Report to Congressional Committees
United States Government Accountability Office
A report to congressional committees
Contact: Sharon M. Silas at silass@gao.gov
What GAO Found
In 2023, the Department of Defense (DOD) directed the military departments—Army, Navy, and Air Force—to update their policies on clinical quality management to align with Defense Health Agency (DHA) procedures to ensure high-quality care in operational settings. In December 2024, GAO reported that the military departments had not yet issued policies, specifically on provider credentialing and privileging, and recommended that they do so. As of March 2026, GAO found that Army and Air Force had not issued updated policies, while Navy issued several policies on aspects of clinical quality management.
GAO maintains that the military departments’ updates to these policies will facilitate a more consistent approach to clinical quality in operational settings. These updates may require more time, as the military departments incorporate additional changes resulting from DOD’s October 2025 implementation of a universal provider privileging program (i.e., the process of reviewing a provider’s qualifications and granting permission to deliver specific services).
For patient safety events and health care risk management investigations, Army and Air Force officials stated that their departments generally follow the processes outlined in DHA’s procedures manual as their policies are being updated. GAO also found that Navy’s policies—which have been updated—align with DHA’s procedures.
· Patient safety events are incidents or conditions that could have resulted, or did result, in harm to a patient, such as a medication error or a wrong-site surgery. Events are entered into a patient safety reporting system and investigated accordingly.
· Health care risk management activities primarily involve provider quality assurance investigations, which could originate from suspected provider misconduct, among other reasons. Army and Air Force leverage DHA for assistance for investigations; Navy relies on its medical staff for support.
Why GAO Did This Study
DOD health care providers deliver critical health care services in settings where military operations take place. These operational settings include hospital ships, field hospitals, and aircraft carriers. To guide efforts to promote health, prevent harm, and provide high-quality care in the military health system, DHA issued a clinical quality management framework in 2019. This framework consists of programs such as provider credentialing and privileging, patient safety, and risk management. Military departments are responsible for updating their policies to align with DHA’s framework and implementing these programs in operational settings.
A House Report accompanying the National Defense Authorization Act for Fiscal Year 2023 includes a provision for GAO to review how the military departments ensure clinical quality in operational settings. GAO reported in GAO-25-106445 on provider credentialing and privileging and recommended that the military departments issue updated policies, which they indicated would be included in overall clinical quality management policies for operational settings. In this report, GAO describes (1) the status of these military department policies on clinical quality management, (2) how the military departments report and manage patient safety events, and (3) how the military departments conduct health care risk management investigations.
GAO interviewed DHA and military department officials and reviewed relevant program documentation. GAO also reviewed available operational patient safety event data reported for fiscal years 2022 through 2024, the most recent available data at the time of this review. These data were not included due to DOD’s concerns about the sensitivity of these data.
Abbreviations
DHA Defense Health Agency
DOD Department of Defense
This is a work of the U.S. government and is not subject to copyright protection in the United States. The published product may be reproduced and distributed in its entirety without further permission from GAO. However, because this work may contain copyrighted images or other material, permission from the copyright holder may be necessary if you wish to reproduce this material separately.
July 13, 2026
The Honorable Roger Wicker
Chairman
The Honorable Jack Reed
Ranking Member
Committee on Armed Services
United States Senate
The Honorable Mike Rogers
Chairman
The Honorable Adam Smith
Ranking Member
Committee on Armed Services
House of Representatives
The Department of Defense’s (DOD) military health system delivers critical health care services to active-duty service members and other eligible beneficiaries in a range of settings, including in military medical treatment facilities and in operational settings. Operational settings are generally geographic locations that are used by the military departments—Army, Navy, and Air Force—to meet the needs of a mission, such as providing humanitarian assistance and trauma care for battle injuries. These locations may be remote, near combat zones, or in areas that have experienced natural disasters.
In operational settings, health care providers deliver care on hospital ships, aircraft carriers, aeromedical evacuation aircraft, and field hospitals, among other places. The type of care delivered can range from first responder care to advanced medical care, such as surgical procedures, depending on the clinical capabilities of the operational setting.
DOD’s Defense Health Agency (DHA) has established policies to help ensure that the military health system provides high-quality care in all settings. Specifically, DHA established a clinical quality management framework that it issued in August 2019.[1] The framework outlines six aspects of clinical quality management, which DHA refers to as programs. These include patient safety—the prevention of patient harm in health care settings—and health care risk management—the mitigation of risk in the clinical aspects of health care delivery—among other programs.[2]
DHA is responsible for implementing its clinical quality management framework at military medical treatment facilities. The military departments are responsible for clinical quality management in operational settings. In July 2023, DOD issued an instruction directing the military departments to update their policies for managing clinical quality in operational settings to align with the DHA procedures manual and to ensure consistency, to the extent practicable, across the military health system.[3] The DOD instruction did not specify a deadline for these updates.
A House Report accompanying the National Defense Authorization Act for Fiscal Year 2023 includes a provision for us to review how the military departments ensure clinical quality in operational settings.[4] In December 2024, we reported on one of the clinical quality management programs—provider credentialing and privileging—and found that the military departments’ policies were outdated and did not align with DHA’s framework.[5] We recommended that the military departments update their policies on provider credentialing and privileging, and DOD concurred with our recommendations. In this report, we describe the status of the military departments’ clinical quality management policies and two more clinical quality management programs—patient safety and health care risk management.[6] Specifically, we describe
1. the status of the military departments’ policies on clinical quality management in operational settings;
2. how the military departments report and manage patient safety events occurring in operational settings; and
3. how the military departments conduct health care risk management investigations for operational settings.
To describe the status of the military departments’ policies on clinical quality management in operational settings, we interviewed Army, Navy, and Air Force officials regarding their progress toward updating these policies. We reviewed recent DHA memorandums on provider privileging and interviewed DHA officials to understand the effects of these memorandums on military department policies.
To describe the military departments’ reporting and management of patient safety events occurring in operational settings, as well as how they conduct health care risk management investigations, we interviewed patient safety and health care risk management officials at Army, Air Force, and Navy about their processes. We were unable to review updated Army and Air Force policies for patient safety and health care risk management, as they had not been issued at the time of our review. Navy issued policies for patient safety in July 2025 and health care risk management in April 2025, which we reviewed. We also reviewed Navy’s clinical quality management program policy released in January 2026, which provides an overview of several of the programs included in the DHA procedures manual but does not address all clinical quality management programs. We interviewed DHA officials about their support of the military departments and reviewed relevant DOD and DHA policies and procedures.
