provide estimates to inform the remainder of its budget projection.
[17]EHCPM estimates encompass a full range of health care services to include prosthetics, dental, prescription drugs, and long-term services and supports in addition to just inpatient and outpatient care.
[18]According to VHA officials, EHCPM cost estimates are based on historical data and information provided by VHA, as well as assumptions from VHA subject matter experts, VA leadership, and VHA’s actuarial consultant.
[19]According to VHA officials, all work performed by VHA’s actuarial consultant is done at the direction of E&F. VHA’s actuarial consultant also maintains and updates the Civilian Health and Medical Program of the Department of Veterans’ Affairs model and the Program of Comprehensive Assistance for Family Caregivers projection model.
[20]When VHA begins developing the health care budget projection in April, it uses model estimates from the EHCPM update that begins in August of the previous year in addition to two other actuarial models: the Civilian Health and Medical Program Veterans Affairs model and the Program of Comprehensive Assistance for Family Caregivers projection model. Activities and programs that are not projected by these models are called “non-modeled” and change annually. In general, they may include non-recurring maintenance, state-based long-term services and supports programs, and readjustment counseling.
[21]31 U.S.C. § 1105. In practice, however, the budget submission sometimes occurs after the first Monday of February.
[22]During the “passback” process, OMB officials notify agencies of their approved budgetary levels, which may differ from the agencies’ budget requests. The “passback” process and the content of “passback” decisions may differ under each administration and each OMB Director. For example, “passback” decisions may also include program policy changes. An agency may appeal these decisions in accordance with the guidance on the appeals process issued by OMB at the time of “passback.” Such processes could include appealing decisions to the relevant OMB examiner or branch chief, the OMB Director, a group of officials, or, in some cases, to the President directly, depending on the procedures established by the OMB Director.
[23]Pub. L. No. 117-168, § 805, 136 Stat. 1759, 1804.
[24]There is a one year lag in projected unit costs data and actual obligations data. For example, for projected fiscal year 2025 unit costs, developed using fiscal year 2022 data, the complete actual obligations data would not be available until the end of fiscal year 2025.
[25]According to VHA officials, during and after the delivery of the initial budget scenario E&F and VHA’s actuarial consultant work collaboratively with VHA’s Office of Finance. VHA’s Office of Finance also provides input on assumptions and data used in the EHCPM.
[26]In addition to the advance appropriations, the President’s annual budget request for VHA includes a second part, called the revised estimate, which is an adjustment to the advance appropriations request based on more current information. In preparing for the fiscal year 2025 President’s budget request, VA did not include a revised estimate for health care.
[27]The Actuarial Standards Board’s actuarial standards of practice describe the procedures an actuary should follow when performing actuarial services and identify what the actuary should disclose when communicating the results of those services. Out of the 58 actuarial standards of practice, we identified eight that are relevant to the actuarial modeling that VHA uses to inform the budget projections for health care services. See appendix II for more information on actuarial standards of practice relevant to VHA’s processes for developing EHCPM estimates and examples of VHA’s actuarial consultant’s work.
[28]See VA OIG 24-03127-66. The VA Office of Inspector General also conducted a review of the circumstances and the underlying conditions that led to the Veterans Benefits Administration announcing a potential funding shortfall and requesting supplemental funding for fiscal year 2024. The Veterans Benefits Administration ultimately did not require this supplemental funding. The VA Office of Inspector General found that the Veterans Benefits Administration had not included realized prior-year recoveries in its monthly status report calculations throughout the year, which would have shown a reduced risk of a shortfall by year-end, among other things. The VA Office of Inspector General found that improved financial oversight, reporting accuracy, and communications may have obviated the need for a supplemental funding request. The VA Office of Inspector General made four recommendations to the Veterans Benefits Administration and VA’s Office of Management to improve financial management practices and communications, such as holding monthly fiscal reviews to routinely assess performance and cost drivers that may affect the status of available funds. As of April 24, 2026, all recommendations have been implemented. See Department of Veterans Affairs, Office of Inspector General, Veterans Benefits Administration: Review of VA’s $2.9 Billion Supplemental Funds Request for FY 2024 to Support Veterans’ Benefits Payments, VA OIG 24-03692-76 (Washington, D.C: Mar. 27, 2025).
[29]Relevant actuarial standards of practice include 23 (Data Quality); 41 (Actuarial Communications); and 56 (Modeling). The relevant federal internal control standards that VHA’s processes do not fully align with are Principle 7 (Identify, Analyze, and Respond to Risks), Principle 10 (Design Control Activities), Principle 12 (Implement Control Activities), Principle 13 (Use Quality Information), and Principle 15 (Communicate Externally). Actuarial Standards of Practice apply to actuaries, whereas the staff from VHA’s Office of Enrollment and Forecasting are not actuaries. Nonetheless, we viewed the actuarial standards as relevant guides to areas where VHA’s processes could potentially be improved. Our examination was focused on VHA’s processes and not VHA’s actuarial consultant’s compliance with Actuarial Standards of Practice. In their reporting, VHA’s actuarial consultant certified that its work was performed in compliance with Actuarial Standards of Practice.
[30]See section 3.3, 3.4, and 3.5 of Actuarial Standard of Practice No. 23.
[31]See Principle 13 in GAO‑25‑107721.
[32]According to E&F officials, VHA’s actuarial consultant reviews the data for reasonableness and consistency, which aligns with the relevant actuarial standards of practice 23 (Data Quality). Actuarial standards of practice No. 23 provides guidance for (1) selecting the data that underlie the actuarial work product; (2) relying on data supplied by others; (3) reviewing data; (4) using data; (5) preparing data to be used by other actuaries in an actuarial work product; and (6) making appropriate disclosures with regard to data quality.
[33]See GAO, VA Health Care: Additional Steps Could Help Improve Community Care Budget Estimates, GAO‑20‑669 (Washington, D.C.: Sept. 30, 2020).
[34]VHA, VHA’s actuarial consultant, the Office of Actuarial Services, VHA Office of Finance, and the Office of Integrated Veteran Care meet monthly to review community care data and address any issues related to data consistency and reliability. During these meetings, participants compare trends in community care claims and payments observed across offices, reconcile discrepancies, and discuss methods for categorizing services to ensure a shared understanding of community care workload and costs.
[35]See section 3.2 of Actuarial Standard of Practice No. 23.
[36]See Principles 10, 12, and 13 in GAO‑25‑107721.
[37]Incorporating newly emerging data may include refreshing some of the baseline data or refreshing one or more assumptions if new information becomes available after the budget scenario is finalized, and before submitting the VHA health care budget projections for the President’s budget request. For example, when new information emerges that might influence key assumptions, such as pharmaceutical trends from the office of VHA’s Pharmacy Benefits Management Services, VHA’s actuarial consultant may make adjustments to these assumptions without necessarily re-baselining the entire model.
[38]For example, according to VHA documents, the 2023 EHCPM model used base year 2022 data (data as of September 30, 2022) to project an estimated total health care cost of $130 billion for fiscal year 2025. However, when the model was updated using newly emerging data from September 30, 2023, the projected total cost was $132.6 billion for fiscal year 2025.
[39]See section 3.1 of Actuarial Standard of Practice No. 56 and section 3.4 of Actuarial Standard of Practice No. 41.
[40]See Principles 7 and 15 in GAO‑25‑107721.
[41]We previously recommended VA establish further steps for assessing and communicating to stakeholders the degree of overall uncertainty associated with actuarial projections for community care that inform the community care budget estimates. VA agreed with our recommendation. To implement this recommendation, E&F developed a risk assessment report to communicate to stakeholders the degree of overall uncertainty associated with the actuarial projections used to support the President’s budget. For more information, see GAO‑20‑669.
[42]Various techniques can be used to develop and communicate overall uncertainty, and some techniques might be more practical and useful than others depending upon facts and circumstances. Techniques from the actuarial literature include scenario analysis under plausible alternative scenarios, stochastic analysis, and stress testing.
[43]Scenario analysis is a process for assessing the impact of one possible event or several simultaneously or sequentially occurring possible events. Scenario analysis may include numerical calculations. Stress testing measures the impact of adverse changes affecting an organization’s financial position.
[44]According to VHA officials, staff from E&F serve as the contracting officer’s representative. The contracting officer’s representative manages labor hours and the quality of the work provided to ensure that the government receives the best value for the work performed. This is done by soliciting information from E&F staff who have led tasks in the performance work statement and have direct knowledge about the level of effort necessary to perform the work, responsiveness of the contractor, and the quality of the work.
[45]VHA documents also show that E&F develops a contractor performance assessment report that is used to help government agencies make objective selection decisions for future contract awards. According to VHA officials and documentation, VHA’s actuarial consultant performs its work under an actuarial support services contract that E&F manages. This federal contract is developed and managed under the Federal Acquisition Regulation and the VA Acquisition Regulation. As part of the contract, the actuarial consultant is responsible for several tasks that are outlined in the performance work statement. See appendix III for a list of project tasks, deliverables, and required due dates for the deliverables of VHA’s actuarial consultant as outlined in the performance work statement.
[46]48 C.F.R. § 46.401.