We also analyzed patient safety data reported by each of the military departments for operational settings in the Joint Patient Safety Reporting system for fiscal years 2022 through 2024, the most recent fiscal years for which data were available at the time of our review. However, due to DOD’s concerns about the sensitivity of these data, we did not include the results of our analyses in this report. A general description of the data we reviewed is included in appendix II.
We conducted this performance audit from December 2024 to July 2026 in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Background
The Military Health System, DHA, and Military Departments
The military health system is a complex, integrated enterprise responsible for health care delivery, combat medicine, medical education, public health, and medical research and development. The military departments and DHA share responsibilities within this system. Specifically, DHA manages and administers military medical treatment facilities worldwide and oversees health care delivery in these locations, among other responsibilities.[7] The military departments are responsible for health care delivered in operational settings.
|
DOD Combatant Commands
DOD’s operational settings may be aligned with one of its 11 unified combatant commands, which are joint military commands that are composed of units from two or more military departments and conduct broad and continuing missions. Six of the combatant commands are responsible for defined geographic areas, such as Africa and Europe. Operational settings are located within the geographic areas covered by these commands. The remaining combatant commands are functional and focus on issues such as cyberspace operations and transportation. Source: GAO analysis of Department of Defense (DOD) information; U.S. Marine Corps photo by Lance Cpl. Justin Cledera. | GAO‑26‑107979 |

Each military department maintains one or more organizational units that carry out health care responsibilities under the leadership of a surgeon general. These organizational units include the U.S. Army’s Medical Command, the Air Force’s Medical Command, and the Navy’s Bureau of Medicine and Surgery. These departments train and equip their own medical personnel to deliver health care in both military medical treatment facilities and operational settings.
Clinical Quality Management
DHA’s clinical quality management framework consists of six programs: patient safety, health care risk management, credentialing and privileging, accreditation and compliance, clinical measurement, and clinical quality improvement.[8]
Patient Safety
Patient safety includes the identification, investigation, and response to patient safety events, which are incidents or conditions that could have resulted, or did result, in harm to a patient in a health care setting. For example, an incident could include a medication error or surgery on the wrong part of the body, known as wrong-site surgery. According to the DHA procedures manual, patient safety events must be reported so they may be used as learning opportunities to prevent future harm.
Patient safety events that occur within the military health system are captured in the Joint Patient Safety Reporting system (patient safety reporting system).[9] Individuals with appropriate credentials are expected to submit a report of any event or unsafe condition into the system. Reporting can be anonymous and includes information regarding the facts of the event, such as the date, location, and description of what occurred. There are four categories of patient safety events:
· Adverse event. Patient experiences harm, which may have occurred by the omission or commission of medical care.
· No-harm event. Patient experiences event but was not harmed.
· Near-miss event. Patient does not experience event (also known as “close call”).[10]
· Unsafe/hazardous condition. Condition or a circumstance (other than a patient’s own disease process or condition) that increases the probability of an adverse event.
Events can only be reported in locations for which the patient safety reporting system has been configured. The military departments are responsible for submitting a request to DHA for the system to be configured to capture all the events occurring within their specific geographic operational locations. If the patient safety reporting system cannot be accessed, the military departments are to use paper records and enter events into the system when it becomes available.[11]
Health Care Risk Management
Health care risk management includes identifying and assessing risks to a health care organization, patients, and staff and implementing risk reduction and process improvement strategies. A primary focus of health care risk management policies is investigations of providers and any actions taken against them, referred to as clinical adverse actions.[12]
Investigations of providers, known as quality assurance investigations, may be initiated when there are concerns about suspected provider misconduct, impairment, incompetence, or any conduct that adversely affects, or could adversely affect, the health or welfare of a patient or staff member. These investigations involve due process professional reviews, based on evidence. They may result in a clinical adverse action, which could leave the provider unable to practice and may result in a report to the state or states of licensure or other applicable certifying or regulatory agencies, among other things.
DHA and DOD Guidance
Two key guidance documents inform the military departments’ policies for clinical quality management.
· DHA Procedures Manual 6025.13. In 2019, DHA published a procedures manual that outlines key activities for clinical quality management in the military health system, including guidance for the six programs.[13]
· DOD Instruction 6025.13. In July 2023, DOD issued a corresponding instruction to further define the military departments’ roles and responsibilities, including that they establish policies for operational settings that align with the DHA procedures manual to the extent practicable.[14] The DOD instruction did not specify a time frame for these updates.
In addition, DOD implemented a universal privileging program for providers in the military health system—referred to as enterprise-wide credentialing and privileging—in October 2025.[15] Under this program, military providers will not have to be re-privileged when changing care locations, for example, between military medical treatment facilities and operational environments. This change of how providers are privileged within the military health system directly affects the clinical quality management program for credentialing and privileging, though it is also relevant to other areas of quality management, such as health care risk management.[16] According to DHA, this change was a significant undertaking for the military health system. The shift to universal privileging was done through a series of memorandums and will require updates to the military departments’ procedures and policies, according to DHA.
The Military Departments Are in Varying Stages of Updating Clinical Quality Management Policies for Operational Settings to Align with DHA Procedures
Army, Air Force, and Navy are in varying stages of updating their clinical quality management policies in response to recommendations we made in December 2024 to align with DHA’s clinical quality management framework.[17] Additionally, according to DHA and the military departments, DOD’s October 2025 implementation of a universal privileging program for providers in the military health system will require updates to relevant clinical quality management instructions, procedures, and policies, which could further delay the military departments’ efforts.
In December 2024, we reported that the military departments had outdated policies to address clinical quality management in operational settings, specifically with respect to provider privileging.[18] Officials from each of the military departments told us that they had been waiting for the DOD instruction on clinical quality management—which was issued in July 2023—before updating and finalizing their department’s policies to align with the DHA procedures manual, as required by the instruction.[19] We recommended that each of the military departments issue, as soon as possible, updated clinical quality management policies for provider privileging in operational settings. DOD concurred with our recommendations.
In response to our recommendations, Army and Air Force indicated that their updated policies for provider privileging would address all clinical quality management programs, including patient safety and health care risk management.[20] In March 2026, Army officials told us they were holding working groups and discussions with stakeholder groups on updates to their policy, but they did not have a time frame for completing their updates. Air Force officials also indicated in March 2026 that they hoped to issue their policy in September 2026, after incorporating revisions to incorporate DOD’s recent universal privileging program. Without these clinical quality management policies, there were no patient safety or health care risk management policies for us to review.
Navy has taken a different approach to updating policies for its clinical quality management programs. During the course of our work, Navy issued separate policies to address aspects of clinical quality management in operational settings. Specifically, the department issued individual policies for patient safety and health care risk management in July 2025 and April 2025, respectively.[21] Navy also issued a clinical quality management program framework in January 2026 which touches on three of the six programs in the DHA procedures manual.[22] As of April 2026, Navy anticipated issuing its specific policy on credentialing and privileging in August 2026, after incorporating any changes needed to comply with DOD’s universal privileging program.[23]
DOD officials stated that the recent universal privileging policy would require the military departments to modify some policies that are under development, such as the clinical quality management policies, as well as some published policies, such as the DHA procedures manual. This will likely add to their time frames for completing their policy updates as required by the DOD instruction on clinical quality management. As a result, it is not clear when the military departments will finalize all their clinical quality management policies for the six programs outlined in DHA’s framework. In accordance with our prior report, we continue to believe that updated policies will facilitate a more consistent approach for the military departments’ clinical quality management across all operational settings which will help to ensure that service members in these settings receive high-quality care.
Military Departments Generally Follow the Same Process to Report and Manage Patient Safety Events
The military departments told us they generally follow the process outlined in the DHA procedures manual to report and manage patient safety events. Army and Air Force officials described their processes and told us their written policies remained under development. Navy released a written patient safety policy in July 2025. All the military departments stated that an April 2026 updated patient safety reporting system is intended to help improve the reporting of patient safety events in operational settings.
Military Departments Generally Follow the DHA Procedures Manual to Report and Manage Patient Safety Events in Operational Settings While Departments Develop Policies
Officials from the three military departments told us they generally follow the processes outlined in the DHA procedures manual for reporting and managing patient safety events that occur in operational settings (see fig. 1). Because Army and Air Force are in the process of updating their policies, officials described to us the processes they follow. Navy released a written patient safety policy in July 2025, and we found that it largely mirrors the DHA procedures manual.[24]
Figure 1: Overview of Defense Health Agency Procedures Manual Process for Reviewing Patient Safety Events Reported in Operational Settings
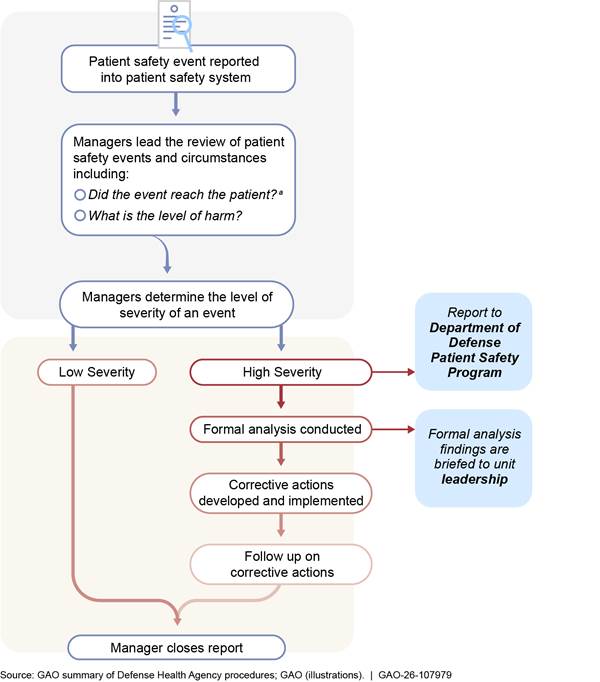
aIf an event reaches a patient, it is also reported to health care risk management for assessment.
According to the DHA procedures manual, all reported patient safety events are to be entered into the authorized patient safety reporting system, the Joint Patient Safety Reporting system. Individuals with appropriate credentials can access the system and are expected to report patient safety events. An online form captures information about the event, such as the date, location, and a description of what occurred. This form is then submitted into the patient safety reporting system and becomes part of the database.
|
Air Force Aeromedical Evacuation
The aeromedical evacuation system works throughout the military health system by moving patients of all military departments to locations that can provide more comprehensive care. When a patient safety event occurs during the movement of a patient, Air Force officials said they follow the same processes for managing patient safety events as in other operational settings. Air Force officials said patient safety events that occur during patient movement may involve additional collaboration and coordination between the military departments. This may include sending an event report to other involved military departments to obtain or provide insight into the event. The other military department may also document the event in the patient safety reporting system to identify gaps they need to address. Source: GAO summary of U.S. Air Force, Army, and Navy information; U.S. Air National Guard photo by Tech. Sgt. Nicole Wright. | GAO‑26‑107979 |

Once the event is reported, a designated individual—the patient safety manager—accesses the system and reviews the event. In operational settings, these managers may not be physically located in the same area where the event occurred. For example, Navy officials said managers may not be on every vessel due to staffing limitations, while Air Force officials said the manager role is an additional duty taken on by a service member based in a deployed location.
The managers review patient safety reports to identify any gaps in systems and processes for patient care. They may conduct follow-up work with involved staff to obtain pertinent incident information or assign other reviewers with relevant knowledge and expertise to examine how and why the event occurred, according to military department officials. After looking over responses, the manager may close the report.[25]
In some instances, a patient safety event may involve more than one military department and may, therefore, be reviewed by multiple departments. Navy officials said such instances commonly occur, for example, during operations where a Navy medical facility requests a patient movement and the Air Force executes an aeromedical evacuation.
The specific responsibilities for the manager during the review of a patient safety event include the following:
· Determining if the event reached the patient or did not reach the patient; assigning the appropriate degree of harm for events that reached a patient (no harm, mild harm, moderate harm, or severe harm); and identifying unsafe conditions or near misses or close calls for events that did not reach a patient.