[47]According to the American Academy of Actuaries, an independent review is an expert evaluation of an actuary’s work by another qualified actuary that strengthens and maintains confidence in actuarial work and the profession, and protects the public interest by ensuring that actuarial opinions are objective and of the highest quality.
[48]See GAO, DHS Office of Inspector General: Actions Needed to Address Long-Standing Management Weaknesses, GAO‑21‑316 (Washington, D.C.: June 3, 2021); Genetically Engineered Crops: USDA Needs to Enhance Oversight and Better Understand Impacts of Unintended Mixing with Other Crops, GAO‑16‑241 (Washington, D.C.: Mar. 15, 2016); Streamlining Government: Key Practices from Select Efficiency Initiatives Should Be Shared Governmentwide, GAO‑11‑908 (Washington, D.C.: Sept. 30, 2011); and Results-Oriented Cultures: Implementation Steps to Assist Mergers and Organizational Transformations, GAO‑03‑669 (Washington, D.C.: July 2, 2003).
[49]See Principle 14 in GAO‑25‑107721.
[50]E&F and its actuarial consultant are responsible for the actuarial model used to develop estimates for VA’s health care funding needs. VHA’s Office of Finance reviews, calculates, and combines both modeled and unmodeled estimates into an overall VHA estimate for review and approval by the Office of the Under Secretary for Health.
[51]Actuarial Standards of Practice apply to actuaries, whereas the staff from VHA’s Office of Enrollment and Forecasting are not actuaries. Nonetheless, we viewed the actuarial standards as relevant guides to areas where VHA’s processes could potentially be improved. Our examination was focused on VHA’s processes and not VHA’s actuarial consultant’s compliance with Actuarial Standards of Practice. In their reporting, VHA’s actuarial consultant certified that its work was performed in compliance with Actuarial Standards of Practice.
[52]The actuarial analyses and reviews in this report were performed by Assistant Director, Actuary Lijia Guo, Ph.D., ASA, MAAA; and Chief Actuary Frank Todisco, FSA, MAAA. Collectively, the actuaries responsible for this review meet the American Academy of Actuaries’ qualification standards with respect to their educational background, designated professional standing, and experience.
[53]Actuarial standards of practice are promulgated by the Actuarial Standards Board. These 58 standards describe the procedures an actuary should follow when performing actuarial services and identify what the actuary should disclose when communicating the results of those services. We selected eight as the most relevant to VHA’s processes for developing EHCPM model estimates. For more information, see Incurred Health and Disability Claims (No. 5), Risk Classification (No. 12), Expert Testimony by Actuaries (No. 17), Data Quality (No. 23), Credibility Procedures (No. 25), Actuarial Communications (No. 41), The Use of Health Status Based Risk Adjustment Methodologies (No. 45), and Modeling (No. 56).
[54]Internal control is a process effected by an entity’s oversight body, management, and other personnel that provides reasonable assurance that the objectives of an entity will be achieved. In this review, we relied specifically on internal control Principle 7, 10, 12, 13, and 15. See GAO, Standards for Internal Control in the Federal Government, GAO‑25‑107721 (Washington, D.C.: May 15, 2025).
[55]The Office of Actuarial Services provides coordination and oversight in the development of actuarial estimates, polices, and services for the department. The Office of Integrated Veteran Care is a national program office that manages and advocates for veterans’ and beneficiaries’ access to health care in both VA and community facilities. The Office of Productivity, Efficiency and Staffing is responsible for developing VA’s clinical productivity metrics and efficiency models. The Pharmacy Benefits Management Services provides leadership for pharmacy activities in VHA. The Prosthetics and Sensory Aids Service provides prosthetic devices and sensory aids service to veterans. The Veterans Benefit Administration provides financial and other forms of assistance to veterans and their dependents.
[56]The Office of Management enables VA to provide a full range of benefits and services to veterans by providing strategic and operational leadership in budget, asset enterprise management, financial management, financial management business transformation service, actuarial services, and business oversight. The Strategic Acquisition Center provides dedicated acquisition and program management expertise and support for life cycle management of non-IT enterprise-wide solutions for VA’s highly complex requirements.
[57]Contracting officers are responsible for ensuring performance of all necessary actions for effective contracting, ensuring compliance with the terms of the contract, and safeguarding the interests of the United States in its contractual relationships. 48 C.F.R. § 1602-2. Contract administration means government actions taken after contract award to obtain compliance with such contract requirements as timely delivery of supplies or services, acceptance, payment, and closing of the contract. These actions include, but are not limited to, technical, financial, audit, legal, administrative, and managerial services in support of the contracting officer. 48 C.F.R. § 842.070. Internal controls include Principle 14.