· Classifying the event type based on the description of what occurred, such as product or device events (e.g., defects in products or devices); environmental events (e.g., shocks or burns); or surgical, invasive procedure, or anesthesia events (e.g., wrong-patient or wrong-site surgery).
· Assigning a risk assessment grade (low, significant, or high) based on the severity of a patient safety event and the probability of recurrence.
Certain patient safety events with a high level of severity or harm—known as DOD reportable events—have specific requirements.[26] These events must be reported to leadership within 24 hours of being identified. Officials from the military departments said they follow this timeline, though Army officials noted this may be difficult to achieve in operational settings. Additionally, DOD reportable events require a formal investigation called a comprehensive systematic analysis to identify causal and contributing factors. Officials from the military departments said these formal investigations may also be undertaken for events of lower severity, if necessary, due to the potential for future harm.
The patient safety manager generally conducts these formal investigations with support from the military departments’ medical commands, according to military department officials. In addition, DHA officials said they can assist the military departments with these investigations. Completed investigations must be sent to military department leadership for review and approval, according to the military departments, and to the DOD patient safety program, according to the procedures manual.
When investigations identify gaps in systems and processes, officials told us that corrective actions are taken to mitigate these gaps and improve processes. In addition, officials said that progress toward these actions is tracked, and the corrective action is not closed until implementation is complete. After a corrective action is implemented, a report is sent to leadership.
Officials from the military departments said they use patient safety event reports to understand patient safety trends and improve processes. Specifically, the patient safety managers track data on patient safety trends and present improvement efforts in regular knowledge sharing sessions. Their efforts may also involve sharing information—such as safety alerts—within and across the military departments for wider awareness.[27]
An Updated Patient Safety Reporting System Is Intended to Facilitate Reporting of Patient Safety Events in Operational Settings
An updated Joint Patient Safety Reporting system, to be implemented in April 2026, could improve the military departments’ ability to enter patient safety events in operational settings, according to DHA and military department officials.[28] The military departments cited limitations to entering patient safety events into the system that was being used at the time of our review, such as not having the system configured to report events in all locations and an inability to access the database in operational settings.
|
Navy Connectivity Issues
Navy officials indicated that connectivity is a particular challenge when ships are at sea and, as a result, not all patient safety events are reported in the system. While paper records may be created in the interim, Navy officials acknowledged these records may not be entered into the system, as required. Officials also acknowledged not all patient safety events may be reported or recorded due to limited personnel on ships. DHA officials said they have plans for an offline reporting capability that is intended to allow patient safety reports to be filled out offline and uploaded once connectivity is restored. Source: GAO Summary of U.S. Navy and Defense Health Agency (DHA) information; U.S. Navy photo by Mass Communication Specialist 2nd Class Kaitlin Young. | GAO‑26‑107979 |

In the updated system, the military departments and DHA have worked to address several of the limitations described by the military departments. According to DHA officials, the updated system is intended to have an expanded list of geographic locations provided by the military departments to facilitate their ability to report patient safety events for operational settings. The patient safety reporting system is location dependent—that is, it can only capture events in specific geographic locations for which it has been configured.[29] If a location is not available as an option in the system, the event cannot be captured. The system used at the time of our review was not configured for all geographic locations where the military departments operate, and, as a result, it did not include all patient safety events that occurred in these operational settings. Specifically, Army officials said that, as of fiscal year 2024, the patient safety system was only configured to capture their patient safety events for operational settings in one geographic area, but the updated system includes all operational settings identified at the time of the system’s release.[30]
The military departments also indicated that individuals might have been unable to report patient safety events if they did not have access to a computer at their location. To improve reporting capability, DHA officials said the updated system is designed to allow users to report patient safety events with a mobile device rather than a computer. DHA officials told us the mobile reporting capability should allow for easier reporting in deployed areas. These planned system changes are positive steps; however, until the updated system is implemented, it is too early to assess the extent to which the system will fully address the identified limitations.
Military Departments Generally Use DHA’s Procedures for Health Care Risk Management Investigations for Operational Settings
Military department officials told us they generally follow the process outlined in the DHA procedures manual for health care risk management investigations into providers. The military departments are responsible for initiating and processing these investigations for operational settings. Army and Air Force leverage DHA for assistance with their investigations and have taken steps to clarify this process through memorandums while their policies for clinical quality management are under development. Navy issued a policy detailing its process for health care risk management investigations in April 2025 and relies on its medical command for support, according to officials.
Military Departments Generally Follow DHA’s Procedures Manual for Health Care Risk Management Investigations in Operational Settings
Military department officials told us they generally follow the process for health care risk management investigations into providers that is outlined in the DHA procedures manual. As a result, the process used in operational settings is largely consistent with the process used at military medical treatment facilities. Because Army and Air Force are in varying stages of updating their clinical quality management policies, officials described to us the investigation process that they use in operational settings. Navy issued an updated policy on clinical adverse actions and health care misconduct in April 2025, which includes a process for health care risk management investigations. We found that it is generally the same process as outlined in the DHA procedures manual.[31]
Provider investigations, commonly referred to as quality assurance investigations, are a key element of the military departments’ health care risk management efforts.[32] These quality assurance investigations focus on the providers’ ability to deliver safe health care, with a goal of mitigating risk to the military health system while providing due process.[33] According to the manual, quality assurance investigations can be done anytime there are concerns of suspected misconduct, impairment, incompetence, or any conduct that adversely affects, or could adversely affect, the health or welfare of a patient, or staff member. Figure 2 details the process for these investigations, which are completed by a peer who formally reviews allegations and issues a report with conclusions and recommendations. The report goes through additional layers of review, and the process allows for provider appeal.[34] Final decisions may be reported to regulatory agencies or state licensure entities.
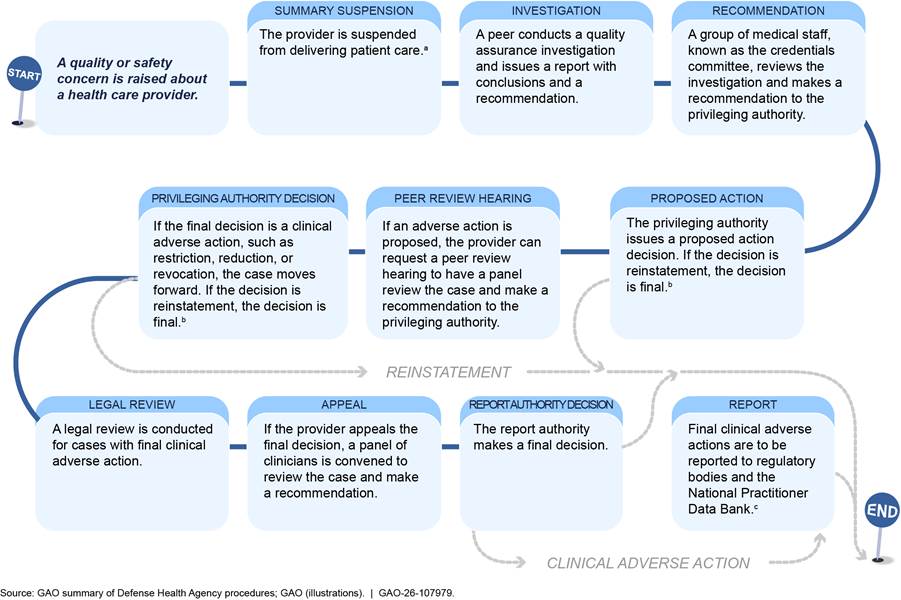
aThe provider is placed in summary suspension—the temporary removal of all or a portion of a health care provider’s privileges or scope of practice. Summary suspensions continue until the clinical adverse action process is complete. The Defense Health Agency requires that summary suspensions that exceed 30 calendar days be reported to the National Practitioner Data Bank—a web-based repository of reports containing information on medical malpractice payments and certain adverse actions related to health care practitioners, providers, and suppliers—and the states of licensure for privileged providers such as physicians and physicians’ assistants. Summary suspensions of non-privileged providers, such as registered nurses, do not need to be reported.
bClinical adverse actions include actions that limit the care a provider can deliver or that prohibit them from delivering care altogether, such as the restriction, reduction, or revocation of a provider’s permission to deliver care. The privileging authority also may decide to reinstate providers with or without a temporary period of performance monitoring.
cThe surgeons general of the military departments are responsible for reporting final clinical adverse actions to the National Practitioner Data bank, as well as any states where the provider holds a medical license, for any providers in operational settings.
Military Departments Are Responsible for Provider Investigations in Operational Settings and Have Taken Steps to Clarify Responsibilities for Investigations While Policies Are Being Updated
The military departments are responsible for provider quality assurance investigations in operational settings. Army and Air Force officials told us that they leverage DHA for assistance because they do not have the capacity to conduct these investigations. Air Force officials also stated that they leverage operational personnel to the maximum extent practicable for peer review panels, since operational personnel may have information pertinent to these investigations. Navy officials indicated that they rely on support from the Navy medical command, the Bureau of Medicine and Surgery, for quality assurance investigations.
|
Privileging Authority
Privileging a provider involves a review of professional credentials—such as medical licenses—and qualifications to ensure the provider is qualified to serve in the specific health care setting. Officials designated as the privileging authority are responsible for deciding whether to grant privileges to providers, following their review and consideration of the locations’ capacities. Within the military health system, the Defense Health Agency director and the surgeons general of the military departments (Army, Air Force, and Navy), or their delegates, serve as privileging authorities. Source: GAO analysis of Defense Health Agency Procedures; Defense Health Agency photo by Robb Agnello. | GAO‑26‑107979 |

DHA officials noted that, while its personnel have assisted the military departments, those departments were ultimately responsible for the investigations and outcomes. To help clarify the responsibilities for these quality assurance investigations, DHA signed memorandums of agreement with Army in February 2025 and Air Force in December 2024. Under these agreements, DHA agreed to conduct the processing of these investigations for the military departments’ review and decision.
According to the DHA procedures manual, the privileging authority initiates a quality assurance investigation when a quality or safety concern is raised. Prior to October 2025, the surgeons general of each military department—who serve as privileging authorities—were required to re-privilege providers for operational settings. With the shift to universal privileging for the military health system in October 2025, the surgeons general no longer need to re-privilege providers in operational settings. However, they will continue to serve as privileging authorities and be responsible for clinical quality in operational settings—to include initiating quality assurance investigations—according to DHA officials.
DHA officials further stated that the implementation of the universal privileging system will require updates to the memorandums of agreement they have with the Army and Air Force. Additionally, they said that clinical quality management instructions, procedures, and policies will need to be updated. These updates may further delay the military departments’ written clinical quality management policies, which they have been in the process of updating in response to our December 2024 recommendations. These policies will be important in guiding cooperation and clarifying roles among the different entities in the military health system, especially for the Army and Air Force.
Concluding Observations
Military department policies to manage clinical quality in operational settings, like field hospitals and aircraft carriers, have been under development for several years. While some progress has been made in response to our December 2024 recommendations, DHA and the military departments will need to make critical updates to ensure a consistent approach for clinical quality management and fully implement our recommendations. These updates are particularly important for clarifying the roles and responsibilities between the military departments and DHA under the new October 2025 universal privileging program. While we understand that updating these policies may take time, the lack of clarity on responsibilities for operational settings could result in implementation challenges in executing clinical quality programs in these locations, potentially impacting the quality of care. Issuing these policies, as soon as possible, would help the military departments to ensure that service members in operational settings are consistently receiving high-quality care.
Agency Comments
We provided a copy of this report to DOD for review and comment. DOD provided technical comments, which we incorporated, as appropriate.
We are sending copies of this report to the appropriate congressional committees, the Secretary of Defense, and other interested parties. In addition, the report will be available at no charge on GAO’s website at http://www.gao.gov.
If you or your staff have any questions about this report, please contact me at SilasS@gao.gov. Contact points for our Offices of Congressional Relations and Public Affairs can be found on the last page of this report. Other major contributors to this report are listed in appendix IV.

Sharon M. Silas,
Director, Health Care
The Defense Health Agency (DHA) established six programs in its clinical quality management framework for the military health system. These programs are outlined in its 2019 procedures manual: 1) credentialing and privileging; 2) patient safety; 3) health care risk management; 4) accreditation and compliance; 5) clinical measurement; and 6) clinical quality improvement.[35] In December 2024, we reported on the military departments’ efforts to implement the credentialing and privileging program.[36] In this report, we describe the departments’ efforts to implement the patient safety and health care risk management programs. In table 1, we summarize the military departments’ efforts to implement the other three programs.
Table 1: Military Departments’ Efforts to Implement Selected Programs in the Military Health System’s Clinical Quality Management Framework, as of March 2026
|
Military department |
Clinical quality management program |
Status |
|
Army |
Accreditation and compliancea |
Developing a comprehensive list of operational clinical services facilities that need to be accredited. |
|
Clinical measurementb |
Developing a clinical measurement program. |
|
|
Clinical quality improvementc |
Developing a clinical quality improvement program. |
|
|
Air Force |
Accreditation and compliance |
For non-deployed settings, conducting a gap analysis to determine what facilities need accreditation; for deployed settings, determining how to meet compliance requirements. |
|
Clinical measurement |
Working to establish additional standardized clinical measures for deployed operational settings; working to collect clinical measures currently tracked in deployed settings. |
|
|
Clinical quality improvement |
Working to establish tracking and oversight for clinical quality improvement in deployed operational settings. |
|
|
Navy |
Accreditation and compliance |
Identifying operational clinical services sites and determining which category of accreditation criteria apply. |
|
Clinical measurement |
Collects six categories of information in operational settings and uses these data for clinical quality improvements. |
|
|
Clinical quality improvement |
Identified examples of clinical quality improvement programs, including operational clinical communities to discuss and enact process improvement initiatives. |
Source: GAO summary of information provided by military departments. | GAO‑26‑107979
aAccreditation is the process of review that allows health care organizations to demonstrate their ability to meet regulatory requirements and standards established by a recognized accrediting organization. Compliance is the ongoing process of meeting the legal, ethical, and professional standards applicable to a particular health care organization.
bClinical quality improvement consists of systematic and continuous actions that lead to measurable improvement in health care services and focuses on the application of several widely accepted process improvement methodologies to improve clinical performance and desired outcomes.
cClinical measurement uses tools to help evaluate and track the quality of health care services provided to beneficiaries in the military health system.
Appendix II: Reported Patient Safety Event Data for Operational Settings, Fiscal Years 2022 Through 2024
We reviewed and analyzed patient safety events from operational settings as reported in the Joint Patient Safety Reporting system for fiscal years 2022 through 2024 by each of the military departments. Military department officials told us that these data may not include all patient safety events occurring in operational settings because the system, which is location dependent, did not include all locations for operational settings during those fiscal years.[37] Additionally, individuals in operational settings may not have been able to access the reporting system because they may not have had a computer, for example. Therefore, our analysis reflects events reported in the system by the military departments and may not be a complete picture of all patient safety events that occurred during that time period.
Army
Army reported 619 patient safety events that occurred in operational settings in the Joint Patient Safety Reporting system for fiscal years 2022 through 2024. Because the patient safety reporting system was only configured for operational settings within one geographic combatant command (U.S. Central Command) during that time period, patient safety events in other operational settings were not reported.[38]
The majority of patient safety events reported each fiscal year for operational settings were classified as care management events, that is, events related to clinical care other than surgery. We also found around half or more of the events reported by Army each fiscal year did not reach a patient. Of the events that reached a patient, over 80 percent each year were classified as no-harm events.
Air Force
Air Force reported 618 patient safety events that occurred in operational settings in the Joint Patient Safety Reporting system for fiscal years 2022 through 2024.[39]
The majority of patient safety events reported each fiscal year for operational settings were classified as care management events. We also found that, depending on the year, between 43 and 50 percent of the events reported by Air Force did not reach a patient. Of those that reached a patient each fiscal year, over 80 percent were classified as no-harm events.
Air Force - Aeromedical Evacuation
Air Force tracks aeromedical evacuation patient safety reports separately from those that occur in their other operational settings in the Joint Patient Safety Reporting system. It reported 1,329 of these events for fiscal years 2022 through 2024. Aeromedical evacuation events may occur whenever a patient is transported via Air Force or contracted aircraft (i.e., at sending location, at destination location, or in flight) and may involve more than one military department.
The majority of Air Force aeromedical evacuation patient safety events reported each fiscal year were considered care management events. We also found that over 69 percent of events reported by Air Force’s Aeromedical Evacuation each fiscal year did not reach a patient. Of those that did reach a patient, over 95 percent each fiscal year were classified as no-harm events.
Navy
Navy reported 163 patient safety events in the Joint Patient Safety Reporting system for fiscal years 2022 through 2024. Navy officials reported events occurring across several different operational settings, such as aircraft carriers and hospital ships. Navy officials said not all patient safety events occurring in operational settings are entered into the patient safety reporting system, as required, as individuals may be unable to access the system in certain operational settings, such as when they are at sea.
The majority of events reported by Navy each fiscal year were classified as care management events. We also found that between 29 and 54 percent of events reported by Navy each fiscal year did not reach a patient. Of those that reached a patient, between 41 and 73 percent were classified as no-harm events.
Each of the military departments told us that they have various activities underway to mitigate health care risk in operational settings, in addition to health care risk management investigations. (See fig. 3 for examples of selected risk management activities.)
Figure 3: Selected Health Care Risk Management Activities for Operational Settings by Military Department
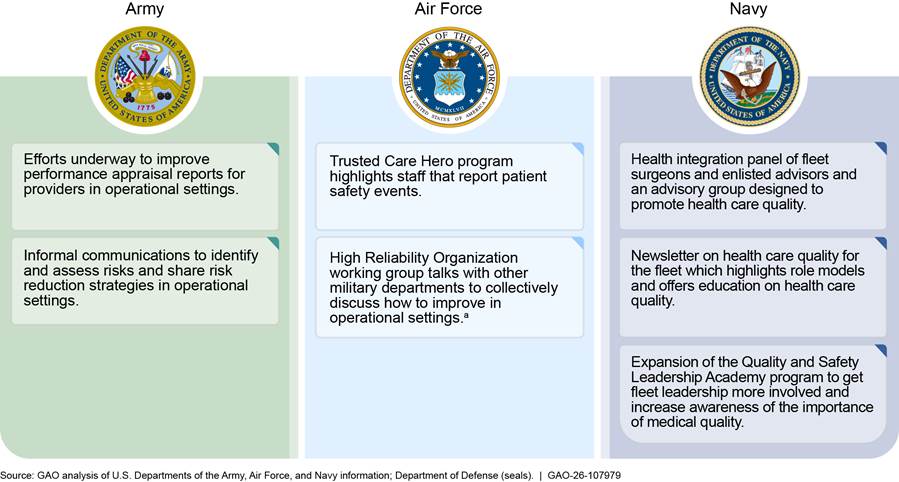
aA high reliability organization is one that experiences fewer than anticipated accidents or events of harm despite operating in highly complex, high-risk environments where even small errors can lead to tragic results.
GAO Contact
Sharon M. Silas, silass@gao.gov
Staff Acknowledgments
In addition to the contact named above, Bonnie Anderson (Assistant Director), Erin C. Henderson (Analyst-in-Charge), Ann Marie Cortez, Ying Hu, Stephanie Lola, and Ethiene Salgado-Rodriguez made key contributions to this report.
The Government Accountability Office, the audit, evaluation, and investigative arm of Congress, exists to support Congress in meeting its constitutional responsibilities and to help improve the performance and accountability of the federal government for the American people. GAO examines the use of public funds; evaluates federal programs and policies; and provides analyses, recommendations, and other assistance to help Congress make informed oversight, policy, and funding decisions. GAO’s commitment to good government is reflected in its core values of accountability, integrity, and reliability.
Obtaining Copies of GAO Reports and Testimony
The fastest and easiest way to obtain copies of GAO documents at no cost is through our website. Each weekday afternoon, GAO posts on its website newly released reports, testimony, and correspondence. You can also subscribe to GAO’s email updates to receive notification of newly posted products.
Order by Phone
The price of each GAO publication reflects GAO’s actual cost of production and distribution and depends on the number of pages in the publication and whether the publication is printed in color or black and white. Pricing and ordering information is posted on GAO’s website, https://www.gao.gov/ordering.htm.
Place orders by calling (202) 512-6000, toll free (866) 801-7077,
or
TDD (202) 512-2537.
Orders may be paid for using American Express, Discover Card, MasterCard, Visa, check, or money order. Call for additional information.
Connect with GAO
Connect with GAO on X,
LinkedIn, Instagram, and YouTube.
Subscribe to our Email Updates. Listen to our Podcasts.
Visit GAO on the web at https://www.gao.gov.
To Report Fraud, Waste, and Abuse in Federal Programs
Contact FraudNet:
Website: https://www.gao.gov/about/what-gao-does/fraudnet
Automated answering system: (800) 424-5454
Media Relations
Sarah Kaczmarek, Managing Director, Media@gao.gov
Congressional Relations
David A. Powner, Acting Managing Director, CongRel@gao.gov
General Inquiries
[1]Department of Defense, Defense Health Agency, Defense Health Agency Procedures Manual 6025.13: Clinical Quality Management in the Military Health System (Falls Church, VA.: Aug. 29, 2019). Clinical quality management provides an organized structure for defining, measuring, assuring, and improving the quality of care delivered in the military health system.
[2] The six aspects of clinical quality management are 1) credentialing and privileging; 2) patient safety; 3) health care risk management; 4) accreditation and compliance; 5) clinical measurement; and 6) clinical quality improvement.
[3]Department of Defense, DOD Instruction 6025.13: Medical Quality Assurance and Clinical Quality Management in the Military Health System (Washington, D.C.: July 26, 2023).
[4]H.R. Rep. No. 117-397, at 204 (2022).
[5]See GAO, Military Health Care: Departments Should Update Policies for Providers in Operational Settings Like Field Hospitals and Aircraft Carriers, GAO‑25‑106445 (Washington, D.C.: Dec. 4, 2024).
[6]We also provide information on military departments’ efforts to address the three remaining programs outlined in the clinical quality management framework (accreditation and compliance, clinical measurement, and clinical quality improvement). See appendix I.
[7]The National Defense Authorization Act for Fiscal Year 2017 included a variety of provisions that aimed to streamline management and improve efficiency across the military health system. In response, DHA took over the management of the military medical treatment facilities from the military departments. Prior to this reorganization, the military departments were responsible for health care in operational and non-operational settings.
[8]For more information on military departments efforts to address credentialing and privileging in operational settings, see GAO‑25‑106445.
[9]The Joint Patient Safety Reporting system is a web-based application used by both DOD and the Department of Veterans Affairs to standardize event capture and data management of medical errors and close calls or near misses.
[10]In a near miss event, an error was committed, but the patient did not experience clinical harm, either through early detection or sheer luck.
[11]The DHA procedures manual states that the reports must be entered within 72 hours. However, this may not be practicable in certain operational settings.
[12]We have previously reported on DHA’s clinical adverse action procedures at military medical treatment facilities. See GAO, Military Health Care: DOD Should Improve Its Process for Clinical Adverse Actions against Providers, GAO‑24‑106107 (Washington, D.C.: April 11, 2024).
[13]Department of Defense, Defense Health Agency, Defense Health Agency Procedures Manual 6025.13.
[14]Department of Defense, DOD Instruction 6025.13.
[15]Privileging a provider is the process of reviewing a provider’s qualifications and granting permission for the provider to perform certain health care services in a specific setting. This program makes all granted privileges portable across all health care facilities and environments throughout the military health system; providers will only need to be re-privileged when their privileges expire. See Assistant Secretary of Defense, Health Affairs, Exception to Policy to Authorize Enterprise-wide Credentialing and Privileging in the Military Health System (Washington, D.C.: Sept. 19, 2025).
[16]For example, according to the health care risk management program in the DHA procedures manual, the privileging authority is responsible for suspending a provider from delivering patient care if a quality or safety concern is raised. Under the new privileging program, the responsibility for taking action on a provider’s privileges is transferred automatically; re-privileging is not required.
[17]The six clinical quality management programs in the framework are 1) credentialing and privileging; 2) patient safety; 3) health care risk management; 4) accreditation and compliance; 5) clinical measurement; and 6) clinical quality improvement.
[18]Current versions of Army, Air Force, and Navy policies addressing provider privileging and evaluation are dated 2004, 2011, and 2015, respectively.
For the current version of Army’s policy, see Department of the Army, Clinical Quality Management, Army Regulation 40-68 (Washington, D.C.: March 2004). Army also issued a rapid action revision of Army Regulation 40-68 in 2009 and an administrative revision in July 2025. See Department of the Army, Clinical Quality Management, Rapid Action Revision, Army Regulation 40-68 (Washington, D.C.: May 2009).
For the current version of Air Force’s policy, see Department of the Air Force, Medical Quality Operations, Air Force Instruction 44-119 (Washington, D.C.: August 2011). Air Force also released a guidance memorandum to accompany this instruction in 2023; see Department of the Air Force, Medical Quality Operations, Department of the Air Force Guidance Memorandum to Department of the Air Force Instruction 44-119 (Washington, D.C.: March 2023). In May 2024, Air Force issued an additional guidance memorandum that extended the 2023 memorandum for another year; see Department of the Air Force, Medical Quality Operations, Department of the Air Force Guidance Memorandum to Department of the Air Force Instruction 44-119 (Washington, D.C.: May 2024).
For the current version of Navy’s policy, see Department of the Navy, Bureau of Medicine and Surgery, Credentialing and Privileging Program, Bureau of Medicine and Surgery Instruction 6010.30 (Falls Church, VA.: March 2015).
[19]Department of Defense, DOD Instruction 6025.13.
[21]See Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6010.23A, Operational Clinical Patient Safety Program (Falls Church, VA.: July 15, 2025) and Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6010.31A: Clinical Adverse Actions and Health Care Related Misconduct (Falls Church, VA.: April 25, 2025).
[22]Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6010.13A: Medical Quality Assurance Program and Clinical Quality Management Program (Falls Church, VA.: Jan. 26, 2026).
[23]While Navy has not yet published its policy on credentialing and privileging, it has issued interim guidance on universal privileging. See Department of the Navy, Bureau of Medicine and Surgery, BUMED Notice 6000, Navy Medicine Enterprise-Wide Privileging Implementation Guidance (Falls Church, VA.: Nov. 25, 2025). Navy also issued medical staff bylaws, which serve as the formal organizational structure for privileging authorities, medical executive committees, and licensed independent providers. See Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6010.17D, Navy Medical Staff Bylaws (Falls Church, VA.: April 24, 2025).
[24]Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6010.23A.
[25]The DHA procedures manual has a goal of closing 80 percent of patient safety events within 30 days, and additional time frames are associated with specific steps in the review process. Military department officials told us they try to meet these timelines; however, they said that time frames may vary due to the unique circumstances of operational settings. Assessing the timeliness of the military departments’ review of patient safety events was not in the scope of our review.
[26]Any patient safety events resulting in death, permanent harm, or severe temporary harm are classified as DOD reportable events. When an event reaches the patient and is likely to present a possible financial loss to the federal government, it is considered a potentially compensable event, which requires further collaboration with health care risk management. We have previously reported on reviews of potentially compensable events at military medical treatment facilities, see GAO, Military Health Care: Improved Procedures and Monitoring Needed to Ensure Provider Qualifications and Competence, GAO‑22‑104668 (Washington, D.C.: Aug. 11, 2022).
[27]Air Force shares information within the department and may also share clinical operational patient safety alerts with the Army and Navy to promote shared awareness. Army officials said they may share information in an all-Army message. Navy officials said they share a regular newsletter highlighting findings from patient safety events.
[28]DHA officials said a second module–for reviews and investigations–is scheduled to be released in late 2026. This module is intended to allow managers to more easily provide reviewers access to the report in the system for collaboration. Air Force officials said investigations are slower when multiple units are involved. Air Force officials believe the updated system should help increase collaboration and streamline the investigation process.
[29]The military departments are responsible for requesting the system be configured to capture all geographic locations.
[30]As of fiscal year 2024, Army only captured events in the U.S. Central Command area of responsibility, which includes operational settings from the Middle East to Central and South Asia. In locations where the department has yet to configure the patient reporting system, Army officials said service members can report patient safety events up the chain of command. However, Army officials acknowledged the patient safety system allows service members to report events and unsafe conditions anonymously. Therefore, the inability to report events or conditions anonymously could limit reporting.
As of fiscal year 2025, Army officials said they configured the system in two more operational settings, one following the occurrence of a severe patient safety event, and another when the Army established operational settings there.
[31]According to Navy officials, the policy differs from the DHA procedures only in that the scope and applicability are slightly different for those providers privileged by Bureau of Medicine. In rare cases, adverse actions can be initiated beyond the 24-month limit in the DHA procedures manual. See Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6010.31A.
Navy has also issued a policy on specialty reviews, when adequacy of the medical care provided is at issue, and a policy that describes the available resources to implement a high reliability organization—an organization that experiences fewer than anticipated accidents or events of harm despite operating in complex, high-risk environments—operating model. See Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 5830.1C, Health Care Investigation Procedures for Specialty Reviews (Falls Church, VA.: Jan. 25, 2025) and Department of the Navy, Bureau of Medicine and Surgery, BUMED Instruction 6000.22, High Reliability Organization Implementation (Falls Church, VA.: Jan. 21, 2026).
[32]In addition to investigations, the military departments also conduct various other health care risk management activities. See appendix III for information on these activities.
[33]Quality assurance investigations are separate from evaluations of clinical proficiency. Routine and regular evaluations of clinical privileges and practice are required and provide a means to validate clinical proficiency. Routine and regular evaluations include ongoing professional practice evaluations, focused professional practice evaluations with monitoring and evaluation, and regular training and education.
[34]An investigation may result in a clinical adverse action, which removes the provider from clinical practice.
[35]Department of Defense, Defense Health Agency, Defense Health Agency Procedures Manual 6025.13: Clinical Quality Management in the Military Health System (Falls Church, VA.: Aug. 29, 2019).
[36]GAO, Military Health Care: Departments Should Update Policies for Providers in Operational Settings Like Field Hospitals and Aircraft Carriers, GAO‑25‑106445 (Washington, D.C.: Dec. 4, 2024).
[37]The military departments are responsible for submitting a request to the Defense Health Agency for the system be configured to capture all the events occurring within their specific geographic operational locations.
[38]Department of Defense (DOD) operational settings may be aligned with one of DOD’s 11 unified combatant commands, which are joint military commands of the DOD that are composed of units from two or more service branches of the United States Armed Forces and conduct broad and continuing missions. U.S. Central Command’s area of responsibility includes operational settings from the Middle East to Central and South Asia.
[39]Air Force reports aeromedical evacuation patient safety events separately.